User login
For MD-IQ use only
Older men more at risk as dangerous falls rise for all seniors
When Senate Minority Leader Mitch McConnell (R-Ky.) fell recently at a dinner event in Washington, he unfortunately joined a large group of his senior citizen peers.
This wasn’t the first tumble the 81-year-old has taken. In 2019, he fell in his home, fracturing his shoulder. This time, he got a concussion and was recently released to an in-patient rehabilitation facility. While Sen. McConnell didn’t fracture his skull, in falling and hitting his head, he became part of an emerging statistic: One that reveals falls are more dangerous for senior men than senior women.
This new research, which appeared in the American Journal of Emergency Medicine, came as a surprise to lead researcher Scott Alter, MD, associate professor of emergency medicine at the Florida Atlantic University, Boca Raton.
“We always hear about lower bone density rates among females, so we didn’t expect to see males with more skull fractures,” he said.
Dr. Alter said that as a clinician in a southern Florida facility, his emergency department was the perfect study grounds to evaluate incoming geriatric patients due to falls. Older “patients are at higher risk of skull fractures and intercranial bleeding, and we wanted to look at any patient presenting with a head injury. Some 80% were fall related, however.”
The statistics bear out the fact that falls of all types are common among the elderly: Some 800,000 seniors wind up in the hospital each year because of falls.
The numbers show death rates from falls are on the rise in the senior citizen age group, too, up 30% from 2007 to 2016. Falls account for 70% of accidental deaths in people 75 and older. They are the leading cause of injury-related visits to emergency departments in the country, too.
Jennifer Stevens, MD, a gerontologist and executive director at Florida-based Abbey Delray South, is aware of the dire numbers and sees their consequences regularly. “The reasons seniors are at a high fall risk are many,” she said. “They include balance issues, declining strength, diseases like Parkinson’s and Alzheimer’s, side effects of their medications, and more.”
In addition, many seniors live in spaces that are not necessarily equipped for their limitations, and hazards exist all over their homes. Put together, and the risks for falls are everywhere. But there are steps seniors, their families, and even middle-aged people can take to mitigate and hopefully prevent dangerous falls.
Starting early
While in many cases the journey to lessen fall risks begins after a fall, the time to begin addressing the issue is long before you hit your senior years. Mary Therese Cole, a physical therapist and certified dementia practitioner at Manual Edge Physical Therapy in Colorado Springs, Colo., says that age 50 is a good time to start paying attention and addressing physical declines.
“This is an age where your vision might begin deteriorating,” she said. “It’s a big reason why elderly people trip and fall.”
As our brains begin to age in our middle years, the neural pathways from brain to extremities start to decline, too. The result is that many people stop picking up their feet as well as they used to do, making them more likely to trip.
“You’re not elderly yet, but you’re not a spring chicken, either,” Ms. Cole said. “Any issues you have now will only get worse if you’re not working on them.”
A good starting point in middle age, then, is to work on both strength training and balance exercises. A certified personal trainer or physical therapist can help get you on a program to ward off many of these declines.
If you’ve reached your later years, however, and are experiencing physical declines, it’s smart to check in with your primary care doctor for an assessment. “He or she can get your started on regular PT to evaluate any shortcomings and then address them,” Ms. Cole said.
She noted that when she’s working with senior patients, she’ll test their strength getting into and out of a chair, do a manual strength test to check on lower extremities, check their walking stride, and ask about conditions such as diabetes, former surgeries, and other conditions.
From there, Ms. Cole said she can write up a plan for the patient. Likewise, Dr. Stevens uses a program called Be Active that allows her to test seniors on a variety of measurements, including flexibility, balance, hand strength, and more.
“Then we match them with classes to address their shortcomings,” she said. “It’s critical that seniors have the ability to recover and not fall if they get knocked off balance.”
Beyond working on your physical limitations, taking a good look at your home is essential, too. “You can have an occupational therapist come to your home and do an evaluation,” Dr. Stevens said. “They can help you rearrange and reorganize for a safer environment.”
Big, common household fall hazards include throw rugs, lack of nightlights for middle-of-the-night visits to the bathroom, a lack of grab bars in the shower/bathtub, and furniture that blocks pathways.
For his part, Dr. Alter likes to point seniors and their doctors to the CDC’s STEADI program, which is aimed at stopping elderly accidents, deaths, and injuries.
“It includes screening for fall risk, assessing factors you can modify or improve, and more tools,” he said.
Dr. Alter also recommended seniors talk to their doctors about medications, particularly blood thinners.
“At a certain point, you need to weigh the benefits of disease prevention with the risk of injury if you fall,” he said. “The bleeding risk might be too high if the patient is at a high risk of falls.”
A version of this article originally appeared on WebMD.com.
When Senate Minority Leader Mitch McConnell (R-Ky.) fell recently at a dinner event in Washington, he unfortunately joined a large group of his senior citizen peers.
This wasn’t the first tumble the 81-year-old has taken. In 2019, he fell in his home, fracturing his shoulder. This time, he got a concussion and was recently released to an in-patient rehabilitation facility. While Sen. McConnell didn’t fracture his skull, in falling and hitting his head, he became part of an emerging statistic: One that reveals falls are more dangerous for senior men than senior women.
This new research, which appeared in the American Journal of Emergency Medicine, came as a surprise to lead researcher Scott Alter, MD, associate professor of emergency medicine at the Florida Atlantic University, Boca Raton.
“We always hear about lower bone density rates among females, so we didn’t expect to see males with more skull fractures,” he said.
Dr. Alter said that as a clinician in a southern Florida facility, his emergency department was the perfect study grounds to evaluate incoming geriatric patients due to falls. Older “patients are at higher risk of skull fractures and intercranial bleeding, and we wanted to look at any patient presenting with a head injury. Some 80% were fall related, however.”
The statistics bear out the fact that falls of all types are common among the elderly: Some 800,000 seniors wind up in the hospital each year because of falls.
The numbers show death rates from falls are on the rise in the senior citizen age group, too, up 30% from 2007 to 2016. Falls account for 70% of accidental deaths in people 75 and older. They are the leading cause of injury-related visits to emergency departments in the country, too.
Jennifer Stevens, MD, a gerontologist and executive director at Florida-based Abbey Delray South, is aware of the dire numbers and sees their consequences regularly. “The reasons seniors are at a high fall risk are many,” she said. “They include balance issues, declining strength, diseases like Parkinson’s and Alzheimer’s, side effects of their medications, and more.”
In addition, many seniors live in spaces that are not necessarily equipped for their limitations, and hazards exist all over their homes. Put together, and the risks for falls are everywhere. But there are steps seniors, their families, and even middle-aged people can take to mitigate and hopefully prevent dangerous falls.
Starting early
While in many cases the journey to lessen fall risks begins after a fall, the time to begin addressing the issue is long before you hit your senior years. Mary Therese Cole, a physical therapist and certified dementia practitioner at Manual Edge Physical Therapy in Colorado Springs, Colo., says that age 50 is a good time to start paying attention and addressing physical declines.
“This is an age where your vision might begin deteriorating,” she said. “It’s a big reason why elderly people trip and fall.”
As our brains begin to age in our middle years, the neural pathways from brain to extremities start to decline, too. The result is that many people stop picking up their feet as well as they used to do, making them more likely to trip.
“You’re not elderly yet, but you’re not a spring chicken, either,” Ms. Cole said. “Any issues you have now will only get worse if you’re not working on them.”
A good starting point in middle age, then, is to work on both strength training and balance exercises. A certified personal trainer or physical therapist can help get you on a program to ward off many of these declines.
If you’ve reached your later years, however, and are experiencing physical declines, it’s smart to check in with your primary care doctor for an assessment. “He or she can get your started on regular PT to evaluate any shortcomings and then address them,” Ms. Cole said.
She noted that when she’s working with senior patients, she’ll test their strength getting into and out of a chair, do a manual strength test to check on lower extremities, check their walking stride, and ask about conditions such as diabetes, former surgeries, and other conditions.
From there, Ms. Cole said she can write up a plan for the patient. Likewise, Dr. Stevens uses a program called Be Active that allows her to test seniors on a variety of measurements, including flexibility, balance, hand strength, and more.
“Then we match them with classes to address their shortcomings,” she said. “It’s critical that seniors have the ability to recover and not fall if they get knocked off balance.”
Beyond working on your physical limitations, taking a good look at your home is essential, too. “You can have an occupational therapist come to your home and do an evaluation,” Dr. Stevens said. “They can help you rearrange and reorganize for a safer environment.”
Big, common household fall hazards include throw rugs, lack of nightlights for middle-of-the-night visits to the bathroom, a lack of grab bars in the shower/bathtub, and furniture that blocks pathways.
For his part, Dr. Alter likes to point seniors and their doctors to the CDC’s STEADI program, which is aimed at stopping elderly accidents, deaths, and injuries.
“It includes screening for fall risk, assessing factors you can modify or improve, and more tools,” he said.
Dr. Alter also recommended seniors talk to their doctors about medications, particularly blood thinners.
“At a certain point, you need to weigh the benefits of disease prevention with the risk of injury if you fall,” he said. “The bleeding risk might be too high if the patient is at a high risk of falls.”
A version of this article originally appeared on WebMD.com.
When Senate Minority Leader Mitch McConnell (R-Ky.) fell recently at a dinner event in Washington, he unfortunately joined a large group of his senior citizen peers.
This wasn’t the first tumble the 81-year-old has taken. In 2019, he fell in his home, fracturing his shoulder. This time, he got a concussion and was recently released to an in-patient rehabilitation facility. While Sen. McConnell didn’t fracture his skull, in falling and hitting his head, he became part of an emerging statistic: One that reveals falls are more dangerous for senior men than senior women.
This new research, which appeared in the American Journal of Emergency Medicine, came as a surprise to lead researcher Scott Alter, MD, associate professor of emergency medicine at the Florida Atlantic University, Boca Raton.
“We always hear about lower bone density rates among females, so we didn’t expect to see males with more skull fractures,” he said.
Dr. Alter said that as a clinician in a southern Florida facility, his emergency department was the perfect study grounds to evaluate incoming geriatric patients due to falls. Older “patients are at higher risk of skull fractures and intercranial bleeding, and we wanted to look at any patient presenting with a head injury. Some 80% were fall related, however.”
The statistics bear out the fact that falls of all types are common among the elderly: Some 800,000 seniors wind up in the hospital each year because of falls.
The numbers show death rates from falls are on the rise in the senior citizen age group, too, up 30% from 2007 to 2016. Falls account for 70% of accidental deaths in people 75 and older. They are the leading cause of injury-related visits to emergency departments in the country, too.
Jennifer Stevens, MD, a gerontologist and executive director at Florida-based Abbey Delray South, is aware of the dire numbers and sees their consequences regularly. “The reasons seniors are at a high fall risk are many,” she said. “They include balance issues, declining strength, diseases like Parkinson’s and Alzheimer’s, side effects of their medications, and more.”
In addition, many seniors live in spaces that are not necessarily equipped for their limitations, and hazards exist all over their homes. Put together, and the risks for falls are everywhere. But there are steps seniors, their families, and even middle-aged people can take to mitigate and hopefully prevent dangerous falls.
Starting early
While in many cases the journey to lessen fall risks begins after a fall, the time to begin addressing the issue is long before you hit your senior years. Mary Therese Cole, a physical therapist and certified dementia practitioner at Manual Edge Physical Therapy in Colorado Springs, Colo., says that age 50 is a good time to start paying attention and addressing physical declines.
“This is an age where your vision might begin deteriorating,” she said. “It’s a big reason why elderly people trip and fall.”
As our brains begin to age in our middle years, the neural pathways from brain to extremities start to decline, too. The result is that many people stop picking up their feet as well as they used to do, making them more likely to trip.
“You’re not elderly yet, but you’re not a spring chicken, either,” Ms. Cole said. “Any issues you have now will only get worse if you’re not working on them.”
A good starting point in middle age, then, is to work on both strength training and balance exercises. A certified personal trainer or physical therapist can help get you on a program to ward off many of these declines.
If you’ve reached your later years, however, and are experiencing physical declines, it’s smart to check in with your primary care doctor for an assessment. “He or she can get your started on regular PT to evaluate any shortcomings and then address them,” Ms. Cole said.
She noted that when she’s working with senior patients, she’ll test their strength getting into and out of a chair, do a manual strength test to check on lower extremities, check their walking stride, and ask about conditions such as diabetes, former surgeries, and other conditions.
From there, Ms. Cole said she can write up a plan for the patient. Likewise, Dr. Stevens uses a program called Be Active that allows her to test seniors on a variety of measurements, including flexibility, balance, hand strength, and more.
“Then we match them with classes to address their shortcomings,” she said. “It’s critical that seniors have the ability to recover and not fall if they get knocked off balance.”
Beyond working on your physical limitations, taking a good look at your home is essential, too. “You can have an occupational therapist come to your home and do an evaluation,” Dr. Stevens said. “They can help you rearrange and reorganize for a safer environment.”
Big, common household fall hazards include throw rugs, lack of nightlights for middle-of-the-night visits to the bathroom, a lack of grab bars in the shower/bathtub, and furniture that blocks pathways.
For his part, Dr. Alter likes to point seniors and their doctors to the CDC’s STEADI program, which is aimed at stopping elderly accidents, deaths, and injuries.
“It includes screening for fall risk, assessing factors you can modify or improve, and more tools,” he said.
Dr. Alter also recommended seniors talk to their doctors about medications, particularly blood thinners.
“At a certain point, you need to weigh the benefits of disease prevention with the risk of injury if you fall,” he said. “The bleeding risk might be too high if the patient is at a high risk of falls.”
A version of this article originally appeared on WebMD.com.
Physician suicide: Investigating its prevalence and cause
Physicians are admired for their sacrifice and dedication. Yet beneath the surface lies a painful, quiet reality:
The Physicians Foundation says that 55% of physicians know a doctor who considered, attempted, or died by suicide. Doctor’s Burden: Medscape Physician Suicide Report 2023 asked more than 9,000 doctors if they had suicidal thoughts. Nine percent of male physicians and 11% of female physicians said yes.
Why do so many doctors take their own lives?
“It’s not a new phenomenon,” says Rajnish Jaiswal, MD, associate chief of emergency medicine at NYC H+H Metropolitan Hospital and assistant professor of emergency medicine at New York Medical College. “There was a paper 150 years ago, published in England, which commented on the high rates of physician suicides compared to other professionals, and that trend has continued.”
Dr. Jaiswal says that the feeling in the physician community is that the numbers are even higher than what’s reported, unfortunately, which is an opinion echoed by other doctors this news organization spoke with for this story.
A perfect storm
Jodie Eckleberry-Hunt, PhD, a board-certified health psychologist, executive coach, and author, says the most significant culprit historically may be a rigid mindset that many physicians have. “There’s black and white, there’s a right answer and a wrong answer, there’s good and bad, and some physicians have a really hard time flexing,” she says.
Psychological flexibility underlies resilience. Dr. Eckleberry-Hunt says, “Think about your bounce factor and how that resilience is protective. Life isn’t always going to go well. You have to be able to flex and bounce, and some physicians (not all of them, of course) tend to be lower on cognitive flexibility.”
Brad Fern, coach and psychotherapist at Fern Executive and Physician Consulting, Minneapolis, says he uses two analogies that help when he works with physicians. One is the evil twins, and the other is the pressure cooker.
Mr. Fern says that the evil twins are silence and isolation and that several professions, including physicians, fall prey to these. To put any dent in suicidal ideations and suicide, Mr. Fern says, these must be addressed.
“Physicians tend not to talk about what’s bothering them, and that’s for many different reasons. They disproportionally tend to be great at helping other people but not great at receiving help themselves.”
On top of that, there’s a pressure cooker where they work. Mr. Fern doesn’t think anyone would argue that the health care system in the United States is not dysfunctional, at least to some degree. He says that this dysfunction acts like the physicians’ pressure cooker.
Add in circumstances, cultures, and day-to-day issues everyone has, like relational issues, parenting issues, and mental health problems. Then, toss in an individual’s lower resiliency, the inability to receive help, and a predicament for good measure – a loss, a divorce, or financial woes, for instance, which can overwhelm. Mr. Fern says it can be a mathematical equation for suicidal ideation.
Is there a why?
“Some people think there’s a reason for suicide, but often, there’s a spectrum of reasons,” says Mr. Fern. He says that some physicians are trying to escape emotional pain. For others, it can be fear or a revenge thing, like, “the hell with you, I’m going to kill myself.” It can be getting attention the way teens do, as professionals have seen. Then there’s the organic component, like brain trauma, brain imbalance, depression, anxiety, or bipolar disorder. And finally, a drug or alcohol issue.
“But the reason why physician suicide is elevated, I think, is because there’s this ethos around being silent and, ‘I’m going to listen to and solve everyone else’s problems, but I’m not going to reach out and get help for my own,’ ” says Mr. Fern. “If you take advantage of mental health services, you’re implying that you’re mentally ill. And most physicians aren’t going to do that.”
On the positive side, Dr. Eckleberry-Hunt says that she sees many younger physicians discussing trauma. As a result, they’re more open to receiving help than previous generations. She speculates whether physicians have always had trauma from their past and whether current-day issues are now triggering it or whether they have more trauma these days. “Are they talking about it more, or is it experienced more?”
The failure of the system
The building blocks for physician suicide may have been there from the beginning. “From your first day of medical school and throughout your career, there was a very rigid system in place that is quite unforgiving, is quite stressful, and demands a lot,” says Dr. Jaiswal. And it’s within this system that physicians must operate.
“You have all the corporations, entities, organizations, [and] medical societies talking about physician wellness, burnout, and suicide, but the reality is it’s not making that much of a difference,” he says.
In her report, “What I’ve Learned From 1,710 Doctor Suicides,” Pamelia Wible, MD, who runs a physician suicide helpline that physicians can email and get an immediate callback, likens the current system to assembly line medicine.
Dr. Eckleberry-Hunt thinks the message has been bungled in health care. Everyone discusses burnout, meditation, self-care, and other essential constructs. “But we don’t deal with the root cause [of suicide]. Instead, we teach you soothing strategies.”
Further, Dr. Jaiswal says that not all physicians who commit suicide experience burnout or are experiencing burnout and that the vast majority of physicians who experience burnout don’t have suicidal ideation. “In the sense, that ‘let’s address physician burnout and that will hopefully translate to a reduced number of physician suicides’ – there is a very tenuous argument to be made for that because that is just one aspect in this complex system,” he says.
We need more than just lip service on suicide
Overall, the experts interviewed for this article acknowledged that the system is at least talking about physician suicide, which is a big first step. However, most agree that where big health entities go wrong is that they set up wellness or mental health programs, they implement a wellness officer, they write up talking points for physicians who need mental health care to get that care, and they think they’ve done their job, that they’ve done what’s required to address the problem.
But Dr. Jaiswal thinks these are often mostly public-relations rebuttals. Mr. Fern suggests, “It’s a show that’s not effective.” And Dr. Eckleberry-Hunt says that “even if you had a legit, well-funded well-being program for health care providers, you would still have a baseline rate of physician suicide, and that gets down to having drug and alcohol education and talking about having a system for physicians to access that doesn’t come along with insurance billing” – one that doesn’t create a paper trail and follow physician licensure and job applications for the rest of their career; one that doesn’t associate their mental health care with their work institution; one that offers confidentiality.
“For most folks, there is still a big distrust in the system. As physicians, very few of them feel that the system that they’re operating in has their best interest at heart. And that is why very few physicians will self-report any mental health issues, depression, or even ideation to colleagues, superiors, or managers,” says Dr. Jaiswal. Many more feel skeptical about the confidentiality of the programs in place.
The experts acknowledge that many people are trying to work on this and bring about change on multiple levels – grassroots, department levels, state, and federal. “But I think the biggest thing that the system has to do is earn back the trust of the physician,” Dr. Jaiswal adds.
“Physician suicide is a very visible problem in a very broken system. So, it’ll be very difficult in isolation to treat it without making any systemic changes, because that’s happening right now, and it’s not working,” says Dr. Jaiswal.
“The thing that I am most hopeful about is that I am seeing an influx of younger physicians who seek me out, and granted, their training programs tell them to come and see me, but they are ready and willing to talk about their mental health separate from work. They’re not coming in saying, ‘Here are all the people who I blame.’ They’re saying, ‘These are my struggles, and I want to be a better, happier physician,’ ” says Dr. Eckleberry-Hunt.
A version of this article originally appeared on Medscape.com.
Physicians are admired for their sacrifice and dedication. Yet beneath the surface lies a painful, quiet reality:
The Physicians Foundation says that 55% of physicians know a doctor who considered, attempted, or died by suicide. Doctor’s Burden: Medscape Physician Suicide Report 2023 asked more than 9,000 doctors if they had suicidal thoughts. Nine percent of male physicians and 11% of female physicians said yes.
Why do so many doctors take their own lives?
“It’s not a new phenomenon,” says Rajnish Jaiswal, MD, associate chief of emergency medicine at NYC H+H Metropolitan Hospital and assistant professor of emergency medicine at New York Medical College. “There was a paper 150 years ago, published in England, which commented on the high rates of physician suicides compared to other professionals, and that trend has continued.”
Dr. Jaiswal says that the feeling in the physician community is that the numbers are even higher than what’s reported, unfortunately, which is an opinion echoed by other doctors this news organization spoke with for this story.
A perfect storm
Jodie Eckleberry-Hunt, PhD, a board-certified health psychologist, executive coach, and author, says the most significant culprit historically may be a rigid mindset that many physicians have. “There’s black and white, there’s a right answer and a wrong answer, there’s good and bad, and some physicians have a really hard time flexing,” she says.
Psychological flexibility underlies resilience. Dr. Eckleberry-Hunt says, “Think about your bounce factor and how that resilience is protective. Life isn’t always going to go well. You have to be able to flex and bounce, and some physicians (not all of them, of course) tend to be lower on cognitive flexibility.”
Brad Fern, coach and psychotherapist at Fern Executive and Physician Consulting, Minneapolis, says he uses two analogies that help when he works with physicians. One is the evil twins, and the other is the pressure cooker.
Mr. Fern says that the evil twins are silence and isolation and that several professions, including physicians, fall prey to these. To put any dent in suicidal ideations and suicide, Mr. Fern says, these must be addressed.
“Physicians tend not to talk about what’s bothering them, and that’s for many different reasons. They disproportionally tend to be great at helping other people but not great at receiving help themselves.”
On top of that, there’s a pressure cooker where they work. Mr. Fern doesn’t think anyone would argue that the health care system in the United States is not dysfunctional, at least to some degree. He says that this dysfunction acts like the physicians’ pressure cooker.
Add in circumstances, cultures, and day-to-day issues everyone has, like relational issues, parenting issues, and mental health problems. Then, toss in an individual’s lower resiliency, the inability to receive help, and a predicament for good measure – a loss, a divorce, or financial woes, for instance, which can overwhelm. Mr. Fern says it can be a mathematical equation for suicidal ideation.
Is there a why?
“Some people think there’s a reason for suicide, but often, there’s a spectrum of reasons,” says Mr. Fern. He says that some physicians are trying to escape emotional pain. For others, it can be fear or a revenge thing, like, “the hell with you, I’m going to kill myself.” It can be getting attention the way teens do, as professionals have seen. Then there’s the organic component, like brain trauma, brain imbalance, depression, anxiety, or bipolar disorder. And finally, a drug or alcohol issue.
“But the reason why physician suicide is elevated, I think, is because there’s this ethos around being silent and, ‘I’m going to listen to and solve everyone else’s problems, but I’m not going to reach out and get help for my own,’ ” says Mr. Fern. “If you take advantage of mental health services, you’re implying that you’re mentally ill. And most physicians aren’t going to do that.”
On the positive side, Dr. Eckleberry-Hunt says that she sees many younger physicians discussing trauma. As a result, they’re more open to receiving help than previous generations. She speculates whether physicians have always had trauma from their past and whether current-day issues are now triggering it or whether they have more trauma these days. “Are they talking about it more, or is it experienced more?”
The failure of the system
The building blocks for physician suicide may have been there from the beginning. “From your first day of medical school and throughout your career, there was a very rigid system in place that is quite unforgiving, is quite stressful, and demands a lot,” says Dr. Jaiswal. And it’s within this system that physicians must operate.
“You have all the corporations, entities, organizations, [and] medical societies talking about physician wellness, burnout, and suicide, but the reality is it’s not making that much of a difference,” he says.
In her report, “What I’ve Learned From 1,710 Doctor Suicides,” Pamelia Wible, MD, who runs a physician suicide helpline that physicians can email and get an immediate callback, likens the current system to assembly line medicine.
Dr. Eckleberry-Hunt thinks the message has been bungled in health care. Everyone discusses burnout, meditation, self-care, and other essential constructs. “But we don’t deal with the root cause [of suicide]. Instead, we teach you soothing strategies.”
Further, Dr. Jaiswal says that not all physicians who commit suicide experience burnout or are experiencing burnout and that the vast majority of physicians who experience burnout don’t have suicidal ideation. “In the sense, that ‘let’s address physician burnout and that will hopefully translate to a reduced number of physician suicides’ – there is a very tenuous argument to be made for that because that is just one aspect in this complex system,” he says.
We need more than just lip service on suicide
Overall, the experts interviewed for this article acknowledged that the system is at least talking about physician suicide, which is a big first step. However, most agree that where big health entities go wrong is that they set up wellness or mental health programs, they implement a wellness officer, they write up talking points for physicians who need mental health care to get that care, and they think they’ve done their job, that they’ve done what’s required to address the problem.
But Dr. Jaiswal thinks these are often mostly public-relations rebuttals. Mr. Fern suggests, “It’s a show that’s not effective.” And Dr. Eckleberry-Hunt says that “even if you had a legit, well-funded well-being program for health care providers, you would still have a baseline rate of physician suicide, and that gets down to having drug and alcohol education and talking about having a system for physicians to access that doesn’t come along with insurance billing” – one that doesn’t create a paper trail and follow physician licensure and job applications for the rest of their career; one that doesn’t associate their mental health care with their work institution; one that offers confidentiality.
“For most folks, there is still a big distrust in the system. As physicians, very few of them feel that the system that they’re operating in has their best interest at heart. And that is why very few physicians will self-report any mental health issues, depression, or even ideation to colleagues, superiors, or managers,” says Dr. Jaiswal. Many more feel skeptical about the confidentiality of the programs in place.
The experts acknowledge that many people are trying to work on this and bring about change on multiple levels – grassroots, department levels, state, and federal. “But I think the biggest thing that the system has to do is earn back the trust of the physician,” Dr. Jaiswal adds.
“Physician suicide is a very visible problem in a very broken system. So, it’ll be very difficult in isolation to treat it without making any systemic changes, because that’s happening right now, and it’s not working,” says Dr. Jaiswal.
“The thing that I am most hopeful about is that I am seeing an influx of younger physicians who seek me out, and granted, their training programs tell them to come and see me, but they are ready and willing to talk about their mental health separate from work. They’re not coming in saying, ‘Here are all the people who I blame.’ They’re saying, ‘These are my struggles, and I want to be a better, happier physician,’ ” says Dr. Eckleberry-Hunt.
A version of this article originally appeared on Medscape.com.
Physicians are admired for their sacrifice and dedication. Yet beneath the surface lies a painful, quiet reality:
The Physicians Foundation says that 55% of physicians know a doctor who considered, attempted, or died by suicide. Doctor’s Burden: Medscape Physician Suicide Report 2023 asked more than 9,000 doctors if they had suicidal thoughts. Nine percent of male physicians and 11% of female physicians said yes.
Why do so many doctors take their own lives?
“It’s not a new phenomenon,” says Rajnish Jaiswal, MD, associate chief of emergency medicine at NYC H+H Metropolitan Hospital and assistant professor of emergency medicine at New York Medical College. “There was a paper 150 years ago, published in England, which commented on the high rates of physician suicides compared to other professionals, and that trend has continued.”
Dr. Jaiswal says that the feeling in the physician community is that the numbers are even higher than what’s reported, unfortunately, which is an opinion echoed by other doctors this news organization spoke with for this story.
A perfect storm
Jodie Eckleberry-Hunt, PhD, a board-certified health psychologist, executive coach, and author, says the most significant culprit historically may be a rigid mindset that many physicians have. “There’s black and white, there’s a right answer and a wrong answer, there’s good and bad, and some physicians have a really hard time flexing,” she says.
Psychological flexibility underlies resilience. Dr. Eckleberry-Hunt says, “Think about your bounce factor and how that resilience is protective. Life isn’t always going to go well. You have to be able to flex and bounce, and some physicians (not all of them, of course) tend to be lower on cognitive flexibility.”
Brad Fern, coach and psychotherapist at Fern Executive and Physician Consulting, Minneapolis, says he uses two analogies that help when he works with physicians. One is the evil twins, and the other is the pressure cooker.
Mr. Fern says that the evil twins are silence and isolation and that several professions, including physicians, fall prey to these. To put any dent in suicidal ideations and suicide, Mr. Fern says, these must be addressed.
“Physicians tend not to talk about what’s bothering them, and that’s for many different reasons. They disproportionally tend to be great at helping other people but not great at receiving help themselves.”
On top of that, there’s a pressure cooker where they work. Mr. Fern doesn’t think anyone would argue that the health care system in the United States is not dysfunctional, at least to some degree. He says that this dysfunction acts like the physicians’ pressure cooker.
Add in circumstances, cultures, and day-to-day issues everyone has, like relational issues, parenting issues, and mental health problems. Then, toss in an individual’s lower resiliency, the inability to receive help, and a predicament for good measure – a loss, a divorce, or financial woes, for instance, which can overwhelm. Mr. Fern says it can be a mathematical equation for suicidal ideation.
Is there a why?
“Some people think there’s a reason for suicide, but often, there’s a spectrum of reasons,” says Mr. Fern. He says that some physicians are trying to escape emotional pain. For others, it can be fear or a revenge thing, like, “the hell with you, I’m going to kill myself.” It can be getting attention the way teens do, as professionals have seen. Then there’s the organic component, like brain trauma, brain imbalance, depression, anxiety, or bipolar disorder. And finally, a drug or alcohol issue.
“But the reason why physician suicide is elevated, I think, is because there’s this ethos around being silent and, ‘I’m going to listen to and solve everyone else’s problems, but I’m not going to reach out and get help for my own,’ ” says Mr. Fern. “If you take advantage of mental health services, you’re implying that you’re mentally ill. And most physicians aren’t going to do that.”
On the positive side, Dr. Eckleberry-Hunt says that she sees many younger physicians discussing trauma. As a result, they’re more open to receiving help than previous generations. She speculates whether physicians have always had trauma from their past and whether current-day issues are now triggering it or whether they have more trauma these days. “Are they talking about it more, or is it experienced more?”
The failure of the system
The building blocks for physician suicide may have been there from the beginning. “From your first day of medical school and throughout your career, there was a very rigid system in place that is quite unforgiving, is quite stressful, and demands a lot,” says Dr. Jaiswal. And it’s within this system that physicians must operate.
“You have all the corporations, entities, organizations, [and] medical societies talking about physician wellness, burnout, and suicide, but the reality is it’s not making that much of a difference,” he says.
In her report, “What I’ve Learned From 1,710 Doctor Suicides,” Pamelia Wible, MD, who runs a physician suicide helpline that physicians can email and get an immediate callback, likens the current system to assembly line medicine.
Dr. Eckleberry-Hunt thinks the message has been bungled in health care. Everyone discusses burnout, meditation, self-care, and other essential constructs. “But we don’t deal with the root cause [of suicide]. Instead, we teach you soothing strategies.”
Further, Dr. Jaiswal says that not all physicians who commit suicide experience burnout or are experiencing burnout and that the vast majority of physicians who experience burnout don’t have suicidal ideation. “In the sense, that ‘let’s address physician burnout and that will hopefully translate to a reduced number of physician suicides’ – there is a very tenuous argument to be made for that because that is just one aspect in this complex system,” he says.
We need more than just lip service on suicide
Overall, the experts interviewed for this article acknowledged that the system is at least talking about physician suicide, which is a big first step. However, most agree that where big health entities go wrong is that they set up wellness or mental health programs, they implement a wellness officer, they write up talking points for physicians who need mental health care to get that care, and they think they’ve done their job, that they’ve done what’s required to address the problem.
But Dr. Jaiswal thinks these are often mostly public-relations rebuttals. Mr. Fern suggests, “It’s a show that’s not effective.” And Dr. Eckleberry-Hunt says that “even if you had a legit, well-funded well-being program for health care providers, you would still have a baseline rate of physician suicide, and that gets down to having drug and alcohol education and talking about having a system for physicians to access that doesn’t come along with insurance billing” – one that doesn’t create a paper trail and follow physician licensure and job applications for the rest of their career; one that doesn’t associate their mental health care with their work institution; one that offers confidentiality.
“For most folks, there is still a big distrust in the system. As physicians, very few of them feel that the system that they’re operating in has their best interest at heart. And that is why very few physicians will self-report any mental health issues, depression, or even ideation to colleagues, superiors, or managers,” says Dr. Jaiswal. Many more feel skeptical about the confidentiality of the programs in place.
The experts acknowledge that many people are trying to work on this and bring about change on multiple levels – grassroots, department levels, state, and federal. “But I think the biggest thing that the system has to do is earn back the trust of the physician,” Dr. Jaiswal adds.
“Physician suicide is a very visible problem in a very broken system. So, it’ll be very difficult in isolation to treat it without making any systemic changes, because that’s happening right now, and it’s not working,” says Dr. Jaiswal.
“The thing that I am most hopeful about is that I am seeing an influx of younger physicians who seek me out, and granted, their training programs tell them to come and see me, but they are ready and willing to talk about their mental health separate from work. They’re not coming in saying, ‘Here are all the people who I blame.’ They’re saying, ‘These are my struggles, and I want to be a better, happier physician,’ ” says Dr. Eckleberry-Hunt.
A version of this article originally appeared on Medscape.com.
The human-looking robot therapist will coach your well-being now
Do android therapists dream of electric employees?
Robots. It can be tough to remember that, when they’re not dooming humanity to apocalypse or just telling you that you’re doomed, robots have real-world uses. There are actual robots in the world, and they can do things beyond bend girders, sing about science, or run the navy.

Look, we’ll stop with the pop-culture references when pop culture runs out of robots to reference. It may take a while.
Robots are indelibly rooted in the public consciousness, and that plays into our expectations when we encounter a real-life robot. This leads us into a recent study conducted by researchers at the University of Cambridge, who developed a robot-led mental well-being program that a tech company utilized for 4 weeks. Why choose a robot? Well, why spring for a qualified therapist who requires a salary when you could simply get a robot to do the job for free? Get with the capitalist agenda here. Surely it won’t backfire.
The 26 people enrolled in the study received coaching from one of two robots, both programmed identically to act like mental health coaches, based on interviews with human therapists. Both acted identically and had identical expressions. The only difference between the two was their appearance. QTRobot was nearly a meter tall and looked like a human child; Misty II was much smaller and looked like a toy.
People who received coaching from Misty II were better able to connect and had a better experience than those who received coaching from QTRobot. According to those in the QTRobot group, their expectations didn’t match reality. The robots are good coaches, but they don’t act human. This wasn’t a problem for Misty II, since it doesn’t look human, but for QTRobot, the participants were expecting “to hell with our orders,” but received “Daisy, Daisy, give me your answer do.” When you’ve been programmed to think of robots as metal humans, it can be off-putting to see them act as, well, robots.
That said, all participants found the exercises helpful and were open to receiving more robot-led therapy in the future. And while we’re sure the technology will advance to make robot therapists more empathetic and more human, hopefully scientists won’t go too far. We don’t need depressed robots.
Birthing experience is all in the mindset
Alexa, play Peer Gynt Suite No. 1, Op. 46 - I. Morning Mood.
Birth.
Giving birth is a common experience for many, if not most, female mammals, but wanting it to be a pleasurable one seems distinctly human. There are many methods and practices that may make giving birth an easier and enjoyable experience for the mother, but a new study suggests that the key could be in her mind.
The mindset of the expectant mother during pregnancy, it seems, has some effect on how smooth or intervention-filled delivery is. If the mothers saw their experience as a natural process, they were less likely to need pain medication or a C-section, but mothers who viewed the experience as more of a “medical procedure” were more likely to require more medical supervision and intervention, according to investigators from the University of Bonn (Germany).
Now, the researchers wanted to be super clear in saying that there’s no right or wrong mindset to have. They just focused on the outcomes of those mindsets and whether they actually do have some effect on occurrences.
Apparently, yes.
“Mindsets can be understood as a kind of mental lense that guide our perception of the world around us and can influence our behavior,” Dr. Lisa Hoffmann said in a statement from the university. “The study highlights the importance of psychological factors in childbirth.”
The researchers surveyed 300 women with an online tool before and after delivery and found the effects of the natural process mindset lingered even after giving birth. They had lower rates of depression and posttraumatic stress, which may have a snowballing effect on mother-child bonding after childbirth.
Preparation for the big day, then, should be about more than gathering diapers and shopping for car seats. Women should prepare their minds as well. If it’s going to make giving birth better, why not?
Becoming a parent is going to create a psychological shift, no matter how you slice it.
Giant inflatable colon reported in Utah
Do not be alarmed! Yes, there is a giant inflatable colon currently at large in the Beehive State, but it will not harm you. The giant inflatable colon is in Utah as part of Intermountain Health’s “Let’s get to the bottom of colon cancer tour” and he only wants to help you.
The giant inflatable colon, whose name happens to be Collin, is 12 feet long and weighs 113 pounds. March is Colon Cancer Awareness Month, so Collin is traveling around Utah and Idaho to raise awareness about colon cancer and the various screening options. He is not going to change local weather patterns, eat small children, or take over local governments and raise your taxes.
Instead, Collin is planning to display “portions of a healthy colon, polyps or bumps on the colon, malignant polyps which look more vascular and have more redness, cancerous cells, advanced cancer cells, and Crohn’s disease,” KSL.com said.
Collin the colon is on loan to Intermountain Health from medical device manufacturer Boston Scientific and will be traveling to Spanish Fork, Provo, and Ogden, among other locations in Utah, as well as Burley and Meridian, Idaho, in the coming days.
Collin the colon’s participation in the tour has created some serious buzz in the Colin/Collin community:
- Colin Powell (four-star general and Secretary of State): “Back then, the second-most important topic among the Joint Chiefs of Staff was colon cancer screening. And the Navy guy – I can’t remember his name – was a huge fan of giant inflatable organs.”
- Colin Jost (comedian and Saturday Night Live “Weekend Update” cohost): “He’s funnier than Tucker Carlson and Pete Davidson combined.”
Do android therapists dream of electric employees?
Robots. It can be tough to remember that, when they’re not dooming humanity to apocalypse or just telling you that you’re doomed, robots have real-world uses. There are actual robots in the world, and they can do things beyond bend girders, sing about science, or run the navy.
Look, we’ll stop with the pop-culture references when pop culture runs out of robots to reference. It may take a while.
Robots are indelibly rooted in the public consciousness, and that plays into our expectations when we encounter a real-life robot. This leads us into a recent study conducted by researchers at the University of Cambridge, who developed a robot-led mental well-being program that a tech company utilized for 4 weeks. Why choose a robot? Well, why spring for a qualified therapist who requires a salary when you could simply get a robot to do the job for free? Get with the capitalist agenda here. Surely it won’t backfire.
The 26 people enrolled in the study received coaching from one of two robots, both programmed identically to act like mental health coaches, based on interviews with human therapists. Both acted identically and had identical expressions. The only difference between the two was their appearance. QTRobot was nearly a meter tall and looked like a human child; Misty II was much smaller and looked like a toy.
People who received coaching from Misty II were better able to connect and had a better experience than those who received coaching from QTRobot. According to those in the QTRobot group, their expectations didn’t match reality. The robots are good coaches, but they don’t act human. This wasn’t a problem for Misty II, since it doesn’t look human, but for QTRobot, the participants were expecting “to hell with our orders,” but received “Daisy, Daisy, give me your answer do.” When you’ve been programmed to think of robots as metal humans, it can be off-putting to see them act as, well, robots.
That said, all participants found the exercises helpful and were open to receiving more robot-led therapy in the future. And while we’re sure the technology will advance to make robot therapists more empathetic and more human, hopefully scientists won’t go too far. We don’t need depressed robots.
Birthing experience is all in the mindset
Alexa, play Peer Gynt Suite No. 1, Op. 46 - I. Morning Mood.
Birth.
Giving birth is a common experience for many, if not most, female mammals, but wanting it to be a pleasurable one seems distinctly human. There are many methods and practices that may make giving birth an easier and enjoyable experience for the mother, but a new study suggests that the key could be in her mind.
The mindset of the expectant mother during pregnancy, it seems, has some effect on how smooth or intervention-filled delivery is. If the mothers saw their experience as a natural process, they were less likely to need pain medication or a C-section, but mothers who viewed the experience as more of a “medical procedure” were more likely to require more medical supervision and intervention, according to investigators from the University of Bonn (Germany).
Now, the researchers wanted to be super clear in saying that there’s no right or wrong mindset to have. They just focused on the outcomes of those mindsets and whether they actually do have some effect on occurrences.
Apparently, yes.
“Mindsets can be understood as a kind of mental lense that guide our perception of the world around us and can influence our behavior,” Dr. Lisa Hoffmann said in a statement from the university. “The study highlights the importance of psychological factors in childbirth.”
The researchers surveyed 300 women with an online tool before and after delivery and found the effects of the natural process mindset lingered even after giving birth. They had lower rates of depression and posttraumatic stress, which may have a snowballing effect on mother-child bonding after childbirth.
Preparation for the big day, then, should be about more than gathering diapers and shopping for car seats. Women should prepare their minds as well. If it’s going to make giving birth better, why not?
Becoming a parent is going to create a psychological shift, no matter how you slice it.
Giant inflatable colon reported in Utah
Do not be alarmed! Yes, there is a giant inflatable colon currently at large in the Beehive State, but it will not harm you. The giant inflatable colon is in Utah as part of Intermountain Health’s “Let’s get to the bottom of colon cancer tour” and he only wants to help you.
The giant inflatable colon, whose name happens to be Collin, is 12 feet long and weighs 113 pounds. March is Colon Cancer Awareness Month, so Collin is traveling around Utah and Idaho to raise awareness about colon cancer and the various screening options. He is not going to change local weather patterns, eat small children, or take over local governments and raise your taxes.
Instead, Collin is planning to display “portions of a healthy colon, polyps or bumps on the colon, malignant polyps which look more vascular and have more redness, cancerous cells, advanced cancer cells, and Crohn’s disease,” KSL.com said.
Collin the colon is on loan to Intermountain Health from medical device manufacturer Boston Scientific and will be traveling to Spanish Fork, Provo, and Ogden, among other locations in Utah, as well as Burley and Meridian, Idaho, in the coming days.
Collin the colon’s participation in the tour has created some serious buzz in the Colin/Collin community:
- Colin Powell (four-star general and Secretary of State): “Back then, the second-most important topic among the Joint Chiefs of Staff was colon cancer screening. And the Navy guy – I can’t remember his name – was a huge fan of giant inflatable organs.”
- Colin Jost (comedian and Saturday Night Live “Weekend Update” cohost): “He’s funnier than Tucker Carlson and Pete Davidson combined.”
Do android therapists dream of electric employees?
Robots. It can be tough to remember that, when they’re not dooming humanity to apocalypse or just telling you that you’re doomed, robots have real-world uses. There are actual robots in the world, and they can do things beyond bend girders, sing about science, or run the navy.
Look, we’ll stop with the pop-culture references when pop culture runs out of robots to reference. It may take a while.
Robots are indelibly rooted in the public consciousness, and that plays into our expectations when we encounter a real-life robot. This leads us into a recent study conducted by researchers at the University of Cambridge, who developed a robot-led mental well-being program that a tech company utilized for 4 weeks. Why choose a robot? Well, why spring for a qualified therapist who requires a salary when you could simply get a robot to do the job for free? Get with the capitalist agenda here. Surely it won’t backfire.
The 26 people enrolled in the study received coaching from one of two robots, both programmed identically to act like mental health coaches, based on interviews with human therapists. Both acted identically and had identical expressions. The only difference between the two was their appearance. QTRobot was nearly a meter tall and looked like a human child; Misty II was much smaller and looked like a toy.
People who received coaching from Misty II were better able to connect and had a better experience than those who received coaching from QTRobot. According to those in the QTRobot group, their expectations didn’t match reality. The robots are good coaches, but they don’t act human. This wasn’t a problem for Misty II, since it doesn’t look human, but for QTRobot, the participants were expecting “to hell with our orders,” but received “Daisy, Daisy, give me your answer do.” When you’ve been programmed to think of robots as metal humans, it can be off-putting to see them act as, well, robots.
That said, all participants found the exercises helpful and were open to receiving more robot-led therapy in the future. And while we’re sure the technology will advance to make robot therapists more empathetic and more human, hopefully scientists won’t go too far. We don’t need depressed robots.
Birthing experience is all in the mindset
Alexa, play Peer Gynt Suite No. 1, Op. 46 - I. Morning Mood.
Birth.
Giving birth is a common experience for many, if not most, female mammals, but wanting it to be a pleasurable one seems distinctly human. There are many methods and practices that may make giving birth an easier and enjoyable experience for the mother, but a new study suggests that the key could be in her mind.
The mindset of the expectant mother during pregnancy, it seems, has some effect on how smooth or intervention-filled delivery is. If the mothers saw their experience as a natural process, they were less likely to need pain medication or a C-section, but mothers who viewed the experience as more of a “medical procedure” were more likely to require more medical supervision and intervention, according to investigators from the University of Bonn (Germany).
Now, the researchers wanted to be super clear in saying that there’s no right or wrong mindset to have. They just focused on the outcomes of those mindsets and whether they actually do have some effect on occurrences.
Apparently, yes.
“Mindsets can be understood as a kind of mental lense that guide our perception of the world around us and can influence our behavior,” Dr. Lisa Hoffmann said in a statement from the university. “The study highlights the importance of psychological factors in childbirth.”
The researchers surveyed 300 women with an online tool before and after delivery and found the effects of the natural process mindset lingered even after giving birth. They had lower rates of depression and posttraumatic stress, which may have a snowballing effect on mother-child bonding after childbirth.
Preparation for the big day, then, should be about more than gathering diapers and shopping for car seats. Women should prepare their minds as well. If it’s going to make giving birth better, why not?
Becoming a parent is going to create a psychological shift, no matter how you slice it.
Giant inflatable colon reported in Utah
Do not be alarmed! Yes, there is a giant inflatable colon currently at large in the Beehive State, but it will not harm you. The giant inflatable colon is in Utah as part of Intermountain Health’s “Let’s get to the bottom of colon cancer tour” and he only wants to help you.
The giant inflatable colon, whose name happens to be Collin, is 12 feet long and weighs 113 pounds. March is Colon Cancer Awareness Month, so Collin is traveling around Utah and Idaho to raise awareness about colon cancer and the various screening options. He is not going to change local weather patterns, eat small children, or take over local governments and raise your taxes.
Instead, Collin is planning to display “portions of a healthy colon, polyps or bumps on the colon, malignant polyps which look more vascular and have more redness, cancerous cells, advanced cancer cells, and Crohn’s disease,” KSL.com said.
Collin the colon is on loan to Intermountain Health from medical device manufacturer Boston Scientific and will be traveling to Spanish Fork, Provo, and Ogden, among other locations in Utah, as well as Burley and Meridian, Idaho, in the coming days.
Collin the colon’s participation in the tour has created some serious buzz in the Colin/Collin community:
- Colin Powell (four-star general and Secretary of State): “Back then, the second-most important topic among the Joint Chiefs of Staff was colon cancer screening. And the Navy guy – I can’t remember his name – was a huge fan of giant inflatable organs.”
- Colin Jost (comedian and Saturday Night Live “Weekend Update” cohost): “He’s funnier than Tucker Carlson and Pete Davidson combined.”
CDC recommends screening all adults for hepatitis B
This is the first update to HBV screening guidelines since 2008, the agency said.
“Risk-based testing alone has not identified most persons living with chronic HBV infection and is considered inefficient for providers to implement,” the authors wrote in the new guidance, published in the CDC’s Morbidity and Mortality Weekly Report. “Universal screening of adults for HBV infection is cost-effective, compared with risk-based screening and averts liver disease and death. Although a curative treatment is not yet available, early diagnosis and treatment of chronic HBV infections reduces the risk for cirrhosis, liver cancer, and death.”
Howard Lee, MD, an assistant professor in the section of gastroenterology and hepatology at Baylor College of Medicine in Houston, agreed that risk-based screening has not been effective. A universal screening approach “is the way to go,” he said. With this new screening approach, patients can get tested without having to admit that they may be at risk for a chronic disease like HIV and HBV, which can be stigmatizing, said Dr. Lee, who was not involved with making these recommendations.
An estimated 580,000 to 2.4 million individuals are living with HBV infection in the United States, and two-thirds may be unaware they are infected, according to the CDC. The virus spreads through contact with blood, semen, and other body fluids of an infected person.
The guidance now recommends using the triple panel (HBsAg, anti-HBs, total anti-HBc) for initial screening.
“It can help identify persons who have an active HBV infection and could be linked to care; have resolved infection and might be susceptible to reactivation (for example, immunosuppressed persons); are susceptible and need vaccination; or are vaccinated,” the authors wrote.
Patients with previous HBV infection can have the infection reactivated with immunosuppressive treatments, Dr. Lee said, which is why detecting prior infection via the triple panel screening is important.
Women who are pregnant should be screened, ideally, in the first trimester of each pregnancy, regardless of vaccination status or testing history. If they have already received timely triple panel screening for hepatitis B and have no new HBV exposures, pregnant women only need HBsAg screening, the guidelines state.
The guidelines also specify that higher risk groups, specifically those incarcerated or formerly incarcerated, adults with current or past hepatitis C virus infection, and those with current or past sexually transmitted infections and multiple sex partners.
People who are susceptible for infection, refuse vaccination and are at higher risk for HBV should be screened periodically, but how often they should be screened should be based on shared decision-making between the provider and patient as well as individual risk and immune status.
Additional research into the optimal frequency of periodic testing is necessary, the authors say.
“Along with vaccination strategies, universal screening of adults and appropriate testing of persons at increased risk for HBV infection will improve health outcomes, reduce the prevalence of HBV infection in the United States, and advance viral hepatitis elimination goals,” the authors wrote.
The new recommendations now contrast with the 2020 screening guidelines issued by the U.S. Preventive Services Task Force (USPSTF) that recommend risk-based screening for hepatitis B.
“When that recommendation was published, the Task Force was aligned with several other organizations, including the CDC, in supporting screening for hepatitis B in high-risk populations — and importantly, we’re all still aligned in making sure that people get the care that they need,” said Michael Barry, MD, chair of the USPSTF, in an emailed statement. “The evidence on clinical preventive services is always changing, and the Task Force aims to keep all recommendations current, updating each recommendation approximately every 5 years.”
“In the meantime, we always encourage clinicians to use their judgment as they provide care for their patients — including those who may benefit from screening for hepatitis B — and to decide together with each patient which preventive services can best help them live a long and healthy life,” Dr. Barry said.
The American Association for the Study of Liver Diseases is currently updating their HBV screening recommendations, Dr. Lee said, and he expects other professional societies to follow the CDC recommendations.
“It’s not uncommon that we see the CDC or societies making recommendations and the USPSTF following along, so hopefully that’s the case for hepatitis B as well,” he said.
The authors reported no potential conflicts of interest.
A version of this article originally appeared on Medscape.com.
This is the first update to HBV screening guidelines since 2008, the agency said.
“Risk-based testing alone has not identified most persons living with chronic HBV infection and is considered inefficient for providers to implement,” the authors wrote in the new guidance, published in the CDC’s Morbidity and Mortality Weekly Report. “Universal screening of adults for HBV infection is cost-effective, compared with risk-based screening and averts liver disease and death. Although a curative treatment is not yet available, early diagnosis and treatment of chronic HBV infections reduces the risk for cirrhosis, liver cancer, and death.”
Howard Lee, MD, an assistant professor in the section of gastroenterology and hepatology at Baylor College of Medicine in Houston, agreed that risk-based screening has not been effective. A universal screening approach “is the way to go,” he said. With this new screening approach, patients can get tested without having to admit that they may be at risk for a chronic disease like HIV and HBV, which can be stigmatizing, said Dr. Lee, who was not involved with making these recommendations.
An estimated 580,000 to 2.4 million individuals are living with HBV infection in the United States, and two-thirds may be unaware they are infected, according to the CDC. The virus spreads through contact with blood, semen, and other body fluids of an infected person.
The guidance now recommends using the triple panel (HBsAg, anti-HBs, total anti-HBc) for initial screening.
“It can help identify persons who have an active HBV infection and could be linked to care; have resolved infection and might be susceptible to reactivation (for example, immunosuppressed persons); are susceptible and need vaccination; or are vaccinated,” the authors wrote.
Patients with previous HBV infection can have the infection reactivated with immunosuppressive treatments, Dr. Lee said, which is why detecting prior infection via the triple panel screening is important.
Women who are pregnant should be screened, ideally, in the first trimester of each pregnancy, regardless of vaccination status or testing history. If they have already received timely triple panel screening for hepatitis B and have no new HBV exposures, pregnant women only need HBsAg screening, the guidelines state.
The guidelines also specify that higher risk groups, specifically those incarcerated or formerly incarcerated, adults with current or past hepatitis C virus infection, and those with current or past sexually transmitted infections and multiple sex partners.
People who are susceptible for infection, refuse vaccination and are at higher risk for HBV should be screened periodically, but how often they should be screened should be based on shared decision-making between the provider and patient as well as individual risk and immune status.
Additional research into the optimal frequency of periodic testing is necessary, the authors say.
“Along with vaccination strategies, universal screening of adults and appropriate testing of persons at increased risk for HBV infection will improve health outcomes, reduce the prevalence of HBV infection in the United States, and advance viral hepatitis elimination goals,” the authors wrote.
The new recommendations now contrast with the 2020 screening guidelines issued by the U.S. Preventive Services Task Force (USPSTF) that recommend risk-based screening for hepatitis B.
“When that recommendation was published, the Task Force was aligned with several other organizations, including the CDC, in supporting screening for hepatitis B in high-risk populations — and importantly, we’re all still aligned in making sure that people get the care that they need,” said Michael Barry, MD, chair of the USPSTF, in an emailed statement. “The evidence on clinical preventive services is always changing, and the Task Force aims to keep all recommendations current, updating each recommendation approximately every 5 years.”
“In the meantime, we always encourage clinicians to use their judgment as they provide care for their patients — including those who may benefit from screening for hepatitis B — and to decide together with each patient which preventive services can best help them live a long and healthy life,” Dr. Barry said.
The American Association for the Study of Liver Diseases is currently updating their HBV screening recommendations, Dr. Lee said, and he expects other professional societies to follow the CDC recommendations.
“It’s not uncommon that we see the CDC or societies making recommendations and the USPSTF following along, so hopefully that’s the case for hepatitis B as well,” he said.
The authors reported no potential conflicts of interest.
A version of this article originally appeared on Medscape.com.
This is the first update to HBV screening guidelines since 2008, the agency said.
“Risk-based testing alone has not identified most persons living with chronic HBV infection and is considered inefficient for providers to implement,” the authors wrote in the new guidance, published in the CDC’s Morbidity and Mortality Weekly Report. “Universal screening of adults for HBV infection is cost-effective, compared with risk-based screening and averts liver disease and death. Although a curative treatment is not yet available, early diagnosis and treatment of chronic HBV infections reduces the risk for cirrhosis, liver cancer, and death.”
Howard Lee, MD, an assistant professor in the section of gastroenterology and hepatology at Baylor College of Medicine in Houston, agreed that risk-based screening has not been effective. A universal screening approach “is the way to go,” he said. With this new screening approach, patients can get tested without having to admit that they may be at risk for a chronic disease like HIV and HBV, which can be stigmatizing, said Dr. Lee, who was not involved with making these recommendations.
An estimated 580,000 to 2.4 million individuals are living with HBV infection in the United States, and two-thirds may be unaware they are infected, according to the CDC. The virus spreads through contact with blood, semen, and other body fluids of an infected person.
The guidance now recommends using the triple panel (HBsAg, anti-HBs, total anti-HBc) for initial screening.
“It can help identify persons who have an active HBV infection and could be linked to care; have resolved infection and might be susceptible to reactivation (for example, immunosuppressed persons); are susceptible and need vaccination; or are vaccinated,” the authors wrote.
Patients with previous HBV infection can have the infection reactivated with immunosuppressive treatments, Dr. Lee said, which is why detecting prior infection via the triple panel screening is important.
Women who are pregnant should be screened, ideally, in the first trimester of each pregnancy, regardless of vaccination status or testing history. If they have already received timely triple panel screening for hepatitis B and have no new HBV exposures, pregnant women only need HBsAg screening, the guidelines state.
The guidelines also specify that higher risk groups, specifically those incarcerated or formerly incarcerated, adults with current or past hepatitis C virus infection, and those with current or past sexually transmitted infections and multiple sex partners.
People who are susceptible for infection, refuse vaccination and are at higher risk for HBV should be screened periodically, but how often they should be screened should be based on shared decision-making between the provider and patient as well as individual risk and immune status.
Additional research into the optimal frequency of periodic testing is necessary, the authors say.
“Along with vaccination strategies, universal screening of adults and appropriate testing of persons at increased risk for HBV infection will improve health outcomes, reduce the prevalence of HBV infection in the United States, and advance viral hepatitis elimination goals,” the authors wrote.
The new recommendations now contrast with the 2020 screening guidelines issued by the U.S. Preventive Services Task Force (USPSTF) that recommend risk-based screening for hepatitis B.
“When that recommendation was published, the Task Force was aligned with several other organizations, including the CDC, in supporting screening for hepatitis B in high-risk populations — and importantly, we’re all still aligned in making sure that people get the care that they need,” said Michael Barry, MD, chair of the USPSTF, in an emailed statement. “The evidence on clinical preventive services is always changing, and the Task Force aims to keep all recommendations current, updating each recommendation approximately every 5 years.”
“In the meantime, we always encourage clinicians to use their judgment as they provide care for their patients — including those who may benefit from screening for hepatitis B — and to decide together with each patient which preventive services can best help them live a long and healthy life,” Dr. Barry said.
The American Association for the Study of Liver Diseases is currently updating their HBV screening recommendations, Dr. Lee said, and he expects other professional societies to follow the CDC recommendations.
“It’s not uncommon that we see the CDC or societies making recommendations and the USPSTF following along, so hopefully that’s the case for hepatitis B as well,” he said.
The authors reported no potential conflicts of interest.
A version of this article originally appeared on Medscape.com.
Adherence to Evidence-Based Outpatient Antimicrobial Prescribing Guidelines at a Tribal Health System
Tuba City Regional Health Care Corporation (TCRHCC) is located on the Navajo Reservation in northeastern Arizona and provides medical coverage to a 6000-square-mile area, serving more than 33,000 residents of the Navajo, Hopi, and San Juan Southern Paiute tribes.1,2 In 2021, there were 334,497 outpatient visits. TCRHCC departments involved in prescribing outpatient antibiotics include the emergency, internal medicine, family medicine, pediatrics, dentistry, surgery, podiatry, obstetrics and gynecology, and midwifery.
Antimicrobial resistance is one of the largest public health threats, causing an estimated 2 million infections and 23,000 deaths every year in the United States.3 This can lead to increased health care costs, morbidity, and mortality. A large, modifiable risk factor is the inappropriate prescribing of antibiotics: An estimated half of all outpatient antibiotics prescribed may be inappropriate in some manner, such as antibiotic choice, dosing, or duration. In addition, at least 30% of US antibiotic prescriptions are unnecessary, leading to significant overuse.3 As such, antimicrobial stewardship is a cornerstone of improving antibiotic use, patient care, and safety.
The goals of antimicrobial stewardship are to measure antimicrobial prescribing, improve clinician prescribing, minimize misdiagnosis or delayed diagnoses, and ensure the right drug, dose, and duration are selected when antimicrobial therapy is appropriate.3 The Centers for Disease Control and Prevention recommends 4 core elements of outpatient antimicrobial stewardship: commitment, action for policy and practice, tracking and reporting, and education and expertise.3 This study focuses on the pillars of action for policy and practice and tracking and reporting.
Methods
The study objectives were not designed to achieve statistical power. A retrospective chart review was performed for patients of any age who were seen in an ambulatory care setting at TCRHCC from August 1, 2020, to August 1, 2021, with a visit diagnosis included in the outpatient antimicrobial prescribing guidelines.4,5 A random sample of 10% of charts of each diagnosis code was used for analysis. An Excel spreadsheet with all patient charts, separated by diagnosis code, was created. Each chart was then assigned a number, and the Excel function RAND was used to select a random number from the pool. This was continued until 10% of each category, or at least 1 chart from diagnosis code categories with less than 10 total charts available, were selected.
Inclusion criteria were patients seen in ambulatory clinics or the emergency department, an infectious disease diagnosis addressed in the facility guidelines, diagnosis and treatment occurred between August 1, 2020, and August 1, 2021, and the patient was discharged home after the visit. Exclusion criteria were patients who required inpatient admission, patient visits to the clinic established solely for COVID-19 vaccination or testing as no other care was ever provided at this location, patients who refused treatment, patients who failed empiric therapy and required treatment adjustments, or patients who were initially treated and received an antibiotic prescription at a facility outside the TCRHCC system.
After chart review and analysis were completed, a prescriber survey and educational intervention were performed from March 2, 2022, to March 31, 2022. This consisted of an anonymous survey to gather demographic data and prescribing habits pre-education, a short educational brief on the existence, location, and recommended use of the outpatient antimicrobial prescribing guidelines, and a posteducation survey to assess knowledge of the guidelines and willingness to adhere to them after the educational intervention.
Results
We reviewed 8779 patient records. A random sample of 10% of the records of each diagnosis code was taken and 876 charts were reviewed. Of the charts reviewed, 351 patients met the inclusion criteria and were included in the analysis. A goal of 90% was established as the target for prescriber adherence for the study based on author consensus for a reasonable goal. Of the 351 evaluated charts, 62 (16.1%) were pediatric patients (aged < 19 years) and 289 (83.9%) were adults (aged ≥ 19 years). Fifty-two (84%) of the pediatric charts and 249 (86%) of the adult charts demonstrated prescribers had appropriately followed guidelines for a combined total of 301 of the 351 charts and an overall adherence rate of 86%. This was 4 points below the established goal of 90%, warranting further investigation. An analysis of prescribers and locations revealed no trends or patterns of nonadherence. A prescriber survey and educational intervention were designed and disseminated to all prescribers at the facility with the approval and assistance of the chief of medicine.
Thirty-nine prescribers responded to the survey. In the pre-educational survey, clinical resources were the most common source of guidance with 36 prescribers (92%) indicating they used them to make an appropriate selection of an antimicrobial; 32 (82%) used personal knowledge, 30 (77%) used culture results, and 24 (62%) used facility guidelines. This was consistent with the posteducational questions: 12 (31%) indicated they were not aware of the facility guidelines before the educational intervention. 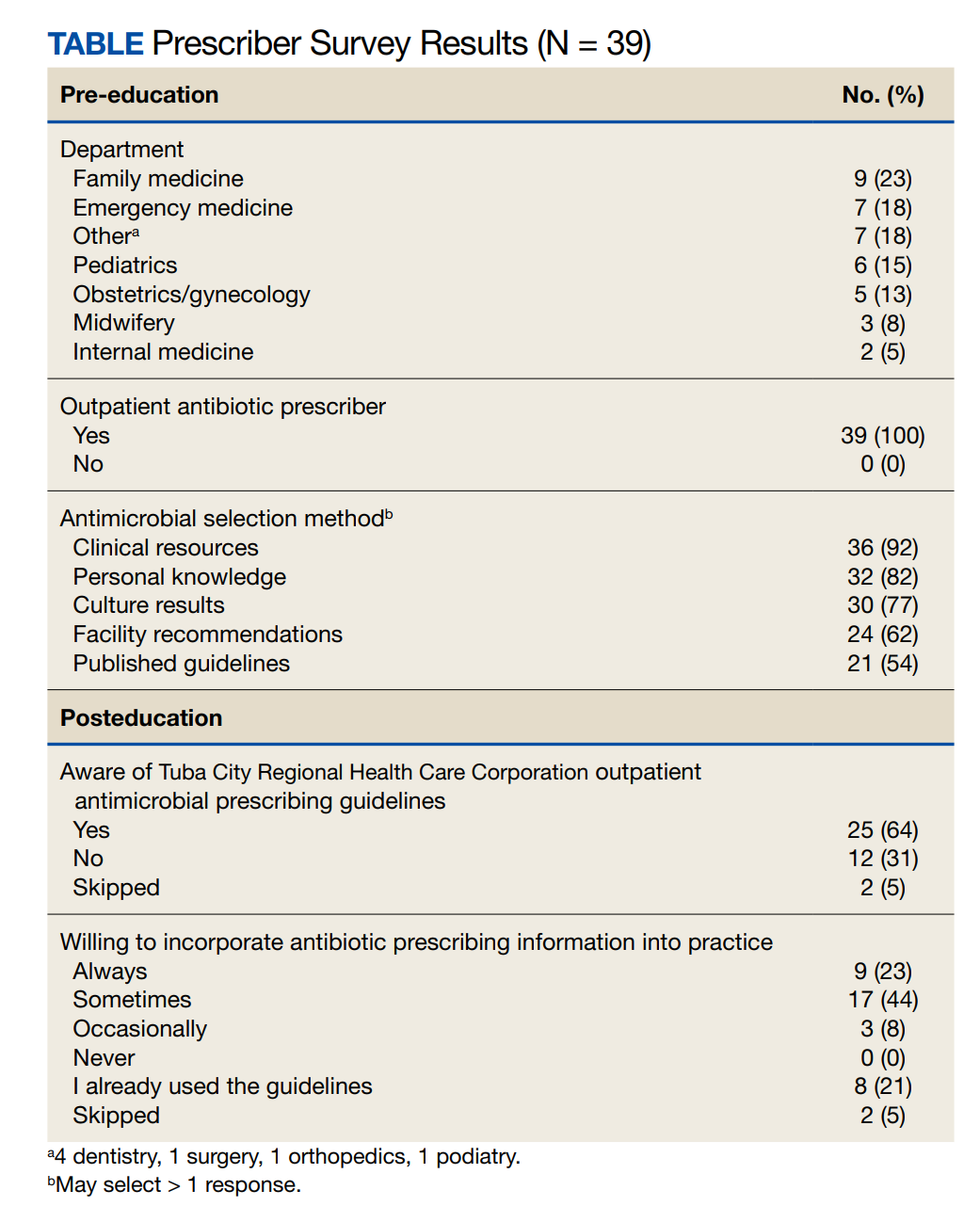
Discussion
This study’s objective was to evaluate prescriber adherence to the facility outpatient prescribing guidelines after they were implemented in 2019 and to plan for interventions if necessary. Overall prescriber adherence was high with 86% of the sampled charts adherent. This was below the goal of 90%, so evaluation of the nonadherent charts was warranted for the determination of any patterns to guide the planned interventions with the facility prescribers. However, no trends were identified, so the intervention was designed as a general survey and educational session for all prescribers. Overall prescriber response was positive, with a total of 34 responding prescribers (87%) indicating a willingness to use the guidelines.
Limitations
This is a retrospective observational study performed through chart review that allowed for frequency analysis but did not allow for statistical analysis, so the significance of results cannot be obtained. Additionally, this study was not able to compare rates of adherence before and after the educational intervention, so the effectiveness of the intervention cannot be assessed.
Conclusions
This retrospective observational study’s data demonstrate that prescribers are adhering at a high rate to recommended empiric antimicrobials for outpatient treatment with an 86% adherence rate. Response to educational intervention indicated a larger proportion of prescribers than previously will use the guidelines. However, the impact this will have on appropriate prescribing rates in the future could not be assessed during this study.
1. Tuba City Regional Health Care Corporation. TCRHCC Annual Report 2021. 2012. Accessed January 25, 2023. Accessed January 30, 2023. https://tchealth.org/pdfdownload/2021_TCRHCC_Annual_Report.pdf
2. Tuba City Regional Health Care Corporation. TCRHCC Annual Report 2013. 2013. Accessed January 25, 2023. Accessed January 30, 2023. https://www.tchealth.org/pdfdownload/2013_Annual_Report.pdf
3. Sanchez GV, Fleming-Dutra KE, Roberts RM, Hicks LA. Core Elements of Outpatient Antibiotic Stewardship. MMWR Recomm Rep. 2016;65(No. RR-6):1–12. doi:10.15585/mmwr.rr6506a1
4. Tuba City Regional Health Care Corporation. Antimicrobial stewardship adult outpatient guidelines. 2019.
5. Tuba City Regional Health Care Corporation. Antimicrobial stewardship pediatric outpatient guidelines. 2019.
Tuba City Regional Health Care Corporation (TCRHCC) is located on the Navajo Reservation in northeastern Arizona and provides medical coverage to a 6000-square-mile area, serving more than 33,000 residents of the Navajo, Hopi, and San Juan Southern Paiute tribes.1,2 In 2021, there were 334,497 outpatient visits. TCRHCC departments involved in prescribing outpatient antibiotics include the emergency, internal medicine, family medicine, pediatrics, dentistry, surgery, podiatry, obstetrics and gynecology, and midwifery.
Antimicrobial resistance is one of the largest public health threats, causing an estimated 2 million infections and 23,000 deaths every year in the United States.3 This can lead to increased health care costs, morbidity, and mortality. A large, modifiable risk factor is the inappropriate prescribing of antibiotics: An estimated half of all outpatient antibiotics prescribed may be inappropriate in some manner, such as antibiotic choice, dosing, or duration. In addition, at least 30% of US antibiotic prescriptions are unnecessary, leading to significant overuse.3 As such, antimicrobial stewardship is a cornerstone of improving antibiotic use, patient care, and safety.
The goals of antimicrobial stewardship are to measure antimicrobial prescribing, improve clinician prescribing, minimize misdiagnosis or delayed diagnoses, and ensure the right drug, dose, and duration are selected when antimicrobial therapy is appropriate.3 The Centers for Disease Control and Prevention recommends 4 core elements of outpatient antimicrobial stewardship: commitment, action for policy and practice, tracking and reporting, and education and expertise.3 This study focuses on the pillars of action for policy and practice and tracking and reporting.
Methods
The study objectives were not designed to achieve statistical power. A retrospective chart review was performed for patients of any age who were seen in an ambulatory care setting at TCRHCC from August 1, 2020, to August 1, 2021, with a visit diagnosis included in the outpatient antimicrobial prescribing guidelines.4,5 A random sample of 10% of charts of each diagnosis code was used for analysis. An Excel spreadsheet with all patient charts, separated by diagnosis code, was created. Each chart was then assigned a number, and the Excel function RAND was used to select a random number from the pool. This was continued until 10% of each category, or at least 1 chart from diagnosis code categories with less than 10 total charts available, were selected.
Inclusion criteria were patients seen in ambulatory clinics or the emergency department, an infectious disease diagnosis addressed in the facility guidelines, diagnosis and treatment occurred between August 1, 2020, and August 1, 2021, and the patient was discharged home after the visit. Exclusion criteria were patients who required inpatient admission, patient visits to the clinic established solely for COVID-19 vaccination or testing as no other care was ever provided at this location, patients who refused treatment, patients who failed empiric therapy and required treatment adjustments, or patients who were initially treated and received an antibiotic prescription at a facility outside the TCRHCC system.
After chart review and analysis were completed, a prescriber survey and educational intervention were performed from March 2, 2022, to March 31, 2022. This consisted of an anonymous survey to gather demographic data and prescribing habits pre-education, a short educational brief on the existence, location, and recommended use of the outpatient antimicrobial prescribing guidelines, and a posteducation survey to assess knowledge of the guidelines and willingness to adhere to them after the educational intervention.
Results
We reviewed 8779 patient records. A random sample of 10% of the records of each diagnosis code was taken and 876 charts were reviewed. Of the charts reviewed, 351 patients met the inclusion criteria and were included in the analysis. A goal of 90% was established as the target for prescriber adherence for the study based on author consensus for a reasonable goal. Of the 351 evaluated charts, 62 (16.1%) were pediatric patients (aged < 19 years) and 289 (83.9%) were adults (aged ≥ 19 years). Fifty-two (84%) of the pediatric charts and 249 (86%) of the adult charts demonstrated prescribers had appropriately followed guidelines for a combined total of 301 of the 351 charts and an overall adherence rate of 86%. This was 4 points below the established goal of 90%, warranting further investigation. An analysis of prescribers and locations revealed no trends or patterns of nonadherence. A prescriber survey and educational intervention were designed and disseminated to all prescribers at the facility with the approval and assistance of the chief of medicine.
Thirty-nine prescribers responded to the survey. In the pre-educational survey, clinical resources were the most common source of guidance with 36 prescribers (92%) indicating they used them to make an appropriate selection of an antimicrobial; 32 (82%) used personal knowledge, 30 (77%) used culture results, and 24 (62%) used facility guidelines. This was consistent with the posteducational questions: 12 (31%) indicated they were not aware of the facility guidelines before the educational intervention.
Discussion
This study’s objective was to evaluate prescriber adherence to the facility outpatient prescribing guidelines after they were implemented in 2019 and to plan for interventions if necessary. Overall prescriber adherence was high with 86% of the sampled charts adherent. This was below the goal of 90%, so evaluation of the nonadherent charts was warranted for the determination of any patterns to guide the planned interventions with the facility prescribers. However, no trends were identified, so the intervention was designed as a general survey and educational session for all prescribers. Overall prescriber response was positive, with a total of 34 responding prescribers (87%) indicating a willingness to use the guidelines.
Limitations
This is a retrospective observational study performed through chart review that allowed for frequency analysis but did not allow for statistical analysis, so the significance of results cannot be obtained. Additionally, this study was not able to compare rates of adherence before and after the educational intervention, so the effectiveness of the intervention cannot be assessed.
Conclusions
This retrospective observational study’s data demonstrate that prescribers are adhering at a high rate to recommended empiric antimicrobials for outpatient treatment with an 86% adherence rate. Response to educational intervention indicated a larger proportion of prescribers than previously will use the guidelines. However, the impact this will have on appropriate prescribing rates in the future could not be assessed during this study.
Tuba City Regional Health Care Corporation (TCRHCC) is located on the Navajo Reservation in northeastern Arizona and provides medical coverage to a 6000-square-mile area, serving more than 33,000 residents of the Navajo, Hopi, and San Juan Southern Paiute tribes.1,2 In 2021, there were 334,497 outpatient visits. TCRHCC departments involved in prescribing outpatient antibiotics include the emergency, internal medicine, family medicine, pediatrics, dentistry, surgery, podiatry, obstetrics and gynecology, and midwifery.
Antimicrobial resistance is one of the largest public health threats, causing an estimated 2 million infections and 23,000 deaths every year in the United States.3 This can lead to increased health care costs, morbidity, and mortality. A large, modifiable risk factor is the inappropriate prescribing of antibiotics: An estimated half of all outpatient antibiotics prescribed may be inappropriate in some manner, such as antibiotic choice, dosing, or duration. In addition, at least 30% of US antibiotic prescriptions are unnecessary, leading to significant overuse.3 As such, antimicrobial stewardship is a cornerstone of improving antibiotic use, patient care, and safety.
The goals of antimicrobial stewardship are to measure antimicrobial prescribing, improve clinician prescribing, minimize misdiagnosis or delayed diagnoses, and ensure the right drug, dose, and duration are selected when antimicrobial therapy is appropriate.3 The Centers for Disease Control and Prevention recommends 4 core elements of outpatient antimicrobial stewardship: commitment, action for policy and practice, tracking and reporting, and education and expertise.3 This study focuses on the pillars of action for policy and practice and tracking and reporting.
Methods
The study objectives were not designed to achieve statistical power. A retrospective chart review was performed for patients of any age who were seen in an ambulatory care setting at TCRHCC from August 1, 2020, to August 1, 2021, with a visit diagnosis included in the outpatient antimicrobial prescribing guidelines.4,5 A random sample of 10% of charts of each diagnosis code was used for analysis. An Excel spreadsheet with all patient charts, separated by diagnosis code, was created. Each chart was then assigned a number, and the Excel function RAND was used to select a random number from the pool. This was continued until 10% of each category, or at least 1 chart from diagnosis code categories with less than 10 total charts available, were selected.
Inclusion criteria were patients seen in ambulatory clinics or the emergency department, an infectious disease diagnosis addressed in the facility guidelines, diagnosis and treatment occurred between August 1, 2020, and August 1, 2021, and the patient was discharged home after the visit. Exclusion criteria were patients who required inpatient admission, patient visits to the clinic established solely for COVID-19 vaccination or testing as no other care was ever provided at this location, patients who refused treatment, patients who failed empiric therapy and required treatment adjustments, or patients who were initially treated and received an antibiotic prescription at a facility outside the TCRHCC system.
After chart review and analysis were completed, a prescriber survey and educational intervention were performed from March 2, 2022, to March 31, 2022. This consisted of an anonymous survey to gather demographic data and prescribing habits pre-education, a short educational brief on the existence, location, and recommended use of the outpatient antimicrobial prescribing guidelines, and a posteducation survey to assess knowledge of the guidelines and willingness to adhere to them after the educational intervention.
Results
We reviewed 8779 patient records. A random sample of 10% of the records of each diagnosis code was taken and 876 charts were reviewed. Of the charts reviewed, 351 patients met the inclusion criteria and were included in the analysis. A goal of 90% was established as the target for prescriber adherence for the study based on author consensus for a reasonable goal. Of the 351 evaluated charts, 62 (16.1%) were pediatric patients (aged < 19 years) and 289 (83.9%) were adults (aged ≥ 19 years). Fifty-two (84%) of the pediatric charts and 249 (86%) of the adult charts demonstrated prescribers had appropriately followed guidelines for a combined total of 301 of the 351 charts and an overall adherence rate of 86%. This was 4 points below the established goal of 90%, warranting further investigation. An analysis of prescribers and locations revealed no trends or patterns of nonadherence. A prescriber survey and educational intervention were designed and disseminated to all prescribers at the facility with the approval and assistance of the chief of medicine.
Thirty-nine prescribers responded to the survey. In the pre-educational survey, clinical resources were the most common source of guidance with 36 prescribers (92%) indicating they used them to make an appropriate selection of an antimicrobial; 32 (82%) used personal knowledge, 30 (77%) used culture results, and 24 (62%) used facility guidelines. This was consistent with the posteducational questions: 12 (31%) indicated they were not aware of the facility guidelines before the educational intervention.
Discussion
This study’s objective was to evaluate prescriber adherence to the facility outpatient prescribing guidelines after they were implemented in 2019 and to plan for interventions if necessary. Overall prescriber adherence was high with 86% of the sampled charts adherent. This was below the goal of 90%, so evaluation of the nonadherent charts was warranted for the determination of any patterns to guide the planned interventions with the facility prescribers. However, no trends were identified, so the intervention was designed as a general survey and educational session for all prescribers. Overall prescriber response was positive, with a total of 34 responding prescribers (87%) indicating a willingness to use the guidelines.
Limitations
This is a retrospective observational study performed through chart review that allowed for frequency analysis but did not allow for statistical analysis, so the significance of results cannot be obtained. Additionally, this study was not able to compare rates of adherence before and after the educational intervention, so the effectiveness of the intervention cannot be assessed.
Conclusions
This retrospective observational study’s data demonstrate that prescribers are adhering at a high rate to recommended empiric antimicrobials for outpatient treatment with an 86% adherence rate. Response to educational intervention indicated a larger proportion of prescribers than previously will use the guidelines. However, the impact this will have on appropriate prescribing rates in the future could not be assessed during this study.
1. Tuba City Regional Health Care Corporation. TCRHCC Annual Report 2021. 2012. Accessed January 25, 2023. Accessed January 30, 2023. https://tchealth.org/pdfdownload/2021_TCRHCC_Annual_Report.pdf
2. Tuba City Regional Health Care Corporation. TCRHCC Annual Report 2013. 2013. Accessed January 25, 2023. Accessed January 30, 2023. https://www.tchealth.org/pdfdownload/2013_Annual_Report.pdf
3. Sanchez GV, Fleming-Dutra KE, Roberts RM, Hicks LA. Core Elements of Outpatient Antibiotic Stewardship. MMWR Recomm Rep. 2016;65(No. RR-6):1–12. doi:10.15585/mmwr.rr6506a1
4. Tuba City Regional Health Care Corporation. Antimicrobial stewardship adult outpatient guidelines. 2019.
5. Tuba City Regional Health Care Corporation. Antimicrobial stewardship pediatric outpatient guidelines. 2019.
1. Tuba City Regional Health Care Corporation. TCRHCC Annual Report 2021. 2012. Accessed January 25, 2023. Accessed January 30, 2023. https://tchealth.org/pdfdownload/2021_TCRHCC_Annual_Report.pdf
2. Tuba City Regional Health Care Corporation. TCRHCC Annual Report 2013. 2013. Accessed January 25, 2023. Accessed January 30, 2023. https://www.tchealth.org/pdfdownload/2013_Annual_Report.pdf
3. Sanchez GV, Fleming-Dutra KE, Roberts RM, Hicks LA. Core Elements of Outpatient Antibiotic Stewardship. MMWR Recomm Rep. 2016;65(No. RR-6):1–12. doi:10.15585/mmwr.rr6506a1
4. Tuba City Regional Health Care Corporation. Antimicrobial stewardship adult outpatient guidelines. 2019.
5. Tuba City Regional Health Care Corporation. Antimicrobial stewardship pediatric outpatient guidelines. 2019.
Augmented Reality Demonstration Survey Results From a Veteran Affairs Medical Center
Building the health care system of the future requires the thoughtful development and integration of innovative technologies to positively transform care.1-4 Extended reality (XR) represents a spectrum of emerging technologies that have the potential to enhance health care. This includes virtual reality (VR), where a computer-generated visual experience fills the screen; augmented reality (AR), which allows users to see computer-generated images superimposed into an otherwise normal real-world field of view; and mixed reality (MR), which allows users to interact and manipulate computer-generated AR images.
Clinicians and researchers have begun exploring the potential of XR to address a wide variety of health care challenges. A recent systematic review concluded that many clinical studies in this area have small sample sizes and are in the preclinical, proof-of-concept stage, but demonstrate the potential and impact of the underlying VR, AR, and MR technologies.5 Common emerging health care uses for XR include medical education, training, presurgical planning, surgical guidance, distraction therapy for pain and anxiety, and home health indications, including rehabilitation.5-39 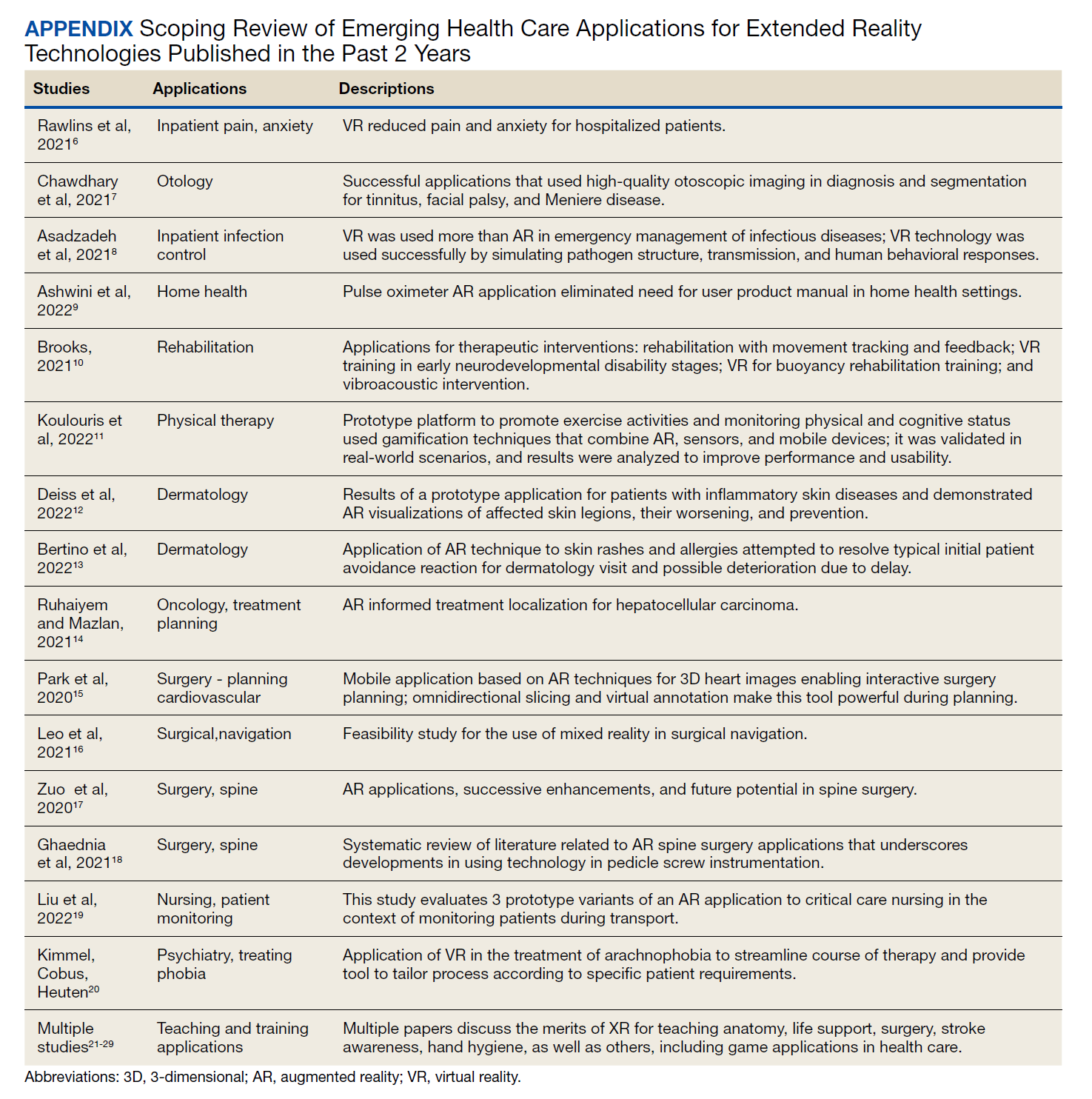
Importantly, some researchers have raised concerns regarding the adaptability of the health care workforce with emerging technologies, and their interest in new methods of delivering care.7,39 Successful deployment of any novel health care technology depends on multiple factors, including alignment with staff needs, receptivity to those solutions, customization to specific preferences, and usability.1,3,40-42 Unfortunately, the implementation of some health care technologies, such as electronic health records that did not account for end-user requirements, resulted in employee fatigue, burnout, and negative staffing turnover.42-44 Conversely, elevated employee morale and operational performance have been directly linked to a climate of inclusion and innovation.45-47 In this assessment, we sought to understand US Department of Veterans Affairs (VA) employees’ perceptions and expert opinions related to the introduction of new AR/MR technology.
Methods
The VA Palo Alto Health Care System (VAPAHCS) consists of 3 inpatient hospitals and 7 outpatient clinics, provides a full range of care services to > 90,000 enrolled veterans with 800 hospital beds, 3 nursing homes, and a 100-bed domiciliary. The facility also runs data-driven care projects in research, innovation, and evidence-based practice group under nursing services.48 This project was performed by the VA National Center for Collaborative Healthcare Innovation at the VAPAHCS campus.
The combined technical system used for this assessment included a wireless communication network, AR/MR hardware, and software. Medivis AnatomyX software displayed an interactive human anatomy atlas segmented into about 6000 individual interactive parts. Medivis SurgicalAR received US Food and Drug Administration clearance for presurgical planning and was used to transform and display deidentified diagnostic images (eg, magnetic resonance images and computed tomography) in 3-dimensional (3D) interactive holograms (Figures 1 and 2). 
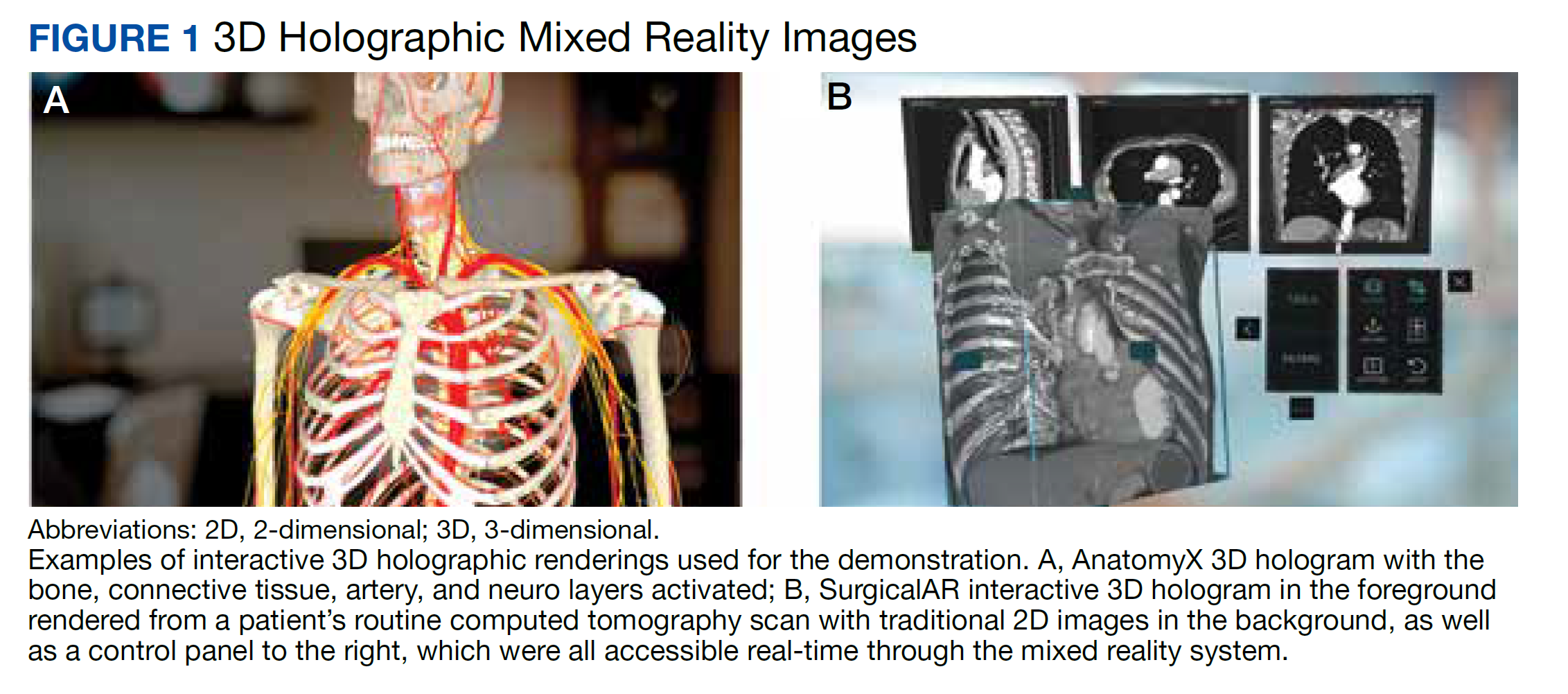
The wireless Microsoft HoloLens 2 AR/MR headset was used for viewing and sensor-enabled collaborative interaction. Multiple participants in the same physical location simultaneously participated and interacted with 3D holograms. The interactive hologram data were enabled for 3D stereoscopic viewing and manipulation.
Setting and Participants
We reviewed published studies that used questionnaires to evaluate institutions’ level of innovation and new technology user acceptance to develop the questionnaire.49-56 Questions and methods were modified, with a focus on understanding the impact on hospital employees. The questionnaire consisted of 2 predemonstration and 3 postdemonstration sections. The first section included background questions. The second (predemonstration) and third (postdemonstration) sections provided matched questions on feelings about the VA. The fourth section included 2 unmatched questions about how the participant felt this technology would impact veterans and whether the VA should implement similar technologies. We used a 5-point Likert scale for sections 2, 3 and 4 (1 = not at all to 5 = extremely). Two unmatched free-text questions asked how the technology could be used in the participant’s hospital service, and another open-ended question asked for any additional comments. To reduce potential reporting bias, 2 VA employees that did not work at VAPAHCS assisted with the survey distribution and collection. VAPAHCS staff were informed by all employee email and facility intranet of the opportunity to participate; the voluntary demonstration and survey took place on February 10 and 11, 2020.
Data Analysis
All matching pre/post questions were analyzed together to determine statistically significant differences using the Wilcoxon signed rank matched pairs test and pooled t test. Survey respondents were also grouped by employment type to evaluate the impact on subgroups. Results were also grouped by VA tenure into 4 categorical 10-year increments (0-10, 11-20, 21-30, 31-40). Additionally, analysis of variance (ANOVA) was performed on employment types and VA tenure to understand whether there was a statistically significant difference in responses by these subgroups. Respondents’ optional free-text answers were manually reviewed by 2 authors (ZPV and DMA), classified, coded by the common themes, and analyzed for comparison.
Results
A total of 166 participants completed the predemonstration survey, which was a requirement for participating in the AR demonstration. Of those, 159 staff members (95.8%) also completed at least part of the postdemonstration paired structured questions, and their results were included in the analysis. 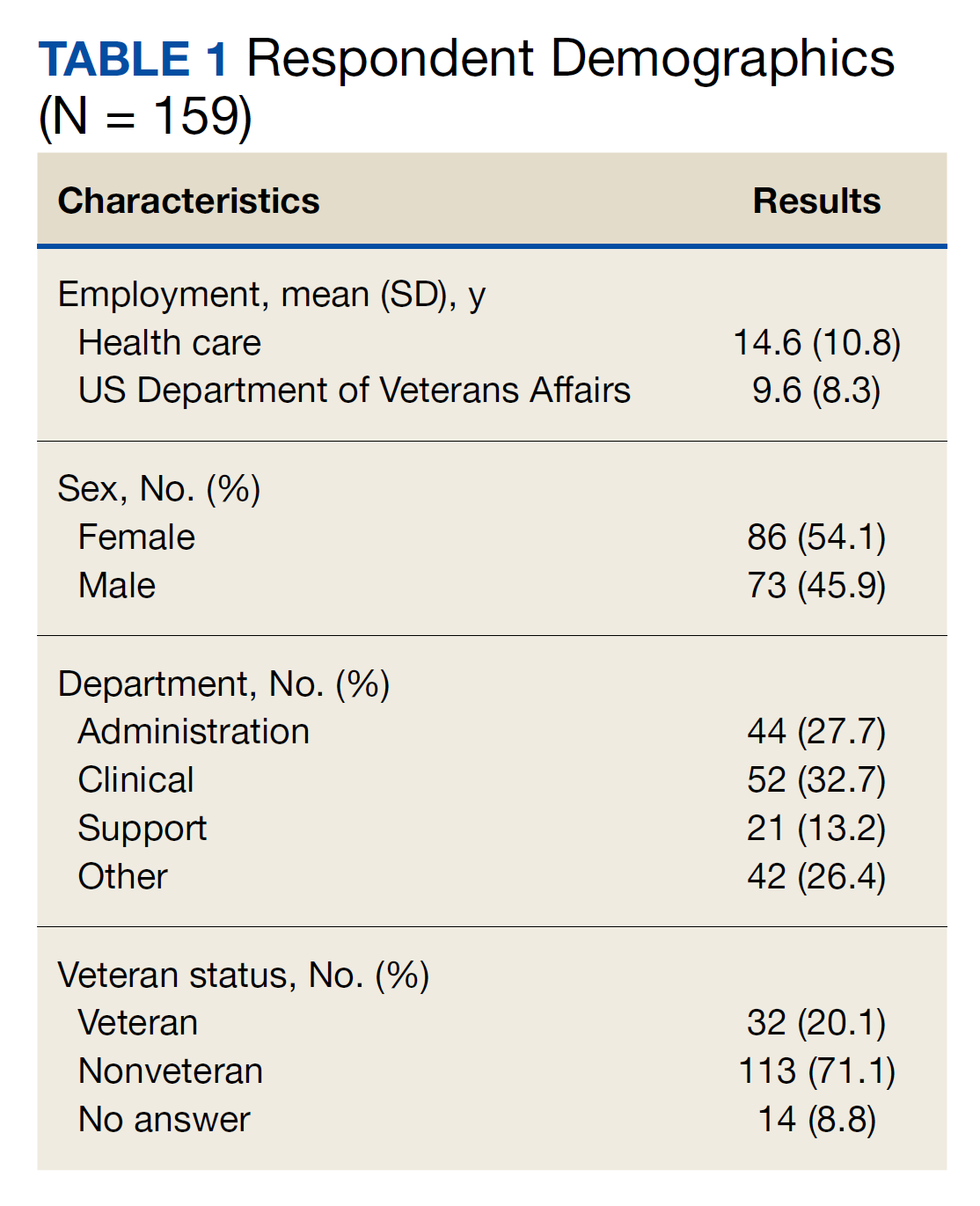
Paired Questions
For questions about how innovative the VA is, 108 of 152 participants (71.1%) provided higher scores after the demonstration, 42 (27.6%) had no change, and 2 (1.3%) provided decreased scores. The mean innovative score increased from 3.4 predemonstration to 4.5 postdemonstration on a Likert scale, which is a 1.1 point increase from predemonstration to postdemonstration (95% CI, 0.9- 1.2) or a 22% increase (95% CI, 18%-24%) (P < .001). Respondents level of excitement about VA also increased with 82 of 157 participants (52.2%) providing higher scores after the demonstration, 71 (45.2%) had no change, and 4 scores (2.5%) decreased. The predemonstration mean excitement score of 3.7 increased to 4.3 postdemonstration, which is a 0.6 point increase from before to after the demonstration (95% CI, 0.5-0.7) or a 12% increase (95% CI, 10%-14%) (P < .001). In the survey, 36 of 149 participants (24.2%) had higher scores for their expectation to continue working at VA postdemonstration, 109 (73.2%) had no change, and 4 scores (2.7%) decreased. The mean employee retention score increased from 4.2 predemonstration to 4.5 postdemonstration, which is a 0.3 point increase between pre/post (95% CI, 0.2-0.4) or a 6% increase (95% CI, 4%-8%) (P < .001)
The pre/post questions were analyzed using 1-way ANOVA by hospital department and VA tenure. The responses by department were not statistically significant. Of the 159 employees assessed, 101 respondents (63.5%) had 0 to 10 years VA tenure, 44 (27.7%) had 11 to 20 years, 10 (6.3%) had 21 to 30 years, and 4 (2.5%) had > 31 to 40 years. Length of VA tenure did not impact respondent excitement. Respondents opinions on innovation in the 0 to 10 year and the 11 to 20 year groups rose from 3.2 and 3.7 predemonstration to 4.3 and 4.6 postdemonstration, respectively (P < .001 for both statistical comparisons) (Table 2). Interestingly, the 0 to 10 group saw a 9% rise from a 4.0 score predemonstration to a 4.4 score postdemonstration (P < .001), indicating that the demonstration had a positive impact on their plans to continue employment at VA (Table 3).
Sex did not play a significant role in how respondents answered questions regarding VA excitement or innovation. However, there was a statistically significant difference in how male and female respondents answered the predemonstration question about their plans to continue VA employment, according to the Wilcoxon rank sum test. Predemonstration, female respondents had a mean score of 4.1, which was 6% lower than the 4.4 score of male colleagues (P = .04). Veteran status did have an impact on how respondents felt about VA innovation, and their plans to continue employment at VA. After the demonstration, veteran staff felt the VA was more innovative compared with nonveterans: 4.7 vs 4.4, respectively, a 6% difference (P = .02) Similarly, for the continued VA employment question, veterans had a mean score of 4.8 vs 4.4 for nonveterans, an 8% difference (P = .03) These results suggest that the demonstration had more of an impact on veteran employees vs nonveteran employees.
Unpaired Questions
There were 2 structured unpaired postdemonstration questions. Respondents agreed that similar technology would impact veteran health care with mean (SD) of 4.6 (0.6) and a median score of 5 on a 5-point Likert scale. Respondents also agreed on the importance of implementing similar innovations with mean (SD) of 4.7 (0.5), and a median score of 5.
The survey asked how this technology could benefit their hospital service department and had 64 responses. Forty-six respondents saw applications for education or patient care/surgery. Other responses shared excitement about the technology and its potential to positively impact patient education. There were 37 responses to the open-ended question: 21 respondents expressed excitement for the technology, and 10 respondents reiterated that the demonstration would be of benefit to patient care/surgery and training.
Discussion
Successful development, design, and deployment of any new health care tool depends on leveraging insights from the employees that will be using and supporting these systems. Correspondingly, understanding the impact that advanced technologies have on health care employees’ satisfaction, morale, and retention is critical to our overall institutional strategy. Our findings show that a one-time experience with AR/MR technology elicited positive employee reactions. Of note, the survey revealed statistically significant improvements in staff’s view of the VA, with the greatest positive impact for questions about innovation, followed by excitement to work at the VA, and likelihood to continue work at the VA. It is very disruptive and costly when health care employees leave, and improving employee satisfaction and morale is important for better patient care and patient satisfaction, which is priority for VAPAHCS leadership.57-62
The paired predemonstration and postdemonstration scores were similarly high, nearing the top threshold available for the Likert scale (4.3 to 4.5). Furthermore, the least incremental improvement for these responses was observed for topics that had the highest initial baseline score. Therefore, the improvements observed for the paired questions may have more to do with the high baseline values.
Of additional interest, the self-reported likelihood of continuing to work at the VA increased the most for female employees, veteran employees, and employees with the least number of years at the VA. These demographic differences have important implications for VA staff recruitment and retention strategies.62 The unpaired questions about the impact on veteran care and whether the VA should continue similar work demonstrated extremely high support with median scores of 5 for both questions. The free-text postdemonstration responses also demonstrate similar positive themes, with a disposition for excitement about both the training and patient care applications for this technology. In addition, respondents felt strongly that this and other similar technologies will positively impact the health care for veterans and that the VA should continue these efforts.
Strengths and Limitations
A strength of this assessment is the ability to evaluate survey responses that were systematically collected and matched from the same individual immediately before and after exposure to the new technology. The free-text responses provided additional important information that both confirmed the results and provided additional valued supplementary guidance for future implementation strategies, which is critical for our translational implementation goals. An additional strength is that the voluntary surveys were managed by non-VAPAHCS colleagues, limiting potential bias. Importantly, the number of respondents allowed a statistically significant assessment of important health care employee metrics. These results have emphasized how being part of an innovative organization, and the introduction of advanced AR/MR technology, improve employees’ satisfaction and morale about where they work as well as their intention to stay at their institution.
A limitation of this assessment was the lack of comparative data for employee acceptance of other technologies at VAPAHCS. This limits our ability to differentiate whether the strong positive results observed in this evaluation were a result of the specific technology assessed, or of new and advanced health care technology in general. Nonetheless, our unpaired questions, which received extremely high scores, also included participant questions about comparing the system with other similar technologies. This assessment was also focused on veteran care, which limits generalizability.
Conclusions
One-time exposure to advanced AR technology for health care significantly increased employee morale as measured by excitement about working at the VA as well as employee intention to continue employment at the VA. These collateral benefits of the technology are particularly important in health care because our employees are our most important asset and improving employee morale equates to better patient care. Positive impacts were most pronounced for women employees, newer VA employees, and employees who are also veterans. These more detailed insights are also positioned to have a direct impact on employee recruitment and retention strategies. Additional valuable insights regarding the most applicable use of the technology in the clinical setting were also obtained.
Acknowledgments
We thank Andrew Spiegelman, Hyewon Kim, Jonathan Sills, and Alexander Erickson for their assistance in developing the survey questions. We also thank Jason Rhodes and Mark Bulson for traveling to our facility to assist with managing the anonymous surveys during the demonstration event.
1. World Economic Forum. Health and healthcare in the fourth industrial revolution: Global Future Council on the future of health and healthcare 2016-2018. April 2019. Accessed January 27, 2023. https://www3.weforum.org/docs/WEF__Shaping_the_Future_of_Health_Council_Report.pdf
2. Iveroth E, Fryk P, Rapp B. Information technology strategy and alignment issues in health care organizations. Health Care Manage Rev. 2013;38(3):188-200. doi:10.1097/HMR.0b013e31826119d7
3. Thakur R, Hsu SH, Fontenot G. Innovation in healthcare: issues and future trends. J Bus Res. 2012;65(4):562-569. doi:10.1016/j.jbusres.2011.02.022
4. Thimbleby H. Technology and the future of healthcare. J Public Health Res. 2013;2(3):e28. Published 2013 Dec 1. doi:10.4081/jphr.2013.e28
5. Viglialoro RM, Condino S, Turini G, Carbone M, Ferrari V, Gesi M. augmented reality, mixed reality, and hybrid approach in healthcare simulation: a systematic review. Applied Sciences. 2021;11(5):2338. doi:10.3390/app11052338
6. Rawlins CR, Veigulis Z, Hebert C, Curtin C, Osborne T. Effect of immersive virtual reality on pain and anxiety at a Veterans Affairs health care facility. Front Virt Real. 2021;(2):136. doi:10.3389/frvir.2021.719681
7. Chawdhary G, Shoman N. Emerging artificial intelligence applications in otological imaging. Curr Opin Otolaryngol Head Neck Surg. 2021;29(5):357-364. doi:10.1097/MOO.0000000000000754
8. Asadzadeh A, Samad-Soltani T, Rezaei-Hachesu P. Applications of virtual and augmented reality in infectious disease epidemics with a focus on the COVID-19 outbreak. Inform Med Unlocked. 2021;24:100579. doi:10.1016/j.imu.2021.100579
9. Ashwini KB, Savitha R, Harish A. Application of augmented reality technology for home healthcare product visualization. ECS Transas. 2022;107(1):10921. doi:10.1149/10701.10921ecst
10. Brooks AL. VR/Technologies for Rehabilitation. In: Brooks AL, Brahman S, Kapralos B, Nakajima A, Tyerman J, Jain LC, eds. Recent Advances in Technologies for Inclusive Well-Being Virtual Patients, Gamification and Simulation. Intelligent Systems Reference Library. Springer; 2021:241-252. doi:10.1007/978-3-030-59608-8_13
11. Koulouris D, Menychtas A, Maglogiannis I. An IoT-enabled platform for the assessment of physical and mental activities utilizing augmented reality exergaming. Sensors (Basel). 2022;22(9):3181. Published 2022 Apr 21. doi:10.3390/s22093181
12. Deiss YR, Korkut S, Inglese T. Increase therapy understanding and medication adherence for patients with inflammatory skin diseases through augmented reality. Digital Human Modeling and Applications in Health, Safety, Ergonomics and Risk Management. Health, Operations Management, and Design: 13th International Conference, DHM 2022, Held as Part of the 24th HCI International Conference, HCII 2022. 2022:21-40. doi:10.1007/978-3-031-06018-2_2
13. Bertino E, Gao W, Steffan B, et al, eds. Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics). Springer; 2022:21-40.
14. Ruhaiyem NIR, Mazlan NA. Image Modeling Through Augmented Reality for Skin Allergies Recognition. Lecture Notes on Data Engineering and Communications Technologies. 2021:72-79. doi: 10.1007/978-3-030-70713-2_8
15. Park BJ, Perkons NR, Profka E, et al. Three-dimensional augmented reality visualization informs locoregional therapy in a translational model of hepatocellular carcinoma. J Vasc Interv Radiol. 2020;31(10):1612-1618.e1. doi:10.1016/j.jvir.2020.01.028
16. Leo J, Zhou Z, Yang H, et al, eds. Interactive cardiovascular surgical planning via augmented reality. 5th Asian CHI Symposium 2021; 2021. doi:10.1145/3429360.3468195
17. Zuo Y, Jiang T, Dou J, et al. A novel evaluation model for a mixed-reality surgical navigation system: where Microsoft Hololens meets the operating room. Surg Innov. 2020;27(2):193-202. doi:10.1177/1553350619893236
18. Ghaednia H, Fourman MS, Lans A, et al. Augmented and virtual reality in spine surgery, current applications and future potentials. Spine J. 2021;21(10):1617-1625. doi:10.1016/j.spinee.2021.03.018
19. Liu Y, Lee MG, Kim JS. Spine surgery assisted by augmented reality: where have we been?. Yonsei Med J. 2022;63(4):305-316. doi:10.3349/ymj.2022.63.4.305
20. Kimmel S, Cobus V, Heuten W, eds. opticARe—augmented reality mobile patient monitoring in intensive care units. Proceedings of the ACM Symposium on Virtual Reality Software and Technology, VRST; 2021. doi:10.1145/3489849.3489852
21. Voštinár P, Horváthová D, Mitter M, Bako M. The look at the various uses of VR. Open Computer Sci. 2021;11(1):241-250. doi:10.1515/comp-2020-0123
22. Zhao J, Xu X, Jiang H, Ding Y. The effectiveness of virtual reality-based technology on anatomy teaching: a meta-analysis of randomized controlled studies. BMC Med Educ. 2020;20(1):127. Published 2020 Apr 25. doi:10.1186/s12909-020-1994-z
23. Ricci S, Calandrino A, Borgonovo G, Chirico M, Casadio M. Viewpoint: virtual and augmented reality in basic and advanced life support training. JMIR Serious Games. 2022;10(1):e28595. Published 2022 Mar 23. doi:10.2196/28595
24. Ricci S, Mobilio GA, Calandrino A, et al. RiNeo MR: A mixed-reality tool for newborn life support training. Annu Int Conf IEEE Eng Med Biol Soc. 2021;2021:5043-5046. doi:10.1109/EMBC46164.2021.9629612
25. Dhar P, Rocks T, Samarasinghe RM, Stephenson G, Smith C. Augmented reality in medical education: students’ experiences and learning outcomes. Med Educ Online. 2021;26(1):1953953. doi:10.1080/10872981.2021.1953953
26. Pears M, Konstantinidis S. The future of immersive technology in global surgery education [published online ahead of print, 2021 Jul 1]. Indian J Surg. 2021;84(suppl 1):1-5. doi:10.1007/s12262-021-02998-6
27. Liang CJ, Start C, Boley H, Kamat VR, Menassa CC, Aebersold M. Enhancing stroke assessment simulation experience in clinical training using augmented reality. Virt Real. 2021;25(3):575-584. doi:10.1007/s10055-020-00475-1
28. Lacey G, Gozdzielewska L, McAloney-Kocaman K, Ruttle J, Cronin S, Price L. Psychomotor learning theory informing the design and evaluation of an interactive augmented reality hand hygiene training app for healthcare workers. Educ Inf Technol. 2022;27(3):3813-3832. doi:10.1007/s10639-021-10752-4
29. Ryan GV, Callaghan S, Rafferty A, Higgins MF, Mangina E, McAuliffe F. Learning outcomes of immersive technologies in health care student education: systematic review of the literature. J Med Internet Res. 2022;24(2):e30082. Published 2022 Feb 1. doi:10.2196/30082
30. Yu FU, Yan HU, Sundstedt V. A Systematic literature review of virtual, augmented, and mixed reality game applications in healthcare. ACM Trans Comput Healthcare. 2022;3(2);1-27. doi:10.1145/3472303
31. Weeks JK, Amiel JM. Enhancing neuroanatomy education with augmented reality. Med Educ. 2019;53(5):516-517. doi:10.1111/medu.13843
32. Williams MA, McVeigh J, Handa AI, Lee R. Augmented reality in surgical training: a systematic review. Postgrad Med J. 2020;96(1139):537-542. doi:10.1136/postgradmedj-2020-137600

33. Triepels CPR, Smeets CFA, Notten KJB, et al. Does three-dimensional anatomy improve student understanding? Clin Anat. 2020;33(1):25-33. doi:10.1002/ca.23405
34. Pietruski P, Majak M, S´wia¸tek-Najwer E, et al. Supporting fibula free flap harvest with augmented reality: A proof-of-concept study. Laryngoscope. 2020;130(5):1173-1179. doi:10.1002/lary.28090
35. Perkins SL, Krajancich B, Yang CJ, Hargreaves BA, Daniel BL, Berry MF. A patient-specific mixed-reality visualization tool for thoracic surgical planning. Ann Thorac Surg. 2020;110(1):290-295. doi:10.1016/j.athoracsur.2020.01.060
36. Müller F, Roner S, Liebmann F, Spirig JM, Fürnstahl P, Farshad M. Augmented reality navigation for spinal pedicle screw instrumentation using intraoperative 3D imaging. Spine J. 2020;20(4):621-628. doi:10.1016/j.spinee.2019.10.012
37. Kaplan AD, Cruit J, Endsley M, Beers SM, Sawyer BD, Hancock PA. The effects of virtual reality, augmented reality, and mixed reality as training enhancement methods: a meta-analysis. Hum Factors. 2021;63(4):706-726. doi:10.1177/0018720820904229
38. Jud L, Fotouhi J, Andronic O, et al. Applicability of augmented reality in orthopedic surgery - a systematic review. BMC Musculoskelet Disord. 2020;21(1):103. Published 2020 Feb 15. doi:10.1186/s12891-020-3110-2
39. Ara J, Karim FB, Alsubaie MSA, et al. Comprehensive analysis of augmented reality technology in modern healthcare system. Int J Adv Comput Sci Appl. 2021;12(6):845-854. doi:10.14569/IJACSA.2021.0120698
40. Webster A, Gardner J. Aligning technology and institutional readiness: the adoption of innovation. Technol Anal Strateg Manag. 2019;31(10):1229-1241. doi:10.1080/09537325.2019.1601694
41. Hastall MR, Dockweiler C, Mühlhaus J. achieving end user acceptance: building blocks for an evidence-based user-centered framework for health technology development and assessment. In: Antona, M, Stephanidis C, eds. Universal Access in Human–Computer Interaction. Human and Technological Environments. UAHCI 2017. Lecture Notes in Computer Science, vol 10279. Springer, Cham; 2017. doi:10.1007/978-3-319-58700-4_2
42. Ratwani RM, Fairbanks RJ, Hettinger AZ, Benda NC. Electronic health record usability: analysis of the user-centered design processes of eleven electronic health record vendors. J Am Med Inform Assoc. 2015;22(6):1179-1182. doi:10.1093/jamia/ocv050
43. Khairat S, Coleman C, Ottmar P, Jayachander DI, Bice T, Carson SS. Association of Electronic Health Record Use With Physician Fatigue and Efficiency. JAMA Netw Open. 2020;3(6):e207385. Published 2020 Jun 1. doi:10.1001/jamanetworkopen.2020.7385
44. Melnick ER, Dyrbye LN, Sinsky CA, et al. The association between perceived electronic health record usability and professional burnout among US physicians. Mayo Clin Proc. 2020;95(3):476-487. doi:10.1016/j.mayocp.2019.09.024
45. Lee YJ. Comparison of job satisfaction between nonprofit and public employees. Nonprofit Volunt Sect Q. 2016;45(2):295-313. doi:10.1177/0899764015584061
46. Brimhall KC. Inclusion is important... but how do I include? Examining the effects of leader engagement on inclusion, innovation, job satisfaction, and perceived quality of care in a diverse nonprofit health care organization. Nonprofit Volunt Sect Q. 2019;48(4):716-737. doi:10.1177/0899764019829834
47. Moreira MR, Gherman M, Sousa PS. Does innovation influence the performance of healthcare organizations?. Innovation (North Syd). 2017;19(3):335-352. doi:10.1080/14479338.2017.1293489
48. US Department of Veterans Affairs. VA Palo Alto Healthcare System. Updated December 29, 2020. Accessed January 27, 2023. https://www.paloalto.va.gov/about/index.asp
49. Siegel SM, Kaemmerer WF. Measuring the perceived support for innovation in organizations. J Appl Psychol. 1978;63(5):553-562. doi:10.1037/0021-9010.63.5.553
50. Anderson NR, West MA. Measuring climate for work group innovation: development and validation of the team climate inventory. J Organ Behav. 1998;19(3):235-258. doi:10.1002/(SICI)1099-1379(199805)19:3<235::AID-JOB837>3.0.CO;2-C
51. Aarons GA. Measuring provider attitudes toward evidence-based practice: consideration of organizational context and individual differences. Child Adolesc Psychiatr Clin N Am. 2005;14(2):255-viii. doi:10.1016/j.chc.2004.04.008
52. Van der Heijden H. User acceptance of hedonic information systems. MIS Q. 2004;28(4):695-704. doi:10.2307/25148660
53. Venkatesh V, Speier C, Morris MG. User acceptance enablers in individual decision making about technology: Toward an integrated model. Decis Sci. 2002;33(2):297-316. doi:10.1111/j.1540-5915.2002.tb01646.x
54. Puri A, Kim B, Nguyen O, Stolee P, Tung J, Lee J. User acceptance of wrist-worn activity trackers among community-dwelling older adults: mixed method study. JMIR Mhealth Uhealth. 2017;5(11):e173. Published 2017 Nov 15. doi:10.2196/mhealth.8211
55. Huang YC, Backman SJ, Backman KF, Moore D. Exploring user acceptance of 3D virtual worlds in travel and tourism marketing. Tourism Management. 2013;36:490-501. doi:10.1016/j.tourman.2012.09.009
56. Rasimah CM, Ahmad A, Zaman HB. Evaluation of user acceptance of mixed reality technology. AJET. 2011;27(8). doi:10.14742/ajet.899
57. Choi J, Boyle DK. RN workgroup job satisfaction and patient falls in acute care hospital units. J Nurs Adm. 2013;43(11):586-591. doi:10.1097/01.NNA.0000434509.66749.7c58. Tzeng HM, Ketefian S. The relationship between nurses’ job satisfaction and inpatient satisfaction: an exploratory study in a Taiwan teaching hospital. J Nurs Care Qual. 2002;16(2):39-49. doi:10.1097/00001786-200201000-00005
59. Williams ES, Skinner AC. Outcomes of physician job satisfaction: a narrative review, implications, and directions for future research. Health Care Manage Rev. 2003;28(2):119-139. doi:10.1097/00004010-200304000-00004
60. Waldman JD, Kelly F, Arora S, Smith HL. The shocking cost of turnover in health care. Health Care Manage Rev. 2004;29(1):2-7. doi:10.1097/00004010-200401000-00002
61. Hayes LJ, O’Brien-Pallas L, Duffield C, et al. Nurse turnover: a literature review - an update. Int J Nurs Stud. 2012;49(7):887-905. doi:10.1016/j.ijnurstu.2011.10.001
62. US Department of Veterans Affairs. FY 2021/FY 2019 Annual performance plan and report. February 2020. Accessed January 27, 2023. https://www.va.gov/oei/docs/VA2019-2021appr.pdf
Building the health care system of the future requires the thoughtful development and integration of innovative technologies to positively transform care.1-4 Extended reality (XR) represents a spectrum of emerging technologies that have the potential to enhance health care. This includes virtual reality (VR), where a computer-generated visual experience fills the screen; augmented reality (AR), which allows users to see computer-generated images superimposed into an otherwise normal real-world field of view; and mixed reality (MR), which allows users to interact and manipulate computer-generated AR images.
Clinicians and researchers have begun exploring the potential of XR to address a wide variety of health care challenges. A recent systematic review concluded that many clinical studies in this area have small sample sizes and are in the preclinical, proof-of-concept stage, but demonstrate the potential and impact of the underlying VR, AR, and MR technologies.5 Common emerging health care uses for XR include medical education, training, presurgical planning, surgical guidance, distraction therapy for pain and anxiety, and home health indications, including rehabilitation.5-39
Importantly, some researchers have raised concerns regarding the adaptability of the health care workforce with emerging technologies, and their interest in new methods of delivering care.7,39 Successful deployment of any novel health care technology depends on multiple factors, including alignment with staff needs, receptivity to those solutions, customization to specific preferences, and usability.1,3,40-42 Unfortunately, the implementation of some health care technologies, such as electronic health records that did not account for end-user requirements, resulted in employee fatigue, burnout, and negative staffing turnover.42-44 Conversely, elevated employee morale and operational performance have been directly linked to a climate of inclusion and innovation.45-47 In this assessment, we sought to understand US Department of Veterans Affairs (VA) employees’ perceptions and expert opinions related to the introduction of new AR/MR technology.
Methods
The VA Palo Alto Health Care System (VAPAHCS) consists of 3 inpatient hospitals and 7 outpatient clinics, provides a full range of care services to > 90,000 enrolled veterans with 800 hospital beds, 3 nursing homes, and a 100-bed domiciliary. The facility also runs data-driven care projects in research, innovation, and evidence-based practice group under nursing services.48 This project was performed by the VA National Center for Collaborative Healthcare Innovation at the VAPAHCS campus.
The combined technical system used for this assessment included a wireless communication network, AR/MR hardware, and software. Medivis AnatomyX software displayed an interactive human anatomy atlas segmented into about 6000 individual interactive parts. Medivis SurgicalAR received US Food and Drug Administration clearance for presurgical planning and was used to transform and display deidentified diagnostic images (eg, magnetic resonance images and computed tomography) in 3-dimensional (3D) interactive holograms (Figures 1 and 2).
The wireless Microsoft HoloLens 2 AR/MR headset was used for viewing and sensor-enabled collaborative interaction. Multiple participants in the same physical location simultaneously participated and interacted with 3D holograms. The interactive hologram data were enabled for 3D stereoscopic viewing and manipulation.
Setting and Participants
We reviewed published studies that used questionnaires to evaluate institutions’ level of innovation and new technology user acceptance to develop the questionnaire.49-56 Questions and methods were modified, with a focus on understanding the impact on hospital employees. The questionnaire consisted of 2 predemonstration and 3 postdemonstration sections. The first section included background questions. The second (predemonstration) and third (postdemonstration) sections provided matched questions on feelings about the VA. The fourth section included 2 unmatched questions about how the participant felt this technology would impact veterans and whether the VA should implement similar technologies. We used a 5-point Likert scale for sections 2, 3 and 4 (1 = not at all to 5 = extremely). Two unmatched free-text questions asked how the technology could be used in the participant’s hospital service, and another open-ended question asked for any additional comments. To reduce potential reporting bias, 2 VA employees that did not work at VAPAHCS assisted with the survey distribution and collection. VAPAHCS staff were informed by all employee email and facility intranet of the opportunity to participate; the voluntary demonstration and survey took place on February 10 and 11, 2020.
Data Analysis
All matching pre/post questions were analyzed together to determine statistically significant differences using the Wilcoxon signed rank matched pairs test and pooled t test. Survey respondents were also grouped by employment type to evaluate the impact on subgroups. Results were also grouped by VA tenure into 4 categorical 10-year increments (0-10, 11-20, 21-30, 31-40). Additionally, analysis of variance (ANOVA) was performed on employment types and VA tenure to understand whether there was a statistically significant difference in responses by these subgroups. Respondents’ optional free-text answers were manually reviewed by 2 authors (ZPV and DMA), classified, coded by the common themes, and analyzed for comparison.
Results
A total of 166 participants completed the predemonstration survey, which was a requirement for participating in the AR demonstration. Of those, 159 staff members (95.8%) also completed at least part of the postdemonstration paired structured questions, and their results were included in the analysis.
Paired Questions
For questions about how innovative the VA is, 108 of 152 participants (71.1%) provided higher scores after the demonstration, 42 (27.6%) had no change, and 2 (1.3%) provided decreased scores. The mean innovative score increased from 3.4 predemonstration to 4.5 postdemonstration on a Likert scale, which is a 1.1 point increase from predemonstration to postdemonstration (95% CI, 0.9- 1.2) or a 22% increase (95% CI, 18%-24%) (P < .001). Respondents level of excitement about VA also increased with 82 of 157 participants (52.2%) providing higher scores after the demonstration, 71 (45.2%) had no change, and 4 scores (2.5%) decreased. The predemonstration mean excitement score of 3.7 increased to 4.3 postdemonstration, which is a 0.6 point increase from before to after the demonstration (95% CI, 0.5-0.7) or a 12% increase (95% CI, 10%-14%) (P < .001). In the survey, 36 of 149 participants (24.2%) had higher scores for their expectation to continue working at VA postdemonstration, 109 (73.2%) had no change, and 4 scores (2.7%) decreased. The mean employee retention score increased from 4.2 predemonstration to 4.5 postdemonstration, which is a 0.3 point increase between pre/post (95% CI, 0.2-0.4) or a 6% increase (95% CI, 4%-8%) (P < .001)
The pre/post questions were analyzed using 1-way ANOVA by hospital department and VA tenure. The responses by department were not statistically significant. Of the 159 employees assessed, 101 respondents (63.5%) had 0 to 10 years VA tenure, 44 (27.7%) had 11 to 20 years, 10 (6.3%) had 21 to 30 years, and 4 (2.5%) had > 31 to 40 years. Length of VA tenure did not impact respondent excitement. Respondents opinions on innovation in the 0 to 10 year and the 11 to 20 year groups rose from 3.2 and 3.7 predemonstration to 4.3 and 4.6 postdemonstration, respectively (P < .001 for both statistical comparisons) (Table 2). Interestingly, the 0 to 10 group saw a 9% rise from a 4.0 score predemonstration to a 4.4 score postdemonstration (P < .001), indicating that the demonstration had a positive impact on their plans to continue employment at VA (Table 3).
Sex did not play a significant role in how respondents answered questions regarding VA excitement or innovation. However, there was a statistically significant difference in how male and female respondents answered the predemonstration question about their plans to continue VA employment, according to the Wilcoxon rank sum test. Predemonstration, female respondents had a mean score of 4.1, which was 6% lower than the 4.4 score of male colleagues (P = .04). Veteran status did have an impact on how respondents felt about VA innovation, and their plans to continue employment at VA. After the demonstration, veteran staff felt the VA was more innovative compared with nonveterans: 4.7 vs 4.4, respectively, a 6% difference (P = .02) Similarly, for the continued VA employment question, veterans had a mean score of 4.8 vs 4.4 for nonveterans, an 8% difference (P = .03) These results suggest that the demonstration had more of an impact on veteran employees vs nonveteran employees.
Unpaired Questions
There were 2 structured unpaired postdemonstration questions. Respondents agreed that similar technology would impact veteran health care with mean (SD) of 4.6 (0.6) and a median score of 5 on a 5-point Likert scale. Respondents also agreed on the importance of implementing similar innovations with mean (SD) of 4.7 (0.5), and a median score of 5.
The survey asked how this technology could benefit their hospital service department and had 64 responses. Forty-six respondents saw applications for education or patient care/surgery. Other responses shared excitement about the technology and its potential to positively impact patient education. There were 37 responses to the open-ended question: 21 respondents expressed excitement for the technology, and 10 respondents reiterated that the demonstration would be of benefit to patient care/surgery and training.
Discussion
Successful development, design, and deployment of any new health care tool depends on leveraging insights from the employees that will be using and supporting these systems. Correspondingly, understanding the impact that advanced technologies have on health care employees’ satisfaction, morale, and retention is critical to our overall institutional strategy. Our findings show that a one-time experience with AR/MR technology elicited positive employee reactions. Of note, the survey revealed statistically significant improvements in staff’s view of the VA, with the greatest positive impact for questions about innovation, followed by excitement to work at the VA, and likelihood to continue work at the VA. It is very disruptive and costly when health care employees leave, and improving employee satisfaction and morale is important for better patient care and patient satisfaction, which is priority for VAPAHCS leadership.57-62
The paired predemonstration and postdemonstration scores were similarly high, nearing the top threshold available for the Likert scale (4.3 to 4.5). Furthermore, the least incremental improvement for these responses was observed for topics that had the highest initial baseline score. Therefore, the improvements observed for the paired questions may have more to do with the high baseline values.
Of additional interest, the self-reported likelihood of continuing to work at the VA increased the most for female employees, veteran employees, and employees with the least number of years at the VA. These demographic differences have important implications for VA staff recruitment and retention strategies.62 The unpaired questions about the impact on veteran care and whether the VA should continue similar work demonstrated extremely high support with median scores of 5 for both questions. The free-text postdemonstration responses also demonstrate similar positive themes, with a disposition for excitement about both the training and patient care applications for this technology. In addition, respondents felt strongly that this and other similar technologies will positively impact the health care for veterans and that the VA should continue these efforts.
Strengths and Limitations
A strength of this assessment is the ability to evaluate survey responses that were systematically collected and matched from the same individual immediately before and after exposure to the new technology. The free-text responses provided additional important information that both confirmed the results and provided additional valued supplementary guidance for future implementation strategies, which is critical for our translational implementation goals. An additional strength is that the voluntary surveys were managed by non-VAPAHCS colleagues, limiting potential bias. Importantly, the number of respondents allowed a statistically significant assessment of important health care employee metrics. These results have emphasized how being part of an innovative organization, and the introduction of advanced AR/MR technology, improve employees’ satisfaction and morale about where they work as well as their intention to stay at their institution.
A limitation of this assessment was the lack of comparative data for employee acceptance of other technologies at VAPAHCS. This limits our ability to differentiate whether the strong positive results observed in this evaluation were a result of the specific technology assessed, or of new and advanced health care technology in general. Nonetheless, our unpaired questions, which received extremely high scores, also included participant questions about comparing the system with other similar technologies. This assessment was also focused on veteran care, which limits generalizability.
Conclusions
One-time exposure to advanced AR technology for health care significantly increased employee morale as measured by excitement about working at the VA as well as employee intention to continue employment at the VA. These collateral benefits of the technology are particularly important in health care because our employees are our most important asset and improving employee morale equates to better patient care. Positive impacts were most pronounced for women employees, newer VA employees, and employees who are also veterans. These more detailed insights are also positioned to have a direct impact on employee recruitment and retention strategies. Additional valuable insights regarding the most applicable use of the technology in the clinical setting were also obtained.
Acknowledgments
We thank Andrew Spiegelman, Hyewon Kim, Jonathan Sills, and Alexander Erickson for their assistance in developing the survey questions. We also thank Jason Rhodes and Mark Bulson for traveling to our facility to assist with managing the anonymous surveys during the demonstration event.
Building the health care system of the future requires the thoughtful development and integration of innovative technologies to positively transform care.1-4 Extended reality (XR) represents a spectrum of emerging technologies that have the potential to enhance health care. This includes virtual reality (VR), where a computer-generated visual experience fills the screen; augmented reality (AR), which allows users to see computer-generated images superimposed into an otherwise normal real-world field of view; and mixed reality (MR), which allows users to interact and manipulate computer-generated AR images.
Clinicians and researchers have begun exploring the potential of XR to address a wide variety of health care challenges. A recent systematic review concluded that many clinical studies in this area have small sample sizes and are in the preclinical, proof-of-concept stage, but demonstrate the potential and impact of the underlying VR, AR, and MR technologies.5 Common emerging health care uses for XR include medical education, training, presurgical planning, surgical guidance, distraction therapy for pain and anxiety, and home health indications, including rehabilitation.5-39
Importantly, some researchers have raised concerns regarding the adaptability of the health care workforce with emerging technologies, and their interest in new methods of delivering care.7,39 Successful deployment of any novel health care technology depends on multiple factors, including alignment with staff needs, receptivity to those solutions, customization to specific preferences, and usability.1,3,40-42 Unfortunately, the implementation of some health care technologies, such as electronic health records that did not account for end-user requirements, resulted in employee fatigue, burnout, and negative staffing turnover.42-44 Conversely, elevated employee morale and operational performance have been directly linked to a climate of inclusion and innovation.45-47 In this assessment, we sought to understand US Department of Veterans Affairs (VA) employees’ perceptions and expert opinions related to the introduction of new AR/MR technology.
Methods
The VA Palo Alto Health Care System (VAPAHCS) consists of 3 inpatient hospitals and 7 outpatient clinics, provides a full range of care services to > 90,000 enrolled veterans with 800 hospital beds, 3 nursing homes, and a 100-bed domiciliary. The facility also runs data-driven care projects in research, innovation, and evidence-based practice group under nursing services.48 This project was performed by the VA National Center for Collaborative Healthcare Innovation at the VAPAHCS campus.
The combined technical system used for this assessment included a wireless communication network, AR/MR hardware, and software. Medivis AnatomyX software displayed an interactive human anatomy atlas segmented into about 6000 individual interactive parts. Medivis SurgicalAR received US Food and Drug Administration clearance for presurgical planning and was used to transform and display deidentified diagnostic images (eg, magnetic resonance images and computed tomography) in 3-dimensional (3D) interactive holograms (Figures 1 and 2).
The wireless Microsoft HoloLens 2 AR/MR headset was used for viewing and sensor-enabled collaborative interaction. Multiple participants in the same physical location simultaneously participated and interacted with 3D holograms. The interactive hologram data were enabled for 3D stereoscopic viewing and manipulation.
Setting and Participants
We reviewed published studies that used questionnaires to evaluate institutions’ level of innovation and new technology user acceptance to develop the questionnaire.49-56 Questions and methods were modified, with a focus on understanding the impact on hospital employees. The questionnaire consisted of 2 predemonstration and 3 postdemonstration sections. The first section included background questions. The second (predemonstration) and third (postdemonstration) sections provided matched questions on feelings about the VA. The fourth section included 2 unmatched questions about how the participant felt this technology would impact veterans and whether the VA should implement similar technologies. We used a 5-point Likert scale for sections 2, 3 and 4 (1 = not at all to 5 = extremely). Two unmatched free-text questions asked how the technology could be used in the participant’s hospital service, and another open-ended question asked for any additional comments. To reduce potential reporting bias, 2 VA employees that did not work at VAPAHCS assisted with the survey distribution and collection. VAPAHCS staff were informed by all employee email and facility intranet of the opportunity to participate; the voluntary demonstration and survey took place on February 10 and 11, 2020.
Data Analysis
All matching pre/post questions were analyzed together to determine statistically significant differences using the Wilcoxon signed rank matched pairs test and pooled t test. Survey respondents were also grouped by employment type to evaluate the impact on subgroups. Results were also grouped by VA tenure into 4 categorical 10-year increments (0-10, 11-20, 21-30, 31-40). Additionally, analysis of variance (ANOVA) was performed on employment types and VA tenure to understand whether there was a statistically significant difference in responses by these subgroups. Respondents’ optional free-text answers were manually reviewed by 2 authors (ZPV and DMA), classified, coded by the common themes, and analyzed for comparison.
Results
A total of 166 participants completed the predemonstration survey, which was a requirement for participating in the AR demonstration. Of those, 159 staff members (95.8%) also completed at least part of the postdemonstration paired structured questions, and their results were included in the analysis.
Paired Questions
For questions about how innovative the VA is, 108 of 152 participants (71.1%) provided higher scores after the demonstration, 42 (27.6%) had no change, and 2 (1.3%) provided decreased scores. The mean innovative score increased from 3.4 predemonstration to 4.5 postdemonstration on a Likert scale, which is a 1.1 point increase from predemonstration to postdemonstration (95% CI, 0.9- 1.2) or a 22% increase (95% CI, 18%-24%) (P < .001). Respondents level of excitement about VA also increased with 82 of 157 participants (52.2%) providing higher scores after the demonstration, 71 (45.2%) had no change, and 4 scores (2.5%) decreased. The predemonstration mean excitement score of 3.7 increased to 4.3 postdemonstration, which is a 0.6 point increase from before to after the demonstration (95% CI, 0.5-0.7) or a 12% increase (95% CI, 10%-14%) (P < .001). In the survey, 36 of 149 participants (24.2%) had higher scores for their expectation to continue working at VA postdemonstration, 109 (73.2%) had no change, and 4 scores (2.7%) decreased. The mean employee retention score increased from 4.2 predemonstration to 4.5 postdemonstration, which is a 0.3 point increase between pre/post (95% CI, 0.2-0.4) or a 6% increase (95% CI, 4%-8%) (P < .001)
The pre/post questions were analyzed using 1-way ANOVA by hospital department and VA tenure. The responses by department were not statistically significant. Of the 159 employees assessed, 101 respondents (63.5%) had 0 to 10 years VA tenure, 44 (27.7%) had 11 to 20 years, 10 (6.3%) had 21 to 30 years, and 4 (2.5%) had > 31 to 40 years. Length of VA tenure did not impact respondent excitement. Respondents opinions on innovation in the 0 to 10 year and the 11 to 20 year groups rose from 3.2 and 3.7 predemonstration to 4.3 and 4.6 postdemonstration, respectively (P < .001 for both statistical comparisons) (Table 2). Interestingly, the 0 to 10 group saw a 9% rise from a 4.0 score predemonstration to a 4.4 score postdemonstration (P < .001), indicating that the demonstration had a positive impact on their plans to continue employment at VA (Table 3).
Sex did not play a significant role in how respondents answered questions regarding VA excitement or innovation. However, there was a statistically significant difference in how male and female respondents answered the predemonstration question about their plans to continue VA employment, according to the Wilcoxon rank sum test. Predemonstration, female respondents had a mean score of 4.1, which was 6% lower than the 4.4 score of male colleagues (P = .04). Veteran status did have an impact on how respondents felt about VA innovation, and their plans to continue employment at VA. After the demonstration, veteran staff felt the VA was more innovative compared with nonveterans: 4.7 vs 4.4, respectively, a 6% difference (P = .02) Similarly, for the continued VA employment question, veterans had a mean score of 4.8 vs 4.4 for nonveterans, an 8% difference (P = .03) These results suggest that the demonstration had more of an impact on veteran employees vs nonveteran employees.
Unpaired Questions
There were 2 structured unpaired postdemonstration questions. Respondents agreed that similar technology would impact veteran health care with mean (SD) of 4.6 (0.6) and a median score of 5 on a 5-point Likert scale. Respondents also agreed on the importance of implementing similar innovations with mean (SD) of 4.7 (0.5), and a median score of 5.
The survey asked how this technology could benefit their hospital service department and had 64 responses. Forty-six respondents saw applications for education or patient care/surgery. Other responses shared excitement about the technology and its potential to positively impact patient education. There were 37 responses to the open-ended question: 21 respondents expressed excitement for the technology, and 10 respondents reiterated that the demonstration would be of benefit to patient care/surgery and training.
Discussion
Successful development, design, and deployment of any new health care tool depends on leveraging insights from the employees that will be using and supporting these systems. Correspondingly, understanding the impact that advanced technologies have on health care employees’ satisfaction, morale, and retention is critical to our overall institutional strategy. Our findings show that a one-time experience with AR/MR technology elicited positive employee reactions. Of note, the survey revealed statistically significant improvements in staff’s view of the VA, with the greatest positive impact for questions about innovation, followed by excitement to work at the VA, and likelihood to continue work at the VA. It is very disruptive and costly when health care employees leave, and improving employee satisfaction and morale is important for better patient care and patient satisfaction, which is priority for VAPAHCS leadership.57-62
The paired predemonstration and postdemonstration scores were similarly high, nearing the top threshold available for the Likert scale (4.3 to 4.5). Furthermore, the least incremental improvement for these responses was observed for topics that had the highest initial baseline score. Therefore, the improvements observed for the paired questions may have more to do with the high baseline values.
Of additional interest, the self-reported likelihood of continuing to work at the VA increased the most for female employees, veteran employees, and employees with the least number of years at the VA. These demographic differences have important implications for VA staff recruitment and retention strategies.62 The unpaired questions about the impact on veteran care and whether the VA should continue similar work demonstrated extremely high support with median scores of 5 for both questions. The free-text postdemonstration responses also demonstrate similar positive themes, with a disposition for excitement about both the training and patient care applications for this technology. In addition, respondents felt strongly that this and other similar technologies will positively impact the health care for veterans and that the VA should continue these efforts.
Strengths and Limitations
A strength of this assessment is the ability to evaluate survey responses that were systematically collected and matched from the same individual immediately before and after exposure to the new technology. The free-text responses provided additional important information that both confirmed the results and provided additional valued supplementary guidance for future implementation strategies, which is critical for our translational implementation goals. An additional strength is that the voluntary surveys were managed by non-VAPAHCS colleagues, limiting potential bias. Importantly, the number of respondents allowed a statistically significant assessment of important health care employee metrics. These results have emphasized how being part of an innovative organization, and the introduction of advanced AR/MR technology, improve employees’ satisfaction and morale about where they work as well as their intention to stay at their institution.
A limitation of this assessment was the lack of comparative data for employee acceptance of other technologies at VAPAHCS. This limits our ability to differentiate whether the strong positive results observed in this evaluation were a result of the specific technology assessed, or of new and advanced health care technology in general. Nonetheless, our unpaired questions, which received extremely high scores, also included participant questions about comparing the system with other similar technologies. This assessment was also focused on veteran care, which limits generalizability.
Conclusions
One-time exposure to advanced AR technology for health care significantly increased employee morale as measured by excitement about working at the VA as well as employee intention to continue employment at the VA. These collateral benefits of the technology are particularly important in health care because our employees are our most important asset and improving employee morale equates to better patient care. Positive impacts were most pronounced for women employees, newer VA employees, and employees who are also veterans. These more detailed insights are also positioned to have a direct impact on employee recruitment and retention strategies. Additional valuable insights regarding the most applicable use of the technology in the clinical setting were also obtained.
Acknowledgments
We thank Andrew Spiegelman, Hyewon Kim, Jonathan Sills, and Alexander Erickson for their assistance in developing the survey questions. We also thank Jason Rhodes and Mark Bulson for traveling to our facility to assist with managing the anonymous surveys during the demonstration event.
1. World Economic Forum. Health and healthcare in the fourth industrial revolution: Global Future Council on the future of health and healthcare 2016-2018. April 2019. Accessed January 27, 2023. https://www3.weforum.org/docs/WEF__Shaping_the_Future_of_Health_Council_Report.pdf
2. Iveroth E, Fryk P, Rapp B. Information technology strategy and alignment issues in health care organizations. Health Care Manage Rev. 2013;38(3):188-200. doi:10.1097/HMR.0b013e31826119d7
3. Thakur R, Hsu SH, Fontenot G. Innovation in healthcare: issues and future trends. J Bus Res. 2012;65(4):562-569. doi:10.1016/j.jbusres.2011.02.022
4. Thimbleby H. Technology and the future of healthcare. J Public Health Res. 2013;2(3):e28. Published 2013 Dec 1. doi:10.4081/jphr.2013.e28
5. Viglialoro RM, Condino S, Turini G, Carbone M, Ferrari V, Gesi M. augmented reality, mixed reality, and hybrid approach in healthcare simulation: a systematic review. Applied Sciences. 2021;11(5):2338. doi:10.3390/app11052338
6. Rawlins CR, Veigulis Z, Hebert C, Curtin C, Osborne T. Effect of immersive virtual reality on pain and anxiety at a Veterans Affairs health care facility. Front Virt Real. 2021;(2):136. doi:10.3389/frvir.2021.719681
7. Chawdhary G, Shoman N. Emerging artificial intelligence applications in otological imaging. Curr Opin Otolaryngol Head Neck Surg. 2021;29(5):357-364. doi:10.1097/MOO.0000000000000754
8. Asadzadeh A, Samad-Soltani T, Rezaei-Hachesu P. Applications of virtual and augmented reality in infectious disease epidemics with a focus on the COVID-19 outbreak. Inform Med Unlocked. 2021;24:100579. doi:10.1016/j.imu.2021.100579
9. Ashwini KB, Savitha R, Harish A. Application of augmented reality technology for home healthcare product visualization. ECS Transas. 2022;107(1):10921. doi:10.1149/10701.10921ecst
10. Brooks AL. VR/Technologies for Rehabilitation. In: Brooks AL, Brahman S, Kapralos B, Nakajima A, Tyerman J, Jain LC, eds. Recent Advances in Technologies for Inclusive Well-Being Virtual Patients, Gamification and Simulation. Intelligent Systems Reference Library. Springer; 2021:241-252. doi:10.1007/978-3-030-59608-8_13
11. Koulouris D, Menychtas A, Maglogiannis I. An IoT-enabled platform for the assessment of physical and mental activities utilizing augmented reality exergaming. Sensors (Basel). 2022;22(9):3181. Published 2022 Apr 21. doi:10.3390/s22093181
12. Deiss YR, Korkut S, Inglese T. Increase therapy understanding and medication adherence for patients with inflammatory skin diseases through augmented reality. Digital Human Modeling and Applications in Health, Safety, Ergonomics and Risk Management. Health, Operations Management, and Design: 13th International Conference, DHM 2022, Held as Part of the 24th HCI International Conference, HCII 2022. 2022:21-40. doi:10.1007/978-3-031-06018-2_2
13. Bertino E, Gao W, Steffan B, et al, eds. Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics). Springer; 2022:21-40.
14. Ruhaiyem NIR, Mazlan NA. Image Modeling Through Augmented Reality for Skin Allergies Recognition. Lecture Notes on Data Engineering and Communications Technologies. 2021:72-79. doi: 10.1007/978-3-030-70713-2_8
15. Park BJ, Perkons NR, Profka E, et al. Three-dimensional augmented reality visualization informs locoregional therapy in a translational model of hepatocellular carcinoma. J Vasc Interv Radiol. 2020;31(10):1612-1618.e1. doi:10.1016/j.jvir.2020.01.028
16. Leo J, Zhou Z, Yang H, et al, eds. Interactive cardiovascular surgical planning via augmented reality. 5th Asian CHI Symposium 2021; 2021. doi:10.1145/3429360.3468195
17. Zuo Y, Jiang T, Dou J, et al. A novel evaluation model for a mixed-reality surgical navigation system: where Microsoft Hololens meets the operating room. Surg Innov. 2020;27(2):193-202. doi:10.1177/1553350619893236
18. Ghaednia H, Fourman MS, Lans A, et al. Augmented and virtual reality in spine surgery, current applications and future potentials. Spine J. 2021;21(10):1617-1625. doi:10.1016/j.spinee.2021.03.018
19. Liu Y, Lee MG, Kim JS. Spine surgery assisted by augmented reality: where have we been?. Yonsei Med J. 2022;63(4):305-316. doi:10.3349/ymj.2022.63.4.305
20. Kimmel S, Cobus V, Heuten W, eds. opticARe—augmented reality mobile patient monitoring in intensive care units. Proceedings of the ACM Symposium on Virtual Reality Software and Technology, VRST; 2021. doi:10.1145/3489849.3489852
21. Voštinár P, Horváthová D, Mitter M, Bako M. The look at the various uses of VR. Open Computer Sci. 2021;11(1):241-250. doi:10.1515/comp-2020-0123
22. Zhao J, Xu X, Jiang H, Ding Y. The effectiveness of virtual reality-based technology on anatomy teaching: a meta-analysis of randomized controlled studies. BMC Med Educ. 2020;20(1):127. Published 2020 Apr 25. doi:10.1186/s12909-020-1994-z
23. Ricci S, Calandrino A, Borgonovo G, Chirico M, Casadio M. Viewpoint: virtual and augmented reality in basic and advanced life support training. JMIR Serious Games. 2022;10(1):e28595. Published 2022 Mar 23. doi:10.2196/28595
24. Ricci S, Mobilio GA, Calandrino A, et al. RiNeo MR: A mixed-reality tool for newborn life support training. Annu Int Conf IEEE Eng Med Biol Soc. 2021;2021:5043-5046. doi:10.1109/EMBC46164.2021.9629612
25. Dhar P, Rocks T, Samarasinghe RM, Stephenson G, Smith C. Augmented reality in medical education: students’ experiences and learning outcomes. Med Educ Online. 2021;26(1):1953953. doi:10.1080/10872981.2021.1953953
26. Pears M, Konstantinidis S. The future of immersive technology in global surgery education [published online ahead of print, 2021 Jul 1]. Indian J Surg. 2021;84(suppl 1):1-5. doi:10.1007/s12262-021-02998-6
27. Liang CJ, Start C, Boley H, Kamat VR, Menassa CC, Aebersold M. Enhancing stroke assessment simulation experience in clinical training using augmented reality. Virt Real. 2021;25(3):575-584. doi:10.1007/s10055-020-00475-1
28. Lacey G, Gozdzielewska L, McAloney-Kocaman K, Ruttle J, Cronin S, Price L. Psychomotor learning theory informing the design and evaluation of an interactive augmented reality hand hygiene training app for healthcare workers. Educ Inf Technol. 2022;27(3):3813-3832. doi:10.1007/s10639-021-10752-4
29. Ryan GV, Callaghan S, Rafferty A, Higgins MF, Mangina E, McAuliffe F. Learning outcomes of immersive technologies in health care student education: systematic review of the literature. J Med Internet Res. 2022;24(2):e30082. Published 2022 Feb 1. doi:10.2196/30082
30. Yu FU, Yan HU, Sundstedt V. A Systematic literature review of virtual, augmented, and mixed reality game applications in healthcare. ACM Trans Comput Healthcare. 2022;3(2);1-27. doi:10.1145/3472303
31. Weeks JK, Amiel JM. Enhancing neuroanatomy education with augmented reality. Med Educ. 2019;53(5):516-517. doi:10.1111/medu.13843
32. Williams MA, McVeigh J, Handa AI, Lee R. Augmented reality in surgical training: a systematic review. Postgrad Med J. 2020;96(1139):537-542. doi:10.1136/postgradmedj-2020-137600
33. Triepels CPR, Smeets CFA, Notten KJB, et al. Does three-dimensional anatomy improve student understanding? Clin Anat. 2020;33(1):25-33. doi:10.1002/ca.23405
34. Pietruski P, Majak M, S´wia¸tek-Najwer E, et al. Supporting fibula free flap harvest with augmented reality: A proof-of-concept study. Laryngoscope. 2020;130(5):1173-1179. doi:10.1002/lary.28090
35. Perkins SL, Krajancich B, Yang CJ, Hargreaves BA, Daniel BL, Berry MF. A patient-specific mixed-reality visualization tool for thoracic surgical planning. Ann Thorac Surg. 2020;110(1):290-295. doi:10.1016/j.athoracsur.2020.01.060
36. Müller F, Roner S, Liebmann F, Spirig JM, Fürnstahl P, Farshad M. Augmented reality navigation for spinal pedicle screw instrumentation using intraoperative 3D imaging. Spine J. 2020;20(4):621-628. doi:10.1016/j.spinee.2019.10.012
37. Kaplan AD, Cruit J, Endsley M, Beers SM, Sawyer BD, Hancock PA. The effects of virtual reality, augmented reality, and mixed reality as training enhancement methods: a meta-analysis. Hum Factors. 2021;63(4):706-726. doi:10.1177/0018720820904229
38. Jud L, Fotouhi J, Andronic O, et al. Applicability of augmented reality in orthopedic surgery - a systematic review. BMC Musculoskelet Disord. 2020;21(1):103. Published 2020 Feb 15. doi:10.1186/s12891-020-3110-2
39. Ara J, Karim FB, Alsubaie MSA, et al. Comprehensive analysis of augmented reality technology in modern healthcare system. Int J Adv Comput Sci Appl. 2021;12(6):845-854. doi:10.14569/IJACSA.2021.0120698
40. Webster A, Gardner J. Aligning technology and institutional readiness: the adoption of innovation. Technol Anal Strateg Manag. 2019;31(10):1229-1241. doi:10.1080/09537325.2019.1601694
41. Hastall MR, Dockweiler C, Mühlhaus J. achieving end user acceptance: building blocks for an evidence-based user-centered framework for health technology development and assessment. In: Antona, M, Stephanidis C, eds. Universal Access in Human–Computer Interaction. Human and Technological Environments. UAHCI 2017. Lecture Notes in Computer Science, vol 10279. Springer, Cham; 2017. doi:10.1007/978-3-319-58700-4_2
42. Ratwani RM, Fairbanks RJ, Hettinger AZ, Benda NC. Electronic health record usability: analysis of the user-centered design processes of eleven electronic health record vendors. J Am Med Inform Assoc. 2015;22(6):1179-1182. doi:10.1093/jamia/ocv050
43. Khairat S, Coleman C, Ottmar P, Jayachander DI, Bice T, Carson SS. Association of Electronic Health Record Use With Physician Fatigue and Efficiency. JAMA Netw Open. 2020;3(6):e207385. Published 2020 Jun 1. doi:10.1001/jamanetworkopen.2020.7385
44. Melnick ER, Dyrbye LN, Sinsky CA, et al. The association between perceived electronic health record usability and professional burnout among US physicians. Mayo Clin Proc. 2020;95(3):476-487. doi:10.1016/j.mayocp.2019.09.024
45. Lee YJ. Comparison of job satisfaction between nonprofit and public employees. Nonprofit Volunt Sect Q. 2016;45(2):295-313. doi:10.1177/0899764015584061
46. Brimhall KC. Inclusion is important... but how do I include? Examining the effects of leader engagement on inclusion, innovation, job satisfaction, and perceived quality of care in a diverse nonprofit health care organization. Nonprofit Volunt Sect Q. 2019;48(4):716-737. doi:10.1177/0899764019829834
47. Moreira MR, Gherman M, Sousa PS. Does innovation influence the performance of healthcare organizations?. Innovation (North Syd). 2017;19(3):335-352. doi:10.1080/14479338.2017.1293489
48. US Department of Veterans Affairs. VA Palo Alto Healthcare System. Updated December 29, 2020. Accessed January 27, 2023. https://www.paloalto.va.gov/about/index.asp
49. Siegel SM, Kaemmerer WF. Measuring the perceived support for innovation in organizations. J Appl Psychol. 1978;63(5):553-562. doi:10.1037/0021-9010.63.5.553
50. Anderson NR, West MA. Measuring climate for work group innovation: development and validation of the team climate inventory. J Organ Behav. 1998;19(3):235-258. doi:10.1002/(SICI)1099-1379(199805)19:3<235::AID-JOB837>3.0.CO;2-C
51. Aarons GA. Measuring provider attitudes toward evidence-based practice: consideration of organizational context and individual differences. Child Adolesc Psychiatr Clin N Am. 2005;14(2):255-viii. doi:10.1016/j.chc.2004.04.008
52. Van der Heijden H. User acceptance of hedonic information systems. MIS Q. 2004;28(4):695-704. doi:10.2307/25148660
53. Venkatesh V, Speier C, Morris MG. User acceptance enablers in individual decision making about technology: Toward an integrated model. Decis Sci. 2002;33(2):297-316. doi:10.1111/j.1540-5915.2002.tb01646.x
54. Puri A, Kim B, Nguyen O, Stolee P, Tung J, Lee J. User acceptance of wrist-worn activity trackers among community-dwelling older adults: mixed method study. JMIR Mhealth Uhealth. 2017;5(11):e173. Published 2017 Nov 15. doi:10.2196/mhealth.8211
55. Huang YC, Backman SJ, Backman KF, Moore D. Exploring user acceptance of 3D virtual worlds in travel and tourism marketing. Tourism Management. 2013;36:490-501. doi:10.1016/j.tourman.2012.09.009
56. Rasimah CM, Ahmad A, Zaman HB. Evaluation of user acceptance of mixed reality technology. AJET. 2011;27(8). doi:10.14742/ajet.899
57. Choi J, Boyle DK. RN workgroup job satisfaction and patient falls in acute care hospital units. J Nurs Adm. 2013;43(11):586-591. doi:10.1097/01.NNA.0000434509.66749.7c58. Tzeng HM, Ketefian S. The relationship between nurses’ job satisfaction and inpatient satisfaction: an exploratory study in a Taiwan teaching hospital. J Nurs Care Qual. 2002;16(2):39-49. doi:10.1097/00001786-200201000-00005
59. Williams ES, Skinner AC. Outcomes of physician job satisfaction: a narrative review, implications, and directions for future research. Health Care Manage Rev. 2003;28(2):119-139. doi:10.1097/00004010-200304000-00004
60. Waldman JD, Kelly F, Arora S, Smith HL. The shocking cost of turnover in health care. Health Care Manage Rev. 2004;29(1):2-7. doi:10.1097/00004010-200401000-00002
61. Hayes LJ, O’Brien-Pallas L, Duffield C, et al. Nurse turnover: a literature review - an update. Int J Nurs Stud. 2012;49(7):887-905. doi:10.1016/j.ijnurstu.2011.10.001
62. US Department of Veterans Affairs. FY 2021/FY 2019 Annual performance plan and report. February 2020. Accessed January 27, 2023. https://www.va.gov/oei/docs/VA2019-2021appr.pdf
1. World Economic Forum. Health and healthcare in the fourth industrial revolution: Global Future Council on the future of health and healthcare 2016-2018. April 2019. Accessed January 27, 2023. https://www3.weforum.org/docs/WEF__Shaping_the_Future_of_Health_Council_Report.pdf
2. Iveroth E, Fryk P, Rapp B. Information technology strategy and alignment issues in health care organizations. Health Care Manage Rev. 2013;38(3):188-200. doi:10.1097/HMR.0b013e31826119d7
3. Thakur R, Hsu SH, Fontenot G. Innovation in healthcare: issues and future trends. J Bus Res. 2012;65(4):562-569. doi:10.1016/j.jbusres.2011.02.022
4. Thimbleby H. Technology and the future of healthcare. J Public Health Res. 2013;2(3):e28. Published 2013 Dec 1. doi:10.4081/jphr.2013.e28
5. Viglialoro RM, Condino S, Turini G, Carbone M, Ferrari V, Gesi M. augmented reality, mixed reality, and hybrid approach in healthcare simulation: a systematic review. Applied Sciences. 2021;11(5):2338. doi:10.3390/app11052338
6. Rawlins CR, Veigulis Z, Hebert C, Curtin C, Osborne T. Effect of immersive virtual reality on pain and anxiety at a Veterans Affairs health care facility. Front Virt Real. 2021;(2):136. doi:10.3389/frvir.2021.719681
7. Chawdhary G, Shoman N. Emerging artificial intelligence applications in otological imaging. Curr Opin Otolaryngol Head Neck Surg. 2021;29(5):357-364. doi:10.1097/MOO.0000000000000754
8. Asadzadeh A, Samad-Soltani T, Rezaei-Hachesu P. Applications of virtual and augmented reality in infectious disease epidemics with a focus on the COVID-19 outbreak. Inform Med Unlocked. 2021;24:100579. doi:10.1016/j.imu.2021.100579
9. Ashwini KB, Savitha R, Harish A. Application of augmented reality technology for home healthcare product visualization. ECS Transas. 2022;107(1):10921. doi:10.1149/10701.10921ecst
10. Brooks AL. VR/Technologies for Rehabilitation. In: Brooks AL, Brahman S, Kapralos B, Nakajima A, Tyerman J, Jain LC, eds. Recent Advances in Technologies for Inclusive Well-Being Virtual Patients, Gamification and Simulation. Intelligent Systems Reference Library. Springer; 2021:241-252. doi:10.1007/978-3-030-59608-8_13
11. Koulouris D, Menychtas A, Maglogiannis I. An IoT-enabled platform for the assessment of physical and mental activities utilizing augmented reality exergaming. Sensors (Basel). 2022;22(9):3181. Published 2022 Apr 21. doi:10.3390/s22093181
12. Deiss YR, Korkut S, Inglese T. Increase therapy understanding and medication adherence for patients with inflammatory skin diseases through augmented reality. Digital Human Modeling and Applications in Health, Safety, Ergonomics and Risk Management. Health, Operations Management, and Design: 13th International Conference, DHM 2022, Held as Part of the 24th HCI International Conference, HCII 2022. 2022:21-40. doi:10.1007/978-3-031-06018-2_2
13. Bertino E, Gao W, Steffan B, et al, eds. Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics). Springer; 2022:21-40.
14. Ruhaiyem NIR, Mazlan NA. Image Modeling Through Augmented Reality for Skin Allergies Recognition. Lecture Notes on Data Engineering and Communications Technologies. 2021:72-79. doi: 10.1007/978-3-030-70713-2_8
15. Park BJ, Perkons NR, Profka E, et al. Three-dimensional augmented reality visualization informs locoregional therapy in a translational model of hepatocellular carcinoma. J Vasc Interv Radiol. 2020;31(10):1612-1618.e1. doi:10.1016/j.jvir.2020.01.028
16. Leo J, Zhou Z, Yang H, et al, eds. Interactive cardiovascular surgical planning via augmented reality. 5th Asian CHI Symposium 2021; 2021. doi:10.1145/3429360.3468195
17. Zuo Y, Jiang T, Dou J, et al. A novel evaluation model for a mixed-reality surgical navigation system: where Microsoft Hololens meets the operating room. Surg Innov. 2020;27(2):193-202. doi:10.1177/1553350619893236
18. Ghaednia H, Fourman MS, Lans A, et al. Augmented and virtual reality in spine surgery, current applications and future potentials. Spine J. 2021;21(10):1617-1625. doi:10.1016/j.spinee.2021.03.018
19. Liu Y, Lee MG, Kim JS. Spine surgery assisted by augmented reality: where have we been?. Yonsei Med J. 2022;63(4):305-316. doi:10.3349/ymj.2022.63.4.305
20. Kimmel S, Cobus V, Heuten W, eds. opticARe—augmented reality mobile patient monitoring in intensive care units. Proceedings of the ACM Symposium on Virtual Reality Software and Technology, VRST; 2021. doi:10.1145/3489849.3489852
21. Voštinár P, Horváthová D, Mitter M, Bako M. The look at the various uses of VR. Open Computer Sci. 2021;11(1):241-250. doi:10.1515/comp-2020-0123
22. Zhao J, Xu X, Jiang H, Ding Y. The effectiveness of virtual reality-based technology on anatomy teaching: a meta-analysis of randomized controlled studies. BMC Med Educ. 2020;20(1):127. Published 2020 Apr 25. doi:10.1186/s12909-020-1994-z
23. Ricci S, Calandrino A, Borgonovo G, Chirico M, Casadio M. Viewpoint: virtual and augmented reality in basic and advanced life support training. JMIR Serious Games. 2022;10(1):e28595. Published 2022 Mar 23. doi:10.2196/28595
24. Ricci S, Mobilio GA, Calandrino A, et al. RiNeo MR: A mixed-reality tool for newborn life support training. Annu Int Conf IEEE Eng Med Biol Soc. 2021;2021:5043-5046. doi:10.1109/EMBC46164.2021.9629612
25. Dhar P, Rocks T, Samarasinghe RM, Stephenson G, Smith C. Augmented reality in medical education: students’ experiences and learning outcomes. Med Educ Online. 2021;26(1):1953953. doi:10.1080/10872981.2021.1953953
26. Pears M, Konstantinidis S. The future of immersive technology in global surgery education [published online ahead of print, 2021 Jul 1]. Indian J Surg. 2021;84(suppl 1):1-5. doi:10.1007/s12262-021-02998-6
27. Liang CJ, Start C, Boley H, Kamat VR, Menassa CC, Aebersold M. Enhancing stroke assessment simulation experience in clinical training using augmented reality. Virt Real. 2021;25(3):575-584. doi:10.1007/s10055-020-00475-1
28. Lacey G, Gozdzielewska L, McAloney-Kocaman K, Ruttle J, Cronin S, Price L. Psychomotor learning theory informing the design and evaluation of an interactive augmented reality hand hygiene training app for healthcare workers. Educ Inf Technol. 2022;27(3):3813-3832. doi:10.1007/s10639-021-10752-4
29. Ryan GV, Callaghan S, Rafferty A, Higgins MF, Mangina E, McAuliffe F. Learning outcomes of immersive technologies in health care student education: systematic review of the literature. J Med Internet Res. 2022;24(2):e30082. Published 2022 Feb 1. doi:10.2196/30082
30. Yu FU, Yan HU, Sundstedt V. A Systematic literature review of virtual, augmented, and mixed reality game applications in healthcare. ACM Trans Comput Healthcare. 2022;3(2);1-27. doi:10.1145/3472303
31. Weeks JK, Amiel JM. Enhancing neuroanatomy education with augmented reality. Med Educ. 2019;53(5):516-517. doi:10.1111/medu.13843
32. Williams MA, McVeigh J, Handa AI, Lee R. Augmented reality in surgical training: a systematic review. Postgrad Med J. 2020;96(1139):537-542. doi:10.1136/postgradmedj-2020-137600
33. Triepels CPR, Smeets CFA, Notten KJB, et al. Does three-dimensional anatomy improve student understanding? Clin Anat. 2020;33(1):25-33. doi:10.1002/ca.23405
34. Pietruski P, Majak M, S´wia¸tek-Najwer E, et al. Supporting fibula free flap harvest with augmented reality: A proof-of-concept study. Laryngoscope. 2020;130(5):1173-1179. doi:10.1002/lary.28090
35. Perkins SL, Krajancich B, Yang CJ, Hargreaves BA, Daniel BL, Berry MF. A patient-specific mixed-reality visualization tool for thoracic surgical planning. Ann Thorac Surg. 2020;110(1):290-295. doi:10.1016/j.athoracsur.2020.01.060
36. Müller F, Roner S, Liebmann F, Spirig JM, Fürnstahl P, Farshad M. Augmented reality navigation for spinal pedicle screw instrumentation using intraoperative 3D imaging. Spine J. 2020;20(4):621-628. doi:10.1016/j.spinee.2019.10.012
37. Kaplan AD, Cruit J, Endsley M, Beers SM, Sawyer BD, Hancock PA. The effects of virtual reality, augmented reality, and mixed reality as training enhancement methods: a meta-analysis. Hum Factors. 2021;63(4):706-726. doi:10.1177/0018720820904229
38. Jud L, Fotouhi J, Andronic O, et al. Applicability of augmented reality in orthopedic surgery - a systematic review. BMC Musculoskelet Disord. 2020;21(1):103. Published 2020 Feb 15. doi:10.1186/s12891-020-3110-2
39. Ara J, Karim FB, Alsubaie MSA, et al. Comprehensive analysis of augmented reality technology in modern healthcare system. Int J Adv Comput Sci Appl. 2021;12(6):845-854. doi:10.14569/IJACSA.2021.0120698
40. Webster A, Gardner J. Aligning technology and institutional readiness: the adoption of innovation. Technol Anal Strateg Manag. 2019;31(10):1229-1241. doi:10.1080/09537325.2019.1601694
41. Hastall MR, Dockweiler C, Mühlhaus J. achieving end user acceptance: building blocks for an evidence-based user-centered framework for health technology development and assessment. In: Antona, M, Stephanidis C, eds. Universal Access in Human–Computer Interaction. Human and Technological Environments. UAHCI 2017. Lecture Notes in Computer Science, vol 10279. Springer, Cham; 2017. doi:10.1007/978-3-319-58700-4_2
42. Ratwani RM, Fairbanks RJ, Hettinger AZ, Benda NC. Electronic health record usability: analysis of the user-centered design processes of eleven electronic health record vendors. J Am Med Inform Assoc. 2015;22(6):1179-1182. doi:10.1093/jamia/ocv050
43. Khairat S, Coleman C, Ottmar P, Jayachander DI, Bice T, Carson SS. Association of Electronic Health Record Use With Physician Fatigue and Efficiency. JAMA Netw Open. 2020;3(6):e207385. Published 2020 Jun 1. doi:10.1001/jamanetworkopen.2020.7385
44. Melnick ER, Dyrbye LN, Sinsky CA, et al. The association between perceived electronic health record usability and professional burnout among US physicians. Mayo Clin Proc. 2020;95(3):476-487. doi:10.1016/j.mayocp.2019.09.024
45. Lee YJ. Comparison of job satisfaction between nonprofit and public employees. Nonprofit Volunt Sect Q. 2016;45(2):295-313. doi:10.1177/0899764015584061
46. Brimhall KC. Inclusion is important... but how do I include? Examining the effects of leader engagement on inclusion, innovation, job satisfaction, and perceived quality of care in a diverse nonprofit health care organization. Nonprofit Volunt Sect Q. 2019;48(4):716-737. doi:10.1177/0899764019829834
47. Moreira MR, Gherman M, Sousa PS. Does innovation influence the performance of healthcare organizations?. Innovation (North Syd). 2017;19(3):335-352. doi:10.1080/14479338.2017.1293489
48. US Department of Veterans Affairs. VA Palo Alto Healthcare System. Updated December 29, 2020. Accessed January 27, 2023. https://www.paloalto.va.gov/about/index.asp
49. Siegel SM, Kaemmerer WF. Measuring the perceived support for innovation in organizations. J Appl Psychol. 1978;63(5):553-562. doi:10.1037/0021-9010.63.5.553
50. Anderson NR, West MA. Measuring climate for work group innovation: development and validation of the team climate inventory. J Organ Behav. 1998;19(3):235-258. doi:10.1002/(SICI)1099-1379(199805)19:3<235::AID-JOB837>3.0.CO;2-C
51. Aarons GA. Measuring provider attitudes toward evidence-based practice: consideration of organizational context and individual differences. Child Adolesc Psychiatr Clin N Am. 2005;14(2):255-viii. doi:10.1016/j.chc.2004.04.008
52. Van der Heijden H. User acceptance of hedonic information systems. MIS Q. 2004;28(4):695-704. doi:10.2307/25148660
53. Venkatesh V, Speier C, Morris MG. User acceptance enablers in individual decision making about technology: Toward an integrated model. Decis Sci. 2002;33(2):297-316. doi:10.1111/j.1540-5915.2002.tb01646.x
54. Puri A, Kim B, Nguyen O, Stolee P, Tung J, Lee J. User acceptance of wrist-worn activity trackers among community-dwelling older adults: mixed method study. JMIR Mhealth Uhealth. 2017;5(11):e173. Published 2017 Nov 15. doi:10.2196/mhealth.8211
55. Huang YC, Backman SJ, Backman KF, Moore D. Exploring user acceptance of 3D virtual worlds in travel and tourism marketing. Tourism Management. 2013;36:490-501. doi:10.1016/j.tourman.2012.09.009
56. Rasimah CM, Ahmad A, Zaman HB. Evaluation of user acceptance of mixed reality technology. AJET. 2011;27(8). doi:10.14742/ajet.899
57. Choi J, Boyle DK. RN workgroup job satisfaction and patient falls in acute care hospital units. J Nurs Adm. 2013;43(11):586-591. doi:10.1097/01.NNA.0000434509.66749.7c58. Tzeng HM, Ketefian S. The relationship between nurses’ job satisfaction and inpatient satisfaction: an exploratory study in a Taiwan teaching hospital. J Nurs Care Qual. 2002;16(2):39-49. doi:10.1097/00001786-200201000-00005
59. Williams ES, Skinner AC. Outcomes of physician job satisfaction: a narrative review, implications, and directions for future research. Health Care Manage Rev. 2003;28(2):119-139. doi:10.1097/00004010-200304000-00004
60. Waldman JD, Kelly F, Arora S, Smith HL. The shocking cost of turnover in health care. Health Care Manage Rev. 2004;29(1):2-7. doi:10.1097/00004010-200401000-00002
61. Hayes LJ, O’Brien-Pallas L, Duffield C, et al. Nurse turnover: a literature review - an update. Int J Nurs Stud. 2012;49(7):887-905. doi:10.1016/j.ijnurstu.2011.10.001
62. US Department of Veterans Affairs. FY 2021/FY 2019 Annual performance plan and report. February 2020. Accessed January 27, 2023. https://www.va.gov/oei/docs/VA2019-2021appr.pdf
Yoga linked with improved gait speed, lower extremity strength in older adults
“Up to 50% of adults aged 80 years or older are estimated to be frail, and the global prevalence is expected to rise given the aging of our population,” therefore more interventions are needed to help with frailty, corresponding author Julia Loewenthal, MD, said in an interview.
Yoga integrates across multiple body systems including the musculoskeletal system, nervous system, and others, said Dr. Loewenthal of Brigham and Women’s Hospital, Boston. Previous research has shown that yoga has a positive effect on cardiovascular risk factors, mood, and quality of life, but the effects of yoga on frailty have not been well studied.
“We wanted to evaluate whether [yoga] might help with frailty, since it touches on so many systems, as frailty does,” she noted.
In a systematic review published in Annals of Internal Medicine, the researchers identified 33 randomized, controlled trials of yoga-based interventions including 2,384 adults aged 65 years and older. The studies mainly involved Iyengar or chair-based yoga methods. The study population included community-dwelling seniors, nursing home residents, and individuals with chronic diseases.
The studies assessed the effect of a range of yoga practices on frailty markers including gait speed, handgrip strength, balance, lower extremity strength and endurance, and multicomponent measures of physical performance.
Overall, individuals who were randomized to engage in a yoga practice showed improved gait speed and lower extremity strength, compared with controls who were inactive or received an education intervention, with moderate-certainty evidence. The researchers also found low-certainty evidence in favor of yoga for improved balance and for a composite measure of physical function, and low-certainty evidence in favor of yoga for improved handgrip strength.
The findings were limited by several factors, mainly the heterogenous study designs, populations, and yoga styles, the researchers noted. Other limitations included the small sample sizes, variation in descriptions of the studies’ randomizations, and a lack of data on race and ethnicity of the participants.
Yoga’s role in healthy aging
“Overall, we were not surprised by the results since we have seen similar findings from other mind-body practices such as tai chi,” Dr. Loewenthal said in an interview. “We were surprised by the degree of improvement many of the participants had with gait speed.
“Yoga practices usually include a mix of poses in the standing, seated, and lying-down positions,” Dr. Loewenthal said. Some of the studies in the review also involved chair-based methods with few standing poses, and some involved gentle or slow-paced practices. “We know that many of the practices helped with leg strength, and perhaps they are also helping with coordination between the brain and body for walking.”
The findings suggest that clinicians can view yoga practice in general as part of a strategy to support healthy aging, Dr. Loewenthal said. “While our work looked at frailty markers and not overall frailty, I think it would be reasonable to offer yoga as a strategy along with already-established interventions such as resistance training and the Mediterranean diet, and if older adults are already practicing yoga, this could help them understand how the practice is impacting the aging process.”
There are many styles of yoga that overlap and are related to one another, so it is hard to make recommendations about a single type, said Dr. Loewenthal. Many of the studies in the review involved Iyengar yoga, named for yoga master B.K.S. Iyengar, which focuses on precise alignment and breath and seems to be conducive for older populations. Iyengar yoga also involves use of props such as blocks, bolsters, straps, and chairs, which makes it well suited for older individuals who may have a chronic condition or other limitations.
“Some styles of yoga are very physical and may reach energy expenditure and cardiovascular effects similar to aerobic exercise, but this is generally not the case for most styles of yoga,” she added.
As for additional research, “I think it is important that trials use a validated definition of frailty as an outcome; all of the trials in our study used markers of frailty but did not look at overall frailty,” said Dr. Loewenthal. In addition, it is important to understand how yoga affects people who have different levels of frailty, since previous research shows that those who are the most frail benefit most from physical activity interventions.
Yoga as an entry point for physical activity
With the increasing population of older adults in the United States and around the world, frailty is a major health concern because its association with significant declines in health and potential loss of independence, Amanda Paluch, PhD, said in an interview.
“Therefore, it is important to identify programs that can prevent frailty to support longevity and living independently for older adults. Yoga can be a feasible solution to promote movement and prevent frailty,” said Dr. Paluch, of the University of Massachusetts, Amherst, an assistant professor in the department of kinesiology and Institute for Applied Life Sciences.
“Other studies have demonstrated that light-intensity movement, as in yoga, may be particularly beneficial for older adults,” Dr. Paluch said. “Additionally, research has demonstrated that balance training activities are important to maintain physical function, prevent falls, and maintain their independence for older adults, so it makes sense that yoga was associated with lower likelihood of frailty.”
Although there may be additional benefits with higher intensity activity, “yoga could be a great place to start for older adults who are starting at low activity levels,” she said.
The takeaway for clinicians is to consider encouraging more physical activity for their patients to support healthy aging, including reducing the risk factors for frailty, said Dr. Paluch. “Particularly for older adults, physical activity may not need to be of high intensity for benefits. Activities such as yoga that focus on flexibility, balance, and movement at lower intensities can support healthy aging, and yoga may be a particularly good option for older adults who are least active.”
The study received no outside funding. The researchers and Dr. Paluch had no financial conflicts to disclose.
“Up to 50% of adults aged 80 years or older are estimated to be frail, and the global prevalence is expected to rise given the aging of our population,” therefore more interventions are needed to help with frailty, corresponding author Julia Loewenthal, MD, said in an interview.
Yoga integrates across multiple body systems including the musculoskeletal system, nervous system, and others, said Dr. Loewenthal of Brigham and Women’s Hospital, Boston. Previous research has shown that yoga has a positive effect on cardiovascular risk factors, mood, and quality of life, but the effects of yoga on frailty have not been well studied.
“We wanted to evaluate whether [yoga] might help with frailty, since it touches on so many systems, as frailty does,” she noted.
In a systematic review published in Annals of Internal Medicine, the researchers identified 33 randomized, controlled trials of yoga-based interventions including 2,384 adults aged 65 years and older. The studies mainly involved Iyengar or chair-based yoga methods. The study population included community-dwelling seniors, nursing home residents, and individuals with chronic diseases.
The studies assessed the effect of a range of yoga practices on frailty markers including gait speed, handgrip strength, balance, lower extremity strength and endurance, and multicomponent measures of physical performance.
Overall, individuals who were randomized to engage in a yoga practice showed improved gait speed and lower extremity strength, compared with controls who were inactive or received an education intervention, with moderate-certainty evidence. The researchers also found low-certainty evidence in favor of yoga for improved balance and for a composite measure of physical function, and low-certainty evidence in favor of yoga for improved handgrip strength.
The findings were limited by several factors, mainly the heterogenous study designs, populations, and yoga styles, the researchers noted. Other limitations included the small sample sizes, variation in descriptions of the studies’ randomizations, and a lack of data on race and ethnicity of the participants.
Yoga’s role in healthy aging
“Overall, we were not surprised by the results since we have seen similar findings from other mind-body practices such as tai chi,” Dr. Loewenthal said in an interview. “We were surprised by the degree of improvement many of the participants had with gait speed.
“Yoga practices usually include a mix of poses in the standing, seated, and lying-down positions,” Dr. Loewenthal said. Some of the studies in the review also involved chair-based methods with few standing poses, and some involved gentle or slow-paced practices. “We know that many of the practices helped with leg strength, and perhaps they are also helping with coordination between the brain and body for walking.”
The findings suggest that clinicians can view yoga practice in general as part of a strategy to support healthy aging, Dr. Loewenthal said. “While our work looked at frailty markers and not overall frailty, I think it would be reasonable to offer yoga as a strategy along with already-established interventions such as resistance training and the Mediterranean diet, and if older adults are already practicing yoga, this could help them understand how the practice is impacting the aging process.”
There are many styles of yoga that overlap and are related to one another, so it is hard to make recommendations about a single type, said Dr. Loewenthal. Many of the studies in the review involved Iyengar yoga, named for yoga master B.K.S. Iyengar, which focuses on precise alignment and breath and seems to be conducive for older populations. Iyengar yoga also involves use of props such as blocks, bolsters, straps, and chairs, which makes it well suited for older individuals who may have a chronic condition or other limitations.
“Some styles of yoga are very physical and may reach energy expenditure and cardiovascular effects similar to aerobic exercise, but this is generally not the case for most styles of yoga,” she added.
As for additional research, “I think it is important that trials use a validated definition of frailty as an outcome; all of the trials in our study used markers of frailty but did not look at overall frailty,” said Dr. Loewenthal. In addition, it is important to understand how yoga affects people who have different levels of frailty, since previous research shows that those who are the most frail benefit most from physical activity interventions.
Yoga as an entry point for physical activity
With the increasing population of older adults in the United States and around the world, frailty is a major health concern because its association with significant declines in health and potential loss of independence, Amanda Paluch, PhD, said in an interview.
“Therefore, it is important to identify programs that can prevent frailty to support longevity and living independently for older adults. Yoga can be a feasible solution to promote movement and prevent frailty,” said Dr. Paluch, of the University of Massachusetts, Amherst, an assistant professor in the department of kinesiology and Institute for Applied Life Sciences.
“Other studies have demonstrated that light-intensity movement, as in yoga, may be particularly beneficial for older adults,” Dr. Paluch said. “Additionally, research has demonstrated that balance training activities are important to maintain physical function, prevent falls, and maintain their independence for older adults, so it makes sense that yoga was associated with lower likelihood of frailty.”
Although there may be additional benefits with higher intensity activity, “yoga could be a great place to start for older adults who are starting at low activity levels,” she said.
The takeaway for clinicians is to consider encouraging more physical activity for their patients to support healthy aging, including reducing the risk factors for frailty, said Dr. Paluch. “Particularly for older adults, physical activity may not need to be of high intensity for benefits. Activities such as yoga that focus on flexibility, balance, and movement at lower intensities can support healthy aging, and yoga may be a particularly good option for older adults who are least active.”
The study received no outside funding. The researchers and Dr. Paluch had no financial conflicts to disclose.
“Up to 50% of adults aged 80 years or older are estimated to be frail, and the global prevalence is expected to rise given the aging of our population,” therefore more interventions are needed to help with frailty, corresponding author Julia Loewenthal, MD, said in an interview.
Yoga integrates across multiple body systems including the musculoskeletal system, nervous system, and others, said Dr. Loewenthal of Brigham and Women’s Hospital, Boston. Previous research has shown that yoga has a positive effect on cardiovascular risk factors, mood, and quality of life, but the effects of yoga on frailty have not been well studied.
“We wanted to evaluate whether [yoga] might help with frailty, since it touches on so many systems, as frailty does,” she noted.
In a systematic review published in Annals of Internal Medicine, the researchers identified 33 randomized, controlled trials of yoga-based interventions including 2,384 adults aged 65 years and older. The studies mainly involved Iyengar or chair-based yoga methods. The study population included community-dwelling seniors, nursing home residents, and individuals with chronic diseases.
The studies assessed the effect of a range of yoga practices on frailty markers including gait speed, handgrip strength, balance, lower extremity strength and endurance, and multicomponent measures of physical performance.
Overall, individuals who were randomized to engage in a yoga practice showed improved gait speed and lower extremity strength, compared with controls who were inactive or received an education intervention, with moderate-certainty evidence. The researchers also found low-certainty evidence in favor of yoga for improved balance and for a composite measure of physical function, and low-certainty evidence in favor of yoga for improved handgrip strength.
The findings were limited by several factors, mainly the heterogenous study designs, populations, and yoga styles, the researchers noted. Other limitations included the small sample sizes, variation in descriptions of the studies’ randomizations, and a lack of data on race and ethnicity of the participants.
Yoga’s role in healthy aging
“Overall, we were not surprised by the results since we have seen similar findings from other mind-body practices such as tai chi,” Dr. Loewenthal said in an interview. “We were surprised by the degree of improvement many of the participants had with gait speed.
“Yoga practices usually include a mix of poses in the standing, seated, and lying-down positions,” Dr. Loewenthal said. Some of the studies in the review also involved chair-based methods with few standing poses, and some involved gentle or slow-paced practices. “We know that many of the practices helped with leg strength, and perhaps they are also helping with coordination between the brain and body for walking.”
The findings suggest that clinicians can view yoga practice in general as part of a strategy to support healthy aging, Dr. Loewenthal said. “While our work looked at frailty markers and not overall frailty, I think it would be reasonable to offer yoga as a strategy along with already-established interventions such as resistance training and the Mediterranean diet, and if older adults are already practicing yoga, this could help them understand how the practice is impacting the aging process.”
There are many styles of yoga that overlap and are related to one another, so it is hard to make recommendations about a single type, said Dr. Loewenthal. Many of the studies in the review involved Iyengar yoga, named for yoga master B.K.S. Iyengar, which focuses on precise alignment and breath and seems to be conducive for older populations. Iyengar yoga also involves use of props such as blocks, bolsters, straps, and chairs, which makes it well suited for older individuals who may have a chronic condition or other limitations.
“Some styles of yoga are very physical and may reach energy expenditure and cardiovascular effects similar to aerobic exercise, but this is generally not the case for most styles of yoga,” she added.
As for additional research, “I think it is important that trials use a validated definition of frailty as an outcome; all of the trials in our study used markers of frailty but did not look at overall frailty,” said Dr. Loewenthal. In addition, it is important to understand how yoga affects people who have different levels of frailty, since previous research shows that those who are the most frail benefit most from physical activity interventions.
Yoga as an entry point for physical activity
With the increasing population of older adults in the United States and around the world, frailty is a major health concern because its association with significant declines in health and potential loss of independence, Amanda Paluch, PhD, said in an interview.
“Therefore, it is important to identify programs that can prevent frailty to support longevity and living independently for older adults. Yoga can be a feasible solution to promote movement and prevent frailty,” said Dr. Paluch, of the University of Massachusetts, Amherst, an assistant professor in the department of kinesiology and Institute for Applied Life Sciences.
“Other studies have demonstrated that light-intensity movement, as in yoga, may be particularly beneficial for older adults,” Dr. Paluch said. “Additionally, research has demonstrated that balance training activities are important to maintain physical function, prevent falls, and maintain their independence for older adults, so it makes sense that yoga was associated with lower likelihood of frailty.”
Although there may be additional benefits with higher intensity activity, “yoga could be a great place to start for older adults who are starting at low activity levels,” she said.
The takeaway for clinicians is to consider encouraging more physical activity for their patients to support healthy aging, including reducing the risk factors for frailty, said Dr. Paluch. “Particularly for older adults, physical activity may not need to be of high intensity for benefits. Activities such as yoga that focus on flexibility, balance, and movement at lower intensities can support healthy aging, and yoga may be a particularly good option for older adults who are least active.”
The study received no outside funding. The researchers and Dr. Paluch had no financial conflicts to disclose.
FROM ANNALS OF INTERNAL MEDICINE
'Zombie viruses': Fascinating and a little frightening
Of all the consequences of climate change, here’s one nobody counted on.
A team of European researchers digging into Siberian permafrost discovered and revived 13 types of prehistoric viruses.
The researchers coined the isn’t-that-just-great term “zombie viruses” to describe previously dormant viruses that had been frozen in ice for tens of thousands of years – 27,000 to 48,500 years, in fact.
The first question is obvious: This is fascinating, but is it a good idea? We’re still dealing with a certain mutating virus our immune systems have never encountered before.
The second question: What does it mean?
No humans were harmed in this study
The quick answer: The viruses observed here were only able to infect amoebae. But viruses that can infect humans do indeed exist in environments like permafrost.
The possibility that an unearthed, unknown virus will one day appear from seemingly nowhere and result in another pandemic is not necessarily zero.
“There is an objective risk, and it is increasing,” says Jean-Michel Claverie, PhD, the lead researcher and an emeritus professor of genomics and bioinformatics at Aix-Marseille University in France. “However, we cannot put a number on this probability, specifically because we refuse to work with and revive human- and animal-infecting viruses. It would be much too dangerous.”
Based on Dr. Claverie and his team’s results, human- and animal-infecting viruses can indeed survive deep within the permafrost for extended periods of time.
“From our research, we can deduce that other viruses present in the permafrost are likely still infectious,” says Dr. Claverie. “By sequencing the total DNA, we can detect the presence of viruses similar to those infecting animals or humans today.”
That said, the chances of something catastrophic happening from, say, humans exposed to thawed permafrost are slim. “[The microbes] would be quick to decay once they’re exposed to heat, UV light, and oxygen,” he says.
Also, in places like Siberia where permafrost exists, people generally do not. So, some science fiction-inspired fears (we see you, fans of John Carpenter’s “The Thing”) are pretty unfounded. But if more people or companies begin to migrate toward the areas where these microbes are being released, the chances of a virus successfully infecting a host could be greater.
But what if ...
So, what would happen – hypothetically – if the next deadly virus to overtake our planet came from the Arctic permafrost? Would we even be remotely prepared?
“There is a small risk that a frozen virus that gets unearthed is able to start an infection chain that ends up in humans,” says Adrian Liston, PhD, an immunologist and senior group leader at the Babraham Institute, a life sciences research institute at the University of Cambridge in England. Dr. Liston was not involved in the research discussed here. “On the one hand, we would not have preexisting immunity against it, so the initial ability to combat the infection is low. On the other hand, the virus would not be adapted to infect (modern-day) humans, so the chance of an initial infection being successful for the virus is extremely low.”
That’s something a lot of folks don’t understand: Today’s viruses and other infectious microbes are infectious only because they exist today. They have evolved to work within our modern immune systems – for either good or ill.
“ ‘Entry events’ do happen, very rarely, and they can shape human evolution,” says Dr. Liston. “Major examples would be smallpox (a virus) and tuberculosis (a bacteria), which strongly influenced human evolution when they entered our species, selecting for the type of immune system that was able to fight them and killing off individuals with the ‘wrong’ type of immune system.”
And not all organisms are harmful.
“There are many, many microbes that are beneficial to humans,” Dr. Liston says. “But generally speaking, these are microbes that have evolved for millions of years to work in harmony with our body, such as our microbiome, or have been selected for thousands of years to do beneficial chores for us, like yeast in making bread or brewing beer.”
Some random frozen microbe is unlikely to affect us directly, but if it does, it is far more likely to be bad, Dr. Liston says.
For now, at least, we can rest easy knowing that Dr. Claverie and his team have no plans to revive dangerous viruses or retrieve more samples. “Because of the Russian-Ukrainian war, all of our collaborations have stopped. We are now focused on studying the viruses already in our lab and understanding how they replicate and interact with their cellular hosts,” he says.
If anything, zombie viruses can at least remind us about the constant increasing effects that climate change will have on our lives and planet in the near future.
“The most important take-home message is that climate change is going to create unexpected problems,” says Dr. Liston. “It isn’t simply changes to weather, climate events, and sea levels rising. A whole cascade of secondary problems will be generated. New infections, some of which could go pandemic, are almost certainly going to happen because of climate change.”
A version of this article first appeared on WebMD.com.
Of all the consequences of climate change, here’s one nobody counted on.
A team of European researchers digging into Siberian permafrost discovered and revived 13 types of prehistoric viruses.
The researchers coined the isn’t-that-just-great term “zombie viruses” to describe previously dormant viruses that had been frozen in ice for tens of thousands of years – 27,000 to 48,500 years, in fact.
The first question is obvious: This is fascinating, but is it a good idea? We’re still dealing with a certain mutating virus our immune systems have never encountered before.
The second question: What does it mean?
No humans were harmed in this study
The quick answer: The viruses observed here were only able to infect amoebae. But viruses that can infect humans do indeed exist in environments like permafrost.
The possibility that an unearthed, unknown virus will one day appear from seemingly nowhere and result in another pandemic is not necessarily zero.
“There is an objective risk, and it is increasing,” says Jean-Michel Claverie, PhD, the lead researcher and an emeritus professor of genomics and bioinformatics at Aix-Marseille University in France. “However, we cannot put a number on this probability, specifically because we refuse to work with and revive human- and animal-infecting viruses. It would be much too dangerous.”
Based on Dr. Claverie and his team’s results, human- and animal-infecting viruses can indeed survive deep within the permafrost for extended periods of time.
“From our research, we can deduce that other viruses present in the permafrost are likely still infectious,” says Dr. Claverie. “By sequencing the total DNA, we can detect the presence of viruses similar to those infecting animals or humans today.”
That said, the chances of something catastrophic happening from, say, humans exposed to thawed permafrost are slim. “[The microbes] would be quick to decay once they’re exposed to heat, UV light, and oxygen,” he says.
Also, in places like Siberia where permafrost exists, people generally do not. So, some science fiction-inspired fears (we see you, fans of John Carpenter’s “The Thing”) are pretty unfounded. But if more people or companies begin to migrate toward the areas where these microbes are being released, the chances of a virus successfully infecting a host could be greater.
But what if ...
So, what would happen – hypothetically – if the next deadly virus to overtake our planet came from the Arctic permafrost? Would we even be remotely prepared?
“There is a small risk that a frozen virus that gets unearthed is able to start an infection chain that ends up in humans,” says Adrian Liston, PhD, an immunologist and senior group leader at the Babraham Institute, a life sciences research institute at the University of Cambridge in England. Dr. Liston was not involved in the research discussed here. “On the one hand, we would not have preexisting immunity against it, so the initial ability to combat the infection is low. On the other hand, the virus would not be adapted to infect (modern-day) humans, so the chance of an initial infection being successful for the virus is extremely low.”
That’s something a lot of folks don’t understand: Today’s viruses and other infectious microbes are infectious only because they exist today. They have evolved to work within our modern immune systems – for either good or ill.
“ ‘Entry events’ do happen, very rarely, and they can shape human evolution,” says Dr. Liston. “Major examples would be smallpox (a virus) and tuberculosis (a bacteria), which strongly influenced human evolution when they entered our species, selecting for the type of immune system that was able to fight them and killing off individuals with the ‘wrong’ type of immune system.”
And not all organisms are harmful.
“There are many, many microbes that are beneficial to humans,” Dr. Liston says. “But generally speaking, these are microbes that have evolved for millions of years to work in harmony with our body, such as our microbiome, or have been selected for thousands of years to do beneficial chores for us, like yeast in making bread or brewing beer.”
Some random frozen microbe is unlikely to affect us directly, but if it does, it is far more likely to be bad, Dr. Liston says.
For now, at least, we can rest easy knowing that Dr. Claverie and his team have no plans to revive dangerous viruses or retrieve more samples. “Because of the Russian-Ukrainian war, all of our collaborations have stopped. We are now focused on studying the viruses already in our lab and understanding how they replicate and interact with their cellular hosts,” he says.
If anything, zombie viruses can at least remind us about the constant increasing effects that climate change will have on our lives and planet in the near future.
“The most important take-home message is that climate change is going to create unexpected problems,” says Dr. Liston. “It isn’t simply changes to weather, climate events, and sea levels rising. A whole cascade of secondary problems will be generated. New infections, some of which could go pandemic, are almost certainly going to happen because of climate change.”
A version of this article first appeared on WebMD.com.
Of all the consequences of climate change, here’s one nobody counted on.
A team of European researchers digging into Siberian permafrost discovered and revived 13 types of prehistoric viruses.
The researchers coined the isn’t-that-just-great term “zombie viruses” to describe previously dormant viruses that had been frozen in ice for tens of thousands of years – 27,000 to 48,500 years, in fact.
The first question is obvious: This is fascinating, but is it a good idea? We’re still dealing with a certain mutating virus our immune systems have never encountered before.
The second question: What does it mean?
No humans were harmed in this study
The quick answer: The viruses observed here were only able to infect amoebae. But viruses that can infect humans do indeed exist in environments like permafrost.
The possibility that an unearthed, unknown virus will one day appear from seemingly nowhere and result in another pandemic is not necessarily zero.
“There is an objective risk, and it is increasing,” says Jean-Michel Claverie, PhD, the lead researcher and an emeritus professor of genomics and bioinformatics at Aix-Marseille University in France. “However, we cannot put a number on this probability, specifically because we refuse to work with and revive human- and animal-infecting viruses. It would be much too dangerous.”
Based on Dr. Claverie and his team’s results, human- and animal-infecting viruses can indeed survive deep within the permafrost for extended periods of time.
“From our research, we can deduce that other viruses present in the permafrost are likely still infectious,” says Dr. Claverie. “By sequencing the total DNA, we can detect the presence of viruses similar to those infecting animals or humans today.”
That said, the chances of something catastrophic happening from, say, humans exposed to thawed permafrost are slim. “[The microbes] would be quick to decay once they’re exposed to heat, UV light, and oxygen,” he says.
Also, in places like Siberia where permafrost exists, people generally do not. So, some science fiction-inspired fears (we see you, fans of John Carpenter’s “The Thing”) are pretty unfounded. But if more people or companies begin to migrate toward the areas where these microbes are being released, the chances of a virus successfully infecting a host could be greater.
But what if ...
So, what would happen – hypothetically – if the next deadly virus to overtake our planet came from the Arctic permafrost? Would we even be remotely prepared?
“There is a small risk that a frozen virus that gets unearthed is able to start an infection chain that ends up in humans,” says Adrian Liston, PhD, an immunologist and senior group leader at the Babraham Institute, a life sciences research institute at the University of Cambridge in England. Dr. Liston was not involved in the research discussed here. “On the one hand, we would not have preexisting immunity against it, so the initial ability to combat the infection is low. On the other hand, the virus would not be adapted to infect (modern-day) humans, so the chance of an initial infection being successful for the virus is extremely low.”
That’s something a lot of folks don’t understand: Today’s viruses and other infectious microbes are infectious only because they exist today. They have evolved to work within our modern immune systems – for either good or ill.
“ ‘Entry events’ do happen, very rarely, and they can shape human evolution,” says Dr. Liston. “Major examples would be smallpox (a virus) and tuberculosis (a bacteria), which strongly influenced human evolution when they entered our species, selecting for the type of immune system that was able to fight them and killing off individuals with the ‘wrong’ type of immune system.”
And not all organisms are harmful.
“There are many, many microbes that are beneficial to humans,” Dr. Liston says. “But generally speaking, these are microbes that have evolved for millions of years to work in harmony with our body, such as our microbiome, or have been selected for thousands of years to do beneficial chores for us, like yeast in making bread or brewing beer.”
Some random frozen microbe is unlikely to affect us directly, but if it does, it is far more likely to be bad, Dr. Liston says.
For now, at least, we can rest easy knowing that Dr. Claverie and his team have no plans to revive dangerous viruses or retrieve more samples. “Because of the Russian-Ukrainian war, all of our collaborations have stopped. We are now focused on studying the viruses already in our lab and understanding how they replicate and interact with their cellular hosts,” he says.
If anything, zombie viruses can at least remind us about the constant increasing effects that climate change will have on our lives and planet in the near future.
“The most important take-home message is that climate change is going to create unexpected problems,” says Dr. Liston. “It isn’t simply changes to weather, climate events, and sea levels rising. A whole cascade of secondary problems will be generated. New infections, some of which could go pandemic, are almost certainly going to happen because of climate change.”
A version of this article first appeared on WebMD.com.
A Systematic Approach to Central Sleep Apnea in an Era of Medical Complexity
In this issue, Regn and colleagues (page 78) have provided a concise resource for primary care professionals (PCPs) on a lesser known sleep disorder that is increasingly common in veterans.1 Their review provides a basic understanding of central sleep apnea (CSA) and a systematic clinical approach to diagnosis and treatment in primary care. We applaud the authors for providing education on sleep disorders to the Federal Practitioner audience, since sleep disorders are prevalent among military service members and veterans, with significant implications for health, wellness, productivity, and cost. The American workforce has a long-held sense of pride in working hard, often at the expense of sleep. Early work start times are common in the military and federal government, and sleep medicine specialists have the expertise necessary to diagnose and treat the myriad of sleep disorders that have come to light recently. A massive shortage of sleep medicine specialists limits the evidence-based sleep treatment implementations in medical care.
Medicine has become increasingly complex, necessitating a highly connected web of people, resources, institutions, and processes to keep up with the demands of growing information and technology. The evolution of a systems approach to health care built momentum during the 21st century.1-3 The National Academy of Medicine has published 2 reports that raised concerns about the quality and safety of medical care.4,5 With this expansion, the potential for medical errors at individual components or relationship nodes between actors in the medical system also has grown. Medical errors encompass more than acts of commission and can also take the form of acts of omission by failing to diagnosis and appropriately treat before long-term or irrevocable health consequences occur. A systems approach seeks to aid clinical decision making to improve the quality of medical care and patient outcomes in an otherwise complex medical system that can be difficult to navigate.
Although awareness of obstructive sleep apnea (OSA) has increased, CSA has not received the same level of attention and may not be recognized by PCPs. A lack of education about CSA can contribute to acts of omission in a health care setting. Although CSA is ultimately diagnosed and managed in specialty care sleep medicine clinics, PCPs play an instrumental role in referring patients for evaluation and then collaborating with specialists to optimize care and outcomes. The multidisciplinary approach of CSA management is important because it overlaps with many conditions that are commonly seen in primary care, including obesity, chronic pain, congestive heart failure (CHF), chronic kidney disease, and hypothyroidism. These chronic conditions are also prevalent among veterans. In a national cross-sectional study, veterans had higher prevalence rates of chronic health conditions, including cardiovascular disease and kidney disease, compared with nonveterans (odds ratios, 1.4 and 1.2, respectively).6
It is important to understand the relationship between CSA and chronic medical conditions because recognizing the signs of CSA can lead to identification of underlying medical conditions. Likewise, the chronic medical conditions that lead to CSA may cue the PCP’s clinical suspicion for CSA and lead to specialty care referrals if needed. The clinician also serves a significant role in the management of CSA by optimizing medical care for the underlying condition prior to pursuing additional specialty care treatments like positive airway pressure (PAP). For example, PCPs are often involved in the management of atrial fibrillation and cardiac dysfunction, which can minimize or exacerbate CSA. PCPs should also be aware of which drugs are associated with the presentation of CSA as withdrawal or reduction of the medication can resolve symptoms without further evaluation by a specialist.
The review by Regn and colleagues updates readers on developments—and lack thereof—in the literature. Treatment options for CSA have been limited. For most patients, continuous PAP (CPAP), which is the gold standard treatment for OSA, is not an effective CSA treatment. Earlier specialty guidelines endorsed adaptive servo-ventilation (ASV), a more sophisticated respiratory assist device, for treating CSA. In 2015, the SERVE-HF trial examined the effects of ASV in combination with guideline-based medical treatment on survival and cardiovascular outcomes for patients who had CSA and HF with reduced ejection fraction.7 They found that ASV had no significant effect on the primary endpoints of first event of death from any cause, lifesaving cardiovascular intervention, or unplanned hospitalization for worsening HF. However, all-cause and cardiovascular mortality were both increased with ASV. There has not been a more recent large clinical trial that either refutes or reinforces those findings (ADVENT-HF found that ASV effectively treated CSA and OSA in patients with CHF but had no impact on the primary endpoint of mortality).7,8 We are unlikely to see more studies soon that will put this issue to rest and change the guidance that is currently available for ASV use.
Regn and colleagues also provide an update on the use of acetazolamide as to assist in CSA treatment. This should be done cautiously and potentially deferred to subspecialists in sleep medicine, cardiology, or nephrology. The theoretical benefit of acetazolamide in CSA is based on its promotion of excretion of sodium bicarbonate, leading to metabolic acidosis, which can stimulate central respiratory drive. Since CSA is characterized by episodic loss of central respiratory drive, it seems logical that a respiratory stimulant would provide benefit. However, acetazolamide is not approved by the US Food and Drug Administration for CSA.9 In those with impaired respiratory mechanics, CHF, chronic obstructive pulmonary disease, and obesity hypoventilation syndrome, this medication has the potential for harm by adding metabolic acidosis to a patient with concurrent respiratory acidosis or respiratory constraints that limit their ability to compensate effectively for additional acid-base derangements.
It is worth noting that Regn and colleagues do not make claims outside the intended scope. It accomplishes the mission of providing all PCPs with an updated streamlined summary for diagnosing and treating CSA. Such tools are important in an age of growing medical information technology because it can improve the quality of medical care and ultimately, patient outcomes with timely diagnosis and treatment. This is particularly significant in a veteran population with a high burden of chronic medical conditions and polypharmacy.
1. Regn DD, Davis AH, Smith WD, Blasser CJ, Ford CM. Central sleep apnea in adults: diagnosis and treatment. Fed Pract. 2023;40(3):76-83. doi:10.12788/fp.0367
2. Clarkson J, Dean J, Ward J, Komashie A, Bashford T. A systems approach to healthcare: from thinking to -practice. Future Healthc J. 2018;5(3):151-155. doi:10.7861/futurehosp.5-3-151 3. Komashie A, Ward J, Bashford T, et al. Systems approach to health service design, delivery and improvement: a systematic review and meta-analysis. BMJ Open. 2021;11(1):e037667. Published 2021 Jan 19. doi:10.1136/bmjopen-2020-037667 4. Institute of Medicine (US) Committee on Quality of Health Care in America, Kohn LT, Corrigan JM, Donaldson MS, eds. To Err Is Human: Building a Safer Health System. National Academies Press; 2000.
5. Institute of Medicine (US) Committee on Crossing the Quality Chasm: Adaptation to Mental Health and Addictive Disorders. Improving the Quality of Health Care for Mental and Substance-Use Conditions: Quality Chasm Series. National Academies Press; 2006.
6. McDaniel M, McDaniel JT. Examining the geographic distribution of six chronic disease risk factors for severe COVID-19: veteran-nonveteran differences. Chronic Illn. 2022;18(3):666-676. doi:10.1177/17423953211028280
7. Cowie MR, Woehrle H, Wegscheider K, et al. Adaptive servo-ventilation for central sleep apnea in systolic heart failure. N Engl J Med. 2015;373(12):1095-1105. doi:10.1056/NEJMoa1506459
8. Lyons OD, Floras JS, Logan AG, et al; ADVENT-HF Investigators. Design of the effect of adaptive servo-ventilation on survival and cardiovascular hospital admissions in patients with heart failure and sleep apnoea: the ADVENT-HF trial. Eur J Heart Fail. 2017;19(4):579-587. doi:10.1002/ejhf.790
9. US Food and Drug Administration. Diomax. Updated May 2022. Accessed Feb 13, 2023. https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/008943s052,009388s038lbl.pdf
In this issue, Regn and colleagues (page 78) have provided a concise resource for primary care professionals (PCPs) on a lesser known sleep disorder that is increasingly common in veterans.1 Their review provides a basic understanding of central sleep apnea (CSA) and a systematic clinical approach to diagnosis and treatment in primary care. We applaud the authors for providing education on sleep disorders to the Federal Practitioner audience, since sleep disorders are prevalent among military service members and veterans, with significant implications for health, wellness, productivity, and cost. The American workforce has a long-held sense of pride in working hard, often at the expense of sleep. Early work start times are common in the military and federal government, and sleep medicine specialists have the expertise necessary to diagnose and treat the myriad of sleep disorders that have come to light recently. A massive shortage of sleep medicine specialists limits the evidence-based sleep treatment implementations in medical care.
Medicine has become increasingly complex, necessitating a highly connected web of people, resources, institutions, and processes to keep up with the demands of growing information and technology. The evolution of a systems approach to health care built momentum during the 21st century.1-3 The National Academy of Medicine has published 2 reports that raised concerns about the quality and safety of medical care.4,5 With this expansion, the potential for medical errors at individual components or relationship nodes between actors in the medical system also has grown. Medical errors encompass more than acts of commission and can also take the form of acts of omission by failing to diagnosis and appropriately treat before long-term or irrevocable health consequences occur. A systems approach seeks to aid clinical decision making to improve the quality of medical care and patient outcomes in an otherwise complex medical system that can be difficult to navigate.
Although awareness of obstructive sleep apnea (OSA) has increased, CSA has not received the same level of attention and may not be recognized by PCPs. A lack of education about CSA can contribute to acts of omission in a health care setting. Although CSA is ultimately diagnosed and managed in specialty care sleep medicine clinics, PCPs play an instrumental role in referring patients for evaluation and then collaborating with specialists to optimize care and outcomes. The multidisciplinary approach of CSA management is important because it overlaps with many conditions that are commonly seen in primary care, including obesity, chronic pain, congestive heart failure (CHF), chronic kidney disease, and hypothyroidism. These chronic conditions are also prevalent among veterans. In a national cross-sectional study, veterans had higher prevalence rates of chronic health conditions, including cardiovascular disease and kidney disease, compared with nonveterans (odds ratios, 1.4 and 1.2, respectively).6
It is important to understand the relationship between CSA and chronic medical conditions because recognizing the signs of CSA can lead to identification of underlying medical conditions. Likewise, the chronic medical conditions that lead to CSA may cue the PCP’s clinical suspicion for CSA and lead to specialty care referrals if needed. The clinician also serves a significant role in the management of CSA by optimizing medical care for the underlying condition prior to pursuing additional specialty care treatments like positive airway pressure (PAP). For example, PCPs are often involved in the management of atrial fibrillation and cardiac dysfunction, which can minimize or exacerbate CSA. PCPs should also be aware of which drugs are associated with the presentation of CSA as withdrawal or reduction of the medication can resolve symptoms without further evaluation by a specialist.
The review by Regn and colleagues updates readers on developments—and lack thereof—in the literature. Treatment options for CSA have been limited. For most patients, continuous PAP (CPAP), which is the gold standard treatment for OSA, is not an effective CSA treatment. Earlier specialty guidelines endorsed adaptive servo-ventilation (ASV), a more sophisticated respiratory assist device, for treating CSA. In 2015, the SERVE-HF trial examined the effects of ASV in combination with guideline-based medical treatment on survival and cardiovascular outcomes for patients who had CSA and HF with reduced ejection fraction.7 They found that ASV had no significant effect on the primary endpoints of first event of death from any cause, lifesaving cardiovascular intervention, or unplanned hospitalization for worsening HF. However, all-cause and cardiovascular mortality were both increased with ASV. There has not been a more recent large clinical trial that either refutes or reinforces those findings (ADVENT-HF found that ASV effectively treated CSA and OSA in patients with CHF but had no impact on the primary endpoint of mortality).7,8 We are unlikely to see more studies soon that will put this issue to rest and change the guidance that is currently available for ASV use.
Regn and colleagues also provide an update on the use of acetazolamide as to assist in CSA treatment. This should be done cautiously and potentially deferred to subspecialists in sleep medicine, cardiology, or nephrology. The theoretical benefit of acetazolamide in CSA is based on its promotion of excretion of sodium bicarbonate, leading to metabolic acidosis, which can stimulate central respiratory drive. Since CSA is characterized by episodic loss of central respiratory drive, it seems logical that a respiratory stimulant would provide benefit. However, acetazolamide is not approved by the US Food and Drug Administration for CSA.9 In those with impaired respiratory mechanics, CHF, chronic obstructive pulmonary disease, and obesity hypoventilation syndrome, this medication has the potential for harm by adding metabolic acidosis to a patient with concurrent respiratory acidosis or respiratory constraints that limit their ability to compensate effectively for additional acid-base derangements.
It is worth noting that Regn and colleagues do not make claims outside the intended scope. It accomplishes the mission of providing all PCPs with an updated streamlined summary for diagnosing and treating CSA. Such tools are important in an age of growing medical information technology because it can improve the quality of medical care and ultimately, patient outcomes with timely diagnosis and treatment. This is particularly significant in a veteran population with a high burden of chronic medical conditions and polypharmacy.
In this issue, Regn and colleagues (page 78) have provided a concise resource for primary care professionals (PCPs) on a lesser known sleep disorder that is increasingly common in veterans.1 Their review provides a basic understanding of central sleep apnea (CSA) and a systematic clinical approach to diagnosis and treatment in primary care. We applaud the authors for providing education on sleep disorders to the Federal Practitioner audience, since sleep disorders are prevalent among military service members and veterans, with significant implications for health, wellness, productivity, and cost. The American workforce has a long-held sense of pride in working hard, often at the expense of sleep. Early work start times are common in the military and federal government, and sleep medicine specialists have the expertise necessary to diagnose and treat the myriad of sleep disorders that have come to light recently. A massive shortage of sleep medicine specialists limits the evidence-based sleep treatment implementations in medical care.
Medicine has become increasingly complex, necessitating a highly connected web of people, resources, institutions, and processes to keep up with the demands of growing information and technology. The evolution of a systems approach to health care built momentum during the 21st century.1-3 The National Academy of Medicine has published 2 reports that raised concerns about the quality and safety of medical care.4,5 With this expansion, the potential for medical errors at individual components or relationship nodes between actors in the medical system also has grown. Medical errors encompass more than acts of commission and can also take the form of acts of omission by failing to diagnosis and appropriately treat before long-term or irrevocable health consequences occur. A systems approach seeks to aid clinical decision making to improve the quality of medical care and patient outcomes in an otherwise complex medical system that can be difficult to navigate.
Although awareness of obstructive sleep apnea (OSA) has increased, CSA has not received the same level of attention and may not be recognized by PCPs. A lack of education about CSA can contribute to acts of omission in a health care setting. Although CSA is ultimately diagnosed and managed in specialty care sleep medicine clinics, PCPs play an instrumental role in referring patients for evaluation and then collaborating with specialists to optimize care and outcomes. The multidisciplinary approach of CSA management is important because it overlaps with many conditions that are commonly seen in primary care, including obesity, chronic pain, congestive heart failure (CHF), chronic kidney disease, and hypothyroidism. These chronic conditions are also prevalent among veterans. In a national cross-sectional study, veterans had higher prevalence rates of chronic health conditions, including cardiovascular disease and kidney disease, compared with nonveterans (odds ratios, 1.4 and 1.2, respectively).6
It is important to understand the relationship between CSA and chronic medical conditions because recognizing the signs of CSA can lead to identification of underlying medical conditions. Likewise, the chronic medical conditions that lead to CSA may cue the PCP’s clinical suspicion for CSA and lead to specialty care referrals if needed. The clinician also serves a significant role in the management of CSA by optimizing medical care for the underlying condition prior to pursuing additional specialty care treatments like positive airway pressure (PAP). For example, PCPs are often involved in the management of atrial fibrillation and cardiac dysfunction, which can minimize or exacerbate CSA. PCPs should also be aware of which drugs are associated with the presentation of CSA as withdrawal or reduction of the medication can resolve symptoms without further evaluation by a specialist.
The review by Regn and colleagues updates readers on developments—and lack thereof—in the literature. Treatment options for CSA have been limited. For most patients, continuous PAP (CPAP), which is the gold standard treatment for OSA, is not an effective CSA treatment. Earlier specialty guidelines endorsed adaptive servo-ventilation (ASV), a more sophisticated respiratory assist device, for treating CSA. In 2015, the SERVE-HF trial examined the effects of ASV in combination with guideline-based medical treatment on survival and cardiovascular outcomes for patients who had CSA and HF with reduced ejection fraction.7 They found that ASV had no significant effect on the primary endpoints of first event of death from any cause, lifesaving cardiovascular intervention, or unplanned hospitalization for worsening HF. However, all-cause and cardiovascular mortality were both increased with ASV. There has not been a more recent large clinical trial that either refutes or reinforces those findings (ADVENT-HF found that ASV effectively treated CSA and OSA in patients with CHF but had no impact on the primary endpoint of mortality).7,8 We are unlikely to see more studies soon that will put this issue to rest and change the guidance that is currently available for ASV use.
Regn and colleagues also provide an update on the use of acetazolamide as to assist in CSA treatment. This should be done cautiously and potentially deferred to subspecialists in sleep medicine, cardiology, or nephrology. The theoretical benefit of acetazolamide in CSA is based on its promotion of excretion of sodium bicarbonate, leading to metabolic acidosis, which can stimulate central respiratory drive. Since CSA is characterized by episodic loss of central respiratory drive, it seems logical that a respiratory stimulant would provide benefit. However, acetazolamide is not approved by the US Food and Drug Administration for CSA.9 In those with impaired respiratory mechanics, CHF, chronic obstructive pulmonary disease, and obesity hypoventilation syndrome, this medication has the potential for harm by adding metabolic acidosis to a patient with concurrent respiratory acidosis or respiratory constraints that limit their ability to compensate effectively for additional acid-base derangements.
It is worth noting that Regn and colleagues do not make claims outside the intended scope. It accomplishes the mission of providing all PCPs with an updated streamlined summary for diagnosing and treating CSA. Such tools are important in an age of growing medical information technology because it can improve the quality of medical care and ultimately, patient outcomes with timely diagnosis and treatment. This is particularly significant in a veteran population with a high burden of chronic medical conditions and polypharmacy.
1. Regn DD, Davis AH, Smith WD, Blasser CJ, Ford CM. Central sleep apnea in adults: diagnosis and treatment. Fed Pract. 2023;40(3):76-83. doi:10.12788/fp.0367
2. Clarkson J, Dean J, Ward J, Komashie A, Bashford T. A systems approach to healthcare: from thinking to -practice. Future Healthc J. 2018;5(3):151-155. doi:10.7861/futurehosp.5-3-151 3. Komashie A, Ward J, Bashford T, et al. Systems approach to health service design, delivery and improvement: a systematic review and meta-analysis. BMJ Open. 2021;11(1):e037667. Published 2021 Jan 19. doi:10.1136/bmjopen-2020-037667 4. Institute of Medicine (US) Committee on Quality of Health Care in America, Kohn LT, Corrigan JM, Donaldson MS, eds. To Err Is Human: Building a Safer Health System. National Academies Press; 2000.
5. Institute of Medicine (US) Committee on Crossing the Quality Chasm: Adaptation to Mental Health and Addictive Disorders. Improving the Quality of Health Care for Mental and Substance-Use Conditions: Quality Chasm Series. National Academies Press; 2006.
6. McDaniel M, McDaniel JT. Examining the geographic distribution of six chronic disease risk factors for severe COVID-19: veteran-nonveteran differences. Chronic Illn. 2022;18(3):666-676. doi:10.1177/17423953211028280
7. Cowie MR, Woehrle H, Wegscheider K, et al. Adaptive servo-ventilation for central sleep apnea in systolic heart failure. N Engl J Med. 2015;373(12):1095-1105. doi:10.1056/NEJMoa1506459
8. Lyons OD, Floras JS, Logan AG, et al; ADVENT-HF Investigators. Design of the effect of adaptive servo-ventilation on survival and cardiovascular hospital admissions in patients with heart failure and sleep apnoea: the ADVENT-HF trial. Eur J Heart Fail. 2017;19(4):579-587. doi:10.1002/ejhf.790
9. US Food and Drug Administration. Diomax. Updated May 2022. Accessed Feb 13, 2023. https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/008943s052,009388s038lbl.pdf
1. Regn DD, Davis AH, Smith WD, Blasser CJ, Ford CM. Central sleep apnea in adults: diagnosis and treatment. Fed Pract. 2023;40(3):76-83. doi:10.12788/fp.0367
2. Clarkson J, Dean J, Ward J, Komashie A, Bashford T. A systems approach to healthcare: from thinking to -practice. Future Healthc J. 2018;5(3):151-155. doi:10.7861/futurehosp.5-3-151 3. Komashie A, Ward J, Bashford T, et al. Systems approach to health service design, delivery and improvement: a systematic review and meta-analysis. BMJ Open. 2021;11(1):e037667. Published 2021 Jan 19. doi:10.1136/bmjopen-2020-037667 4. Institute of Medicine (US) Committee on Quality of Health Care in America, Kohn LT, Corrigan JM, Donaldson MS, eds. To Err Is Human: Building a Safer Health System. National Academies Press; 2000.
5. Institute of Medicine (US) Committee on Crossing the Quality Chasm: Adaptation to Mental Health and Addictive Disorders. Improving the Quality of Health Care for Mental and Substance-Use Conditions: Quality Chasm Series. National Academies Press; 2006.
6. McDaniel M, McDaniel JT. Examining the geographic distribution of six chronic disease risk factors for severe COVID-19: veteran-nonveteran differences. Chronic Illn. 2022;18(3):666-676. doi:10.1177/17423953211028280
7. Cowie MR, Woehrle H, Wegscheider K, et al. Adaptive servo-ventilation for central sleep apnea in systolic heart failure. N Engl J Med. 2015;373(12):1095-1105. doi:10.1056/NEJMoa1506459
8. Lyons OD, Floras JS, Logan AG, et al; ADVENT-HF Investigators. Design of the effect of adaptive servo-ventilation on survival and cardiovascular hospital admissions in patients with heart failure and sleep apnoea: the ADVENT-HF trial. Eur J Heart Fail. 2017;19(4):579-587. doi:10.1002/ejhf.790
9. US Food and Drug Administration. Diomax. Updated May 2022. Accessed Feb 13, 2023. https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/008943s052,009388s038lbl.pdf
Silicone-based film for radiation dermatitis: It works, so why isn’t it used?
Radiation dermatitis is one of the most common side effects of radiotherapy for women with breast cancer. Results from a phase 3 trial add to previous evidence from smaller trials that show that a silicone-based film can protect skin from this side effect.
But it is not being used much in clinical practice. Instead, radiation dermatitis is usually treated after the fact, most often with aqueous creams.
said Edward Chow, MBBS, PhD, of the department of radiation oncology, Odette Cancer Centre, Sunnybrook Health Sciences Centre, Toronto, who was the senior author of the phase 3 study published recently in the Journal of Clinical Oncology.
“Other doctors think that because radiation dermatitis isn’t life-threatening it isn’t as important, but the condition does affect the quality of life for patients,” Dr. Chow said. “If we can lessen the pain and discomfort, why wouldn’t we as physicians?”
Dr. Chow’s open-label, multicenter trial was conducted in 376 women with large breasts (bra cup size C or larger) who were undergoing radiotherapy after lumpectomy or mastectomy. The primary endpoint was grade 2 or 3 radiation dermatitis using the Common Terminology Criteria for Adverse Events. (Grade 2 is described as moderate, whereas grade 3 is severe.)
The film significantly reduced the incidence of grade 2 or 3 radiation dermatitis, down to 15.5% compared with 45.6% in patients receiving standard care (odds ratio, 0.20, 95% confidence interval, 0.12-0.34, P < .0001).
There was also a significant reduction in grade 3 radiation dermatitis (2.8% vs. 13.6%; OR, 0.19; P < .0002) and moist desquamation (8% vs. 19.2%; OR, 0.36; P = .002).
“The film was remarkably effective and helped protect patients from potentially debilitating side effects,” commented Corey Speers, MD, PhD, a radiation oncologist with University Hospitals, Cleveland, who saw the study data presented during a plenary session at the annual meeting of the American Society of Clinical Oncology.
He believes that preventing radiation dermatitis before it develops is the best way to care for patients.
“[Radiation dermatitis] is usually associated with pain and discomfort and can lead to more serious issues like infection or delayed wound healing, and unfortunately, there aren’t effective treatments for it once it’s developed, so preventing it is our most effective strategy,” Dr. Speers said.
One reason for the film not being used much could be that it takes time apply the film, suggested Patries Herst, PhD, department of radiation therapy, University of Otago, Wellington, New Zealand. She was the lead author of a study published in 2014 that also analyzed the effectiveness of the film in preventing radiation dermatitis.
In their trial, a research radiation therapist applied the film to women when they were starting their radiotherapy. The film is applied to a portion of the breast or chest wall, and Dr. Herst emphasized the importance of applying the film correctly, making sure the film is not stretched during application and not overlapping other pieces of the film, while also making sure that it conforms to the breast shape. The film was replaced when it would curl too much around the sides, approximately every 1 or 2 weeks.
“Radiation therapy itself is very short. And so you have about 10 minutes for every patient,” she explained.
“But applying the film adds 20-30 minutes and it’s really awkward to apply properly,” Dr. Herst said. “You have to tap it in and then have to maybe cut it so that it fits better. And hospitals say, ‘We don’t have the time’ and that is still the biggest issue that we’re seeing right now.”
In Dr. Chow’s study, the average time spent applying the film on lumpectomy patients was 55 minutes and was slightly shorter at 45 minutes for mastectomy patients. He acknowledged that it does take time that staff at most hospitals and clinics simply don’t have.
Dr. Chow suggested that perhaps a family member or other caregiver could apply the film, and he referenced an educational video from the manufacturer that provides in-depth instructions on the correct way to apply the film for radiotherapy patients. However, this could lead to errors and a waste of product if not the film was not applied properly.
The cost of Mepitel film may also be a deterrent. Dr. Chow’s study noted that, during the entire course of radiotherapy, the cost for the film was about $80-$100 per patient. However, he believes the benefits outweigh the cost.
In addition, there have been issues with supplies, and it has been difficult for people to get their hands on the actual product.
Currently, the Mayo Clinic is also conducting a study testing Mepitel Film for radiation dermatitis in breast cancer patients following mastectomy. Mayo Clinic principal investigator Kimberly Corbin, MD, could not go into great detail about the ongoing trial, but she said it has been difficult to get the product.
“We have been using the film at Mayo for a number of years,” Dr. Corbin said, but we “have found that it is challenging to get supplies.”
“While we have generally been able to have some supply established through our store here, we know that is not typical and it is difficult for patients to access,” she said. In addition, “there are not a ton of centers with experience in application.”
A representative with Mölnlycke Health Care, Allyson Bower-Willner, could not comment on the distribution of Mepitel film in the United States or if the company plans to increase the amount of product shipped. The film is available “to a limited set of customers,” she said.
A version of this article first appeared on Medscape.com.
Radiation dermatitis is one of the most common side effects of radiotherapy for women with breast cancer. Results from a phase 3 trial add to previous evidence from smaller trials that show that a silicone-based film can protect skin from this side effect.
But it is not being used much in clinical practice. Instead, radiation dermatitis is usually treated after the fact, most often with aqueous creams.
said Edward Chow, MBBS, PhD, of the department of radiation oncology, Odette Cancer Centre, Sunnybrook Health Sciences Centre, Toronto, who was the senior author of the phase 3 study published recently in the Journal of Clinical Oncology.
“Other doctors think that because radiation dermatitis isn’t life-threatening it isn’t as important, but the condition does affect the quality of life for patients,” Dr. Chow said. “If we can lessen the pain and discomfort, why wouldn’t we as physicians?”
Dr. Chow’s open-label, multicenter trial was conducted in 376 women with large breasts (bra cup size C or larger) who were undergoing radiotherapy after lumpectomy or mastectomy. The primary endpoint was grade 2 or 3 radiation dermatitis using the Common Terminology Criteria for Adverse Events. (Grade 2 is described as moderate, whereas grade 3 is severe.)
The film significantly reduced the incidence of grade 2 or 3 radiation dermatitis, down to 15.5% compared with 45.6% in patients receiving standard care (odds ratio, 0.20, 95% confidence interval, 0.12-0.34, P < .0001).
There was also a significant reduction in grade 3 radiation dermatitis (2.8% vs. 13.6%; OR, 0.19; P < .0002) and moist desquamation (8% vs. 19.2%; OR, 0.36; P = .002).
“The film was remarkably effective and helped protect patients from potentially debilitating side effects,” commented Corey Speers, MD, PhD, a radiation oncologist with University Hospitals, Cleveland, who saw the study data presented during a plenary session at the annual meeting of the American Society of Clinical Oncology.
He believes that preventing radiation dermatitis before it develops is the best way to care for patients.
“[Radiation dermatitis] is usually associated with pain and discomfort and can lead to more serious issues like infection or delayed wound healing, and unfortunately, there aren’t effective treatments for it once it’s developed, so preventing it is our most effective strategy,” Dr. Speers said.
One reason for the film not being used much could be that it takes time apply the film, suggested Patries Herst, PhD, department of radiation therapy, University of Otago, Wellington, New Zealand. She was the lead author of a study published in 2014 that also analyzed the effectiveness of the film in preventing radiation dermatitis.
In their trial, a research radiation therapist applied the film to women when they were starting their radiotherapy. The film is applied to a portion of the breast or chest wall, and Dr. Herst emphasized the importance of applying the film correctly, making sure the film is not stretched during application and not overlapping other pieces of the film, while also making sure that it conforms to the breast shape. The film was replaced when it would curl too much around the sides, approximately every 1 or 2 weeks.
“Radiation therapy itself is very short. And so you have about 10 minutes for every patient,” she explained.
“But applying the film adds 20-30 minutes and it’s really awkward to apply properly,” Dr. Herst said. “You have to tap it in and then have to maybe cut it so that it fits better. And hospitals say, ‘We don’t have the time’ and that is still the biggest issue that we’re seeing right now.”
In Dr. Chow’s study, the average time spent applying the film on lumpectomy patients was 55 minutes and was slightly shorter at 45 minutes for mastectomy patients. He acknowledged that it does take time that staff at most hospitals and clinics simply don’t have.
Dr. Chow suggested that perhaps a family member or other caregiver could apply the film, and he referenced an educational video from the manufacturer that provides in-depth instructions on the correct way to apply the film for radiotherapy patients. However, this could lead to errors and a waste of product if not the film was not applied properly.
The cost of Mepitel film may also be a deterrent. Dr. Chow’s study noted that, during the entire course of radiotherapy, the cost for the film was about $80-$100 per patient. However, he believes the benefits outweigh the cost.
In addition, there have been issues with supplies, and it has been difficult for people to get their hands on the actual product.
Currently, the Mayo Clinic is also conducting a study testing Mepitel Film for radiation dermatitis in breast cancer patients following mastectomy. Mayo Clinic principal investigator Kimberly Corbin, MD, could not go into great detail about the ongoing trial, but she said it has been difficult to get the product.
“We have been using the film at Mayo for a number of years,” Dr. Corbin said, but we “have found that it is challenging to get supplies.”
“While we have generally been able to have some supply established through our store here, we know that is not typical and it is difficult for patients to access,” she said. In addition, “there are not a ton of centers with experience in application.”
A representative with Mölnlycke Health Care, Allyson Bower-Willner, could not comment on the distribution of Mepitel film in the United States or if the company plans to increase the amount of product shipped. The film is available “to a limited set of customers,” she said.
A version of this article first appeared on Medscape.com.
Radiation dermatitis is one of the most common side effects of radiotherapy for women with breast cancer. Results from a phase 3 trial add to previous evidence from smaller trials that show that a silicone-based film can protect skin from this side effect.
But it is not being used much in clinical practice. Instead, radiation dermatitis is usually treated after the fact, most often with aqueous creams.
said Edward Chow, MBBS, PhD, of the department of radiation oncology, Odette Cancer Centre, Sunnybrook Health Sciences Centre, Toronto, who was the senior author of the phase 3 study published recently in the Journal of Clinical Oncology.
“Other doctors think that because radiation dermatitis isn’t life-threatening it isn’t as important, but the condition does affect the quality of life for patients,” Dr. Chow said. “If we can lessen the pain and discomfort, why wouldn’t we as physicians?”
Dr. Chow’s open-label, multicenter trial was conducted in 376 women with large breasts (bra cup size C or larger) who were undergoing radiotherapy after lumpectomy or mastectomy. The primary endpoint was grade 2 or 3 radiation dermatitis using the Common Terminology Criteria for Adverse Events. (Grade 2 is described as moderate, whereas grade 3 is severe.)
The film significantly reduced the incidence of grade 2 or 3 radiation dermatitis, down to 15.5% compared with 45.6% in patients receiving standard care (odds ratio, 0.20, 95% confidence interval, 0.12-0.34, P < .0001).
There was also a significant reduction in grade 3 radiation dermatitis (2.8% vs. 13.6%; OR, 0.19; P < .0002) and moist desquamation (8% vs. 19.2%; OR, 0.36; P = .002).
“The film was remarkably effective and helped protect patients from potentially debilitating side effects,” commented Corey Speers, MD, PhD, a radiation oncologist with University Hospitals, Cleveland, who saw the study data presented during a plenary session at the annual meeting of the American Society of Clinical Oncology.
He believes that preventing radiation dermatitis before it develops is the best way to care for patients.
“[Radiation dermatitis] is usually associated with pain and discomfort and can lead to more serious issues like infection or delayed wound healing, and unfortunately, there aren’t effective treatments for it once it’s developed, so preventing it is our most effective strategy,” Dr. Speers said.
One reason for the film not being used much could be that it takes time apply the film, suggested Patries Herst, PhD, department of radiation therapy, University of Otago, Wellington, New Zealand. She was the lead author of a study published in 2014 that also analyzed the effectiveness of the film in preventing radiation dermatitis.
In their trial, a research radiation therapist applied the film to women when they were starting their radiotherapy. The film is applied to a portion of the breast or chest wall, and Dr. Herst emphasized the importance of applying the film correctly, making sure the film is not stretched during application and not overlapping other pieces of the film, while also making sure that it conforms to the breast shape. The film was replaced when it would curl too much around the sides, approximately every 1 or 2 weeks.
“Radiation therapy itself is very short. And so you have about 10 minutes for every patient,” she explained.
“But applying the film adds 20-30 minutes and it’s really awkward to apply properly,” Dr. Herst said. “You have to tap it in and then have to maybe cut it so that it fits better. And hospitals say, ‘We don’t have the time’ and that is still the biggest issue that we’re seeing right now.”
In Dr. Chow’s study, the average time spent applying the film on lumpectomy patients was 55 minutes and was slightly shorter at 45 minutes for mastectomy patients. He acknowledged that it does take time that staff at most hospitals and clinics simply don’t have.
Dr. Chow suggested that perhaps a family member or other caregiver could apply the film, and he referenced an educational video from the manufacturer that provides in-depth instructions on the correct way to apply the film for radiotherapy patients. However, this could lead to errors and a waste of product if not the film was not applied properly.
The cost of Mepitel film may also be a deterrent. Dr. Chow’s study noted that, during the entire course of radiotherapy, the cost for the film was about $80-$100 per patient. However, he believes the benefits outweigh the cost.
In addition, there have been issues with supplies, and it has been difficult for people to get their hands on the actual product.
Currently, the Mayo Clinic is also conducting a study testing Mepitel Film for radiation dermatitis in breast cancer patients following mastectomy. Mayo Clinic principal investigator Kimberly Corbin, MD, could not go into great detail about the ongoing trial, but she said it has been difficult to get the product.
“We have been using the film at Mayo for a number of years,” Dr. Corbin said, but we “have found that it is challenging to get supplies.”
“While we have generally been able to have some supply established through our store here, we know that is not typical and it is difficult for patients to access,” she said. In addition, “there are not a ton of centers with experience in application.”
A representative with Mölnlycke Health Care, Allyson Bower-Willner, could not comment on the distribution of Mepitel film in the United States or if the company plans to increase the amount of product shipped. The film is available “to a limited set of customers,” she said.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL ONCOLOGY