User login
For MD-IQ use only
AAP: ‘Toddler milk’ unnecessary for most kids
WASHINGTON – These products are not nutritionally complete and are not to be confused with formulas for infants younger than 12 months.
“Toddler drinks do not offer anything nutritionally exceptional,” said George J. Fuchs III, MD, a pediatric gastroenterologist at the University of Kentucky, Lexington, who presented a clinical report on toddler formulas from the American Academy of Pediatrics at the group’s annual meeting. The products are not regulated by the U.S. Food and Drug Administration and should not be given to infants younger than 12 months in place of infant formulas, but murky marketing can leave parents and caregivers confused as to whether these products are essential for good health, Dr. Fuchs said.
Despite the rise in marketing of formulas pitched as toddler milks, growth milks, or transition formulas, among other names, the AAP says these formulas are both unregulated and unnecessary for the vast majority of toddlers because they have adequate diets and do not require supplementation.
Clinicians should understand and explain the distinction between products formulated for infants younger than 12 months and those designed for children aged 12 months or older, Dr. Fuchs added.
Formulas for infants younger than 12 months represent a distinct product category for the FDA and are required to be nutritionally complete for this age, Dr. Fuchs said. Infant formulas sold in the United States must meet nutrition requirements as defined by the Infant Formula Act of 1980 (updated in 1986), and the facilities that manufacture them are regularly inspected by the agency.
In contrast, toddler formulas are not regulated or categorized by the FDA and therefore may vary widely in composition and are not nutritionally complete for any age, he said.
One area of concern is that parents or caregivers misunderstand and give these products to infants younger than 12 months instead of infant formulas, he said.
Also, mass-market toddler formulas are inadequate for children with disease-specific requirements, such as malnutrition, gastrointestinal disorders, metabolic disorders, or food allergies.
Questionable composition, misleading marketing
Toddler formulas are not only unnecessary but could be detrimental to children’s health, Dr. Fuchs said. Some formulas have high sodium content relative to cow’s milk or may be high or low in protein. Other products have added sweeteners, which could contribute to an increased preference for sweetened foods as the children get older, he noted.
However, manufacturers of regulated infant products often market them alongside their infant formula, which can be confusing for parents and caregivers. The products often have similar names, images, slogans, and logos, and may suggest benefits such as immune system support, brain development, and digestive health, he added.
A 2020 survey published in Maternal and Child Nutrition found that 60% of approximately 1,000 caregivers of children aged 12-36 months agreed with the marketing claim that toddler formulas or powdered milks provide nutrition that is not available from other food and drinks, Dr. Fuchs said.
Balanced diet is best for healthy children
For infants younger than 12 months, the AAP recommends that the liquid portion of the diet should come from human milk or a standard infant formula that has been reviewed by the FDA based on the Infant Formula Act, Dr. Fuchs said.
Children aged 12 months or older should receive a varied diet with fortified foods. Formula can safely be used as part of a varied diet; however, it offers no nutritional advantage for most children over a well-balanced diet that includes human milk and/or cow milk, “and should not be promoted as such,” Dr. Fuchs noted.
“The category of these toddler drinks has grown and the landscape has changed quite a bit; we thought it was appropriate that we review this category,” Dr. Fuchs said in an interview.
Dr. Fuchs advised pediatricians in practice to follow the AAP’s guidance for breastfeeding infants if possible and progression to formula as needed for infants up to age 1 year, followed by transition to cow milk (or alternatives for those with cow milk allergies) and the addition of a healthy mixed diet.
Formula choices pose practice challenges
In an interview, Cathy Haut, DNP, CPNP-AC, CPNP-PC, a pediatric nurse practitioner in Rehoboth Beach, Del., pointed out that not only are parents often baffled by formula choices, but many are also hesitant to make a switch to regular milk as children get older because they worry that cow’s milk is inadequate for nutrition or is not as “clean” or “sterile” as formula.
In some cases, parents may have had difficulty in acquiring genuine infant formulas, which were relocated to locked cabinets in stores during recent shortages and began using toddler formulas as an alternative for infants younger than 1 year, she added.
“If breastfeeding is not possible, using approved infant formula is preferred, switching to whole cow milk at 1 year of age,” she said. “Nutritional assessment is an important part of well-child visits, with caregiver counseling regarding importance of intake of variety of fortified foods [that] offer vitamins, calcium, iron and zinc,” Ms. Haut added. Although toddler formulas are safe additions to the diets of most young children older than 1 year, supplementation of specific nutrients such as vitamin D if needed is a more effective option, she said.
“National health studies indicate that U.S. toddlers have nutritional gaps in their diet often related to picky eating,” an Abbott spokesperson said in an interview. “When [toddlers] don’t do well transitioning to table foods or won’t drink milk, our toddler drinks contain many of the complementary nutrients, such as vitamins and minerals, that they may be missing in their diet. Toddler drinks may be an option to help fill nutrient gaps for these children 12-36 months of age. Abbott does not recommend or indicate its toddler drinks for infants under 12 months of age,” according to the company.
Dr. Fuchs had no financial conflicts to disclose. Dr. Haut had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
WASHINGTON – These products are not nutritionally complete and are not to be confused with formulas for infants younger than 12 months.
“Toddler drinks do not offer anything nutritionally exceptional,” said George J. Fuchs III, MD, a pediatric gastroenterologist at the University of Kentucky, Lexington, who presented a clinical report on toddler formulas from the American Academy of Pediatrics at the group’s annual meeting. The products are not regulated by the U.S. Food and Drug Administration and should not be given to infants younger than 12 months in place of infant formulas, but murky marketing can leave parents and caregivers confused as to whether these products are essential for good health, Dr. Fuchs said.
Despite the rise in marketing of formulas pitched as toddler milks, growth milks, or transition formulas, among other names, the AAP says these formulas are both unregulated and unnecessary for the vast majority of toddlers because they have adequate diets and do not require supplementation.
Clinicians should understand and explain the distinction between products formulated for infants younger than 12 months and those designed for children aged 12 months or older, Dr. Fuchs added.
Formulas for infants younger than 12 months represent a distinct product category for the FDA and are required to be nutritionally complete for this age, Dr. Fuchs said. Infant formulas sold in the United States must meet nutrition requirements as defined by the Infant Formula Act of 1980 (updated in 1986), and the facilities that manufacture them are regularly inspected by the agency.
In contrast, toddler formulas are not regulated or categorized by the FDA and therefore may vary widely in composition and are not nutritionally complete for any age, he said.
One area of concern is that parents or caregivers misunderstand and give these products to infants younger than 12 months instead of infant formulas, he said.
Also, mass-market toddler formulas are inadequate for children with disease-specific requirements, such as malnutrition, gastrointestinal disorders, metabolic disorders, or food allergies.
Questionable composition, misleading marketing
Toddler formulas are not only unnecessary but could be detrimental to children’s health, Dr. Fuchs said. Some formulas have high sodium content relative to cow’s milk or may be high or low in protein. Other products have added sweeteners, which could contribute to an increased preference for sweetened foods as the children get older, he noted.
However, manufacturers of regulated infant products often market them alongside their infant formula, which can be confusing for parents and caregivers. The products often have similar names, images, slogans, and logos, and may suggest benefits such as immune system support, brain development, and digestive health, he added.
A 2020 survey published in Maternal and Child Nutrition found that 60% of approximately 1,000 caregivers of children aged 12-36 months agreed with the marketing claim that toddler formulas or powdered milks provide nutrition that is not available from other food and drinks, Dr. Fuchs said.
Balanced diet is best for healthy children
For infants younger than 12 months, the AAP recommends that the liquid portion of the diet should come from human milk or a standard infant formula that has been reviewed by the FDA based on the Infant Formula Act, Dr. Fuchs said.
Children aged 12 months or older should receive a varied diet with fortified foods. Formula can safely be used as part of a varied diet; however, it offers no nutritional advantage for most children over a well-balanced diet that includes human milk and/or cow milk, “and should not be promoted as such,” Dr. Fuchs noted.
“The category of these toddler drinks has grown and the landscape has changed quite a bit; we thought it was appropriate that we review this category,” Dr. Fuchs said in an interview.
Dr. Fuchs advised pediatricians in practice to follow the AAP’s guidance for breastfeeding infants if possible and progression to formula as needed for infants up to age 1 year, followed by transition to cow milk (or alternatives for those with cow milk allergies) and the addition of a healthy mixed diet.
Formula choices pose practice challenges
In an interview, Cathy Haut, DNP, CPNP-AC, CPNP-PC, a pediatric nurse practitioner in Rehoboth Beach, Del., pointed out that not only are parents often baffled by formula choices, but many are also hesitant to make a switch to regular milk as children get older because they worry that cow’s milk is inadequate for nutrition or is not as “clean” or “sterile” as formula.
In some cases, parents may have had difficulty in acquiring genuine infant formulas, which were relocated to locked cabinets in stores during recent shortages and began using toddler formulas as an alternative for infants younger than 1 year, she added.
“If breastfeeding is not possible, using approved infant formula is preferred, switching to whole cow milk at 1 year of age,” she said. “Nutritional assessment is an important part of well-child visits, with caregiver counseling regarding importance of intake of variety of fortified foods [that] offer vitamins, calcium, iron and zinc,” Ms. Haut added. Although toddler formulas are safe additions to the diets of most young children older than 1 year, supplementation of specific nutrients such as vitamin D if needed is a more effective option, she said.
“National health studies indicate that U.S. toddlers have nutritional gaps in their diet often related to picky eating,” an Abbott spokesperson said in an interview. “When [toddlers] don’t do well transitioning to table foods or won’t drink milk, our toddler drinks contain many of the complementary nutrients, such as vitamins and minerals, that they may be missing in their diet. Toddler drinks may be an option to help fill nutrient gaps for these children 12-36 months of age. Abbott does not recommend or indicate its toddler drinks for infants under 12 months of age,” according to the company.
Dr. Fuchs had no financial conflicts to disclose. Dr. Haut had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
WASHINGTON – These products are not nutritionally complete and are not to be confused with formulas for infants younger than 12 months.
“Toddler drinks do not offer anything nutritionally exceptional,” said George J. Fuchs III, MD, a pediatric gastroenterologist at the University of Kentucky, Lexington, who presented a clinical report on toddler formulas from the American Academy of Pediatrics at the group’s annual meeting. The products are not regulated by the U.S. Food and Drug Administration and should not be given to infants younger than 12 months in place of infant formulas, but murky marketing can leave parents and caregivers confused as to whether these products are essential for good health, Dr. Fuchs said.
Despite the rise in marketing of formulas pitched as toddler milks, growth milks, or transition formulas, among other names, the AAP says these formulas are both unregulated and unnecessary for the vast majority of toddlers because they have adequate diets and do not require supplementation.
Clinicians should understand and explain the distinction between products formulated for infants younger than 12 months and those designed for children aged 12 months or older, Dr. Fuchs added.
Formulas for infants younger than 12 months represent a distinct product category for the FDA and are required to be nutritionally complete for this age, Dr. Fuchs said. Infant formulas sold in the United States must meet nutrition requirements as defined by the Infant Formula Act of 1980 (updated in 1986), and the facilities that manufacture them are regularly inspected by the agency.
In contrast, toddler formulas are not regulated or categorized by the FDA and therefore may vary widely in composition and are not nutritionally complete for any age, he said.
One area of concern is that parents or caregivers misunderstand and give these products to infants younger than 12 months instead of infant formulas, he said.
Also, mass-market toddler formulas are inadequate for children with disease-specific requirements, such as malnutrition, gastrointestinal disorders, metabolic disorders, or food allergies.
Questionable composition, misleading marketing
Toddler formulas are not only unnecessary but could be detrimental to children’s health, Dr. Fuchs said. Some formulas have high sodium content relative to cow’s milk or may be high or low in protein. Other products have added sweeteners, which could contribute to an increased preference for sweetened foods as the children get older, he noted.
However, manufacturers of regulated infant products often market them alongside their infant formula, which can be confusing for parents and caregivers. The products often have similar names, images, slogans, and logos, and may suggest benefits such as immune system support, brain development, and digestive health, he added.
A 2020 survey published in Maternal and Child Nutrition found that 60% of approximately 1,000 caregivers of children aged 12-36 months agreed with the marketing claim that toddler formulas or powdered milks provide nutrition that is not available from other food and drinks, Dr. Fuchs said.
Balanced diet is best for healthy children
For infants younger than 12 months, the AAP recommends that the liquid portion of the diet should come from human milk or a standard infant formula that has been reviewed by the FDA based on the Infant Formula Act, Dr. Fuchs said.
Children aged 12 months or older should receive a varied diet with fortified foods. Formula can safely be used as part of a varied diet; however, it offers no nutritional advantage for most children over a well-balanced diet that includes human milk and/or cow milk, “and should not be promoted as such,” Dr. Fuchs noted.
“The category of these toddler drinks has grown and the landscape has changed quite a bit; we thought it was appropriate that we review this category,” Dr. Fuchs said in an interview.
Dr. Fuchs advised pediatricians in practice to follow the AAP’s guidance for breastfeeding infants if possible and progression to formula as needed for infants up to age 1 year, followed by transition to cow milk (or alternatives for those with cow milk allergies) and the addition of a healthy mixed diet.
Formula choices pose practice challenges
In an interview, Cathy Haut, DNP, CPNP-AC, CPNP-PC, a pediatric nurse practitioner in Rehoboth Beach, Del., pointed out that not only are parents often baffled by formula choices, but many are also hesitant to make a switch to regular milk as children get older because they worry that cow’s milk is inadequate for nutrition or is not as “clean” or “sterile” as formula.
In some cases, parents may have had difficulty in acquiring genuine infant formulas, which were relocated to locked cabinets in stores during recent shortages and began using toddler formulas as an alternative for infants younger than 1 year, she added.
“If breastfeeding is not possible, using approved infant formula is preferred, switching to whole cow milk at 1 year of age,” she said. “Nutritional assessment is an important part of well-child visits, with caregiver counseling regarding importance of intake of variety of fortified foods [that] offer vitamins, calcium, iron and zinc,” Ms. Haut added. Although toddler formulas are safe additions to the diets of most young children older than 1 year, supplementation of specific nutrients such as vitamin D if needed is a more effective option, she said.
“National health studies indicate that U.S. toddlers have nutritional gaps in their diet often related to picky eating,” an Abbott spokesperson said in an interview. “When [toddlers] don’t do well transitioning to table foods or won’t drink milk, our toddler drinks contain many of the complementary nutrients, such as vitamins and minerals, that they may be missing in their diet. Toddler drinks may be an option to help fill nutrient gaps for these children 12-36 months of age. Abbott does not recommend or indicate its toddler drinks for infants under 12 months of age,” according to the company.
Dr. Fuchs had no financial conflicts to disclose. Dr. Haut had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
AT AAP 2023
Is ChatGPT smarter than a PCP?
GLASGOW –
ChatGPT also provided novel explanations – it frequently “hallucinates” – by describing inaccurate information as if they were facts, according to Shathar Mahmood, BA, a fifth-year medical student at the University of Cambridge, England, who presented the findings at the annual meeting of the Royal College of General Practitioners. The study was published in JMIR Medical Education earlier this year.
“Artificial intelligence has generated impressive results across medicine, and with the release of ChatGPT there is now discussion about these large language models taking over clinicians’ jobs,” Arun James Thirunavukarasu, MB BChir, of the University of Oxford, England, and Oxford University Hospitals NHS Foundation Trust, who is the lead author of the study, told this news organization.
Performance of AI on medical school examinations has prompted much of this discussion, often because performance does not reflect real-world clinical practice, he said. “We used the Applied Knowledge Test instead, and this allowed us to explore the potential and pitfalls of deploying large language models in primary care and to explore what further development of medical large language model applications is required.”
The researchers investigated the strengths and weaknesses of ChatGPT in primary care using the Membership of the Royal College of General Practitioners Applied Knowledge Test. The computer-based, multiple-choice assessment is part of the U.K.’s specialty training to become a general practitioner (GP). It tests knowledge behind general practice within the context of the United Kingdom’s National Health Service.
The researchers entered a series of 674 questions into ChatGPT on two occasions, or “runs.” “By putting the questions into two separate dialogues, we hoped to avoid the influence of one dialogue on the other,” Ms. Mahmood said. To validate that the answers were correct, the ChatGPT responses were compared with the answers provided by the GP self-test and past articles.
Docs 1, AI 0
Overall performance of the algorithm was good across both runs (59.94% and 60.39%); 83.23% of questions produced the same answer on both runs.
But 17% of the answers didn’t match, Ms. Mahmood reported, a statistically significant difference. “And the overall performance of ChatGPT was 10% lower than the average RCGP pass mark in the last few years, which informs one of our conclusions about it not being very precise at expert level recall and decision-making,” she said.
Also, a small percentage of questions (1.48% and 2.25% in each run) produced an uncertain answer or there was no answer.
Say what?
Novel explanations were generated upon running a question through ChatGPT that then provided an extended answer, Ms. Mahmood said. When the accuracy of the extended answers was checked against the correct answers, no correlation was found. “ChatGPT can hallucinate answers, and there’s no way a nonexpert reading this could know it is incorrect,” she said.
Regarding the application of ChatGPT and similar algorithms to clinical practice, Ms. Mahmood was clear. “As they stand, [AI systems] will not be able to replace the health care professional workforce, in primary care at least,” she said. “I think larger and more medically specific datasets are required to improve their outputs in this field.”
Sandip Pramanik, MBcHB, a GP in Watford, Hertfordshire, England, said the study “clearly showed ChatGPT’s struggle to deal with the complexity of the exam questions that is based on the primary care system. In essence, this in indicative of the human factors involved in decision-making in primary care.”
The applied knowledge test is designed to test the knowledge required to be a generalist in the primary care setting, and as such, there are lots of nuances reflecting this within the questions, Dr. Pramanik said.
“ChatGPT may look at these in a more black and white way, whereas the generalist needs to be reflective of the complexities involved and the different possibilities that can present rather than take a binary ‘yes’ or ‘no’ stance,” he said. “In fact, this highlights a lot about the nature of general practice in managing uncertainty, and this is reflected in the questions asked in the exam,” he remarked. He noted, “Being a generalist is about factoring in human emotion and human perception as well as knowledge.”
Ms. Mahmood, Dr. Thirunavukarasu, and Dr. Pramanik have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
GLASGOW –
ChatGPT also provided novel explanations – it frequently “hallucinates” – by describing inaccurate information as if they were facts, according to Shathar Mahmood, BA, a fifth-year medical student at the University of Cambridge, England, who presented the findings at the annual meeting of the Royal College of General Practitioners. The study was published in JMIR Medical Education earlier this year.
“Artificial intelligence has generated impressive results across medicine, and with the release of ChatGPT there is now discussion about these large language models taking over clinicians’ jobs,” Arun James Thirunavukarasu, MB BChir, of the University of Oxford, England, and Oxford University Hospitals NHS Foundation Trust, who is the lead author of the study, told this news organization.
Performance of AI on medical school examinations has prompted much of this discussion, often because performance does not reflect real-world clinical practice, he said. “We used the Applied Knowledge Test instead, and this allowed us to explore the potential and pitfalls of deploying large language models in primary care and to explore what further development of medical large language model applications is required.”
The researchers investigated the strengths and weaknesses of ChatGPT in primary care using the Membership of the Royal College of General Practitioners Applied Knowledge Test. The computer-based, multiple-choice assessment is part of the U.K.’s specialty training to become a general practitioner (GP). It tests knowledge behind general practice within the context of the United Kingdom’s National Health Service.
The researchers entered a series of 674 questions into ChatGPT on two occasions, or “runs.” “By putting the questions into two separate dialogues, we hoped to avoid the influence of one dialogue on the other,” Ms. Mahmood said. To validate that the answers were correct, the ChatGPT responses were compared with the answers provided by the GP self-test and past articles.
Docs 1, AI 0
Overall performance of the algorithm was good across both runs (59.94% and 60.39%); 83.23% of questions produced the same answer on both runs.
But 17% of the answers didn’t match, Ms. Mahmood reported, a statistically significant difference. “And the overall performance of ChatGPT was 10% lower than the average RCGP pass mark in the last few years, which informs one of our conclusions about it not being very precise at expert level recall and decision-making,” she said.
Also, a small percentage of questions (1.48% and 2.25% in each run) produced an uncertain answer or there was no answer.
Say what?
Novel explanations were generated upon running a question through ChatGPT that then provided an extended answer, Ms. Mahmood said. When the accuracy of the extended answers was checked against the correct answers, no correlation was found. “ChatGPT can hallucinate answers, and there’s no way a nonexpert reading this could know it is incorrect,” she said.
Regarding the application of ChatGPT and similar algorithms to clinical practice, Ms. Mahmood was clear. “As they stand, [AI systems] will not be able to replace the health care professional workforce, in primary care at least,” she said. “I think larger and more medically specific datasets are required to improve their outputs in this field.”
Sandip Pramanik, MBcHB, a GP in Watford, Hertfordshire, England, said the study “clearly showed ChatGPT’s struggle to deal with the complexity of the exam questions that is based on the primary care system. In essence, this in indicative of the human factors involved in decision-making in primary care.”
The applied knowledge test is designed to test the knowledge required to be a generalist in the primary care setting, and as such, there are lots of nuances reflecting this within the questions, Dr. Pramanik said.
“ChatGPT may look at these in a more black and white way, whereas the generalist needs to be reflective of the complexities involved and the different possibilities that can present rather than take a binary ‘yes’ or ‘no’ stance,” he said. “In fact, this highlights a lot about the nature of general practice in managing uncertainty, and this is reflected in the questions asked in the exam,” he remarked. He noted, “Being a generalist is about factoring in human emotion and human perception as well as knowledge.”
Ms. Mahmood, Dr. Thirunavukarasu, and Dr. Pramanik have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
GLASGOW –
ChatGPT also provided novel explanations – it frequently “hallucinates” – by describing inaccurate information as if they were facts, according to Shathar Mahmood, BA, a fifth-year medical student at the University of Cambridge, England, who presented the findings at the annual meeting of the Royal College of General Practitioners. The study was published in JMIR Medical Education earlier this year.
“Artificial intelligence has generated impressive results across medicine, and with the release of ChatGPT there is now discussion about these large language models taking over clinicians’ jobs,” Arun James Thirunavukarasu, MB BChir, of the University of Oxford, England, and Oxford University Hospitals NHS Foundation Trust, who is the lead author of the study, told this news organization.
Performance of AI on medical school examinations has prompted much of this discussion, often because performance does not reflect real-world clinical practice, he said. “We used the Applied Knowledge Test instead, and this allowed us to explore the potential and pitfalls of deploying large language models in primary care and to explore what further development of medical large language model applications is required.”
The researchers investigated the strengths and weaknesses of ChatGPT in primary care using the Membership of the Royal College of General Practitioners Applied Knowledge Test. The computer-based, multiple-choice assessment is part of the U.K.’s specialty training to become a general practitioner (GP). It tests knowledge behind general practice within the context of the United Kingdom’s National Health Service.
The researchers entered a series of 674 questions into ChatGPT on two occasions, or “runs.” “By putting the questions into two separate dialogues, we hoped to avoid the influence of one dialogue on the other,” Ms. Mahmood said. To validate that the answers were correct, the ChatGPT responses were compared with the answers provided by the GP self-test and past articles.
Docs 1, AI 0
Overall performance of the algorithm was good across both runs (59.94% and 60.39%); 83.23% of questions produced the same answer on both runs.
But 17% of the answers didn’t match, Ms. Mahmood reported, a statistically significant difference. “And the overall performance of ChatGPT was 10% lower than the average RCGP pass mark in the last few years, which informs one of our conclusions about it not being very precise at expert level recall and decision-making,” she said.
Also, a small percentage of questions (1.48% and 2.25% in each run) produced an uncertain answer or there was no answer.
Say what?
Novel explanations were generated upon running a question through ChatGPT that then provided an extended answer, Ms. Mahmood said. When the accuracy of the extended answers was checked against the correct answers, no correlation was found. “ChatGPT can hallucinate answers, and there’s no way a nonexpert reading this could know it is incorrect,” she said.
Regarding the application of ChatGPT and similar algorithms to clinical practice, Ms. Mahmood was clear. “As they stand, [AI systems] will not be able to replace the health care professional workforce, in primary care at least,” she said. “I think larger and more medically specific datasets are required to improve their outputs in this field.”
Sandip Pramanik, MBcHB, a GP in Watford, Hertfordshire, England, said the study “clearly showed ChatGPT’s struggle to deal with the complexity of the exam questions that is based on the primary care system. In essence, this in indicative of the human factors involved in decision-making in primary care.”
The applied knowledge test is designed to test the knowledge required to be a generalist in the primary care setting, and as such, there are lots of nuances reflecting this within the questions, Dr. Pramanik said.
“ChatGPT may look at these in a more black and white way, whereas the generalist needs to be reflective of the complexities involved and the different possibilities that can present rather than take a binary ‘yes’ or ‘no’ stance,” he said. “In fact, this highlights a lot about the nature of general practice in managing uncertainty, and this is reflected in the questions asked in the exam,” he remarked. He noted, “Being a generalist is about factoring in human emotion and human perception as well as knowledge.”
Ms. Mahmood, Dr. Thirunavukarasu, and Dr. Pramanik have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT RCGP 2023
FDA proposes ban on hair straightener ingredients
The
The proposal specifies that formaldehyde would be banned, as well as other chemicals that release formaldehyde, such as methylene glycol. Using hair smoothing products containing formaldehyde and formaldehyde-releasing chemicals “is linked to short-term adverse health effects, such as sensitization reactions and breathing problems, and long-term adverse health effects, including an increased risk of certain cancers,” the proposal states.
One study published last year showed that repeated use of hair straightening products, also called relaxers, could more than double the risk of uterine cancer. Although that study didn’t find that the uterine cancer risk varied based on a person’s race, the researchers noted that women who are Black are among the most likely to use the products and tend to start using them at younger ages, compared with people of other races and ethnicities.
Hair straightening products have also been linked to elevated risks of hormone-sensitive cancers, such as breast cancer and ovarian cancer.
Rep. Ayanna Pressley (D-Mass.) and Rep. Shontel Brown (D-Ohio) applauded the proposed rule in a statement issued jointly on Oct. 6. “The FDA’s proposal to ban these harmful chemicals in hair straighteners and relaxers is a win for public health – especially the health of Black women who are disproportionately put at risk by these products as a result of systemic racism and anti–Black hair sentiment,” Rep. Pressley said The two congresswomen wrote a letter to the FDA earlier this year requesting the topic be investigated.
“Regardless of how we wear our hair, we should be allowed to show up in the world without putting our health at risk. I applaud the FDA for being responsive to our calls and advancing a rule that will help prevent manufacturers from making a profit at the expense of our health,” Rep. Pressley said in the statement. “The administration should finalize this rule without delay.”
A version of this article appeared on WebMD.com
The
The proposal specifies that formaldehyde would be banned, as well as other chemicals that release formaldehyde, such as methylene glycol. Using hair smoothing products containing formaldehyde and formaldehyde-releasing chemicals “is linked to short-term adverse health effects, such as sensitization reactions and breathing problems, and long-term adverse health effects, including an increased risk of certain cancers,” the proposal states.
One study published last year showed that repeated use of hair straightening products, also called relaxers, could more than double the risk of uterine cancer. Although that study didn’t find that the uterine cancer risk varied based on a person’s race, the researchers noted that women who are Black are among the most likely to use the products and tend to start using them at younger ages, compared with people of other races and ethnicities.
Hair straightening products have also been linked to elevated risks of hormone-sensitive cancers, such as breast cancer and ovarian cancer.
Rep. Ayanna Pressley (D-Mass.) and Rep. Shontel Brown (D-Ohio) applauded the proposed rule in a statement issued jointly on Oct. 6. “The FDA’s proposal to ban these harmful chemicals in hair straighteners and relaxers is a win for public health – especially the health of Black women who are disproportionately put at risk by these products as a result of systemic racism and anti–Black hair sentiment,” Rep. Pressley said The two congresswomen wrote a letter to the FDA earlier this year requesting the topic be investigated.
“Regardless of how we wear our hair, we should be allowed to show up in the world without putting our health at risk. I applaud the FDA for being responsive to our calls and advancing a rule that will help prevent manufacturers from making a profit at the expense of our health,” Rep. Pressley said in the statement. “The administration should finalize this rule without delay.”
A version of this article appeared on WebMD.com
The
The proposal specifies that formaldehyde would be banned, as well as other chemicals that release formaldehyde, such as methylene glycol. Using hair smoothing products containing formaldehyde and formaldehyde-releasing chemicals “is linked to short-term adverse health effects, such as sensitization reactions and breathing problems, and long-term adverse health effects, including an increased risk of certain cancers,” the proposal states.
One study published last year showed that repeated use of hair straightening products, also called relaxers, could more than double the risk of uterine cancer. Although that study didn’t find that the uterine cancer risk varied based on a person’s race, the researchers noted that women who are Black are among the most likely to use the products and tend to start using them at younger ages, compared with people of other races and ethnicities.
Hair straightening products have also been linked to elevated risks of hormone-sensitive cancers, such as breast cancer and ovarian cancer.
Rep. Ayanna Pressley (D-Mass.) and Rep. Shontel Brown (D-Ohio) applauded the proposed rule in a statement issued jointly on Oct. 6. “The FDA’s proposal to ban these harmful chemicals in hair straighteners and relaxers is a win for public health – especially the health of Black women who are disproportionately put at risk by these products as a result of systemic racism and anti–Black hair sentiment,” Rep. Pressley said The two congresswomen wrote a letter to the FDA earlier this year requesting the topic be investigated.
“Regardless of how we wear our hair, we should be allowed to show up in the world without putting our health at risk. I applaud the FDA for being responsive to our calls and advancing a rule that will help prevent manufacturers from making a profit at the expense of our health,” Rep. Pressley said in the statement. “The administration should finalize this rule without delay.”
A version of this article appeared on WebMD.com
Why legal pot makes this physician sick
Last year, my husband and I took a 16-day road trip from Kentucky through Massachusetts to Maine. On our first morning in Boston, we exited the Park Street Station en route to Boston Common, but instead of being greeted by the aroma of molasses, we were hit full-on with a pungent, repulsive odor. “That’s skunk weed,” my husband chuckled as we stepped right into the middle of the Boston Freedom Rally, a celebration of all things cannabis.
As we boarded a hop-on-hop-off bus, we learned that this was the one week of the year that the city skips testing tour bus drivers for tetrahydrocannabinol (THC), “because we all test positive,” the driver quipped. As our open-air bus circled the Common, a crowd of pot enthusiasts displayed signs in support of relaxed regulation for public consumption.
The 34-year-old Boston Freedom Rally is a sign that U.S. culture has transformed forever. Mary Jane is no friend of emergency physicians nor of staff on hospital wards and offices.
Toking boomers and millennials
Researchers at the University of California, San Diego, looked at cannabis-related emergency department visits from all acute-care hospitals in the state from 2005 to 2019 and found an 1,808% increase in patients aged 65 or older (that is not a typo) who were there for complications from cannabis use.
The lead author said in an interview that, “older patients taking marijuana or related products may have dizziness and falls, heart palpitations, panic attacks, confusion, anxiety or worsening of underlying lung diseases, such as asthma or [chronic obstructive pulmonary disease].”
A recent study from Canada suggests that commercialization has been associated with an increase in related hospitalizations, including cannabis-induced psychosis.
According to a National Study of Drug Use and Health, marijuana use in young adults reached an all-time high (pun intended) in 2021. Nearly 10% of eighth graders and 20% of 10th graders reported using marijuana this past year.
The full downside of any drug, legal or illegal, is largely unknown until it infiltrates the mainstream market, but these are the typical cases we see:
Let’s start with the demotivated high school honors student who dropped out of college to work at the local cinema. He stumbled and broke his clavicle outside a bar at 2 AM, but he wasn’t sure if he passed out, so a cardiology consult was requested to “rule out” arrhythmia associated with syncope. He related that his plan to become a railway conductor had been upended because he knew he would be drug tested and just couldn’t give up pot. After a normal cardiac exam, ECG, labs, a Holter, and an echocardiogram were also requested and normal at a significant cost.
Cannabinoid hyperemesis syndrome
One of my Midwest colleagues related her encounter with two middle-aged pot users with ventricular tachycardia (VT). These episodes coincided with potassium levels less than 3.0 mEq/L in the setting of repetitive vomiting. The QTc interval didn’t normalize despite a corrected potassium level in one patient. They were both informed that they should never smoke pot because vomiting would predictably drop their K+ levels again and prolong their QTc intervals. Then began “the circular argument,” as my friend described it. The patient claims, “I smoke pot to relieve my nausea,” to which she explains that “in many folks, pot use induces nausea.” Of course, the classic reply is, “Not me.” Predictably one of these stoners soon returned with more VT, more puking, and more hypokalemia. “Consider yourself ‘allergic’ to pot smoke,” my friend advised, but “was met with no meaningful hint of understanding or hope for transformative change,” she told me.
I’ve seen cannabinoid hyperemesis syndrome several times in the past few years. It occurs in daily to weekly pot users. Very rarely, it can cause cerebral edema, but it is also associated with seizures and dehydration that can lead to hypovolemic shock and kidney failure.
Heart and brain harm
Then there are the young patients who for various reasons have developed heart failure. Unfortunately, some are repetitively tox screen positive with varying trifectas of methamphetamine (meth), cocaine, and THC; opiates, meth, and THC; alcohol, meth, and THC; or heroin, meth, and THC. THC, the ever present and essential third leg of the stool of stupor. These unfortunate patients often need heart failure medications that they can’t afford or won’t take because illicit drug use is expensive and dulls their ability to prioritize their health. Some desperately need a heart transplant, but the necessary negative drug screen is a pipe dream.
And it’s not just the heart that is affected. There are data linking cannabis use to a higher risk for both ischemic and hemorrhagic stroke. A retrospective study published in Stroke, of more than 1,000 people diagnosed with an aneurysmal subarachnoid hemorrhage, found that more than half of the 46 who tested positive for THC at admission developed delayed cerebral ischemia (DCI), which increases the risk for disability or early death. This was after adjusting for several patient characteristics as well as recent exposure to other illicit substances; cocaine, meth, and tobacco use were not associated with DCI.
Natural my ...
I’m certain my anti-cannabis stance will strike a nerve with those who love their recreational THC and push for its legal sale; after all, “It’s perfectly natural.” But I counter with the fact that tornadoes, earthquakes, cyanide, and appendicitis are all natural but certainly not optimal. And what we are seeing in the vascular specialties is completely unnatural. We are treating a different mix of complications than before pot was readily accessible across several states.
Our most effective action is to educate our patients. We should encourage those who don’t currently smoke cannabis to never start and those who do to quit. People who require marijuana for improved quality of life for terminal care or true (not supposed) disorders that mainstream medicine fails should be approached with empathy and caution.
A good rule of thumb is to never breathe anything you can see. Never put anything in your body that comes off the street: Drug dealers who sell cannabis cut with fentanyl will be ecstatic to take someone’s money then merely keep scrolling when their obituary comes up.
Let’s try to reverse the rise of vascular complications, orthopedic injuries, and vomiting across America. We can start by encouraging our patients to avoid “skunk weed” and get back to the sweet smells of nature in our cities and parks.
Some details have been changed to protect the patients’ identities, but the essence of their diagnoses has been preserved.
Dr. Walton-Shirley is a retired clinical cardiologist from Nashville, Tenn. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Last year, my husband and I took a 16-day road trip from Kentucky through Massachusetts to Maine. On our first morning in Boston, we exited the Park Street Station en route to Boston Common, but instead of being greeted by the aroma of molasses, we were hit full-on with a pungent, repulsive odor. “That’s skunk weed,” my husband chuckled as we stepped right into the middle of the Boston Freedom Rally, a celebration of all things cannabis.
As we boarded a hop-on-hop-off bus, we learned that this was the one week of the year that the city skips testing tour bus drivers for tetrahydrocannabinol (THC), “because we all test positive,” the driver quipped. As our open-air bus circled the Common, a crowd of pot enthusiasts displayed signs in support of relaxed regulation for public consumption.
The 34-year-old Boston Freedom Rally is a sign that U.S. culture has transformed forever. Mary Jane is no friend of emergency physicians nor of staff on hospital wards and offices.
Toking boomers and millennials
Researchers at the University of California, San Diego, looked at cannabis-related emergency department visits from all acute-care hospitals in the state from 2005 to 2019 and found an 1,808% increase in patients aged 65 or older (that is not a typo) who were there for complications from cannabis use.
The lead author said in an interview that, “older patients taking marijuana or related products may have dizziness and falls, heart palpitations, panic attacks, confusion, anxiety or worsening of underlying lung diseases, such as asthma or [chronic obstructive pulmonary disease].”
A recent study from Canada suggests that commercialization has been associated with an increase in related hospitalizations, including cannabis-induced psychosis.
According to a National Study of Drug Use and Health, marijuana use in young adults reached an all-time high (pun intended) in 2021. Nearly 10% of eighth graders and 20% of 10th graders reported using marijuana this past year.
The full downside of any drug, legal or illegal, is largely unknown until it infiltrates the mainstream market, but these are the typical cases we see:
Let’s start with the demotivated high school honors student who dropped out of college to work at the local cinema. He stumbled and broke his clavicle outside a bar at 2 AM, but he wasn’t sure if he passed out, so a cardiology consult was requested to “rule out” arrhythmia associated with syncope. He related that his plan to become a railway conductor had been upended because he knew he would be drug tested and just couldn’t give up pot. After a normal cardiac exam, ECG, labs, a Holter, and an echocardiogram were also requested and normal at a significant cost.
Cannabinoid hyperemesis syndrome
One of my Midwest colleagues related her encounter with two middle-aged pot users with ventricular tachycardia (VT). These episodes coincided with potassium levels less than 3.0 mEq/L in the setting of repetitive vomiting. The QTc interval didn’t normalize despite a corrected potassium level in one patient. They were both informed that they should never smoke pot because vomiting would predictably drop their K+ levels again and prolong their QTc intervals. Then began “the circular argument,” as my friend described it. The patient claims, “I smoke pot to relieve my nausea,” to which she explains that “in many folks, pot use induces nausea.” Of course, the classic reply is, “Not me.” Predictably one of these stoners soon returned with more VT, more puking, and more hypokalemia. “Consider yourself ‘allergic’ to pot smoke,” my friend advised, but “was met with no meaningful hint of understanding or hope for transformative change,” she told me.
I’ve seen cannabinoid hyperemesis syndrome several times in the past few years. It occurs in daily to weekly pot users. Very rarely, it can cause cerebral edema, but it is also associated with seizures and dehydration that can lead to hypovolemic shock and kidney failure.
Heart and brain harm
Then there are the young patients who for various reasons have developed heart failure. Unfortunately, some are repetitively tox screen positive with varying trifectas of methamphetamine (meth), cocaine, and THC; opiates, meth, and THC; alcohol, meth, and THC; or heroin, meth, and THC. THC, the ever present and essential third leg of the stool of stupor. These unfortunate patients often need heart failure medications that they can’t afford or won’t take because illicit drug use is expensive and dulls their ability to prioritize their health. Some desperately need a heart transplant, but the necessary negative drug screen is a pipe dream.
And it’s not just the heart that is affected. There are data linking cannabis use to a higher risk for both ischemic and hemorrhagic stroke. A retrospective study published in Stroke, of more than 1,000 people diagnosed with an aneurysmal subarachnoid hemorrhage, found that more than half of the 46 who tested positive for THC at admission developed delayed cerebral ischemia (DCI), which increases the risk for disability or early death. This was after adjusting for several patient characteristics as well as recent exposure to other illicit substances; cocaine, meth, and tobacco use were not associated with DCI.
Natural my ...
I’m certain my anti-cannabis stance will strike a nerve with those who love their recreational THC and push for its legal sale; after all, “It’s perfectly natural.” But I counter with the fact that tornadoes, earthquakes, cyanide, and appendicitis are all natural but certainly not optimal. And what we are seeing in the vascular specialties is completely unnatural. We are treating a different mix of complications than before pot was readily accessible across several states.
Our most effective action is to educate our patients. We should encourage those who don’t currently smoke cannabis to never start and those who do to quit. People who require marijuana for improved quality of life for terminal care or true (not supposed) disorders that mainstream medicine fails should be approached with empathy and caution.
A good rule of thumb is to never breathe anything you can see. Never put anything in your body that comes off the street: Drug dealers who sell cannabis cut with fentanyl will be ecstatic to take someone’s money then merely keep scrolling when their obituary comes up.
Let’s try to reverse the rise of vascular complications, orthopedic injuries, and vomiting across America. We can start by encouraging our patients to avoid “skunk weed” and get back to the sweet smells of nature in our cities and parks.
Some details have been changed to protect the patients’ identities, but the essence of their diagnoses has been preserved.
Dr. Walton-Shirley is a retired clinical cardiologist from Nashville, Tenn. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Last year, my husband and I took a 16-day road trip from Kentucky through Massachusetts to Maine. On our first morning in Boston, we exited the Park Street Station en route to Boston Common, but instead of being greeted by the aroma of molasses, we were hit full-on with a pungent, repulsive odor. “That’s skunk weed,” my husband chuckled as we stepped right into the middle of the Boston Freedom Rally, a celebration of all things cannabis.
As we boarded a hop-on-hop-off bus, we learned that this was the one week of the year that the city skips testing tour bus drivers for tetrahydrocannabinol (THC), “because we all test positive,” the driver quipped. As our open-air bus circled the Common, a crowd of pot enthusiasts displayed signs in support of relaxed regulation for public consumption.
The 34-year-old Boston Freedom Rally is a sign that U.S. culture has transformed forever. Mary Jane is no friend of emergency physicians nor of staff on hospital wards and offices.
Toking boomers and millennials
Researchers at the University of California, San Diego, looked at cannabis-related emergency department visits from all acute-care hospitals in the state from 2005 to 2019 and found an 1,808% increase in patients aged 65 or older (that is not a typo) who were there for complications from cannabis use.
The lead author said in an interview that, “older patients taking marijuana or related products may have dizziness and falls, heart palpitations, panic attacks, confusion, anxiety or worsening of underlying lung diseases, such as asthma or [chronic obstructive pulmonary disease].”
A recent study from Canada suggests that commercialization has been associated with an increase in related hospitalizations, including cannabis-induced psychosis.
According to a National Study of Drug Use and Health, marijuana use in young adults reached an all-time high (pun intended) in 2021. Nearly 10% of eighth graders and 20% of 10th graders reported using marijuana this past year.
The full downside of any drug, legal or illegal, is largely unknown until it infiltrates the mainstream market, but these are the typical cases we see:
Let’s start with the demotivated high school honors student who dropped out of college to work at the local cinema. He stumbled and broke his clavicle outside a bar at 2 AM, but he wasn’t sure if he passed out, so a cardiology consult was requested to “rule out” arrhythmia associated with syncope. He related that his plan to become a railway conductor had been upended because he knew he would be drug tested and just couldn’t give up pot. After a normal cardiac exam, ECG, labs, a Holter, and an echocardiogram were also requested and normal at a significant cost.
Cannabinoid hyperemesis syndrome
One of my Midwest colleagues related her encounter with two middle-aged pot users with ventricular tachycardia (VT). These episodes coincided with potassium levels less than 3.0 mEq/L in the setting of repetitive vomiting. The QTc interval didn’t normalize despite a corrected potassium level in one patient. They were both informed that they should never smoke pot because vomiting would predictably drop their K+ levels again and prolong their QTc intervals. Then began “the circular argument,” as my friend described it. The patient claims, “I smoke pot to relieve my nausea,” to which she explains that “in many folks, pot use induces nausea.” Of course, the classic reply is, “Not me.” Predictably one of these stoners soon returned with more VT, more puking, and more hypokalemia. “Consider yourself ‘allergic’ to pot smoke,” my friend advised, but “was met with no meaningful hint of understanding or hope for transformative change,” she told me.
I’ve seen cannabinoid hyperemesis syndrome several times in the past few years. It occurs in daily to weekly pot users. Very rarely, it can cause cerebral edema, but it is also associated with seizures and dehydration that can lead to hypovolemic shock and kidney failure.
Heart and brain harm
Then there are the young patients who for various reasons have developed heart failure. Unfortunately, some are repetitively tox screen positive with varying trifectas of methamphetamine (meth), cocaine, and THC; opiates, meth, and THC; alcohol, meth, and THC; or heroin, meth, and THC. THC, the ever present and essential third leg of the stool of stupor. These unfortunate patients often need heart failure medications that they can’t afford or won’t take because illicit drug use is expensive and dulls their ability to prioritize their health. Some desperately need a heart transplant, but the necessary negative drug screen is a pipe dream.
And it’s not just the heart that is affected. There are data linking cannabis use to a higher risk for both ischemic and hemorrhagic stroke. A retrospective study published in Stroke, of more than 1,000 people diagnosed with an aneurysmal subarachnoid hemorrhage, found that more than half of the 46 who tested positive for THC at admission developed delayed cerebral ischemia (DCI), which increases the risk for disability or early death. This was after adjusting for several patient characteristics as well as recent exposure to other illicit substances; cocaine, meth, and tobacco use were not associated with DCI.
Natural my ...
I’m certain my anti-cannabis stance will strike a nerve with those who love their recreational THC and push for its legal sale; after all, “It’s perfectly natural.” But I counter with the fact that tornadoes, earthquakes, cyanide, and appendicitis are all natural but certainly not optimal. And what we are seeing in the vascular specialties is completely unnatural. We are treating a different mix of complications than before pot was readily accessible across several states.
Our most effective action is to educate our patients. We should encourage those who don’t currently smoke cannabis to never start and those who do to quit. People who require marijuana for improved quality of life for terminal care or true (not supposed) disorders that mainstream medicine fails should be approached with empathy and caution.
A good rule of thumb is to never breathe anything you can see. Never put anything in your body that comes off the street: Drug dealers who sell cannabis cut with fentanyl will be ecstatic to take someone’s money then merely keep scrolling when their obituary comes up.
Let’s try to reverse the rise of vascular complications, orthopedic injuries, and vomiting across America. We can start by encouraging our patients to avoid “skunk weed” and get back to the sweet smells of nature in our cities and parks.
Some details have been changed to protect the patients’ identities, but the essence of their diagnoses has been preserved.
Dr. Walton-Shirley is a retired clinical cardiologist from Nashville, Tenn. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Artificial intelligence in the office: Part 2
In the year since generative artificial intelligence (AI) software first began to emerge for use, the staggering pace and breadth of development has condensed years of growth and change into months and weeks. Among the settings where these tools may find the greatest straight-line relevance is private medical practice.
. A multitude of generative AI products with potential medical applications are now available, with new ones appearing almost weekly. (As always, I have no financial interest in any product or service mentioned in this column.)

Last month, I discussed ChatGPT, the best-known AI algorithm, and some of its applications in clinical practice, such as generating website, video, and blog content. ChatGPT can also provide rapid and concise answers to general medical questions, like a search engine – but with more natural language processing and contextual understanding. Additionally, the algorithm can draft generic medical documents, including templates for after-visit summaries, postprocedure instructions, referrals, prior authorization appeal letters, and educational handouts.
Another useful feature of ChatGPT is its ability to provide accurate and conversational language translations, thus serving as an interpreter during clinic visits in situations where a human translator is not available. It also has potential uses in clinical research by finding resources, formulating hypotheses, drafting study protocols, and collecting large amounts of data in short periods of time. Other possibilities include survey administration, clinical trial recruitment, and automatic medication monitoring.
GPT-4, the latest version of ChatGPT, is reported to have greater problem-solving abilities and an even broader knowledge base. Among its claimed skills are the ability to find the latest literature in a given area, write a discharge summary for a patient following an uncomplicated surgery, and an image analysis feature to identify objects in photos. GPT-4 has been praised as having “the potential to help drive medical innovation, from aiding with patient discharge notes, summarizing recent clinical trials, providing information on ethical guidelines, and much more.”
Bard, an AI “chat bot” introduced by Google earlier this year, intends to leverage Google’s enormous database to compete with ChatGPT in providing answers to medical questions. Bard also hopes to play a pivotal role in expanding telemedicine and remote care via Google’s secure connections and access to patient records and medical history, and “facilitate seamless communication through appointment scheduling, messaging, and sharing medical images,” according to PackT, a website for IT professionals. The company claims that Bard’s integration of AI and machine learning capabilities will serve to elevate health care efficiency and patient outcomes, PackT says, and “the platform’s AI system quickly and accurately analyzes patient records, identifies patterns and trends, and aids medical professionals in developing effective treatment plans.”
Doximity has introduced an AI engine called DocsGPT, an encrypted, HIPAA-compliant writing assistant that, the company says, can draft any form of professional correspondence, including prior authorization letters, insurance appeals, patient support letters, and patient education materials. The service is available at no charge to all U.S. physicians and medical students through their Doximity accounts.
Microsoft has introduced several AI products. BioGPT is a language model specifically designed for health care. Compared with GPT models that are trained on more general text data, BioGPT is purported to have a deeper understanding of the language used in biomedical research and can generate more accurate and relevant outputs for biomedical tasks, such as drug discovery, disease classification, and clinical decision support. Fabric is another health care–specific data and analytics platform the company described in an announcement in May. It can combine data from sources such as electronic health records, images, lab systems, medical devices, and claims systems so hospitals and offices can standardize it and access it in the same place. Microsoft said the new tools will help eliminate the “time-consuming” process of searching through these sources one by one. Microsoft will also offer a new generative AI chatbot called the Azure Health Bot, which can pull information from a health organization’s own internal data as well as reputable external sources such as the Food and Drug Administration and the National Institutes of Health.
Several other AI products are available for clinicians. Tana served as an administrative aid and a clinical helper during the height of the COVID-19 pandemic, answering frequently asked questions, facilitating appointment management, and gathering preliminary medical information prior to teleconsultations. Dougall GPT is another AI chatbot tailored for health care professionals. It provides clinicians with AI-tuned answers to their queries, augmented by links to relevant, up-to-date, authoritative resources. It also assists in drafting patient instructions, consultation summaries, speeches, and professional correspondence. Wang has created Clinical Camel, an open-source health care–focused chatbot that assembles medical data with a combination of user-shared conversations and synthetic conversations derived from curated clinical articles. The Chinese company Baidu has rolled out Ernie as a potential rival to ChatGPT. You get the idea.
Of course, the inherent drawbacks of AI, such as producing false or biased information, perpetuating harmful stereotypes, and presenting information that has since been proven inaccurate or out-of-date, must always be kept in mind. All AI algorithms have been criticized for giving wrong answers, as their datasets are generally culled from information published in 2021 or earlier. Several of them have been shown to fabricate information – a phenomenon labeled “artificial hallucinations” in one article. “The scientific community must be vigilant in verifying the accuracy and reliability of the information provided by AI tools,” wrote the authors of that paper. “Researchers should use AI as an aid rather than a replacement for critical thinking and fact-checking.”
In the year since generative artificial intelligence (AI) software first began to emerge for use, the staggering pace and breadth of development has condensed years of growth and change into months and weeks. Among the settings where these tools may find the greatest straight-line relevance is private medical practice.
. A multitude of generative AI products with potential medical applications are now available, with new ones appearing almost weekly. (As always, I have no financial interest in any product or service mentioned in this column.)
Last month, I discussed ChatGPT, the best-known AI algorithm, and some of its applications in clinical practice, such as generating website, video, and blog content. ChatGPT can also provide rapid and concise answers to general medical questions, like a search engine – but with more natural language processing and contextual understanding. Additionally, the algorithm can draft generic medical documents, including templates for after-visit summaries, postprocedure instructions, referrals, prior authorization appeal letters, and educational handouts.
Another useful feature of ChatGPT is its ability to provide accurate and conversational language translations, thus serving as an interpreter during clinic visits in situations where a human translator is not available. It also has potential uses in clinical research by finding resources, formulating hypotheses, drafting study protocols, and collecting large amounts of data in short periods of time. Other possibilities include survey administration, clinical trial recruitment, and automatic medication monitoring.
GPT-4, the latest version of ChatGPT, is reported to have greater problem-solving abilities and an even broader knowledge base. Among its claimed skills are the ability to find the latest literature in a given area, write a discharge summary for a patient following an uncomplicated surgery, and an image analysis feature to identify objects in photos. GPT-4 has been praised as having “the potential to help drive medical innovation, from aiding with patient discharge notes, summarizing recent clinical trials, providing information on ethical guidelines, and much more.”
Bard, an AI “chat bot” introduced by Google earlier this year, intends to leverage Google’s enormous database to compete with ChatGPT in providing answers to medical questions. Bard also hopes to play a pivotal role in expanding telemedicine and remote care via Google’s secure connections and access to patient records and medical history, and “facilitate seamless communication through appointment scheduling, messaging, and sharing medical images,” according to PackT, a website for IT professionals. The company claims that Bard’s integration of AI and machine learning capabilities will serve to elevate health care efficiency and patient outcomes, PackT says, and “the platform’s AI system quickly and accurately analyzes patient records, identifies patterns and trends, and aids medical professionals in developing effective treatment plans.”
Doximity has introduced an AI engine called DocsGPT, an encrypted, HIPAA-compliant writing assistant that, the company says, can draft any form of professional correspondence, including prior authorization letters, insurance appeals, patient support letters, and patient education materials. The service is available at no charge to all U.S. physicians and medical students through their Doximity accounts.
Microsoft has introduced several AI products. BioGPT is a language model specifically designed for health care. Compared with GPT models that are trained on more general text data, BioGPT is purported to have a deeper understanding of the language used in biomedical research and can generate more accurate and relevant outputs for biomedical tasks, such as drug discovery, disease classification, and clinical decision support. Fabric is another health care–specific data and analytics platform the company described in an announcement in May. It can combine data from sources such as electronic health records, images, lab systems, medical devices, and claims systems so hospitals and offices can standardize it and access it in the same place. Microsoft said the new tools will help eliminate the “time-consuming” process of searching through these sources one by one. Microsoft will also offer a new generative AI chatbot called the Azure Health Bot, which can pull information from a health organization’s own internal data as well as reputable external sources such as the Food and Drug Administration and the National Institutes of Health.
Several other AI products are available for clinicians. Tana served as an administrative aid and a clinical helper during the height of the COVID-19 pandemic, answering frequently asked questions, facilitating appointment management, and gathering preliminary medical information prior to teleconsultations. Dougall GPT is another AI chatbot tailored for health care professionals. It provides clinicians with AI-tuned answers to their queries, augmented by links to relevant, up-to-date, authoritative resources. It also assists in drafting patient instructions, consultation summaries, speeches, and professional correspondence. Wang has created Clinical Camel, an open-source health care–focused chatbot that assembles medical data with a combination of user-shared conversations and synthetic conversations derived from curated clinical articles. The Chinese company Baidu has rolled out Ernie as a potential rival to ChatGPT. You get the idea.
Of course, the inherent drawbacks of AI, such as producing false or biased information, perpetuating harmful stereotypes, and presenting information that has since been proven inaccurate or out-of-date, must always be kept in mind. All AI algorithms have been criticized for giving wrong answers, as their datasets are generally culled from information published in 2021 or earlier. Several of them have been shown to fabricate information – a phenomenon labeled “artificial hallucinations” in one article. “The scientific community must be vigilant in verifying the accuracy and reliability of the information provided by AI tools,” wrote the authors of that paper. “Researchers should use AI as an aid rather than a replacement for critical thinking and fact-checking.”
In the year since generative artificial intelligence (AI) software first began to emerge for use, the staggering pace and breadth of development has condensed years of growth and change into months and weeks. Among the settings where these tools may find the greatest straight-line relevance is private medical practice.
. A multitude of generative AI products with potential medical applications are now available, with new ones appearing almost weekly. (As always, I have no financial interest in any product or service mentioned in this column.)
Last month, I discussed ChatGPT, the best-known AI algorithm, and some of its applications in clinical practice, such as generating website, video, and blog content. ChatGPT can also provide rapid and concise answers to general medical questions, like a search engine – but with more natural language processing and contextual understanding. Additionally, the algorithm can draft generic medical documents, including templates for after-visit summaries, postprocedure instructions, referrals, prior authorization appeal letters, and educational handouts.
Another useful feature of ChatGPT is its ability to provide accurate and conversational language translations, thus serving as an interpreter during clinic visits in situations where a human translator is not available. It also has potential uses in clinical research by finding resources, formulating hypotheses, drafting study protocols, and collecting large amounts of data in short periods of time. Other possibilities include survey administration, clinical trial recruitment, and automatic medication monitoring.
GPT-4, the latest version of ChatGPT, is reported to have greater problem-solving abilities and an even broader knowledge base. Among its claimed skills are the ability to find the latest literature in a given area, write a discharge summary for a patient following an uncomplicated surgery, and an image analysis feature to identify objects in photos. GPT-4 has been praised as having “the potential to help drive medical innovation, from aiding with patient discharge notes, summarizing recent clinical trials, providing information on ethical guidelines, and much more.”
Bard, an AI “chat bot” introduced by Google earlier this year, intends to leverage Google’s enormous database to compete with ChatGPT in providing answers to medical questions. Bard also hopes to play a pivotal role in expanding telemedicine and remote care via Google’s secure connections and access to patient records and medical history, and “facilitate seamless communication through appointment scheduling, messaging, and sharing medical images,” according to PackT, a website for IT professionals. The company claims that Bard’s integration of AI and machine learning capabilities will serve to elevate health care efficiency and patient outcomes, PackT says, and “the platform’s AI system quickly and accurately analyzes patient records, identifies patterns and trends, and aids medical professionals in developing effective treatment plans.”
Doximity has introduced an AI engine called DocsGPT, an encrypted, HIPAA-compliant writing assistant that, the company says, can draft any form of professional correspondence, including prior authorization letters, insurance appeals, patient support letters, and patient education materials. The service is available at no charge to all U.S. physicians and medical students through their Doximity accounts.
Microsoft has introduced several AI products. BioGPT is a language model specifically designed for health care. Compared with GPT models that are trained on more general text data, BioGPT is purported to have a deeper understanding of the language used in biomedical research and can generate more accurate and relevant outputs for biomedical tasks, such as drug discovery, disease classification, and clinical decision support. Fabric is another health care–specific data and analytics platform the company described in an announcement in May. It can combine data from sources such as electronic health records, images, lab systems, medical devices, and claims systems so hospitals and offices can standardize it and access it in the same place. Microsoft said the new tools will help eliminate the “time-consuming” process of searching through these sources one by one. Microsoft will also offer a new generative AI chatbot called the Azure Health Bot, which can pull information from a health organization’s own internal data as well as reputable external sources such as the Food and Drug Administration and the National Institutes of Health.
Several other AI products are available for clinicians. Tana served as an administrative aid and a clinical helper during the height of the COVID-19 pandemic, answering frequently asked questions, facilitating appointment management, and gathering preliminary medical information prior to teleconsultations. Dougall GPT is another AI chatbot tailored for health care professionals. It provides clinicians with AI-tuned answers to their queries, augmented by links to relevant, up-to-date, authoritative resources. It also assists in drafting patient instructions, consultation summaries, speeches, and professional correspondence. Wang has created Clinical Camel, an open-source health care–focused chatbot that assembles medical data with a combination of user-shared conversations and synthetic conversations derived from curated clinical articles. The Chinese company Baidu has rolled out Ernie as a potential rival to ChatGPT. You get the idea.
Of course, the inherent drawbacks of AI, such as producing false or biased information, perpetuating harmful stereotypes, and presenting information that has since been proven inaccurate or out-of-date, must always be kept in mind. All AI algorithms have been criticized for giving wrong answers, as their datasets are generally culled from information published in 2021 or earlier. Several of them have been shown to fabricate information – a phenomenon labeled “artificial hallucinations” in one article. “The scientific community must be vigilant in verifying the accuracy and reliability of the information provided by AI tools,” wrote the authors of that paper. “Researchers should use AI as an aid rather than a replacement for critical thinking and fact-checking.”

AI chatbot ‘hallucinates’ faulty medical intelligence
Artificial intelligence (AI) models are typically a year out of date and have this “charming problem of hallucinating made-up data and saying it with all the certainty of an attending on rounds,” Isaac Kohane, MD, PhD, Harvard Medical School, Boston, told a packed audience at plenary at an annual scientific meeting on infectious diseases.
Dr. Kohane, chair of the department of biomedical informatics, says the future intersection between AI and health care is “muddy.”
Echoing questions about the accuracy of new AI tools, researchers at the meeting presented the results of their new test of ChatGPT.
To test the accuracy of ChatGPT’s version 3.5, the researchers asked it if there are any boxed warnings on the U.S. Food and Drug Administration’s label for common antibiotics, and if so, what they are.
ChatGPT provided correct answers about FDA boxed warnings for only 12 of the 41 antibiotics queried – a matching rate of just 29%.
For the other 29 antibiotics, ChatGPT either “incorrectly reported that there was an FDA boxed warning when there was not, or inaccurately or incorrectly reported the boxed warning,” Rebecca Linfield, MD, infectious diseases fellow, Stanford (Calif.) University, said in an interview.
Uncritical AI use risky
Nine of the 41 antibiotics included in the query have boxed warnings. And ChatGPT correctly identified all nine, but only three were the matching adverse event (33%). For the 32 antibiotics without an FDA boxed warning, ChatGPT correctly reported that 28% (9 of 32) do not have a boxed warning.
For example, ChatGPT stated that the antibiotic fidaxomicin has a boxed warning for increased risk for Clostridioides difficile, “but it is the first-line antibiotic used to treat C. difficile,” Dr. Linfield pointed out.
ChatGPT also reported that cefepime increased the risk for death in those with pneumonia and fabricated a study supporting that assertion. “However, cefepime is a first-line drug for those with hospital-acquired pneumonia,” Dr. Linfield explained.
“I can imagine a worried family member finding this through ChatGPT, and needing to have extensive reassurances from the patient’s physicians about why this antibiotic was chosen,” she said.
ChatGPT also incorrectly stated that aztreonam has a boxed warning for increased mortality.
“The risk is that both physicians and the public uncritically use ChatGPT as an easily accessible, readable source of clinically validated information, when these large language models are meant to generate fluid text, and not necessarily accurate information,” Dr. Linfield told this news organization.
Dr. Linfield said that the next step is to compare the ChatGPT 3.5 used in this analysis with ChatGPT 4, as well as with Google’s Med-PaLM 2 after it is released to the public.
Advancing fast
At plenary, Dr. Kohane pointed out that AI is a quick learner and improvements in tools are coming fast.
As an example, just 3 years ago, the best AI tool could score about as well as the worst student taking the medical boards, he told the audience. “Three years later, the leading large language models are scoring better than 90% of all the candidates. What’s it going to be doing next year?” he asked.
“I don’t know,” Dr. Kohane said, “but it will be better than this year.” AI will “transform health care.”
A version of this article first appeared on Medscape.com.
Artificial intelligence (AI) models are typically a year out of date and have this “charming problem of hallucinating made-up data and saying it with all the certainty of an attending on rounds,” Isaac Kohane, MD, PhD, Harvard Medical School, Boston, told a packed audience at plenary at an annual scientific meeting on infectious diseases.
Dr. Kohane, chair of the department of biomedical informatics, says the future intersection between AI and health care is “muddy.”
Echoing questions about the accuracy of new AI tools, researchers at the meeting presented the results of their new test of ChatGPT.
To test the accuracy of ChatGPT’s version 3.5, the researchers asked it if there are any boxed warnings on the U.S. Food and Drug Administration’s label for common antibiotics, and if so, what they are.
ChatGPT provided correct answers about FDA boxed warnings for only 12 of the 41 antibiotics queried – a matching rate of just 29%.
For the other 29 antibiotics, ChatGPT either “incorrectly reported that there was an FDA boxed warning when there was not, or inaccurately or incorrectly reported the boxed warning,” Rebecca Linfield, MD, infectious diseases fellow, Stanford (Calif.) University, said in an interview.
Uncritical AI use risky
Nine of the 41 antibiotics included in the query have boxed warnings. And ChatGPT correctly identified all nine, but only three were the matching adverse event (33%). For the 32 antibiotics without an FDA boxed warning, ChatGPT correctly reported that 28% (9 of 32) do not have a boxed warning.
For example, ChatGPT stated that the antibiotic fidaxomicin has a boxed warning for increased risk for Clostridioides difficile, “but it is the first-line antibiotic used to treat C. difficile,” Dr. Linfield pointed out.
ChatGPT also reported that cefepime increased the risk for death in those with pneumonia and fabricated a study supporting that assertion. “However, cefepime is a first-line drug for those with hospital-acquired pneumonia,” Dr. Linfield explained.
“I can imagine a worried family member finding this through ChatGPT, and needing to have extensive reassurances from the patient’s physicians about why this antibiotic was chosen,” she said.
ChatGPT also incorrectly stated that aztreonam has a boxed warning for increased mortality.
“The risk is that both physicians and the public uncritically use ChatGPT as an easily accessible, readable source of clinically validated information, when these large language models are meant to generate fluid text, and not necessarily accurate information,” Dr. Linfield told this news organization.
Dr. Linfield said that the next step is to compare the ChatGPT 3.5 used in this analysis with ChatGPT 4, as well as with Google’s Med-PaLM 2 after it is released to the public.
Advancing fast
At plenary, Dr. Kohane pointed out that AI is a quick learner and improvements in tools are coming fast.
As an example, just 3 years ago, the best AI tool could score about as well as the worst student taking the medical boards, he told the audience. “Three years later, the leading large language models are scoring better than 90% of all the candidates. What’s it going to be doing next year?” he asked.
“I don’t know,” Dr. Kohane said, “but it will be better than this year.” AI will “transform health care.”
A version of this article first appeared on Medscape.com.
Artificial intelligence (AI) models are typically a year out of date and have this “charming problem of hallucinating made-up data and saying it with all the certainty of an attending on rounds,” Isaac Kohane, MD, PhD, Harvard Medical School, Boston, told a packed audience at plenary at an annual scientific meeting on infectious diseases.
Dr. Kohane, chair of the department of biomedical informatics, says the future intersection between AI and health care is “muddy.”
Echoing questions about the accuracy of new AI tools, researchers at the meeting presented the results of their new test of ChatGPT.
To test the accuracy of ChatGPT’s version 3.5, the researchers asked it if there are any boxed warnings on the U.S. Food and Drug Administration’s label for common antibiotics, and if so, what they are.
ChatGPT provided correct answers about FDA boxed warnings for only 12 of the 41 antibiotics queried – a matching rate of just 29%.
For the other 29 antibiotics, ChatGPT either “incorrectly reported that there was an FDA boxed warning when there was not, or inaccurately or incorrectly reported the boxed warning,” Rebecca Linfield, MD, infectious diseases fellow, Stanford (Calif.) University, said in an interview.
Uncritical AI use risky
Nine of the 41 antibiotics included in the query have boxed warnings. And ChatGPT correctly identified all nine, but only three were the matching adverse event (33%). For the 32 antibiotics without an FDA boxed warning, ChatGPT correctly reported that 28% (9 of 32) do not have a boxed warning.
For example, ChatGPT stated that the antibiotic fidaxomicin has a boxed warning for increased risk for Clostridioides difficile, “but it is the first-line antibiotic used to treat C. difficile,” Dr. Linfield pointed out.
ChatGPT also reported that cefepime increased the risk for death in those with pneumonia and fabricated a study supporting that assertion. “However, cefepime is a first-line drug for those with hospital-acquired pneumonia,” Dr. Linfield explained.
“I can imagine a worried family member finding this through ChatGPT, and needing to have extensive reassurances from the patient’s physicians about why this antibiotic was chosen,” she said.
ChatGPT also incorrectly stated that aztreonam has a boxed warning for increased mortality.
“The risk is that both physicians and the public uncritically use ChatGPT as an easily accessible, readable source of clinically validated information, when these large language models are meant to generate fluid text, and not necessarily accurate information,” Dr. Linfield told this news organization.
Dr. Linfield said that the next step is to compare the ChatGPT 3.5 used in this analysis with ChatGPT 4, as well as with Google’s Med-PaLM 2 after it is released to the public.
Advancing fast
At plenary, Dr. Kohane pointed out that AI is a quick learner and improvements in tools are coming fast.
As an example, just 3 years ago, the best AI tool could score about as well as the worst student taking the medical boards, he told the audience. “Three years later, the leading large language models are scoring better than 90% of all the candidates. What’s it going to be doing next year?” he asked.
“I don’t know,” Dr. Kohane said, “but it will be better than this year.” AI will “transform health care.”
A version of this article first appeared on Medscape.com.
FROM IDWEEK 2023
AI in medicine has a major Cassandra problem
This transcript has been edited for clarity.
Today I’m going to talk to you about a study at the cutting edge of modern medicine, one that uses an artificial intelligence (AI) model to guide care. But before I do, I need to take you back to the late Bronze Age, to a city located on the coast of what is now Turkey.
Troy’s towering walls made it seem unassailable, but that would not stop the Achaeans and their fleet of black ships from making landfall, and, after a siege, destroying the city. The destruction of Troy, as told in the Iliad and the Aeneid, was foretold by Cassandra, the daughter of King Priam and Priestess of Troy.
Cassandra had been given the gift of prophecy by the god Apollo in exchange for her favors. But after the gift was bestowed, she rejected the bright god and, in his rage, he added a curse to her blessing: that no one would ever believe her prophecies.
Thus it was that when her brother Paris set off to Sparta to abduct Helen, she warned him that his actions would lead to the downfall of their great city. He, of course, ignored her.
And you know the rest of the story.
Why am I telling you the story of Cassandra of Troy when we’re supposed to be talking about AI in medicine? Because AI has a major Cassandra problem.
The recent history of AI, and particularly the subset of AI known as machine learning in medicine, has been characterized by an accuracy arms race.
The electronic health record allows for the collection of volumes of data orders of magnitude greater than what we have ever been able to collect before. And all that data can be crunched by various algorithms to make predictions about, well, anything – whether a patient will be transferred to the intensive care unit, whether a GI bleed will need an intervention, whether someone will die in the next year.
Studies in this area tend to rely on retrospective datasets, and as time has gone on, better algorithms and more data have led to better and better predictions. In some simpler cases, machine-learning models have achieved near-perfect accuracy – Cassandra-level accuracy – as in the reading of chest x-rays for pneumonia, for example.
But as Cassandra teaches us, even perfect prediction is useless if no one believes you, if they don’t change their behavior. And this is the central problem of AI in medicine today. Many people are focusing on accuracy of the prediction but have forgotten that high accuracy is just table stakes for an AI model to be useful. It has to not only be accurate, but its use also has to change outcomes for patients. We need to be able to save Troy.
The best way to determine whether an AI model will help patients is to treat a model like we treat a new medication and evaluate it through a randomized trial. That’s what researchers, led by Shannon Walker of Vanderbilt University, Nashville, Tenn., did in a paper appearing in JAMA Network Open.
The model in question was one that predicted venous thromboembolism – blood clots – in hospitalized children. The model took in a variety of data points from the health record: a history of blood clot, history of cancer, presence of a central line, a variety of lab values. And the predictive model was very good – maybe not Cassandra good, but it achieved an AUC of 0.90, which means it had very high accuracy.
But again, accuracy is just table stakes.
The authors deployed the model in the live health record and recorded the results. For half of the kids, that was all that happened; no one actually saw the predictions. For those randomized to the intervention, the hematology team would be notified when the risk for clot was calculated to be greater than 2.5%. The hematology team would then contact the primary team to discuss prophylactic anticoagulation.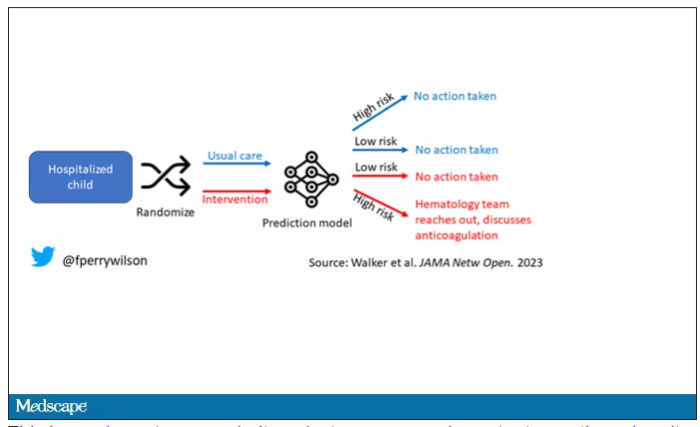
This is an elegant approach.
Let’s start with those table stakes – accuracy. The predictions were, by and large, pretty accurate in this trial. Of the 135 kids who developed blood clots, 121 had been flagged by the model in advance. That’s about 90%. The model flagged about 10% of kids who didn’t get a blood clot as well, but that’s not entirely surprising since the threshold for flagging was a 2.5% risk.
Given that the model preidentified almost every kid who would go on to develop a blood clot, it would make sense that kids randomized to the intervention would do better; after all, Cassandra was calling out her warnings.
But those kids didn’t do better. The rate of blood clot was no different between the group that used the accurate prediction model and the group that did not.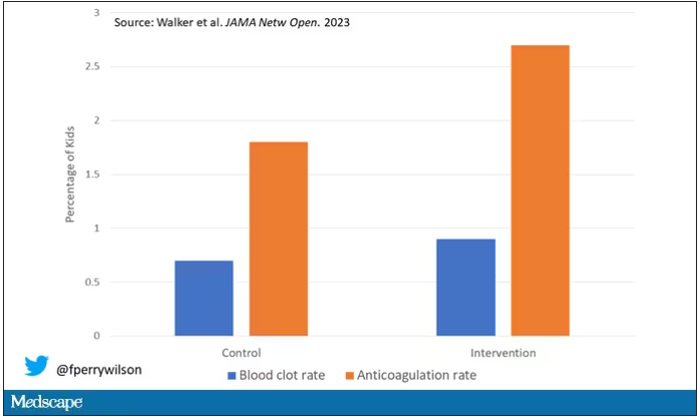
Why? Why does the use of an accurate model not necessarily improve outcomes?
First of all, a warning must lead to some change in management. Indeed, the kids in the intervention group were more likely to receive anticoagulation, but barely so. There were lots of reasons for this: physician preference, imminent discharge, active bleeding, and so on.
But let’s take a look at the 77 kids in the intervention arm who developed blood clots, because I think this is an instructive analysis.
Six of them did not meet the 2.5% threshold criteria, a case where the model missed its mark. Again, accuracy is table stakes.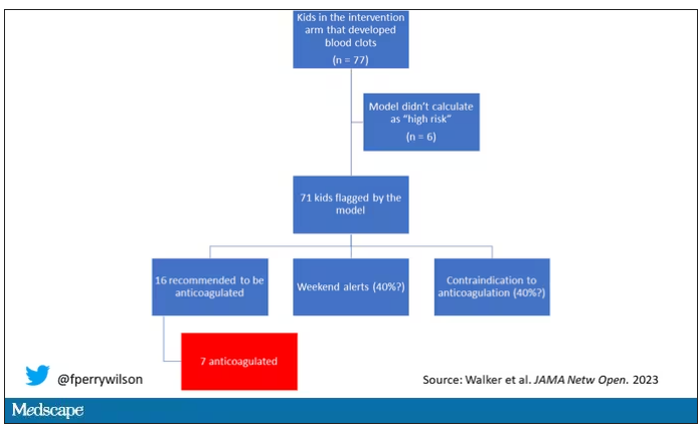
Of the remaining 71, only 16 got a recommendation from the hematologist to start anticoagulation. Why not more? Well, the model identified some of the high-risk kids on the weekend, and it seems that the study team did not contact treatment teams during that time. That may account for about 40% of these cases. The remainder had some contraindication to anticoagulation.
Most tellingly, of the 16 who did get a recommendation to start anticoagulation, the recommendation was followed in only seven patients.
This is the gap between accurate prediction and the ability to change outcomes for patients. A prediction is useless if it is wrong, for sure. But it’s also useless if you don’t tell anyone about it. It’s useless if you tell someone but they can’t do anything about it. And it’s useless if they could do something about it but choose not to.
That’s the gulf that these models need to cross at this point. So, the next time some slick company tells you how accurate their AI model is, ask them if accuracy is really the most important thing. If they say, “Well, yes, of course,” then tell them about Cassandra.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Today I’m going to talk to you about a study at the cutting edge of modern medicine, one that uses an artificial intelligence (AI) model to guide care. But before I do, I need to take you back to the late Bronze Age, to a city located on the coast of what is now Turkey.
Troy’s towering walls made it seem unassailable, but that would not stop the Achaeans and their fleet of black ships from making landfall, and, after a siege, destroying the city. The destruction of Troy, as told in the Iliad and the Aeneid, was foretold by Cassandra, the daughter of King Priam and Priestess of Troy.
Cassandra had been given the gift of prophecy by the god Apollo in exchange for her favors. But after the gift was bestowed, she rejected the bright god and, in his rage, he added a curse to her blessing: that no one would ever believe her prophecies.
Thus it was that when her brother Paris set off to Sparta to abduct Helen, she warned him that his actions would lead to the downfall of their great city. He, of course, ignored her.
And you know the rest of the story.
Why am I telling you the story of Cassandra of Troy when we’re supposed to be talking about AI in medicine? Because AI has a major Cassandra problem.
The recent history of AI, and particularly the subset of AI known as machine learning in medicine, has been characterized by an accuracy arms race.
The electronic health record allows for the collection of volumes of data orders of magnitude greater than what we have ever been able to collect before. And all that data can be crunched by various algorithms to make predictions about, well, anything – whether a patient will be transferred to the intensive care unit, whether a GI bleed will need an intervention, whether someone will die in the next year.
Studies in this area tend to rely on retrospective datasets, and as time has gone on, better algorithms and more data have led to better and better predictions. In some simpler cases, machine-learning models have achieved near-perfect accuracy – Cassandra-level accuracy – as in the reading of chest x-rays for pneumonia, for example.
But as Cassandra teaches us, even perfect prediction is useless if no one believes you, if they don’t change their behavior. And this is the central problem of AI in medicine today. Many people are focusing on accuracy of the prediction but have forgotten that high accuracy is just table stakes for an AI model to be useful. It has to not only be accurate, but its use also has to change outcomes for patients. We need to be able to save Troy.
The best way to determine whether an AI model will help patients is to treat a model like we treat a new medication and evaluate it through a randomized trial. That’s what researchers, led by Shannon Walker of Vanderbilt University, Nashville, Tenn., did in a paper appearing in JAMA Network Open.
The model in question was one that predicted venous thromboembolism – blood clots – in hospitalized children. The model took in a variety of data points from the health record: a history of blood clot, history of cancer, presence of a central line, a variety of lab values. And the predictive model was very good – maybe not Cassandra good, but it achieved an AUC of 0.90, which means it had very high accuracy.
But again, accuracy is just table stakes.
The authors deployed the model in the live health record and recorded the results. For half of the kids, that was all that happened; no one actually saw the predictions. For those randomized to the intervention, the hematology team would be notified when the risk for clot was calculated to be greater than 2.5%. The hematology team would then contact the primary team to discuss prophylactic anticoagulation.
This is an elegant approach.
Let’s start with those table stakes – accuracy. The predictions were, by and large, pretty accurate in this trial. Of the 135 kids who developed blood clots, 121 had been flagged by the model in advance. That’s about 90%. The model flagged about 10% of kids who didn’t get a blood clot as well, but that’s not entirely surprising since the threshold for flagging was a 2.5% risk.
Given that the model preidentified almost every kid who would go on to develop a blood clot, it would make sense that kids randomized to the intervention would do better; after all, Cassandra was calling out her warnings.
But those kids didn’t do better. The rate of blood clot was no different between the group that used the accurate prediction model and the group that did not.
Why? Why does the use of an accurate model not necessarily improve outcomes?
First of all, a warning must lead to some change in management. Indeed, the kids in the intervention group were more likely to receive anticoagulation, but barely so. There were lots of reasons for this: physician preference, imminent discharge, active bleeding, and so on.
But let’s take a look at the 77 kids in the intervention arm who developed blood clots, because I think this is an instructive analysis.
Six of them did not meet the 2.5% threshold criteria, a case where the model missed its mark. Again, accuracy is table stakes.
Of the remaining 71, only 16 got a recommendation from the hematologist to start anticoagulation. Why not more? Well, the model identified some of the high-risk kids on the weekend, and it seems that the study team did not contact treatment teams during that time. That may account for about 40% of these cases. The remainder had some contraindication to anticoagulation.
Most tellingly, of the 16 who did get a recommendation to start anticoagulation, the recommendation was followed in only seven patients.
This is the gap between accurate prediction and the ability to change outcomes for patients. A prediction is useless if it is wrong, for sure. But it’s also useless if you don’t tell anyone about it. It’s useless if you tell someone but they can’t do anything about it. And it’s useless if they could do something about it but choose not to.
That’s the gulf that these models need to cross at this point. So, the next time some slick company tells you how accurate their AI model is, ask them if accuracy is really the most important thing. If they say, “Well, yes, of course,” then tell them about Cassandra.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Today I’m going to talk to you about a study at the cutting edge of modern medicine, one that uses an artificial intelligence (AI) model to guide care. But before I do, I need to take you back to the late Bronze Age, to a city located on the coast of what is now Turkey.
Troy’s towering walls made it seem unassailable, but that would not stop the Achaeans and their fleet of black ships from making landfall, and, after a siege, destroying the city. The destruction of Troy, as told in the Iliad and the Aeneid, was foretold by Cassandra, the daughter of King Priam and Priestess of Troy.
Cassandra had been given the gift of prophecy by the god Apollo in exchange for her favors. But after the gift was bestowed, she rejected the bright god and, in his rage, he added a curse to her blessing: that no one would ever believe her prophecies.
Thus it was that when her brother Paris set off to Sparta to abduct Helen, she warned him that his actions would lead to the downfall of their great city. He, of course, ignored her.
And you know the rest of the story.
Why am I telling you the story of Cassandra of Troy when we’re supposed to be talking about AI in medicine? Because AI has a major Cassandra problem.
The recent history of AI, and particularly the subset of AI known as machine learning in medicine, has been characterized by an accuracy arms race.
The electronic health record allows for the collection of volumes of data orders of magnitude greater than what we have ever been able to collect before. And all that data can be crunched by various algorithms to make predictions about, well, anything – whether a patient will be transferred to the intensive care unit, whether a GI bleed will need an intervention, whether someone will die in the next year.
Studies in this area tend to rely on retrospective datasets, and as time has gone on, better algorithms and more data have led to better and better predictions. In some simpler cases, machine-learning models have achieved near-perfect accuracy – Cassandra-level accuracy – as in the reading of chest x-rays for pneumonia, for example.
But as Cassandra teaches us, even perfect prediction is useless if no one believes you, if they don’t change their behavior. And this is the central problem of AI in medicine today. Many people are focusing on accuracy of the prediction but have forgotten that high accuracy is just table stakes for an AI model to be useful. It has to not only be accurate, but its use also has to change outcomes for patients. We need to be able to save Troy.
The best way to determine whether an AI model will help patients is to treat a model like we treat a new medication and evaluate it through a randomized trial. That’s what researchers, led by Shannon Walker of Vanderbilt University, Nashville, Tenn., did in a paper appearing in JAMA Network Open.
The model in question was one that predicted venous thromboembolism – blood clots – in hospitalized children. The model took in a variety of data points from the health record: a history of blood clot, history of cancer, presence of a central line, a variety of lab values. And the predictive model was very good – maybe not Cassandra good, but it achieved an AUC of 0.90, which means it had very high accuracy.
But again, accuracy is just table stakes.
The authors deployed the model in the live health record and recorded the results. For half of the kids, that was all that happened; no one actually saw the predictions. For those randomized to the intervention, the hematology team would be notified when the risk for clot was calculated to be greater than 2.5%. The hematology team would then contact the primary team to discuss prophylactic anticoagulation.
This is an elegant approach.
Let’s start with those table stakes – accuracy. The predictions were, by and large, pretty accurate in this trial. Of the 135 kids who developed blood clots, 121 had been flagged by the model in advance. That’s about 90%. The model flagged about 10% of kids who didn’t get a blood clot as well, but that’s not entirely surprising since the threshold for flagging was a 2.5% risk.
Given that the model preidentified almost every kid who would go on to develop a blood clot, it would make sense that kids randomized to the intervention would do better; after all, Cassandra was calling out her warnings.
But those kids didn’t do better. The rate of blood clot was no different between the group that used the accurate prediction model and the group that did not.
Why? Why does the use of an accurate model not necessarily improve outcomes?
First of all, a warning must lead to some change in management. Indeed, the kids in the intervention group were more likely to receive anticoagulation, but barely so. There were lots of reasons for this: physician preference, imminent discharge, active bleeding, and so on.
But let’s take a look at the 77 kids in the intervention arm who developed blood clots, because I think this is an instructive analysis.
Six of them did not meet the 2.5% threshold criteria, a case where the model missed its mark. Again, accuracy is table stakes.
Of the remaining 71, only 16 got a recommendation from the hematologist to start anticoagulation. Why not more? Well, the model identified some of the high-risk kids on the weekend, and it seems that the study team did not contact treatment teams during that time. That may account for about 40% of these cases. The remainder had some contraindication to anticoagulation.
Most tellingly, of the 16 who did get a recommendation to start anticoagulation, the recommendation was followed in only seven patients.
This is the gap between accurate prediction and the ability to change outcomes for patients. A prediction is useless if it is wrong, for sure. But it’s also useless if you don’t tell anyone about it. It’s useless if you tell someone but they can’t do anything about it. And it’s useless if they could do something about it but choose not to.
That’s the gulf that these models need to cross at this point. So, the next time some slick company tells you how accurate their AI model is, ask them if accuracy is really the most important thing. If they say, “Well, yes, of course,” then tell them about Cassandra.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
EMA warns that omega-3-acid ethyl esters may cause AFib
In its September meeting, the Should atrial fibrillation develop, intake of the medication must be stopped permanently.
Omega-3-acid ethyl esters are used to treat hypertriglyceridemia if lifestyle changes, particularly those related to nutrition, have not been sufficient to lower the blood triglyceride level. Hypertriglyceridemia is a risk factor for coronary heart disease.
During a Periodic Safety Update Single Assessment Procedure, the EMA safety committee analyzed systematic overviews and meta-analyses of randomized, controlled clinical studies. Experts found a dose-dependent increase in the risk for atrial fibrillation in patients with cardiovascular diseases or cardiovascular risk factors who were being treated with omega-3-acid ethyl esters, compared with those treated with placebo. The observed risk was at its highest at a dose of 4 g/d.
The PRAC will recommend an update to the Summary of Product Characteristics for preparations that contain omega-3-acid ethyl esters. The aim is to inform physicians, pharmacists, and patients of the risk for atrial fibrillation. A notification will be sent to health care professionals soon to inform them of further details.
This article was translated from the Medscape German Edition. A version appeared on Medscape.com.
In its September meeting, the Should atrial fibrillation develop, intake of the medication must be stopped permanently.
Omega-3-acid ethyl esters are used to treat hypertriglyceridemia if lifestyle changes, particularly those related to nutrition, have not been sufficient to lower the blood triglyceride level. Hypertriglyceridemia is a risk factor for coronary heart disease.
During a Periodic Safety Update Single Assessment Procedure, the EMA safety committee analyzed systematic overviews and meta-analyses of randomized, controlled clinical studies. Experts found a dose-dependent increase in the risk for atrial fibrillation in patients with cardiovascular diseases or cardiovascular risk factors who were being treated with omega-3-acid ethyl esters, compared with those treated with placebo. The observed risk was at its highest at a dose of 4 g/d.
The PRAC will recommend an update to the Summary of Product Characteristics for preparations that contain omega-3-acid ethyl esters. The aim is to inform physicians, pharmacists, and patients of the risk for atrial fibrillation. A notification will be sent to health care professionals soon to inform them of further details.
This article was translated from the Medscape German Edition. A version appeared on Medscape.com.
In its September meeting, the Should atrial fibrillation develop, intake of the medication must be stopped permanently.
Omega-3-acid ethyl esters are used to treat hypertriglyceridemia if lifestyle changes, particularly those related to nutrition, have not been sufficient to lower the blood triglyceride level. Hypertriglyceridemia is a risk factor for coronary heart disease.
During a Periodic Safety Update Single Assessment Procedure, the EMA safety committee analyzed systematic overviews and meta-analyses of randomized, controlled clinical studies. Experts found a dose-dependent increase in the risk for atrial fibrillation in patients with cardiovascular diseases or cardiovascular risk factors who were being treated with omega-3-acid ethyl esters, compared with those treated with placebo. The observed risk was at its highest at a dose of 4 g/d.
The PRAC will recommend an update to the Summary of Product Characteristics for preparations that contain omega-3-acid ethyl esters. The aim is to inform physicians, pharmacists, and patients of the risk for atrial fibrillation. A notification will be sent to health care professionals soon to inform them of further details.
This article was translated from the Medscape German Edition. A version appeared on Medscape.com.
Updated pleural disease guidelines from the British Thoracic Society
Thoracic Oncology & Chest Imaging Network
Pleural Disease Section
After more than a decade, the British Thoracic Society (BTS) released updated guidelines for pleural disease (Roberts ME , et al. Thorax 2023; 78, s1-s42). Their focus includes spontaneous pneumothorax, undiagnosed unilateral pleural effusion, pleural infections, and malignant pleural effusion (MPE). Separate statements for pleural procedures (Asciak R et al. Thorax. 2023;78:s43-s68) and pleural mesothelioma (Woolhouse I et al. Thorax. 2018;73:i1-i30) are available.
Major highlights of the recommendations are as follows:
- Conservative management can be considered for minimally symptomatic primary spontaneous pneumothorax regardless of size. A multi-disciplinary approach and shared decision-making is vital, especially when deciding between needle aspiration, intercostal drainage or ambulatory devices. Special recommendations were for pregnancy, cystic fibrosis, catamenial, iatrogenic and familial.
- Undiagnosed unilateral pleural effusion. Besides pleural fluid studies, in those with unclear etiology, thoracoscopic or image-guided pleural biopsy is recommended.
- Pleural infection. Use of renal, age, purulence, infection source, dietary factors (RAPID) scoring may be considered for risk stratification. Drainage of the pleural space with catheter and intrapleural therapy with combination tissue plasminogen activator (TPA) and DNAse in residual pleural fluid should be considered. Medical thoracoscopy not supported due to lack of evidence.
- MPE. Definitive pleural intervention based on symptoms and shared decision making was supported. Modality may include talc slurry via chest tube, talc poudrage via thoracoscopy or talc instillation via indwelling pleural catheter. Intrapleural chemotherapy should not be routinely used for treatment of MPE.
These guidelines provide a comprehensive consensus to the literature and reinforce prior recommendations of other professional societies (Gilbert CR et al. Chest. 2020;158:2221-8. Miller RJ et al.; J Bronchology Interv Pulmonol. 2020;27[4]:229-45. Feller-Kopman DJ et al.; Am J Respir Crit Care Med. 2018;198:839-49).
Munish Sharma, MD
Hiren Mehta, MD, Section Member-at-Large
Philip Ong, MD, Section Member-at-Large
Thoracic Oncology & Chest Imaging Network
Pleural Disease Section
After more than a decade, the British Thoracic Society (BTS) released updated guidelines for pleural disease (Roberts ME , et al. Thorax 2023; 78, s1-s42). Their focus includes spontaneous pneumothorax, undiagnosed unilateral pleural effusion, pleural infections, and malignant pleural effusion (MPE). Separate statements for pleural procedures (Asciak R et al. Thorax. 2023;78:s43-s68) and pleural mesothelioma (Woolhouse I et al. Thorax. 2018;73:i1-i30) are available.
Major highlights of the recommendations are as follows:
- Conservative management can be considered for minimally symptomatic primary spontaneous pneumothorax regardless of size. A multi-disciplinary approach and shared decision-making is vital, especially when deciding between needle aspiration, intercostal drainage or ambulatory devices. Special recommendations were for pregnancy, cystic fibrosis, catamenial, iatrogenic and familial.
- Undiagnosed unilateral pleural effusion. Besides pleural fluid studies, in those with unclear etiology, thoracoscopic or image-guided pleural biopsy is recommended.
- Pleural infection. Use of renal, age, purulence, infection source, dietary factors (RAPID) scoring may be considered for risk stratification. Drainage of the pleural space with catheter and intrapleural therapy with combination tissue plasminogen activator (TPA) and DNAse in residual pleural fluid should be considered. Medical thoracoscopy not supported due to lack of evidence.
- MPE. Definitive pleural intervention based on symptoms and shared decision making was supported. Modality may include talc slurry via chest tube, talc poudrage via thoracoscopy or talc instillation via indwelling pleural catheter. Intrapleural chemotherapy should not be routinely used for treatment of MPE.
These guidelines provide a comprehensive consensus to the literature and reinforce prior recommendations of other professional societies (Gilbert CR et al. Chest. 2020;158:2221-8. Miller RJ et al.; J Bronchology Interv Pulmonol. 2020;27[4]:229-45. Feller-Kopman DJ et al.; Am J Respir Crit Care Med. 2018;198:839-49).
Munish Sharma, MD
Hiren Mehta, MD, Section Member-at-Large
Philip Ong, MD, Section Member-at-Large
Thoracic Oncology & Chest Imaging Network
Pleural Disease Section
After more than a decade, the British Thoracic Society (BTS) released updated guidelines for pleural disease (Roberts ME , et al. Thorax 2023; 78, s1-s42). Their focus includes spontaneous pneumothorax, undiagnosed unilateral pleural effusion, pleural infections, and malignant pleural effusion (MPE). Separate statements for pleural procedures (Asciak R et al. Thorax. 2023;78:s43-s68) and pleural mesothelioma (Woolhouse I et al. Thorax. 2018;73:i1-i30) are available.
Major highlights of the recommendations are as follows:
- Conservative management can be considered for minimally symptomatic primary spontaneous pneumothorax regardless of size. A multi-disciplinary approach and shared decision-making is vital, especially when deciding between needle aspiration, intercostal drainage or ambulatory devices. Special recommendations were for pregnancy, cystic fibrosis, catamenial, iatrogenic and familial.
- Undiagnosed unilateral pleural effusion. Besides pleural fluid studies, in those with unclear etiology, thoracoscopic or image-guided pleural biopsy is recommended.
- Pleural infection. Use of renal, age, purulence, infection source, dietary factors (RAPID) scoring may be considered for risk stratification. Drainage of the pleural space with catheter and intrapleural therapy with combination tissue plasminogen activator (TPA) and DNAse in residual pleural fluid should be considered. Medical thoracoscopy not supported due to lack of evidence.
- MPE. Definitive pleural intervention based on symptoms and shared decision making was supported. Modality may include talc slurry via chest tube, talc poudrage via thoracoscopy or talc instillation via indwelling pleural catheter. Intrapleural chemotherapy should not be routinely used for treatment of MPE.
These guidelines provide a comprehensive consensus to the literature and reinforce prior recommendations of other professional societies (Gilbert CR et al. Chest. 2020;158:2221-8. Miller RJ et al.; J Bronchology Interv Pulmonol. 2020;27[4]:229-45. Feller-Kopman DJ et al.; Am J Respir Crit Care Med. 2018;198:839-49).
Munish Sharma, MD
Hiren Mehta, MD, Section Member-at-Large
Philip Ong, MD, Section Member-at-Large
Rare disease roundup
Can a repurposed Parkinson’s drug slow ALS progression?
Ropinirole, a drug used for Parkinson’s disease, shows promise in slowing the progression of amyotrophic lateral sclerosis (ALS), early research suggests.
Investigators randomly assigned 20 individuals with sporadic ALS to receive either ropinirole or placebo for 24 weeks. During the double-blind period, there was no difference between the groups in terms of decline in functional status.
However, during a further open-label extension period, the ropinirole group showed significant suppression of functional decline and an average of an additional 7 months of progression-free survival.
The researchers were able to predict clinical responsiveness to ropinirole in vitro by analyzing motor neurons derived from participants’ stem cells.
The study was published online in Cell Stem Cell (2023 Jun 1. doi: 10.1016/j.stem.2023.04.017).
The trial was sponsored by K Pharma. The study drug, active drugs, and placebo were supplied free of charge by GlaxoSmithKline.
West Nile infections rising in the U.S.
Several signs are pointing to an impending surge in the number of human cases of West Nile virus in several regions of the United States. West Nile virus is spread by infected mosquitoes and currently there is no cure or virus-specific treatment. In rare cases, it can be deadly. It can infect humans, birds, horses, and other mammals.
West Nile Virus is the leading cause of mosquito-borne disease in the continental United States. As of Aug. 8, 126 human cases had been identified across 22 states, according to the Centers for Disease Control and Prevention.
“Particularly here in California, it’s peak risk right now,” said Vicki Kramer, PhD, chief of vector-borne diseases in the California Department of Public Health. She said scientists there are seeing higher mosquito and infected mosquito numbers.
Dead birds are tested for the virus and by Aug. 4, 181 of the 913 birds tested in California have been positive, three times the total testing positive by that time in 2022.
“Last year at this time, we had 60 positive dead birds out of 817 tested,” Dr. Kramer said.
Myasthenia gravis drug gets FDA nod
The Food and Drug Administration (FDA) has approved rozanolixizumab (Rystiggo, UCB) to treat adults with generalized myasthenia gravis (gMG) who are positive for anti-acetylcholine receptor (AChR) or anti–muscle-specific tyrosine kinase (MuSK) antibody, the drug’s manufacturer, UCB, has announced.
gMG is a rare autoimmune disease of the nerve muscle junction. Anti-AChR and anti-MuSK antibody-positive gMG are the two most common subtypes. Rozanolixizumab is the first FDA-approved treatment for adults with both subtypes.
Rozanolixizumab is a subcutaneous-infused humanized IgG4 monoclonal antibody that binds to the neonatal Fc
receptor (FcRn), reducing the concentration of pathogenic IgG autoantibodies.
U.S. approval is based on results of the phase 3
MycarinG study involving 200 patients with AChR or MuSK autoantibody-positive gMG. Patients were randomly assigned to one of two rozanolixizumab groups (7 mg/kg or 10 mg/kg) or placebo for 6 weeks.
As reported in The Lancet Neurology (2023 May. doi: 10.1016/S1474-4422[23]00077-7), rozanolixizumab led to statistically significant improvements in gMG-specific outcomes, including everyday activities such as breathing, talking, swallowing, and being able to rise from a chair.
Gene therapy promising for reversal of hereditary vision loss
An unapproved gene therapy for Leber hereditary optic neuropathy (LHON) led to a marked improvement in the eyesight of patients with a severe, progressive form of the disease who received the therapy as part of an early access program.
Results of a study of more than 60 patients who received lenadogene nolparvovec (Lumevoq, GenSight Biologics) as a unilateral or bilateral intravitreal injection showed that, at 2-year follow-up, 60% had experienced a clinically relevant improvement in the number of letters they could read on a visual acuity chart.
The results, said study presenter Chiara La Morgia, MD, PhD, IRCCS Istituto delle Scienze Neurologiche di Bologna (Italy), confirm in a “real-life setting” the efficacy and safety of the treatment as previously shown in clinical trials.
The findings were presented at the 2023 Congress of the European Academy of Neurology.
No funding was declared. Dr. La Morgia has relationships with Chiesi Farmaceutici, GenSight Biologics, Regulatory Pharma Net, Thenewway, Santhera Pharmaceuticals, First Class, Biologix, Stoke Therapeutics, and Reneo.
FDA OKs new drug for Fabry disease
The FDA has approved pegunigalsidase alfa (Elfabrio, Chiesi Global Rare Diseases/Protalix BioTherapeutics), an enzyme replacement therapy (ERT) to treat adults with Fabry disease.
Fabry disease is a rare inherited X-linked lysosomal disorder caused by a deficiency of the enzyme alpha-galactosidase A (GLA), which leads to the buildup of globotriaosylceramide (GL-3) in blood vessels, kidneys, heart, nerves, and other organs, increasing the risk for kidney failure, myocardial infarction, stroke, and other problems.
Elfabrio delivers a functional version of GLA. It is given by intravenous infusion every 2 weeks.
Evidence for safety, tolerability, and efficacy of Elfabrio stem from a comprehensive clinical program in more than 140 patients with up to 7.5 years of follow-up treatment.
It has been studied in both ERT-naive and ERT-experienced patients. In one head-to-head trial, Elfabrio was noninferior in safety and efficacy to agalsidase beta (Fabrazyme, Sanofi Genzyme), the companies said in a press statement announcing approval.
U.S. incidence, prevalence of myasthenia gravis are rising
There has been an increase in the incidence and prevalence of myasthenia gravis in the United States, an analysis of new claims data shows. Investigators speculate the rise of this rare disorder may be caused by “increased diagnosis and more awareness of the disease over time, which has been shown in several studies,” said study investigator Ema Rodrigues, DSc, MPH, with Alexion Pharmaceuticals, Boston.
Dr. Rodrigues presented her research at the 2023 annual meeting of the American Academy of Neurology.
Funding for the study was provided by Alexion, AstraZeneca Rare
Disease. Dr. Rodrigues receives compensation and owns stock as an employee of Alexion, AstraZeneca Rare Diseases.
Novel agent offers hope for hereditary ATTR polyneuropathy in pivotal trial
The investigational agent eplontersen (Ionis Pharmaceuticals/AstraZeneca) halted neuropathy disease progression and improved neuropathy impairment and quality of life for patients with hereditary transthyretin-mediated amyloid polyneuropathy (ATTRv-PN) in a pivotal phase 3 trial.
Eplontersen led to “clinically and statistically significant benefits at week 66 with an early and rapid sustained reduction in serum TTR [transthyretin] concentration, a halting of the progression of the neuropathy impairment, and a trend to improvement in quality of life,” said principal investigator Sami Khella, MD, professor of clinical neurology at the University of Pennsylvania, Philadelphia.
Dr. Khella reported final data from the NEURO-TTRansform trial at the annual meeting of the American Academy of Neurology.
The FDA has accepted a new drug application for eplontersen for the treatment of ATTRv-PN. The drug has a Prescription Drug User Fee Act date of Dec. 22, 2023. Eplontersen has orphan drug designation in the United States.
The study was sponsored by Ionis Pharmaceuticals. Dr. Khella has relationships with Ionis, Pfizer, Alnylam, and Eidos.
FDA gives fast-track approval to new ALS drug
The FDA has approved the first treatment that takes a genetics-based approach to slowing or stopping the progression of a rare form of amyotrophic lateral sclerosis (ALS).
The FDA fast-tracked the approval of Qalsody (Biogen) based on early trial results. The agency said in a news release that its decision was based on the demonstrated ability of the drug to reduce a protein in the blood that is a sign of degeneration of brain and nerve cells.
Qalsody is given to people via a spinal injection, with an initial course of three injections every 2 weeks. People then get the injection once every 28 days.
The new treatment is approved only for people with SOD1-ALS, which is known for a genetic mutation. While ALS affects up to 32,000 people in the United States, just 2% of people with ALS have the SOD1 gene mutation. The FDA says the number of people in the United States who could use Qalsody is about 500.
FDA OKs first treatment for Friedreich ataxia
The FDA has approved the first treatment for the neurodegenerative disorder Friedreich ataxia for use in adults and adolescents aged 16 and older.
The recommended dose of omaveloxolone (Skyclarys, Reata Pharmaceuticals) is 150 mg (three capsules) taken orally once daily on an empty stomach.
The FDA approval of omaveloxolone was supported by a randomized double-blind, placebo-controlled study comprising 103 patients with genetically confirmed Friedreich ataxia and baseline modified Friedreich Ataxia Rating Scale (mFARS) scores between 20 and 80.
Treatment with the novel medication led to statistically significant lower mFARS scores, signifying less impairment, relative to placebo, at week 48. The placebo-corrected difference between the two groups was –2.41 points (P = .0138).
Omaveloxolone received priority review and had orphan drug, fast track, and rare pediatric disease designations.
FDA OKs first drug for Rett syndrome
The FDA has approved trofinetide oral solution (Daybue, Acadia Pharmaceuticals) as the first treatment of Rett syndrome in adults and children aged 2 years and older.
Trofinetide is a synthetic analogue of the amino-terminal tripeptide of insulinlike growth factor-1, which occurs naturally in the brain. The drug is designed to treat the core symptoms of Rett syndrome by potentially reducing neuroinflammation and supporting synaptic function.
The approval of trofinetide was supported by results from the pivotal phase 3 LAVENDER study that tested the efficacy and safety of trofinetide versus placebo in 187 female patients with Rett syndrome, aged 5-20 years.
More data back Guillain-Barré risk with Janssen COVID shot
New surveillance data from the Vaccine Adverse Event Reporting System (VAERS) back previous findings of increased risk for Guillain-Barré syndrome (GBS) after receiving the Janssen COVID-19 vaccine (Ad26.COV2.S).
Over 14 months, GBS reporting rates within 21 and 42 days of administration of Janssen’s replication-incompetent adenoviral vector vaccine were approximately 9-12 times higher than after administration of the Pfizer-BioNTech (BNT162b2) or the Moderna (mRNA-1273) mRNA COVID vaccines.
Additionally, observed GBS cases after the Janssen shot were two to three times greater than expected, based on background rates within 21 and 42 days of vaccination.
Conversely, and confirming prior data, there was no increased risk for GBS with the Pfizer or Moderna vaccines and no significant difference between observed and expected numbers of GBS cases after either mRNA COVID-19 vaccine.
The findings were published online in JAMA Network Open (2023 Feb 1. doi: 10.1001/jamanetworkopen.2022.53845).
Diazepam nasal spray effective in Lennox-Gastaut syndrome
A new analysis of data from a phase 3 clinical trial suggests that an inhaled diazepam nasal spray (Valtoco, Neurelis) works about as well among patients with Lennox-Gastaut syndrome (LGS) as it does with other patients with pediatric encephalopathies.
LGS is a severe form of epilepsy that generally begins in early childhood and has a poor prognosis and seizures that are often treatment refractory. The findings of the analysis should be encouraging to physicians who may view patients with LGS as not benefiting from treatment, said Daniel C. Tarquinio, DO, who presented the results at the 2022 annual meeting of the Child Neurology Society.
Novel cannabis oil curbs tics in severe Tourette syndrome
An oral oil containing tetrahydrocannabinol (THC) and cannabidiol (CBD) led to a significant and meaningful reduction in motor and vocal tics in patients with severe Tourette syndrome, results of a double-blind, placebo-controlled, crossover study showed.
“In a methodologically robust manner (and independent of any drug company sponsorship), we provide evidence for the effectiveness of repeated dosing with THC:CBD versus placebo in tic
suppression, as well as reduction of comorbid anxiety and obsessive-compulsive disorder in severe Tourette syndrome,” neuropsychiatrist and lead investigator Philip Mosley, PhD, said in an interview.
The results offer support to people with Tourette syndrome who “want to approach their doctor to try medicinal cannabis when other drugs have not worked or are intolerable,” said
Dr. Mosley, of the Wesley Research Institute and QIMR Berghofer Medical Research Institute, Herston, Australia.
The study was published online in NEJM Evidence (2023 Jun 7. doi: 10.1056/EVIDoa2300012).
Twenty-two adults (mean age, 31 years) with severe Tourette syndrome received THC:CBD oil titrated upward over 6 weeks to a daily dose of 20 mg of THC and 20 mg of CBD, followed by a 6-week course of placebo (or vice versa). Six participants had not previously used cannabis.
The primary outcome was the total tic score on the Yale Global Tic Severity Scale (YGTSS; range, 0-50 with higher scores = greater tic severity).
The mean baseline YGTSS total tic score was 35.7. At 6 weeks, the reduction in total tic score was 8.9 with THC:CBD versus 2.5 with placebo.
A linear mixed-effects model (intention to treat) showed a significant interaction of treatment and visit number (P = .008), indicating a greater decrease (improvement) in tic score over time with THC:CBD, the study team reported.
On average, the magnitude of the tic reduction was “moderate” and comparable with the effect observed with existing treatments such as antipsychotic agents, the investigators noted.
The study was funded by the Wesley Medical Research Institute, Brisbane, and the Lambert Initiative for Cannabinoid Therapeutics, a philanthropically funded research organization at the University of Sydney, Australia.
Dr. Mosley reported no relevant financial relationships.
Can a repurposed Parkinson’s drug slow ALS progression?
Ropinirole, a drug used for Parkinson’s disease, shows promise in slowing the progression of amyotrophic lateral sclerosis (ALS), early research suggests.
Investigators randomly assigned 20 individuals with sporadic ALS to receive either ropinirole or placebo for 24 weeks. During the double-blind period, there was no difference between the groups in terms of decline in functional status.
However, during a further open-label extension period, the ropinirole group showed significant suppression of functional decline and an average of an additional 7 months of progression-free survival.
The researchers were able to predict clinical responsiveness to ropinirole in vitro by analyzing motor neurons derived from participants’ stem cells.
The study was published online in Cell Stem Cell (2023 Jun 1. doi: 10.1016/j.stem.2023.04.017).
The trial was sponsored by K Pharma. The study drug, active drugs, and placebo were supplied free of charge by GlaxoSmithKline.
West Nile infections rising in the U.S.
Several signs are pointing to an impending surge in the number of human cases of West Nile virus in several regions of the United States. West Nile virus is spread by infected mosquitoes and currently there is no cure or virus-specific treatment. In rare cases, it can be deadly. It can infect humans, birds, horses, and other mammals.
West Nile Virus is the leading cause of mosquito-borne disease in the continental United States. As of Aug. 8, 126 human cases had been identified across 22 states, according to the Centers for Disease Control and Prevention.
“Particularly here in California, it’s peak risk right now,” said Vicki Kramer, PhD, chief of vector-borne diseases in the California Department of Public Health. She said scientists there are seeing higher mosquito and infected mosquito numbers.
Dead birds are tested for the virus and by Aug. 4, 181 of the 913 birds tested in California have been positive, three times the total testing positive by that time in 2022.
“Last year at this time, we had 60 positive dead birds out of 817 tested,” Dr. Kramer said.
Myasthenia gravis drug gets FDA nod
The Food and Drug Administration (FDA) has approved rozanolixizumab (Rystiggo, UCB) to treat adults with generalized myasthenia gravis (gMG) who are positive for anti-acetylcholine receptor (AChR) or anti–muscle-specific tyrosine kinase (MuSK) antibody, the drug’s manufacturer, UCB, has announced.
gMG is a rare autoimmune disease of the nerve muscle junction. Anti-AChR and anti-MuSK antibody-positive gMG are the two most common subtypes. Rozanolixizumab is the first FDA-approved treatment for adults with both subtypes.
Rozanolixizumab is a subcutaneous-infused humanized IgG4 monoclonal antibody that binds to the neonatal Fc
receptor (FcRn), reducing the concentration of pathogenic IgG autoantibodies.
U.S. approval is based on results of the phase 3
MycarinG study involving 200 patients with AChR or MuSK autoantibody-positive gMG. Patients were randomly assigned to one of two rozanolixizumab groups (7 mg/kg or 10 mg/kg) or placebo for 6 weeks.
As reported in The Lancet Neurology (2023 May. doi: 10.1016/S1474-4422[23]00077-7), rozanolixizumab led to statistically significant improvements in gMG-specific outcomes, including everyday activities such as breathing, talking, swallowing, and being able to rise from a chair.
Gene therapy promising for reversal of hereditary vision loss
An unapproved gene therapy for Leber hereditary optic neuropathy (LHON) led to a marked improvement in the eyesight of patients with a severe, progressive form of the disease who received the therapy as part of an early access program.
Results of a study of more than 60 patients who received lenadogene nolparvovec (Lumevoq, GenSight Biologics) as a unilateral or bilateral intravitreal injection showed that, at 2-year follow-up, 60% had experienced a clinically relevant improvement in the number of letters they could read on a visual acuity chart.
The results, said study presenter Chiara La Morgia, MD, PhD, IRCCS Istituto delle Scienze Neurologiche di Bologna (Italy), confirm in a “real-life setting” the efficacy and safety of the treatment as previously shown in clinical trials.
The findings were presented at the 2023 Congress of the European Academy of Neurology.
No funding was declared. Dr. La Morgia has relationships with Chiesi Farmaceutici, GenSight Biologics, Regulatory Pharma Net, Thenewway, Santhera Pharmaceuticals, First Class, Biologix, Stoke Therapeutics, and Reneo.
FDA OKs new drug for Fabry disease
The FDA has approved pegunigalsidase alfa (Elfabrio, Chiesi Global Rare Diseases/Protalix BioTherapeutics), an enzyme replacement therapy (ERT) to treat adults with Fabry disease.
Fabry disease is a rare inherited X-linked lysosomal disorder caused by a deficiency of the enzyme alpha-galactosidase A (GLA), which leads to the buildup of globotriaosylceramide (GL-3) in blood vessels, kidneys, heart, nerves, and other organs, increasing the risk for kidney failure, myocardial infarction, stroke, and other problems.
Elfabrio delivers a functional version of GLA. It is given by intravenous infusion every 2 weeks.
Evidence for safety, tolerability, and efficacy of Elfabrio stem from a comprehensive clinical program in more than 140 patients with up to 7.5 years of follow-up treatment.
It has been studied in both ERT-naive and ERT-experienced patients. In one head-to-head trial, Elfabrio was noninferior in safety and efficacy to agalsidase beta (Fabrazyme, Sanofi Genzyme), the companies said in a press statement announcing approval.
U.S. incidence, prevalence of myasthenia gravis are rising
There has been an increase in the incidence and prevalence of myasthenia gravis in the United States, an analysis of new claims data shows. Investigators speculate the rise of this rare disorder may be caused by “increased diagnosis and more awareness of the disease over time, which has been shown in several studies,” said study investigator Ema Rodrigues, DSc, MPH, with Alexion Pharmaceuticals, Boston.
Dr. Rodrigues presented her research at the 2023 annual meeting of the American Academy of Neurology.
Funding for the study was provided by Alexion, AstraZeneca Rare
Disease. Dr. Rodrigues receives compensation and owns stock as an employee of Alexion, AstraZeneca Rare Diseases.
Novel agent offers hope for hereditary ATTR polyneuropathy in pivotal trial
The investigational agent eplontersen (Ionis Pharmaceuticals/AstraZeneca) halted neuropathy disease progression and improved neuropathy impairment and quality of life for patients with hereditary transthyretin-mediated amyloid polyneuropathy (ATTRv-PN) in a pivotal phase 3 trial.
Eplontersen led to “clinically and statistically significant benefits at week 66 with an early and rapid sustained reduction in serum TTR [transthyretin] concentration, a halting of the progression of the neuropathy impairment, and a trend to improvement in quality of life,” said principal investigator Sami Khella, MD, professor of clinical neurology at the University of Pennsylvania, Philadelphia.
Dr. Khella reported final data from the NEURO-TTRansform trial at the annual meeting of the American Academy of Neurology.
The FDA has accepted a new drug application for eplontersen for the treatment of ATTRv-PN. The drug has a Prescription Drug User Fee Act date of Dec. 22, 2023. Eplontersen has orphan drug designation in the United States.
The study was sponsored by Ionis Pharmaceuticals. Dr. Khella has relationships with Ionis, Pfizer, Alnylam, and Eidos.
FDA gives fast-track approval to new ALS drug
The FDA has approved the first treatment that takes a genetics-based approach to slowing or stopping the progression of a rare form of amyotrophic lateral sclerosis (ALS).
The FDA fast-tracked the approval of Qalsody (Biogen) based on early trial results. The agency said in a news release that its decision was based on the demonstrated ability of the drug to reduce a protein in the blood that is a sign of degeneration of brain and nerve cells.
Qalsody is given to people via a spinal injection, with an initial course of three injections every 2 weeks. People then get the injection once every 28 days.
The new treatment is approved only for people with SOD1-ALS, which is known for a genetic mutation. While ALS affects up to 32,000 people in the United States, just 2% of people with ALS have the SOD1 gene mutation. The FDA says the number of people in the United States who could use Qalsody is about 500.
FDA OKs first treatment for Friedreich ataxia
The FDA has approved the first treatment for the neurodegenerative disorder Friedreich ataxia for use in adults and adolescents aged 16 and older.
The recommended dose of omaveloxolone (Skyclarys, Reata Pharmaceuticals) is 150 mg (three capsules) taken orally once daily on an empty stomach.
The FDA approval of omaveloxolone was supported by a randomized double-blind, placebo-controlled study comprising 103 patients with genetically confirmed Friedreich ataxia and baseline modified Friedreich Ataxia Rating Scale (mFARS) scores between 20 and 80.
Treatment with the novel medication led to statistically significant lower mFARS scores, signifying less impairment, relative to placebo, at week 48. The placebo-corrected difference between the two groups was –2.41 points (P = .0138).
Omaveloxolone received priority review and had orphan drug, fast track, and rare pediatric disease designations.
FDA OKs first drug for Rett syndrome
The FDA has approved trofinetide oral solution (Daybue, Acadia Pharmaceuticals) as the first treatment of Rett syndrome in adults and children aged 2 years and older.
Trofinetide is a synthetic analogue of the amino-terminal tripeptide of insulinlike growth factor-1, which occurs naturally in the brain. The drug is designed to treat the core symptoms of Rett syndrome by potentially reducing neuroinflammation and supporting synaptic function.
The approval of trofinetide was supported by results from the pivotal phase 3 LAVENDER study that tested the efficacy and safety of trofinetide versus placebo in 187 female patients with Rett syndrome, aged 5-20 years.
More data back Guillain-Barré risk with Janssen COVID shot
New surveillance data from the Vaccine Adverse Event Reporting System (VAERS) back previous findings of increased risk for Guillain-Barré syndrome (GBS) after receiving the Janssen COVID-19 vaccine (Ad26.COV2.S).
Over 14 months, GBS reporting rates within 21 and 42 days of administration of Janssen’s replication-incompetent adenoviral vector vaccine were approximately 9-12 times higher than after administration of the Pfizer-BioNTech (BNT162b2) or the Moderna (mRNA-1273) mRNA COVID vaccines.
Additionally, observed GBS cases after the Janssen shot were two to three times greater than expected, based on background rates within 21 and 42 days of vaccination.
Conversely, and confirming prior data, there was no increased risk for GBS with the Pfizer or Moderna vaccines and no significant difference between observed and expected numbers of GBS cases after either mRNA COVID-19 vaccine.
The findings were published online in JAMA Network Open (2023 Feb 1. doi: 10.1001/jamanetworkopen.2022.53845).
Diazepam nasal spray effective in Lennox-Gastaut syndrome
A new analysis of data from a phase 3 clinical trial suggests that an inhaled diazepam nasal spray (Valtoco, Neurelis) works about as well among patients with Lennox-Gastaut syndrome (LGS) as it does with other patients with pediatric encephalopathies.
LGS is a severe form of epilepsy that generally begins in early childhood and has a poor prognosis and seizures that are often treatment refractory. The findings of the analysis should be encouraging to physicians who may view patients with LGS as not benefiting from treatment, said Daniel C. Tarquinio, DO, who presented the results at the 2022 annual meeting of the Child Neurology Society.
Novel cannabis oil curbs tics in severe Tourette syndrome
An oral oil containing tetrahydrocannabinol (THC) and cannabidiol (CBD) led to a significant and meaningful reduction in motor and vocal tics in patients with severe Tourette syndrome, results of a double-blind, placebo-controlled, crossover study showed.
“In a methodologically robust manner (and independent of any drug company sponsorship), we provide evidence for the effectiveness of repeated dosing with THC:CBD versus placebo in tic
suppression, as well as reduction of comorbid anxiety and obsessive-compulsive disorder in severe Tourette syndrome,” neuropsychiatrist and lead investigator Philip Mosley, PhD, said in an interview.
The results offer support to people with Tourette syndrome who “want to approach their doctor to try medicinal cannabis when other drugs have not worked or are intolerable,” said
Dr. Mosley, of the Wesley Research Institute and QIMR Berghofer Medical Research Institute, Herston, Australia.
The study was published online in NEJM Evidence (2023 Jun 7. doi: 10.1056/EVIDoa2300012).
Twenty-two adults (mean age, 31 years) with severe Tourette syndrome received THC:CBD oil titrated upward over 6 weeks to a daily dose of 20 mg of THC and 20 mg of CBD, followed by a 6-week course of placebo (or vice versa). Six participants had not previously used cannabis.
The primary outcome was the total tic score on the Yale Global Tic Severity Scale (YGTSS; range, 0-50 with higher scores = greater tic severity).
The mean baseline YGTSS total tic score was 35.7. At 6 weeks, the reduction in total tic score was 8.9 with THC:CBD versus 2.5 with placebo.
A linear mixed-effects model (intention to treat) showed a significant interaction of treatment and visit number (P = .008), indicating a greater decrease (improvement) in tic score over time with THC:CBD, the study team reported.
On average, the magnitude of the tic reduction was “moderate” and comparable with the effect observed with existing treatments such as antipsychotic agents, the investigators noted.
The study was funded by the Wesley Medical Research Institute, Brisbane, and the Lambert Initiative for Cannabinoid Therapeutics, a philanthropically funded research organization at the University of Sydney, Australia.
Dr. Mosley reported no relevant financial relationships.
Can a repurposed Parkinson’s drug slow ALS progression?
Ropinirole, a drug used for Parkinson’s disease, shows promise in slowing the progression of amyotrophic lateral sclerosis (ALS), early research suggests.
Investigators randomly assigned 20 individuals with sporadic ALS to receive either ropinirole or placebo for 24 weeks. During the double-blind period, there was no difference between the groups in terms of decline in functional status.
However, during a further open-label extension period, the ropinirole group showed significant suppression of functional decline and an average of an additional 7 months of progression-free survival.
The researchers were able to predict clinical responsiveness to ropinirole in vitro by analyzing motor neurons derived from participants’ stem cells.
The study was published online in Cell Stem Cell (2023 Jun 1. doi: 10.1016/j.stem.2023.04.017).
The trial was sponsored by K Pharma. The study drug, active drugs, and placebo were supplied free of charge by GlaxoSmithKline.
West Nile infections rising in the U.S.
Several signs are pointing to an impending surge in the number of human cases of West Nile virus in several regions of the United States. West Nile virus is spread by infected mosquitoes and currently there is no cure or virus-specific treatment. In rare cases, it can be deadly. It can infect humans, birds, horses, and other mammals.
West Nile Virus is the leading cause of mosquito-borne disease in the continental United States. As of Aug. 8, 126 human cases had been identified across 22 states, according to the Centers for Disease Control and Prevention.
“Particularly here in California, it’s peak risk right now,” said Vicki Kramer, PhD, chief of vector-borne diseases in the California Department of Public Health. She said scientists there are seeing higher mosquito and infected mosquito numbers.
Dead birds are tested for the virus and by Aug. 4, 181 of the 913 birds tested in California have been positive, three times the total testing positive by that time in 2022.
“Last year at this time, we had 60 positive dead birds out of 817 tested,” Dr. Kramer said.
Myasthenia gravis drug gets FDA nod
The Food and Drug Administration (FDA) has approved rozanolixizumab (Rystiggo, UCB) to treat adults with generalized myasthenia gravis (gMG) who are positive for anti-acetylcholine receptor (AChR) or anti–muscle-specific tyrosine kinase (MuSK) antibody, the drug’s manufacturer, UCB, has announced.
gMG is a rare autoimmune disease of the nerve muscle junction. Anti-AChR and anti-MuSK antibody-positive gMG are the two most common subtypes. Rozanolixizumab is the first FDA-approved treatment for adults with both subtypes.
Rozanolixizumab is a subcutaneous-infused humanized IgG4 monoclonal antibody that binds to the neonatal Fc
receptor (FcRn), reducing the concentration of pathogenic IgG autoantibodies.
U.S. approval is based on results of the phase 3
MycarinG study involving 200 patients with AChR or MuSK autoantibody-positive gMG. Patients were randomly assigned to one of two rozanolixizumab groups (7 mg/kg or 10 mg/kg) or placebo for 6 weeks.
As reported in The Lancet Neurology (2023 May. doi: 10.1016/S1474-4422[23]00077-7), rozanolixizumab led to statistically significant improvements in gMG-specific outcomes, including everyday activities such as breathing, talking, swallowing, and being able to rise from a chair.
Gene therapy promising for reversal of hereditary vision loss
An unapproved gene therapy for Leber hereditary optic neuropathy (LHON) led to a marked improvement in the eyesight of patients with a severe, progressive form of the disease who received the therapy as part of an early access program.
Results of a study of more than 60 patients who received lenadogene nolparvovec (Lumevoq, GenSight Biologics) as a unilateral or bilateral intravitreal injection showed that, at 2-year follow-up, 60% had experienced a clinically relevant improvement in the number of letters they could read on a visual acuity chart.
The results, said study presenter Chiara La Morgia, MD, PhD, IRCCS Istituto delle Scienze Neurologiche di Bologna (Italy), confirm in a “real-life setting” the efficacy and safety of the treatment as previously shown in clinical trials.
The findings were presented at the 2023 Congress of the European Academy of Neurology.
No funding was declared. Dr. La Morgia has relationships with Chiesi Farmaceutici, GenSight Biologics, Regulatory Pharma Net, Thenewway, Santhera Pharmaceuticals, First Class, Biologix, Stoke Therapeutics, and Reneo.
FDA OKs new drug for Fabry disease
The FDA has approved pegunigalsidase alfa (Elfabrio, Chiesi Global Rare Diseases/Protalix BioTherapeutics), an enzyme replacement therapy (ERT) to treat adults with Fabry disease.
Fabry disease is a rare inherited X-linked lysosomal disorder caused by a deficiency of the enzyme alpha-galactosidase A (GLA), which leads to the buildup of globotriaosylceramide (GL-3) in blood vessels, kidneys, heart, nerves, and other organs, increasing the risk for kidney failure, myocardial infarction, stroke, and other problems.
Elfabrio delivers a functional version of GLA. It is given by intravenous infusion every 2 weeks.
Evidence for safety, tolerability, and efficacy of Elfabrio stem from a comprehensive clinical program in more than 140 patients with up to 7.5 years of follow-up treatment.
It has been studied in both ERT-naive and ERT-experienced patients. In one head-to-head trial, Elfabrio was noninferior in safety and efficacy to agalsidase beta (Fabrazyme, Sanofi Genzyme), the companies said in a press statement announcing approval.
U.S. incidence, prevalence of myasthenia gravis are rising
There has been an increase in the incidence and prevalence of myasthenia gravis in the United States, an analysis of new claims data shows. Investigators speculate the rise of this rare disorder may be caused by “increased diagnosis and more awareness of the disease over time, which has been shown in several studies,” said study investigator Ema Rodrigues, DSc, MPH, with Alexion Pharmaceuticals, Boston.
Dr. Rodrigues presented her research at the 2023 annual meeting of the American Academy of Neurology.
Funding for the study was provided by Alexion, AstraZeneca Rare
Disease. Dr. Rodrigues receives compensation and owns stock as an employee of Alexion, AstraZeneca Rare Diseases.
Novel agent offers hope for hereditary ATTR polyneuropathy in pivotal trial
The investigational agent eplontersen (Ionis Pharmaceuticals/AstraZeneca) halted neuropathy disease progression and improved neuropathy impairment and quality of life for patients with hereditary transthyretin-mediated amyloid polyneuropathy (ATTRv-PN) in a pivotal phase 3 trial.
Eplontersen led to “clinically and statistically significant benefits at week 66 with an early and rapid sustained reduction in serum TTR [transthyretin] concentration, a halting of the progression of the neuropathy impairment, and a trend to improvement in quality of life,” said principal investigator Sami Khella, MD, professor of clinical neurology at the University of Pennsylvania, Philadelphia.
Dr. Khella reported final data from the NEURO-TTRansform trial at the annual meeting of the American Academy of Neurology.
The FDA has accepted a new drug application for eplontersen for the treatment of ATTRv-PN. The drug has a Prescription Drug User Fee Act date of Dec. 22, 2023. Eplontersen has orphan drug designation in the United States.
The study was sponsored by Ionis Pharmaceuticals. Dr. Khella has relationships with Ionis, Pfizer, Alnylam, and Eidos.
FDA gives fast-track approval to new ALS drug
The FDA has approved the first treatment that takes a genetics-based approach to slowing or stopping the progression of a rare form of amyotrophic lateral sclerosis (ALS).
The FDA fast-tracked the approval of Qalsody (Biogen) based on early trial results. The agency said in a news release that its decision was based on the demonstrated ability of the drug to reduce a protein in the blood that is a sign of degeneration of brain and nerve cells.
Qalsody is given to people via a spinal injection, with an initial course of three injections every 2 weeks. People then get the injection once every 28 days.
The new treatment is approved only for people with SOD1-ALS, which is known for a genetic mutation. While ALS affects up to 32,000 people in the United States, just 2% of people with ALS have the SOD1 gene mutation. The FDA says the number of people in the United States who could use Qalsody is about 500.
FDA OKs first treatment for Friedreich ataxia
The FDA has approved the first treatment for the neurodegenerative disorder Friedreich ataxia for use in adults and adolescents aged 16 and older.
The recommended dose of omaveloxolone (Skyclarys, Reata Pharmaceuticals) is 150 mg (three capsules) taken orally once daily on an empty stomach.
The FDA approval of omaveloxolone was supported by a randomized double-blind, placebo-controlled study comprising 103 patients with genetically confirmed Friedreich ataxia and baseline modified Friedreich Ataxia Rating Scale (mFARS) scores between 20 and 80.
Treatment with the novel medication led to statistically significant lower mFARS scores, signifying less impairment, relative to placebo, at week 48. The placebo-corrected difference between the two groups was –2.41 points (P = .0138).
Omaveloxolone received priority review and had orphan drug, fast track, and rare pediatric disease designations.
FDA OKs first drug for Rett syndrome
The FDA has approved trofinetide oral solution (Daybue, Acadia Pharmaceuticals) as the first treatment of Rett syndrome in adults and children aged 2 years and older.
Trofinetide is a synthetic analogue of the amino-terminal tripeptide of insulinlike growth factor-1, which occurs naturally in the brain. The drug is designed to treat the core symptoms of Rett syndrome by potentially reducing neuroinflammation and supporting synaptic function.
The approval of trofinetide was supported by results from the pivotal phase 3 LAVENDER study that tested the efficacy and safety of trofinetide versus placebo in 187 female patients with Rett syndrome, aged 5-20 years.
More data back Guillain-Barré risk with Janssen COVID shot
New surveillance data from the Vaccine Adverse Event Reporting System (VAERS) back previous findings of increased risk for Guillain-Barré syndrome (GBS) after receiving the Janssen COVID-19 vaccine (Ad26.COV2.S).
Over 14 months, GBS reporting rates within 21 and 42 days of administration of Janssen’s replication-incompetent adenoviral vector vaccine were approximately 9-12 times higher than after administration of the Pfizer-BioNTech (BNT162b2) or the Moderna (mRNA-1273) mRNA COVID vaccines.
Additionally, observed GBS cases after the Janssen shot were two to three times greater than expected, based on background rates within 21 and 42 days of vaccination.
Conversely, and confirming prior data, there was no increased risk for GBS with the Pfizer or Moderna vaccines and no significant difference between observed and expected numbers of GBS cases after either mRNA COVID-19 vaccine.
The findings were published online in JAMA Network Open (2023 Feb 1. doi: 10.1001/jamanetworkopen.2022.53845).
Diazepam nasal spray effective in Lennox-Gastaut syndrome
A new analysis of data from a phase 3 clinical trial suggests that an inhaled diazepam nasal spray (Valtoco, Neurelis) works about as well among patients with Lennox-Gastaut syndrome (LGS) as it does with other patients with pediatric encephalopathies.
LGS is a severe form of epilepsy that generally begins in early childhood and has a poor prognosis and seizures that are often treatment refractory. The findings of the analysis should be encouraging to physicians who may view patients with LGS as not benefiting from treatment, said Daniel C. Tarquinio, DO, who presented the results at the 2022 annual meeting of the Child Neurology Society.
Novel cannabis oil curbs tics in severe Tourette syndrome
An oral oil containing tetrahydrocannabinol (THC) and cannabidiol (CBD) led to a significant and meaningful reduction in motor and vocal tics in patients with severe Tourette syndrome, results of a double-blind, placebo-controlled, crossover study showed.
“In a methodologically robust manner (and independent of any drug company sponsorship), we provide evidence for the effectiveness of repeated dosing with THC:CBD versus placebo in tic
suppression, as well as reduction of comorbid anxiety and obsessive-compulsive disorder in severe Tourette syndrome,” neuropsychiatrist and lead investigator Philip Mosley, PhD, said in an interview.
The results offer support to people with Tourette syndrome who “want to approach their doctor to try medicinal cannabis when other drugs have not worked or are intolerable,” said
Dr. Mosley, of the Wesley Research Institute and QIMR Berghofer Medical Research Institute, Herston, Australia.
The study was published online in NEJM Evidence (2023 Jun 7. doi: 10.1056/EVIDoa2300012).
Twenty-two adults (mean age, 31 years) with severe Tourette syndrome received THC:CBD oil titrated upward over 6 weeks to a daily dose of 20 mg of THC and 20 mg of CBD, followed by a 6-week course of placebo (or vice versa). Six participants had not previously used cannabis.
The primary outcome was the total tic score on the Yale Global Tic Severity Scale (YGTSS; range, 0-50 with higher scores = greater tic severity).
The mean baseline YGTSS total tic score was 35.7. At 6 weeks, the reduction in total tic score was 8.9 with THC:CBD versus 2.5 with placebo.
A linear mixed-effects model (intention to treat) showed a significant interaction of treatment and visit number (P = .008), indicating a greater decrease (improvement) in tic score over time with THC:CBD, the study team reported.
On average, the magnitude of the tic reduction was “moderate” and comparable with the effect observed with existing treatments such as antipsychotic agents, the investigators noted.
The study was funded by the Wesley Medical Research Institute, Brisbane, and the Lambert Initiative for Cannabinoid Therapeutics, a philanthropically funded research organization at the University of Sydney, Australia.
Dr. Mosley reported no relevant financial relationships.