User login
National poll shows ‘concerning’ impact of COVID on Americans’ mental health
Concern and anxiety around COVID-19 remains high among Americans, with more people reporting mental health effects from the pandemic this year than last, and parents concerned about the mental health of their children, results of a new poll by the American Psychiatric Association show. Although the overall level of anxiety has decreased from last year’s APA poll, “the degree to which anxiety still reigns is concerning,” APA President Jeffrey Geller, MD, MPH, told this news organization.

The results of the latest poll were presented at the American Psychiatric Association 2021 annual meeting and based on an online survey conducted March 26 to April 5 among a sample of 1,000 adults aged 18 years or older.
Serious mental health hit
In the new poll, about 4 in 10 Americans (41%) report they are more anxious than last year, down from just over 60%.
Young adults aged 18-29 years (49%) and Hispanic/Latinos (50%) are more likely to report being more anxious now than a year ago. Those 65 or older (30%) are less apt to say they feel more anxious than last year.
The latest poll also shows that Americans are more anxious about family and loved ones getting COVID-19 (64%) than about catching the virus themselves (49%).
Concern about family and loved ones contracting COVID-19 has increased since last year’s poll (conducted September 2020), rising from 56% then to 64% now. Hispanic/Latinx individuals (73%) and African American/Black individuals (76%) are more anxious about COVID-19 than White people (59%).
In the new poll, 43% of adults report the pandemic has had a serious impact on their mental health, up from 37% in 2020. Younger adults are more apt than older adults to report serious mental health effects.
Slightly fewer Americans report the pandemic is affecting their day-to-day life now as compared to a year ago, in ways such as problems sleeping (19% down from 22%), difficulty concentrating (18% down from 20%), and fighting more with loved ones (16% down from 17%).
The percentage of adults consuming more alcohol or other substances/drugs than normal increased slightly since last year (14%-17%). Additionally, 33% of adults (40% of women) report gaining weight during the pandemic.
Call to action
More than half of adults (53%) with children report they are concerned about the mental state of their children and almost half (48%) report the pandemic has caused mental health problems for one or more of their children, including minor problems for 29% and major problems for 19%.
More than a quarter (26%) of parents have sought professional mental health help for their children because of the pandemic.
; 23% received help from a primary care professional, 18% from a psychiatrist, 15% from a psychologist, 13% from a therapist, 10% from a social worker, and 10% from a school counselor or school psychologist.
More than 1 in 5 parents reported difficulty scheduling appointments for their child with a mental health professional.
“This poll shows that, even as vaccines become more widespread, Americans are still worried about the mental state of their children,” Dr. Geller said in a news release.
“This is a call to action for policymakers, who need to remember that, in our COVID-19 recovery, there’s no health without mental health,” he added.
Just over three-quarters (76%) of those surveyed say they have been or intend to get vaccinated; 22% say they don’t intend to get vaccinated; and 2% didn’t know.
For those who do not intend to get vaccinated, the primary concern (53%) is about side effects of the vaccine. Other reasons for not getting vaccinated include believing the vaccine is not effective (31%), believing the makers of the vaccine aren’t being honest about what’s in it (27%), and fear/anxiety about needles (12%).
Resiliency a finite resource
Reached for comment, Samoon Ahmad, MD, professor in the department of psychiatry, New York University, said it’s not surprising that Americans are still suffering more anxiety than normal.

“The Census Bureau’s Household Pulse Survey has shown that anxiety and depression levels have remained higher than normal since the pandemic began. That 43% of adults now say that the pandemic has had a serious impact on their mental health seems in line with what that survey has been reporting for over a year,” Dr. Ahmad, who serves as unit chief of inpatient psychiatry at Bellevue Hospital Center in New York, said in an interview.
He believes there are several reasons why anxiety levels remain high. One reason is something he’s noticed among his patients for years. “Most people struggle with anxiety especially at night when the noise and distractions of contemporary life fade away. This is the time of introspection,” he explained.
“Quarantine has been kind of like a protracted night because the distractions that are common in the so-called ‘rat race’ have been relatively muted for the past 14 months. I believe this has caused what you might call ‘forced introspection,’ and that this is giving rise to feelings of anxiety as people use their time alone to reassess their careers and their social lives and really begin to fret about some of the decisions that have led them to this point in their lives,” said Dr. Ahmad.
The other finding in the APA survey – that people are more concerned about their loved ones catching the virus than they were a year ago – is also not surprising, Dr. Ahmad said.
“Even though we seem to have turned a corner in the United States and the worst of the pandemic is behind us, the surge that went from roughly November through March of this year was more wide-reaching geographically than previous waves, and I think this made the severity of the virus far more real to people who lived in communities that had been spared severe outbreaks during the surges that we saw in the spring and summer of 2020,” Dr. Ahmad told this news organization.
“There’s also heightened concern over variants and the efficacy of the vaccine in treating these variants. Those who have families in other countries where the virus is surging, such as India or parts of Latin America, are likely experiencing additional stress and anxiety too,” he noted.
While the new APA poll findings are not surprising, they still are “deeply concerning,” Dr. Ahmad said.
“Resiliency is a finite resource, and people can only take so much stress before their mental health begins to suffer. For most people, this is not going to lead to some kind of overdramatic nervous breakdown. Instead, one may notice that they are more irritable than they once were, that they’re not sleeping particularly well, or that they have a nagging sense of discomfort and stress when doing activities that they used to think of as normal,” like taking a trip to the grocery store, meeting up with friends, or going to work, Dr. Ahmad said.
“Overcoming this kind of anxiety and reacclimating ourselves to social situations is going to take more time for some people than others, and that is perfectly natural,” said Dr. Ahmad, founder of the Integrative Center for Wellness in New York.
“I don’t think it’s wise to try to put a limit on what constitutes a normal amount of time to readjust, and I think everyone in the field of mental health needs to avoid pathologizing any lingering sense of unease. No one needs to be medicated or diagnosed with a mental illness because they are nervous about going into public spaces in the immediate aftermath of a pandemic. We need to show a lot of patience and encourage people to readjust at their own pace for the foreseeable future,” Dr. Ahmad said.
Dr. Geller and Dr. Ahmad have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Concern and anxiety around COVID-19 remains high among Americans, with more people reporting mental health effects from the pandemic this year than last, and parents concerned about the mental health of their children, results of a new poll by the American Psychiatric Association show. Although the overall level of anxiety has decreased from last year’s APA poll, “the degree to which anxiety still reigns is concerning,” APA President Jeffrey Geller, MD, MPH, told this news organization.
The results of the latest poll were presented at the American Psychiatric Association 2021 annual meeting and based on an online survey conducted March 26 to April 5 among a sample of 1,000 adults aged 18 years or older.
Serious mental health hit
In the new poll, about 4 in 10 Americans (41%) report they are more anxious than last year, down from just over 60%.
Young adults aged 18-29 years (49%) and Hispanic/Latinos (50%) are more likely to report being more anxious now than a year ago. Those 65 or older (30%) are less apt to say they feel more anxious than last year.
The latest poll also shows that Americans are more anxious about family and loved ones getting COVID-19 (64%) than about catching the virus themselves (49%).
Concern about family and loved ones contracting COVID-19 has increased since last year’s poll (conducted September 2020), rising from 56% then to 64% now. Hispanic/Latinx individuals (73%) and African American/Black individuals (76%) are more anxious about COVID-19 than White people (59%).
In the new poll, 43% of adults report the pandemic has had a serious impact on their mental health, up from 37% in 2020. Younger adults are more apt than older adults to report serious mental health effects.
Slightly fewer Americans report the pandemic is affecting their day-to-day life now as compared to a year ago, in ways such as problems sleeping (19% down from 22%), difficulty concentrating (18% down from 20%), and fighting more with loved ones (16% down from 17%).
The percentage of adults consuming more alcohol or other substances/drugs than normal increased slightly since last year (14%-17%). Additionally, 33% of adults (40% of women) report gaining weight during the pandemic.
Call to action
More than half of adults (53%) with children report they are concerned about the mental state of their children and almost half (48%) report the pandemic has caused mental health problems for one or more of their children, including minor problems for 29% and major problems for 19%.
More than a quarter (26%) of parents have sought professional mental health help for their children because of the pandemic.
; 23% received help from a primary care professional, 18% from a psychiatrist, 15% from a psychologist, 13% from a therapist, 10% from a social worker, and 10% from a school counselor or school psychologist.
More than 1 in 5 parents reported difficulty scheduling appointments for their child with a mental health professional.
“This poll shows that, even as vaccines become more widespread, Americans are still worried about the mental state of their children,” Dr. Geller said in a news release.
“This is a call to action for policymakers, who need to remember that, in our COVID-19 recovery, there’s no health without mental health,” he added.
Just over three-quarters (76%) of those surveyed say they have been or intend to get vaccinated; 22% say they don’t intend to get vaccinated; and 2% didn’t know.
For those who do not intend to get vaccinated, the primary concern (53%) is about side effects of the vaccine. Other reasons for not getting vaccinated include believing the vaccine is not effective (31%), believing the makers of the vaccine aren’t being honest about what’s in it (27%), and fear/anxiety about needles (12%).
Resiliency a finite resource
Reached for comment, Samoon Ahmad, MD, professor in the department of psychiatry, New York University, said it’s not surprising that Americans are still suffering more anxiety than normal.
“The Census Bureau’s Household Pulse Survey has shown that anxiety and depression levels have remained higher than normal since the pandemic began. That 43% of adults now say that the pandemic has had a serious impact on their mental health seems in line with what that survey has been reporting for over a year,” Dr. Ahmad, who serves as unit chief of inpatient psychiatry at Bellevue Hospital Center in New York, said in an interview.
He believes there are several reasons why anxiety levels remain high. One reason is something he’s noticed among his patients for years. “Most people struggle with anxiety especially at night when the noise and distractions of contemporary life fade away. This is the time of introspection,” he explained.
“Quarantine has been kind of like a protracted night because the distractions that are common in the so-called ‘rat race’ have been relatively muted for the past 14 months. I believe this has caused what you might call ‘forced introspection,’ and that this is giving rise to feelings of anxiety as people use their time alone to reassess their careers and their social lives and really begin to fret about some of the decisions that have led them to this point in their lives,” said Dr. Ahmad.
The other finding in the APA survey – that people are more concerned about their loved ones catching the virus than they were a year ago – is also not surprising, Dr. Ahmad said.
“Even though we seem to have turned a corner in the United States and the worst of the pandemic is behind us, the surge that went from roughly November through March of this year was more wide-reaching geographically than previous waves, and I think this made the severity of the virus far more real to people who lived in communities that had been spared severe outbreaks during the surges that we saw in the spring and summer of 2020,” Dr. Ahmad told this news organization.
“There’s also heightened concern over variants and the efficacy of the vaccine in treating these variants. Those who have families in other countries where the virus is surging, such as India or parts of Latin America, are likely experiencing additional stress and anxiety too,” he noted.
While the new APA poll findings are not surprising, they still are “deeply concerning,” Dr. Ahmad said.
“Resiliency is a finite resource, and people can only take so much stress before their mental health begins to suffer. For most people, this is not going to lead to some kind of overdramatic nervous breakdown. Instead, one may notice that they are more irritable than they once were, that they’re not sleeping particularly well, or that they have a nagging sense of discomfort and stress when doing activities that they used to think of as normal,” like taking a trip to the grocery store, meeting up with friends, or going to work, Dr. Ahmad said.
“Overcoming this kind of anxiety and reacclimating ourselves to social situations is going to take more time for some people than others, and that is perfectly natural,” said Dr. Ahmad, founder of the Integrative Center for Wellness in New York.
“I don’t think it’s wise to try to put a limit on what constitutes a normal amount of time to readjust, and I think everyone in the field of mental health needs to avoid pathologizing any lingering sense of unease. No one needs to be medicated or diagnosed with a mental illness because they are nervous about going into public spaces in the immediate aftermath of a pandemic. We need to show a lot of patience and encourage people to readjust at their own pace for the foreseeable future,” Dr. Ahmad said.
Dr. Geller and Dr. Ahmad have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Concern and anxiety around COVID-19 remains high among Americans, with more people reporting mental health effects from the pandemic this year than last, and parents concerned about the mental health of their children, results of a new poll by the American Psychiatric Association show. Although the overall level of anxiety has decreased from last year’s APA poll, “the degree to which anxiety still reigns is concerning,” APA President Jeffrey Geller, MD, MPH, told this news organization.
The results of the latest poll were presented at the American Psychiatric Association 2021 annual meeting and based on an online survey conducted March 26 to April 5 among a sample of 1,000 adults aged 18 years or older.
Serious mental health hit
In the new poll, about 4 in 10 Americans (41%) report they are more anxious than last year, down from just over 60%.
Young adults aged 18-29 years (49%) and Hispanic/Latinos (50%) are more likely to report being more anxious now than a year ago. Those 65 or older (30%) are less apt to say they feel more anxious than last year.
The latest poll also shows that Americans are more anxious about family and loved ones getting COVID-19 (64%) than about catching the virus themselves (49%).
Concern about family and loved ones contracting COVID-19 has increased since last year’s poll (conducted September 2020), rising from 56% then to 64% now. Hispanic/Latinx individuals (73%) and African American/Black individuals (76%) are more anxious about COVID-19 than White people (59%).
In the new poll, 43% of adults report the pandemic has had a serious impact on their mental health, up from 37% in 2020. Younger adults are more apt than older adults to report serious mental health effects.
Slightly fewer Americans report the pandemic is affecting their day-to-day life now as compared to a year ago, in ways such as problems sleeping (19% down from 22%), difficulty concentrating (18% down from 20%), and fighting more with loved ones (16% down from 17%).
The percentage of adults consuming more alcohol or other substances/drugs than normal increased slightly since last year (14%-17%). Additionally, 33% of adults (40% of women) report gaining weight during the pandemic.
Call to action
More than half of adults (53%) with children report they are concerned about the mental state of their children and almost half (48%) report the pandemic has caused mental health problems for one or more of their children, including minor problems for 29% and major problems for 19%.
More than a quarter (26%) of parents have sought professional mental health help for their children because of the pandemic.
; 23% received help from a primary care professional, 18% from a psychiatrist, 15% from a psychologist, 13% from a therapist, 10% from a social worker, and 10% from a school counselor or school psychologist.
More than 1 in 5 parents reported difficulty scheduling appointments for their child with a mental health professional.
“This poll shows that, even as vaccines become more widespread, Americans are still worried about the mental state of their children,” Dr. Geller said in a news release.
“This is a call to action for policymakers, who need to remember that, in our COVID-19 recovery, there’s no health without mental health,” he added.
Just over three-quarters (76%) of those surveyed say they have been or intend to get vaccinated; 22% say they don’t intend to get vaccinated; and 2% didn’t know.
For those who do not intend to get vaccinated, the primary concern (53%) is about side effects of the vaccine. Other reasons for not getting vaccinated include believing the vaccine is not effective (31%), believing the makers of the vaccine aren’t being honest about what’s in it (27%), and fear/anxiety about needles (12%).
Resiliency a finite resource
Reached for comment, Samoon Ahmad, MD, professor in the department of psychiatry, New York University, said it’s not surprising that Americans are still suffering more anxiety than normal.
“The Census Bureau’s Household Pulse Survey has shown that anxiety and depression levels have remained higher than normal since the pandemic began. That 43% of adults now say that the pandemic has had a serious impact on their mental health seems in line with what that survey has been reporting for over a year,” Dr. Ahmad, who serves as unit chief of inpatient psychiatry at Bellevue Hospital Center in New York, said in an interview.
He believes there are several reasons why anxiety levels remain high. One reason is something he’s noticed among his patients for years. “Most people struggle with anxiety especially at night when the noise and distractions of contemporary life fade away. This is the time of introspection,” he explained.
“Quarantine has been kind of like a protracted night because the distractions that are common in the so-called ‘rat race’ have been relatively muted for the past 14 months. I believe this has caused what you might call ‘forced introspection,’ and that this is giving rise to feelings of anxiety as people use their time alone to reassess their careers and their social lives and really begin to fret about some of the decisions that have led them to this point in their lives,” said Dr. Ahmad.
The other finding in the APA survey – that people are more concerned about their loved ones catching the virus than they were a year ago – is also not surprising, Dr. Ahmad said.
“Even though we seem to have turned a corner in the United States and the worst of the pandemic is behind us, the surge that went from roughly November through March of this year was more wide-reaching geographically than previous waves, and I think this made the severity of the virus far more real to people who lived in communities that had been spared severe outbreaks during the surges that we saw in the spring and summer of 2020,” Dr. Ahmad told this news organization.
“There’s also heightened concern over variants and the efficacy of the vaccine in treating these variants. Those who have families in other countries where the virus is surging, such as India or parts of Latin America, are likely experiencing additional stress and anxiety too,” he noted.
While the new APA poll findings are not surprising, they still are “deeply concerning,” Dr. Ahmad said.
“Resiliency is a finite resource, and people can only take so much stress before their mental health begins to suffer. For most people, this is not going to lead to some kind of overdramatic nervous breakdown. Instead, one may notice that they are more irritable than they once were, that they’re not sleeping particularly well, or that they have a nagging sense of discomfort and stress when doing activities that they used to think of as normal,” like taking a trip to the grocery store, meeting up with friends, or going to work, Dr. Ahmad said.
“Overcoming this kind of anxiety and reacclimating ourselves to social situations is going to take more time for some people than others, and that is perfectly natural,” said Dr. Ahmad, founder of the Integrative Center for Wellness in New York.
“I don’t think it’s wise to try to put a limit on what constitutes a normal amount of time to readjust, and I think everyone in the field of mental health needs to avoid pathologizing any lingering sense of unease. No one needs to be medicated or diagnosed with a mental illness because they are nervous about going into public spaces in the immediate aftermath of a pandemic. We need to show a lot of patience and encourage people to readjust at their own pace for the foreseeable future,” Dr. Ahmad said.
Dr. Geller and Dr. Ahmad have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Moral distress in the COVID era weighs on hospitalists
Focus on effort, not just outcomes
Moral distress can result when health professionals like doctors and nurses feel prevented from doing what they know is right and ethically correct – reflecting the values of their profession and their own sense of professional integrity – because of unmanageable caseload demands, lack of resources, coverage limitations, or institutional policies.

Hospitalists are not exempt from moral distress, which is associated with soul-searching, burnout, and even PTSD. It is also associated with a higher likelihood for professionals to report an intention to leave their jobs. But the COVID-19 pandemic has superimposed a whole new layer of challenges, constraints, and frustrations, creating a potent mix of trauma and exhaustion, cumulative unease, depleted job satisfaction, and difficult ethical choices.
These challenges include seeing so many patients die and working with short supplies of personal protective equipment (PPE) – with resulting fears that they could catch the virus or pass it on to others, including loved ones. Also, not having enough ventilators or even beds for patients in hospitals hit hard by COVID surges raises fears that decisions for rationing medical care might become necessary.
In a commentary published in the Journal of General Internal Medicine in October 2019 – shortly before the COVID pandemic burst onto the scene – hospitalist and medical sociologist Elizabeth Dzeng, MD, PhD, MPH, and hospital medicine pioneer Robert Wachter, MD, MHM, both from the University of California, San Francisco, described “moral distress and professional ethical dissonance as root causes of burnout.”1 They characterized moral distress by its emotional exhaustion, depersonalization, reduced sense of accomplishment, and moral apathy, and they called for renewed attention to social and ethical dimensions of practice and threats to physician professionalism.

Prevailing explanations for documented high rates of burnout in doctors have tended to focus on work hours and struggles with electronic medical records and the like, Dr. Dzeng and Dr. Wachter wrote. “We see evidence of an insidious moral distress resulting from physicians’ inability to act in accord with their individual and professional ethical values due to institutional and social constraints.”
COVID has intensified these issues surrounding moral distress. “In a short period of time it created more situations that raise issues of moral distress than I have seen since the early days of HIV,” Dr. Wachter said. “Those of us who work in hospitals often find ourselves in complex circumstances with limited resources. What was so striking about COVID was finding ourselves caring for large volumes of patients who had a condition that was new to us.”
And the fact that constraints imposed by COVID, such as having to don unwieldy PPE and not allowing families to be present with hospitalized loved ones, are explainable and rational only helps a little with the clinician’s distress.
People talk about the need for doctors to be more resilient, Dr. Dzeng added, but that’s too narrow of an approach to these very real challenges. There are huge issues of workforce retention and costs, major mental health issues, suicide – and implications for patient care, because burned-out doctors can be bad doctors.
What is moral distress?
Moral distress is a term from the nursing ethics literature, attributed to philosopher Andrew Jameton in 1984.2 Contributors to moral distress imposed by COVID include having to make difficult medical decisions under stressful circumstances – especially early on, when effective treatment options were few. Doctors felt the demands of the pandemic were putting care quality and patient safety at risk. Poor working conditions overall, being pushed to work beyond their normal physical limits for days at a time, and feelings of not being valued added to this stress. But some say the pandemic has only highlighted and amplified existing inequities and disparities in the health care system.
Experts say moral distress is about feeling powerless, especially in a system driven by market values, and feeling let down by a society that has put them in harm’s way. They work all day under physically and emotionally exhausting conditions and then go home to hear specious conspiracy theories about the pandemic and see other people unwilling to wear masks.

Moral distress is complicated, said Lucia Wocial, PhD, RN, a nurse ethicist and cochair of the ethics consultation subcommittee at Indiana University Health in Indianapolis. “If you say you have moral distress, my first response is: tell me more. It helps to peel back the layers of this complexity. Emotion is only part of moral distress. It’s about the professional’s sense of responsibility and obligation – and the inability to honor that.”
Dr. Wocial, whose research specialty is moral distress, is corresponding author of a study published in the Journal of General Internal Medicine in February 2020, which identified moral distress in 4 out of 10 surveyed physicians who cared for older hospitalized adults and found themselves needing to work with their surrogate decision-makers.3 “We know physician moral distress is higher when people haven’t had the chance to hold conversations about their end-of-life care preferences,” she said, such as whether to continue life support.
“We have also learned that communication is key to diminishing physician moral distress. Our responsibility as clinicians is to guide patients and families through these decisions. If the family feels a high level of support from me, then my moral distress is lower,” she added. “If you think about how COVID has evolved, at first people were dying so quickly. Some patients were going to the ICU on ventilators without ever having a goals-of-care conversation.”
COVID has shifted the usual standard of care in U.S. hospitals in the face of patient surges. “How can you feel okay in accepting a level of care that in the prepandemic world would not have been acceptable?” Dr. Wocial posed. “What if you know the standard of care has shifted, of necessity, but you haven’t had time to prepare for it and nobody’s talking about what that means? Who is going to help you accept that good enough under these circumstances is enough – at least for today?”
What to call it
Michael J. Asken, PhD, director of provider well-being at UPMC Pinnacle Harrisburg (Pa.), has questioned in print the use of the military and wartime term “moral injury” when applied to a variety of less serious physician stressors.4 More recently, however, he observed, “The pandemic has muted or erased many of the distinctions between medical care and military conflict. ... The onslaught and volume of critical patients and resulting deaths is beyond what most providers have ever contemplated as part of care.”5

In a recent interview with the Hospitalist, he said: “While I initially resisted using the term moral injury, especially pre-COVID, because it was not equivalent to the moral injury created by war, I have relented a bit.” The volume of deaths and the apparent dangers to providers themselves reflect some of the critical aspects of war, and repetitive, intense, and/or incessant ethical challenges may have longer term negative psychological or emotional effects.
“Feeling emotional pain in situations of multiple deaths is to be expected and, perhaps, should even be welcomed as a sign of retained humanity and a buffer against burnout and cynicism in these times of unabating stress,” Dr. Asken said. “This is only true, however, if the emotional impact is tolerable and not experienced in repetitive extremes.”

“These things are real,” said Clarissa Barnes, MD, a physician adviser, hospitalist at Avera McKennan Hospital in Sioux Falls, S.D., and former medical director of Avera’s LIGHT Program, a wellness-oriented service for clinicians. Dr. Barnes herself caught the virus on the job but has since recovered.
“Physicians don’t see their work as an occupation. It’s their core identity: I am a doctor; I practice medicine. If things are being done in ways I don’t think are right, that’s fundamentally a breach,” she said. “As internists, we have an opportunity to forestall death whenever we can and, if not, promote a peaceful death. That’s what made me choose this specialty. I think there’s value in allowing a person to end well. But when that doesn’t happen because of social or administrative reasons, that’s hard.”
Where is the leadership?
“A lot of moral injury comes down to the individual health system and its leaders. Some have done well; others you hear saying things that make you question whether these are the people you want leading the organization. Hospitalists need to have a clear value framework and an idea of how to negotiate things when decisions don’t match that framework,” Dr. Barnes said.
“Sometimes administrators have additional information that they’re not sharing,” she added. “They’re caught between a rock and a hard place regarding the decisions they have to make, but they need to be more transparent and not hold things so close to their vest while thinking they are helping clinicians [by doing so]. Physicians need to understand why they are being asked to do things counter to what they believe is appropriate.”
David Oliver, MD, a geriatrics and internal medicine consultant at Royal Berkshire Hospital in Reading, England, also practices as a hospital physician, a role similar to the hospitalist in the United States. “In any system, in any environment, the job of being a doctor, nurse, or other health professional carries a lot of responsibility. That is a timeless, inherent stress of medical practice. With COVID, we’ve seen a lot of emotional burdens – a whole separate set of problems outside of your control, where you are responsible for care but don’t have accountability,” he said.
“People like me, hospital doctors, are used to chronic workforce issues in the National Health Service. But we didn’t sign up to come and get COVID and be hospitalized ourselves.” More than 850 frontline health care providers in the U.K. have so far died from the virus, Dr. Oliver said. “I saw five patients die in 90 minutes one day in April. That’s above and beyond normal human capacity.”
In England specifically, he said, it has exposed underlying structural issues and serious workforce gaps, unfilled vacancies, and a much lower number of ICU beds per 100,000 population than the United States or Europe. And there is consistent pressure to send patients home in order to empty beds for new patients.
But a range of supportive services is offered in U.K. hospitals, such as making senior clinicians available to speak to frontline clinicians, providing mentorship and a sounding board. The Point of Care Foundation has helped to disseminate the practice of Schwartz Rounds, a group reflective practice forum for health care teams developed by the Schwartz Center for Compassionate Healthcare in Boston.
“We don’t need this clap-for-the-NHS heroes stuff,” Dr. Oliver said. “We need an adequate workforce and [better] working conditions. What happened on the front lines of the pandemic was heroic – all done by local clinical teams. But where was the government – the centralized NHS? A lot of frontline clinicians aren’t feeling valued, supported, or listened to.”
What can be done?
What are some things that hospitalists can do, individually and collectively, to try to prevent moral distress from turning into full-scale burnout? Dr. Wocial emphasized the importance of unit-based ethics conversations. “At IU Health we have someone who is available to sit down with frontline clinicians and help unpack what they are experiencing,” she said. Clinicians need to be able to process this terrible experience in order to sort out the feelings of sadness from questions of whether they are doing something wrong.
Hospital chaplains are exquisitely skilled at supporting people and debriefing hospital teams, Dr. Wocial added. Palliative care professionals are also skilled at facilitating goals of care conversations with patients and families and can support hospitalists through coaching and joint family meetings.
“It’s about raising your sense of agency in your job – what in your practice you can control. People need to be able to talk frankly about it. Some managers say to clinicians: ‘Just buck up,’ while others are doing a fabulous job of offering support to their staff,” Dr. Wocial said. Hospitalists have to be willing to say when they’ve had too much. “You may not get help when you first ask for it. Be persistent. Asking for help doesn’t make you weak.”
Most doctors have their own strategies for managing stress on the job, Dr. Wachter noted. “What makes it a little easier is not having to do it alone. Many find solace in community, but community has been constrained by this pandemic. You can’t just go out for a beer after work anymore. So what are other ways to let off steam?”
The people leading hospitalist programs need to work harder at creating community and empathy when the tools allowing people to get together are somewhat limited. “Everybody is tired of Zoom,” he said. “One thing I learned as a manager was to just send messages to people acknowledging that I know this is hard. Try to think from the lens of other people and what they would find useful.”
The pandemic has been terribly unpredictable, Dr. Wachter added, but it won’t go on forever. For some doctors, yoga or mindfulness meditation may be very comforting. “For me, that’s not what I do. Golf or a good Seinfeld episode works for me.”

SHM’s Wellbeing Taskforce has created a “Hospital Medicine COVID Check-in Guide for Self & Peers” to promote both sharing and support for one another. It can be found at SHM’s Wellbeing webpage [www.hospitalmedicine.org/practice-management/wellbeing/]. The Taskforce believes that sharing common stressors as hospitalists can be healing, said its chair, Sarah Richards, MD, assistant professor of medicine at the University of Nebraska, Omaha. “This is especially true in situations where we feel we can’t provide the type of care we know our patients deserve.”
Respect, advocacy, self-care
Dr. Asken encouraged clinicians to focus on the efforts they are making on the job, not just the outcomes. “If someone has done their absolute best in a given circumstance, satisfaction and solace needs to be taken from that,” he said.
“Ongoing support group meetings, which we have called frontline support groups, should occur on a regular basis. Designated for physicians on the medical floors and in critical care units who are directly involved with COVID patients, these provide a brief respite but also engagement, sharing, and strengthening of mutual support.”
A lot of these issues have a fundamental thread, which comes down to respect, Dr. Barnes said. “Hospitalists need to hear their hospital administrators say: ‘I hear what you’re saying [about a problem]. Let’s think together about how to solve it.’ We need to work on being clear, and we need to speak up for what’s right. If you aren’t comfortable doing things you are being asked to do in the hospital, maybe you’re not working in the right place.”
Some efforts in the area of wellness and self-care really are helpful, Dr. Barnes said. “But you can’t exercise you way through a health system that doesn’t respect you. You need to get out of the mindset that you have no ability to make things different. We are not powerless as doctors. We can do a lot, actually. Physicians need to take ownership. If you are a hospitalist and you’re not part of any local or state or national organization that advocates for physicians, you should be.”
References
1. Dzeng L and Wachter RM. Ethics in conflict: Moral distress as a root cause of burnout. J Gen Intern Med. 2020 Feb;35(2):409-11. doi: 10.1007/s11606-019-05505-6.
2. Jameton A, Nursing Practice: The ethical issues. Prentice Hall Series in the Philosophy of Medicine. 1984, Englewood Cliffs, N.J.: Prentice Hall.
3. Wocial LD et al. Factors associated with physician moral distress caring for hospitalized elderly patients needing a surrogate decision-maker: A prospective study. J Gen Intern Med. 2020 May;35(5):1405-12. doi: 10.1007/s11606-020-05652-1.
4. Asken MJ. It’s not moral injury: It’s burnout (or something else). Medical Economics; June 7, 2019.
5. Asken MJ. Now it is moral injury: The COVID-19 pandemic and moral distress. Medical Economics; April 29, 2020.
Focus on effort, not just outcomes
Focus on effort, not just outcomes
Moral distress can result when health professionals like doctors and nurses feel prevented from doing what they know is right and ethically correct – reflecting the values of their profession and their own sense of professional integrity – because of unmanageable caseload demands, lack of resources, coverage limitations, or institutional policies.
Hospitalists are not exempt from moral distress, which is associated with soul-searching, burnout, and even PTSD. It is also associated with a higher likelihood for professionals to report an intention to leave their jobs. But the COVID-19 pandemic has superimposed a whole new layer of challenges, constraints, and frustrations, creating a potent mix of trauma and exhaustion, cumulative unease, depleted job satisfaction, and difficult ethical choices.
These challenges include seeing so many patients die and working with short supplies of personal protective equipment (PPE) – with resulting fears that they could catch the virus or pass it on to others, including loved ones. Also, not having enough ventilators or even beds for patients in hospitals hit hard by COVID surges raises fears that decisions for rationing medical care might become necessary.
In a commentary published in the Journal of General Internal Medicine in October 2019 – shortly before the COVID pandemic burst onto the scene – hospitalist and medical sociologist Elizabeth Dzeng, MD, PhD, MPH, and hospital medicine pioneer Robert Wachter, MD, MHM, both from the University of California, San Francisco, described “moral distress and professional ethical dissonance as root causes of burnout.”1 They characterized moral distress by its emotional exhaustion, depersonalization, reduced sense of accomplishment, and moral apathy, and they called for renewed attention to social and ethical dimensions of practice and threats to physician professionalism.
Prevailing explanations for documented high rates of burnout in doctors have tended to focus on work hours and struggles with electronic medical records and the like, Dr. Dzeng and Dr. Wachter wrote. “We see evidence of an insidious moral distress resulting from physicians’ inability to act in accord with their individual and professional ethical values due to institutional and social constraints.”
COVID has intensified these issues surrounding moral distress. “In a short period of time it created more situations that raise issues of moral distress than I have seen since the early days of HIV,” Dr. Wachter said. “Those of us who work in hospitals often find ourselves in complex circumstances with limited resources. What was so striking about COVID was finding ourselves caring for large volumes of patients who had a condition that was new to us.”
And the fact that constraints imposed by COVID, such as having to don unwieldy PPE and not allowing families to be present with hospitalized loved ones, are explainable and rational only helps a little with the clinician’s distress.
People talk about the need for doctors to be more resilient, Dr. Dzeng added, but that’s too narrow of an approach to these very real challenges. There are huge issues of workforce retention and costs, major mental health issues, suicide – and implications for patient care, because burned-out doctors can be bad doctors.
What is moral distress?
Moral distress is a term from the nursing ethics literature, attributed to philosopher Andrew Jameton in 1984.2 Contributors to moral distress imposed by COVID include having to make difficult medical decisions under stressful circumstances – especially early on, when effective treatment options were few. Doctors felt the demands of the pandemic were putting care quality and patient safety at risk. Poor working conditions overall, being pushed to work beyond their normal physical limits for days at a time, and feelings of not being valued added to this stress. But some say the pandemic has only highlighted and amplified existing inequities and disparities in the health care system.
Experts say moral distress is about feeling powerless, especially in a system driven by market values, and feeling let down by a society that has put them in harm’s way. They work all day under physically and emotionally exhausting conditions and then go home to hear specious conspiracy theories about the pandemic and see other people unwilling to wear masks.
Moral distress is complicated, said Lucia Wocial, PhD, RN, a nurse ethicist and cochair of the ethics consultation subcommittee at Indiana University Health in Indianapolis. “If you say you have moral distress, my first response is: tell me more. It helps to peel back the layers of this complexity. Emotion is only part of moral distress. It’s about the professional’s sense of responsibility and obligation – and the inability to honor that.”
Dr. Wocial, whose research specialty is moral distress, is corresponding author of a study published in the Journal of General Internal Medicine in February 2020, which identified moral distress in 4 out of 10 surveyed physicians who cared for older hospitalized adults and found themselves needing to work with their surrogate decision-makers.3 “We know physician moral distress is higher when people haven’t had the chance to hold conversations about their end-of-life care preferences,” she said, such as whether to continue life support.
“We have also learned that communication is key to diminishing physician moral distress. Our responsibility as clinicians is to guide patients and families through these decisions. If the family feels a high level of support from me, then my moral distress is lower,” she added. “If you think about how COVID has evolved, at first people were dying so quickly. Some patients were going to the ICU on ventilators without ever having a goals-of-care conversation.”
COVID has shifted the usual standard of care in U.S. hospitals in the face of patient surges. “How can you feel okay in accepting a level of care that in the prepandemic world would not have been acceptable?” Dr. Wocial posed. “What if you know the standard of care has shifted, of necessity, but you haven’t had time to prepare for it and nobody’s talking about what that means? Who is going to help you accept that good enough under these circumstances is enough – at least for today?”
What to call it
Michael J. Asken, PhD, director of provider well-being at UPMC Pinnacle Harrisburg (Pa.), has questioned in print the use of the military and wartime term “moral injury” when applied to a variety of less serious physician stressors.4 More recently, however, he observed, “The pandemic has muted or erased many of the distinctions between medical care and military conflict. ... The onslaught and volume of critical patients and resulting deaths is beyond what most providers have ever contemplated as part of care.”5
In a recent interview with the Hospitalist, he said: “While I initially resisted using the term moral injury, especially pre-COVID, because it was not equivalent to the moral injury created by war, I have relented a bit.” The volume of deaths and the apparent dangers to providers themselves reflect some of the critical aspects of war, and repetitive, intense, and/or incessant ethical challenges may have longer term negative psychological or emotional effects.
“Feeling emotional pain in situations of multiple deaths is to be expected and, perhaps, should even be welcomed as a sign of retained humanity and a buffer against burnout and cynicism in these times of unabating stress,” Dr. Asken said. “This is only true, however, if the emotional impact is tolerable and not experienced in repetitive extremes.”
“These things are real,” said Clarissa Barnes, MD, a physician adviser, hospitalist at Avera McKennan Hospital in Sioux Falls, S.D., and former medical director of Avera’s LIGHT Program, a wellness-oriented service for clinicians. Dr. Barnes herself caught the virus on the job but has since recovered.
“Physicians don’t see their work as an occupation. It’s their core identity: I am a doctor; I practice medicine. If things are being done in ways I don’t think are right, that’s fundamentally a breach,” she said. “As internists, we have an opportunity to forestall death whenever we can and, if not, promote a peaceful death. That’s what made me choose this specialty. I think there’s value in allowing a person to end well. But when that doesn’t happen because of social or administrative reasons, that’s hard.”
Where is the leadership?
“A lot of moral injury comes down to the individual health system and its leaders. Some have done well; others you hear saying things that make you question whether these are the people you want leading the organization. Hospitalists need to have a clear value framework and an idea of how to negotiate things when decisions don’t match that framework,” Dr. Barnes said.
“Sometimes administrators have additional information that they’re not sharing,” she added. “They’re caught between a rock and a hard place regarding the decisions they have to make, but they need to be more transparent and not hold things so close to their vest while thinking they are helping clinicians [by doing so]. Physicians need to understand why they are being asked to do things counter to what they believe is appropriate.”
David Oliver, MD, a geriatrics and internal medicine consultant at Royal Berkshire Hospital in Reading, England, also practices as a hospital physician, a role similar to the hospitalist in the United States. “In any system, in any environment, the job of being a doctor, nurse, or other health professional carries a lot of responsibility. That is a timeless, inherent stress of medical practice. With COVID, we’ve seen a lot of emotional burdens – a whole separate set of problems outside of your control, where you are responsible for care but don’t have accountability,” he said.
“People like me, hospital doctors, are used to chronic workforce issues in the National Health Service. But we didn’t sign up to come and get COVID and be hospitalized ourselves.” More than 850 frontline health care providers in the U.K. have so far died from the virus, Dr. Oliver said. “I saw five patients die in 90 minutes one day in April. That’s above and beyond normal human capacity.”
In England specifically, he said, it has exposed underlying structural issues and serious workforce gaps, unfilled vacancies, and a much lower number of ICU beds per 100,000 population than the United States or Europe. And there is consistent pressure to send patients home in order to empty beds for new patients.
But a range of supportive services is offered in U.K. hospitals, such as making senior clinicians available to speak to frontline clinicians, providing mentorship and a sounding board. The Point of Care Foundation has helped to disseminate the practice of Schwartz Rounds, a group reflective practice forum for health care teams developed by the Schwartz Center for Compassionate Healthcare in Boston.
“We don’t need this clap-for-the-NHS heroes stuff,” Dr. Oliver said. “We need an adequate workforce and [better] working conditions. What happened on the front lines of the pandemic was heroic – all done by local clinical teams. But where was the government – the centralized NHS? A lot of frontline clinicians aren’t feeling valued, supported, or listened to.”
What can be done?
What are some things that hospitalists can do, individually and collectively, to try to prevent moral distress from turning into full-scale burnout? Dr. Wocial emphasized the importance of unit-based ethics conversations. “At IU Health we have someone who is available to sit down with frontline clinicians and help unpack what they are experiencing,” she said. Clinicians need to be able to process this terrible experience in order to sort out the feelings of sadness from questions of whether they are doing something wrong.
Hospital chaplains are exquisitely skilled at supporting people and debriefing hospital teams, Dr. Wocial added. Palliative care professionals are also skilled at facilitating goals of care conversations with patients and families and can support hospitalists through coaching and joint family meetings.
“It’s about raising your sense of agency in your job – what in your practice you can control. People need to be able to talk frankly about it. Some managers say to clinicians: ‘Just buck up,’ while others are doing a fabulous job of offering support to their staff,” Dr. Wocial said. Hospitalists have to be willing to say when they’ve had too much. “You may not get help when you first ask for it. Be persistent. Asking for help doesn’t make you weak.”
Most doctors have their own strategies for managing stress on the job, Dr. Wachter noted. “What makes it a little easier is not having to do it alone. Many find solace in community, but community has been constrained by this pandemic. You can’t just go out for a beer after work anymore. So what are other ways to let off steam?”
The people leading hospitalist programs need to work harder at creating community and empathy when the tools allowing people to get together are somewhat limited. “Everybody is tired of Zoom,” he said. “One thing I learned as a manager was to just send messages to people acknowledging that I know this is hard. Try to think from the lens of other people and what they would find useful.”
The pandemic has been terribly unpredictable, Dr. Wachter added, but it won’t go on forever. For some doctors, yoga or mindfulness meditation may be very comforting. “For me, that’s not what I do. Golf or a good Seinfeld episode works for me.”
SHM’s Wellbeing Taskforce has created a “Hospital Medicine COVID Check-in Guide for Self & Peers” to promote both sharing and support for one another. It can be found at SHM’s Wellbeing webpage [www.hospitalmedicine.org/practice-management/wellbeing/]. The Taskforce believes that sharing common stressors as hospitalists can be healing, said its chair, Sarah Richards, MD, assistant professor of medicine at the University of Nebraska, Omaha. “This is especially true in situations where we feel we can’t provide the type of care we know our patients deserve.”
Respect, advocacy, self-care
Dr. Asken encouraged clinicians to focus on the efforts they are making on the job, not just the outcomes. “If someone has done their absolute best in a given circumstance, satisfaction and solace needs to be taken from that,” he said.
“Ongoing support group meetings, which we have called frontline support groups, should occur on a regular basis. Designated for physicians on the medical floors and in critical care units who are directly involved with COVID patients, these provide a brief respite but also engagement, sharing, and strengthening of mutual support.”
A lot of these issues have a fundamental thread, which comes down to respect, Dr. Barnes said. “Hospitalists need to hear their hospital administrators say: ‘I hear what you’re saying [about a problem]. Let’s think together about how to solve it.’ We need to work on being clear, and we need to speak up for what’s right. If you aren’t comfortable doing things you are being asked to do in the hospital, maybe you’re not working in the right place.”
Some efforts in the area of wellness and self-care really are helpful, Dr. Barnes said. “But you can’t exercise you way through a health system that doesn’t respect you. You need to get out of the mindset that you have no ability to make things different. We are not powerless as doctors. We can do a lot, actually. Physicians need to take ownership. If you are a hospitalist and you’re not part of any local or state or national organization that advocates for physicians, you should be.”
References
1. Dzeng L and Wachter RM. Ethics in conflict: Moral distress as a root cause of burnout. J Gen Intern Med. 2020 Feb;35(2):409-11. doi: 10.1007/s11606-019-05505-6.
2. Jameton A, Nursing Practice: The ethical issues. Prentice Hall Series in the Philosophy of Medicine. 1984, Englewood Cliffs, N.J.: Prentice Hall.
3. Wocial LD et al. Factors associated with physician moral distress caring for hospitalized elderly patients needing a surrogate decision-maker: A prospective study. J Gen Intern Med. 2020 May;35(5):1405-12. doi: 10.1007/s11606-020-05652-1.
4. Asken MJ. It’s not moral injury: It’s burnout (or something else). Medical Economics; June 7, 2019.
5. Asken MJ. Now it is moral injury: The COVID-19 pandemic and moral distress. Medical Economics; April 29, 2020.
Moral distress can result when health professionals like doctors and nurses feel prevented from doing what they know is right and ethically correct – reflecting the values of their profession and their own sense of professional integrity – because of unmanageable caseload demands, lack of resources, coverage limitations, or institutional policies.
Hospitalists are not exempt from moral distress, which is associated with soul-searching, burnout, and even PTSD. It is also associated with a higher likelihood for professionals to report an intention to leave their jobs. But the COVID-19 pandemic has superimposed a whole new layer of challenges, constraints, and frustrations, creating a potent mix of trauma and exhaustion, cumulative unease, depleted job satisfaction, and difficult ethical choices.
These challenges include seeing so many patients die and working with short supplies of personal protective equipment (PPE) – with resulting fears that they could catch the virus or pass it on to others, including loved ones. Also, not having enough ventilators or even beds for patients in hospitals hit hard by COVID surges raises fears that decisions for rationing medical care might become necessary.
In a commentary published in the Journal of General Internal Medicine in October 2019 – shortly before the COVID pandemic burst onto the scene – hospitalist and medical sociologist Elizabeth Dzeng, MD, PhD, MPH, and hospital medicine pioneer Robert Wachter, MD, MHM, both from the University of California, San Francisco, described “moral distress and professional ethical dissonance as root causes of burnout.”1 They characterized moral distress by its emotional exhaustion, depersonalization, reduced sense of accomplishment, and moral apathy, and they called for renewed attention to social and ethical dimensions of practice and threats to physician professionalism.
Prevailing explanations for documented high rates of burnout in doctors have tended to focus on work hours and struggles with electronic medical records and the like, Dr. Dzeng and Dr. Wachter wrote. “We see evidence of an insidious moral distress resulting from physicians’ inability to act in accord with their individual and professional ethical values due to institutional and social constraints.”
COVID has intensified these issues surrounding moral distress. “In a short period of time it created more situations that raise issues of moral distress than I have seen since the early days of HIV,” Dr. Wachter said. “Those of us who work in hospitals often find ourselves in complex circumstances with limited resources. What was so striking about COVID was finding ourselves caring for large volumes of patients who had a condition that was new to us.”
And the fact that constraints imposed by COVID, such as having to don unwieldy PPE and not allowing families to be present with hospitalized loved ones, are explainable and rational only helps a little with the clinician’s distress.
People talk about the need for doctors to be more resilient, Dr. Dzeng added, but that’s too narrow of an approach to these very real challenges. There are huge issues of workforce retention and costs, major mental health issues, suicide – and implications for patient care, because burned-out doctors can be bad doctors.
What is moral distress?
Moral distress is a term from the nursing ethics literature, attributed to philosopher Andrew Jameton in 1984.2 Contributors to moral distress imposed by COVID include having to make difficult medical decisions under stressful circumstances – especially early on, when effective treatment options were few. Doctors felt the demands of the pandemic were putting care quality and patient safety at risk. Poor working conditions overall, being pushed to work beyond their normal physical limits for days at a time, and feelings of not being valued added to this stress. But some say the pandemic has only highlighted and amplified existing inequities and disparities in the health care system.
Experts say moral distress is about feeling powerless, especially in a system driven by market values, and feeling let down by a society that has put them in harm’s way. They work all day under physically and emotionally exhausting conditions and then go home to hear specious conspiracy theories about the pandemic and see other people unwilling to wear masks.
Moral distress is complicated, said Lucia Wocial, PhD, RN, a nurse ethicist and cochair of the ethics consultation subcommittee at Indiana University Health in Indianapolis. “If you say you have moral distress, my first response is: tell me more. It helps to peel back the layers of this complexity. Emotion is only part of moral distress. It’s about the professional’s sense of responsibility and obligation – and the inability to honor that.”
Dr. Wocial, whose research specialty is moral distress, is corresponding author of a study published in the Journal of General Internal Medicine in February 2020, which identified moral distress in 4 out of 10 surveyed physicians who cared for older hospitalized adults and found themselves needing to work with their surrogate decision-makers.3 “We know physician moral distress is higher when people haven’t had the chance to hold conversations about their end-of-life care preferences,” she said, such as whether to continue life support.
“We have also learned that communication is key to diminishing physician moral distress. Our responsibility as clinicians is to guide patients and families through these decisions. If the family feels a high level of support from me, then my moral distress is lower,” she added. “If you think about how COVID has evolved, at first people were dying so quickly. Some patients were going to the ICU on ventilators without ever having a goals-of-care conversation.”
COVID has shifted the usual standard of care in U.S. hospitals in the face of patient surges. “How can you feel okay in accepting a level of care that in the prepandemic world would not have been acceptable?” Dr. Wocial posed. “What if you know the standard of care has shifted, of necessity, but you haven’t had time to prepare for it and nobody’s talking about what that means? Who is going to help you accept that good enough under these circumstances is enough – at least for today?”
What to call it
Michael J. Asken, PhD, director of provider well-being at UPMC Pinnacle Harrisburg (Pa.), has questioned in print the use of the military and wartime term “moral injury” when applied to a variety of less serious physician stressors.4 More recently, however, he observed, “The pandemic has muted or erased many of the distinctions between medical care and military conflict. ... The onslaught and volume of critical patients and resulting deaths is beyond what most providers have ever contemplated as part of care.”5
In a recent interview with the Hospitalist, he said: “While I initially resisted using the term moral injury, especially pre-COVID, because it was not equivalent to the moral injury created by war, I have relented a bit.” The volume of deaths and the apparent dangers to providers themselves reflect some of the critical aspects of war, and repetitive, intense, and/or incessant ethical challenges may have longer term negative psychological or emotional effects.
“Feeling emotional pain in situations of multiple deaths is to be expected and, perhaps, should even be welcomed as a sign of retained humanity and a buffer against burnout and cynicism in these times of unabating stress,” Dr. Asken said. “This is only true, however, if the emotional impact is tolerable and not experienced in repetitive extremes.”
“These things are real,” said Clarissa Barnes, MD, a physician adviser, hospitalist at Avera McKennan Hospital in Sioux Falls, S.D., and former medical director of Avera’s LIGHT Program, a wellness-oriented service for clinicians. Dr. Barnes herself caught the virus on the job but has since recovered.
“Physicians don’t see their work as an occupation. It’s their core identity: I am a doctor; I practice medicine. If things are being done in ways I don’t think are right, that’s fundamentally a breach,” she said. “As internists, we have an opportunity to forestall death whenever we can and, if not, promote a peaceful death. That’s what made me choose this specialty. I think there’s value in allowing a person to end well. But when that doesn’t happen because of social or administrative reasons, that’s hard.”
Where is the leadership?
“A lot of moral injury comes down to the individual health system and its leaders. Some have done well; others you hear saying things that make you question whether these are the people you want leading the organization. Hospitalists need to have a clear value framework and an idea of how to negotiate things when decisions don’t match that framework,” Dr. Barnes said.
“Sometimes administrators have additional information that they’re not sharing,” she added. “They’re caught between a rock and a hard place regarding the decisions they have to make, but they need to be more transparent and not hold things so close to their vest while thinking they are helping clinicians [by doing so]. Physicians need to understand why they are being asked to do things counter to what they believe is appropriate.”
David Oliver, MD, a geriatrics and internal medicine consultant at Royal Berkshire Hospital in Reading, England, also practices as a hospital physician, a role similar to the hospitalist in the United States. “In any system, in any environment, the job of being a doctor, nurse, or other health professional carries a lot of responsibility. That is a timeless, inherent stress of medical practice. With COVID, we’ve seen a lot of emotional burdens – a whole separate set of problems outside of your control, where you are responsible for care but don’t have accountability,” he said.
“People like me, hospital doctors, are used to chronic workforce issues in the National Health Service. But we didn’t sign up to come and get COVID and be hospitalized ourselves.” More than 850 frontline health care providers in the U.K. have so far died from the virus, Dr. Oliver said. “I saw five patients die in 90 minutes one day in April. That’s above and beyond normal human capacity.”
In England specifically, he said, it has exposed underlying structural issues and serious workforce gaps, unfilled vacancies, and a much lower number of ICU beds per 100,000 population than the United States or Europe. And there is consistent pressure to send patients home in order to empty beds for new patients.
But a range of supportive services is offered in U.K. hospitals, such as making senior clinicians available to speak to frontline clinicians, providing mentorship and a sounding board. The Point of Care Foundation has helped to disseminate the practice of Schwartz Rounds, a group reflective practice forum for health care teams developed by the Schwartz Center for Compassionate Healthcare in Boston.
“We don’t need this clap-for-the-NHS heroes stuff,” Dr. Oliver said. “We need an adequate workforce and [better] working conditions. What happened on the front lines of the pandemic was heroic – all done by local clinical teams. But where was the government – the centralized NHS? A lot of frontline clinicians aren’t feeling valued, supported, or listened to.”
What can be done?
What are some things that hospitalists can do, individually and collectively, to try to prevent moral distress from turning into full-scale burnout? Dr. Wocial emphasized the importance of unit-based ethics conversations. “At IU Health we have someone who is available to sit down with frontline clinicians and help unpack what they are experiencing,” she said. Clinicians need to be able to process this terrible experience in order to sort out the feelings of sadness from questions of whether they are doing something wrong.
Hospital chaplains are exquisitely skilled at supporting people and debriefing hospital teams, Dr. Wocial added. Palliative care professionals are also skilled at facilitating goals of care conversations with patients and families and can support hospitalists through coaching and joint family meetings.
“It’s about raising your sense of agency in your job – what in your practice you can control. People need to be able to talk frankly about it. Some managers say to clinicians: ‘Just buck up,’ while others are doing a fabulous job of offering support to their staff,” Dr. Wocial said. Hospitalists have to be willing to say when they’ve had too much. “You may not get help when you first ask for it. Be persistent. Asking for help doesn’t make you weak.”
Most doctors have their own strategies for managing stress on the job, Dr. Wachter noted. “What makes it a little easier is not having to do it alone. Many find solace in community, but community has been constrained by this pandemic. You can’t just go out for a beer after work anymore. So what are other ways to let off steam?”
The people leading hospitalist programs need to work harder at creating community and empathy when the tools allowing people to get together are somewhat limited. “Everybody is tired of Zoom,” he said. “One thing I learned as a manager was to just send messages to people acknowledging that I know this is hard. Try to think from the lens of other people and what they would find useful.”
The pandemic has been terribly unpredictable, Dr. Wachter added, but it won’t go on forever. For some doctors, yoga or mindfulness meditation may be very comforting. “For me, that’s not what I do. Golf or a good Seinfeld episode works for me.”
SHM’s Wellbeing Taskforce has created a “Hospital Medicine COVID Check-in Guide for Self & Peers” to promote both sharing and support for one another. It can be found at SHM’s Wellbeing webpage [www.hospitalmedicine.org/practice-management/wellbeing/]. The Taskforce believes that sharing common stressors as hospitalists can be healing, said its chair, Sarah Richards, MD, assistant professor of medicine at the University of Nebraska, Omaha. “This is especially true in situations where we feel we can’t provide the type of care we know our patients deserve.”
Respect, advocacy, self-care
Dr. Asken encouraged clinicians to focus on the efforts they are making on the job, not just the outcomes. “If someone has done their absolute best in a given circumstance, satisfaction and solace needs to be taken from that,” he said.
“Ongoing support group meetings, which we have called frontline support groups, should occur on a regular basis. Designated for physicians on the medical floors and in critical care units who are directly involved with COVID patients, these provide a brief respite but also engagement, sharing, and strengthening of mutual support.”
A lot of these issues have a fundamental thread, which comes down to respect, Dr. Barnes said. “Hospitalists need to hear their hospital administrators say: ‘I hear what you’re saying [about a problem]. Let’s think together about how to solve it.’ We need to work on being clear, and we need to speak up for what’s right. If you aren’t comfortable doing things you are being asked to do in the hospital, maybe you’re not working in the right place.”
Some efforts in the area of wellness and self-care really are helpful, Dr. Barnes said. “But you can’t exercise you way through a health system that doesn’t respect you. You need to get out of the mindset that you have no ability to make things different. We are not powerless as doctors. We can do a lot, actually. Physicians need to take ownership. If you are a hospitalist and you’re not part of any local or state or national organization that advocates for physicians, you should be.”
References
1. Dzeng L and Wachter RM. Ethics in conflict: Moral distress as a root cause of burnout. J Gen Intern Med. 2020 Feb;35(2):409-11. doi: 10.1007/s11606-019-05505-6.
2. Jameton A, Nursing Practice: The ethical issues. Prentice Hall Series in the Philosophy of Medicine. 1984, Englewood Cliffs, N.J.: Prentice Hall.
3. Wocial LD et al. Factors associated with physician moral distress caring for hospitalized elderly patients needing a surrogate decision-maker: A prospective study. J Gen Intern Med. 2020 May;35(5):1405-12. doi: 10.1007/s11606-020-05652-1.
4. Asken MJ. It’s not moral injury: It’s burnout (or something else). Medical Economics; June 7, 2019.
5. Asken MJ. Now it is moral injury: The COVID-19 pandemic and moral distress. Medical Economics; April 29, 2020.
Police contact tied to elevated anxiety in young Black adults
Young Black adults who witness or experience police violence have significantly elevated levels of anxiety, new research shows.

In the first study to quantify the impact of police contact anxiety, investigators found it was associated with moderately severe anxiety levels in this group of individuals, highlighting the need to screen for exposure to police violence in this patient population, study investigator Robert O. Motley Jr, PhD, manager of the Race & Opportunity Lab at Washington University in St. Louis, said in an interview.
“If you’re working in an institution and providing clinical care, mental health care, or behavior health care, these additional measures should be included to get a much more holistic view of the exposure of these individuals in terms of traumatic events. These assessments can inform your decisions around care,” Dr. Motley added.
The findings were presented at the annual meeting of the American Psychiatric Association.
‘Alarming’ rates of exposure
Evidence shows anxiety disorders are among the most prevalent conditions for Black people aged 18-29 years – an age group described as “emergent adulthood” because these individuals haven’t yet taken on full responsibilities of adulthood.
Research shows Black emergent adults are three to four times more likely than other ethnic groups to be exposed to actual or threatened nonfatal police violence, said Dr. Motley. “So they didn’t die, but were exposed to force, which could be things like police yelling at them, hitting or kicking them, pointing a gun at them, or tasing them.”
These individuals are also two to three times more likely to experience exposure to fatal police violence, and to be unarmed and killed, said Dr. Motley.
Evidence shows a clear link between exposure to stressful or traumatic events and anxiety disorders, but there has been little research examining the relationship between exposure to police violence and anxiety disorders among Black emergent adults, he said.
To assess the prevalence and correlates of “police contact anxiety” the investigators used computer-assisted surveys to collect data from 300 young Black college students in St. Louis who had been exposed to police violence at some point in their lives. The mean age of the sample was 20.4 years and included an equal number of men and women.
Work status for the previous year showed almost one-quarter (23.6%) were unemployed and about half worked part time. Almost two-thirds (62.6%) had an annual income of less than $10,000.
Respondents reported they had personally experienced police violence almost twice (a mean of 1.89) during their lifetime. The mean number of times they witnessed police using force against someone else was 7.82. Respondents also reported they had watched videos showing police use of force on the internet or television an average of 34.5 times.
This, said Dr. Motley, isn’t surprising given the growing number of young adults – of all races – who are using social media platforms to upload and share videos.
The researchers also looked at witnessing community violence, unrelated to police violence. Here, respondents had an average of 10.9 exposures.
Protectors or predators?
To examine the impact of police contact anxiety caused either by direct experience, or as a result of witnessing, or seeing a video of police use of violence in the past 30 days, the researchers created a “police contact anxiety” scale.
Respondents were asked six questions pertaining specifically to experiences during, or in anticipation of, police contact and its effects on anxiety levels.
For each of the six questions, participants rated the severity of anxiety on a scale of 0 (least severe) to 3 (most severe) for each exposure type. The final score had a potential range of 0-24.
Results showed police contact anxiety was moderately severe for all three exposure types with scores ranging from 13 to 14.
Ordinary least square regression analyses showed that, compared with unemployed participants, those who worked full time were less likely to have higher police contact anxiety as a result of seeing a video of police use of force (P < .05) – a finding Dr. Motley said was not surprising.
Employment, he noted, promotes individual self-efficacy, social participation, and mental health, which may provide a “buffer” to the effects of watching videos of police violence.
Dr. Motley noted that police officers “have been entrusted to serve and protect” the community, but “rarely face consequences when they use force against Black emergent adults; they’re rarely held accountable.”
These young Black adults “may perceive police officers as more of a threat to personal safety instead of a protector of it.”
Additional bivariate analyses showed that males had significantly higher scores than females for police contact anxiety because of witnessing police use of force.
This, too, was not surprising since males are exposed to more violence in general, said Dr. Motley.
It’s important to replicate the findings using a much larger and more diverse sample, he said. His next research project will be to collect data from a nationally representative sample of emerging adults across different ethnic groups and examining a range of different variables.
Commenting on the findings, Jeffrey Borenstein, MD, president and CEO of the Brain & Behavior Research Foundation and editor in chief of Psychiatric News, called it “outstanding.”
“This is a very important issue,” said Dr. Borenstein, who moderated a press briefing that featured the study.
“We know anxiety is an extremely important condition and symptom, across the board for all groups, and often anxiety isn’t evaluated in the way that it needs to be. This is a great study that will lead to further research in this important area,” he added.
The study was funded by the National Institute on Minority Health and Health Disparities. Dr. Motley and Dr. Borenstein have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Young Black adults who witness or experience police violence have significantly elevated levels of anxiety, new research shows.
In the first study to quantify the impact of police contact anxiety, investigators found it was associated with moderately severe anxiety levels in this group of individuals, highlighting the need to screen for exposure to police violence in this patient population, study investigator Robert O. Motley Jr, PhD, manager of the Race & Opportunity Lab at Washington University in St. Louis, said in an interview.
“If you’re working in an institution and providing clinical care, mental health care, or behavior health care, these additional measures should be included to get a much more holistic view of the exposure of these individuals in terms of traumatic events. These assessments can inform your decisions around care,” Dr. Motley added.
The findings were presented at the annual meeting of the American Psychiatric Association.
‘Alarming’ rates of exposure
Evidence shows anxiety disorders are among the most prevalent conditions for Black people aged 18-29 years – an age group described as “emergent adulthood” because these individuals haven’t yet taken on full responsibilities of adulthood.
Research shows Black emergent adults are three to four times more likely than other ethnic groups to be exposed to actual or threatened nonfatal police violence, said Dr. Motley. “So they didn’t die, but were exposed to force, which could be things like police yelling at them, hitting or kicking them, pointing a gun at them, or tasing them.”
These individuals are also two to three times more likely to experience exposure to fatal police violence, and to be unarmed and killed, said Dr. Motley.
Evidence shows a clear link between exposure to stressful or traumatic events and anxiety disorders, but there has been little research examining the relationship between exposure to police violence and anxiety disorders among Black emergent adults, he said.
To assess the prevalence and correlates of “police contact anxiety” the investigators used computer-assisted surveys to collect data from 300 young Black college students in St. Louis who had been exposed to police violence at some point in their lives. The mean age of the sample was 20.4 years and included an equal number of men and women.
Work status for the previous year showed almost one-quarter (23.6%) were unemployed and about half worked part time. Almost two-thirds (62.6%) had an annual income of less than $10,000.
Respondents reported they had personally experienced police violence almost twice (a mean of 1.89) during their lifetime. The mean number of times they witnessed police using force against someone else was 7.82. Respondents also reported they had watched videos showing police use of force on the internet or television an average of 34.5 times.
This, said Dr. Motley, isn’t surprising given the growing number of young adults – of all races – who are using social media platforms to upload and share videos.
The researchers also looked at witnessing community violence, unrelated to police violence. Here, respondents had an average of 10.9 exposures.
Protectors or predators?
To examine the impact of police contact anxiety caused either by direct experience, or as a result of witnessing, or seeing a video of police use of violence in the past 30 days, the researchers created a “police contact anxiety” scale.
Respondents were asked six questions pertaining specifically to experiences during, or in anticipation of, police contact and its effects on anxiety levels.
For each of the six questions, participants rated the severity of anxiety on a scale of 0 (least severe) to 3 (most severe) for each exposure type. The final score had a potential range of 0-24.
Results showed police contact anxiety was moderately severe for all three exposure types with scores ranging from 13 to 14.
Ordinary least square regression analyses showed that, compared with unemployed participants, those who worked full time were less likely to have higher police contact anxiety as a result of seeing a video of police use of force (P < .05) – a finding Dr. Motley said was not surprising.
Employment, he noted, promotes individual self-efficacy, social participation, and mental health, which may provide a “buffer” to the effects of watching videos of police violence.
Dr. Motley noted that police officers “have been entrusted to serve and protect” the community, but “rarely face consequences when they use force against Black emergent adults; they’re rarely held accountable.”
These young Black adults “may perceive police officers as more of a threat to personal safety instead of a protector of it.”
Additional bivariate analyses showed that males had significantly higher scores than females for police contact anxiety because of witnessing police use of force.
This, too, was not surprising since males are exposed to more violence in general, said Dr. Motley.
It’s important to replicate the findings using a much larger and more diverse sample, he said. His next research project will be to collect data from a nationally representative sample of emerging adults across different ethnic groups and examining a range of different variables.
Commenting on the findings, Jeffrey Borenstein, MD, president and CEO of the Brain & Behavior Research Foundation and editor in chief of Psychiatric News, called it “outstanding.”
“This is a very important issue,” said Dr. Borenstein, who moderated a press briefing that featured the study.
“We know anxiety is an extremely important condition and symptom, across the board for all groups, and often anxiety isn’t evaluated in the way that it needs to be. This is a great study that will lead to further research in this important area,” he added.
The study was funded by the National Institute on Minority Health and Health Disparities. Dr. Motley and Dr. Borenstein have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Young Black adults who witness or experience police violence have significantly elevated levels of anxiety, new research shows.
In the first study to quantify the impact of police contact anxiety, investigators found it was associated with moderately severe anxiety levels in this group of individuals, highlighting the need to screen for exposure to police violence in this patient population, study investigator Robert O. Motley Jr, PhD, manager of the Race & Opportunity Lab at Washington University in St. Louis, said in an interview.
“If you’re working in an institution and providing clinical care, mental health care, or behavior health care, these additional measures should be included to get a much more holistic view of the exposure of these individuals in terms of traumatic events. These assessments can inform your decisions around care,” Dr. Motley added.
The findings were presented at the annual meeting of the American Psychiatric Association.
‘Alarming’ rates of exposure
Evidence shows anxiety disorders are among the most prevalent conditions for Black people aged 18-29 years – an age group described as “emergent adulthood” because these individuals haven’t yet taken on full responsibilities of adulthood.
Research shows Black emergent adults are three to four times more likely than other ethnic groups to be exposed to actual or threatened nonfatal police violence, said Dr. Motley. “So they didn’t die, but were exposed to force, which could be things like police yelling at them, hitting or kicking them, pointing a gun at them, or tasing them.”
These individuals are also two to three times more likely to experience exposure to fatal police violence, and to be unarmed and killed, said Dr. Motley.
Evidence shows a clear link between exposure to stressful or traumatic events and anxiety disorders, but there has been little research examining the relationship between exposure to police violence and anxiety disorders among Black emergent adults, he said.
To assess the prevalence and correlates of “police contact anxiety” the investigators used computer-assisted surveys to collect data from 300 young Black college students in St. Louis who had been exposed to police violence at some point in their lives. The mean age of the sample was 20.4 years and included an equal number of men and women.
Work status for the previous year showed almost one-quarter (23.6%) were unemployed and about half worked part time. Almost two-thirds (62.6%) had an annual income of less than $10,000.
Respondents reported they had personally experienced police violence almost twice (a mean of 1.89) during their lifetime. The mean number of times they witnessed police using force against someone else was 7.82. Respondents also reported they had watched videos showing police use of force on the internet or television an average of 34.5 times.
This, said Dr. Motley, isn’t surprising given the growing number of young adults – of all races – who are using social media platforms to upload and share videos.
The researchers also looked at witnessing community violence, unrelated to police violence. Here, respondents had an average of 10.9 exposures.
Protectors or predators?
To examine the impact of police contact anxiety caused either by direct experience, or as a result of witnessing, or seeing a video of police use of violence in the past 30 days, the researchers created a “police contact anxiety” scale.
Respondents were asked six questions pertaining specifically to experiences during, or in anticipation of, police contact and its effects on anxiety levels.
For each of the six questions, participants rated the severity of anxiety on a scale of 0 (least severe) to 3 (most severe) for each exposure type. The final score had a potential range of 0-24.
Results showed police contact anxiety was moderately severe for all three exposure types with scores ranging from 13 to 14.
Ordinary least square regression analyses showed that, compared with unemployed participants, those who worked full time were less likely to have higher police contact anxiety as a result of seeing a video of police use of force (P < .05) – a finding Dr. Motley said was not surprising.
Employment, he noted, promotes individual self-efficacy, social participation, and mental health, which may provide a “buffer” to the effects of watching videos of police violence.
Dr. Motley noted that police officers “have been entrusted to serve and protect” the community, but “rarely face consequences when they use force against Black emergent adults; they’re rarely held accountable.”
These young Black adults “may perceive police officers as more of a threat to personal safety instead of a protector of it.”
Additional bivariate analyses showed that males had significantly higher scores than females for police contact anxiety because of witnessing police use of force.
This, too, was not surprising since males are exposed to more violence in general, said Dr. Motley.
It’s important to replicate the findings using a much larger and more diverse sample, he said. His next research project will be to collect data from a nationally representative sample of emerging adults across different ethnic groups and examining a range of different variables.
Commenting on the findings, Jeffrey Borenstein, MD, president and CEO of the Brain & Behavior Research Foundation and editor in chief of Psychiatric News, called it “outstanding.”
“This is a very important issue,” said Dr. Borenstein, who moderated a press briefing that featured the study.
“We know anxiety is an extremely important condition and symptom, across the board for all groups, and often anxiety isn’t evaluated in the way that it needs to be. This is a great study that will lead to further research in this important area,” he added.
The study was funded by the National Institute on Minority Health and Health Disparities. Dr. Motley and Dr. Borenstein have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The cloudy role of cannabis as a neuropsychiatric treatment
Although the healing properties of cannabis have been touted for millennia, research into its potential neuropsychiatric applications truly began to take off in the 1990s following the discovery of the cannabinoid system in the brain. This led to speculation that cannabis could play a therapeutic role in regulating dopamine, serotonin, and other neurotransmitters and offer a new means of treating various ailments.

At the same time, efforts to liberalize marijuana laws have successfully played out in several nations, including the United States, where, as of April 29, 36 states provide some access to cannabis. These dual tracks – medical and political – have made cannabis an increasingly accepted part of the cultural fabric.
Yet with this development has come a new quandary for clinicians. Medical cannabis has been made widely available to patients and has largely outpaced the clinical evidence, leaving it unclear how and for which indications it should be used.
The many forms of medical cannabis
Cannabis is a genus of plants that includes marijuana (Cannabis sativa) and hemp. These plants contain over 100 compounds, including terpenes, flavonoids, and – most importantly for medicinal applications – cannabinoids.
The most abundant cannabinoid in marijuana is the psychotropic delta-9-tetrahydrocannabinol (THC), which imparts the “high” sensation. The next most abundant cannabinoid is cannabidiol (CBD), which is the nonpsychotropic. THC and CBD are the most extensively studied cannabinoids, together and in isolation. Evidence suggests that other cannabinoids and terpenoids may also hold medical promise and that cannabis’ various compounds can work synergistically to produce a so-called entourage effect.
Patients walking into a typical medical cannabis dispensary will be faced with several plant-derived and synthetic options, which can differ considerably in terms of the ratios and amounts of THC and CBD they contain, as well in how they are consumed (i.e., via smoke, vapor, ingestion, topical administration, or oromucosal spray), all of which can alter their effects. Further complicating matters is the varying level of oversight each state and country has in how and whether they test for and accurately label products’ potency, cannabinoid content, and possible impurities.
Medically authorized, prescription cannabis products go through an official regulatory review process, and indications/contraindications have been established for them. To date, the Food and Drug Administration has approved one cannabis-derived drug product – Epidiolex (purified CBD) – for the treatment of seizures associated with Lennox-Gastaut syndrome or Dravet syndrome in patients aged 2 years and older. The FDA has also approved three synthetic cannabis-related drug products – Marinol, Syndros (or dronabinol, created from synthetic THC), and Cesamet (or nabilone, a synthetic cannabinoid similar to THC) – all of which are indicated for treatment-related nausea and anorexia associated with weight loss in AIDS patients.
Surveys of medical cannabis consumers indicate that most people cannot distinguish between THC and CBD, so the first role that physicians find themselves in when recommending this treatment may be in helping patients navigate the volume of options.
Promising treatment for pain
Chronic pain is the leading reason patients seek out medical cannabis. It is also the indication that most researchers agree has the strongest evidence to support its use.

“In my mind, the most promising immediate use for medical cannabis is with THC for pain,” Diana M. Martinez, MD, a professor of psychiatry at Columbia University, New York, who specializes in addiction research, said in a recent MDedge podcast. “THC could be added to the armamentarium of pain medications that we use today.”
In a 2015 systematic literature review, researchers assessed 28 randomized, controlled trials (RCTs) of the use of cannabinoids for chronic pain. They reported that a variety of formulations resulted in at least a 30% reduction in the odds of pain, compared with placebo. A meta-analysis of five RCTs involving patients with neuropathic pain found a 30% reduction in pain over placebo with inhaled, vaporized cannabis. Varying results have been reported in additional studies for this indication. The National Academies of Sciences, Engineering, and Medicine concluded that there was a substantial body of evidence that cannabis is an effective treatment for chronic pain in adults.
The ongoing opioid epidemic has lent these results additional relevance.
Seeing this firsthand has caused Mark Steven Wallace, MD, a pain management specialist and chair of the division of pain medicine at the University of California San Diego Health, to reconsider offering cannabis to his patients.
“I think it’s probably more efficacious, just from my personal experience, and it’s a much lower risk of abuse and dependence than the opioids,” he said.
Dr. Wallace advised that clinicians who treat pain consider the ratios of cannabinoids.
“This is anecdotal, but we do find that with the combination of the two, CBD reduces the psychoactive effects of the THC. The ratios we use during the daytime range around 20 mg of CBD to 1 mg of THC,” he said.
In a recent secondary analysis of an RCT involving patients with painful diabetic peripheral neuropathy, Dr. Wallace and colleagues showed that THC’s effects appear to reverse themselves at a certain level.
“As the THC level goes up, the pain reduces until you reach about 16 ng/mL; then it starts going in the opposite direction, and pain will start to increase,” he said. “Even recreational cannabis users have reported that they avoid high doses because it’s very aversive. Using cannabis is all about, start low and go slow.”
A mixed bag for neurologic indications
There are relatively limited data on the use of medical cannabis for other neurologic conditions, and results have varied. For uses other than pain management, the evidence that does exist is strongest regarding epilepsy, said Daniel Freedman, DO, assistant professor of neurology at the University of Texas at Austin. He noted “multiple high-quality RCTs showing that pharmaceutical-grade CBD can reduce seizures associated with two particular epilepsy syndromes: Dravet Syndrome and Lennox Gastaut.”

These findings led to the FDA’s 2018 approval of Epidiolex for these syndromes. In earlier years, interest in CBD for pediatric seizures was largely driven by anecdotal parental reports of its benefits. NASEM’s 2017 overview on medical cannabis found evidence from subsequent RCTs in this indication to be insufficient. Clinicians who prescribe CBD for this indication must be vigilant because it can interact with several commonly used antiepileptic drugs.
Cannabinoid treatments have also shown success in alleviating muscle spasticity resulting from multiple sclerosis, most prominently in the form of nabiximols (Sativex), a standardized oralmucosal spray containing approximately equal quantities of THC and CBD. Nabiximols is approved in Europe but not in the United States. Moderate evidence supports the efficacy of these and other treatments over placebo in reducing muscle spasticity. Patient ratings of its effects tend to be higher than clinician assessment.
Parkinson’s disease has not yet been approved as an indication for treatment with cannabis or cannabinoids, yet a growing body of preclinical data suggests these could influence the dopaminergic system, said Carsten Buhmann, MD, from the department of neurology at the University Medical Center Hamburg-Eppendorf (Germany).
“In general, cannabinoids modulate basal-ganglia function on two levels which are especially relevant in Parkinson’s disease, i.e., the glutamatergic/dopaminergic synaptic neurotransmission and the corticostriatal plasticity,” he said. “Furthermore, activation of the endocannabinoid system might induce neuroprotective effects related to direct receptor-independent mechanisms, activation of anti-inflammatory cascades in glial cells via the cannabinoid receptor type 2, and antiglutamatergic antiexcitotoxic properties.”
Dr. Buhmann said that currently, clinical evidence is scarce, consisting of only four double-blind, placebo-controlled RCTs involving 49 patients. Various cannabinoids and methods of administering treatment were employed. Improvement was only observed in one of these RCTs, which found that the cannabinoid receptor agonist nabilone significantly reduced levodopa-induced dyskinesia for patients with Parkinson’s disease. Subjective data support a beneficial effect. In a nationwide survey of 1,348 respondents conducted by Dr. Buhmann and colleagues, the majority of medical cannabis users reported that it improved their symptoms (54% with oral CBD and 68% with inhaled THC-containing cannabis).
NASEM concluded that there was insufficient evidence to support the efficacy of medical cannabis for other neurologic conditions, including Tourette syndrome, amyotrophic lateral sclerosis, Huntington disease, dystonia, or dementia. A 2020 position statement from the American Academy of Neurology cited the lack of sufficient peer-reviewed research as the reason it could not currently support the use of cannabis for neurologic disorders.
Yet, according to Dr. Freedman, who served as a coauthor of the AAN position statement, this hasn’t stymied research interest in the topic. He’s seen a substantial uptick in studies of CBD over the past 2 years. “The body of evidence grows, but I still see many claims being made without evidence. And no one seems to care about all the negative trials.”
Cannabis as a treatment for, and cause of, psychiatric disorders
Mental health problems – such as anxiety, depression, and PTSD – are among the most common reasons patients seek out medical cannabis. There is an understandable interest in using cannabis and cannabinoids to treat psychiatric disorders. Preclinical studies suggest that the endocannabinoid system plays a prominent role in modulating feelings of anxiety, mood, and fear. As with opioids and chronic pain management, there is hope that medical cannabis may provide a means of reducing prescription anxiolytics and their associated risks.
The authors of the first systematic review (BMC Psychiatry. 2020 Jan 16;20[1]:24) of the use of medical cannabis for major psychiatric disorders noted that the current evidence was “encouraging, albeit embryonic.”
Meta-analyses have indicated a small but positive association between cannabis use and anxiety, although this may reflect the fact that patients with anxiety sought out this treatment. Given the risks for substance use disorders among patients with anxiety, CBD may present a more viable option. Positive results have been shown as treatment for generalized social anxiety disorder.
Limited but encouraging results have also been reported regarding the alleviation of PTSD symptoms with both cannabis and CBD, although the body of high-quality evidence hasn’t notably progressed since 2017, when NASEM declared that the evidence was insufficient. Supportive evidence is similarly lacking regarding the treatment of depression. Longitudinal studies suggest that cannabis use, particularly heavy use, may increase the risk of developing this disorder. Because THC is psychoactive, it is advised that it be avoided by patients at risk for psychotic disorders. However, CBD has yielded limited benefits for patients with treatment-resistant schizophrenia and for young people at risk for psychosis.
The use of medical cannabis for psychiatric conditions requires a complex balancing act, inasmuch as these treatments may exacerbate the very problems they are intended to alleviate.
Marta Di Forti, MD, PhD, professor of psychiatric research at Kings College London, has been at the forefront of determining the mental health risks of continued cannabis use. In 2019, Dr. Di Forti developed the first and only Cannabis Clinic for Patients With Psychosis in London where she and her colleagues have continued to elucidate this connection.
Dr. Di Forti and colleagues have linked daily cannabis use to an increase in the risk of experiencing psychotic disorder, compared with never using it. That risk was further increased among users of high-potency cannabis (≥10% THC). The latter finding has troubling implications, because concentrations of THC have steadily risen since 1970. By contrast, CBD concentrations have remained generally stable. High-potency cannabis products are common in both recreational and medicinal settings.
“For somebody prescribing medicinal cannabis that has a ≥10% concentration of THC, I’d be particularly wary of the risk of psychosis,” said Dr. Di Forti. “If you’re expecting people to use a high content of THC daily to medicate pain or a chronic condition, you even more so need to be aware that this is a potential side effect.”
Dr. Di Forti noted that her findings come from a cohort of recreational users, most of whom were aged 18-35 years.
“There have actually not been studies developed from collecting data in this area from groups specifically using cannabis for medicinal rather than recreational purposes,” she said.
She added that she personally has no concerns about the use of medical cannabis but wants clinicians to be aware of the risk for psychosis, to structure their patient conversations to identify risk factors or family histories of psychosis, and to become knowledgeable in detecting the often subtle signs of its initial onset.
When cannabis-associated psychosis occurs, Dr. Di Forti said it is primarily treated with conventional means, such as antipsychotics and therapeutic interventions and by refraining from using cannabis. Achieving the latter goal can be a challenge for patients who are daily users of high-potency cannabis. Currently, there are no treatment options such as those offered to patients withdrawing from the use of alcohol or opioids. Dr. Di Forti and colleagues are currently researching a solution to that problem through the use of another medical cannabis, the oromucosal spray Sativex, which has been approved in the European Union.
The regulatory obstacles to clarifying cannabis’ role in medicine
That currently there is limited or no evidence to support the use of medical cannabis for the treatment of neuropsychiatric conditions points to the inherent difficulties in conducting high-level research in this area.
“There’s a tremendous shortage of reliable data, largely due to regulatory barriers,” said Dr. Martinez.
Since 1970, cannabis has been listed as a Schedule I drug that is illegal to prescribe (the Agriculture Improvement Act of 2018 removed hemp from such restrictions). The FDA has issued guidance for researchers who wish to investigate treatments using Cannabis sativa or its derivatives in which the THC content is greater than 0.3%. Such research requires regular interactions with several federal agencies, including the Drug Enforcement Administration.
“It’s impossible to do multicenter RCTs with large numbers of patients, because you can’t transport cannabis across state lines,” said Dr. Wallace.
Regulatory restrictions regarding medical cannabis vary considerably throughout the world (the European Monitoring Center for Drugs and Drug Addiction provides a useful breakdown of this on their website). The lack of consistency in regulatory oversight acts as an impediment for conducting large-scale international multicenter studies on the topic.
Dr. Buhmann noted that, in Germany, cannabis has been broadly approved for treatment-resistant conditions with severe symptoms that impair quality of life. In addition, it is easy to be reimbursed for the use of cannabis as a medical treatment. These factors serve as disincentives for the funding of high-quality studies.
“It’s likely that no pharmaceutical company will do an expensive RCT to get an approval for Parkinson’s disease because it is already possible to prescribe medical cannabis of any type of THC-containing cannabinoid, dose, or route of application,” Dr. Buhmann said.
In the face of such restrictions and barriers, researchers are turning to ambitious real-world data projects to better understand medical cannabis’ efficacy and safety. A notable example is ProjectTwenty21, which is supported by the Royal College of Psychiatrists. The project is collecting outcomes of the use of medical cannabis among 20,000 U.K. patients whose conventional treatments of chronic pain, anxiety disorder, epilepsy, multiple sclerosis, PTSD, substance use disorder, and Tourette syndrome failed.
Dr. Freedman noted that the continued lack of high-quality data creates a void that commercial interests fill with unfounded claims.
“The danger is that patients might abandon a medication or intervention backed by robust science in favor of something without any science or evidence behind it,” he said. “There is no reason not to expect the same level of data for claims about cannabis products as we would expect from pharmaceutical products.”
Getting to that point, however, will require that the authorities governing clinical trials begin to view cannabis as the research community does, as a possible treatment with potential value, rather than as an illicit drug that needs to be tamped down.
A version of this article first appeared on Medscape.com.
Although the healing properties of cannabis have been touted for millennia, research into its potential neuropsychiatric applications truly began to take off in the 1990s following the discovery of the cannabinoid system in the brain. This led to speculation that cannabis could play a therapeutic role in regulating dopamine, serotonin, and other neurotransmitters and offer a new means of treating various ailments.
At the same time, efforts to liberalize marijuana laws have successfully played out in several nations, including the United States, where, as of April 29, 36 states provide some access to cannabis. These dual tracks – medical and political – have made cannabis an increasingly accepted part of the cultural fabric.
Yet with this development has come a new quandary for clinicians. Medical cannabis has been made widely available to patients and has largely outpaced the clinical evidence, leaving it unclear how and for which indications it should be used.
The many forms of medical cannabis
Cannabis is a genus of plants that includes marijuana (Cannabis sativa) and hemp. These plants contain over 100 compounds, including terpenes, flavonoids, and – most importantly for medicinal applications – cannabinoids.
The most abundant cannabinoid in marijuana is the psychotropic delta-9-tetrahydrocannabinol (THC), which imparts the “high” sensation. The next most abundant cannabinoid is cannabidiol (CBD), which is the nonpsychotropic. THC and CBD are the most extensively studied cannabinoids, together and in isolation. Evidence suggests that other cannabinoids and terpenoids may also hold medical promise and that cannabis’ various compounds can work synergistically to produce a so-called entourage effect.
Patients walking into a typical medical cannabis dispensary will be faced with several plant-derived and synthetic options, which can differ considerably in terms of the ratios and amounts of THC and CBD they contain, as well in how they are consumed (i.e., via smoke, vapor, ingestion, topical administration, or oromucosal spray), all of which can alter their effects. Further complicating matters is the varying level of oversight each state and country has in how and whether they test for and accurately label products’ potency, cannabinoid content, and possible impurities.
Medically authorized, prescription cannabis products go through an official regulatory review process, and indications/contraindications have been established for them. To date, the Food and Drug Administration has approved one cannabis-derived drug product – Epidiolex (purified CBD) – for the treatment of seizures associated with Lennox-Gastaut syndrome or Dravet syndrome in patients aged 2 years and older. The FDA has also approved three synthetic cannabis-related drug products – Marinol, Syndros (or dronabinol, created from synthetic THC), and Cesamet (or nabilone, a synthetic cannabinoid similar to THC) – all of which are indicated for treatment-related nausea and anorexia associated with weight loss in AIDS patients.
Surveys of medical cannabis consumers indicate that most people cannot distinguish between THC and CBD, so the first role that physicians find themselves in when recommending this treatment may be in helping patients navigate the volume of options.
Promising treatment for pain
Chronic pain is the leading reason patients seek out medical cannabis. It is also the indication that most researchers agree has the strongest evidence to support its use.
“In my mind, the most promising immediate use for medical cannabis is with THC for pain,” Diana M. Martinez, MD, a professor of psychiatry at Columbia University, New York, who specializes in addiction research, said in a recent MDedge podcast. “THC could be added to the armamentarium of pain medications that we use today.”
In a 2015 systematic literature review, researchers assessed 28 randomized, controlled trials (RCTs) of the use of cannabinoids for chronic pain. They reported that a variety of formulations resulted in at least a 30% reduction in the odds of pain, compared with placebo. A meta-analysis of five RCTs involving patients with neuropathic pain found a 30% reduction in pain over placebo with inhaled, vaporized cannabis. Varying results have been reported in additional studies for this indication. The National Academies of Sciences, Engineering, and Medicine concluded that there was a substantial body of evidence that cannabis is an effective treatment for chronic pain in adults.
The ongoing opioid epidemic has lent these results additional relevance.
Seeing this firsthand has caused Mark Steven Wallace, MD, a pain management specialist and chair of the division of pain medicine at the University of California San Diego Health, to reconsider offering cannabis to his patients.
“I think it’s probably more efficacious, just from my personal experience, and it’s a much lower risk of abuse and dependence than the opioids,” he said.
Dr. Wallace advised that clinicians who treat pain consider the ratios of cannabinoids.
“This is anecdotal, but we do find that with the combination of the two, CBD reduces the psychoactive effects of the THC. The ratios we use during the daytime range around 20 mg of CBD to 1 mg of THC,” he said.
In a recent secondary analysis of an RCT involving patients with painful diabetic peripheral neuropathy, Dr. Wallace and colleagues showed that THC’s effects appear to reverse themselves at a certain level.
“As the THC level goes up, the pain reduces until you reach about 16 ng/mL; then it starts going in the opposite direction, and pain will start to increase,” he said. “Even recreational cannabis users have reported that they avoid high doses because it’s very aversive. Using cannabis is all about, start low and go slow.”
A mixed bag for neurologic indications
There are relatively limited data on the use of medical cannabis for other neurologic conditions, and results have varied. For uses other than pain management, the evidence that does exist is strongest regarding epilepsy, said Daniel Freedman, DO, assistant professor of neurology at the University of Texas at Austin. He noted “multiple high-quality RCTs showing that pharmaceutical-grade CBD can reduce seizures associated with two particular epilepsy syndromes: Dravet Syndrome and Lennox Gastaut.”
These findings led to the FDA’s 2018 approval of Epidiolex for these syndromes. In earlier years, interest in CBD for pediatric seizures was largely driven by anecdotal parental reports of its benefits. NASEM’s 2017 overview on medical cannabis found evidence from subsequent RCTs in this indication to be insufficient. Clinicians who prescribe CBD for this indication must be vigilant because it can interact with several commonly used antiepileptic drugs.
Cannabinoid treatments have also shown success in alleviating muscle spasticity resulting from multiple sclerosis, most prominently in the form of nabiximols (Sativex), a standardized oralmucosal spray containing approximately equal quantities of THC and CBD. Nabiximols is approved in Europe but not in the United States. Moderate evidence supports the efficacy of these and other treatments over placebo in reducing muscle spasticity. Patient ratings of its effects tend to be higher than clinician assessment.
Parkinson’s disease has not yet been approved as an indication for treatment with cannabis or cannabinoids, yet a growing body of preclinical data suggests these could influence the dopaminergic system, said Carsten Buhmann, MD, from the department of neurology at the University Medical Center Hamburg-Eppendorf (Germany).
“In general, cannabinoids modulate basal-ganglia function on two levels which are especially relevant in Parkinson’s disease, i.e., the glutamatergic/dopaminergic synaptic neurotransmission and the corticostriatal plasticity,” he said. “Furthermore, activation of the endocannabinoid system might induce neuroprotective effects related to direct receptor-independent mechanisms, activation of anti-inflammatory cascades in glial cells via the cannabinoid receptor type 2, and antiglutamatergic antiexcitotoxic properties.”
Dr. Buhmann said that currently, clinical evidence is scarce, consisting of only four double-blind, placebo-controlled RCTs involving 49 patients. Various cannabinoids and methods of administering treatment were employed. Improvement was only observed in one of these RCTs, which found that the cannabinoid receptor agonist nabilone significantly reduced levodopa-induced dyskinesia for patients with Parkinson’s disease. Subjective data support a beneficial effect. In a nationwide survey of 1,348 respondents conducted by Dr. Buhmann and colleagues, the majority of medical cannabis users reported that it improved their symptoms (54% with oral CBD and 68% with inhaled THC-containing cannabis).
NASEM concluded that there was insufficient evidence to support the efficacy of medical cannabis for other neurologic conditions, including Tourette syndrome, amyotrophic lateral sclerosis, Huntington disease, dystonia, or dementia. A 2020 position statement from the American Academy of Neurology cited the lack of sufficient peer-reviewed research as the reason it could not currently support the use of cannabis for neurologic disorders.
Yet, according to Dr. Freedman, who served as a coauthor of the AAN position statement, this hasn’t stymied research interest in the topic. He’s seen a substantial uptick in studies of CBD over the past 2 years. “The body of evidence grows, but I still see many claims being made without evidence. And no one seems to care about all the negative trials.”
Cannabis as a treatment for, and cause of, psychiatric disorders
Mental health problems – such as anxiety, depression, and PTSD – are among the most common reasons patients seek out medical cannabis. There is an understandable interest in using cannabis and cannabinoids to treat psychiatric disorders. Preclinical studies suggest that the endocannabinoid system plays a prominent role in modulating feelings of anxiety, mood, and fear. As with opioids and chronic pain management, there is hope that medical cannabis may provide a means of reducing prescription anxiolytics and their associated risks.
The authors of the first systematic review (BMC Psychiatry. 2020 Jan 16;20[1]:24) of the use of medical cannabis for major psychiatric disorders noted that the current evidence was “encouraging, albeit embryonic.”
Meta-analyses have indicated a small but positive association between cannabis use and anxiety, although this may reflect the fact that patients with anxiety sought out this treatment. Given the risks for substance use disorders among patients with anxiety, CBD may present a more viable option. Positive results have been shown as treatment for generalized social anxiety disorder.
Limited but encouraging results have also been reported regarding the alleviation of PTSD symptoms with both cannabis and CBD, although the body of high-quality evidence hasn’t notably progressed since 2017, when NASEM declared that the evidence was insufficient. Supportive evidence is similarly lacking regarding the treatment of depression. Longitudinal studies suggest that cannabis use, particularly heavy use, may increase the risk of developing this disorder. Because THC is psychoactive, it is advised that it be avoided by patients at risk for psychotic disorders. However, CBD has yielded limited benefits for patients with treatment-resistant schizophrenia and for young people at risk for psychosis.
The use of medical cannabis for psychiatric conditions requires a complex balancing act, inasmuch as these treatments may exacerbate the very problems they are intended to alleviate.
Marta Di Forti, MD, PhD, professor of psychiatric research at Kings College London, has been at the forefront of determining the mental health risks of continued cannabis use. In 2019, Dr. Di Forti developed the first and only Cannabis Clinic for Patients With Psychosis in London where she and her colleagues have continued to elucidate this connection.
Dr. Di Forti and colleagues have linked daily cannabis use to an increase in the risk of experiencing psychotic disorder, compared with never using it. That risk was further increased among users of high-potency cannabis (≥10% THC). The latter finding has troubling implications, because concentrations of THC have steadily risen since 1970. By contrast, CBD concentrations have remained generally stable. High-potency cannabis products are common in both recreational and medicinal settings.
“For somebody prescribing medicinal cannabis that has a ≥10% concentration of THC, I’d be particularly wary of the risk of psychosis,” said Dr. Di Forti. “If you’re expecting people to use a high content of THC daily to medicate pain or a chronic condition, you even more so need to be aware that this is a potential side effect.”
Dr. Di Forti noted that her findings come from a cohort of recreational users, most of whom were aged 18-35 years.
“There have actually not been studies developed from collecting data in this area from groups specifically using cannabis for medicinal rather than recreational purposes,” she said.
She added that she personally has no concerns about the use of medical cannabis but wants clinicians to be aware of the risk for psychosis, to structure their patient conversations to identify risk factors or family histories of psychosis, and to become knowledgeable in detecting the often subtle signs of its initial onset.
When cannabis-associated psychosis occurs, Dr. Di Forti said it is primarily treated with conventional means, such as antipsychotics and therapeutic interventions and by refraining from using cannabis. Achieving the latter goal can be a challenge for patients who are daily users of high-potency cannabis. Currently, there are no treatment options such as those offered to patients withdrawing from the use of alcohol or opioids. Dr. Di Forti and colleagues are currently researching a solution to that problem through the use of another medical cannabis, the oromucosal spray Sativex, which has been approved in the European Union.
The regulatory obstacles to clarifying cannabis’ role in medicine
That currently there is limited or no evidence to support the use of medical cannabis for the treatment of neuropsychiatric conditions points to the inherent difficulties in conducting high-level research in this area.
“There’s a tremendous shortage of reliable data, largely due to regulatory barriers,” said Dr. Martinez.
Since 1970, cannabis has been listed as a Schedule I drug that is illegal to prescribe (the Agriculture Improvement Act of 2018 removed hemp from such restrictions). The FDA has issued guidance for researchers who wish to investigate treatments using Cannabis sativa or its derivatives in which the THC content is greater than 0.3%. Such research requires regular interactions with several federal agencies, including the Drug Enforcement Administration.
“It’s impossible to do multicenter RCTs with large numbers of patients, because you can’t transport cannabis across state lines,” said Dr. Wallace.
Regulatory restrictions regarding medical cannabis vary considerably throughout the world (the European Monitoring Center for Drugs and Drug Addiction provides a useful breakdown of this on their website). The lack of consistency in regulatory oversight acts as an impediment for conducting large-scale international multicenter studies on the topic.
Dr. Buhmann noted that, in Germany, cannabis has been broadly approved for treatment-resistant conditions with severe symptoms that impair quality of life. In addition, it is easy to be reimbursed for the use of cannabis as a medical treatment. These factors serve as disincentives for the funding of high-quality studies.
“It’s likely that no pharmaceutical company will do an expensive RCT to get an approval for Parkinson’s disease because it is already possible to prescribe medical cannabis of any type of THC-containing cannabinoid, dose, or route of application,” Dr. Buhmann said.
In the face of such restrictions and barriers, researchers are turning to ambitious real-world data projects to better understand medical cannabis’ efficacy and safety. A notable example is ProjectTwenty21, which is supported by the Royal College of Psychiatrists. The project is collecting outcomes of the use of medical cannabis among 20,000 U.K. patients whose conventional treatments of chronic pain, anxiety disorder, epilepsy, multiple sclerosis, PTSD, substance use disorder, and Tourette syndrome failed.
Dr. Freedman noted that the continued lack of high-quality data creates a void that commercial interests fill with unfounded claims.
“The danger is that patients might abandon a medication or intervention backed by robust science in favor of something without any science or evidence behind it,” he said. “There is no reason not to expect the same level of data for claims about cannabis products as we would expect from pharmaceutical products.”
Getting to that point, however, will require that the authorities governing clinical trials begin to view cannabis as the research community does, as a possible treatment with potential value, rather than as an illicit drug that needs to be tamped down.
A version of this article first appeared on Medscape.com.
Although the healing properties of cannabis have been touted for millennia, research into its potential neuropsychiatric applications truly began to take off in the 1990s following the discovery of the cannabinoid system in the brain. This led to speculation that cannabis could play a therapeutic role in regulating dopamine, serotonin, and other neurotransmitters and offer a new means of treating various ailments.
At the same time, efforts to liberalize marijuana laws have successfully played out in several nations, including the United States, where, as of April 29, 36 states provide some access to cannabis. These dual tracks – medical and political – have made cannabis an increasingly accepted part of the cultural fabric.
Yet with this development has come a new quandary for clinicians. Medical cannabis has been made widely available to patients and has largely outpaced the clinical evidence, leaving it unclear how and for which indications it should be used.
The many forms of medical cannabis
Cannabis is a genus of plants that includes marijuana (Cannabis sativa) and hemp. These plants contain over 100 compounds, including terpenes, flavonoids, and – most importantly for medicinal applications – cannabinoids.
The most abundant cannabinoid in marijuana is the psychotropic delta-9-tetrahydrocannabinol (THC), which imparts the “high” sensation. The next most abundant cannabinoid is cannabidiol (CBD), which is the nonpsychotropic. THC and CBD are the most extensively studied cannabinoids, together and in isolation. Evidence suggests that other cannabinoids and terpenoids may also hold medical promise and that cannabis’ various compounds can work synergistically to produce a so-called entourage effect.
Patients walking into a typical medical cannabis dispensary will be faced with several plant-derived and synthetic options, which can differ considerably in terms of the ratios and amounts of THC and CBD they contain, as well in how they are consumed (i.e., via smoke, vapor, ingestion, topical administration, or oromucosal spray), all of which can alter their effects. Further complicating matters is the varying level of oversight each state and country has in how and whether they test for and accurately label products’ potency, cannabinoid content, and possible impurities.
Medically authorized, prescription cannabis products go through an official regulatory review process, and indications/contraindications have been established for them. To date, the Food and Drug Administration has approved one cannabis-derived drug product – Epidiolex (purified CBD) – for the treatment of seizures associated with Lennox-Gastaut syndrome or Dravet syndrome in patients aged 2 years and older. The FDA has also approved three synthetic cannabis-related drug products – Marinol, Syndros (or dronabinol, created from synthetic THC), and Cesamet (or nabilone, a synthetic cannabinoid similar to THC) – all of which are indicated for treatment-related nausea and anorexia associated with weight loss in AIDS patients.
Surveys of medical cannabis consumers indicate that most people cannot distinguish between THC and CBD, so the first role that physicians find themselves in when recommending this treatment may be in helping patients navigate the volume of options.
Promising treatment for pain
Chronic pain is the leading reason patients seek out medical cannabis. It is also the indication that most researchers agree has the strongest evidence to support its use.
“In my mind, the most promising immediate use for medical cannabis is with THC for pain,” Diana M. Martinez, MD, a professor of psychiatry at Columbia University, New York, who specializes in addiction research, said in a recent MDedge podcast. “THC could be added to the armamentarium of pain medications that we use today.”
In a 2015 systematic literature review, researchers assessed 28 randomized, controlled trials (RCTs) of the use of cannabinoids for chronic pain. They reported that a variety of formulations resulted in at least a 30% reduction in the odds of pain, compared with placebo. A meta-analysis of five RCTs involving patients with neuropathic pain found a 30% reduction in pain over placebo with inhaled, vaporized cannabis. Varying results have been reported in additional studies for this indication. The National Academies of Sciences, Engineering, and Medicine concluded that there was a substantial body of evidence that cannabis is an effective treatment for chronic pain in adults.
The ongoing opioid epidemic has lent these results additional relevance.
Seeing this firsthand has caused Mark Steven Wallace, MD, a pain management specialist and chair of the division of pain medicine at the University of California San Diego Health, to reconsider offering cannabis to his patients.
“I think it’s probably more efficacious, just from my personal experience, and it’s a much lower risk of abuse and dependence than the opioids,” he said.
Dr. Wallace advised that clinicians who treat pain consider the ratios of cannabinoids.
“This is anecdotal, but we do find that with the combination of the two, CBD reduces the psychoactive effects of the THC. The ratios we use during the daytime range around 20 mg of CBD to 1 mg of THC,” he said.
In a recent secondary analysis of an RCT involving patients with painful diabetic peripheral neuropathy, Dr. Wallace and colleagues showed that THC’s effects appear to reverse themselves at a certain level.
“As the THC level goes up, the pain reduces until you reach about 16 ng/mL; then it starts going in the opposite direction, and pain will start to increase,” he said. “Even recreational cannabis users have reported that they avoid high doses because it’s very aversive. Using cannabis is all about, start low and go slow.”
A mixed bag for neurologic indications
There are relatively limited data on the use of medical cannabis for other neurologic conditions, and results have varied. For uses other than pain management, the evidence that does exist is strongest regarding epilepsy, said Daniel Freedman, DO, assistant professor of neurology at the University of Texas at Austin. He noted “multiple high-quality RCTs showing that pharmaceutical-grade CBD can reduce seizures associated with two particular epilepsy syndromes: Dravet Syndrome and Lennox Gastaut.”
These findings led to the FDA’s 2018 approval of Epidiolex for these syndromes. In earlier years, interest in CBD for pediatric seizures was largely driven by anecdotal parental reports of its benefits. NASEM’s 2017 overview on medical cannabis found evidence from subsequent RCTs in this indication to be insufficient. Clinicians who prescribe CBD for this indication must be vigilant because it can interact with several commonly used antiepileptic drugs.
Cannabinoid treatments have also shown success in alleviating muscle spasticity resulting from multiple sclerosis, most prominently in the form of nabiximols (Sativex), a standardized oralmucosal spray containing approximately equal quantities of THC and CBD. Nabiximols is approved in Europe but not in the United States. Moderate evidence supports the efficacy of these and other treatments over placebo in reducing muscle spasticity. Patient ratings of its effects tend to be higher than clinician assessment.
Parkinson’s disease has not yet been approved as an indication for treatment with cannabis or cannabinoids, yet a growing body of preclinical data suggests these could influence the dopaminergic system, said Carsten Buhmann, MD, from the department of neurology at the University Medical Center Hamburg-Eppendorf (Germany).
“In general, cannabinoids modulate basal-ganglia function on two levels which are especially relevant in Parkinson’s disease, i.e., the glutamatergic/dopaminergic synaptic neurotransmission and the corticostriatal plasticity,” he said. “Furthermore, activation of the endocannabinoid system might induce neuroprotective effects related to direct receptor-independent mechanisms, activation of anti-inflammatory cascades in glial cells via the cannabinoid receptor type 2, and antiglutamatergic antiexcitotoxic properties.”
Dr. Buhmann said that currently, clinical evidence is scarce, consisting of only four double-blind, placebo-controlled RCTs involving 49 patients. Various cannabinoids and methods of administering treatment were employed. Improvement was only observed in one of these RCTs, which found that the cannabinoid receptor agonist nabilone significantly reduced levodopa-induced dyskinesia for patients with Parkinson’s disease. Subjective data support a beneficial effect. In a nationwide survey of 1,348 respondents conducted by Dr. Buhmann and colleagues, the majority of medical cannabis users reported that it improved their symptoms (54% with oral CBD and 68% with inhaled THC-containing cannabis).
NASEM concluded that there was insufficient evidence to support the efficacy of medical cannabis for other neurologic conditions, including Tourette syndrome, amyotrophic lateral sclerosis, Huntington disease, dystonia, or dementia. A 2020 position statement from the American Academy of Neurology cited the lack of sufficient peer-reviewed research as the reason it could not currently support the use of cannabis for neurologic disorders.
Yet, according to Dr. Freedman, who served as a coauthor of the AAN position statement, this hasn’t stymied research interest in the topic. He’s seen a substantial uptick in studies of CBD over the past 2 years. “The body of evidence grows, but I still see many claims being made without evidence. And no one seems to care about all the negative trials.”
Cannabis as a treatment for, and cause of, psychiatric disorders
Mental health problems – such as anxiety, depression, and PTSD – are among the most common reasons patients seek out medical cannabis. There is an understandable interest in using cannabis and cannabinoids to treat psychiatric disorders. Preclinical studies suggest that the endocannabinoid system plays a prominent role in modulating feelings of anxiety, mood, and fear. As with opioids and chronic pain management, there is hope that medical cannabis may provide a means of reducing prescription anxiolytics and their associated risks.
The authors of the first systematic review (BMC Psychiatry. 2020 Jan 16;20[1]:24) of the use of medical cannabis for major psychiatric disorders noted that the current evidence was “encouraging, albeit embryonic.”
Meta-analyses have indicated a small but positive association between cannabis use and anxiety, although this may reflect the fact that patients with anxiety sought out this treatment. Given the risks for substance use disorders among patients with anxiety, CBD may present a more viable option. Positive results have been shown as treatment for generalized social anxiety disorder.
Limited but encouraging results have also been reported regarding the alleviation of PTSD symptoms with both cannabis and CBD, although the body of high-quality evidence hasn’t notably progressed since 2017, when NASEM declared that the evidence was insufficient. Supportive evidence is similarly lacking regarding the treatment of depression. Longitudinal studies suggest that cannabis use, particularly heavy use, may increase the risk of developing this disorder. Because THC is psychoactive, it is advised that it be avoided by patients at risk for psychotic disorders. However, CBD has yielded limited benefits for patients with treatment-resistant schizophrenia and for young people at risk for psychosis.
The use of medical cannabis for psychiatric conditions requires a complex balancing act, inasmuch as these treatments may exacerbate the very problems they are intended to alleviate.
Marta Di Forti, MD, PhD, professor of psychiatric research at Kings College London, has been at the forefront of determining the mental health risks of continued cannabis use. In 2019, Dr. Di Forti developed the first and only Cannabis Clinic for Patients With Psychosis in London where she and her colleagues have continued to elucidate this connection.
Dr. Di Forti and colleagues have linked daily cannabis use to an increase in the risk of experiencing psychotic disorder, compared with never using it. That risk was further increased among users of high-potency cannabis (≥10% THC). The latter finding has troubling implications, because concentrations of THC have steadily risen since 1970. By contrast, CBD concentrations have remained generally stable. High-potency cannabis products are common in both recreational and medicinal settings.
“For somebody prescribing medicinal cannabis that has a ≥10% concentration of THC, I’d be particularly wary of the risk of psychosis,” said Dr. Di Forti. “If you’re expecting people to use a high content of THC daily to medicate pain or a chronic condition, you even more so need to be aware that this is a potential side effect.”
Dr. Di Forti noted that her findings come from a cohort of recreational users, most of whom were aged 18-35 years.
“There have actually not been studies developed from collecting data in this area from groups specifically using cannabis for medicinal rather than recreational purposes,” she said.
She added that she personally has no concerns about the use of medical cannabis but wants clinicians to be aware of the risk for psychosis, to structure their patient conversations to identify risk factors or family histories of psychosis, and to become knowledgeable in detecting the often subtle signs of its initial onset.
When cannabis-associated psychosis occurs, Dr. Di Forti said it is primarily treated with conventional means, such as antipsychotics and therapeutic interventions and by refraining from using cannabis. Achieving the latter goal can be a challenge for patients who are daily users of high-potency cannabis. Currently, there are no treatment options such as those offered to patients withdrawing from the use of alcohol or opioids. Dr. Di Forti and colleagues are currently researching a solution to that problem through the use of another medical cannabis, the oromucosal spray Sativex, which has been approved in the European Union.
The regulatory obstacles to clarifying cannabis’ role in medicine
That currently there is limited or no evidence to support the use of medical cannabis for the treatment of neuropsychiatric conditions points to the inherent difficulties in conducting high-level research in this area.
“There’s a tremendous shortage of reliable data, largely due to regulatory barriers,” said Dr. Martinez.
Since 1970, cannabis has been listed as a Schedule I drug that is illegal to prescribe (the Agriculture Improvement Act of 2018 removed hemp from such restrictions). The FDA has issued guidance for researchers who wish to investigate treatments using Cannabis sativa or its derivatives in which the THC content is greater than 0.3%. Such research requires regular interactions with several federal agencies, including the Drug Enforcement Administration.
“It’s impossible to do multicenter RCTs with large numbers of patients, because you can’t transport cannabis across state lines,” said Dr. Wallace.
Regulatory restrictions regarding medical cannabis vary considerably throughout the world (the European Monitoring Center for Drugs and Drug Addiction provides a useful breakdown of this on their website). The lack of consistency in regulatory oversight acts as an impediment for conducting large-scale international multicenter studies on the topic.
Dr. Buhmann noted that, in Germany, cannabis has been broadly approved for treatment-resistant conditions with severe symptoms that impair quality of life. In addition, it is easy to be reimbursed for the use of cannabis as a medical treatment. These factors serve as disincentives for the funding of high-quality studies.
“It’s likely that no pharmaceutical company will do an expensive RCT to get an approval for Parkinson’s disease because it is already possible to prescribe medical cannabis of any type of THC-containing cannabinoid, dose, or route of application,” Dr. Buhmann said.
In the face of such restrictions and barriers, researchers are turning to ambitious real-world data projects to better understand medical cannabis’ efficacy and safety. A notable example is ProjectTwenty21, which is supported by the Royal College of Psychiatrists. The project is collecting outcomes of the use of medical cannabis among 20,000 U.K. patients whose conventional treatments of chronic pain, anxiety disorder, epilepsy, multiple sclerosis, PTSD, substance use disorder, and Tourette syndrome failed.
Dr. Freedman noted that the continued lack of high-quality data creates a void that commercial interests fill with unfounded claims.
“The danger is that patients might abandon a medication or intervention backed by robust science in favor of something without any science or evidence behind it,” he said. “There is no reason not to expect the same level of data for claims about cannabis products as we would expect from pharmaceutical products.”
Getting to that point, however, will require that the authorities governing clinical trials begin to view cannabis as the research community does, as a possible treatment with potential value, rather than as an illicit drug that needs to be tamped down.
A version of this article first appeared on Medscape.com.
Distress and Factors Associated with Suicidal Ideation in Veterans Living with Cancer (FULL)
It was estimated that physicians would diagnose a form of invasive cancer > 1.7 million times in 2019. As the second most common cause of death in the US, > 600,000 people were projected to die from cancer in 2019.1 Many individuals with cancer endure distress, which the National Comprehensive Cancer Network (NCCN) defines as a “multifactorial unpleasant experience of a psychological (ie, cognitive, behavioral, emotional), social, spiritual, and/or physical nature that may interfere with the ability to cope effectively with cancer, its physical symptoms, and its treatment.”2,3 Distress in people living with cancer has been attributed to various psychosocial concerns, such as family problems, whichinclude dealing with partners and children; emotional problems, such as depression and anxiety; and physical symptoms, such as pain and fatigue.4-9 Certain factors associated with distress may increase a patient’s risk for suicide.4
Veterans are at particularly high risk for suicide.10 In 2014, veterans accounted for 18% of completed suicides in the US but only were 8.5% of the total population that same year.10 Yet, little research has been done on the relationship between distress and suicide in veterans living with cancer. Aboumrad and colleagues found that 45% of veterans with cancer who completed suicide reported family issues and 41% endorsed chronic pain.11 This study recommended continued efforts to assess and treat distress to lessen risk of suicide in veterans living with cancer; however, to date, only 1 study has specifically evaluated distress and problems endorsed among veterans living with cancer.7
Suicide prevention is of the highest priority to the US Department of Veterans Affairs (VA).12 Consistent with the VA mission to end veteran suicide, the current study aimed to better understand the relationship between distress and suicide within a sample of veterans living with cancer. Findings would additionally be used to tailor clinical assessments and interventions for veterans living with cancer.
This study had 3 primary goals. First, we sought to understand demographic and clinical factors associated with low, moderate, and severe levels of distress in veterans living with cancer who were referred for psychology services. Second, the study investigated the most commonly endorsed problems by veterans living with cancer. Finally, we examined which problems were related to suicidal ideation (SI). It was hypothesized that veterans who reported severe distress would be significantly more likely to endorse SI when compared with veterans who reported mild or moderate distress. Based on existing literature, it was further hypothesized that family, emotional, and physical problems would be significantly associated with SI.7,11
Methods
The current study was conducted at James A. Haley Veterans’ Hospital (JAHVH) in Tampa, Florida. Inclusion criteria included veterans who were diagnosed with cancer, attended an outpatient psychology-oncology evaluation, and completed mental health screening measures provided during their evaluation. Exclusion criteria included veterans who: were seen in response to an inpatient consult, were seen solely for a stem cell transplant evaluation, or did not complete the screening measures.
Measures
A veteran’s demographic (eg, age, sex, ethnicity) and clinical (eg, cancer type, stage of disease, recurrence, cancer treatments received) information was abstracted from their VA medical records. Marital status was assessed during a clinical interview and documented as part of the standardized suicide risk assessment.
The Distress Thermometer (DT) is a subjective measure developed by the NCCN.2 The DT provides a visual representation of a thermometer and asks patients to rate their level of distress over the past week with 0 indicating no distress and 10 indicating extreme distress.
The measurement additionally lists 39 problems nested within 5 domains: practical, family, emotional, spiritual/religious, and physical. Patients may endorse listed items under each problem domain by indicating yes or no. Endorsement of various items are intended to provide more detailed information about sources of distress. Due to the predominantly male and mostly older population included in this study the ability to have children measure was removed from the family problem domain.
SI was assessed in 2 ways. First, by patients’ self-report through item-9 of the Patient Health Questionnaire-9 (PHQ-9).14 Item-9 asks “over the last 2 weeks, how often have you been bothered by thoughts that you would be better off dead or of hurting yourself in some way?” Responses range from 0 (not at all) to 3 (nearly every day).14 Responses > 0 were considered a positive screen for SI.
Procedure
Participants were a sample of veterans who were referred for psychology-oncology services. The NCCN DT and Problems List were administered prior to the start of clinical interviews, which followed a checklist and included standardized assessments of SI and history of a suicide attempt(s). A licensed clinical psychologist or a postdoctoral resident conducted these assessments under the supervision of a licensed psychologist. Data gathered during the clinical interview and from the DT and problems list were documented in health records, which were retrospectively reviewed for relevant information (eg, cancer diagnosis, SI). Therefore, informed consent was waived. This study was approved by the JAHVH Institutional Review Board.
Analysis
Data were analyzed using SPSS Version 25. Data analysis proceeded in 3 steps. First, descriptive statistics included the demographic and clinical factors present in the current sample. Difference between those with and without suicidal ideation were compared using F-statistic for continuous variables and χ2 analyses for categorical variables. Second, to examine relationships between each DT problem domain and SI, χ2 analyses were conducted. Third, DT problem domains that had a significant relationship with SI were entered in a logistic regression. This analysis determined which items, if any, from a DT problem domain predicted SI. In the logistic regression model, history of suicide attempts was entered into the first block, as history of suicide attempts is a well-established risk factor for subsequent suicidal ideation. In the second block, other variables that were significantly related to suicidal ideation in the second step of analyses were included. Before interpreting the results of the logistic regression, model fit was tested using the Hosmer-Lemeshow test. Significance of each individual predictor variable in the model is reported using the Wald χ2 statistic; each Wald statistic is compared with a χ2 distribution with 1 degree of freedom (df). Results of logistic regression models also provide information about the effect of each predictor variable in the regression equation (beta weight), odds a veteran who endorsed each predictor variable in the model would also endorse SI (as indicated by the odds ratio), and an estimate of the amount of variance accounted for by each predictor variable (using Nagelkerke’s pseudo R2, which ranges in value from 0 to 1 with higher values indicating more variance explained). For all analyses, P value of .05 (2-tailed) was used for statistical significance.
Results
The sample consisted of 174 veterans (Table 1). The majority (77.6%) were male with a mean age of nearly 62 years (range, 29-87). Most identified as white (74.1%) with half reporting they were either married or living with a partner.
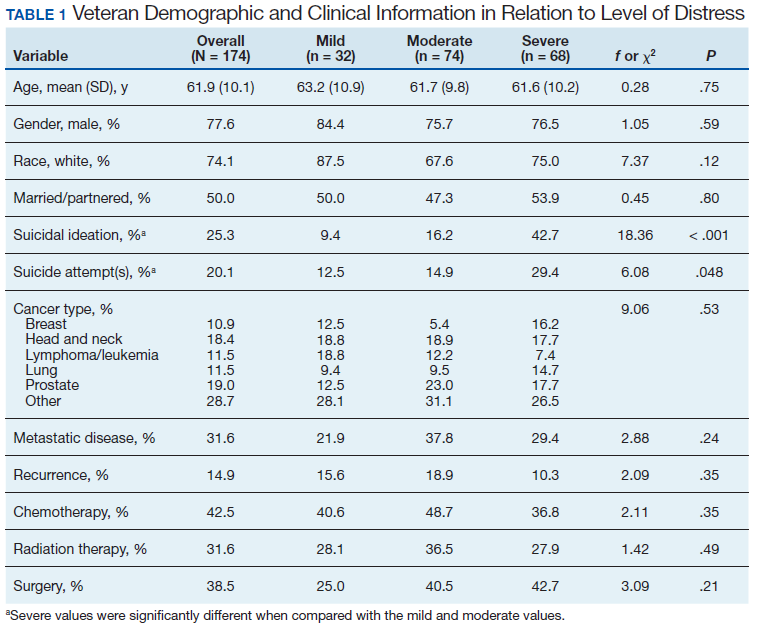
Prostate cancer (19.0%) was the most common type of cancer among study participants followed by head and neck (18.4%), lymphoma/leukemia (11.5%), lung (11.5%), and breast (10.9%); 31.6% had metastatic disease and 14.9% had recurrent disease. Chemotherapy (42.5%) was the most common treatment modality, followed by surgery (38.5%) and radiation (31.6%). The sample was distributed among the 3 distress DT categories: mild (18.4%), moderate (42.5%), and severe (39.1%).
Problems Endorsed
Treatment decisions (44.3%) and insurance/financial concerns (35.1%) were the most frequently endorsed practical problems (Figure 1). Family health issues (33.9%) and dealing with partner (23.0%) were the most frequently endorsed family problems (Figure 2). Worry (73.0%) and depression (69.5%) were the most frequent emotional problems; of note, all emotional problems were endorsed by at least 50% of veterans (Figure 3). Fatigue (71.3%), sleep (70.7%), and pain (69%), were the most frequently endorsed physical problems (Figure 4). Spiritual/religious problems were endorsed by 15% of veterans.
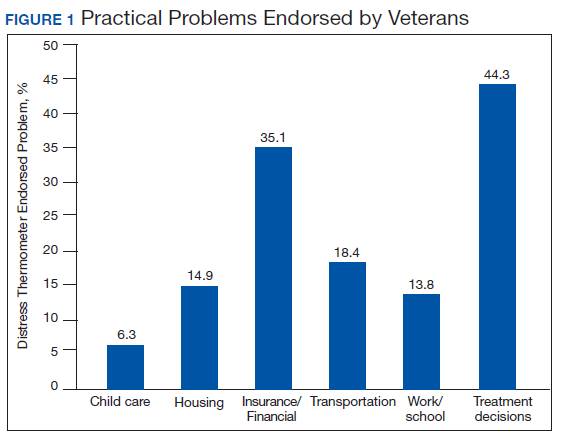
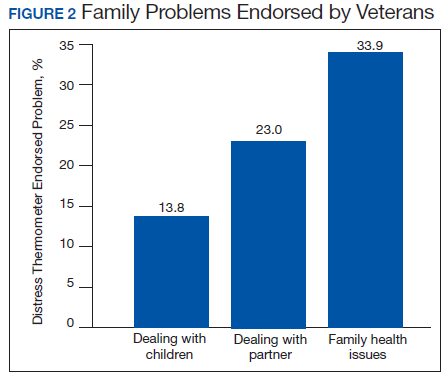
Suicidal Ideation
Overall, 25.3% of veterans endorsed SI. About 20% of veterans reported a history of ≥ 1 suicide attempts in their lifetime. A significant relationship among distress categories and SI was found (χ2 = 18.36, P < .001). Veterans with severe distress were more likely to endorse SI (42.7%) when compared with veterans with mild (9.4%) or moderate (16.2%) distress.
Similarly, a significant relationship among distress categories and a history of a suicide attempt(s) was found (χ2 = 6.08, P = .048). Veterans with severe distress were more likely to have attempted suicide (29.4%) when compared with veterans with mild (12.5%) or moderate (14.9%) distress.
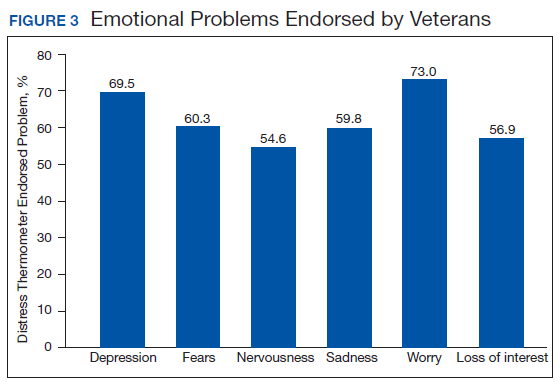
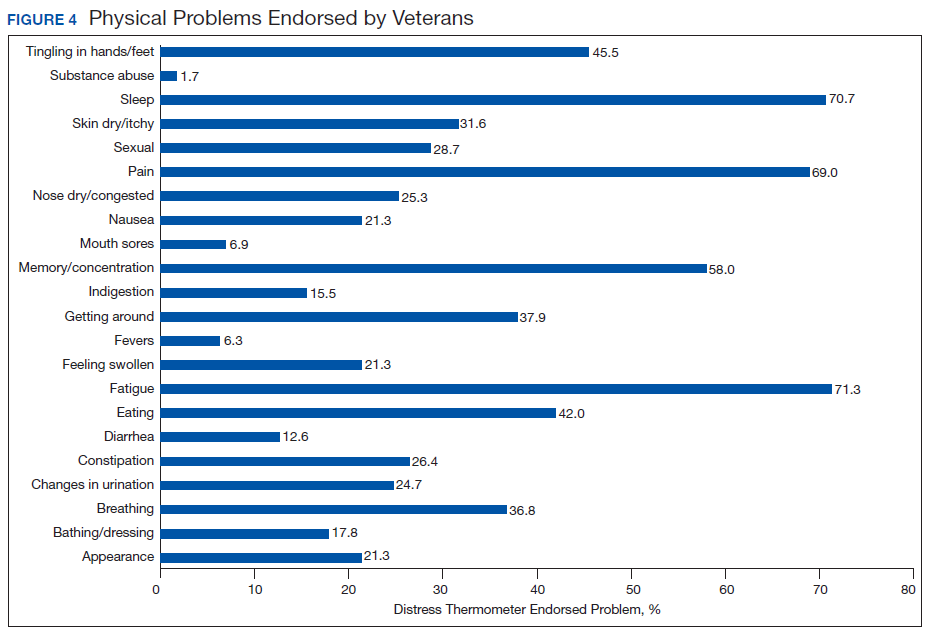
χ2 analyses were conducted to examine the relationships between DT problem domains and SI. A significant relationship was found between family problems and SI (
Logistic regression analyses determined whether items representative of the family problems domain were predictive of SI. Suicide attempt(s) were entered in the first step of the model to evaluate risk factors for SI over this already established risk factor. The assumptions of logistic regression were met.
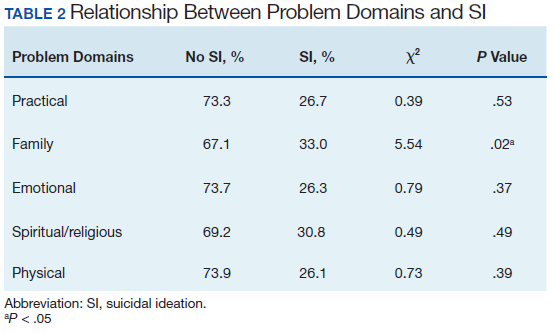
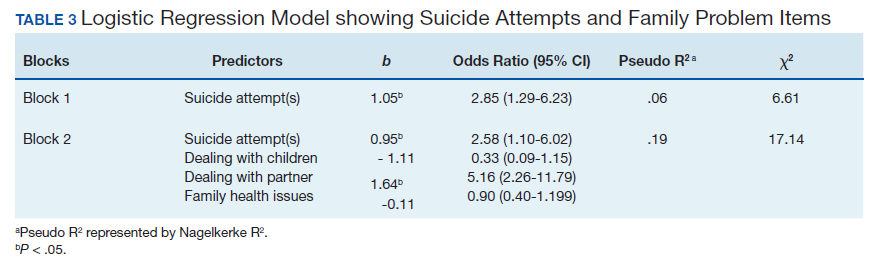
The Hosmer-Lemeshow test (χ2 = 3.66, df = 5, P = .56) demonstrated that the model fit was good. The group of predictors used in the model differentiate between people who were experiencing SI and those who were not experiencing SI at the time of evaluation. A history of a suicide attempt(s) predicted SI, as expected (Wald = 6.821, df = 1, P = .01). The odds that a veteran with a history of a suicide attempt(s) would endorse SI at the time of the evaluation was nearly 3 times greater than that of veterans without a history of a suicide attempt(s). Over and above suicide attempts, problems dealing with partner (Wald = 15.142; df = 1, P < .001) was a second significant predictor of current SI. The odds that a veteran who endorsed problems dealing with partner would also endorse SI was > 5 times higher than that of veterans who did not endorse problems dealing with partner. This finding represents a significant risk factor for SI, over and above a history of a suicide attempt(s). The other items from the family problems domains were not significant (P > .05) (Table 3).
Discussion
This study aimed to understand factors associated with low, moderate, and severe levels of distress in veterans living with cancer who were referred for psychology services. As hypothesized, veterans who endorsed severe distress were significantly more likely to endorse SI. They also were more likely to have a history of a suicide attempt(s) when compared with those with mild or moderate distress.
A second aim of this study was to understand the most commonly endorsed problems. Consistent with prior literature, treatment decisions were the most commonly endorsed practical problem; worry and depression were the most common emotional problems; and fatigue, sleep, and pain were the most common physical problems.7
A finding unique to the current study is that family health issues and dealing with partner were specified as the most common family problems. However, a study by Smith and colleagues did not provide information about the rank of most frequently reported problems within this domain.7
The third aim was to understand which problems were related to SI. It was hypothesized that family, emotional, and physical problems would be related to SI. However, results indicated that only family problems (specifically, problems dealing with a partner) were significantly associated with SI among veterans living with cancer.
Contrary to expectations, emotional and physical problems were not found to have a significant relationship with SI. This is likely because veterans endorsed items nested within these problem domains with similar frequency. The lack of significant findings does not suggest that emotional and physical problems are not significant predictors of SI for veterans living with cancer, but that no specific emotional or physical symptom stood out as a predictor of suicidal ideation above the others.
The finding of a significant relationship between family problems (specifically, problems dealing with a partner) and SI in this study is consistent with findings of Aboumrad and colleagues in a study that examined root-cause analyses of completed suicides by veterans living with cancer.11 They found that nearly half the sample endorsed family problems prior to their death, and a small but notable percentage of veterans who completed suicide reported divorce as a stressor prior to their death.
This finding may be explained by Thomas Joiner's interpersonal-psychological theory of suicidal behavior (IPT), which suggests that completed suicide may result from a thwarted sense of belonging, perceived burdensomeness, and acquired capability for suicide.16 Problems dealing with a partner may impact a veteran’s sense of belonging or social connectedness. Problems dealing with a partner also may be attributed to perceived burdens due to limitations imposed by living with cancer and/or undergoing treatment. In both circumstances, the veteran’s social support system may be negatively impacted, and perceived social support is a well-established protective factor against suicide.17
Partner distress is a second consideration. It is likely that veterans’ partners experienced their own distress in response to the veteran’s cancer diagnosis and/or treatment. The partner’s cause, severity, and expression of distress may contribute to problems for the couple.
Finally, the latter point of the IPT refers to acquired capability, or the ability to inflict deadly harm to oneself.18 A military sample was found to have more acquired capability for suicide when compared with a college undergraduate sample.19 A history of a suicide attempt(s) and male gender have been found to significantly predict acquired capability to complete suicide.18 Furthermore, because veterans living with cancer often are in pain, fear of pain associated with suicide may be reduced and, therefore, acquired capability increased. This suggests that male veterans living with cancer who are in pain, have a history of a suicide attempt(s), and current problems with their partner may be an extremely vulnerable population at-risk for suicide. Results from the current study emphasize the importance of veterans having access to mental health and crisis resources for problems dealing with their partner. Partner problems may foreshadow a potentially lethal type of distress.
Strengths
This study’s aims are consistent with the VA’s mission to end veteran suicide and contributes to literature in several important ways.12 First, veterans living with cancer are an understudied population. The current study addresses a gap in existing literature by researching veterans living with cancer and aims to better understand the relationship between cancer-related distress and SI. Second, to the best of the authors’ knowledge, this study is the first to find that problems dealing with a partner significantly increases a veteran’s risk for SI above a history of a suicide attempt(s). Risk assessments now may be more comprehensive through inclusion of this distress factor.
It is recommended that future research use IPT to further investigate the relationship between problems dealing with a partner and SI.16 Future research may do so by including specific measures to assess for the tenants of the theory, including measurements of burdensomeness and belongingness. An expanded knowledge base about what makes problems dealing with a partner a significant suicide risk factor (eg, increased conflict, lack of support, etc.) would better enable clinicians to intervene effectively. Effective intervention may lessen suicidal behaviors or deaths from suicides within the Veteran population.
Limitations
One limitation is the focus on patients who accepted a mental health referral. This study design may limit the generalizability of results to veterans who would not accept mental health treatment. The homogenous sample of veterans is a second limitation. Most participants were male, white, and had a mean age of 62 years. These demographics are representative of the veterans that most typically utilize VA services; however, more research is needed on veterans living with cancer who are female and of diverse racial and ethnic backgrounds. There are likely differences in problems endorsed and factors associated with SI based on age, race, sex, and other socioeconomic factors. A third limitation is the cross-sectional, retrospective nature of this study. Future studies are advised to assess for distress at multiple time points. This is consistent with NCCN Standards of Care for Distress Management.2 Longitudinal data would enable more findings about distress and SI throughout the course of cancer diagnosis and treatment, therefore enhancing clinical implications and informing future research.
Conclusion
This is among the first of studies to investigate distress and factors associated with SI in veterans living with cancer who were referred for psychology services. The prevalence of distress caused by psychosocial factors (including treatment decisions, worry, and depression) highlights the importance of including mental health services as part of comprehensive cancer treatment.
Distress due to treatment decisions may be attributed to a litany of factors such as a veteran’s consideration of adverse effects, effectiveness of treatments, changes to quality of life or functioning, and inclusion of alternative or complimentary treatments. These types of decisions often are reported to be difficult conversations to have with family members or loved ones, who are likely experiencing distress of their own. The role of a mental health provider to assist veterans in exploring their treatment decisions and the implications of such decisions appears important to lessening distress.
Early intervention for emotional symptoms would likely benefit veterans’ management of distress and may lessen suicide risk as depression is known to place veterans at-risk for SI.20 This underscores the importance of timely distress assessment to prevent mild emotional distress from progressing to potentially severe or life-threatening emotional distress. For veterans with a psychiatric history, timely assessment and intervention is essential because psychiatric history is an established suicide risk factor that may be exacerbated by cancer-related distress.12
Furthermore, management of intolerable physical symptoms may lessen risk for suicide.4 Under medical guidance, fatigue may be improved using exercise.21 Behavioral intervention is commonly used as first-line treatment for sleep problems.22 While pain may be lessened through medication or nonpharmacological interventions.23
Considering the numerous ways that distress may present itself (eg, practical, emotional, or physical) and increase risk for SI, it is essential that all veterans living with cancer are assessed for distress and SI, regardless of their presentation. Although veterans may not outwardly express distress, this does not indicate the absence of either distress or risk for suicide. For example, a veteran may be distressed due to financial concerns, transportation issues, and the health of his/her partner or spouse. This veteran may not exhibit visible symptoms of distress, as would be expected when the source of distress is emotional (eg, depression, anxiety). However, this veteran is equally vulnerable to impairing distress and SI as someone who exhibits emotional distress. Distress assessments should be further developed to capture both the visible and less apparent sources of distress, while also serving the imperative function of screening for suicide. Other researchers also have noted the necessity of this development.24 Currently, the NCCN DT and Problems List does not include any assessment of SI or behavior.
Finally, this study identified a potentially critical factor to include in distress assessment: problems dealing with a partner. Problems dealing with a partner have been noted as a source of distress in existing literature, but this is the first study to find problems dealing with a partner to be a predictor of SI in veterans living with cancer.4-6
Because partners often attend appointments with veterans, it is not surprising that problems dealing with their partner are not disclosed more readily. It is recommended that clinicians ask veterans about potential problems with their partner when they are alone. Directly gathering information about such problems while assessing for distress may assist health care workers in providing the most effective, accurate type of intervention in a timely manner, and potentially mitigate risk for suicide.
As recommended by the NCCN and numerous researchers, findings from the current study underscore the importance of accurate, timely assessment of distress.2,4,8 This study makes several important recommendations about how distress assessment may be strengthened and further developed, specifically for the veteran population. This study also expands the current knowledge base of what is known about veterans living with cancer, and has begun to fill a gap in the existing literature. Consistent with the VA mission to end veteran suicide, results suggest that veterans living with cancer should be regularly screened for distress, asked about distress related to their partner, and assessed for SI. Continued efforts to enhance assessment of and response to distress may lessen suicide risk in veterans with cancer.11
Acknowledgements
This study is the result of work supported with resources and the use of facilities at the James A. Haley Veterans’ Hospital.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7-34.
2. Riba MB, Donovan, KA, Andersen, B. National Comprehensive Cancer Network clinical practice guidelines in oncology. Distress management (Version 3.2019). J Natl Compr Can Net, 2019;17(10):1229-1249.
3. Zabora J, BrintzenhofeSzoc K, Curbow B, Hooker C, Pianta dosi S. The prevalence of psychological distress by cancer site. Psychooncology. 2001;10(1):19–28.
4. Holland JC, Alici Y. Management of distress in cancer patients. J Support Oncol. 2010;8(1):4-12.
5. Bulli F, Miccinesi G, Maruelli A, Katz M, Paci E. The measure of psychological distress in cancer patients: the use of distress thermometer in the oncological rehabilitation center of Florence. Support Care Cancer. 2009;17(7):771–779.
6. Jacobsen PB, Donovan KA, Trask PC, et al. Screening for psychologic distress in ambulatory cancer patients. Cancer. 2005;103(7):1494-1502.
7. Smith J, Berman S, Dimick J, et al. Distress Screening and Management in an Outpatient VA Cancer Clinic: A Pilot Project Involving Ambulatory Patients Across the Disease Trajectory. Fed Pract. 2017;34(Suppl 1):43S–50S.
8. Carlson LE, Waller A, Groff SL, Bultz BD. Screening for distress, the sixth vital sign, in lung cancer patients: effects on pain, fatigue, and common problems--secondary outcomes of a randomized controlled trial. Psychooncology. 2013;22(8):1880-1888.
9. Cooley ME, Short TH, Moriarty HJ. Symptom prevalence, distress, and change over time in adults receiving treatment for lung cancer. Psychooncology. 2003;12(7):694-708.
10. US Department of Veterans Affairs Office of Suicide Prevention. Suicide among veterans and other Americans 2001-2014. https://www.mentalhealth.va.gov/docs/2016suicidedatareport.pdf. Published August 3, 2016. Accessed April 13, 2020.
11. Aboumrad M, Shiner B, Riblet N, Mills, PD, Watts BV. Factors contributing to cancer-related suicide: a study of root-cause-analysis reports. Psychooncology. 2018;27(9):2237-2244.
12. US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention. National Strategy for Preventing Veteran Suicide 2018–2028. https://www.mentalhealth.va.gov/suicide_prevention/docs/Office-of-Mental-Health-and-Suicide-Prevention-National-Strategy-for-Preventing-Veterans-Suicide.pdf Published 2018. Accessed April 13, 2020.
13. Carlson LE, Waller A, Mitchell AJ. Screening for distress and unmet needs in patients with cancer: review and recommendations. J Clin Oncol. 2012;30(11):1160-1177.
14. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613.
15. Martin A, Rief W, Klaiberg A, Braehler E. Validity of the brief patient health questionnaire mood scale (PHQ-9) in the general population. Gen Hosp Psychiatry. 2006;28(1):71-77.
16. Joiner TE. Why People Die by Suicide. Cambridge, MA: Harvard University Press, 2005.
17. Kleiman EM, Riskind JH, Schaefer KE. Social support and positive events as suicide resiliency factors: examination of synergistic buffering effects. Arch Suicide Res. 2014;18(2):144-155.
18. Van Orden KA, Witte TK, Gordon KH, Bender TW, Joiner TE Jr. Suicidal desire and the capability for suicide: tests of the interpersonal-psychological theory of suicidal behavior among adults. J Consult Clin Psychol. 2008;76(1):72–83.
19. Bryan CJ, Morrow CE, Anestis MD, Joiner TE. A preliminary test of the interpersonal -psychological theory of suicidal behavior in a military sample. Personal Individual Differ. 2010;48(3):347-350.
20. Miller SN, Monahan CJ, Phillips KM, Agliata D, Gironda RJ. Mental health utilization among veterans at risk for suicide: Data from a post-deployment clinic [published online ahead of print, 2018 Oct 8]. Psychol Serv. 2018;10.1037/ser0000311.
21. Galvão DA, Newton RU. Review of exercise intervention studies in cancer patients. J Clin Oncol. 2005;23(4):899-909.
22. Qaseem A, Kansagara D, Forciea MA, Cooke M, Denberg TD; Clinical Guidelines Committee of the American College of Physicians. Management of chronic insomnia disorder in adults: A clinical practice guideline from the American College of Physicians. Ann Intern Med. 2016;165(2):125-133.
23. Ngamkham S, Holden JE, Smith EL. A systematic review: Mindfulness intervention for cancer-related pain. Asia Pac J Oncol Nurs. 2019;6(2):161-169.
24. Granek L, Nakash O, Ben-David M, Shapira S, Ariad S. Oncologists’, nurses’, and social workers’ strategies and barriers to identifying suicide risk in cancer patients. Psychooncology. 2018;27(1):148-154.
It was estimated that physicians would diagnose a form of invasive cancer > 1.7 million times in 2019. As the second most common cause of death in the US, > 600,000 people were projected to die from cancer in 2019.1 Many individuals with cancer endure distress, which the National Comprehensive Cancer Network (NCCN) defines as a “multifactorial unpleasant experience of a psychological (ie, cognitive, behavioral, emotional), social, spiritual, and/or physical nature that may interfere with the ability to cope effectively with cancer, its physical symptoms, and its treatment.”2,3 Distress in people living with cancer has been attributed to various psychosocial concerns, such as family problems, whichinclude dealing with partners and children; emotional problems, such as depression and anxiety; and physical symptoms, such as pain and fatigue.4-9 Certain factors associated with distress may increase a patient’s risk for suicide.4
Veterans are at particularly high risk for suicide.10 In 2014, veterans accounted for 18% of completed suicides in the US but only were 8.5% of the total population that same year.10 Yet, little research has been done on the relationship between distress and suicide in veterans living with cancer. Aboumrad and colleagues found that 45% of veterans with cancer who completed suicide reported family issues and 41% endorsed chronic pain.11 This study recommended continued efforts to assess and treat distress to lessen risk of suicide in veterans living with cancer; however, to date, only 1 study has specifically evaluated distress and problems endorsed among veterans living with cancer.7
Suicide prevention is of the highest priority to the US Department of Veterans Affairs (VA).12 Consistent with the VA mission to end veteran suicide, the current study aimed to better understand the relationship between distress and suicide within a sample of veterans living with cancer. Findings would additionally be used to tailor clinical assessments and interventions for veterans living with cancer.
This study had 3 primary goals. First, we sought to understand demographic and clinical factors associated with low, moderate, and severe levels of distress in veterans living with cancer who were referred for psychology services. Second, the study investigated the most commonly endorsed problems by veterans living with cancer. Finally, we examined which problems were related to suicidal ideation (SI). It was hypothesized that veterans who reported severe distress would be significantly more likely to endorse SI when compared with veterans who reported mild or moderate distress. Based on existing literature, it was further hypothesized that family, emotional, and physical problems would be significantly associated with SI.7,11
Methods
The current study was conducted at James A. Haley Veterans’ Hospital (JAHVH) in Tampa, Florida. Inclusion criteria included veterans who were diagnosed with cancer, attended an outpatient psychology-oncology evaluation, and completed mental health screening measures provided during their evaluation. Exclusion criteria included veterans who: were seen in response to an inpatient consult, were seen solely for a stem cell transplant evaluation, or did not complete the screening measures.
Measures
A veteran’s demographic (eg, age, sex, ethnicity) and clinical (eg, cancer type, stage of disease, recurrence, cancer treatments received) information was abstracted from their VA medical records. Marital status was assessed during a clinical interview and documented as part of the standardized suicide risk assessment.
The Distress Thermometer (DT) is a subjective measure developed by the NCCN.2 The DT provides a visual representation of a thermometer and asks patients to rate their level of distress over the past week with 0 indicating no distress and 10 indicating extreme distress.
The measurement additionally lists 39 problems nested within 5 domains: practical, family, emotional, spiritual/religious, and physical. Patients may endorse listed items under each problem domain by indicating yes or no. Endorsement of various items are intended to provide more detailed information about sources of distress. Due to the predominantly male and mostly older population included in this study the ability to have children measure was removed from the family problem domain.
SI was assessed in 2 ways. First, by patients’ self-report through item-9 of the Patient Health Questionnaire-9 (PHQ-9).14 Item-9 asks “over the last 2 weeks, how often have you been bothered by thoughts that you would be better off dead or of hurting yourself in some way?” Responses range from 0 (not at all) to 3 (nearly every day).14 Responses > 0 were considered a positive screen for SI.
Procedure
Participants were a sample of veterans who were referred for psychology-oncology services. The NCCN DT and Problems List were administered prior to the start of clinical interviews, which followed a checklist and included standardized assessments of SI and history of a suicide attempt(s). A licensed clinical psychologist or a postdoctoral resident conducted these assessments under the supervision of a licensed psychologist. Data gathered during the clinical interview and from the DT and problems list were documented in health records, which were retrospectively reviewed for relevant information (eg, cancer diagnosis, SI). Therefore, informed consent was waived. This study was approved by the JAHVH Institutional Review Board.
Analysis
Data were analyzed using SPSS Version 25. Data analysis proceeded in 3 steps. First, descriptive statistics included the demographic and clinical factors present in the current sample. Difference between those with and without suicidal ideation were compared using F-statistic for continuous variables and χ2 analyses for categorical variables. Second, to examine relationships between each DT problem domain and SI, χ2 analyses were conducted. Third, DT problem domains that had a significant relationship with SI were entered in a logistic regression. This analysis determined which items, if any, from a DT problem domain predicted SI. In the logistic regression model, history of suicide attempts was entered into the first block, as history of suicide attempts is a well-established risk factor for subsequent suicidal ideation. In the second block, other variables that were significantly related to suicidal ideation in the second step of analyses were included. Before interpreting the results of the logistic regression, model fit was tested using the Hosmer-Lemeshow test. Significance of each individual predictor variable in the model is reported using the Wald χ2 statistic; each Wald statistic is compared with a χ2 distribution with 1 degree of freedom (df). Results of logistic regression models also provide information about the effect of each predictor variable in the regression equation (beta weight), odds a veteran who endorsed each predictor variable in the model would also endorse SI (as indicated by the odds ratio), and an estimate of the amount of variance accounted for by each predictor variable (using Nagelkerke’s pseudo R2, which ranges in value from 0 to 1 with higher values indicating more variance explained). For all analyses, P value of .05 (2-tailed) was used for statistical significance.
Results
The sample consisted of 174 veterans (Table 1). The majority (77.6%) were male with a mean age of nearly 62 years (range, 29-87). Most identified as white (74.1%) with half reporting they were either married or living with a partner.
Prostate cancer (19.0%) was the most common type of cancer among study participants followed by head and neck (18.4%), lymphoma/leukemia (11.5%), lung (11.5%), and breast (10.9%); 31.6% had metastatic disease and 14.9% had recurrent disease. Chemotherapy (42.5%) was the most common treatment modality, followed by surgery (38.5%) and radiation (31.6%). The sample was distributed among the 3 distress DT categories: mild (18.4%), moderate (42.5%), and severe (39.1%).
Problems Endorsed
Treatment decisions (44.3%) and insurance/financial concerns (35.1%) were the most frequently endorsed practical problems (Figure 1). Family health issues (33.9%) and dealing with partner (23.0%) were the most frequently endorsed family problems (Figure 2). Worry (73.0%) and depression (69.5%) were the most frequent emotional problems; of note, all emotional problems were endorsed by at least 50% of veterans (Figure 3). Fatigue (71.3%), sleep (70.7%), and pain (69%), were the most frequently endorsed physical problems (Figure 4). Spiritual/religious problems were endorsed by 15% of veterans.
Suicidal Ideation
Overall, 25.3% of veterans endorsed SI. About 20% of veterans reported a history of ≥ 1 suicide attempts in their lifetime. A significant relationship among distress categories and SI was found (χ2 = 18.36, P < .001). Veterans with severe distress were more likely to endorse SI (42.7%) when compared with veterans with mild (9.4%) or moderate (16.2%) distress.
Similarly, a significant relationship among distress categories and a history of a suicide attempt(s) was found (χ2 = 6.08, P = .048). Veterans with severe distress were more likely to have attempted suicide (29.4%) when compared with veterans with mild (12.5%) or moderate (14.9%) distress.
χ2 analyses were conducted to examine the relationships between DT problem domains and SI. A significant relationship was found between family problems and SI (
Logistic regression analyses determined whether items representative of the family problems domain were predictive of SI. Suicide attempt(s) were entered in the first step of the model to evaluate risk factors for SI over this already established risk factor. The assumptions of logistic regression were met.
The Hosmer-Lemeshow test (χ2 = 3.66, df = 5, P = .56) demonstrated that the model fit was good. The group of predictors used in the model differentiate between people who were experiencing SI and those who were not experiencing SI at the time of evaluation. A history of a suicide attempt(s) predicted SI, as expected (Wald = 6.821, df = 1, P = .01). The odds that a veteran with a history of a suicide attempt(s) would endorse SI at the time of the evaluation was nearly 3 times greater than that of veterans without a history of a suicide attempt(s). Over and above suicide attempts, problems dealing with partner (Wald = 15.142; df = 1, P < .001) was a second significant predictor of current SI. The odds that a veteran who endorsed problems dealing with partner would also endorse SI was > 5 times higher than that of veterans who did not endorse problems dealing with partner. This finding represents a significant risk factor for SI, over and above a history of a suicide attempt(s). The other items from the family problems domains were not significant (P > .05) (Table 3).
Discussion
This study aimed to understand factors associated with low, moderate, and severe levels of distress in veterans living with cancer who were referred for psychology services. As hypothesized, veterans who endorsed severe distress were significantly more likely to endorse SI. They also were more likely to have a history of a suicide attempt(s) when compared with those with mild or moderate distress.
A second aim of this study was to understand the most commonly endorsed problems. Consistent with prior literature, treatment decisions were the most commonly endorsed practical problem; worry and depression were the most common emotional problems; and fatigue, sleep, and pain were the most common physical problems.7
A finding unique to the current study is that family health issues and dealing with partner were specified as the most common family problems. However, a study by Smith and colleagues did not provide information about the rank of most frequently reported problems within this domain.7
The third aim was to understand which problems were related to SI. It was hypothesized that family, emotional, and physical problems would be related to SI. However, results indicated that only family problems (specifically, problems dealing with a partner) were significantly associated with SI among veterans living with cancer.
Contrary to expectations, emotional and physical problems were not found to have a significant relationship with SI. This is likely because veterans endorsed items nested within these problem domains with similar frequency. The lack of significant findings does not suggest that emotional and physical problems are not significant predictors of SI for veterans living with cancer, but that no specific emotional or physical symptom stood out as a predictor of suicidal ideation above the others.
The finding of a significant relationship between family problems (specifically, problems dealing with a partner) and SI in this study is consistent with findings of Aboumrad and colleagues in a study that examined root-cause analyses of completed suicides by veterans living with cancer.11 They found that nearly half the sample endorsed family problems prior to their death, and a small but notable percentage of veterans who completed suicide reported divorce as a stressor prior to their death.
This finding may be explained by Thomas Joiner's interpersonal-psychological theory of suicidal behavior (IPT), which suggests that completed suicide may result from a thwarted sense of belonging, perceived burdensomeness, and acquired capability for suicide.16 Problems dealing with a partner may impact a veteran’s sense of belonging or social connectedness. Problems dealing with a partner also may be attributed to perceived burdens due to limitations imposed by living with cancer and/or undergoing treatment. In both circumstances, the veteran’s social support system may be negatively impacted, and perceived social support is a well-established protective factor against suicide.17
Partner distress is a second consideration. It is likely that veterans’ partners experienced their own distress in response to the veteran’s cancer diagnosis and/or treatment. The partner’s cause, severity, and expression of distress may contribute to problems for the couple.
Finally, the latter point of the IPT refers to acquired capability, or the ability to inflict deadly harm to oneself.18 A military sample was found to have more acquired capability for suicide when compared with a college undergraduate sample.19 A history of a suicide attempt(s) and male gender have been found to significantly predict acquired capability to complete suicide.18 Furthermore, because veterans living with cancer often are in pain, fear of pain associated with suicide may be reduced and, therefore, acquired capability increased. This suggests that male veterans living with cancer who are in pain, have a history of a suicide attempt(s), and current problems with their partner may be an extremely vulnerable population at-risk for suicide. Results from the current study emphasize the importance of veterans having access to mental health and crisis resources for problems dealing with their partner. Partner problems may foreshadow a potentially lethal type of distress.
Strengths
This study’s aims are consistent with the VA’s mission to end veteran suicide and contributes to literature in several important ways.12 First, veterans living with cancer are an understudied population. The current study addresses a gap in existing literature by researching veterans living with cancer and aims to better understand the relationship between cancer-related distress and SI. Second, to the best of the authors’ knowledge, this study is the first to find that problems dealing with a partner significantly increases a veteran’s risk for SI above a history of a suicide attempt(s). Risk assessments now may be more comprehensive through inclusion of this distress factor.
It is recommended that future research use IPT to further investigate the relationship between problems dealing with a partner and SI.16 Future research may do so by including specific measures to assess for the tenants of the theory, including measurements of burdensomeness and belongingness. An expanded knowledge base about what makes problems dealing with a partner a significant suicide risk factor (eg, increased conflict, lack of support, etc.) would better enable clinicians to intervene effectively. Effective intervention may lessen suicidal behaviors or deaths from suicides within the Veteran population.
Limitations
One limitation is the focus on patients who accepted a mental health referral. This study design may limit the generalizability of results to veterans who would not accept mental health treatment. The homogenous sample of veterans is a second limitation. Most participants were male, white, and had a mean age of 62 years. These demographics are representative of the veterans that most typically utilize VA services; however, more research is needed on veterans living with cancer who are female and of diverse racial and ethnic backgrounds. There are likely differences in problems endorsed and factors associated with SI based on age, race, sex, and other socioeconomic factors. A third limitation is the cross-sectional, retrospective nature of this study. Future studies are advised to assess for distress at multiple time points. This is consistent with NCCN Standards of Care for Distress Management.2 Longitudinal data would enable more findings about distress and SI throughout the course of cancer diagnosis and treatment, therefore enhancing clinical implications and informing future research.
Conclusion
This is among the first of studies to investigate distress and factors associated with SI in veterans living with cancer who were referred for psychology services. The prevalence of distress caused by psychosocial factors (including treatment decisions, worry, and depression) highlights the importance of including mental health services as part of comprehensive cancer treatment.
Distress due to treatment decisions may be attributed to a litany of factors such as a veteran’s consideration of adverse effects, effectiveness of treatments, changes to quality of life or functioning, and inclusion of alternative or complimentary treatments. These types of decisions often are reported to be difficult conversations to have with family members or loved ones, who are likely experiencing distress of their own. The role of a mental health provider to assist veterans in exploring their treatment decisions and the implications of such decisions appears important to lessening distress.
Early intervention for emotional symptoms would likely benefit veterans’ management of distress and may lessen suicide risk as depression is known to place veterans at-risk for SI.20 This underscores the importance of timely distress assessment to prevent mild emotional distress from progressing to potentially severe or life-threatening emotional distress. For veterans with a psychiatric history, timely assessment and intervention is essential because psychiatric history is an established suicide risk factor that may be exacerbated by cancer-related distress.12
Furthermore, management of intolerable physical symptoms may lessen risk for suicide.4 Under medical guidance, fatigue may be improved using exercise.21 Behavioral intervention is commonly used as first-line treatment for sleep problems.22 While pain may be lessened through medication or nonpharmacological interventions.23
Considering the numerous ways that distress may present itself (eg, practical, emotional, or physical) and increase risk for SI, it is essential that all veterans living with cancer are assessed for distress and SI, regardless of their presentation. Although veterans may not outwardly express distress, this does not indicate the absence of either distress or risk for suicide. For example, a veteran may be distressed due to financial concerns, transportation issues, and the health of his/her partner or spouse. This veteran may not exhibit visible symptoms of distress, as would be expected when the source of distress is emotional (eg, depression, anxiety). However, this veteran is equally vulnerable to impairing distress and SI as someone who exhibits emotional distress. Distress assessments should be further developed to capture both the visible and less apparent sources of distress, while also serving the imperative function of screening for suicide. Other researchers also have noted the necessity of this development.24 Currently, the NCCN DT and Problems List does not include any assessment of SI or behavior.
Finally, this study identified a potentially critical factor to include in distress assessment: problems dealing with a partner. Problems dealing with a partner have been noted as a source of distress in existing literature, but this is the first study to find problems dealing with a partner to be a predictor of SI in veterans living with cancer.4-6
Because partners often attend appointments with veterans, it is not surprising that problems dealing with their partner are not disclosed more readily. It is recommended that clinicians ask veterans about potential problems with their partner when they are alone. Directly gathering information about such problems while assessing for distress may assist health care workers in providing the most effective, accurate type of intervention in a timely manner, and potentially mitigate risk for suicide.
As recommended by the NCCN and numerous researchers, findings from the current study underscore the importance of accurate, timely assessment of distress.2,4,8 This study makes several important recommendations about how distress assessment may be strengthened and further developed, specifically for the veteran population. This study also expands the current knowledge base of what is known about veterans living with cancer, and has begun to fill a gap in the existing literature. Consistent with the VA mission to end veteran suicide, results suggest that veterans living with cancer should be regularly screened for distress, asked about distress related to their partner, and assessed for SI. Continued efforts to enhance assessment of and response to distress may lessen suicide risk in veterans with cancer.11
Acknowledgements
This study is the result of work supported with resources and the use of facilities at the James A. Haley Veterans’ Hospital.
It was estimated that physicians would diagnose a form of invasive cancer > 1.7 million times in 2019. As the second most common cause of death in the US, > 600,000 people were projected to die from cancer in 2019.1 Many individuals with cancer endure distress, which the National Comprehensive Cancer Network (NCCN) defines as a “multifactorial unpleasant experience of a psychological (ie, cognitive, behavioral, emotional), social, spiritual, and/or physical nature that may interfere with the ability to cope effectively with cancer, its physical symptoms, and its treatment.”2,3 Distress in people living with cancer has been attributed to various psychosocial concerns, such as family problems, whichinclude dealing with partners and children; emotional problems, such as depression and anxiety; and physical symptoms, such as pain and fatigue.4-9 Certain factors associated with distress may increase a patient’s risk for suicide.4
Veterans are at particularly high risk for suicide.10 In 2014, veterans accounted for 18% of completed suicides in the US but only were 8.5% of the total population that same year.10 Yet, little research has been done on the relationship between distress and suicide in veterans living with cancer. Aboumrad and colleagues found that 45% of veterans with cancer who completed suicide reported family issues and 41% endorsed chronic pain.11 This study recommended continued efforts to assess and treat distress to lessen risk of suicide in veterans living with cancer; however, to date, only 1 study has specifically evaluated distress and problems endorsed among veterans living with cancer.7
Suicide prevention is of the highest priority to the US Department of Veterans Affairs (VA).12 Consistent with the VA mission to end veteran suicide, the current study aimed to better understand the relationship between distress and suicide within a sample of veterans living with cancer. Findings would additionally be used to tailor clinical assessments and interventions for veterans living with cancer.
This study had 3 primary goals. First, we sought to understand demographic and clinical factors associated with low, moderate, and severe levels of distress in veterans living with cancer who were referred for psychology services. Second, the study investigated the most commonly endorsed problems by veterans living with cancer. Finally, we examined which problems were related to suicidal ideation (SI). It was hypothesized that veterans who reported severe distress would be significantly more likely to endorse SI when compared with veterans who reported mild or moderate distress. Based on existing literature, it was further hypothesized that family, emotional, and physical problems would be significantly associated with SI.7,11
Methods
The current study was conducted at James A. Haley Veterans’ Hospital (JAHVH) in Tampa, Florida. Inclusion criteria included veterans who were diagnosed with cancer, attended an outpatient psychology-oncology evaluation, and completed mental health screening measures provided during their evaluation. Exclusion criteria included veterans who: were seen in response to an inpatient consult, were seen solely for a stem cell transplant evaluation, or did not complete the screening measures.
Measures
A veteran’s demographic (eg, age, sex, ethnicity) and clinical (eg, cancer type, stage of disease, recurrence, cancer treatments received) information was abstracted from their VA medical records. Marital status was assessed during a clinical interview and documented as part of the standardized suicide risk assessment.
The Distress Thermometer (DT) is a subjective measure developed by the NCCN.2 The DT provides a visual representation of a thermometer and asks patients to rate their level of distress over the past week with 0 indicating no distress and 10 indicating extreme distress.
The measurement additionally lists 39 problems nested within 5 domains: practical, family, emotional, spiritual/religious, and physical. Patients may endorse listed items under each problem domain by indicating yes or no. Endorsement of various items are intended to provide more detailed information about sources of distress. Due to the predominantly male and mostly older population included in this study the ability to have children measure was removed from the family problem domain.
SI was assessed in 2 ways. First, by patients’ self-report through item-9 of the Patient Health Questionnaire-9 (PHQ-9).14 Item-9 asks “over the last 2 weeks, how often have you been bothered by thoughts that you would be better off dead or of hurting yourself in some way?” Responses range from 0 (not at all) to 3 (nearly every day).14 Responses > 0 were considered a positive screen for SI.
Procedure
Participants were a sample of veterans who were referred for psychology-oncology services. The NCCN DT and Problems List were administered prior to the start of clinical interviews, which followed a checklist and included standardized assessments of SI and history of a suicide attempt(s). A licensed clinical psychologist or a postdoctoral resident conducted these assessments under the supervision of a licensed psychologist. Data gathered during the clinical interview and from the DT and problems list were documented in health records, which were retrospectively reviewed for relevant information (eg, cancer diagnosis, SI). Therefore, informed consent was waived. This study was approved by the JAHVH Institutional Review Board.
Analysis
Data were analyzed using SPSS Version 25. Data analysis proceeded in 3 steps. First, descriptive statistics included the demographic and clinical factors present in the current sample. Difference between those with and without suicidal ideation were compared using F-statistic for continuous variables and χ2 analyses for categorical variables. Second, to examine relationships between each DT problem domain and SI, χ2 analyses were conducted. Third, DT problem domains that had a significant relationship with SI were entered in a logistic regression. This analysis determined which items, if any, from a DT problem domain predicted SI. In the logistic regression model, history of suicide attempts was entered into the first block, as history of suicide attempts is a well-established risk factor for subsequent suicidal ideation. In the second block, other variables that were significantly related to suicidal ideation in the second step of analyses were included. Before interpreting the results of the logistic regression, model fit was tested using the Hosmer-Lemeshow test. Significance of each individual predictor variable in the model is reported using the Wald χ2 statistic; each Wald statistic is compared with a χ2 distribution with 1 degree of freedom (df). Results of logistic regression models also provide information about the effect of each predictor variable in the regression equation (beta weight), odds a veteran who endorsed each predictor variable in the model would also endorse SI (as indicated by the odds ratio), and an estimate of the amount of variance accounted for by each predictor variable (using Nagelkerke’s pseudo R2, which ranges in value from 0 to 1 with higher values indicating more variance explained). For all analyses, P value of .05 (2-tailed) was used for statistical significance.
Results
The sample consisted of 174 veterans (Table 1). The majority (77.6%) were male with a mean age of nearly 62 years (range, 29-87). Most identified as white (74.1%) with half reporting they were either married or living with a partner.
Prostate cancer (19.0%) was the most common type of cancer among study participants followed by head and neck (18.4%), lymphoma/leukemia (11.5%), lung (11.5%), and breast (10.9%); 31.6% had metastatic disease and 14.9% had recurrent disease. Chemotherapy (42.5%) was the most common treatment modality, followed by surgery (38.5%) and radiation (31.6%). The sample was distributed among the 3 distress DT categories: mild (18.4%), moderate (42.5%), and severe (39.1%).
Problems Endorsed
Treatment decisions (44.3%) and insurance/financial concerns (35.1%) were the most frequently endorsed practical problems (Figure 1). Family health issues (33.9%) and dealing with partner (23.0%) were the most frequently endorsed family problems (Figure 2). Worry (73.0%) and depression (69.5%) were the most frequent emotional problems; of note, all emotional problems were endorsed by at least 50% of veterans (Figure 3). Fatigue (71.3%), sleep (70.7%), and pain (69%), were the most frequently endorsed physical problems (Figure 4). Spiritual/religious problems were endorsed by 15% of veterans.
Suicidal Ideation
Overall, 25.3% of veterans endorsed SI. About 20% of veterans reported a history of ≥ 1 suicide attempts in their lifetime. A significant relationship among distress categories and SI was found (χ2 = 18.36, P < .001). Veterans with severe distress were more likely to endorse SI (42.7%) when compared with veterans with mild (9.4%) or moderate (16.2%) distress.
Similarly, a significant relationship among distress categories and a history of a suicide attempt(s) was found (χ2 = 6.08, P = .048). Veterans with severe distress were more likely to have attempted suicide (29.4%) when compared with veterans with mild (12.5%) or moderate (14.9%) distress.
χ2 analyses were conducted to examine the relationships between DT problem domains and SI. A significant relationship was found between family problems and SI (
Logistic regression analyses determined whether items representative of the family problems domain were predictive of SI. Suicide attempt(s) were entered in the first step of the model to evaluate risk factors for SI over this already established risk factor. The assumptions of logistic regression were met.
The Hosmer-Lemeshow test (χ2 = 3.66, df = 5, P = .56) demonstrated that the model fit was good. The group of predictors used in the model differentiate between people who were experiencing SI and those who were not experiencing SI at the time of evaluation. A history of a suicide attempt(s) predicted SI, as expected (Wald = 6.821, df = 1, P = .01). The odds that a veteran with a history of a suicide attempt(s) would endorse SI at the time of the evaluation was nearly 3 times greater than that of veterans without a history of a suicide attempt(s). Over and above suicide attempts, problems dealing with partner (Wald = 15.142; df = 1, P < .001) was a second significant predictor of current SI. The odds that a veteran who endorsed problems dealing with partner would also endorse SI was > 5 times higher than that of veterans who did not endorse problems dealing with partner. This finding represents a significant risk factor for SI, over and above a history of a suicide attempt(s). The other items from the family problems domains were not significant (P > .05) (Table 3).
Discussion
This study aimed to understand factors associated with low, moderate, and severe levels of distress in veterans living with cancer who were referred for psychology services. As hypothesized, veterans who endorsed severe distress were significantly more likely to endorse SI. They also were more likely to have a history of a suicide attempt(s) when compared with those with mild or moderate distress.
A second aim of this study was to understand the most commonly endorsed problems. Consistent with prior literature, treatment decisions were the most commonly endorsed practical problem; worry and depression were the most common emotional problems; and fatigue, sleep, and pain were the most common physical problems.7
A finding unique to the current study is that family health issues and dealing with partner were specified as the most common family problems. However, a study by Smith and colleagues did not provide information about the rank of most frequently reported problems within this domain.7
The third aim was to understand which problems were related to SI. It was hypothesized that family, emotional, and physical problems would be related to SI. However, results indicated that only family problems (specifically, problems dealing with a partner) were significantly associated with SI among veterans living with cancer.
Contrary to expectations, emotional and physical problems were not found to have a significant relationship with SI. This is likely because veterans endorsed items nested within these problem domains with similar frequency. The lack of significant findings does not suggest that emotional and physical problems are not significant predictors of SI for veterans living with cancer, but that no specific emotional or physical symptom stood out as a predictor of suicidal ideation above the others.
The finding of a significant relationship between family problems (specifically, problems dealing with a partner) and SI in this study is consistent with findings of Aboumrad and colleagues in a study that examined root-cause analyses of completed suicides by veterans living with cancer.11 They found that nearly half the sample endorsed family problems prior to their death, and a small but notable percentage of veterans who completed suicide reported divorce as a stressor prior to their death.
This finding may be explained by Thomas Joiner's interpersonal-psychological theory of suicidal behavior (IPT), which suggests that completed suicide may result from a thwarted sense of belonging, perceived burdensomeness, and acquired capability for suicide.16 Problems dealing with a partner may impact a veteran’s sense of belonging or social connectedness. Problems dealing with a partner also may be attributed to perceived burdens due to limitations imposed by living with cancer and/or undergoing treatment. In both circumstances, the veteran’s social support system may be negatively impacted, and perceived social support is a well-established protective factor against suicide.17
Partner distress is a second consideration. It is likely that veterans’ partners experienced their own distress in response to the veteran’s cancer diagnosis and/or treatment. The partner’s cause, severity, and expression of distress may contribute to problems for the couple.
Finally, the latter point of the IPT refers to acquired capability, or the ability to inflict deadly harm to oneself.18 A military sample was found to have more acquired capability for suicide when compared with a college undergraduate sample.19 A history of a suicide attempt(s) and male gender have been found to significantly predict acquired capability to complete suicide.18 Furthermore, because veterans living with cancer often are in pain, fear of pain associated with suicide may be reduced and, therefore, acquired capability increased. This suggests that male veterans living with cancer who are in pain, have a history of a suicide attempt(s), and current problems with their partner may be an extremely vulnerable population at-risk for suicide. Results from the current study emphasize the importance of veterans having access to mental health and crisis resources for problems dealing with their partner. Partner problems may foreshadow a potentially lethal type of distress.
Strengths
This study’s aims are consistent with the VA’s mission to end veteran suicide and contributes to literature in several important ways.12 First, veterans living with cancer are an understudied population. The current study addresses a gap in existing literature by researching veterans living with cancer and aims to better understand the relationship between cancer-related distress and SI. Second, to the best of the authors’ knowledge, this study is the first to find that problems dealing with a partner significantly increases a veteran’s risk for SI above a history of a suicide attempt(s). Risk assessments now may be more comprehensive through inclusion of this distress factor.
It is recommended that future research use IPT to further investigate the relationship between problems dealing with a partner and SI.16 Future research may do so by including specific measures to assess for the tenants of the theory, including measurements of burdensomeness and belongingness. An expanded knowledge base about what makes problems dealing with a partner a significant suicide risk factor (eg, increased conflict, lack of support, etc.) would better enable clinicians to intervene effectively. Effective intervention may lessen suicidal behaviors or deaths from suicides within the Veteran population.
Limitations
One limitation is the focus on patients who accepted a mental health referral. This study design may limit the generalizability of results to veterans who would not accept mental health treatment. The homogenous sample of veterans is a second limitation. Most participants were male, white, and had a mean age of 62 years. These demographics are representative of the veterans that most typically utilize VA services; however, more research is needed on veterans living with cancer who are female and of diverse racial and ethnic backgrounds. There are likely differences in problems endorsed and factors associated with SI based on age, race, sex, and other socioeconomic factors. A third limitation is the cross-sectional, retrospective nature of this study. Future studies are advised to assess for distress at multiple time points. This is consistent with NCCN Standards of Care for Distress Management.2 Longitudinal data would enable more findings about distress and SI throughout the course of cancer diagnosis and treatment, therefore enhancing clinical implications and informing future research.
Conclusion
This is among the first of studies to investigate distress and factors associated with SI in veterans living with cancer who were referred for psychology services. The prevalence of distress caused by psychosocial factors (including treatment decisions, worry, and depression) highlights the importance of including mental health services as part of comprehensive cancer treatment.
Distress due to treatment decisions may be attributed to a litany of factors such as a veteran’s consideration of adverse effects, effectiveness of treatments, changes to quality of life or functioning, and inclusion of alternative or complimentary treatments. These types of decisions often are reported to be difficult conversations to have with family members or loved ones, who are likely experiencing distress of their own. The role of a mental health provider to assist veterans in exploring their treatment decisions and the implications of such decisions appears important to lessening distress.
Early intervention for emotional symptoms would likely benefit veterans’ management of distress and may lessen suicide risk as depression is known to place veterans at-risk for SI.20 This underscores the importance of timely distress assessment to prevent mild emotional distress from progressing to potentially severe or life-threatening emotional distress. For veterans with a psychiatric history, timely assessment and intervention is essential because psychiatric history is an established suicide risk factor that may be exacerbated by cancer-related distress.12
Furthermore, management of intolerable physical symptoms may lessen risk for suicide.4 Under medical guidance, fatigue may be improved using exercise.21 Behavioral intervention is commonly used as first-line treatment for sleep problems.22 While pain may be lessened through medication or nonpharmacological interventions.23
Considering the numerous ways that distress may present itself (eg, practical, emotional, or physical) and increase risk for SI, it is essential that all veterans living with cancer are assessed for distress and SI, regardless of their presentation. Although veterans may not outwardly express distress, this does not indicate the absence of either distress or risk for suicide. For example, a veteran may be distressed due to financial concerns, transportation issues, and the health of his/her partner or spouse. This veteran may not exhibit visible symptoms of distress, as would be expected when the source of distress is emotional (eg, depression, anxiety). However, this veteran is equally vulnerable to impairing distress and SI as someone who exhibits emotional distress. Distress assessments should be further developed to capture both the visible and less apparent sources of distress, while also serving the imperative function of screening for suicide. Other researchers also have noted the necessity of this development.24 Currently, the NCCN DT and Problems List does not include any assessment of SI or behavior.
Finally, this study identified a potentially critical factor to include in distress assessment: problems dealing with a partner. Problems dealing with a partner have been noted as a source of distress in existing literature, but this is the first study to find problems dealing with a partner to be a predictor of SI in veterans living with cancer.4-6
Because partners often attend appointments with veterans, it is not surprising that problems dealing with their partner are not disclosed more readily. It is recommended that clinicians ask veterans about potential problems with their partner when they are alone. Directly gathering information about such problems while assessing for distress may assist health care workers in providing the most effective, accurate type of intervention in a timely manner, and potentially mitigate risk for suicide.
As recommended by the NCCN and numerous researchers, findings from the current study underscore the importance of accurate, timely assessment of distress.2,4,8 This study makes several important recommendations about how distress assessment may be strengthened and further developed, specifically for the veteran population. This study also expands the current knowledge base of what is known about veterans living with cancer, and has begun to fill a gap in the existing literature. Consistent with the VA mission to end veteran suicide, results suggest that veterans living with cancer should be regularly screened for distress, asked about distress related to their partner, and assessed for SI. Continued efforts to enhance assessment of and response to distress may lessen suicide risk in veterans with cancer.11
Acknowledgements
This study is the result of work supported with resources and the use of facilities at the James A. Haley Veterans’ Hospital.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7-34.
2. Riba MB, Donovan, KA, Andersen, B. National Comprehensive Cancer Network clinical practice guidelines in oncology. Distress management (Version 3.2019). J Natl Compr Can Net, 2019;17(10):1229-1249.
3. Zabora J, BrintzenhofeSzoc K, Curbow B, Hooker C, Pianta dosi S. The prevalence of psychological distress by cancer site. Psychooncology. 2001;10(1):19–28.
4. Holland JC, Alici Y. Management of distress in cancer patients. J Support Oncol. 2010;8(1):4-12.
5. Bulli F, Miccinesi G, Maruelli A, Katz M, Paci E. The measure of psychological distress in cancer patients: the use of distress thermometer in the oncological rehabilitation center of Florence. Support Care Cancer. 2009;17(7):771–779.
6. Jacobsen PB, Donovan KA, Trask PC, et al. Screening for psychologic distress in ambulatory cancer patients. Cancer. 2005;103(7):1494-1502.
7. Smith J, Berman S, Dimick J, et al. Distress Screening and Management in an Outpatient VA Cancer Clinic: A Pilot Project Involving Ambulatory Patients Across the Disease Trajectory. Fed Pract. 2017;34(Suppl 1):43S–50S.
8. Carlson LE, Waller A, Groff SL, Bultz BD. Screening for distress, the sixth vital sign, in lung cancer patients: effects on pain, fatigue, and common problems--secondary outcomes of a randomized controlled trial. Psychooncology. 2013;22(8):1880-1888.
9. Cooley ME, Short TH, Moriarty HJ. Symptom prevalence, distress, and change over time in adults receiving treatment for lung cancer. Psychooncology. 2003;12(7):694-708.
10. US Department of Veterans Affairs Office of Suicide Prevention. Suicide among veterans and other Americans 2001-2014. https://www.mentalhealth.va.gov/docs/2016suicidedatareport.pdf. Published August 3, 2016. Accessed April 13, 2020.
11. Aboumrad M, Shiner B, Riblet N, Mills, PD, Watts BV. Factors contributing to cancer-related suicide: a study of root-cause-analysis reports. Psychooncology. 2018;27(9):2237-2244.
12. US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention. National Strategy for Preventing Veteran Suicide 2018–2028. https://www.mentalhealth.va.gov/suicide_prevention/docs/Office-of-Mental-Health-and-Suicide-Prevention-National-Strategy-for-Preventing-Veterans-Suicide.pdf Published 2018. Accessed April 13, 2020.
13. Carlson LE, Waller A, Mitchell AJ. Screening for distress and unmet needs in patients with cancer: review and recommendations. J Clin Oncol. 2012;30(11):1160-1177.
14. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613.
15. Martin A, Rief W, Klaiberg A, Braehler E. Validity of the brief patient health questionnaire mood scale (PHQ-9) in the general population. Gen Hosp Psychiatry. 2006;28(1):71-77.
16. Joiner TE. Why People Die by Suicide. Cambridge, MA: Harvard University Press, 2005.
17. Kleiman EM, Riskind JH, Schaefer KE. Social support and positive events as suicide resiliency factors: examination of synergistic buffering effects. Arch Suicide Res. 2014;18(2):144-155.
18. Van Orden KA, Witte TK, Gordon KH, Bender TW, Joiner TE Jr. Suicidal desire and the capability for suicide: tests of the interpersonal-psychological theory of suicidal behavior among adults. J Consult Clin Psychol. 2008;76(1):72–83.
19. Bryan CJ, Morrow CE, Anestis MD, Joiner TE. A preliminary test of the interpersonal -psychological theory of suicidal behavior in a military sample. Personal Individual Differ. 2010;48(3):347-350.
20. Miller SN, Monahan CJ, Phillips KM, Agliata D, Gironda RJ. Mental health utilization among veterans at risk for suicide: Data from a post-deployment clinic [published online ahead of print, 2018 Oct 8]. Psychol Serv. 2018;10.1037/ser0000311.
21. Galvão DA, Newton RU. Review of exercise intervention studies in cancer patients. J Clin Oncol. 2005;23(4):899-909.
22. Qaseem A, Kansagara D, Forciea MA, Cooke M, Denberg TD; Clinical Guidelines Committee of the American College of Physicians. Management of chronic insomnia disorder in adults: A clinical practice guideline from the American College of Physicians. Ann Intern Med. 2016;165(2):125-133.
23. Ngamkham S, Holden JE, Smith EL. A systematic review: Mindfulness intervention for cancer-related pain. Asia Pac J Oncol Nurs. 2019;6(2):161-169.
24. Granek L, Nakash O, Ben-David M, Shapira S, Ariad S. Oncologists’, nurses’, and social workers’ strategies and barriers to identifying suicide risk in cancer patients. Psychooncology. 2018;27(1):148-154.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7-34.
2. Riba MB, Donovan, KA, Andersen, B. National Comprehensive Cancer Network clinical practice guidelines in oncology. Distress management (Version 3.2019). J Natl Compr Can Net, 2019;17(10):1229-1249.
3. Zabora J, BrintzenhofeSzoc K, Curbow B, Hooker C, Pianta dosi S. The prevalence of psychological distress by cancer site. Psychooncology. 2001;10(1):19–28.
4. Holland JC, Alici Y. Management of distress in cancer patients. J Support Oncol. 2010;8(1):4-12.
5. Bulli F, Miccinesi G, Maruelli A, Katz M, Paci E. The measure of psychological distress in cancer patients: the use of distress thermometer in the oncological rehabilitation center of Florence. Support Care Cancer. 2009;17(7):771–779.
6. Jacobsen PB, Donovan KA, Trask PC, et al. Screening for psychologic distress in ambulatory cancer patients. Cancer. 2005;103(7):1494-1502.
7. Smith J, Berman S, Dimick J, et al. Distress Screening and Management in an Outpatient VA Cancer Clinic: A Pilot Project Involving Ambulatory Patients Across the Disease Trajectory. Fed Pract. 2017;34(Suppl 1):43S–50S.
8. Carlson LE, Waller A, Groff SL, Bultz BD. Screening for distress, the sixth vital sign, in lung cancer patients: effects on pain, fatigue, and common problems--secondary outcomes of a randomized controlled trial. Psychooncology. 2013;22(8):1880-1888.
9. Cooley ME, Short TH, Moriarty HJ. Symptom prevalence, distress, and change over time in adults receiving treatment for lung cancer. Psychooncology. 2003;12(7):694-708.
10. US Department of Veterans Affairs Office of Suicide Prevention. Suicide among veterans and other Americans 2001-2014. https://www.mentalhealth.va.gov/docs/2016suicidedatareport.pdf. Published August 3, 2016. Accessed April 13, 2020.
11. Aboumrad M, Shiner B, Riblet N, Mills, PD, Watts BV. Factors contributing to cancer-related suicide: a study of root-cause-analysis reports. Psychooncology. 2018;27(9):2237-2244.
12. US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention. National Strategy for Preventing Veteran Suicide 2018–2028. https://www.mentalhealth.va.gov/suicide_prevention/docs/Office-of-Mental-Health-and-Suicide-Prevention-National-Strategy-for-Preventing-Veterans-Suicide.pdf Published 2018. Accessed April 13, 2020.
13. Carlson LE, Waller A, Mitchell AJ. Screening for distress and unmet needs in patients with cancer: review and recommendations. J Clin Oncol. 2012;30(11):1160-1177.
14. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613.
15. Martin A, Rief W, Klaiberg A, Braehler E. Validity of the brief patient health questionnaire mood scale (PHQ-9) in the general population. Gen Hosp Psychiatry. 2006;28(1):71-77.
16. Joiner TE. Why People Die by Suicide. Cambridge, MA: Harvard University Press, 2005.
17. Kleiman EM, Riskind JH, Schaefer KE. Social support and positive events as suicide resiliency factors: examination of synergistic buffering effects. Arch Suicide Res. 2014;18(2):144-155.
18. Van Orden KA, Witte TK, Gordon KH, Bender TW, Joiner TE Jr. Suicidal desire and the capability for suicide: tests of the interpersonal-psychological theory of suicidal behavior among adults. J Consult Clin Psychol. 2008;76(1):72–83.
19. Bryan CJ, Morrow CE, Anestis MD, Joiner TE. A preliminary test of the interpersonal -psychological theory of suicidal behavior in a military sample. Personal Individual Differ. 2010;48(3):347-350.
20. Miller SN, Monahan CJ, Phillips KM, Agliata D, Gironda RJ. Mental health utilization among veterans at risk for suicide: Data from a post-deployment clinic [published online ahead of print, 2018 Oct 8]. Psychol Serv. 2018;10.1037/ser0000311.
21. Galvão DA, Newton RU. Review of exercise intervention studies in cancer patients. J Clin Oncol. 2005;23(4):899-909.
22. Qaseem A, Kansagara D, Forciea MA, Cooke M, Denberg TD; Clinical Guidelines Committee of the American College of Physicians. Management of chronic insomnia disorder in adults: A clinical practice guideline from the American College of Physicians. Ann Intern Med. 2016;165(2):125-133.
23. Ngamkham S, Holden JE, Smith EL. A systematic review: Mindfulness intervention for cancer-related pain. Asia Pac J Oncol Nurs. 2019;6(2):161-169.
24. Granek L, Nakash O, Ben-David M, Shapira S, Ariad S. Oncologists’, nurses’, and social workers’ strategies and barriers to identifying suicide risk in cancer patients. Psychooncology. 2018;27(1):148-154.
COVID lockdowns linked to PTSD in patients with eating disorders
COVID-19 and its resulting lockdowns are linked to posttraumatic stress disorder symptoms and other adverse outcomes among patients with eating disorders (EDs), two new studies show.

Results of the first study show that patients with EDs had more stress, anxiety, depression, and PTSD-related symptoms during the lockdowns than their mentally healthy peers.
In the second study, treatment-related symptom improvement among patients with bulimia nervosa (BN) slowed following lockdown. In addition, patients with BN or anorexia nervosa (AN) experienced significant worsening of disorder-specific behaviors, including binge eating and overexercising.
Because of the strict lockdown measures introduced by the Italian government to contain the COVID-19 pandemic, “everyday life of all citizens was disrupted,” Veronica Nisticò, MS, Università Degli Studi Di Milano, who led the first study, told delegates attending the virtual European Psychiatric Association 2021 Congress.

In addition to difficulties in accessing health care, “it became difficult to go to the supermarket, to the gym, and to have the social support we were all used to,” all of which had a well-documented impact on mental health, added Ms. Nisticò, who is also affiliated with Aldo Ravelli Research Center for Neurotechnology and Experimental Brain Therapeutics.
Loss of control
Previous research suggests that individuals with EDs experience high levels of anxiety and an increase in binge eating, exercise, and purging behaviors, said Ms. Nisticò.
To investigate further, the researchers conducted a longitudinal study of the changes in prevalence of adverse outcomes. In the study, two assessments were conducted.
The second group served as the control group.
Participants completed an online survey that included several standardized depression and anxiety scales, as well as an ad hoc survey adapted from the Eating Disorder Examination Questionnaire. This assessed changes in restrictive dieting, control over food, body image, and psychological well-being in comparison with prepandemic levels.
The results, which were also recently published online in Eating and Weight Disorders – Studies on Anorexia, Bulimia and Obesity, showed that patients with EDs experienced significantly more stress, anxiety, depression, and PTSD-related symptoms in comparison with control persons (P < .05 for all).
In addition, the investigators found that those with EDs were more fearful of losing control over their eating behavior, spent more time thinking about food and their body, and became more uncomfortable seeing their body than before the lockdown in comparison with those without EDs (P < .05).
Clinical implications
A second assessment, which occurred in June 2020, after lockdown restrictions were lifted, included 40 patients with EDs who had taken part in the first assessment. This time, participants were asked to compare their current eating behavior with their eating behavior during the lockdown.
Although the lifting of lockdown restrictions was associated with significant improvement in PTSD-related symptoms, the impact on stress, anxiety, and depression persisted.
These findings, said Ms. Nisticó, support the hypothesis that specific conditions that occurred during the lockdown had a direct effect on specific ED symptoms.
These findings, she added, should be considered when developing interventions for EDs in the context of individual psychotherapy and when designing large, preventive interventions.
In the second study, Eleonora Rossi, MD, psychiatric unit, department of health sciences, University of Florence (Italy), and colleagues examined the longitudinal impact of the pandemic on individuals with EDs.
They examined 74 patients with AN or BN who had undergone baseline assessments and had completed a number of questionnaires in the first months of 2019 in conjunction with being enrolled in another study.
Participants were treated with enhanced cognitive-behavioral therapy and were reevaluated between November 2019 and January 2020. They were then compared with 97 healthy individuals.
Bulimia patients more vulnerable
After the outbreak of the pandemic, most treatment was administered online, so patients were able to continue therapy, Dr. Rossi said during her presentation.
All participants were assessed again in April 2020, 6 weeks after the start of Italy’s lockdown.
The results, which were published in the International Journal of Eating Disorders, show that the patients with EDs “underwent a significant improvement in terms of general and eating disorder specific psychopathology” during the first treatment period, Dr. Rossi reported. In addition, among those with AN, body mass index increased significantly (P < .05 for all).
Patients with AN continued to improve during the lockdown when therapy was administered online. However, improvements that had occurred among those with BN slowed, Dr. Rossi noted.
In addition, both groups of patients with EDs experienced a worsening of their pathological eating behaviors during the lockdown, in particular, objective binge eating and compensatory physical exercise (P < .05).
“Indeed, the positive trajectory of improvement observed before lockdown was clearly interrupted during the pandemic period,” Dr. Rossi said. This could “represent a possible hint of an imminent exacerbation of the disease.”
The results also suggest that the occurrence of arguments within the household and fear regarding the safety of loved ones predicted an increase in symptoms during the lockdown, she added.
In addition, patients with BN reported more severe COVID-related PTSD symptoms than did those with AN and the control group. This increase in severity of symptoms was more prevalent among patients who had a history of childhood trauma and among those with insecure attachment, suggesting that such patients may be more vulnerable.
Evidence of recovery
Commenting on the studies, David Spiegel, MD, associate chair of psychiatry, Stanford (Calif.) University, noted that EDs commonly occur after physical or sexual trauma earlier in life.

“It’s a standard thing with trauma-related disorders that any other, even relatively minor, traumatic experience can exacerbate PTSD symptoms,” said Dr. Spiegel, who was not involved in the studies. In addition, the trauma of the COVID pandemic “was not minor.
“The relative isolation and the lack of outside contact may focus many people with eating disorders even more on their struggles with how they are taking care of their bodies,” said Dr. Spiegel.
“It struck me that the anorexia nervosa group were more impervious than the bulimia nervosa group, but I think that’s the case with the disorder. In some ways it’s more severe, obviously a more life-threatening disorder,” he added.
The “hopeful thing is that there seemed to be some evidence of recovery and improvement, particularly with the posttraumatic stress exacerbation, as time went on,” Dr. Spiegel said, “and that’s a good thing.”
The study authors and Dr. Spiegel reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
COVID-19 and its resulting lockdowns are linked to posttraumatic stress disorder symptoms and other adverse outcomes among patients with eating disorders (EDs), two new studies show.
Results of the first study show that patients with EDs had more stress, anxiety, depression, and PTSD-related symptoms during the lockdowns than their mentally healthy peers.
In the second study, treatment-related symptom improvement among patients with bulimia nervosa (BN) slowed following lockdown. In addition, patients with BN or anorexia nervosa (AN) experienced significant worsening of disorder-specific behaviors, including binge eating and overexercising.
Because of the strict lockdown measures introduced by the Italian government to contain the COVID-19 pandemic, “everyday life of all citizens was disrupted,” Veronica Nisticò, MS, Università Degli Studi Di Milano, who led the first study, told delegates attending the virtual European Psychiatric Association 2021 Congress.
In addition to difficulties in accessing health care, “it became difficult to go to the supermarket, to the gym, and to have the social support we were all used to,” all of which had a well-documented impact on mental health, added Ms. Nisticò, who is also affiliated with Aldo Ravelli Research Center for Neurotechnology and Experimental Brain Therapeutics.
Loss of control
Previous research suggests that individuals with EDs experience high levels of anxiety and an increase in binge eating, exercise, and purging behaviors, said Ms. Nisticò.
To investigate further, the researchers conducted a longitudinal study of the changes in prevalence of adverse outcomes. In the study, two assessments were conducted.
The second group served as the control group.
Participants completed an online survey that included several standardized depression and anxiety scales, as well as an ad hoc survey adapted from the Eating Disorder Examination Questionnaire. This assessed changes in restrictive dieting, control over food, body image, and psychological well-being in comparison with prepandemic levels.
The results, which were also recently published online in Eating and Weight Disorders – Studies on Anorexia, Bulimia and Obesity, showed that patients with EDs experienced significantly more stress, anxiety, depression, and PTSD-related symptoms in comparison with control persons (P < .05 for all).
In addition, the investigators found that those with EDs were more fearful of losing control over their eating behavior, spent more time thinking about food and their body, and became more uncomfortable seeing their body than before the lockdown in comparison with those without EDs (P < .05).
Clinical implications
A second assessment, which occurred in June 2020, after lockdown restrictions were lifted, included 40 patients with EDs who had taken part in the first assessment. This time, participants were asked to compare their current eating behavior with their eating behavior during the lockdown.
Although the lifting of lockdown restrictions was associated with significant improvement in PTSD-related symptoms, the impact on stress, anxiety, and depression persisted.
These findings, said Ms. Nisticó, support the hypothesis that specific conditions that occurred during the lockdown had a direct effect on specific ED symptoms.
These findings, she added, should be considered when developing interventions for EDs in the context of individual psychotherapy and when designing large, preventive interventions.
In the second study, Eleonora Rossi, MD, psychiatric unit, department of health sciences, University of Florence (Italy), and colleagues examined the longitudinal impact of the pandemic on individuals with EDs.
They examined 74 patients with AN or BN who had undergone baseline assessments and had completed a number of questionnaires in the first months of 2019 in conjunction with being enrolled in another study.
Participants were treated with enhanced cognitive-behavioral therapy and were reevaluated between November 2019 and January 2020. They were then compared with 97 healthy individuals.
Bulimia patients more vulnerable
After the outbreak of the pandemic, most treatment was administered online, so patients were able to continue therapy, Dr. Rossi said during her presentation.
All participants were assessed again in April 2020, 6 weeks after the start of Italy’s lockdown.
The results, which were published in the International Journal of Eating Disorders, show that the patients with EDs “underwent a significant improvement in terms of general and eating disorder specific psychopathology” during the first treatment period, Dr. Rossi reported. In addition, among those with AN, body mass index increased significantly (P < .05 for all).
Patients with AN continued to improve during the lockdown when therapy was administered online. However, improvements that had occurred among those with BN slowed, Dr. Rossi noted.
In addition, both groups of patients with EDs experienced a worsening of their pathological eating behaviors during the lockdown, in particular, objective binge eating and compensatory physical exercise (P < .05).
“Indeed, the positive trajectory of improvement observed before lockdown was clearly interrupted during the pandemic period,” Dr. Rossi said. This could “represent a possible hint of an imminent exacerbation of the disease.”
The results also suggest that the occurrence of arguments within the household and fear regarding the safety of loved ones predicted an increase in symptoms during the lockdown, she added.
In addition, patients with BN reported more severe COVID-related PTSD symptoms than did those with AN and the control group. This increase in severity of symptoms was more prevalent among patients who had a history of childhood trauma and among those with insecure attachment, suggesting that such patients may be more vulnerable.
Evidence of recovery
Commenting on the studies, David Spiegel, MD, associate chair of psychiatry, Stanford (Calif.) University, noted that EDs commonly occur after physical or sexual trauma earlier in life.
“It’s a standard thing with trauma-related disorders that any other, even relatively minor, traumatic experience can exacerbate PTSD symptoms,” said Dr. Spiegel, who was not involved in the studies. In addition, the trauma of the COVID pandemic “was not minor.
“The relative isolation and the lack of outside contact may focus many people with eating disorders even more on their struggles with how they are taking care of their bodies,” said Dr. Spiegel.
“It struck me that the anorexia nervosa group were more impervious than the bulimia nervosa group, but I think that’s the case with the disorder. In some ways it’s more severe, obviously a more life-threatening disorder,” he added.
The “hopeful thing is that there seemed to be some evidence of recovery and improvement, particularly with the posttraumatic stress exacerbation, as time went on,” Dr. Spiegel said, “and that’s a good thing.”
The study authors and Dr. Spiegel reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
COVID-19 and its resulting lockdowns are linked to posttraumatic stress disorder symptoms and other adverse outcomes among patients with eating disorders (EDs), two new studies show.
Results of the first study show that patients with EDs had more stress, anxiety, depression, and PTSD-related symptoms during the lockdowns than their mentally healthy peers.
In the second study, treatment-related symptom improvement among patients with bulimia nervosa (BN) slowed following lockdown. In addition, patients with BN or anorexia nervosa (AN) experienced significant worsening of disorder-specific behaviors, including binge eating and overexercising.
Because of the strict lockdown measures introduced by the Italian government to contain the COVID-19 pandemic, “everyday life of all citizens was disrupted,” Veronica Nisticò, MS, Università Degli Studi Di Milano, who led the first study, told delegates attending the virtual European Psychiatric Association 2021 Congress.
In addition to difficulties in accessing health care, “it became difficult to go to the supermarket, to the gym, and to have the social support we were all used to,” all of which had a well-documented impact on mental health, added Ms. Nisticò, who is also affiliated with Aldo Ravelli Research Center for Neurotechnology and Experimental Brain Therapeutics.
Loss of control
Previous research suggests that individuals with EDs experience high levels of anxiety and an increase in binge eating, exercise, and purging behaviors, said Ms. Nisticò.
To investigate further, the researchers conducted a longitudinal study of the changes in prevalence of adverse outcomes. In the study, two assessments were conducted.
The second group served as the control group.
Participants completed an online survey that included several standardized depression and anxiety scales, as well as an ad hoc survey adapted from the Eating Disorder Examination Questionnaire. This assessed changes in restrictive dieting, control over food, body image, and psychological well-being in comparison with prepandemic levels.
The results, which were also recently published online in Eating and Weight Disorders – Studies on Anorexia, Bulimia and Obesity, showed that patients with EDs experienced significantly more stress, anxiety, depression, and PTSD-related symptoms in comparison with control persons (P < .05 for all).
In addition, the investigators found that those with EDs were more fearful of losing control over their eating behavior, spent more time thinking about food and their body, and became more uncomfortable seeing their body than before the lockdown in comparison with those without EDs (P < .05).
Clinical implications
A second assessment, which occurred in June 2020, after lockdown restrictions were lifted, included 40 patients with EDs who had taken part in the first assessment. This time, participants were asked to compare their current eating behavior with their eating behavior during the lockdown.
Although the lifting of lockdown restrictions was associated with significant improvement in PTSD-related symptoms, the impact on stress, anxiety, and depression persisted.
These findings, said Ms. Nisticó, support the hypothesis that specific conditions that occurred during the lockdown had a direct effect on specific ED symptoms.
These findings, she added, should be considered when developing interventions for EDs in the context of individual psychotherapy and when designing large, preventive interventions.
In the second study, Eleonora Rossi, MD, psychiatric unit, department of health sciences, University of Florence (Italy), and colleagues examined the longitudinal impact of the pandemic on individuals with EDs.
They examined 74 patients with AN or BN who had undergone baseline assessments and had completed a number of questionnaires in the first months of 2019 in conjunction with being enrolled in another study.
Participants were treated with enhanced cognitive-behavioral therapy and were reevaluated between November 2019 and January 2020. They were then compared with 97 healthy individuals.
Bulimia patients more vulnerable
After the outbreak of the pandemic, most treatment was administered online, so patients were able to continue therapy, Dr. Rossi said during her presentation.
All participants were assessed again in April 2020, 6 weeks after the start of Italy’s lockdown.
The results, which were published in the International Journal of Eating Disorders, show that the patients with EDs “underwent a significant improvement in terms of general and eating disorder specific psychopathology” during the first treatment period, Dr. Rossi reported. In addition, among those with AN, body mass index increased significantly (P < .05 for all).
Patients with AN continued to improve during the lockdown when therapy was administered online. However, improvements that had occurred among those with BN slowed, Dr. Rossi noted.
In addition, both groups of patients with EDs experienced a worsening of their pathological eating behaviors during the lockdown, in particular, objective binge eating and compensatory physical exercise (P < .05).
“Indeed, the positive trajectory of improvement observed before lockdown was clearly interrupted during the pandemic period,” Dr. Rossi said. This could “represent a possible hint of an imminent exacerbation of the disease.”
The results also suggest that the occurrence of arguments within the household and fear regarding the safety of loved ones predicted an increase in symptoms during the lockdown, she added.
In addition, patients with BN reported more severe COVID-related PTSD symptoms than did those with AN and the control group. This increase in severity of symptoms was more prevalent among patients who had a history of childhood trauma and among those with insecure attachment, suggesting that such patients may be more vulnerable.
Evidence of recovery
Commenting on the studies, David Spiegel, MD, associate chair of psychiatry, Stanford (Calif.) University, noted that EDs commonly occur after physical or sexual trauma earlier in life.
“It’s a standard thing with trauma-related disorders that any other, even relatively minor, traumatic experience can exacerbate PTSD symptoms,” said Dr. Spiegel, who was not involved in the studies. In addition, the trauma of the COVID pandemic “was not minor.
“The relative isolation and the lack of outside contact may focus many people with eating disorders even more on their struggles with how they are taking care of their bodies,” said Dr. Spiegel.
“It struck me that the anorexia nervosa group were more impervious than the bulimia nervosa group, but I think that’s the case with the disorder. In some ways it’s more severe, obviously a more life-threatening disorder,” he added.
The “hopeful thing is that there seemed to be some evidence of recovery and improvement, particularly with the posttraumatic stress exacerbation, as time went on,” Dr. Spiegel said, “and that’s a good thing.”
The study authors and Dr. Spiegel reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Suicide in the early months of the pandemic: Unexpected trends
Every psychiatrist knows that this past year has been a challenge. The COVID-19 pandemic altered our lives, practically overnight, in ways that most of us had never anticipated.

There were months of lockdown. A new work-from-home transition. Recommendations to distance and mask. The destruction and recreation of our social lives. And the end of some industries as we have known them.
Over a year later, many children are still in virtual school. This lifestyle and economic toll do not even begin to include the horror experienced by exhausted and distressed health care workers or by the many who have lost a loved one or survived a hospitalization. National and international anxiety are running high. More people are seeking mental health care, and many of the patients we were caring for prior to the pandemic have been distressed.
Rates of both depression and anxiety are up, and the fear has been that the isolation of lockdowns, with their emotional and economic toll, would also increase suicide rates. Despite the increase in psychiatric symptoms and general distress, initial studies in the United States have shown that overall suicide rates in the early months of the pandemic were lower than in prior years.
A study published in The Lancet looked at suicide data from around the world and compared expected suicides, based on data from past years, with observed suicides. The researchers restricted their analysis to the countries, and regions of countries, where real-time suicide data were available through internet searches. Their paper is based on findings from 21 countries, including 16 high-income countries and five upper-middle–income countries (from regions where data were available). The overall analysis showed a drop in suicides by 5% when looking at the first 4 months of the pandemic, defined as April 1, 2020, to July 31, 2020. There were statistically significant increases in suicide only in Vienna, Puerto Rico, and Japan.
Igor Galynker, MD, PhD, directs the Suicide Research and Prevention Lab and the Zirinsky Center for Bipolar Disorder at the Icahn School of Medicine at Mount Sinai. He was not surprised by these findings.
“This is an important study,” Dr. Galynker said. “When it was discovered that U.S. rates went down, it was ‘U.S. specific’ and it was confounded by the fact that there was a dramatic increase in opiate overdose deaths in the U.S., which are not reported as suicides. This study shows that the decrease is international and that the finding in the United States is not related to the spike in overdose deaths.”
The study authors postulated that the drop in suicide may be due to proactive protective measures that societies have put in place, such as improved mental health services and fiscal support to mitigate financial consequences of the pandemic. They explained that “communities might have actively tried to support at-risk individuals, people might have connected in new ways, and some relationships might have been strengthened by households spending more time with each other. For some people, everyday stresses might have been reduced during stay-at-home periods, and for others the collective feeling of ‘we’re all in this together’ might have been beneficial”.
Dr. Galynker noted that, in times of calamity, suicide rates historically go down. “Short-term disasters invoke a fight-or-flight response that mobilizes us and improves our functioning under stress. Those acute responses last 2-3 months and then chronic stress sets in.” He is concerned that there will be increases in suicide rates down the road.
It is possible that individuals who consider social gatherings to be stressful, or who are bullied at school, may have found some relief from social interactions and expectations during the lockdown. “Some people have discovered that they like their families!” Dr. Galynker said.
While suicide rates have gone down, that is not true for all population subsets, and the authors of the Lancet paper noted that they were unable to give breakdowns of rates for different demographics.
Paul Nestadt, MD, is codirector of the Johns Hopkins Anxiety Disorders Clinic and studies suicide, firearms, and opiates. He looked at suicides in Maryland during the first 2 months of the lockdown (March 5, 2020 to May 7, 2020) and found that, Studies in Connecticut and Chicago yielded similar findings. These findings indicate that the overall trends may not reflect the impact on a specific subpopulation.
Dr. Nestadt talked about the disparities of suicide trends. “Communities hit harder by this pandemic in terms of sickness and death may experience more distress in ways that may come out as suicide in the context of other comorbid mood disorders. Also, in line with the idea of suicide as a marker of community- or population-level distress, there’s a general idea that having less of an economic cushion makes the pandemic more of a problem for some than for others. We know that suicide has been correlated to economic distress in general, and it makes sense that it would be community-specific where there is more economic duress.”
It has been a difficult year – not just for the United States, but for the entire world. One thing that may come of it is a unique opportunity to look at how stress and loss affect suicide rates, with the hope that preventive measures will follow.
A version of this article first appeared on Medscape.com.
Every psychiatrist knows that this past year has been a challenge. The COVID-19 pandemic altered our lives, practically overnight, in ways that most of us had never anticipated.
There were months of lockdown. A new work-from-home transition. Recommendations to distance and mask. The destruction and recreation of our social lives. And the end of some industries as we have known them.
Over a year later, many children are still in virtual school. This lifestyle and economic toll do not even begin to include the horror experienced by exhausted and distressed health care workers or by the many who have lost a loved one or survived a hospitalization. National and international anxiety are running high. More people are seeking mental health care, and many of the patients we were caring for prior to the pandemic have been distressed.
Rates of both depression and anxiety are up, and the fear has been that the isolation of lockdowns, with their emotional and economic toll, would also increase suicide rates. Despite the increase in psychiatric symptoms and general distress, initial studies in the United States have shown that overall suicide rates in the early months of the pandemic were lower than in prior years.
A study published in The Lancet looked at suicide data from around the world and compared expected suicides, based on data from past years, with observed suicides. The researchers restricted their analysis to the countries, and regions of countries, where real-time suicide data were available through internet searches. Their paper is based on findings from 21 countries, including 16 high-income countries and five upper-middle–income countries (from regions where data were available). The overall analysis showed a drop in suicides by 5% when looking at the first 4 months of the pandemic, defined as April 1, 2020, to July 31, 2020. There were statistically significant increases in suicide only in Vienna, Puerto Rico, and Japan.
Igor Galynker, MD, PhD, directs the Suicide Research and Prevention Lab and the Zirinsky Center for Bipolar Disorder at the Icahn School of Medicine at Mount Sinai. He was not surprised by these findings.
“This is an important study,” Dr. Galynker said. “When it was discovered that U.S. rates went down, it was ‘U.S. specific’ and it was confounded by the fact that there was a dramatic increase in opiate overdose deaths in the U.S., which are not reported as suicides. This study shows that the decrease is international and that the finding in the United States is not related to the spike in overdose deaths.”
The study authors postulated that the drop in suicide may be due to proactive protective measures that societies have put in place, such as improved mental health services and fiscal support to mitigate financial consequences of the pandemic. They explained that “communities might have actively tried to support at-risk individuals, people might have connected in new ways, and some relationships might have been strengthened by households spending more time with each other. For some people, everyday stresses might have been reduced during stay-at-home periods, and for others the collective feeling of ‘we’re all in this together’ might have been beneficial”.
Dr. Galynker noted that, in times of calamity, suicide rates historically go down. “Short-term disasters invoke a fight-or-flight response that mobilizes us and improves our functioning under stress. Those acute responses last 2-3 months and then chronic stress sets in.” He is concerned that there will be increases in suicide rates down the road.
It is possible that individuals who consider social gatherings to be stressful, or who are bullied at school, may have found some relief from social interactions and expectations during the lockdown. “Some people have discovered that they like their families!” Dr. Galynker said.
While suicide rates have gone down, that is not true for all population subsets, and the authors of the Lancet paper noted that they were unable to give breakdowns of rates for different demographics.
Paul Nestadt, MD, is codirector of the Johns Hopkins Anxiety Disorders Clinic and studies suicide, firearms, and opiates. He looked at suicides in Maryland during the first 2 months of the lockdown (March 5, 2020 to May 7, 2020) and found that, Studies in Connecticut and Chicago yielded similar findings. These findings indicate that the overall trends may not reflect the impact on a specific subpopulation.
Dr. Nestadt talked about the disparities of suicide trends. “Communities hit harder by this pandemic in terms of sickness and death may experience more distress in ways that may come out as suicide in the context of other comorbid mood disorders. Also, in line with the idea of suicide as a marker of community- or population-level distress, there’s a general idea that having less of an economic cushion makes the pandemic more of a problem for some than for others. We know that suicide has been correlated to economic distress in general, and it makes sense that it would be community-specific where there is more economic duress.”
It has been a difficult year – not just for the United States, but for the entire world. One thing that may come of it is a unique opportunity to look at how stress and loss affect suicide rates, with the hope that preventive measures will follow.
A version of this article first appeared on Medscape.com.
Every psychiatrist knows that this past year has been a challenge. The COVID-19 pandemic altered our lives, practically overnight, in ways that most of us had never anticipated.
There were months of lockdown. A new work-from-home transition. Recommendations to distance and mask. The destruction and recreation of our social lives. And the end of some industries as we have known them.
Over a year later, many children are still in virtual school. This lifestyle and economic toll do not even begin to include the horror experienced by exhausted and distressed health care workers or by the many who have lost a loved one or survived a hospitalization. National and international anxiety are running high. More people are seeking mental health care, and many of the patients we were caring for prior to the pandemic have been distressed.
Rates of both depression and anxiety are up, and the fear has been that the isolation of lockdowns, with their emotional and economic toll, would also increase suicide rates. Despite the increase in psychiatric symptoms and general distress, initial studies in the United States have shown that overall suicide rates in the early months of the pandemic were lower than in prior years.
A study published in The Lancet looked at suicide data from around the world and compared expected suicides, based on data from past years, with observed suicides. The researchers restricted their analysis to the countries, and regions of countries, where real-time suicide data were available through internet searches. Their paper is based on findings from 21 countries, including 16 high-income countries and five upper-middle–income countries (from regions where data were available). The overall analysis showed a drop in suicides by 5% when looking at the first 4 months of the pandemic, defined as April 1, 2020, to July 31, 2020. There were statistically significant increases in suicide only in Vienna, Puerto Rico, and Japan.
Igor Galynker, MD, PhD, directs the Suicide Research and Prevention Lab and the Zirinsky Center for Bipolar Disorder at the Icahn School of Medicine at Mount Sinai. He was not surprised by these findings.
“This is an important study,” Dr. Galynker said. “When it was discovered that U.S. rates went down, it was ‘U.S. specific’ and it was confounded by the fact that there was a dramatic increase in opiate overdose deaths in the U.S., which are not reported as suicides. This study shows that the decrease is international and that the finding in the United States is not related to the spike in overdose deaths.”
The study authors postulated that the drop in suicide may be due to proactive protective measures that societies have put in place, such as improved mental health services and fiscal support to mitigate financial consequences of the pandemic. They explained that “communities might have actively tried to support at-risk individuals, people might have connected in new ways, and some relationships might have been strengthened by households spending more time with each other. For some people, everyday stresses might have been reduced during stay-at-home periods, and for others the collective feeling of ‘we’re all in this together’ might have been beneficial”.
Dr. Galynker noted that, in times of calamity, suicide rates historically go down. “Short-term disasters invoke a fight-or-flight response that mobilizes us and improves our functioning under stress. Those acute responses last 2-3 months and then chronic stress sets in.” He is concerned that there will be increases in suicide rates down the road.
It is possible that individuals who consider social gatherings to be stressful, or who are bullied at school, may have found some relief from social interactions and expectations during the lockdown. “Some people have discovered that they like their families!” Dr. Galynker said.
While suicide rates have gone down, that is not true for all population subsets, and the authors of the Lancet paper noted that they were unable to give breakdowns of rates for different demographics.
Paul Nestadt, MD, is codirector of the Johns Hopkins Anxiety Disorders Clinic and studies suicide, firearms, and opiates. He looked at suicides in Maryland during the first 2 months of the lockdown (March 5, 2020 to May 7, 2020) and found that, Studies in Connecticut and Chicago yielded similar findings. These findings indicate that the overall trends may not reflect the impact on a specific subpopulation.
Dr. Nestadt talked about the disparities of suicide trends. “Communities hit harder by this pandemic in terms of sickness and death may experience more distress in ways that may come out as suicide in the context of other comorbid mood disorders. Also, in line with the idea of suicide as a marker of community- or population-level distress, there’s a general idea that having less of an economic cushion makes the pandemic more of a problem for some than for others. We know that suicide has been correlated to economic distress in general, and it makes sense that it would be community-specific where there is more economic duress.”
It has been a difficult year – not just for the United States, but for the entire world. One thing that may come of it is a unique opportunity to look at how stress and loss affect suicide rates, with the hope that preventive measures will follow.
A version of this article first appeared on Medscape.com.
What I want people to know about the Chauvin verdict
I woke up from a nap on Tuesday, April 20, to a barrage of text messages and social media alerts about the Derek Chauvin verdict. Messages varied in content, from “let’s celebrate,” to “just so exciting,” to “finally.” As I took in the sentiments of others, I could barely sense what, if any, sentiments I had of my own.

There I sat, a Black DEI [diversity, equity, and inclusion] consultant who calls herself a “psychiatrist-activist,” but slept through the landmark court decision for policing African Americans and felt almost nothing about it.
However, I did have feelings about other matters such as the slide decks due for my client, sending reassuring text messages about the hospitalization of a friend’s child, and the 2 weeks of patient notes on my to-do list. So why did I feel emotionally flatlined about an issue that should stimulate the opposite – emotional intensity?
The answer to “why” could be attributed to a number of psychological buzz words like trauma, grief, desensitization, dissociation, numbness, or my new favorite term, languishing.
Despite the applicability of any of the above, I think my emotional flattening has more to do with the fact that in addition to the guilty verdict, I also woke up to news that 16-year-old Ma’Khia Bryant had been shot by a police officer in Columbus, Ohio.
I asked myself: How can anyone find time to grieve, nevertheless celebrate when (young) Black people continue to be killed by the police?
While it hurts to see individuals who look like me being shot by police, or even emboldened citizens, my hurt likely pales in comparison to someone who grew up surrounded by police gun violence. I grew up solidly middle class, lived in a house at the end of a cul-de-sac in a semi-gated community, and have many years ahead of me to reach my earning potential as a physician in one of the most liberal cities in the nation. While I have the skin color that puts me at risk of being shot by police due to racism, I am in a cushy position compared to other Black people who live in cities or neighborhoods with more police shootings.
Given this line of thinking, it seems clearer to me why I do not feel like celebrating, but instead, feel grateful to be alive. Not only do I feel grateful to be alive, but alive with the emotional stamina to help White people understand their contributions to the widespread oppression that keeps our society rooted in white supremacy.
This brings me to my point of what I want people, especially physicians, to know about the guilty verdict of Derek Chauvin: Some of us cannot really celebrate until there is actual police reform. This is not to say that anyone is wrong to celebrate, as long as there is an understanding that .
Meanwhile, White men like Kyle Rittenhouse who are peaceably arrested after shooting a man with a semi-automatic weapon receive donations from a Virginia police lieutenant; a policeman who, in a possible world, could one day pull me over while driving through Virginia given its proximity to Washington D.C., where I currently live.
Black and Brown people cannot fully celebrate until there is actual police reform, and reform across American institutions like the health care system. Celebration comes when the leaders who run schools, hospitals, and courtrooms look more like the numbers actually reflected in U.S. racial demographics and look less like Derek Chauvin.
Until there are more doctors who look like the racial breakdown of the nation, Black and Brown patients can never fully trust their primary care doctors, orthopedic surgeons, and psychiatrists who are White. While this reality may sound harsh, it is the reality for many of us who are dealing with trauma, grief, desensitization, dissociation, emotional numbness, or languishment resulting from racist experiences.
People of color cannot and will not stop protesting in the streets, being the one who always brings up race in the meeting, or disagreeing that the new changes are “not enough” until there is actual anti-racist institutional reform. More importantly, the efforts of people of color can be made more powerful working collectively with White allies.
But we need White allies who recognize their tendency to perceive “progress” in racial equality. We need White allies who recognize that despite the passage of the Civil Rights Act, the two-time election of a Black president, and the guilty verdict of Derek Chauvin, there is still so much work to do.
Dr. Cyrus is assistant professor in the department of psychiatry at Johns Hopkins University, Baltimore. She reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
I woke up from a nap on Tuesday, April 20, to a barrage of text messages and social media alerts about the Derek Chauvin verdict. Messages varied in content, from “let’s celebrate,” to “just so exciting,” to “finally.” As I took in the sentiments of others, I could barely sense what, if any, sentiments I had of my own.
There I sat, a Black DEI [diversity, equity, and inclusion] consultant who calls herself a “psychiatrist-activist,” but slept through the landmark court decision for policing African Americans and felt almost nothing about it.
However, I did have feelings about other matters such as the slide decks due for my client, sending reassuring text messages about the hospitalization of a friend’s child, and the 2 weeks of patient notes on my to-do list. So why did I feel emotionally flatlined about an issue that should stimulate the opposite – emotional intensity?
The answer to “why” could be attributed to a number of psychological buzz words like trauma, grief, desensitization, dissociation, numbness, or my new favorite term, languishing.
Despite the applicability of any of the above, I think my emotional flattening has more to do with the fact that in addition to the guilty verdict, I also woke up to news that 16-year-old Ma’Khia Bryant had been shot by a police officer in Columbus, Ohio.
I asked myself: How can anyone find time to grieve, nevertheless celebrate when (young) Black people continue to be killed by the police?
While it hurts to see individuals who look like me being shot by police, or even emboldened citizens, my hurt likely pales in comparison to someone who grew up surrounded by police gun violence. I grew up solidly middle class, lived in a house at the end of a cul-de-sac in a semi-gated community, and have many years ahead of me to reach my earning potential as a physician in one of the most liberal cities in the nation. While I have the skin color that puts me at risk of being shot by police due to racism, I am in a cushy position compared to other Black people who live in cities or neighborhoods with more police shootings.
Given this line of thinking, it seems clearer to me why I do not feel like celebrating, but instead, feel grateful to be alive. Not only do I feel grateful to be alive, but alive with the emotional stamina to help White people understand their contributions to the widespread oppression that keeps our society rooted in white supremacy.
This brings me to my point of what I want people, especially physicians, to know about the guilty verdict of Derek Chauvin: Some of us cannot really celebrate until there is actual police reform. This is not to say that anyone is wrong to celebrate, as long as there is an understanding that .
Meanwhile, White men like Kyle Rittenhouse who are peaceably arrested after shooting a man with a semi-automatic weapon receive donations from a Virginia police lieutenant; a policeman who, in a possible world, could one day pull me over while driving through Virginia given its proximity to Washington D.C., where I currently live.
Black and Brown people cannot fully celebrate until there is actual police reform, and reform across American institutions like the health care system. Celebration comes when the leaders who run schools, hospitals, and courtrooms look more like the numbers actually reflected in U.S. racial demographics and look less like Derek Chauvin.
Until there are more doctors who look like the racial breakdown of the nation, Black and Brown patients can never fully trust their primary care doctors, orthopedic surgeons, and psychiatrists who are White. While this reality may sound harsh, it is the reality for many of us who are dealing with trauma, grief, desensitization, dissociation, emotional numbness, or languishment resulting from racist experiences.
People of color cannot and will not stop protesting in the streets, being the one who always brings up race in the meeting, or disagreeing that the new changes are “not enough” until there is actual anti-racist institutional reform. More importantly, the efforts of people of color can be made more powerful working collectively with White allies.
But we need White allies who recognize their tendency to perceive “progress” in racial equality. We need White allies who recognize that despite the passage of the Civil Rights Act, the two-time election of a Black president, and the guilty verdict of Derek Chauvin, there is still so much work to do.
Dr. Cyrus is assistant professor in the department of psychiatry at Johns Hopkins University, Baltimore. She reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
I woke up from a nap on Tuesday, April 20, to a barrage of text messages and social media alerts about the Derek Chauvin verdict. Messages varied in content, from “let’s celebrate,” to “just so exciting,” to “finally.” As I took in the sentiments of others, I could barely sense what, if any, sentiments I had of my own.
There I sat, a Black DEI [diversity, equity, and inclusion] consultant who calls herself a “psychiatrist-activist,” but slept through the landmark court decision for policing African Americans and felt almost nothing about it.
However, I did have feelings about other matters such as the slide decks due for my client, sending reassuring text messages about the hospitalization of a friend’s child, and the 2 weeks of patient notes on my to-do list. So why did I feel emotionally flatlined about an issue that should stimulate the opposite – emotional intensity?
The answer to “why” could be attributed to a number of psychological buzz words like trauma, grief, desensitization, dissociation, numbness, or my new favorite term, languishing.
Despite the applicability of any of the above, I think my emotional flattening has more to do with the fact that in addition to the guilty verdict, I also woke up to news that 16-year-old Ma’Khia Bryant had been shot by a police officer in Columbus, Ohio.
I asked myself: How can anyone find time to grieve, nevertheless celebrate when (young) Black people continue to be killed by the police?
While it hurts to see individuals who look like me being shot by police, or even emboldened citizens, my hurt likely pales in comparison to someone who grew up surrounded by police gun violence. I grew up solidly middle class, lived in a house at the end of a cul-de-sac in a semi-gated community, and have many years ahead of me to reach my earning potential as a physician in one of the most liberal cities in the nation. While I have the skin color that puts me at risk of being shot by police due to racism, I am in a cushy position compared to other Black people who live in cities or neighborhoods with more police shootings.
Given this line of thinking, it seems clearer to me why I do not feel like celebrating, but instead, feel grateful to be alive. Not only do I feel grateful to be alive, but alive with the emotional stamina to help White people understand their contributions to the widespread oppression that keeps our society rooted in white supremacy.
This brings me to my point of what I want people, especially physicians, to know about the guilty verdict of Derek Chauvin: Some of us cannot really celebrate until there is actual police reform. This is not to say that anyone is wrong to celebrate, as long as there is an understanding that .
Meanwhile, White men like Kyle Rittenhouse who are peaceably arrested after shooting a man with a semi-automatic weapon receive donations from a Virginia police lieutenant; a policeman who, in a possible world, could one day pull me over while driving through Virginia given its proximity to Washington D.C., where I currently live.
Black and Brown people cannot fully celebrate until there is actual police reform, and reform across American institutions like the health care system. Celebration comes when the leaders who run schools, hospitals, and courtrooms look more like the numbers actually reflected in U.S. racial demographics and look less like Derek Chauvin.
Until there are more doctors who look like the racial breakdown of the nation, Black and Brown patients can never fully trust their primary care doctors, orthopedic surgeons, and psychiatrists who are White. While this reality may sound harsh, it is the reality for many of us who are dealing with trauma, grief, desensitization, dissociation, emotional numbness, or languishment resulting from racist experiences.
People of color cannot and will not stop protesting in the streets, being the one who always brings up race in the meeting, or disagreeing that the new changes are “not enough” until there is actual anti-racist institutional reform. More importantly, the efforts of people of color can be made more powerful working collectively with White allies.
But we need White allies who recognize their tendency to perceive “progress” in racial equality. We need White allies who recognize that despite the passage of the Civil Rights Act, the two-time election of a Black president, and the guilty verdict of Derek Chauvin, there is still so much work to do.
Dr. Cyrus is assistant professor in the department of psychiatry at Johns Hopkins University, Baltimore. She reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Are psychiatric disorders a ‘canary in a coal mine’ for Alzheimer’s disease?
, according to findings from a review of 1,500 patients with Alzheimer’s disease from a single-center population.

“Could psychosis symptoms be the proverbial canary in a coal mine?” Emily Eijansantos, a medical student at the University of California, San Francisco, said in reporting results of the chart review at the 2021 annual meeting of the American Academy of Neurology. “Previously in this cohort it was found that neurodevelopmental factors as well as chronic insults such as autoimmunity and seizure were also associated with an early age of onset in Alzheimer’s disease.”
The link between depression and autoimmunity, and anxiety and seizure “beg more questions about underlying pathophysiology,” she said. The study included 750 patients with early-onset Alzheimer’s disease and a similar number of late-onset patients from the UCSF Memory and Aging Center.
An inverse correlation between psychiatric disorders and age of Alzheimer’s onset
In the total study population, 43.5% (n = 652) had a previous diagnosis of depression and 32.3% (n = 485) had been diagnosed with anxiety. That, Ms. Eijansantos said, falls into similar ranges that other studies have reported.
“When we look at individual psychiatric disorders, we find that those with depression, anxiety, or PTSD are younger on average,” she said. “Patients with depression and anxiety are more [likely] female and have less vascular risk factors, and we observed an association between depression and autoimmunity, anxiety, and seizures.”
Specifically, patients with a history of depression were 2.2 years younger, on average, at the age of onset than patients without such history (P = .01); those with anxiety were 3 years younger on average (P = .01); and those with PTSD were 6.8 years younger on average, although only 1% (n = 15) of study subjects had PTSD, making for a small sample to study. These age-of-onset disparities didn’t appear among patients with previously diagnosed bipolar disorder (BPD) or schizophrenia.
Ms. Eijansantos noted that there were no differences in education attained or apolipoprotein-E gene status between the patients with and without a history of psychosis, and, within the subgroups of individual psychiatric disorders, there were no differences between patients with past and current or formal and informal diagnoses.
“When we split the cohort into quintiles based on age of Alzheimer’s disease onset, we find an inverse correlation between the amount of depression, anxiety, and PTSD endorsed and their ages of onset,” Ms. Eijansantos said. For example, the youngest quintile had a greater than 50% rate of depression while the oldest quintile had a depression rate around 36%. A similar spread was found with anxiety: a rate around 46% in the youngest quantile versus around 25% in the oldest, whereas rates of PTSD, BPD, and schizophrenia were similar across the five age-of-onset groups.
Patients with a history of multiple psychiatric disorders had an even younger age of onset. “We see that those with two psychiatric disorder are younger than those with one, and those with three psychiatric disorders are younger still,” Ms. Eijansantos said. “And we find that the Alzheimer’s disease age-at-onset reduction doubles with each additional psychiatric disorder.” Multiple disorders also adversely impacted survival, she said.
Because they found no difference between patients with past versus active symptoms and informal versus formal diagnosis, Ms. Eijansantos explained that they further studied the National Alzheimer’s Coordinating Center cohort of 8,267 patients with Alzheimer’s disease and found a similar relationship between psychiatric history and age of onset among patients with depression or anxiety or both. This cohort also documented symptom severity, she noted. “So when we look at depression and anxiety we find similar reductions in the Alzheimer’s disease age of onset with each increasing degree of symptom severity,” she said.
“Does this mean that psychiatric disease is a risk factor for Alzheimr’s disease?” Ms. Eijansantos said. “We can’t answer that with this study because it was only designed to see if the psychiatric factors modulate the age of onset in those that have Alzheimer’s disease, but taken together we believe that these results fit the framework that there are pathophysiological and profound differences between earlier and later presentations of Alzheimer’s disease.”
She pointed to reports that early-onset Alzheimer’s disease is associated with more aggressive tau pathology and that depression is associated with tau. However, the evidence supporting a link between amyloid and psychiatric disease is less certain, she said.
Preliminary and speculative findings
Senior study author Zachary Miller, MD, an assistant professor in the UCSF Memory and Aging Center, explained the significance of the study findings of potential links between depression and autoimmunity, and anxiety and seizure. “There may be distinct underlying pathophysiological mechanisms in patients with Alzheimer’s disease who have symptoms of depression versus anxiety,” he said, acknowledging the findings “are quite preliminary and our interpretations quite speculative.”

The findings raise the question that the symptomatic presentation of greater amounts of depression in early-onset Alzheimer’s disease may be moderated by an underlying neuroinflammatory insult, he said. “If so, depression symptomatology could then be seen as a possible clinical marker of this inflammatory response and possibly be used in testing clinical endpoints for future intervention trials,” Dr. Miller said. “Similarly, if neuronal hyperexcitability in Alzheimer’s disease manifests itself as either seizure and/or anxiety, this would have significant impact for therapeutic monitoring and treatment.”
He said a multicenter study of Alzheimer’s disease cohorts would validate the findings. “At the same time, we are also interested in looking deeper into these findings, investigating the potential cognitive and neuroanatomical correlates associated with these conditions,” Dr. Miller said.
Clinical phenotyping may provide more insight into the relationship between psychosis and age of Alzheimer’s disease onset, said Vijay K. Ramanan, MD, PhD, an assistant professor of neurology at Mayo Clinic in Rochester, Minn.

“Less typical presentations of Alzheimer’s disease, such as posterior cortical atrophy or dysexecutive Alzheimer’s disease, are associated with younger age of onset and are sometimes misdiagnosed as having pure psychiatric disease,” he said. “It is also possible that, in some cases with psychiatric disease, a younger age of onset of cognitive symptoms is charted, even though there are fundamentally two distinct processes at play – a psychiatric disease and a separate neurodegenerative disease – each having independent but additive impacts on cognition.”
Dr. Ramanan added, “This work is also a good reminder to be on the lookout for neuropsychiatric symptoms, treat where indicated, and be open to the possibility that psychiatric symptoms and Alzheimer’s disease can coexist.”
Ms. Eijansantos, Dr. Miller, and Dr. Ramanan have no relevant financial relationships to disclose.
, according to findings from a review of 1,500 patients with Alzheimer’s disease from a single-center population.
“Could psychosis symptoms be the proverbial canary in a coal mine?” Emily Eijansantos, a medical student at the University of California, San Francisco, said in reporting results of the chart review at the 2021 annual meeting of the American Academy of Neurology. “Previously in this cohort it was found that neurodevelopmental factors as well as chronic insults such as autoimmunity and seizure were also associated with an early age of onset in Alzheimer’s disease.”
The link between depression and autoimmunity, and anxiety and seizure “beg more questions about underlying pathophysiology,” she said. The study included 750 patients with early-onset Alzheimer’s disease and a similar number of late-onset patients from the UCSF Memory and Aging Center.
An inverse correlation between psychiatric disorders and age of Alzheimer’s onset
In the total study population, 43.5% (n = 652) had a previous diagnosis of depression and 32.3% (n = 485) had been diagnosed with anxiety. That, Ms. Eijansantos said, falls into similar ranges that other studies have reported.
“When we look at individual psychiatric disorders, we find that those with depression, anxiety, or PTSD are younger on average,” she said. “Patients with depression and anxiety are more [likely] female and have less vascular risk factors, and we observed an association between depression and autoimmunity, anxiety, and seizures.”
Specifically, patients with a history of depression were 2.2 years younger, on average, at the age of onset than patients without such history (P = .01); those with anxiety were 3 years younger on average (P = .01); and those with PTSD were 6.8 years younger on average, although only 1% (n = 15) of study subjects had PTSD, making for a small sample to study. These age-of-onset disparities didn’t appear among patients with previously diagnosed bipolar disorder (BPD) or schizophrenia.
Ms. Eijansantos noted that there were no differences in education attained or apolipoprotein-E gene status between the patients with and without a history of psychosis, and, within the subgroups of individual psychiatric disorders, there were no differences between patients with past and current or formal and informal diagnoses.
“When we split the cohort into quintiles based on age of Alzheimer’s disease onset, we find an inverse correlation between the amount of depression, anxiety, and PTSD endorsed and their ages of onset,” Ms. Eijansantos said. For example, the youngest quintile had a greater than 50% rate of depression while the oldest quintile had a depression rate around 36%. A similar spread was found with anxiety: a rate around 46% in the youngest quantile versus around 25% in the oldest, whereas rates of PTSD, BPD, and schizophrenia were similar across the five age-of-onset groups.
Patients with a history of multiple psychiatric disorders had an even younger age of onset. “We see that those with two psychiatric disorder are younger than those with one, and those with three psychiatric disorders are younger still,” Ms. Eijansantos said. “And we find that the Alzheimer’s disease age-at-onset reduction doubles with each additional psychiatric disorder.” Multiple disorders also adversely impacted survival, she said.
Because they found no difference between patients with past versus active symptoms and informal versus formal diagnosis, Ms. Eijansantos explained that they further studied the National Alzheimer’s Coordinating Center cohort of 8,267 patients with Alzheimer’s disease and found a similar relationship between psychiatric history and age of onset among patients with depression or anxiety or both. This cohort also documented symptom severity, she noted. “So when we look at depression and anxiety we find similar reductions in the Alzheimer’s disease age of onset with each increasing degree of symptom severity,” she said.
“Does this mean that psychiatric disease is a risk factor for Alzheimr’s disease?” Ms. Eijansantos said. “We can’t answer that with this study because it was only designed to see if the psychiatric factors modulate the age of onset in those that have Alzheimer’s disease, but taken together we believe that these results fit the framework that there are pathophysiological and profound differences between earlier and later presentations of Alzheimer’s disease.”
She pointed to reports that early-onset Alzheimer’s disease is associated with more aggressive tau pathology and that depression is associated with tau. However, the evidence supporting a link between amyloid and psychiatric disease is less certain, she said.
Preliminary and speculative findings
Senior study author Zachary Miller, MD, an assistant professor in the UCSF Memory and Aging Center, explained the significance of the study findings of potential links between depression and autoimmunity, and anxiety and seizure. “There may be distinct underlying pathophysiological mechanisms in patients with Alzheimer’s disease who have symptoms of depression versus anxiety,” he said, acknowledging the findings “are quite preliminary and our interpretations quite speculative.”
The findings raise the question that the symptomatic presentation of greater amounts of depression in early-onset Alzheimer’s disease may be moderated by an underlying neuroinflammatory insult, he said. “If so, depression symptomatology could then be seen as a possible clinical marker of this inflammatory response and possibly be used in testing clinical endpoints for future intervention trials,” Dr. Miller said. “Similarly, if neuronal hyperexcitability in Alzheimer’s disease manifests itself as either seizure and/or anxiety, this would have significant impact for therapeutic monitoring and treatment.”
He said a multicenter study of Alzheimer’s disease cohorts would validate the findings. “At the same time, we are also interested in looking deeper into these findings, investigating the potential cognitive and neuroanatomical correlates associated with these conditions,” Dr. Miller said.
Clinical phenotyping may provide more insight into the relationship between psychosis and age of Alzheimer’s disease onset, said Vijay K. Ramanan, MD, PhD, an assistant professor of neurology at Mayo Clinic in Rochester, Minn.
“Less typical presentations of Alzheimer’s disease, such as posterior cortical atrophy or dysexecutive Alzheimer’s disease, are associated with younger age of onset and are sometimes misdiagnosed as having pure psychiatric disease,” he said. “It is also possible that, in some cases with psychiatric disease, a younger age of onset of cognitive symptoms is charted, even though there are fundamentally two distinct processes at play – a psychiatric disease and a separate neurodegenerative disease – each having independent but additive impacts on cognition.”
Dr. Ramanan added, “This work is also a good reminder to be on the lookout for neuropsychiatric symptoms, treat where indicated, and be open to the possibility that psychiatric symptoms and Alzheimer’s disease can coexist.”
Ms. Eijansantos, Dr. Miller, and Dr. Ramanan have no relevant financial relationships to disclose.
, according to findings from a review of 1,500 patients with Alzheimer’s disease from a single-center population.
“Could psychosis symptoms be the proverbial canary in a coal mine?” Emily Eijansantos, a medical student at the University of California, San Francisco, said in reporting results of the chart review at the 2021 annual meeting of the American Academy of Neurology. “Previously in this cohort it was found that neurodevelopmental factors as well as chronic insults such as autoimmunity and seizure were also associated with an early age of onset in Alzheimer’s disease.”
The link between depression and autoimmunity, and anxiety and seizure “beg more questions about underlying pathophysiology,” she said. The study included 750 patients with early-onset Alzheimer’s disease and a similar number of late-onset patients from the UCSF Memory and Aging Center.
An inverse correlation between psychiatric disorders and age of Alzheimer’s onset
In the total study population, 43.5% (n = 652) had a previous diagnosis of depression and 32.3% (n = 485) had been diagnosed with anxiety. That, Ms. Eijansantos said, falls into similar ranges that other studies have reported.
“When we look at individual psychiatric disorders, we find that those with depression, anxiety, or PTSD are younger on average,” she said. “Patients with depression and anxiety are more [likely] female and have less vascular risk factors, and we observed an association between depression and autoimmunity, anxiety, and seizures.”
Specifically, patients with a history of depression were 2.2 years younger, on average, at the age of onset than patients without such history (P = .01); those with anxiety were 3 years younger on average (P = .01); and those with PTSD were 6.8 years younger on average, although only 1% (n = 15) of study subjects had PTSD, making for a small sample to study. These age-of-onset disparities didn’t appear among patients with previously diagnosed bipolar disorder (BPD) or schizophrenia.
Ms. Eijansantos noted that there were no differences in education attained or apolipoprotein-E gene status between the patients with and without a history of psychosis, and, within the subgroups of individual psychiatric disorders, there were no differences between patients with past and current or formal and informal diagnoses.
“When we split the cohort into quintiles based on age of Alzheimer’s disease onset, we find an inverse correlation between the amount of depression, anxiety, and PTSD endorsed and their ages of onset,” Ms. Eijansantos said. For example, the youngest quintile had a greater than 50% rate of depression while the oldest quintile had a depression rate around 36%. A similar spread was found with anxiety: a rate around 46% in the youngest quantile versus around 25% in the oldest, whereas rates of PTSD, BPD, and schizophrenia were similar across the five age-of-onset groups.
Patients with a history of multiple psychiatric disorders had an even younger age of onset. “We see that those with two psychiatric disorder are younger than those with one, and those with three psychiatric disorders are younger still,” Ms. Eijansantos said. “And we find that the Alzheimer’s disease age-at-onset reduction doubles with each additional psychiatric disorder.” Multiple disorders also adversely impacted survival, she said.
Because they found no difference between patients with past versus active symptoms and informal versus formal diagnosis, Ms. Eijansantos explained that they further studied the National Alzheimer’s Coordinating Center cohort of 8,267 patients with Alzheimer’s disease and found a similar relationship between psychiatric history and age of onset among patients with depression or anxiety or both. This cohort also documented symptom severity, she noted. “So when we look at depression and anxiety we find similar reductions in the Alzheimer’s disease age of onset with each increasing degree of symptom severity,” she said.
“Does this mean that psychiatric disease is a risk factor for Alzheimr’s disease?” Ms. Eijansantos said. “We can’t answer that with this study because it was only designed to see if the psychiatric factors modulate the age of onset in those that have Alzheimer’s disease, but taken together we believe that these results fit the framework that there are pathophysiological and profound differences between earlier and later presentations of Alzheimer’s disease.”
She pointed to reports that early-onset Alzheimer’s disease is associated with more aggressive tau pathology and that depression is associated with tau. However, the evidence supporting a link between amyloid and psychiatric disease is less certain, she said.
Preliminary and speculative findings
Senior study author Zachary Miller, MD, an assistant professor in the UCSF Memory and Aging Center, explained the significance of the study findings of potential links between depression and autoimmunity, and anxiety and seizure. “There may be distinct underlying pathophysiological mechanisms in patients with Alzheimer’s disease who have symptoms of depression versus anxiety,” he said, acknowledging the findings “are quite preliminary and our interpretations quite speculative.”
The findings raise the question that the symptomatic presentation of greater amounts of depression in early-onset Alzheimer’s disease may be moderated by an underlying neuroinflammatory insult, he said. “If so, depression symptomatology could then be seen as a possible clinical marker of this inflammatory response and possibly be used in testing clinical endpoints for future intervention trials,” Dr. Miller said. “Similarly, if neuronal hyperexcitability in Alzheimer’s disease manifests itself as either seizure and/or anxiety, this would have significant impact for therapeutic monitoring and treatment.”
He said a multicenter study of Alzheimer’s disease cohorts would validate the findings. “At the same time, we are also interested in looking deeper into these findings, investigating the potential cognitive and neuroanatomical correlates associated with these conditions,” Dr. Miller said.
Clinical phenotyping may provide more insight into the relationship between psychosis and age of Alzheimer’s disease onset, said Vijay K. Ramanan, MD, PhD, an assistant professor of neurology at Mayo Clinic in Rochester, Minn.
“Less typical presentations of Alzheimer’s disease, such as posterior cortical atrophy or dysexecutive Alzheimer’s disease, are associated with younger age of onset and are sometimes misdiagnosed as having pure psychiatric disease,” he said. “It is also possible that, in some cases with psychiatric disease, a younger age of onset of cognitive symptoms is charted, even though there are fundamentally two distinct processes at play – a psychiatric disease and a separate neurodegenerative disease – each having independent but additive impacts on cognition.”
Dr. Ramanan added, “This work is also a good reminder to be on the lookout for neuropsychiatric symptoms, treat where indicated, and be open to the possibility that psychiatric symptoms and Alzheimer’s disease can coexist.”
Ms. Eijansantos, Dr. Miller, and Dr. Ramanan have no relevant financial relationships to disclose.
FROM AAN 2021

Nurses or physicians: Who are at highest suicide risk?
Female nurses are at significantly greater risk of dying by suicide than physicians in findings that contradict previous research suggesting doctors are at greatest risk.

Results of a large retrospective cohort study show that nurses of both sexes were 18% more likely to die by suicide, compared with individuals in the general population. In addition, compared with female physicians, the suicide risk among female nurses was 70% higher.
“The main takeaway is that the risk of suicide among nurses is twice that of the general population and even higher than that among physicians, a population known to be at high risk,” lead author Matthew Davis, MPH, PhD, associate professor, department of systems, populations, and leadership, University of Michigan, Ann Arbor, said in an interview.
The study was published online April 14, 2021, in JAMA Psychiatry.
Focus on physicians
Compared with the general public, health care workers are at higher risk for suicide, but most studies of suicide have focused on physicians, Dr. Davis said.
Although “there were several older studies hinting that there might be a difference in suicide risk among nurses,” the data were insufficient to “make an overall conclusion,” he noted.
For that reason, his group “set out to make the best estimates possible” by using a large dataset from the National Violent Death Reporting System of the Centers for Disease Control and Prevention spanning the years 2007-2018 and focusing on suicides by individuals aged 30 years and older (n = 159,372 suicides).
Additional workforce data were acquired from the Bureau of Labor Statistics and the Association of Medical Colleges State Physician Workforce Data.
An important area of focus was method of suicide.
“ and know how to use them to overdose, which also increases their risk,” Dr. Davis said in a press release.
Enormous job strain
The researchers identified 2,374 suicides among nurses, 857 suicides among physicians, and 156,141 suicides in the general population.
Compared with the general population, nurses who died by suicide were more likely to be women, less racially diverse (non-Hispanic White), and more likely to have been married.
Rates of suicide were higher among nurses than among the general population, with a sex-adjusted incidence for 2017-2018 of 23.8 per 100,000 versus 20.1 per 100,000 (relative risk, 1.18; 95% confidence interval, 1.03-1.36).
The difference between suicide rates among female nurses and among women in the general population was even more striking: In 2017-2018, the suicide incidence among nurses was 17.1 per 100,000 versus 8.6 per 100,000 in the population at large (RR, 1.99; 95% CI, 1.82-2.18).
“In absolute terms, being a female nurse was associated with an additional 8.5 suicides per 100,000 (7.0-10.0), compared with the general population,” the authors reported.
In contrast, overall physician suicide rates were not statistically different from those of the general population (RR, 1.01; 95% CI, 0.79-1.30) except during the period 2011-2012 (11.7 per 100,000; 95% CI, 6.6-16.8 vs. 7.5 per 100,000; 95% CI, 7.2-7.7).
Clinicians of both sexes were more likely to use poisoning and less likely to use a firearm, compared with individuals in the general population who died by suicide. For example, 24.9% (23.5%-26.4%) of nurse suicides involved poisoning, compared to 16.8% (16.6%-17.0%) of suicides in the general population.
Toxicology reports showed that the presence of antidepressants, benzodiazepines, barbiturates, and opiates was more common in clinician suicides than suicides in the general population.
Dr. Davis suggested the higher risk for suicide among nurses, compared with physicians, might be attributed to “high job demands – for example, nurses provide the majority of bedside care, work long shifts in stressful environments, and have less autonomy.
“Health care workers and friends and family of health care workers need to be aware of mental health issues and suicide risk that can be associated with the job and, most importantly, recognize those who may be struggling and encourage them to get help by calling the National Suicide Prevention Lifeline,” he said.
Other potential contributors include “avoidance of mental health services due to stigma and greater access to the means to commit suicide via medication,” Dr. Davis noted.
Benchmark research
Commenting on the study, Constance Guille, MD, MSCR, professor in the department of psychiatry and behavioral science, Medical University of South Carolina, Charleston, noted that nurses are “predominantly female” and that women tend to be twice as likely as men to experience depression, which is a major risk factor for suicide. Thus, this population is particularly vulnerable.
One reason the investigators did not find that suicide rates were higher among physicians is that the health care professionals whom the researchers studied were older than 30 years. Thus, the study “excludes younger physicians in early practice or training, who likely do have higher suicide rates than the general population,” she suggested.
Dr. Guille, who is the author of an accompanying editorial and was not involved with the study, recommended “taking a public health approach, implementing preventative interventions, identifying people at high risk, providing treatment for health care professionals struggling with mental health problems, and destigmatizing help seeking.”
She encouraged clinicians to “reach out to colleagues who are struggling in a way to help them seek services and check in with them because it’s helpful when peers reach out.”
Dr. Davis noted that these disturbing trends will likely increase in the aftermath of the COVID-19 pandemic. “The pandemic has placed enormous strain on the health care workforce, and we fear this may have made the situation even worse.”
The current findings “will serve as a benchmark for future comparisons,” he said.
No source of funding for the study was reported. Dr. Davis has received consulting fees as a statistical reviewer for the journal Regional Anesthesia and Pain Medicine. His coauthors disclosed no relevant financial relationships. Dr. Guille has received grants from the National Institute on Drug Abuse, the American Foundation on Suicide Prevention, and the Duke Endowment and serves on the advisory board and speakers bureau of Sage Therapeutics.
A version of this article first appeared on Medscape.com.
Female nurses are at significantly greater risk of dying by suicide than physicians in findings that contradict previous research suggesting doctors are at greatest risk.
Results of a large retrospective cohort study show that nurses of both sexes were 18% more likely to die by suicide, compared with individuals in the general population. In addition, compared with female physicians, the suicide risk among female nurses was 70% higher.
“The main takeaway is that the risk of suicide among nurses is twice that of the general population and even higher than that among physicians, a population known to be at high risk,” lead author Matthew Davis, MPH, PhD, associate professor, department of systems, populations, and leadership, University of Michigan, Ann Arbor, said in an interview.
The study was published online April 14, 2021, in JAMA Psychiatry.
Focus on physicians
Compared with the general public, health care workers are at higher risk for suicide, but most studies of suicide have focused on physicians, Dr. Davis said.
Although “there were several older studies hinting that there might be a difference in suicide risk among nurses,” the data were insufficient to “make an overall conclusion,” he noted.
For that reason, his group “set out to make the best estimates possible” by using a large dataset from the National Violent Death Reporting System of the Centers for Disease Control and Prevention spanning the years 2007-2018 and focusing on suicides by individuals aged 30 years and older (n = 159,372 suicides).
Additional workforce data were acquired from the Bureau of Labor Statistics and the Association of Medical Colleges State Physician Workforce Data.
An important area of focus was method of suicide.
“ and know how to use them to overdose, which also increases their risk,” Dr. Davis said in a press release.
Enormous job strain
The researchers identified 2,374 suicides among nurses, 857 suicides among physicians, and 156,141 suicides in the general population.
Compared with the general population, nurses who died by suicide were more likely to be women, less racially diverse (non-Hispanic White), and more likely to have been married.
Rates of suicide were higher among nurses than among the general population, with a sex-adjusted incidence for 2017-2018 of 23.8 per 100,000 versus 20.1 per 100,000 (relative risk, 1.18; 95% confidence interval, 1.03-1.36).
The difference between suicide rates among female nurses and among women in the general population was even more striking: In 2017-2018, the suicide incidence among nurses was 17.1 per 100,000 versus 8.6 per 100,000 in the population at large (RR, 1.99; 95% CI, 1.82-2.18).
“In absolute terms, being a female nurse was associated with an additional 8.5 suicides per 100,000 (7.0-10.0), compared with the general population,” the authors reported.
In contrast, overall physician suicide rates were not statistically different from those of the general population (RR, 1.01; 95% CI, 0.79-1.30) except during the period 2011-2012 (11.7 per 100,000; 95% CI, 6.6-16.8 vs. 7.5 per 100,000; 95% CI, 7.2-7.7).
Clinicians of both sexes were more likely to use poisoning and less likely to use a firearm, compared with individuals in the general population who died by suicide. For example, 24.9% (23.5%-26.4%) of nurse suicides involved poisoning, compared to 16.8% (16.6%-17.0%) of suicides in the general population.
Toxicology reports showed that the presence of antidepressants, benzodiazepines, barbiturates, and opiates was more common in clinician suicides than suicides in the general population.
Dr. Davis suggested the higher risk for suicide among nurses, compared with physicians, might be attributed to “high job demands – for example, nurses provide the majority of bedside care, work long shifts in stressful environments, and have less autonomy.
“Health care workers and friends and family of health care workers need to be aware of mental health issues and suicide risk that can be associated with the job and, most importantly, recognize those who may be struggling and encourage them to get help by calling the National Suicide Prevention Lifeline,” he said.
Other potential contributors include “avoidance of mental health services due to stigma and greater access to the means to commit suicide via medication,” Dr. Davis noted.
Benchmark research
Commenting on the study, Constance Guille, MD, MSCR, professor in the department of psychiatry and behavioral science, Medical University of South Carolina, Charleston, noted that nurses are “predominantly female” and that women tend to be twice as likely as men to experience depression, which is a major risk factor for suicide. Thus, this population is particularly vulnerable.
One reason the investigators did not find that suicide rates were higher among physicians is that the health care professionals whom the researchers studied were older than 30 years. Thus, the study “excludes younger physicians in early practice or training, who likely do have higher suicide rates than the general population,” she suggested.
Dr. Guille, who is the author of an accompanying editorial and was not involved with the study, recommended “taking a public health approach, implementing preventative interventions, identifying people at high risk, providing treatment for health care professionals struggling with mental health problems, and destigmatizing help seeking.”
She encouraged clinicians to “reach out to colleagues who are struggling in a way to help them seek services and check in with them because it’s helpful when peers reach out.”
Dr. Davis noted that these disturbing trends will likely increase in the aftermath of the COVID-19 pandemic. “The pandemic has placed enormous strain on the health care workforce, and we fear this may have made the situation even worse.”
The current findings “will serve as a benchmark for future comparisons,” he said.
No source of funding for the study was reported. Dr. Davis has received consulting fees as a statistical reviewer for the journal Regional Anesthesia and Pain Medicine. His coauthors disclosed no relevant financial relationships. Dr. Guille has received grants from the National Institute on Drug Abuse, the American Foundation on Suicide Prevention, and the Duke Endowment and serves on the advisory board and speakers bureau of Sage Therapeutics.
A version of this article first appeared on Medscape.com.
Female nurses are at significantly greater risk of dying by suicide than physicians in findings that contradict previous research suggesting doctors are at greatest risk.
Results of a large retrospective cohort study show that nurses of both sexes were 18% more likely to die by suicide, compared with individuals in the general population. In addition, compared with female physicians, the suicide risk among female nurses was 70% higher.
“The main takeaway is that the risk of suicide among nurses is twice that of the general population and even higher than that among physicians, a population known to be at high risk,” lead author Matthew Davis, MPH, PhD, associate professor, department of systems, populations, and leadership, University of Michigan, Ann Arbor, said in an interview.
The study was published online April 14, 2021, in JAMA Psychiatry.
Focus on physicians
Compared with the general public, health care workers are at higher risk for suicide, but most studies of suicide have focused on physicians, Dr. Davis said.
Although “there were several older studies hinting that there might be a difference in suicide risk among nurses,” the data were insufficient to “make an overall conclusion,” he noted.
For that reason, his group “set out to make the best estimates possible” by using a large dataset from the National Violent Death Reporting System of the Centers for Disease Control and Prevention spanning the years 2007-2018 and focusing on suicides by individuals aged 30 years and older (n = 159,372 suicides).
Additional workforce data were acquired from the Bureau of Labor Statistics and the Association of Medical Colleges State Physician Workforce Data.
An important area of focus was method of suicide.
“ and know how to use them to overdose, which also increases their risk,” Dr. Davis said in a press release.
Enormous job strain
The researchers identified 2,374 suicides among nurses, 857 suicides among physicians, and 156,141 suicides in the general population.
Compared with the general population, nurses who died by suicide were more likely to be women, less racially diverse (non-Hispanic White), and more likely to have been married.
Rates of suicide were higher among nurses than among the general population, with a sex-adjusted incidence for 2017-2018 of 23.8 per 100,000 versus 20.1 per 100,000 (relative risk, 1.18; 95% confidence interval, 1.03-1.36).
The difference between suicide rates among female nurses and among women in the general population was even more striking: In 2017-2018, the suicide incidence among nurses was 17.1 per 100,000 versus 8.6 per 100,000 in the population at large (RR, 1.99; 95% CI, 1.82-2.18).
“In absolute terms, being a female nurse was associated with an additional 8.5 suicides per 100,000 (7.0-10.0), compared with the general population,” the authors reported.
In contrast, overall physician suicide rates were not statistically different from those of the general population (RR, 1.01; 95% CI, 0.79-1.30) except during the period 2011-2012 (11.7 per 100,000; 95% CI, 6.6-16.8 vs. 7.5 per 100,000; 95% CI, 7.2-7.7).
Clinicians of both sexes were more likely to use poisoning and less likely to use a firearm, compared with individuals in the general population who died by suicide. For example, 24.9% (23.5%-26.4%) of nurse suicides involved poisoning, compared to 16.8% (16.6%-17.0%) of suicides in the general population.
Toxicology reports showed that the presence of antidepressants, benzodiazepines, barbiturates, and opiates was more common in clinician suicides than suicides in the general population.
Dr. Davis suggested the higher risk for suicide among nurses, compared with physicians, might be attributed to “high job demands – for example, nurses provide the majority of bedside care, work long shifts in stressful environments, and have less autonomy.
“Health care workers and friends and family of health care workers need to be aware of mental health issues and suicide risk that can be associated with the job and, most importantly, recognize those who may be struggling and encourage them to get help by calling the National Suicide Prevention Lifeline,” he said.
Other potential contributors include “avoidance of mental health services due to stigma and greater access to the means to commit suicide via medication,” Dr. Davis noted.
Benchmark research
Commenting on the study, Constance Guille, MD, MSCR, professor in the department of psychiatry and behavioral science, Medical University of South Carolina, Charleston, noted that nurses are “predominantly female” and that women tend to be twice as likely as men to experience depression, which is a major risk factor for suicide. Thus, this population is particularly vulnerable.
One reason the investigators did not find that suicide rates were higher among physicians is that the health care professionals whom the researchers studied were older than 30 years. Thus, the study “excludes younger physicians in early practice or training, who likely do have higher suicide rates than the general population,” she suggested.
Dr. Guille, who is the author of an accompanying editorial and was not involved with the study, recommended “taking a public health approach, implementing preventative interventions, identifying people at high risk, providing treatment for health care professionals struggling with mental health problems, and destigmatizing help seeking.”
She encouraged clinicians to “reach out to colleagues who are struggling in a way to help them seek services and check in with them because it’s helpful when peers reach out.”
Dr. Davis noted that these disturbing trends will likely increase in the aftermath of the COVID-19 pandemic. “The pandemic has placed enormous strain on the health care workforce, and we fear this may have made the situation even worse.”
The current findings “will serve as a benchmark for future comparisons,” he said.
No source of funding for the study was reported. Dr. Davis has received consulting fees as a statistical reviewer for the journal Regional Anesthesia and Pain Medicine. His coauthors disclosed no relevant financial relationships. Dr. Guille has received grants from the National Institute on Drug Abuse, the American Foundation on Suicide Prevention, and the Duke Endowment and serves on the advisory board and speakers bureau of Sage Therapeutics.
A version of this article first appeared on Medscape.com.