User login
Asian children less likely to receive ADHD treatment
A study of U.S. children across ethnic and racial groups found that Asians were least likely to receive therapy for ADHD, compared with White children – who had the highest odds of getting some kind of treatment over other groups.
Other studies have identified disparity problems in ADHD diagnosis, although results have varied on inequality metrics. Few studies have looked at Asians separately, according to the study’s lead author, Yu Shi, MD, MPH. “They were usually just classified as ‘other’ or as non-White,” Dr. Shi, a consultant with the Mayo Clinic’s division of pediatric anesthesia in Rochester, Minn., said in an interview.
, and the way in which clinicians interpret behavior and apply diagnostic criteria.
“Further understanding of how treatment patterns for ADHD may differ based on race, at the time of initial diagnosis and in the early stages of treatment, may help all children receive appropriate evidence-based care,” Dr. Shi and colleagues reported in JAMA Network Open.
Researchers develop large birth cohort
Dr. Shi and colleagues hypothesized that non-Hispanic White children had a greater chance of getting diagnosed and treated within the first year of diagnosis than that of other ethnic and racial cohorts. Using administrative claims data with socioeconomic status information from a national commercial insurance warehouse, they constructed a retrospective birth cohort of children born between Jan. 1, 2006, and Dec. 31, 2012. The children had continuous insurance coverage for at least 4 years, and represented non-Hispanic Whites, Blacks, Hispanics, and Asians. Self-reporting identified the race/ethnicity groups.
Investigators analyzed ADHD diagnosis and treatment data on 238,011 children between October 2019 and December 2020, using a multivariate Cox regression model to adjust for sex, region, and household income. Primary and secondary outcomes included ADHD diagnosis as defined by recent ICD codes, ADHD behavior, and medication therapies in the clinical setting after initial diagnosis, respectively.
Whites made up most of the cohort (72.7%), followed by Hispanics (9.8%), Asians (6.7%), and Blacks (6.2%). Nearly half the population was female (48.8%). During the follow-up period with these children, 11,401, or 4.8%, had received an ADHD diagnosis. Mean age of diagnosis was 6.5 years, and overall incidence of ADHD was 69 per 10,000 person years (95% confidence interval, 68-70).
Pediatricians were most likely to make an ADHD diagnosis, although the study cited other clinicians, such as psychiatrists, neurologists, psychologists, and family practice clinicians, as responsible for these decisions.
Children diagnosed with ADHD had more years of coverage in the data set, and were more likely to be White and male. The Southern census region had a higher representation of diagnoses (50.6%) than did the Northeast region (11.8%).
Asians at highest odds for no treatment
Taking a closer look at race and ethnicity, Whites had the highest cumulative incidence of ADHD (14.19%), versus Asian children, who had lowest incidence (6.08%). “The curves for Black and Hispanic children were similar in shape and slightly lower than that for White children,” reported the investigators.
White children had higher odds of receiving some kind of treatment, compared with the other groups.
Incidence of medication treatment was lower among Asians and Hispanics. In a striking finding, Asians were most likely to receive no treatment at all (odds ratio compared with White children, 0.54; 95% confidence interval, 0.42-0.70). “However, the percentage of Asian children receiving psychotherapy was not significantly lower than other groups, which is different than a 2013 study finding that Asian children with ADHD were less likely to use mental health services,” they noted.
Most of the patients received medication (32.4%) in the first year after diagnosis, whereas (19.4%) received behavioral therapy only. Nineteen percent had both. More than 29% of these cases had no claims associated with either treatment. Among school-aged children, 65.5% were prescribed medications, compared with just 14.4% who received therapy. Twenty percent had no treatment.
Diagnosis with another disorder often preceded ADHD diagnosis. Results varied among racial groups. White children were more likely than were Black children to be diagnosed with an anxiety or adjustment disorder. Relative to White children, Asians were more likely to be diagnosed with autism spectrum disorder, speech sound disorders, or unspecified neurodevelopmental disorders. Even after an ADHD diagnosis, clinicians were more likely to diagnose Asian children with autism.
Parents may influence treatment decisions
Parental views and preferences may explain some of the variations in diagnosis and treatment among the racial/ethnic groups.
“In order for a diagnosis of ADHD to happen, a parent has first to recognize a problem and bring a child for clinical evaluation,” said Dr. Shi. “A certain behavior could be viewed as normal or a problem depending on a person’s cultural or racial background.” It’s unclear whether clinicians played any role in diagnosis disparities, he added. Patients’ concerns about racism might also influence the desire to get treated in health care systems.
Overall, the findings underscore the presence of racial and ethnic disparities in ADHD diagnosis and treatment. Future research should explore the underlying mechanisms, Dr. Shi suggested. While he and his colleagues have no immediate plans to do another ADHD study, “we’re planning on research to understand disparities in surgery in children,” he said.
The authors cited numerous limitations with their study. Use of ICD codes to identify cases might not have represented true clinical diagnosis, since the data were collected for billing, not research purposes. Investigators drew participants from a commercial insurance database, which did not necessarily reflect all U.S. children. The results might not represent a large number of children covered by Medicaid, for example, noted Dr. Shi. “It is more difficult to work with Medicaid data because there’s no national-level Medicaid data for research. Only state-level data is available.”
Because of other data gaps, Dr. Shi and colleagues might have underestimated the number of children in therapy.
A need for ‘culturally sensitive care’
The findings “ultimately demonstrate the need for culturally sensitive care in the diagnosis and treatment of children and adolescents,” said Tiffani L. Bell, MD, a psychiatrist in Winston-Salem, N.C., who was not involved with the study. She specializes in child and adolescent psychiatry.

The exact cause for racial disparity in diagnosis and treatment of ADHD is unknown and likely multifaceted, she continued. “It may be due to differences in the way that disruptive behaviors are interrupted based on factors such as race. This study found that Asian parents often brought their children in for evaluation for reasons other than ADHD. Concerns surrounding the stigma of mental health treatment and racism also could contribute to the disparity in diagnosis and treatment,” she said.
Dr. Bell said she hopes to see future studies that address the impact of social determinants of health on mental illness and investigate underlying causes that contribute to disparities in treatment and diagnosis.
The Mayo Clinic supported the study but had no role in its design or research methods. The authors reported no conflicts of interest.
A study of U.S. children across ethnic and racial groups found that Asians were least likely to receive therapy for ADHD, compared with White children – who had the highest odds of getting some kind of treatment over other groups.
Other studies have identified disparity problems in ADHD diagnosis, although results have varied on inequality metrics. Few studies have looked at Asians separately, according to the study’s lead author, Yu Shi, MD, MPH. “They were usually just classified as ‘other’ or as non-White,” Dr. Shi, a consultant with the Mayo Clinic’s division of pediatric anesthesia in Rochester, Minn., said in an interview.
, and the way in which clinicians interpret behavior and apply diagnostic criteria.
“Further understanding of how treatment patterns for ADHD may differ based on race, at the time of initial diagnosis and in the early stages of treatment, may help all children receive appropriate evidence-based care,” Dr. Shi and colleagues reported in JAMA Network Open.
Researchers develop large birth cohort
Dr. Shi and colleagues hypothesized that non-Hispanic White children had a greater chance of getting diagnosed and treated within the first year of diagnosis than that of other ethnic and racial cohorts. Using administrative claims data with socioeconomic status information from a national commercial insurance warehouse, they constructed a retrospective birth cohort of children born between Jan. 1, 2006, and Dec. 31, 2012. The children had continuous insurance coverage for at least 4 years, and represented non-Hispanic Whites, Blacks, Hispanics, and Asians. Self-reporting identified the race/ethnicity groups.
Investigators analyzed ADHD diagnosis and treatment data on 238,011 children between October 2019 and December 2020, using a multivariate Cox regression model to adjust for sex, region, and household income. Primary and secondary outcomes included ADHD diagnosis as defined by recent ICD codes, ADHD behavior, and medication therapies in the clinical setting after initial diagnosis, respectively.
Whites made up most of the cohort (72.7%), followed by Hispanics (9.8%), Asians (6.7%), and Blacks (6.2%). Nearly half the population was female (48.8%). During the follow-up period with these children, 11,401, or 4.8%, had received an ADHD diagnosis. Mean age of diagnosis was 6.5 years, and overall incidence of ADHD was 69 per 10,000 person years (95% confidence interval, 68-70).
Pediatricians were most likely to make an ADHD diagnosis, although the study cited other clinicians, such as psychiatrists, neurologists, psychologists, and family practice clinicians, as responsible for these decisions.
Children diagnosed with ADHD had more years of coverage in the data set, and were more likely to be White and male. The Southern census region had a higher representation of diagnoses (50.6%) than did the Northeast region (11.8%).
Asians at highest odds for no treatment
Taking a closer look at race and ethnicity, Whites had the highest cumulative incidence of ADHD (14.19%), versus Asian children, who had lowest incidence (6.08%). “The curves for Black and Hispanic children were similar in shape and slightly lower than that for White children,” reported the investigators.
White children had higher odds of receiving some kind of treatment, compared with the other groups.
Incidence of medication treatment was lower among Asians and Hispanics. In a striking finding, Asians were most likely to receive no treatment at all (odds ratio compared with White children, 0.54; 95% confidence interval, 0.42-0.70). “However, the percentage of Asian children receiving psychotherapy was not significantly lower than other groups, which is different than a 2013 study finding that Asian children with ADHD were less likely to use mental health services,” they noted.
Most of the patients received medication (32.4%) in the first year after diagnosis, whereas (19.4%) received behavioral therapy only. Nineteen percent had both. More than 29% of these cases had no claims associated with either treatment. Among school-aged children, 65.5% were prescribed medications, compared with just 14.4% who received therapy. Twenty percent had no treatment.
Diagnosis with another disorder often preceded ADHD diagnosis. Results varied among racial groups. White children were more likely than were Black children to be diagnosed with an anxiety or adjustment disorder. Relative to White children, Asians were more likely to be diagnosed with autism spectrum disorder, speech sound disorders, or unspecified neurodevelopmental disorders. Even after an ADHD diagnosis, clinicians were more likely to diagnose Asian children with autism.
Parents may influence treatment decisions
Parental views and preferences may explain some of the variations in diagnosis and treatment among the racial/ethnic groups.
“In order for a diagnosis of ADHD to happen, a parent has first to recognize a problem and bring a child for clinical evaluation,” said Dr. Shi. “A certain behavior could be viewed as normal or a problem depending on a person’s cultural or racial background.” It’s unclear whether clinicians played any role in diagnosis disparities, he added. Patients’ concerns about racism might also influence the desire to get treated in health care systems.
Overall, the findings underscore the presence of racial and ethnic disparities in ADHD diagnosis and treatment. Future research should explore the underlying mechanisms, Dr. Shi suggested. While he and his colleagues have no immediate plans to do another ADHD study, “we’re planning on research to understand disparities in surgery in children,” he said.
The authors cited numerous limitations with their study. Use of ICD codes to identify cases might not have represented true clinical diagnosis, since the data were collected for billing, not research purposes. Investigators drew participants from a commercial insurance database, which did not necessarily reflect all U.S. children. The results might not represent a large number of children covered by Medicaid, for example, noted Dr. Shi. “It is more difficult to work with Medicaid data because there’s no national-level Medicaid data for research. Only state-level data is available.”
Because of other data gaps, Dr. Shi and colleagues might have underestimated the number of children in therapy.
A need for ‘culturally sensitive care’
The findings “ultimately demonstrate the need for culturally sensitive care in the diagnosis and treatment of children and adolescents,” said Tiffani L. Bell, MD, a psychiatrist in Winston-Salem, N.C., who was not involved with the study. She specializes in child and adolescent psychiatry.
The exact cause for racial disparity in diagnosis and treatment of ADHD is unknown and likely multifaceted, she continued. “It may be due to differences in the way that disruptive behaviors are interrupted based on factors such as race. This study found that Asian parents often brought their children in for evaluation for reasons other than ADHD. Concerns surrounding the stigma of mental health treatment and racism also could contribute to the disparity in diagnosis and treatment,” she said.
Dr. Bell said she hopes to see future studies that address the impact of social determinants of health on mental illness and investigate underlying causes that contribute to disparities in treatment and diagnosis.
The Mayo Clinic supported the study but had no role in its design or research methods. The authors reported no conflicts of interest.
A study of U.S. children across ethnic and racial groups found that Asians were least likely to receive therapy for ADHD, compared with White children – who had the highest odds of getting some kind of treatment over other groups.
Other studies have identified disparity problems in ADHD diagnosis, although results have varied on inequality metrics. Few studies have looked at Asians separately, according to the study’s lead author, Yu Shi, MD, MPH. “They were usually just classified as ‘other’ or as non-White,” Dr. Shi, a consultant with the Mayo Clinic’s division of pediatric anesthesia in Rochester, Minn., said in an interview.
, and the way in which clinicians interpret behavior and apply diagnostic criteria.
“Further understanding of how treatment patterns for ADHD may differ based on race, at the time of initial diagnosis and in the early stages of treatment, may help all children receive appropriate evidence-based care,” Dr. Shi and colleagues reported in JAMA Network Open.
Researchers develop large birth cohort
Dr. Shi and colleagues hypothesized that non-Hispanic White children had a greater chance of getting diagnosed and treated within the first year of diagnosis than that of other ethnic and racial cohorts. Using administrative claims data with socioeconomic status information from a national commercial insurance warehouse, they constructed a retrospective birth cohort of children born between Jan. 1, 2006, and Dec. 31, 2012. The children had continuous insurance coverage for at least 4 years, and represented non-Hispanic Whites, Blacks, Hispanics, and Asians. Self-reporting identified the race/ethnicity groups.
Investigators analyzed ADHD diagnosis and treatment data on 238,011 children between October 2019 and December 2020, using a multivariate Cox regression model to adjust for sex, region, and household income. Primary and secondary outcomes included ADHD diagnosis as defined by recent ICD codes, ADHD behavior, and medication therapies in the clinical setting after initial diagnosis, respectively.
Whites made up most of the cohort (72.7%), followed by Hispanics (9.8%), Asians (6.7%), and Blacks (6.2%). Nearly half the population was female (48.8%). During the follow-up period with these children, 11,401, or 4.8%, had received an ADHD diagnosis. Mean age of diagnosis was 6.5 years, and overall incidence of ADHD was 69 per 10,000 person years (95% confidence interval, 68-70).
Pediatricians were most likely to make an ADHD diagnosis, although the study cited other clinicians, such as psychiatrists, neurologists, psychologists, and family practice clinicians, as responsible for these decisions.
Children diagnosed with ADHD had more years of coverage in the data set, and were more likely to be White and male. The Southern census region had a higher representation of diagnoses (50.6%) than did the Northeast region (11.8%).
Asians at highest odds for no treatment
Taking a closer look at race and ethnicity, Whites had the highest cumulative incidence of ADHD (14.19%), versus Asian children, who had lowest incidence (6.08%). “The curves for Black and Hispanic children were similar in shape and slightly lower than that for White children,” reported the investigators.
White children had higher odds of receiving some kind of treatment, compared with the other groups.
Incidence of medication treatment was lower among Asians and Hispanics. In a striking finding, Asians were most likely to receive no treatment at all (odds ratio compared with White children, 0.54; 95% confidence interval, 0.42-0.70). “However, the percentage of Asian children receiving psychotherapy was not significantly lower than other groups, which is different than a 2013 study finding that Asian children with ADHD were less likely to use mental health services,” they noted.
Most of the patients received medication (32.4%) in the first year after diagnosis, whereas (19.4%) received behavioral therapy only. Nineteen percent had both. More than 29% of these cases had no claims associated with either treatment. Among school-aged children, 65.5% were prescribed medications, compared with just 14.4% who received therapy. Twenty percent had no treatment.
Diagnosis with another disorder often preceded ADHD diagnosis. Results varied among racial groups. White children were more likely than were Black children to be diagnosed with an anxiety or adjustment disorder. Relative to White children, Asians were more likely to be diagnosed with autism spectrum disorder, speech sound disorders, or unspecified neurodevelopmental disorders. Even after an ADHD diagnosis, clinicians were more likely to diagnose Asian children with autism.
Parents may influence treatment decisions
Parental views and preferences may explain some of the variations in diagnosis and treatment among the racial/ethnic groups.
“In order for a diagnosis of ADHD to happen, a parent has first to recognize a problem and bring a child for clinical evaluation,” said Dr. Shi. “A certain behavior could be viewed as normal or a problem depending on a person’s cultural or racial background.” It’s unclear whether clinicians played any role in diagnosis disparities, he added. Patients’ concerns about racism might also influence the desire to get treated in health care systems.
Overall, the findings underscore the presence of racial and ethnic disparities in ADHD diagnosis and treatment. Future research should explore the underlying mechanisms, Dr. Shi suggested. While he and his colleagues have no immediate plans to do another ADHD study, “we’re planning on research to understand disparities in surgery in children,” he said.
The authors cited numerous limitations with their study. Use of ICD codes to identify cases might not have represented true clinical diagnosis, since the data were collected for billing, not research purposes. Investigators drew participants from a commercial insurance database, which did not necessarily reflect all U.S. children. The results might not represent a large number of children covered by Medicaid, for example, noted Dr. Shi. “It is more difficult to work with Medicaid data because there’s no national-level Medicaid data for research. Only state-level data is available.”
Because of other data gaps, Dr. Shi and colleagues might have underestimated the number of children in therapy.
A need for ‘culturally sensitive care’
The findings “ultimately demonstrate the need for culturally sensitive care in the diagnosis and treatment of children and adolescents,” said Tiffani L. Bell, MD, a psychiatrist in Winston-Salem, N.C., who was not involved with the study. She specializes in child and adolescent psychiatry.
The exact cause for racial disparity in diagnosis and treatment of ADHD is unknown and likely multifaceted, she continued. “It may be due to differences in the way that disruptive behaviors are interrupted based on factors such as race. This study found that Asian parents often brought their children in for evaluation for reasons other than ADHD. Concerns surrounding the stigma of mental health treatment and racism also could contribute to the disparity in diagnosis and treatment,” she said.
Dr. Bell said she hopes to see future studies that address the impact of social determinants of health on mental illness and investigate underlying causes that contribute to disparities in treatment and diagnosis.
The Mayo Clinic supported the study but had no role in its design or research methods. The authors reported no conflicts of interest.
FROM JAMA NETWORK OPEN
Chauvin guilty verdict: Now it’s time to get to work
On Tuesday, April 20, the country braced for the impact of the trial verdict in death of George Floyd. Despite the case having what many would consider an overwhelming amount of evidence pointing toward conviction, if we’re completely honest, the country – and particularly the African American community – had significant doubts that the jury would render a guilty verdict.

In the hour leading up to the announcement, people and images dominated my thoughts; Tamir Rice, Breonna Taylor, Eric Garner, Rashard Brooks, and most recently, Daunte Wright. With the deaths of these Black Americans and many others as historical context, I took a stoic stance and held my breath as the verdict was read. Former Minneapolis Police Officer Derek Chauvin was found guilty of second-degree murder, third-degree murder, and second-degree manslaughter.
As Mr. Chauvin was remanded to custody and led away in handcuffs, it was clear there were no “winners” in this verdict. Mr. Floyd is still dead, and violent encounters experienced by Black Americans continue at a vastly disproportionate rate. The result is far from true justice, but what we as a country do have is a moment of accountability – and perhaps an opportunity for true system-level reform.
The final report of the President’s Task Force on 21st Century Policing, released in May 2015, recommended major policy changes at the federal level and developed key pillars aimed at promoting effective crime reduction while building public trust. Based on this report, four key takeaways are relevant to any discussion of police reform. All are vitally important, but two stand out as particularly relevant in the aftermath of the verdict. One of the key recommendations was “embracing a guardian – rather than a warrior mindset” in an effort to build trust and legitimacy. Another was ensuring that “peace officer and standards training (POST) boards include mandatory Crisis Intervention Training.”
As health professionals, we know that the ultimate effectiveness of any intervention is based upon the amount of shared trust and collaboration in the patient-physician relationship. As a consultation-liaison psychiatrist, I’ve been trained to recognize that, when requested to consult on a case, I’m frequently not making a medical diagnosis or delivering an intervention; I’m helping the team and patient reestablish trust in each other. Communication skills and techniques help start a dialogue, but you will ultimately fall short of shared understanding without trust. The underpinning of trust could begin with a commitment to procedural justice. Procedural justice, as described in The Justice Collaboratory of Yale Law School, “speaks to the idea of fair processes and how the quality of their experiences strongly impacts people’s perception of fairness.” There are four central tenets of procedural justice:
- Whether they were treated with dignity and respect.
- Whether they were given voice.
- Whether the decision-maker was neutral and transparent.
- Whether the decision-maker conveyed trustworthy motives.
These four tenets have been researched and shown to improve the trust and confidence a community has in police, and lay the foundation for creating a standard set of shared interests and values.

As health professionals, there are many aspects of procedural justice that we can and should embrace, particularly as we come to our reckoning with the use of restraints in medical settings.
Building on the work of the Task Force on 21st Century Policing, the National Initiative for Building Community Trust and Justice, from January 2015 through December 2018, implemented a six-city intervention aimed at generating measurable improvements in officer behavior, public safety, and community trust in police. The National Initiative was organized around three principal ideas: procedural justice, implicit bias training, and reconciliation and candid conversations about law enforcement’s historic role in racial tensions.
In addition to the recommendations of the federal government and independent institutions, national-level health policy organizations have made clear statements regarding police brutality and the need for systemic reform to address police brutality and systemic racism. In 2018, the American Psychiatric Association released a position statement on Police Brutality and Black Males. This was then followed in 2020 with a joint statement from the National Medical Association and the APA condemning systemic racism and police violence against Black Americans. Other health policy associations, including the American Medical Association and the American Association of Medical Colleges, have made clear statements condemning systemic racism and police brutality.
In the aftermath of the verdict, we also saw something very different. In our partisan country, there appeared to be uniform common ground. Statements were made acknowledging the importance of this historic moment, from police unions, and both political parties, and various invested grassroots organizations. In short, we may have true agreement and motivation to take the next hard steps in police reform for this country. There will be policy discussions and new mandates for training, and certainly a push to ban the use of lethal techniques, such as choke holds. While helpful, these will ultimately fall short unless we hold ourselves accountable for a true culture change.
The challenge of implementing procedural justice shouldn’t be just a law enforcement challenge, and it shouldn’t fall on the shoulders of communities with high crime areas. In other words, no single racial group should own it. Ultimately, procedural justice will need to be embraced by all of us.
On April 20, as I watched the verdict, my oldest daughter watched with me, and she asked, “What do you think, Dad?” I responded: “It’s accountability and an opportunity.” She nodded her head with resolve. She then grabbed her smartphone and jumped into social media and proclaimed in her very knowledgeable teenage voice, “See Dad, one voice is cool, but many voices in unison is better; time to get to work!” To Darnella Frazier, who captured the crime on video at age 17, and all in your generation who dare to hold us accountable, I salute you. I thank you for forcing us to look even when it was painful and not ignore the humanity of our fellow man. It is indeed time to get to work.
Dr. Norris is associate dean of student affairs and administration at George Washington University, Washington. He has no disclosures.
On Tuesday, April 20, the country braced for the impact of the trial verdict in death of George Floyd. Despite the case having what many would consider an overwhelming amount of evidence pointing toward conviction, if we’re completely honest, the country – and particularly the African American community – had significant doubts that the jury would render a guilty verdict.
In the hour leading up to the announcement, people and images dominated my thoughts; Tamir Rice, Breonna Taylor, Eric Garner, Rashard Brooks, and most recently, Daunte Wright. With the deaths of these Black Americans and many others as historical context, I took a stoic stance and held my breath as the verdict was read. Former Minneapolis Police Officer Derek Chauvin was found guilty of second-degree murder, third-degree murder, and second-degree manslaughter.
As Mr. Chauvin was remanded to custody and led away in handcuffs, it was clear there were no “winners” in this verdict. Mr. Floyd is still dead, and violent encounters experienced by Black Americans continue at a vastly disproportionate rate. The result is far from true justice, but what we as a country do have is a moment of accountability – and perhaps an opportunity for true system-level reform.
The final report of the President’s Task Force on 21st Century Policing, released in May 2015, recommended major policy changes at the federal level and developed key pillars aimed at promoting effective crime reduction while building public trust. Based on this report, four key takeaways are relevant to any discussion of police reform. All are vitally important, but two stand out as particularly relevant in the aftermath of the verdict. One of the key recommendations was “embracing a guardian – rather than a warrior mindset” in an effort to build trust and legitimacy. Another was ensuring that “peace officer and standards training (POST) boards include mandatory Crisis Intervention Training.”
As health professionals, we know that the ultimate effectiveness of any intervention is based upon the amount of shared trust and collaboration in the patient-physician relationship. As a consultation-liaison psychiatrist, I’ve been trained to recognize that, when requested to consult on a case, I’m frequently not making a medical diagnosis or delivering an intervention; I’m helping the team and patient reestablish trust in each other. Communication skills and techniques help start a dialogue, but you will ultimately fall short of shared understanding without trust. The underpinning of trust could begin with a commitment to procedural justice. Procedural justice, as described in The Justice Collaboratory of Yale Law School, “speaks to the idea of fair processes and how the quality of their experiences strongly impacts people’s perception of fairness.” There are four central tenets of procedural justice:
- Whether they were treated with dignity and respect.
- Whether they were given voice.
- Whether the decision-maker was neutral and transparent.
- Whether the decision-maker conveyed trustworthy motives.
These four tenets have been researched and shown to improve the trust and confidence a community has in police, and lay the foundation for creating a standard set of shared interests and values.
As health professionals, there are many aspects of procedural justice that we can and should embrace, particularly as we come to our reckoning with the use of restraints in medical settings.
Building on the work of the Task Force on 21st Century Policing, the National Initiative for Building Community Trust and Justice, from January 2015 through December 2018, implemented a six-city intervention aimed at generating measurable improvements in officer behavior, public safety, and community trust in police. The National Initiative was organized around three principal ideas: procedural justice, implicit bias training, and reconciliation and candid conversations about law enforcement’s historic role in racial tensions.
In addition to the recommendations of the federal government and independent institutions, national-level health policy organizations have made clear statements regarding police brutality and the need for systemic reform to address police brutality and systemic racism. In 2018, the American Psychiatric Association released a position statement on Police Brutality and Black Males. This was then followed in 2020 with a joint statement from the National Medical Association and the APA condemning systemic racism and police violence against Black Americans. Other health policy associations, including the American Medical Association and the American Association of Medical Colleges, have made clear statements condemning systemic racism and police brutality.
In the aftermath of the verdict, we also saw something very different. In our partisan country, there appeared to be uniform common ground. Statements were made acknowledging the importance of this historic moment, from police unions, and both political parties, and various invested grassroots organizations. In short, we may have true agreement and motivation to take the next hard steps in police reform for this country. There will be policy discussions and new mandates for training, and certainly a push to ban the use of lethal techniques, such as choke holds. While helpful, these will ultimately fall short unless we hold ourselves accountable for a true culture change.
The challenge of implementing procedural justice shouldn’t be just a law enforcement challenge, and it shouldn’t fall on the shoulders of communities with high crime areas. In other words, no single racial group should own it. Ultimately, procedural justice will need to be embraced by all of us.
On April 20, as I watched the verdict, my oldest daughter watched with me, and she asked, “What do you think, Dad?” I responded: “It’s accountability and an opportunity.” She nodded her head with resolve. She then grabbed her smartphone and jumped into social media and proclaimed in her very knowledgeable teenage voice, “See Dad, one voice is cool, but many voices in unison is better; time to get to work!” To Darnella Frazier, who captured the crime on video at age 17, and all in your generation who dare to hold us accountable, I salute you. I thank you for forcing us to look even when it was painful and not ignore the humanity of our fellow man. It is indeed time to get to work.
Dr. Norris is associate dean of student affairs and administration at George Washington University, Washington. He has no disclosures.
On Tuesday, April 20, the country braced for the impact of the trial verdict in death of George Floyd. Despite the case having what many would consider an overwhelming amount of evidence pointing toward conviction, if we’re completely honest, the country – and particularly the African American community – had significant doubts that the jury would render a guilty verdict.
In the hour leading up to the announcement, people and images dominated my thoughts; Tamir Rice, Breonna Taylor, Eric Garner, Rashard Brooks, and most recently, Daunte Wright. With the deaths of these Black Americans and many others as historical context, I took a stoic stance and held my breath as the verdict was read. Former Minneapolis Police Officer Derek Chauvin was found guilty of second-degree murder, third-degree murder, and second-degree manslaughter.
As Mr. Chauvin was remanded to custody and led away in handcuffs, it was clear there were no “winners” in this verdict. Mr. Floyd is still dead, and violent encounters experienced by Black Americans continue at a vastly disproportionate rate. The result is far from true justice, but what we as a country do have is a moment of accountability – and perhaps an opportunity for true system-level reform.
The final report of the President’s Task Force on 21st Century Policing, released in May 2015, recommended major policy changes at the federal level and developed key pillars aimed at promoting effective crime reduction while building public trust. Based on this report, four key takeaways are relevant to any discussion of police reform. All are vitally important, but two stand out as particularly relevant in the aftermath of the verdict. One of the key recommendations was “embracing a guardian – rather than a warrior mindset” in an effort to build trust and legitimacy. Another was ensuring that “peace officer and standards training (POST) boards include mandatory Crisis Intervention Training.”
As health professionals, we know that the ultimate effectiveness of any intervention is based upon the amount of shared trust and collaboration in the patient-physician relationship. As a consultation-liaison psychiatrist, I’ve been trained to recognize that, when requested to consult on a case, I’m frequently not making a medical diagnosis or delivering an intervention; I’m helping the team and patient reestablish trust in each other. Communication skills and techniques help start a dialogue, but you will ultimately fall short of shared understanding without trust. The underpinning of trust could begin with a commitment to procedural justice. Procedural justice, as described in The Justice Collaboratory of Yale Law School, “speaks to the idea of fair processes and how the quality of their experiences strongly impacts people’s perception of fairness.” There are four central tenets of procedural justice:
- Whether they were treated with dignity and respect.
- Whether they were given voice.
- Whether the decision-maker was neutral and transparent.
- Whether the decision-maker conveyed trustworthy motives.
These four tenets have been researched and shown to improve the trust and confidence a community has in police, and lay the foundation for creating a standard set of shared interests and values.
As health professionals, there are many aspects of procedural justice that we can and should embrace, particularly as we come to our reckoning with the use of restraints in medical settings.
Building on the work of the Task Force on 21st Century Policing, the National Initiative for Building Community Trust and Justice, from January 2015 through December 2018, implemented a six-city intervention aimed at generating measurable improvements in officer behavior, public safety, and community trust in police. The National Initiative was organized around three principal ideas: procedural justice, implicit bias training, and reconciliation and candid conversations about law enforcement’s historic role in racial tensions.
In addition to the recommendations of the federal government and independent institutions, national-level health policy organizations have made clear statements regarding police brutality and the need for systemic reform to address police brutality and systemic racism. In 2018, the American Psychiatric Association released a position statement on Police Brutality and Black Males. This was then followed in 2020 with a joint statement from the National Medical Association and the APA condemning systemic racism and police violence against Black Americans. Other health policy associations, including the American Medical Association and the American Association of Medical Colleges, have made clear statements condemning systemic racism and police brutality.
In the aftermath of the verdict, we also saw something very different. In our partisan country, there appeared to be uniform common ground. Statements were made acknowledging the importance of this historic moment, from police unions, and both political parties, and various invested grassroots organizations. In short, we may have true agreement and motivation to take the next hard steps in police reform for this country. There will be policy discussions and new mandates for training, and certainly a push to ban the use of lethal techniques, such as choke holds. While helpful, these will ultimately fall short unless we hold ourselves accountable for a true culture change.
The challenge of implementing procedural justice shouldn’t be just a law enforcement challenge, and it shouldn’t fall on the shoulders of communities with high crime areas. In other words, no single racial group should own it. Ultimately, procedural justice will need to be embraced by all of us.
On April 20, as I watched the verdict, my oldest daughter watched with me, and she asked, “What do you think, Dad?” I responded: “It’s accountability and an opportunity.” She nodded her head with resolve. She then grabbed her smartphone and jumped into social media and proclaimed in her very knowledgeable teenage voice, “See Dad, one voice is cool, but many voices in unison is better; time to get to work!” To Darnella Frazier, who captured the crime on video at age 17, and all in your generation who dare to hold us accountable, I salute you. I thank you for forcing us to look even when it was painful and not ignore the humanity of our fellow man. It is indeed time to get to work.
Dr. Norris is associate dean of student affairs and administration at George Washington University, Washington. He has no disclosures.

Psilocybin matches SSRI for moderate to severe depression in phase 2 study
The psychedelic drug psilocybin performed just as well as a widely used antidepressant in easing the symptoms of major depression, and outperformed the selective serotonin reuptake inhibitor on a range of secondary measures, results of a small-scale, phase 2 study show.

In a 6-week trial that included 59 patients with moderate to severe depression, there was no significant difference between the impact of high-dose psilocybin on the study’s primary yardstick – the 16-item Quick Inventory of Depressive Symptomatology–Self-Report – and that of the SSRI escitalopram.
Patients in the psilocybin cohort did show a much more rapid improvement in the main measure than those taking escitalopram, but this gap narrowed over the span of the trial until it was no longer statistically significant.
“It’s very clear that psilocybin therapy has a faster antidepressant onset than escitalopram. And psilocybin was consistently superior on the ancillary outcomes, but it wasn’t different on the primary,” the study’s lead author Robin Carhart-Harris, PhD, head of the Centre for Psychedelic Research at Imperial College London, told reporters attending a news briefing.
Results of the phase 2, double-blind, randomized study were published online April 15, 2021, in the New England Journal of Medicine.
Secondary outcomes
Investigators found that psilocybin bested escitalopram in several secondary outcomes, including feelings of well-being, the ability to express emotion, and social functioning.

Still, Larger and longer trials are required.
“But the secondaries were highly suggestive – tantalizingly suggestive – of the potential superiority of psilocybin therapy to treat not just depression, but these ancillary symptoms,” Dr. Carhart-Harris said.
After they were selected from 1000 screening calls, the 59 patients were randomly assigned to receive psilocybin and 29 patients to receive escitalopram. Every procedure was mirrored in both groups.
At the 2 “dosing days” scheduled during the 6-week trial, all patients received an oral dose of psilocybin in a clinical setting. However, the escitalopram group received 1 mg versus 25 mg for the psilocybin group.
“And the reason why we did that is because we can standardize expectation. We say to everyone, you will receive psilocybin. It’s just the dosage might differ,” Dr. Carhart-Harris said.
He conceded that most patients – though not all – were able to determine which group they were in following the first dosing day based on the drugs’ effects.
Supportive therapy
Following the oral dose, volunteers would spend 6 hours reclining on a bed, surrounded by pillows and a curated selection of music and supported by two “guides” or therapists. The guides were on hand to support patients through their psychedelic experience but did not chat or otherwise interfere.
The next day, patients attended a session with their two therapists to talk through their experiences.
Between dosing days, patients in the high-dose psilocybin group would take daily capsules containing a placebo. The low-dose group received a course of escitalopram.
The incidence of adverse effects was similar in each group. None was serious.
The study’s principal investigator David Nutt, DM, FRCP, FRCPsych, FSB, FMedSci, the Edmond J. Safra Chair in Neuropsychopharmacology at Imperial College London, said that many patients in the psilocybin group reported revelatory insights during dosing days.
“Very often, for the first time, people have actually come to understand why they’re depressed,” he said.
The word psychedelic, coined in 1957 by psychiatrist Humphry Osmond, derives from the Greek words “psyche,” which means “soul” or “mind,” and “delos,” which means “reveal.”
'Profound experiences'
Certainly, patients in the psilocybin group received enough of the compound to induce what Dr. Carhart-Harris called “very profound experiences.”
The researchers said that the results, while promising, should not encourage anyone to self-medicate with psychedelic substances, which are still illegal in most jurisdictions.
“I view this very much – and I think most colleagues do as well – as a combination treatment,” Dr. Carhart-Harris said. “And we strongly believe that the psychotherapy component is as important as the drug action.”
He said the study was inspired by his earlier research into the effects of psilocybin on brain function along with a small open-label trial of the compound’s effects on treatment-resistant depression published in The Lancet Psychiatry in July 2016.
The team stressed that the cohort and the absence of an entirely placebo group limit conclusions that can be drawn about either treatment.
Dr. Carhart-Harris also said he would have liked a more diverse group of patients. Participants were mostly White and mostly male, with a mean age of 41, and a high educational attainment. Of the 59 enrolled, only 34% were women.
Volunteers underwent functional MRI scans at the start and end of the trial. The team will now analyze these results to gain insight into impact on brain function and will gather and assess follow-up data. They also plan a trial examining the effect of psilocybin on anorexia.
“I think it’s fair to say the results signal hope that we may be looking at a promising alternative treatment for depression,” Dr. Carhart-Harris said. “It’s often said that we need novel treatments to treat depression because too many new drugs are what [are] sometimes called ‘me too’ drugs: They work in the same way as drugs that have preceded them. Psilocybin therapy seems to work fundamentally in a different way to SSRIs.”
Unanswered questions
In an accompanying editorial, Jeffrey A. Lieberman, MD, Lawrence C. Kolb Professor and chairman of the department of psychiatry at Columbia University, New York, warned that there remain many unanswered questions about using psychedelics for medical purposes.
They were considered potential miracle cures for a range of mental disorders in the 1960s, only to be banned in 1970s America because of “the perceived dangers and corrosive effects” on society, he wrote.
“The Carhart-Harris study notwithstanding, we are still awaiting definitive proof of the therapeutic efficacy of psychedelics and their capacity to improve the human condition,” Dr. Lieberman wrote. “Should the mind-bending properties of the psychedelics prove to be the panacea their proponents professed, informed consent and safety standards must be established. How do we explain mystical, ineffable, and potentially transformative experiences to patients, particularly if they are in a vulnerable state of mind? What is their potential for addiction?”
David Owens, MD, PhD, professor emeritus of clinical psychiatry at the University of Edinburgh, described Lieberman’s comments as “spot on.”
“This is a small, exploratory study with numbers too small to analyze fully,” he said. “The population is not recruited randomly from, for example, consecutive admissions or presentations, and screening of volunteers was by telephone, not face to face. One might say this is an ‘interested’ population, willing to go for novel approaches and with no placebo group, the extent of the placebo response cannot be assessed.”
The study was funded by the Alexander Mosley Charitable Trust and the founders of the Centre for Psychedelic Research. Infrastructure support was provided by the National Institute for Health Research Imperial Biomedical Research Centre and NIHR Imperial Clinical Research Facility.
A version of this article first appeared on Medscape.com.
The psychedelic drug psilocybin performed just as well as a widely used antidepressant in easing the symptoms of major depression, and outperformed the selective serotonin reuptake inhibitor on a range of secondary measures, results of a small-scale, phase 2 study show.
In a 6-week trial that included 59 patients with moderate to severe depression, there was no significant difference between the impact of high-dose psilocybin on the study’s primary yardstick – the 16-item Quick Inventory of Depressive Symptomatology–Self-Report – and that of the SSRI escitalopram.
Patients in the psilocybin cohort did show a much more rapid improvement in the main measure than those taking escitalopram, but this gap narrowed over the span of the trial until it was no longer statistically significant.
“It’s very clear that psilocybin therapy has a faster antidepressant onset than escitalopram. And psilocybin was consistently superior on the ancillary outcomes, but it wasn’t different on the primary,” the study’s lead author Robin Carhart-Harris, PhD, head of the Centre for Psychedelic Research at Imperial College London, told reporters attending a news briefing.
Results of the phase 2, double-blind, randomized study were published online April 15, 2021, in the New England Journal of Medicine.
Secondary outcomes
Investigators found that psilocybin bested escitalopram in several secondary outcomes, including feelings of well-being, the ability to express emotion, and social functioning.
Still, Larger and longer trials are required.
“But the secondaries were highly suggestive – tantalizingly suggestive – of the potential superiority of psilocybin therapy to treat not just depression, but these ancillary symptoms,” Dr. Carhart-Harris said.
After they were selected from 1000 screening calls, the 59 patients were randomly assigned to receive psilocybin and 29 patients to receive escitalopram. Every procedure was mirrored in both groups.
At the 2 “dosing days” scheduled during the 6-week trial, all patients received an oral dose of psilocybin in a clinical setting. However, the escitalopram group received 1 mg versus 25 mg for the psilocybin group.
“And the reason why we did that is because we can standardize expectation. We say to everyone, you will receive psilocybin. It’s just the dosage might differ,” Dr. Carhart-Harris said.
He conceded that most patients – though not all – were able to determine which group they were in following the first dosing day based on the drugs’ effects.
Supportive therapy
Following the oral dose, volunteers would spend 6 hours reclining on a bed, surrounded by pillows and a curated selection of music and supported by two “guides” or therapists. The guides were on hand to support patients through their psychedelic experience but did not chat or otherwise interfere.
The next day, patients attended a session with their two therapists to talk through their experiences.
Between dosing days, patients in the high-dose psilocybin group would take daily capsules containing a placebo. The low-dose group received a course of escitalopram.
The incidence of adverse effects was similar in each group. None was serious.
The study’s principal investigator David Nutt, DM, FRCP, FRCPsych, FSB, FMedSci, the Edmond J. Safra Chair in Neuropsychopharmacology at Imperial College London, said that many patients in the psilocybin group reported revelatory insights during dosing days.
“Very often, for the first time, people have actually come to understand why they’re depressed,” he said.
The word psychedelic, coined in 1957 by psychiatrist Humphry Osmond, derives from the Greek words “psyche,” which means “soul” or “mind,” and “delos,” which means “reveal.”
'Profound experiences'
Certainly, patients in the psilocybin group received enough of the compound to induce what Dr. Carhart-Harris called “very profound experiences.”
The researchers said that the results, while promising, should not encourage anyone to self-medicate with psychedelic substances, which are still illegal in most jurisdictions.
“I view this very much – and I think most colleagues do as well – as a combination treatment,” Dr. Carhart-Harris said. “And we strongly believe that the psychotherapy component is as important as the drug action.”
He said the study was inspired by his earlier research into the effects of psilocybin on brain function along with a small open-label trial of the compound’s effects on treatment-resistant depression published in The Lancet Psychiatry in July 2016.
The team stressed that the cohort and the absence of an entirely placebo group limit conclusions that can be drawn about either treatment.
Dr. Carhart-Harris also said he would have liked a more diverse group of patients. Participants were mostly White and mostly male, with a mean age of 41, and a high educational attainment. Of the 59 enrolled, only 34% were women.
Volunteers underwent functional MRI scans at the start and end of the trial. The team will now analyze these results to gain insight into impact on brain function and will gather and assess follow-up data. They also plan a trial examining the effect of psilocybin on anorexia.
“I think it’s fair to say the results signal hope that we may be looking at a promising alternative treatment for depression,” Dr. Carhart-Harris said. “It’s often said that we need novel treatments to treat depression because too many new drugs are what [are] sometimes called ‘me too’ drugs: They work in the same way as drugs that have preceded them. Psilocybin therapy seems to work fundamentally in a different way to SSRIs.”
Unanswered questions
In an accompanying editorial, Jeffrey A. Lieberman, MD, Lawrence C. Kolb Professor and chairman of the department of psychiatry at Columbia University, New York, warned that there remain many unanswered questions about using psychedelics for medical purposes.
They were considered potential miracle cures for a range of mental disorders in the 1960s, only to be banned in 1970s America because of “the perceived dangers and corrosive effects” on society, he wrote.
“The Carhart-Harris study notwithstanding, we are still awaiting definitive proof of the therapeutic efficacy of psychedelics and their capacity to improve the human condition,” Dr. Lieberman wrote. “Should the mind-bending properties of the psychedelics prove to be the panacea their proponents professed, informed consent and safety standards must be established. How do we explain mystical, ineffable, and potentially transformative experiences to patients, particularly if they are in a vulnerable state of mind? What is their potential for addiction?”
David Owens, MD, PhD, professor emeritus of clinical psychiatry at the University of Edinburgh, described Lieberman’s comments as “spot on.”
“This is a small, exploratory study with numbers too small to analyze fully,” he said. “The population is not recruited randomly from, for example, consecutive admissions or presentations, and screening of volunteers was by telephone, not face to face. One might say this is an ‘interested’ population, willing to go for novel approaches and with no placebo group, the extent of the placebo response cannot be assessed.”
The study was funded by the Alexander Mosley Charitable Trust and the founders of the Centre for Psychedelic Research. Infrastructure support was provided by the National Institute for Health Research Imperial Biomedical Research Centre and NIHR Imperial Clinical Research Facility.
A version of this article first appeared on Medscape.com.
The psychedelic drug psilocybin performed just as well as a widely used antidepressant in easing the symptoms of major depression, and outperformed the selective serotonin reuptake inhibitor on a range of secondary measures, results of a small-scale, phase 2 study show.
In a 6-week trial that included 59 patients with moderate to severe depression, there was no significant difference between the impact of high-dose psilocybin on the study’s primary yardstick – the 16-item Quick Inventory of Depressive Symptomatology–Self-Report – and that of the SSRI escitalopram.
Patients in the psilocybin cohort did show a much more rapid improvement in the main measure than those taking escitalopram, but this gap narrowed over the span of the trial until it was no longer statistically significant.
“It’s very clear that psilocybin therapy has a faster antidepressant onset than escitalopram. And psilocybin was consistently superior on the ancillary outcomes, but it wasn’t different on the primary,” the study’s lead author Robin Carhart-Harris, PhD, head of the Centre for Psychedelic Research at Imperial College London, told reporters attending a news briefing.
Results of the phase 2, double-blind, randomized study were published online April 15, 2021, in the New England Journal of Medicine.
Secondary outcomes
Investigators found that psilocybin bested escitalopram in several secondary outcomes, including feelings of well-being, the ability to express emotion, and social functioning.
Still, Larger and longer trials are required.
“But the secondaries were highly suggestive – tantalizingly suggestive – of the potential superiority of psilocybin therapy to treat not just depression, but these ancillary symptoms,” Dr. Carhart-Harris said.
After they were selected from 1000 screening calls, the 59 patients were randomly assigned to receive psilocybin and 29 patients to receive escitalopram. Every procedure was mirrored in both groups.
At the 2 “dosing days” scheduled during the 6-week trial, all patients received an oral dose of psilocybin in a clinical setting. However, the escitalopram group received 1 mg versus 25 mg for the psilocybin group.
“And the reason why we did that is because we can standardize expectation. We say to everyone, you will receive psilocybin. It’s just the dosage might differ,” Dr. Carhart-Harris said.
He conceded that most patients – though not all – were able to determine which group they were in following the first dosing day based on the drugs’ effects.
Supportive therapy
Following the oral dose, volunteers would spend 6 hours reclining on a bed, surrounded by pillows and a curated selection of music and supported by two “guides” or therapists. The guides were on hand to support patients through their psychedelic experience but did not chat or otherwise interfere.
The next day, patients attended a session with their two therapists to talk through their experiences.
Between dosing days, patients in the high-dose psilocybin group would take daily capsules containing a placebo. The low-dose group received a course of escitalopram.
The incidence of adverse effects was similar in each group. None was serious.
The study’s principal investigator David Nutt, DM, FRCP, FRCPsych, FSB, FMedSci, the Edmond J. Safra Chair in Neuropsychopharmacology at Imperial College London, said that many patients in the psilocybin group reported revelatory insights during dosing days.
“Very often, for the first time, people have actually come to understand why they’re depressed,” he said.
The word psychedelic, coined in 1957 by psychiatrist Humphry Osmond, derives from the Greek words “psyche,” which means “soul” or “mind,” and “delos,” which means “reveal.”
'Profound experiences'
Certainly, patients in the psilocybin group received enough of the compound to induce what Dr. Carhart-Harris called “very profound experiences.”
The researchers said that the results, while promising, should not encourage anyone to self-medicate with psychedelic substances, which are still illegal in most jurisdictions.
“I view this very much – and I think most colleagues do as well – as a combination treatment,” Dr. Carhart-Harris said. “And we strongly believe that the psychotherapy component is as important as the drug action.”
He said the study was inspired by his earlier research into the effects of psilocybin on brain function along with a small open-label trial of the compound’s effects on treatment-resistant depression published in The Lancet Psychiatry in July 2016.
The team stressed that the cohort and the absence of an entirely placebo group limit conclusions that can be drawn about either treatment.
Dr. Carhart-Harris also said he would have liked a more diverse group of patients. Participants were mostly White and mostly male, with a mean age of 41, and a high educational attainment. Of the 59 enrolled, only 34% were women.
Volunteers underwent functional MRI scans at the start and end of the trial. The team will now analyze these results to gain insight into impact on brain function and will gather and assess follow-up data. They also plan a trial examining the effect of psilocybin on anorexia.
“I think it’s fair to say the results signal hope that we may be looking at a promising alternative treatment for depression,” Dr. Carhart-Harris said. “It’s often said that we need novel treatments to treat depression because too many new drugs are what [are] sometimes called ‘me too’ drugs: They work in the same way as drugs that have preceded them. Psilocybin therapy seems to work fundamentally in a different way to SSRIs.”
Unanswered questions
In an accompanying editorial, Jeffrey A. Lieberman, MD, Lawrence C. Kolb Professor and chairman of the department of psychiatry at Columbia University, New York, warned that there remain many unanswered questions about using psychedelics for medical purposes.
They were considered potential miracle cures for a range of mental disorders in the 1960s, only to be banned in 1970s America because of “the perceived dangers and corrosive effects” on society, he wrote.
“The Carhart-Harris study notwithstanding, we are still awaiting definitive proof of the therapeutic efficacy of psychedelics and their capacity to improve the human condition,” Dr. Lieberman wrote. “Should the mind-bending properties of the psychedelics prove to be the panacea their proponents professed, informed consent and safety standards must be established. How do we explain mystical, ineffable, and potentially transformative experiences to patients, particularly if they are in a vulnerable state of mind? What is their potential for addiction?”
David Owens, MD, PhD, professor emeritus of clinical psychiatry at the University of Edinburgh, described Lieberman’s comments as “spot on.”
“This is a small, exploratory study with numbers too small to analyze fully,” he said. “The population is not recruited randomly from, for example, consecutive admissions or presentations, and screening of volunteers was by telephone, not face to face. One might say this is an ‘interested’ population, willing to go for novel approaches and with no placebo group, the extent of the placebo response cannot be assessed.”
The study was funded by the Alexander Mosley Charitable Trust and the founders of the Centre for Psychedelic Research. Infrastructure support was provided by the National Institute for Health Research Imperial Biomedical Research Centre and NIHR Imperial Clinical Research Facility.
A version of this article first appeared on Medscape.com.
PTSD linked to ischemic heart disease
A study using data from Veterans Health Administration (VHA) electronic medical records shows a significant association between posttraumatic stress disorder (PTSD) among female veterans and an increased risk for incident ischemic heart disease (IHD).
The increased risk for IHD was highest among women younger than 40 with PTSD, and among racial and ethnic minorities.
“These women have been emerging as important targets for cardiovascular prevention, and our study suggests that PTSD may be an important psychosocial risk factor for IHD in these individuals,” wrote the researchers, led by Ramin Ebrahimi, MD, department of medicine, cardiology section, Veterans Affairs Greater Los Angeles Health Care System. “With the number of women veterans growing, it is critical to appreciate the health care needs of this relatively young and diverse patient population.”
The study results also have “important implications for earlier and more aggressive IHD risk assessment, monitoring and management in vulnerable women veterans,” they added. “Indeed, our findings support recent calls for cardiovascular risk screening in younger individuals and for the need to harness a broad range of clinicians who routinely treat younger women to maximize prevention efforts.”
The article was published online in JAMA Cardiology on March 17.
Increasing number of VHA users
“As an interventional cardiologist and the director of the cardiac catheterization laboratory, I noticed a significant number of the patients referred to the cath lab carried a diagnosis of posttraumatic stress disorder,” Dr. Ebrahimi said in an interview. “This intrigued me and started my journey into trying to understand how psychiatric disorders in general, and PTSD, may impact/interact with cardiovascular disorders,” he added.
The number of female veterans in the military has been increasing, and they now make up about 10% of the 20 million American veterans; that number is projected to exceed 2.2 million in the next 20 years, the authors wrote. Female veterans are also the fastest growing group of users of the VHA, they added.
IHD is the leading cause of death in women in the United States, despite the advancements in prevention and treatment. Although women are twice as likely to develop PTSD as are men, and it is even more likely in female veterans, much of the research has predominately been on male veterans, the authors wrote.
For this retrospective study, which used data from the VHA Corporate Data Warehouse, the authors examined a cohort of female veterans who were 18 years or older who had used the VHA health care system between Jan. 1, 2000, and Dec. 31, 2017.
Of the 828,997 female veterans, 151,030 had PTSD. Women excluded from the study were those who did not have any clinical encounters after their index visit, participants who had a diagnosis of IHD at or before the index visit, and those with incident IHD within 90 days of the index visit, allowing time between a PTSD diagnosis and IHD.
Propensity score matching on age at index visit, the number of previous visits, and the presence of traditional and female-specific cardiovascular risk factors, as well as mental and physical health conditions, was conducted to identify female veterans ever diagnosed with PTSD, who were matched in a 1:2 ratio to those never diagnosed with PTSD. In all, 132,923 women with PTSD and 265,846 women without PTSD were included, and data were analyzed for the period of Oct. 1, 2018, to Oct. 30, 2020.
IHD was defined as new-onset coronary artery disease, angina, or myocardial infarction–based ICD-9 and ICD-10 diagnostic codes. Age, race, and ethnicity were self-reported.
The analytic sample consisted of relatively young female veterans (mean [SD] age at baseline, 40.1 [12.2] years) of various races (White, 57.6%; Black, 29.8%) and ethnicities, the authors reported.
Of the 9,940 women who experienced incident IHD during follow-up, 5,559 did not have PTSD (2.1% of the overall population examined) and 4,381 had PTSD (3.3%). PTSD was significantly associated with an increased risk for IHD. Over the median follow-up of 4.9 years, female veterans with PTSD had a 44% higher rate of developing incident IHD compared with the female veterans without PTSD (hazard ratio [HR], 1.44; 95% confidence interval [CI], 1.38-1.50).
In addition, those with PTSD who developed IHD were younger at diagnosis (mean [SD] age, 55.5 [9.7]) than were patients without PTSD (mean [SD] age, 57.8 [10.7]). Effect sizes were largest in the group younger than 40 years (HR, 1.72; 95% CI, 1.55-1.90) and decreased for older participants (HR for those ≥60 years, 1.24; 95% CI, 1.12-1.38)
The authors found a 49% to 66% increase in risk for IHD associated with PTSD in Black women (HR, 1.49; 95% CI, 1.38-1.62) and those identified as non-White and non-Black (HR, 1.66; 95%, 1.33-2.08).
Women of all ethnic groups with PTSD were at higher risk of developing IHD, but this was especially true for Hispanic/Latina women (HR, 1.50; 95% CI 1.22-1.84), they noted.
The authors reported some limitations to their findings. The analytic sample could result in a lower ascertainment of certain conditions, such as psychiatric disorders, they wrote. Substance disorders were low in this study, possibly because of the younger age of female veterans in the sample. Because this study used VHA electronic medical records data, medical care outside of the VHA that was not paid for by the VHA could not be considered.
In addition, although this study used a large sample of female veterans, the findings cannot be generalized to female veterans outside of the VHA system, nonveteran women, or men, the researchers wrote.
A call to action
In an accompanying comment, Beth E. Cohen, MD, of the University of California, San Francisco, and the San Francisco Veterans Affairs Health Care System, points out that the physical implications for psychosocial conditions, including depression and PTSD, have been recognized for quite some time. For example, results of the INTERHEART case-control study of 30,000 people showed stress, depression, and stressful life events accounted for one-third the population-attributable risk for myocardial infarction.
As was also noted by Dr. Ebrahimi and colleagues, much of the current research has been on male veterans, yet types of trauma differ among genders; women experience higher rates of military sexual trauma but lower rates of combat trauma, Dr. Cohen wrote. The PTSD symptoms, trajectory, and biological effects can differ for women and men, as can the pathogenesis, presentation, and outcomes of cardiovascular disease (CVD).
These findings, she said, “are an important extension of the prior literature and represent the largest study in female veterans to date. Although methods differ across studies, the magnitude of risk associated with PTSD was consistent with that found in prior studies of male veterans and nonveteran samples.”
The assessment of age-specific risk is also a strength of the study, “and has implications for clinical practice, because PTSD-associated risk was greatest in a younger group in whom CVD may be overlooked.”
Dr. Cohen addressed the limitations outlined by the authors, including ascertainment bias, severity of PTSD symptoms, and their chronicity, but added that “even in the context of these limitations, this study illustrates the importance of PTSD to the health of women veterans and the additional work needed to reduce their CVD risk.”
Clinical questions remain, she added. Screens for PTSD are widely used in the VHA, yet no studies have examined whether screening or early detection decrease CVD risk. In addition, no evidence suggests that screening for or treatment of PTSD improves cardiovascular outcomes.
“Given the challenges of answering these questions in observational studies, it will be important to incorporate measures of CVD risk and outcomes in trials of behavioral and medical therapies for patients with PTSD,” she wrote.
She added that collaborations among multidisciplinary patient care teams will be important. “The findings of this study represent a call to action for this important work to understand the cardiovascular effects of PTSD and improve the health and well-being of women veterans,” Dr. Cohen concluded.
This research was supported by Investigator-Initiated Research Award from the Department of Defense U.S. Army Medical Research and Material Command Congressionally Directed Medical Research Programs (Dr. Ebrahimi) and in part by grants from the VA Informatics and Computing Infrastructure and the Offices of Research and Development at the Northport, Durham, and Greater Los Angeles Veterans Affairs medical centers. Dr. Ebrahimi reported receiving grants from the Department of Defense during the conduct of the study. Disclosures for other authors are available in the paper. Dr. Cohen reports no disclosures.
A version of this article first appeared on Medscape.com.
A study using data from Veterans Health Administration (VHA) electronic medical records shows a significant association between posttraumatic stress disorder (PTSD) among female veterans and an increased risk for incident ischemic heart disease (IHD).
The increased risk for IHD was highest among women younger than 40 with PTSD, and among racial and ethnic minorities.
“These women have been emerging as important targets for cardiovascular prevention, and our study suggests that PTSD may be an important psychosocial risk factor for IHD in these individuals,” wrote the researchers, led by Ramin Ebrahimi, MD, department of medicine, cardiology section, Veterans Affairs Greater Los Angeles Health Care System. “With the number of women veterans growing, it is critical to appreciate the health care needs of this relatively young and diverse patient population.”
The study results also have “important implications for earlier and more aggressive IHD risk assessment, monitoring and management in vulnerable women veterans,” they added. “Indeed, our findings support recent calls for cardiovascular risk screening in younger individuals and for the need to harness a broad range of clinicians who routinely treat younger women to maximize prevention efforts.”
The article was published online in JAMA Cardiology on March 17.
Increasing number of VHA users
“As an interventional cardiologist and the director of the cardiac catheterization laboratory, I noticed a significant number of the patients referred to the cath lab carried a diagnosis of posttraumatic stress disorder,” Dr. Ebrahimi said in an interview. “This intrigued me and started my journey into trying to understand how psychiatric disorders in general, and PTSD, may impact/interact with cardiovascular disorders,” he added.
The number of female veterans in the military has been increasing, and they now make up about 10% of the 20 million American veterans; that number is projected to exceed 2.2 million in the next 20 years, the authors wrote. Female veterans are also the fastest growing group of users of the VHA, they added.
IHD is the leading cause of death in women in the United States, despite the advancements in prevention and treatment. Although women are twice as likely to develop PTSD as are men, and it is even more likely in female veterans, much of the research has predominately been on male veterans, the authors wrote.
For this retrospective study, which used data from the VHA Corporate Data Warehouse, the authors examined a cohort of female veterans who were 18 years or older who had used the VHA health care system between Jan. 1, 2000, and Dec. 31, 2017.
Of the 828,997 female veterans, 151,030 had PTSD. Women excluded from the study were those who did not have any clinical encounters after their index visit, participants who had a diagnosis of IHD at or before the index visit, and those with incident IHD within 90 days of the index visit, allowing time between a PTSD diagnosis and IHD.
Propensity score matching on age at index visit, the number of previous visits, and the presence of traditional and female-specific cardiovascular risk factors, as well as mental and physical health conditions, was conducted to identify female veterans ever diagnosed with PTSD, who were matched in a 1:2 ratio to those never diagnosed with PTSD. In all, 132,923 women with PTSD and 265,846 women without PTSD were included, and data were analyzed for the period of Oct. 1, 2018, to Oct. 30, 2020.
IHD was defined as new-onset coronary artery disease, angina, or myocardial infarction–based ICD-9 and ICD-10 diagnostic codes. Age, race, and ethnicity were self-reported.
The analytic sample consisted of relatively young female veterans (mean [SD] age at baseline, 40.1 [12.2] years) of various races (White, 57.6%; Black, 29.8%) and ethnicities, the authors reported.
Of the 9,940 women who experienced incident IHD during follow-up, 5,559 did not have PTSD (2.1% of the overall population examined) and 4,381 had PTSD (3.3%). PTSD was significantly associated with an increased risk for IHD. Over the median follow-up of 4.9 years, female veterans with PTSD had a 44% higher rate of developing incident IHD compared with the female veterans without PTSD (hazard ratio [HR], 1.44; 95% confidence interval [CI], 1.38-1.50).
In addition, those with PTSD who developed IHD were younger at diagnosis (mean [SD] age, 55.5 [9.7]) than were patients without PTSD (mean [SD] age, 57.8 [10.7]). Effect sizes were largest in the group younger than 40 years (HR, 1.72; 95% CI, 1.55-1.90) and decreased for older participants (HR for those ≥60 years, 1.24; 95% CI, 1.12-1.38)
The authors found a 49% to 66% increase in risk for IHD associated with PTSD in Black women (HR, 1.49; 95% CI, 1.38-1.62) and those identified as non-White and non-Black (HR, 1.66; 95%, 1.33-2.08).
Women of all ethnic groups with PTSD were at higher risk of developing IHD, but this was especially true for Hispanic/Latina women (HR, 1.50; 95% CI 1.22-1.84), they noted.
The authors reported some limitations to their findings. The analytic sample could result in a lower ascertainment of certain conditions, such as psychiatric disorders, they wrote. Substance disorders were low in this study, possibly because of the younger age of female veterans in the sample. Because this study used VHA electronic medical records data, medical care outside of the VHA that was not paid for by the VHA could not be considered.
In addition, although this study used a large sample of female veterans, the findings cannot be generalized to female veterans outside of the VHA system, nonveteran women, or men, the researchers wrote.
A call to action
In an accompanying comment, Beth E. Cohen, MD, of the University of California, San Francisco, and the San Francisco Veterans Affairs Health Care System, points out that the physical implications for psychosocial conditions, including depression and PTSD, have been recognized for quite some time. For example, results of the INTERHEART case-control study of 30,000 people showed stress, depression, and stressful life events accounted for one-third the population-attributable risk for myocardial infarction.
As was also noted by Dr. Ebrahimi and colleagues, much of the current research has been on male veterans, yet types of trauma differ among genders; women experience higher rates of military sexual trauma but lower rates of combat trauma, Dr. Cohen wrote. The PTSD symptoms, trajectory, and biological effects can differ for women and men, as can the pathogenesis, presentation, and outcomes of cardiovascular disease (CVD).
These findings, she said, “are an important extension of the prior literature and represent the largest study in female veterans to date. Although methods differ across studies, the magnitude of risk associated with PTSD was consistent with that found in prior studies of male veterans and nonveteran samples.”
The assessment of age-specific risk is also a strength of the study, “and has implications for clinical practice, because PTSD-associated risk was greatest in a younger group in whom CVD may be overlooked.”
Dr. Cohen addressed the limitations outlined by the authors, including ascertainment bias, severity of PTSD symptoms, and their chronicity, but added that “even in the context of these limitations, this study illustrates the importance of PTSD to the health of women veterans and the additional work needed to reduce their CVD risk.”
Clinical questions remain, she added. Screens for PTSD are widely used in the VHA, yet no studies have examined whether screening or early detection decrease CVD risk. In addition, no evidence suggests that screening for or treatment of PTSD improves cardiovascular outcomes.
“Given the challenges of answering these questions in observational studies, it will be important to incorporate measures of CVD risk and outcomes in trials of behavioral and medical therapies for patients with PTSD,” she wrote.
She added that collaborations among multidisciplinary patient care teams will be important. “The findings of this study represent a call to action for this important work to understand the cardiovascular effects of PTSD and improve the health and well-being of women veterans,” Dr. Cohen concluded.
This research was supported by Investigator-Initiated Research Award from the Department of Defense U.S. Army Medical Research and Material Command Congressionally Directed Medical Research Programs (Dr. Ebrahimi) and in part by grants from the VA Informatics and Computing Infrastructure and the Offices of Research and Development at the Northport, Durham, and Greater Los Angeles Veterans Affairs medical centers. Dr. Ebrahimi reported receiving grants from the Department of Defense during the conduct of the study. Disclosures for other authors are available in the paper. Dr. Cohen reports no disclosures.
A version of this article first appeared on Medscape.com.
A study using data from Veterans Health Administration (VHA) electronic medical records shows a significant association between posttraumatic stress disorder (PTSD) among female veterans and an increased risk for incident ischemic heart disease (IHD).
The increased risk for IHD was highest among women younger than 40 with PTSD, and among racial and ethnic minorities.
“These women have been emerging as important targets for cardiovascular prevention, and our study suggests that PTSD may be an important psychosocial risk factor for IHD in these individuals,” wrote the researchers, led by Ramin Ebrahimi, MD, department of medicine, cardiology section, Veterans Affairs Greater Los Angeles Health Care System. “With the number of women veterans growing, it is critical to appreciate the health care needs of this relatively young and diverse patient population.”
The study results also have “important implications for earlier and more aggressive IHD risk assessment, monitoring and management in vulnerable women veterans,” they added. “Indeed, our findings support recent calls for cardiovascular risk screening in younger individuals and for the need to harness a broad range of clinicians who routinely treat younger women to maximize prevention efforts.”
The article was published online in JAMA Cardiology on March 17.
Increasing number of VHA users
“As an interventional cardiologist and the director of the cardiac catheterization laboratory, I noticed a significant number of the patients referred to the cath lab carried a diagnosis of posttraumatic stress disorder,” Dr. Ebrahimi said in an interview. “This intrigued me and started my journey into trying to understand how psychiatric disorders in general, and PTSD, may impact/interact with cardiovascular disorders,” he added.
The number of female veterans in the military has been increasing, and they now make up about 10% of the 20 million American veterans; that number is projected to exceed 2.2 million in the next 20 years, the authors wrote. Female veterans are also the fastest growing group of users of the VHA, they added.
IHD is the leading cause of death in women in the United States, despite the advancements in prevention and treatment. Although women are twice as likely to develop PTSD as are men, and it is even more likely in female veterans, much of the research has predominately been on male veterans, the authors wrote.
For this retrospective study, which used data from the VHA Corporate Data Warehouse, the authors examined a cohort of female veterans who were 18 years or older who had used the VHA health care system between Jan. 1, 2000, and Dec. 31, 2017.
Of the 828,997 female veterans, 151,030 had PTSD. Women excluded from the study were those who did not have any clinical encounters after their index visit, participants who had a diagnosis of IHD at or before the index visit, and those with incident IHD within 90 days of the index visit, allowing time between a PTSD diagnosis and IHD.
Propensity score matching on age at index visit, the number of previous visits, and the presence of traditional and female-specific cardiovascular risk factors, as well as mental and physical health conditions, was conducted to identify female veterans ever diagnosed with PTSD, who were matched in a 1:2 ratio to those never diagnosed with PTSD. In all, 132,923 women with PTSD and 265,846 women without PTSD were included, and data were analyzed for the period of Oct. 1, 2018, to Oct. 30, 2020.
IHD was defined as new-onset coronary artery disease, angina, or myocardial infarction–based ICD-9 and ICD-10 diagnostic codes. Age, race, and ethnicity were self-reported.
The analytic sample consisted of relatively young female veterans (mean [SD] age at baseline, 40.1 [12.2] years) of various races (White, 57.6%; Black, 29.8%) and ethnicities, the authors reported.
Of the 9,940 women who experienced incident IHD during follow-up, 5,559 did not have PTSD (2.1% of the overall population examined) and 4,381 had PTSD (3.3%). PTSD was significantly associated with an increased risk for IHD. Over the median follow-up of 4.9 years, female veterans with PTSD had a 44% higher rate of developing incident IHD compared with the female veterans without PTSD (hazard ratio [HR], 1.44; 95% confidence interval [CI], 1.38-1.50).
In addition, those with PTSD who developed IHD were younger at diagnosis (mean [SD] age, 55.5 [9.7]) than were patients without PTSD (mean [SD] age, 57.8 [10.7]). Effect sizes were largest in the group younger than 40 years (HR, 1.72; 95% CI, 1.55-1.90) and decreased for older participants (HR for those ≥60 years, 1.24; 95% CI, 1.12-1.38)
The authors found a 49% to 66% increase in risk for IHD associated with PTSD in Black women (HR, 1.49; 95% CI, 1.38-1.62) and those identified as non-White and non-Black (HR, 1.66; 95%, 1.33-2.08).
Women of all ethnic groups with PTSD were at higher risk of developing IHD, but this was especially true for Hispanic/Latina women (HR, 1.50; 95% CI 1.22-1.84), they noted.
The authors reported some limitations to their findings. The analytic sample could result in a lower ascertainment of certain conditions, such as psychiatric disorders, they wrote. Substance disorders were low in this study, possibly because of the younger age of female veterans in the sample. Because this study used VHA electronic medical records data, medical care outside of the VHA that was not paid for by the VHA could not be considered.
In addition, although this study used a large sample of female veterans, the findings cannot be generalized to female veterans outside of the VHA system, nonveteran women, or men, the researchers wrote.
A call to action
In an accompanying comment, Beth E. Cohen, MD, of the University of California, San Francisco, and the San Francisco Veterans Affairs Health Care System, points out that the physical implications for psychosocial conditions, including depression and PTSD, have been recognized for quite some time. For example, results of the INTERHEART case-control study of 30,000 people showed stress, depression, and stressful life events accounted for one-third the population-attributable risk for myocardial infarction.
As was also noted by Dr. Ebrahimi and colleagues, much of the current research has been on male veterans, yet types of trauma differ among genders; women experience higher rates of military sexual trauma but lower rates of combat trauma, Dr. Cohen wrote. The PTSD symptoms, trajectory, and biological effects can differ for women and men, as can the pathogenesis, presentation, and outcomes of cardiovascular disease (CVD).
These findings, she said, “are an important extension of the prior literature and represent the largest study in female veterans to date. Although methods differ across studies, the magnitude of risk associated with PTSD was consistent with that found in prior studies of male veterans and nonveteran samples.”
The assessment of age-specific risk is also a strength of the study, “and has implications for clinical practice, because PTSD-associated risk was greatest in a younger group in whom CVD may be overlooked.”
Dr. Cohen addressed the limitations outlined by the authors, including ascertainment bias, severity of PTSD symptoms, and their chronicity, but added that “even in the context of these limitations, this study illustrates the importance of PTSD to the health of women veterans and the additional work needed to reduce their CVD risk.”
Clinical questions remain, she added. Screens for PTSD are widely used in the VHA, yet no studies have examined whether screening or early detection decrease CVD risk. In addition, no evidence suggests that screening for or treatment of PTSD improves cardiovascular outcomes.
“Given the challenges of answering these questions in observational studies, it will be important to incorporate measures of CVD risk and outcomes in trials of behavioral and medical therapies for patients with PTSD,” she wrote.
She added that collaborations among multidisciplinary patient care teams will be important. “The findings of this study represent a call to action for this important work to understand the cardiovascular effects of PTSD and improve the health and well-being of women veterans,” Dr. Cohen concluded.
This research was supported by Investigator-Initiated Research Award from the Department of Defense U.S. Army Medical Research and Material Command Congressionally Directed Medical Research Programs (Dr. Ebrahimi) and in part by grants from the VA Informatics and Computing Infrastructure and the Offices of Research and Development at the Northport, Durham, and Greater Los Angeles Veterans Affairs medical centers. Dr. Ebrahimi reported receiving grants from the Department of Defense during the conduct of the study. Disclosures for other authors are available in the paper. Dr. Cohen reports no disclosures.
A version of this article first appeared on Medscape.com.
Study: Spanking may change children’s brains
Rare is the parent who has never so much as thought about spanking an unruly child. But a new study provides another reason to avoid corporal punishment: Spanking may cause changes in the same areas of a child’s brain that are affected by more severe physical and sexual abuse.
Previous research has consistently found links between spanking and behavioral problems, aggression, depression, and anxiety, says Jorge Cuartas, a doctoral candidate at the Harvard Graduate School of Education and first author of the study. “We wanted to look at one potential mechanism, brain development, that might explain how corporal punishment can impact children’s behavior and cognitive development.”
The study, published in Child Development, used functional MRIs to map brain changes in 147 tweens who’d never experienced physical or sexual abuse. Researchers tracked which parts of the children’s brains activated in response to neutral or fearful facial expressions. When shown pictures of someone looking fearful, kids who reported having been spanked had a larger response in certain parts of the brain than kids who hadn’t been. Those areas drive the response to environmental cues, recognizing threats and reacting to them. If a child’s brain overreacts, behavioral challenges can result.
“We saw those changes in the same areas as more severe forms of abuse or domestic violence. It suggests the difference is of degree rather than type,” Mr. Cuartas says. As far as a child’s brain is concerned, “It’s all violence.”
It’s a significant finding because many parents don’t think of spanking as being violent, says Vincent J. Palusci, MD, a pediatrician and editor-in-chief of the journal Child Maltreatment. “We want to raise kids who are happy and healthy, and many parents who use spanking are doing it with that goal.”
Spanking in the U.S.
Around the world, 62 states and countries have outlawed corporal punishment. While the U.S. has no such protections, both the American Academy of Pediatrics and the American Psychological Association have condemned the practice. Acceptance of spanking seems to be shrinking: The percentage of parents in this country who say they spank their children is trending downward. In 1993, 50% of parents surveyed said they did, but by 2017 that number had fallen to 35%. Still far too many, Mr. Cuartas and Dr. Palusci say, but a promising trend.
“While we wouldn’t as parents want to hurt our kids,” Dr. Palusci says, “we need to understand that spanking can be just as bad as things we’d never do.”
Discipline vs. punishment
For some parents, it may require a shift in thinking, differentiating between discipline and punishment. “Discipline changes behavior – it teaches positive behavior, empathy, essential social skills. But that’s different from punishment,” Mr. Cuartas says. “That makes somebody feel pain or shame. We have to start thinking about spanking as punishment.”
That can be difficult, especially for adults who’ve been spanked themselves. They may believe that since they turned out fine, spanking must be fine, too. But the study doesn’t suggest that every child who’s spanked will have these difficulties – it just shows they happen, Mr. Cuartas says. “Compare this to smoking. We all know someone who smokes who’s healthy, but that doesn’t mean smoking is good,” he says. “Individual cases aren’t enough to understand whether certain experiences are good or bad.”
Dr. Palusci draws parallels to the advice pregnant women receive about taking medications: If it hasn’t been tested in pregnancy specifically, no amount can be considered safe. “We don’t have the studies to say how much spanking is dangerous, so we have to think that any amount has this potential.”
A version of this article first appeared on Medscape.com.
Rare is the parent who has never so much as thought about spanking an unruly child. But a new study provides another reason to avoid corporal punishment: Spanking may cause changes in the same areas of a child’s brain that are affected by more severe physical and sexual abuse.
Previous research has consistently found links between spanking and behavioral problems, aggression, depression, and anxiety, says Jorge Cuartas, a doctoral candidate at the Harvard Graduate School of Education and first author of the study. “We wanted to look at one potential mechanism, brain development, that might explain how corporal punishment can impact children’s behavior and cognitive development.”
The study, published in Child Development, used functional MRIs to map brain changes in 147 tweens who’d never experienced physical or sexual abuse. Researchers tracked which parts of the children’s brains activated in response to neutral or fearful facial expressions. When shown pictures of someone looking fearful, kids who reported having been spanked had a larger response in certain parts of the brain than kids who hadn’t been. Those areas drive the response to environmental cues, recognizing threats and reacting to them. If a child’s brain overreacts, behavioral challenges can result.
“We saw those changes in the same areas as more severe forms of abuse or domestic violence. It suggests the difference is of degree rather than type,” Mr. Cuartas says. As far as a child’s brain is concerned, “It’s all violence.”
It’s a significant finding because many parents don’t think of spanking as being violent, says Vincent J. Palusci, MD, a pediatrician and editor-in-chief of the journal Child Maltreatment. “We want to raise kids who are happy and healthy, and many parents who use spanking are doing it with that goal.”
Spanking in the U.S.
Around the world, 62 states and countries have outlawed corporal punishment. While the U.S. has no such protections, both the American Academy of Pediatrics and the American Psychological Association have condemned the practice. Acceptance of spanking seems to be shrinking: The percentage of parents in this country who say they spank their children is trending downward. In 1993, 50% of parents surveyed said they did, but by 2017 that number had fallen to 35%. Still far too many, Mr. Cuartas and Dr. Palusci say, but a promising trend.
“While we wouldn’t as parents want to hurt our kids,” Dr. Palusci says, “we need to understand that spanking can be just as bad as things we’d never do.”
Discipline vs. punishment
For some parents, it may require a shift in thinking, differentiating between discipline and punishment. “Discipline changes behavior – it teaches positive behavior, empathy, essential social skills. But that’s different from punishment,” Mr. Cuartas says. “That makes somebody feel pain or shame. We have to start thinking about spanking as punishment.”
That can be difficult, especially for adults who’ve been spanked themselves. They may believe that since they turned out fine, spanking must be fine, too. But the study doesn’t suggest that every child who’s spanked will have these difficulties – it just shows they happen, Mr. Cuartas says. “Compare this to smoking. We all know someone who smokes who’s healthy, but that doesn’t mean smoking is good,” he says. “Individual cases aren’t enough to understand whether certain experiences are good or bad.”
Dr. Palusci draws parallels to the advice pregnant women receive about taking medications: If it hasn’t been tested in pregnancy specifically, no amount can be considered safe. “We don’t have the studies to say how much spanking is dangerous, so we have to think that any amount has this potential.”
A version of this article first appeared on Medscape.com.
Rare is the parent who has never so much as thought about spanking an unruly child. But a new study provides another reason to avoid corporal punishment: Spanking may cause changes in the same areas of a child’s brain that are affected by more severe physical and sexual abuse.
Previous research has consistently found links between spanking and behavioral problems, aggression, depression, and anxiety, says Jorge Cuartas, a doctoral candidate at the Harvard Graduate School of Education and first author of the study. “We wanted to look at one potential mechanism, brain development, that might explain how corporal punishment can impact children’s behavior and cognitive development.”
The study, published in Child Development, used functional MRIs to map brain changes in 147 tweens who’d never experienced physical or sexual abuse. Researchers tracked which parts of the children’s brains activated in response to neutral or fearful facial expressions. When shown pictures of someone looking fearful, kids who reported having been spanked had a larger response in certain parts of the brain than kids who hadn’t been. Those areas drive the response to environmental cues, recognizing threats and reacting to them. If a child’s brain overreacts, behavioral challenges can result.
“We saw those changes in the same areas as more severe forms of abuse or domestic violence. It suggests the difference is of degree rather than type,” Mr. Cuartas says. As far as a child’s brain is concerned, “It’s all violence.”
It’s a significant finding because many parents don’t think of spanking as being violent, says Vincent J. Palusci, MD, a pediatrician and editor-in-chief of the journal Child Maltreatment. “We want to raise kids who are happy and healthy, and many parents who use spanking are doing it with that goal.”
Spanking in the U.S.
Around the world, 62 states and countries have outlawed corporal punishment. While the U.S. has no such protections, both the American Academy of Pediatrics and the American Psychological Association have condemned the practice. Acceptance of spanking seems to be shrinking: The percentage of parents in this country who say they spank their children is trending downward. In 1993, 50% of parents surveyed said they did, but by 2017 that number had fallen to 35%. Still far too many, Mr. Cuartas and Dr. Palusci say, but a promising trend.
“While we wouldn’t as parents want to hurt our kids,” Dr. Palusci says, “we need to understand that spanking can be just as bad as things we’d never do.”
Discipline vs. punishment
For some parents, it may require a shift in thinking, differentiating between discipline and punishment. “Discipline changes behavior – it teaches positive behavior, empathy, essential social skills. But that’s different from punishment,” Mr. Cuartas says. “That makes somebody feel pain or shame. We have to start thinking about spanking as punishment.”
That can be difficult, especially for adults who’ve been spanked themselves. They may believe that since they turned out fine, spanking must be fine, too. But the study doesn’t suggest that every child who’s spanked will have these difficulties – it just shows they happen, Mr. Cuartas says. “Compare this to smoking. We all know someone who smokes who’s healthy, but that doesn’t mean smoking is good,” he says. “Individual cases aren’t enough to understand whether certain experiences are good or bad.”
Dr. Palusci draws parallels to the advice pregnant women receive about taking medications: If it hasn’t been tested in pregnancy specifically, no amount can be considered safe. “We don’t have the studies to say how much spanking is dangerous, so we have to think that any amount has this potential.”
A version of this article first appeared on Medscape.com.
How often should we check EKGs in patients starting antipsychotic medications?
Determining relative risk with available data
Case
An 88-year-old woman with history of osteoporosis, hyperlipidemia, and a remote myocardial infarction presents to the ED with altered mental status and agitation. The patient is admitted to the medicine service for further management. Her current medications include a thiazide and a statin. Psychiatry is consulted and recommends administering intravenous haloperidol. A baseline EKG shows a corrected QT interval (QTc) of 486 milliseconds (ms). How often should subsequent EKGs be ordered?
Overview of issue
A prolonged QT interval can predispose a patient to dangerous arrhythmias such as Torsades de pointes (TdP), which results in sudden cardiac death in about 10% of cases.1,2 A prolonged QTc interval can be caused by cardiac, renal, or hepatic dysfunction; congenital Long QT Syndrome (LQTS)2; electrolyte abnormalities; or as a result of many drugs, including most antipsychotic medications such as quetiapine, olanzapine, risperidone and haloperidol.

To diminish risk of TdP while taking these medications, it is necessary to monitor the QTc interval. Before commencing a QT-prolonging medication, it is recommended to get a baseline EKG, then perform EKG monitoring after administering the medication.
According to American Heart Association guidelines, a prolonged QT interval is considered more than 460 ms in women or above 450 ms in men.3 If an abnormal rhythm and/or prolonged QTc is detected via EKG monitoring, then the drug dosage can be changed or an alternative therapy selected.4 However, there are no current guidelines recommending how often EKG monitoring should be performed after a QT-prolonging antipsychotic medication is administered on an inpatient medicine unit. Without guidelines, there is potential for health care providers to under- or over-order EKG monitoring, possibly putting patients at risk of TdP or wasting hospital resources, respectively.

Overview of the data
There are currently no universally accepted guidelines regarding inpatient EKG monitoring for patients started on QTc prolonging antipsychotic medications. A 2018 review of the literature surrounding assessment and management of patients on QTc prolonging medications was performed to analyze the available data and make recommendations; notably the evidence was limited as none of the studies were randomized controlled trials.
The authors recommend assessing the drug for QTc prolonging potential, and if possible, choosing alternative treatment in patients with baseline prolonged QTc. If the QT prolonging medication is the best or only option, then the next step is assessing the patient’s risk for QTc prolongation based on that person’s current condition and medical history.5 They recommend using the QTc prolonging risk point system developed by Tisdale and colleagues, which identified patient risk factors for elevated QTc intervals based on EKG findings in cardiac care units at a large tertiary hospital center.6

Based on the patient’s demographics, current condition, and medication list, the score can be used to stratify patients into low-, medium-, and high-risk categories (see Table 1). 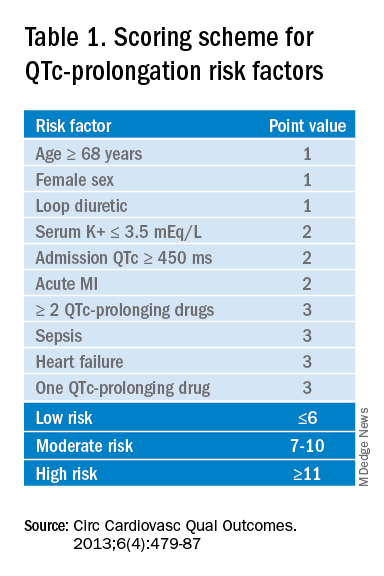
Risk factors include age over 68 years, female sex, prior MI, concurrent use of other QTc prolonging medications, and sepsis, all of which have differing ability to cause QTc prolongation and thus are weighted differentially. This scoring system is helpful in identifying high risk patients; however, the review does not include recommendations for management of these patients beyond removing the offending drug or monitoring EKGs more aggressively in higher risk patients once identified.6

Low-risk patients can be managed expectantly. If the baseline QTc is < 500 ms, then the provider may administer the medication, but should obtain follow-up EKG monitoring to ensure the QTc does not rise above 500 ms; if it does, a management change is necessitated. For moderate- to high-risk patients with a baseline QTc > 500 ms, they recommend not administering the medication and consulting a cardiologist. The review does not provide a recommendation on how often EKG monitoring should be performed after prescribing an antipsychotic medication in an inpatient setting.5
A 2018 review article explored patient risk factors for a prolonged QTc in the setting of prescribing potentially QTc prolonging antipsychotics.7 The authors reiterate that QTc prolonging risk factors are important considerations when prescribing antipsychotics that can lead to adverse events, though they note that much of the literature associating antipsychotics with negative outcomes consists of case reports in which patients had independent risk factors for development of TdP, such as preexisting ventricular arrhythmias.
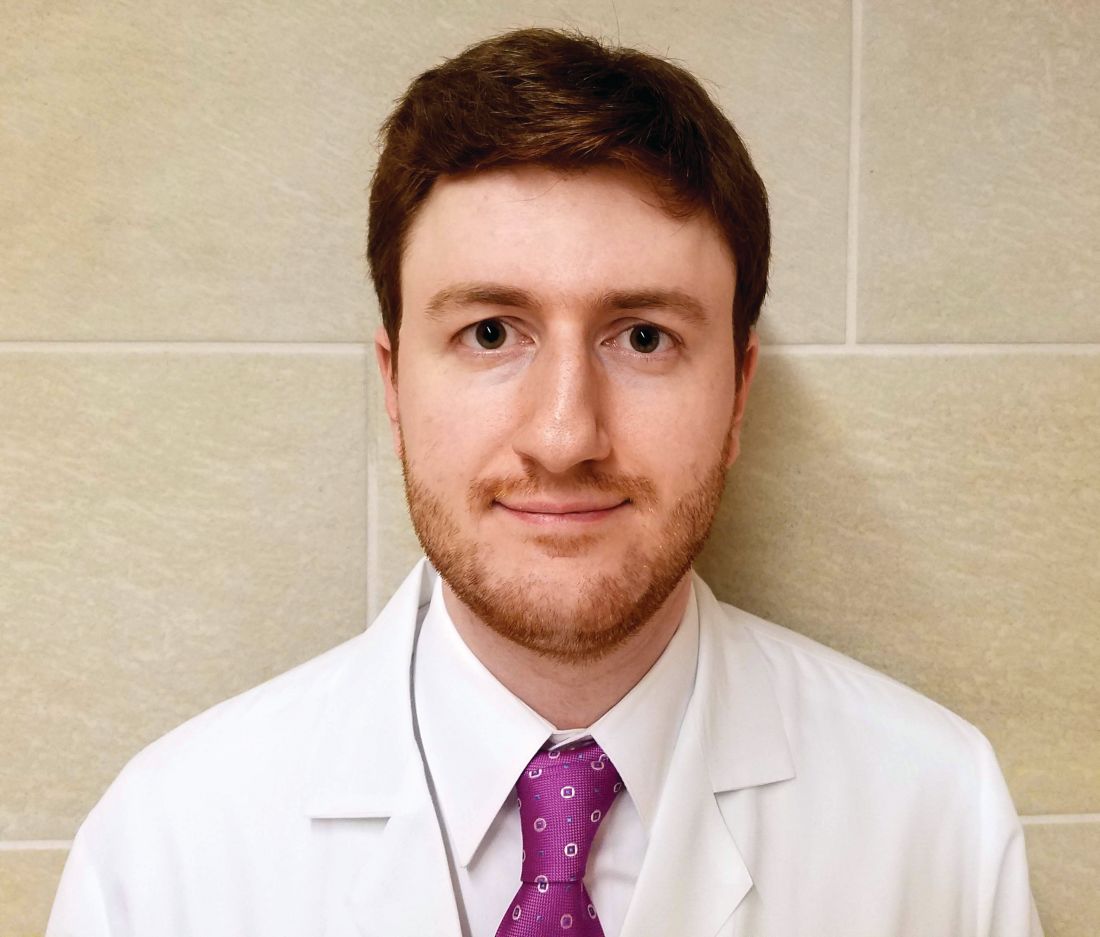
In addition, the data regarding the risk of each individual antipsychotic agent are not comprehensive. Some medications that have been deemed “QTc prolonging” were identified as such in only a handful of cases where patients had confounding comorbid risk factors. This raises concern that some medications are being unduly stigmatized in situations where there is little chance of TdP. If there is no equivalent or alternate treatment available, this may lead to an antipsychotic medication being held unnecessarily, which may exacerbate the psychiatric illness.
The authors note that the trend toward ordering baseline EKGs in the inpatient setting following administration of a new antipsychotic may be partly attributed to the ready availability of EKG testing in hospitals. They recommend a baseline EKG to assess the patient’s risk. For most agents, they recommend no further EKG monitoring unless there is a change in patient risk factors. Follow-up EKGs should be done in patients with multiple or significant risk factors to assess their QTc stability. In patients with a QTc > 500 ms on a follow-up EKG, daily monitoring is encouraged alongside reassessment of the current treatment regimen.7
Overall, the current literature suggests that providers should know which antipsychotics carry a risk for QTc prolongation and what other treatment options are available. The risk of QTc prolongation for common antipsychotic agents is provided in Table 2.
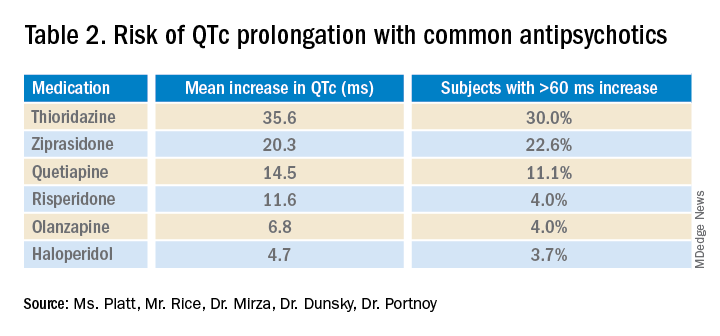
Providers should assess their patients’ risk factors for QTc prolongation and order a baseline EKG to help quantify the cardiac risk associated with prescribing the drug. In patients with many risk factors or complicated medication regimens, a follow-up EKG should be performed to assess the new QTc baseline. If the subsequent QTc is > 500 ms, then an alternative medication should be strongly considered. The majority of patients, however, will not have a clinically significant increase in their QTc, in which case there is no need for a change in medication and monitoring frequency can be deescalated.
Application of data to the case
Our 88-year-old patient has multiple risk factors for a prolonged QTc, and according to the Tisdale scoring system is at moderate risk (7-10 points). Her risk of developing TdP increases with the addition of IV haloperidol to her regimen.
Because of her increased risk, it is reasonable to consider alternative management. If she can cooperate with PO medications, then olanzapine could be given, which has a lesser effect on the QTc interval. If unable to take oral medications, she could be given haloperidol intramuscularly, which causes less QTc prolongation than the IV formulation. If an antipsychotic is administered, she should receive EKG monitoring.
Given the lack of evidence on the optimal monitoring strategy, a protocol should be utilized that balances the ability to capture a clinically meaningful increase in the QTc with appropriate stewardship of resources. Our practice is to initially monitor the EKG every 3 days in moderate- to high-risk patients with baseline QTc < 500 ms. If the QTc remains below 500 ms over three EKGs, then treatment may continue with EKG monitoring weekly while the patient is hospitalized. If the QTc rises above 500 ms, then a management change would be indicated (either dose reduction or a change of agents). If antipsychotic medications are continued, we check the EKG daily while the QTc is >500 ms until there are three unchanged EKGS, and then consider deescalating monitoring to every 3 days.
Bottom line
Prior to prescribing, perform a baseline EKG and assess the patient’s risk of QTc prolongation. If the patient is at increased risk, avoid prescribing QTc prolonging medications where alternatives exist. If a QTc prolonging medication is used in a patient with a moderate- to high-risk score, check an EKG every 3 days or daily if the QTc increases to > 500 ms.
Ms. Platt is a medical student at the Icahn School of Medicine at Mount Sinai in New York. Mr. Rice is a medical student at the Icahn School of Medicine. Dr. Mirza is assistant clinical professor of psychiatry at the Icahn School of Medicine. Dr. Dunsky is a cardiologist and assistant professor at the Icahn School of Medicine. Dr. Portnoy is a hospitalist and assistant professor at the Icahn School of Medicine.
References
1. Darpö B. Spectrum of drugs prolonging QT interval and the incidence of torsades de pointes. Eur Heart J Supplements. 2001;3(suppl_K):K70-K80. doi: 10.1016/S1520-765X(01)90009-4.
2. Schwartz PJ, Woosley RL. Predicting the unpredictable: Drug-induced QT prolongation and torsades de pointes. J Am Coll Cardiol. 2016;67(13):1639-50. doi: 10.1016/j.jacc.2015.12.063.
3. Rautaharju PM et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram. Part IV: The ST Segment, T and U Waves, and the QT Interval A Scientific Statement From the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society Endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol. 2009 Mar 17;53(11):982-91. doi: 10.1016/j.jacc.2008.12.014.
4. Drew BJ et al. Prevention of torsades de pointes in hospital settings: A scientific statement from the American Heart Association and the American College of Cardiology Foundation. Circulation. 2010;121(8):1047-60. doi: 10.1161/CIRCULATIONAHA.109.192704.
5. Zolezzi M, Cheung L. A literature-based algorithm for the assessment, management, and monitoring of drug-induced QTc prolongation in the psychiatric population. Neuropsychiatr Dis Treat. 2019;15:105-14. doi: 10.2147/NDT.S186474.
6. Tisdale JE et al. Development and validation of a risk score to predict QT interval prolongation in hospitalized patients. Circ Cardiovasc Qual Outcomes. 2013;6(4):479-87. doi: 10.1161/CIRCOUTCOMES.113.000152.
7. Beach SR et al. QT prolongation, torsades de pointes, and psychotropic medications: A 5-year update. Psychosomatics. 2018;59(2):105-22. doi: 10.1016/j.psym.2017.10.009.
Key points
- An increased QTc interval can lead to TdP, ventricular fibrillation and cardiac death.
- The relative risk of each antipsychotic medication should be determined based on available data and the Tisdale scoring system can provide a system to assess a patient’s risk of QTc prolongation.
- Low-risk patients with a baseline QTc <500 ms should receive a baseline EKG and inpatient EKG monitoring weekly while moderate- to high-risk patients should receive EKG monitoring every 3 days.
- A QTc > 500 ms suggests the need for a management change (drug discontinuation, dose reduction, or a switch to another agent). If the antipsychotic is absolutely necessary, perform daily EKG monitoring until there are three unchanged EKGs, and then consider deescalating monitoring to every 3 days.
Additional reading
Beach SR et al. QT Prolongation, torsades de pointes, and psychotropic medications: A 5-year update. Psychosomatics. 2018;59(2):105-22. doi: 10.1016/j.psym.2017.10.009.
Drew BJ et al. Prevention of torsades de pointes in hospital settings: A scientific statement from the American Heart Association and the American College of Cardiology Foundation. Circulation. 2010;121(8):1047-60. doi: 10.1161/CIRCULATIONAHA.109.192704.
Zolezzi M, Cheung L. A literature-based algorithm for the assessment, management, and monitoring of drug-induced QTc prolongation in the psychiatric population. Neuropsychiatr Dis Treat. 2019;15:105-14. doi: 10.2147/NDT.S186474.
Quiz
A 70-year-old male inpatient on furosemide with last known potassium level of 3.3 is going to be started on olanzapine. His baseline EKG has a QTc of 470 ms.
How often should he receive EKG monitoring?
A. Daily
B. Every 3 days
C. Weekly
D. Monthly
Answer (C): He is a low risk patient (6 points: over 70 yrs, loop diuretic, K+< 3.5, QTc > 450 ms), so he should receive weekly EKG monitoring.
Determining relative risk with available data
Determining relative risk with available data
Case
An 88-year-old woman with history of osteoporosis, hyperlipidemia, and a remote myocardial infarction presents to the ED with altered mental status and agitation. The patient is admitted to the medicine service for further management. Her current medications include a thiazide and a statin. Psychiatry is consulted and recommends administering intravenous haloperidol. A baseline EKG shows a corrected QT interval (QTc) of 486 milliseconds (ms). How often should subsequent EKGs be ordered?
Overview of issue
A prolonged QT interval can predispose a patient to dangerous arrhythmias such as Torsades de pointes (TdP), which results in sudden cardiac death in about 10% of cases.1,2 A prolonged QTc interval can be caused by cardiac, renal, or hepatic dysfunction; congenital Long QT Syndrome (LQTS)2; electrolyte abnormalities; or as a result of many drugs, including most antipsychotic medications such as quetiapine, olanzapine, risperidone and haloperidol.
To diminish risk of TdP while taking these medications, it is necessary to monitor the QTc interval. Before commencing a QT-prolonging medication, it is recommended to get a baseline EKG, then perform EKG monitoring after administering the medication.
According to American Heart Association guidelines, a prolonged QT interval is considered more than 460 ms in women or above 450 ms in men.3 If an abnormal rhythm and/or prolonged QTc is detected via EKG monitoring, then the drug dosage can be changed or an alternative therapy selected.4 However, there are no current guidelines recommending how often EKG monitoring should be performed after a QT-prolonging antipsychotic medication is administered on an inpatient medicine unit. Without guidelines, there is potential for health care providers to under- or over-order EKG monitoring, possibly putting patients at risk of TdP or wasting hospital resources, respectively.
Overview of the data
There are currently no universally accepted guidelines regarding inpatient EKG monitoring for patients started on QTc prolonging antipsychotic medications. A 2018 review of the literature surrounding assessment and management of patients on QTc prolonging medications was performed to analyze the available data and make recommendations; notably the evidence was limited as none of the studies were randomized controlled trials.
The authors recommend assessing the drug for QTc prolonging potential, and if possible, choosing alternative treatment in patients with baseline prolonged QTc. If the QT prolonging medication is the best or only option, then the next step is assessing the patient’s risk for QTc prolongation based on that person’s current condition and medical history.5 They recommend using the QTc prolonging risk point system developed by Tisdale and colleagues, which identified patient risk factors for elevated QTc intervals based on EKG findings in cardiac care units at a large tertiary hospital center.6
Based on the patient’s demographics, current condition, and medication list, the score can be used to stratify patients into low-, medium-, and high-risk categories (see Table 1).
Risk factors include age over 68 years, female sex, prior MI, concurrent use of other QTc prolonging medications, and sepsis, all of which have differing ability to cause QTc prolongation and thus are weighted differentially. This scoring system is helpful in identifying high risk patients; however, the review does not include recommendations for management of these patients beyond removing the offending drug or monitoring EKGs more aggressively in higher risk patients once identified.6
Low-risk patients can be managed expectantly. If the baseline QTc is < 500 ms, then the provider may administer the medication, but should obtain follow-up EKG monitoring to ensure the QTc does not rise above 500 ms; if it does, a management change is necessitated. For moderate- to high-risk patients with a baseline QTc > 500 ms, they recommend not administering the medication and consulting a cardiologist. The review does not provide a recommendation on how often EKG monitoring should be performed after prescribing an antipsychotic medication in an inpatient setting.5
A 2018 review article explored patient risk factors for a prolonged QTc in the setting of prescribing potentially QTc prolonging antipsychotics.7 The authors reiterate that QTc prolonging risk factors are important considerations when prescribing antipsychotics that can lead to adverse events, though they note that much of the literature associating antipsychotics with negative outcomes consists of case reports in which patients had independent risk factors for development of TdP, such as preexisting ventricular arrhythmias.
In addition, the data regarding the risk of each individual antipsychotic agent are not comprehensive. Some medications that have been deemed “QTc prolonging” were identified as such in only a handful of cases where patients had confounding comorbid risk factors. This raises concern that some medications are being unduly stigmatized in situations where there is little chance of TdP. If there is no equivalent or alternate treatment available, this may lead to an antipsychotic medication being held unnecessarily, which may exacerbate the psychiatric illness.
The authors note that the trend toward ordering baseline EKGs in the inpatient setting following administration of a new antipsychotic may be partly attributed to the ready availability of EKG testing in hospitals. They recommend a baseline EKG to assess the patient’s risk. For most agents, they recommend no further EKG monitoring unless there is a change in patient risk factors. Follow-up EKGs should be done in patients with multiple or significant risk factors to assess their QTc stability. In patients with a QTc > 500 ms on a follow-up EKG, daily monitoring is encouraged alongside reassessment of the current treatment regimen.7
Overall, the current literature suggests that providers should know which antipsychotics carry a risk for QTc prolongation and what other treatment options are available. The risk of QTc prolongation for common antipsychotic agents is provided in Table 2.
Providers should assess their patients’ risk factors for QTc prolongation and order a baseline EKG to help quantify the cardiac risk associated with prescribing the drug. In patients with many risk factors or complicated medication regimens, a follow-up EKG should be performed to assess the new QTc baseline. If the subsequent QTc is > 500 ms, then an alternative medication should be strongly considered. The majority of patients, however, will not have a clinically significant increase in their QTc, in which case there is no need for a change in medication and monitoring frequency can be deescalated.
Application of data to the case
Our 88-year-old patient has multiple risk factors for a prolonged QTc, and according to the Tisdale scoring system is at moderate risk (7-10 points). Her risk of developing TdP increases with the addition of IV haloperidol to her regimen.
Because of her increased risk, it is reasonable to consider alternative management. If she can cooperate with PO medications, then olanzapine could be given, which has a lesser effect on the QTc interval. If unable to take oral medications, she could be given haloperidol intramuscularly, which causes less QTc prolongation than the IV formulation. If an antipsychotic is administered, she should receive EKG monitoring.
Given the lack of evidence on the optimal monitoring strategy, a protocol should be utilized that balances the ability to capture a clinically meaningful increase in the QTc with appropriate stewardship of resources. Our practice is to initially monitor the EKG every 3 days in moderate- to high-risk patients with baseline QTc < 500 ms. If the QTc remains below 500 ms over three EKGs, then treatment may continue with EKG monitoring weekly while the patient is hospitalized. If the QTc rises above 500 ms, then a management change would be indicated (either dose reduction or a change of agents). If antipsychotic medications are continued, we check the EKG daily while the QTc is >500 ms until there are three unchanged EKGS, and then consider deescalating monitoring to every 3 days.
Bottom line
Prior to prescribing, perform a baseline EKG and assess the patient’s risk of QTc prolongation. If the patient is at increased risk, avoid prescribing QTc prolonging medications where alternatives exist. If a QTc prolonging medication is used in a patient with a moderate- to high-risk score, check an EKG every 3 days or daily if the QTc increases to > 500 ms.
Ms. Platt is a medical student at the Icahn School of Medicine at Mount Sinai in New York. Mr. Rice is a medical student at the Icahn School of Medicine. Dr. Mirza is assistant clinical professor of psychiatry at the Icahn School of Medicine. Dr. Dunsky is a cardiologist and assistant professor at the Icahn School of Medicine. Dr. Portnoy is a hospitalist and assistant professor at the Icahn School of Medicine.
References
1. Darpö B. Spectrum of drugs prolonging QT interval and the incidence of torsades de pointes. Eur Heart J Supplements. 2001;3(suppl_K):K70-K80. doi: 10.1016/S1520-765X(01)90009-4.
2. Schwartz PJ, Woosley RL. Predicting the unpredictable: Drug-induced QT prolongation and torsades de pointes. J Am Coll Cardiol. 2016;67(13):1639-50. doi: 10.1016/j.jacc.2015.12.063.
3. Rautaharju PM et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram. Part IV: The ST Segment, T and U Waves, and the QT Interval A Scientific Statement From the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society Endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol. 2009 Mar 17;53(11):982-91. doi: 10.1016/j.jacc.2008.12.014.
4. Drew BJ et al. Prevention of torsades de pointes in hospital settings: A scientific statement from the American Heart Association and the American College of Cardiology Foundation. Circulation. 2010;121(8):1047-60. doi: 10.1161/CIRCULATIONAHA.109.192704.
5. Zolezzi M, Cheung L. A literature-based algorithm for the assessment, management, and monitoring of drug-induced QTc prolongation in the psychiatric population. Neuropsychiatr Dis Treat. 2019;15:105-14. doi: 10.2147/NDT.S186474.
6. Tisdale JE et al. Development and validation of a risk score to predict QT interval prolongation in hospitalized patients. Circ Cardiovasc Qual Outcomes. 2013;6(4):479-87. doi: 10.1161/CIRCOUTCOMES.113.000152.
7. Beach SR et al. QT prolongation, torsades de pointes, and psychotropic medications: A 5-year update. Psychosomatics. 2018;59(2):105-22. doi: 10.1016/j.psym.2017.10.009.
Key points
- An increased QTc interval can lead to TdP, ventricular fibrillation and cardiac death.
- The relative risk of each antipsychotic medication should be determined based on available data and the Tisdale scoring system can provide a system to assess a patient’s risk of QTc prolongation.
- Low-risk patients with a baseline QTc <500 ms should receive a baseline EKG and inpatient EKG monitoring weekly while moderate- to high-risk patients should receive EKG monitoring every 3 days.
- A QTc > 500 ms suggests the need for a management change (drug discontinuation, dose reduction, or a switch to another agent). If the antipsychotic is absolutely necessary, perform daily EKG monitoring until there are three unchanged EKGs, and then consider deescalating monitoring to every 3 days.
Additional reading
Beach SR et al. QT Prolongation, torsades de pointes, and psychotropic medications: A 5-year update. Psychosomatics. 2018;59(2):105-22. doi: 10.1016/j.psym.2017.10.009.
Drew BJ et al. Prevention of torsades de pointes in hospital settings: A scientific statement from the American Heart Association and the American College of Cardiology Foundation. Circulation. 2010;121(8):1047-60. doi: 10.1161/CIRCULATIONAHA.109.192704.
Zolezzi M, Cheung L. A literature-based algorithm for the assessment, management, and monitoring of drug-induced QTc prolongation in the psychiatric population. Neuropsychiatr Dis Treat. 2019;15:105-14. doi: 10.2147/NDT.S186474.
Quiz
A 70-year-old male inpatient on furosemide with last known potassium level of 3.3 is going to be started on olanzapine. His baseline EKG has a QTc of 470 ms.
How often should he receive EKG monitoring?
A. Daily
B. Every 3 days
C. Weekly
D. Monthly
Answer (C): He is a low risk patient (6 points: over 70 yrs, loop diuretic, K+< 3.5, QTc > 450 ms), so he should receive weekly EKG monitoring.
Case
An 88-year-old woman with history of osteoporosis, hyperlipidemia, and a remote myocardial infarction presents to the ED with altered mental status and agitation. The patient is admitted to the medicine service for further management. Her current medications include a thiazide and a statin. Psychiatry is consulted and recommends administering intravenous haloperidol. A baseline EKG shows a corrected QT interval (QTc) of 486 milliseconds (ms). How often should subsequent EKGs be ordered?
Overview of issue
A prolonged QT interval can predispose a patient to dangerous arrhythmias such as Torsades de pointes (TdP), which results in sudden cardiac death in about 10% of cases.1,2 A prolonged QTc interval can be caused by cardiac, renal, or hepatic dysfunction; congenital Long QT Syndrome (LQTS)2; electrolyte abnormalities; or as a result of many drugs, including most antipsychotic medications such as quetiapine, olanzapine, risperidone and haloperidol.
To diminish risk of TdP while taking these medications, it is necessary to monitor the QTc interval. Before commencing a QT-prolonging medication, it is recommended to get a baseline EKG, then perform EKG monitoring after administering the medication.
According to American Heart Association guidelines, a prolonged QT interval is considered more than 460 ms in women or above 450 ms in men.3 If an abnormal rhythm and/or prolonged QTc is detected via EKG monitoring, then the drug dosage can be changed or an alternative therapy selected.4 However, there are no current guidelines recommending how often EKG monitoring should be performed after a QT-prolonging antipsychotic medication is administered on an inpatient medicine unit. Without guidelines, there is potential for health care providers to under- or over-order EKG monitoring, possibly putting patients at risk of TdP or wasting hospital resources, respectively.
Overview of the data
There are currently no universally accepted guidelines regarding inpatient EKG monitoring for patients started on QTc prolonging antipsychotic medications. A 2018 review of the literature surrounding assessment and management of patients on QTc prolonging medications was performed to analyze the available data and make recommendations; notably the evidence was limited as none of the studies were randomized controlled trials.
The authors recommend assessing the drug for QTc prolonging potential, and if possible, choosing alternative treatment in patients with baseline prolonged QTc. If the QT prolonging medication is the best or only option, then the next step is assessing the patient’s risk for QTc prolongation based on that person’s current condition and medical history.5 They recommend using the QTc prolonging risk point system developed by Tisdale and colleagues, which identified patient risk factors for elevated QTc intervals based on EKG findings in cardiac care units at a large tertiary hospital center.6
Based on the patient’s demographics, current condition, and medication list, the score can be used to stratify patients into low-, medium-, and high-risk categories (see Table 1).
Risk factors include age over 68 years, female sex, prior MI, concurrent use of other QTc prolonging medications, and sepsis, all of which have differing ability to cause QTc prolongation and thus are weighted differentially. This scoring system is helpful in identifying high risk patients; however, the review does not include recommendations for management of these patients beyond removing the offending drug or monitoring EKGs more aggressively in higher risk patients once identified.6
Low-risk patients can be managed expectantly. If the baseline QTc is < 500 ms, then the provider may administer the medication, but should obtain follow-up EKG monitoring to ensure the QTc does not rise above 500 ms; if it does, a management change is necessitated. For moderate- to high-risk patients with a baseline QTc > 500 ms, they recommend not administering the medication and consulting a cardiologist. The review does not provide a recommendation on how often EKG monitoring should be performed after prescribing an antipsychotic medication in an inpatient setting.5
A 2018 review article explored patient risk factors for a prolonged QTc in the setting of prescribing potentially QTc prolonging antipsychotics.7 The authors reiterate that QTc prolonging risk factors are important considerations when prescribing antipsychotics that can lead to adverse events, though they note that much of the literature associating antipsychotics with negative outcomes consists of case reports in which patients had independent risk factors for development of TdP, such as preexisting ventricular arrhythmias.
In addition, the data regarding the risk of each individual antipsychotic agent are not comprehensive. Some medications that have been deemed “QTc prolonging” were identified as such in only a handful of cases where patients had confounding comorbid risk factors. This raises concern that some medications are being unduly stigmatized in situations where there is little chance of TdP. If there is no equivalent or alternate treatment available, this may lead to an antipsychotic medication being held unnecessarily, which may exacerbate the psychiatric illness.
The authors note that the trend toward ordering baseline EKGs in the inpatient setting following administration of a new antipsychotic may be partly attributed to the ready availability of EKG testing in hospitals. They recommend a baseline EKG to assess the patient’s risk. For most agents, they recommend no further EKG monitoring unless there is a change in patient risk factors. Follow-up EKGs should be done in patients with multiple or significant risk factors to assess their QTc stability. In patients with a QTc > 500 ms on a follow-up EKG, daily monitoring is encouraged alongside reassessment of the current treatment regimen.7
Overall, the current literature suggests that providers should know which antipsychotics carry a risk for QTc prolongation and what other treatment options are available. The risk of QTc prolongation for common antipsychotic agents is provided in Table 2.
Providers should assess their patients’ risk factors for QTc prolongation and order a baseline EKG to help quantify the cardiac risk associated with prescribing the drug. In patients with many risk factors or complicated medication regimens, a follow-up EKG should be performed to assess the new QTc baseline. If the subsequent QTc is > 500 ms, then an alternative medication should be strongly considered. The majority of patients, however, will not have a clinically significant increase in their QTc, in which case there is no need for a change in medication and monitoring frequency can be deescalated.
Application of data to the case
Our 88-year-old patient has multiple risk factors for a prolonged QTc, and according to the Tisdale scoring system is at moderate risk (7-10 points). Her risk of developing TdP increases with the addition of IV haloperidol to her regimen.
Because of her increased risk, it is reasonable to consider alternative management. If she can cooperate with PO medications, then olanzapine could be given, which has a lesser effect on the QTc interval. If unable to take oral medications, she could be given haloperidol intramuscularly, which causes less QTc prolongation than the IV formulation. If an antipsychotic is administered, she should receive EKG monitoring.
Given the lack of evidence on the optimal monitoring strategy, a protocol should be utilized that balances the ability to capture a clinically meaningful increase in the QTc with appropriate stewardship of resources. Our practice is to initially monitor the EKG every 3 days in moderate- to high-risk patients with baseline QTc < 500 ms. If the QTc remains below 500 ms over three EKGs, then treatment may continue with EKG monitoring weekly while the patient is hospitalized. If the QTc rises above 500 ms, then a management change would be indicated (either dose reduction or a change of agents). If antipsychotic medications are continued, we check the EKG daily while the QTc is >500 ms until there are three unchanged EKGS, and then consider deescalating monitoring to every 3 days.
Bottom line
Prior to prescribing, perform a baseline EKG and assess the patient’s risk of QTc prolongation. If the patient is at increased risk, avoid prescribing QTc prolonging medications where alternatives exist. If a QTc prolonging medication is used in a patient with a moderate- to high-risk score, check an EKG every 3 days or daily if the QTc increases to > 500 ms.
Ms. Platt is a medical student at the Icahn School of Medicine at Mount Sinai in New York. Mr. Rice is a medical student at the Icahn School of Medicine. Dr. Mirza is assistant clinical professor of psychiatry at the Icahn School of Medicine. Dr. Dunsky is a cardiologist and assistant professor at the Icahn School of Medicine. Dr. Portnoy is a hospitalist and assistant professor at the Icahn School of Medicine.
References
1. Darpö B. Spectrum of drugs prolonging QT interval and the incidence of torsades de pointes. Eur Heart J Supplements. 2001;3(suppl_K):K70-K80. doi: 10.1016/S1520-765X(01)90009-4.
2. Schwartz PJ, Woosley RL. Predicting the unpredictable: Drug-induced QT prolongation and torsades de pointes. J Am Coll Cardiol. 2016;67(13):1639-50. doi: 10.1016/j.jacc.2015.12.063.
3. Rautaharju PM et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram. Part IV: The ST Segment, T and U Waves, and the QT Interval A Scientific Statement From the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society Endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol. 2009 Mar 17;53(11):982-91. doi: 10.1016/j.jacc.2008.12.014.
4. Drew BJ et al. Prevention of torsades de pointes in hospital settings: A scientific statement from the American Heart Association and the American College of Cardiology Foundation. Circulation. 2010;121(8):1047-60. doi: 10.1161/CIRCULATIONAHA.109.192704.
5. Zolezzi M, Cheung L. A literature-based algorithm for the assessment, management, and monitoring of drug-induced QTc prolongation in the psychiatric population. Neuropsychiatr Dis Treat. 2019;15:105-14. doi: 10.2147/NDT.S186474.
6. Tisdale JE et al. Development and validation of a risk score to predict QT interval prolongation in hospitalized patients. Circ Cardiovasc Qual Outcomes. 2013;6(4):479-87. doi: 10.1161/CIRCOUTCOMES.113.000152.
7. Beach SR et al. QT prolongation, torsades de pointes, and psychotropic medications: A 5-year update. Psychosomatics. 2018;59(2):105-22. doi: 10.1016/j.psym.2017.10.009.
Key points
- An increased QTc interval can lead to TdP, ventricular fibrillation and cardiac death.
- The relative risk of each antipsychotic medication should be determined based on available data and the Tisdale scoring system can provide a system to assess a patient’s risk of QTc prolongation.
- Low-risk patients with a baseline QTc <500 ms should receive a baseline EKG and inpatient EKG monitoring weekly while moderate- to high-risk patients should receive EKG monitoring every 3 days.
- A QTc > 500 ms suggests the need for a management change (drug discontinuation, dose reduction, or a switch to another agent). If the antipsychotic is absolutely necessary, perform daily EKG monitoring until there are three unchanged EKGs, and then consider deescalating monitoring to every 3 days.
Additional reading
Beach SR et al. QT Prolongation, torsades de pointes, and psychotropic medications: A 5-year update. Psychosomatics. 2018;59(2):105-22. doi: 10.1016/j.psym.2017.10.009.
Drew BJ et al. Prevention of torsades de pointes in hospital settings: A scientific statement from the American Heart Association and the American College of Cardiology Foundation. Circulation. 2010;121(8):1047-60. doi: 10.1161/CIRCULATIONAHA.109.192704.
Zolezzi M, Cheung L. A literature-based algorithm for the assessment, management, and monitoring of drug-induced QTc prolongation in the psychiatric population. Neuropsychiatr Dis Treat. 2019;15:105-14. doi: 10.2147/NDT.S186474.
Quiz
A 70-year-old male inpatient on furosemide with last known potassium level of 3.3 is going to be started on olanzapine. His baseline EKG has a QTc of 470 ms.
How often should he receive EKG monitoring?
A. Daily
B. Every 3 days
C. Weekly
D. Monthly
Answer (C): He is a low risk patient (6 points: over 70 yrs, loop diuretic, K+< 3.5, QTc > 450 ms), so he should receive weekly EKG monitoring.
Preventing the psychosocial effects of adult ADHD during the pandemic
As some countries brace for yet another possible surge in the COVID-19 pandemic – particularly among young adults who have not yet been vaccinated – clinicians should remain wary of the cardinal symptoms of adult ADHD.
Research from an Israeli study shows that individuals with unmedicated ADHD are 52% more likely to test positive for the virus.1,2

The symptoms of ADHD, including impulsiveness and inability to follow directions, combined with the tendency to leave adults with ADHD on their own to sort out COVID-19–related protocols – make these individuals susceptible to exposure.
As we know, ADHD is a condition characterized by a pervasive pattern of impulsivity and/or inattention, which greatly reduces organizational capabilities by interfering at the developmental level.3 Other key symptoms include short attention span, hyperactivity, restlessness, difficulty in prioritizing tasks, and an absence of time awareness. Symptom presentation of ADHD is contingent upon the nature of the individual’s overall mental health and etiologic issues that may be traced back to the brain’s development.4

Diagnosing ADHD in adults is relatively difficult, because a formal diagnosis generally requires symptoms to show up between the ages of 6 and 12.5 Also, clinicians can interview parents and family members to assess whether the classical features of ADHD were present in childhood for those suspected of having the condition.
Early vs. late presentation
Among the preschool population, it has been observed that emerging ADHD symptoms may progress with time or remain relatively constant with respect to the activities that children partake in. In some instances, impulsive behavior, especially compared with other symptoms, might be identified quickly by the attentive parent or caregiver. However, when ADHD appears in adulthood, it is possible that prior ADHD symptoms escaped detection – only to be diagnosed later in life because of varying presentations and the increased organizational demands of adulthood.
Meanwhile, diagnosis in adolescence can bring a different set of challenges to the forefront as teenagers face problems with self-management and responsibilities of daily living. These young people must cope with academic6 and social pressures – and a host of new societal expectations.
It is essential to understand how all of those societal factors have affected ADHD and its aspects, especially within the context of COVID-19. The coronavirus has introduced myriad challenges at the global level. Individuals with ADHD exhibit neurodevelopmental and corollary attention deficit issues that make them more susceptible to environmental stressors. Physical distancing practices might aggravate existing behavioral problems.
Distance forced by pandemic offers challenges
Despite the widespread adoption of telemedicine during the pandemic, some physicians think that the delivery of optimal care and the ability to adequately address patients’ health-related concerns have been compromised. Certainly, in the case of addressing the needs of patients with ADHD or related learning disorders, in-person examinations and clinical visits are best.
That is also the case for ADHD patients with comorbid sleep disorders. For those patients, it might be prudent to explore lifestyle changes (for example, improvements in sleep hygiene practices) before resorting to the use of pharmacologic agents such as hypnotics and melatonin. Along similar lines, the European ADHD Guideline Group (EAGG) advises the use of pharmacotherapy after the successful completion of a physical exam; patients already adhering to a treatment plan should continue therapy without interruption. Clinicians caring for patients with adult ADHD have faced a dilemma because treatment breaks increase the likelihood of illnesses resulting from the pandemic. Also, the inability to conduct treatment in person because of the pandemic raises concerns about pharmacotherapy.
The pandemic has affected the course of pediatric care and also has presented new challenges for adolescents as they begin to tackle unique problems related to their health concerns. In prepandemic times, teachers played integral roles in the diagnostic process, because they were able to readily identify children and teenagers with mental and physical challenges. In stark contrast, connecting with students online may not allow teachers to identify skill deficits in young patients or in adults with ADHD.
Furthermore, adults with ADHD and medical comorbidities may be at increased risk of disease exposure directly resulting from an inability to address their social and/or emotional well-being adequately. The social distancing and other mitigation measures advised by public health experts ensure safety and protection but also can present numerous hurdles for children, teenagers, adults – and their respective families.
Individuals with adult ADHD and other psychiatric disorders may downplay their psychological distress7 [for example, sleep dysfunction, issues concerning activities of daily living], and view it as being the natural product of the COVID-19 environment. As a result of their misconceptions, they may avoid increasing their medication dose to control emergent symptoms of hyperactivity and impulsivity, instead opting to manage stress without aid from health care professionals. The absence of patient-provider interactivity and the integration of telemedicine has introduced unnecessary obstacles with respect to medication management and therapy as well as general access to expert advice. It is of utmost importance for clinicians to identify at-risk patients and reeducate the adult ADHD patient on issues concerning medication intake and psychological wellness.
Individuals with developmental disorders may experience numerous setbacks when trying to navigate their environments. The lack of correct feedback, supervision, and guidance may adversely affect adults with ADHD, contributing toward a lack of self-esteem and social awareness.
Individuals with adult ADHD are more likely than are their younger counterparts to have medical comorbidities, such as cardiovascular disease8 and type 2 diabetes,9 so it is crucial to prescribe dietary instructions to patients. Sometimes patients with adult ADHD lack support in the form of acceptance by family and peers, so it is critical for the patient to come to terms with his/her condition and seek professional help, incorporating effective strategies wherever needed to maintain day-to-day functioning.
Other possible comorbidities
There can be risk factors associated with isolation of adults who have depression and/or anxiety, poor eating habits, and maladaptive behaviors. Other adverse health-related issues may include substance use disorder.10 Drug use suppresses developmental growth and may induce ADHD symptom exacerbation. Consistent with Khantzian’s self-medication hypothesis, among individuals with ADHD, including those who lack a formal diagnosis, there is a tendency to gravitate toward illicit substances, in particular, stimulants.11
We also know that adolescents are known to engage in normal risk-taking and social experimentation. Given that, the notion of boundary setting becomes a complicated affair during a pandemic. Adults may no longer be involved in the same types of risk-taking behaviors, but enforced self-isolation coupled with unchecked consumption of various social medial platforms continue to take a toll on personal development. Socialization plays an enormous role in maintaining psychological health, and social media is no substitute for in-person interactions. Such platforms can reduce mental growth opportunities and affect ADHD adults unfavorably.
For instance, it has been reported that women with adult ADHD are more likely to present with negative cognitive biases and symptoms of anxiety as a function of social media use.12,13 As clinicians, we should recommend introducing activities with the aim of enhancing self-acceptance, mindfulness, and the ability to engage in healthy lifestyles. A holistic framework that focuses on psychological wellness and physical fitness will ensure treatment success. Medication management may prove to be a challenge because of differences in dosing, response schedules, and agreed-upon diagnostic criteria used for young patients, compared with those needed for adults.
Treatment strategies
Before the pandemic, researchers were observing an increase globally in the ADHD diagnosis,14 and clinicians have been exploring the efficacy of select medications, sometimes with limited success.15 Stimulant medication, combined with behavioral interventions, is supported by evidenced-based medicine and is the treatment of choice for childhood ADHD.
The stimulant remedy considered to be the most efficacious for adult ADHD is methylphenidate or dextroamphetamine.
However, be sure to proceed with caution and prepare a thorough work-up, because there can be cardiovascular risk factors associated with these medications with a pronounced increase in heart rate and blood pressure.
Stimulant medications are known to increase the risk of stroke or myocardial infarction for individuals with preexisting cardiovascular anomalies or structural anomalies. The American Heart Association no longer recommends a baseline EKG before commencing stimulant therapy with the exception of preexisting cardiac risk. Nonstimulant medications such as atomoxetine are available as alternatives.
The process of finding therapies that will reduce symptoms of ADHD takes considerable time, and individuals may fail to notice improvements, at least initially.
Before prescribing any medicine or therapies, it is important to evaluate for factors that are specific to ADHD and rule out the presence of other learning or developmental disorders, to prevent negative consequences.
Health care professionals can introduce nonspecific interventions as a means of tackling complicated cases of adult ADHD, especially those that coincide with underlying medical conditions (for example, cardiovascular disease, seizure disorders, and/or eating disorders). In such cases, stimulant medications may lead to symptom exacerbation, and the health care professional should carry out a systematic evaluation (risks vs. benefits of drug classes), despite the limitations of online appointments over the course of the pandemic.
Moreover, ADHD symptoms can take on a more severe form within the context of preexisting mood and anxiety disorders. Unfortunately, these comorbidities may have a negative prognostic outcome, too, thereby increasing other health-related risk factors. Psychological interventions can be implemented via online assessments because of recent technological advances worldwide, providing a new level of confidence and social engagement. EEG-assisted biofeedback is an example of new technological modalities that may help improve the overall performance and functionality of individuals with adult ADHD.16 Numerous services and resources are available to patients and their families that can improve mental health and well-being.
Other nonpharmacologic choices also play an instrumental role in bringing harmony and organization into a patient’s life through the use of daily planners, alarms, and to-do lists. In addition, therapists can provide treatment that helps individuals get motivated and reduce their anxiety levels. Behavioral therapies support patient initiatives by increasing their productivity, activity management, and satisfaction. Cognitive-behavioral therapy (CBT), and marriage counseling and family therapy are modalities that may help adults with ADHD change underlying thoughts and perceptions and develop coping skills and self-esteem.
Appropriate to the pandemic situation is another treatment, e-therapy, which includes text-based communication, video calling, and phone calls. It is a low-cost and convenient alternative for people. For some patients, traveling to a particular clinic or counseling center can be difficult, and there is a shortage of counselors worldwide, so it is beneficial to talk with a counselor on a video/phone call or through social media. It is crucial for the ADHD coach to be trained with relevant knowledge to make plans, set goals, and manage a patient’s schedule of activities. For the counselor, sharing tips based on personal experience and making the appropriate suggestions allows adults with ADHD to stay motivated and focus on the task at hand. It should be noted that counselors play an important role in reducing stress levels for those diagnosed with ADHD, allowing patients to lead productive lives and achieve career goals.
Various online support communities can provide patients and their parents with educational resources, to address issues connected to ADHD in a professional manner.17
The road to treatment success
Any delays in treating adults with ADHD can lead to a frustrating situation in which the entire family will be affected. As stated earlier, numerous support groups are available to adults with ADHD, and some of those groups can offer valuable tips about addressing stress management and the diverse roles that parents and family members may play in patient care.18 These groups provide a network for people to exchange ideas and recommend strategies. Online support groups may connect patients directly with key opinion leaders and health care providers.
Individuals with ADHD often experience problems with organization and concentration – especially within the context of the pandemic – and receiving guidance from counselors will provide an opportunity to learn valuable coping strategies and manage symptoms, recognizing and mitigating any mood swings associated with anxiety or depression that emerge alongside their ADHD. Psychotherapy is instrumental in patient care, and individuals with adult ADHD should be taught to acknowledge the role of medications (for example, neglect, divert, or self-medicate). A holistic approach to managing ADHD symptoms is necessary for optimal functioning and independence.
Dr. Aman is a faculty member in the biology department of City Colleges of Chicago. She is a postdoctoral researcher at the International Maternal and Child Health Foundation (IMCHF), Montreal; a fellow, medical staff development, from the American Academy of Medical Management; and a Masters Online Teacher, University of Illinois at Chicago. Dr. Aman disclosed no relevant financial relationships. Dr. Islam is a medical adviser for the IMCHF, Montreal, and is based in New York. He is a postdoctoral fellow, psychopharmacologist, and a board-certified medical affairs specialist. Dr. Islam disclosed no relevant financial relationships. Dr. Karama is a psychiatrist at the Douglas Mental Health University Institute, Montreal. He is an assistant professor at the department of psychiatry, McGill University, also in Montreal. He has no disclosures. Dr. Choudhry is the chief scientific officer and head of the department of mental health and clinical research at the IMCHF. He has no disclosures.
References
1. J Atten Disord. 2020. doi: 10.1177/1087054720943271.
2. ADDitude Magazine. 2020 Jul 23.
3. Management of ADHD in Adults: What the Science Says. 2007 Oct 9. Guilford Press.
4. N Engl J Med. 2013 Nov 14;369(20):1935-44.
5. J Clin Psychiatry. 2002;63 Suppl 12:29-35.
6. J Atten Dis. 2015 Jan 12. doi: 10.1177/1087054144566076.
7. Psychiatry Res. 2020 Oct;292. doi: 10.1016/j.psychres.2020.113345.
8. Case Rep Cardiol. 2016. doi: 10.1155/2016/2343691.
9. Curr Diab Rep. 2019 Jun 27;19(8):46. doi: 10.1007/s11892-019-1174-x.
10. Curr Psychiatry Rep. 2014 Mar;16(3):436. doi: 10.1007/s/11920-013-0436-6.
11. Current Psychiatry. 2014 Dec;13(12):e3-4.
12. BMC Psychiatry. 2020;20(40). doi: 10.1186/s/12888-020-02707-9.
13. Psychol Addict Behav. 2016 Mar;30(2):252–62.
14. ADDitude Magazine. 2017 Apr 6.
15. Harv Mental Health Letter. 2009 Nov.
16. MGM J Med Sci. 2020 Jul 17(3):161-2.
17. J Child Psychol Psychiatry. 2020 Jul 7.
18. Int J Disaster Risk Reduct. 2020 Dec;51. doi: 10.1016/j.ijdrr.2020.101845.
As some countries brace for yet another possible surge in the COVID-19 pandemic – particularly among young adults who have not yet been vaccinated – clinicians should remain wary of the cardinal symptoms of adult ADHD.
Research from an Israeli study shows that individuals with unmedicated ADHD are 52% more likely to test positive for the virus.1,2
The symptoms of ADHD, including impulsiveness and inability to follow directions, combined with the tendency to leave adults with ADHD on their own to sort out COVID-19–related protocols – make these individuals susceptible to exposure.
As we know, ADHD is a condition characterized by a pervasive pattern of impulsivity and/or inattention, which greatly reduces organizational capabilities by interfering at the developmental level.3 Other key symptoms include short attention span, hyperactivity, restlessness, difficulty in prioritizing tasks, and an absence of time awareness. Symptom presentation of ADHD is contingent upon the nature of the individual’s overall mental health and etiologic issues that may be traced back to the brain’s development.4
Diagnosing ADHD in adults is relatively difficult, because a formal diagnosis generally requires symptoms to show up between the ages of 6 and 12.5 Also, clinicians can interview parents and family members to assess whether the classical features of ADHD were present in childhood for those suspected of having the condition.
Early vs. late presentation
Among the preschool population, it has been observed that emerging ADHD symptoms may progress with time or remain relatively constant with respect to the activities that children partake in. In some instances, impulsive behavior, especially compared with other symptoms, might be identified quickly by the attentive parent or caregiver. However, when ADHD appears in adulthood, it is possible that prior ADHD symptoms escaped detection – only to be diagnosed later in life because of varying presentations and the increased organizational demands of adulthood.
Meanwhile, diagnosis in adolescence can bring a different set of challenges to the forefront as teenagers face problems with self-management and responsibilities of daily living. These young people must cope with academic6 and social pressures – and a host of new societal expectations.
It is essential to understand how all of those societal factors have affected ADHD and its aspects, especially within the context of COVID-19. The coronavirus has introduced myriad challenges at the global level. Individuals with ADHD exhibit neurodevelopmental and corollary attention deficit issues that make them more susceptible to environmental stressors. Physical distancing practices might aggravate existing behavioral problems.
Distance forced by pandemic offers challenges
Despite the widespread adoption of telemedicine during the pandemic, some physicians think that the delivery of optimal care and the ability to adequately address patients’ health-related concerns have been compromised. Certainly, in the case of addressing the needs of patients with ADHD or related learning disorders, in-person examinations and clinical visits are best.
That is also the case for ADHD patients with comorbid sleep disorders. For those patients, it might be prudent to explore lifestyle changes (for example, improvements in sleep hygiene practices) before resorting to the use of pharmacologic agents such as hypnotics and melatonin. Along similar lines, the European ADHD Guideline Group (EAGG) advises the use of pharmacotherapy after the successful completion of a physical exam; patients already adhering to a treatment plan should continue therapy without interruption. Clinicians caring for patients with adult ADHD have faced a dilemma because treatment breaks increase the likelihood of illnesses resulting from the pandemic. Also, the inability to conduct treatment in person because of the pandemic raises concerns about pharmacotherapy.
The pandemic has affected the course of pediatric care and also has presented new challenges for adolescents as they begin to tackle unique problems related to their health concerns. In prepandemic times, teachers played integral roles in the diagnostic process, because they were able to readily identify children and teenagers with mental and physical challenges. In stark contrast, connecting with students online may not allow teachers to identify skill deficits in young patients or in adults with ADHD.
Furthermore, adults with ADHD and medical comorbidities may be at increased risk of disease exposure directly resulting from an inability to address their social and/or emotional well-being adequately. The social distancing and other mitigation measures advised by public health experts ensure safety and protection but also can present numerous hurdles for children, teenagers, adults – and their respective families.
Individuals with adult ADHD and other psychiatric disorders may downplay their psychological distress7 [for example, sleep dysfunction, issues concerning activities of daily living], and view it as being the natural product of the COVID-19 environment. As a result of their misconceptions, they may avoid increasing their medication dose to control emergent symptoms of hyperactivity and impulsivity, instead opting to manage stress without aid from health care professionals. The absence of patient-provider interactivity and the integration of telemedicine has introduced unnecessary obstacles with respect to medication management and therapy as well as general access to expert advice. It is of utmost importance for clinicians to identify at-risk patients and reeducate the adult ADHD patient on issues concerning medication intake and psychological wellness.
Individuals with developmental disorders may experience numerous setbacks when trying to navigate their environments. The lack of correct feedback, supervision, and guidance may adversely affect adults with ADHD, contributing toward a lack of self-esteem and social awareness.
Individuals with adult ADHD are more likely than are their younger counterparts to have medical comorbidities, such as cardiovascular disease8 and type 2 diabetes,9 so it is crucial to prescribe dietary instructions to patients. Sometimes patients with adult ADHD lack support in the form of acceptance by family and peers, so it is critical for the patient to come to terms with his/her condition and seek professional help, incorporating effective strategies wherever needed to maintain day-to-day functioning.
Other possible comorbidities
There can be risk factors associated with isolation of adults who have depression and/or anxiety, poor eating habits, and maladaptive behaviors. Other adverse health-related issues may include substance use disorder.10 Drug use suppresses developmental growth and may induce ADHD symptom exacerbation. Consistent with Khantzian’s self-medication hypothesis, among individuals with ADHD, including those who lack a formal diagnosis, there is a tendency to gravitate toward illicit substances, in particular, stimulants.11
We also know that adolescents are known to engage in normal risk-taking and social experimentation. Given that, the notion of boundary setting becomes a complicated affair during a pandemic. Adults may no longer be involved in the same types of risk-taking behaviors, but enforced self-isolation coupled with unchecked consumption of various social medial platforms continue to take a toll on personal development. Socialization plays an enormous role in maintaining psychological health, and social media is no substitute for in-person interactions. Such platforms can reduce mental growth opportunities and affect ADHD adults unfavorably.
For instance, it has been reported that women with adult ADHD are more likely to present with negative cognitive biases and symptoms of anxiety as a function of social media use.12,13 As clinicians, we should recommend introducing activities with the aim of enhancing self-acceptance, mindfulness, and the ability to engage in healthy lifestyles. A holistic framework that focuses on psychological wellness and physical fitness will ensure treatment success. Medication management may prove to be a challenge because of differences in dosing, response schedules, and agreed-upon diagnostic criteria used for young patients, compared with those needed for adults.
Treatment strategies
Before the pandemic, researchers were observing an increase globally in the ADHD diagnosis,14 and clinicians have been exploring the efficacy of select medications, sometimes with limited success.15 Stimulant medication, combined with behavioral interventions, is supported by evidenced-based medicine and is the treatment of choice for childhood ADHD.
The stimulant remedy considered to be the most efficacious for adult ADHD is methylphenidate or dextroamphetamine.
However, be sure to proceed with caution and prepare a thorough work-up, because there can be cardiovascular risk factors associated with these medications with a pronounced increase in heart rate and blood pressure.
Stimulant medications are known to increase the risk of stroke or myocardial infarction for individuals with preexisting cardiovascular anomalies or structural anomalies. The American Heart Association no longer recommends a baseline EKG before commencing stimulant therapy with the exception of preexisting cardiac risk. Nonstimulant medications such as atomoxetine are available as alternatives.
The process of finding therapies that will reduce symptoms of ADHD takes considerable time, and individuals may fail to notice improvements, at least initially.
Before prescribing any medicine or therapies, it is important to evaluate for factors that are specific to ADHD and rule out the presence of other learning or developmental disorders, to prevent negative consequences.
Health care professionals can introduce nonspecific interventions as a means of tackling complicated cases of adult ADHD, especially those that coincide with underlying medical conditions (for example, cardiovascular disease, seizure disorders, and/or eating disorders). In such cases, stimulant medications may lead to symptom exacerbation, and the health care professional should carry out a systematic evaluation (risks vs. benefits of drug classes), despite the limitations of online appointments over the course of the pandemic.
Moreover, ADHD symptoms can take on a more severe form within the context of preexisting mood and anxiety disorders. Unfortunately, these comorbidities may have a negative prognostic outcome, too, thereby increasing other health-related risk factors. Psychological interventions can be implemented via online assessments because of recent technological advances worldwide, providing a new level of confidence and social engagement. EEG-assisted biofeedback is an example of new technological modalities that may help improve the overall performance and functionality of individuals with adult ADHD.16 Numerous services and resources are available to patients and their families that can improve mental health and well-being.
Other nonpharmacologic choices also play an instrumental role in bringing harmony and organization into a patient’s life through the use of daily planners, alarms, and to-do lists. In addition, therapists can provide treatment that helps individuals get motivated and reduce their anxiety levels. Behavioral therapies support patient initiatives by increasing their productivity, activity management, and satisfaction. Cognitive-behavioral therapy (CBT), and marriage counseling and family therapy are modalities that may help adults with ADHD change underlying thoughts and perceptions and develop coping skills and self-esteem.
Appropriate to the pandemic situation is another treatment, e-therapy, which includes text-based communication, video calling, and phone calls. It is a low-cost and convenient alternative for people. For some patients, traveling to a particular clinic or counseling center can be difficult, and there is a shortage of counselors worldwide, so it is beneficial to talk with a counselor on a video/phone call or through social media. It is crucial for the ADHD coach to be trained with relevant knowledge to make plans, set goals, and manage a patient’s schedule of activities. For the counselor, sharing tips based on personal experience and making the appropriate suggestions allows adults with ADHD to stay motivated and focus on the task at hand. It should be noted that counselors play an important role in reducing stress levels for those diagnosed with ADHD, allowing patients to lead productive lives and achieve career goals.
Various online support communities can provide patients and their parents with educational resources, to address issues connected to ADHD in a professional manner.17
The road to treatment success
Any delays in treating adults with ADHD can lead to a frustrating situation in which the entire family will be affected. As stated earlier, numerous support groups are available to adults with ADHD, and some of those groups can offer valuable tips about addressing stress management and the diverse roles that parents and family members may play in patient care.18 These groups provide a network for people to exchange ideas and recommend strategies. Online support groups may connect patients directly with key opinion leaders and health care providers.
Individuals with ADHD often experience problems with organization and concentration – especially within the context of the pandemic – and receiving guidance from counselors will provide an opportunity to learn valuable coping strategies and manage symptoms, recognizing and mitigating any mood swings associated with anxiety or depression that emerge alongside their ADHD. Psychotherapy is instrumental in patient care, and individuals with adult ADHD should be taught to acknowledge the role of medications (for example, neglect, divert, or self-medicate). A holistic approach to managing ADHD symptoms is necessary for optimal functioning and independence.
Dr. Aman is a faculty member in the biology department of City Colleges of Chicago. She is a postdoctoral researcher at the International Maternal and Child Health Foundation (IMCHF), Montreal; a fellow, medical staff development, from the American Academy of Medical Management; and a Masters Online Teacher, University of Illinois at Chicago. Dr. Aman disclosed no relevant financial relationships. Dr. Islam is a medical adviser for the IMCHF, Montreal, and is based in New York. He is a postdoctoral fellow, psychopharmacologist, and a board-certified medical affairs specialist. Dr. Islam disclosed no relevant financial relationships. Dr. Karama is a psychiatrist at the Douglas Mental Health University Institute, Montreal. He is an assistant professor at the department of psychiatry, McGill University, also in Montreal. He has no disclosures. Dr. Choudhry is the chief scientific officer and head of the department of mental health and clinical research at the IMCHF. He has no disclosures.
References
1. J Atten Disord. 2020. doi: 10.1177/1087054720943271.
2. ADDitude Magazine. 2020 Jul 23.
3. Management of ADHD in Adults: What the Science Says. 2007 Oct 9. Guilford Press.
4. N Engl J Med. 2013 Nov 14;369(20):1935-44.
5. J Clin Psychiatry. 2002;63 Suppl 12:29-35.
6. J Atten Dis. 2015 Jan 12. doi: 10.1177/1087054144566076.
7. Psychiatry Res. 2020 Oct;292. doi: 10.1016/j.psychres.2020.113345.
8. Case Rep Cardiol. 2016. doi: 10.1155/2016/2343691.
9. Curr Diab Rep. 2019 Jun 27;19(8):46. doi: 10.1007/s11892-019-1174-x.
10. Curr Psychiatry Rep. 2014 Mar;16(3):436. doi: 10.1007/s/11920-013-0436-6.
11. Current Psychiatry. 2014 Dec;13(12):e3-4.
12. BMC Psychiatry. 2020;20(40). doi: 10.1186/s/12888-020-02707-9.
13. Psychol Addict Behav. 2016 Mar;30(2):252–62.
14. ADDitude Magazine. 2017 Apr 6.
15. Harv Mental Health Letter. 2009 Nov.
16. MGM J Med Sci. 2020 Jul 17(3):161-2.
17. J Child Psychol Psychiatry. 2020 Jul 7.
18. Int J Disaster Risk Reduct. 2020 Dec;51. doi: 10.1016/j.ijdrr.2020.101845.
As some countries brace for yet another possible surge in the COVID-19 pandemic – particularly among young adults who have not yet been vaccinated – clinicians should remain wary of the cardinal symptoms of adult ADHD.
Research from an Israeli study shows that individuals with unmedicated ADHD are 52% more likely to test positive for the virus.1,2
The symptoms of ADHD, including impulsiveness and inability to follow directions, combined with the tendency to leave adults with ADHD on their own to sort out COVID-19–related protocols – make these individuals susceptible to exposure.
As we know, ADHD is a condition characterized by a pervasive pattern of impulsivity and/or inattention, which greatly reduces organizational capabilities by interfering at the developmental level.3 Other key symptoms include short attention span, hyperactivity, restlessness, difficulty in prioritizing tasks, and an absence of time awareness. Symptom presentation of ADHD is contingent upon the nature of the individual’s overall mental health and etiologic issues that may be traced back to the brain’s development.4
Diagnosing ADHD in adults is relatively difficult, because a formal diagnosis generally requires symptoms to show up between the ages of 6 and 12.5 Also, clinicians can interview parents and family members to assess whether the classical features of ADHD were present in childhood for those suspected of having the condition.
Early vs. late presentation
Among the preschool population, it has been observed that emerging ADHD symptoms may progress with time or remain relatively constant with respect to the activities that children partake in. In some instances, impulsive behavior, especially compared with other symptoms, might be identified quickly by the attentive parent or caregiver. However, when ADHD appears in adulthood, it is possible that prior ADHD symptoms escaped detection – only to be diagnosed later in life because of varying presentations and the increased organizational demands of adulthood.
Meanwhile, diagnosis in adolescence can bring a different set of challenges to the forefront as teenagers face problems with self-management and responsibilities of daily living. These young people must cope with academic6 and social pressures – and a host of new societal expectations.
It is essential to understand how all of those societal factors have affected ADHD and its aspects, especially within the context of COVID-19. The coronavirus has introduced myriad challenges at the global level. Individuals with ADHD exhibit neurodevelopmental and corollary attention deficit issues that make them more susceptible to environmental stressors. Physical distancing practices might aggravate existing behavioral problems.
Distance forced by pandemic offers challenges
Despite the widespread adoption of telemedicine during the pandemic, some physicians think that the delivery of optimal care and the ability to adequately address patients’ health-related concerns have been compromised. Certainly, in the case of addressing the needs of patients with ADHD or related learning disorders, in-person examinations and clinical visits are best.
That is also the case for ADHD patients with comorbid sleep disorders. For those patients, it might be prudent to explore lifestyle changes (for example, improvements in sleep hygiene practices) before resorting to the use of pharmacologic agents such as hypnotics and melatonin. Along similar lines, the European ADHD Guideline Group (EAGG) advises the use of pharmacotherapy after the successful completion of a physical exam; patients already adhering to a treatment plan should continue therapy without interruption. Clinicians caring for patients with adult ADHD have faced a dilemma because treatment breaks increase the likelihood of illnesses resulting from the pandemic. Also, the inability to conduct treatment in person because of the pandemic raises concerns about pharmacotherapy.
The pandemic has affected the course of pediatric care and also has presented new challenges for adolescents as they begin to tackle unique problems related to their health concerns. In prepandemic times, teachers played integral roles in the diagnostic process, because they were able to readily identify children and teenagers with mental and physical challenges. In stark contrast, connecting with students online may not allow teachers to identify skill deficits in young patients or in adults with ADHD.
Furthermore, adults with ADHD and medical comorbidities may be at increased risk of disease exposure directly resulting from an inability to address their social and/or emotional well-being adequately. The social distancing and other mitigation measures advised by public health experts ensure safety and protection but also can present numerous hurdles for children, teenagers, adults – and their respective families.
Individuals with adult ADHD and other psychiatric disorders may downplay their psychological distress7 [for example, sleep dysfunction, issues concerning activities of daily living], and view it as being the natural product of the COVID-19 environment. As a result of their misconceptions, they may avoid increasing their medication dose to control emergent symptoms of hyperactivity and impulsivity, instead opting to manage stress without aid from health care professionals. The absence of patient-provider interactivity and the integration of telemedicine has introduced unnecessary obstacles with respect to medication management and therapy as well as general access to expert advice. It is of utmost importance for clinicians to identify at-risk patients and reeducate the adult ADHD patient on issues concerning medication intake and psychological wellness.
Individuals with developmental disorders may experience numerous setbacks when trying to navigate their environments. The lack of correct feedback, supervision, and guidance may adversely affect adults with ADHD, contributing toward a lack of self-esteem and social awareness.
Individuals with adult ADHD are more likely than are their younger counterparts to have medical comorbidities, such as cardiovascular disease8 and type 2 diabetes,9 so it is crucial to prescribe dietary instructions to patients. Sometimes patients with adult ADHD lack support in the form of acceptance by family and peers, so it is critical for the patient to come to terms with his/her condition and seek professional help, incorporating effective strategies wherever needed to maintain day-to-day functioning.
Other possible comorbidities
There can be risk factors associated with isolation of adults who have depression and/or anxiety, poor eating habits, and maladaptive behaviors. Other adverse health-related issues may include substance use disorder.10 Drug use suppresses developmental growth and may induce ADHD symptom exacerbation. Consistent with Khantzian’s self-medication hypothesis, among individuals with ADHD, including those who lack a formal diagnosis, there is a tendency to gravitate toward illicit substances, in particular, stimulants.11
We also know that adolescents are known to engage in normal risk-taking and social experimentation. Given that, the notion of boundary setting becomes a complicated affair during a pandemic. Adults may no longer be involved in the same types of risk-taking behaviors, but enforced self-isolation coupled with unchecked consumption of various social medial platforms continue to take a toll on personal development. Socialization plays an enormous role in maintaining psychological health, and social media is no substitute for in-person interactions. Such platforms can reduce mental growth opportunities and affect ADHD adults unfavorably.
For instance, it has been reported that women with adult ADHD are more likely to present with negative cognitive biases and symptoms of anxiety as a function of social media use.12,13 As clinicians, we should recommend introducing activities with the aim of enhancing self-acceptance, mindfulness, and the ability to engage in healthy lifestyles. A holistic framework that focuses on psychological wellness and physical fitness will ensure treatment success. Medication management may prove to be a challenge because of differences in dosing, response schedules, and agreed-upon diagnostic criteria used for young patients, compared with those needed for adults.
Treatment strategies
Before the pandemic, researchers were observing an increase globally in the ADHD diagnosis,14 and clinicians have been exploring the efficacy of select medications, sometimes with limited success.15 Stimulant medication, combined with behavioral interventions, is supported by evidenced-based medicine and is the treatment of choice for childhood ADHD.
The stimulant remedy considered to be the most efficacious for adult ADHD is methylphenidate or dextroamphetamine.
However, be sure to proceed with caution and prepare a thorough work-up, because there can be cardiovascular risk factors associated with these medications with a pronounced increase in heart rate and blood pressure.
Stimulant medications are known to increase the risk of stroke or myocardial infarction for individuals with preexisting cardiovascular anomalies or structural anomalies. The American Heart Association no longer recommends a baseline EKG before commencing stimulant therapy with the exception of preexisting cardiac risk. Nonstimulant medications such as atomoxetine are available as alternatives.
The process of finding therapies that will reduce symptoms of ADHD takes considerable time, and individuals may fail to notice improvements, at least initially.
Before prescribing any medicine or therapies, it is important to evaluate for factors that are specific to ADHD and rule out the presence of other learning or developmental disorders, to prevent negative consequences.
Health care professionals can introduce nonspecific interventions as a means of tackling complicated cases of adult ADHD, especially those that coincide with underlying medical conditions (for example, cardiovascular disease, seizure disorders, and/or eating disorders). In such cases, stimulant medications may lead to symptom exacerbation, and the health care professional should carry out a systematic evaluation (risks vs. benefits of drug classes), despite the limitations of online appointments over the course of the pandemic.
Moreover, ADHD symptoms can take on a more severe form within the context of preexisting mood and anxiety disorders. Unfortunately, these comorbidities may have a negative prognostic outcome, too, thereby increasing other health-related risk factors. Psychological interventions can be implemented via online assessments because of recent technological advances worldwide, providing a new level of confidence and social engagement. EEG-assisted biofeedback is an example of new technological modalities that may help improve the overall performance and functionality of individuals with adult ADHD.16 Numerous services and resources are available to patients and their families that can improve mental health and well-being.
Other nonpharmacologic choices also play an instrumental role in bringing harmony and organization into a patient’s life through the use of daily planners, alarms, and to-do lists. In addition, therapists can provide treatment that helps individuals get motivated and reduce their anxiety levels. Behavioral therapies support patient initiatives by increasing their productivity, activity management, and satisfaction. Cognitive-behavioral therapy (CBT), and marriage counseling and family therapy are modalities that may help adults with ADHD change underlying thoughts and perceptions and develop coping skills and self-esteem.
Appropriate to the pandemic situation is another treatment, e-therapy, which includes text-based communication, video calling, and phone calls. It is a low-cost and convenient alternative for people. For some patients, traveling to a particular clinic or counseling center can be difficult, and there is a shortage of counselors worldwide, so it is beneficial to talk with a counselor on a video/phone call or through social media. It is crucial for the ADHD coach to be trained with relevant knowledge to make plans, set goals, and manage a patient’s schedule of activities. For the counselor, sharing tips based on personal experience and making the appropriate suggestions allows adults with ADHD to stay motivated and focus on the task at hand. It should be noted that counselors play an important role in reducing stress levels for those diagnosed with ADHD, allowing patients to lead productive lives and achieve career goals.
Various online support communities can provide patients and their parents with educational resources, to address issues connected to ADHD in a professional manner.17
The road to treatment success
Any delays in treating adults with ADHD can lead to a frustrating situation in which the entire family will be affected. As stated earlier, numerous support groups are available to adults with ADHD, and some of those groups can offer valuable tips about addressing stress management and the diverse roles that parents and family members may play in patient care.18 These groups provide a network for people to exchange ideas and recommend strategies. Online support groups may connect patients directly with key opinion leaders and health care providers.
Individuals with ADHD often experience problems with organization and concentration – especially within the context of the pandemic – and receiving guidance from counselors will provide an opportunity to learn valuable coping strategies and manage symptoms, recognizing and mitigating any mood swings associated with anxiety or depression that emerge alongside their ADHD. Psychotherapy is instrumental in patient care, and individuals with adult ADHD should be taught to acknowledge the role of medications (for example, neglect, divert, or self-medicate). A holistic approach to managing ADHD symptoms is necessary for optimal functioning and independence.
Dr. Aman is a faculty member in the biology department of City Colleges of Chicago. She is a postdoctoral researcher at the International Maternal and Child Health Foundation (IMCHF), Montreal; a fellow, medical staff development, from the American Academy of Medical Management; and a Masters Online Teacher, University of Illinois at Chicago. Dr. Aman disclosed no relevant financial relationships. Dr. Islam is a medical adviser for the IMCHF, Montreal, and is based in New York. He is a postdoctoral fellow, psychopharmacologist, and a board-certified medical affairs specialist. Dr. Islam disclosed no relevant financial relationships. Dr. Karama is a psychiatrist at the Douglas Mental Health University Institute, Montreal. He is an assistant professor at the department of psychiatry, McGill University, also in Montreal. He has no disclosures. Dr. Choudhry is the chief scientific officer and head of the department of mental health and clinical research at the IMCHF. He has no disclosures.
References
1. J Atten Disord. 2020. doi: 10.1177/1087054720943271.
2. ADDitude Magazine. 2020 Jul 23.
3. Management of ADHD in Adults: What the Science Says. 2007 Oct 9. Guilford Press.
4. N Engl J Med. 2013 Nov 14;369(20):1935-44.
5. J Clin Psychiatry. 2002;63 Suppl 12:29-35.
6. J Atten Dis. 2015 Jan 12. doi: 10.1177/1087054144566076.
7. Psychiatry Res. 2020 Oct;292. doi: 10.1016/j.psychres.2020.113345.
8. Case Rep Cardiol. 2016. doi: 10.1155/2016/2343691.
9. Curr Diab Rep. 2019 Jun 27;19(8):46. doi: 10.1007/s11892-019-1174-x.
10. Curr Psychiatry Rep. 2014 Mar;16(3):436. doi: 10.1007/s/11920-013-0436-6.
11. Current Psychiatry. 2014 Dec;13(12):e3-4.
12. BMC Psychiatry. 2020;20(40). doi: 10.1186/s/12888-020-02707-9.
13. Psychol Addict Behav. 2016 Mar;30(2):252–62.
14. ADDitude Magazine. 2017 Apr 6.
15. Harv Mental Health Letter. 2009 Nov.
16. MGM J Med Sci. 2020 Jul 17(3):161-2.
17. J Child Psychol Psychiatry. 2020 Jul 7.
18. Int J Disaster Risk Reduct. 2020 Dec;51. doi: 10.1016/j.ijdrr.2020.101845.
Antipsychotics protective against COVID-19?
Antipsychotics may protect against SARS-CoV-2 infection or lead to a milder course of illness, new research suggests.
“Counterintuitively,” the investigators noted, vulnerable people with severe mental illness “on antipsychotic treatment showed a lower risk of SARS-CoV-2 infection and a likely better COVID-19 prognosis.”
“These are very interesting findings that reflect a clinical reality where we see few patients with severe COVID-19, despite the presence of various risk factors,” study investigator Manuel Canal-Rivero, PhD, clinical psychologist, Virgen del Rocio University Hospital, Sevilla, Spain, said in a news release.
“The number of COVID-19 patients is lower than expected among this group of people and in cases where a proven infection does occur, the evolution is benign and does not reach a life-threatening clinical situation. These data as a whole seem to point to the protective effect of the medication,” Dr. Canal-Rivero added.
The study was published online as a letter to the editor February 19, 2021, in Schizophrenia Research.
A ‘striking’ finding
The researchers assessed the prevalence and prognosis of COVID-19 in 698 patients with serious mental disorders (SMDs) receiving treatment with long-acting injectable antipsychotic medication. The non-SMD population included the catchment area population of 557,576 individuals.
From February to November 2020, 4.1% of the non-SMD population were infected with SARS-CoV-2 versus just 1.3% of the SMD population (9 of 698 patients). All but one patient with SMD had asymptomatic illness (8 of 9, 89%). Accurate information on asymptomatic illness in the non-SMD population was not available.
There were also fewer hospital admissions in the SMD population (0% vs. 8.5%), ICU admissions (0% vs. 0.9%) and deaths because of COVID-19 (0% vs. 1.1%), although the differences were not statistically significant.
In related research, the same investigators found that many of the genes whose expression is altered by SARS-CoV-2 infection are significantly down-regulated by antipsychotic drugs.
“In a striking way, we have shown how antipsychotics reduce the activation of genes involved in many of the inflammatory and immunological pathways associated with the severity of COVID-19 infection,” Benedicto Crespo-Facorro, MD, PhD, University of Sevilla, who led the study, said in the news release.
“Although this finding requires replication, the discovery could be very significant because the treatment of COVID-19 with drugs originally indicated for unrelated clinical situations, that is to say drug repositioning, has been shown to be an interesting source of effective treatments for COVID-19 patients,” he added.
Antiviral properties?
In a comment, Samoon Ahmad, MD, professor, department of psychiatry, New York University, said the findings are “fascinating” and should be explored further.

While the findings on long-acting injectable antipsychotic treatment “seem counterintuitive at first, they are in line with other studies,” said Dr. Ahmad, who heads the inpatient psychiatry unit at Bellevue Hospital Center and is founder of the Integrative Center for Wellness in New York.
“ and antidepressant medications appear to activate key cellular proteins that the SARS-CoV-2 virus uses for replication,” explained Dr. Ahmad, who was not associated with the study.
For example, as reported by this news organization, a preliminary study published in 2020 showed that early treatment with the antidepressant fluvoxamine prevented clinical deterioration in adult outpatients with confirmed COVID-19.
The antipsychotic aripiprazole has also shown potential to treat severe COVID-19 infection.
“Consequently, there appears to be a possible explanation as to why these drugs afford patients with severe mental disorders increased protection against the SARS-CoV-2 virus,” Dr. Ahmad said in an interview.
However, he cautioned, there are several factors at play that could influence the results. Therefore, more research is needed before drawing any firm conclusions.
“Still, the possibility that psychiatric medications may have antiviral properties is a tremendous development and I really hope that additional studies confirm the preliminary findings,” Dr. Ahmad said.
The study had no specific funding. The authors and Dr. Ahmad disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Antipsychotics may protect against SARS-CoV-2 infection or lead to a milder course of illness, new research suggests.
“Counterintuitively,” the investigators noted, vulnerable people with severe mental illness “on antipsychotic treatment showed a lower risk of SARS-CoV-2 infection and a likely better COVID-19 prognosis.”
“These are very interesting findings that reflect a clinical reality where we see few patients with severe COVID-19, despite the presence of various risk factors,” study investigator Manuel Canal-Rivero, PhD, clinical psychologist, Virgen del Rocio University Hospital, Sevilla, Spain, said in a news release.
“The number of COVID-19 patients is lower than expected among this group of people and in cases where a proven infection does occur, the evolution is benign and does not reach a life-threatening clinical situation. These data as a whole seem to point to the protective effect of the medication,” Dr. Canal-Rivero added.
The study was published online as a letter to the editor February 19, 2021, in Schizophrenia Research.
A ‘striking’ finding
The researchers assessed the prevalence and prognosis of COVID-19 in 698 patients with serious mental disorders (SMDs) receiving treatment with long-acting injectable antipsychotic medication. The non-SMD population included the catchment area population of 557,576 individuals.
From February to November 2020, 4.1% of the non-SMD population were infected with SARS-CoV-2 versus just 1.3% of the SMD population (9 of 698 patients). All but one patient with SMD had asymptomatic illness (8 of 9, 89%). Accurate information on asymptomatic illness in the non-SMD population was not available.
There were also fewer hospital admissions in the SMD population (0% vs. 8.5%), ICU admissions (0% vs. 0.9%) and deaths because of COVID-19 (0% vs. 1.1%), although the differences were not statistically significant.
In related research, the same investigators found that many of the genes whose expression is altered by SARS-CoV-2 infection are significantly down-regulated by antipsychotic drugs.
“In a striking way, we have shown how antipsychotics reduce the activation of genes involved in many of the inflammatory and immunological pathways associated with the severity of COVID-19 infection,” Benedicto Crespo-Facorro, MD, PhD, University of Sevilla, who led the study, said in the news release.
“Although this finding requires replication, the discovery could be very significant because the treatment of COVID-19 with drugs originally indicated for unrelated clinical situations, that is to say drug repositioning, has been shown to be an interesting source of effective treatments for COVID-19 patients,” he added.
Antiviral properties?
In a comment, Samoon Ahmad, MD, professor, department of psychiatry, New York University, said the findings are “fascinating” and should be explored further.
While the findings on long-acting injectable antipsychotic treatment “seem counterintuitive at first, they are in line with other studies,” said Dr. Ahmad, who heads the inpatient psychiatry unit at Bellevue Hospital Center and is founder of the Integrative Center for Wellness in New York.
“ and antidepressant medications appear to activate key cellular proteins that the SARS-CoV-2 virus uses for replication,” explained Dr. Ahmad, who was not associated with the study.
For example, as reported by this news organization, a preliminary study published in 2020 showed that early treatment with the antidepressant fluvoxamine prevented clinical deterioration in adult outpatients with confirmed COVID-19.
The antipsychotic aripiprazole has also shown potential to treat severe COVID-19 infection.
“Consequently, there appears to be a possible explanation as to why these drugs afford patients with severe mental disorders increased protection against the SARS-CoV-2 virus,” Dr. Ahmad said in an interview.
However, he cautioned, there are several factors at play that could influence the results. Therefore, more research is needed before drawing any firm conclusions.
“Still, the possibility that psychiatric medications may have antiviral properties is a tremendous development and I really hope that additional studies confirm the preliminary findings,” Dr. Ahmad said.
The study had no specific funding. The authors and Dr. Ahmad disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Antipsychotics may protect against SARS-CoV-2 infection or lead to a milder course of illness, new research suggests.
“Counterintuitively,” the investigators noted, vulnerable people with severe mental illness “on antipsychotic treatment showed a lower risk of SARS-CoV-2 infection and a likely better COVID-19 prognosis.”
“These are very interesting findings that reflect a clinical reality where we see few patients with severe COVID-19, despite the presence of various risk factors,” study investigator Manuel Canal-Rivero, PhD, clinical psychologist, Virgen del Rocio University Hospital, Sevilla, Spain, said in a news release.
“The number of COVID-19 patients is lower than expected among this group of people and in cases where a proven infection does occur, the evolution is benign and does not reach a life-threatening clinical situation. These data as a whole seem to point to the protective effect of the medication,” Dr. Canal-Rivero added.
The study was published online as a letter to the editor February 19, 2021, in Schizophrenia Research.
A ‘striking’ finding
The researchers assessed the prevalence and prognosis of COVID-19 in 698 patients with serious mental disorders (SMDs) receiving treatment with long-acting injectable antipsychotic medication. The non-SMD population included the catchment area population of 557,576 individuals.
From February to November 2020, 4.1% of the non-SMD population were infected with SARS-CoV-2 versus just 1.3% of the SMD population (9 of 698 patients). All but one patient with SMD had asymptomatic illness (8 of 9, 89%). Accurate information on asymptomatic illness in the non-SMD population was not available.
There were also fewer hospital admissions in the SMD population (0% vs. 8.5%), ICU admissions (0% vs. 0.9%) and deaths because of COVID-19 (0% vs. 1.1%), although the differences were not statistically significant.
In related research, the same investigators found that many of the genes whose expression is altered by SARS-CoV-2 infection are significantly down-regulated by antipsychotic drugs.
“In a striking way, we have shown how antipsychotics reduce the activation of genes involved in many of the inflammatory and immunological pathways associated with the severity of COVID-19 infection,” Benedicto Crespo-Facorro, MD, PhD, University of Sevilla, who led the study, said in the news release.
“Although this finding requires replication, the discovery could be very significant because the treatment of COVID-19 with drugs originally indicated for unrelated clinical situations, that is to say drug repositioning, has been shown to be an interesting source of effective treatments for COVID-19 patients,” he added.
Antiviral properties?
In a comment, Samoon Ahmad, MD, professor, department of psychiatry, New York University, said the findings are “fascinating” and should be explored further.
While the findings on long-acting injectable antipsychotic treatment “seem counterintuitive at first, they are in line with other studies,” said Dr. Ahmad, who heads the inpatient psychiatry unit at Bellevue Hospital Center and is founder of the Integrative Center for Wellness in New York.
“ and antidepressant medications appear to activate key cellular proteins that the SARS-CoV-2 virus uses for replication,” explained Dr. Ahmad, who was not associated with the study.
For example, as reported by this news organization, a preliminary study published in 2020 showed that early treatment with the antidepressant fluvoxamine prevented clinical deterioration in adult outpatients with confirmed COVID-19.
The antipsychotic aripiprazole has also shown potential to treat severe COVID-19 infection.
“Consequently, there appears to be a possible explanation as to why these drugs afford patients with severe mental disorders increased protection against the SARS-CoV-2 virus,” Dr. Ahmad said in an interview.
However, he cautioned, there are several factors at play that could influence the results. Therefore, more research is needed before drawing any firm conclusions.
“Still, the possibility that psychiatric medications may have antiviral properties is a tremendous development and I really hope that additional studies confirm the preliminary findings,” Dr. Ahmad said.
The study had no specific funding. The authors and Dr. Ahmad disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Let me tell you about my vaccine
Welcome to our national obsession: Vaccines! You may have noticed – it’s all talk, all the time, with short breaks to discuss what we’re watching on Netflix.

For months, every session with almost every patient includes a commentary on someone they know who has gotten “the shot.” Before our state expanded eligibility to all adults, the discussion might include thoughts about who deserves to go first, who “cut the line,” how they did it, what vaccine is best, and worries about side effects.

And it’s not just my patients: With every friend, with every acquaintance, and even just walking by strangers who are conversing, the topic of discussion is vaccines. The narratives are similar; people want to talk about who has gotten vaccinated, why they qualified, where they went, which one they got, and what side effects they experienced. This is followed by a discussion about what they are now doing that they weren’t doing before being vaccinated, if anything. Some have returned to indoor restaurant dining, others only dine outdoors, still others continue to avoid public settings. There are the fully vaccinated, the partially vaccinated, and those scheduled for the first shot. In the unvaccinated/unregistered group there are the vaccine-hesitants and vaccine-refusers, with their concerns about everything from the safety of the agent to whether the government is using this as a way to insert tracker chips into all of us. There is enthusiasm, trepidation, anxiety, fear, excitement, relief, and absolute joy.
Recently I opened two emails from old friends I have not communicated with in a long time. Both emails began with, “I am fully vaccinated.” And yes, I heard the status of his wife and two children. In the course of one work day, I received distressed text messages from two patients about vaccines – one was anxious about having received the Janssen vaccine that was paused that morning, another was worried about getting a second dose of the Pfizer vaccine later in the week because he was having a symptom that could be indicative of COVID-19. I suggested that his primary care physician might be a better resource for this, but then added that he should probably get tested and delay having the second dose if positive. It seems I did have thoughts about a course of action after all.
Some psychiatrists have wondered how to handle patient questions about their own vaccination status. I have taken the stance that we are physicians, and that patients who may be seeing us – now or in the future – for in-person appointments are entitled to know if we pose a risk to their health, and so I have chosen to answer, without further exploration, when patients ask if I’ve received that coronavirus vaccine. Some psychiatrists feel it is our responsibility to share this information with our patients as a way of modeling safe behavior, and I have had one patient who said she would not be getting vaccinated until I told her that I thought she should.
“Did you get it?” she asked.
“I did,” I responded.
“Okay, if you got it, I will.” She soon discovered that vaccinations were hard to come by and that in her social group, being vaccinated was something of a status symbol. In addition to the worry about contracting a potentially fatal virus, her hesitancy yielded to “vaccine FOMO” or fear of missing out.
Some psychiatrists have felt uneasy with a question that pertains to their personal health, or have used the question as a springboard for exploration. Nicole Leistikow, MD (fully vaccinated, Moderna), is a psychiatrist in private practice in Baltimore. She notes, “Recently, I was discussing vaccination with a patient who wasn’t sure what information to believe or how much to trust the U.S. government. My careful exploration comparing different risks was not very helpful. I mentioned that I was vaccinated and that if he got vaccinated, he could come for a low-risk, in-person appointment after a year of telephone visits. This proved to be a winning argument and he called back later that day to say he had already had his first shot from leftover vaccine at his pharmacy.”
I grew up in a world that did not question vaccines. You got them and they were good things. No one asked which pharmaceutical company manufactured the vaccine. We trusted the system and our physicians. Schools asked for proof of vaccination, and it never occurred to me not to be vaccinated. Life has grown more complicated in the last 30 years, and the groups of people who are opposed to being vaccinated are more diverse. Those opposed to getting a COVID-19 vaccine are not necessarily the same as the broader group of anti-vaxxers that spawned from the fear that childhood vaccines cause autism. For some, it’s a personal issue related to their own health and risk perception, for others it’s a polarized political issue, and for another group there is the question of where their trust lies.
What lies ahead in our postvaccine world? This will be our next national conversation, and just as we negotiated our own levels of comfort with regard to working and socializing during the pandemic, I imagine the postvaccine world will have the same adjustment. There already are cases of COVID-19 in those who have been fully vaccinated, as well as the rare hospitalizations and deaths – we simply cannot expect a vaccine that did so well in controlled studies of tens of thousands of study subjects to do as well when given to tens of millions of uncontrolled citizens. One of the first deaths in a fully vaccinated person in late March was an older psychologist, and it remains unclear how effective the vaccine is for immunocompromised patients. Some people will play it very safe, eschewing all activities that entail risk, while others will choose to adhere to either their own intuition about what is safe, or to the recommendations of Anthony S. Fauci, MD, and the Centers for Disease Control and Prevention.
I’ll end with a final thought from the Twitter feed of Ashish K. Jha, MD, dean of the School of Public Health at Brown University, Providence, R.I. Dr. Jha tweeted, “Once you get fully vaccinated, it absolutely changes what you can do safely.” It seems our national conversation is not slated to change anytime soon.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore.
Welcome to our national obsession: Vaccines! You may have noticed – it’s all talk, all the time, with short breaks to discuss what we’re watching on Netflix.
For months, every session with almost every patient includes a commentary on someone they know who has gotten “the shot.” Before our state expanded eligibility to all adults, the discussion might include thoughts about who deserves to go first, who “cut the line,” how they did it, what vaccine is best, and worries about side effects.
And it’s not just my patients: With every friend, with every acquaintance, and even just walking by strangers who are conversing, the topic of discussion is vaccines. The narratives are similar; people want to talk about who has gotten vaccinated, why they qualified, where they went, which one they got, and what side effects they experienced. This is followed by a discussion about what they are now doing that they weren’t doing before being vaccinated, if anything. Some have returned to indoor restaurant dining, others only dine outdoors, still others continue to avoid public settings. There are the fully vaccinated, the partially vaccinated, and those scheduled for the first shot. In the unvaccinated/unregistered group there are the vaccine-hesitants and vaccine-refusers, with their concerns about everything from the safety of the agent to whether the government is using this as a way to insert tracker chips into all of us. There is enthusiasm, trepidation, anxiety, fear, excitement, relief, and absolute joy.
Recently I opened two emails from old friends I have not communicated with in a long time. Both emails began with, “I am fully vaccinated.” And yes, I heard the status of his wife and two children. In the course of one work day, I received distressed text messages from two patients about vaccines – one was anxious about having received the Janssen vaccine that was paused that morning, another was worried about getting a second dose of the Pfizer vaccine later in the week because he was having a symptom that could be indicative of COVID-19. I suggested that his primary care physician might be a better resource for this, but then added that he should probably get tested and delay having the second dose if positive. It seems I did have thoughts about a course of action after all.
Some psychiatrists have wondered how to handle patient questions about their own vaccination status. I have taken the stance that we are physicians, and that patients who may be seeing us – now or in the future – for in-person appointments are entitled to know if we pose a risk to their health, and so I have chosen to answer, without further exploration, when patients ask if I’ve received that coronavirus vaccine. Some psychiatrists feel it is our responsibility to share this information with our patients as a way of modeling safe behavior, and I have had one patient who said she would not be getting vaccinated until I told her that I thought she should.
“Did you get it?” she asked.
“I did,” I responded.
“Okay, if you got it, I will.” She soon discovered that vaccinations were hard to come by and that in her social group, being vaccinated was something of a status symbol. In addition to the worry about contracting a potentially fatal virus, her hesitancy yielded to “vaccine FOMO” or fear of missing out.
Some psychiatrists have felt uneasy with a question that pertains to their personal health, or have used the question as a springboard for exploration. Nicole Leistikow, MD (fully vaccinated, Moderna), is a psychiatrist in private practice in Baltimore. She notes, “Recently, I was discussing vaccination with a patient who wasn’t sure what information to believe or how much to trust the U.S. government. My careful exploration comparing different risks was not very helpful. I mentioned that I was vaccinated and that if he got vaccinated, he could come for a low-risk, in-person appointment after a year of telephone visits. This proved to be a winning argument and he called back later that day to say he had already had his first shot from leftover vaccine at his pharmacy.”
I grew up in a world that did not question vaccines. You got them and they were good things. No one asked which pharmaceutical company manufactured the vaccine. We trusted the system and our physicians. Schools asked for proof of vaccination, and it never occurred to me not to be vaccinated. Life has grown more complicated in the last 30 years, and the groups of people who are opposed to being vaccinated are more diverse. Those opposed to getting a COVID-19 vaccine are not necessarily the same as the broader group of anti-vaxxers that spawned from the fear that childhood vaccines cause autism. For some, it’s a personal issue related to their own health and risk perception, for others it’s a polarized political issue, and for another group there is the question of where their trust lies.
What lies ahead in our postvaccine world? This will be our next national conversation, and just as we negotiated our own levels of comfort with regard to working and socializing during the pandemic, I imagine the postvaccine world will have the same adjustment. There already are cases of COVID-19 in those who have been fully vaccinated, as well as the rare hospitalizations and deaths – we simply cannot expect a vaccine that did so well in controlled studies of tens of thousands of study subjects to do as well when given to tens of millions of uncontrolled citizens. One of the first deaths in a fully vaccinated person in late March was an older psychologist, and it remains unclear how effective the vaccine is for immunocompromised patients. Some people will play it very safe, eschewing all activities that entail risk, while others will choose to adhere to either their own intuition about what is safe, or to the recommendations of Anthony S. Fauci, MD, and the Centers for Disease Control and Prevention.
I’ll end with a final thought from the Twitter feed of Ashish K. Jha, MD, dean of the School of Public Health at Brown University, Providence, R.I. Dr. Jha tweeted, “Once you get fully vaccinated, it absolutely changes what you can do safely.” It seems our national conversation is not slated to change anytime soon.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore.
Welcome to our national obsession: Vaccines! You may have noticed – it’s all talk, all the time, with short breaks to discuss what we’re watching on Netflix.
For months, every session with almost every patient includes a commentary on someone they know who has gotten “the shot.” Before our state expanded eligibility to all adults, the discussion might include thoughts about who deserves to go first, who “cut the line,” how they did it, what vaccine is best, and worries about side effects.
And it’s not just my patients: With every friend, with every acquaintance, and even just walking by strangers who are conversing, the topic of discussion is vaccines. The narratives are similar; people want to talk about who has gotten vaccinated, why they qualified, where they went, which one they got, and what side effects they experienced. This is followed by a discussion about what they are now doing that they weren’t doing before being vaccinated, if anything. Some have returned to indoor restaurant dining, others only dine outdoors, still others continue to avoid public settings. There are the fully vaccinated, the partially vaccinated, and those scheduled for the first shot. In the unvaccinated/unregistered group there are the vaccine-hesitants and vaccine-refusers, with their concerns about everything from the safety of the agent to whether the government is using this as a way to insert tracker chips into all of us. There is enthusiasm, trepidation, anxiety, fear, excitement, relief, and absolute joy.
Recently I opened two emails from old friends I have not communicated with in a long time. Both emails began with, “I am fully vaccinated.” And yes, I heard the status of his wife and two children. In the course of one work day, I received distressed text messages from two patients about vaccines – one was anxious about having received the Janssen vaccine that was paused that morning, another was worried about getting a second dose of the Pfizer vaccine later in the week because he was having a symptom that could be indicative of COVID-19. I suggested that his primary care physician might be a better resource for this, but then added that he should probably get tested and delay having the second dose if positive. It seems I did have thoughts about a course of action after all.
Some psychiatrists have wondered how to handle patient questions about their own vaccination status. I have taken the stance that we are physicians, and that patients who may be seeing us – now or in the future – for in-person appointments are entitled to know if we pose a risk to their health, and so I have chosen to answer, without further exploration, when patients ask if I’ve received that coronavirus vaccine. Some psychiatrists feel it is our responsibility to share this information with our patients as a way of modeling safe behavior, and I have had one patient who said she would not be getting vaccinated until I told her that I thought she should.
“Did you get it?” she asked.
“I did,” I responded.
“Okay, if you got it, I will.” She soon discovered that vaccinations were hard to come by and that in her social group, being vaccinated was something of a status symbol. In addition to the worry about contracting a potentially fatal virus, her hesitancy yielded to “vaccine FOMO” or fear of missing out.
Some psychiatrists have felt uneasy with a question that pertains to their personal health, or have used the question as a springboard for exploration. Nicole Leistikow, MD (fully vaccinated, Moderna), is a psychiatrist in private practice in Baltimore. She notes, “Recently, I was discussing vaccination with a patient who wasn’t sure what information to believe or how much to trust the U.S. government. My careful exploration comparing different risks was not very helpful. I mentioned that I was vaccinated and that if he got vaccinated, he could come for a low-risk, in-person appointment after a year of telephone visits. This proved to be a winning argument and he called back later that day to say he had already had his first shot from leftover vaccine at his pharmacy.”
I grew up in a world that did not question vaccines. You got them and they were good things. No one asked which pharmaceutical company manufactured the vaccine. We trusted the system and our physicians. Schools asked for proof of vaccination, and it never occurred to me not to be vaccinated. Life has grown more complicated in the last 30 years, and the groups of people who are opposed to being vaccinated are more diverse. Those opposed to getting a COVID-19 vaccine are not necessarily the same as the broader group of anti-vaxxers that spawned from the fear that childhood vaccines cause autism. For some, it’s a personal issue related to their own health and risk perception, for others it’s a polarized political issue, and for another group there is the question of where their trust lies.
What lies ahead in our postvaccine world? This will be our next national conversation, and just as we negotiated our own levels of comfort with regard to working and socializing during the pandemic, I imagine the postvaccine world will have the same adjustment. There already are cases of COVID-19 in those who have been fully vaccinated, as well as the rare hospitalizations and deaths – we simply cannot expect a vaccine that did so well in controlled studies of tens of thousands of study subjects to do as well when given to tens of millions of uncontrolled citizens. One of the first deaths in a fully vaccinated person in late March was an older psychologist, and it remains unclear how effective the vaccine is for immunocompromised patients. Some people will play it very safe, eschewing all activities that entail risk, while others will choose to adhere to either their own intuition about what is safe, or to the recommendations of Anthony S. Fauci, MD, and the Centers for Disease Control and Prevention.
I’ll end with a final thought from the Twitter feed of Ashish K. Jha, MD, dean of the School of Public Health at Brown University, Providence, R.I. Dr. Jha tweeted, “Once you get fully vaccinated, it absolutely changes what you can do safely.” It seems our national conversation is not slated to change anytime soon.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore.
Adolescent substance use and the COVID-19 pandemic
During the past year, adolescents, families, educators, and health care providers have had to press forward through myriad challenges and stressors with flexibility and adaptability. With appropriate concern, we ask ourselves how children and youth are coping emotionally with the unprecedented changes of the past year.

Adolescent substance use represents an important area of concern. What has happened during the pandemic? Has youth substance use increased or decreased? Has access to substances increased or decreased, has monitoring and support for at-risk youth increased or decreased?
The answers to these questions are mixed. If anything, the pandemic has highlighted the heterogeneity of adolescent substance use. Now is a key time for assessment, support, and conversation with teens and families.
Monitoring the Future (MTF), a nationally representative annual survey, has provided a broad perspective on trends of adolescent substance use for decades.1 The MTF data is usually collected from February to May and was cut short in 2020 because of school closures associated with the pandemic. The sample size, though still nationally representative, was about a quarter of the typical volume. Some of the data are encouraging, including a flattening out of previous years’ stark increase in vaping of both nicotine and cannabis products (though overall numbers remain alarmingly high). Other data are more concerning including a continued increase in misuse of cough medicine, amphetamines, and inhalants among the youngest cohort surveyed (eighth graders). However, these data were largely representative of prepandemic circumstances.
The COVID-19 pandemic has significantly affected risk and protective factors for teen drug and alcohol use. Most notably, it has had a widely observed negative impact on adolescent mental health, across multiple disease categories.2 In addition, the cancellation of in-person academic and extracurricular activities such as arts and athletics markedly increased unstructured time, a known associated factor for higher-risk activities including substance use. This has also led to decreased contact with many supportive adults such as teachers and coaches. On the other hand, some adolescents now have more time with supportive parents and caregivers, more meals together, and more supervision, all of which are associated with decreased likelihood of substance use disorders.
The highly variable reasons for substance use affect highly variable pandemic-related changes in use. Understanding the impetus for use is a good place to start conversation and can help providers assess risk of escalation during the pandemic. Some teens primarily use for social enhancement while others use as a means of coping with stress or to mask or escape negative emotions. Still others continue use because of physiological dependence, craving, and other symptoms consistent with use disorders.
Highlighting the heterogeneity of this issue, one study assessing use early in the pandemic showed a decrease in the percentage of teens who use substances but an increase in frequency of use for those who are using.3 Though expected, an increase in frequency of use by oneself as compared with peers was also notable. Using substances alone is associated with more severe use disorders, carries greater risk of overdose, and can increase shame and secrecy, further fueling use disorders.
The pandemic has thus represented a protective pause for some experimental or socially motivated substance-using teens who have experienced a period of abstinence even if not fully by choice. For others, it has represented an acute amplification of risk factors and use has accelerated. This latter group includes those whose use represents an effort to cope with depression, anxiety, and loneliness or for whom isolation at home represents less monitoring, increased access, and greater exposure to substances.
Over the past year, in the treatment of adolescents struggling with substance use, many clinicians have observed a sifting effect during these unprecedented social changes. Many youth, who no longer have access to substances, have found they can “take it or leave it”. Other youth have been observed engaging in additional risk or going to greater lengths to access substances and continue their use. For both groups and everyone in between, this is an important time for screening, clinical assessment, and support.
While anticipating further research and data regarding broad substance use trends, including MTF data from 2021, recognizing that the impact of the COVID-19 pandemic is individual, with marked differences from adolescent to adolescent, will help us continue to act now to assess this important area of adolescent health. The first step for primary care providers is unchanged: to routinely screen for and discuss substance use in clinical settings.
Two brief, validated, easily accessible screening tools are available for primary care settings. They can both be self-administered and take less than 2 minutes to complete. Screening, Brief Intervention and Referral to Treatment and the Brief Screener for Tobacco, Alcohol and other Drugs can both be used for youth aged 12-17 years.4,5 Both screens are available online at drugabuse.gov.6
Routine screening will normalize conversations about substance use and healthy choices, provide opportunities for positive reinforcement, identify adolescents at risk, increase comfort and competence in providing brief intervention, and expedite referrals for additional support and treatment.
A false assumption that a particular adolescent isn’t using substances creates a missed opportunity to offer guidance and treatment. An oft-overlooked opportunity is that of providing positive reinforcement for an adolescent who isn’t using any substances or experimenting at all. Positive reinforcement is a strong component of reinforcing health maintenance.
Parent guidance and family assessment will also be critical tools. Parents and caregivers play a primary role in substance use treatment for teens and have a contributory impact on risk through both genes and environment. Of note, research suggests a moderate overall increase in adult substance use during the pandemic, particularly substances that are widely available such as alcohol. Adolescents may thus have greater access and exposure to substance use. A remarkably high percentage, 42%, of substance-using teens surveyed early in the pandemic indicated that they were using substances with their parents.3 Parents, who have equally been challenged by the pandemic, may need guidance in balancing compassion and support for struggling youth, while setting appropriate limits and maintaining expectations of healthy activities.
Unprecedented change and uncertainty provide an opportunity to reassess risks and openly discuss substance use with youth and families. Even with much on our minds during the COVID-19 pandemic, we can maintain focus on this significant risk to adolescent health and wellness. Our efforts now, from screening to treatment for adolescent substance use should be reinforced rather than delayed.
Dr. Jackson is assistant professor of psychiatry at the University of Vermont, Burlington.
References
1. Monitoringthefuture.org
2. Jones EAK et al. Int J Environ Res Public Health, 2021;18(5):2470.
3. Dumas TM et al. J Adolesc Health, 2020;67(3):354-61.
4. Levy S et al. JAMA Pediatr. 2014;168(9):822-8.
5. Kelly SM et al. Pediatrics. 2014;133(5):819-26.
6. National Institute on Drug Abuse. Adolescent Substance Use Screening Tools. 2016 Apr 27. https://www.drugabuse.gov/nidamed-medical-health-professionals/screening-tools-prevention/screening-tools-adolescent-substance-use/adolescent-substance-use-screening-tools
During the past year, adolescents, families, educators, and health care providers have had to press forward through myriad challenges and stressors with flexibility and adaptability. With appropriate concern, we ask ourselves how children and youth are coping emotionally with the unprecedented changes of the past year.
Adolescent substance use represents an important area of concern. What has happened during the pandemic? Has youth substance use increased or decreased? Has access to substances increased or decreased, has monitoring and support for at-risk youth increased or decreased?
The answers to these questions are mixed. If anything, the pandemic has highlighted the heterogeneity of adolescent substance use. Now is a key time for assessment, support, and conversation with teens and families.
Monitoring the Future (MTF), a nationally representative annual survey, has provided a broad perspective on trends of adolescent substance use for decades.1 The MTF data is usually collected from February to May and was cut short in 2020 because of school closures associated with the pandemic. The sample size, though still nationally representative, was about a quarter of the typical volume. Some of the data are encouraging, including a flattening out of previous years’ stark increase in vaping of both nicotine and cannabis products (though overall numbers remain alarmingly high). Other data are more concerning including a continued increase in misuse of cough medicine, amphetamines, and inhalants among the youngest cohort surveyed (eighth graders). However, these data were largely representative of prepandemic circumstances.
The COVID-19 pandemic has significantly affected risk and protective factors for teen drug and alcohol use. Most notably, it has had a widely observed negative impact on adolescent mental health, across multiple disease categories.2 In addition, the cancellation of in-person academic and extracurricular activities such as arts and athletics markedly increased unstructured time, a known associated factor for higher-risk activities including substance use. This has also led to decreased contact with many supportive adults such as teachers and coaches. On the other hand, some adolescents now have more time with supportive parents and caregivers, more meals together, and more supervision, all of which are associated with decreased likelihood of substance use disorders.
The highly variable reasons for substance use affect highly variable pandemic-related changes in use. Understanding the impetus for use is a good place to start conversation and can help providers assess risk of escalation during the pandemic. Some teens primarily use for social enhancement while others use as a means of coping with stress or to mask or escape negative emotions. Still others continue use because of physiological dependence, craving, and other symptoms consistent with use disorders.
Highlighting the heterogeneity of this issue, one study assessing use early in the pandemic showed a decrease in the percentage of teens who use substances but an increase in frequency of use for those who are using.3 Though expected, an increase in frequency of use by oneself as compared with peers was also notable. Using substances alone is associated with more severe use disorders, carries greater risk of overdose, and can increase shame and secrecy, further fueling use disorders.
The pandemic has thus represented a protective pause for some experimental or socially motivated substance-using teens who have experienced a period of abstinence even if not fully by choice. For others, it has represented an acute amplification of risk factors and use has accelerated. This latter group includes those whose use represents an effort to cope with depression, anxiety, and loneliness or for whom isolation at home represents less monitoring, increased access, and greater exposure to substances.
Over the past year, in the treatment of adolescents struggling with substance use, many clinicians have observed a sifting effect during these unprecedented social changes. Many youth, who no longer have access to substances, have found they can “take it or leave it”. Other youth have been observed engaging in additional risk or going to greater lengths to access substances and continue their use. For both groups and everyone in between, this is an important time for screening, clinical assessment, and support.
While anticipating further research and data regarding broad substance use trends, including MTF data from 2021, recognizing that the impact of the COVID-19 pandemic is individual, with marked differences from adolescent to adolescent, will help us continue to act now to assess this important area of adolescent health. The first step for primary care providers is unchanged: to routinely screen for and discuss substance use in clinical settings.
Two brief, validated, easily accessible screening tools are available for primary care settings. They can both be self-administered and take less than 2 minutes to complete. Screening, Brief Intervention and Referral to Treatment and the Brief Screener for Tobacco, Alcohol and other Drugs can both be used for youth aged 12-17 years.4,5 Both screens are available online at drugabuse.gov.6
Routine screening will normalize conversations about substance use and healthy choices, provide opportunities for positive reinforcement, identify adolescents at risk, increase comfort and competence in providing brief intervention, and expedite referrals for additional support and treatment.
A false assumption that a particular adolescent isn’t using substances creates a missed opportunity to offer guidance and treatment. An oft-overlooked opportunity is that of providing positive reinforcement for an adolescent who isn’t using any substances or experimenting at all. Positive reinforcement is a strong component of reinforcing health maintenance.
Parent guidance and family assessment will also be critical tools. Parents and caregivers play a primary role in substance use treatment for teens and have a contributory impact on risk through both genes and environment. Of note, research suggests a moderate overall increase in adult substance use during the pandemic, particularly substances that are widely available such as alcohol. Adolescents may thus have greater access and exposure to substance use. A remarkably high percentage, 42%, of substance-using teens surveyed early in the pandemic indicated that they were using substances with their parents.3 Parents, who have equally been challenged by the pandemic, may need guidance in balancing compassion and support for struggling youth, while setting appropriate limits and maintaining expectations of healthy activities.
Unprecedented change and uncertainty provide an opportunity to reassess risks and openly discuss substance use with youth and families. Even with much on our minds during the COVID-19 pandemic, we can maintain focus on this significant risk to adolescent health and wellness. Our efforts now, from screening to treatment for adolescent substance use should be reinforced rather than delayed.
Dr. Jackson is assistant professor of psychiatry at the University of Vermont, Burlington.
References
1. Monitoringthefuture.org
2. Jones EAK et al. Int J Environ Res Public Health, 2021;18(5):2470.
3. Dumas TM et al. J Adolesc Health, 2020;67(3):354-61.
4. Levy S et al. JAMA Pediatr. 2014;168(9):822-8.
5. Kelly SM et al. Pediatrics. 2014;133(5):819-26.
6. National Institute on Drug Abuse. Adolescent Substance Use Screening Tools. 2016 Apr 27. https://www.drugabuse.gov/nidamed-medical-health-professionals/screening-tools-prevention/screening-tools-adolescent-substance-use/adolescent-substance-use-screening-tools
During the past year, adolescents, families, educators, and health care providers have had to press forward through myriad challenges and stressors with flexibility and adaptability. With appropriate concern, we ask ourselves how children and youth are coping emotionally with the unprecedented changes of the past year.
Adolescent substance use represents an important area of concern. What has happened during the pandemic? Has youth substance use increased or decreased? Has access to substances increased or decreased, has monitoring and support for at-risk youth increased or decreased?
The answers to these questions are mixed. If anything, the pandemic has highlighted the heterogeneity of adolescent substance use. Now is a key time for assessment, support, and conversation with teens and families.
Monitoring the Future (MTF), a nationally representative annual survey, has provided a broad perspective on trends of adolescent substance use for decades.1 The MTF data is usually collected from February to May and was cut short in 2020 because of school closures associated with the pandemic. The sample size, though still nationally representative, was about a quarter of the typical volume. Some of the data are encouraging, including a flattening out of previous years’ stark increase in vaping of both nicotine and cannabis products (though overall numbers remain alarmingly high). Other data are more concerning including a continued increase in misuse of cough medicine, amphetamines, and inhalants among the youngest cohort surveyed (eighth graders). However, these data were largely representative of prepandemic circumstances.
The COVID-19 pandemic has significantly affected risk and protective factors for teen drug and alcohol use. Most notably, it has had a widely observed negative impact on adolescent mental health, across multiple disease categories.2 In addition, the cancellation of in-person academic and extracurricular activities such as arts and athletics markedly increased unstructured time, a known associated factor for higher-risk activities including substance use. This has also led to decreased contact with many supportive adults such as teachers and coaches. On the other hand, some adolescents now have more time with supportive parents and caregivers, more meals together, and more supervision, all of which are associated with decreased likelihood of substance use disorders.
The highly variable reasons for substance use affect highly variable pandemic-related changes in use. Understanding the impetus for use is a good place to start conversation and can help providers assess risk of escalation during the pandemic. Some teens primarily use for social enhancement while others use as a means of coping with stress or to mask or escape negative emotions. Still others continue use because of physiological dependence, craving, and other symptoms consistent with use disorders.
Highlighting the heterogeneity of this issue, one study assessing use early in the pandemic showed a decrease in the percentage of teens who use substances but an increase in frequency of use for those who are using.3 Though expected, an increase in frequency of use by oneself as compared with peers was also notable. Using substances alone is associated with more severe use disorders, carries greater risk of overdose, and can increase shame and secrecy, further fueling use disorders.
The pandemic has thus represented a protective pause for some experimental or socially motivated substance-using teens who have experienced a period of abstinence even if not fully by choice. For others, it has represented an acute amplification of risk factors and use has accelerated. This latter group includes those whose use represents an effort to cope with depression, anxiety, and loneliness or for whom isolation at home represents less monitoring, increased access, and greater exposure to substances.
Over the past year, in the treatment of adolescents struggling with substance use, many clinicians have observed a sifting effect during these unprecedented social changes. Many youth, who no longer have access to substances, have found they can “take it or leave it”. Other youth have been observed engaging in additional risk or going to greater lengths to access substances and continue their use. For both groups and everyone in between, this is an important time for screening, clinical assessment, and support.
While anticipating further research and data regarding broad substance use trends, including MTF data from 2021, recognizing that the impact of the COVID-19 pandemic is individual, with marked differences from adolescent to adolescent, will help us continue to act now to assess this important area of adolescent health. The first step for primary care providers is unchanged: to routinely screen for and discuss substance use in clinical settings.
Two brief, validated, easily accessible screening tools are available for primary care settings. They can both be self-administered and take less than 2 minutes to complete. Screening, Brief Intervention and Referral to Treatment and the Brief Screener for Tobacco, Alcohol and other Drugs can both be used for youth aged 12-17 years.4,5 Both screens are available online at drugabuse.gov.6
Routine screening will normalize conversations about substance use and healthy choices, provide opportunities for positive reinforcement, identify adolescents at risk, increase comfort and competence in providing brief intervention, and expedite referrals for additional support and treatment.
A false assumption that a particular adolescent isn’t using substances creates a missed opportunity to offer guidance and treatment. An oft-overlooked opportunity is that of providing positive reinforcement for an adolescent who isn’t using any substances or experimenting at all. Positive reinforcement is a strong component of reinforcing health maintenance.
Parent guidance and family assessment will also be critical tools. Parents and caregivers play a primary role in substance use treatment for teens and have a contributory impact on risk through both genes and environment. Of note, research suggests a moderate overall increase in adult substance use during the pandemic, particularly substances that are widely available such as alcohol. Adolescents may thus have greater access and exposure to substance use. A remarkably high percentage, 42%, of substance-using teens surveyed early in the pandemic indicated that they were using substances with their parents.3 Parents, who have equally been challenged by the pandemic, may need guidance in balancing compassion and support for struggling youth, while setting appropriate limits and maintaining expectations of healthy activities.
Unprecedented change and uncertainty provide an opportunity to reassess risks and openly discuss substance use with youth and families. Even with much on our minds during the COVID-19 pandemic, we can maintain focus on this significant risk to adolescent health and wellness. Our efforts now, from screening to treatment for adolescent substance use should be reinforced rather than delayed.
Dr. Jackson is assistant professor of psychiatry at the University of Vermont, Burlington.
References
1. Monitoringthefuture.org
2. Jones EAK et al. Int J Environ Res Public Health, 2021;18(5):2470.
3. Dumas TM et al. J Adolesc Health, 2020;67(3):354-61.
4. Levy S et al. JAMA Pediatr. 2014;168(9):822-8.
5. Kelly SM et al. Pediatrics. 2014;133(5):819-26.
6. National Institute on Drug Abuse. Adolescent Substance Use Screening Tools. 2016 Apr 27. https://www.drugabuse.gov/nidamed-medical-health-professionals/screening-tools-prevention/screening-tools-adolescent-substance-use/adolescent-substance-use-screening-tools