User login
Early onset of atopic dermatitis linked to poorer control
according to a study published in the Journal of the American Academy of Dermatology.
Atopic dermatitis most commonly arises in infancy but also can emerge in later childhood and even adolescence, leading to a distinction between early- and late-onset disease, wrote Joy Wan, MD, of the University of Pennsylvania, Philadelphia, and coauthors.
“Early-onset, mid-onset, and late-onset AD appear to differ in the presence of active disease over time; however, whether these groups also differ in terms of the severity of AD is unknown,” they wrote.
In this observational cohort study, 8,015 individuals with childhood-onset atopic dermatitis – 53% of whom were female – were assessed twice-yearly for up to 10 years. Nearly three-quarters (72%) of the group had early-onset atopic dermatitis – defined as onset before 2 years of age – while 19% had mid-onset disease (3-7 years) and 9% had late-onset disease (8-17 years).
The study found that older age of onset was associated with better control, such that for each additional year of age at the onset of disease, there was a 7% reduction in the odds of poorer control of disease. Those who had mid-onset disease had a 29% lower odds of poorer control compared with those with early-onset, while those with late-onset disease had a 49% lower odds of poorer control.
The likelihood of atopic dermatitis persisting beyond childhood also appeared to be linked to the age of onset. Those with mid-onset disease had a 55% lower odds of persistent atopic dermatitis, compared with those with early-onset disease, while those with late-onset disease had an 81% lower odds.
“In all 3 groups, the proportion of subjects reporting persistent AD generally declined with older age, and the differences among the 3 onset age groups were most pronounced from early adolescence onward,” the authors wrote.
They noted that there was considerable research currently focused on identifying distinct atopic dermatitis phenotypes and endotypes, and their evidence on the different disease course for early-, mid-, and late-onset disease supported this idea of disease subtypes.
“However, additional research is needed to understand whether and how early-, mid-, and late-onset AD differ molecularly or immunologically, and whether they respond differentially to treatment,” they wrote. They also suggested that the timing of onset could help identify patients who were at greater risk of persistent or poorly controlled disease, and who benefits from more intensive monitoring or treatment.
The study was partly supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases and the Dermatology Foundation. Three authors declared funding, consultancies, or advisory board positions with the pharmaceutical sector. No other conflicts of interest were declared.
SOURCE: Wan J et al. J Am Acad Dermatol. 2019 Dec;81(6):1292-9.
according to a study published in the Journal of the American Academy of Dermatology.
Atopic dermatitis most commonly arises in infancy but also can emerge in later childhood and even adolescence, leading to a distinction between early- and late-onset disease, wrote Joy Wan, MD, of the University of Pennsylvania, Philadelphia, and coauthors.
“Early-onset, mid-onset, and late-onset AD appear to differ in the presence of active disease over time; however, whether these groups also differ in terms of the severity of AD is unknown,” they wrote.
In this observational cohort study, 8,015 individuals with childhood-onset atopic dermatitis – 53% of whom were female – were assessed twice-yearly for up to 10 years. Nearly three-quarters (72%) of the group had early-onset atopic dermatitis – defined as onset before 2 years of age – while 19% had mid-onset disease (3-7 years) and 9% had late-onset disease (8-17 years).
The study found that older age of onset was associated with better control, such that for each additional year of age at the onset of disease, there was a 7% reduction in the odds of poorer control of disease. Those who had mid-onset disease had a 29% lower odds of poorer control compared with those with early-onset, while those with late-onset disease had a 49% lower odds of poorer control.
The likelihood of atopic dermatitis persisting beyond childhood also appeared to be linked to the age of onset. Those with mid-onset disease had a 55% lower odds of persistent atopic dermatitis, compared with those with early-onset disease, while those with late-onset disease had an 81% lower odds.
“In all 3 groups, the proportion of subjects reporting persistent AD generally declined with older age, and the differences among the 3 onset age groups were most pronounced from early adolescence onward,” the authors wrote.
They noted that there was considerable research currently focused on identifying distinct atopic dermatitis phenotypes and endotypes, and their evidence on the different disease course for early-, mid-, and late-onset disease supported this idea of disease subtypes.
“However, additional research is needed to understand whether and how early-, mid-, and late-onset AD differ molecularly or immunologically, and whether they respond differentially to treatment,” they wrote. They also suggested that the timing of onset could help identify patients who were at greater risk of persistent or poorly controlled disease, and who benefits from more intensive monitoring or treatment.
The study was partly supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases and the Dermatology Foundation. Three authors declared funding, consultancies, or advisory board positions with the pharmaceutical sector. No other conflicts of interest were declared.
SOURCE: Wan J et al. J Am Acad Dermatol. 2019 Dec;81(6):1292-9.
according to a study published in the Journal of the American Academy of Dermatology.
Atopic dermatitis most commonly arises in infancy but also can emerge in later childhood and even adolescence, leading to a distinction between early- and late-onset disease, wrote Joy Wan, MD, of the University of Pennsylvania, Philadelphia, and coauthors.
“Early-onset, mid-onset, and late-onset AD appear to differ in the presence of active disease over time; however, whether these groups also differ in terms of the severity of AD is unknown,” they wrote.
In this observational cohort study, 8,015 individuals with childhood-onset atopic dermatitis – 53% of whom were female – were assessed twice-yearly for up to 10 years. Nearly three-quarters (72%) of the group had early-onset atopic dermatitis – defined as onset before 2 years of age – while 19% had mid-onset disease (3-7 years) and 9% had late-onset disease (8-17 years).
The study found that older age of onset was associated with better control, such that for each additional year of age at the onset of disease, there was a 7% reduction in the odds of poorer control of disease. Those who had mid-onset disease had a 29% lower odds of poorer control compared with those with early-onset, while those with late-onset disease had a 49% lower odds of poorer control.
The likelihood of atopic dermatitis persisting beyond childhood also appeared to be linked to the age of onset. Those with mid-onset disease had a 55% lower odds of persistent atopic dermatitis, compared with those with early-onset disease, while those with late-onset disease had an 81% lower odds.
“In all 3 groups, the proportion of subjects reporting persistent AD generally declined with older age, and the differences among the 3 onset age groups were most pronounced from early adolescence onward,” the authors wrote.
They noted that there was considerable research currently focused on identifying distinct atopic dermatitis phenotypes and endotypes, and their evidence on the different disease course for early-, mid-, and late-onset disease supported this idea of disease subtypes.
“However, additional research is needed to understand whether and how early-, mid-, and late-onset AD differ molecularly or immunologically, and whether they respond differentially to treatment,” they wrote. They also suggested that the timing of onset could help identify patients who were at greater risk of persistent or poorly controlled disease, and who benefits from more intensive monitoring or treatment.
The study was partly supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases and the Dermatology Foundation. Three authors declared funding, consultancies, or advisory board positions with the pharmaceutical sector. No other conflicts of interest were declared.
SOURCE: Wan J et al. J Am Acad Dermatol. 2019 Dec;81(6):1292-9.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
IL-1 alpha is a new target in atopic dermatitis
MADRID – on the basis of an encouraging phase 2, proof-of-concept study involving bermekimab, an investigational monoclonal antibody directed at that cytokine.

The mechanism of benefit is unclear, although there are a number of plausible possibilities, all orbiting around the notion that AD is not only a Th2 immunity–mediated disease, but that Th1 immunity plays a role, too.
“The ultimate proof, as you will see, is that it works,” Alice B. Gottlieb, MD, PhD, observed in presenting the phase 2 study findings at the annual congress of the European Academy of Dermatology and Venereology.
Bermekimab is a monoclonal antibody cloned from human peripheral B lymphocytes. Sources of its target – IL-1 alpha – that are of therapeutic relevance include neutrophils, keratinocytes, platelets, and monocytes.
The study included 10 adults with moderate to severe AD who received a single subcutaneous injection of 200 mg of bermekimab and 28 who received 400 mg weekly for 8 weeks. Lumping together the various outcome measures employed in the study, the 400-mg dose was three times more effective than the 200-mg dose, a finding explainable by the 240% higher serum levels at 400 mg, according to Dr. Gottlieb, medical director of Mount Sinai Beth Israel Dermatology in the department of dermatology at the Icahn School of Medicine at Mount Sinai, New York.
This was a small, uncontrolled, proof-of-concept study; at this early stage, results painted a favorable picture of efficacy and safety. For example, scores on the Eczema Area and Severity Index dropped by a mean of 65% from baseline at week 4 of bermekimab at 400 mg/week and by 80% at week 8. Scoring Atopic Dermatitis scores dropped by about 55% at week 4 and by nearly 70% at 8 weeks. Scores on the 0-4 Investigator Global Assessment improved by 1.2 points at week 4 and 1.4 points by week 8. Dermatology Life Quality Index scores improved by a mean of 70% by week 8, at which point 61% of patients had a DLQI of 0-1, indicating that AD had no or only a slight impact on quality of life. Scores on the Hospital Anxiety and Depression Scale improved by about 45% at 4 weeks and 65% at 8 weeks.
At baseline, most patients rated their pain as 7 out of 10. By week 8, pain scores had dropped by an average of 80%, and 80% of patients experienced a 4-point drop or greater. Similarly, 80% of patients had at least a 4-point drop in their self-rated worst itch scores on a 0-10 scale. The greatest improvement in both pain and itch scores occurred in the first 4 weeks, after which further improvement continued, albeit at a slower rate.
Adverse events consisted of grade 2 wheezing in two patients, grade 1 nausea in two patients, and a 3% rate of mild injection-site reactions.
An audience member rose to comment: “This is really interesting data, and it goes against everything that we think about atopic dermatitis. But we know from allergic contact dermatitis that IL-1 is a very early signal coming out of keratinocytes. It almost makes you wonder whether that’s not a primary problem in atopic dermatitis that we haven’t realized – that the keratinocytes are under stress because of damage to the skin barrier or other functions, and by alleviating that stress by blocking IL-1, you block the progression into what we previously thought was an Th2-mediated disease, atopic dermatitis.”
“I was thinking that, too – that the keratinocytes could be playing a role in atopic dermatitis through IL-1,” Dr. Gottlieb replied.
She noted that her Mount Sinai colleague Emma Guttman-Yassky, MD, PhD, and coinvestigators have demonstrated that a monoclonal antibody that blocks IL-17C is effective in treating AD, and that IL-17C causes keratinocytes to release proinflammatory IL-1 alpha. High levels of IL-1 alpha have been shown to drive leukocyte recruitment into the skin, promote breakdown of the skin barrier through production of matrix metalloproteinase, stimulate itch by a direct effect on nerves, and cause leaky vascular endothelium.
A phase 2 study of bermekimab for treatment of AD enrolled the first patient in mid-November. In addition, Dr. Gottlieb has led a positive phase 2 study of the monoclonal antibody in patients with hidradenitis suppurativa, with a phase 3 trial in the works.
She reported receiving research funding from and serving as a consultant without personal compensation to XBiotech, which sponsored the AD and hidradenitis suppurativa studies. She has similar financial relationships with numerous pharmaceutical companies developing psoriasis medications.
MADRID – on the basis of an encouraging phase 2, proof-of-concept study involving bermekimab, an investigational monoclonal antibody directed at that cytokine.
The mechanism of benefit is unclear, although there are a number of plausible possibilities, all orbiting around the notion that AD is not only a Th2 immunity–mediated disease, but that Th1 immunity plays a role, too.
“The ultimate proof, as you will see, is that it works,” Alice B. Gottlieb, MD, PhD, observed in presenting the phase 2 study findings at the annual congress of the European Academy of Dermatology and Venereology.
Bermekimab is a monoclonal antibody cloned from human peripheral B lymphocytes. Sources of its target – IL-1 alpha – that are of therapeutic relevance include neutrophils, keratinocytes, platelets, and monocytes.
The study included 10 adults with moderate to severe AD who received a single subcutaneous injection of 200 mg of bermekimab and 28 who received 400 mg weekly for 8 weeks. Lumping together the various outcome measures employed in the study, the 400-mg dose was three times more effective than the 200-mg dose, a finding explainable by the 240% higher serum levels at 400 mg, according to Dr. Gottlieb, medical director of Mount Sinai Beth Israel Dermatology in the department of dermatology at the Icahn School of Medicine at Mount Sinai, New York.
This was a small, uncontrolled, proof-of-concept study; at this early stage, results painted a favorable picture of efficacy and safety. For example, scores on the Eczema Area and Severity Index dropped by a mean of 65% from baseline at week 4 of bermekimab at 400 mg/week and by 80% at week 8. Scoring Atopic Dermatitis scores dropped by about 55% at week 4 and by nearly 70% at 8 weeks. Scores on the 0-4 Investigator Global Assessment improved by 1.2 points at week 4 and 1.4 points by week 8. Dermatology Life Quality Index scores improved by a mean of 70% by week 8, at which point 61% of patients had a DLQI of 0-1, indicating that AD had no or only a slight impact on quality of life. Scores on the Hospital Anxiety and Depression Scale improved by about 45% at 4 weeks and 65% at 8 weeks.
At baseline, most patients rated their pain as 7 out of 10. By week 8, pain scores had dropped by an average of 80%, and 80% of patients experienced a 4-point drop or greater. Similarly, 80% of patients had at least a 4-point drop in their self-rated worst itch scores on a 0-10 scale. The greatest improvement in both pain and itch scores occurred in the first 4 weeks, after which further improvement continued, albeit at a slower rate.
Adverse events consisted of grade 2 wheezing in two patients, grade 1 nausea in two patients, and a 3% rate of mild injection-site reactions.
An audience member rose to comment: “This is really interesting data, and it goes against everything that we think about atopic dermatitis. But we know from allergic contact dermatitis that IL-1 is a very early signal coming out of keratinocytes. It almost makes you wonder whether that’s not a primary problem in atopic dermatitis that we haven’t realized – that the keratinocytes are under stress because of damage to the skin barrier or other functions, and by alleviating that stress by blocking IL-1, you block the progression into what we previously thought was an Th2-mediated disease, atopic dermatitis.”
“I was thinking that, too – that the keratinocytes could be playing a role in atopic dermatitis through IL-1,” Dr. Gottlieb replied.
She noted that her Mount Sinai colleague Emma Guttman-Yassky, MD, PhD, and coinvestigators have demonstrated that a monoclonal antibody that blocks IL-17C is effective in treating AD, and that IL-17C causes keratinocytes to release proinflammatory IL-1 alpha. High levels of IL-1 alpha have been shown to drive leukocyte recruitment into the skin, promote breakdown of the skin barrier through production of matrix metalloproteinase, stimulate itch by a direct effect on nerves, and cause leaky vascular endothelium.
A phase 2 study of bermekimab for treatment of AD enrolled the first patient in mid-November. In addition, Dr. Gottlieb has led a positive phase 2 study of the monoclonal antibody in patients with hidradenitis suppurativa, with a phase 3 trial in the works.
She reported receiving research funding from and serving as a consultant without personal compensation to XBiotech, which sponsored the AD and hidradenitis suppurativa studies. She has similar financial relationships with numerous pharmaceutical companies developing psoriasis medications.
MADRID – on the basis of an encouraging phase 2, proof-of-concept study involving bermekimab, an investigational monoclonal antibody directed at that cytokine.
The mechanism of benefit is unclear, although there are a number of plausible possibilities, all orbiting around the notion that AD is not only a Th2 immunity–mediated disease, but that Th1 immunity plays a role, too.
“The ultimate proof, as you will see, is that it works,” Alice B. Gottlieb, MD, PhD, observed in presenting the phase 2 study findings at the annual congress of the European Academy of Dermatology and Venereology.
Bermekimab is a monoclonal antibody cloned from human peripheral B lymphocytes. Sources of its target – IL-1 alpha – that are of therapeutic relevance include neutrophils, keratinocytes, platelets, and monocytes.
The study included 10 adults with moderate to severe AD who received a single subcutaneous injection of 200 mg of bermekimab and 28 who received 400 mg weekly for 8 weeks. Lumping together the various outcome measures employed in the study, the 400-mg dose was three times more effective than the 200-mg dose, a finding explainable by the 240% higher serum levels at 400 mg, according to Dr. Gottlieb, medical director of Mount Sinai Beth Israel Dermatology in the department of dermatology at the Icahn School of Medicine at Mount Sinai, New York.
This was a small, uncontrolled, proof-of-concept study; at this early stage, results painted a favorable picture of efficacy and safety. For example, scores on the Eczema Area and Severity Index dropped by a mean of 65% from baseline at week 4 of bermekimab at 400 mg/week and by 80% at week 8. Scoring Atopic Dermatitis scores dropped by about 55% at week 4 and by nearly 70% at 8 weeks. Scores on the 0-4 Investigator Global Assessment improved by 1.2 points at week 4 and 1.4 points by week 8. Dermatology Life Quality Index scores improved by a mean of 70% by week 8, at which point 61% of patients had a DLQI of 0-1, indicating that AD had no or only a slight impact on quality of life. Scores on the Hospital Anxiety and Depression Scale improved by about 45% at 4 weeks and 65% at 8 weeks.
At baseline, most patients rated their pain as 7 out of 10. By week 8, pain scores had dropped by an average of 80%, and 80% of patients experienced a 4-point drop or greater. Similarly, 80% of patients had at least a 4-point drop in their self-rated worst itch scores on a 0-10 scale. The greatest improvement in both pain and itch scores occurred in the first 4 weeks, after which further improvement continued, albeit at a slower rate.
Adverse events consisted of grade 2 wheezing in two patients, grade 1 nausea in two patients, and a 3% rate of mild injection-site reactions.
An audience member rose to comment: “This is really interesting data, and it goes against everything that we think about atopic dermatitis. But we know from allergic contact dermatitis that IL-1 is a very early signal coming out of keratinocytes. It almost makes you wonder whether that’s not a primary problem in atopic dermatitis that we haven’t realized – that the keratinocytes are under stress because of damage to the skin barrier or other functions, and by alleviating that stress by blocking IL-1, you block the progression into what we previously thought was an Th2-mediated disease, atopic dermatitis.”
“I was thinking that, too – that the keratinocytes could be playing a role in atopic dermatitis through IL-1,” Dr. Gottlieb replied.
She noted that her Mount Sinai colleague Emma Guttman-Yassky, MD, PhD, and coinvestigators have demonstrated that a monoclonal antibody that blocks IL-17C is effective in treating AD, and that IL-17C causes keratinocytes to release proinflammatory IL-1 alpha. High levels of IL-1 alpha have been shown to drive leukocyte recruitment into the skin, promote breakdown of the skin barrier through production of matrix metalloproteinase, stimulate itch by a direct effect on nerves, and cause leaky vascular endothelium.
A phase 2 study of bermekimab for treatment of AD enrolled the first patient in mid-November. In addition, Dr. Gottlieb has led a positive phase 2 study of the monoclonal antibody in patients with hidradenitis suppurativa, with a phase 3 trial in the works.
She reported receiving research funding from and serving as a consultant without personal compensation to XBiotech, which sponsored the AD and hidradenitis suppurativa studies. She has similar financial relationships with numerous pharmaceutical companies developing psoriasis medications.
REPORTING FROM EADV 2019
Skin barrier dysfunction mutations vary by race, disease persistence in children with AD
Among children with atopic dermatitis, genetic variants associated with skin barrier dysfunction vary significantly by race and by their influence on disease persistence, according to authors of a cohort study.
In the study, which was based on data from a pediatric eczema registry, The investigators remarked on “profound” differences by race in the study, which used a high-throughput sequencing method to identify FLG LoF variants, some of which were common in white children but not so frequently seen in black children.
Conversely, some variants common in black children were completely absent in the white children, according to the investigators, led by David J. Margolis, MD, PhD, professor of dermatology at the University of Pennsylvania, Philadelphia. The study was published in JAMA Dermatology.
These findings imply that any genetic tests developed for AD should be “inclusive,” they wrote, and shouldn’t simply rely on the most common variants associated with patients of European ancestry, namely p.R501*, c.2282del4[p.S761fs], p.S3247*, and p.R2447*.
“Relying on the classic 4 FLG LoF variants would result in approximately 8% of white children and 64% of black children with an FLG LoF variant being improperly classified,” Dr. Margolis and coinvestigators wrote.
Their comprehensive analysis of FLG LoF variants was based on a U.S. cohort of 741 children with mild to moderate AD in the Pediatric Eczema Elective Registry (PEER), enrolled from 2005 to 2017. The mean age of onset of AD among the children was almost 2 years. Using massively parallel sequencing, the investigators identified a total of 23 FLG LoF variants in 177 children, or 23.9% of the overall cohort.
White children had a higher frequency of FLG LoF variants, according to the investigators. The prevalence of variants was 31.5% in white and 15.3% in black participants, translating into an odds ratio of 2.44 for carrying any variant in a white versus black child (95% confidence interval, 1.76-3.39).
In previous studies, FLG LoF variants are seen in 25%-30% of people with AD who have European and Asian ancestry; by contrast, they are “uncommonly” exhibited in individuals of African ancestry, the investigators wrote.
Persistent AD was more likely among children with FLG LoF variants, with an odds ratio of 0.67 (95% CI, 0.56-0.80), according to Dr. Margolis and coauthors. However, the black children in this cohort had more persistent disease, compared with white children, regardless of whether they had FLG LoF variants or not.
Exon 3 FLG LoF are known to be the most common variants linked to skin barrier dysfunction, the investigators noted.
“However, all FLG LoF variants might not confer an increased risk of AD, and further, they may not all have the same effect on the persistence of AD over time,” they added in a discussion of their results.
The study was supported by a grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. The PEER cohort is funded by Valeant Pharmaceuticals. Dr. Margolis reported receiving research funding as the principal investigator via the trustees of the University of Pennsylvania, and receiving funding from the National Institutes of Health and Valeant; disclosures not related to the study included consulting activities primarily as a member of a data monitoring or scientific advisory boards for several pharmaceutical companies.
SOURCE: Margolis DJ et al. JAMA Dermatol. 2019 Jul 31. doi: 10.1011/jamadermatol.2019.1946.
Among children with atopic dermatitis, genetic variants associated with skin barrier dysfunction vary significantly by race and by their influence on disease persistence, according to authors of a cohort study.
In the study, which was based on data from a pediatric eczema registry, The investigators remarked on “profound” differences by race in the study, which used a high-throughput sequencing method to identify FLG LoF variants, some of which were common in white children but not so frequently seen in black children.
Conversely, some variants common in black children were completely absent in the white children, according to the investigators, led by David J. Margolis, MD, PhD, professor of dermatology at the University of Pennsylvania, Philadelphia. The study was published in JAMA Dermatology.
These findings imply that any genetic tests developed for AD should be “inclusive,” they wrote, and shouldn’t simply rely on the most common variants associated with patients of European ancestry, namely p.R501*, c.2282del4[p.S761fs], p.S3247*, and p.R2447*.
“Relying on the classic 4 FLG LoF variants would result in approximately 8% of white children and 64% of black children with an FLG LoF variant being improperly classified,” Dr. Margolis and coinvestigators wrote.
Their comprehensive analysis of FLG LoF variants was based on a U.S. cohort of 741 children with mild to moderate AD in the Pediatric Eczema Elective Registry (PEER), enrolled from 2005 to 2017. The mean age of onset of AD among the children was almost 2 years. Using massively parallel sequencing, the investigators identified a total of 23 FLG LoF variants in 177 children, or 23.9% of the overall cohort.
White children had a higher frequency of FLG LoF variants, according to the investigators. The prevalence of variants was 31.5% in white and 15.3% in black participants, translating into an odds ratio of 2.44 for carrying any variant in a white versus black child (95% confidence interval, 1.76-3.39).
In previous studies, FLG LoF variants are seen in 25%-30% of people with AD who have European and Asian ancestry; by contrast, they are “uncommonly” exhibited in individuals of African ancestry, the investigators wrote.
Persistent AD was more likely among children with FLG LoF variants, with an odds ratio of 0.67 (95% CI, 0.56-0.80), according to Dr. Margolis and coauthors. However, the black children in this cohort had more persistent disease, compared with white children, regardless of whether they had FLG LoF variants or not.
Exon 3 FLG LoF are known to be the most common variants linked to skin barrier dysfunction, the investigators noted.
“However, all FLG LoF variants might not confer an increased risk of AD, and further, they may not all have the same effect on the persistence of AD over time,” they added in a discussion of their results.
The study was supported by a grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. The PEER cohort is funded by Valeant Pharmaceuticals. Dr. Margolis reported receiving research funding as the principal investigator via the trustees of the University of Pennsylvania, and receiving funding from the National Institutes of Health and Valeant; disclosures not related to the study included consulting activities primarily as a member of a data monitoring or scientific advisory boards for several pharmaceutical companies.
SOURCE: Margolis DJ et al. JAMA Dermatol. 2019 Jul 31. doi: 10.1011/jamadermatol.2019.1946.
Among children with atopic dermatitis, genetic variants associated with skin barrier dysfunction vary significantly by race and by their influence on disease persistence, according to authors of a cohort study.
In the study, which was based on data from a pediatric eczema registry, The investigators remarked on “profound” differences by race in the study, which used a high-throughput sequencing method to identify FLG LoF variants, some of which were common in white children but not so frequently seen in black children.
Conversely, some variants common in black children were completely absent in the white children, according to the investigators, led by David J. Margolis, MD, PhD, professor of dermatology at the University of Pennsylvania, Philadelphia. The study was published in JAMA Dermatology.
These findings imply that any genetic tests developed for AD should be “inclusive,” they wrote, and shouldn’t simply rely on the most common variants associated with patients of European ancestry, namely p.R501*, c.2282del4[p.S761fs], p.S3247*, and p.R2447*.
“Relying on the classic 4 FLG LoF variants would result in approximately 8% of white children and 64% of black children with an FLG LoF variant being improperly classified,” Dr. Margolis and coinvestigators wrote.
Their comprehensive analysis of FLG LoF variants was based on a U.S. cohort of 741 children with mild to moderate AD in the Pediatric Eczema Elective Registry (PEER), enrolled from 2005 to 2017. The mean age of onset of AD among the children was almost 2 years. Using massively parallel sequencing, the investigators identified a total of 23 FLG LoF variants in 177 children, or 23.9% of the overall cohort.
White children had a higher frequency of FLG LoF variants, according to the investigators. The prevalence of variants was 31.5% in white and 15.3% in black participants, translating into an odds ratio of 2.44 for carrying any variant in a white versus black child (95% confidence interval, 1.76-3.39).
In previous studies, FLG LoF variants are seen in 25%-30% of people with AD who have European and Asian ancestry; by contrast, they are “uncommonly” exhibited in individuals of African ancestry, the investigators wrote.
Persistent AD was more likely among children with FLG LoF variants, with an odds ratio of 0.67 (95% CI, 0.56-0.80), according to Dr. Margolis and coauthors. However, the black children in this cohort had more persistent disease, compared with white children, regardless of whether they had FLG LoF variants or not.
Exon 3 FLG LoF are known to be the most common variants linked to skin barrier dysfunction, the investigators noted.
“However, all FLG LoF variants might not confer an increased risk of AD, and further, they may not all have the same effect on the persistence of AD over time,” they added in a discussion of their results.
The study was supported by a grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. The PEER cohort is funded by Valeant Pharmaceuticals. Dr. Margolis reported receiving research funding as the principal investigator via the trustees of the University of Pennsylvania, and receiving funding from the National Institutes of Health and Valeant; disclosures not related to the study included consulting activities primarily as a member of a data monitoring or scientific advisory boards for several pharmaceutical companies.
SOURCE: Margolis DJ et al. JAMA Dermatol. 2019 Jul 31. doi: 10.1011/jamadermatol.2019.1946.
FROM JAMA DERMATOLOGY
In age of biologics, don’t forget traditional AD treatments
LAS VEGAS – Biologics are revolutionizing the treatment of atopic dermatitis (AD), but a dermatologist urged colleagues to keep in mind the value of traditional topical and systemic treatments.

Joseph F. Fowler Jr., MD, of the University of Louisville, Ky., offered these tips about AD treatment in a presentation at the Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar:
- Keep the epidermal skin barrier in mind.
The epidermal skin barrier is abnormal in patients with AD, Dr. Fowler said, because of several possible factors: altered levels of natural moisturizing factor (which can be caused by a genetic mutation), imbalances between ceramides and lipids, and reduced aquaporin levels.
Enhancing the skin barrier is crucial in treating AD, he said, and products with these ingredients may help: ceramides, glycerin/glycerol (glucoside), colloidal oatmeal, and components of natural moisturizing factor.
- Expensive products are probably better.
“These products are available over the counter and via prescription,” he said. “Do they make the skin barrier stronger? The answer is they probably they do. But most do tend to be expensive, especially Rx products.”
Not all patients, of course, can afford the most expensive options. “You and your patients have to decide whether it’s better to get something like plain old Vaseline or a very inexpensive cream at Walmart that may be more accessible,” he said. “I tell patients that if the cost is not a big issue, these other products are probably better, and they will make your skin heal better and feel better. But if cost is a problem, use what you can afford.”
- Don’t forget about hypochlorous acid.
While it’s chemically similar to bleach, this product “doesn’t bleach your clothes or smell bleachy,” Dr. Fowler said. “It does have antibiotic and antipruritic effects.”
- For predictability, try methotrexate.
Methotrexate, an old workhorse in dermatology, remains an option, especially for patients who need alternatives to biologics, Dr. Fowler said. “I’ve used it much more in the last 10 years for eczema than for psoriasis and anything else. We’re used to using it, and I find it predictably effective at a dosage that’s similar to that for psoriasis.”
- Mycophenolate mofetil (CellCept) may be helpful.
Dr. Fowler’s research has shown that mycophenolate mofetil is useful in about 50% of chronic AD cases. “The problem with the drug is that you couldn’t tell which ones would get better and which ones wouldn’t.” Still, it can be an alternative to methotrexate and cyclosporine, he said.
- Cyclosporine is a short-term treatment.
“It’s like steroids on steroids,” Dr. Fowler said. “I’ve had to use it sometimes even in the age of biologics, which may not work as fast as we’d like in someone who’s really miserable.” The drug is linked to liver and kidney risks, he cautioned, and “you don’t want to be on it very long.”
- Ultraviolet light therapy can help.
This strategy works well “if they come in and get to the office and do it,” Dr. Fowler said. “We should remember it as an option.”
A patient who’s over 80 years old with bad AD has been getting narrow-band UVB treatments for at least 5 years, he said. “I just look at him every 3-4 months. Every time he says, ‘Can I keep coming and get my light treatments?’ and I say sure. At 80-plus, I’m not too worried about cutaneous malignancy or any other side effects.”
Dr. Fowler reported relationships with the speaker’s bureau of SmartPractice and ties with Asana, Johnson & Johnson, Lilly, Novartis and Pfizer. SDEF and this news organization are owned by the same parent company.
LAS VEGAS – Biologics are revolutionizing the treatment of atopic dermatitis (AD), but a dermatologist urged colleagues to keep in mind the value of traditional topical and systemic treatments.
Joseph F. Fowler Jr., MD, of the University of Louisville, Ky., offered these tips about AD treatment in a presentation at the Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar:
- Keep the epidermal skin barrier in mind.
The epidermal skin barrier is abnormal in patients with AD, Dr. Fowler said, because of several possible factors: altered levels of natural moisturizing factor (which can be caused by a genetic mutation), imbalances between ceramides and lipids, and reduced aquaporin levels.
Enhancing the skin barrier is crucial in treating AD, he said, and products with these ingredients may help: ceramides, glycerin/glycerol (glucoside), colloidal oatmeal, and components of natural moisturizing factor.
- Expensive products are probably better.
“These products are available over the counter and via prescription,” he said. “Do they make the skin barrier stronger? The answer is they probably they do. But most do tend to be expensive, especially Rx products.”
Not all patients, of course, can afford the most expensive options. “You and your patients have to decide whether it’s better to get something like plain old Vaseline or a very inexpensive cream at Walmart that may be more accessible,” he said. “I tell patients that if the cost is not a big issue, these other products are probably better, and they will make your skin heal better and feel better. But if cost is a problem, use what you can afford.”
- Don’t forget about hypochlorous acid.
While it’s chemically similar to bleach, this product “doesn’t bleach your clothes or smell bleachy,” Dr. Fowler said. “It does have antibiotic and antipruritic effects.”
- For predictability, try methotrexate.
Methotrexate, an old workhorse in dermatology, remains an option, especially for patients who need alternatives to biologics, Dr. Fowler said. “I’ve used it much more in the last 10 years for eczema than for psoriasis and anything else. We’re used to using it, and I find it predictably effective at a dosage that’s similar to that for psoriasis.”
- Mycophenolate mofetil (CellCept) may be helpful.
Dr. Fowler’s research has shown that mycophenolate mofetil is useful in about 50% of chronic AD cases. “The problem with the drug is that you couldn’t tell which ones would get better and which ones wouldn’t.” Still, it can be an alternative to methotrexate and cyclosporine, he said.
- Cyclosporine is a short-term treatment.
“It’s like steroids on steroids,” Dr. Fowler said. “I’ve had to use it sometimes even in the age of biologics, which may not work as fast as we’d like in someone who’s really miserable.” The drug is linked to liver and kidney risks, he cautioned, and “you don’t want to be on it very long.”
- Ultraviolet light therapy can help.
This strategy works well “if they come in and get to the office and do it,” Dr. Fowler said. “We should remember it as an option.”
A patient who’s over 80 years old with bad AD has been getting narrow-band UVB treatments for at least 5 years, he said. “I just look at him every 3-4 months. Every time he says, ‘Can I keep coming and get my light treatments?’ and I say sure. At 80-plus, I’m not too worried about cutaneous malignancy or any other side effects.”
Dr. Fowler reported relationships with the speaker’s bureau of SmartPractice and ties with Asana, Johnson & Johnson, Lilly, Novartis and Pfizer. SDEF and this news organization are owned by the same parent company.
LAS VEGAS – Biologics are revolutionizing the treatment of atopic dermatitis (AD), but a dermatologist urged colleagues to keep in mind the value of traditional topical and systemic treatments.
Joseph F. Fowler Jr., MD, of the University of Louisville, Ky., offered these tips about AD treatment in a presentation at the Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar:
- Keep the epidermal skin barrier in mind.
The epidermal skin barrier is abnormal in patients with AD, Dr. Fowler said, because of several possible factors: altered levels of natural moisturizing factor (which can be caused by a genetic mutation), imbalances between ceramides and lipids, and reduced aquaporin levels.
Enhancing the skin barrier is crucial in treating AD, he said, and products with these ingredients may help: ceramides, glycerin/glycerol (glucoside), colloidal oatmeal, and components of natural moisturizing factor.
- Expensive products are probably better.
“These products are available over the counter and via prescription,” he said. “Do they make the skin barrier stronger? The answer is they probably they do. But most do tend to be expensive, especially Rx products.”
Not all patients, of course, can afford the most expensive options. “You and your patients have to decide whether it’s better to get something like plain old Vaseline or a very inexpensive cream at Walmart that may be more accessible,” he said. “I tell patients that if the cost is not a big issue, these other products are probably better, and they will make your skin heal better and feel better. But if cost is a problem, use what you can afford.”
- Don’t forget about hypochlorous acid.
While it’s chemically similar to bleach, this product “doesn’t bleach your clothes or smell bleachy,” Dr. Fowler said. “It does have antibiotic and antipruritic effects.”
- For predictability, try methotrexate.
Methotrexate, an old workhorse in dermatology, remains an option, especially for patients who need alternatives to biologics, Dr. Fowler said. “I’ve used it much more in the last 10 years for eczema than for psoriasis and anything else. We’re used to using it, and I find it predictably effective at a dosage that’s similar to that for psoriasis.”
- Mycophenolate mofetil (CellCept) may be helpful.
Dr. Fowler’s research has shown that mycophenolate mofetil is useful in about 50% of chronic AD cases. “The problem with the drug is that you couldn’t tell which ones would get better and which ones wouldn’t.” Still, it can be an alternative to methotrexate and cyclosporine, he said.
- Cyclosporine is a short-term treatment.
“It’s like steroids on steroids,” Dr. Fowler said. “I’ve had to use it sometimes even in the age of biologics, which may not work as fast as we’d like in someone who’s really miserable.” The drug is linked to liver and kidney risks, he cautioned, and “you don’t want to be on it very long.”
- Ultraviolet light therapy can help.
This strategy works well “if they come in and get to the office and do it,” Dr. Fowler said. “We should remember it as an option.”
A patient who’s over 80 years old with bad AD has been getting narrow-band UVB treatments for at least 5 years, he said. “I just look at him every 3-4 months. Every time he says, ‘Can I keep coming and get my light treatments?’ and I say sure. At 80-plus, I’m not too worried about cutaneous malignancy or any other side effects.”
Dr. Fowler reported relationships with the speaker’s bureau of SmartPractice and ties with Asana, Johnson & Johnson, Lilly, Novartis and Pfizer. SDEF and this news organization are owned by the same parent company.
REPORTING FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR
Seborrhea Herpeticum: Cutaneous Herpes Simplex Virus Infection Within Infantile Seborrheic Dermatitis
Classically, eczema herpeticum is associated with atopic dermatitis (AD), but it also has been previously reported in the setting of pemphigus vulgaris, Darier disease, ichthyosis vulgaris, burns, psoriasis, and irritant contact dermatitis.1,2 Descriptions of cutaneous herpes simplex virus (HSV) in the setting of seborrheic dermatitis are lacking.
Case Report
A 2-month-old infant boy who was otherwise healthy presented to the emergency department with a new rash on the scalp. Initially there were a few clusters of small fluid-filled lesions that evolved over several days into diffuse clusters covering the scalp and extending onto the forehead and upper chest (Figure). The patient’s medical history was notable for infantile seborrheic dermatitis and a family history of AD. His grandmother, who was his primary caretaker, had a recent history of herpes labialis.

Physical examination revealed numerous discrete, erythematous, and punched-out erosions diffusely on the scalp. There were fewer similar erosions on the forehead and upper chest. There were no oral or periocular lesions. There were no areas of lichenification or eczematous plaques on the remainder of the trunk or extremities. Laboratory testing was positive for HSV type 1 polymerase chain reaction and positive for HSV type 1 viral culture. Liver enzymes were elevated with alanine aminotransferase at 107 U/L (reference range, 7–52 U/L) and aspartate aminotransferase at 94 U/L (reference range, 13–39 U/L).
The patient was admitted to the hospital and was treated by the dermatology and infectious disease services. Intravenous acyclovir 60 mg/kg daily was administered for 3 days until all lesions had crusted over. On the day of discharge, the patient was transitioned to oral valacyclovir 20 mg/kg daily for 7 days with resolution. One month later he developed a recurrence that was within his existing seborrheic dermatitis. After a repeat 7-day course of oral valacyclovir 20 mg/kg daily, he was placed on prophylaxis therapy of oral acyclovir 10 mg/kg daily. Gentle skin care precautions also were recommended.
Comment
Eczema herpeticum refers to disseminated cutaneous infection with HSV types 1 or 2 in the setting of underlying dermatosis.2 Although it is classically associated with AD, it has been reported in a number of other chronic skin disorders and can lead to serious complications, including hepatitis, keratoconjunctivitis, and meningitis. In those with AD who develop HSV, presentation may occur in active dermatitis locations because of skin barrier disruption, which may lead to increased susceptibility to viral infection.3
Herpes simplex virus in a background of seborrheic dermatitis has not been well described. Although the pathogenesis of seborrheic dermatitis has not been fully reported, several gene mutations and protein deficiencies have been identified in patients and animal models that are associated with immune response or epidermal differentiation.4 Therefore, it is possible that, as with AD, a disruption in the skin barrier increases susceptibility to viral infection.
It also has been suggested that infantile seborrheic dermatitis and AD represent the same spectrum of disease.5 Given our patient’s family history of AD, it is possible his presentation represents early underlying AD. Providers should be aware that cutaneous HSV can be confined to a seborrheic distribution and may represent underlying epidermal dysfunction secondary to seborrheic dermatitis.
- Wheeler CE, Abele DC. Eczema herpeticum, primary and recurrent. Arch Dermatol. 1966;93:162-173.
- Santmyire-Rosenberger BR, Nigra TP. Psoriasis herpeticum: three cases of Kaposi’s varicelliform eruption in psoriasis. J Am Acad Dermatol. 2005;53:52-56.
- Wollenberg A, Wetzel S, Burgdorf WH, et al. Viral infections in atopic dermatitis: pathogenic aspects and clinical management. J Allergy Clin Immunol. 2003;112:667-674.
- Karakadze M, Hirt P, Wikramanayake T. The genetic basis of seborrhoeic dermatitis: a review. J Eur Acad Dermatol Venereol. 2017;32:529-536.
- Alexopoulos A, Kakourou T, Orfanou I, et al. Retrospective analysis of the relationship between infantile seborrheic dermatitis and atopic dermatitis. Pediatr Dermatol. 2013;31:125-130.
Classically, eczema herpeticum is associated with atopic dermatitis (AD), but it also has been previously reported in the setting of pemphigus vulgaris, Darier disease, ichthyosis vulgaris, burns, psoriasis, and irritant contact dermatitis.1,2 Descriptions of cutaneous herpes simplex virus (HSV) in the setting of seborrheic dermatitis are lacking.
Case Report
A 2-month-old infant boy who was otherwise healthy presented to the emergency department with a new rash on the scalp. Initially there were a few clusters of small fluid-filled lesions that evolved over several days into diffuse clusters covering the scalp and extending onto the forehead and upper chest (Figure). The patient’s medical history was notable for infantile seborrheic dermatitis and a family history of AD. His grandmother, who was his primary caretaker, had a recent history of herpes labialis.
Physical examination revealed numerous discrete, erythematous, and punched-out erosions diffusely on the scalp. There were fewer similar erosions on the forehead and upper chest. There were no oral or periocular lesions. There were no areas of lichenification or eczematous plaques on the remainder of the trunk or extremities. Laboratory testing was positive for HSV type 1 polymerase chain reaction and positive for HSV type 1 viral culture. Liver enzymes were elevated with alanine aminotransferase at 107 U/L (reference range, 7–52 U/L) and aspartate aminotransferase at 94 U/L (reference range, 13–39 U/L).
The patient was admitted to the hospital and was treated by the dermatology and infectious disease services. Intravenous acyclovir 60 mg/kg daily was administered for 3 days until all lesions had crusted over. On the day of discharge, the patient was transitioned to oral valacyclovir 20 mg/kg daily for 7 days with resolution. One month later he developed a recurrence that was within his existing seborrheic dermatitis. After a repeat 7-day course of oral valacyclovir 20 mg/kg daily, he was placed on prophylaxis therapy of oral acyclovir 10 mg/kg daily. Gentle skin care precautions also were recommended.
Comment
Eczema herpeticum refers to disseminated cutaneous infection with HSV types 1 or 2 in the setting of underlying dermatosis.2 Although it is classically associated with AD, it has been reported in a number of other chronic skin disorders and can lead to serious complications, including hepatitis, keratoconjunctivitis, and meningitis. In those with AD who develop HSV, presentation may occur in active dermatitis locations because of skin barrier disruption, which may lead to increased susceptibility to viral infection.3
Herpes simplex virus in a background of seborrheic dermatitis has not been well described. Although the pathogenesis of seborrheic dermatitis has not been fully reported, several gene mutations and protein deficiencies have been identified in patients and animal models that are associated with immune response or epidermal differentiation.4 Therefore, it is possible that, as with AD, a disruption in the skin barrier increases susceptibility to viral infection.
It also has been suggested that infantile seborrheic dermatitis and AD represent the same spectrum of disease.5 Given our patient’s family history of AD, it is possible his presentation represents early underlying AD. Providers should be aware that cutaneous HSV can be confined to a seborrheic distribution and may represent underlying epidermal dysfunction secondary to seborrheic dermatitis.
Classically, eczema herpeticum is associated with atopic dermatitis (AD), but it also has been previously reported in the setting of pemphigus vulgaris, Darier disease, ichthyosis vulgaris, burns, psoriasis, and irritant contact dermatitis.1,2 Descriptions of cutaneous herpes simplex virus (HSV) in the setting of seborrheic dermatitis are lacking.
Case Report
A 2-month-old infant boy who was otherwise healthy presented to the emergency department with a new rash on the scalp. Initially there were a few clusters of small fluid-filled lesions that evolved over several days into diffuse clusters covering the scalp and extending onto the forehead and upper chest (Figure). The patient’s medical history was notable for infantile seborrheic dermatitis and a family history of AD. His grandmother, who was his primary caretaker, had a recent history of herpes labialis.
Physical examination revealed numerous discrete, erythematous, and punched-out erosions diffusely on the scalp. There were fewer similar erosions on the forehead and upper chest. There were no oral or periocular lesions. There were no areas of lichenification or eczematous plaques on the remainder of the trunk or extremities. Laboratory testing was positive for HSV type 1 polymerase chain reaction and positive for HSV type 1 viral culture. Liver enzymes were elevated with alanine aminotransferase at 107 U/L (reference range, 7–52 U/L) and aspartate aminotransferase at 94 U/L (reference range, 13–39 U/L).
The patient was admitted to the hospital and was treated by the dermatology and infectious disease services. Intravenous acyclovir 60 mg/kg daily was administered for 3 days until all lesions had crusted over. On the day of discharge, the patient was transitioned to oral valacyclovir 20 mg/kg daily for 7 days with resolution. One month later he developed a recurrence that was within his existing seborrheic dermatitis. After a repeat 7-day course of oral valacyclovir 20 mg/kg daily, he was placed on prophylaxis therapy of oral acyclovir 10 mg/kg daily. Gentle skin care precautions also were recommended.
Comment
Eczema herpeticum refers to disseminated cutaneous infection with HSV types 1 or 2 in the setting of underlying dermatosis.2 Although it is classically associated with AD, it has been reported in a number of other chronic skin disorders and can lead to serious complications, including hepatitis, keratoconjunctivitis, and meningitis. In those with AD who develop HSV, presentation may occur in active dermatitis locations because of skin barrier disruption, which may lead to increased susceptibility to viral infection.3
Herpes simplex virus in a background of seborrheic dermatitis has not been well described. Although the pathogenesis of seborrheic dermatitis has not been fully reported, several gene mutations and protein deficiencies have been identified in patients and animal models that are associated with immune response or epidermal differentiation.4 Therefore, it is possible that, as with AD, a disruption in the skin barrier increases susceptibility to viral infection.
It also has been suggested that infantile seborrheic dermatitis and AD represent the same spectrum of disease.5 Given our patient’s family history of AD, it is possible his presentation represents early underlying AD. Providers should be aware that cutaneous HSV can be confined to a seborrheic distribution and may represent underlying epidermal dysfunction secondary to seborrheic dermatitis.
- Wheeler CE, Abele DC. Eczema herpeticum, primary and recurrent. Arch Dermatol. 1966;93:162-173.
- Santmyire-Rosenberger BR, Nigra TP. Psoriasis herpeticum: three cases of Kaposi’s varicelliform eruption in psoriasis. J Am Acad Dermatol. 2005;53:52-56.
- Wollenberg A, Wetzel S, Burgdorf WH, et al. Viral infections in atopic dermatitis: pathogenic aspects and clinical management. J Allergy Clin Immunol. 2003;112:667-674.
- Karakadze M, Hirt P, Wikramanayake T. The genetic basis of seborrhoeic dermatitis: a review. J Eur Acad Dermatol Venereol. 2017;32:529-536.
- Alexopoulos A, Kakourou T, Orfanou I, et al. Retrospective analysis of the relationship between infantile seborrheic dermatitis and atopic dermatitis. Pediatr Dermatol. 2013;31:125-130.
- Wheeler CE, Abele DC. Eczema herpeticum, primary and recurrent. Arch Dermatol. 1966;93:162-173.
- Santmyire-Rosenberger BR, Nigra TP. Psoriasis herpeticum: three cases of Kaposi’s varicelliform eruption in psoriasis. J Am Acad Dermatol. 2005;53:52-56.
- Wollenberg A, Wetzel S, Burgdorf WH, et al. Viral infections in atopic dermatitis: pathogenic aspects and clinical management. J Allergy Clin Immunol. 2003;112:667-674.
- Karakadze M, Hirt P, Wikramanayake T. The genetic basis of seborrhoeic dermatitis: a review. J Eur Acad Dermatol Venereol. 2017;32:529-536.
- Alexopoulos A, Kakourou T, Orfanou I, et al. Retrospective analysis of the relationship between infantile seborrheic dermatitis and atopic dermatitis. Pediatr Dermatol. 2013;31:125-130.
Practice Points
- Cutaneous herpes simplex virus may present in a seborrheic distribution within infantile seborrheic dermatitis, suggesting underlying dysfunction secondary to seborrheic dermatitis.
- Treatment of seborrhea herpeticum involves antiviral therapy to treat the secondary viral infection and gentle skin care precautions for the primary condition.

Pediatric Molluscum: An Update
Molluscum contagiosum virus (MCV) infection causes the cutaneous lesions we call molluscum. Molluscum has become common in the last 30 years. Deciding the best course of therapy requires some fundamental understanding about how MCV relates to the following factors: epidemiology, childhood immunity and vaccination, clinical features, comorbidities, and quality of life. Treatment depends on many factors, including presence or absence of atopic dermatitis (AD) and/or pruritus, other symptoms, cosmetic location, and the child’s concern about the lesions. Therapeutics include destructive and immunologic therapies, the latter geared toward increasing immune response.
Epidemiology
Molluscum contagiosum virus is the solo member of the Molluscipoxvirus genus. Infection with MCV causes benign growth or tumors in the skin (ie, molluscum). The infection is slow to clear because the virus reduces the host’s immunity.1,2 Molluscum contagiosum virus is a double-stranded DNA virus that affects keratinocytes and genetically carries the tools for its own replication (ie, DNA-dependent RNA polymerase). The virus has a few subtypes—I/Ia, II, III, and IV—with MCV-I predominating in children and healthy humans and MCV-II in patients with human immunodeficiency virus.1,2 Typing is experimental and is not standardly performed in clinical practice. Molluscum contagiosum virus produces a variety of factors that block the host’s immune response, prolonging infection and preventing erythema and inflammatory response.3
Molluscum contagiosum virus is transmitted through skin-to-skin contact and fomites, including shared towels, bathtubs, spas, bath sponges, and pool equipment.2,4,5 Transmission from household contact and bathing together has been noted in pediatric patients with MCV. Based on the data it can be posited that the lesions are softer when wet and more readily release viral particles or fomites, and fomites may be left on surfaces, especially when a child is wet.6,7 Propensity for infection occurs in patients with AD and in immunosuppressed hosts, including children with human immunodeficiency virus and iatrogenic immunosuppression caused by chemotherapy.1,2,8 Contact sports can increase the risk of transmission, and outbreaks have occurred in pools,5,9 day-care facilities,10 and sports settings.11 Cases of congenital and vertically transmitted molluscum have been documented.12,13 Sexual transmission of MCV may be seen in adolescents who are sexually active. Although child-to-child transmission can occur in the groin area from shared equipment, transmission via sexual abuse also is possible.14 Bargman15 has mentioned the isolated genital location and lack of contact with other infected children as concerning features. Latency of new lesion appearance is anywhere from 1 to 50 days from the date of inoculation; therefore, new lesions are possible and expected even after therapy has been effective in eradicating visible lesions.10 Although clearance has been reported in 6 to 12 months, one pediatric study demonstrated 70% clearance by 1.5 years, suggesting the disease often is more prolonged.16 One-third of children will experience signs of inflammation, such as pruritus and/or erythema. Rare side effects include bacterial superinfection and hypersensitivity.2
One Dutch study from 1994, the largest database survey of children to date, cited a 17% cumulative incidence of molluscum in children by reviewing the data from 103 general practices.17 In a survey and review of molluscum by Braue et al,18 annual rates in populations vary but seem to maximize at approximately 6% to 7%. Sturt et al19 reviewed the prevalence in the indigenous West Sepik section of New Guinea and noted annual incidence rates of 6% in children younger than 10 years (range, 1.8%–10.9%). Epidemics occur and can produce large numbers of cases in a short time period.18 The cumulative prevalence in early childhood may be as high as 22%, as Sturt et al19 observed in children younger than 10 years.
Rising incidence and therefore rising lifetime prevalence appear to have been an issue in the last few decades. Data from the Indian Health Service have demonstrated increases in MCV in Native American children between 2001 and 2005.20 In adults, the data support a steady increase of molluscum from 1988-2007, with a 3-fold increase from 1988-1997 to 1998-2007 in a Spanish study.21 Better population-based data are needed.
Childhood Immunity and Vaccination
Sequence homology between MC133L, a protein of MCV, with vaccinia virus suggests overlapping genes.22 Therefore, it is conceptually possible that the rise in incidence of MCV since the 1980s relates to the loss of herd immunity to variola due to lack of vaccination for smallpox, which has not been offered in the United States since 1972.23 Childhood immunity to MCV varies among studies, but it appears that children do develop antibodies to molluscum in the setting of forming an immune response. Because the rise in molluscum incidence began after the smallpox vaccine was discontinued, the factors appear related; however, the scientific data do not support the theory of a relationship. Mitchell24 has shown that a patient can develop antibodies in response to ground molluscum bodies inoculated into the skin; however, vaccination against molluscum and natural infection do not appear to produce antibodies that would cross-react and protect against other poxviruses, including vaccinia or fowl pox infections.25 Cell-mediated immunity also is required to clear MCV and may account for the inflammatory appearance of lesions as they resolve.26
Demonstrated factors that account for the rise in MCV incidence, aside from alterations in vaccination practices, include spread through sports,9 swimming,11 and AD,7 which have become more commonplace in the United States in the last few decades, supporting the theory that they may be the cause of the increase in childhood MCV infections. Another cause may be the ability of MCV to create factors that stem host immune response.1
Clinical Features
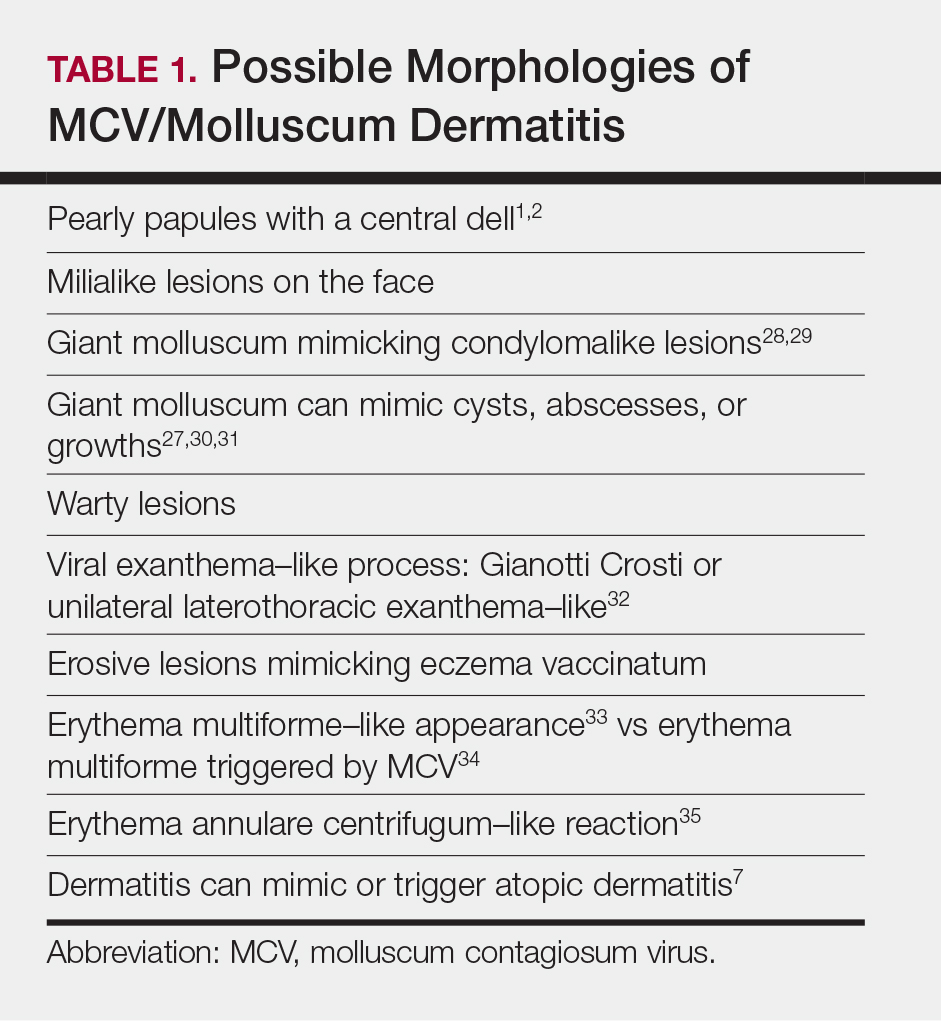
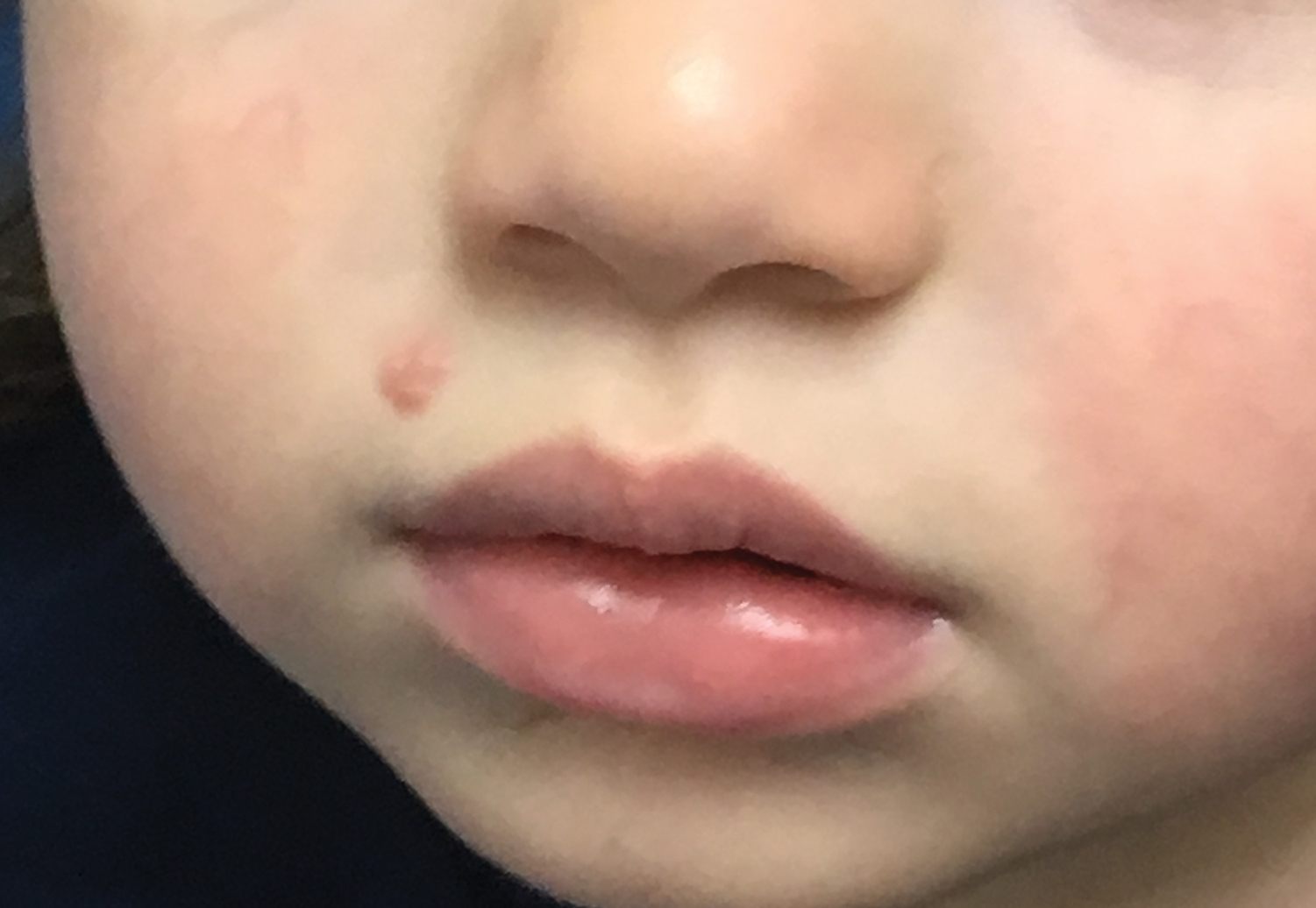
Molluscum lesions have a typical appearance of pearly papules with a central dell. These lesions are lighter to flesh colored and measure 1 to 3 mm.2,4,5 The lesions cluster in the axillae and extremities and average from 10 to 20 per child.6 Lesions clear spontaneously, but new ones will continue to form until immunity is developed. Specific clinical appearances of lesions that are not pearly papules are not infrequent. Table 1 contains a short list of the manifold clinical appearances of molluscum lesions in children.1,2,7,27-35 In particular, certain clinical appearances should be considered. In small children, head and neck lesions resembling milia are not uncommon. Giant or wartlike lesions can appear on the head, neck, or gluteal region in children and are clinical mimics of condyloma or other warts (Figure 1). Giant lesions also can grow in the subcutaneous space and mimic a cyst or abscess.27 Erosive lesions mimicking eczema vaccinatum can be seen (Figure 2), but dermoscopy may demonstrate central dells in some lesions. Other viral processes mimicked include Gianotti Crosti–like lesions (Figure 3) that appear when a papular id reaction forms over the extremities or a localized version in the axilla, mimicking unilateral laterothoracic exanthema.2,36,37 Hypersensitivity reactions are commonly noted with clearance and can be papular or demonstrate swelling and erythema, termed the beginning-of-the-end sign.38


Pruritus, erythema, and swelling can occur with clearance but do not appear in all patients. Addressing pruritus is important to prevent disease spread, as patients are likely to inoculate other areas of the skin with virus when they scratch, and lesion number is reduced with dermatitis interventions.36
Comorbidities
Molluscum lesions can occur in any child; however, the impaired immunologic status and skin barrier in patients with AD is ripe for the extensive spread of lesions that is associated with higher lesion count.36 Children with molluscum infection can experience new-onset dermatitis or triggering of AD flares, especially on the extremities, such as the antecubital and popliteal regions.7 A study of children with MCV infection demonstrated that treatment of active dermatitis reduced spread. The authors mentioned autoinoculation as the mechanism; however, these data also suggest supporting barrier state as a factor in disease spread.36 Superinfection can occur prior to6 or after therapy for lesions,37 but it is unclear if this relates to the underlying atopic diathesis. Children with molluscum have been described to have warts, psoriasis, family history of atopy, diabetes mellitus, and pityriasis alba,7 while immunosuppression of any kind is associated with molluscum and high lesion count or prolonged disease in childhood.1,2
Quality of Life
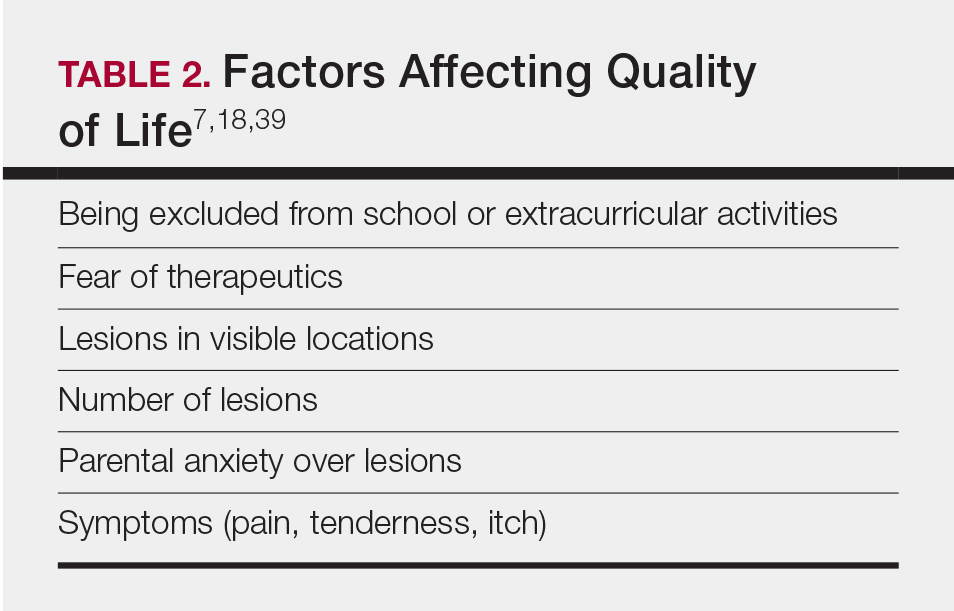
Children with molluscum who have higher lesion counts appear to be at risk for severe effects on their quality of life. Approximately 10% of children with MCV infection have been documented to have severe impairments on quality of life.39 In my practice, quality of life in children with MCV appears to be affected by many factors (Table 2).7,18,39
Treatments
Proper Skin Care and Treatment of AD
Therapy for AD and/or pruritus appears to limit lesion number in children with MCV and rashes or itch.7,36 I recommend barrier repair agents, including emollients and syndet bar cleansers, to prevent small breaks in the skin that occur with xerosis and AD and that increase itch and risk of spread. Therapy for AD and molluscum dermatitis is similar and overlapping. There is always a concern about the spread of MCV when using topical calcineurin inhibitors. I, therefore, focus the dermatitis therapeutics on topical corticosteroid–based care.6,40
Prevention of Spread
Prevention of spread begins with hygiene interventions. Cobathing is common in children with MCV and should be held off when possible. It is important for the child with MCV to avoid sharing bath towels and equipment23 and having bare skin come in contact with mats in sports. I request that children with MCV wear bathing suits that cover the areas affected.
Reassurance
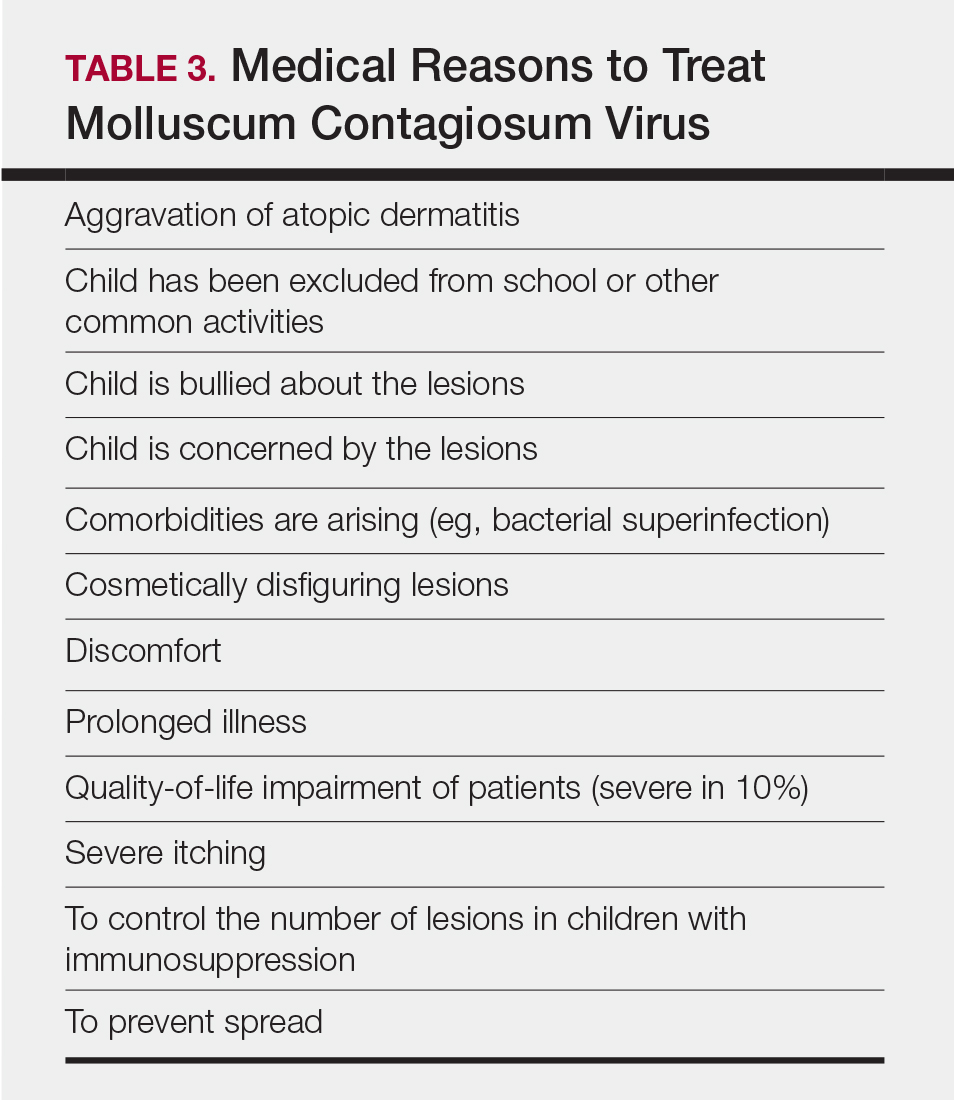
The most important therapy is reassurance.41 Many parents/guardians are truly unaware that the MCV infection can last for more than a year and therefore worry over normal disease course. When counseled as to the benign course of illness and given instructions on proper skin care, the parent/guardian of a child with MCV will often opt against therapy of uncomplicated cases. On the other hand, there are medical reasons for treatment, and they support the need for intervention (Table 3). Seventy percent of lesions resolve in 1.5 years; however, of the residual infections, some may last as long as 4 years.16 It is not recommended to stop children from attending school because of MCV.
Interventional Therapy
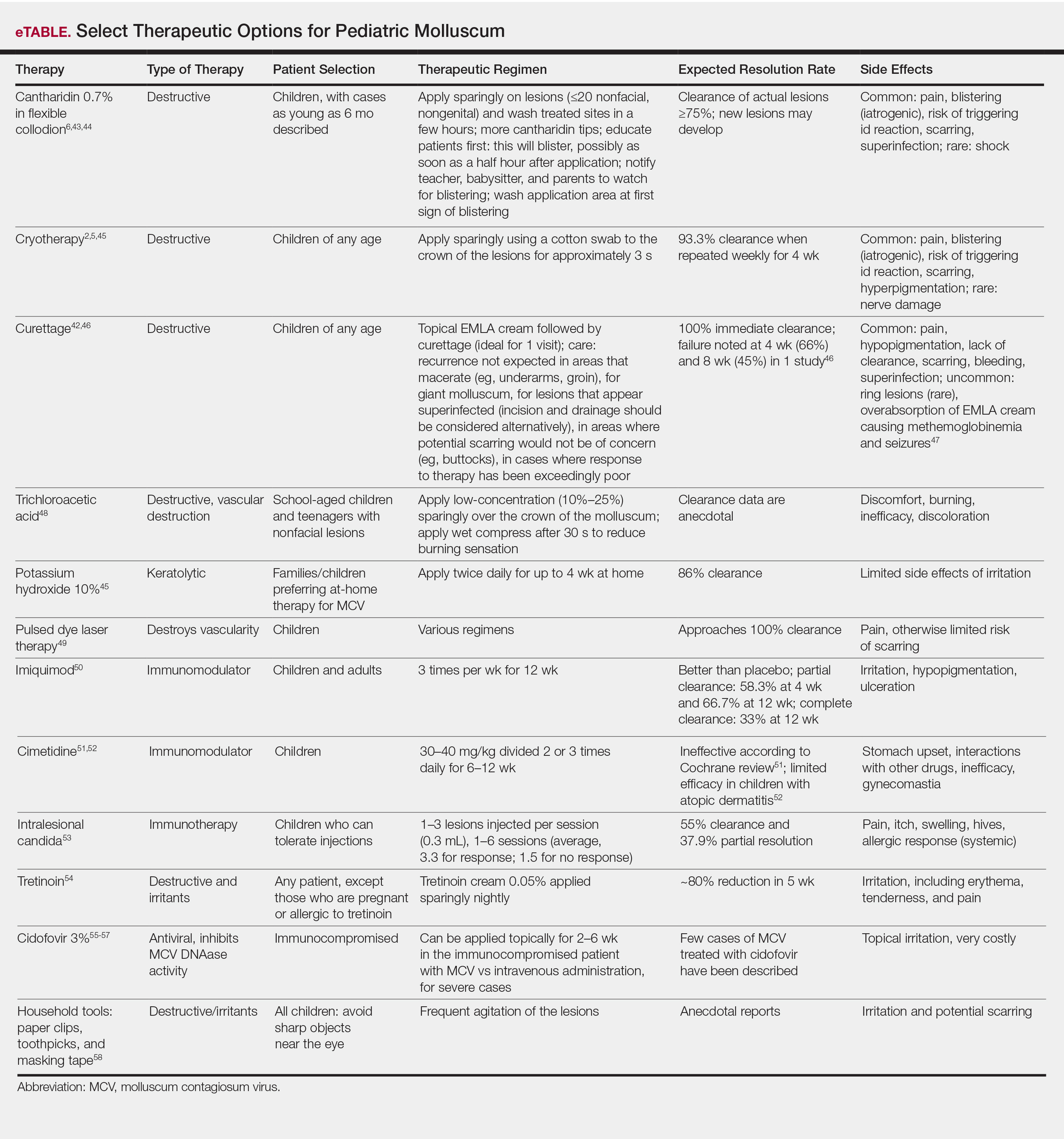
Therapeutics of MCV include destructive therapies in office (ie, cantharidin, cryotherapy, curettage, trichloroacetic acid, and glycolic acid) and at-home therapies (ie, topical retinoids, nitric oxide releasers)(eTable).2,5,6,42-58 When there are many lesions or spread is noted, immunotherapies can be used, including topical imiquimod, oral cimetidine, and intralesional Candida antigen.2,4,7 Pulsed dye laser cuts off the lesion vascular supply, while cidofovir is directly antiviral both topically and systemically, the latter reserved for severe cases in immunosuppressed adults.59 Head-to-head studies of cantharidin, curettage, topical peeling agents, and imiquimod demonstrated better satisfaction and fewer office visits with topical anesthetic and curettage on the first visit. Side effects were greatest for salicylic acid and glycolic acid; therefore, these agents are less desirable.42
Conclusion
Molluscum is a cutaneous viral infection that is common in children and has associated morbidities, including AD, pruritus, poor quality of life in some cases, and risk of contagion. Addressing the disease includes understanding its natural history and explaining it to parents/guardians. Therapeutics can be offered in cases where need is demonstrated, such as with lesions that spread and cause discomfort. Choice of therapeutics depends on the practitioner’s experience, the child’s clinical appearance, availability of therapy, and review of options with the parents/guardians. When avoidance of intervention is desired, barrier enhancement and treatment of symptomatic dermatitis are still beneficial, as are household (eg, not sharing towels) and activity (eg, adhesive bandages over active lesions) interventions to reduce transmission.
- Shisler JL. Immune evasion strategies of molluscum contagiosum virus. Adv Virus Res. 2015;92:201-252.
- Brown J, Janniger CK, Schwartz RA, et al. Childhood molluscum contagiosum. Int J Dermatol. 2006;45:93-99.
- Moss B, Shisler JL, Xiang Y, et al. Immune-defense molecules of molluscum contagiosum virus, a human poxvirus. Trends Microbiol. 2000;8:473-477.
- Silverberg NB. Warts and molluscum in children. Adv Dermatol. 2004;20:23-73.
- Choong KY, Roberts LJ. Molluscum contagiosum, swimming and bathing: a clinical analysis. Australas J Dermatol. 1999;40:89-92.
- Silverberg NB, Sidbury R, Mancini AJ. Childhood molluscum contagiosum: experience with cantharidin therapy in 300 patients. J Am Acad Dermatol. 2000;43:503-507.
- Silverberg NB. Molluscum contagiosum virus infection can trigger atopic dermatitis disease onset or flare. Cutis. 2018;102:191-194.
- Ajithkumar VT, Sasidharanpillai S, Muhammed K, et al. Disseminated molluscum contagiosum following chemotherapy: a therapeutic challenge. Indian J Dermatol Venereol Leprol. 2017;83:516.
- Oren B, Wende SO. An outbreak of molluscum contagiosum in a kibbutz. Infection. 1991;19:159-161.
- Molluscum contagiosum. Healthy Children website. https://www.healthychildren.org/English/health-issues/conditions/skin/Pages/Molluscum-Contagiosum.aspx. Updated November 21, 2015. Accessed October 16, 2019.
- Peterson AR, Nash E, Anderson BJ. Infectious disease in contact sports. Sports Health. 2019;11:47-58.
- Connell CO, Oranje A, Van Gysel D, et al. Congenital molluscum contagiosum: report of four cases and review of the literature. Pediatr Dermatol. 2008;25:553-556.
- Luke JD, Silverberg NB. Vertically transmitted molluscum contagiosum infection. Pediatrics. 2010;125:E423-E425.
- Mendiratta V, Agarwal S, Chander R. Reappraisal of sexually transmitted infections in children: a hospital-based study from an urban area. Indian J Sex Transm Dis AIDS. 2014;35:25-28.
- Bargman H. Genital molluscum contagiosum in children: evidence of sexual abuse? CMAJ. 1986;135:432-433.
- Basdag H, Rainer BM, Cohen BA. Molluscum contagiosum: to treat or not to treat? experience with 170 children in an outpatient clinic setting in the northeastern United States. Pediatr Dermatol. 2015;32:353-357.
- Koning S, Bruijnzeels MA, van Suijlekom-Smit LW, et al. Molluscum contagiosum in Dutch general practice. Br J Gen Pract. 1994;44:417-419.
- Braue A, Ross G, Varigos G, et al. Epidemiology and impact of childhood molluscum contagiosum: a case series and critical review of the literature. Pediatr Dermatol. 2005;22:287-294.
- Sturt RJ, Muller HK, Francis GD. Molluscum contagiosum in villages of the West Sepik District of New Guinea. Med J Aust. 1971;2:751-754.
- Reynolds MG, Homan RC, Yorita Christensen KL, et al. The incidence of molluscum contagiosum among American Indians and Alaska Natives. PLoS One. 2009;4:e5255.
- Villa L, Varela JA, Otero L, et al. Molluscum contagiosum: a 20-year study in a sexually transmitted infections unit. Sex Transm Dis. 2010;37:423-424.
- Watanabe T, Morikawa S, Suzuki K, et al. Two major antigenic polypeptides of molluscum contagiosum virus. J Infect Dis. 1998;177:284-292.
- Vaccine basics. Centers for Disease Control and Prevention website. https://www.cdc.gov/smallpox/vaccine-basics/index.html. Updated July 12, 2017. Accessed October 16, 2019.
- Mitchell JC. Observations on the virus of molluscum contagiosum. Br J Exp Pathol. 1953;34:44-49.
- Konya J, Thompson CH. Molluscum contagiosum virus: antibody responses in patients with clinical lesions and its sero-epidemiology in a representative Australian population. J Infect Dis. 1999;179:701-704.
- Steffen C, Markman JA. Spontaneous disappearance of molluscum contagiosum. Arch Dermatol. 1980;116:923-924.
- Uzuncakmak TK, Kuru BC, Zemheri EI, et al. Isolated giant molluscum contagiosum mimicking epidermoid cyst. Dermatol Pract Concept. 2016;6:71-73.
- Persechino S, Abruzzese C, Caperchi C, et al. Condyloma acuminata and mollusca contagiosa: a giant manifestation in a patient with lupus. Skinmed. 2014;12:310-311.
- Kim SK, Do JE, Kang HY, et al. Giant molluscum contagiosum of immunocompetent children occurring on the anogenital area. Eur J Dermatol. 2007;17:537-538.
- Alam MS, Shrirao N. Giant molluscum contagiosum presenting as lid neoplasm in an immunocompetent child. Dermatol Online J. 2016;22. pii:13030/qt56v567gn.
- Krishnamurthy J, Nagappa DK. The cytology of molluscum contagiosum mimicking skin adnexal tumor. J Cytol. 2010;27:74-75.
- Baek YS, Oh CH, Song HJ, et al. Asymmetrical periflexural exanthem of childhood with concurrence of molluscum contagiosum infection. Clin Exp Dermatol. 2011;36:676-677.
- Lee HJ, Kwon JA, Kim JW. Erythema multiforme-like molluscum dermatitis. Acta Derm Venereol. 2002;82:217-218.
- Lee YB, Choi HJ, Park HJ, et al. Two cases of erythema multiforme associated with molluscum contagiosum. Int J Dermatol. 2009;48:659-660.
- Vasily DB, Bhatia SG. Erythema annulare centrifugum and molluscum contagiosum.
- Berger EM, Orlow SJ, Patel RR, et al. Experience with molluscum contagiosum and associated inflammatory reactions in a pediatric dermatology practice: the bump that rashes. Arch Dermatol. 2012;148:1257-1264.
- Groner A, Laing-Grayman D, Silverberg NB. Outpatient pediatric community-acquired methicillin-resistant Staphylococcus aureus: a polymorphous clinical disease. Cutis. 2008;81:115-122.
- Butala N, Siegfried E, Weissler A. Molluscum BOTE sign: a predictor of imminent resolution. Pediatrics. 2013;131:E1650-E1653.
- Olsen JR, Gallagher J, Finlay AY, et al. Time to resolution and effect on quality of life of molluscum contagiosum in children in the UK: a prospective community cohort study. Lancet Infect Dis. 2015;15:190-195.
- Goksugur N, Ozbostanci B, Goksugur SB. Molluscum contagiosum infection associated with pimecrolimus use in pityriasis alba. Pediatr Dermatol. 2007;24:E63-E65.
- Lee R, Schwartz RA. Pediatric molluscum contagiosum: reflections on the last challenging poxvirus infection, part 1. Cutis. 2010;86:230-236.
- Hanna D, Hatami A, Powell J, et al. A prospective randomized trial comparing the efficacy and adverse effects of four recognized treatments of molluscum contagiosum in children. Pediatr Dermatol. 2006;23:574-579.
- Coloe Dosal J, Stewart PW, Lin JA, et al. Cantharidin for the treatment of molluscum contagiosum: a prospective, double-blinded, placebo-controlled trial. Pediatr Dermatol. 2014;31:440-449.
- Vakharia PP, Chopra R, Silverberg NB, et al. Efficacy and safety of topical cantharidin treatment for molluscum contagiosum and warts: a systematic review. Am J Clin Dermatol. 2018;19:791-803.
- Handjani F, Behazin E, Sadati MS. Comparison of 10% potassium hydroxide solution versus cryotherapy in the treatment of molluscum contagiosum: an open randomized clinical trial. J Dermatolog Treat. 2014;25:249-250.
- Simonart T, De Maertelaer V. Curettage treatment for molluscum contagiosum: a follow-up survey study. Br J Dermatol. 2008;159:1144-1147.
- Cho YS, Chung BY, Park CW, et al. Seizures and methemoglobinemia after topical application of eutectic mixture of lidocaine and prilocaine on a 3.5-year-old child with molluscum contagiosum and atopic dermatitis. Pediatr Dermatol. 2016;33:E284-E285.
- Bard S, Shiman MI, Bellman B, et al. Treatment of facial molluscum contagiosum with trichloroacetic acid. Pediatr Dermatol. 2009;26:425-426.
- Griffith RD, Yazdani Abyaneh MA, Falto-Aizpurua L, et al. Pulsed dye laser therapy for molluscum contagiosum: a systematic review. J Drugs Dermatol. 2014;13:1349-1352.
- Theos AU, Cummins R, Silverberg NB, et al. Effectiveness of imiquimod cream 5% for treating childhood molluscum contagiosum in a double-blind, randomized pilot trial. Cutis. 2004;74:134-138, 141-142.
- van der Wouden JC, Menke J, Gajadin S, et al. Interventions for cutaneous molluscum contagiosum. Cochrane Database Syst Rev. 2006:CD004767.
- Cunningham BB, Paller AS, Garzon M. Inefficacy of oral cimetidine for nonatopic children with molluscum contagiosum. Pediatr Dermatol. 1998;15:71-72.
- Enns LL, Evans MS. Intralesional immunotherapy with Candida antigen for the treatment of molluscum contagiosum in children. Pediatr Dermatol. 2011;28:254-258.
- Rajouria EA, Amatya A, Karn D. Comparative study of 5% potassium hydroxide solution versus 0.05% tretinoin cream for molluscum contagiosum in children. Kathmandu Univ Med J (KUMJ). 2011;9:291-294.
- Briand S, Milpied B, Navas D, et al. 1% topical cidofovir used as last alternative to treat viral infections. J Eur Acad Dermatol Venereol. 2008;22:249-250.
- Zabawski EJ Jr, Cockerell CJ. Topical cidofovir for molluscum contagiosum in children. Pediatr Dermatol. 1999;16:414-415.
- Watanabe T. Cidofovir diphosphate inhibits molluscum contagiosum virus DNA polymerase activity. J Invest Dermatol. 2008;128:1327-1329.
- Lindau MS, Munar MY. Use of duct tape occlusion in the treatment of recurrent molluscum contagiosum. Pediatr Dermatol. 2004;21:609.
- Silverberg N. Pediatric molluscum contagiosum: optimal treatment strategies. Paediatr Drugs. 2003;5:505-512.
Molluscum contagiosum virus (MCV) infection causes the cutaneous lesions we call molluscum. Molluscum has become common in the last 30 years. Deciding the best course of therapy requires some fundamental understanding about how MCV relates to the following factors: epidemiology, childhood immunity and vaccination, clinical features, comorbidities, and quality of life. Treatment depends on many factors, including presence or absence of atopic dermatitis (AD) and/or pruritus, other symptoms, cosmetic location, and the child’s concern about the lesions. Therapeutics include destructive and immunologic therapies, the latter geared toward increasing immune response.
Epidemiology
Molluscum contagiosum virus is the solo member of the Molluscipoxvirus genus. Infection with MCV causes benign growth or tumors in the skin (ie, molluscum). The infection is slow to clear because the virus reduces the host’s immunity.1,2 Molluscum contagiosum virus is a double-stranded DNA virus that affects keratinocytes and genetically carries the tools for its own replication (ie, DNA-dependent RNA polymerase). The virus has a few subtypes—I/Ia, II, III, and IV—with MCV-I predominating in children and healthy humans and MCV-II in patients with human immunodeficiency virus.1,2 Typing is experimental and is not standardly performed in clinical practice. Molluscum contagiosum virus produces a variety of factors that block the host’s immune response, prolonging infection and preventing erythema and inflammatory response.3
Molluscum contagiosum virus is transmitted through skin-to-skin contact and fomites, including shared towels, bathtubs, spas, bath sponges, and pool equipment.2,4,5 Transmission from household contact and bathing together has been noted in pediatric patients with MCV. Based on the data it can be posited that the lesions are softer when wet and more readily release viral particles or fomites, and fomites may be left on surfaces, especially when a child is wet.6,7 Propensity for infection occurs in patients with AD and in immunosuppressed hosts, including children with human immunodeficiency virus and iatrogenic immunosuppression caused by chemotherapy.1,2,8 Contact sports can increase the risk of transmission, and outbreaks have occurred in pools,5,9 day-care facilities,10 and sports settings.11 Cases of congenital and vertically transmitted molluscum have been documented.12,13 Sexual transmission of MCV may be seen in adolescents who are sexually active. Although child-to-child transmission can occur in the groin area from shared equipment, transmission via sexual abuse also is possible.14 Bargman15 has mentioned the isolated genital location and lack of contact with other infected children as concerning features. Latency of new lesion appearance is anywhere from 1 to 50 days from the date of inoculation; therefore, new lesions are possible and expected even after therapy has been effective in eradicating visible lesions.10 Although clearance has been reported in 6 to 12 months, one pediatric study demonstrated 70% clearance by 1.5 years, suggesting the disease often is more prolonged.16 One-third of children will experience signs of inflammation, such as pruritus and/or erythema. Rare side effects include bacterial superinfection and hypersensitivity.2
One Dutch study from 1994, the largest database survey of children to date, cited a 17% cumulative incidence of molluscum in children by reviewing the data from 103 general practices.17 In a survey and review of molluscum by Braue et al,18 annual rates in populations vary but seem to maximize at approximately 6% to 7%. Sturt et al19 reviewed the prevalence in the indigenous West Sepik section of New Guinea and noted annual incidence rates of 6% in children younger than 10 years (range, 1.8%–10.9%). Epidemics occur and can produce large numbers of cases in a short time period.18 The cumulative prevalence in early childhood may be as high as 22%, as Sturt et al19 observed in children younger than 10 years.
Rising incidence and therefore rising lifetime prevalence appear to have been an issue in the last few decades. Data from the Indian Health Service have demonstrated increases in MCV in Native American children between 2001 and 2005.20 In adults, the data support a steady increase of molluscum from 1988-2007, with a 3-fold increase from 1988-1997 to 1998-2007 in a Spanish study.21 Better population-based data are needed.
Childhood Immunity and Vaccination
Sequence homology between MC133L, a protein of MCV, with vaccinia virus suggests overlapping genes.22 Therefore, it is conceptually possible that the rise in incidence of MCV since the 1980s relates to the loss of herd immunity to variola due to lack of vaccination for smallpox, which has not been offered in the United States since 1972.23 Childhood immunity to MCV varies among studies, but it appears that children do develop antibodies to molluscum in the setting of forming an immune response. Because the rise in molluscum incidence began after the smallpox vaccine was discontinued, the factors appear related; however, the scientific data do not support the theory of a relationship. Mitchell24 has shown that a patient can develop antibodies in response to ground molluscum bodies inoculated into the skin; however, vaccination against molluscum and natural infection do not appear to produce antibodies that would cross-react and protect against other poxviruses, including vaccinia or fowl pox infections.25 Cell-mediated immunity also is required to clear MCV and may account for the inflammatory appearance of lesions as they resolve.26
Demonstrated factors that account for the rise in MCV incidence, aside from alterations in vaccination practices, include spread through sports,9 swimming,11 and AD,7 which have become more commonplace in the United States in the last few decades, supporting the theory that they may be the cause of the increase in childhood MCV infections. Another cause may be the ability of MCV to create factors that stem host immune response.1
Clinical Features
Molluscum lesions have a typical appearance of pearly papules with a central dell. These lesions are lighter to flesh colored and measure 1 to 3 mm.2,4,5 The lesions cluster in the axillae and extremities and average from 10 to 20 per child.6 Lesions clear spontaneously, but new ones will continue to form until immunity is developed. Specific clinical appearances of lesions that are not pearly papules are not infrequent. Table 1 contains a short list of the manifold clinical appearances of molluscum lesions in children.1,2,7,27-35 In particular, certain clinical appearances should be considered. In small children, head and neck lesions resembling milia are not uncommon. Giant or wartlike lesions can appear on the head, neck, or gluteal region in children and are clinical mimics of condyloma or other warts (Figure 1). Giant lesions also can grow in the subcutaneous space and mimic a cyst or abscess.27 Erosive lesions mimicking eczema vaccinatum can be seen (Figure 2), but dermoscopy may demonstrate central dells in some lesions. Other viral processes mimicked include Gianotti Crosti–like lesions (Figure 3) that appear when a papular id reaction forms over the extremities or a localized version in the axilla, mimicking unilateral laterothoracic exanthema.2,36,37 Hypersensitivity reactions are commonly noted with clearance and can be papular or demonstrate swelling and erythema, termed the beginning-of-the-end sign.38
Pruritus, erythema, and swelling can occur with clearance but do not appear in all patients. Addressing pruritus is important to prevent disease spread, as patients are likely to inoculate other areas of the skin with virus when they scratch, and lesion number is reduced with dermatitis interventions.36
Comorbidities
Molluscum lesions can occur in any child; however, the impaired immunologic status and skin barrier in patients with AD is ripe for the extensive spread of lesions that is associated with higher lesion count.36 Children with molluscum infection can experience new-onset dermatitis or triggering of AD flares, especially on the extremities, such as the antecubital and popliteal regions.7 A study of children with MCV infection demonstrated that treatment of active dermatitis reduced spread. The authors mentioned autoinoculation as the mechanism; however, these data also suggest supporting barrier state as a factor in disease spread.36 Superinfection can occur prior to6 or after therapy for lesions,37 but it is unclear if this relates to the underlying atopic diathesis. Children with molluscum have been described to have warts, psoriasis, family history of atopy, diabetes mellitus, and pityriasis alba,7 while immunosuppression of any kind is associated with molluscum and high lesion count or prolonged disease in childhood.1,2
Quality of Life
Children with molluscum who have higher lesion counts appear to be at risk for severe effects on their quality of life. Approximately 10% of children with MCV infection have been documented to have severe impairments on quality of life.39 In my practice, quality of life in children with MCV appears to be affected by many factors (Table 2).7,18,39
Treatments
Proper Skin Care and Treatment of AD
Therapy for AD and/or pruritus appears to limit lesion number in children with MCV and rashes or itch.7,36 I recommend barrier repair agents, including emollients and syndet bar cleansers, to prevent small breaks in the skin that occur with xerosis and AD and that increase itch and risk of spread. Therapy for AD and molluscum dermatitis is similar and overlapping. There is always a concern about the spread of MCV when using topical calcineurin inhibitors. I, therefore, focus the dermatitis therapeutics on topical corticosteroid–based care.6,40
Prevention of Spread
Prevention of spread begins with hygiene interventions. Cobathing is common in children with MCV and should be held off when possible. It is important for the child with MCV to avoid sharing bath towels and equipment23 and having bare skin come in contact with mats in sports. I request that children with MCV wear bathing suits that cover the areas affected.
Reassurance
The most important therapy is reassurance.41 Many parents/guardians are truly unaware that the MCV infection can last for more than a year and therefore worry over normal disease course. When counseled as to the benign course of illness and given instructions on proper skin care, the parent/guardian of a child with MCV will often opt against therapy of uncomplicated cases. On the other hand, there are medical reasons for treatment, and they support the need for intervention (Table 3). Seventy percent of lesions resolve in 1.5 years; however, of the residual infections, some may last as long as 4 years.16 It is not recommended to stop children from attending school because of MCV.
Interventional Therapy
Therapeutics of MCV include destructive therapies in office (ie, cantharidin, cryotherapy, curettage, trichloroacetic acid, and glycolic acid) and at-home therapies (ie, topical retinoids, nitric oxide releasers)(eTable).2,5,6,42-58 When there are many lesions or spread is noted, immunotherapies can be used, including topical imiquimod, oral cimetidine, and intralesional Candida antigen.2,4,7 Pulsed dye laser cuts off the lesion vascular supply, while cidofovir is directly antiviral both topically and systemically, the latter reserved for severe cases in immunosuppressed adults.59 Head-to-head studies of cantharidin, curettage, topical peeling agents, and imiquimod demonstrated better satisfaction and fewer office visits with topical anesthetic and curettage on the first visit. Side effects were greatest for salicylic acid and glycolic acid; therefore, these agents are less desirable.42
Conclusion
Molluscum is a cutaneous viral infection that is common in children and has associated morbidities, including AD, pruritus, poor quality of life in some cases, and risk of contagion. Addressing the disease includes understanding its natural history and explaining it to parents/guardians. Therapeutics can be offered in cases where need is demonstrated, such as with lesions that spread and cause discomfort. Choice of therapeutics depends on the practitioner’s experience, the child’s clinical appearance, availability of therapy, and review of options with the parents/guardians. When avoidance of intervention is desired, barrier enhancement and treatment of symptomatic dermatitis are still beneficial, as are household (eg, not sharing towels) and activity (eg, adhesive bandages over active lesions) interventions to reduce transmission.
Molluscum contagiosum virus (MCV) infection causes the cutaneous lesions we call molluscum. Molluscum has become common in the last 30 years. Deciding the best course of therapy requires some fundamental understanding about how MCV relates to the following factors: epidemiology, childhood immunity and vaccination, clinical features, comorbidities, and quality of life. Treatment depends on many factors, including presence or absence of atopic dermatitis (AD) and/or pruritus, other symptoms, cosmetic location, and the child’s concern about the lesions. Therapeutics include destructive and immunologic therapies, the latter geared toward increasing immune response.
Epidemiology
Molluscum contagiosum virus is the solo member of the Molluscipoxvirus genus. Infection with MCV causes benign growth or tumors in the skin (ie, molluscum). The infection is slow to clear because the virus reduces the host’s immunity.1,2 Molluscum contagiosum virus is a double-stranded DNA virus that affects keratinocytes and genetically carries the tools for its own replication (ie, DNA-dependent RNA polymerase). The virus has a few subtypes—I/Ia, II, III, and IV—with MCV-I predominating in children and healthy humans and MCV-II in patients with human immunodeficiency virus.1,2 Typing is experimental and is not standardly performed in clinical practice. Molluscum contagiosum virus produces a variety of factors that block the host’s immune response, prolonging infection and preventing erythema and inflammatory response.3
Molluscum contagiosum virus is transmitted through skin-to-skin contact and fomites, including shared towels, bathtubs, spas, bath sponges, and pool equipment.2,4,5 Transmission from household contact and bathing together has been noted in pediatric patients with MCV. Based on the data it can be posited that the lesions are softer when wet and more readily release viral particles or fomites, and fomites may be left on surfaces, especially when a child is wet.6,7 Propensity for infection occurs in patients with AD and in immunosuppressed hosts, including children with human immunodeficiency virus and iatrogenic immunosuppression caused by chemotherapy.1,2,8 Contact sports can increase the risk of transmission, and outbreaks have occurred in pools,5,9 day-care facilities,10 and sports settings.11 Cases of congenital and vertically transmitted molluscum have been documented.12,13 Sexual transmission of MCV may be seen in adolescents who are sexually active. Although child-to-child transmission can occur in the groin area from shared equipment, transmission via sexual abuse also is possible.14 Bargman15 has mentioned the isolated genital location and lack of contact with other infected children as concerning features. Latency of new lesion appearance is anywhere from 1 to 50 days from the date of inoculation; therefore, new lesions are possible and expected even after therapy has been effective in eradicating visible lesions.10 Although clearance has been reported in 6 to 12 months, one pediatric study demonstrated 70% clearance by 1.5 years, suggesting the disease often is more prolonged.16 One-third of children will experience signs of inflammation, such as pruritus and/or erythema. Rare side effects include bacterial superinfection and hypersensitivity.2
One Dutch study from 1994, the largest database survey of children to date, cited a 17% cumulative incidence of molluscum in children by reviewing the data from 103 general practices.17 In a survey and review of molluscum by Braue et al,18 annual rates in populations vary but seem to maximize at approximately 6% to 7%. Sturt et al19 reviewed the prevalence in the indigenous West Sepik section of New Guinea and noted annual incidence rates of 6% in children younger than 10 years (range, 1.8%–10.9%). Epidemics occur and can produce large numbers of cases in a short time period.18 The cumulative prevalence in early childhood may be as high as 22%, as Sturt et al19 observed in children younger than 10 years.
Rising incidence and therefore rising lifetime prevalence appear to have been an issue in the last few decades. Data from the Indian Health Service have demonstrated increases in MCV in Native American children between 2001 and 2005.20 In adults, the data support a steady increase of molluscum from 1988-2007, with a 3-fold increase from 1988-1997 to 1998-2007 in a Spanish study.21 Better population-based data are needed.
Childhood Immunity and Vaccination
Sequence homology between MC133L, a protein of MCV, with vaccinia virus suggests overlapping genes.22 Therefore, it is conceptually possible that the rise in incidence of MCV since the 1980s relates to the loss of herd immunity to variola due to lack of vaccination for smallpox, which has not been offered in the United States since 1972.23 Childhood immunity to MCV varies among studies, but it appears that children do develop antibodies to molluscum in the setting of forming an immune response. Because the rise in molluscum incidence began after the smallpox vaccine was discontinued, the factors appear related; however, the scientific data do not support the theory of a relationship. Mitchell24 has shown that a patient can develop antibodies in response to ground molluscum bodies inoculated into the skin; however, vaccination against molluscum and natural infection do not appear to produce antibodies that would cross-react and protect against other poxviruses, including vaccinia or fowl pox infections.25 Cell-mediated immunity also is required to clear MCV and may account for the inflammatory appearance of lesions as they resolve.26
Demonstrated factors that account for the rise in MCV incidence, aside from alterations in vaccination practices, include spread through sports,9 swimming,11 and AD,7 which have become more commonplace in the United States in the last few decades, supporting the theory that they may be the cause of the increase in childhood MCV infections. Another cause may be the ability of MCV to create factors that stem host immune response.1
Clinical Features
Molluscum lesions have a typical appearance of pearly papules with a central dell. These lesions are lighter to flesh colored and measure 1 to 3 mm.2,4,5 The lesions cluster in the axillae and extremities and average from 10 to 20 per child.6 Lesions clear spontaneously, but new ones will continue to form until immunity is developed. Specific clinical appearances of lesions that are not pearly papules are not infrequent. Table 1 contains a short list of the manifold clinical appearances of molluscum lesions in children.1,2,7,27-35 In particular, certain clinical appearances should be considered. In small children, head and neck lesions resembling milia are not uncommon. Giant or wartlike lesions can appear on the head, neck, or gluteal region in children and are clinical mimics of condyloma or other warts (Figure 1). Giant lesions also can grow in the subcutaneous space and mimic a cyst or abscess.27 Erosive lesions mimicking eczema vaccinatum can be seen (Figure 2), but dermoscopy may demonstrate central dells in some lesions. Other viral processes mimicked include Gianotti Crosti–like lesions (Figure 3) that appear when a papular id reaction forms over the extremities or a localized version in the axilla, mimicking unilateral laterothoracic exanthema.2,36,37 Hypersensitivity reactions are commonly noted with clearance and can be papular or demonstrate swelling and erythema, termed the beginning-of-the-end sign.38
Pruritus, erythema, and swelling can occur with clearance but do not appear in all patients. Addressing pruritus is important to prevent disease spread, as patients are likely to inoculate other areas of the skin with virus when they scratch, and lesion number is reduced with dermatitis interventions.36
Comorbidities
Molluscum lesions can occur in any child; however, the impaired immunologic status and skin barrier in patients with AD is ripe for the extensive spread of lesions that is associated with higher lesion count.36 Children with molluscum infection can experience new-onset dermatitis or triggering of AD flares, especially on the extremities, such as the antecubital and popliteal regions.7 A study of children with MCV infection demonstrated that treatment of active dermatitis reduced spread. The authors mentioned autoinoculation as the mechanism; however, these data also suggest supporting barrier state as a factor in disease spread.36 Superinfection can occur prior to6 or after therapy for lesions,37 but it is unclear if this relates to the underlying atopic diathesis. Children with molluscum have been described to have warts, psoriasis, family history of atopy, diabetes mellitus, and pityriasis alba,7 while immunosuppression of any kind is associated with molluscum and high lesion count or prolonged disease in childhood.1,2
Quality of Life
Children with molluscum who have higher lesion counts appear to be at risk for severe effects on their quality of life. Approximately 10% of children with MCV infection have been documented to have severe impairments on quality of life.39 In my practice, quality of life in children with MCV appears to be affected by many factors (Table 2).7,18,39
Treatments
Proper Skin Care and Treatment of AD
Therapy for AD and/or pruritus appears to limit lesion number in children with MCV and rashes or itch.7,36 I recommend barrier repair agents, including emollients and syndet bar cleansers, to prevent small breaks in the skin that occur with xerosis and AD and that increase itch and risk of spread. Therapy for AD and molluscum dermatitis is similar and overlapping. There is always a concern about the spread of MCV when using topical calcineurin inhibitors. I, therefore, focus the dermatitis therapeutics on topical corticosteroid–based care.6,40
Prevention of Spread
Prevention of spread begins with hygiene interventions. Cobathing is common in children with MCV and should be held off when possible. It is important for the child with MCV to avoid sharing bath towels and equipment23 and having bare skin come in contact with mats in sports. I request that children with MCV wear bathing suits that cover the areas affected.
Reassurance
The most important therapy is reassurance.41 Many parents/guardians are truly unaware that the MCV infection can last for more than a year and therefore worry over normal disease course. When counseled as to the benign course of illness and given instructions on proper skin care, the parent/guardian of a child with MCV will often opt against therapy of uncomplicated cases. On the other hand, there are medical reasons for treatment, and they support the need for intervention (Table 3). Seventy percent of lesions resolve in 1.5 years; however, of the residual infections, some may last as long as 4 years.16 It is not recommended to stop children from attending school because of MCV.
Interventional Therapy
Therapeutics of MCV include destructive therapies in office (ie, cantharidin, cryotherapy, curettage, trichloroacetic acid, and glycolic acid) and at-home therapies (ie, topical retinoids, nitric oxide releasers)(eTable).2,5,6,42-58 When there are many lesions or spread is noted, immunotherapies can be used, including topical imiquimod, oral cimetidine, and intralesional Candida antigen.2,4,7 Pulsed dye laser cuts off the lesion vascular supply, while cidofovir is directly antiviral both topically and systemically, the latter reserved for severe cases in immunosuppressed adults.59 Head-to-head studies of cantharidin, curettage, topical peeling agents, and imiquimod demonstrated better satisfaction and fewer office visits with topical anesthetic and curettage on the first visit. Side effects were greatest for salicylic acid and glycolic acid; therefore, these agents are less desirable.42
Conclusion
Molluscum is a cutaneous viral infection that is common in children and has associated morbidities, including AD, pruritus, poor quality of life in some cases, and risk of contagion. Addressing the disease includes understanding its natural history and explaining it to parents/guardians. Therapeutics can be offered in cases where need is demonstrated, such as with lesions that spread and cause discomfort. Choice of therapeutics depends on the practitioner’s experience, the child’s clinical appearance, availability of therapy, and review of options with the parents/guardians. When avoidance of intervention is desired, barrier enhancement and treatment of symptomatic dermatitis are still beneficial, as are household (eg, not sharing towels) and activity (eg, adhesive bandages over active lesions) interventions to reduce transmission.
- Shisler JL. Immune evasion strategies of molluscum contagiosum virus. Adv Virus Res. 2015;92:201-252.
- Brown J, Janniger CK, Schwartz RA, et al. Childhood molluscum contagiosum. Int J Dermatol. 2006;45:93-99.
- Moss B, Shisler JL, Xiang Y, et al. Immune-defense molecules of molluscum contagiosum virus, a human poxvirus. Trends Microbiol. 2000;8:473-477.
- Silverberg NB. Warts and molluscum in children. Adv Dermatol. 2004;20:23-73.
- Choong KY, Roberts LJ. Molluscum contagiosum, swimming and bathing: a clinical analysis. Australas J Dermatol. 1999;40:89-92.
- Silverberg NB, Sidbury R, Mancini AJ. Childhood molluscum contagiosum: experience with cantharidin therapy in 300 patients. J Am Acad Dermatol. 2000;43:503-507.
- Silverberg NB. Molluscum contagiosum virus infection can trigger atopic dermatitis disease onset or flare. Cutis. 2018;102:191-194.
- Ajithkumar VT, Sasidharanpillai S, Muhammed K, et al. Disseminated molluscum contagiosum following chemotherapy: a therapeutic challenge. Indian J Dermatol Venereol Leprol. 2017;83:516.
- Oren B, Wende SO. An outbreak of molluscum contagiosum in a kibbutz. Infection. 1991;19:159-161.
- Molluscum contagiosum. Healthy Children website. https://www.healthychildren.org/English/health-issues/conditions/skin/Pages/Molluscum-Contagiosum.aspx. Updated November 21, 2015. Accessed October 16, 2019.
- Peterson AR, Nash E, Anderson BJ. Infectious disease in contact sports. Sports Health. 2019;11:47-58.
- Connell CO, Oranje A, Van Gysel D, et al. Congenital molluscum contagiosum: report of four cases and review of the literature. Pediatr Dermatol. 2008;25:553-556.
- Luke JD, Silverberg NB. Vertically transmitted molluscum contagiosum infection. Pediatrics. 2010;125:E423-E425.
- Mendiratta V, Agarwal S, Chander R. Reappraisal of sexually transmitted infections in children: a hospital-based study from an urban area. Indian J Sex Transm Dis AIDS. 2014;35:25-28.
- Bargman H. Genital molluscum contagiosum in children: evidence of sexual abuse? CMAJ. 1986;135:432-433.
- Basdag H, Rainer BM, Cohen BA. Molluscum contagiosum: to treat or not to treat? experience with 170 children in an outpatient clinic setting in the northeastern United States. Pediatr Dermatol. 2015;32:353-357.
- Koning S, Bruijnzeels MA, van Suijlekom-Smit LW, et al. Molluscum contagiosum in Dutch general practice. Br J Gen Pract. 1994;44:417-419.
- Braue A, Ross G, Varigos G, et al. Epidemiology and impact of childhood molluscum contagiosum: a case series and critical review of the literature. Pediatr Dermatol. 2005;22:287-294.
- Sturt RJ, Muller HK, Francis GD. Molluscum contagiosum in villages of the West Sepik District of New Guinea. Med J Aust. 1971;2:751-754.
- Reynolds MG, Homan RC, Yorita Christensen KL, et al. The incidence of molluscum contagiosum among American Indians and Alaska Natives. PLoS One. 2009;4:e5255.
- Villa L, Varela JA, Otero L, et al. Molluscum contagiosum: a 20-year study in a sexually transmitted infections unit. Sex Transm Dis. 2010;37:423-424.
- Watanabe T, Morikawa S, Suzuki K, et al. Two major antigenic polypeptides of molluscum contagiosum virus. J Infect Dis. 1998;177:284-292.
- Vaccine basics. Centers for Disease Control and Prevention website. https://www.cdc.gov/smallpox/vaccine-basics/index.html. Updated July 12, 2017. Accessed October 16, 2019.
- Mitchell JC. Observations on the virus of molluscum contagiosum. Br J Exp Pathol. 1953;34:44-49.
- Konya J, Thompson CH. Molluscum contagiosum virus: antibody responses in patients with clinical lesions and its sero-epidemiology in a representative Australian population. J Infect Dis. 1999;179:701-704.
- Steffen C, Markman JA. Spontaneous disappearance of molluscum contagiosum. Arch Dermatol. 1980;116:923-924.
- Uzuncakmak TK, Kuru BC, Zemheri EI, et al. Isolated giant molluscum contagiosum mimicking epidermoid cyst. Dermatol Pract Concept. 2016;6:71-73.
- Persechino S, Abruzzese C, Caperchi C, et al. Condyloma acuminata and mollusca contagiosa: a giant manifestation in a patient with lupus. Skinmed. 2014;12:310-311.
- Kim SK, Do JE, Kang HY, et al. Giant molluscum contagiosum of immunocompetent children occurring on the anogenital area. Eur J Dermatol. 2007;17:537-538.
- Alam MS, Shrirao N. Giant molluscum contagiosum presenting as lid neoplasm in an immunocompetent child. Dermatol Online J. 2016;22. pii:13030/qt56v567gn.
- Krishnamurthy J, Nagappa DK. The cytology of molluscum contagiosum mimicking skin adnexal tumor. J Cytol. 2010;27:74-75.
- Baek YS, Oh CH, Song HJ, et al. Asymmetrical periflexural exanthem of childhood with concurrence of molluscum contagiosum infection. Clin Exp Dermatol. 2011;36:676-677.
- Lee HJ, Kwon JA, Kim JW. Erythema multiforme-like molluscum dermatitis. Acta Derm Venereol. 2002;82:217-218.
- Lee YB, Choi HJ, Park HJ, et al. Two cases of erythema multiforme associated with molluscum contagiosum. Int J Dermatol. 2009;48:659-660.
- Vasily DB, Bhatia SG. Erythema annulare centrifugum and molluscum contagiosum.
- Berger EM, Orlow SJ, Patel RR, et al. Experience with molluscum contagiosum and associated inflammatory reactions in a pediatric dermatology practice: the bump that rashes. Arch Dermatol. 2012;148:1257-1264.
- Groner A, Laing-Grayman D, Silverberg NB. Outpatient pediatric community-acquired methicillin-resistant Staphylococcus aureus: a polymorphous clinical disease. Cutis. 2008;81:115-122.
- Butala N, Siegfried E, Weissler A. Molluscum BOTE sign: a predictor of imminent resolution. Pediatrics. 2013;131:E1650-E1653.
- Olsen JR, Gallagher J, Finlay AY, et al. Time to resolution and effect on quality of life of molluscum contagiosum in children in the UK: a prospective community cohort study. Lancet Infect Dis. 2015;15:190-195.
- Goksugur N, Ozbostanci B, Goksugur SB. Molluscum contagiosum infection associated with pimecrolimus use in pityriasis alba. Pediatr Dermatol. 2007;24:E63-E65.
- Lee R, Schwartz RA. Pediatric molluscum contagiosum: reflections on the last challenging poxvirus infection, part 1. Cutis. 2010;86:230-236.
- Hanna D, Hatami A, Powell J, et al. A prospective randomized trial comparing the efficacy and adverse effects of four recognized treatments of molluscum contagiosum in children. Pediatr Dermatol. 2006;23:574-579.
- Coloe Dosal J, Stewart PW, Lin JA, et al. Cantharidin for the treatment of molluscum contagiosum: a prospective, double-blinded, placebo-controlled trial. Pediatr Dermatol. 2014;31:440-449.
- Vakharia PP, Chopra R, Silverberg NB, et al. Efficacy and safety of topical cantharidin treatment for molluscum contagiosum and warts: a systematic review. Am J Clin Dermatol. 2018;19:791-803.
- Handjani F, Behazin E, Sadati MS. Comparison of 10% potassium hydroxide solution versus cryotherapy in the treatment of molluscum contagiosum: an open randomized clinical trial. J Dermatolog Treat. 2014;25:249-250.
- Simonart T, De Maertelaer V. Curettage treatment for molluscum contagiosum: a follow-up survey study. Br J Dermatol. 2008;159:1144-1147.
- Cho YS, Chung BY, Park CW, et al. Seizures and methemoglobinemia after topical application of eutectic mixture of lidocaine and prilocaine on a 3.5-year-old child with molluscum contagiosum and atopic dermatitis. Pediatr Dermatol. 2016;33:E284-E285.
- Bard S, Shiman MI, Bellman B, et al. Treatment of facial molluscum contagiosum with trichloroacetic acid. Pediatr Dermatol. 2009;26:425-426.
- Griffith RD, Yazdani Abyaneh MA, Falto-Aizpurua L, et al. Pulsed dye laser therapy for molluscum contagiosum: a systematic review. J Drugs Dermatol. 2014;13:1349-1352.
- Theos AU, Cummins R, Silverberg NB, et al. Effectiveness of imiquimod cream 5% for treating childhood molluscum contagiosum in a double-blind, randomized pilot trial. Cutis. 2004;74:134-138, 141-142.
- van der Wouden JC, Menke J, Gajadin S, et al. Interventions for cutaneous molluscum contagiosum. Cochrane Database Syst Rev. 2006:CD004767.
- Cunningham BB, Paller AS, Garzon M. Inefficacy of oral cimetidine for nonatopic children with molluscum contagiosum. Pediatr Dermatol. 1998;15:71-72.
- Enns LL, Evans MS. Intralesional immunotherapy with Candida antigen for the treatment of molluscum contagiosum in children. Pediatr Dermatol. 2011;28:254-258.
- Rajouria EA, Amatya A, Karn D. Comparative study of 5% potassium hydroxide solution versus 0.05% tretinoin cream for molluscum contagiosum in children. Kathmandu Univ Med J (KUMJ). 2011;9:291-294.
- Briand S, Milpied B, Navas D, et al. 1% topical cidofovir used as last alternative to treat viral infections. J Eur Acad Dermatol Venereol. 2008;22:249-250.
- Zabawski EJ Jr, Cockerell CJ. Topical cidofovir for molluscum contagiosum in children. Pediatr Dermatol. 1999;16:414-415.
- Watanabe T. Cidofovir diphosphate inhibits molluscum contagiosum virus DNA polymerase activity. J Invest Dermatol. 2008;128:1327-1329.
- Lindau MS, Munar MY. Use of duct tape occlusion in the treatment of recurrent molluscum contagiosum. Pediatr Dermatol. 2004;21:609.
- Silverberg N. Pediatric molluscum contagiosum: optimal treatment strategies. Paediatr Drugs. 2003;5:505-512.
- Shisler JL. Immune evasion strategies of molluscum contagiosum virus. Adv Virus Res. 2015;92:201-252.
- Brown J, Janniger CK, Schwartz RA, et al. Childhood molluscum contagiosum. Int J Dermatol. 2006;45:93-99.
- Moss B, Shisler JL, Xiang Y, et al. Immune-defense molecules of molluscum contagiosum virus, a human poxvirus. Trends Microbiol. 2000;8:473-477.
- Silverberg NB. Warts and molluscum in children. Adv Dermatol. 2004;20:23-73.
- Choong KY, Roberts LJ. Molluscum contagiosum, swimming and bathing: a clinical analysis. Australas J Dermatol. 1999;40:89-92.
- Silverberg NB, Sidbury R, Mancini AJ. Childhood molluscum contagiosum: experience with cantharidin therapy in 300 patients. J Am Acad Dermatol. 2000;43:503-507.
- Silverberg NB. Molluscum contagiosum virus infection can trigger atopic dermatitis disease onset or flare. Cutis. 2018;102:191-194.
- Ajithkumar VT, Sasidharanpillai S, Muhammed K, et al. Disseminated molluscum contagiosum following chemotherapy: a therapeutic challenge. Indian J Dermatol Venereol Leprol. 2017;83:516.
- Oren B, Wende SO. An outbreak of molluscum contagiosum in a kibbutz. Infection. 1991;19:159-161.
- Molluscum contagiosum. Healthy Children website. https://www.healthychildren.org/English/health-issues/conditions/skin/Pages/Molluscum-Contagiosum.aspx. Updated November 21, 2015. Accessed October 16, 2019.
- Peterson AR, Nash E, Anderson BJ. Infectious disease in contact sports. Sports Health. 2019;11:47-58.
- Connell CO, Oranje A, Van Gysel D, et al. Congenital molluscum contagiosum: report of four cases and review of the literature. Pediatr Dermatol. 2008;25:553-556.
- Luke JD, Silverberg NB. Vertically transmitted molluscum contagiosum infection. Pediatrics. 2010;125:E423-E425.
- Mendiratta V, Agarwal S, Chander R. Reappraisal of sexually transmitted infections in children: a hospital-based study from an urban area. Indian J Sex Transm Dis AIDS. 2014;35:25-28.
- Bargman H. Genital molluscum contagiosum in children: evidence of sexual abuse? CMAJ. 1986;135:432-433.
- Basdag H, Rainer BM, Cohen BA. Molluscum contagiosum: to treat or not to treat? experience with 170 children in an outpatient clinic setting in the northeastern United States. Pediatr Dermatol. 2015;32:353-357.
- Koning S, Bruijnzeels MA, van Suijlekom-Smit LW, et al. Molluscum contagiosum in Dutch general practice. Br J Gen Pract. 1994;44:417-419.
- Braue A, Ross G, Varigos G, et al. Epidemiology and impact of childhood molluscum contagiosum: a case series and critical review of the literature. Pediatr Dermatol. 2005;22:287-294.
- Sturt RJ, Muller HK, Francis GD. Molluscum contagiosum in villages of the West Sepik District of New Guinea. Med J Aust. 1971;2:751-754.
- Reynolds MG, Homan RC, Yorita Christensen KL, et al. The incidence of molluscum contagiosum among American Indians and Alaska Natives. PLoS One. 2009;4:e5255.
- Villa L, Varela JA, Otero L, et al. Molluscum contagiosum: a 20-year study in a sexually transmitted infections unit. Sex Transm Dis. 2010;37:423-424.
- Watanabe T, Morikawa S, Suzuki K, et al. Two major antigenic polypeptides of molluscum contagiosum virus. J Infect Dis. 1998;177:284-292.
- Vaccine basics. Centers for Disease Control and Prevention website. https://www.cdc.gov/smallpox/vaccine-basics/index.html. Updated July 12, 2017. Accessed October 16, 2019.
- Mitchell JC. Observations on the virus of molluscum contagiosum. Br J Exp Pathol. 1953;34:44-49.
- Konya J, Thompson CH. Molluscum contagiosum virus: antibody responses in patients with clinical lesions and its sero-epidemiology in a representative Australian population. J Infect Dis. 1999;179:701-704.
- Steffen C, Markman JA. Spontaneous disappearance of molluscum contagiosum. Arch Dermatol. 1980;116:923-924.
- Uzuncakmak TK, Kuru BC, Zemheri EI, et al. Isolated giant molluscum contagiosum mimicking epidermoid cyst. Dermatol Pract Concept. 2016;6:71-73.
- Persechino S, Abruzzese C, Caperchi C, et al. Condyloma acuminata and mollusca contagiosa: a giant manifestation in a patient with lupus. Skinmed. 2014;12:310-311.
- Kim SK, Do JE, Kang HY, et al. Giant molluscum contagiosum of immunocompetent children occurring on the anogenital area. Eur J Dermatol. 2007;17:537-538.
- Alam MS, Shrirao N. Giant molluscum contagiosum presenting as lid neoplasm in an immunocompetent child. Dermatol Online J. 2016;22. pii:13030/qt56v567gn.
- Krishnamurthy J, Nagappa DK. The cytology of molluscum contagiosum mimicking skin adnexal tumor. J Cytol. 2010;27:74-75.
- Baek YS, Oh CH, Song HJ, et al. Asymmetrical periflexural exanthem of childhood with concurrence of molluscum contagiosum infection. Clin Exp Dermatol. 2011;36:676-677.
- Lee HJ, Kwon JA, Kim JW. Erythema multiforme-like molluscum dermatitis. Acta Derm Venereol. 2002;82:217-218.
- Lee YB, Choi HJ, Park HJ, et al. Two cases of erythema multiforme associated with molluscum contagiosum. Int J Dermatol. 2009;48:659-660.
- Vasily DB, Bhatia SG. Erythema annulare centrifugum and molluscum contagiosum.
- Berger EM, Orlow SJ, Patel RR, et al. Experience with molluscum contagiosum and associated inflammatory reactions in a pediatric dermatology practice: the bump that rashes. Arch Dermatol. 2012;148:1257-1264.
- Groner A, Laing-Grayman D, Silverberg NB. Outpatient pediatric community-acquired methicillin-resistant Staphylococcus aureus: a polymorphous clinical disease. Cutis. 2008;81:115-122.
- Butala N, Siegfried E, Weissler A. Molluscum BOTE sign: a predictor of imminent resolution. Pediatrics. 2013;131:E1650-E1653.
- Olsen JR, Gallagher J, Finlay AY, et al. Time to resolution and effect on quality of life of molluscum contagiosum in children in the UK: a prospective community cohort study. Lancet Infect Dis. 2015;15:190-195.
- Goksugur N, Ozbostanci B, Goksugur SB. Molluscum contagiosum infection associated with pimecrolimus use in pityriasis alba. Pediatr Dermatol. 2007;24:E63-E65.
- Lee R, Schwartz RA. Pediatric molluscum contagiosum: reflections on the last challenging poxvirus infection, part 1. Cutis. 2010;86:230-236.
- Hanna D, Hatami A, Powell J, et al. A prospective randomized trial comparing the efficacy and adverse effects of four recognized treatments of molluscum contagiosum in children. Pediatr Dermatol. 2006;23:574-579.
- Coloe Dosal J, Stewart PW, Lin JA, et al. Cantharidin for the treatment of molluscum contagiosum: a prospective, double-blinded, placebo-controlled trial. Pediatr Dermatol. 2014;31:440-449.
- Vakharia PP, Chopra R, Silverberg NB, et al. Efficacy and safety of topical cantharidin treatment for molluscum contagiosum and warts: a systematic review. Am J Clin Dermatol. 2018;19:791-803.
- Handjani F, Behazin E, Sadati MS. Comparison of 10% potassium hydroxide solution versus cryotherapy in the treatment of molluscum contagiosum: an open randomized clinical trial. J Dermatolog Treat. 2014;25:249-250.
- Simonart T, De Maertelaer V. Curettage treatment for molluscum contagiosum: a follow-up survey study. Br J Dermatol. 2008;159:1144-1147.
- Cho YS, Chung BY, Park CW, et al. Seizures and methemoglobinemia after topical application of eutectic mixture of lidocaine and prilocaine on a 3.5-year-old child with molluscum contagiosum and atopic dermatitis. Pediatr Dermatol. 2016;33:E284-E285.
- Bard S, Shiman MI, Bellman B, et al. Treatment of facial molluscum contagiosum with trichloroacetic acid. Pediatr Dermatol. 2009;26:425-426.
- Griffith RD, Yazdani Abyaneh MA, Falto-Aizpurua L, et al. Pulsed dye laser therapy for molluscum contagiosum: a systematic review. J Drugs Dermatol. 2014;13:1349-1352.
- Theos AU, Cummins R, Silverberg NB, et al. Effectiveness of imiquimod cream 5% for treating childhood molluscum contagiosum in a double-blind, randomized pilot trial. Cutis. 2004;74:134-138, 141-142.
- van der Wouden JC, Menke J, Gajadin S, et al. Interventions for cutaneous molluscum contagiosum. Cochrane Database Syst Rev. 2006:CD004767.
- Cunningham BB, Paller AS, Garzon M. Inefficacy of oral cimetidine for nonatopic children with molluscum contagiosum. Pediatr Dermatol. 1998;15:71-72.
- Enns LL, Evans MS. Intralesional immunotherapy with Candida antigen for the treatment of molluscum contagiosum in children. Pediatr Dermatol. 2011;28:254-258.
- Rajouria EA, Amatya A, Karn D. Comparative study of 5% potassium hydroxide solution versus 0.05% tretinoin cream for molluscum contagiosum in children. Kathmandu Univ Med J (KUMJ). 2011;9:291-294.
- Briand S, Milpied B, Navas D, et al. 1% topical cidofovir used as last alternative to treat viral infections. J Eur Acad Dermatol Venereol. 2008;22:249-250.
- Zabawski EJ Jr, Cockerell CJ. Topical cidofovir for molluscum contagiosum in children. Pediatr Dermatol. 1999;16:414-415.
- Watanabe T. Cidofovir diphosphate inhibits molluscum contagiosum virus DNA polymerase activity. J Invest Dermatol. 2008;128:1327-1329.
- Lindau MS, Munar MY. Use of duct tape occlusion in the treatment of recurrent molluscum contagiosum. Pediatr Dermatol. 2004;21:609.
- Silverberg N. Pediatric molluscum contagiosum: optimal treatment strategies. Paediatr Drugs. 2003;5:505-512.
Practice Points
- Molluscum appears as pearly papules with a central dell (ie, umbilicated).
- Caused by a poxvirus, the disease is very contagious and transferred via skin-to-skin contact or fomites.
- One-third of children with molluscum will develop symptoms of local erythema, swelling, or pruritus.
- Diagnosis usually is clinical.
- Children are primarily managed through observation; however, cantharidin, cryotherapy, or curettage can be used for symptomatic or cosmetically concerning lesions.

Etokimab trial highlights IL-33 targeting as potential new AD therapy
Patients with moderate to severe atopic dermatitis who received the immunoglobulin G1 anti–interleukin-33 monoclonal antibody etokimab showed significant disease improvement 29 days after receiving a single systemic administration, according to results from a recent proof-of-concept, phase IIa study.
“Most of the focus for IL-33 pathway inhibition has been on the type 2 cytokine axis because of significant supporting genetic and functional data in both human and murine systems,” Yi-Ling Chen, a DPhil student at the University of Oxford (England), and colleagues wrote in Science Translational Medicine. “Our findings might also provide a further dimension to explain how etokimab, by inhibiting IL-33, could provide such a rapid and persistent clinical benefit as described in this report.”
In their study, 12 patients with moderate to severe AD received etokimab in a single intravenous dose of 300 mg. Prior to receiving etokimab, patients received a placebo dose and then underwent saline or house dust mite intraepidermal challenge, with researchers obtaining blister samples 1 day after challenge following placebo administration and again after patients received etokimab.
At 29 days, 83% of patients reached rapid and sustained clinical benefit under Eczema Area and Severity Index (EASI ) 50 and 33% in EASI 75, including peripheral eosinophil reduction. There also was significant reduction in skin neutrophil infiltration after patients received etokimab and then house dust mite challenge, compared with after they received placebo, .
“These findings open new therapeutic possible applications of etokimab to sterile neutrophilic disease as well as other inflammatory diseases with a clear neutrophilic involvement such as neutrophilic asthma,” the researchers said. “This first-in-class experimental medicine study has shown that in vivo in human tissue IL-33 has key upstream effects which broadly influence different and relevant inflammatory cascades and thus widen the potential of this treatment to a larger than anticipated group of diseases.
“Although excellent previous studies have demonstrated in vitro and in murine models that IL-33 is involved in neutrophil migration, the translation here to human tissue immunology shows that IL-33 plays a dominant role and effects are in part likely to be mediated instead by CXCR1,” concluded Ms. Chen and colleagues. “Therefore, specific IL-33 therapeutic intervention is not targeting a redundant system and is worthy of further investigation.”
This study was funded by AnaptysBio, which was responsible for the conception and design of the study. AnaptysBio also helped in part to analyze and interpret the data from the study, and approved it for submission. Dr. Ogg reported having served on an advisory board, as a consultant, or holds equity in Eli Lilly, Novartis, Janssen, Orbit Discovery, and UCB Pharma. Ms. Marquette and Dr. Londei reported being employees of AnaptysBio.
SOURCE: Chen Y-L et al. Sci Transl Med. 2019. doi: 10.1126/scitranslmed.aax2945.
Patients with moderate to severe atopic dermatitis who received the immunoglobulin G1 anti–interleukin-33 monoclonal antibody etokimab showed significant disease improvement 29 days after receiving a single systemic administration, according to results from a recent proof-of-concept, phase IIa study.
“Most of the focus for IL-33 pathway inhibition has been on the type 2 cytokine axis because of significant supporting genetic and functional data in both human and murine systems,” Yi-Ling Chen, a DPhil student at the University of Oxford (England), and colleagues wrote in Science Translational Medicine. “Our findings might also provide a further dimension to explain how etokimab, by inhibiting IL-33, could provide such a rapid and persistent clinical benefit as described in this report.”
In their study, 12 patients with moderate to severe AD received etokimab in a single intravenous dose of 300 mg. Prior to receiving etokimab, patients received a placebo dose and then underwent saline or house dust mite intraepidermal challenge, with researchers obtaining blister samples 1 day after challenge following placebo administration and again after patients received etokimab.
At 29 days, 83% of patients reached rapid and sustained clinical benefit under Eczema Area and Severity Index (EASI ) 50 and 33% in EASI 75, including peripheral eosinophil reduction. There also was significant reduction in skin neutrophil infiltration after patients received etokimab and then house dust mite challenge, compared with after they received placebo, .
“These findings open new therapeutic possible applications of etokimab to sterile neutrophilic disease as well as other inflammatory diseases with a clear neutrophilic involvement such as neutrophilic asthma,” the researchers said. “This first-in-class experimental medicine study has shown that in vivo in human tissue IL-33 has key upstream effects which broadly influence different and relevant inflammatory cascades and thus widen the potential of this treatment to a larger than anticipated group of diseases.
“Although excellent previous studies have demonstrated in vitro and in murine models that IL-33 is involved in neutrophil migration, the translation here to human tissue immunology shows that IL-33 plays a dominant role and effects are in part likely to be mediated instead by CXCR1,” concluded Ms. Chen and colleagues. “Therefore, specific IL-33 therapeutic intervention is not targeting a redundant system and is worthy of further investigation.”
This study was funded by AnaptysBio, which was responsible for the conception and design of the study. AnaptysBio also helped in part to analyze and interpret the data from the study, and approved it for submission. Dr. Ogg reported having served on an advisory board, as a consultant, or holds equity in Eli Lilly, Novartis, Janssen, Orbit Discovery, and UCB Pharma. Ms. Marquette and Dr. Londei reported being employees of AnaptysBio.
SOURCE: Chen Y-L et al. Sci Transl Med. 2019. doi: 10.1126/scitranslmed.aax2945.
Patients with moderate to severe atopic dermatitis who received the immunoglobulin G1 anti–interleukin-33 monoclonal antibody etokimab showed significant disease improvement 29 days after receiving a single systemic administration, according to results from a recent proof-of-concept, phase IIa study.
“Most of the focus for IL-33 pathway inhibition has been on the type 2 cytokine axis because of significant supporting genetic and functional data in both human and murine systems,” Yi-Ling Chen, a DPhil student at the University of Oxford (England), and colleagues wrote in Science Translational Medicine. “Our findings might also provide a further dimension to explain how etokimab, by inhibiting IL-33, could provide such a rapid and persistent clinical benefit as described in this report.”
In their study, 12 patients with moderate to severe AD received etokimab in a single intravenous dose of 300 mg. Prior to receiving etokimab, patients received a placebo dose and then underwent saline or house dust mite intraepidermal challenge, with researchers obtaining blister samples 1 day after challenge following placebo administration and again after patients received etokimab.
At 29 days, 83% of patients reached rapid and sustained clinical benefit under Eczema Area and Severity Index (EASI ) 50 and 33% in EASI 75, including peripheral eosinophil reduction. There also was significant reduction in skin neutrophil infiltration after patients received etokimab and then house dust mite challenge, compared with after they received placebo, .
“These findings open new therapeutic possible applications of etokimab to sterile neutrophilic disease as well as other inflammatory diseases with a clear neutrophilic involvement such as neutrophilic asthma,” the researchers said. “This first-in-class experimental medicine study has shown that in vivo in human tissue IL-33 has key upstream effects which broadly influence different and relevant inflammatory cascades and thus widen the potential of this treatment to a larger than anticipated group of diseases.
“Although excellent previous studies have demonstrated in vitro and in murine models that IL-33 is involved in neutrophil migration, the translation here to human tissue immunology shows that IL-33 plays a dominant role and effects are in part likely to be mediated instead by CXCR1,” concluded Ms. Chen and colleagues. “Therefore, specific IL-33 therapeutic intervention is not targeting a redundant system and is worthy of further investigation.”
This study was funded by AnaptysBio, which was responsible for the conception and design of the study. AnaptysBio also helped in part to analyze and interpret the data from the study, and approved it for submission. Dr. Ogg reported having served on an advisory board, as a consultant, or holds equity in Eli Lilly, Novartis, Janssen, Orbit Discovery, and UCB Pharma. Ms. Marquette and Dr. Londei reported being employees of AnaptysBio.
SOURCE: Chen Y-L et al. Sci Transl Med. 2019. doi: 10.1126/scitranslmed.aax2945.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point:
Major finding: At 29 days, 83% of patients reached rapid and sustained clinical benefit under Eczema Area and Severity Index (EASI) 50 and 33% in EASI 75, including peripheral eosinophil reduction. There also was significant reduction in skin neutrophil infiltration after patients received etokimab and then house dust mite challenge, compared with the response after they received placebo.
Study details: An analysis of 12 patients with moderate to severe atopic dermatitis who received a single 300 mg IV dose of etokimab, an IgG1 anti–IL-33 monoclonal antibody.
Disclosures: This study was funded by AnaptysBio, which was responsible for the conception and design of the study. AnaptysBio also helped in part to analyze and interpret the data from the study, and approved it for submission. Dr. Ogg reported having served on an advisory board, as a consultant, or holds equity in Eli Lilly, Novartis, Janssen, Orbit Discovery, and UCB Pharma. Ms. Marquette and Dr. Londei reported being employees of AnaptysBio.
Source: Chen Y-L et al. Sci Transl Med. 2019. doi: 10.1126/scitranslmed.aax2945.
No tacrolimus/cancer link in atopic dermatitis in 10-year study
MADRID – participating in the large, prospective, observational APPLES study, Regina Folster-Holst, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.

With nearly 45,000 person-years of follow-up in APPLES (A Prospective Pediatric Longitudinal Evaluation Study), there were no lymphomas and just a single case of skin cancer. That’s highly reassuring, since those were the two types of malignancies singled out as being of particular concern in the boxed warnings for the topical calcineurin inhibitors tacrolimus and pimecrolimus mandated by U.S. and European regulatory agencies in 2005, noted Dr. Folster-Holst, professor of dermatology at Christian Albrechts University of Kiel (Germany).
APPLES included 7,954 children with moderate or severe AD who were a median of 6 years old at enrollment in the study, conducted at 314 sites in the United States, Canada, and seven European countries. This was a naturalistic study in which patients used the topical calcineurin inhibitor as needed, with no restrictions.
A total of six cancers were diagnosed in six individuals during 44,629 person-years of prospective follow-up: one case each of chronic myeloid leukemia, alveolar rhabdomyosarcoma, malignant paraganglioma, carcinoid tumor of the appendix, spinal cord neoplasm, and Spitzoid melanoma. None of those malignancies are classically associated with immunosuppressive therapy.
The primary outcome in APPLES was the standardized incidence ratio of observed cancers to the expected number based upon extrapolation from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) database, as well as national cancer registries in the other countries where the study was carried out. The expected number of cancers was 5.95, yielding a standardized incidence ratio of 1.01.
Only 27% of patients completed the study. Investigators had anticipated a substantial attrition rate and recalculated their statistics based upon a range of hypothetically increased cancer rates among the dropouts. Even if the cancer rate was 2.5-fold higher in dropouts than in those who remained in the study – a far-fetched possibility – the standardized incidence ratio would not be significantly affected, according to Dr. Folster-Holst.
The new APPLES findings were preceded by a favorable report on long-term use of topical pimecrolimus from the Pediatric Eczema Elective Registry (PEER). The study included 7,457 pimecrolimus-using children with AD followed for 26,792 person-years. The standardized incidence ratio for all cancers was not significantly increased at 1.2. The investigators concluded “it seems unlikely” that topical pimecrolimus as generally used for treatment of AD is associated with an increased risk of malignancy (JAMA Dermatol. 2015 Jun;151[6]:594-9).
The boxed warnings for the topical calcineurin inhibitors have been the source of enormous frustration for dermatologists. The warnings were ordered because of regulatory concern about an increased risk of malignancy in organ transplant recipients on systemic calcineurin inhibitors for immunosuppression, even though the topical agents – unlike the systemic versions – are used intermittently, their systemic absorption is low to nil, and no plausible mechanism by which they could cause cancer has been put forth. Many physicians believe these drugs are probably safer than topical corticosteroids, so the first question put to Dr. Folster-Holst from the audience was, When will the boxed warnings be removed?
“That’s a good question,” she replied. “Patients and parents are afraid. But I think we have now a good argument to move forward with topically applied calcineurin inhibitors.”
Dr. Folster-Holst reported having no financial conflicts of interest regarding the APPLES study, funded by LEO Pharma.
MADRID – participating in the large, prospective, observational APPLES study, Regina Folster-Holst, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
With nearly 45,000 person-years of follow-up in APPLES (A Prospective Pediatric Longitudinal Evaluation Study), there were no lymphomas and just a single case of skin cancer. That’s highly reassuring, since those were the two types of malignancies singled out as being of particular concern in the boxed warnings for the topical calcineurin inhibitors tacrolimus and pimecrolimus mandated by U.S. and European regulatory agencies in 2005, noted Dr. Folster-Holst, professor of dermatology at Christian Albrechts University of Kiel (Germany).
APPLES included 7,954 children with moderate or severe AD who were a median of 6 years old at enrollment in the study, conducted at 314 sites in the United States, Canada, and seven European countries. This was a naturalistic study in which patients used the topical calcineurin inhibitor as needed, with no restrictions.
A total of six cancers were diagnosed in six individuals during 44,629 person-years of prospective follow-up: one case each of chronic myeloid leukemia, alveolar rhabdomyosarcoma, malignant paraganglioma, carcinoid tumor of the appendix, spinal cord neoplasm, and Spitzoid melanoma. None of those malignancies are classically associated with immunosuppressive therapy.
The primary outcome in APPLES was the standardized incidence ratio of observed cancers to the expected number based upon extrapolation from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) database, as well as national cancer registries in the other countries where the study was carried out. The expected number of cancers was 5.95, yielding a standardized incidence ratio of 1.01.
Only 27% of patients completed the study. Investigators had anticipated a substantial attrition rate and recalculated their statistics based upon a range of hypothetically increased cancer rates among the dropouts. Even if the cancer rate was 2.5-fold higher in dropouts than in those who remained in the study – a far-fetched possibility – the standardized incidence ratio would not be significantly affected, according to Dr. Folster-Holst.
The new APPLES findings were preceded by a favorable report on long-term use of topical pimecrolimus from the Pediatric Eczema Elective Registry (PEER). The study included 7,457 pimecrolimus-using children with AD followed for 26,792 person-years. The standardized incidence ratio for all cancers was not significantly increased at 1.2. The investigators concluded “it seems unlikely” that topical pimecrolimus as generally used for treatment of AD is associated with an increased risk of malignancy (JAMA Dermatol. 2015 Jun;151[6]:594-9).
The boxed warnings for the topical calcineurin inhibitors have been the source of enormous frustration for dermatologists. The warnings were ordered because of regulatory concern about an increased risk of malignancy in organ transplant recipients on systemic calcineurin inhibitors for immunosuppression, even though the topical agents – unlike the systemic versions – are used intermittently, their systemic absorption is low to nil, and no plausible mechanism by which they could cause cancer has been put forth. Many physicians believe these drugs are probably safer than topical corticosteroids, so the first question put to Dr. Folster-Holst from the audience was, When will the boxed warnings be removed?
“That’s a good question,” she replied. “Patients and parents are afraid. But I think we have now a good argument to move forward with topically applied calcineurin inhibitors.”
Dr. Folster-Holst reported having no financial conflicts of interest regarding the APPLES study, funded by LEO Pharma.
MADRID – participating in the large, prospective, observational APPLES study, Regina Folster-Holst, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
With nearly 45,000 person-years of follow-up in APPLES (A Prospective Pediatric Longitudinal Evaluation Study), there were no lymphomas and just a single case of skin cancer. That’s highly reassuring, since those were the two types of malignancies singled out as being of particular concern in the boxed warnings for the topical calcineurin inhibitors tacrolimus and pimecrolimus mandated by U.S. and European regulatory agencies in 2005, noted Dr. Folster-Holst, professor of dermatology at Christian Albrechts University of Kiel (Germany).
APPLES included 7,954 children with moderate or severe AD who were a median of 6 years old at enrollment in the study, conducted at 314 sites in the United States, Canada, and seven European countries. This was a naturalistic study in which patients used the topical calcineurin inhibitor as needed, with no restrictions.
A total of six cancers were diagnosed in six individuals during 44,629 person-years of prospective follow-up: one case each of chronic myeloid leukemia, alveolar rhabdomyosarcoma, malignant paraganglioma, carcinoid tumor of the appendix, spinal cord neoplasm, and Spitzoid melanoma. None of those malignancies are classically associated with immunosuppressive therapy.
The primary outcome in APPLES was the standardized incidence ratio of observed cancers to the expected number based upon extrapolation from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) database, as well as national cancer registries in the other countries where the study was carried out. The expected number of cancers was 5.95, yielding a standardized incidence ratio of 1.01.
Only 27% of patients completed the study. Investigators had anticipated a substantial attrition rate and recalculated their statistics based upon a range of hypothetically increased cancer rates among the dropouts. Even if the cancer rate was 2.5-fold higher in dropouts than in those who remained in the study – a far-fetched possibility – the standardized incidence ratio would not be significantly affected, according to Dr. Folster-Holst.
The new APPLES findings were preceded by a favorable report on long-term use of topical pimecrolimus from the Pediatric Eczema Elective Registry (PEER). The study included 7,457 pimecrolimus-using children with AD followed for 26,792 person-years. The standardized incidence ratio for all cancers was not significantly increased at 1.2. The investigators concluded “it seems unlikely” that topical pimecrolimus as generally used for treatment of AD is associated with an increased risk of malignancy (JAMA Dermatol. 2015 Jun;151[6]:594-9).
The boxed warnings for the topical calcineurin inhibitors have been the source of enormous frustration for dermatologists. The warnings were ordered because of regulatory concern about an increased risk of malignancy in organ transplant recipients on systemic calcineurin inhibitors for immunosuppression, even though the topical agents – unlike the systemic versions – are used intermittently, their systemic absorption is low to nil, and no plausible mechanism by which they could cause cancer has been put forth. Many physicians believe these drugs are probably safer than topical corticosteroids, so the first question put to Dr. Folster-Holst from the audience was, When will the boxed warnings be removed?
“That’s a good question,” she replied. “Patients and parents are afraid. But I think we have now a good argument to move forward with topically applied calcineurin inhibitors.”
Dr. Folster-Holst reported having no financial conflicts of interest regarding the APPLES study, funded by LEO Pharma.
REPORTING FROM THE EADV CONGRESS
Adjunctive therapy is among the roles for topical agents in psoriasis
SEATTLE – is not dead,” Linda Stein Gold, MD, said at the annual Coastal Dermatology Symposium.

“We have to remember when we think back to our practice, how many topical prescriptions do we write, compared to preventive prescriptions? Probably most are topical,” said Dr. Stein Gold, director of dermatology clinical research at the Henry Ford Hospital Center, Detroit.
Topical agents have a place when a patient is doing well on treatment with a biologic but is not responding completely, she noted. One open-label, single-arm study looked at adjunctive calcipotriene 0.005%/betamethasone dipropionate 0.064% (Enstilar) foam, applied once daily for 4 week, then twice a week on consecutive days for 12 weeks in 25 patients with psoriasis who had a mean body surface area (BSA) of less than 5% but significant remaining disease despite treatment with biologics.
At week 4, 76% achieved a BSA of 1% or less and Physician’s Global Assessment score of 1 or less at week 4, as did 68% at week 16. This was compared with 12% and 4%, respectively (J Drugs Dermatol. 2018 Aug 1;17[8]:845-50). “They found that a good potent topical on top of a biologic does really well. That can really kick up the last part of the efficacy to get the patients almost to clear,” she observed.
At the meeting, jointly presented by the University of Louisville and Global Academy for Medical Education, Dr. Stein Gold also discussed tazarotene, a topical retinoid approved by the Food and Drug Administration for treating psoriasis and is available as a 0.1% and 0.05% cream and gel. About 10%-30% of patients experience side effects with tazarotene, such as pruritus, stinging, and burning. Topical corticosteroids can help, which prompted development of a combined product, she noted.
She referred to a phase 2 study of patients with moderate to severe plaque psoriasis, which compared the fixed combination lotion formulation of tazarotene plus halobetasol propionate to the two components alone. The investigators found almost a 9% rate of treatment success with tazarotene alone, versus about 23% with halobetasol propionate alone and about 43% with the combined product. The combined individual effect of the two drugs was about 32%, so the 43% efficacy of the combined product had an absolute synergistic effect of about 11%, Dr. Stein Gold pointed out.
Two phase 3 trials of adults with moderate to severe psoriasis supported the phase 2 results of the combined lotion formulation (halobetasol 0.01% with tazarotene 0.045%), said Dr. Stein Gold, the first author (J Am Acad Dermatol. 2018 Aug;79[2]:287-93). Treatment success was defined as at least a 2-grade Investigator’s Global Assessment score and improvement from baseline and a score of “clear” or “almost clear.” In one of the studies, 36% of those on the combination versus 7% of those on the vehicle met this endpoint at week 8, as did 45% versus 13%, respectively, in the second study (P less than .001 for both studies).
Patients also had less itching, drying, and stinging than typically seen with tazarotene alone, Dr. Stein Gold said. In the studies, contact dermatitis was the most common side effect associated with treatment, reported in 6.3%
Dr. Stein Gold has received research support from Galderma, Leo, Novan, Valeant, Dermira, Novartis, Celgene, Allergan, and Foamix. She has been a consultant for Sol-gel, Galderma, Leo, Novan, Valeant, Dermira, Novartis, Celgene, Allergan, Foamix, Promis, Anacor, and Medimetriks. She has been on the speakers bureau of Galderma, Leo, Valeant, Novartis, Celgene, and Allergan. She has been a member of scientific advisory boards for Galderma, Leo, Novan, Valeant, Dermira, Novartis, Celgene, Allergan, Foamix, and Promius.
This publication and Global Academy for Medical Education are owned by the same parent company.
SEATTLE – is not dead,” Linda Stein Gold, MD, said at the annual Coastal Dermatology Symposium.
“We have to remember when we think back to our practice, how many topical prescriptions do we write, compared to preventive prescriptions? Probably most are topical,” said Dr. Stein Gold, director of dermatology clinical research at the Henry Ford Hospital Center, Detroit.
Topical agents have a place when a patient is doing well on treatment with a biologic but is not responding completely, she noted. One open-label, single-arm study looked at adjunctive calcipotriene 0.005%/betamethasone dipropionate 0.064% (Enstilar) foam, applied once daily for 4 week, then twice a week on consecutive days for 12 weeks in 25 patients with psoriasis who had a mean body surface area (BSA) of less than 5% but significant remaining disease despite treatment with biologics.
At week 4, 76% achieved a BSA of 1% or less and Physician’s Global Assessment score of 1 or less at week 4, as did 68% at week 16. This was compared with 12% and 4%, respectively (J Drugs Dermatol. 2018 Aug 1;17[8]:845-50). “They found that a good potent topical on top of a biologic does really well. That can really kick up the last part of the efficacy to get the patients almost to clear,” she observed.
At the meeting, jointly presented by the University of Louisville and Global Academy for Medical Education, Dr. Stein Gold also discussed tazarotene, a topical retinoid approved by the Food and Drug Administration for treating psoriasis and is available as a 0.1% and 0.05% cream and gel. About 10%-30% of patients experience side effects with tazarotene, such as pruritus, stinging, and burning. Topical corticosteroids can help, which prompted development of a combined product, she noted.
She referred to a phase 2 study of patients with moderate to severe plaque psoriasis, which compared the fixed combination lotion formulation of tazarotene plus halobetasol propionate to the two components alone. The investigators found almost a 9% rate of treatment success with tazarotene alone, versus about 23% with halobetasol propionate alone and about 43% with the combined product. The combined individual effect of the two drugs was about 32%, so the 43% efficacy of the combined product had an absolute synergistic effect of about 11%, Dr. Stein Gold pointed out.
Two phase 3 trials of adults with moderate to severe psoriasis supported the phase 2 results of the combined lotion formulation (halobetasol 0.01% with tazarotene 0.045%), said Dr. Stein Gold, the first author (J Am Acad Dermatol. 2018 Aug;79[2]:287-93). Treatment success was defined as at least a 2-grade Investigator’s Global Assessment score and improvement from baseline and a score of “clear” or “almost clear.” In one of the studies, 36% of those on the combination versus 7% of those on the vehicle met this endpoint at week 8, as did 45% versus 13%, respectively, in the second study (P less than .001 for both studies).
Patients also had less itching, drying, and stinging than typically seen with tazarotene alone, Dr. Stein Gold said. In the studies, contact dermatitis was the most common side effect associated with treatment, reported in 6.3%
Dr. Stein Gold has received research support from Galderma, Leo, Novan, Valeant, Dermira, Novartis, Celgene, Allergan, and Foamix. She has been a consultant for Sol-gel, Galderma, Leo, Novan, Valeant, Dermira, Novartis, Celgene, Allergan, Foamix, Promis, Anacor, and Medimetriks. She has been on the speakers bureau of Galderma, Leo, Valeant, Novartis, Celgene, and Allergan. She has been a member of scientific advisory boards for Galderma, Leo, Novan, Valeant, Dermira, Novartis, Celgene, Allergan, Foamix, and Promius.
This publication and Global Academy for Medical Education are owned by the same parent company.
SEATTLE – is not dead,” Linda Stein Gold, MD, said at the annual Coastal Dermatology Symposium.
“We have to remember when we think back to our practice, how many topical prescriptions do we write, compared to preventive prescriptions? Probably most are topical,” said Dr. Stein Gold, director of dermatology clinical research at the Henry Ford Hospital Center, Detroit.
Topical agents have a place when a patient is doing well on treatment with a biologic but is not responding completely, she noted. One open-label, single-arm study looked at adjunctive calcipotriene 0.005%/betamethasone dipropionate 0.064% (Enstilar) foam, applied once daily for 4 week, then twice a week on consecutive days for 12 weeks in 25 patients with psoriasis who had a mean body surface area (BSA) of less than 5% but significant remaining disease despite treatment with biologics.
At week 4, 76% achieved a BSA of 1% or less and Physician’s Global Assessment score of 1 or less at week 4, as did 68% at week 16. This was compared with 12% and 4%, respectively (J Drugs Dermatol. 2018 Aug 1;17[8]:845-50). “They found that a good potent topical on top of a biologic does really well. That can really kick up the last part of the efficacy to get the patients almost to clear,” she observed.
At the meeting, jointly presented by the University of Louisville and Global Academy for Medical Education, Dr. Stein Gold also discussed tazarotene, a topical retinoid approved by the Food and Drug Administration for treating psoriasis and is available as a 0.1% and 0.05% cream and gel. About 10%-30% of patients experience side effects with tazarotene, such as pruritus, stinging, and burning. Topical corticosteroids can help, which prompted development of a combined product, she noted.
She referred to a phase 2 study of patients with moderate to severe plaque psoriasis, which compared the fixed combination lotion formulation of tazarotene plus halobetasol propionate to the two components alone. The investigators found almost a 9% rate of treatment success with tazarotene alone, versus about 23% with halobetasol propionate alone and about 43% with the combined product. The combined individual effect of the two drugs was about 32%, so the 43% efficacy of the combined product had an absolute synergistic effect of about 11%, Dr. Stein Gold pointed out.
Two phase 3 trials of adults with moderate to severe psoriasis supported the phase 2 results of the combined lotion formulation (halobetasol 0.01% with tazarotene 0.045%), said Dr. Stein Gold, the first author (J Am Acad Dermatol. 2018 Aug;79[2]:287-93). Treatment success was defined as at least a 2-grade Investigator’s Global Assessment score and improvement from baseline and a score of “clear” or “almost clear.” In one of the studies, 36% of those on the combination versus 7% of those on the vehicle met this endpoint at week 8, as did 45% versus 13%, respectively, in the second study (P less than .001 for both studies).
Patients also had less itching, drying, and stinging than typically seen with tazarotene alone, Dr. Stein Gold said. In the studies, contact dermatitis was the most common side effect associated with treatment, reported in 6.3%
Dr. Stein Gold has received research support from Galderma, Leo, Novan, Valeant, Dermira, Novartis, Celgene, Allergan, and Foamix. She has been a consultant for Sol-gel, Galderma, Leo, Novan, Valeant, Dermira, Novartis, Celgene, Allergan, Foamix, Promis, Anacor, and Medimetriks. She has been on the speakers bureau of Galderma, Leo, Valeant, Novartis, Celgene, and Allergan. She has been a member of scientific advisory boards for Galderma, Leo, Novan, Valeant, Dermira, Novartis, Celgene, Allergan, Foamix, and Promius.
This publication and Global Academy for Medical Education are owned by the same parent company.
EXPERT ANALYSIS FROM COASTAL DERM
Once-daily oral JAK inhibitor for atopic dermatitis effective in phase 3 study
MADRID – (AD) on the strength of its knockout performance in the pivotal phase 3 JADE MONO-1 trial, presented at the annual congress of the European Academy of Dermatology and Venereology.

“The IGA [Investigator Global Assessment] and EASI [Eczema Area and Severity Index]-75 responses for both doses of abrocitinib were significantly greater than placebo as early as week 2 and continued to increase until week 12 with no plateau. This study stopped at week 12. I would have liked to see what happened at 16 weeks or further. I don’t know where this is going to end up maxing out,” commented principal investigator Eric Simpson, MD, professor of dermatology at Oregon Health & Science University, Portland.
JADE MONO-1 (JAK1 Atopic Dermatitis Efficacy and Safety Monotherapy–1) was a 12-week, double-blind, multicenter study which included 387 adolescents and adults with moderate or severe AD randomized 2:2:1 to abrocitinib at 200 mg or 100 mg once daily, or to placebo. Overall, this was a fairly severely affected population, with a mean baseline EASI (Eczema Area and Severity Index) score of about 30, a peak pruritus numeric rating scale score of 7 out of 10, and a mean Dermatology Quality Life Index score greater than 14. Nonetheless, this was a rigorous abrocitinib monotherapy trial, as participants were not allowed to take even a single dose of topical corticosteroids.
The coprimary endpoints in JADE MONO-1 were achievement of an IGA score of 0 or 1 – that is, clear or almost clear – at week 12 plus at least a 2-point improvement, compared with baseline on the 0-4 scale, and an EASI-75 response as defined by a 75% or greater improvement from baseline.
A clear-cut dose response was evident: the IGA response rate was 43.8% in the group on abrocitinib at 200 mg/day, 23.7% with 100 mg, and 7.9% with placebo. The EASI-75 response rates were 62.7%, 39.7%, and 11.8%, respectively, with a statistically significant separation from placebo by week 2.
Key secondary endpoints included the rigorous EASI-90 response rate: 38.6% with the higher dose of abrocitinib, 18.6% at 100 mg per day, and 5.3% with placebo. And again, that’s without resort to topical steroids, Dr. Simpson noted.
Another important secondary endpoint was the proportion of patients who achieved at least a 4-point improvement in itch on the pruritus self-rating scale by week 12: 57.2%, 37.7%, and 15.3%. The rapidity of the improvement was notable: By week 2, this endpoint was achieved in 45.6% of patients on abrocitinib on the 200-mg dose, 20.4% on the 100-mg dose, and 2.7% of placebo-treated controls.
“By day 2, 1 day after taking the first pill, you can see really nice reductions in itch at both doses, compared with placebo,” the dermatologist said.
Study dropout rates were low despite the inability to utilize topical steroids: 11% in the higher-dose abrocitinib group and 13.5% with abrocitinib at 100 mg/day, both of which were lower than in controls.
Turning to safety results, Dr. Simpson noted that the 9.1% rate of discontinuations because of adverse events in the placebo group was significantly higher than the 5.8% rates in each of the active treatment arms. The serious adverse event rate was 3.2% in each of the abrocitinib groups and 1.9% with placebo. Among the serious adverse events in abrocitinib-treated patients Dr. Simpson considered worthy of special mention were a single case of inflammatory bowel disease, which resolved after halting treatment; one case of peritonsillitis; and a case of pancreatitis in an alcoholic patient. No deaths, major adverse cardiovascular events, or malignancies occurred in this brief 12-week trial. Nor were there any cases of deep vein thrombosis or pulmonary embolism, which has been an issue with some other JAK inhibitors.
“We need long-term safety data, of course,” he said.
Laboratory findings were generally unremarkable, with no clinically significant changes. Platelet counts dropped to a nadir at about 4 weeks while staying within normal range, then came back up. Mean LDL cholesterol levels rose by about 10%, an unwelcome event that was counterbalanced by a favorable 20% rise in HDL cholesterol.
Asked about the efficacy rates in the 20%-plus adolescent study participants, compared with the adults, Dr. Simpson replied that a detailed analysis is planned, adding: “I can say that things are looking pretty similar.”
Abrocitinib is selective for inhibition of JAK1, with resultant modulation of interleukins-4, -13, and -31, as well as interferon-gamma, all of which are cytokines involved in the pathophysiology of AD.
Of note, Pfizer, the drug’s developer, has announced positive results from the sister pivotal phase 3 trial, JADE MONO-2, with full details forthcoming in early 2020. Results of a phase 2b study of abrocitinib were also recently published (JAMA Dermatol. 2019 Oct 2. doi: 10.1001/jamadermatol.2019.2855).
Dr. Simpson reported receiving research grants from and serving as a consultant to Pfizer, the study sponsor. He has similar financial relationships with close to a dozen other pharmaceutical companies.
MADRID – (AD) on the strength of its knockout performance in the pivotal phase 3 JADE MONO-1 trial, presented at the annual congress of the European Academy of Dermatology and Venereology.
“The IGA [Investigator Global Assessment] and EASI [Eczema Area and Severity Index]-75 responses for both doses of abrocitinib were significantly greater than placebo as early as week 2 and continued to increase until week 12 with no plateau. This study stopped at week 12. I would have liked to see what happened at 16 weeks or further. I don’t know where this is going to end up maxing out,” commented principal investigator Eric Simpson, MD, professor of dermatology at Oregon Health & Science University, Portland.
JADE MONO-1 (JAK1 Atopic Dermatitis Efficacy and Safety Monotherapy–1) was a 12-week, double-blind, multicenter study which included 387 adolescents and adults with moderate or severe AD randomized 2:2:1 to abrocitinib at 200 mg or 100 mg once daily, or to placebo. Overall, this was a fairly severely affected population, with a mean baseline EASI (Eczema Area and Severity Index) score of about 30, a peak pruritus numeric rating scale score of 7 out of 10, and a mean Dermatology Quality Life Index score greater than 14. Nonetheless, this was a rigorous abrocitinib monotherapy trial, as participants were not allowed to take even a single dose of topical corticosteroids.
The coprimary endpoints in JADE MONO-1 were achievement of an IGA score of 0 or 1 – that is, clear or almost clear – at week 12 plus at least a 2-point improvement, compared with baseline on the 0-4 scale, and an EASI-75 response as defined by a 75% or greater improvement from baseline.
A clear-cut dose response was evident: the IGA response rate was 43.8% in the group on abrocitinib at 200 mg/day, 23.7% with 100 mg, and 7.9% with placebo. The EASI-75 response rates were 62.7%, 39.7%, and 11.8%, respectively, with a statistically significant separation from placebo by week 2.
Key secondary endpoints included the rigorous EASI-90 response rate: 38.6% with the higher dose of abrocitinib, 18.6% at 100 mg per day, and 5.3% with placebo. And again, that’s without resort to topical steroids, Dr. Simpson noted.
Another important secondary endpoint was the proportion of patients who achieved at least a 4-point improvement in itch on the pruritus self-rating scale by week 12: 57.2%, 37.7%, and 15.3%. The rapidity of the improvement was notable: By week 2, this endpoint was achieved in 45.6% of patients on abrocitinib on the 200-mg dose, 20.4% on the 100-mg dose, and 2.7% of placebo-treated controls.
“By day 2, 1 day after taking the first pill, you can see really nice reductions in itch at both doses, compared with placebo,” the dermatologist said.
Study dropout rates were low despite the inability to utilize topical steroids: 11% in the higher-dose abrocitinib group and 13.5% with abrocitinib at 100 mg/day, both of which were lower than in controls.
Turning to safety results, Dr. Simpson noted that the 9.1% rate of discontinuations because of adverse events in the placebo group was significantly higher than the 5.8% rates in each of the active treatment arms. The serious adverse event rate was 3.2% in each of the abrocitinib groups and 1.9% with placebo. Among the serious adverse events in abrocitinib-treated patients Dr. Simpson considered worthy of special mention were a single case of inflammatory bowel disease, which resolved after halting treatment; one case of peritonsillitis; and a case of pancreatitis in an alcoholic patient. No deaths, major adverse cardiovascular events, or malignancies occurred in this brief 12-week trial. Nor were there any cases of deep vein thrombosis or pulmonary embolism, which has been an issue with some other JAK inhibitors.
“We need long-term safety data, of course,” he said.
Laboratory findings were generally unremarkable, with no clinically significant changes. Platelet counts dropped to a nadir at about 4 weeks while staying within normal range, then came back up. Mean LDL cholesterol levels rose by about 10%, an unwelcome event that was counterbalanced by a favorable 20% rise in HDL cholesterol.
Asked about the efficacy rates in the 20%-plus adolescent study participants, compared with the adults, Dr. Simpson replied that a detailed analysis is planned, adding: “I can say that things are looking pretty similar.”
Abrocitinib is selective for inhibition of JAK1, with resultant modulation of interleukins-4, -13, and -31, as well as interferon-gamma, all of which are cytokines involved in the pathophysiology of AD.
Of note, Pfizer, the drug’s developer, has announced positive results from the sister pivotal phase 3 trial, JADE MONO-2, with full details forthcoming in early 2020. Results of a phase 2b study of abrocitinib were also recently published (JAMA Dermatol. 2019 Oct 2. doi: 10.1001/jamadermatol.2019.2855).
Dr. Simpson reported receiving research grants from and serving as a consultant to Pfizer, the study sponsor. He has similar financial relationships with close to a dozen other pharmaceutical companies.
MADRID – (AD) on the strength of its knockout performance in the pivotal phase 3 JADE MONO-1 trial, presented at the annual congress of the European Academy of Dermatology and Venereology.
“The IGA [Investigator Global Assessment] and EASI [Eczema Area and Severity Index]-75 responses for both doses of abrocitinib were significantly greater than placebo as early as week 2 and continued to increase until week 12 with no plateau. This study stopped at week 12. I would have liked to see what happened at 16 weeks or further. I don’t know where this is going to end up maxing out,” commented principal investigator Eric Simpson, MD, professor of dermatology at Oregon Health & Science University, Portland.
JADE MONO-1 (JAK1 Atopic Dermatitis Efficacy and Safety Monotherapy–1) was a 12-week, double-blind, multicenter study which included 387 adolescents and adults with moderate or severe AD randomized 2:2:1 to abrocitinib at 200 mg or 100 mg once daily, or to placebo. Overall, this was a fairly severely affected population, with a mean baseline EASI (Eczema Area and Severity Index) score of about 30, a peak pruritus numeric rating scale score of 7 out of 10, and a mean Dermatology Quality Life Index score greater than 14. Nonetheless, this was a rigorous abrocitinib monotherapy trial, as participants were not allowed to take even a single dose of topical corticosteroids.
The coprimary endpoints in JADE MONO-1 were achievement of an IGA score of 0 or 1 – that is, clear or almost clear – at week 12 plus at least a 2-point improvement, compared with baseline on the 0-4 scale, and an EASI-75 response as defined by a 75% or greater improvement from baseline.
A clear-cut dose response was evident: the IGA response rate was 43.8% in the group on abrocitinib at 200 mg/day, 23.7% with 100 mg, and 7.9% with placebo. The EASI-75 response rates were 62.7%, 39.7%, and 11.8%, respectively, with a statistically significant separation from placebo by week 2.
Key secondary endpoints included the rigorous EASI-90 response rate: 38.6% with the higher dose of abrocitinib, 18.6% at 100 mg per day, and 5.3% with placebo. And again, that’s without resort to topical steroids, Dr. Simpson noted.
Another important secondary endpoint was the proportion of patients who achieved at least a 4-point improvement in itch on the pruritus self-rating scale by week 12: 57.2%, 37.7%, and 15.3%. The rapidity of the improvement was notable: By week 2, this endpoint was achieved in 45.6% of patients on abrocitinib on the 200-mg dose, 20.4% on the 100-mg dose, and 2.7% of placebo-treated controls.
“By day 2, 1 day after taking the first pill, you can see really nice reductions in itch at both doses, compared with placebo,” the dermatologist said.
Study dropout rates were low despite the inability to utilize topical steroids: 11% in the higher-dose abrocitinib group and 13.5% with abrocitinib at 100 mg/day, both of which were lower than in controls.
Turning to safety results, Dr. Simpson noted that the 9.1% rate of discontinuations because of adverse events in the placebo group was significantly higher than the 5.8% rates in each of the active treatment arms. The serious adverse event rate was 3.2% in each of the abrocitinib groups and 1.9% with placebo. Among the serious adverse events in abrocitinib-treated patients Dr. Simpson considered worthy of special mention were a single case of inflammatory bowel disease, which resolved after halting treatment; one case of peritonsillitis; and a case of pancreatitis in an alcoholic patient. No deaths, major adverse cardiovascular events, or malignancies occurred in this brief 12-week trial. Nor were there any cases of deep vein thrombosis or pulmonary embolism, which has been an issue with some other JAK inhibitors.
“We need long-term safety data, of course,” he said.
Laboratory findings were generally unremarkable, with no clinically significant changes. Platelet counts dropped to a nadir at about 4 weeks while staying within normal range, then came back up. Mean LDL cholesterol levels rose by about 10%, an unwelcome event that was counterbalanced by a favorable 20% rise in HDL cholesterol.
Asked about the efficacy rates in the 20%-plus adolescent study participants, compared with the adults, Dr. Simpson replied that a detailed analysis is planned, adding: “I can say that things are looking pretty similar.”
Abrocitinib is selective for inhibition of JAK1, with resultant modulation of interleukins-4, -13, and -31, as well as interferon-gamma, all of which are cytokines involved in the pathophysiology of AD.
Of note, Pfizer, the drug’s developer, has announced positive results from the sister pivotal phase 3 trial, JADE MONO-2, with full details forthcoming in early 2020. Results of a phase 2b study of abrocitinib were also recently published (JAMA Dermatol. 2019 Oct 2. doi: 10.1001/jamadermatol.2019.2855).
Dr. Simpson reported receiving research grants from and serving as a consultant to Pfizer, the study sponsor. He has similar financial relationships with close to a dozen other pharmaceutical companies.
REPORTING FROM THE EADV CONGRESS