User login
Severe Site Reaction After Injecting Hyaluronic Acid—Based Soft Tissue Filler
Ten Years in Academic Dermatology [editorial]
Ischemia Predicts Poor Functional Outcomes in Diabetic Foot Ulcers
PALM BEACH, Fla. - Neuropathic diabetic foot ulcers can be treated with revascularization, but successful surgery doesn't always translate into good long-term outcomes, a study has shown.
In the review of 917 such ulcers, the 219 revascularized lesions had no better healing or survival outcomes than that of ischemic wounds that were not revascularized, Dr. Spence Taylor said at the annual meeting of the Southern Surgical Association. Just 35% of the revascularized ulcers healed completely, and 32% of the patients eventually needed an amputation.

"Assessing this treatment, we must conclude that while revascularization is important to wound healing, favorable functional outcomes can't be assumed," said Dr. Taylor of the Greenville (S.C.) Hospital System. "This suggests that we should realign our financial incentives [away from procedures and] toward foot care and wound prevention, affording a better opportunity of prevention and preservation of functional outcomes."
Dr. Taylor and his colleagues presented a review of 917 limbs with new diabetic foot ulcers that occurred among 706 patients. Most of the patients (87%) had type 2 diabetes, and more than half (52%) were smokers. Other comorbidities included hyperlipidemia (53%), hypertension (90%), and end-stage renal disease (26%).
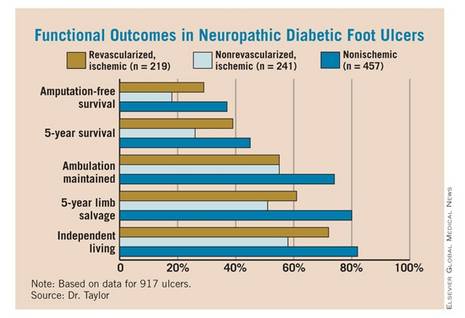
Of the 917 ulcers, 457 were nonischemic and 460 were ischemic. Of the ischemic lesions, 241 were not revascularized and 219 were – 137 by angioplasty and 82 by open surgery. Outcomes measured included primary healing, functional healing (defined as healing to clinical insignificance), limb salvage, amputation-free survival, 5-year survival, and maintenance of ambulation and independent living.
Overall, the data showed primary wound healing in 27%, functional healing in 53%, minor amputations in 28%, and major amputations in 20% of patients. The time to achieve healing was 7-8 months.
For patients with the revascularized ulcers, the 5-year survival rate was 39%, and 5-year limb salvage rate was 61%. The 5-year rate of amputation-free survival was 29%, while 55% of patients maintained ambulation and 72% maintained independent living at 5 years.
When the investigators compared the different groups (nonischemic, revascularized ischemic, and nonrevascularized ischemic), they found no significant differences in the rate of wound healing. But ischemia was a significant predictor of poor functional outcomes, which revascularization did not completely mitigate. "Ischemic patients had twice as many amputations and 50% higher mortality than nonischemic patients, whether they were revascularized or not. It was quite remarkable morbidity," Dr. Taylor said.
The presence of ischemia conferred a 26% increase in the risk of death by 5 years. Also, patients with end-stage renal disease were 2.5 times more likely to die than were those without. However, functional healing was associated with a 42% decreased risk of death.
Those same factors were independent predictors of amputation-free survival. Ischemia conferred a 57% increased risk of losing a limb, while end-stage renal disease doubled that risk. Functional healing, however, decreased the risk of amputation by 58%.
"Patients who were able to heal their wound significantly outperformed those who did not – not only for limb salvage and survival, which is intuitive, but also for amputation-free survival and maintenance of ambulation and independent living status, which is not intuitive," Dr. Taylor said. "The poorest outcomes were in ischemic nonrevascularized patients, whose 5-year mortality was 75% and amputation-free survival only 18% – as bad as any cancer outcomes presented at this meeting."
Conventional wisdom holds that patients who do have revascularization will almost always heal their ulcers. Therefore, Dr. Taylor said, reimbursement has been structured to favor surgical intervention rather than diabetic foot care and prevention.
"Reimbursement is very robust for procedures, while for wound care, it barely covers the cost, implying that revascularization does all the heavy lifting."
His review shows that this is not always the case. "Our functional outcomes were disappointing at best and really reflect an opportunity for improvement. Realigning the financial incentives toward foot wound care and prevention may give us a better opportunity to make these improvements."
Dr. Taylor had no financial disclosures.
PALM BEACH, Fla. - Neuropathic diabetic foot ulcers can be treated with revascularization, but successful surgery doesn't always translate into good long-term outcomes, a study has shown.
In the review of 917 such ulcers, the 219 revascularized lesions had no better healing or survival outcomes than that of ischemic wounds that were not revascularized, Dr. Spence Taylor said at the annual meeting of the Southern Surgical Association. Just 35% of the revascularized ulcers healed completely, and 32% of the patients eventually needed an amputation.
"Assessing this treatment, we must conclude that while revascularization is important to wound healing, favorable functional outcomes can't be assumed," said Dr. Taylor of the Greenville (S.C.) Hospital System. "This suggests that we should realign our financial incentives [away from procedures and] toward foot care and wound prevention, affording a better opportunity of prevention and preservation of functional outcomes."
Dr. Taylor and his colleagues presented a review of 917 limbs with new diabetic foot ulcers that occurred among 706 patients. Most of the patients (87%) had type 2 diabetes, and more than half (52%) were smokers. Other comorbidities included hyperlipidemia (53%), hypertension (90%), and end-stage renal disease (26%).
Of the 917 ulcers, 457 were nonischemic and 460 were ischemic. Of the ischemic lesions, 241 were not revascularized and 219 were – 137 by angioplasty and 82 by open surgery. Outcomes measured included primary healing, functional healing (defined as healing to clinical insignificance), limb salvage, amputation-free survival, 5-year survival, and maintenance of ambulation and independent living.
Overall, the data showed primary wound healing in 27%, functional healing in 53%, minor amputations in 28%, and major amputations in 20% of patients. The time to achieve healing was 7-8 months.
For patients with the revascularized ulcers, the 5-year survival rate was 39%, and 5-year limb salvage rate was 61%. The 5-year rate of amputation-free survival was 29%, while 55% of patients maintained ambulation and 72% maintained independent living at 5 years.
When the investigators compared the different groups (nonischemic, revascularized ischemic, and nonrevascularized ischemic), they found no significant differences in the rate of wound healing. But ischemia was a significant predictor of poor functional outcomes, which revascularization did not completely mitigate. "Ischemic patients had twice as many amputations and 50% higher mortality than nonischemic patients, whether they were revascularized or not. It was quite remarkable morbidity," Dr. Taylor said.
The presence of ischemia conferred a 26% increase in the risk of death by 5 years. Also, patients with end-stage renal disease were 2.5 times more likely to die than were those without. However, functional healing was associated with a 42% decreased risk of death.
Those same factors were independent predictors of amputation-free survival. Ischemia conferred a 57% increased risk of losing a limb, while end-stage renal disease doubled that risk. Functional healing, however, decreased the risk of amputation by 58%.
"Patients who were able to heal their wound significantly outperformed those who did not – not only for limb salvage and survival, which is intuitive, but also for amputation-free survival and maintenance of ambulation and independent living status, which is not intuitive," Dr. Taylor said. "The poorest outcomes were in ischemic nonrevascularized patients, whose 5-year mortality was 75% and amputation-free survival only 18% – as bad as any cancer outcomes presented at this meeting."
Conventional wisdom holds that patients who do have revascularization will almost always heal their ulcers. Therefore, Dr. Taylor said, reimbursement has been structured to favor surgical intervention rather than diabetic foot care and prevention.
"Reimbursement is very robust for procedures, while for wound care, it barely covers the cost, implying that revascularization does all the heavy lifting."
His review shows that this is not always the case. "Our functional outcomes were disappointing at best and really reflect an opportunity for improvement. Realigning the financial incentives toward foot wound care and prevention may give us a better opportunity to make these improvements."
Dr. Taylor had no financial disclosures.
PALM BEACH, Fla. - Neuropathic diabetic foot ulcers can be treated with revascularization, but successful surgery doesn't always translate into good long-term outcomes, a study has shown.
In the review of 917 such ulcers, the 219 revascularized lesions had no better healing or survival outcomes than that of ischemic wounds that were not revascularized, Dr. Spence Taylor said at the annual meeting of the Southern Surgical Association. Just 35% of the revascularized ulcers healed completely, and 32% of the patients eventually needed an amputation.
"Assessing this treatment, we must conclude that while revascularization is important to wound healing, favorable functional outcomes can't be assumed," said Dr. Taylor of the Greenville (S.C.) Hospital System. "This suggests that we should realign our financial incentives [away from procedures and] toward foot care and wound prevention, affording a better opportunity of prevention and preservation of functional outcomes."
Dr. Taylor and his colleagues presented a review of 917 limbs with new diabetic foot ulcers that occurred among 706 patients. Most of the patients (87%) had type 2 diabetes, and more than half (52%) were smokers. Other comorbidities included hyperlipidemia (53%), hypertension (90%), and end-stage renal disease (26%).
Of the 917 ulcers, 457 were nonischemic and 460 were ischemic. Of the ischemic lesions, 241 were not revascularized and 219 were – 137 by angioplasty and 82 by open surgery. Outcomes measured included primary healing, functional healing (defined as healing to clinical insignificance), limb salvage, amputation-free survival, 5-year survival, and maintenance of ambulation and independent living.
Overall, the data showed primary wound healing in 27%, functional healing in 53%, minor amputations in 28%, and major amputations in 20% of patients. The time to achieve healing was 7-8 months.
For patients with the revascularized ulcers, the 5-year survival rate was 39%, and 5-year limb salvage rate was 61%. The 5-year rate of amputation-free survival was 29%, while 55% of patients maintained ambulation and 72% maintained independent living at 5 years.
When the investigators compared the different groups (nonischemic, revascularized ischemic, and nonrevascularized ischemic), they found no significant differences in the rate of wound healing. But ischemia was a significant predictor of poor functional outcomes, which revascularization did not completely mitigate. "Ischemic patients had twice as many amputations and 50% higher mortality than nonischemic patients, whether they were revascularized or not. It was quite remarkable morbidity," Dr. Taylor said.
The presence of ischemia conferred a 26% increase in the risk of death by 5 years. Also, patients with end-stage renal disease were 2.5 times more likely to die than were those without. However, functional healing was associated with a 42% decreased risk of death.
Those same factors were independent predictors of amputation-free survival. Ischemia conferred a 57% increased risk of losing a limb, while end-stage renal disease doubled that risk. Functional healing, however, decreased the risk of amputation by 58%.
"Patients who were able to heal their wound significantly outperformed those who did not – not only for limb salvage and survival, which is intuitive, but also for amputation-free survival and maintenance of ambulation and independent living status, which is not intuitive," Dr. Taylor said. "The poorest outcomes were in ischemic nonrevascularized patients, whose 5-year mortality was 75% and amputation-free survival only 18% – as bad as any cancer outcomes presented at this meeting."
Conventional wisdom holds that patients who do have revascularization will almost always heal their ulcers. Therefore, Dr. Taylor said, reimbursement has been structured to favor surgical intervention rather than diabetic foot care and prevention.
"Reimbursement is very robust for procedures, while for wound care, it barely covers the cost, implying that revascularization does all the heavy lifting."
His review shows that this is not always the case. "Our functional outcomes were disappointing at best and really reflect an opportunity for improvement. Realigning the financial incentives toward foot wound care and prevention may give us a better opportunity to make these improvements."
Dr. Taylor had no financial disclosures.
FROM THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: Only 35% of revascularized ulcers healed completely, and 32% of the patients eventually needed an amputation because of the ulcer.
Data Source: A review of 917 diabetic foot ulcers in 706 patients.
Disclosures: Dr. Spence Taylor had no financial disclosures.
Shave Biopsies Accurately Identify Most Melanomas
PALM BEACH, FLA. - Shave biopsy of possible melanomas usually provides enough diagnostic information to plan a successful surgical treatment, judging by a retrospective study of 600 patients.
The procedure has been controversial, because many surgeons believe it fails to give a full clinical picture of the lesion – especially thickness, said Dr. Stephen Grobmyer of the University of Florida, Gainesville. However, in his review of 600 patients who had shave biopsies at two surgical centers in 2006-2009, just 22% of patients had residual melanoma after the procedure, with tumor upstaging required in 2% and a wider margin excision in 1%.
"We feel the definitive treatment planning for melanoma can be reliably made on results of shave biopsy. We advocate the liberal use of shave biopsy for suspicious cutaneous lesions; this should be emphasized over other techniques of biopsy, as this would advance the early diagnosis of melanoma and improve outcomes," Dr. Grobmyer said at the annual meeting of the Southern Surgical Association.
Dermatologists and family physicians can easily perform the shave biopsy, which Dr. Grobmyer said is "easy, quick, cheap, safe, and doesn't require suture closure or postoperative follow-up."
All patients in the study had undergone shave biopsies of lesions less than 2 mm in depth. This was considered the cut-off point because patients with deeper lesions usually go on to have a wide excision and sentinel node biopsy, Dr. Grobmyer said.
The patients' median age was 62 years, and 40% were female. "It's interesting to note that dermatologists performed about 90% of the shave biopsies on patients who were referred, and that on clinical exam, more than two-thirds did not have a diagnosis of melanoma. Most had a diagnosis of nonmelanoma skin cancer or a benign skin lesion."
Based on the results of the shave biopsy, however, 88% of the lesions were confirmed as melanoma. Of these, 11% were invasive, with a median Breslow depth of 0.73 mm. Ulceration was present in 6% of patients, and 37% had a positive deep margin on the shave biopsy.
All who had the shave biopsy went to initial surgical management based on the depth of the shave. "After the sentinel node biopsy, only 3% of patients needed additional surgery," Dr. Grobmyer pointed out.
The researchers especially wanted to analyze the subset of patients who had a diagnosis of melanoma made on clinical observation before the biopsy was done – a total of 179 patients (30%). "On shave, we found that 22% had a positive deep margin, which is statistically significantly less than those patients who did not have a preshave diagnosis of melanoma, suggesting that the shaves were done in a way as to more completely excise the lesion."
Evaluation of these patients after initial surgical management revealed that there were very few instances of tumor upstaging (3%), need for wider excision (3%), or a change in the need for sentinel node biopsy (1%).
Dr. Grobmyer acknowledged that the study's 12-month follow-up period was fairly short. "We saw a 2.3% overall recurrence rate with 1.7% local regional and 0.7% distant recurrences. It’s also important to note that the patients with recurrence had much deeper lesions than those who did not, with an average depth of 1.7 mm."
"It may be time to stop bashing shave biopsies," Dr. Kelly McMasters said during the discussion period. "The conventional dogma among melanoma experts against shave biopsy has been that they're bad because they underestimate true tumor thickness," said Dr. McMasters of the University of Louisville (Ky.) "This suggests that shave biopsies fall below the standard of care, but nearly every melanoma patient I've seen has had a shave biopsy for diagnosis. Are all these physicians practicing below the standard of care? It seems [that] because shave biopsies are what’s being performed most commonly, they are the standard of care."
The most important point of the study, however, is that the easily accessible shave biopsy, in the hands of primary care physicians, can get melanoma patients into surgical treatment faster – and time is life in this case, said Dr. Hiram C. Polk Jr.
"The only improvement in survival in melanoma has been due to earlier diagnosis, and you don't want to do anything to discourage the dermatologists or the family physicians from doing a biopsy," said Dr. Polk, the Ben A. Reid Sr. Professor of Surgery at the University of Louisville. "The worst thing they can do is say 'come back in 3 months,' or cauterize them. This paper encourages people with lesser surgical skills to get any piece of the lesion, as long as they won't be doing the diagnosis. The shave biopsy is a good thing, and we need to share this and encourage those in dermatology and family medicine to do more of them."
Dr. Grobmyer had no financial conflicts.
PALM BEACH, FLA. - Shave biopsy of possible melanomas usually provides enough diagnostic information to plan a successful surgical treatment, judging by a retrospective study of 600 patients.
The procedure has been controversial, because many surgeons believe it fails to give a full clinical picture of the lesion – especially thickness, said Dr. Stephen Grobmyer of the University of Florida, Gainesville. However, in his review of 600 patients who had shave biopsies at two surgical centers in 2006-2009, just 22% of patients had residual melanoma after the procedure, with tumor upstaging required in 2% and a wider margin excision in 1%.
"We feel the definitive treatment planning for melanoma can be reliably made on results of shave biopsy. We advocate the liberal use of shave biopsy for suspicious cutaneous lesions; this should be emphasized over other techniques of biopsy, as this would advance the early diagnosis of melanoma and improve outcomes," Dr. Grobmyer said at the annual meeting of the Southern Surgical Association.
Dermatologists and family physicians can easily perform the shave biopsy, which Dr. Grobmyer said is "easy, quick, cheap, safe, and doesn't require suture closure or postoperative follow-up."
All patients in the study had undergone shave biopsies of lesions less than 2 mm in depth. This was considered the cut-off point because patients with deeper lesions usually go on to have a wide excision and sentinel node biopsy, Dr. Grobmyer said.
The patients' median age was 62 years, and 40% were female. "It's interesting to note that dermatologists performed about 90% of the shave biopsies on patients who were referred, and that on clinical exam, more than two-thirds did not have a diagnosis of melanoma. Most had a diagnosis of nonmelanoma skin cancer or a benign skin lesion."
Based on the results of the shave biopsy, however, 88% of the lesions were confirmed as melanoma. Of these, 11% were invasive, with a median Breslow depth of 0.73 mm. Ulceration was present in 6% of patients, and 37% had a positive deep margin on the shave biopsy.
All who had the shave biopsy went to initial surgical management based on the depth of the shave. "After the sentinel node biopsy, only 3% of patients needed additional surgery," Dr. Grobmyer pointed out.
The researchers especially wanted to analyze the subset of patients who had a diagnosis of melanoma made on clinical observation before the biopsy was done – a total of 179 patients (30%). "On shave, we found that 22% had a positive deep margin, which is statistically significantly less than those patients who did not have a preshave diagnosis of melanoma, suggesting that the shaves were done in a way as to more completely excise the lesion."
Evaluation of these patients after initial surgical management revealed that there were very few instances of tumor upstaging (3%), need for wider excision (3%), or a change in the need for sentinel node biopsy (1%).
Dr. Grobmyer acknowledged that the study's 12-month follow-up period was fairly short. "We saw a 2.3% overall recurrence rate with 1.7% local regional and 0.7% distant recurrences. It’s also important to note that the patients with recurrence had much deeper lesions than those who did not, with an average depth of 1.7 mm."
"It may be time to stop bashing shave biopsies," Dr. Kelly McMasters said during the discussion period. "The conventional dogma among melanoma experts against shave biopsy has been that they're bad because they underestimate true tumor thickness," said Dr. McMasters of the University of Louisville (Ky.) "This suggests that shave biopsies fall below the standard of care, but nearly every melanoma patient I've seen has had a shave biopsy for diagnosis. Are all these physicians practicing below the standard of care? It seems [that] because shave biopsies are what’s being performed most commonly, they are the standard of care."
The most important point of the study, however, is that the easily accessible shave biopsy, in the hands of primary care physicians, can get melanoma patients into surgical treatment faster – and time is life in this case, said Dr. Hiram C. Polk Jr.
"The only improvement in survival in melanoma has been due to earlier diagnosis, and you don't want to do anything to discourage the dermatologists or the family physicians from doing a biopsy," said Dr. Polk, the Ben A. Reid Sr. Professor of Surgery at the University of Louisville. "The worst thing they can do is say 'come back in 3 months,' or cauterize them. This paper encourages people with lesser surgical skills to get any piece of the lesion, as long as they won't be doing the diagnosis. The shave biopsy is a good thing, and we need to share this and encourage those in dermatology and family medicine to do more of them."
Dr. Grobmyer had no financial conflicts.
PALM BEACH, FLA. - Shave biopsy of possible melanomas usually provides enough diagnostic information to plan a successful surgical treatment, judging by a retrospective study of 600 patients.
The procedure has been controversial, because many surgeons believe it fails to give a full clinical picture of the lesion – especially thickness, said Dr. Stephen Grobmyer of the University of Florida, Gainesville. However, in his review of 600 patients who had shave biopsies at two surgical centers in 2006-2009, just 22% of patients had residual melanoma after the procedure, with tumor upstaging required in 2% and a wider margin excision in 1%.
"We feel the definitive treatment planning for melanoma can be reliably made on results of shave biopsy. We advocate the liberal use of shave biopsy for suspicious cutaneous lesions; this should be emphasized over other techniques of biopsy, as this would advance the early diagnosis of melanoma and improve outcomes," Dr. Grobmyer said at the annual meeting of the Southern Surgical Association.
Dermatologists and family physicians can easily perform the shave biopsy, which Dr. Grobmyer said is "easy, quick, cheap, safe, and doesn't require suture closure or postoperative follow-up."
All patients in the study had undergone shave biopsies of lesions less than 2 mm in depth. This was considered the cut-off point because patients with deeper lesions usually go on to have a wide excision and sentinel node biopsy, Dr. Grobmyer said.
The patients' median age was 62 years, and 40% were female. "It's interesting to note that dermatologists performed about 90% of the shave biopsies on patients who were referred, and that on clinical exam, more than two-thirds did not have a diagnosis of melanoma. Most had a diagnosis of nonmelanoma skin cancer or a benign skin lesion."
Based on the results of the shave biopsy, however, 88% of the lesions were confirmed as melanoma. Of these, 11% were invasive, with a median Breslow depth of 0.73 mm. Ulceration was present in 6% of patients, and 37% had a positive deep margin on the shave biopsy.
All who had the shave biopsy went to initial surgical management based on the depth of the shave. "After the sentinel node biopsy, only 3% of patients needed additional surgery," Dr. Grobmyer pointed out.
The researchers especially wanted to analyze the subset of patients who had a diagnosis of melanoma made on clinical observation before the biopsy was done – a total of 179 patients (30%). "On shave, we found that 22% had a positive deep margin, which is statistically significantly less than those patients who did not have a preshave diagnosis of melanoma, suggesting that the shaves were done in a way as to more completely excise the lesion."
Evaluation of these patients after initial surgical management revealed that there were very few instances of tumor upstaging (3%), need for wider excision (3%), or a change in the need for sentinel node biopsy (1%).
Dr. Grobmyer acknowledged that the study's 12-month follow-up period was fairly short. "We saw a 2.3% overall recurrence rate with 1.7% local regional and 0.7% distant recurrences. It’s also important to note that the patients with recurrence had much deeper lesions than those who did not, with an average depth of 1.7 mm."
"It may be time to stop bashing shave biopsies," Dr. Kelly McMasters said during the discussion period. "The conventional dogma among melanoma experts against shave biopsy has been that they're bad because they underestimate true tumor thickness," said Dr. McMasters of the University of Louisville (Ky.) "This suggests that shave biopsies fall below the standard of care, but nearly every melanoma patient I've seen has had a shave biopsy for diagnosis. Are all these physicians practicing below the standard of care? It seems [that] because shave biopsies are what’s being performed most commonly, they are the standard of care."
The most important point of the study, however, is that the easily accessible shave biopsy, in the hands of primary care physicians, can get melanoma patients into surgical treatment faster – and time is life in this case, said Dr. Hiram C. Polk Jr.
"The only improvement in survival in melanoma has been due to earlier diagnosis, and you don't want to do anything to discourage the dermatologists or the family physicians from doing a biopsy," said Dr. Polk, the Ben A. Reid Sr. Professor of Surgery at the University of Louisville. "The worst thing they can do is say 'come back in 3 months,' or cauterize them. This paper encourages people with lesser surgical skills to get any piece of the lesion, as long as they won't be doing the diagnosis. The shave biopsy is a good thing, and we need to share this and encourage those in dermatology and family medicine to do more of them."
Dr. Grobmyer had no financial conflicts.
FROM THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: Eighty-eight percent of shaved biopsy lesions were confirmed as melanoma. Of these, 11% were invasive.
Data Source: A retrospective study of 600 patients with prediagnostic shave biopsies.
Disclosures: Dr.
Grobmyer had no financial conflicts.
Nd:YAG Laser Targets Sweat Gland Disorders
CHICAGO – An Nd:YAG laser used for facial fat plasty and laser liposuction treatment has shown promise for targeting axillary bromhidrosis and hyperhidrosis, according to the first prospective, long-term follow-up study for these indications.
After an iodine starch test at baseline, researchers treated both axillae of 18 patients with the disorders with a 1,444-nm pulsed Nd:YAG laser (AccuSculpt, Lutronic). Each operative field was anesthetized. Participants were then assessed at day 1, 7, 30, 60, and 180 for clinical effects.
"Outcome was good in this study" Dr. Sang Min Yi said. Patients rated 61% of axillary bromhidrosis and 86% of hyperhidrosis results as excellent or good.
Patients judged the severity of their condition at baseline and regular intervals using a 10-point scale (10 being the most severe). For example, average bromhidrosis severity was 1.2 on day 7 and 1.7 on day 60. Patients also rated their average pain severity as 1.2 on day 7 and 0.3 on day 60. Severity of limitation on movement was an average 2.6 on day 7 after treatment and 0.4 on day 60.
Participants also rated the severity of remaining sweating as 1.4 on day 7 and 1.7 on day 60. Overall satisfaction was an average 9 out of 10 on both days 7 and 60. Results at day 180 are pending.
The 1,444-nm pulsed Nd:YAG laser targets apocrine sweat glands in the deep dermis and subcutaneous fat layer. Pulse energy was 175 mJ, pulse rate was 40 Hz, power was 7 watts, and the energy density ranged from 20 J/cm2 to 30 J/cm2.
Other treatments for axillary bromhidrosis and hyperhidrosis include local topical medications, botulinum toxin injections, ultrasonic therapy, and liposuction curettage. However, this laser is one of the best modalities to treat these disorders, said Dr. Yi, of the department of dermatology, Korea University, Ansan Hospital, South Korea.
Most adverse events were temporary and mild. Bullae, mild ecchymoses, and bruises on the operative sites all resolved within 30 days, Dr. Yi said. "The most severe and unwanted complication was skin necrosis." This occurred in two patients. Necrosis is preventable if the tip of the probe is held properly and delivery of excess energy to any unit area is avoided, he noted.
Dr. Yi received research funding from Lutronic, which also funded the study.
CHICAGO – An Nd:YAG laser used for facial fat plasty and laser liposuction treatment has shown promise for targeting axillary bromhidrosis and hyperhidrosis, according to the first prospective, long-term follow-up study for these indications.
After an iodine starch test at baseline, researchers treated both axillae of 18 patients with the disorders with a 1,444-nm pulsed Nd:YAG laser (AccuSculpt, Lutronic). Each operative field was anesthetized. Participants were then assessed at day 1, 7, 30, 60, and 180 for clinical effects.
"Outcome was good in this study" Dr. Sang Min Yi said. Patients rated 61% of axillary bromhidrosis and 86% of hyperhidrosis results as excellent or good.
Patients judged the severity of their condition at baseline and regular intervals using a 10-point scale (10 being the most severe). For example, average bromhidrosis severity was 1.2 on day 7 and 1.7 on day 60. Patients also rated their average pain severity as 1.2 on day 7 and 0.3 on day 60. Severity of limitation on movement was an average 2.6 on day 7 after treatment and 0.4 on day 60.
Participants also rated the severity of remaining sweating as 1.4 on day 7 and 1.7 on day 60. Overall satisfaction was an average 9 out of 10 on both days 7 and 60. Results at day 180 are pending.
The 1,444-nm pulsed Nd:YAG laser targets apocrine sweat glands in the deep dermis and subcutaneous fat layer. Pulse energy was 175 mJ, pulse rate was 40 Hz, power was 7 watts, and the energy density ranged from 20 J/cm2 to 30 J/cm2.
Other treatments for axillary bromhidrosis and hyperhidrosis include local topical medications, botulinum toxin injections, ultrasonic therapy, and liposuction curettage. However, this laser is one of the best modalities to treat these disorders, said Dr. Yi, of the department of dermatology, Korea University, Ansan Hospital, South Korea.
Most adverse events were temporary and mild. Bullae, mild ecchymoses, and bruises on the operative sites all resolved within 30 days, Dr. Yi said. "The most severe and unwanted complication was skin necrosis." This occurred in two patients. Necrosis is preventable if the tip of the probe is held properly and delivery of excess energy to any unit area is avoided, he noted.
Dr. Yi received research funding from Lutronic, which also funded the study.
CHICAGO – An Nd:YAG laser used for facial fat plasty and laser liposuction treatment has shown promise for targeting axillary bromhidrosis and hyperhidrosis, according to the first prospective, long-term follow-up study for these indications.
After an iodine starch test at baseline, researchers treated both axillae of 18 patients with the disorders with a 1,444-nm pulsed Nd:YAG laser (AccuSculpt, Lutronic). Each operative field was anesthetized. Participants were then assessed at day 1, 7, 30, 60, and 180 for clinical effects.
"Outcome was good in this study" Dr. Sang Min Yi said. Patients rated 61% of axillary bromhidrosis and 86% of hyperhidrosis results as excellent or good.
Patients judged the severity of their condition at baseline and regular intervals using a 10-point scale (10 being the most severe). For example, average bromhidrosis severity was 1.2 on day 7 and 1.7 on day 60. Patients also rated their average pain severity as 1.2 on day 7 and 0.3 on day 60. Severity of limitation on movement was an average 2.6 on day 7 after treatment and 0.4 on day 60.
Participants also rated the severity of remaining sweating as 1.4 on day 7 and 1.7 on day 60. Overall satisfaction was an average 9 out of 10 on both days 7 and 60. Results at day 180 are pending.
The 1,444-nm pulsed Nd:YAG laser targets apocrine sweat glands in the deep dermis and subcutaneous fat layer. Pulse energy was 175 mJ, pulse rate was 40 Hz, power was 7 watts, and the energy density ranged from 20 J/cm2 to 30 J/cm2.
Other treatments for axillary bromhidrosis and hyperhidrosis include local topical medications, botulinum toxin injections, ultrasonic therapy, and liposuction curettage. However, this laser is one of the best modalities to treat these disorders, said Dr. Yi, of the department of dermatology, Korea University, Ansan Hospital, South Korea.
Most adverse events were temporary and mild. Bullae, mild ecchymoses, and bruises on the operative sites all resolved within 30 days, Dr. Yi said. "The most severe and unwanted complication was skin necrosis." This occurred in two patients. Necrosis is preventable if the tip of the probe is held properly and delivery of excess energy to any unit area is avoided, he noted.
Dr. Yi received research funding from Lutronic, which also funded the study.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR DERMATOLOGIC SURGERY
Major Finding: Patients rated 61% of axillary bromhidrosis and 86% of hyperhidrosis results as excellent or good.
Data Source: 18 patients with axillary bromhidrosis or hyperhidrosis.
Disclosures: Dr. Yi received research funding from Lutronic, which also funded the study.
Expert Reveals Secrets to Mohs Coding
SAN DIEGO – To receive appropriate payment for Mohs surgery, using the correct codes is key.
While there are not many CPT codes for Mohs, it is crucial to use the right ones, and the right add-on codes, to get full payment for work and to avoid the headache of resubmission and third-payer arguments, Denise Harriman Koger said at a meeting sponsored by the American Society for Mohs Surgery.
One aspect of Mohs makes it unique among all other dermatologic surgeries, said Ms. Kroger, a billing specialist from San Diego. "You must act as both surgeon and pathologist for this, and if you don't, you are not doing Mohs, and you can’t use Mohs codes to bill. If either of these responsibilities is delegated to another physician who reports his services separately, these codes are not appropriate."
The money trail begins with clear documentation of why Mohs is the best treatment, she said. "You need to document this – whether it's an aggressive tumor, one with poorly defined margins – whatever it is. If you are subject to a post-review audit after submitting the claim, they will want to see your reasoning about why you chose Mohs rather than a simple excision."
CPT code 17311 is probably the "most-utilized code for stage I Mohs," she said. It covers procedures on the head, neck, hands, feet, genitals, or any other location that directly involves any of those areas – including muscle, cartilage, bone, tendon, major nerves, or blood vessels. "These are the areas where Mohs is most indicated, especially the face, because lesions on the face are where you want to preserve as much tissue as possible." This code covers up to five tissue blocks from stage I.
For every additional stage performed, use the 17312 code and bill it in units. "For example, if you do three more stages, you would bill 17312 times three," Ms. Koger said. Code 17312 is only used in conjunction with 17311. "That primary code is rarely billed in units unless you are doing two separate lesions. And a lot of insurance companies won't pay for two first stages on the same day." But if two separate lesions are addressed on the same day, continue to bill each one as a unit of the 17312 code.
Again, each additional stage is covered for up to five tissue blocks. Since 17312 is an add-on code, it is not subject to the multiple surgical reduction rules. "If your billing staff sees the payer reducing the fee on this code, they should appeal," Ms. Koger advised.
Code 17313 covers the first stage of Mohs surgery on the trunk, arms, or legs. Again, up to five tissue blocks are covered. The add-on code for additional stages is 17314, which should be billed in units and is not subject to the multiple surgical reduction rule.
"Sometimes you might get a lot of referred patients, who may or may not arrive with a biopsy slide and report," she said. "If you don’t have it, there are some rules as to whether you can bill for a biopsy and frozen section done on the same day as Mohs."
If a biopsy has been done in the previous 60 days and the surgeon has access to it, then no billing can be submitted for a same-day biopsy. "But if you've tried to get it and were not able to, document that and do another biopsy that day."
In order to get paid for that biopsy, however, the billing code modifier 59 is necessary. "This is very important because it's how you get paid for those same-day biopsies and frozen sections. If you bill 17311 without the 59 modifier [after a same-day biopsy] it will be denied because the payer will consider it bundled in."
If more than five tissue blocks are required for any stage, the billing code is 17315. This billing code should be listed separately in addition to the primary procedural code.
Three other important modifier codes are 58, 78 and 79, Ms. Koger said. Modifier 58 covers related procedures done by the same physician during the 90-day postoperative period, including major surgery. It also covers Mohs on a different site, or an incision or excision on the day of Mohs surgery.
If a patient needs to return for a related procedure to the operating room in an outpatient surgery center or hospital during the post-op period, code 78 is the one to use. "Modifier 79 is used if you are doing Mohs during the global period of a previous surgery; it tells the payer that the Mohs is unrelated to the prior work. You need to use that to tell them it’s unrelated to the work you did. For example, if you perform Mohs on the scalp and repair the defect and then 3 weeks later you excise a cyst somewhere else."
The patient who needs to go home overnight and have Mohs completed the next day can be a billing problem, she added. "It might not make sense, but if you have this situation, on the second day you have to start all over again with the stage I code, even though it’s not really a stage I procedure," she said. "Then you follow with the code for additional stages. It seems wrong but that is the only way you can get paid." Staggering patients to force them to come back the next day, to take advantage of this rule, is sometimes done by "unscrupulous" surgeons trying to increase their payment, she said.
Finally she offered a few caveats about billing propriety.
"Excising really small lesions or every basal or squamous cell lesion with Mohs is not a good idea; it looks really suspicious. And don't divide really small specimens into a lot of blocks to be able to bill that. That is definitely not a good idea," she said
Ms. Koger disclosed having no financial disclosures.
SAN DIEGO – To receive appropriate payment for Mohs surgery, using the correct codes is key.
While there are not many CPT codes for Mohs, it is crucial to use the right ones, and the right add-on codes, to get full payment for work and to avoid the headache of resubmission and third-payer arguments, Denise Harriman Koger said at a meeting sponsored by the American Society for Mohs Surgery.
One aspect of Mohs makes it unique among all other dermatologic surgeries, said Ms. Kroger, a billing specialist from San Diego. "You must act as both surgeon and pathologist for this, and if you don't, you are not doing Mohs, and you can’t use Mohs codes to bill. If either of these responsibilities is delegated to another physician who reports his services separately, these codes are not appropriate."
The money trail begins with clear documentation of why Mohs is the best treatment, she said. "You need to document this – whether it's an aggressive tumor, one with poorly defined margins – whatever it is. If you are subject to a post-review audit after submitting the claim, they will want to see your reasoning about why you chose Mohs rather than a simple excision."
CPT code 17311 is probably the "most-utilized code for stage I Mohs," she said. It covers procedures on the head, neck, hands, feet, genitals, or any other location that directly involves any of those areas – including muscle, cartilage, bone, tendon, major nerves, or blood vessels. "These are the areas where Mohs is most indicated, especially the face, because lesions on the face are where you want to preserve as much tissue as possible." This code covers up to five tissue blocks from stage I.
For every additional stage performed, use the 17312 code and bill it in units. "For example, if you do three more stages, you would bill 17312 times three," Ms. Koger said. Code 17312 is only used in conjunction with 17311. "That primary code is rarely billed in units unless you are doing two separate lesions. And a lot of insurance companies won't pay for two first stages on the same day." But if two separate lesions are addressed on the same day, continue to bill each one as a unit of the 17312 code.
Again, each additional stage is covered for up to five tissue blocks. Since 17312 is an add-on code, it is not subject to the multiple surgical reduction rules. "If your billing staff sees the payer reducing the fee on this code, they should appeal," Ms. Koger advised.
Code 17313 covers the first stage of Mohs surgery on the trunk, arms, or legs. Again, up to five tissue blocks are covered. The add-on code for additional stages is 17314, which should be billed in units and is not subject to the multiple surgical reduction rule.
"Sometimes you might get a lot of referred patients, who may or may not arrive with a biopsy slide and report," she said. "If you don’t have it, there are some rules as to whether you can bill for a biopsy and frozen section done on the same day as Mohs."
If a biopsy has been done in the previous 60 days and the surgeon has access to it, then no billing can be submitted for a same-day biopsy. "But if you've tried to get it and were not able to, document that and do another biopsy that day."
In order to get paid for that biopsy, however, the billing code modifier 59 is necessary. "This is very important because it's how you get paid for those same-day biopsies and frozen sections. If you bill 17311 without the 59 modifier [after a same-day biopsy] it will be denied because the payer will consider it bundled in."
If more than five tissue blocks are required for any stage, the billing code is 17315. This billing code should be listed separately in addition to the primary procedural code.
Three other important modifier codes are 58, 78 and 79, Ms. Koger said. Modifier 58 covers related procedures done by the same physician during the 90-day postoperative period, including major surgery. It also covers Mohs on a different site, or an incision or excision on the day of Mohs surgery.
If a patient needs to return for a related procedure to the operating room in an outpatient surgery center or hospital during the post-op period, code 78 is the one to use. "Modifier 79 is used if you are doing Mohs during the global period of a previous surgery; it tells the payer that the Mohs is unrelated to the prior work. You need to use that to tell them it’s unrelated to the work you did. For example, if you perform Mohs on the scalp and repair the defect and then 3 weeks later you excise a cyst somewhere else."
The patient who needs to go home overnight and have Mohs completed the next day can be a billing problem, she added. "It might not make sense, but if you have this situation, on the second day you have to start all over again with the stage I code, even though it’s not really a stage I procedure," she said. "Then you follow with the code for additional stages. It seems wrong but that is the only way you can get paid." Staggering patients to force them to come back the next day, to take advantage of this rule, is sometimes done by "unscrupulous" surgeons trying to increase their payment, she said.
Finally she offered a few caveats about billing propriety.
"Excising really small lesions or every basal or squamous cell lesion with Mohs is not a good idea; it looks really suspicious. And don't divide really small specimens into a lot of blocks to be able to bill that. That is definitely not a good idea," she said
Ms. Koger disclosed having no financial disclosures.
SAN DIEGO – To receive appropriate payment for Mohs surgery, using the correct codes is key.
While there are not many CPT codes for Mohs, it is crucial to use the right ones, and the right add-on codes, to get full payment for work and to avoid the headache of resubmission and third-payer arguments, Denise Harriman Koger said at a meeting sponsored by the American Society for Mohs Surgery.
One aspect of Mohs makes it unique among all other dermatologic surgeries, said Ms. Kroger, a billing specialist from San Diego. "You must act as both surgeon and pathologist for this, and if you don't, you are not doing Mohs, and you can’t use Mohs codes to bill. If either of these responsibilities is delegated to another physician who reports his services separately, these codes are not appropriate."
The money trail begins with clear documentation of why Mohs is the best treatment, she said. "You need to document this – whether it's an aggressive tumor, one with poorly defined margins – whatever it is. If you are subject to a post-review audit after submitting the claim, they will want to see your reasoning about why you chose Mohs rather than a simple excision."
CPT code 17311 is probably the "most-utilized code for stage I Mohs," she said. It covers procedures on the head, neck, hands, feet, genitals, or any other location that directly involves any of those areas – including muscle, cartilage, bone, tendon, major nerves, or blood vessels. "These are the areas where Mohs is most indicated, especially the face, because lesions on the face are where you want to preserve as much tissue as possible." This code covers up to five tissue blocks from stage I.
For every additional stage performed, use the 17312 code and bill it in units. "For example, if you do three more stages, you would bill 17312 times three," Ms. Koger said. Code 17312 is only used in conjunction with 17311. "That primary code is rarely billed in units unless you are doing two separate lesions. And a lot of insurance companies won't pay for two first stages on the same day." But if two separate lesions are addressed on the same day, continue to bill each one as a unit of the 17312 code.
Again, each additional stage is covered for up to five tissue blocks. Since 17312 is an add-on code, it is not subject to the multiple surgical reduction rules. "If your billing staff sees the payer reducing the fee on this code, they should appeal," Ms. Koger advised.
Code 17313 covers the first stage of Mohs surgery on the trunk, arms, or legs. Again, up to five tissue blocks are covered. The add-on code for additional stages is 17314, which should be billed in units and is not subject to the multiple surgical reduction rule.
"Sometimes you might get a lot of referred patients, who may or may not arrive with a biopsy slide and report," she said. "If you don’t have it, there are some rules as to whether you can bill for a biopsy and frozen section done on the same day as Mohs."
If a biopsy has been done in the previous 60 days and the surgeon has access to it, then no billing can be submitted for a same-day biopsy. "But if you've tried to get it and were not able to, document that and do another biopsy that day."
In order to get paid for that biopsy, however, the billing code modifier 59 is necessary. "This is very important because it's how you get paid for those same-day biopsies and frozen sections. If you bill 17311 without the 59 modifier [after a same-day biopsy] it will be denied because the payer will consider it bundled in."
If more than five tissue blocks are required for any stage, the billing code is 17315. This billing code should be listed separately in addition to the primary procedural code.
Three other important modifier codes are 58, 78 and 79, Ms. Koger said. Modifier 58 covers related procedures done by the same physician during the 90-day postoperative period, including major surgery. It also covers Mohs on a different site, or an incision or excision on the day of Mohs surgery.
If a patient needs to return for a related procedure to the operating room in an outpatient surgery center or hospital during the post-op period, code 78 is the one to use. "Modifier 79 is used if you are doing Mohs during the global period of a previous surgery; it tells the payer that the Mohs is unrelated to the prior work. You need to use that to tell them it’s unrelated to the work you did. For example, if you perform Mohs on the scalp and repair the defect and then 3 weeks later you excise a cyst somewhere else."
The patient who needs to go home overnight and have Mohs completed the next day can be a billing problem, she added. "It might not make sense, but if you have this situation, on the second day you have to start all over again with the stage I code, even though it’s not really a stage I procedure," she said. "Then you follow with the code for additional stages. It seems wrong but that is the only way you can get paid." Staggering patients to force them to come back the next day, to take advantage of this rule, is sometimes done by "unscrupulous" surgeons trying to increase their payment, she said.
Finally she offered a few caveats about billing propriety.
"Excising really small lesions or every basal or squamous cell lesion with Mohs is not a good idea; it looks really suspicious. And don't divide really small specimens into a lot of blocks to be able to bill that. That is definitely not a good idea," she said
Ms. Koger disclosed having no financial disclosures.
EXPERT ANALYSIS FROM A MEETING SPONSORED BY THE AMERICAN SOCIETY FOR MOHS SURGERY
Botulinum Toxin Complications on the Rise
Botulinum toxins, including Botox and Dysport, are being associated with increasing reports of paralysis away from injection sites, difficulties in swallowing, incontinence, and breathing problems, according to the Institute for Safe Medication Practices.
The institute reviews and analyzes reports to the Food and Drug Administration's MedWatch Safety Information and Adverse Event Reporting Program.

The group cited 6 deaths, 18 cases of disability, and 100 other serious injuries in the first quarter of 2010. Previous quarters have averaged 30-50 adverse events and one patient death associated with the toxin. Seventy-nine of the cases (64%) in the latest quarter were associated with Botox, 26 (21%) with Botox Cosmetic, 17 (14%) with Dysport, and 2 cases with undetermined brands.
The watchdog group charged that the Botox label downplays the potential for the drug to spread during dermatologic use.
Botulinum toxins, including Botox and Dysport, are being associated with increasing reports of paralysis away from injection sites, difficulties in swallowing, incontinence, and breathing problems, according to the Institute for Safe Medication Practices.
The institute reviews and analyzes reports to the Food and Drug Administration's MedWatch Safety Information and Adverse Event Reporting Program.
The group cited 6 deaths, 18 cases of disability, and 100 other serious injuries in the first quarter of 2010. Previous quarters have averaged 30-50 adverse events and one patient death associated with the toxin. Seventy-nine of the cases (64%) in the latest quarter were associated with Botox, 26 (21%) with Botox Cosmetic, 17 (14%) with Dysport, and 2 cases with undetermined brands.
The watchdog group charged that the Botox label downplays the potential for the drug to spread during dermatologic use.
Botulinum toxins, including Botox and Dysport, are being associated with increasing reports of paralysis away from injection sites, difficulties in swallowing, incontinence, and breathing problems, according to the Institute for Safe Medication Practices.
The institute reviews and analyzes reports to the Food and Drug Administration's MedWatch Safety Information and Adverse Event Reporting Program.
The group cited 6 deaths, 18 cases of disability, and 100 other serious injuries in the first quarter of 2010. Previous quarters have averaged 30-50 adverse events and one patient death associated with the toxin. Seventy-nine of the cases (64%) in the latest quarter were associated with Botox, 26 (21%) with Botox Cosmetic, 17 (14%) with Dysport, and 2 cases with undetermined brands.
The watchdog group charged that the Botox label downplays the potential for the drug to spread during dermatologic use.
FROM THE INSTITUTE FOR SAFE MEDICATION PRACTICES
New Data Support Safety of Dermatologic Office-Based Surgery
CHICAGO – Office-based surgery is safe when performed by dermatologists, according to a study of 10 years of complication and death reports from Florida and 6 years of data from Alabama.
Dermatologic surgeons could use the findings to combat any legislative attempts to curtail office procedures, including liposuction, Dr. Brett Coldiron said.
Some plastic surgeons, for example, are trying to restrict what types of office surgeries dermatologists can legally perform, said Dr. Coldiron, a private practice dermatologic surgeon and member of the dermatology faculty at the University of Cincinnati.
The study indicates procedures performed by plastic surgeons actually carry a greater risk for adverse events and death, compared with dermatologic surgeries, Dr. Coldiron said.
A plastic surgeon contacted for comment, Dr. Michael McGuire, said the comparison is unfair given the differing complexity of surgeries done by the two specialties. "It’s a total misrepresentation of the statistics. There is no question that the incidence and even the deaths are smaller with dermatology than with any other specialty."
"Comparing an abdominoplasty – a tummy tuck – with a skin cancer excision or even a small volume of liposuction is ridiculous. To compare that with doing tummy tucks, and 4- or 5-hour facelifts, or major breast reconstructive surgery, all of which are done in outpatient surgery centers, is apples and oranges. They are totally different procedures," said Dr. McGuire, who is in private practice in Santa Monica, Calif., and director of The American Board of Plastic Surgeons.
The prospectively collected data show "that any claims by plastic surgeons or anesthesiologists that dermatologists are doing unsafe things and injuring patients in the office is unfounded," Dr. Coldiron said. "And ... if they are going to make such claims, they should have some data to back them up."
Both Alabama and Florida require notification when an outpatient experiences serious injury, transfer to a hospital, or death related to surgery. These mandatory reports are part of public record in the state of Florida, for example.
Dr. Coldiron found 46 deaths and 263 complications that required hospital transfers in Florida. Cosmetic (nonmedically necessary) procedures were associated with 57% of these deaths and almost 50% of such transfers in the state. Liposuction or liposuction with another cosmetic procedure (abdominoplasty, for example) resulted in death for 10 patients and hospital transfer in another 34 cases.
The majority of cosmetic procedure deaths (67%) and hospital transfers (74%) in Florida were performed under general anesthesia, said Dr. Coldiron.
This is relevant because some physicians who perform liposuction under general anesthesia are trying to restrict liposuction under local or tumescent anesthesia, he said. "There have been legislative attempts to prohibit this. The state of New York recently passed a law restricting liposuction in offices, under local anesthesia to 500 cc, which paradoxically will increase the number of injuries and deaths."
"When you try to restrict the use of local anesthesia or tumescent anesthesia ... you will force more people into using general anesthesia, which has more complications. Hospital transfers or deaths with the use of local anesthesia are incredibly rare," Dr. Coldiron said in an interview. "In fact, I’m only aware of a couple that occurred after anaphylactic reactions."
"They [dermatologists] like to blame the general anesthesia," Dr. McGuire said. "It’s not the general anesthesia that is the difference; it’s the magnitude of the surgery. Clearly there are going to be more risks and complications with major surgery compared to minor surgery under any kind of anesthesia." Plastic surgeons in Florida reported the most adverse events (45% of the total), compared with 1.3% reported by dermatologists.
A meeting attendee questioned a direct comparison between specialties, citing the higher complexity of cases typically performed by plastic surgeons. "Yes, the plastic surgeons do more big, multiple procedures and have more problems," Dr. Coldiron replied. "That does not give them the right to try and restrict our practices under the guise of patient safety at the level of the state medical boards and legislatures that is preposterous."
The current study is in press, and represents an update of Dr. Coldiron’s previously reported 7-year Florida data (Dermatol. Surg. 2008;34:285-91).
Additional information is available on the website for Dr. Coldiron's practice, including real adverse event incident reports.
Alabama reports support and validate the Florida data, Dr. Coldiron said. There were three deaths and 52 adverse events that required an office-to-hospital transfer in Alabama. Cosmetic procedures were associated with zero deaths and 42% of hospital transfers during the 6 years. The Alabama medical board provided Dr. Coldiron with the data upon request.
A majority of cosmetic procedure adverse events (86%) were from cases performed under general anesthesia.
Plastic surgery was the specialty most often involved in adverse event reports (42% of all complications), compared with 1.9% for dermatologists in that state (one report associated with tumescent anesthesia).
"Certainly we are not a major contributor in any sense. Dermatologic surgery is extremely safe," Dr. Coldiron said at the meeting, which was jointly sponsored by the American Society of Cosmetic Dermatology and Aesthetic Surgery.
Dr. McGuire said that office-based surgery is safe when performed at centers accredited by the American Association for Accreditation of Ambulatory Surgery Facilities (AAAASF). Studies cited on the organization's website reported 23 deaths of 1,141,418 outpatient procedures in the United States over 5.5 years.
Dr. McGuire is past president of the AAASF. Dr. Coldiron said he had no disclosures.
CHICAGO – Office-based surgery is safe when performed by dermatologists, according to a study of 10 years of complication and death reports from Florida and 6 years of data from Alabama.
Dermatologic surgeons could use the findings to combat any legislative attempts to curtail office procedures, including liposuction, Dr. Brett Coldiron said.
Some plastic surgeons, for example, are trying to restrict what types of office surgeries dermatologists can legally perform, said Dr. Coldiron, a private practice dermatologic surgeon and member of the dermatology faculty at the University of Cincinnati.
The study indicates procedures performed by plastic surgeons actually carry a greater risk for adverse events and death, compared with dermatologic surgeries, Dr. Coldiron said.
A plastic surgeon contacted for comment, Dr. Michael McGuire, said the comparison is unfair given the differing complexity of surgeries done by the two specialties. "It’s a total misrepresentation of the statistics. There is no question that the incidence and even the deaths are smaller with dermatology than with any other specialty."
"Comparing an abdominoplasty – a tummy tuck – with a skin cancer excision or even a small volume of liposuction is ridiculous. To compare that with doing tummy tucks, and 4- or 5-hour facelifts, or major breast reconstructive surgery, all of which are done in outpatient surgery centers, is apples and oranges. They are totally different procedures," said Dr. McGuire, who is in private practice in Santa Monica, Calif., and director of The American Board of Plastic Surgeons.
The prospectively collected data show "that any claims by plastic surgeons or anesthesiologists that dermatologists are doing unsafe things and injuring patients in the office is unfounded," Dr. Coldiron said. "And ... if they are going to make such claims, they should have some data to back them up."
Both Alabama and Florida require notification when an outpatient experiences serious injury, transfer to a hospital, or death related to surgery. These mandatory reports are part of public record in the state of Florida, for example.
Dr. Coldiron found 46 deaths and 263 complications that required hospital transfers in Florida. Cosmetic (nonmedically necessary) procedures were associated with 57% of these deaths and almost 50% of such transfers in the state. Liposuction or liposuction with another cosmetic procedure (abdominoplasty, for example) resulted in death for 10 patients and hospital transfer in another 34 cases.
The majority of cosmetic procedure deaths (67%) and hospital transfers (74%) in Florida were performed under general anesthesia, said Dr. Coldiron.
This is relevant because some physicians who perform liposuction under general anesthesia are trying to restrict liposuction under local or tumescent anesthesia, he said. "There have been legislative attempts to prohibit this. The state of New York recently passed a law restricting liposuction in offices, under local anesthesia to 500 cc, which paradoxically will increase the number of injuries and deaths."
"When you try to restrict the use of local anesthesia or tumescent anesthesia ... you will force more people into using general anesthesia, which has more complications. Hospital transfers or deaths with the use of local anesthesia are incredibly rare," Dr. Coldiron said in an interview. "In fact, I’m only aware of a couple that occurred after anaphylactic reactions."
"They [dermatologists] like to blame the general anesthesia," Dr. McGuire said. "It’s not the general anesthesia that is the difference; it’s the magnitude of the surgery. Clearly there are going to be more risks and complications with major surgery compared to minor surgery under any kind of anesthesia." Plastic surgeons in Florida reported the most adverse events (45% of the total), compared with 1.3% reported by dermatologists.
A meeting attendee questioned a direct comparison between specialties, citing the higher complexity of cases typically performed by plastic surgeons. "Yes, the plastic surgeons do more big, multiple procedures and have more problems," Dr. Coldiron replied. "That does not give them the right to try and restrict our practices under the guise of patient safety at the level of the state medical boards and legislatures that is preposterous."
The current study is in press, and represents an update of Dr. Coldiron’s previously reported 7-year Florida data (Dermatol. Surg. 2008;34:285-91).
Additional information is available on the website for Dr. Coldiron's practice, including real adverse event incident reports.
Alabama reports support and validate the Florida data, Dr. Coldiron said. There were three deaths and 52 adverse events that required an office-to-hospital transfer in Alabama. Cosmetic procedures were associated with zero deaths and 42% of hospital transfers during the 6 years. The Alabama medical board provided Dr. Coldiron with the data upon request.
A majority of cosmetic procedure adverse events (86%) were from cases performed under general anesthesia.
Plastic surgery was the specialty most often involved in adverse event reports (42% of all complications), compared with 1.9% for dermatologists in that state (one report associated with tumescent anesthesia).
"Certainly we are not a major contributor in any sense. Dermatologic surgery is extremely safe," Dr. Coldiron said at the meeting, which was jointly sponsored by the American Society of Cosmetic Dermatology and Aesthetic Surgery.
Dr. McGuire said that office-based surgery is safe when performed at centers accredited by the American Association for Accreditation of Ambulatory Surgery Facilities (AAAASF). Studies cited on the organization's website reported 23 deaths of 1,141,418 outpatient procedures in the United States over 5.5 years.
Dr. McGuire is past president of the AAASF. Dr. Coldiron said he had no disclosures.
CHICAGO – Office-based surgery is safe when performed by dermatologists, according to a study of 10 years of complication and death reports from Florida and 6 years of data from Alabama.
Dermatologic surgeons could use the findings to combat any legislative attempts to curtail office procedures, including liposuction, Dr. Brett Coldiron said.
Some plastic surgeons, for example, are trying to restrict what types of office surgeries dermatologists can legally perform, said Dr. Coldiron, a private practice dermatologic surgeon and member of the dermatology faculty at the University of Cincinnati.
The study indicates procedures performed by plastic surgeons actually carry a greater risk for adverse events and death, compared with dermatologic surgeries, Dr. Coldiron said.
A plastic surgeon contacted for comment, Dr. Michael McGuire, said the comparison is unfair given the differing complexity of surgeries done by the two specialties. "It’s a total misrepresentation of the statistics. There is no question that the incidence and even the deaths are smaller with dermatology than with any other specialty."
"Comparing an abdominoplasty – a tummy tuck – with a skin cancer excision or even a small volume of liposuction is ridiculous. To compare that with doing tummy tucks, and 4- or 5-hour facelifts, or major breast reconstructive surgery, all of which are done in outpatient surgery centers, is apples and oranges. They are totally different procedures," said Dr. McGuire, who is in private practice in Santa Monica, Calif., and director of The American Board of Plastic Surgeons.
The prospectively collected data show "that any claims by plastic surgeons or anesthesiologists that dermatologists are doing unsafe things and injuring patients in the office is unfounded," Dr. Coldiron said. "And ... if they are going to make such claims, they should have some data to back them up."
Both Alabama and Florida require notification when an outpatient experiences serious injury, transfer to a hospital, or death related to surgery. These mandatory reports are part of public record in the state of Florida, for example.
Dr. Coldiron found 46 deaths and 263 complications that required hospital transfers in Florida. Cosmetic (nonmedically necessary) procedures were associated with 57% of these deaths and almost 50% of such transfers in the state. Liposuction or liposuction with another cosmetic procedure (abdominoplasty, for example) resulted in death for 10 patients and hospital transfer in another 34 cases.
The majority of cosmetic procedure deaths (67%) and hospital transfers (74%) in Florida were performed under general anesthesia, said Dr. Coldiron.
This is relevant because some physicians who perform liposuction under general anesthesia are trying to restrict liposuction under local or tumescent anesthesia, he said. "There have been legislative attempts to prohibit this. The state of New York recently passed a law restricting liposuction in offices, under local anesthesia to 500 cc, which paradoxically will increase the number of injuries and deaths."
"When you try to restrict the use of local anesthesia or tumescent anesthesia ... you will force more people into using general anesthesia, which has more complications. Hospital transfers or deaths with the use of local anesthesia are incredibly rare," Dr. Coldiron said in an interview. "In fact, I’m only aware of a couple that occurred after anaphylactic reactions."
"They [dermatologists] like to blame the general anesthesia," Dr. McGuire said. "It’s not the general anesthesia that is the difference; it’s the magnitude of the surgery. Clearly there are going to be more risks and complications with major surgery compared to minor surgery under any kind of anesthesia." Plastic surgeons in Florida reported the most adverse events (45% of the total), compared with 1.3% reported by dermatologists.
A meeting attendee questioned a direct comparison between specialties, citing the higher complexity of cases typically performed by plastic surgeons. "Yes, the plastic surgeons do more big, multiple procedures and have more problems," Dr. Coldiron replied. "That does not give them the right to try and restrict our practices under the guise of patient safety at the level of the state medical boards and legislatures that is preposterous."
The current study is in press, and represents an update of Dr. Coldiron’s previously reported 7-year Florida data (Dermatol. Surg. 2008;34:285-91).
Additional information is available on the website for Dr. Coldiron's practice, including real adverse event incident reports.
Alabama reports support and validate the Florida data, Dr. Coldiron said. There were three deaths and 52 adverse events that required an office-to-hospital transfer in Alabama. Cosmetic procedures were associated with zero deaths and 42% of hospital transfers during the 6 years. The Alabama medical board provided Dr. Coldiron with the data upon request.
A majority of cosmetic procedure adverse events (86%) were from cases performed under general anesthesia.
Plastic surgery was the specialty most often involved in adverse event reports (42% of all complications), compared with 1.9% for dermatologists in that state (one report associated with tumescent anesthesia).
"Certainly we are not a major contributor in any sense. Dermatologic surgery is extremely safe," Dr. Coldiron said at the meeting, which was jointly sponsored by the American Society of Cosmetic Dermatology and Aesthetic Surgery.
Dr. McGuire said that office-based surgery is safe when performed at centers accredited by the American Association for Accreditation of Ambulatory Surgery Facilities (AAAASF). Studies cited on the organization's website reported 23 deaths of 1,141,418 outpatient procedures in the United States over 5.5 years.
Dr. McGuire is past president of the AAASF. Dr. Coldiron said he had no disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR DERMATOLOGIC SURGERY
Major Finding: Forty-six deaths and 263 complications required hospital transfers in Florida. Cosmetic procedures were associated with 57% of these deaths and almost 50% of such transfers in the state.
Data Source: Ten years of complication and death reports from Florida and 6 years of data from Alabama
Disclosures: Dr. McGuire is past president of the AAASF. Dr. Coldiron said he had no disclosures.