User login
Great Saphenous Vein Diameter Poor Indicator for Varicose Vein Treatment
SAN DIEGO – Great saphenous vein diameter is a poor surrogate marker for assessing the impact of superficial venous incompetence on a patient's quality of life, results from a study of 91 patients showed.
The finding runs counter to the current practice of some health insurance carriers that use great saphenous vein (GSV) diameter to determine coverage for treatment of axial venous insufficiency.
"It is inappropriate to use GSV diameter as a sole criterion for determining medical necessity for the treatment of GSV reflux," Dr. Kathleen Gibson said at the annual meeting of the American Venous Forum. "Further investigation should be undertaken to look for more appropriate surrogate markers to guide treatment decisions."
Dr. Gibson and her associates collected data from the charts of 91 patients who were prospectively enrolled in two varicose vein trials that examined changes in quality-of-life measures with different varicose vein treatments. It was the first study of its kind, said Dr. Gibson, a vascular surgeon at Lake Washington Vascular in Bellevue, Wash.
The current analysis looked for correlations between GSV diameter and quality-of-life measures prior to any vein treatment.
GSV diameter was measured on duplex ultrasound within 5 cm of the saphenofemoral junction, while the patient was standing. Clinicians also determined Venous Clinical Severity Score (VCSS), and patients completed the Chronic Venous Insufficiency Questionnaire 2 (CIVIQ-2), the Venous Insufficiency Epidemiological and Economic Study-Quality of Life (VEINES-QOL) questionnaire, and the VEINES Symptoms (VEINES-SYM) questionnaire prior to treatment.
Values for VCSS range from 0 to 30, with 30 being the most severe. Scores on the CIVIQ-2 range from 0 to 100, with 100 being the most severe. Higher scores on both the 25-item VEINES-QOL and the 10-item VEINES-SYM indicate better outcomes.
The mean age of patients was 45 years, 72 were women, and the mean GSV diameter was 6.77 mm.
Dr. Gibson reported that the mean VCSS value was 6.4 (range 2-12). The mean CIVIQ-2 score was 42.5 (range 20-85), the mean VEINES-QOL score was 82.7 (range 35-188), and the VEINES-SYM scores had a mean value of 40.5 (range 12-60).
Before vein treatment, there was a moderate correlation between VCSS and QOL measures, she said, and a strong correlation between VCSS and patient-derived quality-of-life measures, which were both significant (P less than .01).
Scatter plot analysis and Pearson correlation coefficients revealed a poor correlation between GSV diameter and VCSS, and no correlation between GSV diameter and any of the following: CIVIQ-2, VEINES-SYM, or VEINES-QOL.
"The only statistically significant findings we had for correlation were a weak correlation between height and body mass index and GSV diameter," Dr. Gibson said. "There was no statistical significance with the weak correlation we saw with VCSS and GSV diameter, and no correlation with any of the quality-of-life surveys. For reflux time, there was a trend toward a weak correlation inversely with height and BMI."
Dr. Gibson said that she had no relevant financial disclosures.
SAN DIEGO – Great saphenous vein diameter is a poor surrogate marker for assessing the impact of superficial venous incompetence on a patient's quality of life, results from a study of 91 patients showed.
The finding runs counter to the current practice of some health insurance carriers that use great saphenous vein (GSV) diameter to determine coverage for treatment of axial venous insufficiency.
"It is inappropriate to use GSV diameter as a sole criterion for determining medical necessity for the treatment of GSV reflux," Dr. Kathleen Gibson said at the annual meeting of the American Venous Forum. "Further investigation should be undertaken to look for more appropriate surrogate markers to guide treatment decisions."
Dr. Gibson and her associates collected data from the charts of 91 patients who were prospectively enrolled in two varicose vein trials that examined changes in quality-of-life measures with different varicose vein treatments. It was the first study of its kind, said Dr. Gibson, a vascular surgeon at Lake Washington Vascular in Bellevue, Wash.
The current analysis looked for correlations between GSV diameter and quality-of-life measures prior to any vein treatment.
GSV diameter was measured on duplex ultrasound within 5 cm of the saphenofemoral junction, while the patient was standing. Clinicians also determined Venous Clinical Severity Score (VCSS), and patients completed the Chronic Venous Insufficiency Questionnaire 2 (CIVIQ-2), the Venous Insufficiency Epidemiological and Economic Study-Quality of Life (VEINES-QOL) questionnaire, and the VEINES Symptoms (VEINES-SYM) questionnaire prior to treatment.
Values for VCSS range from 0 to 30, with 30 being the most severe. Scores on the CIVIQ-2 range from 0 to 100, with 100 being the most severe. Higher scores on both the 25-item VEINES-QOL and the 10-item VEINES-SYM indicate better outcomes.
The mean age of patients was 45 years, 72 were women, and the mean GSV diameter was 6.77 mm.
Dr. Gibson reported that the mean VCSS value was 6.4 (range 2-12). The mean CIVIQ-2 score was 42.5 (range 20-85), the mean VEINES-QOL score was 82.7 (range 35-188), and the VEINES-SYM scores had a mean value of 40.5 (range 12-60).
Before vein treatment, there was a moderate correlation between VCSS and QOL measures, she said, and a strong correlation between VCSS and patient-derived quality-of-life measures, which were both significant (P less than .01).
Scatter plot analysis and Pearson correlation coefficients revealed a poor correlation between GSV diameter and VCSS, and no correlation between GSV diameter and any of the following: CIVIQ-2, VEINES-SYM, or VEINES-QOL.
"The only statistically significant findings we had for correlation were a weak correlation between height and body mass index and GSV diameter," Dr. Gibson said. "There was no statistical significance with the weak correlation we saw with VCSS and GSV diameter, and no correlation with any of the quality-of-life surveys. For reflux time, there was a trend toward a weak correlation inversely with height and BMI."
Dr. Gibson said that she had no relevant financial disclosures.
SAN DIEGO – Great saphenous vein diameter is a poor surrogate marker for assessing the impact of superficial venous incompetence on a patient's quality of life, results from a study of 91 patients showed.
The finding runs counter to the current practice of some health insurance carriers that use great saphenous vein (GSV) diameter to determine coverage for treatment of axial venous insufficiency.
"It is inappropriate to use GSV diameter as a sole criterion for determining medical necessity for the treatment of GSV reflux," Dr. Kathleen Gibson said at the annual meeting of the American Venous Forum. "Further investigation should be undertaken to look for more appropriate surrogate markers to guide treatment decisions."
Dr. Gibson and her associates collected data from the charts of 91 patients who were prospectively enrolled in two varicose vein trials that examined changes in quality-of-life measures with different varicose vein treatments. It was the first study of its kind, said Dr. Gibson, a vascular surgeon at Lake Washington Vascular in Bellevue, Wash.
The current analysis looked for correlations between GSV diameter and quality-of-life measures prior to any vein treatment.
GSV diameter was measured on duplex ultrasound within 5 cm of the saphenofemoral junction, while the patient was standing. Clinicians also determined Venous Clinical Severity Score (VCSS), and patients completed the Chronic Venous Insufficiency Questionnaire 2 (CIVIQ-2), the Venous Insufficiency Epidemiological and Economic Study-Quality of Life (VEINES-QOL) questionnaire, and the VEINES Symptoms (VEINES-SYM) questionnaire prior to treatment.
Values for VCSS range from 0 to 30, with 30 being the most severe. Scores on the CIVIQ-2 range from 0 to 100, with 100 being the most severe. Higher scores on both the 25-item VEINES-QOL and the 10-item VEINES-SYM indicate better outcomes.
The mean age of patients was 45 years, 72 were women, and the mean GSV diameter was 6.77 mm.
Dr. Gibson reported that the mean VCSS value was 6.4 (range 2-12). The mean CIVIQ-2 score was 42.5 (range 20-85), the mean VEINES-QOL score was 82.7 (range 35-188), and the VEINES-SYM scores had a mean value of 40.5 (range 12-60).
Before vein treatment, there was a moderate correlation between VCSS and QOL measures, she said, and a strong correlation between VCSS and patient-derived quality-of-life measures, which were both significant (P less than .01).
Scatter plot analysis and Pearson correlation coefficients revealed a poor correlation between GSV diameter and VCSS, and no correlation between GSV diameter and any of the following: CIVIQ-2, VEINES-SYM, or VEINES-QOL.
"The only statistically significant findings we had for correlation were a weak correlation between height and body mass index and GSV diameter," Dr. Gibson said. "There was no statistical significance with the weak correlation we saw with VCSS and GSV diameter, and no correlation with any of the quality-of-life surveys. For reflux time, there was a trend toward a weak correlation inversely with height and BMI."
Dr. Gibson said that she had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN VENOUS FORUM
Major Finding: No correlation was found between great saphenous vein diameter and any of three quality-of-life measures known as CIVIQ-2, VEINES-SYM, and VEINES-QOL, all measured prior to any vein treatment.
Data Source: A study of 91 patients who were prospectively enrolled in two varicose vein trials.
Disclosures: Dr. Gibson said that she had no relevant financial disclosures.
Minimally Invasive Cosmetic Procedures Down in 2010
As the economy rebounds, so is interest in cosmetic plastic surgery, according to statistics from the American Society for Aesthetic Plastic Surgery.
The latest figures show that cosmetic surgical procedures increased nearly 9% in 2010. More than 1.6 million cosmetic surgical procedures were performed in the United States last year, with breast augmentation remaining the most popular. Liposuction, eyelid surgery, abdominoplasty, and breast reduction rounded out the top five procedures in 2010.
"Patients who put off surgery because of uncertainty in the economy and the job market are coming back for tried and true procedures," Dr. Felmont Eaves III, ASAPS president, said in a statement. "Growth in demand will likely continue as the recession eases and baby boomers and their offspring begin to explore surgical and nonsurgical options."
But demand for some minimally invasive procedures, such as laser hair removal, dropped in 2010. Overall, cosmetic minimally invasive procedures decreased nearly 9%. A total of 8 million procedures were performed last year, representing about 39% of the total spending on cosmetic surgery. Fewer patients underwent injections of botulinum toxin type A, laser hair removal, laser skin resurfacing, and chemical peels than in previous years. However, the number of procedures performed with hyaluronic acid increased.
Cosmetic surgery remains big business. In 2010, Americans spent close to $10.7 billion on cosmetic procedures. The bulk – $6.6 billion – was spent on surgical procedures. An additional $1.9 billion was spent on injectable procedures, $1.8 billion on skin rejuvenation procedures, and nearly $500 million on other nonsurgical procedures.
The 2010 figures are based on a survey of more than 900 plastic surgeons, dermatologists, and otolaryngologists. The ASAPS has compiled cosmetic surgery procedure data since 1997.
As the economy rebounds, so is interest in cosmetic plastic surgery, according to statistics from the American Society for Aesthetic Plastic Surgery.
The latest figures show that cosmetic surgical procedures increased nearly 9% in 2010. More than 1.6 million cosmetic surgical procedures were performed in the United States last year, with breast augmentation remaining the most popular. Liposuction, eyelid surgery, abdominoplasty, and breast reduction rounded out the top five procedures in 2010.
"Patients who put off surgery because of uncertainty in the economy and the job market are coming back for tried and true procedures," Dr. Felmont Eaves III, ASAPS president, said in a statement. "Growth in demand will likely continue as the recession eases and baby boomers and their offspring begin to explore surgical and nonsurgical options."
But demand for some minimally invasive procedures, such as laser hair removal, dropped in 2010. Overall, cosmetic minimally invasive procedures decreased nearly 9%. A total of 8 million procedures were performed last year, representing about 39% of the total spending on cosmetic surgery. Fewer patients underwent injections of botulinum toxin type A, laser hair removal, laser skin resurfacing, and chemical peels than in previous years. However, the number of procedures performed with hyaluronic acid increased.
Cosmetic surgery remains big business. In 2010, Americans spent close to $10.7 billion on cosmetic procedures. The bulk – $6.6 billion – was spent on surgical procedures. An additional $1.9 billion was spent on injectable procedures, $1.8 billion on skin rejuvenation procedures, and nearly $500 million on other nonsurgical procedures.
The 2010 figures are based on a survey of more than 900 plastic surgeons, dermatologists, and otolaryngologists. The ASAPS has compiled cosmetic surgery procedure data since 1997.
As the economy rebounds, so is interest in cosmetic plastic surgery, according to statistics from the American Society for Aesthetic Plastic Surgery.
The latest figures show that cosmetic surgical procedures increased nearly 9% in 2010. More than 1.6 million cosmetic surgical procedures were performed in the United States last year, with breast augmentation remaining the most popular. Liposuction, eyelid surgery, abdominoplasty, and breast reduction rounded out the top five procedures in 2010.
"Patients who put off surgery because of uncertainty in the economy and the job market are coming back for tried and true procedures," Dr. Felmont Eaves III, ASAPS president, said in a statement. "Growth in demand will likely continue as the recession eases and baby boomers and their offspring begin to explore surgical and nonsurgical options."
But demand for some minimally invasive procedures, such as laser hair removal, dropped in 2010. Overall, cosmetic minimally invasive procedures decreased nearly 9%. A total of 8 million procedures were performed last year, representing about 39% of the total spending on cosmetic surgery. Fewer patients underwent injections of botulinum toxin type A, laser hair removal, laser skin resurfacing, and chemical peels than in previous years. However, the number of procedures performed with hyaluronic acid increased.
Cosmetic surgery remains big business. In 2010, Americans spent close to $10.7 billion on cosmetic procedures. The bulk – $6.6 billion – was spent on surgical procedures. An additional $1.9 billion was spent on injectable procedures, $1.8 billion on skin rejuvenation procedures, and nearly $500 million on other nonsurgical procedures.
The 2010 figures are based on a survey of more than 900 plastic surgeons, dermatologists, and otolaryngologists. The ASAPS has compiled cosmetic surgery procedure data since 1997.
Novel Device Uses Cold Therapy to Reduce Forehead Wrinkles
GRAPEVINE, TEX. – An investigational cryoprobe device reduced dynamic forehead wrinkles immediately after application in a pilot study of 36 patients that was presented at the annual meeting of the American Society for Laser Medicine and Surgery.
The self-contained, hand-held device, made by MyoScience Inc., uses a 27-gauge needle to deliver cooling to the temporal branch of the facial nerve that controls the frontalis muscle, rather than directly into the muscle as is done with botulinum toxins. The duration of effect is similar to that of botulinum toxins, about 3-4 months.
"Basically, it's a green alternative. There's no chemical, no toxin, it's only cold therapy," principal investigator Dr. Francis Palmer said in an interview.

Results from the use of a first-generation version of the device were reported by Dr. Vic Narurkar, who directs the Bay Area Laser Institute in San Francisco. The 36 patients were aged 35-70 years, all with forehead lines during animation. Some were at risk for brow ptosis.
After lidocaine administration, the probe was inserted for 30-45 seconds, and the subsequent reduction in muscle contractility was monitored to see if additional cryoprobe insertions were needed. All patients had immediate dynamic line reduction after two to four cryoprobe insertions, Dr. Narurkar reported.
The most common adverse events were headaches and small focal areas of minor epidermal cold injury, attributed to limitations in the prototype design. No patient experienced ptosis. "Cold has the unique natural property of selectively affecting the axon, yet preserves the endoneurial sheath. ... [It] has no impact on collagen-based structures," Dr. Narurkar explained.
According to Dr. Palmer, both the absence of ptosis risk and the immediacy of the response represent significant advantages over botulinum toxins, for which peak of action is typically 4-7 days following injection.
However, "I don't see this as a replacement for toxin, but as a complement. Physicians now have something to give patients who don't want a toxin, or for use in combination in areas where you can’t use a toxin. Botox is fabulous. It doesn't need to be replaced," said Dr. Palmer, director of the Beverly Hills (Calif.) International Center for Aesthetic Surgery.
Moreover, he noted, at this point, the injection of neurotoxin is easier and somewhat less invasive, although that could change with further revision of the cryoprobe's design. "We think it offers additional things toxin therapy doesn't offer, but it’s in a very early stage. It will be refined further before it hits the market."
MyoScience plans to seek a CE marking for the cryoprobe later this year before approaching the U.S. Food and Drug Administration, he said.
Both Dr. Palmer and Dr. Narurkar are paid consultants for MyoScience, which funded the study.
GRAPEVINE, TEX. – An investigational cryoprobe device reduced dynamic forehead wrinkles immediately after application in a pilot study of 36 patients that was presented at the annual meeting of the American Society for Laser Medicine and Surgery.
The self-contained, hand-held device, made by MyoScience Inc., uses a 27-gauge needle to deliver cooling to the temporal branch of the facial nerve that controls the frontalis muscle, rather than directly into the muscle as is done with botulinum toxins. The duration of effect is similar to that of botulinum toxins, about 3-4 months.
"Basically, it's a green alternative. There's no chemical, no toxin, it's only cold therapy," principal investigator Dr. Francis Palmer said in an interview.
Results from the use of a first-generation version of the device were reported by Dr. Vic Narurkar, who directs the Bay Area Laser Institute in San Francisco. The 36 patients were aged 35-70 years, all with forehead lines during animation. Some were at risk for brow ptosis.
After lidocaine administration, the probe was inserted for 30-45 seconds, and the subsequent reduction in muscle contractility was monitored to see if additional cryoprobe insertions were needed. All patients had immediate dynamic line reduction after two to four cryoprobe insertions, Dr. Narurkar reported.
The most common adverse events were headaches and small focal areas of minor epidermal cold injury, attributed to limitations in the prototype design. No patient experienced ptosis. "Cold has the unique natural property of selectively affecting the axon, yet preserves the endoneurial sheath. ... [It] has no impact on collagen-based structures," Dr. Narurkar explained.
According to Dr. Palmer, both the absence of ptosis risk and the immediacy of the response represent significant advantages over botulinum toxins, for which peak of action is typically 4-7 days following injection.
However, "I don't see this as a replacement for toxin, but as a complement. Physicians now have something to give patients who don't want a toxin, or for use in combination in areas where you can’t use a toxin. Botox is fabulous. It doesn't need to be replaced," said Dr. Palmer, director of the Beverly Hills (Calif.) International Center for Aesthetic Surgery.
Moreover, he noted, at this point, the injection of neurotoxin is easier and somewhat less invasive, although that could change with further revision of the cryoprobe's design. "We think it offers additional things toxin therapy doesn't offer, but it’s in a very early stage. It will be refined further before it hits the market."
MyoScience plans to seek a CE marking for the cryoprobe later this year before approaching the U.S. Food and Drug Administration, he said.
Both Dr. Palmer and Dr. Narurkar are paid consultants for MyoScience, which funded the study.
GRAPEVINE, TEX. – An investigational cryoprobe device reduced dynamic forehead wrinkles immediately after application in a pilot study of 36 patients that was presented at the annual meeting of the American Society for Laser Medicine and Surgery.
The self-contained, hand-held device, made by MyoScience Inc., uses a 27-gauge needle to deliver cooling to the temporal branch of the facial nerve that controls the frontalis muscle, rather than directly into the muscle as is done with botulinum toxins. The duration of effect is similar to that of botulinum toxins, about 3-4 months.
"Basically, it's a green alternative. There's no chemical, no toxin, it's only cold therapy," principal investigator Dr. Francis Palmer said in an interview.
Results from the use of a first-generation version of the device were reported by Dr. Vic Narurkar, who directs the Bay Area Laser Institute in San Francisco. The 36 patients were aged 35-70 years, all with forehead lines during animation. Some were at risk for brow ptosis.
After lidocaine administration, the probe was inserted for 30-45 seconds, and the subsequent reduction in muscle contractility was monitored to see if additional cryoprobe insertions were needed. All patients had immediate dynamic line reduction after two to four cryoprobe insertions, Dr. Narurkar reported.
The most common adverse events were headaches and small focal areas of minor epidermal cold injury, attributed to limitations in the prototype design. No patient experienced ptosis. "Cold has the unique natural property of selectively affecting the axon, yet preserves the endoneurial sheath. ... [It] has no impact on collagen-based structures," Dr. Narurkar explained.
According to Dr. Palmer, both the absence of ptosis risk and the immediacy of the response represent significant advantages over botulinum toxins, for which peak of action is typically 4-7 days following injection.
However, "I don't see this as a replacement for toxin, but as a complement. Physicians now have something to give patients who don't want a toxin, or for use in combination in areas where you can’t use a toxin. Botox is fabulous. It doesn't need to be replaced," said Dr. Palmer, director of the Beverly Hills (Calif.) International Center for Aesthetic Surgery.
Moreover, he noted, at this point, the injection of neurotoxin is easier and somewhat less invasive, although that could change with further revision of the cryoprobe's design. "We think it offers additional things toxin therapy doesn't offer, but it’s in a very early stage. It will be refined further before it hits the market."
MyoScience plans to seek a CE marking for the cryoprobe later this year before approaching the U.S. Food and Drug Administration, he said.
Both Dr. Palmer and Dr. Narurkar are paid consultants for MyoScience, which funded the study.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR LASER MEDICINE AND SURGERY
Major Finding: All patients experienced immediate reduction in wrinkles with two to four cryoprobe insertions.
Data Source: Pilot study of 36 adults (aged 35-70 years) with dynamic forehead wrinkles.
Disclosures: Both Dr. Palmer and Dr. Narurkar are paid consultants for MyoScience, which funded the study.
Nd:YAG Provides Best Outcomes for Mucosal Venous Malformations
GRAPEVINE, TEX. – In a prospective evaluation of 59 children with venous malformations, the long-pulsed neodymium:YAG laser was more effective in treating mucosal venous malformations than lesions on the limbs.
Venous malformations present in many forms that vary in depth, location, and extent, and treatment is largely symptomatic rather than curative. "It is, therefore, important that treatments given are effective in improving the symptoms medium or long term, with as few side effects as possible," said Dr. Stratos Sofos of Alder Hey Children's Hospital in Liverpool, England.
The long-pulsed Nd:YAG laser has become popular for the treatment of small- to medium-size vessels. Its longer pulse duration provides deeper penetration and weaker melanin absorption, allowing it to heat the vessels slowly and uniformly, thus avoiding the vessel rupture with subsequent purpura and hyperpigmentation that can occur with other lasers.
However, published data do not address whether treatment with a long-pulsed Nd:YAG laser provides long-term symptom relief, nor which types of venous malformations respond better than do others, Dr. Sofos said at the annual meeting of the American Society for Laser Medicine and Surgery.
All children who met criteria such as functional impairment, large facial deformities, and painful or bleeding lesions were treated with Candela Corp.'s GentleYAG 1064-nm laser. They received one to three treatments under general anesthesia, delivered in six to eight weekly intervals. Prior to Nd:YAG laser treatment, 32 of the children had received multiple other treatments, including pulsed dye lasers and sclerotherapy.
The 59 patients were aged 2-18 years (mean, 12.3 years). Venous malformations were present on the head and neck in 23, of which 18 (31% of the total) were mucosal. Malformations were on the upper limbs in 15 and on the lower limbs in 18 (total with limb lesions, 56%). The other three had lesions on the chest wall. Average follow up was 24 months (range, 6 months–9 years).
Based on objective assessment, 18% in the upper- and lower-limb group had excellent results and 27% patients had good results, whereas 55% of patients had no change. For the mucosal group, 28% had excellent results, 56% had good results, and 17% had no improvement, Dr. Sofos reported.
The overall complication rate from the Nd:YAG laser treatment was 20% (12 of 59), including skin blistering in 10%, ulceration in 7%, and hypertrophic scarring in 3%. Overall, 83% of the complications occurred in either upper or lower limbs, he noted.
Recurrence was defined by patients for whom symptoms had improved (with good or excellent results) but subsequently recurred. Of the 15 patients who had good or excellent results in the limbs, 4 had a recurrence (recurrence rate, 27%). Of 15 in the mucosa group who had been treated successfully, one had a recurrence (7%).
Subjective and objective evaluation of efficacy correlated well, and the vast majority of patients found the treatment to be successful and would opt to have it again if necessary, Dr. Sofos said.
"Due to the high risk of complications of treatment, however, we feel that treatment should be offered to a [select] group of patients, and should be carried out with caution. Further study will hopefully help us in establishing the best parameters to achieve better results, with minimal complications," he concluded.
This study was funded by the U.K. National Health Service. Dr. Sofos stated that he had no other disclosures.
GRAPEVINE, TEX. – In a prospective evaluation of 59 children with venous malformations, the long-pulsed neodymium:YAG laser was more effective in treating mucosal venous malformations than lesions on the limbs.
Venous malformations present in many forms that vary in depth, location, and extent, and treatment is largely symptomatic rather than curative. "It is, therefore, important that treatments given are effective in improving the symptoms medium or long term, with as few side effects as possible," said Dr. Stratos Sofos of Alder Hey Children's Hospital in Liverpool, England.
The long-pulsed Nd:YAG laser has become popular for the treatment of small- to medium-size vessels. Its longer pulse duration provides deeper penetration and weaker melanin absorption, allowing it to heat the vessels slowly and uniformly, thus avoiding the vessel rupture with subsequent purpura and hyperpigmentation that can occur with other lasers.
However, published data do not address whether treatment with a long-pulsed Nd:YAG laser provides long-term symptom relief, nor which types of venous malformations respond better than do others, Dr. Sofos said at the annual meeting of the American Society for Laser Medicine and Surgery.
All children who met criteria such as functional impairment, large facial deformities, and painful or bleeding lesions were treated with Candela Corp.'s GentleYAG 1064-nm laser. They received one to three treatments under general anesthesia, delivered in six to eight weekly intervals. Prior to Nd:YAG laser treatment, 32 of the children had received multiple other treatments, including pulsed dye lasers and sclerotherapy.
The 59 patients were aged 2-18 years (mean, 12.3 years). Venous malformations were present on the head and neck in 23, of which 18 (31% of the total) were mucosal. Malformations were on the upper limbs in 15 and on the lower limbs in 18 (total with limb lesions, 56%). The other three had lesions on the chest wall. Average follow up was 24 months (range, 6 months–9 years).
Based on objective assessment, 18% in the upper- and lower-limb group had excellent results and 27% patients had good results, whereas 55% of patients had no change. For the mucosal group, 28% had excellent results, 56% had good results, and 17% had no improvement, Dr. Sofos reported.
The overall complication rate from the Nd:YAG laser treatment was 20% (12 of 59), including skin blistering in 10%, ulceration in 7%, and hypertrophic scarring in 3%. Overall, 83% of the complications occurred in either upper or lower limbs, he noted.
Recurrence was defined by patients for whom symptoms had improved (with good or excellent results) but subsequently recurred. Of the 15 patients who had good or excellent results in the limbs, 4 had a recurrence (recurrence rate, 27%). Of 15 in the mucosa group who had been treated successfully, one had a recurrence (7%).
Subjective and objective evaluation of efficacy correlated well, and the vast majority of patients found the treatment to be successful and would opt to have it again if necessary, Dr. Sofos said.
"Due to the high risk of complications of treatment, however, we feel that treatment should be offered to a [select] group of patients, and should be carried out with caution. Further study will hopefully help us in establishing the best parameters to achieve better results, with minimal complications," he concluded.
This study was funded by the U.K. National Health Service. Dr. Sofos stated that he had no other disclosures.
GRAPEVINE, TEX. – In a prospective evaluation of 59 children with venous malformations, the long-pulsed neodymium:YAG laser was more effective in treating mucosal venous malformations than lesions on the limbs.
Venous malformations present in many forms that vary in depth, location, and extent, and treatment is largely symptomatic rather than curative. "It is, therefore, important that treatments given are effective in improving the symptoms medium or long term, with as few side effects as possible," said Dr. Stratos Sofos of Alder Hey Children's Hospital in Liverpool, England.
The long-pulsed Nd:YAG laser has become popular for the treatment of small- to medium-size vessels. Its longer pulse duration provides deeper penetration and weaker melanin absorption, allowing it to heat the vessels slowly and uniformly, thus avoiding the vessel rupture with subsequent purpura and hyperpigmentation that can occur with other lasers.
However, published data do not address whether treatment with a long-pulsed Nd:YAG laser provides long-term symptom relief, nor which types of venous malformations respond better than do others, Dr. Sofos said at the annual meeting of the American Society for Laser Medicine and Surgery.
All children who met criteria such as functional impairment, large facial deformities, and painful or bleeding lesions were treated with Candela Corp.'s GentleYAG 1064-nm laser. They received one to three treatments under general anesthesia, delivered in six to eight weekly intervals. Prior to Nd:YAG laser treatment, 32 of the children had received multiple other treatments, including pulsed dye lasers and sclerotherapy.
The 59 patients were aged 2-18 years (mean, 12.3 years). Venous malformations were present on the head and neck in 23, of which 18 (31% of the total) were mucosal. Malformations were on the upper limbs in 15 and on the lower limbs in 18 (total with limb lesions, 56%). The other three had lesions on the chest wall. Average follow up was 24 months (range, 6 months–9 years).
Based on objective assessment, 18% in the upper- and lower-limb group had excellent results and 27% patients had good results, whereas 55% of patients had no change. For the mucosal group, 28% had excellent results, 56% had good results, and 17% had no improvement, Dr. Sofos reported.
The overall complication rate from the Nd:YAG laser treatment was 20% (12 of 59), including skin blistering in 10%, ulceration in 7%, and hypertrophic scarring in 3%. Overall, 83% of the complications occurred in either upper or lower limbs, he noted.
Recurrence was defined by patients for whom symptoms had improved (with good or excellent results) but subsequently recurred. Of the 15 patients who had good or excellent results in the limbs, 4 had a recurrence (recurrence rate, 27%). Of 15 in the mucosa group who had been treated successfully, one had a recurrence (7%).
Subjective and objective evaluation of efficacy correlated well, and the vast majority of patients found the treatment to be successful and would opt to have it again if necessary, Dr. Sofos said.
"Due to the high risk of complications of treatment, however, we feel that treatment should be offered to a [select] group of patients, and should be carried out with caution. Further study will hopefully help us in establishing the best parameters to achieve better results, with minimal complications," he concluded.
This study was funded by the U.K. National Health Service. Dr. Sofos stated that he had no other disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR LASER MEDICINE AND SURGERY
Major Finding: Based on objective assessment, 18% in the upper- and lower-limb group had excellent results and 27% of patients had good results, whereas 55% of patients had no change. In the mucosal group, 28% had excellent results, 56% had good results, and 17% had no improvement.
Data Source: Prospective evaluation of 59 children with venous malformations who were seen at a single hospital.
Disclosures: The study was funded by the U.K. National Health Service. Dr. Sofos stated that he had no other disclosures.
All-in-One Skin and Hair Care Products
Sublative Rejuvenation Strikes Efficacy, Adverse Event Balance
MIAMI BEACH – Sublative skin rejuvenation is a resurfacing technology that seeks to provide the best of both worlds – efficacy closer to more intensive ablative procedures and an adverse event profile more akin to gentler, nonablative techniques.
Sublative rejuvenation can be performed on the full face, with good results around the eyes and the neck, Dr. Robert A. Weiss said at the symposium.

"We've gotten some very nice skin contraction and smoothing in the periorbital area," he said.
The fractional radiofrequency eMatrix system (Syneron) offers deep volumetric heating into the dermis with minimal epidermal disruption, said Dr. Weiss, director of the Maryland Laser, Skin, and Vein Institute in Hunt Valley. Subsequent dermal remodeling with minimal downtime are other advantages of this treatment.
The Food and Drug Administration cleared marketing of the applicator for use in dermatologic procedures requiring ablation of soft tissue and skin resurfacing.
The device tip is a grid of negatively- and positively-charged electrodes between which bipolar radiofrequency energy flows. The current can be controlled and varied depending on individual patient factors. Because this is a fractional technology, intact tissue is left between the electrode pins to speed healing and recovery.
The standard protocol is three to four treatment sessions spaced 4-6 weeks apart. Touch-up sessions, as indicated, are generally every 6 months or so.
The full face can be treated in 20 minutes, said Dr. Weiss, also of the department of dermatology at Johns Hopkins University, Baltimore. Improvements in acne scarring and wrinkles can be observed as well.
Ask patients to return 2-3 days after treatment to check for any adverse events, he said. Postoperative discomfort, significant pain, erythema, edema, and pigmentary changes can arise in the short or long term. Patient discomfort is usually tolerable and can be managed with topical anesthetics.
Postprocedure redness with nonablative techniques typically lasts a few hours to 1-2 days; with ablative procedures, 5-7 days (and sometimes up to 10 days); and with sublative treatment, a patient will have red dots on their skin and redness that lasts for a day or 2, Dr. Weiss said. "So it's really somewhere in the middle between ablative and nonablative."
Contraindications include any facelift or eyelid surgery 1 year prior to sublative resurfacing; injections of botulinum toxin, collagen, or fat (or any biomaterial augmentation) within the last 6 months; and any facial dermabrasion, resurfacing, or deep chemical peeling within the last 3 months.
Treat a hidden test spot to gauge individual response prior to full treatment, Dr. Weiss recommended. Gauge response after 24-48 hours for skin types I-III and 5-7 days for skin types IV-VI to ensure safety.
Cold packs or Synercool (Syneron) can be used immediately after treatment to cool the area if patients are uncomfortable. Advise patients to apply emollient cream and to use at least 30 SPF or greater sunscreen for at least a month.
"It's a promising technology, and I think we will know more a year from now," Dr. Weiss said.
He is a researcher for Syneron and received some initial free use of equipment.
MIAMI BEACH – Sublative skin rejuvenation is a resurfacing technology that seeks to provide the best of both worlds – efficacy closer to more intensive ablative procedures and an adverse event profile more akin to gentler, nonablative techniques.
Sublative rejuvenation can be performed on the full face, with good results around the eyes and the neck, Dr. Robert A. Weiss said at the symposium.
"We've gotten some very nice skin contraction and smoothing in the periorbital area," he said.
The fractional radiofrequency eMatrix system (Syneron) offers deep volumetric heating into the dermis with minimal epidermal disruption, said Dr. Weiss, director of the Maryland Laser, Skin, and Vein Institute in Hunt Valley. Subsequent dermal remodeling with minimal downtime are other advantages of this treatment.
The Food and Drug Administration cleared marketing of the applicator for use in dermatologic procedures requiring ablation of soft tissue and skin resurfacing.
The device tip is a grid of negatively- and positively-charged electrodes between which bipolar radiofrequency energy flows. The current can be controlled and varied depending on individual patient factors. Because this is a fractional technology, intact tissue is left between the electrode pins to speed healing and recovery.
The standard protocol is three to four treatment sessions spaced 4-6 weeks apart. Touch-up sessions, as indicated, are generally every 6 months or so.
The full face can be treated in 20 minutes, said Dr. Weiss, also of the department of dermatology at Johns Hopkins University, Baltimore. Improvements in acne scarring and wrinkles can be observed as well.
Ask patients to return 2-3 days after treatment to check for any adverse events, he said. Postoperative discomfort, significant pain, erythema, edema, and pigmentary changes can arise in the short or long term. Patient discomfort is usually tolerable and can be managed with topical anesthetics.
Postprocedure redness with nonablative techniques typically lasts a few hours to 1-2 days; with ablative procedures, 5-7 days (and sometimes up to 10 days); and with sublative treatment, a patient will have red dots on their skin and redness that lasts for a day or 2, Dr. Weiss said. "So it's really somewhere in the middle between ablative and nonablative."
Contraindications include any facelift or eyelid surgery 1 year prior to sublative resurfacing; injections of botulinum toxin, collagen, or fat (or any biomaterial augmentation) within the last 6 months; and any facial dermabrasion, resurfacing, or deep chemical peeling within the last 3 months.
Treat a hidden test spot to gauge individual response prior to full treatment, Dr. Weiss recommended. Gauge response after 24-48 hours for skin types I-III and 5-7 days for skin types IV-VI to ensure safety.
Cold packs or Synercool (Syneron) can be used immediately after treatment to cool the area if patients are uncomfortable. Advise patients to apply emollient cream and to use at least 30 SPF or greater sunscreen for at least a month.
"It's a promising technology, and I think we will know more a year from now," Dr. Weiss said.
He is a researcher for Syneron and received some initial free use of equipment.
MIAMI BEACH – Sublative skin rejuvenation is a resurfacing technology that seeks to provide the best of both worlds – efficacy closer to more intensive ablative procedures and an adverse event profile more akin to gentler, nonablative techniques.
Sublative rejuvenation can be performed on the full face, with good results around the eyes and the neck, Dr. Robert A. Weiss said at the symposium.
"We've gotten some very nice skin contraction and smoothing in the periorbital area," he said.
The fractional radiofrequency eMatrix system (Syneron) offers deep volumetric heating into the dermis with minimal epidermal disruption, said Dr. Weiss, director of the Maryland Laser, Skin, and Vein Institute in Hunt Valley. Subsequent dermal remodeling with minimal downtime are other advantages of this treatment.
The Food and Drug Administration cleared marketing of the applicator for use in dermatologic procedures requiring ablation of soft tissue and skin resurfacing.
The device tip is a grid of negatively- and positively-charged electrodes between which bipolar radiofrequency energy flows. The current can be controlled and varied depending on individual patient factors. Because this is a fractional technology, intact tissue is left between the electrode pins to speed healing and recovery.
The standard protocol is three to four treatment sessions spaced 4-6 weeks apart. Touch-up sessions, as indicated, are generally every 6 months or so.
The full face can be treated in 20 minutes, said Dr. Weiss, also of the department of dermatology at Johns Hopkins University, Baltimore. Improvements in acne scarring and wrinkles can be observed as well.
Ask patients to return 2-3 days after treatment to check for any adverse events, he said. Postoperative discomfort, significant pain, erythema, edema, and pigmentary changes can arise in the short or long term. Patient discomfort is usually tolerable and can be managed with topical anesthetics.
Postprocedure redness with nonablative techniques typically lasts a few hours to 1-2 days; with ablative procedures, 5-7 days (and sometimes up to 10 days); and with sublative treatment, a patient will have red dots on their skin and redness that lasts for a day or 2, Dr. Weiss said. "So it's really somewhere in the middle between ablative and nonablative."
Contraindications include any facelift or eyelid surgery 1 year prior to sublative resurfacing; injections of botulinum toxin, collagen, or fat (or any biomaterial augmentation) within the last 6 months; and any facial dermabrasion, resurfacing, or deep chemical peeling within the last 3 months.
Treat a hidden test spot to gauge individual response prior to full treatment, Dr. Weiss recommended. Gauge response after 24-48 hours for skin types I-III and 5-7 days for skin types IV-VI to ensure safety.
Cold packs or Synercool (Syneron) can be used immediately after treatment to cool the area if patients are uncomfortable. Advise patients to apply emollient cream and to use at least 30 SPF or greater sunscreen for at least a month.
"It's a promising technology, and I think we will know more a year from now," Dr. Weiss said.
He is a researcher for Syneron and received some initial free use of equipment.
EXPERT ANALYSIS FROM THE SOUTH BEACH SYMPOSIUM
Melatonin
Melatonin (N-acetyl-5-methoxytryptamine) is a hormone produced naturally by the pineal gland in humans. Production of the hormone is stimulated by beta-adrenergic receptors. Research in recent years has offered some intriguing and in some cases promising results that may one day be utilized for dermatologic treatments and products.
Also found in various animal and plant species, melatonin is probably best known for its daily fluctuations in circulating levels that play an important role in circadian rhythms. In recent years, melatonin has been gaining increased attention in antiaging medicine and dermatology because it has been found to exert antioxidant activity, particularly against hydroxyl radicals (Hautarzt. 1999;50:5-11), the most harmful of free radicals. Melatonin levels are known to decrease with age. In addition to its antioxidative and regulatory roles, including in seasonal reproduction control, melatonin modulates the immune system and inhibits inflammation (J. Pineal Res. 2009;47:324-9).
Melatonin and UV-Induced Erythema
In 1996, Bangha et al. conducted a randomized double-blind study with 20 healthy volunteers to examine the efficacy of topically applied melatonin in hindering UV-induced erythema. Each subject was irradiated with UVB (0.099 J/cm2) on 4-cm2 areas on the lower back, and then treated with different concentrations of melatonin. The investigators observed a dose-response relationship between melatonin concentration and the degree of erythema, with significantly less redness found in the areas treated with 0.5% melatonin, compared with melatonin 0.05% or just the vehicle gel (Arch. Dermatol. Res. 1996;288:522-9).
The next year, Bangha et al. performed another randomized double-blind study on topical melatonin and its antierythema effect, this time to ascertain the role of the application time in exerting the effect. Again using 20 volunteers, the researchers treated small areas of the lower back with 0.6 mg/cm2 melatonin 15 minutes before or 1, 30, or 240 minutes after simulated UVA and UVB irradiation at twice the individual minimal erythema dose. The authors found that post-treatment with melatonin imparted no protective effect but pretreatment 15 minutes prior to irradiation yielded significant protection against erythema (Dermatology 1997;195:248-52). That same year, Bangha et al. also studied the penetration kinetics of topical melatonin in six healthy volunteers between the ages of 26 and 34 years, and found that melatonin has the potential to accumulate in the stratum corneum with extended release into the bloodstream through cutaneous delivery (Skin Pharmacol. 1997;10:298-302).
In 1998, Dreher et al. conducted a randomized double-blind study in 12 healthy adults (6 women and 6 men, all white, ranging in age from 29 to 49 years). The researchers looked at the short-term photoprotective effects of topically applied vitamin C; vitamin E; and melatnonin; alone or in combination. All formulations were applied 30 minutes after UV exposure. A dose-dependent photoprotective effect was associated with melatonin, with modest effects seen with the vitamins alone. Photoprotective activity was clearly enhanced when melatonin was combined with vitamins C and E (Br. J. Dermatol. 1998;139:332-9).
The following year, Dreher et al. performed a similar experiment to assess the short-term photoprotective effects of the same compounds. This placebo-controlled, randomized double-blind human study entailed the topical use of each antioxidant alone or in combination after UV exposure in a single application (immediately or 30 minutes after UV exposure) or in multiple applications 30 minutes, 1 hour, and 2 hours after UV exposure (totaling three applications).
Interestingly, no photoprotective effects were observed regardless of the number of applications of antioxidants. The investigators concluded that given the speed of damage to skin from UV radiation, antioxidants probably must be delivered at the appropriate site in sufficient concentrations at the outset of and during active oxidative insult (Dermatology 1999;198:52-5).
Similarly, in 2006 Howes et al. studied the effects of topical melatonin applied after solar-simulated UV exposure in 16 healthy Mantoux-positive volunteers, and found that melatonin imparted no protection against sunburn or immune suppression (Photodermatol. Photoimmunol. Photomed. 2006;22:267-9).
Antioxidant Properties
Morganti et al. conducted an 8-week placebo-controlled, randomized double-blind study on 30 xerotic female volunteers (between ages 48 and 59 years) to determine the effects of topical and systemic antioxidant-enriched formulation administration on the skin. Subjects applied a nanocolloidal gel twice daily and/or took two capsules per day of an oral diet supplement. The antioxidant-enriched formulations included vitamins C and E, alpha-lipoic acid, emblica, and melatonin.
Investigators found that oxidative stress and lipid peroxidation declined 30%-40% in the blood serum of all participants who used the topical or systemic antioxidant formulation. Those treated with the antioxidants also showed reductions in free radicals recovered in blood serum and on skin, as well as decreases in reactive oxygen species engendered by UVB irradiation of leukocytes (in vitro). The researchers concluded that the tested compounds indeed exerted topical and systemic photoprotection and represent promising ingredients for combating oxidative stress and photoaging (Int. J. Cosmet. Sci. 2002;24:331-9).
Uses of Melatonin for Skin Lesions
In 2004, Fischer et al. conducted a clinical study in 15 healthy volunteers to consider the skin penetration activity of melatonin 0.01% in a cream and 0.01% and 0.03% in a solution. In a 24-hour time window, investigators took blood samples for melatonin measurement prior to application at 9:00 a.m., as well as 1, 4, 8, and 24 hours after application. Preapplication serum melatonin levels ranged from 0.6 to 15.9 pg/mL.
The mean serum value 24 hours after application of the 0.01% melatonin cream was 9.0 pg/mL. For the 0.01% solution group, the mean melatonin level was 12.7 pg/mL 24 hours after application. Melatonin levels also markedly increased just 1 and 8 hours later in the 0.03% solution group, with cumulative melatonin noted as 7.1 pg/mL in the 0.01% cream subjects, 8.6 pg/mL in the 0.01% solution participants, and 15.7 pg/mL in the 0.03% group. The investigators concluded that potently lipophilic melatonin penetrates the skin, with serum blood levels increasing in a dose- and galenic-dependent manner without causing increases above the physiological range (Skin Pharmacol. Physiol. 2004;17:190-4).
In a more recent study using NC/Nga mice, researchers investigated whether melatonin inhibits the development of 2,4-dinitrofluorobenzene (DNFB)-induced atopic dermatitis-like skin lesions. Topically administered melatonin hindered ear thickness increases and skin lesions engendered by DNFB treatment. Melatonin was also found to significantly inhibit interleukin (IL)-4 and interferon (IFN)-gamma secretion by activated CD4(+) T cells from the draining lymph nodes of DNFB-treated mice, and to diminish serum total IgE levels. The investigators concluded that topically administered melatonin, by lowering total IgE in serum, and IL-4 and IFN-gamma synthesis by activated CD4(+) T cells, suppresses atopic dermatitis-like skin lesion development provoked by DNFB treatment in NC/Nga mice (J. Pineal. Res. 2009;47:324-9).
In 2006, Sener et al. studied the effects of melatonin in treating pressure ulcers in rats. Animals were treated twice daily during reperfusion periods with a locally applied ointment or received intraperitoneal administration of the antioxidant.
Topical melatonin treatment was associated with suppressed malondialdehyde levels and attenuated decreases in glutathione in the skin induced by the pressure ulcers. Melatonin treatment also prevented significant increases in alanine aminotransferase, aspartate aminotransferase, blood urea nitrogen, creatinine, lactate dehydrogenase, and collagen levels. In addition, the researchers noted degenerative changes in the dermis and epidermis of the rats, with marked decreases in tissue injury in the animals that received topical melatonin. They concluded that melatonin, delivered topically or systemically, warrants consideration as a pressure ulcer treatment (J. Pineal Res. 2006;40:280-7).
Finally, in a 2010 study Ozler et al. compared systemic and topical administration of melatonin in chronic wound models in rats with pinealectomy that suppressed basal melatonin. The researchers found that hydroxyproline levels were significantly lower in rats that underwent pinealectomy and wound formation, compared with controls (with wound formation only), with increased wound surface areas. In addition, compared with the control group, these animals exhibited increased malondialdehyde levels and decreases in superoxide dismutase and glutathione peroxidase. However, superoxide dismutase and glutathione peroxidase enzymes increased in the groups treated with melatonin, and malondialdehyde decreased.
The researchers concluded that melatonin exerts a positive effect on wound healing, as the absence of melatonin prolonged the healing process. Topical and systemic administration methods were equally effective (Scand. J. Clin. Lab. Invest. 2010;70:447-52).
Conclusion
There is a good deal of research on the biological functions of melatonin. There is also an interesting, emerging body of evidence on the dermatologic effectiveness of the topical application of this hormone. In fact, there seem to be a wide variety of potential cutaneous uses for melatonin. However, most of the clinical studies have been extremely small, including a couple of investigations that indicated no photoprotective effect associated with melatonin.
Clearly, much more research, preferably in the form of randomized double-blind studies larger than those that have thus far appeared in the literature, is necessary. But the prospect of melatonin conferring dermatologic benefits is intriguing and more than likely promising.
Melatonin (N-acetyl-5-methoxytryptamine) is a hormone produced naturally by the pineal gland in humans. Production of the hormone is stimulated by beta-adrenergic receptors. Research in recent years has offered some intriguing and in some cases promising results that may one day be utilized for dermatologic treatments and products.
Also found in various animal and plant species, melatonin is probably best known for its daily fluctuations in circulating levels that play an important role in circadian rhythms. In recent years, melatonin has been gaining increased attention in antiaging medicine and dermatology because it has been found to exert antioxidant activity, particularly against hydroxyl radicals (Hautarzt. 1999;50:5-11), the most harmful of free radicals. Melatonin levels are known to decrease with age. In addition to its antioxidative and regulatory roles, including in seasonal reproduction control, melatonin modulates the immune system and inhibits inflammation (J. Pineal Res. 2009;47:324-9).
Melatonin and UV-Induced Erythema
In 1996, Bangha et al. conducted a randomized double-blind study with 20 healthy volunteers to examine the efficacy of topically applied melatonin in hindering UV-induced erythema. Each subject was irradiated with UVB (0.099 J/cm2) on 4-cm2 areas on the lower back, and then treated with different concentrations of melatonin. The investigators observed a dose-response relationship between melatonin concentration and the degree of erythema, with significantly less redness found in the areas treated with 0.5% melatonin, compared with melatonin 0.05% or just the vehicle gel (Arch. Dermatol. Res. 1996;288:522-9).
The next year, Bangha et al. performed another randomized double-blind study on topical melatonin and its antierythema effect, this time to ascertain the role of the application time in exerting the effect. Again using 20 volunteers, the researchers treated small areas of the lower back with 0.6 mg/cm2 melatonin 15 minutes before or 1, 30, or 240 minutes after simulated UVA and UVB irradiation at twice the individual minimal erythema dose. The authors found that post-treatment with melatonin imparted no protective effect but pretreatment 15 minutes prior to irradiation yielded significant protection against erythema (Dermatology 1997;195:248-52). That same year, Bangha et al. also studied the penetration kinetics of topical melatonin in six healthy volunteers between the ages of 26 and 34 years, and found that melatonin has the potential to accumulate in the stratum corneum with extended release into the bloodstream through cutaneous delivery (Skin Pharmacol. 1997;10:298-302).
In 1998, Dreher et al. conducted a randomized double-blind study in 12 healthy adults (6 women and 6 men, all white, ranging in age from 29 to 49 years). The researchers looked at the short-term photoprotective effects of topically applied vitamin C; vitamin E; and melatnonin; alone or in combination. All formulations were applied 30 minutes after UV exposure. A dose-dependent photoprotective effect was associated with melatonin, with modest effects seen with the vitamins alone. Photoprotective activity was clearly enhanced when melatonin was combined with vitamins C and E (Br. J. Dermatol. 1998;139:332-9).
The following year, Dreher et al. performed a similar experiment to assess the short-term photoprotective effects of the same compounds. This placebo-controlled, randomized double-blind human study entailed the topical use of each antioxidant alone or in combination after UV exposure in a single application (immediately or 30 minutes after UV exposure) or in multiple applications 30 minutes, 1 hour, and 2 hours after UV exposure (totaling three applications).
Interestingly, no photoprotective effects were observed regardless of the number of applications of antioxidants. The investigators concluded that given the speed of damage to skin from UV radiation, antioxidants probably must be delivered at the appropriate site in sufficient concentrations at the outset of and during active oxidative insult (Dermatology 1999;198:52-5).
Similarly, in 2006 Howes et al. studied the effects of topical melatonin applied after solar-simulated UV exposure in 16 healthy Mantoux-positive volunteers, and found that melatonin imparted no protection against sunburn or immune suppression (Photodermatol. Photoimmunol. Photomed. 2006;22:267-9).
Antioxidant Properties
Morganti et al. conducted an 8-week placebo-controlled, randomized double-blind study on 30 xerotic female volunteers (between ages 48 and 59 years) to determine the effects of topical and systemic antioxidant-enriched formulation administration on the skin. Subjects applied a nanocolloidal gel twice daily and/or took two capsules per day of an oral diet supplement. The antioxidant-enriched formulations included vitamins C and E, alpha-lipoic acid, emblica, and melatonin.
Investigators found that oxidative stress and lipid peroxidation declined 30%-40% in the blood serum of all participants who used the topical or systemic antioxidant formulation. Those treated with the antioxidants also showed reductions in free radicals recovered in blood serum and on skin, as well as decreases in reactive oxygen species engendered by UVB irradiation of leukocytes (in vitro). The researchers concluded that the tested compounds indeed exerted topical and systemic photoprotection and represent promising ingredients for combating oxidative stress and photoaging (Int. J. Cosmet. Sci. 2002;24:331-9).
Uses of Melatonin for Skin Lesions
In 2004, Fischer et al. conducted a clinical study in 15 healthy volunteers to consider the skin penetration activity of melatonin 0.01% in a cream and 0.01% and 0.03% in a solution. In a 24-hour time window, investigators took blood samples for melatonin measurement prior to application at 9:00 a.m., as well as 1, 4, 8, and 24 hours after application. Preapplication serum melatonin levels ranged from 0.6 to 15.9 pg/mL.
The mean serum value 24 hours after application of the 0.01% melatonin cream was 9.0 pg/mL. For the 0.01% solution group, the mean melatonin level was 12.7 pg/mL 24 hours after application. Melatonin levels also markedly increased just 1 and 8 hours later in the 0.03% solution group, with cumulative melatonin noted as 7.1 pg/mL in the 0.01% cream subjects, 8.6 pg/mL in the 0.01% solution participants, and 15.7 pg/mL in the 0.03% group. The investigators concluded that potently lipophilic melatonin penetrates the skin, with serum blood levels increasing in a dose- and galenic-dependent manner without causing increases above the physiological range (Skin Pharmacol. Physiol. 2004;17:190-4).
In a more recent study using NC/Nga mice, researchers investigated whether melatonin inhibits the development of 2,4-dinitrofluorobenzene (DNFB)-induced atopic dermatitis-like skin lesions. Topically administered melatonin hindered ear thickness increases and skin lesions engendered by DNFB treatment. Melatonin was also found to significantly inhibit interleukin (IL)-4 and interferon (IFN)-gamma secretion by activated CD4(+) T cells from the draining lymph nodes of DNFB-treated mice, and to diminish serum total IgE levels. The investigators concluded that topically administered melatonin, by lowering total IgE in serum, and IL-4 and IFN-gamma synthesis by activated CD4(+) T cells, suppresses atopic dermatitis-like skin lesion development provoked by DNFB treatment in NC/Nga mice (J. Pineal. Res. 2009;47:324-9).
In 2006, Sener et al. studied the effects of melatonin in treating pressure ulcers in rats. Animals were treated twice daily during reperfusion periods with a locally applied ointment or received intraperitoneal administration of the antioxidant.
Topical melatonin treatment was associated with suppressed malondialdehyde levels and attenuated decreases in glutathione in the skin induced by the pressure ulcers. Melatonin treatment also prevented significant increases in alanine aminotransferase, aspartate aminotransferase, blood urea nitrogen, creatinine, lactate dehydrogenase, and collagen levels. In addition, the researchers noted degenerative changes in the dermis and epidermis of the rats, with marked decreases in tissue injury in the animals that received topical melatonin. They concluded that melatonin, delivered topically or systemically, warrants consideration as a pressure ulcer treatment (J. Pineal Res. 2006;40:280-7).
Finally, in a 2010 study Ozler et al. compared systemic and topical administration of melatonin in chronic wound models in rats with pinealectomy that suppressed basal melatonin. The researchers found that hydroxyproline levels were significantly lower in rats that underwent pinealectomy and wound formation, compared with controls (with wound formation only), with increased wound surface areas. In addition, compared with the control group, these animals exhibited increased malondialdehyde levels and decreases in superoxide dismutase and glutathione peroxidase. However, superoxide dismutase and glutathione peroxidase enzymes increased in the groups treated with melatonin, and malondialdehyde decreased.
The researchers concluded that melatonin exerts a positive effect on wound healing, as the absence of melatonin prolonged the healing process. Topical and systemic administration methods were equally effective (Scand. J. Clin. Lab. Invest. 2010;70:447-52).
Conclusion
There is a good deal of research on the biological functions of melatonin. There is also an interesting, emerging body of evidence on the dermatologic effectiveness of the topical application of this hormone. In fact, there seem to be a wide variety of potential cutaneous uses for melatonin. However, most of the clinical studies have been extremely small, including a couple of investigations that indicated no photoprotective effect associated with melatonin.
Clearly, much more research, preferably in the form of randomized double-blind studies larger than those that have thus far appeared in the literature, is necessary. But the prospect of melatonin conferring dermatologic benefits is intriguing and more than likely promising.
Melatonin (N-acetyl-5-methoxytryptamine) is a hormone produced naturally by the pineal gland in humans. Production of the hormone is stimulated by beta-adrenergic receptors. Research in recent years has offered some intriguing and in some cases promising results that may one day be utilized for dermatologic treatments and products.
Also found in various animal and plant species, melatonin is probably best known for its daily fluctuations in circulating levels that play an important role in circadian rhythms. In recent years, melatonin has been gaining increased attention in antiaging medicine and dermatology because it has been found to exert antioxidant activity, particularly against hydroxyl radicals (Hautarzt. 1999;50:5-11), the most harmful of free radicals. Melatonin levels are known to decrease with age. In addition to its antioxidative and regulatory roles, including in seasonal reproduction control, melatonin modulates the immune system and inhibits inflammation (J. Pineal Res. 2009;47:324-9).
Melatonin and UV-Induced Erythema
In 1996, Bangha et al. conducted a randomized double-blind study with 20 healthy volunteers to examine the efficacy of topically applied melatonin in hindering UV-induced erythema. Each subject was irradiated with UVB (0.099 J/cm2) on 4-cm2 areas on the lower back, and then treated with different concentrations of melatonin. The investigators observed a dose-response relationship between melatonin concentration and the degree of erythema, with significantly less redness found in the areas treated with 0.5% melatonin, compared with melatonin 0.05% or just the vehicle gel (Arch. Dermatol. Res. 1996;288:522-9).
The next year, Bangha et al. performed another randomized double-blind study on topical melatonin and its antierythema effect, this time to ascertain the role of the application time in exerting the effect. Again using 20 volunteers, the researchers treated small areas of the lower back with 0.6 mg/cm2 melatonin 15 minutes before or 1, 30, or 240 minutes after simulated UVA and UVB irradiation at twice the individual minimal erythema dose. The authors found that post-treatment with melatonin imparted no protective effect but pretreatment 15 minutes prior to irradiation yielded significant protection against erythema (Dermatology 1997;195:248-52). That same year, Bangha et al. also studied the penetration kinetics of topical melatonin in six healthy volunteers between the ages of 26 and 34 years, and found that melatonin has the potential to accumulate in the stratum corneum with extended release into the bloodstream through cutaneous delivery (Skin Pharmacol. 1997;10:298-302).
In 1998, Dreher et al. conducted a randomized double-blind study in 12 healthy adults (6 women and 6 men, all white, ranging in age from 29 to 49 years). The researchers looked at the short-term photoprotective effects of topically applied vitamin C; vitamin E; and melatnonin; alone or in combination. All formulations were applied 30 minutes after UV exposure. A dose-dependent photoprotective effect was associated with melatonin, with modest effects seen with the vitamins alone. Photoprotective activity was clearly enhanced when melatonin was combined with vitamins C and E (Br. J. Dermatol. 1998;139:332-9).
The following year, Dreher et al. performed a similar experiment to assess the short-term photoprotective effects of the same compounds. This placebo-controlled, randomized double-blind human study entailed the topical use of each antioxidant alone or in combination after UV exposure in a single application (immediately or 30 minutes after UV exposure) or in multiple applications 30 minutes, 1 hour, and 2 hours after UV exposure (totaling three applications).
Interestingly, no photoprotective effects were observed regardless of the number of applications of antioxidants. The investigators concluded that given the speed of damage to skin from UV radiation, antioxidants probably must be delivered at the appropriate site in sufficient concentrations at the outset of and during active oxidative insult (Dermatology 1999;198:52-5).
Similarly, in 2006 Howes et al. studied the effects of topical melatonin applied after solar-simulated UV exposure in 16 healthy Mantoux-positive volunteers, and found that melatonin imparted no protection against sunburn or immune suppression (Photodermatol. Photoimmunol. Photomed. 2006;22:267-9).
Antioxidant Properties
Morganti et al. conducted an 8-week placebo-controlled, randomized double-blind study on 30 xerotic female volunteers (between ages 48 and 59 years) to determine the effects of topical and systemic antioxidant-enriched formulation administration on the skin. Subjects applied a nanocolloidal gel twice daily and/or took two capsules per day of an oral diet supplement. The antioxidant-enriched formulations included vitamins C and E, alpha-lipoic acid, emblica, and melatonin.
Investigators found that oxidative stress and lipid peroxidation declined 30%-40% in the blood serum of all participants who used the topical or systemic antioxidant formulation. Those treated with the antioxidants also showed reductions in free radicals recovered in blood serum and on skin, as well as decreases in reactive oxygen species engendered by UVB irradiation of leukocytes (in vitro). The researchers concluded that the tested compounds indeed exerted topical and systemic photoprotection and represent promising ingredients for combating oxidative stress and photoaging (Int. J. Cosmet. Sci. 2002;24:331-9).
Uses of Melatonin for Skin Lesions
In 2004, Fischer et al. conducted a clinical study in 15 healthy volunteers to consider the skin penetration activity of melatonin 0.01% in a cream and 0.01% and 0.03% in a solution. In a 24-hour time window, investigators took blood samples for melatonin measurement prior to application at 9:00 a.m., as well as 1, 4, 8, and 24 hours after application. Preapplication serum melatonin levels ranged from 0.6 to 15.9 pg/mL.
The mean serum value 24 hours after application of the 0.01% melatonin cream was 9.0 pg/mL. For the 0.01% solution group, the mean melatonin level was 12.7 pg/mL 24 hours after application. Melatonin levels also markedly increased just 1 and 8 hours later in the 0.03% solution group, with cumulative melatonin noted as 7.1 pg/mL in the 0.01% cream subjects, 8.6 pg/mL in the 0.01% solution participants, and 15.7 pg/mL in the 0.03% group. The investigators concluded that potently lipophilic melatonin penetrates the skin, with serum blood levels increasing in a dose- and galenic-dependent manner without causing increases above the physiological range (Skin Pharmacol. Physiol. 2004;17:190-4).
In a more recent study using NC/Nga mice, researchers investigated whether melatonin inhibits the development of 2,4-dinitrofluorobenzene (DNFB)-induced atopic dermatitis-like skin lesions. Topically administered melatonin hindered ear thickness increases and skin lesions engendered by DNFB treatment. Melatonin was also found to significantly inhibit interleukin (IL)-4 and interferon (IFN)-gamma secretion by activated CD4(+) T cells from the draining lymph nodes of DNFB-treated mice, and to diminish serum total IgE levels. The investigators concluded that topically administered melatonin, by lowering total IgE in serum, and IL-4 and IFN-gamma synthesis by activated CD4(+) T cells, suppresses atopic dermatitis-like skin lesion development provoked by DNFB treatment in NC/Nga mice (J. Pineal. Res. 2009;47:324-9).
In 2006, Sener et al. studied the effects of melatonin in treating pressure ulcers in rats. Animals were treated twice daily during reperfusion periods with a locally applied ointment or received intraperitoneal administration of the antioxidant.
Topical melatonin treatment was associated with suppressed malondialdehyde levels and attenuated decreases in glutathione in the skin induced by the pressure ulcers. Melatonin treatment also prevented significant increases in alanine aminotransferase, aspartate aminotransferase, blood urea nitrogen, creatinine, lactate dehydrogenase, and collagen levels. In addition, the researchers noted degenerative changes in the dermis and epidermis of the rats, with marked decreases in tissue injury in the animals that received topical melatonin. They concluded that melatonin, delivered topically or systemically, warrants consideration as a pressure ulcer treatment (J. Pineal Res. 2006;40:280-7).
Finally, in a 2010 study Ozler et al. compared systemic and topical administration of melatonin in chronic wound models in rats with pinealectomy that suppressed basal melatonin. The researchers found that hydroxyproline levels were significantly lower in rats that underwent pinealectomy and wound formation, compared with controls (with wound formation only), with increased wound surface areas. In addition, compared with the control group, these animals exhibited increased malondialdehyde levels and decreases in superoxide dismutase and glutathione peroxidase. However, superoxide dismutase and glutathione peroxidase enzymes increased in the groups treated with melatonin, and malondialdehyde decreased.
The researchers concluded that melatonin exerts a positive effect on wound healing, as the absence of melatonin prolonged the healing process. Topical and systemic administration methods were equally effective (Scand. J. Clin. Lab. Invest. 2010;70:447-52).
Conclusion
There is a good deal of research on the biological functions of melatonin. There is also an interesting, emerging body of evidence on the dermatologic effectiveness of the topical application of this hormone. In fact, there seem to be a wide variety of potential cutaneous uses for melatonin. However, most of the clinical studies have been extremely small, including a couple of investigations that indicated no photoprotective effect associated with melatonin.
Clearly, much more research, preferably in the form of randomized double-blind studies larger than those that have thus far appeared in the literature, is necessary. But the prospect of melatonin conferring dermatologic benefits is intriguing and more than likely promising.
Body Dysmorphic Disorder Criteria May Expand in DSM-5
SAN FRANCISCO – Three criteria for diagnosing body dysmorphic disorder could increase to four under a proposal aimed at requiring that the patient demonstrate repetitive behaviors or mental acts in response to appearance concerns at some point during the course of the disorder.
Acts like mirror checking, excessive grooming, skin picking, or reassurance seeking would be considered repetitive behaviors. "Mental acts" could include comparing one's appearance with that of others, Dr. Katharine A. Phillips said at the annual meeting of the American College of Psychiatrists.

The proposed change for the fifth Diagnostic and Statistical Manual of Mental Disorders (DSM-5) would retain the three existing criteria for body dysmorphic disorder. The first criterion is a preoccupation with an imagined defect in appearance. If a slight physical anomaly is present, the person's concern is markedly excessive.
Second, the person's preoccupation causes clinically significant distress or impairment in social, occupational, or other important areas of functioning. Third, the preoccupation is not better accounted for by another mental disorder (such as anorexia nervosa, which involves dissatisfaction with body shape and size), said Dr. Phillips, director of the Body Dysmorphic Disorder Program at Rhode Island Hospital, Providence.
Making the diagnosis matters, because the disorder is common and very distressing, markedly impairing a person's functioning and quality of life, said Dr. Phillips, also professor of psychiatry and human behavior at Brown University, Providence.
The prevalence of body dysmorphic disorder has been reported as approximately 2% in nationwide epidemiologic studies, 2%-13% in nonclinical student samples, and 13%-16% in psychiatric inpatients. Suicide attempts are common, in 24%-28% of people with body dysmorphic disorder. Preliminary, unpublished data from Dr. Phillips and her associates suggest that the annual rate of completed suicides is 22-36 times higher among people with body dysmorphic disorder, compared with the general population, she said.
Body dysmorphic disorder most commonly first appears at 13 years of age. "Impulsivity and distress can quickly lead to a suicide attempt," she said. It might be equally common among males and females, or somewhat more common in females.
The obsessional, distressing preoccupation with appearance can focus on any body area but most often involves the skin, hair, and nose. Patients find it difficult to resist or control the preoccupation with appearance, which consumes 3-8 hours of their attention each day, on average. They spend much of this time in ritualistic behaviors such as checking mirrors, excessive grooming, camouflaging their alleged defect, skin picking, comparing themselves to others, and seeking reassurance about their appearance.
Accounts of body dysmorphic disorder have surfaced from around the world for more than a century, but there is little research to guide management, Dr. Phillips said. Recommended therapy starts with selective serotonin reuptake inhibitors and/or cognitive-behavioral therapy (CBT) tailored specifically to body dysmorphic disorder.
Cosmetic treatment is not recommended, whether it's dermatologic, surgical, dental, or another form. Two-thirds of people with body dysmorphic disorder already will have tried cosmetic treatment before seeing a psychiatrist, and the cosmetic treatment seems to be ineffective in 92%, some data suggest.
Two controlled studies and four open-label trials report that SSRIs are effective in 53%-77% of patients with body dysmorphic disorder (including those with delusions), though relatively high doses often are needed in at least a 12-week trial of SSRI therapy.
The recommendation for tailored CBT as a first-line treatment is backed only by data from case series and three "not well-controlled" studies that used people on waiting lists for treatment, she said. Both cognitive and behavioral elements of CBT are recommended.
Dr. Phillips highly recommended that anyone doing CBT with patients who have body dysmorphic disorder read the book "Cognitive Therapy for Suicidal Patients: Scientific and Clinical Applications" (Washington: American Psychological Association, 2008).
If first-line therapy fails, the best treatment strategies are unknown. "This is very underresearched," she said.
Monotherapy with either venlafaxine or levetiracetam seemed helpful in 17 open-label trials of each.
SSRI augmentation could be considered. Small case series suggest that buspirone might be an effective augmentation agent at average doses of 50-60 mg/day, she said. Minimal data on antipsychotics to augment SSRI therapy mostly suggest that antipsychotics are not helpful, though some clinical experience hints at a possible role for atypicals.
Other augmenting agents that have shown some promise in limited reports include clomipramine, venlafaxine, lithium, and levetiracetam. Stimulants also have had positive results.
Dr. Phillips said she has received donated medications for studies from Forest Laboratories. She also reported receiving royalties from three publishers: The Free Press, Guilford Press, and Oxford University Press.
SAN FRANCISCO – Three criteria for diagnosing body dysmorphic disorder could increase to four under a proposal aimed at requiring that the patient demonstrate repetitive behaviors or mental acts in response to appearance concerns at some point during the course of the disorder.
Acts like mirror checking, excessive grooming, skin picking, or reassurance seeking would be considered repetitive behaviors. "Mental acts" could include comparing one's appearance with that of others, Dr. Katharine A. Phillips said at the annual meeting of the American College of Psychiatrists.
The proposed change for the fifth Diagnostic and Statistical Manual of Mental Disorders (DSM-5) would retain the three existing criteria for body dysmorphic disorder. The first criterion is a preoccupation with an imagined defect in appearance. If a slight physical anomaly is present, the person's concern is markedly excessive.
Second, the person's preoccupation causes clinically significant distress or impairment in social, occupational, or other important areas of functioning. Third, the preoccupation is not better accounted for by another mental disorder (such as anorexia nervosa, which involves dissatisfaction with body shape and size), said Dr. Phillips, director of the Body Dysmorphic Disorder Program at Rhode Island Hospital, Providence.
Making the diagnosis matters, because the disorder is common and very distressing, markedly impairing a person's functioning and quality of life, said Dr. Phillips, also professor of psychiatry and human behavior at Brown University, Providence.
The prevalence of body dysmorphic disorder has been reported as approximately 2% in nationwide epidemiologic studies, 2%-13% in nonclinical student samples, and 13%-16% in psychiatric inpatients. Suicide attempts are common, in 24%-28% of people with body dysmorphic disorder. Preliminary, unpublished data from Dr. Phillips and her associates suggest that the annual rate of completed suicides is 22-36 times higher among people with body dysmorphic disorder, compared with the general population, she said.
Body dysmorphic disorder most commonly first appears at 13 years of age. "Impulsivity and distress can quickly lead to a suicide attempt," she said. It might be equally common among males and females, or somewhat more common in females.
The obsessional, distressing preoccupation with appearance can focus on any body area but most often involves the skin, hair, and nose. Patients find it difficult to resist or control the preoccupation with appearance, which consumes 3-8 hours of their attention each day, on average. They spend much of this time in ritualistic behaviors such as checking mirrors, excessive grooming, camouflaging their alleged defect, skin picking, comparing themselves to others, and seeking reassurance about their appearance.
Accounts of body dysmorphic disorder have surfaced from around the world for more than a century, but there is little research to guide management, Dr. Phillips said. Recommended therapy starts with selective serotonin reuptake inhibitors and/or cognitive-behavioral therapy (CBT) tailored specifically to body dysmorphic disorder.
Cosmetic treatment is not recommended, whether it's dermatologic, surgical, dental, or another form. Two-thirds of people with body dysmorphic disorder already will have tried cosmetic treatment before seeing a psychiatrist, and the cosmetic treatment seems to be ineffective in 92%, some data suggest.
Two controlled studies and four open-label trials report that SSRIs are effective in 53%-77% of patients with body dysmorphic disorder (including those with delusions), though relatively high doses often are needed in at least a 12-week trial of SSRI therapy.
The recommendation for tailored CBT as a first-line treatment is backed only by data from case series and three "not well-controlled" studies that used people on waiting lists for treatment, she said. Both cognitive and behavioral elements of CBT are recommended.
Dr. Phillips highly recommended that anyone doing CBT with patients who have body dysmorphic disorder read the book "Cognitive Therapy for Suicidal Patients: Scientific and Clinical Applications" (Washington: American Psychological Association, 2008).
If first-line therapy fails, the best treatment strategies are unknown. "This is very underresearched," she said.
Monotherapy with either venlafaxine or levetiracetam seemed helpful in 17 open-label trials of each.
SSRI augmentation could be considered. Small case series suggest that buspirone might be an effective augmentation agent at average doses of 50-60 mg/day, she said. Minimal data on antipsychotics to augment SSRI therapy mostly suggest that antipsychotics are not helpful, though some clinical experience hints at a possible role for atypicals.
Other augmenting agents that have shown some promise in limited reports include clomipramine, venlafaxine, lithium, and levetiracetam. Stimulants also have had positive results.
Dr. Phillips said she has received donated medications for studies from Forest Laboratories. She also reported receiving royalties from three publishers: The Free Press, Guilford Press, and Oxford University Press.
SAN FRANCISCO – Three criteria for diagnosing body dysmorphic disorder could increase to four under a proposal aimed at requiring that the patient demonstrate repetitive behaviors or mental acts in response to appearance concerns at some point during the course of the disorder.
Acts like mirror checking, excessive grooming, skin picking, or reassurance seeking would be considered repetitive behaviors. "Mental acts" could include comparing one's appearance with that of others, Dr. Katharine A. Phillips said at the annual meeting of the American College of Psychiatrists.
The proposed change for the fifth Diagnostic and Statistical Manual of Mental Disorders (DSM-5) would retain the three existing criteria for body dysmorphic disorder. The first criterion is a preoccupation with an imagined defect in appearance. If a slight physical anomaly is present, the person's concern is markedly excessive.
Second, the person's preoccupation causes clinically significant distress or impairment in social, occupational, or other important areas of functioning. Third, the preoccupation is not better accounted for by another mental disorder (such as anorexia nervosa, which involves dissatisfaction with body shape and size), said Dr. Phillips, director of the Body Dysmorphic Disorder Program at Rhode Island Hospital, Providence.
Making the diagnosis matters, because the disorder is common and very distressing, markedly impairing a person's functioning and quality of life, said Dr. Phillips, also professor of psychiatry and human behavior at Brown University, Providence.
The prevalence of body dysmorphic disorder has been reported as approximately 2% in nationwide epidemiologic studies, 2%-13% in nonclinical student samples, and 13%-16% in psychiatric inpatients. Suicide attempts are common, in 24%-28% of people with body dysmorphic disorder. Preliminary, unpublished data from Dr. Phillips and her associates suggest that the annual rate of completed suicides is 22-36 times higher among people with body dysmorphic disorder, compared with the general population, she said.
Body dysmorphic disorder most commonly first appears at 13 years of age. "Impulsivity and distress can quickly lead to a suicide attempt," she said. It might be equally common among males and females, or somewhat more common in females.
The obsessional, distressing preoccupation with appearance can focus on any body area but most often involves the skin, hair, and nose. Patients find it difficult to resist or control the preoccupation with appearance, which consumes 3-8 hours of their attention each day, on average. They spend much of this time in ritualistic behaviors such as checking mirrors, excessive grooming, camouflaging their alleged defect, skin picking, comparing themselves to others, and seeking reassurance about their appearance.
Accounts of body dysmorphic disorder have surfaced from around the world for more than a century, but there is little research to guide management, Dr. Phillips said. Recommended therapy starts with selective serotonin reuptake inhibitors and/or cognitive-behavioral therapy (CBT) tailored specifically to body dysmorphic disorder.
Cosmetic treatment is not recommended, whether it's dermatologic, surgical, dental, or another form. Two-thirds of people with body dysmorphic disorder already will have tried cosmetic treatment before seeing a psychiatrist, and the cosmetic treatment seems to be ineffective in 92%, some data suggest.
Two controlled studies and four open-label trials report that SSRIs are effective in 53%-77% of patients with body dysmorphic disorder (including those with delusions), though relatively high doses often are needed in at least a 12-week trial of SSRI therapy.
The recommendation for tailored CBT as a first-line treatment is backed only by data from case series and three "not well-controlled" studies that used people on waiting lists for treatment, she said. Both cognitive and behavioral elements of CBT are recommended.
Dr. Phillips highly recommended that anyone doing CBT with patients who have body dysmorphic disorder read the book "Cognitive Therapy for Suicidal Patients: Scientific and Clinical Applications" (Washington: American Psychological Association, 2008).
If first-line therapy fails, the best treatment strategies are unknown. "This is very underresearched," she said.
Monotherapy with either venlafaxine or levetiracetam seemed helpful in 17 open-label trials of each.
SSRI augmentation could be considered. Small case series suggest that buspirone might be an effective augmentation agent at average doses of 50-60 mg/day, she said. Minimal data on antipsychotics to augment SSRI therapy mostly suggest that antipsychotics are not helpful, though some clinical experience hints at a possible role for atypicals.
Other augmenting agents that have shown some promise in limited reports include clomipramine, venlafaxine, lithium, and levetiracetam. Stimulants also have had positive results.
Dr. Phillips said she has received donated medications for studies from Forest Laboratories. She also reported receiving royalties from three publishers: The Free Press, Guilford Press, and Oxford University Press.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF PSYCHIATRISTS
High-Dose PDT May Offer "Cure" for Acne
WAILEA, HAWAII - Aggressively dosed red light photodynamic therapy effectively destroys sebaceous glands, resulting in prolonged inhibition of sebum output and la asting cure of moderate-to-severe acne, according to Dr. R. Rox Anderson said.
"I don't use the word 'cure' lightly. I think there really are patients you can cure with high-dose aggressive photodynamic therapy. In my experience, it's more effective than oral retinoids. It's something you want to reserve for patients who have more severe acne, though," said Dr. Anderson, professor of dermatology at Harvard Medical School, Boston, and director of the Wellman Center for Photomedicine at Massachusetts General Hospital.
High-dose red light PDT needs to be employed selectively because it is a time consuming office-based procedure with substantial side effects. These include marked pain, several days of erythema and edema, crusting, sterile pustules, and sensitivity to light that keeps patients indoors for 48 hours post treatment; because of their daunting appearance, they actually welcome being temporarily shut in. Complete healing is typical a week after treatment, he explained at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
This therapy is different from the low-dose version of PDT that improves acne temporarily via its anti-inflammatory effect. High-dose red light PDT is akin to a necrotizing folliculitis that results in histologically confirmed destruction of many of the deeply placed sebaceous glands.
Having first demonstrated that high-dose red light PDT is capable of curing acne in a small clinical trial 11 years ago (J. Invest. Dermatol. 2000;15:183-92), lately, Dr. Anderson has focused on optimizing the treatment. He is varying the topical photosensitizer agent and dose, contact time, light fluence, and other factors in an effort to make a faster therapy with fewer side effects, while preserving the unmatched effectiveness.
"We're not done with this yet. We're still tweaking," he said. "This work is not funded by any drug or device company. I'm doing it because I just want to help people with severe acne. It's still the number-one disease we face. We're losing Accutane [isotretinoin] because of medicolegal issues, and we need to come up with an alternative."
An important step has been the discovery in his laboratory that low-level blue light, shined on the skin during incubation with the photosensitizing agent, appears to inhibit porphyrin synthesis selectively in the epidermis. This turns off unwanted epidermal photosensitization and greatly lessens the epidermal inflammatory reaction responsible for many of the most florid treatment side effects. At the same time, the dim blue light, which cannot penetrate far into the skin, allows continued production of porphyrin deep into the sebaceous follicles, where the red light is aimed.
"Pain scores go from 7 or 8 on a 10-point scale down to 1 or 2 with blue light," according to Dr. Anderson.
The only Food and Drug Administration-approved dermatologic indication for the two topical PDT photosensitizing agents—aminolevulinic acid (Levulan) and methyl aminolevulinate (Metvixia)—is treatment of actinic keratoses.
For dermatologists interested in using high-dose red light PDT off-label to treat severe acne, Dr. Anderson provided several practical tips. First degrease the skin, then apply the photosensitizing agent under plastic wrap occlusion for 1-3 hours with low-level blue light, and apply 5%-7% topical lidocaine 30 minutes before putting on the red PDT light for 10-30 minutes. Use a red light LED array having a 635-nm wavelength and a fluence of at least 50 J/cm2. The topical lidocaine has the side benefit of greatly enhancing the PDT response for reasons that are not understood.
Also, keep the treatment room warm. Porphyrin is the target in PDT, and porphyrin synthesis varies tremendously depending upon skin temperature. A chilly room will essentially shut it down. Dr. Anderson said he keeps the room warm and dimly lit with a low-level blue LED light source. The optimal features of the blue light in terms of wavelength and output level are still under study.
The two available photosensitizing agents appear to be essentially equivalent for this form of therapy, although methyl aminolevulinate tends to be more selective for the sebaceous glands.
The treatment course consists of four sessions at roughly 2-week intervals. The first two sessions elicit the big inflammatory reaction. The third and fourth generate only a mild sunburn-like reaction.
Asked if he is concerned about possible long-term adverse health consequences resulting from destroying sebaceous glands, Dr. Anderson said he used to be until he asked the late Dr. Albert Kligman for his thoughts.
"He said if you want to know what skin is like with no sebaceous gland function, look at any child. The glands are there but they're turned off because they haven't yet seen the androgen of puberty," recalled Dr. Anderson. "So, I think functionally, the sebaceous gland is just there as God's curse on teenagers."
A blinded, split-face comparative study of high-dose red light PDT testing various parameters is underway at Massachusetts General Hospital and should be completed in about 6 months.
Dr. Anderson has been awarded more than 60 patents and is responsible for numerous seminal advances in laser medicine. Many top laser experts have trained under him, a process they call "getting Roxified," in which they acquire a spirit of open-minded inquiry.
Dr. Anderson declared having no relevant financial interests. SDEF and this news organization are owned by Elsevier.
WAILEA, HAWAII - Aggressively dosed red light photodynamic therapy effectively destroys sebaceous glands, resulting in prolonged inhibition of sebum output and la asting cure of moderate-to-severe acne, according to Dr. R. Rox Anderson said.
"I don't use the word 'cure' lightly. I think there really are patients you can cure with high-dose aggressive photodynamic therapy. In my experience, it's more effective than oral retinoids. It's something you want to reserve for patients who have more severe acne, though," said Dr. Anderson, professor of dermatology at Harvard Medical School, Boston, and director of the Wellman Center for Photomedicine at Massachusetts General Hospital.
High-dose red light PDT needs to be employed selectively because it is a time consuming office-based procedure with substantial side effects. These include marked pain, several days of erythema and edema, crusting, sterile pustules, and sensitivity to light that keeps patients indoors for 48 hours post treatment; because of their daunting appearance, they actually welcome being temporarily shut in. Complete healing is typical a week after treatment, he explained at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
This therapy is different from the low-dose version of PDT that improves acne temporarily via its anti-inflammatory effect. High-dose red light PDT is akin to a necrotizing folliculitis that results in histologically confirmed destruction of many of the deeply placed sebaceous glands.
Having first demonstrated that high-dose red light PDT is capable of curing acne in a small clinical trial 11 years ago (J. Invest. Dermatol. 2000;15:183-92), lately, Dr. Anderson has focused on optimizing the treatment. He is varying the topical photosensitizer agent and dose, contact time, light fluence, and other factors in an effort to make a faster therapy with fewer side effects, while preserving the unmatched effectiveness.
"We're not done with this yet. We're still tweaking," he said. "This work is not funded by any drug or device company. I'm doing it because I just want to help people with severe acne. It's still the number-one disease we face. We're losing Accutane [isotretinoin] because of medicolegal issues, and we need to come up with an alternative."
An important step has been the discovery in his laboratory that low-level blue light, shined on the skin during incubation with the photosensitizing agent, appears to inhibit porphyrin synthesis selectively in the epidermis. This turns off unwanted epidermal photosensitization and greatly lessens the epidermal inflammatory reaction responsible for many of the most florid treatment side effects. At the same time, the dim blue light, which cannot penetrate far into the skin, allows continued production of porphyrin deep into the sebaceous follicles, where the red light is aimed.
"Pain scores go from 7 or 8 on a 10-point scale down to 1 or 2 with blue light," according to Dr. Anderson.
The only Food and Drug Administration-approved dermatologic indication for the two topical PDT photosensitizing agents—aminolevulinic acid (Levulan) and methyl aminolevulinate (Metvixia)—is treatment of actinic keratoses.
For dermatologists interested in using high-dose red light PDT off-label to treat severe acne, Dr. Anderson provided several practical tips. First degrease the skin, then apply the photosensitizing agent under plastic wrap occlusion for 1-3 hours with low-level blue light, and apply 5%-7% topical lidocaine 30 minutes before putting on the red PDT light for 10-30 minutes. Use a red light LED array having a 635-nm wavelength and a fluence of at least 50 J/cm2. The topical lidocaine has the side benefit of greatly enhancing the PDT response for reasons that are not understood.
Also, keep the treatment room warm. Porphyrin is the target in PDT, and porphyrin synthesis varies tremendously depending upon skin temperature. A chilly room will essentially shut it down. Dr. Anderson said he keeps the room warm and dimly lit with a low-level blue LED light source. The optimal features of the blue light in terms of wavelength and output level are still under study.
The two available photosensitizing agents appear to be essentially equivalent for this form of therapy, although methyl aminolevulinate tends to be more selective for the sebaceous glands.
The treatment course consists of four sessions at roughly 2-week intervals. The first two sessions elicit the big inflammatory reaction. The third and fourth generate only a mild sunburn-like reaction.
Asked if he is concerned about possible long-term adverse health consequences resulting from destroying sebaceous glands, Dr. Anderson said he used to be until he asked the late Dr. Albert Kligman for his thoughts.
"He said if you want to know what skin is like with no sebaceous gland function, look at any child. The glands are there but they're turned off because they haven't yet seen the androgen of puberty," recalled Dr. Anderson. "So, I think functionally, the sebaceous gland is just there as God's curse on teenagers."
A blinded, split-face comparative study of high-dose red light PDT testing various parameters is underway at Massachusetts General Hospital and should be completed in about 6 months.
Dr. Anderson has been awarded more than 60 patents and is responsible for numerous seminal advances in laser medicine. Many top laser experts have trained under him, a process they call "getting Roxified," in which they acquire a spirit of open-minded inquiry.
Dr. Anderson declared having no relevant financial interests. SDEF and this news organization are owned by Elsevier.
WAILEA, HAWAII - Aggressively dosed red light photodynamic therapy effectively destroys sebaceous glands, resulting in prolonged inhibition of sebum output and la asting cure of moderate-to-severe acne, according to Dr. R. Rox Anderson said.
"I don't use the word 'cure' lightly. I think there really are patients you can cure with high-dose aggressive photodynamic therapy. In my experience, it's more effective than oral retinoids. It's something you want to reserve for patients who have more severe acne, though," said Dr. Anderson, professor of dermatology at Harvard Medical School, Boston, and director of the Wellman Center for Photomedicine at Massachusetts General Hospital.
High-dose red light PDT needs to be employed selectively because it is a time consuming office-based procedure with substantial side effects. These include marked pain, several days of erythema and edema, crusting, sterile pustules, and sensitivity to light that keeps patients indoors for 48 hours post treatment; because of their daunting appearance, they actually welcome being temporarily shut in. Complete healing is typical a week after treatment, he explained at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
This therapy is different from the low-dose version of PDT that improves acne temporarily via its anti-inflammatory effect. High-dose red light PDT is akin to a necrotizing folliculitis that results in histologically confirmed destruction of many of the deeply placed sebaceous glands.
Having first demonstrated that high-dose red light PDT is capable of curing acne in a small clinical trial 11 years ago (J. Invest. Dermatol. 2000;15:183-92), lately, Dr. Anderson has focused on optimizing the treatment. He is varying the topical photosensitizer agent and dose, contact time, light fluence, and other factors in an effort to make a faster therapy with fewer side effects, while preserving the unmatched effectiveness.
"We're not done with this yet. We're still tweaking," he said. "This work is not funded by any drug or device company. I'm doing it because I just want to help people with severe acne. It's still the number-one disease we face. We're losing Accutane [isotretinoin] because of medicolegal issues, and we need to come up with an alternative."
An important step has been the discovery in his laboratory that low-level blue light, shined on the skin during incubation with the photosensitizing agent, appears to inhibit porphyrin synthesis selectively in the epidermis. This turns off unwanted epidermal photosensitization and greatly lessens the epidermal inflammatory reaction responsible for many of the most florid treatment side effects. At the same time, the dim blue light, which cannot penetrate far into the skin, allows continued production of porphyrin deep into the sebaceous follicles, where the red light is aimed.
"Pain scores go from 7 or 8 on a 10-point scale down to 1 or 2 with blue light," according to Dr. Anderson.
The only Food and Drug Administration-approved dermatologic indication for the two topical PDT photosensitizing agents—aminolevulinic acid (Levulan) and methyl aminolevulinate (Metvixia)—is treatment of actinic keratoses.
For dermatologists interested in using high-dose red light PDT off-label to treat severe acne, Dr. Anderson provided several practical tips. First degrease the skin, then apply the photosensitizing agent under plastic wrap occlusion for 1-3 hours with low-level blue light, and apply 5%-7% topical lidocaine 30 minutes before putting on the red PDT light for 10-30 minutes. Use a red light LED array having a 635-nm wavelength and a fluence of at least 50 J/cm2. The topical lidocaine has the side benefit of greatly enhancing the PDT response for reasons that are not understood.
Also, keep the treatment room warm. Porphyrin is the target in PDT, and porphyrin synthesis varies tremendously depending upon skin temperature. A chilly room will essentially shut it down. Dr. Anderson said he keeps the room warm and dimly lit with a low-level blue LED light source. The optimal features of the blue light in terms of wavelength and output level are still under study.
The two available photosensitizing agents appear to be essentially equivalent for this form of therapy, although methyl aminolevulinate tends to be more selective for the sebaceous glands.
The treatment course consists of four sessions at roughly 2-week intervals. The first two sessions elicit the big inflammatory reaction. The third and fourth generate only a mild sunburn-like reaction.
Asked if he is concerned about possible long-term adverse health consequences resulting from destroying sebaceous glands, Dr. Anderson said he used to be until he asked the late Dr. Albert Kligman for his thoughts.
"He said if you want to know what skin is like with no sebaceous gland function, look at any child. The glands are there but they're turned off because they haven't yet seen the androgen of puberty," recalled Dr. Anderson. "So, I think functionally, the sebaceous gland is just there as God's curse on teenagers."
A blinded, split-face comparative study of high-dose red light PDT testing various parameters is underway at Massachusetts General Hospital and should be completed in about 6 months.
Dr. Anderson has been awarded more than 60 patents and is responsible for numerous seminal advances in laser medicine. Many top laser experts have trained under him, a process they call "getting Roxified," in which they acquire a spirit of open-minded inquiry.
Dr. Anderson declared having no relevant financial interests. SDEF and this news organization are owned by Elsevier.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR
SDEF: Leg Vein Treatment Requires Algorithmic Approach
Newer agents, approaches, and techniques have made sclerotherapy more effective with fewer complications than ever before, whereas the basic goal of this therapy remains the same as it was 100 years ago, according to Dr. Margaret Mann.
Sclerotherapy remains the preferred treatment for spider and reticular veins. And with the recent Food and Drug Administration approval of polidocanol, there has been a resurgence of interest in sclerotherapy, she said at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
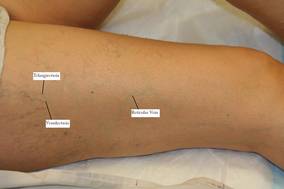
A successful outcome, however, requires the proper patient and sclerosant selection and concentration based on the size of the vessel to be treated, said Dr. Mann, codirector of dermatologic surgery and chief of clinical services in dermatology at the University of California, Irvine.
Also, because the superficial venous system is an interconnected network, the treatment of leg veins should follow a logical algorithmic approach. Patients with great saphenous vein incompetency or perforator disease, for example, should be treated with endovenous ablation and phlebectomy prior to treatment of their spider veins, she explained, noting that it is a myth that unwanted veins can be treated independently of each other.
"Indeed, treating vessels independently results in higher rates of failure, pigmentation, and matting," she said, explaining that a successful outcome requires that the most proximal point of reflux be recognized and treated.
Sclerotherapy is ideal for those with only spider veins and reticular veins, those with minimal or no symptoms, those with a history of successful sclerotherapy, and those with isolated spider veins along the lateral subdermic system.
Consider further testing prior to sclerotherapy in those with significant symptoms, veins that are refractory to multiple sclerotherapy treatments, palpable varicose veins, and/or the presence of corona phlebectasia, as these factors are suggestive of venous insufficiency. Duplex ultrasound for venous reflux should be performed in these patients to help guide treatment, she added.
In those patients for whom sclerotherapy is suitable, Dr. Mann advised using the detergent sclerosants STS (sodium tetradecyl sulfate) or polidocanol when possible for spider and reticular veins, as these are the safest and most efficacious of the FDA-approved sclerosants. Detergent sclerosants have an added advantage, as they can be made into foam.
Foam sclerosants are ideal for larger vessels because the tiny air bubbles trap the sclerosant temporarily, thus increasing contact time between the sclerosant and vein endothelium, and allowing a lower concentration and volume of foam to be used, compared with liquid sclerosant, she explained.
This in turns reduces the risk of complications such as necrosis and pigmentation.

"Match the sclerosant to the caliber of the vessel, and use the lowest effective concentration and volume to optimize outcomes and minimize side effects," she said.
Remember that the goal of sclerotherapy is to induce damage to the endothelial wall resulting in permanent fibrous occlusion of the vessel, she said, explaining that too little damage – from either low concentration or low volume of sclerosant – will result in thrombosis of the vessel, which will recanalize and be ineffective, whereas too much damage – from either high concentration or high volume of sclerosant – will cause extravasation and side effects such as necrosis and pigmentation.
Detergent sclerosants are the ideal sclerosants in most cases, with a few exceptions: For matting or fine telangiectasias, glycerin is often more effective, Dr. Mann said.
For patients with severe allergies, she recommended using hypertonic saline, as there have been documented cases of allergic reaction to both sodium tetradecyl sulfate and polidocanol.
Also, use compression (20-30 mm Hg) following sclerotherapy in all patients to minimize complications, she said.
This reduces the thrombophlebitic reaction and risk of deep vein thrombosis, increases the direct apposition of the treated vein wall, and thus enhances the effectiveness of the sclerosant while decreasing the incidence of recanalization and hyperpigmentation.
Patients' expectations can be managed by reminding them that multiple treatments are usually required, that final results may not be seen for weeks or months, and that treatment induces improvement – not perfection – and doesn't eliminate a genetic tendency to form more troublesome leg veins, she said.
Dr. Mann disclosed that she is a consultant for Bioform/Mertz Aesthetics. She discussed off-label and non–FDA approved sclerosants. SDEF and this news organization are owned by Elsevier.
Newer agents, approaches, and techniques have made sclerotherapy more effective with fewer complications than ever before, whereas the basic goal of this therapy remains the same as it was 100 years ago, according to Dr. Margaret Mann.
Sclerotherapy remains the preferred treatment for spider and reticular veins. And with the recent Food and Drug Administration approval of polidocanol, there has been a resurgence of interest in sclerotherapy, she said at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
A successful outcome, however, requires the proper patient and sclerosant selection and concentration based on the size of the vessel to be treated, said Dr. Mann, codirector of dermatologic surgery and chief of clinical services in dermatology at the University of California, Irvine.
Also, because the superficial venous system is an interconnected network, the treatment of leg veins should follow a logical algorithmic approach. Patients with great saphenous vein incompetency or perforator disease, for example, should be treated with endovenous ablation and phlebectomy prior to treatment of their spider veins, she explained, noting that it is a myth that unwanted veins can be treated independently of each other.
"Indeed, treating vessels independently results in higher rates of failure, pigmentation, and matting," she said, explaining that a successful outcome requires that the most proximal point of reflux be recognized and treated.
Sclerotherapy is ideal for those with only spider veins and reticular veins, those with minimal or no symptoms, those with a history of successful sclerotherapy, and those with isolated spider veins along the lateral subdermic system.
Consider further testing prior to sclerotherapy in those with significant symptoms, veins that are refractory to multiple sclerotherapy treatments, palpable varicose veins, and/or the presence of corona phlebectasia, as these factors are suggestive of venous insufficiency. Duplex ultrasound for venous reflux should be performed in these patients to help guide treatment, she added.
In those patients for whom sclerotherapy is suitable, Dr. Mann advised using the detergent sclerosants STS (sodium tetradecyl sulfate) or polidocanol when possible for spider and reticular veins, as these are the safest and most efficacious of the FDA-approved sclerosants. Detergent sclerosants have an added advantage, as they can be made into foam.
Foam sclerosants are ideal for larger vessels because the tiny air bubbles trap the sclerosant temporarily, thus increasing contact time between the sclerosant and vein endothelium, and allowing a lower concentration and volume of foam to be used, compared with liquid sclerosant, she explained.
This in turns reduces the risk of complications such as necrosis and pigmentation.
"Match the sclerosant to the caliber of the vessel, and use the lowest effective concentration and volume to optimize outcomes and minimize side effects," she said.
Remember that the goal of sclerotherapy is to induce damage to the endothelial wall resulting in permanent fibrous occlusion of the vessel, she said, explaining that too little damage – from either low concentration or low volume of sclerosant – will result in thrombosis of the vessel, which will recanalize and be ineffective, whereas too much damage – from either high concentration or high volume of sclerosant – will cause extravasation and side effects such as necrosis and pigmentation.
Detergent sclerosants are the ideal sclerosants in most cases, with a few exceptions: For matting or fine telangiectasias, glycerin is often more effective, Dr. Mann said.
For patients with severe allergies, she recommended using hypertonic saline, as there have been documented cases of allergic reaction to both sodium tetradecyl sulfate and polidocanol.
Also, use compression (20-30 mm Hg) following sclerotherapy in all patients to minimize complications, she said.
This reduces the thrombophlebitic reaction and risk of deep vein thrombosis, increases the direct apposition of the treated vein wall, and thus enhances the effectiveness of the sclerosant while decreasing the incidence of recanalization and hyperpigmentation.
Patients' expectations can be managed by reminding them that multiple treatments are usually required, that final results may not be seen for weeks or months, and that treatment induces improvement – not perfection – and doesn't eliminate a genetic tendency to form more troublesome leg veins, she said.
Dr. Mann disclosed that she is a consultant for Bioform/Mertz Aesthetics. She discussed off-label and non–FDA approved sclerosants. SDEF and this news organization are owned by Elsevier.
Newer agents, approaches, and techniques have made sclerotherapy more effective with fewer complications than ever before, whereas the basic goal of this therapy remains the same as it was 100 years ago, according to Dr. Margaret Mann.
Sclerotherapy remains the preferred treatment for spider and reticular veins. And with the recent Food and Drug Administration approval of polidocanol, there has been a resurgence of interest in sclerotherapy, she said at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
A successful outcome, however, requires the proper patient and sclerosant selection and concentration based on the size of the vessel to be treated, said Dr. Mann, codirector of dermatologic surgery and chief of clinical services in dermatology at the University of California, Irvine.
Also, because the superficial venous system is an interconnected network, the treatment of leg veins should follow a logical algorithmic approach. Patients with great saphenous vein incompetency or perforator disease, for example, should be treated with endovenous ablation and phlebectomy prior to treatment of their spider veins, she explained, noting that it is a myth that unwanted veins can be treated independently of each other.
"Indeed, treating vessels independently results in higher rates of failure, pigmentation, and matting," she said, explaining that a successful outcome requires that the most proximal point of reflux be recognized and treated.
Sclerotherapy is ideal for those with only spider veins and reticular veins, those with minimal or no symptoms, those with a history of successful sclerotherapy, and those with isolated spider veins along the lateral subdermic system.
Consider further testing prior to sclerotherapy in those with significant symptoms, veins that are refractory to multiple sclerotherapy treatments, palpable varicose veins, and/or the presence of corona phlebectasia, as these factors are suggestive of venous insufficiency. Duplex ultrasound for venous reflux should be performed in these patients to help guide treatment, she added.
In those patients for whom sclerotherapy is suitable, Dr. Mann advised using the detergent sclerosants STS (sodium tetradecyl sulfate) or polidocanol when possible for spider and reticular veins, as these are the safest and most efficacious of the FDA-approved sclerosants. Detergent sclerosants have an added advantage, as they can be made into foam.
Foam sclerosants are ideal for larger vessels because the tiny air bubbles trap the sclerosant temporarily, thus increasing contact time between the sclerosant and vein endothelium, and allowing a lower concentration and volume of foam to be used, compared with liquid sclerosant, she explained.
This in turns reduces the risk of complications such as necrosis and pigmentation.
"Match the sclerosant to the caliber of the vessel, and use the lowest effective concentration and volume to optimize outcomes and minimize side effects," she said.
Remember that the goal of sclerotherapy is to induce damage to the endothelial wall resulting in permanent fibrous occlusion of the vessel, she said, explaining that too little damage – from either low concentration or low volume of sclerosant – will result in thrombosis of the vessel, which will recanalize and be ineffective, whereas too much damage – from either high concentration or high volume of sclerosant – will cause extravasation and side effects such as necrosis and pigmentation.
Detergent sclerosants are the ideal sclerosants in most cases, with a few exceptions: For matting or fine telangiectasias, glycerin is often more effective, Dr. Mann said.
For patients with severe allergies, she recommended using hypertonic saline, as there have been documented cases of allergic reaction to both sodium tetradecyl sulfate and polidocanol.
Also, use compression (20-30 mm Hg) following sclerotherapy in all patients to minimize complications, she said.
This reduces the thrombophlebitic reaction and risk of deep vein thrombosis, increases the direct apposition of the treated vein wall, and thus enhances the effectiveness of the sclerosant while decreasing the incidence of recanalization and hyperpigmentation.
Patients' expectations can be managed by reminding them that multiple treatments are usually required, that final results may not be seen for weeks or months, and that treatment induces improvement – not perfection – and doesn't eliminate a genetic tendency to form more troublesome leg veins, she said.
Dr. Mann disclosed that she is a consultant for Bioform/Mertz Aesthetics. She discussed off-label and non–FDA approved sclerosants. SDEF and this news organization are owned by Elsevier.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR