User login
Reflections on My VA Experience and Why I See the Proverbial Glass as Half Full
Veterans Health Administration (VA) hospitals have received notoriety due to episodes of misdiagnosis, poor management, and negligent care described in many recent reports and news articles.1-3 While veterans are appropriately the primary focus of these investigative reports, physicians are also challenged in this setting, as they often meet resistance when advocating for patients and attempting to improve a flawed system.2 Although my residency training includes 6 months at a VA hospital mired in controversy, the hospital has played a critical role in my training.3
Despite my many frustrations with the VA and the daily stresses incurred because of barriers impeding the timing and quality of care, I have several reasons to see the glass as “half full” when reflecting on my experiences as an orthopedic surgery resident at a VA medical center. This editorial will focus on the most important of these reasons—the special opportunity and pride associated with caring for veterans and these patients’ extremely appreciative nature.
The VA is one of the largest integrated health care systems in the United States, offering both inpatient and outpatient care to eligible veterans. Although eligibility has historically been based on military service–related medical conditions, disability, and financial need, reforms from 1996 to 2002 expanded enrollment to veteran populations previously deemed ineligible for VA care.4,5 Despite this, studies suggest that some uninsured veterans do not seek VA care, even when eligible for VA coverage. This troubling notion is further complicated by research suggesting that veterans who use the VA for all of their health care are more likely to be from poor, less-educated, and minority populations, and are more likely to report fair or poor health and seek more disability days.6
Such disheartening realities can mask the most important attributes of VA patients, which pertain to their selfless commitment to our country. Orthopedic surgery residents must appreciate these attributes as well as the tremendous need for musculoskeletal care in this setting, as musculoskeletal conditions are some of the most common reasons for patient visits at the VA.7 Although combat-related high-energy blast injuries and the reconstructive procedures used to treat them have received a lot of attention, it is the more common musculoskeletal disorders that are most responsible for the tremendous burden of musculoskeletal disease in the VA. In a study by Dominick and colleagues,8 veterans had significantly greater odds of reporting doctor-diagnosed arthritis compared with nonveterans. Furthermore, veterans are also more vulnerable to overuse injuries, a finding attributed to the intense physical activity associated with military training and service.9
The busy orthopedic surgery clinic at my VA hospital is a fulfilling experience and a reminder of the large demand for musculoskeletal care. However, it is the patient population that makes it most gratifying. Most of the veterans seeking care are appreciative, regularly expressing their gratitude. They view me and the other residents as their physicians, not simply as doctors in training, like so many other non-VA patients do. Despite the fact that VA patients sometimes have to wait several hours to be seen in clinic and several months for surgery, I have never been subjected to their inevitable disdain or frustration. This is true in even the most trying and infuriating times, such as when an operation is cancelled on the day of surgery for reasons that many surgeons in non-VA hospitals would consider trivial. And even when witness to my visible irritation with the VA system, the veterans remain respectful and understanding; if they ever share similar feelings, they most certainly never voice them to me.
I cannot refute the notion that the VA must change and that the veterans deserve an improved health care system. However, this editorial is not written as a call to action. Instead, I hope it helps to humanize the patients of the VA, serving as a reminder to residents and other providers that the VA is a unique and extraordinary opportunity to give back and say thank you to veterans.
This editorial is dedicated to CPT David Huskie, USAR (Ret.), a veteran of Operation Desert Storm and orthopedic nurse at my VA hospital. It was he who first reminded me, and the other orthopedic residents, of the importance of our time at the VA. The Figure depicts the letter he gives to orthopedic residents at our program, along with a pewter coin, after their first VA rotation.
1. Pearson M. The VA’s troubled history. Cable News Network (CNN) website. http://www.cnn.com/2014/05/23/politics/va-scandals-timeline. Updated May 30, 2014. Accessed August 28, 2015.
2. Scherz H. Doctors’ war stories from VA hospitals. The Wall Street Journal website. http://www.wsj.com/articles/hal-scherz-doctors-war-stories-from-va-hospitals-1401233147. Published May 27, 2014. Accessed August 28, 2015.
3. Riviello V. Nurse exposes VA hospital: stolen drugs, tortured veterans. New York Post website. http://nypost.com/2014/07/12/nurse-exposes-va-hospital-stolen-drugs-tortured-veterans. Published July 12, 2014. Accessed August 28, 2015.
4. Enrollment—provision of hospital and outpatient care to veterans—VA. Proposed rule. Fed Regist. 1998;63(132):37299-37307.
5. US Department of Veterans Affairs, Veterans Health Administration, Office of Assistant Deputy Under Secretary for Health for Policy and Planning. 2003 Survey of Veteran Enrollees’ Health and Reliance Upon VA With Selected Comparisons to the 1999 and 2002 Surveys. US Department of Veterans Affairs website. www.va.gov/healthpolicyplanning/Docs/SOE2003_Report.pdf. Published December 2004. Accessed August 28, 2015.
6. Nelson KM, Starkebaum GA, Reiber GE. Veterans using and uninsured veterans not using Veterans Affairs (VA) health care. Public Health Rep. 2007;122(1):93-100.
7. Wasserman GM, Martin BL, Hyams KC, Merrill BR, Oaks HG, McAdoo HA. A survey of outpatient visits in a United States Army forward unit during Operation Desert Shield. Mil Med. 1997;162(6):374-379.
8. Dominick KL, Golightly YM, Jackson GL. Arthritis prevalence and symptoms among US non-veterans, veterans, and veterans receiving Department of Veterans Affairs Healthcare. J Rheumatol. 2006;33(2):348-354.
9. West SG. Rheumatic disorders during Operation Desert Storm. Arthritis Rheum. 1993;36(10):1487-1488.
Veterans Health Administration (VA) hospitals have received notoriety due to episodes of misdiagnosis, poor management, and negligent care described in many recent reports and news articles.1-3 While veterans are appropriately the primary focus of these investigative reports, physicians are also challenged in this setting, as they often meet resistance when advocating for patients and attempting to improve a flawed system.2 Although my residency training includes 6 months at a VA hospital mired in controversy, the hospital has played a critical role in my training.3
Despite my many frustrations with the VA and the daily stresses incurred because of barriers impeding the timing and quality of care, I have several reasons to see the glass as “half full” when reflecting on my experiences as an orthopedic surgery resident at a VA medical center. This editorial will focus on the most important of these reasons—the special opportunity and pride associated with caring for veterans and these patients’ extremely appreciative nature.
The VA is one of the largest integrated health care systems in the United States, offering both inpatient and outpatient care to eligible veterans. Although eligibility has historically been based on military service–related medical conditions, disability, and financial need, reforms from 1996 to 2002 expanded enrollment to veteran populations previously deemed ineligible for VA care.4,5 Despite this, studies suggest that some uninsured veterans do not seek VA care, even when eligible for VA coverage. This troubling notion is further complicated by research suggesting that veterans who use the VA for all of their health care are more likely to be from poor, less-educated, and minority populations, and are more likely to report fair or poor health and seek more disability days.6
Such disheartening realities can mask the most important attributes of VA patients, which pertain to their selfless commitment to our country. Orthopedic surgery residents must appreciate these attributes as well as the tremendous need for musculoskeletal care in this setting, as musculoskeletal conditions are some of the most common reasons for patient visits at the VA.7 Although combat-related high-energy blast injuries and the reconstructive procedures used to treat them have received a lot of attention, it is the more common musculoskeletal disorders that are most responsible for the tremendous burden of musculoskeletal disease in the VA. In a study by Dominick and colleagues,8 veterans had significantly greater odds of reporting doctor-diagnosed arthritis compared with nonveterans. Furthermore, veterans are also more vulnerable to overuse injuries, a finding attributed to the intense physical activity associated with military training and service.9
The busy orthopedic surgery clinic at my VA hospital is a fulfilling experience and a reminder of the large demand for musculoskeletal care. However, it is the patient population that makes it most gratifying. Most of the veterans seeking care are appreciative, regularly expressing their gratitude. They view me and the other residents as their physicians, not simply as doctors in training, like so many other non-VA patients do. Despite the fact that VA patients sometimes have to wait several hours to be seen in clinic and several months for surgery, I have never been subjected to their inevitable disdain or frustration. This is true in even the most trying and infuriating times, such as when an operation is cancelled on the day of surgery for reasons that many surgeons in non-VA hospitals would consider trivial. And even when witness to my visible irritation with the VA system, the veterans remain respectful and understanding; if they ever share similar feelings, they most certainly never voice them to me.
I cannot refute the notion that the VA must change and that the veterans deserve an improved health care system. However, this editorial is not written as a call to action. Instead, I hope it helps to humanize the patients of the VA, serving as a reminder to residents and other providers that the VA is a unique and extraordinary opportunity to give back and say thank you to veterans.
This editorial is dedicated to CPT David Huskie, USAR (Ret.), a veteran of Operation Desert Storm and orthopedic nurse at my VA hospital. It was he who first reminded me, and the other orthopedic residents, of the importance of our time at the VA. The Figure depicts the letter he gives to orthopedic residents at our program, along with a pewter coin, after their first VA rotation.
Veterans Health Administration (VA) hospitals have received notoriety due to episodes of misdiagnosis, poor management, and negligent care described in many recent reports and news articles.1-3 While veterans are appropriately the primary focus of these investigative reports, physicians are also challenged in this setting, as they often meet resistance when advocating for patients and attempting to improve a flawed system.2 Although my residency training includes 6 months at a VA hospital mired in controversy, the hospital has played a critical role in my training.3
Despite my many frustrations with the VA and the daily stresses incurred because of barriers impeding the timing and quality of care, I have several reasons to see the glass as “half full” when reflecting on my experiences as an orthopedic surgery resident at a VA medical center. This editorial will focus on the most important of these reasons—the special opportunity and pride associated with caring for veterans and these patients’ extremely appreciative nature.
The VA is one of the largest integrated health care systems in the United States, offering both inpatient and outpatient care to eligible veterans. Although eligibility has historically been based on military service–related medical conditions, disability, and financial need, reforms from 1996 to 2002 expanded enrollment to veteran populations previously deemed ineligible for VA care.4,5 Despite this, studies suggest that some uninsured veterans do not seek VA care, even when eligible for VA coverage. This troubling notion is further complicated by research suggesting that veterans who use the VA for all of their health care are more likely to be from poor, less-educated, and minority populations, and are more likely to report fair or poor health and seek more disability days.6
Such disheartening realities can mask the most important attributes of VA patients, which pertain to their selfless commitment to our country. Orthopedic surgery residents must appreciate these attributes as well as the tremendous need for musculoskeletal care in this setting, as musculoskeletal conditions are some of the most common reasons for patient visits at the VA.7 Although combat-related high-energy blast injuries and the reconstructive procedures used to treat them have received a lot of attention, it is the more common musculoskeletal disorders that are most responsible for the tremendous burden of musculoskeletal disease in the VA. In a study by Dominick and colleagues,8 veterans had significantly greater odds of reporting doctor-diagnosed arthritis compared with nonveterans. Furthermore, veterans are also more vulnerable to overuse injuries, a finding attributed to the intense physical activity associated with military training and service.9
The busy orthopedic surgery clinic at my VA hospital is a fulfilling experience and a reminder of the large demand for musculoskeletal care. However, it is the patient population that makes it most gratifying. Most of the veterans seeking care are appreciative, regularly expressing their gratitude. They view me and the other residents as their physicians, not simply as doctors in training, like so many other non-VA patients do. Despite the fact that VA patients sometimes have to wait several hours to be seen in clinic and several months for surgery, I have never been subjected to their inevitable disdain or frustration. This is true in even the most trying and infuriating times, such as when an operation is cancelled on the day of surgery for reasons that many surgeons in non-VA hospitals would consider trivial. And even when witness to my visible irritation with the VA system, the veterans remain respectful and understanding; if they ever share similar feelings, they most certainly never voice them to me.
I cannot refute the notion that the VA must change and that the veterans deserve an improved health care system. However, this editorial is not written as a call to action. Instead, I hope it helps to humanize the patients of the VA, serving as a reminder to residents and other providers that the VA is a unique and extraordinary opportunity to give back and say thank you to veterans.
This editorial is dedicated to CPT David Huskie, USAR (Ret.), a veteran of Operation Desert Storm and orthopedic nurse at my VA hospital. It was he who first reminded me, and the other orthopedic residents, of the importance of our time at the VA. The Figure depicts the letter he gives to orthopedic residents at our program, along with a pewter coin, after their first VA rotation.
1. Pearson M. The VA’s troubled history. Cable News Network (CNN) website. http://www.cnn.com/2014/05/23/politics/va-scandals-timeline. Updated May 30, 2014. Accessed August 28, 2015.
2. Scherz H. Doctors’ war stories from VA hospitals. The Wall Street Journal website. http://www.wsj.com/articles/hal-scherz-doctors-war-stories-from-va-hospitals-1401233147. Published May 27, 2014. Accessed August 28, 2015.
3. Riviello V. Nurse exposes VA hospital: stolen drugs, tortured veterans. New York Post website. http://nypost.com/2014/07/12/nurse-exposes-va-hospital-stolen-drugs-tortured-veterans. Published July 12, 2014. Accessed August 28, 2015.
4. Enrollment—provision of hospital and outpatient care to veterans—VA. Proposed rule. Fed Regist. 1998;63(132):37299-37307.
5. US Department of Veterans Affairs, Veterans Health Administration, Office of Assistant Deputy Under Secretary for Health for Policy and Planning. 2003 Survey of Veteran Enrollees’ Health and Reliance Upon VA With Selected Comparisons to the 1999 and 2002 Surveys. US Department of Veterans Affairs website. www.va.gov/healthpolicyplanning/Docs/SOE2003_Report.pdf. Published December 2004. Accessed August 28, 2015.
6. Nelson KM, Starkebaum GA, Reiber GE. Veterans using and uninsured veterans not using Veterans Affairs (VA) health care. Public Health Rep. 2007;122(1):93-100.
7. Wasserman GM, Martin BL, Hyams KC, Merrill BR, Oaks HG, McAdoo HA. A survey of outpatient visits in a United States Army forward unit during Operation Desert Shield. Mil Med. 1997;162(6):374-379.
8. Dominick KL, Golightly YM, Jackson GL. Arthritis prevalence and symptoms among US non-veterans, veterans, and veterans receiving Department of Veterans Affairs Healthcare. J Rheumatol. 2006;33(2):348-354.
9. West SG. Rheumatic disorders during Operation Desert Storm. Arthritis Rheum. 1993;36(10):1487-1488.
1. Pearson M. The VA’s troubled history. Cable News Network (CNN) website. http://www.cnn.com/2014/05/23/politics/va-scandals-timeline. Updated May 30, 2014. Accessed August 28, 2015.
2. Scherz H. Doctors’ war stories from VA hospitals. The Wall Street Journal website. http://www.wsj.com/articles/hal-scherz-doctors-war-stories-from-va-hospitals-1401233147. Published May 27, 2014. Accessed August 28, 2015.
3. Riviello V. Nurse exposes VA hospital: stolen drugs, tortured veterans. New York Post website. http://nypost.com/2014/07/12/nurse-exposes-va-hospital-stolen-drugs-tortured-veterans. Published July 12, 2014. Accessed August 28, 2015.
4. Enrollment—provision of hospital and outpatient care to veterans—VA. Proposed rule. Fed Regist. 1998;63(132):37299-37307.
5. US Department of Veterans Affairs, Veterans Health Administration, Office of Assistant Deputy Under Secretary for Health for Policy and Planning. 2003 Survey of Veteran Enrollees’ Health and Reliance Upon VA With Selected Comparisons to the 1999 and 2002 Surveys. US Department of Veterans Affairs website. www.va.gov/healthpolicyplanning/Docs/SOE2003_Report.pdf. Published December 2004. Accessed August 28, 2015.
6. Nelson KM, Starkebaum GA, Reiber GE. Veterans using and uninsured veterans not using Veterans Affairs (VA) health care. Public Health Rep. 2007;122(1):93-100.
7. Wasserman GM, Martin BL, Hyams KC, Merrill BR, Oaks HG, McAdoo HA. A survey of outpatient visits in a United States Army forward unit during Operation Desert Shield. Mil Med. 1997;162(6):374-379.
8. Dominick KL, Golightly YM, Jackson GL. Arthritis prevalence and symptoms among US non-veterans, veterans, and veterans receiving Department of Veterans Affairs Healthcare. J Rheumatol. 2006;33(2):348-354.
9. West SG. Rheumatic disorders during Operation Desert Storm. Arthritis Rheum. 1993;36(10):1487-1488.

Enhancing Dermatology Education: Resident Presentation Opportunities
Dermatology residency is busy with 3 years of clinical duties, academic responsibilities, and administrative work. In addition, it is a time to maximize educational experiences in dermatology from didactics to hands-on learning. It also is a time to take advantage of special opportunities that are available to residents, including attending academic meetings and giving oral and/or poster presentations. Major dermatology conferences often have designated sessions for residents that provide an excellent chance for residents to share interesting cases or present their research. This article provides a review of selected presentation opportunities available to residents at the major academic dermatology meetings.
American Academy of Dermatology
The Annual Meeting of the American Academy of Dermatology (AAD) accepts abstracts for oral presentation from both residents and fellows for its “Residents and Fellows Symposium” and “Gross and Microscopic Symposium.” The “Residents and Fellows Symposium” is an opportunity to present either clinical or laboratory research in a 9-minute oral format. Up to 20 abstracts are chosen for presentation along with 4 alternate abstracts. Furthermore, awards are given to the top 3 abstracts in both the clinical and laboratory categories. Those accepted for the “Gross and Microscopic Symposium” give a 5-minute oral presentation of a case with interesting clinical and histopathological findings. Submission guidelines for these presentations are available on the AAD Web site (https://www.aad.org/symposium/am2016).
Residents and fellows also are eligible to submit abstracts for the AAD’s electronic poster exhibits and presentations. The posters are presented electronically and are displayed and/or are available to be viewed throughout the meeting. The abstracts are blind reviewed by the Poster Exhibits Task Force on a scale from 1 (unsatisfactory) to 10 (outstanding). Presenters with abstracts that receive a passing score (2.5 or higher) by judges are allowed to discuss their poster in a live 5-minute oral presentation.
The AAD’s Summer Academy Meeting, which also takes place annually, does not have separate resident-specific poster or oral presentation sessions; however, it does offer an electronic poster exhibit and presentation session.
Pediatric Dermatology
The Annual Meeting of the Society for Pediatric Dermatology (https://pedsderm.net/meetings/annual-meeting/) accepts abstract submissions for its “Cases of the Year” session as well as poster presentations. Residents, medical students, and fellows who are chosen for a “Cases of the Year” or poster presentation are eligible for a travel award that is available on a competitive basis. The American Academy of Pediatrics’ Section on Dermatology also offers an additional travel award for a resident or fellow who presents a case or poster at the Annual Meeting of the Society for Pediatric Dermatology.
American Society for Dermatologic Surgery
The American Society for Dermatologic Surgery has an Annual Meeting (https://www.asds.net/ annualmeeting/) that includes a competitive “Resident Oral Abstracts” session. If selected, residents give a 5-minute presentation and abstracts are published in the Annual Meeting program book.
American Society of Dermatopathology
The American Society of Dermatopathology Annual Meeting has several opportunities for residents and fellows to present abstracts (https://www.asdp.org/meetings-events/annual-meeting/52nd/call-for -abtracts/). Submissions to the “General Abstracts” category are selected for either oral or poster presentation. Ambitious dermatology or pathology residents may choose to submit their case report abstracts to the “Duel in Dermatopathology” competition, which includes an oral presentation and publication of abstracts in the meeting program book. Finally, the “Dermatopathology Fellows Abstract” category is a special category for dermatopathology fellows to present an oral or poster presentation. Any resident or fellow who is accepted for oral or poster presentations is eligible for a “Physician-in-Training Award” (except winners of the “Duel in Dermatopathology” competition), which are granted to the best oral and poster presentations.
Conclusion
Beyond dermatology residency, there are many opportunities for resident education through attendance at academic meetings as well as presentation of case reports and research. The major dermatology meetings often have specific sessions to give residents a chance to share their work or interesting cases. This guide may be helpful to residents who are hoping for such venues to enhance their education and even their curriculum vitae.
Dermatology residency is busy with 3 years of clinical duties, academic responsibilities, and administrative work. In addition, it is a time to maximize educational experiences in dermatology from didactics to hands-on learning. It also is a time to take advantage of special opportunities that are available to residents, including attending academic meetings and giving oral and/or poster presentations. Major dermatology conferences often have designated sessions for residents that provide an excellent chance for residents to share interesting cases or present their research. This article provides a review of selected presentation opportunities available to residents at the major academic dermatology meetings.
American Academy of Dermatology
The Annual Meeting of the American Academy of Dermatology (AAD) accepts abstracts for oral presentation from both residents and fellows for its “Residents and Fellows Symposium” and “Gross and Microscopic Symposium.” The “Residents and Fellows Symposium” is an opportunity to present either clinical or laboratory research in a 9-minute oral format. Up to 20 abstracts are chosen for presentation along with 4 alternate abstracts. Furthermore, awards are given to the top 3 abstracts in both the clinical and laboratory categories. Those accepted for the “Gross and Microscopic Symposium” give a 5-minute oral presentation of a case with interesting clinical and histopathological findings. Submission guidelines for these presentations are available on the AAD Web site (https://www.aad.org/symposium/am2016).
Residents and fellows also are eligible to submit abstracts for the AAD’s electronic poster exhibits and presentations. The posters are presented electronically and are displayed and/or are available to be viewed throughout the meeting. The abstracts are blind reviewed by the Poster Exhibits Task Force on a scale from 1 (unsatisfactory) to 10 (outstanding). Presenters with abstracts that receive a passing score (2.5 or higher) by judges are allowed to discuss their poster in a live 5-minute oral presentation.
The AAD’s Summer Academy Meeting, which also takes place annually, does not have separate resident-specific poster or oral presentation sessions; however, it does offer an electronic poster exhibit and presentation session.
Pediatric Dermatology
The Annual Meeting of the Society for Pediatric Dermatology (https://pedsderm.net/meetings/annual-meeting/) accepts abstract submissions for its “Cases of the Year” session as well as poster presentations. Residents, medical students, and fellows who are chosen for a “Cases of the Year” or poster presentation are eligible for a travel award that is available on a competitive basis. The American Academy of Pediatrics’ Section on Dermatology also offers an additional travel award for a resident or fellow who presents a case or poster at the Annual Meeting of the Society for Pediatric Dermatology.
American Society for Dermatologic Surgery
The American Society for Dermatologic Surgery has an Annual Meeting (https://www.asds.net/ annualmeeting/) that includes a competitive “Resident Oral Abstracts” session. If selected, residents give a 5-minute presentation and abstracts are published in the Annual Meeting program book.
American Society of Dermatopathology
The American Society of Dermatopathology Annual Meeting has several opportunities for residents and fellows to present abstracts (https://www.asdp.org/meetings-events/annual-meeting/52nd/call-for -abtracts/). Submissions to the “General Abstracts” category are selected for either oral or poster presentation. Ambitious dermatology or pathology residents may choose to submit their case report abstracts to the “Duel in Dermatopathology” competition, which includes an oral presentation and publication of abstracts in the meeting program book. Finally, the “Dermatopathology Fellows Abstract” category is a special category for dermatopathology fellows to present an oral or poster presentation. Any resident or fellow who is accepted for oral or poster presentations is eligible for a “Physician-in-Training Award” (except winners of the “Duel in Dermatopathology” competition), which are granted to the best oral and poster presentations.
Conclusion
Beyond dermatology residency, there are many opportunities for resident education through attendance at academic meetings as well as presentation of case reports and research. The major dermatology meetings often have specific sessions to give residents a chance to share their work or interesting cases. This guide may be helpful to residents who are hoping for such venues to enhance their education and even their curriculum vitae.
Dermatology residency is busy with 3 years of clinical duties, academic responsibilities, and administrative work. In addition, it is a time to maximize educational experiences in dermatology from didactics to hands-on learning. It also is a time to take advantage of special opportunities that are available to residents, including attending academic meetings and giving oral and/or poster presentations. Major dermatology conferences often have designated sessions for residents that provide an excellent chance for residents to share interesting cases or present their research. This article provides a review of selected presentation opportunities available to residents at the major academic dermatology meetings.
American Academy of Dermatology
The Annual Meeting of the American Academy of Dermatology (AAD) accepts abstracts for oral presentation from both residents and fellows for its “Residents and Fellows Symposium” and “Gross and Microscopic Symposium.” The “Residents and Fellows Symposium” is an opportunity to present either clinical or laboratory research in a 9-minute oral format. Up to 20 abstracts are chosen for presentation along with 4 alternate abstracts. Furthermore, awards are given to the top 3 abstracts in both the clinical and laboratory categories. Those accepted for the “Gross and Microscopic Symposium” give a 5-minute oral presentation of a case with interesting clinical and histopathological findings. Submission guidelines for these presentations are available on the AAD Web site (https://www.aad.org/symposium/am2016).
Residents and fellows also are eligible to submit abstracts for the AAD’s electronic poster exhibits and presentations. The posters are presented electronically and are displayed and/or are available to be viewed throughout the meeting. The abstracts are blind reviewed by the Poster Exhibits Task Force on a scale from 1 (unsatisfactory) to 10 (outstanding). Presenters with abstracts that receive a passing score (2.5 or higher) by judges are allowed to discuss their poster in a live 5-minute oral presentation.
The AAD’s Summer Academy Meeting, which also takes place annually, does not have separate resident-specific poster or oral presentation sessions; however, it does offer an electronic poster exhibit and presentation session.
Pediatric Dermatology
The Annual Meeting of the Society for Pediatric Dermatology (https://pedsderm.net/meetings/annual-meeting/) accepts abstract submissions for its “Cases of the Year” session as well as poster presentations. Residents, medical students, and fellows who are chosen for a “Cases of the Year” or poster presentation are eligible for a travel award that is available on a competitive basis. The American Academy of Pediatrics’ Section on Dermatology also offers an additional travel award for a resident or fellow who presents a case or poster at the Annual Meeting of the Society for Pediatric Dermatology.
American Society for Dermatologic Surgery
The American Society for Dermatologic Surgery has an Annual Meeting (https://www.asds.net/ annualmeeting/) that includes a competitive “Resident Oral Abstracts” session. If selected, residents give a 5-minute presentation and abstracts are published in the Annual Meeting program book.
American Society of Dermatopathology
The American Society of Dermatopathology Annual Meeting has several opportunities for residents and fellows to present abstracts (https://www.asdp.org/meetings-events/annual-meeting/52nd/call-for -abtracts/). Submissions to the “General Abstracts” category are selected for either oral or poster presentation. Ambitious dermatology or pathology residents may choose to submit their case report abstracts to the “Duel in Dermatopathology” competition, which includes an oral presentation and publication of abstracts in the meeting program book. Finally, the “Dermatopathology Fellows Abstract” category is a special category for dermatopathology fellows to present an oral or poster presentation. Any resident or fellow who is accepted for oral or poster presentations is eligible for a “Physician-in-Training Award” (except winners of the “Duel in Dermatopathology” competition), which are granted to the best oral and poster presentations.
Conclusion
Beyond dermatology residency, there are many opportunities for resident education through attendance at academic meetings as well as presentation of case reports and research. The major dermatology meetings often have specific sessions to give residents a chance to share their work or interesting cases. This guide may be helpful to residents who are hoping for such venues to enhance their education and even their curriculum vitae.

A Picture Is Worth a Thousand Words: Unconscious Bias in the Residency Application Process?
Applying for a residency program can be a stressful process for medical students. It is a combination of applying for a job in the “real world” and applying to a college or medical school. In certain fields of medicine or surgery, there may be over 600 residency applications for 40 to 80 interviewee slots. Different specialties, as well as programs within a given specialty, take a different number of residents per year. This can vary from 1 to over 20 available spots, depending on the field of medicine or surgery as well as the specific program. Orthopedic surgery residencies, for example, can match between 2 and 12 residents each year. During the 2013–2014 academic year at our institution, there were over 600 applications received for approximately 50 interview slots for a class of 5 orthopedic surgery residents. Nationally, according to publicly available 2013 National Resident Matching Program (NRMP) data, a total of 1038 applicants (833 US medical school seniors) applied for 693 spots in orthopedic surgery, of which 692 were filled, indicating that orthopedic surgery remains one of the most desired fields among medical school seniors.1 Looking at the statistics provided by the NRMP data, orthopedic applicants remain some of the most competitive, with proportionally higher board scores, publication numbers, and grades, among other factors.1
Each individual program has its own method for sifting through the applications. At some institutions, the individual “in charge” of the selection committee may look through all applications initially, narrow them down, and then distribute them to the other members of the selection committee to determine the final interviewee list. At other institutions, the initial group of applications may be divided and distributed to the committee members so that each member reviews the applications and ultimately decides upon the interview candidates.
The Electronic Residency Application Service (ERAS) application includes the applicant’s name, birth city, current place of residence, education history, standardized test scores, grades achieved during medical school, letters of recommendation, personal statement, extracurricular activities, volunteer activities, research experience, and languages spoken, along with several other pieces of data, all intended to be able to give the committee a better understanding of the applicant. Interestingly, however, the application also includes a photograph of the applicant.
Countless authors have demonstrated that we make assumptions and reach conclusions without even being aware that this is occurring. This is the theory of “unconscious bias.”2-5 Unconscious bias applies to how we perceive other people, and occurs when subconscious beliefs or unrecognized stereotypes about specific characteristics, including gender, ethnicity, religion, socioeconomic status, age, and sexual orientation, result in an automatic and unconscious reaction and/or behavior.6 Unconscious bias has the ability to affect everything from how health care is delivered to how employees are hired.7-12 We are all biased, and becoming aware of our biases will help us mitigate them in the workplace.
Title VII of the Civil Rights Act of 1964 requires that employers rely solely on job-related qualifications, and not physical characteristics, in their interviewing and hiring process. The US Equal Employment Opportunity Commission (EEOC), the federal agency that enforces Title VII, includes asking for photographs during the application stage on its list of prohibited practices for employers.13 It is our belief that including a photograph in the ERAS application, prior to the selection of interview candidates, may produce unconscious bias in the decision for granting (or not granting) an interview, and this component of the application should be eliminated.
Using a wide spectrum of cultural backgrounds in employers, Dion and colleagues14 demonstrated that the “what is beautiful is good” bias is present in all cultures when prospective employees are closely matched in qualification. Attractive individuals are thought to have better professional lives and stable marital relationships and personalities, according to previous studies.14 There has been much research aimed at determining if physical attractiveness is a factor in hiring, and the evidence suggests that the more attractive the applicant is, the greater the chances of being hired.15 Specifically, Watkins and Johnston15 have found that attractive people are thought to have better personalities than less attractive people, and that a photograph can influence the hiring decision process.
Bradley Ruffle at Ben-Gurion University and Ze’ev Shtudiner at Ariel University looked at what happens when job hunters include photographs with their curricula vitae (CV), as is the norm in much of Europe and Asia.16 For over 2500 job postings, they sent 2 identical résumés: one with a photograph and one without a photograph. An equal number of male and female applicants were sent to each posting, as were an equal number of attractive and plain-looking photographs; applications without photographs were also sent as a control group. For men, the results were as expected: CVs of “attractive” men were more likely to elicit a response from the employer (19.7%) compared with those of no-picture men (13.7%) and plain-looking men (9.2%). Interestingly, men who were viewed as “plain-looking” were better off not including a photograph. For the female applicants, however, the results were unexpected: CVs of women without a picture elicited the highest response rate (16.6%), while CVs of “plain-looking” women (13.6%) and of “attractive” women (12.8%) were less likely to receive a response.16
It is an unfortunate reality that personal preference, bias, and, in some cases, discriminatory hiring practices all factor into the selection process.17 This is why, as described above, the EEOC includes asking for photographs during the application stage on its list of prohibited practices for employers.13 The EEOC website also states: “If needed for identification purposes, a photograph may be obtained after an offer of employment is made and accepted.”13 In the residency application scenario, once an applicant has been granted an interview, a photograph can be taken on the day of the interview. With so many interviewees, this may help the interviewers to remember the interviewee. At this point in the process, the applicant has already been granted the interview. The bias associated with merely looking at a photograph is thus eliminated. This is in accordance with Title VII and is clearly different than including a photograph in the initial application, which directly violates Title VII.
Reviewers of applicants may have an unconscious bias due to the applicant’s attractiveness, race, sex, ethnicity, etc. Other, subtler forms of bias may also be present. Without realizing it, people may judge the quality of the photograph, or even what the applicant was wearing in the photograph. In orthopedic surgery, for example, there may be bias in the “size” of the applicant regardless of sex. Reviewers may unconsciously think how is he/she going to hold the leg, cut a rod, reduce a hip, etc. Without even realizing it, this may sway the person reviewing the application to choose one applicant over another. This may occur regardless of the applicant’s actual qualifications as based on the previously described factors, including test scores, grades during medical school, letters of recommendation, personal statement, extracurricular activities, volunteer activities, and research experience.
Unconscious bias is present in everyone. In an ideal world, one would be able to eliminate all sources of unconscious bias in the application process. Bias due to attending an Ivy League school versus a state school, bias due to where the applicant is from, bias due to who wrote the letter of recommendation, along with various other sources of unconscious bias, would be able to be eliminated. Unfortunately, this is not possible. What is possible, however, is to remove the photograph from the application process and to comply with Title VII of the Civil Rights Act of 1964.
1. National Resident Matching Program, Data Release and Research Committee. Results of the 2013 NRMP Applicant Survey by Preferred Specialty and Applicant Type. Washington, DC: National Resident Matching Program; 2013. www.nrmp.org/wp-content/uploads/2013/08/applicantresultsbyspecialty2013.pdf. Accessed July 20, 2015.
2. Santry HP, Wren SM. The role of unconscious bias in surgical safety and outcomes. Surg Clin North Am. 2012;92(1):137–151.
3. Greenwald AG, McGhee DE, Schwartz JL. Measuring individual differences in implicit cognition: the implicit association test. J Pers Soc Psychol. 1998;74(6):1464–1480.
4. Greenwald AG, Poehlman TA, Uhlmann EL, Banaji MR. Understanding and using the Implicit Association Test: III. Meta-analysis of predictive validity. J Pers Soc Psychol. 2009;97(1):17–41.
5. Plessner H, Banse R. Attitude measurement using the Implicit Association Test (IAT). Z Exp Psychol. 2001;48(2):82–84.
6. Chapman EN, Kaatz A, Carnes M. Physicians and implicit bias: how doctors may unwittingly perpetuate health care disparities. J Gen Intern Med. 2013;28(11):1504–1510.
7. What you don’t know: the science of unconscious bias and what to do about it in the search and recruitment process [e-learning seminar]. Association of American Medical Colleges website. https://www.aamc.org/members/leadership/catalog/178420/unconscious_bias.html. Accessed July 14, 2015.
8. Haider AH, Schneider EB, Sriram N, et al. Unconscious race and class bias: its association with decision making by trauma and acute care surgeons. J Trauma Acute Care Surg. 2014;77(3):409–416.
9. Blair IV, Steiner JF, Hanratty R, et al. An investigation of associations between clinicians’ ethnic or racial bias and hypertension treatment, medication adherence and blood pressure control. J Gen Intern Med. 2014;29(7):987–995.
10. Ravenell J, Ogedegbe G. Unconscious bias and real-world hypertension outcomes: advancing disparities research. J Gen Intern Med. 2014;29(7):973–975.
11. van Ryn M, Saha S. Exploring unconscious bias in disparities research and medical education. JAMA. 2011;306(9):995–996.
12. Puhl RM, Moss-Racusin CA, Schwartz MB, Brownell KD. Weight stigmatization and bias reduction: perspectives of overweight and obese adults. Health Educ Res. 2008;23(2):347–358.
13. Prohibited employment policies/practices. US Equal Employment Opportunity Commission website. http://www.eeoc.gov/laws/practices/. Accessed July 14, 2015.
14. Dion K, Berscheid E, Walster E. What is beautiful is good. J Pers Soc Psychol. 1972;24(3):285–290.
15. Watkins LM, Johnston L. Screening job applicants: the impact of physical attractiveness and application quality. Int J Selection Assess. 2000;8(2):76–84.
16. Ruffle BJ, Shtudiner Z. Are good-looking people more employable? Manage Sci. http://dx.doi.org/10.1287/mnsc.2014.1927. Published May 29, 2014. Accessed July 14, 2015.
17. Lemay EP Jr, Clark MS, Greenberg A. What is beautiful is good because what is beautiful is desired: physical attractiveness stereotyping as projection of interpersonal goals. Pers Soc Psychol Bull. 2010;36(3):339–353.
Applying for a residency program can be a stressful process for medical students. It is a combination of applying for a job in the “real world” and applying to a college or medical school. In certain fields of medicine or surgery, there may be over 600 residency applications for 40 to 80 interviewee slots. Different specialties, as well as programs within a given specialty, take a different number of residents per year. This can vary from 1 to over 20 available spots, depending on the field of medicine or surgery as well as the specific program. Orthopedic surgery residencies, for example, can match between 2 and 12 residents each year. During the 2013–2014 academic year at our institution, there were over 600 applications received for approximately 50 interview slots for a class of 5 orthopedic surgery residents. Nationally, according to publicly available 2013 National Resident Matching Program (NRMP) data, a total of 1038 applicants (833 US medical school seniors) applied for 693 spots in orthopedic surgery, of which 692 were filled, indicating that orthopedic surgery remains one of the most desired fields among medical school seniors.1 Looking at the statistics provided by the NRMP data, orthopedic applicants remain some of the most competitive, with proportionally higher board scores, publication numbers, and grades, among other factors.1
Each individual program has its own method for sifting through the applications. At some institutions, the individual “in charge” of the selection committee may look through all applications initially, narrow them down, and then distribute them to the other members of the selection committee to determine the final interviewee list. At other institutions, the initial group of applications may be divided and distributed to the committee members so that each member reviews the applications and ultimately decides upon the interview candidates.
The Electronic Residency Application Service (ERAS) application includes the applicant’s name, birth city, current place of residence, education history, standardized test scores, grades achieved during medical school, letters of recommendation, personal statement, extracurricular activities, volunteer activities, research experience, and languages spoken, along with several other pieces of data, all intended to be able to give the committee a better understanding of the applicant. Interestingly, however, the application also includes a photograph of the applicant.
Countless authors have demonstrated that we make assumptions and reach conclusions without even being aware that this is occurring. This is the theory of “unconscious bias.”2-5 Unconscious bias applies to how we perceive other people, and occurs when subconscious beliefs or unrecognized stereotypes about specific characteristics, including gender, ethnicity, religion, socioeconomic status, age, and sexual orientation, result in an automatic and unconscious reaction and/or behavior.6 Unconscious bias has the ability to affect everything from how health care is delivered to how employees are hired.7-12 We are all biased, and becoming aware of our biases will help us mitigate them in the workplace.
Title VII of the Civil Rights Act of 1964 requires that employers rely solely on job-related qualifications, and not physical characteristics, in their interviewing and hiring process. The US Equal Employment Opportunity Commission (EEOC), the federal agency that enforces Title VII, includes asking for photographs during the application stage on its list of prohibited practices for employers.13 It is our belief that including a photograph in the ERAS application, prior to the selection of interview candidates, may produce unconscious bias in the decision for granting (or not granting) an interview, and this component of the application should be eliminated.
Using a wide spectrum of cultural backgrounds in employers, Dion and colleagues14 demonstrated that the “what is beautiful is good” bias is present in all cultures when prospective employees are closely matched in qualification. Attractive individuals are thought to have better professional lives and stable marital relationships and personalities, according to previous studies.14 There has been much research aimed at determining if physical attractiveness is a factor in hiring, and the evidence suggests that the more attractive the applicant is, the greater the chances of being hired.15 Specifically, Watkins and Johnston15 have found that attractive people are thought to have better personalities than less attractive people, and that a photograph can influence the hiring decision process.
Bradley Ruffle at Ben-Gurion University and Ze’ev Shtudiner at Ariel University looked at what happens when job hunters include photographs with their curricula vitae (CV), as is the norm in much of Europe and Asia.16 For over 2500 job postings, they sent 2 identical résumés: one with a photograph and one without a photograph. An equal number of male and female applicants were sent to each posting, as were an equal number of attractive and plain-looking photographs; applications without photographs were also sent as a control group. For men, the results were as expected: CVs of “attractive” men were more likely to elicit a response from the employer (19.7%) compared with those of no-picture men (13.7%) and plain-looking men (9.2%). Interestingly, men who were viewed as “plain-looking” were better off not including a photograph. For the female applicants, however, the results were unexpected: CVs of women without a picture elicited the highest response rate (16.6%), while CVs of “plain-looking” women (13.6%) and of “attractive” women (12.8%) were less likely to receive a response.16
It is an unfortunate reality that personal preference, bias, and, in some cases, discriminatory hiring practices all factor into the selection process.17 This is why, as described above, the EEOC includes asking for photographs during the application stage on its list of prohibited practices for employers.13 The EEOC website also states: “If needed for identification purposes, a photograph may be obtained after an offer of employment is made and accepted.”13 In the residency application scenario, once an applicant has been granted an interview, a photograph can be taken on the day of the interview. With so many interviewees, this may help the interviewers to remember the interviewee. At this point in the process, the applicant has already been granted the interview. The bias associated with merely looking at a photograph is thus eliminated. This is in accordance with Title VII and is clearly different than including a photograph in the initial application, which directly violates Title VII.
Reviewers of applicants may have an unconscious bias due to the applicant’s attractiveness, race, sex, ethnicity, etc. Other, subtler forms of bias may also be present. Without realizing it, people may judge the quality of the photograph, or even what the applicant was wearing in the photograph. In orthopedic surgery, for example, there may be bias in the “size” of the applicant regardless of sex. Reviewers may unconsciously think how is he/she going to hold the leg, cut a rod, reduce a hip, etc. Without even realizing it, this may sway the person reviewing the application to choose one applicant over another. This may occur regardless of the applicant’s actual qualifications as based on the previously described factors, including test scores, grades during medical school, letters of recommendation, personal statement, extracurricular activities, volunteer activities, and research experience.
Unconscious bias is present in everyone. In an ideal world, one would be able to eliminate all sources of unconscious bias in the application process. Bias due to attending an Ivy League school versus a state school, bias due to where the applicant is from, bias due to who wrote the letter of recommendation, along with various other sources of unconscious bias, would be able to be eliminated. Unfortunately, this is not possible. What is possible, however, is to remove the photograph from the application process and to comply with Title VII of the Civil Rights Act of 1964.
Applying for a residency program can be a stressful process for medical students. It is a combination of applying for a job in the “real world” and applying to a college or medical school. In certain fields of medicine or surgery, there may be over 600 residency applications for 40 to 80 interviewee slots. Different specialties, as well as programs within a given specialty, take a different number of residents per year. This can vary from 1 to over 20 available spots, depending on the field of medicine or surgery as well as the specific program. Orthopedic surgery residencies, for example, can match between 2 and 12 residents each year. During the 2013–2014 academic year at our institution, there were over 600 applications received for approximately 50 interview slots for a class of 5 orthopedic surgery residents. Nationally, according to publicly available 2013 National Resident Matching Program (NRMP) data, a total of 1038 applicants (833 US medical school seniors) applied for 693 spots in orthopedic surgery, of which 692 were filled, indicating that orthopedic surgery remains one of the most desired fields among medical school seniors.1 Looking at the statistics provided by the NRMP data, orthopedic applicants remain some of the most competitive, with proportionally higher board scores, publication numbers, and grades, among other factors.1
Each individual program has its own method for sifting through the applications. At some institutions, the individual “in charge” of the selection committee may look through all applications initially, narrow them down, and then distribute them to the other members of the selection committee to determine the final interviewee list. At other institutions, the initial group of applications may be divided and distributed to the committee members so that each member reviews the applications and ultimately decides upon the interview candidates.
The Electronic Residency Application Service (ERAS) application includes the applicant’s name, birth city, current place of residence, education history, standardized test scores, grades achieved during medical school, letters of recommendation, personal statement, extracurricular activities, volunteer activities, research experience, and languages spoken, along with several other pieces of data, all intended to be able to give the committee a better understanding of the applicant. Interestingly, however, the application also includes a photograph of the applicant.
Countless authors have demonstrated that we make assumptions and reach conclusions without even being aware that this is occurring. This is the theory of “unconscious bias.”2-5 Unconscious bias applies to how we perceive other people, and occurs when subconscious beliefs or unrecognized stereotypes about specific characteristics, including gender, ethnicity, religion, socioeconomic status, age, and sexual orientation, result in an automatic and unconscious reaction and/or behavior.6 Unconscious bias has the ability to affect everything from how health care is delivered to how employees are hired.7-12 We are all biased, and becoming aware of our biases will help us mitigate them in the workplace.
Title VII of the Civil Rights Act of 1964 requires that employers rely solely on job-related qualifications, and not physical characteristics, in their interviewing and hiring process. The US Equal Employment Opportunity Commission (EEOC), the federal agency that enforces Title VII, includes asking for photographs during the application stage on its list of prohibited practices for employers.13 It is our belief that including a photograph in the ERAS application, prior to the selection of interview candidates, may produce unconscious bias in the decision for granting (or not granting) an interview, and this component of the application should be eliminated.
Using a wide spectrum of cultural backgrounds in employers, Dion and colleagues14 demonstrated that the “what is beautiful is good” bias is present in all cultures when prospective employees are closely matched in qualification. Attractive individuals are thought to have better professional lives and stable marital relationships and personalities, according to previous studies.14 There has been much research aimed at determining if physical attractiveness is a factor in hiring, and the evidence suggests that the more attractive the applicant is, the greater the chances of being hired.15 Specifically, Watkins and Johnston15 have found that attractive people are thought to have better personalities than less attractive people, and that a photograph can influence the hiring decision process.
Bradley Ruffle at Ben-Gurion University and Ze’ev Shtudiner at Ariel University looked at what happens when job hunters include photographs with their curricula vitae (CV), as is the norm in much of Europe and Asia.16 For over 2500 job postings, they sent 2 identical résumés: one with a photograph and one without a photograph. An equal number of male and female applicants were sent to each posting, as were an equal number of attractive and plain-looking photographs; applications without photographs were also sent as a control group. For men, the results were as expected: CVs of “attractive” men were more likely to elicit a response from the employer (19.7%) compared with those of no-picture men (13.7%) and plain-looking men (9.2%). Interestingly, men who were viewed as “plain-looking” were better off not including a photograph. For the female applicants, however, the results were unexpected: CVs of women without a picture elicited the highest response rate (16.6%), while CVs of “plain-looking” women (13.6%) and of “attractive” women (12.8%) were less likely to receive a response.16
It is an unfortunate reality that personal preference, bias, and, in some cases, discriminatory hiring practices all factor into the selection process.17 This is why, as described above, the EEOC includes asking for photographs during the application stage on its list of prohibited practices for employers.13 The EEOC website also states: “If needed for identification purposes, a photograph may be obtained after an offer of employment is made and accepted.”13 In the residency application scenario, once an applicant has been granted an interview, a photograph can be taken on the day of the interview. With so many interviewees, this may help the interviewers to remember the interviewee. At this point in the process, the applicant has already been granted the interview. The bias associated with merely looking at a photograph is thus eliminated. This is in accordance with Title VII and is clearly different than including a photograph in the initial application, which directly violates Title VII.
Reviewers of applicants may have an unconscious bias due to the applicant’s attractiveness, race, sex, ethnicity, etc. Other, subtler forms of bias may also be present. Without realizing it, people may judge the quality of the photograph, or even what the applicant was wearing in the photograph. In orthopedic surgery, for example, there may be bias in the “size” of the applicant regardless of sex. Reviewers may unconsciously think how is he/she going to hold the leg, cut a rod, reduce a hip, etc. Without even realizing it, this may sway the person reviewing the application to choose one applicant over another. This may occur regardless of the applicant’s actual qualifications as based on the previously described factors, including test scores, grades during medical school, letters of recommendation, personal statement, extracurricular activities, volunteer activities, and research experience.
Unconscious bias is present in everyone. In an ideal world, one would be able to eliminate all sources of unconscious bias in the application process. Bias due to attending an Ivy League school versus a state school, bias due to where the applicant is from, bias due to who wrote the letter of recommendation, along with various other sources of unconscious bias, would be able to be eliminated. Unfortunately, this is not possible. What is possible, however, is to remove the photograph from the application process and to comply with Title VII of the Civil Rights Act of 1964.
1. National Resident Matching Program, Data Release and Research Committee. Results of the 2013 NRMP Applicant Survey by Preferred Specialty and Applicant Type. Washington, DC: National Resident Matching Program; 2013. www.nrmp.org/wp-content/uploads/2013/08/applicantresultsbyspecialty2013.pdf. Accessed July 20, 2015.
2. Santry HP, Wren SM. The role of unconscious bias in surgical safety and outcomes. Surg Clin North Am. 2012;92(1):137–151.
3. Greenwald AG, McGhee DE, Schwartz JL. Measuring individual differences in implicit cognition: the implicit association test. J Pers Soc Psychol. 1998;74(6):1464–1480.
4. Greenwald AG, Poehlman TA, Uhlmann EL, Banaji MR. Understanding and using the Implicit Association Test: III. Meta-analysis of predictive validity. J Pers Soc Psychol. 2009;97(1):17–41.
5. Plessner H, Banse R. Attitude measurement using the Implicit Association Test (IAT). Z Exp Psychol. 2001;48(2):82–84.
6. Chapman EN, Kaatz A, Carnes M. Physicians and implicit bias: how doctors may unwittingly perpetuate health care disparities. J Gen Intern Med. 2013;28(11):1504–1510.
7. What you don’t know: the science of unconscious bias and what to do about it in the search and recruitment process [e-learning seminar]. Association of American Medical Colleges website. https://www.aamc.org/members/leadership/catalog/178420/unconscious_bias.html. Accessed July 14, 2015.
8. Haider AH, Schneider EB, Sriram N, et al. Unconscious race and class bias: its association with decision making by trauma and acute care surgeons. J Trauma Acute Care Surg. 2014;77(3):409–416.
9. Blair IV, Steiner JF, Hanratty R, et al. An investigation of associations between clinicians’ ethnic or racial bias and hypertension treatment, medication adherence and blood pressure control. J Gen Intern Med. 2014;29(7):987–995.
10. Ravenell J, Ogedegbe G. Unconscious bias and real-world hypertension outcomes: advancing disparities research. J Gen Intern Med. 2014;29(7):973–975.
11. van Ryn M, Saha S. Exploring unconscious bias in disparities research and medical education. JAMA. 2011;306(9):995–996.
12. Puhl RM, Moss-Racusin CA, Schwartz MB, Brownell KD. Weight stigmatization and bias reduction: perspectives of overweight and obese adults. Health Educ Res. 2008;23(2):347–358.
13. Prohibited employment policies/practices. US Equal Employment Opportunity Commission website. http://www.eeoc.gov/laws/practices/. Accessed July 14, 2015.
14. Dion K, Berscheid E, Walster E. What is beautiful is good. J Pers Soc Psychol. 1972;24(3):285–290.
15. Watkins LM, Johnston L. Screening job applicants: the impact of physical attractiveness and application quality. Int J Selection Assess. 2000;8(2):76–84.
16. Ruffle BJ, Shtudiner Z. Are good-looking people more employable? Manage Sci. http://dx.doi.org/10.1287/mnsc.2014.1927. Published May 29, 2014. Accessed July 14, 2015.
17. Lemay EP Jr, Clark MS, Greenberg A. What is beautiful is good because what is beautiful is desired: physical attractiveness stereotyping as projection of interpersonal goals. Pers Soc Psychol Bull. 2010;36(3):339–353.
1. National Resident Matching Program, Data Release and Research Committee. Results of the 2013 NRMP Applicant Survey by Preferred Specialty and Applicant Type. Washington, DC: National Resident Matching Program; 2013. www.nrmp.org/wp-content/uploads/2013/08/applicantresultsbyspecialty2013.pdf. Accessed July 20, 2015.
2. Santry HP, Wren SM. The role of unconscious bias in surgical safety and outcomes. Surg Clin North Am. 2012;92(1):137–151.
3. Greenwald AG, McGhee DE, Schwartz JL. Measuring individual differences in implicit cognition: the implicit association test. J Pers Soc Psychol. 1998;74(6):1464–1480.
4. Greenwald AG, Poehlman TA, Uhlmann EL, Banaji MR. Understanding and using the Implicit Association Test: III. Meta-analysis of predictive validity. J Pers Soc Psychol. 2009;97(1):17–41.
5. Plessner H, Banse R. Attitude measurement using the Implicit Association Test (IAT). Z Exp Psychol. 2001;48(2):82–84.
6. Chapman EN, Kaatz A, Carnes M. Physicians and implicit bias: how doctors may unwittingly perpetuate health care disparities. J Gen Intern Med. 2013;28(11):1504–1510.
7. What you don’t know: the science of unconscious bias and what to do about it in the search and recruitment process [e-learning seminar]. Association of American Medical Colleges website. https://www.aamc.org/members/leadership/catalog/178420/unconscious_bias.html. Accessed July 14, 2015.
8. Haider AH, Schneider EB, Sriram N, et al. Unconscious race and class bias: its association with decision making by trauma and acute care surgeons. J Trauma Acute Care Surg. 2014;77(3):409–416.
9. Blair IV, Steiner JF, Hanratty R, et al. An investigation of associations between clinicians’ ethnic or racial bias and hypertension treatment, medication adherence and blood pressure control. J Gen Intern Med. 2014;29(7):987–995.
10. Ravenell J, Ogedegbe G. Unconscious bias and real-world hypertension outcomes: advancing disparities research. J Gen Intern Med. 2014;29(7):973–975.
11. van Ryn M, Saha S. Exploring unconscious bias in disparities research and medical education. JAMA. 2011;306(9):995–996.
12. Puhl RM, Moss-Racusin CA, Schwartz MB, Brownell KD. Weight stigmatization and bias reduction: perspectives of overweight and obese adults. Health Educ Res. 2008;23(2):347–358.
13. Prohibited employment policies/practices. US Equal Employment Opportunity Commission website. http://www.eeoc.gov/laws/practices/. Accessed July 14, 2015.
14. Dion K, Berscheid E, Walster E. What is beautiful is good. J Pers Soc Psychol. 1972;24(3):285–290.
15. Watkins LM, Johnston L. Screening job applicants: the impact of physical attractiveness and application quality. Int J Selection Assess. 2000;8(2):76–84.
16. Ruffle BJ, Shtudiner Z. Are good-looking people more employable? Manage Sci. http://dx.doi.org/10.1287/mnsc.2014.1927. Published May 29, 2014. Accessed July 14, 2015.
17. Lemay EP Jr, Clark MS, Greenberg A. What is beautiful is good because what is beautiful is desired: physical attractiveness stereotyping as projection of interpersonal goals. Pers Soc Psychol Bull. 2010;36(3):339–353.

The value and veracity of psychiatric themes depicted in modern cinema
Perhaps more than any other medical specialty, psychiatry enjoys a longstanding and, at times, complicated relationship with cinema. Recent award-winning films, such as Still Alice, Silver Linings Playbook, and Birdman: Or (The Unexpected Virtue of Ignorance) continue traditions rooted in One Flew Over the Cuckoo’s Nest, Martha Marcy May Marlene, Spellbound, and dozens of other films. Through these films, psychiatry is afforded exposure unavailable to most medical specialties. This exposure has proven to be a double-edged sword, however.
Exposure vs accurate portrayal
Relative benefits and disadvantages of psychiatry’s position in film and popular media are difficult to calculate. A film such as Still Alice can provide a vivid, concrete personal narrative of a patient with Alzheimer’s disease, equipping millions of viewers with knowledge that might otherwise remain esoteric and inaccessible. Martha Marcy May Marlene offers a similar stage for posttraumatic stress disorder (PTSD), as does Spellbound for dissociative amnesia.
Such exposure comes at a cost, inevitably, because information about psychiatry is incorporated into a dramatic storyline assembled by filmmakers who are not medical professionals and who are bound by conflicting pressures. At times, those pressures outweigh the desire to accurately portray psychiatric illness.
‘Magical realism’
Two of last year’s celebrated films, Birdman and Still Alice, have continued the longstanding tradition of portraying mental illness in film. Medicine often is touted as art and science; film likewise sits at this intersection. However, filmmakers are artists, primarily, and the nature of storytelling is to emphasize art over scientific accuracy.
The main character in Birdman, for example, manifests psychosis, but many of his presenting signs and symptoms are incongruent with any diagnosable form of psychosis. To tell its story, the film employs magical realism, a celebrated literary and film technique. Although magical realism might detract from the accuracy of the condition portrayed, it adds cinematic appeal to the film, likely creates more entertainment value, and, in turn, garners appreciation from a broader audience.
Expansion of medical information, accurate and otherwise
As in the 1970’s, we are, today, in the midst of rapidly evolving societal norms. One of the most rapid changes is in how the public acquires information. We are in the midst of the “Googlification” of medical knowledge and the expansion of online medical resources. These resources can, simultaneously, inform and mislead the public.
Popular films behave in much the same way. There is no motion picture-guild requirement that mentally ill characters in films such as Birdman meet any set of psychiatric criteria, from DSM-5 or elsewhere. Similarly, the fact that psychiatrists do not control the information in films that portray mental illness comes as no surprise.
‘One flew East, one flew West…’
The tension between engaging storytelling and medical accuracy certainly is not a new phenomenon, extending not only to representations of disease but to representations of treatment. Consider director Miloš Forman’s seminal 1975 film, One Flew Over the Cuckoo’s Nest, whose chief importance for psychiatry rests not in its individualized representations of patients but in a portrayal of the environment in which they are treated. Louise Fletcher’s Academy Award-winning portrayal of cruel Nurse Ratched has lingered in the public consciousness, remaining a prominent image for many Americans when they think of a psychiatric institution.
When Cuckoo’s Nest was released, it was considered by critics to be an “exploration of society’s enforcement of conformism” that “almost willfully overlooked the realities of mental illness”1 so that it could vivify its protagonist’s struggle against tyrannical Nurse Ratched. The film’s primary intent might not have been to make a statement about the injustices of the time, but it has certainly had a lasting effect on the public’s perception of psychiatric illness and treatment.
Films offer an opportunity for discussion
Films on the theme of psychiatry and mental illness have long held a distinctive position in the canon of Western cinema. In this vein, films from the past year have made timely contributions to the genre. Although Still Alice and Birdman might prove to be ground-breaking in changing societal views over time, we must not expect them to do so.
Nevertheless, psychiatry ought to take advantage of popular films’ wide exposure and ability to destigmatize mental illness—rather than lament medical inaccuracies in these films.
Cinema is, first and foremost, an art. Although patients and the public might pick up misconceptions about psychosis, Alzheimer’s disease, or PTSD because popular films take artistic liberty about mental illness, psychiatrists are available to set the record straight. After all, psychiatry has long been about managing perceptions, and patient education is at the core of our specialty.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Reference
1. Ebert R. “One Flew Over The Cuckoo’s Nest (review). http://www.rogerebert.com/reviews/great-movie-one-flew-overthe-cuckoos-nest-1975. February 2, 2003. Accessed September 9, 2015.
Perhaps more than any other medical specialty, psychiatry enjoys a longstanding and, at times, complicated relationship with cinema. Recent award-winning films, such as Still Alice, Silver Linings Playbook, and Birdman: Or (The Unexpected Virtue of Ignorance) continue traditions rooted in One Flew Over the Cuckoo’s Nest, Martha Marcy May Marlene, Spellbound, and dozens of other films. Through these films, psychiatry is afforded exposure unavailable to most medical specialties. This exposure has proven to be a double-edged sword, however.
Exposure vs accurate portrayal
Relative benefits and disadvantages of psychiatry’s position in film and popular media are difficult to calculate. A film such as Still Alice can provide a vivid, concrete personal narrative of a patient with Alzheimer’s disease, equipping millions of viewers with knowledge that might otherwise remain esoteric and inaccessible. Martha Marcy May Marlene offers a similar stage for posttraumatic stress disorder (PTSD), as does Spellbound for dissociative amnesia.
Such exposure comes at a cost, inevitably, because information about psychiatry is incorporated into a dramatic storyline assembled by filmmakers who are not medical professionals and who are bound by conflicting pressures. At times, those pressures outweigh the desire to accurately portray psychiatric illness.
‘Magical realism’
Two of last year’s celebrated films, Birdman and Still Alice, have continued the longstanding tradition of portraying mental illness in film. Medicine often is touted as art and science; film likewise sits at this intersection. However, filmmakers are artists, primarily, and the nature of storytelling is to emphasize art over scientific accuracy.
The main character in Birdman, for example, manifests psychosis, but many of his presenting signs and symptoms are incongruent with any diagnosable form of psychosis. To tell its story, the film employs magical realism, a celebrated literary and film technique. Although magical realism might detract from the accuracy of the condition portrayed, it adds cinematic appeal to the film, likely creates more entertainment value, and, in turn, garners appreciation from a broader audience.
Expansion of medical information, accurate and otherwise
As in the 1970’s, we are, today, in the midst of rapidly evolving societal norms. One of the most rapid changes is in how the public acquires information. We are in the midst of the “Googlification” of medical knowledge and the expansion of online medical resources. These resources can, simultaneously, inform and mislead the public.
Popular films behave in much the same way. There is no motion picture-guild requirement that mentally ill characters in films such as Birdman meet any set of psychiatric criteria, from DSM-5 or elsewhere. Similarly, the fact that psychiatrists do not control the information in films that portray mental illness comes as no surprise.
‘One flew East, one flew West…’
The tension between engaging storytelling and medical accuracy certainly is not a new phenomenon, extending not only to representations of disease but to representations of treatment. Consider director Miloš Forman’s seminal 1975 film, One Flew Over the Cuckoo’s Nest, whose chief importance for psychiatry rests not in its individualized representations of patients but in a portrayal of the environment in which they are treated. Louise Fletcher’s Academy Award-winning portrayal of cruel Nurse Ratched has lingered in the public consciousness, remaining a prominent image for many Americans when they think of a psychiatric institution.
When Cuckoo’s Nest was released, it was considered by critics to be an “exploration of society’s enforcement of conformism” that “almost willfully overlooked the realities of mental illness”1 so that it could vivify its protagonist’s struggle against tyrannical Nurse Ratched. The film’s primary intent might not have been to make a statement about the injustices of the time, but it has certainly had a lasting effect on the public’s perception of psychiatric illness and treatment.
Films offer an opportunity for discussion
Films on the theme of psychiatry and mental illness have long held a distinctive position in the canon of Western cinema. In this vein, films from the past year have made timely contributions to the genre. Although Still Alice and Birdman might prove to be ground-breaking in changing societal views over time, we must not expect them to do so.
Nevertheless, psychiatry ought to take advantage of popular films’ wide exposure and ability to destigmatize mental illness—rather than lament medical inaccuracies in these films.
Cinema is, first and foremost, an art. Although patients and the public might pick up misconceptions about psychosis, Alzheimer’s disease, or PTSD because popular films take artistic liberty about mental illness, psychiatrists are available to set the record straight. After all, psychiatry has long been about managing perceptions, and patient education is at the core of our specialty.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Perhaps more than any other medical specialty, psychiatry enjoys a longstanding and, at times, complicated relationship with cinema. Recent award-winning films, such as Still Alice, Silver Linings Playbook, and Birdman: Or (The Unexpected Virtue of Ignorance) continue traditions rooted in One Flew Over the Cuckoo’s Nest, Martha Marcy May Marlene, Spellbound, and dozens of other films. Through these films, psychiatry is afforded exposure unavailable to most medical specialties. This exposure has proven to be a double-edged sword, however.
Exposure vs accurate portrayal
Relative benefits and disadvantages of psychiatry’s position in film and popular media are difficult to calculate. A film such as Still Alice can provide a vivid, concrete personal narrative of a patient with Alzheimer’s disease, equipping millions of viewers with knowledge that might otherwise remain esoteric and inaccessible. Martha Marcy May Marlene offers a similar stage for posttraumatic stress disorder (PTSD), as does Spellbound for dissociative amnesia.
Such exposure comes at a cost, inevitably, because information about psychiatry is incorporated into a dramatic storyline assembled by filmmakers who are not medical professionals and who are bound by conflicting pressures. At times, those pressures outweigh the desire to accurately portray psychiatric illness.
‘Magical realism’
Two of last year’s celebrated films, Birdman and Still Alice, have continued the longstanding tradition of portraying mental illness in film. Medicine often is touted as art and science; film likewise sits at this intersection. However, filmmakers are artists, primarily, and the nature of storytelling is to emphasize art over scientific accuracy.
The main character in Birdman, for example, manifests psychosis, but many of his presenting signs and symptoms are incongruent with any diagnosable form of psychosis. To tell its story, the film employs magical realism, a celebrated literary and film technique. Although magical realism might detract from the accuracy of the condition portrayed, it adds cinematic appeal to the film, likely creates more entertainment value, and, in turn, garners appreciation from a broader audience.
Expansion of medical information, accurate and otherwise
As in the 1970’s, we are, today, in the midst of rapidly evolving societal norms. One of the most rapid changes is in how the public acquires information. We are in the midst of the “Googlification” of medical knowledge and the expansion of online medical resources. These resources can, simultaneously, inform and mislead the public.
Popular films behave in much the same way. There is no motion picture-guild requirement that mentally ill characters in films such as Birdman meet any set of psychiatric criteria, from DSM-5 or elsewhere. Similarly, the fact that psychiatrists do not control the information in films that portray mental illness comes as no surprise.
‘One flew East, one flew West…’
The tension between engaging storytelling and medical accuracy certainly is not a new phenomenon, extending not only to representations of disease but to representations of treatment. Consider director Miloš Forman’s seminal 1975 film, One Flew Over the Cuckoo’s Nest, whose chief importance for psychiatry rests not in its individualized representations of patients but in a portrayal of the environment in which they are treated. Louise Fletcher’s Academy Award-winning portrayal of cruel Nurse Ratched has lingered in the public consciousness, remaining a prominent image for many Americans when they think of a psychiatric institution.
When Cuckoo’s Nest was released, it was considered by critics to be an “exploration of society’s enforcement of conformism” that “almost willfully overlooked the realities of mental illness”1 so that it could vivify its protagonist’s struggle against tyrannical Nurse Ratched. The film’s primary intent might not have been to make a statement about the injustices of the time, but it has certainly had a lasting effect on the public’s perception of psychiatric illness and treatment.
Films offer an opportunity for discussion
Films on the theme of psychiatry and mental illness have long held a distinctive position in the canon of Western cinema. In this vein, films from the past year have made timely contributions to the genre. Although Still Alice and Birdman might prove to be ground-breaking in changing societal views over time, we must not expect them to do so.
Nevertheless, psychiatry ought to take advantage of popular films’ wide exposure and ability to destigmatize mental illness—rather than lament medical inaccuracies in these films.
Cinema is, first and foremost, an art. Although patients and the public might pick up misconceptions about psychosis, Alzheimer’s disease, or PTSD because popular films take artistic liberty about mental illness, psychiatrists are available to set the record straight. After all, psychiatry has long been about managing perceptions, and patient education is at the core of our specialty.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Reference
1. Ebert R. “One Flew Over The Cuckoo’s Nest (review). http://www.rogerebert.com/reviews/great-movie-one-flew-overthe-cuckoos-nest-1975. February 2, 2003. Accessed September 9, 2015.
Reference
1. Ebert R. “One Flew Over The Cuckoo’s Nest (review). http://www.rogerebert.com/reviews/great-movie-one-flew-overthe-cuckoos-nest-1975. February 2, 2003. Accessed September 9, 2015.

Don’t Forget About Syphilis
Case Report
A 42-year-old man presented to our dermatology clinic for evaluation of “dark spots” on both hands for 2 months (Figure 1). He had been treated 1 month earlier with various topical agents, including mid-potency steroids and lightening agents, and had not seen a change. Interestingly, he reported recent-onset of similar lesions on the feet (Figure 2). Initially, our differential diagnosis indicated some form of postinflammatory hyperpigmentation, but the recent onset of the lesions on the feet 1 week prior, the distribution of the lesions, and the absence of an inciting factor did not fit the clinical picture. Among various laboratory tests, rapid plasma reagin was positive, and the patient was appropriately diagnosed and treated for secondary syphilis with 2.4 million U of benzathine penicillin.

|

|
The Great Masquerader
Syphilis has been called “the great masquerader” or “the great imitator” because it is protean in appearance, manifests in different stages, and can affect different parts of the body.1 In fact, another case of secondary syphilis I saw prior to this patient appeared different. Secondary syphilis has variable clinical presentations and thus is difficult to recognize. It is estimated that approximately half of community physicians will not clinically suspect secondary syphilis.2
Resurgence of Syphilis
It is not every day that you may diagnose syphilis in an outpatient clinic or consultation service, but it recently has been making resurgence, particularly in inner-city settings. Although syphilis is one of the oldest sexually transmitted diseases and has established and effective treatment options, it is now reemerging as a major public health problem in urban communities. A 2001 study by Williams and Ekundayo3 evaluated the distribution of and factors affecting the syphilis epidemic among inner-city minorities in Baltimore, Maryland, and found that it was the city with the highest number of syphilis cases in the nation, surpassing the national average of 2.6 cases per 100,000 population. The factors that particularly favored syphilis infectivity were poverty, poor communication with health care providers, exchanging sex for drugs, lower educational background, and inadequate health education.3 Although syphilis should not be forgotten as part of a differential diagnosis, preventative health education should be undertaken.
Diagnostic Approach
The best way to approach a possible case of syphilis is to have a high index of suspicion (Table). The skin findings of secondary syphilis may mimic other skin conditions (as described above), including pityriasis rosea, erythema multiforme, drug reactions, psoriasis, pityriasis lichenoides et varioliformis acuta, and dyshidrotic eczema, among others. Although the disease usually begins approximately 6 weeks after the onset of a primary chancre, approximately 25% of patients with secondary syphilis will not recall a chancre, and in other cases, the primary chancre will still be present.5 The case reported above did not have any other associated symptoms, but commonly reported symptoms in other cases have included headaches, fevers, pruritus, loss of appetite, and malaise.6
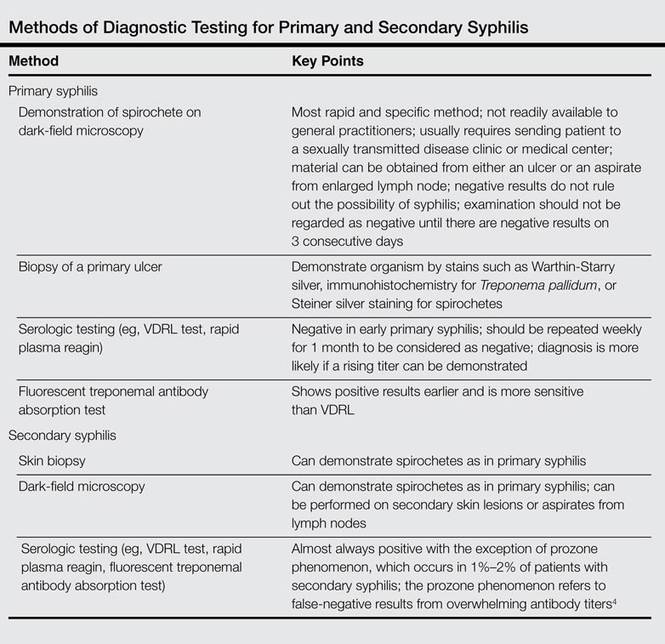
Clinical Features of Secondary Syphilis
Usually, the lesions of syphiloderms consist of variably scaly macules and papules that can be annular, pustular, or psoriasiform. They typically are widespread and symmetric, though in some cases they can remain localized. The appearance also may vary depending on immunocompromised status, which may cause a more aggressive and quicker appearance of the rash.
The Connection to Human Immunodeficiency Virus and AIDS
It is known that patients with syphilis have an increased incidence of other sexually transmitted infections such as venereal warts, gonorrhea, and human immunodeficiency virus (HIV) infection, thus patients should be tested for these conditions as part of their course of treatment. It has been shown that cutaneous sores/chancres facilitate transmission and acquisition of HIV infection. The risk for acquiring HIV increases 2- to 5-fold if exposure occurs when syphilis is present.7 Additionally, syphilis will increase viral loads in patients who are already infected with HIV. These data are concerning, particularly because many patients with syphilis also are infected with HIV.8
Final Thoughts
Although syphilis is known to present with highly variable clinical presentations, early diagnosis, appropriate treatment, and patient education are crucial to avoid further complications.9 Social factors have contributed to a resurgence of syphilis; although easily treatable, it can lead to great suffering and morbidity. In summary, syphilis is a treatable infectious disease and physicians should test for it when investigating a patient, particularly one with risk factors as well as a symmetric hyperpigmented rash on the acral surfaces. There are uncommon presentations of syphilis, thus it is important to consider it early on and treat appropriately to prevent life-threatening complications.
1. Tampa M, Sarbu I, Matei C, et al. Brief history of syphilis. J Med Life. 2014;7:4-10.
2. Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2007. Atlanta, GA: US Department of Health and Human Services; 2008.
3. Williams PB, Ekundayo O. Study of distribution and factors affecting syphilis epidemic among inner-city minorities of Baltimore. Public Health. 2001;115:387-393.
4. Ruchi S, Mangala HC, Murugesh SB, et al. Prozone phenomenon in secondary syphilis. Indian J Sex Trans Dis. 2011;32:47-49.
5. Lee V, Kinghorn G. Syphilis: an update. Clin Med. 2008;8:330-333.
6. Chapel TA. The signs and symptoms of secondary syphilis. Sex Transm Dis. 1980;7:161-164.
7. Bolan G. Syphilis and HIV: a dangerous duo affecting gay and bisexual men. https://blog.aids.gov/2012/12/ syphilis-and-hiv-a-dangerous-duo-affecting-gay-and -bisexual-men.html. Published December 13, 2012. Accessed August 19, 2015.
8. Zetola NM, Klausner JD. Syphilis and HIV infection: an update. Clin Infect Dis. 2007;44:1222-1228.
9. Green CB, Fitzpatrick J. Syphilis. In: Fitzpatrick J, Morelli J, eds. Dermatology Secrets Plus. Philadelphia, PA: Elsevier Mosby; 2011:195-200.
Case Report
A 42-year-old man presented to our dermatology clinic for evaluation of “dark spots” on both hands for 2 months (Figure 1). He had been treated 1 month earlier with various topical agents, including mid-potency steroids and lightening agents, and had not seen a change. Interestingly, he reported recent-onset of similar lesions on the feet (Figure 2). Initially, our differential diagnosis indicated some form of postinflammatory hyperpigmentation, but the recent onset of the lesions on the feet 1 week prior, the distribution of the lesions, and the absence of an inciting factor did not fit the clinical picture. Among various laboratory tests, rapid plasma reagin was positive, and the patient was appropriately diagnosed and treated for secondary syphilis with 2.4 million U of benzathine penicillin.
|
|
|
|
The Great Masquerader
Syphilis has been called “the great masquerader” or “the great imitator” because it is protean in appearance, manifests in different stages, and can affect different parts of the body.1 In fact, another case of secondary syphilis I saw prior to this patient appeared different. Secondary syphilis has variable clinical presentations and thus is difficult to recognize. It is estimated that approximately half of community physicians will not clinically suspect secondary syphilis.2
Resurgence of Syphilis
It is not every day that you may diagnose syphilis in an outpatient clinic or consultation service, but it recently has been making resurgence, particularly in inner-city settings. Although syphilis is one of the oldest sexually transmitted diseases and has established and effective treatment options, it is now reemerging as a major public health problem in urban communities. A 2001 study by Williams and Ekundayo3 evaluated the distribution of and factors affecting the syphilis epidemic among inner-city minorities in Baltimore, Maryland, and found that it was the city with the highest number of syphilis cases in the nation, surpassing the national average of 2.6 cases per 100,000 population. The factors that particularly favored syphilis infectivity were poverty, poor communication with health care providers, exchanging sex for drugs, lower educational background, and inadequate health education.3 Although syphilis should not be forgotten as part of a differential diagnosis, preventative health education should be undertaken.
Diagnostic Approach
The best way to approach a possible case of syphilis is to have a high index of suspicion (Table). The skin findings of secondary syphilis may mimic other skin conditions (as described above), including pityriasis rosea, erythema multiforme, drug reactions, psoriasis, pityriasis lichenoides et varioliformis acuta, and dyshidrotic eczema, among others. Although the disease usually begins approximately 6 weeks after the onset of a primary chancre, approximately 25% of patients with secondary syphilis will not recall a chancre, and in other cases, the primary chancre will still be present.5 The case reported above did not have any other associated symptoms, but commonly reported symptoms in other cases have included headaches, fevers, pruritus, loss of appetite, and malaise.6
Clinical Features of Secondary Syphilis
Usually, the lesions of syphiloderms consist of variably scaly macules and papules that can be annular, pustular, or psoriasiform. They typically are widespread and symmetric, though in some cases they can remain localized. The appearance also may vary depending on immunocompromised status, which may cause a more aggressive and quicker appearance of the rash.
The Connection to Human Immunodeficiency Virus and AIDS
It is known that patients with syphilis have an increased incidence of other sexually transmitted infections such as venereal warts, gonorrhea, and human immunodeficiency virus (HIV) infection, thus patients should be tested for these conditions as part of their course of treatment. It has been shown that cutaneous sores/chancres facilitate transmission and acquisition of HIV infection. The risk for acquiring HIV increases 2- to 5-fold if exposure occurs when syphilis is present.7 Additionally, syphilis will increase viral loads in patients who are already infected with HIV. These data are concerning, particularly because many patients with syphilis also are infected with HIV.8
Final Thoughts
Although syphilis is known to present with highly variable clinical presentations, early diagnosis, appropriate treatment, and patient education are crucial to avoid further complications.9 Social factors have contributed to a resurgence of syphilis; although easily treatable, it can lead to great suffering and morbidity. In summary, syphilis is a treatable infectious disease and physicians should test for it when investigating a patient, particularly one with risk factors as well as a symmetric hyperpigmented rash on the acral surfaces. There are uncommon presentations of syphilis, thus it is important to consider it early on and treat appropriately to prevent life-threatening complications.
Case Report
A 42-year-old man presented to our dermatology clinic for evaluation of “dark spots” on both hands for 2 months (Figure 1). He had been treated 1 month earlier with various topical agents, including mid-potency steroids and lightening agents, and had not seen a change. Interestingly, he reported recent-onset of similar lesions on the feet (Figure 2). Initially, our differential diagnosis indicated some form of postinflammatory hyperpigmentation, but the recent onset of the lesions on the feet 1 week prior, the distribution of the lesions, and the absence of an inciting factor did not fit the clinical picture. Among various laboratory tests, rapid plasma reagin was positive, and the patient was appropriately diagnosed and treated for secondary syphilis with 2.4 million U of benzathine penicillin.
|
|
|
|
The Great Masquerader
Syphilis has been called “the great masquerader” or “the great imitator” because it is protean in appearance, manifests in different stages, and can affect different parts of the body.1 In fact, another case of secondary syphilis I saw prior to this patient appeared different. Secondary syphilis has variable clinical presentations and thus is difficult to recognize. It is estimated that approximately half of community physicians will not clinically suspect secondary syphilis.2
Resurgence of Syphilis
It is not every day that you may diagnose syphilis in an outpatient clinic or consultation service, but it recently has been making resurgence, particularly in inner-city settings. Although syphilis is one of the oldest sexually transmitted diseases and has established and effective treatment options, it is now reemerging as a major public health problem in urban communities. A 2001 study by Williams and Ekundayo3 evaluated the distribution of and factors affecting the syphilis epidemic among inner-city minorities in Baltimore, Maryland, and found that it was the city with the highest number of syphilis cases in the nation, surpassing the national average of 2.6 cases per 100,000 population. The factors that particularly favored syphilis infectivity were poverty, poor communication with health care providers, exchanging sex for drugs, lower educational background, and inadequate health education.3 Although syphilis should not be forgotten as part of a differential diagnosis, preventative health education should be undertaken.
Diagnostic Approach
The best way to approach a possible case of syphilis is to have a high index of suspicion (Table). The skin findings of secondary syphilis may mimic other skin conditions (as described above), including pityriasis rosea, erythema multiforme, drug reactions, psoriasis, pityriasis lichenoides et varioliformis acuta, and dyshidrotic eczema, among others. Although the disease usually begins approximately 6 weeks after the onset of a primary chancre, approximately 25% of patients with secondary syphilis will not recall a chancre, and in other cases, the primary chancre will still be present.5 The case reported above did not have any other associated symptoms, but commonly reported symptoms in other cases have included headaches, fevers, pruritus, loss of appetite, and malaise.6
Clinical Features of Secondary Syphilis
Usually, the lesions of syphiloderms consist of variably scaly macules and papules that can be annular, pustular, or psoriasiform. They typically are widespread and symmetric, though in some cases they can remain localized. The appearance also may vary depending on immunocompromised status, which may cause a more aggressive and quicker appearance of the rash.
The Connection to Human Immunodeficiency Virus and AIDS
It is known that patients with syphilis have an increased incidence of other sexually transmitted infections such as venereal warts, gonorrhea, and human immunodeficiency virus (HIV) infection, thus patients should be tested for these conditions as part of their course of treatment. It has been shown that cutaneous sores/chancres facilitate transmission and acquisition of HIV infection. The risk for acquiring HIV increases 2- to 5-fold if exposure occurs when syphilis is present.7 Additionally, syphilis will increase viral loads in patients who are already infected with HIV. These data are concerning, particularly because many patients with syphilis also are infected with HIV.8
Final Thoughts
Although syphilis is known to present with highly variable clinical presentations, early diagnosis, appropriate treatment, and patient education are crucial to avoid further complications.9 Social factors have contributed to a resurgence of syphilis; although easily treatable, it can lead to great suffering and morbidity. In summary, syphilis is a treatable infectious disease and physicians should test for it when investigating a patient, particularly one with risk factors as well as a symmetric hyperpigmented rash on the acral surfaces. There are uncommon presentations of syphilis, thus it is important to consider it early on and treat appropriately to prevent life-threatening complications.
1. Tampa M, Sarbu I, Matei C, et al. Brief history of syphilis. J Med Life. 2014;7:4-10.
2. Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2007. Atlanta, GA: US Department of Health and Human Services; 2008.
3. Williams PB, Ekundayo O. Study of distribution and factors affecting syphilis epidemic among inner-city minorities of Baltimore. Public Health. 2001;115:387-393.
4. Ruchi S, Mangala HC, Murugesh SB, et al. Prozone phenomenon in secondary syphilis. Indian J Sex Trans Dis. 2011;32:47-49.
5. Lee V, Kinghorn G. Syphilis: an update. Clin Med. 2008;8:330-333.
6. Chapel TA. The signs and symptoms of secondary syphilis. Sex Transm Dis. 1980;7:161-164.
7. Bolan G. Syphilis and HIV: a dangerous duo affecting gay and bisexual men. https://blog.aids.gov/2012/12/ syphilis-and-hiv-a-dangerous-duo-affecting-gay-and -bisexual-men.html. Published December 13, 2012. Accessed August 19, 2015.
8. Zetola NM, Klausner JD. Syphilis and HIV infection: an update. Clin Infect Dis. 2007;44:1222-1228.
9. Green CB, Fitzpatrick J. Syphilis. In: Fitzpatrick J, Morelli J, eds. Dermatology Secrets Plus. Philadelphia, PA: Elsevier Mosby; 2011:195-200.
1. Tampa M, Sarbu I, Matei C, et al. Brief history of syphilis. J Med Life. 2014;7:4-10.
2. Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2007. Atlanta, GA: US Department of Health and Human Services; 2008.
3. Williams PB, Ekundayo O. Study of distribution and factors affecting syphilis epidemic among inner-city minorities of Baltimore. Public Health. 2001;115:387-393.
4. Ruchi S, Mangala HC, Murugesh SB, et al. Prozone phenomenon in secondary syphilis. Indian J Sex Trans Dis. 2011;32:47-49.
5. Lee V, Kinghorn G. Syphilis: an update. Clin Med. 2008;8:330-333.
6. Chapel TA. The signs and symptoms of secondary syphilis. Sex Transm Dis. 1980;7:161-164.
7. Bolan G. Syphilis and HIV: a dangerous duo affecting gay and bisexual men. https://blog.aids.gov/2012/12/ syphilis-and-hiv-a-dangerous-duo-affecting-gay-and -bisexual-men.html. Published December 13, 2012. Accessed August 19, 2015.
8. Zetola NM, Klausner JD. Syphilis and HIV infection: an update. Clin Infect Dis. 2007;44:1222-1228.
9. Green CB, Fitzpatrick J. Syphilis. In: Fitzpatrick J, Morelli J, eds. Dermatology Secrets Plus. Philadelphia, PA: Elsevier Mosby; 2011:195-200.

The Challenge of Surgeon Self-Improvement
At the end of a journey 3,650 days long, there is a path leading into the wilderness. From the first day of medical school until the last day of fellowship, we safely follow the well-paved and often-traveled road of medical education with its preset and regimented responsibilities, objectives, and milestones. We become comfortable in the academic routine of newly prescribed goals and responsibilities every year of training. We continually push forward with the stated desire of completing our education, beginning our dream job, and discovering our personas as physicians and human beings along the way. Balance, while an ideal to aspire to, is often put aside for the perceived greater glory of practical knowledge, competition, and the finish line. The assumption all along is that happiness is preordained by this path. However, when the routine comes to an end and we take our first steps into life as an attending surgeon, we can come face to face with an inexplicable void.
It is often said that the best period of training is the first years of practice. We spend those initial years drinking from the fire hose that is the attending surgeon learning curve, but that learning curve often too quickly plateaus. We can be paralyzed by the uncertainty of what the future may bring and of our roles in it. At that moment we have a profound new choice to make: to relish the freedom to reinvent ourselves and create new adventures, or to succumb to the unhealthy temptations and outside influences that abound. Bad decisions are inevitable if we never spend any time reflecting on what actually makes us happy. The sesquipedalian prose of self-improvement books often belabors the fact that we are all at risk of becoming clichés. To fight the cliché, we believe the essence of healthy success in practice after training lies in 3 principles: reinvention, passion, and inspiration. The rest is filler.
Reinvent yourself within medicine. As physicians, part of our identities is built upon our abilities to compassionately care for patients and effectively treat disease. However, the vast majority of procedures and skills we acquire during training will be obsolete in a decade or less. Therefore, it is imperative that we change with time, or else we will become stagnant. If we choose to compare ourselves only to those around us and similar to us, we can be unaware of our standing still as the world moves forward. Medicine as a career can remain exciting if we persistently demand that we improve every day in some way, no matter how small. Previous training cannot limit future learning, and we must strive to never give in to excuses and constantly seek out new skills. Research, teaching, administration, society involvement, politics, governance, and business can all serve as catalysts in our work lives to instigate meaningful change and discover new challenges. The pursuit of new experiences in medicine is the lifeblood of our future careers and constant reinvention is the heartbeat that sustains it. No talented person in the business or technology sectors would ever be asked to do the exact same job for an entire career. Therefore, why should we? Reinvention every 5 to 7 years is a must.
Find passion outside of medicine. Our interests outside of medicine are assets no different than finances, property, and material goods. As such, we need a plan for asset allocation and diversification that involves more than just numbers and percentages. We need healthy passions that evoke emotions and solidify memories. A busy practice can be a jealous mistress. Therefore, be careful to allocate time in your calendar to develop your identity outside of the practice environment. The overwhelming urge is to ignore the lack of attention to life outside medicine because it’s not as comfortable as seeing familiar patients who need your help. As ignoring an infection can be deadly for patients, this approach can pull us inescapably far away from the things and people that we love. While a simple hike in the woods, a dinner with friends, or quiet conversation with family can seem trivial and easily pushed aside for clinics and cases, these are the anchors in our lives that will prevent us from going astray. As we develop healthy passions in our personal lives outside of medicine, we in turn create more anchors, keeping us grounded and true to ourselves and to those around us. When we decide what is important in our personal lives we must ensure that our schedules diligently protect the time devoted to these priorities. Control your schedule or your schedule will control you.
Create your own inspiration. To put it simply and honestly as Andy Dufresne once did in the film The Shawshank Redemption, we have to “get busy living or get busy dying.” There is a widely held misconception that by completing our training and graduating for the final time, we will be imbued with a sense of purpose to guide us for the rest of our careers. However, the reality is that, if we do the same thing every day for years, medicine can become simply a job, and the world around us can lose some of its luster. Inspiration is hard to come by, which is why we must create our own in the moments we can. Nothing should be taken for granted, as inspiration has no prerequisite size or form. It can be as simple as a novel observation or as grandiose as a revolutionary treatment. It can be as guileless as a beloved child’s success or a spouse’s love. Actively sharing ideas with mentors, colleagues, friends, and patients empowers each of us with a voice to create change. However, what matters more than the final outcome is our perception of the process and how we lead it. The constant and deliberate pursuit of new sources of motivation is paramount to staying excited and engaged in our work and our lives. Enjoy the journey—it can be well worth it.
In the end, if we change nothing, nothing will ever change. This adage is harder to follow than any surgical skill we perform. We can never give up on our personal growth in and out of medicine, as both are vitally important for our mental, spiritual, and physical health. A vibrant optimism is contagious and good for patients and physicians alike. As we travel deeper into the wilderness, remember that failures need not be daunting and perilous. They can be embraced and lead to learning and success that make us stronger and more hopeful than we ever thought possible. Be bold, be brave, and commit to fighting the cliché for your entire unique career. ◾
At the end of a journey 3,650 days long, there is a path leading into the wilderness. From the first day of medical school until the last day of fellowship, we safely follow the well-paved and often-traveled road of medical education with its preset and regimented responsibilities, objectives, and milestones. We become comfortable in the academic routine of newly prescribed goals and responsibilities every year of training. We continually push forward with the stated desire of completing our education, beginning our dream job, and discovering our personas as physicians and human beings along the way. Balance, while an ideal to aspire to, is often put aside for the perceived greater glory of practical knowledge, competition, and the finish line. The assumption all along is that happiness is preordained by this path. However, when the routine comes to an end and we take our first steps into life as an attending surgeon, we can come face to face with an inexplicable void.
It is often said that the best period of training is the first years of practice. We spend those initial years drinking from the fire hose that is the attending surgeon learning curve, but that learning curve often too quickly plateaus. We can be paralyzed by the uncertainty of what the future may bring and of our roles in it. At that moment we have a profound new choice to make: to relish the freedom to reinvent ourselves and create new adventures, or to succumb to the unhealthy temptations and outside influences that abound. Bad decisions are inevitable if we never spend any time reflecting on what actually makes us happy. The sesquipedalian prose of self-improvement books often belabors the fact that we are all at risk of becoming clichés. To fight the cliché, we believe the essence of healthy success in practice after training lies in 3 principles: reinvention, passion, and inspiration. The rest is filler.
Reinvent yourself within medicine. As physicians, part of our identities is built upon our abilities to compassionately care for patients and effectively treat disease. However, the vast majority of procedures and skills we acquire during training will be obsolete in a decade or less. Therefore, it is imperative that we change with time, or else we will become stagnant. If we choose to compare ourselves only to those around us and similar to us, we can be unaware of our standing still as the world moves forward. Medicine as a career can remain exciting if we persistently demand that we improve every day in some way, no matter how small. Previous training cannot limit future learning, and we must strive to never give in to excuses and constantly seek out new skills. Research, teaching, administration, society involvement, politics, governance, and business can all serve as catalysts in our work lives to instigate meaningful change and discover new challenges. The pursuit of new experiences in medicine is the lifeblood of our future careers and constant reinvention is the heartbeat that sustains it. No talented person in the business or technology sectors would ever be asked to do the exact same job for an entire career. Therefore, why should we? Reinvention every 5 to 7 years is a must.
Find passion outside of medicine. Our interests outside of medicine are assets no different than finances, property, and material goods. As such, we need a plan for asset allocation and diversification that involves more than just numbers and percentages. We need healthy passions that evoke emotions and solidify memories. A busy practice can be a jealous mistress. Therefore, be careful to allocate time in your calendar to develop your identity outside of the practice environment. The overwhelming urge is to ignore the lack of attention to life outside medicine because it’s not as comfortable as seeing familiar patients who need your help. As ignoring an infection can be deadly for patients, this approach can pull us inescapably far away from the things and people that we love. While a simple hike in the woods, a dinner with friends, or quiet conversation with family can seem trivial and easily pushed aside for clinics and cases, these are the anchors in our lives that will prevent us from going astray. As we develop healthy passions in our personal lives outside of medicine, we in turn create more anchors, keeping us grounded and true to ourselves and to those around us. When we decide what is important in our personal lives we must ensure that our schedules diligently protect the time devoted to these priorities. Control your schedule or your schedule will control you.
Create your own inspiration. To put it simply and honestly as Andy Dufresne once did in the film The Shawshank Redemption, we have to “get busy living or get busy dying.” There is a widely held misconception that by completing our training and graduating for the final time, we will be imbued with a sense of purpose to guide us for the rest of our careers. However, the reality is that, if we do the same thing every day for years, medicine can become simply a job, and the world around us can lose some of its luster. Inspiration is hard to come by, which is why we must create our own in the moments we can. Nothing should be taken for granted, as inspiration has no prerequisite size or form. It can be as simple as a novel observation or as grandiose as a revolutionary treatment. It can be as guileless as a beloved child’s success or a spouse’s love. Actively sharing ideas with mentors, colleagues, friends, and patients empowers each of us with a voice to create change. However, what matters more than the final outcome is our perception of the process and how we lead it. The constant and deliberate pursuit of new sources of motivation is paramount to staying excited and engaged in our work and our lives. Enjoy the journey—it can be well worth it.
In the end, if we change nothing, nothing will ever change. This adage is harder to follow than any surgical skill we perform. We can never give up on our personal growth in and out of medicine, as both are vitally important for our mental, spiritual, and physical health. A vibrant optimism is contagious and good for patients and physicians alike. As we travel deeper into the wilderness, remember that failures need not be daunting and perilous. They can be embraced and lead to learning and success that make us stronger and more hopeful than we ever thought possible. Be bold, be brave, and commit to fighting the cliché for your entire unique career. ◾
At the end of a journey 3,650 days long, there is a path leading into the wilderness. From the first day of medical school until the last day of fellowship, we safely follow the well-paved and often-traveled road of medical education with its preset and regimented responsibilities, objectives, and milestones. We become comfortable in the academic routine of newly prescribed goals and responsibilities every year of training. We continually push forward with the stated desire of completing our education, beginning our dream job, and discovering our personas as physicians and human beings along the way. Balance, while an ideal to aspire to, is often put aside for the perceived greater glory of practical knowledge, competition, and the finish line. The assumption all along is that happiness is preordained by this path. However, when the routine comes to an end and we take our first steps into life as an attending surgeon, we can come face to face with an inexplicable void.
It is often said that the best period of training is the first years of practice. We spend those initial years drinking from the fire hose that is the attending surgeon learning curve, but that learning curve often too quickly plateaus. We can be paralyzed by the uncertainty of what the future may bring and of our roles in it. At that moment we have a profound new choice to make: to relish the freedom to reinvent ourselves and create new adventures, or to succumb to the unhealthy temptations and outside influences that abound. Bad decisions are inevitable if we never spend any time reflecting on what actually makes us happy. The sesquipedalian prose of self-improvement books often belabors the fact that we are all at risk of becoming clichés. To fight the cliché, we believe the essence of healthy success in practice after training lies in 3 principles: reinvention, passion, and inspiration. The rest is filler.
Reinvent yourself within medicine. As physicians, part of our identities is built upon our abilities to compassionately care for patients and effectively treat disease. However, the vast majority of procedures and skills we acquire during training will be obsolete in a decade or less. Therefore, it is imperative that we change with time, or else we will become stagnant. If we choose to compare ourselves only to those around us and similar to us, we can be unaware of our standing still as the world moves forward. Medicine as a career can remain exciting if we persistently demand that we improve every day in some way, no matter how small. Previous training cannot limit future learning, and we must strive to never give in to excuses and constantly seek out new skills. Research, teaching, administration, society involvement, politics, governance, and business can all serve as catalysts in our work lives to instigate meaningful change and discover new challenges. The pursuit of new experiences in medicine is the lifeblood of our future careers and constant reinvention is the heartbeat that sustains it. No talented person in the business or technology sectors would ever be asked to do the exact same job for an entire career. Therefore, why should we? Reinvention every 5 to 7 years is a must.
Find passion outside of medicine. Our interests outside of medicine are assets no different than finances, property, and material goods. As such, we need a plan for asset allocation and diversification that involves more than just numbers and percentages. We need healthy passions that evoke emotions and solidify memories. A busy practice can be a jealous mistress. Therefore, be careful to allocate time in your calendar to develop your identity outside of the practice environment. The overwhelming urge is to ignore the lack of attention to life outside medicine because it’s not as comfortable as seeing familiar patients who need your help. As ignoring an infection can be deadly for patients, this approach can pull us inescapably far away from the things and people that we love. While a simple hike in the woods, a dinner with friends, or quiet conversation with family can seem trivial and easily pushed aside for clinics and cases, these are the anchors in our lives that will prevent us from going astray. As we develop healthy passions in our personal lives outside of medicine, we in turn create more anchors, keeping us grounded and true to ourselves and to those around us. When we decide what is important in our personal lives we must ensure that our schedules diligently protect the time devoted to these priorities. Control your schedule or your schedule will control you.
Create your own inspiration. To put it simply and honestly as Andy Dufresne once did in the film The Shawshank Redemption, we have to “get busy living or get busy dying.” There is a widely held misconception that by completing our training and graduating for the final time, we will be imbued with a sense of purpose to guide us for the rest of our careers. However, the reality is that, if we do the same thing every day for years, medicine can become simply a job, and the world around us can lose some of its luster. Inspiration is hard to come by, which is why we must create our own in the moments we can. Nothing should be taken for granted, as inspiration has no prerequisite size or form. It can be as simple as a novel observation or as grandiose as a revolutionary treatment. It can be as guileless as a beloved child’s success or a spouse’s love. Actively sharing ideas with mentors, colleagues, friends, and patients empowers each of us with a voice to create change. However, what matters more than the final outcome is our perception of the process and how we lead it. The constant and deliberate pursuit of new sources of motivation is paramount to staying excited and engaged in our work and our lives. Enjoy the journey—it can be well worth it.
In the end, if we change nothing, nothing will ever change. This adage is harder to follow than any surgical skill we perform. We can never give up on our personal growth in and out of medicine, as both are vitally important for our mental, spiritual, and physical health. A vibrant optimism is contagious and good for patients and physicians alike. As we travel deeper into the wilderness, remember that failures need not be daunting and perilous. They can be embraced and lead to learning and success that make us stronger and more hopeful than we ever thought possible. Be bold, be brave, and commit to fighting the cliché for your entire unique career. ◾

Allergic Contact Dermatitis for Residents
Allergic contact dermatitis (ACD) is a common inflammatory skin condition that affects more than 14 million Americans each year.1 It has been estimated that the economic burden of ACD is nearly $3 billion per year due to school absences, work time lost, and medical expenditures.1,2 In fact, skin diseases rank second to traumatic injuries as the most common type of occupational disease.3 As dermatology residents, we will encounter many patients with ACD, a potentially debilitating skin condition. In this column, I will discuss the different types of ACD as well as their differential diagnoses and management options according to the American Academy of Allergy, Asthma & Immunology’s updated practice parameter for contact dermatitis.4 The 2015 American Contact Dermatitis Society (ACDS) Allergen of the Year and the ACDS’s Contact Allergen Management Program also will be discussed.
Clinical Presentation and Pathophysiology
Allergic contact dermatitis is a widespread skin condition characterized by erythematous and pruritic skin lesions that occur after contact with external stimuli.5 It is caused by a type IV, T cell–mediated, delayed hypersensitivity reaction in which a foreign substance comes into contact with the skin and forms an antigen complex that subsequently leads to sensitization. Upon reexposure to the antigen, the sensitized T cells induce an inflammatory cascade causing the skin changes associated with ACD. Clinical presentations of ACD include vesicles and bullae with distinct angles, lines, and borders.6
Differential Diagnosis
In contrast to ACD, irritant contact dermatitis (the more common form of contact dermatitis) is a non–immune-modulated skin reaction that occurs when an individual is exposed to a substance that causes irritation and damage to the keratinocytes.6,7 It can be an acute reaction to a household cleaning product or a chronic reaction to soap if the patient has had exposure to the product for a prolonged period of time.7 The clinical presentation of irritant contact dermatitis includes dry and fissured skin with less distinct borders and negative patch test results.6
Some other skin diseases that should be considered in the differential diagnosis for suspected ACD include atopic dermatitis, dyshidrotic eczema, inverse psoriasis, latex allergy, palmoplantar psoriasis, scabies, and tinea pedis.5 When ACD is suspected, our diagnostic approach as dermatology residents should be based on a combination of the following factors: the clinical features of the skin reaction (eg, morphology, location, symptoms), the patient’s history of exposure to an alleged allergen and lack of exposure after treatment and/or avoidance, patch test results, laboratory test results, and/or histopathologic examination to exclude other disorders with similar clinical features.8
Management
Localized acute lesions of ACD can be successfully treated with mid- or high-potency topical steroids such as triamcinolone 0.1% or clobetasol 0.05%. If an extensive area of the skin (>20%) is affected, systemic steroid therapy often is required, generally offering relief within 12 to 24 hours. Caution should be taken when prescribing oral prednisone, such as for poison ivy, as it should be tapered over a few weeks to prevent rebound dermatitis. If treatment fails and the diagnosis or specific allergen remains unknown, patch testing should be performed.3,5
Updated Practice Parameter
Practice parameters for contact dermatitis were updated in 2015, as commissioned by the Joint Task Force on Practice Parameters, to address recent advances in the field of contact dermatitis and the most recommended methods for diagnosis and management based on the current scientific literature.4 Prior to this update, the most recent recommendations were from 2006.3
Since the publication of the original practice parameter, new questions have been addressed related to emerging clinical problems such as preoperative screening and postimplantation patch testing for metal allergy in patients undergoing joint replacement surgery. In the updated practice parameter, statements have been added that more comprehensively address evaluation and management of occupational contact dermatitis.4 The potential benefits and limitations of drug patch testing in patients with maculopapular rashes, erythroderma, and nonimmediate cutaneous reactions also have been addressed. New summary statements have been included that make recommendations on the management of ACD, particularly avoidance and prevention.4
ACDS Allergen of the Year
The purpose of this “award” is to recognize the agents that cause the most remarkable clinical effects, those that draw less attention, or those that exhibit exposure patterns that have changed. The ACDS’s 2015 Allergen of the Year is formaldehyde, an inexpensive biocidal preservative used in a wide range of products such as tissue specimen and cadaveric preservation solutions, nail polish, hair-smoothing treatments, and wrinkle-free fabrics.9
Formaldehyde-releasing preservatives (FRPs) are among the leading contact allergens and are found in many personal hygiene products, medications, and household cleansers.8 Specific sources of FRPs include shampoos, bodywashes, hand soaps, lotions, creams, baby wipes, mascara, disinfectants, fabric softeners, topical wart remedies, adhesives, and tissue specimen preservation solutions.10-13 According to de Groot et al,14 the US Food and Drug Administration’s Voluntary Cosmetic Registration Program database has estimated that approximately 20% of personal hygiene products and cosmetics contain an FRP, with imidazolidinyl urea as the most common.
It is important for patients to be aware of sources of formaldehyde exposure and understand that many products containing formaldehyde or FRPs may not list this information on their labels. In fact, one study reported that 33% of 67 moisturizers evaluated did not have proper labeling with regard to their formaldehyde/FRP content.15
Contact Allergen Management Program
During medical school I served as the Dermatology Interest Group Contact Dermatitis Awareness Chair at the University of Texas Medical Branch (Galveston, Texas) and was fortunate to have attended the annual meeting of the ACDS where I learned about the ACDS Contact Allergen Management Program (CAMP), an online resource for dermatologists to access that provides patients a printout list of allergen and cross-reactivity information for more than 1200 products (http://www.contactderm.org/i4a/pages/indexcfm?pageID=3489). This information helps consumers to choose the right products based on their allergies.
Final Thoughts
A thorough review of a patient’s medical history and, if needed, skin patch testing can identify the responsible allergen and initiate an appropriate avoidance plan for the patient. With appropriate avoidance, patients can achieve resolution of their dermatitis and prevent further episodes to substantially improve their quality of life and decrease health care costs.1 If left untreated, ACD can evolve from an acute form to a subacute form and eventually chronic eczematous dermatitis or progression to systemic disease.16,17 Allergic contact dermatitis can negatively impact an individual’s health-related quality of life, particularly in social functioning and psychological well-being.18,19 Therefore, it is pertinent in our role as dermatology residents to recognize ACD before its progression to a chronic state.
1. Bickers DR, Lim HW, Margolis D, et al. The burden of skin diseases: 2004 a joint project of the American Academy of Dermatology and the Society for Investigative Dermatology. J Am Acad Dermatol. 2006;55:490-500.
2. Jacob SE. The lanolin-wool wax alcohol update. The Dermatologist. February 2014;22. http://www.the-dermatologist.com/content/lanolin-wool-wax-alcohol-update. Accessed June 26, 2015.
3. Beltrani VS, Bernstein IL, Cohen DE, et al. Contact dermatitis: a practice parameter [published correction appears in Ann Allergy Asthma Immunol. 2006;97:819]. Ann Allergy Asthma Immunol. 2006;97(3, suppl 2):S1-S38.
4. Fonacier L, Bernstein DI, Pacheco K, et al. Contact dermatitis: a practice parameter—update 2015. J Allergy Clin Immunol Pract. 2015;3(suppl 3):S1-S39.
5. Usatine R, Riojas M. Diagnosis and management of contact dermatitis. Am Fam Physician. 2010;82:249-255.
6. Usatine RP. Contact dermatitis. In: Usatine RP, Smith M, Mayeaux EJ Jr, et al, eds. Color Atlas of Family Medicine. New York, NY: McGraw-Hill; 2009. http://accessmedicine.mhmedical.com/content.aspx?bookid=378&Sectionid=40419504. Accessed June 26, 2015.
7. Vazirnia A, Jacob SE. Review of ACDS’ allergen of the year 2010-2015. The Dermatologist. November 2014;22. http://www.the-dermatologist.com/content/review-acds%E2%80%99-allergen-od-year-2000-2015. Accessed June 26, 2015.
8. Yiannias J. Clinical features and diagnosis of allergic contact dermatitis. UpToDate Web site. http://www.uptodate.com/contents/clinical-features-and-diagnosis-of-allergic-contact-dermatitis?source=search_result&search=allergic+contact+dermatitis&selectedTitle=2~142#. Updated May 20, 2014. Accessed June 18, 2015.
9. Pontén A, Bruze M. Formaldehyde. Dermatitis. 2015;26:3-6.
10. Maier LE, Lampel HP, Bhutani T, et al. Hand dermatitis: a focus on allergic contact dermatitis to biocides. Dermatol Clin. 2009;27:251-264.
11. Marks JG, Elsner P, DeLeo VA. Contact & Occupational Dermatology. 3rd ed. St. Louis, MO: Mosby; 2002.
12. Rietschel RL, Fowler JF Jr, eds. Fisher’s Contact Dermatitis. 6th ed. Hamilton, ON: BC Decker Inc; 2008.
13. Sasseville D. Hypersensitivity to preservatives. Dermatol Ther. 2004;17:251-263.
14. de Groot AC, White IR, Flyvholm MA, et al. Formaldehyde-releasers in cosmetics: relationship to formaldehyde contact allergy. part 1. characterization, frequency and relevance of sensitization, and frequency of use in cosmetics. Contact Dermatitis. 2010;62:2-17.
15. Rastogi SC. Analytical control of preservative labeling on skin creams. Contact Dermatitis. 2000;43:339-343.
16. Hsu JW, Matiz C, Jacob SE. Nickel allergy: localized, id, and systemic manifestations in children. Pediatr Dermatol. 2011;28:276-280.
17. Salam TN, Fowler JF Jr. Balsam-related systemic contact dermatitis. J Am Acad Dermatol. 2001;45:377-381.
18. Kiebert G, Sorensen SV, Revicki D, et al. Atopic dermatitis is associated with a decrement in health-related quality of life. Int J Dermatol. 2002;41:151-158.
19. Hutchings CV, Shum KW, Gawkrodger DJ. Occupational contact dermatitis has an appreciable impact on quality of life. Contact Dermatitis. 2001;45:17-20.
Allergic contact dermatitis (ACD) is a common inflammatory skin condition that affects more than 14 million Americans each year.1 It has been estimated that the economic burden of ACD is nearly $3 billion per year due to school absences, work time lost, and medical expenditures.1,2 In fact, skin diseases rank second to traumatic injuries as the most common type of occupational disease.3 As dermatology residents, we will encounter many patients with ACD, a potentially debilitating skin condition. In this column, I will discuss the different types of ACD as well as their differential diagnoses and management options according to the American Academy of Allergy, Asthma & Immunology’s updated practice parameter for contact dermatitis.4 The 2015 American Contact Dermatitis Society (ACDS) Allergen of the Year and the ACDS’s Contact Allergen Management Program also will be discussed.
Clinical Presentation and Pathophysiology
Allergic contact dermatitis is a widespread skin condition characterized by erythematous and pruritic skin lesions that occur after contact with external stimuli.5 It is caused by a type IV, T cell–mediated, delayed hypersensitivity reaction in which a foreign substance comes into contact with the skin and forms an antigen complex that subsequently leads to sensitization. Upon reexposure to the antigen, the sensitized T cells induce an inflammatory cascade causing the skin changes associated with ACD. Clinical presentations of ACD include vesicles and bullae with distinct angles, lines, and borders.6
Differential Diagnosis
In contrast to ACD, irritant contact dermatitis (the more common form of contact dermatitis) is a non–immune-modulated skin reaction that occurs when an individual is exposed to a substance that causes irritation and damage to the keratinocytes.6,7 It can be an acute reaction to a household cleaning product or a chronic reaction to soap if the patient has had exposure to the product for a prolonged period of time.7 The clinical presentation of irritant contact dermatitis includes dry and fissured skin with less distinct borders and negative patch test results.6
Some other skin diseases that should be considered in the differential diagnosis for suspected ACD include atopic dermatitis, dyshidrotic eczema, inverse psoriasis, latex allergy, palmoplantar psoriasis, scabies, and tinea pedis.5 When ACD is suspected, our diagnostic approach as dermatology residents should be based on a combination of the following factors: the clinical features of the skin reaction (eg, morphology, location, symptoms), the patient’s history of exposure to an alleged allergen and lack of exposure after treatment and/or avoidance, patch test results, laboratory test results, and/or histopathologic examination to exclude other disorders with similar clinical features.8
Management
Localized acute lesions of ACD can be successfully treated with mid- or high-potency topical steroids such as triamcinolone 0.1% or clobetasol 0.05%. If an extensive area of the skin (>20%) is affected, systemic steroid therapy often is required, generally offering relief within 12 to 24 hours. Caution should be taken when prescribing oral prednisone, such as for poison ivy, as it should be tapered over a few weeks to prevent rebound dermatitis. If treatment fails and the diagnosis or specific allergen remains unknown, patch testing should be performed.3,5
Updated Practice Parameter
Practice parameters for contact dermatitis were updated in 2015, as commissioned by the Joint Task Force on Practice Parameters, to address recent advances in the field of contact dermatitis and the most recommended methods for diagnosis and management based on the current scientific literature.4 Prior to this update, the most recent recommendations were from 2006.3
Since the publication of the original practice parameter, new questions have been addressed related to emerging clinical problems such as preoperative screening and postimplantation patch testing for metal allergy in patients undergoing joint replacement surgery. In the updated practice parameter, statements have been added that more comprehensively address evaluation and management of occupational contact dermatitis.4 The potential benefits and limitations of drug patch testing in patients with maculopapular rashes, erythroderma, and nonimmediate cutaneous reactions also have been addressed. New summary statements have been included that make recommendations on the management of ACD, particularly avoidance and prevention.4
ACDS Allergen of the Year
The purpose of this “award” is to recognize the agents that cause the most remarkable clinical effects, those that draw less attention, or those that exhibit exposure patterns that have changed. The ACDS’s 2015 Allergen of the Year is formaldehyde, an inexpensive biocidal preservative used in a wide range of products such as tissue specimen and cadaveric preservation solutions, nail polish, hair-smoothing treatments, and wrinkle-free fabrics.9
Formaldehyde-releasing preservatives (FRPs) are among the leading contact allergens and are found in many personal hygiene products, medications, and household cleansers.8 Specific sources of FRPs include shampoos, bodywashes, hand soaps, lotions, creams, baby wipes, mascara, disinfectants, fabric softeners, topical wart remedies, adhesives, and tissue specimen preservation solutions.10-13 According to de Groot et al,14 the US Food and Drug Administration’s Voluntary Cosmetic Registration Program database has estimated that approximately 20% of personal hygiene products and cosmetics contain an FRP, with imidazolidinyl urea as the most common.
It is important for patients to be aware of sources of formaldehyde exposure and understand that many products containing formaldehyde or FRPs may not list this information on their labels. In fact, one study reported that 33% of 67 moisturizers evaluated did not have proper labeling with regard to their formaldehyde/FRP content.15
Contact Allergen Management Program
During medical school I served as the Dermatology Interest Group Contact Dermatitis Awareness Chair at the University of Texas Medical Branch (Galveston, Texas) and was fortunate to have attended the annual meeting of the ACDS where I learned about the ACDS Contact Allergen Management Program (CAMP), an online resource for dermatologists to access that provides patients a printout list of allergen and cross-reactivity information for more than 1200 products (http://www.contactderm.org/i4a/pages/indexcfm?pageID=3489). This information helps consumers to choose the right products based on their allergies.
Final Thoughts
A thorough review of a patient’s medical history and, if needed, skin patch testing can identify the responsible allergen and initiate an appropriate avoidance plan for the patient. With appropriate avoidance, patients can achieve resolution of their dermatitis and prevent further episodes to substantially improve their quality of life and decrease health care costs.1 If left untreated, ACD can evolve from an acute form to a subacute form and eventually chronic eczematous dermatitis or progression to systemic disease.16,17 Allergic contact dermatitis can negatively impact an individual’s health-related quality of life, particularly in social functioning and psychological well-being.18,19 Therefore, it is pertinent in our role as dermatology residents to recognize ACD before its progression to a chronic state.
Allergic contact dermatitis (ACD) is a common inflammatory skin condition that affects more than 14 million Americans each year.1 It has been estimated that the economic burden of ACD is nearly $3 billion per year due to school absences, work time lost, and medical expenditures.1,2 In fact, skin diseases rank second to traumatic injuries as the most common type of occupational disease.3 As dermatology residents, we will encounter many patients with ACD, a potentially debilitating skin condition. In this column, I will discuss the different types of ACD as well as their differential diagnoses and management options according to the American Academy of Allergy, Asthma & Immunology’s updated practice parameter for contact dermatitis.4 The 2015 American Contact Dermatitis Society (ACDS) Allergen of the Year and the ACDS’s Contact Allergen Management Program also will be discussed.
Clinical Presentation and Pathophysiology
Allergic contact dermatitis is a widespread skin condition characterized by erythematous and pruritic skin lesions that occur after contact with external stimuli.5 It is caused by a type IV, T cell–mediated, delayed hypersensitivity reaction in which a foreign substance comes into contact with the skin and forms an antigen complex that subsequently leads to sensitization. Upon reexposure to the antigen, the sensitized T cells induce an inflammatory cascade causing the skin changes associated with ACD. Clinical presentations of ACD include vesicles and bullae with distinct angles, lines, and borders.6
Differential Diagnosis
In contrast to ACD, irritant contact dermatitis (the more common form of contact dermatitis) is a non–immune-modulated skin reaction that occurs when an individual is exposed to a substance that causes irritation and damage to the keratinocytes.6,7 It can be an acute reaction to a household cleaning product or a chronic reaction to soap if the patient has had exposure to the product for a prolonged period of time.7 The clinical presentation of irritant contact dermatitis includes dry and fissured skin with less distinct borders and negative patch test results.6
Some other skin diseases that should be considered in the differential diagnosis for suspected ACD include atopic dermatitis, dyshidrotic eczema, inverse psoriasis, latex allergy, palmoplantar psoriasis, scabies, and tinea pedis.5 When ACD is suspected, our diagnostic approach as dermatology residents should be based on a combination of the following factors: the clinical features of the skin reaction (eg, morphology, location, symptoms), the patient’s history of exposure to an alleged allergen and lack of exposure after treatment and/or avoidance, patch test results, laboratory test results, and/or histopathologic examination to exclude other disorders with similar clinical features.8
Management
Localized acute lesions of ACD can be successfully treated with mid- or high-potency topical steroids such as triamcinolone 0.1% or clobetasol 0.05%. If an extensive area of the skin (>20%) is affected, systemic steroid therapy often is required, generally offering relief within 12 to 24 hours. Caution should be taken when prescribing oral prednisone, such as for poison ivy, as it should be tapered over a few weeks to prevent rebound dermatitis. If treatment fails and the diagnosis or specific allergen remains unknown, patch testing should be performed.3,5
Updated Practice Parameter
Practice parameters for contact dermatitis were updated in 2015, as commissioned by the Joint Task Force on Practice Parameters, to address recent advances in the field of contact dermatitis and the most recommended methods for diagnosis and management based on the current scientific literature.4 Prior to this update, the most recent recommendations were from 2006.3
Since the publication of the original practice parameter, new questions have been addressed related to emerging clinical problems such as preoperative screening and postimplantation patch testing for metal allergy in patients undergoing joint replacement surgery. In the updated practice parameter, statements have been added that more comprehensively address evaluation and management of occupational contact dermatitis.4 The potential benefits and limitations of drug patch testing in patients with maculopapular rashes, erythroderma, and nonimmediate cutaneous reactions also have been addressed. New summary statements have been included that make recommendations on the management of ACD, particularly avoidance and prevention.4
ACDS Allergen of the Year
The purpose of this “award” is to recognize the agents that cause the most remarkable clinical effects, those that draw less attention, or those that exhibit exposure patterns that have changed. The ACDS’s 2015 Allergen of the Year is formaldehyde, an inexpensive biocidal preservative used in a wide range of products such as tissue specimen and cadaveric preservation solutions, nail polish, hair-smoothing treatments, and wrinkle-free fabrics.9
Formaldehyde-releasing preservatives (FRPs) are among the leading contact allergens and are found in many personal hygiene products, medications, and household cleansers.8 Specific sources of FRPs include shampoos, bodywashes, hand soaps, lotions, creams, baby wipes, mascara, disinfectants, fabric softeners, topical wart remedies, adhesives, and tissue specimen preservation solutions.10-13 According to de Groot et al,14 the US Food and Drug Administration’s Voluntary Cosmetic Registration Program database has estimated that approximately 20% of personal hygiene products and cosmetics contain an FRP, with imidazolidinyl urea as the most common.
It is important for patients to be aware of sources of formaldehyde exposure and understand that many products containing formaldehyde or FRPs may not list this information on their labels. In fact, one study reported that 33% of 67 moisturizers evaluated did not have proper labeling with regard to their formaldehyde/FRP content.15
Contact Allergen Management Program
During medical school I served as the Dermatology Interest Group Contact Dermatitis Awareness Chair at the University of Texas Medical Branch (Galveston, Texas) and was fortunate to have attended the annual meeting of the ACDS where I learned about the ACDS Contact Allergen Management Program (CAMP), an online resource for dermatologists to access that provides patients a printout list of allergen and cross-reactivity information for more than 1200 products (http://www.contactderm.org/i4a/pages/indexcfm?pageID=3489). This information helps consumers to choose the right products based on their allergies.
Final Thoughts
A thorough review of a patient’s medical history and, if needed, skin patch testing can identify the responsible allergen and initiate an appropriate avoidance plan for the patient. With appropriate avoidance, patients can achieve resolution of their dermatitis and prevent further episodes to substantially improve their quality of life and decrease health care costs.1 If left untreated, ACD can evolve from an acute form to a subacute form and eventually chronic eczematous dermatitis or progression to systemic disease.16,17 Allergic contact dermatitis can negatively impact an individual’s health-related quality of life, particularly in social functioning and psychological well-being.18,19 Therefore, it is pertinent in our role as dermatology residents to recognize ACD before its progression to a chronic state.
1. Bickers DR, Lim HW, Margolis D, et al. The burden of skin diseases: 2004 a joint project of the American Academy of Dermatology and the Society for Investigative Dermatology. J Am Acad Dermatol. 2006;55:490-500.
2. Jacob SE. The lanolin-wool wax alcohol update. The Dermatologist. February 2014;22. http://www.the-dermatologist.com/content/lanolin-wool-wax-alcohol-update. Accessed June 26, 2015.
3. Beltrani VS, Bernstein IL, Cohen DE, et al. Contact dermatitis: a practice parameter [published correction appears in Ann Allergy Asthma Immunol. 2006;97:819]. Ann Allergy Asthma Immunol. 2006;97(3, suppl 2):S1-S38.
4. Fonacier L, Bernstein DI, Pacheco K, et al. Contact dermatitis: a practice parameter—update 2015. J Allergy Clin Immunol Pract. 2015;3(suppl 3):S1-S39.
5. Usatine R, Riojas M. Diagnosis and management of contact dermatitis. Am Fam Physician. 2010;82:249-255.
6. Usatine RP. Contact dermatitis. In: Usatine RP, Smith M, Mayeaux EJ Jr, et al, eds. Color Atlas of Family Medicine. New York, NY: McGraw-Hill; 2009. http://accessmedicine.mhmedical.com/content.aspx?bookid=378&Sectionid=40419504. Accessed June 26, 2015.
7. Vazirnia A, Jacob SE. Review of ACDS’ allergen of the year 2010-2015. The Dermatologist. November 2014;22. http://www.the-dermatologist.com/content/review-acds%E2%80%99-allergen-od-year-2000-2015. Accessed June 26, 2015.
8. Yiannias J. Clinical features and diagnosis of allergic contact dermatitis. UpToDate Web site. http://www.uptodate.com/contents/clinical-features-and-diagnosis-of-allergic-contact-dermatitis?source=search_result&search=allergic+contact+dermatitis&selectedTitle=2~142#. Updated May 20, 2014. Accessed June 18, 2015.
9. Pontén A, Bruze M. Formaldehyde. Dermatitis. 2015;26:3-6.
10. Maier LE, Lampel HP, Bhutani T, et al. Hand dermatitis: a focus on allergic contact dermatitis to biocides. Dermatol Clin. 2009;27:251-264.
11. Marks JG, Elsner P, DeLeo VA. Contact & Occupational Dermatology. 3rd ed. St. Louis, MO: Mosby; 2002.
12. Rietschel RL, Fowler JF Jr, eds. Fisher’s Contact Dermatitis. 6th ed. Hamilton, ON: BC Decker Inc; 2008.
13. Sasseville D. Hypersensitivity to preservatives. Dermatol Ther. 2004;17:251-263.
14. de Groot AC, White IR, Flyvholm MA, et al. Formaldehyde-releasers in cosmetics: relationship to formaldehyde contact allergy. part 1. characterization, frequency and relevance of sensitization, and frequency of use in cosmetics. Contact Dermatitis. 2010;62:2-17.
15. Rastogi SC. Analytical control of preservative labeling on skin creams. Contact Dermatitis. 2000;43:339-343.
16. Hsu JW, Matiz C, Jacob SE. Nickel allergy: localized, id, and systemic manifestations in children. Pediatr Dermatol. 2011;28:276-280.
17. Salam TN, Fowler JF Jr. Balsam-related systemic contact dermatitis. J Am Acad Dermatol. 2001;45:377-381.
18. Kiebert G, Sorensen SV, Revicki D, et al. Atopic dermatitis is associated with a decrement in health-related quality of life. Int J Dermatol. 2002;41:151-158.
19. Hutchings CV, Shum KW, Gawkrodger DJ. Occupational contact dermatitis has an appreciable impact on quality of life. Contact Dermatitis. 2001;45:17-20.
1. Bickers DR, Lim HW, Margolis D, et al. The burden of skin diseases: 2004 a joint project of the American Academy of Dermatology and the Society for Investigative Dermatology. J Am Acad Dermatol. 2006;55:490-500.
2. Jacob SE. The lanolin-wool wax alcohol update. The Dermatologist. February 2014;22. http://www.the-dermatologist.com/content/lanolin-wool-wax-alcohol-update. Accessed June 26, 2015.
3. Beltrani VS, Bernstein IL, Cohen DE, et al. Contact dermatitis: a practice parameter [published correction appears in Ann Allergy Asthma Immunol. 2006;97:819]. Ann Allergy Asthma Immunol. 2006;97(3, suppl 2):S1-S38.
4. Fonacier L, Bernstein DI, Pacheco K, et al. Contact dermatitis: a practice parameter—update 2015. J Allergy Clin Immunol Pract. 2015;3(suppl 3):S1-S39.
5. Usatine R, Riojas M. Diagnosis and management of contact dermatitis. Am Fam Physician. 2010;82:249-255.
6. Usatine RP. Contact dermatitis. In: Usatine RP, Smith M, Mayeaux EJ Jr, et al, eds. Color Atlas of Family Medicine. New York, NY: McGraw-Hill; 2009. http://accessmedicine.mhmedical.com/content.aspx?bookid=378&Sectionid=40419504. Accessed June 26, 2015.
7. Vazirnia A, Jacob SE. Review of ACDS’ allergen of the year 2010-2015. The Dermatologist. November 2014;22. http://www.the-dermatologist.com/content/review-acds%E2%80%99-allergen-od-year-2000-2015. Accessed June 26, 2015.
8. Yiannias J. Clinical features and diagnosis of allergic contact dermatitis. UpToDate Web site. http://www.uptodate.com/contents/clinical-features-and-diagnosis-of-allergic-contact-dermatitis?source=search_result&search=allergic+contact+dermatitis&selectedTitle=2~142#. Updated May 20, 2014. Accessed June 18, 2015.
9. Pontén A, Bruze M. Formaldehyde. Dermatitis. 2015;26:3-6.
10. Maier LE, Lampel HP, Bhutani T, et al. Hand dermatitis: a focus on allergic contact dermatitis to biocides. Dermatol Clin. 2009;27:251-264.
11. Marks JG, Elsner P, DeLeo VA. Contact & Occupational Dermatology. 3rd ed. St. Louis, MO: Mosby; 2002.
12. Rietschel RL, Fowler JF Jr, eds. Fisher’s Contact Dermatitis. 6th ed. Hamilton, ON: BC Decker Inc; 2008.
13. Sasseville D. Hypersensitivity to preservatives. Dermatol Ther. 2004;17:251-263.
14. de Groot AC, White IR, Flyvholm MA, et al. Formaldehyde-releasers in cosmetics: relationship to formaldehyde contact allergy. part 1. characterization, frequency and relevance of sensitization, and frequency of use in cosmetics. Contact Dermatitis. 2010;62:2-17.
15. Rastogi SC. Analytical control of preservative labeling on skin creams. Contact Dermatitis. 2000;43:339-343.
16. Hsu JW, Matiz C, Jacob SE. Nickel allergy: localized, id, and systemic manifestations in children. Pediatr Dermatol. 2011;28:276-280.
17. Salam TN, Fowler JF Jr. Balsam-related systemic contact dermatitis. J Am Acad Dermatol. 2001;45:377-381.
18. Kiebert G, Sorensen SV, Revicki D, et al. Atopic dermatitis is associated with a decrement in health-related quality of life. Int J Dermatol. 2002;41:151-158.
19. Hutchings CV, Shum KW, Gawkrodger DJ. Occupational contact dermatitis has an appreciable impact on quality of life. Contact Dermatitis. 2001;45:17-20.

Orthopedic Resident Education and Patient Safety
The mantra “See one, do one, teach one” is a longstanding cliché in surgical education. Although this mantra does not apply literally in the case of complex modern orthopedic procedures, the reality is that all surgical education, including orthopedic surgery residency, involves learning “on the job” in the clinic, emergency room, and operating room. In conjunction with a sound basis of textbook learning and observation, orthopedic residents receive graduated patient care responsibilities leading to the goal of entering independent practice at the conclusion of 5 years of residency.
Moreover, the academic medical centers involved in orthopedic resident education often also serve as referral centers for patients with challenging problems and multiple comorbidities, so that attending physicians teaching orthopedic residents must balance educating residents with caring for complex patients. In contrast to their physicians’ dual focus on patient care and resident education, some patients are hesitant to allow residents to participate in their surgical care, fearing increased errors and complications due to resident inexperience.1,2 How do we address these patients’ legitimate concerns while continuing to provide the on-the-job training experience so important to resident education?
Does Orthopedic Resident Surgical Education Affect Patient Safety?
The sparse literature generally suggests that orthopedic resident involvement in patient care may lengthen procedures but is not associated with substantively worse patient outcomes. Studies at single centers found that resident involvement in adolescent idiopathic scoliosis surgery and hip and knee arthroplasty leads to slightly longer operative times, without increased complication rates or clinical outcomes.3,4 One study found significantly less acetabular anteversion in resident-involved total hip arthroplasty cases, although there was no difference in dislocation rate, other complications, or patient clinical outcome.5 These single-center studies showing no change in patient complications or outcomes based on resident involvement could reflect unique experiences that do not generalize beyond a few academic medical centers. Alternatively, the relatively small patient samples may leave these studies underpowered to detect small changes in patient complication rates.
Recently, several studies in the orthopedic literature have addressed the role of resident involvement in patient complications using the large American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database.6-11 This database contains high-quality information from over 400 hospitals across the United States about whether residents were involved with a surgery, as well as patient comorbidities, operative variables, and 30-day postoperative complications. These studies have found that resident participation is associated with either a decreased rate of complications or no change in the complication rate for common orthopedic surgeries, though the studies have corroborated the small increase in operative time associated with resident involvement.6-9 Interestingly, other ACS-NSQIP database studies failed to identify a “July effect” of increased complications due to resident inexperience at the beginning of the residency academic year.10,11
These studies suggest that, based on current evidence, patients can be reassured that orthopedic resident participation in surgery does not increase complication rates. Moreover, there is no evidence that having orthopedic surgery at the beginning of the residency academic year in July results in a higher complication rate. Although operative time for cases involving residents is on the order of 10 to 15 minutes longer, this small difference in operative time has not translated into differences in patient outcomes or complications. It is worth noting that hospital billing for surgical procedures may take operative time into account based on duration of anesthesia. Appropriate resident training, then, should not be expected to harm patient safety. Resident training should include educational preparation prior to the operating room, intraoperative supervision, and graduated responsibility appropriate to resident training level and skill level.
Have Recent Changes in Orthopedic Resident Education Improved Patient Safety?
Fifteen years ago, the Institute of Medicine published its seminal work, To Err is Human: Building a Safer Health System, highlighting medical errors leading to patient injury and death.12 In 2003, the Accreditation Council for Graduate Medical Education (ACGME) implemented resident work-hour restrictions (subsequently refined in 2011) designed to improve resident education, promote resident well-being, and maximize patient safety.13 The work-hour regulations have been met with mixed reactions, with orthopedic surgeon–authors expressing concerns that the work-hour limits compromise resident education and professionalism in patient care without leading to any proven increase in patient safety.13-15 These views are supported by a recent systematic review of the orthopedic literature, which found that, while work-hour changes have subjectively improved resident quality of life and fatigue, there has been no clear benefit to resident education or patient safety.14 A review of the overall surgery literature similarly found no benefit for resident education and no improvement in patient outcomes associated with the work-hour regulations, with some of the literature suggesting increased complications for high-acuity patients.16 Patient safety, a major impetus behind the work-hour regulations, appears not to be impacted by the regulations except in limited circumstances, though additional studies more specific to common orthopedic procedures and to orthopedic patients could provide additional insight.
Orthopedic resident education standards are constantly changing in an effort to improve education, quality of care, and patient safety. Recently, the ACGME and American Board of Orthopaedic Surgery (ABOS) have implemented clinical “milestones” for evaluating residents’ competency based on knowledge and skill rather than postgraduate year (PGY).15,17 Education of orthopedic PGY-1 residents (interns) has evolved in the last 2 years as well, with 6 months of orthopedic rotations and surgical skills training now required.18 Additionally, the use of surgical simulation in orthopedic resident education has been rapidly increasing, particularly for arthroscopic surgery.19 Whether these recent changes improve patient care remains unclear, and future studies should address whether these changes objectively improve orthopedic surgical education, patient care, and patient safety.
Conclusions
Patients inquiring about resident involvement in their orthopedic procedure can be counseled that available evidence shows resident involvement does not hinder patient safety and does not increase complications. In the author’s opinion, academic medical centers with orthopedic residents involved in patient care may provide superior patient care and expertise in complex, challenging cases. In addition, we should strive to improve patients’ awareness of the orthopedic resident education process and the multiple recent changes designed to improve both resident education and patient care and safety.
1. Holt G, Nunn T, Gregori A. Ethical dilemmas in orthopaedic surgical training. J Bone Joint Surg Am. 2008;90(12):2798-2803. doi:10.2106/JBJS.H.00910.
2. Chiong W. Justifying patient risks associated with medical education. JAMA. 2007;298(9):1046-1048. doi:10.1001/jama.298.9.1046.
3. Woolson ST, Kang MN. A comparison of the results of total hip and knee arthroplasty performed on a teaching service or a private practice service. J Bone Joint Surg Am. 2007;89(3):601-607. doi:10.2106/JBJS.F.00584.
4. Auerbach JD, Lonner BS, Antonacci MD, Kean KE. Perioperative outcomes and complications related to teaching residents and fellows in scoliosis surgery. Spine. 2008;33(10):1113-1118. doi:10.1097/BRS.0b013e31816f69cf.
5. Moran M, Yap SL, Walmsley P, Brenkel IJ. Clinical and radiologic outcome of total hip arthroplasty performed by trainee compared with consultant orthopedic surgeons. J Arthroplasty. 2004;19(7):853-857. doi:10.1016/j.arth.2004.06.026.
6. Haughom BD, Schairer WW, Hellman MD, Yi PH, Levine BR. Does resident involvement impact post-operative complications following primary total knee arthroplasty? An analysis of 24,529 cases. J Arthroplasty. 2014;29(7):1468-1472.e2. doi:10.1016/j.arth.2014.02.036.
7. Edelstein AI, Lovecchio FC, Saha S, Hsu WK, Kim JYS. Impact of resident involvement on orthopaedic surgery outcomes: an analysis of 30,628 patients from the American College of Surgeons National Surgical Quality Improvement Program Database. J Bone Joint Surg Am. 2014;96(15):e131. doi:10.2106/JBJS.M.00660.
8. Haughom BD, Schairer WW, Hellman MD, Yi PH, Levine BR. Resident involvement does not influence complication after total hip arthroplasty: an analysis of 13,109 cases. J Arthroplasty. 2014;29(10):1919-1924. doi:10.1016/j.arth.2014.06.003.
9. Pugely AJ, Gao Y, Martin CT, Callagh JJ, Weinstein SL, Marsh JL. The effect of resident participation on short-term outcomes after orthopaedic surgery. Clin Orthop Relat Res. 2014;472(7):2290-2300. doi:10.1007/s11999-014-3567-0.
10. Bohl DD, Fu MC, Gruskay JA, Basques BA, Golinvaux NS, Grauer JN. “July effect” in elective spine surgery: analysis of the American College of Surgeons National Surgical Quality Improvement Program database. Spine. 2014;39(7):603-611. doi:10.1097/BRS.0000000000000196.
11. Bohl DD, Fu MC, Golinvaux NS, Basques BA, Gruskay JA, Grauer JN. The “July effect” in primary total hip and knee arthroplasty: analysis of 21,434 cases from the ACS-NSQIP database. J Arthroplasty. 2014;29(7):1332-1338. doi:10.1016/j.arth.2014.02.008.
12. Institute of Medicine Committee on Quality of Health Care in America. To Err Is Human: Building a Safer Health System. Kohn LT, Corrigan JM, Donaldson MS, eds. Washington, DC: National Academies Press; 2000.
13. Levine WN, Spang RC. ACGME duty hour requirements: perceptions and impact on resident training and patient care. J Am Acad Orthop Surg. 2014;22(9):535-544. doi:10.5435/JAAOS-22-09-535.
14. Harris JD, Staheli G, LeClere L, Andersone D, McCormick F. What effects have resident work-hour changes had on education, quality of life, and safety? A systematic review. Clin Orthop Relat Res. 2015;473(5):1600-1608. doi:10.1007/s11999-014-3968-0.
15. Peabody T, Nestler S, Marx C, Pellegrini V. Resident duty-hour restrictions-who are we protecting?: AOA critical issues. J Bone Joint Surg Am. 2012;94(17):e131. doi:10.2106/JBJS.J.01685.
16. Ahmed N, Devitt KS, Keshet I, et al. A systematic review of the effects of resident duty hour restrictions in surgery: impact on resident wellness, training, and patient outcomes. Ann Surg. 2014;259(6):1041-1053. doi:10.1097/SLA.0000000000000595.
17. Tosti R. Will the new milestone requirements improve residency training? Am J Orthop. 2013;42(12):E109-E110.
18. Dougherty PJ, Marcus RE. ACGME and ABOS changes for the orthopaedic surgery PGY-1 (intern) year. Clin Orthop Relat Res. 2013;471(11):3412-3416. doi:10.1007/s11999-013-3227-9.
19. Frank RM, Erickson B, Frank JM, et al. Utility of modern arthroscopic simulator training models. Arthroscopy. 2014;30(1):121-133. doi:10.1016/j.arthro.2013.09.084.
The mantra “See one, do one, teach one” is a longstanding cliché in surgical education. Although this mantra does not apply literally in the case of complex modern orthopedic procedures, the reality is that all surgical education, including orthopedic surgery residency, involves learning “on the job” in the clinic, emergency room, and operating room. In conjunction with a sound basis of textbook learning and observation, orthopedic residents receive graduated patient care responsibilities leading to the goal of entering independent practice at the conclusion of 5 years of residency.
Moreover, the academic medical centers involved in orthopedic resident education often also serve as referral centers for patients with challenging problems and multiple comorbidities, so that attending physicians teaching orthopedic residents must balance educating residents with caring for complex patients. In contrast to their physicians’ dual focus on patient care and resident education, some patients are hesitant to allow residents to participate in their surgical care, fearing increased errors and complications due to resident inexperience.1,2 How do we address these patients’ legitimate concerns while continuing to provide the on-the-job training experience so important to resident education?
Does Orthopedic Resident Surgical Education Affect Patient Safety?
The sparse literature generally suggests that orthopedic resident involvement in patient care may lengthen procedures but is not associated with substantively worse patient outcomes. Studies at single centers found that resident involvement in adolescent idiopathic scoliosis surgery and hip and knee arthroplasty leads to slightly longer operative times, without increased complication rates or clinical outcomes.3,4 One study found significantly less acetabular anteversion in resident-involved total hip arthroplasty cases, although there was no difference in dislocation rate, other complications, or patient clinical outcome.5 These single-center studies showing no change in patient complications or outcomes based on resident involvement could reflect unique experiences that do not generalize beyond a few academic medical centers. Alternatively, the relatively small patient samples may leave these studies underpowered to detect small changes in patient complication rates.
Recently, several studies in the orthopedic literature have addressed the role of resident involvement in patient complications using the large American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database.6-11 This database contains high-quality information from over 400 hospitals across the United States about whether residents were involved with a surgery, as well as patient comorbidities, operative variables, and 30-day postoperative complications. These studies have found that resident participation is associated with either a decreased rate of complications or no change in the complication rate for common orthopedic surgeries, though the studies have corroborated the small increase in operative time associated with resident involvement.6-9 Interestingly, other ACS-NSQIP database studies failed to identify a “July effect” of increased complications due to resident inexperience at the beginning of the residency academic year.10,11
These studies suggest that, based on current evidence, patients can be reassured that orthopedic resident participation in surgery does not increase complication rates. Moreover, there is no evidence that having orthopedic surgery at the beginning of the residency academic year in July results in a higher complication rate. Although operative time for cases involving residents is on the order of 10 to 15 minutes longer, this small difference in operative time has not translated into differences in patient outcomes or complications. It is worth noting that hospital billing for surgical procedures may take operative time into account based on duration of anesthesia. Appropriate resident training, then, should not be expected to harm patient safety. Resident training should include educational preparation prior to the operating room, intraoperative supervision, and graduated responsibility appropriate to resident training level and skill level.
Have Recent Changes in Orthopedic Resident Education Improved Patient Safety?
Fifteen years ago, the Institute of Medicine published its seminal work, To Err is Human: Building a Safer Health System, highlighting medical errors leading to patient injury and death.12 In 2003, the Accreditation Council for Graduate Medical Education (ACGME) implemented resident work-hour restrictions (subsequently refined in 2011) designed to improve resident education, promote resident well-being, and maximize patient safety.13 The work-hour regulations have been met with mixed reactions, with orthopedic surgeon–authors expressing concerns that the work-hour limits compromise resident education and professionalism in patient care without leading to any proven increase in patient safety.13-15 These views are supported by a recent systematic review of the orthopedic literature, which found that, while work-hour changes have subjectively improved resident quality of life and fatigue, there has been no clear benefit to resident education or patient safety.14 A review of the overall surgery literature similarly found no benefit for resident education and no improvement in patient outcomes associated with the work-hour regulations, with some of the literature suggesting increased complications for high-acuity patients.16 Patient safety, a major impetus behind the work-hour regulations, appears not to be impacted by the regulations except in limited circumstances, though additional studies more specific to common orthopedic procedures and to orthopedic patients could provide additional insight.
Orthopedic resident education standards are constantly changing in an effort to improve education, quality of care, and patient safety. Recently, the ACGME and American Board of Orthopaedic Surgery (ABOS) have implemented clinical “milestones” for evaluating residents’ competency based on knowledge and skill rather than postgraduate year (PGY).15,17 Education of orthopedic PGY-1 residents (interns) has evolved in the last 2 years as well, with 6 months of orthopedic rotations and surgical skills training now required.18 Additionally, the use of surgical simulation in orthopedic resident education has been rapidly increasing, particularly for arthroscopic surgery.19 Whether these recent changes improve patient care remains unclear, and future studies should address whether these changes objectively improve orthopedic surgical education, patient care, and patient safety.
Conclusions
Patients inquiring about resident involvement in their orthopedic procedure can be counseled that available evidence shows resident involvement does not hinder patient safety and does not increase complications. In the author’s opinion, academic medical centers with orthopedic residents involved in patient care may provide superior patient care and expertise in complex, challenging cases. In addition, we should strive to improve patients’ awareness of the orthopedic resident education process and the multiple recent changes designed to improve both resident education and patient care and safety.
The mantra “See one, do one, teach one” is a longstanding cliché in surgical education. Although this mantra does not apply literally in the case of complex modern orthopedic procedures, the reality is that all surgical education, including orthopedic surgery residency, involves learning “on the job” in the clinic, emergency room, and operating room. In conjunction with a sound basis of textbook learning and observation, orthopedic residents receive graduated patient care responsibilities leading to the goal of entering independent practice at the conclusion of 5 years of residency.
Moreover, the academic medical centers involved in orthopedic resident education often also serve as referral centers for patients with challenging problems and multiple comorbidities, so that attending physicians teaching orthopedic residents must balance educating residents with caring for complex patients. In contrast to their physicians’ dual focus on patient care and resident education, some patients are hesitant to allow residents to participate in their surgical care, fearing increased errors and complications due to resident inexperience.1,2 How do we address these patients’ legitimate concerns while continuing to provide the on-the-job training experience so important to resident education?
Does Orthopedic Resident Surgical Education Affect Patient Safety?
The sparse literature generally suggests that orthopedic resident involvement in patient care may lengthen procedures but is not associated with substantively worse patient outcomes. Studies at single centers found that resident involvement in adolescent idiopathic scoliosis surgery and hip and knee arthroplasty leads to slightly longer operative times, without increased complication rates or clinical outcomes.3,4 One study found significantly less acetabular anteversion in resident-involved total hip arthroplasty cases, although there was no difference in dislocation rate, other complications, or patient clinical outcome.5 These single-center studies showing no change in patient complications or outcomes based on resident involvement could reflect unique experiences that do not generalize beyond a few academic medical centers. Alternatively, the relatively small patient samples may leave these studies underpowered to detect small changes in patient complication rates.
Recently, several studies in the orthopedic literature have addressed the role of resident involvement in patient complications using the large American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database.6-11 This database contains high-quality information from over 400 hospitals across the United States about whether residents were involved with a surgery, as well as patient comorbidities, operative variables, and 30-day postoperative complications. These studies have found that resident participation is associated with either a decreased rate of complications or no change in the complication rate for common orthopedic surgeries, though the studies have corroborated the small increase in operative time associated with resident involvement.6-9 Interestingly, other ACS-NSQIP database studies failed to identify a “July effect” of increased complications due to resident inexperience at the beginning of the residency academic year.10,11
These studies suggest that, based on current evidence, patients can be reassured that orthopedic resident participation in surgery does not increase complication rates. Moreover, there is no evidence that having orthopedic surgery at the beginning of the residency academic year in July results in a higher complication rate. Although operative time for cases involving residents is on the order of 10 to 15 minutes longer, this small difference in operative time has not translated into differences in patient outcomes or complications. It is worth noting that hospital billing for surgical procedures may take operative time into account based on duration of anesthesia. Appropriate resident training, then, should not be expected to harm patient safety. Resident training should include educational preparation prior to the operating room, intraoperative supervision, and graduated responsibility appropriate to resident training level and skill level.
Have Recent Changes in Orthopedic Resident Education Improved Patient Safety?
Fifteen years ago, the Institute of Medicine published its seminal work, To Err is Human: Building a Safer Health System, highlighting medical errors leading to patient injury and death.12 In 2003, the Accreditation Council for Graduate Medical Education (ACGME) implemented resident work-hour restrictions (subsequently refined in 2011) designed to improve resident education, promote resident well-being, and maximize patient safety.13 The work-hour regulations have been met with mixed reactions, with orthopedic surgeon–authors expressing concerns that the work-hour limits compromise resident education and professionalism in patient care without leading to any proven increase in patient safety.13-15 These views are supported by a recent systematic review of the orthopedic literature, which found that, while work-hour changes have subjectively improved resident quality of life and fatigue, there has been no clear benefit to resident education or patient safety.14 A review of the overall surgery literature similarly found no benefit for resident education and no improvement in patient outcomes associated with the work-hour regulations, with some of the literature suggesting increased complications for high-acuity patients.16 Patient safety, a major impetus behind the work-hour regulations, appears not to be impacted by the regulations except in limited circumstances, though additional studies more specific to common orthopedic procedures and to orthopedic patients could provide additional insight.
Orthopedic resident education standards are constantly changing in an effort to improve education, quality of care, and patient safety. Recently, the ACGME and American Board of Orthopaedic Surgery (ABOS) have implemented clinical “milestones” for evaluating residents’ competency based on knowledge and skill rather than postgraduate year (PGY).15,17 Education of orthopedic PGY-1 residents (interns) has evolved in the last 2 years as well, with 6 months of orthopedic rotations and surgical skills training now required.18 Additionally, the use of surgical simulation in orthopedic resident education has been rapidly increasing, particularly for arthroscopic surgery.19 Whether these recent changes improve patient care remains unclear, and future studies should address whether these changes objectively improve orthopedic surgical education, patient care, and patient safety.
Conclusions
Patients inquiring about resident involvement in their orthopedic procedure can be counseled that available evidence shows resident involvement does not hinder patient safety and does not increase complications. In the author’s opinion, academic medical centers with orthopedic residents involved in patient care may provide superior patient care and expertise in complex, challenging cases. In addition, we should strive to improve patients’ awareness of the orthopedic resident education process and the multiple recent changes designed to improve both resident education and patient care and safety.
1. Holt G, Nunn T, Gregori A. Ethical dilemmas in orthopaedic surgical training. J Bone Joint Surg Am. 2008;90(12):2798-2803. doi:10.2106/JBJS.H.00910.
2. Chiong W. Justifying patient risks associated with medical education. JAMA. 2007;298(9):1046-1048. doi:10.1001/jama.298.9.1046.
3. Woolson ST, Kang MN. A comparison of the results of total hip and knee arthroplasty performed on a teaching service or a private practice service. J Bone Joint Surg Am. 2007;89(3):601-607. doi:10.2106/JBJS.F.00584.
4. Auerbach JD, Lonner BS, Antonacci MD, Kean KE. Perioperative outcomes and complications related to teaching residents and fellows in scoliosis surgery. Spine. 2008;33(10):1113-1118. doi:10.1097/BRS.0b013e31816f69cf.
5. Moran M, Yap SL, Walmsley P, Brenkel IJ. Clinical and radiologic outcome of total hip arthroplasty performed by trainee compared with consultant orthopedic surgeons. J Arthroplasty. 2004;19(7):853-857. doi:10.1016/j.arth.2004.06.026.
6. Haughom BD, Schairer WW, Hellman MD, Yi PH, Levine BR. Does resident involvement impact post-operative complications following primary total knee arthroplasty? An analysis of 24,529 cases. J Arthroplasty. 2014;29(7):1468-1472.e2. doi:10.1016/j.arth.2014.02.036.
7. Edelstein AI, Lovecchio FC, Saha S, Hsu WK, Kim JYS. Impact of resident involvement on orthopaedic surgery outcomes: an analysis of 30,628 patients from the American College of Surgeons National Surgical Quality Improvement Program Database. J Bone Joint Surg Am. 2014;96(15):e131. doi:10.2106/JBJS.M.00660.
8. Haughom BD, Schairer WW, Hellman MD, Yi PH, Levine BR. Resident involvement does not influence complication after total hip arthroplasty: an analysis of 13,109 cases. J Arthroplasty. 2014;29(10):1919-1924. doi:10.1016/j.arth.2014.06.003.
9. Pugely AJ, Gao Y, Martin CT, Callagh JJ, Weinstein SL, Marsh JL. The effect of resident participation on short-term outcomes after orthopaedic surgery. Clin Orthop Relat Res. 2014;472(7):2290-2300. doi:10.1007/s11999-014-3567-0.
10. Bohl DD, Fu MC, Gruskay JA, Basques BA, Golinvaux NS, Grauer JN. “July effect” in elective spine surgery: analysis of the American College of Surgeons National Surgical Quality Improvement Program database. Spine. 2014;39(7):603-611. doi:10.1097/BRS.0000000000000196.
11. Bohl DD, Fu MC, Golinvaux NS, Basques BA, Gruskay JA, Grauer JN. The “July effect” in primary total hip and knee arthroplasty: analysis of 21,434 cases from the ACS-NSQIP database. J Arthroplasty. 2014;29(7):1332-1338. doi:10.1016/j.arth.2014.02.008.
12. Institute of Medicine Committee on Quality of Health Care in America. To Err Is Human: Building a Safer Health System. Kohn LT, Corrigan JM, Donaldson MS, eds. Washington, DC: National Academies Press; 2000.
13. Levine WN, Spang RC. ACGME duty hour requirements: perceptions and impact on resident training and patient care. J Am Acad Orthop Surg. 2014;22(9):535-544. doi:10.5435/JAAOS-22-09-535.
14. Harris JD, Staheli G, LeClere L, Andersone D, McCormick F. What effects have resident work-hour changes had on education, quality of life, and safety? A systematic review. Clin Orthop Relat Res. 2015;473(5):1600-1608. doi:10.1007/s11999-014-3968-0.
15. Peabody T, Nestler S, Marx C, Pellegrini V. Resident duty-hour restrictions-who are we protecting?: AOA critical issues. J Bone Joint Surg Am. 2012;94(17):e131. doi:10.2106/JBJS.J.01685.
16. Ahmed N, Devitt KS, Keshet I, et al. A systematic review of the effects of resident duty hour restrictions in surgery: impact on resident wellness, training, and patient outcomes. Ann Surg. 2014;259(6):1041-1053. doi:10.1097/SLA.0000000000000595.
17. Tosti R. Will the new milestone requirements improve residency training? Am J Orthop. 2013;42(12):E109-E110.
18. Dougherty PJ, Marcus RE. ACGME and ABOS changes for the orthopaedic surgery PGY-1 (intern) year. Clin Orthop Relat Res. 2013;471(11):3412-3416. doi:10.1007/s11999-013-3227-9.
19. Frank RM, Erickson B, Frank JM, et al. Utility of modern arthroscopic simulator training models. Arthroscopy. 2014;30(1):121-133. doi:10.1016/j.arthro.2013.09.084.
1. Holt G, Nunn T, Gregori A. Ethical dilemmas in orthopaedic surgical training. J Bone Joint Surg Am. 2008;90(12):2798-2803. doi:10.2106/JBJS.H.00910.
2. Chiong W. Justifying patient risks associated with medical education. JAMA. 2007;298(9):1046-1048. doi:10.1001/jama.298.9.1046.
3. Woolson ST, Kang MN. A comparison of the results of total hip and knee arthroplasty performed on a teaching service or a private practice service. J Bone Joint Surg Am. 2007;89(3):601-607. doi:10.2106/JBJS.F.00584.
4. Auerbach JD, Lonner BS, Antonacci MD, Kean KE. Perioperative outcomes and complications related to teaching residents and fellows in scoliosis surgery. Spine. 2008;33(10):1113-1118. doi:10.1097/BRS.0b013e31816f69cf.
5. Moran M, Yap SL, Walmsley P, Brenkel IJ. Clinical and radiologic outcome of total hip arthroplasty performed by trainee compared with consultant orthopedic surgeons. J Arthroplasty. 2004;19(7):853-857. doi:10.1016/j.arth.2004.06.026.
6. Haughom BD, Schairer WW, Hellman MD, Yi PH, Levine BR. Does resident involvement impact post-operative complications following primary total knee arthroplasty? An analysis of 24,529 cases. J Arthroplasty. 2014;29(7):1468-1472.e2. doi:10.1016/j.arth.2014.02.036.
7. Edelstein AI, Lovecchio FC, Saha S, Hsu WK, Kim JYS. Impact of resident involvement on orthopaedic surgery outcomes: an analysis of 30,628 patients from the American College of Surgeons National Surgical Quality Improvement Program Database. J Bone Joint Surg Am. 2014;96(15):e131. doi:10.2106/JBJS.M.00660.
8. Haughom BD, Schairer WW, Hellman MD, Yi PH, Levine BR. Resident involvement does not influence complication after total hip arthroplasty: an analysis of 13,109 cases. J Arthroplasty. 2014;29(10):1919-1924. doi:10.1016/j.arth.2014.06.003.
9. Pugely AJ, Gao Y, Martin CT, Callagh JJ, Weinstein SL, Marsh JL. The effect of resident participation on short-term outcomes after orthopaedic surgery. Clin Orthop Relat Res. 2014;472(7):2290-2300. doi:10.1007/s11999-014-3567-0.
10. Bohl DD, Fu MC, Gruskay JA, Basques BA, Golinvaux NS, Grauer JN. “July effect” in elective spine surgery: analysis of the American College of Surgeons National Surgical Quality Improvement Program database. Spine. 2014;39(7):603-611. doi:10.1097/BRS.0000000000000196.
11. Bohl DD, Fu MC, Golinvaux NS, Basques BA, Gruskay JA, Grauer JN. The “July effect” in primary total hip and knee arthroplasty: analysis of 21,434 cases from the ACS-NSQIP database. J Arthroplasty. 2014;29(7):1332-1338. doi:10.1016/j.arth.2014.02.008.
12. Institute of Medicine Committee on Quality of Health Care in America. To Err Is Human: Building a Safer Health System. Kohn LT, Corrigan JM, Donaldson MS, eds. Washington, DC: National Academies Press; 2000.
13. Levine WN, Spang RC. ACGME duty hour requirements: perceptions and impact on resident training and patient care. J Am Acad Orthop Surg. 2014;22(9):535-544. doi:10.5435/JAAOS-22-09-535.
14. Harris JD, Staheli G, LeClere L, Andersone D, McCormick F. What effects have resident work-hour changes had on education, quality of life, and safety? A systematic review. Clin Orthop Relat Res. 2015;473(5):1600-1608. doi:10.1007/s11999-014-3968-0.
15. Peabody T, Nestler S, Marx C, Pellegrini V. Resident duty-hour restrictions-who are we protecting?: AOA critical issues. J Bone Joint Surg Am. 2012;94(17):e131. doi:10.2106/JBJS.J.01685.
16. Ahmed N, Devitt KS, Keshet I, et al. A systematic review of the effects of resident duty hour restrictions in surgery: impact on resident wellness, training, and patient outcomes. Ann Surg. 2014;259(6):1041-1053. doi:10.1097/SLA.0000000000000595.
17. Tosti R. Will the new milestone requirements improve residency training? Am J Orthop. 2013;42(12):E109-E110.
18. Dougherty PJ, Marcus RE. ACGME and ABOS changes for the orthopaedic surgery PGY-1 (intern) year. Clin Orthop Relat Res. 2013;471(11):3412-3416. doi:10.1007/s11999-013-3227-9.
19. Frank RM, Erickson B, Frank JM, et al. Utility of modern arthroscopic simulator training models. Arthroscopy. 2014;30(1):121-133. doi:10.1016/j.arthro.2013.09.084.

For residents, technology can put professionalism and reputation at risk
As mobile devices permeate our professional lives, resident disengagement, social media, and communications with patients all present a risk of breaches in professionalism for unwary trainees.
Encroaching technology and resident disengagement
It is pointless to be some kind of Luddite and reject the transformative tide of technology—mobile devices in particular—in psychiatry.1 Yet commentators have remarked on the potential that technology has to damage the professionalism of physicians.2
We are dismayed to observe that, nationally, residents seem at times more absorbed with their social media accounts, e-mail, text messages, and Web browsers than by Grand Rounds and didactic lectures provided by faculty. We believe that this electronic preoccupation shows a level of disrespect; indeed, self-control does matter, and is an inherent facet of professionalism.3
We are under no illusion that, when we give small-group didactic presentations to medical students, they will stop surfing the Internet, e-mailing, and texting: Frankly, we aren’t that riveting. We certainly appreciate, however, students’ discretion by generally using their mobile devices out of our view.
Last, we find it interesting that, despite the greater formality of national medical meetings, we see more blatant use of mobile devices by residents when greater respect is, arguably, warranted. Perhaps the anonymity of a larger audience is to blame for that phenomenon.
Social media
The rise of social media presents particular concerns for the professionalism of residents. In a recent study of applicants to residency, 46% of all applicants maintained a Facebook profile; 16% of those who maintained a profile have posted unprofessional content there.4 (In our experience, the percentage of residents who have a social media or other online presence is considerably greater than 46%.)
Using social media presents risks: for example, if a resident were to post to her (his) social media profile that she (he) was “tired” or had been out “partying with friends.” Like it or not, we, as residents, speak not just as individuals but as representatives of our training program and institution. Should a resident’s patient suffer an adverse outcome the day after the physician posts a 3 AM image of herself out drinking, she might be exposing herself, her institution, or both, to liability.
Correspondence with patients
E-mail and texting correspondence with patients present their own professionalism dilemmas, with regard to legal liability, confidentiality, boundary violations, and “netiquette” issues.5-7 In our experience, the rapid-fire nature of texting can lead a resident to write without appropriate deliberation or to respond outside of business hours. In doing so, the boundary between what is professional and what is purely personal can be blurred. Furthermore, unless our patients have signed a consent form that articulates the acceptable uses of e-mail and text communication,7 we risk exposing ourselves to liability if a patient notifies us of an urgent matter by e-mail at a time when we are inaccessible.
Our residency class is fairly divided on texting patients. However, we (the authors) sometimes feel comfortable exchanging text messages about scheduling with our psychotherapy patients.
Admittedly, texting with a patient can easily become a slippery slope when a patient texts about a scheduling matter well outside of business hours. The path of least resistance would be to reply at the moment, but we have learned that the wiser course is to wait and reply during business hours (even though that adds another item to the to-do list).
Even more challenging is when a psychotherapy patient pushes boundaries further, for example, by texting about a non-emergent psychotherapy concern that should be addressed in a therapy session. Although non-emergent texts about a psychotherapy matter clearly represent a pressing concern to the patient, boundaries can be blurred if a resident, reluctant to risk offending a patient, addresses the matter directly. The benefit of having these experiences during residency is that a psychotherapy supervisor is available to provide guidance.
Better understanding of these risks is needed
Resident disengagement, social media, and correspondence with patients can present pitfalls for unwary residents. They have the potential to create a breach in professionalism and, as a result, increase our exposure to liability. The solution? We believe it isn’t to restrict use of technology, but to continue to study these slippery slopes and how we should address them. Ultimately, by continuing to embrace professionalism, we enhance the reputation of psychiatry and of medicine broadly.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. DeJong SM. Networking, professionalism and the internet: what practicing psychiatrists need to know about Facebook, LinkedIn,and beyond. Psychiatric Times. http://www.psychiatrictimes.com/career/networking-professionalism-and-internet.Published December 7, 2012. Accessed June 22, 2015.
2. Blumenthal D. Doctors in a wired world: can professionalism survive connectivity? Milbank Q. 2002;80(3):525-546, iv.
3. Hershberger PJ, Zryd TW, Rodes MB, et al. Professionalism: self-control matters. Med Teach. 2010;32(1):e36-e41.
4. Ponce BA, Determann JR, Boohaker HA, et al. Social networking profiles and professionalism issues in residency applicants: an original study-cohort study. J Surg Educ. 2013;70(4):502-507.
5. DeJong SM, Benjamin S, Anzia JM, et al. Professionalism and the internet in psychiatry: what to teach and how to teach it. Acad Psychiatry. 2012;36(5):356-362.
6. DeJong SM, Gorrindo T. To text or not to text: applying clinical and professionalism principles to decisions about text messaging with patients. J Am Acad Child Adolesc Psychiatry.2014;53(7):713-715.
7. Reynolds A, Mossman D. Before you hit ‘send’: will an e-mail to your patient put you at legal risk? Current Psychiatry. 2015;14(6):33,38,39,42.
As mobile devices permeate our professional lives, resident disengagement, social media, and communications with patients all present a risk of breaches in professionalism for unwary trainees.
Encroaching technology and resident disengagement
It is pointless to be some kind of Luddite and reject the transformative tide of technology—mobile devices in particular—in psychiatry.1 Yet commentators have remarked on the potential that technology has to damage the professionalism of physicians.2
We are dismayed to observe that, nationally, residents seem at times more absorbed with their social media accounts, e-mail, text messages, and Web browsers than by Grand Rounds and didactic lectures provided by faculty. We believe that this electronic preoccupation shows a level of disrespect; indeed, self-control does matter, and is an inherent facet of professionalism.3
We are under no illusion that, when we give small-group didactic presentations to medical students, they will stop surfing the Internet, e-mailing, and texting: Frankly, we aren’t that riveting. We certainly appreciate, however, students’ discretion by generally using their mobile devices out of our view.
Last, we find it interesting that, despite the greater formality of national medical meetings, we see more blatant use of mobile devices by residents when greater respect is, arguably, warranted. Perhaps the anonymity of a larger audience is to blame for that phenomenon.
Social media
The rise of social media presents particular concerns for the professionalism of residents. In a recent study of applicants to residency, 46% of all applicants maintained a Facebook profile; 16% of those who maintained a profile have posted unprofessional content there.4 (In our experience, the percentage of residents who have a social media or other online presence is considerably greater than 46%.)
Using social media presents risks: for example, if a resident were to post to her (his) social media profile that she (he) was “tired” or had been out “partying with friends.” Like it or not, we, as residents, speak not just as individuals but as representatives of our training program and institution. Should a resident’s patient suffer an adverse outcome the day after the physician posts a 3 AM image of herself out drinking, she might be exposing herself, her institution, or both, to liability.
Correspondence with patients
E-mail and texting correspondence with patients present their own professionalism dilemmas, with regard to legal liability, confidentiality, boundary violations, and “netiquette” issues.5-7 In our experience, the rapid-fire nature of texting can lead a resident to write without appropriate deliberation or to respond outside of business hours. In doing so, the boundary between what is professional and what is purely personal can be blurred. Furthermore, unless our patients have signed a consent form that articulates the acceptable uses of e-mail and text communication,7 we risk exposing ourselves to liability if a patient notifies us of an urgent matter by e-mail at a time when we are inaccessible.
Our residency class is fairly divided on texting patients. However, we (the authors) sometimes feel comfortable exchanging text messages about scheduling with our psychotherapy patients.
Admittedly, texting with a patient can easily become a slippery slope when a patient texts about a scheduling matter well outside of business hours. The path of least resistance would be to reply at the moment, but we have learned that the wiser course is to wait and reply during business hours (even though that adds another item to the to-do list).
Even more challenging is when a psychotherapy patient pushes boundaries further, for example, by texting about a non-emergent psychotherapy concern that should be addressed in a therapy session. Although non-emergent texts about a psychotherapy matter clearly represent a pressing concern to the patient, boundaries can be blurred if a resident, reluctant to risk offending a patient, addresses the matter directly. The benefit of having these experiences during residency is that a psychotherapy supervisor is available to provide guidance.
Better understanding of these risks is needed
Resident disengagement, social media, and correspondence with patients can present pitfalls for unwary residents. They have the potential to create a breach in professionalism and, as a result, increase our exposure to liability. The solution? We believe it isn’t to restrict use of technology, but to continue to study these slippery slopes and how we should address them. Ultimately, by continuing to embrace professionalism, we enhance the reputation of psychiatry and of medicine broadly.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
As mobile devices permeate our professional lives, resident disengagement, social media, and communications with patients all present a risk of breaches in professionalism for unwary trainees.
Encroaching technology and resident disengagement
It is pointless to be some kind of Luddite and reject the transformative tide of technology—mobile devices in particular—in psychiatry.1 Yet commentators have remarked on the potential that technology has to damage the professionalism of physicians.2
We are dismayed to observe that, nationally, residents seem at times more absorbed with their social media accounts, e-mail, text messages, and Web browsers than by Grand Rounds and didactic lectures provided by faculty. We believe that this electronic preoccupation shows a level of disrespect; indeed, self-control does matter, and is an inherent facet of professionalism.3
We are under no illusion that, when we give small-group didactic presentations to medical students, they will stop surfing the Internet, e-mailing, and texting: Frankly, we aren’t that riveting. We certainly appreciate, however, students’ discretion by generally using their mobile devices out of our view.
Last, we find it interesting that, despite the greater formality of national medical meetings, we see more blatant use of mobile devices by residents when greater respect is, arguably, warranted. Perhaps the anonymity of a larger audience is to blame for that phenomenon.
Social media
The rise of social media presents particular concerns for the professionalism of residents. In a recent study of applicants to residency, 46% of all applicants maintained a Facebook profile; 16% of those who maintained a profile have posted unprofessional content there.4 (In our experience, the percentage of residents who have a social media or other online presence is considerably greater than 46%.)
Using social media presents risks: for example, if a resident were to post to her (his) social media profile that she (he) was “tired” or had been out “partying with friends.” Like it or not, we, as residents, speak not just as individuals but as representatives of our training program and institution. Should a resident’s patient suffer an adverse outcome the day after the physician posts a 3 AM image of herself out drinking, she might be exposing herself, her institution, or both, to liability.
Correspondence with patients
E-mail and texting correspondence with patients present their own professionalism dilemmas, with regard to legal liability, confidentiality, boundary violations, and “netiquette” issues.5-7 In our experience, the rapid-fire nature of texting can lead a resident to write without appropriate deliberation or to respond outside of business hours. In doing so, the boundary between what is professional and what is purely personal can be blurred. Furthermore, unless our patients have signed a consent form that articulates the acceptable uses of e-mail and text communication,7 we risk exposing ourselves to liability if a patient notifies us of an urgent matter by e-mail at a time when we are inaccessible.
Our residency class is fairly divided on texting patients. However, we (the authors) sometimes feel comfortable exchanging text messages about scheduling with our psychotherapy patients.
Admittedly, texting with a patient can easily become a slippery slope when a patient texts about a scheduling matter well outside of business hours. The path of least resistance would be to reply at the moment, but we have learned that the wiser course is to wait and reply during business hours (even though that adds another item to the to-do list).
Even more challenging is when a psychotherapy patient pushes boundaries further, for example, by texting about a non-emergent psychotherapy concern that should be addressed in a therapy session. Although non-emergent texts about a psychotherapy matter clearly represent a pressing concern to the patient, boundaries can be blurred if a resident, reluctant to risk offending a patient, addresses the matter directly. The benefit of having these experiences during residency is that a psychotherapy supervisor is available to provide guidance.
Better understanding of these risks is needed
Resident disengagement, social media, and correspondence with patients can present pitfalls for unwary residents. They have the potential to create a breach in professionalism and, as a result, increase our exposure to liability. The solution? We believe it isn’t to restrict use of technology, but to continue to study these slippery slopes and how we should address them. Ultimately, by continuing to embrace professionalism, we enhance the reputation of psychiatry and of medicine broadly.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. DeJong SM. Networking, professionalism and the internet: what practicing psychiatrists need to know about Facebook, LinkedIn,and beyond. Psychiatric Times. http://www.psychiatrictimes.com/career/networking-professionalism-and-internet.Published December 7, 2012. Accessed June 22, 2015.
2. Blumenthal D. Doctors in a wired world: can professionalism survive connectivity? Milbank Q. 2002;80(3):525-546, iv.
3. Hershberger PJ, Zryd TW, Rodes MB, et al. Professionalism: self-control matters. Med Teach. 2010;32(1):e36-e41.
4. Ponce BA, Determann JR, Boohaker HA, et al. Social networking profiles and professionalism issues in residency applicants: an original study-cohort study. J Surg Educ. 2013;70(4):502-507.
5. DeJong SM, Benjamin S, Anzia JM, et al. Professionalism and the internet in psychiatry: what to teach and how to teach it. Acad Psychiatry. 2012;36(5):356-362.
6. DeJong SM, Gorrindo T. To text or not to text: applying clinical and professionalism principles to decisions about text messaging with patients. J Am Acad Child Adolesc Psychiatry.2014;53(7):713-715.
7. Reynolds A, Mossman D. Before you hit ‘send’: will an e-mail to your patient put you at legal risk? Current Psychiatry. 2015;14(6):33,38,39,42.
1. DeJong SM. Networking, professionalism and the internet: what practicing psychiatrists need to know about Facebook, LinkedIn,and beyond. Psychiatric Times. http://www.psychiatrictimes.com/career/networking-professionalism-and-internet.Published December 7, 2012. Accessed June 22, 2015.
2. Blumenthal D. Doctors in a wired world: can professionalism survive connectivity? Milbank Q. 2002;80(3):525-546, iv.
3. Hershberger PJ, Zryd TW, Rodes MB, et al. Professionalism: self-control matters. Med Teach. 2010;32(1):e36-e41.
4. Ponce BA, Determann JR, Boohaker HA, et al. Social networking profiles and professionalism issues in residency applicants: an original study-cohort study. J Surg Educ. 2013;70(4):502-507.
5. DeJong SM, Benjamin S, Anzia JM, et al. Professionalism and the internet in psychiatry: what to teach and how to teach it. Acad Psychiatry. 2012;36(5):356-362.
6. DeJong SM, Gorrindo T. To text or not to text: applying clinical and professionalism principles to decisions about text messaging with patients. J Am Acad Child Adolesc Psychiatry.2014;53(7):713-715.
7. Reynolds A, Mossman D. Before you hit ‘send’: will an e-mail to your patient put you at legal risk? Current Psychiatry. 2015;14(6):33,38,39,42.
Minimize That “Pinch and Burn”: Tips and Tricks to Reduce Injection Pain With Local Anesthetics
The use of local anesthetics, particularly local anesthetic injections, is a core part of the practice of dermatology. The use of anesthetics in both diagnosis and management make the administration and usage of these medications a foundational skill for all dermatology residents. Minimizing that familiar “pinch and burn” and giving patients a nearly pain-free experience can result in satisfaction for both patients and physicians. This column describes several useful and easily implemented techniques that residents can incorporate into their daily practice.
Buffer
Plain lidocaine is less acidic than the more commonly utilized lidocaine 1% with 1:100,000 epinephrine. When the latter is buffered with sodium bicarbonate in a 10:1 dilution, it is superior to its unbuffered counterpart.1 This method works by raising the pH of the solution, which is normally 4.2, to a physiologic and more comfortable 7.4.2 Of note, bupivacaine is more acidic than lidocaine.3
Warm
Warming anesthetics has been shown to reduce injection pain. Warming anesthetics to body temperature or up to 40°C to 54.4°C (104°F–130°F) has been studied and recommended.4-7 Warming combined with buffering may result in the least painful injection.4-6
Use Smaller-Gauge Needles
A more obvious tip, using smaller-gauge needles can reduce injection pain. Generally, 27- or 30-gauge needles are commonly recommended.8,9
Limit Repeated Use of the Same Needle
Switch to a fresh needle when you have to inject multiple times in the same lesion or when you have multiple injection sites. In addition, use different needles for drawing up and for the actual injection procedure. A dull needle means more pain.
Perpendicular Injection Technique
Compared to a 45° injection angle, lidocaine injected at a 90° angle reduces pain,10 as this technique minimizes the number of nerve endings that come in contact with the needle.8
Inject Slowly
A slow injection technique using small volumes can substantially minimize pain, as it allows for the nerve endings in the skin to accommodate for the distortion caused by anesthetic infiltration.2
Pulse Injection
Pulse injections can be less painful than injecting an anesthetic in a continuous fashion. It has been recommended that 0.1 cc of anesthetic be injected followed by a 3-second pause, then repeating this step 2 to 3 times. More volumes may subsequently be administered.8
Thoughtful Reinsertion
When larger surface areas must be anesthetized, the needle may have to be reinserted multiple times. In these instances, injection within 1 cm of the visibly blanched area of skin ensures that lidocaine (and epinephrine, if such a solution is used) has already infiltrated that area.2
Distraction
There is merit to the idea of distracting the patient when injecting local anesthetics. Distraction methods including engaging in simple conversation with the patient, having the patient look away, playing background music, and even suggesting that the procedure is painless or has minimal pain have shown utility in minimizing injection pain.8,11
Other distraction techniques are physical, including stretching and scratching the skin, pinching, local vibration, and pressure.12,13
Combination Anesthetic Technique
Topical anesthetic application, such as lidocaine 2.5%–prilocaine 2.5% cream, can be applied 60 to 120 minutes prior to intralesional anesthetic injection to attenuate injection pain.2,8 Ice or ethyl chloride spray also can be utilized and has a faster onset of action than topical anesthetics.2,8
Conclusion
The knowledge and application of techniques to minimize pain associated with local anesthetic injection can greatly enhance a resident’s practice. Learning and incorporating these techniques early on in resident training can help instill these skills that can be useful for the remainder of a dermatologist’s career.
1. Burns CA, Ferris G, Feng C, et al. Decreasing the pain of local anesthesia: a prospective, double-blind comparison of buffered, premixed 1% lidocaine with epinephrine versus 1% lidocaine freshly mixed with epinephrine. J Am Acad Dermatol. 2006;54:128-131.
2. Strazar R, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013;132:675-684.
3. Knowles WR. Minimizing pain due to local anesthesia. J Dermatol Surg Oncol. 1990;16:489.
4. Colaric KB, Overton DT, Moore K. Pain reduction in lidocaine administration through buffering and warming. Am J Emerg Med. 1998;16:353-356.
5. Mader TJ, Playe SJ, Garb JL. Reducing the pain of local anesthetic infiltration: warming and buffering have a synergistic effect. Ann Emerg Med. 1994;23:550-554.
6. Yang CH, Hsu HC, Shen SC, et al. Warm and neutral tumescent anesthetic solutions are essential factors for a less painful injection. Dermatol Surg. 2006;32:1119-1122.
7. Krathen RA, Donnelly HB. Warmed local anesthetic for dermatologic surgery. Dermatol Surg. 2008;34:1239-1240.
8. Zilinsky I, Bar-Meir E, Zaslansky R, et al. Ten commandments for minimal pain during administration of local anesthetics. J Drugs Dermatol. 2005;4:212-216.
9. Mustoe TA, Buck DW II, Lalonde DH. The safe management of anesthesia, sedation, and pain in plastic surgery. Plast Reconstr Surg. 2010;126:e165-e176.
10. Martires KJ, Malbasa CL, Bordeaux JS. A randomized controlled crossover trial: lidocaine injected at a 90-degree angle causes less pain than lidocaine injected at a 45-degree angle. J Am Acad Dermatol. 2011;65:1231-1233.
11. Uman LS, Chambers CT, McGrath PJ, et al. A systematic review of randomized controlled trials examining psychological interventions for needle-related procedural pain and distress in children and adolescents: an abbreviated Cochrane review. J Pediatr Psychol. 2008;33:842-854.
12. Ong EL, Lim NL, Koay CK. Towards a pain-free venepuncture. Anaesthesia. 2000;55:260-262.
13. Strazar R, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013;132:675-684.
The use of local anesthetics, particularly local anesthetic injections, is a core part of the practice of dermatology. The use of anesthetics in both diagnosis and management make the administration and usage of these medications a foundational skill for all dermatology residents. Minimizing that familiar “pinch and burn” and giving patients a nearly pain-free experience can result in satisfaction for both patients and physicians. This column describes several useful and easily implemented techniques that residents can incorporate into their daily practice.
Buffer
Plain lidocaine is less acidic than the more commonly utilized lidocaine 1% with 1:100,000 epinephrine. When the latter is buffered with sodium bicarbonate in a 10:1 dilution, it is superior to its unbuffered counterpart.1 This method works by raising the pH of the solution, which is normally 4.2, to a physiologic and more comfortable 7.4.2 Of note, bupivacaine is more acidic than lidocaine.3
Warm
Warming anesthetics has been shown to reduce injection pain. Warming anesthetics to body temperature or up to 40°C to 54.4°C (104°F–130°F) has been studied and recommended.4-7 Warming combined with buffering may result in the least painful injection.4-6
Use Smaller-Gauge Needles
A more obvious tip, using smaller-gauge needles can reduce injection pain. Generally, 27- or 30-gauge needles are commonly recommended.8,9
Limit Repeated Use of the Same Needle
Switch to a fresh needle when you have to inject multiple times in the same lesion or when you have multiple injection sites. In addition, use different needles for drawing up and for the actual injection procedure. A dull needle means more pain.
Perpendicular Injection Technique
Compared to a 45° injection angle, lidocaine injected at a 90° angle reduces pain,10 as this technique minimizes the number of nerve endings that come in contact with the needle.8
Inject Slowly
A slow injection technique using small volumes can substantially minimize pain, as it allows for the nerve endings in the skin to accommodate for the distortion caused by anesthetic infiltration.2
Pulse Injection
Pulse injections can be less painful than injecting an anesthetic in a continuous fashion. It has been recommended that 0.1 cc of anesthetic be injected followed by a 3-second pause, then repeating this step 2 to 3 times. More volumes may subsequently be administered.8
Thoughtful Reinsertion
When larger surface areas must be anesthetized, the needle may have to be reinserted multiple times. In these instances, injection within 1 cm of the visibly blanched area of skin ensures that lidocaine (and epinephrine, if such a solution is used) has already infiltrated that area.2
Distraction
There is merit to the idea of distracting the patient when injecting local anesthetics. Distraction methods including engaging in simple conversation with the patient, having the patient look away, playing background music, and even suggesting that the procedure is painless or has minimal pain have shown utility in minimizing injection pain.8,11
Other distraction techniques are physical, including stretching and scratching the skin, pinching, local vibration, and pressure.12,13
Combination Anesthetic Technique
Topical anesthetic application, such as lidocaine 2.5%–prilocaine 2.5% cream, can be applied 60 to 120 minutes prior to intralesional anesthetic injection to attenuate injection pain.2,8 Ice or ethyl chloride spray also can be utilized and has a faster onset of action than topical anesthetics.2,8
Conclusion
The knowledge and application of techniques to minimize pain associated with local anesthetic injection can greatly enhance a resident’s practice. Learning and incorporating these techniques early on in resident training can help instill these skills that can be useful for the remainder of a dermatologist’s career.
The use of local anesthetics, particularly local anesthetic injections, is a core part of the practice of dermatology. The use of anesthetics in both diagnosis and management make the administration and usage of these medications a foundational skill for all dermatology residents. Minimizing that familiar “pinch and burn” and giving patients a nearly pain-free experience can result in satisfaction for both patients and physicians. This column describes several useful and easily implemented techniques that residents can incorporate into their daily practice.
Buffer
Plain lidocaine is less acidic than the more commonly utilized lidocaine 1% with 1:100,000 epinephrine. When the latter is buffered with sodium bicarbonate in a 10:1 dilution, it is superior to its unbuffered counterpart.1 This method works by raising the pH of the solution, which is normally 4.2, to a physiologic and more comfortable 7.4.2 Of note, bupivacaine is more acidic than lidocaine.3
Warm
Warming anesthetics has been shown to reduce injection pain. Warming anesthetics to body temperature or up to 40°C to 54.4°C (104°F–130°F) has been studied and recommended.4-7 Warming combined with buffering may result in the least painful injection.4-6
Use Smaller-Gauge Needles
A more obvious tip, using smaller-gauge needles can reduce injection pain. Generally, 27- or 30-gauge needles are commonly recommended.8,9
Limit Repeated Use of the Same Needle
Switch to a fresh needle when you have to inject multiple times in the same lesion or when you have multiple injection sites. In addition, use different needles for drawing up and for the actual injection procedure. A dull needle means more pain.
Perpendicular Injection Technique
Compared to a 45° injection angle, lidocaine injected at a 90° angle reduces pain,10 as this technique minimizes the number of nerve endings that come in contact with the needle.8
Inject Slowly
A slow injection technique using small volumes can substantially minimize pain, as it allows for the nerve endings in the skin to accommodate for the distortion caused by anesthetic infiltration.2
Pulse Injection
Pulse injections can be less painful than injecting an anesthetic in a continuous fashion. It has been recommended that 0.1 cc of anesthetic be injected followed by a 3-second pause, then repeating this step 2 to 3 times. More volumes may subsequently be administered.8
Thoughtful Reinsertion
When larger surface areas must be anesthetized, the needle may have to be reinserted multiple times. In these instances, injection within 1 cm of the visibly blanched area of skin ensures that lidocaine (and epinephrine, if such a solution is used) has already infiltrated that area.2
Distraction
There is merit to the idea of distracting the patient when injecting local anesthetics. Distraction methods including engaging in simple conversation with the patient, having the patient look away, playing background music, and even suggesting that the procedure is painless or has minimal pain have shown utility in minimizing injection pain.8,11
Other distraction techniques are physical, including stretching and scratching the skin, pinching, local vibration, and pressure.12,13
Combination Anesthetic Technique
Topical anesthetic application, such as lidocaine 2.5%–prilocaine 2.5% cream, can be applied 60 to 120 minutes prior to intralesional anesthetic injection to attenuate injection pain.2,8 Ice or ethyl chloride spray also can be utilized and has a faster onset of action than topical anesthetics.2,8
Conclusion
The knowledge and application of techniques to minimize pain associated with local anesthetic injection can greatly enhance a resident’s practice. Learning and incorporating these techniques early on in resident training can help instill these skills that can be useful for the remainder of a dermatologist’s career.
1. Burns CA, Ferris G, Feng C, et al. Decreasing the pain of local anesthesia: a prospective, double-blind comparison of buffered, premixed 1% lidocaine with epinephrine versus 1% lidocaine freshly mixed with epinephrine. J Am Acad Dermatol. 2006;54:128-131.
2. Strazar R, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013;132:675-684.
3. Knowles WR. Minimizing pain due to local anesthesia. J Dermatol Surg Oncol. 1990;16:489.
4. Colaric KB, Overton DT, Moore K. Pain reduction in lidocaine administration through buffering and warming. Am J Emerg Med. 1998;16:353-356.
5. Mader TJ, Playe SJ, Garb JL. Reducing the pain of local anesthetic infiltration: warming and buffering have a synergistic effect. Ann Emerg Med. 1994;23:550-554.
6. Yang CH, Hsu HC, Shen SC, et al. Warm and neutral tumescent anesthetic solutions are essential factors for a less painful injection. Dermatol Surg. 2006;32:1119-1122.
7. Krathen RA, Donnelly HB. Warmed local anesthetic for dermatologic surgery. Dermatol Surg. 2008;34:1239-1240.
8. Zilinsky I, Bar-Meir E, Zaslansky R, et al. Ten commandments for minimal pain during administration of local anesthetics. J Drugs Dermatol. 2005;4:212-216.
9. Mustoe TA, Buck DW II, Lalonde DH. The safe management of anesthesia, sedation, and pain in plastic surgery. Plast Reconstr Surg. 2010;126:e165-e176.
10. Martires KJ, Malbasa CL, Bordeaux JS. A randomized controlled crossover trial: lidocaine injected at a 90-degree angle causes less pain than lidocaine injected at a 45-degree angle. J Am Acad Dermatol. 2011;65:1231-1233.
11. Uman LS, Chambers CT, McGrath PJ, et al. A systematic review of randomized controlled trials examining psychological interventions for needle-related procedural pain and distress in children and adolescents: an abbreviated Cochrane review. J Pediatr Psychol. 2008;33:842-854.
12. Ong EL, Lim NL, Koay CK. Towards a pain-free venepuncture. Anaesthesia. 2000;55:260-262.
13. Strazar R, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013;132:675-684.
1. Burns CA, Ferris G, Feng C, et al. Decreasing the pain of local anesthesia: a prospective, double-blind comparison of buffered, premixed 1% lidocaine with epinephrine versus 1% lidocaine freshly mixed with epinephrine. J Am Acad Dermatol. 2006;54:128-131.
2. Strazar R, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013;132:675-684.
3. Knowles WR. Minimizing pain due to local anesthesia. J Dermatol Surg Oncol. 1990;16:489.
4. Colaric KB, Overton DT, Moore K. Pain reduction in lidocaine administration through buffering and warming. Am J Emerg Med. 1998;16:353-356.
5. Mader TJ, Playe SJ, Garb JL. Reducing the pain of local anesthetic infiltration: warming and buffering have a synergistic effect. Ann Emerg Med. 1994;23:550-554.
6. Yang CH, Hsu HC, Shen SC, et al. Warm and neutral tumescent anesthetic solutions are essential factors for a less painful injection. Dermatol Surg. 2006;32:1119-1122.
7. Krathen RA, Donnelly HB. Warmed local anesthetic for dermatologic surgery. Dermatol Surg. 2008;34:1239-1240.
8. Zilinsky I, Bar-Meir E, Zaslansky R, et al. Ten commandments for minimal pain during administration of local anesthetics. J Drugs Dermatol. 2005;4:212-216.
9. Mustoe TA, Buck DW II, Lalonde DH. The safe management of anesthesia, sedation, and pain in plastic surgery. Plast Reconstr Surg. 2010;126:e165-e176.
10. Martires KJ, Malbasa CL, Bordeaux JS. A randomized controlled crossover trial: lidocaine injected at a 90-degree angle causes less pain than lidocaine injected at a 45-degree angle. J Am Acad Dermatol. 2011;65:1231-1233.
11. Uman LS, Chambers CT, McGrath PJ, et al. A systematic review of randomized controlled trials examining psychological interventions for needle-related procedural pain and distress in children and adolescents: an abbreviated Cochrane review. J Pediatr Psychol. 2008;33:842-854.
12. Ong EL, Lim NL, Koay CK. Towards a pain-free venepuncture. Anaesthesia. 2000;55:260-262.
13. Strazar R, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013;132:675-684.