User login
What is the VA? The Largest Educator of Health Care Professionals in the U.S.
This July, medical students, residents, and fellows in almost every medical and surgical specialty will join nurses at all levels of training, undergraduate and graduate pharmacists, dentists, and allied health students to train at a VA hospital. The VA Office of Academic Affiliations (OAA), which coordinates this massive educational effort, reported that in 2015, the last year for which data are available, 123,552 health care trainees were enrolled in VA programs.1 That’s in addition to the hundreds of health care professionals trained in the 4 branches of the armed services, including students at the Uniformed Services University of the Health Sciences and those receiving a health care education through the PHS. Federal institutions are easily the largest contributors to health care education in the nation and very likely in the world.
This mission to educate the U.S. health care workforce is not new. This year marks the 70th anniversary of the collaboration between the VA and academic affiliates across the country to ensure a highly qualified cadre of health care professionals care, not only for veterans, but also for the public. Hence, the OAA motto: To educate for VA and for the nation.
When allopathic and osteopathic medical schools are combined, there are partnerships between the VA and 90% of U.S. medical schools. More than 70% of all U.S. practicing physicians trained at a VA facility at some time.2 Currently, the VA has more than 40 different health care professional training programs under its auspices.
This educational mission is a core VA function that is enshrined in law as are VA’s other 3 core charges. According to the statute, the VA secretary shall “to the extent feasible without interfering with the medical care and treatment of veterans, develop and carry out a program of education and training of health personnel.” The primary clinical care, education, and research functions of the VA are inseparable, and none can be carried out without an adequate number of qualified staff.
Government reports and the media have identified the shortage of VA health care professionals as a major contributor to the wait times crisis of the past several years.3 Section 301 of the Veterans Access, Choice, and Accountability Act of 2014 actually requires the VA Office of Inspector General (OIG) to conduct assessments of the staffing shortages in the department. Reports from the OIG have identified 5 critical need occupations: medical officer, nurse, psychologist, physician assistant, and physical therapist.4
From my perspective as a medical officer, I am certain that the reason I went straight to the VA after my residency in psychiatry and have never left is my overwhelmingly positive experience as a medical student and resident. The VA had many of the best teachers in my training programs. The patients were—and still are nearly 20 years later—among the most respectful and appreciative of any I have treated.
Many VA patients considered us, even as trainees, their doctors and often asked us when we were residents whether they could “keep us,” although they knew that as former members of the military, most of us would rotate out of their lives. Yet they also knew that because of the strength of the training programs, a new young doctor would come to take care of them. Even now when the occasional angry patient says, “all you doctors care about is money,” I am proud to say that I could probably make more money in the private sector, but I choose to work at the VA.
Many of my fine colleagues in medicine, nursing, psychology, and allied health also remained at the VA after their training, inspired to provide public health to those who served and were underserved. Those who entered military medicine or the PHS had similar ideals borne of the role models who taught them in those federal institutions. One of the often unappreciated negative consequences of the VA scandal is that it may discouarge students in the health care professions from rotating through or seriously considering careers in the VA.
The VA and the military often do not receive the recognition they deserve as academic medical institutions. Some of the most renowned and accomplished faculty of prestigious medical universities also work at VA facilities. The ability to simultaneously teach gifted students, conduct cutting-edge research, and practice high-quality medicine all in a public health setting are what attracted me and many other idealistic health care professionals to the VA.
The VA, however, has taken active steps to restore its reputation as one of the best places to learn and work. Three outstanding initiatives deserve special attention. The first being a series of visits to medical schools that Carolyn M. Clancy, MD, made when she was the interim under secretary for health. Fortunately for me, she spoke at the academic affiliate of my VAMC (the University of New Mexico School of Medicine), where she talked about the excitement and rewards of VA clinical care and research.5
The VA Nursing Academic Partnerships (VANAP) is another initiative to promote VA as an educator and employer of health professionals. Comprised of 18 competitively selected nursing schools in the nation and the VA, VANAP’s objective is “increasing recruitment and retention of VA nurses as a result of enhanced roles in nursing education.” The New Mexico VA Health Care System, the hospital I practice at, had the honor of being awarded one of these partnerships, and I have been encouraged to see many student nurses choose the training track at the VA and express interest in employment.
According to a nurse at the Oregon Health & Science University VA partnership, “One thing I learned that I did not expect was about the wars the clients had served in. I gained a greater respect for our men and women in the service past and present…I have now an understanding of not only the physical, but also the mental and emotional effects war has on an individual.”6 It is important to realize that even if physicians and nurses in training do not ultimately enter the VA workforce, they still leave their educational experience with a more empathic understanding of the health care needs of veterans.
The salience of the third endeavor, however, has not been widely recognized. In March, Secretary Robert McDonald spoke at a meeting of the Association of American Medical Colleges Council of Deans. His speech traced the history of academic collaboration with the VA; acknowledged the bureaucratic, information technology, and other challenges faced by the VA and its academic affiliates; and reaffirmed the VA’s commitment to academic partnerships. He recognized the significant and lasting contributions the relationship with academic medical centers has had on the care of veterans and the community for decades. His remarks concluded with a vision of the potential the partnership has to transform health education and the delivery of care in the years to come. But perhaps the most hopeful remarks in the speech came not from Secretary McDonald but from the comments of medical students who had rotated at the San Diego VAMC, which he shared:
“The emphasis on teaching was fantastic, and far superior to most other rotations.”
“The vets were a wonderful patient population who really allowed us a great opportunity to learn.”
“The VA is the best place for medical students to work.”7
1. U.S. Veterans Health Administration Office of Academic Affiliations. 2015 statistics: health professions traineees. U.S. Department of Veterans Affairs website. http://www.va.gov/oaa/docs/OAA_Statistics.pdf. Accessed June 14, 2016.
2. Office of Academic Affiliations. 70th anniversary of academic affiliations. U.S. Department of Veterans Affairs website. http://www.va.gov/OAA/OAA_70th_Anniversary.asp. Update February 18, 2016. Accessed June 4, 2016.
3. Oppel RA, Goodnough A. Doctor shortage is cited in delays at V.A. hospitals. The New York Times. May 29, 2014.
4. Zonana HV, Wells JA, Getz MA, Buchanan J. Part I: The NGRI Registry: initial analyses of data collected on Connecticut insanity acquittees. Bull Am Acad Psychiatry Law. 1990;18(2):115-128.
5. Foster C. V.A. official visits HSC, as agency seeks to hire health care workers. UNM HSC Newsbeat. November 11, 2014.
6. VA Nursing Academic Partnerships. Oregon Health and Science University website. http://www.ohsu.edu/xd/education/schools/school-of-nursing/about/loader.cfm?csModule=security/getfile&pageid=2301310. Accessed June 14, 2016.
7. McDonald R. McDonald: Academic affiliations a source of strength for VA, medical schools. U.S. Department of Veterans Affairs website. http://www.blogs.va.gov/VAntage/18655/mcdonald-academic-affiliations-a-source-of-strength-for-the-va-medical-schools. Updated March 30, 2015. Accessed June 14, 2016.
This July, medical students, residents, and fellows in almost every medical and surgical specialty will join nurses at all levels of training, undergraduate and graduate pharmacists, dentists, and allied health students to train at a VA hospital. The VA Office of Academic Affiliations (OAA), which coordinates this massive educational effort, reported that in 2015, the last year for which data are available, 123,552 health care trainees were enrolled in VA programs.1 That’s in addition to the hundreds of health care professionals trained in the 4 branches of the armed services, including students at the Uniformed Services University of the Health Sciences and those receiving a health care education through the PHS. Federal institutions are easily the largest contributors to health care education in the nation and very likely in the world.
This mission to educate the U.S. health care workforce is not new. This year marks the 70th anniversary of the collaboration between the VA and academic affiliates across the country to ensure a highly qualified cadre of health care professionals care, not only for veterans, but also for the public. Hence, the OAA motto: To educate for VA and for the nation.
When allopathic and osteopathic medical schools are combined, there are partnerships between the VA and 90% of U.S. medical schools. More than 70% of all U.S. practicing physicians trained at a VA facility at some time.2 Currently, the VA has more than 40 different health care professional training programs under its auspices.
This educational mission is a core VA function that is enshrined in law as are VA’s other 3 core charges. According to the statute, the VA secretary shall “to the extent feasible without interfering with the medical care and treatment of veterans, develop and carry out a program of education and training of health personnel.” The primary clinical care, education, and research functions of the VA are inseparable, and none can be carried out without an adequate number of qualified staff.
Government reports and the media have identified the shortage of VA health care professionals as a major contributor to the wait times crisis of the past several years.3 Section 301 of the Veterans Access, Choice, and Accountability Act of 2014 actually requires the VA Office of Inspector General (OIG) to conduct assessments of the staffing shortages in the department. Reports from the OIG have identified 5 critical need occupations: medical officer, nurse, psychologist, physician assistant, and physical therapist.4
From my perspective as a medical officer, I am certain that the reason I went straight to the VA after my residency in psychiatry and have never left is my overwhelmingly positive experience as a medical student and resident. The VA had many of the best teachers in my training programs. The patients were—and still are nearly 20 years later—among the most respectful and appreciative of any I have treated.
Many VA patients considered us, even as trainees, their doctors and often asked us when we were residents whether they could “keep us,” although they knew that as former members of the military, most of us would rotate out of their lives. Yet they also knew that because of the strength of the training programs, a new young doctor would come to take care of them. Even now when the occasional angry patient says, “all you doctors care about is money,” I am proud to say that I could probably make more money in the private sector, but I choose to work at the VA.
Many of my fine colleagues in medicine, nursing, psychology, and allied health also remained at the VA after their training, inspired to provide public health to those who served and were underserved. Those who entered military medicine or the PHS had similar ideals borne of the role models who taught them in those federal institutions. One of the often unappreciated negative consequences of the VA scandal is that it may discouarge students in the health care professions from rotating through or seriously considering careers in the VA.
The VA and the military often do not receive the recognition they deserve as academic medical institutions. Some of the most renowned and accomplished faculty of prestigious medical universities also work at VA facilities. The ability to simultaneously teach gifted students, conduct cutting-edge research, and practice high-quality medicine all in a public health setting are what attracted me and many other idealistic health care professionals to the VA.
The VA, however, has taken active steps to restore its reputation as one of the best places to learn and work. Three outstanding initiatives deserve special attention. The first being a series of visits to medical schools that Carolyn M. Clancy, MD, made when she was the interim under secretary for health. Fortunately for me, she spoke at the academic affiliate of my VAMC (the University of New Mexico School of Medicine), where she talked about the excitement and rewards of VA clinical care and research.5
The VA Nursing Academic Partnerships (VANAP) is another initiative to promote VA as an educator and employer of health professionals. Comprised of 18 competitively selected nursing schools in the nation and the VA, VANAP’s objective is “increasing recruitment and retention of VA nurses as a result of enhanced roles in nursing education.” The New Mexico VA Health Care System, the hospital I practice at, had the honor of being awarded one of these partnerships, and I have been encouraged to see many student nurses choose the training track at the VA and express interest in employment.
According to a nurse at the Oregon Health & Science University VA partnership, “One thing I learned that I did not expect was about the wars the clients had served in. I gained a greater respect for our men and women in the service past and present…I have now an understanding of not only the physical, but also the mental and emotional effects war has on an individual.”6 It is important to realize that even if physicians and nurses in training do not ultimately enter the VA workforce, they still leave their educational experience with a more empathic understanding of the health care needs of veterans.
The salience of the third endeavor, however, has not been widely recognized. In March, Secretary Robert McDonald spoke at a meeting of the Association of American Medical Colleges Council of Deans. His speech traced the history of academic collaboration with the VA; acknowledged the bureaucratic, information technology, and other challenges faced by the VA and its academic affiliates; and reaffirmed the VA’s commitment to academic partnerships. He recognized the significant and lasting contributions the relationship with academic medical centers has had on the care of veterans and the community for decades. His remarks concluded with a vision of the potential the partnership has to transform health education and the delivery of care in the years to come. But perhaps the most hopeful remarks in the speech came not from Secretary McDonald but from the comments of medical students who had rotated at the San Diego VAMC, which he shared:
“The emphasis on teaching was fantastic, and far superior to most other rotations.”
“The vets were a wonderful patient population who really allowed us a great opportunity to learn.”
“The VA is the best place for medical students to work.”7
This July, medical students, residents, and fellows in almost every medical and surgical specialty will join nurses at all levels of training, undergraduate and graduate pharmacists, dentists, and allied health students to train at a VA hospital. The VA Office of Academic Affiliations (OAA), which coordinates this massive educational effort, reported that in 2015, the last year for which data are available, 123,552 health care trainees were enrolled in VA programs.1 That’s in addition to the hundreds of health care professionals trained in the 4 branches of the armed services, including students at the Uniformed Services University of the Health Sciences and those receiving a health care education through the PHS. Federal institutions are easily the largest contributors to health care education in the nation and very likely in the world.
This mission to educate the U.S. health care workforce is not new. This year marks the 70th anniversary of the collaboration between the VA and academic affiliates across the country to ensure a highly qualified cadre of health care professionals care, not only for veterans, but also for the public. Hence, the OAA motto: To educate for VA and for the nation.
When allopathic and osteopathic medical schools are combined, there are partnerships between the VA and 90% of U.S. medical schools. More than 70% of all U.S. practicing physicians trained at a VA facility at some time.2 Currently, the VA has more than 40 different health care professional training programs under its auspices.
This educational mission is a core VA function that is enshrined in law as are VA’s other 3 core charges. According to the statute, the VA secretary shall “to the extent feasible without interfering with the medical care and treatment of veterans, develop and carry out a program of education and training of health personnel.” The primary clinical care, education, and research functions of the VA are inseparable, and none can be carried out without an adequate number of qualified staff.
Government reports and the media have identified the shortage of VA health care professionals as a major contributor to the wait times crisis of the past several years.3 Section 301 of the Veterans Access, Choice, and Accountability Act of 2014 actually requires the VA Office of Inspector General (OIG) to conduct assessments of the staffing shortages in the department. Reports from the OIG have identified 5 critical need occupations: medical officer, nurse, psychologist, physician assistant, and physical therapist.4
From my perspective as a medical officer, I am certain that the reason I went straight to the VA after my residency in psychiatry and have never left is my overwhelmingly positive experience as a medical student and resident. The VA had many of the best teachers in my training programs. The patients were—and still are nearly 20 years later—among the most respectful and appreciative of any I have treated.
Many VA patients considered us, even as trainees, their doctors and often asked us when we were residents whether they could “keep us,” although they knew that as former members of the military, most of us would rotate out of their lives. Yet they also knew that because of the strength of the training programs, a new young doctor would come to take care of them. Even now when the occasional angry patient says, “all you doctors care about is money,” I am proud to say that I could probably make more money in the private sector, but I choose to work at the VA.
Many of my fine colleagues in medicine, nursing, psychology, and allied health also remained at the VA after their training, inspired to provide public health to those who served and were underserved. Those who entered military medicine or the PHS had similar ideals borne of the role models who taught them in those federal institutions. One of the often unappreciated negative consequences of the VA scandal is that it may discouarge students in the health care professions from rotating through or seriously considering careers in the VA.
The VA and the military often do not receive the recognition they deserve as academic medical institutions. Some of the most renowned and accomplished faculty of prestigious medical universities also work at VA facilities. The ability to simultaneously teach gifted students, conduct cutting-edge research, and practice high-quality medicine all in a public health setting are what attracted me and many other idealistic health care professionals to the VA.
The VA, however, has taken active steps to restore its reputation as one of the best places to learn and work. Three outstanding initiatives deserve special attention. The first being a series of visits to medical schools that Carolyn M. Clancy, MD, made when she was the interim under secretary for health. Fortunately for me, she spoke at the academic affiliate of my VAMC (the University of New Mexico School of Medicine), where she talked about the excitement and rewards of VA clinical care and research.5
The VA Nursing Academic Partnerships (VANAP) is another initiative to promote VA as an educator and employer of health professionals. Comprised of 18 competitively selected nursing schools in the nation and the VA, VANAP’s objective is “increasing recruitment and retention of VA nurses as a result of enhanced roles in nursing education.” The New Mexico VA Health Care System, the hospital I practice at, had the honor of being awarded one of these partnerships, and I have been encouraged to see many student nurses choose the training track at the VA and express interest in employment.
According to a nurse at the Oregon Health & Science University VA partnership, “One thing I learned that I did not expect was about the wars the clients had served in. I gained a greater respect for our men and women in the service past and present…I have now an understanding of not only the physical, but also the mental and emotional effects war has on an individual.”6 It is important to realize that even if physicians and nurses in training do not ultimately enter the VA workforce, they still leave their educational experience with a more empathic understanding of the health care needs of veterans.
The salience of the third endeavor, however, has not been widely recognized. In March, Secretary Robert McDonald spoke at a meeting of the Association of American Medical Colleges Council of Deans. His speech traced the history of academic collaboration with the VA; acknowledged the bureaucratic, information technology, and other challenges faced by the VA and its academic affiliates; and reaffirmed the VA’s commitment to academic partnerships. He recognized the significant and lasting contributions the relationship with academic medical centers has had on the care of veterans and the community for decades. His remarks concluded with a vision of the potential the partnership has to transform health education and the delivery of care in the years to come. But perhaps the most hopeful remarks in the speech came not from Secretary McDonald but from the comments of medical students who had rotated at the San Diego VAMC, which he shared:
“The emphasis on teaching was fantastic, and far superior to most other rotations.”
“The vets were a wonderful patient population who really allowed us a great opportunity to learn.”
“The VA is the best place for medical students to work.”7
1. U.S. Veterans Health Administration Office of Academic Affiliations. 2015 statistics: health professions traineees. U.S. Department of Veterans Affairs website. http://www.va.gov/oaa/docs/OAA_Statistics.pdf. Accessed June 14, 2016.
2. Office of Academic Affiliations. 70th anniversary of academic affiliations. U.S. Department of Veterans Affairs website. http://www.va.gov/OAA/OAA_70th_Anniversary.asp. Update February 18, 2016. Accessed June 4, 2016.
3. Oppel RA, Goodnough A. Doctor shortage is cited in delays at V.A. hospitals. The New York Times. May 29, 2014.
4. Zonana HV, Wells JA, Getz MA, Buchanan J. Part I: The NGRI Registry: initial analyses of data collected on Connecticut insanity acquittees. Bull Am Acad Psychiatry Law. 1990;18(2):115-128.
5. Foster C. V.A. official visits HSC, as agency seeks to hire health care workers. UNM HSC Newsbeat. November 11, 2014.
6. VA Nursing Academic Partnerships. Oregon Health and Science University website. http://www.ohsu.edu/xd/education/schools/school-of-nursing/about/loader.cfm?csModule=security/getfile&pageid=2301310. Accessed June 14, 2016.
7. McDonald R. McDonald: Academic affiliations a source of strength for VA, medical schools. U.S. Department of Veterans Affairs website. http://www.blogs.va.gov/VAntage/18655/mcdonald-academic-affiliations-a-source-of-strength-for-the-va-medical-schools. Updated March 30, 2015. Accessed June 14, 2016.
1. U.S. Veterans Health Administration Office of Academic Affiliations. 2015 statistics: health professions traineees. U.S. Department of Veterans Affairs website. http://www.va.gov/oaa/docs/OAA_Statistics.pdf. Accessed June 14, 2016.
2. Office of Academic Affiliations. 70th anniversary of academic affiliations. U.S. Department of Veterans Affairs website. http://www.va.gov/OAA/OAA_70th_Anniversary.asp. Update February 18, 2016. Accessed June 4, 2016.
3. Oppel RA, Goodnough A. Doctor shortage is cited in delays at V.A. hospitals. The New York Times. May 29, 2014.
4. Zonana HV, Wells JA, Getz MA, Buchanan J. Part I: The NGRI Registry: initial analyses of data collected on Connecticut insanity acquittees. Bull Am Acad Psychiatry Law. 1990;18(2):115-128.
5. Foster C. V.A. official visits HSC, as agency seeks to hire health care workers. UNM HSC Newsbeat. November 11, 2014.
6. VA Nursing Academic Partnerships. Oregon Health and Science University website. http://www.ohsu.edu/xd/education/schools/school-of-nursing/about/loader.cfm?csModule=security/getfile&pageid=2301310. Accessed June 14, 2016.
7. McDonald R. McDonald: Academic affiliations a source of strength for VA, medical schools. U.S. Department of Veterans Affairs website. http://www.blogs.va.gov/VAntage/18655/mcdonald-academic-affiliations-a-source-of-strength-for-the-va-medical-schools. Updated March 30, 2015. Accessed June 14, 2016.

The Unique Value of Externships to Nursing Education and Health Care Organizations
New nurse graduates often have difficulty transitioning to the role of registered nurse (RN).1 Given the complexity of the health care environment, the need is growing to prepare nursing students for nursing practice. Although nursing education provides students with a basis for practice, school alone cannot prepare them for actual practice in the hospital setting.2 Compared with nurse residency programs, which provide extended postlicensure training, the national Veterans Affairs Learning Opportunity Residency (VALOR) program provides externships independent of nursing school. Externships allow students to train in a hospital setting (generally during the summer months) before becoming a licensed RN. Nursing students who are entering their senior year of coursework in a bachelor of science nursing program and who have a minimum 3.0 grade point average can apply for this competitive national scholarship offered at VAMCs. The VALOR program is a paid learning opportunity, and students gain hands-on clinical experience under the guidance of preceptors.
Little externship research exists in the nursing literature.3,4 The authors conducted the present study to help fill the gaps in the literature and to add to the only other study findings on VALOR.3 This program, started in 1990 to aid in nursing recruitment and retention, offers students early exposure to the complexities of nursing practice.
The authors investigated RNs’ experience in the VALOR prelicensure externship during the nurses’ senior year of coursework and the impact of this experience on their nursing practice. The program offers 800 hours of hospital-based experience outside the classroom. New nurses who gained only limited clinical exposure in nursing school may feel insecure about their clinical skills.5 Casey and colleagues found that students want more clinical experience than offered by nursing school practicums.6 The VALOR participants obtain additional clinical time, which contributes to their self-confidence when transitioning to the RN role.7
Literature Review
New graduate nurses work in complex health care environments with unfamiliar technologies, shift hours, heavy patient loads, psychological and professional stressors, socialization problems, and patient safety issues.8 They often are unable to connect their educational experience with the realities of practice and find the work environment incongruent with their nursing school education.9 Although new nurses’ difficulty in transitioning to their professional role has been addressed in the literature, transitional experience has not improved.10 Studies have found that new graduate nurses want more support than is given and have suggested that unfamiliar workplace dynamics create stress for new nurses.11
Anxiety, insecurity, and fear of failure are associated with the transition from student to practicing nurse.10 Because of the additional clinical experience gained in an externship, students likely are more self-confident when they assume the RN role.12 White suggested self-confident students see themselves as nurses and feel capable of caring for patients.13 Externship experience makes the transition to professional nursing less stressful, because externship students obtain an inside view of nursing culture.14 Students increase their understanding of nurses’ multiple roles and responsibilities, because these programs focus on increasing clinical skills and competency.15 To perform successfully as RNs, new graduates need competencies and knowledge beyond those obtained in nursing school.16
In the nursing profession, an association between job satisfaction and turnover exists.17,18 Of new graduate nurses, 35% to 69% leave their position within the first year of employment.19 Replacing nurses reduces hospital productivity and efficiency and increases cost.20 New graduate nurses leave because they are dissatisfied with and overwhelmed by the complexity of the work environment.21 Prelicensure nurse externships can aid in recruiting and retaining new graduate nurses for the hospitals that host these programs.22 For host facilities, recruitment rates of 50% to 79% have been reported.23,24
In a quantitative study, Nuttall surveyed 133 RNs about job satisfaction, role socialization, professionalism, and sense of belonging.3 Of these RNs, 34 had participated in VALOR and 99 had not. There was no evidence that the RNs with VALOR experience had a higher degree of professionalism, job satisfaction, or role socialization; only sense of belonging (age-adjusted) was higher for the VALOR group. The conflicting data on prelicensure externship outcomes call for further analysis of these programs.3 Nuttall noted that her study “was the first... to evaluate the VALOR program and future research [using a qualitative approach] is needed to identify additional outcomes related to this program.”3
Methods
This study using hermeneutic phenomenology was approved by the Salem VAMC in Virginia and by the institutional review board at Nova Southeastern University.24 Study participants provided written informed consent before being interviewed.
Interviewees
Data Collection and Analysis
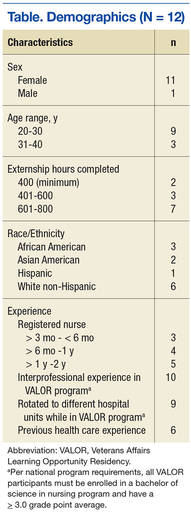
Data collection began in March 2013 with a pilot test of the interview questions for appropriateness. Open-ended, semistructured questions were used to elicit nurses’ descriptions of their experience. Field notes were written, and all interviews were tape-recorded and professionally transcribed verbatim. Data saturation was reached after 12 nurses were interviewed. Transcripts were analyzed and interpreted using van Manen’s line-by-line approach.26 All 12 interviewees were invited to review the findings of the data analysis. Eleven of the 12 interviewees verified and validated the study findings.
Rigor using Lincoln and Guba’s criteria of credibility, dependability, transferability, and confirmability added trustworthiness to the study findings. Bracketing helped eliminate potential bias.27 Credibility was achieved with prolonged engagement and triangulation. To further enhance credibility, the authors invited qualitative research experts to validate the emerging themes and create an audit trail. For dependability, a flow chart was created for use by researchers who might want to replicate the study. Rich, lengthy descriptions and interviewees’ quotations were provided so researchers could judge the study’s transferability to other settings. Maintaining an audit trail and having a doctor of nursing practice independently code the data aided with confirmability. This study used findings from the literature, audio recordings, member checking, and field notes to assess data accuracy.
Results
The overarching theme discovered in this study was confidence. Subthemes were transitioning to the RN role, making decisions, and interacting with interprofessional staff.
Confidence
Interviewees felt confident in transitioning to the RN role, making decisions, and interacting with interprofessional staff. They shared that they had applied to the externship to gain additional clinical experience and that the program increased their self-confidence with respect to transitioning to the new role as RN. However, it is possible that these interviewees were highly motivated and would not have had difficulty transitioning to the RN role—this is addressed in the Limitations section of this article.
Interviewees said they initially approached VALOR with fear and apprehension but completed it feeling confident about becoming an RN. One interviewee stated, “The VALOR program gave me the confidence in my own abilities, so I was not scared and had confidence that, yes, I could do this job.” Another said, “Honestly, the entire externship program, regardless of which question you ask, my answer is going to always fall back on confidence. I became prepared for the RN job, I feel, before I graduated because of the [externship] experiences.”
Transitioning to RN Role
Transitioning involved understanding the RN’s scope of practice and feeling clinically competent. Students worked 40 hours a week over the summer and gained firsthand insight into working as an RN daily. Interviewees believed completing the externship made it easy to transition to the RN role because they knew what to expect.
Working side-by-side with nurses, students gained insight into RNs’ responsibilities and scope of practice. Interviewees reported that, after the externship, they had a better understanding of their patient care and licensure legal responsibilities.
Students began to feel clinically competent during the externship. Interviewees shared that they had had several opportunities to practice basic skills, such as giving injections. One interviewee said, “I don’t think I tried to stick a single IV when I was in school or in clinical [training].” Interviewees also commented that repeatedly practicing skills increased their self-confidence.
Students also gained firsthand insight into working with veterans and their families. During the externship, they learned about communicating therapeutically, providing education for caregivers, and advocating for patients and their families. Before the externship, they felt apprehensive about communicating with patients. One interviewee said that after the program, “Eventually you had to talk to patients, and eventually figured it out that it wasn’t so scary.”
Students found that patients were not always happy with their care, and procedures did not always go as planned. They also discovered that education did not end with the patient; family members needed education as well. The externship experience heightened students’ awareness of the RN’s role as patient advocate. One interviewee explained it is the RN’s responsibility to intervene on the patient’s behalf. Interviewees were surprised that patients would not tell their health care provider that they did not understand what was said or that they wanted another course of treatment.
The externship helped decrease learning-related stress. Interviewees indicated they had learned without fear of reprisal. One described feeling free to learn: “Uninhibited learning...you can ask what you need to without fear of not graduating.” Externship students were able to focus on learning the RN role without worrying about the next test or grade. They felt free to ask questions without fear of failing their clinical rotation.
The supportive and nurturing relationships that students developed in VALOR also increased their confidence when transitioning to the RN role. One interviewee said, “There was never the sense of, no, you learn my way, or I don’t want you here.” Interviewees shared that they felt comfortable and supported.
Decision Making
Interviewees reported that after VALOR, it was easy to make decisions regarding nursing practice, delegation, care prioritization, and career choice. As students, they found the school clinical setting did not provide the decision-making opportunities VALOR did, and they quickly realized nursing practice involved more than making patient-care decisions. One interviewee said, “In a classroom, a picture is painted of an idealistic environment that may not truly mimic the hospital unit.”
Students became familiar with the practice of delegating care to the appropriate staff and the next shift. One interviewee said VALOR “provided me with a better understanding of delegation in my RN role.” VALOR participants discovered that, as new nurses, they were less anxious when delegating to others.
Before RN licensure, VALOR participants learned about prioritizing patient care. One interviewee said, “It’s like everybody has to be charted on, and all the medications have to be passed out, but it’s a matter of getting everything done while doing the more important and more dire things first.” Students learned that all aspects of nursing are important, but they had to make rational decisions.
Interacting With Professionals
Interviewees who had been in VALOR said interacting with interprofessional (different disciplines) staff contributed to their working comfortably in teams and collaborating with others. Their collaborative relationships with physicians would help them later, when as new graduate nurses they again needed to work together with doctors. Typical comments were, “When I started as an RN, I felt I was not new at it because I had communicated with doctors in the externship program.”
Discussion
The present study found that nursing students who had been in the VALOR externship felt confident in their clinical skills when they were transitioning to the RN role. Other studies similarly have found that externship students were self-confident assuming the RN role, owing to their additional clinical experience.12,28 The VALOR program allows students to work alongside nurses and receive hands-on experience while interacting with interprofessional health care teams. Findings of Nuttall’s quantitative study contradict those of the present, qualitative study. Nuttall used surveys and a control group, whereas this phenomenologic study captured the essence of study participants’ experiences through interviews.
The RNs interviewed in the present study discovered that, unlike nursing school, VALOR provided a realistic view of full-time work as an RN. This finding aligns with Starr and Conley’s finding that, before participating in an externship, most students were unaware of the extent of RNs’ roles and responsibilities, whereas after the program they understood these roles and responsibilities better.28
The interviewees in this study thought VALOR improved their skills in communicating with patients, families, and interprofessional team members. Interviewees shared that they learned patient advocacy skills and that, through firsthand experience, realized nurses provide patients with a voice. Externships can help new graduate nurses become better communicators and can teach students the importance of patient communication and advocacy.12
This study also found that students wanted more exposure to realistic nursing environments, additional nursing skills practice, and more interaction with interprofessional team members. VALOR helped bridge the theory–practice gap by providing real-world nursing experience outside the academic environment and extra time for nursing skills development. In a study by Casey and colleagues, students indicated that the time allowed for nursing skills practice during school was inadequate.6
The VALOR program helped students learn about delegating work, whereas nursing school did not provide the opportunity to practice delegation. Other studies have corroborated that students do not practice delegation during nursing school clinical time.29,30
Study respondents noted they could focus on learning without the fear of passing their clinical rotation. They felt supported by staff and were comfortable asking questions. White suggested that externship students who feel supported by nursing staff are able to focus on patients instead of on their discomfort.13 Rush and colleagues found that constraints on the student experience in traditional academic clinical rotations were replaced with “freedom and fearlessness in learning” in externships.31
Ten of the 12 study participants applied for a new graduate nurse position at the VAMC where they had their externship. A potential benefit to organizations that sponsor a nursing externship is the recruitment of new graduate nurses.14 Before applying for a full-time position, VALOR students had the opportunity to become familiar with the work environment and assess their fit with the employer. One student found staff nurse work “scary” and “stressful” and decided against it. She said the VALOR externship helped her realize exactly what nursing entailed: “Until this experience, I did not realize I would not like the hospital environment. This was a reality check for me.” Another student decided that working different shifts and working holidays would be difficult for her. These 2 students’ externship experience convinced them to seek other nursing positions.
Limitations
All participants in this study were nurses with excellent academic grades. It is possible they were highly motivated and might not have had any difficulty transitioning to the RN role. The principal investigator in this study was a VALOR program coordinator who knew 3 of the study participants—a potential source of bias. It is possible participants did not want to speak negatively about the program for several reasons: the interviewer was their coordinator, they received a salary during the externship, and several worked for the VA at the time of the survey.
Researchers have acknowledged the likelihood that not all VALOR students have positive experiences. It is possible that students with negative experiences did not discuss them or did not participate in the study. Increasing the size of the study sample may have brought in students with negative experiences. There is also the possibility of researcher misinterpretation and bias. Although bracketing was used, it was not possible to eliminate all potential sources of bias from this qualitative study.
Future Research
This is 1 of only 2 studies on the VALOR externship. Given the contradictory findings of these studies—Nuttall reported VALOR experience did not affect students’ transition to the RN role,3 whereas in the present study VALOR students thought the program positively affected their successful transition—additional quantitative and qualitative research is needed.
In addition, the low recruitment rate of VALOR students should be compared with other studies’ recruitment rates. The 38% VALOR extern recruitment rate for the period 2007 to 2012 is lower than the rate for other programs (G. Fuller, August 27, 2014, e-mail communication). The VALOR program does not track retention of participants after employment. Longitudinal studies should compare VALOR participants’ length of employment with that of nonparticipants’.
Conclusion
Externships provide clinical experience outside the classroom, expose students to the realities of nursing practice before graduation, and serve as a recruitment tool for hospitals. These programs, in conjunction with school-based practicums, increase exposure to the clinical environment. Before graduation, students have the opportunity to practice skills, interact with interprofessional staff, and experience different hospital units, all of which contribute to career decisions. The present study found that the VALOR externship helped new graduate nurses with their transition to the workplace. However, it is important to recognize the limitations of this study.
Interviewees indicated they were confident when they were transitioning to their new nurse role and caring for patients before receiving their RN licensure. New graduate nurses discovered they acclimated to the hospital environment quicker. The reality of working day-to-day in a hospital setting allowed students to select a compatible work environment and understand the daily challenges health care professionals encounter. Interviewees shared that they felt “like the RN” during the externship, which lessened the shock of actually assuming the RN role.
Van Manen asserted there is no conclusion or ending to a phenomenological study.26 Continued research on hospital-based externships will demonstrate how these programs can assist in the development of new graduate nurses, ease their transition to practice, and benefit nursing education, practice, research, and public policy.
1. Clark CM, Springer PJ. Nurse residents' first-hand accounts on transition to practice. Nurs Outlook. 2012;60(4):e2-e8.
2. Myers S, Reidy P, French B, McHale J, Chisholm M, Griffin M. Safety concerns of hospital-based new-to-practice registered nurses and their preceptors. J Contin Educ Nurs. 2010;41(4):163-171.
3. Nuttall CM. A Comparative Study Evaluating the Impact of Participation in a VALOR Nurse Externship on Job Satisfaction, Sense of Belonging, Role Socialization and Sense of Professionalism: Transition From Graduate to Registered Nurse [dissertation]. Albuquerque: University of New Mexico; 2010.
4. Steen JE, Gould EW, Raingruber B, Hill J. Effect of student nurse intern position on ease of transition from student nurse to registered nurse. J Nurs Staff Dev. 2011;27(4):181-186.
5. Ulrich B, Krozek C, Early S, Ashlock CH, Africa LM, Carman ML. Improving retention, confidence, and competence of new graduate nurses: results from a 10-year longitudinal database. Nurs Econ. 2010;28(6):363-375.
6. Casey K, Fink R, Jaynes C, Campbell L, Cook P, Wilson V. Readiness for practice: the senior practicum experience. J Nurs Educ. 2011;50(11):646-652.
7. Shipman D, Hooten J, Stanley S. The VALOR program: preparing nursing students to care for our veterans. Fed Pract. 2014;31(9):35-38.
8. Walker A, Earl C, Costa B, Cuddihy L. Graduate nurses' transition and integration into the workplace: a qualitative comparison of graduate nurses' and nurse unit managers' perspectives. Nurs Educ Today. 2013;33(3):291-296.
9. Welding NM. Creating a nursing residency: decrease turnover and increase clinical competence. Medsurg Nurs. 2011;20(1):37-40.
10. Morrow S. New graduate transitions: leaving the nest, joining the flight. J Nurs Manag. 2009;17(3):278-287.
11. Parker V, Giles M, Lantry G, McMillan M. New graduate nurses' experience in their first year of practice. Nurs Educ Today. 2014;34(1):150-156.
12. Ruth-Sahd LA, Beck J, McCall C. Transformative learning during a nursing externship program: the reflections of senior nursing students. Nurs Educ Perspect. 2010;31(2):78-83.
13. White AH. Clinical decision making among fourth-year nursing students: an interpretive study. J Nurs Educ. 2003;42(3):113-121.
14. Kropkowski LR, Most R. Set for success: nurse "externs." Nurs Manag. 2008;39(7):8-9.
15. Rhoads J, Sensenig K, Ruth-Sahd L, Thompson E. Nursing externship: a collaborative endeavor between nursing education and nursing administration. Dimens Crit Care Nurs. 2003;22(6):255-258.
16. Hillman L, Foster RR. The impact of a nursing transitions programme on retention and cost savings. J Nurs Manag. 2011;19(1):50-56.
17. Baernholdt M, Mark BA. The nurse work environment, job satisfaction and turnover rates in rural and urban nursing units. J Nurs Manag. 2009;17(8):994-1001.
18. Jones CB. Revisiting nurse turnover costs: adjusting for inflation. J Nurs Adm. 2008;38(1):11-18.
19. Pine R, Tart K. Return on investment: benefits and challenges of baccalaureate nurse residency program. Nurs Econ. 2007;25(1):13-18, 39.
20. Beecroft PC, Dorey F, Wenten M. Turnover intention in new graduate nurses: a multivariate analysis. J Adv Nurs, 2008;62(1):41-52.
21. Phillips C, Esterman A, Kenny A. The theory of organisational socialisation and its potential for improving transition experiences for new graduate nurses. Nurs Educ Today. 2015;35(1):118-124.
22. Diefenbeck CA, Plowfield LA, Herrman JW. Clinical immersion: a residency model for nursing education. Nurs Educ Perspect. 2006;27(2):72-79.
23. Cantrell MA, Browne AM. The impact of a nurse externship on the transition process from graduate to registered nurse: part III. Recruitment and retention effects. J Nurs Staff Dev. 2006;22(1):11-14.
24. Kilpatrick K, Frunchak V. The nursing extern program: innovative strategies for students in transition. Health Care Manag (Frederick). 2006;25(3):236-242.
25. Kovner CT, Brewer CS, Fairchild S, Poornima S, Kim H, Djukic CM. Newly licensed RN's characteristics, work attitudes, and intentions to work. Am J Nurs. 2007;107(9):58-70
26. van Manen M. Researching Lived Experience: Human Science for an Action Sensitive Pedagogy. Albany: State University of New York Press; 1990.
27. Lincoln YS, Guba EG. Naturalistic Inquiry. Beverly Hills, CA: Sage; 1985.
28. Starr K, Conley VM. Becoming a registered nurse: the nurse extern experience. J Contin Educ Nurs. 2006;37(2):86-92.
29. Hasson F, McKenna HP, Keeney S. Delegating and supervising unregistered professionals: the student nurse experience. Nurs Educ Today. 2013;33(3):229-235.
30. Kramer M, Maguire P, Halfer D, et al. The organizational transformative power of nurse residency programs. Nurs Adm Q. 2012;36(2):155-168.
31. Rush KL, Peel K, McCracken B. Empowered learning on the inside: an externship experience. Nurs Educ Perspect. 2004;25(6):284-291
New nurse graduates often have difficulty transitioning to the role of registered nurse (RN).1 Given the complexity of the health care environment, the need is growing to prepare nursing students for nursing practice. Although nursing education provides students with a basis for practice, school alone cannot prepare them for actual practice in the hospital setting.2 Compared with nurse residency programs, which provide extended postlicensure training, the national Veterans Affairs Learning Opportunity Residency (VALOR) program provides externships independent of nursing school. Externships allow students to train in a hospital setting (generally during the summer months) before becoming a licensed RN. Nursing students who are entering their senior year of coursework in a bachelor of science nursing program and who have a minimum 3.0 grade point average can apply for this competitive national scholarship offered at VAMCs. The VALOR program is a paid learning opportunity, and students gain hands-on clinical experience under the guidance of preceptors.
Little externship research exists in the nursing literature.3,4 The authors conducted the present study to help fill the gaps in the literature and to add to the only other study findings on VALOR.3 This program, started in 1990 to aid in nursing recruitment and retention, offers students early exposure to the complexities of nursing practice.
The authors investigated RNs’ experience in the VALOR prelicensure externship during the nurses’ senior year of coursework and the impact of this experience on their nursing practice. The program offers 800 hours of hospital-based experience outside the classroom. New nurses who gained only limited clinical exposure in nursing school may feel insecure about their clinical skills.5 Casey and colleagues found that students want more clinical experience than offered by nursing school practicums.6 The VALOR participants obtain additional clinical time, which contributes to their self-confidence when transitioning to the RN role.7
Literature Review
New graduate nurses work in complex health care environments with unfamiliar technologies, shift hours, heavy patient loads, psychological and professional stressors, socialization problems, and patient safety issues.8 They often are unable to connect their educational experience with the realities of practice and find the work environment incongruent with their nursing school education.9 Although new nurses’ difficulty in transitioning to their professional role has been addressed in the literature, transitional experience has not improved.10 Studies have found that new graduate nurses want more support than is given and have suggested that unfamiliar workplace dynamics create stress for new nurses.11
Anxiety, insecurity, and fear of failure are associated with the transition from student to practicing nurse.10 Because of the additional clinical experience gained in an externship, students likely are more self-confident when they assume the RN role.12 White suggested self-confident students see themselves as nurses and feel capable of caring for patients.13 Externship experience makes the transition to professional nursing less stressful, because externship students obtain an inside view of nursing culture.14 Students increase their understanding of nurses’ multiple roles and responsibilities, because these programs focus on increasing clinical skills and competency.15 To perform successfully as RNs, new graduates need competencies and knowledge beyond those obtained in nursing school.16
In the nursing profession, an association between job satisfaction and turnover exists.17,18 Of new graduate nurses, 35% to 69% leave their position within the first year of employment.19 Replacing nurses reduces hospital productivity and efficiency and increases cost.20 New graduate nurses leave because they are dissatisfied with and overwhelmed by the complexity of the work environment.21 Prelicensure nurse externships can aid in recruiting and retaining new graduate nurses for the hospitals that host these programs.22 For host facilities, recruitment rates of 50% to 79% have been reported.23,24
In a quantitative study, Nuttall surveyed 133 RNs about job satisfaction, role socialization, professionalism, and sense of belonging.3 Of these RNs, 34 had participated in VALOR and 99 had not. There was no evidence that the RNs with VALOR experience had a higher degree of professionalism, job satisfaction, or role socialization; only sense of belonging (age-adjusted) was higher for the VALOR group. The conflicting data on prelicensure externship outcomes call for further analysis of these programs.3 Nuttall noted that her study “was the first... to evaluate the VALOR program and future research [using a qualitative approach] is needed to identify additional outcomes related to this program.”3
Methods
This study using hermeneutic phenomenology was approved by the Salem VAMC in Virginia and by the institutional review board at Nova Southeastern University.24 Study participants provided written informed consent before being interviewed.
Interviewees
Data Collection and Analysis
Data collection began in March 2013 with a pilot test of the interview questions for appropriateness. Open-ended, semistructured questions were used to elicit nurses’ descriptions of their experience. Field notes were written, and all interviews were tape-recorded and professionally transcribed verbatim. Data saturation was reached after 12 nurses were interviewed. Transcripts were analyzed and interpreted using van Manen’s line-by-line approach.26 All 12 interviewees were invited to review the findings of the data analysis. Eleven of the 12 interviewees verified and validated the study findings.
Rigor using Lincoln and Guba’s criteria of credibility, dependability, transferability, and confirmability added trustworthiness to the study findings. Bracketing helped eliminate potential bias.27 Credibility was achieved with prolonged engagement and triangulation. To further enhance credibility, the authors invited qualitative research experts to validate the emerging themes and create an audit trail. For dependability, a flow chart was created for use by researchers who might want to replicate the study. Rich, lengthy descriptions and interviewees’ quotations were provided so researchers could judge the study’s transferability to other settings. Maintaining an audit trail and having a doctor of nursing practice independently code the data aided with confirmability. This study used findings from the literature, audio recordings, member checking, and field notes to assess data accuracy.
Results
The overarching theme discovered in this study was confidence. Subthemes were transitioning to the RN role, making decisions, and interacting with interprofessional staff.
Confidence
Interviewees felt confident in transitioning to the RN role, making decisions, and interacting with interprofessional staff. They shared that they had applied to the externship to gain additional clinical experience and that the program increased their self-confidence with respect to transitioning to the new role as RN. However, it is possible that these interviewees were highly motivated and would not have had difficulty transitioning to the RN role—this is addressed in the Limitations section of this article.
Interviewees said they initially approached VALOR with fear and apprehension but completed it feeling confident about becoming an RN. One interviewee stated, “The VALOR program gave me the confidence in my own abilities, so I was not scared and had confidence that, yes, I could do this job.” Another said, “Honestly, the entire externship program, regardless of which question you ask, my answer is going to always fall back on confidence. I became prepared for the RN job, I feel, before I graduated because of the [externship] experiences.”
Transitioning to RN Role
Transitioning involved understanding the RN’s scope of practice and feeling clinically competent. Students worked 40 hours a week over the summer and gained firsthand insight into working as an RN daily. Interviewees believed completing the externship made it easy to transition to the RN role because they knew what to expect.
Working side-by-side with nurses, students gained insight into RNs’ responsibilities and scope of practice. Interviewees reported that, after the externship, they had a better understanding of their patient care and licensure legal responsibilities.
Students began to feel clinically competent during the externship. Interviewees shared that they had had several opportunities to practice basic skills, such as giving injections. One interviewee said, “I don’t think I tried to stick a single IV when I was in school or in clinical [training].” Interviewees also commented that repeatedly practicing skills increased their self-confidence.
Students also gained firsthand insight into working with veterans and their families. During the externship, they learned about communicating therapeutically, providing education for caregivers, and advocating for patients and their families. Before the externship, they felt apprehensive about communicating with patients. One interviewee said that after the program, “Eventually you had to talk to patients, and eventually figured it out that it wasn’t so scary.”
Students found that patients were not always happy with their care, and procedures did not always go as planned. They also discovered that education did not end with the patient; family members needed education as well. The externship experience heightened students’ awareness of the RN’s role as patient advocate. One interviewee explained it is the RN’s responsibility to intervene on the patient’s behalf. Interviewees were surprised that patients would not tell their health care provider that they did not understand what was said or that they wanted another course of treatment.
The externship helped decrease learning-related stress. Interviewees indicated they had learned without fear of reprisal. One described feeling free to learn: “Uninhibited learning...you can ask what you need to without fear of not graduating.” Externship students were able to focus on learning the RN role without worrying about the next test or grade. They felt free to ask questions without fear of failing their clinical rotation.
The supportive and nurturing relationships that students developed in VALOR also increased their confidence when transitioning to the RN role. One interviewee said, “There was never the sense of, no, you learn my way, or I don’t want you here.” Interviewees shared that they felt comfortable and supported.
Decision Making
Interviewees reported that after VALOR, it was easy to make decisions regarding nursing practice, delegation, care prioritization, and career choice. As students, they found the school clinical setting did not provide the decision-making opportunities VALOR did, and they quickly realized nursing practice involved more than making patient-care decisions. One interviewee said, “In a classroom, a picture is painted of an idealistic environment that may not truly mimic the hospital unit.”
Students became familiar with the practice of delegating care to the appropriate staff and the next shift. One interviewee said VALOR “provided me with a better understanding of delegation in my RN role.” VALOR participants discovered that, as new nurses, they were less anxious when delegating to others.
Before RN licensure, VALOR participants learned about prioritizing patient care. One interviewee said, “It’s like everybody has to be charted on, and all the medications have to be passed out, but it’s a matter of getting everything done while doing the more important and more dire things first.” Students learned that all aspects of nursing are important, but they had to make rational decisions.
Interacting With Professionals
Interviewees who had been in VALOR said interacting with interprofessional (different disciplines) staff contributed to their working comfortably in teams and collaborating with others. Their collaborative relationships with physicians would help them later, when as new graduate nurses they again needed to work together with doctors. Typical comments were, “When I started as an RN, I felt I was not new at it because I had communicated with doctors in the externship program.”
Discussion
The present study found that nursing students who had been in the VALOR externship felt confident in their clinical skills when they were transitioning to the RN role. Other studies similarly have found that externship students were self-confident assuming the RN role, owing to their additional clinical experience.12,28 The VALOR program allows students to work alongside nurses and receive hands-on experience while interacting with interprofessional health care teams. Findings of Nuttall’s quantitative study contradict those of the present, qualitative study. Nuttall used surveys and a control group, whereas this phenomenologic study captured the essence of study participants’ experiences through interviews.
The RNs interviewed in the present study discovered that, unlike nursing school, VALOR provided a realistic view of full-time work as an RN. This finding aligns with Starr and Conley’s finding that, before participating in an externship, most students were unaware of the extent of RNs’ roles and responsibilities, whereas after the program they understood these roles and responsibilities better.28
The interviewees in this study thought VALOR improved their skills in communicating with patients, families, and interprofessional team members. Interviewees shared that they learned patient advocacy skills and that, through firsthand experience, realized nurses provide patients with a voice. Externships can help new graduate nurses become better communicators and can teach students the importance of patient communication and advocacy.12
This study also found that students wanted more exposure to realistic nursing environments, additional nursing skills practice, and more interaction with interprofessional team members. VALOR helped bridge the theory–practice gap by providing real-world nursing experience outside the academic environment and extra time for nursing skills development. In a study by Casey and colleagues, students indicated that the time allowed for nursing skills practice during school was inadequate.6
The VALOR program helped students learn about delegating work, whereas nursing school did not provide the opportunity to practice delegation. Other studies have corroborated that students do not practice delegation during nursing school clinical time.29,30
Study respondents noted they could focus on learning without the fear of passing their clinical rotation. They felt supported by staff and were comfortable asking questions. White suggested that externship students who feel supported by nursing staff are able to focus on patients instead of on their discomfort.13 Rush and colleagues found that constraints on the student experience in traditional academic clinical rotations were replaced with “freedom and fearlessness in learning” in externships.31
Ten of the 12 study participants applied for a new graduate nurse position at the VAMC where they had their externship. A potential benefit to organizations that sponsor a nursing externship is the recruitment of new graduate nurses.14 Before applying for a full-time position, VALOR students had the opportunity to become familiar with the work environment and assess their fit with the employer. One student found staff nurse work “scary” and “stressful” and decided against it. She said the VALOR externship helped her realize exactly what nursing entailed: “Until this experience, I did not realize I would not like the hospital environment. This was a reality check for me.” Another student decided that working different shifts and working holidays would be difficult for her. These 2 students’ externship experience convinced them to seek other nursing positions.
Limitations
All participants in this study were nurses with excellent academic grades. It is possible they were highly motivated and might not have had any difficulty transitioning to the RN role. The principal investigator in this study was a VALOR program coordinator who knew 3 of the study participants—a potential source of bias. It is possible participants did not want to speak negatively about the program for several reasons: the interviewer was their coordinator, they received a salary during the externship, and several worked for the VA at the time of the survey.
Researchers have acknowledged the likelihood that not all VALOR students have positive experiences. It is possible that students with negative experiences did not discuss them or did not participate in the study. Increasing the size of the study sample may have brought in students with negative experiences. There is also the possibility of researcher misinterpretation and bias. Although bracketing was used, it was not possible to eliminate all potential sources of bias from this qualitative study.
Future Research
This is 1 of only 2 studies on the VALOR externship. Given the contradictory findings of these studies—Nuttall reported VALOR experience did not affect students’ transition to the RN role,3 whereas in the present study VALOR students thought the program positively affected their successful transition—additional quantitative and qualitative research is needed.
In addition, the low recruitment rate of VALOR students should be compared with other studies’ recruitment rates. The 38% VALOR extern recruitment rate for the period 2007 to 2012 is lower than the rate for other programs (G. Fuller, August 27, 2014, e-mail communication). The VALOR program does not track retention of participants after employment. Longitudinal studies should compare VALOR participants’ length of employment with that of nonparticipants’.
Conclusion
Externships provide clinical experience outside the classroom, expose students to the realities of nursing practice before graduation, and serve as a recruitment tool for hospitals. These programs, in conjunction with school-based practicums, increase exposure to the clinical environment. Before graduation, students have the opportunity to practice skills, interact with interprofessional staff, and experience different hospital units, all of which contribute to career decisions. The present study found that the VALOR externship helped new graduate nurses with their transition to the workplace. However, it is important to recognize the limitations of this study.
Interviewees indicated they were confident when they were transitioning to their new nurse role and caring for patients before receiving their RN licensure. New graduate nurses discovered they acclimated to the hospital environment quicker. The reality of working day-to-day in a hospital setting allowed students to select a compatible work environment and understand the daily challenges health care professionals encounter. Interviewees shared that they felt “like the RN” during the externship, which lessened the shock of actually assuming the RN role.
Van Manen asserted there is no conclusion or ending to a phenomenological study.26 Continued research on hospital-based externships will demonstrate how these programs can assist in the development of new graduate nurses, ease their transition to practice, and benefit nursing education, practice, research, and public policy.
New nurse graduates often have difficulty transitioning to the role of registered nurse (RN).1 Given the complexity of the health care environment, the need is growing to prepare nursing students for nursing practice. Although nursing education provides students with a basis for practice, school alone cannot prepare them for actual practice in the hospital setting.2 Compared with nurse residency programs, which provide extended postlicensure training, the national Veterans Affairs Learning Opportunity Residency (VALOR) program provides externships independent of nursing school. Externships allow students to train in a hospital setting (generally during the summer months) before becoming a licensed RN. Nursing students who are entering their senior year of coursework in a bachelor of science nursing program and who have a minimum 3.0 grade point average can apply for this competitive national scholarship offered at VAMCs. The VALOR program is a paid learning opportunity, and students gain hands-on clinical experience under the guidance of preceptors.
Little externship research exists in the nursing literature.3,4 The authors conducted the present study to help fill the gaps in the literature and to add to the only other study findings on VALOR.3 This program, started in 1990 to aid in nursing recruitment and retention, offers students early exposure to the complexities of nursing practice.
The authors investigated RNs’ experience in the VALOR prelicensure externship during the nurses’ senior year of coursework and the impact of this experience on their nursing practice. The program offers 800 hours of hospital-based experience outside the classroom. New nurses who gained only limited clinical exposure in nursing school may feel insecure about their clinical skills.5 Casey and colleagues found that students want more clinical experience than offered by nursing school practicums.6 The VALOR participants obtain additional clinical time, which contributes to their self-confidence when transitioning to the RN role.7
Literature Review
New graduate nurses work in complex health care environments with unfamiliar technologies, shift hours, heavy patient loads, psychological and professional stressors, socialization problems, and patient safety issues.8 They often are unable to connect their educational experience with the realities of practice and find the work environment incongruent with their nursing school education.9 Although new nurses’ difficulty in transitioning to their professional role has been addressed in the literature, transitional experience has not improved.10 Studies have found that new graduate nurses want more support than is given and have suggested that unfamiliar workplace dynamics create stress for new nurses.11
Anxiety, insecurity, and fear of failure are associated with the transition from student to practicing nurse.10 Because of the additional clinical experience gained in an externship, students likely are more self-confident when they assume the RN role.12 White suggested self-confident students see themselves as nurses and feel capable of caring for patients.13 Externship experience makes the transition to professional nursing less stressful, because externship students obtain an inside view of nursing culture.14 Students increase their understanding of nurses’ multiple roles and responsibilities, because these programs focus on increasing clinical skills and competency.15 To perform successfully as RNs, new graduates need competencies and knowledge beyond those obtained in nursing school.16
In the nursing profession, an association between job satisfaction and turnover exists.17,18 Of new graduate nurses, 35% to 69% leave their position within the first year of employment.19 Replacing nurses reduces hospital productivity and efficiency and increases cost.20 New graduate nurses leave because they are dissatisfied with and overwhelmed by the complexity of the work environment.21 Prelicensure nurse externships can aid in recruiting and retaining new graduate nurses for the hospitals that host these programs.22 For host facilities, recruitment rates of 50% to 79% have been reported.23,24
In a quantitative study, Nuttall surveyed 133 RNs about job satisfaction, role socialization, professionalism, and sense of belonging.3 Of these RNs, 34 had participated in VALOR and 99 had not. There was no evidence that the RNs with VALOR experience had a higher degree of professionalism, job satisfaction, or role socialization; only sense of belonging (age-adjusted) was higher for the VALOR group. The conflicting data on prelicensure externship outcomes call for further analysis of these programs.3 Nuttall noted that her study “was the first... to evaluate the VALOR program and future research [using a qualitative approach] is needed to identify additional outcomes related to this program.”3
Methods
This study using hermeneutic phenomenology was approved by the Salem VAMC in Virginia and by the institutional review board at Nova Southeastern University.24 Study participants provided written informed consent before being interviewed.
Interviewees
Data Collection and Analysis
Data collection began in March 2013 with a pilot test of the interview questions for appropriateness. Open-ended, semistructured questions were used to elicit nurses’ descriptions of their experience. Field notes were written, and all interviews were tape-recorded and professionally transcribed verbatim. Data saturation was reached after 12 nurses were interviewed. Transcripts were analyzed and interpreted using van Manen’s line-by-line approach.26 All 12 interviewees were invited to review the findings of the data analysis. Eleven of the 12 interviewees verified and validated the study findings.
Rigor using Lincoln and Guba’s criteria of credibility, dependability, transferability, and confirmability added trustworthiness to the study findings. Bracketing helped eliminate potential bias.27 Credibility was achieved with prolonged engagement and triangulation. To further enhance credibility, the authors invited qualitative research experts to validate the emerging themes and create an audit trail. For dependability, a flow chart was created for use by researchers who might want to replicate the study. Rich, lengthy descriptions and interviewees’ quotations were provided so researchers could judge the study’s transferability to other settings. Maintaining an audit trail and having a doctor of nursing practice independently code the data aided with confirmability. This study used findings from the literature, audio recordings, member checking, and field notes to assess data accuracy.
Results
The overarching theme discovered in this study was confidence. Subthemes were transitioning to the RN role, making decisions, and interacting with interprofessional staff.
Confidence
Interviewees felt confident in transitioning to the RN role, making decisions, and interacting with interprofessional staff. They shared that they had applied to the externship to gain additional clinical experience and that the program increased their self-confidence with respect to transitioning to the new role as RN. However, it is possible that these interviewees were highly motivated and would not have had difficulty transitioning to the RN role—this is addressed in the Limitations section of this article.
Interviewees said they initially approached VALOR with fear and apprehension but completed it feeling confident about becoming an RN. One interviewee stated, “The VALOR program gave me the confidence in my own abilities, so I was not scared and had confidence that, yes, I could do this job.” Another said, “Honestly, the entire externship program, regardless of which question you ask, my answer is going to always fall back on confidence. I became prepared for the RN job, I feel, before I graduated because of the [externship] experiences.”
Transitioning to RN Role
Transitioning involved understanding the RN’s scope of practice and feeling clinically competent. Students worked 40 hours a week over the summer and gained firsthand insight into working as an RN daily. Interviewees believed completing the externship made it easy to transition to the RN role because they knew what to expect.
Working side-by-side with nurses, students gained insight into RNs’ responsibilities and scope of practice. Interviewees reported that, after the externship, they had a better understanding of their patient care and licensure legal responsibilities.
Students began to feel clinically competent during the externship. Interviewees shared that they had had several opportunities to practice basic skills, such as giving injections. One interviewee said, “I don’t think I tried to stick a single IV when I was in school or in clinical [training].” Interviewees also commented that repeatedly practicing skills increased their self-confidence.
Students also gained firsthand insight into working with veterans and their families. During the externship, they learned about communicating therapeutically, providing education for caregivers, and advocating for patients and their families. Before the externship, they felt apprehensive about communicating with patients. One interviewee said that after the program, “Eventually you had to talk to patients, and eventually figured it out that it wasn’t so scary.”
Students found that patients were not always happy with their care, and procedures did not always go as planned. They also discovered that education did not end with the patient; family members needed education as well. The externship experience heightened students’ awareness of the RN’s role as patient advocate. One interviewee explained it is the RN’s responsibility to intervene on the patient’s behalf. Interviewees were surprised that patients would not tell their health care provider that they did not understand what was said or that they wanted another course of treatment.
The externship helped decrease learning-related stress. Interviewees indicated they had learned without fear of reprisal. One described feeling free to learn: “Uninhibited learning...you can ask what you need to without fear of not graduating.” Externship students were able to focus on learning the RN role without worrying about the next test or grade. They felt free to ask questions without fear of failing their clinical rotation.
The supportive and nurturing relationships that students developed in VALOR also increased their confidence when transitioning to the RN role. One interviewee said, “There was never the sense of, no, you learn my way, or I don’t want you here.” Interviewees shared that they felt comfortable and supported.
Decision Making
Interviewees reported that after VALOR, it was easy to make decisions regarding nursing practice, delegation, care prioritization, and career choice. As students, they found the school clinical setting did not provide the decision-making opportunities VALOR did, and they quickly realized nursing practice involved more than making patient-care decisions. One interviewee said, “In a classroom, a picture is painted of an idealistic environment that may not truly mimic the hospital unit.”
Students became familiar with the practice of delegating care to the appropriate staff and the next shift. One interviewee said VALOR “provided me with a better understanding of delegation in my RN role.” VALOR participants discovered that, as new nurses, they were less anxious when delegating to others.
Before RN licensure, VALOR participants learned about prioritizing patient care. One interviewee said, “It’s like everybody has to be charted on, and all the medications have to be passed out, but it’s a matter of getting everything done while doing the more important and more dire things first.” Students learned that all aspects of nursing are important, but they had to make rational decisions.
Interacting With Professionals
Interviewees who had been in VALOR said interacting with interprofessional (different disciplines) staff contributed to their working comfortably in teams and collaborating with others. Their collaborative relationships with physicians would help them later, when as new graduate nurses they again needed to work together with doctors. Typical comments were, “When I started as an RN, I felt I was not new at it because I had communicated with doctors in the externship program.”
Discussion
The present study found that nursing students who had been in the VALOR externship felt confident in their clinical skills when they were transitioning to the RN role. Other studies similarly have found that externship students were self-confident assuming the RN role, owing to their additional clinical experience.12,28 The VALOR program allows students to work alongside nurses and receive hands-on experience while interacting with interprofessional health care teams. Findings of Nuttall’s quantitative study contradict those of the present, qualitative study. Nuttall used surveys and a control group, whereas this phenomenologic study captured the essence of study participants’ experiences through interviews.
The RNs interviewed in the present study discovered that, unlike nursing school, VALOR provided a realistic view of full-time work as an RN. This finding aligns with Starr and Conley’s finding that, before participating in an externship, most students were unaware of the extent of RNs’ roles and responsibilities, whereas after the program they understood these roles and responsibilities better.28
The interviewees in this study thought VALOR improved their skills in communicating with patients, families, and interprofessional team members. Interviewees shared that they learned patient advocacy skills and that, through firsthand experience, realized nurses provide patients with a voice. Externships can help new graduate nurses become better communicators and can teach students the importance of patient communication and advocacy.12
This study also found that students wanted more exposure to realistic nursing environments, additional nursing skills practice, and more interaction with interprofessional team members. VALOR helped bridge the theory–practice gap by providing real-world nursing experience outside the academic environment and extra time for nursing skills development. In a study by Casey and colleagues, students indicated that the time allowed for nursing skills practice during school was inadequate.6
The VALOR program helped students learn about delegating work, whereas nursing school did not provide the opportunity to practice delegation. Other studies have corroborated that students do not practice delegation during nursing school clinical time.29,30
Study respondents noted they could focus on learning without the fear of passing their clinical rotation. They felt supported by staff and were comfortable asking questions. White suggested that externship students who feel supported by nursing staff are able to focus on patients instead of on their discomfort.13 Rush and colleagues found that constraints on the student experience in traditional academic clinical rotations were replaced with “freedom and fearlessness in learning” in externships.31
Ten of the 12 study participants applied for a new graduate nurse position at the VAMC where they had their externship. A potential benefit to organizations that sponsor a nursing externship is the recruitment of new graduate nurses.14 Before applying for a full-time position, VALOR students had the opportunity to become familiar with the work environment and assess their fit with the employer. One student found staff nurse work “scary” and “stressful” and decided against it. She said the VALOR externship helped her realize exactly what nursing entailed: “Until this experience, I did not realize I would not like the hospital environment. This was a reality check for me.” Another student decided that working different shifts and working holidays would be difficult for her. These 2 students’ externship experience convinced them to seek other nursing positions.
Limitations
All participants in this study were nurses with excellent academic grades. It is possible they were highly motivated and might not have had any difficulty transitioning to the RN role. The principal investigator in this study was a VALOR program coordinator who knew 3 of the study participants—a potential source of bias. It is possible participants did not want to speak negatively about the program for several reasons: the interviewer was their coordinator, they received a salary during the externship, and several worked for the VA at the time of the survey.
Researchers have acknowledged the likelihood that not all VALOR students have positive experiences. It is possible that students with negative experiences did not discuss them or did not participate in the study. Increasing the size of the study sample may have brought in students with negative experiences. There is also the possibility of researcher misinterpretation and bias. Although bracketing was used, it was not possible to eliminate all potential sources of bias from this qualitative study.
Future Research
This is 1 of only 2 studies on the VALOR externship. Given the contradictory findings of these studies—Nuttall reported VALOR experience did not affect students’ transition to the RN role,3 whereas in the present study VALOR students thought the program positively affected their successful transition—additional quantitative and qualitative research is needed.
In addition, the low recruitment rate of VALOR students should be compared with other studies’ recruitment rates. The 38% VALOR extern recruitment rate for the period 2007 to 2012 is lower than the rate for other programs (G. Fuller, August 27, 2014, e-mail communication). The VALOR program does not track retention of participants after employment. Longitudinal studies should compare VALOR participants’ length of employment with that of nonparticipants’.
Conclusion
Externships provide clinical experience outside the classroom, expose students to the realities of nursing practice before graduation, and serve as a recruitment tool for hospitals. These programs, in conjunction with school-based practicums, increase exposure to the clinical environment. Before graduation, students have the opportunity to practice skills, interact with interprofessional staff, and experience different hospital units, all of which contribute to career decisions. The present study found that the VALOR externship helped new graduate nurses with their transition to the workplace. However, it is important to recognize the limitations of this study.
Interviewees indicated they were confident when they were transitioning to their new nurse role and caring for patients before receiving their RN licensure. New graduate nurses discovered they acclimated to the hospital environment quicker. The reality of working day-to-day in a hospital setting allowed students to select a compatible work environment and understand the daily challenges health care professionals encounter. Interviewees shared that they felt “like the RN” during the externship, which lessened the shock of actually assuming the RN role.
Van Manen asserted there is no conclusion or ending to a phenomenological study.26 Continued research on hospital-based externships will demonstrate how these programs can assist in the development of new graduate nurses, ease their transition to practice, and benefit nursing education, practice, research, and public policy.
1. Clark CM, Springer PJ. Nurse residents' first-hand accounts on transition to practice. Nurs Outlook. 2012;60(4):e2-e8.
2. Myers S, Reidy P, French B, McHale J, Chisholm M, Griffin M. Safety concerns of hospital-based new-to-practice registered nurses and their preceptors. J Contin Educ Nurs. 2010;41(4):163-171.
3. Nuttall CM. A Comparative Study Evaluating the Impact of Participation in a VALOR Nurse Externship on Job Satisfaction, Sense of Belonging, Role Socialization and Sense of Professionalism: Transition From Graduate to Registered Nurse [dissertation]. Albuquerque: University of New Mexico; 2010.
4. Steen JE, Gould EW, Raingruber B, Hill J. Effect of student nurse intern position on ease of transition from student nurse to registered nurse. J Nurs Staff Dev. 2011;27(4):181-186.
5. Ulrich B, Krozek C, Early S, Ashlock CH, Africa LM, Carman ML. Improving retention, confidence, and competence of new graduate nurses: results from a 10-year longitudinal database. Nurs Econ. 2010;28(6):363-375.
6. Casey K, Fink R, Jaynes C, Campbell L, Cook P, Wilson V. Readiness for practice: the senior practicum experience. J Nurs Educ. 2011;50(11):646-652.
7. Shipman D, Hooten J, Stanley S. The VALOR program: preparing nursing students to care for our veterans. Fed Pract. 2014;31(9):35-38.
8. Walker A, Earl C, Costa B, Cuddihy L. Graduate nurses' transition and integration into the workplace: a qualitative comparison of graduate nurses' and nurse unit managers' perspectives. Nurs Educ Today. 2013;33(3):291-296.
9. Welding NM. Creating a nursing residency: decrease turnover and increase clinical competence. Medsurg Nurs. 2011;20(1):37-40.
10. Morrow S. New graduate transitions: leaving the nest, joining the flight. J Nurs Manag. 2009;17(3):278-287.
11. Parker V, Giles M, Lantry G, McMillan M. New graduate nurses' experience in their first year of practice. Nurs Educ Today. 2014;34(1):150-156.
12. Ruth-Sahd LA, Beck J, McCall C. Transformative learning during a nursing externship program: the reflections of senior nursing students. Nurs Educ Perspect. 2010;31(2):78-83.
13. White AH. Clinical decision making among fourth-year nursing students: an interpretive study. J Nurs Educ. 2003;42(3):113-121.
14. Kropkowski LR, Most R. Set for success: nurse "externs." Nurs Manag. 2008;39(7):8-9.
15. Rhoads J, Sensenig K, Ruth-Sahd L, Thompson E. Nursing externship: a collaborative endeavor between nursing education and nursing administration. Dimens Crit Care Nurs. 2003;22(6):255-258.
16. Hillman L, Foster RR. The impact of a nursing transitions programme on retention and cost savings. J Nurs Manag. 2011;19(1):50-56.
17. Baernholdt M, Mark BA. The nurse work environment, job satisfaction and turnover rates in rural and urban nursing units. J Nurs Manag. 2009;17(8):994-1001.
18. Jones CB. Revisiting nurse turnover costs: adjusting for inflation. J Nurs Adm. 2008;38(1):11-18.
19. Pine R, Tart K. Return on investment: benefits and challenges of baccalaureate nurse residency program. Nurs Econ. 2007;25(1):13-18, 39.
20. Beecroft PC, Dorey F, Wenten M. Turnover intention in new graduate nurses: a multivariate analysis. J Adv Nurs, 2008;62(1):41-52.
21. Phillips C, Esterman A, Kenny A. The theory of organisational socialisation and its potential for improving transition experiences for new graduate nurses. Nurs Educ Today. 2015;35(1):118-124.
22. Diefenbeck CA, Plowfield LA, Herrman JW. Clinical immersion: a residency model for nursing education. Nurs Educ Perspect. 2006;27(2):72-79.
23. Cantrell MA, Browne AM. The impact of a nurse externship on the transition process from graduate to registered nurse: part III. Recruitment and retention effects. J Nurs Staff Dev. 2006;22(1):11-14.
24. Kilpatrick K, Frunchak V. The nursing extern program: innovative strategies for students in transition. Health Care Manag (Frederick). 2006;25(3):236-242.
25. Kovner CT, Brewer CS, Fairchild S, Poornima S, Kim H, Djukic CM. Newly licensed RN's characteristics, work attitudes, and intentions to work. Am J Nurs. 2007;107(9):58-70
26. van Manen M. Researching Lived Experience: Human Science for an Action Sensitive Pedagogy. Albany: State University of New York Press; 1990.
27. Lincoln YS, Guba EG. Naturalistic Inquiry. Beverly Hills, CA: Sage; 1985.
28. Starr K, Conley VM. Becoming a registered nurse: the nurse extern experience. J Contin Educ Nurs. 2006;37(2):86-92.
29. Hasson F, McKenna HP, Keeney S. Delegating and supervising unregistered professionals: the student nurse experience. Nurs Educ Today. 2013;33(3):229-235.
30. Kramer M, Maguire P, Halfer D, et al. The organizational transformative power of nurse residency programs. Nurs Adm Q. 2012;36(2):155-168.
31. Rush KL, Peel K, McCracken B. Empowered learning on the inside: an externship experience. Nurs Educ Perspect. 2004;25(6):284-291
1. Clark CM, Springer PJ. Nurse residents' first-hand accounts on transition to practice. Nurs Outlook. 2012;60(4):e2-e8.
2. Myers S, Reidy P, French B, McHale J, Chisholm M, Griffin M. Safety concerns of hospital-based new-to-practice registered nurses and their preceptors. J Contin Educ Nurs. 2010;41(4):163-171.
3. Nuttall CM. A Comparative Study Evaluating the Impact of Participation in a VALOR Nurse Externship on Job Satisfaction, Sense of Belonging, Role Socialization and Sense of Professionalism: Transition From Graduate to Registered Nurse [dissertation]. Albuquerque: University of New Mexico; 2010.
4. Steen JE, Gould EW, Raingruber B, Hill J. Effect of student nurse intern position on ease of transition from student nurse to registered nurse. J Nurs Staff Dev. 2011;27(4):181-186.
5. Ulrich B, Krozek C, Early S, Ashlock CH, Africa LM, Carman ML. Improving retention, confidence, and competence of new graduate nurses: results from a 10-year longitudinal database. Nurs Econ. 2010;28(6):363-375.
6. Casey K, Fink R, Jaynes C, Campbell L, Cook P, Wilson V. Readiness for practice: the senior practicum experience. J Nurs Educ. 2011;50(11):646-652.
7. Shipman D, Hooten J, Stanley S. The VALOR program: preparing nursing students to care for our veterans. Fed Pract. 2014;31(9):35-38.
8. Walker A, Earl C, Costa B, Cuddihy L. Graduate nurses' transition and integration into the workplace: a qualitative comparison of graduate nurses' and nurse unit managers' perspectives. Nurs Educ Today. 2013;33(3):291-296.
9. Welding NM. Creating a nursing residency: decrease turnover and increase clinical competence. Medsurg Nurs. 2011;20(1):37-40.
10. Morrow S. New graduate transitions: leaving the nest, joining the flight. J Nurs Manag. 2009;17(3):278-287.
11. Parker V, Giles M, Lantry G, McMillan M. New graduate nurses' experience in their first year of practice. Nurs Educ Today. 2014;34(1):150-156.
12. Ruth-Sahd LA, Beck J, McCall C. Transformative learning during a nursing externship program: the reflections of senior nursing students. Nurs Educ Perspect. 2010;31(2):78-83.
13. White AH. Clinical decision making among fourth-year nursing students: an interpretive study. J Nurs Educ. 2003;42(3):113-121.
14. Kropkowski LR, Most R. Set for success: nurse "externs." Nurs Manag. 2008;39(7):8-9.
15. Rhoads J, Sensenig K, Ruth-Sahd L, Thompson E. Nursing externship: a collaborative endeavor between nursing education and nursing administration. Dimens Crit Care Nurs. 2003;22(6):255-258.
16. Hillman L, Foster RR. The impact of a nursing transitions programme on retention and cost savings. J Nurs Manag. 2011;19(1):50-56.
17. Baernholdt M, Mark BA. The nurse work environment, job satisfaction and turnover rates in rural and urban nursing units. J Nurs Manag. 2009;17(8):994-1001.
18. Jones CB. Revisiting nurse turnover costs: adjusting for inflation. J Nurs Adm. 2008;38(1):11-18.
19. Pine R, Tart K. Return on investment: benefits and challenges of baccalaureate nurse residency program. Nurs Econ. 2007;25(1):13-18, 39.
20. Beecroft PC, Dorey F, Wenten M. Turnover intention in new graduate nurses: a multivariate analysis. J Adv Nurs, 2008;62(1):41-52.
21. Phillips C, Esterman A, Kenny A. The theory of organisational socialisation and its potential for improving transition experiences for new graduate nurses. Nurs Educ Today. 2015;35(1):118-124.
22. Diefenbeck CA, Plowfield LA, Herrman JW. Clinical immersion: a residency model for nursing education. Nurs Educ Perspect. 2006;27(2):72-79.
23. Cantrell MA, Browne AM. The impact of a nurse externship on the transition process from graduate to registered nurse: part III. Recruitment and retention effects. J Nurs Staff Dev. 2006;22(1):11-14.
24. Kilpatrick K, Frunchak V. The nursing extern program: innovative strategies for students in transition. Health Care Manag (Frederick). 2006;25(3):236-242.
25. Kovner CT, Brewer CS, Fairchild S, Poornima S, Kim H, Djukic CM. Newly licensed RN's characteristics, work attitudes, and intentions to work. Am J Nurs. 2007;107(9):58-70
26. van Manen M. Researching Lived Experience: Human Science for an Action Sensitive Pedagogy. Albany: State University of New York Press; 1990.
27. Lincoln YS, Guba EG. Naturalistic Inquiry. Beverly Hills, CA: Sage; 1985.
28. Starr K, Conley VM. Becoming a registered nurse: the nurse extern experience. J Contin Educ Nurs. 2006;37(2):86-92.
29. Hasson F, McKenna HP, Keeney S. Delegating and supervising unregistered professionals: the student nurse experience. Nurs Educ Today. 2013;33(3):229-235.
30. Kramer M, Maguire P, Halfer D, et al. The organizational transformative power of nurse residency programs. Nurs Adm Q. 2012;36(2):155-168.
31. Rush KL, Peel K, McCracken B. Empowered learning on the inside: an externship experience. Nurs Educ Perspect. 2004;25(6):284-291
Cognitive Biases in Dermatology Training
As young physicians, we are taught to be as objective as possible when evaluating a patient; however, cognitive biases are regularly encountered in day-to-day patient experiences and can unfortunately influence our clinical decision-making skills to be subpar.
Consider the following case: An overweight 74-year-old man with diabetes mellitus and a nonhealing ulceration on the left lower extremity presented to the emergency department for repeat evaluation. He previously had been treated by an outside dermatologist for stasis dermatitis and was being managed with compression, elevation, and lubrication of both lower extremities. Often, the initial reaction is to conclude that the patient does in fact have an ulceration associated with stasis dermatitis and changing the management strategy or performing a biopsy would not change the outcome. However, this response limits the potential to provide the patient with a thorough examination. If the patient is treated with the same management strategies that previously failed rather than delving into all the causes for nonhealing ulceration on the left lower extremity, a vital diagnosis could be missed. In this scenario, when the patient was ultimately biopsied, the diagnosis was an ulcerative squamous cell carcinoma.
These subconscious predetermined decisions regarding difficult patient encounters come from the physician’s heuristics, a process of decision-making wherein a snap judgment about a patient occurs because it is similar to prior patient encounters or a set of views from prior knowledge of the disease.1,2
A recent article by Cohen and Burgin3 elucidated a set of cognitive biases that often are encountered in dermatology practices, including affective, anchoring, availability, and confirmation biases; zebra retreat; and Sutton’s slip.
Affective Bias
Affective bias is a process in which emotions regarding a patient interaction alter the objective prospective and reasoning of a patient. For example, consider the case of a pemphigus vulgaris patient who does not want to be on prednisone due to weight gain and persistently presents to the dermatology clinic insisting that the physician taper the dosage. To avoid the constant frustration and upsetting the patient further, the dermatologist tapers the dosage of prednisone prematurely and the patient has a flare.
Anchoring Bias
Anchoring bias occurs when initial information regarding a patient causes one to jump to a conclusion rather than developing a thorough history. An example may be if an infant presents with a mole on the nasal dorsum that the patient’s father reports has only been present for a short while. Without performing imaging studies or asking for further history, the physician decides to biopsy the lesion. The biopsy results show a neural mass, such that a nasal glioma cannot be ruled out. In this bias, magnetic resonance imaging would have been prudent prior to biopsy and premature action.
Availability Bias
Availability bias refers to a diagnosis that immediately comes to mind, as it is common or recently encountered, such as in the example presented at the beginning of this column about the patient with squamous cell carcinoma.
Confirmation Bias
Confirmation bias caters to elucidating information that confirms your own clinical suspicion as opposed to determining the true cause of the disease etiology. Consider the following example: An obese patient presents with a history of painful sores on the bilateral lower extremities. The physician asks specifically about diabetes mellitus and mobility. When the patient answers yes to poor mobility and diabetes mellitus, the physician asks questions confirming an initial suspected diagnosis of stasis dermatitis. Unfortunately, as the patient continues to get worse, it is revealed that his medication history indicates he has been taking sulfasalazine for several years, and it is eventually determined that the patient has cutaneous Crohn disease.
Zebra Retreat
This bias describes a physician’s unwillingness to consider a diagnosis because it is very obscure, even if it is correct. For example, the case of the patient described in the previous example with a diagnosis of cutaneous Crohn disease also can be considered as an example of zebra retreat. Because the clinician may rarely think of this diagnosis due to its infrequent presentation, he/she may not consider doing a biopsy or investigate further.
Sutton’s Slip
This bias describes a situation in which a physician disregards a problem because a thorough examination is not performed, which is classically noted when physicians treat their family and friends. If asked about a mole or lesion regarding its questionable nature, a dermatologist may either disregard it or not evaluate it carefully, as the person is in a casual setting.
Final Thoughts
Although there are several other types of cognitive biases, those described here show that on several occasions, dermatologists can be swayed toward an incorrect diagnosis simply because of a subconscious thought process. Often times, such as in multiple-choice examinations, initial guesses are usually the best answers, but care has to be taken when in a clinical setting. Our patients rarely are good historians and do not present in well-written question stems. The biases emphasize that dermatologists in training should keep their minds open, focus on getting a clear and concise history, and use their knowledge as a tool to derive a well thought-out answer.
1. Croskerry P. The importance of cognitive errors in diagnosis and strategies to minimize them. Acad Med. 2003;78:775-780.
2. Hicks EP, Kluemper GT. Heuristic reasoning and cognitive biases: are they hindrances to judgments and decision making in orthodontics? Am J Orthod Dentofacial Orthop. 2011;139:297-304.
3. Cohen JM, Burgin S. Cognitive biases in clinical decision making: a primer for the practicing dermatologist. JAMA Dermatol. 2016;152:253-254.
As young physicians, we are taught to be as objective as possible when evaluating a patient; however, cognitive biases are regularly encountered in day-to-day patient experiences and can unfortunately influence our clinical decision-making skills to be subpar.
Consider the following case: An overweight 74-year-old man with diabetes mellitus and a nonhealing ulceration on the left lower extremity presented to the emergency department for repeat evaluation. He previously had been treated by an outside dermatologist for stasis dermatitis and was being managed with compression, elevation, and lubrication of both lower extremities. Often, the initial reaction is to conclude that the patient does in fact have an ulceration associated with stasis dermatitis and changing the management strategy or performing a biopsy would not change the outcome. However, this response limits the potential to provide the patient with a thorough examination. If the patient is treated with the same management strategies that previously failed rather than delving into all the causes for nonhealing ulceration on the left lower extremity, a vital diagnosis could be missed. In this scenario, when the patient was ultimately biopsied, the diagnosis was an ulcerative squamous cell carcinoma.
These subconscious predetermined decisions regarding difficult patient encounters come from the physician’s heuristics, a process of decision-making wherein a snap judgment about a patient occurs because it is similar to prior patient encounters or a set of views from prior knowledge of the disease.1,2
A recent article by Cohen and Burgin3 elucidated a set of cognitive biases that often are encountered in dermatology practices, including affective, anchoring, availability, and confirmation biases; zebra retreat; and Sutton’s slip.
Affective Bias
Affective bias is a process in which emotions regarding a patient interaction alter the objective prospective and reasoning of a patient. For example, consider the case of a pemphigus vulgaris patient who does not want to be on prednisone due to weight gain and persistently presents to the dermatology clinic insisting that the physician taper the dosage. To avoid the constant frustration and upsetting the patient further, the dermatologist tapers the dosage of prednisone prematurely and the patient has a flare.
Anchoring Bias
Anchoring bias occurs when initial information regarding a patient causes one to jump to a conclusion rather than developing a thorough history. An example may be if an infant presents with a mole on the nasal dorsum that the patient’s father reports has only been present for a short while. Without performing imaging studies or asking for further history, the physician decides to biopsy the lesion. The biopsy results show a neural mass, such that a nasal glioma cannot be ruled out. In this bias, magnetic resonance imaging would have been prudent prior to biopsy and premature action.
Availability Bias
Availability bias refers to a diagnosis that immediately comes to mind, as it is common or recently encountered, such as in the example presented at the beginning of this column about the patient with squamous cell carcinoma.
Confirmation Bias
Confirmation bias caters to elucidating information that confirms your own clinical suspicion as opposed to determining the true cause of the disease etiology. Consider the following example: An obese patient presents with a history of painful sores on the bilateral lower extremities. The physician asks specifically about diabetes mellitus and mobility. When the patient answers yes to poor mobility and diabetes mellitus, the physician asks questions confirming an initial suspected diagnosis of stasis dermatitis. Unfortunately, as the patient continues to get worse, it is revealed that his medication history indicates he has been taking sulfasalazine for several years, and it is eventually determined that the patient has cutaneous Crohn disease.
Zebra Retreat
This bias describes a physician’s unwillingness to consider a diagnosis because it is very obscure, even if it is correct. For example, the case of the patient described in the previous example with a diagnosis of cutaneous Crohn disease also can be considered as an example of zebra retreat. Because the clinician may rarely think of this diagnosis due to its infrequent presentation, he/she may not consider doing a biopsy or investigate further.
Sutton’s Slip
This bias describes a situation in which a physician disregards a problem because a thorough examination is not performed, which is classically noted when physicians treat their family and friends. If asked about a mole or lesion regarding its questionable nature, a dermatologist may either disregard it or not evaluate it carefully, as the person is in a casual setting.
Final Thoughts
Although there are several other types of cognitive biases, those described here show that on several occasions, dermatologists can be swayed toward an incorrect diagnosis simply because of a subconscious thought process. Often times, such as in multiple-choice examinations, initial guesses are usually the best answers, but care has to be taken when in a clinical setting. Our patients rarely are good historians and do not present in well-written question stems. The biases emphasize that dermatologists in training should keep their minds open, focus on getting a clear and concise history, and use their knowledge as a tool to derive a well thought-out answer.
As young physicians, we are taught to be as objective as possible when evaluating a patient; however, cognitive biases are regularly encountered in day-to-day patient experiences and can unfortunately influence our clinical decision-making skills to be subpar.
Consider the following case: An overweight 74-year-old man with diabetes mellitus and a nonhealing ulceration on the left lower extremity presented to the emergency department for repeat evaluation. He previously had been treated by an outside dermatologist for stasis dermatitis and was being managed with compression, elevation, and lubrication of both lower extremities. Often, the initial reaction is to conclude that the patient does in fact have an ulceration associated with stasis dermatitis and changing the management strategy or performing a biopsy would not change the outcome. However, this response limits the potential to provide the patient with a thorough examination. If the patient is treated with the same management strategies that previously failed rather than delving into all the causes for nonhealing ulceration on the left lower extremity, a vital diagnosis could be missed. In this scenario, when the patient was ultimately biopsied, the diagnosis was an ulcerative squamous cell carcinoma.
These subconscious predetermined decisions regarding difficult patient encounters come from the physician’s heuristics, a process of decision-making wherein a snap judgment about a patient occurs because it is similar to prior patient encounters or a set of views from prior knowledge of the disease.1,2
A recent article by Cohen and Burgin3 elucidated a set of cognitive biases that often are encountered in dermatology practices, including affective, anchoring, availability, and confirmation biases; zebra retreat; and Sutton’s slip.
Affective Bias
Affective bias is a process in which emotions regarding a patient interaction alter the objective prospective and reasoning of a patient. For example, consider the case of a pemphigus vulgaris patient who does not want to be on prednisone due to weight gain and persistently presents to the dermatology clinic insisting that the physician taper the dosage. To avoid the constant frustration and upsetting the patient further, the dermatologist tapers the dosage of prednisone prematurely and the patient has a flare.
Anchoring Bias
Anchoring bias occurs when initial information regarding a patient causes one to jump to a conclusion rather than developing a thorough history. An example may be if an infant presents with a mole on the nasal dorsum that the patient’s father reports has only been present for a short while. Without performing imaging studies or asking for further history, the physician decides to biopsy the lesion. The biopsy results show a neural mass, such that a nasal glioma cannot be ruled out. In this bias, magnetic resonance imaging would have been prudent prior to biopsy and premature action.
Availability Bias
Availability bias refers to a diagnosis that immediately comes to mind, as it is common or recently encountered, such as in the example presented at the beginning of this column about the patient with squamous cell carcinoma.
Confirmation Bias
Confirmation bias caters to elucidating information that confirms your own clinical suspicion as opposed to determining the true cause of the disease etiology. Consider the following example: An obese patient presents with a history of painful sores on the bilateral lower extremities. The physician asks specifically about diabetes mellitus and mobility. When the patient answers yes to poor mobility and diabetes mellitus, the physician asks questions confirming an initial suspected diagnosis of stasis dermatitis. Unfortunately, as the patient continues to get worse, it is revealed that his medication history indicates he has been taking sulfasalazine for several years, and it is eventually determined that the patient has cutaneous Crohn disease.
Zebra Retreat
This bias describes a physician’s unwillingness to consider a diagnosis because it is very obscure, even if it is correct. For example, the case of the patient described in the previous example with a diagnosis of cutaneous Crohn disease also can be considered as an example of zebra retreat. Because the clinician may rarely think of this diagnosis due to its infrequent presentation, he/she may not consider doing a biopsy or investigate further.
Sutton’s Slip
This bias describes a situation in which a physician disregards a problem because a thorough examination is not performed, which is classically noted when physicians treat their family and friends. If asked about a mole or lesion regarding its questionable nature, a dermatologist may either disregard it or not evaluate it carefully, as the person is in a casual setting.
Final Thoughts
Although there are several other types of cognitive biases, those described here show that on several occasions, dermatologists can be swayed toward an incorrect diagnosis simply because of a subconscious thought process. Often times, such as in multiple-choice examinations, initial guesses are usually the best answers, but care has to be taken when in a clinical setting. Our patients rarely are good historians and do not present in well-written question stems. The biases emphasize that dermatologists in training should keep their minds open, focus on getting a clear and concise history, and use their knowledge as a tool to derive a well thought-out answer.
1. Croskerry P. The importance of cognitive errors in diagnosis and strategies to minimize them. Acad Med. 2003;78:775-780.
2. Hicks EP, Kluemper GT. Heuristic reasoning and cognitive biases: are they hindrances to judgments and decision making in orthodontics? Am J Orthod Dentofacial Orthop. 2011;139:297-304.
3. Cohen JM, Burgin S. Cognitive biases in clinical decision making: a primer for the practicing dermatologist. JAMA Dermatol. 2016;152:253-254.
1. Croskerry P. The importance of cognitive errors in diagnosis and strategies to minimize them. Acad Med. 2003;78:775-780.
2. Hicks EP, Kluemper GT. Heuristic reasoning and cognitive biases: are they hindrances to judgments and decision making in orthodontics? Am J Orthod Dentofacial Orthop. 2011;139:297-304.
3. Cohen JM, Burgin S. Cognitive biases in clinical decision making: a primer for the practicing dermatologist. JAMA Dermatol. 2016;152:253-254.

The importance of ‘delivery factors’ and ‘patient factors’ in the therapeutic alliance
The therapeutic alliance (interchangeably, the therapeutic relationship) is a subjective measure of the relationship between a clinician and a patient. It is an indicator of clinical trustworthiness: what a patient is referring to when she (he) expresses trust in her provider. The therapeutic alliance also is known as the working alliance, the therapeutic bond, and the helping alliance,1 and it is an important factor in patient satisfaction ratings—the gauging parameter through which clinicians and institutions measure the quality of care they provide.2
A therapeutic alliance is essential to the delivery of psychiatric care. Itself, it can be a healing factor3 and has been linked to patients’ adherence to treatment and continuation of care.4 For example, psychiatric patients who perceive the therapeutic alliance more positively have:
- a better long-term health outcome after discharge
- a significantly better psychological quality of life5
- a better follow-up record of outpatient care after inpatient discharge4,6
- better adherence to prescribed treatment7
- a reduced likelihood of relapse and readmission.6
Patient satisfaction is an indirect measure of the therapeutic alliance; many variables of the therapeutic relationship can affect that satisfaction. In this article, we call those variables patient factors and delivery factors; our aim, using the example of 2 hypothetical cases, is to highlight their importance in patients’ perception of the therapeutic alliance they have with providers.
CASE Paranoid delusions lead to termination of care
Mr. D, age 21, unmarried, unemployed, and with no medical or psychiatric history, is transferred from the medical floor to the inpatient psychiatric unit after coming to the hospital’s emergency room (ER) with a report of chest pain. Workup on the medical floor was negative for a serious cardiac event.
On questioning, Mr. D tells the team that his chest pain is caused by National Security Agency (NSA) satellites “locking” onto his heart and causing veins in his heart to “pop.”
Mr. D agrees to be transferred to the psychiatric unit. Once there, however, he refuses to take the psychotropic medications that have been prescribed or to comply with the balance of the treatment protocol. He is adamant about the influence of NSA satellites, and requests daily imaging to locate evidence of the path of the satellite tracking device that he claims is inside his body.
The treatment team repeatedly refuses to comply with Mr. D’s demand for imaging. He becomes angry and says that he does not think he is getting proper care because the nature of his problem is medical, not psychiatric.
Mr. D repeatedly asserts that he will not take any of the psychotropic medications that have been prescribed for him and will not attend follow-up appointments with the psychiatry team because he does not need treatment. He accuses the treatment team of conspiring with the NSA and causing his chest pain.
Mr. D asks to be discharged.
Patient factors: Unmodifiable and static
As Mr. D’s case exemplifies, patient factors are a set of elements, intrinsic to a given patient, that affect that patient’s perceptions independent of the quality of the care delivered. Included among patient factors are personal sociodemographic and psychopathological characteristics. These patient factors influence the therapeutic relationship in many ways.
Sociodemographics. It has been reported that patients of minority heritage and those who are male, young, and unmarried tend to be less satisfied with medical treatment in general and with psychiatric inpatient treatment in particular.8,9 Females and older patients, on the other hand, are more likely to be satisfied with the perceived delivery of care and the therapeutic alliance.8-10
Psychopathology affects patients’ perception of the delivery of care and the therapeutic alliance. Patients who are highly distressed psychologically and those who suffer chronic psychiatric illness, for example, tend to perceive themselves as having benefitted less from treatment than healthier counterparts.9,11 Such patients also tend to see their therapeutic outcome in a much less favorable light.11,12 Patients with borderline personality disorder and antisocial personality disorder12-14 and those hospitalized involuntarily8 tend to (1) be less satisfied with their therapeutic outcome and (2) see the therapeutic alliance less favorably compared with those who do not have these psychopathologies.
CASE Denied a blanket, she feels like a 'burden'
Ms. X, age 34, married and a homemaker, has a history of bipolar I disorder. She brings herself to the ER complaining of depression and suicidal ideation.
After Ms. X is seen by the psychiatry consult service in the ER, she reports that she feels frustrated and angry and thinks that the hospital’s physicians do not really want to help her. She states that she felt that the ER staff “dismissed” her, in part because she spent 4 hours in the ER waiting room before she was given a bed.
Ms. X says that, once she was placed in a room, she felt that the nursing staff and medical assistants ignored her because they did not give her the extra blanket she requested. She said she was cold as a result, while she waited to see the psychiatrist and the ER physician.
Ms. X states that she came to the ER seeking help because she felt depressed and thought that no one cared about her. Coming to the hospital made her feel worse, after all, she said, because there she has been treated like she is a burden, much like she is treated at home.
Delivery factors: Amenable to change
These mutable elements of the therapeutic alliance are dependent on the quality of the care, as they were in Ms. X’s case; they can be changed. Included among delivery factors is the quality of the relationship between provider and patient—that is, how the psychiatrist and the nursing staff relate to the patient.
Perceptions are key. Delivery factors rank as one of the most important elements that influence the patient’s perception of the therapeutic alliance.15,16 Given the objectives of psychiatric treatment—to relieve psychiatric symptoms, improve patient functioning, and alleviate psychological distress—it is no wonder that delivery factors play an important role in the perception of the therapeutic alliance: The quality of the provider−patient relationship is the axis around which treatment takes place. This relationship constantly ranks high on surveys of what is important to patients15—especially in an inpatient psychiatric setting.
Attitudes are modifiable. From the treating psychiatrist to nursing and ancillary staffs, all team members need to express attitudes and behaviors that reflect positively on the patient.17 Behaviors such as involving the patient fully in therapeutic decision-making; exuding an attitude of caring, equanimity, empathy, sincerity, and respect; and listening to the patient’s concerns can go a long way to improving the therapeutic relationship. Displaying such attitudes and behaviors also help improve the larger vision of psychiatric intervention: to bring about positive therapeutic changes.
Summing up
Ratings of the therapeutic alliance are the currency of patient satisfaction. The value of this therapeutic currency is affected by delivery factors, which are adjustable, and patient factors, which are not. Taken together, however, both types of factors are the foundation of patient satisfaction and the therapeutic alliance.
1. Martin DJ, Garske JP, Davis MK. Relation of the therapeutic alliance with outcome and other variables: a meta-analytic review. J Consult Clin Psychol. 2000;68(3):438-450.
2. Chue P. The relationship between patient satisfaction and treatment outcomes in schizophrenia. J Psychopharmacol. 2006;20(suppl 6):38-56.
3. Priebe S, McCabe R. The therapeutic relationship in psychiatric settings. Acta Psychiatrica Scandinavica Suppl. 2006;113(429):69-72.
4. Bowersox NW, Bohnert AS, Ganoczy D, et al. Inpatient psychiatric care experience and its relationship to posthospitalization treatment participation. Psychiatr Serv. 2013;64(6):554-562.
5. Zendjidjian XY, Baumstarck K, Auquier P, et al. Satisfaction of hospitalized psychiatry patients: why should clinicians care? Patient Preference Adherence. 2014;8:575-583.
6. Druss BG, Rosenheck RA, Stolar M. Patient satisfaction and administrative measures as indicators of the quality of mental health care. Psychiatr Serv. 1999;50(8):1053-1058.
7. Sapra M, Weiden PJ, Schooler NR, et al. Reasons for adherence and nonadherence: a pilot study comparing first- and multi-episode schizophrenia patients. Clin Schizophr Relat Psychoses. 2014;7(4):199-206.
8. Rosenheck R, Wilson NJ, Meterko M. Influence of patient and hospital factors on consumer satisfaction with inpatient mental health treatment. Psychiatr Serv. 1997;48(12):1553-1561.
9. Hoff RA, Rosenheck RA, Meterko M, et al. Mental illness as a predictor of satisfaction with inpatient care at Veterans Affairs hospitals. Psychiatr Serv. 1999;50(5):680-685.
10. Bjørngaard JH, Ruud T, Friis S. The impact of mental illness on patient satisfaction with the therapeutic relationship: a multilevel analysis. Soc Psychiatry Psychiatr Epidemiol. 2007;42(10):803-809.
11. Greenley JR, Young TB, Schoenherr RA. Psychological distress and patient satisfaction. Med Care. 1982;20(4):373-385.
12. Svensson B, Hansson L. Patient satisfaction with inpatient psychiatric care. The influence of personality traits, diagnosis and perceived coercion. Acta Psychiatr Scand. 1994;90(5):379-384.
13. Köhler S, Unger T, Hoffmann S, et al. Patient satisfaction with inpatient psychiatric treatment and its relation to treatment outcome in unipolar depression and schizophrenia. Int J Psychiatry Clin Pract. 2015;19(2):119-123.
14. Holcomb WR, Parker JC, Leong GB, et al. Customer satisfaction and self-reported treatment outcomes among psychiatric inpatients. Psychiatr Serv. 1998;49(7):929-934.
15. Hansson L, Björkman T, Berglund I. What is important in psychiatric inpatient care? Quality of care from the patient’s perspective. Qual Assur Health Care. 1993;5(1):41-48.
16. Remnik Y, Melamed Y, Swartz M, et al. Patients’ satisfaction with psychiatric inpatient care. Isr J Psychiatry Relat Sci. 2003;41(3):208-212.
17. Norcross JC, ed. Psychotherapy relationships that work: therapist contributions and responsiveness to patients. New York, NY: Oxford University Press; 2002.
The therapeutic alliance (interchangeably, the therapeutic relationship) is a subjective measure of the relationship between a clinician and a patient. It is an indicator of clinical trustworthiness: what a patient is referring to when she (he) expresses trust in her provider. The therapeutic alliance also is known as the working alliance, the therapeutic bond, and the helping alliance,1 and it is an important factor in patient satisfaction ratings—the gauging parameter through which clinicians and institutions measure the quality of care they provide.2
A therapeutic alliance is essential to the delivery of psychiatric care. Itself, it can be a healing factor3 and has been linked to patients’ adherence to treatment and continuation of care.4 For example, psychiatric patients who perceive the therapeutic alliance more positively have:
- a better long-term health outcome after discharge
- a significantly better psychological quality of life5
- a better follow-up record of outpatient care after inpatient discharge4,6
- better adherence to prescribed treatment7
- a reduced likelihood of relapse and readmission.6
Patient satisfaction is an indirect measure of the therapeutic alliance; many variables of the therapeutic relationship can affect that satisfaction. In this article, we call those variables patient factors and delivery factors; our aim, using the example of 2 hypothetical cases, is to highlight their importance in patients’ perception of the therapeutic alliance they have with providers.
CASE Paranoid delusions lead to termination of care
Mr. D, age 21, unmarried, unemployed, and with no medical or psychiatric history, is transferred from the medical floor to the inpatient psychiatric unit after coming to the hospital’s emergency room (ER) with a report of chest pain. Workup on the medical floor was negative for a serious cardiac event.
On questioning, Mr. D tells the team that his chest pain is caused by National Security Agency (NSA) satellites “locking” onto his heart and causing veins in his heart to “pop.”
Mr. D agrees to be transferred to the psychiatric unit. Once there, however, he refuses to take the psychotropic medications that have been prescribed or to comply with the balance of the treatment protocol. He is adamant about the influence of NSA satellites, and requests daily imaging to locate evidence of the path of the satellite tracking device that he claims is inside his body.
The treatment team repeatedly refuses to comply with Mr. D’s demand for imaging. He becomes angry and says that he does not think he is getting proper care because the nature of his problem is medical, not psychiatric.
Mr. D repeatedly asserts that he will not take any of the psychotropic medications that have been prescribed for him and will not attend follow-up appointments with the psychiatry team because he does not need treatment. He accuses the treatment team of conspiring with the NSA and causing his chest pain.
Mr. D asks to be discharged.
Patient factors: Unmodifiable and static
As Mr. D’s case exemplifies, patient factors are a set of elements, intrinsic to a given patient, that affect that patient’s perceptions independent of the quality of the care delivered. Included among patient factors are personal sociodemographic and psychopathological characteristics. These patient factors influence the therapeutic relationship in many ways.
Sociodemographics. It has been reported that patients of minority heritage and those who are male, young, and unmarried tend to be less satisfied with medical treatment in general and with psychiatric inpatient treatment in particular.8,9 Females and older patients, on the other hand, are more likely to be satisfied with the perceived delivery of care and the therapeutic alliance.8-10
Psychopathology affects patients’ perception of the delivery of care and the therapeutic alliance. Patients who are highly distressed psychologically and those who suffer chronic psychiatric illness, for example, tend to perceive themselves as having benefitted less from treatment than healthier counterparts.9,11 Such patients also tend to see their therapeutic outcome in a much less favorable light.11,12 Patients with borderline personality disorder and antisocial personality disorder12-14 and those hospitalized involuntarily8 tend to (1) be less satisfied with their therapeutic outcome and (2) see the therapeutic alliance less favorably compared with those who do not have these psychopathologies.
CASE Denied a blanket, she feels like a 'burden'
Ms. X, age 34, married and a homemaker, has a history of bipolar I disorder. She brings herself to the ER complaining of depression and suicidal ideation.
After Ms. X is seen by the psychiatry consult service in the ER, she reports that she feels frustrated and angry and thinks that the hospital’s physicians do not really want to help her. She states that she felt that the ER staff “dismissed” her, in part because she spent 4 hours in the ER waiting room before she was given a bed.
Ms. X says that, once she was placed in a room, she felt that the nursing staff and medical assistants ignored her because they did not give her the extra blanket she requested. She said she was cold as a result, while she waited to see the psychiatrist and the ER physician.
Ms. X states that she came to the ER seeking help because she felt depressed and thought that no one cared about her. Coming to the hospital made her feel worse, after all, she said, because there she has been treated like she is a burden, much like she is treated at home.
Delivery factors: Amenable to change
These mutable elements of the therapeutic alliance are dependent on the quality of the care, as they were in Ms. X’s case; they can be changed. Included among delivery factors is the quality of the relationship between provider and patient—that is, how the psychiatrist and the nursing staff relate to the patient.
Perceptions are key. Delivery factors rank as one of the most important elements that influence the patient’s perception of the therapeutic alliance.15,16 Given the objectives of psychiatric treatment—to relieve psychiatric symptoms, improve patient functioning, and alleviate psychological distress—it is no wonder that delivery factors play an important role in the perception of the therapeutic alliance: The quality of the provider−patient relationship is the axis around which treatment takes place. This relationship constantly ranks high on surveys of what is important to patients15—especially in an inpatient psychiatric setting.
Attitudes are modifiable. From the treating psychiatrist to nursing and ancillary staffs, all team members need to express attitudes and behaviors that reflect positively on the patient.17 Behaviors such as involving the patient fully in therapeutic decision-making; exuding an attitude of caring, equanimity, empathy, sincerity, and respect; and listening to the patient’s concerns can go a long way to improving the therapeutic relationship. Displaying such attitudes and behaviors also help improve the larger vision of psychiatric intervention: to bring about positive therapeutic changes.
Summing up
Ratings of the therapeutic alliance are the currency of patient satisfaction. The value of this therapeutic currency is affected by delivery factors, which are adjustable, and patient factors, which are not. Taken together, however, both types of factors are the foundation of patient satisfaction and the therapeutic alliance.
The therapeutic alliance (interchangeably, the therapeutic relationship) is a subjective measure of the relationship between a clinician and a patient. It is an indicator of clinical trustworthiness: what a patient is referring to when she (he) expresses trust in her provider. The therapeutic alliance also is known as the working alliance, the therapeutic bond, and the helping alliance,1 and it is an important factor in patient satisfaction ratings—the gauging parameter through which clinicians and institutions measure the quality of care they provide.2
A therapeutic alliance is essential to the delivery of psychiatric care. Itself, it can be a healing factor3 and has been linked to patients’ adherence to treatment and continuation of care.4 For example, psychiatric patients who perceive the therapeutic alliance more positively have:
- a better long-term health outcome after discharge
- a significantly better psychological quality of life5
- a better follow-up record of outpatient care after inpatient discharge4,6
- better adherence to prescribed treatment7
- a reduced likelihood of relapse and readmission.6
Patient satisfaction is an indirect measure of the therapeutic alliance; many variables of the therapeutic relationship can affect that satisfaction. In this article, we call those variables patient factors and delivery factors; our aim, using the example of 2 hypothetical cases, is to highlight their importance in patients’ perception of the therapeutic alliance they have with providers.
CASE Paranoid delusions lead to termination of care
Mr. D, age 21, unmarried, unemployed, and with no medical or psychiatric history, is transferred from the medical floor to the inpatient psychiatric unit after coming to the hospital’s emergency room (ER) with a report of chest pain. Workup on the medical floor was negative for a serious cardiac event.
On questioning, Mr. D tells the team that his chest pain is caused by National Security Agency (NSA) satellites “locking” onto his heart and causing veins in his heart to “pop.”
Mr. D agrees to be transferred to the psychiatric unit. Once there, however, he refuses to take the psychotropic medications that have been prescribed or to comply with the balance of the treatment protocol. He is adamant about the influence of NSA satellites, and requests daily imaging to locate evidence of the path of the satellite tracking device that he claims is inside his body.
The treatment team repeatedly refuses to comply with Mr. D’s demand for imaging. He becomes angry and says that he does not think he is getting proper care because the nature of his problem is medical, not psychiatric.
Mr. D repeatedly asserts that he will not take any of the psychotropic medications that have been prescribed for him and will not attend follow-up appointments with the psychiatry team because he does not need treatment. He accuses the treatment team of conspiring with the NSA and causing his chest pain.
Mr. D asks to be discharged.
Patient factors: Unmodifiable and static
As Mr. D’s case exemplifies, patient factors are a set of elements, intrinsic to a given patient, that affect that patient’s perceptions independent of the quality of the care delivered. Included among patient factors are personal sociodemographic and psychopathological characteristics. These patient factors influence the therapeutic relationship in many ways.
Sociodemographics. It has been reported that patients of minority heritage and those who are male, young, and unmarried tend to be less satisfied with medical treatment in general and with psychiatric inpatient treatment in particular.8,9 Females and older patients, on the other hand, are more likely to be satisfied with the perceived delivery of care and the therapeutic alliance.8-10
Psychopathology affects patients’ perception of the delivery of care and the therapeutic alliance. Patients who are highly distressed psychologically and those who suffer chronic psychiatric illness, for example, tend to perceive themselves as having benefitted less from treatment than healthier counterparts.9,11 Such patients also tend to see their therapeutic outcome in a much less favorable light.11,12 Patients with borderline personality disorder and antisocial personality disorder12-14 and those hospitalized involuntarily8 tend to (1) be less satisfied with their therapeutic outcome and (2) see the therapeutic alliance less favorably compared with those who do not have these psychopathologies.
CASE Denied a blanket, she feels like a 'burden'
Ms. X, age 34, married and a homemaker, has a history of bipolar I disorder. She brings herself to the ER complaining of depression and suicidal ideation.
After Ms. X is seen by the psychiatry consult service in the ER, she reports that she feels frustrated and angry and thinks that the hospital’s physicians do not really want to help her. She states that she felt that the ER staff “dismissed” her, in part because she spent 4 hours in the ER waiting room before she was given a bed.
Ms. X says that, once she was placed in a room, she felt that the nursing staff and medical assistants ignored her because they did not give her the extra blanket she requested. She said she was cold as a result, while she waited to see the psychiatrist and the ER physician.
Ms. X states that she came to the ER seeking help because she felt depressed and thought that no one cared about her. Coming to the hospital made her feel worse, after all, she said, because there she has been treated like she is a burden, much like she is treated at home.
Delivery factors: Amenable to change
These mutable elements of the therapeutic alliance are dependent on the quality of the care, as they were in Ms. X’s case; they can be changed. Included among delivery factors is the quality of the relationship between provider and patient—that is, how the psychiatrist and the nursing staff relate to the patient.
Perceptions are key. Delivery factors rank as one of the most important elements that influence the patient’s perception of the therapeutic alliance.15,16 Given the objectives of psychiatric treatment—to relieve psychiatric symptoms, improve patient functioning, and alleviate psychological distress—it is no wonder that delivery factors play an important role in the perception of the therapeutic alliance: The quality of the provider−patient relationship is the axis around which treatment takes place. This relationship constantly ranks high on surveys of what is important to patients15—especially in an inpatient psychiatric setting.
Attitudes are modifiable. From the treating psychiatrist to nursing and ancillary staffs, all team members need to express attitudes and behaviors that reflect positively on the patient.17 Behaviors such as involving the patient fully in therapeutic decision-making; exuding an attitude of caring, equanimity, empathy, sincerity, and respect; and listening to the patient’s concerns can go a long way to improving the therapeutic relationship. Displaying such attitudes and behaviors also help improve the larger vision of psychiatric intervention: to bring about positive therapeutic changes.
Summing up
Ratings of the therapeutic alliance are the currency of patient satisfaction. The value of this therapeutic currency is affected by delivery factors, which are adjustable, and patient factors, which are not. Taken together, however, both types of factors are the foundation of patient satisfaction and the therapeutic alliance.
1. Martin DJ, Garske JP, Davis MK. Relation of the therapeutic alliance with outcome and other variables: a meta-analytic review. J Consult Clin Psychol. 2000;68(3):438-450.
2. Chue P. The relationship between patient satisfaction and treatment outcomes in schizophrenia. J Psychopharmacol. 2006;20(suppl 6):38-56.
3. Priebe S, McCabe R. The therapeutic relationship in psychiatric settings. Acta Psychiatrica Scandinavica Suppl. 2006;113(429):69-72.
4. Bowersox NW, Bohnert AS, Ganoczy D, et al. Inpatient psychiatric care experience and its relationship to posthospitalization treatment participation. Psychiatr Serv. 2013;64(6):554-562.
5. Zendjidjian XY, Baumstarck K, Auquier P, et al. Satisfaction of hospitalized psychiatry patients: why should clinicians care? Patient Preference Adherence. 2014;8:575-583.
6. Druss BG, Rosenheck RA, Stolar M. Patient satisfaction and administrative measures as indicators of the quality of mental health care. Psychiatr Serv. 1999;50(8):1053-1058.
7. Sapra M, Weiden PJ, Schooler NR, et al. Reasons for adherence and nonadherence: a pilot study comparing first- and multi-episode schizophrenia patients. Clin Schizophr Relat Psychoses. 2014;7(4):199-206.
8. Rosenheck R, Wilson NJ, Meterko M. Influence of patient and hospital factors on consumer satisfaction with inpatient mental health treatment. Psychiatr Serv. 1997;48(12):1553-1561.
9. Hoff RA, Rosenheck RA, Meterko M, et al. Mental illness as a predictor of satisfaction with inpatient care at Veterans Affairs hospitals. Psychiatr Serv. 1999;50(5):680-685.
10. Bjørngaard JH, Ruud T, Friis S. The impact of mental illness on patient satisfaction with the therapeutic relationship: a multilevel analysis. Soc Psychiatry Psychiatr Epidemiol. 2007;42(10):803-809.
11. Greenley JR, Young TB, Schoenherr RA. Psychological distress and patient satisfaction. Med Care. 1982;20(4):373-385.
12. Svensson B, Hansson L. Patient satisfaction with inpatient psychiatric care. The influence of personality traits, diagnosis and perceived coercion. Acta Psychiatr Scand. 1994;90(5):379-384.
13. Köhler S, Unger T, Hoffmann S, et al. Patient satisfaction with inpatient psychiatric treatment and its relation to treatment outcome in unipolar depression and schizophrenia. Int J Psychiatry Clin Pract. 2015;19(2):119-123.
14. Holcomb WR, Parker JC, Leong GB, et al. Customer satisfaction and self-reported treatment outcomes among psychiatric inpatients. Psychiatr Serv. 1998;49(7):929-934.
15. Hansson L, Björkman T, Berglund I. What is important in psychiatric inpatient care? Quality of care from the patient’s perspective. Qual Assur Health Care. 1993;5(1):41-48.
16. Remnik Y, Melamed Y, Swartz M, et al. Patients’ satisfaction with psychiatric inpatient care. Isr J Psychiatry Relat Sci. 2003;41(3):208-212.
17. Norcross JC, ed. Psychotherapy relationships that work: therapist contributions and responsiveness to patients. New York, NY: Oxford University Press; 2002.
1. Martin DJ, Garske JP, Davis MK. Relation of the therapeutic alliance with outcome and other variables: a meta-analytic review. J Consult Clin Psychol. 2000;68(3):438-450.
2. Chue P. The relationship between patient satisfaction and treatment outcomes in schizophrenia. J Psychopharmacol. 2006;20(suppl 6):38-56.
3. Priebe S, McCabe R. The therapeutic relationship in psychiatric settings. Acta Psychiatrica Scandinavica Suppl. 2006;113(429):69-72.
4. Bowersox NW, Bohnert AS, Ganoczy D, et al. Inpatient psychiatric care experience and its relationship to posthospitalization treatment participation. Psychiatr Serv. 2013;64(6):554-562.
5. Zendjidjian XY, Baumstarck K, Auquier P, et al. Satisfaction of hospitalized psychiatry patients: why should clinicians care? Patient Preference Adherence. 2014;8:575-583.
6. Druss BG, Rosenheck RA, Stolar M. Patient satisfaction and administrative measures as indicators of the quality of mental health care. Psychiatr Serv. 1999;50(8):1053-1058.
7. Sapra M, Weiden PJ, Schooler NR, et al. Reasons for adherence and nonadherence: a pilot study comparing first- and multi-episode schizophrenia patients. Clin Schizophr Relat Psychoses. 2014;7(4):199-206.
8. Rosenheck R, Wilson NJ, Meterko M. Influence of patient and hospital factors on consumer satisfaction with inpatient mental health treatment. Psychiatr Serv. 1997;48(12):1553-1561.
9. Hoff RA, Rosenheck RA, Meterko M, et al. Mental illness as a predictor of satisfaction with inpatient care at Veterans Affairs hospitals. Psychiatr Serv. 1999;50(5):680-685.
10. Bjørngaard JH, Ruud T, Friis S. The impact of mental illness on patient satisfaction with the therapeutic relationship: a multilevel analysis. Soc Psychiatry Psychiatr Epidemiol. 2007;42(10):803-809.
11. Greenley JR, Young TB, Schoenherr RA. Psychological distress and patient satisfaction. Med Care. 1982;20(4):373-385.
12. Svensson B, Hansson L. Patient satisfaction with inpatient psychiatric care. The influence of personality traits, diagnosis and perceived coercion. Acta Psychiatr Scand. 1994;90(5):379-384.
13. Köhler S, Unger T, Hoffmann S, et al. Patient satisfaction with inpatient psychiatric treatment and its relation to treatment outcome in unipolar depression and schizophrenia. Int J Psychiatry Clin Pract. 2015;19(2):119-123.
14. Holcomb WR, Parker JC, Leong GB, et al. Customer satisfaction and self-reported treatment outcomes among psychiatric inpatients. Psychiatr Serv. 1998;49(7):929-934.
15. Hansson L, Björkman T, Berglund I. What is important in psychiatric inpatient care? Quality of care from the patient’s perspective. Qual Assur Health Care. 1993;5(1):41-48.
16. Remnik Y, Melamed Y, Swartz M, et al. Patients’ satisfaction with psychiatric inpatient care. Isr J Psychiatry Relat Sci. 2003;41(3):208-212.
17. Norcross JC, ed. Psychotherapy relationships that work: therapist contributions and responsiveness to patients. New York, NY: Oxford University Press; 2002.

Preventing, Identifying, and Managing Cosmetic Procedure Complications, Part 1: Soft-Tissue Augmentation and Botulinum Toxin Injections
The primary cosmetic procedures that dermatology residents will perform or assist in performing during their training are soft-tissue augmentation, botulinum toxin injections, chemical peels, and laser therapy. Because complications can occur from these procedures, it is important for residents to learn how to prevent, identify, and manage them for optimal patient outcomes. In part 1 of this 2-part series, soft-tissue augmentation and botulinum toxin injections are discussed. Chemical peels and laser therapy will be addressed in part 2.
Soft-Tissue Augmentation
Soft-tissue fillers include those that are made from collagen (bovine or human), hyaluronic acid (HA), poly-L-lactic acid, calcium hydroxylapatite, silicone, and polymethylmethacrylate. In general, acute complications of soft-tissue filler injections include erythema, swelling, and bruising.1-3 Patients who take blood thinners or supplements (eg, vitamin E, ginseng, garlic, ginger) should be asked to discontinue use 1 week prior to the procedure. Patients who take blood thinners also should be counseled to expect some bruising. Prior to injection, the skin should be thoroughly cleansed to avoid introducing skin bacteria into the injection site and to reduce infection risk. Postinjection erythema may be related to mast cell activation, which is temporary and should resolve after a few days.1-3
If you find yourself injecting the filler too superficially, you may notice that the skin begins to take on a blue-gray hue1-3 that is known as the Tyndall effect and can be prevented by injecting the filler at the proper level. For example, collagen-based fillers should be placed at the mid dermis, thicker HA fillers should be placed in the deep dermis, and calcium hydroxylapatite should be placed at the junction of the dermis and subcutaneous tissue. Polymethylmethacrylate and poly-L-lactic acid should both be placed subdermally.1-3
The gravest immediate complications associated with soft-tissue filler injections are occlusion of the central retinal artery and/or skin necrosis.1-4 Residents should never inject filler to the glabella or to the nose.1-3 Injections at these sites are sometimes performed but should only be performed by experienced dermatologists. The perioral and tear trough regions also are high-risk injection areas that require a high degree of experience and should only be injected with proper supervision by an experienced dermatologist.1-3 Residents generally can avoid these complications, though not with a 100% guarantee, by avoiding injections in high-risk areas, aspirating to check for blood, and slowly injecting a small amount of filler into the treatment area.1-3 A consensus statement on management of injection-induced necrosis advises to apply a nitropaste ointment 2% to the treatment site or administer an oral aspirin if the patient develops severe pain; vision loss; or acute skin discoloration, especially blanching.4 For HA-based fillers, at least 200 U of hyaluronidase should be injected. It has been suggested that saline can be injected to flush out calcium hydroxylapatite fillers.3 Warm compresses should be placed on the involved area. Following these interventions, any patient with vision loss or orbital pain should immediately undergo ophthalmologic evaluation.3 The most important intervention occurs in the first 24 hours.3,4 After 24 hours, careful wound care, oral anticoagulants, and hyperbaric oxygen therapy have been suggested as management options.3
There are 2 major chronic complications of soft-tissue filler injection, including delayed-onset infection, which occurs 2 weeks or more postinjection, and granuloma formation.1-3 Chronic low-grade infection at the injection site may be indicative of biofilm formation. If an HA filler was used, it should be dissolved with hyaluronidase to help break up the biofilm nidus.3 A course of oral antibiotics also may be indicated.1-3 Intralesional steroids may be used but only after antibiotics have been administered. A biofilm that develops from more permanent fillers may be more difficult to manage. Atypical mycobacterial infections have been known to develop at injection sites, which should be considered in refractory cases.1-3,5
Calcium hydroxylapatite, polymethylmethacrylate, and silicone can stimulate chronic immune system activation, which makes them more prone to granuloma formation.1-3 Once infection is ruled out, granulomas may be treated with intralesional steroids, surgical excision (if the results would be cosmetically acceptable), laser therapy, or potentially local injection of an immunosuppressant (eg, methotrexate, 5-fluorouracil).3
Botulinum Toxin Injections
Patients who are pregnant, lactating, or have neuromuscular disease are not candidates for botulinum toxin injections. There also is a risk that patients taking calcium channel blockers or aminoglycoside antibiotics may experience potentiated effects of the botulinum toxin.6
Patients should be informed that a postinjection headache may occur and should be treated with over-the-counter medications.6 Complication-free botulinum toxin procedures depend heavily on the physician’s knowledge of facial anatomy.1,6 The diagrams provided by Hirsch and Stier1 offer an excellent guide on where to place the injections. Brow droop, eyelid ptosis, and “Spock brow” (eyebrows that are overarched) largely can be avoided by proper injection point placement. A Spock brow may be corrected by injecting the lateral upper forehead with a few units to correct the exaggerated arch.6,7 For eyelid ptosis, apraclonidine 0.05% drops (1–2 drops 3 times daily) should be used until the ptosis resolves.6 Phenylephrine hydrochloride drops may be used should a patient have a documented sensitivity to apraclonidine but should not be used in a patient with acute angle-closure glaucoma or aneurysms.6
Final Thoughts
Learning to perform soft-tissue augmentation and botulinum toxin injections can be a satisfying and fun part of dermatology residency. Preventing, identifying, and managing any complications that may occur is an integral part of performing these procedures.
- Hirsch R, Stier M. Complications and their management in cosmetic dermatology. Dermatol Clin. 2009;27:507-520.
- Gladstone HB, Cohen JL. Adverse effects when injecting facial fillers. Semin Cutan Med Surg. 2007;26:34-39.
- Boulle K, Heydenrych I. Patient factors influencing dermal filler complications: prevention, assessment, and treatment. Clin Cosmet Investig Dermatol. 2015;8:205-214.
- Cohen JL, Biesman BS, Dayan SH, et al. Treatment of hyaluronic acid filler–induced impending necrosis with hyaluronidase: consensus recommendations [published online May 10, 2015]. Aesthet Surg J. 2015;35:844-849.
- Rodriguez JM, Xie YL, Winthrop KL, et al. Mycobacterium chelonae facial infections following injection of dermal filler. Aesthet Surg J. 2013;33:265-269.
- Nigam PK, Nigam A. Botulinum toxin. Indian J Dermatol. 2010;55:8-14.
- Carruthers A, Carruthers J. Update on the botulinum neurotoxins. Skin Therapy Lett. 2001;6:1-2.
The primary cosmetic procedures that dermatology residents will perform or assist in performing during their training are soft-tissue augmentation, botulinum toxin injections, chemical peels, and laser therapy. Because complications can occur from these procedures, it is important for residents to learn how to prevent, identify, and manage them for optimal patient outcomes. In part 1 of this 2-part series, soft-tissue augmentation and botulinum toxin injections are discussed. Chemical peels and laser therapy will be addressed in part 2.
Soft-Tissue Augmentation
Soft-tissue fillers include those that are made from collagen (bovine or human), hyaluronic acid (HA), poly-L-lactic acid, calcium hydroxylapatite, silicone, and polymethylmethacrylate. In general, acute complications of soft-tissue filler injections include erythema, swelling, and bruising.1-3 Patients who take blood thinners or supplements (eg, vitamin E, ginseng, garlic, ginger) should be asked to discontinue use 1 week prior to the procedure. Patients who take blood thinners also should be counseled to expect some bruising. Prior to injection, the skin should be thoroughly cleansed to avoid introducing skin bacteria into the injection site and to reduce infection risk. Postinjection erythema may be related to mast cell activation, which is temporary and should resolve after a few days.1-3
If you find yourself injecting the filler too superficially, you may notice that the skin begins to take on a blue-gray hue1-3 that is known as the Tyndall effect and can be prevented by injecting the filler at the proper level. For example, collagen-based fillers should be placed at the mid dermis, thicker HA fillers should be placed in the deep dermis, and calcium hydroxylapatite should be placed at the junction of the dermis and subcutaneous tissue. Polymethylmethacrylate and poly-L-lactic acid should both be placed subdermally.1-3
The gravest immediate complications associated with soft-tissue filler injections are occlusion of the central retinal artery and/or skin necrosis.1-4 Residents should never inject filler to the glabella or to the nose.1-3 Injections at these sites are sometimes performed but should only be performed by experienced dermatologists. The perioral and tear trough regions also are high-risk injection areas that require a high degree of experience and should only be injected with proper supervision by an experienced dermatologist.1-3 Residents generally can avoid these complications, though not with a 100% guarantee, by avoiding injections in high-risk areas, aspirating to check for blood, and slowly injecting a small amount of filler into the treatment area.1-3 A consensus statement on management of injection-induced necrosis advises to apply a nitropaste ointment 2% to the treatment site or administer an oral aspirin if the patient develops severe pain; vision loss; or acute skin discoloration, especially blanching.4 For HA-based fillers, at least 200 U of hyaluronidase should be injected. It has been suggested that saline can be injected to flush out calcium hydroxylapatite fillers.3 Warm compresses should be placed on the involved area. Following these interventions, any patient with vision loss or orbital pain should immediately undergo ophthalmologic evaluation.3 The most important intervention occurs in the first 24 hours.3,4 After 24 hours, careful wound care, oral anticoagulants, and hyperbaric oxygen therapy have been suggested as management options.3
There are 2 major chronic complications of soft-tissue filler injection, including delayed-onset infection, which occurs 2 weeks or more postinjection, and granuloma formation.1-3 Chronic low-grade infection at the injection site may be indicative of biofilm formation. If an HA filler was used, it should be dissolved with hyaluronidase to help break up the biofilm nidus.3 A course of oral antibiotics also may be indicated.1-3 Intralesional steroids may be used but only after antibiotics have been administered. A biofilm that develops from more permanent fillers may be more difficult to manage. Atypical mycobacterial infections have been known to develop at injection sites, which should be considered in refractory cases.1-3,5
Calcium hydroxylapatite, polymethylmethacrylate, and silicone can stimulate chronic immune system activation, which makes them more prone to granuloma formation.1-3 Once infection is ruled out, granulomas may be treated with intralesional steroids, surgical excision (if the results would be cosmetically acceptable), laser therapy, or potentially local injection of an immunosuppressant (eg, methotrexate, 5-fluorouracil).3
Botulinum Toxin Injections
Patients who are pregnant, lactating, or have neuromuscular disease are not candidates for botulinum toxin injections. There also is a risk that patients taking calcium channel blockers or aminoglycoside antibiotics may experience potentiated effects of the botulinum toxin.6
Patients should be informed that a postinjection headache may occur and should be treated with over-the-counter medications.6 Complication-free botulinum toxin procedures depend heavily on the physician’s knowledge of facial anatomy.1,6 The diagrams provided by Hirsch and Stier1 offer an excellent guide on where to place the injections. Brow droop, eyelid ptosis, and “Spock brow” (eyebrows that are overarched) largely can be avoided by proper injection point placement. A Spock brow may be corrected by injecting the lateral upper forehead with a few units to correct the exaggerated arch.6,7 For eyelid ptosis, apraclonidine 0.05% drops (1–2 drops 3 times daily) should be used until the ptosis resolves.6 Phenylephrine hydrochloride drops may be used should a patient have a documented sensitivity to apraclonidine but should not be used in a patient with acute angle-closure glaucoma or aneurysms.6
Final Thoughts
Learning to perform soft-tissue augmentation and botulinum toxin injections can be a satisfying and fun part of dermatology residency. Preventing, identifying, and managing any complications that may occur is an integral part of performing these procedures.
The primary cosmetic procedures that dermatology residents will perform or assist in performing during their training are soft-tissue augmentation, botulinum toxin injections, chemical peels, and laser therapy. Because complications can occur from these procedures, it is important for residents to learn how to prevent, identify, and manage them for optimal patient outcomes. In part 1 of this 2-part series, soft-tissue augmentation and botulinum toxin injections are discussed. Chemical peels and laser therapy will be addressed in part 2.
Soft-Tissue Augmentation
Soft-tissue fillers include those that are made from collagen (bovine or human), hyaluronic acid (HA), poly-L-lactic acid, calcium hydroxylapatite, silicone, and polymethylmethacrylate. In general, acute complications of soft-tissue filler injections include erythema, swelling, and bruising.1-3 Patients who take blood thinners or supplements (eg, vitamin E, ginseng, garlic, ginger) should be asked to discontinue use 1 week prior to the procedure. Patients who take blood thinners also should be counseled to expect some bruising. Prior to injection, the skin should be thoroughly cleansed to avoid introducing skin bacteria into the injection site and to reduce infection risk. Postinjection erythema may be related to mast cell activation, which is temporary and should resolve after a few days.1-3
If you find yourself injecting the filler too superficially, you may notice that the skin begins to take on a blue-gray hue1-3 that is known as the Tyndall effect and can be prevented by injecting the filler at the proper level. For example, collagen-based fillers should be placed at the mid dermis, thicker HA fillers should be placed in the deep dermis, and calcium hydroxylapatite should be placed at the junction of the dermis and subcutaneous tissue. Polymethylmethacrylate and poly-L-lactic acid should both be placed subdermally.1-3
The gravest immediate complications associated with soft-tissue filler injections are occlusion of the central retinal artery and/or skin necrosis.1-4 Residents should never inject filler to the glabella or to the nose.1-3 Injections at these sites are sometimes performed but should only be performed by experienced dermatologists. The perioral and tear trough regions also are high-risk injection areas that require a high degree of experience and should only be injected with proper supervision by an experienced dermatologist.1-3 Residents generally can avoid these complications, though not with a 100% guarantee, by avoiding injections in high-risk areas, aspirating to check for blood, and slowly injecting a small amount of filler into the treatment area.1-3 A consensus statement on management of injection-induced necrosis advises to apply a nitropaste ointment 2% to the treatment site or administer an oral aspirin if the patient develops severe pain; vision loss; or acute skin discoloration, especially blanching.4 For HA-based fillers, at least 200 U of hyaluronidase should be injected. It has been suggested that saline can be injected to flush out calcium hydroxylapatite fillers.3 Warm compresses should be placed on the involved area. Following these interventions, any patient with vision loss or orbital pain should immediately undergo ophthalmologic evaluation.3 The most important intervention occurs in the first 24 hours.3,4 After 24 hours, careful wound care, oral anticoagulants, and hyperbaric oxygen therapy have been suggested as management options.3
There are 2 major chronic complications of soft-tissue filler injection, including delayed-onset infection, which occurs 2 weeks or more postinjection, and granuloma formation.1-3 Chronic low-grade infection at the injection site may be indicative of biofilm formation. If an HA filler was used, it should be dissolved with hyaluronidase to help break up the biofilm nidus.3 A course of oral antibiotics also may be indicated.1-3 Intralesional steroids may be used but only after antibiotics have been administered. A biofilm that develops from more permanent fillers may be more difficult to manage. Atypical mycobacterial infections have been known to develop at injection sites, which should be considered in refractory cases.1-3,5
Calcium hydroxylapatite, polymethylmethacrylate, and silicone can stimulate chronic immune system activation, which makes them more prone to granuloma formation.1-3 Once infection is ruled out, granulomas may be treated with intralesional steroids, surgical excision (if the results would be cosmetically acceptable), laser therapy, or potentially local injection of an immunosuppressant (eg, methotrexate, 5-fluorouracil).3
Botulinum Toxin Injections
Patients who are pregnant, lactating, or have neuromuscular disease are not candidates for botulinum toxin injections. There also is a risk that patients taking calcium channel blockers or aminoglycoside antibiotics may experience potentiated effects of the botulinum toxin.6
Patients should be informed that a postinjection headache may occur and should be treated with over-the-counter medications.6 Complication-free botulinum toxin procedures depend heavily on the physician’s knowledge of facial anatomy.1,6 The diagrams provided by Hirsch and Stier1 offer an excellent guide on where to place the injections. Brow droop, eyelid ptosis, and “Spock brow” (eyebrows that are overarched) largely can be avoided by proper injection point placement. A Spock brow may be corrected by injecting the lateral upper forehead with a few units to correct the exaggerated arch.6,7 For eyelid ptosis, apraclonidine 0.05% drops (1–2 drops 3 times daily) should be used until the ptosis resolves.6 Phenylephrine hydrochloride drops may be used should a patient have a documented sensitivity to apraclonidine but should not be used in a patient with acute angle-closure glaucoma or aneurysms.6
Final Thoughts
Learning to perform soft-tissue augmentation and botulinum toxin injections can be a satisfying and fun part of dermatology residency. Preventing, identifying, and managing any complications that may occur is an integral part of performing these procedures.
- Hirsch R, Stier M. Complications and their management in cosmetic dermatology. Dermatol Clin. 2009;27:507-520.
- Gladstone HB, Cohen JL. Adverse effects when injecting facial fillers. Semin Cutan Med Surg. 2007;26:34-39.
- Boulle K, Heydenrych I. Patient factors influencing dermal filler complications: prevention, assessment, and treatment. Clin Cosmet Investig Dermatol. 2015;8:205-214.
- Cohen JL, Biesman BS, Dayan SH, et al. Treatment of hyaluronic acid filler–induced impending necrosis with hyaluronidase: consensus recommendations [published online May 10, 2015]. Aesthet Surg J. 2015;35:844-849.
- Rodriguez JM, Xie YL, Winthrop KL, et al. Mycobacterium chelonae facial infections following injection of dermal filler. Aesthet Surg J. 2013;33:265-269.
- Nigam PK, Nigam A. Botulinum toxin. Indian J Dermatol. 2010;55:8-14.
- Carruthers A, Carruthers J. Update on the botulinum neurotoxins. Skin Therapy Lett. 2001;6:1-2.
- Hirsch R, Stier M. Complications and their management in cosmetic dermatology. Dermatol Clin. 2009;27:507-520.
- Gladstone HB, Cohen JL. Adverse effects when injecting facial fillers. Semin Cutan Med Surg. 2007;26:34-39.
- Boulle K, Heydenrych I. Patient factors influencing dermal filler complications: prevention, assessment, and treatment. Clin Cosmet Investig Dermatol. 2015;8:205-214.
- Cohen JL, Biesman BS, Dayan SH, et al. Treatment of hyaluronic acid filler–induced impending necrosis with hyaluronidase: consensus recommendations [published online May 10, 2015]. Aesthet Surg J. 2015;35:844-849.
- Rodriguez JM, Xie YL, Winthrop KL, et al. Mycobacterium chelonae facial infections following injection of dermal filler. Aesthet Surg J. 2013;33:265-269.
- Nigam PK, Nigam A. Botulinum toxin. Indian J Dermatol. 2010;55:8-14.
- Carruthers A, Carruthers J. Update on the botulinum neurotoxins. Skin Therapy Lett. 2001;6:1-2.

Maximizing Efficiency in the Operating Room for Total Joint Arthroplasty
Developing a high-efficiency operating room (OR) is both a challenging and rewarding goal for any healthcare system. The OR is traditionally a high-cost/high-revenue environment1 and operative efficacy has been correlated with low complication rates and surgical success.2 An efficient OR is one that maximizes utilization while providing safe, reproducible, cost-effective, high-quality care. Total joint arthroplasty (TJA) has occupied the center stage for OR efficiency research, in part due to increasing demands from our aging population3 and economic pressures related to high implant costs, decreased reimbursement, and competition for market shares when OR time and space are limited.
A PubMed search on OR efficiency in TJA shows a disproportionately high focus on surgical technique, such as use of patient-specific instrumentation (PSI), computer-assisted surgery (CAS), minimally invasive surgery, and closure with barbed suture. In a retrospective review of 352 TKA patients who had PSI vs conventional instrumentation, DeHaan and colleagues4 found that PSI was associated with significantly decreased operative and room turnover times (20.4 minutes and 6.4 minutes, respectively). In another prospective multicenter study, Mont and colleagues5 showed a reduction in surgical time by 8.90 min for navigated total knee arthroplasty (TKA) performed with single-use instruments, cutting blocks, and trials. Other investigators compared PSI to CAS in TKA and found PSI to be 1.45 times more profitable than CAS, with 3 PSI cases performed in an 8-hour OR day compared to 2 CAS cases.6
There is no question that improved surgical technique can enhance OR efficiency. However, this model, while promising, is difficult to implement on a wide scale due to surgeon preferences, vendor limitations, and added costs related to the advanced preoperative imaging studies, manufacturing of the custom guides, and maintenance of navigation equipment. In addition, while interventions such as the use of barbed suture have the potential for speeding closure time, the time saved (4.7 minutes in one randomized trial)7 may not be enough to affect major utilization differences per OR per day. These technologies are also frequently employed by high-volume surgeons with high-volume teams and institutions.
Ideally, we need investment in the human capital and a collective change in work cultures to produce high-quality, well-choreographed, easily reproducible routines. An efficient OR requires the synchronous involvement of a large team of individuals, including hospital administrators, surgery schedulers, surgeons, anesthesiologists, preoperative holding area staff, OR nurses, surgical attendants, sterile processing personnel, and recovery room nurses. Case schedulers should match allocated block time with time required for surgery based on the historical performance of the individual surgeon, preferably scheduling similar cases on the same day. Preoperative work-up and medical clearance should be completed prior to scheduling to avoid last-minute cancellations. Patient reminders and accommodations for those traveling from long distances can further minimize late arrivals. Prompt initiation of the perioperative clinical pathway upon a patient’s check-in is important. The surgical site should be marked and the anesthesia plan confirmed upon arrival in the preoperative holding area. Necessary products need to be ready and/or administrated in time for transfer to the OR. These include prophylactic antibiotics, coagulation factors (eg, tranexamic acid), and blood products as indicated. Spinal anesthesia, regional nerve blocks, and intravenous (IV) lines should be completed before transfer to the OR. A “block room” close to the OR can allow concurrent induction of anesthesia and has been shown to increase the number of surgical cases performed during a regular workday.8 Hair clipping within the surgical site and pre-scrubbing of the operative extremity should also be performed prior to transfer to the OR in order to minimize micro-organisms and dispersal of loose hair onto the sterile field.
Upon arrival of the patient to the OR, instrument tables based on the surgeon preference cards should be opened, instrument count and implant templating completed, necessary imaging displayed, and OR staff ready with specific responsibilities assigned to each member. Small and colleagues9 showed that using dedicated orthopedic staff familiar with the surgical routine decreased operative time by 19 minutes per procedure, or 1.25 hours for a surgeon performing 4 primary TJAs per day. Practices such as routine placement of a urinary catheter should be seriously scrutinized. In a randomized prospective study of patients undergoing total hip arthroplasty under spinal anesthesia, Miller and colleagues10 found no benefit for indwelling catheters in preventing urinary retention. In another randomized prospective study, Huang and colleagues11 found the prevalence of urinary tract infections was significantly higher in TJA patients who received indwelling urinary catheters.
A scrub nurse familiar with the instruments, their assembly, and the sequence of events can ensure efficient surgical flow. The scrub nurse needs to anticipate missing or defective tools and call for them, ideally before the incision is made. Direct comparison studies are needed to assess the efficacy of routine intraoperative imaging vs commercially available universal cup alignment guides or clinical examinations in determining acceptable component positioning and limb length. Following component implantation and before wound closure, the circulating nurse should initiate the process of acquisition of a recovery room bed, make sure dressing supplies and necessary equipment are available, and call for surgical attendants. Lack of surgical attendants, delayed transfer from the OR table to hospital bed, and prolonged acquisition of a recovery room bed have been identified as major OR inefficiencies in a retrospective study by Attarian and colleagues.12
In summary, time is the OR’s most valuable resource.13 We believe that a consistent, almost automated attitude to the above procedures decreases variability and improves efficiency. By providing clear communication of the surgical needs with the team, having consistent anesthesia and nursing staff, implementing consistent perioperative protocols, and insuring that all necessary instruments and modalities are available prior to starting the procedure, we were able to sustainably increase OR throughput in a large teaching hospital.9,14 This process, however, requires constant review to identify and eliminate new gaps, with each member of the team sharing a frank desire to improve. In this regard, hospital administrators share the duty to facilitate the implementation of any necessary changes, allocation of needed resources, and rewarding good effort, which could ultimately increase staff satisfaction and retention. Because efficiency is the ratio of benefits (eg, revenue, safety, etc.) to investment (eg, implant costs, wages, etc.), raises the question: what would be the effect of transitioning from hourly-wage to a salary-based system for key support staff? Unlike hourly-wage personnel, who have no incentive for productivity, a salaried employee assigned to a high-efficiency OR will inherently strive for improvement, employing higher organizational skills to accomplish a common goal. To our knowledge, there is no published data on this topic.
1. Krupka DC, Sandberg WS. Operating room design and its impact on operating room economics. Curr Opin Anaesthesiol. 2006;19(2):185-191.
2. Scott WN, Booth RE Jr, Dalury DF, Healy WL, Lonner JH. Efficiency and economics in joint arthroplasty. J Bone Joint Surg Am. 2009;91 Suppl 5:33-36.
3. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780-785.
4. DeHaan AM, Adams JR, DeHart ML, Huff TW. Patient-specific versus conventional instrumentation for total knee arthroplasty: peri-operative and cost differences. J Arthroplasty. 2014;29(11):2065-2069.
5. Mont MA, McElroy MJ, Johnson AJ, Pivec R; Single-Use Multicenter Trial Group Writing Group. Single-use instruments, cutting blocks, and trials increase efficiency in the operating room during total knee arthroplasty: a prospective comparison of navigated and non-navigated cases. J Arthroplasty. 2013;28(7):1135-1140.
6. Lionberger DR, Crocker CL, Chen V. Patient specific instrumentation. J Arthroplasty. 2014;29(9):1699-1704.
7. Sah AP. Is there an advantage to knotless barbed suture in TKA wound closure? A randomized trial in simultaneous bilateral TKAs. Clin Orthop Relat Res. 2015;473(6):2019-2027.
8. Torkki PM, Marjamaa RA, Torkki MI, Kallio PE, Kirvelä OA. Use of anesthesia induction rooms can increase the number of urgent orthopedic cases completed within 7 hours. Anesthesiology. 2005;103(2):401-405.
9. Small TJ, Gad BV, Klika AK, Mounir-Soliman LS, Gerritsen RL, Barsoum WK. Dedicated orthopedic operating room unit improves operating room efficiency. J Arthroplasty. 2013;28(7):1066-1071.e2.
10. Miller AG, McKenzie J, Greenky M, et al. Spinal anesthesia: should everyone receive a urinary catheter?: a randomized, prospective study of patients undergoing total hip arthroplasty. J Bone Joint Surg Am. 2013;95(16):1498-1503.
11. Huang Z, Ma J, Shen B, Pei F. General anesthesia: to catheterize or not? A prospective randomized controlled study of patients undergoing total knee arthroplasty. J Arthroplasty. 2015;30(3):502-506.
12. Attarian DE, Wahl JE, Wellman SS, Bolognesi MP. Developing a high-efficiency operating room for total joint arthroplasty in an academic setting. Clin Orthop Relat Res. 2013;471(6):1832-1836.
13. Gamble M. 6 cornerstones of operating room efficiency: best practices for each. Becker’s Hospital Review Web site. http://www.beckershospitalreview.com/or-efficiencies/6-cornerstones-of-operating-room-efficiency-best-practices-for-each.html. Updated January 18, 2013. Accessed September 3, 2015.
14. Smith MP, Sandberg WS, Foss J, et al. High-throughput operating room system for joint arthroplasties durably outperforms routine processes. Anesthesiology. 2008;109(1):25-35.
Developing a high-efficiency operating room (OR) is both a challenging and rewarding goal for any healthcare system. The OR is traditionally a high-cost/high-revenue environment1 and operative efficacy has been correlated with low complication rates and surgical success.2 An efficient OR is one that maximizes utilization while providing safe, reproducible, cost-effective, high-quality care. Total joint arthroplasty (TJA) has occupied the center stage for OR efficiency research, in part due to increasing demands from our aging population3 and economic pressures related to high implant costs, decreased reimbursement, and competition for market shares when OR time and space are limited.
A PubMed search on OR efficiency in TJA shows a disproportionately high focus on surgical technique, such as use of patient-specific instrumentation (PSI), computer-assisted surgery (CAS), minimally invasive surgery, and closure with barbed suture. In a retrospective review of 352 TKA patients who had PSI vs conventional instrumentation, DeHaan and colleagues4 found that PSI was associated with significantly decreased operative and room turnover times (20.4 minutes and 6.4 minutes, respectively). In another prospective multicenter study, Mont and colleagues5 showed a reduction in surgical time by 8.90 min for navigated total knee arthroplasty (TKA) performed with single-use instruments, cutting blocks, and trials. Other investigators compared PSI to CAS in TKA and found PSI to be 1.45 times more profitable than CAS, with 3 PSI cases performed in an 8-hour OR day compared to 2 CAS cases.6
There is no question that improved surgical technique can enhance OR efficiency. However, this model, while promising, is difficult to implement on a wide scale due to surgeon preferences, vendor limitations, and added costs related to the advanced preoperative imaging studies, manufacturing of the custom guides, and maintenance of navigation equipment. In addition, while interventions such as the use of barbed suture have the potential for speeding closure time, the time saved (4.7 minutes in one randomized trial)7 may not be enough to affect major utilization differences per OR per day. These technologies are also frequently employed by high-volume surgeons with high-volume teams and institutions.
Ideally, we need investment in the human capital and a collective change in work cultures to produce high-quality, well-choreographed, easily reproducible routines. An efficient OR requires the synchronous involvement of a large team of individuals, including hospital administrators, surgery schedulers, surgeons, anesthesiologists, preoperative holding area staff, OR nurses, surgical attendants, sterile processing personnel, and recovery room nurses. Case schedulers should match allocated block time with time required for surgery based on the historical performance of the individual surgeon, preferably scheduling similar cases on the same day. Preoperative work-up and medical clearance should be completed prior to scheduling to avoid last-minute cancellations. Patient reminders and accommodations for those traveling from long distances can further minimize late arrivals. Prompt initiation of the perioperative clinical pathway upon a patient’s check-in is important. The surgical site should be marked and the anesthesia plan confirmed upon arrival in the preoperative holding area. Necessary products need to be ready and/or administrated in time for transfer to the OR. These include prophylactic antibiotics, coagulation factors (eg, tranexamic acid), and blood products as indicated. Spinal anesthesia, regional nerve blocks, and intravenous (IV) lines should be completed before transfer to the OR. A “block room” close to the OR can allow concurrent induction of anesthesia and has been shown to increase the number of surgical cases performed during a regular workday.8 Hair clipping within the surgical site and pre-scrubbing of the operative extremity should also be performed prior to transfer to the OR in order to minimize micro-organisms and dispersal of loose hair onto the sterile field.
Upon arrival of the patient to the OR, instrument tables based on the surgeon preference cards should be opened, instrument count and implant templating completed, necessary imaging displayed, and OR staff ready with specific responsibilities assigned to each member. Small and colleagues9 showed that using dedicated orthopedic staff familiar with the surgical routine decreased operative time by 19 minutes per procedure, or 1.25 hours for a surgeon performing 4 primary TJAs per day. Practices such as routine placement of a urinary catheter should be seriously scrutinized. In a randomized prospective study of patients undergoing total hip arthroplasty under spinal anesthesia, Miller and colleagues10 found no benefit for indwelling catheters in preventing urinary retention. In another randomized prospective study, Huang and colleagues11 found the prevalence of urinary tract infections was significantly higher in TJA patients who received indwelling urinary catheters.
A scrub nurse familiar with the instruments, their assembly, and the sequence of events can ensure efficient surgical flow. The scrub nurse needs to anticipate missing or defective tools and call for them, ideally before the incision is made. Direct comparison studies are needed to assess the efficacy of routine intraoperative imaging vs commercially available universal cup alignment guides or clinical examinations in determining acceptable component positioning and limb length. Following component implantation and before wound closure, the circulating nurse should initiate the process of acquisition of a recovery room bed, make sure dressing supplies and necessary equipment are available, and call for surgical attendants. Lack of surgical attendants, delayed transfer from the OR table to hospital bed, and prolonged acquisition of a recovery room bed have been identified as major OR inefficiencies in a retrospective study by Attarian and colleagues.12
In summary, time is the OR’s most valuable resource.13 We believe that a consistent, almost automated attitude to the above procedures decreases variability and improves efficiency. By providing clear communication of the surgical needs with the team, having consistent anesthesia and nursing staff, implementing consistent perioperative protocols, and insuring that all necessary instruments and modalities are available prior to starting the procedure, we were able to sustainably increase OR throughput in a large teaching hospital.9,14 This process, however, requires constant review to identify and eliminate new gaps, with each member of the team sharing a frank desire to improve. In this regard, hospital administrators share the duty to facilitate the implementation of any necessary changes, allocation of needed resources, and rewarding good effort, which could ultimately increase staff satisfaction and retention. Because efficiency is the ratio of benefits (eg, revenue, safety, etc.) to investment (eg, implant costs, wages, etc.), raises the question: what would be the effect of transitioning from hourly-wage to a salary-based system for key support staff? Unlike hourly-wage personnel, who have no incentive for productivity, a salaried employee assigned to a high-efficiency OR will inherently strive for improvement, employing higher organizational skills to accomplish a common goal. To our knowledge, there is no published data on this topic.
Developing a high-efficiency operating room (OR) is both a challenging and rewarding goal for any healthcare system. The OR is traditionally a high-cost/high-revenue environment1 and operative efficacy has been correlated with low complication rates and surgical success.2 An efficient OR is one that maximizes utilization while providing safe, reproducible, cost-effective, high-quality care. Total joint arthroplasty (TJA) has occupied the center stage for OR efficiency research, in part due to increasing demands from our aging population3 and economic pressures related to high implant costs, decreased reimbursement, and competition for market shares when OR time and space are limited.
A PubMed search on OR efficiency in TJA shows a disproportionately high focus on surgical technique, such as use of patient-specific instrumentation (PSI), computer-assisted surgery (CAS), minimally invasive surgery, and closure with barbed suture. In a retrospective review of 352 TKA patients who had PSI vs conventional instrumentation, DeHaan and colleagues4 found that PSI was associated with significantly decreased operative and room turnover times (20.4 minutes and 6.4 minutes, respectively). In another prospective multicenter study, Mont and colleagues5 showed a reduction in surgical time by 8.90 min for navigated total knee arthroplasty (TKA) performed with single-use instruments, cutting blocks, and trials. Other investigators compared PSI to CAS in TKA and found PSI to be 1.45 times more profitable than CAS, with 3 PSI cases performed in an 8-hour OR day compared to 2 CAS cases.6
There is no question that improved surgical technique can enhance OR efficiency. However, this model, while promising, is difficult to implement on a wide scale due to surgeon preferences, vendor limitations, and added costs related to the advanced preoperative imaging studies, manufacturing of the custom guides, and maintenance of navigation equipment. In addition, while interventions such as the use of barbed suture have the potential for speeding closure time, the time saved (4.7 minutes in one randomized trial)7 may not be enough to affect major utilization differences per OR per day. These technologies are also frequently employed by high-volume surgeons with high-volume teams and institutions.
Ideally, we need investment in the human capital and a collective change in work cultures to produce high-quality, well-choreographed, easily reproducible routines. An efficient OR requires the synchronous involvement of a large team of individuals, including hospital administrators, surgery schedulers, surgeons, anesthesiologists, preoperative holding area staff, OR nurses, surgical attendants, sterile processing personnel, and recovery room nurses. Case schedulers should match allocated block time with time required for surgery based on the historical performance of the individual surgeon, preferably scheduling similar cases on the same day. Preoperative work-up and medical clearance should be completed prior to scheduling to avoid last-minute cancellations. Patient reminders and accommodations for those traveling from long distances can further minimize late arrivals. Prompt initiation of the perioperative clinical pathway upon a patient’s check-in is important. The surgical site should be marked and the anesthesia plan confirmed upon arrival in the preoperative holding area. Necessary products need to be ready and/or administrated in time for transfer to the OR. These include prophylactic antibiotics, coagulation factors (eg, tranexamic acid), and blood products as indicated. Spinal anesthesia, regional nerve blocks, and intravenous (IV) lines should be completed before transfer to the OR. A “block room” close to the OR can allow concurrent induction of anesthesia and has been shown to increase the number of surgical cases performed during a regular workday.8 Hair clipping within the surgical site and pre-scrubbing of the operative extremity should also be performed prior to transfer to the OR in order to minimize micro-organisms and dispersal of loose hair onto the sterile field.
Upon arrival of the patient to the OR, instrument tables based on the surgeon preference cards should be opened, instrument count and implant templating completed, necessary imaging displayed, and OR staff ready with specific responsibilities assigned to each member. Small and colleagues9 showed that using dedicated orthopedic staff familiar with the surgical routine decreased operative time by 19 minutes per procedure, or 1.25 hours for a surgeon performing 4 primary TJAs per day. Practices such as routine placement of a urinary catheter should be seriously scrutinized. In a randomized prospective study of patients undergoing total hip arthroplasty under spinal anesthesia, Miller and colleagues10 found no benefit for indwelling catheters in preventing urinary retention. In another randomized prospective study, Huang and colleagues11 found the prevalence of urinary tract infections was significantly higher in TJA patients who received indwelling urinary catheters.
A scrub nurse familiar with the instruments, their assembly, and the sequence of events can ensure efficient surgical flow. The scrub nurse needs to anticipate missing or defective tools and call for them, ideally before the incision is made. Direct comparison studies are needed to assess the efficacy of routine intraoperative imaging vs commercially available universal cup alignment guides or clinical examinations in determining acceptable component positioning and limb length. Following component implantation and before wound closure, the circulating nurse should initiate the process of acquisition of a recovery room bed, make sure dressing supplies and necessary equipment are available, and call for surgical attendants. Lack of surgical attendants, delayed transfer from the OR table to hospital bed, and prolonged acquisition of a recovery room bed have been identified as major OR inefficiencies in a retrospective study by Attarian and colleagues.12
In summary, time is the OR’s most valuable resource.13 We believe that a consistent, almost automated attitude to the above procedures decreases variability and improves efficiency. By providing clear communication of the surgical needs with the team, having consistent anesthesia and nursing staff, implementing consistent perioperative protocols, and insuring that all necessary instruments and modalities are available prior to starting the procedure, we were able to sustainably increase OR throughput in a large teaching hospital.9,14 This process, however, requires constant review to identify and eliminate new gaps, with each member of the team sharing a frank desire to improve. In this regard, hospital administrators share the duty to facilitate the implementation of any necessary changes, allocation of needed resources, and rewarding good effort, which could ultimately increase staff satisfaction and retention. Because efficiency is the ratio of benefits (eg, revenue, safety, etc.) to investment (eg, implant costs, wages, etc.), raises the question: what would be the effect of transitioning from hourly-wage to a salary-based system for key support staff? Unlike hourly-wage personnel, who have no incentive for productivity, a salaried employee assigned to a high-efficiency OR will inherently strive for improvement, employing higher organizational skills to accomplish a common goal. To our knowledge, there is no published data on this topic.
1. Krupka DC, Sandberg WS. Operating room design and its impact on operating room economics. Curr Opin Anaesthesiol. 2006;19(2):185-191.
2. Scott WN, Booth RE Jr, Dalury DF, Healy WL, Lonner JH. Efficiency and economics in joint arthroplasty. J Bone Joint Surg Am. 2009;91 Suppl 5:33-36.
3. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780-785.
4. DeHaan AM, Adams JR, DeHart ML, Huff TW. Patient-specific versus conventional instrumentation for total knee arthroplasty: peri-operative and cost differences. J Arthroplasty. 2014;29(11):2065-2069.
5. Mont MA, McElroy MJ, Johnson AJ, Pivec R; Single-Use Multicenter Trial Group Writing Group. Single-use instruments, cutting blocks, and trials increase efficiency in the operating room during total knee arthroplasty: a prospective comparison of navigated and non-navigated cases. J Arthroplasty. 2013;28(7):1135-1140.
6. Lionberger DR, Crocker CL, Chen V. Patient specific instrumentation. J Arthroplasty. 2014;29(9):1699-1704.
7. Sah AP. Is there an advantage to knotless barbed suture in TKA wound closure? A randomized trial in simultaneous bilateral TKAs. Clin Orthop Relat Res. 2015;473(6):2019-2027.
8. Torkki PM, Marjamaa RA, Torkki MI, Kallio PE, Kirvelä OA. Use of anesthesia induction rooms can increase the number of urgent orthopedic cases completed within 7 hours. Anesthesiology. 2005;103(2):401-405.
9. Small TJ, Gad BV, Klika AK, Mounir-Soliman LS, Gerritsen RL, Barsoum WK. Dedicated orthopedic operating room unit improves operating room efficiency. J Arthroplasty. 2013;28(7):1066-1071.e2.
10. Miller AG, McKenzie J, Greenky M, et al. Spinal anesthesia: should everyone receive a urinary catheter?: a randomized, prospective study of patients undergoing total hip arthroplasty. J Bone Joint Surg Am. 2013;95(16):1498-1503.
11. Huang Z, Ma J, Shen B, Pei F. General anesthesia: to catheterize or not? A prospective randomized controlled study of patients undergoing total knee arthroplasty. J Arthroplasty. 2015;30(3):502-506.
12. Attarian DE, Wahl JE, Wellman SS, Bolognesi MP. Developing a high-efficiency operating room for total joint arthroplasty in an academic setting. Clin Orthop Relat Res. 2013;471(6):1832-1836.
13. Gamble M. 6 cornerstones of operating room efficiency: best practices for each. Becker’s Hospital Review Web site. http://www.beckershospitalreview.com/or-efficiencies/6-cornerstones-of-operating-room-efficiency-best-practices-for-each.html. Updated January 18, 2013. Accessed September 3, 2015.
14. Smith MP, Sandberg WS, Foss J, et al. High-throughput operating room system for joint arthroplasties durably outperforms routine processes. Anesthesiology. 2008;109(1):25-35.
1. Krupka DC, Sandberg WS. Operating room design and its impact on operating room economics. Curr Opin Anaesthesiol. 2006;19(2):185-191.
2. Scott WN, Booth RE Jr, Dalury DF, Healy WL, Lonner JH. Efficiency and economics in joint arthroplasty. J Bone Joint Surg Am. 2009;91 Suppl 5:33-36.
3. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780-785.
4. DeHaan AM, Adams JR, DeHart ML, Huff TW. Patient-specific versus conventional instrumentation for total knee arthroplasty: peri-operative and cost differences. J Arthroplasty. 2014;29(11):2065-2069.
5. Mont MA, McElroy MJ, Johnson AJ, Pivec R; Single-Use Multicenter Trial Group Writing Group. Single-use instruments, cutting blocks, and trials increase efficiency in the operating room during total knee arthroplasty: a prospective comparison of navigated and non-navigated cases. J Arthroplasty. 2013;28(7):1135-1140.
6. Lionberger DR, Crocker CL, Chen V. Patient specific instrumentation. J Arthroplasty. 2014;29(9):1699-1704.
7. Sah AP. Is there an advantage to knotless barbed suture in TKA wound closure? A randomized trial in simultaneous bilateral TKAs. Clin Orthop Relat Res. 2015;473(6):2019-2027.
8. Torkki PM, Marjamaa RA, Torkki MI, Kallio PE, Kirvelä OA. Use of anesthesia induction rooms can increase the number of urgent orthopedic cases completed within 7 hours. Anesthesiology. 2005;103(2):401-405.
9. Small TJ, Gad BV, Klika AK, Mounir-Soliman LS, Gerritsen RL, Barsoum WK. Dedicated orthopedic operating room unit improves operating room efficiency. J Arthroplasty. 2013;28(7):1066-1071.e2.
10. Miller AG, McKenzie J, Greenky M, et al. Spinal anesthesia: should everyone receive a urinary catheter?: a randomized, prospective study of patients undergoing total hip arthroplasty. J Bone Joint Surg Am. 2013;95(16):1498-1503.
11. Huang Z, Ma J, Shen B, Pei F. General anesthesia: to catheterize or not? A prospective randomized controlled study of patients undergoing total knee arthroplasty. J Arthroplasty. 2015;30(3):502-506.
12. Attarian DE, Wahl JE, Wellman SS, Bolognesi MP. Developing a high-efficiency operating room for total joint arthroplasty in an academic setting. Clin Orthop Relat Res. 2013;471(6):1832-1836.
13. Gamble M. 6 cornerstones of operating room efficiency: best practices for each. Becker’s Hospital Review Web site. http://www.beckershospitalreview.com/or-efficiencies/6-cornerstones-of-operating-room-efficiency-best-practices-for-each.html. Updated January 18, 2013. Accessed September 3, 2015.
14. Smith MP, Sandberg WS, Foss J, et al. High-throughput operating room system for joint arthroplasties durably outperforms routine processes. Anesthesiology. 2008;109(1):25-35.
Lessons learned working in the clinical trial industry
As a resident in psychiatry, I am being trained in the art of diagnosis, treatment, and prevention of mental illness and emotional problems. As part of my training, research and scholarly activities are encouraged—reminding us that clinical medicine is always evolving and that it is every physician’s duty to be at the forefront of advancements in medical science.
Last year, I worked in the clinical trial industry under a seasoned principal investigator. I learned several lessons from my time with him and in the industry. Here, I present these lessons as a starting point for residents who are looking to gain experience or contemplating a career as an expert trialist or principal investigator.
Lesson 1: Know the lingo
To make the transition from physician to principal investigator go more smoothly, I recommend taking the time to learn the language of the industry. The good news? Clinical trials involve patients who have a medical history and take medications, which you are well acquainted with. In addition to medical jargon, the industry has developed its own distinctive terminology and abbreviations: adverse drug reaction (ADR), good clinical practice (GCP), contract research organization (CRO), and more.
Don’t stop there, however. I recommend that you read FDA research guidelines and guidelines of the International Conference on Harmonisation of Good Clinical Practice (ICH-GCP) to be familiar with the ethics and standard regulations of the industry.
Lesson 2: When in doubt, refer to the Protocol
Every clinical trial has a manual, so to speak, known as the Study Protocol, which outlines approved methods of performing diagnostic tests and procedures; provides information on the study timeline; and specifies patient inclusion and exclusion criteria. This document ensures conformity across all study sites, helps prevent errors, limits bias, and answers questions that might come up during the study. It’s worth noting that, in my experience, many of the questions about exclusionary medications arise when psychiatric drugs are involved.
Lesson 3: Document. Document. And document.
The golden rule in clinical practice and research is: “If it isn’t documented, it didn’t happen.” (Recall what I said about reading FDA and ICH-GCP guidelines to learn about regulations.) Documentation of all study-related activities must be meticulous. At any time, your documents might be subject to external or internal audit, conducted to preserve conformity to the protocol and maintain patient safety. Improper documentation can delay, even invalidate, your research.
Lesson 4: Remember that advertising is an art
The real work begins when your site is ready to accept patients. To fill the study, patients need to be aware that you are recruiting participants. A good starting point is to inform likely candidates from your existing patient population about any studies from which they might benefit.
Most times, however, recruiting among your patients is not enough to meet necessary enrollment numbers. You will have to advertise the study to the general public. Advertisements must target the specific patient population, informing them of the study but, at the same time, not be coercive or make false promises. The advertisements must be approved by the study’s institutional review board, which is responsible for protecting the rights and welfare of study participants.
Advertising can be tricky. If an advertisement is too vague, you will get a huge response, causing time and resources to be spent screening patients—most of whom might not be suitable for the study. If an advertisement is too specific, on the other hand, the response might be poor or none at all.
Advertising is its own industry. It might be best to hire an advertising expert who can help you decide on the selection of media (radio, television, print, digital) and can design a campaign that best suits your needs. If you decide to hire a professional, I recommend close collaboration with him (her), to help him understand the medical nature of the study.
Related Resources
• ClinicalTrials.gov. About clinical studies. https://clinicaltrials.gov/ct2/about-studies.
• U.S. Food and Drug Administration. Clinical trials and human subject protection. http://www.fda.gov/ScienceResearch/SpecialTopics/RunningClinicalTrials/default.htm.
• ICH GCP. International Conference on Harmonisation of technical requirements for registration of pharmaceuticals for human use. http://ichgcp.net/.
As a resident in psychiatry, I am being trained in the art of diagnosis, treatment, and prevention of mental illness and emotional problems. As part of my training, research and scholarly activities are encouraged—reminding us that clinical medicine is always evolving and that it is every physician’s duty to be at the forefront of advancements in medical science.
Last year, I worked in the clinical trial industry under a seasoned principal investigator. I learned several lessons from my time with him and in the industry. Here, I present these lessons as a starting point for residents who are looking to gain experience or contemplating a career as an expert trialist or principal investigator.
Lesson 1: Know the lingo
To make the transition from physician to principal investigator go more smoothly, I recommend taking the time to learn the language of the industry. The good news? Clinical trials involve patients who have a medical history and take medications, which you are well acquainted with. In addition to medical jargon, the industry has developed its own distinctive terminology and abbreviations: adverse drug reaction (ADR), good clinical practice (GCP), contract research organization (CRO), and more.
Don’t stop there, however. I recommend that you read FDA research guidelines and guidelines of the International Conference on Harmonisation of Good Clinical Practice (ICH-GCP) to be familiar with the ethics and standard regulations of the industry.
Lesson 2: When in doubt, refer to the Protocol
Every clinical trial has a manual, so to speak, known as the Study Protocol, which outlines approved methods of performing diagnostic tests and procedures; provides information on the study timeline; and specifies patient inclusion and exclusion criteria. This document ensures conformity across all study sites, helps prevent errors, limits bias, and answers questions that might come up during the study. It’s worth noting that, in my experience, many of the questions about exclusionary medications arise when psychiatric drugs are involved.
Lesson 3: Document. Document. And document.
The golden rule in clinical practice and research is: “If it isn’t documented, it didn’t happen.” (Recall what I said about reading FDA and ICH-GCP guidelines to learn about regulations.) Documentation of all study-related activities must be meticulous. At any time, your documents might be subject to external or internal audit, conducted to preserve conformity to the protocol and maintain patient safety. Improper documentation can delay, even invalidate, your research.
Lesson 4: Remember that advertising is an art
The real work begins when your site is ready to accept patients. To fill the study, patients need to be aware that you are recruiting participants. A good starting point is to inform likely candidates from your existing patient population about any studies from which they might benefit.
Most times, however, recruiting among your patients is not enough to meet necessary enrollment numbers. You will have to advertise the study to the general public. Advertisements must target the specific patient population, informing them of the study but, at the same time, not be coercive or make false promises. The advertisements must be approved by the study’s institutional review board, which is responsible for protecting the rights and welfare of study participants.
Advertising can be tricky. If an advertisement is too vague, you will get a huge response, causing time and resources to be spent screening patients—most of whom might not be suitable for the study. If an advertisement is too specific, on the other hand, the response might be poor or none at all.
Advertising is its own industry. It might be best to hire an advertising expert who can help you decide on the selection of media (radio, television, print, digital) and can design a campaign that best suits your needs. If you decide to hire a professional, I recommend close collaboration with him (her), to help him understand the medical nature of the study.
Related Resources
• ClinicalTrials.gov. About clinical studies. https://clinicaltrials.gov/ct2/about-studies.
• U.S. Food and Drug Administration. Clinical trials and human subject protection. http://www.fda.gov/ScienceResearch/SpecialTopics/RunningClinicalTrials/default.htm.
• ICH GCP. International Conference on Harmonisation of technical requirements for registration of pharmaceuticals for human use. http://ichgcp.net/.
As a resident in psychiatry, I am being trained in the art of diagnosis, treatment, and prevention of mental illness and emotional problems. As part of my training, research and scholarly activities are encouraged—reminding us that clinical medicine is always evolving and that it is every physician’s duty to be at the forefront of advancements in medical science.
Last year, I worked in the clinical trial industry under a seasoned principal investigator. I learned several lessons from my time with him and in the industry. Here, I present these lessons as a starting point for residents who are looking to gain experience or contemplating a career as an expert trialist or principal investigator.
Lesson 1: Know the lingo
To make the transition from physician to principal investigator go more smoothly, I recommend taking the time to learn the language of the industry. The good news? Clinical trials involve patients who have a medical history and take medications, which you are well acquainted with. In addition to medical jargon, the industry has developed its own distinctive terminology and abbreviations: adverse drug reaction (ADR), good clinical practice (GCP), contract research organization (CRO), and more.
Don’t stop there, however. I recommend that you read FDA research guidelines and guidelines of the International Conference on Harmonisation of Good Clinical Practice (ICH-GCP) to be familiar with the ethics and standard regulations of the industry.
Lesson 2: When in doubt, refer to the Protocol
Every clinical trial has a manual, so to speak, known as the Study Protocol, which outlines approved methods of performing diagnostic tests and procedures; provides information on the study timeline; and specifies patient inclusion and exclusion criteria. This document ensures conformity across all study sites, helps prevent errors, limits bias, and answers questions that might come up during the study. It’s worth noting that, in my experience, many of the questions about exclusionary medications arise when psychiatric drugs are involved.
Lesson 3: Document. Document. And document.
The golden rule in clinical practice and research is: “If it isn’t documented, it didn’t happen.” (Recall what I said about reading FDA and ICH-GCP guidelines to learn about regulations.) Documentation of all study-related activities must be meticulous. At any time, your documents might be subject to external or internal audit, conducted to preserve conformity to the protocol and maintain patient safety. Improper documentation can delay, even invalidate, your research.
Lesson 4: Remember that advertising is an art
The real work begins when your site is ready to accept patients. To fill the study, patients need to be aware that you are recruiting participants. A good starting point is to inform likely candidates from your existing patient population about any studies from which they might benefit.
Most times, however, recruiting among your patients is not enough to meet necessary enrollment numbers. You will have to advertise the study to the general public. Advertisements must target the specific patient population, informing them of the study but, at the same time, not be coercive or make false promises. The advertisements must be approved by the study’s institutional review board, which is responsible for protecting the rights and welfare of study participants.
Advertising can be tricky. If an advertisement is too vague, you will get a huge response, causing time and resources to be spent screening patients—most of whom might not be suitable for the study. If an advertisement is too specific, on the other hand, the response might be poor or none at all.
Advertising is its own industry. It might be best to hire an advertising expert who can help you decide on the selection of media (radio, television, print, digital) and can design a campaign that best suits your needs. If you decide to hire a professional, I recommend close collaboration with him (her), to help him understand the medical nature of the study.
Related Resources
• ClinicalTrials.gov. About clinical studies. https://clinicaltrials.gov/ct2/about-studies.
• U.S. Food and Drug Administration. Clinical trials and human subject protection. http://www.fda.gov/ScienceResearch/SpecialTopics/RunningClinicalTrials/default.htm.
• ICH GCP. International Conference on Harmonisation of technical requirements for registration of pharmaceuticals for human use. http://ichgcp.net/.

Mentally ill and behind bars
The measure of a country’s greatness, Mahatma Gandhi said, should be based on how well it cares for its most vulnerable. Recently, I had the opportunity to work with members of a vulnerable population: men and women who have a mental illness and languish in jails and prisons around the country. My experience was eye-opening and heartbreaking.
Widespread incarceration of the mentally ill in a developed country such as the United States should be a national embarrassment. But this tragedy, which has reached an epidemic level, has been effectively shut out of the national conversation.
The problem has grown, and is enormous
By the estimate of the U.S. Department of Justice, more than one-half of people incarcerated in the United States are mentally ill and approximately 20% suffer from a serious mental illness.1,2 In fact, there are now 3 times as many mentally ill people in jail and prison as there are occupying psychiatric beds in hospitals.3 These numbers represent a considerable increase over the past 6 decades, and can be attributed to 2 major factors:
- A program of deinstitutionalization set in motion by the federal government in the 1950s called for shuttering of state psychiatric facilities around the country. This was a period of renewed national discourse on civil rights; for many people, the practice of institutionalization was considered a violation of civil rights. (Coincidentally, chlorpromazine was introduced about this time, and many experts believed that the drug would revolutionize outpatient management of psychiatric disorders.)
- More recently, heavy criminal penalties have been attached to convictions for possession and distribution of illegal substances—part of the government’s “war on drugs.”
As a consequence of these programs and policies, the United States has come full circle—routinely incarcerating the mentally ill as it did in the early 19th century, before reforms were initiated in response to the lobbying efforts of activist Dorothea Dix and her contemporaries.
My distressing, eye-opening experience
The time I spent with the incarcerated mentally ill was limited to a 6-month period at a county jail during residency. Yet the contrast between services provided to this population and those that are available to people in the community was immediately evident—and stark. The sheer number of adults in jails and prisons who require mental health care is such that the ratio of patients to psychiatrists, psychologists, and other mental health clinicians is shockingly skewed.
It does not take years of experience to figure out that a brief interview with an 18-year-old who is being jailed for the first time, has never seen a psychiatrist, and suffers panic attacks (or hallucinations, or suicidal thoughts) is a less-than-ideal clinical situation. Making that situation even more hazardous is that inmates have a high risk of suicide, particularly in the first 24 to 48 hours of incarceration.4
Other ethical issues arose during my stint in the correctional system: My patients frequently would be charged with prison-rule violations (there is evidence that mentally ill inmates are more likely to be charged with such violations2); on many such occasions, they would be placed in solitary confinement (“the hole”), a practice the United Nations has called “cruel, inhuman, and degrading: for the mentally ill5 and that, in turn, exacerbates the inmate’s psychiatric illness.6-11
Last, there are restrictions on the types of formulations of medications that can be prescribed, involuntary treatment, and other critical aspects of care that make the experience of providing care in this system frustrating for mental health providers.
Are there solutions?
One way to tackle this crisis might be to insert more psychiatrists and psychologists into the correctional system. A more sensible approach, however, would be to tackle the root cause and divert the mentally ill away from incarceration and into treatment—moving from a model of retribution and incapacitation to one of rehabilitation. For example:
- Several counties nationwide have adopted diversion programs that include so-called mental health courts and drug courts, with encouraging results12
- Police departments are establishing Crisis Intervention Teams
- Assisted outpatient treatment programs are growing in popularity.
Far more needs to be done, however. In the absence of a national debate on the problem of the incarcerated mentally ill, there is real risk that this population will continue to be ignored and that our mental health care infrastructure will remain inadequate for meeting their need for services.
1. American Psychiatric Association. Psychiatric services in jails and prisons: a task force report of the American Psychiatric Association. 2nd ed. Washington, DC: American Psychiatric Association; 2000:XIX.
2. U.S. Department of Justice. Bureau of Justice Statistics: special report. Mental health problems of prison and jail inmates. http://www.bjs.gov/content/pub/pdf/mhppji.pdf. Updated December 14, 2006. Accessed April 8, 2016.|
3. Torrey FE, Kennard AD, Eslinger D, et al. More mentally ill persons are in jails and prisons than hospitals: a survey of the states. http://www.treatmentadvocacycenter.org/storage/documents/final_jails_v_hospitals_study.pdf. Published May 2010. Accessed April 8, 2016.
4. U.S. Department of Justice. National study of jail suicide: 20 years later. http://static.nicic.gov/Library/024308.pdf. Published April 2010. Accessed April 8, 2016.
5. Méndez JE. Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment. http://www.ohchr.org/EN/Issues/Torture/SRTorture/Pages/SRTortureIndex.aspx. Published 2011. Accessed April 8, 2016.
6. Daniel AE. Preventing suicide in prison: a collaborative responsibility of administrative, custodial, and clinical staff. J Am Acad Psychiatry Law. 2006;34(2):165-175.
7. White TW, Schimmel DJ, Frickey R. A comprehensive analysis of suicide in federal prisons: a fifteen-year review. J Correct Health Care. 2002;9(3):321-345.
8. Smith PS. The effects of solitary confinement on prison inmates: a brief history and review of the literature, crime and justice. Crime and Justice. 2006;34(1):441-528.
9. Grassian S. Psychopathological effects of solitary confinement. Am J Psychiatry. 1983;140(11):1450-1454.
10. Patterson RF, Hughes K. Review of completed suicides in the California Department of Corrections and Rehabilitation, 1999 to 2004. Psychiatr Serv. 2008;59(6):676-682.
11. Kaba F, Lewis A, Glowa-Kollisch S, et al. Solitary confinement and risk of self-harm among jail inmates. Am J Public Health. 2014;104(3):442-447.
12. McNiel DE, Binder RL. Effectiveness of a mental health court in reducing criminal recidivism and violence. Am J Psychiatry. 2007;164(9):1395-1403.
The measure of a country’s greatness, Mahatma Gandhi said, should be based on how well it cares for its most vulnerable. Recently, I had the opportunity to work with members of a vulnerable population: men and women who have a mental illness and languish in jails and prisons around the country. My experience was eye-opening and heartbreaking.
Widespread incarceration of the mentally ill in a developed country such as the United States should be a national embarrassment. But this tragedy, which has reached an epidemic level, has been effectively shut out of the national conversation.
The problem has grown, and is enormous
By the estimate of the U.S. Department of Justice, more than one-half of people incarcerated in the United States are mentally ill and approximately 20% suffer from a serious mental illness.1,2 In fact, there are now 3 times as many mentally ill people in jail and prison as there are occupying psychiatric beds in hospitals.3 These numbers represent a considerable increase over the past 6 decades, and can be attributed to 2 major factors:
- A program of deinstitutionalization set in motion by the federal government in the 1950s called for shuttering of state psychiatric facilities around the country. This was a period of renewed national discourse on civil rights; for many people, the practice of institutionalization was considered a violation of civil rights. (Coincidentally, chlorpromazine was introduced about this time, and many experts believed that the drug would revolutionize outpatient management of psychiatric disorders.)
- More recently, heavy criminal penalties have been attached to convictions for possession and distribution of illegal substances—part of the government’s “war on drugs.”
As a consequence of these programs and policies, the United States has come full circle—routinely incarcerating the mentally ill as it did in the early 19th century, before reforms were initiated in response to the lobbying efforts of activist Dorothea Dix and her contemporaries.
My distressing, eye-opening experience
The time I spent with the incarcerated mentally ill was limited to a 6-month period at a county jail during residency. Yet the contrast between services provided to this population and those that are available to people in the community was immediately evident—and stark. The sheer number of adults in jails and prisons who require mental health care is such that the ratio of patients to psychiatrists, psychologists, and other mental health clinicians is shockingly skewed.
It does not take years of experience to figure out that a brief interview with an 18-year-old who is being jailed for the first time, has never seen a psychiatrist, and suffers panic attacks (or hallucinations, or suicidal thoughts) is a less-than-ideal clinical situation. Making that situation even more hazardous is that inmates have a high risk of suicide, particularly in the first 24 to 48 hours of incarceration.4
Other ethical issues arose during my stint in the correctional system: My patients frequently would be charged with prison-rule violations (there is evidence that mentally ill inmates are more likely to be charged with such violations2); on many such occasions, they would be placed in solitary confinement (“the hole”), a practice the United Nations has called “cruel, inhuman, and degrading: for the mentally ill5 and that, in turn, exacerbates the inmate’s psychiatric illness.6-11
Last, there are restrictions on the types of formulations of medications that can be prescribed, involuntary treatment, and other critical aspects of care that make the experience of providing care in this system frustrating for mental health providers.
Are there solutions?
One way to tackle this crisis might be to insert more psychiatrists and psychologists into the correctional system. A more sensible approach, however, would be to tackle the root cause and divert the mentally ill away from incarceration and into treatment—moving from a model of retribution and incapacitation to one of rehabilitation. For example:
- Several counties nationwide have adopted diversion programs that include so-called mental health courts and drug courts, with encouraging results12
- Police departments are establishing Crisis Intervention Teams
- Assisted outpatient treatment programs are growing in popularity.
Far more needs to be done, however. In the absence of a national debate on the problem of the incarcerated mentally ill, there is real risk that this population will continue to be ignored and that our mental health care infrastructure will remain inadequate for meeting their need for services.
The measure of a country’s greatness, Mahatma Gandhi said, should be based on how well it cares for its most vulnerable. Recently, I had the opportunity to work with members of a vulnerable population: men and women who have a mental illness and languish in jails and prisons around the country. My experience was eye-opening and heartbreaking.
Widespread incarceration of the mentally ill in a developed country such as the United States should be a national embarrassment. But this tragedy, which has reached an epidemic level, has been effectively shut out of the national conversation.
The problem has grown, and is enormous
By the estimate of the U.S. Department of Justice, more than one-half of people incarcerated in the United States are mentally ill and approximately 20% suffer from a serious mental illness.1,2 In fact, there are now 3 times as many mentally ill people in jail and prison as there are occupying psychiatric beds in hospitals.3 These numbers represent a considerable increase over the past 6 decades, and can be attributed to 2 major factors:
- A program of deinstitutionalization set in motion by the federal government in the 1950s called for shuttering of state psychiatric facilities around the country. This was a period of renewed national discourse on civil rights; for many people, the practice of institutionalization was considered a violation of civil rights. (Coincidentally, chlorpromazine was introduced about this time, and many experts believed that the drug would revolutionize outpatient management of psychiatric disorders.)
- More recently, heavy criminal penalties have been attached to convictions for possession and distribution of illegal substances—part of the government’s “war on drugs.”
As a consequence of these programs and policies, the United States has come full circle—routinely incarcerating the mentally ill as it did in the early 19th century, before reforms were initiated in response to the lobbying efforts of activist Dorothea Dix and her contemporaries.
My distressing, eye-opening experience
The time I spent with the incarcerated mentally ill was limited to a 6-month period at a county jail during residency. Yet the contrast between services provided to this population and those that are available to people in the community was immediately evident—and stark. The sheer number of adults in jails and prisons who require mental health care is such that the ratio of patients to psychiatrists, psychologists, and other mental health clinicians is shockingly skewed.
It does not take years of experience to figure out that a brief interview with an 18-year-old who is being jailed for the first time, has never seen a psychiatrist, and suffers panic attacks (or hallucinations, or suicidal thoughts) is a less-than-ideal clinical situation. Making that situation even more hazardous is that inmates have a high risk of suicide, particularly in the first 24 to 48 hours of incarceration.4
Other ethical issues arose during my stint in the correctional system: My patients frequently would be charged with prison-rule violations (there is evidence that mentally ill inmates are more likely to be charged with such violations2); on many such occasions, they would be placed in solitary confinement (“the hole”), a practice the United Nations has called “cruel, inhuman, and degrading: for the mentally ill5 and that, in turn, exacerbates the inmate’s psychiatric illness.6-11
Last, there are restrictions on the types of formulations of medications that can be prescribed, involuntary treatment, and other critical aspects of care that make the experience of providing care in this system frustrating for mental health providers.
Are there solutions?
One way to tackle this crisis might be to insert more psychiatrists and psychologists into the correctional system. A more sensible approach, however, would be to tackle the root cause and divert the mentally ill away from incarceration and into treatment—moving from a model of retribution and incapacitation to one of rehabilitation. For example:
- Several counties nationwide have adopted diversion programs that include so-called mental health courts and drug courts, with encouraging results12
- Police departments are establishing Crisis Intervention Teams
- Assisted outpatient treatment programs are growing in popularity.
Far more needs to be done, however. In the absence of a national debate on the problem of the incarcerated mentally ill, there is real risk that this population will continue to be ignored and that our mental health care infrastructure will remain inadequate for meeting their need for services.
1. American Psychiatric Association. Psychiatric services in jails and prisons: a task force report of the American Psychiatric Association. 2nd ed. Washington, DC: American Psychiatric Association; 2000:XIX.
2. U.S. Department of Justice. Bureau of Justice Statistics: special report. Mental health problems of prison and jail inmates. http://www.bjs.gov/content/pub/pdf/mhppji.pdf. Updated December 14, 2006. Accessed April 8, 2016.|
3. Torrey FE, Kennard AD, Eslinger D, et al. More mentally ill persons are in jails and prisons than hospitals: a survey of the states. http://www.treatmentadvocacycenter.org/storage/documents/final_jails_v_hospitals_study.pdf. Published May 2010. Accessed April 8, 2016.
4. U.S. Department of Justice. National study of jail suicide: 20 years later. http://static.nicic.gov/Library/024308.pdf. Published April 2010. Accessed April 8, 2016.
5. Méndez JE. Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment. http://www.ohchr.org/EN/Issues/Torture/SRTorture/Pages/SRTortureIndex.aspx. Published 2011. Accessed April 8, 2016.
6. Daniel AE. Preventing suicide in prison: a collaborative responsibility of administrative, custodial, and clinical staff. J Am Acad Psychiatry Law. 2006;34(2):165-175.
7. White TW, Schimmel DJ, Frickey R. A comprehensive analysis of suicide in federal prisons: a fifteen-year review. J Correct Health Care. 2002;9(3):321-345.
8. Smith PS. The effects of solitary confinement on prison inmates: a brief history and review of the literature, crime and justice. Crime and Justice. 2006;34(1):441-528.
9. Grassian S. Psychopathological effects of solitary confinement. Am J Psychiatry. 1983;140(11):1450-1454.
10. Patterson RF, Hughes K. Review of completed suicides in the California Department of Corrections and Rehabilitation, 1999 to 2004. Psychiatr Serv. 2008;59(6):676-682.
11. Kaba F, Lewis A, Glowa-Kollisch S, et al. Solitary confinement and risk of self-harm among jail inmates. Am J Public Health. 2014;104(3):442-447.
12. McNiel DE, Binder RL. Effectiveness of a mental health court in reducing criminal recidivism and violence. Am J Psychiatry. 2007;164(9):1395-1403.
1. American Psychiatric Association. Psychiatric services in jails and prisons: a task force report of the American Psychiatric Association. 2nd ed. Washington, DC: American Psychiatric Association; 2000:XIX.
2. U.S. Department of Justice. Bureau of Justice Statistics: special report. Mental health problems of prison and jail inmates. http://www.bjs.gov/content/pub/pdf/mhppji.pdf. Updated December 14, 2006. Accessed April 8, 2016.|
3. Torrey FE, Kennard AD, Eslinger D, et al. More mentally ill persons are in jails and prisons than hospitals: a survey of the states. http://www.treatmentadvocacycenter.org/storage/documents/final_jails_v_hospitals_study.pdf. Published May 2010. Accessed April 8, 2016.
4. U.S. Department of Justice. National study of jail suicide: 20 years later. http://static.nicic.gov/Library/024308.pdf. Published April 2010. Accessed April 8, 2016.
5. Méndez JE. Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment. http://www.ohchr.org/EN/Issues/Torture/SRTorture/Pages/SRTortureIndex.aspx. Published 2011. Accessed April 8, 2016.
6. Daniel AE. Preventing suicide in prison: a collaborative responsibility of administrative, custodial, and clinical staff. J Am Acad Psychiatry Law. 2006;34(2):165-175.
7. White TW, Schimmel DJ, Frickey R. A comprehensive analysis of suicide in federal prisons: a fifteen-year review. J Correct Health Care. 2002;9(3):321-345.
8. Smith PS. The effects of solitary confinement on prison inmates: a brief history and review of the literature, crime and justice. Crime and Justice. 2006;34(1):441-528.
9. Grassian S. Psychopathological effects of solitary confinement. Am J Psychiatry. 1983;140(11):1450-1454.
10. Patterson RF, Hughes K. Review of completed suicides in the California Department of Corrections and Rehabilitation, 1999 to 2004. Psychiatr Serv. 2008;59(6):676-682.
11. Kaba F, Lewis A, Glowa-Kollisch S, et al. Solitary confinement and risk of self-harm among jail inmates. Am J Public Health. 2014;104(3):442-447.
12. McNiel DE, Binder RL. Effectiveness of a mental health court in reducing criminal recidivism and violence. Am J Psychiatry. 2007;164(9):1395-1403.

Management of Vitiligo Patients With Surgical Interventions
Vitiligo is a common, asymptomatic, acquired depigmentation disorder that is caused by an unknown etiology. Lesions appear as sharply demarcated, depigmented macules and patches that are scattered symmetrically or unsymmetrically over the body. The presentation can be delineated based on the segmental or nonsegmental nature of the disease. According to the revised classification/nomenclature of vitiligo,1 the disorder can be classified as nonsegmental, segmental, mixed, or unclassified. The pathogenesis of the vitiligo disease process is due to multiple modalities that contribute to melanocyte loss. Theories for melanocyte destruction include but are not limited to autoimmunity, biochemicals, epidermal cytokines, increased hydrogen peroxide and free radicals, and humoral and cellular immune alteration.2,3
Despite its long history, the most frustrating aspect of the vitiligo disease process remains its treatment due to limited efficacy, frequent application of topicals, and the need for high-potency steroids. Medical therapies usually are the first line of treatment and are most effective with few side effects for bilateral nonsegmental or evolving vitiligo.2 Some of the primary therapies with the highest efficacies appear to be calcipotriene and psoralen plus UVA, psoralen plus UVA as monotherapy, excimer laser, narrowband UVB, oral steroids, 8-methoxypsoralen, tacrolimus, and topical steroids.4 The theory is that these treatments would be successful if the patient had active melanocytes in the external root sheath that would be able to repigment a patch of vitiligo.5 Hence, it would be more difficult to treat areas such as the dorsal aspect of the fingers and toes because they lack hair-bearing areas with melanocytes.6 The alternative approach to treating vitiligo patches would be surgical intervention techniques, as they provide melanocytic cells to a previously depigmented area.3,5 The focus of this article is to evaluate the efficacy and appropriate use of some of the surgical procedures that can be used in the treatment of vitiligo patients.
Candidate Selection
First, vitiligo patients for whom first-line treatment with medical therapies has failed are candidates for surgical techniques. The second vital component is to clinically confirm the diagnosis of vitiligo as opposed to other genetic, infectious, or autoimmune causes of pigment loss. Lastly, the vitiligo patch should be stable. A stable vitiligo patch does not continue to progress and is no longer responsive to topical medications that are meant to repigment for a discernible period of time.7
Classification of Disease Stage
To classify the stage of vitiligo prior to surgical intervention, Gauthier8 created a basic grading system: grade I, with partial depletion of epidermal melanocytes in a vitiligo patch that responds to repigmentation in a follicular pattern evenly such as on the face and neck; grade II, with complete depletion of epidermal melanocytes with a usual follicular pattern of repigmentation; and grade III, indicating complete depletion of follicular melanocytes with no hope of response to medical therapy. According to Rusfianti and Wirohadidjodjo,2 the surgical techniques that have developed over the years for treatment of grade III vitiligo patients include split-thickness skin grafting, suction blister grafting, miniature punch grafting, and cultured melanocyte transplantation.
Surgical Techniques
Split-thickness skin grafting is an older procedure that entails the use of a harvesting graft site with no pigment loss and dermabrasion of the recipient area to allow interaction with the wound bed.9 With proper care and minimal movement or wrinkling of the graft site, patients can have repigmentation without skip areas.
Suction blister grafting is another tried and tested surgical intervention. Hasegawa et al10 conducted a study of 15 patients (13 males, 2 females; age range, 16–38 years) diagnosed with segmental vitiligo who were treated using the suction blister grafting technique with CO2 laser resurfacing. Patients were recruited 1 month prior to initiating therapy and no other treatments were used during the month or in conjunction with the surgical intervention. Suction blisters were harvested from the left thigh and transferred in saline to the recipient site, which was abraded with 1 pass of the short-pulse CO2 laser system. The recipient sites were then closed with 7-0 nylon sutures and covered tightly with tie-over dressings for at least 1 week. Within 6 months of the procedure, a treatment response of 100% was seen in 15 patients, making it an effective method for treatment-resistant vitiligo patients.10
Miniature punch grafting is another possible treatment option for resistant cases of vitiligo. Mapar et al11 conducted a study in 25 patients (21 women, 4 men; age range, 20–47 years) who had been diagnosed with stable vitiligo (ie, no progression in the last 2 years) and were treated with single hair follicle transplant versus miniature punch grafting. The theory behind the study was to use the melanocytic reservoir noted in the normal hair follicle to repigment the vitiligo patch. With follow-up of both methods of treatment, there was no statistical difference in treatment results.11 A similar study was conducted by Malakar and Lahiri12 in patients with lip leukoderma (a variant of vitiligo). One hundred eight patients (41 males, 67 females; age range, 14–62 years) who had been diagnosed with stable lip leukoderma (ie, stable vitiligo for at least 6 months) underwent treatment via autologous miniature punch grafting. Punch biopsies were performed in donor sites of the buttocks and upper thighs with 72% of patients noting complete repigmentation. Complications noted were herpes labialis–induced lip leukoderma, which ultimately led to rejection of the graft site.12 Overall, however, miniature punch grafting is a viable surgical option in stable vitiligo patients.
Cultured melanocyte transplantation, or a noncultured epidermal suspension, was first initiated in 1992.13 Silpa-Archa et al14 conducted an open, split-comparison study of 6 vitiligo patients (5 women, 1 man; age range, 20–65 years) with stable lesions. Fifty percent of patients received autologous pigmented skin cellular suspension, which was applied to vitiligo-affected skin that was treated with a fractionated CO2 laser, and 50% received dermabrasion. Composite dressing was placed overlying the site with dressing removal in 1 week. The degree of repigmentation was based on a modified vitiligo area scoring index scale of poor (0%–25%), fair (26%–50%), good (51%–75%), very good (76%–90%), or excellent (91%–100%). Overall repigmentation was very good to excellent in all 6 patients.14 Potentially, this method can far improve the surgical treatment options for future vitiligo patients.
Final Thoughts
Overall, when evaluating surgical interventions for the treatment of vitiligo, careful consideration of the patient’s disease progression, failed therapies, outcome expectations, and repigmentation is warranted prior to initiating any procedure. For appropriate candidates, a range of surgical methodologies has proven to be effective in treatment of stable vitiligo patients.
- Taïeb A, Picardo M; VETF members. The definition and assessment of vitiligo: a consensus report of the Vitiligo European Task Force. Pigment Cell Res. 2007;20:27-35. Cited by: Ezzedine K, Lim HW, Suzuki T, et al; Vitiligo Global Issue Consensus Conference Panelists. Revised classification/nomenclature of vitiligo and related issues: the Vitiligo Global Issues Consensus Conference. Pigment Cell Melanoma Res. 2012;25:E1-E13.
- Rusfianti M, Wirohadidjodjo YW. Dermatosurgical techniques for repigmentation of vitiligo. Int J Dermatol. 2006;45:411-417.
- Falabella R. Surgical therapies for vitiligo. Clin Dermatol. 1997;15:927-939.
- Whitton ME, Pinart M, Batchelor J, et al. Interventions for vitiligo. Cochrane Database Syst Rev. 2015;2:CD003263.
- Mulekar SV, Isedeh P. Surgical interventions for vitiligo: an evidence-based review. Br J Dermatol. 2013;169(suppl 3):57-66.
- Dutta AK, Mandal SB. A clinical study of 650 vitiligo cases and their classification. Indian J Dermatol. 1969;14:103-111.
- Falabella R, Arrunategui A, Barona MI, et al. The minigrafting test for vitiligo: detection of stable lesions for melanocyte transplantation. J Am Acad Dermatol. 1995;32:228-232.
- Gauthier Y. Le vitiligo. Gaz Med. 1994;101:8-12.
- Malakar S, Malakar RS. Surgical pearl: composite film and graft unit for the recipient area dressing after split-thickness skin grafting in vitiligo. J Am Acad Dermatol. 2001;44:856-858.
- Hasegawa T, Suga Y, Ikejima A, et al. Suction blister grafting with CO2 laser resurfacing of the graft recipient site for vitiligo. J Dermatol. 2007;34:490-492.
- Mapar MA, Safarpour M, Mapar M, et al. A comparative study of the mini-punch grafting and hair follicle transplantation in the treatment of refractory and stable vitiligo. J Am Acad Dermatol. 2014;70:743-747.
- Malakar S, Lahiri K. Punch grafting for lip leukoderma. Dermatology. 2004;208:125-128.
- Gauthier Y, Surleve-Bazeille JE. Autologous grafting with noncultured melanocytes: a simplified method for treatment of depigmented lesions. J Am Acad Dermatol. 1992;26(2, pt 1):191-194.
- Silpa-Archa N, Griffith JL, Williams MS, et al. Prospective comparison of recipient-site preparation with fractional carbon dioxide laser versus dermabrasion and recipient-site dressing composition in melanocyte-keratinocyte transplantation procedure in vitiligo: a preliminary study [published online January 24, 2016]. Br J Dermatol. 2016;174:895-897.
Vitiligo is a common, asymptomatic, acquired depigmentation disorder that is caused by an unknown etiology. Lesions appear as sharply demarcated, depigmented macules and patches that are scattered symmetrically or unsymmetrically over the body. The presentation can be delineated based on the segmental or nonsegmental nature of the disease. According to the revised classification/nomenclature of vitiligo,1 the disorder can be classified as nonsegmental, segmental, mixed, or unclassified. The pathogenesis of the vitiligo disease process is due to multiple modalities that contribute to melanocyte loss. Theories for melanocyte destruction include but are not limited to autoimmunity, biochemicals, epidermal cytokines, increased hydrogen peroxide and free radicals, and humoral and cellular immune alteration.2,3
Despite its long history, the most frustrating aspect of the vitiligo disease process remains its treatment due to limited efficacy, frequent application of topicals, and the need for high-potency steroids. Medical therapies usually are the first line of treatment and are most effective with few side effects for bilateral nonsegmental or evolving vitiligo.2 Some of the primary therapies with the highest efficacies appear to be calcipotriene and psoralen plus UVA, psoralen plus UVA as monotherapy, excimer laser, narrowband UVB, oral steroids, 8-methoxypsoralen, tacrolimus, and topical steroids.4 The theory is that these treatments would be successful if the patient had active melanocytes in the external root sheath that would be able to repigment a patch of vitiligo.5 Hence, it would be more difficult to treat areas such as the dorsal aspect of the fingers and toes because they lack hair-bearing areas with melanocytes.6 The alternative approach to treating vitiligo patches would be surgical intervention techniques, as they provide melanocytic cells to a previously depigmented area.3,5 The focus of this article is to evaluate the efficacy and appropriate use of some of the surgical procedures that can be used in the treatment of vitiligo patients.
Candidate Selection
First, vitiligo patients for whom first-line treatment with medical therapies has failed are candidates for surgical techniques. The second vital component is to clinically confirm the diagnosis of vitiligo as opposed to other genetic, infectious, or autoimmune causes of pigment loss. Lastly, the vitiligo patch should be stable. A stable vitiligo patch does not continue to progress and is no longer responsive to topical medications that are meant to repigment for a discernible period of time.7
Classification of Disease Stage
To classify the stage of vitiligo prior to surgical intervention, Gauthier8 created a basic grading system: grade I, with partial depletion of epidermal melanocytes in a vitiligo patch that responds to repigmentation in a follicular pattern evenly such as on the face and neck; grade II, with complete depletion of epidermal melanocytes with a usual follicular pattern of repigmentation; and grade III, indicating complete depletion of follicular melanocytes with no hope of response to medical therapy. According to Rusfianti and Wirohadidjodjo,2 the surgical techniques that have developed over the years for treatment of grade III vitiligo patients include split-thickness skin grafting, suction blister grafting, miniature punch grafting, and cultured melanocyte transplantation.
Surgical Techniques
Split-thickness skin grafting is an older procedure that entails the use of a harvesting graft site with no pigment loss and dermabrasion of the recipient area to allow interaction with the wound bed.9 With proper care and minimal movement or wrinkling of the graft site, patients can have repigmentation without skip areas.
Suction blister grafting is another tried and tested surgical intervention. Hasegawa et al10 conducted a study of 15 patients (13 males, 2 females; age range, 16–38 years) diagnosed with segmental vitiligo who were treated using the suction blister grafting technique with CO2 laser resurfacing. Patients were recruited 1 month prior to initiating therapy and no other treatments were used during the month or in conjunction with the surgical intervention. Suction blisters were harvested from the left thigh and transferred in saline to the recipient site, which was abraded with 1 pass of the short-pulse CO2 laser system. The recipient sites were then closed with 7-0 nylon sutures and covered tightly with tie-over dressings for at least 1 week. Within 6 months of the procedure, a treatment response of 100% was seen in 15 patients, making it an effective method for treatment-resistant vitiligo patients.10
Miniature punch grafting is another possible treatment option for resistant cases of vitiligo. Mapar et al11 conducted a study in 25 patients (21 women, 4 men; age range, 20–47 years) who had been diagnosed with stable vitiligo (ie, no progression in the last 2 years) and were treated with single hair follicle transplant versus miniature punch grafting. The theory behind the study was to use the melanocytic reservoir noted in the normal hair follicle to repigment the vitiligo patch. With follow-up of both methods of treatment, there was no statistical difference in treatment results.11 A similar study was conducted by Malakar and Lahiri12 in patients with lip leukoderma (a variant of vitiligo). One hundred eight patients (41 males, 67 females; age range, 14–62 years) who had been diagnosed with stable lip leukoderma (ie, stable vitiligo for at least 6 months) underwent treatment via autologous miniature punch grafting. Punch biopsies were performed in donor sites of the buttocks and upper thighs with 72% of patients noting complete repigmentation. Complications noted were herpes labialis–induced lip leukoderma, which ultimately led to rejection of the graft site.12 Overall, however, miniature punch grafting is a viable surgical option in stable vitiligo patients.
Cultured melanocyte transplantation, or a noncultured epidermal suspension, was first initiated in 1992.13 Silpa-Archa et al14 conducted an open, split-comparison study of 6 vitiligo patients (5 women, 1 man; age range, 20–65 years) with stable lesions. Fifty percent of patients received autologous pigmented skin cellular suspension, which was applied to vitiligo-affected skin that was treated with a fractionated CO2 laser, and 50% received dermabrasion. Composite dressing was placed overlying the site with dressing removal in 1 week. The degree of repigmentation was based on a modified vitiligo area scoring index scale of poor (0%–25%), fair (26%–50%), good (51%–75%), very good (76%–90%), or excellent (91%–100%). Overall repigmentation was very good to excellent in all 6 patients.14 Potentially, this method can far improve the surgical treatment options for future vitiligo patients.
Final Thoughts
Overall, when evaluating surgical interventions for the treatment of vitiligo, careful consideration of the patient’s disease progression, failed therapies, outcome expectations, and repigmentation is warranted prior to initiating any procedure. For appropriate candidates, a range of surgical methodologies has proven to be effective in treatment of stable vitiligo patients.
Vitiligo is a common, asymptomatic, acquired depigmentation disorder that is caused by an unknown etiology. Lesions appear as sharply demarcated, depigmented macules and patches that are scattered symmetrically or unsymmetrically over the body. The presentation can be delineated based on the segmental or nonsegmental nature of the disease. According to the revised classification/nomenclature of vitiligo,1 the disorder can be classified as nonsegmental, segmental, mixed, or unclassified. The pathogenesis of the vitiligo disease process is due to multiple modalities that contribute to melanocyte loss. Theories for melanocyte destruction include but are not limited to autoimmunity, biochemicals, epidermal cytokines, increased hydrogen peroxide and free radicals, and humoral and cellular immune alteration.2,3
Despite its long history, the most frustrating aspect of the vitiligo disease process remains its treatment due to limited efficacy, frequent application of topicals, and the need for high-potency steroids. Medical therapies usually are the first line of treatment and are most effective with few side effects for bilateral nonsegmental or evolving vitiligo.2 Some of the primary therapies with the highest efficacies appear to be calcipotriene and psoralen plus UVA, psoralen plus UVA as monotherapy, excimer laser, narrowband UVB, oral steroids, 8-methoxypsoralen, tacrolimus, and topical steroids.4 The theory is that these treatments would be successful if the patient had active melanocytes in the external root sheath that would be able to repigment a patch of vitiligo.5 Hence, it would be more difficult to treat areas such as the dorsal aspect of the fingers and toes because they lack hair-bearing areas with melanocytes.6 The alternative approach to treating vitiligo patches would be surgical intervention techniques, as they provide melanocytic cells to a previously depigmented area.3,5 The focus of this article is to evaluate the efficacy and appropriate use of some of the surgical procedures that can be used in the treatment of vitiligo patients.
Candidate Selection
First, vitiligo patients for whom first-line treatment with medical therapies has failed are candidates for surgical techniques. The second vital component is to clinically confirm the diagnosis of vitiligo as opposed to other genetic, infectious, or autoimmune causes of pigment loss. Lastly, the vitiligo patch should be stable. A stable vitiligo patch does not continue to progress and is no longer responsive to topical medications that are meant to repigment for a discernible period of time.7
Classification of Disease Stage
To classify the stage of vitiligo prior to surgical intervention, Gauthier8 created a basic grading system: grade I, with partial depletion of epidermal melanocytes in a vitiligo patch that responds to repigmentation in a follicular pattern evenly such as on the face and neck; grade II, with complete depletion of epidermal melanocytes with a usual follicular pattern of repigmentation; and grade III, indicating complete depletion of follicular melanocytes with no hope of response to medical therapy. According to Rusfianti and Wirohadidjodjo,2 the surgical techniques that have developed over the years for treatment of grade III vitiligo patients include split-thickness skin grafting, suction blister grafting, miniature punch grafting, and cultured melanocyte transplantation.
Surgical Techniques
Split-thickness skin grafting is an older procedure that entails the use of a harvesting graft site with no pigment loss and dermabrasion of the recipient area to allow interaction with the wound bed.9 With proper care and minimal movement or wrinkling of the graft site, patients can have repigmentation without skip areas.
Suction blister grafting is another tried and tested surgical intervention. Hasegawa et al10 conducted a study of 15 patients (13 males, 2 females; age range, 16–38 years) diagnosed with segmental vitiligo who were treated using the suction blister grafting technique with CO2 laser resurfacing. Patients were recruited 1 month prior to initiating therapy and no other treatments were used during the month or in conjunction with the surgical intervention. Suction blisters were harvested from the left thigh and transferred in saline to the recipient site, which was abraded with 1 pass of the short-pulse CO2 laser system. The recipient sites were then closed with 7-0 nylon sutures and covered tightly with tie-over dressings for at least 1 week. Within 6 months of the procedure, a treatment response of 100% was seen in 15 patients, making it an effective method for treatment-resistant vitiligo patients.10
Miniature punch grafting is another possible treatment option for resistant cases of vitiligo. Mapar et al11 conducted a study in 25 patients (21 women, 4 men; age range, 20–47 years) who had been diagnosed with stable vitiligo (ie, no progression in the last 2 years) and were treated with single hair follicle transplant versus miniature punch grafting. The theory behind the study was to use the melanocytic reservoir noted in the normal hair follicle to repigment the vitiligo patch. With follow-up of both methods of treatment, there was no statistical difference in treatment results.11 A similar study was conducted by Malakar and Lahiri12 in patients with lip leukoderma (a variant of vitiligo). One hundred eight patients (41 males, 67 females; age range, 14–62 years) who had been diagnosed with stable lip leukoderma (ie, stable vitiligo for at least 6 months) underwent treatment via autologous miniature punch grafting. Punch biopsies were performed in donor sites of the buttocks and upper thighs with 72% of patients noting complete repigmentation. Complications noted were herpes labialis–induced lip leukoderma, which ultimately led to rejection of the graft site.12 Overall, however, miniature punch grafting is a viable surgical option in stable vitiligo patients.
Cultured melanocyte transplantation, or a noncultured epidermal suspension, was first initiated in 1992.13 Silpa-Archa et al14 conducted an open, split-comparison study of 6 vitiligo patients (5 women, 1 man; age range, 20–65 years) with stable lesions. Fifty percent of patients received autologous pigmented skin cellular suspension, which was applied to vitiligo-affected skin that was treated with a fractionated CO2 laser, and 50% received dermabrasion. Composite dressing was placed overlying the site with dressing removal in 1 week. The degree of repigmentation was based on a modified vitiligo area scoring index scale of poor (0%–25%), fair (26%–50%), good (51%–75%), very good (76%–90%), or excellent (91%–100%). Overall repigmentation was very good to excellent in all 6 patients.14 Potentially, this method can far improve the surgical treatment options for future vitiligo patients.
Final Thoughts
Overall, when evaluating surgical interventions for the treatment of vitiligo, careful consideration of the patient’s disease progression, failed therapies, outcome expectations, and repigmentation is warranted prior to initiating any procedure. For appropriate candidates, a range of surgical methodologies has proven to be effective in treatment of stable vitiligo patients.
- Taïeb A, Picardo M; VETF members. The definition and assessment of vitiligo: a consensus report of the Vitiligo European Task Force. Pigment Cell Res. 2007;20:27-35. Cited by: Ezzedine K, Lim HW, Suzuki T, et al; Vitiligo Global Issue Consensus Conference Panelists. Revised classification/nomenclature of vitiligo and related issues: the Vitiligo Global Issues Consensus Conference. Pigment Cell Melanoma Res. 2012;25:E1-E13.
- Rusfianti M, Wirohadidjodjo YW. Dermatosurgical techniques for repigmentation of vitiligo. Int J Dermatol. 2006;45:411-417.
- Falabella R. Surgical therapies for vitiligo. Clin Dermatol. 1997;15:927-939.
- Whitton ME, Pinart M, Batchelor J, et al. Interventions for vitiligo. Cochrane Database Syst Rev. 2015;2:CD003263.
- Mulekar SV, Isedeh P. Surgical interventions for vitiligo: an evidence-based review. Br J Dermatol. 2013;169(suppl 3):57-66.
- Dutta AK, Mandal SB. A clinical study of 650 vitiligo cases and their classification. Indian J Dermatol. 1969;14:103-111.
- Falabella R, Arrunategui A, Barona MI, et al. The minigrafting test for vitiligo: detection of stable lesions for melanocyte transplantation. J Am Acad Dermatol. 1995;32:228-232.
- Gauthier Y. Le vitiligo. Gaz Med. 1994;101:8-12.
- Malakar S, Malakar RS. Surgical pearl: composite film and graft unit for the recipient area dressing after split-thickness skin grafting in vitiligo. J Am Acad Dermatol. 2001;44:856-858.
- Hasegawa T, Suga Y, Ikejima A, et al. Suction blister grafting with CO2 laser resurfacing of the graft recipient site for vitiligo. J Dermatol. 2007;34:490-492.
- Mapar MA, Safarpour M, Mapar M, et al. A comparative study of the mini-punch grafting and hair follicle transplantation in the treatment of refractory and stable vitiligo. J Am Acad Dermatol. 2014;70:743-747.
- Malakar S, Lahiri K. Punch grafting for lip leukoderma. Dermatology. 2004;208:125-128.
- Gauthier Y, Surleve-Bazeille JE. Autologous grafting with noncultured melanocytes: a simplified method for treatment of depigmented lesions. J Am Acad Dermatol. 1992;26(2, pt 1):191-194.
- Silpa-Archa N, Griffith JL, Williams MS, et al. Prospective comparison of recipient-site preparation with fractional carbon dioxide laser versus dermabrasion and recipient-site dressing composition in melanocyte-keratinocyte transplantation procedure in vitiligo: a preliminary study [published online January 24, 2016]. Br J Dermatol. 2016;174:895-897.
- Taïeb A, Picardo M; VETF members. The definition and assessment of vitiligo: a consensus report of the Vitiligo European Task Force. Pigment Cell Res. 2007;20:27-35. Cited by: Ezzedine K, Lim HW, Suzuki T, et al; Vitiligo Global Issue Consensus Conference Panelists. Revised classification/nomenclature of vitiligo and related issues: the Vitiligo Global Issues Consensus Conference. Pigment Cell Melanoma Res. 2012;25:E1-E13.
- Rusfianti M, Wirohadidjodjo YW. Dermatosurgical techniques for repigmentation of vitiligo. Int J Dermatol. 2006;45:411-417.
- Falabella R. Surgical therapies for vitiligo. Clin Dermatol. 1997;15:927-939.
- Whitton ME, Pinart M, Batchelor J, et al. Interventions for vitiligo. Cochrane Database Syst Rev. 2015;2:CD003263.
- Mulekar SV, Isedeh P. Surgical interventions for vitiligo: an evidence-based review. Br J Dermatol. 2013;169(suppl 3):57-66.
- Dutta AK, Mandal SB. A clinical study of 650 vitiligo cases and their classification. Indian J Dermatol. 1969;14:103-111.
- Falabella R, Arrunategui A, Barona MI, et al. The minigrafting test for vitiligo: detection of stable lesions for melanocyte transplantation. J Am Acad Dermatol. 1995;32:228-232.
- Gauthier Y. Le vitiligo. Gaz Med. 1994;101:8-12.
- Malakar S, Malakar RS. Surgical pearl: composite film and graft unit for the recipient area dressing after split-thickness skin grafting in vitiligo. J Am Acad Dermatol. 2001;44:856-858.
- Hasegawa T, Suga Y, Ikejima A, et al. Suction blister grafting with CO2 laser resurfacing of the graft recipient site for vitiligo. J Dermatol. 2007;34:490-492.
- Mapar MA, Safarpour M, Mapar M, et al. A comparative study of the mini-punch grafting and hair follicle transplantation in the treatment of refractory and stable vitiligo. J Am Acad Dermatol. 2014;70:743-747.
- Malakar S, Lahiri K. Punch grafting for lip leukoderma. Dermatology. 2004;208:125-128.
- Gauthier Y, Surleve-Bazeille JE. Autologous grafting with noncultured melanocytes: a simplified method for treatment of depigmented lesions. J Am Acad Dermatol. 1992;26(2, pt 1):191-194.
- Silpa-Archa N, Griffith JL, Williams MS, et al. Prospective comparison of recipient-site preparation with fractional carbon dioxide laser versus dermabrasion and recipient-site dressing composition in melanocyte-keratinocyte transplantation procedure in vitiligo: a preliminary study [published online January 24, 2016]. Br J Dermatol. 2016;174:895-897.
Why VA Health Care Is Different
Is VA health care really “all that different” from what veterans would find in the private sector?
As someone who spent more than 25 years managing private sector health care organizations and recently joined VA as its under secretary for health, I’ve had the unique opportunity to compare the health care systems. Over the past several months, I’ve met with veterans and their families, veterans service organizations, VA clinicians, facility staff, and veteran employees at all levels. Through these meetings and travel to dozens of facilities, I’ve come to realize that many of the essential services provided by the VA cannot be found in or even replicated in the private sector.
Over time and in partnership with successive generations of veterans, the VA has evolved into an interconnected, institutionalized system of care and services. And while many of these services aren’t unique to the VA, ours is the only health care organization that combines these services “under one roof” and integrates them in a way that is veteran-centric.
Further, as our country continues to struggle with improving health outcomes and unsustainable increases in health care costs, the VA can play a crucial role. As a long-standing, highly integrated, and patient-focused provider of care, the VA can lead the way in advancing the nation’s health care. This is the appropriate role for government: Do what the private sector cannot or will not do, given the nature of its enterprise.
The VA has 3 core strengths that distinguish its services from those of the private sector in caring for veterans: (1) systemwide clinical expertise regarding service-connected conditions and disorders; (2) a team approach to primary care that is veteran-centric; and (3) a holistic view of the veteran that includes physical, psychosocial, and economic determinants of health, as well as critical support services for family members and caregivers.
First, the VA brings together comprehensive expertise on service-connected health issues in a single health care system. Our clinicians are trained to identify, assess, and treat a wide spectrum of health issues, such as spinal cord injury and limb loss, conditions arising from environmentalexposures, and traumatic brain injury. Additionally, VA specialists have expertise in the treatment of mental health issues, substance abuse, suicide prevention, and posttraumatic stress disorder (PTSD). Further, the VA has a long track record that includes national programs in audiology and speech pathology, blind rehabilitation, chiropractic care, physical med-icine and rehabilitation, prostheticand sensory aids services, recreation therapy, and polytrauma care.
In contrast, knowledge of and expertise in these crucially important health care issues are not nearly as widespread in the private sector. For example, less than 50% of private practice primary care providers (PCPs) regularly perform screening tests for PTSD and depression.1 In addition, only 15% of community-based mental health providers are proficient in treating military and deployment-related issues such as PTSD, and less than 20% of PCPs have sufficient military culture competence to take a veteran’s military history.1
The VA’s second core strength is its team-based, veteran-centric model of primary care that focuses on patient-driven, proactive, and personalized care. This patient aligned care team (PACT) addresses not only disease management, but also disease prevention, wellness, and health promotion. The PACT model often includes PCPs, nurse care managers, social workers, pharmacists, nutritionists, behavioral health professionals, administrative clerks, as well as the veteran, family members, and caregivers. Through PACT, veterans can attend group clinics and educational seminars, access web-based information via a personalized patient portal, and directly communicate with their care team by phone, secure messaging, or telehealth. The PACT approach has proven effective: Several studies examined its impact on reducing avoidable hospitalizations, emergency department visits, and behavioral health issues and on improving communication among health care professionals.2-4
The VA’s third core strength—a holistic approach to patient care— also is not uniformly seen in the private sector. All too often the private sector health care system addresses only the patient’s chief complaint, focusing on the physical manifestation of an illness or the patient’s psychological condition. Ensuring a patient’s well-being requires the integration of the physical, psychological, social, and economic aspects of health and a thorough understanding of how these factors impact treatment compliance. As any health care professional knows, even the best treatment plan cannot succeed without patient compliance. In this regard, the ability to address nonmedical issues is as important as the treatment plan.
By taking a holistic view of health and inviting veterans to do the same, the VA addresses these and other compliance issues head-on. The VA is positioned to provide help, as appropriate, with transportation; caregiver support; homelessness; pharmaceutical benefits; clothing allowances; counseling in readjustment centers; and a full range of physical, psychological, dental, and social services.
As someone who has spent considerable time in the private sector, I can report that delivery of such services is the exception, not the rule, especially given the current system of health care reimbursement. The benefit of a holistic view is underscored by numerous outcome studies showing that the VA performs as well as, if not better than, the private sector. For example, screening and prevention outcomes at the VA have been consistently better than those at community care sites.5
Studies also suggest that standard care measures, such as control of blood pressure and hemoglobin A1c levels, are often better in VA patients compared with non-VA patients. Studies of risk-adjusted mortality rates generally found improved outcomes for VA care or little difference between VA and non-VA care.6-9 Moreover, a recent independent assessment of the VA reported that the VA performed as well as, and in some cases better than, the private sector on a number of key indicators.10
In my first year as the VA under secretary for health, I have come to appreciate these strengths even more and to sharpen my understanding of what makes VA care different from private sector care. Five distinctions are clear:
1. Veteran Patients Are Inherently Different
The VA manages a patient mix that is distinct from what civilian community providers typically treat. The majority of veterans who utilize VA health care are collectively sicker and poorer and have fewer support services than age-matched non-veteran patients.10,11 When compared with the general population, veterans are more likely to have as many as 3 additional comorbid physical conditions as well as a possible mental health diagnosis.
Similarly, the VA also cares for a higher percentage of minorities who, as a group, too often encounter barriers to care in community settings. Given these disproportionately higher numbers of patients facing access issues, the VA has done better than the private sector in reducing barriers to care for many health measures.12 For many veterans, the VA has become a lifeline of health care support and service.
2. Reimbursement and Incentives
The veteran patient population typically requires more time during a typical doctor visit than private sector physicians generally can provide. Ever-changing reimbursement schedules have forced many private sector PCPs to shorten patient visits in order to survive economically. Because VA physicians are salaried, they don’t face the same constraints on time spent with patients. Further, there is less of a mismatch between financial performance and clinical performance and, therefore, less likelihood of inappropriate tests and services.
3. VA Employees’ Sense of Mission
Almost 95% of VA staff believe the work they do is important.13 In annual employee surveys, the VA sees a high commitment to service from its employees. Additionally, 40% of VA staff are veterans, who can relate to veteran patients in ways nonveterans cannot. As under secretary for health, it has been a remarkable experience seeing this sense of mission translated into everyday care and observing the very personal connection between VA employees and patients.
This sense of mission, embedded throughout the organization, has a far-reaching impact that includes the relationships formed with veterans. In stark contrast to the private sector, where patients may receive care from multiple sources and switch providers and insurance companies with increasing frequency, veterans tend to forge lifelong relationships with the VA. In turn, this stable and consistent relationship strengthens doctor-patient communications and provides a solid foundation for shared decision making. These long-term relationships also may improve the continuity of care and the ability to track long-term outcomes.
4. VA’s Unique Integration of Clinical Practice With Education & Research
As someone whose residency included training at VA, I’ve long appreciated the VA’s ability to advance health care, incorporate new learning, and promote best practices. These capabilities are fortified by its 70-year partnership with academic affiliates. Through academic partnerships, the VA trains tens of thousands of health care professionals yearly and conducts cutting-edge research on all the service-connected issues described above, as well as chronic illness, disparities in care, and emerging areas such as personalized medicine.
The VA Research and Development Program is the nation’s only intramural research program entirely dedicated to the health of veterans. Further, more than 60% of VA researchers are clinicians, which means their studies are framed by daily interaction with patients, and their study findings are put into practice more quickly.
5. VA Investment in Large-Scale Capabilities
As the largest integrated health care system in the U.S., the VA can invest in capabilities that are difficult for smaller systems to undertake. For example, the VA electronic medical record platform has enabled the organization to capture veteran health data systemwide for more than 2 decades, longer than almost any other health care enterprise in the country. Additionally, the ability of the VA to house and analyze “big data” is more advanced than that of most other health care systems, in part because of its considerably larger scale. This capability supports the holistic approach to care noted above and makes it possible to consider the numerous social and economic determinants of health and to track outcomes over time. This capability also supports the VA Million Veteran Program (MVP), a research effort that is building a genomic database of 1 million users of VA health care. Through the MVP, researchers will be able to use genomic and clinical data to develop personalized therapies for veterans and address some of America’s most significant research questions.14
As we continue to transform the VA and improve veterans’ health care, it is essential to understand that VA care is different from private sector care. It also is essential to understand—particularly given an environment of intense public scrutiny—that this fundamental distinction is embedded in the VA mission “to care for those who have borne the battle for their country.”
At the same time, it also is crucial to recognize that, although VA care is distinctly different from private sector care, our ongoing transformation means closer collaboration with the private sector—that is, for veterans seeking care from community providers. In this regard, we are working to achieve a tighter integration of the care offered to veterans in both sectors by working to develop a high-performance network that includes care from both VA and the private sector.15
Finally, in the midst of such a transformation, it is imperative to underscore that one factor will remain the same: our long-standing and unwavering commitment to provide patient-centric care and value to every veteran. As the under secretary for health, it is my great privilege to see this commitment daily and to better position the VA to serve our veterans and the nation.
1. Tanielian T, Farris C, Batka C, et al. Ready to Serve: Community-Based Provider Capacity to Deliver Culturally Competent, Quality Mental Health Care to Veterans and Their Families. San Francisco, CA: Rand Corporation; 2014.
2. Kearney LK, Post EP, Pomerantz AS, Zeiss AM. Applying the interprofessional patient aligned care team in the Department of Veterans Affairs: transforming primary care. Am Psychol. 2014;69(4):399-408.
3. Chaiyachati KH, Gordon K, Long T, et al. Continuity in a VA patient-centered medical home reduces emergency department visits. PloS One. 2014;9(5):e96356.
4. Yano EM. Implementation and impact of VA patient centered medical home. U.S. Department of Veterans Affairs website. http://www.hsrd.research.va.gov/research/abstracts.cfm?Project_ID=2141701013. Updated March 24, 2014. Accessed April 5, 2016.
5. Evidence-Based Synthesis Program Center. Comparison of Quality of Care in VA and Non-VA Settings: A Systematic Review. Los Angeles, CA: West Los Angeles VA Medical Center; 2010.
6. Nuti SV, Qin L, Rumsfeld JS, et al. Association of admission to Veterans Affairs hospitals vs non-Veterans Affairs hospitals with mortality and readmission rates among older men hospitalized with acute myocardial infarction, heart failure, or pneumonia. JAMA. 2016;315(6):582-592.
7. Kazis LE, Ren XS, Lee A, et al. Health status in VA patients: results from the Veterans Health Study. Am J Med Qual. 1999;14(1):28-38.
8. Payne SM, Lee A, Clark JA, et al. Utilization of medical services by Veterans Health Study (VHS) respondents. J Ambul Care Manage. 2005;28(2):125-140.
9. Keyhani S, Cheng E, Arling G, et al. Does the inclusion of stroke severity in a 30-day mortality model change standardized mortality rates at Veterans Affairs hospitals? Circ Cardiovasc Qual Outcomes. 2012;5(4):508-513.
10. CMS Alliance to Modernize Healthcare. Independent Assessment of the Healthcare Delivery Systems and Management Processes of the Department of Veterans Affairs. Volume 1: Integrated Report. U.S. Department of Veterans Affairs website. http://www.va.gov/opa/choiceact/documents/assessments/integrated_report.pdf. Published September 2015. Accessed April 4, 2016.
11. Jha AK. Learning from the past to improve VA health care. JAMA. 2016;315(6):560-561.
12. Trivedi AN, Grebla RC, Wright SM, Washington DL. Despite improved quality of care in the Veterans Affairs health system, racial disparity persists for important clinical outcomes. Health Aff (Millwood). 2011;30(4):707-715.
13. U.S. Department of Veterans Affairs. Department of Veterans Affairs 2015 Federal Employee Viewpoint Results. U.S. Department of Veterans Affairs website. http://www.va.gov/OHRM/docs/2015FEVSReportVA.pdf. Accessed April 4, 2016.
14. Kupersmith J, O’Leary T. The Million Veteran Program: building VA’s mega-database for genomic medicine. Health Affairs website. http://healthaffairs.org/blog/2012/11/19/the-million-veteran-program-building-vas-mega-database-for-genomic-medicine. Published November 19, 2012. Accessed February 18, 2016.
15. Shulkin D. Beyond the VA crisis: becoming a high-performance network. N Engl J Med. 2016;374(11):1003-1005.
Is VA health care really “all that different” from what veterans would find in the private sector?
As someone who spent more than 25 years managing private sector health care organizations and recently joined VA as its under secretary for health, I’ve had the unique opportunity to compare the health care systems. Over the past several months, I’ve met with veterans and their families, veterans service organizations, VA clinicians, facility staff, and veteran employees at all levels. Through these meetings and travel to dozens of facilities, I’ve come to realize that many of the essential services provided by the VA cannot be found in or even replicated in the private sector.
Over time and in partnership with successive generations of veterans, the VA has evolved into an interconnected, institutionalized system of care and services. And while many of these services aren’t unique to the VA, ours is the only health care organization that combines these services “under one roof” and integrates them in a way that is veteran-centric.
Further, as our country continues to struggle with improving health outcomes and unsustainable increases in health care costs, the VA can play a crucial role. As a long-standing, highly integrated, and patient-focused provider of care, the VA can lead the way in advancing the nation’s health care. This is the appropriate role for government: Do what the private sector cannot or will not do, given the nature of its enterprise.
The VA has 3 core strengths that distinguish its services from those of the private sector in caring for veterans: (1) systemwide clinical expertise regarding service-connected conditions and disorders; (2) a team approach to primary care that is veteran-centric; and (3) a holistic view of the veteran that includes physical, psychosocial, and economic determinants of health, as well as critical support services for family members and caregivers.
First, the VA brings together comprehensive expertise on service-connected health issues in a single health care system. Our clinicians are trained to identify, assess, and treat a wide spectrum of health issues, such as spinal cord injury and limb loss, conditions arising from environmentalexposures, and traumatic brain injury. Additionally, VA specialists have expertise in the treatment of mental health issues, substance abuse, suicide prevention, and posttraumatic stress disorder (PTSD). Further, the VA has a long track record that includes national programs in audiology and speech pathology, blind rehabilitation, chiropractic care, physical med-icine and rehabilitation, prostheticand sensory aids services, recreation therapy, and polytrauma care.
In contrast, knowledge of and expertise in these crucially important health care issues are not nearly as widespread in the private sector. For example, less than 50% of private practice primary care providers (PCPs) regularly perform screening tests for PTSD and depression.1 In addition, only 15% of community-based mental health providers are proficient in treating military and deployment-related issues such as PTSD, and less than 20% of PCPs have sufficient military culture competence to take a veteran’s military history.1
The VA’s second core strength is its team-based, veteran-centric model of primary care that focuses on patient-driven, proactive, and personalized care. This patient aligned care team (PACT) addresses not only disease management, but also disease prevention, wellness, and health promotion. The PACT model often includes PCPs, nurse care managers, social workers, pharmacists, nutritionists, behavioral health professionals, administrative clerks, as well as the veteran, family members, and caregivers. Through PACT, veterans can attend group clinics and educational seminars, access web-based information via a personalized patient portal, and directly communicate with their care team by phone, secure messaging, or telehealth. The PACT approach has proven effective: Several studies examined its impact on reducing avoidable hospitalizations, emergency department visits, and behavioral health issues and on improving communication among health care professionals.2-4
The VA’s third core strength—a holistic approach to patient care— also is not uniformly seen in the private sector. All too often the private sector health care system addresses only the patient’s chief complaint, focusing on the physical manifestation of an illness or the patient’s psychological condition. Ensuring a patient’s well-being requires the integration of the physical, psychological, social, and economic aspects of health and a thorough understanding of how these factors impact treatment compliance. As any health care professional knows, even the best treatment plan cannot succeed without patient compliance. In this regard, the ability to address nonmedical issues is as important as the treatment plan.
By taking a holistic view of health and inviting veterans to do the same, the VA addresses these and other compliance issues head-on. The VA is positioned to provide help, as appropriate, with transportation; caregiver support; homelessness; pharmaceutical benefits; clothing allowances; counseling in readjustment centers; and a full range of physical, psychological, dental, and social services.
As someone who has spent considerable time in the private sector, I can report that delivery of such services is the exception, not the rule, especially given the current system of health care reimbursement. The benefit of a holistic view is underscored by numerous outcome studies showing that the VA performs as well as, if not better than, the private sector. For example, screening and prevention outcomes at the VA have been consistently better than those at community care sites.5
Studies also suggest that standard care measures, such as control of blood pressure and hemoglobin A1c levels, are often better in VA patients compared with non-VA patients. Studies of risk-adjusted mortality rates generally found improved outcomes for VA care or little difference between VA and non-VA care.6-9 Moreover, a recent independent assessment of the VA reported that the VA performed as well as, and in some cases better than, the private sector on a number of key indicators.10
In my first year as the VA under secretary for health, I have come to appreciate these strengths even more and to sharpen my understanding of what makes VA care different from private sector care. Five distinctions are clear:
1. Veteran Patients Are Inherently Different
The VA manages a patient mix that is distinct from what civilian community providers typically treat. The majority of veterans who utilize VA health care are collectively sicker and poorer and have fewer support services than age-matched non-veteran patients.10,11 When compared with the general population, veterans are more likely to have as many as 3 additional comorbid physical conditions as well as a possible mental health diagnosis.
Similarly, the VA also cares for a higher percentage of minorities who, as a group, too often encounter barriers to care in community settings. Given these disproportionately higher numbers of patients facing access issues, the VA has done better than the private sector in reducing barriers to care for many health measures.12 For many veterans, the VA has become a lifeline of health care support and service.
2. Reimbursement and Incentives
The veteran patient population typically requires more time during a typical doctor visit than private sector physicians generally can provide. Ever-changing reimbursement schedules have forced many private sector PCPs to shorten patient visits in order to survive economically. Because VA physicians are salaried, they don’t face the same constraints on time spent with patients. Further, there is less of a mismatch between financial performance and clinical performance and, therefore, less likelihood of inappropriate tests and services.
3. VA Employees’ Sense of Mission
Almost 95% of VA staff believe the work they do is important.13 In annual employee surveys, the VA sees a high commitment to service from its employees. Additionally, 40% of VA staff are veterans, who can relate to veteran patients in ways nonveterans cannot. As under secretary for health, it has been a remarkable experience seeing this sense of mission translated into everyday care and observing the very personal connection between VA employees and patients.
This sense of mission, embedded throughout the organization, has a far-reaching impact that includes the relationships formed with veterans. In stark contrast to the private sector, where patients may receive care from multiple sources and switch providers and insurance companies with increasing frequency, veterans tend to forge lifelong relationships with the VA. In turn, this stable and consistent relationship strengthens doctor-patient communications and provides a solid foundation for shared decision making. These long-term relationships also may improve the continuity of care and the ability to track long-term outcomes.
4. VA’s Unique Integration of Clinical Practice With Education & Research
As someone whose residency included training at VA, I’ve long appreciated the VA’s ability to advance health care, incorporate new learning, and promote best practices. These capabilities are fortified by its 70-year partnership with academic affiliates. Through academic partnerships, the VA trains tens of thousands of health care professionals yearly and conducts cutting-edge research on all the service-connected issues described above, as well as chronic illness, disparities in care, and emerging areas such as personalized medicine.
The VA Research and Development Program is the nation’s only intramural research program entirely dedicated to the health of veterans. Further, more than 60% of VA researchers are clinicians, which means their studies are framed by daily interaction with patients, and their study findings are put into practice more quickly.
5. VA Investment in Large-Scale Capabilities
As the largest integrated health care system in the U.S., the VA can invest in capabilities that are difficult for smaller systems to undertake. For example, the VA electronic medical record platform has enabled the organization to capture veteran health data systemwide for more than 2 decades, longer than almost any other health care enterprise in the country. Additionally, the ability of the VA to house and analyze “big data” is more advanced than that of most other health care systems, in part because of its considerably larger scale. This capability supports the holistic approach to care noted above and makes it possible to consider the numerous social and economic determinants of health and to track outcomes over time. This capability also supports the VA Million Veteran Program (MVP), a research effort that is building a genomic database of 1 million users of VA health care. Through the MVP, researchers will be able to use genomic and clinical data to develop personalized therapies for veterans and address some of America’s most significant research questions.14
As we continue to transform the VA and improve veterans’ health care, it is essential to understand that VA care is different from private sector care. It also is essential to understand—particularly given an environment of intense public scrutiny—that this fundamental distinction is embedded in the VA mission “to care for those who have borne the battle for their country.”
At the same time, it also is crucial to recognize that, although VA care is distinctly different from private sector care, our ongoing transformation means closer collaboration with the private sector—that is, for veterans seeking care from community providers. In this regard, we are working to achieve a tighter integration of the care offered to veterans in both sectors by working to develop a high-performance network that includes care from both VA and the private sector.15
Finally, in the midst of such a transformation, it is imperative to underscore that one factor will remain the same: our long-standing and unwavering commitment to provide patient-centric care and value to every veteran. As the under secretary for health, it is my great privilege to see this commitment daily and to better position the VA to serve our veterans and the nation.
Is VA health care really “all that different” from what veterans would find in the private sector?
As someone who spent more than 25 years managing private sector health care organizations and recently joined VA as its under secretary for health, I’ve had the unique opportunity to compare the health care systems. Over the past several months, I’ve met with veterans and their families, veterans service organizations, VA clinicians, facility staff, and veteran employees at all levels. Through these meetings and travel to dozens of facilities, I’ve come to realize that many of the essential services provided by the VA cannot be found in or even replicated in the private sector.
Over time and in partnership with successive generations of veterans, the VA has evolved into an interconnected, institutionalized system of care and services. And while many of these services aren’t unique to the VA, ours is the only health care organization that combines these services “under one roof” and integrates them in a way that is veteran-centric.
Further, as our country continues to struggle with improving health outcomes and unsustainable increases in health care costs, the VA can play a crucial role. As a long-standing, highly integrated, and patient-focused provider of care, the VA can lead the way in advancing the nation’s health care. This is the appropriate role for government: Do what the private sector cannot or will not do, given the nature of its enterprise.
The VA has 3 core strengths that distinguish its services from those of the private sector in caring for veterans: (1) systemwide clinical expertise regarding service-connected conditions and disorders; (2) a team approach to primary care that is veteran-centric; and (3) a holistic view of the veteran that includes physical, psychosocial, and economic determinants of health, as well as critical support services for family members and caregivers.
First, the VA brings together comprehensive expertise on service-connected health issues in a single health care system. Our clinicians are trained to identify, assess, and treat a wide spectrum of health issues, such as spinal cord injury and limb loss, conditions arising from environmentalexposures, and traumatic brain injury. Additionally, VA specialists have expertise in the treatment of mental health issues, substance abuse, suicide prevention, and posttraumatic stress disorder (PTSD). Further, the VA has a long track record that includes national programs in audiology and speech pathology, blind rehabilitation, chiropractic care, physical med-icine and rehabilitation, prostheticand sensory aids services, recreation therapy, and polytrauma care.
In contrast, knowledge of and expertise in these crucially important health care issues are not nearly as widespread in the private sector. For example, less than 50% of private practice primary care providers (PCPs) regularly perform screening tests for PTSD and depression.1 In addition, only 15% of community-based mental health providers are proficient in treating military and deployment-related issues such as PTSD, and less than 20% of PCPs have sufficient military culture competence to take a veteran’s military history.1
The VA’s second core strength is its team-based, veteran-centric model of primary care that focuses on patient-driven, proactive, and personalized care. This patient aligned care team (PACT) addresses not only disease management, but also disease prevention, wellness, and health promotion. The PACT model often includes PCPs, nurse care managers, social workers, pharmacists, nutritionists, behavioral health professionals, administrative clerks, as well as the veteran, family members, and caregivers. Through PACT, veterans can attend group clinics and educational seminars, access web-based information via a personalized patient portal, and directly communicate with their care team by phone, secure messaging, or telehealth. The PACT approach has proven effective: Several studies examined its impact on reducing avoidable hospitalizations, emergency department visits, and behavioral health issues and on improving communication among health care professionals.2-4
The VA’s third core strength—a holistic approach to patient care— also is not uniformly seen in the private sector. All too often the private sector health care system addresses only the patient’s chief complaint, focusing on the physical manifestation of an illness or the patient’s psychological condition. Ensuring a patient’s well-being requires the integration of the physical, psychological, social, and economic aspects of health and a thorough understanding of how these factors impact treatment compliance. As any health care professional knows, even the best treatment plan cannot succeed without patient compliance. In this regard, the ability to address nonmedical issues is as important as the treatment plan.
By taking a holistic view of health and inviting veterans to do the same, the VA addresses these and other compliance issues head-on. The VA is positioned to provide help, as appropriate, with transportation; caregiver support; homelessness; pharmaceutical benefits; clothing allowances; counseling in readjustment centers; and a full range of physical, psychological, dental, and social services.
As someone who has spent considerable time in the private sector, I can report that delivery of such services is the exception, not the rule, especially given the current system of health care reimbursement. The benefit of a holistic view is underscored by numerous outcome studies showing that the VA performs as well as, if not better than, the private sector. For example, screening and prevention outcomes at the VA have been consistently better than those at community care sites.5
Studies also suggest that standard care measures, such as control of blood pressure and hemoglobin A1c levels, are often better in VA patients compared with non-VA patients. Studies of risk-adjusted mortality rates generally found improved outcomes for VA care or little difference between VA and non-VA care.6-9 Moreover, a recent independent assessment of the VA reported that the VA performed as well as, and in some cases better than, the private sector on a number of key indicators.10
In my first year as the VA under secretary for health, I have come to appreciate these strengths even more and to sharpen my understanding of what makes VA care different from private sector care. Five distinctions are clear:
1. Veteran Patients Are Inherently Different
The VA manages a patient mix that is distinct from what civilian community providers typically treat. The majority of veterans who utilize VA health care are collectively sicker and poorer and have fewer support services than age-matched non-veteran patients.10,11 When compared with the general population, veterans are more likely to have as many as 3 additional comorbid physical conditions as well as a possible mental health diagnosis.
Similarly, the VA also cares for a higher percentage of minorities who, as a group, too often encounter barriers to care in community settings. Given these disproportionately higher numbers of patients facing access issues, the VA has done better than the private sector in reducing barriers to care for many health measures.12 For many veterans, the VA has become a lifeline of health care support and service.
2. Reimbursement and Incentives
The veteran patient population typically requires more time during a typical doctor visit than private sector physicians generally can provide. Ever-changing reimbursement schedules have forced many private sector PCPs to shorten patient visits in order to survive economically. Because VA physicians are salaried, they don’t face the same constraints on time spent with patients. Further, there is less of a mismatch between financial performance and clinical performance and, therefore, less likelihood of inappropriate tests and services.
3. VA Employees’ Sense of Mission
Almost 95% of VA staff believe the work they do is important.13 In annual employee surveys, the VA sees a high commitment to service from its employees. Additionally, 40% of VA staff are veterans, who can relate to veteran patients in ways nonveterans cannot. As under secretary for health, it has been a remarkable experience seeing this sense of mission translated into everyday care and observing the very personal connection between VA employees and patients.
This sense of mission, embedded throughout the organization, has a far-reaching impact that includes the relationships formed with veterans. In stark contrast to the private sector, where patients may receive care from multiple sources and switch providers and insurance companies with increasing frequency, veterans tend to forge lifelong relationships with the VA. In turn, this stable and consistent relationship strengthens doctor-patient communications and provides a solid foundation for shared decision making. These long-term relationships also may improve the continuity of care and the ability to track long-term outcomes.
4. VA’s Unique Integration of Clinical Practice With Education & Research
As someone whose residency included training at VA, I’ve long appreciated the VA’s ability to advance health care, incorporate new learning, and promote best practices. These capabilities are fortified by its 70-year partnership with academic affiliates. Through academic partnerships, the VA trains tens of thousands of health care professionals yearly and conducts cutting-edge research on all the service-connected issues described above, as well as chronic illness, disparities in care, and emerging areas such as personalized medicine.
The VA Research and Development Program is the nation’s only intramural research program entirely dedicated to the health of veterans. Further, more than 60% of VA researchers are clinicians, which means their studies are framed by daily interaction with patients, and their study findings are put into practice more quickly.
5. VA Investment in Large-Scale Capabilities
As the largest integrated health care system in the U.S., the VA can invest in capabilities that are difficult for smaller systems to undertake. For example, the VA electronic medical record platform has enabled the organization to capture veteran health data systemwide for more than 2 decades, longer than almost any other health care enterprise in the country. Additionally, the ability of the VA to house and analyze “big data” is more advanced than that of most other health care systems, in part because of its considerably larger scale. This capability supports the holistic approach to care noted above and makes it possible to consider the numerous social and economic determinants of health and to track outcomes over time. This capability also supports the VA Million Veteran Program (MVP), a research effort that is building a genomic database of 1 million users of VA health care. Through the MVP, researchers will be able to use genomic and clinical data to develop personalized therapies for veterans and address some of America’s most significant research questions.14
As we continue to transform the VA and improve veterans’ health care, it is essential to understand that VA care is different from private sector care. It also is essential to understand—particularly given an environment of intense public scrutiny—that this fundamental distinction is embedded in the VA mission “to care for those who have borne the battle for their country.”
At the same time, it also is crucial to recognize that, although VA care is distinctly different from private sector care, our ongoing transformation means closer collaboration with the private sector—that is, for veterans seeking care from community providers. In this regard, we are working to achieve a tighter integration of the care offered to veterans in both sectors by working to develop a high-performance network that includes care from both VA and the private sector.15
Finally, in the midst of such a transformation, it is imperative to underscore that one factor will remain the same: our long-standing and unwavering commitment to provide patient-centric care and value to every veteran. As the under secretary for health, it is my great privilege to see this commitment daily and to better position the VA to serve our veterans and the nation.
1. Tanielian T, Farris C, Batka C, et al. Ready to Serve: Community-Based Provider Capacity to Deliver Culturally Competent, Quality Mental Health Care to Veterans and Their Families. San Francisco, CA: Rand Corporation; 2014.
2. Kearney LK, Post EP, Pomerantz AS, Zeiss AM. Applying the interprofessional patient aligned care team in the Department of Veterans Affairs: transforming primary care. Am Psychol. 2014;69(4):399-408.
3. Chaiyachati KH, Gordon K, Long T, et al. Continuity in a VA patient-centered medical home reduces emergency department visits. PloS One. 2014;9(5):e96356.
4. Yano EM. Implementation and impact of VA patient centered medical home. U.S. Department of Veterans Affairs website. http://www.hsrd.research.va.gov/research/abstracts.cfm?Project_ID=2141701013. Updated March 24, 2014. Accessed April 5, 2016.
5. Evidence-Based Synthesis Program Center. Comparison of Quality of Care in VA and Non-VA Settings: A Systematic Review. Los Angeles, CA: West Los Angeles VA Medical Center; 2010.
6. Nuti SV, Qin L, Rumsfeld JS, et al. Association of admission to Veterans Affairs hospitals vs non-Veterans Affairs hospitals with mortality and readmission rates among older men hospitalized with acute myocardial infarction, heart failure, or pneumonia. JAMA. 2016;315(6):582-592.
7. Kazis LE, Ren XS, Lee A, et al. Health status in VA patients: results from the Veterans Health Study. Am J Med Qual. 1999;14(1):28-38.
8. Payne SM, Lee A, Clark JA, et al. Utilization of medical services by Veterans Health Study (VHS) respondents. J Ambul Care Manage. 2005;28(2):125-140.
9. Keyhani S, Cheng E, Arling G, et al. Does the inclusion of stroke severity in a 30-day mortality model change standardized mortality rates at Veterans Affairs hospitals? Circ Cardiovasc Qual Outcomes. 2012;5(4):508-513.
10. CMS Alliance to Modernize Healthcare. Independent Assessment of the Healthcare Delivery Systems and Management Processes of the Department of Veterans Affairs. Volume 1: Integrated Report. U.S. Department of Veterans Affairs website. http://www.va.gov/opa/choiceact/documents/assessments/integrated_report.pdf. Published September 2015. Accessed April 4, 2016.
11. Jha AK. Learning from the past to improve VA health care. JAMA. 2016;315(6):560-561.
12. Trivedi AN, Grebla RC, Wright SM, Washington DL. Despite improved quality of care in the Veterans Affairs health system, racial disparity persists for important clinical outcomes. Health Aff (Millwood). 2011;30(4):707-715.
13. U.S. Department of Veterans Affairs. Department of Veterans Affairs 2015 Federal Employee Viewpoint Results. U.S. Department of Veterans Affairs website. http://www.va.gov/OHRM/docs/2015FEVSReportVA.pdf. Accessed April 4, 2016.
14. Kupersmith J, O’Leary T. The Million Veteran Program: building VA’s mega-database for genomic medicine. Health Affairs website. http://healthaffairs.org/blog/2012/11/19/the-million-veteran-program-building-vas-mega-database-for-genomic-medicine. Published November 19, 2012. Accessed February 18, 2016.
15. Shulkin D. Beyond the VA crisis: becoming a high-performance network. N Engl J Med. 2016;374(11):1003-1005.
1. Tanielian T, Farris C, Batka C, et al. Ready to Serve: Community-Based Provider Capacity to Deliver Culturally Competent, Quality Mental Health Care to Veterans and Their Families. San Francisco, CA: Rand Corporation; 2014.
2. Kearney LK, Post EP, Pomerantz AS, Zeiss AM. Applying the interprofessional patient aligned care team in the Department of Veterans Affairs: transforming primary care. Am Psychol. 2014;69(4):399-408.
3. Chaiyachati KH, Gordon K, Long T, et al. Continuity in a VA patient-centered medical home reduces emergency department visits. PloS One. 2014;9(5):e96356.
4. Yano EM. Implementation and impact of VA patient centered medical home. U.S. Department of Veterans Affairs website. http://www.hsrd.research.va.gov/research/abstracts.cfm?Project_ID=2141701013. Updated March 24, 2014. Accessed April 5, 2016.
5. Evidence-Based Synthesis Program Center. Comparison of Quality of Care in VA and Non-VA Settings: A Systematic Review. Los Angeles, CA: West Los Angeles VA Medical Center; 2010.
6. Nuti SV, Qin L, Rumsfeld JS, et al. Association of admission to Veterans Affairs hospitals vs non-Veterans Affairs hospitals with mortality and readmission rates among older men hospitalized with acute myocardial infarction, heart failure, or pneumonia. JAMA. 2016;315(6):582-592.
7. Kazis LE, Ren XS, Lee A, et al. Health status in VA patients: results from the Veterans Health Study. Am J Med Qual. 1999;14(1):28-38.
8. Payne SM, Lee A, Clark JA, et al. Utilization of medical services by Veterans Health Study (VHS) respondents. J Ambul Care Manage. 2005;28(2):125-140.
9. Keyhani S, Cheng E, Arling G, et al. Does the inclusion of stroke severity in a 30-day mortality model change standardized mortality rates at Veterans Affairs hospitals? Circ Cardiovasc Qual Outcomes. 2012;5(4):508-513.
10. CMS Alliance to Modernize Healthcare. Independent Assessment of the Healthcare Delivery Systems and Management Processes of the Department of Veterans Affairs. Volume 1: Integrated Report. U.S. Department of Veterans Affairs website. http://www.va.gov/opa/choiceact/documents/assessments/integrated_report.pdf. Published September 2015. Accessed April 4, 2016.
11. Jha AK. Learning from the past to improve VA health care. JAMA. 2016;315(6):560-561.
12. Trivedi AN, Grebla RC, Wright SM, Washington DL. Despite improved quality of care in the Veterans Affairs health system, racial disparity persists for important clinical outcomes. Health Aff (Millwood). 2011;30(4):707-715.
13. U.S. Department of Veterans Affairs. Department of Veterans Affairs 2015 Federal Employee Viewpoint Results. U.S. Department of Veterans Affairs website. http://www.va.gov/OHRM/docs/2015FEVSReportVA.pdf. Accessed April 4, 2016.
14. Kupersmith J, O’Leary T. The Million Veteran Program: building VA’s mega-database for genomic medicine. Health Affairs website. http://healthaffairs.org/blog/2012/11/19/the-million-veteran-program-building-vas-mega-database-for-genomic-medicine. Published November 19, 2012. Accessed February 18, 2016.
15. Shulkin D. Beyond the VA crisis: becoming a high-performance network. N Engl J Med. 2016;374(11):1003-1005.
