User login
Grind it out
“And five more, four more, three more, two more, one more, and done!” Just when you thought you could not stand the searing pain any longer, it ends. Your spin instructor is not only helping you be fit, she is also teaching you an important lesson for life: Sometimes you just need to grind it out.
. College basketball teams need to simply grind it out to advance in the NCAA championship tournament. How might Tiger Woods recover from a disastrous few holes at the Masters? “He’ll just have to grind it out on the back nine.” How will you finally finish your PhD thesis? You’ll have to grind it out this month. It’s how I’m writing this column, how I got my taxes in on time, and, sometimes, how I get through clinic.
The phrase is used to describe something which needs to be done that is tedious, laborious, or joyless. Although the outcome of grinding it out is always pleasant, the task is often considered arduous.
In my dermatology practice, patient demand came in like a lion this March, and to meet our awesome access goals, we needed to add clinics on Saturdays, early mornings, and even a few nights. We met our goal, with supply to spare, and felt proud of our accomplishments. Physician wellness gurus (this author not included) say that, to avoid burnout from such excess work, you must find meaning in your work. Be grateful to help that 24-year-old with acne at 8:15 p.m. Think about how lucky you are to serve that lawyer with hand dermatitis at 8:45 p.m. Celebrate the mom’s cancer-free skin screening at 9:00 p.m. By finding meaning in our work, we’re told, we can achieve clinic nirvana. Except it doesn’t always work, and sometimes it serves us badly.

For the long days that ended in night clinic last month, I found myself counting down those last few patients – “four more, three more, two more, and last one.” I love my work and care about my patients, but sometimes I just have to grind it out. I’m proud of what I’ve accomplished.
Now it’s on to spin class.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@MDedge.com.
“And five more, four more, three more, two more, one more, and done!” Just when you thought you could not stand the searing pain any longer, it ends. Your spin instructor is not only helping you be fit, she is also teaching you an important lesson for life: Sometimes you just need to grind it out.
. College basketball teams need to simply grind it out to advance in the NCAA championship tournament. How might Tiger Woods recover from a disastrous few holes at the Masters? “He’ll just have to grind it out on the back nine.” How will you finally finish your PhD thesis? You’ll have to grind it out this month. It’s how I’m writing this column, how I got my taxes in on time, and, sometimes, how I get through clinic.
The phrase is used to describe something which needs to be done that is tedious, laborious, or joyless. Although the outcome of grinding it out is always pleasant, the task is often considered arduous.
In my dermatology practice, patient demand came in like a lion this March, and to meet our awesome access goals, we needed to add clinics on Saturdays, early mornings, and even a few nights. We met our goal, with supply to spare, and felt proud of our accomplishments. Physician wellness gurus (this author not included) say that, to avoid burnout from such excess work, you must find meaning in your work. Be grateful to help that 24-year-old with acne at 8:15 p.m. Think about how lucky you are to serve that lawyer with hand dermatitis at 8:45 p.m. Celebrate the mom’s cancer-free skin screening at 9:00 p.m. By finding meaning in our work, we’re told, we can achieve clinic nirvana. Except it doesn’t always work, and sometimes it serves us badly.
For the long days that ended in night clinic last month, I found myself counting down those last few patients – “four more, three more, two more, and last one.” I love my work and care about my patients, but sometimes I just have to grind it out. I’m proud of what I’ve accomplished.
Now it’s on to spin class.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@MDedge.com.
“And five more, four more, three more, two more, one more, and done!” Just when you thought you could not stand the searing pain any longer, it ends. Your spin instructor is not only helping you be fit, she is also teaching you an important lesson for life: Sometimes you just need to grind it out.
. College basketball teams need to simply grind it out to advance in the NCAA championship tournament. How might Tiger Woods recover from a disastrous few holes at the Masters? “He’ll just have to grind it out on the back nine.” How will you finally finish your PhD thesis? You’ll have to grind it out this month. It’s how I’m writing this column, how I got my taxes in on time, and, sometimes, how I get through clinic.
The phrase is used to describe something which needs to be done that is tedious, laborious, or joyless. Although the outcome of grinding it out is always pleasant, the task is often considered arduous.
In my dermatology practice, patient demand came in like a lion this March, and to meet our awesome access goals, we needed to add clinics on Saturdays, early mornings, and even a few nights. We met our goal, with supply to spare, and felt proud of our accomplishments. Physician wellness gurus (this author not included) say that, to avoid burnout from such excess work, you must find meaning in your work. Be grateful to help that 24-year-old with acne at 8:15 p.m. Think about how lucky you are to serve that lawyer with hand dermatitis at 8:45 p.m. Celebrate the mom’s cancer-free skin screening at 9:00 p.m. By finding meaning in our work, we’re told, we can achieve clinic nirvana. Except it doesn’t always work, and sometimes it serves us badly.
For the long days that ended in night clinic last month, I found myself counting down those last few patients – “four more, three more, two more, and last one.” I love my work and care about my patients, but sometimes I just have to grind it out. I’m proud of what I’ve accomplished.
Now it’s on to spin class.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@MDedge.com.

Take action to prevent maternal mortality
The facts
While other industrialized nations are seeing a decrease in their maternal mortality rates, the United States has noted a 26% increase over a 15-year period. This is especially true for women of color: black women are nearly 4 times as likely to die from pregnancy related causes as compared to non-Hispanic white women. Postpartum hemorrhage and preeclampsia are often the leading causes of maternal death; however, suicide and overdoses are becoming increasingly more common. This information is highlighted in the March 2018 OBG Management article “Factors critical to reducing US maternal mortality and morbidity,” by Lucia DiVenere, MA, Government and Political Affairs, at the American College of Obstetricians and Gynecologists (ACOG).1
Although there are efforts to improve these outcomes, programs vary by state. One initiative is the perinatal quality collaboratives (PQCs), state or multistate networks of teams working to improve the quality of care for mothers and babies (see “Has your state established a perinatal quality collaborative?”).
Currently, only 33 states have a maternal mortality review committee (MMRC) comprised of an interdisciplinary team of ObGyns, nurses, and other stakeholders. The MMRC reviews each maternal death in their state and provides recommendations and policy changes to help prevent further loss of life.
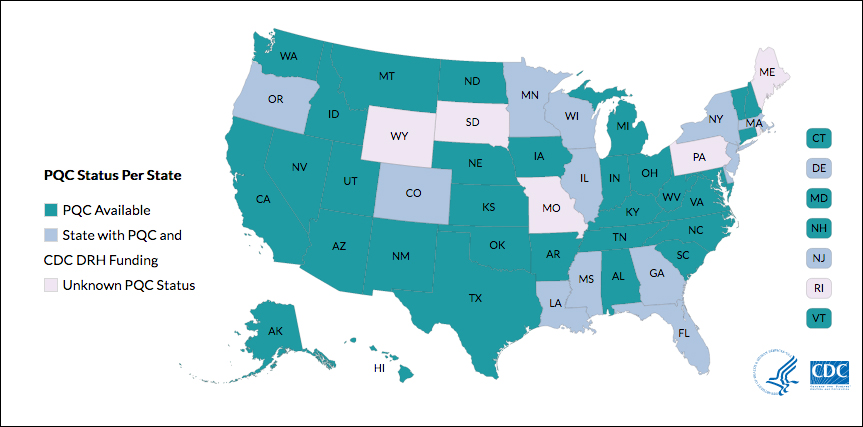
Many states currently have active collaboratives, and others are in development. The CDC’s Division of Reproductive Health (DRH) currently provides support for state-based PQCs in Colorado, Delaware, Florida, Georgia, Illinois, Louisiana, Massachusetts, Minnesota, Mississippi, New Jersey, New York, Oregon, and Wisconsin. The status of PQCs in Maine, Rhode Island, Pennsylvania, Missouri, South Dakota, and Wyoming is unknown.1
The CDC can help people establish a collaborative. Visit: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pqc-states.html.
Reference
- Centers for Disease Control and Prevention. Reproductive health: State Perinatal Quality Collaboratives. CDC website. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pqc-states.html Updated October 17, 2017. Accessed April 4, 2018.
The bill
Preventing Maternal Deaths Act/Maternal Health Accountability Act (H.R. 1318/S. 1112) is a bipartisan, bicameral effort to reduce maternal mortality and reduce health care disparities.
The bills authorize the Centers for Disease Control and Prevention (CDC) to help states create or expand state MMRCs through annual grant funding of $7 million through fiscal year 2022. Through the MMRCs, the CDC would have the ability to gather data on maternal mortality and health care disparities, allowing the agency to better understand leading causes of maternal death as well as a state’s successes and pitfalls in interventions.
Currently the House bill (H.R. 1318) has 102 cosponsors (https://cqrcengage.com/acog/app/bill/903056?0) and the Senate bill (S. 1112) has 17 cosponsors (https://cqrcengage.com/acog/app/bill/943204?1). Click these links to see if your representative is a cosponsor.
Not sure who your representative is? Click here to find out: http://cqrcengage.com/acog/app/lookup?1&m=29525.
Take action
Both the Senate and House bills have been referred to health committees. However, no advances have been made since March 2017. In order for the bills to move forward, your representatives need to hear from you.
If your representative is a cosponsor of the bill, thank them for their support, but also ask what we can do to ensure this bill becomes law.
If your representative is not a cosponsor, follow this link to email your representative: http://cqrcengage.com/acog/app/onestep-write-a-letter?0&engagementId=306574. You also can call your representative’s office and speak directly to a staff member.
When calling or emailing, highlight the following:
- I am an ObGyn and I am asking [your Representative/Senator] to support H.R. 1318 or S. 1112.
- While maternal mortality rates are decreasing in other parts of the world, they are increasing in the United States. We have the highest maternal mortality rate in the developing world.
- This bill gives all states the opportunity to have a maternal mortality review committee, allowing health care leaders to review each maternal death and analyze how further deaths can be prevented.
- Congress has invested in programs addressing infant mortality, birth defects, and preterm birth. It is time we put the same investment into saving our nation’s mothers.
- As an ObGyn, I urge you to support this bill.
More from ACOG
Want to know what other advocacy opportunities are available? Check out ACOG action at http://cqrcengage.com/acog/home?3.
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
- DiVenere L. Factors critical to reducing US maternal mortality and morbidity. OBG Manag. 2018;30(3):30−33.
The facts
While other industrialized nations are seeing a decrease in their maternal mortality rates, the United States has noted a 26% increase over a 15-year period. This is especially true for women of color: black women are nearly 4 times as likely to die from pregnancy related causes as compared to non-Hispanic white women. Postpartum hemorrhage and preeclampsia are often the leading causes of maternal death; however, suicide and overdoses are becoming increasingly more common. This information is highlighted in the March 2018 OBG Management article “Factors critical to reducing US maternal mortality and morbidity,” by Lucia DiVenere, MA, Government and Political Affairs, at the American College of Obstetricians and Gynecologists (ACOG).1
Although there are efforts to improve these outcomes, programs vary by state. One initiative is the perinatal quality collaboratives (PQCs), state or multistate networks of teams working to improve the quality of care for mothers and babies (see “Has your state established a perinatal quality collaborative?”).
Currently, only 33 states have a maternal mortality review committee (MMRC) comprised of an interdisciplinary team of ObGyns, nurses, and other stakeholders. The MMRC reviews each maternal death in their state and provides recommendations and policy changes to help prevent further loss of life.
Many states currently have active collaboratives, and others are in development. The CDC’s Division of Reproductive Health (DRH) currently provides support for state-based PQCs in Colorado, Delaware, Florida, Georgia, Illinois, Louisiana, Massachusetts, Minnesota, Mississippi, New Jersey, New York, Oregon, and Wisconsin. The status of PQCs in Maine, Rhode Island, Pennsylvania, Missouri, South Dakota, and Wyoming is unknown.1
The CDC can help people establish a collaborative. Visit: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pqc-states.html.
Reference
- Centers for Disease Control and Prevention. Reproductive health: State Perinatal Quality Collaboratives. CDC website. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pqc-states.html Updated October 17, 2017. Accessed April 4, 2018.
The bill
Preventing Maternal Deaths Act/Maternal Health Accountability Act (H.R. 1318/S. 1112) is a bipartisan, bicameral effort to reduce maternal mortality and reduce health care disparities.
The bills authorize the Centers for Disease Control and Prevention (CDC) to help states create or expand state MMRCs through annual grant funding of $7 million through fiscal year 2022. Through the MMRCs, the CDC would have the ability to gather data on maternal mortality and health care disparities, allowing the agency to better understand leading causes of maternal death as well as a state’s successes and pitfalls in interventions.
Currently the House bill (H.R. 1318) has 102 cosponsors (https://cqrcengage.com/acog/app/bill/903056?0) and the Senate bill (S. 1112) has 17 cosponsors (https://cqrcengage.com/acog/app/bill/943204?1). Click these links to see if your representative is a cosponsor.
Not sure who your representative is? Click here to find out: http://cqrcengage.com/acog/app/lookup?1&m=29525.
Take action
Both the Senate and House bills have been referred to health committees. However, no advances have been made since March 2017. In order for the bills to move forward, your representatives need to hear from you.
If your representative is a cosponsor of the bill, thank them for their support, but also ask what we can do to ensure this bill becomes law.
If your representative is not a cosponsor, follow this link to email your representative: http://cqrcengage.com/acog/app/onestep-write-a-letter?0&engagementId=306574. You also can call your representative’s office and speak directly to a staff member.
When calling or emailing, highlight the following:
- I am an ObGyn and I am asking [your Representative/Senator] to support H.R. 1318 or S. 1112.
- While maternal mortality rates are decreasing in other parts of the world, they are increasing in the United States. We have the highest maternal mortality rate in the developing world.
- This bill gives all states the opportunity to have a maternal mortality review committee, allowing health care leaders to review each maternal death and analyze how further deaths can be prevented.
- Congress has invested in programs addressing infant mortality, birth defects, and preterm birth. It is time we put the same investment into saving our nation’s mothers.
- As an ObGyn, I urge you to support this bill.
More from ACOG
Want to know what other advocacy opportunities are available? Check out ACOG action at http://cqrcengage.com/acog/home?3.
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
The facts
While other industrialized nations are seeing a decrease in their maternal mortality rates, the United States has noted a 26% increase over a 15-year period. This is especially true for women of color: black women are nearly 4 times as likely to die from pregnancy related causes as compared to non-Hispanic white women. Postpartum hemorrhage and preeclampsia are often the leading causes of maternal death; however, suicide and overdoses are becoming increasingly more common. This information is highlighted in the March 2018 OBG Management article “Factors critical to reducing US maternal mortality and morbidity,” by Lucia DiVenere, MA, Government and Political Affairs, at the American College of Obstetricians and Gynecologists (ACOG).1
Although there are efforts to improve these outcomes, programs vary by state. One initiative is the perinatal quality collaboratives (PQCs), state or multistate networks of teams working to improve the quality of care for mothers and babies (see “Has your state established a perinatal quality collaborative?”).
Currently, only 33 states have a maternal mortality review committee (MMRC) comprised of an interdisciplinary team of ObGyns, nurses, and other stakeholders. The MMRC reviews each maternal death in their state and provides recommendations and policy changes to help prevent further loss of life.
Many states currently have active collaboratives, and others are in development. The CDC’s Division of Reproductive Health (DRH) currently provides support for state-based PQCs in Colorado, Delaware, Florida, Georgia, Illinois, Louisiana, Massachusetts, Minnesota, Mississippi, New Jersey, New York, Oregon, and Wisconsin. The status of PQCs in Maine, Rhode Island, Pennsylvania, Missouri, South Dakota, and Wyoming is unknown.1
The CDC can help people establish a collaborative. Visit: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pqc-states.html.
Reference
- Centers for Disease Control and Prevention. Reproductive health: State Perinatal Quality Collaboratives. CDC website. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pqc-states.html Updated October 17, 2017. Accessed April 4, 2018.
The bill
Preventing Maternal Deaths Act/Maternal Health Accountability Act (H.R. 1318/S. 1112) is a bipartisan, bicameral effort to reduce maternal mortality and reduce health care disparities.
The bills authorize the Centers for Disease Control and Prevention (CDC) to help states create or expand state MMRCs through annual grant funding of $7 million through fiscal year 2022. Through the MMRCs, the CDC would have the ability to gather data on maternal mortality and health care disparities, allowing the agency to better understand leading causes of maternal death as well as a state’s successes and pitfalls in interventions.
Currently the House bill (H.R. 1318) has 102 cosponsors (https://cqrcengage.com/acog/app/bill/903056?0) and the Senate bill (S. 1112) has 17 cosponsors (https://cqrcengage.com/acog/app/bill/943204?1). Click these links to see if your representative is a cosponsor.
Not sure who your representative is? Click here to find out: http://cqrcengage.com/acog/app/lookup?1&m=29525.
Take action
Both the Senate and House bills have been referred to health committees. However, no advances have been made since March 2017. In order for the bills to move forward, your representatives need to hear from you.
If your representative is a cosponsor of the bill, thank them for their support, but also ask what we can do to ensure this bill becomes law.
If your representative is not a cosponsor, follow this link to email your representative: http://cqrcengage.com/acog/app/onestep-write-a-letter?0&engagementId=306574. You also can call your representative’s office and speak directly to a staff member.
When calling or emailing, highlight the following:
- I am an ObGyn and I am asking [your Representative/Senator] to support H.R. 1318 or S. 1112.
- While maternal mortality rates are decreasing in other parts of the world, they are increasing in the United States. We have the highest maternal mortality rate in the developing world.
- This bill gives all states the opportunity to have a maternal mortality review committee, allowing health care leaders to review each maternal death and analyze how further deaths can be prevented.
- Congress has invested in programs addressing infant mortality, birth defects, and preterm birth. It is time we put the same investment into saving our nation’s mothers.
- As an ObGyn, I urge you to support this bill.
More from ACOG
Want to know what other advocacy opportunities are available? Check out ACOG action at http://cqrcengage.com/acog/home?3.
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
- DiVenere L. Factors critical to reducing US maternal mortality and morbidity. OBG Manag. 2018;30(3):30−33.
- DiVenere L. Factors critical to reducing US maternal mortality and morbidity. OBG Manag. 2018;30(3):30−33.
Dermatology practice gaps: improving medication management
KAUAI, HAWAII – Dermatologists don’t ordinarily peruse the ophthalmology literature. So they may be unaware that the American Academy of Ophthalmology has issued Erik J. Stratman, MD, noted at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
Most dermatologists routinely dose hydroxychloroquine at 400 mg/day, regardless of body weight. The former AAO recommendation, which dates back to 2011, called for dosing at up to 6.5 mg/kg of ideal body weight or 400 mg/day, whichever is lower. However, the AAO recommendation has changed in light of a large, retrospective case-control study that suggested this practice may be overdosing thin patients – thereby exposing them to increased risk of retinal toxicity and other drug-related adverse events – while at the same time possibly underdosing some obese patients, said Dr. Stratman, chairman of the department of dermatology at the Marshfield (Wisc.) Clinic.
This was one of two dermatology practice gaps he highlighted involving suboptimal medication management, the other being most dermatologists’ failure to protect their patients’ gut when prescribing prednisone.
“I think the push over the last 5 years has been ‘protect the bones, protect the bones, protect the bones.’ We’ve done better and better about protecting the bones and getting that into our conversations with patients on prednisone. But we’re not thinking so much about the gut,” the dermatologist said.
Hydroxychloroquine dosing
The former AAO recommendation was revised in response to a retrospective case-control study of retinal toxicity rates in 2,361 patients on the drug continuously for longer than 5 years. The study demonstrated that the risk of retinopathy jumped 5.7-fold with daily consumption of hydroxychloroquine at more than 5.0 mg/kg (JAMA Ophthalmol. 2014 Dec;132[12]:1453-60).
The current AAO recommendation (Ophthalmology. 2016 Jun;123[6]:1386-94) is to dose hydroxychloroquine at a daily maximum of 5.0 mg/kg of real weight, which correlated better with retinopathy risk in the case-control study than did ideal body weight. Hydroxychloroquine doesn’t accumulate well in fat.
Until now, most dermatologists have not routinely measured patients’ body weight in the office or calculated their body mass index. But Dr. Stratman advised against reliance upon a patient’s self-reported body weight, which may diverge substantially from reality. “Get yourself a good office scale – they’re not that expensive – and use it when prescribing drugs with a tight therapeutic window,” he urged.
Another key to minimizing retinopathy risk in patients on hydroxychloroquine is to pay careful attention to how long they’ve been on the drug. As the years go by in patients being treated for cutaneous lupus or other dermatologic disorders where decades-long therapy is often a mainstay, it’s important to check with patients and make sure they’re getting annual ophthalmologic screening for irreversible retinal toxicity by both threshold visual fields and spectral domain optical coherence tomography. In the large, practice-changing retrospective study, patients on hydroxychloroquine at 4.0-5.0 mg/kg daily had a prevalence of retinopathy of less than 2% during the first 10 years of therapy, but the rate shot up to nearly 20% after 20 years of use, Dr. Stratman observed.
He highlighted as helpful an updated review of the use of hydroxychloroquine in dermatology recently published by Anthony P. Fernandez, MD, PhD, of the department of dermatology at the Cleveland Clinic (J Am Acad Dermatol. 2017 Jun;76[6]:1176-82).
Dr. Fernandez recommends following the AAO guidance to dose the drug at 5.0 mg/kg or less of actual body weight in thin or normal-weight patients; however, he departed from the ophthalmologists with regard to treatment of obese patients. Because dosing based on actual weight could potentially lead to relative overdosing in obese patients, in that growing population he recommends calculating the dose based upon 5.0 mg/kg of actual body weight, as well as the dose based on 6.5 mg/kg of ideal body weight, then prescribing the lower of the two, up to a maximum of 400 mg/day.
“The current recommendation is really about not overdosing thin patients. Basically, dosing is not so difficult for obese people because if you weigh more than 175 pounds, you’re going to get 400 mg/day,” Dr. Stratman explained.
That 400 mg/day ceiling is not cast in stone, he continued. The guideline recommends that, if a patient is a nonresponder to several months of hydroxychloroquine at 400 mg/day, it’s worthwhile to order a drug blood level. If it’s not above the efficacy threshold of more than 750 ng/mL, it’s appropriate to titrate up.
Protecting against prednisone-induced gastritis
“We underprotect the gut,” Dr. Stratman asserted.
He referred to a recent comprehensive dermatologic review of the prevention and management of glucocorticoid-related side effects, especially the part on peptic ulcer disease (J Am Acad Dermatol. 2017 Jan;76[1]:11-6). This is an issue that heretofore hadn’t been much emphasized in the dermatology literature.
“I read this and thought, ‘Gosh, I’m not really having a conversation with my patients about a review of systems for gut protection as I should. And I certainly haven’t been thinking about prescribing PPIs [proton pump inhibitors] for my patients,’” he recalled.
Dr. Stratman polled his Hawaii Dermatology Seminar audience as to who had ever prescribed a PPI. Most indicated with their electronic clickers that they had never done so.
“This is what a practice gap is,” he commented. “You read the literature and you say, ‘Oh, I guess that makes sense. Maybe I should be doing that more often, or making sure it gets done.’”
“I don’t want to come across as saying, ‘For everybody we put on prednisone we should be giving vitamin D, calcium, and a PPI.’ That’s not the message. The message is, assess your patient – or make sure your patient is being assessed – for risk of peptic ulcer disease. And if you don’t feel comfortable prescribing a PPI, please get the patient connected with their primary care provider, who should,” Dr. Stratman said.
The authors of the dermatology review made a case for screening for GI risk factors in every patient who is going to receive an oral glucocorticoid. The ones who absolutely should be prescribed a PPI unless contraindicated include patients who are taking daily aspirin or NSAIDs for an essential reason, such as cardiovascular protection or significant arthritic pain. The authors suggest consideration of a PPI in patients with other, less potent risk factors for peptic ulcer disease, including a history of ulcer disease, gastroesophageal reflux disease, Barrett’s esophagus, heavy smoking, heavy alcohol consumption, age greater than 65, and concomitant use of other medications with an associated risk of peptic ulcer disease – such as bisphosphonates, “which you may have just put them on to protect their bones,” Dr. Stratman noted.
Of course, PPIs come with side effects of their own, including increased fracture risk, Clostridium difficile infections, and rebound acid secretion.
Dr. Stratman reported having no financial conflicts regarding his presentation.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – Dermatologists don’t ordinarily peruse the ophthalmology literature. So they may be unaware that the American Academy of Ophthalmology has issued Erik J. Stratman, MD, noted at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
Most dermatologists routinely dose hydroxychloroquine at 400 mg/day, regardless of body weight. The former AAO recommendation, which dates back to 2011, called for dosing at up to 6.5 mg/kg of ideal body weight or 400 mg/day, whichever is lower. However, the AAO recommendation has changed in light of a large, retrospective case-control study that suggested this practice may be overdosing thin patients – thereby exposing them to increased risk of retinal toxicity and other drug-related adverse events – while at the same time possibly underdosing some obese patients, said Dr. Stratman, chairman of the department of dermatology at the Marshfield (Wisc.) Clinic.
This was one of two dermatology practice gaps he highlighted involving suboptimal medication management, the other being most dermatologists’ failure to protect their patients’ gut when prescribing prednisone.
“I think the push over the last 5 years has been ‘protect the bones, protect the bones, protect the bones.’ We’ve done better and better about protecting the bones and getting that into our conversations with patients on prednisone. But we’re not thinking so much about the gut,” the dermatologist said.
Hydroxychloroquine dosing
The former AAO recommendation was revised in response to a retrospective case-control study of retinal toxicity rates in 2,361 patients on the drug continuously for longer than 5 years. The study demonstrated that the risk of retinopathy jumped 5.7-fold with daily consumption of hydroxychloroquine at more than 5.0 mg/kg (JAMA Ophthalmol. 2014 Dec;132[12]:1453-60).
The current AAO recommendation (Ophthalmology. 2016 Jun;123[6]:1386-94) is to dose hydroxychloroquine at a daily maximum of 5.0 mg/kg of real weight, which correlated better with retinopathy risk in the case-control study than did ideal body weight. Hydroxychloroquine doesn’t accumulate well in fat.
Until now, most dermatologists have not routinely measured patients’ body weight in the office or calculated their body mass index. But Dr. Stratman advised against reliance upon a patient’s self-reported body weight, which may diverge substantially from reality. “Get yourself a good office scale – they’re not that expensive – and use it when prescribing drugs with a tight therapeutic window,” he urged.
Another key to minimizing retinopathy risk in patients on hydroxychloroquine is to pay careful attention to how long they’ve been on the drug. As the years go by in patients being treated for cutaneous lupus or other dermatologic disorders where decades-long therapy is often a mainstay, it’s important to check with patients and make sure they’re getting annual ophthalmologic screening for irreversible retinal toxicity by both threshold visual fields and spectral domain optical coherence tomography. In the large, practice-changing retrospective study, patients on hydroxychloroquine at 4.0-5.0 mg/kg daily had a prevalence of retinopathy of less than 2% during the first 10 years of therapy, but the rate shot up to nearly 20% after 20 years of use, Dr. Stratman observed.
He highlighted as helpful an updated review of the use of hydroxychloroquine in dermatology recently published by Anthony P. Fernandez, MD, PhD, of the department of dermatology at the Cleveland Clinic (J Am Acad Dermatol. 2017 Jun;76[6]:1176-82).
Dr. Fernandez recommends following the AAO guidance to dose the drug at 5.0 mg/kg or less of actual body weight in thin or normal-weight patients; however, he departed from the ophthalmologists with regard to treatment of obese patients. Because dosing based on actual weight could potentially lead to relative overdosing in obese patients, in that growing population he recommends calculating the dose based upon 5.0 mg/kg of actual body weight, as well as the dose based on 6.5 mg/kg of ideal body weight, then prescribing the lower of the two, up to a maximum of 400 mg/day.
“The current recommendation is really about not overdosing thin patients. Basically, dosing is not so difficult for obese people because if you weigh more than 175 pounds, you’re going to get 400 mg/day,” Dr. Stratman explained.
That 400 mg/day ceiling is not cast in stone, he continued. The guideline recommends that, if a patient is a nonresponder to several months of hydroxychloroquine at 400 mg/day, it’s worthwhile to order a drug blood level. If it’s not above the efficacy threshold of more than 750 ng/mL, it’s appropriate to titrate up.
Protecting against prednisone-induced gastritis
“We underprotect the gut,” Dr. Stratman asserted.
He referred to a recent comprehensive dermatologic review of the prevention and management of glucocorticoid-related side effects, especially the part on peptic ulcer disease (J Am Acad Dermatol. 2017 Jan;76[1]:11-6). This is an issue that heretofore hadn’t been much emphasized in the dermatology literature.
“I read this and thought, ‘Gosh, I’m not really having a conversation with my patients about a review of systems for gut protection as I should. And I certainly haven’t been thinking about prescribing PPIs [proton pump inhibitors] for my patients,’” he recalled.
Dr. Stratman polled his Hawaii Dermatology Seminar audience as to who had ever prescribed a PPI. Most indicated with their electronic clickers that they had never done so.
“This is what a practice gap is,” he commented. “You read the literature and you say, ‘Oh, I guess that makes sense. Maybe I should be doing that more often, or making sure it gets done.’”
“I don’t want to come across as saying, ‘For everybody we put on prednisone we should be giving vitamin D, calcium, and a PPI.’ That’s not the message. The message is, assess your patient – or make sure your patient is being assessed – for risk of peptic ulcer disease. And if you don’t feel comfortable prescribing a PPI, please get the patient connected with their primary care provider, who should,” Dr. Stratman said.
The authors of the dermatology review made a case for screening for GI risk factors in every patient who is going to receive an oral glucocorticoid. The ones who absolutely should be prescribed a PPI unless contraindicated include patients who are taking daily aspirin or NSAIDs for an essential reason, such as cardiovascular protection or significant arthritic pain. The authors suggest consideration of a PPI in patients with other, less potent risk factors for peptic ulcer disease, including a history of ulcer disease, gastroesophageal reflux disease, Barrett’s esophagus, heavy smoking, heavy alcohol consumption, age greater than 65, and concomitant use of other medications with an associated risk of peptic ulcer disease – such as bisphosphonates, “which you may have just put them on to protect their bones,” Dr. Stratman noted.
Of course, PPIs come with side effects of their own, including increased fracture risk, Clostridium difficile infections, and rebound acid secretion.
Dr. Stratman reported having no financial conflicts regarding his presentation.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – Dermatologists don’t ordinarily peruse the ophthalmology literature. So they may be unaware that the American Academy of Ophthalmology has issued Erik J. Stratman, MD, noted at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
Most dermatologists routinely dose hydroxychloroquine at 400 mg/day, regardless of body weight. The former AAO recommendation, which dates back to 2011, called for dosing at up to 6.5 mg/kg of ideal body weight or 400 mg/day, whichever is lower. However, the AAO recommendation has changed in light of a large, retrospective case-control study that suggested this practice may be overdosing thin patients – thereby exposing them to increased risk of retinal toxicity and other drug-related adverse events – while at the same time possibly underdosing some obese patients, said Dr. Stratman, chairman of the department of dermatology at the Marshfield (Wisc.) Clinic.
This was one of two dermatology practice gaps he highlighted involving suboptimal medication management, the other being most dermatologists’ failure to protect their patients’ gut when prescribing prednisone.
“I think the push over the last 5 years has been ‘protect the bones, protect the bones, protect the bones.’ We’ve done better and better about protecting the bones and getting that into our conversations with patients on prednisone. But we’re not thinking so much about the gut,” the dermatologist said.
Hydroxychloroquine dosing
The former AAO recommendation was revised in response to a retrospective case-control study of retinal toxicity rates in 2,361 patients on the drug continuously for longer than 5 years. The study demonstrated that the risk of retinopathy jumped 5.7-fold with daily consumption of hydroxychloroquine at more than 5.0 mg/kg (JAMA Ophthalmol. 2014 Dec;132[12]:1453-60).
The current AAO recommendation (Ophthalmology. 2016 Jun;123[6]:1386-94) is to dose hydroxychloroquine at a daily maximum of 5.0 mg/kg of real weight, which correlated better with retinopathy risk in the case-control study than did ideal body weight. Hydroxychloroquine doesn’t accumulate well in fat.
Until now, most dermatologists have not routinely measured patients’ body weight in the office or calculated their body mass index. But Dr. Stratman advised against reliance upon a patient’s self-reported body weight, which may diverge substantially from reality. “Get yourself a good office scale – they’re not that expensive – and use it when prescribing drugs with a tight therapeutic window,” he urged.
Another key to minimizing retinopathy risk in patients on hydroxychloroquine is to pay careful attention to how long they’ve been on the drug. As the years go by in patients being treated for cutaneous lupus or other dermatologic disorders where decades-long therapy is often a mainstay, it’s important to check with patients and make sure they’re getting annual ophthalmologic screening for irreversible retinal toxicity by both threshold visual fields and spectral domain optical coherence tomography. In the large, practice-changing retrospective study, patients on hydroxychloroquine at 4.0-5.0 mg/kg daily had a prevalence of retinopathy of less than 2% during the first 10 years of therapy, but the rate shot up to nearly 20% after 20 years of use, Dr. Stratman observed.
He highlighted as helpful an updated review of the use of hydroxychloroquine in dermatology recently published by Anthony P. Fernandez, MD, PhD, of the department of dermatology at the Cleveland Clinic (J Am Acad Dermatol. 2017 Jun;76[6]:1176-82).
Dr. Fernandez recommends following the AAO guidance to dose the drug at 5.0 mg/kg or less of actual body weight in thin or normal-weight patients; however, he departed from the ophthalmologists with regard to treatment of obese patients. Because dosing based on actual weight could potentially lead to relative overdosing in obese patients, in that growing population he recommends calculating the dose based upon 5.0 mg/kg of actual body weight, as well as the dose based on 6.5 mg/kg of ideal body weight, then prescribing the lower of the two, up to a maximum of 400 mg/day.
“The current recommendation is really about not overdosing thin patients. Basically, dosing is not so difficult for obese people because if you weigh more than 175 pounds, you’re going to get 400 mg/day,” Dr. Stratman explained.
That 400 mg/day ceiling is not cast in stone, he continued. The guideline recommends that, if a patient is a nonresponder to several months of hydroxychloroquine at 400 mg/day, it’s worthwhile to order a drug blood level. If it’s not above the efficacy threshold of more than 750 ng/mL, it’s appropriate to titrate up.
Protecting against prednisone-induced gastritis
“We underprotect the gut,” Dr. Stratman asserted.
He referred to a recent comprehensive dermatologic review of the prevention and management of glucocorticoid-related side effects, especially the part on peptic ulcer disease (J Am Acad Dermatol. 2017 Jan;76[1]:11-6). This is an issue that heretofore hadn’t been much emphasized in the dermatology literature.
“I read this and thought, ‘Gosh, I’m not really having a conversation with my patients about a review of systems for gut protection as I should. And I certainly haven’t been thinking about prescribing PPIs [proton pump inhibitors] for my patients,’” he recalled.
Dr. Stratman polled his Hawaii Dermatology Seminar audience as to who had ever prescribed a PPI. Most indicated with their electronic clickers that they had never done so.
“This is what a practice gap is,” he commented. “You read the literature and you say, ‘Oh, I guess that makes sense. Maybe I should be doing that more often, or making sure it gets done.’”
“I don’t want to come across as saying, ‘For everybody we put on prednisone we should be giving vitamin D, calcium, and a PPI.’ That’s not the message. The message is, assess your patient – or make sure your patient is being assessed – for risk of peptic ulcer disease. And if you don’t feel comfortable prescribing a PPI, please get the patient connected with their primary care provider, who should,” Dr. Stratman said.
The authors of the dermatology review made a case for screening for GI risk factors in every patient who is going to receive an oral glucocorticoid. The ones who absolutely should be prescribed a PPI unless contraindicated include patients who are taking daily aspirin or NSAIDs for an essential reason, such as cardiovascular protection or significant arthritic pain. The authors suggest consideration of a PPI in patients with other, less potent risk factors for peptic ulcer disease, including a history of ulcer disease, gastroesophageal reflux disease, Barrett’s esophagus, heavy smoking, heavy alcohol consumption, age greater than 65, and concomitant use of other medications with an associated risk of peptic ulcer disease – such as bisphosphonates, “which you may have just put them on to protect their bones,” Dr. Stratman noted.
Of course, PPIs come with side effects of their own, including increased fracture risk, Clostridium difficile infections, and rebound acid secretion.
Dr. Stratman reported having no financial conflicts regarding his presentation.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR
Neurology faculty gender gap confirmed, but explanations remain scant
Despite a wide gap between male and female neurologists, both in terms of academic faculty rank and number of publications, there may be some good news for women in this medical field.
A recent study of the 1,712 academic neurologists across 29 top-ranked neurology programs revealed that 1,184 (69%) were men and 528 (31%) were women, and men outnumbered women in all academic faculty ranks with a gap that increased as the rank advanced. For example, at the rank of instructor/lecturer, the male-to-female ratio was 59% to 41%. The gap only widens from there: assistant professor (57% male), associate professor (70%), and professor (86%).
Additionally, unadjusted analyses showed that men had significantly more publications listed in PubMed than women at the positions of assistant professor, associate professor, and full professor.
The investigators compiled their list of programs and faculty members by combining the top 20 programs listed on either the 2016 or 2017 Doximity Residency Navigator tool with the top 20 programs listed in the U.S. News and World Report ranking of Best Graduate Schools and a search of the programs’ departmental websites between December 1, 2015, and April 30, 2016.
The study was not able to account for many potential explanations for the gender gap, suggesting that the findings may not necessarily be indicative of bad news.
The results “can be viewed as either disappointing or encouraging, depending on whether they reflect persistent barriers to women trying to achieve similar goals as men, or whether they reflect a system that supports women with different goals altogether,” Dr. McDermott and her colleagues wrote.
For example, the authors note that there are a variety of explanations for the gender gap in both rank and publication, including asymmetric home or childcare responsibilities, cultural stereotypes, professional isolation, and different career motivations, though the study was not able to account for those variables.
“Compared with men, women may be more likely to be recruited for employment positions that emphasize teaching and mentoring rather than research, or women may be more inclined to choose such positions,” the authors noted, adding that academic institutions are moving beyond traditional measures of academic productivity (publication rate, publication impact, and grant support) to recognize other factors, such as the quality and quantity of teaching, the development of educational resources, and administrative effectiveness.
If the numbers reflect persistent barriers to women, “it will be important to develop programs to heighten awareness of diversity in academic neurology,” the authors stated. On the flip side, if the numbers reflect a system that is supporting different goals, “academic neurology departments should be encouraged to foster a variety of career paths and expectations for all faculty.”
The authors reported no conflicts of interest. The study was funded by the Jerry Isler Neuromuscular Fund.
SOURCE: McDermott M et al. JAMA Neurol. 2018 Apr 2. doi: 10.1001/jamaneurol.2018.0275.
While there may be positive ways to interpret the data, challenges remain for women who want to pursue a career path that features more traditional ways of being recognized. These include ensuring that career paths that require protected time for research and depend on publication and grant support are carefully monitored; and determining that barriers do not hinder women from advancing.
Training programs also must be revisited to ensure that parity across the wider spectrum of careers in neurology is maintained and opportunities continue to exist for both men and women as the specialty continues to grow.
Frances Jensen, MD , is with the University of Pennsylvania, Philadelphia. Her remarks are derived from an editorial accompanying the report by Dr. McDermott and colleagues (JAMA Neurol. 2018 Apr 2. doi: 10.1001/jamaneurol.2018.0300). She reported no disclosures.
While there may be positive ways to interpret the data, challenges remain for women who want to pursue a career path that features more traditional ways of being recognized. These include ensuring that career paths that require protected time for research and depend on publication and grant support are carefully monitored; and determining that barriers do not hinder women from advancing.
Training programs also must be revisited to ensure that parity across the wider spectrum of careers in neurology is maintained and opportunities continue to exist for both men and women as the specialty continues to grow.
Frances Jensen, MD , is with the University of Pennsylvania, Philadelphia. Her remarks are derived from an editorial accompanying the report by Dr. McDermott and colleagues (JAMA Neurol. 2018 Apr 2. doi: 10.1001/jamaneurol.2018.0300). She reported no disclosures.
While there may be positive ways to interpret the data, challenges remain for women who want to pursue a career path that features more traditional ways of being recognized. These include ensuring that career paths that require protected time for research and depend on publication and grant support are carefully monitored; and determining that barriers do not hinder women from advancing.
Training programs also must be revisited to ensure that parity across the wider spectrum of careers in neurology is maintained and opportunities continue to exist for both men and women as the specialty continues to grow.
Frances Jensen, MD , is with the University of Pennsylvania, Philadelphia. Her remarks are derived from an editorial accompanying the report by Dr. McDermott and colleagues (JAMA Neurol. 2018 Apr 2. doi: 10.1001/jamaneurol.2018.0300). She reported no disclosures.
Despite a wide gap between male and female neurologists, both in terms of academic faculty rank and number of publications, there may be some good news for women in this medical field.
A recent study of the 1,712 academic neurologists across 29 top-ranked neurology programs revealed that 1,184 (69%) were men and 528 (31%) were women, and men outnumbered women in all academic faculty ranks with a gap that increased as the rank advanced. For example, at the rank of instructor/lecturer, the male-to-female ratio was 59% to 41%. The gap only widens from there: assistant professor (57% male), associate professor (70%), and professor (86%).
Additionally, unadjusted analyses showed that men had significantly more publications listed in PubMed than women at the positions of assistant professor, associate professor, and full professor.
The investigators compiled their list of programs and faculty members by combining the top 20 programs listed on either the 2016 or 2017 Doximity Residency Navigator tool with the top 20 programs listed in the U.S. News and World Report ranking of Best Graduate Schools and a search of the programs’ departmental websites between December 1, 2015, and April 30, 2016.
The study was not able to account for many potential explanations for the gender gap, suggesting that the findings may not necessarily be indicative of bad news.
The results “can be viewed as either disappointing or encouraging, depending on whether they reflect persistent barriers to women trying to achieve similar goals as men, or whether they reflect a system that supports women with different goals altogether,” Dr. McDermott and her colleagues wrote.
For example, the authors note that there are a variety of explanations for the gender gap in both rank and publication, including asymmetric home or childcare responsibilities, cultural stereotypes, professional isolation, and different career motivations, though the study was not able to account for those variables.
“Compared with men, women may be more likely to be recruited for employment positions that emphasize teaching and mentoring rather than research, or women may be more inclined to choose such positions,” the authors noted, adding that academic institutions are moving beyond traditional measures of academic productivity (publication rate, publication impact, and grant support) to recognize other factors, such as the quality and quantity of teaching, the development of educational resources, and administrative effectiveness.
If the numbers reflect persistent barriers to women, “it will be important to develop programs to heighten awareness of diversity in academic neurology,” the authors stated. On the flip side, if the numbers reflect a system that is supporting different goals, “academic neurology departments should be encouraged to foster a variety of career paths and expectations for all faculty.”
The authors reported no conflicts of interest. The study was funded by the Jerry Isler Neuromuscular Fund.
SOURCE: McDermott M et al. JAMA Neurol. 2018 Apr 2. doi: 10.1001/jamaneurol.2018.0275.
Despite a wide gap between male and female neurologists, both in terms of academic faculty rank and number of publications, there may be some good news for women in this medical field.
A recent study of the 1,712 academic neurologists across 29 top-ranked neurology programs revealed that 1,184 (69%) were men and 528 (31%) were women, and men outnumbered women in all academic faculty ranks with a gap that increased as the rank advanced. For example, at the rank of instructor/lecturer, the male-to-female ratio was 59% to 41%. The gap only widens from there: assistant professor (57% male), associate professor (70%), and professor (86%).
Additionally, unadjusted analyses showed that men had significantly more publications listed in PubMed than women at the positions of assistant professor, associate professor, and full professor.
The investigators compiled their list of programs and faculty members by combining the top 20 programs listed on either the 2016 or 2017 Doximity Residency Navigator tool with the top 20 programs listed in the U.S. News and World Report ranking of Best Graduate Schools and a search of the programs’ departmental websites between December 1, 2015, and April 30, 2016.
The study was not able to account for many potential explanations for the gender gap, suggesting that the findings may not necessarily be indicative of bad news.
The results “can be viewed as either disappointing or encouraging, depending on whether they reflect persistent barriers to women trying to achieve similar goals as men, or whether they reflect a system that supports women with different goals altogether,” Dr. McDermott and her colleagues wrote.
For example, the authors note that there are a variety of explanations for the gender gap in both rank and publication, including asymmetric home or childcare responsibilities, cultural stereotypes, professional isolation, and different career motivations, though the study was not able to account for those variables.
“Compared with men, women may be more likely to be recruited for employment positions that emphasize teaching and mentoring rather than research, or women may be more inclined to choose such positions,” the authors noted, adding that academic institutions are moving beyond traditional measures of academic productivity (publication rate, publication impact, and grant support) to recognize other factors, such as the quality and quantity of teaching, the development of educational resources, and administrative effectiveness.
If the numbers reflect persistent barriers to women, “it will be important to develop programs to heighten awareness of diversity in academic neurology,” the authors stated. On the flip side, if the numbers reflect a system that is supporting different goals, “academic neurology departments should be encouraged to foster a variety of career paths and expectations for all faculty.”
The authors reported no conflicts of interest. The study was funded by the Jerry Isler Neuromuscular Fund.
SOURCE: McDermott M et al. JAMA Neurol. 2018 Apr 2. doi: 10.1001/jamaneurol.2018.0275.
FROM JAMA NEUROLOGY
Major finding: Male-to-female ratio widens as rank advances, from 59% male at instructor/lecturer to 86% male at full professor.
Study details: An examination of 1,712 academic neurologists across 29 top-ranked academic institutions.
Disclosures: The study authors reported no conflicts of interest. The study was funded by the Jerry Isler Neuromuscular Fund.
Source: McDermott M et al. JAMA Neurol. 2018 Apr 2. doi: 10.1001/jamaneurol.2018.0275.
Career Choices: Community mental health in an urban/public setting
Editor’s note : Career Choices features a psychiatry resident/fellow interviewing a psychiatrist about why he or she has chosen a specific career path. The goal is to inform trainees about the various psychiatric career options, and to give them a feel for the pros and cons of the various paths.
In this Career Choices, Cornel Stanciu, MD, talked with Mufida Wadhwania, MD. Dr. Wadhwania is an adult psychiatrist practicing in an urban/public setting in metro Atlanta, Georgia, at DeKalb Community Service Board. She manages a variety of uninsured and underinsured patients in an outpatient setting.
Dr. Stanciu: What attracted you to practice community mental health in an urban-public setting?
Dr. Wadhwania: A high portion of the population here has no health insurance, and hence there is a great need in the community. The psychopathology severity is high, so one can see a wide range of disorders. One can also build on the skill to pull together resources, such as linking patients to community resources and patient assistance programs, finding food banks, and finding ways to secure stable housing. There is continuity of care, and when a staff member leaves the agency, patients are linked to the next provider in an adequate time frame so that the patient’s quality of care is not compromised. The new provider is also given notification so that he or she is aware of the transfer of the patient and is able to review the chart in advance.
Along with medication management, we also provide psychotherapy. We utilize a single electronic health record (EHR) throughout the agency and we are able to contribute to changes in the EHR to make it more user-friendly. We have monthly journal club meetings and meetings with other staff members to review and discuss the progress of our organization. There are also numerous online resources through which we can keep ourselves updated with current research and earn CME. Some of the providers at our agency have academic affiliations, and hence there are opportunities to teach medical students and residents who rotate at some of our sites.
Dr. Stanciu: What are some of the more prevalent disorders you encounter?
Dr. Wadhwania: We see a wide range of disorders, such as affective disorders, schizophrenia, and comorbid disorders, specifically comorbid substance use disorders. So we encounter a high number of chronic mental illnesses.
Continue to: What are some challenges in working with this population?
Dr. Stanciu: What are some challenges in working with this population?
Dr. Wadhwania: Based on the high volume of patients we encounter, the resources available in the community are limited. But this challenges us to be creative and maximize what we have available to create new resources, such as having on-site case managers rather than just in the community, and building psychosocial rehabilitation programs near our various clinics for the patients to bring them the best care possible. Other challenges include a lack of education on and awareness of mental illness; there is still a lot of stigma surrounding mental illness in the community.
Dr. Stanciu: How would you describe your experience working in this setting?
Dr. Wadhwania: It’s a very rewarding experience, as you get to be creative, and patients appreciate your efforts. We use a patient-centered approach, and we work as a team. Each team member brings in a unique set of skills, and we bounce ideas off each other. There is a sense of satisfaction when you help people who don’t have easy access to health care. Finally, in a setting like this, young psychiatrists are able to gain more opportunities earlier than they would while working in other settings.
Continue to: How did you career path prepare you to work in such a challenging setting?
Dr. Stanciu: How did your career path prepare you to work in such a challenging setting?
Dr. Wadhwania: While at East Carolina University
Dr. Stanciu: How would you describe a psychiatric physician who is well-suited for such a setting?
Dr. Wadhwania: A perfect fit would be someone who is able to harness and build resources for the patients in the community and in the practice and wants to continue to build that skill. This individual is someone who is a team player, is flexible, and has a high professional frustration tolerance. The physician’s main aim would be to serve, and his or her mission would not be monetarily driven.
Continue to: What is the typical reimbursement model for your practice, and do you run into difficulties with health insurance providers in this setting?
Dr. Stanciu: What is the typical reimbursement model for your practice, and do you run into difficulties with health insurance providers in this setting?
Dr. Wadhwania: Approximately 40% of the patients we treat have no health insurance, and approximately 60% have Medicaid or managed Medicaid or Medicare. There is no burden of health insurance. Full-time employees are salaried, and part-time employees are compensated on an hourly model. There is also an incentive bonus system based on quality and productivity.
Dr. Stanciu: What model does your clinic use to overcome the shortage of services?
Dr. Wadhwania: There are approximately 37 medical staff members in the agency, most of whom are MDs, but this group also includes nurse practitioners and clinical nurse specialists, so there is no shortage within our agency. We do contract for telepsychiatry services, but because our agency’s clinics are located throughout the county, most of our patients have easy access to any one of our clinics. We have a number of social workers, therapists, nurses, case managers, and pharmacists. We have a crisis center where unstable patients who require admission to an inpatient unit can be admitted; we also are able to refer patients directly to other inpatient psychiatric units. Our agency also has an addiction clinic and a residential substance abuse program catering specifically to patients with substance use disorders. We have educational, therapeutic, and behavioral support services, including residential services, for patients who have developmental disabilities. Our agency also has residential services for patients who are homeless or have a lower income and would benefit from support in a residential setting.
Our therapists are able to refer patients to state-contracted Assertive Community Treatment teams that serve our county. We are also able to set up intensive case management for patients in the community, as well as other community support services, peer support programs, and psychosocial rehabilitation programs.
Continue to: What advice do you have for early career psychiatrists and trainees who are contemplating working in an urban-public setting?
Dr. Stanciu: What advice do you have for early career psychiatrists and trainees who are contemplating working in an urban-public setting?
Dr. Wadhwania: First of all, realize that there are many misconceptions about serving in the public sector, such as there is no access to new medications, etc. It is important to establish whether public sector service is “in your heart.” You need to learn the organization’s philosophy, mission, and vision, and figure out whether these views align with yours. Getting to know the leadership and how they value psychiatrists and other staff members is also very important. Also, make sure that there are opportunities for you to become a leader in the organization, that there is room for growth, and that it’s a stable organization.
Editor’s note : Career Choices features a psychiatry resident/fellow interviewing a psychiatrist about why he or she has chosen a specific career path. The goal is to inform trainees about the various psychiatric career options, and to give them a feel for the pros and cons of the various paths.
In this Career Choices, Cornel Stanciu, MD, talked with Mufida Wadhwania, MD. Dr. Wadhwania is an adult psychiatrist practicing in an urban/public setting in metro Atlanta, Georgia, at DeKalb Community Service Board. She manages a variety of uninsured and underinsured patients in an outpatient setting.
Dr. Stanciu: What attracted you to practice community mental health in an urban-public setting?
Dr. Wadhwania: A high portion of the population here has no health insurance, and hence there is a great need in the community. The psychopathology severity is high, so one can see a wide range of disorders. One can also build on the skill to pull together resources, such as linking patients to community resources and patient assistance programs, finding food banks, and finding ways to secure stable housing. There is continuity of care, and when a staff member leaves the agency, patients are linked to the next provider in an adequate time frame so that the patient’s quality of care is not compromised. The new provider is also given notification so that he or she is aware of the transfer of the patient and is able to review the chart in advance.
Along with medication management, we also provide psychotherapy. We utilize a single electronic health record (EHR) throughout the agency and we are able to contribute to changes in the EHR to make it more user-friendly. We have monthly journal club meetings and meetings with other staff members to review and discuss the progress of our organization. There are also numerous online resources through which we can keep ourselves updated with current research and earn CME. Some of the providers at our agency have academic affiliations, and hence there are opportunities to teach medical students and residents who rotate at some of our sites.
Dr. Stanciu: What are some of the more prevalent disorders you encounter?
Dr. Wadhwania: We see a wide range of disorders, such as affective disorders, schizophrenia, and comorbid disorders, specifically comorbid substance use disorders. So we encounter a high number of chronic mental illnesses.
Continue to: What are some challenges in working with this population?
Dr. Stanciu: What are some challenges in working with this population?
Dr. Wadhwania: Based on the high volume of patients we encounter, the resources available in the community are limited. But this challenges us to be creative and maximize what we have available to create new resources, such as having on-site case managers rather than just in the community, and building psychosocial rehabilitation programs near our various clinics for the patients to bring them the best care possible. Other challenges include a lack of education on and awareness of mental illness; there is still a lot of stigma surrounding mental illness in the community.
Dr. Stanciu: How would you describe your experience working in this setting?
Dr. Wadhwania: It’s a very rewarding experience, as you get to be creative, and patients appreciate your efforts. We use a patient-centered approach, and we work as a team. Each team member brings in a unique set of skills, and we bounce ideas off each other. There is a sense of satisfaction when you help people who don’t have easy access to health care. Finally, in a setting like this, young psychiatrists are able to gain more opportunities earlier than they would while working in other settings.
Continue to: How did you career path prepare you to work in such a challenging setting?
Dr. Stanciu: How did your career path prepare you to work in such a challenging setting?
Dr. Wadhwania: While at East Carolina University
Dr. Stanciu: How would you describe a psychiatric physician who is well-suited for such a setting?
Dr. Wadhwania: A perfect fit would be someone who is able to harness and build resources for the patients in the community and in the practice and wants to continue to build that skill. This individual is someone who is a team player, is flexible, and has a high professional frustration tolerance. The physician’s main aim would be to serve, and his or her mission would not be monetarily driven.
Continue to: What is the typical reimbursement model for your practice, and do you run into difficulties with health insurance providers in this setting?
Dr. Stanciu: What is the typical reimbursement model for your practice, and do you run into difficulties with health insurance providers in this setting?
Dr. Wadhwania: Approximately 40% of the patients we treat have no health insurance, and approximately 60% have Medicaid or managed Medicaid or Medicare. There is no burden of health insurance. Full-time employees are salaried, and part-time employees are compensated on an hourly model. There is also an incentive bonus system based on quality and productivity.
Dr. Stanciu: What model does your clinic use to overcome the shortage of services?
Dr. Wadhwania: There are approximately 37 medical staff members in the agency, most of whom are MDs, but this group also includes nurse practitioners and clinical nurse specialists, so there is no shortage within our agency. We do contract for telepsychiatry services, but because our agency’s clinics are located throughout the county, most of our patients have easy access to any one of our clinics. We have a number of social workers, therapists, nurses, case managers, and pharmacists. We have a crisis center where unstable patients who require admission to an inpatient unit can be admitted; we also are able to refer patients directly to other inpatient psychiatric units. Our agency also has an addiction clinic and a residential substance abuse program catering specifically to patients with substance use disorders. We have educational, therapeutic, and behavioral support services, including residential services, for patients who have developmental disabilities. Our agency also has residential services for patients who are homeless or have a lower income and would benefit from support in a residential setting.
Our therapists are able to refer patients to state-contracted Assertive Community Treatment teams that serve our county. We are also able to set up intensive case management for patients in the community, as well as other community support services, peer support programs, and psychosocial rehabilitation programs.
Continue to: What advice do you have for early career psychiatrists and trainees who are contemplating working in an urban-public setting?
Dr. Stanciu: What advice do you have for early career psychiatrists and trainees who are contemplating working in an urban-public setting?
Dr. Wadhwania: First of all, realize that there are many misconceptions about serving in the public sector, such as there is no access to new medications, etc. It is important to establish whether public sector service is “in your heart.” You need to learn the organization’s philosophy, mission, and vision, and figure out whether these views align with yours. Getting to know the leadership and how they value psychiatrists and other staff members is also very important. Also, make sure that there are opportunities for you to become a leader in the organization, that there is room for growth, and that it’s a stable organization.
Editor’s note : Career Choices features a psychiatry resident/fellow interviewing a psychiatrist about why he or she has chosen a specific career path. The goal is to inform trainees about the various psychiatric career options, and to give them a feel for the pros and cons of the various paths.
In this Career Choices, Cornel Stanciu, MD, talked with Mufida Wadhwania, MD. Dr. Wadhwania is an adult psychiatrist practicing in an urban/public setting in metro Atlanta, Georgia, at DeKalb Community Service Board. She manages a variety of uninsured and underinsured patients in an outpatient setting.
Dr. Stanciu: What attracted you to practice community mental health in an urban-public setting?
Dr. Wadhwania: A high portion of the population here has no health insurance, and hence there is a great need in the community. The psychopathology severity is high, so one can see a wide range of disorders. One can also build on the skill to pull together resources, such as linking patients to community resources and patient assistance programs, finding food banks, and finding ways to secure stable housing. There is continuity of care, and when a staff member leaves the agency, patients are linked to the next provider in an adequate time frame so that the patient’s quality of care is not compromised. The new provider is also given notification so that he or she is aware of the transfer of the patient and is able to review the chart in advance.
Along with medication management, we also provide psychotherapy. We utilize a single electronic health record (EHR) throughout the agency and we are able to contribute to changes in the EHR to make it more user-friendly. We have monthly journal club meetings and meetings with other staff members to review and discuss the progress of our organization. There are also numerous online resources through which we can keep ourselves updated with current research and earn CME. Some of the providers at our agency have academic affiliations, and hence there are opportunities to teach medical students and residents who rotate at some of our sites.
Dr. Stanciu: What are some of the more prevalent disorders you encounter?
Dr. Wadhwania: We see a wide range of disorders, such as affective disorders, schizophrenia, and comorbid disorders, specifically comorbid substance use disorders. So we encounter a high number of chronic mental illnesses.
Continue to: What are some challenges in working with this population?
Dr. Stanciu: What are some challenges in working with this population?
Dr. Wadhwania: Based on the high volume of patients we encounter, the resources available in the community are limited. But this challenges us to be creative and maximize what we have available to create new resources, such as having on-site case managers rather than just in the community, and building psychosocial rehabilitation programs near our various clinics for the patients to bring them the best care possible. Other challenges include a lack of education on and awareness of mental illness; there is still a lot of stigma surrounding mental illness in the community.
Dr. Stanciu: How would you describe your experience working in this setting?
Dr. Wadhwania: It’s a very rewarding experience, as you get to be creative, and patients appreciate your efforts. We use a patient-centered approach, and we work as a team. Each team member brings in a unique set of skills, and we bounce ideas off each other. There is a sense of satisfaction when you help people who don’t have easy access to health care. Finally, in a setting like this, young psychiatrists are able to gain more opportunities earlier than they would while working in other settings.
Continue to: How did you career path prepare you to work in such a challenging setting?
Dr. Stanciu: How did your career path prepare you to work in such a challenging setting?
Dr. Wadhwania: While at East Carolina University
Dr. Stanciu: How would you describe a psychiatric physician who is well-suited for such a setting?
Dr. Wadhwania: A perfect fit would be someone who is able to harness and build resources for the patients in the community and in the practice and wants to continue to build that skill. This individual is someone who is a team player, is flexible, and has a high professional frustration tolerance. The physician’s main aim would be to serve, and his or her mission would not be monetarily driven.
Continue to: What is the typical reimbursement model for your practice, and do you run into difficulties with health insurance providers in this setting?
Dr. Stanciu: What is the typical reimbursement model for your practice, and do you run into difficulties with health insurance providers in this setting?
Dr. Wadhwania: Approximately 40% of the patients we treat have no health insurance, and approximately 60% have Medicaid or managed Medicaid or Medicare. There is no burden of health insurance. Full-time employees are salaried, and part-time employees are compensated on an hourly model. There is also an incentive bonus system based on quality and productivity.
Dr. Stanciu: What model does your clinic use to overcome the shortage of services?
Dr. Wadhwania: There are approximately 37 medical staff members in the agency, most of whom are MDs, but this group also includes nurse practitioners and clinical nurse specialists, so there is no shortage within our agency. We do contract for telepsychiatry services, but because our agency’s clinics are located throughout the county, most of our patients have easy access to any one of our clinics. We have a number of social workers, therapists, nurses, case managers, and pharmacists. We have a crisis center where unstable patients who require admission to an inpatient unit can be admitted; we also are able to refer patients directly to other inpatient psychiatric units. Our agency also has an addiction clinic and a residential substance abuse program catering specifically to patients with substance use disorders. We have educational, therapeutic, and behavioral support services, including residential services, for patients who have developmental disabilities. Our agency also has residential services for patients who are homeless or have a lower income and would benefit from support in a residential setting.
Our therapists are able to refer patients to state-contracted Assertive Community Treatment teams that serve our county. We are also able to set up intensive case management for patients in the community, as well as other community support services, peer support programs, and psychosocial rehabilitation programs.
Continue to: What advice do you have for early career psychiatrists and trainees who are contemplating working in an urban-public setting?
Dr. Stanciu: What advice do you have for early career psychiatrists and trainees who are contemplating working in an urban-public setting?
Dr. Wadhwania: First of all, realize that there are many misconceptions about serving in the public sector, such as there is no access to new medications, etc. It is important to establish whether public sector service is “in your heart.” You need to learn the organization’s philosophy, mission, and vision, and figure out whether these views align with yours. Getting to know the leadership and how they value psychiatrists and other staff members is also very important. Also, make sure that there are opportunities for you to become a leader in the organization, that there is room for growth, and that it’s a stable organization.

A Mission for Graduate Medical Education at VA
More than 65% of all physicians who train in the U.S. rotate through a VA hospital at some point during their training. In 2015 alone, more than 43,000 residents received some or all of their clinical training through VA.1 Of the approximately 120 VAMCs that hold academic affiliations
with medical schools and residency training programs, several hold affiliations with multiple institutions, including VA Boston Healthcare System (VABHS) in Massachusetts. The West Roxbury campus is the home of VA Boston’s acute care hospital, where residents and fellows from Boston Medical Center (BMC), Beth Israel Deaconess Medical Center (BIDMC), and Brigham and Women’s Hospital (BWH) train together. These are 3 of the largest medical training programs in Boston, though each provides a unique training experience for residents due to differences in patient population, faculty expertise, and hospital network affiliations (Table 1). 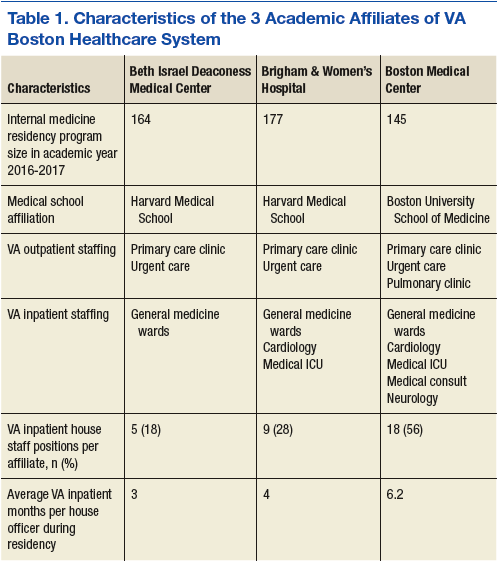
This diversity brings differences in cultural norms, institutional preferences, and educational expectations. Furthermore, residents from different programs who work together at VA Boston are often meeting one another for the first time, as opportunities for interinstitutional collaboration among these 3 training programs do not exist outside of VA. This training environment presents both an opportunity
and a challenge for medical educators: offering the best possible learning experience for physiciansin-training from multiple programs while providing the best possible care for U.S. veterans.
To guide educators charged with meeting this challenge, the VA Office of Academic Affiliations put forth a mission statement describing its overarching teaching mission (Table 2).2 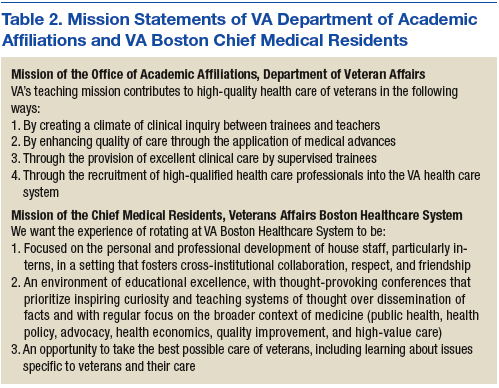
To address this gap, chief medical residents from the 3 affiliate residency training programs came together to develop a shared mission statement for what we envision as the educational experience for all medical trainees rotating through VABHS (Table 2). In this article, we describe the development of a mission statement for graduate medical education in internal medicine at VABHS and provides examples of how our mission statement guided educational programming.
Methods
Whereas the affiliated institutions assign generic competency-based learning objectives to rotations at VABHS, no specific overarching educational objectives for residents have been defined previously. The directors of the internal medicine residency programs at each of the VABHS affiliate institutions grant their respective VA-based chief medical residents the autonomy to deliver graduate medical education at VA as they see fit, in collaboration with their colleagues from the other affiliated institutions and the VA director of medical resident education. This autonomy and flexibility allowed each of the chief medical residents to articulate an individual vision for VA graduate medical education based on their affiliate program’s goals, values, and mission.
At the beginning of the 2016/2017 academic year, in partnership with the director of medical resident education at VABHS, the chief medical residents met to reconcile these into a single shared mission statement. Special attention was paid to educational gaps at each affiliate institution that could be filled while residents were rotating at VABHS. Once all educational goals and priorities of the shared mission statement were identified, the chief medical residents and director of medical resident education adopted the mission statement as the blueprint for all educational programming for the academic year. Progress toward enacting the various components of the mission statement was reviewed monthly and changes in educational programming to ensure adequate emphasis of all components were made accordingly.
Results
Our first goal was to promote the personal and professional development of residents who rotate through VABHS, particularly interns, in a setting that fosters cross-institutional collaboration, respect, and friendship. The West Roxbury campus of VABHS is the only hospital in the city where internal medicine residents from 3 large training programs work together on teams that have been intentionally built to place residents from different institutions with one another. In educational conferences, we encouraged residents from different training programs to share their experiences with patient populations that others may not see at their home institutions, based on the specialized care that each institution provides. The conferences also give residents the opportunity to provide and receive near-peer teaching in a collegial environment.
Our second goal was to maintain an environment of educational excellence. We produced thought-provoking conferences that prioritized inspiring curiosity and teaching systems of thought over the dissemination of facts. We regularly focused on the broader context of medicine in case conferences and journal club, including topics such as public health, health policy, advocacy, health economics, quality improvement (QI), and high-value care. Our morning reports were interactive and participatory, emphasizing both technical skill practice and sophisticated clinical reasoning.
We embraced the principles of cognitive learning theory by priming learners with preconference “teasers” that previewed conference topics to be discussed. Every Friday, we played a medical version of Jeopardy!, which used spaced learning to consolidate the week’s teaching points in a fun, collaborative, and collegial atmosphere. Our dedicated patient safety conference gave residents the chance to use QI tools to dissect and tackle real problems in the hospital, and our monthly Morbidity and Mortality conference served as inspiration for many of the resident-driven QI projects.
Our third goal was to challenge physicians to provide the best possible care to veterans, including learning about issues unique to this often-marginalized population. We emphasized that training at a VA hospital is a privilege and that the best way to honor our veterans is to take advantage of the unique learning opportunities available at VA. To that end, we exposed residents to veteran-specific educational content, ranging from the structure and payment model of VHA to service-related medical conditions, such as posttraumatic stress disorder, other mental health issues, traumatic brain injury, Agent Orange exposure, and Gulf War Syndrome.
Discussion
Findings from the recently published Accreditation Council for Graduate Medical Education’s (ACGME) 2016 Clinical Learning Environment Review (CLER) Report support the need for mission statements like ours to guide the delivery of graduate medical education.3 A major finding of this report was that the development and implementation of graduate medical education largely occurs separately from other areas of organizational and strategic focus within clinical learning environments. Our mission statement has served as a road map for aligning the delivery of graduate medical education at VABHS with the specific strengths of the clinical learning environment that VA affords.
Additionally, the 2016 CLER report identified a lack of specificity in training on health care disparities and cultural competency for the specific populations served by the surveyed residency programs. The emphasis we placed on learning about issues specific to the care of the veteran population highlights the potential for other mission statements like ours to bridge the gap between articulation and execution of educational priorities. Finally, through the academic partnerships it holds with more than 90% of medical schools in the U.S., VA already has an integral role in both undergraduate and graduate medical education that positions its hospitals as ideal training environments in which to address shortcomings in medical training like those identified by the ACGME.4
Conclusion
We propose this mission statement as a model for the delivery of graduate medical education throughout all VA hospitals with academic affiliations and especially those where trainees from multiple institutions work together. As embodied in our mission statement, our goal was to provide a clinical training experience at VA that complements that of our residents’ home institutions and fosters a respect for and interest in the special care provided at VA. The development of a shared mission statement provides an invaluable tool in accomplishing that goal. We encourage chief medical residents and other leaders in medical education in all specialties at VAMCs to develop their own mission statements that reflect and embody the values of each affiliated training program. For our residents, rotating at VA is an opportunity to learn the practice of medicine for veterans, rather than practicing medicine on veterans. It is our sincere hope that shaping our residents’ educational experience in this fashion will foster a greater appreciation for the care of our nation’s veterans.
1. VA Office of Academic Affiliations. 2015 statistics: health professions trainees. http://www.va.gov/oaa/docs/OAA_Statistics.pdf. Published 2016. Accessed September 18, 2017.
2. VA Office of Academic Affiliations. Mission of the Office of Academic Affiliations. http://www.va.gov/oaa/oaa_mission.asp. Updated June 23, 2017. Accessed September 18, 2017.
3. Accreditation Council for Graduate Medical Education. Clinical learning environment review – national report of findings 2016 – executive summary. https://www.acgme.org/Portals/0/PDFs/CLER/ACGME-CLER-ExecutiveSummary.pdf. Published 2016. Accessed September 18, 2017.
4. Association of American Medical Colleges. The VA and academic medicine: partners in health care, training, and research. https://www.aamc.org/download/385612/data/07182014.pdf. Accessed September 14, 2017.
More than 65% of all physicians who train in the U.S. rotate through a VA hospital at some point during their training. In 2015 alone, more than 43,000 residents received some or all of their clinical training through VA.1 Of the approximately 120 VAMCs that hold academic affiliations
with medical schools and residency training programs, several hold affiliations with multiple institutions, including VA Boston Healthcare System (VABHS) in Massachusetts. The West Roxbury campus is the home of VA Boston’s acute care hospital, where residents and fellows from Boston Medical Center (BMC), Beth Israel Deaconess Medical Center (BIDMC), and Brigham and Women’s Hospital (BWH) train together. These are 3 of the largest medical training programs in Boston, though each provides a unique training experience for residents due to differences in patient population, faculty expertise, and hospital network affiliations (Table 1).
This diversity brings differences in cultural norms, institutional preferences, and educational expectations. Furthermore, residents from different programs who work together at VA Boston are often meeting one another for the first time, as opportunities for interinstitutional collaboration among these 3 training programs do not exist outside of VA. This training environment presents both an opportunity
and a challenge for medical educators: offering the best possible learning experience for physiciansin-training from multiple programs while providing the best possible care for U.S. veterans.
To guide educators charged with meeting this challenge, the VA Office of Academic Affiliations put forth a mission statement describing its overarching teaching mission (Table 2).2
To address this gap, chief medical residents from the 3 affiliate residency training programs came together to develop a shared mission statement for what we envision as the educational experience for all medical trainees rotating through VABHS (Table 2). In this article, we describe the development of a mission statement for graduate medical education in internal medicine at VABHS and provides examples of how our mission statement guided educational programming.
Methods
Whereas the affiliated institutions assign generic competency-based learning objectives to rotations at VABHS, no specific overarching educational objectives for residents have been defined previously. The directors of the internal medicine residency programs at each of the VABHS affiliate institutions grant their respective VA-based chief medical residents the autonomy to deliver graduate medical education at VA as they see fit, in collaboration with their colleagues from the other affiliated institutions and the VA director of medical resident education. This autonomy and flexibility allowed each of the chief medical residents to articulate an individual vision for VA graduate medical education based on their affiliate program’s goals, values, and mission.
At the beginning of the 2016/2017 academic year, in partnership with the director of medical resident education at VABHS, the chief medical residents met to reconcile these into a single shared mission statement. Special attention was paid to educational gaps at each affiliate institution that could be filled while residents were rotating at VABHS. Once all educational goals and priorities of the shared mission statement were identified, the chief medical residents and director of medical resident education adopted the mission statement as the blueprint for all educational programming for the academic year. Progress toward enacting the various components of the mission statement was reviewed monthly and changes in educational programming to ensure adequate emphasis of all components were made accordingly.
Results
Our first goal was to promote the personal and professional development of residents who rotate through VABHS, particularly interns, in a setting that fosters cross-institutional collaboration, respect, and friendship. The West Roxbury campus of VABHS is the only hospital in the city where internal medicine residents from 3 large training programs work together on teams that have been intentionally built to place residents from different institutions with one another. In educational conferences, we encouraged residents from different training programs to share their experiences with patient populations that others may not see at their home institutions, based on the specialized care that each institution provides. The conferences also give residents the opportunity to provide and receive near-peer teaching in a collegial environment.
Our second goal was to maintain an environment of educational excellence. We produced thought-provoking conferences that prioritized inspiring curiosity and teaching systems of thought over the dissemination of facts. We regularly focused on the broader context of medicine in case conferences and journal club, including topics such as public health, health policy, advocacy, health economics, quality improvement (QI), and high-value care. Our morning reports were interactive and participatory, emphasizing both technical skill practice and sophisticated clinical reasoning.
We embraced the principles of cognitive learning theory by priming learners with preconference “teasers” that previewed conference topics to be discussed. Every Friday, we played a medical version of Jeopardy!, which used spaced learning to consolidate the week’s teaching points in a fun, collaborative, and collegial atmosphere. Our dedicated patient safety conference gave residents the chance to use QI tools to dissect and tackle real problems in the hospital, and our monthly Morbidity and Mortality conference served as inspiration for many of the resident-driven QI projects.
Our third goal was to challenge physicians to provide the best possible care to veterans, including learning about issues unique to this often-marginalized population. We emphasized that training at a VA hospital is a privilege and that the best way to honor our veterans is to take advantage of the unique learning opportunities available at VA. To that end, we exposed residents to veteran-specific educational content, ranging from the structure and payment model of VHA to service-related medical conditions, such as posttraumatic stress disorder, other mental health issues, traumatic brain injury, Agent Orange exposure, and Gulf War Syndrome.
Discussion
Findings from the recently published Accreditation Council for Graduate Medical Education’s (ACGME) 2016 Clinical Learning Environment Review (CLER) Report support the need for mission statements like ours to guide the delivery of graduate medical education.3 A major finding of this report was that the development and implementation of graduate medical education largely occurs separately from other areas of organizational and strategic focus within clinical learning environments. Our mission statement has served as a road map for aligning the delivery of graduate medical education at VABHS with the specific strengths of the clinical learning environment that VA affords.
Additionally, the 2016 CLER report identified a lack of specificity in training on health care disparities and cultural competency for the specific populations served by the surveyed residency programs. The emphasis we placed on learning about issues specific to the care of the veteran population highlights the potential for other mission statements like ours to bridge the gap between articulation and execution of educational priorities. Finally, through the academic partnerships it holds with more than 90% of medical schools in the U.S., VA already has an integral role in both undergraduate and graduate medical education that positions its hospitals as ideal training environments in which to address shortcomings in medical training like those identified by the ACGME.4
Conclusion
We propose this mission statement as a model for the delivery of graduate medical education throughout all VA hospitals with academic affiliations and especially those where trainees from multiple institutions work together. As embodied in our mission statement, our goal was to provide a clinical training experience at VA that complements that of our residents’ home institutions and fosters a respect for and interest in the special care provided at VA. The development of a shared mission statement provides an invaluable tool in accomplishing that goal. We encourage chief medical residents and other leaders in medical education in all specialties at VAMCs to develop their own mission statements that reflect and embody the values of each affiliated training program. For our residents, rotating at VA is an opportunity to learn the practice of medicine for veterans, rather than practicing medicine on veterans. It is our sincere hope that shaping our residents’ educational experience in this fashion will foster a greater appreciation for the care of our nation’s veterans.
More than 65% of all physicians who train in the U.S. rotate through a VA hospital at some point during their training. In 2015 alone, more than 43,000 residents received some or all of their clinical training through VA.1 Of the approximately 120 VAMCs that hold academic affiliations
with medical schools and residency training programs, several hold affiliations with multiple institutions, including VA Boston Healthcare System (VABHS) in Massachusetts. The West Roxbury campus is the home of VA Boston’s acute care hospital, where residents and fellows from Boston Medical Center (BMC), Beth Israel Deaconess Medical Center (BIDMC), and Brigham and Women’s Hospital (BWH) train together. These are 3 of the largest medical training programs in Boston, though each provides a unique training experience for residents due to differences in patient population, faculty expertise, and hospital network affiliations (Table 1).
This diversity brings differences in cultural norms, institutional preferences, and educational expectations. Furthermore, residents from different programs who work together at VA Boston are often meeting one another for the first time, as opportunities for interinstitutional collaboration among these 3 training programs do not exist outside of VA. This training environment presents both an opportunity
and a challenge for medical educators: offering the best possible learning experience for physiciansin-training from multiple programs while providing the best possible care for U.S. veterans.
To guide educators charged with meeting this challenge, the VA Office of Academic Affiliations put forth a mission statement describing its overarching teaching mission (Table 2).2
To address this gap, chief medical residents from the 3 affiliate residency training programs came together to develop a shared mission statement for what we envision as the educational experience for all medical trainees rotating through VABHS (Table 2). In this article, we describe the development of a mission statement for graduate medical education in internal medicine at VABHS and provides examples of how our mission statement guided educational programming.
Methods
Whereas the affiliated institutions assign generic competency-based learning objectives to rotations at VABHS, no specific overarching educational objectives for residents have been defined previously. The directors of the internal medicine residency programs at each of the VABHS affiliate institutions grant their respective VA-based chief medical residents the autonomy to deliver graduate medical education at VA as they see fit, in collaboration with their colleagues from the other affiliated institutions and the VA director of medical resident education. This autonomy and flexibility allowed each of the chief medical residents to articulate an individual vision for VA graduate medical education based on their affiliate program’s goals, values, and mission.
At the beginning of the 2016/2017 academic year, in partnership with the director of medical resident education at VABHS, the chief medical residents met to reconcile these into a single shared mission statement. Special attention was paid to educational gaps at each affiliate institution that could be filled while residents were rotating at VABHS. Once all educational goals and priorities of the shared mission statement were identified, the chief medical residents and director of medical resident education adopted the mission statement as the blueprint for all educational programming for the academic year. Progress toward enacting the various components of the mission statement was reviewed monthly and changes in educational programming to ensure adequate emphasis of all components were made accordingly.
Results
Our first goal was to promote the personal and professional development of residents who rotate through VABHS, particularly interns, in a setting that fosters cross-institutional collaboration, respect, and friendship. The West Roxbury campus of VABHS is the only hospital in the city where internal medicine residents from 3 large training programs work together on teams that have been intentionally built to place residents from different institutions with one another. In educational conferences, we encouraged residents from different training programs to share their experiences with patient populations that others may not see at their home institutions, based on the specialized care that each institution provides. The conferences also give residents the opportunity to provide and receive near-peer teaching in a collegial environment.
Our second goal was to maintain an environment of educational excellence. We produced thought-provoking conferences that prioritized inspiring curiosity and teaching systems of thought over the dissemination of facts. We regularly focused on the broader context of medicine in case conferences and journal club, including topics such as public health, health policy, advocacy, health economics, quality improvement (QI), and high-value care. Our morning reports were interactive and participatory, emphasizing both technical skill practice and sophisticated clinical reasoning.
We embraced the principles of cognitive learning theory by priming learners with preconference “teasers” that previewed conference topics to be discussed. Every Friday, we played a medical version of Jeopardy!, which used spaced learning to consolidate the week’s teaching points in a fun, collaborative, and collegial atmosphere. Our dedicated patient safety conference gave residents the chance to use QI tools to dissect and tackle real problems in the hospital, and our monthly Morbidity and Mortality conference served as inspiration for many of the resident-driven QI projects.
Our third goal was to challenge physicians to provide the best possible care to veterans, including learning about issues unique to this often-marginalized population. We emphasized that training at a VA hospital is a privilege and that the best way to honor our veterans is to take advantage of the unique learning opportunities available at VA. To that end, we exposed residents to veteran-specific educational content, ranging from the structure and payment model of VHA to service-related medical conditions, such as posttraumatic stress disorder, other mental health issues, traumatic brain injury, Agent Orange exposure, and Gulf War Syndrome.
Discussion
Findings from the recently published Accreditation Council for Graduate Medical Education’s (ACGME) 2016 Clinical Learning Environment Review (CLER) Report support the need for mission statements like ours to guide the delivery of graduate medical education.3 A major finding of this report was that the development and implementation of graduate medical education largely occurs separately from other areas of organizational and strategic focus within clinical learning environments. Our mission statement has served as a road map for aligning the delivery of graduate medical education at VABHS with the specific strengths of the clinical learning environment that VA affords.
Additionally, the 2016 CLER report identified a lack of specificity in training on health care disparities and cultural competency for the specific populations served by the surveyed residency programs. The emphasis we placed on learning about issues specific to the care of the veteran population highlights the potential for other mission statements like ours to bridge the gap between articulation and execution of educational priorities. Finally, through the academic partnerships it holds with more than 90% of medical schools in the U.S., VA already has an integral role in both undergraduate and graduate medical education that positions its hospitals as ideal training environments in which to address shortcomings in medical training like those identified by the ACGME.4
Conclusion
We propose this mission statement as a model for the delivery of graduate medical education throughout all VA hospitals with academic affiliations and especially those where trainees from multiple institutions work together. As embodied in our mission statement, our goal was to provide a clinical training experience at VA that complements that of our residents’ home institutions and fosters a respect for and interest in the special care provided at VA. The development of a shared mission statement provides an invaluable tool in accomplishing that goal. We encourage chief medical residents and other leaders in medical education in all specialties at VAMCs to develop their own mission statements that reflect and embody the values of each affiliated training program. For our residents, rotating at VA is an opportunity to learn the practice of medicine for veterans, rather than practicing medicine on veterans. It is our sincere hope that shaping our residents’ educational experience in this fashion will foster a greater appreciation for the care of our nation’s veterans.
1. VA Office of Academic Affiliations. 2015 statistics: health professions trainees. http://www.va.gov/oaa/docs/OAA_Statistics.pdf. Published 2016. Accessed September 18, 2017.
2. VA Office of Academic Affiliations. Mission of the Office of Academic Affiliations. http://www.va.gov/oaa/oaa_mission.asp. Updated June 23, 2017. Accessed September 18, 2017.
3. Accreditation Council for Graduate Medical Education. Clinical learning environment review – national report of findings 2016 – executive summary. https://www.acgme.org/Portals/0/PDFs/CLER/ACGME-CLER-ExecutiveSummary.pdf. Published 2016. Accessed September 18, 2017.
4. Association of American Medical Colleges. The VA and academic medicine: partners in health care, training, and research. https://www.aamc.org/download/385612/data/07182014.pdf. Accessed September 14, 2017.
1. VA Office of Academic Affiliations. 2015 statistics: health professions trainees. http://www.va.gov/oaa/docs/OAA_Statistics.pdf. Published 2016. Accessed September 18, 2017.
2. VA Office of Academic Affiliations. Mission of the Office of Academic Affiliations. http://www.va.gov/oaa/oaa_mission.asp. Updated June 23, 2017. Accessed September 18, 2017.
3. Accreditation Council for Graduate Medical Education. Clinical learning environment review – national report of findings 2016 – executive summary. https://www.acgme.org/Portals/0/PDFs/CLER/ACGME-CLER-ExecutiveSummary.pdf. Published 2016. Accessed September 18, 2017.
4. Association of American Medical Colleges. The VA and academic medicine: partners in health care, training, and research. https://www.aamc.org/download/385612/data/07182014.pdf. Accessed September 14, 2017.
Podcasts
you need no effort to enjoy them. Indeed, you can be actively engaged elsewhere: running, cycling, commuting, or simply loafing. The detail and richness of the sound also creates an intimate connection with the host in a way other mediums cannot. It feels like they are talking only to you.
Yet, there is a problem with podcasts: There are too many of them. If I listened continuously to the episodes in my queue it would take 6 months. I suppose I could see patients and listen at the same time. (Yes, I have a problem.) I also own far more books than I’ll ever read. Aspirational, I call it.
If, like me, you’re unable to dedicate your life to consuming podcasts, you might appreciate a few recommendations. Here’s a charcuterie board of tasty bits, carefully curated to avoid political allergies and Dunning-Kruger references.
1. Physicians Practice. It’s one of the oldest podcasts running and addresses a wide range of issues affecting health care professionals and the industry at large. Episodes are short (typically under 10 minutes) and address a range of issues relevant to both young and seasoned physicians With scores of podcasts from which to choose, I suggest just selecting one and jumping in. With episode titles such as “The Patient Empathy Problem Physicians Must Face” and “EHRs Not Designed with Real People in Mind, Expert Opines,” it’s easy to do.
2. UpToDate. If you’re looking for straight clinical talk buttressed with scientific evidence, then download UpToDate. Episodes typically feature interviews with one or two respected physician leaders who share their clinical findings. You can select episode topics based upon clinical specialty or simply start listening. Here is a sampling of topics: sentinel lymph node metastasis in melanoma; dexamethasone and acute pharyngitis pain in adults; management of anticoagulation for patients with nonvalvular atrial fibrillation. UpToDate states that it is entirely funded by user subscriptions and does not accept advertising or funding unrelated to subscriptions.
3. Bedside Rounds. The tagline for the podcast Bedside Rounds is “Because medicine is awesome.” This is not meant to be ironic. Creator and host, Adam Rodman, MD, a global health hospitalist who divides his time between Boston (at the Beth Israel Deaconess Medical Center) and Botswana, is that eager kid in the classroom who sits in the front row just because he’s so excited to be there. Unlike UpToDate, which focuses on current advances in clinical medicine, Bedside Rounds explores both the science and art of medicine through captivating stories heavily rooted in the history of medicine. Instead of brushing the dust off of your old medical books, tune in to Bedside Rounds to hear stories such as “Bone Portraits,” which explores the history of radiation, and “Curse of the Ninth,” which explores whether or not composer Gustav Mahler, worked his heart murmur into his famous Ninth Symphony.
4. The Adventures of Memento Mori. Creator and host, D.S. Moss, has created a podcast about death, or, to be more upbeat, the quest for the meaning of life. A screenwriter/producer, Mr. Moss deep dives into all things death. But it’s not as depressing as it sounds. “Memento mori,” he explains, is Latin for being mindful that you will die. As a result, Mr. Moss has created his podcast with the goal of encouraging listeners to live a more engaged, mindful, and meaningful life. We can apply many of these lessons to our own professional and personal lives and perhaps learn some ways to help our patients cope with terminal illness and mortality. Topics range from the emotional (“Thoughts in Passing,” which features several hospice patients) to the technological (“Digital Afterlife,” which explores what our digital legacies say about us), to the scientific (“The Science of Immortality,” which explores venture capital’s movement in the science of living forever).
5. Invisibilia. Invisibilia – Latin for invisible things – is an exploration of the “unseeable forces” that shape human behavior – our beliefs, thoughts, and assumptions. Hosts Alix Spiegel and Hanna Rosin, both of National Public Radio, seamlessly weave storytelling, interviewing, and scientific data to tackle a wide range of topics such as prejudice and implicit bias in “The Culture Inside” to people’s desire for radical change in “Bubble Hopping.” Part behavioral economics, part neuroscience, part sociology, part pop culture, fully fascinating.
6. Jocko Podcast. Jocko Willink, a retired Navy SEAL and motivational author and speaker, along with Echo Charles, conduct compelling interviews with leaders from various fields including the military, sports, medicine, and the arts. Mr. Willink’s style of motivation is refreshingly honest and direct. I have taken tips from his podcasts that have helped me become a more efficient and energetic physician and leader. Two fundamental themes that run through his podcast are the value of treating people well and of living your life with discipline. It gets you a long way as a Navy SEAL, as well as a doctor. One of my personal favorites is Episode 69: “The Real Top Gun. Battlefield, Work, and Life are Identical” with Elite Marine Fighter Pilot, David Berke. If that doesn’t pique your interest, no worries; there are over 100 episodes from which to choose.
There are many, many more podcasts I’d like to recommend, but I’ll show some discipline (thanks, Jocko) and save them for next time.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@frontlinemedcom.com.
you need no effort to enjoy them. Indeed, you can be actively engaged elsewhere: running, cycling, commuting, or simply loafing. The detail and richness of the sound also creates an intimate connection with the host in a way other mediums cannot. It feels like they are talking only to you.
Yet, there is a problem with podcasts: There are too many of them. If I listened continuously to the episodes in my queue it would take 6 months. I suppose I could see patients and listen at the same time. (Yes, I have a problem.) I also own far more books than I’ll ever read. Aspirational, I call it.
If, like me, you’re unable to dedicate your life to consuming podcasts, you might appreciate a few recommendations. Here’s a charcuterie board of tasty bits, carefully curated to avoid political allergies and Dunning-Kruger references.
1. Physicians Practice. It’s one of the oldest podcasts running and addresses a wide range of issues affecting health care professionals and the industry at large. Episodes are short (typically under 10 minutes) and address a range of issues relevant to both young and seasoned physicians With scores of podcasts from which to choose, I suggest just selecting one and jumping in. With episode titles such as “The Patient Empathy Problem Physicians Must Face” and “EHRs Not Designed with Real People in Mind, Expert Opines,” it’s easy to do.
2. UpToDate. If you’re looking for straight clinical talk buttressed with scientific evidence, then download UpToDate. Episodes typically feature interviews with one or two respected physician leaders who share their clinical findings. You can select episode topics based upon clinical specialty or simply start listening. Here is a sampling of topics: sentinel lymph node metastasis in melanoma; dexamethasone and acute pharyngitis pain in adults; management of anticoagulation for patients with nonvalvular atrial fibrillation. UpToDate states that it is entirely funded by user subscriptions and does not accept advertising or funding unrelated to subscriptions.
3. Bedside Rounds. The tagline for the podcast Bedside Rounds is “Because medicine is awesome.” This is not meant to be ironic. Creator and host, Adam Rodman, MD, a global health hospitalist who divides his time between Boston (at the Beth Israel Deaconess Medical Center) and Botswana, is that eager kid in the classroom who sits in the front row just because he’s so excited to be there. Unlike UpToDate, which focuses on current advances in clinical medicine, Bedside Rounds explores both the science and art of medicine through captivating stories heavily rooted in the history of medicine. Instead of brushing the dust off of your old medical books, tune in to Bedside Rounds to hear stories such as “Bone Portraits,” which explores the history of radiation, and “Curse of the Ninth,” which explores whether or not composer Gustav Mahler, worked his heart murmur into his famous Ninth Symphony.
4. The Adventures of Memento Mori. Creator and host, D.S. Moss, has created a podcast about death, or, to be more upbeat, the quest for the meaning of life. A screenwriter/producer, Mr. Moss deep dives into all things death. But it’s not as depressing as it sounds. “Memento mori,” he explains, is Latin for being mindful that you will die. As a result, Mr. Moss has created his podcast with the goal of encouraging listeners to live a more engaged, mindful, and meaningful life. We can apply many of these lessons to our own professional and personal lives and perhaps learn some ways to help our patients cope with terminal illness and mortality. Topics range from the emotional (“Thoughts in Passing,” which features several hospice patients) to the technological (“Digital Afterlife,” which explores what our digital legacies say about us), to the scientific (“The Science of Immortality,” which explores venture capital’s movement in the science of living forever).
5. Invisibilia. Invisibilia – Latin for invisible things – is an exploration of the “unseeable forces” that shape human behavior – our beliefs, thoughts, and assumptions. Hosts Alix Spiegel and Hanna Rosin, both of National Public Radio, seamlessly weave storytelling, interviewing, and scientific data to tackle a wide range of topics such as prejudice and implicit bias in “The Culture Inside” to people’s desire for radical change in “Bubble Hopping.” Part behavioral economics, part neuroscience, part sociology, part pop culture, fully fascinating.
6. Jocko Podcast. Jocko Willink, a retired Navy SEAL and motivational author and speaker, along with Echo Charles, conduct compelling interviews with leaders from various fields including the military, sports, medicine, and the arts. Mr. Willink’s style of motivation is refreshingly honest and direct. I have taken tips from his podcasts that have helped me become a more efficient and energetic physician and leader. Two fundamental themes that run through his podcast are the value of treating people well and of living your life with discipline. It gets you a long way as a Navy SEAL, as well as a doctor. One of my personal favorites is Episode 69: “The Real Top Gun. Battlefield, Work, and Life are Identical” with Elite Marine Fighter Pilot, David Berke. If that doesn’t pique your interest, no worries; there are over 100 episodes from which to choose.
There are many, many more podcasts I’d like to recommend, but I’ll show some discipline (thanks, Jocko) and save them for next time.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@frontlinemedcom.com.
you need no effort to enjoy them. Indeed, you can be actively engaged elsewhere: running, cycling, commuting, or simply loafing. The detail and richness of the sound also creates an intimate connection with the host in a way other mediums cannot. It feels like they are talking only to you.
Yet, there is a problem with podcasts: There are too many of them. If I listened continuously to the episodes in my queue it would take 6 months. I suppose I could see patients and listen at the same time. (Yes, I have a problem.) I also own far more books than I’ll ever read. Aspirational, I call it.
If, like me, you’re unable to dedicate your life to consuming podcasts, you might appreciate a few recommendations. Here’s a charcuterie board of tasty bits, carefully curated to avoid political allergies and Dunning-Kruger references.
1. Physicians Practice. It’s one of the oldest podcasts running and addresses a wide range of issues affecting health care professionals and the industry at large. Episodes are short (typically under 10 minutes) and address a range of issues relevant to both young and seasoned physicians With scores of podcasts from which to choose, I suggest just selecting one and jumping in. With episode titles such as “The Patient Empathy Problem Physicians Must Face” and “EHRs Not Designed with Real People in Mind, Expert Opines,” it’s easy to do.
2. UpToDate. If you’re looking for straight clinical talk buttressed with scientific evidence, then download UpToDate. Episodes typically feature interviews with one or two respected physician leaders who share their clinical findings. You can select episode topics based upon clinical specialty or simply start listening. Here is a sampling of topics: sentinel lymph node metastasis in melanoma; dexamethasone and acute pharyngitis pain in adults; management of anticoagulation for patients with nonvalvular atrial fibrillation. UpToDate states that it is entirely funded by user subscriptions and does not accept advertising or funding unrelated to subscriptions.
3. Bedside Rounds. The tagline for the podcast Bedside Rounds is “Because medicine is awesome.” This is not meant to be ironic. Creator and host, Adam Rodman, MD, a global health hospitalist who divides his time between Boston (at the Beth Israel Deaconess Medical Center) and Botswana, is that eager kid in the classroom who sits in the front row just because he’s so excited to be there. Unlike UpToDate, which focuses on current advances in clinical medicine, Bedside Rounds explores both the science and art of medicine through captivating stories heavily rooted in the history of medicine. Instead of brushing the dust off of your old medical books, tune in to Bedside Rounds to hear stories such as “Bone Portraits,” which explores the history of radiation, and “Curse of the Ninth,” which explores whether or not composer Gustav Mahler, worked his heart murmur into his famous Ninth Symphony.
4. The Adventures of Memento Mori. Creator and host, D.S. Moss, has created a podcast about death, or, to be more upbeat, the quest for the meaning of life. A screenwriter/producer, Mr. Moss deep dives into all things death. But it’s not as depressing as it sounds. “Memento mori,” he explains, is Latin for being mindful that you will die. As a result, Mr. Moss has created his podcast with the goal of encouraging listeners to live a more engaged, mindful, and meaningful life. We can apply many of these lessons to our own professional and personal lives and perhaps learn some ways to help our patients cope with terminal illness and mortality. Topics range from the emotional (“Thoughts in Passing,” which features several hospice patients) to the technological (“Digital Afterlife,” which explores what our digital legacies say about us), to the scientific (“The Science of Immortality,” which explores venture capital’s movement in the science of living forever).
5. Invisibilia. Invisibilia – Latin for invisible things – is an exploration of the “unseeable forces” that shape human behavior – our beliefs, thoughts, and assumptions. Hosts Alix Spiegel and Hanna Rosin, both of National Public Radio, seamlessly weave storytelling, interviewing, and scientific data to tackle a wide range of topics such as prejudice and implicit bias in “The Culture Inside” to people’s desire for radical change in “Bubble Hopping.” Part behavioral economics, part neuroscience, part sociology, part pop culture, fully fascinating.
6. Jocko Podcast. Jocko Willink, a retired Navy SEAL and motivational author and speaker, along with Echo Charles, conduct compelling interviews with leaders from various fields including the military, sports, medicine, and the arts. Mr. Willink’s style of motivation is refreshingly honest and direct. I have taken tips from his podcasts that have helped me become a more efficient and energetic physician and leader. Two fundamental themes that run through his podcast are the value of treating people well and of living your life with discipline. It gets you a long way as a Navy SEAL, as well as a doctor. One of my personal favorites is Episode 69: “The Real Top Gun. Battlefield, Work, and Life are Identical” with Elite Marine Fighter Pilot, David Berke. If that doesn’t pique your interest, no worries; there are over 100 episodes from which to choose.
There are many, many more podcasts I’d like to recommend, but I’ll show some discipline (thanks, Jocko) and save them for next time.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@frontlinemedcom.com.
Match Day 2018: Big increases for neurology
Neurology helped to make the 2018 Main Residency Match the largest ever as the specialty offered and filled over 12% more residency slots than in 2017, according to the National Resident Matching Program (NRMP).
The third consecutive year with a double-digit increase in PGY-1 positions enabled neurology to bring 552 slots to the Match Day party this year: 50.7% were filled with U.S. graduates and the overall fill rate was 97.6%. For all specialties, U.S. graduates filled 58.7% of the record-high 30,232 available spots, and the overall fill rate was 96.1%, the NRMP said in its 2018 Main Residency Match report.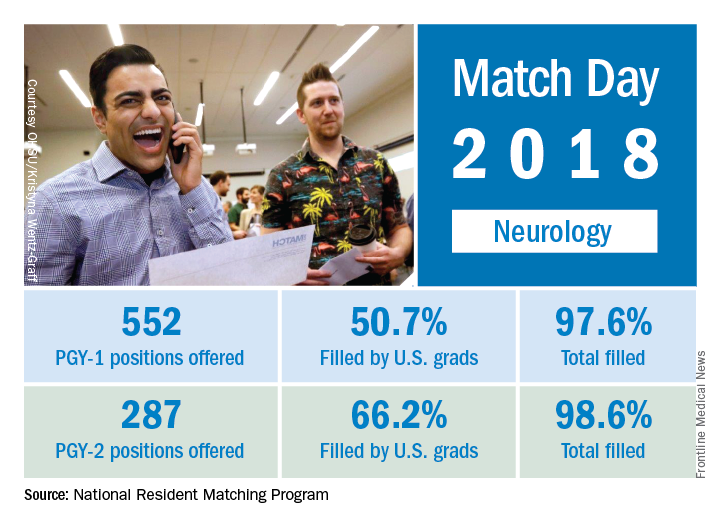
The total number of child neurology PGY-1 positions offered rose to 134, of which 96.3% were filled (75.4% by U.S. graduates). Another seven of eight PGY-2 child neurology positions were filled. Of 26 PGY-2 physician positions offered for child neurology, 12 were filled.
The 2018 Match also set new highs for total positions offered (up 4.4% over last year), total (up 4.7%) and PGY-1 positions (up 4.9%) filled, and total applicants (up 1.7%). “The results of the Match are closely watched because they can be predictors of future physician workforce supply. There also is significant interest in the competitiveness of specialties, as measured by the percentage of positions filled overall and the percentage filled by senior students in U.S. allopathic medical schools,” the NRMP said.
Neurology helped to make the 2018 Main Residency Match the largest ever as the specialty offered and filled over 12% more residency slots than in 2017, according to the National Resident Matching Program (NRMP).
The third consecutive year with a double-digit increase in PGY-1 positions enabled neurology to bring 552 slots to the Match Day party this year: 50.7% were filled with U.S. graduates and the overall fill rate was 97.6%. For all specialties, U.S. graduates filled 58.7% of the record-high 30,232 available spots, and the overall fill rate was 96.1%, the NRMP said in its 2018 Main Residency Match report.
The total number of child neurology PGY-1 positions offered rose to 134, of which 96.3% were filled (75.4% by U.S. graduates). Another seven of eight PGY-2 child neurology positions were filled. Of 26 PGY-2 physician positions offered for child neurology, 12 were filled.
The 2018 Match also set new highs for total positions offered (up 4.4% over last year), total (up 4.7%) and PGY-1 positions (up 4.9%) filled, and total applicants (up 1.7%). “The results of the Match are closely watched because they can be predictors of future physician workforce supply. There also is significant interest in the competitiveness of specialties, as measured by the percentage of positions filled overall and the percentage filled by senior students in U.S. allopathic medical schools,” the NRMP said.
Neurology helped to make the 2018 Main Residency Match the largest ever as the specialty offered and filled over 12% more residency slots than in 2017, according to the National Resident Matching Program (NRMP).
The third consecutive year with a double-digit increase in PGY-1 positions enabled neurology to bring 552 slots to the Match Day party this year: 50.7% were filled with U.S. graduates and the overall fill rate was 97.6%. For all specialties, U.S. graduates filled 58.7% of the record-high 30,232 available spots, and the overall fill rate was 96.1%, the NRMP said in its 2018 Main Residency Match report.
The total number of child neurology PGY-1 positions offered rose to 134, of which 96.3% were filled (75.4% by U.S. graduates). Another seven of eight PGY-2 child neurology positions were filled. Of 26 PGY-2 physician positions offered for child neurology, 12 were filled.
The 2018 Match also set new highs for total positions offered (up 4.4% over last year), total (up 4.7%) and PGY-1 positions (up 4.9%) filled, and total applicants (up 1.7%). “The results of the Match are closely watched because they can be predictors of future physician workforce supply. There also is significant interest in the competitiveness of specialties, as measured by the percentage of positions filled overall and the percentage filled by senior students in U.S. allopathic medical schools,” the NRMP said.
Dermatology residency match: Is the glut of applications for limited positions corrupting the process?
SAN DIEGO – Whether was the topic of discussion at a session on dermatoethics at the annual meeting of the American Academy of Dermatology.
“I think it is unethical and we need to address it,” Jane M. Grant-Kels, MD, said during the session. “What we are doing through the process of physicians getting into dermatology residency programs is telling them to lie to us and to do well on a single examination,” the United States Medical Licensing Examination.

Lionel G. Bercovitch, MD, is among the dermatologists who acknowledge the unarguable fact that application rates are high but don’t see it as a crisis of credibility.
“I don’t believe that dermatology match is broken, unethical, or unfair. The match is not perfect, but it’s fair,” contended Dr. Bercovitch, professor of dermatology at Brown University, Providence, R.I. “The problem [of an application glut] is real, but it’s not an ethical issue.”
Dr. Grant-Kels sees it in ethical terms because, in her view, “everyone is gaming the system. It makes applicants liars” when they profess interest in moving to a remote location or planning to practice a certain type of dermatology.

The “extremely competitive” process leads a majority of applicants to “shot gun” their filings to many programs such that dermatology residency programs are “deluged” with applications, Dr. Grant-Kels said. Data from the Association of American Medical Colleges for 2017 showed an average of just over 500 applications received by each U.S. dermatology residency program.
As a result, residency programs feel forced to apply blind filters that generally cull out more than a third of the applications received. Dr. Grant-Kels decried the need for programs to impose arbitrary barriers to entering dermatology based on a score from a single examination or other criteria like membership in Alpha Omega Alpha or current location.
“Blanket screening methods run the risk of excluding genuinely interested and qualified candidates who do not fall above a threshold. This violates the principal of nonmaleficence,” she said. “Screens are unfair.”
[polldaddy:{"method":"iframe","type":"survey","src":"//newspolls2017.polldaddy.com/s/dermatology-residency-match?iframe=1"}]
Dr. Grant-Kels proposed a pair of potential remedies: putting a cap on the number of applications someone can make and – a more realistic approach – mentors’ giving guidance to prospective applicants.
“It’s a problem that kids are applying to dermatology programs who have no business applying, who really don’t have a chance,” she said.
Dr. Bercovitch noted that most dermatology residency programs are too small and that, while the number of residency slots has been rising, it has not kept pace with increasing demand from physicians seeking residency slots. He saw no ethical reason for physicians to feel they should rein in the number of applications they file, and he said the only obligations for residency programs are to strictly adhere to the Match rules and both federal and state civil rights and labor laws and to be nondiscriminatory and avoid nepotism and conflicts of interest. Because programs cannot seriously consider nor interview several hundred applicants each year, some type of filtering is needed, and no filter is fair or perfect, he conceded.
“Filters are inherently unfair” to certain applicants, “but how else to effectively screen” hundreds of applications, Dr. Bercovitch asked.
“We need to talk about this. It’s not a good system. If we don’t talk about it, it will never change,” Dr. Grant-Kels said.
Dr. Grant-Kels and Dr. Bercovitch had no disclosures.
SAN DIEGO – Whether was the topic of discussion at a session on dermatoethics at the annual meeting of the American Academy of Dermatology.
“I think it is unethical and we need to address it,” Jane M. Grant-Kels, MD, said during the session. “What we are doing through the process of physicians getting into dermatology residency programs is telling them to lie to us and to do well on a single examination,” the United States Medical Licensing Examination.
Lionel G. Bercovitch, MD, is among the dermatologists who acknowledge the unarguable fact that application rates are high but don’t see it as a crisis of credibility.
“I don’t believe that dermatology match is broken, unethical, or unfair. The match is not perfect, but it’s fair,” contended Dr. Bercovitch, professor of dermatology at Brown University, Providence, R.I. “The problem [of an application glut] is real, but it’s not an ethical issue.”
Dr. Grant-Kels sees it in ethical terms because, in her view, “everyone is gaming the system. It makes applicants liars” when they profess interest in moving to a remote location or planning to practice a certain type of dermatology.
The “extremely competitive” process leads a majority of applicants to “shot gun” their filings to many programs such that dermatology residency programs are “deluged” with applications, Dr. Grant-Kels said. Data from the Association of American Medical Colleges for 2017 showed an average of just over 500 applications received by each U.S. dermatology residency program.
As a result, residency programs feel forced to apply blind filters that generally cull out more than a third of the applications received. Dr. Grant-Kels decried the need for programs to impose arbitrary barriers to entering dermatology based on a score from a single examination or other criteria like membership in Alpha Omega Alpha or current location.
“Blanket screening methods run the risk of excluding genuinely interested and qualified candidates who do not fall above a threshold. This violates the principal of nonmaleficence,” she said. “Screens are unfair.”
[polldaddy:{"method":"iframe","type":"survey","src":"//newspolls2017.polldaddy.com/s/dermatology-residency-match?iframe=1"}]
Dr. Grant-Kels proposed a pair of potential remedies: putting a cap on the number of applications someone can make and – a more realistic approach – mentors’ giving guidance to prospective applicants.
“It’s a problem that kids are applying to dermatology programs who have no business applying, who really don’t have a chance,” she said.
Dr. Bercovitch noted that most dermatology residency programs are too small and that, while the number of residency slots has been rising, it has not kept pace with increasing demand from physicians seeking residency slots. He saw no ethical reason for physicians to feel they should rein in the number of applications they file, and he said the only obligations for residency programs are to strictly adhere to the Match rules and both federal and state civil rights and labor laws and to be nondiscriminatory and avoid nepotism and conflicts of interest. Because programs cannot seriously consider nor interview several hundred applicants each year, some type of filtering is needed, and no filter is fair or perfect, he conceded.
“Filters are inherently unfair” to certain applicants, “but how else to effectively screen” hundreds of applications, Dr. Bercovitch asked.
“We need to talk about this. It’s not a good system. If we don’t talk about it, it will never change,” Dr. Grant-Kels said.
Dr. Grant-Kels and Dr. Bercovitch had no disclosures.
SAN DIEGO – Whether was the topic of discussion at a session on dermatoethics at the annual meeting of the American Academy of Dermatology.
“I think it is unethical and we need to address it,” Jane M. Grant-Kels, MD, said during the session. “What we are doing through the process of physicians getting into dermatology residency programs is telling them to lie to us and to do well on a single examination,” the United States Medical Licensing Examination.
Lionel G. Bercovitch, MD, is among the dermatologists who acknowledge the unarguable fact that application rates are high but don’t see it as a crisis of credibility.
“I don’t believe that dermatology match is broken, unethical, or unfair. The match is not perfect, but it’s fair,” contended Dr. Bercovitch, professor of dermatology at Brown University, Providence, R.I. “The problem [of an application glut] is real, but it’s not an ethical issue.”
Dr. Grant-Kels sees it in ethical terms because, in her view, “everyone is gaming the system. It makes applicants liars” when they profess interest in moving to a remote location or planning to practice a certain type of dermatology.
The “extremely competitive” process leads a majority of applicants to “shot gun” their filings to many programs such that dermatology residency programs are “deluged” with applications, Dr. Grant-Kels said. Data from the Association of American Medical Colleges for 2017 showed an average of just over 500 applications received by each U.S. dermatology residency program.
As a result, residency programs feel forced to apply blind filters that generally cull out more than a third of the applications received. Dr. Grant-Kels decried the need for programs to impose arbitrary barriers to entering dermatology based on a score from a single examination or other criteria like membership in Alpha Omega Alpha or current location.
“Blanket screening methods run the risk of excluding genuinely interested and qualified candidates who do not fall above a threshold. This violates the principal of nonmaleficence,” she said. “Screens are unfair.”
[polldaddy:{"method":"iframe","type":"survey","src":"//newspolls2017.polldaddy.com/s/dermatology-residency-match?iframe=1"}]
Dr. Grant-Kels proposed a pair of potential remedies: putting a cap on the number of applications someone can make and – a more realistic approach – mentors’ giving guidance to prospective applicants.
“It’s a problem that kids are applying to dermatology programs who have no business applying, who really don’t have a chance,” she said.
Dr. Bercovitch noted that most dermatology residency programs are too small and that, while the number of residency slots has been rising, it has not kept pace with increasing demand from physicians seeking residency slots. He saw no ethical reason for physicians to feel they should rein in the number of applications they file, and he said the only obligations for residency programs are to strictly adhere to the Match rules and both federal and state civil rights and labor laws and to be nondiscriminatory and avoid nepotism and conflicts of interest. Because programs cannot seriously consider nor interview several hundred applicants each year, some type of filtering is needed, and no filter is fair or perfect, he conceded.
“Filters are inherently unfair” to certain applicants, “but how else to effectively screen” hundreds of applications, Dr. Bercovitch asked.
“We need to talk about this. It’s not a good system. If we don’t talk about it, it will never change,” Dr. Grant-Kels said.
Dr. Grant-Kels and Dr. Bercovitch had no disclosures.
EXPERT ANALYSIS FROM AAD 18
ACOG app and applets: Tools to augment your practice
The American College of Obstetricians and Gynecologists (ACOG) is a nonprofit organization of women’s health care physicians advocating the highest standards of practice, continuing member education, and public awareness of women’s health care issues.1 The organization has long recognized the impact that social media and mobile technology would have for itself as well as its membership. ACOG published a Social Media Guide in 2012, featuring a section on how to use apps in ObGyn practice and provided a list of apps for ObGyns and their patients.2
ACOG introduced its own app 4 years ago and has since updated the app several times, most recently on December 6, 2017. The ACOG app has a useful search function, a home button, and a place for users to email feedback (TABLE 1). The app most importantly contains several applets (small applications designed to perform a specific function within the main application). These applets encompass 3 types of apps for health care providers: clinical decision-making apps (Practice Bulletins, Committee Opinions, an Estimated Due Date Calculator that was featured in a prior review,3 Indicated Delivery, and Immunize) (TABLE 2), reference and information gathering apps (Today’s Headlines), and member support apps (ACOG Contacts, Careers, Annual Meeting, Districts, Council on Resident Education in Obstetrics and Gynecology [CREOG], and Website).4
This review will focus on the main ACOG app, which is evaluated by a shortened version of the APPLICATIONS scoring system, APPLI (app comprehensiveness, price, platform, literature use, and important special features).5 In addition, the clinical decision-making applets will be highlighted in a second table. I commend ACOG for developing these useful tools to augment their members’ practices. Of note, for the Practice Bulletins and Indicated Delivery applets, users will need to input their ACOG log-in access information.

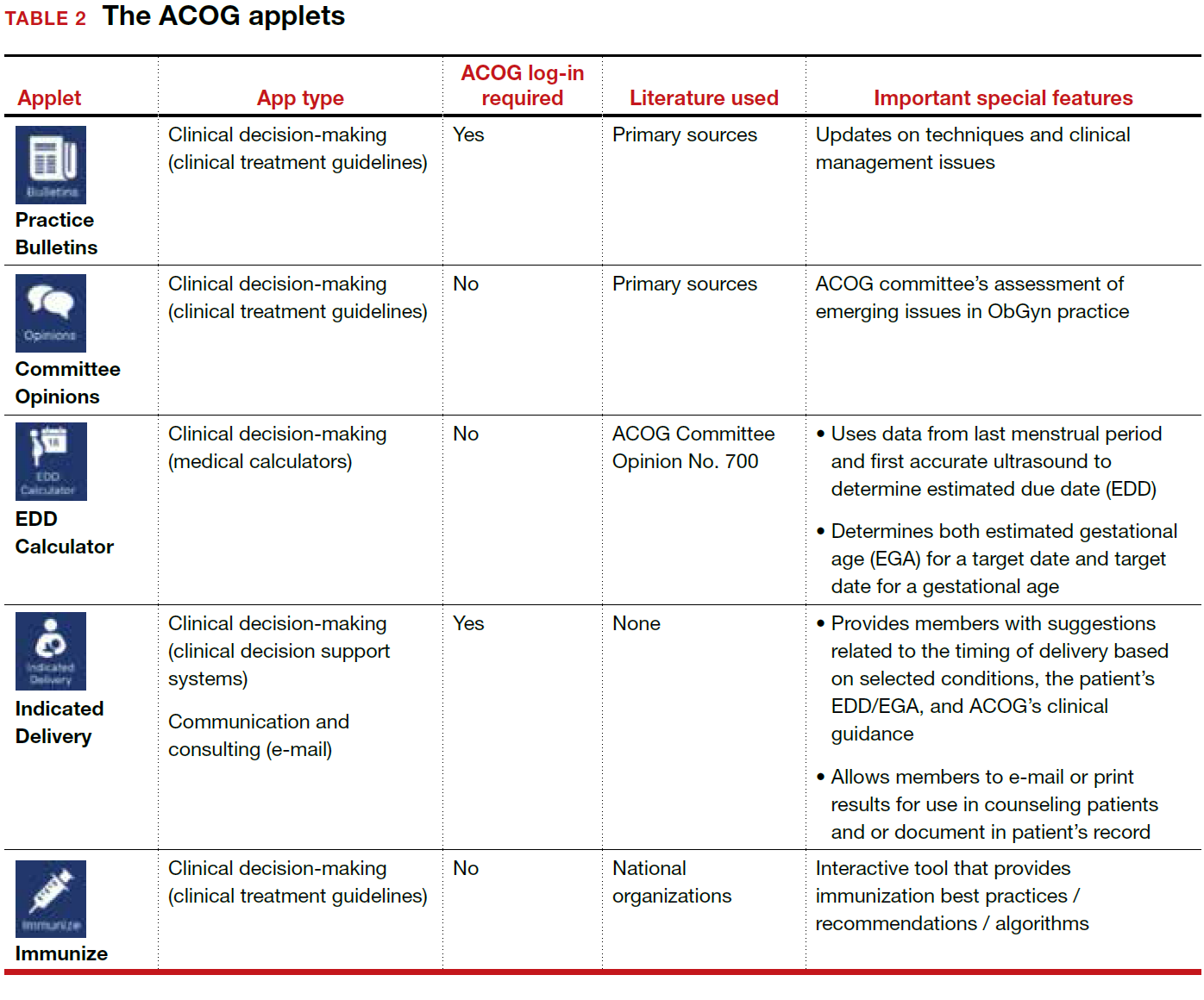
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- The American College of Obstetricians and Gynecologists web site. https://www.acog.org/About-ACOG. Updated 2017. Accessed February 12, 2018.
- ACOG today. The American College of Obstetricians and Gynecologists https://www.acog.org/-/media/ACOG-Today /acogToday201211.pdf. Published November 2012. Accessed February 12, 2018.
- Chen KT. Three good apps for calculating the date of delivery. OBG Manag. 2017;29(1):45–46.
- Ventola CL. Mobile devices and apps for health care professionals: Uses and benefits. P T. 2014;39(5):356–364.
- Chyjek K, Farag S, Chen KT. Rating pregnancy wheel applications using the APPLICATIONS scoring system. Obstet Gynecol. 2015;125(6):1478–1483.

Dr. Chen is Professor of Obstetrics, Gynecology, and Reproductive Science and Medical Education, Vice-Chair of Ob-Gyn Education for the Mount Sinai Health System, Icahn School of Medicine, Mount Sinai, New York, New York. She is an OBG
The author reports receiving royalties from UpToDate, Inc.
Dr. Chen is Professor of Obstetrics, Gynecology, and Reproductive Science and Medical Education, Vice-Chair of Ob-Gyn Education for the Mount Sinai Health System, Icahn School of Medicine, Mount Sinai, New York, New York. She is an OBG
The author reports receiving royalties from UpToDate, Inc.
Dr. Chen is Professor of Obstetrics, Gynecology, and Reproductive Science and Medical Education, Vice-Chair of Ob-Gyn Education for the Mount Sinai Health System, Icahn School of Medicine, Mount Sinai, New York, New York. She is an OBG
The author reports receiving royalties from UpToDate, Inc.
The American College of Obstetricians and Gynecologists (ACOG) is a nonprofit organization of women’s health care physicians advocating the highest standards of practice, continuing member education, and public awareness of women’s health care issues.1 The organization has long recognized the impact that social media and mobile technology would have for itself as well as its membership. ACOG published a Social Media Guide in 2012, featuring a section on how to use apps in ObGyn practice and provided a list of apps for ObGyns and their patients.2
ACOG introduced its own app 4 years ago and has since updated the app several times, most recently on December 6, 2017. The ACOG app has a useful search function, a home button, and a place for users to email feedback (TABLE 1). The app most importantly contains several applets (small applications designed to perform a specific function within the main application). These applets encompass 3 types of apps for health care providers: clinical decision-making apps (Practice Bulletins, Committee Opinions, an Estimated Due Date Calculator that was featured in a prior review,3 Indicated Delivery, and Immunize) (TABLE 2), reference and information gathering apps (Today’s Headlines), and member support apps (ACOG Contacts, Careers, Annual Meeting, Districts, Council on Resident Education in Obstetrics and Gynecology [CREOG], and Website).4
This review will focus on the main ACOG app, which is evaluated by a shortened version of the APPLICATIONS scoring system, APPLI (app comprehensiveness, price, platform, literature use, and important special features).5 In addition, the clinical decision-making applets will be highlighted in a second table. I commend ACOG for developing these useful tools to augment their members’ practices. Of note, for the Practice Bulletins and Indicated Delivery applets, users will need to input their ACOG log-in access information.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
The American College of Obstetricians and Gynecologists (ACOG) is a nonprofit organization of women’s health care physicians advocating the highest standards of practice, continuing member education, and public awareness of women’s health care issues.1 The organization has long recognized the impact that social media and mobile technology would have for itself as well as its membership. ACOG published a Social Media Guide in 2012, featuring a section on how to use apps in ObGyn practice and provided a list of apps for ObGyns and their patients.2
ACOG introduced its own app 4 years ago and has since updated the app several times, most recently on December 6, 2017. The ACOG app has a useful search function, a home button, and a place for users to email feedback (TABLE 1). The app most importantly contains several applets (small applications designed to perform a specific function within the main application). These applets encompass 3 types of apps for health care providers: clinical decision-making apps (Practice Bulletins, Committee Opinions, an Estimated Due Date Calculator that was featured in a prior review,3 Indicated Delivery, and Immunize) (TABLE 2), reference and information gathering apps (Today’s Headlines), and member support apps (ACOG Contacts, Careers, Annual Meeting, Districts, Council on Resident Education in Obstetrics and Gynecology [CREOG], and Website).4
This review will focus on the main ACOG app, which is evaluated by a shortened version of the APPLICATIONS scoring system, APPLI (app comprehensiveness, price, platform, literature use, and important special features).5 In addition, the clinical decision-making applets will be highlighted in a second table. I commend ACOG for developing these useful tools to augment their members’ practices. Of note, for the Practice Bulletins and Indicated Delivery applets, users will need to input their ACOG log-in access information.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- The American College of Obstetricians and Gynecologists web site. https://www.acog.org/About-ACOG. Updated 2017. Accessed February 12, 2018.
- ACOG today. The American College of Obstetricians and Gynecologists https://www.acog.org/-/media/ACOG-Today /acogToday201211.pdf. Published November 2012. Accessed February 12, 2018.
- Chen KT. Three good apps for calculating the date of delivery. OBG Manag. 2017;29(1):45–46.
- Ventola CL. Mobile devices and apps for health care professionals: Uses and benefits. P T. 2014;39(5):356–364.
- Chyjek K, Farag S, Chen KT. Rating pregnancy wheel applications using the APPLICATIONS scoring system. Obstet Gynecol. 2015;125(6):1478–1483.
- The American College of Obstetricians and Gynecologists web site. https://www.acog.org/About-ACOG. Updated 2017. Accessed February 12, 2018.
- ACOG today. The American College of Obstetricians and Gynecologists https://www.acog.org/-/media/ACOG-Today /acogToday201211.pdf. Published November 2012. Accessed February 12, 2018.
- Chen KT. Three good apps for calculating the date of delivery. OBG Manag. 2017;29(1):45–46.
- Ventola CL. Mobile devices and apps for health care professionals: Uses and benefits. P T. 2014;39(5):356–364.
- Chyjek K, Farag S, Chen KT. Rating pregnancy wheel applications using the APPLICATIONS scoring system. Obstet Gynecol. 2015;125(6):1478–1483.
