User login
Sen. Cardin hears doctors’ concerns on ACA
On Oct. 1, the Affordable Care Act’s health insurance exchanges will be open for business in all 50 states and the District of Columbia. Some members of Congress have been meeting with constituents to talk about this milestone and what it means to them. Sen. Ben Cardin (D-Md.) recently held an open forum on health reform with physicians and administrators at the Prince George’s Hospital Center in Cheverly, Md.
The hospital is a safety net facility, treating many underinsured and uninsured patients. Sen. Cardin listened to doctors’ concerns about being able to meet their patients’ needs and also let them know that Democrats were aiming to make sure that the law would continue to be implemented.
On Twitter @aliciaault
On Oct. 1, the Affordable Care Act’s health insurance exchanges will be open for business in all 50 states and the District of Columbia. Some members of Congress have been meeting with constituents to talk about this milestone and what it means to them. Sen. Ben Cardin (D-Md.) recently held an open forum on health reform with physicians and administrators at the Prince George’s Hospital Center in Cheverly, Md.
The hospital is a safety net facility, treating many underinsured and uninsured patients. Sen. Cardin listened to doctors’ concerns about being able to meet their patients’ needs and also let them know that Democrats were aiming to make sure that the law would continue to be implemented.
On Twitter @aliciaault
On Oct. 1, the Affordable Care Act’s health insurance exchanges will be open for business in all 50 states and the District of Columbia. Some members of Congress have been meeting with constituents to talk about this milestone and what it means to them. Sen. Ben Cardin (D-Md.) recently held an open forum on health reform with physicians and administrators at the Prince George’s Hospital Center in Cheverly, Md.
The hospital is a safety net facility, treating many underinsured and uninsured patients. Sen. Cardin listened to doctors’ concerns about being able to meet their patients’ needs and also let them know that Democrats were aiming to make sure that the law would continue to be implemented.
On Twitter @aliciaault

Inside Hospitalists' Evolving Scope of Practice

In the October 2012 issue of The Hospitalist, the “Survey Insights” article discussed hospitalists’ evolving scope of practice based on information published in the 2012 State of Hospital Medicine report. The report remains the most authoritative, comprehensive source of information about our rapidly developing specialty, and this important topic is worthy of continued attention.
As I begin to orient a new class of hospitalists in my own HM group (HMG), I emphasize the five S’s of HMGs: scope, salary, schedule, structure, and society. HMGs define who they are largely by these constructs. As a specialty, we will define who we are by how we develop these constructs as a community. And it may indeed be the scope that most confirms our identity.
The survey (www.hospitalmedicine.org/survey) paints a self-portrait: What do we see when we look at that image? Figure 1 (below) lists information about services routinely provided by hospitalists, and one could divide the findings into three general categories.
First and foremost, there is the core work. It is clear that virtually all HMGs attended to primary-care-physician referrals and unassigned ED hospitalizations, and they also served as at least consultants for surgical comanagement. Most HMGs are now doing medical subspecialty comanagement, and the data would indicate that we are admitting and attending many of these patients. This raises the question about whether our identity will morph to that of the “universal admitter.” Many contend that health-care change forces will continue to pressure in this direction unless, and until, medical subspecialties develop their own dedicated hospitalists. Many hospitals may not be able to resource this; hence, there will likely be persistent pressure for the HMGs to provide this scope of care.
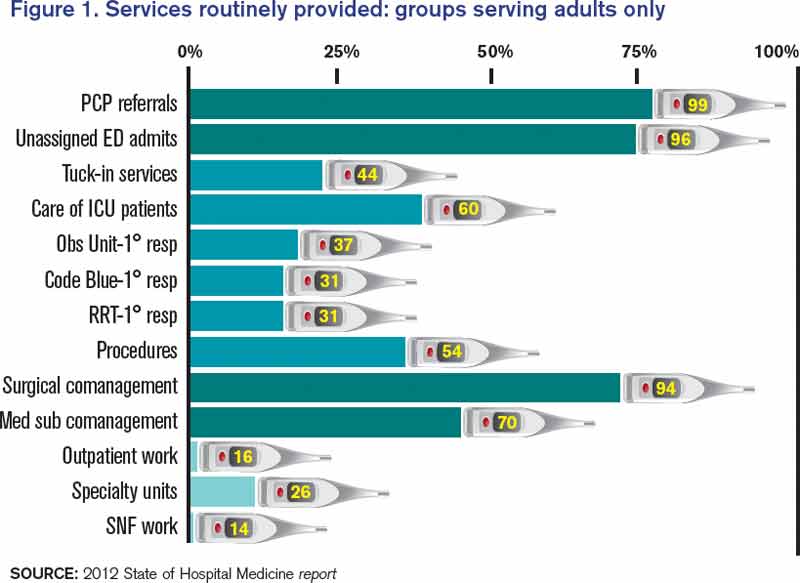
Perhaps half of HMGs provide the second group of services, which includes primary clinical care for rapid-response teams, code blue teams, and observation units. Forty-four percent of adult hospitalist programs provide a “tuck-in” service (nighttime coverage for other providers), and about 50% of HMGs reported performing procedures. Although this graph might suggest a decline in the proportion of groups caring for ICU patients compared with the 78% that was reported in 2011, this data set includes academic practices (the 2011 data didn’t). For nonacademic adult medicine practices, the proportion doing ICU work actually rose to 83.5% in 2012 from 78% in 2011. Larger hospitals and university settings are increasingly employing intensivists for ICU coverage, but the national deficit of intensivists will likely continue the external pressure for hospitalists to provide ICU care in many settings.
The final group of services represents the “road less traveled”—work in outpatient settings in such specialty units as long-term acute care, psychiatric wings, and skilled nursing facilities. These might prove to be niche opportunities or possible distractions.
There remains, however, the core work that identifies our specialty. We all do it, people depend on us to have it done, and it largely defines who we are as individuals, as HMGs, and as the fastest-growing specialty in American medical history.
Dr. Landis is medical director of Wellspan Hospitalists in York, Pa., and a member of SHM’s Practice Analysis Committee.
In the October 2012 issue of The Hospitalist, the “Survey Insights” article discussed hospitalists’ evolving scope of practice based on information published in the 2012 State of Hospital Medicine report. The report remains the most authoritative, comprehensive source of information about our rapidly developing specialty, and this important topic is worthy of continued attention.
As I begin to orient a new class of hospitalists in my own HM group (HMG), I emphasize the five S’s of HMGs: scope, salary, schedule, structure, and society. HMGs define who they are largely by these constructs. As a specialty, we will define who we are by how we develop these constructs as a community. And it may indeed be the scope that most confirms our identity.
The survey (www.hospitalmedicine.org/survey) paints a self-portrait: What do we see when we look at that image? Figure 1 (below) lists information about services routinely provided by hospitalists, and one could divide the findings into three general categories.
First and foremost, there is the core work. It is clear that virtually all HMGs attended to primary-care-physician referrals and unassigned ED hospitalizations, and they also served as at least consultants for surgical comanagement. Most HMGs are now doing medical subspecialty comanagement, and the data would indicate that we are admitting and attending many of these patients. This raises the question about whether our identity will morph to that of the “universal admitter.” Many contend that health-care change forces will continue to pressure in this direction unless, and until, medical subspecialties develop their own dedicated hospitalists. Many hospitals may not be able to resource this; hence, there will likely be persistent pressure for the HMGs to provide this scope of care.
Perhaps half of HMGs provide the second group of services, which includes primary clinical care for rapid-response teams, code blue teams, and observation units. Forty-four percent of adult hospitalist programs provide a “tuck-in” service (nighttime coverage for other providers), and about 50% of HMGs reported performing procedures. Although this graph might suggest a decline in the proportion of groups caring for ICU patients compared with the 78% that was reported in 2011, this data set includes academic practices (the 2011 data didn’t). For nonacademic adult medicine practices, the proportion doing ICU work actually rose to 83.5% in 2012 from 78% in 2011. Larger hospitals and university settings are increasingly employing intensivists for ICU coverage, but the national deficit of intensivists will likely continue the external pressure for hospitalists to provide ICU care in many settings.
The final group of services represents the “road less traveled”—work in outpatient settings in such specialty units as long-term acute care, psychiatric wings, and skilled nursing facilities. These might prove to be niche opportunities or possible distractions.
There remains, however, the core work that identifies our specialty. We all do it, people depend on us to have it done, and it largely defines who we are as individuals, as HMGs, and as the fastest-growing specialty in American medical history.
Dr. Landis is medical director of Wellspan Hospitalists in York, Pa., and a member of SHM’s Practice Analysis Committee.
In the October 2012 issue of The Hospitalist, the “Survey Insights” article discussed hospitalists’ evolving scope of practice based on information published in the 2012 State of Hospital Medicine report. The report remains the most authoritative, comprehensive source of information about our rapidly developing specialty, and this important topic is worthy of continued attention.
As I begin to orient a new class of hospitalists in my own HM group (HMG), I emphasize the five S’s of HMGs: scope, salary, schedule, structure, and society. HMGs define who they are largely by these constructs. As a specialty, we will define who we are by how we develop these constructs as a community. And it may indeed be the scope that most confirms our identity.
The survey (www.hospitalmedicine.org/survey) paints a self-portrait: What do we see when we look at that image? Figure 1 (below) lists information about services routinely provided by hospitalists, and one could divide the findings into three general categories.
First and foremost, there is the core work. It is clear that virtually all HMGs attended to primary-care-physician referrals and unassigned ED hospitalizations, and they also served as at least consultants for surgical comanagement. Most HMGs are now doing medical subspecialty comanagement, and the data would indicate that we are admitting and attending many of these patients. This raises the question about whether our identity will morph to that of the “universal admitter.” Many contend that health-care change forces will continue to pressure in this direction unless, and until, medical subspecialties develop their own dedicated hospitalists. Many hospitals may not be able to resource this; hence, there will likely be persistent pressure for the HMGs to provide this scope of care.
Perhaps half of HMGs provide the second group of services, which includes primary clinical care for rapid-response teams, code blue teams, and observation units. Forty-four percent of adult hospitalist programs provide a “tuck-in” service (nighttime coverage for other providers), and about 50% of HMGs reported performing procedures. Although this graph might suggest a decline in the proportion of groups caring for ICU patients compared with the 78% that was reported in 2011, this data set includes academic practices (the 2011 data didn’t). For nonacademic adult medicine practices, the proportion doing ICU work actually rose to 83.5% in 2012 from 78% in 2011. Larger hospitals and university settings are increasingly employing intensivists for ICU coverage, but the national deficit of intensivists will likely continue the external pressure for hospitalists to provide ICU care in many settings.
The final group of services represents the “road less traveled”—work in outpatient settings in such specialty units as long-term acute care, psychiatric wings, and skilled nursing facilities. These might prove to be niche opportunities or possible distractions.
There remains, however, the core work that identifies our specialty. We all do it, people depend on us to have it done, and it largely defines who we are as individuals, as HMGs, and as the fastest-growing specialty in American medical history.
Dr. Landis is medical director of Wellspan Hospitalists in York, Pa., and a member of SHM’s Practice Analysis Committee.
Multiple Approaches to Combat High Hospital Patient Census

In this age of cost containment and fiscal frugality, how do you handle high-census periods without jeopardizing patient care?
–Michael P. Mason, Tulsa, Okla.
Dr. Hospitalist responds:
Your group must first define the term “high census,” because workload is based on many factors. Seeing 20 patients a day in a large inner-city hospital is much different from seeing 20 patients in a suburban hospital in an affluent part of town. Also, seeing 20 patients geographically located on the same floor is much easier than 20 patients spread all over the hospital. Mid-level or nurse case-management support also makes a difference.
Once defined, there are many different ways to handle the high census; each hospitalist group must decide what works for them.
Many groups rely on their compensation structure to entice their physicians to see higher numbers of patients. The pay structure may be production-based and entice many of the group members to see more patients. Typically, for the member that does not want to see the large volumes, there are usually colleagues who are more than happy to cover the excess patients.
Some groups employ a hybrid system, with their compensation based on production and salary. Generally, bonuses or incentives are applied after meeting a specific relative value unit (RVU) threshold. These thresholds vary and usually are raised periodically based on the percentage of staff able to collect. Again, some group members may volunteer to see the excess patients for higher compensation. It is up to the group to develop mechanisms to measure the quality of care of these high producers and monitor for burnout.
Then there are groups that have no volume incentives and everyone is paid a salary. Many groups that utilize any of these compensation models have group members “on call” to come in when needed and see the excess patients. Many pay the on-call person some nominal amount just for being on call, or a per-patient or hourly rate if they have to come in. Others make it a mandatory part of the schedule without any additional compensation.
Many groups have integrated advanced-practice providers (nurse practitioners and physician assistants) into their systems. They can help hospitalists improve efficiency by seeing patients that are less ill or awaiting placement, or by performing such labor-intensive tasks as admissions and discharges.
HM groups should collaborate with the hospital’s chief financial officer. Like clinicians, most administrators recognize it is very difficult to deliver high-quality and efficient care when the numbers get high. It is in their best interest to help devise strategies and models that deliver quality care and the metrics needed to sustain support.
HM has become such a large specialty that there is no-one-size-fits-all solution to high censuses. In the end, you have to be comfortable with the system created by your group, work to help improve it, or seek a better fit.
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to drhospit@wiley.com.
In this age of cost containment and fiscal frugality, how do you handle high-census periods without jeopardizing patient care?
–Michael P. Mason, Tulsa, Okla.
Dr. Hospitalist responds:
Your group must first define the term “high census,” because workload is based on many factors. Seeing 20 patients a day in a large inner-city hospital is much different from seeing 20 patients in a suburban hospital in an affluent part of town. Also, seeing 20 patients geographically located on the same floor is much easier than 20 patients spread all over the hospital. Mid-level or nurse case-management support also makes a difference.
Once defined, there are many different ways to handle the high census; each hospitalist group must decide what works for them.
Many groups rely on their compensation structure to entice their physicians to see higher numbers of patients. The pay structure may be production-based and entice many of the group members to see more patients. Typically, for the member that does not want to see the large volumes, there are usually colleagues who are more than happy to cover the excess patients.
Some groups employ a hybrid system, with their compensation based on production and salary. Generally, bonuses or incentives are applied after meeting a specific relative value unit (RVU) threshold. These thresholds vary and usually are raised periodically based on the percentage of staff able to collect. Again, some group members may volunteer to see the excess patients for higher compensation. It is up to the group to develop mechanisms to measure the quality of care of these high producers and monitor for burnout.
Then there are groups that have no volume incentives and everyone is paid a salary. Many groups that utilize any of these compensation models have group members “on call” to come in when needed and see the excess patients. Many pay the on-call person some nominal amount just for being on call, or a per-patient or hourly rate if they have to come in. Others make it a mandatory part of the schedule without any additional compensation.
Many groups have integrated advanced-practice providers (nurse practitioners and physician assistants) into their systems. They can help hospitalists improve efficiency by seeing patients that are less ill or awaiting placement, or by performing such labor-intensive tasks as admissions and discharges.
HM groups should collaborate with the hospital’s chief financial officer. Like clinicians, most administrators recognize it is very difficult to deliver high-quality and efficient care when the numbers get high. It is in their best interest to help devise strategies and models that deliver quality care and the metrics needed to sustain support.
HM has become such a large specialty that there is no-one-size-fits-all solution to high censuses. In the end, you have to be comfortable with the system created by your group, work to help improve it, or seek a better fit.
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to drhospit@wiley.com.
In this age of cost containment and fiscal frugality, how do you handle high-census periods without jeopardizing patient care?
–Michael P. Mason, Tulsa, Okla.
Dr. Hospitalist responds:
Your group must first define the term “high census,” because workload is based on many factors. Seeing 20 patients a day in a large inner-city hospital is much different from seeing 20 patients in a suburban hospital in an affluent part of town. Also, seeing 20 patients geographically located on the same floor is much easier than 20 patients spread all over the hospital. Mid-level or nurse case-management support also makes a difference.
Once defined, there are many different ways to handle the high census; each hospitalist group must decide what works for them.
Many groups rely on their compensation structure to entice their physicians to see higher numbers of patients. The pay structure may be production-based and entice many of the group members to see more patients. Typically, for the member that does not want to see the large volumes, there are usually colleagues who are more than happy to cover the excess patients.
Some groups employ a hybrid system, with their compensation based on production and salary. Generally, bonuses or incentives are applied after meeting a specific relative value unit (RVU) threshold. These thresholds vary and usually are raised periodically based on the percentage of staff able to collect. Again, some group members may volunteer to see the excess patients for higher compensation. It is up to the group to develop mechanisms to measure the quality of care of these high producers and monitor for burnout.
Then there are groups that have no volume incentives and everyone is paid a salary. Many groups that utilize any of these compensation models have group members “on call” to come in when needed and see the excess patients. Many pay the on-call person some nominal amount just for being on call, or a per-patient or hourly rate if they have to come in. Others make it a mandatory part of the schedule without any additional compensation.
Many groups have integrated advanced-practice providers (nurse practitioners and physician assistants) into their systems. They can help hospitalists improve efficiency by seeing patients that are less ill or awaiting placement, or by performing such labor-intensive tasks as admissions and discharges.
HM groups should collaborate with the hospital’s chief financial officer. Like clinicians, most administrators recognize it is very difficult to deliver high-quality and efficient care when the numbers get high. It is in their best interest to help devise strategies and models that deliver quality care and the metrics needed to sustain support.
HM has become such a large specialty that there is no-one-size-fits-all solution to high censuses. In the end, you have to be comfortable with the system created by your group, work to help improve it, or seek a better fit.
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to drhospit@wiley.com.
MGMA Physician Compensation Survey Raises Questions About Performance Pay

Sorting out whether a hospitalist’s bonus and other compensation elements are in line with survey data often leads to confusion. The 2013 MGMA Physician Compensation and Production Survey report, based on 2012 data, shows median compensation of $240,352 for internal-medicine hospitalists (I’ll round it to $240,000 for the rest of this piece). So is your compensation in line with survey medians if your base pay is $230,000 and you have a performance bonus of up to $20,000?
The problem is that you can’t know in advance how much of the $20,000 performance bonus you will earn. And isn’t a bonus supposed to be on top of typical compensation? To be in line with the survey, shouldn’t your base pay equal the $240,000 median, with any available bonus dollars on top of that? (Base pay means all forms of compensation other than a performance bonus; it could be productivity-based compensation, pay connected to numbers of shifts or hours worked, or a fixed annual salary, etc.)
The short answer is no, and to demonstrate why, I’ll first review some facts about the survey itself, then apply that knowledge to the hospitalist marketplace.
I want to emphasize that in this article, I’m not taking a position on the right amount of workload, compensation, or bonus for any hospitalist practice. And I’m using survey medians just to simplify the discussion, not because they’re optimal for any particular practice.
Survey Data
The most important thing to know about the survey data is that the $240,000 figure takes into account all forms of pay, including extra shift pay and any bonuses that might have been paid to each provider in the data set. Such benefits as health insurance and retirement-plan contribution are not included in this figure.
There are several ways a hospitalist might have earned compensation that matches the survey median. He or she might have a fixed annual salary equal to the median with no bonus available or had a meaningful bonus (e.g. $10,000 to $20,000) available and failed to earn any of it. Or the base might have come to $230,000, and he or she earned half of the available $20,000 performance bonus. Many other permutations of bonus and other salary elements could occur to arrive at the same $240,000 figure.
The important thing to remember is that whatever bonus dollars were paid, they are included in the salary figure from the survey—not added on top of that figure. So if all bonus dollars earned were subtracted from the survey, the total “nonbonus” compensation would be lower than $240,000.
How much lower?
Typical Hospitalist Bonus Amounts
The MGMA survey doesn’t report the portion of compensation tied to a bonus, but SHM’s does. SHM’s 2012 State of Hospital Medicine Report, based on 2011 data (www.hospitalmedicine.org/survey), is based on the most recent data available, and it showed (on page 60) that an average of 7% of pay was tied to performance for nonacademic hospitalist groups serving adults only. This included any payments for good individual or group performance on quality, efficiency, service, satisfaction, and/or other nonproduction measures. In conversation, this often is referred to as a “bonus” rather than “performance compensation.”
One way to estimate the nonbonus compensation would be to reduce the total pay by 7%, which comes to $223,200. Keep in mind that there are all kinds of mathematical and methodological problems in manipulating the reported survey numbers from two separate surveys to derive additional benchmarks. But this seems like a reasonable guess.
An increasing portion of hospitalist groups have some pay tied to performance, and the portion of total pay tied to performance seems to be going up at least a little. It was 5% of pay in 2010 and 4% in 2011, compared with 7% in the 2012 survey.
Keep in mind two things. First, this 7% reflects the performance or bonus dollars actually paid out, not the total amount available. In other words, even if the median total bonus dollars available were 20% of compensation, hospitalists earned less than that. Some hospitalists earned all dollars available, and some earned only a portion of what was available. And second, some hospitalists fail to earn any bonus or don’t have one available at all. So the survey would show for them zero compensation tied to bonus.
Making Sense of the Numbers
If you follow the reasoning above, then you probably agree that if your goal is to match mean compensation from the MGMA survey (I’m not suggesting that is the best goal, merely using it for simplicity), then you would set nonbonus compensation 7% below median—as long as you’re likely to get the same portion of a bonus as the median practice.
In some practices, performance thresholds are set at a level that is very easy to achieve, meaning the hospitalists are almost guaranteed to get all of the bonus compensation available. To be consistent with survey medians, it would be appropriate for them to set nonbonus compensation by subtracting all bonus dollars from the survey median. For example, if a $20,000 bonus is available and all of it is likely to be earned by the hospitalists, then total nonbonus compensation would be $220,000.
However, what if the bonus requires significant improvements in performance by the doctors (which seems most appropriate to me; why have a bonus otherwise?) and it is likely they will earn only 25% of all bonus dollars available? If the total available bonus is $20,000, then something like 25%, or $5,000, should be subtracted from the median to yield a total nonbonus compensation of $235,000.
Simple Thinking
I think it makes most sense to set total nonbonus compensation below the targeted total compensation. Failure to achieve any performance thresholds means no bonus and compensation will be below target that year. Meeting some thresholds (some improvement in performance) should result in matching the target compensation, and truly terrific performance that meets or exceeds all thresholds should result in the doctor being paid above the target.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Sorting out whether a hospitalist’s bonus and other compensation elements are in line with survey data often leads to confusion. The 2013 MGMA Physician Compensation and Production Survey report, based on 2012 data, shows median compensation of $240,352 for internal-medicine hospitalists (I’ll round it to $240,000 for the rest of this piece). So is your compensation in line with survey medians if your base pay is $230,000 and you have a performance bonus of up to $20,000?
The problem is that you can’t know in advance how much of the $20,000 performance bonus you will earn. And isn’t a bonus supposed to be on top of typical compensation? To be in line with the survey, shouldn’t your base pay equal the $240,000 median, with any available bonus dollars on top of that? (Base pay means all forms of compensation other than a performance bonus; it could be productivity-based compensation, pay connected to numbers of shifts or hours worked, or a fixed annual salary, etc.)
The short answer is no, and to demonstrate why, I’ll first review some facts about the survey itself, then apply that knowledge to the hospitalist marketplace.
I want to emphasize that in this article, I’m not taking a position on the right amount of workload, compensation, or bonus for any hospitalist practice. And I’m using survey medians just to simplify the discussion, not because they’re optimal for any particular practice.
Survey Data
The most important thing to know about the survey data is that the $240,000 figure takes into account all forms of pay, including extra shift pay and any bonuses that might have been paid to each provider in the data set. Such benefits as health insurance and retirement-plan contribution are not included in this figure.
There are several ways a hospitalist might have earned compensation that matches the survey median. He or she might have a fixed annual salary equal to the median with no bonus available or had a meaningful bonus (e.g. $10,000 to $20,000) available and failed to earn any of it. Or the base might have come to $230,000, and he or she earned half of the available $20,000 performance bonus. Many other permutations of bonus and other salary elements could occur to arrive at the same $240,000 figure.
The important thing to remember is that whatever bonus dollars were paid, they are included in the salary figure from the survey—not added on top of that figure. So if all bonus dollars earned were subtracted from the survey, the total “nonbonus” compensation would be lower than $240,000.
How much lower?
Typical Hospitalist Bonus Amounts
The MGMA survey doesn’t report the portion of compensation tied to a bonus, but SHM’s does. SHM’s 2012 State of Hospital Medicine Report, based on 2011 data (www.hospitalmedicine.org/survey), is based on the most recent data available, and it showed (on page 60) that an average of 7% of pay was tied to performance for nonacademic hospitalist groups serving adults only. This included any payments for good individual or group performance on quality, efficiency, service, satisfaction, and/or other nonproduction measures. In conversation, this often is referred to as a “bonus” rather than “performance compensation.”
One way to estimate the nonbonus compensation would be to reduce the total pay by 7%, which comes to $223,200. Keep in mind that there are all kinds of mathematical and methodological problems in manipulating the reported survey numbers from two separate surveys to derive additional benchmarks. But this seems like a reasonable guess.
An increasing portion of hospitalist groups have some pay tied to performance, and the portion of total pay tied to performance seems to be going up at least a little. It was 5% of pay in 2010 and 4% in 2011, compared with 7% in the 2012 survey.
Keep in mind two things. First, this 7% reflects the performance or bonus dollars actually paid out, not the total amount available. In other words, even if the median total bonus dollars available were 20% of compensation, hospitalists earned less than that. Some hospitalists earned all dollars available, and some earned only a portion of what was available. And second, some hospitalists fail to earn any bonus or don’t have one available at all. So the survey would show for them zero compensation tied to bonus.
Making Sense of the Numbers
If you follow the reasoning above, then you probably agree that if your goal is to match mean compensation from the MGMA survey (I’m not suggesting that is the best goal, merely using it for simplicity), then you would set nonbonus compensation 7% below median—as long as you’re likely to get the same portion of a bonus as the median practice.
In some practices, performance thresholds are set at a level that is very easy to achieve, meaning the hospitalists are almost guaranteed to get all of the bonus compensation available. To be consistent with survey medians, it would be appropriate for them to set nonbonus compensation by subtracting all bonus dollars from the survey median. For example, if a $20,000 bonus is available and all of it is likely to be earned by the hospitalists, then total nonbonus compensation would be $220,000.
However, what if the bonus requires significant improvements in performance by the doctors (which seems most appropriate to me; why have a bonus otherwise?) and it is likely they will earn only 25% of all bonus dollars available? If the total available bonus is $20,000, then something like 25%, or $5,000, should be subtracted from the median to yield a total nonbonus compensation of $235,000.
Simple Thinking
I think it makes most sense to set total nonbonus compensation below the targeted total compensation. Failure to achieve any performance thresholds means no bonus and compensation will be below target that year. Meeting some thresholds (some improvement in performance) should result in matching the target compensation, and truly terrific performance that meets or exceeds all thresholds should result in the doctor being paid above the target.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Sorting out whether a hospitalist’s bonus and other compensation elements are in line with survey data often leads to confusion. The 2013 MGMA Physician Compensation and Production Survey report, based on 2012 data, shows median compensation of $240,352 for internal-medicine hospitalists (I’ll round it to $240,000 for the rest of this piece). So is your compensation in line with survey medians if your base pay is $230,000 and you have a performance bonus of up to $20,000?
The problem is that you can’t know in advance how much of the $20,000 performance bonus you will earn. And isn’t a bonus supposed to be on top of typical compensation? To be in line with the survey, shouldn’t your base pay equal the $240,000 median, with any available bonus dollars on top of that? (Base pay means all forms of compensation other than a performance bonus; it could be productivity-based compensation, pay connected to numbers of shifts or hours worked, or a fixed annual salary, etc.)
The short answer is no, and to demonstrate why, I’ll first review some facts about the survey itself, then apply that knowledge to the hospitalist marketplace.
I want to emphasize that in this article, I’m not taking a position on the right amount of workload, compensation, or bonus for any hospitalist practice. And I’m using survey medians just to simplify the discussion, not because they’re optimal for any particular practice.
Survey Data
The most important thing to know about the survey data is that the $240,000 figure takes into account all forms of pay, including extra shift pay and any bonuses that might have been paid to each provider in the data set. Such benefits as health insurance and retirement-plan contribution are not included in this figure.
There are several ways a hospitalist might have earned compensation that matches the survey median. He or she might have a fixed annual salary equal to the median with no bonus available or had a meaningful bonus (e.g. $10,000 to $20,000) available and failed to earn any of it. Or the base might have come to $230,000, and he or she earned half of the available $20,000 performance bonus. Many other permutations of bonus and other salary elements could occur to arrive at the same $240,000 figure.
The important thing to remember is that whatever bonus dollars were paid, they are included in the salary figure from the survey—not added on top of that figure. So if all bonus dollars earned were subtracted from the survey, the total “nonbonus” compensation would be lower than $240,000.
How much lower?
Typical Hospitalist Bonus Amounts
The MGMA survey doesn’t report the portion of compensation tied to a bonus, but SHM’s does. SHM’s 2012 State of Hospital Medicine Report, based on 2011 data (www.hospitalmedicine.org/survey), is based on the most recent data available, and it showed (on page 60) that an average of 7% of pay was tied to performance for nonacademic hospitalist groups serving adults only. This included any payments for good individual or group performance on quality, efficiency, service, satisfaction, and/or other nonproduction measures. In conversation, this often is referred to as a “bonus” rather than “performance compensation.”
One way to estimate the nonbonus compensation would be to reduce the total pay by 7%, which comes to $223,200. Keep in mind that there are all kinds of mathematical and methodological problems in manipulating the reported survey numbers from two separate surveys to derive additional benchmarks. But this seems like a reasonable guess.
An increasing portion of hospitalist groups have some pay tied to performance, and the portion of total pay tied to performance seems to be going up at least a little. It was 5% of pay in 2010 and 4% in 2011, compared with 7% in the 2012 survey.
Keep in mind two things. First, this 7% reflects the performance or bonus dollars actually paid out, not the total amount available. In other words, even if the median total bonus dollars available were 20% of compensation, hospitalists earned less than that. Some hospitalists earned all dollars available, and some earned only a portion of what was available. And second, some hospitalists fail to earn any bonus or don’t have one available at all. So the survey would show for them zero compensation tied to bonus.
Making Sense of the Numbers
If you follow the reasoning above, then you probably agree that if your goal is to match mean compensation from the MGMA survey (I’m not suggesting that is the best goal, merely using it for simplicity), then you would set nonbonus compensation 7% below median—as long as you’re likely to get the same portion of a bonus as the median practice.
In some practices, performance thresholds are set at a level that is very easy to achieve, meaning the hospitalists are almost guaranteed to get all of the bonus compensation available. To be consistent with survey medians, it would be appropriate for them to set nonbonus compensation by subtracting all bonus dollars from the survey median. For example, if a $20,000 bonus is available and all of it is likely to be earned by the hospitalists, then total nonbonus compensation would be $220,000.
However, what if the bonus requires significant improvements in performance by the doctors (which seems most appropriate to me; why have a bonus otherwise?) and it is likely they will earn only 25% of all bonus dollars available? If the total available bonus is $20,000, then something like 25%, or $5,000, should be subtracted from the median to yield a total nonbonus compensation of $235,000.
Simple Thinking
I think it makes most sense to set total nonbonus compensation below the targeted total compensation. Failure to achieve any performance thresholds means no bonus and compensation will be below target that year. Meeting some thresholds (some improvement in performance) should result in matching the target compensation, and truly terrific performance that meets or exceeds all thresholds should result in the doctor being paid above the target.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Patient Satisfaction Surveys Not Accurate Measure of Hospitalists’ Performance

Feeling frustrated with your group’s patient-satisfaction performance? Wondering why your chief (fill in the blank) officer glazes over when you try to explain why your hospitalist group’s Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS) scores for doctor communication are in a percentile rivaling the numeric age of your children?
It is likely that the C-suite administrator overseeing your hospitalist group has a portion of their pay based on HCAHPS or other patient-satisfaction (also called patient experience) scores. And for good reason: The Centers for Medicare & Medicaid Services (CMS) Hospital Value-Based Purchasing (HVBP) program that started Oct. 1, 2012, has placed your hospital’s Medicare reimbursement at risk based on its HCAHPS scores.
HVBP and Patient Satisfaction
Patient satisfaction will remain an important part of HVBP in the coming years. Table 1 (below) shows the domains that will be included in fiscal years 2014 (which starts Oct. 1, 2013), 2015, and 2016. Table 2 (below) depicts the percent weighting the patient-satisfaction domain will receive through 2016. You may recall that HVBP is a program in which all hospitals place 1% to 2% (2013 through 2017, starting at 1% and increasing each year by 0.25% so that by 2017%, it is 2%) of their CMS inpatient payments in a withhold pool and, based on performance, can make back some, all, or an amount in excess of the amount placed in the withhold pool.
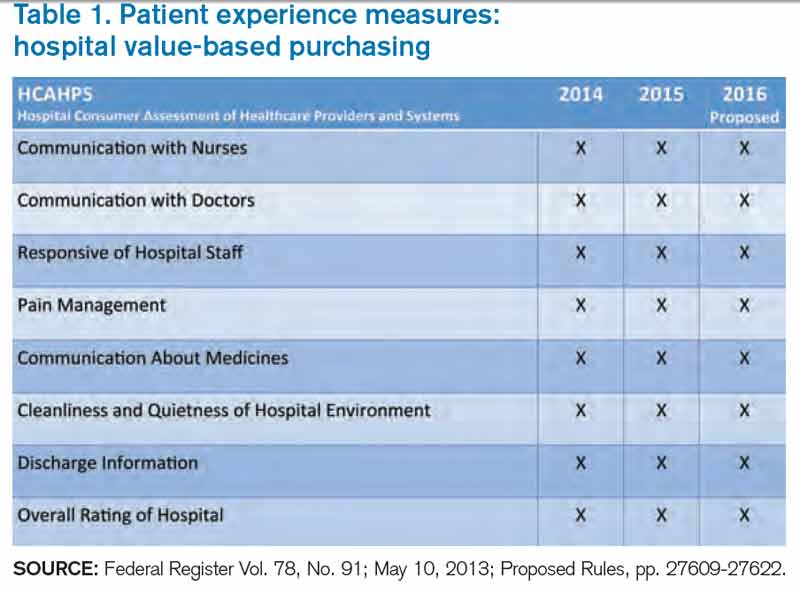
Source: Federal Register Vol. 78, No. 91; May 10, 2013; Proposed Rules, pp. 27609-27622.
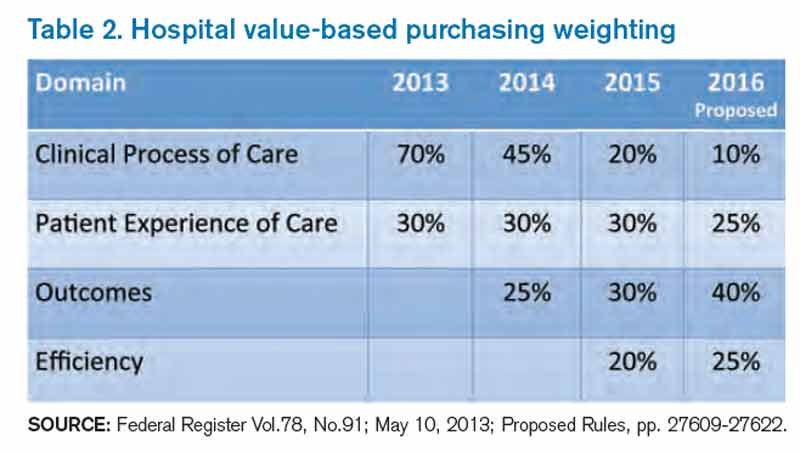
Source: Federal Register Vol.78, No.91; May 10, 2013; Proposed Rules, pp. 27609-27622.
End In Itself
A colleague of mine recently asked, “Is an increase in patient satisfaction associated with higher quality of care and better patient safety?” The point here: It doesn’t matter. Patient satisfaction is an end in itself, and we should strive to maximize it, or at least put ourselves in the place of the patient and design care accordingly.
For Hospitalists: A Starting Point
There is a conundrum for hospitalists vis-à-vis patient satisfaction. Follow this chain of logic: The hospitals at which we work are incented to perform well on the HCAHPS domains. Hospitals pay a lot for hospitalists. Hospitalists can impact many of the HCAHPS domains. So shouldn’t hospitalists be judged according to HCAHPS scores?
Yes and no.
HCAHPS as a survey is intended to measure a patient’s overall experience of receiving care in the hospital. For example, from the “Doctor Communication” domain, we have questions like “how often did doctors treat you with courtesy and respect?” And “how often did doctors explain things in a way you could understand?”
These questions, like all in HCAHPS, are not designed to get at individual doctor performance, or even performance of a group of doctors, such as hospitalists. Instead, they are designed to measure a patient’s overall experience with the hospitalization, and “Doctor Communication” questions are designed to assess satisfaction with “doctors” collectively.
The Need for Hospitalist-Specific Satisfaction Surveys
So while HCAHPS is not designed to measure hospitalist performance with regard to patient satisfaction, it is a reasonable interim step for hospitals to judge hospitalists according to HCAHPS. However, this should be a bridge to a strategy that adopts hospitalist-specific patient-satisfaction questionnaires in the future and not an end in itself.
Why? Perhaps the biggest reason is that HCAHPS scores are neither specific nor timely enough to form the basis of improvement efforts for hospitalists. If a hospitalist receives a low score on the “Doctor Communication” domain, the scores are likely to be three to nine months old. How can we legitimately assign (and then modify) behaviors based on those scores?
Further, because the survey is not built to measure patient satisfaction specifically with hospitalists, the results are unlikely to engender meaningful and sustained behavior change. Hospitalists I talk to are generally bewildered and confused by HCAHPS scores attributed to them or their groups. Even if they understand the scores, I almost never see true quality improvement (plan-do-study-act) based on specific HCAHPS results. Instead, I see hospitalists trying to adhere to “best practices,” with no adjustments made along the way based on performance.
Nearly all the prominent patient satisfaction vendors have developed a survey instrument specifically designed for hospitalists. Each has an approach to appropriately attribute performance to the hospitalist in question, and each has a battery of questions that is designed to capture patient satisfaction with the hospitalist. Although use of these surveys involves an added financial commitment, I submit that because hospitalists have an unparalleled proximity to hospitalized patients, such an investment is worthy of consideration and has an accompanying business case, thanks to HVBP. The results of these surveys may form the basis of legitimate, targeted feedback to hospitalists, who may then adjust their approach to patient interactions. Such performance improvement should result in improved HCAHPS scores.
In sum, hospitalists should pay close attention to patient satisfaction and embrace HCAHPS. However, we should be looking beyond HCAHPS to survey instruments that fairly and accurately measure our performance. Such surveys will be more widely accepted by the hospitalists they are measuring, and will allow hospitalists to perform meaningful quality improvement based on the results. Although hospitalist-specific surveys will require an investment, the increased patient satisfaction that results should be the basis of a favorable return on that investment.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Feeling frustrated with your group’s patient-satisfaction performance? Wondering why your chief (fill in the blank) officer glazes over when you try to explain why your hospitalist group’s Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS) scores for doctor communication are in a percentile rivaling the numeric age of your children?
It is likely that the C-suite administrator overseeing your hospitalist group has a portion of their pay based on HCAHPS or other patient-satisfaction (also called patient experience) scores. And for good reason: The Centers for Medicare & Medicaid Services (CMS) Hospital Value-Based Purchasing (HVBP) program that started Oct. 1, 2012, has placed your hospital’s Medicare reimbursement at risk based on its HCAHPS scores.
HVBP and Patient Satisfaction
Patient satisfaction will remain an important part of HVBP in the coming years. Table 1 (below) shows the domains that will be included in fiscal years 2014 (which starts Oct. 1, 2013), 2015, and 2016. Table 2 (below) depicts the percent weighting the patient-satisfaction domain will receive through 2016. You may recall that HVBP is a program in which all hospitals place 1% to 2% (2013 through 2017, starting at 1% and increasing each year by 0.25% so that by 2017%, it is 2%) of their CMS inpatient payments in a withhold pool and, based on performance, can make back some, all, or an amount in excess of the amount placed in the withhold pool.
Source: Federal Register Vol. 78, No. 91; May 10, 2013; Proposed Rules, pp. 27609-27622.
Source: Federal Register Vol.78, No.91; May 10, 2013; Proposed Rules, pp. 27609-27622.
End In Itself
A colleague of mine recently asked, “Is an increase in patient satisfaction associated with higher quality of care and better patient safety?” The point here: It doesn’t matter. Patient satisfaction is an end in itself, and we should strive to maximize it, or at least put ourselves in the place of the patient and design care accordingly.
For Hospitalists: A Starting Point
There is a conundrum for hospitalists vis-à-vis patient satisfaction. Follow this chain of logic: The hospitals at which we work are incented to perform well on the HCAHPS domains. Hospitals pay a lot for hospitalists. Hospitalists can impact many of the HCAHPS domains. So shouldn’t hospitalists be judged according to HCAHPS scores?
Yes and no.
HCAHPS as a survey is intended to measure a patient’s overall experience of receiving care in the hospital. For example, from the “Doctor Communication” domain, we have questions like “how often did doctors treat you with courtesy and respect?” And “how often did doctors explain things in a way you could understand?”
These questions, like all in HCAHPS, are not designed to get at individual doctor performance, or even performance of a group of doctors, such as hospitalists. Instead, they are designed to measure a patient’s overall experience with the hospitalization, and “Doctor Communication” questions are designed to assess satisfaction with “doctors” collectively.
The Need for Hospitalist-Specific Satisfaction Surveys
So while HCAHPS is not designed to measure hospitalist performance with regard to patient satisfaction, it is a reasonable interim step for hospitals to judge hospitalists according to HCAHPS. However, this should be a bridge to a strategy that adopts hospitalist-specific patient-satisfaction questionnaires in the future and not an end in itself.
Why? Perhaps the biggest reason is that HCAHPS scores are neither specific nor timely enough to form the basis of improvement efforts for hospitalists. If a hospitalist receives a low score on the “Doctor Communication” domain, the scores are likely to be three to nine months old. How can we legitimately assign (and then modify) behaviors based on those scores?
Further, because the survey is not built to measure patient satisfaction specifically with hospitalists, the results are unlikely to engender meaningful and sustained behavior change. Hospitalists I talk to are generally bewildered and confused by HCAHPS scores attributed to them or their groups. Even if they understand the scores, I almost never see true quality improvement (plan-do-study-act) based on specific HCAHPS results. Instead, I see hospitalists trying to adhere to “best practices,” with no adjustments made along the way based on performance.
Nearly all the prominent patient satisfaction vendors have developed a survey instrument specifically designed for hospitalists. Each has an approach to appropriately attribute performance to the hospitalist in question, and each has a battery of questions that is designed to capture patient satisfaction with the hospitalist. Although use of these surveys involves an added financial commitment, I submit that because hospitalists have an unparalleled proximity to hospitalized patients, such an investment is worthy of consideration and has an accompanying business case, thanks to HVBP. The results of these surveys may form the basis of legitimate, targeted feedback to hospitalists, who may then adjust their approach to patient interactions. Such performance improvement should result in improved HCAHPS scores.
In sum, hospitalists should pay close attention to patient satisfaction and embrace HCAHPS. However, we should be looking beyond HCAHPS to survey instruments that fairly and accurately measure our performance. Such surveys will be more widely accepted by the hospitalists they are measuring, and will allow hospitalists to perform meaningful quality improvement based on the results. Although hospitalist-specific surveys will require an investment, the increased patient satisfaction that results should be the basis of a favorable return on that investment.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Feeling frustrated with your group’s patient-satisfaction performance? Wondering why your chief (fill in the blank) officer glazes over when you try to explain why your hospitalist group’s Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS) scores for doctor communication are in a percentile rivaling the numeric age of your children?
It is likely that the C-suite administrator overseeing your hospitalist group has a portion of their pay based on HCAHPS or other patient-satisfaction (also called patient experience) scores. And for good reason: The Centers for Medicare & Medicaid Services (CMS) Hospital Value-Based Purchasing (HVBP) program that started Oct. 1, 2012, has placed your hospital’s Medicare reimbursement at risk based on its HCAHPS scores.
HVBP and Patient Satisfaction
Patient satisfaction will remain an important part of HVBP in the coming years. Table 1 (below) shows the domains that will be included in fiscal years 2014 (which starts Oct. 1, 2013), 2015, and 2016. Table 2 (below) depicts the percent weighting the patient-satisfaction domain will receive through 2016. You may recall that HVBP is a program in which all hospitals place 1% to 2% (2013 through 2017, starting at 1% and increasing each year by 0.25% so that by 2017%, it is 2%) of their CMS inpatient payments in a withhold pool and, based on performance, can make back some, all, or an amount in excess of the amount placed in the withhold pool.
Source: Federal Register Vol. 78, No. 91; May 10, 2013; Proposed Rules, pp. 27609-27622.
Source: Federal Register Vol.78, No.91; May 10, 2013; Proposed Rules, pp. 27609-27622.
End In Itself
A colleague of mine recently asked, “Is an increase in patient satisfaction associated with higher quality of care and better patient safety?” The point here: It doesn’t matter. Patient satisfaction is an end in itself, and we should strive to maximize it, or at least put ourselves in the place of the patient and design care accordingly.
For Hospitalists: A Starting Point
There is a conundrum for hospitalists vis-à-vis patient satisfaction. Follow this chain of logic: The hospitals at which we work are incented to perform well on the HCAHPS domains. Hospitals pay a lot for hospitalists. Hospitalists can impact many of the HCAHPS domains. So shouldn’t hospitalists be judged according to HCAHPS scores?
Yes and no.
HCAHPS as a survey is intended to measure a patient’s overall experience of receiving care in the hospital. For example, from the “Doctor Communication” domain, we have questions like “how often did doctors treat you with courtesy and respect?” And “how often did doctors explain things in a way you could understand?”
These questions, like all in HCAHPS, are not designed to get at individual doctor performance, or even performance of a group of doctors, such as hospitalists. Instead, they are designed to measure a patient’s overall experience with the hospitalization, and “Doctor Communication” questions are designed to assess satisfaction with “doctors” collectively.
The Need for Hospitalist-Specific Satisfaction Surveys
So while HCAHPS is not designed to measure hospitalist performance with regard to patient satisfaction, it is a reasonable interim step for hospitals to judge hospitalists according to HCAHPS. However, this should be a bridge to a strategy that adopts hospitalist-specific patient-satisfaction questionnaires in the future and not an end in itself.
Why? Perhaps the biggest reason is that HCAHPS scores are neither specific nor timely enough to form the basis of improvement efforts for hospitalists. If a hospitalist receives a low score on the “Doctor Communication” domain, the scores are likely to be three to nine months old. How can we legitimately assign (and then modify) behaviors based on those scores?
Further, because the survey is not built to measure patient satisfaction specifically with hospitalists, the results are unlikely to engender meaningful and sustained behavior change. Hospitalists I talk to are generally bewildered and confused by HCAHPS scores attributed to them or their groups. Even if they understand the scores, I almost never see true quality improvement (plan-do-study-act) based on specific HCAHPS results. Instead, I see hospitalists trying to adhere to “best practices,” with no adjustments made along the way based on performance.
Nearly all the prominent patient satisfaction vendors have developed a survey instrument specifically designed for hospitalists. Each has an approach to appropriately attribute performance to the hospitalist in question, and each has a battery of questions that is designed to capture patient satisfaction with the hospitalist. Although use of these surveys involves an added financial commitment, I submit that because hospitalists have an unparalleled proximity to hospitalized patients, such an investment is worthy of consideration and has an accompanying business case, thanks to HVBP. The results of these surveys may form the basis of legitimate, targeted feedback to hospitalists, who may then adjust their approach to patient interactions. Such performance improvement should result in improved HCAHPS scores.
In sum, hospitalists should pay close attention to patient satisfaction and embrace HCAHPS. However, we should be looking beyond HCAHPS to survey instruments that fairly and accurately measure our performance. Such surveys will be more widely accepted by the hospitalists they are measuring, and will allow hospitalists to perform meaningful quality improvement based on the results. Although hospitalist-specific surveys will require an investment, the increased patient satisfaction that results should be the basis of a favorable return on that investment.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Pediatric Hospital Medicine Marks 10th Anniversary

With a record number of attendees, Pediatric Hospital Medicine 2013 (PHM) swept into New Orleans last month, carrying with it unbridled enthusiasm about the past, present, and future.
Virginia Moyer, MD, MPH, vice president for maintenance of certification and quality for the American Board of Pediatrics (ABP) and professor of pediatrics and chief of academic general pediatrics at Texas Children’s Hospital, delivered a keynote address to 700 attendees that focused on the challenges and opportunities of providing evidence-based, high-quality care in the hospital, as well as ABP’s role in meeting these challenges.
“If evidence-based medicine is an individual sport,” Dr. Moyer said, “then quality improvement is a team sport.”
Barriers to quality improvement (QI)— such as lack of will, lack of data, and lack of training—can be surmounted in a team environment, she said. ABP is continuing in its efforts to support QI education through its Maintenance of Certification (MOC) Part 4 modules, as well as other educational activities.
Other highlights of the 10th annual Pediatric Hospital Medicine meeting:
- The addition of a new “Community Hospitalists” track was given high marks by those in attendance. It covered such topics as perioperative management of medically complex pediatric patients, community-acquired pneumonia, and osteomyelitis.
- A 10-year retrospective of pediatric hospital medicine was given by a panel of notable pediatric hospitalists, including Erin Stucky Fisher, MD, FAAP, MHM, chief of hospital medicine at Rady Children’s Hospital in San Diego; Mary Ottolini, MD, MPH, chief of hospital medicine at Children’s National Medical Center in Washington; Jack Percelay, MD, MPH, FAAP, associate clinical professor at Pace University; and Daniel Rauch, MD, FAAP, pediatric hospitalist program director at the NYU School of Medicine in New York City. A host of new programs has been established by the PHM community, including the Quality Improvement Innovation Networks (QuIIN); the Value in Pediatrics (VIP) network; the International Network for Simulation-Based Pediatric Innovation, Research, and Education (INSPIRE); patient- and family-centered rounds; and the I-PASS Handoff Program. The panel also discussed future challenges, including reduction of unnecessary treatments, interfacing, and perhaps incorporating “hyphen hospitalists,” and learning from advances made by the adult HM community.
- The ever-popular “Top Articles in Pediatric Hospital Medicine” session was presented by H. Barrett Fromme, MD, associate professor of pediatrics at the University of Chicago, and Ben Bauer, MD, director of pediatric hospital medicine at Riley Hospital for Children at Indiana University Health in Indianapolis, which was met with raucous approval by the audience. The presentation not only educated those in attendance about the most cutting-edge pediatric literature, but it also included dance moves most likely to attract the opposite sex and clothing appropriate for the Australian pediatric hospitalist.
- The three presidents of the sponsoring societies—Thomas McInerney, MD, FAAP, of the American Academy of Pediatrics, David Keller, MD, of the Academic Pediatric Association, and Eric Howell, MD, SFHM, of SHM—presented each society’s contributions to the growth of PHM, as well as future areas for cooperative sponsorship. These include the development of the AAP Section of Hospital Medicine Library website (sohmlibrary.org), the APA Quality Scholars program, and SHM’s efforts to increase interest in hospital medicine in medical students and trainees. “Ask not what hospital medicine can do for you,” Dr. Howell implored, “ask what you can do for hospital medicine!”
- Members of the Joint Council of Pediatric Hospital Medicine (JCPHM) presented the recent recommendations of the council arising from an April 2013 meeting with the ABP in Chapel Hill, N.C. Despite acknowledgements that no decision will be met with uniform satisfaction by all the stakeholders, the JCPHM concluded that the path that would best advance the field of PHM, provide for high-quality care of hospitalized children, and ensure the public trust would be a two-year fellowship sponsored by ABP. This would ultimately lead to approved certification eligibility for fellowship graduates by the American Board of Medical Specialties (ABMS); it would also make provisions for “grandfathering” in current pediatric hospitalists. Concerns from med-peds, community hospitalists, and recent residency graduate communities were addressed by the panel.
- A recurrent theme of reducing unnecessary treatments, interventions, and, perhaps, hospitalizations was summarized eloquently by Alan Schroeder, MD, director of the pediatric ICU and chief of pediatric inpatient care at Santa Clara (Calif.) Valley Health. Barriers to reducing unnecessary care can be substantial, including pressure from families, pressure from colleagues, profit motive, and the “n’s of 1,” according to Dr. Schroeder. Ultimately, however, avoiding testing and treatments that have no benefit to children will improve care. “Ask, ‘How will this test benefit my patient?’ not ‘How will this test change management?’” Dr. Schroeder advised.
Dr. Chang is The Hospitalist’s pediatric editor and a med-peds-trained hospitalist working at the University of California San Diego and Rady Children’s Hospital.
With a record number of attendees, Pediatric Hospital Medicine 2013 (PHM) swept into New Orleans last month, carrying with it unbridled enthusiasm about the past, present, and future.
Virginia Moyer, MD, MPH, vice president for maintenance of certification and quality for the American Board of Pediatrics (ABP) and professor of pediatrics and chief of academic general pediatrics at Texas Children’s Hospital, delivered a keynote address to 700 attendees that focused on the challenges and opportunities of providing evidence-based, high-quality care in the hospital, as well as ABP’s role in meeting these challenges.
“If evidence-based medicine is an individual sport,” Dr. Moyer said, “then quality improvement is a team sport.”
Barriers to quality improvement (QI)— such as lack of will, lack of data, and lack of training—can be surmounted in a team environment, she said. ABP is continuing in its efforts to support QI education through its Maintenance of Certification (MOC) Part 4 modules, as well as other educational activities.
Other highlights of the 10th annual Pediatric Hospital Medicine meeting:
- The addition of a new “Community Hospitalists” track was given high marks by those in attendance. It covered such topics as perioperative management of medically complex pediatric patients, community-acquired pneumonia, and osteomyelitis.
- A 10-year retrospective of pediatric hospital medicine was given by a panel of notable pediatric hospitalists, including Erin Stucky Fisher, MD, FAAP, MHM, chief of hospital medicine at Rady Children’s Hospital in San Diego; Mary Ottolini, MD, MPH, chief of hospital medicine at Children’s National Medical Center in Washington; Jack Percelay, MD, MPH, FAAP, associate clinical professor at Pace University; and Daniel Rauch, MD, FAAP, pediatric hospitalist program director at the NYU School of Medicine in New York City. A host of new programs has been established by the PHM community, including the Quality Improvement Innovation Networks (QuIIN); the Value in Pediatrics (VIP) network; the International Network for Simulation-Based Pediatric Innovation, Research, and Education (INSPIRE); patient- and family-centered rounds; and the I-PASS Handoff Program. The panel also discussed future challenges, including reduction of unnecessary treatments, interfacing, and perhaps incorporating “hyphen hospitalists,” and learning from advances made by the adult HM community.
- The ever-popular “Top Articles in Pediatric Hospital Medicine” session was presented by H. Barrett Fromme, MD, associate professor of pediatrics at the University of Chicago, and Ben Bauer, MD, director of pediatric hospital medicine at Riley Hospital for Children at Indiana University Health in Indianapolis, which was met with raucous approval by the audience. The presentation not only educated those in attendance about the most cutting-edge pediatric literature, but it also included dance moves most likely to attract the opposite sex and clothing appropriate for the Australian pediatric hospitalist.
- The three presidents of the sponsoring societies—Thomas McInerney, MD, FAAP, of the American Academy of Pediatrics, David Keller, MD, of the Academic Pediatric Association, and Eric Howell, MD, SFHM, of SHM—presented each society’s contributions to the growth of PHM, as well as future areas for cooperative sponsorship. These include the development of the AAP Section of Hospital Medicine Library website (sohmlibrary.org), the APA Quality Scholars program, and SHM’s efforts to increase interest in hospital medicine in medical students and trainees. “Ask not what hospital medicine can do for you,” Dr. Howell implored, “ask what you can do for hospital medicine!”
- Members of the Joint Council of Pediatric Hospital Medicine (JCPHM) presented the recent recommendations of the council arising from an April 2013 meeting with the ABP in Chapel Hill, N.C. Despite acknowledgements that no decision will be met with uniform satisfaction by all the stakeholders, the JCPHM concluded that the path that would best advance the field of PHM, provide for high-quality care of hospitalized children, and ensure the public trust would be a two-year fellowship sponsored by ABP. This would ultimately lead to approved certification eligibility for fellowship graduates by the American Board of Medical Specialties (ABMS); it would also make provisions for “grandfathering” in current pediatric hospitalists. Concerns from med-peds, community hospitalists, and recent residency graduate communities were addressed by the panel.
- A recurrent theme of reducing unnecessary treatments, interventions, and, perhaps, hospitalizations was summarized eloquently by Alan Schroeder, MD, director of the pediatric ICU and chief of pediatric inpatient care at Santa Clara (Calif.) Valley Health. Barriers to reducing unnecessary care can be substantial, including pressure from families, pressure from colleagues, profit motive, and the “n’s of 1,” according to Dr. Schroeder. Ultimately, however, avoiding testing and treatments that have no benefit to children will improve care. “Ask, ‘How will this test benefit my patient?’ not ‘How will this test change management?’” Dr. Schroeder advised.
Dr. Chang is The Hospitalist’s pediatric editor and a med-peds-trained hospitalist working at the University of California San Diego and Rady Children’s Hospital.
With a record number of attendees, Pediatric Hospital Medicine 2013 (PHM) swept into New Orleans last month, carrying with it unbridled enthusiasm about the past, present, and future.
Virginia Moyer, MD, MPH, vice president for maintenance of certification and quality for the American Board of Pediatrics (ABP) and professor of pediatrics and chief of academic general pediatrics at Texas Children’s Hospital, delivered a keynote address to 700 attendees that focused on the challenges and opportunities of providing evidence-based, high-quality care in the hospital, as well as ABP’s role in meeting these challenges.
“If evidence-based medicine is an individual sport,” Dr. Moyer said, “then quality improvement is a team sport.”
Barriers to quality improvement (QI)— such as lack of will, lack of data, and lack of training—can be surmounted in a team environment, she said. ABP is continuing in its efforts to support QI education through its Maintenance of Certification (MOC) Part 4 modules, as well as other educational activities.
Other highlights of the 10th annual Pediatric Hospital Medicine meeting:
- The addition of a new “Community Hospitalists” track was given high marks by those in attendance. It covered such topics as perioperative management of medically complex pediatric patients, community-acquired pneumonia, and osteomyelitis.
- A 10-year retrospective of pediatric hospital medicine was given by a panel of notable pediatric hospitalists, including Erin Stucky Fisher, MD, FAAP, MHM, chief of hospital medicine at Rady Children’s Hospital in San Diego; Mary Ottolini, MD, MPH, chief of hospital medicine at Children’s National Medical Center in Washington; Jack Percelay, MD, MPH, FAAP, associate clinical professor at Pace University; and Daniel Rauch, MD, FAAP, pediatric hospitalist program director at the NYU School of Medicine in New York City. A host of new programs has been established by the PHM community, including the Quality Improvement Innovation Networks (QuIIN); the Value in Pediatrics (VIP) network; the International Network for Simulation-Based Pediatric Innovation, Research, and Education (INSPIRE); patient- and family-centered rounds; and the I-PASS Handoff Program. The panel also discussed future challenges, including reduction of unnecessary treatments, interfacing, and perhaps incorporating “hyphen hospitalists,” and learning from advances made by the adult HM community.
- The ever-popular “Top Articles in Pediatric Hospital Medicine” session was presented by H. Barrett Fromme, MD, associate professor of pediatrics at the University of Chicago, and Ben Bauer, MD, director of pediatric hospital medicine at Riley Hospital for Children at Indiana University Health in Indianapolis, which was met with raucous approval by the audience. The presentation not only educated those in attendance about the most cutting-edge pediatric literature, but it also included dance moves most likely to attract the opposite sex and clothing appropriate for the Australian pediatric hospitalist.
- The three presidents of the sponsoring societies—Thomas McInerney, MD, FAAP, of the American Academy of Pediatrics, David Keller, MD, of the Academic Pediatric Association, and Eric Howell, MD, SFHM, of SHM—presented each society’s contributions to the growth of PHM, as well as future areas for cooperative sponsorship. These include the development of the AAP Section of Hospital Medicine Library website (sohmlibrary.org), the APA Quality Scholars program, and SHM’s efforts to increase interest in hospital medicine in medical students and trainees. “Ask not what hospital medicine can do for you,” Dr. Howell implored, “ask what you can do for hospital medicine!”
- Members of the Joint Council of Pediatric Hospital Medicine (JCPHM) presented the recent recommendations of the council arising from an April 2013 meeting with the ABP in Chapel Hill, N.C. Despite acknowledgements that no decision will be met with uniform satisfaction by all the stakeholders, the JCPHM concluded that the path that would best advance the field of PHM, provide for high-quality care of hospitalized children, and ensure the public trust would be a two-year fellowship sponsored by ABP. This would ultimately lead to approved certification eligibility for fellowship graduates by the American Board of Medical Specialties (ABMS); it would also make provisions for “grandfathering” in current pediatric hospitalists. Concerns from med-peds, community hospitalists, and recent residency graduate communities were addressed by the panel.
- A recurrent theme of reducing unnecessary treatments, interventions, and, perhaps, hospitalizations was summarized eloquently by Alan Schroeder, MD, director of the pediatric ICU and chief of pediatric inpatient care at Santa Clara (Calif.) Valley Health. Barriers to reducing unnecessary care can be substantial, including pressure from families, pressure from colleagues, profit motive, and the “n’s of 1,” according to Dr. Schroeder. Ultimately, however, avoiding testing and treatments that have no benefit to children will improve care. “Ask, ‘How will this test benefit my patient?’ not ‘How will this test change management?’” Dr. Schroeder advised.
Dr. Chang is The Hospitalist’s pediatric editor and a med-peds-trained hospitalist working at the University of California San Diego and Rady Children’s Hospital.
ACO spillover effect: Lower spending for all
Implementing the requirements of an accountable care organization for one group of patients may lower costs and improve care for every patient seen in a physician’s practice, according to a study published online Aug. 27 in JAMA.
Dr. J. Michael McWilliams of Harvard Medical School, Boston, and his colleagues looked at whether the Blue Cross Blue Shield of Massachusetts’ Alternative Quality Contract (ACQ), a successful ACO started in 2009, was associated with changes in spending or quality of care for Medicare beneficiaries who were not part of the ACO.
In the AQC, physicians and other providers assumed financial risk if they spent more than a global budget, but shared savings with the insurer if spending was under budget. Physicians could also receive bonuses for meeting quality targets.

The investigators compared total quarterly medical spending per beneficiary between two groups: beneficiaries who received care through the AQC in 2009 or 2010 (1.7 million person-years) and controls who received care from other providers (JAMA 2013;310:829-836).
Quarterly spending per beneficiary in 2007 and 2008 (prior to the AQC contracts) was $150 higher for the AQC group than the control group. Two years after the ACQ contracts went into effect, the difference was $51 per quarter. The biggest reduction in spending was for beneficiaries with five or more conditions, and in spending on outpatient care. Spending was significantly reduced for office visits, emergency department visits, minor procedures, imaging, and lab tests.
Some improvement was seen on quality measures. The number of beneficiaries tested for low-density lipoprotein levels increased. Prior to the AQC, LDL testing rates for diabetic beneficiaries in the AQC group were 2.2% higher than for controls. By the second year, the testing rate was 5.2% higher for those in the AQC. LDL testing rates also improved for cardiovascular disease patients in the AQC.
No improvement was seen on other quality measures, including hospitalization for an ambulatory care–sensitive condition related to cardiovascular disease or diabetes; readmission within 30 days of discharge; screening mammography for women aged 65-69 years; LDL testing for beneficiaries with a history of ischemic heart disease, myocardial infarction, or stroke; and hemoglobin A1c testing and retinal exams for beneficiaries with diabetes.
"These findings suggest that global payment incentives in the AQC elicited responses from participating organizations that extended beyond targeted case management of BCBS enrollees," the authors wrote.
Overall, the study "suggests that organizations in Massachusetts willing to assume greater financial risk were capable of achieving modest reductions in spending for Medicare beneficiaries without compromising quality of care," wrote Dr. McWilliams and his colleagues.
The study also showed that physicians and provider organizations who see spillover effects from one ACO contract might be willing "to enter similar contracts with additional insurers."
But there is a potential downside to the spillover effect, according to the authors: Because cost and quality may be improved overall, "competing insurers with similar provider networks could offer lower premiums without incurring the costs of managing an ACO."
The study was supported by grants from the National Institute on Aging, the American Federation for Aging Research, the Doris Duke Charitable Foundation, and the Commonwealth Fund. The investigators reported no relevant conflicts of interest.
On Twitter @aliciaault
Implementing the requirements of an accountable care organization for one group of patients may lower costs and improve care for every patient seen in a physician’s practice, according to a study published online Aug. 27 in JAMA.
Dr. J. Michael McWilliams of Harvard Medical School, Boston, and his colleagues looked at whether the Blue Cross Blue Shield of Massachusetts’ Alternative Quality Contract (ACQ), a successful ACO started in 2009, was associated with changes in spending or quality of care for Medicare beneficiaries who were not part of the ACO.
In the AQC, physicians and other providers assumed financial risk if they spent more than a global budget, but shared savings with the insurer if spending was under budget. Physicians could also receive bonuses for meeting quality targets.
The investigators compared total quarterly medical spending per beneficiary between two groups: beneficiaries who received care through the AQC in 2009 or 2010 (1.7 million person-years) and controls who received care from other providers (JAMA 2013;310:829-836).
Quarterly spending per beneficiary in 2007 and 2008 (prior to the AQC contracts) was $150 higher for the AQC group than the control group. Two years after the ACQ contracts went into effect, the difference was $51 per quarter. The biggest reduction in spending was for beneficiaries with five or more conditions, and in spending on outpatient care. Spending was significantly reduced for office visits, emergency department visits, minor procedures, imaging, and lab tests.
Some improvement was seen on quality measures. The number of beneficiaries tested for low-density lipoprotein levels increased. Prior to the AQC, LDL testing rates for diabetic beneficiaries in the AQC group were 2.2% higher than for controls. By the second year, the testing rate was 5.2% higher for those in the AQC. LDL testing rates also improved for cardiovascular disease patients in the AQC.
No improvement was seen on other quality measures, including hospitalization for an ambulatory care–sensitive condition related to cardiovascular disease or diabetes; readmission within 30 days of discharge; screening mammography for women aged 65-69 years; LDL testing for beneficiaries with a history of ischemic heart disease, myocardial infarction, or stroke; and hemoglobin A1c testing and retinal exams for beneficiaries with diabetes.
"These findings suggest that global payment incentives in the AQC elicited responses from participating organizations that extended beyond targeted case management of BCBS enrollees," the authors wrote.
Overall, the study "suggests that organizations in Massachusetts willing to assume greater financial risk were capable of achieving modest reductions in spending for Medicare beneficiaries without compromising quality of care," wrote Dr. McWilliams and his colleagues.
The study also showed that physicians and provider organizations who see spillover effects from one ACO contract might be willing "to enter similar contracts with additional insurers."
But there is a potential downside to the spillover effect, according to the authors: Because cost and quality may be improved overall, "competing insurers with similar provider networks could offer lower premiums without incurring the costs of managing an ACO."
The study was supported by grants from the National Institute on Aging, the American Federation for Aging Research, the Doris Duke Charitable Foundation, and the Commonwealth Fund. The investigators reported no relevant conflicts of interest.
On Twitter @aliciaault
Implementing the requirements of an accountable care organization for one group of patients may lower costs and improve care for every patient seen in a physician’s practice, according to a study published online Aug. 27 in JAMA.
Dr. J. Michael McWilliams of Harvard Medical School, Boston, and his colleagues looked at whether the Blue Cross Blue Shield of Massachusetts’ Alternative Quality Contract (ACQ), a successful ACO started in 2009, was associated with changes in spending or quality of care for Medicare beneficiaries who were not part of the ACO.
In the AQC, physicians and other providers assumed financial risk if they spent more than a global budget, but shared savings with the insurer if spending was under budget. Physicians could also receive bonuses for meeting quality targets.
The investigators compared total quarterly medical spending per beneficiary between two groups: beneficiaries who received care through the AQC in 2009 or 2010 (1.7 million person-years) and controls who received care from other providers (JAMA 2013;310:829-836).
Quarterly spending per beneficiary in 2007 and 2008 (prior to the AQC contracts) was $150 higher for the AQC group than the control group. Two years after the ACQ contracts went into effect, the difference was $51 per quarter. The biggest reduction in spending was for beneficiaries with five or more conditions, and in spending on outpatient care. Spending was significantly reduced for office visits, emergency department visits, minor procedures, imaging, and lab tests.
Some improvement was seen on quality measures. The number of beneficiaries tested for low-density lipoprotein levels increased. Prior to the AQC, LDL testing rates for diabetic beneficiaries in the AQC group were 2.2% higher than for controls. By the second year, the testing rate was 5.2% higher for those in the AQC. LDL testing rates also improved for cardiovascular disease patients in the AQC.
No improvement was seen on other quality measures, including hospitalization for an ambulatory care–sensitive condition related to cardiovascular disease or diabetes; readmission within 30 days of discharge; screening mammography for women aged 65-69 years; LDL testing for beneficiaries with a history of ischemic heart disease, myocardial infarction, or stroke; and hemoglobin A1c testing and retinal exams for beneficiaries with diabetes.
"These findings suggest that global payment incentives in the AQC elicited responses from participating organizations that extended beyond targeted case management of BCBS enrollees," the authors wrote.
Overall, the study "suggests that organizations in Massachusetts willing to assume greater financial risk were capable of achieving modest reductions in spending for Medicare beneficiaries without compromising quality of care," wrote Dr. McWilliams and his colleagues.
The study also showed that physicians and provider organizations who see spillover effects from one ACO contract might be willing "to enter similar contracts with additional insurers."
But there is a potential downside to the spillover effect, according to the authors: Because cost and quality may be improved overall, "competing insurers with similar provider networks could offer lower premiums without incurring the costs of managing an ACO."
The study was supported by grants from the National Institute on Aging, the American Federation for Aging Research, the Doris Duke Charitable Foundation, and the Commonwealth Fund. The investigators reported no relevant conflicts of interest.
On Twitter @aliciaault
FROM JAMA
Major finding: Quarterly spending per Medicare beneficiary was reduced by about $100 for those who were receiving care in a practice that had a contract with Blues Cross Blue Shield of Massachusetts’ Alternative Quality Contract.
Data source: Quasi-experimental comparisons from 2007-2010 of Medicare beneficiaries served by 11 provider organizations who entered the AQC in 2009 or 2010, compared to those served by other providers.
Disclosures: The study was supported by grants from the National Institute on Aging, the American Federation for Aging Research, the Doris Duke Charitable Foundation, and the Commonwealth Fund. The investigators reported no relevant conflicts of interest.

Public Citizen: Malpractice payouts hit record lows
Malpractice lawsuit awards are at an all-time low, according to an analysis from the consumer watchdog group Public Citizen.
But the news isn’t all good. Despite the fact that malpractice awards fell 28.8% between 2003 and 2012, the drop in payments isn’t translating into a decline in overall health care costs or improvements in safety, according to Public Citizen.
"We now have a decade’s worth of data debunking the litigation canard," said Taylor Lincoln, research director for Public Citizen’s Congress Watch division and the report’s author. "Policy makers need to focus on reducing medical errors, not reducing accountability for medical errors."

Examining data from the National Practitioner Data Bank, Public Citizen found that in 2012, both the number of awards (9,379) and the amount of those payouts ($3.1 billion) was the lowest on record, once adjusted for inflation. In 2012, the average payment was about $335,000.
The big driver for the drop in malpractice awards is likely state laws that have imposed caps on the amount of noneconomic damages that patients can receive, according to Public Citizen.
The decline in litigation awards appears to be good news for doctors, who overall experienced a decrease in medical liability insurance premiums during the same period. Physician premiums fell to 0.36% of health care costs, the lowest amount in a decade, the report said.
But consumers are losing out, Public Citizen argued, because health care costs are up 58.3% over the last decade. And reports continue to be published showing high rates of adverse events in U.S. hospitals.
Public Citizen cited a 2010 report from the inspector general of the federal Department of Health and Human Services that found that one in seven hospitalized Medicare beneficiaries experienced a serious adverse event, which contributed to death in 1.5% of patients.
But Texas Medical Association President Stephen L. Brotherton countered that medical liability reform actually creates a safer health care environment by improving access to care.
Texas voters approved comprehensive medical liability reform in 2003, including a cap on noneconomic damages. Before that law was enacted, the state had been losing physicians who couldn’t afford their rising malpractice premiums or feared the personal and professional upheaval of a lawsuit, said Dr. Brotherton, an orthopedic surgeon in Fort Worth.
"We were losing people in the prime of their practice," Dr. Brotherton explained.
Many Texas counties had no access to high-risk specialty care, including ob.gyns and neurosurgeons, he noted. And hospitals were having difficulty finding physicians willing to take call in the emergency department. As a result, patients in rural areas couldn’t get access to high-risk specialty care, and some physicians were increasing the volume in their practice to unsafe levels to meet financial pressures from rising insurance premiums, Dr. Brotherton said.
A decade after medical liability reform was passed, physicians are returning to Texas, according to the TMA. Since Texas voters passed Proposition 12 in 2003, Texas has licensed more than 28,000 new physicians, an average of about 3,135 per year. And many of these new doctors are filling the gaps in high-risk areas such as obstetrics, Dr. Brotherton said. Since 2003, 35 rural counties have added at least one obstetrician, including 16 counties that previously had no obstetricians.
There’s no evidence that having an active plaintiff’s bar in a state promotes safer medicine, Dr. Brotherton asserted. "Good doctors are going to where they are wanted," he said.
Dr. Brotherton didn’t dispute the Public Citizen charge that medical liability reform has not brought down health care costs. There are many factors driving rising health care costs, he said, from lifestyle and diet to medication compliance. But reducing overall health care costs was never an argument in favor of reforming the tort system, at least not in Texas, he said.
"No tort reform in the world is going to reduce the number of diabetics," Dr. Brotherton noted.
mschneider@frontlinemedcom.com
On Twitter @MaryEllenNY
Malpractice lawsuit awards are at an all-time low, according to an analysis from the consumer watchdog group Public Citizen.
But the news isn’t all good. Despite the fact that malpractice awards fell 28.8% between 2003 and 2012, the drop in payments isn’t translating into a decline in overall health care costs or improvements in safety, according to Public Citizen.
"We now have a decade’s worth of data debunking the litigation canard," said Taylor Lincoln, research director for Public Citizen’s Congress Watch division and the report’s author. "Policy makers need to focus on reducing medical errors, not reducing accountability for medical errors."
Examining data from the National Practitioner Data Bank, Public Citizen found that in 2012, both the number of awards (9,379) and the amount of those payouts ($3.1 billion) was the lowest on record, once adjusted for inflation. In 2012, the average payment was about $335,000.
The big driver for the drop in malpractice awards is likely state laws that have imposed caps on the amount of noneconomic damages that patients can receive, according to Public Citizen.
The decline in litigation awards appears to be good news for doctors, who overall experienced a decrease in medical liability insurance premiums during the same period. Physician premiums fell to 0.36% of health care costs, the lowest amount in a decade, the report said.
But consumers are losing out, Public Citizen argued, because health care costs are up 58.3% over the last decade. And reports continue to be published showing high rates of adverse events in U.S. hospitals.
Public Citizen cited a 2010 report from the inspector general of the federal Department of Health and Human Services that found that one in seven hospitalized Medicare beneficiaries experienced a serious adverse event, which contributed to death in 1.5% of patients.
But Texas Medical Association President Stephen L. Brotherton countered that medical liability reform actually creates a safer health care environment by improving access to care.
Texas voters approved comprehensive medical liability reform in 2003, including a cap on noneconomic damages. Before that law was enacted, the state had been losing physicians who couldn’t afford their rising malpractice premiums or feared the personal and professional upheaval of a lawsuit, said Dr. Brotherton, an orthopedic surgeon in Fort Worth.
"We were losing people in the prime of their practice," Dr. Brotherton explained.
Many Texas counties had no access to high-risk specialty care, including ob.gyns and neurosurgeons, he noted. And hospitals were having difficulty finding physicians willing to take call in the emergency department. As a result, patients in rural areas couldn’t get access to high-risk specialty care, and some physicians were increasing the volume in their practice to unsafe levels to meet financial pressures from rising insurance premiums, Dr. Brotherton said.
A decade after medical liability reform was passed, physicians are returning to Texas, according to the TMA. Since Texas voters passed Proposition 12 in 2003, Texas has licensed more than 28,000 new physicians, an average of about 3,135 per year. And many of these new doctors are filling the gaps in high-risk areas such as obstetrics, Dr. Brotherton said. Since 2003, 35 rural counties have added at least one obstetrician, including 16 counties that previously had no obstetricians.
There’s no evidence that having an active plaintiff’s bar in a state promotes safer medicine, Dr. Brotherton asserted. "Good doctors are going to where they are wanted," he said.
Dr. Brotherton didn’t dispute the Public Citizen charge that medical liability reform has not brought down health care costs. There are many factors driving rising health care costs, he said, from lifestyle and diet to medication compliance. But reducing overall health care costs was never an argument in favor of reforming the tort system, at least not in Texas, he said.
"No tort reform in the world is going to reduce the number of diabetics," Dr. Brotherton noted.
mschneider@frontlinemedcom.com
On Twitter @MaryEllenNY
Malpractice lawsuit awards are at an all-time low, according to an analysis from the consumer watchdog group Public Citizen.
But the news isn’t all good. Despite the fact that malpractice awards fell 28.8% between 2003 and 2012, the drop in payments isn’t translating into a decline in overall health care costs or improvements in safety, according to Public Citizen.
"We now have a decade’s worth of data debunking the litigation canard," said Taylor Lincoln, research director for Public Citizen’s Congress Watch division and the report’s author. "Policy makers need to focus on reducing medical errors, not reducing accountability for medical errors."
Examining data from the National Practitioner Data Bank, Public Citizen found that in 2012, both the number of awards (9,379) and the amount of those payouts ($3.1 billion) was the lowest on record, once adjusted for inflation. In 2012, the average payment was about $335,000.
The big driver for the drop in malpractice awards is likely state laws that have imposed caps on the amount of noneconomic damages that patients can receive, according to Public Citizen.
The decline in litigation awards appears to be good news for doctors, who overall experienced a decrease in medical liability insurance premiums during the same period. Physician premiums fell to 0.36% of health care costs, the lowest amount in a decade, the report said.
But consumers are losing out, Public Citizen argued, because health care costs are up 58.3% over the last decade. And reports continue to be published showing high rates of adverse events in U.S. hospitals.
Public Citizen cited a 2010 report from the inspector general of the federal Department of Health and Human Services that found that one in seven hospitalized Medicare beneficiaries experienced a serious adverse event, which contributed to death in 1.5% of patients.
But Texas Medical Association President Stephen L. Brotherton countered that medical liability reform actually creates a safer health care environment by improving access to care.
Texas voters approved comprehensive medical liability reform in 2003, including a cap on noneconomic damages. Before that law was enacted, the state had been losing physicians who couldn’t afford their rising malpractice premiums or feared the personal and professional upheaval of a lawsuit, said Dr. Brotherton, an orthopedic surgeon in Fort Worth.
"We were losing people in the prime of their practice," Dr. Brotherton explained.
Many Texas counties had no access to high-risk specialty care, including ob.gyns and neurosurgeons, he noted. And hospitals were having difficulty finding physicians willing to take call in the emergency department. As a result, patients in rural areas couldn’t get access to high-risk specialty care, and some physicians were increasing the volume in their practice to unsafe levels to meet financial pressures from rising insurance premiums, Dr. Brotherton said.
A decade after medical liability reform was passed, physicians are returning to Texas, according to the TMA. Since Texas voters passed Proposition 12 in 2003, Texas has licensed more than 28,000 new physicians, an average of about 3,135 per year. And many of these new doctors are filling the gaps in high-risk areas such as obstetrics, Dr. Brotherton said. Since 2003, 35 rural counties have added at least one obstetrician, including 16 counties that previously had no obstetricians.
There’s no evidence that having an active plaintiff’s bar in a state promotes safer medicine, Dr. Brotherton asserted. "Good doctors are going to where they are wanted," he said.
Dr. Brotherton didn’t dispute the Public Citizen charge that medical liability reform has not brought down health care costs. There are many factors driving rising health care costs, he said, from lifestyle and diet to medication compliance. But reducing overall health care costs was never an argument in favor of reforming the tort system, at least not in Texas, he said.
"No tort reform in the world is going to reduce the number of diabetics," Dr. Brotherton noted.
mschneider@frontlinemedcom.com
On Twitter @MaryEllenNY

Listen to Project BOOST lead analyst Luke Hansen, MD, MPH, discuss the outcomes study published in JHM
Click here to listen to our interview with Dr. Hansen
Click here to listen to our interview with Dr. Hansen
Click here to listen to our interview with Dr. Hansen
11 Things Neurologists Think Hospitalists Need To Know

11 Things: At a Glance
- You might be overdiagnosing transient ischemic attacks (TIA).
- Early mobilization after a stroke might be better for some patients.
- MRI is the best tool to evaluate TIA patients.
- Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
- Tracking the time a hospitalized patient was last seen to be normal is crucial.
- Consider neuromuscular disorders when a patient presents with weakness.
- Urinary tract infections (UTIs) are not the only cause of altered mental status.
- Take care in distinguishing aphasia from general confusion.
- A simple checklist might eliminate the need to consult the neurologist.
- Calling a neurologist earlier is way better than calling later.
- Hire a neurohospitalist if your institution doesn’t have one already.
When a patient is admitted to the hospital with neurological symptoms, such as altered mental status, he or she might not be the only one who is confused. Hospitalists might be a little confused, too.
Of all the subspecialties to which hospitalists are exposed, none might make them more uncomfortable than neurology. Because of what often is a dearth of training in this area, and because of the vexing and sometimes fleeting nature of symptoms, hospitalists might be inclined to lean on neurologists more than other specialists.
The Hospitalist spoke with a half-dozen experts, gathering their words of guidance and clinical tips. Here’s hoping they give you a little extra confidence the next time you see a patient with altered mental status.
You might be overdiagnosing transient ischemic attacks (TIA).
Ira Chang, MD, a neurohospitalist with Blue Sky Neurology in Englewood, Colo., and assistant clinical professor at the University of Colorado Health Sciences Center in Denver, says TIA is all too commonly a go-to diagnosis, frequently when there’s another cause.
“I think that hospitalists, and maybe medical internists in general, are very quick to diagnose anything that has a neurologic symptom that comes and goes as a TIA,” she says. “Patients have to have specific neurologic symptoms that we think are due to arterial blood flow or ischemia problems.”
Near-fainting spells and dizzy spells involving confusion commonly are diagnosed as TIA when these symptoms could be due to “a number of other causes,” Dr. Chang adds.

Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says the suspicion of a TIA should be greater if the patient is older or has traditional cardiovascular risk factors, such as hyptertension, diabetes, hyperlipidemia, or tobacco use.
A TIA typically causes symptoms referable to common arterial distributions. Carotid-distribution TIA often causes ipsilateral loss of vision and contralateral weakness or numbness. Posterior-circulation TIAs bring on symptoms such as ataxia, unilateral or bilateral limb weakness, diplopia, and slurred or slow speech.
TIA diagnoses can be tricky even for those trained in neurology, Dr. Barrett says.
“Even among fellowship-trained vascular neurologists, TIA can be a challenging diagnosis, often with poor inter-observer agreement,” he notes.
Early mobilization after a stroke might be better for some patients.
After receiving tissue plasminogen activator (tPA) therapy for stroke, patients historically were kept on bed rest for 24 hours to reduce the risk of hemorrhage. Evidence now is coming to light that some patients might benefit from getting out of bed sooner, Dr. Barrett says.1
“We’re learning that in selected patients, they can actually be mobilized at 12 hours,” he says. “In some cases, that would not only reduce the risk of complications related to immobilization like DVT but shorten length of stay. These are all important metrics for anybody who practices primarily within an inpatient setting.”
Early mobilization generally is more suitable for patients with less severe deficits and who are hemodynamically stable.
MRI is the best tool to evaluate TIA patients.
TIA patients who have transient symptoms and normal diffusion-weighted imaging (DWI) abnormalities on an MRI are at a very low risk. “Less than 1% of those patients have a stroke within the subsequent seven days,” Dr. Barrett says.2 “But those patients who do have a DWI abnormality, they’re at very high risk: 7.1% at seven days.
“The utility of MRI following TIA is becoming very much apparent. It is something that hospitalists should be aware of.”
Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
Patients experiencing confusion or speech disturbance or altered mentation—particularly if they’re elderly or have dementia—could be having a partial seizure, Dr. Chang says. Dementia patients have a 10% to 15% incidence of complex partial seizures, she says.
“I see that underdiagnosed a lot,” she says. “They keep coming back, and everybody diagnoses them with TIAs. So they keep getting put on aspirin, and they get switched to Aggrenox [to prevent clotting]. They keep coming back with the same symptoms.”
Tracking the time a hospitalized patient was last seen to be normal is crucial.
About 10% to 15% of strokes occur in patients who are in the hospital.
“While a lot of those strokes are perioperative, there also are patients who are going to be on hospitalist services,” says Eric Adelman, MD, assistant professor of neurology at the University of Michigan in Ann Arbor.

Hospitalists should note that patients suffering strokes are found not just in the ED but also on the floor, where all the tools for treatment might not be as readily available. That makes those cases a challenge and makes forethought that much more important, Dr. Adelman says.
“It’s a matter of trying to track down last normal times,” he says. “If they’re eligible for tPA and they’re within the therapeutic window, we should be able to do that within a hospital.”
Establishing a neurological baseline is particularly important for patients who are at higher stroke risk, like those with atrial fibrillation and other cardiovascular risk factors.
“In case something does happen,” Dr. Adelman says, “at least you have a baseline so you can [know that] at time X, we knew they had full strength in their right arm, and now they don’t.”
Consider neuromuscular disorders when a patient presents with weakness.
It’s safe to say some hospitalists might miss a neuromuscular disorder, Dr. Chang says.
“A lot of disorders that are harder for hospitalists to diagnose and that tend to take longer to call a neurologist [on] are things that are due to myasthenia gravis [a breakdown between nerves and muscles leading to muscle fatigue], myopathy, or ALS,” she says. “Many patients present with weakness. I think a lot of times there will be a lot of tests on and a lot of treatment for general medical conditions that can cause weakness.”
And that might be a case of misdirected attention. Patients with weakness accompanied by persistent swallowing problems, slurred speech with no other obvious cause, or the inability to lift their head off the bed without an obvious cause may end up with a neuromuscular diagnosis, she says.
It would be helpful to have a neurologist’s input in these cases, she says, where “nothing’s getting better, and three, four, five days later, the patient’s still weak.
“I think a neurologist would be more in tune with something like that,” she adds.
Urinary tract infections (UTIs) are not the only cause of altered mental status.
That might seem obvious, but too often, a UTI can be pegged as the source of altered mental status when it should not be, Dr. Chang says.
“We get a lot of people who come in with confusion and they have a slightly abnormal urinalysis and they diagnose them with UTI,” Dr. Chang says. “And it turns out that they actually had a stroke or they had a seizure.”
Significantly altered mentation should show a significantly abnormal urine with a positive culture, she says. “They ought to have significant laboratory support for a urinary tract infection.”
Dr. Barrett says a neurologic review of systems, or at least a neurologic exam, should be the physician’s guide.
“Those are key parts of a hospitalist’s practice,” he says, “because that’s what’s truly going to guide them to consider primary neurological causes of altered mental status.”
Take care in distinguishing aphasia from general confusion.
If a patient is still talking and is fairly fluent, that doesn’t mean they aren’t suffering from certain types of aphasia, a disorder caused by damage to parts of the brain that control language, Dr. Adelman says.
“Oftentimes, when you’re dealing with a patient with confusion, you want to make sure that it’s confusion, or encephalopathy, rather than a focal neurologic problem like aphasia,” he says. “Frequently patients with aphasia will have other symptoms such as a facial drop or weakness in the arm, but stroke can present as isolated aphasia.”
A good habit to get into is to determine whether the patient can repeat a phrase, follow a command, or name objects, he says. If they can, they probably do not have aphasia.
“The thing that you worry about with aphasia, particularly acute onset aphasia, is an ischemic stroke,” Dr. Adelman says.
A simple checklist might eliminate the need to consult the neurologist.
When Edgar Kenton, MD, now director of the stroke program at Geisinger Health System in Danville, Pa., was at Emory University Hospital in Atlanta, he found he was getting snowed under with consults from hospitalists. There were about 15 hospitalists for just one or two neurologists.
“There was no way I was able to see these patients, particularly in follow-up, because you might get five consults every day,” he says. “By the middle of the week, that’s 15 consults. You don’t get a chance to go back and see the patients because you’re just going from one consult to the other.”
The situation improved with a checklist of things to consider when a patient presents with altered mental status. Before seeking a consult, neurologists suggested the hospitalists check the electrolytes, blood pressure, and urine, and use CT scans as a screening test. That might uncover the root of the patient’s problems. If those are clear, by all means get the neurologist involved, he says.
“We were able to educate the hospitalists so they knew when to call; they knew when it was beyond their expertise to take care of the patient, so we weren’t getting called for every patient with altered mental status when all they needed to do was to check the electrolytes,” Dr. Kenton says.
Calling a neurologist earlier is way better than calling later.
Once the decision is made to consult with a neurologist, the consult should be done right away, Dr. Kenton says, not after a few days when symptoms don’t appear to be improving.
“We’ll get the call on a Friday afternoon because they thought, finally, ‘Well, you know, we need to get neurology involved because we a) haven’t solved the problem and b) there may be some other tests we should be getting,’” he says of common situations. “That has been a problem. If you don’t have a neurohospitalist involved day by day, working with the patient and the general hospitalist, neurology becomes an afterthought.”
He says accurate and early diagnosis is paramount to the patient.
“If the diagnosis is delayed, obviously there’s more insult to the patients, more persistent insult,” he says, noting the timing is particularly important in neurological conditions “because things can get bad in a hurry.”
He strongly urges hospitalists to consult with a neurologist before ordering an entire battery of tests.
At Geisinger, neurologists are encouraging hospitalists to chat informally with neurosurgeons about cases for guidance at the outset rather than after several days.
Hire a neurohospitalist if your institution doesn’t have one already.
At the top of the list of Dr. Kenton’s suggestions on caring for hospitalized neurology patients is this declaration: “Get a neurohospitalist.”
“It’s important to have the neurologist involved from the time the patient’s admitted,” he says. “That’s the value of connecting the general hospitalist with neurologists.”
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says his colleagues are team players and improve patient care.
“Neurology consultations can be called very quickly, and a nice partnership can develop between internal medicine hospitalists and neurohospitalists to care for those patients who have those medical and neurologic problems,” he says.
He also says having a neurohospitalist on board can ease some of the tension.
“No longer if there’s a neurologic condition does a hospitalist have to think about, ‘Well, does this rise to the level of something that I need to get the neurologist to drive across the city to come see?’” he explains. “‘Or is this something we should try to manage ourselves?’”
Tom Collins is a freelance writer in South Florida.
“Neurophobia” a Challenge for Hospitalists, Other Physicians

The unease that many hospitalists, internal-medicine doctors, and other providers feel about treating neurologic conditions is so readily recognized that a term has been coined to describe it: “neurophobia.”
The term has been used in published literature for at least two decades. A 2010 survey found that medical students and residents felt that neurology was the specialty they had the least knowledge about and was the one that was the most difficult.3 And trainees had the least confidence in treating patients with neurological complaints.
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says internal-medicine hospitalists are “increasingly feeling uncomfortable with requests that they have to care for patients with a wide range of primary neurologic conditions in some instances.”
That has helped lead to the emergence of neurohospitalists, he says.
John Vazquez, MD, medical director of the division hospital medicine of Emory University Hospital in Atlanta, says neurophobia is real.
“Every hospitalist has different subspecialty areas that they’re less comfortable with, and I think neurology specifically is one that does scare a lot of hospitalists,” he says. “I think on one side there are hospitalists that might ignore a neurologic problem because they don’t really know what they don’t know. On the other side are the hospitalists who I think are just concerned that they don’t know the field very well and may not feel comfortable.”
Dr. Vazquez did rotations in nephrology, pulmonology, cardiology, and rheumatology but, like many hospitalists, not neurology.
“Neurology is not one that you have to go through,” he says.
He made these suggestions:
- Know what you don’t know and get guidance when necessary.
- Do your own neurologic assessment. Even if a neurologist decides confusion is due to a patient being elderly and having a urinary tract infection, that doesn’t mean that they didn’t actually have a stroke. So if something seems not quite right, be willing to challenge the neurologist.
- Use the resources available to widen your knowledge base.
“You can utilize the consultants for your own education if you have neurologists in your hospital, and many at least have some that rotate in,” Dr. Vazquez says. “You can pick their brain on what they would do with different strokes and what’s the newest thing and ongoing treatment and whatever it is you’re concerned about.”
—Thomas R. Collins
John Vazquez, MD, of Emory University Hospital talks about neurophobia and provides tips for adjusting to the discomfort of working with neurology patients.
References
- Bernhardt J, Dewey H, Thrift A, Collier J, Donnan G. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke. 2008;39;390-396.
- Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs. time-defined TIA: a multicenter study. Neurology. 2011;77(13):1222-1228.
- Zinchuk AV, Flanagan EP, Tubridy NJ, Miller WA, McCullough LD. Attitudes of US medical trainees towards neurology education: “Neurophobia”—a global issue. BMC Med Educ. 2010;10:49.
11 Things: At a Glance
- You might be overdiagnosing transient ischemic attacks (TIA).
- Early mobilization after a stroke might be better for some patients.
- MRI is the best tool to evaluate TIA patients.
- Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
- Tracking the time a hospitalized patient was last seen to be normal is crucial.
- Consider neuromuscular disorders when a patient presents with weakness.
- Urinary tract infections (UTIs) are not the only cause of altered mental status.
- Take care in distinguishing aphasia from general confusion.
- A simple checklist might eliminate the need to consult the neurologist.
- Calling a neurologist earlier is way better than calling later.
- Hire a neurohospitalist if your institution doesn’t have one already.
When a patient is admitted to the hospital with neurological symptoms, such as altered mental status, he or she might not be the only one who is confused. Hospitalists might be a little confused, too.
Of all the subspecialties to which hospitalists are exposed, none might make them more uncomfortable than neurology. Because of what often is a dearth of training in this area, and because of the vexing and sometimes fleeting nature of symptoms, hospitalists might be inclined to lean on neurologists more than other specialists.
The Hospitalist spoke with a half-dozen experts, gathering their words of guidance and clinical tips. Here’s hoping they give you a little extra confidence the next time you see a patient with altered mental status.
You might be overdiagnosing transient ischemic attacks (TIA).
Ira Chang, MD, a neurohospitalist with Blue Sky Neurology in Englewood, Colo., and assistant clinical professor at the University of Colorado Health Sciences Center in Denver, says TIA is all too commonly a go-to diagnosis, frequently when there’s another cause.
“I think that hospitalists, and maybe medical internists in general, are very quick to diagnose anything that has a neurologic symptom that comes and goes as a TIA,” she says. “Patients have to have specific neurologic symptoms that we think are due to arterial blood flow or ischemia problems.”
Near-fainting spells and dizzy spells involving confusion commonly are diagnosed as TIA when these symptoms could be due to “a number of other causes,” Dr. Chang adds.
Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says the suspicion of a TIA should be greater if the patient is older or has traditional cardiovascular risk factors, such as hyptertension, diabetes, hyperlipidemia, or tobacco use.
A TIA typically causes symptoms referable to common arterial distributions. Carotid-distribution TIA often causes ipsilateral loss of vision and contralateral weakness or numbness. Posterior-circulation TIAs bring on symptoms such as ataxia, unilateral or bilateral limb weakness, diplopia, and slurred or slow speech.
TIA diagnoses can be tricky even for those trained in neurology, Dr. Barrett says.
“Even among fellowship-trained vascular neurologists, TIA can be a challenging diagnosis, often with poor inter-observer agreement,” he notes.
Early mobilization after a stroke might be better for some patients.
After receiving tissue plasminogen activator (tPA) therapy for stroke, patients historically were kept on bed rest for 24 hours to reduce the risk of hemorrhage. Evidence now is coming to light that some patients might benefit from getting out of bed sooner, Dr. Barrett says.1
“We’re learning that in selected patients, they can actually be mobilized at 12 hours,” he says. “In some cases, that would not only reduce the risk of complications related to immobilization like DVT but shorten length of stay. These are all important metrics for anybody who practices primarily within an inpatient setting.”
Early mobilization generally is more suitable for patients with less severe deficits and who are hemodynamically stable.
MRI is the best tool to evaluate TIA patients.
TIA patients who have transient symptoms and normal diffusion-weighted imaging (DWI) abnormalities on an MRI are at a very low risk. “Less than 1% of those patients have a stroke within the subsequent seven days,” Dr. Barrett says.2 “But those patients who do have a DWI abnormality, they’re at very high risk: 7.1% at seven days.
“The utility of MRI following TIA is becoming very much apparent. It is something that hospitalists should be aware of.”
Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
Patients experiencing confusion or speech disturbance or altered mentation—particularly if they’re elderly or have dementia—could be having a partial seizure, Dr. Chang says. Dementia patients have a 10% to 15% incidence of complex partial seizures, she says.
“I see that underdiagnosed a lot,” she says. “They keep coming back, and everybody diagnoses them with TIAs. So they keep getting put on aspirin, and they get switched to Aggrenox [to prevent clotting]. They keep coming back with the same symptoms.”
Tracking the time a hospitalized patient was last seen to be normal is crucial.
About 10% to 15% of strokes occur in patients who are in the hospital.
“While a lot of those strokes are perioperative, there also are patients who are going to be on hospitalist services,” says Eric Adelman, MD, assistant professor of neurology at the University of Michigan in Ann Arbor.
Hospitalists should note that patients suffering strokes are found not just in the ED but also on the floor, where all the tools for treatment might not be as readily available. That makes those cases a challenge and makes forethought that much more important, Dr. Adelman says.
“It’s a matter of trying to track down last normal times,” he says. “If they’re eligible for tPA and they’re within the therapeutic window, we should be able to do that within a hospital.”
Establishing a neurological baseline is particularly important for patients who are at higher stroke risk, like those with atrial fibrillation and other cardiovascular risk factors.
“In case something does happen,” Dr. Adelman says, “at least you have a baseline so you can [know that] at time X, we knew they had full strength in their right arm, and now they don’t.”
Consider neuromuscular disorders when a patient presents with weakness.
It’s safe to say some hospitalists might miss a neuromuscular disorder, Dr. Chang says.
“A lot of disorders that are harder for hospitalists to diagnose and that tend to take longer to call a neurologist [on] are things that are due to myasthenia gravis [a breakdown between nerves and muscles leading to muscle fatigue], myopathy, or ALS,” she says. “Many patients present with weakness. I think a lot of times there will be a lot of tests on and a lot of treatment for general medical conditions that can cause weakness.”
And that might be a case of misdirected attention. Patients with weakness accompanied by persistent swallowing problems, slurred speech with no other obvious cause, or the inability to lift their head off the bed without an obvious cause may end up with a neuromuscular diagnosis, she says.
It would be helpful to have a neurologist’s input in these cases, she says, where “nothing’s getting better, and three, four, five days later, the patient’s still weak.
“I think a neurologist would be more in tune with something like that,” she adds.
Urinary tract infections (UTIs) are not the only cause of altered mental status.
That might seem obvious, but too often, a UTI can be pegged as the source of altered mental status when it should not be, Dr. Chang says.
“We get a lot of people who come in with confusion and they have a slightly abnormal urinalysis and they diagnose them with UTI,” Dr. Chang says. “And it turns out that they actually had a stroke or they had a seizure.”
Significantly altered mentation should show a significantly abnormal urine with a positive culture, she says. “They ought to have significant laboratory support for a urinary tract infection.”
Dr. Barrett says a neurologic review of systems, or at least a neurologic exam, should be the physician’s guide.
“Those are key parts of a hospitalist’s practice,” he says, “because that’s what’s truly going to guide them to consider primary neurological causes of altered mental status.”
Take care in distinguishing aphasia from general confusion.
If a patient is still talking and is fairly fluent, that doesn’t mean they aren’t suffering from certain types of aphasia, a disorder caused by damage to parts of the brain that control language, Dr. Adelman says.
“Oftentimes, when you’re dealing with a patient with confusion, you want to make sure that it’s confusion, or encephalopathy, rather than a focal neurologic problem like aphasia,” he says. “Frequently patients with aphasia will have other symptoms such as a facial drop or weakness in the arm, but stroke can present as isolated aphasia.”
A good habit to get into is to determine whether the patient can repeat a phrase, follow a command, or name objects, he says. If they can, they probably do not have aphasia.
“The thing that you worry about with aphasia, particularly acute onset aphasia, is an ischemic stroke,” Dr. Adelman says.
A simple checklist might eliminate the need to consult the neurologist.
When Edgar Kenton, MD, now director of the stroke program at Geisinger Health System in Danville, Pa., was at Emory University Hospital in Atlanta, he found he was getting snowed under with consults from hospitalists. There were about 15 hospitalists for just one or two neurologists.
“There was no way I was able to see these patients, particularly in follow-up, because you might get five consults every day,” he says. “By the middle of the week, that’s 15 consults. You don’t get a chance to go back and see the patients because you’re just going from one consult to the other.”
The situation improved with a checklist of things to consider when a patient presents with altered mental status. Before seeking a consult, neurologists suggested the hospitalists check the electrolytes, blood pressure, and urine, and use CT scans as a screening test. That might uncover the root of the patient’s problems. If those are clear, by all means get the neurologist involved, he says.
“We were able to educate the hospitalists so they knew when to call; they knew when it was beyond their expertise to take care of the patient, so we weren’t getting called for every patient with altered mental status when all they needed to do was to check the electrolytes,” Dr. Kenton says.
Calling a neurologist earlier is way better than calling later.
Once the decision is made to consult with a neurologist, the consult should be done right away, Dr. Kenton says, not after a few days when symptoms don’t appear to be improving.
“We’ll get the call on a Friday afternoon because they thought, finally, ‘Well, you know, we need to get neurology involved because we a) haven’t solved the problem and b) there may be some other tests we should be getting,’” he says of common situations. “That has been a problem. If you don’t have a neurohospitalist involved day by day, working with the patient and the general hospitalist, neurology becomes an afterthought.”
He says accurate and early diagnosis is paramount to the patient.
“If the diagnosis is delayed, obviously there’s more insult to the patients, more persistent insult,” he says, noting the timing is particularly important in neurological conditions “because things can get bad in a hurry.”
He strongly urges hospitalists to consult with a neurologist before ordering an entire battery of tests.
At Geisinger, neurologists are encouraging hospitalists to chat informally with neurosurgeons about cases for guidance at the outset rather than after several days.
Hire a neurohospitalist if your institution doesn’t have one already.
At the top of the list of Dr. Kenton’s suggestions on caring for hospitalized neurology patients is this declaration: “Get a neurohospitalist.”
“It’s important to have the neurologist involved from the time the patient’s admitted,” he says. “That’s the value of connecting the general hospitalist with neurologists.”
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says his colleagues are team players and improve patient care.
“Neurology consultations can be called very quickly, and a nice partnership can develop between internal medicine hospitalists and neurohospitalists to care for those patients who have those medical and neurologic problems,” he says.
He also says having a neurohospitalist on board can ease some of the tension.
“No longer if there’s a neurologic condition does a hospitalist have to think about, ‘Well, does this rise to the level of something that I need to get the neurologist to drive across the city to come see?’” he explains. “‘Or is this something we should try to manage ourselves?’”
Tom Collins is a freelance writer in South Florida.
“Neurophobia” a Challenge for Hospitalists, Other Physicians
The unease that many hospitalists, internal-medicine doctors, and other providers feel about treating neurologic conditions is so readily recognized that a term has been coined to describe it: “neurophobia.”
The term has been used in published literature for at least two decades. A 2010 survey found that medical students and residents felt that neurology was the specialty they had the least knowledge about and was the one that was the most difficult.3 And trainees had the least confidence in treating patients with neurological complaints.
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says internal-medicine hospitalists are “increasingly feeling uncomfortable with requests that they have to care for patients with a wide range of primary neurologic conditions in some instances.”
That has helped lead to the emergence of neurohospitalists, he says.
John Vazquez, MD, medical director of the division hospital medicine of Emory University Hospital in Atlanta, says neurophobia is real.
“Every hospitalist has different subspecialty areas that they’re less comfortable with, and I think neurology specifically is one that does scare a lot of hospitalists,” he says. “I think on one side there are hospitalists that might ignore a neurologic problem because they don’t really know what they don’t know. On the other side are the hospitalists who I think are just concerned that they don’t know the field very well and may not feel comfortable.”
Dr. Vazquez did rotations in nephrology, pulmonology, cardiology, and rheumatology but, like many hospitalists, not neurology.
“Neurology is not one that you have to go through,” he says.
He made these suggestions:
- Know what you don’t know and get guidance when necessary.
- Do your own neurologic assessment. Even if a neurologist decides confusion is due to a patient being elderly and having a urinary tract infection, that doesn’t mean that they didn’t actually have a stroke. So if something seems not quite right, be willing to challenge the neurologist.
- Use the resources available to widen your knowledge base.
“You can utilize the consultants for your own education if you have neurologists in your hospital, and many at least have some that rotate in,” Dr. Vazquez says. “You can pick their brain on what they would do with different strokes and what’s the newest thing and ongoing treatment and whatever it is you’re concerned about.”
—Thomas R. Collins
John Vazquez, MD, of Emory University Hospital talks about neurophobia and provides tips for adjusting to the discomfort of working with neurology patients.
References
- Bernhardt J, Dewey H, Thrift A, Collier J, Donnan G. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke. 2008;39;390-396.
- Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs. time-defined TIA: a multicenter study. Neurology. 2011;77(13):1222-1228.
- Zinchuk AV, Flanagan EP, Tubridy NJ, Miller WA, McCullough LD. Attitudes of US medical trainees towards neurology education: “Neurophobia”—a global issue. BMC Med Educ. 2010;10:49.
11 Things: At a Glance
- You might be overdiagnosing transient ischemic attacks (TIA).
- Early mobilization after a stroke might be better for some patients.
- MRI is the best tool to evaluate TIA patients.
- Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
- Tracking the time a hospitalized patient was last seen to be normal is crucial.
- Consider neuromuscular disorders when a patient presents with weakness.
- Urinary tract infections (UTIs) are not the only cause of altered mental status.
- Take care in distinguishing aphasia from general confusion.
- A simple checklist might eliminate the need to consult the neurologist.
- Calling a neurologist earlier is way better than calling later.
- Hire a neurohospitalist if your institution doesn’t have one already.
When a patient is admitted to the hospital with neurological symptoms, such as altered mental status, he or she might not be the only one who is confused. Hospitalists might be a little confused, too.
Of all the subspecialties to which hospitalists are exposed, none might make them more uncomfortable than neurology. Because of what often is a dearth of training in this area, and because of the vexing and sometimes fleeting nature of symptoms, hospitalists might be inclined to lean on neurologists more than other specialists.
The Hospitalist spoke with a half-dozen experts, gathering their words of guidance and clinical tips. Here’s hoping they give you a little extra confidence the next time you see a patient with altered mental status.
You might be overdiagnosing transient ischemic attacks (TIA).
Ira Chang, MD, a neurohospitalist with Blue Sky Neurology in Englewood, Colo., and assistant clinical professor at the University of Colorado Health Sciences Center in Denver, says TIA is all too commonly a go-to diagnosis, frequently when there’s another cause.
“I think that hospitalists, and maybe medical internists in general, are very quick to diagnose anything that has a neurologic symptom that comes and goes as a TIA,” she says. “Patients have to have specific neurologic symptoms that we think are due to arterial blood flow or ischemia problems.”
Near-fainting spells and dizzy spells involving confusion commonly are diagnosed as TIA when these symptoms could be due to “a number of other causes,” Dr. Chang adds.
Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says the suspicion of a TIA should be greater if the patient is older or has traditional cardiovascular risk factors, such as hyptertension, diabetes, hyperlipidemia, or tobacco use.
A TIA typically causes symptoms referable to common arterial distributions. Carotid-distribution TIA often causes ipsilateral loss of vision and contralateral weakness or numbness. Posterior-circulation TIAs bring on symptoms such as ataxia, unilateral or bilateral limb weakness, diplopia, and slurred or slow speech.
TIA diagnoses can be tricky even for those trained in neurology, Dr. Barrett says.
“Even among fellowship-trained vascular neurologists, TIA can be a challenging diagnosis, often with poor inter-observer agreement,” he notes.
Early mobilization after a stroke might be better for some patients.
After receiving tissue plasminogen activator (tPA) therapy for stroke, patients historically were kept on bed rest for 24 hours to reduce the risk of hemorrhage. Evidence now is coming to light that some patients might benefit from getting out of bed sooner, Dr. Barrett says.1
“We’re learning that in selected patients, they can actually be mobilized at 12 hours,” he says. “In some cases, that would not only reduce the risk of complications related to immobilization like DVT but shorten length of stay. These are all important metrics for anybody who practices primarily within an inpatient setting.”
Early mobilization generally is more suitable for patients with less severe deficits and who are hemodynamically stable.
MRI is the best tool to evaluate TIA patients.
TIA patients who have transient symptoms and normal diffusion-weighted imaging (DWI) abnormalities on an MRI are at a very low risk. “Less than 1% of those patients have a stroke within the subsequent seven days,” Dr. Barrett says.2 “But those patients who do have a DWI abnormality, they’re at very high risk: 7.1% at seven days.
“The utility of MRI following TIA is becoming very much apparent. It is something that hospitalists should be aware of.”
Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
Patients experiencing confusion or speech disturbance or altered mentation—particularly if they’re elderly or have dementia—could be having a partial seizure, Dr. Chang says. Dementia patients have a 10% to 15% incidence of complex partial seizures, she says.
“I see that underdiagnosed a lot,” she says. “They keep coming back, and everybody diagnoses them with TIAs. So they keep getting put on aspirin, and they get switched to Aggrenox [to prevent clotting]. They keep coming back with the same symptoms.”
Tracking the time a hospitalized patient was last seen to be normal is crucial.
About 10% to 15% of strokes occur in patients who are in the hospital.
“While a lot of those strokes are perioperative, there also are patients who are going to be on hospitalist services,” says Eric Adelman, MD, assistant professor of neurology at the University of Michigan in Ann Arbor.
Hospitalists should note that patients suffering strokes are found not just in the ED but also on the floor, where all the tools for treatment might not be as readily available. That makes those cases a challenge and makes forethought that much more important, Dr. Adelman says.
“It’s a matter of trying to track down last normal times,” he says. “If they’re eligible for tPA and they’re within the therapeutic window, we should be able to do that within a hospital.”
Establishing a neurological baseline is particularly important for patients who are at higher stroke risk, like those with atrial fibrillation and other cardiovascular risk factors.
“In case something does happen,” Dr. Adelman says, “at least you have a baseline so you can [know that] at time X, we knew they had full strength in their right arm, and now they don’t.”
Consider neuromuscular disorders when a patient presents with weakness.
It’s safe to say some hospitalists might miss a neuromuscular disorder, Dr. Chang says.
“A lot of disorders that are harder for hospitalists to diagnose and that tend to take longer to call a neurologist [on] are things that are due to myasthenia gravis [a breakdown between nerves and muscles leading to muscle fatigue], myopathy, or ALS,” she says. “Many patients present with weakness. I think a lot of times there will be a lot of tests on and a lot of treatment for general medical conditions that can cause weakness.”
And that might be a case of misdirected attention. Patients with weakness accompanied by persistent swallowing problems, slurred speech with no other obvious cause, or the inability to lift their head off the bed without an obvious cause may end up with a neuromuscular diagnosis, she says.
It would be helpful to have a neurologist’s input in these cases, she says, where “nothing’s getting better, and three, four, five days later, the patient’s still weak.
“I think a neurologist would be more in tune with something like that,” she adds.
Urinary tract infections (UTIs) are not the only cause of altered mental status.
That might seem obvious, but too often, a UTI can be pegged as the source of altered mental status when it should not be, Dr. Chang says.
“We get a lot of people who come in with confusion and they have a slightly abnormal urinalysis and they diagnose them with UTI,” Dr. Chang says. “And it turns out that they actually had a stroke or they had a seizure.”
Significantly altered mentation should show a significantly abnormal urine with a positive culture, she says. “They ought to have significant laboratory support for a urinary tract infection.”
Dr. Barrett says a neurologic review of systems, or at least a neurologic exam, should be the physician’s guide.
“Those are key parts of a hospitalist’s practice,” he says, “because that’s what’s truly going to guide them to consider primary neurological causes of altered mental status.”
Take care in distinguishing aphasia from general confusion.
If a patient is still talking and is fairly fluent, that doesn’t mean they aren’t suffering from certain types of aphasia, a disorder caused by damage to parts of the brain that control language, Dr. Adelman says.
“Oftentimes, when you’re dealing with a patient with confusion, you want to make sure that it’s confusion, or encephalopathy, rather than a focal neurologic problem like aphasia,” he says. “Frequently patients with aphasia will have other symptoms such as a facial drop or weakness in the arm, but stroke can present as isolated aphasia.”
A good habit to get into is to determine whether the patient can repeat a phrase, follow a command, or name objects, he says. If they can, they probably do not have aphasia.
“The thing that you worry about with aphasia, particularly acute onset aphasia, is an ischemic stroke,” Dr. Adelman says.
A simple checklist might eliminate the need to consult the neurologist.
When Edgar Kenton, MD, now director of the stroke program at Geisinger Health System in Danville, Pa., was at Emory University Hospital in Atlanta, he found he was getting snowed under with consults from hospitalists. There were about 15 hospitalists for just one or two neurologists.
“There was no way I was able to see these patients, particularly in follow-up, because you might get five consults every day,” he says. “By the middle of the week, that’s 15 consults. You don’t get a chance to go back and see the patients because you’re just going from one consult to the other.”
The situation improved with a checklist of things to consider when a patient presents with altered mental status. Before seeking a consult, neurologists suggested the hospitalists check the electrolytes, blood pressure, and urine, and use CT scans as a screening test. That might uncover the root of the patient’s problems. If those are clear, by all means get the neurologist involved, he says.
“We were able to educate the hospitalists so they knew when to call; they knew when it was beyond their expertise to take care of the patient, so we weren’t getting called for every patient with altered mental status when all they needed to do was to check the electrolytes,” Dr. Kenton says.
Calling a neurologist earlier is way better than calling later.
Once the decision is made to consult with a neurologist, the consult should be done right away, Dr. Kenton says, not after a few days when symptoms don’t appear to be improving.
“We’ll get the call on a Friday afternoon because they thought, finally, ‘Well, you know, we need to get neurology involved because we a) haven’t solved the problem and b) there may be some other tests we should be getting,’” he says of common situations. “That has been a problem. If you don’t have a neurohospitalist involved day by day, working with the patient and the general hospitalist, neurology becomes an afterthought.”
He says accurate and early diagnosis is paramount to the patient.
“If the diagnosis is delayed, obviously there’s more insult to the patients, more persistent insult,” he says, noting the timing is particularly important in neurological conditions “because things can get bad in a hurry.”
He strongly urges hospitalists to consult with a neurologist before ordering an entire battery of tests.
At Geisinger, neurologists are encouraging hospitalists to chat informally with neurosurgeons about cases for guidance at the outset rather than after several days.
Hire a neurohospitalist if your institution doesn’t have one already.
At the top of the list of Dr. Kenton’s suggestions on caring for hospitalized neurology patients is this declaration: “Get a neurohospitalist.”
“It’s important to have the neurologist involved from the time the patient’s admitted,” he says. “That’s the value of connecting the general hospitalist with neurologists.”
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says his colleagues are team players and improve patient care.
“Neurology consultations can be called very quickly, and a nice partnership can develop between internal medicine hospitalists and neurohospitalists to care for those patients who have those medical and neurologic problems,” he says.
He also says having a neurohospitalist on board can ease some of the tension.
“No longer if there’s a neurologic condition does a hospitalist have to think about, ‘Well, does this rise to the level of something that I need to get the neurologist to drive across the city to come see?’” he explains. “‘Or is this something we should try to manage ourselves?’”
Tom Collins is a freelance writer in South Florida.
“Neurophobia” a Challenge for Hospitalists, Other Physicians
The unease that many hospitalists, internal-medicine doctors, and other providers feel about treating neurologic conditions is so readily recognized that a term has been coined to describe it: “neurophobia.”
The term has been used in published literature for at least two decades. A 2010 survey found that medical students and residents felt that neurology was the specialty they had the least knowledge about and was the one that was the most difficult.3 And trainees had the least confidence in treating patients with neurological complaints.
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says internal-medicine hospitalists are “increasingly feeling uncomfortable with requests that they have to care for patients with a wide range of primary neurologic conditions in some instances.”
That has helped lead to the emergence of neurohospitalists, he says.
John Vazquez, MD, medical director of the division hospital medicine of Emory University Hospital in Atlanta, says neurophobia is real.
“Every hospitalist has different subspecialty areas that they’re less comfortable with, and I think neurology specifically is one that does scare a lot of hospitalists,” he says. “I think on one side there are hospitalists that might ignore a neurologic problem because they don’t really know what they don’t know. On the other side are the hospitalists who I think are just concerned that they don’t know the field very well and may not feel comfortable.”
Dr. Vazquez did rotations in nephrology, pulmonology, cardiology, and rheumatology but, like many hospitalists, not neurology.
“Neurology is not one that you have to go through,” he says.
He made these suggestions:
- Know what you don’t know and get guidance when necessary.
- Do your own neurologic assessment. Even if a neurologist decides confusion is due to a patient being elderly and having a urinary tract infection, that doesn’t mean that they didn’t actually have a stroke. So if something seems not quite right, be willing to challenge the neurologist.
- Use the resources available to widen your knowledge base.
“You can utilize the consultants for your own education if you have neurologists in your hospital, and many at least have some that rotate in,” Dr. Vazquez says. “You can pick their brain on what they would do with different strokes and what’s the newest thing and ongoing treatment and whatever it is you’re concerned about.”
—Thomas R. Collins
John Vazquez, MD, of Emory University Hospital talks about neurophobia and provides tips for adjusting to the discomfort of working with neurology patients.
References
- Bernhardt J, Dewey H, Thrift A, Collier J, Donnan G. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke. 2008;39;390-396.
- Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs. time-defined TIA: a multicenter study. Neurology. 2011;77(13):1222-1228.
- Zinchuk AV, Flanagan EP, Tubridy NJ, Miller WA, McCullough LD. Attitudes of US medical trainees towards neurology education: “Neurophobia”—a global issue. BMC Med Educ. 2010;10:49.