User login
How to Handle Medicare Documentation Audits

The recent announcement of a settlement by a physician firm should cause the HM community to pause and take inventory. The settlement “addressed allegations that, between 2004 and 2012, [the firm] knowingly submitted to federal health benefits programs inflated claims on behalf of its hospitalist employees for higher and more expensive levels of service than were documented by hospitalists in patient medical records.”1
This civil settlement highlights the vigilance being exercised against healthcare fraud and demonstrates the coordinated efforts in place to tackle the issue. To put the weight of this case in perspective, consider the breadth of legal entities involved: the U.S. Department of Justice; the U.S. Attorney’s Office; the U.S. Department of Health and Human Services; the U.S. Department of Defense; the U.S. Office of Personnel Management; the U.S. Department of Veterans’ Affairs; and the TRICARE Management Activity Office of General Counsel.1
The underlying factor in the settlement is a common issue routinely identified by Medicare-initiated review programs such as CERT (Comprehensive Error Rate Testing). CERT selects a stratified, random sample of approximately 40,000 claims submitted to Part A/B Medicare Administrative Contractors (MACs) and Durable Medical Equipment MACs (DME MACs) during each reporting period and allows the Centers for Medicare and Medicaid Services (CMS) to calculate a national improper payment rate and contractor- and service-specific improper payment rates.2 The CERT-determined improper payment rate identifies services that have not satisfied Medicare requirements, but it cannot label a claim fraudulent.2
Incorrect coding errors involving hospitalists are related to inpatient evaluation and management (E/M) services that do not adequately reflect the documentation in the medical record. For example, WPS Medicare identified the following error rates for claims submitted 7/1/11 to 6/30/12: 45% of 99223 (initial hospital care, per day, for the evaluation and management of a patient, which requires these three key components: a comprehensive history, a comprehensive exam, and medical decision-making of high complexity); and 34% of 99233 (subsequent hospital care, per day, for the evaluation and management of a patient, which requires at least two of these three key components: a detailed interval history, a detailed examination, and medical decision-making of high complexity).3,4 More recent WPS Medicare data in first quarter of FY2013 reveals a continuing problem but an improved error rate.5 Novitas Solutions offers additional support of these findings.6
Based on efforts that identify improper payments, MACs are encouraged to initiate targeted service-specific prepayment review to prevent improper payments for services identified by CERT or recovery audit contractors (RACs) as problem areas, as well as problem areas identified by their own data analysis.7 For this reason, hospitalists may see prepayment requests for documentation by Medicare for services that are most “problematic” (e.g., 99223 and 99233). This occurs when a claim involving these services is submitted to Medicare. The MAC suspends all or part of a claim so that a trained clinician or claims analyst can review the claim and associated documentation in order to make determinations about coverage and payment.7 Responding to these requests in a timely manner is crucial in preventing claim denials.
Responding to Requests
When documentation is requested by the payor, take note of the date and the provider for whom the service is requested. Be certain to include all pertinent information in support of the claim. The payor request letter will typically include a generic list of items that should be submitted with the documentation request. Consider these particular items when submitting documentation for targeted services typically provided by hospitalists:
- Initial Hospital Care (99223)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify any referenced sources of information (e.g., physician referencing a family history documented in the ED record);
- Dictations, when performed;
- Admitting orders; and
- Labs or diagnostic test reports performed on admission.
- Subsequent Hospital Care (99233)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify multiple encounters/entries recorded on a given date;
- Physician orders; and
- Labs or diagnostic test reports performed on the requested date.
Documentation Tips
Because it is the primary communication tool for providers involved in the patient’s care, documentation must be entered in a timely manner and must be decipherable to members of the healthcare team as well as other individuals who may need to review the information (e.g., auditors). Proper credit cannot be given for documentation that is difficult to read.
Information should include historical review of past/interim events, a physical exam, medical decision-making as related to the patient’s progress/response to intervention, and modification of the care plan (as necessary). The reason for the encounter should be evident to support the medical necessity of the service. Because various specialists may participate in patient care, documentation for each provider’s encounter should demonstrate personalized and non-duplicative care.
Each individual provider must exhibit a personal contribution to the case to prevent payors from viewing the documentation as overlapping and indistinguishable from care already provided by another physician. Each entry should be dated and signed with a legible identifier (i.e., signature with a printed name).
The next several articles will address each of the key components (history, exam, and decision-making) and serve as a “documentation refresher” for providers who wish to compare their documentation to current standards.
References
- Department of Justice, Office of Public Affairs. Tacoma, Wash., Medical Firm to Pay $14.5 Million to Settle Overbilling Allegations. Available at: www.justice.gov/opa/pr/2013/July/13-civ-758.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Comprehensive Error Rate Testing (CERT). Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/CERT/index.html?redirect=/cert. Accessed September 20, 2013.
- WPS Medicare, Legacy Part B. Are you billing these evaluation and management (e/m) services correctly? Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2011-0912-billemservices.shtml. Accessed September 20, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis, L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012:15-17.
- WPS Medicare, Legacy Part B. 1st Qtr. 2013 (Jan. - Mar.) - CERT Error Summary. Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2013-1st-quarter-summary.shtml. Accessed September 20, 2013.
- Novitas Solutions. Analysis of JL Part B Comprehensive Error Rate Testing (CERT) Data - January thru March 2013. Available at: https://www.novitas-solutions.com/cert/errors/2013/b-jan-mar-j12.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Program Integrity Manual, Chapter 3, Section 3.2. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/pim83c03.pdf. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual, Chapter 11, Section 40.1.2 Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed September 20, 2013.
The recent announcement of a settlement by a physician firm should cause the HM community to pause and take inventory. The settlement “addressed allegations that, between 2004 and 2012, [the firm] knowingly submitted to federal health benefits programs inflated claims on behalf of its hospitalist employees for higher and more expensive levels of service than were documented by hospitalists in patient medical records.”1
This civil settlement highlights the vigilance being exercised against healthcare fraud and demonstrates the coordinated efforts in place to tackle the issue. To put the weight of this case in perspective, consider the breadth of legal entities involved: the U.S. Department of Justice; the U.S. Attorney’s Office; the U.S. Department of Health and Human Services; the U.S. Department of Defense; the U.S. Office of Personnel Management; the U.S. Department of Veterans’ Affairs; and the TRICARE Management Activity Office of General Counsel.1
The underlying factor in the settlement is a common issue routinely identified by Medicare-initiated review programs such as CERT (Comprehensive Error Rate Testing). CERT selects a stratified, random sample of approximately 40,000 claims submitted to Part A/B Medicare Administrative Contractors (MACs) and Durable Medical Equipment MACs (DME MACs) during each reporting period and allows the Centers for Medicare and Medicaid Services (CMS) to calculate a national improper payment rate and contractor- and service-specific improper payment rates.2 The CERT-determined improper payment rate identifies services that have not satisfied Medicare requirements, but it cannot label a claim fraudulent.2
Incorrect coding errors involving hospitalists are related to inpatient evaluation and management (E/M) services that do not adequately reflect the documentation in the medical record. For example, WPS Medicare identified the following error rates for claims submitted 7/1/11 to 6/30/12: 45% of 99223 (initial hospital care, per day, for the evaluation and management of a patient, which requires these three key components: a comprehensive history, a comprehensive exam, and medical decision-making of high complexity); and 34% of 99233 (subsequent hospital care, per day, for the evaluation and management of a patient, which requires at least two of these three key components: a detailed interval history, a detailed examination, and medical decision-making of high complexity).3,4 More recent WPS Medicare data in first quarter of FY2013 reveals a continuing problem but an improved error rate.5 Novitas Solutions offers additional support of these findings.6
Based on efforts that identify improper payments, MACs are encouraged to initiate targeted service-specific prepayment review to prevent improper payments for services identified by CERT or recovery audit contractors (RACs) as problem areas, as well as problem areas identified by their own data analysis.7 For this reason, hospitalists may see prepayment requests for documentation by Medicare for services that are most “problematic” (e.g., 99223 and 99233). This occurs when a claim involving these services is submitted to Medicare. The MAC suspends all or part of a claim so that a trained clinician or claims analyst can review the claim and associated documentation in order to make determinations about coverage and payment.7 Responding to these requests in a timely manner is crucial in preventing claim denials.
Responding to Requests
When documentation is requested by the payor, take note of the date and the provider for whom the service is requested. Be certain to include all pertinent information in support of the claim. The payor request letter will typically include a generic list of items that should be submitted with the documentation request. Consider these particular items when submitting documentation for targeted services typically provided by hospitalists:
- Initial Hospital Care (99223)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify any referenced sources of information (e.g., physician referencing a family history documented in the ED record);
- Dictations, when performed;
- Admitting orders; and
- Labs or diagnostic test reports performed on admission.
- Subsequent Hospital Care (99233)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify multiple encounters/entries recorded on a given date;
- Physician orders; and
- Labs or diagnostic test reports performed on the requested date.
Documentation Tips
Because it is the primary communication tool for providers involved in the patient’s care, documentation must be entered in a timely manner and must be decipherable to members of the healthcare team as well as other individuals who may need to review the information (e.g., auditors). Proper credit cannot be given for documentation that is difficult to read.
Information should include historical review of past/interim events, a physical exam, medical decision-making as related to the patient’s progress/response to intervention, and modification of the care plan (as necessary). The reason for the encounter should be evident to support the medical necessity of the service. Because various specialists may participate in patient care, documentation for each provider’s encounter should demonstrate personalized and non-duplicative care.
Each individual provider must exhibit a personal contribution to the case to prevent payors from viewing the documentation as overlapping and indistinguishable from care already provided by another physician. Each entry should be dated and signed with a legible identifier (i.e., signature with a printed name).
The next several articles will address each of the key components (history, exam, and decision-making) and serve as a “documentation refresher” for providers who wish to compare their documentation to current standards.
References
- Department of Justice, Office of Public Affairs. Tacoma, Wash., Medical Firm to Pay $14.5 Million to Settle Overbilling Allegations. Available at: www.justice.gov/opa/pr/2013/July/13-civ-758.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Comprehensive Error Rate Testing (CERT). Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/CERT/index.html?redirect=/cert. Accessed September 20, 2013.
- WPS Medicare, Legacy Part B. Are you billing these evaluation and management (e/m) services correctly? Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2011-0912-billemservices.shtml. Accessed September 20, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis, L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012:15-17.
- WPS Medicare, Legacy Part B. 1st Qtr. 2013 (Jan. - Mar.) - CERT Error Summary. Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2013-1st-quarter-summary.shtml. Accessed September 20, 2013.
- Novitas Solutions. Analysis of JL Part B Comprehensive Error Rate Testing (CERT) Data - January thru March 2013. Available at: https://www.novitas-solutions.com/cert/errors/2013/b-jan-mar-j12.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Program Integrity Manual, Chapter 3, Section 3.2. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/pim83c03.pdf. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual, Chapter 11, Section 40.1.2 Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed September 20, 2013.
The recent announcement of a settlement by a physician firm should cause the HM community to pause and take inventory. The settlement “addressed allegations that, between 2004 and 2012, [the firm] knowingly submitted to federal health benefits programs inflated claims on behalf of its hospitalist employees for higher and more expensive levels of service than were documented by hospitalists in patient medical records.”1
This civil settlement highlights the vigilance being exercised against healthcare fraud and demonstrates the coordinated efforts in place to tackle the issue. To put the weight of this case in perspective, consider the breadth of legal entities involved: the U.S. Department of Justice; the U.S. Attorney’s Office; the U.S. Department of Health and Human Services; the U.S. Department of Defense; the U.S. Office of Personnel Management; the U.S. Department of Veterans’ Affairs; and the TRICARE Management Activity Office of General Counsel.1
The underlying factor in the settlement is a common issue routinely identified by Medicare-initiated review programs such as CERT (Comprehensive Error Rate Testing). CERT selects a stratified, random sample of approximately 40,000 claims submitted to Part A/B Medicare Administrative Contractors (MACs) and Durable Medical Equipment MACs (DME MACs) during each reporting period and allows the Centers for Medicare and Medicaid Services (CMS) to calculate a national improper payment rate and contractor- and service-specific improper payment rates.2 The CERT-determined improper payment rate identifies services that have not satisfied Medicare requirements, but it cannot label a claim fraudulent.2
Incorrect coding errors involving hospitalists are related to inpatient evaluation and management (E/M) services that do not adequately reflect the documentation in the medical record. For example, WPS Medicare identified the following error rates for claims submitted 7/1/11 to 6/30/12: 45% of 99223 (initial hospital care, per day, for the evaluation and management of a patient, which requires these three key components: a comprehensive history, a comprehensive exam, and medical decision-making of high complexity); and 34% of 99233 (subsequent hospital care, per day, for the evaluation and management of a patient, which requires at least two of these three key components: a detailed interval history, a detailed examination, and medical decision-making of high complexity).3,4 More recent WPS Medicare data in first quarter of FY2013 reveals a continuing problem but an improved error rate.5 Novitas Solutions offers additional support of these findings.6
Based on efforts that identify improper payments, MACs are encouraged to initiate targeted service-specific prepayment review to prevent improper payments for services identified by CERT or recovery audit contractors (RACs) as problem areas, as well as problem areas identified by their own data analysis.7 For this reason, hospitalists may see prepayment requests for documentation by Medicare for services that are most “problematic” (e.g., 99223 and 99233). This occurs when a claim involving these services is submitted to Medicare. The MAC suspends all or part of a claim so that a trained clinician or claims analyst can review the claim and associated documentation in order to make determinations about coverage and payment.7 Responding to these requests in a timely manner is crucial in preventing claim denials.
Responding to Requests
When documentation is requested by the payor, take note of the date and the provider for whom the service is requested. Be certain to include all pertinent information in support of the claim. The payor request letter will typically include a generic list of items that should be submitted with the documentation request. Consider these particular items when submitting documentation for targeted services typically provided by hospitalists:
- Initial Hospital Care (99223)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify any referenced sources of information (e.g., physician referencing a family history documented in the ED record);
- Dictations, when performed;
- Admitting orders; and
- Labs or diagnostic test reports performed on admission.
- Subsequent Hospital Care (99233)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify multiple encounters/entries recorded on a given date;
- Physician orders; and
- Labs or diagnostic test reports performed on the requested date.
Documentation Tips
Because it is the primary communication tool for providers involved in the patient’s care, documentation must be entered in a timely manner and must be decipherable to members of the healthcare team as well as other individuals who may need to review the information (e.g., auditors). Proper credit cannot be given for documentation that is difficult to read.
Information should include historical review of past/interim events, a physical exam, medical decision-making as related to the patient’s progress/response to intervention, and modification of the care plan (as necessary). The reason for the encounter should be evident to support the medical necessity of the service. Because various specialists may participate in patient care, documentation for each provider’s encounter should demonstrate personalized and non-duplicative care.
Each individual provider must exhibit a personal contribution to the case to prevent payors from viewing the documentation as overlapping and indistinguishable from care already provided by another physician. Each entry should be dated and signed with a legible identifier (i.e., signature with a printed name).
The next several articles will address each of the key components (history, exam, and decision-making) and serve as a “documentation refresher” for providers who wish to compare their documentation to current standards.
References
- Department of Justice, Office of Public Affairs. Tacoma, Wash., Medical Firm to Pay $14.5 Million to Settle Overbilling Allegations. Available at: www.justice.gov/opa/pr/2013/July/13-civ-758.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Comprehensive Error Rate Testing (CERT). Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/CERT/index.html?redirect=/cert. Accessed September 20, 2013.
- WPS Medicare, Legacy Part B. Are you billing these evaluation and management (e/m) services correctly? Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2011-0912-billemservices.shtml. Accessed September 20, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis, L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012:15-17.
- WPS Medicare, Legacy Part B. 1st Qtr. 2013 (Jan. - Mar.) - CERT Error Summary. Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2013-1st-quarter-summary.shtml. Accessed September 20, 2013.
- Novitas Solutions. Analysis of JL Part B Comprehensive Error Rate Testing (CERT) Data - January thru March 2013. Available at: https://www.novitas-solutions.com/cert/errors/2013/b-jan-mar-j12.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Program Integrity Manual, Chapter 3, Section 3.2. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/pim83c03.pdf. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual, Chapter 11, Section 40.1.2 Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed September 20, 2013.
San Francisco Medical Center Adapts Choosing Wisely List for Waste Reduction Campaign


A University of California at San Francisco (UCSF) quality initiative targeting waste and overuse of healthcare resources plans to focus on four of five questionable treatments identified by the Society of Hospital Medicine for the ABIM Foundation’s Choosing Wisely campaign. The UCSF Division of Hospital Medicine’s High Value Care Committee grew out of efforts to operationalize a curriculum for teaching medical trainees about the actual costs of treatments they commonly order. UCSF hospitalist Christopher Moriates, MD, developed the curriculum when he was a resident.
The committee brings together physicians, who have historically focused on quality improvement, and finance administrators, who focus on cost reduction. Together they are pursuing performance improvement projects serving both goals, Dr. Moriates says. The committee identified six waste targets initially and has already reduced the use of ionized calcium blood tests, formerly administered to numerous patients at UCSF Medical Center whether they needed it or not, and the unnecessary use of nebulizers, by more than half.
“When the Choosing Wisely list came out, it fit with what we were doing, although I wasn’t sure that these things were problems for us,” Dr. Moriates explains.
The data, however, show that UCSF was significantly better than its peers for only one of the five treatments on the list: utilization of Foley catheters and corresponding rates of catheter-related urinary tract infections. The committee is focused on more judicious, evidence-based ordering of the other Choosing Wisely treatments: medications for stress ulcer prophylaxis, blood transfusions, continuous telemetry monitoring outside of the ICU, and certain lab tests.
Dr. Moriates recommends the Choosing Wisely list for other hospitals and hospitalists starting to tackle unnecessary medical treatments and tests. Data is essential to these efforts, he says, stressing the need to consider not just utilization rates but actual dollars spent.
“That shouldn’t be a major hurdle, given hospital information technology, but often it is,” he says, adding that waste initiatives are more successful when they are led by frontline champions, rather than just assigned by the department’s chair.
Read more about Dr. Moriates’ waste control efforts in HealthLeaders Media, and learn about another waste reduction strategy called the Teaching Value Project at www.teachingvalue.org.1
Reference
A University of California at San Francisco (UCSF) quality initiative targeting waste and overuse of healthcare resources plans to focus on four of five questionable treatments identified by the Society of Hospital Medicine for the ABIM Foundation’s Choosing Wisely campaign. The UCSF Division of Hospital Medicine’s High Value Care Committee grew out of efforts to operationalize a curriculum for teaching medical trainees about the actual costs of treatments they commonly order. UCSF hospitalist Christopher Moriates, MD, developed the curriculum when he was a resident.
The committee brings together physicians, who have historically focused on quality improvement, and finance administrators, who focus on cost reduction. Together they are pursuing performance improvement projects serving both goals, Dr. Moriates says. The committee identified six waste targets initially and has already reduced the use of ionized calcium blood tests, formerly administered to numerous patients at UCSF Medical Center whether they needed it or not, and the unnecessary use of nebulizers, by more than half.
“When the Choosing Wisely list came out, it fit with what we were doing, although I wasn’t sure that these things were problems for us,” Dr. Moriates explains.
The data, however, show that UCSF was significantly better than its peers for only one of the five treatments on the list: utilization of Foley catheters and corresponding rates of catheter-related urinary tract infections. The committee is focused on more judicious, evidence-based ordering of the other Choosing Wisely treatments: medications for stress ulcer prophylaxis, blood transfusions, continuous telemetry monitoring outside of the ICU, and certain lab tests.
Dr. Moriates recommends the Choosing Wisely list for other hospitals and hospitalists starting to tackle unnecessary medical treatments and tests. Data is essential to these efforts, he says, stressing the need to consider not just utilization rates but actual dollars spent.
“That shouldn’t be a major hurdle, given hospital information technology, but often it is,” he says, adding that waste initiatives are more successful when they are led by frontline champions, rather than just assigned by the department’s chair.
Read more about Dr. Moriates’ waste control efforts in HealthLeaders Media, and learn about another waste reduction strategy called the Teaching Value Project at www.teachingvalue.org.1
Reference
A University of California at San Francisco (UCSF) quality initiative targeting waste and overuse of healthcare resources plans to focus on four of five questionable treatments identified by the Society of Hospital Medicine for the ABIM Foundation’s Choosing Wisely campaign. The UCSF Division of Hospital Medicine’s High Value Care Committee grew out of efforts to operationalize a curriculum for teaching medical trainees about the actual costs of treatments they commonly order. UCSF hospitalist Christopher Moriates, MD, developed the curriculum when he was a resident.
The committee brings together physicians, who have historically focused on quality improvement, and finance administrators, who focus on cost reduction. Together they are pursuing performance improvement projects serving both goals, Dr. Moriates says. The committee identified six waste targets initially and has already reduced the use of ionized calcium blood tests, formerly administered to numerous patients at UCSF Medical Center whether they needed it or not, and the unnecessary use of nebulizers, by more than half.
“When the Choosing Wisely list came out, it fit with what we were doing, although I wasn’t sure that these things were problems for us,” Dr. Moriates explains.
The data, however, show that UCSF was significantly better than its peers for only one of the five treatments on the list: utilization of Foley catheters and corresponding rates of catheter-related urinary tract infections. The committee is focused on more judicious, evidence-based ordering of the other Choosing Wisely treatments: medications for stress ulcer prophylaxis, blood transfusions, continuous telemetry monitoring outside of the ICU, and certain lab tests.
Dr. Moriates recommends the Choosing Wisely list for other hospitals and hospitalists starting to tackle unnecessary medical treatments and tests. Data is essential to these efforts, he says, stressing the need to consider not just utilization rates but actual dollars spent.
“That shouldn’t be a major hurdle, given hospital information technology, but often it is,” he says, adding that waste initiatives are more successful when they are led by frontline champions, rather than just assigned by the department’s chair.
Read more about Dr. Moriates’ waste control efforts in HealthLeaders Media, and learn about another waste reduction strategy called the Teaching Value Project at www.teachingvalue.org.1
Reference
PIAA Director of Research and Loss Prevention Discusses Hospitalist Insurance Premiums
Click here to listen to more of our interview with Divya Parikh
Click here to listen to more of our interview with Divya Parikh
Click here to listen to more of our interview with Divya Parikh
Hospitalists' Role in PQRS, Pay for Performance Gets Boost
With the voluntary and incentive period for participating in the Physician Quality Reporting System (PQRS) quickly coming to a close, hospitalists are finding a limited number of PQRS measures broadly applicable to their practice. SHM, through its Performance Measurement and Reporting Committee (PMRC), is actively working on behalf of hospitalists to change that. At the same time, it is critical that hospitalists be proactive and participate in PQRS, not just to avoid the 2015 penalty, but to position themselves for success as the Value-Based Payment Modifier (VBPM) expands to all physicians by 2017.
In the current PQRS, the PMRC has identified the following measures that have appropriate inpatient codes for reporting and have potential relevance to hospitalists:
- Congestive Heart Failure (CHF): #5, ACE/ARB for LV systolic dysfunction; #8, beta-blocker prescribed for LV systolic dysfunction; #228, assessment of LV function.
- Stroke: #31, DVT prophylaxis; #32, discharge on antiplatelet therapy; #33, anticoagulation for atrial fibrillation; #35, dysphagia screening; #36, consideration of rehab; #187, thrombolytic therapy.
- Others: #47, advance care plan documented; #76, use of a central venous catheter insertion protocol.
Some of these measures are only reportable by registry. For groups who do not take care of stroke patients, the field is clearly limited. More detail on PQRS reporting and available codes can be found at the Centers for Medicare and Medicaid Services (CMS) website (www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/MeasuresCodes.html).
The committee is deeply concerned about the limited number of PQRS measures broadly applicable to hospitalists, and we are working to change this disparity. Over the past several months, the PMRC has successfully advocated to add inpatient codes to existing measures that will expand the field for hospitalists. So far, we have achieved the following changes for future PQRS reporting years:
- Community-acquired pneumonia (CAP): Measures #56 (vital signs) and #59 (empiric antibiotics) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Osteoporosis/fractures: Measure #24 (communication with the outpatient provider) and #40 (DXA scan ordered or therapy initiated) will have discharge codes 99238 and 99239 added to their denominator, in recognition of the fact that many hospitalists partner with their orthopedic colleagues in the care of patients post-hip fracture.
- Medication reconciliation: Measure #130 (documentation of current medication list) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Anticoagulation for acute pulmonary embolism: Measure #252, intended for use by ED physicians, is being retired by CMS due to a loss of National Quality Forum endorsement. SHM is working with the American College of Emergency Physicians (ACEP) to appeal the decision, possibly maintain the measure, and add inpatient admission codes to the denominator. This remains a work in progress.
Finally, in response to SHM advocacy efforts, the recent FY2014 Physician Fee Schedule proposed rule sought comments from stakeholders about retooling certain hospital-based measures to allow for physician-level reporting. SHM supports the concept of allowing physician-level performance reporting on hospital metrics and recommended the inclusion of multiple measures from the Inpatient Quality Reporting Program.
The PMRC is charged with monitoring the rapidly evolving provider performance and measurement landscape to ensure that hospitalists are adequately represented. We will continue to work diligently with key stakeholders on behalf of our field.
Dr. Seymann is chief of the division of hospital medicine at the University of California San Diego and chair of SHM’s Performance Measurement and Reporting Committee. Josh Boswell is SHM’s senior manager of government relations.
With the voluntary and incentive period for participating in the Physician Quality Reporting System (PQRS) quickly coming to a close, hospitalists are finding a limited number of PQRS measures broadly applicable to their practice. SHM, through its Performance Measurement and Reporting Committee (PMRC), is actively working on behalf of hospitalists to change that. At the same time, it is critical that hospitalists be proactive and participate in PQRS, not just to avoid the 2015 penalty, but to position themselves for success as the Value-Based Payment Modifier (VBPM) expands to all physicians by 2017.
In the current PQRS, the PMRC has identified the following measures that have appropriate inpatient codes for reporting and have potential relevance to hospitalists:
- Congestive Heart Failure (CHF): #5, ACE/ARB for LV systolic dysfunction; #8, beta-blocker prescribed for LV systolic dysfunction; #228, assessment of LV function.
- Stroke: #31, DVT prophylaxis; #32, discharge on antiplatelet therapy; #33, anticoagulation for atrial fibrillation; #35, dysphagia screening; #36, consideration of rehab; #187, thrombolytic therapy.
- Others: #47, advance care plan documented; #76, use of a central venous catheter insertion protocol.
Some of these measures are only reportable by registry. For groups who do not take care of stroke patients, the field is clearly limited. More detail on PQRS reporting and available codes can be found at the Centers for Medicare and Medicaid Services (CMS) website (www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/MeasuresCodes.html).
The committee is deeply concerned about the limited number of PQRS measures broadly applicable to hospitalists, and we are working to change this disparity. Over the past several months, the PMRC has successfully advocated to add inpatient codes to existing measures that will expand the field for hospitalists. So far, we have achieved the following changes for future PQRS reporting years:
- Community-acquired pneumonia (CAP): Measures #56 (vital signs) and #59 (empiric antibiotics) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Osteoporosis/fractures: Measure #24 (communication with the outpatient provider) and #40 (DXA scan ordered or therapy initiated) will have discharge codes 99238 and 99239 added to their denominator, in recognition of the fact that many hospitalists partner with their orthopedic colleagues in the care of patients post-hip fracture.
- Medication reconciliation: Measure #130 (documentation of current medication list) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Anticoagulation for acute pulmonary embolism: Measure #252, intended for use by ED physicians, is being retired by CMS due to a loss of National Quality Forum endorsement. SHM is working with the American College of Emergency Physicians (ACEP) to appeal the decision, possibly maintain the measure, and add inpatient admission codes to the denominator. This remains a work in progress.
Finally, in response to SHM advocacy efforts, the recent FY2014 Physician Fee Schedule proposed rule sought comments from stakeholders about retooling certain hospital-based measures to allow for physician-level reporting. SHM supports the concept of allowing physician-level performance reporting on hospital metrics and recommended the inclusion of multiple measures from the Inpatient Quality Reporting Program.
The PMRC is charged with monitoring the rapidly evolving provider performance and measurement landscape to ensure that hospitalists are adequately represented. We will continue to work diligently with key stakeholders on behalf of our field.
Dr. Seymann is chief of the division of hospital medicine at the University of California San Diego and chair of SHM’s Performance Measurement and Reporting Committee. Josh Boswell is SHM’s senior manager of government relations.
With the voluntary and incentive period for participating in the Physician Quality Reporting System (PQRS) quickly coming to a close, hospitalists are finding a limited number of PQRS measures broadly applicable to their practice. SHM, through its Performance Measurement and Reporting Committee (PMRC), is actively working on behalf of hospitalists to change that. At the same time, it is critical that hospitalists be proactive and participate in PQRS, not just to avoid the 2015 penalty, but to position themselves for success as the Value-Based Payment Modifier (VBPM) expands to all physicians by 2017.
In the current PQRS, the PMRC has identified the following measures that have appropriate inpatient codes for reporting and have potential relevance to hospitalists:
- Congestive Heart Failure (CHF): #5, ACE/ARB for LV systolic dysfunction; #8, beta-blocker prescribed for LV systolic dysfunction; #228, assessment of LV function.
- Stroke: #31, DVT prophylaxis; #32, discharge on antiplatelet therapy; #33, anticoagulation for atrial fibrillation; #35, dysphagia screening; #36, consideration of rehab; #187, thrombolytic therapy.
- Others: #47, advance care plan documented; #76, use of a central venous catheter insertion protocol.
Some of these measures are only reportable by registry. For groups who do not take care of stroke patients, the field is clearly limited. More detail on PQRS reporting and available codes can be found at the Centers for Medicare and Medicaid Services (CMS) website (www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/MeasuresCodes.html).
The committee is deeply concerned about the limited number of PQRS measures broadly applicable to hospitalists, and we are working to change this disparity. Over the past several months, the PMRC has successfully advocated to add inpatient codes to existing measures that will expand the field for hospitalists. So far, we have achieved the following changes for future PQRS reporting years:
- Community-acquired pneumonia (CAP): Measures #56 (vital signs) and #59 (empiric antibiotics) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Osteoporosis/fractures: Measure #24 (communication with the outpatient provider) and #40 (DXA scan ordered or therapy initiated) will have discharge codes 99238 and 99239 added to their denominator, in recognition of the fact that many hospitalists partner with their orthopedic colleagues in the care of patients post-hip fracture.
- Medication reconciliation: Measure #130 (documentation of current medication list) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Anticoagulation for acute pulmonary embolism: Measure #252, intended for use by ED physicians, is being retired by CMS due to a loss of National Quality Forum endorsement. SHM is working with the American College of Emergency Physicians (ACEP) to appeal the decision, possibly maintain the measure, and add inpatient admission codes to the denominator. This remains a work in progress.
Finally, in response to SHM advocacy efforts, the recent FY2014 Physician Fee Schedule proposed rule sought comments from stakeholders about retooling certain hospital-based measures to allow for physician-level reporting. SHM supports the concept of allowing physician-level performance reporting on hospital metrics and recommended the inclusion of multiple measures from the Inpatient Quality Reporting Program.
The PMRC is charged with monitoring the rapidly evolving provider performance and measurement landscape to ensure that hospitalists are adequately represented. We will continue to work diligently with key stakeholders on behalf of our field.
Dr. Seymann is chief of the division of hospital medicine at the University of California San Diego and chair of SHM’s Performance Measurement and Reporting Committee. Josh Boswell is SHM’s senior manager of government relations.
SHM Report Provides New Insights About Physician Practice Leaders
The Society of Hospital Medicine’s 2012 State of Hospital Medicine report (SOHM) offers new insights about physician practice leaders.
Physician Leader Presence
“Choose a hospitalist leader with the right skills and experience. Selecting the right leader is fundamental to a successful hospitalist practice. These individuals are hard to find. They must be excellent clinically and have superb communication skills.”1
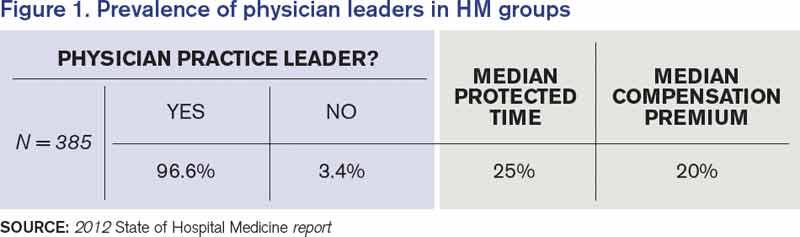
The SOHM survey shows that the vast majority (97%) of hospital medicine groups (HMGs) in the U.S. now have a designated physician leader (see Figure 1). Given this high percentage, examining the outliers is intriguing. Of the 13 adult medicine HMGs that reported not having a physician leader, the large majority were hospital-owned, located in the South region, and situated in non-teaching hospitals. The size of the HMG impacted the presence of a physician leader: 100% of groups with 20 or more full-time equivalents had physician leaders.
Source: 2012 State of Hospital Medicine report
Dedicated Leadership Time
“The medical director of the hospitalist program needs sufficient, non-clinical time to address administrative and leadership issues.”1
The 2007/2008 SOHM survey reported a median of 20% administrative time for physician leaders. In the 2012 survey, the median amount of time was 25% for adult medicine HMGs. The percentages were higher in the East and West regions, in hospital-owned programs, and in non- academic programs. The percentage of protected time also went up with group size.

Compensation
The 2012 SOHM shows median compensation premiums for physician leaders of 20%; that is, leader compensation is 120% of the average salary in their group. The numbers across regions and sizes were remarkably consistent. Overall, it seems that a 15% to 20% compensation premium for hospitalist leaders is standard.
Key Takeaways
No. 1, hospitalist groups need physician hospitalist leaders with protected leadership, but who also work clinically as a hospitalist. Why? Because hospitalists need a leader they respect, someone that they believe understands their specific issues. Unless the physician in charge has worked those 12-hour overnight shifts, argued with the consultants, tried to discharge an ornery patient, received 20 pages in an hour about medication reconciliation, or disagreed with an ED doc about the appropriateness of an admission, it would be hard for that leader to fully understand the stresses hospitalists encounter on a daily basis.
Hospitalist leaders are taking on increasingly important roles to help their organizations realize key performance improvement goals.
Additionally, the roles of outpatient doctors are changing: “Many physicians are no longer able or willing to serve on hospital committees or play a leadership role for the medical staff. Hospitalists have the potential to step in and help address these key issues”1
No. 2, size matters. Given increased responsibilities that include handling focused and ongoing professional practice evaluations, designing pathways to reduce adverse events, counseling, mentoring, disciplining, conducting yearly reviews, and investigating patient and staff complaints, it makes sense that larger programs also have leaders with more protected time and commensurate compensation.
As our healthcare systems ask hospitalists to offer higher reliability and to champion more administrative, safety, and quality projects, HM leaders—who are perfectly placed to organize and manage those projects—need the time and the compensation to do so. To borrow from hospitalist pioneer Bob Wachter, MD, MHM, our future C-suite leaders are percolating in hospitalist programs, learning the skills we will need to participate in the high reliability hospitals of our present and future.
Dr. Lovins is chief of hospital medicine at Middlesex Hospital in Middletown, Conn., and assistant clinical professor of medicine at Yale University School of Medicine. She is a member of SHM’s Practice Analysis Committee.
Reference
The Society of Hospital Medicine’s 2012 State of Hospital Medicine report (SOHM) offers new insights about physician practice leaders.
Physician Leader Presence
“Choose a hospitalist leader with the right skills and experience. Selecting the right leader is fundamental to a successful hospitalist practice. These individuals are hard to find. They must be excellent clinically and have superb communication skills.”1
The SOHM survey shows that the vast majority (97%) of hospital medicine groups (HMGs) in the U.S. now have a designated physician leader (see Figure 1). Given this high percentage, examining the outliers is intriguing. Of the 13 adult medicine HMGs that reported not having a physician leader, the large majority were hospital-owned, located in the South region, and situated in non-teaching hospitals. The size of the HMG impacted the presence of a physician leader: 100% of groups with 20 or more full-time equivalents had physician leaders.
Source: 2012 State of Hospital Medicine report
Dedicated Leadership Time
“The medical director of the hospitalist program needs sufficient, non-clinical time to address administrative and leadership issues.”1
The 2007/2008 SOHM survey reported a median of 20% administrative time for physician leaders. In the 2012 survey, the median amount of time was 25% for adult medicine HMGs. The percentages were higher in the East and West regions, in hospital-owned programs, and in non- academic programs. The percentage of protected time also went up with group size.
Compensation
The 2012 SOHM shows median compensation premiums for physician leaders of 20%; that is, leader compensation is 120% of the average salary in their group. The numbers across regions and sizes were remarkably consistent. Overall, it seems that a 15% to 20% compensation premium for hospitalist leaders is standard.
Key Takeaways
No. 1, hospitalist groups need physician hospitalist leaders with protected leadership, but who also work clinically as a hospitalist. Why? Because hospitalists need a leader they respect, someone that they believe understands their specific issues. Unless the physician in charge has worked those 12-hour overnight shifts, argued with the consultants, tried to discharge an ornery patient, received 20 pages in an hour about medication reconciliation, or disagreed with an ED doc about the appropriateness of an admission, it would be hard for that leader to fully understand the stresses hospitalists encounter on a daily basis.
Hospitalist leaders are taking on increasingly important roles to help their organizations realize key performance improvement goals.
Additionally, the roles of outpatient doctors are changing: “Many physicians are no longer able or willing to serve on hospital committees or play a leadership role for the medical staff. Hospitalists have the potential to step in and help address these key issues”1
No. 2, size matters. Given increased responsibilities that include handling focused and ongoing professional practice evaluations, designing pathways to reduce adverse events, counseling, mentoring, disciplining, conducting yearly reviews, and investigating patient and staff complaints, it makes sense that larger programs also have leaders with more protected time and commensurate compensation.
As our healthcare systems ask hospitalists to offer higher reliability and to champion more administrative, safety, and quality projects, HM leaders—who are perfectly placed to organize and manage those projects—need the time and the compensation to do so. To borrow from hospitalist pioneer Bob Wachter, MD, MHM, our future C-suite leaders are percolating in hospitalist programs, learning the skills we will need to participate in the high reliability hospitals of our present and future.
Dr. Lovins is chief of hospital medicine at Middlesex Hospital in Middletown, Conn., and assistant clinical professor of medicine at Yale University School of Medicine. She is a member of SHM’s Practice Analysis Committee.
Reference
The Society of Hospital Medicine’s 2012 State of Hospital Medicine report (SOHM) offers new insights about physician practice leaders.
Physician Leader Presence
“Choose a hospitalist leader with the right skills and experience. Selecting the right leader is fundamental to a successful hospitalist practice. These individuals are hard to find. They must be excellent clinically and have superb communication skills.”1
The SOHM survey shows that the vast majority (97%) of hospital medicine groups (HMGs) in the U.S. now have a designated physician leader (see Figure 1). Given this high percentage, examining the outliers is intriguing. Of the 13 adult medicine HMGs that reported not having a physician leader, the large majority were hospital-owned, located in the South region, and situated in non-teaching hospitals. The size of the HMG impacted the presence of a physician leader: 100% of groups with 20 or more full-time equivalents had physician leaders.
Source: 2012 State of Hospital Medicine report
Dedicated Leadership Time
“The medical director of the hospitalist program needs sufficient, non-clinical time to address administrative and leadership issues.”1
The 2007/2008 SOHM survey reported a median of 20% administrative time for physician leaders. In the 2012 survey, the median amount of time was 25% for adult medicine HMGs. The percentages were higher in the East and West regions, in hospital-owned programs, and in non- academic programs. The percentage of protected time also went up with group size.
Compensation
The 2012 SOHM shows median compensation premiums for physician leaders of 20%; that is, leader compensation is 120% of the average salary in their group. The numbers across regions and sizes were remarkably consistent. Overall, it seems that a 15% to 20% compensation premium for hospitalist leaders is standard.
Key Takeaways
No. 1, hospitalist groups need physician hospitalist leaders with protected leadership, but who also work clinically as a hospitalist. Why? Because hospitalists need a leader they respect, someone that they believe understands their specific issues. Unless the physician in charge has worked those 12-hour overnight shifts, argued with the consultants, tried to discharge an ornery patient, received 20 pages in an hour about medication reconciliation, or disagreed with an ED doc about the appropriateness of an admission, it would be hard for that leader to fully understand the stresses hospitalists encounter on a daily basis.
Hospitalist leaders are taking on increasingly important roles to help their organizations realize key performance improvement goals.
Additionally, the roles of outpatient doctors are changing: “Many physicians are no longer able or willing to serve on hospital committees or play a leadership role for the medical staff. Hospitalists have the potential to step in and help address these key issues”1
No. 2, size matters. Given increased responsibilities that include handling focused and ongoing professional practice evaluations, designing pathways to reduce adverse events, counseling, mentoring, disciplining, conducting yearly reviews, and investigating patient and staff complaints, it makes sense that larger programs also have leaders with more protected time and commensurate compensation.
As our healthcare systems ask hospitalists to offer higher reliability and to champion more administrative, safety, and quality projects, HM leaders—who are perfectly placed to organize and manage those projects—need the time and the compensation to do so. To borrow from hospitalist pioneer Bob Wachter, MD, MHM, our future C-suite leaders are percolating in hospitalist programs, learning the skills we will need to participate in the high reliability hospitals of our present and future.
Dr. Lovins is chief of hospital medicine at Middlesex Hospital in Middletown, Conn., and assistant clinical professor of medicine at Yale University School of Medicine. She is a member of SHM’s Practice Analysis Committee.
Reference
Culture Shift Required to Defeat Defensive Medicine
Hospitalist Allen Kachalia, MD, JD, of Brigham and Women’s Hospital in Boston, sees defensive medicine as a source of unnecessary costs—and a threat to patient safety.
In fact, he and his colleagues offered an oral presentation at HM13 earlier this year titled, “Overutilization and Defensive Medicine in U.S. Hospitals: A Randomized National Survey of Hospitalists.” In a survey of 1,020 hospitalists, it was reported that defensive medicine was practiced in 37% of pre-operative evaluations and 58% of syncope cases.
Dr. Kachalia says he understands the pressures that can lead physicians to order unnecessary tests, particularly when patients request them. So what does he say about those requests?

“The answer is a simple one but takes time and effort: If you don’t think that something is clinically indicated, you should talk with the patient, explaining to them why you don’t think it’s necessary,” he says. “And, hopefully, you can come to mutual agreement. Ordering things just for the sake of preventing legal liability is just not the right thing to do.”
Dr. Kachalia says he believes that a paradigm shift in how medical liability is handled in this country is needed to change those habits.
But culture change also takes time.
Bryan Weiss, MBA, managing director of the consulting services practice at Irving, Texas-based MedSynergies, says the first step of that change may be having physicians admit that few doctors know a lot about malpractice issues, because they are typically negotiated, arranged, and paid for by their employers, whether that’s a hospital or large management companies.
“It’s not me versus them,” says Weiss, a Team Hospitalist member. “As a specialty, we need to be in this together, to push the education and awareness that it’s OK not to know, so let’s work together to make it better. But it’s not going to happen overnight.”
Hospitalist Allen Kachalia, MD, JD, of Brigham and Women’s Hospital in Boston, sees defensive medicine as a source of unnecessary costs—and a threat to patient safety.
In fact, he and his colleagues offered an oral presentation at HM13 earlier this year titled, “Overutilization and Defensive Medicine in U.S. Hospitals: A Randomized National Survey of Hospitalists.” In a survey of 1,020 hospitalists, it was reported that defensive medicine was practiced in 37% of pre-operative evaluations and 58% of syncope cases.
Dr. Kachalia says he understands the pressures that can lead physicians to order unnecessary tests, particularly when patients request them. So what does he say about those requests?
“The answer is a simple one but takes time and effort: If you don’t think that something is clinically indicated, you should talk with the patient, explaining to them why you don’t think it’s necessary,” he says. “And, hopefully, you can come to mutual agreement. Ordering things just for the sake of preventing legal liability is just not the right thing to do.”
Dr. Kachalia says he believes that a paradigm shift in how medical liability is handled in this country is needed to change those habits.
But culture change also takes time.
Bryan Weiss, MBA, managing director of the consulting services practice at Irving, Texas-based MedSynergies, says the first step of that change may be having physicians admit that few doctors know a lot about malpractice issues, because they are typically negotiated, arranged, and paid for by their employers, whether that’s a hospital or large management companies.
“It’s not me versus them,” says Weiss, a Team Hospitalist member. “As a specialty, we need to be in this together, to push the education and awareness that it’s OK not to know, so let’s work together to make it better. But it’s not going to happen overnight.”
Hospitalist Allen Kachalia, MD, JD, of Brigham and Women’s Hospital in Boston, sees defensive medicine as a source of unnecessary costs—and a threat to patient safety.
In fact, he and his colleagues offered an oral presentation at HM13 earlier this year titled, “Overutilization and Defensive Medicine in U.S. Hospitals: A Randomized National Survey of Hospitalists.” In a survey of 1,020 hospitalists, it was reported that defensive medicine was practiced in 37% of pre-operative evaluations and 58% of syncope cases.
Dr. Kachalia says he understands the pressures that can lead physicians to order unnecessary tests, particularly when patients request them. So what does he say about those requests?
“The answer is a simple one but takes time and effort: If you don’t think that something is clinically indicated, you should talk with the patient, explaining to them why you don’t think it’s necessary,” he says. “And, hopefully, you can come to mutual agreement. Ordering things just for the sake of preventing legal liability is just not the right thing to do.”
Dr. Kachalia says he believes that a paradigm shift in how medical liability is handled in this country is needed to change those habits.
But culture change also takes time.
Bryan Weiss, MBA, managing director of the consulting services practice at Irving, Texas-based MedSynergies, says the first step of that change may be having physicians admit that few doctors know a lot about malpractice issues, because they are typically negotiated, arranged, and paid for by their employers, whether that’s a hospital or large management companies.
“It’s not me versus them,” says Weiss, a Team Hospitalist member. “As a specialty, we need to be in this together, to push the education and awareness that it’s OK not to know, so let’s work together to make it better. But it’s not going to happen overnight.”
Why Hospitalists Remain Outside Malpractice Insurers' High-Risk Categories, For Now

Source: The Doctors Company
Ten years ago, the national headlines on malpractice insurance were staggering. Media reports catalogued OB-GYNs who proclaimed they were shutting down their private practices in the face of runaway premiums. Surgeons and other proceduralists decried payments tied to lawsuits they’d argue were arbitrary and capricious. And the American Medical Association (AMA) made announcement after announcement about states being in a “malpractice crisis.”
In recent years, premiums have actually dropped and stabilized at levels that most physicians agree are manageable for bottom lines. But, in that time, there has been scant discussion about hospital medicine’s relationship with malpractice. It’s not because the issue isn’t omnipresent for all healthcare practitioners, including the relatively nascent specialty that is HM.
Practice management experts say anecdotally that delayed diagnosis of, or treatment for, a spinal epidural abscess (SEA) is likely to get more than a few hospitalists sued. And, the proliferation of co-management of other specialties—particularly those with higher risk of incidence and higher premiums than internal medicine—open up hospitalists to further liability.
The issue is that at less than 20 years as a specialty, HM is in its infancy when it comes to its interaction with malpractice premiums. Health insurance companies and trade groups that track the insurance industry are just beginning to have enough data on claims, premiums, and payouts to make recommendations on risk factors, risk mitigation, and potential trends.
Still, even in a landscape of limited information, there are a few rules of thumb hospitalist group leaders should live by when it comes to managing exposure to malpractice cases, according to interviews with a half dozen healthcare professionals:
- Know how your coverage works. Is there “tail coverage” that ensures you have protection for incidents that happened at an institution where you no longer practice? Even though hospital-employed physicians rarely have rate discussions directly (the hospital typically covers premiums as part of the compensation package), take the time to learn the basic details.
- Be diligent in documentation. Note concerns in charts when appropriate, and stand up for your point of view. There’s a fine line between picking fights with other physicians involved in a patient’s care and making your concerns known, but don’t be afraid to put your clinical view on the record.
- Avoid the practice of “defensive medicine.” Ordering tests and procedures that aren’t clinically necessary might seem like it can serve as a protection from later lawsuits, but it adds to healthcare costs and is just not the right thing to do, says hospitalist Allen Kachalia, MD, JD, of Brigham and Women’s Hospital in Boston, who has studied the phenomenon (see “Culture Shift Necessary to Defeat “Defensive” Medicine,” on p. 38).
- Recognize the risks associated with co-management. Caring for neurology, cardiology, and other subspecialty patients is a revenue boost for HM groups, but when some of those complex cases have adverse events, the hospitalist who interacted with the patient daily could be included in a lawsuit.
- Focus on communication skills. An analysis of claims data by The Doctors Company (TDC) (www.thedoctors.com), a medical malpractice insurance company exclusively endorsed by SHM, reports that the second most common factor contributing to patient injury by hospitalists is “communication breakdown among healthcare professionals.”
- Manage workloads to avoid burnout. Don’t take on too many patients at the expense of being involved in hospital committees or quality initiatives.
To be sure, many of the same tenets of being a productive hospitalist with high patient satisfaction scores—maintain manageable censuses; focus on patient centeredness; and use checklists, technology, and regimented protocols to reduce adverse events—translate very well to being a lower-risk hospitalist in relation to malpractice cases.
When you’re “thinking of patient satisfaction strategies, also think of them as risk mitigation strategies,” says John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash., an SHM co-founder and practice management columnist for The Hospitalist. “They overlap tremendously.”
A History Lesson
Medical malpractice has been around for centuries and has two prevailing goals: 1) to provide monetary remuneration to patients who have been injured via substandard care and 2) to deter that poor treatment through fiscal punishment.
Malpractice lawsuits were not prevalent enough to be a major medical concern until the early 1800s. By the middle of the 19th century, the country hit its first periods of crisis.1 Cycles ebbed and flowed from there, with malpractice premiums causing crises in the 1980s and again in the early 2000s.
continued below...
Now, rates for medical professional liability insurance have been dropping for seven years, and an eighth straight annual decline is expected this year, according to Mike Matray, the editor of trade publication Medical Liability Monitor and the chief content officer of its associated website, www.mymedicalmalpracticeinsurance.com.
“We are in the longest, deepest soft market that the malpractice insurance industry has ever been in,” he says. “Right now, things are really good for the doctors, as far as rates coming down.”
Matray says he understands that declining rates may seem immaterial to a physician who receives an insurance bill that eats into the bottom line. For some specialties, that premium can be as high as $200,000 per physician, per year—or more.
“I’m not saying it isn’t expensive,” he adds. “It’s expensive to run a medical practice. At the same time, medical malpractice insurance is less expensive in today’s dollars than it was in 2005.”
The reduction in rates is multi-faceted. Prominently, state-level tort reforms like non-economic damage caps, health courts, and arbitration hearings are making it harder to bring cases to trial, particularly for lawyers who take cases on contingency. Second, frivolous lawsuits “are making an impression on jury pools,” Matray says, which means fewer filed claims and fewer cases that make it to trial. Third, this soft cycle has outlasted the typical pattern of rates falling for three to four years before rebounding.
“A lot of smart actuaries keep saying this has to change soon, because in a soft market there is a lot of competition,” he says, noting that in order to compete for low rates, insurance companies offer credits to clients and use their own reserve cash piles. “So things are really going to change in the next couple of years.”

—Robin Diamond, senior vice president and chief patient safety officer, The Doctors Company
In Need of Data, Patience
So what does it all mean for hospitalists and HM group leaders looking to be proactive about medical malpractice liability insurance? Patience is required.
For starters, there is no designated premium category for hospitalists. Much like the situation that exists for coding issues, the closest proxy for HM is internal medicine. According to Medical Liability Monitor, the premium paid by internal medicine physicians as of July 1, 2012, varied widely across the country. In South Florida, internal medicine insurance premiums in Miami, Dade, and Broward counties were between $42,000 and $46,000 per year. In South Dakota, one insurer reported rates of just under $4,000 per year. There is no average or median figure available, and Matray notes that actual rates paid can vary from county to county.
Moreover, it is difficult for group leaders or hospital executives to use past history to negotiate rates with insurers because of a shortage of reliable data. In its spring 2013 newsletter, the PIAA (formerly known as the Physician Insurers Association of America) published its first report on hospitalist claims reported to its Data Sharing Project. Of the 92,868 closed claims reported from 2002-2011, just 312, or 0.3%, named hospitalists as the defendant.
The data also showed that, of those claims, 20% were settled through insurance company payments. Those payments totaled $17.1 million, with an average payout to a claimant (known as the indemnity) of $272,553 per claim. Overall, hospitalists had a 20% paid-to-closed ratio, totaling more than $17.1 million. By comparison, the percent of paid-to-closed claims for all physicians was 29.3%, according to PIAA.
In a separate data set compiled this year by TDC, 34% of allegations against hospitalists were related to missed or failed diagnoses, with 28% tied to “improper management of treatment.” Twelve percent of allegations were the result of either improper medication management or ordering errors.
Robin Diamond, TDC’s senior vice president and chief patient safety officer, says that teasing out trends from the initial data can be challenging. Hospitalists, she says, can deal with so many different patients, diseases, and severity levels that it is difficult to draw conclusions.
“Hospital medicine is different than other specialties, because the hospitalist treats a broad range of patients in an acute care setting—from a pediatric patient to an adult patient with many chronic illnesses,” she says.
Divya Parikh, PIAA’s director of research and loss prevention, says HM group leaders should avoid reading too much into the first batch of data, because it’s a small sample size.
“A big part of that is we feel that a lot of hospitalists are intermingled into the other medical specialties,” she says. “So this becomes a very small subset where they are distinctly identified as hospitalists. And that’s the challenge.”
In particular, Parikh is curious to see whether HM’s rate of claims paid through insurance payments drops from 20% (already below the overall healthcare industry average). “It will be interesting as we proceed...to see if they begin to mitigate areas of risk where we used to see a lot of claims,” she adds. “If you look at a hospital setting, there has been some shift change in what the errors are. And, what you’d hope with hospitalists within these environments who are really owning this specialty, is that you’d see a decrease in that. There would be that connective care. There would be the patient that felt that they had an individual who was their go-to individual throughout their care at a hospital.”
A Peek at the Future
Insurers have begun compiling claims data on hospitalists and are taking a longer-term view of the specialty. TDC, for example, has analyzed its data and identified characteristics it says make a low-risk hospitalist, an analysis the company says is the first of its kind (see Figure 1). The insurer adds that it sees its responsibility as making sure everyone understands the hospitalist’s role within the acute care setting so that its pricing is commensurate with the liability risk.
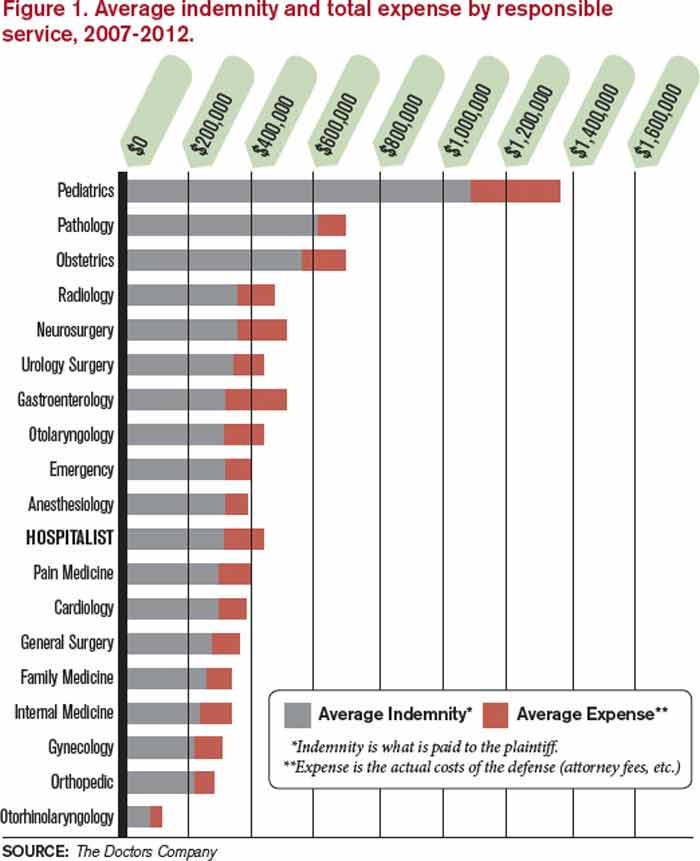
Source: The Doctors Company
“We’re looking at the systems within the hospitalist group, as well as how well that group is integrating with the hospital where they’re practicing,” Diamond says. “What kind of patient mix is this particular hospitalist group seeing in that particular hospital, because it can be different in a large healthcare corporation in Manhattan, New York, from a community hospital in rural Texas.”
The growing popularity of hospitalists taking on co-management responsibilities for other specialties is another trend to keep an eye on, as it creates what insurers call “vicarious liability.” Working together in teams with other specialties can improve communication, reduce errors during transitions of care, and create better outcomes. However, in instances where there are problems, being on a care team means hospitalists can open themselves to liability. To mitigate that risk, hospitalists can look to other groups that have dealt with shared liability issues in the past, Parikh says.
“Historically, you would have seen it with anesthesiology,” she explains. “And one huge improvement anesthesiologists have made when a patient comes in for a surgery now is they come out, introduce themselves, say hello, and tell you what’s going on. They put a face to the name, so that it’s not just a no-name anesthesiologist who gets included in the lawsuit as well because they’re naming everybody in the group.”
But, holistically, the best long-term mitigation strategy appears to be tort reform and new ways of looking at the way in which healthcare liability issues are handled in the U.S., says Anupam Jena, MD, PhD, assistant professor of healthcare policy and medicine at Harvard Medical School, and an internist at Massachusetts General Hospital, both in Boston. Dr. Jena says that there is limited evidence that enacted malpractice reforms have produced more than a 2% to 5% reduction in healthcare spending compared to states that have not.2 Instead, healthcare leaders should push for the elimination of defensive medicine, which he says contributes the lion’s share of the estimated $50 billion annual cost of malpractice liability across the country.
“Do I think the country is in a malpractice crisis? No,” he says. “Do I think that defensive medicine is larger than we think it is? Yes.
“If physicians practice as they felt they should practice without ordering extra tests and procedures, my guess would be you could reduce healthcare spending by substantially more than $50 billion.”
Richard Quinn is a freelance writer in New Jersey.
References
- Spiegel AD, Kavaler F. America’s first medical malpractice crisis, 1835-1865. J Community Health. 1997;22:283-308.
- Chandra A, Jena A, Seabury, S. Defensive medicine may be costlier than it seems. The Wall Street Journal website. http://online.wsj.com/article/SB10001424127887323701904578280112638373302.html. Accessed September 21, 2013.
Source: The Doctors Company
Ten years ago, the national headlines on malpractice insurance were staggering. Media reports catalogued OB-GYNs who proclaimed they were shutting down their private practices in the face of runaway premiums. Surgeons and other proceduralists decried payments tied to lawsuits they’d argue were arbitrary and capricious. And the American Medical Association (AMA) made announcement after announcement about states being in a “malpractice crisis.”
In recent years, premiums have actually dropped and stabilized at levels that most physicians agree are manageable for bottom lines. But, in that time, there has been scant discussion about hospital medicine’s relationship with malpractice. It’s not because the issue isn’t omnipresent for all healthcare practitioners, including the relatively nascent specialty that is HM.
Practice management experts say anecdotally that delayed diagnosis of, or treatment for, a spinal epidural abscess (SEA) is likely to get more than a few hospitalists sued. And, the proliferation of co-management of other specialties—particularly those with higher risk of incidence and higher premiums than internal medicine—open up hospitalists to further liability.
The issue is that at less than 20 years as a specialty, HM is in its infancy when it comes to its interaction with malpractice premiums. Health insurance companies and trade groups that track the insurance industry are just beginning to have enough data on claims, premiums, and payouts to make recommendations on risk factors, risk mitigation, and potential trends.
Still, even in a landscape of limited information, there are a few rules of thumb hospitalist group leaders should live by when it comes to managing exposure to malpractice cases, according to interviews with a half dozen healthcare professionals:
- Know how your coverage works. Is there “tail coverage” that ensures you have protection for incidents that happened at an institution where you no longer practice? Even though hospital-employed physicians rarely have rate discussions directly (the hospital typically covers premiums as part of the compensation package), take the time to learn the basic details.
- Be diligent in documentation. Note concerns in charts when appropriate, and stand up for your point of view. There’s a fine line between picking fights with other physicians involved in a patient’s care and making your concerns known, but don’t be afraid to put your clinical view on the record.
- Avoid the practice of “defensive medicine.” Ordering tests and procedures that aren’t clinically necessary might seem like it can serve as a protection from later lawsuits, but it adds to healthcare costs and is just not the right thing to do, says hospitalist Allen Kachalia, MD, JD, of Brigham and Women’s Hospital in Boston, who has studied the phenomenon (see “Culture Shift Necessary to Defeat “Defensive” Medicine,” on p. 38).
- Recognize the risks associated with co-management. Caring for neurology, cardiology, and other subspecialty patients is a revenue boost for HM groups, but when some of those complex cases have adverse events, the hospitalist who interacted with the patient daily could be included in a lawsuit.
- Focus on communication skills. An analysis of claims data by The Doctors Company (TDC) (www.thedoctors.com), a medical malpractice insurance company exclusively endorsed by SHM, reports that the second most common factor contributing to patient injury by hospitalists is “communication breakdown among healthcare professionals.”
- Manage workloads to avoid burnout. Don’t take on too many patients at the expense of being involved in hospital committees or quality initiatives.
To be sure, many of the same tenets of being a productive hospitalist with high patient satisfaction scores—maintain manageable censuses; focus on patient centeredness; and use checklists, technology, and regimented protocols to reduce adverse events—translate very well to being a lower-risk hospitalist in relation to malpractice cases.
When you’re “thinking of patient satisfaction strategies, also think of them as risk mitigation strategies,” says John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash., an SHM co-founder and practice management columnist for The Hospitalist. “They overlap tremendously.”
A History Lesson
Medical malpractice has been around for centuries and has two prevailing goals: 1) to provide monetary remuneration to patients who have been injured via substandard care and 2) to deter that poor treatment through fiscal punishment.
Malpractice lawsuits were not prevalent enough to be a major medical concern until the early 1800s. By the middle of the 19th century, the country hit its first periods of crisis.1 Cycles ebbed and flowed from there, with malpractice premiums causing crises in the 1980s and again in the early 2000s.
continued below...
Now, rates for medical professional liability insurance have been dropping for seven years, and an eighth straight annual decline is expected this year, according to Mike Matray, the editor of trade publication Medical Liability Monitor and the chief content officer of its associated website, www.mymedicalmalpracticeinsurance.com.
“We are in the longest, deepest soft market that the malpractice insurance industry has ever been in,” he says. “Right now, things are really good for the doctors, as far as rates coming down.”
Matray says he understands that declining rates may seem immaterial to a physician who receives an insurance bill that eats into the bottom line. For some specialties, that premium can be as high as $200,000 per physician, per year—or more.
“I’m not saying it isn’t expensive,” he adds. “It’s expensive to run a medical practice. At the same time, medical malpractice insurance is less expensive in today’s dollars than it was in 2005.”
The reduction in rates is multi-faceted. Prominently, state-level tort reforms like non-economic damage caps, health courts, and arbitration hearings are making it harder to bring cases to trial, particularly for lawyers who take cases on contingency. Second, frivolous lawsuits “are making an impression on jury pools,” Matray says, which means fewer filed claims and fewer cases that make it to trial. Third, this soft cycle has outlasted the typical pattern of rates falling for three to four years before rebounding.
“A lot of smart actuaries keep saying this has to change soon, because in a soft market there is a lot of competition,” he says, noting that in order to compete for low rates, insurance companies offer credits to clients and use their own reserve cash piles. “So things are really going to change in the next couple of years.”
—Robin Diamond, senior vice president and chief patient safety officer, The Doctors Company
In Need of Data, Patience
So what does it all mean for hospitalists and HM group leaders looking to be proactive about medical malpractice liability insurance? Patience is required.
For starters, there is no designated premium category for hospitalists. Much like the situation that exists for coding issues, the closest proxy for HM is internal medicine. According to Medical Liability Monitor, the premium paid by internal medicine physicians as of July 1, 2012, varied widely across the country. In South Florida, internal medicine insurance premiums in Miami, Dade, and Broward counties were between $42,000 and $46,000 per year. In South Dakota, one insurer reported rates of just under $4,000 per year. There is no average or median figure available, and Matray notes that actual rates paid can vary from county to county.
Moreover, it is difficult for group leaders or hospital executives to use past history to negotiate rates with insurers because of a shortage of reliable data. In its spring 2013 newsletter, the PIAA (formerly known as the Physician Insurers Association of America) published its first report on hospitalist claims reported to its Data Sharing Project. Of the 92,868 closed claims reported from 2002-2011, just 312, or 0.3%, named hospitalists as the defendant.
The data also showed that, of those claims, 20% were settled through insurance company payments. Those payments totaled $17.1 million, with an average payout to a claimant (known as the indemnity) of $272,553 per claim. Overall, hospitalists had a 20% paid-to-closed ratio, totaling more than $17.1 million. By comparison, the percent of paid-to-closed claims for all physicians was 29.3%, according to PIAA.
In a separate data set compiled this year by TDC, 34% of allegations against hospitalists were related to missed or failed diagnoses, with 28% tied to “improper management of treatment.” Twelve percent of allegations were the result of either improper medication management or ordering errors.
Robin Diamond, TDC’s senior vice president and chief patient safety officer, says that teasing out trends from the initial data can be challenging. Hospitalists, she says, can deal with so many different patients, diseases, and severity levels that it is difficult to draw conclusions.
“Hospital medicine is different than other specialties, because the hospitalist treats a broad range of patients in an acute care setting—from a pediatric patient to an adult patient with many chronic illnesses,” she says.
Divya Parikh, PIAA’s director of research and loss prevention, says HM group leaders should avoid reading too much into the first batch of data, because it’s a small sample size.
“A big part of that is we feel that a lot of hospitalists are intermingled into the other medical specialties,” she says. “So this becomes a very small subset where they are distinctly identified as hospitalists. And that’s the challenge.”
In particular, Parikh is curious to see whether HM’s rate of claims paid through insurance payments drops from 20% (already below the overall healthcare industry average). “It will be interesting as we proceed...to see if they begin to mitigate areas of risk where we used to see a lot of claims,” she adds. “If you look at a hospital setting, there has been some shift change in what the errors are. And, what you’d hope with hospitalists within these environments who are really owning this specialty, is that you’d see a decrease in that. There would be that connective care. There would be the patient that felt that they had an individual who was their go-to individual throughout their care at a hospital.”
A Peek at the Future
Insurers have begun compiling claims data on hospitalists and are taking a longer-term view of the specialty. TDC, for example, has analyzed its data and identified characteristics it says make a low-risk hospitalist, an analysis the company says is the first of its kind (see Figure 1). The insurer adds that it sees its responsibility as making sure everyone understands the hospitalist’s role within the acute care setting so that its pricing is commensurate with the liability risk.
Source: The Doctors Company
“We’re looking at the systems within the hospitalist group, as well as how well that group is integrating with the hospital where they’re practicing,” Diamond says. “What kind of patient mix is this particular hospitalist group seeing in that particular hospital, because it can be different in a large healthcare corporation in Manhattan, New York, from a community hospital in rural Texas.”
The growing popularity of hospitalists taking on co-management responsibilities for other specialties is another trend to keep an eye on, as it creates what insurers call “vicarious liability.” Working together in teams with other specialties can improve communication, reduce errors during transitions of care, and create better outcomes. However, in instances where there are problems, being on a care team means hospitalists can open themselves to liability. To mitigate that risk, hospitalists can look to other groups that have dealt with shared liability issues in the past, Parikh says.
“Historically, you would have seen it with anesthesiology,” she explains. “And one huge improvement anesthesiologists have made when a patient comes in for a surgery now is they come out, introduce themselves, say hello, and tell you what’s going on. They put a face to the name, so that it’s not just a no-name anesthesiologist who gets included in the lawsuit as well because they’re naming everybody in the group.”
But, holistically, the best long-term mitigation strategy appears to be tort reform and new ways of looking at the way in which healthcare liability issues are handled in the U.S., says Anupam Jena, MD, PhD, assistant professor of healthcare policy and medicine at Harvard Medical School, and an internist at Massachusetts General Hospital, both in Boston. Dr. Jena says that there is limited evidence that enacted malpractice reforms have produced more than a 2% to 5% reduction in healthcare spending compared to states that have not.2 Instead, healthcare leaders should push for the elimination of defensive medicine, which he says contributes the lion’s share of the estimated $50 billion annual cost of malpractice liability across the country.
“Do I think the country is in a malpractice crisis? No,” he says. “Do I think that defensive medicine is larger than we think it is? Yes.
“If physicians practice as they felt they should practice without ordering extra tests and procedures, my guess would be you could reduce healthcare spending by substantially more than $50 billion.”
Richard Quinn is a freelance writer in New Jersey.
References
- Spiegel AD, Kavaler F. America’s first medical malpractice crisis, 1835-1865. J Community Health. 1997;22:283-308.
- Chandra A, Jena A, Seabury, S. Defensive medicine may be costlier than it seems. The Wall Street Journal website. http://online.wsj.com/article/SB10001424127887323701904578280112638373302.html. Accessed September 21, 2013.
Source: The Doctors Company
Ten years ago, the national headlines on malpractice insurance were staggering. Media reports catalogued OB-GYNs who proclaimed they were shutting down their private practices in the face of runaway premiums. Surgeons and other proceduralists decried payments tied to lawsuits they’d argue were arbitrary and capricious. And the American Medical Association (AMA) made announcement after announcement about states being in a “malpractice crisis.”
In recent years, premiums have actually dropped and stabilized at levels that most physicians agree are manageable for bottom lines. But, in that time, there has been scant discussion about hospital medicine’s relationship with malpractice. It’s not because the issue isn’t omnipresent for all healthcare practitioners, including the relatively nascent specialty that is HM.
Practice management experts say anecdotally that delayed diagnosis of, or treatment for, a spinal epidural abscess (SEA) is likely to get more than a few hospitalists sued. And, the proliferation of co-management of other specialties—particularly those with higher risk of incidence and higher premiums than internal medicine—open up hospitalists to further liability.
The issue is that at less than 20 years as a specialty, HM is in its infancy when it comes to its interaction with malpractice premiums. Health insurance companies and trade groups that track the insurance industry are just beginning to have enough data on claims, premiums, and payouts to make recommendations on risk factors, risk mitigation, and potential trends.
Still, even in a landscape of limited information, there are a few rules of thumb hospitalist group leaders should live by when it comes to managing exposure to malpractice cases, according to interviews with a half dozen healthcare professionals:
- Know how your coverage works. Is there “tail coverage” that ensures you have protection for incidents that happened at an institution where you no longer practice? Even though hospital-employed physicians rarely have rate discussions directly (the hospital typically covers premiums as part of the compensation package), take the time to learn the basic details.
- Be diligent in documentation. Note concerns in charts when appropriate, and stand up for your point of view. There’s a fine line between picking fights with other physicians involved in a patient’s care and making your concerns known, but don’t be afraid to put your clinical view on the record.
- Avoid the practice of “defensive medicine.” Ordering tests and procedures that aren’t clinically necessary might seem like it can serve as a protection from later lawsuits, but it adds to healthcare costs and is just not the right thing to do, says hospitalist Allen Kachalia, MD, JD, of Brigham and Women’s Hospital in Boston, who has studied the phenomenon (see “Culture Shift Necessary to Defeat “Defensive” Medicine,” on p. 38).
- Recognize the risks associated with co-management. Caring for neurology, cardiology, and other subspecialty patients is a revenue boost for HM groups, but when some of those complex cases have adverse events, the hospitalist who interacted with the patient daily could be included in a lawsuit.
- Focus on communication skills. An analysis of claims data by The Doctors Company (TDC) (www.thedoctors.com), a medical malpractice insurance company exclusively endorsed by SHM, reports that the second most common factor contributing to patient injury by hospitalists is “communication breakdown among healthcare professionals.”
- Manage workloads to avoid burnout. Don’t take on too many patients at the expense of being involved in hospital committees or quality initiatives.
To be sure, many of the same tenets of being a productive hospitalist with high patient satisfaction scores—maintain manageable censuses; focus on patient centeredness; and use checklists, technology, and regimented protocols to reduce adverse events—translate very well to being a lower-risk hospitalist in relation to malpractice cases.
When you’re “thinking of patient satisfaction strategies, also think of them as risk mitigation strategies,” says John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash., an SHM co-founder and practice management columnist for The Hospitalist. “They overlap tremendously.”
A History Lesson
Medical malpractice has been around for centuries and has two prevailing goals: 1) to provide monetary remuneration to patients who have been injured via substandard care and 2) to deter that poor treatment through fiscal punishment.
Malpractice lawsuits were not prevalent enough to be a major medical concern until the early 1800s. By the middle of the 19th century, the country hit its first periods of crisis.1 Cycles ebbed and flowed from there, with malpractice premiums causing crises in the 1980s and again in the early 2000s.
continued below...
Now, rates for medical professional liability insurance have been dropping for seven years, and an eighth straight annual decline is expected this year, according to Mike Matray, the editor of trade publication Medical Liability Monitor and the chief content officer of its associated website, www.mymedicalmalpracticeinsurance.com.
“We are in the longest, deepest soft market that the malpractice insurance industry has ever been in,” he says. “Right now, things are really good for the doctors, as far as rates coming down.”
Matray says he understands that declining rates may seem immaterial to a physician who receives an insurance bill that eats into the bottom line. For some specialties, that premium can be as high as $200,000 per physician, per year—or more.
“I’m not saying it isn’t expensive,” he adds. “It’s expensive to run a medical practice. At the same time, medical malpractice insurance is less expensive in today’s dollars than it was in 2005.”
The reduction in rates is multi-faceted. Prominently, state-level tort reforms like non-economic damage caps, health courts, and arbitration hearings are making it harder to bring cases to trial, particularly for lawyers who take cases on contingency. Second, frivolous lawsuits “are making an impression on jury pools,” Matray says, which means fewer filed claims and fewer cases that make it to trial. Third, this soft cycle has outlasted the typical pattern of rates falling for three to four years before rebounding.
“A lot of smart actuaries keep saying this has to change soon, because in a soft market there is a lot of competition,” he says, noting that in order to compete for low rates, insurance companies offer credits to clients and use their own reserve cash piles. “So things are really going to change in the next couple of years.”
—Robin Diamond, senior vice president and chief patient safety officer, The Doctors Company
In Need of Data, Patience
So what does it all mean for hospitalists and HM group leaders looking to be proactive about medical malpractice liability insurance? Patience is required.
For starters, there is no designated premium category for hospitalists. Much like the situation that exists for coding issues, the closest proxy for HM is internal medicine. According to Medical Liability Monitor, the premium paid by internal medicine physicians as of July 1, 2012, varied widely across the country. In South Florida, internal medicine insurance premiums in Miami, Dade, and Broward counties were between $42,000 and $46,000 per year. In South Dakota, one insurer reported rates of just under $4,000 per year. There is no average or median figure available, and Matray notes that actual rates paid can vary from county to county.
Moreover, it is difficult for group leaders or hospital executives to use past history to negotiate rates with insurers because of a shortage of reliable data. In its spring 2013 newsletter, the PIAA (formerly known as the Physician Insurers Association of America) published its first report on hospitalist claims reported to its Data Sharing Project. Of the 92,868 closed claims reported from 2002-2011, just 312, or 0.3%, named hospitalists as the defendant.
The data also showed that, of those claims, 20% were settled through insurance company payments. Those payments totaled $17.1 million, with an average payout to a claimant (known as the indemnity) of $272,553 per claim. Overall, hospitalists had a 20% paid-to-closed ratio, totaling more than $17.1 million. By comparison, the percent of paid-to-closed claims for all physicians was 29.3%, according to PIAA.
In a separate data set compiled this year by TDC, 34% of allegations against hospitalists were related to missed or failed diagnoses, with 28% tied to “improper management of treatment.” Twelve percent of allegations were the result of either improper medication management or ordering errors.
Robin Diamond, TDC’s senior vice president and chief patient safety officer, says that teasing out trends from the initial data can be challenging. Hospitalists, she says, can deal with so many different patients, diseases, and severity levels that it is difficult to draw conclusions.
“Hospital medicine is different than other specialties, because the hospitalist treats a broad range of patients in an acute care setting—from a pediatric patient to an adult patient with many chronic illnesses,” she says.
Divya Parikh, PIAA’s director of research and loss prevention, says HM group leaders should avoid reading too much into the first batch of data, because it’s a small sample size.
“A big part of that is we feel that a lot of hospitalists are intermingled into the other medical specialties,” she says. “So this becomes a very small subset where they are distinctly identified as hospitalists. And that’s the challenge.”
In particular, Parikh is curious to see whether HM’s rate of claims paid through insurance payments drops from 20% (already below the overall healthcare industry average). “It will be interesting as we proceed...to see if they begin to mitigate areas of risk where we used to see a lot of claims,” she adds. “If you look at a hospital setting, there has been some shift change in what the errors are. And, what you’d hope with hospitalists within these environments who are really owning this specialty, is that you’d see a decrease in that. There would be that connective care. There would be the patient that felt that they had an individual who was their go-to individual throughout their care at a hospital.”
A Peek at the Future
Insurers have begun compiling claims data on hospitalists and are taking a longer-term view of the specialty. TDC, for example, has analyzed its data and identified characteristics it says make a low-risk hospitalist, an analysis the company says is the first of its kind (see Figure 1). The insurer adds that it sees its responsibility as making sure everyone understands the hospitalist’s role within the acute care setting so that its pricing is commensurate with the liability risk.
Source: The Doctors Company
“We’re looking at the systems within the hospitalist group, as well as how well that group is integrating with the hospital where they’re practicing,” Diamond says. “What kind of patient mix is this particular hospitalist group seeing in that particular hospital, because it can be different in a large healthcare corporation in Manhattan, New York, from a community hospital in rural Texas.”
The growing popularity of hospitalists taking on co-management responsibilities for other specialties is another trend to keep an eye on, as it creates what insurers call “vicarious liability.” Working together in teams with other specialties can improve communication, reduce errors during transitions of care, and create better outcomes. However, in instances where there are problems, being on a care team means hospitalists can open themselves to liability. To mitigate that risk, hospitalists can look to other groups that have dealt with shared liability issues in the past, Parikh says.
“Historically, you would have seen it with anesthesiology,” she explains. “And one huge improvement anesthesiologists have made when a patient comes in for a surgery now is they come out, introduce themselves, say hello, and tell you what’s going on. They put a face to the name, so that it’s not just a no-name anesthesiologist who gets included in the lawsuit as well because they’re naming everybody in the group.”
But, holistically, the best long-term mitigation strategy appears to be tort reform and new ways of looking at the way in which healthcare liability issues are handled in the U.S., says Anupam Jena, MD, PhD, assistant professor of healthcare policy and medicine at Harvard Medical School, and an internist at Massachusetts General Hospital, both in Boston. Dr. Jena says that there is limited evidence that enacted malpractice reforms have produced more than a 2% to 5% reduction in healthcare spending compared to states that have not.2 Instead, healthcare leaders should push for the elimination of defensive medicine, which he says contributes the lion’s share of the estimated $50 billion annual cost of malpractice liability across the country.
“Do I think the country is in a malpractice crisis? No,” he says. “Do I think that defensive medicine is larger than we think it is? Yes.
“If physicians practice as they felt they should practice without ordering extra tests and procedures, my guess would be you could reduce healthcare spending by substantially more than $50 billion.”
Richard Quinn is a freelance writer in New Jersey.
References
- Spiegel AD, Kavaler F. America’s first medical malpractice crisis, 1835-1865. J Community Health. 1997;22:283-308.
- Chandra A, Jena A, Seabury, S. Defensive medicine may be costlier than it seems. The Wall Street Journal website. http://online.wsj.com/article/SB10001424127887323701904578280112638373302.html. Accessed September 21, 2013.
Lawmakers unveil bipartisan SGR repeal plan
A new bipartisan, bicameral plan to repeal the Medicare Sustainable Growth Rate formula has surfaced on Capitol Hill.
On Oct. 30, the Senate Finance Committee and the House Ways and Means Committee jointly released a legislative framework that would scrap Medicare’s Sustainable Growth Rate (SGR) formula and freeze physician payments for the next decade.

Starting in 2017, physicians would see their payments tied to cost and quality of care using a single quality incentive program. Under the proposal, Medicare would create the Value-Based Performance Payment Program to adjust physician payments based on quality, resource use, clinical practice improvement activities, and the use of electronic health records.
Since the program is budget neutral, some physicians would see increases while others would see cuts.
At the end of 2016, Medicare would end a group of existing incentive programs including the Physician Quality Reporting System; the Value-Based Modifier Program; and the Electronic Health Record (EHR) Incentive Program, which requires the meaningful use of certified EHR technology.
Physicians who treat few Medicare patients or who receive a significant portion of their payments from advanced alternative payment models, such as accountable care organizations, would be excluded from the new Value-Based Performance Payment Program. Physicians in ACOs and other models that involved taking on financial risk and reporting on quality measures would instead be eligible for bonus payments under the proposal.
After 2023, physicians who participate in these advanced alternative payment models would see an annual 2% payment increase, and other physicians would earn updates of 1% each year, according to the proposal circulated by the two committees.
"This discussion draft is an important step in a long-term solution to this failed policy," Rep. Dave Camp, chairman of the House Ways and Means Committee, said in a statement. "Creating a policy that rewards providers for delivering high-quality, efficient health care is the ultimate goal, and this draft brings us one step closer to that reality."

The release of the proposal follows a summer of feverish activity in the House on the issue of the SGR. After months of hearings, the Energy and Commerce Committee unanimously approved a bill on July 31 (H.R. 2810) that would repeal the SGR and provide 0.5% payment increases for physicians through 2018.
Momentum slowed after Labor Day with the continuing debate over the Affordable Care Act and the federal government shutdown that began on Oct. 1. This latest plan incorporates ideas from both the Democratic-led Senate and the GOP-controlled House.
While physician groups were still reviewing the proposal at press time, they hailed the renewed focus on the SGR as a move in the right direction.
"Congress is demonstrating that they understand that ending the failed SGR this year is fiscally responsible, and that the current Medicare payment system is a barrier to adoption of health care delivery and payment reforms that will improve health care for America’s seniors and rein in overall costs," Dr. Ardis Dee Hoven, president of the American Medical Association, said in a statement.
Physicians can comment on the proposal until Nov. 12. Send comments to the Senate Finance Committee at sgrcomments@finance.senate.gov and to the House Ways and Means Committee at sgrwhitepaper@mail.house.gov.
A new bipartisan, bicameral plan to repeal the Medicare Sustainable Growth Rate formula has surfaced on Capitol Hill.
On Oct. 30, the Senate Finance Committee and the House Ways and Means Committee jointly released a legislative framework that would scrap Medicare’s Sustainable Growth Rate (SGR) formula and freeze physician payments for the next decade.
Starting in 2017, physicians would see their payments tied to cost and quality of care using a single quality incentive program. Under the proposal, Medicare would create the Value-Based Performance Payment Program to adjust physician payments based on quality, resource use, clinical practice improvement activities, and the use of electronic health records.
Since the program is budget neutral, some physicians would see increases while others would see cuts.
At the end of 2016, Medicare would end a group of existing incentive programs including the Physician Quality Reporting System; the Value-Based Modifier Program; and the Electronic Health Record (EHR) Incentive Program, which requires the meaningful use of certified EHR technology.
Physicians who treat few Medicare patients or who receive a significant portion of their payments from advanced alternative payment models, such as accountable care organizations, would be excluded from the new Value-Based Performance Payment Program. Physicians in ACOs and other models that involved taking on financial risk and reporting on quality measures would instead be eligible for bonus payments under the proposal.
After 2023, physicians who participate in these advanced alternative payment models would see an annual 2% payment increase, and other physicians would earn updates of 1% each year, according to the proposal circulated by the two committees.
"This discussion draft is an important step in a long-term solution to this failed policy," Rep. Dave Camp, chairman of the House Ways and Means Committee, said in a statement. "Creating a policy that rewards providers for delivering high-quality, efficient health care is the ultimate goal, and this draft brings us one step closer to that reality."
The release of the proposal follows a summer of feverish activity in the House on the issue of the SGR. After months of hearings, the Energy and Commerce Committee unanimously approved a bill on July 31 (H.R. 2810) that would repeal the SGR and provide 0.5% payment increases for physicians through 2018.
Momentum slowed after Labor Day with the continuing debate over the Affordable Care Act and the federal government shutdown that began on Oct. 1. This latest plan incorporates ideas from both the Democratic-led Senate and the GOP-controlled House.
While physician groups were still reviewing the proposal at press time, they hailed the renewed focus on the SGR as a move in the right direction.
"Congress is demonstrating that they understand that ending the failed SGR this year is fiscally responsible, and that the current Medicare payment system is a barrier to adoption of health care delivery and payment reforms that will improve health care for America’s seniors and rein in overall costs," Dr. Ardis Dee Hoven, president of the American Medical Association, said in a statement.
Physicians can comment on the proposal until Nov. 12. Send comments to the Senate Finance Committee at sgrcomments@finance.senate.gov and to the House Ways and Means Committee at sgrwhitepaper@mail.house.gov.
A new bipartisan, bicameral plan to repeal the Medicare Sustainable Growth Rate formula has surfaced on Capitol Hill.
On Oct. 30, the Senate Finance Committee and the House Ways and Means Committee jointly released a legislative framework that would scrap Medicare’s Sustainable Growth Rate (SGR) formula and freeze physician payments for the next decade.
Starting in 2017, physicians would see their payments tied to cost and quality of care using a single quality incentive program. Under the proposal, Medicare would create the Value-Based Performance Payment Program to adjust physician payments based on quality, resource use, clinical practice improvement activities, and the use of electronic health records.
Since the program is budget neutral, some physicians would see increases while others would see cuts.
At the end of 2016, Medicare would end a group of existing incentive programs including the Physician Quality Reporting System; the Value-Based Modifier Program; and the Electronic Health Record (EHR) Incentive Program, which requires the meaningful use of certified EHR technology.
Physicians who treat few Medicare patients or who receive a significant portion of their payments from advanced alternative payment models, such as accountable care organizations, would be excluded from the new Value-Based Performance Payment Program. Physicians in ACOs and other models that involved taking on financial risk and reporting on quality measures would instead be eligible for bonus payments under the proposal.
After 2023, physicians who participate in these advanced alternative payment models would see an annual 2% payment increase, and other physicians would earn updates of 1% each year, according to the proposal circulated by the two committees.
"This discussion draft is an important step in a long-term solution to this failed policy," Rep. Dave Camp, chairman of the House Ways and Means Committee, said in a statement. "Creating a policy that rewards providers for delivering high-quality, efficient health care is the ultimate goal, and this draft brings us one step closer to that reality."
The release of the proposal follows a summer of feverish activity in the House on the issue of the SGR. After months of hearings, the Energy and Commerce Committee unanimously approved a bill on July 31 (H.R. 2810) that would repeal the SGR and provide 0.5% payment increases for physicians through 2018.
Momentum slowed after Labor Day with the continuing debate over the Affordable Care Act and the federal government shutdown that began on Oct. 1. This latest plan incorporates ideas from both the Democratic-led Senate and the GOP-controlled House.
While physician groups were still reviewing the proposal at press time, they hailed the renewed focus on the SGR as a move in the right direction.
"Congress is demonstrating that they understand that ending the failed SGR this year is fiscally responsible, and that the current Medicare payment system is a barrier to adoption of health care delivery and payment reforms that will improve health care for America’s seniors and rein in overall costs," Dr. Ardis Dee Hoven, president of the American Medical Association, said in a statement.
Physicians can comment on the proposal until Nov. 12. Send comments to the Senate Finance Committee at sgrcomments@finance.senate.gov and to the House Ways and Means Committee at sgrwhitepaper@mail.house.gov.

Proposed FDA measures aim to reduce drug shortages
The Food and Drug Administration announced on Oct. 31 two initiatives aimed at cutting down on drug shortages and improving communications with drug companies.
The first is a proposed rule to require drug manufacturers to alert the FDA if certain "medically important drug products" are running low, Dr. Margaret Hamburg, commissioner of the agency, said during a teleconference announcing the initiatives. This proposal expands on early notification requirements included in the Food and Drug Administration Safety and Innovation Act of 2012 (FDASIA), which created a task force designated to deal with drug shortages. The proposal also would extend those requirements to biologically manufactured drugs.

The second initiative is a strategic plan to improve communications between the FDA and drug manufacturers, develop short- and long-term contingency plans for drug shortages, and revamp communications processes within the agency to improve response times to potential shortages.
The strategy was developed with both internal and external input and analysis from work groups, drug manufacturers, and health care organizations. For the plan to work "this has to be a group effort," Dr. Hamburg said.
Drug shortages have declined significantly since 2012, with 117 drug shortages in 2012, down from 212 in 2011. But early notification from manufacturers about possible shortages can help drive those numbers down even further, said FDA representatives.
The strategic plan, which was required by FDASIA and is being sent to Congress Oct. 31, also includes new ideas such as the development of a smartphone app for real-time drug shortage news, a proposal for rewarding drug manufacturers based on cooperation with the FDA, and a new office within the Center for Drug Evaluation and Research focused exclusively on pharmaceutical quality.
Members of the public may comment on the proposed rule, which is scheduled to be published in the Federal Register on Nov. 4.
The Food and Drug Administration announced on Oct. 31 two initiatives aimed at cutting down on drug shortages and improving communications with drug companies.
The first is a proposed rule to require drug manufacturers to alert the FDA if certain "medically important drug products" are running low, Dr. Margaret Hamburg, commissioner of the agency, said during a teleconference announcing the initiatives. This proposal expands on early notification requirements included in the Food and Drug Administration Safety and Innovation Act of 2012 (FDASIA), which created a task force designated to deal with drug shortages. The proposal also would extend those requirements to biologically manufactured drugs.
The second initiative is a strategic plan to improve communications between the FDA and drug manufacturers, develop short- and long-term contingency plans for drug shortages, and revamp communications processes within the agency to improve response times to potential shortages.
The strategy was developed with both internal and external input and analysis from work groups, drug manufacturers, and health care organizations. For the plan to work "this has to be a group effort," Dr. Hamburg said.
Drug shortages have declined significantly since 2012, with 117 drug shortages in 2012, down from 212 in 2011. But early notification from manufacturers about possible shortages can help drive those numbers down even further, said FDA representatives.
The strategic plan, which was required by FDASIA and is being sent to Congress Oct. 31, also includes new ideas such as the development of a smartphone app for real-time drug shortage news, a proposal for rewarding drug manufacturers based on cooperation with the FDA, and a new office within the Center for Drug Evaluation and Research focused exclusively on pharmaceutical quality.
Members of the public may comment on the proposed rule, which is scheduled to be published in the Federal Register on Nov. 4.
The Food and Drug Administration announced on Oct. 31 two initiatives aimed at cutting down on drug shortages and improving communications with drug companies.
The first is a proposed rule to require drug manufacturers to alert the FDA if certain "medically important drug products" are running low, Dr. Margaret Hamburg, commissioner of the agency, said during a teleconference announcing the initiatives. This proposal expands on early notification requirements included in the Food and Drug Administration Safety and Innovation Act of 2012 (FDASIA), which created a task force designated to deal with drug shortages. The proposal also would extend those requirements to biologically manufactured drugs.
The second initiative is a strategic plan to improve communications between the FDA and drug manufacturers, develop short- and long-term contingency plans for drug shortages, and revamp communications processes within the agency to improve response times to potential shortages.
The strategy was developed with both internal and external input and analysis from work groups, drug manufacturers, and health care organizations. For the plan to work "this has to be a group effort," Dr. Hamburg said.
Drug shortages have declined significantly since 2012, with 117 drug shortages in 2012, down from 212 in 2011. But early notification from manufacturers about possible shortages can help drive those numbers down even further, said FDA representatives.
The strategic plan, which was required by FDASIA and is being sent to Congress Oct. 31, also includes new ideas such as the development of a smartphone app for real-time drug shortage news, a proposal for rewarding drug manufacturers based on cooperation with the FDA, and a new office within the Center for Drug Evaluation and Research focused exclusively on pharmaceutical quality.
Members of the public may comment on the proposed rule, which is scheduled to be published in the Federal Register on Nov. 4.

Sebelius: Hold me accountable for healthcare.gov
WASHINGTON – Testifying before a House committee, Health and Human Services Secretary Kathleen Sebelius said that she is accountable for the failures of the healthcare.gov website.
"In these early weeks, access to healthcare.gov has been a miserably frustrating experience for way too many Americans," Ms. Sebelius said at an Oct. 30 hearing of the House Energy and Commerce Committee. "I’m as frustrated and angry as anyone with the flawed launch of healthcare.gov."
Ms. Sebelius apologized and said that she wanted Americans to know that "I’m accountable to you for fixing these problems." She added that she was "committed to earning your confidence back by fixing the site."

It was the second consecutive day that an Obama administration official fielded tough questions from Congress on the problems with healthcare.gov, the main avenue for Americans in 36 states to shop for and enroll in health plans offered under the Affordable Care Act’s (ACA’s) insurance exchanges.
When asked by Rep. Marsha Blackburn (R-Tenn.) who was "responsible for this debacle" surrounding healthcare.gov, Ms. Sebelius said, "Hold me accountable for the debacle. I’m responsible."
When asked whether anyone had suggested delaying the site’s Oct. 1 launch, Ms. Sebelius said that neither officials from the Centers for Medicare and Medicaid Services (CMS) nor information technology contractors had given such advice.
The Health and Human Services (HHS) secretary also refused repeatedly to state how many Americans have enrolled in a plan through the website – or by phone or in person – claiming there is no reliable or confirmed data yet.
"The system isn’t functioning, so we are not getting that reliable data," she said, adding that good numbers will be available in mid-November. HHS has spent $118 million on healthcare.gov and $56 million on "other IT" to support the website, Ms. Sebelius said.
Republicans in Congress also questioned Ms. Sebelius about the insurance cancellation notices that thousands of Americans have received since Oct. 1.
"Americans are scared and frustrated," said Energy and Commerce Committee Chairman Fred Upton (R-Mich.). "There are also millions of Americans coast to coast who no doubt believed the president’s repeated promise that if they liked their plan, they’d be able to keep it, no matter what. They are now receiving termination notices, and for those who lose the coverage they like, they may also be losing faith in their government."
Ms. Sebelius said insurers were cancelling policies in the individual market because the plans did not meet ACA criteria.
Rep. Frank Pallone (D-N.J.) called the cancellation issue "another red herring." He said the real explanation is that "insurance companies are cancelling lousy policies with high prices because they can’t compete."
Rep. Michael Burgess (R-Tex.) said he believed that administration officials had misled the committee and asked if Ms. Sebelius would seek the resignation of Gary Cohen, director of the Center for Consumer Information and Insurance Oversight at the CMS. Mr. Cohen’s office oversees the exchanges.
"I will not, sir," Ms. Sebelius responded.
On Twitter @aliciaault
WASHINGTON – Testifying before a House committee, Health and Human Services Secretary Kathleen Sebelius said that she is accountable for the failures of the healthcare.gov website.
"In these early weeks, access to healthcare.gov has been a miserably frustrating experience for way too many Americans," Ms. Sebelius said at an Oct. 30 hearing of the House Energy and Commerce Committee. "I’m as frustrated and angry as anyone with the flawed launch of healthcare.gov."
Ms. Sebelius apologized and said that she wanted Americans to know that "I’m accountable to you for fixing these problems." She added that she was "committed to earning your confidence back by fixing the site."
It was the second consecutive day that an Obama administration official fielded tough questions from Congress on the problems with healthcare.gov, the main avenue for Americans in 36 states to shop for and enroll in health plans offered under the Affordable Care Act’s (ACA’s) insurance exchanges.
When asked by Rep. Marsha Blackburn (R-Tenn.) who was "responsible for this debacle" surrounding healthcare.gov, Ms. Sebelius said, "Hold me accountable for the debacle. I’m responsible."
When asked whether anyone had suggested delaying the site’s Oct. 1 launch, Ms. Sebelius said that neither officials from the Centers for Medicare and Medicaid Services (CMS) nor information technology contractors had given such advice.
The Health and Human Services (HHS) secretary also refused repeatedly to state how many Americans have enrolled in a plan through the website – or by phone or in person – claiming there is no reliable or confirmed data yet.
"The system isn’t functioning, so we are not getting that reliable data," she said, adding that good numbers will be available in mid-November. HHS has spent $118 million on healthcare.gov and $56 million on "other IT" to support the website, Ms. Sebelius said.
Republicans in Congress also questioned Ms. Sebelius about the insurance cancellation notices that thousands of Americans have received since Oct. 1.
"Americans are scared and frustrated," said Energy and Commerce Committee Chairman Fred Upton (R-Mich.). "There are also millions of Americans coast to coast who no doubt believed the president’s repeated promise that if they liked their plan, they’d be able to keep it, no matter what. They are now receiving termination notices, and for those who lose the coverage they like, they may also be losing faith in their government."
Ms. Sebelius said insurers were cancelling policies in the individual market because the plans did not meet ACA criteria.
Rep. Frank Pallone (D-N.J.) called the cancellation issue "another red herring." He said the real explanation is that "insurance companies are cancelling lousy policies with high prices because they can’t compete."
Rep. Michael Burgess (R-Tex.) said he believed that administration officials had misled the committee and asked if Ms. Sebelius would seek the resignation of Gary Cohen, director of the Center for Consumer Information and Insurance Oversight at the CMS. Mr. Cohen’s office oversees the exchanges.
"I will not, sir," Ms. Sebelius responded.
On Twitter @aliciaault
WASHINGTON – Testifying before a House committee, Health and Human Services Secretary Kathleen Sebelius said that she is accountable for the failures of the healthcare.gov website.
"In these early weeks, access to healthcare.gov has been a miserably frustrating experience for way too many Americans," Ms. Sebelius said at an Oct. 30 hearing of the House Energy and Commerce Committee. "I’m as frustrated and angry as anyone with the flawed launch of healthcare.gov."
Ms. Sebelius apologized and said that she wanted Americans to know that "I’m accountable to you for fixing these problems." She added that she was "committed to earning your confidence back by fixing the site."
It was the second consecutive day that an Obama administration official fielded tough questions from Congress on the problems with healthcare.gov, the main avenue for Americans in 36 states to shop for and enroll in health plans offered under the Affordable Care Act’s (ACA’s) insurance exchanges.
When asked by Rep. Marsha Blackburn (R-Tenn.) who was "responsible for this debacle" surrounding healthcare.gov, Ms. Sebelius said, "Hold me accountable for the debacle. I’m responsible."
When asked whether anyone had suggested delaying the site’s Oct. 1 launch, Ms. Sebelius said that neither officials from the Centers for Medicare and Medicaid Services (CMS) nor information technology contractors had given such advice.
The Health and Human Services (HHS) secretary also refused repeatedly to state how many Americans have enrolled in a plan through the website – or by phone or in person – claiming there is no reliable or confirmed data yet.
"The system isn’t functioning, so we are not getting that reliable data," she said, adding that good numbers will be available in mid-November. HHS has spent $118 million on healthcare.gov and $56 million on "other IT" to support the website, Ms. Sebelius said.
Republicans in Congress also questioned Ms. Sebelius about the insurance cancellation notices that thousands of Americans have received since Oct. 1.
"Americans are scared and frustrated," said Energy and Commerce Committee Chairman Fred Upton (R-Mich.). "There are also millions of Americans coast to coast who no doubt believed the president’s repeated promise that if they liked their plan, they’d be able to keep it, no matter what. They are now receiving termination notices, and for those who lose the coverage they like, they may also be losing faith in their government."
Ms. Sebelius said insurers were cancelling policies in the individual market because the plans did not meet ACA criteria.
Rep. Frank Pallone (D-N.J.) called the cancellation issue "another red herring." He said the real explanation is that "insurance companies are cancelling lousy policies with high prices because they can’t compete."
Rep. Michael Burgess (R-Tex.) said he believed that administration officials had misled the committee and asked if Ms. Sebelius would seek the resignation of Gary Cohen, director of the Center for Consumer Information and Insurance Oversight at the CMS. Mr. Cohen’s office oversees the exchanges.
"I will not, sir," Ms. Sebelius responded.
On Twitter @aliciaault
AT A HOUSE ENERGY AND COMMERCE COMMITTEE HEARING