User login
How Will New Physician Value-Based Payment Modifier Affect Medicare Reimbursements?

We talk a lot about value in healthcare—about how to enhance quality and reduce cost—because we all know both need an incredible amount of work. One tactic Medicare is using to improve the value equation on a large scale is aggregating and displaying physician-specific “value” metrics. These metrics, which will be used to deduct or enhance reimbursement for physicians, are known as the Physician Value-Based Payment Modifier (PVBM).
This program has been enacted fairly rapidly since the passage of the Affordable Care Act; it is being rolled out first to large physician practices, then to all groups by 2017. Those with superior performance in both quality and cost will experience as much as a 2% higher reimbursement, while groups with average performance will remain financially neutral and those who show lower performance or choose not to report will be penalized up to 1% of Medicare reimbursement. This first round, for larger groups of 100-plus physicians, will affect about 30% of all U.S. physicians. The second round, for groups of 10 or more physicians, will affect about another third of physicians. The last round, for groups with fewer than 10 physicians, will be applicable to the remaining physicians practicing in the U.S.
On the face of it, the program does seem to be a potentially effective tactic for improving value on a large scale, holding individual physicians accountable for their own individual patient-care performance. A few fatal flaws in the program as it currently stands make it extraordinarily unlikely to be universally adopted by all physicians, however. Here are a few of those flaws:1,2
1 Uncertain yield: Because it is essentially a “zero-sum game” for Medicare, the incentive or penalty for a physician (or the physician’s group) depends on the performance of all the other physicians’ or groups’ performance. As a result, there is incredible uncertainty as to how strong a physician’s performance actually needs to be, year to year, to result in a bonus payment. Given that many of the metrics will require some type of investment to perform well, such as information technology infrastructure or a quality coordinator, there is an equal amount of uncertainty about how much investment will be needed to get a certain budgetary yield. For smaller physician practices, taking a 1% to 2% reduction in Medicare reimbursements may be easier to weather financially than investing in the infrastructure needed to reliably hit the quality metrics for every relevant patient.
2 Uncertain benchmarks: Unlike many hospital quality metrics, which have been publicly displayed for years, physician-level value metrics are just now being reported publicly. This leaves uncertainty about how strong a physician’s performance needs to be in order to be better than average. In the hospital value-based purchasing program, “average” performance is extremely good, in the 98% to 99% compliance range for most metrics. It is less clear what compliance range will be “average” in the physician-based program.
3 Physician variability: More than a half million physicians in the U.S. bill Medicare, and their practice types range from primary care solo practice to multi-group specialty practice. Motivating all brands to understand, measure, report, and improve quality metrics is a yeoman’s task, unlikely to be successful in the short term. Most physicians have not received any formal education or training in quality improvement, so they may not even have the skill set required to improve their metrics into a highly reliable range, worthy of bonus designation.
4 Metric identity and attribution: Because the repertoire of physician types is broad, the ability of each physician type to have a set of metrics that they understand and can identify with is extremely unlikely. In addition, attribution of patients and their associated metrics to any single physician is complicated, especially for patients who are cared for by many different physicians across a number of settings. For hospitalists, the attribution issue is a fatal flaw, as many groups routinely “hand off” patients among other hospitalists in their group, at least once if not several times during a typical hospital stay. The same is true of many other hospital-based specialty physicians.
5 Playing to the test: As with other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to play to the test, so that their efforts to perform exceedingly well at a few metrics will crowd out and hinder their performance on unmeasured metrics. This tendency can result in lower-value care in the sum total, even if the metrics show stellar performance.
6 Reducing the risk: As seen in other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to avoid caring for patients who are likely to be unpredictable, including those with multiple co-morbid conditions or with complex social situations; these patients are likely to perform less well on any metric, despite risk adjusting (which is inherently imperfect). This is a well-known and documented risk of publicly reported programs, and there is no reason to believe the PVBM program will be immune to this risk.
In Sum
Because these flaws seem so daunting at first glance, many physicians and physician groups will be tempted to reject the program outright and take the financial hit induced by nonparticipation. An alternative approach is to embrace all of the value programs outright, investing time and energy in improving the metrics that are truly valuable to both patients and providers.
Regardless of which regulatory agency is demanding performance, we need to be active participants in foraging out what metrics and attribution logic are most appropriate. For hospitalists, these could include risk-adjusted device days, appropriate prescribing and unprescribing of antibiotics, judicious utilization of diagnostic testing, and measurements of patient functional status and/or mobility.
Value metrics are here to stay, including those attributable to individual physicians; our job now is to advocate for meaningful metrics and meaningful attribution, which can and should motivate hospitalists to enhance their patients’ quality of life at a lower cost.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
We talk a lot about value in healthcare—about how to enhance quality and reduce cost—because we all know both need an incredible amount of work. One tactic Medicare is using to improve the value equation on a large scale is aggregating and displaying physician-specific “value” metrics. These metrics, which will be used to deduct or enhance reimbursement for physicians, are known as the Physician Value-Based Payment Modifier (PVBM).
This program has been enacted fairly rapidly since the passage of the Affordable Care Act; it is being rolled out first to large physician practices, then to all groups by 2017. Those with superior performance in both quality and cost will experience as much as a 2% higher reimbursement, while groups with average performance will remain financially neutral and those who show lower performance or choose not to report will be penalized up to 1% of Medicare reimbursement. This first round, for larger groups of 100-plus physicians, will affect about 30% of all U.S. physicians. The second round, for groups of 10 or more physicians, will affect about another third of physicians. The last round, for groups with fewer than 10 physicians, will be applicable to the remaining physicians practicing in the U.S.
On the face of it, the program does seem to be a potentially effective tactic for improving value on a large scale, holding individual physicians accountable for their own individual patient-care performance. A few fatal flaws in the program as it currently stands make it extraordinarily unlikely to be universally adopted by all physicians, however. Here are a few of those flaws:1,2
1 Uncertain yield: Because it is essentially a “zero-sum game” for Medicare, the incentive or penalty for a physician (or the physician’s group) depends on the performance of all the other physicians’ or groups’ performance. As a result, there is incredible uncertainty as to how strong a physician’s performance actually needs to be, year to year, to result in a bonus payment. Given that many of the metrics will require some type of investment to perform well, such as information technology infrastructure or a quality coordinator, there is an equal amount of uncertainty about how much investment will be needed to get a certain budgetary yield. For smaller physician practices, taking a 1% to 2% reduction in Medicare reimbursements may be easier to weather financially than investing in the infrastructure needed to reliably hit the quality metrics for every relevant patient.
2 Uncertain benchmarks: Unlike many hospital quality metrics, which have been publicly displayed for years, physician-level value metrics are just now being reported publicly. This leaves uncertainty about how strong a physician’s performance needs to be in order to be better than average. In the hospital value-based purchasing program, “average” performance is extremely good, in the 98% to 99% compliance range for most metrics. It is less clear what compliance range will be “average” in the physician-based program.
3 Physician variability: More than a half million physicians in the U.S. bill Medicare, and their practice types range from primary care solo practice to multi-group specialty practice. Motivating all brands to understand, measure, report, and improve quality metrics is a yeoman’s task, unlikely to be successful in the short term. Most physicians have not received any formal education or training in quality improvement, so they may not even have the skill set required to improve their metrics into a highly reliable range, worthy of bonus designation.
4 Metric identity and attribution: Because the repertoire of physician types is broad, the ability of each physician type to have a set of metrics that they understand and can identify with is extremely unlikely. In addition, attribution of patients and their associated metrics to any single physician is complicated, especially for patients who are cared for by many different physicians across a number of settings. For hospitalists, the attribution issue is a fatal flaw, as many groups routinely “hand off” patients among other hospitalists in their group, at least once if not several times during a typical hospital stay. The same is true of many other hospital-based specialty physicians.
5 Playing to the test: As with other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to play to the test, so that their efforts to perform exceedingly well at a few metrics will crowd out and hinder their performance on unmeasured metrics. This tendency can result in lower-value care in the sum total, even if the metrics show stellar performance.
6 Reducing the risk: As seen in other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to avoid caring for patients who are likely to be unpredictable, including those with multiple co-morbid conditions or with complex social situations; these patients are likely to perform less well on any metric, despite risk adjusting (which is inherently imperfect). This is a well-known and documented risk of publicly reported programs, and there is no reason to believe the PVBM program will be immune to this risk.
In Sum
Because these flaws seem so daunting at first glance, many physicians and physician groups will be tempted to reject the program outright and take the financial hit induced by nonparticipation. An alternative approach is to embrace all of the value programs outright, investing time and energy in improving the metrics that are truly valuable to both patients and providers.
Regardless of which regulatory agency is demanding performance, we need to be active participants in foraging out what metrics and attribution logic are most appropriate. For hospitalists, these could include risk-adjusted device days, appropriate prescribing and unprescribing of antibiotics, judicious utilization of diagnostic testing, and measurements of patient functional status and/or mobility.
Value metrics are here to stay, including those attributable to individual physicians; our job now is to advocate for meaningful metrics and meaningful attribution, which can and should motivate hospitalists to enhance their patients’ quality of life at a lower cost.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
We talk a lot about value in healthcare—about how to enhance quality and reduce cost—because we all know both need an incredible amount of work. One tactic Medicare is using to improve the value equation on a large scale is aggregating and displaying physician-specific “value” metrics. These metrics, which will be used to deduct or enhance reimbursement for physicians, are known as the Physician Value-Based Payment Modifier (PVBM).
This program has been enacted fairly rapidly since the passage of the Affordable Care Act; it is being rolled out first to large physician practices, then to all groups by 2017. Those with superior performance in both quality and cost will experience as much as a 2% higher reimbursement, while groups with average performance will remain financially neutral and those who show lower performance or choose not to report will be penalized up to 1% of Medicare reimbursement. This first round, for larger groups of 100-plus physicians, will affect about 30% of all U.S. physicians. The second round, for groups of 10 or more physicians, will affect about another third of physicians. The last round, for groups with fewer than 10 physicians, will be applicable to the remaining physicians practicing in the U.S.
On the face of it, the program does seem to be a potentially effective tactic for improving value on a large scale, holding individual physicians accountable for their own individual patient-care performance. A few fatal flaws in the program as it currently stands make it extraordinarily unlikely to be universally adopted by all physicians, however. Here are a few of those flaws:1,2
1 Uncertain yield: Because it is essentially a “zero-sum game” for Medicare, the incentive or penalty for a physician (or the physician’s group) depends on the performance of all the other physicians’ or groups’ performance. As a result, there is incredible uncertainty as to how strong a physician’s performance actually needs to be, year to year, to result in a bonus payment. Given that many of the metrics will require some type of investment to perform well, such as information technology infrastructure or a quality coordinator, there is an equal amount of uncertainty about how much investment will be needed to get a certain budgetary yield. For smaller physician practices, taking a 1% to 2% reduction in Medicare reimbursements may be easier to weather financially than investing in the infrastructure needed to reliably hit the quality metrics for every relevant patient.
2 Uncertain benchmarks: Unlike many hospital quality metrics, which have been publicly displayed for years, physician-level value metrics are just now being reported publicly. This leaves uncertainty about how strong a physician’s performance needs to be in order to be better than average. In the hospital value-based purchasing program, “average” performance is extremely good, in the 98% to 99% compliance range for most metrics. It is less clear what compliance range will be “average” in the physician-based program.
3 Physician variability: More than a half million physicians in the U.S. bill Medicare, and their practice types range from primary care solo practice to multi-group specialty practice. Motivating all brands to understand, measure, report, and improve quality metrics is a yeoman’s task, unlikely to be successful in the short term. Most physicians have not received any formal education or training in quality improvement, so they may not even have the skill set required to improve their metrics into a highly reliable range, worthy of bonus designation.
4 Metric identity and attribution: Because the repertoire of physician types is broad, the ability of each physician type to have a set of metrics that they understand and can identify with is extremely unlikely. In addition, attribution of patients and their associated metrics to any single physician is complicated, especially for patients who are cared for by many different physicians across a number of settings. For hospitalists, the attribution issue is a fatal flaw, as many groups routinely “hand off” patients among other hospitalists in their group, at least once if not several times during a typical hospital stay. The same is true of many other hospital-based specialty physicians.
5 Playing to the test: As with other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to play to the test, so that their efforts to perform exceedingly well at a few metrics will crowd out and hinder their performance on unmeasured metrics. This tendency can result in lower-value care in the sum total, even if the metrics show stellar performance.
6 Reducing the risk: As seen in other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to avoid caring for patients who are likely to be unpredictable, including those with multiple co-morbid conditions or with complex social situations; these patients are likely to perform less well on any metric, despite risk adjusting (which is inherently imperfect). This is a well-known and documented risk of publicly reported programs, and there is no reason to believe the PVBM program will be immune to this risk.
In Sum
Because these flaws seem so daunting at first glance, many physicians and physician groups will be tempted to reject the program outright and take the financial hit induced by nonparticipation. An alternative approach is to embrace all of the value programs outright, investing time and energy in improving the metrics that are truly valuable to both patients and providers.
Regardless of which regulatory agency is demanding performance, we need to be active participants in foraging out what metrics and attribution logic are most appropriate. For hospitalists, these could include risk-adjusted device days, appropriate prescribing and unprescribing of antibiotics, judicious utilization of diagnostic testing, and measurements of patient functional status and/or mobility.
Value metrics are here to stay, including those attributable to individual physicians; our job now is to advocate for meaningful metrics and meaningful attribution, which can and should motivate hospitalists to enhance their patients’ quality of life at a lower cost.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
Centers for Medicare & Medicaid Services Modify Physician Quality Reporting System

Only 27% of eligible providers participated in the Physician Quality Reporting System (PQRS) in 2011—roughly 26,500 medical practices and 266,500 medical professionals, according to the Centers for Medicare & Medicaid Services (CMS).
“A lot of physicians have walked away [from PQRS] feeling like there are not sufficient measures for them to be measured against,” says Cheryl Damberg, senior principal researcher at RAND corporation and professor at the Pardee RAND Graduate School in Santa Monica, Calif.
Encouraging more participation from hospitalists has been the goal of the Society of Hospital Medicine (SHM) for the last several years, says Gregory Seymann, MD, SFHM, clinical professor and chief in the division of hospital medicine at University of California San Diego Health Sciences and chair of SHM’s Performance Measurement and Reporting Committee (PMRC).
“The committee has tried to champion it the best we can, making sure the measures that are there and in development meet the needs of the specialty,” Dr. Seymann says.
In just one year, the SHM committee managed to increase hospitalist reportable measures in PQRS from a paltry 11—half of which were only for stroke patients—to 21, which now includes things like diabetes exams, osteoporosis management, documentation of current medications, and community-acquired pneumonia treatment.
For Comparison’s Sake
For the first couple of phases of PQRS reporting, very few measures were relevant to hospitalists, Dr. Seymann says. The committee worked to ensure that more measures were added and billing codes modified to include those used by the specialty. Hospital medicine is relatively new, not officially recognized by the American Board of Medical Specialties (ABMS), and hospitalists serve a unique role. Most hospitalists are in internal medicine, family medicine, or pediatrics, but they aren’t doing what the average primary care doctor does, like referral for breast cancer or colon cancer screening, Dr. Seymann adds. Additionally, they aren’t always the provider performing specific cardiac or neurological care.
Hospitalists’ patients usually are in the hospital because they are sick. They may have chronic disease or more complex medical needs (e.g. osteoporosis-related hip fracture) than the average population seen by a non-hospitalist PCP.
If hospitalists are compared to other PCPs, as is the plan in the Physician Value-Based Payment Modifier, it “looks like our patients are dying a lot more frequently, we’re spending a lot of money, and we’re not doing primary care,” Dr. Seymann explains.
New Brand, New Push
PQRS is not new; it is the rebranding of CMS’ Physician Quality Reporting Initiative (PQRI), launched in 2006. But changes to the program are part of a national push to improve healthcare quality and patient care while reimbursing for performance on outcome- and process-based measures instead of simply for the volume of services provided. Each year, CMS updates PQRS rules.
This year is the last one in which providers will receive a bonus for reporting through PQRS. Beginning next year, practitioners that don’t meet the reporting requirements for 2013 will incur a 1.5% penalty—with additional penalties for physicians in groups of 100 or more from the value-based payment modifier. This year also serves as the performance year for 2016, when a 2% penalty for insufficient reporting will be assessed.
In early December 2013, the Centers for Medicare & Medicaid Services (CMS) published the 2014 Physician Fee Schedule and, with it, the final rules for the PQRS. Although many physicians and specialist groups believed the measures included in PQRS in previous years were too limited, CMS has added the additional reporting methodology of qualified clinical data registries (QCDR), which can include measures outside of the PQRS—a marked shift from previous policies.
The rule change, Damberg says, should take some energy out of the discussion surrounding the program and allow more physicians to participate.
“From CMS’ perspective, they want doctors delivering the recommended care and they want doctors to be able to report it out easily,” Damberg says.
Moving Forward
In 2014, providers can submit measures through the new QCDR option, or submit PQRS-identified measures through a Medicare qualified registry, through electronic health records, through the group practice reporting option (GPRO), and through claims-based reporting (though this last option is expected to be phased out over time).
Registries themselves are not new, but they can cost millions of dollars to establish and as much as a million a year to maintain. They typically contain more clinical depth and specificity than claims data, and numerous studies show the use of registries leads to improved patient outcomes.
“We don’t know how many [existing] registries are going to qualify to become these qualified clinical data registries,” says Tom Granatir, senior vice president for health policy and external relations at ABMS. “It’s going to take some time for these registries to evolve.”
Qualified clinical data registries must be in operation for at least one year to be eligible for certification by Medicare. They must include performance data from other payers beyond Medicare. Not only must QCDRs be capable of capturing and sending data, they must also provide national benchmarks to those who submit and must report back at least four times per year.
Granatir believes the QCDR rule, which allows QCDR’s to report measures beyond those included in the PQRS program, will help increase participation and will lead to more practice-based measures, but he fears it may exclude some important nuances of day-to-day patient care.
“The whole point [of quality measure reporting] is to create more public transparency…but if you have measures that are not relevant to what is actually done in practices, then it’s not a useful dataset,” he says.
Ideally, Damberg says, PQRS and other performance measures should enable physicians to do what they do better.
“I think this is really going to raise the stakes for [hospitalists] if they want to control their destiny,” Damberg says. “I think they have to get really engaged in this game and take a pro-active role in looking at where the quality gaps are and how can they better benefit patients. That’s the ultimate goal.”
Kelly April Tyrrell is a freelance writer in Wilmington, Del.
Only 27% of eligible providers participated in the Physician Quality Reporting System (PQRS) in 2011—roughly 26,500 medical practices and 266,500 medical professionals, according to the Centers for Medicare & Medicaid Services (CMS).
“A lot of physicians have walked away [from PQRS] feeling like there are not sufficient measures for them to be measured against,” says Cheryl Damberg, senior principal researcher at RAND corporation and professor at the Pardee RAND Graduate School in Santa Monica, Calif.
Encouraging more participation from hospitalists has been the goal of the Society of Hospital Medicine (SHM) for the last several years, says Gregory Seymann, MD, SFHM, clinical professor and chief in the division of hospital medicine at University of California San Diego Health Sciences and chair of SHM’s Performance Measurement and Reporting Committee (PMRC).
“The committee has tried to champion it the best we can, making sure the measures that are there and in development meet the needs of the specialty,” Dr. Seymann says.
In just one year, the SHM committee managed to increase hospitalist reportable measures in PQRS from a paltry 11—half of which were only for stroke patients—to 21, which now includes things like diabetes exams, osteoporosis management, documentation of current medications, and community-acquired pneumonia treatment.
For Comparison’s Sake
For the first couple of phases of PQRS reporting, very few measures were relevant to hospitalists, Dr. Seymann says. The committee worked to ensure that more measures were added and billing codes modified to include those used by the specialty. Hospital medicine is relatively new, not officially recognized by the American Board of Medical Specialties (ABMS), and hospitalists serve a unique role. Most hospitalists are in internal medicine, family medicine, or pediatrics, but they aren’t doing what the average primary care doctor does, like referral for breast cancer or colon cancer screening, Dr. Seymann adds. Additionally, they aren’t always the provider performing specific cardiac or neurological care.
Hospitalists’ patients usually are in the hospital because they are sick. They may have chronic disease or more complex medical needs (e.g. osteoporosis-related hip fracture) than the average population seen by a non-hospitalist PCP.
If hospitalists are compared to other PCPs, as is the plan in the Physician Value-Based Payment Modifier, it “looks like our patients are dying a lot more frequently, we’re spending a lot of money, and we’re not doing primary care,” Dr. Seymann explains.
New Brand, New Push
PQRS is not new; it is the rebranding of CMS’ Physician Quality Reporting Initiative (PQRI), launched in 2006. But changes to the program are part of a national push to improve healthcare quality and patient care while reimbursing for performance on outcome- and process-based measures instead of simply for the volume of services provided. Each year, CMS updates PQRS rules.
This year is the last one in which providers will receive a bonus for reporting through PQRS. Beginning next year, practitioners that don’t meet the reporting requirements for 2013 will incur a 1.5% penalty—with additional penalties for physicians in groups of 100 or more from the value-based payment modifier. This year also serves as the performance year for 2016, when a 2% penalty for insufficient reporting will be assessed.
In early December 2013, the Centers for Medicare & Medicaid Services (CMS) published the 2014 Physician Fee Schedule and, with it, the final rules for the PQRS. Although many physicians and specialist groups believed the measures included in PQRS in previous years were too limited, CMS has added the additional reporting methodology of qualified clinical data registries (QCDR), which can include measures outside of the PQRS—a marked shift from previous policies.
The rule change, Damberg says, should take some energy out of the discussion surrounding the program and allow more physicians to participate.
“From CMS’ perspective, they want doctors delivering the recommended care and they want doctors to be able to report it out easily,” Damberg says.
Moving Forward
In 2014, providers can submit measures through the new QCDR option, or submit PQRS-identified measures through a Medicare qualified registry, through electronic health records, through the group practice reporting option (GPRO), and through claims-based reporting (though this last option is expected to be phased out over time).
Registries themselves are not new, but they can cost millions of dollars to establish and as much as a million a year to maintain. They typically contain more clinical depth and specificity than claims data, and numerous studies show the use of registries leads to improved patient outcomes.
“We don’t know how many [existing] registries are going to qualify to become these qualified clinical data registries,” says Tom Granatir, senior vice president for health policy and external relations at ABMS. “It’s going to take some time for these registries to evolve.”
Qualified clinical data registries must be in operation for at least one year to be eligible for certification by Medicare. They must include performance data from other payers beyond Medicare. Not only must QCDRs be capable of capturing and sending data, they must also provide national benchmarks to those who submit and must report back at least four times per year.
Granatir believes the QCDR rule, which allows QCDR’s to report measures beyond those included in the PQRS program, will help increase participation and will lead to more practice-based measures, but he fears it may exclude some important nuances of day-to-day patient care.
“The whole point [of quality measure reporting] is to create more public transparency…but if you have measures that are not relevant to what is actually done in practices, then it’s not a useful dataset,” he says.
Ideally, Damberg says, PQRS and other performance measures should enable physicians to do what they do better.
“I think this is really going to raise the stakes for [hospitalists] if they want to control their destiny,” Damberg says. “I think they have to get really engaged in this game and take a pro-active role in looking at where the quality gaps are and how can they better benefit patients. That’s the ultimate goal.”
Kelly April Tyrrell is a freelance writer in Wilmington, Del.
Only 27% of eligible providers participated in the Physician Quality Reporting System (PQRS) in 2011—roughly 26,500 medical practices and 266,500 medical professionals, according to the Centers for Medicare & Medicaid Services (CMS).
“A lot of physicians have walked away [from PQRS] feeling like there are not sufficient measures for them to be measured against,” says Cheryl Damberg, senior principal researcher at RAND corporation and professor at the Pardee RAND Graduate School in Santa Monica, Calif.
Encouraging more participation from hospitalists has been the goal of the Society of Hospital Medicine (SHM) for the last several years, says Gregory Seymann, MD, SFHM, clinical professor and chief in the division of hospital medicine at University of California San Diego Health Sciences and chair of SHM’s Performance Measurement and Reporting Committee (PMRC).
“The committee has tried to champion it the best we can, making sure the measures that are there and in development meet the needs of the specialty,” Dr. Seymann says.
In just one year, the SHM committee managed to increase hospitalist reportable measures in PQRS from a paltry 11—half of which were only for stroke patients—to 21, which now includes things like diabetes exams, osteoporosis management, documentation of current medications, and community-acquired pneumonia treatment.
For Comparison’s Sake
For the first couple of phases of PQRS reporting, very few measures were relevant to hospitalists, Dr. Seymann says. The committee worked to ensure that more measures were added and billing codes modified to include those used by the specialty. Hospital medicine is relatively new, not officially recognized by the American Board of Medical Specialties (ABMS), and hospitalists serve a unique role. Most hospitalists are in internal medicine, family medicine, or pediatrics, but they aren’t doing what the average primary care doctor does, like referral for breast cancer or colon cancer screening, Dr. Seymann adds. Additionally, they aren’t always the provider performing specific cardiac or neurological care.
Hospitalists’ patients usually are in the hospital because they are sick. They may have chronic disease or more complex medical needs (e.g. osteoporosis-related hip fracture) than the average population seen by a non-hospitalist PCP.
If hospitalists are compared to other PCPs, as is the plan in the Physician Value-Based Payment Modifier, it “looks like our patients are dying a lot more frequently, we’re spending a lot of money, and we’re not doing primary care,” Dr. Seymann explains.
New Brand, New Push
PQRS is not new; it is the rebranding of CMS’ Physician Quality Reporting Initiative (PQRI), launched in 2006. But changes to the program are part of a national push to improve healthcare quality and patient care while reimbursing for performance on outcome- and process-based measures instead of simply for the volume of services provided. Each year, CMS updates PQRS rules.
This year is the last one in which providers will receive a bonus for reporting through PQRS. Beginning next year, practitioners that don’t meet the reporting requirements for 2013 will incur a 1.5% penalty—with additional penalties for physicians in groups of 100 or more from the value-based payment modifier. This year also serves as the performance year for 2016, when a 2% penalty for insufficient reporting will be assessed.
In early December 2013, the Centers for Medicare & Medicaid Services (CMS) published the 2014 Physician Fee Schedule and, with it, the final rules for the PQRS. Although many physicians and specialist groups believed the measures included in PQRS in previous years were too limited, CMS has added the additional reporting methodology of qualified clinical data registries (QCDR), which can include measures outside of the PQRS—a marked shift from previous policies.
The rule change, Damberg says, should take some energy out of the discussion surrounding the program and allow more physicians to participate.
“From CMS’ perspective, they want doctors delivering the recommended care and they want doctors to be able to report it out easily,” Damberg says.
Moving Forward
In 2014, providers can submit measures through the new QCDR option, or submit PQRS-identified measures through a Medicare qualified registry, through electronic health records, through the group practice reporting option (GPRO), and through claims-based reporting (though this last option is expected to be phased out over time).
Registries themselves are not new, but they can cost millions of dollars to establish and as much as a million a year to maintain. They typically contain more clinical depth and specificity than claims data, and numerous studies show the use of registries leads to improved patient outcomes.
“We don’t know how many [existing] registries are going to qualify to become these qualified clinical data registries,” says Tom Granatir, senior vice president for health policy and external relations at ABMS. “It’s going to take some time for these registries to evolve.”
Qualified clinical data registries must be in operation for at least one year to be eligible for certification by Medicare. They must include performance data from other payers beyond Medicare. Not only must QCDRs be capable of capturing and sending data, they must also provide national benchmarks to those who submit and must report back at least four times per year.
Granatir believes the QCDR rule, which allows QCDR’s to report measures beyond those included in the PQRS program, will help increase participation and will lead to more practice-based measures, but he fears it may exclude some important nuances of day-to-day patient care.
“The whole point [of quality measure reporting] is to create more public transparency…but if you have measures that are not relevant to what is actually done in practices, then it’s not a useful dataset,” he says.
Ideally, Damberg says, PQRS and other performance measures should enable physicians to do what they do better.
“I think this is really going to raise the stakes for [hospitalists] if they want to control their destiny,” Damberg says. “I think they have to get really engaged in this game and take a pro-active role in looking at where the quality gaps are and how can they better benefit patients. That’s the ultimate goal.”
Kelly April Tyrrell is a freelance writer in Wilmington, Del.
Hospitalist Pay Shifts from Volume to Value with Global Payment System

The move to paying hospitals and physicians based on value instead of volume is well underway. As programs ultimately designed to offer a global payment for a population (ACOs) or an episode of care (bundled payment) expand, we are left with this paradox: How do we reward physicians for working harder and seeing more patients under a global payment system that encourages physicians and hospitals to do less?
It appears that the existing fee-for-service payment system will need to form the scaffolding of any new, value-based system. Physicians must document the services they provide, leaving a “footprint” that can be recognized and rewarded. Without a record of the volume of services, physicians will have no incentive to see more patients during times of increased demand. This is what we often experience with straight-salary arrangements—physicians question why they should work harder for no additional compensation.
Through the ACO lens, Bruce Landon, professor of health care policy at Harvard Medical School, states the challenge in a different way: “The fundamental questions become how ACOs will divide their global budgets and how their physicians and service providers will be reimbursed. Thus, this system for determining who has earned what portion of payments—keeping score—is likely to be crucially important to the success of these new models of care.”1
In another article addressing value-based payment for physicians, Eric Stecker, MD, MPH, and Steve Schroeder, MD, argue that, due to their longevity and resilience, relative value units (RVUs), instead of physician-level capitation, straight salary, or salary with pay for performance incentives, should be the preferred mechanism to reimburse physicians based on value.2
I’d like to further develop the idea of an RVU-centric approach to value-based physician reimbursement, specifically discussing the case of hospitalists.
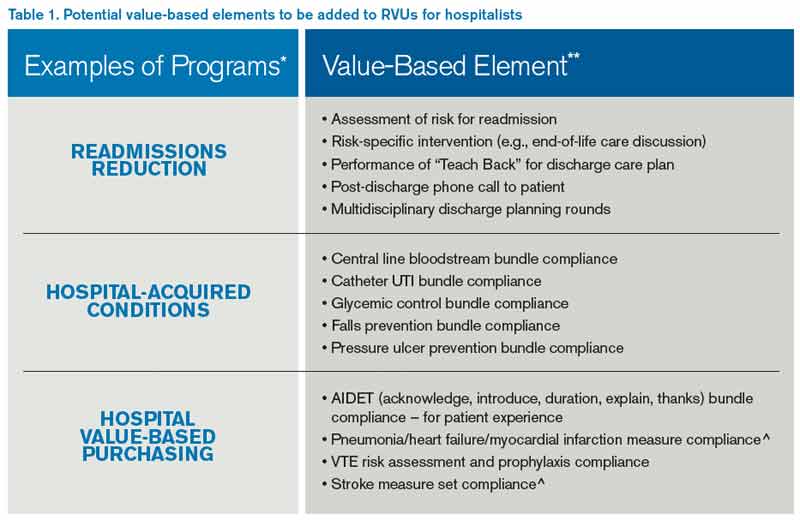
In Table 1, I provide examples of “value-based elements” to be added to an RVU reimbursement system. I chose measures related to three hospital-based quality programs: readmission reduction, hospital-acquired conditions, and value-based purchasing; however, one could choose hospitalist-relevant quality measures from other programs, such as ACOs, meaningful use, outpatient quality reporting (for observation patients), bundled payments, or a broad range of other domains. I selected only process measures, because outcome measures such as mortality or readmission rates suffer from sample size that is too small and risk adjustment too inadequate to be applied to individual physician payment.
Drs. Stecker and Schroeder offer an observation that is especially important to hospitalists: “Although RVUs are traditionally used for episodes of care provided by individual clinicians for individual patients, activities linked to RVUs could be more broadly defined to include team-based and supervisory clinical activities as well.”2 In the table, I include “multidisciplinary discharge planning rounds” as a potential measure. One can envision other team-based or supervisory activities involving hospitalists collaborating with nurses, pharmacists, or case managers working on a catheter-UTI bundle, high-risk medication counseling, or readmission risk assessment—with each activity linked to RVUs.
The implementation of an RVU system incorporating quality measures would be aided by documentation templates in the electronic medical record, similar to templates emerging for care bundles like central line blood stream infection. Value-based RVUs would have challenges, such as the need to change the measures over time and the system gaming inherent in any incentive design. Details of implementing the program would need to be worked out, such as attributing measures to individual physicians/providers or limiting to one the number of times certain measures are fulfilled per hospitalization.
Once established, a value-based RVU system could replace the complex and variable physician compensation landscape that exists today. As has always been the case, an RVU system could form the basis of a production incentive. Such a system could be implemented on existing billing software systems, would not require additional resources to administer, and is likely to find acceptance among hospitalists, because it is something most are already accustomed to.
Current efforts to pay physicians based on value are facing substantial headwinds. The Value-Based Payment Modifier has been criticized for being too complex, while the Physician Quality Reporting System, in place since 2007, has been plagued by a “dismal” adoption rate by physicians and has been noted to “reflect a vanishingly small part of professional activities in most clinical specialties.”3 The time may be right to rethink physician value-based payment and integrate it into the existing, time-honored RVU payment system.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
References
- Landon BE. Keeping score under a global payment system. N Engl J Med. 2012;366(5):393-395.
- Stecker EC, Schroeder SA. Adding value to relative-value units. N Engl J Med. 2013;369(23):2176-2179.
- Berenson RA, Kaye DR. Grading a physician’s value — the misapplication of performance measurement. N Engl J Med. 2013;369(22):2079-2078.
The move to paying hospitals and physicians based on value instead of volume is well underway. As programs ultimately designed to offer a global payment for a population (ACOs) or an episode of care (bundled payment) expand, we are left with this paradox: How do we reward physicians for working harder and seeing more patients under a global payment system that encourages physicians and hospitals to do less?
It appears that the existing fee-for-service payment system will need to form the scaffolding of any new, value-based system. Physicians must document the services they provide, leaving a “footprint” that can be recognized and rewarded. Without a record of the volume of services, physicians will have no incentive to see more patients during times of increased demand. This is what we often experience with straight-salary arrangements—physicians question why they should work harder for no additional compensation.
Through the ACO lens, Bruce Landon, professor of health care policy at Harvard Medical School, states the challenge in a different way: “The fundamental questions become how ACOs will divide their global budgets and how their physicians and service providers will be reimbursed. Thus, this system for determining who has earned what portion of payments—keeping score—is likely to be crucially important to the success of these new models of care.”1
In another article addressing value-based payment for physicians, Eric Stecker, MD, MPH, and Steve Schroeder, MD, argue that, due to their longevity and resilience, relative value units (RVUs), instead of physician-level capitation, straight salary, or salary with pay for performance incentives, should be the preferred mechanism to reimburse physicians based on value.2
I’d like to further develop the idea of an RVU-centric approach to value-based physician reimbursement, specifically discussing the case of hospitalists.
In Table 1, I provide examples of “value-based elements” to be added to an RVU reimbursement system. I chose measures related to three hospital-based quality programs: readmission reduction, hospital-acquired conditions, and value-based purchasing; however, one could choose hospitalist-relevant quality measures from other programs, such as ACOs, meaningful use, outpatient quality reporting (for observation patients), bundled payments, or a broad range of other domains. I selected only process measures, because outcome measures such as mortality or readmission rates suffer from sample size that is too small and risk adjustment too inadequate to be applied to individual physician payment.
Drs. Stecker and Schroeder offer an observation that is especially important to hospitalists: “Although RVUs are traditionally used for episodes of care provided by individual clinicians for individual patients, activities linked to RVUs could be more broadly defined to include team-based and supervisory clinical activities as well.”2 In the table, I include “multidisciplinary discharge planning rounds” as a potential measure. One can envision other team-based or supervisory activities involving hospitalists collaborating with nurses, pharmacists, or case managers working on a catheter-UTI bundle, high-risk medication counseling, or readmission risk assessment—with each activity linked to RVUs.
The implementation of an RVU system incorporating quality measures would be aided by documentation templates in the electronic medical record, similar to templates emerging for care bundles like central line blood stream infection. Value-based RVUs would have challenges, such as the need to change the measures over time and the system gaming inherent in any incentive design. Details of implementing the program would need to be worked out, such as attributing measures to individual physicians/providers or limiting to one the number of times certain measures are fulfilled per hospitalization.
Once established, a value-based RVU system could replace the complex and variable physician compensation landscape that exists today. As has always been the case, an RVU system could form the basis of a production incentive. Such a system could be implemented on existing billing software systems, would not require additional resources to administer, and is likely to find acceptance among hospitalists, because it is something most are already accustomed to.
Current efforts to pay physicians based on value are facing substantial headwinds. The Value-Based Payment Modifier has been criticized for being too complex, while the Physician Quality Reporting System, in place since 2007, has been plagued by a “dismal” adoption rate by physicians and has been noted to “reflect a vanishingly small part of professional activities in most clinical specialties.”3 The time may be right to rethink physician value-based payment and integrate it into the existing, time-honored RVU payment system.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
References
- Landon BE. Keeping score under a global payment system. N Engl J Med. 2012;366(5):393-395.
- Stecker EC, Schroeder SA. Adding value to relative-value units. N Engl J Med. 2013;369(23):2176-2179.
- Berenson RA, Kaye DR. Grading a physician’s value — the misapplication of performance measurement. N Engl J Med. 2013;369(22):2079-2078.
The move to paying hospitals and physicians based on value instead of volume is well underway. As programs ultimately designed to offer a global payment for a population (ACOs) or an episode of care (bundled payment) expand, we are left with this paradox: How do we reward physicians for working harder and seeing more patients under a global payment system that encourages physicians and hospitals to do less?
It appears that the existing fee-for-service payment system will need to form the scaffolding of any new, value-based system. Physicians must document the services they provide, leaving a “footprint” that can be recognized and rewarded. Without a record of the volume of services, physicians will have no incentive to see more patients during times of increased demand. This is what we often experience with straight-salary arrangements—physicians question why they should work harder for no additional compensation.
Through the ACO lens, Bruce Landon, professor of health care policy at Harvard Medical School, states the challenge in a different way: “The fundamental questions become how ACOs will divide their global budgets and how their physicians and service providers will be reimbursed. Thus, this system for determining who has earned what portion of payments—keeping score—is likely to be crucially important to the success of these new models of care.”1
In another article addressing value-based payment for physicians, Eric Stecker, MD, MPH, and Steve Schroeder, MD, argue that, due to their longevity and resilience, relative value units (RVUs), instead of physician-level capitation, straight salary, or salary with pay for performance incentives, should be the preferred mechanism to reimburse physicians based on value.2
I’d like to further develop the idea of an RVU-centric approach to value-based physician reimbursement, specifically discussing the case of hospitalists.
In Table 1, I provide examples of “value-based elements” to be added to an RVU reimbursement system. I chose measures related to three hospital-based quality programs: readmission reduction, hospital-acquired conditions, and value-based purchasing; however, one could choose hospitalist-relevant quality measures from other programs, such as ACOs, meaningful use, outpatient quality reporting (for observation patients), bundled payments, or a broad range of other domains. I selected only process measures, because outcome measures such as mortality or readmission rates suffer from sample size that is too small and risk adjustment too inadequate to be applied to individual physician payment.
Drs. Stecker and Schroeder offer an observation that is especially important to hospitalists: “Although RVUs are traditionally used for episodes of care provided by individual clinicians for individual patients, activities linked to RVUs could be more broadly defined to include team-based and supervisory clinical activities as well.”2 In the table, I include “multidisciplinary discharge planning rounds” as a potential measure. One can envision other team-based or supervisory activities involving hospitalists collaborating with nurses, pharmacists, or case managers working on a catheter-UTI bundle, high-risk medication counseling, or readmission risk assessment—with each activity linked to RVUs.
The implementation of an RVU system incorporating quality measures would be aided by documentation templates in the electronic medical record, similar to templates emerging for care bundles like central line blood stream infection. Value-based RVUs would have challenges, such as the need to change the measures over time and the system gaming inherent in any incentive design. Details of implementing the program would need to be worked out, such as attributing measures to individual physicians/providers or limiting to one the number of times certain measures are fulfilled per hospitalization.
Once established, a value-based RVU system could replace the complex and variable physician compensation landscape that exists today. As has always been the case, an RVU system could form the basis of a production incentive. Such a system could be implemented on existing billing software systems, would not require additional resources to administer, and is likely to find acceptance among hospitalists, because it is something most are already accustomed to.
Current efforts to pay physicians based on value are facing substantial headwinds. The Value-Based Payment Modifier has been criticized for being too complex, while the Physician Quality Reporting System, in place since 2007, has been plagued by a “dismal” adoption rate by physicians and has been noted to “reflect a vanishingly small part of professional activities in most clinical specialties.”3 The time may be right to rethink physician value-based payment and integrate it into the existing, time-honored RVU payment system.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
References
- Landon BE. Keeping score under a global payment system. N Engl J Med. 2012;366(5):393-395.
- Stecker EC, Schroeder SA. Adding value to relative-value units. N Engl J Med. 2013;369(23):2176-2179.
- Berenson RA, Kaye DR. Grading a physician’s value — the misapplication of performance measurement. N Engl J Med. 2013;369(22):2079-2078.
Flexibility – but no passes – on meaningful use Stage 2
ORLANDO – The government can be a bit more flexible on physicians meeting Stage 2 of meaningful use of electronic health records, but won’t give blanket permission to slide on deadlines.
That’s according to Marilyn Tavenner, administrator of the Centers for Medicare & Medicaid Services (CMS), who spoke Feb. 27 at the annual meeting of the Healthcare Information and Management Systems Society.

Physicians have been seeking more leeway from CMS on participating in meaningful use this year, in part because they must purchase or upgrade to the 2014 edition of certified EHR (electronic health records) technology, and in part because they must get ready to switch over to the ICD-10 coding set on Oct. 1.
Physicians who participate in meaningful use get incentive payments from Medicare or Medicaid. If they don’t participate this year, they’ll be penalized starting in 2015.
On Feb. 21, 48 physician organizations wrote to the Health and Human Services department, asking for delays in some of the deadlines for meaningful use this year and for more flexibility from the CMS.
Ms. Tavenner said that CMS officials had heard many concerns about moving forward with Stage 2, and "are sensitive to those concerns." She noted that over the past few years, the agency had delayed the start of Stage 1 and Stage 2, and most recently pushed back implementation of Stage 3 to 2017.
"But now is not the time to stop moving forward," she said. Ms. Tavenner said that it was understood that some health care providers and vendors "may legitimately have issues with establishing Stage 2 reporting deadlines."
Because of that, the CMS has "decided to permit flexibility in how hardship exemptions will be granted in the 2014 reporting year," she said.
The agency will look at hardship requests case-by-case, as is required by law. And it is expected to issue further guidance on what qualifies as a hardship very soon.
But Ms. Tavenner said the agency would not give everyone a pass.
"I must stress to you that we do expect all eligible Stage 2 providers to fully meet all requirements in 2015," Ms. Tavenner said. "And I urge all of you to do everything you can to meet the Stage 2 requirements this year."
aault@frontlinemedcom.com
On Twitter @aliciaault
ORLANDO – The government can be a bit more flexible on physicians meeting Stage 2 of meaningful use of electronic health records, but won’t give blanket permission to slide on deadlines.
That’s according to Marilyn Tavenner, administrator of the Centers for Medicare & Medicaid Services (CMS), who spoke Feb. 27 at the annual meeting of the Healthcare Information and Management Systems Society.
Physicians have been seeking more leeway from CMS on participating in meaningful use this year, in part because they must purchase or upgrade to the 2014 edition of certified EHR (electronic health records) technology, and in part because they must get ready to switch over to the ICD-10 coding set on Oct. 1.
Physicians who participate in meaningful use get incentive payments from Medicare or Medicaid. If they don’t participate this year, they’ll be penalized starting in 2015.
On Feb. 21, 48 physician organizations wrote to the Health and Human Services department, asking for delays in some of the deadlines for meaningful use this year and for more flexibility from the CMS.
Ms. Tavenner said that CMS officials had heard many concerns about moving forward with Stage 2, and "are sensitive to those concerns." She noted that over the past few years, the agency had delayed the start of Stage 1 and Stage 2, and most recently pushed back implementation of Stage 3 to 2017.
"But now is not the time to stop moving forward," she said. Ms. Tavenner said that it was understood that some health care providers and vendors "may legitimately have issues with establishing Stage 2 reporting deadlines."
Because of that, the CMS has "decided to permit flexibility in how hardship exemptions will be granted in the 2014 reporting year," she said.
The agency will look at hardship requests case-by-case, as is required by law. And it is expected to issue further guidance on what qualifies as a hardship very soon.
But Ms. Tavenner said the agency would not give everyone a pass.
"I must stress to you that we do expect all eligible Stage 2 providers to fully meet all requirements in 2015," Ms. Tavenner said. "And I urge all of you to do everything you can to meet the Stage 2 requirements this year."
aault@frontlinemedcom.com
On Twitter @aliciaault
ORLANDO – The government can be a bit more flexible on physicians meeting Stage 2 of meaningful use of electronic health records, but won’t give blanket permission to slide on deadlines.
That’s according to Marilyn Tavenner, administrator of the Centers for Medicare & Medicaid Services (CMS), who spoke Feb. 27 at the annual meeting of the Healthcare Information and Management Systems Society.
Physicians have been seeking more leeway from CMS on participating in meaningful use this year, in part because they must purchase or upgrade to the 2014 edition of certified EHR (electronic health records) technology, and in part because they must get ready to switch over to the ICD-10 coding set on Oct. 1.
Physicians who participate in meaningful use get incentive payments from Medicare or Medicaid. If they don’t participate this year, they’ll be penalized starting in 2015.
On Feb. 21, 48 physician organizations wrote to the Health and Human Services department, asking for delays in some of the deadlines for meaningful use this year and for more flexibility from the CMS.
Ms. Tavenner said that CMS officials had heard many concerns about moving forward with Stage 2, and "are sensitive to those concerns." She noted that over the past few years, the agency had delayed the start of Stage 1 and Stage 2, and most recently pushed back implementation of Stage 3 to 2017.
"But now is not the time to stop moving forward," she said. Ms. Tavenner said that it was understood that some health care providers and vendors "may legitimately have issues with establishing Stage 2 reporting deadlines."
Because of that, the CMS has "decided to permit flexibility in how hardship exemptions will be granted in the 2014 reporting year," she said.
The agency will look at hardship requests case-by-case, as is required by law. And it is expected to issue further guidance on what qualifies as a hardship very soon.
But Ms. Tavenner said the agency would not give everyone a pass.
"I must stress to you that we do expect all eligible Stage 2 providers to fully meet all requirements in 2015," Ms. Tavenner said. "And I urge all of you to do everything you can to meet the Stage 2 requirements this year."
aault@frontlinemedcom.com
On Twitter @aliciaault
AT HIMSS14

Stage 2 of meaningful use: Expect tougher objectives, pre-payment audits
ORLANDO – Expect a more rigorous process of certification for Stage 2 of meaningful use and be prepared for audits that will withhold incentive payments until all issues are resolved, federal officials advised.
This year is the first that physicians can work to meet the requirements for Stage 2 of meaningful use. Stage 1 was about data capture, but Stage 2 is about sharing information across care settings and between patients and providers, Robert Anthony, deputy director of the Health IT Initiatives Group at the Centers for Medicare and Medicaid Services’ Office of E-Health Standards and Services, said at the annual meeting of the Healthcare Information and Management Systems Society.
Among the core requirements for Stage 2 are establishing a patient portal and ensuring and using secure messaging between patients and providers. Physicians must be able to link to imaging results, report to a registry, and record electronic progress notes.

Mr. Anthony said that CMS purposely set what he called a "low bar" for patient engagement in Stage 2. To demonstrate meaningful use, 5% of patients must use the practice’s patient portal and 5% must participate in secure messaging beyond appointment booking, he said.
Even so, meeting that target might not be easy. Mr. Anthony said that he had heard from some physicians that they are sitting down with patients at the end of a visit and walking them through use of the portal or the messaging process. Those encounters, he added, can be counted toward the target.
Requirements for documenting care transitions are stricter as well, Mr. Anthony said.
"In Stage 1, ‘transitions of care’ was a menu objective, and virtually none of you selected transitions of care," he said. "We know why everybody didn’t select it – because it’s a difficult objective to achieve."
Care transitions, though, are "the Holy Grail" for showing that systems and clinicians can talk to each other, so the measure was moved into the core objectives for stage 2, he said.
Under Stage 1, physicians could send a summary of care to the next provider by any method, as long as it arrived, said Mr. Anthony. Under Stage 2, summaries must be electronically transmitted 10% or more of the time. At least some have to be sent to clinicians using a different electronic health record system.
Finally, CMS will be performing more audits under Stage 2. The agency must be accountable for the $21 billion spent on incentive payments so far, he said. In stage 1, the audits for Medicare were primarily post payment. Now, payments will be withheld until the audits are resolved. Some 5%-10% of physicians will be subject to an audit. They will be chosen at random or through risk profiling.
And, "no, we’re not going to talk about what raises a red flag, because that’s the point of an oversight program," he added.
So far, documentation has been the primary deficiency found through the audit process, Mr. Anthony said.
"I am shocked by the number of people who do not retain any documentation related to their attestation figures," he said. Physicians need to document the numerators and denominators they use for attestation and then keep that documentation for 6 years.
There are no consultants or companies that have any special knowledge about how to avoid audits or resolve an audit more quickly. They also don’t know anything special about the appeals process. "The process is the same for everybody and is transparent and public for everybody," he said.
"Anybody who is telling you separately that they have some kind of inside line to CMS is drumming up business and nothing more," Mr. Anthony said.
He also said that there is no secret process to getting an appeal. The agency spells out what it is looking for in the appeals documentation available on the CMS ICD-10 website. There’s also a sample audit letter from the CMS contractor, Figliozzi and Co.
On Twitter @aliciaault
ORLANDO – Expect a more rigorous process of certification for Stage 2 of meaningful use and be prepared for audits that will withhold incentive payments until all issues are resolved, federal officials advised.
This year is the first that physicians can work to meet the requirements for Stage 2 of meaningful use. Stage 1 was about data capture, but Stage 2 is about sharing information across care settings and between patients and providers, Robert Anthony, deputy director of the Health IT Initiatives Group at the Centers for Medicare and Medicaid Services’ Office of E-Health Standards and Services, said at the annual meeting of the Healthcare Information and Management Systems Society.
Among the core requirements for Stage 2 are establishing a patient portal and ensuring and using secure messaging between patients and providers. Physicians must be able to link to imaging results, report to a registry, and record electronic progress notes.
Mr. Anthony said that CMS purposely set what he called a "low bar" for patient engagement in Stage 2. To demonstrate meaningful use, 5% of patients must use the practice’s patient portal and 5% must participate in secure messaging beyond appointment booking, he said.
Even so, meeting that target might not be easy. Mr. Anthony said that he had heard from some physicians that they are sitting down with patients at the end of a visit and walking them through use of the portal or the messaging process. Those encounters, he added, can be counted toward the target.
Requirements for documenting care transitions are stricter as well, Mr. Anthony said.
"In Stage 1, ‘transitions of care’ was a menu objective, and virtually none of you selected transitions of care," he said. "We know why everybody didn’t select it – because it’s a difficult objective to achieve."
Care transitions, though, are "the Holy Grail" for showing that systems and clinicians can talk to each other, so the measure was moved into the core objectives for stage 2, he said.
Under Stage 1, physicians could send a summary of care to the next provider by any method, as long as it arrived, said Mr. Anthony. Under Stage 2, summaries must be electronically transmitted 10% or more of the time. At least some have to be sent to clinicians using a different electronic health record system.
Finally, CMS will be performing more audits under Stage 2. The agency must be accountable for the $21 billion spent on incentive payments so far, he said. In stage 1, the audits for Medicare were primarily post payment. Now, payments will be withheld until the audits are resolved. Some 5%-10% of physicians will be subject to an audit. They will be chosen at random or through risk profiling.
And, "no, we’re not going to talk about what raises a red flag, because that’s the point of an oversight program," he added.
So far, documentation has been the primary deficiency found through the audit process, Mr. Anthony said.
"I am shocked by the number of people who do not retain any documentation related to their attestation figures," he said. Physicians need to document the numerators and denominators they use for attestation and then keep that documentation for 6 years.
There are no consultants or companies that have any special knowledge about how to avoid audits or resolve an audit more quickly. They also don’t know anything special about the appeals process. "The process is the same for everybody and is transparent and public for everybody," he said.
"Anybody who is telling you separately that they have some kind of inside line to CMS is drumming up business and nothing more," Mr. Anthony said.
He also said that there is no secret process to getting an appeal. The agency spells out what it is looking for in the appeals documentation available on the CMS ICD-10 website. There’s also a sample audit letter from the CMS contractor, Figliozzi and Co.
On Twitter @aliciaault
ORLANDO – Expect a more rigorous process of certification for Stage 2 of meaningful use and be prepared for audits that will withhold incentive payments until all issues are resolved, federal officials advised.
This year is the first that physicians can work to meet the requirements for Stage 2 of meaningful use. Stage 1 was about data capture, but Stage 2 is about sharing information across care settings and between patients and providers, Robert Anthony, deputy director of the Health IT Initiatives Group at the Centers for Medicare and Medicaid Services’ Office of E-Health Standards and Services, said at the annual meeting of the Healthcare Information and Management Systems Society.
Among the core requirements for Stage 2 are establishing a patient portal and ensuring and using secure messaging between patients and providers. Physicians must be able to link to imaging results, report to a registry, and record electronic progress notes.
Mr. Anthony said that CMS purposely set what he called a "low bar" for patient engagement in Stage 2. To demonstrate meaningful use, 5% of patients must use the practice’s patient portal and 5% must participate in secure messaging beyond appointment booking, he said.
Even so, meeting that target might not be easy. Mr. Anthony said that he had heard from some physicians that they are sitting down with patients at the end of a visit and walking them through use of the portal or the messaging process. Those encounters, he added, can be counted toward the target.
Requirements for documenting care transitions are stricter as well, Mr. Anthony said.
"In Stage 1, ‘transitions of care’ was a menu objective, and virtually none of you selected transitions of care," he said. "We know why everybody didn’t select it – because it’s a difficult objective to achieve."
Care transitions, though, are "the Holy Grail" for showing that systems and clinicians can talk to each other, so the measure was moved into the core objectives for stage 2, he said.
Under Stage 1, physicians could send a summary of care to the next provider by any method, as long as it arrived, said Mr. Anthony. Under Stage 2, summaries must be electronically transmitted 10% or more of the time. At least some have to be sent to clinicians using a different electronic health record system.
Finally, CMS will be performing more audits under Stage 2. The agency must be accountable for the $21 billion spent on incentive payments so far, he said. In stage 1, the audits for Medicare were primarily post payment. Now, payments will be withheld until the audits are resolved. Some 5%-10% of physicians will be subject to an audit. They will be chosen at random or through risk profiling.
And, "no, we’re not going to talk about what raises a red flag, because that’s the point of an oversight program," he added.
So far, documentation has been the primary deficiency found through the audit process, Mr. Anthony said.
"I am shocked by the number of people who do not retain any documentation related to their attestation figures," he said. Physicians need to document the numerators and denominators they use for attestation and then keep that documentation for 6 years.
There are no consultants or companies that have any special knowledge about how to avoid audits or resolve an audit more quickly. They also don’t know anything special about the appeals process. "The process is the same for everybody and is transparent and public for everybody," he said.
"Anybody who is telling you separately that they have some kind of inside line to CMS is drumming up business and nothing more," Mr. Anthony said.
He also said that there is no secret process to getting an appeal. The agency spells out what it is looking for in the appeals documentation available on the CMS ICD-10 website. There’s also a sample audit letter from the CMS contractor, Figliozzi and Co.
On Twitter @aliciaault
AT HIMSS14

New guidelines issued for geriatric care in the ED
New consensus-based guidelines aim to provide a standardized approach to improving the care of patients in geriatric emergency departments.
The Geriatric Emergency Department Guidelines are the result of a 2-year effort by representatives from the American College of Emergency Physicians, the American Geriatrics Society, the Society for Academic Emergency Medicine, and the Emergency Nurses Association. According to 2010 Census data, more than 40 million Americans are now over the age of 65 years. Further, the populations of adults aged 65 years and older and those aged 85 years and older are increasing at rates substantially greater than those of the general population.

"The subsequent increased need for health care for this burgeoning geriatric population represents an unprecedented and overwhelming challenge to the American health care system as a whole and to emergency departments [EDs] specifically," the authors state.
In response to this challenge, geriatric EDs are becoming increasingly common. The new guidelines address the special needs of the geriatric population, and propose methods for ensuring that those needs are met, as "the contemporary emergency medicine management model may not be adequate for geriatric adults."
"Similar programs designed for other age groups (pediatric) or directed toward specific diseases (STEMI [ST segment elevation myocardial infarction], stroke, and trauma) have improved care both in individual EDs and system wide, resulting in better, more cost-effective care and ultimately, better patient outcomes," the guideline writers note.
Among the topics addressed in detail in the guidelines are geriatric ED staffing, equipment, education, policies and procedures, follow-up care, and performance improvement measures.
According to the guidelines, an effective program will:
• Involve hospital site-specific staff and overall local coordination resources.
The guidelines spell out qualifications and responsibilities for the geriatric ED medical director, nurse manager, and staff physicians, nurses, specialists, and ancillary service providers.
• Decrease hospital admissions through effective follow-up and care transition plans.
The guidelines state that clinical patient information should be provided in a format best suited for elder adults and that department leaders should maintain relationships and resources in the community that can be used by patients to facilitate care following discharge.
• Include specialty-specific education and training of a multidisciplinary staff, with assessment for interdisciplinary core competencies.
Education should include "go-live" implementation sessions, as well as community awareness, involvement, and outreach, and regular educational assessment and implementation of site-specific educational needs.
• Assess quality, and implement an effective quality improvement program that involves collection and monitoring of relevant data.
The guidelines provide an explicit geriatric program quality-improvement plan designed to be conducive to staff education and program success.
• Utilize equipment designed for a patient population with specific needs.
For example, effective and comfortable evaluation requires equipment that takes into consideration issues of mobility, incontinence, and behavioral needs while minimizing iatrogenic complications. The physical plant of a geriatric ED should similarly promote safety, comfort, mobility, memory cues, and sensorial perception for elders, according to the guidelines.
• Put in place readily available and easily accessed policies, procedures, and protocols that address the challenges involved in caring for geriatric patients in the ED.
These might address screening for risk of added needs assessment, consultation, and intervention, for example. The guidelines offer specific recommendations and tools for medication management, fall assessment, use of urinary catheters, addressing delirium and dementia, and providing palliative care.
The detailed recommendations provided for each of these topics represent research- and consensus-based best practices from the perspectives of the agencies involved in their development, the authors note.
"Improved attention to the needs of this challenging population has the opportunity to more effectively allocate health care resources, optimize admission and readmission rates, while simultaneously decreasing iatrogenic complications and the resultant increased length-of-stay and decreased reimbursement," they wrote, concluding that with implementation of the recommendations, "hospitals, regardless of size, will positively impact the care of the geriatric emergency patients."
New consensus-based guidelines aim to provide a standardized approach to improving the care of patients in geriatric emergency departments.
The Geriatric Emergency Department Guidelines are the result of a 2-year effort by representatives from the American College of Emergency Physicians, the American Geriatrics Society, the Society for Academic Emergency Medicine, and the Emergency Nurses Association. According to 2010 Census data, more than 40 million Americans are now over the age of 65 years. Further, the populations of adults aged 65 years and older and those aged 85 years and older are increasing at rates substantially greater than those of the general population.
"The subsequent increased need for health care for this burgeoning geriatric population represents an unprecedented and overwhelming challenge to the American health care system as a whole and to emergency departments [EDs] specifically," the authors state.
In response to this challenge, geriatric EDs are becoming increasingly common. The new guidelines address the special needs of the geriatric population, and propose methods for ensuring that those needs are met, as "the contemporary emergency medicine management model may not be adequate for geriatric adults."
"Similar programs designed for other age groups (pediatric) or directed toward specific diseases (STEMI [ST segment elevation myocardial infarction], stroke, and trauma) have improved care both in individual EDs and system wide, resulting in better, more cost-effective care and ultimately, better patient outcomes," the guideline writers note.
Among the topics addressed in detail in the guidelines are geriatric ED staffing, equipment, education, policies and procedures, follow-up care, and performance improvement measures.
According to the guidelines, an effective program will:
• Involve hospital site-specific staff and overall local coordination resources.
The guidelines spell out qualifications and responsibilities for the geriatric ED medical director, nurse manager, and staff physicians, nurses, specialists, and ancillary service providers.
• Decrease hospital admissions through effective follow-up and care transition plans.
The guidelines state that clinical patient information should be provided in a format best suited for elder adults and that department leaders should maintain relationships and resources in the community that can be used by patients to facilitate care following discharge.
• Include specialty-specific education and training of a multidisciplinary staff, with assessment for interdisciplinary core competencies.
Education should include "go-live" implementation sessions, as well as community awareness, involvement, and outreach, and regular educational assessment and implementation of site-specific educational needs.
• Assess quality, and implement an effective quality improvement program that involves collection and monitoring of relevant data.
The guidelines provide an explicit geriatric program quality-improvement plan designed to be conducive to staff education and program success.
• Utilize equipment designed for a patient population with specific needs.
For example, effective and comfortable evaluation requires equipment that takes into consideration issues of mobility, incontinence, and behavioral needs while minimizing iatrogenic complications. The physical plant of a geriatric ED should similarly promote safety, comfort, mobility, memory cues, and sensorial perception for elders, according to the guidelines.
• Put in place readily available and easily accessed policies, procedures, and protocols that address the challenges involved in caring for geriatric patients in the ED.
These might address screening for risk of added needs assessment, consultation, and intervention, for example. The guidelines offer specific recommendations and tools for medication management, fall assessment, use of urinary catheters, addressing delirium and dementia, and providing palliative care.
The detailed recommendations provided for each of these topics represent research- and consensus-based best practices from the perspectives of the agencies involved in their development, the authors note.
"Improved attention to the needs of this challenging population has the opportunity to more effectively allocate health care resources, optimize admission and readmission rates, while simultaneously decreasing iatrogenic complications and the resultant increased length-of-stay and decreased reimbursement," they wrote, concluding that with implementation of the recommendations, "hospitals, regardless of size, will positively impact the care of the geriatric emergency patients."
New consensus-based guidelines aim to provide a standardized approach to improving the care of patients in geriatric emergency departments.
The Geriatric Emergency Department Guidelines are the result of a 2-year effort by representatives from the American College of Emergency Physicians, the American Geriatrics Society, the Society for Academic Emergency Medicine, and the Emergency Nurses Association. According to 2010 Census data, more than 40 million Americans are now over the age of 65 years. Further, the populations of adults aged 65 years and older and those aged 85 years and older are increasing at rates substantially greater than those of the general population.
"The subsequent increased need for health care for this burgeoning geriatric population represents an unprecedented and overwhelming challenge to the American health care system as a whole and to emergency departments [EDs] specifically," the authors state.
In response to this challenge, geriatric EDs are becoming increasingly common. The new guidelines address the special needs of the geriatric population, and propose methods for ensuring that those needs are met, as "the contemporary emergency medicine management model may not be adequate for geriatric adults."
"Similar programs designed for other age groups (pediatric) or directed toward specific diseases (STEMI [ST segment elevation myocardial infarction], stroke, and trauma) have improved care both in individual EDs and system wide, resulting in better, more cost-effective care and ultimately, better patient outcomes," the guideline writers note.
Among the topics addressed in detail in the guidelines are geriatric ED staffing, equipment, education, policies and procedures, follow-up care, and performance improvement measures.
According to the guidelines, an effective program will:
• Involve hospital site-specific staff and overall local coordination resources.
The guidelines spell out qualifications and responsibilities for the geriatric ED medical director, nurse manager, and staff physicians, nurses, specialists, and ancillary service providers.
• Decrease hospital admissions through effective follow-up and care transition plans.
The guidelines state that clinical patient information should be provided in a format best suited for elder adults and that department leaders should maintain relationships and resources in the community that can be used by patients to facilitate care following discharge.
• Include specialty-specific education and training of a multidisciplinary staff, with assessment for interdisciplinary core competencies.
Education should include "go-live" implementation sessions, as well as community awareness, involvement, and outreach, and regular educational assessment and implementation of site-specific educational needs.
• Assess quality, and implement an effective quality improvement program that involves collection and monitoring of relevant data.
The guidelines provide an explicit geriatric program quality-improvement plan designed to be conducive to staff education and program success.
• Utilize equipment designed for a patient population with specific needs.
For example, effective and comfortable evaluation requires equipment that takes into consideration issues of mobility, incontinence, and behavioral needs while minimizing iatrogenic complications. The physical plant of a geriatric ED should similarly promote safety, comfort, mobility, memory cues, and sensorial perception for elders, according to the guidelines.
• Put in place readily available and easily accessed policies, procedures, and protocols that address the challenges involved in caring for geriatric patients in the ED.
These might address screening for risk of added needs assessment, consultation, and intervention, for example. The guidelines offer specific recommendations and tools for medication management, fall assessment, use of urinary catheters, addressing delirium and dementia, and providing palliative care.
The detailed recommendations provided for each of these topics represent research- and consensus-based best practices from the perspectives of the agencies involved in their development, the authors note.
"Improved attention to the needs of this challenging population has the opportunity to more effectively allocate health care resources, optimize admission and readmission rates, while simultaneously decreasing iatrogenic complications and the resultant increased length-of-stay and decreased reimbursement," they wrote, concluding that with implementation of the recommendations, "hospitals, regardless of size, will positively impact the care of the geriatric emergency patients."

Doctors seek to delay 2014 meaningful use deadlines
ORLANDO – Several dozen physician organizations are imploring the Department of Health and Human Services to slow down implementation of the meaningful use program for electronic health records, saying that the pace is overwhelming doctors’ ability to keep up.
The request comes as more than 35,500 attendees gather for the annual meeting of the Healthcare Information and Management Systems Society to learn more about government and private efforts to digitize the U.S. health care system.
In a letter to HHS Secretary Kathleen Sebelius, the physician groups said that doctors are struggling to make the investments needed to meet the federal targets. The groups want the government to give physicians through 2015 to transition to new EHR software and to meet stage 1 and 2 meaningful use requirements. They are also seeking more flexibility in how physicians meet those requirements.
Under the meaningful use program, eligible providers – physicians, nurse practitioners, and physician assistants who meet specific criteria – can receive incentive payments from Medicare and Medicaid. In 2014, the Medicare payment can be up to $23,520.

Centers for Medicare & Medicaid Services (CMS) officials at the HIMSS meeting said that 267,029 eligible providers have received Medicare incentive payments and 142,801 have received Medicaid payments since the program began in 2011, amounting to some $21 billion in payouts.
Providers will be penalized in 2015 if they do not sign up to be a meaningful user by March 31, said Elizabeth Holland, director of the HIT initiatives group at the CMS Office of E-Health Standards and Services. That date was recently extended by a month. Doctors who have never participated in the meaningful use program have until Oct. 1 to sign up to avoid penalties next year, and many physicians may be eligible for hardship exemptions that give them even more time to sign up, Ms. Holland said.
The physician groups still want more leeway. A big sticking point: Currently, eligible professionals have to adopt the 2014 Edition of Certified Electronic Health Record Technology (CEHRT) and also meet more stringent meaningful use standards by the end of the year. Most providers are still working with the last edition – the 2011 CEHRT. The Office of the National Coordinator for Health Information Technology (ONC) created the CEHRT program to guide providers to EHRs that contain all the elements necessary to achieve meaningful use. The 2014 edition supports stage 2 of meaningful use, which started this year.
"With only a fraction of 2011 Edition products currently certified to 2014 Edition standards, it is clear the pace and scope of change have outstripped the ability of vendors to support providers," according to the letter from the physician groups. If doctors can’t easily move on to the 2014 edition, they might "either abandon the possibility of meeting meaningful use criteria in 2014 or be forced to implement a system much more rapidly than would otherwise be the case."
While physicians worry about the 2014 edition, the ONC on Feb. 21 proposed to move forward again, spelling out standards for the 2015 edition of the CEHRT.
The ONC said that compliance with the 2015 edition would be voluntary – providers would not have to upgrade to be able to get incentive payments.
"This provides the opportunity for developers and health care providers to move to the 2015 Edition on their own terms and at their own pace," Dr. Karen DeSalvo, national coordinator for health IT, said in a statement.
The rule on the 2015 edition will be published in the Federal Register on Feb. 26, and the ONC will take comments at www.regulations.gov until April 28. The final rule will be published this summer.
On Twitter @aliciaault
ORLANDO – Several dozen physician organizations are imploring the Department of Health and Human Services to slow down implementation of the meaningful use program for electronic health records, saying that the pace is overwhelming doctors’ ability to keep up.
The request comes as more than 35,500 attendees gather for the annual meeting of the Healthcare Information and Management Systems Society to learn more about government and private efforts to digitize the U.S. health care system.
In a letter to HHS Secretary Kathleen Sebelius, the physician groups said that doctors are struggling to make the investments needed to meet the federal targets. The groups want the government to give physicians through 2015 to transition to new EHR software and to meet stage 1 and 2 meaningful use requirements. They are also seeking more flexibility in how physicians meet those requirements.
Under the meaningful use program, eligible providers – physicians, nurse practitioners, and physician assistants who meet specific criteria – can receive incentive payments from Medicare and Medicaid. In 2014, the Medicare payment can be up to $23,520.
Centers for Medicare & Medicaid Services (CMS) officials at the HIMSS meeting said that 267,029 eligible providers have received Medicare incentive payments and 142,801 have received Medicaid payments since the program began in 2011, amounting to some $21 billion in payouts.
Providers will be penalized in 2015 if they do not sign up to be a meaningful user by March 31, said Elizabeth Holland, director of the HIT initiatives group at the CMS Office of E-Health Standards and Services. That date was recently extended by a month. Doctors who have never participated in the meaningful use program have until Oct. 1 to sign up to avoid penalties next year, and many physicians may be eligible for hardship exemptions that give them even more time to sign up, Ms. Holland said.
The physician groups still want more leeway. A big sticking point: Currently, eligible professionals have to adopt the 2014 Edition of Certified Electronic Health Record Technology (CEHRT) and also meet more stringent meaningful use standards by the end of the year. Most providers are still working with the last edition – the 2011 CEHRT. The Office of the National Coordinator for Health Information Technology (ONC) created the CEHRT program to guide providers to EHRs that contain all the elements necessary to achieve meaningful use. The 2014 edition supports stage 2 of meaningful use, which started this year.
"With only a fraction of 2011 Edition products currently certified to 2014 Edition standards, it is clear the pace and scope of change have outstripped the ability of vendors to support providers," according to the letter from the physician groups. If doctors can’t easily move on to the 2014 edition, they might "either abandon the possibility of meeting meaningful use criteria in 2014 or be forced to implement a system much more rapidly than would otherwise be the case."
While physicians worry about the 2014 edition, the ONC on Feb. 21 proposed to move forward again, spelling out standards for the 2015 edition of the CEHRT.
The ONC said that compliance with the 2015 edition would be voluntary – providers would not have to upgrade to be able to get incentive payments.
"This provides the opportunity for developers and health care providers to move to the 2015 Edition on their own terms and at their own pace," Dr. Karen DeSalvo, national coordinator for health IT, said in a statement.
The rule on the 2015 edition will be published in the Federal Register on Feb. 26, and the ONC will take comments at www.regulations.gov until April 28. The final rule will be published this summer.
On Twitter @aliciaault
ORLANDO – Several dozen physician organizations are imploring the Department of Health and Human Services to slow down implementation of the meaningful use program for electronic health records, saying that the pace is overwhelming doctors’ ability to keep up.
The request comes as more than 35,500 attendees gather for the annual meeting of the Healthcare Information and Management Systems Society to learn more about government and private efforts to digitize the U.S. health care system.
In a letter to HHS Secretary Kathleen Sebelius, the physician groups said that doctors are struggling to make the investments needed to meet the federal targets. The groups want the government to give physicians through 2015 to transition to new EHR software and to meet stage 1 and 2 meaningful use requirements. They are also seeking more flexibility in how physicians meet those requirements.
Under the meaningful use program, eligible providers – physicians, nurse practitioners, and physician assistants who meet specific criteria – can receive incentive payments from Medicare and Medicaid. In 2014, the Medicare payment can be up to $23,520.
Centers for Medicare & Medicaid Services (CMS) officials at the HIMSS meeting said that 267,029 eligible providers have received Medicare incentive payments and 142,801 have received Medicaid payments since the program began in 2011, amounting to some $21 billion in payouts.
Providers will be penalized in 2015 if they do not sign up to be a meaningful user by March 31, said Elizabeth Holland, director of the HIT initiatives group at the CMS Office of E-Health Standards and Services. That date was recently extended by a month. Doctors who have never participated in the meaningful use program have until Oct. 1 to sign up to avoid penalties next year, and many physicians may be eligible for hardship exemptions that give them even more time to sign up, Ms. Holland said.
The physician groups still want more leeway. A big sticking point: Currently, eligible professionals have to adopt the 2014 Edition of Certified Electronic Health Record Technology (CEHRT) and also meet more stringent meaningful use standards by the end of the year. Most providers are still working with the last edition – the 2011 CEHRT. The Office of the National Coordinator for Health Information Technology (ONC) created the CEHRT program to guide providers to EHRs that contain all the elements necessary to achieve meaningful use. The 2014 edition supports stage 2 of meaningful use, which started this year.
"With only a fraction of 2011 Edition products currently certified to 2014 Edition standards, it is clear the pace and scope of change have outstripped the ability of vendors to support providers," according to the letter from the physician groups. If doctors can’t easily move on to the 2014 edition, they might "either abandon the possibility of meeting meaningful use criteria in 2014 or be forced to implement a system much more rapidly than would otherwise be the case."
While physicians worry about the 2014 edition, the ONC on Feb. 21 proposed to move forward again, spelling out standards for the 2015 edition of the CEHRT.
The ONC said that compliance with the 2015 edition would be voluntary – providers would not have to upgrade to be able to get incentive payments.
"This provides the opportunity for developers and health care providers to move to the 2015 Edition on their own terms and at their own pace," Dr. Karen DeSalvo, national coordinator for health IT, said in a statement.
The rule on the 2015 edition will be published in the Federal Register on Feb. 26, and the ONC will take comments at www.regulations.gov until April 28. The final rule will be published this summer.
On Twitter @aliciaault
AT HIMSS14

Physician Compare site adds quality scores
Physician Compare, Medicare’s online portal for checking on physician qualifications, has added quality scores for physicians in some group practices and Accountable Care Organizations.
The site now displays how a group of physicians has performed on five quality indicators related to management of diabetes and heart disease.
The website will display the ratings using stars, as well as the actual percentage score on the measure.
"This is an important first step in publicly reporting quality measures on Physician Compare," Dr. Patrick Conway, chief medical officer and deputy administrator for innovation and quality at the Centers for Medicare and Medicaid Services, said in a statement. "Offering a strong set of meaningful quality measures on the site will ultimately help consumers make decisions and it will encourage quality improvement among the clinician community, who shares CMS’s strong commitment to the best possible patient care."
The Physician Compare site, which was created under the Affordable Care Act, already displays the specialties offered by physicians, their board certification, and hospital affiliations. It also displays whether physicians participate in Medicare quality programs such as the Physician Quality Reporting System, the Electronic Prescribing Incentive Program, and the Electronic Health Records Incentive Program.
The information comes primarily from the Provider, Enrollment, Chain, and Ownership System (PECOS) and is checked against Medicare claims data. The site includes information on physicians enrolled in the Medicare program only.
This year, CMS is posting quality data from 66 group practices and 141 ACOs. The data is reported at the group practice and ACO level.
The quality measures include:
• Controlling hemoglobin A1c in patients with diabetes.
• Controlling blood pressure in patients with diabetes.
• Prescribing aspirin to patients with diabetes and heart disease.
• Reporting the number of diabetic patients who do not use tobacco.
• Prescribing medicine to improve the pumping action of the heart in patients who have both heart disease and certain other conditions.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
Physician Compare, Medicare’s online portal for checking on physician qualifications, has added quality scores for physicians in some group practices and Accountable Care Organizations.
The site now displays how a group of physicians has performed on five quality indicators related to management of diabetes and heart disease.
The website will display the ratings using stars, as well as the actual percentage score on the measure.
"This is an important first step in publicly reporting quality measures on Physician Compare," Dr. Patrick Conway, chief medical officer and deputy administrator for innovation and quality at the Centers for Medicare and Medicaid Services, said in a statement. "Offering a strong set of meaningful quality measures on the site will ultimately help consumers make decisions and it will encourage quality improvement among the clinician community, who shares CMS’s strong commitment to the best possible patient care."
The Physician Compare site, which was created under the Affordable Care Act, already displays the specialties offered by physicians, their board certification, and hospital affiliations. It also displays whether physicians participate in Medicare quality programs such as the Physician Quality Reporting System, the Electronic Prescribing Incentive Program, and the Electronic Health Records Incentive Program.
The information comes primarily from the Provider, Enrollment, Chain, and Ownership System (PECOS) and is checked against Medicare claims data. The site includes information on physicians enrolled in the Medicare program only.
This year, CMS is posting quality data from 66 group practices and 141 ACOs. The data is reported at the group practice and ACO level.
The quality measures include:
• Controlling hemoglobin A1c in patients with diabetes.
• Controlling blood pressure in patients with diabetes.
• Prescribing aspirin to patients with diabetes and heart disease.
• Reporting the number of diabetic patients who do not use tobacco.
• Prescribing medicine to improve the pumping action of the heart in patients who have both heart disease and certain other conditions.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
Physician Compare, Medicare’s online portal for checking on physician qualifications, has added quality scores for physicians in some group practices and Accountable Care Organizations.
The site now displays how a group of physicians has performed on five quality indicators related to management of diabetes and heart disease.
The website will display the ratings using stars, as well as the actual percentage score on the measure.
"This is an important first step in publicly reporting quality measures on Physician Compare," Dr. Patrick Conway, chief medical officer and deputy administrator for innovation and quality at the Centers for Medicare and Medicaid Services, said in a statement. "Offering a strong set of meaningful quality measures on the site will ultimately help consumers make decisions and it will encourage quality improvement among the clinician community, who shares CMS’s strong commitment to the best possible patient care."
The Physician Compare site, which was created under the Affordable Care Act, already displays the specialties offered by physicians, their board certification, and hospital affiliations. It also displays whether physicians participate in Medicare quality programs such as the Physician Quality Reporting System, the Electronic Prescribing Incentive Program, and the Electronic Health Records Incentive Program.
The information comes primarily from the Provider, Enrollment, Chain, and Ownership System (PECOS) and is checked against Medicare claims data. The site includes information on physicians enrolled in the Medicare program only.
This year, CMS is posting quality data from 66 group practices and 141 ACOs. The data is reported at the group practice and ACO level.
The quality measures include:
• Controlling hemoglobin A1c in patients with diabetes.
• Controlling blood pressure in patients with diabetes.
• Prescribing aspirin to patients with diabetes and heart disease.
• Reporting the number of diabetic patients who do not use tobacco.
• Prescribing medicine to improve the pumping action of the heart in patients who have both heart disease and certain other conditions.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
ICD-10: CMS to hold end-to-end testing
To address concerns about the upcoming transition to ICD-10, the Centers for Medicare and Medicaid Services announced Feb. 20 that it would conduct full end-to-end testing this summer.
End-to-end testing will allow selected physicians, health care providers, hospitals, clearing houses, and billing agents to submit claims with ICD-10 codes, have those claims processed, and receive accurate remittance advice regarding payment.

The test will be conducted by a statistically significant sample of providers gleaned from a pool of volunteers, CMS officials said during a webinar on ICD-10.
Providers can apply to participate through one of the 16 Medicare Administrative Contractors (MACs) in March; the agency will announce those selected sometime in April. More details will be available on the CMS ICD-10 website in a few weeks, CMS officials said.
Physician groups have sought such thorough testing and heralded the CMS announcement.
"The AMA believes end-to-end testing is essential for ensuring the health care industry will not suffer massive disruptions in claims and payment processing and ultimately risk physicians’ ability to care for their patients," said Dr. Ardis Dee Hoven, president of the American Medical Association, in a statement. "The AMA urges CMS to conduct the testing as soon as possible and to ensure that there is an adequate sample which includes a variety of different-sized medical practices and specialties."
The Medical Group Management Association also supports end-to-end testing, according to Dr. Susan Turney, president and CEO. However, the MGMA would like to see the CMS expand the scope of the testing "to include any provider who wishes to test with them," Dr. Turney said in a statement. That would minimize the possibility of "potential operational problems similar to what was experienced with the rollout of healthcare.gov," and "help to decrease the potential of catastrophic cash flow disruption that could impact the ability of practices to treat patients."
The AMA said that it continues to seek a delay in the Oct. 1 implementation of the new coding set, but CMS officials said that would not happen.
"I want to make really clear that the Oct. 1, 2014, date is firm," said Robert Tagalicod, director of the Office of eHealth Standards and Services at the CMS. "If you are a medical practice and haven’t talked with your vendors, clearing houses, and payers, now is the time to act."
CMS officials also noted that acknowledgment testing for interested providers starts soon. The first official period will be March 3-7. The test will let physicians determine whether their ICD-10 coded claims would be accepted or rejected. The claims will not be adjudicated. Doctors can apply through their MAC website for the testing; so far, some 2,500 have signed up for the March dates.
The agency will offer more official test periods, and will provide information on those soon, officials said. Physicians also can request unofficial testing with their MAC any time between March and October. The results of those tests won’t be included as part of the CMS’s official statistics.
Denesecia Green, of the CMS Office of eHealth Standards and Services, said that the agency wanted to reach out more to small physician practices. The agency is collaborating with state medical societies and national physician organizations to do so.
She also said that the CMS offers specific training for physician offices, and free billing software. More information about those programs can be found on the ICD-10 website.
Both the AMA and the MGMA also provide tools to help physicians make the transition.
But, Dr. Hoven said, although adopting the new code set "may provide benefits to others in the health care system, [it] is unlikely to improve the care physicians provide their patients and takes valuable resources away from implementing delivery reforms and health information technology."
On Twitter @aliciaault
To address concerns about the upcoming transition to ICD-10, the Centers for Medicare and Medicaid Services announced Feb. 20 that it would conduct full end-to-end testing this summer.
End-to-end testing will allow selected physicians, health care providers, hospitals, clearing houses, and billing agents to submit claims with ICD-10 codes, have those claims processed, and receive accurate remittance advice regarding payment.
The test will be conducted by a statistically significant sample of providers gleaned from a pool of volunteers, CMS officials said during a webinar on ICD-10.
Providers can apply to participate through one of the 16 Medicare Administrative Contractors (MACs) in March; the agency will announce those selected sometime in April. More details will be available on the CMS ICD-10 website in a few weeks, CMS officials said.
Physician groups have sought such thorough testing and heralded the CMS announcement.
"The AMA believes end-to-end testing is essential for ensuring the health care industry will not suffer massive disruptions in claims and payment processing and ultimately risk physicians’ ability to care for their patients," said Dr. Ardis Dee Hoven, president of the American Medical Association, in a statement. "The AMA urges CMS to conduct the testing as soon as possible and to ensure that there is an adequate sample which includes a variety of different-sized medical practices and specialties."
The Medical Group Management Association also supports end-to-end testing, according to Dr. Susan Turney, president and CEO. However, the MGMA would like to see the CMS expand the scope of the testing "to include any provider who wishes to test with them," Dr. Turney said in a statement. That would minimize the possibility of "potential operational problems similar to what was experienced with the rollout of healthcare.gov," and "help to decrease the potential of catastrophic cash flow disruption that could impact the ability of practices to treat patients."
The AMA said that it continues to seek a delay in the Oct. 1 implementation of the new coding set, but CMS officials said that would not happen.
"I want to make really clear that the Oct. 1, 2014, date is firm," said Robert Tagalicod, director of the Office of eHealth Standards and Services at the CMS. "If you are a medical practice and haven’t talked with your vendors, clearing houses, and payers, now is the time to act."
CMS officials also noted that acknowledgment testing for interested providers starts soon. The first official period will be March 3-7. The test will let physicians determine whether their ICD-10 coded claims would be accepted or rejected. The claims will not be adjudicated. Doctors can apply through their MAC website for the testing; so far, some 2,500 have signed up for the March dates.
The agency will offer more official test periods, and will provide information on those soon, officials said. Physicians also can request unofficial testing with their MAC any time between March and October. The results of those tests won’t be included as part of the CMS’s official statistics.
Denesecia Green, of the CMS Office of eHealth Standards and Services, said that the agency wanted to reach out more to small physician practices. The agency is collaborating with state medical societies and national physician organizations to do so.
She also said that the CMS offers specific training for physician offices, and free billing software. More information about those programs can be found on the ICD-10 website.
Both the AMA and the MGMA also provide tools to help physicians make the transition.
But, Dr. Hoven said, although adopting the new code set "may provide benefits to others in the health care system, [it] is unlikely to improve the care physicians provide their patients and takes valuable resources away from implementing delivery reforms and health information technology."
On Twitter @aliciaault
To address concerns about the upcoming transition to ICD-10, the Centers for Medicare and Medicaid Services announced Feb. 20 that it would conduct full end-to-end testing this summer.
End-to-end testing will allow selected physicians, health care providers, hospitals, clearing houses, and billing agents to submit claims with ICD-10 codes, have those claims processed, and receive accurate remittance advice regarding payment.
The test will be conducted by a statistically significant sample of providers gleaned from a pool of volunteers, CMS officials said during a webinar on ICD-10.
Providers can apply to participate through one of the 16 Medicare Administrative Contractors (MACs) in March; the agency will announce those selected sometime in April. More details will be available on the CMS ICD-10 website in a few weeks, CMS officials said.
Physician groups have sought such thorough testing and heralded the CMS announcement.
"The AMA believes end-to-end testing is essential for ensuring the health care industry will not suffer massive disruptions in claims and payment processing and ultimately risk physicians’ ability to care for their patients," said Dr. Ardis Dee Hoven, president of the American Medical Association, in a statement. "The AMA urges CMS to conduct the testing as soon as possible and to ensure that there is an adequate sample which includes a variety of different-sized medical practices and specialties."
The Medical Group Management Association also supports end-to-end testing, according to Dr. Susan Turney, president and CEO. However, the MGMA would like to see the CMS expand the scope of the testing "to include any provider who wishes to test with them," Dr. Turney said in a statement. That would minimize the possibility of "potential operational problems similar to what was experienced with the rollout of healthcare.gov," and "help to decrease the potential of catastrophic cash flow disruption that could impact the ability of practices to treat patients."
The AMA said that it continues to seek a delay in the Oct. 1 implementation of the new coding set, but CMS officials said that would not happen.
"I want to make really clear that the Oct. 1, 2014, date is firm," said Robert Tagalicod, director of the Office of eHealth Standards and Services at the CMS. "If you are a medical practice and haven’t talked with your vendors, clearing houses, and payers, now is the time to act."
CMS officials also noted that acknowledgment testing for interested providers starts soon. The first official period will be March 3-7. The test will let physicians determine whether their ICD-10 coded claims would be accepted or rejected. The claims will not be adjudicated. Doctors can apply through their MAC website for the testing; so far, some 2,500 have signed up for the March dates.
The agency will offer more official test periods, and will provide information on those soon, officials said. Physicians also can request unofficial testing with their MAC any time between March and October. The results of those tests won’t be included as part of the CMS’s official statistics.
Denesecia Green, of the CMS Office of eHealth Standards and Services, said that the agency wanted to reach out more to small physician practices. The agency is collaborating with state medical societies and national physician organizations to do so.
She also said that the CMS offers specific training for physician offices, and free billing software. More information about those programs can be found on the ICD-10 website.
Both the AMA and the MGMA also provide tools to help physicians make the transition.
But, Dr. Hoven said, although adopting the new code set "may provide benefits to others in the health care system, [it] is unlikely to improve the care physicians provide their patients and takes valuable resources away from implementing delivery reforms and health information technology."
On Twitter @aliciaault
FROM A CMS WEBINAR ON ICD-10

ACA hassles, payment cuts are top reasons physicians sell practices
When a hospital approached Georgia surgeon Ian Hamilton Jr. about buying his vascular surgery practice, the proposal was too appealing for him to turn down. At the time, Dr. Hamilton’s practice was facing the challenges of meeting new regulatory and business requirements, including the need for a new electronic health record system that would meet meaningful use requirements.
"I didn’t feel that I was going to be able to maintain a solo practice indefinitely," said Dr. Hamilton, who sold his practice in 2013. "I felt something was going to have to change. The reality of what’s happening in American medicine right now makes it very difficult for a solo practitioner at many different levels. It’s become very expensive to be compliant with the Affordable Care Act and the other regulations that are associated with it."
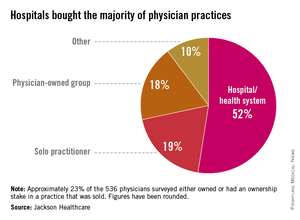
Dr. Hamilton is far from alone in closing up shop because of a more complex and changing health care landscape. Thirty-two percent of physicians who sold their practice within the past 3 years cited the complexities of the ACA as a primary motivator for the sale, according to a nationwide survey by Jackson Healthcare, a health care staffing firm. Of physicians who sold their practices more than 3 years ago, 10% said the law was a factor, according to the survey.
A second survey by Jackson Healthcare found 60% of practice acquisitions by hospitals in 2013 were initiated by the sellers.
"The practice of medicine has increasingly become more complex," said Sheri Sorrell, director of market research for Jackson Healthcare. This includes "getting reimbursement and the amount of paperwork and the amount of regulations [doctors] have to deal with. They can’t keep up with all the regulations. At least if they are selling to a hospital, the hospital has those resources" to comply.
Budding and completed practice acquisitions varied by specialty, the survey found. Nearly 25% of physicians actively seeking to sell their practices described themselves as internal medicine subspecialists, 14% as primary care physicians, and 12% as surgeons. Of the internal medicine subspecialists seeking to sell, 23% described themselves as otolaryngologists, 17% as urologists, and 13% as cardiologists, the survey found.
Hospitals are keen to acquire primary care practices, the second survey found. Family medicine practices made up 58% of practices acquired by hospitals in 2013, while internal medicine made up 40%.
Cardiology practices also are being acquired as physicians seek to avoid significant reimbursement gaps, Dallas health law attorney Cheryl Camin Murray said. Ms. Murray is a shareholder in the health care industry group and corporate securities/mergers and acquisitions practice group of Texas law firm Winstead PC. Hospitals are paid at a higher rate by Medicare than cardiology practices for the same procedures, Ms. Murray said.
While physicians who sell their practices face their share of challenges, the Jackson Healthcare survey found that the majority of doctors who sold are happy with their decision. Fifty-five percent of physicians who sold said they do not miss private practice, and 60% said they are satisfied or very satisfied. Overall, 76% of physician sellers said they would make the same choice again.
One of those physicians is Dr. Hamilton. In the end, he chose not to become an employee of the hospital he sold his practice to, and he is job hunting for nonclinical positions. The sale came at the right time in his practice and career, Dr. Hamilton said.
"For me it was a very good decision," he said. "I’m very happy I was able to get the equity out of my practice that I built over 11 years. For me it was a very timely and very wonderful opportunity."
Data in the first survey were collected from 536 physicians across the United States who responded to a survey about practice acquisitions in 2013. The second survey analyzed responses from 123 hospital executives who had completed acquisitions in 2013 or had acquisitions planned for 2014.
When a hospital approached Georgia surgeon Ian Hamilton Jr. about buying his vascular surgery practice, the proposal was too appealing for him to turn down. At the time, Dr. Hamilton’s practice was facing the challenges of meeting new regulatory and business requirements, including the need for a new electronic health record system that would meet meaningful use requirements.
"I didn’t feel that I was going to be able to maintain a solo practice indefinitely," said Dr. Hamilton, who sold his practice in 2013. "I felt something was going to have to change. The reality of what’s happening in American medicine right now makes it very difficult for a solo practitioner at many different levels. It’s become very expensive to be compliant with the Affordable Care Act and the other regulations that are associated with it."
Dr. Hamilton is far from alone in closing up shop because of a more complex and changing health care landscape. Thirty-two percent of physicians who sold their practice within the past 3 years cited the complexities of the ACA as a primary motivator for the sale, according to a nationwide survey by Jackson Healthcare, a health care staffing firm. Of physicians who sold their practices more than 3 years ago, 10% said the law was a factor, according to the survey.
A second survey by Jackson Healthcare found 60% of practice acquisitions by hospitals in 2013 were initiated by the sellers.
"The practice of medicine has increasingly become more complex," said Sheri Sorrell, director of market research for Jackson Healthcare. This includes "getting reimbursement and the amount of paperwork and the amount of regulations [doctors] have to deal with. They can’t keep up with all the regulations. At least if they are selling to a hospital, the hospital has those resources" to comply.
Budding and completed practice acquisitions varied by specialty, the survey found. Nearly 25% of physicians actively seeking to sell their practices described themselves as internal medicine subspecialists, 14% as primary care physicians, and 12% as surgeons. Of the internal medicine subspecialists seeking to sell, 23% described themselves as otolaryngologists, 17% as urologists, and 13% as cardiologists, the survey found.
Hospitals are keen to acquire primary care practices, the second survey found. Family medicine practices made up 58% of practices acquired by hospitals in 2013, while internal medicine made up 40%.
Cardiology practices also are being acquired as physicians seek to avoid significant reimbursement gaps, Dallas health law attorney Cheryl Camin Murray said. Ms. Murray is a shareholder in the health care industry group and corporate securities/mergers and acquisitions practice group of Texas law firm Winstead PC. Hospitals are paid at a higher rate by Medicare than cardiology practices for the same procedures, Ms. Murray said.
While physicians who sell their practices face their share of challenges, the Jackson Healthcare survey found that the majority of doctors who sold are happy with their decision. Fifty-five percent of physicians who sold said they do not miss private practice, and 60% said they are satisfied or very satisfied. Overall, 76% of physician sellers said they would make the same choice again.
One of those physicians is Dr. Hamilton. In the end, he chose not to become an employee of the hospital he sold his practice to, and he is job hunting for nonclinical positions. The sale came at the right time in his practice and career, Dr. Hamilton said.
"For me it was a very good decision," he said. "I’m very happy I was able to get the equity out of my practice that I built over 11 years. For me it was a very timely and very wonderful opportunity."
Data in the first survey were collected from 536 physicians across the United States who responded to a survey about practice acquisitions in 2013. The second survey analyzed responses from 123 hospital executives who had completed acquisitions in 2013 or had acquisitions planned for 2014.
When a hospital approached Georgia surgeon Ian Hamilton Jr. about buying his vascular surgery practice, the proposal was too appealing for him to turn down. At the time, Dr. Hamilton’s practice was facing the challenges of meeting new regulatory and business requirements, including the need for a new electronic health record system that would meet meaningful use requirements.
"I didn’t feel that I was going to be able to maintain a solo practice indefinitely," said Dr. Hamilton, who sold his practice in 2013. "I felt something was going to have to change. The reality of what’s happening in American medicine right now makes it very difficult for a solo practitioner at many different levels. It’s become very expensive to be compliant with the Affordable Care Act and the other regulations that are associated with it."
Dr. Hamilton is far from alone in closing up shop because of a more complex and changing health care landscape. Thirty-two percent of physicians who sold their practice within the past 3 years cited the complexities of the ACA as a primary motivator for the sale, according to a nationwide survey by Jackson Healthcare, a health care staffing firm. Of physicians who sold their practices more than 3 years ago, 10% said the law was a factor, according to the survey.
A second survey by Jackson Healthcare found 60% of practice acquisitions by hospitals in 2013 were initiated by the sellers.
"The practice of medicine has increasingly become more complex," said Sheri Sorrell, director of market research for Jackson Healthcare. This includes "getting reimbursement and the amount of paperwork and the amount of regulations [doctors] have to deal with. They can’t keep up with all the regulations. At least if they are selling to a hospital, the hospital has those resources" to comply.
Budding and completed practice acquisitions varied by specialty, the survey found. Nearly 25% of physicians actively seeking to sell their practices described themselves as internal medicine subspecialists, 14% as primary care physicians, and 12% as surgeons. Of the internal medicine subspecialists seeking to sell, 23% described themselves as otolaryngologists, 17% as urologists, and 13% as cardiologists, the survey found.
Hospitals are keen to acquire primary care practices, the second survey found. Family medicine practices made up 58% of practices acquired by hospitals in 2013, while internal medicine made up 40%.
Cardiology practices also are being acquired as physicians seek to avoid significant reimbursement gaps, Dallas health law attorney Cheryl Camin Murray said. Ms. Murray is a shareholder in the health care industry group and corporate securities/mergers and acquisitions practice group of Texas law firm Winstead PC. Hospitals are paid at a higher rate by Medicare than cardiology practices for the same procedures, Ms. Murray said.
While physicians who sell their practices face their share of challenges, the Jackson Healthcare survey found that the majority of doctors who sold are happy with their decision. Fifty-five percent of physicians who sold said they do not miss private practice, and 60% said they are satisfied or very satisfied. Overall, 76% of physician sellers said they would make the same choice again.
One of those physicians is Dr. Hamilton. In the end, he chose not to become an employee of the hospital he sold his practice to, and he is job hunting for nonclinical positions. The sale came at the right time in his practice and career, Dr. Hamilton said.
"For me it was a very good decision," he said. "I’m very happy I was able to get the equity out of my practice that I built over 11 years. For me it was a very timely and very wonderful opportunity."
Data in the first survey were collected from 536 physicians across the United States who responded to a survey about practice acquisitions in 2013. The second survey analyzed responses from 123 hospital executives who had completed acquisitions in 2013 or had acquisitions planned for 2014.