User login
Swamp coolers not linked to dust mite sensitization in atopic children
ORLANDO – Swamp coolers – a low-cost alternative to air-conditioning in dry regions – weren’t found to increase sensitization to house dust mites or mold in atopic pediatric patients, researchers reported.
Neema Izadi, MD, and his associates say the findings, seen in a pediatric Colorado population in a study evaluating data over 10 years, could mean that not everyone at risk of dust mite and mold sensitization needs to avoid these cooling systems.

“Evaporative coolers have been shown to raise relative humidity by about 10%,” said Dr. Izadi, a pediatric allergy and immunology fellow at National Jewish Health, Denver, presenting at the joint congress of the American Academy of Asthma, Allergy and Immunology and the World Asthma Organization. “They work best in environments where the air is very warm and dry.”
House dust mites and mold thrive in higher humidity. Small studies performed in Colorado, Utah, and other locations have shown that the swamp coolers increase house dust mite allergen content, but there have been very few studies that have looked at actual sensitization. One smaller study in Nevada did find that the coolers increased sensitization to dust mites and mold.
In this study – thought to be the largest ever to look at this question – Dr. Izadi and his colleagues assessed data on patients aged 21 years and younger who were seen at National Jewish Health during 2008-2017 and who had at least one positive environmental skin-prick test. The average age was about 9 years. The cohort included 8,503 patients with sensitization to house dust mites and 9,286 with sensitization to mold. Researchers examined data on swamp coolers in their homes.
The researchers found that 29% of those with swamp coolers were dust-mite positive on skin testing, and 28% of those without one were positive. This was not a significant difference (P = .85). They found that 45% of those with the coolers were positive for sensitization to any mold, compared with 44% without one – also not a significant difference (P = .43).
They also found no difference according to age group, sex, or individually for atopic dermatitis, asthma, or allergic rhinitis.
He acknowledged that the study had no way to reliably account for patients who were transplants to Colorado, having moved there from somewhere else. The study also didn’t examine the age of homes, whether it had carpeting, or other factors.
He noted that the amount of time the coolers were run in the home was not examined and that “it might matter how much it is on.” This, he said, might account for differences in these results, compared with the Nevada study that did find a sensitization increase cause by the coolers.
“Evaporative coolers or swamp coolers are a great low-cost alternative in semiarid and arid environments – they can cut costs from 15%-35%,” Dr. Izadi said. “These data may indicate that it may be unnecessary to recommend that patients remove their swamp cooler, at least from a dust-mite and mold-sensitization standpoint.”
Dr. Izadi had no relevant financial disclosures.
SOURCE: Izadi N et al. AAAAI/WAO Joint Congress, Abstract 586

Susan Millard, MD, FCCP, comments: Swamp coolers are used in semi-arid and arid climates like Arizona, where I did my fellowship training but they didn't work well to keep apartments and homes cool enough if over about 100°F outside! The system is cheaper than air conditioning. So it is great to know that this type of cooling system does not cause more mold and dust mite allergies.
Susan Millard, MD, FCCP, comments: Swamp coolers are used in semi-arid and arid climates like Arizona, where I did my fellowship training but they didn't work well to keep apartments and homes cool enough if over about 100°F outside! The system is cheaper than air conditioning. So it is great to know that this type of cooling system does not cause more mold and dust mite allergies.
Susan Millard, MD, FCCP, comments: Swamp coolers are used in semi-arid and arid climates like Arizona, where I did my fellowship training but they didn't work well to keep apartments and homes cool enough if over about 100°F outside! The system is cheaper than air conditioning. So it is great to know that this type of cooling system does not cause more mold and dust mite allergies.
ORLANDO – Swamp coolers – a low-cost alternative to air-conditioning in dry regions – weren’t found to increase sensitization to house dust mites or mold in atopic pediatric patients, researchers reported.
Neema Izadi, MD, and his associates say the findings, seen in a pediatric Colorado population in a study evaluating data over 10 years, could mean that not everyone at risk of dust mite and mold sensitization needs to avoid these cooling systems.
“Evaporative coolers have been shown to raise relative humidity by about 10%,” said Dr. Izadi, a pediatric allergy and immunology fellow at National Jewish Health, Denver, presenting at the joint congress of the American Academy of Asthma, Allergy and Immunology and the World Asthma Organization. “They work best in environments where the air is very warm and dry.”
House dust mites and mold thrive in higher humidity. Small studies performed in Colorado, Utah, and other locations have shown that the swamp coolers increase house dust mite allergen content, but there have been very few studies that have looked at actual sensitization. One smaller study in Nevada did find that the coolers increased sensitization to dust mites and mold.
In this study – thought to be the largest ever to look at this question – Dr. Izadi and his colleagues assessed data on patients aged 21 years and younger who were seen at National Jewish Health during 2008-2017 and who had at least one positive environmental skin-prick test. The average age was about 9 years. The cohort included 8,503 patients with sensitization to house dust mites and 9,286 with sensitization to mold. Researchers examined data on swamp coolers in their homes.
The researchers found that 29% of those with swamp coolers were dust-mite positive on skin testing, and 28% of those without one were positive. This was not a significant difference (P = .85). They found that 45% of those with the coolers were positive for sensitization to any mold, compared with 44% without one – also not a significant difference (P = .43).
They also found no difference according to age group, sex, or individually for atopic dermatitis, asthma, or allergic rhinitis.
He acknowledged that the study had no way to reliably account for patients who were transplants to Colorado, having moved there from somewhere else. The study also didn’t examine the age of homes, whether it had carpeting, or other factors.
He noted that the amount of time the coolers were run in the home was not examined and that “it might matter how much it is on.” This, he said, might account for differences in these results, compared with the Nevada study that did find a sensitization increase cause by the coolers.
“Evaporative coolers or swamp coolers are a great low-cost alternative in semiarid and arid environments – they can cut costs from 15%-35%,” Dr. Izadi said. “These data may indicate that it may be unnecessary to recommend that patients remove their swamp cooler, at least from a dust-mite and mold-sensitization standpoint.”
Dr. Izadi had no relevant financial disclosures.
SOURCE: Izadi N et al. AAAAI/WAO Joint Congress, Abstract 586
ORLANDO – Swamp coolers – a low-cost alternative to air-conditioning in dry regions – weren’t found to increase sensitization to house dust mites or mold in atopic pediatric patients, researchers reported.
Neema Izadi, MD, and his associates say the findings, seen in a pediatric Colorado population in a study evaluating data over 10 years, could mean that not everyone at risk of dust mite and mold sensitization needs to avoid these cooling systems.
“Evaporative coolers have been shown to raise relative humidity by about 10%,” said Dr. Izadi, a pediatric allergy and immunology fellow at National Jewish Health, Denver, presenting at the joint congress of the American Academy of Asthma, Allergy and Immunology and the World Asthma Organization. “They work best in environments where the air is very warm and dry.”
House dust mites and mold thrive in higher humidity. Small studies performed in Colorado, Utah, and other locations have shown that the swamp coolers increase house dust mite allergen content, but there have been very few studies that have looked at actual sensitization. One smaller study in Nevada did find that the coolers increased sensitization to dust mites and mold.
In this study – thought to be the largest ever to look at this question – Dr. Izadi and his colleagues assessed data on patients aged 21 years and younger who were seen at National Jewish Health during 2008-2017 and who had at least one positive environmental skin-prick test. The average age was about 9 years. The cohort included 8,503 patients with sensitization to house dust mites and 9,286 with sensitization to mold. Researchers examined data on swamp coolers in their homes.
The researchers found that 29% of those with swamp coolers were dust-mite positive on skin testing, and 28% of those without one were positive. This was not a significant difference (P = .85). They found that 45% of those with the coolers were positive for sensitization to any mold, compared with 44% without one – also not a significant difference (P = .43).
They also found no difference according to age group, sex, or individually for atopic dermatitis, asthma, or allergic rhinitis.
He acknowledged that the study had no way to reliably account for patients who were transplants to Colorado, having moved there from somewhere else. The study also didn’t examine the age of homes, whether it had carpeting, or other factors.
He noted that the amount of time the coolers were run in the home was not examined and that “it might matter how much it is on.” This, he said, might account for differences in these results, compared with the Nevada study that did find a sensitization increase cause by the coolers.
“Evaporative coolers or swamp coolers are a great low-cost alternative in semiarid and arid environments – they can cut costs from 15%-35%,” Dr. Izadi said. “These data may indicate that it may be unnecessary to recommend that patients remove their swamp cooler, at least from a dust-mite and mold-sensitization standpoint.”
Dr. Izadi had no relevant financial disclosures.
SOURCE: Izadi N et al. AAAAI/WAO Joint Congress, Abstract 586
REPORTING FROM AAAAI/WAO JOINT CONGRESS
Key clinical point:
Major finding: Researchers found that 29% of those with swamp coolers were dust-mite positive on skin testing, and 28% of those without one were as well. This was not a significant difference (P = .85).
Study details: A retrospective review of more than 17,000 cases of atopic children aged 21 years and younger who were seen at National Jewish Health and had a positive environmental skin prick test.
Disclosures: Dr. Izadi had no relevant financial disclosures.
Source: Izadi N et al. AAAAI/WAO Joint Congress, Abstract 586
Does Your Work Trigger Asthma?
As many as 1 in 5 asthma-related deaths in the US is due to occupational exposure—and many could be prevented, according to CDC researchers.
The researchers analyzed reports from 1999-2016 of asthma-related mortality and occupations of the people involved. Of 3,396 deaths (3,396 in 2015 alone), between 11% and 21% were due to occupational exposures. Health care workers and construction workers were at highest risk.
By industry, the highest number of deaths were among men working in construction (13%) and women in health care (14%). By occupation, the most deaths were among men construction trades workers (11%) and women office and administrative support workers (9%).
The researchers note that ongoing exposure to cleaners, disinfectants, and antibiotics, all can trigger asthma. But they also point out that steps can be successfully taken to limit the type of exposure that exacerbates asthma symptoms, such as replacing powdered latex gloves with powder-free natural rubber latex or nonlatex gloves.
In an interview with MD Magazine, principle investigator Jacek Mazurek, MD, PhD, said there’s also an opportunity for health care providers to intervene more effectively. “Inadequate screening of workers for occupational exposures by health providers and lack of recognition of associations between workplace exposures and asthma symptoms remain the main reasons for underrecognition and underdiagnosis of work-related asthma.”
The Occupational Safety and Health Administration offers guidance for diagnosing work-related asthma at https://www.osha.gov/SLTC/occupationalasthma/.
As many as 1 in 5 asthma-related deaths in the US is due to occupational exposure—and many could be prevented, according to CDC researchers.
The researchers analyzed reports from 1999-2016 of asthma-related mortality and occupations of the people involved. Of 3,396 deaths (3,396 in 2015 alone), between 11% and 21% were due to occupational exposures. Health care workers and construction workers were at highest risk.
By industry, the highest number of deaths were among men working in construction (13%) and women in health care (14%). By occupation, the most deaths were among men construction trades workers (11%) and women office and administrative support workers (9%).
The researchers note that ongoing exposure to cleaners, disinfectants, and antibiotics, all can trigger asthma. But they also point out that steps can be successfully taken to limit the type of exposure that exacerbates asthma symptoms, such as replacing powdered latex gloves with powder-free natural rubber latex or nonlatex gloves.
In an interview with MD Magazine, principle investigator Jacek Mazurek, MD, PhD, said there’s also an opportunity for health care providers to intervene more effectively. “Inadequate screening of workers for occupational exposures by health providers and lack of recognition of associations between workplace exposures and asthma symptoms remain the main reasons for underrecognition and underdiagnosis of work-related asthma.”
The Occupational Safety and Health Administration offers guidance for diagnosing work-related asthma at https://www.osha.gov/SLTC/occupationalasthma/.
As many as 1 in 5 asthma-related deaths in the US is due to occupational exposure—and many could be prevented, according to CDC researchers.
The researchers analyzed reports from 1999-2016 of asthma-related mortality and occupations of the people involved. Of 3,396 deaths (3,396 in 2015 alone), between 11% and 21% were due to occupational exposures. Health care workers and construction workers were at highest risk.
By industry, the highest number of deaths were among men working in construction (13%) and women in health care (14%). By occupation, the most deaths were among men construction trades workers (11%) and women office and administrative support workers (9%).
The researchers note that ongoing exposure to cleaners, disinfectants, and antibiotics, all can trigger asthma. But they also point out that steps can be successfully taken to limit the type of exposure that exacerbates asthma symptoms, such as replacing powdered latex gloves with powder-free natural rubber latex or nonlatex gloves.
In an interview with MD Magazine, principle investigator Jacek Mazurek, MD, PhD, said there’s also an opportunity for health care providers to intervene more effectively. “Inadequate screening of workers for occupational exposures by health providers and lack of recognition of associations between workplace exposures and asthma symptoms remain the main reasons for underrecognition and underdiagnosis of work-related asthma.”
The Occupational Safety and Health Administration offers guidance for diagnosing work-related asthma at https://www.osha.gov/SLTC/occupationalasthma/.
Teleconference is effective in assessing penicillin allergy
ORLANDO – and resulted in almost every patient having their allergy label removed, researchers reported.
In what the researchers said was the first study showing the utility of telemedicine in evaluating patient-reported penicillin allergies, allergy and immunology physicians did a secure telemedicine consultation with patients after they underwent penicillin skin testing with a physician assistant; an approach which, on average, took 123 minutes fewer each time than if the physician had done the consultation face-to-face. The teleconference can be done on a laptop or smartphone.

She said the approach is sensible and effective, and it is a good alternative to the traditional way of doing these tests. “What this takes out of that is the travel part. Someone else is doing the travel and the technique of testing,” added that people often are labeled in childhood after getting a rash that was thought to be related to penicillin, but actually was just a coincidence that was unrelated. Then the false allergy label is attached to them for life.
“This is so overlabeled,” Dr. Ramsey said. “Ten percent of the population thinks they’re allergic to penicillin, and 90% of them are not.”
A stark difference was found in the types of medicines administered before and after the evaluations, with aminopenicillin therapy jumping from 0 days of use to 188 days, and vancomycin – a more potent, but more costly alternative – dropping from 130 days of use to 16 days (P less than .05 for both).
Dr. Ramsey noted that, in part because of the time-consuming nature of the penicillin skin tests, they often are simply not done, so the false allergy labels are not caught, leading to pointless costs and exposure to more potent and potentially harmful forms of antibiotic therapy.
“Some hospitals don’t have allergists who will come in to do testing,” she said. “Sometimes patients are on medications that may interfere. And then a lot of times it’s just underrecognized – the implications of a penicillin allergy label. That is a very hot topic in our field and also in infectious disease.”
She hopes the telemedicine approach catches on more widely, which would help minimize the multitude of problems linked to penicillin allergy labels.
“Patients that avoid penicillin, they’re on more costly second-line antibiotics that are, in general, less effective, depending on which infection you’re talking about,” Dr. Ramsey said. “The [second-line antibiotics] have more side effects. And there’s data to show that patients with [a] penicillin allergy label have longer hospital stays, more costly hospital stays, are at risk for more resistant infections. And it breeds antimicrobial resistance in the long-term.”
Dr. Ramsey had no relevant financial disclosures.
SOURCE: Ramsey AC et al. AAAAI/WAO Joint Congress, Abstract 104.
ORLANDO – and resulted in almost every patient having their allergy label removed, researchers reported.
In what the researchers said was the first study showing the utility of telemedicine in evaluating patient-reported penicillin allergies, allergy and immunology physicians did a secure telemedicine consultation with patients after they underwent penicillin skin testing with a physician assistant; an approach which, on average, took 123 minutes fewer each time than if the physician had done the consultation face-to-face. The teleconference can be done on a laptop or smartphone.
She said the approach is sensible and effective, and it is a good alternative to the traditional way of doing these tests. “What this takes out of that is the travel part. Someone else is doing the travel and the technique of testing,” added that people often are labeled in childhood after getting a rash that was thought to be related to penicillin, but actually was just a coincidence that was unrelated. Then the false allergy label is attached to them for life.
“This is so overlabeled,” Dr. Ramsey said. “Ten percent of the population thinks they’re allergic to penicillin, and 90% of them are not.”
A stark difference was found in the types of medicines administered before and after the evaluations, with aminopenicillin therapy jumping from 0 days of use to 188 days, and vancomycin – a more potent, but more costly alternative – dropping from 130 days of use to 16 days (P less than .05 for both).
Dr. Ramsey noted that, in part because of the time-consuming nature of the penicillin skin tests, they often are simply not done, so the false allergy labels are not caught, leading to pointless costs and exposure to more potent and potentially harmful forms of antibiotic therapy.
“Some hospitals don’t have allergists who will come in to do testing,” she said. “Sometimes patients are on medications that may interfere. And then a lot of times it’s just underrecognized – the implications of a penicillin allergy label. That is a very hot topic in our field and also in infectious disease.”
She hopes the telemedicine approach catches on more widely, which would help minimize the multitude of problems linked to penicillin allergy labels.
“Patients that avoid penicillin, they’re on more costly second-line antibiotics that are, in general, less effective, depending on which infection you’re talking about,” Dr. Ramsey said. “The [second-line antibiotics] have more side effects. And there’s data to show that patients with [a] penicillin allergy label have longer hospital stays, more costly hospital stays, are at risk for more resistant infections. And it breeds antimicrobial resistance in the long-term.”
Dr. Ramsey had no relevant financial disclosures.
SOURCE: Ramsey AC et al. AAAAI/WAO Joint Congress, Abstract 104.
ORLANDO – and resulted in almost every patient having their allergy label removed, researchers reported.
In what the researchers said was the first study showing the utility of telemedicine in evaluating patient-reported penicillin allergies, allergy and immunology physicians did a secure telemedicine consultation with patients after they underwent penicillin skin testing with a physician assistant; an approach which, on average, took 123 minutes fewer each time than if the physician had done the consultation face-to-face. The teleconference can be done on a laptop or smartphone.
She said the approach is sensible and effective, and it is a good alternative to the traditional way of doing these tests. “What this takes out of that is the travel part. Someone else is doing the travel and the technique of testing,” added that people often are labeled in childhood after getting a rash that was thought to be related to penicillin, but actually was just a coincidence that was unrelated. Then the false allergy label is attached to them for life.
“This is so overlabeled,” Dr. Ramsey said. “Ten percent of the population thinks they’re allergic to penicillin, and 90% of them are not.”
A stark difference was found in the types of medicines administered before and after the evaluations, with aminopenicillin therapy jumping from 0 days of use to 188 days, and vancomycin – a more potent, but more costly alternative – dropping from 130 days of use to 16 days (P less than .05 for both).
Dr. Ramsey noted that, in part because of the time-consuming nature of the penicillin skin tests, they often are simply not done, so the false allergy labels are not caught, leading to pointless costs and exposure to more potent and potentially harmful forms of antibiotic therapy.
“Some hospitals don’t have allergists who will come in to do testing,” she said. “Sometimes patients are on medications that may interfere. And then a lot of times it’s just underrecognized – the implications of a penicillin allergy label. That is a very hot topic in our field and also in infectious disease.”
She hopes the telemedicine approach catches on more widely, which would help minimize the multitude of problems linked to penicillin allergy labels.
“Patients that avoid penicillin, they’re on more costly second-line antibiotics that are, in general, less effective, depending on which infection you’re talking about,” Dr. Ramsey said. “The [second-line antibiotics] have more side effects. And there’s data to show that patients with [a] penicillin allergy label have longer hospital stays, more costly hospital stays, are at risk for more resistant infections. And it breeds antimicrobial resistance in the long-term.”
Dr. Ramsey had no relevant financial disclosures.
SOURCE: Ramsey AC et al. AAAAI/WAO Joint Congress, Abstract 104.
REPORTING FROM AAAAI/WAO JOINT CONGRESS
Key clinical point: Teleconferencing to assess patient-reported penicillin allergies saves time and results in 9 out of 10 patients being delabeled.
Major finding: Of 50 patients prospectively assessed with this approach over a 4-month period last year, 46 were delabeled, with $23,000 in direct antibiotic cost savings, or $360 per patient.
Study details: A prospective study conducted over 4 months in 2017.
Disclosures: Dr. Ramsey had no relevant financial disclosures.
Source: Ramsey AC et al. AAAAI/WAO Joint Congress, Abstract 104.
OSA may provide cardioprotection
, according to researchers.
In a study of 127 patients presenting with acute coronary syndromes (ACS), median peak cardiac troponin-I (cTn-I) values were significantly higher in patients without obstructive sleep apnea, compared with OSA patients (10.7; interquartile range: 1.78-40.1, vs. 3.79; IQR: 0.37-24.3, respectively; P = .04 ). The findings were published Feb. 5 in the journal CHEST®.
The study comprised 89 OSA patients and 38 non-OSA patients who were admitted to a hospital for acute coronary syndromes. The OSA group had a median apnea-hypopnea index (AHI) of 32, while the non-OSA group had a median AHI of 4.8. There was no significant difference between the two groups in gender, age, or cardiovascular risk factors such as hypertension, diabetes mellitus, body mass index, dyslipidemia, and smoking.
The cohort was part of the Continuous Positive Airway Pressure (CPAP) in Patients With Acute Coronary Syndrome and Obstructive Sleep Apnea (ISAACC) study, a prior randomized, controlled trial that evaluated the effect of CPAP treatment on new cardiovascular events in patients with an episode of ACS and OSA, reported Alicia Sánchez-de-la-Torre, PhD, of the respiratory department at Hospital Universitari Arnau de Vilanova and Santa Maria in Catalonia, Spain, and her coauthors.
Respiratory polygraphy was performed in the first 24-72 hours after hospital admission, and patients with an AHI of at least 15 events per hour were considered to have OSA. Those with an AHI less than 15 events per hour were included in the non-OSA group.
The OSA patients were randomized to conservative or CPAP treatment. An obstructive apnea “episode” was defined as a complete cessation of airflow for 10 seconds or longer, and an episode of hypopnea was defined as a reduction in airflow for at least 10 seconds associated with a greater than 4% decrease in arterial oxygen saturation.
Blood samples were collected from patients every 6 hours until two consecutive cTn-I measurements showed a decrease, with the highest measurement considered the peak cTn-I value.
Peak cTn-I value was significantly higher in non-OSA patients than in OSA patients. Median infarct size, measured by calculating the area under the cTn-I curve, was significantly different between the two groups (451 for non-OSA patients vs. 143 in OSA patients; P = .049), wrote Dr. Sánchez-de-la-Torre and her colleagues.
As cTn-I levels decreased, there was a trend toward increased OSA severity (P = .058). In the multivariable linear regression model used to assess OSA severity, patients with severe OSA had 61% lower cTn-I levels than non-OSA patients, the authors noted.
“The effects of chronic hypoxia in individual organ systems are not well understood. While chronic sustained hypoxia as seen with COPD may lead to pulmonary hypertension, chronic intermittent hypoxia (CIH) as seen predominantly in sleep apnea has been attributed to causing widespread effects ranging from systemic hypertension to metabolic dysfunction and systemic inflammation,” noted Krishna Sundar, MD, FCCP. “Despite these associations, an increased risk of major cardiovascular events from untreated OSA is yet to be definitively established.”

In this article, a protective effect from OSA on myocardial ischemic events is demonstrated in a group of 127 consecutively admitted patients with acute coronary syndrome (ACS). While it is interesting that a high proportion of those admitted for ACS had OSA, there were no significant differences in the age, sex, BMI, usage of antihypertensive or antiplatelet agents, presence of hypertension, DM, dyslipidemia or smoking status between those with and without OSA. “OSA appeared to confer a protective effect on the size of myocardial injury with those having higher AHI values demonstrating lower peak cardiac troponin values,” said Dr. Sundar, who is an associate clinical professor of pulmonary, critical care and sleep medicine at the University of Utah.“An effect of age (mean age in this study being 64 years) and BMI (mean being 27) on the occurrence of preconditioning effects of OSA is not excluded given deleterious effects of untreated OSA on infarct size in other studies on obese or younger patients with ACS. Further understanding of molecular effects of chronic hypoxia exposure (high altitude, chronic lung disease, OSA) is required before the complex and often contradictory effects of chronic hypoxia can be affirmed as being protective or deleterious,” added Dr. Sundar, who is also medical director of the Sleep-Wake Center at the University of Utah and a member of CHEST Physician’s editorial advisory board.
According to the study’s authors, their findings “suggest that patients with higher AHI are significantly more likely to have low cTn-I levels than patients without evidence of OSA, which could imply that patients with elevated AHI, particularly those with severe OSA, may experience less severe myocardial injury.”Limitations of the study include exclusion of patients with severe ACS, exclusion of sleepy subjects, and assessment of myocardial injury using cTn-I as a biomarker, without further data to determine infarct size.
“The possible role of OSA in cardioprotection should be explored in future studies,” the authors concluded.
The authors disclosed relationships with ResMed, Spanish Ministry of Health, Spanish Respiratory Society, Catalonian Cardiology Society, and ALLER. No other disclosures were reported.
chestphysiciannews@chestnet.org
SOURCE: Chest. 2018 Feb 5;153[2]:329-38. doi: 10.1016/j.chest.2017.06.046.
Although this study cannot definitively establish a clinically meaningful protective effect, it does provide important “preliminary evidence supporting the concept of OSA-induced cardioprotection” and challenges existing research, according to an editorial by Doron Aronson, MD, of the department of cardiology at Rambam Medical Center, Haifa, Israel, and coauthors (CHEST. 2018 Feb 153[2]:295-7. doi: 10.1016/j.chest.2017.07.036).
The results should be interpreted with caution, especially since accurate assessment of infarct size poses a challenge, they wrote.
“Myocardial infarct size is highly variable and is influenced by the duration of coronary occlusion, ST-segment elevation or non–ST elevation myocardial infarction, infarct location, residual antegrade infarct-related artery flow, collateral flow, the presence of non–culprit vessel coronary artery disease and myocardial metabolic demand,” they wrote. “Without accounting for these variables in a small study, results may be affected by variation in the characteristics of the patients.”
Though further study is needed, the findings may have “profound clinical implications regarding our therapeutic approach to patients with sleep apnea” if confirmed, the authors concluded.
Although this study cannot definitively establish a clinically meaningful protective effect, it does provide important “preliminary evidence supporting the concept of OSA-induced cardioprotection” and challenges existing research, according to an editorial by Doron Aronson, MD, of the department of cardiology at Rambam Medical Center, Haifa, Israel, and coauthors (CHEST. 2018 Feb 153[2]:295-7. doi: 10.1016/j.chest.2017.07.036).
The results should be interpreted with caution, especially since accurate assessment of infarct size poses a challenge, they wrote.
“Myocardial infarct size is highly variable and is influenced by the duration of coronary occlusion, ST-segment elevation or non–ST elevation myocardial infarction, infarct location, residual antegrade infarct-related artery flow, collateral flow, the presence of non–culprit vessel coronary artery disease and myocardial metabolic demand,” they wrote. “Without accounting for these variables in a small study, results may be affected by variation in the characteristics of the patients.”
Though further study is needed, the findings may have “profound clinical implications regarding our therapeutic approach to patients with sleep apnea” if confirmed, the authors concluded.
Although this study cannot definitively establish a clinically meaningful protective effect, it does provide important “preliminary evidence supporting the concept of OSA-induced cardioprotection” and challenges existing research, according to an editorial by Doron Aronson, MD, of the department of cardiology at Rambam Medical Center, Haifa, Israel, and coauthors (CHEST. 2018 Feb 153[2]:295-7. doi: 10.1016/j.chest.2017.07.036).
The results should be interpreted with caution, especially since accurate assessment of infarct size poses a challenge, they wrote.
“Myocardial infarct size is highly variable and is influenced by the duration of coronary occlusion, ST-segment elevation or non–ST elevation myocardial infarction, infarct location, residual antegrade infarct-related artery flow, collateral flow, the presence of non–culprit vessel coronary artery disease and myocardial metabolic demand,” they wrote. “Without accounting for these variables in a small study, results may be affected by variation in the characteristics of the patients.”
Though further study is needed, the findings may have “profound clinical implications regarding our therapeutic approach to patients with sleep apnea” if confirmed, the authors concluded.
, according to researchers.
In a study of 127 patients presenting with acute coronary syndromes (ACS), median peak cardiac troponin-I (cTn-I) values were significantly higher in patients without obstructive sleep apnea, compared with OSA patients (10.7; interquartile range: 1.78-40.1, vs. 3.79; IQR: 0.37-24.3, respectively; P = .04 ). The findings were published Feb. 5 in the journal CHEST®.
The study comprised 89 OSA patients and 38 non-OSA patients who were admitted to a hospital for acute coronary syndromes. The OSA group had a median apnea-hypopnea index (AHI) of 32, while the non-OSA group had a median AHI of 4.8. There was no significant difference between the two groups in gender, age, or cardiovascular risk factors such as hypertension, diabetes mellitus, body mass index, dyslipidemia, and smoking.
The cohort was part of the Continuous Positive Airway Pressure (CPAP) in Patients With Acute Coronary Syndrome and Obstructive Sleep Apnea (ISAACC) study, a prior randomized, controlled trial that evaluated the effect of CPAP treatment on new cardiovascular events in patients with an episode of ACS and OSA, reported Alicia Sánchez-de-la-Torre, PhD, of the respiratory department at Hospital Universitari Arnau de Vilanova and Santa Maria in Catalonia, Spain, and her coauthors.
Respiratory polygraphy was performed in the first 24-72 hours after hospital admission, and patients with an AHI of at least 15 events per hour were considered to have OSA. Those with an AHI less than 15 events per hour were included in the non-OSA group.
The OSA patients were randomized to conservative or CPAP treatment. An obstructive apnea “episode” was defined as a complete cessation of airflow for 10 seconds or longer, and an episode of hypopnea was defined as a reduction in airflow for at least 10 seconds associated with a greater than 4% decrease in arterial oxygen saturation.
Blood samples were collected from patients every 6 hours until two consecutive cTn-I measurements showed a decrease, with the highest measurement considered the peak cTn-I value.
Peak cTn-I value was significantly higher in non-OSA patients than in OSA patients. Median infarct size, measured by calculating the area under the cTn-I curve, was significantly different between the two groups (451 for non-OSA patients vs. 143 in OSA patients; P = .049), wrote Dr. Sánchez-de-la-Torre and her colleagues.
As cTn-I levels decreased, there was a trend toward increased OSA severity (P = .058). In the multivariable linear regression model used to assess OSA severity, patients with severe OSA had 61% lower cTn-I levels than non-OSA patients, the authors noted.
“The effects of chronic hypoxia in individual organ systems are not well understood. While chronic sustained hypoxia as seen with COPD may lead to pulmonary hypertension, chronic intermittent hypoxia (CIH) as seen predominantly in sleep apnea has been attributed to causing widespread effects ranging from systemic hypertension to metabolic dysfunction and systemic inflammation,” noted Krishna Sundar, MD, FCCP. “Despite these associations, an increased risk of major cardiovascular events from untreated OSA is yet to be definitively established.”
In this article, a protective effect from OSA on myocardial ischemic events is demonstrated in a group of 127 consecutively admitted patients with acute coronary syndrome (ACS). While it is interesting that a high proportion of those admitted for ACS had OSA, there were no significant differences in the age, sex, BMI, usage of antihypertensive or antiplatelet agents, presence of hypertension, DM, dyslipidemia or smoking status between those with and without OSA. “OSA appeared to confer a protective effect on the size of myocardial injury with those having higher AHI values demonstrating lower peak cardiac troponin values,” said Dr. Sundar, who is an associate clinical professor of pulmonary, critical care and sleep medicine at the University of Utah.“An effect of age (mean age in this study being 64 years) and BMI (mean being 27) on the occurrence of preconditioning effects of OSA is not excluded given deleterious effects of untreated OSA on infarct size in other studies on obese or younger patients with ACS. Further understanding of molecular effects of chronic hypoxia exposure (high altitude, chronic lung disease, OSA) is required before the complex and often contradictory effects of chronic hypoxia can be affirmed as being protective or deleterious,” added Dr. Sundar, who is also medical director of the Sleep-Wake Center at the University of Utah and a member of CHEST Physician’s editorial advisory board.
According to the study’s authors, their findings “suggest that patients with higher AHI are significantly more likely to have low cTn-I levels than patients without evidence of OSA, which could imply that patients with elevated AHI, particularly those with severe OSA, may experience less severe myocardial injury.”Limitations of the study include exclusion of patients with severe ACS, exclusion of sleepy subjects, and assessment of myocardial injury using cTn-I as a biomarker, without further data to determine infarct size.
“The possible role of OSA in cardioprotection should be explored in future studies,” the authors concluded.
The authors disclosed relationships with ResMed, Spanish Ministry of Health, Spanish Respiratory Society, Catalonian Cardiology Society, and ALLER. No other disclosures were reported.
chestphysiciannews@chestnet.org
SOURCE: Chest. 2018 Feb 5;153[2]:329-38. doi: 10.1016/j.chest.2017.06.046.
, according to researchers.
In a study of 127 patients presenting with acute coronary syndromes (ACS), median peak cardiac troponin-I (cTn-I) values were significantly higher in patients without obstructive sleep apnea, compared with OSA patients (10.7; interquartile range: 1.78-40.1, vs. 3.79; IQR: 0.37-24.3, respectively; P = .04 ). The findings were published Feb. 5 in the journal CHEST®.
The study comprised 89 OSA patients and 38 non-OSA patients who were admitted to a hospital for acute coronary syndromes. The OSA group had a median apnea-hypopnea index (AHI) of 32, while the non-OSA group had a median AHI of 4.8. There was no significant difference between the two groups in gender, age, or cardiovascular risk factors such as hypertension, diabetes mellitus, body mass index, dyslipidemia, and smoking.
The cohort was part of the Continuous Positive Airway Pressure (CPAP) in Patients With Acute Coronary Syndrome and Obstructive Sleep Apnea (ISAACC) study, a prior randomized, controlled trial that evaluated the effect of CPAP treatment on new cardiovascular events in patients with an episode of ACS and OSA, reported Alicia Sánchez-de-la-Torre, PhD, of the respiratory department at Hospital Universitari Arnau de Vilanova and Santa Maria in Catalonia, Spain, and her coauthors.
Respiratory polygraphy was performed in the first 24-72 hours after hospital admission, and patients with an AHI of at least 15 events per hour were considered to have OSA. Those with an AHI less than 15 events per hour were included in the non-OSA group.
The OSA patients were randomized to conservative or CPAP treatment. An obstructive apnea “episode” was defined as a complete cessation of airflow for 10 seconds or longer, and an episode of hypopnea was defined as a reduction in airflow for at least 10 seconds associated with a greater than 4% decrease in arterial oxygen saturation.
Blood samples were collected from patients every 6 hours until two consecutive cTn-I measurements showed a decrease, with the highest measurement considered the peak cTn-I value.
Peak cTn-I value was significantly higher in non-OSA patients than in OSA patients. Median infarct size, measured by calculating the area under the cTn-I curve, was significantly different between the two groups (451 for non-OSA patients vs. 143 in OSA patients; P = .049), wrote Dr. Sánchez-de-la-Torre and her colleagues.
As cTn-I levels decreased, there was a trend toward increased OSA severity (P = .058). In the multivariable linear regression model used to assess OSA severity, patients with severe OSA had 61% lower cTn-I levels than non-OSA patients, the authors noted.
“The effects of chronic hypoxia in individual organ systems are not well understood. While chronic sustained hypoxia as seen with COPD may lead to pulmonary hypertension, chronic intermittent hypoxia (CIH) as seen predominantly in sleep apnea has been attributed to causing widespread effects ranging from systemic hypertension to metabolic dysfunction and systemic inflammation,” noted Krishna Sundar, MD, FCCP. “Despite these associations, an increased risk of major cardiovascular events from untreated OSA is yet to be definitively established.”
In this article, a protective effect from OSA on myocardial ischemic events is demonstrated in a group of 127 consecutively admitted patients with acute coronary syndrome (ACS). While it is interesting that a high proportion of those admitted for ACS had OSA, there were no significant differences in the age, sex, BMI, usage of antihypertensive or antiplatelet agents, presence of hypertension, DM, dyslipidemia or smoking status between those with and without OSA. “OSA appeared to confer a protective effect on the size of myocardial injury with those having higher AHI values demonstrating lower peak cardiac troponin values,” said Dr. Sundar, who is an associate clinical professor of pulmonary, critical care and sleep medicine at the University of Utah.“An effect of age (mean age in this study being 64 years) and BMI (mean being 27) on the occurrence of preconditioning effects of OSA is not excluded given deleterious effects of untreated OSA on infarct size in other studies on obese or younger patients with ACS. Further understanding of molecular effects of chronic hypoxia exposure (high altitude, chronic lung disease, OSA) is required before the complex and often contradictory effects of chronic hypoxia can be affirmed as being protective or deleterious,” added Dr. Sundar, who is also medical director of the Sleep-Wake Center at the University of Utah and a member of CHEST Physician’s editorial advisory board.
According to the study’s authors, their findings “suggest that patients with higher AHI are significantly more likely to have low cTn-I levels than patients without evidence of OSA, which could imply that patients with elevated AHI, particularly those with severe OSA, may experience less severe myocardial injury.”Limitations of the study include exclusion of patients with severe ACS, exclusion of sleepy subjects, and assessment of myocardial injury using cTn-I as a biomarker, without further data to determine infarct size.
“The possible role of OSA in cardioprotection should be explored in future studies,” the authors concluded.
The authors disclosed relationships with ResMed, Spanish Ministry of Health, Spanish Respiratory Society, Catalonian Cardiology Society, and ALLER. No other disclosures were reported.
chestphysiciannews@chestnet.org
SOURCE: Chest. 2018 Feb 5;153[2]:329-38. doi: 10.1016/j.chest.2017.06.046.

Unassigned school epinephrine used more than assigned injectors
ORLANDO –
In the 2015-2016 and 2016-2017 school years, epinephrine was administered to students 31 times at schools in the Austin Independent School District, which began to stock unassigned epinephrine in its schools after state legislators approved a law in 2015 allowing, but not requiring, school districts to do so. In 21 of those cases, or 68% of the time, it was the unassigned stockpile that was used, Kathryn Neupert, MD, said at the joint congress of the American Academy of Allergy, Asthma, and Immunology and the World Asthma Organization.

She drew attention to the finding that 22% of the time in the study, the epinephrine use involved the unassigned stock for children with no history of anaphylaxis or allergy.
“It kind of argues that, for those people that we don’t know have anaphylaxis to anything, it’s definitely important to have it available to them,” reported Dr. Neupert, a resident at the University of Texas, Austin.
In 45% of the cases, epinephrine was administered to children who had a known history of allergic reactions but, for whatever reason, did not have an epinephrine injector assigned to them.
Food was the most common trigger for use of epinephrine, accounting for 48% of the injections, with fragrance at 16%, insect stings at 10%, and exercise and overheating at 7%.
Dr. Neupert and her associates said the frequency with which epinephrine was administered after exposure to a fragrance – seen in about the same amount for unassigned and assigned epinephrine – might signal a need for greater education.
She emphasized the importance of follow-up after the use of unassigned injectors. If children get epinephrine that was unassigned and they have known allergies, “be sure that they subsequently get back in with their pediatrician or their allergist [and] that they’re getting their up-to-date epinephrine pens renewed,” she noted.
Carla Davis, MD, a pediatrician at Baylor College of Medicine, Houston, said she hopes more school districts adopt the stock epinephrine policy, despite barriers of cost and education. “I do think that it’s important for these schools to have these, because 20% of children will have their first episode of food allergic reaction – and in some of those cases it will be anaphylaxis – in schools.”
Dr. Neupert had no relevant financial disclosures.
SOURCE: AAAAI/WAO Joint Congress Abstract 465.
ORLANDO –
In the 2015-2016 and 2016-2017 school years, epinephrine was administered to students 31 times at schools in the Austin Independent School District, which began to stock unassigned epinephrine in its schools after state legislators approved a law in 2015 allowing, but not requiring, school districts to do so. In 21 of those cases, or 68% of the time, it was the unassigned stockpile that was used, Kathryn Neupert, MD, said at the joint congress of the American Academy of Allergy, Asthma, and Immunology and the World Asthma Organization.
She drew attention to the finding that 22% of the time in the study, the epinephrine use involved the unassigned stock for children with no history of anaphylaxis or allergy.
“It kind of argues that, for those people that we don’t know have anaphylaxis to anything, it’s definitely important to have it available to them,” reported Dr. Neupert, a resident at the University of Texas, Austin.
In 45% of the cases, epinephrine was administered to children who had a known history of allergic reactions but, for whatever reason, did not have an epinephrine injector assigned to them.
Food was the most common trigger for use of epinephrine, accounting for 48% of the injections, with fragrance at 16%, insect stings at 10%, and exercise and overheating at 7%.
Dr. Neupert and her associates said the frequency with which epinephrine was administered after exposure to a fragrance – seen in about the same amount for unassigned and assigned epinephrine – might signal a need for greater education.
She emphasized the importance of follow-up after the use of unassigned injectors. If children get epinephrine that was unassigned and they have known allergies, “be sure that they subsequently get back in with their pediatrician or their allergist [and] that they’re getting their up-to-date epinephrine pens renewed,” she noted.
Carla Davis, MD, a pediatrician at Baylor College of Medicine, Houston, said she hopes more school districts adopt the stock epinephrine policy, despite barriers of cost and education. “I do think that it’s important for these schools to have these, because 20% of children will have their first episode of food allergic reaction – and in some of those cases it will be anaphylaxis – in schools.”
Dr. Neupert had no relevant financial disclosures.
SOURCE: AAAAI/WAO Joint Congress Abstract 465.
ORLANDO –
In the 2015-2016 and 2016-2017 school years, epinephrine was administered to students 31 times at schools in the Austin Independent School District, which began to stock unassigned epinephrine in its schools after state legislators approved a law in 2015 allowing, but not requiring, school districts to do so. In 21 of those cases, or 68% of the time, it was the unassigned stockpile that was used, Kathryn Neupert, MD, said at the joint congress of the American Academy of Allergy, Asthma, and Immunology and the World Asthma Organization.
She drew attention to the finding that 22% of the time in the study, the epinephrine use involved the unassigned stock for children with no history of anaphylaxis or allergy.
“It kind of argues that, for those people that we don’t know have anaphylaxis to anything, it’s definitely important to have it available to them,” reported Dr. Neupert, a resident at the University of Texas, Austin.
In 45% of the cases, epinephrine was administered to children who had a known history of allergic reactions but, for whatever reason, did not have an epinephrine injector assigned to them.
Food was the most common trigger for use of epinephrine, accounting for 48% of the injections, with fragrance at 16%, insect stings at 10%, and exercise and overheating at 7%.
Dr. Neupert and her associates said the frequency with which epinephrine was administered after exposure to a fragrance – seen in about the same amount for unassigned and assigned epinephrine – might signal a need for greater education.
She emphasized the importance of follow-up after the use of unassigned injectors. If children get epinephrine that was unassigned and they have known allergies, “be sure that they subsequently get back in with their pediatrician or their allergist [and] that they’re getting their up-to-date epinephrine pens renewed,” she noted.
Carla Davis, MD, a pediatrician at Baylor College of Medicine, Houston, said she hopes more school districts adopt the stock epinephrine policy, despite barriers of cost and education. “I do think that it’s important for these schools to have these, because 20% of children will have their first episode of food allergic reaction – and in some of those cases it will be anaphylaxis – in schools.”
Dr. Neupert had no relevant financial disclosures.
SOURCE: AAAAI/WAO Joint Congress Abstract 465.
REPORTING FROM AAAAI/WAO JOINT CONGRESS
Key clinical point: Unassigned epinephrine was used more often in a Texas school district than assigned epinephrine.
Major finding: Over 2 years, 31 epinephrine injections were administered, and in 68% of the cases, it was the unassigned stock that was used.
Study details: A review of nursing records for the Austin Independent School District.
Disclosures: Dr. Kathryn Neupert had no relevant financial disclosures.
Source: Neupert K et al. Abstract 465.
Flu activity continues to decline
The 2017-2018 flu season continued to loosen its grip on the country as both outpatient activity and pediatric deaths dropped during the week ending March 3, according to the Centers for Disease Control and Prevention.
After five consecutive weeks of double-digit pediatric deaths related to influenza-like illness (ILI), five deaths were reported for the week ending March 3, four of which occurred in previous weeks. The total for the 2017-2018 season is now 119, the CDC said in its weekly surveillance report.
The proportion of outpatient visits for ILI was 3.7% for the week, which is down from 4.9% the week before and less than half of the seasonal high of 7.5% that was recorded for the week of Feb. 3, CDC data show. The national baseline level of outpatient activity is 2.2%.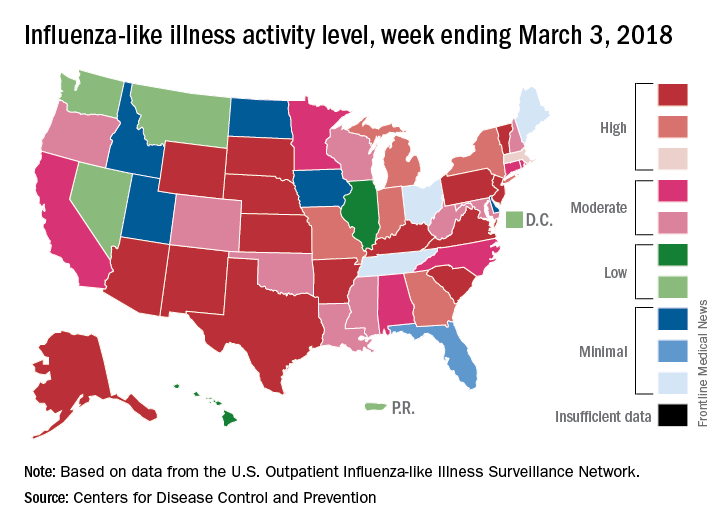
The cumulative hospitalization rate for the 2017-2018 flu season climbed from 84.2 the previous week to 86.3 per 100,000 population – well above the rate of 57.2 per 100,000 that was recorded for the corresponding week of the hospitalization-record-setting 2014-2015 season, FluView data show.
The 2017-2018 flu season continued to loosen its grip on the country as both outpatient activity and pediatric deaths dropped during the week ending March 3, according to the Centers for Disease Control and Prevention.
After five consecutive weeks of double-digit pediatric deaths related to influenza-like illness (ILI), five deaths were reported for the week ending March 3, four of which occurred in previous weeks. The total for the 2017-2018 season is now 119, the CDC said in its weekly surveillance report.
The proportion of outpatient visits for ILI was 3.7% for the week, which is down from 4.9% the week before and less than half of the seasonal high of 7.5% that was recorded for the week of Feb. 3, CDC data show. The national baseline level of outpatient activity is 2.2%.
The cumulative hospitalization rate for the 2017-2018 flu season climbed from 84.2 the previous week to 86.3 per 100,000 population – well above the rate of 57.2 per 100,000 that was recorded for the corresponding week of the hospitalization-record-setting 2014-2015 season, FluView data show.
The 2017-2018 flu season continued to loosen its grip on the country as both outpatient activity and pediatric deaths dropped during the week ending March 3, according to the Centers for Disease Control and Prevention.
After five consecutive weeks of double-digit pediatric deaths related to influenza-like illness (ILI), five deaths were reported for the week ending March 3, four of which occurred in previous weeks. The total for the 2017-2018 season is now 119, the CDC said in its weekly surveillance report.
The proportion of outpatient visits for ILI was 3.7% for the week, which is down from 4.9% the week before and less than half of the seasonal high of 7.5% that was recorded for the week of Feb. 3, CDC data show. The national baseline level of outpatient activity is 2.2%.
The cumulative hospitalization rate for the 2017-2018 flu season climbed from 84.2 the previous week to 86.3 per 100,000 population – well above the rate of 57.2 per 100,000 that was recorded for the corresponding week of the hospitalization-record-setting 2014-2015 season, FluView data show.
Peanut is most prevalent culprit in anaphylaxis PICU admits
ORLANDO – Food was found to be the most commonly identified trigger, with peanuts the most prevalent food cause, in what researchers say is the largest comprehensive review of anaphylaxis episodes in North America that led to pediatric intensive-care unit stays.
Researchers examined the Virtual Pediatrics Systems database, an international database of pediatric intensive care unit (PICU) information, said Carla M. Davis, MD, a pediatrician at Baylor College of Medicine, Houston. During 2010-2015, there were 1,989 pediatric anaphylaxis admissions to these units in North America, she reported at the joint congress of the American Academy of Allergy, Asthma and Immunology and the World Asthma Organization.

“Because anaphylaxis is one of the most severe consequences of allergic disease, we decided that this study needed to be done to see really what the landscape was in the most critically ill children,” she said.
Peanuts accounted for 45% of the food triggers, followed by tree nuts and seeds at 19%, and milk at 10%.
Common causes aside from food included drug, blood products, and venom, Dr. Davis said.
Anaphylaxis accounted for 0.3% of all PICU admissions over the 5-year period, researchers found. Dr. Davis said this was “higher than what we anticipated.”
The overall mortality rate was 1%, and researchers found that peanuts and dairy were main causes of death of all the food-induced cases.
Anaphylaxis occurred more often in children ages 6-18 years than in kids of other ages and was least common among those aged 2-5 years. Asian children were disproportionately represented among the PICU anaphylaxis patients, but the mortality rate didn’t vary by any demographic factors.
Admissions were most likely to happen in the fall and were more common in the Northeast and Western regions of the United States, Dr. Davis reported.
She said the deep look at the causes of these severe cases should help drive home the importance of counseling patients and families about prevention.
“For patients that have had a history of an allergic reaction to food or medication, but specifically food, I think really stressing avoidance measures will be something that will be very helpful, as well as counseling about epinephrine injectors and carrying them is going to help,” she said. “I think having a little more knowledge, pediatricians should be able to counsel and refer to allergists when they don’t feel they have all the necessary skills.”
Dr. Davis reports financial relationships with Aimmune Therapeutics and DBV Technologies.
SOURCE: Davis CM et al. 2018 AAAAI/WAO Joint Congress Abstract 775.
ORLANDO – Food was found to be the most commonly identified trigger, with peanuts the most prevalent food cause, in what researchers say is the largest comprehensive review of anaphylaxis episodes in North America that led to pediatric intensive-care unit stays.
Researchers examined the Virtual Pediatrics Systems database, an international database of pediatric intensive care unit (PICU) information, said Carla M. Davis, MD, a pediatrician at Baylor College of Medicine, Houston. During 2010-2015, there were 1,989 pediatric anaphylaxis admissions to these units in North America, she reported at the joint congress of the American Academy of Allergy, Asthma and Immunology and the World Asthma Organization.
“Because anaphylaxis is one of the most severe consequences of allergic disease, we decided that this study needed to be done to see really what the landscape was in the most critically ill children,” she said.
Peanuts accounted for 45% of the food triggers, followed by tree nuts and seeds at 19%, and milk at 10%.
Common causes aside from food included drug, blood products, and venom, Dr. Davis said.
Anaphylaxis accounted for 0.3% of all PICU admissions over the 5-year period, researchers found. Dr. Davis said this was “higher than what we anticipated.”
The overall mortality rate was 1%, and researchers found that peanuts and dairy were main causes of death of all the food-induced cases.
Anaphylaxis occurred more often in children ages 6-18 years than in kids of other ages and was least common among those aged 2-5 years. Asian children were disproportionately represented among the PICU anaphylaxis patients, but the mortality rate didn’t vary by any demographic factors.
Admissions were most likely to happen in the fall and were more common in the Northeast and Western regions of the United States, Dr. Davis reported.
She said the deep look at the causes of these severe cases should help drive home the importance of counseling patients and families about prevention.
“For patients that have had a history of an allergic reaction to food or medication, but specifically food, I think really stressing avoidance measures will be something that will be very helpful, as well as counseling about epinephrine injectors and carrying them is going to help,” she said. “I think having a little more knowledge, pediatricians should be able to counsel and refer to allergists when they don’t feel they have all the necessary skills.”
Dr. Davis reports financial relationships with Aimmune Therapeutics and DBV Technologies.
SOURCE: Davis CM et al. 2018 AAAAI/WAO Joint Congress Abstract 775.
ORLANDO – Food was found to be the most commonly identified trigger, with peanuts the most prevalent food cause, in what researchers say is the largest comprehensive review of anaphylaxis episodes in North America that led to pediatric intensive-care unit stays.
Researchers examined the Virtual Pediatrics Systems database, an international database of pediatric intensive care unit (PICU) information, said Carla M. Davis, MD, a pediatrician at Baylor College of Medicine, Houston. During 2010-2015, there were 1,989 pediatric anaphylaxis admissions to these units in North America, she reported at the joint congress of the American Academy of Allergy, Asthma and Immunology and the World Asthma Organization.
“Because anaphylaxis is one of the most severe consequences of allergic disease, we decided that this study needed to be done to see really what the landscape was in the most critically ill children,” she said.
Peanuts accounted for 45% of the food triggers, followed by tree nuts and seeds at 19%, and milk at 10%.
Common causes aside from food included drug, blood products, and venom, Dr. Davis said.
Anaphylaxis accounted for 0.3% of all PICU admissions over the 5-year period, researchers found. Dr. Davis said this was “higher than what we anticipated.”
The overall mortality rate was 1%, and researchers found that peanuts and dairy were main causes of death of all the food-induced cases.
Anaphylaxis occurred more often in children ages 6-18 years than in kids of other ages and was least common among those aged 2-5 years. Asian children were disproportionately represented among the PICU anaphylaxis patients, but the mortality rate didn’t vary by any demographic factors.
Admissions were most likely to happen in the fall and were more common in the Northeast and Western regions of the United States, Dr. Davis reported.
She said the deep look at the causes of these severe cases should help drive home the importance of counseling patients and families about prevention.
“For patients that have had a history of an allergic reaction to food or medication, but specifically food, I think really stressing avoidance measures will be something that will be very helpful, as well as counseling about epinephrine injectors and carrying them is going to help,” she said. “I think having a little more knowledge, pediatricians should be able to counsel and refer to allergists when they don’t feel they have all the necessary skills.”
Dr. Davis reports financial relationships with Aimmune Therapeutics and DBV Technologies.
SOURCE: Davis CM et al. 2018 AAAAI/WAO Joint Congress Abstract 775.
REPORTING FROM AAAAI/WAO JOINT CONGRESS
Key clinical point:
Major finding: Researchers found that 45% of these PICU stays from food were caused by reactions to peanuts.
Study details: A review of 1,989 cases during 2010-2015 in the Virtual Pediatrics Systems database, which collects international PICU information.
Disclosures: Dr. Davis reports financial relationships with Aimmune Therapeutics and DBV Technologies.
Source: Davis CM et al. 2018 AAAAI/WAO Joint Congress, Abstract 775.
Phosphodiesterase-5 inhibitors often prescribed inappropriately
While most veterans with pulmonary hypertension are treated in accordance with clinical guidelines, almost two-thirds who are prescribed therapy are being treated with pulmonary vasodilators inappropriately, an analysis of veteran prescription data reveals.
Little was known about how pulmonary vasodilators were used in practice prior to the publication of this study. While pulmonary vasodilators are considered effective for group 1 pulmonary hypertension (PH), clinical guidelines and advice from the Choosing Wisely campaign recommend against their routine use for PH patients classified into the most common types of PH – groups 2 and 3 – because of a lack of benefit, potential for harm, and high cost, the authors wrote. The report was published in Annals of the American Thoracic Society.
The new analysis shows that patients with PH are potentially being exposed to unnecessary harm, according to study author Renda Soylemez Wiener, MD, MPH, of the Center for Healthcare Organization & Implementation Research at Bedford (Mass.) Veterans Affairs Medical Center, and her colleagues. Their findings also reveal that inappropriate prescribing of pulmonary vasodilators, mostly by specialist clinicians, is contributing to the financial burden of an already stretched health system.
The research team looked at prescription data for veterans prescribed a phosphodiesterase-5 inhibitor (PDE5i), which causes pulmonary vasodilation, between 2005 and 2012 at any VA site. The primary outcome of the study was the proportion of patients who received potentially inappropriate PDE5i as classified in guideline recommendations. Patients with group 1 PH were deemed to have been treated appropriately, while those with group 2 and 3 PH were deemed to have been potentially treated inappropriately. Those with groups 4 and 5 PH were thought to have received treatment of “uncertain value.”

In a chart abstraction analysis from a randomly selected subset of PDE5i-treated patients, half (110/230, 47.8% [41.3%-54.5%]) had documented right heart catheterization to confirm the presence of PH. After factoring this into their algorithm, the investigators determined that only 11.7% [8.0%-16.8%] of these patients received clearly appropriate treatment.
Over the 8-year study period, the number of patients with PH group 2 or 3 prescribed PDE5i rose more than 14-fold, the researchers said. They speculated that this figure was likely to continue to rise with the increasing use of echocardiography and detection of PH.
According to the authors, the cost of treating one PH patient for 1 year with PDE5i therapy was between $10,000 and $13,000.
The 1,711 PH patients classified as being treated inappropriately in the study translated into a cost of over $20 million, if each patient were treated for only 1 year, but many of the patients were treated for a longer period of time.
The researchers suggested that there were several reasons why clinicians might choose to deviate from the guidelines, including lacking familiarity with them or disagreeing with them.
“While guidelines do allow trials of PDE5i in treatment for groups 2 or 3 PH on a case-by-case basis after consultation with a PH expert and a confirmatory [right heart catheterization], even PH experts disagree about whether a trial of PDE5i therapy is reasonable and appropriate for patients with group 3 PH,” they wrote.
They may also overestimate the potential benefits of treatment and/or underestimate potential harm.
Clinicians may believe that guidelines developed for a general population do not apply to the patients they are treating.
“It is understandable why clinicians may offer unproven therapies like PDE5i in hopes of providing relief to very sick patients with groups 2 or 3 PH, especially if they do not believe the recommendation applies to their individual patient or they are not convinced about the potential harms of pulmonary vasodilators,” they said.
The authors expressed concern about VA clinicians’ allowing patients to take PDE5i therapy that had been initially prescribed by clinicians outside of VA hospitals. The researchers said such drugs, which potentially had been prescribed inappropriately, “were continued by VA clinicians without much apparent scrutiny.”
The chart abstraction analysis also showed that specialists prescribed the majority of potentially inappropriate PDE5i treatment, suggesting “that other interventions to prevent inappropriate use may be required.”
The researchers concluded that “[the] time has come to develop interventions to optimize prescribing for PH in order to improve the value, quality, and safety of care.”
One potential intervention suggested by the researchers was to require patients with PH to be evaluated at a PH expert center, as recommended by treatment guidelines.
The study was funded by the Department of Veterans Affairs with resources from the Edith Nourse Rogers Memorial VA Hospital. Elizabeth S. Klings, MD, one of the study’s authors, declared receiving research support from several pharmaceutical companies.
SOURCE: Wiener RS et al. Ann Am Thorac Soc. 2018 Feb 27. doi: 10.1513/AnnalsATS.201710-762OC.
While most veterans with pulmonary hypertension are treated in accordance with clinical guidelines, almost two-thirds who are prescribed therapy are being treated with pulmonary vasodilators inappropriately, an analysis of veteran prescription data reveals.
Little was known about how pulmonary vasodilators were used in practice prior to the publication of this study. While pulmonary vasodilators are considered effective for group 1 pulmonary hypertension (PH), clinical guidelines and advice from the Choosing Wisely campaign recommend against their routine use for PH patients classified into the most common types of PH – groups 2 and 3 – because of a lack of benefit, potential for harm, and high cost, the authors wrote. The report was published in Annals of the American Thoracic Society.
The new analysis shows that patients with PH are potentially being exposed to unnecessary harm, according to study author Renda Soylemez Wiener, MD, MPH, of the Center for Healthcare Organization & Implementation Research at Bedford (Mass.) Veterans Affairs Medical Center, and her colleagues. Their findings also reveal that inappropriate prescribing of pulmonary vasodilators, mostly by specialist clinicians, is contributing to the financial burden of an already stretched health system.
The research team looked at prescription data for veterans prescribed a phosphodiesterase-5 inhibitor (PDE5i), which causes pulmonary vasodilation, between 2005 and 2012 at any VA site. The primary outcome of the study was the proportion of patients who received potentially inappropriate PDE5i as classified in guideline recommendations. Patients with group 1 PH were deemed to have been treated appropriately, while those with group 2 and 3 PH were deemed to have been potentially treated inappropriately. Those with groups 4 and 5 PH were thought to have received treatment of “uncertain value.”
In a chart abstraction analysis from a randomly selected subset of PDE5i-treated patients, half (110/230, 47.8% [41.3%-54.5%]) had documented right heart catheterization to confirm the presence of PH. After factoring this into their algorithm, the investigators determined that only 11.7% [8.0%-16.8%] of these patients received clearly appropriate treatment.
Over the 8-year study period, the number of patients with PH group 2 or 3 prescribed PDE5i rose more than 14-fold, the researchers said. They speculated that this figure was likely to continue to rise with the increasing use of echocardiography and detection of PH.
According to the authors, the cost of treating one PH patient for 1 year with PDE5i therapy was between $10,000 and $13,000.
The 1,711 PH patients classified as being treated inappropriately in the study translated into a cost of over $20 million, if each patient were treated for only 1 year, but many of the patients were treated for a longer period of time.
The researchers suggested that there were several reasons why clinicians might choose to deviate from the guidelines, including lacking familiarity with them or disagreeing with them.
“While guidelines do allow trials of PDE5i in treatment for groups 2 or 3 PH on a case-by-case basis after consultation with a PH expert and a confirmatory [right heart catheterization], even PH experts disagree about whether a trial of PDE5i therapy is reasonable and appropriate for patients with group 3 PH,” they wrote.
They may also overestimate the potential benefits of treatment and/or underestimate potential harm.
Clinicians may believe that guidelines developed for a general population do not apply to the patients they are treating.
“It is understandable why clinicians may offer unproven therapies like PDE5i in hopes of providing relief to very sick patients with groups 2 or 3 PH, especially if they do not believe the recommendation applies to their individual patient or they are not convinced about the potential harms of pulmonary vasodilators,” they said.
The authors expressed concern about VA clinicians’ allowing patients to take PDE5i therapy that had been initially prescribed by clinicians outside of VA hospitals. The researchers said such drugs, which potentially had been prescribed inappropriately, “were continued by VA clinicians without much apparent scrutiny.”
The chart abstraction analysis also showed that specialists prescribed the majority of potentially inappropriate PDE5i treatment, suggesting “that other interventions to prevent inappropriate use may be required.”
The researchers concluded that “[the] time has come to develop interventions to optimize prescribing for PH in order to improve the value, quality, and safety of care.”
One potential intervention suggested by the researchers was to require patients with PH to be evaluated at a PH expert center, as recommended by treatment guidelines.
The study was funded by the Department of Veterans Affairs with resources from the Edith Nourse Rogers Memorial VA Hospital. Elizabeth S. Klings, MD, one of the study’s authors, declared receiving research support from several pharmaceutical companies.
SOURCE: Wiener RS et al. Ann Am Thorac Soc. 2018 Feb 27. doi: 10.1513/AnnalsATS.201710-762OC.
While most veterans with pulmonary hypertension are treated in accordance with clinical guidelines, almost two-thirds who are prescribed therapy are being treated with pulmonary vasodilators inappropriately, an analysis of veteran prescription data reveals.
Little was known about how pulmonary vasodilators were used in practice prior to the publication of this study. While pulmonary vasodilators are considered effective for group 1 pulmonary hypertension (PH), clinical guidelines and advice from the Choosing Wisely campaign recommend against their routine use for PH patients classified into the most common types of PH – groups 2 and 3 – because of a lack of benefit, potential for harm, and high cost, the authors wrote. The report was published in Annals of the American Thoracic Society.
The new analysis shows that patients with PH are potentially being exposed to unnecessary harm, according to study author Renda Soylemez Wiener, MD, MPH, of the Center for Healthcare Organization & Implementation Research at Bedford (Mass.) Veterans Affairs Medical Center, and her colleagues. Their findings also reveal that inappropriate prescribing of pulmonary vasodilators, mostly by specialist clinicians, is contributing to the financial burden of an already stretched health system.
The research team looked at prescription data for veterans prescribed a phosphodiesterase-5 inhibitor (PDE5i), which causes pulmonary vasodilation, between 2005 and 2012 at any VA site. The primary outcome of the study was the proportion of patients who received potentially inappropriate PDE5i as classified in guideline recommendations. Patients with group 1 PH were deemed to have been treated appropriately, while those with group 2 and 3 PH were deemed to have been potentially treated inappropriately. Those with groups 4 and 5 PH were thought to have received treatment of “uncertain value.”
In a chart abstraction analysis from a randomly selected subset of PDE5i-treated patients, half (110/230, 47.8% [41.3%-54.5%]) had documented right heart catheterization to confirm the presence of PH. After factoring this into their algorithm, the investigators determined that only 11.7% [8.0%-16.8%] of these patients received clearly appropriate treatment.
Over the 8-year study period, the number of patients with PH group 2 or 3 prescribed PDE5i rose more than 14-fold, the researchers said. They speculated that this figure was likely to continue to rise with the increasing use of echocardiography and detection of PH.
According to the authors, the cost of treating one PH patient for 1 year with PDE5i therapy was between $10,000 and $13,000.
The 1,711 PH patients classified as being treated inappropriately in the study translated into a cost of over $20 million, if each patient were treated for only 1 year, but many of the patients were treated for a longer period of time.
The researchers suggested that there were several reasons why clinicians might choose to deviate from the guidelines, including lacking familiarity with them or disagreeing with them.
“While guidelines do allow trials of PDE5i in treatment for groups 2 or 3 PH on a case-by-case basis after consultation with a PH expert and a confirmatory [right heart catheterization], even PH experts disagree about whether a trial of PDE5i therapy is reasonable and appropriate for patients with group 3 PH,” they wrote.
They may also overestimate the potential benefits of treatment and/or underestimate potential harm.
Clinicians may believe that guidelines developed for a general population do not apply to the patients they are treating.
“It is understandable why clinicians may offer unproven therapies like PDE5i in hopes of providing relief to very sick patients with groups 2 or 3 PH, especially if they do not believe the recommendation applies to their individual patient or they are not convinced about the potential harms of pulmonary vasodilators,” they said.
The authors expressed concern about VA clinicians’ allowing patients to take PDE5i therapy that had been initially prescribed by clinicians outside of VA hospitals. The researchers said such drugs, which potentially had been prescribed inappropriately, “were continued by VA clinicians without much apparent scrutiny.”
The chart abstraction analysis also showed that specialists prescribed the majority of potentially inappropriate PDE5i treatment, suggesting “that other interventions to prevent inappropriate use may be required.”
The researchers concluded that “[the] time has come to develop interventions to optimize prescribing for PH in order to improve the value, quality, and safety of care.”
One potential intervention suggested by the researchers was to require patients with PH to be evaluated at a PH expert center, as recommended by treatment guidelines.
The study was funded by the Department of Veterans Affairs with resources from the Edith Nourse Rogers Memorial VA Hospital. Elizabeth S. Klings, MD, one of the study’s authors, declared receiving research support from several pharmaceutical companies.
SOURCE: Wiener RS et al. Ann Am Thorac Soc. 2018 Feb 27. doi: 10.1513/AnnalsATS.201710-762OC.
FROM ANNALS OF THE AMERICAN THORACIC SOCIETY
Key clinical point: Inappropriate prescribing of phosphodiesterase-5 inhibitor (PDE5i) therapy has risen 14-fold in 8 years, at a cost of $20 million per year.
Major finding:
Study details: A retrospective analysis of veterans prescribed phosphodiesterase-5 inhibitors for pulmonary hypertension between 2005 and 2012.
Disclosures: The study was funded by the Department of Veterans Affairs with resources from the Edith Nourse Rogers Memorial Veterans Hospital. Elizabeth S. Klings, MD, one of the study’s authors, declared receiving research support from several pharmaceutical companies.
Source: Wiener RS et al. Ann Am Thorac Soc. 2018 Feb 27. doi: 10.1513/AnnalsATS.201710-762OC.
Windows to the Brain
“We were kind of astounded by this—it’s a very unrecognized phenomenon,” said Richard Leigh, MD, assistant clinical investigator at the National Institute of Neurological Disorders and Stroke (NINDS). Dr. Leigh and his co-researchers had discovered that gadolinium, used in brain scans for stroke patients, sometimes leaks into eyes—literally highlighting abnormalities. The finding could lead to more accurate stroke treatment.
The researchers performed MRI scans on 167 stroke patients on admission to the hospital without administering gadolinium and compared those scans to scans taken using gadolinium 2 hours and 24 hours later.
They found that the gadolinium made some eyes glow brightly, marking the location of brain damage. It appeared that the stroke could compromise the blood-ocular barrier. “It looks like the stroke is influencing the eye, and so the eye is reflective of what is going on in the brain,” said Dr. Leigh.
In about three-fourths of patients, gadolinium leaked into the eyes on 1 of the scans: 66% in the 2-hour scan (typically leaking in the aqueous chamber, in the front of the eye) and 75% in the 24-hour scan (typically in in the vitreous chamber, in the back of the eye).
Older patients, those with hypertension and those with brighter spots on their brain scans (associated with brain aging) were more likely to show gadolinium in the vitreous chamber at 24 hours. In a minority of patients, both eye chambers showed gadolinium at 2 hours. In those patients, stroke tended to affect a larger portion of the brain and cause more damage to the blood-brain barrier than did strokes in patients with a slower pattern of gadolinium leakage or no leakage. The researchers observed the phenomenon in both untreated patients and in those who received tPA.
The findings raise the possibility that clinicians could administer a substance to patients that would collect in the eye, like gadolinium, and quickly yield information about the stroke without the need for an MRI, the researchers say. “It’s much easier for us to look inside somebody’s eye than to look into somebody’s brain,” Dr. Leigh said. “So if the eye truly is a window to the brain, we can use one to learn about the other.”
“We were kind of astounded by this—it’s a very unrecognized phenomenon,” said Richard Leigh, MD, assistant clinical investigator at the National Institute of Neurological Disorders and Stroke (NINDS). Dr. Leigh and his co-researchers had discovered that gadolinium, used in brain scans for stroke patients, sometimes leaks into eyes—literally highlighting abnormalities. The finding could lead to more accurate stroke treatment.
The researchers performed MRI scans on 167 stroke patients on admission to the hospital without administering gadolinium and compared those scans to scans taken using gadolinium 2 hours and 24 hours later.
They found that the gadolinium made some eyes glow brightly, marking the location of brain damage. It appeared that the stroke could compromise the blood-ocular barrier. “It looks like the stroke is influencing the eye, and so the eye is reflective of what is going on in the brain,” said Dr. Leigh.
In about three-fourths of patients, gadolinium leaked into the eyes on 1 of the scans: 66% in the 2-hour scan (typically leaking in the aqueous chamber, in the front of the eye) and 75% in the 24-hour scan (typically in in the vitreous chamber, in the back of the eye).
Older patients, those with hypertension and those with brighter spots on their brain scans (associated with brain aging) were more likely to show gadolinium in the vitreous chamber at 24 hours. In a minority of patients, both eye chambers showed gadolinium at 2 hours. In those patients, stroke tended to affect a larger portion of the brain and cause more damage to the blood-brain barrier than did strokes in patients with a slower pattern of gadolinium leakage or no leakage. The researchers observed the phenomenon in both untreated patients and in those who received tPA.
The findings raise the possibility that clinicians could administer a substance to patients that would collect in the eye, like gadolinium, and quickly yield information about the stroke without the need for an MRI, the researchers say. “It’s much easier for us to look inside somebody’s eye than to look into somebody’s brain,” Dr. Leigh said. “So if the eye truly is a window to the brain, we can use one to learn about the other.”
“We were kind of astounded by this—it’s a very unrecognized phenomenon,” said Richard Leigh, MD, assistant clinical investigator at the National Institute of Neurological Disorders and Stroke (NINDS). Dr. Leigh and his co-researchers had discovered that gadolinium, used in brain scans for stroke patients, sometimes leaks into eyes—literally highlighting abnormalities. The finding could lead to more accurate stroke treatment.
The researchers performed MRI scans on 167 stroke patients on admission to the hospital without administering gadolinium and compared those scans to scans taken using gadolinium 2 hours and 24 hours later.
They found that the gadolinium made some eyes glow brightly, marking the location of brain damage. It appeared that the stroke could compromise the blood-ocular barrier. “It looks like the stroke is influencing the eye, and so the eye is reflective of what is going on in the brain,” said Dr. Leigh.
In about three-fourths of patients, gadolinium leaked into the eyes on 1 of the scans: 66% in the 2-hour scan (typically leaking in the aqueous chamber, in the front of the eye) and 75% in the 24-hour scan (typically in in the vitreous chamber, in the back of the eye).
Older patients, those with hypertension and those with brighter spots on their brain scans (associated with brain aging) were more likely to show gadolinium in the vitreous chamber at 24 hours. In a minority of patients, both eye chambers showed gadolinium at 2 hours. In those patients, stroke tended to affect a larger portion of the brain and cause more damage to the blood-brain barrier than did strokes in patients with a slower pattern of gadolinium leakage or no leakage. The researchers observed the phenomenon in both untreated patients and in those who received tPA.
The findings raise the possibility that clinicians could administer a substance to patients that would collect in the eye, like gadolinium, and quickly yield information about the stroke without the need for an MRI, the researchers say. “It’s much easier for us to look inside somebody’s eye than to look into somebody’s brain,” Dr. Leigh said. “So if the eye truly is a window to the brain, we can use one to learn about the other.”
Climate change is worsening allergies, expert says
ORLANDO – Climate change is not just eroding coastlines and threatening seaside cities and taking lives with increasingly powerful hurricanes, but appears to be contributing to increases in allergy and asthma, an expert told the audience at the joint congress of the American Academy of Allergy, Asthma and Immunology and the World Asthma Organization.
Longer pollen seasons, allergens unleashed by felled trees and ripped-up plants, mold growth following floods, and irritants launched into the air by wildfires are some of the concerns that should be alarming physicians and policy makers, said Nelson A. Rosario, MD, PhD, professor of pediatrics at Federal University of Paraná (Brazil).

And evidence suggests that his fellow allergists and their patients agree.
A 2015 international survey found that 80% of rhinitis patients blamed climate change for contributing to their symptoms.
Only 11% said that climate change wasn’t relevant at all. Asked how patients have been affected by climate change, about two-thirds said “increased care for allergic sensitization and symptoms on exposure to plants or mold.”
Science supports these views, Dr. Rosario said.
A 2011 study of North American pollen seasons found that some cities had significant increases of 11-27 days, compared with 15 years before.

And a 2017 review noted the impacts of the consequences of climate change, from increased allergies due to heavy precipitation events, asthma prompted by intense tropical cyclones, and allergic conditions caused by extremely high sea levels.
Dr. Rosario suggested that, rather than wait for official agencies to take action, physicians need to adapt and help their patients adapt. A team of doctors wrote in 2013 that while “improved governmental controls” could lead to cleaner air, they “meet strong opposition because of their effect on business and productivity.” So, they said, the allergy community should adjust, by “anticipating the needs of patients and by adopting practices and research methods to meet changing environmental conditions.”
Dr. Rosario urged physicians to think of the climate-change effects on allergy and asthma as a “collective action” problem, not an individual one.
“The consequences will come,” he said. “There must be international cooperation.”
ORLANDO – Climate change is not just eroding coastlines and threatening seaside cities and taking lives with increasingly powerful hurricanes, but appears to be contributing to increases in allergy and asthma, an expert told the audience at the joint congress of the American Academy of Allergy, Asthma and Immunology and the World Asthma Organization.
Longer pollen seasons, allergens unleashed by felled trees and ripped-up plants, mold growth following floods, and irritants launched into the air by wildfires are some of the concerns that should be alarming physicians and policy makers, said Nelson A. Rosario, MD, PhD, professor of pediatrics at Federal University of Paraná (Brazil).
And evidence suggests that his fellow allergists and their patients agree.
A 2015 international survey found that 80% of rhinitis patients blamed climate change for contributing to their symptoms.
Only 11% said that climate change wasn’t relevant at all. Asked how patients have been affected by climate change, about two-thirds said “increased care for allergic sensitization and symptoms on exposure to plants or mold.”
Science supports these views, Dr. Rosario said.
A 2011 study of North American pollen seasons found that some cities had significant increases of 11-27 days, compared with 15 years before.
And a 2017 review noted the impacts of the consequences of climate change, from increased allergies due to heavy precipitation events, asthma prompted by intense tropical cyclones, and allergic conditions caused by extremely high sea levels.
Dr. Rosario suggested that, rather than wait for official agencies to take action, physicians need to adapt and help their patients adapt. A team of doctors wrote in 2013 that while “improved governmental controls” could lead to cleaner air, they “meet strong opposition because of their effect on business and productivity.” So, they said, the allergy community should adjust, by “anticipating the needs of patients and by adopting practices and research methods to meet changing environmental conditions.”
Dr. Rosario urged physicians to think of the climate-change effects on allergy and asthma as a “collective action” problem, not an individual one.
“The consequences will come,” he said. “There must be international cooperation.”
ORLANDO – Climate change is not just eroding coastlines and threatening seaside cities and taking lives with increasingly powerful hurricanes, but appears to be contributing to increases in allergy and asthma, an expert told the audience at the joint congress of the American Academy of Allergy, Asthma and Immunology and the World Asthma Organization.
Longer pollen seasons, allergens unleashed by felled trees and ripped-up plants, mold growth following floods, and irritants launched into the air by wildfires are some of the concerns that should be alarming physicians and policy makers, said Nelson A. Rosario, MD, PhD, professor of pediatrics at Federal University of Paraná (Brazil).
And evidence suggests that his fellow allergists and their patients agree.
A 2015 international survey found that 80% of rhinitis patients blamed climate change for contributing to their symptoms.
Only 11% said that climate change wasn’t relevant at all. Asked how patients have been affected by climate change, about two-thirds said “increased care for allergic sensitization and symptoms on exposure to plants or mold.”
Science supports these views, Dr. Rosario said.
A 2011 study of North American pollen seasons found that some cities had significant increases of 11-27 days, compared with 15 years before.
And a 2017 review noted the impacts of the consequences of climate change, from increased allergies due to heavy precipitation events, asthma prompted by intense tropical cyclones, and allergic conditions caused by extremely high sea levels.
Dr. Rosario suggested that, rather than wait for official agencies to take action, physicians need to adapt and help their patients adapt. A team of doctors wrote in 2013 that while “improved governmental controls” could lead to cleaner air, they “meet strong opposition because of their effect on business and productivity.” So, they said, the allergy community should adjust, by “anticipating the needs of patients and by adopting practices and research methods to meet changing environmental conditions.”
Dr. Rosario urged physicians to think of the climate-change effects on allergy and asthma as a “collective action” problem, not an individual one.
“The consequences will come,” he said. “There must be international cooperation.”
EXPERT ANALYSIS FROM AAAAI/WAO JOINT CONGRESS