User login
2018-2019 flu season: Going but not gone yet
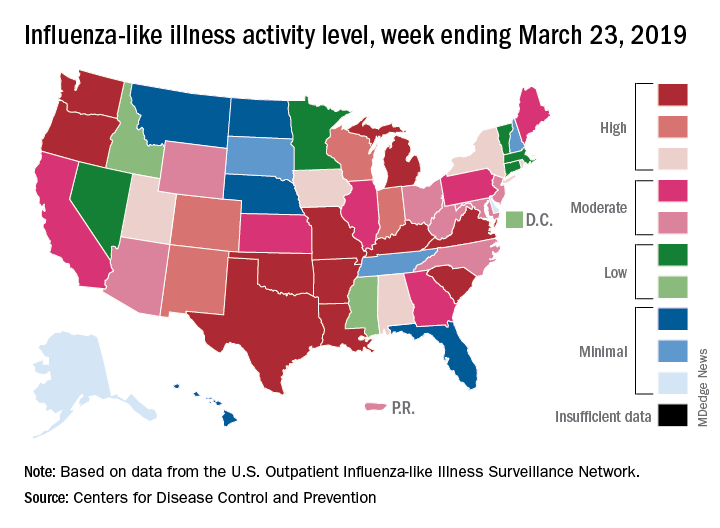
The 2018-2019 flu season again showed real signs of ending as influenza activity levels dropped during the week ending March 23, according to the Centers for Disease Control and Prevention.
Despite those declines, however, current levels of influenza-like illness (ILI) activity are still elevated enough that the CDC issued a health advisory on March 28 to inform clinicians about the “increasing proportion of activity due to influenza A(H3N2) viruses, continued circulation of influenza A(H1N1) viruses, and low levels of influenza B viruses.”
The CDC’s weekly flu report, released March 29, does show that the overall burden is improving. The national proportion of outpatient visits for ILI dropped from 4.3% for the week ending March 16 to 3.8% for the latest reporting week, the CDC’s influenza division reported. The figure for March 16 was originally reported to be 4.4% but was revised in the new report.
The length of this years’ flu season, when measured as the number of weeks at or above the baseline level of 2.2%, is now 18 weeks. By this measure, the last five seasons have averaged 16 weeks, the CDC noted.
Influenza was considered widespread in 34 states and Puerto Rico for the week ending March 23, down from 44 states the previous week. The number of states at the highest level of ILI activity on the CDC’s 1-10 scale dropped from 20 to 11, and those in the high range (8-10) dropped from 26 to 20, data from the CDC’s Outpatient ILI Surveillance Network show.
There was one flu-related pediatric death during the week of March 23 but none reported from earlier weeks, which brings the total to 77 for the 2018-2019 season, the CDC said.
The 2018-2019 flu season again showed real signs of ending as influenza activity levels dropped during the week ending March 23, according to the Centers for Disease Control and Prevention.
Despite those declines, however, current levels of influenza-like illness (ILI) activity are still elevated enough that the CDC issued a health advisory on March 28 to inform clinicians about the “increasing proportion of activity due to influenza A(H3N2) viruses, continued circulation of influenza A(H1N1) viruses, and low levels of influenza B viruses.”
The CDC’s weekly flu report, released March 29, does show that the overall burden is improving. The national proportion of outpatient visits for ILI dropped from 4.3% for the week ending March 16 to 3.8% for the latest reporting week, the CDC’s influenza division reported. The figure for March 16 was originally reported to be 4.4% but was revised in the new report.
The length of this years’ flu season, when measured as the number of weeks at or above the baseline level of 2.2%, is now 18 weeks. By this measure, the last five seasons have averaged 16 weeks, the CDC noted.
Influenza was considered widespread in 34 states and Puerto Rico for the week ending March 23, down from 44 states the previous week. The number of states at the highest level of ILI activity on the CDC’s 1-10 scale dropped from 20 to 11, and those in the high range (8-10) dropped from 26 to 20, data from the CDC’s Outpatient ILI Surveillance Network show.
There was one flu-related pediatric death during the week of March 23 but none reported from earlier weeks, which brings the total to 77 for the 2018-2019 season, the CDC said.
The 2018-2019 flu season again showed real signs of ending as influenza activity levels dropped during the week ending March 23, according to the Centers for Disease Control and Prevention.
Despite those declines, however, current levels of influenza-like illness (ILI) activity are still elevated enough that the CDC issued a health advisory on March 28 to inform clinicians about the “increasing proportion of activity due to influenza A(H3N2) viruses, continued circulation of influenza A(H1N1) viruses, and low levels of influenza B viruses.”
The CDC’s weekly flu report, released March 29, does show that the overall burden is improving. The national proportion of outpatient visits for ILI dropped from 4.3% for the week ending March 16 to 3.8% for the latest reporting week, the CDC’s influenza division reported. The figure for March 16 was originally reported to be 4.4% but was revised in the new report.
The length of this years’ flu season, when measured as the number of weeks at or above the baseline level of 2.2%, is now 18 weeks. By this measure, the last five seasons have averaged 16 weeks, the CDC noted.
Influenza was considered widespread in 34 states and Puerto Rico for the week ending March 23, down from 44 states the previous week. The number of states at the highest level of ILI activity on the CDC’s 1-10 scale dropped from 20 to 11, and those in the high range (8-10) dropped from 26 to 20, data from the CDC’s Outpatient ILI Surveillance Network show.
There was one flu-related pediatric death during the week of March 23 but none reported from earlier weeks, which brings the total to 77 for the 2018-2019 season, the CDC said.
Do Collaborative Models Work for Mental Health in a General Clinical Setting?
Collaborative chronic care models (CCMs) are effective in serious mental illnesses, which has been shown in extensive randomized clinical trials. Much of their effectiveness comes from the emphasis on flexibility: They are implemented according to local needs, capabilities, and priorities. Collaborative chronic care models also provide support: for redesigned work roles that promote “anticipatory” continuous care, for self-management, and for clinical decision making at a local level.
In 2013, the VA Office of Mental Health and Suicide Prevention (OMHSP) began an initiative to enhance care coordination in general mental health clinics with mixed-diagnosis populations. It established interdisciplinary teams in each VA medical center throughout the US. Although providing centrally developed guidance, VAOMHSP gave facilities “broad latitude” to develop their team processes. In 2015, VAOMHSP adopted the CCM.
But most of the data on how well CCMs work for mental health conditions come from depression treatment in primary care—and the effects seem to be inconsistent. So researchers from Veterans Affairs Boston Healthcare System and others partnered with VAOMHSP to find out whether the CCM model would be effective in a general clinical setting.
They recruited 9 VA facilities for a 2-year study conducted in 3 waves. The implementation strategy was based on the premise that “health care is a complex adaptive system rather than a highly controlled machine.” That is, it would work best if local solutions for local challenges could be developed in accordance with evidence-based guidance. The multifaceted approach included an external facilitator who provided guidance and quality improvement expertise and an on-site internal facilitator to direct the implementation.
In the study, 5,596 veterans treated by outpatient general mental health teams were included in hospitalization analyses. A randomly selected sample of 1,050 (including 210 women) was identified for health status interviews.
The researchers found a “robust” and sustained reduction in mental health hospitalization. However, the effects on self-reported health outcomes were “limited,” the researchers say. The mental component score (the primary intervention outcome) did not change statistically significantly with implementation support in adjusted or unadjusted models, nor did other interview measures. The researchers say they saw no difference in the way veterans were treated between higher and lower implementing teams.
In post hoc analyses, though, patients with more complex problems, defined as receiving treatment for ≥ 3 mental health diagnoses in the previous year, did show statistically significant improvements in the facilitation year (by a magnitude of 0.31 SD). By contrast, those with ≤ 2 diagnoses declined nonsignificantly during the same time. The researchers note that other studies have found that CCM-based teams in patient-centered medical homes have also shown more benefit among higher morbidity patients.
Overall, the model was shown to be effectively implemented with “practical, scalable support” for clinicians. Another benefit was that teams performed better, the researchers found. They assessed team function at baseline and during the second 6 months on measures, including communication, cohesion, role clarity, and team primacy (prioritizing team over individual goals). The subscales showed high ratings for cohesion and communication at baseline, which did not change with implementation support. However, role clarity and team primacy improved significantly. The researchers conclude that under typical practice conditions CCMs can help the clinicians help the sickest patients.
Collaborative chronic care models (CCMs) are effective in serious mental illnesses, which has been shown in extensive randomized clinical trials. Much of their effectiveness comes from the emphasis on flexibility: They are implemented according to local needs, capabilities, and priorities. Collaborative chronic care models also provide support: for redesigned work roles that promote “anticipatory” continuous care, for self-management, and for clinical decision making at a local level.
In 2013, the VA Office of Mental Health and Suicide Prevention (OMHSP) began an initiative to enhance care coordination in general mental health clinics with mixed-diagnosis populations. It established interdisciplinary teams in each VA medical center throughout the US. Although providing centrally developed guidance, VAOMHSP gave facilities “broad latitude” to develop their team processes. In 2015, VAOMHSP adopted the CCM.
But most of the data on how well CCMs work for mental health conditions come from depression treatment in primary care—and the effects seem to be inconsistent. So researchers from Veterans Affairs Boston Healthcare System and others partnered with VAOMHSP to find out whether the CCM model would be effective in a general clinical setting.
They recruited 9 VA facilities for a 2-year study conducted in 3 waves. The implementation strategy was based on the premise that “health care is a complex adaptive system rather than a highly controlled machine.” That is, it would work best if local solutions for local challenges could be developed in accordance with evidence-based guidance. The multifaceted approach included an external facilitator who provided guidance and quality improvement expertise and an on-site internal facilitator to direct the implementation.
In the study, 5,596 veterans treated by outpatient general mental health teams were included in hospitalization analyses. A randomly selected sample of 1,050 (including 210 women) was identified for health status interviews.
The researchers found a “robust” and sustained reduction in mental health hospitalization. However, the effects on self-reported health outcomes were “limited,” the researchers say. The mental component score (the primary intervention outcome) did not change statistically significantly with implementation support in adjusted or unadjusted models, nor did other interview measures. The researchers say they saw no difference in the way veterans were treated between higher and lower implementing teams.
In post hoc analyses, though, patients with more complex problems, defined as receiving treatment for ≥ 3 mental health diagnoses in the previous year, did show statistically significant improvements in the facilitation year (by a magnitude of 0.31 SD). By contrast, those with ≤ 2 diagnoses declined nonsignificantly during the same time. The researchers note that other studies have found that CCM-based teams in patient-centered medical homes have also shown more benefit among higher morbidity patients.
Overall, the model was shown to be effectively implemented with “practical, scalable support” for clinicians. Another benefit was that teams performed better, the researchers found. They assessed team function at baseline and during the second 6 months on measures, including communication, cohesion, role clarity, and team primacy (prioritizing team over individual goals). The subscales showed high ratings for cohesion and communication at baseline, which did not change with implementation support. However, role clarity and team primacy improved significantly. The researchers conclude that under typical practice conditions CCMs can help the clinicians help the sickest patients.
Collaborative chronic care models (CCMs) are effective in serious mental illnesses, which has been shown in extensive randomized clinical trials. Much of their effectiveness comes from the emphasis on flexibility: They are implemented according to local needs, capabilities, and priorities. Collaborative chronic care models also provide support: for redesigned work roles that promote “anticipatory” continuous care, for self-management, and for clinical decision making at a local level.
In 2013, the VA Office of Mental Health and Suicide Prevention (OMHSP) began an initiative to enhance care coordination in general mental health clinics with mixed-diagnosis populations. It established interdisciplinary teams in each VA medical center throughout the US. Although providing centrally developed guidance, VAOMHSP gave facilities “broad latitude” to develop their team processes. In 2015, VAOMHSP adopted the CCM.
But most of the data on how well CCMs work for mental health conditions come from depression treatment in primary care—and the effects seem to be inconsistent. So researchers from Veterans Affairs Boston Healthcare System and others partnered with VAOMHSP to find out whether the CCM model would be effective in a general clinical setting.
They recruited 9 VA facilities for a 2-year study conducted in 3 waves. The implementation strategy was based on the premise that “health care is a complex adaptive system rather than a highly controlled machine.” That is, it would work best if local solutions for local challenges could be developed in accordance with evidence-based guidance. The multifaceted approach included an external facilitator who provided guidance and quality improvement expertise and an on-site internal facilitator to direct the implementation.
In the study, 5,596 veterans treated by outpatient general mental health teams were included in hospitalization analyses. A randomly selected sample of 1,050 (including 210 women) was identified for health status interviews.
The researchers found a “robust” and sustained reduction in mental health hospitalization. However, the effects on self-reported health outcomes were “limited,” the researchers say. The mental component score (the primary intervention outcome) did not change statistically significantly with implementation support in adjusted or unadjusted models, nor did other interview measures. The researchers say they saw no difference in the way veterans were treated between higher and lower implementing teams.
In post hoc analyses, though, patients with more complex problems, defined as receiving treatment for ≥ 3 mental health diagnoses in the previous year, did show statistically significant improvements in the facilitation year (by a magnitude of 0.31 SD). By contrast, those with ≤ 2 diagnoses declined nonsignificantly during the same time. The researchers note that other studies have found that CCM-based teams in patient-centered medical homes have also shown more benefit among higher morbidity patients.
Overall, the model was shown to be effectively implemented with “practical, scalable support” for clinicians. Another benefit was that teams performed better, the researchers found. They assessed team function at baseline and during the second 6 months on measures, including communication, cohesion, role clarity, and team primacy (prioritizing team over individual goals). The subscales showed high ratings for cohesion and communication at baseline, which did not change with implementation support. However, role clarity and team primacy improved significantly. The researchers conclude that under typical practice conditions CCMs can help the clinicians help the sickest patients.
VA Community Living Centers Health Care Reports Are Now Public
Although VA nursing homes, on the whole, have sicker patients than do those in private sector nursing homes, they compare closely in terms of quality of care—and in some cases, VA health care gets higher marks. VA has more higher performing facilities (17% vs 11%) and fewer low-performing facilities (17% vs 20%).
Those figures come from the health care inspection reports and staffing data for its 134 community living centers (CLCs) that the VA is, for the first time, posting publicly. So far, VA has posted 101 health inspection reports; the remainder are scheduled for later this year. The reports cover April 2018 to the present.
The VA reports are based on yearly, unannounced inspections conducted by an outside contracted agency. The survey teams assess a variety of aspects of life at VA nursing homes, such as the care of residents and the processes used to give that care, how the staff and residents interact, and the nursing home environment. The surveyors also review residents’ clinical records and interview residents, family members, caregivers, and staff.
VA nursing homes also had a significantly lower percentage (6%) of 1-star (lowest rated) nursing homes compared with 15,487 private sector nursing homes rated by the Centers for Medicare and Medicaid Services. Both Medicare-certified skilled nursing facilities and VA CLCs must meet federal standards, such as having enough staff to provide adequate care. “There is significant evidence of a relationship between resident outcomes and staffing levels in nursing homes,” the VA says in its description of survey criteria.
Many VA nursing home residents are being treated for conditions rarely seen in private sector nursing homes, the VA says, including veteran-specific conditions, such as posttraumatic stress disorder (12% vs 0.5%) and traumatic brain injury (2% vs 0.8%). In 2018, 42% of 41,076 VA CLC residents had a service-connected disability rating of ≥ 50%. CLCs also provide more hospice care and care for conditions related to homelessness.
However, the VA notes that “quality measures are not the same as quality standards.” According to Medicare Nursing Home Compare, the quality of resident care measures are not benchmarks, thresholds, guidelines, or standards of care—they are a “snapshot at a point in time” of the average condition of residents. For instance, individual CLCs may serve special populations and have a higher rate of certain conditions. A CLC that specializes in complex skin and wound care may admit veterans with severe pressure ulcers that occurred at home or another hospital.
Detailed information on individual quality measures and how VA facilities compare with others in their areas are available at www.accesstocare.va.gov/healthcare/qualityofcare. That site also has an interactive searchable map that can be used to locate CLCs by zip code or distance. The health inspection reports are available at www.va.gov/qualityofcare/apps/aspire/clcsurvey.aspx.
Although VA nursing homes, on the whole, have sicker patients than do those in private sector nursing homes, they compare closely in terms of quality of care—and in some cases, VA health care gets higher marks. VA has more higher performing facilities (17% vs 11%) and fewer low-performing facilities (17% vs 20%).
Those figures come from the health care inspection reports and staffing data for its 134 community living centers (CLCs) that the VA is, for the first time, posting publicly. So far, VA has posted 101 health inspection reports; the remainder are scheduled for later this year. The reports cover April 2018 to the present.
The VA reports are based on yearly, unannounced inspections conducted by an outside contracted agency. The survey teams assess a variety of aspects of life at VA nursing homes, such as the care of residents and the processes used to give that care, how the staff and residents interact, and the nursing home environment. The surveyors also review residents’ clinical records and interview residents, family members, caregivers, and staff.
VA nursing homes also had a significantly lower percentage (6%) of 1-star (lowest rated) nursing homes compared with 15,487 private sector nursing homes rated by the Centers for Medicare and Medicaid Services. Both Medicare-certified skilled nursing facilities and VA CLCs must meet federal standards, such as having enough staff to provide adequate care. “There is significant evidence of a relationship between resident outcomes and staffing levels in nursing homes,” the VA says in its description of survey criteria.
Many VA nursing home residents are being treated for conditions rarely seen in private sector nursing homes, the VA says, including veteran-specific conditions, such as posttraumatic stress disorder (12% vs 0.5%) and traumatic brain injury (2% vs 0.8%). In 2018, 42% of 41,076 VA CLC residents had a service-connected disability rating of ≥ 50%. CLCs also provide more hospice care and care for conditions related to homelessness.
However, the VA notes that “quality measures are not the same as quality standards.” According to Medicare Nursing Home Compare, the quality of resident care measures are not benchmarks, thresholds, guidelines, or standards of care—they are a “snapshot at a point in time” of the average condition of residents. For instance, individual CLCs may serve special populations and have a higher rate of certain conditions. A CLC that specializes in complex skin and wound care may admit veterans with severe pressure ulcers that occurred at home or another hospital.
Detailed information on individual quality measures and how VA facilities compare with others in their areas are available at www.accesstocare.va.gov/healthcare/qualityofcare. That site also has an interactive searchable map that can be used to locate CLCs by zip code or distance. The health inspection reports are available at www.va.gov/qualityofcare/apps/aspire/clcsurvey.aspx.
Although VA nursing homes, on the whole, have sicker patients than do those in private sector nursing homes, they compare closely in terms of quality of care—and in some cases, VA health care gets higher marks. VA has more higher performing facilities (17% vs 11%) and fewer low-performing facilities (17% vs 20%).
Those figures come from the health care inspection reports and staffing data for its 134 community living centers (CLCs) that the VA is, for the first time, posting publicly. So far, VA has posted 101 health inspection reports; the remainder are scheduled for later this year. The reports cover April 2018 to the present.
The VA reports are based on yearly, unannounced inspections conducted by an outside contracted agency. The survey teams assess a variety of aspects of life at VA nursing homes, such as the care of residents and the processes used to give that care, how the staff and residents interact, and the nursing home environment. The surveyors also review residents’ clinical records and interview residents, family members, caregivers, and staff.
VA nursing homes also had a significantly lower percentage (6%) of 1-star (lowest rated) nursing homes compared with 15,487 private sector nursing homes rated by the Centers for Medicare and Medicaid Services. Both Medicare-certified skilled nursing facilities and VA CLCs must meet federal standards, such as having enough staff to provide adequate care. “There is significant evidence of a relationship between resident outcomes and staffing levels in nursing homes,” the VA says in its description of survey criteria.
Many VA nursing home residents are being treated for conditions rarely seen in private sector nursing homes, the VA says, including veteran-specific conditions, such as posttraumatic stress disorder (12% vs 0.5%) and traumatic brain injury (2% vs 0.8%). In 2018, 42% of 41,076 VA CLC residents had a service-connected disability rating of ≥ 50%. CLCs also provide more hospice care and care for conditions related to homelessness.
However, the VA notes that “quality measures are not the same as quality standards.” According to Medicare Nursing Home Compare, the quality of resident care measures are not benchmarks, thresholds, guidelines, or standards of care—they are a “snapshot at a point in time” of the average condition of residents. For instance, individual CLCs may serve special populations and have a higher rate of certain conditions. A CLC that specializes in complex skin and wound care may admit veterans with severe pressure ulcers that occurred at home or another hospital.
Detailed information on individual quality measures and how VA facilities compare with others in their areas are available at www.accesstocare.va.gov/healthcare/qualityofcare. That site also has an interactive searchable map that can be used to locate CLCs by zip code or distance. The health inspection reports are available at www.va.gov/qualityofcare/apps/aspire/clcsurvey.aspx.
Atypical used in Parkinson’s lifts hallucinations, delusions in refractory schizophrenia
Pimavanserin (Nuplazid), an atypical antipsychotic approved to treat hallucinations and delusions in Parkinson’s disease, shows promise as a treatment for patients with refractory schizophrenia who fail to respond to clozapine, a retrospective study suggests.
“Within a month, sometimes 2 months, hallucinations and delusions that have persisted for years were completely gone,” said lead author Henry A. Nasrallah, MD, in an interview. The study was published in Schizophrenia Research.
Dr. Nasrallah and his colleagues launched the study in a bid to help “the most desperate group of patients” with schizophrenia – the 60% of those with refractory psychosis who do not respond to clozapine.
“This group of patients is so desperate that psychiatrists have used everything in our pharmacopeia,” said Dr. Nasrallah, the Sydney W. Souers Endowed Chair and professor and chairman of the department of psychiatry and behavioral neuroscience at Saint Louis University. “Nothing has been shown to work. We decided to give them this medication [pimavanserin], which was approved by the FDA [Food and Drug Administration] 2 years ago for hallucinations and delusions for Parkinson’s disease.”
For the new study, Dr. Nasrallah and his coauthors gave 34 mg/day of pimavanserin to 10 patients, aged 21-77 years, with schizophrenia or schizoaffective disorder and refractory hallucinations and delusions. The subjects, all of whom live in a residential group home, had either failed clozapine (n = 6) or failed several antipsychotics but had not yet received clozapine (n = 4).
The results, Dr. Nasrallah said, were remarkable. “Not only did they get relief from their delusions and hallucinations, but nursing staff reported they were much more sociable and affable, getting out of their rooms, and mixing and mingling. It seems to help them beyond suppressing delusions and hallucinations. It made them more sociable and pleasant.”
Patients were able to avoid blood tests and the “sometimes life-threatening side effects of clozapine,” he said. According to the study, no patients needed to discontinue treatment because of safety or tolerability.
However, pimavanserin is expensive. According to GoodRx.com, monthly prices for 60 tablets of 17 mg pimavanserin – equal to the daily dose in this study – run from $2,759 to $2,907 with a free coupon.
Should psychiatrists prescribe the drug now for treatment-resistant schizophrenia? “We use drugs off label all the time for patients who do not have any FDA-approved medication,” Dr. Nasrallah said. “Sometimes, off-label use in psychiatry is a necessity, because around 80% of DSM-5 disorders do not have any approved drugs at this time.”
“It would also be interesting to test pimavanserin in first-episode psychosis to identify a ‘serotonergic subtype’ of the schizophrenia syndrome but also to completely avoid the extrapyramidal side effects of dopamine antagonists, to which first-episode psychosis patients are especially susceptible.”
No outside funding was reported. Dr. Nasrallah reported advisory board and consultant and speaker’s bureau relationships with Acadia, Alkermes, Allergan, Janssen, Lundbeck, Neurocrine Biosciences, Otsuka Pharmaceutical, Sunovion, and Teva. Another author reported no disclosures, and a third author reported numerous disclosures.
SOURCE: Nasrallah HA et al. Schizophr Res. 2019 Mar 2. doi: 10/1016/j.schres.2019.02.018.
Pimavanserin (Nuplazid), an atypical antipsychotic approved to treat hallucinations and delusions in Parkinson’s disease, shows promise as a treatment for patients with refractory schizophrenia who fail to respond to clozapine, a retrospective study suggests.
“Within a month, sometimes 2 months, hallucinations and delusions that have persisted for years were completely gone,” said lead author Henry A. Nasrallah, MD, in an interview. The study was published in Schizophrenia Research.
Dr. Nasrallah and his colleagues launched the study in a bid to help “the most desperate group of patients” with schizophrenia – the 60% of those with refractory psychosis who do not respond to clozapine.
“This group of patients is so desperate that psychiatrists have used everything in our pharmacopeia,” said Dr. Nasrallah, the Sydney W. Souers Endowed Chair and professor and chairman of the department of psychiatry and behavioral neuroscience at Saint Louis University. “Nothing has been shown to work. We decided to give them this medication [pimavanserin], which was approved by the FDA [Food and Drug Administration] 2 years ago for hallucinations and delusions for Parkinson’s disease.”
For the new study, Dr. Nasrallah and his coauthors gave 34 mg/day of pimavanserin to 10 patients, aged 21-77 years, with schizophrenia or schizoaffective disorder and refractory hallucinations and delusions. The subjects, all of whom live in a residential group home, had either failed clozapine (n = 6) or failed several antipsychotics but had not yet received clozapine (n = 4).
The results, Dr. Nasrallah said, were remarkable. “Not only did they get relief from their delusions and hallucinations, but nursing staff reported they were much more sociable and affable, getting out of their rooms, and mixing and mingling. It seems to help them beyond suppressing delusions and hallucinations. It made them more sociable and pleasant.”
Patients were able to avoid blood tests and the “sometimes life-threatening side effects of clozapine,” he said. According to the study, no patients needed to discontinue treatment because of safety or tolerability.
However, pimavanserin is expensive. According to GoodRx.com, monthly prices for 60 tablets of 17 mg pimavanserin – equal to the daily dose in this study – run from $2,759 to $2,907 with a free coupon.
Should psychiatrists prescribe the drug now for treatment-resistant schizophrenia? “We use drugs off label all the time for patients who do not have any FDA-approved medication,” Dr. Nasrallah said. “Sometimes, off-label use in psychiatry is a necessity, because around 80% of DSM-5 disorders do not have any approved drugs at this time.”
“It would also be interesting to test pimavanserin in first-episode psychosis to identify a ‘serotonergic subtype’ of the schizophrenia syndrome but also to completely avoid the extrapyramidal side effects of dopamine antagonists, to which first-episode psychosis patients are especially susceptible.”
No outside funding was reported. Dr. Nasrallah reported advisory board and consultant and speaker’s bureau relationships with Acadia, Alkermes, Allergan, Janssen, Lundbeck, Neurocrine Biosciences, Otsuka Pharmaceutical, Sunovion, and Teva. Another author reported no disclosures, and a third author reported numerous disclosures.
SOURCE: Nasrallah HA et al. Schizophr Res. 2019 Mar 2. doi: 10/1016/j.schres.2019.02.018.
Pimavanserin (Nuplazid), an atypical antipsychotic approved to treat hallucinations and delusions in Parkinson’s disease, shows promise as a treatment for patients with refractory schizophrenia who fail to respond to clozapine, a retrospective study suggests.
“Within a month, sometimes 2 months, hallucinations and delusions that have persisted for years were completely gone,” said lead author Henry A. Nasrallah, MD, in an interview. The study was published in Schizophrenia Research.
Dr. Nasrallah and his colleagues launched the study in a bid to help “the most desperate group of patients” with schizophrenia – the 60% of those with refractory psychosis who do not respond to clozapine.
“This group of patients is so desperate that psychiatrists have used everything in our pharmacopeia,” said Dr. Nasrallah, the Sydney W. Souers Endowed Chair and professor and chairman of the department of psychiatry and behavioral neuroscience at Saint Louis University. “Nothing has been shown to work. We decided to give them this medication [pimavanserin], which was approved by the FDA [Food and Drug Administration] 2 years ago for hallucinations and delusions for Parkinson’s disease.”
For the new study, Dr. Nasrallah and his coauthors gave 34 mg/day of pimavanserin to 10 patients, aged 21-77 years, with schizophrenia or schizoaffective disorder and refractory hallucinations and delusions. The subjects, all of whom live in a residential group home, had either failed clozapine (n = 6) or failed several antipsychotics but had not yet received clozapine (n = 4).
The results, Dr. Nasrallah said, were remarkable. “Not only did they get relief from their delusions and hallucinations, but nursing staff reported they were much more sociable and affable, getting out of their rooms, and mixing and mingling. It seems to help them beyond suppressing delusions and hallucinations. It made them more sociable and pleasant.”
Patients were able to avoid blood tests and the “sometimes life-threatening side effects of clozapine,” he said. According to the study, no patients needed to discontinue treatment because of safety or tolerability.
However, pimavanserin is expensive. According to GoodRx.com, monthly prices for 60 tablets of 17 mg pimavanserin – equal to the daily dose in this study – run from $2,759 to $2,907 with a free coupon.
Should psychiatrists prescribe the drug now for treatment-resistant schizophrenia? “We use drugs off label all the time for patients who do not have any FDA-approved medication,” Dr. Nasrallah said. “Sometimes, off-label use in psychiatry is a necessity, because around 80% of DSM-5 disorders do not have any approved drugs at this time.”
“It would also be interesting to test pimavanserin in first-episode psychosis to identify a ‘serotonergic subtype’ of the schizophrenia syndrome but also to completely avoid the extrapyramidal side effects of dopamine antagonists, to which first-episode psychosis patients are especially susceptible.”
No outside funding was reported. Dr. Nasrallah reported advisory board and consultant and speaker’s bureau relationships with Acadia, Alkermes, Allergan, Janssen, Lundbeck, Neurocrine Biosciences, Otsuka Pharmaceutical, Sunovion, and Teva. Another author reported no disclosures, and a third author reported numerous disclosures.
SOURCE: Nasrallah HA et al. Schizophr Res. 2019 Mar 2. doi: 10/1016/j.schres.2019.02.018.
FROM SCHIZOPHRENIA RESEARCH
Universal “Test-and-Treat” Strategy Cuts Down New HIV Infections
The findings suggest that a universal “test-and-treat” strategy could be “an important addition to our toolbox of proven HIV prevention modalities,” said Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases.
The National Institute of Allergy and Infectious Diseases (NIAID)-sponsored study, Population Effects of Antiretroviral Therapy to Reduce HIV Transmission (PopART), was conducted from 2013 to 2018 in 21 urban and peri-urban communities in Zambia and South Africa, each with about 50,000 residents.
The communities were grouped as 7 “triplets” matched by geographic location and estimated HIV prevalence. The first group received annual house-to-house voluntary HIV testing and counseling, linkage to care for those testing positive, and the offer of a suite of proven prevention measures for those who tested negative. The second group received the same services as the first except treatment was offered according to national guidelines. The third group served as a control and received HIV prevention and testing services according to the local standard of care and HIV treatment according to national guidelines.
At the start of the study, the national guidelines for HIV treatment in Zambia and South Africa specified starting ART when the CD4+ T-cell count had declined to 350 cells/µL. In 2014, that threshold was raised to 500 cells/µL. In 2016, both countries recommended that everyone diagnosed with HIV begin ART immediately regardless of CD4+ T-cell count. Consequently, the first and second groups received the same intervention during the last 2 years of the study.
The researchers also recruited a random sample of about 2,300 adults from each community and visited them once a year for 3 years to collect data and test blood.
In the first 3 years, during nearly 40,000 person-years of follow-up, 553 people developed HIV infection (1.4 infections per 100 person-years). HIV incidence was 7% lower in group 1 than in the control group, although the difference was not statistically significant. However, HIV incidence was 30% lower in group 2 compared with that in the control group—a highly statistically significant and consistent result. (The researchers can’t explain why new HIV infections didn’t decline in all the communities where people who tested positive were offered immediate treatment.)
Of participants who tested positive by year 2, 72% of group 1, 68% of group 2, and 60% of the control group had achieved viral suppression.
The findings suggest that a universal “test-and-treat” strategy could be “an important addition to our toolbox of proven HIV prevention modalities,” said Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases.
The National Institute of Allergy and Infectious Diseases (NIAID)-sponsored study, Population Effects of Antiretroviral Therapy to Reduce HIV Transmission (PopART), was conducted from 2013 to 2018 in 21 urban and peri-urban communities in Zambia and South Africa, each with about 50,000 residents.
The communities were grouped as 7 “triplets” matched by geographic location and estimated HIV prevalence. The first group received annual house-to-house voluntary HIV testing and counseling, linkage to care for those testing positive, and the offer of a suite of proven prevention measures for those who tested negative. The second group received the same services as the first except treatment was offered according to national guidelines. The third group served as a control and received HIV prevention and testing services according to the local standard of care and HIV treatment according to national guidelines.
At the start of the study, the national guidelines for HIV treatment in Zambia and South Africa specified starting ART when the CD4+ T-cell count had declined to 350 cells/µL. In 2014, that threshold was raised to 500 cells/µL. In 2016, both countries recommended that everyone diagnosed with HIV begin ART immediately regardless of CD4+ T-cell count. Consequently, the first and second groups received the same intervention during the last 2 years of the study.
The researchers also recruited a random sample of about 2,300 adults from each community and visited them once a year for 3 years to collect data and test blood.
In the first 3 years, during nearly 40,000 person-years of follow-up, 553 people developed HIV infection (1.4 infections per 100 person-years). HIV incidence was 7% lower in group 1 than in the control group, although the difference was not statistically significant. However, HIV incidence was 30% lower in group 2 compared with that in the control group—a highly statistically significant and consistent result. (The researchers can’t explain why new HIV infections didn’t decline in all the communities where people who tested positive were offered immediate treatment.)
Of participants who tested positive by year 2, 72% of group 1, 68% of group 2, and 60% of the control group had achieved viral suppression.
The findings suggest that a universal “test-and-treat” strategy could be “an important addition to our toolbox of proven HIV prevention modalities,” said Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases.
The National Institute of Allergy and Infectious Diseases (NIAID)-sponsored study, Population Effects of Antiretroviral Therapy to Reduce HIV Transmission (PopART), was conducted from 2013 to 2018 in 21 urban and peri-urban communities in Zambia and South Africa, each with about 50,000 residents.
The communities were grouped as 7 “triplets” matched by geographic location and estimated HIV prevalence. The first group received annual house-to-house voluntary HIV testing and counseling, linkage to care for those testing positive, and the offer of a suite of proven prevention measures for those who tested negative. The second group received the same services as the first except treatment was offered according to national guidelines. The third group served as a control and received HIV prevention and testing services according to the local standard of care and HIV treatment according to national guidelines.
At the start of the study, the national guidelines for HIV treatment in Zambia and South Africa specified starting ART when the CD4+ T-cell count had declined to 350 cells/µL. In 2014, that threshold was raised to 500 cells/µL. In 2016, both countries recommended that everyone diagnosed with HIV begin ART immediately regardless of CD4+ T-cell count. Consequently, the first and second groups received the same intervention during the last 2 years of the study.
The researchers also recruited a random sample of about 2,300 adults from each community and visited them once a year for 3 years to collect data and test blood.
In the first 3 years, during nearly 40,000 person-years of follow-up, 553 people developed HIV infection (1.4 infections per 100 person-years). HIV incidence was 7% lower in group 1 than in the control group, although the difference was not statistically significant. However, HIV incidence was 30% lower in group 2 compared with that in the control group—a highly statistically significant and consistent result. (The researchers can’t explain why new HIV infections didn’t decline in all the communities where people who tested positive were offered immediate treatment.)
Of participants who tested positive by year 2, 72% of group 1, 68% of group 2, and 60% of the control group had achieved viral suppression.
Occurrence of pulmonary embolisms in hospitalized patients nearly doubled during 2004-2015
NEW ORLEANS –
During 2004-2015 the incidence of all diagnosed pulmonary embolism (PE), based on discharge diagnoses, rose from 5.4 cases/1,000 hospitalized patients in 2004 to 9.7 cases/1,000 hospitalized patients in 2015, an 80% increase, Joshua B. Goldberg, MD said at the annual meeting of the American College of Cardiology. The incidence of major PE – defined as a patient who needed vasopressor treatment, mechanical ventilation, or had nonseptic shock – rose from 7.9% of all hospitalized PE diagnoses in 2004 to 9.7% in 2015, a 23% relative increase.

The data also documented a shifting pattern of treatment for all hospitalized patients with PE, and especially among patients with major PE. During the study period, treatment with systemic thrombolysis for all PE rose nearly threefold, and catheter-directed therapy began to show a steady rise in use from 0.2% of all patients in 2011 (and before) to 1% of all patients by 2015. Surgical intervention remained lightly used throughout, with about 0.2% of all PE patients undergoing surgery annually.
Most of these intervention options focused on patients with major PE. Among patients in this subgroup with more severe disease, use of one of these three types of interventions rose from 6% in 2004 to 12% in 2015, mostly driven by a rise in systemic thrombolysis, which jumped from 3% of major PE in 2004 to 9% in 2015. However, the efficacy of systemic thrombolysis in patients with major PE remains suspect. In 2004, 39% of patients with major PE treated with systemic thrombolysis died in hospital; in 2015 the number was 47%. “The data don’t support using systemic thrombolysis to treat major PE; the mortality is high,” noted Dr. Goldberg, a cardiothoracic surgeon at Westchester Medical Center in Valhalla, N.Y.
Although catheter-directed therapy began to be much more widely used in U.S. practice starting in about 2015, during the period studied its use for major PE held fairly steady at roughly 2%-3%, but this approach also showed substantial shortcomings for the major PE population. These sicker patients treated with catheter-directed therapy had 37% mortality in 2004 and a 31% mortality in 2015, a difference that was not statistically significant. In general, PE patients enrolled in the catheter-directed therapy trials were not as sick as the major PE patients who get treated with surgery in routine practice, Dr. Goldberg said in an interview.
The data showed much better performance using surgery, although only 1,237 patients of the entire group of 713,083 PE patients studied in the database underwent surgical embolectomy. Overall, in-hospital mortality in these patients was 22%, but in a time trend analysis, mortality among all PE patients treated with surgery fell from 32% in 2004 to 14% in 2015; among patients with major PE treated with surgery, mortality fell from 52% in 2004 to 21% in 2015.
Dr. Goldberg attributed the success of surgery in severe PE patients to the definitive nature of embolectomy and the concurrent use of extracorporeal membrane oxygenation that helps stabilize acutely ill PE patients. He also cited refinements that surgery underwent during the 2004-2015 period based on the experience managing chronic thromboembolic pulmonary hypertension, including routine use of cardiopulmonary bypass during surgery. “Very high risk [PE] patients should go straight to surgery, unless the patient is at high risk for surgery because of conditions like prior sternotomy or very advanced age, in which case catheter-directed therapy may be a safer option, he said. He cited a recent 5% death rate after surgery at his center among patients with major PE who did not require cardiopulmonary resuscitation.
The database Dr. Goldberg and his collaborator reviewed included 12,735 patients treated by systemic thrombolysis, and 2,595 treated by catheter-directed therapy. Patients averaged 63 years old. The most common indicator of major PE was mechanical ventilation, used on 8% of all PE patients in the study. Non-septic shock occurred in 2%, and just under 1% needed vasopressor treatment.
Published guidelines on PE management from several medical groups are “vague and have numerous caveats,” Dr. Goldberg said. He is participating in an update to the 2011 PE management statement from the American College of Cardiology and American Heart Association (Circulation. 2011 April 26;123[16]:1788-1830).
The study received no commercial funding. Dr. Goldberg had no disclosures.
SOURCE: Haider A et al. J Amer Coll Cardiol. 2019 March;73:9[suppl 1]: doi: 10.1016/S0735-1097(19)32507-0
At my center, Allegheny General Hospital, we often rely on catheter-directed therapy to treat major pulmonary embolism. We now perform more catheter-directed interventions than surgical embolectomies. Generally, when treating patients with major pulmonary embolism it comes down to a choice between those two options. We rarely use systemic thrombolysis for major pulmonary embolism any more.
Raymond L. Benza, MD , is professor of medicine at Temple University College of Medicine and program director for advanced heart failure at the Allegheny Health Network in Pittsburgh. He has been a consultant to Actelion, Gilead, and United Therapeutics, and he has received research funding from Bayer. He made these comments in an interview.
At my center, Allegheny General Hospital, we often rely on catheter-directed therapy to treat major pulmonary embolism. We now perform more catheter-directed interventions than surgical embolectomies. Generally, when treating patients with major pulmonary embolism it comes down to a choice between those two options. We rarely use systemic thrombolysis for major pulmonary embolism any more.
Raymond L. Benza, MD , is professor of medicine at Temple University College of Medicine and program director for advanced heart failure at the Allegheny Health Network in Pittsburgh. He has been a consultant to Actelion, Gilead, and United Therapeutics, and he has received research funding from Bayer. He made these comments in an interview.
At my center, Allegheny General Hospital, we often rely on catheter-directed therapy to treat major pulmonary embolism. We now perform more catheter-directed interventions than surgical embolectomies. Generally, when treating patients with major pulmonary embolism it comes down to a choice between those two options. We rarely use systemic thrombolysis for major pulmonary embolism any more.
Raymond L. Benza, MD , is professor of medicine at Temple University College of Medicine and program director for advanced heart failure at the Allegheny Health Network in Pittsburgh. He has been a consultant to Actelion, Gilead, and United Therapeutics, and he has received research funding from Bayer. He made these comments in an interview.
NEW ORLEANS –
During 2004-2015 the incidence of all diagnosed pulmonary embolism (PE), based on discharge diagnoses, rose from 5.4 cases/1,000 hospitalized patients in 2004 to 9.7 cases/1,000 hospitalized patients in 2015, an 80% increase, Joshua B. Goldberg, MD said at the annual meeting of the American College of Cardiology. The incidence of major PE – defined as a patient who needed vasopressor treatment, mechanical ventilation, or had nonseptic shock – rose from 7.9% of all hospitalized PE diagnoses in 2004 to 9.7% in 2015, a 23% relative increase.
The data also documented a shifting pattern of treatment for all hospitalized patients with PE, and especially among patients with major PE. During the study period, treatment with systemic thrombolysis for all PE rose nearly threefold, and catheter-directed therapy began to show a steady rise in use from 0.2% of all patients in 2011 (and before) to 1% of all patients by 2015. Surgical intervention remained lightly used throughout, with about 0.2% of all PE patients undergoing surgery annually.
Most of these intervention options focused on patients with major PE. Among patients in this subgroup with more severe disease, use of one of these three types of interventions rose from 6% in 2004 to 12% in 2015, mostly driven by a rise in systemic thrombolysis, which jumped from 3% of major PE in 2004 to 9% in 2015. However, the efficacy of systemic thrombolysis in patients with major PE remains suspect. In 2004, 39% of patients with major PE treated with systemic thrombolysis died in hospital; in 2015 the number was 47%. “The data don’t support using systemic thrombolysis to treat major PE; the mortality is high,” noted Dr. Goldberg, a cardiothoracic surgeon at Westchester Medical Center in Valhalla, N.Y.
Although catheter-directed therapy began to be much more widely used in U.S. practice starting in about 2015, during the period studied its use for major PE held fairly steady at roughly 2%-3%, but this approach also showed substantial shortcomings for the major PE population. These sicker patients treated with catheter-directed therapy had 37% mortality in 2004 and a 31% mortality in 2015, a difference that was not statistically significant. In general, PE patients enrolled in the catheter-directed therapy trials were not as sick as the major PE patients who get treated with surgery in routine practice, Dr. Goldberg said in an interview.
The data showed much better performance using surgery, although only 1,237 patients of the entire group of 713,083 PE patients studied in the database underwent surgical embolectomy. Overall, in-hospital mortality in these patients was 22%, but in a time trend analysis, mortality among all PE patients treated with surgery fell from 32% in 2004 to 14% in 2015; among patients with major PE treated with surgery, mortality fell from 52% in 2004 to 21% in 2015.
Dr. Goldberg attributed the success of surgery in severe PE patients to the definitive nature of embolectomy and the concurrent use of extracorporeal membrane oxygenation that helps stabilize acutely ill PE patients. He also cited refinements that surgery underwent during the 2004-2015 period based on the experience managing chronic thromboembolic pulmonary hypertension, including routine use of cardiopulmonary bypass during surgery. “Very high risk [PE] patients should go straight to surgery, unless the patient is at high risk for surgery because of conditions like prior sternotomy or very advanced age, in which case catheter-directed therapy may be a safer option, he said. He cited a recent 5% death rate after surgery at his center among patients with major PE who did not require cardiopulmonary resuscitation.
The database Dr. Goldberg and his collaborator reviewed included 12,735 patients treated by systemic thrombolysis, and 2,595 treated by catheter-directed therapy. Patients averaged 63 years old. The most common indicator of major PE was mechanical ventilation, used on 8% of all PE patients in the study. Non-septic shock occurred in 2%, and just under 1% needed vasopressor treatment.
Published guidelines on PE management from several medical groups are “vague and have numerous caveats,” Dr. Goldberg said. He is participating in an update to the 2011 PE management statement from the American College of Cardiology and American Heart Association (Circulation. 2011 April 26;123[16]:1788-1830).
The study received no commercial funding. Dr. Goldberg had no disclosures.
SOURCE: Haider A et al. J Amer Coll Cardiol. 2019 March;73:9[suppl 1]: doi: 10.1016/S0735-1097(19)32507-0
NEW ORLEANS –
During 2004-2015 the incidence of all diagnosed pulmonary embolism (PE), based on discharge diagnoses, rose from 5.4 cases/1,000 hospitalized patients in 2004 to 9.7 cases/1,000 hospitalized patients in 2015, an 80% increase, Joshua B. Goldberg, MD said at the annual meeting of the American College of Cardiology. The incidence of major PE – defined as a patient who needed vasopressor treatment, mechanical ventilation, or had nonseptic shock – rose from 7.9% of all hospitalized PE diagnoses in 2004 to 9.7% in 2015, a 23% relative increase.
The data also documented a shifting pattern of treatment for all hospitalized patients with PE, and especially among patients with major PE. During the study period, treatment with systemic thrombolysis for all PE rose nearly threefold, and catheter-directed therapy began to show a steady rise in use from 0.2% of all patients in 2011 (and before) to 1% of all patients by 2015. Surgical intervention remained lightly used throughout, with about 0.2% of all PE patients undergoing surgery annually.
Most of these intervention options focused on patients with major PE. Among patients in this subgroup with more severe disease, use of one of these three types of interventions rose from 6% in 2004 to 12% in 2015, mostly driven by a rise in systemic thrombolysis, which jumped from 3% of major PE in 2004 to 9% in 2015. However, the efficacy of systemic thrombolysis in patients with major PE remains suspect. In 2004, 39% of patients with major PE treated with systemic thrombolysis died in hospital; in 2015 the number was 47%. “The data don’t support using systemic thrombolysis to treat major PE; the mortality is high,” noted Dr. Goldberg, a cardiothoracic surgeon at Westchester Medical Center in Valhalla, N.Y.
Although catheter-directed therapy began to be much more widely used in U.S. practice starting in about 2015, during the period studied its use for major PE held fairly steady at roughly 2%-3%, but this approach also showed substantial shortcomings for the major PE population. These sicker patients treated with catheter-directed therapy had 37% mortality in 2004 and a 31% mortality in 2015, a difference that was not statistically significant. In general, PE patients enrolled in the catheter-directed therapy trials were not as sick as the major PE patients who get treated with surgery in routine practice, Dr. Goldberg said in an interview.
The data showed much better performance using surgery, although only 1,237 patients of the entire group of 713,083 PE patients studied in the database underwent surgical embolectomy. Overall, in-hospital mortality in these patients was 22%, but in a time trend analysis, mortality among all PE patients treated with surgery fell from 32% in 2004 to 14% in 2015; among patients with major PE treated with surgery, mortality fell from 52% in 2004 to 21% in 2015.
Dr. Goldberg attributed the success of surgery in severe PE patients to the definitive nature of embolectomy and the concurrent use of extracorporeal membrane oxygenation that helps stabilize acutely ill PE patients. He also cited refinements that surgery underwent during the 2004-2015 period based on the experience managing chronic thromboembolic pulmonary hypertension, including routine use of cardiopulmonary bypass during surgery. “Very high risk [PE] patients should go straight to surgery, unless the patient is at high risk for surgery because of conditions like prior sternotomy or very advanced age, in which case catheter-directed therapy may be a safer option, he said. He cited a recent 5% death rate after surgery at his center among patients with major PE who did not require cardiopulmonary resuscitation.
The database Dr. Goldberg and his collaborator reviewed included 12,735 patients treated by systemic thrombolysis, and 2,595 treated by catheter-directed therapy. Patients averaged 63 years old. The most common indicator of major PE was mechanical ventilation, used on 8% of all PE patients in the study. Non-septic shock occurred in 2%, and just under 1% needed vasopressor treatment.
Published guidelines on PE management from several medical groups are “vague and have numerous caveats,” Dr. Goldberg said. He is participating in an update to the 2011 PE management statement from the American College of Cardiology and American Heart Association (Circulation. 2011 April 26;123[16]:1788-1830).
The study received no commercial funding. Dr. Goldberg had no disclosures.
SOURCE: Haider A et al. J Amer Coll Cardiol. 2019 March;73:9[suppl 1]: doi: 10.1016/S0735-1097(19)32507-0
REPORTING FROM ACC 2019
Algorithm ruled out PE, averts radiation exposure in pregnant women
A diagnostic algorithm adapted for use in pregnancy safely ruled out acute pulmonary embolism in nearly 500 women with suspected pulmonary embolism enrolled in a recent prospective study, investigators are reporting.
Using the adapted algorithm, there was only one deep-vein thrombosis (DVT) and no pulmonary embolism (PE) in follow-up among those women, according to the investigators, including senior author Menno V. Huisman, MD, PhD, of the department of thrombosis and hemostasis at Leiden (Netherlands) University Medical Center and his coauthors.

The main advantage of the algorithm is that it averted CT pulmonary angiography in nearly 40% of patients, thus sparing radiation exposure to mother and fetus in many cases, the investigators added.
“Our algorithm provides solid evidence for the safe management of suspected PE in pregnant women, with selective use of CT pulmonary angiography,” Dr. Huisman and colleagues said in their March 21 report in the New England Journal of Medicine.
In a previous clinical trial, known as the YEARS study, a specialized diagnostic algorithm had a low incidence of failure in men and women with clinically suspected PE, as shown by a venous thromboembolism (VTE) rate of just 0.61% at 3 months and by use of CT pulmonary angiography that was 14 percentage points lower than with a conventional algorithmic approach.
For the current study, Dr. Huisman and his coinvestigators took the YEARS algorithm and adapted it for use in pregnant women with suspected PE presenting at 1 of 18 centers in the Netherlands, France, and Ireland.
Their adapted algorithm was based on the three criteria investigators said were most predictive in the YEARS trial, namely, clinical signs of symptoms of DVT, hemoptysis, and PE as the most likely diagnosis. Patients also underwent D-dimer testing, and if they had clinical signs and symptoms of DVT, underwent compression utrasonography of the symptomatic leg.
Pulmonary embolism was considered ruled out in patients who met none of the three YEARS criteria and had a D-dimer under 1,000 ng/mL, or if they met one to three YEARS criteria and had a D-dimer under 500 ng/mL. Otherwise, patients underwent CT pulmonary angiography and started anticoagulant treatment if results of that test indicated PE.
The primary endpoint of the study was the cumulative 3-month incidence of symptomatic VTE among patients with PE ruled out by this algorithm.
Of 498 patients participating in the study, 477 (96%) had a negative result on the adapted YEARS algorithm at baseline, while 20 (4.0%) received a diagnosis of PE, according to results of the study. One patient was lost to follow-up.
Of the 477 patients with negative results, 1 patient (0.21%) had a diagnosis of symptomatic DVT over the 3 months of follow-up, investigators reported, adding that there were no PE diagnoses over the follow-up period.
That patient with the DVT diagnosis met none of the three YEARS criteria and had a D-dimer level of 480 ng/mL, and so did not undergo CT pulmonary angiography, investigators said.
In the worst-case scenario, the VTE incidence would have been 0.42%, assuming the one patient lost to follow-up would have had a VTE diagnosis over the 3-month follow-up period, they added.
“These data meet the proposed criteria for assessing the safety of diagnostic methods in VTE, even in the context of a low baseline prevalence of disease,” Dr. Huisman and his colleagues wrote.
Overall, CT pulmonary angiography was avoided – avoiding potential radiation exposure-related harms– in 39% of the patients, the investigators said, noting that the proportion of women avoiding the diagnostic test decreased from 65% for those evaluated in the third trimester, 46% in the second trimester, and 32% in the third.
“This decreasing specificity can be explained by the physiological rise in the D-dimer level that commonly occurs during pregnancy,” said Dr. Huisman and his coauthors.
The study was supported by unrestricted grants from Leiden University Medical Center and 17 other participating hospitals. Many authors reported financial ties to the pharmaceutical industry.
SOURCE: van der Pol LM et al. N Engl J Med. 2019;380:1139-49
A diagnostic algorithm adapted for use in pregnancy safely ruled out acute pulmonary embolism in nearly 500 women with suspected pulmonary embolism enrolled in a recent prospective study, investigators are reporting.
Using the adapted algorithm, there was only one deep-vein thrombosis (DVT) and no pulmonary embolism (PE) in follow-up among those women, according to the investigators, including senior author Menno V. Huisman, MD, PhD, of the department of thrombosis and hemostasis at Leiden (Netherlands) University Medical Center and his coauthors.
The main advantage of the algorithm is that it averted CT pulmonary angiography in nearly 40% of patients, thus sparing radiation exposure to mother and fetus in many cases, the investigators added.
“Our algorithm provides solid evidence for the safe management of suspected PE in pregnant women, with selective use of CT pulmonary angiography,” Dr. Huisman and colleagues said in their March 21 report in the New England Journal of Medicine.
In a previous clinical trial, known as the YEARS study, a specialized diagnostic algorithm had a low incidence of failure in men and women with clinically suspected PE, as shown by a venous thromboembolism (VTE) rate of just 0.61% at 3 months and by use of CT pulmonary angiography that was 14 percentage points lower than with a conventional algorithmic approach.
For the current study, Dr. Huisman and his coinvestigators took the YEARS algorithm and adapted it for use in pregnant women with suspected PE presenting at 1 of 18 centers in the Netherlands, France, and Ireland.
Their adapted algorithm was based on the three criteria investigators said were most predictive in the YEARS trial, namely, clinical signs of symptoms of DVT, hemoptysis, and PE as the most likely diagnosis. Patients also underwent D-dimer testing, and if they had clinical signs and symptoms of DVT, underwent compression utrasonography of the symptomatic leg.
Pulmonary embolism was considered ruled out in patients who met none of the three YEARS criteria and had a D-dimer under 1,000 ng/mL, or if they met one to three YEARS criteria and had a D-dimer under 500 ng/mL. Otherwise, patients underwent CT pulmonary angiography and started anticoagulant treatment if results of that test indicated PE.
The primary endpoint of the study was the cumulative 3-month incidence of symptomatic VTE among patients with PE ruled out by this algorithm.
Of 498 patients participating in the study, 477 (96%) had a negative result on the adapted YEARS algorithm at baseline, while 20 (4.0%) received a diagnosis of PE, according to results of the study. One patient was lost to follow-up.
Of the 477 patients with negative results, 1 patient (0.21%) had a diagnosis of symptomatic DVT over the 3 months of follow-up, investigators reported, adding that there were no PE diagnoses over the follow-up period.
That patient with the DVT diagnosis met none of the three YEARS criteria and had a D-dimer level of 480 ng/mL, and so did not undergo CT pulmonary angiography, investigators said.
In the worst-case scenario, the VTE incidence would have been 0.42%, assuming the one patient lost to follow-up would have had a VTE diagnosis over the 3-month follow-up period, they added.
“These data meet the proposed criteria for assessing the safety of diagnostic methods in VTE, even in the context of a low baseline prevalence of disease,” Dr. Huisman and his colleagues wrote.
Overall, CT pulmonary angiography was avoided – avoiding potential radiation exposure-related harms– in 39% of the patients, the investigators said, noting that the proportion of women avoiding the diagnostic test decreased from 65% for those evaluated in the third trimester, 46% in the second trimester, and 32% in the third.
“This decreasing specificity can be explained by the physiological rise in the D-dimer level that commonly occurs during pregnancy,” said Dr. Huisman and his coauthors.
The study was supported by unrestricted grants from Leiden University Medical Center and 17 other participating hospitals. Many authors reported financial ties to the pharmaceutical industry.
SOURCE: van der Pol LM et al. N Engl J Med. 2019;380:1139-49
A diagnostic algorithm adapted for use in pregnancy safely ruled out acute pulmonary embolism in nearly 500 women with suspected pulmonary embolism enrolled in a recent prospective study, investigators are reporting.
Using the adapted algorithm, there was only one deep-vein thrombosis (DVT) and no pulmonary embolism (PE) in follow-up among those women, according to the investigators, including senior author Menno V. Huisman, MD, PhD, of the department of thrombosis and hemostasis at Leiden (Netherlands) University Medical Center and his coauthors.
The main advantage of the algorithm is that it averted CT pulmonary angiography in nearly 40% of patients, thus sparing radiation exposure to mother and fetus in many cases, the investigators added.
“Our algorithm provides solid evidence for the safe management of suspected PE in pregnant women, with selective use of CT pulmonary angiography,” Dr. Huisman and colleagues said in their March 21 report in the New England Journal of Medicine.
In a previous clinical trial, known as the YEARS study, a specialized diagnostic algorithm had a low incidence of failure in men and women with clinically suspected PE, as shown by a venous thromboembolism (VTE) rate of just 0.61% at 3 months and by use of CT pulmonary angiography that was 14 percentage points lower than with a conventional algorithmic approach.
For the current study, Dr. Huisman and his coinvestigators took the YEARS algorithm and adapted it for use in pregnant women with suspected PE presenting at 1 of 18 centers in the Netherlands, France, and Ireland.
Their adapted algorithm was based on the three criteria investigators said were most predictive in the YEARS trial, namely, clinical signs of symptoms of DVT, hemoptysis, and PE as the most likely diagnosis. Patients also underwent D-dimer testing, and if they had clinical signs and symptoms of DVT, underwent compression utrasonography of the symptomatic leg.
Pulmonary embolism was considered ruled out in patients who met none of the three YEARS criteria and had a D-dimer under 1,000 ng/mL, or if they met one to three YEARS criteria and had a D-dimer under 500 ng/mL. Otherwise, patients underwent CT pulmonary angiography and started anticoagulant treatment if results of that test indicated PE.
The primary endpoint of the study was the cumulative 3-month incidence of symptomatic VTE among patients with PE ruled out by this algorithm.
Of 498 patients participating in the study, 477 (96%) had a negative result on the adapted YEARS algorithm at baseline, while 20 (4.0%) received a diagnosis of PE, according to results of the study. One patient was lost to follow-up.
Of the 477 patients with negative results, 1 patient (0.21%) had a diagnosis of symptomatic DVT over the 3 months of follow-up, investigators reported, adding that there were no PE diagnoses over the follow-up period.
That patient with the DVT diagnosis met none of the three YEARS criteria and had a D-dimer level of 480 ng/mL, and so did not undergo CT pulmonary angiography, investigators said.
In the worst-case scenario, the VTE incidence would have been 0.42%, assuming the one patient lost to follow-up would have had a VTE diagnosis over the 3-month follow-up period, they added.
“These data meet the proposed criteria for assessing the safety of diagnostic methods in VTE, even in the context of a low baseline prevalence of disease,” Dr. Huisman and his colleagues wrote.
Overall, CT pulmonary angiography was avoided – avoiding potential radiation exposure-related harms– in 39% of the patients, the investigators said, noting that the proportion of women avoiding the diagnostic test decreased from 65% for those evaluated in the third trimester, 46% in the second trimester, and 32% in the third.
“This decreasing specificity can be explained by the physiological rise in the D-dimer level that commonly occurs during pregnancy,” said Dr. Huisman and his coauthors.
The study was supported by unrestricted grants from Leiden University Medical Center and 17 other participating hospitals. Many authors reported financial ties to the pharmaceutical industry.
SOURCE: van der Pol LM et al. N Engl J Med. 2019;380:1139-49
FROM The New England Journal of Medicine
H3N2 putting a damper on flu season’s departure
The decline of influenza activity remains slow, largely “driven by a wave of H3N2 virus activity” in recent weeks, according to the Centers for Disease Control and Prevention.
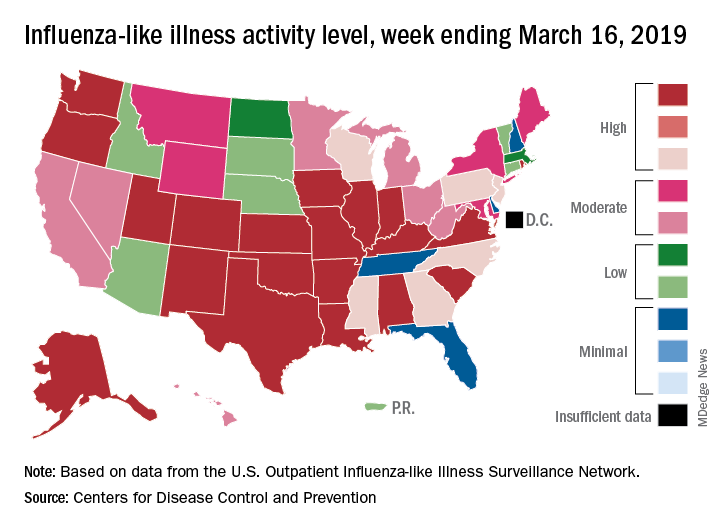
Fewer states reported the highest level of influenza-like illness (ILI) activity on the CDC’s 1-10 scale for the week ending March 16, but the national proportion of outpatient visits for ILI was 4.4% for the second consecutive week, the CDC’s influenza division reported March 22. The outpatient-visit figure for the week ending March 9 was originally reported as 4.5% last week, but it has been revised down to 4.4% this week.
Another measure of activity – the percentage of respiratory specimens testing positive for influenza viruses in clinical laboratories – actually increased slightly during the week ending March 16, the CDC noted.
For the current week, there were 26 states in the high (8-10) range of activity – 20 states were at level 10 and another 6 states were at level 8 – compared with the previous week, when 21 states were at level 10 and 30 states were in the high range, the CDC’s Outpatient ILI Surveillance Network reported.
There were eight ILI-related deaths in children reported during the week ending March 16, seven of which occurred in previous weeks. The total for the 2018-2019 season so far is 76, the CDC said.
New preliminary estimates on influenza’s burden nationally put the total number of deaths at 25,000-41,500 since the beginning of the season on Oct. 1, 2018. There also have been 375,000-454,000 flu-related hospitalizations, 13.2 million to 15.4 million medical visits, and 28.5 to 32.8 million individual illnesses, the CDC said.
Since the CDC “expects flu activity to remain elevated for a number of weeks,” it continues to recommend flu vaccination and the use of influenza antiviral drugs as “an important second line of defense that can be used to treat flu illness. H3N2 viruses are typically associated with more severe illness in older adults, and flu vaccine may protect less well against H3N2 illness in older adults, making prompt treatment with flu antivirals in this age group especially important during the current period of H3N2 predominance.”
The decline of influenza activity remains slow, largely “driven by a wave of H3N2 virus activity” in recent weeks, according to the Centers for Disease Control and Prevention.
Fewer states reported the highest level of influenza-like illness (ILI) activity on the CDC’s 1-10 scale for the week ending March 16, but the national proportion of outpatient visits for ILI was 4.4% for the second consecutive week, the CDC’s influenza division reported March 22. The outpatient-visit figure for the week ending March 9 was originally reported as 4.5% last week, but it has been revised down to 4.4% this week.
Another measure of activity – the percentage of respiratory specimens testing positive for influenza viruses in clinical laboratories – actually increased slightly during the week ending March 16, the CDC noted.
For the current week, there were 26 states in the high (8-10) range of activity – 20 states were at level 10 and another 6 states were at level 8 – compared with the previous week, when 21 states were at level 10 and 30 states were in the high range, the CDC’s Outpatient ILI Surveillance Network reported.
There were eight ILI-related deaths in children reported during the week ending March 16, seven of which occurred in previous weeks. The total for the 2018-2019 season so far is 76, the CDC said.
New preliminary estimates on influenza’s burden nationally put the total number of deaths at 25,000-41,500 since the beginning of the season on Oct. 1, 2018. There also have been 375,000-454,000 flu-related hospitalizations, 13.2 million to 15.4 million medical visits, and 28.5 to 32.8 million individual illnesses, the CDC said.
Since the CDC “expects flu activity to remain elevated for a number of weeks,” it continues to recommend flu vaccination and the use of influenza antiviral drugs as “an important second line of defense that can be used to treat flu illness. H3N2 viruses are typically associated with more severe illness in older adults, and flu vaccine may protect less well against H3N2 illness in older adults, making prompt treatment with flu antivirals in this age group especially important during the current period of H3N2 predominance.”
The decline of influenza activity remains slow, largely “driven by a wave of H3N2 virus activity” in recent weeks, according to the Centers for Disease Control and Prevention.
Fewer states reported the highest level of influenza-like illness (ILI) activity on the CDC’s 1-10 scale for the week ending March 16, but the national proportion of outpatient visits for ILI was 4.4% for the second consecutive week, the CDC’s influenza division reported March 22. The outpatient-visit figure for the week ending March 9 was originally reported as 4.5% last week, but it has been revised down to 4.4% this week.
Another measure of activity – the percentage of respiratory specimens testing positive for influenza viruses in clinical laboratories – actually increased slightly during the week ending March 16, the CDC noted.
For the current week, there were 26 states in the high (8-10) range of activity – 20 states were at level 10 and another 6 states were at level 8 – compared with the previous week, when 21 states were at level 10 and 30 states were in the high range, the CDC’s Outpatient ILI Surveillance Network reported.
There were eight ILI-related deaths in children reported during the week ending March 16, seven of which occurred in previous weeks. The total for the 2018-2019 season so far is 76, the CDC said.
New preliminary estimates on influenza’s burden nationally put the total number of deaths at 25,000-41,500 since the beginning of the season on Oct. 1, 2018. There also have been 375,000-454,000 flu-related hospitalizations, 13.2 million to 15.4 million medical visits, and 28.5 to 32.8 million individual illnesses, the CDC said.
Since the CDC “expects flu activity to remain elevated for a number of weeks,” it continues to recommend flu vaccination and the use of influenza antiviral drugs as “an important second line of defense that can be used to treat flu illness. H3N2 viruses are typically associated with more severe illness in older adults, and flu vaccine may protect less well against H3N2 illness in older adults, making prompt treatment with flu antivirals in this age group especially important during the current period of H3N2 predominance.”
FDA approves solriamfetol for daytime sleepiness treatment
The. It is the first dopamine and norepinephrine reuptake inhibitor approved to treat those conditions.

Approval was based on results from TONES (Treatment of Obstructive Sleep Apnea and Narcolepsy Excessive Sleepiness), a phase 3 study that combined four randomized, placebo-controlled trials assessing solriamfetol at various doses, compared with a placebo. After 12 weeks, 68%-74% of patients taking solriamfetol at 75 mg and 78%-90% of those taking solriamfetol at 150 mg reported improvement as assessed by the Patient Global Impression of Change scale.
Solriamfetol is approved at 75 mg and 150 mg for patients with narcolepsy and at 37.5 mg, 75 mg, and 150 mg for patients with obstructive sleep apnea. The most common adverse events associated with solriamfetol are headache, nausea, decreased appetite, and anxiety.
“Excessive daytime sleepiness can negatively impact the daily lives of people living with narcolepsy or obstructive sleep apnea at work, at home, or in daily activities. With this approval, a new, daytime medicine that can provide sustained wakefulness throughout the day will be available for patients,” Bruce Cozadd, chairman and CEO of Jazz Pharmaceuticals, said in the press release.
Find the full press release on the Jazz Pharmaceuticals website.
The. It is the first dopamine and norepinephrine reuptake inhibitor approved to treat those conditions.
Approval was based on results from TONES (Treatment of Obstructive Sleep Apnea and Narcolepsy Excessive Sleepiness), a phase 3 study that combined four randomized, placebo-controlled trials assessing solriamfetol at various doses, compared with a placebo. After 12 weeks, 68%-74% of patients taking solriamfetol at 75 mg and 78%-90% of those taking solriamfetol at 150 mg reported improvement as assessed by the Patient Global Impression of Change scale.
Solriamfetol is approved at 75 mg and 150 mg for patients with narcolepsy and at 37.5 mg, 75 mg, and 150 mg for patients with obstructive sleep apnea. The most common adverse events associated with solriamfetol are headache, nausea, decreased appetite, and anxiety.
“Excessive daytime sleepiness can negatively impact the daily lives of people living with narcolepsy or obstructive sleep apnea at work, at home, or in daily activities. With this approval, a new, daytime medicine that can provide sustained wakefulness throughout the day will be available for patients,” Bruce Cozadd, chairman and CEO of Jazz Pharmaceuticals, said in the press release.
Find the full press release on the Jazz Pharmaceuticals website.
The. It is the first dopamine and norepinephrine reuptake inhibitor approved to treat those conditions.
Approval was based on results from TONES (Treatment of Obstructive Sleep Apnea and Narcolepsy Excessive Sleepiness), a phase 3 study that combined four randomized, placebo-controlled trials assessing solriamfetol at various doses, compared with a placebo. After 12 weeks, 68%-74% of patients taking solriamfetol at 75 mg and 78%-90% of those taking solriamfetol at 150 mg reported improvement as assessed by the Patient Global Impression of Change scale.
Solriamfetol is approved at 75 mg and 150 mg for patients with narcolepsy and at 37.5 mg, 75 mg, and 150 mg for patients with obstructive sleep apnea. The most common adverse events associated with solriamfetol are headache, nausea, decreased appetite, and anxiety.
“Excessive daytime sleepiness can negatively impact the daily lives of people living with narcolepsy or obstructive sleep apnea at work, at home, or in daily activities. With this approval, a new, daytime medicine that can provide sustained wakefulness throughout the day will be available for patients,” Bruce Cozadd, chairman and CEO of Jazz Pharmaceuticals, said in the press release.
Find the full press release on the Jazz Pharmaceuticals website.
Survey: Americans support regulation of vaping products
Almost 70% of adults believe that the Food and Drug Administration should raise the legal age to purchase e-cigarettes and tobacco, according to a new survey by NORC at the University of Chicago, a nonpartisan research institution.
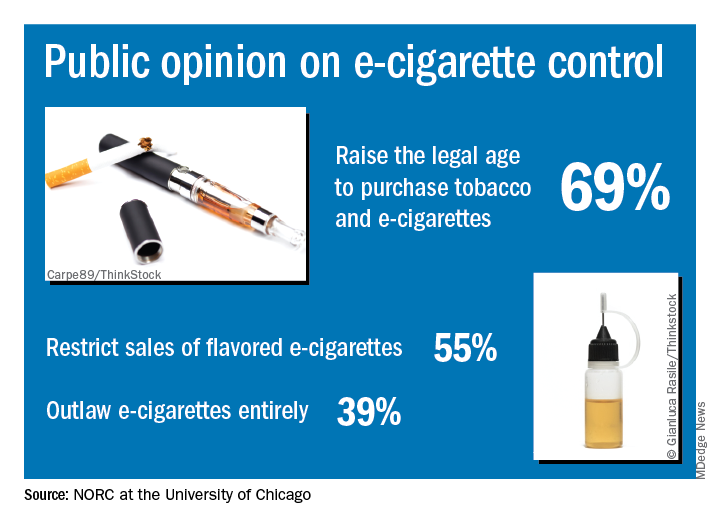
“Americans are particularly concerned about teens becoming newly addicted to e-cigarettes, and they support a range of actions the federal government could take to make vaping products less available, less addictive, and less appealing,” Caroline Pearson, senior vice president at NORC, said in a written statement.
The AmeriSpeak Spotlight on Health Poll, conducted Feb. 14-18, 2019 (margin of error, plus or minus 4.12%), showed that 69% of adults strongly or somewhat support raising the age limit to purchase e-cigarettes and tobacco and 55% support restricting sales of flavored e-cigarettes, NORC reported. Almost 40% of the 1,004 respondents expressed support for a complete ban on e-cigarettes.
Despite FDA efforts under Commissioner Scott Gottlieb, MD, to raise awareness of teen vaping, only 21% of those surveyed correctly responded that e-cigarettes generally contain more nicotine that regular cigarettes. Dr. Gottlieb announced his resignation recently, “but he indicated that the Trump Administration will continue efforts to increase regulation of e-cigarettes,” NORC said.
Almost 70% of adults believe that the Food and Drug Administration should raise the legal age to purchase e-cigarettes and tobacco, according to a new survey by NORC at the University of Chicago, a nonpartisan research institution.
“Americans are particularly concerned about teens becoming newly addicted to e-cigarettes, and they support a range of actions the federal government could take to make vaping products less available, less addictive, and less appealing,” Caroline Pearson, senior vice president at NORC, said in a written statement.
The AmeriSpeak Spotlight on Health Poll, conducted Feb. 14-18, 2019 (margin of error, plus or minus 4.12%), showed that 69% of adults strongly or somewhat support raising the age limit to purchase e-cigarettes and tobacco and 55% support restricting sales of flavored e-cigarettes, NORC reported. Almost 40% of the 1,004 respondents expressed support for a complete ban on e-cigarettes.
Despite FDA efforts under Commissioner Scott Gottlieb, MD, to raise awareness of teen vaping, only 21% of those surveyed correctly responded that e-cigarettes generally contain more nicotine that regular cigarettes. Dr. Gottlieb announced his resignation recently, “but he indicated that the Trump Administration will continue efforts to increase regulation of e-cigarettes,” NORC said.
Almost 70% of adults believe that the Food and Drug Administration should raise the legal age to purchase e-cigarettes and tobacco, according to a new survey by NORC at the University of Chicago, a nonpartisan research institution.
“Americans are particularly concerned about teens becoming newly addicted to e-cigarettes, and they support a range of actions the federal government could take to make vaping products less available, less addictive, and less appealing,” Caroline Pearson, senior vice president at NORC, said in a written statement.
The AmeriSpeak Spotlight on Health Poll, conducted Feb. 14-18, 2019 (margin of error, plus or minus 4.12%), showed that 69% of adults strongly or somewhat support raising the age limit to purchase e-cigarettes and tobacco and 55% support restricting sales of flavored e-cigarettes, NORC reported. Almost 40% of the 1,004 respondents expressed support for a complete ban on e-cigarettes.
Despite FDA efforts under Commissioner Scott Gottlieb, MD, to raise awareness of teen vaping, only 21% of those surveyed correctly responded that e-cigarettes generally contain more nicotine that regular cigarettes. Dr. Gottlieb announced his resignation recently, “but he indicated that the Trump Administration will continue efforts to increase regulation of e-cigarettes,” NORC said.