User login
Match Day 2019: Another strong year for neurology
according to the National Resident Matching Program (NRMP).
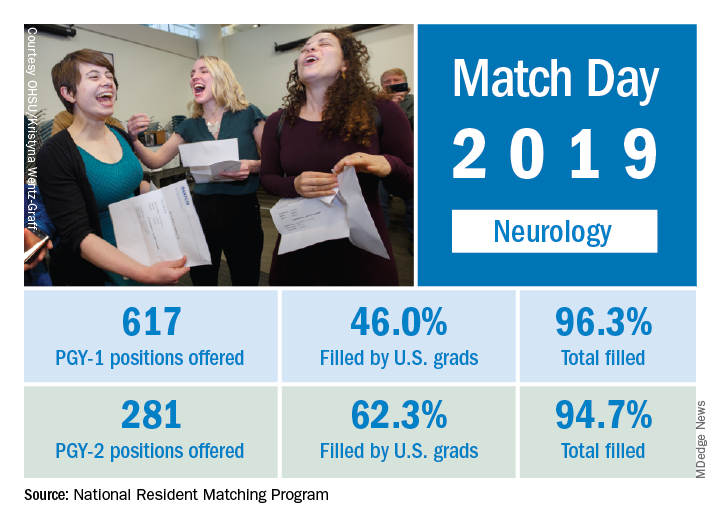
This year, 617 first-year (PGY-1) neurology slots were offered, an increase of 11.8% over the 552 offered in 2018 and well above the 6.5% gain recorded for the Match as whole. The 114 neurology programs participating this year filled 96.3% of those PGY-1 positions, compared with 94.7% for the 52 programs that offered PGY-2 positions, the NRMP reported.
“The results of the Match are closely watched because they can be predictors of future physician workforce supply. There also is significant interest in the competitiveness of specialties, as measured by the percentage of positions filled overall and the percentage filled by senior students in U.S. allopathic medical schools,” the NRMP said.
The proportion of PGY-1 neurology positions filled by U.S. seniors dropped to 46.0% from 50.7% last year, although the number of U.S. seniors filling spots actually went up from 280 in 2018 to 284. The PGY-2 positions saw declines in both cases: The 175 U.S. seniors represented 62.3% of the 2019 spots, compared with the 190 U.S. seniors who filled 66.2% of slots in 2018, the NRMP data show.
The total numbers of applicants (38,376) and positions offered (35,185) were both record highs for the Match, although they were affected, in part, by “increased numbers of osteopathic programs that joined the Main Residency Match as a result of the ongoing transition to a single accreditation system for graduate medical education programs,” the NRMP noted.
according to the National Resident Matching Program (NRMP).
This year, 617 first-year (PGY-1) neurology slots were offered, an increase of 11.8% over the 552 offered in 2018 and well above the 6.5% gain recorded for the Match as whole. The 114 neurology programs participating this year filled 96.3% of those PGY-1 positions, compared with 94.7% for the 52 programs that offered PGY-2 positions, the NRMP reported.
“The results of the Match are closely watched because they can be predictors of future physician workforce supply. There also is significant interest in the competitiveness of specialties, as measured by the percentage of positions filled overall and the percentage filled by senior students in U.S. allopathic medical schools,” the NRMP said.
The proportion of PGY-1 neurology positions filled by U.S. seniors dropped to 46.0% from 50.7% last year, although the number of U.S. seniors filling spots actually went up from 280 in 2018 to 284. The PGY-2 positions saw declines in both cases: The 175 U.S. seniors represented 62.3% of the 2019 spots, compared with the 190 U.S. seniors who filled 66.2% of slots in 2018, the NRMP data show.
The total numbers of applicants (38,376) and positions offered (35,185) were both record highs for the Match, although they were affected, in part, by “increased numbers of osteopathic programs that joined the Main Residency Match as a result of the ongoing transition to a single accreditation system for graduate medical education programs,” the NRMP noted.
according to the National Resident Matching Program (NRMP).
This year, 617 first-year (PGY-1) neurology slots were offered, an increase of 11.8% over the 552 offered in 2018 and well above the 6.5% gain recorded for the Match as whole. The 114 neurology programs participating this year filled 96.3% of those PGY-1 positions, compared with 94.7% for the 52 programs that offered PGY-2 positions, the NRMP reported.
“The results of the Match are closely watched because they can be predictors of future physician workforce supply. There also is significant interest in the competitiveness of specialties, as measured by the percentage of positions filled overall and the percentage filled by senior students in U.S. allopathic medical schools,” the NRMP said.
The proportion of PGY-1 neurology positions filled by U.S. seniors dropped to 46.0% from 50.7% last year, although the number of U.S. seniors filling spots actually went up from 280 in 2018 to 284. The PGY-2 positions saw declines in both cases: The 175 U.S. seniors represented 62.3% of the 2019 spots, compared with the 190 U.S. seniors who filled 66.2% of slots in 2018, the NRMP data show.
The total numbers of applicants (38,376) and positions offered (35,185) were both record highs for the Match, although they were affected, in part, by “increased numbers of osteopathic programs that joined the Main Residency Match as a result of the ongoing transition to a single accreditation system for graduate medical education programs,” the NRMP noted.
VEText 1 Year Later—Still Growing
Nearly 6 million veterans get health care scheduling reminders via VEText, an interactive mobile program launched a year ago. More than 70 million text messages later, how is VEText doing? Apparently, well. The VA says an “overwhelming majority” of veterans like the enhanced access. Only 4% have opted out.
The VA has worked to improve the user experience along the way. The latest enhancement allows the VA to send facility and clinic location in the unsecured text message appointment reminders. One user, James Preston, interviewed for a VA article, says at the Loma Linda VA Medical Center veterans still had to use the information desk to find out exactly where they needed to go. “Now it’s almost perfect,” he says, “because it provides all the necessary information.” Deanna Callahan, innovation specialist and National Program Manager for VEText, says before VEText, the VA was relying on phone calls, robocalls, and mail. “We wanted to modernize our efforts to not only bring text message appointment reminders but go above and beyond and positively affect the No Show rate.” It worked—the No Show rate has dropped from 13.7% to 11.7% in the year the program has been active.
The system automatically enrolls veterans based on phone information already on file, but they can opt out by replying STOP to a reminder. Accidentally opting out is easily reversed by replying START to a previous reminder. Reminders are sent for clinical appointments at local medical centers and outpatient clinics, but not for Lab, Community Care, Research, Telephone Clinics, or Home-based Primary Care. (The reminders are additional—they do not replace letters, postcards, or automated phone call reminders.) VEText itself does not cost the veteran anything, but text messaging rates may apply, depending on individual cell phone plans. For more information, go to www.va.gov/HEALTH/vetext_faqs.asp.
Nearly 6 million veterans get health care scheduling reminders via VEText, an interactive mobile program launched a year ago. More than 70 million text messages later, how is VEText doing? Apparently, well. The VA says an “overwhelming majority” of veterans like the enhanced access. Only 4% have opted out.
The VA has worked to improve the user experience along the way. The latest enhancement allows the VA to send facility and clinic location in the unsecured text message appointment reminders. One user, James Preston, interviewed for a VA article, says at the Loma Linda VA Medical Center veterans still had to use the information desk to find out exactly where they needed to go. “Now it’s almost perfect,” he says, “because it provides all the necessary information.” Deanna Callahan, innovation specialist and National Program Manager for VEText, says before VEText, the VA was relying on phone calls, robocalls, and mail. “We wanted to modernize our efforts to not only bring text message appointment reminders but go above and beyond and positively affect the No Show rate.” It worked—the No Show rate has dropped from 13.7% to 11.7% in the year the program has been active.
The system automatically enrolls veterans based on phone information already on file, but they can opt out by replying STOP to a reminder. Accidentally opting out is easily reversed by replying START to a previous reminder. Reminders are sent for clinical appointments at local medical centers and outpatient clinics, but not for Lab, Community Care, Research, Telephone Clinics, or Home-based Primary Care. (The reminders are additional—they do not replace letters, postcards, or automated phone call reminders.) VEText itself does not cost the veteran anything, but text messaging rates may apply, depending on individual cell phone plans. For more information, go to www.va.gov/HEALTH/vetext_faqs.asp.
Nearly 6 million veterans get health care scheduling reminders via VEText, an interactive mobile program launched a year ago. More than 70 million text messages later, how is VEText doing? Apparently, well. The VA says an “overwhelming majority” of veterans like the enhanced access. Only 4% have opted out.
The VA has worked to improve the user experience along the way. The latest enhancement allows the VA to send facility and clinic location in the unsecured text message appointment reminders. One user, James Preston, interviewed for a VA article, says at the Loma Linda VA Medical Center veterans still had to use the information desk to find out exactly where they needed to go. “Now it’s almost perfect,” he says, “because it provides all the necessary information.” Deanna Callahan, innovation specialist and National Program Manager for VEText, says before VEText, the VA was relying on phone calls, robocalls, and mail. “We wanted to modernize our efforts to not only bring text message appointment reminders but go above and beyond and positively affect the No Show rate.” It worked—the No Show rate has dropped from 13.7% to 11.7% in the year the program has been active.
The system automatically enrolls veterans based on phone information already on file, but they can opt out by replying STOP to a reminder. Accidentally opting out is easily reversed by replying START to a previous reminder. Reminders are sent for clinical appointments at local medical centers and outpatient clinics, but not for Lab, Community Care, Research, Telephone Clinics, or Home-based Primary Care. (The reminders are additional—they do not replace letters, postcards, or automated phone call reminders.) VEText itself does not cost the veteran anything, but text messaging rates may apply, depending on individual cell phone plans. For more information, go to www.va.gov/HEALTH/vetext_faqs.asp.
Flu activity levels down, but outpatient visits highest since 1998-99
Influenza activity measures declined for a third consecutive week, but levels are higher than usual at this point in the flu season, according to the Centers for Disease Control and Prevention.
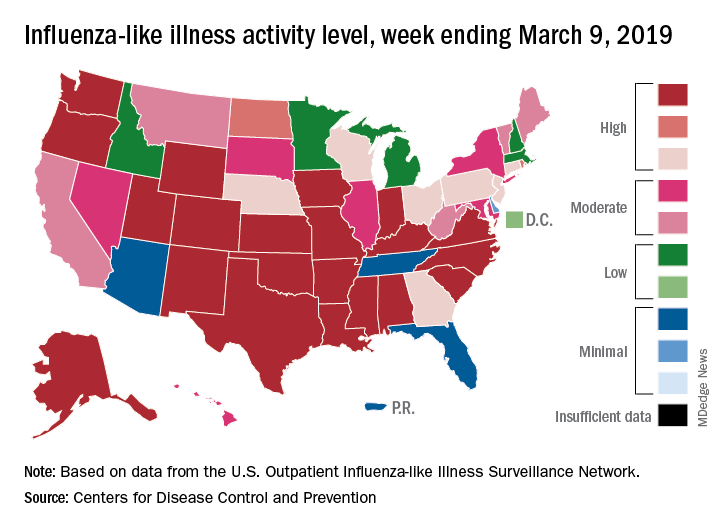
For the week ending March 9, an estimated 4.5% of outpatient visits were for influenza-like illness (ILI), which was down from 4.6% the previous week, the CDC’s influenza division reported March 15, but that is higher than the comparable week for any year since 1998-1999. During last year’s very severe flu season, the outpatient visit rate was just under 3.2% for the week ending March 10.
Although the number of states at level 10 on the CDC’s 1-10 scale remained at 21, the activity map actually looks more red than last week since Rhode Island and West Virgina were replaced by the much larger states of Iowa and Washington. The number of states in the high range (8-10), did go down from 32 to 30, data from the CDC’s Outpatient ILI Surveillance Network show.
Of those four deaths, only one occurred during the most recent reporting week, the CDC said.
Influenza activity measures declined for a third consecutive week, but levels are higher than usual at this point in the flu season, according to the Centers for Disease Control and Prevention.
For the week ending March 9, an estimated 4.5% of outpatient visits were for influenza-like illness (ILI), which was down from 4.6% the previous week, the CDC’s influenza division reported March 15, but that is higher than the comparable week for any year since 1998-1999. During last year’s very severe flu season, the outpatient visit rate was just under 3.2% for the week ending March 10.
Although the number of states at level 10 on the CDC’s 1-10 scale remained at 21, the activity map actually looks more red than last week since Rhode Island and West Virgina were replaced by the much larger states of Iowa and Washington. The number of states in the high range (8-10), did go down from 32 to 30, data from the CDC’s Outpatient ILI Surveillance Network show.
Of those four deaths, only one occurred during the most recent reporting week, the CDC said.
Influenza activity measures declined for a third consecutive week, but levels are higher than usual at this point in the flu season, according to the Centers for Disease Control and Prevention.
For the week ending March 9, an estimated 4.5% of outpatient visits were for influenza-like illness (ILI), which was down from 4.6% the previous week, the CDC’s influenza division reported March 15, but that is higher than the comparable week for any year since 1998-1999. During last year’s very severe flu season, the outpatient visit rate was just under 3.2% for the week ending March 10.
Although the number of states at level 10 on the CDC’s 1-10 scale remained at 21, the activity map actually looks more red than last week since Rhode Island and West Virgina were replaced by the much larger states of Iowa and Washington. The number of states in the high range (8-10), did go down from 32 to 30, data from the CDC’s Outpatient ILI Surveillance Network show.
Of those four deaths, only one occurred during the most recent reporting week, the CDC said.
When a Public Health Alert Goes Wrong
At 8:07 am on January 13, 2018, people in Hawaii received an emergency alert advising them to seek shelter from an incoming ballistic missile.
A very long 38 minutes later, the message was retracted via the same systems that had sent it—the Wireless Emergency Alert system, which sends location-based warnings to wireless carrier systems, and the Emergency Alert System, which sends television and radio alerts.
The Federal Communications Commission report that covered the debacle noted that, among other errors, the employee responsible for triggering the false alert believed the missile threat was real. Moreover, the exercise plans did not document a process for disseminating an all-clear message. And on top of that, the established ballistic missile alert checklist did not include a step to notify the Hawaii Emergency Management Agency’s public information officer responsible for communicating with the public, media, other agencies, and other stakeholders during an incident.
Researchers from the CDC and Hawaii Department of Health analyzed tweets sent during 2 periods: early (8:07-8:45 am), the 38 minutes during which the alert circulated; and the late period (8:46-9:24 am), the same amount of elapsed time after the correction had been issued.
They found 4 themes dominated the early period: information processing, information sharing, authentication, and emotional reaction (shock, fear, panic, terror). Information processing was defined as any indication of initial mental processing of the alert. Many of the tweets dealt with coming to terms with the threat.
During the late period, information sharing and emotional reaction persisted, but they were joined by new themes that, according to the researchers, were “fundamentally different” from the early-period themes and reflected reactions to misinformation: denunciation, insufficient knowledge to act, and mistrust of authority. “Insufficient knowledge to act” involved reacting to the lack of a response plan, particularly not knowing how to properly take shelter. Denunciations blamed the emergency warning and response, especially the time it took to correct the mistake. Mistrust of authority involved doubting the emergency alert system or governmental response.
How can a situation like this be better handled? The researchers say public health messaging during an emergency is complicated. For instance, it is influenced by how messages are perceived and interpreted by different people, and by the fact that messages need to be sent over multiple platforms to ensure that the information is disseminated accurately and quickly.
Which is why social media is both a handicap and a boon in public health emergencies. Tweets spread misinformation as fast as information (if not faster), so the first messages are critical. In addition to conveying timely messages, the researchers advise, public health authorities need to address the reactions during each phase of a crisis. They also need to establish credibility to prevent the public from mistrusting the public health message and its issuers.
Most important, perhaps: Alerts should carry clear instructions for persons in the affected area to carry out during an emergency.
At 8:07 am on January 13, 2018, people in Hawaii received an emergency alert advising them to seek shelter from an incoming ballistic missile.
A very long 38 minutes later, the message was retracted via the same systems that had sent it—the Wireless Emergency Alert system, which sends location-based warnings to wireless carrier systems, and the Emergency Alert System, which sends television and radio alerts.
The Federal Communications Commission report that covered the debacle noted that, among other errors, the employee responsible for triggering the false alert believed the missile threat was real. Moreover, the exercise plans did not document a process for disseminating an all-clear message. And on top of that, the established ballistic missile alert checklist did not include a step to notify the Hawaii Emergency Management Agency’s public information officer responsible for communicating with the public, media, other agencies, and other stakeholders during an incident.
Researchers from the CDC and Hawaii Department of Health analyzed tweets sent during 2 periods: early (8:07-8:45 am), the 38 minutes during which the alert circulated; and the late period (8:46-9:24 am), the same amount of elapsed time after the correction had been issued.
They found 4 themes dominated the early period: information processing, information sharing, authentication, and emotional reaction (shock, fear, panic, terror). Information processing was defined as any indication of initial mental processing of the alert. Many of the tweets dealt with coming to terms with the threat.
During the late period, information sharing and emotional reaction persisted, but they were joined by new themes that, according to the researchers, were “fundamentally different” from the early-period themes and reflected reactions to misinformation: denunciation, insufficient knowledge to act, and mistrust of authority. “Insufficient knowledge to act” involved reacting to the lack of a response plan, particularly not knowing how to properly take shelter. Denunciations blamed the emergency warning and response, especially the time it took to correct the mistake. Mistrust of authority involved doubting the emergency alert system or governmental response.
How can a situation like this be better handled? The researchers say public health messaging during an emergency is complicated. For instance, it is influenced by how messages are perceived and interpreted by different people, and by the fact that messages need to be sent over multiple platforms to ensure that the information is disseminated accurately and quickly.
Which is why social media is both a handicap and a boon in public health emergencies. Tweets spread misinformation as fast as information (if not faster), so the first messages are critical. In addition to conveying timely messages, the researchers advise, public health authorities need to address the reactions during each phase of a crisis. They also need to establish credibility to prevent the public from mistrusting the public health message and its issuers.
Most important, perhaps: Alerts should carry clear instructions for persons in the affected area to carry out during an emergency.
At 8:07 am on January 13, 2018, people in Hawaii received an emergency alert advising them to seek shelter from an incoming ballistic missile.
A very long 38 minutes later, the message was retracted via the same systems that had sent it—the Wireless Emergency Alert system, which sends location-based warnings to wireless carrier systems, and the Emergency Alert System, which sends television and radio alerts.
The Federal Communications Commission report that covered the debacle noted that, among other errors, the employee responsible for triggering the false alert believed the missile threat was real. Moreover, the exercise plans did not document a process for disseminating an all-clear message. And on top of that, the established ballistic missile alert checklist did not include a step to notify the Hawaii Emergency Management Agency’s public information officer responsible for communicating with the public, media, other agencies, and other stakeholders during an incident.
Researchers from the CDC and Hawaii Department of Health analyzed tweets sent during 2 periods: early (8:07-8:45 am), the 38 minutes during which the alert circulated; and the late period (8:46-9:24 am), the same amount of elapsed time after the correction had been issued.
They found 4 themes dominated the early period: information processing, information sharing, authentication, and emotional reaction (shock, fear, panic, terror). Information processing was defined as any indication of initial mental processing of the alert. Many of the tweets dealt with coming to terms with the threat.
During the late period, information sharing and emotional reaction persisted, but they were joined by new themes that, according to the researchers, were “fundamentally different” from the early-period themes and reflected reactions to misinformation: denunciation, insufficient knowledge to act, and mistrust of authority. “Insufficient knowledge to act” involved reacting to the lack of a response plan, particularly not knowing how to properly take shelter. Denunciations blamed the emergency warning and response, especially the time it took to correct the mistake. Mistrust of authority involved doubting the emergency alert system or governmental response.
How can a situation like this be better handled? The researchers say public health messaging during an emergency is complicated. For instance, it is influenced by how messages are perceived and interpreted by different people, and by the fact that messages need to be sent over multiple platforms to ensure that the information is disseminated accurately and quickly.
Which is why social media is both a handicap and a boon in public health emergencies. Tweets spread misinformation as fast as information (if not faster), so the first messages are critical. In addition to conveying timely messages, the researchers advise, public health authorities need to address the reactions during each phase of a crisis. They also need to establish credibility to prevent the public from mistrusting the public health message and its issuers.
Most important, perhaps: Alerts should carry clear instructions for persons in the affected area to carry out during an emergency.
Funduscopy: Critical to the Right Diagnosis
It is always good to look the patient in the eye, say researchers from Texas Tech University in Odessa, Texas, and Centro Policlinico Valencia in Venezuela. They report on the case of a patient with atheroembolism, a “rare but feared complication of arteriography.” Most commonly, it affects small-diameter vessels in the skin and kidneys.
The patient, a 69-year-old man, had a history of hypertension, type 2 diabetes, and unstable angina; he had a drug-eluting stent placed in the left anterior descending coronary artery 10 days before he was admitted to the hospital. He arrived at the emergency department with intense abdominal pain, nausea, vomiting, oliguria, and pain in his legs and feet.
Physical examination revealed livedo reticularis (which is caused by small blood clots) in his left foot, and a tender abdomen. His creatinine and blood urea nitrogen levels were increased. Funduscopy showed a Hollenhorst crystal in the right inferotemporal quadrant.
He was treated with methylprednisolone, which improved the abdominal symptoms, renal function, and skin findings; then prednisone. His initial symptoms resolved over the next year.
The clinicians say the usual treatment for atheroembolism is supportive and depends on the affected organ. To their knowledge, they say, no formal studies have evaluated the use of anti-inflammatory therapies for this complication.
Funduscopy was an essential part of their examination, the researchers note, and spared the patient from invasive diagnostic studies such as biopsies. They also say that contrast-induced renal failure might have been the cause of the majority of his symptoms, but the combination of physical exam and differential diagnosis led them to the appropriate cause, as well as allowing for opportune treatment.
It is always good to look the patient in the eye, say researchers from Texas Tech University in Odessa, Texas, and Centro Policlinico Valencia in Venezuela. They report on the case of a patient with atheroembolism, a “rare but feared complication of arteriography.” Most commonly, it affects small-diameter vessels in the skin and kidneys.
The patient, a 69-year-old man, had a history of hypertension, type 2 diabetes, and unstable angina; he had a drug-eluting stent placed in the left anterior descending coronary artery 10 days before he was admitted to the hospital. He arrived at the emergency department with intense abdominal pain, nausea, vomiting, oliguria, and pain in his legs and feet.
Physical examination revealed livedo reticularis (which is caused by small blood clots) in his left foot, and a tender abdomen. His creatinine and blood urea nitrogen levels were increased. Funduscopy showed a Hollenhorst crystal in the right inferotemporal quadrant.
He was treated with methylprednisolone, which improved the abdominal symptoms, renal function, and skin findings; then prednisone. His initial symptoms resolved over the next year.
The clinicians say the usual treatment for atheroembolism is supportive and depends on the affected organ. To their knowledge, they say, no formal studies have evaluated the use of anti-inflammatory therapies for this complication.
Funduscopy was an essential part of their examination, the researchers note, and spared the patient from invasive diagnostic studies such as biopsies. They also say that contrast-induced renal failure might have been the cause of the majority of his symptoms, but the combination of physical exam and differential diagnosis led them to the appropriate cause, as well as allowing for opportune treatment.
It is always good to look the patient in the eye, say researchers from Texas Tech University in Odessa, Texas, and Centro Policlinico Valencia in Venezuela. They report on the case of a patient with atheroembolism, a “rare but feared complication of arteriography.” Most commonly, it affects small-diameter vessels in the skin and kidneys.
The patient, a 69-year-old man, had a history of hypertension, type 2 diabetes, and unstable angina; he had a drug-eluting stent placed in the left anterior descending coronary artery 10 days before he was admitted to the hospital. He arrived at the emergency department with intense abdominal pain, nausea, vomiting, oliguria, and pain in his legs and feet.
Physical examination revealed livedo reticularis (which is caused by small blood clots) in his left foot, and a tender abdomen. His creatinine and blood urea nitrogen levels were increased. Funduscopy showed a Hollenhorst crystal in the right inferotemporal quadrant.
He was treated with methylprednisolone, which improved the abdominal symptoms, renal function, and skin findings; then prednisone. His initial symptoms resolved over the next year.
The clinicians say the usual treatment for atheroembolism is supportive and depends on the affected organ. To their knowledge, they say, no formal studies have evaluated the use of anti-inflammatory therapies for this complication.
Funduscopy was an essential part of their examination, the researchers note, and spared the patient from invasive diagnostic studies such as biopsies. They also say that contrast-induced renal failure might have been the cause of the majority of his symptoms, but the combination of physical exam and differential diagnosis led them to the appropriate cause, as well as allowing for opportune treatment.
HHS Updates Decontamination Guidance With New Research
With help from researchers from the University of Hertfordshire in the United Kingdom, The US Department of Health and Human Services (HHS) has updated guidance on how best to decontaminate after mass chemical exposure. This second edition of Primary Response Incident Scene Management (PRISM) incorporates new scientific evidence on emergency self-decontamination, hair decontamination, and the interactions of chemicals with hair.
The goal of working with the University of Hertfordshire was to help emergency managers and first responders make “fundamental and fast decisions on how to save the greatest number of lives in chemical emergencies,” says Rick Bright, PhD, director of the Biomedical Advanced Research and Development Authority (BARDA).
The study included a large-scale exercise in which > 80 volunteers were dosed with a chemical warfare agent simulant to quantify the efficacy of different forms of decontamination.
Notably, the research demonstrates that immediate “dry” decontamination—wiping down the victim with any absorbent material (eg, toilet paper, paper towels, wound dressings) can be highly effective on its own and can be done by affected individuals themselves under the instruction of first responders. The dry decontamination step removes up to 99% of contamination and minimizes the accumulation of hazardous material in the subsequent steps.
The new guidance also expands on the effects of the “triple protocol,” a combined decontamination strategy. The 3 steps of that protocol—dry decontamination, wet decontamination using water deluges from fire trucks, and technical decontamination—have been shown to remove 99.9% of chemical contamination. Moreover, the latest clinical evidence indicates that the 3-step approach is faster and more effective than traditional methods for treating chemically contaminated patients.
The guideline also addresses how communities can prepare for chemical emergencies and what to do after the event, such as providing washcloths, towels, blankets, and temporary clothing.
Federal experts and the researchers devised the Algorithm Suggesting Proportionate Incident Response Engagement (ASPIRE), a decision-support tool to help emergency management planners and responders decide which decontamination approach suits a given situation. Using the algorithm, they can tailor plans and responses based on the chemical and type of exposure, how quickly the chemical evaporates, and the amount of time passed since exposure.
ASPIRE and the guidance are integrated into the Chemical Hazards Emergency Medical Management (CHEMM), a web-based resource and suite of preparedness and emergency response tools. The developers also plan to incorporate them into a mobile app.
PRISM is available at www.medicalcountermeasures.gov.
With help from researchers from the University of Hertfordshire in the United Kingdom, The US Department of Health and Human Services (HHS) has updated guidance on how best to decontaminate after mass chemical exposure. This second edition of Primary Response Incident Scene Management (PRISM) incorporates new scientific evidence on emergency self-decontamination, hair decontamination, and the interactions of chemicals with hair.
The goal of working with the University of Hertfordshire was to help emergency managers and first responders make “fundamental and fast decisions on how to save the greatest number of lives in chemical emergencies,” says Rick Bright, PhD, director of the Biomedical Advanced Research and Development Authority (BARDA).
The study included a large-scale exercise in which > 80 volunteers were dosed with a chemical warfare agent simulant to quantify the efficacy of different forms of decontamination.
Notably, the research demonstrates that immediate “dry” decontamination—wiping down the victim with any absorbent material (eg, toilet paper, paper towels, wound dressings) can be highly effective on its own and can be done by affected individuals themselves under the instruction of first responders. The dry decontamination step removes up to 99% of contamination and minimizes the accumulation of hazardous material in the subsequent steps.
The new guidance also expands on the effects of the “triple protocol,” a combined decontamination strategy. The 3 steps of that protocol—dry decontamination, wet decontamination using water deluges from fire trucks, and technical decontamination—have been shown to remove 99.9% of chemical contamination. Moreover, the latest clinical evidence indicates that the 3-step approach is faster and more effective than traditional methods for treating chemically contaminated patients.
The guideline also addresses how communities can prepare for chemical emergencies and what to do after the event, such as providing washcloths, towels, blankets, and temporary clothing.
Federal experts and the researchers devised the Algorithm Suggesting Proportionate Incident Response Engagement (ASPIRE), a decision-support tool to help emergency management planners and responders decide which decontamination approach suits a given situation. Using the algorithm, they can tailor plans and responses based on the chemical and type of exposure, how quickly the chemical evaporates, and the amount of time passed since exposure.
ASPIRE and the guidance are integrated into the Chemical Hazards Emergency Medical Management (CHEMM), a web-based resource and suite of preparedness and emergency response tools. The developers also plan to incorporate them into a mobile app.
PRISM is available at www.medicalcountermeasures.gov.
With help from researchers from the University of Hertfordshire in the United Kingdom, The US Department of Health and Human Services (HHS) has updated guidance on how best to decontaminate after mass chemical exposure. This second edition of Primary Response Incident Scene Management (PRISM) incorporates new scientific evidence on emergency self-decontamination, hair decontamination, and the interactions of chemicals with hair.
The goal of working with the University of Hertfordshire was to help emergency managers and first responders make “fundamental and fast decisions on how to save the greatest number of lives in chemical emergencies,” says Rick Bright, PhD, director of the Biomedical Advanced Research and Development Authority (BARDA).
The study included a large-scale exercise in which > 80 volunteers were dosed with a chemical warfare agent simulant to quantify the efficacy of different forms of decontamination.
Notably, the research demonstrates that immediate “dry” decontamination—wiping down the victim with any absorbent material (eg, toilet paper, paper towels, wound dressings) can be highly effective on its own and can be done by affected individuals themselves under the instruction of first responders. The dry decontamination step removes up to 99% of contamination and minimizes the accumulation of hazardous material in the subsequent steps.
The new guidance also expands on the effects of the “triple protocol,” a combined decontamination strategy. The 3 steps of that protocol—dry decontamination, wet decontamination using water deluges from fire trucks, and technical decontamination—have been shown to remove 99.9% of chemical contamination. Moreover, the latest clinical evidence indicates that the 3-step approach is faster and more effective than traditional methods for treating chemically contaminated patients.
The guideline also addresses how communities can prepare for chemical emergencies and what to do after the event, such as providing washcloths, towels, blankets, and temporary clothing.
Federal experts and the researchers devised the Algorithm Suggesting Proportionate Incident Response Engagement (ASPIRE), a decision-support tool to help emergency management planners and responders decide which decontamination approach suits a given situation. Using the algorithm, they can tailor plans and responses based on the chemical and type of exposure, how quickly the chemical evaporates, and the amount of time passed since exposure.
ASPIRE and the guidance are integrated into the Chemical Hazards Emergency Medical Management (CHEMM), a web-based resource and suite of preparedness and emergency response tools. The developers also plan to incorporate them into a mobile app.
PRISM is available at www.medicalcountermeasures.gov.
Military Doctors In Crosshairs of a Budget Battle
The move inside the military coincides with efforts by the Trump administration to privatize care for veterans. The Department of Veterans Affairs in February proposed rules that would allow veterans to use private hospitals and clinics if government primary care facilities are not nearby or if they have to wait too long for an appointment.
Shrinking the medical corps within the armed forces is proving more contentious and complex. In 2017, a Republican-controlled Congress mandated changes in what a Senate Armed Services Committee report described as “an under-performing, disjointed health system” with “bloated medical headquarters staffs” and “inevitable turf wars.” The directive sought a greater emphasis for military doctors on combat-related needs while transferring other care to civilian providers.
Details of reductions have yet to be finalized, a military spokeswoman said. But within the system and among alumni, trepidation has increased since Military.com, an online military and veterans organization, reported in January that the Department of Defense had drafted proposals to convert more than 17,000 medical positions into fighting and support positions – a 13 percent reduction in medical personnel.
“That would be a drastic first cut,” said Dr. David Lane, a retired rear admiral and former director of the Walter Reed National Military Medical Center in Bethesda, Md.
At most risk in the current planning are positions that aren’t considered essential to troops overseas, such as training spots for new doctors and jobs that can be outsourced to private physicians and hospitals – obstetricians and primary care doctors, for example. The reductions may also limit the military’s medical humanitarian assistance and relief for foreign natural disasters and disease outbreaks.
Even in war zones, Lane warned, it would be a mistake to downplay the importance of contributions by doctors who do not specialize in trauma. In the 1991 invasion of Kuwait, for instance, cases of diseases and non-battle injuries rather than combat injuries created the most medical work, he said.
Doctors who train in the military’s highly regarded medical school – who have committed to serve in the armed forces after training – and those who do military residencies account for much of the staff serving troops overseas. A major deployment could leave the military flatfooted, said Dr. John Prescott, a former Army physician.
“The majority of folks in the military don’t stay in for their whole career, they stay in for a few years,” Prescott said. “I’m concerned there will be a very small cohort that will be available for deployment in the future.”
The military health system is responsible for more than 1.4 million active-duty and 331,000 reserve personnel, with 54 hospitals and 377 military clinics around the world. Split among the Navy, Army and Air Force, each with its own doctors and hospitals, the service has been targeted for years for overhaul to reduce redundancies and save costs.
The department has already started moving administrative functions under one bureaucracy, called the Defense Health Agency, which is slated to take over the service branch hospitals in 2021.
The budget for the next fiscal year is still being developed and final decisions have not yet been made, a Department of Defense spokeswoman, Lt. Col. Carla Gleason, said in an email. “Any reforms that do result will be driven by the Department’s efforts to ensure our medical personnel are ready to provide battlefield care in support of our forces, and to provide the outstanding medical benefits that Service members, retirees and their families deserve,” she said.
For years, critics of the broad role of the military health services have argued that many medical corps services – such as maternity care and pediatrics on bases – could be provided more effectively by civilian doctors and hospitals.
But Lane said there is too much focus on the high-profile trauma cases on the battlefield “that at the end of the day are a small portion” of medical care. “When we’re trying to put things back together that got broken during a war,” he said, “that’s what you need the most of – pediatricians, public health doctors, primary care doctors.”
Some studies commissioned by the department have concluded private hospitals could deliver less costly care, in part because doctors at hospitals take care of more patients. But the Congressional Budget Office said savings were not at all certain and that military hospitals might be less expensive if the government arranged for greater use of them.
Brad Carson and Morgan Plummer, who held senior jobs in the Department of Defense during President Barack Obama’s administration, argued in a 2016 essay that the military isn’t the best training for surgeons because it doesn’t provide them with a sufficient number of cases to develop expertise.
The military health system “has too much infrastructure, the wrong mix of providers, and predominantly serves the needs of beneficiaries who could easily have their health care needs satisfied by civilian providers at far less cost and with equal or better quality,” they wrote.
The government this year is spending $50 billion on the military health system, including Tricare insurance for more than 9 million active-duty service members, veterans, families and survivors, according to Congress’ budget office. That is roughly a tenth of the military budget. The CBO projected costs are on track to increase to $63 billion in 2033.
Defenders of the system reject the idea that non-wartime jobs can be eliminated without it hurting that core mission.
“Military health care providers between deployments maintain their clinical skills by treating service members and millions of beneficiaries,” Dr. Arthur Kellermann, dean of the school of medicine at the Uniformed Services University in Bethesda, wrote in a 2017 Health Affairs article. “Military hospitals provide valuable platforms for teaching the next generation of uniformed health care professionals and standby capacity for combat casualties.”
Prescott, the former Army doctor, said that the military may have trouble turning to civilian doctors in some regions given physician shortages, which he said the military cuts would exacerbate.
“Most hospitals are already pretty full, most health care providers are pretty busy,” said Prescott, now chief academic officer at the Association of American Medical Colleges.
Doctor shortages would increase if the military cut the slots it now has to train doctors, because there wouldn’t be new civilian residencies created to compensate. “Those positions basically disappear,” he said.
Kathryn Beasley, a retired Navy captain who is director of government relations for health affairs at the Military Officers Association of America, said she was also concerned with unforeseen consequences of dramatic cuts.
“Everything’s tied together, there’s a lot of interdependencies in these things,” she said. “You pull a string on one and you might feel it in an area you don’t expect.”
Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
The move inside the military coincides with efforts by the Trump administration to privatize care for veterans. The Department of Veterans Affairs in February proposed rules that would allow veterans to use private hospitals and clinics if government primary care facilities are not nearby or if they have to wait too long for an appointment.
Shrinking the medical corps within the armed forces is proving more contentious and complex. In 2017, a Republican-controlled Congress mandated changes in what a Senate Armed Services Committee report described as “an under-performing, disjointed health system” with “bloated medical headquarters staffs” and “inevitable turf wars.” The directive sought a greater emphasis for military doctors on combat-related needs while transferring other care to civilian providers.
Details of reductions have yet to be finalized, a military spokeswoman said. But within the system and among alumni, trepidation has increased since Military.com, an online military and veterans organization, reported in January that the Department of Defense had drafted proposals to convert more than 17,000 medical positions into fighting and support positions – a 13 percent reduction in medical personnel.
“That would be a drastic first cut,” said Dr. David Lane, a retired rear admiral and former director of the Walter Reed National Military Medical Center in Bethesda, Md.
At most risk in the current planning are positions that aren’t considered essential to troops overseas, such as training spots for new doctors and jobs that can be outsourced to private physicians and hospitals – obstetricians and primary care doctors, for example. The reductions may also limit the military’s medical humanitarian assistance and relief for foreign natural disasters and disease outbreaks.
Even in war zones, Lane warned, it would be a mistake to downplay the importance of contributions by doctors who do not specialize in trauma. In the 1991 invasion of Kuwait, for instance, cases of diseases and non-battle injuries rather than combat injuries created the most medical work, he said.
Doctors who train in the military’s highly regarded medical school – who have committed to serve in the armed forces after training – and those who do military residencies account for much of the staff serving troops overseas. A major deployment could leave the military flatfooted, said Dr. John Prescott, a former Army physician.
“The majority of folks in the military don’t stay in for their whole career, they stay in for a few years,” Prescott said. “I’m concerned there will be a very small cohort that will be available for deployment in the future.”
The military health system is responsible for more than 1.4 million active-duty and 331,000 reserve personnel, with 54 hospitals and 377 military clinics around the world. Split among the Navy, Army and Air Force, each with its own doctors and hospitals, the service has been targeted for years for overhaul to reduce redundancies and save costs.
The department has already started moving administrative functions under one bureaucracy, called the Defense Health Agency, which is slated to take over the service branch hospitals in 2021.
The budget for the next fiscal year is still being developed and final decisions have not yet been made, a Department of Defense spokeswoman, Lt. Col. Carla Gleason, said in an email. “Any reforms that do result will be driven by the Department’s efforts to ensure our medical personnel are ready to provide battlefield care in support of our forces, and to provide the outstanding medical benefits that Service members, retirees and their families deserve,” she said.
For years, critics of the broad role of the military health services have argued that many medical corps services – such as maternity care and pediatrics on bases – could be provided more effectively by civilian doctors and hospitals.
But Lane said there is too much focus on the high-profile trauma cases on the battlefield “that at the end of the day are a small portion” of medical care. “When we’re trying to put things back together that got broken during a war,” he said, “that’s what you need the most of – pediatricians, public health doctors, primary care doctors.”
Some studies commissioned by the department have concluded private hospitals could deliver less costly care, in part because doctors at hospitals take care of more patients. But the Congressional Budget Office said savings were not at all certain and that military hospitals might be less expensive if the government arranged for greater use of them.
Brad Carson and Morgan Plummer, who held senior jobs in the Department of Defense during President Barack Obama’s administration, argued in a 2016 essay that the military isn’t the best training for surgeons because it doesn’t provide them with a sufficient number of cases to develop expertise.
The military health system “has too much infrastructure, the wrong mix of providers, and predominantly serves the needs of beneficiaries who could easily have their health care needs satisfied by civilian providers at far less cost and with equal or better quality,” they wrote.
The government this year is spending $50 billion on the military health system, including Tricare insurance for more than 9 million active-duty service members, veterans, families and survivors, according to Congress’ budget office. That is roughly a tenth of the military budget. The CBO projected costs are on track to increase to $63 billion in 2033.
Defenders of the system reject the idea that non-wartime jobs can be eliminated without it hurting that core mission.
“Military health care providers between deployments maintain their clinical skills by treating service members and millions of beneficiaries,” Dr. Arthur Kellermann, dean of the school of medicine at the Uniformed Services University in Bethesda, wrote in a 2017 Health Affairs article. “Military hospitals provide valuable platforms for teaching the next generation of uniformed health care professionals and standby capacity for combat casualties.”
Prescott, the former Army doctor, said that the military may have trouble turning to civilian doctors in some regions given physician shortages, which he said the military cuts would exacerbate.
“Most hospitals are already pretty full, most health care providers are pretty busy,” said Prescott, now chief academic officer at the Association of American Medical Colleges.
Doctor shortages would increase if the military cut the slots it now has to train doctors, because there wouldn’t be new civilian residencies created to compensate. “Those positions basically disappear,” he said.
Kathryn Beasley, a retired Navy captain who is director of government relations for health affairs at the Military Officers Association of America, said she was also concerned with unforeseen consequences of dramatic cuts.
“Everything’s tied together, there’s a lot of interdependencies in these things,” she said. “You pull a string on one and you might feel it in an area you don’t expect.”
Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
The move inside the military coincides with efforts by the Trump administration to privatize care for veterans. The Department of Veterans Affairs in February proposed rules that would allow veterans to use private hospitals and clinics if government primary care facilities are not nearby or if they have to wait too long for an appointment.
Shrinking the medical corps within the armed forces is proving more contentious and complex. In 2017, a Republican-controlled Congress mandated changes in what a Senate Armed Services Committee report described as “an under-performing, disjointed health system” with “bloated medical headquarters staffs” and “inevitable turf wars.” The directive sought a greater emphasis for military doctors on combat-related needs while transferring other care to civilian providers.
Details of reductions have yet to be finalized, a military spokeswoman said. But within the system and among alumni, trepidation has increased since Military.com, an online military and veterans organization, reported in January that the Department of Defense had drafted proposals to convert more than 17,000 medical positions into fighting and support positions – a 13 percent reduction in medical personnel.
“That would be a drastic first cut,” said Dr. David Lane, a retired rear admiral and former director of the Walter Reed National Military Medical Center in Bethesda, Md.
At most risk in the current planning are positions that aren’t considered essential to troops overseas, such as training spots for new doctors and jobs that can be outsourced to private physicians and hospitals – obstetricians and primary care doctors, for example. The reductions may also limit the military’s medical humanitarian assistance and relief for foreign natural disasters and disease outbreaks.
Even in war zones, Lane warned, it would be a mistake to downplay the importance of contributions by doctors who do not specialize in trauma. In the 1991 invasion of Kuwait, for instance, cases of diseases and non-battle injuries rather than combat injuries created the most medical work, he said.
Doctors who train in the military’s highly regarded medical school – who have committed to serve in the armed forces after training – and those who do military residencies account for much of the staff serving troops overseas. A major deployment could leave the military flatfooted, said Dr. John Prescott, a former Army physician.
“The majority of folks in the military don’t stay in for their whole career, they stay in for a few years,” Prescott said. “I’m concerned there will be a very small cohort that will be available for deployment in the future.”
The military health system is responsible for more than 1.4 million active-duty and 331,000 reserve personnel, with 54 hospitals and 377 military clinics around the world. Split among the Navy, Army and Air Force, each with its own doctors and hospitals, the service has been targeted for years for overhaul to reduce redundancies and save costs.
The department has already started moving administrative functions under one bureaucracy, called the Defense Health Agency, which is slated to take over the service branch hospitals in 2021.
The budget for the next fiscal year is still being developed and final decisions have not yet been made, a Department of Defense spokeswoman, Lt. Col. Carla Gleason, said in an email. “Any reforms that do result will be driven by the Department’s efforts to ensure our medical personnel are ready to provide battlefield care in support of our forces, and to provide the outstanding medical benefits that Service members, retirees and their families deserve,” she said.
For years, critics of the broad role of the military health services have argued that many medical corps services – such as maternity care and pediatrics on bases – could be provided more effectively by civilian doctors and hospitals.
But Lane said there is too much focus on the high-profile trauma cases on the battlefield “that at the end of the day are a small portion” of medical care. “When we’re trying to put things back together that got broken during a war,” he said, “that’s what you need the most of – pediatricians, public health doctors, primary care doctors.”
Some studies commissioned by the department have concluded private hospitals could deliver less costly care, in part because doctors at hospitals take care of more patients. But the Congressional Budget Office said savings were not at all certain and that military hospitals might be less expensive if the government arranged for greater use of them.
Brad Carson and Morgan Plummer, who held senior jobs in the Department of Defense during President Barack Obama’s administration, argued in a 2016 essay that the military isn’t the best training for surgeons because it doesn’t provide them with a sufficient number of cases to develop expertise.
The military health system “has too much infrastructure, the wrong mix of providers, and predominantly serves the needs of beneficiaries who could easily have their health care needs satisfied by civilian providers at far less cost and with equal or better quality,” they wrote.
The government this year is spending $50 billion on the military health system, including Tricare insurance for more than 9 million active-duty service members, veterans, families and survivors, according to Congress’ budget office. That is roughly a tenth of the military budget. The CBO projected costs are on track to increase to $63 billion in 2033.
Defenders of the system reject the idea that non-wartime jobs can be eliminated without it hurting that core mission.
“Military health care providers between deployments maintain their clinical skills by treating service members and millions of beneficiaries,” Dr. Arthur Kellermann, dean of the school of medicine at the Uniformed Services University in Bethesda, wrote in a 2017 Health Affairs article. “Military hospitals provide valuable platforms for teaching the next generation of uniformed health care professionals and standby capacity for combat casualties.”
Prescott, the former Army doctor, said that the military may have trouble turning to civilian doctors in some regions given physician shortages, which he said the military cuts would exacerbate.
“Most hospitals are already pretty full, most health care providers are pretty busy,” said Prescott, now chief academic officer at the Association of American Medical Colleges.
Doctor shortages would increase if the military cut the slots it now has to train doctors, because there wouldn’t be new civilian residencies created to compensate. “Those positions basically disappear,” he said.
Kathryn Beasley, a retired Navy captain who is director of government relations for health affairs at the Military Officers Association of America, said she was also concerned with unforeseen consequences of dramatic cuts.
“Everything’s tied together, there’s a lot of interdependencies in these things,” she said. “You pull a string on one and you might feel it in an area you don’t expect.”
Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Daily aspirin associated with lower risk of COPD flareup
Daily aspirin use could reduce the risk of acute exacerbations of chronic obstructive pulmonary disease, new data suggest.

Researchers reported the outcomes of an observational cohort study of 1,698 individuals with COPD, 45% of whom said they were taking daily aspirin at baseline. Their findings were published in Chest.
After a median follow up of 2.7 years, aspirin users had an overall 22% lower incidence of acute COPD exacerbations compared with nonusers. This was largely accounted for by a 25% reduction in moderate exacerbations, but there was no significant difference between aspirin users and nonusers in severe exacerbations.
A similar pattern was seen after just 1 year of follow-up, with an overall 30% reduction in the incidence of exacerbations, a 37% reduction in moderate exacerbations, but no significant reduction in severe exacerbations.
“Though aspirin use has previously been linked with reduced mortality risk in patients with COPD, to our knowledge, this is the first study to investigate the association of daily aspirin use with respiratory morbidity in COPD,” wrote Ashraf Fawzy, MD, of the division of pulmonary and critical care medicine at Johns Hopkins University, Baltimore, and his coauthors.
The association between aspirin use and reduced incidence of exacerbations was stronger among individuals with chronic bronchitis, which prompted the authors to suggest that future studies of aspirin in COPD should focus on participants with chronic bronchitis.
However, the association was not affected by COPD severity, emphysema presence or severity, or cardiometabolic phenotype.
Aspirin users reported better respiratory-specific quality of life than that of nonusers, including 34% lower odds of reporting moderate to severe dyspnea, and better baseline COPD health status.
“Findings of this study add to the existing literature by highlighting that aspirin use is also associated with reduced respiratory morbidity across several domains – including exacerbation risk, quality of life, and dyspnea – factors related to patient well-being and healthcare utilization,” the authors wrote.
Aspirin users were more likely to be white, male, and obese, and less likely to be smokers. They had better lung function but more cardiovascular comorbidities at baseline, although the aspirin users and nonusers were matched on baseline characteristics.
Speculating on the mechanisms by which aspirin might impact COPD exacerbations, the authors noted that the drug has both systemic and local pulmonary mechanisms of action.
For example, a pathway that results in elevated levels of a urinary metabolite in patients with COPD is irreversibly blocked by aspirin. Aspirin also attenuates the elevation of inflammatory markers interleukin-6 and C-reactive protein, which are part of the inflammatory phenotype of COPD. Aspirin has been shown to reduce proinflammatory cytokines in the lung.
The authors did note that aspirin use was self-reported, so they did not have data on dosage or duration of use.
The National Institutes of Health funded the study. Six authors declared advisory board positions, research support, and other funding from the pharmaceutical sector. One author was also a founder of a company commercializing lung image analysis software. No other conflicts of interest were declared.
SOURCE: Fawzy A et al. Chest. 2019 Mar;155(3): 519-27. doi: 10.1016/j.chest.2018.11.028.
Daily aspirin use could reduce the risk of acute exacerbations of chronic obstructive pulmonary disease, new data suggest.
Researchers reported the outcomes of an observational cohort study of 1,698 individuals with COPD, 45% of whom said they were taking daily aspirin at baseline. Their findings were published in Chest.
After a median follow up of 2.7 years, aspirin users had an overall 22% lower incidence of acute COPD exacerbations compared with nonusers. This was largely accounted for by a 25% reduction in moderate exacerbations, but there was no significant difference between aspirin users and nonusers in severe exacerbations.
A similar pattern was seen after just 1 year of follow-up, with an overall 30% reduction in the incidence of exacerbations, a 37% reduction in moderate exacerbations, but no significant reduction in severe exacerbations.
“Though aspirin use has previously been linked with reduced mortality risk in patients with COPD, to our knowledge, this is the first study to investigate the association of daily aspirin use with respiratory morbidity in COPD,” wrote Ashraf Fawzy, MD, of the division of pulmonary and critical care medicine at Johns Hopkins University, Baltimore, and his coauthors.
The association between aspirin use and reduced incidence of exacerbations was stronger among individuals with chronic bronchitis, which prompted the authors to suggest that future studies of aspirin in COPD should focus on participants with chronic bronchitis.
However, the association was not affected by COPD severity, emphysema presence or severity, or cardiometabolic phenotype.
Aspirin users reported better respiratory-specific quality of life than that of nonusers, including 34% lower odds of reporting moderate to severe dyspnea, and better baseline COPD health status.
“Findings of this study add to the existing literature by highlighting that aspirin use is also associated with reduced respiratory morbidity across several domains – including exacerbation risk, quality of life, and dyspnea – factors related to patient well-being and healthcare utilization,” the authors wrote.
Aspirin users were more likely to be white, male, and obese, and less likely to be smokers. They had better lung function but more cardiovascular comorbidities at baseline, although the aspirin users and nonusers were matched on baseline characteristics.
Speculating on the mechanisms by which aspirin might impact COPD exacerbations, the authors noted that the drug has both systemic and local pulmonary mechanisms of action.
For example, a pathway that results in elevated levels of a urinary metabolite in patients with COPD is irreversibly blocked by aspirin. Aspirin also attenuates the elevation of inflammatory markers interleukin-6 and C-reactive protein, which are part of the inflammatory phenotype of COPD. Aspirin has been shown to reduce proinflammatory cytokines in the lung.
The authors did note that aspirin use was self-reported, so they did not have data on dosage or duration of use.
The National Institutes of Health funded the study. Six authors declared advisory board positions, research support, and other funding from the pharmaceutical sector. One author was also a founder of a company commercializing lung image analysis software. No other conflicts of interest were declared.
SOURCE: Fawzy A et al. Chest. 2019 Mar;155(3): 519-27. doi: 10.1016/j.chest.2018.11.028.
Daily aspirin use could reduce the risk of acute exacerbations of chronic obstructive pulmonary disease, new data suggest.
Researchers reported the outcomes of an observational cohort study of 1,698 individuals with COPD, 45% of whom said they were taking daily aspirin at baseline. Their findings were published in Chest.
After a median follow up of 2.7 years, aspirin users had an overall 22% lower incidence of acute COPD exacerbations compared with nonusers. This was largely accounted for by a 25% reduction in moderate exacerbations, but there was no significant difference between aspirin users and nonusers in severe exacerbations.
A similar pattern was seen after just 1 year of follow-up, with an overall 30% reduction in the incidence of exacerbations, a 37% reduction in moderate exacerbations, but no significant reduction in severe exacerbations.
“Though aspirin use has previously been linked with reduced mortality risk in patients with COPD, to our knowledge, this is the first study to investigate the association of daily aspirin use with respiratory morbidity in COPD,” wrote Ashraf Fawzy, MD, of the division of pulmonary and critical care medicine at Johns Hopkins University, Baltimore, and his coauthors.
The association between aspirin use and reduced incidence of exacerbations was stronger among individuals with chronic bronchitis, which prompted the authors to suggest that future studies of aspirin in COPD should focus on participants with chronic bronchitis.
However, the association was not affected by COPD severity, emphysema presence or severity, or cardiometabolic phenotype.
Aspirin users reported better respiratory-specific quality of life than that of nonusers, including 34% lower odds of reporting moderate to severe dyspnea, and better baseline COPD health status.
“Findings of this study add to the existing literature by highlighting that aspirin use is also associated with reduced respiratory morbidity across several domains – including exacerbation risk, quality of life, and dyspnea – factors related to patient well-being and healthcare utilization,” the authors wrote.
Aspirin users were more likely to be white, male, and obese, and less likely to be smokers. They had better lung function but more cardiovascular comorbidities at baseline, although the aspirin users and nonusers were matched on baseline characteristics.
Speculating on the mechanisms by which aspirin might impact COPD exacerbations, the authors noted that the drug has both systemic and local pulmonary mechanisms of action.
For example, a pathway that results in elevated levels of a urinary metabolite in patients with COPD is irreversibly blocked by aspirin. Aspirin also attenuates the elevation of inflammatory markers interleukin-6 and C-reactive protein, which are part of the inflammatory phenotype of COPD. Aspirin has been shown to reduce proinflammatory cytokines in the lung.
The authors did note that aspirin use was self-reported, so they did not have data on dosage or duration of use.
The National Institutes of Health funded the study. Six authors declared advisory board positions, research support, and other funding from the pharmaceutical sector. One author was also a founder of a company commercializing lung image analysis software. No other conflicts of interest were declared.
SOURCE: Fawzy A et al. Chest. 2019 Mar;155(3): 519-27. doi: 10.1016/j.chest.2018.11.028.
FROM CHEST
Thyroid Hormones Predict Readmission After Aortic Surgery
Thoracic endovascular aortic repair (TEVAR) is a “young technology with several unknowns,” say researchers from Shantou University Medical College, and Wuhan Asia Heart Hospital, both China. One of those unknowns is the risk factors for prognosis after TEVAR.
After all, thyroid hormones are critical to many areas of heart health, such as vascular remodeling; hypothyroidism can aggravate hypertension; and low levels of free thyroxine (FT4) influence arterial stiffness and C-reactive protein. In spite of the many links, however, the relationship between subclinical hypothyroidism and cardiovascular disease has not been fully elucidated, the researchers say. They conducted a study to evaluate whether thyroid hormones predicted early (30 days) and mid-term (12 months) aorta-related adverse events (AEs), such as death, progression of aortic disease, organ failure, or lower limb ischemia; and aorta-related readmissions.
In their study, 338 patients were stratified according to their levels of FT4 before undergoing TEVAR. Of the enrolled patients, 288 were followed up at 12 months for readmission; 292 were followed up on AEs.
Patients with low normal levels of FT4 had a greater risk of readmission after thoracic endovascular aortic repair. Within 30 days, the incidence of AEs and readmission were 2.7% and 4.1%; within 12 months, 8.9% and 13.5%. After the researchers adjusted for confounders, the patients with the lowest FT4 quartile were at significantly greater risk for readmission than those in the highest-quartile group, at both early and mid-term follow-up.
The same did not hold true for AEs. The researchers say this is not uncommon in studies of predictors of AEs and readmission: Factors that are weak predictors of readmission tend to be strong predictors of AEs, and vice versa.
Thoracic endovascular aortic repair (TEVAR) is a “young technology with several unknowns,” say researchers from Shantou University Medical College, and Wuhan Asia Heart Hospital, both China. One of those unknowns is the risk factors for prognosis after TEVAR.
After all, thyroid hormones are critical to many areas of heart health, such as vascular remodeling; hypothyroidism can aggravate hypertension; and low levels of free thyroxine (FT4) influence arterial stiffness and C-reactive protein. In spite of the many links, however, the relationship between subclinical hypothyroidism and cardiovascular disease has not been fully elucidated, the researchers say. They conducted a study to evaluate whether thyroid hormones predicted early (30 days) and mid-term (12 months) aorta-related adverse events (AEs), such as death, progression of aortic disease, organ failure, or lower limb ischemia; and aorta-related readmissions.
In their study, 338 patients were stratified according to their levels of FT4 before undergoing TEVAR. Of the enrolled patients, 288 were followed up at 12 months for readmission; 292 were followed up on AEs.
Patients with low normal levels of FT4 had a greater risk of readmission after thoracic endovascular aortic repair. Within 30 days, the incidence of AEs and readmission were 2.7% and 4.1%; within 12 months, 8.9% and 13.5%. After the researchers adjusted for confounders, the patients with the lowest FT4 quartile were at significantly greater risk for readmission than those in the highest-quartile group, at both early and mid-term follow-up.
The same did not hold true for AEs. The researchers say this is not uncommon in studies of predictors of AEs and readmission: Factors that are weak predictors of readmission tend to be strong predictors of AEs, and vice versa.
Thoracic endovascular aortic repair (TEVAR) is a “young technology with several unknowns,” say researchers from Shantou University Medical College, and Wuhan Asia Heart Hospital, both China. One of those unknowns is the risk factors for prognosis after TEVAR.
After all, thyroid hormones are critical to many areas of heart health, such as vascular remodeling; hypothyroidism can aggravate hypertension; and low levels of free thyroxine (FT4) influence arterial stiffness and C-reactive protein. In spite of the many links, however, the relationship between subclinical hypothyroidism and cardiovascular disease has not been fully elucidated, the researchers say. They conducted a study to evaluate whether thyroid hormones predicted early (30 days) and mid-term (12 months) aorta-related adverse events (AEs), such as death, progression of aortic disease, organ failure, or lower limb ischemia; and aorta-related readmissions.
In their study, 338 patients were stratified according to their levels of FT4 before undergoing TEVAR. Of the enrolled patients, 288 were followed up at 12 months for readmission; 292 were followed up on AEs.
Patients with low normal levels of FT4 had a greater risk of readmission after thoracic endovascular aortic repair. Within 30 days, the incidence of AEs and readmission were 2.7% and 4.1%; within 12 months, 8.9% and 13.5%. After the researchers adjusted for confounders, the patients with the lowest FT4 quartile were at significantly greater risk for readmission than those in the highest-quartile group, at both early and mid-term follow-up.
The same did not hold true for AEs. The researchers say this is not uncommon in studies of predictors of AEs and readmission: Factors that are weak predictors of readmission tend to be strong predictors of AEs, and vice versa.
Nonadherent Diabetes Patients: An Unexpected Group
“Time-specific” dosing of insulin can be an obstacle to adherence for patients with complicated, busy lives. More than half of patients with type 2 diabetes do not achieve their target HbA1c of 7% after insulin is added to their treatment regimen. Researchers from CAPHRI School for Public Health and Primary Care, and CARIM Institute in The Netherlands, who surveyed 1,483 adults with diabetes suggest that it may be time to rethink both prescribing and patient education, in part because of who fell into the nonadherent group.
The researchers conducted a web-based self-report survey. Of the respondents, 58% used bolus insulin before meals, 24% after meals, and 18% before, during, or after meals. The researchers excluded the “mixed” cohort, including 1,218 in the analysis.
Half the respondents in the postmeal cohort reported experiencing minor hypoglycemic events at least once a week compared with 35% of the premeal cohort. Similarly, more in the postmeal group had had major hypoglycemic events (38% vs 26%). The postmeal respondents also were more likely to have HbA1c ≥ 9% (40% vs 29%). And they were less likely to report always testing their blood glucose before injecting insulin (36% vs 54%).
Perhaps contrary to some expectations, the respondents who injected insulin postmeal were younger, had shorter duration of diabetes, had the highest level of college or university education, were more likely to be employed, and more frequently participated in diabetes education programs (including one-on-one programs).
The researchers say those data suggest that factors other than lack of diabetes education, education, or low socioeconomic status should be considered in explaining the nonadherence. They add that some research has shown that education programs have an “inconsistent relationship with patient adherence.” They suggest that such programs might be improved by placing greater emphasis on the importance of dosing insulin before meals.
Of the nearly 20% of patients who use insulin treatment, > 90% receive bolus insulin. The researchers note that respondents preferred a form of bolus insulin they can administer before, after, or during meals as they see fit. The respondents who injected postmeal were more likely than the premeal respondents to prefer this formulation.
“Time-specific” dosing of insulin can be an obstacle to adherence for patients with complicated, busy lives. More than half of patients with type 2 diabetes do not achieve their target HbA1c of 7% after insulin is added to their treatment regimen. Researchers from CAPHRI School for Public Health and Primary Care, and CARIM Institute in The Netherlands, who surveyed 1,483 adults with diabetes suggest that it may be time to rethink both prescribing and patient education, in part because of who fell into the nonadherent group.
The researchers conducted a web-based self-report survey. Of the respondents, 58% used bolus insulin before meals, 24% after meals, and 18% before, during, or after meals. The researchers excluded the “mixed” cohort, including 1,218 in the analysis.
Half the respondents in the postmeal cohort reported experiencing minor hypoglycemic events at least once a week compared with 35% of the premeal cohort. Similarly, more in the postmeal group had had major hypoglycemic events (38% vs 26%). The postmeal respondents also were more likely to have HbA1c ≥ 9% (40% vs 29%). And they were less likely to report always testing their blood glucose before injecting insulin (36% vs 54%).
Perhaps contrary to some expectations, the respondents who injected insulin postmeal were younger, had shorter duration of diabetes, had the highest level of college or university education, were more likely to be employed, and more frequently participated in diabetes education programs (including one-on-one programs).
The researchers say those data suggest that factors other than lack of diabetes education, education, or low socioeconomic status should be considered in explaining the nonadherence. They add that some research has shown that education programs have an “inconsistent relationship with patient adherence.” They suggest that such programs might be improved by placing greater emphasis on the importance of dosing insulin before meals.
Of the nearly 20% of patients who use insulin treatment, > 90% receive bolus insulin. The researchers note that respondents preferred a form of bolus insulin they can administer before, after, or during meals as they see fit. The respondents who injected postmeal were more likely than the premeal respondents to prefer this formulation.
“Time-specific” dosing of insulin can be an obstacle to adherence for patients with complicated, busy lives. More than half of patients with type 2 diabetes do not achieve their target HbA1c of 7% after insulin is added to their treatment regimen. Researchers from CAPHRI School for Public Health and Primary Care, and CARIM Institute in The Netherlands, who surveyed 1,483 adults with diabetes suggest that it may be time to rethink both prescribing and patient education, in part because of who fell into the nonadherent group.
The researchers conducted a web-based self-report survey. Of the respondents, 58% used bolus insulin before meals, 24% after meals, and 18% before, during, or after meals. The researchers excluded the “mixed” cohort, including 1,218 in the analysis.
Half the respondents in the postmeal cohort reported experiencing minor hypoglycemic events at least once a week compared with 35% of the premeal cohort. Similarly, more in the postmeal group had had major hypoglycemic events (38% vs 26%). The postmeal respondents also were more likely to have HbA1c ≥ 9% (40% vs 29%). And they were less likely to report always testing their blood glucose before injecting insulin (36% vs 54%).
Perhaps contrary to some expectations, the respondents who injected insulin postmeal were younger, had shorter duration of diabetes, had the highest level of college or university education, were more likely to be employed, and more frequently participated in diabetes education programs (including one-on-one programs).
The researchers say those data suggest that factors other than lack of diabetes education, education, or low socioeconomic status should be considered in explaining the nonadherence. They add that some research has shown that education programs have an “inconsistent relationship with patient adherence.” They suggest that such programs might be improved by placing greater emphasis on the importance of dosing insulin before meals.
Of the nearly 20% of patients who use insulin treatment, > 90% receive bolus insulin. The researchers note that respondents preferred a form of bolus insulin they can administer before, after, or during meals as they see fit. The respondents who injected postmeal were more likely than the premeal respondents to prefer this formulation.