User login
NSAID continuation linked to less knee OA pain
in a randomized trial.
The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain score was 6.7 out of a possible total of 20 for patients who continued meloxicam for 4 weeks versus 7.8 in those who stopped and switched to a placebo. The estimated mean difference in pain score was 1.4 (P = .92 for noninferiority), which is below the threshold of 2.1 that is considered to be the minimum clinically important difference.
Furthermore, patients who had switched to placebo and then subsequently participated in a telephone-based cognitive behavior therapy (CBT) program for another 10 weeks had higher pain levels compared with those who continued meloxicam. WOMAC scores were 12.1 and 11.8, respectively with a mean difference of 0.8 (P = .28 for noninferiority).
“Among patients with knee osteoarthritis, placebo and CBT (after placebo) are inferior to meloxicam,” Liana Fraenkel, MD, MPH, of Yale University, New Haven, Conn., and coinvestigators concluded in their article, published in JAMA Internal Medicine.
They observed that the WOMAC pain score differences between the two groups were small, however, and that there were no statistically significant differences in participants’ global impression of change or function after 14 weeks.
“Although the overall results of the trial are negative, they provide clinicians with data to support shared decision-making and reassure patients willing to taper NSAIDs and consider self-management approaches such as CBT,” Dr. Fraenkel and coauthors suggested.
The Stopping NSAIDs for Arthritis Pain trial had ultimately included 364 participants, 86% of whom were men, recruited from four veterans affairs health care systems. All had been taking NSAIDs for knee OA pain for at least 3 months and had participated in a 2-week run-in period where the NSAID they had been taking was switched to meloxicam, 15 mg once daily.
The aim of the trial had been to see if discontinuing NSAIDs and starting a CBT program would be noninferior to continuing NSAIDs in patients with knee OA.
The trial does not provide robust information on the use of CBT, David Walsh, a rheumatologist and director of the Pain Centre Versus Arthritis at the University of Nottingham, England, said in an interview.
“It can’t tell you about efficacy of CBT,” Dr. Walsh said as the CBT part of the study was not randomized, was not controlled, and was unblinded. ”It would be a different task to design a CBT trial aiming to help people to stop taking tablets,” he added.
Dr. Fraenkel and coinvestigators had reported that, at week 14, the adjusted mean difference in WOMAC pain score between the placebo (followed by CBT) and meloxicam groups was 0.8 (P = .28 for noninferiority).
“What the trial’s really doing is seeing whether people who’ve been on long-term nonsteroidals, can they just stop them without getting any worse? The conclusion for that is actually they are more likely to get worse than not if you just stop the nonsteroidals,” Dr. Walsh said.
“The withdrawal trial protocol is an important one. You can’t run a prospective trial for years to see whether something works for years. It is just not feasible. So actually, the protocol they’ve got of switching to placebo, or continuing with a nonsteroidal, is probably the best way of working out if an anti-inflammatory still has a pharmacological effect after actually being on it for X years,” Dr. Walsh said.
Dr. Walsh, who was not involved in the trial, observed that while the difference in pain scores between the groups was small, the deterioration in scores might be important for individual patients. Some may do worse, although granted that there may be some that might do better, he said.
“It is suggesting to me that nonsteroidals are still working in people who are on long-term treatment. It is not a very big pharmacological effect, but we already know from the RCTs of anti-inflammatory tablets, that they can be beneficial,” Dr. Walsh noted.
He also pointed out that patients’ pain had been improved after being switched from their current NSAID to meloxicam – the overall WOMAC pain score at recruitment was 9.6 and was 5.6 after the 2-week meloxicam run-in phase.
“Now, whether that’s because they’ve been switched to meloxicam, or whether it’s because they’re in a trial,” is an important question, Dr. Walsh suggested, adding that “it looks as though it’s more likely to be because they’re in a trial, because improvement was maintained during the following 4 weeks on placebo.”
Another point he made was that there was a higher percentage of patients in the placebo group that started taking other types of painkillers, just under half (46%) used acetaminophen versus a quarter (26%) of those who continued using meloxicam.
It is an interesting trial, “trying to tackle some really difficult questions and I think that there are really important implications from it that we can build on, but is it actually going to change the lives of patients at the moment? Not massively,” Dr. Walsh said, ”but it’s another step in the right direction.”
Dr. Fraenkel disclosed receiving research funding from the VA Office of Research and Development, the sponsor of the trial.
SOURCE: Fraenkel L et al. JAMA Intern Med. 2020 Jul 20. doi:10.1001/jamainternmed.2020.2821.
in a randomized trial.
The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain score was 6.7 out of a possible total of 20 for patients who continued meloxicam for 4 weeks versus 7.8 in those who stopped and switched to a placebo. The estimated mean difference in pain score was 1.4 (P = .92 for noninferiority), which is below the threshold of 2.1 that is considered to be the minimum clinically important difference.
Furthermore, patients who had switched to placebo and then subsequently participated in a telephone-based cognitive behavior therapy (CBT) program for another 10 weeks had higher pain levels compared with those who continued meloxicam. WOMAC scores were 12.1 and 11.8, respectively with a mean difference of 0.8 (P = .28 for noninferiority).
“Among patients with knee osteoarthritis, placebo and CBT (after placebo) are inferior to meloxicam,” Liana Fraenkel, MD, MPH, of Yale University, New Haven, Conn., and coinvestigators concluded in their article, published in JAMA Internal Medicine.
They observed that the WOMAC pain score differences between the two groups were small, however, and that there were no statistically significant differences in participants’ global impression of change or function after 14 weeks.
“Although the overall results of the trial are negative, they provide clinicians with data to support shared decision-making and reassure patients willing to taper NSAIDs and consider self-management approaches such as CBT,” Dr. Fraenkel and coauthors suggested.
The Stopping NSAIDs for Arthritis Pain trial had ultimately included 364 participants, 86% of whom were men, recruited from four veterans affairs health care systems. All had been taking NSAIDs for knee OA pain for at least 3 months and had participated in a 2-week run-in period where the NSAID they had been taking was switched to meloxicam, 15 mg once daily.
The aim of the trial had been to see if discontinuing NSAIDs and starting a CBT program would be noninferior to continuing NSAIDs in patients with knee OA.
The trial does not provide robust information on the use of CBT, David Walsh, a rheumatologist and director of the Pain Centre Versus Arthritis at the University of Nottingham, England, said in an interview.
“It can’t tell you about efficacy of CBT,” Dr. Walsh said as the CBT part of the study was not randomized, was not controlled, and was unblinded. ”It would be a different task to design a CBT trial aiming to help people to stop taking tablets,” he added.
Dr. Fraenkel and coinvestigators had reported that, at week 14, the adjusted mean difference in WOMAC pain score between the placebo (followed by CBT) and meloxicam groups was 0.8 (P = .28 for noninferiority).
“What the trial’s really doing is seeing whether people who’ve been on long-term nonsteroidals, can they just stop them without getting any worse? The conclusion for that is actually they are more likely to get worse than not if you just stop the nonsteroidals,” Dr. Walsh said.
“The withdrawal trial protocol is an important one. You can’t run a prospective trial for years to see whether something works for years. It is just not feasible. So actually, the protocol they’ve got of switching to placebo, or continuing with a nonsteroidal, is probably the best way of working out if an anti-inflammatory still has a pharmacological effect after actually being on it for X years,” Dr. Walsh said.
Dr. Walsh, who was not involved in the trial, observed that while the difference in pain scores between the groups was small, the deterioration in scores might be important for individual patients. Some may do worse, although granted that there may be some that might do better, he said.
“It is suggesting to me that nonsteroidals are still working in people who are on long-term treatment. It is not a very big pharmacological effect, but we already know from the RCTs of anti-inflammatory tablets, that they can be beneficial,” Dr. Walsh noted.
He also pointed out that patients’ pain had been improved after being switched from their current NSAID to meloxicam – the overall WOMAC pain score at recruitment was 9.6 and was 5.6 after the 2-week meloxicam run-in phase.
“Now, whether that’s because they’ve been switched to meloxicam, or whether it’s because they’re in a trial,” is an important question, Dr. Walsh suggested, adding that “it looks as though it’s more likely to be because they’re in a trial, because improvement was maintained during the following 4 weeks on placebo.”
Another point he made was that there was a higher percentage of patients in the placebo group that started taking other types of painkillers, just under half (46%) used acetaminophen versus a quarter (26%) of those who continued using meloxicam.
It is an interesting trial, “trying to tackle some really difficult questions and I think that there are really important implications from it that we can build on, but is it actually going to change the lives of patients at the moment? Not massively,” Dr. Walsh said, ”but it’s another step in the right direction.”
Dr. Fraenkel disclosed receiving research funding from the VA Office of Research and Development, the sponsor of the trial.
SOURCE: Fraenkel L et al. JAMA Intern Med. 2020 Jul 20. doi:10.1001/jamainternmed.2020.2821.
in a randomized trial.
The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain score was 6.7 out of a possible total of 20 for patients who continued meloxicam for 4 weeks versus 7.8 in those who stopped and switched to a placebo. The estimated mean difference in pain score was 1.4 (P = .92 for noninferiority), which is below the threshold of 2.1 that is considered to be the minimum clinically important difference.
Furthermore, patients who had switched to placebo and then subsequently participated in a telephone-based cognitive behavior therapy (CBT) program for another 10 weeks had higher pain levels compared with those who continued meloxicam. WOMAC scores were 12.1 and 11.8, respectively with a mean difference of 0.8 (P = .28 for noninferiority).
“Among patients with knee osteoarthritis, placebo and CBT (after placebo) are inferior to meloxicam,” Liana Fraenkel, MD, MPH, of Yale University, New Haven, Conn., and coinvestigators concluded in their article, published in JAMA Internal Medicine.
They observed that the WOMAC pain score differences between the two groups were small, however, and that there were no statistically significant differences in participants’ global impression of change or function after 14 weeks.
“Although the overall results of the trial are negative, they provide clinicians with data to support shared decision-making and reassure patients willing to taper NSAIDs and consider self-management approaches such as CBT,” Dr. Fraenkel and coauthors suggested.
The Stopping NSAIDs for Arthritis Pain trial had ultimately included 364 participants, 86% of whom were men, recruited from four veterans affairs health care systems. All had been taking NSAIDs for knee OA pain for at least 3 months and had participated in a 2-week run-in period where the NSAID they had been taking was switched to meloxicam, 15 mg once daily.
The aim of the trial had been to see if discontinuing NSAIDs and starting a CBT program would be noninferior to continuing NSAIDs in patients with knee OA.
The trial does not provide robust information on the use of CBT, David Walsh, a rheumatologist and director of the Pain Centre Versus Arthritis at the University of Nottingham, England, said in an interview.
“It can’t tell you about efficacy of CBT,” Dr. Walsh said as the CBT part of the study was not randomized, was not controlled, and was unblinded. ”It would be a different task to design a CBT trial aiming to help people to stop taking tablets,” he added.
Dr. Fraenkel and coinvestigators had reported that, at week 14, the adjusted mean difference in WOMAC pain score between the placebo (followed by CBT) and meloxicam groups was 0.8 (P = .28 for noninferiority).
“What the trial’s really doing is seeing whether people who’ve been on long-term nonsteroidals, can they just stop them without getting any worse? The conclusion for that is actually they are more likely to get worse than not if you just stop the nonsteroidals,” Dr. Walsh said.
“The withdrawal trial protocol is an important one. You can’t run a prospective trial for years to see whether something works for years. It is just not feasible. So actually, the protocol they’ve got of switching to placebo, or continuing with a nonsteroidal, is probably the best way of working out if an anti-inflammatory still has a pharmacological effect after actually being on it for X years,” Dr. Walsh said.
Dr. Walsh, who was not involved in the trial, observed that while the difference in pain scores between the groups was small, the deterioration in scores might be important for individual patients. Some may do worse, although granted that there may be some that might do better, he said.
“It is suggesting to me that nonsteroidals are still working in people who are on long-term treatment. It is not a very big pharmacological effect, but we already know from the RCTs of anti-inflammatory tablets, that they can be beneficial,” Dr. Walsh noted.
He also pointed out that patients’ pain had been improved after being switched from their current NSAID to meloxicam – the overall WOMAC pain score at recruitment was 9.6 and was 5.6 after the 2-week meloxicam run-in phase.
“Now, whether that’s because they’ve been switched to meloxicam, or whether it’s because they’re in a trial,” is an important question, Dr. Walsh suggested, adding that “it looks as though it’s more likely to be because they’re in a trial, because improvement was maintained during the following 4 weeks on placebo.”
Another point he made was that there was a higher percentage of patients in the placebo group that started taking other types of painkillers, just under half (46%) used acetaminophen versus a quarter (26%) of those who continued using meloxicam.
It is an interesting trial, “trying to tackle some really difficult questions and I think that there are really important implications from it that we can build on, but is it actually going to change the lives of patients at the moment? Not massively,” Dr. Walsh said, ”but it’s another step in the right direction.”
Dr. Fraenkel disclosed receiving research funding from the VA Office of Research and Development, the sponsor of the trial.
SOURCE: Fraenkel L et al. JAMA Intern Med. 2020 Jul 20. doi:10.1001/jamainternmed.2020.2821.
FROM JAMA INTERNAL MEDICINE
Physician recruitment drops by 30% because of pandemic
the firm reported.
“Rather than having many practice opportunities to choose from, physicians now may have to compete to secure practice opportunities that meet their needs,” the authors wrote in Merritt Hawkins’ report on the impact of COVID-19.
Most of the report concerns physician recruitment from April 1, 2019, to March 31, 2020. The data were mostly derived from searches that Merritt Hawkins conducted before the effects of the pandemic was fully felt.
Family medicine was again the most sought-after specialty, as it has been for the past 14 years. But demand for primary care doctors – including family physicians, internists, and pediatricians – leveled off, and average starting salaries for primary care doctors dropped during 2019-2020. In contrast, the number of searches conducted for nurse practitioners (NPs) and physician assistants (PAs) increased by 54%, and their salaries increased slightly.
To explain the lackluster prospects for primary care before the pandemic, the authors cited research showing that patients were turning away from the traditional office visit model. At the same time, there was a rise in visits to NPs and PAs, including those in urgent care centers and retail clinics.
As a result of decreased demand for primary care physicians and the rising prevalence of telehealth, Merritt Hawkins expects primary care salaries to drop overall. With telehealth generating a larger portion of revenues, “it is uncertain whether primary care physicians will be able to sustain levels of reimbursement that were prevalent pre-COVID even at such time as the economy is improved and utilization increases,” the authors reported.
Demand for specialists was increasing prior to the COVID-19 crisis, partly as a result of the aging of the population. Seventy-eight percent of all searches were for medical specialists, compared with 67% 5 years ago. However, the pandemic has set back specialist searches. “Demand and compensation for specialists also will change as a result of COVID-19 in response to declines in the volume of medical procedures,” according to the authors.
In contrast, the recruitment of doctors who are on the front line of COVID-19 care is expected to increase. Among the fields anticipated to be in demand are emergency department specialists, infectious disease specialists, and pulmonology/critical care physicians. Travis Singleton, executive vice president of Merritt Hawkins, said in an interview that this trend is already happening and will accelerate as COVID-19 hot spots arise across the country.
Specialists in different fields received either higher or lower offers than during the previous year. Starting salaries for noninvasive cardiologists, for example, dropped 7.3%; gastroenterologists earned 7.7% less; and neurologists, 6.9% less. In contrast, orthopedic surgeons saw offers surge 16.7%; radiologists, 9.3%; and pulmonologists/critical care specialists, 7.7%.
Physicians were offered salaries plus bonuses in three-quarters of searches. Relative value unit–based production remained the most common basis for bonuses. Quality/value-based metrics were used in computing 64% of bonuses – up from 56% the previous year – but still determined only 11% of total physician compensation.
Pandemic outlook
Whereas health care helped drive the U.S. economy in 2018-2019, the pace of job growth in health care has decreased since March. As a result of the pandemic, health care spending in the United States declined by 18% in the first quarter of 2020. Physician practice revenue dropped by 55% during the first quarter, and many small and solo practices are still struggling.
In a 2018 Merritt Hawkins survey, 18% of physicians said they had used telehealth to treat patients. Because of the pandemic, that percentage jumped to 48% in April 2020. But telehealth hasn’t made up for the loss of patient revenue from in-office procedures, tests, and other services, and it still isn’t being reimbursed at the same level as in-office visits.
With practices under severe financial strain, the authors explained, “A majority of private practices have curtailed most physician recruiting activity since the virus emerged.”
In some states, many specialty practices have been adversely affected by the suspension of elective procedures, and specialty practices that rely on nonessential procedures are unlikely to recruit additional physicians.
One-third of practices could close
The survival of many private practices is now in question. “Based on the losses physician practices have sustained as a result of COVID-19, some markets could lose up to 35% or more of their most vulnerable group practices while a large percent of others will be acquired,” the authors wrote.
Hospitals and health systems will acquire the bulk of these practices, in many cases at fire-sale prices, Mr. Singleton predicted. This enormous shift from private practice to employment, he added, “will have as much to do with the [physician] income levels we’re going to see as the demand for the specialties themselves.”
Right now, he said, Merritt Hawkins is fielding a huge number of requests from doctors seeking employment, but there aren’t many jobs out there. “We haven’t seen an employer-friendly market like this since the 1970s,” he noted. “Before the pandemic, a physician might have had five to 10 jobs to choose from. Now it’s the opposite: We have one job, and 5 to 10 physicians are applying for it.”
Singleton believes the market will adjust by the second quarter of next year. Even if the pandemic worsens, he said, the system will have made the necessary corrections and adjustments “because we have to start seeing patients again, both in terms of demand and economics. So these doctors will be in demand again and will have work.”
Contingent employment
Although the COVID-related falloff in revenue has hit private practices the hardest, some employed physicians have also found themselves in a bind. According to a Merritt Hawkins/Physicians Foundation survey conducted in April, 21% of physicians said they had been furloughed or had taken a pay cut.
Mr. Singleton views this trend as part of hospitals’ reassessment of how they’re going to deal with labor going forward. To cope with utilization ebbs and flows in response to the virus, hospitals are now considering what the report calls a “contingent labor/flex staffing model.”
Under this type of arrangement, which some hospitals have already adopted, physicians may no longer work full time in a single setting, Mr. Singleton said. They may be asked to conduct telehealth visits on nights and weekends and work 20 hours a week in the clinic, or they may have shifts in multiple hospitals or clinics.
“You can make as much or more on a temporary basis as on a permanent basis,” he said. “But you have to be more flexible. You may have to travel or do a different scope of work, or work in different settings.”
A version of this article originally appeared on Medscape.com.
the firm reported.
“Rather than having many practice opportunities to choose from, physicians now may have to compete to secure practice opportunities that meet their needs,” the authors wrote in Merritt Hawkins’ report on the impact of COVID-19.
Most of the report concerns physician recruitment from April 1, 2019, to March 31, 2020. The data were mostly derived from searches that Merritt Hawkins conducted before the effects of the pandemic was fully felt.
Family medicine was again the most sought-after specialty, as it has been for the past 14 years. But demand for primary care doctors – including family physicians, internists, and pediatricians – leveled off, and average starting salaries for primary care doctors dropped during 2019-2020. In contrast, the number of searches conducted for nurse practitioners (NPs) and physician assistants (PAs) increased by 54%, and their salaries increased slightly.
To explain the lackluster prospects for primary care before the pandemic, the authors cited research showing that patients were turning away from the traditional office visit model. At the same time, there was a rise in visits to NPs and PAs, including those in urgent care centers and retail clinics.
As a result of decreased demand for primary care physicians and the rising prevalence of telehealth, Merritt Hawkins expects primary care salaries to drop overall. With telehealth generating a larger portion of revenues, “it is uncertain whether primary care physicians will be able to sustain levels of reimbursement that were prevalent pre-COVID even at such time as the economy is improved and utilization increases,” the authors reported.
Demand for specialists was increasing prior to the COVID-19 crisis, partly as a result of the aging of the population. Seventy-eight percent of all searches were for medical specialists, compared with 67% 5 years ago. However, the pandemic has set back specialist searches. “Demand and compensation for specialists also will change as a result of COVID-19 in response to declines in the volume of medical procedures,” according to the authors.
In contrast, the recruitment of doctors who are on the front line of COVID-19 care is expected to increase. Among the fields anticipated to be in demand are emergency department specialists, infectious disease specialists, and pulmonology/critical care physicians. Travis Singleton, executive vice president of Merritt Hawkins, said in an interview that this trend is already happening and will accelerate as COVID-19 hot spots arise across the country.
Specialists in different fields received either higher or lower offers than during the previous year. Starting salaries for noninvasive cardiologists, for example, dropped 7.3%; gastroenterologists earned 7.7% less; and neurologists, 6.9% less. In contrast, orthopedic surgeons saw offers surge 16.7%; radiologists, 9.3%; and pulmonologists/critical care specialists, 7.7%.
Physicians were offered salaries plus bonuses in three-quarters of searches. Relative value unit–based production remained the most common basis for bonuses. Quality/value-based metrics were used in computing 64% of bonuses – up from 56% the previous year – but still determined only 11% of total physician compensation.
Pandemic outlook
Whereas health care helped drive the U.S. economy in 2018-2019, the pace of job growth in health care has decreased since March. As a result of the pandemic, health care spending in the United States declined by 18% in the first quarter of 2020. Physician practice revenue dropped by 55% during the first quarter, and many small and solo practices are still struggling.
In a 2018 Merritt Hawkins survey, 18% of physicians said they had used telehealth to treat patients. Because of the pandemic, that percentage jumped to 48% in April 2020. But telehealth hasn’t made up for the loss of patient revenue from in-office procedures, tests, and other services, and it still isn’t being reimbursed at the same level as in-office visits.
With practices under severe financial strain, the authors explained, “A majority of private practices have curtailed most physician recruiting activity since the virus emerged.”
In some states, many specialty practices have been adversely affected by the suspension of elective procedures, and specialty practices that rely on nonessential procedures are unlikely to recruit additional physicians.
One-third of practices could close
The survival of many private practices is now in question. “Based on the losses physician practices have sustained as a result of COVID-19, some markets could lose up to 35% or more of their most vulnerable group practices while a large percent of others will be acquired,” the authors wrote.
Hospitals and health systems will acquire the bulk of these practices, in many cases at fire-sale prices, Mr. Singleton predicted. This enormous shift from private practice to employment, he added, “will have as much to do with the [physician] income levels we’re going to see as the demand for the specialties themselves.”
Right now, he said, Merritt Hawkins is fielding a huge number of requests from doctors seeking employment, but there aren’t many jobs out there. “We haven’t seen an employer-friendly market like this since the 1970s,” he noted. “Before the pandemic, a physician might have had five to 10 jobs to choose from. Now it’s the opposite: We have one job, and 5 to 10 physicians are applying for it.”
Singleton believes the market will adjust by the second quarter of next year. Even if the pandemic worsens, he said, the system will have made the necessary corrections and adjustments “because we have to start seeing patients again, both in terms of demand and economics. So these doctors will be in demand again and will have work.”
Contingent employment
Although the COVID-related falloff in revenue has hit private practices the hardest, some employed physicians have also found themselves in a bind. According to a Merritt Hawkins/Physicians Foundation survey conducted in April, 21% of physicians said they had been furloughed or had taken a pay cut.
Mr. Singleton views this trend as part of hospitals’ reassessment of how they’re going to deal with labor going forward. To cope with utilization ebbs and flows in response to the virus, hospitals are now considering what the report calls a “contingent labor/flex staffing model.”
Under this type of arrangement, which some hospitals have already adopted, physicians may no longer work full time in a single setting, Mr. Singleton said. They may be asked to conduct telehealth visits on nights and weekends and work 20 hours a week in the clinic, or they may have shifts in multiple hospitals or clinics.
“You can make as much or more on a temporary basis as on a permanent basis,” he said. “But you have to be more flexible. You may have to travel or do a different scope of work, or work in different settings.”
A version of this article originally appeared on Medscape.com.
the firm reported.
“Rather than having many practice opportunities to choose from, physicians now may have to compete to secure practice opportunities that meet their needs,” the authors wrote in Merritt Hawkins’ report on the impact of COVID-19.
Most of the report concerns physician recruitment from April 1, 2019, to March 31, 2020. The data were mostly derived from searches that Merritt Hawkins conducted before the effects of the pandemic was fully felt.
Family medicine was again the most sought-after specialty, as it has been for the past 14 years. But demand for primary care doctors – including family physicians, internists, and pediatricians – leveled off, and average starting salaries for primary care doctors dropped during 2019-2020. In contrast, the number of searches conducted for nurse practitioners (NPs) and physician assistants (PAs) increased by 54%, and their salaries increased slightly.
To explain the lackluster prospects for primary care before the pandemic, the authors cited research showing that patients were turning away from the traditional office visit model. At the same time, there was a rise in visits to NPs and PAs, including those in urgent care centers and retail clinics.
As a result of decreased demand for primary care physicians and the rising prevalence of telehealth, Merritt Hawkins expects primary care salaries to drop overall. With telehealth generating a larger portion of revenues, “it is uncertain whether primary care physicians will be able to sustain levels of reimbursement that were prevalent pre-COVID even at such time as the economy is improved and utilization increases,” the authors reported.
Demand for specialists was increasing prior to the COVID-19 crisis, partly as a result of the aging of the population. Seventy-eight percent of all searches were for medical specialists, compared with 67% 5 years ago. However, the pandemic has set back specialist searches. “Demand and compensation for specialists also will change as a result of COVID-19 in response to declines in the volume of medical procedures,” according to the authors.
In contrast, the recruitment of doctors who are on the front line of COVID-19 care is expected to increase. Among the fields anticipated to be in demand are emergency department specialists, infectious disease specialists, and pulmonology/critical care physicians. Travis Singleton, executive vice president of Merritt Hawkins, said in an interview that this trend is already happening and will accelerate as COVID-19 hot spots arise across the country.
Specialists in different fields received either higher or lower offers than during the previous year. Starting salaries for noninvasive cardiologists, for example, dropped 7.3%; gastroenterologists earned 7.7% less; and neurologists, 6.9% less. In contrast, orthopedic surgeons saw offers surge 16.7%; radiologists, 9.3%; and pulmonologists/critical care specialists, 7.7%.
Physicians were offered salaries plus bonuses in three-quarters of searches. Relative value unit–based production remained the most common basis for bonuses. Quality/value-based metrics were used in computing 64% of bonuses – up from 56% the previous year – but still determined only 11% of total physician compensation.
Pandemic outlook
Whereas health care helped drive the U.S. economy in 2018-2019, the pace of job growth in health care has decreased since March. As a result of the pandemic, health care spending in the United States declined by 18% in the first quarter of 2020. Physician practice revenue dropped by 55% during the first quarter, and many small and solo practices are still struggling.
In a 2018 Merritt Hawkins survey, 18% of physicians said they had used telehealth to treat patients. Because of the pandemic, that percentage jumped to 48% in April 2020. But telehealth hasn’t made up for the loss of patient revenue from in-office procedures, tests, and other services, and it still isn’t being reimbursed at the same level as in-office visits.
With practices under severe financial strain, the authors explained, “A majority of private practices have curtailed most physician recruiting activity since the virus emerged.”
In some states, many specialty practices have been adversely affected by the suspension of elective procedures, and specialty practices that rely on nonessential procedures are unlikely to recruit additional physicians.
One-third of practices could close
The survival of many private practices is now in question. “Based on the losses physician practices have sustained as a result of COVID-19, some markets could lose up to 35% or more of their most vulnerable group practices while a large percent of others will be acquired,” the authors wrote.
Hospitals and health systems will acquire the bulk of these practices, in many cases at fire-sale prices, Mr. Singleton predicted. This enormous shift from private practice to employment, he added, “will have as much to do with the [physician] income levels we’re going to see as the demand for the specialties themselves.”
Right now, he said, Merritt Hawkins is fielding a huge number of requests from doctors seeking employment, but there aren’t many jobs out there. “We haven’t seen an employer-friendly market like this since the 1970s,” he noted. “Before the pandemic, a physician might have had five to 10 jobs to choose from. Now it’s the opposite: We have one job, and 5 to 10 physicians are applying for it.”
Singleton believes the market will adjust by the second quarter of next year. Even if the pandemic worsens, he said, the system will have made the necessary corrections and adjustments “because we have to start seeing patients again, both in terms of demand and economics. So these doctors will be in demand again and will have work.”
Contingent employment
Although the COVID-related falloff in revenue has hit private practices the hardest, some employed physicians have also found themselves in a bind. According to a Merritt Hawkins/Physicians Foundation survey conducted in April, 21% of physicians said they had been furloughed or had taken a pay cut.
Mr. Singleton views this trend as part of hospitals’ reassessment of how they’re going to deal with labor going forward. To cope with utilization ebbs and flows in response to the virus, hospitals are now considering what the report calls a “contingent labor/flex staffing model.”
Under this type of arrangement, which some hospitals have already adopted, physicians may no longer work full time in a single setting, Mr. Singleton said. They may be asked to conduct telehealth visits on nights and weekends and work 20 hours a week in the clinic, or they may have shifts in multiple hospitals or clinics.
“You can make as much or more on a temporary basis as on a permanent basis,” he said. “But you have to be more flexible. You may have to travel or do a different scope of work, or work in different settings.”
A version of this article originally appeared on Medscape.com.
Diary of a rheumatologist who briefly became a COVID hospitalist
When the coronavirus pandemic hit New York City in early March, the Hospital for Special Surgery leadership decided that the best way to serve the city was to stop elective orthopedic procedures temporarily and use the facility to take on patients from its sister institution, NewYork–Presbyterian Hospital.
As in other institutions, it was all hands on deck. , other internal medicine subspecialists were asked to volunteer, including rheumatologists and primary care sports medicine doctors.
As a rheumatologist, it had been well over 10 years since I had last done any inpatient work. I was filled with trepidation, but I was also excited to dive in.
April 4:
Feeling very unmoored. I am in unfamiliar territory, and it’s terrifying. There are so many things that I no longer know how to do. Thankfully, the hospitalists are gracious, extremely supportive, and helpful.
My N95 doesn’t fit well. It’s never fit — not during residency or fellowship, not in any job I’ve had, and not today. The lady fit-testing me said she was sorry, but the look on her face said, “I’m sorry, but you’re going to die.”
April 7:
We don’t know how to treat coronavirus. I’ve sent some patients home, others I’ve sent to the ICU. Thank goodness for treatment algorithms from leadership, but we are sorely lacking good-quality data.
Our infectious disease doctor doesn’t think hydroxychloroquine works at all; I suspect he is right. The guidance right now is to give hydroxychloroquine and azithromycin to everyone who is sick enough to be admitted, but there are methodologic flaws in the early enthusiastic preprints, and so far, I’ve not noticed any demonstrable benefit.
The only thing that seems to be happening is that I am seeing more QT prolongation — not something I previously counseled my rheumatology patients on.
April 9:
The patients have been, with a few exceptions, alone in the room. They’re not allowed to have visitors and are required to wear masks all the time. Anyone who enters their rooms is fully covered up so you can barely see them. It’s anonymous and dehumanizing.
We’re instructed to take histories by phone in order to limit the time spent in each room. I buck this instruction; I still take histories in person because human contact seems more important now than ever.
Except maybe I should be smarter about this. One of my patients refuses any treatment, including oxygen support. She firmly believes this is a result of 5G networks — something I later discovered was a common conspiracy theory. She refused to wear a mask despite having a very bad cough. She coughed in my face a lot when we were chatting. My face with my ill-fitting N95 mask. Maybe the fit-testing lady’s eyes weren’t lying and I will die after all.
April 15:
On the days when I’m not working as a hospitalist, I am still doing remote visits with my rheumatology patients. It feels good to be doing something familiar and something I’m actually good at. But it is surreal to be faced with the quotidian on one hand and life and death on the other.
I recently saw a fairly new patient, and I still haven’t figured out if she has a rheumatic condition or if her symptoms all stem from an alcohol use disorder. In our previous visits, she could barely acknowledge that her drinking was an issue. On today’s visit, she told me she was 1½ months sober.
I don’t know her very well, but it was the happiest news I’d heard in a long time. I was so beside myself with joy that I cried, which says more about my current emotional state than anything else, really.
April 21:
On my panel of patients, I have three women with COVID-19 — all of whom lost their husbands to COVID-19, and none of whom were able to say their goodbyes. I cannot even begin to imagine what it must be like to survive this period of illness, isolation, and fear, only to be met on the other side by grief.
Rheumatology doesn’t lend itself too well to such existential concerns; I am not equipped for this. Perhaps my only advantage as a rheumatologist is that I know how to use IVIG, anakinra, and tocilizumab.
Someone on my panel was started on anakinra, and it turned his case around. Would he have gotten better without it anyway? We’ll never know for sure.
April 28:
Patients seem to be requiring prolonged intubation. We have now reached the stage where patients are alive but trached and PEGed. One of my patients had been intubated for close to 3 weeks. She was one of four people in her family who contracted the illness (they had had a dinner party before New York’s state of emergency was declared). We thought she might die once she was extubated, but she is still fighting. Unconscious, unarousable, but breathing on her own.
Will she ever wake up? We don’t know. We put the onus on her family to make decisions about placing a PEG tube in. They can only do so from a distance with imperfect information gleaned from periodic, brief FaceTime interactions — where no interaction happens at all.
May 4:
It’s my last day as a “COVID hospitalist.” When I first started, I felt like I was being helpful. Walking home in the middle of the 7 PM cheers for healthcare workers frequently left me teary eyed. As horrible as the situation was, I was proud of myself for volunteering to help and appreciative of a broken city’s gratitude toward all healthcare workers in general. Maybe I bought into the idea that, like many others around me, I am a hero.
I don’t feel like a hero, though. The stuff I saw was easy compared with the stuff that my colleagues in critical care saw. Our hospital accepted the more stable patient transfers from our sister hospitals. Patients who remained in the NewYork–Presbyterian system were sicker, with encephalitis, thrombotic complications, multiorgan failure, and cytokine release syndrome. It’s the doctors who took care of those patients who deserve to be called heroes.
No, I am no hero. But did my volunteering make a difference? It made a difference to me. The overwhelming feeling I am left with isn’t pride; it’s humility. I feel humbled that I could feel so unexpectedly touched by the lives of people that I had no idea I could feel touched by.
Postscript:
My patient Esther [name changed to hide her identity] died from COVID-19. She was MY patient — not a patient I met as a COVID hospitalist, but a patient with rheumatoid arthritis whom I cared for for years.
She had scleromalacia and multiple failed scleral grafts, which made her profoundly sad. She fought her anxiety fiercely and always with poise and panache. One way she dealt with her anxiety was that she constantly messaged me via our EHR portal. She ran everything by me and trusted me to be her rock.
The past month has been so busy that I just now noticed it had been a month since I last heard from her. I tried to call her but got her voicemail. It wasn’t until I exchanged messages with her ophthalmologist that I found out she had passed away from complications of COVID-19.
She was taking rituximab and mycophenolate. I wonder if these drugs made her sicker than she would have been otherwise; it fills me with sadness. I wonder if she was alone like my other COVID-19 patients. I wonder if she was afraid. I am sorry that I wasn’t able to say goodbye.
Karmela Kim Chan, MD, is an assistant professor at Weill Cornell Medical College and an attending physician at Hospital for Special Surgery and Memorial Sloan Kettering Cancer Center in New York City. Before moving to New York City, she spent 7 years in private practice in Rhode Island and was a columnist for this rheumatology publication, writing about the challenges of starting life as a full-fledged rheumatologist in a private practice.
A version of this article originally appeared on Medscape.com. This article is part of a partnership between Medscape and Hospital for Special Surgery.
When the coronavirus pandemic hit New York City in early March, the Hospital for Special Surgery leadership decided that the best way to serve the city was to stop elective orthopedic procedures temporarily and use the facility to take on patients from its sister institution, NewYork–Presbyterian Hospital.
As in other institutions, it was all hands on deck. , other internal medicine subspecialists were asked to volunteer, including rheumatologists and primary care sports medicine doctors.
As a rheumatologist, it had been well over 10 years since I had last done any inpatient work. I was filled with trepidation, but I was also excited to dive in.
April 4:
Feeling very unmoored. I am in unfamiliar territory, and it’s terrifying. There are so many things that I no longer know how to do. Thankfully, the hospitalists are gracious, extremely supportive, and helpful.
My N95 doesn’t fit well. It’s never fit — not during residency or fellowship, not in any job I’ve had, and not today. The lady fit-testing me said she was sorry, but the look on her face said, “I’m sorry, but you’re going to die.”
April 7:
We don’t know how to treat coronavirus. I’ve sent some patients home, others I’ve sent to the ICU. Thank goodness for treatment algorithms from leadership, but we are sorely lacking good-quality data.
Our infectious disease doctor doesn’t think hydroxychloroquine works at all; I suspect he is right. The guidance right now is to give hydroxychloroquine and azithromycin to everyone who is sick enough to be admitted, but there are methodologic flaws in the early enthusiastic preprints, and so far, I’ve not noticed any demonstrable benefit.
The only thing that seems to be happening is that I am seeing more QT prolongation — not something I previously counseled my rheumatology patients on.
April 9:
The patients have been, with a few exceptions, alone in the room. They’re not allowed to have visitors and are required to wear masks all the time. Anyone who enters their rooms is fully covered up so you can barely see them. It’s anonymous and dehumanizing.
We’re instructed to take histories by phone in order to limit the time spent in each room. I buck this instruction; I still take histories in person because human contact seems more important now than ever.
Except maybe I should be smarter about this. One of my patients refuses any treatment, including oxygen support. She firmly believes this is a result of 5G networks — something I later discovered was a common conspiracy theory. She refused to wear a mask despite having a very bad cough. She coughed in my face a lot when we were chatting. My face with my ill-fitting N95 mask. Maybe the fit-testing lady’s eyes weren’t lying and I will die after all.
April 15:
On the days when I’m not working as a hospitalist, I am still doing remote visits with my rheumatology patients. It feels good to be doing something familiar and something I’m actually good at. But it is surreal to be faced with the quotidian on one hand and life and death on the other.
I recently saw a fairly new patient, and I still haven’t figured out if she has a rheumatic condition or if her symptoms all stem from an alcohol use disorder. In our previous visits, she could barely acknowledge that her drinking was an issue. On today’s visit, she told me she was 1½ months sober.
I don’t know her very well, but it was the happiest news I’d heard in a long time. I was so beside myself with joy that I cried, which says more about my current emotional state than anything else, really.
April 21:
On my panel of patients, I have three women with COVID-19 — all of whom lost their husbands to COVID-19, and none of whom were able to say their goodbyes. I cannot even begin to imagine what it must be like to survive this period of illness, isolation, and fear, only to be met on the other side by grief.
Rheumatology doesn’t lend itself too well to such existential concerns; I am not equipped for this. Perhaps my only advantage as a rheumatologist is that I know how to use IVIG, anakinra, and tocilizumab.
Someone on my panel was started on anakinra, and it turned his case around. Would he have gotten better without it anyway? We’ll never know for sure.
April 28:
Patients seem to be requiring prolonged intubation. We have now reached the stage where patients are alive but trached and PEGed. One of my patients had been intubated for close to 3 weeks. She was one of four people in her family who contracted the illness (they had had a dinner party before New York’s state of emergency was declared). We thought she might die once she was extubated, but she is still fighting. Unconscious, unarousable, but breathing on her own.
Will she ever wake up? We don’t know. We put the onus on her family to make decisions about placing a PEG tube in. They can only do so from a distance with imperfect information gleaned from periodic, brief FaceTime interactions — where no interaction happens at all.
May 4:
It’s my last day as a “COVID hospitalist.” When I first started, I felt like I was being helpful. Walking home in the middle of the 7 PM cheers for healthcare workers frequently left me teary eyed. As horrible as the situation was, I was proud of myself for volunteering to help and appreciative of a broken city’s gratitude toward all healthcare workers in general. Maybe I bought into the idea that, like many others around me, I am a hero.
I don’t feel like a hero, though. The stuff I saw was easy compared with the stuff that my colleagues in critical care saw. Our hospital accepted the more stable patient transfers from our sister hospitals. Patients who remained in the NewYork–Presbyterian system were sicker, with encephalitis, thrombotic complications, multiorgan failure, and cytokine release syndrome. It’s the doctors who took care of those patients who deserve to be called heroes.
No, I am no hero. But did my volunteering make a difference? It made a difference to me. The overwhelming feeling I am left with isn’t pride; it’s humility. I feel humbled that I could feel so unexpectedly touched by the lives of people that I had no idea I could feel touched by.
Postscript:
My patient Esther [name changed to hide her identity] died from COVID-19. She was MY patient — not a patient I met as a COVID hospitalist, but a patient with rheumatoid arthritis whom I cared for for years.
She had scleromalacia and multiple failed scleral grafts, which made her profoundly sad. She fought her anxiety fiercely and always with poise and panache. One way she dealt with her anxiety was that she constantly messaged me via our EHR portal. She ran everything by me and trusted me to be her rock.
The past month has been so busy that I just now noticed it had been a month since I last heard from her. I tried to call her but got her voicemail. It wasn’t until I exchanged messages with her ophthalmologist that I found out she had passed away from complications of COVID-19.
She was taking rituximab and mycophenolate. I wonder if these drugs made her sicker than she would have been otherwise; it fills me with sadness. I wonder if she was alone like my other COVID-19 patients. I wonder if she was afraid. I am sorry that I wasn’t able to say goodbye.
Karmela Kim Chan, MD, is an assistant professor at Weill Cornell Medical College and an attending physician at Hospital for Special Surgery and Memorial Sloan Kettering Cancer Center in New York City. Before moving to New York City, she spent 7 years in private practice in Rhode Island and was a columnist for this rheumatology publication, writing about the challenges of starting life as a full-fledged rheumatologist in a private practice.
A version of this article originally appeared on Medscape.com. This article is part of a partnership between Medscape and Hospital for Special Surgery.
When the coronavirus pandemic hit New York City in early March, the Hospital for Special Surgery leadership decided that the best way to serve the city was to stop elective orthopedic procedures temporarily and use the facility to take on patients from its sister institution, NewYork–Presbyterian Hospital.
As in other institutions, it was all hands on deck. , other internal medicine subspecialists were asked to volunteer, including rheumatologists and primary care sports medicine doctors.
As a rheumatologist, it had been well over 10 years since I had last done any inpatient work. I was filled with trepidation, but I was also excited to dive in.
April 4:
Feeling very unmoored. I am in unfamiliar territory, and it’s terrifying. There are so many things that I no longer know how to do. Thankfully, the hospitalists are gracious, extremely supportive, and helpful.
My N95 doesn’t fit well. It’s never fit — not during residency or fellowship, not in any job I’ve had, and not today. The lady fit-testing me said she was sorry, but the look on her face said, “I’m sorry, but you’re going to die.”
April 7:
We don’t know how to treat coronavirus. I’ve sent some patients home, others I’ve sent to the ICU. Thank goodness for treatment algorithms from leadership, but we are sorely lacking good-quality data.
Our infectious disease doctor doesn’t think hydroxychloroquine works at all; I suspect he is right. The guidance right now is to give hydroxychloroquine and azithromycin to everyone who is sick enough to be admitted, but there are methodologic flaws in the early enthusiastic preprints, and so far, I’ve not noticed any demonstrable benefit.
The only thing that seems to be happening is that I am seeing more QT prolongation — not something I previously counseled my rheumatology patients on.
April 9:
The patients have been, with a few exceptions, alone in the room. They’re not allowed to have visitors and are required to wear masks all the time. Anyone who enters their rooms is fully covered up so you can barely see them. It’s anonymous and dehumanizing.
We’re instructed to take histories by phone in order to limit the time spent in each room. I buck this instruction; I still take histories in person because human contact seems more important now than ever.
Except maybe I should be smarter about this. One of my patients refuses any treatment, including oxygen support. She firmly believes this is a result of 5G networks — something I later discovered was a common conspiracy theory. She refused to wear a mask despite having a very bad cough. She coughed in my face a lot when we were chatting. My face with my ill-fitting N95 mask. Maybe the fit-testing lady’s eyes weren’t lying and I will die after all.
April 15:
On the days when I’m not working as a hospitalist, I am still doing remote visits with my rheumatology patients. It feels good to be doing something familiar and something I’m actually good at. But it is surreal to be faced with the quotidian on one hand and life and death on the other.
I recently saw a fairly new patient, and I still haven’t figured out if she has a rheumatic condition or if her symptoms all stem from an alcohol use disorder. In our previous visits, she could barely acknowledge that her drinking was an issue. On today’s visit, she told me she was 1½ months sober.
I don’t know her very well, but it was the happiest news I’d heard in a long time. I was so beside myself with joy that I cried, which says more about my current emotional state than anything else, really.
April 21:
On my panel of patients, I have three women with COVID-19 — all of whom lost their husbands to COVID-19, and none of whom were able to say their goodbyes. I cannot even begin to imagine what it must be like to survive this period of illness, isolation, and fear, only to be met on the other side by grief.
Rheumatology doesn’t lend itself too well to such existential concerns; I am not equipped for this. Perhaps my only advantage as a rheumatologist is that I know how to use IVIG, anakinra, and tocilizumab.
Someone on my panel was started on anakinra, and it turned his case around. Would he have gotten better without it anyway? We’ll never know for sure.
April 28:
Patients seem to be requiring prolonged intubation. We have now reached the stage where patients are alive but trached and PEGed. One of my patients had been intubated for close to 3 weeks. She was one of four people in her family who contracted the illness (they had had a dinner party before New York’s state of emergency was declared). We thought she might die once she was extubated, but she is still fighting. Unconscious, unarousable, but breathing on her own.
Will she ever wake up? We don’t know. We put the onus on her family to make decisions about placing a PEG tube in. They can only do so from a distance with imperfect information gleaned from periodic, brief FaceTime interactions — where no interaction happens at all.
May 4:
It’s my last day as a “COVID hospitalist.” When I first started, I felt like I was being helpful. Walking home in the middle of the 7 PM cheers for healthcare workers frequently left me teary eyed. As horrible as the situation was, I was proud of myself for volunteering to help and appreciative of a broken city’s gratitude toward all healthcare workers in general. Maybe I bought into the idea that, like many others around me, I am a hero.
I don’t feel like a hero, though. The stuff I saw was easy compared with the stuff that my colleagues in critical care saw. Our hospital accepted the more stable patient transfers from our sister hospitals. Patients who remained in the NewYork–Presbyterian system were sicker, with encephalitis, thrombotic complications, multiorgan failure, and cytokine release syndrome. It’s the doctors who took care of those patients who deserve to be called heroes.
No, I am no hero. But did my volunteering make a difference? It made a difference to me. The overwhelming feeling I am left with isn’t pride; it’s humility. I feel humbled that I could feel so unexpectedly touched by the lives of people that I had no idea I could feel touched by.
Postscript:
My patient Esther [name changed to hide her identity] died from COVID-19. She was MY patient — not a patient I met as a COVID hospitalist, but a patient with rheumatoid arthritis whom I cared for for years.
She had scleromalacia and multiple failed scleral grafts, which made her profoundly sad. She fought her anxiety fiercely and always with poise and panache. One way she dealt with her anxiety was that she constantly messaged me via our EHR portal. She ran everything by me and trusted me to be her rock.
The past month has been so busy that I just now noticed it had been a month since I last heard from her. I tried to call her but got her voicemail. It wasn’t until I exchanged messages with her ophthalmologist that I found out she had passed away from complications of COVID-19.
She was taking rituximab and mycophenolate. I wonder if these drugs made her sicker than she would have been otherwise; it fills me with sadness. I wonder if she was alone like my other COVID-19 patients. I wonder if she was afraid. I am sorry that I wasn’t able to say goodbye.
Karmela Kim Chan, MD, is an assistant professor at Weill Cornell Medical College and an attending physician at Hospital for Special Surgery and Memorial Sloan Kettering Cancer Center in New York City. Before moving to New York City, she spent 7 years in private practice in Rhode Island and was a columnist for this rheumatology publication, writing about the challenges of starting life as a full-fledged rheumatologist in a private practice.
A version of this article originally appeared on Medscape.com. This article is part of a partnership between Medscape and Hospital for Special Surgery.
Delaying denosumab dose boosts risk for vertebral fractures
a new study confirms. Physicians say they are especially concerned about the risk facing patients who are delaying the treatment during the coronavirus pandemic.

The recommended doses of denosumab are at 6-month intervals. Patients who delayed a dose by more than 16 weeks were nearly four times more likely to suffer vertebral fractures, compared with those who received on-time injections, according to the study, which was published in Annals of Internal Medicine.
“Because patients who used denosumab were at high risk for vertebral fracture, strategies to improve timely administration of denosumab in routine clinical settings are needed,” wrote the study authors, led by Houchen Lyu, MD, PhD, of National Clinical Research Center for Orthopedics, Sports Medicine & Rehabilitation at General Hospital of Chinese PLA in Beijing.
Denosumab, a human monoclonal antibody, is used to reduce bone loss in osteoporosis. The manufacturer of Prolia, a brand of the drug, recommends it be given every 6 months, but the study reports that it’s common for injections to be delayed.
Researchers have linked cessation of denosumab to higher risk of fractures, and Dr. Lyu led a study published earlier this year that linked less-frequent doses to less bone mineral density improvement. “However,” the authors of the new study wrote, “whether delaying subsequent injections beyond the recommended 6-month interval is associated with fractures is unknown.”
For their new study, researchers retrospectively analyzed data from 2,594 patients in the U.K. 45 years or older (mean age, 76; 94% female; 53% with a history of major osteoporotic fracture) who began taking denosumab between 2010 and 2019. They used a design that aimed to emulate a clinical trial, comparing three dosing intervals: “on time” (within 4 weeks of the recommended 6-month interval), “short delay” (within 4-16 weeks) and “long delay” (16 weeks to 6 months).
The study found that the risk of composite fracture over 6 months out of 1,000 was 27.3 for on-time dosing, 32.2 for short-delay dosing, and 42.4 for long-delay dosing. The hazard ratio for long-delay versus on-time was 1.44 (95% confidence interval, 0.96-2.17; P = .093).
Vertebral fractures were less likely, but delays boosted the risk significantly: Over 6 months, it grew from 2.2 in 1,000 (on time) to 3.6 in 1,000 (short delay) and 10.1 in 1,000 (long delay). The HR for long delay versus on time was 3.91 (95% CI, 1.62-9.45; P = .005).
“This study had limited statistical power for composite fracture and several secondary end points ... except for vertebral fracture. Thus, evidence was insufficient to conclude that fracture risk was increased at other anatomical sites.”
In an accompanying editorial, two physicians from the University of Minnesota, Minneapolis, noted that the study is “timely and relevant” since the coronavirus pandemic may disrupt dosage schedules more than usual. While the study has limitations, the “findings are consistent with known denosumab pharmacokinetics and prior studies of fracture incidence after denosumab treatment discontinuation, wrote Kristine E. Ensrud, MD, MPH, who is also of Minneapolis VA Health Care System, and John T. Schousboe, MD, PhD, who is also of HealthPartners Institute.
The editorial authors noted that, in light of the pandemic, “some organizations recommend temporary transition to an oral bisphosphonate in patients receiving denosumab treatment for whom continued treatment is not feasible within 7 to 8 months of their most recent injection.”
In an interview, endocrinologist and osteoporosis specialist Ethel Siris, MD, of Columbia University, New York, said many of her patients aren’t coming in for denosumab injections during the pandemic. “It’s hard enough to get people to show up every 6 months to get their shot when things are going nicely,” she said. “We’re talking older women who may be on a lot of other medications. People forget, and it’s difficult for the office to constantly remind some of them to get their shots at an infusion center.”
The lack of symptoms is another challenge to getting patients to return for doses, she said. “In osteoporosis, the only time something hurts is if you break it.”
Since the pandemic began, many patients have been avoiding medical offices because of fear of getting the coronavirus.
The new research is helpful because it shows that patients are “more likely to fracture if they delay,” Dr. Siris noted. The endocrinologist added that she has successfully convinced some patients to give themselves subcutaneous injections in the abdomen at home.
Dr. Siris said she has been able to watch patients do these injections on video to check their technique. Her patients have been impressed by “how easy it is and delighted to have accomplished it,” she said.
The study was funded by the National Institutes of Health China’s National Clinical Research Center for Orthopedics, Sports Medicine & Rehabilitation. The study authors, commentary authors, and Dr. Siris report no relevant disclosures.
SOURCE: Lyu H et al. Ann Intern Med. 2020 Jul 28. doi: 10.7326/M20-0882.
a new study confirms. Physicians say they are especially concerned about the risk facing patients who are delaying the treatment during the coronavirus pandemic.
The recommended doses of denosumab are at 6-month intervals. Patients who delayed a dose by more than 16 weeks were nearly four times more likely to suffer vertebral fractures, compared with those who received on-time injections, according to the study, which was published in Annals of Internal Medicine.
“Because patients who used denosumab were at high risk for vertebral fracture, strategies to improve timely administration of denosumab in routine clinical settings are needed,” wrote the study authors, led by Houchen Lyu, MD, PhD, of National Clinical Research Center for Orthopedics, Sports Medicine & Rehabilitation at General Hospital of Chinese PLA in Beijing.
Denosumab, a human monoclonal antibody, is used to reduce bone loss in osteoporosis. The manufacturer of Prolia, a brand of the drug, recommends it be given every 6 months, but the study reports that it’s common for injections to be delayed.
Researchers have linked cessation of denosumab to higher risk of fractures, and Dr. Lyu led a study published earlier this year that linked less-frequent doses to less bone mineral density improvement. “However,” the authors of the new study wrote, “whether delaying subsequent injections beyond the recommended 6-month interval is associated with fractures is unknown.”
For their new study, researchers retrospectively analyzed data from 2,594 patients in the U.K. 45 years or older (mean age, 76; 94% female; 53% with a history of major osteoporotic fracture) who began taking denosumab between 2010 and 2019. They used a design that aimed to emulate a clinical trial, comparing three dosing intervals: “on time” (within 4 weeks of the recommended 6-month interval), “short delay” (within 4-16 weeks) and “long delay” (16 weeks to 6 months).
The study found that the risk of composite fracture over 6 months out of 1,000 was 27.3 for on-time dosing, 32.2 for short-delay dosing, and 42.4 for long-delay dosing. The hazard ratio for long-delay versus on-time was 1.44 (95% confidence interval, 0.96-2.17; P = .093).
Vertebral fractures were less likely, but delays boosted the risk significantly: Over 6 months, it grew from 2.2 in 1,000 (on time) to 3.6 in 1,000 (short delay) and 10.1 in 1,000 (long delay). The HR for long delay versus on time was 3.91 (95% CI, 1.62-9.45; P = .005).
“This study had limited statistical power for composite fracture and several secondary end points ... except for vertebral fracture. Thus, evidence was insufficient to conclude that fracture risk was increased at other anatomical sites.”
In an accompanying editorial, two physicians from the University of Minnesota, Minneapolis, noted that the study is “timely and relevant” since the coronavirus pandemic may disrupt dosage schedules more than usual. While the study has limitations, the “findings are consistent with known denosumab pharmacokinetics and prior studies of fracture incidence after denosumab treatment discontinuation, wrote Kristine E. Ensrud, MD, MPH, who is also of Minneapolis VA Health Care System, and John T. Schousboe, MD, PhD, who is also of HealthPartners Institute.
The editorial authors noted that, in light of the pandemic, “some organizations recommend temporary transition to an oral bisphosphonate in patients receiving denosumab treatment for whom continued treatment is not feasible within 7 to 8 months of their most recent injection.”
In an interview, endocrinologist and osteoporosis specialist Ethel Siris, MD, of Columbia University, New York, said many of her patients aren’t coming in for denosumab injections during the pandemic. “It’s hard enough to get people to show up every 6 months to get their shot when things are going nicely,” she said. “We’re talking older women who may be on a lot of other medications. People forget, and it’s difficult for the office to constantly remind some of them to get their shots at an infusion center.”
The lack of symptoms is another challenge to getting patients to return for doses, she said. “In osteoporosis, the only time something hurts is if you break it.”
Since the pandemic began, many patients have been avoiding medical offices because of fear of getting the coronavirus.
The new research is helpful because it shows that patients are “more likely to fracture if they delay,” Dr. Siris noted. The endocrinologist added that she has successfully convinced some patients to give themselves subcutaneous injections in the abdomen at home.
Dr. Siris said she has been able to watch patients do these injections on video to check their technique. Her patients have been impressed by “how easy it is and delighted to have accomplished it,” she said.
The study was funded by the National Institutes of Health China’s National Clinical Research Center for Orthopedics, Sports Medicine & Rehabilitation. The study authors, commentary authors, and Dr. Siris report no relevant disclosures.
SOURCE: Lyu H et al. Ann Intern Med. 2020 Jul 28. doi: 10.7326/M20-0882.
a new study confirms. Physicians say they are especially concerned about the risk facing patients who are delaying the treatment during the coronavirus pandemic.
The recommended doses of denosumab are at 6-month intervals. Patients who delayed a dose by more than 16 weeks were nearly four times more likely to suffer vertebral fractures, compared with those who received on-time injections, according to the study, which was published in Annals of Internal Medicine.
“Because patients who used denosumab were at high risk for vertebral fracture, strategies to improve timely administration of denosumab in routine clinical settings are needed,” wrote the study authors, led by Houchen Lyu, MD, PhD, of National Clinical Research Center for Orthopedics, Sports Medicine & Rehabilitation at General Hospital of Chinese PLA in Beijing.
Denosumab, a human monoclonal antibody, is used to reduce bone loss in osteoporosis. The manufacturer of Prolia, a brand of the drug, recommends it be given every 6 months, but the study reports that it’s common for injections to be delayed.
Researchers have linked cessation of denosumab to higher risk of fractures, and Dr. Lyu led a study published earlier this year that linked less-frequent doses to less bone mineral density improvement. “However,” the authors of the new study wrote, “whether delaying subsequent injections beyond the recommended 6-month interval is associated with fractures is unknown.”
For their new study, researchers retrospectively analyzed data from 2,594 patients in the U.K. 45 years or older (mean age, 76; 94% female; 53% with a history of major osteoporotic fracture) who began taking denosumab between 2010 and 2019. They used a design that aimed to emulate a clinical trial, comparing three dosing intervals: “on time” (within 4 weeks of the recommended 6-month interval), “short delay” (within 4-16 weeks) and “long delay” (16 weeks to 6 months).
The study found that the risk of composite fracture over 6 months out of 1,000 was 27.3 for on-time dosing, 32.2 for short-delay dosing, and 42.4 for long-delay dosing. The hazard ratio for long-delay versus on-time was 1.44 (95% confidence interval, 0.96-2.17; P = .093).
Vertebral fractures were less likely, but delays boosted the risk significantly: Over 6 months, it grew from 2.2 in 1,000 (on time) to 3.6 in 1,000 (short delay) and 10.1 in 1,000 (long delay). The HR for long delay versus on time was 3.91 (95% CI, 1.62-9.45; P = .005).
“This study had limited statistical power for composite fracture and several secondary end points ... except for vertebral fracture. Thus, evidence was insufficient to conclude that fracture risk was increased at other anatomical sites.”
In an accompanying editorial, two physicians from the University of Minnesota, Minneapolis, noted that the study is “timely and relevant” since the coronavirus pandemic may disrupt dosage schedules more than usual. While the study has limitations, the “findings are consistent with known denosumab pharmacokinetics and prior studies of fracture incidence after denosumab treatment discontinuation, wrote Kristine E. Ensrud, MD, MPH, who is also of Minneapolis VA Health Care System, and John T. Schousboe, MD, PhD, who is also of HealthPartners Institute.
The editorial authors noted that, in light of the pandemic, “some organizations recommend temporary transition to an oral bisphosphonate in patients receiving denosumab treatment for whom continued treatment is not feasible within 7 to 8 months of their most recent injection.”
In an interview, endocrinologist and osteoporosis specialist Ethel Siris, MD, of Columbia University, New York, said many of her patients aren’t coming in for denosumab injections during the pandemic. “It’s hard enough to get people to show up every 6 months to get their shot when things are going nicely,” she said. “We’re talking older women who may be on a lot of other medications. People forget, and it’s difficult for the office to constantly remind some of them to get their shots at an infusion center.”
The lack of symptoms is another challenge to getting patients to return for doses, she said. “In osteoporosis, the only time something hurts is if you break it.”
Since the pandemic began, many patients have been avoiding medical offices because of fear of getting the coronavirus.
The new research is helpful because it shows that patients are “more likely to fracture if they delay,” Dr. Siris noted. The endocrinologist added that she has successfully convinced some patients to give themselves subcutaneous injections in the abdomen at home.
Dr. Siris said she has been able to watch patients do these injections on video to check their technique. Her patients have been impressed by “how easy it is and delighted to have accomplished it,” she said.
The study was funded by the National Institutes of Health China’s National Clinical Research Center for Orthopedics, Sports Medicine & Rehabilitation. The study authors, commentary authors, and Dr. Siris report no relevant disclosures.
SOURCE: Lyu H et al. Ann Intern Med. 2020 Jul 28. doi: 10.7326/M20-0882.
FROM ANNALS OF INTERNAL MEDICINE
Key clinical point: Patients with osteoporosis who delay denosumab doses are at much higher risk for vertebral fractures.
Major finding: Over 6 months, the risk of vertebral fractures grew from 2.2 in 1,000 (on-time doses) to 10.1 in 1,000 (delay of more than 16 weeks) – a hazard ratio of 3.91 (confidence interval, 1.62 to 9.45; P = .005).
Study details: Retrospective analysis of 2,594 patients in the U.K. 45 years or older who began taking denosumab between 2010 and 2019.
Disclosures: The study was funded by the National Institutes of Health China’s National Clinical Research Center for Orthopedics, Sports Medicine & Rehabilitation. The study authors report no relevant disclosures.
Source: Lyu H et al. Ann Intern Med. 2020 Jul 28. doi: 10.7326/M20-0882.
FDA allows qualified claims for UTI risk reduction with cranberry products
The Food and Drug Administration will not object to qualified health claims that consumption of certain cranberry juice products and cranberry supplement products may reduce the risk of recurrent urinary tract infections in otherwise healthy women.

In a letter of enforcement discretion issued on July 21, the FDA responded to a health claim petition submitted by Ocean Spray Cranberries. “A health claim characterizes the relationship between a substance and a disease or health-related condition,” according to the FDA. Ocean Spray Cranberries asked the FDA for an authorized health claim regarding the relationship between the consumption of cranberry beverages and supplements and a reduction in the risk of recurrent urinary tract infections (UTIs) in healthy women.
After reviewing the evidence, the FDA determined that the existing science did not support an authorized health claim, but did allow for a qualified health claim for certain cranberry juice beverages and supplements. A qualified health claim does not constitute an FDA approval; the FDA instead issues a Letter of Enforcement Discretion that includes language reflecting the level of scientific evidence for the claim.
The currently available scientific evidence for a relationship between cranberry and recurrent UTIs includes five intervention studies, according to the FDA letter. Two of these were high-quality, randomized, controlled trials in which daily consumption of a cranberry juice beverage was significantly associated with a reduced risk of recurrent UTIs. Another randomized, controlled trial yielded mixed results, and two other intervention studies that were moderate-quality, randomized, controlled trials showed no effect of cranberry juice consumption on UTI risk reduction.
The FDA’s letter of enforcement discretion states that, with regard to cranberry juice beverages, “Limited and inconsistent scientific evidence shows that by consuming one serving (8 oz) each day of a cranberry juice beverage, healthy women who have had a urinary tract infection may reduce their risk of recurrent UTI.”
Similarly, for cranberry dietary supplements, the FDA states that “Limited scientific evidence shows that, by consuming 500 mg each day of cranberry dietary supplement, healthy women who have had a urinary tract infection may reduce their risk of recurrent UTI.”
The qualified health claims apply specifically to cranberry juice beverages that contain at least 27% cranberry juice, and cranberry dietary supplements containing at least 500 mg of cranberry fruit powder. “The claims do not include other conventional foods or food products made from or containing cranberries, such as dried cranberries or cranberry sauce,” according to the FDA statement.
“With recurrent UTI, a major concern is the frequent use of antibiotics,” Constance Bohon, MD, an ob.gyn. in private practice in Washington and an assistant clinical professor at George Washington University, Washington, said in an interview.
“The challenge is to identify habits and/or nonantibiotic treatment to prevent recurrent UTI and decrease the need for antibiotics,” she said. “The regular use of cranberry can decrease the frequency of UTI in some, but not all, people.
“It does not appear to mask the symptoms of a UTI, so if it is not effective to prevent the infection, the presumptive diagnosis can be made based on the common symptoms,” she explained.
Dr. Bohon said that she has recommended the use of cranberry to some of her patients who have recurrent UTIs and has had success with many of them.
“I think it is important to make it clear that cranberry can be beneficial for some patients to decrease the frequency of UTI. It will not be effective for everyone who has frequent UTI, but for those who use it and have fewer UTIs, there will be less frequent exposure to antibiotics,” she emphasized. “What we need to know is who benefits the most from cranberry to prevent recurrent UTIs; whether age, race, coexisting health problems [such as diabetes], and use of hormonal contraception or menopause impact on its success.”
Dr. Bohon had no relevant financial conflicts to disclose.
The Food and Drug Administration will not object to qualified health claims that consumption of certain cranberry juice products and cranberry supplement products may reduce the risk of recurrent urinary tract infections in otherwise healthy women.
In a letter of enforcement discretion issued on July 21, the FDA responded to a health claim petition submitted by Ocean Spray Cranberries. “A health claim characterizes the relationship between a substance and a disease or health-related condition,” according to the FDA. Ocean Spray Cranberries asked the FDA for an authorized health claim regarding the relationship between the consumption of cranberry beverages and supplements and a reduction in the risk of recurrent urinary tract infections (UTIs) in healthy women.
After reviewing the evidence, the FDA determined that the existing science did not support an authorized health claim, but did allow for a qualified health claim for certain cranberry juice beverages and supplements. A qualified health claim does not constitute an FDA approval; the FDA instead issues a Letter of Enforcement Discretion that includes language reflecting the level of scientific evidence for the claim.
The currently available scientific evidence for a relationship between cranberry and recurrent UTIs includes five intervention studies, according to the FDA letter. Two of these were high-quality, randomized, controlled trials in which daily consumption of a cranberry juice beverage was significantly associated with a reduced risk of recurrent UTIs. Another randomized, controlled trial yielded mixed results, and two other intervention studies that were moderate-quality, randomized, controlled trials showed no effect of cranberry juice consumption on UTI risk reduction.
The FDA’s letter of enforcement discretion states that, with regard to cranberry juice beverages, “Limited and inconsistent scientific evidence shows that by consuming one serving (8 oz) each day of a cranberry juice beverage, healthy women who have had a urinary tract infection may reduce their risk of recurrent UTI.”
Similarly, for cranberry dietary supplements, the FDA states that “Limited scientific evidence shows that, by consuming 500 mg each day of cranberry dietary supplement, healthy women who have had a urinary tract infection may reduce their risk of recurrent UTI.”
The qualified health claims apply specifically to cranberry juice beverages that contain at least 27% cranberry juice, and cranberry dietary supplements containing at least 500 mg of cranberry fruit powder. “The claims do not include other conventional foods or food products made from or containing cranberries, such as dried cranberries or cranberry sauce,” according to the FDA statement.
“With recurrent UTI, a major concern is the frequent use of antibiotics,” Constance Bohon, MD, an ob.gyn. in private practice in Washington and an assistant clinical professor at George Washington University, Washington, said in an interview.
“The challenge is to identify habits and/or nonantibiotic treatment to prevent recurrent UTI and decrease the need for antibiotics,” she said. “The regular use of cranberry can decrease the frequency of UTI in some, but not all, people.
“It does not appear to mask the symptoms of a UTI, so if it is not effective to prevent the infection, the presumptive diagnosis can be made based on the common symptoms,” she explained.
Dr. Bohon said that she has recommended the use of cranberry to some of her patients who have recurrent UTIs and has had success with many of them.
“I think it is important to make it clear that cranberry can be beneficial for some patients to decrease the frequency of UTI. It will not be effective for everyone who has frequent UTI, but for those who use it and have fewer UTIs, there will be less frequent exposure to antibiotics,” she emphasized. “What we need to know is who benefits the most from cranberry to prevent recurrent UTIs; whether age, race, coexisting health problems [such as diabetes], and use of hormonal contraception or menopause impact on its success.”
Dr. Bohon had no relevant financial conflicts to disclose.
The Food and Drug Administration will not object to qualified health claims that consumption of certain cranberry juice products and cranberry supplement products may reduce the risk of recurrent urinary tract infections in otherwise healthy women.
In a letter of enforcement discretion issued on July 21, the FDA responded to a health claim petition submitted by Ocean Spray Cranberries. “A health claim characterizes the relationship between a substance and a disease or health-related condition,” according to the FDA. Ocean Spray Cranberries asked the FDA for an authorized health claim regarding the relationship between the consumption of cranberry beverages and supplements and a reduction in the risk of recurrent urinary tract infections (UTIs) in healthy women.
After reviewing the evidence, the FDA determined that the existing science did not support an authorized health claim, but did allow for a qualified health claim for certain cranberry juice beverages and supplements. A qualified health claim does not constitute an FDA approval; the FDA instead issues a Letter of Enforcement Discretion that includes language reflecting the level of scientific evidence for the claim.
The currently available scientific evidence for a relationship between cranberry and recurrent UTIs includes five intervention studies, according to the FDA letter. Two of these were high-quality, randomized, controlled trials in which daily consumption of a cranberry juice beverage was significantly associated with a reduced risk of recurrent UTIs. Another randomized, controlled trial yielded mixed results, and two other intervention studies that were moderate-quality, randomized, controlled trials showed no effect of cranberry juice consumption on UTI risk reduction.
The FDA’s letter of enforcement discretion states that, with regard to cranberry juice beverages, “Limited and inconsistent scientific evidence shows that by consuming one serving (8 oz) each day of a cranberry juice beverage, healthy women who have had a urinary tract infection may reduce their risk of recurrent UTI.”
Similarly, for cranberry dietary supplements, the FDA states that “Limited scientific evidence shows that, by consuming 500 mg each day of cranberry dietary supplement, healthy women who have had a urinary tract infection may reduce their risk of recurrent UTI.”
The qualified health claims apply specifically to cranberry juice beverages that contain at least 27% cranberry juice, and cranberry dietary supplements containing at least 500 mg of cranberry fruit powder. “The claims do not include other conventional foods or food products made from or containing cranberries, such as dried cranberries or cranberry sauce,” according to the FDA statement.
“With recurrent UTI, a major concern is the frequent use of antibiotics,” Constance Bohon, MD, an ob.gyn. in private practice in Washington and an assistant clinical professor at George Washington University, Washington, said in an interview.
“The challenge is to identify habits and/or nonantibiotic treatment to prevent recurrent UTI and decrease the need for antibiotics,” she said. “The regular use of cranberry can decrease the frequency of UTI in some, but not all, people.
“It does not appear to mask the symptoms of a UTI, so if it is not effective to prevent the infection, the presumptive diagnosis can be made based on the common symptoms,” she explained.
Dr. Bohon said that she has recommended the use of cranberry to some of her patients who have recurrent UTIs and has had success with many of them.
“I think it is important to make it clear that cranberry can be beneficial for some patients to decrease the frequency of UTI. It will not be effective for everyone who has frequent UTI, but for those who use it and have fewer UTIs, there will be less frequent exposure to antibiotics,” she emphasized. “What we need to know is who benefits the most from cranberry to prevent recurrent UTIs; whether age, race, coexisting health problems [such as diabetes], and use of hormonal contraception or menopause impact on its success.”
Dr. Bohon had no relevant financial conflicts to disclose.
Internists still low for earnings and net worth, report finds
according to the Medscape Internist Debt and Net Worth Report 2020.
The results are from a larger survey that tracked physicians’ efforts to reduce or eliminate debt, save, invest, purchase property, and prepare for retirement. The annual survey was completed just as the COVID-19 pandemic was taking hold, and the findings provide a baseline against which to view the effects of the pandemic, which turned the lives of many physicians upside down.
Conducted from Oct. 4, 2019, until Feb. 10, 2020, the survey represents 17,461 physicians from 29 areas of medicine, including family practice, internal medicine, pediatrics, and obstetrics and gynecology.
Earnings and net worth
Internists earned on average $251,000 annually, sixth from the bottom of the list and approximately half the amount of the most lucrative specialty, orthopedics. The annual salary increased from $243,000 in 2019.
The average annual salary for internists represents a 2.5% increase, compared with the 1.5% increase for specialists, whose annual income rose from $341,000 in 2019 to $346,000 in 2020.
The low earnings for internists are echoed in the findings for net worth: 58% of internists have a net worth of less than $1 million, 37% have between $1 million and $5 million, and 5% have more than $5 million. For comparison, half of all physicians have a net worth of less than $1 million, 42% have between $1 million and $5 million, and 8% have over $5 million.
About 40% of internists indicated that their net worth was less than $500,000, which is the fourth highest of the 29 medical fields surveyed. About 44% of pediatricians, 46% of family practitioners, and 30% of ob.gyns. also reported their net worth at less than $500,000, so the primary care providers share low net worth compared with their colleagues. About 41% of neurologists reported a net worth of less than $500,000.
Only 5% of internists reported a net worth of more than $5 million. The specialties with the most physicians with net worth exceeding $5 million are orthopedists, at 19%, and plastic surgeons and gastroenterologists, each at 16%.
Gender disparity in net worth appears to be lower among internists than in other fields. Among all physicians, 56% of men and 39% of women reported a net worth in excess of $1 million, but among internists, 46% of men and 36% of women did so. About 64% of the internists who took the survey are men, and 34% are women.
Higher net worth tracks clearly with age group, as expected in light of diminishing debt over time and an accumulation of wealth.
Expenses
The top three expenses that internists face are mortgage on primary residence (60%), car loans (36%), and credit card debt (26%); 12% of respondents reported no debt or expenses. Among all physicians, the breakdown of expenses by category is very similar to that for internists.
Paying off school loans affects 24% of internists, which was in the middle of the 29 physician groups. The percentage ranges from physical medicine and rehabilitation at 34% to rheumatology at 15%.
About 42% of internists have a mortgage of less than $300,000, and 30% have no mortgage at all. Figures are similar for all physicians.
Internists are apparently savers and not spenders. Only 8% reported living above their means; 39% indicated that they live below their means. These figures are similar for all physicians who responded to the survey.
About 60% of internists put more than $1,000 a month into tax-deferred accounts. Most internists also contribute to taxable savings accounts, which might reflect the fact that they had contributed the maximum amount to tax-deferred accounts.
Two-fifths of the internists reported having worked with a financial planner. Of the nearly three fourths of responding internists who share finances with a spouse or partner, a few more than half pool resources.
In the world before COVID-19, 31% of internists reported significant financial losses over the previous year, most because of bad investments or problems relating to their practice. Financial losses since that time obviously have another predominant cause – the direct and ripple effects of the pandemic.
As of July 22, primary care providers reported a 55% decrease in revenue and a 20%-30% decrease in patient volume, according to Travis Singleton, senior vice president of Merritt Hawkins, a physician placement and recruiting company. Some practitioners have closed their physical offices because patient demand has plummeted and nonessential office procedures and exams have been postponed or canceled. The use of telemedicine has soared.
Medscape’s Internist Debt and Net Worth Report 2020, and the larger report from which it was derived, may come to serve as a marker between two very different financial worlds for clinical medicine.
A version of this article originally appeared on Medscape.com.
according to the Medscape Internist Debt and Net Worth Report 2020.
The results are from a larger survey that tracked physicians’ efforts to reduce or eliminate debt, save, invest, purchase property, and prepare for retirement. The annual survey was completed just as the COVID-19 pandemic was taking hold, and the findings provide a baseline against which to view the effects of the pandemic, which turned the lives of many physicians upside down.
Conducted from Oct. 4, 2019, until Feb. 10, 2020, the survey represents 17,461 physicians from 29 areas of medicine, including family practice, internal medicine, pediatrics, and obstetrics and gynecology.
Earnings and net worth
Internists earned on average $251,000 annually, sixth from the bottom of the list and approximately half the amount of the most lucrative specialty, orthopedics. The annual salary increased from $243,000 in 2019.
The average annual salary for internists represents a 2.5% increase, compared with the 1.5% increase for specialists, whose annual income rose from $341,000 in 2019 to $346,000 in 2020.
The low earnings for internists are echoed in the findings for net worth: 58% of internists have a net worth of less than $1 million, 37% have between $1 million and $5 million, and 5% have more than $5 million. For comparison, half of all physicians have a net worth of less than $1 million, 42% have between $1 million and $5 million, and 8% have over $5 million.
About 40% of internists indicated that their net worth was less than $500,000, which is the fourth highest of the 29 medical fields surveyed. About 44% of pediatricians, 46% of family practitioners, and 30% of ob.gyns. also reported their net worth at less than $500,000, so the primary care providers share low net worth compared with their colleagues. About 41% of neurologists reported a net worth of less than $500,000.
Only 5% of internists reported a net worth of more than $5 million. The specialties with the most physicians with net worth exceeding $5 million are orthopedists, at 19%, and plastic surgeons and gastroenterologists, each at 16%.
Gender disparity in net worth appears to be lower among internists than in other fields. Among all physicians, 56% of men and 39% of women reported a net worth in excess of $1 million, but among internists, 46% of men and 36% of women did so. About 64% of the internists who took the survey are men, and 34% are women.
Higher net worth tracks clearly with age group, as expected in light of diminishing debt over time and an accumulation of wealth.
Expenses
The top three expenses that internists face are mortgage on primary residence (60%), car loans (36%), and credit card debt (26%); 12% of respondents reported no debt or expenses. Among all physicians, the breakdown of expenses by category is very similar to that for internists.
Paying off school loans affects 24% of internists, which was in the middle of the 29 physician groups. The percentage ranges from physical medicine and rehabilitation at 34% to rheumatology at 15%.
About 42% of internists have a mortgage of less than $300,000, and 30% have no mortgage at all. Figures are similar for all physicians.
Internists are apparently savers and not spenders. Only 8% reported living above their means; 39% indicated that they live below their means. These figures are similar for all physicians who responded to the survey.
About 60% of internists put more than $1,000 a month into tax-deferred accounts. Most internists also contribute to taxable savings accounts, which might reflect the fact that they had contributed the maximum amount to tax-deferred accounts.
Two-fifths of the internists reported having worked with a financial planner. Of the nearly three fourths of responding internists who share finances with a spouse or partner, a few more than half pool resources.
In the world before COVID-19, 31% of internists reported significant financial losses over the previous year, most because of bad investments or problems relating to their practice. Financial losses since that time obviously have another predominant cause – the direct and ripple effects of the pandemic.
As of July 22, primary care providers reported a 55% decrease in revenue and a 20%-30% decrease in patient volume, according to Travis Singleton, senior vice president of Merritt Hawkins, a physician placement and recruiting company. Some practitioners have closed their physical offices because patient demand has plummeted and nonessential office procedures and exams have been postponed or canceled. The use of telemedicine has soared.
Medscape’s Internist Debt and Net Worth Report 2020, and the larger report from which it was derived, may come to serve as a marker between two very different financial worlds for clinical medicine.
A version of this article originally appeared on Medscape.com.
according to the Medscape Internist Debt and Net Worth Report 2020.
The results are from a larger survey that tracked physicians’ efforts to reduce or eliminate debt, save, invest, purchase property, and prepare for retirement. The annual survey was completed just as the COVID-19 pandemic was taking hold, and the findings provide a baseline against which to view the effects of the pandemic, which turned the lives of many physicians upside down.
Conducted from Oct. 4, 2019, until Feb. 10, 2020, the survey represents 17,461 physicians from 29 areas of medicine, including family practice, internal medicine, pediatrics, and obstetrics and gynecology.
Earnings and net worth
Internists earned on average $251,000 annually, sixth from the bottom of the list and approximately half the amount of the most lucrative specialty, orthopedics. The annual salary increased from $243,000 in 2019.
The average annual salary for internists represents a 2.5% increase, compared with the 1.5% increase for specialists, whose annual income rose from $341,000 in 2019 to $346,000 in 2020.
The low earnings for internists are echoed in the findings for net worth: 58% of internists have a net worth of less than $1 million, 37% have between $1 million and $5 million, and 5% have more than $5 million. For comparison, half of all physicians have a net worth of less than $1 million, 42% have between $1 million and $5 million, and 8% have over $5 million.
About 40% of internists indicated that their net worth was less than $500,000, which is the fourth highest of the 29 medical fields surveyed. About 44% of pediatricians, 46% of family practitioners, and 30% of ob.gyns. also reported their net worth at less than $500,000, so the primary care providers share low net worth compared with their colleagues. About 41% of neurologists reported a net worth of less than $500,000.
Only 5% of internists reported a net worth of more than $5 million. The specialties with the most physicians with net worth exceeding $5 million are orthopedists, at 19%, and plastic surgeons and gastroenterologists, each at 16%.
Gender disparity in net worth appears to be lower among internists than in other fields. Among all physicians, 56% of men and 39% of women reported a net worth in excess of $1 million, but among internists, 46% of men and 36% of women did so. About 64% of the internists who took the survey are men, and 34% are women.
Higher net worth tracks clearly with age group, as expected in light of diminishing debt over time and an accumulation of wealth.
Expenses
The top three expenses that internists face are mortgage on primary residence (60%), car loans (36%), and credit card debt (26%); 12% of respondents reported no debt or expenses. Among all physicians, the breakdown of expenses by category is very similar to that for internists.
Paying off school loans affects 24% of internists, which was in the middle of the 29 physician groups. The percentage ranges from physical medicine and rehabilitation at 34% to rheumatology at 15%.
About 42% of internists have a mortgage of less than $300,000, and 30% have no mortgage at all. Figures are similar for all physicians.
Internists are apparently savers and not spenders. Only 8% reported living above their means; 39% indicated that they live below their means. These figures are similar for all physicians who responded to the survey.
About 60% of internists put more than $1,000 a month into tax-deferred accounts. Most internists also contribute to taxable savings accounts, which might reflect the fact that they had contributed the maximum amount to tax-deferred accounts.
Two-fifths of the internists reported having worked with a financial planner. Of the nearly three fourths of responding internists who share finances with a spouse or partner, a few more than half pool resources.
In the world before COVID-19, 31% of internists reported significant financial losses over the previous year, most because of bad investments or problems relating to their practice. Financial losses since that time obviously have another predominant cause – the direct and ripple effects of the pandemic.
As of July 22, primary care providers reported a 55% decrease in revenue and a 20%-30% decrease in patient volume, according to Travis Singleton, senior vice president of Merritt Hawkins, a physician placement and recruiting company. Some practitioners have closed their physical offices because patient demand has plummeted and nonessential office procedures and exams have been postponed or canceled. The use of telemedicine has soared.
Medscape’s Internist Debt and Net Worth Report 2020, and the larger report from which it was derived, may come to serve as a marker between two very different financial worlds for clinical medicine.
A version of this article originally appeared on Medscape.com.
Marked improvements seen for women in dermatology since the 1970s
Wilma F. Bergfeld, MD, one of only five women in her medical school class of 1964 and the third female in her dermatology residency program, had recently been appointed as a junior clinical dermatologist and head of dermatopathology at the Cleveland Clinic when she was told by a superior that she would not be promoted or invited to serve on any committee or decision-making group.

“I was told I should go home at night and take care of my husband and two children,” she recalled of that moment in the 1970s. The comment made her feel “outraged,” and it drove her, calmly and steadily, to work harder and to “challenge the system.”
Dr. Bergfeld not only was elected to the Cleveland Clinic’s board of governors and board of trustees and served as president of the Clinic’s staff in 1990, she also became the first woman president of the American Academy of Dermatology (1992) and led numerous other dermatologic organizations. Much earlier on, in 1973, to help fulfill her vision of “women helping women,” she had also founded the Women’s Dermatologic Society (WDS). Three years earlier, in 1970, 6.9% of the approximately 4,000 dermatologists in the United States were women, according to the American Medical Association.
Today, when she goes to work as the long-time director of the Clinic’s dermatopathology fellowship and professor of dermatology and pathology at the Cleveland Clinic Educational Foundation, she sees a transformed staff and, more broadly, a national physician workforce in which women made up almost 50% of active dermatologists in 2017 and almost 60% of dermatology residents in 2018, according to data from the American Association of Medical Colleges.
It’s a different and better world, she and other women dermatologists said, but one in which women must continue to mentor other women and continue to challenge the system. Achieving work-life balance, fairer compensation, and a greater proportion of women in the higher ranks of academia are all on their work list.
Women’s impact on the specialty
Dr. Bergfeld and Molly Hinshaw, MD, the current president of the WDS, said they believe women are drawn to dermatology for its visual nature, the growth in diagnostic tests and therapies, and the opportunity to diagnose early and prevent progression of disease in patients of all ages. “It’s a small but mighty specialty,” said Dr. Hinshaw, associate professor of dermatology and section chief of dermatopathology at the University of Wisconsin–Madison.

It’s also a versatile specialty with a variety of subspecialties and niches to pursue – and women have been stepping in to fill unmet needs, Dr. Hinshaw said. “Women dermatologists are directing vulvar specialty clinics across the country, for example. There aren’t that many, but they’re filling an important niche. We have one at [our university] and it is packed.”
Women have also been drawn to the in-demand subspecialty of pediatric dermatology, she noted. They now make up more than two-thirds of all pediatric dermatologists, and many in practice have trained the old-fashioned way, completing two residencies. “That’s [involved] self-selection into an additional year of years training and a commitment to caring for special populations that, quite honestly, takes more time,” said Dr. Hinshaw, who, as part of her dermatology practice, runs a nail clinic at UW Health in Madison.
Amy S. Paller, MD, who chairs the department of dermatology at Northwestern University, Chicago, where she is professor of dermatology and pediatrics and directs the Skin Biology & Diseases Resource-Based Center, is one of these women. She took a long and determined journey into the subspecialty, encountering bias and discouragement while actively seeking out mentors who helped her advance.

While in medical school at Stanford (Calif.) University in the late 1970s in a class “very progressively” made up of about one-third women, Dr. Paller met Alvin Jacobs, MD, who, in 1975, had founded the Society for Pediatric Dermatology. “There wasn’t much pediatric dermatology in the world at the time, and it was Al who helped [me realize] that it combined my love of genetic research with my [desire] to work with children,” she recalled.
Per Dr. Jacob’s advice, she went to Northwestern to train in both pediatrics and dermatology under Nancy Esterly, MD, who “is considered by many to be the mother of pediatric dermatology.” And knowing that she wanted to do research, Dr. Paller also worked with Ruth Freinkel, MD, who “was the strongest bench researcher” at Northwestern. (Dr. Freinkel had been one of the first female dermatology residents at Harvard and was the first full-time faculty member in dermatology at Northwestern).
After completing postdoctoral research at the University of North Carolina at Chapel Hill, Dr. Paller returned to Chicago and assumed Dr. Esterly’s position as chief of dermatology at the Children’s National Hospital of Chicago. It was there that “someone in a leadership position questioned me about how I could possibly be a scientist, a strong clinician, and a good mother to my three children – and suggested that I drop research,” Dr. Paller recalled.
“I think this person was trying to be helpful to me, but I was shocked,” she said. Just as Dr. Bergfeld had done, Dr. Paller channeled her frustration into new pursuits.
“It made me go home and think, how could I strengthen myself? What else could I do?” she said. “Soon after, with a highly supportive husband, I did a ‘pseudosabbatical,’ basically spending every ounce of spare time I had working with one of the premier female scientists in the country, Elaine Fuchs, and learning molecular biology” in her lab at the University of Chicago.
“I think we’ve all had discrimination along the way. Sometimes there’s implicit bias and sometimes there’s overt bias,” said Dr. Paller, who in 2004 led the society which her mentor Dr. Jacobs had founded several decades earlier. “I just jumped right in, and that’s enabled me to find good role models.”
Across dermatology broadly, the often holistic nature of the specialty – of the ability to peer into the body and its internal health – is another quality that women have been drawn to and advanced, Dr. Hinshaw said. “One of the reasons why I chose dermatology is because it’s a window to total patient health. Patients often see their dermatologists as physicians who help them identify next steps in their health care, who can help them address issues related to their overall health and well-being, including their mental health.”
In a WDS membership survey conducted in 2018, most respondents reported that they frequently or occasionally detect and diagnose systemic/internal diseases and conditions in their female patients, and that they consult and collaborate with different kinds of physicians (Int J Womens Dermatol. 2018 Nov 15;4[4]:189-92).
And in a March 2019 “Dialogues in Dermatology” podcast episode on the history and advancement of women in dermatology produced by the American Academy of Dermatology, Pearl Grimes, MD, a clinical professor of dermatology of the University of California, Los Angeles, and then-president of the WDS, described why “total women’s health” had become an additional focus for the society.
“We’re already gatekeepers” in many respects, Dr. Grimes said. “In addition to my addressing specific skin issues, my patients query me on hormone issues, on nutrition, on stress-related issues….and on [what other physicians they should see].”

Phoebe Rich, MD, who owns a small all-woman practice and a research center in Portland, Oregon, said that, in general, many women also communicate and practice in a way that facilitates holistic care. “These qualities aren’t exclusive to women, but women are very caring. We take time and are interested in [patients’] lives in general, not just their disease.”
Disparities in academia
Dermatology departments in academic medicine have burgeoned in size in the past 50 years, and women are well represented overall. In 2018, women comprised 51.2% of dermatology department faculty – up from 10.8% in 1970 – a current proportion that ranks fifth among specialties for the proportion of female faculty, according to a cross-sectional study of faculty diversity trends using data from the AAMC faculty roster (JAMA Dermatol. 2020 Jan 8;156[3]:280-7).
The AAMC data show the share of women dermatology faculty declining at each subsequent rank, however – a finding that suggests that women are not promoted as quickly or to the same levels of leadership as men, the report’s authors noted. (Dermatology isn’t alone: The AAMC issued a call to action on gender equity in medicine this year, citing this inverse association.)
Another recently published study of gender trends in academic dermatology – this one looking at a smaller sample of data from 15 institutions – similarly found that women dermatologists made up a majority of faculty (53.6%) and were well represented as assistant professors (60.7%) but underrepresented as full professors (17%).
This study differed from the larger AAMC study, however, in that it controlled for “achievement indicators” – career duration, publications per year, and National Institutes of Health research funding – and found that gender alone was not associated with higher rank. Instead, promotions were correlated most significantly with NIH research funding and also with career duration and publications per year.
“If research achievement is to be used as a benchmark for academic promotion, increased efforts are needed to support the research activities of women,” the authors wrote, adding that recognition should be given to other factors as well.
Dr. Paller and Dr. Hinshaw both described the situation as complex and multifaceted. Some research on promotion in academia in general – but not all – has suggested that women do need to publish more than men in order to be promoted. But “the promotion process also has within it the ability to use judgment [about] the impact and merits of work,” said Dr. Hinshaw. “Not all publications [and levels of authorship] may be considered equal, for instance.”
Dr. Hinshaw said she is also concerned by data showing that women still perform the majority of household duties, “even in households in which both partners work outside the home equivalently.” As long as this is the case, women may be “inherently disadvantaged” in their ability to have adequate research time and to advance.
From where she sits, Dr. Paller sees several factors at play: “The pipeline, achievement during the pipeline, and decision-making about advancement” on the part of women themselves. Having served on search committees for top leadership in specialties in which women are well represented, she said, “I’ve seen fewer women who’ve come forward and been interested in rising into a chair or a dean position.”
And “having talked to so many women,” Dr. Paller added, “I think there’s a phenomenon where it’s harder for women to accept positions [that require] a significant change.”
Women “are nurturers, which makes them extremely good [leaders] and chairs, but it also makes it harder to make life changes that affect the people they love,” she said, noting that becoming a department chair or a dean often involves moving. “I also think that women in general are happier and committed to what they’re [currently] doing.”
Dr. Paller is optimistic that, with the support of department chairs and continued attention to role modeling and mentoring, the portrait of women in academic dermatology will continue to improve. Currently, 34 chairs of dermatology departments are female, she noted. “That number was 11 less 15 years ago.”
In the meantime, researchers are increasingly documenting trends in women’s editorships of journals as well as leadership and speaking opportunities at professional conferences.
The authors of one study published this year, for instance, reviewed the editorial boards of dermatology journals and found that women occupied 18% of editor in chief roles, 36% of deputy editor positions, and 22% of overall editorial board roles (Int J Womens Dermatol. 2019 Sep 12;6[1]:20-4). Other research shows women comprising 43% of all authorships across 23 dermatologic journals from 2008 to May 2017, 50.2% of first authorships, and 33.1% of last authorships (BMJ Open. 2018 Apr 13;8[4]:e020089).
Both in academic medicine and in practice, a gender pay gap still affects women physicians across the board. Medscape’s 2020 dermatologist compensation report shows male dermatologists earning about 12% more than their female peers (average, $435,000 vs. $387,000, respectively), while the average number of hours per week spent seeing patients is similar (36.2 vs. 35.6 hours, respectively).
And in its 2020 statement on gender equity, the AAMC said that women in academic medicine are offered less in starting salary, negotiated pay, and other forms of compensation than men “despite equal effort, rank, training, and experience.”
It’s complicated to tease apart all the factors that may be involved – but important to keep challenging the system, said Dr. Bergfeld, who was a long-time board adviser for Dermatology News. “I was underpaid,” she noted, and “this was only rectified in the last 10 years.”
Work-life balance
In the AAD podcast on women in dermatology, Dr. Grimes said that achieving a healthy and balanced work life remains one of the greatest challenges for women dermatologists – and it may be even greater than in the past given the growing numbers of group practices. “When women enter the realm of group practice, they have less flexibility in controlling their time and their own schedules.”
If Anna Hare, MD, is any indication, younger dermatologists may buck this trend. The daughter of Dr. Rich in Portland, Dr. Hare joined her mother’s dermatology practice and research center knowing that she’d have “the respect and flexibility for deciding how I want to practice.”
Younger dermatologists, she said, place “more of an emphasis on work-life balance and quality of life.”
Fortunately, said Dr. Bergfeld, women have advanced enough in the ranks of dermatology that, in networking, in mentorship, and in workplace settings, attention can be paid more fully to discussions about work-life management – “how to manage your life when you’re working with family and kids and parents.”
In the 1970s, at the Cleveland Clinic, “there were only five women on staff and we were fighting for [basic] rights,” she said. “We wanted equality – we were [perceived as] little worker bees….We needed to climb as the men did to positions of leadership and address the problems of women.”
In pursuing their goals and making further progress, women dermatologists today should be “steady and calm,” she advised. Formally acquiring leadership skills and communication skills is a timeless need. And when there are biases or conflicts, “you cannot have righteous indignation, you cannot have revenge. You have to calm yourself and move forward.”
Wilma F. Bergfeld, MD, one of only five women in her medical school class of 1964 and the third female in her dermatology residency program, had recently been appointed as a junior clinical dermatologist and head of dermatopathology at the Cleveland Clinic when she was told by a superior that she would not be promoted or invited to serve on any committee or decision-making group.
“I was told I should go home at night and take care of my husband and two children,” she recalled of that moment in the 1970s. The comment made her feel “outraged,” and it drove her, calmly and steadily, to work harder and to “challenge the system.”
Dr. Bergfeld not only was elected to the Cleveland Clinic’s board of governors and board of trustees and served as president of the Clinic’s staff in 1990, she also became the first woman president of the American Academy of Dermatology (1992) and led numerous other dermatologic organizations. Much earlier on, in 1973, to help fulfill her vision of “women helping women,” she had also founded the Women’s Dermatologic Society (WDS). Three years earlier, in 1970, 6.9% of the approximately 4,000 dermatologists in the United States were women, according to the American Medical Association.
Today, when she goes to work as the long-time director of the Clinic’s dermatopathology fellowship and professor of dermatology and pathology at the Cleveland Clinic Educational Foundation, she sees a transformed staff and, more broadly, a national physician workforce in which women made up almost 50% of active dermatologists in 2017 and almost 60% of dermatology residents in 2018, according to data from the American Association of Medical Colleges.
It’s a different and better world, she and other women dermatologists said, but one in which women must continue to mentor other women and continue to challenge the system. Achieving work-life balance, fairer compensation, and a greater proportion of women in the higher ranks of academia are all on their work list.
Women’s impact on the specialty
Dr. Bergfeld and Molly Hinshaw, MD, the current president of the WDS, said they believe women are drawn to dermatology for its visual nature, the growth in diagnostic tests and therapies, and the opportunity to diagnose early and prevent progression of disease in patients of all ages. “It’s a small but mighty specialty,” said Dr. Hinshaw, associate professor of dermatology and section chief of dermatopathology at the University of Wisconsin–Madison.
It’s also a versatile specialty with a variety of subspecialties and niches to pursue – and women have been stepping in to fill unmet needs, Dr. Hinshaw said. “Women dermatologists are directing vulvar specialty clinics across the country, for example. There aren’t that many, but they’re filling an important niche. We have one at [our university] and it is packed.”
Women have also been drawn to the in-demand subspecialty of pediatric dermatology, she noted. They now make up more than two-thirds of all pediatric dermatologists, and many in practice have trained the old-fashioned way, completing two residencies. “That’s [involved] self-selection into an additional year of years training and a commitment to caring for special populations that, quite honestly, takes more time,” said Dr. Hinshaw, who, as part of her dermatology practice, runs a nail clinic at UW Health in Madison.
Amy S. Paller, MD, who chairs the department of dermatology at Northwestern University, Chicago, where she is professor of dermatology and pediatrics and directs the Skin Biology & Diseases Resource-Based Center, is one of these women. She took a long and determined journey into the subspecialty, encountering bias and discouragement while actively seeking out mentors who helped her advance.
While in medical school at Stanford (Calif.) University in the late 1970s in a class “very progressively” made up of about one-third women, Dr. Paller met Alvin Jacobs, MD, who, in 1975, had founded the Society for Pediatric Dermatology. “There wasn’t much pediatric dermatology in the world at the time, and it was Al who helped [me realize] that it combined my love of genetic research with my [desire] to work with children,” she recalled.
Per Dr. Jacob’s advice, she went to Northwestern to train in both pediatrics and dermatology under Nancy Esterly, MD, who “is considered by many to be the mother of pediatric dermatology.” And knowing that she wanted to do research, Dr. Paller also worked with Ruth Freinkel, MD, who “was the strongest bench researcher” at Northwestern. (Dr. Freinkel had been one of the first female dermatology residents at Harvard and was the first full-time faculty member in dermatology at Northwestern).
After completing postdoctoral research at the University of North Carolina at Chapel Hill, Dr. Paller returned to Chicago and assumed Dr. Esterly’s position as chief of dermatology at the Children’s National Hospital of Chicago. It was there that “someone in a leadership position questioned me about how I could possibly be a scientist, a strong clinician, and a good mother to my three children – and suggested that I drop research,” Dr. Paller recalled.
“I think this person was trying to be helpful to me, but I was shocked,” she said. Just as Dr. Bergfeld had done, Dr. Paller channeled her frustration into new pursuits.
“It made me go home and think, how could I strengthen myself? What else could I do?” she said. “Soon after, with a highly supportive husband, I did a ‘pseudosabbatical,’ basically spending every ounce of spare time I had working with one of the premier female scientists in the country, Elaine Fuchs, and learning molecular biology” in her lab at the University of Chicago.
“I think we’ve all had discrimination along the way. Sometimes there’s implicit bias and sometimes there’s overt bias,” said Dr. Paller, who in 2004 led the society which her mentor Dr. Jacobs had founded several decades earlier. “I just jumped right in, and that’s enabled me to find good role models.”
Across dermatology broadly, the often holistic nature of the specialty – of the ability to peer into the body and its internal health – is another quality that women have been drawn to and advanced, Dr. Hinshaw said. “One of the reasons why I chose dermatology is because it’s a window to total patient health. Patients often see their dermatologists as physicians who help them identify next steps in their health care, who can help them address issues related to their overall health and well-being, including their mental health.”
In a WDS membership survey conducted in 2018, most respondents reported that they frequently or occasionally detect and diagnose systemic/internal diseases and conditions in their female patients, and that they consult and collaborate with different kinds of physicians (Int J Womens Dermatol. 2018 Nov 15;4[4]:189-92).
And in a March 2019 “Dialogues in Dermatology” podcast episode on the history and advancement of women in dermatology produced by the American Academy of Dermatology, Pearl Grimes, MD, a clinical professor of dermatology of the University of California, Los Angeles, and then-president of the WDS, described why “total women’s health” had become an additional focus for the society.
“We’re already gatekeepers” in many respects, Dr. Grimes said. “In addition to my addressing specific skin issues, my patients query me on hormone issues, on nutrition, on stress-related issues….and on [what other physicians they should see].”
Phoebe Rich, MD, who owns a small all-woman practice and a research center in Portland, Oregon, said that, in general, many women also communicate and practice in a way that facilitates holistic care. “These qualities aren’t exclusive to women, but women are very caring. We take time and are interested in [patients’] lives in general, not just their disease.”
Disparities in academia
Dermatology departments in academic medicine have burgeoned in size in the past 50 years, and women are well represented overall. In 2018, women comprised 51.2% of dermatology department faculty – up from 10.8% in 1970 – a current proportion that ranks fifth among specialties for the proportion of female faculty, according to a cross-sectional study of faculty diversity trends using data from the AAMC faculty roster (JAMA Dermatol. 2020 Jan 8;156[3]:280-7).
The AAMC data show the share of women dermatology faculty declining at each subsequent rank, however – a finding that suggests that women are not promoted as quickly or to the same levels of leadership as men, the report’s authors noted. (Dermatology isn’t alone: The AAMC issued a call to action on gender equity in medicine this year, citing this inverse association.)
Another recently published study of gender trends in academic dermatology – this one looking at a smaller sample of data from 15 institutions – similarly found that women dermatologists made up a majority of faculty (53.6%) and were well represented as assistant professors (60.7%) but underrepresented as full professors (17%).
This study differed from the larger AAMC study, however, in that it controlled for “achievement indicators” – career duration, publications per year, and National Institutes of Health research funding – and found that gender alone was not associated with higher rank. Instead, promotions were correlated most significantly with NIH research funding and also with career duration and publications per year.
“If research achievement is to be used as a benchmark for academic promotion, increased efforts are needed to support the research activities of women,” the authors wrote, adding that recognition should be given to other factors as well.
Dr. Paller and Dr. Hinshaw both described the situation as complex and multifaceted. Some research on promotion in academia in general – but not all – has suggested that women do need to publish more than men in order to be promoted. But “the promotion process also has within it the ability to use judgment [about] the impact and merits of work,” said Dr. Hinshaw. “Not all publications [and levels of authorship] may be considered equal, for instance.”
Dr. Hinshaw said she is also concerned by data showing that women still perform the majority of household duties, “even in households in which both partners work outside the home equivalently.” As long as this is the case, women may be “inherently disadvantaged” in their ability to have adequate research time and to advance.
From where she sits, Dr. Paller sees several factors at play: “The pipeline, achievement during the pipeline, and decision-making about advancement” on the part of women themselves. Having served on search committees for top leadership in specialties in which women are well represented, she said, “I’ve seen fewer women who’ve come forward and been interested in rising into a chair or a dean position.”
And “having talked to so many women,” Dr. Paller added, “I think there’s a phenomenon where it’s harder for women to accept positions [that require] a significant change.”
Women “are nurturers, which makes them extremely good [leaders] and chairs, but it also makes it harder to make life changes that affect the people they love,” she said, noting that becoming a department chair or a dean often involves moving. “I also think that women in general are happier and committed to what they’re [currently] doing.”
Dr. Paller is optimistic that, with the support of department chairs and continued attention to role modeling and mentoring, the portrait of women in academic dermatology will continue to improve. Currently, 34 chairs of dermatology departments are female, she noted. “That number was 11 less 15 years ago.”
In the meantime, researchers are increasingly documenting trends in women’s editorships of journals as well as leadership and speaking opportunities at professional conferences.
The authors of one study published this year, for instance, reviewed the editorial boards of dermatology journals and found that women occupied 18% of editor in chief roles, 36% of deputy editor positions, and 22% of overall editorial board roles (Int J Womens Dermatol. 2019 Sep 12;6[1]:20-4). Other research shows women comprising 43% of all authorships across 23 dermatologic journals from 2008 to May 2017, 50.2% of first authorships, and 33.1% of last authorships (BMJ Open. 2018 Apr 13;8[4]:e020089).
Both in academic medicine and in practice, a gender pay gap still affects women physicians across the board. Medscape’s 2020 dermatologist compensation report shows male dermatologists earning about 12% more than their female peers (average, $435,000 vs. $387,000, respectively), while the average number of hours per week spent seeing patients is similar (36.2 vs. 35.6 hours, respectively).
And in its 2020 statement on gender equity, the AAMC said that women in academic medicine are offered less in starting salary, negotiated pay, and other forms of compensation than men “despite equal effort, rank, training, and experience.”
It’s complicated to tease apart all the factors that may be involved – but important to keep challenging the system, said Dr. Bergfeld, who was a long-time board adviser for Dermatology News. “I was underpaid,” she noted, and “this was only rectified in the last 10 years.”
Work-life balance
In the AAD podcast on women in dermatology, Dr. Grimes said that achieving a healthy and balanced work life remains one of the greatest challenges for women dermatologists – and it may be even greater than in the past given the growing numbers of group practices. “When women enter the realm of group practice, they have less flexibility in controlling their time and their own schedules.”
If Anna Hare, MD, is any indication, younger dermatologists may buck this trend. The daughter of Dr. Rich in Portland, Dr. Hare joined her mother’s dermatology practice and research center knowing that she’d have “the respect and flexibility for deciding how I want to practice.”
Younger dermatologists, she said, place “more of an emphasis on work-life balance and quality of life.”
Fortunately, said Dr. Bergfeld, women have advanced enough in the ranks of dermatology that, in networking, in mentorship, and in workplace settings, attention can be paid more fully to discussions about work-life management – “how to manage your life when you’re working with family and kids and parents.”
In the 1970s, at the Cleveland Clinic, “there were only five women on staff and we were fighting for [basic] rights,” she said. “We wanted equality – we were [perceived as] little worker bees….We needed to climb as the men did to positions of leadership and address the problems of women.”
In pursuing their goals and making further progress, women dermatologists today should be “steady and calm,” she advised. Formally acquiring leadership skills and communication skills is a timeless need. And when there are biases or conflicts, “you cannot have righteous indignation, you cannot have revenge. You have to calm yourself and move forward.”
Wilma F. Bergfeld, MD, one of only five women in her medical school class of 1964 and the third female in her dermatology residency program, had recently been appointed as a junior clinical dermatologist and head of dermatopathology at the Cleveland Clinic when she was told by a superior that she would not be promoted or invited to serve on any committee or decision-making group.
“I was told I should go home at night and take care of my husband and two children,” she recalled of that moment in the 1970s. The comment made her feel “outraged,” and it drove her, calmly and steadily, to work harder and to “challenge the system.”
Dr. Bergfeld not only was elected to the Cleveland Clinic’s board of governors and board of trustees and served as president of the Clinic’s staff in 1990, she also became the first woman president of the American Academy of Dermatology (1992) and led numerous other dermatologic organizations. Much earlier on, in 1973, to help fulfill her vision of “women helping women,” she had also founded the Women’s Dermatologic Society (WDS). Three years earlier, in 1970, 6.9% of the approximately 4,000 dermatologists in the United States were women, according to the American Medical Association.
Today, when she goes to work as the long-time director of the Clinic’s dermatopathology fellowship and professor of dermatology and pathology at the Cleveland Clinic Educational Foundation, she sees a transformed staff and, more broadly, a national physician workforce in which women made up almost 50% of active dermatologists in 2017 and almost 60% of dermatology residents in 2018, according to data from the American Association of Medical Colleges.
It’s a different and better world, she and other women dermatologists said, but one in which women must continue to mentor other women and continue to challenge the system. Achieving work-life balance, fairer compensation, and a greater proportion of women in the higher ranks of academia are all on their work list.
Women’s impact on the specialty
Dr. Bergfeld and Molly Hinshaw, MD, the current president of the WDS, said they believe women are drawn to dermatology for its visual nature, the growth in diagnostic tests and therapies, and the opportunity to diagnose early and prevent progression of disease in patients of all ages. “It’s a small but mighty specialty,” said Dr. Hinshaw, associate professor of dermatology and section chief of dermatopathology at the University of Wisconsin–Madison.
It’s also a versatile specialty with a variety of subspecialties and niches to pursue – and women have been stepping in to fill unmet needs, Dr. Hinshaw said. “Women dermatologists are directing vulvar specialty clinics across the country, for example. There aren’t that many, but they’re filling an important niche. We have one at [our university] and it is packed.”
Women have also been drawn to the in-demand subspecialty of pediatric dermatology, she noted. They now make up more than two-thirds of all pediatric dermatologists, and many in practice have trained the old-fashioned way, completing two residencies. “That’s [involved] self-selection into an additional year of years training and a commitment to caring for special populations that, quite honestly, takes more time,” said Dr. Hinshaw, who, as part of her dermatology practice, runs a nail clinic at UW Health in Madison.
Amy S. Paller, MD, who chairs the department of dermatology at Northwestern University, Chicago, where she is professor of dermatology and pediatrics and directs the Skin Biology & Diseases Resource-Based Center, is one of these women. She took a long and determined journey into the subspecialty, encountering bias and discouragement while actively seeking out mentors who helped her advance.
While in medical school at Stanford (Calif.) University in the late 1970s in a class “very progressively” made up of about one-third women, Dr. Paller met Alvin Jacobs, MD, who, in 1975, had founded the Society for Pediatric Dermatology. “There wasn’t much pediatric dermatology in the world at the time, and it was Al who helped [me realize] that it combined my love of genetic research with my [desire] to work with children,” she recalled.
Per Dr. Jacob’s advice, she went to Northwestern to train in both pediatrics and dermatology under Nancy Esterly, MD, who “is considered by many to be the mother of pediatric dermatology.” And knowing that she wanted to do research, Dr. Paller also worked with Ruth Freinkel, MD, who “was the strongest bench researcher” at Northwestern. (Dr. Freinkel had been one of the first female dermatology residents at Harvard and was the first full-time faculty member in dermatology at Northwestern).
After completing postdoctoral research at the University of North Carolina at Chapel Hill, Dr. Paller returned to Chicago and assumed Dr. Esterly’s position as chief of dermatology at the Children’s National Hospital of Chicago. It was there that “someone in a leadership position questioned me about how I could possibly be a scientist, a strong clinician, and a good mother to my three children – and suggested that I drop research,” Dr. Paller recalled.
“I think this person was trying to be helpful to me, but I was shocked,” she said. Just as Dr. Bergfeld had done, Dr. Paller channeled her frustration into new pursuits.
“It made me go home and think, how could I strengthen myself? What else could I do?” she said. “Soon after, with a highly supportive husband, I did a ‘pseudosabbatical,’ basically spending every ounce of spare time I had working with one of the premier female scientists in the country, Elaine Fuchs, and learning molecular biology” in her lab at the University of Chicago.
“I think we’ve all had discrimination along the way. Sometimes there’s implicit bias and sometimes there’s overt bias,” said Dr. Paller, who in 2004 led the society which her mentor Dr. Jacobs had founded several decades earlier. “I just jumped right in, and that’s enabled me to find good role models.”
Across dermatology broadly, the often holistic nature of the specialty – of the ability to peer into the body and its internal health – is another quality that women have been drawn to and advanced, Dr. Hinshaw said. “One of the reasons why I chose dermatology is because it’s a window to total patient health. Patients often see their dermatologists as physicians who help them identify next steps in their health care, who can help them address issues related to their overall health and well-being, including their mental health.”
In a WDS membership survey conducted in 2018, most respondents reported that they frequently or occasionally detect and diagnose systemic/internal diseases and conditions in their female patients, and that they consult and collaborate with different kinds of physicians (Int J Womens Dermatol. 2018 Nov 15;4[4]:189-92).
And in a March 2019 “Dialogues in Dermatology” podcast episode on the history and advancement of women in dermatology produced by the American Academy of Dermatology, Pearl Grimes, MD, a clinical professor of dermatology of the University of California, Los Angeles, and then-president of the WDS, described why “total women’s health” had become an additional focus for the society.
“We’re already gatekeepers” in many respects, Dr. Grimes said. “In addition to my addressing specific skin issues, my patients query me on hormone issues, on nutrition, on stress-related issues….and on [what other physicians they should see].”
Phoebe Rich, MD, who owns a small all-woman practice and a research center in Portland, Oregon, said that, in general, many women also communicate and practice in a way that facilitates holistic care. “These qualities aren’t exclusive to women, but women are very caring. We take time and are interested in [patients’] lives in general, not just their disease.”
Disparities in academia
Dermatology departments in academic medicine have burgeoned in size in the past 50 years, and women are well represented overall. In 2018, women comprised 51.2% of dermatology department faculty – up from 10.8% in 1970 – a current proportion that ranks fifth among specialties for the proportion of female faculty, according to a cross-sectional study of faculty diversity trends using data from the AAMC faculty roster (JAMA Dermatol. 2020 Jan 8;156[3]:280-7).
The AAMC data show the share of women dermatology faculty declining at each subsequent rank, however – a finding that suggests that women are not promoted as quickly or to the same levels of leadership as men, the report’s authors noted. (Dermatology isn’t alone: The AAMC issued a call to action on gender equity in medicine this year, citing this inverse association.)
Another recently published study of gender trends in academic dermatology – this one looking at a smaller sample of data from 15 institutions – similarly found that women dermatologists made up a majority of faculty (53.6%) and were well represented as assistant professors (60.7%) but underrepresented as full professors (17%).
This study differed from the larger AAMC study, however, in that it controlled for “achievement indicators” – career duration, publications per year, and National Institutes of Health research funding – and found that gender alone was not associated with higher rank. Instead, promotions were correlated most significantly with NIH research funding and also with career duration and publications per year.
“If research achievement is to be used as a benchmark for academic promotion, increased efforts are needed to support the research activities of women,” the authors wrote, adding that recognition should be given to other factors as well.
Dr. Paller and Dr. Hinshaw both described the situation as complex and multifaceted. Some research on promotion in academia in general – but not all – has suggested that women do need to publish more than men in order to be promoted. But “the promotion process also has within it the ability to use judgment [about] the impact and merits of work,” said Dr. Hinshaw. “Not all publications [and levels of authorship] may be considered equal, for instance.”
Dr. Hinshaw said she is also concerned by data showing that women still perform the majority of household duties, “even in households in which both partners work outside the home equivalently.” As long as this is the case, women may be “inherently disadvantaged” in their ability to have adequate research time and to advance.
From where she sits, Dr. Paller sees several factors at play: “The pipeline, achievement during the pipeline, and decision-making about advancement” on the part of women themselves. Having served on search committees for top leadership in specialties in which women are well represented, she said, “I’ve seen fewer women who’ve come forward and been interested in rising into a chair or a dean position.”
And “having talked to so many women,” Dr. Paller added, “I think there’s a phenomenon where it’s harder for women to accept positions [that require] a significant change.”
Women “are nurturers, which makes them extremely good [leaders] and chairs, but it also makes it harder to make life changes that affect the people they love,” she said, noting that becoming a department chair or a dean often involves moving. “I also think that women in general are happier and committed to what they’re [currently] doing.”
Dr. Paller is optimistic that, with the support of department chairs and continued attention to role modeling and mentoring, the portrait of women in academic dermatology will continue to improve. Currently, 34 chairs of dermatology departments are female, she noted. “That number was 11 less 15 years ago.”
In the meantime, researchers are increasingly documenting trends in women’s editorships of journals as well as leadership and speaking opportunities at professional conferences.
The authors of one study published this year, for instance, reviewed the editorial boards of dermatology journals and found that women occupied 18% of editor in chief roles, 36% of deputy editor positions, and 22% of overall editorial board roles (Int J Womens Dermatol. 2019 Sep 12;6[1]:20-4). Other research shows women comprising 43% of all authorships across 23 dermatologic journals from 2008 to May 2017, 50.2% of first authorships, and 33.1% of last authorships (BMJ Open. 2018 Apr 13;8[4]:e020089).
Both in academic medicine and in practice, a gender pay gap still affects women physicians across the board. Medscape’s 2020 dermatologist compensation report shows male dermatologists earning about 12% more than their female peers (average, $435,000 vs. $387,000, respectively), while the average number of hours per week spent seeing patients is similar (36.2 vs. 35.6 hours, respectively).
And in its 2020 statement on gender equity, the AAMC said that women in academic medicine are offered less in starting salary, negotiated pay, and other forms of compensation than men “despite equal effort, rank, training, and experience.”
It’s complicated to tease apart all the factors that may be involved – but important to keep challenging the system, said Dr. Bergfeld, who was a long-time board adviser for Dermatology News. “I was underpaid,” she noted, and “this was only rectified in the last 10 years.”
Work-life balance
In the AAD podcast on women in dermatology, Dr. Grimes said that achieving a healthy and balanced work life remains one of the greatest challenges for women dermatologists – and it may be even greater than in the past given the growing numbers of group practices. “When women enter the realm of group practice, they have less flexibility in controlling their time and their own schedules.”
If Anna Hare, MD, is any indication, younger dermatologists may buck this trend. The daughter of Dr. Rich in Portland, Dr. Hare joined her mother’s dermatology practice and research center knowing that she’d have “the respect and flexibility for deciding how I want to practice.”
Younger dermatologists, she said, place “more of an emphasis on work-life balance and quality of life.”
Fortunately, said Dr. Bergfeld, women have advanced enough in the ranks of dermatology that, in networking, in mentorship, and in workplace settings, attention can be paid more fully to discussions about work-life management – “how to manage your life when you’re working with family and kids and parents.”
In the 1970s, at the Cleveland Clinic, “there were only five women on staff and we were fighting for [basic] rights,” she said. “We wanted equality – we were [perceived as] little worker bees….We needed to climb as the men did to positions of leadership and address the problems of women.”
In pursuing their goals and making further progress, women dermatologists today should be “steady and calm,” she advised. Formally acquiring leadership skills and communication skills is a timeless need. And when there are biases or conflicts, “you cannot have righteous indignation, you cannot have revenge. You have to calm yourself and move forward.”
Internists’ use of ultrasound can reduce radiology referrals
researchers say.
“It’s a safe and very useful tool,” Marco Barchiesi, MD, an internal medicine resident at Luigi Sacco Hospital in Milan, said in an interview. “We had a great reduction in chest x-rays because of the use of ultrasound.”
The finding addresses concerns that ultrasound used in primary care could consume more health care resources or put patients at risk.
Dr. Barchiesi and colleagues published their findings July 20 in the European Journal of Internal Medicine.
Point-of-care ultrasound has become increasingly common as miniaturization of devices has made them more portable. The approach has caught on particularly in emergency departments where quick decisions are of the essence.
Its use in internal medicine has been more controversial, with concerns raised that improperly trained practitioners may miss diagnoses or refer patients for unnecessary tests as a result of uncertainty about their findings.
To measure the effect of point-of-care ultrasound in an internal medicine hospital ward, Dr. Barchiesi and colleagues alternated months when point-of-care ultrasound was allowed with months when it was not allowed, for a total of 4 months each, on an internal medicine unit. They allowed the ultrasound to be used for invasive procedures and excluded patients whose critical condition made point-of-care ultrasound crucial.
The researchers analyzed data on 263 patients in the “on” months when point-of-care ultrasound was used, and 255 in the “off” months when it wasn’t used. The two groups were well balanced in age, sex, comorbidity, and clinical impairment.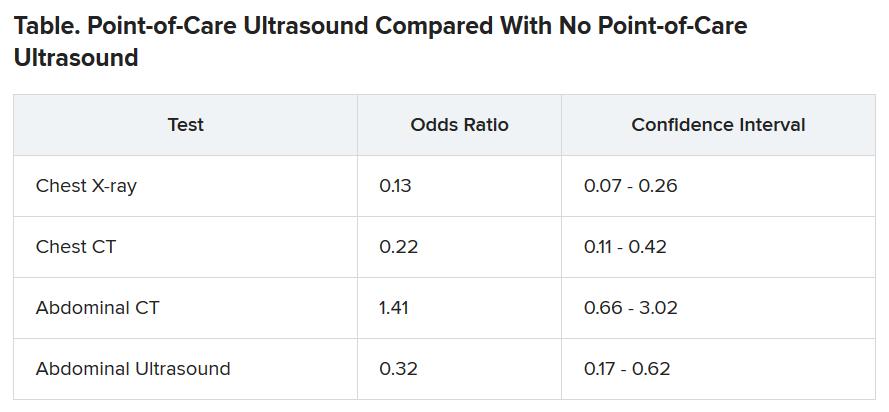
During the on months, the internists ordered 113 diagnostic tests (0.43 per patient). During the off months they ordered 329 tests (1.29 per patient).
The odds of being referred for a chest x-ray were 87% less in the “on” months, compared with the off months, a statistically significant finding (P < .001). The risk for a chest CT scan and abdominal ultrasound were also reduced during the on months, but the risk for an abdominal CT was increased.
Nineteen patients died during the o” months and 10 during the off months, a difference that was not statistically significant (P = .15). The median length of stay in the hospital was almost the same for the two groups: 9 days for the on months and 9 days for the off months. The difference was also not statistically significant (P = .094).
Point-of-care ultrasound is particularly accurate in identifying cardiac abnormalities and pleural fluid and pneumonia, and it can be used effectively for monitoring heart conditions, the researchers wrote. This could explain the reduction in chest x-rays and CT scans.
On the other hand, ultrasound cannot address such questions as staging in an abdominal malignancy, and unexpected findings are more common with abdominal than chest ultrasound. This could explain why the point-of-care ultrasound did not reduce the use of abdominal CT, the researchers speculated.
They acknowledged that the patients in their sample had an average age of 81 years, raising questions about how well their data could be applied to a younger population. And they noted that they used point-of-care ultrasound frequently, so they were particularly adept with it. “We use it almost every day in our clinical practice,” said Dr. Barchiesi.
Those factors may have played a key role in the success of point-of-care ultrasound in this study, said Michael Wagner, MD, an assistant professor of medicine at the University of South Carolina, Greenville, who has helped colleagues incorporate ultrasound into their practices.
Elderly patients often present with multiple comorbidities and atypical signs and symptoms, he said. “Sometimes they can be very confusing as to the underlying clinical picture. Ultrasound is being used frequently to better assess these complicated patients.”
Dr. Wagner said extensive training is required to use point-of-care ultrasound accurately.
Dr. Barchiesi also acknowledged that the devices used in this study were large portable machines, not the simpler and less expensive hand-held versions that are also available for similar purposes.
Point-of-care ultrasound is a promising innovation, said Thomas Melgar, MD, a professor of medicine at Western Michigan University, Kalamazoo. “The advantage is that the exam is being done by someone who knows the patient and specifically what they’re looking for. It’s done at the bedside so you don’t have to move the patient.”
The study could help address opposition to internal medicine residents being trained in the technique, he said, adding that “I think it’s very exciting.”
The study was partially supported by Philips, which provided the ultrasound devices. Dr. Barchiesi, Dr. Melgar, and Dr. Wagner disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
researchers say.
“It’s a safe and very useful tool,” Marco Barchiesi, MD, an internal medicine resident at Luigi Sacco Hospital in Milan, said in an interview. “We had a great reduction in chest x-rays because of the use of ultrasound.”
The finding addresses concerns that ultrasound used in primary care could consume more health care resources or put patients at risk.
Dr. Barchiesi and colleagues published their findings July 20 in the European Journal of Internal Medicine.
Point-of-care ultrasound has become increasingly common as miniaturization of devices has made them more portable. The approach has caught on particularly in emergency departments where quick decisions are of the essence.
Its use in internal medicine has been more controversial, with concerns raised that improperly trained practitioners may miss diagnoses or refer patients for unnecessary tests as a result of uncertainty about their findings.
To measure the effect of point-of-care ultrasound in an internal medicine hospital ward, Dr. Barchiesi and colleagues alternated months when point-of-care ultrasound was allowed with months when it was not allowed, for a total of 4 months each, on an internal medicine unit. They allowed the ultrasound to be used for invasive procedures and excluded patients whose critical condition made point-of-care ultrasound crucial.
The researchers analyzed data on 263 patients in the “on” months when point-of-care ultrasound was used, and 255 in the “off” months when it wasn’t used. The two groups were well balanced in age, sex, comorbidity, and clinical impairment.
During the on months, the internists ordered 113 diagnostic tests (0.43 per patient). During the off months they ordered 329 tests (1.29 per patient).
The odds of being referred for a chest x-ray were 87% less in the “on” months, compared with the off months, a statistically significant finding (P < .001). The risk for a chest CT scan and abdominal ultrasound were also reduced during the on months, but the risk for an abdominal CT was increased.
Nineteen patients died during the o” months and 10 during the off months, a difference that was not statistically significant (P = .15). The median length of stay in the hospital was almost the same for the two groups: 9 days for the on months and 9 days for the off months. The difference was also not statistically significant (P = .094).
Point-of-care ultrasound is particularly accurate in identifying cardiac abnormalities and pleural fluid and pneumonia, and it can be used effectively for monitoring heart conditions, the researchers wrote. This could explain the reduction in chest x-rays and CT scans.
On the other hand, ultrasound cannot address such questions as staging in an abdominal malignancy, and unexpected findings are more common with abdominal than chest ultrasound. This could explain why the point-of-care ultrasound did not reduce the use of abdominal CT, the researchers speculated.
They acknowledged that the patients in their sample had an average age of 81 years, raising questions about how well their data could be applied to a younger population. And they noted that they used point-of-care ultrasound frequently, so they were particularly adept with it. “We use it almost every day in our clinical practice,” said Dr. Barchiesi.
Those factors may have played a key role in the success of point-of-care ultrasound in this study, said Michael Wagner, MD, an assistant professor of medicine at the University of South Carolina, Greenville, who has helped colleagues incorporate ultrasound into their practices.
Elderly patients often present with multiple comorbidities and atypical signs and symptoms, he said. “Sometimes they can be very confusing as to the underlying clinical picture. Ultrasound is being used frequently to better assess these complicated patients.”
Dr. Wagner said extensive training is required to use point-of-care ultrasound accurately.
Dr. Barchiesi also acknowledged that the devices used in this study were large portable machines, not the simpler and less expensive hand-held versions that are also available for similar purposes.
Point-of-care ultrasound is a promising innovation, said Thomas Melgar, MD, a professor of medicine at Western Michigan University, Kalamazoo. “The advantage is that the exam is being done by someone who knows the patient and specifically what they’re looking for. It’s done at the bedside so you don’t have to move the patient.”
The study could help address opposition to internal medicine residents being trained in the technique, he said, adding that “I think it’s very exciting.”
The study was partially supported by Philips, which provided the ultrasound devices. Dr. Barchiesi, Dr. Melgar, and Dr. Wagner disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
researchers say.
“It’s a safe and very useful tool,” Marco Barchiesi, MD, an internal medicine resident at Luigi Sacco Hospital in Milan, said in an interview. “We had a great reduction in chest x-rays because of the use of ultrasound.”
The finding addresses concerns that ultrasound used in primary care could consume more health care resources or put patients at risk.
Dr. Barchiesi and colleagues published their findings July 20 in the European Journal of Internal Medicine.
Point-of-care ultrasound has become increasingly common as miniaturization of devices has made them more portable. The approach has caught on particularly in emergency departments where quick decisions are of the essence.
Its use in internal medicine has been more controversial, with concerns raised that improperly trained practitioners may miss diagnoses or refer patients for unnecessary tests as a result of uncertainty about their findings.
To measure the effect of point-of-care ultrasound in an internal medicine hospital ward, Dr. Barchiesi and colleagues alternated months when point-of-care ultrasound was allowed with months when it was not allowed, for a total of 4 months each, on an internal medicine unit. They allowed the ultrasound to be used for invasive procedures and excluded patients whose critical condition made point-of-care ultrasound crucial.
The researchers analyzed data on 263 patients in the “on” months when point-of-care ultrasound was used, and 255 in the “off” months when it wasn’t used. The two groups were well balanced in age, sex, comorbidity, and clinical impairment.
During the on months, the internists ordered 113 diagnostic tests (0.43 per patient). During the off months they ordered 329 tests (1.29 per patient).
The odds of being referred for a chest x-ray were 87% less in the “on” months, compared with the off months, a statistically significant finding (P < .001). The risk for a chest CT scan and abdominal ultrasound were also reduced during the on months, but the risk for an abdominal CT was increased.
Nineteen patients died during the o” months and 10 during the off months, a difference that was not statistically significant (P = .15). The median length of stay in the hospital was almost the same for the two groups: 9 days for the on months and 9 days for the off months. The difference was also not statistically significant (P = .094).
Point-of-care ultrasound is particularly accurate in identifying cardiac abnormalities and pleural fluid and pneumonia, and it can be used effectively for monitoring heart conditions, the researchers wrote. This could explain the reduction in chest x-rays and CT scans.
On the other hand, ultrasound cannot address such questions as staging in an abdominal malignancy, and unexpected findings are more common with abdominal than chest ultrasound. This could explain why the point-of-care ultrasound did not reduce the use of abdominal CT, the researchers speculated.
They acknowledged that the patients in their sample had an average age of 81 years, raising questions about how well their data could be applied to a younger population. And they noted that they used point-of-care ultrasound frequently, so they were particularly adept with it. “We use it almost every day in our clinical practice,” said Dr. Barchiesi.
Those factors may have played a key role in the success of point-of-care ultrasound in this study, said Michael Wagner, MD, an assistant professor of medicine at the University of South Carolina, Greenville, who has helped colleagues incorporate ultrasound into their practices.
Elderly patients often present with multiple comorbidities and atypical signs and symptoms, he said. “Sometimes they can be very confusing as to the underlying clinical picture. Ultrasound is being used frequently to better assess these complicated patients.”
Dr. Wagner said extensive training is required to use point-of-care ultrasound accurately.
Dr. Barchiesi also acknowledged that the devices used in this study were large portable machines, not the simpler and less expensive hand-held versions that are also available for similar purposes.
Point-of-care ultrasound is a promising innovation, said Thomas Melgar, MD, a professor of medicine at Western Michigan University, Kalamazoo. “The advantage is that the exam is being done by someone who knows the patient and specifically what they’re looking for. It’s done at the bedside so you don’t have to move the patient.”
The study could help address opposition to internal medicine residents being trained in the technique, he said, adding that “I think it’s very exciting.”
The study was partially supported by Philips, which provided the ultrasound devices. Dr. Barchiesi, Dr. Melgar, and Dr. Wagner disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Ob.gyns. struggle to keep pace with changing COVID-19 knowledge
In early April, Maura Quinlan, MD, was working nights on the labor and delivery unit at Northwestern Medicine Prentice Women’s Hospital in Chicago. At the time, hospital policy was to test only patients with known COVID-19 symptoms for SARS-CoV-2. Women in labor wore N95 masks, but only while pushing – and practitioners didn’t always don proper protection in time.
Babies came and families rejoiced. But Dr. Quinlan looks back on those weeks with a degree of horror. “We were laboring a bunch of patients that probably had COVID,” she said, and they were doing so without proper protection.
She’s probably right. According to one study in the New England Journal of Medicine, 13.7% of 211 women who came into the labor and delivery unit at one New York City hospital between March 22 and April 2 were asymptomatic but infected, potentially putting staff and doctors at risk.
Dr. Quinlan already knew she and her fellow ob.gyns. had been walking a thin line and, upon seeing that research, her heart sank. In the middle of a pandemic, they had been racing to keep up with the reality of delivering babies. But despite their efforts to protect both practitioners and patients, some aspects slipped through the cracks. Today, every laboring patient admitted to Northwestern is now tested for the novel coronavirus.
Across the country, hospital labor and delivery wards have been working to find a careful and informed balance among multiple competing interests: the safety of their health care workers, the health of tiny and vulnerable new humans, and the stability of a birthing mother. Each hospital has been making the best decisions it can based on available data. The result is a patchwork of policies, but all of them center around rapid testing and appropriate protection.
Shifting recommendations
One case study of women in a New York City hospital during the height of the city’s surge found that, of seven confirmed COVID-19–positive patients, two were asymptomatic upon admission to the obstetrical service, and these same two patients ultimately required unplanned ICU admission. The women’s care prior to their positive diagnosis had exposed multiple health care workers, all of whom lacked appropriate personal protective equipment (PPE), the study authors wrote. “Further, five of seven confirmed COVID-19–positive women were afebrile on initial screen, and four did not first report a cough. In some locations where testing availability remains limited, the minimal symptoms reported for some of these cases might have been insufficient to prompt COVID-19 testing.”
As studies like this pour in, societies continue to update their recommendations accordingly. The latest guidance from the American College of Obstetricians and Gynecologists came on July 1. The group suggests testing all labor and delivery patients, particularly in high-prevalence areas. If tests are in short supply, it recommends prioritizing testing pregnant women with suspected COVID-19 and those who develop symptoms during admission.
At Northwestern, the hospital requests patients stay home and quarantine for the weeks leading up to their delivery date. Then, they rapidly test every patient who comes in for delivery and aim to have results available within a few hours.
The hospital’s 30-room labor and delivery wing remains reserved for patients who test negative. Those with positive COVID-19 results are sent to a 6-bed COVID labor and delivery unit elsewhere in the hospital. “We were lucky we had the space to do that, because smaller community hospitals wouldn’t have a separate unused unit where they could put these women,” Dr. Quinlan said.
In the COVID unit, women deliver without a support person – no partner, doula, or family member can join. Doctors and nurses wear full PPE and work only in that ward. And because some research shows that pregnant women who are asymptomatic or presymptomatic may develop symptoms quickly after starting labor with no measurable illness, Dr. Quinlan must decide on a case-by-case basis what to do, if anything at all.
Delaying an induction could allow the infection to resolve or it could result in her patient moving from presymptomatic disease to full-blown pneumonia. Accelerating labor could bring on symptoms or it could allow a mother to deliver safely and get out of the hospital as quickly as possible. “There is an advantage to having the baby now if you feel okay – even if it’s alone – and getting home,” Dr. Quinlan said.
The hospital also tests the partners of women who are COVID-19 positive. Those with negative results can take the newborn home and try to maintain distance until the mother is no longer symptomatic.
In different parts of the country, hospitals have developed different approaches. Southern California is experiencing its own surge, but at the Ronald Reagan University of California, Los Angeles, Medical Center there still haven’t been enough COVID-19 patients to warrant a separate labor and delivery unit.
At UCLA, staff swab patients when they enter the labor and delivery ward — those who test positive have specific room designations. For both COVID-19–positive patients and women who progress faster than test results can be returned, the goals are the same, said Rashmi Rao, MD, an ob.gyn. at UCLA: Deliver in the safest way possible for both mother and baby.
All women, positive or negative, must wear masks during labor – as much as they can tolerate, at least. For patients who are only mildly ill or asymptomatic, the only difference is that everyone wears protective gear. But if a patient’s oxygen levels dip, or her baby is in distress, the team moves more quickly to a cesarean delivery than they’d do with a healthy patient.
Just as hospital policies have been evolving, rules for visitors have been constantly changing too. Initially, UCLA allowed a support person to be present during delivery but had to leave immediately following. Now, each new mother is allowed one visitor for the duration of their stay. And the hospital suggests that patients who are COVID-19 positive recover in separate rooms from their babies and encourages them to maintain distance from their infants, except when breastfeeding.
“We respect and understand that this is a joyous occasion and we’re trying to keep families together as much as possible,” Dr. Rao said.
Care conundrums
How hospitals protect their smallest charges keeps changing too. Reports have been circulating about newborns being taken away from COVID-19-positive mothers, especially in marginalized communities. The stories have led many to worry they’d be forcibly separated from their babies. Most hospitals, however, leave it up to the woman and her doctors to decide how much separation is needed. “After delivery, it depends on how someone is feeling,” Dr. Rao said.
The American Academy of Pediatrics recommends that mothers who are COVID-19–positive pump breast milk and have a healthy caregiver use that milk, or formula, to bottle-feed the baby, with the new mother remaining 6 feet away from the child as much as she can. If that’s not possible, she should wear gloves and a mask while breastfeeding until she has been naturally afebrile for 72 hours and at least 1 week removed from the first appearance of her symptoms.
“It’s tragically hard,” said Dr. Quinlan, to keep a COVID-19–positive mother even 6 feet away from her newborn baby. “If a mother declines separation, we ask the acting pediatric team to discuss the theoretical risks and paucity of data.”
Until recently, research indicated that SARS-CoV-2 wasn’t being transmitted through the uterus from mothers to their babies. And despite a recent case study reporting transplacental transmission between a mother and her fetus in France, researchers still say that the risk of transference is low. To ensure newborn risk remains as low as possible, UCLA’s policy is to swab the baby when he/she is 24 hours old and keep watch for signs of infection: increased lethargy, difficulty waking, or gastrointestinal symptoms like vomiting.
Transmission via breast milk has also, to date, proven relatively unlikely. One study in The Lancet detected the novel coronavirus in breast milk, although it’s not clear that the virus can be passed on in the fluid, says Christina Chambers, PhD, a professor of pediatrics at the University of California, San Diego. Dr. Chambers is studying breast milk to see if the virus or antibodies to it are present. She is also investigating how infection with SARS-CoV-2 impacts women at different times in pregnancy, something that’s still an open question.
“[In] pregnant women with a deteriorating infection, the decisions are the same you would make with any delivery: Save the mom and save the baby,” Dr. Chambers said. “Beyond that, I am encouraged to see that pregnant women are prioritized to being tested,” something that will help researchers understand prevalence of disease in order to better understand whether some symptoms are more dangerous than others.
The situation is evolving so quickly that hospitals and providers are simply trying to stay abreast of the flood of new research. In the absence of definitive answers, they are using the information available and adjusting on the fly. “We are cautiously waiting for more data,” said Dr. Rao. “With the information we have we are doing the best we can to keep our patients safe. And we’re just going to keep at it.”
A version of this article originally appeared on Medscape.com.
In early April, Maura Quinlan, MD, was working nights on the labor and delivery unit at Northwestern Medicine Prentice Women’s Hospital in Chicago. At the time, hospital policy was to test only patients with known COVID-19 symptoms for SARS-CoV-2. Women in labor wore N95 masks, but only while pushing – and practitioners didn’t always don proper protection in time.
Babies came and families rejoiced. But Dr. Quinlan looks back on those weeks with a degree of horror. “We were laboring a bunch of patients that probably had COVID,” she said, and they were doing so without proper protection.
She’s probably right. According to one study in the New England Journal of Medicine, 13.7% of 211 women who came into the labor and delivery unit at one New York City hospital between March 22 and April 2 were asymptomatic but infected, potentially putting staff and doctors at risk.
Dr. Quinlan already knew she and her fellow ob.gyns. had been walking a thin line and, upon seeing that research, her heart sank. In the middle of a pandemic, they had been racing to keep up with the reality of delivering babies. But despite their efforts to protect both practitioners and patients, some aspects slipped through the cracks. Today, every laboring patient admitted to Northwestern is now tested for the novel coronavirus.
Across the country, hospital labor and delivery wards have been working to find a careful and informed balance among multiple competing interests: the safety of their health care workers, the health of tiny and vulnerable new humans, and the stability of a birthing mother. Each hospital has been making the best decisions it can based on available data. The result is a patchwork of policies, but all of them center around rapid testing and appropriate protection.
Shifting recommendations
One case study of women in a New York City hospital during the height of the city’s surge found that, of seven confirmed COVID-19–positive patients, two were asymptomatic upon admission to the obstetrical service, and these same two patients ultimately required unplanned ICU admission. The women’s care prior to their positive diagnosis had exposed multiple health care workers, all of whom lacked appropriate personal protective equipment (PPE), the study authors wrote. “Further, five of seven confirmed COVID-19–positive women were afebrile on initial screen, and four did not first report a cough. In some locations where testing availability remains limited, the minimal symptoms reported for some of these cases might have been insufficient to prompt COVID-19 testing.”
As studies like this pour in, societies continue to update their recommendations accordingly. The latest guidance from the American College of Obstetricians and Gynecologists came on July 1. The group suggests testing all labor and delivery patients, particularly in high-prevalence areas. If tests are in short supply, it recommends prioritizing testing pregnant women with suspected COVID-19 and those who develop symptoms during admission.
At Northwestern, the hospital requests patients stay home and quarantine for the weeks leading up to their delivery date. Then, they rapidly test every patient who comes in for delivery and aim to have results available within a few hours.
The hospital’s 30-room labor and delivery wing remains reserved for patients who test negative. Those with positive COVID-19 results are sent to a 6-bed COVID labor and delivery unit elsewhere in the hospital. “We were lucky we had the space to do that, because smaller community hospitals wouldn’t have a separate unused unit where they could put these women,” Dr. Quinlan said.
In the COVID unit, women deliver without a support person – no partner, doula, or family member can join. Doctors and nurses wear full PPE and work only in that ward. And because some research shows that pregnant women who are asymptomatic or presymptomatic may develop symptoms quickly after starting labor with no measurable illness, Dr. Quinlan must decide on a case-by-case basis what to do, if anything at all.
Delaying an induction could allow the infection to resolve or it could result in her patient moving from presymptomatic disease to full-blown pneumonia. Accelerating labor could bring on symptoms or it could allow a mother to deliver safely and get out of the hospital as quickly as possible. “There is an advantage to having the baby now if you feel okay – even if it’s alone – and getting home,” Dr. Quinlan said.
The hospital also tests the partners of women who are COVID-19 positive. Those with negative results can take the newborn home and try to maintain distance until the mother is no longer symptomatic.
In different parts of the country, hospitals have developed different approaches. Southern California is experiencing its own surge, but at the Ronald Reagan University of California, Los Angeles, Medical Center there still haven’t been enough COVID-19 patients to warrant a separate labor and delivery unit.
At UCLA, staff swab patients when they enter the labor and delivery ward — those who test positive have specific room designations. For both COVID-19–positive patients and women who progress faster than test results can be returned, the goals are the same, said Rashmi Rao, MD, an ob.gyn. at UCLA: Deliver in the safest way possible for both mother and baby.
All women, positive or negative, must wear masks during labor – as much as they can tolerate, at least. For patients who are only mildly ill or asymptomatic, the only difference is that everyone wears protective gear. But if a patient’s oxygen levels dip, or her baby is in distress, the team moves more quickly to a cesarean delivery than they’d do with a healthy patient.
Just as hospital policies have been evolving, rules for visitors have been constantly changing too. Initially, UCLA allowed a support person to be present during delivery but had to leave immediately following. Now, each new mother is allowed one visitor for the duration of their stay. And the hospital suggests that patients who are COVID-19 positive recover in separate rooms from their babies and encourages them to maintain distance from their infants, except when breastfeeding.
“We respect and understand that this is a joyous occasion and we’re trying to keep families together as much as possible,” Dr. Rao said.
Care conundrums
How hospitals protect their smallest charges keeps changing too. Reports have been circulating about newborns being taken away from COVID-19-positive mothers, especially in marginalized communities. The stories have led many to worry they’d be forcibly separated from their babies. Most hospitals, however, leave it up to the woman and her doctors to decide how much separation is needed. “After delivery, it depends on how someone is feeling,” Dr. Rao said.
The American Academy of Pediatrics recommends that mothers who are COVID-19–positive pump breast milk and have a healthy caregiver use that milk, or formula, to bottle-feed the baby, with the new mother remaining 6 feet away from the child as much as she can. If that’s not possible, she should wear gloves and a mask while breastfeeding until she has been naturally afebrile for 72 hours and at least 1 week removed from the first appearance of her symptoms.
“It’s tragically hard,” said Dr. Quinlan, to keep a COVID-19–positive mother even 6 feet away from her newborn baby. “If a mother declines separation, we ask the acting pediatric team to discuss the theoretical risks and paucity of data.”
Until recently, research indicated that SARS-CoV-2 wasn’t being transmitted through the uterus from mothers to their babies. And despite a recent case study reporting transplacental transmission between a mother and her fetus in France, researchers still say that the risk of transference is low. To ensure newborn risk remains as low as possible, UCLA’s policy is to swab the baby when he/she is 24 hours old and keep watch for signs of infection: increased lethargy, difficulty waking, or gastrointestinal symptoms like vomiting.
Transmission via breast milk has also, to date, proven relatively unlikely. One study in The Lancet detected the novel coronavirus in breast milk, although it’s not clear that the virus can be passed on in the fluid, says Christina Chambers, PhD, a professor of pediatrics at the University of California, San Diego. Dr. Chambers is studying breast milk to see if the virus or antibodies to it are present. She is also investigating how infection with SARS-CoV-2 impacts women at different times in pregnancy, something that’s still an open question.
“[In] pregnant women with a deteriorating infection, the decisions are the same you would make with any delivery: Save the mom and save the baby,” Dr. Chambers said. “Beyond that, I am encouraged to see that pregnant women are prioritized to being tested,” something that will help researchers understand prevalence of disease in order to better understand whether some symptoms are more dangerous than others.
The situation is evolving so quickly that hospitals and providers are simply trying to stay abreast of the flood of new research. In the absence of definitive answers, they are using the information available and adjusting on the fly. “We are cautiously waiting for more data,” said Dr. Rao. “With the information we have we are doing the best we can to keep our patients safe. And we’re just going to keep at it.”
A version of this article originally appeared on Medscape.com.
In early April, Maura Quinlan, MD, was working nights on the labor and delivery unit at Northwestern Medicine Prentice Women’s Hospital in Chicago. At the time, hospital policy was to test only patients with known COVID-19 symptoms for SARS-CoV-2. Women in labor wore N95 masks, but only while pushing – and practitioners didn’t always don proper protection in time.
Babies came and families rejoiced. But Dr. Quinlan looks back on those weeks with a degree of horror. “We were laboring a bunch of patients that probably had COVID,” she said, and they were doing so without proper protection.
She’s probably right. According to one study in the New England Journal of Medicine, 13.7% of 211 women who came into the labor and delivery unit at one New York City hospital between March 22 and April 2 were asymptomatic but infected, potentially putting staff and doctors at risk.
Dr. Quinlan already knew she and her fellow ob.gyns. had been walking a thin line and, upon seeing that research, her heart sank. In the middle of a pandemic, they had been racing to keep up with the reality of delivering babies. But despite their efforts to protect both practitioners and patients, some aspects slipped through the cracks. Today, every laboring patient admitted to Northwestern is now tested for the novel coronavirus.
Across the country, hospital labor and delivery wards have been working to find a careful and informed balance among multiple competing interests: the safety of their health care workers, the health of tiny and vulnerable new humans, and the stability of a birthing mother. Each hospital has been making the best decisions it can based on available data. The result is a patchwork of policies, but all of them center around rapid testing and appropriate protection.
Shifting recommendations
One case study of women in a New York City hospital during the height of the city’s surge found that, of seven confirmed COVID-19–positive patients, two were asymptomatic upon admission to the obstetrical service, and these same two patients ultimately required unplanned ICU admission. The women’s care prior to their positive diagnosis had exposed multiple health care workers, all of whom lacked appropriate personal protective equipment (PPE), the study authors wrote. “Further, five of seven confirmed COVID-19–positive women were afebrile on initial screen, and four did not first report a cough. In some locations where testing availability remains limited, the minimal symptoms reported for some of these cases might have been insufficient to prompt COVID-19 testing.”
As studies like this pour in, societies continue to update their recommendations accordingly. The latest guidance from the American College of Obstetricians and Gynecologists came on July 1. The group suggests testing all labor and delivery patients, particularly in high-prevalence areas. If tests are in short supply, it recommends prioritizing testing pregnant women with suspected COVID-19 and those who develop symptoms during admission.
At Northwestern, the hospital requests patients stay home and quarantine for the weeks leading up to their delivery date. Then, they rapidly test every patient who comes in for delivery and aim to have results available within a few hours.
The hospital’s 30-room labor and delivery wing remains reserved for patients who test negative. Those with positive COVID-19 results are sent to a 6-bed COVID labor and delivery unit elsewhere in the hospital. “We were lucky we had the space to do that, because smaller community hospitals wouldn’t have a separate unused unit where they could put these women,” Dr. Quinlan said.
In the COVID unit, women deliver without a support person – no partner, doula, or family member can join. Doctors and nurses wear full PPE and work only in that ward. And because some research shows that pregnant women who are asymptomatic or presymptomatic may develop symptoms quickly after starting labor with no measurable illness, Dr. Quinlan must decide on a case-by-case basis what to do, if anything at all.
Delaying an induction could allow the infection to resolve or it could result in her patient moving from presymptomatic disease to full-blown pneumonia. Accelerating labor could bring on symptoms or it could allow a mother to deliver safely and get out of the hospital as quickly as possible. “There is an advantage to having the baby now if you feel okay – even if it’s alone – and getting home,” Dr. Quinlan said.
The hospital also tests the partners of women who are COVID-19 positive. Those with negative results can take the newborn home and try to maintain distance until the mother is no longer symptomatic.
In different parts of the country, hospitals have developed different approaches. Southern California is experiencing its own surge, but at the Ronald Reagan University of California, Los Angeles, Medical Center there still haven’t been enough COVID-19 patients to warrant a separate labor and delivery unit.
At UCLA, staff swab patients when they enter the labor and delivery ward — those who test positive have specific room designations. For both COVID-19–positive patients and women who progress faster than test results can be returned, the goals are the same, said Rashmi Rao, MD, an ob.gyn. at UCLA: Deliver in the safest way possible for both mother and baby.
All women, positive or negative, must wear masks during labor – as much as they can tolerate, at least. For patients who are only mildly ill or asymptomatic, the only difference is that everyone wears protective gear. But if a patient’s oxygen levels dip, or her baby is in distress, the team moves more quickly to a cesarean delivery than they’d do with a healthy patient.
Just as hospital policies have been evolving, rules for visitors have been constantly changing too. Initially, UCLA allowed a support person to be present during delivery but had to leave immediately following. Now, each new mother is allowed one visitor for the duration of their stay. And the hospital suggests that patients who are COVID-19 positive recover in separate rooms from their babies and encourages them to maintain distance from their infants, except when breastfeeding.
“We respect and understand that this is a joyous occasion and we’re trying to keep families together as much as possible,” Dr. Rao said.
Care conundrums
How hospitals protect their smallest charges keeps changing too. Reports have been circulating about newborns being taken away from COVID-19-positive mothers, especially in marginalized communities. The stories have led many to worry they’d be forcibly separated from their babies. Most hospitals, however, leave it up to the woman and her doctors to decide how much separation is needed. “After delivery, it depends on how someone is feeling,” Dr. Rao said.
The American Academy of Pediatrics recommends that mothers who are COVID-19–positive pump breast milk and have a healthy caregiver use that milk, or formula, to bottle-feed the baby, with the new mother remaining 6 feet away from the child as much as she can. If that’s not possible, she should wear gloves and a mask while breastfeeding until she has been naturally afebrile for 72 hours and at least 1 week removed from the first appearance of her symptoms.
“It’s tragically hard,” said Dr. Quinlan, to keep a COVID-19–positive mother even 6 feet away from her newborn baby. “If a mother declines separation, we ask the acting pediatric team to discuss the theoretical risks and paucity of data.”
Until recently, research indicated that SARS-CoV-2 wasn’t being transmitted through the uterus from mothers to their babies. And despite a recent case study reporting transplacental transmission between a mother and her fetus in France, researchers still say that the risk of transference is low. To ensure newborn risk remains as low as possible, UCLA’s policy is to swab the baby when he/she is 24 hours old and keep watch for signs of infection: increased lethargy, difficulty waking, or gastrointestinal symptoms like vomiting.
Transmission via breast milk has also, to date, proven relatively unlikely. One study in The Lancet detected the novel coronavirus in breast milk, although it’s not clear that the virus can be passed on in the fluid, says Christina Chambers, PhD, a professor of pediatrics at the University of California, San Diego. Dr. Chambers is studying breast milk to see if the virus or antibodies to it are present. She is also investigating how infection with SARS-CoV-2 impacts women at different times in pregnancy, something that’s still an open question.
“[In] pregnant women with a deteriorating infection, the decisions are the same you would make with any delivery: Save the mom and save the baby,” Dr. Chambers said. “Beyond that, I am encouraged to see that pregnant women are prioritized to being tested,” something that will help researchers understand prevalence of disease in order to better understand whether some symptoms are more dangerous than others.
The situation is evolving so quickly that hospitals and providers are simply trying to stay abreast of the flood of new research. In the absence of definitive answers, they are using the information available and adjusting on the fly. “We are cautiously waiting for more data,” said Dr. Rao. “With the information we have we are doing the best we can to keep our patients safe. And we’re just going to keep at it.”
A version of this article originally appeared on Medscape.com.
Survey: Most FPs live at or below their means
a Medscape survey has found.
According to the Medscape Family Physician Debt and Net Worth Report 2020, almost half of FPs (46%) reported having that amount as their net worth, compared with the 18% of gastroenterologists and 19% of urologists who fell into that category.
And whereas 19% of orthopedists reported at least $5 million in net worth, only 3% of FPs did.
A third are paying off student loans
FPs were also more likely, along with physical medicine and rehabilitation physicians, at 34%, to report that they are continuing to pay off student loans. Conversely, 14% of gastroenterologists and 15% of nephrologists and rheumatologists said they were still paying off the loans.
Student loan debt was third on the list for FPs. Two-thirds of FPs were paying off a mortgage, and 41% had car loan payments.
Overall, FPs appear to manage their finances well and are living within their means. Only 6% of FPs said they live above their means, whereas 51% said they live at their means, and 42% said they live below that threshold.
Joel Greenwald, MD, CEO of Greenwald Wealth Management in St. Louis Park, Minn., said in an interview he recommends saving 20% of gross salary each year.
The survey was completed before Feb. 11 and before the financial effects of the COVID-19 pandemic could be known. The report is based on responses from more than 17,000 physicians across 30 specialties.
A lower level of net worth among FPs corresponds with their being close to the bottom among physicians in compensation. They made $234,000 on average, according to the report. By contrast, orthopedists made more than twice as much, at $511,000.
Smaller homes, less mortgage debt
FPs were among the least likely to indicate that they had a home of more than 5,000 square feet. That was true for only 6% of FPs; it was true for 22% of plastic surgeons and orthopedists. Most (61%) lived in dwellings of 3,000 square feet or less.
At the same time, FPs reported smaller mortgages than many of their colleagues.
Nearly half (49%) of FPs have mortgages of $300,000 or less; 26% have no mortgage at all. That figure was much higher than the 37% of physicians overall who had mortgages of $300,000 or less, although almost the same percentage had no mortgage at all.
Most had no financial loss in the past year
In further good news, most FPs (70%) said they did not experience a financial loss in the past year. Of those who did experience a loss, the top reasons were problems with their practice, such as reimbursement changes or changes in practice situations, or bad investments.
FPs socked away more into tax-deferred than taxable accounts, the survey showed.
More than half (54%) of FPs put at least $1,000 into tax-deferred accounts, such as college savings or retirement accounts, although 14% said they do not regularly contribute to such accounts.
Fewer (29%) contributed at least $1,000 to a taxable account.
As for who pays the day-to-day bills in households, 56% of FPs said they pool resources with a spouse or partner and pay bills from a common fund. Only 4% split the bills equally, no matter the income difference. One in four said they do not have joint finances with a spouse or partner.
FPs were divided as to whether they are currently working with a financial planner (38%) or had not worked with one (37%); the remainder said they had met with or used one in the past.
A version of this article originally appeared on Medscape.com.
a Medscape survey has found.
According to the Medscape Family Physician Debt and Net Worth Report 2020, almost half of FPs (46%) reported having that amount as their net worth, compared with the 18% of gastroenterologists and 19% of urologists who fell into that category.
And whereas 19% of orthopedists reported at least $5 million in net worth, only 3% of FPs did.
A third are paying off student loans
FPs were also more likely, along with physical medicine and rehabilitation physicians, at 34%, to report that they are continuing to pay off student loans. Conversely, 14% of gastroenterologists and 15% of nephrologists and rheumatologists said they were still paying off the loans.
Student loan debt was third on the list for FPs. Two-thirds of FPs were paying off a mortgage, and 41% had car loan payments.
Overall, FPs appear to manage their finances well and are living within their means. Only 6% of FPs said they live above their means, whereas 51% said they live at their means, and 42% said they live below that threshold.
Joel Greenwald, MD, CEO of Greenwald Wealth Management in St. Louis Park, Minn., said in an interview he recommends saving 20% of gross salary each year.
The survey was completed before Feb. 11 and before the financial effects of the COVID-19 pandemic could be known. The report is based on responses from more than 17,000 physicians across 30 specialties.
A lower level of net worth among FPs corresponds with their being close to the bottom among physicians in compensation. They made $234,000 on average, according to the report. By contrast, orthopedists made more than twice as much, at $511,000.
Smaller homes, less mortgage debt
FPs were among the least likely to indicate that they had a home of more than 5,000 square feet. That was true for only 6% of FPs; it was true for 22% of plastic surgeons and orthopedists. Most (61%) lived in dwellings of 3,000 square feet or less.
At the same time, FPs reported smaller mortgages than many of their colleagues.
Nearly half (49%) of FPs have mortgages of $300,000 or less; 26% have no mortgage at all. That figure was much higher than the 37% of physicians overall who had mortgages of $300,000 or less, although almost the same percentage had no mortgage at all.
Most had no financial loss in the past year
In further good news, most FPs (70%) said they did not experience a financial loss in the past year. Of those who did experience a loss, the top reasons were problems with their practice, such as reimbursement changes or changes in practice situations, or bad investments.
FPs socked away more into tax-deferred than taxable accounts, the survey showed.
More than half (54%) of FPs put at least $1,000 into tax-deferred accounts, such as college savings or retirement accounts, although 14% said they do not regularly contribute to such accounts.
Fewer (29%) contributed at least $1,000 to a taxable account.
As for who pays the day-to-day bills in households, 56% of FPs said they pool resources with a spouse or partner and pay bills from a common fund. Only 4% split the bills equally, no matter the income difference. One in four said they do not have joint finances with a spouse or partner.
FPs were divided as to whether they are currently working with a financial planner (38%) or had not worked with one (37%); the remainder said they had met with or used one in the past.
A version of this article originally appeared on Medscape.com.
a Medscape survey has found.
According to the Medscape Family Physician Debt and Net Worth Report 2020, almost half of FPs (46%) reported having that amount as their net worth, compared with the 18% of gastroenterologists and 19% of urologists who fell into that category.
And whereas 19% of orthopedists reported at least $5 million in net worth, only 3% of FPs did.
A third are paying off student loans
FPs were also more likely, along with physical medicine and rehabilitation physicians, at 34%, to report that they are continuing to pay off student loans. Conversely, 14% of gastroenterologists and 15% of nephrologists and rheumatologists said they were still paying off the loans.
Student loan debt was third on the list for FPs. Two-thirds of FPs were paying off a mortgage, and 41% had car loan payments.
Overall, FPs appear to manage their finances well and are living within their means. Only 6% of FPs said they live above their means, whereas 51% said they live at their means, and 42% said they live below that threshold.
Joel Greenwald, MD, CEO of Greenwald Wealth Management in St. Louis Park, Minn., said in an interview he recommends saving 20% of gross salary each year.
The survey was completed before Feb. 11 and before the financial effects of the COVID-19 pandemic could be known. The report is based on responses from more than 17,000 physicians across 30 specialties.
A lower level of net worth among FPs corresponds with their being close to the bottom among physicians in compensation. They made $234,000 on average, according to the report. By contrast, orthopedists made more than twice as much, at $511,000.
Smaller homes, less mortgage debt
FPs were among the least likely to indicate that they had a home of more than 5,000 square feet. That was true for only 6% of FPs; it was true for 22% of plastic surgeons and orthopedists. Most (61%) lived in dwellings of 3,000 square feet or less.
At the same time, FPs reported smaller mortgages than many of their colleagues.
Nearly half (49%) of FPs have mortgages of $300,000 or less; 26% have no mortgage at all. That figure was much higher than the 37% of physicians overall who had mortgages of $300,000 or less, although almost the same percentage had no mortgage at all.
Most had no financial loss in the past year
In further good news, most FPs (70%) said they did not experience a financial loss in the past year. Of those who did experience a loss, the top reasons were problems with their practice, such as reimbursement changes or changes in practice situations, or bad investments.
FPs socked away more into tax-deferred than taxable accounts, the survey showed.
More than half (54%) of FPs put at least $1,000 into tax-deferred accounts, such as college savings or retirement accounts, although 14% said they do not regularly contribute to such accounts.
Fewer (29%) contributed at least $1,000 to a taxable account.
As for who pays the day-to-day bills in households, 56% of FPs said they pool resources with a spouse or partner and pay bills from a common fund. Only 4% split the bills equally, no matter the income difference. One in four said they do not have joint finances with a spouse or partner.
FPs were divided as to whether they are currently working with a financial planner (38%) or had not worked with one (37%); the remainder said they had met with or used one in the past.
A version of this article originally appeared on Medscape.com.