User login
New road map for CRC screening: Use more stool tests, says AGA
where the default screening modality to date has been colonoscopy.
Instead, the American Gastroenterological Association is proposing new approaches that combine better risk assessment, more use of noninvasive testing (such as fecal occult blood tests), and more targeted referrals for colonoscopy. Such changes could increase patient compliance and “save countless lives.”
“We need to improve our strategies to curb the cancer that ranks second for deaths in the U.S.,” commented Srinadh Komanduri, MD, chair of the AGA Center for GI Innovation and Technology, in a statement.
“Approximately 67% of eligible Americans are screened for colorectal cancer,” he said, which means that a third (33%) are not.
During the COVID-19 pandemic, the proportion of individuals not being screened has increased. One report of medical claims data showed that colonoscopies dropped by 90% during April.
The proposed changes are outlined in an AGA white paper: “Roadmap for the Future of Colorectal Cancer Screening in the United States.”
The report, written following consultation with 60 gastroenterology and research experts, was published online in Clinical Gastroenterology and Hepatology.
It proposed that alternative testing modalities to colonoscopy will need to be integrated into organized screening programs.
Rather than offering colonoscopy as the default screening method for all patients at risk, the AGA advised that it be offered initially only to patients at high risk, which would increase access for those who need it most. For patients at lower risk, noninvasive screening methods, such as fecal occult blood testing, could be offered initially and then integrated with colonoscopy.
“If we offered tests that were convenient, accurate, and of lower cost, and we could help people choose the best option based on their individual cancer risks, we would save more lives,” Joshua E. Melson, MD, MPH, lead author of the AGA white paper and professor at Rush University Medical Center, Chicago, said in an interview.
Screening can reduce CRC mortality by more than 50%, he added.
“Screening should be thought of as a process over time, not a single test isolated in time,” Dr. Melson commented. A clinical practice that has historically used only colonoscopy will need an organized, structured program to incorporate noninvasive testing, he said.
To date, efforts to increase CRC screening uptake have met with limited success, the AGA says. In 2014, the National Colorectal Cancer Round Table set the bar high with a 2018 screening goal of 80% for adults 50 years of age and older. As of 2020, some states had almost reached this goal, but most had not.
“In the opportunistic screening environment in the U.S., where colonoscopy is the most prevalent method, CRC screening has not reached aspirational goals in terms of uptake, reduction in CRC incidence, and disease burden,” the AGA said. “It is questionable if 80% uptake is achievable in a primarily opportunistic screening environment.”
In the proposed revamping of the current CRC screening infrastructure, patients whose physicians recommend CRC screening would no longer be left to their own devices to follow up. Clinicians would initiate CRC screening and oversee follow-up testing at defined intervals and would employ ongoing surveillance.
Ensuring that appropriate screening is readily available to at-risk individuals with no social, racial, or economic disparities is crucial, the AGA says. Racial disparities in access to screening disproportionately burden Blacks and Latin Americans as well as people living in rural areas. Screening differences account for 42% of the disparity in CRC incidence between Black and White Americans and 19% of the disparity in CRC mortality.
Compared with colonoscopy, which requires bowel preparation, time off from work, and a hospital or clinic procedure, the fecal immunochemical test (FIT), for which a patient provides stool samples that are examined for the presence of blood, is much less stressful: it is noninvasive, and the patients collect the samples themselves in their own home. Studies show that, in diverse environments, patients prefer FIT over colonoscopy.
In a controlled trial that involved more than 55,000 patients who were randomly assigned to undergo either FIT or colonoscopy, the participation rate in the first cycle was greater for FIT than for colonoscopy (34.2% vs. 24.6%). This partially offset the lower single-application sensitivity for CRC of FIT, the researchers said.
Results from a study with a cluster randomized design showed that offering up-front stool testing as an option in addition to colonoscopy increased screening uptake. Of patients offered fecal occult blood testing or colonoscopy, 69% completed the noninvasive screening, compared with 38% of those offered colonoscopy alone. Notably, non-White participants were more adherent to stool testing.
The success of the AGA’s new initiative hinges largely upon the development of affordable, highly accurate, easy-to-use, noninvasive tests. In this regard, the organization has challenged scientists and industry partners with an aspirational target that is “far superior to current methodologies in terms of sensitivity and specificity,” said Dr. Melson, who is associate professor at Rush Medical College, Chicago, and a member of the AGA Center for GI Innovation and Technology.
The AGA wants new CRC screening tests that are capable of detecting advanced adenomas and advanced serrated lesions with a one-time sensitivity and specificity of 90% or higher, which is comparable with colonoscopy.
The FIT test has a sensitivity of less than 50% for detecting an advanced polyp of 10 mm or larger, said Dr. Melson.
The multitarget stool DNA (MT-sDNA) test may offer some improvement.
In a 2014 pivotal trial that compared FIT with the MT-sDNA in patients at average risk, the MT-sDNA test had higher sensitivity for detecting nonadvanced CRC lesions than FIT (92% vs. 74%) but less specificity (87% vs. 95%). The rate of detection of polyps with high-grade dysplasia was 69.2% with DNA testing and 46.2% with FIT.
However, the MT-sDNA test costs more than $500, compared with $25 for the FIT test, Dr. Melson pointed out.
To help identify the most appropriate screening for individual patients, better understanding and more thorough identification of risk factors are needed. “Risk assessment is definitely not where it could be,” Dr. Melson said.
The accuracy of risk assessment can be improved by sharing information from electronic health records on past colonoscopy polyp data, the presence of molecular markers, and family history, the AGA said. “With clearer risk assessment, shared decision-making on the most appropriate test becomes more clear and screening rates would benefit from patient buy-in and from easier access.”
The AGA recommended that research focus on the cost-effectiveness of screening younger patients, because the proportion of CRC cases in adults aged younger than 50 years has doubled since 1990.
This has raised the question as to whether the age for initial CRC screening should be lowered to 45 years (it already has been by the American Cancer Society), but there is much debate over this move.
Dr. Melson has received consulting fees from Clinical Genomics and research support from Boston Scientific Corporation and holds stocks in Virgo Imaging. A number of AGA white paper coauthors have disclosed relevant financial relationships.
A version of this article originally appeared on Medscape.com.
where the default screening modality to date has been colonoscopy.
Instead, the American Gastroenterological Association is proposing new approaches that combine better risk assessment, more use of noninvasive testing (such as fecal occult blood tests), and more targeted referrals for colonoscopy. Such changes could increase patient compliance and “save countless lives.”
“We need to improve our strategies to curb the cancer that ranks second for deaths in the U.S.,” commented Srinadh Komanduri, MD, chair of the AGA Center for GI Innovation and Technology, in a statement.
“Approximately 67% of eligible Americans are screened for colorectal cancer,” he said, which means that a third (33%) are not.
During the COVID-19 pandemic, the proportion of individuals not being screened has increased. One report of medical claims data showed that colonoscopies dropped by 90% during April.
The proposed changes are outlined in an AGA white paper: “Roadmap for the Future of Colorectal Cancer Screening in the United States.”
The report, written following consultation with 60 gastroenterology and research experts, was published online in Clinical Gastroenterology and Hepatology.
It proposed that alternative testing modalities to colonoscopy will need to be integrated into organized screening programs.
Rather than offering colonoscopy as the default screening method for all patients at risk, the AGA advised that it be offered initially only to patients at high risk, which would increase access for those who need it most. For patients at lower risk, noninvasive screening methods, such as fecal occult blood testing, could be offered initially and then integrated with colonoscopy.
“If we offered tests that were convenient, accurate, and of lower cost, and we could help people choose the best option based on their individual cancer risks, we would save more lives,” Joshua E. Melson, MD, MPH, lead author of the AGA white paper and professor at Rush University Medical Center, Chicago, said in an interview.
Screening can reduce CRC mortality by more than 50%, he added.
“Screening should be thought of as a process over time, not a single test isolated in time,” Dr. Melson commented. A clinical practice that has historically used only colonoscopy will need an organized, structured program to incorporate noninvasive testing, he said.
To date, efforts to increase CRC screening uptake have met with limited success, the AGA says. In 2014, the National Colorectal Cancer Round Table set the bar high with a 2018 screening goal of 80% for adults 50 years of age and older. As of 2020, some states had almost reached this goal, but most had not.
“In the opportunistic screening environment in the U.S., where colonoscopy is the most prevalent method, CRC screening has not reached aspirational goals in terms of uptake, reduction in CRC incidence, and disease burden,” the AGA said. “It is questionable if 80% uptake is achievable in a primarily opportunistic screening environment.”
In the proposed revamping of the current CRC screening infrastructure, patients whose physicians recommend CRC screening would no longer be left to their own devices to follow up. Clinicians would initiate CRC screening and oversee follow-up testing at defined intervals and would employ ongoing surveillance.
Ensuring that appropriate screening is readily available to at-risk individuals with no social, racial, or economic disparities is crucial, the AGA says. Racial disparities in access to screening disproportionately burden Blacks and Latin Americans as well as people living in rural areas. Screening differences account for 42% of the disparity in CRC incidence between Black and White Americans and 19% of the disparity in CRC mortality.
Compared with colonoscopy, which requires bowel preparation, time off from work, and a hospital or clinic procedure, the fecal immunochemical test (FIT), for which a patient provides stool samples that are examined for the presence of blood, is much less stressful: it is noninvasive, and the patients collect the samples themselves in their own home. Studies show that, in diverse environments, patients prefer FIT over colonoscopy.
In a controlled trial that involved more than 55,000 patients who were randomly assigned to undergo either FIT or colonoscopy, the participation rate in the first cycle was greater for FIT than for colonoscopy (34.2% vs. 24.6%). This partially offset the lower single-application sensitivity for CRC of FIT, the researchers said.
Results from a study with a cluster randomized design showed that offering up-front stool testing as an option in addition to colonoscopy increased screening uptake. Of patients offered fecal occult blood testing or colonoscopy, 69% completed the noninvasive screening, compared with 38% of those offered colonoscopy alone. Notably, non-White participants were more adherent to stool testing.
The success of the AGA’s new initiative hinges largely upon the development of affordable, highly accurate, easy-to-use, noninvasive tests. In this regard, the organization has challenged scientists and industry partners with an aspirational target that is “far superior to current methodologies in terms of sensitivity and specificity,” said Dr. Melson, who is associate professor at Rush Medical College, Chicago, and a member of the AGA Center for GI Innovation and Technology.
The AGA wants new CRC screening tests that are capable of detecting advanced adenomas and advanced serrated lesions with a one-time sensitivity and specificity of 90% or higher, which is comparable with colonoscopy.
The FIT test has a sensitivity of less than 50% for detecting an advanced polyp of 10 mm or larger, said Dr. Melson.
The multitarget stool DNA (MT-sDNA) test may offer some improvement.
In a 2014 pivotal trial that compared FIT with the MT-sDNA in patients at average risk, the MT-sDNA test had higher sensitivity for detecting nonadvanced CRC lesions than FIT (92% vs. 74%) but less specificity (87% vs. 95%). The rate of detection of polyps with high-grade dysplasia was 69.2% with DNA testing and 46.2% with FIT.
However, the MT-sDNA test costs more than $500, compared with $25 for the FIT test, Dr. Melson pointed out.
To help identify the most appropriate screening for individual patients, better understanding and more thorough identification of risk factors are needed. “Risk assessment is definitely not where it could be,” Dr. Melson said.
The accuracy of risk assessment can be improved by sharing information from electronic health records on past colonoscopy polyp data, the presence of molecular markers, and family history, the AGA said. “With clearer risk assessment, shared decision-making on the most appropriate test becomes more clear and screening rates would benefit from patient buy-in and from easier access.”
The AGA recommended that research focus on the cost-effectiveness of screening younger patients, because the proportion of CRC cases in adults aged younger than 50 years has doubled since 1990.
This has raised the question as to whether the age for initial CRC screening should be lowered to 45 years (it already has been by the American Cancer Society), but there is much debate over this move.
Dr. Melson has received consulting fees from Clinical Genomics and research support from Boston Scientific Corporation and holds stocks in Virgo Imaging. A number of AGA white paper coauthors have disclosed relevant financial relationships.
A version of this article originally appeared on Medscape.com.
where the default screening modality to date has been colonoscopy.
Instead, the American Gastroenterological Association is proposing new approaches that combine better risk assessment, more use of noninvasive testing (such as fecal occult blood tests), and more targeted referrals for colonoscopy. Such changes could increase patient compliance and “save countless lives.”
“We need to improve our strategies to curb the cancer that ranks second for deaths in the U.S.,” commented Srinadh Komanduri, MD, chair of the AGA Center for GI Innovation and Technology, in a statement.
“Approximately 67% of eligible Americans are screened for colorectal cancer,” he said, which means that a third (33%) are not.
During the COVID-19 pandemic, the proportion of individuals not being screened has increased. One report of medical claims data showed that colonoscopies dropped by 90% during April.
The proposed changes are outlined in an AGA white paper: “Roadmap for the Future of Colorectal Cancer Screening in the United States.”
The report, written following consultation with 60 gastroenterology and research experts, was published online in Clinical Gastroenterology and Hepatology.
It proposed that alternative testing modalities to colonoscopy will need to be integrated into organized screening programs.
Rather than offering colonoscopy as the default screening method for all patients at risk, the AGA advised that it be offered initially only to patients at high risk, which would increase access for those who need it most. For patients at lower risk, noninvasive screening methods, such as fecal occult blood testing, could be offered initially and then integrated with colonoscopy.
“If we offered tests that were convenient, accurate, and of lower cost, and we could help people choose the best option based on their individual cancer risks, we would save more lives,” Joshua E. Melson, MD, MPH, lead author of the AGA white paper and professor at Rush University Medical Center, Chicago, said in an interview.
Screening can reduce CRC mortality by more than 50%, he added.
“Screening should be thought of as a process over time, not a single test isolated in time,” Dr. Melson commented. A clinical practice that has historically used only colonoscopy will need an organized, structured program to incorporate noninvasive testing, he said.
To date, efforts to increase CRC screening uptake have met with limited success, the AGA says. In 2014, the National Colorectal Cancer Round Table set the bar high with a 2018 screening goal of 80% for adults 50 years of age and older. As of 2020, some states had almost reached this goal, but most had not.
“In the opportunistic screening environment in the U.S., where colonoscopy is the most prevalent method, CRC screening has not reached aspirational goals in terms of uptake, reduction in CRC incidence, and disease burden,” the AGA said. “It is questionable if 80% uptake is achievable in a primarily opportunistic screening environment.”
In the proposed revamping of the current CRC screening infrastructure, patients whose physicians recommend CRC screening would no longer be left to their own devices to follow up. Clinicians would initiate CRC screening and oversee follow-up testing at defined intervals and would employ ongoing surveillance.
Ensuring that appropriate screening is readily available to at-risk individuals with no social, racial, or economic disparities is crucial, the AGA says. Racial disparities in access to screening disproportionately burden Blacks and Latin Americans as well as people living in rural areas. Screening differences account for 42% of the disparity in CRC incidence between Black and White Americans and 19% of the disparity in CRC mortality.
Compared with colonoscopy, which requires bowel preparation, time off from work, and a hospital or clinic procedure, the fecal immunochemical test (FIT), for which a patient provides stool samples that are examined for the presence of blood, is much less stressful: it is noninvasive, and the patients collect the samples themselves in their own home. Studies show that, in diverse environments, patients prefer FIT over colonoscopy.
In a controlled trial that involved more than 55,000 patients who were randomly assigned to undergo either FIT or colonoscopy, the participation rate in the first cycle was greater for FIT than for colonoscopy (34.2% vs. 24.6%). This partially offset the lower single-application sensitivity for CRC of FIT, the researchers said.
Results from a study with a cluster randomized design showed that offering up-front stool testing as an option in addition to colonoscopy increased screening uptake. Of patients offered fecal occult blood testing or colonoscopy, 69% completed the noninvasive screening, compared with 38% of those offered colonoscopy alone. Notably, non-White participants were more adherent to stool testing.
The success of the AGA’s new initiative hinges largely upon the development of affordable, highly accurate, easy-to-use, noninvasive tests. In this regard, the organization has challenged scientists and industry partners with an aspirational target that is “far superior to current methodologies in terms of sensitivity and specificity,” said Dr. Melson, who is associate professor at Rush Medical College, Chicago, and a member of the AGA Center for GI Innovation and Technology.
The AGA wants new CRC screening tests that are capable of detecting advanced adenomas and advanced serrated lesions with a one-time sensitivity and specificity of 90% or higher, which is comparable with colonoscopy.
The FIT test has a sensitivity of less than 50% for detecting an advanced polyp of 10 mm or larger, said Dr. Melson.
The multitarget stool DNA (MT-sDNA) test may offer some improvement.
In a 2014 pivotal trial that compared FIT with the MT-sDNA in patients at average risk, the MT-sDNA test had higher sensitivity for detecting nonadvanced CRC lesions than FIT (92% vs. 74%) but less specificity (87% vs. 95%). The rate of detection of polyps with high-grade dysplasia was 69.2% with DNA testing and 46.2% with FIT.
However, the MT-sDNA test costs more than $500, compared with $25 for the FIT test, Dr. Melson pointed out.
To help identify the most appropriate screening for individual patients, better understanding and more thorough identification of risk factors are needed. “Risk assessment is definitely not where it could be,” Dr. Melson said.
The accuracy of risk assessment can be improved by sharing information from electronic health records on past colonoscopy polyp data, the presence of molecular markers, and family history, the AGA said. “With clearer risk assessment, shared decision-making on the most appropriate test becomes more clear and screening rates would benefit from patient buy-in and from easier access.”
The AGA recommended that research focus on the cost-effectiveness of screening younger patients, because the proportion of CRC cases in adults aged younger than 50 years has doubled since 1990.
This has raised the question as to whether the age for initial CRC screening should be lowered to 45 years (it already has been by the American Cancer Society), but there is much debate over this move.
Dr. Melson has received consulting fees from Clinical Genomics and research support from Boston Scientific Corporation and holds stocks in Virgo Imaging. A number of AGA white paper coauthors have disclosed relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Telemedicine meets menopause in customized patient care service
Women facing issues related to perimenopause and menopause can consult their primary care physicians or ob.gyns. through telemedicine visits, but
The Cusp doesn’t claim to replace routine gynecologic care. Rather, it focuses on perimenopause and menopause symptoms specifically, and states that its physicians, some of whom are certified by the North American Menopause Society, provide expertise in menopause beyond what patients might receive as part of a typical ob.gyn. visit.
The Cusp is a for-profit organization, a group of physicians, nurse practitioners, and technologists who focus on integrated care for women in perimenopause and beyond. The aim is to leverage technology as a way to connect women to the care platform to book physician and nurse practitioner visits virtually and to have all of the information about their care centralized in one place.
According to the website, most patients who sign up for a care plan check in with their providers at least once a month to monitor their symptoms and tweak treatment strategies. Patients who sign up are prompted to download an app, which then becomes the main tool for scheduling future visits, tracking symptoms, and communicating with providers.

The Cusp launched in early 2019, before the advent of the COVID-19 pandemic, but the pandemic has accelerated the acceptance across medical specialties, suggesting that telemedicine is here to stay, according to Mindy Goldman, MD, professor of gynecology and gynecologic surgery at the University of California, San Francisco, and director of the Gynecology Center for Cancer Survivors and At-Risk Women at UCSF, who also serves as a medical adviser to the Cusp.
Partnering with technology companies allows opportunities to provide care in areas where there are gaps, such as menopause management, she said. Many clinicians in primary care and ob.gyn. care don’t have the time or training to discuss menopause management in depth with patients, and patient interviews conducted by the Cusp before launching the site showed that this was an area of need.
“One thing that is really unique about the Cusp is that we brought together experts to provide care in both in an evidence-based and holistic fashion,” Dr. Goldman emphasized.
The Cusp’s medical team includes physician and nurse practitioner menopause experts with backgrounds including not only ob.gyn. but also psychiatry, integrative medicine, and naturopathic medicine, with plans to add endocrinology and dermatology as well. This holistic approach allows the Cusp to tailor care based on what each woman is looking for, with evidence-based expertise to support treatment decisions, said Dr. Goldman, whose advisory role includes helping to develop patient treatment protocols and services.
If a woman wants to begin treating symptoms with a naturopathic approach, the team will provide protocols that take current guidelines into account. Regular visits, approximately once a month or as needed, allow for collaboration with the Cusp’s specialists to provide consistent care that is very comprehensive, she said.
One of the benefits of the Cusp is the opportunity for “frequent touchpoints” in which providers reach out to patients via text, email, or video. Although a traditional medical visit may include some initial discussion of menopause and treatment plans, the Cusp offers “a more seamless way to address needs on an ongoing basis,” to provide more complete patient care, Dr. Goldman said.
“We are constantly asking women what they are looking for in menopause care,” and a recurring question was about hormone testing, she said. Nontraditional practitioners may offer hormone testing as a way of individualizing care that also involves compounded formulations, and other treatments that are not standard of care. “In all of our protocols we follow what is recommended by standard organizations such as ACOG [American College of Obstetricians and Gynecologists] and NAMS.”
The Cusp’s newest service is an at-home hormone test currently for women in New York and California, but the company plans to expand this service. The hormone test, while not essential, is another tool to guide menopause management, and having a sense of when menopause will occur “gives us a chance to talk to people about behavioral changes and time to personalize a treatment protocol,” Dr. Goldman said.
The test is based in part on the anti-Müllerian hormone, which recent studies have shown is useful in predicting time to menopause. This, in combination with other hormone tests and other clinical information, will allow the Cusp’s menopause specialists to help women in perimenopause gain perspective on their symptoms and design a treatment plan that can evolve as their needs change, she explained.
“The more information you know about when menopause is going to be happening, you can tailor your treatment plan,” Dr. Goldman said. For example, a woman who may be 2 years away from menopause might consider a naturopathic approach at first, and switch to a different therapy as menopause occurs. “We know that the risks of cardiovascular disease and bone loss increase after menopause, and knowing the time to menopause gives us more guidance when educating patients about healthy lifestyle habits such as exercise and dietary changes that can help reduce these risks.”
The Cusp allows patients to use money in flexible spending accounts or health savings accounts to pay for the program. If doctors require lab tests or other procedures, these are covered through the patients’ regular health insurance as they would be if requested by a primary care physician or other health care professional.

Lubna Pal, MBBS, director of the menopause program at Yale University, New Haven, Conn., commented that part of the value in a telehealth site such as the Cusp is to serve as “a resource for reproductively aging women to understand what is happening to them.”
Any way to improve education on the topic of menopause is empowering to women, said Dr. Pal, professor of obstetrics, gynecology, and reproductive sciences at Yale. “This is an opportunity for patients to have access to a directed evaluation” of menopause-related symptoms. Then, when women visit their regular health care provider in person, they are well-equipped with knowledge to ask more informed questions and discuss a wide range of treatment options.
Dr. Pal noted that the hormone test is less valuable than the interaction between physicians and patients, whether online or in person.
“Menopause is a Monday morning quarterback diagnosis,” she said, emphasizing that, not only is a year without menses part of the diagnosis of menopause, many women in perimenopause can have wide fluctuations in hormone levels, so a test is more of a snapshot than a diagnostic tool, and that the results might cause unnecessary angst and concerns for patients.
However, part of the value of a telehealth site that focuses on menopause is that it gives women a place to learn more about their biology and to clarify their questions about symptoms and become aware of a range of treatment options. Telehealth consultations also can help women recognize how other factors such as lifestyle modifications can play a role in menopause symptoms, and how modifying these factors may provide some relief, she said.
Dr. Pal said she would be cautious about the idea of prescribing without seeing the patient in person, but noted that telehealth sites such as the Cusp can be a win-win to enhance women’s health when used in combination with regular in-person visits to an ob.gyn. The added value in patients’ being able to discuss their concerns and to learn more about their symptoms means that they will be better informed to develop a menopause management strategy in partnership with their providers, said Dr. Pal, who is not associated with the Cusp.
Dr. Goldman disclosed receiving compensation from the Cusp for her advisory work. She also holds stock options in the company. Dr. Pal, who is a member of the Ob.Gyn. News editorial advisory board, had no financial conflicts to disclose.
Women facing issues related to perimenopause and menopause can consult their primary care physicians or ob.gyns. through telemedicine visits, but
The Cusp doesn’t claim to replace routine gynecologic care. Rather, it focuses on perimenopause and menopause symptoms specifically, and states that its physicians, some of whom are certified by the North American Menopause Society, provide expertise in menopause beyond what patients might receive as part of a typical ob.gyn. visit.
The Cusp is a for-profit organization, a group of physicians, nurse practitioners, and technologists who focus on integrated care for women in perimenopause and beyond. The aim is to leverage technology as a way to connect women to the care platform to book physician and nurse practitioner visits virtually and to have all of the information about their care centralized in one place.
According to the website, most patients who sign up for a care plan check in with their providers at least once a month to monitor their symptoms and tweak treatment strategies. Patients who sign up are prompted to download an app, which then becomes the main tool for scheduling future visits, tracking symptoms, and communicating with providers.
The Cusp launched in early 2019, before the advent of the COVID-19 pandemic, but the pandemic has accelerated the acceptance across medical specialties, suggesting that telemedicine is here to stay, according to Mindy Goldman, MD, professor of gynecology and gynecologic surgery at the University of California, San Francisco, and director of the Gynecology Center for Cancer Survivors and At-Risk Women at UCSF, who also serves as a medical adviser to the Cusp.
Partnering with technology companies allows opportunities to provide care in areas where there are gaps, such as menopause management, she said. Many clinicians in primary care and ob.gyn. care don’t have the time or training to discuss menopause management in depth with patients, and patient interviews conducted by the Cusp before launching the site showed that this was an area of need.
“One thing that is really unique about the Cusp is that we brought together experts to provide care in both in an evidence-based and holistic fashion,” Dr. Goldman emphasized.
The Cusp’s medical team includes physician and nurse practitioner menopause experts with backgrounds including not only ob.gyn. but also psychiatry, integrative medicine, and naturopathic medicine, with plans to add endocrinology and dermatology as well. This holistic approach allows the Cusp to tailor care based on what each woman is looking for, with evidence-based expertise to support treatment decisions, said Dr. Goldman, whose advisory role includes helping to develop patient treatment protocols and services.
If a woman wants to begin treating symptoms with a naturopathic approach, the team will provide protocols that take current guidelines into account. Regular visits, approximately once a month or as needed, allow for collaboration with the Cusp’s specialists to provide consistent care that is very comprehensive, she said.
One of the benefits of the Cusp is the opportunity for “frequent touchpoints” in which providers reach out to patients via text, email, or video. Although a traditional medical visit may include some initial discussion of menopause and treatment plans, the Cusp offers “a more seamless way to address needs on an ongoing basis,” to provide more complete patient care, Dr. Goldman said.
“We are constantly asking women what they are looking for in menopause care,” and a recurring question was about hormone testing, she said. Nontraditional practitioners may offer hormone testing as a way of individualizing care that also involves compounded formulations, and other treatments that are not standard of care. “In all of our protocols we follow what is recommended by standard organizations such as ACOG [American College of Obstetricians and Gynecologists] and NAMS.”
The Cusp’s newest service is an at-home hormone test currently for women in New York and California, but the company plans to expand this service. The hormone test, while not essential, is another tool to guide menopause management, and having a sense of when menopause will occur “gives us a chance to talk to people about behavioral changes and time to personalize a treatment protocol,” Dr. Goldman said.
The test is based in part on the anti-Müllerian hormone, which recent studies have shown is useful in predicting time to menopause. This, in combination with other hormone tests and other clinical information, will allow the Cusp’s menopause specialists to help women in perimenopause gain perspective on their symptoms and design a treatment plan that can evolve as their needs change, she explained.
“The more information you know about when menopause is going to be happening, you can tailor your treatment plan,” Dr. Goldman said. For example, a woman who may be 2 years away from menopause might consider a naturopathic approach at first, and switch to a different therapy as menopause occurs. “We know that the risks of cardiovascular disease and bone loss increase after menopause, and knowing the time to menopause gives us more guidance when educating patients about healthy lifestyle habits such as exercise and dietary changes that can help reduce these risks.”
The Cusp allows patients to use money in flexible spending accounts or health savings accounts to pay for the program. If doctors require lab tests or other procedures, these are covered through the patients’ regular health insurance as they would be if requested by a primary care physician or other health care professional.
Lubna Pal, MBBS, director of the menopause program at Yale University, New Haven, Conn., commented that part of the value in a telehealth site such as the Cusp is to serve as “a resource for reproductively aging women to understand what is happening to them.”
Any way to improve education on the topic of menopause is empowering to women, said Dr. Pal, professor of obstetrics, gynecology, and reproductive sciences at Yale. “This is an opportunity for patients to have access to a directed evaluation” of menopause-related symptoms. Then, when women visit their regular health care provider in person, they are well-equipped with knowledge to ask more informed questions and discuss a wide range of treatment options.
Dr. Pal noted that the hormone test is less valuable than the interaction between physicians and patients, whether online or in person.
“Menopause is a Monday morning quarterback diagnosis,” she said, emphasizing that, not only is a year without menses part of the diagnosis of menopause, many women in perimenopause can have wide fluctuations in hormone levels, so a test is more of a snapshot than a diagnostic tool, and that the results might cause unnecessary angst and concerns for patients.
However, part of the value of a telehealth site that focuses on menopause is that it gives women a place to learn more about their biology and to clarify their questions about symptoms and become aware of a range of treatment options. Telehealth consultations also can help women recognize how other factors such as lifestyle modifications can play a role in menopause symptoms, and how modifying these factors may provide some relief, she said.
Dr. Pal said she would be cautious about the idea of prescribing without seeing the patient in person, but noted that telehealth sites such as the Cusp can be a win-win to enhance women’s health when used in combination with regular in-person visits to an ob.gyn. The added value in patients’ being able to discuss their concerns and to learn more about their symptoms means that they will be better informed to develop a menopause management strategy in partnership with their providers, said Dr. Pal, who is not associated with the Cusp.
Dr. Goldman disclosed receiving compensation from the Cusp for her advisory work. She also holds stock options in the company. Dr. Pal, who is a member of the Ob.Gyn. News editorial advisory board, had no financial conflicts to disclose.
Women facing issues related to perimenopause and menopause can consult their primary care physicians or ob.gyns. through telemedicine visits, but
The Cusp doesn’t claim to replace routine gynecologic care. Rather, it focuses on perimenopause and menopause symptoms specifically, and states that its physicians, some of whom are certified by the North American Menopause Society, provide expertise in menopause beyond what patients might receive as part of a typical ob.gyn. visit.
The Cusp is a for-profit organization, a group of physicians, nurse practitioners, and technologists who focus on integrated care for women in perimenopause and beyond. The aim is to leverage technology as a way to connect women to the care platform to book physician and nurse practitioner visits virtually and to have all of the information about their care centralized in one place.
According to the website, most patients who sign up for a care plan check in with their providers at least once a month to monitor their symptoms and tweak treatment strategies. Patients who sign up are prompted to download an app, which then becomes the main tool for scheduling future visits, tracking symptoms, and communicating with providers.
The Cusp launched in early 2019, before the advent of the COVID-19 pandemic, but the pandemic has accelerated the acceptance across medical specialties, suggesting that telemedicine is here to stay, according to Mindy Goldman, MD, professor of gynecology and gynecologic surgery at the University of California, San Francisco, and director of the Gynecology Center for Cancer Survivors and At-Risk Women at UCSF, who also serves as a medical adviser to the Cusp.
Partnering with technology companies allows opportunities to provide care in areas where there are gaps, such as menopause management, she said. Many clinicians in primary care and ob.gyn. care don’t have the time or training to discuss menopause management in depth with patients, and patient interviews conducted by the Cusp before launching the site showed that this was an area of need.
“One thing that is really unique about the Cusp is that we brought together experts to provide care in both in an evidence-based and holistic fashion,” Dr. Goldman emphasized.
The Cusp’s medical team includes physician and nurse practitioner menopause experts with backgrounds including not only ob.gyn. but also psychiatry, integrative medicine, and naturopathic medicine, with plans to add endocrinology and dermatology as well. This holistic approach allows the Cusp to tailor care based on what each woman is looking for, with evidence-based expertise to support treatment decisions, said Dr. Goldman, whose advisory role includes helping to develop patient treatment protocols and services.
If a woman wants to begin treating symptoms with a naturopathic approach, the team will provide protocols that take current guidelines into account. Regular visits, approximately once a month or as needed, allow for collaboration with the Cusp’s specialists to provide consistent care that is very comprehensive, she said.
One of the benefits of the Cusp is the opportunity for “frequent touchpoints” in which providers reach out to patients via text, email, or video. Although a traditional medical visit may include some initial discussion of menopause and treatment plans, the Cusp offers “a more seamless way to address needs on an ongoing basis,” to provide more complete patient care, Dr. Goldman said.
“We are constantly asking women what they are looking for in menopause care,” and a recurring question was about hormone testing, she said. Nontraditional practitioners may offer hormone testing as a way of individualizing care that also involves compounded formulations, and other treatments that are not standard of care. “In all of our protocols we follow what is recommended by standard organizations such as ACOG [American College of Obstetricians and Gynecologists] and NAMS.”
The Cusp’s newest service is an at-home hormone test currently for women in New York and California, but the company plans to expand this service. The hormone test, while not essential, is another tool to guide menopause management, and having a sense of when menopause will occur “gives us a chance to talk to people about behavioral changes and time to personalize a treatment protocol,” Dr. Goldman said.
The test is based in part on the anti-Müllerian hormone, which recent studies have shown is useful in predicting time to menopause. This, in combination with other hormone tests and other clinical information, will allow the Cusp’s menopause specialists to help women in perimenopause gain perspective on their symptoms and design a treatment plan that can evolve as their needs change, she explained.
“The more information you know about when menopause is going to be happening, you can tailor your treatment plan,” Dr. Goldman said. For example, a woman who may be 2 years away from menopause might consider a naturopathic approach at first, and switch to a different therapy as menopause occurs. “We know that the risks of cardiovascular disease and bone loss increase after menopause, and knowing the time to menopause gives us more guidance when educating patients about healthy lifestyle habits such as exercise and dietary changes that can help reduce these risks.”
The Cusp allows patients to use money in flexible spending accounts or health savings accounts to pay for the program. If doctors require lab tests or other procedures, these are covered through the patients’ regular health insurance as they would be if requested by a primary care physician or other health care professional.
Lubna Pal, MBBS, director of the menopause program at Yale University, New Haven, Conn., commented that part of the value in a telehealth site such as the Cusp is to serve as “a resource for reproductively aging women to understand what is happening to them.”
Any way to improve education on the topic of menopause is empowering to women, said Dr. Pal, professor of obstetrics, gynecology, and reproductive sciences at Yale. “This is an opportunity for patients to have access to a directed evaluation” of menopause-related symptoms. Then, when women visit their regular health care provider in person, they are well-equipped with knowledge to ask more informed questions and discuss a wide range of treatment options.
Dr. Pal noted that the hormone test is less valuable than the interaction between physicians and patients, whether online or in person.
“Menopause is a Monday morning quarterback diagnosis,” she said, emphasizing that, not only is a year without menses part of the diagnosis of menopause, many women in perimenopause can have wide fluctuations in hormone levels, so a test is more of a snapshot than a diagnostic tool, and that the results might cause unnecessary angst and concerns for patients.
However, part of the value of a telehealth site that focuses on menopause is that it gives women a place to learn more about their biology and to clarify their questions about symptoms and become aware of a range of treatment options. Telehealth consultations also can help women recognize how other factors such as lifestyle modifications can play a role in menopause symptoms, and how modifying these factors may provide some relief, she said.
Dr. Pal said she would be cautious about the idea of prescribing without seeing the patient in person, but noted that telehealth sites such as the Cusp can be a win-win to enhance women’s health when used in combination with regular in-person visits to an ob.gyn. The added value in patients’ being able to discuss their concerns and to learn more about their symptoms means that they will be better informed to develop a menopause management strategy in partnership with their providers, said Dr. Pal, who is not associated with the Cusp.
Dr. Goldman disclosed receiving compensation from the Cusp for her advisory work. She also holds stock options in the company. Dr. Pal, who is a member of the Ob.Gyn. News editorial advisory board, had no financial conflicts to disclose.
Medicare sticks with E/M pay plan over some groups’ objections
The Trump administration is sticking with a plan to boost certain Medicare pay for many primary care and other specialties focused heavily on office visits while lowering that for other groups to balance these increased costs.
On Aug. 4, the Centers for Medicare & Medicaid Services posted on the Federal Register draft versions of two of its major annual payment measures: the physician fee schedule and the payment rule for hospital outpatient services. On Aug. 3, the CMS informally posted a copy of the physician fee schedule on its own website, allowing medical groups to begin reading the more than 1,300-page rule.
Federal officials normally use annual Medicare payment rules to make many revisions to policies as well as adjust reimbursement.
The draft 2021 physician fee schedule, for example, calls for broadening the authority of clinicians other than physicians to authorize testing of people enrolled in Medicare.
The CMS intends to allow nurse practitioners, physician assistants, and certain other health care professionals to more widely supervise diagnostic psychological and neuropsychological tests, in keeping with applicable state laws.
The draft 2021 hospital outpatient rule proposes a gradual changeover to allow more procedures to be performed on an outpatient basis. This shift could save money for Medicare as well as for the people enrolled in the giant federal health program who need these services, the CMS explained.
Medicare would begin with a change in status for almost 300 musculoskeletal-related services, making them eligible for payment in the hospital outpatient setting when appropriate, CMS wrote in a fact sheet.
The initial reaction to Medicare’s proposed 2021 rules centered on its planned redistribution of funds among medical specialties. The CMS had outlined this plan last year. It is part of longstanding efforts to boost pay for primary care specialists and other physicians whose practice centers more around office visits than procedures.
There is broad support in health policy circles for raising pay for these specialties, but there also are strong objections to the cuts the CMS plans to offset the cost of rising pay for some fields.
Susan R. Bailey, MD, president of the American Medical Association, addressed both of these ideas in an AMA news release on the proposed 2021 physician fee schedule. The increase in pay for office visits, covered under evaluation and management services (E/M), stems from recommendations on resource costs from the AMA/Specialty Society RVS Update Committee, Dr. Bailey said.
“Unfortunately, these office visit payment increases, and a multitude of other new CMS proposed payment increases, are required by statute to be offset by payment reductions to other services, through an unsustainable reduction of nearly 11% to the Medicare conversion factor,” Dr. Bailey explained.
In the news release, Dr. Bailey asked Congress to waive Medicare’s budget-neutrality requirements to allow increases without the cuts.
“Physicians are already experiencing substantial economic hardships due to COVID-19, so these pay cuts could not come at a worse time,” she said.
Winners and losers
The CMS details the possible winners and losers in its payment reshuffle in Table 90 of the proposed 2021 physician fee schedule. In the proposed rule, CMS notes in the draft that these figures are based upon estimates of aggregate allowed charges across all services furnished by physicians and other clinicians.
“Therefore, they are averages, and may not necessarily be representative of what is happening to the particular services furnished by a single practitioner within any given specialty,” the CMS said.
Specialties in line for increases under the 2021 draft rule include allergy/immunology (9%), endocrinology (17%), family practice (13%), general practice (8%), geriatrics (4%), hematology/oncology (14%), internal medicine (4%), nephrology (6%), physician assistants (8%), psychiatry (8%), rheumatology (16%), and urology (8%).
In line for cuts would be anesthesiology (–8%), cardiac surgery (–9%), emergency medicine (–6%), general surgery (–7%), infectious disease (–4%), neurosurgery (–7%), physical/occupational therapy (–9%), plastic surgery (–7%), radiology (–11%), and thoracic surgery (–8%).
An umbrella group, the Surgical Care Coalition, on Aug. 3 had a quick statement ready about the CMS proposal. Writing on behalf of the group was David B. Hoyt, MD, executive director of the American College of Surgeons.
“Today’s proposed rule ignores both patients and the surgeons who care for them. The middle of a pandemic is no time for cuts to any form of health care, but today’s announcement moves ahead as if nothing has changed,” Hoyt said in the statement. “The Surgical Care Coalition believes no physician should see payment cuts that will reduce patients’ access to care.”
The Surgical Care Coalition already has been asking Congress to waive budget-neutrality requirements. Making a similar request Aug. 4 in a unified statement were the American Physical Therapy Association (APTA), the American Occupational Therapy Association (AOTA), and the American Speech-Language-Hearing Association (ASHA).
“Our organizations call on Congress and CMS to advance well-reasoned fee schedule payment policies and waive budget neutrality,” the groups said. “While APTA, AOTA, and ASHA do not oppose payment increases for primary care physicians, we believe these increases can be implemented without imposing payment reductions on other providers.”
A version of this article originally appeared on Medscape.com.
The Trump administration is sticking with a plan to boost certain Medicare pay for many primary care and other specialties focused heavily on office visits while lowering that for other groups to balance these increased costs.
On Aug. 4, the Centers for Medicare & Medicaid Services posted on the Federal Register draft versions of two of its major annual payment measures: the physician fee schedule and the payment rule for hospital outpatient services. On Aug. 3, the CMS informally posted a copy of the physician fee schedule on its own website, allowing medical groups to begin reading the more than 1,300-page rule.
Federal officials normally use annual Medicare payment rules to make many revisions to policies as well as adjust reimbursement.
The draft 2021 physician fee schedule, for example, calls for broadening the authority of clinicians other than physicians to authorize testing of people enrolled in Medicare.
The CMS intends to allow nurse practitioners, physician assistants, and certain other health care professionals to more widely supervise diagnostic psychological and neuropsychological tests, in keeping with applicable state laws.
The draft 2021 hospital outpatient rule proposes a gradual changeover to allow more procedures to be performed on an outpatient basis. This shift could save money for Medicare as well as for the people enrolled in the giant federal health program who need these services, the CMS explained.
Medicare would begin with a change in status for almost 300 musculoskeletal-related services, making them eligible for payment in the hospital outpatient setting when appropriate, CMS wrote in a fact sheet.
The initial reaction to Medicare’s proposed 2021 rules centered on its planned redistribution of funds among medical specialties. The CMS had outlined this plan last year. It is part of longstanding efforts to boost pay for primary care specialists and other physicians whose practice centers more around office visits than procedures.
There is broad support in health policy circles for raising pay for these specialties, but there also are strong objections to the cuts the CMS plans to offset the cost of rising pay for some fields.
Susan R. Bailey, MD, president of the American Medical Association, addressed both of these ideas in an AMA news release on the proposed 2021 physician fee schedule. The increase in pay for office visits, covered under evaluation and management services (E/M), stems from recommendations on resource costs from the AMA/Specialty Society RVS Update Committee, Dr. Bailey said.
“Unfortunately, these office visit payment increases, and a multitude of other new CMS proposed payment increases, are required by statute to be offset by payment reductions to other services, through an unsustainable reduction of nearly 11% to the Medicare conversion factor,” Dr. Bailey explained.
In the news release, Dr. Bailey asked Congress to waive Medicare’s budget-neutrality requirements to allow increases without the cuts.
“Physicians are already experiencing substantial economic hardships due to COVID-19, so these pay cuts could not come at a worse time,” she said.
Winners and losers
The CMS details the possible winners and losers in its payment reshuffle in Table 90 of the proposed 2021 physician fee schedule. In the proposed rule, CMS notes in the draft that these figures are based upon estimates of aggregate allowed charges across all services furnished by physicians and other clinicians.
“Therefore, they are averages, and may not necessarily be representative of what is happening to the particular services furnished by a single practitioner within any given specialty,” the CMS said.
Specialties in line for increases under the 2021 draft rule include allergy/immunology (9%), endocrinology (17%), family practice (13%), general practice (8%), geriatrics (4%), hematology/oncology (14%), internal medicine (4%), nephrology (6%), physician assistants (8%), psychiatry (8%), rheumatology (16%), and urology (8%).
In line for cuts would be anesthesiology (–8%), cardiac surgery (–9%), emergency medicine (–6%), general surgery (–7%), infectious disease (–4%), neurosurgery (–7%), physical/occupational therapy (–9%), plastic surgery (–7%), radiology (–11%), and thoracic surgery (–8%).
An umbrella group, the Surgical Care Coalition, on Aug. 3 had a quick statement ready about the CMS proposal. Writing on behalf of the group was David B. Hoyt, MD, executive director of the American College of Surgeons.
“Today’s proposed rule ignores both patients and the surgeons who care for them. The middle of a pandemic is no time for cuts to any form of health care, but today’s announcement moves ahead as if nothing has changed,” Hoyt said in the statement. “The Surgical Care Coalition believes no physician should see payment cuts that will reduce patients’ access to care.”
The Surgical Care Coalition already has been asking Congress to waive budget-neutrality requirements. Making a similar request Aug. 4 in a unified statement were the American Physical Therapy Association (APTA), the American Occupational Therapy Association (AOTA), and the American Speech-Language-Hearing Association (ASHA).
“Our organizations call on Congress and CMS to advance well-reasoned fee schedule payment policies and waive budget neutrality,” the groups said. “While APTA, AOTA, and ASHA do not oppose payment increases for primary care physicians, we believe these increases can be implemented without imposing payment reductions on other providers.”
A version of this article originally appeared on Medscape.com.
The Trump administration is sticking with a plan to boost certain Medicare pay for many primary care and other specialties focused heavily on office visits while lowering that for other groups to balance these increased costs.
On Aug. 4, the Centers for Medicare & Medicaid Services posted on the Federal Register draft versions of two of its major annual payment measures: the physician fee schedule and the payment rule for hospital outpatient services. On Aug. 3, the CMS informally posted a copy of the physician fee schedule on its own website, allowing medical groups to begin reading the more than 1,300-page rule.
Federal officials normally use annual Medicare payment rules to make many revisions to policies as well as adjust reimbursement.
The draft 2021 physician fee schedule, for example, calls for broadening the authority of clinicians other than physicians to authorize testing of people enrolled in Medicare.
The CMS intends to allow nurse practitioners, physician assistants, and certain other health care professionals to more widely supervise diagnostic psychological and neuropsychological tests, in keeping with applicable state laws.
The draft 2021 hospital outpatient rule proposes a gradual changeover to allow more procedures to be performed on an outpatient basis. This shift could save money for Medicare as well as for the people enrolled in the giant federal health program who need these services, the CMS explained.
Medicare would begin with a change in status for almost 300 musculoskeletal-related services, making them eligible for payment in the hospital outpatient setting when appropriate, CMS wrote in a fact sheet.
The initial reaction to Medicare’s proposed 2021 rules centered on its planned redistribution of funds among medical specialties. The CMS had outlined this plan last year. It is part of longstanding efforts to boost pay for primary care specialists and other physicians whose practice centers more around office visits than procedures.
There is broad support in health policy circles for raising pay for these specialties, but there also are strong objections to the cuts the CMS plans to offset the cost of rising pay for some fields.
Susan R. Bailey, MD, president of the American Medical Association, addressed both of these ideas in an AMA news release on the proposed 2021 physician fee schedule. The increase in pay for office visits, covered under evaluation and management services (E/M), stems from recommendations on resource costs from the AMA/Specialty Society RVS Update Committee, Dr. Bailey said.
“Unfortunately, these office visit payment increases, and a multitude of other new CMS proposed payment increases, are required by statute to be offset by payment reductions to other services, through an unsustainable reduction of nearly 11% to the Medicare conversion factor,” Dr. Bailey explained.
In the news release, Dr. Bailey asked Congress to waive Medicare’s budget-neutrality requirements to allow increases without the cuts.
“Physicians are already experiencing substantial economic hardships due to COVID-19, so these pay cuts could not come at a worse time,” she said.
Winners and losers
The CMS details the possible winners and losers in its payment reshuffle in Table 90 of the proposed 2021 physician fee schedule. In the proposed rule, CMS notes in the draft that these figures are based upon estimates of aggregate allowed charges across all services furnished by physicians and other clinicians.
“Therefore, they are averages, and may not necessarily be representative of what is happening to the particular services furnished by a single practitioner within any given specialty,” the CMS said.
Specialties in line for increases under the 2021 draft rule include allergy/immunology (9%), endocrinology (17%), family practice (13%), general practice (8%), geriatrics (4%), hematology/oncology (14%), internal medicine (4%), nephrology (6%), physician assistants (8%), psychiatry (8%), rheumatology (16%), and urology (8%).
In line for cuts would be anesthesiology (–8%), cardiac surgery (–9%), emergency medicine (–6%), general surgery (–7%), infectious disease (–4%), neurosurgery (–7%), physical/occupational therapy (–9%), plastic surgery (–7%), radiology (–11%), and thoracic surgery (–8%).
An umbrella group, the Surgical Care Coalition, on Aug. 3 had a quick statement ready about the CMS proposal. Writing on behalf of the group was David B. Hoyt, MD, executive director of the American College of Surgeons.
“Today’s proposed rule ignores both patients and the surgeons who care for them. The middle of a pandemic is no time for cuts to any form of health care, but today’s announcement moves ahead as if nothing has changed,” Hoyt said in the statement. “The Surgical Care Coalition believes no physician should see payment cuts that will reduce patients’ access to care.”
The Surgical Care Coalition already has been asking Congress to waive budget-neutrality requirements. Making a similar request Aug. 4 in a unified statement were the American Physical Therapy Association (APTA), the American Occupational Therapy Association (AOTA), and the American Speech-Language-Hearing Association (ASHA).
“Our organizations call on Congress and CMS to advance well-reasoned fee schedule payment policies and waive budget neutrality,” the groups said. “While APTA, AOTA, and ASHA do not oppose payment increases for primary care physicians, we believe these increases can be implemented without imposing payment reductions on other providers.”
A version of this article originally appeared on Medscape.com.
Septicemia first among hospital inpatient costs
according to a recent analysis from the Agency for Healthcare Research and Quality.
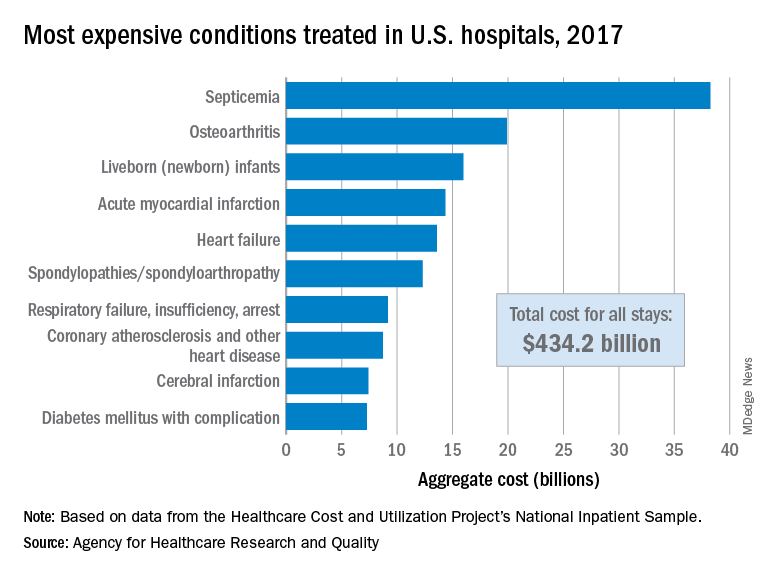
The single most expensive inpatient condition that year, representing about 8.8% of all hospital costs, was septicemia at $38.2 billion, nearly double the $19.9 billion spent on the next most expensive condition, osteoarthritis, Lan Liang, PhD, of the AHRQ, and associates said in a statistical brief.
These figures “represent the hospital’s costs to produce the services – not the amount paid for services by payers – and they do not include separately billed physician fees associated with the hospitalization,” they noted.
Third in overall cost for 2017 but first in total number of stays were live-born infants, with 3.7 million admissions costing just under $16 billion. Hospital costs for acute myocardial infarction ($14.3 billion) made it the fourth most expensive condition, with heart failure fifth at $13.6 billion, based on data from the Healthcare Cost and Utilization Project’s National Inpatient Sample.
The 20 most expensive conditions, which also included coronary atherosclerosis, pneumonia, renal failure, and lower-limb fracture, accounted for close to 47% of all hospital costs and over 43% of all stays in 2017. The total amount spent by hospitals that year, $1.1 trillion, constituted nearly a third of all health care expenditures and was 4.7% higher than in 2016, Dr. Liang and associates reported.
“Although this growth represented deceleration, compared with the 5.8% increase between 2014 and 2015, the consistent year-to-year rise in hospital-related expenses remains a central concern among policymakers,” they wrote.
according to a recent analysis from the Agency for Healthcare Research and Quality.
The single most expensive inpatient condition that year, representing about 8.8% of all hospital costs, was septicemia at $38.2 billion, nearly double the $19.9 billion spent on the next most expensive condition, osteoarthritis, Lan Liang, PhD, of the AHRQ, and associates said in a statistical brief.
These figures “represent the hospital’s costs to produce the services – not the amount paid for services by payers – and they do not include separately billed physician fees associated with the hospitalization,” they noted.
Third in overall cost for 2017 but first in total number of stays were live-born infants, with 3.7 million admissions costing just under $16 billion. Hospital costs for acute myocardial infarction ($14.3 billion) made it the fourth most expensive condition, with heart failure fifth at $13.6 billion, based on data from the Healthcare Cost and Utilization Project’s National Inpatient Sample.
The 20 most expensive conditions, which also included coronary atherosclerosis, pneumonia, renal failure, and lower-limb fracture, accounted for close to 47% of all hospital costs and over 43% of all stays in 2017. The total amount spent by hospitals that year, $1.1 trillion, constituted nearly a third of all health care expenditures and was 4.7% higher than in 2016, Dr. Liang and associates reported.
“Although this growth represented deceleration, compared with the 5.8% increase between 2014 and 2015, the consistent year-to-year rise in hospital-related expenses remains a central concern among policymakers,” they wrote.
according to a recent analysis from the Agency for Healthcare Research and Quality.
The single most expensive inpatient condition that year, representing about 8.8% of all hospital costs, was septicemia at $38.2 billion, nearly double the $19.9 billion spent on the next most expensive condition, osteoarthritis, Lan Liang, PhD, of the AHRQ, and associates said in a statistical brief.
These figures “represent the hospital’s costs to produce the services – not the amount paid for services by payers – and they do not include separately billed physician fees associated with the hospitalization,” they noted.
Third in overall cost for 2017 but first in total number of stays were live-born infants, with 3.7 million admissions costing just under $16 billion. Hospital costs for acute myocardial infarction ($14.3 billion) made it the fourth most expensive condition, with heart failure fifth at $13.6 billion, based on data from the Healthcare Cost and Utilization Project’s National Inpatient Sample.
The 20 most expensive conditions, which also included coronary atherosclerosis, pneumonia, renal failure, and lower-limb fracture, accounted for close to 47% of all hospital costs and over 43% of all stays in 2017. The total amount spent by hospitals that year, $1.1 trillion, constituted nearly a third of all health care expenditures and was 4.7% higher than in 2016, Dr. Liang and associates reported.
“Although this growth represented deceleration, compared with the 5.8% increase between 2014 and 2015, the consistent year-to-year rise in hospital-related expenses remains a central concern among policymakers,” they wrote.
SGLT2 inhibitors have a breakout year
The benefits from sodium-glucose cotransporter 2 inhibitor drugs proven during the past year for cutting heart failure hospitalization rates substantially in patients with heart failure with reduced ejection fraction and slowing progression of chronic kidney disease, all regardless of diabetes status, have thrust this drug class into the top tier of agents for potentially treating millions of patients with cardiac or renal disease.
The sodium-glucose cotransporter 2 (SGLT2) inhibitors, first licensed for U.S. marketing in 2013 purely for glycemic control, have, during the 5 years since the first cardiovascular outcome trial results for the class came out, shown benefits in a range of patients reminiscent of what’s been established for ACE inhibitors and angiotensin receptor blockers (ARBs).
The wide-reaching benefits of SGLT2 inhibitors have recently become even more relevant by showing clinically meaningful effects in patients without type 2 diabetes (T2D). And in an uncanny coincidence, the SGLT2 inhibitors appear to act in complementary harmony with the ACE inhibitors and ARBs for preserving heart and renal function. These properties have made the SGLT2 inhibitors especially attractive as a new weapon for controlling the ascendant disorder of cardiorenal syndrome.
“SGLT2 inhibitors have a relatively greater impact on cardiovascular outcomes, compared with ACE inhibitors and ARBs, but the effects [of the two classes] are synergistic and ideally patients receive both,” said Peter McCullough, MD, a specialist in treating cardiorenal syndrome and other cardiovascular and renal disorders at Baylor, Scott, and White Heart and Vascular Hospital in Dallas. The SGLT2 inhibitors are among the drugs best suited to both treating and preventing cardiorenal syndrome by targeting both ends of the disorder, said Dr. McCullough, who chaired an American Heart Association panel that last year issued a scientific statement on cardiorenal syndrome (Circulation. 2019 Apr 16;139[16]:e840-78).
Although data on the SGLT2 inhibitors “are evolving,” the drug class is “going in the direction” of being “reasonably compared” with the ACE inhibitors and ARBs, said Javed Butler, MD, professor and chair of medicine at the University of Mississippi Medical Center, Jackson. “There are certainly complementary benefits that we see for both cardiovascular and renal outcomes.”

“We’ll think more and more about the SGLT2 inhibitors like renin-angiotensin system [RAS] inhibitors,” said David Z. Cherney, MD, referring to the drug class that includes ACE inhibitors and ARBs. “We should start to approach SGLT2 inhibitors like RAS inhibitors, with pleiotropic effects that go beyond glucose,” said Dr. Cherney, a nephrologist and professor of medicine at the University of Toronto, during the virtual annual scientific sessions of the American Diabetes Association in June 2020.
Working together in the nephron
One of the clearest complementary interactions between the SGLT2 inhibitors and the RAS inhibitors is their ability to reduce intraglomerular pressure, a key mechanism that slows nephron loss and progression of chronic kidney disease. SGLT2 inhibitors reduce sodium absorption in the proximal tubule that causes, through tubuloglomerular feedback, afferent arteriole constriction that lowers intraglomerular pressure, while the RAS inhibitors inhibit efferent arteriole constriction mediated by angiotensin II, also cutting intraglomerular pressure. Together, “they almost work in tandem,” explained Janani Rangaswami, MD, a nephrologist at Einstein Medical Center in Philadelphia, vice chair of the Kidney Council of the AHA, and first author of the 2019 cardiorenal syndrome AHA statement.
“Many had worried that if we target both the afferent and efferent arterioles simultaneously, it might increase the risk for acute kidney injury. What has been reassuring in both the recent data from the DAPA-HF trial and in recent meta-analysis was no evidence of increased risk for acute kidney injury with use of the SGLT2 inhibitor,” Dr. Rangaswami said in an interview. For example, a recent report on more than 39,000 Canadian patients with T2D who were at least 66 years old and newly begun on either an SGLT2 inhibitor or a different oral diabetes drug (a dipeptidyl peptidase–4 inhibitor), found a statistically significant 21% lower rate of acute kidney injury during the first 90 days on treatment with an SGLT2 inhibitor in a propensity score–matched analysis (CMAJ. 2020 Apr 6;192: e351-60).
Much of the concern about possible acute kidney injury stemmed from a property that the SGLT2 inhibitors share with RAS inhibitors: They cause an initial, reversible decline in glomerular filtration rate (GFR), followed by longer-term nephron preservation, a pattern attributable to reduced intraglomerular pressure. The question early on was: “ ‘Does this harm the kidney?’ But what we’ve seen is that patients do better over time, even with this initial hit. Whenever you offload the glomerulus you cut barotrauma and protect renal function,” explained Silvio E. Inzucchi, MD, professor of medicine at Yale University, New Haven, Conn., and director of the Yale Medicine Diabetes Center.
Dr. Inzucchi cautioned, however, that a small number of patients starting treatment with an SGLT2 inhibitor may have their GFR drop too sharply, especially if their GFR was low to start with. “You need to be careful, especially at the lower end of the GFR range. I recheck renal function after 1 month” after a patient starts an SGLT2. Patients whose level falls too low may need to discontinue. He added that it’s hard to set a uniform threshold for alarm, and instead assess patients on a case-by-case basis, but “you need some threshold in mind, where you will stop” treatment.
A smarter diuretic
One of the most intriguing renal effects of SGLT2 inhibitors is their diuretic action. During a talk at the virtual ADA scientific sessions, cardiologist Jeffrey Testani, MD, called them “smart” diuretics, because their effect on diuresis is relatively modest but comes without the neurohormonal price paid when patients take conventional loop diuretics.
”Loop diuretics are particularly bad,” causing neurohormonal activation that includes norepinephrine, renin, and vasopressin, said Dr. Testani, director of heart failure research at Yale. They also fail to produce a meaningful drop in blood volume despite causing substantial natriuresis.
In contrast, SGLT2 inhibitors cause “moderate” natriuresis while producing a significant cut in blood volume. “The body seems content with this lower plasma volume without activating catecholamines or renin, and that’s how the SGLT2 inhibitors differ from other diuretics,” said Dr. Inzucchi.
The class also maintains serum levels of potassium and magnesium, produces significant improvements in serum uric acid levels, and avoids the electrolyte abnormalities, volume depletion, and acute kidney injury that can occur with conventional distal diuretics, Dr. Testani said.
In short, the SGLT2 inhibitors “are safe and easy-to-use diuretics,” which allows them to fill a “huge unmet need for patients with heart failure.” As evidence accumulates for the benefits of the drug class in patients with heart failure and renal disease, “uptake will be extensive,” Dr. Testani predicted, driven in part by how easy it is to add the class to existing cardiorenal drug regimens.
Other standard therapies for patients with heart failure with reduced ejection fraction (HFrEF) risk electrolyte abnormalities, renal dysfunction, significantly lower blood pressure, often make patients feel worse, and involve a slow and laborious titration process, Dr. Testani noted. The SGLT2 inhibitor agents avoid these issues, a property that has played out in quality of life assessments of patients with HFrEF who received a drug from this class.
Outcomes met in trial after trial

In the DAPA-HF trial, with 4,443 patients with HFrEF and divided roughly equally between those with or without T2D, treatment with dapagliflozin (Farxiga) linked with significant improvements in health status and quality of life measured by the Kansas City Cardiomyopathy Questionnaire (Circulation. 2020 Jan 14;141[2]:90-9). “Not all treatments for HFrEF improve symptoms,” but in this study the SGTL2 inhibitor dapagliflozin did, boosting the Kansas City Cardiomyopathy Questionnaire score by about the same magnitude as treatment with a cardiac resynchronization device in patients with HFrEF, said Mikhail N. Kosiborod, MD, director of Cardiometabolic Research at Saint Luke’s Mid America Heart Institute in Kansas City, Mo., speaking at the virtual ADA scientific sessions.
Two more recent renal observations have further solidified the growing role of these drugs for kidney protection. Results from the CREDENCE trial that looked at canagliflozin (Invokana) treatment in 4,401 patients with T2D and albuminuria and chronic kidney disease showed canagliflozin treatment cut the primary, composite renal endpoint by a statistically significant 30%, compared with placebo (N Engl J Med. 2019 Jun 13;380[24]:2295-306). The study stopped earlier than planned because of how effective canagliflozin appeared.

“Never before has a renal protection clinical trial stopped for overwhelming efficacy,” noted nephrologist Katherine R. Tuttle, MD, executive director for research at Providence Health Care in Spokane, Wash. “It’s very exciting to have a treatment that works on both the heart and kidney, given their interrelationship,” she said during the ADA sessions. Dr. Tuttle called the cardiorenal effects from the SGLT2 inhibitors “amazing.”
Just as the DAPA-HF trial’s primary outcome showed the ability of at least one drug from the class, dapagliflozin, to improve outcomes in HFrEF patients without T2D, topline results recently reported from the DAPA-CDK trial showed for the first time renal protection by an SGLT2 inhibitor in patients with chronic kidney disease but no T2D, in a study with about 4,300 patients.
Although detailed results from DAPA-CKD are not yet available, so far the outcomes seem consistent with the CREDENCE findings, and the cumulative renal findings for the class show the SGLT2 inhibitors have “potential for a profound impact on the patients we see in every nephrology clinic, and with dual cardiorenal disease,” said Dr. Rangaswami. The class is now established as “standard of care for patients with chronic kidney disease. The CREDENCE results made that clear.”

The DAPA-CKD findings in patients with chronic kidney disease regardless of their diabetes status “are very important. We really have not had any advances in this space for some time, and chronic kidney disease patients have very poor outcomes, both cardiovascular and renal,” commented Dr. Butler. The advantage from using this drug class in these patients “is huge.”
The DAPA-CKD findings are a “major advance,” agreed Dr. McCullough.
SGLT2 inhibitor use needs to grow
Experts lament that although the evidence favoring the class has been very bullish, prescribing uptake has been slow, perhaps partly explained by the retail U.S. cost for most of these agents, generally about $17/day.
Cost is, unfortunately, an issue right now for these drugs, said Dr. Butler. Generic formulations are imminent, “but we cannot accept waiting. Providing this therapy when insurance coverage is available,” is essential.
The FDA has already granted tentative approval to some generic formulations, although resolution of patent issues can delay generics actually reaching the market. “Generic dapagliflozin will have a major impact; the marketplace for these drugs will shift very quickly,” predicted Dr. McCullough.
But price may not be the sole barrier, cautioned Dr. Rangaswami. “I don’t think it’s just a cost issue. Several factors explain the slow uptake,” of the SGLT2 inhibitors. “The biggest barrier is that this is a new drug class, and understanding how to use the class is not yet where it needs to be in the physician community.” One of the biggest problems is that the SGLT2 inhibitors are still primarily regarded as drugs to treat hyperglycemia.
Physicians who treat patients with heart or renal disease “need to wrap their head around the idea that a drug with antihyperglycemic effects is now in their practice territory, and something they need to prescribe,” she noted. Currently “there is a reluctance to prescribe these drugs given the perception that they are antihyperglycemic agents, and usually get deferred to primary care physicians or endocrinologists. This results in huge missed opportunities by cardiologists and nephrologists in initiating these agents that have major cardiorenal risk reduction effects.”
The key role that cardiologists need to play in prescribing the SGLT2 inhibitors was brought home in a recent study of two representative U.S. health systems that showed patients with T2D were far more likely to see a cardiologist than an endocrinologist (Cardiovasc Endocrinol Metab. 2020 Jun;9[2]:56-9).
“The SGLT2 inhibitors are definitely a game-changing drug class,” summed up Dr. Rangaswami. “We’re going to see a lot of use in patients with heart and kidney disease.”
Dr. Cherney has been a consultant to or has received honoraria from AstraZeneca, Boehringer Ingelheim, Janssen, Lilly, Merck, Mitsubishi Tanabe Pharma, and Sanofi. Dr. Butler has had financial relationships with numerous pharmaceutical companies. Dr. McCullough and Dr. Rangaswami had no disclosures. Dr. Inzucchi has been a consultant to or helped run trials for Abbott, AstraZeneca, Boehringer Ingelheim, Merck, Novo Nordisk, Sanofi/Lexicon, and vTv Therapeutics. Dr. Testani has been a consultant to AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, cardionomic, FIRE1 Magenta Med, Novartis, Reprieve, Sanofi, and W.L. Gore. Dr. Kosiborod has been a consultant to or led trials for Amarin, Amgen, Applied Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Glytec, Janssen, Eli Lilly, Merck, Novartis, Novo Nordisk, Sanofi, and Vifor. Dr. Tuttle has been a consultant to AstraZeneca, Boehringer Ingelheim, Gilead, Goldfinch Bio, Eli Lilly, and Novo Nordisk.
mzoler@mdedge.com
The benefits from sodium-glucose cotransporter 2 inhibitor drugs proven during the past year for cutting heart failure hospitalization rates substantially in patients with heart failure with reduced ejection fraction and slowing progression of chronic kidney disease, all regardless of diabetes status, have thrust this drug class into the top tier of agents for potentially treating millions of patients with cardiac or renal disease.
The sodium-glucose cotransporter 2 (SGLT2) inhibitors, first licensed for U.S. marketing in 2013 purely for glycemic control, have, during the 5 years since the first cardiovascular outcome trial results for the class came out, shown benefits in a range of patients reminiscent of what’s been established for ACE inhibitors and angiotensin receptor blockers (ARBs).
The wide-reaching benefits of SGLT2 inhibitors have recently become even more relevant by showing clinically meaningful effects in patients without type 2 diabetes (T2D). And in an uncanny coincidence, the SGLT2 inhibitors appear to act in complementary harmony with the ACE inhibitors and ARBs for preserving heart and renal function. These properties have made the SGLT2 inhibitors especially attractive as a new weapon for controlling the ascendant disorder of cardiorenal syndrome.
“SGLT2 inhibitors have a relatively greater impact on cardiovascular outcomes, compared with ACE inhibitors and ARBs, but the effects [of the two classes] are synergistic and ideally patients receive both,” said Peter McCullough, MD, a specialist in treating cardiorenal syndrome and other cardiovascular and renal disorders at Baylor, Scott, and White Heart and Vascular Hospital in Dallas. The SGLT2 inhibitors are among the drugs best suited to both treating and preventing cardiorenal syndrome by targeting both ends of the disorder, said Dr. McCullough, who chaired an American Heart Association panel that last year issued a scientific statement on cardiorenal syndrome (Circulation. 2019 Apr 16;139[16]:e840-78).
Although data on the SGLT2 inhibitors “are evolving,” the drug class is “going in the direction” of being “reasonably compared” with the ACE inhibitors and ARBs, said Javed Butler, MD, professor and chair of medicine at the University of Mississippi Medical Center, Jackson. “There are certainly complementary benefits that we see for both cardiovascular and renal outcomes.”
“We’ll think more and more about the SGLT2 inhibitors like renin-angiotensin system [RAS] inhibitors,” said David Z. Cherney, MD, referring to the drug class that includes ACE inhibitors and ARBs. “We should start to approach SGLT2 inhibitors like RAS inhibitors, with pleiotropic effects that go beyond glucose,” said Dr. Cherney, a nephrologist and professor of medicine at the University of Toronto, during the virtual annual scientific sessions of the American Diabetes Association in June 2020.
Working together in the nephron
One of the clearest complementary interactions between the SGLT2 inhibitors and the RAS inhibitors is their ability to reduce intraglomerular pressure, a key mechanism that slows nephron loss and progression of chronic kidney disease. SGLT2 inhibitors reduce sodium absorption in the proximal tubule that causes, through tubuloglomerular feedback, afferent arteriole constriction that lowers intraglomerular pressure, while the RAS inhibitors inhibit efferent arteriole constriction mediated by angiotensin II, also cutting intraglomerular pressure. Together, “they almost work in tandem,” explained Janani Rangaswami, MD, a nephrologist at Einstein Medical Center in Philadelphia, vice chair of the Kidney Council of the AHA, and first author of the 2019 cardiorenal syndrome AHA statement.
“Many had worried that if we target both the afferent and efferent arterioles simultaneously, it might increase the risk for acute kidney injury. What has been reassuring in both the recent data from the DAPA-HF trial and in recent meta-analysis was no evidence of increased risk for acute kidney injury with use of the SGLT2 inhibitor,” Dr. Rangaswami said in an interview. For example, a recent report on more than 39,000 Canadian patients with T2D who were at least 66 years old and newly begun on either an SGLT2 inhibitor or a different oral diabetes drug (a dipeptidyl peptidase–4 inhibitor), found a statistically significant 21% lower rate of acute kidney injury during the first 90 days on treatment with an SGLT2 inhibitor in a propensity score–matched analysis (CMAJ. 2020 Apr 6;192: e351-60).
Much of the concern about possible acute kidney injury stemmed from a property that the SGLT2 inhibitors share with RAS inhibitors: They cause an initial, reversible decline in glomerular filtration rate (GFR), followed by longer-term nephron preservation, a pattern attributable to reduced intraglomerular pressure. The question early on was: “ ‘Does this harm the kidney?’ But what we’ve seen is that patients do better over time, even with this initial hit. Whenever you offload the glomerulus you cut barotrauma and protect renal function,” explained Silvio E. Inzucchi, MD, professor of medicine at Yale University, New Haven, Conn., and director of the Yale Medicine Diabetes Center.
Dr. Inzucchi cautioned, however, that a small number of patients starting treatment with an SGLT2 inhibitor may have their GFR drop too sharply, especially if their GFR was low to start with. “You need to be careful, especially at the lower end of the GFR range. I recheck renal function after 1 month” after a patient starts an SGLT2. Patients whose level falls too low may need to discontinue. He added that it’s hard to set a uniform threshold for alarm, and instead assess patients on a case-by-case basis, but “you need some threshold in mind, where you will stop” treatment.
A smarter diuretic
One of the most intriguing renal effects of SGLT2 inhibitors is their diuretic action. During a talk at the virtual ADA scientific sessions, cardiologist Jeffrey Testani, MD, called them “smart” diuretics, because their effect on diuresis is relatively modest but comes without the neurohormonal price paid when patients take conventional loop diuretics.
”Loop diuretics are particularly bad,” causing neurohormonal activation that includes norepinephrine, renin, and vasopressin, said Dr. Testani, director of heart failure research at Yale. They also fail to produce a meaningful drop in blood volume despite causing substantial natriuresis.
In contrast, SGLT2 inhibitors cause “moderate” natriuresis while producing a significant cut in blood volume. “The body seems content with this lower plasma volume without activating catecholamines or renin, and that’s how the SGLT2 inhibitors differ from other diuretics,” said Dr. Inzucchi.
The class also maintains serum levels of potassium and magnesium, produces significant improvements in serum uric acid levels, and avoids the electrolyte abnormalities, volume depletion, and acute kidney injury that can occur with conventional distal diuretics, Dr. Testani said.
In short, the SGLT2 inhibitors “are safe and easy-to-use diuretics,” which allows them to fill a “huge unmet need for patients with heart failure.” As evidence accumulates for the benefits of the drug class in patients with heart failure and renal disease, “uptake will be extensive,” Dr. Testani predicted, driven in part by how easy it is to add the class to existing cardiorenal drug regimens.
Other standard therapies for patients with heart failure with reduced ejection fraction (HFrEF) risk electrolyte abnormalities, renal dysfunction, significantly lower blood pressure, often make patients feel worse, and involve a slow and laborious titration process, Dr. Testani noted. The SGLT2 inhibitor agents avoid these issues, a property that has played out in quality of life assessments of patients with HFrEF who received a drug from this class.
Outcomes met in trial after trial
In the DAPA-HF trial, with 4,443 patients with HFrEF and divided roughly equally between those with or without T2D, treatment with dapagliflozin (Farxiga) linked with significant improvements in health status and quality of life measured by the Kansas City Cardiomyopathy Questionnaire (Circulation. 2020 Jan 14;141[2]:90-9). “Not all treatments for HFrEF improve symptoms,” but in this study the SGTL2 inhibitor dapagliflozin did, boosting the Kansas City Cardiomyopathy Questionnaire score by about the same magnitude as treatment with a cardiac resynchronization device in patients with HFrEF, said Mikhail N. Kosiborod, MD, director of Cardiometabolic Research at Saint Luke’s Mid America Heart Institute in Kansas City, Mo., speaking at the virtual ADA scientific sessions.
Two more recent renal observations have further solidified the growing role of these drugs for kidney protection. Results from the CREDENCE trial that looked at canagliflozin (Invokana) treatment in 4,401 patients with T2D and albuminuria and chronic kidney disease showed canagliflozin treatment cut the primary, composite renal endpoint by a statistically significant 30%, compared with placebo (N Engl J Med. 2019 Jun 13;380[24]:2295-306). The study stopped earlier than planned because of how effective canagliflozin appeared.
“Never before has a renal protection clinical trial stopped for overwhelming efficacy,” noted nephrologist Katherine R. Tuttle, MD, executive director for research at Providence Health Care in Spokane, Wash. “It’s very exciting to have a treatment that works on both the heart and kidney, given their interrelationship,” she said during the ADA sessions. Dr. Tuttle called the cardiorenal effects from the SGLT2 inhibitors “amazing.”
Just as the DAPA-HF trial’s primary outcome showed the ability of at least one drug from the class, dapagliflozin, to improve outcomes in HFrEF patients without T2D, topline results recently reported from the DAPA-CDK trial showed for the first time renal protection by an SGLT2 inhibitor in patients with chronic kidney disease but no T2D, in a study with about 4,300 patients.
Although detailed results from DAPA-CKD are not yet available, so far the outcomes seem consistent with the CREDENCE findings, and the cumulative renal findings for the class show the SGLT2 inhibitors have “potential for a profound impact on the patients we see in every nephrology clinic, and with dual cardiorenal disease,” said Dr. Rangaswami. The class is now established as “standard of care for patients with chronic kidney disease. The CREDENCE results made that clear.”
The DAPA-CKD findings in patients with chronic kidney disease regardless of their diabetes status “are very important. We really have not had any advances in this space for some time, and chronic kidney disease patients have very poor outcomes, both cardiovascular and renal,” commented Dr. Butler. The advantage from using this drug class in these patients “is huge.”
The DAPA-CKD findings are a “major advance,” agreed Dr. McCullough.
SGLT2 inhibitor use needs to grow
Experts lament that although the evidence favoring the class has been very bullish, prescribing uptake has been slow, perhaps partly explained by the retail U.S. cost for most of these agents, generally about $17/day.
Cost is, unfortunately, an issue right now for these drugs, said Dr. Butler. Generic formulations are imminent, “but we cannot accept waiting. Providing this therapy when insurance coverage is available,” is essential.
The FDA has already granted tentative approval to some generic formulations, although resolution of patent issues can delay generics actually reaching the market. “Generic dapagliflozin will have a major impact; the marketplace for these drugs will shift very quickly,” predicted Dr. McCullough.
But price may not be the sole barrier, cautioned Dr. Rangaswami. “I don’t think it’s just a cost issue. Several factors explain the slow uptake,” of the SGLT2 inhibitors. “The biggest barrier is that this is a new drug class, and understanding how to use the class is not yet where it needs to be in the physician community.” One of the biggest problems is that the SGLT2 inhibitors are still primarily regarded as drugs to treat hyperglycemia.
Physicians who treat patients with heart or renal disease “need to wrap their head around the idea that a drug with antihyperglycemic effects is now in their practice territory, and something they need to prescribe,” she noted. Currently “there is a reluctance to prescribe these drugs given the perception that they are antihyperglycemic agents, and usually get deferred to primary care physicians or endocrinologists. This results in huge missed opportunities by cardiologists and nephrologists in initiating these agents that have major cardiorenal risk reduction effects.”
The key role that cardiologists need to play in prescribing the SGLT2 inhibitors was brought home in a recent study of two representative U.S. health systems that showed patients with T2D were far more likely to see a cardiologist than an endocrinologist (Cardiovasc Endocrinol Metab. 2020 Jun;9[2]:56-9).
“The SGLT2 inhibitors are definitely a game-changing drug class,” summed up Dr. Rangaswami. “We’re going to see a lot of use in patients with heart and kidney disease.”
Dr. Cherney has been a consultant to or has received honoraria from AstraZeneca, Boehringer Ingelheim, Janssen, Lilly, Merck, Mitsubishi Tanabe Pharma, and Sanofi. Dr. Butler has had financial relationships with numerous pharmaceutical companies. Dr. McCullough and Dr. Rangaswami had no disclosures. Dr. Inzucchi has been a consultant to or helped run trials for Abbott, AstraZeneca, Boehringer Ingelheim, Merck, Novo Nordisk, Sanofi/Lexicon, and vTv Therapeutics. Dr. Testani has been a consultant to AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, cardionomic, FIRE1 Magenta Med, Novartis, Reprieve, Sanofi, and W.L. Gore. Dr. Kosiborod has been a consultant to or led trials for Amarin, Amgen, Applied Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Glytec, Janssen, Eli Lilly, Merck, Novartis, Novo Nordisk, Sanofi, and Vifor. Dr. Tuttle has been a consultant to AstraZeneca, Boehringer Ingelheim, Gilead, Goldfinch Bio, Eli Lilly, and Novo Nordisk.
mzoler@mdedge.com
The benefits from sodium-glucose cotransporter 2 inhibitor drugs proven during the past year for cutting heart failure hospitalization rates substantially in patients with heart failure with reduced ejection fraction and slowing progression of chronic kidney disease, all regardless of diabetes status, have thrust this drug class into the top tier of agents for potentially treating millions of patients with cardiac or renal disease.
The sodium-glucose cotransporter 2 (SGLT2) inhibitors, first licensed for U.S. marketing in 2013 purely for glycemic control, have, during the 5 years since the first cardiovascular outcome trial results for the class came out, shown benefits in a range of patients reminiscent of what’s been established for ACE inhibitors and angiotensin receptor blockers (ARBs).
The wide-reaching benefits of SGLT2 inhibitors have recently become even more relevant by showing clinically meaningful effects in patients without type 2 diabetes (T2D). And in an uncanny coincidence, the SGLT2 inhibitors appear to act in complementary harmony with the ACE inhibitors and ARBs for preserving heart and renal function. These properties have made the SGLT2 inhibitors especially attractive as a new weapon for controlling the ascendant disorder of cardiorenal syndrome.
“SGLT2 inhibitors have a relatively greater impact on cardiovascular outcomes, compared with ACE inhibitors and ARBs, but the effects [of the two classes] are synergistic and ideally patients receive both,” said Peter McCullough, MD, a specialist in treating cardiorenal syndrome and other cardiovascular and renal disorders at Baylor, Scott, and White Heart and Vascular Hospital in Dallas. The SGLT2 inhibitors are among the drugs best suited to both treating and preventing cardiorenal syndrome by targeting both ends of the disorder, said Dr. McCullough, who chaired an American Heart Association panel that last year issued a scientific statement on cardiorenal syndrome (Circulation. 2019 Apr 16;139[16]:e840-78).
Although data on the SGLT2 inhibitors “are evolving,” the drug class is “going in the direction” of being “reasonably compared” with the ACE inhibitors and ARBs, said Javed Butler, MD, professor and chair of medicine at the University of Mississippi Medical Center, Jackson. “There are certainly complementary benefits that we see for both cardiovascular and renal outcomes.”
“We’ll think more and more about the SGLT2 inhibitors like renin-angiotensin system [RAS] inhibitors,” said David Z. Cherney, MD, referring to the drug class that includes ACE inhibitors and ARBs. “We should start to approach SGLT2 inhibitors like RAS inhibitors, with pleiotropic effects that go beyond glucose,” said Dr. Cherney, a nephrologist and professor of medicine at the University of Toronto, during the virtual annual scientific sessions of the American Diabetes Association in June 2020.
Working together in the nephron
One of the clearest complementary interactions between the SGLT2 inhibitors and the RAS inhibitors is their ability to reduce intraglomerular pressure, a key mechanism that slows nephron loss and progression of chronic kidney disease. SGLT2 inhibitors reduce sodium absorption in the proximal tubule that causes, through tubuloglomerular feedback, afferent arteriole constriction that lowers intraglomerular pressure, while the RAS inhibitors inhibit efferent arteriole constriction mediated by angiotensin II, also cutting intraglomerular pressure. Together, “they almost work in tandem,” explained Janani Rangaswami, MD, a nephrologist at Einstein Medical Center in Philadelphia, vice chair of the Kidney Council of the AHA, and first author of the 2019 cardiorenal syndrome AHA statement.
“Many had worried that if we target both the afferent and efferent arterioles simultaneously, it might increase the risk for acute kidney injury. What has been reassuring in both the recent data from the DAPA-HF trial and in recent meta-analysis was no evidence of increased risk for acute kidney injury with use of the SGLT2 inhibitor,” Dr. Rangaswami said in an interview. For example, a recent report on more than 39,000 Canadian patients with T2D who were at least 66 years old and newly begun on either an SGLT2 inhibitor or a different oral diabetes drug (a dipeptidyl peptidase–4 inhibitor), found a statistically significant 21% lower rate of acute kidney injury during the first 90 days on treatment with an SGLT2 inhibitor in a propensity score–matched analysis (CMAJ. 2020 Apr 6;192: e351-60).
Much of the concern about possible acute kidney injury stemmed from a property that the SGLT2 inhibitors share with RAS inhibitors: They cause an initial, reversible decline in glomerular filtration rate (GFR), followed by longer-term nephron preservation, a pattern attributable to reduced intraglomerular pressure. The question early on was: “ ‘Does this harm the kidney?’ But what we’ve seen is that patients do better over time, even with this initial hit. Whenever you offload the glomerulus you cut barotrauma and protect renal function,” explained Silvio E. Inzucchi, MD, professor of medicine at Yale University, New Haven, Conn., and director of the Yale Medicine Diabetes Center.
Dr. Inzucchi cautioned, however, that a small number of patients starting treatment with an SGLT2 inhibitor may have their GFR drop too sharply, especially if their GFR was low to start with. “You need to be careful, especially at the lower end of the GFR range. I recheck renal function after 1 month” after a patient starts an SGLT2. Patients whose level falls too low may need to discontinue. He added that it’s hard to set a uniform threshold for alarm, and instead assess patients on a case-by-case basis, but “you need some threshold in mind, where you will stop” treatment.
A smarter diuretic
One of the most intriguing renal effects of SGLT2 inhibitors is their diuretic action. During a talk at the virtual ADA scientific sessions, cardiologist Jeffrey Testani, MD, called them “smart” diuretics, because their effect on diuresis is relatively modest but comes without the neurohormonal price paid when patients take conventional loop diuretics.
”Loop diuretics are particularly bad,” causing neurohormonal activation that includes norepinephrine, renin, and vasopressin, said Dr. Testani, director of heart failure research at Yale. They also fail to produce a meaningful drop in blood volume despite causing substantial natriuresis.
In contrast, SGLT2 inhibitors cause “moderate” natriuresis while producing a significant cut in blood volume. “The body seems content with this lower plasma volume without activating catecholamines or renin, and that’s how the SGLT2 inhibitors differ from other diuretics,” said Dr. Inzucchi.
The class also maintains serum levels of potassium and magnesium, produces significant improvements in serum uric acid levels, and avoids the electrolyte abnormalities, volume depletion, and acute kidney injury that can occur with conventional distal diuretics, Dr. Testani said.
In short, the SGLT2 inhibitors “are safe and easy-to-use diuretics,” which allows them to fill a “huge unmet need for patients with heart failure.” As evidence accumulates for the benefits of the drug class in patients with heart failure and renal disease, “uptake will be extensive,” Dr. Testani predicted, driven in part by how easy it is to add the class to existing cardiorenal drug regimens.
Other standard therapies for patients with heart failure with reduced ejection fraction (HFrEF) risk electrolyte abnormalities, renal dysfunction, significantly lower blood pressure, often make patients feel worse, and involve a slow and laborious titration process, Dr. Testani noted. The SGLT2 inhibitor agents avoid these issues, a property that has played out in quality of life assessments of patients with HFrEF who received a drug from this class.
Outcomes met in trial after trial
In the DAPA-HF trial, with 4,443 patients with HFrEF and divided roughly equally between those with or without T2D, treatment with dapagliflozin (Farxiga) linked with significant improvements in health status and quality of life measured by the Kansas City Cardiomyopathy Questionnaire (Circulation. 2020 Jan 14;141[2]:90-9). “Not all treatments for HFrEF improve symptoms,” but in this study the SGTL2 inhibitor dapagliflozin did, boosting the Kansas City Cardiomyopathy Questionnaire score by about the same magnitude as treatment with a cardiac resynchronization device in patients with HFrEF, said Mikhail N. Kosiborod, MD, director of Cardiometabolic Research at Saint Luke’s Mid America Heart Institute in Kansas City, Mo., speaking at the virtual ADA scientific sessions.
Two more recent renal observations have further solidified the growing role of these drugs for kidney protection. Results from the CREDENCE trial that looked at canagliflozin (Invokana) treatment in 4,401 patients with T2D and albuminuria and chronic kidney disease showed canagliflozin treatment cut the primary, composite renal endpoint by a statistically significant 30%, compared with placebo (N Engl J Med. 2019 Jun 13;380[24]:2295-306). The study stopped earlier than planned because of how effective canagliflozin appeared.
“Never before has a renal protection clinical trial stopped for overwhelming efficacy,” noted nephrologist Katherine R. Tuttle, MD, executive director for research at Providence Health Care in Spokane, Wash. “It’s very exciting to have a treatment that works on both the heart and kidney, given their interrelationship,” she said during the ADA sessions. Dr. Tuttle called the cardiorenal effects from the SGLT2 inhibitors “amazing.”
Just as the DAPA-HF trial’s primary outcome showed the ability of at least one drug from the class, dapagliflozin, to improve outcomes in HFrEF patients without T2D, topline results recently reported from the DAPA-CDK trial showed for the first time renal protection by an SGLT2 inhibitor in patients with chronic kidney disease but no T2D, in a study with about 4,300 patients.
Although detailed results from DAPA-CKD are not yet available, so far the outcomes seem consistent with the CREDENCE findings, and the cumulative renal findings for the class show the SGLT2 inhibitors have “potential for a profound impact on the patients we see in every nephrology clinic, and with dual cardiorenal disease,” said Dr. Rangaswami. The class is now established as “standard of care for patients with chronic kidney disease. The CREDENCE results made that clear.”
The DAPA-CKD findings in patients with chronic kidney disease regardless of their diabetes status “are very important. We really have not had any advances in this space for some time, and chronic kidney disease patients have very poor outcomes, both cardiovascular and renal,” commented Dr. Butler. The advantage from using this drug class in these patients “is huge.”
The DAPA-CKD findings are a “major advance,” agreed Dr. McCullough.
SGLT2 inhibitor use needs to grow
Experts lament that although the evidence favoring the class has been very bullish, prescribing uptake has been slow, perhaps partly explained by the retail U.S. cost for most of these agents, generally about $17/day.
Cost is, unfortunately, an issue right now for these drugs, said Dr. Butler. Generic formulations are imminent, “but we cannot accept waiting. Providing this therapy when insurance coverage is available,” is essential.
The FDA has already granted tentative approval to some generic formulations, although resolution of patent issues can delay generics actually reaching the market. “Generic dapagliflozin will have a major impact; the marketplace for these drugs will shift very quickly,” predicted Dr. McCullough.
But price may not be the sole barrier, cautioned Dr. Rangaswami. “I don’t think it’s just a cost issue. Several factors explain the slow uptake,” of the SGLT2 inhibitors. “The biggest barrier is that this is a new drug class, and understanding how to use the class is not yet where it needs to be in the physician community.” One of the biggest problems is that the SGLT2 inhibitors are still primarily regarded as drugs to treat hyperglycemia.
Physicians who treat patients with heart or renal disease “need to wrap their head around the idea that a drug with antihyperglycemic effects is now in their practice territory, and something they need to prescribe,” she noted. Currently “there is a reluctance to prescribe these drugs given the perception that they are antihyperglycemic agents, and usually get deferred to primary care physicians or endocrinologists. This results in huge missed opportunities by cardiologists and nephrologists in initiating these agents that have major cardiorenal risk reduction effects.”
The key role that cardiologists need to play in prescribing the SGLT2 inhibitors was brought home in a recent study of two representative U.S. health systems that showed patients with T2D were far more likely to see a cardiologist than an endocrinologist (Cardiovasc Endocrinol Metab. 2020 Jun;9[2]:56-9).
“The SGLT2 inhibitors are definitely a game-changing drug class,” summed up Dr. Rangaswami. “We’re going to see a lot of use in patients with heart and kidney disease.”
Dr. Cherney has been a consultant to or has received honoraria from AstraZeneca, Boehringer Ingelheim, Janssen, Lilly, Merck, Mitsubishi Tanabe Pharma, and Sanofi. Dr. Butler has had financial relationships with numerous pharmaceutical companies. Dr. McCullough and Dr. Rangaswami had no disclosures. Dr. Inzucchi has been a consultant to or helped run trials for Abbott, AstraZeneca, Boehringer Ingelheim, Merck, Novo Nordisk, Sanofi/Lexicon, and vTv Therapeutics. Dr. Testani has been a consultant to AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, cardionomic, FIRE1 Magenta Med, Novartis, Reprieve, Sanofi, and W.L. Gore. Dr. Kosiborod has been a consultant to or led trials for Amarin, Amgen, Applied Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Glytec, Janssen, Eli Lilly, Merck, Novartis, Novo Nordisk, Sanofi, and Vifor. Dr. Tuttle has been a consultant to AstraZeneca, Boehringer Ingelheim, Gilead, Goldfinch Bio, Eli Lilly, and Novo Nordisk.
mzoler@mdedge.com
ASCO says ‘no’ to home infusions of cancer treatment, with exceptions
in a new policy statement issued July 31.
At the same time, it supports exceptions: namely, when individual physicians and patients, having jointly discussed risks and benefits, agree to have treatments administered in the home.
The new policy is limited to intravenous infusions of anticancer agents such as chemotherapy, monoclonal antibodies, and other drugs — administered by health care personnel. It does not refer to injections.
The policy was prompted by regulatory flexibilities from the Centers for Medicare & Medicaid Services made in response to the accelerating COVID-19 pandemic. “Among these flexibilities were new provisions that enabled providers to deliver care in a setting most appropriate – and safest – for individual patient circumstances,” which has “opened the path for potential increases in use of home infusion for anticancer therapy,” says ASCO.
“We’re not ready to endorse [chemo at home] as a general policy until we have evidence that it’s safe. At the same time, the policy gives physicians and patients autonomy to respond to whatever situation they find themselves in,” Stephen Grubbs, MD, ASCO’s senior director of clinical affairs, said in an interview.
“Antineoplastic drugs are effective at treating cancer but can be extremely toxic to normal human cells,” reads the statement, which was written by a group of about 25 professionals, including Grubbs and other ASCO staff as well as independent advisers.
“There is a paucity of evidence directly comparing the safety of chemotherapy infusions in the home and outpatient settings,” the ASCO policy explains.
ASCO’s policy acknowledges that there are data “from other countries demonstrating that ... home infusion can be safe, well-tolerated, and may be preferred by some patients.” But such data are limited and only apply “to certain circumstances and for specific agents,” it adds.
One US cancer center (in Philadelphia) already has an established chemo-at-home program and has seen an increase in its use during the pandemic, as reported by Medscape Medical News. Approached for comment, Justin Bekelman, MD, director of the Penn Center for Cancer Care Innovation in Philadelphia, interpreted the new ASCO policy in a positive light.
“Physicians at the Abramson Cancer Center of the University of Pennsylvania and ASCO agree – home-based cancer therapy with oncologist oversight and well-designed safety protocols can be a safe option for patients with cancer,” he said in a statement.
ASCO says its existing safety standards “may be difficult to satisfy in the home infusion context,” including for safely resolving life-threatening emergencies.
Grubbs said that in the worst-case scenario, such as anaphylaxis, “you can die from [it] if you don’t manage it quickly and properly.”
“When I was practicing, we always had a physician present right next to the infusion area because these are severe reactions that happen very quickly,” he said, adding that “several a year” occurred when he practiced full-time.
Also, chemotherapy spills are a “big deal” in the home, as clean-up may be complex and difficult, added Grubbs.
Data from ASCO’s PracticeNET program show that in the first months (March and April) of the COVID-19 pandemic, chemotherapy visits to infusion suites were not reduced in a dataset of 16 US practices, he noted. However, there are exceptions and variance based on location, Grubbs said, such as “hot spots” including New York City in April.
While the pandemic has no end in sight, ASCO issued a set of six recommendations for use of anticancer therapies infused in the home. First, they call for independent, publicly funded research to evaluate the safety and effectiveness of home infusion of anticancer therapy.
Next in importance, ASCO wants the current temporary regulation change from CMS due to the pandemic to end.
“CMS should not extend the temporary flexibility related to home infusion for Part B cancer drugs that was approved as part of their response to the public health emergency,” they state.
Even before the pandemic, changes were afoot. Under the 21st Century Cures Act, which was passed in 2019 and will be implemented in 2021, CMS instituted a permanent home infusion therapy services benefit, which includes anticancer therapies. It “remains to be seen what, if any, shift away from outpatient infusion facilities will occur,” observes ASCO in its policy statement.
This article first appeared on Medscape.com.
in a new policy statement issued July 31.
At the same time, it supports exceptions: namely, when individual physicians and patients, having jointly discussed risks and benefits, agree to have treatments administered in the home.
The new policy is limited to intravenous infusions of anticancer agents such as chemotherapy, monoclonal antibodies, and other drugs — administered by health care personnel. It does not refer to injections.
The policy was prompted by regulatory flexibilities from the Centers for Medicare & Medicaid Services made in response to the accelerating COVID-19 pandemic. “Among these flexibilities were new provisions that enabled providers to deliver care in a setting most appropriate – and safest – for individual patient circumstances,” which has “opened the path for potential increases in use of home infusion for anticancer therapy,” says ASCO.
“We’re not ready to endorse [chemo at home] as a general policy until we have evidence that it’s safe. At the same time, the policy gives physicians and patients autonomy to respond to whatever situation they find themselves in,” Stephen Grubbs, MD, ASCO’s senior director of clinical affairs, said in an interview.
“Antineoplastic drugs are effective at treating cancer but can be extremely toxic to normal human cells,” reads the statement, which was written by a group of about 25 professionals, including Grubbs and other ASCO staff as well as independent advisers.
“There is a paucity of evidence directly comparing the safety of chemotherapy infusions in the home and outpatient settings,” the ASCO policy explains.
ASCO’s policy acknowledges that there are data “from other countries demonstrating that ... home infusion can be safe, well-tolerated, and may be preferred by some patients.” But such data are limited and only apply “to certain circumstances and for specific agents,” it adds.
One US cancer center (in Philadelphia) already has an established chemo-at-home program and has seen an increase in its use during the pandemic, as reported by Medscape Medical News. Approached for comment, Justin Bekelman, MD, director of the Penn Center for Cancer Care Innovation in Philadelphia, interpreted the new ASCO policy in a positive light.
“Physicians at the Abramson Cancer Center of the University of Pennsylvania and ASCO agree – home-based cancer therapy with oncologist oversight and well-designed safety protocols can be a safe option for patients with cancer,” he said in a statement.
ASCO says its existing safety standards “may be difficult to satisfy in the home infusion context,” including for safely resolving life-threatening emergencies.
Grubbs said that in the worst-case scenario, such as anaphylaxis, “you can die from [it] if you don’t manage it quickly and properly.”
“When I was practicing, we always had a physician present right next to the infusion area because these are severe reactions that happen very quickly,” he said, adding that “several a year” occurred when he practiced full-time.
Also, chemotherapy spills are a “big deal” in the home, as clean-up may be complex and difficult, added Grubbs.
Data from ASCO’s PracticeNET program show that in the first months (March and April) of the COVID-19 pandemic, chemotherapy visits to infusion suites were not reduced in a dataset of 16 US practices, he noted. However, there are exceptions and variance based on location, Grubbs said, such as “hot spots” including New York City in April.
While the pandemic has no end in sight, ASCO issued a set of six recommendations for use of anticancer therapies infused in the home. First, they call for independent, publicly funded research to evaluate the safety and effectiveness of home infusion of anticancer therapy.
Next in importance, ASCO wants the current temporary regulation change from CMS due to the pandemic to end.
“CMS should not extend the temporary flexibility related to home infusion for Part B cancer drugs that was approved as part of their response to the public health emergency,” they state.
Even before the pandemic, changes were afoot. Under the 21st Century Cures Act, which was passed in 2019 and will be implemented in 2021, CMS instituted a permanent home infusion therapy services benefit, which includes anticancer therapies. It “remains to be seen what, if any, shift away from outpatient infusion facilities will occur,” observes ASCO in its policy statement.
This article first appeared on Medscape.com.
in a new policy statement issued July 31.
At the same time, it supports exceptions: namely, when individual physicians and patients, having jointly discussed risks and benefits, agree to have treatments administered in the home.
The new policy is limited to intravenous infusions of anticancer agents such as chemotherapy, monoclonal antibodies, and other drugs — administered by health care personnel. It does not refer to injections.
The policy was prompted by regulatory flexibilities from the Centers for Medicare & Medicaid Services made in response to the accelerating COVID-19 pandemic. “Among these flexibilities were new provisions that enabled providers to deliver care in a setting most appropriate – and safest – for individual patient circumstances,” which has “opened the path for potential increases in use of home infusion for anticancer therapy,” says ASCO.
“We’re not ready to endorse [chemo at home] as a general policy until we have evidence that it’s safe. At the same time, the policy gives physicians and patients autonomy to respond to whatever situation they find themselves in,” Stephen Grubbs, MD, ASCO’s senior director of clinical affairs, said in an interview.
“Antineoplastic drugs are effective at treating cancer but can be extremely toxic to normal human cells,” reads the statement, which was written by a group of about 25 professionals, including Grubbs and other ASCO staff as well as independent advisers.
“There is a paucity of evidence directly comparing the safety of chemotherapy infusions in the home and outpatient settings,” the ASCO policy explains.
ASCO’s policy acknowledges that there are data “from other countries demonstrating that ... home infusion can be safe, well-tolerated, and may be preferred by some patients.” But such data are limited and only apply “to certain circumstances and for specific agents,” it adds.
One US cancer center (in Philadelphia) already has an established chemo-at-home program and has seen an increase in its use during the pandemic, as reported by Medscape Medical News. Approached for comment, Justin Bekelman, MD, director of the Penn Center for Cancer Care Innovation in Philadelphia, interpreted the new ASCO policy in a positive light.
“Physicians at the Abramson Cancer Center of the University of Pennsylvania and ASCO agree – home-based cancer therapy with oncologist oversight and well-designed safety protocols can be a safe option for patients with cancer,” he said in a statement.
ASCO says its existing safety standards “may be difficult to satisfy in the home infusion context,” including for safely resolving life-threatening emergencies.
Grubbs said that in the worst-case scenario, such as anaphylaxis, “you can die from [it] if you don’t manage it quickly and properly.”
“When I was practicing, we always had a physician present right next to the infusion area because these are severe reactions that happen very quickly,” he said, adding that “several a year” occurred when he practiced full-time.
Also, chemotherapy spills are a “big deal” in the home, as clean-up may be complex and difficult, added Grubbs.
Data from ASCO’s PracticeNET program show that in the first months (March and April) of the COVID-19 pandemic, chemotherapy visits to infusion suites were not reduced in a dataset of 16 US practices, he noted. However, there are exceptions and variance based on location, Grubbs said, such as “hot spots” including New York City in April.
While the pandemic has no end in sight, ASCO issued a set of six recommendations for use of anticancer therapies infused in the home. First, they call for independent, publicly funded research to evaluate the safety and effectiveness of home infusion of anticancer therapy.
Next in importance, ASCO wants the current temporary regulation change from CMS due to the pandemic to end.
“CMS should not extend the temporary flexibility related to home infusion for Part B cancer drugs that was approved as part of their response to the public health emergency,” they state.
Even before the pandemic, changes were afoot. Under the 21st Century Cures Act, which was passed in 2019 and will be implemented in 2021, CMS instituted a permanent home infusion therapy services benefit, which includes anticancer therapies. It “remains to be seen what, if any, shift away from outpatient infusion facilities will occur,” observes ASCO in its policy statement.
This article first appeared on Medscape.com.
How three cardiac procedures changed in the COVID era
When Virginia’s governor directed the postponement of all elective surgeries in late March, Wayne Batchelor, MD and his colleagues at the Inova Heart and Vascular Institute in Falls Church, Va., canceled about two-thirds of their transcatheter aortic valve replacement (TAVR) procedures.

They then categorized patients by tiers to gauge which procedures could safely be postponed and to guide triaging. And while they did not deviate from the practice of having both an interventional cardiologist and a cardiothoracic surgeon present for TAVR, they slimmed down preprocedural testing when feasible and delayed some 30-day post-TAVR echocardiographic assessments. “It was a delicate dance, very difficult dance. But luckily, we were able to navigate the challenges effectively,” said Dr. Batchelor, the institute’s director of interventional cardiology and interventional cardiology research.
A “system capacity dashboard” that merged bed and staffing data from interventional cardiology spaces with cardiovascular and noncardiovascular ICU beds, operating rooms, and other resources – and daily cross-department meetings – enabled them to proceed with the most urgent TAVR procedures while “keeping a buffer of ICU beds to accommodate an anticipated surge of COVID-19,” he explained.
Such adaptations in cardiac procedures and processes are occurring in hospitals across the country as efforts are made to minimize the risk of COVID-19 exposure for patients and staff. Dr. Batchelor is one of four cardiologists who shared their experiences and advice on common cardiac procedures across three locales: TAVR in Virginia, percutaneous coronary intervention (PCI) in New York City, and atrial fibrillation (AFib) ablation in Kentucky.
More on TAVR in Virginia
Inova’s framework for triaging structural heart disease interventions (largely TAVR and/or percutaneous mitral valve repair) comprised three tiers. Tier 1 captured “emergent cases that had to be done, no questions asked,” Dr. Batchelor said. For TAVR, these were inpatients with severe to critical symptomatic aortic stenosis and advanced congestive heart failure who could not safely be discharged, as well as other patients “with refractory symptoms of heart failure that were compelling.” Many had associated left ventricular systolic dysfunction.
Those who could delay 14-30 days were placed in tier 2, and patients who “we felt were fairly stable and could wait at least 30 days” were placed in tier 3. “For TAVR, a tier 3 patient might be the one … who has severe aortic stenosis but is walking around and doing well at home with only stable exertional symptoms,” he said.
Patients whose procedures were delayed were contacted weekly by the valve clinic’s advanced practice practitioners through video visits or telephone calls, and tier categorization was reevaluated if symptoms worsened. “We had to keep in close contact with them,” Dr. Batchelor said. “These patients can deteriorate quite rapidly and sometimes without much warning.”
Virtual video visits were often used for 30-day postprocedural follow-ups, taking the place of in-person visits during which post-TAVR echocardiographic assessments would normally be performed. “For follow-up, we’d often just do a quick visit to check the vascular access site within 7-10 days, and then, if they were doing okay we’d delay the 30-day echo to a later time frame,” he said.
Preprocedural testing was streamlined to minimize the number of patient-provider interactions, with pulmonary function testing and pre-TAVR catheterization omitted unless absolutely necessary. “A TAVR CT angiogram [performed within the prior year] is the only test you really absolutely need,” Dr. Batchelor said. “We were much less likely to order a heart catheterization unless the patient was having angina and high risk or suspicion for significant coronary artery disease.”
This approach was not associated with any compromise in postprocedural outcomes, he noted. Prior to the pandemic, Inova routinely employed a minimalist approach to TAVR with moderate conscious sedation and avoiding transesophageal echocardiography – steps that were recommended for structural heart procedures in the COVID-19 era in a published review by the heart team at New York-Presbyterian Hospital/Columbia University Irving Medical Center.
The New York review is useful for cardiologists in areas with rising case burdens of COVID-19, Dr. Batchelor said, as is a position statement he coauthored from the American College of Cardiology and the Society for Cardiology and Angiography Interventions (SCAI) on triage considerations for structural heart disease interventions during the pandemic.
TAVR’s resource-heavy nature made the “system capacity dashboard” and daily meetings critical, Dr. Batchelor explained. At one point during the hold on elective procedures, the Falls Church INOVA facility had approximately 300 patients with COVID-19, a significant proportion of whom were in cardiac ICU beds.
“Everyone has to be flexible and learn,” he said. “We trained our cardiologists on managing ventilators in case some of the [critical care] staff got ill or were overwhelmed by the surge.”
More than 2 months after the surge eased and the ban on elective surgery was lifted, Dr. Batchelor and his colleagues are still using the dashboard and continue to meet daily to discuss COVID-19 prevalence in the hospital and the community as they work through the backlog of delayed procedures. They also routinely review the status of COVID-19 testing for inpatients and outpatients and the donning and doffing of personal protective equipment.
“You have to communicate early and often across the whole system of care because you’re competing for the same resources,” he advised. “And you have to be flexible and reassess. A policy that works at the beginning of the pandemic might have to change.”
PCI in New York
Before the pandemic, the cardiac catheterization laboratory at Mount Sinai Morningside Hospital in New York handled a monthly average of 140-150 PCIs, including 6-10 primary PCIs for ST-segment elevation myocardial infarction.

When electives were halted by the hospital in March and the City became the global epicenter for COVID-19, the cath lab went quiet. “Even though we were still able to do urgent cases or emergent cases, the case volume dropped tremendously,” said Jacqueline E. Tamis-Holland, MD, associate director of the cardiac catheterization laboratory and director of the interventional cardiology fellowship. “There weren’t many outpatients in our hospital … and by late March and through April, there wasn’t a single acute infarction.”
She and Tak W. Kwan, MD, director of the cardiac catheterization laboratory and professor of medicine at Icahn School of Medicine at Mount Sinai, New York, were prepared to move true STEMI patients into the cath lab for primary PCI without delay unless the staff or system were overrun.
That primary PCI should remain the first-line treatment for STEMI even in cases of confirmed or suspected COVID-19 was recommended by SCAI guidance issued in March and by a consensus statement released by the SCAI, ACC, and American College of Emergency Physicians in April – and “we were very much of the same frame of mind,” Dr. Tamis-Holland said.
Deciding which elective cases could not be delayed required a completely individualized approach, the cardiologists emphasized. Dr. Tamis-Holland had a few patients scheduled for elective PCI when the hold began, and “we spoke every few days or once a week in the beginning, then transitioned to once every 2 weeks,” she said. “With medical therapy and given that they were relatively sedentary, my patients did okay [with the delays].”
For subsequent patients, she considered their symptoms or stress test results. “If it’s someone who I’d [normally] wait until next week to schedule the cath, then we would wait 2 or 3 more weeks, or a month more with careful monitoring,” she said. “Certainly, there was a decrease in the number of abnormal stress tests that I referred to the cath lab during [the surge period].”
Dr. Kwan described one patient who had new-onset congestive heart failure in late March “with a markedly positive nuclear stress test.” The patient was monitored with twice-weekly telemedicine visits and office visits, and a cardiac catheterization was performed in early May as an urgent elective case. “He had severe three-vessel and left main disease,” he said. “Subsequently, [coronary artery bypass surgery] was done.”
There were no changes in the PCI procedure itself in terms of hospital stay (most elective cases at Mt. Sinai are same-day procedures) or in staffing, other than a ban on visiting students or residents. The most important changes during the surge – in addition to stocking enough personal protective equipment – concerned testing. Patients undergoing elective PCI are tested for the novel coronavirus 72 hours before the procedure, and rapid testing is performed in the emergency room for STEMI patients to determine patient disposition after the procedure.
“Until we have the results back we should treat all patients as if they are a patient under investigation or have COVID,” said Dr. Tamis-Holland, who helped develop emergency guidance on STEMI systems of care during the pandemic for the American Heart Association.
In early May, the hospital freed up additional space for cardiac care, allowing more “urgent-elective” PCIs to be done. Some patients were reluctant to proceed, the cardiologists said, because of a no-visitor policy. In mid-June, the hold on elective procedures was lifted, and around the same time, the hospital shifted to a one-visitor policy. Still, some patients opted to continue longer with medical therapy.
Patients need to feel comfortable, and “there is a lag time from the time everything opens up and when patients get their stress tests and their evaluations, and then arrive for PCI,” said Dr. Tamis-Holland.
By mid-July, the cardiologists were anticipating an increase in complications from infarctions among patients who “waited them out at home” – heart failure or mitral valve regurgitation, for instance – but, in their hospital at least, “we haven’t really seen that,” she added.
AFib ablation in Kentucky
As New York experienced its surge, John Mandrola, MD, and other electrophysiologists across the Baptist Health system in Kentucky reached a consensus on how to categorize their procedures. Electrophysiology interventions were classified urgent, emergent, and truly elective in the event that the state’s relatively low case burden of COVID-19 were to significantly worsen.
There was no doubt where AFib ablation sat. “It’s one of the most elective procedures there is” in terms of scheduling under normal circumstances, and it almost always requires an overnight stay and general anesthesia – factors that upped the ante on an elective classification, said Dr. Mandrola.
All AF ablations were deemed elective unless the patient required immediate hospitalization. For 8-10 weeks during the state’s shutdown of elective care, Dr. Mandrola and his partner successfully monitored patients with phone calls. “To be honest,” he said, “most patients did not want to have their AFib ablation anyway until the pandemic slowed and they knew it was safe.”
In some cases, patients reported that their symptoms were improving: “There are so many things to speculate about. ... Was it that everyone took their foot off the accelerator?” Dr. Mandrola thinks that postpandemic outcomes analyses may drive more scrutiny of the necessity of some AFib ablations and other procedures and tests. AFib ablation “has its place but is probably overused,” he said.
During the pause on electives, “the vast majority of procedures we did were pacemaker procedures,” he said. “We also did some atrial flutter ablations, and ablations for ventricular tachycardia and supraventricular tachycardia.” In mid-July, as the COVID-19 case burden in Kentucky remained relatively low, Dr. Mandrola was “up to 120%” of his pre-COVID electrophysiology volume – but ready to scale back again if needed.
Dr. Batchelor reported consulting fees from Boston Scientific, Abbott Medical, Medtronic, and V-wave. Dr. Kwan, Dr. Mandrola, and Dr. Tamis-Holland reported no relevant financial disclosures.
This article is a collaboration between Medscape and MDedge. A version of it originally appeared on Medscape.com.
When Virginia’s governor directed the postponement of all elective surgeries in late March, Wayne Batchelor, MD and his colleagues at the Inova Heart and Vascular Institute in Falls Church, Va., canceled about two-thirds of their transcatheter aortic valve replacement (TAVR) procedures.
They then categorized patients by tiers to gauge which procedures could safely be postponed and to guide triaging. And while they did not deviate from the practice of having both an interventional cardiologist and a cardiothoracic surgeon present for TAVR, they slimmed down preprocedural testing when feasible and delayed some 30-day post-TAVR echocardiographic assessments. “It was a delicate dance, very difficult dance. But luckily, we were able to navigate the challenges effectively,” said Dr. Batchelor, the institute’s director of interventional cardiology and interventional cardiology research.
A “system capacity dashboard” that merged bed and staffing data from interventional cardiology spaces with cardiovascular and noncardiovascular ICU beds, operating rooms, and other resources – and daily cross-department meetings – enabled them to proceed with the most urgent TAVR procedures while “keeping a buffer of ICU beds to accommodate an anticipated surge of COVID-19,” he explained.
Such adaptations in cardiac procedures and processes are occurring in hospitals across the country as efforts are made to minimize the risk of COVID-19 exposure for patients and staff. Dr. Batchelor is one of four cardiologists who shared their experiences and advice on common cardiac procedures across three locales: TAVR in Virginia, percutaneous coronary intervention (PCI) in New York City, and atrial fibrillation (AFib) ablation in Kentucky.
More on TAVR in Virginia
Inova’s framework for triaging structural heart disease interventions (largely TAVR and/or percutaneous mitral valve repair) comprised three tiers. Tier 1 captured “emergent cases that had to be done, no questions asked,” Dr. Batchelor said. For TAVR, these were inpatients with severe to critical symptomatic aortic stenosis and advanced congestive heart failure who could not safely be discharged, as well as other patients “with refractory symptoms of heart failure that were compelling.” Many had associated left ventricular systolic dysfunction.
Those who could delay 14-30 days were placed in tier 2, and patients who “we felt were fairly stable and could wait at least 30 days” were placed in tier 3. “For TAVR, a tier 3 patient might be the one … who has severe aortic stenosis but is walking around and doing well at home with only stable exertional symptoms,” he said.
Patients whose procedures were delayed were contacted weekly by the valve clinic’s advanced practice practitioners through video visits or telephone calls, and tier categorization was reevaluated if symptoms worsened. “We had to keep in close contact with them,” Dr. Batchelor said. “These patients can deteriorate quite rapidly and sometimes without much warning.”
Virtual video visits were often used for 30-day postprocedural follow-ups, taking the place of in-person visits during which post-TAVR echocardiographic assessments would normally be performed. “For follow-up, we’d often just do a quick visit to check the vascular access site within 7-10 days, and then, if they were doing okay we’d delay the 30-day echo to a later time frame,” he said.
Preprocedural testing was streamlined to minimize the number of patient-provider interactions, with pulmonary function testing and pre-TAVR catheterization omitted unless absolutely necessary. “A TAVR CT angiogram [performed within the prior year] is the only test you really absolutely need,” Dr. Batchelor said. “We were much less likely to order a heart catheterization unless the patient was having angina and high risk or suspicion for significant coronary artery disease.”
This approach was not associated with any compromise in postprocedural outcomes, he noted. Prior to the pandemic, Inova routinely employed a minimalist approach to TAVR with moderate conscious sedation and avoiding transesophageal echocardiography – steps that were recommended for structural heart procedures in the COVID-19 era in a published review by the heart team at New York-Presbyterian Hospital/Columbia University Irving Medical Center.
The New York review is useful for cardiologists in areas with rising case burdens of COVID-19, Dr. Batchelor said, as is a position statement he coauthored from the American College of Cardiology and the Society for Cardiology and Angiography Interventions (SCAI) on triage considerations for structural heart disease interventions during the pandemic.
TAVR’s resource-heavy nature made the “system capacity dashboard” and daily meetings critical, Dr. Batchelor explained. At one point during the hold on elective procedures, the Falls Church INOVA facility had approximately 300 patients with COVID-19, a significant proportion of whom were in cardiac ICU beds.
“Everyone has to be flexible and learn,” he said. “We trained our cardiologists on managing ventilators in case some of the [critical care] staff got ill or were overwhelmed by the surge.”
More than 2 months after the surge eased and the ban on elective surgery was lifted, Dr. Batchelor and his colleagues are still using the dashboard and continue to meet daily to discuss COVID-19 prevalence in the hospital and the community as they work through the backlog of delayed procedures. They also routinely review the status of COVID-19 testing for inpatients and outpatients and the donning and doffing of personal protective equipment.
“You have to communicate early and often across the whole system of care because you’re competing for the same resources,” he advised. “And you have to be flexible and reassess. A policy that works at the beginning of the pandemic might have to change.”
PCI in New York
Before the pandemic, the cardiac catheterization laboratory at Mount Sinai Morningside Hospital in New York handled a monthly average of 140-150 PCIs, including 6-10 primary PCIs for ST-segment elevation myocardial infarction.
When electives were halted by the hospital in March and the City became the global epicenter for COVID-19, the cath lab went quiet. “Even though we were still able to do urgent cases or emergent cases, the case volume dropped tremendously,” said Jacqueline E. Tamis-Holland, MD, associate director of the cardiac catheterization laboratory and director of the interventional cardiology fellowship. “There weren’t many outpatients in our hospital … and by late March and through April, there wasn’t a single acute infarction.”
She and Tak W. Kwan, MD, director of the cardiac catheterization laboratory and professor of medicine at Icahn School of Medicine at Mount Sinai, New York, were prepared to move true STEMI patients into the cath lab for primary PCI without delay unless the staff or system were overrun.
That primary PCI should remain the first-line treatment for STEMI even in cases of confirmed or suspected COVID-19 was recommended by SCAI guidance issued in March and by a consensus statement released by the SCAI, ACC, and American College of Emergency Physicians in April – and “we were very much of the same frame of mind,” Dr. Tamis-Holland said.
Deciding which elective cases could not be delayed required a completely individualized approach, the cardiologists emphasized. Dr. Tamis-Holland had a few patients scheduled for elective PCI when the hold began, and “we spoke every few days or once a week in the beginning, then transitioned to once every 2 weeks,” she said. “With medical therapy and given that they were relatively sedentary, my patients did okay [with the delays].”
For subsequent patients, she considered their symptoms or stress test results. “If it’s someone who I’d [normally] wait until next week to schedule the cath, then we would wait 2 or 3 more weeks, or a month more with careful monitoring,” she said. “Certainly, there was a decrease in the number of abnormal stress tests that I referred to the cath lab during [the surge period].”
Dr. Kwan described one patient who had new-onset congestive heart failure in late March “with a markedly positive nuclear stress test.” The patient was monitored with twice-weekly telemedicine visits and office visits, and a cardiac catheterization was performed in early May as an urgent elective case. “He had severe three-vessel and left main disease,” he said. “Subsequently, [coronary artery bypass surgery] was done.”
There were no changes in the PCI procedure itself in terms of hospital stay (most elective cases at Mt. Sinai are same-day procedures) or in staffing, other than a ban on visiting students or residents. The most important changes during the surge – in addition to stocking enough personal protective equipment – concerned testing. Patients undergoing elective PCI are tested for the novel coronavirus 72 hours before the procedure, and rapid testing is performed in the emergency room for STEMI patients to determine patient disposition after the procedure.
“Until we have the results back we should treat all patients as if they are a patient under investigation or have COVID,” said Dr. Tamis-Holland, who helped develop emergency guidance on STEMI systems of care during the pandemic for the American Heart Association.
In early May, the hospital freed up additional space for cardiac care, allowing more “urgent-elective” PCIs to be done. Some patients were reluctant to proceed, the cardiologists said, because of a no-visitor policy. In mid-June, the hold on elective procedures was lifted, and around the same time, the hospital shifted to a one-visitor policy. Still, some patients opted to continue longer with medical therapy.
Patients need to feel comfortable, and “there is a lag time from the time everything opens up and when patients get their stress tests and their evaluations, and then arrive for PCI,” said Dr. Tamis-Holland.
By mid-July, the cardiologists were anticipating an increase in complications from infarctions among patients who “waited them out at home” – heart failure or mitral valve regurgitation, for instance – but, in their hospital at least, “we haven’t really seen that,” she added.
AFib ablation in Kentucky
As New York experienced its surge, John Mandrola, MD, and other electrophysiologists across the Baptist Health system in Kentucky reached a consensus on how to categorize their procedures. Electrophysiology interventions were classified urgent, emergent, and truly elective in the event that the state’s relatively low case burden of COVID-19 were to significantly worsen.
There was no doubt where AFib ablation sat. “It’s one of the most elective procedures there is” in terms of scheduling under normal circumstances, and it almost always requires an overnight stay and general anesthesia – factors that upped the ante on an elective classification, said Dr. Mandrola.
All AF ablations were deemed elective unless the patient required immediate hospitalization. For 8-10 weeks during the state’s shutdown of elective care, Dr. Mandrola and his partner successfully monitored patients with phone calls. “To be honest,” he said, “most patients did not want to have their AFib ablation anyway until the pandemic slowed and they knew it was safe.”
In some cases, patients reported that their symptoms were improving: “There are so many things to speculate about. ... Was it that everyone took their foot off the accelerator?” Dr. Mandrola thinks that postpandemic outcomes analyses may drive more scrutiny of the necessity of some AFib ablations and other procedures and tests. AFib ablation “has its place but is probably overused,” he said.
During the pause on electives, “the vast majority of procedures we did were pacemaker procedures,” he said. “We also did some atrial flutter ablations, and ablations for ventricular tachycardia and supraventricular tachycardia.” In mid-July, as the COVID-19 case burden in Kentucky remained relatively low, Dr. Mandrola was “up to 120%” of his pre-COVID electrophysiology volume – but ready to scale back again if needed.
Dr. Batchelor reported consulting fees from Boston Scientific, Abbott Medical, Medtronic, and V-wave. Dr. Kwan, Dr. Mandrola, and Dr. Tamis-Holland reported no relevant financial disclosures.
This article is a collaboration between Medscape and MDedge. A version of it originally appeared on Medscape.com.
When Virginia’s governor directed the postponement of all elective surgeries in late March, Wayne Batchelor, MD and his colleagues at the Inova Heart and Vascular Institute in Falls Church, Va., canceled about two-thirds of their transcatheter aortic valve replacement (TAVR) procedures.
They then categorized patients by tiers to gauge which procedures could safely be postponed and to guide triaging. And while they did not deviate from the practice of having both an interventional cardiologist and a cardiothoracic surgeon present for TAVR, they slimmed down preprocedural testing when feasible and delayed some 30-day post-TAVR echocardiographic assessments. “It was a delicate dance, very difficult dance. But luckily, we were able to navigate the challenges effectively,” said Dr. Batchelor, the institute’s director of interventional cardiology and interventional cardiology research.
A “system capacity dashboard” that merged bed and staffing data from interventional cardiology spaces with cardiovascular and noncardiovascular ICU beds, operating rooms, and other resources – and daily cross-department meetings – enabled them to proceed with the most urgent TAVR procedures while “keeping a buffer of ICU beds to accommodate an anticipated surge of COVID-19,” he explained.
Such adaptations in cardiac procedures and processes are occurring in hospitals across the country as efforts are made to minimize the risk of COVID-19 exposure for patients and staff. Dr. Batchelor is one of four cardiologists who shared their experiences and advice on common cardiac procedures across three locales: TAVR in Virginia, percutaneous coronary intervention (PCI) in New York City, and atrial fibrillation (AFib) ablation in Kentucky.
More on TAVR in Virginia
Inova’s framework for triaging structural heart disease interventions (largely TAVR and/or percutaneous mitral valve repair) comprised three tiers. Tier 1 captured “emergent cases that had to be done, no questions asked,” Dr. Batchelor said. For TAVR, these were inpatients with severe to critical symptomatic aortic stenosis and advanced congestive heart failure who could not safely be discharged, as well as other patients “with refractory symptoms of heart failure that were compelling.” Many had associated left ventricular systolic dysfunction.
Those who could delay 14-30 days were placed in tier 2, and patients who “we felt were fairly stable and could wait at least 30 days” were placed in tier 3. “For TAVR, a tier 3 patient might be the one … who has severe aortic stenosis but is walking around and doing well at home with only stable exertional symptoms,” he said.
Patients whose procedures were delayed were contacted weekly by the valve clinic’s advanced practice practitioners through video visits or telephone calls, and tier categorization was reevaluated if symptoms worsened. “We had to keep in close contact with them,” Dr. Batchelor said. “These patients can deteriorate quite rapidly and sometimes without much warning.”
Virtual video visits were often used for 30-day postprocedural follow-ups, taking the place of in-person visits during which post-TAVR echocardiographic assessments would normally be performed. “For follow-up, we’d often just do a quick visit to check the vascular access site within 7-10 days, and then, if they were doing okay we’d delay the 30-day echo to a later time frame,” he said.
Preprocedural testing was streamlined to minimize the number of patient-provider interactions, with pulmonary function testing and pre-TAVR catheterization omitted unless absolutely necessary. “A TAVR CT angiogram [performed within the prior year] is the only test you really absolutely need,” Dr. Batchelor said. “We were much less likely to order a heart catheterization unless the patient was having angina and high risk or suspicion for significant coronary artery disease.”
This approach was not associated with any compromise in postprocedural outcomes, he noted. Prior to the pandemic, Inova routinely employed a minimalist approach to TAVR with moderate conscious sedation and avoiding transesophageal echocardiography – steps that were recommended for structural heart procedures in the COVID-19 era in a published review by the heart team at New York-Presbyterian Hospital/Columbia University Irving Medical Center.
The New York review is useful for cardiologists in areas with rising case burdens of COVID-19, Dr. Batchelor said, as is a position statement he coauthored from the American College of Cardiology and the Society for Cardiology and Angiography Interventions (SCAI) on triage considerations for structural heart disease interventions during the pandemic.
TAVR’s resource-heavy nature made the “system capacity dashboard” and daily meetings critical, Dr. Batchelor explained. At one point during the hold on elective procedures, the Falls Church INOVA facility had approximately 300 patients with COVID-19, a significant proportion of whom were in cardiac ICU beds.
“Everyone has to be flexible and learn,” he said. “We trained our cardiologists on managing ventilators in case some of the [critical care] staff got ill or were overwhelmed by the surge.”
More than 2 months after the surge eased and the ban on elective surgery was lifted, Dr. Batchelor and his colleagues are still using the dashboard and continue to meet daily to discuss COVID-19 prevalence in the hospital and the community as they work through the backlog of delayed procedures. They also routinely review the status of COVID-19 testing for inpatients and outpatients and the donning and doffing of personal protective equipment.
“You have to communicate early and often across the whole system of care because you’re competing for the same resources,” he advised. “And you have to be flexible and reassess. A policy that works at the beginning of the pandemic might have to change.”
PCI in New York
Before the pandemic, the cardiac catheterization laboratory at Mount Sinai Morningside Hospital in New York handled a monthly average of 140-150 PCIs, including 6-10 primary PCIs for ST-segment elevation myocardial infarction.
When electives were halted by the hospital in March and the City became the global epicenter for COVID-19, the cath lab went quiet. “Even though we were still able to do urgent cases or emergent cases, the case volume dropped tremendously,” said Jacqueline E. Tamis-Holland, MD, associate director of the cardiac catheterization laboratory and director of the interventional cardiology fellowship. “There weren’t many outpatients in our hospital … and by late March and through April, there wasn’t a single acute infarction.”
She and Tak W. Kwan, MD, director of the cardiac catheterization laboratory and professor of medicine at Icahn School of Medicine at Mount Sinai, New York, were prepared to move true STEMI patients into the cath lab for primary PCI without delay unless the staff or system were overrun.
That primary PCI should remain the first-line treatment for STEMI even in cases of confirmed or suspected COVID-19 was recommended by SCAI guidance issued in March and by a consensus statement released by the SCAI, ACC, and American College of Emergency Physicians in April – and “we were very much of the same frame of mind,” Dr. Tamis-Holland said.
Deciding which elective cases could not be delayed required a completely individualized approach, the cardiologists emphasized. Dr. Tamis-Holland had a few patients scheduled for elective PCI when the hold began, and “we spoke every few days or once a week in the beginning, then transitioned to once every 2 weeks,” she said. “With medical therapy and given that they were relatively sedentary, my patients did okay [with the delays].”
For subsequent patients, she considered their symptoms or stress test results. “If it’s someone who I’d [normally] wait until next week to schedule the cath, then we would wait 2 or 3 more weeks, or a month more with careful monitoring,” she said. “Certainly, there was a decrease in the number of abnormal stress tests that I referred to the cath lab during [the surge period].”
Dr. Kwan described one patient who had new-onset congestive heart failure in late March “with a markedly positive nuclear stress test.” The patient was monitored with twice-weekly telemedicine visits and office visits, and a cardiac catheterization was performed in early May as an urgent elective case. “He had severe three-vessel and left main disease,” he said. “Subsequently, [coronary artery bypass surgery] was done.”
There were no changes in the PCI procedure itself in terms of hospital stay (most elective cases at Mt. Sinai are same-day procedures) or in staffing, other than a ban on visiting students or residents. The most important changes during the surge – in addition to stocking enough personal protective equipment – concerned testing. Patients undergoing elective PCI are tested for the novel coronavirus 72 hours before the procedure, and rapid testing is performed in the emergency room for STEMI patients to determine patient disposition after the procedure.
“Until we have the results back we should treat all patients as if they are a patient under investigation or have COVID,” said Dr. Tamis-Holland, who helped develop emergency guidance on STEMI systems of care during the pandemic for the American Heart Association.
In early May, the hospital freed up additional space for cardiac care, allowing more “urgent-elective” PCIs to be done. Some patients were reluctant to proceed, the cardiologists said, because of a no-visitor policy. In mid-June, the hold on elective procedures was lifted, and around the same time, the hospital shifted to a one-visitor policy. Still, some patients opted to continue longer with medical therapy.
Patients need to feel comfortable, and “there is a lag time from the time everything opens up and when patients get their stress tests and their evaluations, and then arrive for PCI,” said Dr. Tamis-Holland.
By mid-July, the cardiologists were anticipating an increase in complications from infarctions among patients who “waited them out at home” – heart failure or mitral valve regurgitation, for instance – but, in their hospital at least, “we haven’t really seen that,” she added.
AFib ablation in Kentucky
As New York experienced its surge, John Mandrola, MD, and other electrophysiologists across the Baptist Health system in Kentucky reached a consensus on how to categorize their procedures. Electrophysiology interventions were classified urgent, emergent, and truly elective in the event that the state’s relatively low case burden of COVID-19 were to significantly worsen.
There was no doubt where AFib ablation sat. “It’s one of the most elective procedures there is” in terms of scheduling under normal circumstances, and it almost always requires an overnight stay and general anesthesia – factors that upped the ante on an elective classification, said Dr. Mandrola.
All AF ablations were deemed elective unless the patient required immediate hospitalization. For 8-10 weeks during the state’s shutdown of elective care, Dr. Mandrola and his partner successfully monitored patients with phone calls. “To be honest,” he said, “most patients did not want to have their AFib ablation anyway until the pandemic slowed and they knew it was safe.”
In some cases, patients reported that their symptoms were improving: “There are so many things to speculate about. ... Was it that everyone took their foot off the accelerator?” Dr. Mandrola thinks that postpandemic outcomes analyses may drive more scrutiny of the necessity of some AFib ablations and other procedures and tests. AFib ablation “has its place but is probably overused,” he said.
During the pause on electives, “the vast majority of procedures we did were pacemaker procedures,” he said. “We also did some atrial flutter ablations, and ablations for ventricular tachycardia and supraventricular tachycardia.” In mid-July, as the COVID-19 case burden in Kentucky remained relatively low, Dr. Mandrola was “up to 120%” of his pre-COVID electrophysiology volume – but ready to scale back again if needed.
Dr. Batchelor reported consulting fees from Boston Scientific, Abbott Medical, Medtronic, and V-wave. Dr. Kwan, Dr. Mandrola, and Dr. Tamis-Holland reported no relevant financial disclosures.
This article is a collaboration between Medscape and MDedge. A version of it originally appeared on Medscape.com.
The best and worst states for health care in 2020
according to the personal finance website WalletHub.
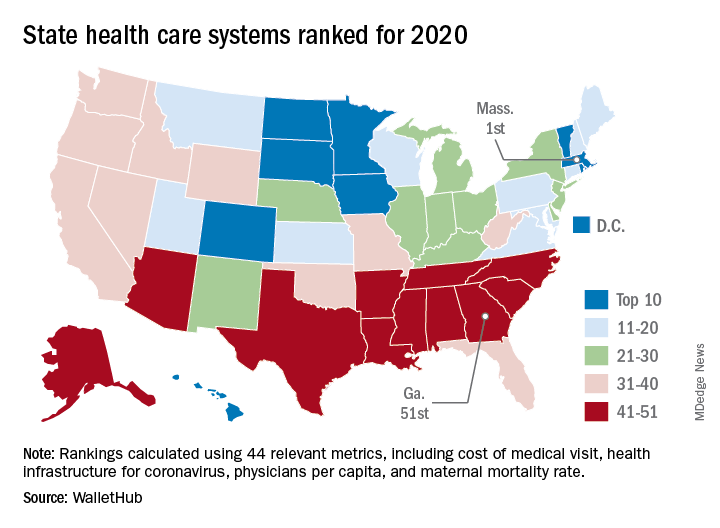
The Bay State finds itself at the top of the company’s annual ranking of state health care systems this year after finishing second in 2019 to Minnesota, which is now ranked second. Rhode Island is third this year, followed by Washington, D.C., and North Dakota, WalletHub reported Aug. 3.
The inclusion of Washington, D.C., allowed Georgia to finish 51st out of 50 states, just below the quartet of Louisiana (50th), Alabama (49th), North Carolina (48th), and Mississippi (47th). Alaska, which occupied the bottom spot in 2019, moved up to 42nd this year, the analysis showed.
The rankings are based on 44 (up from 43 last year) metrics that are grouped into three broad categories: cost (6 metrics), access (24 metrics), and outcomes (14 metrics). The one new measure added for 2020? That would be health infrastructure for coronavirus, which is itself based on a different WalletHub ranking.
Massachusetts’ top finish this year was driven by strong showings in such metrics as average monthly insurance premium (first), physicians per capita (second), insured children (first) and adults (first), and infant mortality rate (fourth). The state was 1st overall in outcomes and 4th in access but only 20th in cost, the company said.
Positive signs among the lowest-ranked states include Louisiana’s 18th-place finish in access, ahead of such top 10 states as Iowa and Hawaii, and Mississippi’s 17th in cost, which is higher than four of the states in the top 10, including Massachusetts, WalletHub said in the report.
Data for the analysis came from 22 different sources, including the Institute for Health Metrics and Evaluation, Centers for Medicare & Medicaid Services, Association of American Medical Colleges, and the American Telemedicine Association.
according to the personal finance website WalletHub.
The Bay State finds itself at the top of the company’s annual ranking of state health care systems this year after finishing second in 2019 to Minnesota, which is now ranked second. Rhode Island is third this year, followed by Washington, D.C., and North Dakota, WalletHub reported Aug. 3.
The inclusion of Washington, D.C., allowed Georgia to finish 51st out of 50 states, just below the quartet of Louisiana (50th), Alabama (49th), North Carolina (48th), and Mississippi (47th). Alaska, which occupied the bottom spot in 2019, moved up to 42nd this year, the analysis showed.
The rankings are based on 44 (up from 43 last year) metrics that are grouped into three broad categories: cost (6 metrics), access (24 metrics), and outcomes (14 metrics). The one new measure added for 2020? That would be health infrastructure for coronavirus, which is itself based on a different WalletHub ranking.
Massachusetts’ top finish this year was driven by strong showings in such metrics as average monthly insurance premium (first), physicians per capita (second), insured children (first) and adults (first), and infant mortality rate (fourth). The state was 1st overall in outcomes and 4th in access but only 20th in cost, the company said.
Positive signs among the lowest-ranked states include Louisiana’s 18th-place finish in access, ahead of such top 10 states as Iowa and Hawaii, and Mississippi’s 17th in cost, which is higher than four of the states in the top 10, including Massachusetts, WalletHub said in the report.
Data for the analysis came from 22 different sources, including the Institute for Health Metrics and Evaluation, Centers for Medicare & Medicaid Services, Association of American Medical Colleges, and the American Telemedicine Association.
according to the personal finance website WalletHub.
The Bay State finds itself at the top of the company’s annual ranking of state health care systems this year after finishing second in 2019 to Minnesota, which is now ranked second. Rhode Island is third this year, followed by Washington, D.C., and North Dakota, WalletHub reported Aug. 3.
The inclusion of Washington, D.C., allowed Georgia to finish 51st out of 50 states, just below the quartet of Louisiana (50th), Alabama (49th), North Carolina (48th), and Mississippi (47th). Alaska, which occupied the bottom spot in 2019, moved up to 42nd this year, the analysis showed.
The rankings are based on 44 (up from 43 last year) metrics that are grouped into three broad categories: cost (6 metrics), access (24 metrics), and outcomes (14 metrics). The one new measure added for 2020? That would be health infrastructure for coronavirus, which is itself based on a different WalletHub ranking.
Massachusetts’ top finish this year was driven by strong showings in such metrics as average monthly insurance premium (first), physicians per capita (second), insured children (first) and adults (first), and infant mortality rate (fourth). The state was 1st overall in outcomes and 4th in access but only 20th in cost, the company said.
Positive signs among the lowest-ranked states include Louisiana’s 18th-place finish in access, ahead of such top 10 states as Iowa and Hawaii, and Mississippi’s 17th in cost, which is higher than four of the states in the top 10, including Massachusetts, WalletHub said in the report.
Data for the analysis came from 22 different sources, including the Institute for Health Metrics and Evaluation, Centers for Medicare & Medicaid Services, Association of American Medical Colleges, and the American Telemedicine Association.
Real-world data show SGLT2 inhibitors for diabetes triple DKA risk
according to a new large database analysis.

The findings, which include data on the use of three different SGLT2 inhibitors in Canada and the United Kingdom and suggest a class effect, were published online July 27 in Annals of Internal Medicine by Antonios Douros, MD, PhD, of McGill University and the Centre for Clinical Epidemiology, Lady Davis Institute, Montreal, and colleagues.
“Our results provide robust evidence that SGLT2 inhibitors are associated with an increased risk for DKA. Of note, increased risks were observed in all molecule-specific analyses, with canagliflozin [Invokana, Janssen] showing the highest effect estimate,” they noted.
And because the beneficial effects of SGLT2 inhibitors in the prevention of cardiovascular and renal disease will probably increase their uptake in the coming years, “Physicians should be aware of DKA as a potential adverse effect,” Dr. Douros and colleagues wrote.
Analysis “generally confirms what has already been published”
Asked for comment, Simeon I. Taylor, MD, PhD, professor of medicine at the University of Maryland, Baltimore, said that the study “generally confirms what has already been published” on the topic. He noted that overall “the risk of SGLT2 inhibitor–induced ketoacidosis is quite low in type 2 diabetes, perhaps on the order of 1 episode per 1000 patient-years.”
However, Dr. Taylor cautioned: “Published evidence suggests that the risk of DKA is increased if patients are unable to eat,” such as when hospitalized patients are not permitted to eat.
“In that setting, it is probably prudent to discontinue an SGLT2 inhibitor. Also, it may be prudent not to prescribe SGLT2 inhibitors to patients with a history of DKA,” he added.
Dr. Taylor also advised: “Although not necessarily supported by this publication, I think that caution should be exercised in prescribing SGLT2 inhibitors to insulin-dependent type 2 diabetes patients. ... Some late-stage type 2 diabetes patients may have severe insulin deficiency, and their physiology may resemble that of a type 1 diabetes patient.”
Dr. Taylor has previously advised against using SGLT2 inhibitors altogether in patients with type 1 diabetes.
Increased DKA risk seen across all SGLT2 inhibitors
The study involved electronic health care databases from seven Canadian provinces and the United Kingdom, from which 208,757 new users of SGLT2 inhibitors were propensity-matched 1:1 to new dipeptidyl peptidase-4 (DPP-4) inhibitor users.
Of those taking an SGLT2 inhibitor, 42.3% took canagliflozin, 30.7% dapagliflozin (Farxiga/Forxiga, AstraZeneca), and 27.0% empagliflozin (Jardiance, Boehringer Ingelheim).
Over a mean 0.9-year follow-up, 521 patients were hospitalized with DKA, for an overall incidence rate of 1.41 per 1,000 person-years.
The rate with SGLT2 inhibitors, 2.03 per 1,000 person-years, was nearly three times that seen with DPP-4 inhibitors, at 0.75 per 1,000 person-years, a significant difference (hazard ratio, 2.85).
By individual SGLT2 inhibitor, the hazard ratios compared with DPP-4 inhibitors were 1.86 for dapagliflozin, 2.52 for empagliflozin, and 3.58 for canagliflozin, all statistically significant. Stratification by age, sex, and incident versus prevalent user did not change the association between SGLT2 inhibitors and DKA.
Asked about the higher rate for canagliflozin, Dr. Taylor commented: “It is hard to know whether there are real and reproducible differences in the risks of DKA among the various SGLT2 inhibitors. The differences are not huge and the populations are not well matched.”
But, he noted, “If canagliflozin triggers more glucosuria, it is not surprising that it would also induce more ketosis and possibly ketoacidosis.”
He also noted that the threefold relative increase in DKA with canagliflozin versus comparators is consistent with Janssen’s data, published in 2015.
“It is, of course, reassuring that both [randomized clinical trials] and epidemiology produce similar estimates of the risk of drug-induced adverse events. Interestingly, the incidence of DKA is approximately threefold higher in the Canadian [data] as compared to Janssen’s clinical trials.”
Dr. Taylor also pointed out that, in the Janssen studies, the risk of canagliflozin-induced DKA appeared to be higher among patients with anti-islet antibodies, which suggests that some may have actually had autoimmune (type 1) diabetes. “So the overall risk of SGLT2 inhibitor-induced DKA may depend at least in part on the mix of patients.”
In the current study, individuals who never used insulin had a greater relative increase in risk of DKA with SGLT2 inhibitors, compared with DPP-4 inhibitors, than did those who did use insulin (hazard ratios, 3.96 vs. 2.24, both compared with DPP-4 inhibitors). However, just among those taking SGLT2 inhibitors, the absolute risk for DKA was higher for those with prior insulin use (3.52 vs. 1.43 per 1,000 person-years).
The results of sensitivity analyses were consistent with those of the primary analysis.
The study was funded by the Canadian Institutes of Health Research and supported by ICES. Dr. Douros has reported receiving a salary support award from Fonds de recherche du Quebec – sante. Dr. Taylor was previously employed at Bristol-Myers Squibb. He is currently a consultant for Ionis Pharmaceuticals and has reported receiving research support provided to the University of Maryland School of Medicine by Regeneron.
A version of this article originally appeared on Medscape.com.
according to a new large database analysis.
The findings, which include data on the use of three different SGLT2 inhibitors in Canada and the United Kingdom and suggest a class effect, were published online July 27 in Annals of Internal Medicine by Antonios Douros, MD, PhD, of McGill University and the Centre for Clinical Epidemiology, Lady Davis Institute, Montreal, and colleagues.
“Our results provide robust evidence that SGLT2 inhibitors are associated with an increased risk for DKA. Of note, increased risks were observed in all molecule-specific analyses, with canagliflozin [Invokana, Janssen] showing the highest effect estimate,” they noted.
And because the beneficial effects of SGLT2 inhibitors in the prevention of cardiovascular and renal disease will probably increase their uptake in the coming years, “Physicians should be aware of DKA as a potential adverse effect,” Dr. Douros and colleagues wrote.
Analysis “generally confirms what has already been published”
Asked for comment, Simeon I. Taylor, MD, PhD, professor of medicine at the University of Maryland, Baltimore, said that the study “generally confirms what has already been published” on the topic. He noted that overall “the risk of SGLT2 inhibitor–induced ketoacidosis is quite low in type 2 diabetes, perhaps on the order of 1 episode per 1000 patient-years.”
However, Dr. Taylor cautioned: “Published evidence suggests that the risk of DKA is increased if patients are unable to eat,” such as when hospitalized patients are not permitted to eat.
“In that setting, it is probably prudent to discontinue an SGLT2 inhibitor. Also, it may be prudent not to prescribe SGLT2 inhibitors to patients with a history of DKA,” he added.
Dr. Taylor also advised: “Although not necessarily supported by this publication, I think that caution should be exercised in prescribing SGLT2 inhibitors to insulin-dependent type 2 diabetes patients. ... Some late-stage type 2 diabetes patients may have severe insulin deficiency, and their physiology may resemble that of a type 1 diabetes patient.”
Dr. Taylor has previously advised against using SGLT2 inhibitors altogether in patients with type 1 diabetes.
Increased DKA risk seen across all SGLT2 inhibitors
The study involved electronic health care databases from seven Canadian provinces and the United Kingdom, from which 208,757 new users of SGLT2 inhibitors were propensity-matched 1:1 to new dipeptidyl peptidase-4 (DPP-4) inhibitor users.
Of those taking an SGLT2 inhibitor, 42.3% took canagliflozin, 30.7% dapagliflozin (Farxiga/Forxiga, AstraZeneca), and 27.0% empagliflozin (Jardiance, Boehringer Ingelheim).
Over a mean 0.9-year follow-up, 521 patients were hospitalized with DKA, for an overall incidence rate of 1.41 per 1,000 person-years.
The rate with SGLT2 inhibitors, 2.03 per 1,000 person-years, was nearly three times that seen with DPP-4 inhibitors, at 0.75 per 1,000 person-years, a significant difference (hazard ratio, 2.85).
By individual SGLT2 inhibitor, the hazard ratios compared with DPP-4 inhibitors were 1.86 for dapagliflozin, 2.52 for empagliflozin, and 3.58 for canagliflozin, all statistically significant. Stratification by age, sex, and incident versus prevalent user did not change the association between SGLT2 inhibitors and DKA.
Asked about the higher rate for canagliflozin, Dr. Taylor commented: “It is hard to know whether there are real and reproducible differences in the risks of DKA among the various SGLT2 inhibitors. The differences are not huge and the populations are not well matched.”
But, he noted, “If canagliflozin triggers more glucosuria, it is not surprising that it would also induce more ketosis and possibly ketoacidosis.”
He also noted that the threefold relative increase in DKA with canagliflozin versus comparators is consistent with Janssen’s data, published in 2015.
“It is, of course, reassuring that both [randomized clinical trials] and epidemiology produce similar estimates of the risk of drug-induced adverse events. Interestingly, the incidence of DKA is approximately threefold higher in the Canadian [data] as compared to Janssen’s clinical trials.”
Dr. Taylor also pointed out that, in the Janssen studies, the risk of canagliflozin-induced DKA appeared to be higher among patients with anti-islet antibodies, which suggests that some may have actually had autoimmune (type 1) diabetes. “So the overall risk of SGLT2 inhibitor-induced DKA may depend at least in part on the mix of patients.”
In the current study, individuals who never used insulin had a greater relative increase in risk of DKA with SGLT2 inhibitors, compared with DPP-4 inhibitors, than did those who did use insulin (hazard ratios, 3.96 vs. 2.24, both compared with DPP-4 inhibitors). However, just among those taking SGLT2 inhibitors, the absolute risk for DKA was higher for those with prior insulin use (3.52 vs. 1.43 per 1,000 person-years).
The results of sensitivity analyses were consistent with those of the primary analysis.
The study was funded by the Canadian Institutes of Health Research and supported by ICES. Dr. Douros has reported receiving a salary support award from Fonds de recherche du Quebec – sante. Dr. Taylor was previously employed at Bristol-Myers Squibb. He is currently a consultant for Ionis Pharmaceuticals and has reported receiving research support provided to the University of Maryland School of Medicine by Regeneron.
A version of this article originally appeared on Medscape.com.
according to a new large database analysis.
The findings, which include data on the use of three different SGLT2 inhibitors in Canada and the United Kingdom and suggest a class effect, were published online July 27 in Annals of Internal Medicine by Antonios Douros, MD, PhD, of McGill University and the Centre for Clinical Epidemiology, Lady Davis Institute, Montreal, and colleagues.
“Our results provide robust evidence that SGLT2 inhibitors are associated with an increased risk for DKA. Of note, increased risks were observed in all molecule-specific analyses, with canagliflozin [Invokana, Janssen] showing the highest effect estimate,” they noted.
And because the beneficial effects of SGLT2 inhibitors in the prevention of cardiovascular and renal disease will probably increase their uptake in the coming years, “Physicians should be aware of DKA as a potential adverse effect,” Dr. Douros and colleagues wrote.
Analysis “generally confirms what has already been published”
Asked for comment, Simeon I. Taylor, MD, PhD, professor of medicine at the University of Maryland, Baltimore, said that the study “generally confirms what has already been published” on the topic. He noted that overall “the risk of SGLT2 inhibitor–induced ketoacidosis is quite low in type 2 diabetes, perhaps on the order of 1 episode per 1000 patient-years.”
However, Dr. Taylor cautioned: “Published evidence suggests that the risk of DKA is increased if patients are unable to eat,” such as when hospitalized patients are not permitted to eat.
“In that setting, it is probably prudent to discontinue an SGLT2 inhibitor. Also, it may be prudent not to prescribe SGLT2 inhibitors to patients with a history of DKA,” he added.
Dr. Taylor also advised: “Although not necessarily supported by this publication, I think that caution should be exercised in prescribing SGLT2 inhibitors to insulin-dependent type 2 diabetes patients. ... Some late-stage type 2 diabetes patients may have severe insulin deficiency, and their physiology may resemble that of a type 1 diabetes patient.”
Dr. Taylor has previously advised against using SGLT2 inhibitors altogether in patients with type 1 diabetes.
Increased DKA risk seen across all SGLT2 inhibitors
The study involved electronic health care databases from seven Canadian provinces and the United Kingdom, from which 208,757 new users of SGLT2 inhibitors were propensity-matched 1:1 to new dipeptidyl peptidase-4 (DPP-4) inhibitor users.
Of those taking an SGLT2 inhibitor, 42.3% took canagliflozin, 30.7% dapagliflozin (Farxiga/Forxiga, AstraZeneca), and 27.0% empagliflozin (Jardiance, Boehringer Ingelheim).
Over a mean 0.9-year follow-up, 521 patients were hospitalized with DKA, for an overall incidence rate of 1.41 per 1,000 person-years.
The rate with SGLT2 inhibitors, 2.03 per 1,000 person-years, was nearly three times that seen with DPP-4 inhibitors, at 0.75 per 1,000 person-years, a significant difference (hazard ratio, 2.85).
By individual SGLT2 inhibitor, the hazard ratios compared with DPP-4 inhibitors were 1.86 for dapagliflozin, 2.52 for empagliflozin, and 3.58 for canagliflozin, all statistically significant. Stratification by age, sex, and incident versus prevalent user did not change the association between SGLT2 inhibitors and DKA.
Asked about the higher rate for canagliflozin, Dr. Taylor commented: “It is hard to know whether there are real and reproducible differences in the risks of DKA among the various SGLT2 inhibitors. The differences are not huge and the populations are not well matched.”
But, he noted, “If canagliflozin triggers more glucosuria, it is not surprising that it would also induce more ketosis and possibly ketoacidosis.”
He also noted that the threefold relative increase in DKA with canagliflozin versus comparators is consistent with Janssen’s data, published in 2015.
“It is, of course, reassuring that both [randomized clinical trials] and epidemiology produce similar estimates of the risk of drug-induced adverse events. Interestingly, the incidence of DKA is approximately threefold higher in the Canadian [data] as compared to Janssen’s clinical trials.”
Dr. Taylor also pointed out that, in the Janssen studies, the risk of canagliflozin-induced DKA appeared to be higher among patients with anti-islet antibodies, which suggests that some may have actually had autoimmune (type 1) diabetes. “So the overall risk of SGLT2 inhibitor-induced DKA may depend at least in part on the mix of patients.”
In the current study, individuals who never used insulin had a greater relative increase in risk of DKA with SGLT2 inhibitors, compared with DPP-4 inhibitors, than did those who did use insulin (hazard ratios, 3.96 vs. 2.24, both compared with DPP-4 inhibitors). However, just among those taking SGLT2 inhibitors, the absolute risk for DKA was higher for those with prior insulin use (3.52 vs. 1.43 per 1,000 person-years).
The results of sensitivity analyses were consistent with those of the primary analysis.
The study was funded by the Canadian Institutes of Health Research and supported by ICES. Dr. Douros has reported receiving a salary support award from Fonds de recherche du Quebec – sante. Dr. Taylor was previously employed at Bristol-Myers Squibb. He is currently a consultant for Ionis Pharmaceuticals and has reported receiving research support provided to the University of Maryland School of Medicine by Regeneron.
A version of this article originally appeared on Medscape.com.
The fix is in: AIM bundles to combat maternal morbidity and mortality
“Anytime you have a maternal death, it sticks with you for life,” said Elliott Main, MD, a maternal fetal medicine specialist at Stanford (Calif.) University and one of the nation’s leaders in combating maternal mortality.

Dr. Main has had two maternal deaths in his career, years ago. One woman had a fatal stroke because of severe hypertension, and another died of cardiac complications. “We tried to do everything we possibly could, but you scrounge your memory for years and years [afterward]. To have a young healthy person go into labor and delivery and not come out is a tragedy at all levels. It charged me to not ever want to see that happen again,” he said.
Today, Dr. Main is the medical director of the California Maternal Quality Care Collaborative (CMQCC), a wide-ranging group of clinicians, state officials, hospitals, and others who have come together to address the issue. About 30 states have similar perinatal quality collaboratives (PQCs), and other states are forming them.
They work in collaboration with maternal mortality review committees (MMRCs), state-level groups that review maternal deaths, identify problems to address, and make recommendations to the quality collaboratives on how to prevent maternal deaths.
About 600-800 women die in the United States each year due to pregnancy-related complications, which ranks the United States behind other industrialized nations. Leading causes include hemorrhage and hemorrhagic strokes secondary to hypertension. It’s estimated that the majority of maternal deaths could be prevented with proper care.
To that end, states are enacting safety bundles from the Alliance for Innovation on Maternal Health (AIM), which was established by the American College of Obstetricians and Gynecologist several years ago. There are bundles that address obstetric hypertension, hemorrhage, mental health, venous thromboembolism, opioid use, racial disparities, and other problems. They were developed by experts in the field and published in multiple journals. California and other states have issued toolkits on how to implement them based on local circumstances.
Dr. Main said.
AIM bundle implementation is “what’s happening in New Mexico and a lot of states, mostly through the efforts of state level quality care collaboratives. Some [states] are further ahead than others,” said Eve Espey, MD, professor and chair of the department of obstetrics and gynecology at the University of New Mexico, Albuquerque, and president of the New Mexico PQC.
“Most states now have a [MMRC] that collects maternal mortality and near-miss data. Those data are used by the action arm,” which is the PQC. “If the review committee says” opioid use disorder is a significant contributor “like in our state, the collaborative rolls out the opioid use disorder bundle,” she said.
Beginning next January, the Joint Commission, formerly known as the Joint Commission on Accreditation of Healthcare Organizations, will require that accredited hospitals enact key elements of the AIM bundles for both obstetric hemorrhage and severe hypertension. “Everyone’s [now] motivated to get on that bandwagon,” Dr. Espey said.
“The bundles are here to stay,” and the Joint Commission requirements are “a really important step for sustainability and basic implementation. We really want to get them adopted everywhere,” said Dr. Main, who is also the national implementation director for the AIM initiative.
“The key thing is to work on implementing the hemorrhage and hypertension bundles in your hospital. I would suggest contacting [your] state” PQC, he said.
The California model
California, which has been working to reduce maternal mortality and morbidity since the mid 2000s, has produced among the strongest evidence to date that the efforts make a difference.
By 2013, the state had halved its maternal mortality rate to a 3-year average of 7 deaths per 100,000 live births, which is comparable with the average Western Europe rate of 7.2 deaths. Nationwide, the rate was about 17.4 deaths per 100,000 live births in 2018, according to the Centers for Disease Control and Prevention
The reasons are multifactorial, but “we think” the quality improvement efforts have been “an important contributor,” Dr. Main said.
Improvements especially for Black women
Among the success stories has been California’s implementation of the AIM obstetric hemorrhage bundle about 5 years ago. Among other steps, the 17 evidence-based recommendations included early recognition, immediate access to oxytocin and other medications, immediate access to a hemorrhage cart with instructions for intrauterine balloons and compression stitches, the establishment of a hemorrhage response protocol and team, and regular unit-based drills with debriefing sessions afterward.
Mentoring teams consisting of a physician and nurse with maternal quality improvement experience were created to help hospitals come on board, with each team working with five to eight hospitals. Efforts included monthly telephone calls and face-to-face meetings, and providers were held accountable for progress. Hospitals shared data and tips on implementation, under the aegis of the CMQCC.
When the baseline period of 2011-2014 to the postintervention period of October 2015 to December 2016 were compared, the rate of severe maternal morbidity from hemorrhage fell from 22.1% to 18.5% across 99 hospitals and 73,476 women.
The benefit among Black women exceeded that among White women, with a 9% absolute rate reduction versus 2.1%. “If you adjusted for risk factors, [we found] you could eliminate [racial differences] completely,” which is something that hadn’t been shown before. “This is a really big deal,” Dr. Main said, because the risk of maternal morbidity and mortality is three to four times higher among Black women, compared with White women.
Dr. Main and his team found that the biggest clinical risk factor that accounted for racial differences was a higher rate of cesarean deliveries among Black women, followed by higher rates of anemia at hospital admission. “If you have a C-section when you are anemic, you are going to have a transfusion,” he explained.
More recently, there’s been a push in California to reduce the rate of primary cesarean deliveries by enacting the associated AIM bundle with use of the same approach as with the hemorrhage bundle. Dr. Main and his team recently reported a rate reduction from 29.3% to 25% without compromising birth outcomes.
However, “some changes are easier than others. Hemorrhage was an easy one to change because it didn’t deal with physician autonomy as much, and you saw more immediate results” with fewer hemorrhages. Reducing cesarean delivery rates is “a bigger lift” because “it’s really changing the culture of labor and delivery. It involves more group pressure and more reinforcing, but we were able to do that,” he said.
Problems in the Show Me State
“We’ve patterned a lot” of what’s being done in New Mexico “after California,” Dr. Espey said.

The AIM hemorrhage bundle, for instance, is being rolled out to New Mexico hospitals, with the help of virtual meetings and mentoring programs, plus outreach to the Navajo and others reservations because, as with Black women, rates of maternal morbidity and mortality are higher among Native American women.
It’s been tougher going, however, in states such as Missouri, which recently ranked 44th in the country for maternal mortality.
“We started a little bit late, and we are a little bit behind,” said ob.gyn. Karen L. Florio, DO, at the University of Missouri–Kansas City and also a leader of the state MMRC and member of its PQC.
The main problem is money. California’s efforts are funded by the Centers for Disease Control and Prevention, the state health department, and hospitals, among others.
But Missouri is “not as well funded as California for our mortality review board, and our [PQC] is mostly not funded. If we could get that funding, we would have more resources to implement these AIM bundles,” she said.
In addition to the issue, Missouri didn’t expand Medicaid under the Accountable Care Act – something that’s been linked to reduced maternal morbidity and mortality – and there are entire rural areas with no maternity care. Plus after generations of mistreatment, “our African American population has a valid distrust of the medical system that contributes to maternal mortality,” she said.
Obesity-related heart disease is also prevalent in Missouri, even among young people. “I cannot tell you how many women I have had who have had a heart attack at the age of 30 and who have had stents placed,” Dr. Florio said.
Dr. Florio and her colleagues are currently using teleconferences and other means to roll out the AIM hypertension bundle but can do so only selectively. “We don’t have the resources to reach every single rural hospital all over the state,” she said; they are working to address the funding issues.
For rural hospitals, implementation is “daunting”
Meanwhile, rural hospitals have been a particular concern in South Dakota, said Kimberlee McKay, MD, an ob.gyn. who is the clinical vice president of the ob.gyn. service line at Avera Health, a hospital system based in Sioux Falls, S.D.
She’s been overseeing Avera’s implementation of the hypertension, hemorrhage, and venous thromboembolism bundles. “What’s hard is that” the AIM protocols come “out of academic centers. Implementation of complex algorithms is daunting” for hospitals that only do a couple hundred deliveries a year, she said.
For small hospitals, the approach she’s found that works is to first assess what they can offer, and then have them “do what’s reasonable” for their resources. The second part is making sure high-risk women get to a regional center – with an adequate blood supply, in the case of hemorrhage, for instance – for complications. Dr. McKay and colleagues are working on a system by which regional centers can monitor smaller hospitals for potential maternity problems, and contact them proactively before they emerge.
They’ve also made access to hemorrhage and hypertension drugs easier on labor and delivery units with the help of close-by dedicated medicine boxes, and standardized protocols and order sets across Avera. “We try to make the right thing the easy thing to do,” Dr. McKay said.
Dr. Espey is an editorial adviser for Ob.Gyn. News. The physicians have no relevant financial disclosures.
“Anytime you have a maternal death, it sticks with you for life,” said Elliott Main, MD, a maternal fetal medicine specialist at Stanford (Calif.) University and one of the nation’s leaders in combating maternal mortality.
Dr. Main has had two maternal deaths in his career, years ago. One woman had a fatal stroke because of severe hypertension, and another died of cardiac complications. “We tried to do everything we possibly could, but you scrounge your memory for years and years [afterward]. To have a young healthy person go into labor and delivery and not come out is a tragedy at all levels. It charged me to not ever want to see that happen again,” he said.
Today, Dr. Main is the medical director of the California Maternal Quality Care Collaborative (CMQCC), a wide-ranging group of clinicians, state officials, hospitals, and others who have come together to address the issue. About 30 states have similar perinatal quality collaboratives (PQCs), and other states are forming them.
They work in collaboration with maternal mortality review committees (MMRCs), state-level groups that review maternal deaths, identify problems to address, and make recommendations to the quality collaboratives on how to prevent maternal deaths.
About 600-800 women die in the United States each year due to pregnancy-related complications, which ranks the United States behind other industrialized nations. Leading causes include hemorrhage and hemorrhagic strokes secondary to hypertension. It’s estimated that the majority of maternal deaths could be prevented with proper care.
To that end, states are enacting safety bundles from the Alliance for Innovation on Maternal Health (AIM), which was established by the American College of Obstetricians and Gynecologist several years ago. There are bundles that address obstetric hypertension, hemorrhage, mental health, venous thromboembolism, opioid use, racial disparities, and other problems. They were developed by experts in the field and published in multiple journals. California and other states have issued toolkits on how to implement them based on local circumstances.
Dr. Main said.
AIM bundle implementation is “what’s happening in New Mexico and a lot of states, mostly through the efforts of state level quality care collaboratives. Some [states] are further ahead than others,” said Eve Espey, MD, professor and chair of the department of obstetrics and gynecology at the University of New Mexico, Albuquerque, and president of the New Mexico PQC.
“Most states now have a [MMRC] that collects maternal mortality and near-miss data. Those data are used by the action arm,” which is the PQC. “If the review committee says” opioid use disorder is a significant contributor “like in our state, the collaborative rolls out the opioid use disorder bundle,” she said.
Beginning next January, the Joint Commission, formerly known as the Joint Commission on Accreditation of Healthcare Organizations, will require that accredited hospitals enact key elements of the AIM bundles for both obstetric hemorrhage and severe hypertension. “Everyone’s [now] motivated to get on that bandwagon,” Dr. Espey said.
“The bundles are here to stay,” and the Joint Commission requirements are “a really important step for sustainability and basic implementation. We really want to get them adopted everywhere,” said Dr. Main, who is also the national implementation director for the AIM initiative.
“The key thing is to work on implementing the hemorrhage and hypertension bundles in your hospital. I would suggest contacting [your] state” PQC, he said.
The California model
California, which has been working to reduce maternal mortality and morbidity since the mid 2000s, has produced among the strongest evidence to date that the efforts make a difference.
By 2013, the state had halved its maternal mortality rate to a 3-year average of 7 deaths per 100,000 live births, which is comparable with the average Western Europe rate of 7.2 deaths. Nationwide, the rate was about 17.4 deaths per 100,000 live births in 2018, according to the Centers for Disease Control and Prevention
The reasons are multifactorial, but “we think” the quality improvement efforts have been “an important contributor,” Dr. Main said.
Improvements especially for Black women
Among the success stories has been California’s implementation of the AIM obstetric hemorrhage bundle about 5 years ago. Among other steps, the 17 evidence-based recommendations included early recognition, immediate access to oxytocin and other medications, immediate access to a hemorrhage cart with instructions for intrauterine balloons and compression stitches, the establishment of a hemorrhage response protocol and team, and regular unit-based drills with debriefing sessions afterward.
Mentoring teams consisting of a physician and nurse with maternal quality improvement experience were created to help hospitals come on board, with each team working with five to eight hospitals. Efforts included monthly telephone calls and face-to-face meetings, and providers were held accountable for progress. Hospitals shared data and tips on implementation, under the aegis of the CMQCC.
When the baseline period of 2011-2014 to the postintervention period of October 2015 to December 2016 were compared, the rate of severe maternal morbidity from hemorrhage fell from 22.1% to 18.5% across 99 hospitals and 73,476 women.
The benefit among Black women exceeded that among White women, with a 9% absolute rate reduction versus 2.1%. “If you adjusted for risk factors, [we found] you could eliminate [racial differences] completely,” which is something that hadn’t been shown before. “This is a really big deal,” Dr. Main said, because the risk of maternal morbidity and mortality is three to four times higher among Black women, compared with White women.
Dr. Main and his team found that the biggest clinical risk factor that accounted for racial differences was a higher rate of cesarean deliveries among Black women, followed by higher rates of anemia at hospital admission. “If you have a C-section when you are anemic, you are going to have a transfusion,” he explained.
More recently, there’s been a push in California to reduce the rate of primary cesarean deliveries by enacting the associated AIM bundle with use of the same approach as with the hemorrhage bundle. Dr. Main and his team recently reported a rate reduction from 29.3% to 25% without compromising birth outcomes.
However, “some changes are easier than others. Hemorrhage was an easy one to change because it didn’t deal with physician autonomy as much, and you saw more immediate results” with fewer hemorrhages. Reducing cesarean delivery rates is “a bigger lift” because “it’s really changing the culture of labor and delivery. It involves more group pressure and more reinforcing, but we were able to do that,” he said.
Problems in the Show Me State
“We’ve patterned a lot” of what’s being done in New Mexico “after California,” Dr. Espey said.
The AIM hemorrhage bundle, for instance, is being rolled out to New Mexico hospitals, with the help of virtual meetings and mentoring programs, plus outreach to the Navajo and others reservations because, as with Black women, rates of maternal morbidity and mortality are higher among Native American women.
It’s been tougher going, however, in states such as Missouri, which recently ranked 44th in the country for maternal mortality.
“We started a little bit late, and we are a little bit behind,” said ob.gyn. Karen L. Florio, DO, at the University of Missouri–Kansas City and also a leader of the state MMRC and member of its PQC.
The main problem is money. California’s efforts are funded by the Centers for Disease Control and Prevention, the state health department, and hospitals, among others.
But Missouri is “not as well funded as California for our mortality review board, and our [PQC] is mostly not funded. If we could get that funding, we would have more resources to implement these AIM bundles,” she said.
In addition to the issue, Missouri didn’t expand Medicaid under the Accountable Care Act – something that’s been linked to reduced maternal morbidity and mortality – and there are entire rural areas with no maternity care. Plus after generations of mistreatment, “our African American population has a valid distrust of the medical system that contributes to maternal mortality,” she said.
Obesity-related heart disease is also prevalent in Missouri, even among young people. “I cannot tell you how many women I have had who have had a heart attack at the age of 30 and who have had stents placed,” Dr. Florio said.
Dr. Florio and her colleagues are currently using teleconferences and other means to roll out the AIM hypertension bundle but can do so only selectively. “We don’t have the resources to reach every single rural hospital all over the state,” she said; they are working to address the funding issues.
For rural hospitals, implementation is “daunting”
Meanwhile, rural hospitals have been a particular concern in South Dakota, said Kimberlee McKay, MD, an ob.gyn. who is the clinical vice president of the ob.gyn. service line at Avera Health, a hospital system based in Sioux Falls, S.D.
She’s been overseeing Avera’s implementation of the hypertension, hemorrhage, and venous thromboembolism bundles. “What’s hard is that” the AIM protocols come “out of academic centers. Implementation of complex algorithms is daunting” for hospitals that only do a couple hundred deliveries a year, she said.
For small hospitals, the approach she’s found that works is to first assess what they can offer, and then have them “do what’s reasonable” for their resources. The second part is making sure high-risk women get to a regional center – with an adequate blood supply, in the case of hemorrhage, for instance – for complications. Dr. McKay and colleagues are working on a system by which regional centers can monitor smaller hospitals for potential maternity problems, and contact them proactively before they emerge.
They’ve also made access to hemorrhage and hypertension drugs easier on labor and delivery units with the help of close-by dedicated medicine boxes, and standardized protocols and order sets across Avera. “We try to make the right thing the easy thing to do,” Dr. McKay said.
Dr. Espey is an editorial adviser for Ob.Gyn. News. The physicians have no relevant financial disclosures.
“Anytime you have a maternal death, it sticks with you for life,” said Elliott Main, MD, a maternal fetal medicine specialist at Stanford (Calif.) University and one of the nation’s leaders in combating maternal mortality.
Dr. Main has had two maternal deaths in his career, years ago. One woman had a fatal stroke because of severe hypertension, and another died of cardiac complications. “We tried to do everything we possibly could, but you scrounge your memory for years and years [afterward]. To have a young healthy person go into labor and delivery and not come out is a tragedy at all levels. It charged me to not ever want to see that happen again,” he said.
Today, Dr. Main is the medical director of the California Maternal Quality Care Collaborative (CMQCC), a wide-ranging group of clinicians, state officials, hospitals, and others who have come together to address the issue. About 30 states have similar perinatal quality collaboratives (PQCs), and other states are forming them.
They work in collaboration with maternal mortality review committees (MMRCs), state-level groups that review maternal deaths, identify problems to address, and make recommendations to the quality collaboratives on how to prevent maternal deaths.
About 600-800 women die in the United States each year due to pregnancy-related complications, which ranks the United States behind other industrialized nations. Leading causes include hemorrhage and hemorrhagic strokes secondary to hypertension. It’s estimated that the majority of maternal deaths could be prevented with proper care.
To that end, states are enacting safety bundles from the Alliance for Innovation on Maternal Health (AIM), which was established by the American College of Obstetricians and Gynecologist several years ago. There are bundles that address obstetric hypertension, hemorrhage, mental health, venous thromboembolism, opioid use, racial disparities, and other problems. They were developed by experts in the field and published in multiple journals. California and other states have issued toolkits on how to implement them based on local circumstances.
Dr. Main said.
AIM bundle implementation is “what’s happening in New Mexico and a lot of states, mostly through the efforts of state level quality care collaboratives. Some [states] are further ahead than others,” said Eve Espey, MD, professor and chair of the department of obstetrics and gynecology at the University of New Mexico, Albuquerque, and president of the New Mexico PQC.
“Most states now have a [MMRC] that collects maternal mortality and near-miss data. Those data are used by the action arm,” which is the PQC. “If the review committee says” opioid use disorder is a significant contributor “like in our state, the collaborative rolls out the opioid use disorder bundle,” she said.
Beginning next January, the Joint Commission, formerly known as the Joint Commission on Accreditation of Healthcare Organizations, will require that accredited hospitals enact key elements of the AIM bundles for both obstetric hemorrhage and severe hypertension. “Everyone’s [now] motivated to get on that bandwagon,” Dr. Espey said.
“The bundles are here to stay,” and the Joint Commission requirements are “a really important step for sustainability and basic implementation. We really want to get them adopted everywhere,” said Dr. Main, who is also the national implementation director for the AIM initiative.
“The key thing is to work on implementing the hemorrhage and hypertension bundles in your hospital. I would suggest contacting [your] state” PQC, he said.
The California model
California, which has been working to reduce maternal mortality and morbidity since the mid 2000s, has produced among the strongest evidence to date that the efforts make a difference.
By 2013, the state had halved its maternal mortality rate to a 3-year average of 7 deaths per 100,000 live births, which is comparable with the average Western Europe rate of 7.2 deaths. Nationwide, the rate was about 17.4 deaths per 100,000 live births in 2018, according to the Centers for Disease Control and Prevention
The reasons are multifactorial, but “we think” the quality improvement efforts have been “an important contributor,” Dr. Main said.
Improvements especially for Black women
Among the success stories has been California’s implementation of the AIM obstetric hemorrhage bundle about 5 years ago. Among other steps, the 17 evidence-based recommendations included early recognition, immediate access to oxytocin and other medications, immediate access to a hemorrhage cart with instructions for intrauterine balloons and compression stitches, the establishment of a hemorrhage response protocol and team, and regular unit-based drills with debriefing sessions afterward.
Mentoring teams consisting of a physician and nurse with maternal quality improvement experience were created to help hospitals come on board, with each team working with five to eight hospitals. Efforts included monthly telephone calls and face-to-face meetings, and providers were held accountable for progress. Hospitals shared data and tips on implementation, under the aegis of the CMQCC.
When the baseline period of 2011-2014 to the postintervention period of October 2015 to December 2016 were compared, the rate of severe maternal morbidity from hemorrhage fell from 22.1% to 18.5% across 99 hospitals and 73,476 women.
The benefit among Black women exceeded that among White women, with a 9% absolute rate reduction versus 2.1%. “If you adjusted for risk factors, [we found] you could eliminate [racial differences] completely,” which is something that hadn’t been shown before. “This is a really big deal,” Dr. Main said, because the risk of maternal morbidity and mortality is three to four times higher among Black women, compared with White women.
Dr. Main and his team found that the biggest clinical risk factor that accounted for racial differences was a higher rate of cesarean deliveries among Black women, followed by higher rates of anemia at hospital admission. “If you have a C-section when you are anemic, you are going to have a transfusion,” he explained.
More recently, there’s been a push in California to reduce the rate of primary cesarean deliveries by enacting the associated AIM bundle with use of the same approach as with the hemorrhage bundle. Dr. Main and his team recently reported a rate reduction from 29.3% to 25% without compromising birth outcomes.
However, “some changes are easier than others. Hemorrhage was an easy one to change because it didn’t deal with physician autonomy as much, and you saw more immediate results” with fewer hemorrhages. Reducing cesarean delivery rates is “a bigger lift” because “it’s really changing the culture of labor and delivery. It involves more group pressure and more reinforcing, but we were able to do that,” he said.
Problems in the Show Me State
“We’ve patterned a lot” of what’s being done in New Mexico “after California,” Dr. Espey said.
The AIM hemorrhage bundle, for instance, is being rolled out to New Mexico hospitals, with the help of virtual meetings and mentoring programs, plus outreach to the Navajo and others reservations because, as with Black women, rates of maternal morbidity and mortality are higher among Native American women.
It’s been tougher going, however, in states such as Missouri, which recently ranked 44th in the country for maternal mortality.
“We started a little bit late, and we are a little bit behind,” said ob.gyn. Karen L. Florio, DO, at the University of Missouri–Kansas City and also a leader of the state MMRC and member of its PQC.
The main problem is money. California’s efforts are funded by the Centers for Disease Control and Prevention, the state health department, and hospitals, among others.
But Missouri is “not as well funded as California for our mortality review board, and our [PQC] is mostly not funded. If we could get that funding, we would have more resources to implement these AIM bundles,” she said.
In addition to the issue, Missouri didn’t expand Medicaid under the Accountable Care Act – something that’s been linked to reduced maternal morbidity and mortality – and there are entire rural areas with no maternity care. Plus after generations of mistreatment, “our African American population has a valid distrust of the medical system that contributes to maternal mortality,” she said.
Obesity-related heart disease is also prevalent in Missouri, even among young people. “I cannot tell you how many women I have had who have had a heart attack at the age of 30 and who have had stents placed,” Dr. Florio said.
Dr. Florio and her colleagues are currently using teleconferences and other means to roll out the AIM hypertension bundle but can do so only selectively. “We don’t have the resources to reach every single rural hospital all over the state,” she said; they are working to address the funding issues.
For rural hospitals, implementation is “daunting”
Meanwhile, rural hospitals have been a particular concern in South Dakota, said Kimberlee McKay, MD, an ob.gyn. who is the clinical vice president of the ob.gyn. service line at Avera Health, a hospital system based in Sioux Falls, S.D.
She’s been overseeing Avera’s implementation of the hypertension, hemorrhage, and venous thromboembolism bundles. “What’s hard is that” the AIM protocols come “out of academic centers. Implementation of complex algorithms is daunting” for hospitals that only do a couple hundred deliveries a year, she said.
For small hospitals, the approach she’s found that works is to first assess what they can offer, and then have them “do what’s reasonable” for their resources. The second part is making sure high-risk women get to a regional center – with an adequate blood supply, in the case of hemorrhage, for instance – for complications. Dr. McKay and colleagues are working on a system by which regional centers can monitor smaller hospitals for potential maternity problems, and contact them proactively before they emerge.
They’ve also made access to hemorrhage and hypertension drugs easier on labor and delivery units with the help of close-by dedicated medicine boxes, and standardized protocols and order sets across Avera. “We try to make the right thing the easy thing to do,” Dr. McKay said.
Dr. Espey is an editorial adviser for Ob.Gyn. News. The physicians have no relevant financial disclosures.