User login
COVID-19 child case count now over 400,000
according to a new report from the American Academy of Pediatrics and the Children’s Hospital Association.
The 406,000 children who have tested positive for COVID-19 represent 9.1% of all cases reported so far by 49 states (New York does not provide age distribution), New York City, the District of Columbia, Puerto Rico, and Guam. Since the proportion of child cases also was 9.1% on Aug. 6, the most recent week is the first without an increase since tracking began in mid-April, the report shows.
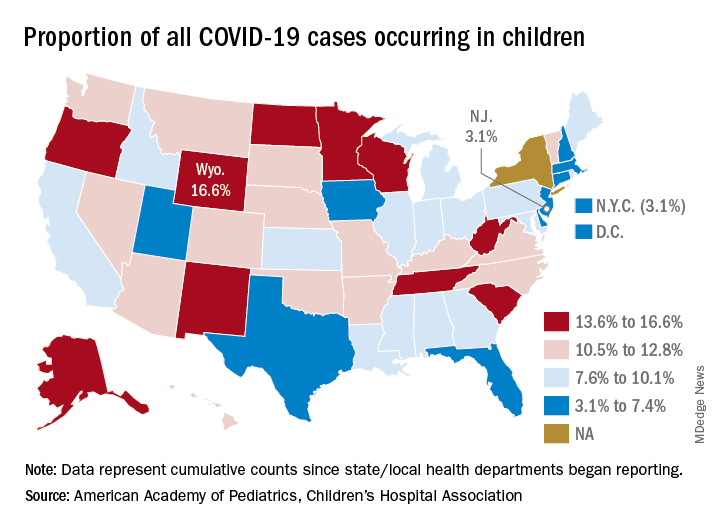
State-level data show that Wyoming has the highest percentage of child cases (16.6%) after Alabama changed its “definition of child case from 0-24 to 0-17 years, resulting in a downward revision of cumulative child cases,” the AAP and the CHA said. Alabama’s proportion of such cases dropped from 22.5% to 9.0%.
New Jersey had the lowest rate (3.1%) again this week, along with New York City, but both were up slightly from the week before, when New Jersey was at 2.9% and N.Y.C. was 3.0%. The only states, other than Alabama, that saw declines over the last week were Arkansas, Massachusetts, Mississippi, South Dakota, Texas, and West Virginia. Texas, however, has reported age for only 8% of its confirmed cases, the report noted.
The overall rate of child COVID-19 cases as of Aug. 13 was 538 per 100,000 children, up from 500.7 per 100,000 a week earlier. Arizona was again highest among the states with a rate of 1,254 per 100,000 (up from 1,206) and Vermont was lowest at 121, although Puerto Rico (114) and Guam (88) were lower still, the AAP/CHA data indicate.
For the nine states that report testing information for children, Arizona has the highest positivity rate at 18.3% and West Virginia has the lowest at 3.6%. Data on hospitalizations – available from 21 states and N.Y.C. – show that 3,849 children have been admitted, with rates varying from 0.2% of children in Hawaii to 8.8% in the Big Apple, according to the report.
More specific information on child cases, such as symptoms or underlying conditions, is not being provided by states at this time, the AAP and CHA pointed out.
according to a new report from the American Academy of Pediatrics and the Children’s Hospital Association.
The 406,000 children who have tested positive for COVID-19 represent 9.1% of all cases reported so far by 49 states (New York does not provide age distribution), New York City, the District of Columbia, Puerto Rico, and Guam. Since the proportion of child cases also was 9.1% on Aug. 6, the most recent week is the first without an increase since tracking began in mid-April, the report shows.
State-level data show that Wyoming has the highest percentage of child cases (16.6%) after Alabama changed its “definition of child case from 0-24 to 0-17 years, resulting in a downward revision of cumulative child cases,” the AAP and the CHA said. Alabama’s proportion of such cases dropped from 22.5% to 9.0%.
New Jersey had the lowest rate (3.1%) again this week, along with New York City, but both were up slightly from the week before, when New Jersey was at 2.9% and N.Y.C. was 3.0%. The only states, other than Alabama, that saw declines over the last week were Arkansas, Massachusetts, Mississippi, South Dakota, Texas, and West Virginia. Texas, however, has reported age for only 8% of its confirmed cases, the report noted.
The overall rate of child COVID-19 cases as of Aug. 13 was 538 per 100,000 children, up from 500.7 per 100,000 a week earlier. Arizona was again highest among the states with a rate of 1,254 per 100,000 (up from 1,206) and Vermont was lowest at 121, although Puerto Rico (114) and Guam (88) were lower still, the AAP/CHA data indicate.
For the nine states that report testing information for children, Arizona has the highest positivity rate at 18.3% and West Virginia has the lowest at 3.6%. Data on hospitalizations – available from 21 states and N.Y.C. – show that 3,849 children have been admitted, with rates varying from 0.2% of children in Hawaii to 8.8% in the Big Apple, according to the report.
More specific information on child cases, such as symptoms or underlying conditions, is not being provided by states at this time, the AAP and CHA pointed out.
according to a new report from the American Academy of Pediatrics and the Children’s Hospital Association.
The 406,000 children who have tested positive for COVID-19 represent 9.1% of all cases reported so far by 49 states (New York does not provide age distribution), New York City, the District of Columbia, Puerto Rico, and Guam. Since the proportion of child cases also was 9.1% on Aug. 6, the most recent week is the first without an increase since tracking began in mid-April, the report shows.
State-level data show that Wyoming has the highest percentage of child cases (16.6%) after Alabama changed its “definition of child case from 0-24 to 0-17 years, resulting in a downward revision of cumulative child cases,” the AAP and the CHA said. Alabama’s proportion of such cases dropped from 22.5% to 9.0%.
New Jersey had the lowest rate (3.1%) again this week, along with New York City, but both were up slightly from the week before, when New Jersey was at 2.9% and N.Y.C. was 3.0%. The only states, other than Alabama, that saw declines over the last week were Arkansas, Massachusetts, Mississippi, South Dakota, Texas, and West Virginia. Texas, however, has reported age for only 8% of its confirmed cases, the report noted.
The overall rate of child COVID-19 cases as of Aug. 13 was 538 per 100,000 children, up from 500.7 per 100,000 a week earlier. Arizona was again highest among the states with a rate of 1,254 per 100,000 (up from 1,206) and Vermont was lowest at 121, although Puerto Rico (114) and Guam (88) were lower still, the AAP/CHA data indicate.
For the nine states that report testing information for children, Arizona has the highest positivity rate at 18.3% and West Virginia has the lowest at 3.6%. Data on hospitalizations – available from 21 states and N.Y.C. – show that 3,849 children have been admitted, with rates varying from 0.2% of children in Hawaii to 8.8% in the Big Apple, according to the report.
More specific information on child cases, such as symptoms or underlying conditions, is not being provided by states at this time, the AAP and CHA pointed out.
Severe obesity ups risk for death in younger men with COVID-19
In a large California health care plan, among patients with COVID-19, men aged 60 years and younger had a much higher risk of dying within 3 weeks of diagnosis if they had severe obesity as opposed to being of normal weight, independently of other risk factors.
reported Sara Y. Tartof, PhD, MPH, Kaiser Permanente Southern California, Pasadena, Calif., and coauthors.
The data “highlight the leading role of severe obesity over correlated risk factors, providing a target for early intervention,” they concluded in an article published online Aug. 12 in Annals of Internal Medicine.
This work adds to nearly 300 articles that have shown that severe obesity is associated with an increased risk for morbidity and mortality from COVID-19.
In an accompanying editorial, David A. Kass, MD, said: “Consistency of this new study and prior research should put to rest the contention that obesity is common in severe COVID-19 because it is common in the population.”
Rather, these findings show that “obesity is an important independent risk factor for serious COVID-19 disease,” he pointed out.
On the basis of this evidence, “arguably the hardest question to answer is: What is to be done?” wondered Kass, of Johns Hopkins University, Baltimore.
Although data consistently show that a body mass index >35 kg/m2 is predictive of major health risks, “weight reduction at that level of obesity is difficult and certainly is not achieved rapidly,” Dr. Kass stressed.
“Therefore ... social distancing; altering behaviors to reduce viral exposure and transmission, such as wearing masks; and instituting policies and health care approaches that recognize the potential effects of obesity should be implemented,” he emphasized. “These actions should help and are certainly doable.”
Similarly, Dr. Tartof and colleagues said their “findings also reveal the distressing collision of two pandemics: COVID-19 and obesity.
“As COVID-19 continues to spread unabated, we must focus our immediate efforts on containing the crisis at hand,” they urged.
However, the findings also “underscore the need for future collective efforts to combat the equally devastating, and potentially synergistic, force of the obesity epidemic.”
COVID-19 pandemic collides with obesity epidemic
Previous studies of obesity and COVID-19 were small, did not adjust for multiple confounders, or did not include nonhospitalized patients, Dr. Tartof and coauthors wrote.
Their study included 6,916 members of the Kaiser Permanente Southern California health care plan who were diagnosed with COVID-19 from Feb. 13 to May 2, 2020.
The researchers calculated the risk for death at 21 days after a COVID-19 diagnosis; findings were corrected for age, sex, race/ethnicity, smoking, myocardial infarction, heart failure, peripheral vascular disease, cerebrovascular disease, chronic pulmonary disease, renal disease, metastatic tumor or malignancy, other immune disease, hyperlipidemia, hypertension, asthma, organ transplant, and diabetes status.
On the basis of BMI, the patients were classified as being underweight, of normal weight, overweight, or as having class 1, 2, or 3 obesity. BMI of 18.5 to 24 kg/m2 is defined as normal weight.
Class 3 obesity, also called severe obesity, included moderately severe obesity (BMI, 40-44 kg/m2) and extremely severe obesity (≥45 kg/m2).
A little more than half of the patients were women (55%), and more than 50% were Hispanic (54%).
A total of 206 patients (3%) died within 21 days of being diagnosed with COVID-19; of these, 67% had been hospitalized, and 43% had been intubated.
Overall, the COVID-19 patients with moderately severe or extremely severe obesity had a 2.7-fold and 4.2-fold increased risk for death, respectively, within 3 weeks compared with patients of normal weight.
Patients in the other BMI categories did not have a significantly higher risk of dying during follow-up.
However, each decade of increasing age after age 40 was associated with a stepwise increased risk for death within 3 weeks of the COVID-19 diagnosis.
Risk stratified by age and sex
Further analysis showed that, “most strikingly,” among patients aged 60 and younger, those with moderately severe obesity and extremely severe obesity had significant 17-fold and 12-fold higher risks of dying during follow-up, respectively, compared with patients of normal weight, the researchers reported.
In patients older than 60, moderately severe obesity did not confer a significant increased risk for imminent death from COVID-19; extremely severe obesity conferred a smaller, threefold increased risk for this.
“Our finding that severe obesity, particularly among younger patients, eclipses the mortality risk posed by other obesity-related conditions, such as history of myocardial infarction (MI), diabetes, hypertension, or hyperlipidemia, suggests a significant pathophysiologic link between excess adiposity and severe COVID-19 illness,” the researchers noted.
This independent increased risk for death with severe obesity was seen in men but not in women.
Men with moderately severe and extremely severe obesity had significant 4.8-fold and 10-fold higher risks of dying within 3 weeks, respectively, compared with men of normal weight.
“That the risks are higher in younger patients is probably not because obesity is particularly damaging in this age group; it is more likely that other serious comorbidities that evolve later in life take over as dominant risk factors,” Dr. Kass suggested in his editorial.
“That males are particularly affected may reflect their greater visceral adiposity over females, given that this fat is notably proinflammatory and contributes to metabolic and vascular disease,” he added.
“As a cardiologist who studies heart failure,” Dr. Kass wrote, “I am struck by how many of the mechanisms that are mentioned in reviews of obesity risk and heart disease are also mentioned in reviews of obesity and COVID-19.”
The study was funded by Roche-Genentech. Kass has disclosed no relevant financial relationships. Disclosures of the authors are listed in the article.
A version of this article originally appeared on Medscape.com.
In a large California health care plan, among patients with COVID-19, men aged 60 years and younger had a much higher risk of dying within 3 weeks of diagnosis if they had severe obesity as opposed to being of normal weight, independently of other risk factors.
reported Sara Y. Tartof, PhD, MPH, Kaiser Permanente Southern California, Pasadena, Calif., and coauthors.
The data “highlight the leading role of severe obesity over correlated risk factors, providing a target for early intervention,” they concluded in an article published online Aug. 12 in Annals of Internal Medicine.
This work adds to nearly 300 articles that have shown that severe obesity is associated with an increased risk for morbidity and mortality from COVID-19.
In an accompanying editorial, David A. Kass, MD, said: “Consistency of this new study and prior research should put to rest the contention that obesity is common in severe COVID-19 because it is common in the population.”
Rather, these findings show that “obesity is an important independent risk factor for serious COVID-19 disease,” he pointed out.
On the basis of this evidence, “arguably the hardest question to answer is: What is to be done?” wondered Kass, of Johns Hopkins University, Baltimore.
Although data consistently show that a body mass index >35 kg/m2 is predictive of major health risks, “weight reduction at that level of obesity is difficult and certainly is not achieved rapidly,” Dr. Kass stressed.
“Therefore ... social distancing; altering behaviors to reduce viral exposure and transmission, such as wearing masks; and instituting policies and health care approaches that recognize the potential effects of obesity should be implemented,” he emphasized. “These actions should help and are certainly doable.”
Similarly, Dr. Tartof and colleagues said their “findings also reveal the distressing collision of two pandemics: COVID-19 and obesity.
“As COVID-19 continues to spread unabated, we must focus our immediate efforts on containing the crisis at hand,” they urged.
However, the findings also “underscore the need for future collective efforts to combat the equally devastating, and potentially synergistic, force of the obesity epidemic.”
COVID-19 pandemic collides with obesity epidemic
Previous studies of obesity and COVID-19 were small, did not adjust for multiple confounders, or did not include nonhospitalized patients, Dr. Tartof and coauthors wrote.
Their study included 6,916 members of the Kaiser Permanente Southern California health care plan who were diagnosed with COVID-19 from Feb. 13 to May 2, 2020.
The researchers calculated the risk for death at 21 days after a COVID-19 diagnosis; findings were corrected for age, sex, race/ethnicity, smoking, myocardial infarction, heart failure, peripheral vascular disease, cerebrovascular disease, chronic pulmonary disease, renal disease, metastatic tumor or malignancy, other immune disease, hyperlipidemia, hypertension, asthma, organ transplant, and diabetes status.
On the basis of BMI, the patients were classified as being underweight, of normal weight, overweight, or as having class 1, 2, or 3 obesity. BMI of 18.5 to 24 kg/m2 is defined as normal weight.
Class 3 obesity, also called severe obesity, included moderately severe obesity (BMI, 40-44 kg/m2) and extremely severe obesity (≥45 kg/m2).
A little more than half of the patients were women (55%), and more than 50% were Hispanic (54%).
A total of 206 patients (3%) died within 21 days of being diagnosed with COVID-19; of these, 67% had been hospitalized, and 43% had been intubated.
Overall, the COVID-19 patients with moderately severe or extremely severe obesity had a 2.7-fold and 4.2-fold increased risk for death, respectively, within 3 weeks compared with patients of normal weight.
Patients in the other BMI categories did not have a significantly higher risk of dying during follow-up.
However, each decade of increasing age after age 40 was associated with a stepwise increased risk for death within 3 weeks of the COVID-19 diagnosis.
Risk stratified by age and sex
Further analysis showed that, “most strikingly,” among patients aged 60 and younger, those with moderately severe obesity and extremely severe obesity had significant 17-fold and 12-fold higher risks of dying during follow-up, respectively, compared with patients of normal weight, the researchers reported.
In patients older than 60, moderately severe obesity did not confer a significant increased risk for imminent death from COVID-19; extremely severe obesity conferred a smaller, threefold increased risk for this.
“Our finding that severe obesity, particularly among younger patients, eclipses the mortality risk posed by other obesity-related conditions, such as history of myocardial infarction (MI), diabetes, hypertension, or hyperlipidemia, suggests a significant pathophysiologic link between excess adiposity and severe COVID-19 illness,” the researchers noted.
This independent increased risk for death with severe obesity was seen in men but not in women.
Men with moderately severe and extremely severe obesity had significant 4.8-fold and 10-fold higher risks of dying within 3 weeks, respectively, compared with men of normal weight.
“That the risks are higher in younger patients is probably not because obesity is particularly damaging in this age group; it is more likely that other serious comorbidities that evolve later in life take over as dominant risk factors,” Dr. Kass suggested in his editorial.
“That males are particularly affected may reflect their greater visceral adiposity over females, given that this fat is notably proinflammatory and contributes to metabolic and vascular disease,” he added.
“As a cardiologist who studies heart failure,” Dr. Kass wrote, “I am struck by how many of the mechanisms that are mentioned in reviews of obesity risk and heart disease are also mentioned in reviews of obesity and COVID-19.”
The study was funded by Roche-Genentech. Kass has disclosed no relevant financial relationships. Disclosures of the authors are listed in the article.
A version of this article originally appeared on Medscape.com.
In a large California health care plan, among patients with COVID-19, men aged 60 years and younger had a much higher risk of dying within 3 weeks of diagnosis if they had severe obesity as opposed to being of normal weight, independently of other risk factors.
reported Sara Y. Tartof, PhD, MPH, Kaiser Permanente Southern California, Pasadena, Calif., and coauthors.
The data “highlight the leading role of severe obesity over correlated risk factors, providing a target for early intervention,” they concluded in an article published online Aug. 12 in Annals of Internal Medicine.
This work adds to nearly 300 articles that have shown that severe obesity is associated with an increased risk for morbidity and mortality from COVID-19.
In an accompanying editorial, David A. Kass, MD, said: “Consistency of this new study and prior research should put to rest the contention that obesity is common in severe COVID-19 because it is common in the population.”
Rather, these findings show that “obesity is an important independent risk factor for serious COVID-19 disease,” he pointed out.
On the basis of this evidence, “arguably the hardest question to answer is: What is to be done?” wondered Kass, of Johns Hopkins University, Baltimore.
Although data consistently show that a body mass index >35 kg/m2 is predictive of major health risks, “weight reduction at that level of obesity is difficult and certainly is not achieved rapidly,” Dr. Kass stressed.
“Therefore ... social distancing; altering behaviors to reduce viral exposure and transmission, such as wearing masks; and instituting policies and health care approaches that recognize the potential effects of obesity should be implemented,” he emphasized. “These actions should help and are certainly doable.”
Similarly, Dr. Tartof and colleagues said their “findings also reveal the distressing collision of two pandemics: COVID-19 and obesity.
“As COVID-19 continues to spread unabated, we must focus our immediate efforts on containing the crisis at hand,” they urged.
However, the findings also “underscore the need for future collective efforts to combat the equally devastating, and potentially synergistic, force of the obesity epidemic.”
COVID-19 pandemic collides with obesity epidemic
Previous studies of obesity and COVID-19 were small, did not adjust for multiple confounders, or did not include nonhospitalized patients, Dr. Tartof and coauthors wrote.
Their study included 6,916 members of the Kaiser Permanente Southern California health care plan who were diagnosed with COVID-19 from Feb. 13 to May 2, 2020.
The researchers calculated the risk for death at 21 days after a COVID-19 diagnosis; findings were corrected for age, sex, race/ethnicity, smoking, myocardial infarction, heart failure, peripheral vascular disease, cerebrovascular disease, chronic pulmonary disease, renal disease, metastatic tumor or malignancy, other immune disease, hyperlipidemia, hypertension, asthma, organ transplant, and diabetes status.
On the basis of BMI, the patients were classified as being underweight, of normal weight, overweight, or as having class 1, 2, or 3 obesity. BMI of 18.5 to 24 kg/m2 is defined as normal weight.
Class 3 obesity, also called severe obesity, included moderately severe obesity (BMI, 40-44 kg/m2) and extremely severe obesity (≥45 kg/m2).
A little more than half of the patients were women (55%), and more than 50% were Hispanic (54%).
A total of 206 patients (3%) died within 21 days of being diagnosed with COVID-19; of these, 67% had been hospitalized, and 43% had been intubated.
Overall, the COVID-19 patients with moderately severe or extremely severe obesity had a 2.7-fold and 4.2-fold increased risk for death, respectively, within 3 weeks compared with patients of normal weight.
Patients in the other BMI categories did not have a significantly higher risk of dying during follow-up.
However, each decade of increasing age after age 40 was associated with a stepwise increased risk for death within 3 weeks of the COVID-19 diagnosis.
Risk stratified by age and sex
Further analysis showed that, “most strikingly,” among patients aged 60 and younger, those with moderately severe obesity and extremely severe obesity had significant 17-fold and 12-fold higher risks of dying during follow-up, respectively, compared with patients of normal weight, the researchers reported.
In patients older than 60, moderately severe obesity did not confer a significant increased risk for imminent death from COVID-19; extremely severe obesity conferred a smaller, threefold increased risk for this.
“Our finding that severe obesity, particularly among younger patients, eclipses the mortality risk posed by other obesity-related conditions, such as history of myocardial infarction (MI), diabetes, hypertension, or hyperlipidemia, suggests a significant pathophysiologic link between excess adiposity and severe COVID-19 illness,” the researchers noted.
This independent increased risk for death with severe obesity was seen in men but not in women.
Men with moderately severe and extremely severe obesity had significant 4.8-fold and 10-fold higher risks of dying within 3 weeks, respectively, compared with men of normal weight.
“That the risks are higher in younger patients is probably not because obesity is particularly damaging in this age group; it is more likely that other serious comorbidities that evolve later in life take over as dominant risk factors,” Dr. Kass suggested in his editorial.
“That males are particularly affected may reflect their greater visceral adiposity over females, given that this fat is notably proinflammatory and contributes to metabolic and vascular disease,” he added.
“As a cardiologist who studies heart failure,” Dr. Kass wrote, “I am struck by how many of the mechanisms that are mentioned in reviews of obesity risk and heart disease are also mentioned in reviews of obesity and COVID-19.”
The study was funded by Roche-Genentech. Kass has disclosed no relevant financial relationships. Disclosures of the authors are listed in the article.
A version of this article originally appeared on Medscape.com.
Only 40% of residents said training prepped them for COVID-19
Most residents who were asked whether their training prepared them for COVID-19 in a Medscape survey said it had not or they weren’t sure.
Whereas 40% said they felt prepared, 30% said they did not feel prepared and 31% answered they were unsure. (Numbers were rounded, so some answers pushed above 100%.)
One quarter have $300,000 or more in student debt
The Medscape Residents Salary & Debt Report 2020, with data collected April 3 to June 1, found that nearly one in four residents (24%) had medical school debt of more than $300,000. Half (49%) had more than $200,000.
The data include answers from 1,659 U.S. medical residents.
For the sixth straight year, female residents were more satisfied with their pay than were their male colleagues. This year the satisfaction gap was 45% female compared with 42% male. That imbalance came despite their making nearly the same pay overall ($63,700 for men and $63,000 for women).
Among practicing physicians, the pay gap is much wider: Men make 25% more in primary care and 31% more in specialties.
Ten percent thought they should earn 76%-100% more.
For those not satisfied with pay, the top reasons were feeling the pay was too low for the hours worked (81%) or too low compared with other medical staff, such as physician assistants (PAs) or nurses (77% chose that answer).
As for hours worked, 31% of residents reported they spend more than 60 hours/week seeing patients.
The top-paying specialties, averaging $69,500, were allergy and immunology, hematology, plastic surgery, aesthetic medicine, rheumatology, and specialized surgery. The lowest paid were family medicine residents at $58,500.
In primary care, overall, most residents said they planned to specialize. Only 47% planned to continue to work in primary care. Male residents were much more likely to say they will subspecialize than were their female colleagues (52% vs. 35%).
More than 90% of residents say future pay has influenced their choice of specialty, though more men than women felt that way (93% vs. 86%).
Good relationships with others
Overall, residents reported good relationships with attending physicians and nurses.
Most (88%) said they had good or very good relationships with attending physicians, 10% said the relationships were fair, and 2% said they were poor.
In addition, 89% of residents said the amount of supervision was appropriate, 4% said there was too much, and 7% said there was too little.
Relationships with nurses/PAs were slightly less positive overall: Eighty-two percent reported good or very good relationships with nurses/PAs, 15% said those relationships were fair, and 3% said they were poor.
One respondent said: “Our relationships could be better, but I think everyone is just overwhelmed with COVID-19, so emotions are heightened.”
Another said: “It takes time to earn the respect from nurses.”
Seventy-seven percent said they were satisfied with their learning experience overall, 12% were neutral on the question, and 11% said they were dissatisfied or very dissatisfied.
Work-life balance is the top concern
Work-life balance continues to be the top concern for residents. More than one-quarter (27%) in residency years 1 through 4 listed that as the top concern, and even more (32%) of those in years 5 through 8 agreed.
That was followed by demands on time and fear of failure or making a serious mistake.
The survey indicates that benefit packages for residents have stayed much the same over the past 2 years with health insurance and paid time off for sick leave, vacation, and personal time most commonly reported at 89% and 87%, respectively.
Much less common were benefits including commuter assistance (parking, public transportation) at 24%, housing allowance (8%), and child care (4%).
The vast majority of residents reported doing scut work (unskilled tasks): More than half (54%) reported doing 1-10 hours/week and 22% did 11-20 hours/week. Regardless of the number of hours, however, 62% said the time spent performing these tasks was appropriate.
A version of this article originally appeared on Medscape.com.
Most residents who were asked whether their training prepared them for COVID-19 in a Medscape survey said it had not or they weren’t sure.
Whereas 40% said they felt prepared, 30% said they did not feel prepared and 31% answered they were unsure. (Numbers were rounded, so some answers pushed above 100%.)
One quarter have $300,000 or more in student debt
The Medscape Residents Salary & Debt Report 2020, with data collected April 3 to June 1, found that nearly one in four residents (24%) had medical school debt of more than $300,000. Half (49%) had more than $200,000.
The data include answers from 1,659 U.S. medical residents.
For the sixth straight year, female residents were more satisfied with their pay than were their male colleagues. This year the satisfaction gap was 45% female compared with 42% male. That imbalance came despite their making nearly the same pay overall ($63,700 for men and $63,000 for women).
Among practicing physicians, the pay gap is much wider: Men make 25% more in primary care and 31% more in specialties.
Ten percent thought they should earn 76%-100% more.
For those not satisfied with pay, the top reasons were feeling the pay was too low for the hours worked (81%) or too low compared with other medical staff, such as physician assistants (PAs) or nurses (77% chose that answer).
As for hours worked, 31% of residents reported they spend more than 60 hours/week seeing patients.
The top-paying specialties, averaging $69,500, were allergy and immunology, hematology, plastic surgery, aesthetic medicine, rheumatology, and specialized surgery. The lowest paid were family medicine residents at $58,500.
In primary care, overall, most residents said they planned to specialize. Only 47% planned to continue to work in primary care. Male residents were much more likely to say they will subspecialize than were their female colleagues (52% vs. 35%).
More than 90% of residents say future pay has influenced their choice of specialty, though more men than women felt that way (93% vs. 86%).
Good relationships with others
Overall, residents reported good relationships with attending physicians and nurses.
Most (88%) said they had good or very good relationships with attending physicians, 10% said the relationships were fair, and 2% said they were poor.
In addition, 89% of residents said the amount of supervision was appropriate, 4% said there was too much, and 7% said there was too little.
Relationships with nurses/PAs were slightly less positive overall: Eighty-two percent reported good or very good relationships with nurses/PAs, 15% said those relationships were fair, and 3% said they were poor.
One respondent said: “Our relationships could be better, but I think everyone is just overwhelmed with COVID-19, so emotions are heightened.”
Another said: “It takes time to earn the respect from nurses.”
Seventy-seven percent said they were satisfied with their learning experience overall, 12% were neutral on the question, and 11% said they were dissatisfied or very dissatisfied.
Work-life balance is the top concern
Work-life balance continues to be the top concern for residents. More than one-quarter (27%) in residency years 1 through 4 listed that as the top concern, and even more (32%) of those in years 5 through 8 agreed.
That was followed by demands on time and fear of failure or making a serious mistake.
The survey indicates that benefit packages for residents have stayed much the same over the past 2 years with health insurance and paid time off for sick leave, vacation, and personal time most commonly reported at 89% and 87%, respectively.
Much less common were benefits including commuter assistance (parking, public transportation) at 24%, housing allowance (8%), and child care (4%).
The vast majority of residents reported doing scut work (unskilled tasks): More than half (54%) reported doing 1-10 hours/week and 22% did 11-20 hours/week. Regardless of the number of hours, however, 62% said the time spent performing these tasks was appropriate.
A version of this article originally appeared on Medscape.com.
Most residents who were asked whether their training prepared them for COVID-19 in a Medscape survey said it had not or they weren’t sure.
Whereas 40% said they felt prepared, 30% said they did not feel prepared and 31% answered they were unsure. (Numbers were rounded, so some answers pushed above 100%.)
One quarter have $300,000 or more in student debt
The Medscape Residents Salary & Debt Report 2020, with data collected April 3 to June 1, found that nearly one in four residents (24%) had medical school debt of more than $300,000. Half (49%) had more than $200,000.
The data include answers from 1,659 U.S. medical residents.
For the sixth straight year, female residents were more satisfied with their pay than were their male colleagues. This year the satisfaction gap was 45% female compared with 42% male. That imbalance came despite their making nearly the same pay overall ($63,700 for men and $63,000 for women).
Among practicing physicians, the pay gap is much wider: Men make 25% more in primary care and 31% more in specialties.
Ten percent thought they should earn 76%-100% more.
For those not satisfied with pay, the top reasons were feeling the pay was too low for the hours worked (81%) or too low compared with other medical staff, such as physician assistants (PAs) or nurses (77% chose that answer).
As for hours worked, 31% of residents reported they spend more than 60 hours/week seeing patients.
The top-paying specialties, averaging $69,500, were allergy and immunology, hematology, plastic surgery, aesthetic medicine, rheumatology, and specialized surgery. The lowest paid were family medicine residents at $58,500.
In primary care, overall, most residents said they planned to specialize. Only 47% planned to continue to work in primary care. Male residents were much more likely to say they will subspecialize than were their female colleagues (52% vs. 35%).
More than 90% of residents say future pay has influenced their choice of specialty, though more men than women felt that way (93% vs. 86%).
Good relationships with others
Overall, residents reported good relationships with attending physicians and nurses.
Most (88%) said they had good or very good relationships with attending physicians, 10% said the relationships were fair, and 2% said they were poor.
In addition, 89% of residents said the amount of supervision was appropriate, 4% said there was too much, and 7% said there was too little.
Relationships with nurses/PAs were slightly less positive overall: Eighty-two percent reported good or very good relationships with nurses/PAs, 15% said those relationships were fair, and 3% said they were poor.
One respondent said: “Our relationships could be better, but I think everyone is just overwhelmed with COVID-19, so emotions are heightened.”
Another said: “It takes time to earn the respect from nurses.”
Seventy-seven percent said they were satisfied with their learning experience overall, 12% were neutral on the question, and 11% said they were dissatisfied or very dissatisfied.
Work-life balance is the top concern
Work-life balance continues to be the top concern for residents. More than one-quarter (27%) in residency years 1 through 4 listed that as the top concern, and even more (32%) of those in years 5 through 8 agreed.
That was followed by demands on time and fear of failure or making a serious mistake.
The survey indicates that benefit packages for residents have stayed much the same over the past 2 years with health insurance and paid time off for sick leave, vacation, and personal time most commonly reported at 89% and 87%, respectively.
Much less common were benefits including commuter assistance (parking, public transportation) at 24%, housing allowance (8%), and child care (4%).
The vast majority of residents reported doing scut work (unskilled tasks): More than half (54%) reported doing 1-10 hours/week and 22% did 11-20 hours/week. Regardless of the number of hours, however, 62% said the time spent performing these tasks was appropriate.
A version of this article originally appeared on Medscape.com.
Telemedicine checklist may smooth visits with older patients
During the pandemic, physicians have raced to set up or expand telemedicine, uncovering both advantages and shortcomings.
Although many of the suggestions, published online in Annals of Internal Medicine, are useful for all patients, Carrie Nieman, MD, MPH, and Esther S. Oh, MD, PhD, developed the list with older patients in mind.
“I have a number of patients into their 90s and with hearing loss, and we have had very successful video-based telemedicine visits,” Dr. Nieman, with the Cochlear Center for Hearing and Public Health at Johns Hopkins Bloomberg School of Public Health in Baltimore said in an interview. “Age should not be considered synonymous with inability or unwillingness to use technology.”
Their recommendations included the following:
- Assume some degree of hearing loss, which affects about two-thirds of adults aged 70 years and older.
- Ask patients to wear headphones or a headset or confirm that they are wearing their hearing aids and are in a quiet location.
- Use a headset.
- When possible, use video and have the camera focused on your face.
- Use captioning when available and provide a written summary of key points and instructions.
- Pay attention to cues, such as nodding along or looking to a loved one, that suggest a patient may not be following the conversation.
“If cognitive impairment is suspected, several screening tools can be used over the telephone to identify individuals who may need more comprehensive, in-person assessment,” wrote Dr. Nieman and Dr. Oh, who is with the division of geriatric medicine and gerontology at Johns Hopkins University School of Medicine. For example, data suggest that a modified version of the Mini–Mental State Examination and the Delirium Symptom Interview could be useful tools. “A formal diagnosis of dementia is not recommended solely based on a telephone-based cognitive screening,” however, Dr. Nieman and Dr. Oh said.
For patients with hearing loss, video visits avoid a current limitation of in-person visits: face masks that hinder patients’ ability to read lips and other visual cues. “For many of us, we rely on these types of cues more than we think,” Dr. Nieman said in an interview.
“When you have doubts about whether you and your patient are on the same page, check in with the patient,” Dr. Nieman said. “When appropriate, having a loved one or a care partner join an encounter, or at least a portion of the encounter, can be helpful to both the patient and the provider.”
Many older patients unprepared
Millions of older patients may not have been ready for the rapid shift to telemedicine brought on by COVID-19, a recent study in JAMA Internal Medicine suggests. Between 32% and 38% of older adults in the United States may not have been ready for video visits, largely because of inexperience with technology. Approximately 20% could have difficulty with telephone visits because of problems hearing or communicating or because of dementia.
Kenneth Lam, MD, of the division of geriatrics at the University of California, San Francisco (UCSF), and colleagues arrived at these estimates after analyzing data from more than 4,500 participants in the National Health and Aging Trends Study that was conducted in 2018. The study is nationally representative of Medicare beneficiaries 65 years or older.
The aim of the study “was to call attention to what clinicians were already experiencing on the front lines,” Dr. Lam said. In an interview, he imagined two scenarios based on his colleagues’ accounts of telemedicine visits.
In one case, a 72-year-old woman logs into Zoom Health on her iPad without any trouble. “She explains she just pushed on the URL and everything loaded up and you have a great visit,” Dr. Lam said. “This is likely to be the case for over 50% of the older people you see; I share this picture to combat ageism, which is, truthfully, just inaccurate stereotyping of older people and gets in the way of actionable, data-driven policies.
“However, for around one in three older adults (and closer to three out of every four of those over the age of 85), you will book an appointment and they will say they don’t have an email address or a computer or know how to go online,” Dr. Lam said. “Or suppose they decide to try it out. ... Come appointment time, you log on and they pick up, but now their sound doesn’t work. They keep saying they can see you but they can’t hear you. ... They accidentally hang up. You place another call, and they ask if you can switch to a phone conversation instead.”
By phone, the physician can address concerns about the patient’s blood pressure, which the patient has been measuring daily. “But when it comes to looking at the swelling in their legs, you’re out of luck, and you’ve been on this call for 45 minutes,” Dr. Lam said.
Have a backup plan
Making sure patients are prepared and having a backup plan can help, said Kaitlin Willham, MD, of UCSF and the San Francisco VA Medical Center.
She says older patients fall into a wide range of categories in terms of skills and access to equipment. Knowing which category a patient falls into and having relevant support available to troubleshoot are important.
During the pandemic, Dr. Willham has conducted many more telemedicine visits with patients who are at their place of residence, whether a private home or a residential care facility. “Even outside of the current crisis, there are benefits to home video visits,” Dr. Willham said. “A home video visit can provide a more holistic view of the patient than an office visit, allowing the clinician to see how the person lives, what they might be challenged by. It allows the clinician to identify areas of intervention and, if there is a care partner, involving that person in the plan. If the visit starts without major technical or communication barriers, they are generally very well received.”
For patients with problems hearing for whom headphones or amplification devices are not available, “using a landline for the audio portion of the visit can help, as can having someone with the patient reiterate what was said,” Dr. Willham suggested. “Many video platforms also enable the clinician to type messages or share a screen with a live document. These options can work well when there is very severe or complete lack of hearing.”
Sometimes an in-person visit is the right way to go, even when technical hurdles can be overcome.
“Although many older adults are willing and able to learn to use telemedicine, an equitable health system should recognize that for some, such as those with dementia and social isolation, in-person visits are already difficult and telemedicine may be impossible,” Dr. Lam and coauthors wrote. “For these patients, clinics and geriatric models of care such as home visits are essential.”
Dr. Nieman, Dr. Oh, and one of Dr. Lam’s coauthors have received funding from the National Institutes of Health. Dr. Oh also has received funding from the Roberts Family Fund. Dr. Nieman serves as a board member of the nonprofit organization Access HEARS and is on the board of trustees of the Hearing Loss Association of America.
A version of this article originally appeared on Medscape.com.
During the pandemic, physicians have raced to set up or expand telemedicine, uncovering both advantages and shortcomings.
Although many of the suggestions, published online in Annals of Internal Medicine, are useful for all patients, Carrie Nieman, MD, MPH, and Esther S. Oh, MD, PhD, developed the list with older patients in mind.
“I have a number of patients into their 90s and with hearing loss, and we have had very successful video-based telemedicine visits,” Dr. Nieman, with the Cochlear Center for Hearing and Public Health at Johns Hopkins Bloomberg School of Public Health in Baltimore said in an interview. “Age should not be considered synonymous with inability or unwillingness to use technology.”
Their recommendations included the following:
- Assume some degree of hearing loss, which affects about two-thirds of adults aged 70 years and older.
- Ask patients to wear headphones or a headset or confirm that they are wearing their hearing aids and are in a quiet location.
- Use a headset.
- When possible, use video and have the camera focused on your face.
- Use captioning when available and provide a written summary of key points and instructions.
- Pay attention to cues, such as nodding along or looking to a loved one, that suggest a patient may not be following the conversation.
“If cognitive impairment is suspected, several screening tools can be used over the telephone to identify individuals who may need more comprehensive, in-person assessment,” wrote Dr. Nieman and Dr. Oh, who is with the division of geriatric medicine and gerontology at Johns Hopkins University School of Medicine. For example, data suggest that a modified version of the Mini–Mental State Examination and the Delirium Symptom Interview could be useful tools. “A formal diagnosis of dementia is not recommended solely based on a telephone-based cognitive screening,” however, Dr. Nieman and Dr. Oh said.
For patients with hearing loss, video visits avoid a current limitation of in-person visits: face masks that hinder patients’ ability to read lips and other visual cues. “For many of us, we rely on these types of cues more than we think,” Dr. Nieman said in an interview.
“When you have doubts about whether you and your patient are on the same page, check in with the patient,” Dr. Nieman said. “When appropriate, having a loved one or a care partner join an encounter, or at least a portion of the encounter, can be helpful to both the patient and the provider.”
Many older patients unprepared
Millions of older patients may not have been ready for the rapid shift to telemedicine brought on by COVID-19, a recent study in JAMA Internal Medicine suggests. Between 32% and 38% of older adults in the United States may not have been ready for video visits, largely because of inexperience with technology. Approximately 20% could have difficulty with telephone visits because of problems hearing or communicating or because of dementia.
Kenneth Lam, MD, of the division of geriatrics at the University of California, San Francisco (UCSF), and colleagues arrived at these estimates after analyzing data from more than 4,500 participants in the National Health and Aging Trends Study that was conducted in 2018. The study is nationally representative of Medicare beneficiaries 65 years or older.
The aim of the study “was to call attention to what clinicians were already experiencing on the front lines,” Dr. Lam said. In an interview, he imagined two scenarios based on his colleagues’ accounts of telemedicine visits.
In one case, a 72-year-old woman logs into Zoom Health on her iPad without any trouble. “She explains she just pushed on the URL and everything loaded up and you have a great visit,” Dr. Lam said. “This is likely to be the case for over 50% of the older people you see; I share this picture to combat ageism, which is, truthfully, just inaccurate stereotyping of older people and gets in the way of actionable, data-driven policies.
“However, for around one in three older adults (and closer to three out of every four of those over the age of 85), you will book an appointment and they will say they don’t have an email address or a computer or know how to go online,” Dr. Lam said. “Or suppose they decide to try it out. ... Come appointment time, you log on and they pick up, but now their sound doesn’t work. They keep saying they can see you but they can’t hear you. ... They accidentally hang up. You place another call, and they ask if you can switch to a phone conversation instead.”
By phone, the physician can address concerns about the patient’s blood pressure, which the patient has been measuring daily. “But when it comes to looking at the swelling in their legs, you’re out of luck, and you’ve been on this call for 45 minutes,” Dr. Lam said.
Have a backup plan
Making sure patients are prepared and having a backup plan can help, said Kaitlin Willham, MD, of UCSF and the San Francisco VA Medical Center.
She says older patients fall into a wide range of categories in terms of skills and access to equipment. Knowing which category a patient falls into and having relevant support available to troubleshoot are important.
During the pandemic, Dr. Willham has conducted many more telemedicine visits with patients who are at their place of residence, whether a private home or a residential care facility. “Even outside of the current crisis, there are benefits to home video visits,” Dr. Willham said. “A home video visit can provide a more holistic view of the patient than an office visit, allowing the clinician to see how the person lives, what they might be challenged by. It allows the clinician to identify areas of intervention and, if there is a care partner, involving that person in the plan. If the visit starts without major technical or communication barriers, they are generally very well received.”
For patients with problems hearing for whom headphones or amplification devices are not available, “using a landline for the audio portion of the visit can help, as can having someone with the patient reiterate what was said,” Dr. Willham suggested. “Many video platforms also enable the clinician to type messages or share a screen with a live document. These options can work well when there is very severe or complete lack of hearing.”
Sometimes an in-person visit is the right way to go, even when technical hurdles can be overcome.
“Although many older adults are willing and able to learn to use telemedicine, an equitable health system should recognize that for some, such as those with dementia and social isolation, in-person visits are already difficult and telemedicine may be impossible,” Dr. Lam and coauthors wrote. “For these patients, clinics and geriatric models of care such as home visits are essential.”
Dr. Nieman, Dr. Oh, and one of Dr. Lam’s coauthors have received funding from the National Institutes of Health. Dr. Oh also has received funding from the Roberts Family Fund. Dr. Nieman serves as a board member of the nonprofit organization Access HEARS and is on the board of trustees of the Hearing Loss Association of America.
A version of this article originally appeared on Medscape.com.
During the pandemic, physicians have raced to set up or expand telemedicine, uncovering both advantages and shortcomings.
Although many of the suggestions, published online in Annals of Internal Medicine, are useful for all patients, Carrie Nieman, MD, MPH, and Esther S. Oh, MD, PhD, developed the list with older patients in mind.
“I have a number of patients into their 90s and with hearing loss, and we have had very successful video-based telemedicine visits,” Dr. Nieman, with the Cochlear Center for Hearing and Public Health at Johns Hopkins Bloomberg School of Public Health in Baltimore said in an interview. “Age should not be considered synonymous with inability or unwillingness to use technology.”
Their recommendations included the following:
- Assume some degree of hearing loss, which affects about two-thirds of adults aged 70 years and older.
- Ask patients to wear headphones or a headset or confirm that they are wearing their hearing aids and are in a quiet location.
- Use a headset.
- When possible, use video and have the camera focused on your face.
- Use captioning when available and provide a written summary of key points and instructions.
- Pay attention to cues, such as nodding along or looking to a loved one, that suggest a patient may not be following the conversation.
“If cognitive impairment is suspected, several screening tools can be used over the telephone to identify individuals who may need more comprehensive, in-person assessment,” wrote Dr. Nieman and Dr. Oh, who is with the division of geriatric medicine and gerontology at Johns Hopkins University School of Medicine. For example, data suggest that a modified version of the Mini–Mental State Examination and the Delirium Symptom Interview could be useful tools. “A formal diagnosis of dementia is not recommended solely based on a telephone-based cognitive screening,” however, Dr. Nieman and Dr. Oh said.
For patients with hearing loss, video visits avoid a current limitation of in-person visits: face masks that hinder patients’ ability to read lips and other visual cues. “For many of us, we rely on these types of cues more than we think,” Dr. Nieman said in an interview.
“When you have doubts about whether you and your patient are on the same page, check in with the patient,” Dr. Nieman said. “When appropriate, having a loved one or a care partner join an encounter, or at least a portion of the encounter, can be helpful to both the patient and the provider.”
Many older patients unprepared
Millions of older patients may not have been ready for the rapid shift to telemedicine brought on by COVID-19, a recent study in JAMA Internal Medicine suggests. Between 32% and 38% of older adults in the United States may not have been ready for video visits, largely because of inexperience with technology. Approximately 20% could have difficulty with telephone visits because of problems hearing or communicating or because of dementia.
Kenneth Lam, MD, of the division of geriatrics at the University of California, San Francisco (UCSF), and colleagues arrived at these estimates after analyzing data from more than 4,500 participants in the National Health and Aging Trends Study that was conducted in 2018. The study is nationally representative of Medicare beneficiaries 65 years or older.
The aim of the study “was to call attention to what clinicians were already experiencing on the front lines,” Dr. Lam said. In an interview, he imagined two scenarios based on his colleagues’ accounts of telemedicine visits.
In one case, a 72-year-old woman logs into Zoom Health on her iPad without any trouble. “She explains she just pushed on the URL and everything loaded up and you have a great visit,” Dr. Lam said. “This is likely to be the case for over 50% of the older people you see; I share this picture to combat ageism, which is, truthfully, just inaccurate stereotyping of older people and gets in the way of actionable, data-driven policies.
“However, for around one in three older adults (and closer to three out of every four of those over the age of 85), you will book an appointment and they will say they don’t have an email address or a computer or know how to go online,” Dr. Lam said. “Or suppose they decide to try it out. ... Come appointment time, you log on and they pick up, but now their sound doesn’t work. They keep saying they can see you but they can’t hear you. ... They accidentally hang up. You place another call, and they ask if you can switch to a phone conversation instead.”
By phone, the physician can address concerns about the patient’s blood pressure, which the patient has been measuring daily. “But when it comes to looking at the swelling in their legs, you’re out of luck, and you’ve been on this call for 45 minutes,” Dr. Lam said.
Have a backup plan
Making sure patients are prepared and having a backup plan can help, said Kaitlin Willham, MD, of UCSF and the San Francisco VA Medical Center.
She says older patients fall into a wide range of categories in terms of skills and access to equipment. Knowing which category a patient falls into and having relevant support available to troubleshoot are important.
During the pandemic, Dr. Willham has conducted many more telemedicine visits with patients who are at their place of residence, whether a private home or a residential care facility. “Even outside of the current crisis, there are benefits to home video visits,” Dr. Willham said. “A home video visit can provide a more holistic view of the patient than an office visit, allowing the clinician to see how the person lives, what they might be challenged by. It allows the clinician to identify areas of intervention and, if there is a care partner, involving that person in the plan. If the visit starts without major technical or communication barriers, they are generally very well received.”
For patients with problems hearing for whom headphones or amplification devices are not available, “using a landline for the audio portion of the visit can help, as can having someone with the patient reiterate what was said,” Dr. Willham suggested. “Many video platforms also enable the clinician to type messages or share a screen with a live document. These options can work well when there is very severe or complete lack of hearing.”
Sometimes an in-person visit is the right way to go, even when technical hurdles can be overcome.
“Although many older adults are willing and able to learn to use telemedicine, an equitable health system should recognize that for some, such as those with dementia and social isolation, in-person visits are already difficult and telemedicine may be impossible,” Dr. Lam and coauthors wrote. “For these patients, clinics and geriatric models of care such as home visits are essential.”
Dr. Nieman, Dr. Oh, and one of Dr. Lam’s coauthors have received funding from the National Institutes of Health. Dr. Oh also has received funding from the Roberts Family Fund. Dr. Nieman serves as a board member of the nonprofit organization Access HEARS and is on the board of trustees of the Hearing Loss Association of America.
A version of this article originally appeared on Medscape.com.
PPE shortage could last years without strategic plan, experts warn

Officials said logistical challenges continue 7 months after the coronavirus reached the United States, as the flu season approaches and as some state emergency management agencies prepare for a fall surge in COVID-19 cases.
Although the disarray is not as widespread as it was this spring, hospitals said rolling shortages of supplies range from specialized beds to disposable isolation gowns to thermometers.
“A few weeks ago, we were having a very difficult time getting the sanitary wipes. You just couldn’t get them,” said Bernard Klein, MD, chief executive of Providence Holy Cross Medical Center in Mission Hills, Calif., near Los Angeles. “We actually had to manufacture our own.”
This same dynamic has played out across a number of critical supplies in his hospital. First masks, then isolation gowns and now a specialized bed that allows nurses to turn COVID-19 patients onto their bellies – equipment that helps workers with what can otherwise be a six-person job.
“We’ve seen whole families come to our hospital with COVID, and several members hospitalized at the same time,” said Dr. Klein. “It’s very, very sad.”
Testing supplies ran short as the predominantly Latino community served by Providence Holy Cross was hit hard by COVID, and even as nearby hospitals could process 15-minute tests.
“If we had a more coordinated response with a partnership between the medical field, the government and the private industry, it would help improve the supply chain to the areas that need it most,” Dr. Klein said.
Dr. Klein said he expected to deal with equipment and supply shortages throughout 2021, especially as flu season approaches.
“Most people focus on those N95 respirators,” said Carmela Coyle, CEO of the California Hospital Association, an industry group that represents more than 400 hospitals across one of America’s hardest-hit states.
She said she believed COVID-19-related supply challenges will persist through 2022.
“We have been challenged with shortages of isolation gowns, face shields, which you’re now starting to see in public places. Any one piece that’s in shortage or not available creates risk for patients and for health care workers,” said Ms. Coyle.
At the same time, trade associations representing manufacturers said persuading customers to shift to American suppliers had been difficult.
“I also have industry that’s working only at 10-20% capacity, who can make PPE in our own backyard, but have no orders,” said Kim Glas, CEO of the National Council of Textile Organizations, whose members make reusable cloth gowns.
Manufacturers in her organization have made “hundreds of millions of products,” but, without long-term government contracts, many are apprehensive to invest in the equipment needed to scale up the business and eventually lower prices.
“If there continues to be an upward trajectory of COVID-19 cases, not just in the U.S. but globally, you can see those supply chains breaking down again,” Ms. Glas said. “It is a health care security issue.”
For the past 2 decades, personal protective equipment was supplied to health care institutions in lean supply chains in the same way toilet paper was to grocery stores. Chains between major manufacturers and end users were so efficient, there was no need to stockpile goods.
But in March, the supply chain broke when major Asian PPE exporters embargoed materials or shut down just as demand increased exponentially. Thus, health care institutions were in much the same position as regular grocery shoppers, who were trying to buy great quantities of a product they never needed to stockpile before.
“I am very concerned about long-term PPE shortages for the foreseeable future,” said Susan Bailey, MD, president of the American Medical Association.
“There’s no question the situation is better than it was a couple of months ago,” said Bailey. However, many health care organizations, including her own, have struggled to obtain PPE. Bailey practices at a 10-doctor allergy clinic and was met with a 10,000-mask minimum when they tried to order N95 respirators.
“We have not seen evidence of a long-term strategic plan for the manufacture, acquisition and distribution of PPE” from the government, said Dr. Bailey. “The supply chain needs to be strengthened dramatically, and we need less dependence on foreign goods to manufacture our own PPE in the U.S.”
Some products have now come back to be made in the United States – although factories are not expected to be able to reach demand until mid-2021.
“A lot has been done in the last 6 months. We are largely out of the hole, and we have planted the seeds to render the United States self-sufficient,” said Dave Rousse, president of the Association of the Nonwoven Fabrics Industry.
In 2019, 850 tons of the material used in disposable masks was made in the United States. Around 10,000 tons is expected to be made in 2021, satisfying perhaps 80% of demand. But PPE is a suite of items – including gloves, gowns and face shields – not all of which have seen the same success.
“Thermometers are becoming a real issue,” said Cindy Juhas, chief strategy officer of CME, an American health care product distributor. “They’re expecting even a problem with needles and syringes for the amount of vaccines they have to make.”
Federal government efforts to address the supply chain have foundered. The Federal Emergency Management Agency, in charge of the COVID-19 response, told congressional interviewers in June it had “no involvement” in distributing PPE to hot spots.
Project Airbridge, an initiative headed by Jared Kushner, President Donald Trump’s son-in-law, flew PPE from international suppliers to the U.S. at taxpayer expense but was phased out. And the government has not responded to the AMA’s calls for more distribution data.
Arguably, Dr. Klein is among the best placed to weather such disruptions. He is part of a 51-hospital chain with purchasing power, and among the institutions that distributors prioritize when selling supplies. But tribulations continue even in hospitals, as shortages have pushed buyers to look directly for manufacturers, often through a swamp of companies that have sprung up overnight.
Now distributors are being called upon not just by their traditional customers – hospitals and long-term care homes – but by nearly every segment of society. First responders, schools, clinics and even food businesses are all buying medical equipment now.
“There’s going to be lots of other shortages we haven’t even thought about,” said Ms. Juhas.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Officials said logistical challenges continue 7 months after the coronavirus reached the United States, as the flu season approaches and as some state emergency management agencies prepare for a fall surge in COVID-19 cases.
Although the disarray is not as widespread as it was this spring, hospitals said rolling shortages of supplies range from specialized beds to disposable isolation gowns to thermometers.
“A few weeks ago, we were having a very difficult time getting the sanitary wipes. You just couldn’t get them,” said Bernard Klein, MD, chief executive of Providence Holy Cross Medical Center in Mission Hills, Calif., near Los Angeles. “We actually had to manufacture our own.”
This same dynamic has played out across a number of critical supplies in his hospital. First masks, then isolation gowns and now a specialized bed that allows nurses to turn COVID-19 patients onto their bellies – equipment that helps workers with what can otherwise be a six-person job.
“We’ve seen whole families come to our hospital with COVID, and several members hospitalized at the same time,” said Dr. Klein. “It’s very, very sad.”
Testing supplies ran short as the predominantly Latino community served by Providence Holy Cross was hit hard by COVID, and even as nearby hospitals could process 15-minute tests.
“If we had a more coordinated response with a partnership between the medical field, the government and the private industry, it would help improve the supply chain to the areas that need it most,” Dr. Klein said.
Dr. Klein said he expected to deal with equipment and supply shortages throughout 2021, especially as flu season approaches.
“Most people focus on those N95 respirators,” said Carmela Coyle, CEO of the California Hospital Association, an industry group that represents more than 400 hospitals across one of America’s hardest-hit states.
She said she believed COVID-19-related supply challenges will persist through 2022.
“We have been challenged with shortages of isolation gowns, face shields, which you’re now starting to see in public places. Any one piece that’s in shortage or not available creates risk for patients and for health care workers,” said Ms. Coyle.
At the same time, trade associations representing manufacturers said persuading customers to shift to American suppliers had been difficult.
“I also have industry that’s working only at 10-20% capacity, who can make PPE in our own backyard, but have no orders,” said Kim Glas, CEO of the National Council of Textile Organizations, whose members make reusable cloth gowns.
Manufacturers in her organization have made “hundreds of millions of products,” but, without long-term government contracts, many are apprehensive to invest in the equipment needed to scale up the business and eventually lower prices.
“If there continues to be an upward trajectory of COVID-19 cases, not just in the U.S. but globally, you can see those supply chains breaking down again,” Ms. Glas said. “It is a health care security issue.”
For the past 2 decades, personal protective equipment was supplied to health care institutions in lean supply chains in the same way toilet paper was to grocery stores. Chains between major manufacturers and end users were so efficient, there was no need to stockpile goods.
But in March, the supply chain broke when major Asian PPE exporters embargoed materials or shut down just as demand increased exponentially. Thus, health care institutions were in much the same position as regular grocery shoppers, who were trying to buy great quantities of a product they never needed to stockpile before.
“I am very concerned about long-term PPE shortages for the foreseeable future,” said Susan Bailey, MD, president of the American Medical Association.
“There’s no question the situation is better than it was a couple of months ago,” said Bailey. However, many health care organizations, including her own, have struggled to obtain PPE. Bailey practices at a 10-doctor allergy clinic and was met with a 10,000-mask minimum when they tried to order N95 respirators.
“We have not seen evidence of a long-term strategic plan for the manufacture, acquisition and distribution of PPE” from the government, said Dr. Bailey. “The supply chain needs to be strengthened dramatically, and we need less dependence on foreign goods to manufacture our own PPE in the U.S.”
Some products have now come back to be made in the United States – although factories are not expected to be able to reach demand until mid-2021.
“A lot has been done in the last 6 months. We are largely out of the hole, and we have planted the seeds to render the United States self-sufficient,” said Dave Rousse, president of the Association of the Nonwoven Fabrics Industry.
In 2019, 850 tons of the material used in disposable masks was made in the United States. Around 10,000 tons is expected to be made in 2021, satisfying perhaps 80% of demand. But PPE is a suite of items – including gloves, gowns and face shields – not all of which have seen the same success.
“Thermometers are becoming a real issue,” said Cindy Juhas, chief strategy officer of CME, an American health care product distributor. “They’re expecting even a problem with needles and syringes for the amount of vaccines they have to make.”
Federal government efforts to address the supply chain have foundered. The Federal Emergency Management Agency, in charge of the COVID-19 response, told congressional interviewers in June it had “no involvement” in distributing PPE to hot spots.
Project Airbridge, an initiative headed by Jared Kushner, President Donald Trump’s son-in-law, flew PPE from international suppliers to the U.S. at taxpayer expense but was phased out. And the government has not responded to the AMA’s calls for more distribution data.
Arguably, Dr. Klein is among the best placed to weather such disruptions. He is part of a 51-hospital chain with purchasing power, and among the institutions that distributors prioritize when selling supplies. But tribulations continue even in hospitals, as shortages have pushed buyers to look directly for manufacturers, often through a swamp of companies that have sprung up overnight.
Now distributors are being called upon not just by their traditional customers – hospitals and long-term care homes – but by nearly every segment of society. First responders, schools, clinics and even food businesses are all buying medical equipment now.
“There’s going to be lots of other shortages we haven’t even thought about,” said Ms. Juhas.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Officials said logistical challenges continue 7 months after the coronavirus reached the United States, as the flu season approaches and as some state emergency management agencies prepare for a fall surge in COVID-19 cases.
Although the disarray is not as widespread as it was this spring, hospitals said rolling shortages of supplies range from specialized beds to disposable isolation gowns to thermometers.
“A few weeks ago, we were having a very difficult time getting the sanitary wipes. You just couldn’t get them,” said Bernard Klein, MD, chief executive of Providence Holy Cross Medical Center in Mission Hills, Calif., near Los Angeles. “We actually had to manufacture our own.”
This same dynamic has played out across a number of critical supplies in his hospital. First masks, then isolation gowns and now a specialized bed that allows nurses to turn COVID-19 patients onto their bellies – equipment that helps workers with what can otherwise be a six-person job.
“We’ve seen whole families come to our hospital with COVID, and several members hospitalized at the same time,” said Dr. Klein. “It’s very, very sad.”
Testing supplies ran short as the predominantly Latino community served by Providence Holy Cross was hit hard by COVID, and even as nearby hospitals could process 15-minute tests.
“If we had a more coordinated response with a partnership between the medical field, the government and the private industry, it would help improve the supply chain to the areas that need it most,” Dr. Klein said.
Dr. Klein said he expected to deal with equipment and supply shortages throughout 2021, especially as flu season approaches.
“Most people focus on those N95 respirators,” said Carmela Coyle, CEO of the California Hospital Association, an industry group that represents more than 400 hospitals across one of America’s hardest-hit states.
She said she believed COVID-19-related supply challenges will persist through 2022.
“We have been challenged with shortages of isolation gowns, face shields, which you’re now starting to see in public places. Any one piece that’s in shortage or not available creates risk for patients and for health care workers,” said Ms. Coyle.
At the same time, trade associations representing manufacturers said persuading customers to shift to American suppliers had been difficult.
“I also have industry that’s working only at 10-20% capacity, who can make PPE in our own backyard, but have no orders,” said Kim Glas, CEO of the National Council of Textile Organizations, whose members make reusable cloth gowns.
Manufacturers in her organization have made “hundreds of millions of products,” but, without long-term government contracts, many are apprehensive to invest in the equipment needed to scale up the business and eventually lower prices.
“If there continues to be an upward trajectory of COVID-19 cases, not just in the U.S. but globally, you can see those supply chains breaking down again,” Ms. Glas said. “It is a health care security issue.”
For the past 2 decades, personal protective equipment was supplied to health care institutions in lean supply chains in the same way toilet paper was to grocery stores. Chains between major manufacturers and end users were so efficient, there was no need to stockpile goods.
But in March, the supply chain broke when major Asian PPE exporters embargoed materials or shut down just as demand increased exponentially. Thus, health care institutions were in much the same position as regular grocery shoppers, who were trying to buy great quantities of a product they never needed to stockpile before.
“I am very concerned about long-term PPE shortages for the foreseeable future,” said Susan Bailey, MD, president of the American Medical Association.
“There’s no question the situation is better than it was a couple of months ago,” said Bailey. However, many health care organizations, including her own, have struggled to obtain PPE. Bailey practices at a 10-doctor allergy clinic and was met with a 10,000-mask minimum when they tried to order N95 respirators.
“We have not seen evidence of a long-term strategic plan for the manufacture, acquisition and distribution of PPE” from the government, said Dr. Bailey. “The supply chain needs to be strengthened dramatically, and we need less dependence on foreign goods to manufacture our own PPE in the U.S.”
Some products have now come back to be made in the United States – although factories are not expected to be able to reach demand until mid-2021.
“A lot has been done in the last 6 months. We are largely out of the hole, and we have planted the seeds to render the United States self-sufficient,” said Dave Rousse, president of the Association of the Nonwoven Fabrics Industry.
In 2019, 850 tons of the material used in disposable masks was made in the United States. Around 10,000 tons is expected to be made in 2021, satisfying perhaps 80% of demand. But PPE is a suite of items – including gloves, gowns and face shields – not all of which have seen the same success.
“Thermometers are becoming a real issue,” said Cindy Juhas, chief strategy officer of CME, an American health care product distributor. “They’re expecting even a problem with needles and syringes for the amount of vaccines they have to make.”
Federal government efforts to address the supply chain have foundered. The Federal Emergency Management Agency, in charge of the COVID-19 response, told congressional interviewers in June it had “no involvement” in distributing PPE to hot spots.
Project Airbridge, an initiative headed by Jared Kushner, President Donald Trump’s son-in-law, flew PPE from international suppliers to the U.S. at taxpayer expense but was phased out. And the government has not responded to the AMA’s calls for more distribution data.
Arguably, Dr. Klein is among the best placed to weather such disruptions. He is part of a 51-hospital chain with purchasing power, and among the institutions that distributors prioritize when selling supplies. But tribulations continue even in hospitals, as shortages have pushed buyers to look directly for manufacturers, often through a swamp of companies that have sprung up overnight.
Now distributors are being called upon not just by their traditional customers – hospitals and long-term care homes – but by nearly every segment of society. First responders, schools, clinics and even food businesses are all buying medical equipment now.
“There’s going to be lots of other shortages we haven’t even thought about,” said Ms. Juhas.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
COVID-19 and masks: Doctor, may I be excused?

In the last 2 months, at least 10 patients have asked Constantine George, MD, for a written medical exemption so they won’t have to wear a mask in public. Dr. George, the chief medical officer of Vedius, an app for a travelers’ concierge medical service in Las Vegas, turned them all down.
Elena Christofides, MD, an endocrinologist in Columbus, Ohio, has also refused patients’ requests for exemptions.
“It’s very rare for someone to need an exemption,” says Albert Rizzo, MD, chief medical officer for the American Lung Association and a lung specialist at ChristianaCare Health System in Newark, Del.
The opposition is sometimes strong. Recently, a video of Lenka Koloma of Laguna Niguel, Calif., who founded the antimask Freedom to Breathe Agency, went viral. She was in a California supermarket, maskless, telling an employee she was breaking the law by requiring patrons to wear masks.
“People need oxygen,” she said. “That alone is a medical condition.” Her webpage has a “Face Mask Exempt Card” that cites the Americans with Disabilities Act and posts a Department of Justice ADA violation reporting number. The DOJ issued a statement calling the cards fraudulent.
Figuring out if a patient’s request to opt out of wearing a mask is legitimate is a ‘’new frontier” for doctors, says Mical Raz, MD, a professor in public policy and health at the University of Rochester (N.Y.), and a hospitalist at the university medical center.
Should some people skip masks?
Experts say there are very few medical reasons for people to skip masks. “If you look at the research, patients with COPD [chronic obstructive pulmonary disorder], those with reactive airway, even those can breathe through a mask,” Dr. George said. Requests for exemptions due to medical reasons are usually without basis. “Obviously, if someone is incapacitated, for example, with mental health issues, that’s case by case.”
Dr. Christofides said one of her patients cited anxiety and the other cited headaches as reasons not to wear a mask. “I told the one who asked for anxiety [reasons] that she could wear ones that were less tight.” The patient with headaches told Dr. Christofides that she had a buildup of carbon dioxide in the mask because of industrial exposure. Baloney, Dr. Christofides told her.
Dr. Rizzo says one rare example of someone who can’t wear a mask might be a patient with an advanced lung condition so severe, they need extra oxygen. “These are the extreme patients where any change in oxygen and carbon dioxide could make a difference,” he said. But “that’s also the population that shouldn’t be going out in the first place.”
Dr. Raz cowrote a commentary about mask exemptions, saying doctors are faced with difficult decisions and must keep a delicate balance between public health and individual disability needs. “Inappropriate medical exemptions may inadvertently hasten viral spread and threaten public health,” she wrote.
In an interview, she says that some people do have a hard time tolerating a mask. “Probably the most common reasons are mental health issues, such as anxiety, panic and PTSD, and children with sensory processing disorders (making them oversensitive to their environment). I think there are very few pulmonary reasons.”
CDC, professional organization guidelines
The CDC says people should wear masks in public and when around people who don’t live in the same household. Beyond that, it simply says masks should not be worn by children under age 2, “or anyone who has trouble breathing, is unconscious, incapacitated, or otherwise unable to remove the mask without assistance.”
In mid-July, four professional organizations released a statement in response to the CDC recommendation for facial coverings. Jointly issued by the American College of Chest Physicians, the American Lung Association, the American Thoracic Society and the COPD Foundation, it states in part that people with normal lungs and “even many individuals with underlying chronic lung disease should be able to wear a non-N95 facial covering without affecting their oxygen or carbon dioxide levels.”
It acknowledges that some people will seek an exemption and doctors must weigh the patient’s concerns against the need to stop the spread of the virus. “In some instances, physician reassurance regarding the safety of the facial coverings may be all that is needed,” it states.
Addressing the excuses
Here are some of the common medical reasons people give for not being able to tolerate a mask:
Claustrophobia or anxiety. Dr. Raz and others suggests a “desensitizing” period, wearing the mask for longer and longer periods of time to get used to it. Parents could suggest kids wear a mask when doing something they like, such as watching television, so they equate it with something pleasant. Switching to a different kind of mask or one that fits better could also help.
Masks cause Legionnaires’ disease. Not true, experts say. Legionnaires’ is a severe form of pneumonia, the result of inhaling tiny water droplets with legionella bacteria.
It’s difficult to read lips. People can buy masks with a clear window that makes their mouth and lips visible.
Trouble breathing. Brief periods of mask use won’t have a bad effect on oxygen levels for most people.
“There is not an inherent right to be out in a pandemic with an unmasked face,” Dr. Raz says. But “you are entitled to an accommodation.” That might be using curbside pickup for food and medication. That requires much less time wearing a mask than entering a store would.
There are no “boilerplate” cards or letters to excuse people provided by the four organizations that addressed the issue, Dr. Rizzo said. If he were to write a letter asking for an exemption, he would personalize it for an individual patient’s medical condition. As to whether a state would honor it, he cannot say. The states have a patchwork of recommendations, making it difficult to say.
Dr. Rizzo tells lung disease patients who are able to go out that wearing a mask for 15-20 minutes to do an errand won’t harm their oxygen levels. And he reminds them that having an exemption, in the form of a doctor’s letter, may bring more problems. “Even with an exemption, someone may confront them” for their lack of a face covering. People with COPD have a higher risk of getting a severe illness from COVID-19, according to the CDC.
This article first appeared on WebMD.com.
In the last 2 months, at least 10 patients have asked Constantine George, MD, for a written medical exemption so they won’t have to wear a mask in public. Dr. George, the chief medical officer of Vedius, an app for a travelers’ concierge medical service in Las Vegas, turned them all down.
Elena Christofides, MD, an endocrinologist in Columbus, Ohio, has also refused patients’ requests for exemptions.
“It’s very rare for someone to need an exemption,” says Albert Rizzo, MD, chief medical officer for the American Lung Association and a lung specialist at ChristianaCare Health System in Newark, Del.
The opposition is sometimes strong. Recently, a video of Lenka Koloma of Laguna Niguel, Calif., who founded the antimask Freedom to Breathe Agency, went viral. She was in a California supermarket, maskless, telling an employee she was breaking the law by requiring patrons to wear masks.
“People need oxygen,” she said. “That alone is a medical condition.” Her webpage has a “Face Mask Exempt Card” that cites the Americans with Disabilities Act and posts a Department of Justice ADA violation reporting number. The DOJ issued a statement calling the cards fraudulent.
Figuring out if a patient’s request to opt out of wearing a mask is legitimate is a ‘’new frontier” for doctors, says Mical Raz, MD, a professor in public policy and health at the University of Rochester (N.Y.), and a hospitalist at the university medical center.
Should some people skip masks?
Experts say there are very few medical reasons for people to skip masks. “If you look at the research, patients with COPD [chronic obstructive pulmonary disorder], those with reactive airway, even those can breathe through a mask,” Dr. George said. Requests for exemptions due to medical reasons are usually without basis. “Obviously, if someone is incapacitated, for example, with mental health issues, that’s case by case.”
Dr. Christofides said one of her patients cited anxiety and the other cited headaches as reasons not to wear a mask. “I told the one who asked for anxiety [reasons] that she could wear ones that were less tight.” The patient with headaches told Dr. Christofides that she had a buildup of carbon dioxide in the mask because of industrial exposure. Baloney, Dr. Christofides told her.
Dr. Rizzo says one rare example of someone who can’t wear a mask might be a patient with an advanced lung condition so severe, they need extra oxygen. “These are the extreme patients where any change in oxygen and carbon dioxide could make a difference,” he said. But “that’s also the population that shouldn’t be going out in the first place.”
Dr. Raz cowrote a commentary about mask exemptions, saying doctors are faced with difficult decisions and must keep a delicate balance between public health and individual disability needs. “Inappropriate medical exemptions may inadvertently hasten viral spread and threaten public health,” she wrote.
In an interview, she says that some people do have a hard time tolerating a mask. “Probably the most common reasons are mental health issues, such as anxiety, panic and PTSD, and children with sensory processing disorders (making them oversensitive to their environment). I think there are very few pulmonary reasons.”
CDC, professional organization guidelines
The CDC says people should wear masks in public and when around people who don’t live in the same household. Beyond that, it simply says masks should not be worn by children under age 2, “or anyone who has trouble breathing, is unconscious, incapacitated, or otherwise unable to remove the mask without assistance.”
In mid-July, four professional organizations released a statement in response to the CDC recommendation for facial coverings. Jointly issued by the American College of Chest Physicians, the American Lung Association, the American Thoracic Society and the COPD Foundation, it states in part that people with normal lungs and “even many individuals with underlying chronic lung disease should be able to wear a non-N95 facial covering without affecting their oxygen or carbon dioxide levels.”
It acknowledges that some people will seek an exemption and doctors must weigh the patient’s concerns against the need to stop the spread of the virus. “In some instances, physician reassurance regarding the safety of the facial coverings may be all that is needed,” it states.
Addressing the excuses
Here are some of the common medical reasons people give for not being able to tolerate a mask:
Claustrophobia or anxiety. Dr. Raz and others suggests a “desensitizing” period, wearing the mask for longer and longer periods of time to get used to it. Parents could suggest kids wear a mask when doing something they like, such as watching television, so they equate it with something pleasant. Switching to a different kind of mask or one that fits better could also help.
Masks cause Legionnaires’ disease. Not true, experts say. Legionnaires’ is a severe form of pneumonia, the result of inhaling tiny water droplets with legionella bacteria.
It’s difficult to read lips. People can buy masks with a clear window that makes their mouth and lips visible.
Trouble breathing. Brief periods of mask use won’t have a bad effect on oxygen levels for most people.
“There is not an inherent right to be out in a pandemic with an unmasked face,” Dr. Raz says. But “you are entitled to an accommodation.” That might be using curbside pickup for food and medication. That requires much less time wearing a mask than entering a store would.
There are no “boilerplate” cards or letters to excuse people provided by the four organizations that addressed the issue, Dr. Rizzo said. If he were to write a letter asking for an exemption, he would personalize it for an individual patient’s medical condition. As to whether a state would honor it, he cannot say. The states have a patchwork of recommendations, making it difficult to say.
Dr. Rizzo tells lung disease patients who are able to go out that wearing a mask for 15-20 minutes to do an errand won’t harm their oxygen levels. And he reminds them that having an exemption, in the form of a doctor’s letter, may bring more problems. “Even with an exemption, someone may confront them” for their lack of a face covering. People with COPD have a higher risk of getting a severe illness from COVID-19, according to the CDC.
This article first appeared on WebMD.com.
In the last 2 months, at least 10 patients have asked Constantine George, MD, for a written medical exemption so they won’t have to wear a mask in public. Dr. George, the chief medical officer of Vedius, an app for a travelers’ concierge medical service in Las Vegas, turned them all down.
Elena Christofides, MD, an endocrinologist in Columbus, Ohio, has also refused patients’ requests for exemptions.
“It’s very rare for someone to need an exemption,” says Albert Rizzo, MD, chief medical officer for the American Lung Association and a lung specialist at ChristianaCare Health System in Newark, Del.
The opposition is sometimes strong. Recently, a video of Lenka Koloma of Laguna Niguel, Calif., who founded the antimask Freedom to Breathe Agency, went viral. She was in a California supermarket, maskless, telling an employee she was breaking the law by requiring patrons to wear masks.
“People need oxygen,” she said. “That alone is a medical condition.” Her webpage has a “Face Mask Exempt Card” that cites the Americans with Disabilities Act and posts a Department of Justice ADA violation reporting number. The DOJ issued a statement calling the cards fraudulent.
Figuring out if a patient’s request to opt out of wearing a mask is legitimate is a ‘’new frontier” for doctors, says Mical Raz, MD, a professor in public policy and health at the University of Rochester (N.Y.), and a hospitalist at the university medical center.
Should some people skip masks?
Experts say there are very few medical reasons for people to skip masks. “If you look at the research, patients with COPD [chronic obstructive pulmonary disorder], those with reactive airway, even those can breathe through a mask,” Dr. George said. Requests for exemptions due to medical reasons are usually without basis. “Obviously, if someone is incapacitated, for example, with mental health issues, that’s case by case.”
Dr. Christofides said one of her patients cited anxiety and the other cited headaches as reasons not to wear a mask. “I told the one who asked for anxiety [reasons] that she could wear ones that were less tight.” The patient with headaches told Dr. Christofides that she had a buildup of carbon dioxide in the mask because of industrial exposure. Baloney, Dr. Christofides told her.
Dr. Rizzo says one rare example of someone who can’t wear a mask might be a patient with an advanced lung condition so severe, they need extra oxygen. “These are the extreme patients where any change in oxygen and carbon dioxide could make a difference,” he said. But “that’s also the population that shouldn’t be going out in the first place.”
Dr. Raz cowrote a commentary about mask exemptions, saying doctors are faced with difficult decisions and must keep a delicate balance between public health and individual disability needs. “Inappropriate medical exemptions may inadvertently hasten viral spread and threaten public health,” she wrote.
In an interview, she says that some people do have a hard time tolerating a mask. “Probably the most common reasons are mental health issues, such as anxiety, panic and PTSD, and children with sensory processing disorders (making them oversensitive to their environment). I think there are very few pulmonary reasons.”
CDC, professional organization guidelines
The CDC says people should wear masks in public and when around people who don’t live in the same household. Beyond that, it simply says masks should not be worn by children under age 2, “or anyone who has trouble breathing, is unconscious, incapacitated, or otherwise unable to remove the mask without assistance.”
In mid-July, four professional organizations released a statement in response to the CDC recommendation for facial coverings. Jointly issued by the American College of Chest Physicians, the American Lung Association, the American Thoracic Society and the COPD Foundation, it states in part that people with normal lungs and “even many individuals with underlying chronic lung disease should be able to wear a non-N95 facial covering without affecting their oxygen or carbon dioxide levels.”
It acknowledges that some people will seek an exemption and doctors must weigh the patient’s concerns against the need to stop the spread of the virus. “In some instances, physician reassurance regarding the safety of the facial coverings may be all that is needed,” it states.
Addressing the excuses
Here are some of the common medical reasons people give for not being able to tolerate a mask:
Claustrophobia or anxiety. Dr. Raz and others suggests a “desensitizing” period, wearing the mask for longer and longer periods of time to get used to it. Parents could suggest kids wear a mask when doing something they like, such as watching television, so they equate it with something pleasant. Switching to a different kind of mask or one that fits better could also help.
Masks cause Legionnaires’ disease. Not true, experts say. Legionnaires’ is a severe form of pneumonia, the result of inhaling tiny water droplets with legionella bacteria.
It’s difficult to read lips. People can buy masks with a clear window that makes their mouth and lips visible.
Trouble breathing. Brief periods of mask use won’t have a bad effect on oxygen levels for most people.
“There is not an inherent right to be out in a pandemic with an unmasked face,” Dr. Raz says. But “you are entitled to an accommodation.” That might be using curbside pickup for food and medication. That requires much less time wearing a mask than entering a store would.
There are no “boilerplate” cards or letters to excuse people provided by the four organizations that addressed the issue, Dr. Rizzo said. If he were to write a letter asking for an exemption, he would personalize it for an individual patient’s medical condition. As to whether a state would honor it, he cannot say. The states have a patchwork of recommendations, making it difficult to say.
Dr. Rizzo tells lung disease patients who are able to go out that wearing a mask for 15-20 minutes to do an errand won’t harm their oxygen levels. And he reminds them that having an exemption, in the form of a doctor’s letter, may bring more problems. “Even with an exemption, someone may confront them” for their lack of a face covering. People with COPD have a higher risk of getting a severe illness from COVID-19, according to the CDC.
This article first appeared on WebMD.com.
APA tackles structural racism in psychiatry, itself
Amanda Calhoun, MD, recalls noticing a distinct empathy gap while she trained at a youth psychiatric unit.

A White male patient hurled the N-word at a Black patient, and the majority White staff did nothing. “And then [they] told me the White patient was struggling and that’s why they allowed it, even though he was aggressive,” said Dr. Calhoun, psychiatry resident at Yale University in New Haven, Conn. But Dr. Calhoun noticed less restraint on the part of her colleagues while she was treating an angry female Black Latinx patient.
“I remember staff saying she was a nightmare; they called her the B-word; she was ‘a terror.’ How is that this patient isn’t viewed as struggling, where the other patient is? I don’t understand the difference here.”
And, Dr. Calhoun said, “when a patient can complain that they feel they were treated differently based on skin color, [the White majority staff] would just say they have borderline personality disorder or they’re depressed.
“When the staff is not diverse, I really see differential treatment in who gets the benefit of the doubt and their empathy.”
Psychiatrists such as Dr. Calhoun can list countless other examples of institutional racism, interpersonal racism, and prejudice in psychiatry. They see signs of institutional racism in clinical care, academia, and in research. Some are questioning the American Psychiatric Association decision to put on hiatus the Institute on Psychiatric Services, its fall annual meeting that has traditionally served as a vehicle for examining the treatment of underserved communities.
Against that backdrop – and after the killing of George Floyd and amid the disproportionate impact of COVID-19 on communities of color – the APA launched an effort the group says is aimed at reforming itself and psychiatry as a whole. In June, the APA announced the formation of the Presidential Task Force to Address Structural Racism Throughout Psychiatry, and the panel – focused on anti-Black racism – has begun its yearlong work.
A specialty with inherent contradictions
Jeffrey Geller, MD, MPH, the APA’s president, acknowledged in an interview that racism in psychiatry is older than the APA – which celebrated its 175th anniversary as an association last year.

As Dr. Geller pointed out recently, Benjamin Rush, MD, a founding father of the United States and the father of American psychiatry, was an abolitionist who owned one enslaved man – and thought the intelligence and morality of Black people were equal to that of their White counterparts.1 Dr. Rush also thought the skin color of Black people was a manifestation of a type of leprosy that he called “Negritude.”2 “Rush was a remarkable mix of contradictions,” Dr. Geller wrote.
Altha J. Stewart, MD, the first and only Black president of the APA, declined to be interviewed for this article.

But as Dr. Stewart was wrapping up her term as president, she reportedly3 said that a 1970 paper titled “Dimensions of Institutional Racism in Psychiatry” by the late Melvin Sabshin, MD, and associates was essentially a blueprint for moving the specialty forward.
That paper, published in the American Journal of Psychiatry, took psychiatry to task on many levels. One of the barriers that Black psychiatric patients must overcome, according to Dr. Sabshin and associates, is the “biases of the White therapist, who must overcome his cultural blind spots, reactive guilt, and unconscious prejudice.” They called community psychiatry paternalistic. Furthermore, Dr. Sabshin, who would later serve as medical director of the APA for almost 25 years, criticized White mental health professionals for viewing Black communities as “seething cauldrons of psychopathology”:
“They create stereotypes of absent fathers, primitive rage, psychopathy, self-depreciation, promiscuity, deficits in intellectual capacity, and lack of psychological sensitivity,” Dr. Sabshin and his associates wrote. “Gross pathological caricaturization ignores the enormous variation of behavior in black communities. ... The obsession with black psychopathology has been so great that it has retarded serious consideration of racism as it pertains to white psychopathology.”4
In other words, White American psychiatrists adopted the prevailing views of society at large toward Black people. More recently, “there was a period in this country where Black people were thought to be at higher risk of developing issues like schizophrenia5 instead of depression,” said Gregory Scott Brown, MD, of the Center for Green Psychiatry and the University of Texas in Austin.

“Pharmaceutical companies developed ads for antipsychotic medications that portrayed angry Black men or women. This got into the heads of who may have been conditioned without knowing it,” he said.
In addition, psychiatry has failed to diversify its ranks. To this day, Dr. Geller said, “Black psychiatrists are underrepresented in academic settings, leadership positions, hospitals, and clinics. Black patients are suffering because of inequities in access to care in treatment, and even those who receive treatment are often misdiagnosed since we don’t account for the extended community’s trauma.” About 2% of U.S. psychiatrists are Black, and Black people make up 13% of the U.S. population.6
The low percentage of Black psychiatrists hurts the field for many reasons, said task force member Steven Starks, MD, clinical assistant professor of psychiatry at the University of Houston, and not solely because the gap forces many Black patients to be treated by non-Black psychiatrists. “The association has a large, broad impact on our field and profession through the DSM, and work in areas like government relations and access to care and insurance,” Dr. Starks said.
Task force gets mixed reviews
After the announcement, Dr. Geller named the psychiatrists who will serve, and the task force, chaired by Cheryl D. Wills, MD, assistant professor of psychiatry at Case Western Reserve University in Cleveland, got to work quickly.
The task force has conducted an online town hall and will conduct another one on Aug. 24. It also released the results of a survey of nearly 500 members about the top three areas that the task force should address.
“Access to Healthcare/Mental Healthcare” received the most votes (97) as the recommended top priority, followed by “Socio-Economic Conditions and Factors” (49). These two areas also received the most first-, second- and third-priority votes overall (173 and 166, respectively).
The other areas with high numbers of first priority votes were “Lack of Minority Psychiatrists, Faculty and Leaders” and “Education for Psychiatrists,” both tied at 46. Those areas received 142 and 122 total votes supporting them as first, second, and third priorities.
Thirty-seven members said “Racism within the APA/APA Actions” should be the top priority. A small number of respondents appeared to doubt the need for such a task force: Nineteen thought the top priority should be “Questioning the Concept of Structural Racism/Task Force.”
Meanwhile, some psychiatrists are raising questions about the task force’s makeup.
Ruth S. Shim, MD, MPH, the Luke & Grace Kim Professor of Cultural Psychiatry at the University of California, Davis, said that she was disappointed by the task force’s membership. Specifically, Dr. Shim said, the task force does not include enough APA members she sees as qualified to address structural racism.
“While many of the Black psychiatrists who are members of the task force are experts in issues of diversity, inclusion, and equity, other members of the board of trustees who were appointed to this task force do not have any expertise in this area,” said Dr. Shim, who wrote a scathing commentary7 in July about the APA’s failures regarding structural racism. “I believe the selection of members could have been more thoughtful and more inclusive of diverse perspectives and voices.”
Dr. Geller countered that the task force includes a mix of APA board members and non–board members with various types of expertise. “Certain board members were chosen because their colleagues on the board “were already involved in task forces and other projects,” he said.
How the task force is envisioned
Dr. Geller’s goals for the task force, which will operate at least through his 1-year term as president, are ambitious.
“I hope the task force will identify structural racism wherever it’s taking place – where psychiatrists practice, within the APA itself,” Dr. Geller said. “It will be an educational process so we can inform members and ourselves about clear and subtle structural racism. Then we’re going to proffer solutions in several areas that can rectify some of what we’ve been doing and the negative outcomes that have resulted in areas of leadership such as access to care, treatment, hospital and clinic administration, health insurance, and academia. It’s clear that this is a massive undertaking.”
For her part, Dr. Shim thinks the task force might chip around the edges of the structural problems in the specialty – rather than focusing on the roots. “The task force is set up to fail,” she said. “To truly dismantle structural racism in the APA, the leadership of the organization – the CEO, the executive committee, and the board of trustees – must do the hard work of deep self-reflection and self-study to recognize the role that they have played in perpetuating and upholding White supremacy in the organization.
“I do not believe the task force will be capable of doing this, as this is not what they have been tasked to do,” Dr. Shim said.
Task force member Dr. Starks said he believes there is potential for progress within the APA. While Black members have been frustrated by an APA power structure that seems both harmful and unchangeable, he said, “this is an opportunity for us to re-root and achieve equity in mental health.”
He added that the priorities of the task force are not set in stone. “Those things that are listed on the website may change and evolve over time as we report back to the board and develop our functions internally,” said Dr. Starks, who praised Dr. Shim’s commentary as “courageous.”
The website lists these initial charges for the task force:
- Providing education and resources on APA’s and psychiatry’s history regarding structural racism.
- Explaining the current impact of structural racism on the mental health of our patients and colleagues.
- Developing achievable and actionable recommendations for change to eliminate structural racism in the APA and psychiatry now and in the future.
- Providing reports with specific recommendations for achievable actions to the APA board of trustees at each of its meetings through May 2021.
- Monitoring the implementation of tasks.
Meanwhile, the task force is reporting to the APA board of directors each month. The entity is tied to the 1-year presidential term of Dr. Geller, which ends in spring 2021, but Dr. Starks said he hopes it will continue in another form – such as a formal committee.
Importance of cultural competence
Dr. Brown highlighted the importance of cultural competence – “making sure that we are looking at patients in the context of their cultural background, their religion, their race, so we can make informed decisions without jumping to conclusions too soon.”
For example, if an African American man or woman talks about hearing God’s voice, “we shouldn’t necessarily brush it off or diminish it as psychiatric illness if it’s in the context of that person’s religious background,” Dr. Brown said.
Francis G. Lu, MD, agreed. He said the task force should explore cultural competency on both clinical and systems levels.
“An antidote to structural racism would be systems cultural competence involving organizations, clinics, and teams looking beyond patient care issues,” said Dr. Lu, the Luke & Grace Kim Professor in Cultural Psychiatry Emeritus at the University of California, Davis. A good starting point, he said, is the National Standards for Culturally and Linguistically Appropriate Services in Health and Health Care, also known as the National CLAS Standards.
Looking forward, Olusola Ajilore, MD, PhD, called for a focus on targeted efforts aimed at encouraging more minority medical students to become psychiatrists.

“We have a field with a lot of crucial questions that have yet to be answered,” said Dr. Ajilore, associate director of residency training and education at the University of Illinois at Chicago. “With more Black psychiatrists, we might be more aware of some of the research questions that affect our community, such as the mental health consequences of exposure to racism and prejudice.”
However, the role of White psychiatrists cannot be overemphasized, said Constance E. Dunlap, MD, clinical professor of psychiatry and behavioral sciences at George Washington University in Washington.

“Whites can make a difference by acknowledging the racial hierarchy that ‘unfairly disadvantages some ... and unfairly advantages others’ – to use the language8 offered by Dr. Camara Phyllis Jones, said Dr. Dunlap.
“As psychiatrists – as physicians – we are obligated to help patients see themselves and the world more clearly. This starts with our own self-appraisal and extends to our work, whether it is in a psychodynamic space or a community psychiatry setting,” Dr. Dunlap said. “Bottom line, instead of focusing on guilt, I tell my White colleagues and patients: You have privilege, use it constructively to benefit the world.”
Dr. Calhoun said she hopes to see mandated integration of training about racism into psychiatric education. “Rather than a special racism lecture, I’d like to see instruction implemented throughout. It should be essential for psychiatrists to learn about the historical racism of psychiatry and the current racial inequities that exist among psychiatric patients.”
The practice of community psychiatry,9 almost by definition, is uniquely positioned to break through some of those structural issues. “The community psychiatry approach to treatment is not specific to any race or cultural group – because each person is treated as an individual,” said Stephanie Le Melle, MD, MS, director of public psychiatry education at Columbia University and the New York Psychiatric Institute. “The social determinants of health, culture, and social justice experience of each person is taken into consideration,” said Dr. Le Melle.
“Community psychiatry steps outside of the traditional medical model of symptoms and illness, and focuses on understanding the person’s strengths and goals – and helps them to live their best lives.”
Dr. Le Melle also views diversifying the psychiatric workforce as imperative.
“For many African American, Latinx, and other marginalized populations that have had to deal with systemic and structural racism, discrimination, and historical abuse at the hands of psychiatry, it can be difficult to establish trust,” said Dr. Le Melle. “Therefore, diversity of our workforce and cultural humility are also crucial for engagement.”
The APA’s decision to not go forward with this year’s Institute on Psychiatric Services: The Mental Health Services Conference undermines the group’s credibility on these issues, according to some psychiatrists.
The IPS meeting, founded in 1948, is “where we traditionally teach and present about the social determinants of health and racism,” said Dr. Le Melle. “If the APA is serious about addressing the social determinants of health, bias, and discrimination against marginalized people and cultural humility, it needs to embrace and grow community psychiatry, not cut it.”
When asked about the IPS conference, Dr. Geller said that it has been scheduled for October 2021 in New York City. He also said the decision to skip the 2020 conference was made 2 years ago. The conference’s organizing committee decided to cancel the event when hotel space in the preferred city could not be arranged, Dr. Geller said.
Meanwhile, in a widely circulated letter that was sent to the APA board of trustees on Aug. 7, numerous leaders in psychiatry from across the country are citing steps they say the APA must take from “continuing impacts of structural racism that will greatly harm underserved patients, [minority and underrepresented] (M/UR) psychiatrists, and the APA as a whole.”
One step the leaders asked the APA to take was to hire an independent entity to investigate the organization’s “workplace culture, staff morale, and experiences of staff members and M/UR psychiatrists who support and/or work at the organization or have previously been dismissed or departed.”
Dr. Calhoun said she agrees that an internal examination would be productive.
“I’d like to see multiple people in positions of power (in the APA) in order to forward agendas,” Dr. Calhoun said. “Unless we do, we’ll have no way to achieve the goal of getting rid of structural racism.”
Dr. Calhoun, Dr. Geller, Dr. Brown, Dr. Starks, Dr. Lu, Dr. Ajilore, Dr. Dunlap, and Dr. Le Melle reported no relevant disclosures. Dr. Shim disclosed receiving royalties from American Psychiatric Association Publishing. Dr. Stewart is a coeditor of “Black Mental Health: Patients, Providers, and Systems” (American Psychiatric Association Publishing, 2018).
References
1. Geller J. Psychiatric News. 2020 Jun 23.
2. Washington HA. Medical Apartheid: The Dark History of Medical Experimentation on Black Americans From Colonial Times to the Present. (New York: Doubleday), 2006.
3. ”Stewart brings a robust and eventful presidential year to a close.” Psychiatric News Daily. 2019 May 18.
4. Sabshin M et al. Am J Psychiatry. 1970 Dec;127:6.
5. Metzl JM. The Protest Psychosis: How Schizophrenia Became a Black Disease. (Boston: Beacon Press), 2009.
6. U.S. Census Bureau. Population estimates. 2019 Jul 1.
7. Shim RS. “Structural racism is why I’m leaving organized psychiatry. statnews.com. 2020 Jul 1.
8. Jones CP. Ethn Dis;28(Suppl):231-4.
9. Ewalt JR and Ewalt PA. Am J Psychiatry. 2006 Apr 1. doi: 10.1176/ajp.126.1.43.
Amanda Calhoun, MD, recalls noticing a distinct empathy gap while she trained at a youth psychiatric unit.
A White male patient hurled the N-word at a Black patient, and the majority White staff did nothing. “And then [they] told me the White patient was struggling and that’s why they allowed it, even though he was aggressive,” said Dr. Calhoun, psychiatry resident at Yale University in New Haven, Conn. But Dr. Calhoun noticed less restraint on the part of her colleagues while she was treating an angry female Black Latinx patient.
“I remember staff saying she was a nightmare; they called her the B-word; she was ‘a terror.’ How is that this patient isn’t viewed as struggling, where the other patient is? I don’t understand the difference here.”
And, Dr. Calhoun said, “when a patient can complain that they feel they were treated differently based on skin color, [the White majority staff] would just say they have borderline personality disorder or they’re depressed.
“When the staff is not diverse, I really see differential treatment in who gets the benefit of the doubt and their empathy.”
Psychiatrists such as Dr. Calhoun can list countless other examples of institutional racism, interpersonal racism, and prejudice in psychiatry. They see signs of institutional racism in clinical care, academia, and in research. Some are questioning the American Psychiatric Association decision to put on hiatus the Institute on Psychiatric Services, its fall annual meeting that has traditionally served as a vehicle for examining the treatment of underserved communities.
Against that backdrop – and after the killing of George Floyd and amid the disproportionate impact of COVID-19 on communities of color – the APA launched an effort the group says is aimed at reforming itself and psychiatry as a whole. In June, the APA announced the formation of the Presidential Task Force to Address Structural Racism Throughout Psychiatry, and the panel – focused on anti-Black racism – has begun its yearlong work.
A specialty with inherent contradictions
Jeffrey Geller, MD, MPH, the APA’s president, acknowledged in an interview that racism in psychiatry is older than the APA – which celebrated its 175th anniversary as an association last year.
As Dr. Geller pointed out recently, Benjamin Rush, MD, a founding father of the United States and the father of American psychiatry, was an abolitionist who owned one enslaved man – and thought the intelligence and morality of Black people were equal to that of their White counterparts.1 Dr. Rush also thought the skin color of Black people was a manifestation of a type of leprosy that he called “Negritude.”2 “Rush was a remarkable mix of contradictions,” Dr. Geller wrote.
Altha J. Stewart, MD, the first and only Black president of the APA, declined to be interviewed for this article.
But as Dr. Stewart was wrapping up her term as president, she reportedly3 said that a 1970 paper titled “Dimensions of Institutional Racism in Psychiatry” by the late Melvin Sabshin, MD, and associates was essentially a blueprint for moving the specialty forward.
That paper, published in the American Journal of Psychiatry, took psychiatry to task on many levels. One of the barriers that Black psychiatric patients must overcome, according to Dr. Sabshin and associates, is the “biases of the White therapist, who must overcome his cultural blind spots, reactive guilt, and unconscious prejudice.” They called community psychiatry paternalistic. Furthermore, Dr. Sabshin, who would later serve as medical director of the APA for almost 25 years, criticized White mental health professionals for viewing Black communities as “seething cauldrons of psychopathology”:
“They create stereotypes of absent fathers, primitive rage, psychopathy, self-depreciation, promiscuity, deficits in intellectual capacity, and lack of psychological sensitivity,” Dr. Sabshin and his associates wrote. “Gross pathological caricaturization ignores the enormous variation of behavior in black communities. ... The obsession with black psychopathology has been so great that it has retarded serious consideration of racism as it pertains to white psychopathology.”4
In other words, White American psychiatrists adopted the prevailing views of society at large toward Black people. More recently, “there was a period in this country where Black people were thought to be at higher risk of developing issues like schizophrenia5 instead of depression,” said Gregory Scott Brown, MD, of the Center for Green Psychiatry and the University of Texas in Austin.
“Pharmaceutical companies developed ads for antipsychotic medications that portrayed angry Black men or women. This got into the heads of who may have been conditioned without knowing it,” he said.
In addition, psychiatry has failed to diversify its ranks. To this day, Dr. Geller said, “Black psychiatrists are underrepresented in academic settings, leadership positions, hospitals, and clinics. Black patients are suffering because of inequities in access to care in treatment, and even those who receive treatment are often misdiagnosed since we don’t account for the extended community’s trauma.” About 2% of U.S. psychiatrists are Black, and Black people make up 13% of the U.S. population.6
The low percentage of Black psychiatrists hurts the field for many reasons, said task force member Steven Starks, MD, clinical assistant professor of psychiatry at the University of Houston, and not solely because the gap forces many Black patients to be treated by non-Black psychiatrists. “The association has a large, broad impact on our field and profession through the DSM, and work in areas like government relations and access to care and insurance,” Dr. Starks said.
Task force gets mixed reviews
After the announcement, Dr. Geller named the psychiatrists who will serve, and the task force, chaired by Cheryl D. Wills, MD, assistant professor of psychiatry at Case Western Reserve University in Cleveland, got to work quickly.
The task force has conducted an online town hall and will conduct another one on Aug. 24. It also released the results of a survey of nearly 500 members about the top three areas that the task force should address.
“Access to Healthcare/Mental Healthcare” received the most votes (97) as the recommended top priority, followed by “Socio-Economic Conditions and Factors” (49). These two areas also received the most first-, second- and third-priority votes overall (173 and 166, respectively).
The other areas with high numbers of first priority votes were “Lack of Minority Psychiatrists, Faculty and Leaders” and “Education for Psychiatrists,” both tied at 46. Those areas received 142 and 122 total votes supporting them as first, second, and third priorities.
Thirty-seven members said “Racism within the APA/APA Actions” should be the top priority. A small number of respondents appeared to doubt the need for such a task force: Nineteen thought the top priority should be “Questioning the Concept of Structural Racism/Task Force.”
Meanwhile, some psychiatrists are raising questions about the task force’s makeup.
Ruth S. Shim, MD, MPH, the Luke & Grace Kim Professor of Cultural Psychiatry at the University of California, Davis, said that she was disappointed by the task force’s membership. Specifically, Dr. Shim said, the task force does not include enough APA members she sees as qualified to address structural racism.
“While many of the Black psychiatrists who are members of the task force are experts in issues of diversity, inclusion, and equity, other members of the board of trustees who were appointed to this task force do not have any expertise in this area,” said Dr. Shim, who wrote a scathing commentary7 in July about the APA’s failures regarding structural racism. “I believe the selection of members could have been more thoughtful and more inclusive of diverse perspectives and voices.”
Dr. Geller countered that the task force includes a mix of APA board members and non–board members with various types of expertise. “Certain board members were chosen because their colleagues on the board “were already involved in task forces and other projects,” he said.
How the task force is envisioned
Dr. Geller’s goals for the task force, which will operate at least through his 1-year term as president, are ambitious.
“I hope the task force will identify structural racism wherever it’s taking place – where psychiatrists practice, within the APA itself,” Dr. Geller said. “It will be an educational process so we can inform members and ourselves about clear and subtle structural racism. Then we’re going to proffer solutions in several areas that can rectify some of what we’ve been doing and the negative outcomes that have resulted in areas of leadership such as access to care, treatment, hospital and clinic administration, health insurance, and academia. It’s clear that this is a massive undertaking.”
For her part, Dr. Shim thinks the task force might chip around the edges of the structural problems in the specialty – rather than focusing on the roots. “The task force is set up to fail,” she said. “To truly dismantle structural racism in the APA, the leadership of the organization – the CEO, the executive committee, and the board of trustees – must do the hard work of deep self-reflection and self-study to recognize the role that they have played in perpetuating and upholding White supremacy in the organization.
“I do not believe the task force will be capable of doing this, as this is not what they have been tasked to do,” Dr. Shim said.
Task force member Dr. Starks said he believes there is potential for progress within the APA. While Black members have been frustrated by an APA power structure that seems both harmful and unchangeable, he said, “this is an opportunity for us to re-root and achieve equity in mental health.”
He added that the priorities of the task force are not set in stone. “Those things that are listed on the website may change and evolve over time as we report back to the board and develop our functions internally,” said Dr. Starks, who praised Dr. Shim’s commentary as “courageous.”
The website lists these initial charges for the task force:
- Providing education and resources on APA’s and psychiatry’s history regarding structural racism.
- Explaining the current impact of structural racism on the mental health of our patients and colleagues.
- Developing achievable and actionable recommendations for change to eliminate structural racism in the APA and psychiatry now and in the future.
- Providing reports with specific recommendations for achievable actions to the APA board of trustees at each of its meetings through May 2021.
- Monitoring the implementation of tasks.
Meanwhile, the task force is reporting to the APA board of directors each month. The entity is tied to the 1-year presidential term of Dr. Geller, which ends in spring 2021, but Dr. Starks said he hopes it will continue in another form – such as a formal committee.
Importance of cultural competence
Dr. Brown highlighted the importance of cultural competence – “making sure that we are looking at patients in the context of their cultural background, their religion, their race, so we can make informed decisions without jumping to conclusions too soon.”
For example, if an African American man or woman talks about hearing God’s voice, “we shouldn’t necessarily brush it off or diminish it as psychiatric illness if it’s in the context of that person’s religious background,” Dr. Brown said.
Francis G. Lu, MD, agreed. He said the task force should explore cultural competency on both clinical and systems levels.
“An antidote to structural racism would be systems cultural competence involving organizations, clinics, and teams looking beyond patient care issues,” said Dr. Lu, the Luke & Grace Kim Professor in Cultural Psychiatry Emeritus at the University of California, Davis. A good starting point, he said, is the National Standards for Culturally and Linguistically Appropriate Services in Health and Health Care, also known as the National CLAS Standards.
Looking forward, Olusola Ajilore, MD, PhD, called for a focus on targeted efforts aimed at encouraging more minority medical students to become psychiatrists.
“We have a field with a lot of crucial questions that have yet to be answered,” said Dr. Ajilore, associate director of residency training and education at the University of Illinois at Chicago. “With more Black psychiatrists, we might be more aware of some of the research questions that affect our community, such as the mental health consequences of exposure to racism and prejudice.”
However, the role of White psychiatrists cannot be overemphasized, said Constance E. Dunlap, MD, clinical professor of psychiatry and behavioral sciences at George Washington University in Washington.
“Whites can make a difference by acknowledging the racial hierarchy that ‘unfairly disadvantages some ... and unfairly advantages others’ – to use the language8 offered by Dr. Camara Phyllis Jones, said Dr. Dunlap.
“As psychiatrists – as physicians – we are obligated to help patients see themselves and the world more clearly. This starts with our own self-appraisal and extends to our work, whether it is in a psychodynamic space or a community psychiatry setting,” Dr. Dunlap said. “Bottom line, instead of focusing on guilt, I tell my White colleagues and patients: You have privilege, use it constructively to benefit the world.”
Dr. Calhoun said she hopes to see mandated integration of training about racism into psychiatric education. “Rather than a special racism lecture, I’d like to see instruction implemented throughout. It should be essential for psychiatrists to learn about the historical racism of psychiatry and the current racial inequities that exist among psychiatric patients.”
The practice of community psychiatry,9 almost by definition, is uniquely positioned to break through some of those structural issues. “The community psychiatry approach to treatment is not specific to any race or cultural group – because each person is treated as an individual,” said Stephanie Le Melle, MD, MS, director of public psychiatry education at Columbia University and the New York Psychiatric Institute. “The social determinants of health, culture, and social justice experience of each person is taken into consideration,” said Dr. Le Melle.
“Community psychiatry steps outside of the traditional medical model of symptoms and illness, and focuses on understanding the person’s strengths and goals – and helps them to live their best lives.”
Dr. Le Melle also views diversifying the psychiatric workforce as imperative.
“For many African American, Latinx, and other marginalized populations that have had to deal with systemic and structural racism, discrimination, and historical abuse at the hands of psychiatry, it can be difficult to establish trust,” said Dr. Le Melle. “Therefore, diversity of our workforce and cultural humility are also crucial for engagement.”
The APA’s decision to not go forward with this year’s Institute on Psychiatric Services: The Mental Health Services Conference undermines the group’s credibility on these issues, according to some psychiatrists.
The IPS meeting, founded in 1948, is “where we traditionally teach and present about the social determinants of health and racism,” said Dr. Le Melle. “If the APA is serious about addressing the social determinants of health, bias, and discrimination against marginalized people and cultural humility, it needs to embrace and grow community psychiatry, not cut it.”
When asked about the IPS conference, Dr. Geller said that it has been scheduled for October 2021 in New York City. He also said the decision to skip the 2020 conference was made 2 years ago. The conference’s organizing committee decided to cancel the event when hotel space in the preferred city could not be arranged, Dr. Geller said.
Meanwhile, in a widely circulated letter that was sent to the APA board of trustees on Aug. 7, numerous leaders in psychiatry from across the country are citing steps they say the APA must take from “continuing impacts of structural racism that will greatly harm underserved patients, [minority and underrepresented] (M/UR) psychiatrists, and the APA as a whole.”
One step the leaders asked the APA to take was to hire an independent entity to investigate the organization’s “workplace culture, staff morale, and experiences of staff members and M/UR psychiatrists who support and/or work at the organization or have previously been dismissed or departed.”
Dr. Calhoun said she agrees that an internal examination would be productive.
“I’d like to see multiple people in positions of power (in the APA) in order to forward agendas,” Dr. Calhoun said. “Unless we do, we’ll have no way to achieve the goal of getting rid of structural racism.”
Dr. Calhoun, Dr. Geller, Dr. Brown, Dr. Starks, Dr. Lu, Dr. Ajilore, Dr. Dunlap, and Dr. Le Melle reported no relevant disclosures. Dr. Shim disclosed receiving royalties from American Psychiatric Association Publishing. Dr. Stewart is a coeditor of “Black Mental Health: Patients, Providers, and Systems” (American Psychiatric Association Publishing, 2018).
References
1. Geller J. Psychiatric News. 2020 Jun 23.
2. Washington HA. Medical Apartheid: The Dark History of Medical Experimentation on Black Americans From Colonial Times to the Present. (New York: Doubleday), 2006.
3. ”Stewart brings a robust and eventful presidential year to a close.” Psychiatric News Daily. 2019 May 18.
4. Sabshin M et al. Am J Psychiatry. 1970 Dec;127:6.
5. Metzl JM. The Protest Psychosis: How Schizophrenia Became a Black Disease. (Boston: Beacon Press), 2009.
6. U.S. Census Bureau. Population estimates. 2019 Jul 1.
7. Shim RS. “Structural racism is why I’m leaving organized psychiatry. statnews.com. 2020 Jul 1.
8. Jones CP. Ethn Dis;28(Suppl):231-4.
9. Ewalt JR and Ewalt PA. Am J Psychiatry. 2006 Apr 1. doi: 10.1176/ajp.126.1.43.
Amanda Calhoun, MD, recalls noticing a distinct empathy gap while she trained at a youth psychiatric unit.
A White male patient hurled the N-word at a Black patient, and the majority White staff did nothing. “And then [they] told me the White patient was struggling and that’s why they allowed it, even though he was aggressive,” said Dr. Calhoun, psychiatry resident at Yale University in New Haven, Conn. But Dr. Calhoun noticed less restraint on the part of her colleagues while she was treating an angry female Black Latinx patient.
“I remember staff saying she was a nightmare; they called her the B-word; she was ‘a terror.’ How is that this patient isn’t viewed as struggling, where the other patient is? I don’t understand the difference here.”
And, Dr. Calhoun said, “when a patient can complain that they feel they were treated differently based on skin color, [the White majority staff] would just say they have borderline personality disorder or they’re depressed.
“When the staff is not diverse, I really see differential treatment in who gets the benefit of the doubt and their empathy.”
Psychiatrists such as Dr. Calhoun can list countless other examples of institutional racism, interpersonal racism, and prejudice in psychiatry. They see signs of institutional racism in clinical care, academia, and in research. Some are questioning the American Psychiatric Association decision to put on hiatus the Institute on Psychiatric Services, its fall annual meeting that has traditionally served as a vehicle for examining the treatment of underserved communities.
Against that backdrop – and after the killing of George Floyd and amid the disproportionate impact of COVID-19 on communities of color – the APA launched an effort the group says is aimed at reforming itself and psychiatry as a whole. In June, the APA announced the formation of the Presidential Task Force to Address Structural Racism Throughout Psychiatry, and the panel – focused on anti-Black racism – has begun its yearlong work.
A specialty with inherent contradictions
Jeffrey Geller, MD, MPH, the APA’s president, acknowledged in an interview that racism in psychiatry is older than the APA – which celebrated its 175th anniversary as an association last year.
As Dr. Geller pointed out recently, Benjamin Rush, MD, a founding father of the United States and the father of American psychiatry, was an abolitionist who owned one enslaved man – and thought the intelligence and morality of Black people were equal to that of their White counterparts.1 Dr. Rush also thought the skin color of Black people was a manifestation of a type of leprosy that he called “Negritude.”2 “Rush was a remarkable mix of contradictions,” Dr. Geller wrote.
Altha J. Stewart, MD, the first and only Black president of the APA, declined to be interviewed for this article.
But as Dr. Stewart was wrapping up her term as president, she reportedly3 said that a 1970 paper titled “Dimensions of Institutional Racism in Psychiatry” by the late Melvin Sabshin, MD, and associates was essentially a blueprint for moving the specialty forward.
That paper, published in the American Journal of Psychiatry, took psychiatry to task on many levels. One of the barriers that Black psychiatric patients must overcome, according to Dr. Sabshin and associates, is the “biases of the White therapist, who must overcome his cultural blind spots, reactive guilt, and unconscious prejudice.” They called community psychiatry paternalistic. Furthermore, Dr. Sabshin, who would later serve as medical director of the APA for almost 25 years, criticized White mental health professionals for viewing Black communities as “seething cauldrons of psychopathology”:
“They create stereotypes of absent fathers, primitive rage, psychopathy, self-depreciation, promiscuity, deficits in intellectual capacity, and lack of psychological sensitivity,” Dr. Sabshin and his associates wrote. “Gross pathological caricaturization ignores the enormous variation of behavior in black communities. ... The obsession with black psychopathology has been so great that it has retarded serious consideration of racism as it pertains to white psychopathology.”4
In other words, White American psychiatrists adopted the prevailing views of society at large toward Black people. More recently, “there was a period in this country where Black people were thought to be at higher risk of developing issues like schizophrenia5 instead of depression,” said Gregory Scott Brown, MD, of the Center for Green Psychiatry and the University of Texas in Austin.
“Pharmaceutical companies developed ads for antipsychotic medications that portrayed angry Black men or women. This got into the heads of who may have been conditioned without knowing it,” he said.
In addition, psychiatry has failed to diversify its ranks. To this day, Dr. Geller said, “Black psychiatrists are underrepresented in academic settings, leadership positions, hospitals, and clinics. Black patients are suffering because of inequities in access to care in treatment, and even those who receive treatment are often misdiagnosed since we don’t account for the extended community’s trauma.” About 2% of U.S. psychiatrists are Black, and Black people make up 13% of the U.S. population.6
The low percentage of Black psychiatrists hurts the field for many reasons, said task force member Steven Starks, MD, clinical assistant professor of psychiatry at the University of Houston, and not solely because the gap forces many Black patients to be treated by non-Black psychiatrists. “The association has a large, broad impact on our field and profession through the DSM, and work in areas like government relations and access to care and insurance,” Dr. Starks said.
Task force gets mixed reviews
After the announcement, Dr. Geller named the psychiatrists who will serve, and the task force, chaired by Cheryl D. Wills, MD, assistant professor of psychiatry at Case Western Reserve University in Cleveland, got to work quickly.
The task force has conducted an online town hall and will conduct another one on Aug. 24. It also released the results of a survey of nearly 500 members about the top three areas that the task force should address.
“Access to Healthcare/Mental Healthcare” received the most votes (97) as the recommended top priority, followed by “Socio-Economic Conditions and Factors” (49). These two areas also received the most first-, second- and third-priority votes overall (173 and 166, respectively).
The other areas with high numbers of first priority votes were “Lack of Minority Psychiatrists, Faculty and Leaders” and “Education for Psychiatrists,” both tied at 46. Those areas received 142 and 122 total votes supporting them as first, second, and third priorities.
Thirty-seven members said “Racism within the APA/APA Actions” should be the top priority. A small number of respondents appeared to doubt the need for such a task force: Nineteen thought the top priority should be “Questioning the Concept of Structural Racism/Task Force.”
Meanwhile, some psychiatrists are raising questions about the task force’s makeup.
Ruth S. Shim, MD, MPH, the Luke & Grace Kim Professor of Cultural Psychiatry at the University of California, Davis, said that she was disappointed by the task force’s membership. Specifically, Dr. Shim said, the task force does not include enough APA members she sees as qualified to address structural racism.
“While many of the Black psychiatrists who are members of the task force are experts in issues of diversity, inclusion, and equity, other members of the board of trustees who were appointed to this task force do not have any expertise in this area,” said Dr. Shim, who wrote a scathing commentary7 in July about the APA’s failures regarding structural racism. “I believe the selection of members could have been more thoughtful and more inclusive of diverse perspectives and voices.”
Dr. Geller countered that the task force includes a mix of APA board members and non–board members with various types of expertise. “Certain board members were chosen because their colleagues on the board “were already involved in task forces and other projects,” he said.
How the task force is envisioned
Dr. Geller’s goals for the task force, which will operate at least through his 1-year term as president, are ambitious.
“I hope the task force will identify structural racism wherever it’s taking place – where psychiatrists practice, within the APA itself,” Dr. Geller said. “It will be an educational process so we can inform members and ourselves about clear and subtle structural racism. Then we’re going to proffer solutions in several areas that can rectify some of what we’ve been doing and the negative outcomes that have resulted in areas of leadership such as access to care, treatment, hospital and clinic administration, health insurance, and academia. It’s clear that this is a massive undertaking.”
For her part, Dr. Shim thinks the task force might chip around the edges of the structural problems in the specialty – rather than focusing on the roots. “The task force is set up to fail,” she said. “To truly dismantle structural racism in the APA, the leadership of the organization – the CEO, the executive committee, and the board of trustees – must do the hard work of deep self-reflection and self-study to recognize the role that they have played in perpetuating and upholding White supremacy in the organization.
“I do not believe the task force will be capable of doing this, as this is not what they have been tasked to do,” Dr. Shim said.
Task force member Dr. Starks said he believes there is potential for progress within the APA. While Black members have been frustrated by an APA power structure that seems both harmful and unchangeable, he said, “this is an opportunity for us to re-root and achieve equity in mental health.”
He added that the priorities of the task force are not set in stone. “Those things that are listed on the website may change and evolve over time as we report back to the board and develop our functions internally,” said Dr. Starks, who praised Dr. Shim’s commentary as “courageous.”
The website lists these initial charges for the task force:
- Providing education and resources on APA’s and psychiatry’s history regarding structural racism.
- Explaining the current impact of structural racism on the mental health of our patients and colleagues.
- Developing achievable and actionable recommendations for change to eliminate structural racism in the APA and psychiatry now and in the future.
- Providing reports with specific recommendations for achievable actions to the APA board of trustees at each of its meetings through May 2021.
- Monitoring the implementation of tasks.
Meanwhile, the task force is reporting to the APA board of directors each month. The entity is tied to the 1-year presidential term of Dr. Geller, which ends in spring 2021, but Dr. Starks said he hopes it will continue in another form – such as a formal committee.
Importance of cultural competence
Dr. Brown highlighted the importance of cultural competence – “making sure that we are looking at patients in the context of their cultural background, their religion, their race, so we can make informed decisions without jumping to conclusions too soon.”
For example, if an African American man or woman talks about hearing God’s voice, “we shouldn’t necessarily brush it off or diminish it as psychiatric illness if it’s in the context of that person’s religious background,” Dr. Brown said.
Francis G. Lu, MD, agreed. He said the task force should explore cultural competency on both clinical and systems levels.
“An antidote to structural racism would be systems cultural competence involving organizations, clinics, and teams looking beyond patient care issues,” said Dr. Lu, the Luke & Grace Kim Professor in Cultural Psychiatry Emeritus at the University of California, Davis. A good starting point, he said, is the National Standards for Culturally and Linguistically Appropriate Services in Health and Health Care, also known as the National CLAS Standards.
Looking forward, Olusola Ajilore, MD, PhD, called for a focus on targeted efforts aimed at encouraging more minority medical students to become psychiatrists.
“We have a field with a lot of crucial questions that have yet to be answered,” said Dr. Ajilore, associate director of residency training and education at the University of Illinois at Chicago. “With more Black psychiatrists, we might be more aware of some of the research questions that affect our community, such as the mental health consequences of exposure to racism and prejudice.”
However, the role of White psychiatrists cannot be overemphasized, said Constance E. Dunlap, MD, clinical professor of psychiatry and behavioral sciences at George Washington University in Washington.
“Whites can make a difference by acknowledging the racial hierarchy that ‘unfairly disadvantages some ... and unfairly advantages others’ – to use the language8 offered by Dr. Camara Phyllis Jones, said Dr. Dunlap.
“As psychiatrists – as physicians – we are obligated to help patients see themselves and the world more clearly. This starts with our own self-appraisal and extends to our work, whether it is in a psychodynamic space or a community psychiatry setting,” Dr. Dunlap said. “Bottom line, instead of focusing on guilt, I tell my White colleagues and patients: You have privilege, use it constructively to benefit the world.”
Dr. Calhoun said she hopes to see mandated integration of training about racism into psychiatric education. “Rather than a special racism lecture, I’d like to see instruction implemented throughout. It should be essential for psychiatrists to learn about the historical racism of psychiatry and the current racial inequities that exist among psychiatric patients.”
The practice of community psychiatry,9 almost by definition, is uniquely positioned to break through some of those structural issues. “The community psychiatry approach to treatment is not specific to any race or cultural group – because each person is treated as an individual,” said Stephanie Le Melle, MD, MS, director of public psychiatry education at Columbia University and the New York Psychiatric Institute. “The social determinants of health, culture, and social justice experience of each person is taken into consideration,” said Dr. Le Melle.
“Community psychiatry steps outside of the traditional medical model of symptoms and illness, and focuses on understanding the person’s strengths and goals – and helps them to live their best lives.”
Dr. Le Melle also views diversifying the psychiatric workforce as imperative.
“For many African American, Latinx, and other marginalized populations that have had to deal with systemic and structural racism, discrimination, and historical abuse at the hands of psychiatry, it can be difficult to establish trust,” said Dr. Le Melle. “Therefore, diversity of our workforce and cultural humility are also crucial for engagement.”
The APA’s decision to not go forward with this year’s Institute on Psychiatric Services: The Mental Health Services Conference undermines the group’s credibility on these issues, according to some psychiatrists.
The IPS meeting, founded in 1948, is “where we traditionally teach and present about the social determinants of health and racism,” said Dr. Le Melle. “If the APA is serious about addressing the social determinants of health, bias, and discrimination against marginalized people and cultural humility, it needs to embrace and grow community psychiatry, not cut it.”
When asked about the IPS conference, Dr. Geller said that it has been scheduled for October 2021 in New York City. He also said the decision to skip the 2020 conference was made 2 years ago. The conference’s organizing committee decided to cancel the event when hotel space in the preferred city could not be arranged, Dr. Geller said.
Meanwhile, in a widely circulated letter that was sent to the APA board of trustees on Aug. 7, numerous leaders in psychiatry from across the country are citing steps they say the APA must take from “continuing impacts of structural racism that will greatly harm underserved patients, [minority and underrepresented] (M/UR) psychiatrists, and the APA as a whole.”
One step the leaders asked the APA to take was to hire an independent entity to investigate the organization’s “workplace culture, staff morale, and experiences of staff members and M/UR psychiatrists who support and/or work at the organization or have previously been dismissed or departed.”
Dr. Calhoun said she agrees that an internal examination would be productive.
“I’d like to see multiple people in positions of power (in the APA) in order to forward agendas,” Dr. Calhoun said. “Unless we do, we’ll have no way to achieve the goal of getting rid of structural racism.”
Dr. Calhoun, Dr. Geller, Dr. Brown, Dr. Starks, Dr. Lu, Dr. Ajilore, Dr. Dunlap, and Dr. Le Melle reported no relevant disclosures. Dr. Shim disclosed receiving royalties from American Psychiatric Association Publishing. Dr. Stewart is a coeditor of “Black Mental Health: Patients, Providers, and Systems” (American Psychiatric Association Publishing, 2018).
References
1. Geller J. Psychiatric News. 2020 Jun 23.
2. Washington HA. Medical Apartheid: The Dark History of Medical Experimentation on Black Americans From Colonial Times to the Present. (New York: Doubleday), 2006.
3. ”Stewart brings a robust and eventful presidential year to a close.” Psychiatric News Daily. 2019 May 18.
4. Sabshin M et al. Am J Psychiatry. 1970 Dec;127:6.
5. Metzl JM. The Protest Psychosis: How Schizophrenia Became a Black Disease. (Boston: Beacon Press), 2009.
6. U.S. Census Bureau. Population estimates. 2019 Jul 1.
7. Shim RS. “Structural racism is why I’m leaving organized psychiatry. statnews.com. 2020 Jul 1.
8. Jones CP. Ethn Dis;28(Suppl):231-4.
9. Ewalt JR and Ewalt PA. Am J Psychiatry. 2006 Apr 1. doi: 10.1176/ajp.126.1.43.
COVID-19 cases in children nearly doubled in just 4 weeks
The cumulative number of new COVID-19 cases among children in the United States jumped by 90% during a recent 4-week period, according to a report that confirms children are not immune to the coronavirus.
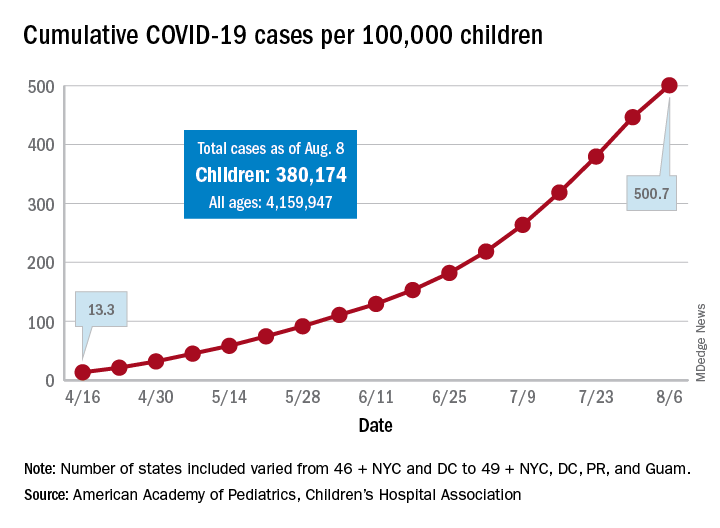
“In areas with rapid community spread, it’s likely that more children will also be infected, and these data show that,” Sally Goza, MD, president of the American Academy of Pediatrics, said in a written statement. “I urge people to wear cloth face coverings and be diligent in social distancing and hand-washing. It is up to us to make the difference, community by community.”
The joint report from the AAP and the Children’s Hospital Association draws on data from state and local health departments in 49 states, New York City, the District of Columbia, Puerto Rico, and Guam.
The cumulative number of COVID-19 cases in children as of Aug. 6, 2020, was 380,174, and that number is 90% higher – an increase of 179,990 cases – than the total on July 9, just 4 weeks earlier, the two organizations said in the report.
and 27 states out of 47 with available data now report that over 10% of their cases were children, with Wyoming the highest at 16.5% and New Jersey the lowest at 2.9%, the report data show.
Alabama has a higher percentage of 22.5%, but the state has been reporting cases in individuals aged 0-24 years as child cases since May 7. The report’s findings are somewhat limited by differences in reporting among the states and by “gaps in the data they are reporting [that affect] how the data can be interpreted,” the AAP said in its statement.
The cumulative number of cases per 100,000 children has risen from 13.3 in mid-April, when the total number was 9,259 cases, to 500.7 per 100,000 as of Aug. 6, and there are now 21 states, along with the District of Columbia, reporting a rate of over 500 cases per 100,000 children. Arizona has the highest rate at 1,206.4, followed by South Carolina (1,074.4) and Tennessee (1,050.8), the AAP and the CHA said.
In New York City, the early epicenter of the pandemic, the 390.5 cases per 100,000 children have been reported, and in New Jersey, which joined New York in the initial surge of cases, the number is 269.5. As of Aug. 6, Hawaii had the fewest cases of any state at 91.2 per 100,000, according to the report.
Children continue to represent a very low proportion of COVID-19 deaths, “but as case counts rise across the board, that is likely to impact more children with severe illness as well,” Sean O’Leary, MD, MPH, vice chair of the AAP’s committee on infectious diseases, said in the AAP statement.
It is possible that “some of the increase in numbers of cases in children could be due to more testing. Early in the pandemic, testing only occurred for the sickest individuals. Now that there is more testing capacity … the numbers reflect a broader slice of the population, including children who may have mild or few symptoms,” the AAP suggested.
This article was updated on 8/17/2020.
The cumulative number of new COVID-19 cases among children in the United States jumped by 90% during a recent 4-week period, according to a report that confirms children are not immune to the coronavirus.
“In areas with rapid community spread, it’s likely that more children will also be infected, and these data show that,” Sally Goza, MD, president of the American Academy of Pediatrics, said in a written statement. “I urge people to wear cloth face coverings and be diligent in social distancing and hand-washing. It is up to us to make the difference, community by community.”
The joint report from the AAP and the Children’s Hospital Association draws on data from state and local health departments in 49 states, New York City, the District of Columbia, Puerto Rico, and Guam.
The cumulative number of COVID-19 cases in children as of Aug. 6, 2020, was 380,174, and that number is 90% higher – an increase of 179,990 cases – than the total on July 9, just 4 weeks earlier, the two organizations said in the report.
and 27 states out of 47 with available data now report that over 10% of their cases were children, with Wyoming the highest at 16.5% and New Jersey the lowest at 2.9%, the report data show.
Alabama has a higher percentage of 22.5%, but the state has been reporting cases in individuals aged 0-24 years as child cases since May 7. The report’s findings are somewhat limited by differences in reporting among the states and by “gaps in the data they are reporting [that affect] how the data can be interpreted,” the AAP said in its statement.
The cumulative number of cases per 100,000 children has risen from 13.3 in mid-April, when the total number was 9,259 cases, to 500.7 per 100,000 as of Aug. 6, and there are now 21 states, along with the District of Columbia, reporting a rate of over 500 cases per 100,000 children. Arizona has the highest rate at 1,206.4, followed by South Carolina (1,074.4) and Tennessee (1,050.8), the AAP and the CHA said.
In New York City, the early epicenter of the pandemic, the 390.5 cases per 100,000 children have been reported, and in New Jersey, which joined New York in the initial surge of cases, the number is 269.5. As of Aug. 6, Hawaii had the fewest cases of any state at 91.2 per 100,000, according to the report.
Children continue to represent a very low proportion of COVID-19 deaths, “but as case counts rise across the board, that is likely to impact more children with severe illness as well,” Sean O’Leary, MD, MPH, vice chair of the AAP’s committee on infectious diseases, said in the AAP statement.
It is possible that “some of the increase in numbers of cases in children could be due to more testing. Early in the pandemic, testing only occurred for the sickest individuals. Now that there is more testing capacity … the numbers reflect a broader slice of the population, including children who may have mild or few symptoms,” the AAP suggested.
This article was updated on 8/17/2020.
The cumulative number of new COVID-19 cases among children in the United States jumped by 90% during a recent 4-week period, according to a report that confirms children are not immune to the coronavirus.
“In areas with rapid community spread, it’s likely that more children will also be infected, and these data show that,” Sally Goza, MD, president of the American Academy of Pediatrics, said in a written statement. “I urge people to wear cloth face coverings and be diligent in social distancing and hand-washing. It is up to us to make the difference, community by community.”
The joint report from the AAP and the Children’s Hospital Association draws on data from state and local health departments in 49 states, New York City, the District of Columbia, Puerto Rico, and Guam.
The cumulative number of COVID-19 cases in children as of Aug. 6, 2020, was 380,174, and that number is 90% higher – an increase of 179,990 cases – than the total on July 9, just 4 weeks earlier, the two organizations said in the report.
and 27 states out of 47 with available data now report that over 10% of their cases were children, with Wyoming the highest at 16.5% and New Jersey the lowest at 2.9%, the report data show.
Alabama has a higher percentage of 22.5%, but the state has been reporting cases in individuals aged 0-24 years as child cases since May 7. The report’s findings are somewhat limited by differences in reporting among the states and by “gaps in the data they are reporting [that affect] how the data can be interpreted,” the AAP said in its statement.
The cumulative number of cases per 100,000 children has risen from 13.3 in mid-April, when the total number was 9,259 cases, to 500.7 per 100,000 as of Aug. 6, and there are now 21 states, along with the District of Columbia, reporting a rate of over 500 cases per 100,000 children. Arizona has the highest rate at 1,206.4, followed by South Carolina (1,074.4) and Tennessee (1,050.8), the AAP and the CHA said.
In New York City, the early epicenter of the pandemic, the 390.5 cases per 100,000 children have been reported, and in New Jersey, which joined New York in the initial surge of cases, the number is 269.5. As of Aug. 6, Hawaii had the fewest cases of any state at 91.2 per 100,000, according to the report.
Children continue to represent a very low proportion of COVID-19 deaths, “but as case counts rise across the board, that is likely to impact more children with severe illness as well,” Sean O’Leary, MD, MPH, vice chair of the AAP’s committee on infectious diseases, said in the AAP statement.
It is possible that “some of the increase in numbers of cases in children could be due to more testing. Early in the pandemic, testing only occurred for the sickest individuals. Now that there is more testing capacity … the numbers reflect a broader slice of the population, including children who may have mild or few symptoms,” the AAP suggested.
This article was updated on 8/17/2020.
Antibiotic resistance: Personal responsibility in somewhat short supply
Most primary care physicians agree that antibiotic resistance and inappropriate prescribing are problems in the United States, but they are much less inclined to recognize these issues in their own practices, according to the results of a nationwide survey.
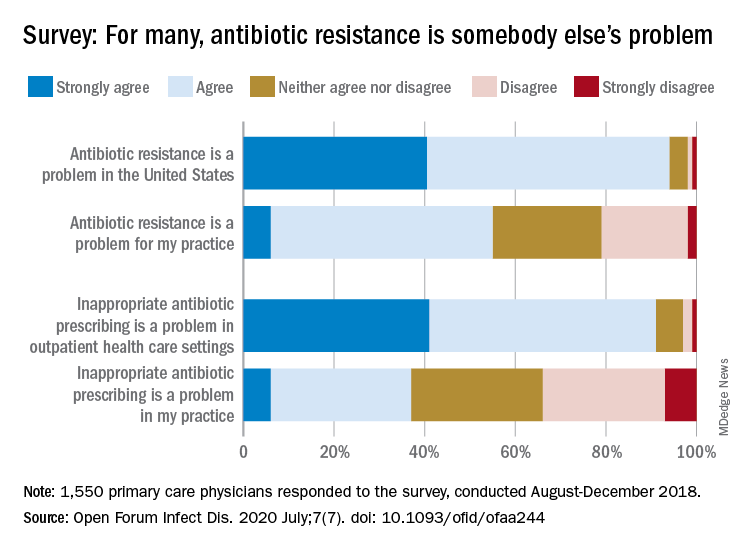
Rachel M. Zetts, MPH, of the Pew Charitable Trusts, Washington, D.C., and associates wrote in Open Forum Infectious Diseases.
Almost all (94%) of the 1,550 internists, family physicians, and pediatricians who responded to the survey said that antibiotic resistance is a national problem, and nearly that many (91%) agreed that “inappropriate antibiotic prescribing is a problem in outpatient health care settings,” the investigators acknowledged.
Narrowing the focus to their own practices, however, changed some opinions. At that level, only 55% of the respondents said that resistance was a problem for their practices, and just 37% said that there any sort of inappropriate prescribing going on, based on data from the survey, which was conducted from August to October 2018 by Pew and the American Medical Association.
Antibiotic stewardship, defined as activities meant to ensure appropriate prescribing of antibiotics, should include “staff and patient education, clinician-level antibiotic prescribing feedback, and communications training on how to discuss antibiotic prescribing with patients,” Ms. Zetts and associates explained.
The need for such stewardship in health care settings was acknowledged by 72% of respondents, but 53% of those surveyed also said that all they need to do to support such efforts “is to talk with their patients about the value of an antibiotic for their symptoms,” they noted.
The bacteria, it seems, are not the only ones with some resistance. Half of the primary care physicians believe that it would be difficult to fairly and accurately track the appropriate use of antibiotics, and 52% agreed with the statement that “practice-based reporting requirements for antibiotic use would be too onerous,” the researchers pointed out.
“Antibiotic resistance is an impending public health crisis. We are seeing today, as we respond to the COVID-19 pandemic, what our health system looks like with no or limited treatments available to tackle an outbreak. … We must all remain vigilant in combating the spread of antibiotic resistant bacteria and be prudent when prescribing antibiotics,” AMA President Susan R. Bailey, MD, said in a written statement.
SOURCE: Zetts RM et al. Open Forum Infect Dis. 2020 July;7(7). doi: 10.1093/ofid/ofaa244.
Most primary care physicians agree that antibiotic resistance and inappropriate prescribing are problems in the United States, but they are much less inclined to recognize these issues in their own practices, according to the results of a nationwide survey.
Rachel M. Zetts, MPH, of the Pew Charitable Trusts, Washington, D.C., and associates wrote in Open Forum Infectious Diseases.
Almost all (94%) of the 1,550 internists, family physicians, and pediatricians who responded to the survey said that antibiotic resistance is a national problem, and nearly that many (91%) agreed that “inappropriate antibiotic prescribing is a problem in outpatient health care settings,” the investigators acknowledged.
Narrowing the focus to their own practices, however, changed some opinions. At that level, only 55% of the respondents said that resistance was a problem for their practices, and just 37% said that there any sort of inappropriate prescribing going on, based on data from the survey, which was conducted from August to October 2018 by Pew and the American Medical Association.
Antibiotic stewardship, defined as activities meant to ensure appropriate prescribing of antibiotics, should include “staff and patient education, clinician-level antibiotic prescribing feedback, and communications training on how to discuss antibiotic prescribing with patients,” Ms. Zetts and associates explained.
The need for such stewardship in health care settings was acknowledged by 72% of respondents, but 53% of those surveyed also said that all they need to do to support such efforts “is to talk with their patients about the value of an antibiotic for their symptoms,” they noted.
The bacteria, it seems, are not the only ones with some resistance. Half of the primary care physicians believe that it would be difficult to fairly and accurately track the appropriate use of antibiotics, and 52% agreed with the statement that “practice-based reporting requirements for antibiotic use would be too onerous,” the researchers pointed out.
“Antibiotic resistance is an impending public health crisis. We are seeing today, as we respond to the COVID-19 pandemic, what our health system looks like with no or limited treatments available to tackle an outbreak. … We must all remain vigilant in combating the spread of antibiotic resistant bacteria and be prudent when prescribing antibiotics,” AMA President Susan R. Bailey, MD, said in a written statement.
SOURCE: Zetts RM et al. Open Forum Infect Dis. 2020 July;7(7). doi: 10.1093/ofid/ofaa244.
Most primary care physicians agree that antibiotic resistance and inappropriate prescribing are problems in the United States, but they are much less inclined to recognize these issues in their own practices, according to the results of a nationwide survey.
Rachel M. Zetts, MPH, of the Pew Charitable Trusts, Washington, D.C., and associates wrote in Open Forum Infectious Diseases.
Almost all (94%) of the 1,550 internists, family physicians, and pediatricians who responded to the survey said that antibiotic resistance is a national problem, and nearly that many (91%) agreed that “inappropriate antibiotic prescribing is a problem in outpatient health care settings,” the investigators acknowledged.
Narrowing the focus to their own practices, however, changed some opinions. At that level, only 55% of the respondents said that resistance was a problem for their practices, and just 37% said that there any sort of inappropriate prescribing going on, based on data from the survey, which was conducted from August to October 2018 by Pew and the American Medical Association.
Antibiotic stewardship, defined as activities meant to ensure appropriate prescribing of antibiotics, should include “staff and patient education, clinician-level antibiotic prescribing feedback, and communications training on how to discuss antibiotic prescribing with patients,” Ms. Zetts and associates explained.
The need for such stewardship in health care settings was acknowledged by 72% of respondents, but 53% of those surveyed also said that all they need to do to support such efforts “is to talk with their patients about the value of an antibiotic for their symptoms,” they noted.
The bacteria, it seems, are not the only ones with some resistance. Half of the primary care physicians believe that it would be difficult to fairly and accurately track the appropriate use of antibiotics, and 52% agreed with the statement that “practice-based reporting requirements for antibiotic use would be too onerous,” the researchers pointed out.
“Antibiotic resistance is an impending public health crisis. We are seeing today, as we respond to the COVID-19 pandemic, what our health system looks like with no or limited treatments available to tackle an outbreak. … We must all remain vigilant in combating the spread of antibiotic resistant bacteria and be prudent when prescribing antibiotics,” AMA President Susan R. Bailey, MD, said in a written statement.
SOURCE: Zetts RM et al. Open Forum Infect Dis. 2020 July;7(7). doi: 10.1093/ofid/ofaa244.
FROM OPEN FORUM INFECTIOUS DISEASES
Pandemic hampers reopening of joint replacement gold mine
Dr. Ira Weintraub, a recently retired orthopedic surgeon who now works at a medical billing consultancy, saw a hip replacement bill for over $400,000 earlier this year.
“The patient stayed in the hospital 17 days, which is only 17 times normal. The bill got paid,” mused Weintraub, chief medical officer of Portland, Oregon-based WellRithms, which helps self-funded employers and workers’ compensation insurers make sense of large, complex medical bills and ensure they pay the fair amount.
Charges like that go a long way toward explaining why hospitals are eager to restore joint replacements to pre-COVID levels as quickly as possible – an eagerness tempered only by safety concerns amid a resurgence of the coronavirus in some regions of the country. Revenue losses at hospitals and outpatient surgery centers may have exceeded $5 billion from canceled knee and hip replacements alone during a roughly two-month hiatus on elective procedures earlier this year.
The cost of joint replacement surgery varies widely – though, on average, it is in the tens, not hundreds, of thousands of dollars. Still, given the high and rapidly growing volume, it’s easy to see why joint replacement operations have become a vital chunk of revenue at most U.S. hospitals.
The rate of knee and hip replacements more than doubled from 2000 to 2015, according to inpatient discharge data from the Agency for Healthcare Research and Quality. And that growth is likely to continue: Knee replacements are expected to triple between now and 2040, with hip replacements not far behind, according to projections published last year in the Journal of Rheumatology.
Joint procedures are usually not emergencies, and they were among the first to be scrubbed or delayed when hospitals froze elective surgeries in March – and again in July in some areas plagued by renewed COVID outbreaks.
“Without orthopedic volumes returning to something near their pre-pandemic levels, it will make it difficult for health systems to get back to anywhere near break-even from a bottom-line perspective,” said Stephen Thome, a principal in health care consulting at Grant Thornton, an advisory, audit and tax firm.
It’s impossible to know exactly how much knee and hip replacements are worth to hospitals, because no definitive data on total volume or price exists.
But using published estimates of volume, extrapolating average commercial payments from published Medicare rates based on a study, and making an educated guess of patient coinsurance, Thome helped KHN arrive at an annual market value for American hospitals and surgery centers of between $15.5 billion and $21.5 billion for knee replacements alone.
That suggests a revenue loss of $1.3 billion to $1.8 billion per month for the period the surgeries were shut down. These figures include ambulatory surgery centers not owned by hospitals, which also suspended most operations in late March, all of April and into May.
If you add hip replacements, which account for about half the volume of knees and are paid at similar rates, the total annual value rises to a range of $23 billion to $32 billion, with monthly revenue losses from $1.9 billion to $2.7 billion.
The American Hospital Association projects total revenue lost at U.S. hospitals will reach $323 billion by year’s end, not counting additional losses from surgeries canceled during the current coronavirus spike. That amount is partially offset by $69 billion in federal relief dollars hospitals have received so far, according to the association. The California Hospital Association puts the net revenue loss for hospitals in that state at about $10.5 billion, said spokesperson Jan Emerson-Shea.
Hospitals resumed joint replacement surgeries in early to mid-May, with the timing and ramp-up speed varying by region and hospital. Some hospitals restored volume quickly; others took a more cautious route and continue to lose revenue. Still others have had to shut down again.
At the NYU Langone Orthopedic Hospital in New York City, “people are starting to come in and you see the operating rooms full again,” said Dr. Claudette Lajam, chief orthopedic safety officer.
At St. Jude Medical Center in Fullerton, California, where the coronavirus is raging, inpatient joint replacements resumed in the second or third week of May – cautiously at first, but volume is “very close to pre-pandemic levels at this point,” said Dr. Kevin Khajavi, chairman of the hospital’s orthopedic surgery department. However, “we are constantly monitoring the situation to determine if we have to scale back once again,” he said.
In large swaths of Texas, elective surgeries were once again suspended in July because of the COVID-19 resurgence. The same is true at many hospitals in Florida, Alabama, South Carolina and Nevada.
The Mayo Clinic in Phoenix suspended nonemergency joint replacement surgeries in early July. It resumed outpatient replacement procedures the week of July 27, but still has not resumed nonemergency inpatient procedures, said Dr. Mark Spangehl, an orthopedic surgeon there. In terms of medical urgency, joint replacements are “at the bottom of the totem pole,” Spangehl said.
In terms of cash flow, however, joint replacements are decidedly not at the bottom of the totem pole. They have become a cash cow as the number of patients undergoing them has skyrocketed in recent decades.
The volume is being driven by an aging population, an epidemic of obesity and a significant rise in the number of younger people replacing joints worn out by years of sports and exercise.
It’s also being driven by the cash. Once only done in hospitals, the operations are now increasingly performed at ambulatory surgery centers – especially on younger, healthier patients who don’t require hospitalization.
The surgery centers are often physician-owned, but private equity groups such as Bain Capital and KKR & Co. have taken an interest in them, drawn by their high growth potential, robust financial returns and ability to offer competitive prices.
“[G]enerally the savings should be very good – but I do see a lot of outlier surgery centers where they are charging exorbitant amounts of money – $100,000 wouldn’t be too much,” said WellRithm’s Weintraub, who co-owned such a surgery center in Portland.
Fear of catching the coronavirus in a hospital is reinforcing the outpatient trend. Matthew Davis, a 58-year-old resident of Washington, was scheduled for a hip replacement on March 30 but got cold feet because of COVID-19, and canceled just before all elective surgeries were halted. When it came time to reschedule in June, he overcame his reservations in large part because the surgeon planned to perform the procedure at a free-standing surgery center.
“That was key to me – avoiding an overnight hospital stay to minimize my exposure,” Davis said. “These joint replacements are almost industrial-scale. They are cranking out joint replacements 9 to 5. I went in at 6:30 a.m. and I was walking out the door at 11:30.”
Acutely aware of the financial benefits, hospitals and surgery clinics have been marketing joint replacements for years, competing for coveted rankings and running ads that show healthy aging people, all smiles, engaged in vigorous activity.
However, a 2014 study concluded that one-third of knee replacements were not warranted, mainly because the symptoms of the patients were not severe enough to justify the procedures.
“The whole marketing of health care is so manipulative to the consuming public,” said Lisa McGiffert, a longtime consumer advocate and co-founder of the Patient Safety Action Network. “People might be encouraged to get a knee replacement, when in reality something less invasive could have improved their condition.”
McGiffert recounted a conversation with an orthopedic surgeon in Washington state who told her about a patient who requested a knee replacement, even though he had not tried any lower-impact treatments to fix the problem. “I asked the surgeon, ‘You didn’t do it, did you?’ And he said, ‘Of course I did. He would just have gone to somebody else.’ ”
This Kaiser Health News story first published on California Healthline, a service of the California Health Care Foundation.
Dr. Ira Weintraub, a recently retired orthopedic surgeon who now works at a medical billing consultancy, saw a hip replacement bill for over $400,000 earlier this year.
“The patient stayed in the hospital 17 days, which is only 17 times normal. The bill got paid,” mused Weintraub, chief medical officer of Portland, Oregon-based WellRithms, which helps self-funded employers and workers’ compensation insurers make sense of large, complex medical bills and ensure they pay the fair amount.
Charges like that go a long way toward explaining why hospitals are eager to restore joint replacements to pre-COVID levels as quickly as possible – an eagerness tempered only by safety concerns amid a resurgence of the coronavirus in some regions of the country. Revenue losses at hospitals and outpatient surgery centers may have exceeded $5 billion from canceled knee and hip replacements alone during a roughly two-month hiatus on elective procedures earlier this year.
The cost of joint replacement surgery varies widely – though, on average, it is in the tens, not hundreds, of thousands of dollars. Still, given the high and rapidly growing volume, it’s easy to see why joint replacement operations have become a vital chunk of revenue at most U.S. hospitals.
The rate of knee and hip replacements more than doubled from 2000 to 2015, according to inpatient discharge data from the Agency for Healthcare Research and Quality. And that growth is likely to continue: Knee replacements are expected to triple between now and 2040, with hip replacements not far behind, according to projections published last year in the Journal of Rheumatology.
Joint procedures are usually not emergencies, and they were among the first to be scrubbed or delayed when hospitals froze elective surgeries in March – and again in July in some areas plagued by renewed COVID outbreaks.
“Without orthopedic volumes returning to something near their pre-pandemic levels, it will make it difficult for health systems to get back to anywhere near break-even from a bottom-line perspective,” said Stephen Thome, a principal in health care consulting at Grant Thornton, an advisory, audit and tax firm.
It’s impossible to know exactly how much knee and hip replacements are worth to hospitals, because no definitive data on total volume or price exists.
But using published estimates of volume, extrapolating average commercial payments from published Medicare rates based on a study, and making an educated guess of patient coinsurance, Thome helped KHN arrive at an annual market value for American hospitals and surgery centers of between $15.5 billion and $21.5 billion for knee replacements alone.
That suggests a revenue loss of $1.3 billion to $1.8 billion per month for the period the surgeries were shut down. These figures include ambulatory surgery centers not owned by hospitals, which also suspended most operations in late March, all of April and into May.
If you add hip replacements, which account for about half the volume of knees and are paid at similar rates, the total annual value rises to a range of $23 billion to $32 billion, with monthly revenue losses from $1.9 billion to $2.7 billion.
The American Hospital Association projects total revenue lost at U.S. hospitals will reach $323 billion by year’s end, not counting additional losses from surgeries canceled during the current coronavirus spike. That amount is partially offset by $69 billion in federal relief dollars hospitals have received so far, according to the association. The California Hospital Association puts the net revenue loss for hospitals in that state at about $10.5 billion, said spokesperson Jan Emerson-Shea.
Hospitals resumed joint replacement surgeries in early to mid-May, with the timing and ramp-up speed varying by region and hospital. Some hospitals restored volume quickly; others took a more cautious route and continue to lose revenue. Still others have had to shut down again.
At the NYU Langone Orthopedic Hospital in New York City, “people are starting to come in and you see the operating rooms full again,” said Dr. Claudette Lajam, chief orthopedic safety officer.
At St. Jude Medical Center in Fullerton, California, where the coronavirus is raging, inpatient joint replacements resumed in the second or third week of May – cautiously at first, but volume is “very close to pre-pandemic levels at this point,” said Dr. Kevin Khajavi, chairman of the hospital’s orthopedic surgery department. However, “we are constantly monitoring the situation to determine if we have to scale back once again,” he said.
In large swaths of Texas, elective surgeries were once again suspended in July because of the COVID-19 resurgence. The same is true at many hospitals in Florida, Alabama, South Carolina and Nevada.
The Mayo Clinic in Phoenix suspended nonemergency joint replacement surgeries in early July. It resumed outpatient replacement procedures the week of July 27, but still has not resumed nonemergency inpatient procedures, said Dr. Mark Spangehl, an orthopedic surgeon there. In terms of medical urgency, joint replacements are “at the bottom of the totem pole,” Spangehl said.
In terms of cash flow, however, joint replacements are decidedly not at the bottom of the totem pole. They have become a cash cow as the number of patients undergoing them has skyrocketed in recent decades.
The volume is being driven by an aging population, an epidemic of obesity and a significant rise in the number of younger people replacing joints worn out by years of sports and exercise.
It’s also being driven by the cash. Once only done in hospitals, the operations are now increasingly performed at ambulatory surgery centers – especially on younger, healthier patients who don’t require hospitalization.
The surgery centers are often physician-owned, but private equity groups such as Bain Capital and KKR & Co. have taken an interest in them, drawn by their high growth potential, robust financial returns and ability to offer competitive prices.
“[G]enerally the savings should be very good – but I do see a lot of outlier surgery centers where they are charging exorbitant amounts of money – $100,000 wouldn’t be too much,” said WellRithm’s Weintraub, who co-owned such a surgery center in Portland.
Fear of catching the coronavirus in a hospital is reinforcing the outpatient trend. Matthew Davis, a 58-year-old resident of Washington, was scheduled for a hip replacement on March 30 but got cold feet because of COVID-19, and canceled just before all elective surgeries were halted. When it came time to reschedule in June, he overcame his reservations in large part because the surgeon planned to perform the procedure at a free-standing surgery center.
“That was key to me – avoiding an overnight hospital stay to minimize my exposure,” Davis said. “These joint replacements are almost industrial-scale. They are cranking out joint replacements 9 to 5. I went in at 6:30 a.m. and I was walking out the door at 11:30.”
Acutely aware of the financial benefits, hospitals and surgery clinics have been marketing joint replacements for years, competing for coveted rankings and running ads that show healthy aging people, all smiles, engaged in vigorous activity.
However, a 2014 study concluded that one-third of knee replacements were not warranted, mainly because the symptoms of the patients were not severe enough to justify the procedures.
“The whole marketing of health care is so manipulative to the consuming public,” said Lisa McGiffert, a longtime consumer advocate and co-founder of the Patient Safety Action Network. “People might be encouraged to get a knee replacement, when in reality something less invasive could have improved their condition.”
McGiffert recounted a conversation with an orthopedic surgeon in Washington state who told her about a patient who requested a knee replacement, even though he had not tried any lower-impact treatments to fix the problem. “I asked the surgeon, ‘You didn’t do it, did you?’ And he said, ‘Of course I did. He would just have gone to somebody else.’ ”
This Kaiser Health News story first published on California Healthline, a service of the California Health Care Foundation.
Dr. Ira Weintraub, a recently retired orthopedic surgeon who now works at a medical billing consultancy, saw a hip replacement bill for over $400,000 earlier this year.
“The patient stayed in the hospital 17 days, which is only 17 times normal. The bill got paid,” mused Weintraub, chief medical officer of Portland, Oregon-based WellRithms, which helps self-funded employers and workers’ compensation insurers make sense of large, complex medical bills and ensure they pay the fair amount.
Charges like that go a long way toward explaining why hospitals are eager to restore joint replacements to pre-COVID levels as quickly as possible – an eagerness tempered only by safety concerns amid a resurgence of the coronavirus in some regions of the country. Revenue losses at hospitals and outpatient surgery centers may have exceeded $5 billion from canceled knee and hip replacements alone during a roughly two-month hiatus on elective procedures earlier this year.
The cost of joint replacement surgery varies widely – though, on average, it is in the tens, not hundreds, of thousands of dollars. Still, given the high and rapidly growing volume, it’s easy to see why joint replacement operations have become a vital chunk of revenue at most U.S. hospitals.
The rate of knee and hip replacements more than doubled from 2000 to 2015, according to inpatient discharge data from the Agency for Healthcare Research and Quality. And that growth is likely to continue: Knee replacements are expected to triple between now and 2040, with hip replacements not far behind, according to projections published last year in the Journal of Rheumatology.
Joint procedures are usually not emergencies, and they were among the first to be scrubbed or delayed when hospitals froze elective surgeries in March – and again in July in some areas plagued by renewed COVID outbreaks.
“Without orthopedic volumes returning to something near their pre-pandemic levels, it will make it difficult for health systems to get back to anywhere near break-even from a bottom-line perspective,” said Stephen Thome, a principal in health care consulting at Grant Thornton, an advisory, audit and tax firm.
It’s impossible to know exactly how much knee and hip replacements are worth to hospitals, because no definitive data on total volume or price exists.
But using published estimates of volume, extrapolating average commercial payments from published Medicare rates based on a study, and making an educated guess of patient coinsurance, Thome helped KHN arrive at an annual market value for American hospitals and surgery centers of between $15.5 billion and $21.5 billion for knee replacements alone.
That suggests a revenue loss of $1.3 billion to $1.8 billion per month for the period the surgeries were shut down. These figures include ambulatory surgery centers not owned by hospitals, which also suspended most operations in late March, all of April and into May.
If you add hip replacements, which account for about half the volume of knees and are paid at similar rates, the total annual value rises to a range of $23 billion to $32 billion, with monthly revenue losses from $1.9 billion to $2.7 billion.
The American Hospital Association projects total revenue lost at U.S. hospitals will reach $323 billion by year’s end, not counting additional losses from surgeries canceled during the current coronavirus spike. That amount is partially offset by $69 billion in federal relief dollars hospitals have received so far, according to the association. The California Hospital Association puts the net revenue loss for hospitals in that state at about $10.5 billion, said spokesperson Jan Emerson-Shea.
Hospitals resumed joint replacement surgeries in early to mid-May, with the timing and ramp-up speed varying by region and hospital. Some hospitals restored volume quickly; others took a more cautious route and continue to lose revenue. Still others have had to shut down again.
At the NYU Langone Orthopedic Hospital in New York City, “people are starting to come in and you see the operating rooms full again,” said Dr. Claudette Lajam, chief orthopedic safety officer.
At St. Jude Medical Center in Fullerton, California, where the coronavirus is raging, inpatient joint replacements resumed in the second or third week of May – cautiously at first, but volume is “very close to pre-pandemic levels at this point,” said Dr. Kevin Khajavi, chairman of the hospital’s orthopedic surgery department. However, “we are constantly monitoring the situation to determine if we have to scale back once again,” he said.
In large swaths of Texas, elective surgeries were once again suspended in July because of the COVID-19 resurgence. The same is true at many hospitals in Florida, Alabama, South Carolina and Nevada.
The Mayo Clinic in Phoenix suspended nonemergency joint replacement surgeries in early July. It resumed outpatient replacement procedures the week of July 27, but still has not resumed nonemergency inpatient procedures, said Dr. Mark Spangehl, an orthopedic surgeon there. In terms of medical urgency, joint replacements are “at the bottom of the totem pole,” Spangehl said.
In terms of cash flow, however, joint replacements are decidedly not at the bottom of the totem pole. They have become a cash cow as the number of patients undergoing them has skyrocketed in recent decades.
The volume is being driven by an aging population, an epidemic of obesity and a significant rise in the number of younger people replacing joints worn out by years of sports and exercise.
It’s also being driven by the cash. Once only done in hospitals, the operations are now increasingly performed at ambulatory surgery centers – especially on younger, healthier patients who don’t require hospitalization.
The surgery centers are often physician-owned, but private equity groups such as Bain Capital and KKR & Co. have taken an interest in them, drawn by their high growth potential, robust financial returns and ability to offer competitive prices.
“[G]enerally the savings should be very good – but I do see a lot of outlier surgery centers where they are charging exorbitant amounts of money – $100,000 wouldn’t be too much,” said WellRithm’s Weintraub, who co-owned such a surgery center in Portland.
Fear of catching the coronavirus in a hospital is reinforcing the outpatient trend. Matthew Davis, a 58-year-old resident of Washington, was scheduled for a hip replacement on March 30 but got cold feet because of COVID-19, and canceled just before all elective surgeries were halted. When it came time to reschedule in June, he overcame his reservations in large part because the surgeon planned to perform the procedure at a free-standing surgery center.
“That was key to me – avoiding an overnight hospital stay to minimize my exposure,” Davis said. “These joint replacements are almost industrial-scale. They are cranking out joint replacements 9 to 5. I went in at 6:30 a.m. and I was walking out the door at 11:30.”
Acutely aware of the financial benefits, hospitals and surgery clinics have been marketing joint replacements for years, competing for coveted rankings and running ads that show healthy aging people, all smiles, engaged in vigorous activity.
However, a 2014 study concluded that one-third of knee replacements were not warranted, mainly because the symptoms of the patients were not severe enough to justify the procedures.
“The whole marketing of health care is so manipulative to the consuming public,” said Lisa McGiffert, a longtime consumer advocate and co-founder of the Patient Safety Action Network. “People might be encouraged to get a knee replacement, when in reality something less invasive could have improved their condition.”
McGiffert recounted a conversation with an orthopedic surgeon in Washington state who told her about a patient who requested a knee replacement, even though he had not tried any lower-impact treatments to fix the problem. “I asked the surgeon, ‘You didn’t do it, did you?’ And he said, ‘Of course I did. He would just have gone to somebody else.’ ”
This Kaiser Health News story first published on California Healthline, a service of the California Health Care Foundation.