User login
Trump and Biden face off over COVID-19, ACA in final debate
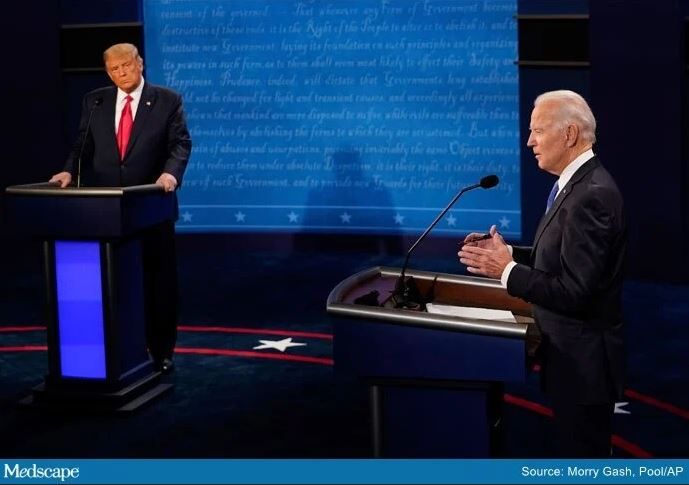
The COVID-19 pandemic figured prominently in the final debate between President Donald Trump and former Vice President Joe Biden when they met on stage for a 90-minute debate in Nashville, Tennessee, Thursday evening.
The adequacy of the COVID-19 response to date, the likely timeline for vaccine availability, and how to reopen businesses while keeping Americans safe were among the points on which the two candidates disagreed. The two candidates also sparred over the value of the Affordable Care Act (ACA) and the future of healthcare in the United States.
Trump and Biden also differed on whether or not the country is facing a “dark winter” because of the pandemic.
Moderator Kristen Welker, NBC News White House correspondent, asked Trump to comment on the fact that 40,000 people are in the hospital on debate night with COVID-19 and that 16,000 have died since the last presidential debate.
Trump said, “2.2 million people modeled out were expected to die.” He said COVID-19 is a worldwide disease that does not only affect the United States.
“The mortality rate is down 85%, and the excess mortality is also down,” he added. He pointed out that previous spikes in Florida, Texas, and Arizona are now gone, and “spikes and surges in other places will soon be gone.
“It will go away, we are rounding the corner,” Trump said. “From personal experience, I was in the hospital, I had it, and they gave me a therapeutic, some would call it a cure...and now they say I’m immune. Whether it’s for a month or lifetime, nobody has been able to say that, but I’m immune.”
Biden countered by saying that “220,000 people are dead. If you hear nothing else I say tonight, hear this: Anyone who’s responsible for that many deaths should not remain president of the United States of America.”
Biden said there are a thousand deaths a day now and that there are over 70K new cases per day. “The expectation is we will have another 200,000 people down before the end of this year. If we just all wore these masks, we could save 100,000.”
“The New England Journal of Medicine said the way the president has handled this is absolutely tragic,” Biden added.
Vaccine timeline
Welker asked Trump if he could guarantee that there will be a COVID-19 vaccine within weeks.
“I can’t guarantee that, but it will be by end of the year. It will be distributed very quickly,” Trump said. He added that three leading vaccine developers, Johnson & Johnson, Moderna, and Pfizer, “are doing very well.”
“We’re about to go into a dark winter and he has no clear plan,” Biden said. “There is no prospect there will be a vaccine for most Americans by middle of next year.”
“It will not be a dark winter,” Trump responded.
Reopening the economy
Trump and Biden disagreed on how aggressively the economy should be reopened in light of the pandemic.
“I want to open the schools. We can’t keep this country closed,” Trump said. “This is a massive country with a massive economy.” He pointed out that rates of depression and suicide have risen because of the economic shutdown. “The cure cannot be worse than the problem.
“His Democrat governors...shut down so tight, and they’re dying,” the president added, gesturing toward Biden. “We are not going to shut down. We are going to open the schools.” As an example of the resiliency of young people, he mentioned that his son Barron tested positive for COVID-19 and recovered.
“I would shut down the virus, not the country,” Biden said. “It’s his ineptitude that caused so many schools and businesses to close in large part. Instead of being in a sand trap playing golf, he should have been negotiating with Nancy Pelosi.”
“He says we’re learning to live with it,” the former vice president said, but instead, “people are learning to die with it.”
Biden added that reopening the economy and minimizing transmission of COVID-19 are not mutually exclusive. “We can walk and chew gum at the same time.”
Divergence over the ACA
The fate of the ACA also garnered considerable attention. The discussion underlined a vast difference of opinion between the two candidates on the US healthcare system.
The moderator asked Trump what he would do for the 20 million Americans who get their healthcare through the ACA if it’s taken away.
“Through the legislature, I terminated the individual mandate, the worst part of Obamacare,” Trump said. “And now it’s in court because Obamacare is no good.
“Preexisting conditions will stay,” Trump added.
“I want to terminate Obamacare, and I want to come up with a beautiful healthcare [plan],” Trump added, turning the discussion toward private health insurance. “One thing that is very important is we have 180 million out there who have great private healthcare. Joe Biden will terminate all of their healthcare.”
Trump described Biden’s plan as “socialized medicine.” He also emphasized that protections for people with preexisting conditions “will stay.”
The Trump administration is supporting a lawsuit to overturn the ACA. The suit was filed by 18 Republican-led states. Arguments before the US Supreme Court on the constitutionality of the ACA are scheduled for November 10.
The moderator asked what Biden plans to do if the ACA is struck down. “I will pass Obamacare with a public option ― that will be ‘Bidencare.’ “ He said his plan will reduce premiums and drug prices. “I support private insurance. No one lost their private insurance under Obamacare.
“There is no way he can protect preexisting conditions,” Biden said. He added that 10 million people have already lost their private healthcare through unemployment during the pandemic.
Muting the mic
Following what many described as a chaotic first debate at the Cleveland Clinic in Ohio on September 29, the Commission on Presidential Debate opted to allow the muting of the microphone during the first 2 minutes of remarks made by each candidate during each debate segment.
The muting of the microphones appeared to prevent crosstalk during the beginning of each segment of the debate. The candidates did manage to talk over and interrupt each other, as well as the moderator, during portions of the debate.
This article first appeared on Medscape.com.
The COVID-19 pandemic figured prominently in the final debate between President Donald Trump and former Vice President Joe Biden when they met on stage for a 90-minute debate in Nashville, Tennessee, Thursday evening.
The adequacy of the COVID-19 response to date, the likely timeline for vaccine availability, and how to reopen businesses while keeping Americans safe were among the points on which the two candidates disagreed. The two candidates also sparred over the value of the Affordable Care Act (ACA) and the future of healthcare in the United States.
Trump and Biden also differed on whether or not the country is facing a “dark winter” because of the pandemic.
Moderator Kristen Welker, NBC News White House correspondent, asked Trump to comment on the fact that 40,000 people are in the hospital on debate night with COVID-19 and that 16,000 have died since the last presidential debate.
Trump said, “2.2 million people modeled out were expected to die.” He said COVID-19 is a worldwide disease that does not only affect the United States.
“The mortality rate is down 85%, and the excess mortality is also down,” he added. He pointed out that previous spikes in Florida, Texas, and Arizona are now gone, and “spikes and surges in other places will soon be gone.
“It will go away, we are rounding the corner,” Trump said. “From personal experience, I was in the hospital, I had it, and they gave me a therapeutic, some would call it a cure...and now they say I’m immune. Whether it’s for a month or lifetime, nobody has been able to say that, but I’m immune.”
Biden countered by saying that “220,000 people are dead. If you hear nothing else I say tonight, hear this: Anyone who’s responsible for that many deaths should not remain president of the United States of America.”
Biden said there are a thousand deaths a day now and that there are over 70K new cases per day. “The expectation is we will have another 200,000 people down before the end of this year. If we just all wore these masks, we could save 100,000.”
“The New England Journal of Medicine said the way the president has handled this is absolutely tragic,” Biden added.
Vaccine timeline
Welker asked Trump if he could guarantee that there will be a COVID-19 vaccine within weeks.
“I can’t guarantee that, but it will be by end of the year. It will be distributed very quickly,” Trump said. He added that three leading vaccine developers, Johnson & Johnson, Moderna, and Pfizer, “are doing very well.”
“We’re about to go into a dark winter and he has no clear plan,” Biden said. “There is no prospect there will be a vaccine for most Americans by middle of next year.”
“It will not be a dark winter,” Trump responded.
Reopening the economy
Trump and Biden disagreed on how aggressively the economy should be reopened in light of the pandemic.
“I want to open the schools. We can’t keep this country closed,” Trump said. “This is a massive country with a massive economy.” He pointed out that rates of depression and suicide have risen because of the economic shutdown. “The cure cannot be worse than the problem.
“His Democrat governors...shut down so tight, and they’re dying,” the president added, gesturing toward Biden. “We are not going to shut down. We are going to open the schools.” As an example of the resiliency of young people, he mentioned that his son Barron tested positive for COVID-19 and recovered.
“I would shut down the virus, not the country,” Biden said. “It’s his ineptitude that caused so many schools and businesses to close in large part. Instead of being in a sand trap playing golf, he should have been negotiating with Nancy Pelosi.”
“He says we’re learning to live with it,” the former vice president said, but instead, “people are learning to die with it.”
Biden added that reopening the economy and minimizing transmission of COVID-19 are not mutually exclusive. “We can walk and chew gum at the same time.”
Divergence over the ACA
The fate of the ACA also garnered considerable attention. The discussion underlined a vast difference of opinion between the two candidates on the US healthcare system.
The moderator asked Trump what he would do for the 20 million Americans who get their healthcare through the ACA if it’s taken away.
“Through the legislature, I terminated the individual mandate, the worst part of Obamacare,” Trump said. “And now it’s in court because Obamacare is no good.
“Preexisting conditions will stay,” Trump added.
“I want to terminate Obamacare, and I want to come up with a beautiful healthcare [plan],” Trump added, turning the discussion toward private health insurance. “One thing that is very important is we have 180 million out there who have great private healthcare. Joe Biden will terminate all of their healthcare.”
Trump described Biden’s plan as “socialized medicine.” He also emphasized that protections for people with preexisting conditions “will stay.”
The Trump administration is supporting a lawsuit to overturn the ACA. The suit was filed by 18 Republican-led states. Arguments before the US Supreme Court on the constitutionality of the ACA are scheduled for November 10.
The moderator asked what Biden plans to do if the ACA is struck down. “I will pass Obamacare with a public option ― that will be ‘Bidencare.’ “ He said his plan will reduce premiums and drug prices. “I support private insurance. No one lost their private insurance under Obamacare.
“There is no way he can protect preexisting conditions,” Biden said. He added that 10 million people have already lost their private healthcare through unemployment during the pandemic.
Muting the mic
Following what many described as a chaotic first debate at the Cleveland Clinic in Ohio on September 29, the Commission on Presidential Debate opted to allow the muting of the microphone during the first 2 minutes of remarks made by each candidate during each debate segment.
The muting of the microphones appeared to prevent crosstalk during the beginning of each segment of the debate. The candidates did manage to talk over and interrupt each other, as well as the moderator, during portions of the debate.
This article first appeared on Medscape.com.
The COVID-19 pandemic figured prominently in the final debate between President Donald Trump and former Vice President Joe Biden when they met on stage for a 90-minute debate in Nashville, Tennessee, Thursday evening.
The adequacy of the COVID-19 response to date, the likely timeline for vaccine availability, and how to reopen businesses while keeping Americans safe were among the points on which the two candidates disagreed. The two candidates also sparred over the value of the Affordable Care Act (ACA) and the future of healthcare in the United States.
Trump and Biden also differed on whether or not the country is facing a “dark winter” because of the pandemic.
Moderator Kristen Welker, NBC News White House correspondent, asked Trump to comment on the fact that 40,000 people are in the hospital on debate night with COVID-19 and that 16,000 have died since the last presidential debate.
Trump said, “2.2 million people modeled out were expected to die.” He said COVID-19 is a worldwide disease that does not only affect the United States.
“The mortality rate is down 85%, and the excess mortality is also down,” he added. He pointed out that previous spikes in Florida, Texas, and Arizona are now gone, and “spikes and surges in other places will soon be gone.
“It will go away, we are rounding the corner,” Trump said. “From personal experience, I was in the hospital, I had it, and they gave me a therapeutic, some would call it a cure...and now they say I’m immune. Whether it’s for a month or lifetime, nobody has been able to say that, but I’m immune.”
Biden countered by saying that “220,000 people are dead. If you hear nothing else I say tonight, hear this: Anyone who’s responsible for that many deaths should not remain president of the United States of America.”
Biden said there are a thousand deaths a day now and that there are over 70K new cases per day. “The expectation is we will have another 200,000 people down before the end of this year. If we just all wore these masks, we could save 100,000.”
“The New England Journal of Medicine said the way the president has handled this is absolutely tragic,” Biden added.
Vaccine timeline
Welker asked Trump if he could guarantee that there will be a COVID-19 vaccine within weeks.
“I can’t guarantee that, but it will be by end of the year. It will be distributed very quickly,” Trump said. He added that three leading vaccine developers, Johnson & Johnson, Moderna, and Pfizer, “are doing very well.”
“We’re about to go into a dark winter and he has no clear plan,” Biden said. “There is no prospect there will be a vaccine for most Americans by middle of next year.”
“It will not be a dark winter,” Trump responded.
Reopening the economy
Trump and Biden disagreed on how aggressively the economy should be reopened in light of the pandemic.
“I want to open the schools. We can’t keep this country closed,” Trump said. “This is a massive country with a massive economy.” He pointed out that rates of depression and suicide have risen because of the economic shutdown. “The cure cannot be worse than the problem.
“His Democrat governors...shut down so tight, and they’re dying,” the president added, gesturing toward Biden. “We are not going to shut down. We are going to open the schools.” As an example of the resiliency of young people, he mentioned that his son Barron tested positive for COVID-19 and recovered.
“I would shut down the virus, not the country,” Biden said. “It’s his ineptitude that caused so many schools and businesses to close in large part. Instead of being in a sand trap playing golf, he should have been negotiating with Nancy Pelosi.”
“He says we’re learning to live with it,” the former vice president said, but instead, “people are learning to die with it.”
Biden added that reopening the economy and minimizing transmission of COVID-19 are not mutually exclusive. “We can walk and chew gum at the same time.”
Divergence over the ACA
The fate of the ACA also garnered considerable attention. The discussion underlined a vast difference of opinion between the two candidates on the US healthcare system.
The moderator asked Trump what he would do for the 20 million Americans who get their healthcare through the ACA if it’s taken away.
“Through the legislature, I terminated the individual mandate, the worst part of Obamacare,” Trump said. “And now it’s in court because Obamacare is no good.
“Preexisting conditions will stay,” Trump added.
“I want to terminate Obamacare, and I want to come up with a beautiful healthcare [plan],” Trump added, turning the discussion toward private health insurance. “One thing that is very important is we have 180 million out there who have great private healthcare. Joe Biden will terminate all of their healthcare.”
Trump described Biden’s plan as “socialized medicine.” He also emphasized that protections for people with preexisting conditions “will stay.”
The Trump administration is supporting a lawsuit to overturn the ACA. The suit was filed by 18 Republican-led states. Arguments before the US Supreme Court on the constitutionality of the ACA are scheduled for November 10.
The moderator asked what Biden plans to do if the ACA is struck down. “I will pass Obamacare with a public option ― that will be ‘Bidencare.’ “ He said his plan will reduce premiums and drug prices. “I support private insurance. No one lost their private insurance under Obamacare.
“There is no way he can protect preexisting conditions,” Biden said. He added that 10 million people have already lost their private healthcare through unemployment during the pandemic.
Muting the mic
Following what many described as a chaotic first debate at the Cleveland Clinic in Ohio on September 29, the Commission on Presidential Debate opted to allow the muting of the microphone during the first 2 minutes of remarks made by each candidate during each debate segment.
The muting of the microphones appeared to prevent crosstalk during the beginning of each segment of the debate. The candidates did manage to talk over and interrupt each other, as well as the moderator, during portions of the debate.
This article first appeared on Medscape.com.
Florida will investigate all COVID-19 deaths
The Florida Department of Health will investigate the state’s 16,000 coronavirus deaths due to questions about the integrity of the data, according to an announcement issued Wednesday.
State health department officials said the “fatality data reported to the state consistently presents confusion and warrants a rigorous review.” The review is meant to “ensure data integrity.”
“During a pandemic, the public must be able to rely on accurate public health data to make informed decisions,” Scott Rivkees, the surgeon general for Florida, said in the statement.
Among the 95 deaths reported Wednesday for instance, 16 had more than a 2-month separation between the time of testing positive for COVID-19 and passing away, and 5 cases had a 3-month gap. In addition, 11 of the deaths occurred more than a month ago.
The health department then listed data for all 95 cases, including the age, gender, county and the dates of test positivity and death. Palm Beach County had 50 of the COVID-19 deaths.
“To ensure the accuracy of COVID-19 related deaths, the department will be performing additional reviews of all deaths,” Rivkees said. “Timely and accurate data remains a top priority of the Department of Health.”
Last week, Jose Oliva, speaker of the Florida House of Representatives, said medical examiner reports were “often lacking in rigor.” House Democrats then said Republicans were trying to “downplay the death toll,” according to the South Florida Sun Sentinel .
Fred Piccolo Jr., a spokesman for Florida Gov. Ron DeSantis, told the newspaper Wednesday that officials have struggled to obtain timely data. Labs sometimes report test results from weeks before, he added.
“It’s really one of those things that you gotta know if someone is dying of COVID or if they’re not,” Piccolo said. “Then you can legitimately say, here are the numbers.”
Sources
Florida Department of Health, “Florida Surgeon General Implements Additional Review Process for Fatalities Attributed to COVID-19 to Ensure Data Integrity.”
South Florida Sun Sentinel, “Florida to investigate all COVID-19 deaths after questions about ‘integrity’ of data.”
WebMD Health News © 2020
This article first appeared on Medscape.com.
The Florida Department of Health will investigate the state’s 16,000 coronavirus deaths due to questions about the integrity of the data, according to an announcement issued Wednesday.
State health department officials said the “fatality data reported to the state consistently presents confusion and warrants a rigorous review.” The review is meant to “ensure data integrity.”
“During a pandemic, the public must be able to rely on accurate public health data to make informed decisions,” Scott Rivkees, the surgeon general for Florida, said in the statement.
Among the 95 deaths reported Wednesday for instance, 16 had more than a 2-month separation between the time of testing positive for COVID-19 and passing away, and 5 cases had a 3-month gap. In addition, 11 of the deaths occurred more than a month ago.
The health department then listed data for all 95 cases, including the age, gender, county and the dates of test positivity and death. Palm Beach County had 50 of the COVID-19 deaths.
“To ensure the accuracy of COVID-19 related deaths, the department will be performing additional reviews of all deaths,” Rivkees said. “Timely and accurate data remains a top priority of the Department of Health.”
Last week, Jose Oliva, speaker of the Florida House of Representatives, said medical examiner reports were “often lacking in rigor.” House Democrats then said Republicans were trying to “downplay the death toll,” according to the South Florida Sun Sentinel .
Fred Piccolo Jr., a spokesman for Florida Gov. Ron DeSantis, told the newspaper Wednesday that officials have struggled to obtain timely data. Labs sometimes report test results from weeks before, he added.
“It’s really one of those things that you gotta know if someone is dying of COVID or if they’re not,” Piccolo said. “Then you can legitimately say, here are the numbers.”
Sources
Florida Department of Health, “Florida Surgeon General Implements Additional Review Process for Fatalities Attributed to COVID-19 to Ensure Data Integrity.”
South Florida Sun Sentinel, “Florida to investigate all COVID-19 deaths after questions about ‘integrity’ of data.”
WebMD Health News © 2020
This article first appeared on Medscape.com.
The Florida Department of Health will investigate the state’s 16,000 coronavirus deaths due to questions about the integrity of the data, according to an announcement issued Wednesday.
State health department officials said the “fatality data reported to the state consistently presents confusion and warrants a rigorous review.” The review is meant to “ensure data integrity.”
“During a pandemic, the public must be able to rely on accurate public health data to make informed decisions,” Scott Rivkees, the surgeon general for Florida, said in the statement.
Among the 95 deaths reported Wednesday for instance, 16 had more than a 2-month separation between the time of testing positive for COVID-19 and passing away, and 5 cases had a 3-month gap. In addition, 11 of the deaths occurred more than a month ago.
The health department then listed data for all 95 cases, including the age, gender, county and the dates of test positivity and death. Palm Beach County had 50 of the COVID-19 deaths.
“To ensure the accuracy of COVID-19 related deaths, the department will be performing additional reviews of all deaths,” Rivkees said. “Timely and accurate data remains a top priority of the Department of Health.”
Last week, Jose Oliva, speaker of the Florida House of Representatives, said medical examiner reports were “often lacking in rigor.” House Democrats then said Republicans were trying to “downplay the death toll,” according to the South Florida Sun Sentinel .
Fred Piccolo Jr., a spokesman for Florida Gov. Ron DeSantis, told the newspaper Wednesday that officials have struggled to obtain timely data. Labs sometimes report test results from weeks before, he added.
“It’s really one of those things that you gotta know if someone is dying of COVID or if they’re not,” Piccolo said. “Then you can legitimately say, here are the numbers.”
Sources
Florida Department of Health, “Florida Surgeon General Implements Additional Review Process for Fatalities Attributed to COVID-19 to Ensure Data Integrity.”
South Florida Sun Sentinel, “Florida to investigate all COVID-19 deaths after questions about ‘integrity’ of data.”
WebMD Health News © 2020
This article first appeared on Medscape.com.
Dr. Anique K. Forrester joins editorial advisory board of Clinical Psychiatry News
Clinical Psychiatry News is pleased to announce that Anique K. Forrester, MD, has joined its editorial advisory board.

Dr. Forrester, who is board certified in the subspecialty of psychosomatic medicine (consultation-liaison psychiatry), holds numerous leadership positions at the University of Maryland, Baltimore. She is director of the consultation-liaison psychiatry fellowship at the university and serves as director of education for the C-L psychiatry PGY-2 rotation. Dr. Forrester, an assistant professor, also serves as chair of the department of psychiatry’s diversity committee and is the coordinator of the cultural psychiatry resident course.
Dr. Forrester completed her psychiatry residency training as well as psychosomatic medicine fellowship training at Sidney Kimmel Medical College, Philadelphia. She is a diplomate of the American Board of Psychiatry and Neurology. In addition, Dr. Forrester is a member of the Academy of Consultation-Liaison Psychiatry. She is a graduate of Howard University, Washington.
Her research interests include perinatal psychiatry, psycho-oncology, and cultural competence in medicine.
Welcome aboard, Dr. Forrester!
Clinical Psychiatry News is pleased to announce that Anique K. Forrester, MD, has joined its editorial advisory board.
Dr. Forrester, who is board certified in the subspecialty of psychosomatic medicine (consultation-liaison psychiatry), holds numerous leadership positions at the University of Maryland, Baltimore. She is director of the consultation-liaison psychiatry fellowship at the university and serves as director of education for the C-L psychiatry PGY-2 rotation. Dr. Forrester, an assistant professor, also serves as chair of the department of psychiatry’s diversity committee and is the coordinator of the cultural psychiatry resident course.
Dr. Forrester completed her psychiatry residency training as well as psychosomatic medicine fellowship training at Sidney Kimmel Medical College, Philadelphia. She is a diplomate of the American Board of Psychiatry and Neurology. In addition, Dr. Forrester is a member of the Academy of Consultation-Liaison Psychiatry. She is a graduate of Howard University, Washington.
Her research interests include perinatal psychiatry, psycho-oncology, and cultural competence in medicine.
Welcome aboard, Dr. Forrester!
Clinical Psychiatry News is pleased to announce that Anique K. Forrester, MD, has joined its editorial advisory board.
Dr. Forrester, who is board certified in the subspecialty of psychosomatic medicine (consultation-liaison psychiatry), holds numerous leadership positions at the University of Maryland, Baltimore. She is director of the consultation-liaison psychiatry fellowship at the university and serves as director of education for the C-L psychiatry PGY-2 rotation. Dr. Forrester, an assistant professor, also serves as chair of the department of psychiatry’s diversity committee and is the coordinator of the cultural psychiatry resident course.
Dr. Forrester completed her psychiatry residency training as well as psychosomatic medicine fellowship training at Sidney Kimmel Medical College, Philadelphia. She is a diplomate of the American Board of Psychiatry and Neurology. In addition, Dr. Forrester is a member of the Academy of Consultation-Liaison Psychiatry. She is a graduate of Howard University, Washington.
Her research interests include perinatal psychiatry, psycho-oncology, and cultural competence in medicine.
Welcome aboard, Dr. Forrester!
Patients can read your clinical notes starting Nov. 2
Starting Nov. 2, all patients in the United States will have immediate access to clinical notes and thus will be able to read their doctors’ writings, as well as test results and reports from pathology and imaging.

The 21st Century Cures Act mandates that patients have fast, electronic access to the following types of notes: consultations, discharge summaries, history, physical examination findings, imaging narratives, laboratory and pathology report narratives, and procedure and progress notes.
But this federal mandate, called “open notes” by many, is potentially confusing and frightening for patients, say some physicians. Others worry that the change will increase workload as clinicians tailor notes for patients and answer related questions.
The law means that inpatient and outpatient notes will be released immediately and that patients will have immediate access to testing and imaging results, including results from sexually transmitted disease tests, Pap tests, cancer biopsies, CT and PET scans, fetal ultrasounds, pneumonia cultures, and mammograms.
Such notes could contain sensitive information, and there is concern that patients could be shocked, confused, or annoyed by what they read, even with more run-of-the-mill notes.
Champions of open notes say that the benefits, including better provider-patient communication, greatly outweigh such risks.
“This is about convenience – a bit like online banking,” commented Charlotte Blease, PhD, resident scholar at OpenNotes, an advocacy nonprofit organization headquartered at the Beth Israel–Deaconess Medical Center in Boston. “But it’s a culture shift for doctors,” she said in an interview.
“It turns physician paternalism on its head,” said C. T. Lin, MD, chief medical information officer, UCHealth, Denver. The change requires “some letting go of old traditions” in medicine, he wrote in an August blog post, referring to the fact that a computer screen – and not a physician – may tell patients about a new health problem.
Dr. Lin summarized the experience at the University of Colorado Cancer Center, which has allowed patients to have access to oncology notes for the past 5 years: “No issues and highly appreciated by patients. We have nothing to fear but fear itself.”
A new audience
Other institutions have also been voluntarily implementing open notes.
UC Davis Health in Sacramento, Calif., has run an optional program for the past year. However, only about two dozen of approximately 1,000 staff physicians opted in to the program.
“This illustrates the point that it’s a new thing that physicians aren’t used to doing. They’ve traditionally written notes for the benefit of their colleagues, for billing, for their own reference,” Scott MacDonald, MD, an internist and electronic health record medical director at UC Davis Health, told this news organization.
“They’ve never –until recently – had the patient as one of the audiences for a note,” he said.
Liam Keating, MD, an otolaryngologist in Martinez, Calif., recalls that he once wrote “globus hystericus,” and the patient wanted to sue him for saying that the patient was hysterical. “I now just code ‘Globus’ (if I don’t jump straight to LPD [lateral pharyngeal diverticulum]),” he commented in response to a commentary on open notes.
Sensitive information occurs more often in certain specialties, for example, psychiatry, genetics, adolescent medicine, and oncology, experts say.
“Cancer is an area that is highly charged for patients and doctors alike,” Dr. MacDonald pointed out. When reading pathology or imaging notes, patients may learn that they have been diagnosed with cancer or that they have a recurrence “without the physician being able to contextualize it and explain things – that’s just new and scary,” he said.
California law dictates that providers cannot post cancer test results without talking with the patient first, said Dr. MacDonald, but not all states have such laws.
Adjustments needed – or not – with open notes
At UCHealth in Aurora, Colo., Robert Breeze, MD, vice-chair of neurosurgery, said he has adjusted his practice to accommodate open notes and to anticipate trouble spots.*
“When I order imaging or send pathology specimens, I have already discussed with the patient the possibilities, including cancer, and what we will do next. Patients deeply appreciate these discussions, before they see the results,” he commented in an institutional white paper issued in anticipation of the changes on Nov. 2.
This is called precounseling, said Trent Rosenbloom, MD, MPH, director of patient portals at Vanderbilt University Medical Center, Nashville, Tenn., which has been a pioneer in information sharing with patients. Their system does delay the release of information in the case of “complicated” results, such as from cancer biopsies, he said in an interview.
However, Christiaan Hoff, MD, PhD, a surgeon at the Medical Center Leeuwarden (the Netherlands), wonders how important it is for the physician to be present when the patient receives bad news, including news about cancer. “We may overestimate our added value in these situations,” he suggested.
“Our empathy may not outweigh” the disadvantages of the situation, and the “finer points of our explanation will often go unnoticed” by the stressed patient, he commented. Dr. Hoff was also responding to the commentary about open notes.
In that commentary, Jack West, MD, a medical oncologist at City of Hope Cancer Center, Duarte, Calif., was concerned about misunderstandings. Oncology is complex, and patients can struggle to understand their prognosis and planned treatment efficacy, especially in cases of metastatic disease, he wrote.
This concern is somewhat refuted by a study published Oct. 5 in Cancer Cell. Responses to two surveys involving 96 oncology clinicians at three U.S. centers found that almost half (44%) believed that their patients “would be confused” by open notes.
However, only 4% of the 3,418 cancer patients from the same surveys reported being confused by open notes. (A majority of participants had more than a high school education, and English was their primary language.)
“Patient and clinician views about open notes in oncology are not aligned, with patients expressing considerably more enthusiasm,” wrote the authors, led by Liz Salmi, senior strategist at OpenNotes, who has been treated for brain cancer.
“All clinicians are anxious at first,” Ms. Salmi told this news organization. “Those patients who have more serious or chronic conditions … are more likely to read their notes.”
The survey results echo the early experience reported from Sweden, where open notes was launched in 2012. “Patients have loved it from the beginning,” said Maria Haggland, PhD, of Uppsala MedTech Science Innovation Center.
However, when the scheme first launched, it was considered to be “very controversial,” and “there were a lot of complaints, from health care professionals, especially,” she added.
Over time, clinicians have embraced open notes, and the program has 7.2 million patient accounts in a country of 10 million people, she observed during an Oct. 5 webinar on open notes.
More work for already overworked clinicians?
An outstanding concern about open notes is that it will cause more work for health care professionals.
Traditionally, doctors have written notes using medical lexicon, including a lot of abbreviations and jargon for efficiency’s sake. Now that patients will read the notes, will clinicians have to spell out things in lay terms, alter their writing so as not to offend, and generally do more work?
William Harvey, MD, chief medical information officer, Tufts Medical Center, Boston, acknowledged that that may be the case.
In a forthcoming note to staff about the Nov. 2 start of open notes, Dr. Harvey will include a reminder to accommodate the patient as a reader. But that may or may not mean an increase in work volume, depending on the provider. “Clinical note writing is highly personal. There’s an art to it,” he said in an interview. “So it’s hard to give standard advice.”
Steven Reidbord, MD, a psychiatrist in private practice in San Francisco and a lecturer at California Pacific Medical Center, is particularly concerned about the impact of open notes on progress notes, which he calls a tool to develop strategies and make observations while working with a patient.
By watering down the language for patients, “you are trading away the technical precision and other advantages of having a professional language,” he told this news organization.
“These notes serve many masters already,” he said, referring to purposes such as utilization review and billing. “The more masters they serve, the less useful they are to get medical work done.”
Dr. MacDonald, the medical information officer, said the new law doesn’t mandate a change in writing style.
In a study published last year, researchers analyzed notes written by oncologists before and after adoption of open notes. They found that, on average, clinicians did not change their note writing. The investigators analyzed more than 100,000 clinical notes written by 35 oncologists at a single center.
Advocates for open notes emphasize that there are benefits for clinicians.
“Doctors are overworked. They’re overburdened. But empowered patients can help the doctor,” said OpenNotes’ Dr. Blease. She cited survey data that show that patients better understand their treatment plan and medication, which can cut down on physician workload.
Open notes are “what you make of it,” said Marlene Millen, MD, an internist at UC San Diego Health, which has had a pilot program for 3 years. Each day, Dr. Millen discusses a shared note with two or three patients. “I actually end all of my appointments with, ‘Don’t forget to read your note later,’ ” she told this news organization.
“I was a little afraid of this initially,” she said, but within the first 3 months of the pilot, about 15 patients gave her direct feedback on how much they appreciated her notes. “It seemed to really reassure them that they were getting good care.”
The persons quoted in this article have disclosed no relevant financial relationships.
Correction, 10/23/20: An earlier version of this article misstated the campus' location.
A version of this article originally appeared on Medscape.com.
Starting Nov. 2, all patients in the United States will have immediate access to clinical notes and thus will be able to read their doctors’ writings, as well as test results and reports from pathology and imaging.
The 21st Century Cures Act mandates that patients have fast, electronic access to the following types of notes: consultations, discharge summaries, history, physical examination findings, imaging narratives, laboratory and pathology report narratives, and procedure and progress notes.
But this federal mandate, called “open notes” by many, is potentially confusing and frightening for patients, say some physicians. Others worry that the change will increase workload as clinicians tailor notes for patients and answer related questions.
The law means that inpatient and outpatient notes will be released immediately and that patients will have immediate access to testing and imaging results, including results from sexually transmitted disease tests, Pap tests, cancer biopsies, CT and PET scans, fetal ultrasounds, pneumonia cultures, and mammograms.
Such notes could contain sensitive information, and there is concern that patients could be shocked, confused, or annoyed by what they read, even with more run-of-the-mill notes.
Champions of open notes say that the benefits, including better provider-patient communication, greatly outweigh such risks.
“This is about convenience – a bit like online banking,” commented Charlotte Blease, PhD, resident scholar at OpenNotes, an advocacy nonprofit organization headquartered at the Beth Israel–Deaconess Medical Center in Boston. “But it’s a culture shift for doctors,” she said in an interview.
“It turns physician paternalism on its head,” said C. T. Lin, MD, chief medical information officer, UCHealth, Denver. The change requires “some letting go of old traditions” in medicine, he wrote in an August blog post, referring to the fact that a computer screen – and not a physician – may tell patients about a new health problem.
Dr. Lin summarized the experience at the University of Colorado Cancer Center, which has allowed patients to have access to oncology notes for the past 5 years: “No issues and highly appreciated by patients. We have nothing to fear but fear itself.”
A new audience
Other institutions have also been voluntarily implementing open notes.
UC Davis Health in Sacramento, Calif., has run an optional program for the past year. However, only about two dozen of approximately 1,000 staff physicians opted in to the program.
“This illustrates the point that it’s a new thing that physicians aren’t used to doing. They’ve traditionally written notes for the benefit of their colleagues, for billing, for their own reference,” Scott MacDonald, MD, an internist and electronic health record medical director at UC Davis Health, told this news organization.
“They’ve never –until recently – had the patient as one of the audiences for a note,” he said.
Liam Keating, MD, an otolaryngologist in Martinez, Calif., recalls that he once wrote “globus hystericus,” and the patient wanted to sue him for saying that the patient was hysterical. “I now just code ‘Globus’ (if I don’t jump straight to LPD [lateral pharyngeal diverticulum]),” he commented in response to a commentary on open notes.
Sensitive information occurs more often in certain specialties, for example, psychiatry, genetics, adolescent medicine, and oncology, experts say.
“Cancer is an area that is highly charged for patients and doctors alike,” Dr. MacDonald pointed out. When reading pathology or imaging notes, patients may learn that they have been diagnosed with cancer or that they have a recurrence “without the physician being able to contextualize it and explain things – that’s just new and scary,” he said.
California law dictates that providers cannot post cancer test results without talking with the patient first, said Dr. MacDonald, but not all states have such laws.
Adjustments needed – or not – with open notes
At UCHealth in Aurora, Colo., Robert Breeze, MD, vice-chair of neurosurgery, said he has adjusted his practice to accommodate open notes and to anticipate trouble spots.*
“When I order imaging or send pathology specimens, I have already discussed with the patient the possibilities, including cancer, and what we will do next. Patients deeply appreciate these discussions, before they see the results,” he commented in an institutional white paper issued in anticipation of the changes on Nov. 2.
This is called precounseling, said Trent Rosenbloom, MD, MPH, director of patient portals at Vanderbilt University Medical Center, Nashville, Tenn., which has been a pioneer in information sharing with patients. Their system does delay the release of information in the case of “complicated” results, such as from cancer biopsies, he said in an interview.
However, Christiaan Hoff, MD, PhD, a surgeon at the Medical Center Leeuwarden (the Netherlands), wonders how important it is for the physician to be present when the patient receives bad news, including news about cancer. “We may overestimate our added value in these situations,” he suggested.
“Our empathy may not outweigh” the disadvantages of the situation, and the “finer points of our explanation will often go unnoticed” by the stressed patient, he commented. Dr. Hoff was also responding to the commentary about open notes.
In that commentary, Jack West, MD, a medical oncologist at City of Hope Cancer Center, Duarte, Calif., was concerned about misunderstandings. Oncology is complex, and patients can struggle to understand their prognosis and planned treatment efficacy, especially in cases of metastatic disease, he wrote.
This concern is somewhat refuted by a study published Oct. 5 in Cancer Cell. Responses to two surveys involving 96 oncology clinicians at three U.S. centers found that almost half (44%) believed that their patients “would be confused” by open notes.
However, only 4% of the 3,418 cancer patients from the same surveys reported being confused by open notes. (A majority of participants had more than a high school education, and English was their primary language.)
“Patient and clinician views about open notes in oncology are not aligned, with patients expressing considerably more enthusiasm,” wrote the authors, led by Liz Salmi, senior strategist at OpenNotes, who has been treated for brain cancer.
“All clinicians are anxious at first,” Ms. Salmi told this news organization. “Those patients who have more serious or chronic conditions … are more likely to read their notes.”
The survey results echo the early experience reported from Sweden, where open notes was launched in 2012. “Patients have loved it from the beginning,” said Maria Haggland, PhD, of Uppsala MedTech Science Innovation Center.
However, when the scheme first launched, it was considered to be “very controversial,” and “there were a lot of complaints, from health care professionals, especially,” she added.
Over time, clinicians have embraced open notes, and the program has 7.2 million patient accounts in a country of 10 million people, she observed during an Oct. 5 webinar on open notes.
More work for already overworked clinicians?
An outstanding concern about open notes is that it will cause more work for health care professionals.
Traditionally, doctors have written notes using medical lexicon, including a lot of abbreviations and jargon for efficiency’s sake. Now that patients will read the notes, will clinicians have to spell out things in lay terms, alter their writing so as not to offend, and generally do more work?
William Harvey, MD, chief medical information officer, Tufts Medical Center, Boston, acknowledged that that may be the case.
In a forthcoming note to staff about the Nov. 2 start of open notes, Dr. Harvey will include a reminder to accommodate the patient as a reader. But that may or may not mean an increase in work volume, depending on the provider. “Clinical note writing is highly personal. There’s an art to it,” he said in an interview. “So it’s hard to give standard advice.”
Steven Reidbord, MD, a psychiatrist in private practice in San Francisco and a lecturer at California Pacific Medical Center, is particularly concerned about the impact of open notes on progress notes, which he calls a tool to develop strategies and make observations while working with a patient.
By watering down the language for patients, “you are trading away the technical precision and other advantages of having a professional language,” he told this news organization.
“These notes serve many masters already,” he said, referring to purposes such as utilization review and billing. “The more masters they serve, the less useful they are to get medical work done.”
Dr. MacDonald, the medical information officer, said the new law doesn’t mandate a change in writing style.
In a study published last year, researchers analyzed notes written by oncologists before and after adoption of open notes. They found that, on average, clinicians did not change their note writing. The investigators analyzed more than 100,000 clinical notes written by 35 oncologists at a single center.
Advocates for open notes emphasize that there are benefits for clinicians.
“Doctors are overworked. They’re overburdened. But empowered patients can help the doctor,” said OpenNotes’ Dr. Blease. She cited survey data that show that patients better understand their treatment plan and medication, which can cut down on physician workload.
Open notes are “what you make of it,” said Marlene Millen, MD, an internist at UC San Diego Health, which has had a pilot program for 3 years. Each day, Dr. Millen discusses a shared note with two or three patients. “I actually end all of my appointments with, ‘Don’t forget to read your note later,’ ” she told this news organization.
“I was a little afraid of this initially,” she said, but within the first 3 months of the pilot, about 15 patients gave her direct feedback on how much they appreciated her notes. “It seemed to really reassure them that they were getting good care.”
The persons quoted in this article have disclosed no relevant financial relationships.
Correction, 10/23/20: An earlier version of this article misstated the campus' location.
A version of this article originally appeared on Medscape.com.
Starting Nov. 2, all patients in the United States will have immediate access to clinical notes and thus will be able to read their doctors’ writings, as well as test results and reports from pathology and imaging.
The 21st Century Cures Act mandates that patients have fast, electronic access to the following types of notes: consultations, discharge summaries, history, physical examination findings, imaging narratives, laboratory and pathology report narratives, and procedure and progress notes.
But this federal mandate, called “open notes” by many, is potentially confusing and frightening for patients, say some physicians. Others worry that the change will increase workload as clinicians tailor notes for patients and answer related questions.
The law means that inpatient and outpatient notes will be released immediately and that patients will have immediate access to testing and imaging results, including results from sexually transmitted disease tests, Pap tests, cancer biopsies, CT and PET scans, fetal ultrasounds, pneumonia cultures, and mammograms.
Such notes could contain sensitive information, and there is concern that patients could be shocked, confused, or annoyed by what they read, even with more run-of-the-mill notes.
Champions of open notes say that the benefits, including better provider-patient communication, greatly outweigh such risks.
“This is about convenience – a bit like online banking,” commented Charlotte Blease, PhD, resident scholar at OpenNotes, an advocacy nonprofit organization headquartered at the Beth Israel–Deaconess Medical Center in Boston. “But it’s a culture shift for doctors,” she said in an interview.
“It turns physician paternalism on its head,” said C. T. Lin, MD, chief medical information officer, UCHealth, Denver. The change requires “some letting go of old traditions” in medicine, he wrote in an August blog post, referring to the fact that a computer screen – and not a physician – may tell patients about a new health problem.
Dr. Lin summarized the experience at the University of Colorado Cancer Center, which has allowed patients to have access to oncology notes for the past 5 years: “No issues and highly appreciated by patients. We have nothing to fear but fear itself.”
A new audience
Other institutions have also been voluntarily implementing open notes.
UC Davis Health in Sacramento, Calif., has run an optional program for the past year. However, only about two dozen of approximately 1,000 staff physicians opted in to the program.
“This illustrates the point that it’s a new thing that physicians aren’t used to doing. They’ve traditionally written notes for the benefit of their colleagues, for billing, for their own reference,” Scott MacDonald, MD, an internist and electronic health record medical director at UC Davis Health, told this news organization.
“They’ve never –until recently – had the patient as one of the audiences for a note,” he said.
Liam Keating, MD, an otolaryngologist in Martinez, Calif., recalls that he once wrote “globus hystericus,” and the patient wanted to sue him for saying that the patient was hysterical. “I now just code ‘Globus’ (if I don’t jump straight to LPD [lateral pharyngeal diverticulum]),” he commented in response to a commentary on open notes.
Sensitive information occurs more often in certain specialties, for example, psychiatry, genetics, adolescent medicine, and oncology, experts say.
“Cancer is an area that is highly charged for patients and doctors alike,” Dr. MacDonald pointed out. When reading pathology or imaging notes, patients may learn that they have been diagnosed with cancer or that they have a recurrence “without the physician being able to contextualize it and explain things – that’s just new and scary,” he said.
California law dictates that providers cannot post cancer test results without talking with the patient first, said Dr. MacDonald, but not all states have such laws.
Adjustments needed – or not – with open notes
At UCHealth in Aurora, Colo., Robert Breeze, MD, vice-chair of neurosurgery, said he has adjusted his practice to accommodate open notes and to anticipate trouble spots.*
“When I order imaging or send pathology specimens, I have already discussed with the patient the possibilities, including cancer, and what we will do next. Patients deeply appreciate these discussions, before they see the results,” he commented in an institutional white paper issued in anticipation of the changes on Nov. 2.
This is called precounseling, said Trent Rosenbloom, MD, MPH, director of patient portals at Vanderbilt University Medical Center, Nashville, Tenn., which has been a pioneer in information sharing with patients. Their system does delay the release of information in the case of “complicated” results, such as from cancer biopsies, he said in an interview.
However, Christiaan Hoff, MD, PhD, a surgeon at the Medical Center Leeuwarden (the Netherlands), wonders how important it is for the physician to be present when the patient receives bad news, including news about cancer. “We may overestimate our added value in these situations,” he suggested.
“Our empathy may not outweigh” the disadvantages of the situation, and the “finer points of our explanation will often go unnoticed” by the stressed patient, he commented. Dr. Hoff was also responding to the commentary about open notes.
In that commentary, Jack West, MD, a medical oncologist at City of Hope Cancer Center, Duarte, Calif., was concerned about misunderstandings. Oncology is complex, and patients can struggle to understand their prognosis and planned treatment efficacy, especially in cases of metastatic disease, he wrote.
This concern is somewhat refuted by a study published Oct. 5 in Cancer Cell. Responses to two surveys involving 96 oncology clinicians at three U.S. centers found that almost half (44%) believed that their patients “would be confused” by open notes.
However, only 4% of the 3,418 cancer patients from the same surveys reported being confused by open notes. (A majority of participants had more than a high school education, and English was their primary language.)
“Patient and clinician views about open notes in oncology are not aligned, with patients expressing considerably more enthusiasm,” wrote the authors, led by Liz Salmi, senior strategist at OpenNotes, who has been treated for brain cancer.
“All clinicians are anxious at first,” Ms. Salmi told this news organization. “Those patients who have more serious or chronic conditions … are more likely to read their notes.”
The survey results echo the early experience reported from Sweden, where open notes was launched in 2012. “Patients have loved it from the beginning,” said Maria Haggland, PhD, of Uppsala MedTech Science Innovation Center.
However, when the scheme first launched, it was considered to be “very controversial,” and “there were a lot of complaints, from health care professionals, especially,” she added.
Over time, clinicians have embraced open notes, and the program has 7.2 million patient accounts in a country of 10 million people, she observed during an Oct. 5 webinar on open notes.
More work for already overworked clinicians?
An outstanding concern about open notes is that it will cause more work for health care professionals.
Traditionally, doctors have written notes using medical lexicon, including a lot of abbreviations and jargon for efficiency’s sake. Now that patients will read the notes, will clinicians have to spell out things in lay terms, alter their writing so as not to offend, and generally do more work?
William Harvey, MD, chief medical information officer, Tufts Medical Center, Boston, acknowledged that that may be the case.
In a forthcoming note to staff about the Nov. 2 start of open notes, Dr. Harvey will include a reminder to accommodate the patient as a reader. But that may or may not mean an increase in work volume, depending on the provider. “Clinical note writing is highly personal. There’s an art to it,” he said in an interview. “So it’s hard to give standard advice.”
Steven Reidbord, MD, a psychiatrist in private practice in San Francisco and a lecturer at California Pacific Medical Center, is particularly concerned about the impact of open notes on progress notes, which he calls a tool to develop strategies and make observations while working with a patient.
By watering down the language for patients, “you are trading away the technical precision and other advantages of having a professional language,” he told this news organization.
“These notes serve many masters already,” he said, referring to purposes such as utilization review and billing. “The more masters they serve, the less useful they are to get medical work done.”
Dr. MacDonald, the medical information officer, said the new law doesn’t mandate a change in writing style.
In a study published last year, researchers analyzed notes written by oncologists before and after adoption of open notes. They found that, on average, clinicians did not change their note writing. The investigators analyzed more than 100,000 clinical notes written by 35 oncologists at a single center.
Advocates for open notes emphasize that there are benefits for clinicians.
“Doctors are overworked. They’re overburdened. But empowered patients can help the doctor,” said OpenNotes’ Dr. Blease. She cited survey data that show that patients better understand their treatment plan and medication, which can cut down on physician workload.
Open notes are “what you make of it,” said Marlene Millen, MD, an internist at UC San Diego Health, which has had a pilot program for 3 years. Each day, Dr. Millen discusses a shared note with two or three patients. “I actually end all of my appointments with, ‘Don’t forget to read your note later,’ ” she told this news organization.
“I was a little afraid of this initially,” she said, but within the first 3 months of the pilot, about 15 patients gave her direct feedback on how much they appreciated her notes. “It seemed to really reassure them that they were getting good care.”
The persons quoted in this article have disclosed no relevant financial relationships.
Correction, 10/23/20: An earlier version of this article misstated the campus' location.
A version of this article originally appeared on Medscape.com.
Popularity of virtual conferences may mean a permanent shift
Fifteen days. That’s how much time the American College of Cardiology (ACC) had to convert its annual conference, scheduled for the end of March this year in Chicago, into a virtual meeting for the estimated 17,000 people who had planned to attend.
Because of the coronavirus pandemic, Illinois announced restrictions on the size of gatherings on March 13, causing the ACC to pivot to an online-only model.
“One big advantage was that we already had all of our content planned,” Janice Sibley, the ACC’s executive vice president of education, told Medscape Medical News. “We knew who the faculty would be for different sessions, and many of them had already planned their slides.”
But determining how to present those hundreds of presentations at an online conference, not to mention addressing the logistics related to registrations, tech platforms, exhibit hall sponsors, and other aspects of an annual meeting, would be no small task.
But according to a Medscape poll, many physicians think that, while the virtual experience is worthwhile and getting better, it’s never going to be the same as spending several days on site, immersed in the experience of an annual meeting.
As one respondent commented, “I miss the intellectual excitement, the electricity in the room, when there is a live presentation that announces a major breakthrough.”
Large medical societies have an advantage
As ACC rapidly prepared for its virtual conference, the society first refunded all registration and expo fees and worked with the vendor partners to resolve the cancellation of rental space, food and beverage services, and decorating. Then they organized a team of 15 people split into three groups. One group focused on the intellectual, scientific, and educational elements of the virtual conference. They chose 24 sessions to livestream and decided to prerecord the rest for on-demand access, limiting the number of presenters they needed to train for online presentation.
A second team focused on business and worked with industry partners on how to translate a large expo into digital offerings. They developed virtual pages, advertisements, promotions, and industry-sponsored education.
The third team’s focus, Ms. Sibley said, was most critical, and the hardest: addressing socio-emotional needs.
“That group was responsible for trying to create the buzz and excitement we would have had at the event,” she said, “pivoting that experience we would have had in a live event to a virtual environment. What we were worried about was, would anyone even come?”
But ACC built it, and they did indeed come. Within a half hour of the opening session, nearly 13,000 people logged on from around the world. “It worked beautifully,” Ms. Sibley said.
By the end of the 3-day event, approximately 34,000 unique visitors had logged in for live or prerecorded sessions. Although ACC worried at first about technical glitches and bandwidth needs, everything ran smoothly. By 90 days after the meeting, 63,000 unique users had logged in to access the conference content.
ACC was among the first organizations forced to switch from an in-person to all-online meeting, but dozens of other organizations have now done the same, discovering the benefits and drawbacks of a virtual environment while experimenting with different formats and offerings. Talks with a few large medical societies about the experience revealed several common themes, including the following:
- Finding new ways to attract and measure attendance.
- Ensuring the actual scientific content was as robust online as in person.
- Realizing the value of social media in enhancing the socio-emotional experience.
- Believing that virtual meetings will become a permanent fixture in a future of “hybrid” conferences.
New ways of attracting and measuring attendance
Previous ways to measure meeting attendance were straightforward: number of registrations and number of people physically walking into sessions. An online conference, however, offers dozens of ways to measure attendance. While the number of registrations remained one tool – and all the organizations interviewed reported record numbers of registrations – organizations also used other metrics to measure success, such as “participation,” “engagement,” and “viewing time.”
ACC defined “participation” as a unique user logging in, and it defined “engagement” as sticking around for a while, possibly using chat functions or discussing the content on social media. The American Society of Clinical Oncology (ASCO) annual conference in May, which attracted more than 44,000 registered attendees, also measured total content views – more than 2.5 million during the meeting – and monitored social media. More than 8,800 Twitter users posted more than 45,000 tweets with the #ASCO20 hashtag during the meeting, generating 750 million likes, shares, and comments. The European League Against Rheumatism (EULAR) annual congress registered a record 18,700 delegates – up from 14,500 in 2019 – but it also measured attendance by average viewing time and visits by congress day and by category.
Organizations shifted fee structures as well. While ACC refunded fees for its first online meeting, it has since developed tiers to match fees to anticipated value, such as charging more for livestreamed sessions that allow interactivity than for viewing recordings. ASCO offered a one-time fee waiver for members plus free registration to cancer survivors and caregivers, discounted registration for patient advocates, and reduced fees for other categories. But adjusting how to measure attendance and charge for events were the easy parts of transitioning to online.
Priority for having robust content
The biggest difficulty for most organizations was the short time they had to move online, with a host of challenges accompanying the switch, said the executive director of EULAR, Julia Rautenstrauch, DrMed. These included technical requirements, communication, training, finances, legal issues, compliance rules, and other logistics.
“The year 2020 will be remembered for being the year of unexpected transformation,” said a spokesperson from European Society for Medical Oncology (ESMO), who declined to be named. “The number of fundamental questions we had to ask ourselves is pages long. The solutions we have implemented so far have been successful, but we won’t rest on our laurels.”
ASCO had an advantage in the pivot, despite only 6 weeks to make the switch, because they already had a robust online platform to build on. “We weren’t starting from scratch, but we were sure changing the way we prepared,” ASCO CEO Clifford Hudis, MD, said.
All of the organizations made the breadth and quality of scientific and educational content a top priority, and those who have already hosted meetings this year report positive feedback.
“The rating of the scientific content was excellent, and the event did indeed fulfill the educational goals and expected learning outcomes for the vast majority of delegates,” EULAR’s Dr. Rautenstrauch said.
“Our goal, when we went into this, was that, in the future when somebody looks back at ASCO20, they should not be able to tell that it was a different year from any other in terms of the science,” Dr. Hudis said.
Missing out on networking and social interaction
Even when logistics run smoothly, virtual conferences must overcome two other challenges: the loss of in-person interactions and the potential for “Zoom burnout.”
“You do miss that human contact, the unsaid reactions in the room when you’re speaking or providing a controversial statement, even the facial expression or seeing people lean in or being distracted,” Ms. Sibley said.
Taher Modarressi, MD, an endocrinologist with Diabetes and Endocrine Associates of Hunterdon in Flemington, N.J., said all the digital conferences he has attended were missing those key social elements: “seeing old friends, sideline discussions that generate new ideas, and meeting new colleagues. However, this has been partly alleviated with the robust rise of social media and ‘MedTwitter,’ in particular, where these discussions and interactions continue.”
To attempt to meet that need for social interaction, societies came up with a variety of options. EULAR offered chatrooms, “Meet the Expert” sessions, and other virtual opportunities for live interaction. ASCO hosted discussion groups with subsets of participants, such as virtual meetings with oncology fellows, and it plans to offer networking sessions and “poster walks” during future meetings.
“The value of an in-person meeting is connecting with people, exchanging ideas over coffee, and making new contacts,” ASCO’s Dr. Hudis said. While virtual meetings lose many of those personal interactions, knowledge can also be shared with more people, he said.
The key to combating digital fatigue is focusing on opportunities for interactivity, ACC’s Ms. Sibley said. “When you are creating a virtual environment, it’s important that you offer choices.” Online learners tend to have shorter attention spans than in-person learners, so people need opportunities to flip between sessions, like flipping between TV channels. Different engagement options are also essential, such as chat functions on the video platforms, asking questions of presenters orally or in writing, and using the familiar hashtags for social media discussion.
“We set up all those different ways to interact, and you allow the user to choose,” Ms. Sibley said.
Some conferences, however, had less time or fewer resources to adjust to a virtual format and couldn’t make up for the lost social interaction. Andy Bowman, MD, a neonatologist in Lubbock, Tex., was supposed to attend the Neonatal & Pediatric Airborne Transport Conference sponsored by International Biomed in the spring, but it was canceled at the last minute. Several weeks later, the organizers released videos of scheduled speakers giving their talks, but it was less engaging and too easy to get distracted, Dr. Bowman said.
“There is a noticeable decrease in energy – you can’t look around to feed off other’s reactions when a speaker says something off the wall, or new, or contrary to expectations,” he said. He also especially missed the social interactions, such as “missing out on the chance encounters in the hallway or seeing the same face in back-to-back sessions and figuring out you have shared interest.” He was also sorry to miss the expo because neonatal transport requires a lot of specialty equipment, and he appreciates the chance to actually touch and see it in person.
Advantages of an online meeting
Despite the challenges, online meetings can overcome obstacles of in-person meetings, particularly for those in low- and middle-income countries, such as travel and registration costs, the hardships of being away from practice, and visa restrictions.
“You really have the potential to broaden your reach,” Ms. Sibley said, noting that people in 157 countries participated in ACC.20.
Another advantage is keeping the experience available to people after the livestreamed event.
“Virtual events have demonstrated the potential for a more democratic conference world, expanding the dissemination of information to a much wider community of stakeholders,” ESMO’s spokesperson said.
Not traveling can actually mean getting more out of the conference, said Atisha Patel Manhas, MD, a hematologist/oncologist in Dallas, who attended ASCO. “I have really enjoyed the access aspect – on the virtual platform there is so much more content available to you, and travel time doesn’t cut into conference time,” she said, though she also missed the interaction with colleagues.
Others found that virtual conferences provided more engagement than in-person conferences. Marwah Abdalla, MD, MPH, an assistant professor of medicine and director of education for the Cardiac Intensive Care Unit at Columbia University Medical Center, New York, felt that moderated Q&A sessions offered more interaction among participants. She attended and spoke on a panel during virtual SLEEP 2020, a joint meeting of the American Academy of Sleep Medicine (AASM) and the Sleep Research Society (SRS).
“Usually during in-person sessions, only a few questions are possible, and participants rarely have an opportunity to discuss the presentations within the session due to time limits,” Dr. Abdalla said. “Because the conference presentations can also be viewed asynchronously, participants have been able to comment on lectures and continue the discussion offline, either via social media or via email.” She acknowledged drawbacks of the virtual experience, such as an inability to socialize in person and participate in activities but appreciated the new opportunities to network and learn from international colleagues who would not have been able to attend in person.
Ritu Thamman, MD, assistant professor of medicine at the University of Pittsburgh School of Medicine, pointed out that many institutions have cut their travel budgets, and physicians would be unable to attend in-person conferences for financial or other reasons. She especially appreciated that the European Society of Cardiology had no registration fee for ESC 2020 and made their content free for all of September, which led to more than 100,000 participants.
“That meant anyone anywhere could learn,” she said. “It makes it much more diverse and more egalitarian. That feels like a good step in the right direction for all of us.”
Dr. Modarressi, who found ESC “exhilarating,” similarly noted the benefit of such an equitably accessible conference. “Decreasing barriers and improving access to top-line results and up-to-date information has always been a challenge to the global health community,” he said, noting that the map of attendance for the virtual meeting was “astonishing.”
Given these benefits, organizers said they expect a future of hybrid conferences: physical meetings for those able to attend in person and virtual ones for those who cannot.
“We also expect that the hybrid congress will cater to the needs of people on-site by allowing them additional access to more scientific content than by physical attendance alone,” Dr. Rautenstrauch said.
Everyone has been in reactive mode this year, Ms. Sibley said, but the future looks bright as they seek ways to overcome challenges such as socio-emotional needs and virtual expo spaces.
“We’ve been thrust into the virtual world much faster than we expected, but we’re finding it’s opening more opportunities than we had live,” Ms. Sibley said. “This has catapulted us, for better or worse, into a new way to deliver education and other types of information.
“I think, if we’re smart, we’ll continue to think of ways this can augment our live environment and not replace it.”
A version of this article originally appeared on Medscape.com.
Fifteen days. That’s how much time the American College of Cardiology (ACC) had to convert its annual conference, scheduled for the end of March this year in Chicago, into a virtual meeting for the estimated 17,000 people who had planned to attend.
Because of the coronavirus pandemic, Illinois announced restrictions on the size of gatherings on March 13, causing the ACC to pivot to an online-only model.
“One big advantage was that we already had all of our content planned,” Janice Sibley, the ACC’s executive vice president of education, told Medscape Medical News. “We knew who the faculty would be for different sessions, and many of them had already planned their slides.”
But determining how to present those hundreds of presentations at an online conference, not to mention addressing the logistics related to registrations, tech platforms, exhibit hall sponsors, and other aspects of an annual meeting, would be no small task.
But according to a Medscape poll, many physicians think that, while the virtual experience is worthwhile and getting better, it’s never going to be the same as spending several days on site, immersed in the experience of an annual meeting.
As one respondent commented, “I miss the intellectual excitement, the electricity in the room, when there is a live presentation that announces a major breakthrough.”
Large medical societies have an advantage
As ACC rapidly prepared for its virtual conference, the society first refunded all registration and expo fees and worked with the vendor partners to resolve the cancellation of rental space, food and beverage services, and decorating. Then they organized a team of 15 people split into three groups. One group focused on the intellectual, scientific, and educational elements of the virtual conference. They chose 24 sessions to livestream and decided to prerecord the rest for on-demand access, limiting the number of presenters they needed to train for online presentation.
A second team focused on business and worked with industry partners on how to translate a large expo into digital offerings. They developed virtual pages, advertisements, promotions, and industry-sponsored education.
The third team’s focus, Ms. Sibley said, was most critical, and the hardest: addressing socio-emotional needs.
“That group was responsible for trying to create the buzz and excitement we would have had at the event,” she said, “pivoting that experience we would have had in a live event to a virtual environment. What we were worried about was, would anyone even come?”
But ACC built it, and they did indeed come. Within a half hour of the opening session, nearly 13,000 people logged on from around the world. “It worked beautifully,” Ms. Sibley said.
By the end of the 3-day event, approximately 34,000 unique visitors had logged in for live or prerecorded sessions. Although ACC worried at first about technical glitches and bandwidth needs, everything ran smoothly. By 90 days after the meeting, 63,000 unique users had logged in to access the conference content.
ACC was among the first organizations forced to switch from an in-person to all-online meeting, but dozens of other organizations have now done the same, discovering the benefits and drawbacks of a virtual environment while experimenting with different formats and offerings. Talks with a few large medical societies about the experience revealed several common themes, including the following:
- Finding new ways to attract and measure attendance.
- Ensuring the actual scientific content was as robust online as in person.
- Realizing the value of social media in enhancing the socio-emotional experience.
- Believing that virtual meetings will become a permanent fixture in a future of “hybrid” conferences.
New ways of attracting and measuring attendance
Previous ways to measure meeting attendance were straightforward: number of registrations and number of people physically walking into sessions. An online conference, however, offers dozens of ways to measure attendance. While the number of registrations remained one tool – and all the organizations interviewed reported record numbers of registrations – organizations also used other metrics to measure success, such as “participation,” “engagement,” and “viewing time.”
ACC defined “participation” as a unique user logging in, and it defined “engagement” as sticking around for a while, possibly using chat functions or discussing the content on social media. The American Society of Clinical Oncology (ASCO) annual conference in May, which attracted more than 44,000 registered attendees, also measured total content views – more than 2.5 million during the meeting – and monitored social media. More than 8,800 Twitter users posted more than 45,000 tweets with the #ASCO20 hashtag during the meeting, generating 750 million likes, shares, and comments. The European League Against Rheumatism (EULAR) annual congress registered a record 18,700 delegates – up from 14,500 in 2019 – but it also measured attendance by average viewing time and visits by congress day and by category.
Organizations shifted fee structures as well. While ACC refunded fees for its first online meeting, it has since developed tiers to match fees to anticipated value, such as charging more for livestreamed sessions that allow interactivity than for viewing recordings. ASCO offered a one-time fee waiver for members plus free registration to cancer survivors and caregivers, discounted registration for patient advocates, and reduced fees for other categories. But adjusting how to measure attendance and charge for events were the easy parts of transitioning to online.
Priority for having robust content
The biggest difficulty for most organizations was the short time they had to move online, with a host of challenges accompanying the switch, said the executive director of EULAR, Julia Rautenstrauch, DrMed. These included technical requirements, communication, training, finances, legal issues, compliance rules, and other logistics.
“The year 2020 will be remembered for being the year of unexpected transformation,” said a spokesperson from European Society for Medical Oncology (ESMO), who declined to be named. “The number of fundamental questions we had to ask ourselves is pages long. The solutions we have implemented so far have been successful, but we won’t rest on our laurels.”
ASCO had an advantage in the pivot, despite only 6 weeks to make the switch, because they already had a robust online platform to build on. “We weren’t starting from scratch, but we were sure changing the way we prepared,” ASCO CEO Clifford Hudis, MD, said.
All of the organizations made the breadth and quality of scientific and educational content a top priority, and those who have already hosted meetings this year report positive feedback.
“The rating of the scientific content was excellent, and the event did indeed fulfill the educational goals and expected learning outcomes for the vast majority of delegates,” EULAR’s Dr. Rautenstrauch said.
“Our goal, when we went into this, was that, in the future when somebody looks back at ASCO20, they should not be able to tell that it was a different year from any other in terms of the science,” Dr. Hudis said.
Missing out on networking and social interaction
Even when logistics run smoothly, virtual conferences must overcome two other challenges: the loss of in-person interactions and the potential for “Zoom burnout.”
“You do miss that human contact, the unsaid reactions in the room when you’re speaking or providing a controversial statement, even the facial expression or seeing people lean in or being distracted,” Ms. Sibley said.
Taher Modarressi, MD, an endocrinologist with Diabetes and Endocrine Associates of Hunterdon in Flemington, N.J., said all the digital conferences he has attended were missing those key social elements: “seeing old friends, sideline discussions that generate new ideas, and meeting new colleagues. However, this has been partly alleviated with the robust rise of social media and ‘MedTwitter,’ in particular, where these discussions and interactions continue.”
To attempt to meet that need for social interaction, societies came up with a variety of options. EULAR offered chatrooms, “Meet the Expert” sessions, and other virtual opportunities for live interaction. ASCO hosted discussion groups with subsets of participants, such as virtual meetings with oncology fellows, and it plans to offer networking sessions and “poster walks” during future meetings.
“The value of an in-person meeting is connecting with people, exchanging ideas over coffee, and making new contacts,” ASCO’s Dr. Hudis said. While virtual meetings lose many of those personal interactions, knowledge can also be shared with more people, he said.
The key to combating digital fatigue is focusing on opportunities for interactivity, ACC’s Ms. Sibley said. “When you are creating a virtual environment, it’s important that you offer choices.” Online learners tend to have shorter attention spans than in-person learners, so people need opportunities to flip between sessions, like flipping between TV channels. Different engagement options are also essential, such as chat functions on the video platforms, asking questions of presenters orally or in writing, and using the familiar hashtags for social media discussion.
“We set up all those different ways to interact, and you allow the user to choose,” Ms. Sibley said.
Some conferences, however, had less time or fewer resources to adjust to a virtual format and couldn’t make up for the lost social interaction. Andy Bowman, MD, a neonatologist in Lubbock, Tex., was supposed to attend the Neonatal & Pediatric Airborne Transport Conference sponsored by International Biomed in the spring, but it was canceled at the last minute. Several weeks later, the organizers released videos of scheduled speakers giving their talks, but it was less engaging and too easy to get distracted, Dr. Bowman said.
“There is a noticeable decrease in energy – you can’t look around to feed off other’s reactions when a speaker says something off the wall, or new, or contrary to expectations,” he said. He also especially missed the social interactions, such as “missing out on the chance encounters in the hallway or seeing the same face in back-to-back sessions and figuring out you have shared interest.” He was also sorry to miss the expo because neonatal transport requires a lot of specialty equipment, and he appreciates the chance to actually touch and see it in person.
Advantages of an online meeting
Despite the challenges, online meetings can overcome obstacles of in-person meetings, particularly for those in low- and middle-income countries, such as travel and registration costs, the hardships of being away from practice, and visa restrictions.
“You really have the potential to broaden your reach,” Ms. Sibley said, noting that people in 157 countries participated in ACC.20.
Another advantage is keeping the experience available to people after the livestreamed event.
“Virtual events have demonstrated the potential for a more democratic conference world, expanding the dissemination of information to a much wider community of stakeholders,” ESMO’s spokesperson said.
Not traveling can actually mean getting more out of the conference, said Atisha Patel Manhas, MD, a hematologist/oncologist in Dallas, who attended ASCO. “I have really enjoyed the access aspect – on the virtual platform there is so much more content available to you, and travel time doesn’t cut into conference time,” she said, though she also missed the interaction with colleagues.
Others found that virtual conferences provided more engagement than in-person conferences. Marwah Abdalla, MD, MPH, an assistant professor of medicine and director of education for the Cardiac Intensive Care Unit at Columbia University Medical Center, New York, felt that moderated Q&A sessions offered more interaction among participants. She attended and spoke on a panel during virtual SLEEP 2020, a joint meeting of the American Academy of Sleep Medicine (AASM) and the Sleep Research Society (SRS).
“Usually during in-person sessions, only a few questions are possible, and participants rarely have an opportunity to discuss the presentations within the session due to time limits,” Dr. Abdalla said. “Because the conference presentations can also be viewed asynchronously, participants have been able to comment on lectures and continue the discussion offline, either via social media or via email.” She acknowledged drawbacks of the virtual experience, such as an inability to socialize in person and participate in activities but appreciated the new opportunities to network and learn from international colleagues who would not have been able to attend in person.
Ritu Thamman, MD, assistant professor of medicine at the University of Pittsburgh School of Medicine, pointed out that many institutions have cut their travel budgets, and physicians would be unable to attend in-person conferences for financial or other reasons. She especially appreciated that the European Society of Cardiology had no registration fee for ESC 2020 and made their content free for all of September, which led to more than 100,000 participants.
“That meant anyone anywhere could learn,” she said. “It makes it much more diverse and more egalitarian. That feels like a good step in the right direction for all of us.”
Dr. Modarressi, who found ESC “exhilarating,” similarly noted the benefit of such an equitably accessible conference. “Decreasing barriers and improving access to top-line results and up-to-date information has always been a challenge to the global health community,” he said, noting that the map of attendance for the virtual meeting was “astonishing.”
Given these benefits, organizers said they expect a future of hybrid conferences: physical meetings for those able to attend in person and virtual ones for those who cannot.
“We also expect that the hybrid congress will cater to the needs of people on-site by allowing them additional access to more scientific content than by physical attendance alone,” Dr. Rautenstrauch said.
Everyone has been in reactive mode this year, Ms. Sibley said, but the future looks bright as they seek ways to overcome challenges such as socio-emotional needs and virtual expo spaces.
“We’ve been thrust into the virtual world much faster than we expected, but we’re finding it’s opening more opportunities than we had live,” Ms. Sibley said. “This has catapulted us, for better or worse, into a new way to deliver education and other types of information.
“I think, if we’re smart, we’ll continue to think of ways this can augment our live environment and not replace it.”
A version of this article originally appeared on Medscape.com.
Fifteen days. That’s how much time the American College of Cardiology (ACC) had to convert its annual conference, scheduled for the end of March this year in Chicago, into a virtual meeting for the estimated 17,000 people who had planned to attend.
Because of the coronavirus pandemic, Illinois announced restrictions on the size of gatherings on March 13, causing the ACC to pivot to an online-only model.
“One big advantage was that we already had all of our content planned,” Janice Sibley, the ACC’s executive vice president of education, told Medscape Medical News. “We knew who the faculty would be for different sessions, and many of them had already planned their slides.”
But determining how to present those hundreds of presentations at an online conference, not to mention addressing the logistics related to registrations, tech platforms, exhibit hall sponsors, and other aspects of an annual meeting, would be no small task.
But according to a Medscape poll, many physicians think that, while the virtual experience is worthwhile and getting better, it’s never going to be the same as spending several days on site, immersed in the experience of an annual meeting.
As one respondent commented, “I miss the intellectual excitement, the electricity in the room, when there is a live presentation that announces a major breakthrough.”
Large medical societies have an advantage
As ACC rapidly prepared for its virtual conference, the society first refunded all registration and expo fees and worked with the vendor partners to resolve the cancellation of rental space, food and beverage services, and decorating. Then they organized a team of 15 people split into three groups. One group focused on the intellectual, scientific, and educational elements of the virtual conference. They chose 24 sessions to livestream and decided to prerecord the rest for on-demand access, limiting the number of presenters they needed to train for online presentation.
A second team focused on business and worked with industry partners on how to translate a large expo into digital offerings. They developed virtual pages, advertisements, promotions, and industry-sponsored education.
The third team’s focus, Ms. Sibley said, was most critical, and the hardest: addressing socio-emotional needs.
“That group was responsible for trying to create the buzz and excitement we would have had at the event,” she said, “pivoting that experience we would have had in a live event to a virtual environment. What we were worried about was, would anyone even come?”
But ACC built it, and they did indeed come. Within a half hour of the opening session, nearly 13,000 people logged on from around the world. “It worked beautifully,” Ms. Sibley said.
By the end of the 3-day event, approximately 34,000 unique visitors had logged in for live or prerecorded sessions. Although ACC worried at first about technical glitches and bandwidth needs, everything ran smoothly. By 90 days after the meeting, 63,000 unique users had logged in to access the conference content.
ACC was among the first organizations forced to switch from an in-person to all-online meeting, but dozens of other organizations have now done the same, discovering the benefits and drawbacks of a virtual environment while experimenting with different formats and offerings. Talks with a few large medical societies about the experience revealed several common themes, including the following:
- Finding new ways to attract and measure attendance.
- Ensuring the actual scientific content was as robust online as in person.
- Realizing the value of social media in enhancing the socio-emotional experience.
- Believing that virtual meetings will become a permanent fixture in a future of “hybrid” conferences.
New ways of attracting and measuring attendance
Previous ways to measure meeting attendance were straightforward: number of registrations and number of people physically walking into sessions. An online conference, however, offers dozens of ways to measure attendance. While the number of registrations remained one tool – and all the organizations interviewed reported record numbers of registrations – organizations also used other metrics to measure success, such as “participation,” “engagement,” and “viewing time.”
ACC defined “participation” as a unique user logging in, and it defined “engagement” as sticking around for a while, possibly using chat functions or discussing the content on social media. The American Society of Clinical Oncology (ASCO) annual conference in May, which attracted more than 44,000 registered attendees, also measured total content views – more than 2.5 million during the meeting – and monitored social media. More than 8,800 Twitter users posted more than 45,000 tweets with the #ASCO20 hashtag during the meeting, generating 750 million likes, shares, and comments. The European League Against Rheumatism (EULAR) annual congress registered a record 18,700 delegates – up from 14,500 in 2019 – but it also measured attendance by average viewing time and visits by congress day and by category.
Organizations shifted fee structures as well. While ACC refunded fees for its first online meeting, it has since developed tiers to match fees to anticipated value, such as charging more for livestreamed sessions that allow interactivity than for viewing recordings. ASCO offered a one-time fee waiver for members plus free registration to cancer survivors and caregivers, discounted registration for patient advocates, and reduced fees for other categories. But adjusting how to measure attendance and charge for events were the easy parts of transitioning to online.
Priority for having robust content
The biggest difficulty for most organizations was the short time they had to move online, with a host of challenges accompanying the switch, said the executive director of EULAR, Julia Rautenstrauch, DrMed. These included technical requirements, communication, training, finances, legal issues, compliance rules, and other logistics.
“The year 2020 will be remembered for being the year of unexpected transformation,” said a spokesperson from European Society for Medical Oncology (ESMO), who declined to be named. “The number of fundamental questions we had to ask ourselves is pages long. The solutions we have implemented so far have been successful, but we won’t rest on our laurels.”
ASCO had an advantage in the pivot, despite only 6 weeks to make the switch, because they already had a robust online platform to build on. “We weren’t starting from scratch, but we were sure changing the way we prepared,” ASCO CEO Clifford Hudis, MD, said.
All of the organizations made the breadth and quality of scientific and educational content a top priority, and those who have already hosted meetings this year report positive feedback.
“The rating of the scientific content was excellent, and the event did indeed fulfill the educational goals and expected learning outcomes for the vast majority of delegates,” EULAR’s Dr. Rautenstrauch said.
“Our goal, when we went into this, was that, in the future when somebody looks back at ASCO20, they should not be able to tell that it was a different year from any other in terms of the science,” Dr. Hudis said.
Missing out on networking and social interaction
Even when logistics run smoothly, virtual conferences must overcome two other challenges: the loss of in-person interactions and the potential for “Zoom burnout.”
“You do miss that human contact, the unsaid reactions in the room when you’re speaking or providing a controversial statement, even the facial expression or seeing people lean in or being distracted,” Ms. Sibley said.
Taher Modarressi, MD, an endocrinologist with Diabetes and Endocrine Associates of Hunterdon in Flemington, N.J., said all the digital conferences he has attended were missing those key social elements: “seeing old friends, sideline discussions that generate new ideas, and meeting new colleagues. However, this has been partly alleviated with the robust rise of social media and ‘MedTwitter,’ in particular, where these discussions and interactions continue.”
To attempt to meet that need for social interaction, societies came up with a variety of options. EULAR offered chatrooms, “Meet the Expert” sessions, and other virtual opportunities for live interaction. ASCO hosted discussion groups with subsets of participants, such as virtual meetings with oncology fellows, and it plans to offer networking sessions and “poster walks” during future meetings.
“The value of an in-person meeting is connecting with people, exchanging ideas over coffee, and making new contacts,” ASCO’s Dr. Hudis said. While virtual meetings lose many of those personal interactions, knowledge can also be shared with more people, he said.
The key to combating digital fatigue is focusing on opportunities for interactivity, ACC’s Ms. Sibley said. “When you are creating a virtual environment, it’s important that you offer choices.” Online learners tend to have shorter attention spans than in-person learners, so people need opportunities to flip between sessions, like flipping between TV channels. Different engagement options are also essential, such as chat functions on the video platforms, asking questions of presenters orally or in writing, and using the familiar hashtags for social media discussion.
“We set up all those different ways to interact, and you allow the user to choose,” Ms. Sibley said.
Some conferences, however, had less time or fewer resources to adjust to a virtual format and couldn’t make up for the lost social interaction. Andy Bowman, MD, a neonatologist in Lubbock, Tex., was supposed to attend the Neonatal & Pediatric Airborne Transport Conference sponsored by International Biomed in the spring, but it was canceled at the last minute. Several weeks later, the organizers released videos of scheduled speakers giving their talks, but it was less engaging and too easy to get distracted, Dr. Bowman said.
“There is a noticeable decrease in energy – you can’t look around to feed off other’s reactions when a speaker says something off the wall, or new, or contrary to expectations,” he said. He also especially missed the social interactions, such as “missing out on the chance encounters in the hallway or seeing the same face in back-to-back sessions and figuring out you have shared interest.” He was also sorry to miss the expo because neonatal transport requires a lot of specialty equipment, and he appreciates the chance to actually touch and see it in person.
Advantages of an online meeting
Despite the challenges, online meetings can overcome obstacles of in-person meetings, particularly for those in low- and middle-income countries, such as travel and registration costs, the hardships of being away from practice, and visa restrictions.
“You really have the potential to broaden your reach,” Ms. Sibley said, noting that people in 157 countries participated in ACC.20.
Another advantage is keeping the experience available to people after the livestreamed event.
“Virtual events have demonstrated the potential for a more democratic conference world, expanding the dissemination of information to a much wider community of stakeholders,” ESMO’s spokesperson said.
Not traveling can actually mean getting more out of the conference, said Atisha Patel Manhas, MD, a hematologist/oncologist in Dallas, who attended ASCO. “I have really enjoyed the access aspect – on the virtual platform there is so much more content available to you, and travel time doesn’t cut into conference time,” she said, though she also missed the interaction with colleagues.
Others found that virtual conferences provided more engagement than in-person conferences. Marwah Abdalla, MD, MPH, an assistant professor of medicine and director of education for the Cardiac Intensive Care Unit at Columbia University Medical Center, New York, felt that moderated Q&A sessions offered more interaction among participants. She attended and spoke on a panel during virtual SLEEP 2020, a joint meeting of the American Academy of Sleep Medicine (AASM) and the Sleep Research Society (SRS).
“Usually during in-person sessions, only a few questions are possible, and participants rarely have an opportunity to discuss the presentations within the session due to time limits,” Dr. Abdalla said. “Because the conference presentations can also be viewed asynchronously, participants have been able to comment on lectures and continue the discussion offline, either via social media or via email.” She acknowledged drawbacks of the virtual experience, such as an inability to socialize in person and participate in activities but appreciated the new opportunities to network and learn from international colleagues who would not have been able to attend in person.
Ritu Thamman, MD, assistant professor of medicine at the University of Pittsburgh School of Medicine, pointed out that many institutions have cut their travel budgets, and physicians would be unable to attend in-person conferences for financial or other reasons. She especially appreciated that the European Society of Cardiology had no registration fee for ESC 2020 and made their content free for all of September, which led to more than 100,000 participants.
“That meant anyone anywhere could learn,” she said. “It makes it much more diverse and more egalitarian. That feels like a good step in the right direction for all of us.”
Dr. Modarressi, who found ESC “exhilarating,” similarly noted the benefit of such an equitably accessible conference. “Decreasing barriers and improving access to top-line results and up-to-date information has always been a challenge to the global health community,” he said, noting that the map of attendance for the virtual meeting was “astonishing.”
Given these benefits, organizers said they expect a future of hybrid conferences: physical meetings for those able to attend in person and virtual ones for those who cannot.
“We also expect that the hybrid congress will cater to the needs of people on-site by allowing them additional access to more scientific content than by physical attendance alone,” Dr. Rautenstrauch said.
Everyone has been in reactive mode this year, Ms. Sibley said, but the future looks bright as they seek ways to overcome challenges such as socio-emotional needs and virtual expo spaces.
“We’ve been thrust into the virtual world much faster than we expected, but we’re finding it’s opening more opportunities than we had live,” Ms. Sibley said. “This has catapulted us, for better or worse, into a new way to deliver education and other types of information.
“I think, if we’re smart, we’ll continue to think of ways this can augment our live environment and not replace it.”
A version of this article originally appeared on Medscape.com.
Novel study explores link between primary immunodeficiencies, rheumatic diseases
Fully 48% of patients with autoimmune rheumatic diseases who developed persistent hypogammaglobulinemia after initiating treatment with immunomodulatory agents harbored gene variants associated with inborn errors of immunity, according to the findings of a single-center study published in Annals of the Rheumatic Diseases.
The results raise the possibility of a shared genetic etiology between “primary” and “secondary” hypogammaglobulinemia and suggest that some cases of autoimmune rheumatic disease may result from inborn errors of immunity. “In other words, a rheumatologist may be treating the rheumatic manifestations of a primary immunodeficiency disorder,” the study’s lead author, Georgios Sogkas, MD, PhD, said in an interview.

Experts now widely acknowledge an association between rheumatic diseases and inborn errors of immunity, or primary immunodeficiencies (PIDs). In one recent large retrospective study, 26% of patients with PIDs had at least one autoimmune or inflammatory disorder, and at least 13% of patients with PIDs had autoimmune rheumatic diseases. However, few studies have sought explanations for this link.
Only a minority of patients develop persistent hypogammaglobulinemia in response to immunomodulatory treatments for rheumatic diseases, suggesting a genetic basis for this outcome, according to Dr. Sogkas of the clinic for rheumatology and immunology at Hannover (Germany) Medical University. To explore this possibility, he and his associates measured the serum IgG levels of 1,008 Hannover University Hospital outpatients with autoimmune rheumatic diseases. In all, 64 patients had “persistent secondary hypogammaglobulinemia,” defined as at least a 12-month history of having serum IgG levels less than 7 g/L that began after the patients started on prednisolone or one or more synthetic or biologic disease-modifying antirheumatic drugs (DMARDs). Using next-generation sequencing (NGS), the researchers screened for known or candidate genes associated with primary antibody deficiencies by testing peripheral blood samples from this cohort and from 64 randomly selected patients with rheumatic diseases who did not have persistent hypogammaglobulinemia.
Among the patients with hypogammaglobulinemia, 31 (48%) had one or more potentially pathogenic variants (35 variants in total, all of them monoallelic). Notably, 10 patients (nearly 16%) harbored variants linked to autosomal dominant PIDs, and five patients harbored variants in NFKB1, which encodes the p51 subunit of the associated transcription factor. Among the 64 patients without hypogammaglobulinemia, only 7 (11%) harbored variants in the same PID-related genes, and only 1 had an autosomal dominant variant. This patient, who had a history of recurrent herpes infections, harbored a variant in the IRF2BP2 gene that does not necessarily lead to hypogammaglobulinemia, the researchers said.
‘Striking’ findings suggest a future in personalized medicine
Experts who were not involved in the study called the results noteworthy. “The fact that half of patients with rheumatic disease who developed secondary hypogammaglobulinemia were found to have a functionally relevant mutation in a known PID gene is striking, albeit purely circumstantial given the absence of any functional or mechanistic data,” said Michael J. Ombrello, MD, principal investigator and head of the translational genetics and genomics unit at the National Institute of Arthritis and Musculoskeletal and Skin Diseases, who was not involved in the study.

The findings, if they are validated by additional studies, might help clinicians personalize medicine by avoiding hypogammaglobulinemia-inducing immunomodulatory regimens in genetically predisposed patients, or by targeting Janus kinase (JAK) inhibitor therapy for patients with STAT3 gain-of-function variants, or PI3K delta inhibitors for patients with variants leading to hyperactivation of the PI3Kdelta gene, Dr. Sogkas said.
Dr. Ombrello agreed: “Whether the hypogammaglobulinemia is classified as primary or secondary, the presence of these genetic variants in half of patients with hypogammaglobulinemia suggests an opportunity to improve clinical care. Although far off at this point, one can imagine a day where genetic data allows a rheumatologist to identify new-onset rheumatic disease patients carrying PID gene mutations and cater their therapy and monitoring accordingly.”
If further research validates these findings, they would add to a growing body of support for incorporating expanded or universal exome or genome sequencing in the care of medically complex patients, such as those with rheumatic diseases, Dr. Ombrello said. However, he cautioned that the investigators could have “overstated” the relationship in their study between secondary hypogammaglobulinemia and immunomodulatory treatment. The fact that a small group of study participants (about 7%) developed hypogammaglobulinemia after initiating immunomodulatory therapy does not confirm a causal relationship, he emphasized. Common variable immune deficiency (CVID) can develop in adults as late as the fifth and sixth decade of life, he noted, making it “not implausible that a small number of rheumatic disease patients would develop CVID while under the care of a rheumatologist. Would these patients have developed hypogammaglobulinemia even without treatment with immunomodulators, purely related to their genetic mutations? If so, they would be better classified as having primary immune deficiency, although that distinction is largely one of semantics.”
‘Rheumatologists are obliged to step up’
Interestingly, only 23% of the patients with hypogammaglobulinemia in the study had a clinically significant history of infections even though only 9% were receiving prophylactic antibiotics. Such findings highlight the complexity of PIDs, according to experts. “A long generation ago, we thought of immunodeficiencies as infections. Now we see them as autoimmune diseases, inflammatory diseases, allergic diseases – the spectrum continues to enlarge,” said Leonard H. Calabrese, DO, the RJ Fasenmyer chair of clinical immunology at the Cleveland Clinic, who was not involved in the study.

Dr. Calabrese noted that more than 450 monogenic variants have been linked to inborn errors of immunity. “Because these [PIDs] can mimic autoinflammatory presentations, rheumatologists are obliged to step up and gain a greater understanding, to be able to recognize and diagnose them and sort them out.”
Future goals should include quantifying the prevalence of genetic variants underlying hypogammaglobulinemia among patients with rheumatic diseases, and better characterizing outcomes and phenotypes of patients harboring variants linked to inborn errors of immunity, Dr. Sogkas said. “Whether these patients actually have a different disease than what they are being treated for, I can’t tell from this paper, and that’s an important question for the future,” added Dr. Calabrese. “I also do wonder about the effects of different drugs,” he said, noting that many patients with PID-associated autosomal gene variants developed persistent secondary hypogammaglobulinemia after initiating methotrexate. “It makes me wonder whether some of these genes have a specific interaction with methotrexate,” he said. “That could be a biomarker for drug toxicity.”
Study funders included the German Research Foundation, the German multiorgan Autoimmunity Network, Hannover Medical School, the Rosemarie-Germscheid Foundation, the German Academic Exchange Service, HBRS, the Center for Infection Biology, and the German Center for Infection Research. The investigators reported having no competing interests.
SOURCE: Sogkas G et al. Ann Rheum Dis. 2020 Oct 12. doi: 10.1136/annrheumdis-2020-218280.
Fully 48% of patients with autoimmune rheumatic diseases who developed persistent hypogammaglobulinemia after initiating treatment with immunomodulatory agents harbored gene variants associated with inborn errors of immunity, according to the findings of a single-center study published in Annals of the Rheumatic Diseases.
The results raise the possibility of a shared genetic etiology between “primary” and “secondary” hypogammaglobulinemia and suggest that some cases of autoimmune rheumatic disease may result from inborn errors of immunity. “In other words, a rheumatologist may be treating the rheumatic manifestations of a primary immunodeficiency disorder,” the study’s lead author, Georgios Sogkas, MD, PhD, said in an interview.
Experts now widely acknowledge an association between rheumatic diseases and inborn errors of immunity, or primary immunodeficiencies (PIDs). In one recent large retrospective study, 26% of patients with PIDs had at least one autoimmune or inflammatory disorder, and at least 13% of patients with PIDs had autoimmune rheumatic diseases. However, few studies have sought explanations for this link.
Only a minority of patients develop persistent hypogammaglobulinemia in response to immunomodulatory treatments for rheumatic diseases, suggesting a genetic basis for this outcome, according to Dr. Sogkas of the clinic for rheumatology and immunology at Hannover (Germany) Medical University. To explore this possibility, he and his associates measured the serum IgG levels of 1,008 Hannover University Hospital outpatients with autoimmune rheumatic diseases. In all, 64 patients had “persistent secondary hypogammaglobulinemia,” defined as at least a 12-month history of having serum IgG levels less than 7 g/L that began after the patients started on prednisolone or one or more synthetic or biologic disease-modifying antirheumatic drugs (DMARDs). Using next-generation sequencing (NGS), the researchers screened for known or candidate genes associated with primary antibody deficiencies by testing peripheral blood samples from this cohort and from 64 randomly selected patients with rheumatic diseases who did not have persistent hypogammaglobulinemia.
Among the patients with hypogammaglobulinemia, 31 (48%) had one or more potentially pathogenic variants (35 variants in total, all of them monoallelic). Notably, 10 patients (nearly 16%) harbored variants linked to autosomal dominant PIDs, and five patients harbored variants in NFKB1, which encodes the p51 subunit of the associated transcription factor. Among the 64 patients without hypogammaglobulinemia, only 7 (11%) harbored variants in the same PID-related genes, and only 1 had an autosomal dominant variant. This patient, who had a history of recurrent herpes infections, harbored a variant in the IRF2BP2 gene that does not necessarily lead to hypogammaglobulinemia, the researchers said.
‘Striking’ findings suggest a future in personalized medicine
Experts who were not involved in the study called the results noteworthy. “The fact that half of patients with rheumatic disease who developed secondary hypogammaglobulinemia were found to have a functionally relevant mutation in a known PID gene is striking, albeit purely circumstantial given the absence of any functional or mechanistic data,” said Michael J. Ombrello, MD, principal investigator and head of the translational genetics and genomics unit at the National Institute of Arthritis and Musculoskeletal and Skin Diseases, who was not involved in the study.
The findings, if they are validated by additional studies, might help clinicians personalize medicine by avoiding hypogammaglobulinemia-inducing immunomodulatory regimens in genetically predisposed patients, or by targeting Janus kinase (JAK) inhibitor therapy for patients with STAT3 gain-of-function variants, or PI3K delta inhibitors for patients with variants leading to hyperactivation of the PI3Kdelta gene, Dr. Sogkas said.
Dr. Ombrello agreed: “Whether the hypogammaglobulinemia is classified as primary or secondary, the presence of these genetic variants in half of patients with hypogammaglobulinemia suggests an opportunity to improve clinical care. Although far off at this point, one can imagine a day where genetic data allows a rheumatologist to identify new-onset rheumatic disease patients carrying PID gene mutations and cater their therapy and monitoring accordingly.”
If further research validates these findings, they would add to a growing body of support for incorporating expanded or universal exome or genome sequencing in the care of medically complex patients, such as those with rheumatic diseases, Dr. Ombrello said. However, he cautioned that the investigators could have “overstated” the relationship in their study between secondary hypogammaglobulinemia and immunomodulatory treatment. The fact that a small group of study participants (about 7%) developed hypogammaglobulinemia after initiating immunomodulatory therapy does not confirm a causal relationship, he emphasized. Common variable immune deficiency (CVID) can develop in adults as late as the fifth and sixth decade of life, he noted, making it “not implausible that a small number of rheumatic disease patients would develop CVID while under the care of a rheumatologist. Would these patients have developed hypogammaglobulinemia even without treatment with immunomodulators, purely related to their genetic mutations? If so, they would be better classified as having primary immune deficiency, although that distinction is largely one of semantics.”
‘Rheumatologists are obliged to step up’
Interestingly, only 23% of the patients with hypogammaglobulinemia in the study had a clinically significant history of infections even though only 9% were receiving prophylactic antibiotics. Such findings highlight the complexity of PIDs, according to experts. “A long generation ago, we thought of immunodeficiencies as infections. Now we see them as autoimmune diseases, inflammatory diseases, allergic diseases – the spectrum continues to enlarge,” said Leonard H. Calabrese, DO, the RJ Fasenmyer chair of clinical immunology at the Cleveland Clinic, who was not involved in the study.
Dr. Calabrese noted that more than 450 monogenic variants have been linked to inborn errors of immunity. “Because these [PIDs] can mimic autoinflammatory presentations, rheumatologists are obliged to step up and gain a greater understanding, to be able to recognize and diagnose them and sort them out.”
Future goals should include quantifying the prevalence of genetic variants underlying hypogammaglobulinemia among patients with rheumatic diseases, and better characterizing outcomes and phenotypes of patients harboring variants linked to inborn errors of immunity, Dr. Sogkas said. “Whether these patients actually have a different disease than what they are being treated for, I can’t tell from this paper, and that’s an important question for the future,” added Dr. Calabrese. “I also do wonder about the effects of different drugs,” he said, noting that many patients with PID-associated autosomal gene variants developed persistent secondary hypogammaglobulinemia after initiating methotrexate. “It makes me wonder whether some of these genes have a specific interaction with methotrexate,” he said. “That could be a biomarker for drug toxicity.”
Study funders included the German Research Foundation, the German multiorgan Autoimmunity Network, Hannover Medical School, the Rosemarie-Germscheid Foundation, the German Academic Exchange Service, HBRS, the Center for Infection Biology, and the German Center for Infection Research. The investigators reported having no competing interests.
SOURCE: Sogkas G et al. Ann Rheum Dis. 2020 Oct 12. doi: 10.1136/annrheumdis-2020-218280.
Fully 48% of patients with autoimmune rheumatic diseases who developed persistent hypogammaglobulinemia after initiating treatment with immunomodulatory agents harbored gene variants associated with inborn errors of immunity, according to the findings of a single-center study published in Annals of the Rheumatic Diseases.
The results raise the possibility of a shared genetic etiology between “primary” and “secondary” hypogammaglobulinemia and suggest that some cases of autoimmune rheumatic disease may result from inborn errors of immunity. “In other words, a rheumatologist may be treating the rheumatic manifestations of a primary immunodeficiency disorder,” the study’s lead author, Georgios Sogkas, MD, PhD, said in an interview.
Experts now widely acknowledge an association between rheumatic diseases and inborn errors of immunity, or primary immunodeficiencies (PIDs). In one recent large retrospective study, 26% of patients with PIDs had at least one autoimmune or inflammatory disorder, and at least 13% of patients with PIDs had autoimmune rheumatic diseases. However, few studies have sought explanations for this link.
Only a minority of patients develop persistent hypogammaglobulinemia in response to immunomodulatory treatments for rheumatic diseases, suggesting a genetic basis for this outcome, according to Dr. Sogkas of the clinic for rheumatology and immunology at Hannover (Germany) Medical University. To explore this possibility, he and his associates measured the serum IgG levels of 1,008 Hannover University Hospital outpatients with autoimmune rheumatic diseases. In all, 64 patients had “persistent secondary hypogammaglobulinemia,” defined as at least a 12-month history of having serum IgG levels less than 7 g/L that began after the patients started on prednisolone or one or more synthetic or biologic disease-modifying antirheumatic drugs (DMARDs). Using next-generation sequencing (NGS), the researchers screened for known or candidate genes associated with primary antibody deficiencies by testing peripheral blood samples from this cohort and from 64 randomly selected patients with rheumatic diseases who did not have persistent hypogammaglobulinemia.
Among the patients with hypogammaglobulinemia, 31 (48%) had one or more potentially pathogenic variants (35 variants in total, all of them monoallelic). Notably, 10 patients (nearly 16%) harbored variants linked to autosomal dominant PIDs, and five patients harbored variants in NFKB1, which encodes the p51 subunit of the associated transcription factor. Among the 64 patients without hypogammaglobulinemia, only 7 (11%) harbored variants in the same PID-related genes, and only 1 had an autosomal dominant variant. This patient, who had a history of recurrent herpes infections, harbored a variant in the IRF2BP2 gene that does not necessarily lead to hypogammaglobulinemia, the researchers said.
‘Striking’ findings suggest a future in personalized medicine
Experts who were not involved in the study called the results noteworthy. “The fact that half of patients with rheumatic disease who developed secondary hypogammaglobulinemia were found to have a functionally relevant mutation in a known PID gene is striking, albeit purely circumstantial given the absence of any functional or mechanistic data,” said Michael J. Ombrello, MD, principal investigator and head of the translational genetics and genomics unit at the National Institute of Arthritis and Musculoskeletal and Skin Diseases, who was not involved in the study.
The findings, if they are validated by additional studies, might help clinicians personalize medicine by avoiding hypogammaglobulinemia-inducing immunomodulatory regimens in genetically predisposed patients, or by targeting Janus kinase (JAK) inhibitor therapy for patients with STAT3 gain-of-function variants, or PI3K delta inhibitors for patients with variants leading to hyperactivation of the PI3Kdelta gene, Dr. Sogkas said.
Dr. Ombrello agreed: “Whether the hypogammaglobulinemia is classified as primary or secondary, the presence of these genetic variants in half of patients with hypogammaglobulinemia suggests an opportunity to improve clinical care. Although far off at this point, one can imagine a day where genetic data allows a rheumatologist to identify new-onset rheumatic disease patients carrying PID gene mutations and cater their therapy and monitoring accordingly.”
If further research validates these findings, they would add to a growing body of support for incorporating expanded or universal exome or genome sequencing in the care of medically complex patients, such as those with rheumatic diseases, Dr. Ombrello said. However, he cautioned that the investigators could have “overstated” the relationship in their study between secondary hypogammaglobulinemia and immunomodulatory treatment. The fact that a small group of study participants (about 7%) developed hypogammaglobulinemia after initiating immunomodulatory therapy does not confirm a causal relationship, he emphasized. Common variable immune deficiency (CVID) can develop in adults as late as the fifth and sixth decade of life, he noted, making it “not implausible that a small number of rheumatic disease patients would develop CVID while under the care of a rheumatologist. Would these patients have developed hypogammaglobulinemia even without treatment with immunomodulators, purely related to their genetic mutations? If so, they would be better classified as having primary immune deficiency, although that distinction is largely one of semantics.”
‘Rheumatologists are obliged to step up’
Interestingly, only 23% of the patients with hypogammaglobulinemia in the study had a clinically significant history of infections even though only 9% were receiving prophylactic antibiotics. Such findings highlight the complexity of PIDs, according to experts. “A long generation ago, we thought of immunodeficiencies as infections. Now we see them as autoimmune diseases, inflammatory diseases, allergic diseases – the spectrum continues to enlarge,” said Leonard H. Calabrese, DO, the RJ Fasenmyer chair of clinical immunology at the Cleveland Clinic, who was not involved in the study.
Dr. Calabrese noted that more than 450 monogenic variants have been linked to inborn errors of immunity. “Because these [PIDs] can mimic autoinflammatory presentations, rheumatologists are obliged to step up and gain a greater understanding, to be able to recognize and diagnose them and sort them out.”
Future goals should include quantifying the prevalence of genetic variants underlying hypogammaglobulinemia among patients with rheumatic diseases, and better characterizing outcomes and phenotypes of patients harboring variants linked to inborn errors of immunity, Dr. Sogkas said. “Whether these patients actually have a different disease than what they are being treated for, I can’t tell from this paper, and that’s an important question for the future,” added Dr. Calabrese. “I also do wonder about the effects of different drugs,” he said, noting that many patients with PID-associated autosomal gene variants developed persistent secondary hypogammaglobulinemia after initiating methotrexate. “It makes me wonder whether some of these genes have a specific interaction with methotrexate,” he said. “That could be a biomarker for drug toxicity.”
Study funders included the German Research Foundation, the German multiorgan Autoimmunity Network, Hannover Medical School, the Rosemarie-Germscheid Foundation, the German Academic Exchange Service, HBRS, the Center for Infection Biology, and the German Center for Infection Research. The investigators reported having no competing interests.
SOURCE: Sogkas G et al. Ann Rheum Dis. 2020 Oct 12. doi: 10.1136/annrheumdis-2020-218280.
FROM ANNALS OF THE RHEUMATIC DISEASES
National three-digit suicide lifeline to take effect in 2022
Beginning in July 2022, Americans experiencing a mental health crisis will be able to dial 9-8-8 and be connected to the services and counselors at the National Suicide Prevention Lifeline.
The number was finalized when President Donald J. Trump signed the National Suicide Hotline Designation Act on Oct. 17. It completes what has been a multiyear effort by Republican and Democratic lawmakers to make it easier for individuals to reach out during mental health emergencies.
“When your house is on fire, you can get help by calling 9-1-1,” noted Rep. Seth Moulton (D-Mass.), a key sponsor of the legislation, in a statement. The new number “is a national step forward out of the shadows of stigma that prevent too many people from getting help and into a new era when mental health care is easy to get and normal to talk about,” said Rep. Moulton, a combat veteran who has openly discussed his struggles with PTSD.
The law requires the Department of Health & Human Services to develop a strategy to provide access to specialized services for high-risk populations such as LGBTQ youth, minorities, and people who live in rural areas.
“This law is a historic victory, as this is the first explicitly LGBTQ-inclusive bill to pass unanimously in history – and 9-8-8 will undoubtedly save countless lives,” said Sam Brinton, vice president of advocacy and government affairs for the Trevor Project, in a statement, also noting that “More than half of transgender and nonbinary youth having seriously considered it.”
Robert Gebbia, CEO of the American Foundation for Suicide Prevention, said in a statement: “This easy-to-remember number will increase public access to mental health and suicide prevention crisis resources, encourage help-seeking for individuals in need, and is a crucial entry point for establishing a continuum of crisis care.”
Mr. Gabbia called for more funding for local crisis centers to “respond to what we expect will be an increased call volume and provide effective crisis services to those in need when 9-8-8 is made available in July 2022.”
In 2017, then-Senator Orrin Hatch (R-Utah) and colleague Joe Donnelly (D-Ind.) pushed for a three-digit number for people having mental health crises. Their legislation passed in the Senate that fall and passed in the House in July 2018.
The bill directed the Federal Communications Commission to submit a report to Congress that would include a recommended number, a cost-benefit analysis comparing the three-digit code with the current hotline, and an assessment of how much it might cost service providers, states, local towns, and cities.
Mr. Trump signed that bill in 2018. The FCC unanimously approved the 9-8-8 number in July 2020.
Until the new number is active in July 2022, those in crisis should continue to call the National Suicide Lifeline at 1-800-273-TALK (8255).
A version of this article originally appeared on Medscape.com.
Beginning in July 2022, Americans experiencing a mental health crisis will be able to dial 9-8-8 and be connected to the services and counselors at the National Suicide Prevention Lifeline.
The number was finalized when President Donald J. Trump signed the National Suicide Hotline Designation Act on Oct. 17. It completes what has been a multiyear effort by Republican and Democratic lawmakers to make it easier for individuals to reach out during mental health emergencies.
“When your house is on fire, you can get help by calling 9-1-1,” noted Rep. Seth Moulton (D-Mass.), a key sponsor of the legislation, in a statement. The new number “is a national step forward out of the shadows of stigma that prevent too many people from getting help and into a new era when mental health care is easy to get and normal to talk about,” said Rep. Moulton, a combat veteran who has openly discussed his struggles with PTSD.
The law requires the Department of Health & Human Services to develop a strategy to provide access to specialized services for high-risk populations such as LGBTQ youth, minorities, and people who live in rural areas.
“This law is a historic victory, as this is the first explicitly LGBTQ-inclusive bill to pass unanimously in history – and 9-8-8 will undoubtedly save countless lives,” said Sam Brinton, vice president of advocacy and government affairs for the Trevor Project, in a statement, also noting that “More than half of transgender and nonbinary youth having seriously considered it.”
Robert Gebbia, CEO of the American Foundation for Suicide Prevention, said in a statement: “This easy-to-remember number will increase public access to mental health and suicide prevention crisis resources, encourage help-seeking for individuals in need, and is a crucial entry point for establishing a continuum of crisis care.”
Mr. Gabbia called for more funding for local crisis centers to “respond to what we expect will be an increased call volume and provide effective crisis services to those in need when 9-8-8 is made available in July 2022.”
In 2017, then-Senator Orrin Hatch (R-Utah) and colleague Joe Donnelly (D-Ind.) pushed for a three-digit number for people having mental health crises. Their legislation passed in the Senate that fall and passed in the House in July 2018.
The bill directed the Federal Communications Commission to submit a report to Congress that would include a recommended number, a cost-benefit analysis comparing the three-digit code with the current hotline, and an assessment of how much it might cost service providers, states, local towns, and cities.
Mr. Trump signed that bill in 2018. The FCC unanimously approved the 9-8-8 number in July 2020.
Until the new number is active in July 2022, those in crisis should continue to call the National Suicide Lifeline at 1-800-273-TALK (8255).
A version of this article originally appeared on Medscape.com.
Beginning in July 2022, Americans experiencing a mental health crisis will be able to dial 9-8-8 and be connected to the services and counselors at the National Suicide Prevention Lifeline.
The number was finalized when President Donald J. Trump signed the National Suicide Hotline Designation Act on Oct. 17. It completes what has been a multiyear effort by Republican and Democratic lawmakers to make it easier for individuals to reach out during mental health emergencies.
“When your house is on fire, you can get help by calling 9-1-1,” noted Rep. Seth Moulton (D-Mass.), a key sponsor of the legislation, in a statement. The new number “is a national step forward out of the shadows of stigma that prevent too many people from getting help and into a new era when mental health care is easy to get and normal to talk about,” said Rep. Moulton, a combat veteran who has openly discussed his struggles with PTSD.
The law requires the Department of Health & Human Services to develop a strategy to provide access to specialized services for high-risk populations such as LGBTQ youth, minorities, and people who live in rural areas.
“This law is a historic victory, as this is the first explicitly LGBTQ-inclusive bill to pass unanimously in history – and 9-8-8 will undoubtedly save countless lives,” said Sam Brinton, vice president of advocacy and government affairs for the Trevor Project, in a statement, also noting that “More than half of transgender and nonbinary youth having seriously considered it.”
Robert Gebbia, CEO of the American Foundation for Suicide Prevention, said in a statement: “This easy-to-remember number will increase public access to mental health and suicide prevention crisis resources, encourage help-seeking for individuals in need, and is a crucial entry point for establishing a continuum of crisis care.”
Mr. Gabbia called for more funding for local crisis centers to “respond to what we expect will be an increased call volume and provide effective crisis services to those in need when 9-8-8 is made available in July 2022.”
In 2017, then-Senator Orrin Hatch (R-Utah) and colleague Joe Donnelly (D-Ind.) pushed for a three-digit number for people having mental health crises. Their legislation passed in the Senate that fall and passed in the House in July 2018.
The bill directed the Federal Communications Commission to submit a report to Congress that would include a recommended number, a cost-benefit analysis comparing the three-digit code with the current hotline, and an assessment of how much it might cost service providers, states, local towns, and cities.
Mr. Trump signed that bill in 2018. The FCC unanimously approved the 9-8-8 number in July 2020.
Until the new number is active in July 2022, those in crisis should continue to call the National Suicide Lifeline at 1-800-273-TALK (8255).
A version of this article originally appeared on Medscape.com.
EMA panel backs peanut allergy desensitizing powder Palforzia
The product is intended for desensitizing children and adolescents to peanut allergy.
Palforzia will be available as an oral powder in capsules (0.5, 1, 10, 20, and 100 mg) and as oral powder in sachet (300 mg). The active substance is defatted powder of Arachis hypogaea.
Through use of the product, children with a peanut allergy receive controlled exposure to precise, increasing amounts of peanut protein, mixed with soft food, every day. Over time, this may help to decrease their sensitivity to small amounts of peanuts.
According to the press release from the EMA, Palforzia can mitigate accidental exposure to small amounts of peanut protein. “[A] single dose of a least 1 gram of peanut protein would cause no more than mild allergy symptoms,” the EMA said.
The treatment is indicated for patients aged 4 to 17 years who have received a confirmed diagnosis of peanut allergy. Treatment may be continued for patients aged 18 years or older, according to the press release.
It should be administered under the supervision of a healthcare provider qualified in the diagnosis and treatment of allergic diseases and should be used in conjunction with a peanut-avoidant diet, the EMA notes.
The most common side effects that have been reported are abdominal pain, throat irritation, itch, nausea, vomiting, urticaria, and upper abdominal discomfort.
The next step in the approval process is to obtain market authorization from the European Commission. Detailed recommendations for use will be described in the summary of product characteristics, which will be published in the European public assessment report and will be made available throughout Europe.
“We are encouraged by the CHMP opinion, which recommends Palforzia as the first and only treatment option in the European Union for patients with peanut allergy and their families,” Andrew Oxtoby, president and chief executive officer of Aimmune Therapeutics, said in a statement. “Today’s decision underscores the strong and compelling data from our Palforzia clinical trials and follows the US FDA approval of Palforzia earlier this year. We look forward to the European Commission’s final decision for the marketing approval of Palforzia, which we expect later this year.”
The FDA said in granting its approval that patients, parents, or caregivers must be counseled on the need for always-available injectable epinephrine, the need for continued peanut avoidance, and on how to recognize signs of anaphylaxis.
This article originally appeared on Medscape.com.
The product is intended for desensitizing children and adolescents to peanut allergy.
Palforzia will be available as an oral powder in capsules (0.5, 1, 10, 20, and 100 mg) and as oral powder in sachet (300 mg). The active substance is defatted powder of Arachis hypogaea.
Through use of the product, children with a peanut allergy receive controlled exposure to precise, increasing amounts of peanut protein, mixed with soft food, every day. Over time, this may help to decrease their sensitivity to small amounts of peanuts.
According to the press release from the EMA, Palforzia can mitigate accidental exposure to small amounts of peanut protein. “[A] single dose of a least 1 gram of peanut protein would cause no more than mild allergy symptoms,” the EMA said.
The treatment is indicated for patients aged 4 to 17 years who have received a confirmed diagnosis of peanut allergy. Treatment may be continued for patients aged 18 years or older, according to the press release.
It should be administered under the supervision of a healthcare provider qualified in the diagnosis and treatment of allergic diseases and should be used in conjunction with a peanut-avoidant diet, the EMA notes.
The most common side effects that have been reported are abdominal pain, throat irritation, itch, nausea, vomiting, urticaria, and upper abdominal discomfort.
The next step in the approval process is to obtain market authorization from the European Commission. Detailed recommendations for use will be described in the summary of product characteristics, which will be published in the European public assessment report and will be made available throughout Europe.
“We are encouraged by the CHMP opinion, which recommends Palforzia as the first and only treatment option in the European Union for patients with peanut allergy and their families,” Andrew Oxtoby, president and chief executive officer of Aimmune Therapeutics, said in a statement. “Today’s decision underscores the strong and compelling data from our Palforzia clinical trials and follows the US FDA approval of Palforzia earlier this year. We look forward to the European Commission’s final decision for the marketing approval of Palforzia, which we expect later this year.”
The FDA said in granting its approval that patients, parents, or caregivers must be counseled on the need for always-available injectable epinephrine, the need for continued peanut avoidance, and on how to recognize signs of anaphylaxis.
This article originally appeared on Medscape.com.
The product is intended for desensitizing children and adolescents to peanut allergy.
Palforzia will be available as an oral powder in capsules (0.5, 1, 10, 20, and 100 mg) and as oral powder in sachet (300 mg). The active substance is defatted powder of Arachis hypogaea.
Through use of the product, children with a peanut allergy receive controlled exposure to precise, increasing amounts of peanut protein, mixed with soft food, every day. Over time, this may help to decrease their sensitivity to small amounts of peanuts.
According to the press release from the EMA, Palforzia can mitigate accidental exposure to small amounts of peanut protein. “[A] single dose of a least 1 gram of peanut protein would cause no more than mild allergy symptoms,” the EMA said.
The treatment is indicated for patients aged 4 to 17 years who have received a confirmed diagnosis of peanut allergy. Treatment may be continued for patients aged 18 years or older, according to the press release.
It should be administered under the supervision of a healthcare provider qualified in the diagnosis and treatment of allergic diseases and should be used in conjunction with a peanut-avoidant diet, the EMA notes.
The most common side effects that have been reported are abdominal pain, throat irritation, itch, nausea, vomiting, urticaria, and upper abdominal discomfort.
The next step in the approval process is to obtain market authorization from the European Commission. Detailed recommendations for use will be described in the summary of product characteristics, which will be published in the European public assessment report and will be made available throughout Europe.
“We are encouraged by the CHMP opinion, which recommends Palforzia as the first and only treatment option in the European Union for patients with peanut allergy and their families,” Andrew Oxtoby, president and chief executive officer of Aimmune Therapeutics, said in a statement. “Today’s decision underscores the strong and compelling data from our Palforzia clinical trials and follows the US FDA approval of Palforzia earlier this year. We look forward to the European Commission’s final decision for the marketing approval of Palforzia, which we expect later this year.”
The FDA said in granting its approval that patients, parents, or caregivers must be counseled on the need for always-available injectable epinephrine, the need for continued peanut avoidance, and on how to recognize signs of anaphylaxis.
This article originally appeared on Medscape.com.
Are oncologists ready to confront a second wave of COVID-19?
Canceled appointments, postponed surgeries, and delayed cancer diagnoses – all are a recipe for exhaustion for oncologists around the world, struggling to reach and treat their patients during the pandemic. Physicians and their teams felt the pain as COVID-19 took its initial march around the globe.
“We saw the distress of people with cancer who could no longer get to anyone on the phone. Their medical visit was usually canceled. Their radiotherapy session was postponed or modified, and chemotherapy postponed,” says Axel Kahn, MD, chairman of the board of directors of La Ligue Nationale Contre le Cancer (National League Against Cancer). “In the vast majority of cases, cancer treatment can be postponed or readjusted, without affecting the patient’s chances of survival, but there has been a lot of anxiety because the patients do not know that.”
The stay-at-home factor was one that played out across many months during the first wave.
“I believe that the ‘stay-home’ message that we transmitted was rigorously followed by patients who should have come to the emergency room much earlier and who, therefore, were admitted with a much more deteriorated general condition than in non-COVID-19 times,” says Benjamín Domingo Arrué, MD, from the department of medical oncology at Hospital Universitari i Politècnic La Fe in Valencia, Spain.
And in Brazil, some of the impact from the initial hit of COVID-19 on oncology is only now being felt, according to Laura Testa, MD, head of breast medical oncology, Instituto do Câncer do Estado de São Paulo.
“We are starting to see a lot of cancer cases that didn’t show up at the beginning of the pandemic, but now they are arriving to us already in advanced stages,” she said. “These patients need hospital care. If the situation worsens and goes back to what we saw at the peak of the curve, I fear the public system won’t be able to treat properly the oncology patients that need hospital care and the patients with cancer who also have COVID-19.”
But even as health care worker fatigue and concerns linger, oncologists say that what they have learned in the last 6 months has helped them prepare as COVID-19 cases increase and a second global wave kicks up.
Lessons from the first wave
In the United States, COVID-19 hit different regions at different times and to different degrees. One of the areas hit first was Seattle.
“We jumped on top of this, we were evidence based, we put things in place very, very quickly,” said Julie Gralow, MD, professor at the University of Washington and the Fred Hutchinson Cancer Research Center, both in Seattle.
“We did a really good job keeping COVID out of our cancer centers,” Dr. Gralow said. “We learned how to be super safe, and to keep symptomatic people out of the building, and to limit the extra people they could bring with them. It’s all about the number of contacts you have.”
The story was different, though, for oncologists in several other countries, and sometimes it varied immensely within each nation.
“We treated fewer patients with cancer during the first wave,” says Dirk Arnold, MD, medical director of the Asklepios Tumor Center Hamburg (Germany), in an interview. “In part, this was because staff were quarantined and because we had a completely different infrastructure in all of the hospitals. But also fewer patients with cancer came to the clinic at all. A lot of resources were directed toward COVID-19.”
In Spain, telemedicine helped keep up with visits, but other areas felt the effect of COVID-19 patient loads.
“At least in the oncology department of our center, we have practically maintained 100% of visits, mostly by telephone,” says Dr. Arrué, “but the reality is that our country has not yet been prepared for telemedicine.”
Laura Mezquita, MD, of the department of medical oncology at Hospital Clinic de Barcelona, describes a more dramatic situation: “We have seen how some of our patients, especially with metastatic disease, have been dismissed for intensive care and life-support treatments, as well as specific treatments against COVID-19 (tocilizumab, remdesivir, etc.) due to the general health collapse of the former wave,” she said. She adds that specific oncologic populations, such as those with thoracic tumors, have been more affected.
Distress among oncologists
Many oncologists are still feeling stressed and fatigued after the first wave, just as a second string of outbreaks is on its way.
A survey presented at last month’s ESMO 2020 Congress found that, in July-August, moral distress was reported by one-third of the oncologists who responded, and more than half reported a feeling of exhaustion.
“The tiredness and team exhaustion is noticeable,” said Dr. Arnold. “We recently had a task force discussion about what will happen when we have a second wave and how the department and our services will adapt. It was clear that those who were at the very front in the first wave had only a limited desire to do that again in the second wave.”
Another concern: COVID-19’s effect on staffing levels.
“We have a population of young caregivers who are affected by the COVID-19 disease with an absenteeism rate that is quite unprecedented,” said Sophie Beaupère, general delegate of Unicancer since January.
She said that, in general, the absenteeism rate in the cancer centers averages 5%-6%, depending on the year. But that rate is now skyrocketing.
Stop-start cycle for surgery
As caregivers quarantined around the world, more than 10% of patients with cancer had treatment canceled or delayed during the first wave of the pandemic, according to another survey from ESMO, involving 109 oncologists from 18 countries.
Difficulties were reported for surgeries by 34% of the centers, but also difficulties with delivering chemotherapy (22% of centers), radiotherapy (13.7%), and therapy with checkpoint inhibitors (9.1%), monoclonal antibodies (9%), and oral targeted therapy (3.7%).
Stopping surgery is a real concern in France, noted Dr. Kahn, the National League Against Cancer chair. He says that in regions that were badly hit by COVID-19, “it was not possible to have access to the operating room for people who absolutely needed surgery; for example, patients with lung cancer that was still operable. Most of the recovery rooms were mobilized for resuscitation.”
There may be some solutions, suggested Thierry Breton, director general of the National Institute of Cancer in France. “We are getting prepared, with the health ministry, for a possible increase in hospital tension, which would lead to a situation where we would have to reschedule operations. Nationally, regionally, and locally, we are seeing how we can resume and prioritize surgeries that have not been done.”
Delays in cancer diagnosis
While COVID-19 affected treatment, many oncologists say the major impact of the first wave was a delay in diagnosing cancer. Some of this was a result of the suspension of cancer screening programs, but there was also fear among the general public about visiting clinics and hospitals during a pandemic.
“We didn’t do so well with cancer during the first wave here in the U.K.,” said Karol Sikora, PhD, MBBChir, professor of cancer medicine and founding dean at the University of Buckingham Medical School, London. “Cancer diagnostic pathways virtually stalled partly because patients didn’t seek help, but getting scans and biopsies was also very difficult. Even patients referred urgently under the ‘2-weeks-wait’ rule were turned down.”
In France, “the delay in diagnosis is indisputable,” said Dr. Kahn. “About 50% of the cancer diagnoses one would expect during this period were missed.”
“I am worried that there remains a major traffic jam that has not been caught up with, and, in the meantime, the health crisis is worsening,” he added.
In Seattle, Dr. Gralow said the first COVID-19 wave had little impact on treatment for breast cancer, but it was in screening for breast cancer “where things really got messed up.”
“Even though we’ve been fully ramped up again,” she said, concerns remain. To ensure that screening mammography is maintained, “we have spaced out the visits to keep our waiting rooms less populated, with a longer time between using the machine so we can clean it. To do this, we have extended operating hours and are now opening on Saturday.
“So we’re actually at 100% of our capacity, but I’m really nervous, though, that a lot of people put off their screening mammogram and aren’t going to come in and get it.
“Not only did people get the message to stay home and not do nonessential things, but I think a lot of people lost their health insurance when they lost their jobs,” she said, and without health insurance, they are not covered for cancer screening.
Looking ahead, with a plan
Many oncologists agree that access to care can and must be improved – and there were some positive moves.
“Some regimens changed during the first months of the pandemic, and I don’t see them going back to the way they were anytime soon,” said Dr. Testa. “The changes/adaptations that were made to minimize the chance of SARS-CoV-2 infection are still in place and will go on for a while. In this context, telemedicine helped a lot. The pandemic forced the stakeholders to step up and put it in place in March. And now it’s here to stay.”
The experience gained in the last several months has driven preparation for the next wave.
“We are not going to see the disorganization that we saw during the first wave,” said Florence Joly, MD, PhD, head of medical oncology at the Centre François Baclesse in Caen, France. “The difference between now and earlier this year is that COVID diagnostic tests are available. That was one of the problems in the first wave. We had no way to diagnose.”
On the East Coast of the United States, medical oncologist Charu Aggarwal, MD, MPH, is also optimistic: “I think we’re at a place where we can manage.”
“I believe if there was going to be a new wave of COVID-19 cases we would be: better psychologically prepared and better organized,” said Dr. Aggarwal, assistant professor of medicine in the hematology-oncology division at the University of Pennsylvania, Philadelphia. “We already have experience with all of the tools, we have telemedicine available, we have screening protocols available, we have testing, we are already universally masking, everyone’s hand-washing, so I do think that means we would be okay.”
Dr. Arnold agreed that “we are much better prepared than for the first wave, but … we have immense tasks in the area of patient management, the digitization of patient care, the clear allocation of resources when there is a second or third wave. In many areas of preparation, I believe, unfortunately, we are not as well positioned as we had actually hoped.”
The first wave of COVID hit cancer services in the United Kingdom particularly hard: One modeling study suggested that delays in cancer referrals will lead to thousands of additional deaths and tens of thousands of life-years lost.
“Cancer services are working at near normal levels now, but they are still fragile and could be severely compromised again if the NHS [National Health Service] gets flooded by COVID patients,” said Dr. Sikora.
The second wave may be different. “Although the number of infections has increased, the hospitalizations have only risen a little. Let’s see what happens,” he said in an interview. Since then, however, infections have continued to rise, and there has been an increase in hospitalizations. New social distancing measures in the United Kingdom were put into place on Oct. 12, with the aim of protecting the NHS from overload.
Dr. Arrué describes it this way: “The reality is that the ‘second wave’ has left behind the initial grief and shock that both patients and health professionals experienced when faced with something that, until now, we had only seen in the movies.” The second wave has led to new restrictions – including a partial lockdown since the beginning of October.
Dr. Aggarwal says her department recently had a conference with Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, about the impact of COVID-19 on oncology.
“I asked him what advice he’d give oncologists, and he said to go back to as much screening as you were doing previously as quickly as possible. That’s what must be relayed to our oncologists in the community – and also to primary care physicians – because they are often the ones who are ordering and championing the screening efforts.”
This article was originated by Aude Lecrubier, Medscape French edition, and developed by Zosia Chustecka, Medscape Oncology. With additional reporting by Kate Johnson, freelance medical journalist, Claudia Gottschling for Medscape Germany, Leoleli Schwartz for Medscape em português, Tim Locke for Medscape United Kingdom, and Carla Nieto Martínez, freelance medical journalist for Medscape Spanish edition.
This article first appeared on Medscape.com.
Canceled appointments, postponed surgeries, and delayed cancer diagnoses – all are a recipe for exhaustion for oncologists around the world, struggling to reach and treat their patients during the pandemic. Physicians and their teams felt the pain as COVID-19 took its initial march around the globe.
“We saw the distress of people with cancer who could no longer get to anyone on the phone. Their medical visit was usually canceled. Their radiotherapy session was postponed or modified, and chemotherapy postponed,” says Axel Kahn, MD, chairman of the board of directors of La Ligue Nationale Contre le Cancer (National League Against Cancer). “In the vast majority of cases, cancer treatment can be postponed or readjusted, without affecting the patient’s chances of survival, but there has been a lot of anxiety because the patients do not know that.”
The stay-at-home factor was one that played out across many months during the first wave.
“I believe that the ‘stay-home’ message that we transmitted was rigorously followed by patients who should have come to the emergency room much earlier and who, therefore, were admitted with a much more deteriorated general condition than in non-COVID-19 times,” says Benjamín Domingo Arrué, MD, from the department of medical oncology at Hospital Universitari i Politècnic La Fe in Valencia, Spain.
And in Brazil, some of the impact from the initial hit of COVID-19 on oncology is only now being felt, according to Laura Testa, MD, head of breast medical oncology, Instituto do Câncer do Estado de São Paulo.
“We are starting to see a lot of cancer cases that didn’t show up at the beginning of the pandemic, but now they are arriving to us already in advanced stages,” she said. “These patients need hospital care. If the situation worsens and goes back to what we saw at the peak of the curve, I fear the public system won’t be able to treat properly the oncology patients that need hospital care and the patients with cancer who also have COVID-19.”
But even as health care worker fatigue and concerns linger, oncologists say that what they have learned in the last 6 months has helped them prepare as COVID-19 cases increase and a second global wave kicks up.
Lessons from the first wave
In the United States, COVID-19 hit different regions at different times and to different degrees. One of the areas hit first was Seattle.
“We jumped on top of this, we were evidence based, we put things in place very, very quickly,” said Julie Gralow, MD, professor at the University of Washington and the Fred Hutchinson Cancer Research Center, both in Seattle.
“We did a really good job keeping COVID out of our cancer centers,” Dr. Gralow said. “We learned how to be super safe, and to keep symptomatic people out of the building, and to limit the extra people they could bring with them. It’s all about the number of contacts you have.”
The story was different, though, for oncologists in several other countries, and sometimes it varied immensely within each nation.
“We treated fewer patients with cancer during the first wave,” says Dirk Arnold, MD, medical director of the Asklepios Tumor Center Hamburg (Germany), in an interview. “In part, this was because staff were quarantined and because we had a completely different infrastructure in all of the hospitals. But also fewer patients with cancer came to the clinic at all. A lot of resources were directed toward COVID-19.”
In Spain, telemedicine helped keep up with visits, but other areas felt the effect of COVID-19 patient loads.
“At least in the oncology department of our center, we have practically maintained 100% of visits, mostly by telephone,” says Dr. Arrué, “but the reality is that our country has not yet been prepared for telemedicine.”
Laura Mezquita, MD, of the department of medical oncology at Hospital Clinic de Barcelona, describes a more dramatic situation: “We have seen how some of our patients, especially with metastatic disease, have been dismissed for intensive care and life-support treatments, as well as specific treatments against COVID-19 (tocilizumab, remdesivir, etc.) due to the general health collapse of the former wave,” she said. She adds that specific oncologic populations, such as those with thoracic tumors, have been more affected.
Distress among oncologists
Many oncologists are still feeling stressed and fatigued after the first wave, just as a second string of outbreaks is on its way.
A survey presented at last month’s ESMO 2020 Congress found that, in July-August, moral distress was reported by one-third of the oncologists who responded, and more than half reported a feeling of exhaustion.
“The tiredness and team exhaustion is noticeable,” said Dr. Arnold. “We recently had a task force discussion about what will happen when we have a second wave and how the department and our services will adapt. It was clear that those who were at the very front in the first wave had only a limited desire to do that again in the second wave.”
Another concern: COVID-19’s effect on staffing levels.
“We have a population of young caregivers who are affected by the COVID-19 disease with an absenteeism rate that is quite unprecedented,” said Sophie Beaupère, general delegate of Unicancer since January.
She said that, in general, the absenteeism rate in the cancer centers averages 5%-6%, depending on the year. But that rate is now skyrocketing.
Stop-start cycle for surgery
As caregivers quarantined around the world, more than 10% of patients with cancer had treatment canceled or delayed during the first wave of the pandemic, according to another survey from ESMO, involving 109 oncologists from 18 countries.
Difficulties were reported for surgeries by 34% of the centers, but also difficulties with delivering chemotherapy (22% of centers), radiotherapy (13.7%), and therapy with checkpoint inhibitors (9.1%), monoclonal antibodies (9%), and oral targeted therapy (3.7%).
Stopping surgery is a real concern in France, noted Dr. Kahn, the National League Against Cancer chair. He says that in regions that were badly hit by COVID-19, “it was not possible to have access to the operating room for people who absolutely needed surgery; for example, patients with lung cancer that was still operable. Most of the recovery rooms were mobilized for resuscitation.”
There may be some solutions, suggested Thierry Breton, director general of the National Institute of Cancer in France. “We are getting prepared, with the health ministry, for a possible increase in hospital tension, which would lead to a situation where we would have to reschedule operations. Nationally, regionally, and locally, we are seeing how we can resume and prioritize surgeries that have not been done.”
Delays in cancer diagnosis
While COVID-19 affected treatment, many oncologists say the major impact of the first wave was a delay in diagnosing cancer. Some of this was a result of the suspension of cancer screening programs, but there was also fear among the general public about visiting clinics and hospitals during a pandemic.
“We didn’t do so well with cancer during the first wave here in the U.K.,” said Karol Sikora, PhD, MBBChir, professor of cancer medicine and founding dean at the University of Buckingham Medical School, London. “Cancer diagnostic pathways virtually stalled partly because patients didn’t seek help, but getting scans and biopsies was also very difficult. Even patients referred urgently under the ‘2-weeks-wait’ rule were turned down.”
In France, “the delay in diagnosis is indisputable,” said Dr. Kahn. “About 50% of the cancer diagnoses one would expect during this period were missed.”
“I am worried that there remains a major traffic jam that has not been caught up with, and, in the meantime, the health crisis is worsening,” he added.
In Seattle, Dr. Gralow said the first COVID-19 wave had little impact on treatment for breast cancer, but it was in screening for breast cancer “where things really got messed up.”
“Even though we’ve been fully ramped up again,” she said, concerns remain. To ensure that screening mammography is maintained, “we have spaced out the visits to keep our waiting rooms less populated, with a longer time between using the machine so we can clean it. To do this, we have extended operating hours and are now opening on Saturday.
“So we’re actually at 100% of our capacity, but I’m really nervous, though, that a lot of people put off their screening mammogram and aren’t going to come in and get it.
“Not only did people get the message to stay home and not do nonessential things, but I think a lot of people lost their health insurance when they lost their jobs,” she said, and without health insurance, they are not covered for cancer screening.
Looking ahead, with a plan
Many oncologists agree that access to care can and must be improved – and there were some positive moves.
“Some regimens changed during the first months of the pandemic, and I don’t see them going back to the way they were anytime soon,” said Dr. Testa. “The changes/adaptations that were made to minimize the chance of SARS-CoV-2 infection are still in place and will go on for a while. In this context, telemedicine helped a lot. The pandemic forced the stakeholders to step up and put it in place in March. And now it’s here to stay.”
The experience gained in the last several months has driven preparation for the next wave.
“We are not going to see the disorganization that we saw during the first wave,” said Florence Joly, MD, PhD, head of medical oncology at the Centre François Baclesse in Caen, France. “The difference between now and earlier this year is that COVID diagnostic tests are available. That was one of the problems in the first wave. We had no way to diagnose.”
On the East Coast of the United States, medical oncologist Charu Aggarwal, MD, MPH, is also optimistic: “I think we’re at a place where we can manage.”
“I believe if there was going to be a new wave of COVID-19 cases we would be: better psychologically prepared and better organized,” said Dr. Aggarwal, assistant professor of medicine in the hematology-oncology division at the University of Pennsylvania, Philadelphia. “We already have experience with all of the tools, we have telemedicine available, we have screening protocols available, we have testing, we are already universally masking, everyone’s hand-washing, so I do think that means we would be okay.”
Dr. Arnold agreed that “we are much better prepared than for the first wave, but … we have immense tasks in the area of patient management, the digitization of patient care, the clear allocation of resources when there is a second or third wave. In many areas of preparation, I believe, unfortunately, we are not as well positioned as we had actually hoped.”
The first wave of COVID hit cancer services in the United Kingdom particularly hard: One modeling study suggested that delays in cancer referrals will lead to thousands of additional deaths and tens of thousands of life-years lost.
“Cancer services are working at near normal levels now, but they are still fragile and could be severely compromised again if the NHS [National Health Service] gets flooded by COVID patients,” said Dr. Sikora.
The second wave may be different. “Although the number of infections has increased, the hospitalizations have only risen a little. Let’s see what happens,” he said in an interview. Since then, however, infections have continued to rise, and there has been an increase in hospitalizations. New social distancing measures in the United Kingdom were put into place on Oct. 12, with the aim of protecting the NHS from overload.
Dr. Arrué describes it this way: “The reality is that the ‘second wave’ has left behind the initial grief and shock that both patients and health professionals experienced when faced with something that, until now, we had only seen in the movies.” The second wave has led to new restrictions – including a partial lockdown since the beginning of October.
Dr. Aggarwal says her department recently had a conference with Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, about the impact of COVID-19 on oncology.
“I asked him what advice he’d give oncologists, and he said to go back to as much screening as you were doing previously as quickly as possible. That’s what must be relayed to our oncologists in the community – and also to primary care physicians – because they are often the ones who are ordering and championing the screening efforts.”
This article was originated by Aude Lecrubier, Medscape French edition, and developed by Zosia Chustecka, Medscape Oncology. With additional reporting by Kate Johnson, freelance medical journalist, Claudia Gottschling for Medscape Germany, Leoleli Schwartz for Medscape em português, Tim Locke for Medscape United Kingdom, and Carla Nieto Martínez, freelance medical journalist for Medscape Spanish edition.
This article first appeared on Medscape.com.
Canceled appointments, postponed surgeries, and delayed cancer diagnoses – all are a recipe for exhaustion for oncologists around the world, struggling to reach and treat their patients during the pandemic. Physicians and their teams felt the pain as COVID-19 took its initial march around the globe.
“We saw the distress of people with cancer who could no longer get to anyone on the phone. Their medical visit was usually canceled. Their radiotherapy session was postponed or modified, and chemotherapy postponed,” says Axel Kahn, MD, chairman of the board of directors of La Ligue Nationale Contre le Cancer (National League Against Cancer). “In the vast majority of cases, cancer treatment can be postponed or readjusted, without affecting the patient’s chances of survival, but there has been a lot of anxiety because the patients do not know that.”
The stay-at-home factor was one that played out across many months during the first wave.
“I believe that the ‘stay-home’ message that we transmitted was rigorously followed by patients who should have come to the emergency room much earlier and who, therefore, were admitted with a much more deteriorated general condition than in non-COVID-19 times,” says Benjamín Domingo Arrué, MD, from the department of medical oncology at Hospital Universitari i Politècnic La Fe in Valencia, Spain.
And in Brazil, some of the impact from the initial hit of COVID-19 on oncology is only now being felt, according to Laura Testa, MD, head of breast medical oncology, Instituto do Câncer do Estado de São Paulo.
“We are starting to see a lot of cancer cases that didn’t show up at the beginning of the pandemic, but now they are arriving to us already in advanced stages,” she said. “These patients need hospital care. If the situation worsens and goes back to what we saw at the peak of the curve, I fear the public system won’t be able to treat properly the oncology patients that need hospital care and the patients with cancer who also have COVID-19.”
But even as health care worker fatigue and concerns linger, oncologists say that what they have learned in the last 6 months has helped them prepare as COVID-19 cases increase and a second global wave kicks up.
Lessons from the first wave
In the United States, COVID-19 hit different regions at different times and to different degrees. One of the areas hit first was Seattle.
“We jumped on top of this, we were evidence based, we put things in place very, very quickly,” said Julie Gralow, MD, professor at the University of Washington and the Fred Hutchinson Cancer Research Center, both in Seattle.
“We did a really good job keeping COVID out of our cancer centers,” Dr. Gralow said. “We learned how to be super safe, and to keep symptomatic people out of the building, and to limit the extra people they could bring with them. It’s all about the number of contacts you have.”
The story was different, though, for oncologists in several other countries, and sometimes it varied immensely within each nation.
“We treated fewer patients with cancer during the first wave,” says Dirk Arnold, MD, medical director of the Asklepios Tumor Center Hamburg (Germany), in an interview. “In part, this was because staff were quarantined and because we had a completely different infrastructure in all of the hospitals. But also fewer patients with cancer came to the clinic at all. A lot of resources were directed toward COVID-19.”
In Spain, telemedicine helped keep up with visits, but other areas felt the effect of COVID-19 patient loads.
“At least in the oncology department of our center, we have practically maintained 100% of visits, mostly by telephone,” says Dr. Arrué, “but the reality is that our country has not yet been prepared for telemedicine.”
Laura Mezquita, MD, of the department of medical oncology at Hospital Clinic de Barcelona, describes a more dramatic situation: “We have seen how some of our patients, especially with metastatic disease, have been dismissed for intensive care and life-support treatments, as well as specific treatments against COVID-19 (tocilizumab, remdesivir, etc.) due to the general health collapse of the former wave,” she said. She adds that specific oncologic populations, such as those with thoracic tumors, have been more affected.
Distress among oncologists
Many oncologists are still feeling stressed and fatigued after the first wave, just as a second string of outbreaks is on its way.
A survey presented at last month’s ESMO 2020 Congress found that, in July-August, moral distress was reported by one-third of the oncologists who responded, and more than half reported a feeling of exhaustion.
“The tiredness and team exhaustion is noticeable,” said Dr. Arnold. “We recently had a task force discussion about what will happen when we have a second wave and how the department and our services will adapt. It was clear that those who were at the very front in the first wave had only a limited desire to do that again in the second wave.”
Another concern: COVID-19’s effect on staffing levels.
“We have a population of young caregivers who are affected by the COVID-19 disease with an absenteeism rate that is quite unprecedented,” said Sophie Beaupère, general delegate of Unicancer since January.
She said that, in general, the absenteeism rate in the cancer centers averages 5%-6%, depending on the year. But that rate is now skyrocketing.
Stop-start cycle for surgery
As caregivers quarantined around the world, more than 10% of patients with cancer had treatment canceled or delayed during the first wave of the pandemic, according to another survey from ESMO, involving 109 oncologists from 18 countries.
Difficulties were reported for surgeries by 34% of the centers, but also difficulties with delivering chemotherapy (22% of centers), radiotherapy (13.7%), and therapy with checkpoint inhibitors (9.1%), monoclonal antibodies (9%), and oral targeted therapy (3.7%).
Stopping surgery is a real concern in France, noted Dr. Kahn, the National League Against Cancer chair. He says that in regions that were badly hit by COVID-19, “it was not possible to have access to the operating room for people who absolutely needed surgery; for example, patients with lung cancer that was still operable. Most of the recovery rooms were mobilized for resuscitation.”
There may be some solutions, suggested Thierry Breton, director general of the National Institute of Cancer in France. “We are getting prepared, with the health ministry, for a possible increase in hospital tension, which would lead to a situation where we would have to reschedule operations. Nationally, regionally, and locally, we are seeing how we can resume and prioritize surgeries that have not been done.”
Delays in cancer diagnosis
While COVID-19 affected treatment, many oncologists say the major impact of the first wave was a delay in diagnosing cancer. Some of this was a result of the suspension of cancer screening programs, but there was also fear among the general public about visiting clinics and hospitals during a pandemic.
“We didn’t do so well with cancer during the first wave here in the U.K.,” said Karol Sikora, PhD, MBBChir, professor of cancer medicine and founding dean at the University of Buckingham Medical School, London. “Cancer diagnostic pathways virtually stalled partly because patients didn’t seek help, but getting scans and biopsies was also very difficult. Even patients referred urgently under the ‘2-weeks-wait’ rule were turned down.”
In France, “the delay in diagnosis is indisputable,” said Dr. Kahn. “About 50% of the cancer diagnoses one would expect during this period were missed.”
“I am worried that there remains a major traffic jam that has not been caught up with, and, in the meantime, the health crisis is worsening,” he added.
In Seattle, Dr. Gralow said the first COVID-19 wave had little impact on treatment for breast cancer, but it was in screening for breast cancer “where things really got messed up.”
“Even though we’ve been fully ramped up again,” she said, concerns remain. To ensure that screening mammography is maintained, “we have spaced out the visits to keep our waiting rooms less populated, with a longer time between using the machine so we can clean it. To do this, we have extended operating hours and are now opening on Saturday.
“So we’re actually at 100% of our capacity, but I’m really nervous, though, that a lot of people put off their screening mammogram and aren’t going to come in and get it.
“Not only did people get the message to stay home and not do nonessential things, but I think a lot of people lost their health insurance when they lost their jobs,” she said, and without health insurance, they are not covered for cancer screening.
Looking ahead, with a plan
Many oncologists agree that access to care can and must be improved – and there were some positive moves.
“Some regimens changed during the first months of the pandemic, and I don’t see them going back to the way they were anytime soon,” said Dr. Testa. “The changes/adaptations that were made to minimize the chance of SARS-CoV-2 infection are still in place and will go on for a while. In this context, telemedicine helped a lot. The pandemic forced the stakeholders to step up and put it in place in March. And now it’s here to stay.”
The experience gained in the last several months has driven preparation for the next wave.
“We are not going to see the disorganization that we saw during the first wave,” said Florence Joly, MD, PhD, head of medical oncology at the Centre François Baclesse in Caen, France. “The difference between now and earlier this year is that COVID diagnostic tests are available. That was one of the problems in the first wave. We had no way to diagnose.”
On the East Coast of the United States, medical oncologist Charu Aggarwal, MD, MPH, is also optimistic: “I think we’re at a place where we can manage.”
“I believe if there was going to be a new wave of COVID-19 cases we would be: better psychologically prepared and better organized,” said Dr. Aggarwal, assistant professor of medicine in the hematology-oncology division at the University of Pennsylvania, Philadelphia. “We already have experience with all of the tools, we have telemedicine available, we have screening protocols available, we have testing, we are already universally masking, everyone’s hand-washing, so I do think that means we would be okay.”
Dr. Arnold agreed that “we are much better prepared than for the first wave, but … we have immense tasks in the area of patient management, the digitization of patient care, the clear allocation of resources when there is a second or third wave. In many areas of preparation, I believe, unfortunately, we are not as well positioned as we had actually hoped.”
The first wave of COVID hit cancer services in the United Kingdom particularly hard: One modeling study suggested that delays in cancer referrals will lead to thousands of additional deaths and tens of thousands of life-years lost.
“Cancer services are working at near normal levels now, but they are still fragile and could be severely compromised again if the NHS [National Health Service] gets flooded by COVID patients,” said Dr. Sikora.
The second wave may be different. “Although the number of infections has increased, the hospitalizations have only risen a little. Let’s see what happens,” he said in an interview. Since then, however, infections have continued to rise, and there has been an increase in hospitalizations. New social distancing measures in the United Kingdom were put into place on Oct. 12, with the aim of protecting the NHS from overload.
Dr. Arrué describes it this way: “The reality is that the ‘second wave’ has left behind the initial grief and shock that both patients and health professionals experienced when faced with something that, until now, we had only seen in the movies.” The second wave has led to new restrictions – including a partial lockdown since the beginning of October.
Dr. Aggarwal says her department recently had a conference with Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, about the impact of COVID-19 on oncology.
“I asked him what advice he’d give oncologists, and he said to go back to as much screening as you were doing previously as quickly as possible. That’s what must be relayed to our oncologists in the community – and also to primary care physicians – because they are often the ones who are ordering and championing the screening efforts.”
This article was originated by Aude Lecrubier, Medscape French edition, and developed by Zosia Chustecka, Medscape Oncology. With additional reporting by Kate Johnson, freelance medical journalist, Claudia Gottschling for Medscape Germany, Leoleli Schwartz for Medscape em português, Tim Locke for Medscape United Kingdom, and Carla Nieto Martínez, freelance medical journalist for Medscape Spanish edition.
This article first appeared on Medscape.com.
Survey: Acceptance of COVID-19 vaccine dips below 50%
Less than half of Americans now say that they would get a coronavirus vaccine if one became available, according to a survey conducted Oct. 8-10.
the lowest number since the weekly survey began at the end of February, digital media company Morning Consult reported.
Americans’ willingness to receive such a vaccine reached its high point, 72%, in early April but has been steadily dropping. “Overall willingness has hovered around 50% throughout September, fueled primarily by a sharp drop among Democrats since mid-August, around the time reports of White House interference at the Food and Drug Administration and other federal health agencies began to command more public attention,” Morning Consult noted.
Despite that drop, a majority of Democrats (55%) are still willing to get a COVID-19 vaccine, compared with 48% of Republicans and just 41% of independents. The willingness gap between the two parties was quite a bit wider in the previous poll, conducted Oct. 1-4: 60% of Democrats versus 48% for Republicans, the company said.
“Keeping with longstanding trends, the survey also shows women were less likely to say they’d seek a vaccine than men (42% to 55%), as were people with lower education levels and those who live in rural areas,” the news outlet added.
The latest poll results also show that 33% of respondents (43% of Republicans/25% of Democrats) are socializing in public places. The overall number was just 8% in mid-April but was up to 27% by mid-June. The proportion of all adults who believe in the effectiveness of face masks has been around 80% since April, but there is a significant gap between those who strongly approve of President Trump (66%) and those who strongly disapprove (95%), Morning Consult said.
Less than half of Americans now say that they would get a coronavirus vaccine if one became available, according to a survey conducted Oct. 8-10.
the lowest number since the weekly survey began at the end of February, digital media company Morning Consult reported.
Americans’ willingness to receive such a vaccine reached its high point, 72%, in early April but has been steadily dropping. “Overall willingness has hovered around 50% throughout September, fueled primarily by a sharp drop among Democrats since mid-August, around the time reports of White House interference at the Food and Drug Administration and other federal health agencies began to command more public attention,” Morning Consult noted.
Despite that drop, a majority of Democrats (55%) are still willing to get a COVID-19 vaccine, compared with 48% of Republicans and just 41% of independents. The willingness gap between the two parties was quite a bit wider in the previous poll, conducted Oct. 1-4: 60% of Democrats versus 48% for Republicans, the company said.
“Keeping with longstanding trends, the survey also shows women were less likely to say they’d seek a vaccine than men (42% to 55%), as were people with lower education levels and those who live in rural areas,” the news outlet added.
The latest poll results also show that 33% of respondents (43% of Republicans/25% of Democrats) are socializing in public places. The overall number was just 8% in mid-April but was up to 27% by mid-June. The proportion of all adults who believe in the effectiveness of face masks has been around 80% since April, but there is a significant gap between those who strongly approve of President Trump (66%) and those who strongly disapprove (95%), Morning Consult said.
Less than half of Americans now say that they would get a coronavirus vaccine if one became available, according to a survey conducted Oct. 8-10.
the lowest number since the weekly survey began at the end of February, digital media company Morning Consult reported.
Americans’ willingness to receive such a vaccine reached its high point, 72%, in early April but has been steadily dropping. “Overall willingness has hovered around 50% throughout September, fueled primarily by a sharp drop among Democrats since mid-August, around the time reports of White House interference at the Food and Drug Administration and other federal health agencies began to command more public attention,” Morning Consult noted.
Despite that drop, a majority of Democrats (55%) are still willing to get a COVID-19 vaccine, compared with 48% of Republicans and just 41% of independents. The willingness gap between the two parties was quite a bit wider in the previous poll, conducted Oct. 1-4: 60% of Democrats versus 48% for Republicans, the company said.
“Keeping with longstanding trends, the survey also shows women were less likely to say they’d seek a vaccine than men (42% to 55%), as were people with lower education levels and those who live in rural areas,” the news outlet added.
The latest poll results also show that 33% of respondents (43% of Republicans/25% of Democrats) are socializing in public places. The overall number was just 8% in mid-April but was up to 27% by mid-June. The proportion of all adults who believe in the effectiveness of face masks has been around 80% since April, but there is a significant gap between those who strongly approve of President Trump (66%) and those who strongly disapprove (95%), Morning Consult said.