User login
COVID frontline physicians afraid to seek mental health care
A new poll of emergency physicians on the front lines of the COVID-19 pandemic shows many are fearful of seeking mental health care for fear of stigma and the potential career impact.

The results of the nationally representative poll, conducted Oct. 7-13 by the American College of Emergency Physicians, showed almost half (45%) of 862 emergency physician respondents reported being uncomfortable seeking available psychiatric care. The poll had a margin of error of plus or minus 3 percentage points.
The findings provide new insight into both the challenges of serving in emergency medicine during the pandemic and the persistent barriers to mental health care in terms of stigma and concerns about potential career setbacks.
In the poll, with another 45% report they were feeling somewhat more stressed.
When asked about causes of stress related directly to COVID-19, 83% cited concerns about family and friends contracting COVID-19. Also factoring into emergency physicians’ stress and burnout were concerns about their own safety (80%) and lack of personal protective equipment or other needed resources (60%).
In the poll, 29% of respondents reported having excellent access to mental health treatment and 42% reported having good access. Despite this, 30% of respondents still reported feeling there was a lot of stigma in their workplace about seeking mental health treatment, with another 43% reporting they felt there was some stigma.
Poll results also showed that 24% of respondents were very concerned about what might happen with their employment if they were to seek mental health treatment, with another 33% saying they were somewhat concerned.
In recent years there have been efforts to break down cultural roadblocks in medicine that deter many physicians from seeking mental health treatment, but more needs to be done, said Mark Rosenberg, DO, MBA, who was elected president of ACEP at last weekend’s annual meeting, ACEP20.
“The pandemic emphatically underscores our need to change the status quo when it comes to physicians’ mental health,” Dr. Rosenberg said.
As previously reported by Medscape Medical News, current efforts to remove such barriers include initiatives to limit inquiries into clinicians’ past or present mental health treatment.
In May, the influential Joint Commission issued a statement urging organizations to refrain from asking about any history of mental health conditions or treatment. The Joint Commission said it supports recommendations already made by the Federation of State Medical Boards and the American Medical Association to limit inquiries on licensing applications to conditions that currently impair a clinician’s ability to perform their job.
Also supporting these efforts is the Dr. Lorna Breen Heroes’ Foundation, created in honor of an emergency physician who died by suicide in April amid the pandemic.
Lorna Breen, MD, had been working intensely in the response to the pandemic. During one shift, she covered two EDs in Manhattan at locations 5 miles apart, according to a backgrounder on the foundation’s web site.
At an ACEP press conference this week, Dr. Breen’s brother-in-law, J. Corey Feist, JD, MBA, cofounder of the foundation, noted that some states’ licensing applications for physicians include questions that fall outside of the boundaries of the Americans With Disabilities Act. He cited an analysis of state medical boards’ initial licensing questions published in 2018 in the Journal of the American Academy of Psychiatry and the Law.
In many cases, states have posed questions that extend beyond an assessment of a physician’s current ability to care for patients, creating a needless hurdle to seeking care, wrote the paper’s lead author, Carol North, MD, of the University of Texas Southwestern Medical Center, Dallas.
“Over the years, many medical licensure boards have asked applicants intrusive questions about whether they have any psychiatric history. This has created a major problem for applicants, and unfortunately this has discouraged many of those who need psychiatric treatment from seeking it because of fear of the questions,” Dr. North and colleagues noted. They cited Ohio as an example of a state that had overhauled its approach to questioning to bring it in compliance with the ADA.
Ohio previously required applicants to answer lengthy questions about their mental health, including:
- Within the last 10 years, have you been diagnosed with or have you been treated for bipolar disorder, schizophrenia, paranoia, or any other psychotic disorder?
- Have you, since attaining the age of eighteen or within the last 10 years, whichever period is shorter, been admitted to a hospital or other facility for the treatment of bipolar disorder, schizophrenia, paranoia, or any other psychotic disorder?
- Do you have, or have you been diagnosed as having, a medical condition which in any way impairs or limits your ability to practice medicine with reasonable skill and safety?
In the new version, the single question reads: “In the past 5 years, have you been diagnosed as having, or been hospitalized for, a medical condition which in any way impairs or limits your ability to practice medicine with reasonable skill and safety?”
Other states such as New York pose no mental health questions on applications for licensure.
Still, even when states have nondiscriminatory laws, physicians may not be aware of them, said Mr. Feist at an ACEP press conference. In addition to his work with the foundation, Mr. Feist is the CEO of the University of Virginia Physicians Group.
He said his sister-in-law Dr. Breen may have worried without cause about potential consequences of seeking psychiatric treatment during the pandemic. In addition, physicians in need of psychiatric care may worry about encountering hitches with medical organizations and insurers.
“This stigma and this fear of professional action on your license or your credentialing or privileging is pervasive throughout the industry,” he said.
A version of this article originally appeared on Medscape.com.
A new poll of emergency physicians on the front lines of the COVID-19 pandemic shows many are fearful of seeking mental health care for fear of stigma and the potential career impact.
The results of the nationally representative poll, conducted Oct. 7-13 by the American College of Emergency Physicians, showed almost half (45%) of 862 emergency physician respondents reported being uncomfortable seeking available psychiatric care. The poll had a margin of error of plus or minus 3 percentage points.
The findings provide new insight into both the challenges of serving in emergency medicine during the pandemic and the persistent barriers to mental health care in terms of stigma and concerns about potential career setbacks.
In the poll, with another 45% report they were feeling somewhat more stressed.
When asked about causes of stress related directly to COVID-19, 83% cited concerns about family and friends contracting COVID-19. Also factoring into emergency physicians’ stress and burnout were concerns about their own safety (80%) and lack of personal protective equipment or other needed resources (60%).
In the poll, 29% of respondents reported having excellent access to mental health treatment and 42% reported having good access. Despite this, 30% of respondents still reported feeling there was a lot of stigma in their workplace about seeking mental health treatment, with another 43% reporting they felt there was some stigma.
Poll results also showed that 24% of respondents were very concerned about what might happen with their employment if they were to seek mental health treatment, with another 33% saying they were somewhat concerned.
In recent years there have been efforts to break down cultural roadblocks in medicine that deter many physicians from seeking mental health treatment, but more needs to be done, said Mark Rosenberg, DO, MBA, who was elected president of ACEP at last weekend’s annual meeting, ACEP20.
“The pandemic emphatically underscores our need to change the status quo when it comes to physicians’ mental health,” Dr. Rosenberg said.
As previously reported by Medscape Medical News, current efforts to remove such barriers include initiatives to limit inquiries into clinicians’ past or present mental health treatment.
In May, the influential Joint Commission issued a statement urging organizations to refrain from asking about any history of mental health conditions or treatment. The Joint Commission said it supports recommendations already made by the Federation of State Medical Boards and the American Medical Association to limit inquiries on licensing applications to conditions that currently impair a clinician’s ability to perform their job.
Also supporting these efforts is the Dr. Lorna Breen Heroes’ Foundation, created in honor of an emergency physician who died by suicide in April amid the pandemic.
Lorna Breen, MD, had been working intensely in the response to the pandemic. During one shift, she covered two EDs in Manhattan at locations 5 miles apart, according to a backgrounder on the foundation’s web site.
At an ACEP press conference this week, Dr. Breen’s brother-in-law, J. Corey Feist, JD, MBA, cofounder of the foundation, noted that some states’ licensing applications for physicians include questions that fall outside of the boundaries of the Americans With Disabilities Act. He cited an analysis of state medical boards’ initial licensing questions published in 2018 in the Journal of the American Academy of Psychiatry and the Law.
In many cases, states have posed questions that extend beyond an assessment of a physician’s current ability to care for patients, creating a needless hurdle to seeking care, wrote the paper’s lead author, Carol North, MD, of the University of Texas Southwestern Medical Center, Dallas.
“Over the years, many medical licensure boards have asked applicants intrusive questions about whether they have any psychiatric history. This has created a major problem for applicants, and unfortunately this has discouraged many of those who need psychiatric treatment from seeking it because of fear of the questions,” Dr. North and colleagues noted. They cited Ohio as an example of a state that had overhauled its approach to questioning to bring it in compliance with the ADA.
Ohio previously required applicants to answer lengthy questions about their mental health, including:
- Within the last 10 years, have you been diagnosed with or have you been treated for bipolar disorder, schizophrenia, paranoia, or any other psychotic disorder?
- Have you, since attaining the age of eighteen or within the last 10 years, whichever period is shorter, been admitted to a hospital or other facility for the treatment of bipolar disorder, schizophrenia, paranoia, or any other psychotic disorder?
- Do you have, or have you been diagnosed as having, a medical condition which in any way impairs or limits your ability to practice medicine with reasonable skill and safety?
In the new version, the single question reads: “In the past 5 years, have you been diagnosed as having, or been hospitalized for, a medical condition which in any way impairs or limits your ability to practice medicine with reasonable skill and safety?”
Other states such as New York pose no mental health questions on applications for licensure.
Still, even when states have nondiscriminatory laws, physicians may not be aware of them, said Mr. Feist at an ACEP press conference. In addition to his work with the foundation, Mr. Feist is the CEO of the University of Virginia Physicians Group.
He said his sister-in-law Dr. Breen may have worried without cause about potential consequences of seeking psychiatric treatment during the pandemic. In addition, physicians in need of psychiatric care may worry about encountering hitches with medical organizations and insurers.
“This stigma and this fear of professional action on your license or your credentialing or privileging is pervasive throughout the industry,” he said.
A version of this article originally appeared on Medscape.com.
A new poll of emergency physicians on the front lines of the COVID-19 pandemic shows many are fearful of seeking mental health care for fear of stigma and the potential career impact.
The results of the nationally representative poll, conducted Oct. 7-13 by the American College of Emergency Physicians, showed almost half (45%) of 862 emergency physician respondents reported being uncomfortable seeking available psychiatric care. The poll had a margin of error of plus or minus 3 percentage points.
The findings provide new insight into both the challenges of serving in emergency medicine during the pandemic and the persistent barriers to mental health care in terms of stigma and concerns about potential career setbacks.
In the poll, with another 45% report they were feeling somewhat more stressed.
When asked about causes of stress related directly to COVID-19, 83% cited concerns about family and friends contracting COVID-19. Also factoring into emergency physicians’ stress and burnout were concerns about their own safety (80%) and lack of personal protective equipment or other needed resources (60%).
In the poll, 29% of respondents reported having excellent access to mental health treatment and 42% reported having good access. Despite this, 30% of respondents still reported feeling there was a lot of stigma in their workplace about seeking mental health treatment, with another 43% reporting they felt there was some stigma.
Poll results also showed that 24% of respondents were very concerned about what might happen with their employment if they were to seek mental health treatment, with another 33% saying they were somewhat concerned.
In recent years there have been efforts to break down cultural roadblocks in medicine that deter many physicians from seeking mental health treatment, but more needs to be done, said Mark Rosenberg, DO, MBA, who was elected president of ACEP at last weekend’s annual meeting, ACEP20.
“The pandemic emphatically underscores our need to change the status quo when it comes to physicians’ mental health,” Dr. Rosenberg said.
As previously reported by Medscape Medical News, current efforts to remove such barriers include initiatives to limit inquiries into clinicians’ past or present mental health treatment.
In May, the influential Joint Commission issued a statement urging organizations to refrain from asking about any history of mental health conditions or treatment. The Joint Commission said it supports recommendations already made by the Federation of State Medical Boards and the American Medical Association to limit inquiries on licensing applications to conditions that currently impair a clinician’s ability to perform their job.
Also supporting these efforts is the Dr. Lorna Breen Heroes’ Foundation, created in honor of an emergency physician who died by suicide in April amid the pandemic.
Lorna Breen, MD, had been working intensely in the response to the pandemic. During one shift, she covered two EDs in Manhattan at locations 5 miles apart, according to a backgrounder on the foundation’s web site.
At an ACEP press conference this week, Dr. Breen’s brother-in-law, J. Corey Feist, JD, MBA, cofounder of the foundation, noted that some states’ licensing applications for physicians include questions that fall outside of the boundaries of the Americans With Disabilities Act. He cited an analysis of state medical boards’ initial licensing questions published in 2018 in the Journal of the American Academy of Psychiatry and the Law.
In many cases, states have posed questions that extend beyond an assessment of a physician’s current ability to care for patients, creating a needless hurdle to seeking care, wrote the paper’s lead author, Carol North, MD, of the University of Texas Southwestern Medical Center, Dallas.
“Over the years, many medical licensure boards have asked applicants intrusive questions about whether they have any psychiatric history. This has created a major problem for applicants, and unfortunately this has discouraged many of those who need psychiatric treatment from seeking it because of fear of the questions,” Dr. North and colleagues noted. They cited Ohio as an example of a state that had overhauled its approach to questioning to bring it in compliance with the ADA.
Ohio previously required applicants to answer lengthy questions about their mental health, including:
- Within the last 10 years, have you been diagnosed with or have you been treated for bipolar disorder, schizophrenia, paranoia, or any other psychotic disorder?
- Have you, since attaining the age of eighteen or within the last 10 years, whichever period is shorter, been admitted to a hospital or other facility for the treatment of bipolar disorder, schizophrenia, paranoia, or any other psychotic disorder?
- Do you have, or have you been diagnosed as having, a medical condition which in any way impairs or limits your ability to practice medicine with reasonable skill and safety?
In the new version, the single question reads: “In the past 5 years, have you been diagnosed as having, or been hospitalized for, a medical condition which in any way impairs or limits your ability to practice medicine with reasonable skill and safety?”
Other states such as New York pose no mental health questions on applications for licensure.
Still, even when states have nondiscriminatory laws, physicians may not be aware of them, said Mr. Feist at an ACEP press conference. In addition to his work with the foundation, Mr. Feist is the CEO of the University of Virginia Physicians Group.
He said his sister-in-law Dr. Breen may have worried without cause about potential consequences of seeking psychiatric treatment during the pandemic. In addition, physicians in need of psychiatric care may worry about encountering hitches with medical organizations and insurers.
“This stigma and this fear of professional action on your license or your credentialing or privileging is pervasive throughout the industry,” he said.
A version of this article originally appeared on Medscape.com.
Lilly stops antibody trial in hospitalized COVID-19 patients, other trials continue
Eli Lilly announced it will halt its ACTIV-3 trial evaluating the antibody bamlanivimab in combination with remdesivir for people hospitalized with COVID-19, after new evidence regarding efficacy emerged.
The new data from the National Institutes of Health suggest that the experimental neutralizing antibody therapy does not offer significant clinical benefit for people with more advanced COVID-19 illness, according to a company statement.
Eli Lilly also announced it plans to continue its other trials evaluating the antibody, including those assessing a potential role in treating people in the earlier stages of COVID-19.
“While there was insufficient evidence that bamlanivimab improved clinical outcomes when added to other treatments in hospitalized patients with COVID-19, we remain confident based on data from Lilly’s BLAZE-1 study that bamlanivimab monotherapy may prevent progression of disease for those earlier in the course of COVID-19,” the statement reads.
The ACTIV-3 trial was paused on October 13 after a data and safety monitoring board cited safety concerns.
The most recent data update that triggered an end to the trial did not reveal any significant differences in safety, though.
This article first appeared on Medscape.com.
Eli Lilly announced it will halt its ACTIV-3 trial evaluating the antibody bamlanivimab in combination with remdesivir for people hospitalized with COVID-19, after new evidence regarding efficacy emerged.
The new data from the National Institutes of Health suggest that the experimental neutralizing antibody therapy does not offer significant clinical benefit for people with more advanced COVID-19 illness, according to a company statement.
Eli Lilly also announced it plans to continue its other trials evaluating the antibody, including those assessing a potential role in treating people in the earlier stages of COVID-19.
“While there was insufficient evidence that bamlanivimab improved clinical outcomes when added to other treatments in hospitalized patients with COVID-19, we remain confident based on data from Lilly’s BLAZE-1 study that bamlanivimab monotherapy may prevent progression of disease for those earlier in the course of COVID-19,” the statement reads.
The ACTIV-3 trial was paused on October 13 after a data and safety monitoring board cited safety concerns.
The most recent data update that triggered an end to the trial did not reveal any significant differences in safety, though.
This article first appeared on Medscape.com.
Eli Lilly announced it will halt its ACTIV-3 trial evaluating the antibody bamlanivimab in combination with remdesivir for people hospitalized with COVID-19, after new evidence regarding efficacy emerged.
The new data from the National Institutes of Health suggest that the experimental neutralizing antibody therapy does not offer significant clinical benefit for people with more advanced COVID-19 illness, according to a company statement.
Eli Lilly also announced it plans to continue its other trials evaluating the antibody, including those assessing a potential role in treating people in the earlier stages of COVID-19.
“While there was insufficient evidence that bamlanivimab improved clinical outcomes when added to other treatments in hospitalized patients with COVID-19, we remain confident based on data from Lilly’s BLAZE-1 study that bamlanivimab monotherapy may prevent progression of disease for those earlier in the course of COVID-19,” the statement reads.
The ACTIV-3 trial was paused on October 13 after a data and safety monitoring board cited safety concerns.
The most recent data update that triggered an end to the trial did not reveal any significant differences in safety, though.
This article first appeared on Medscape.com.
Security breach in Finland leads to psychiatric patient blackmail
Hackers have accessed patient records at Finland’s largest private psychotherapy system, emailing some patients to pay up or face having their private medical records released online.
Vastaamo treats about 40,000 patients and runs 25 centers across the country. Hackers emailed some of the centers’ patients asking for a blackmail payment of 200 euro in bitcoin, The Guardian reports.
Agencies such as the country’s National Bureau of Investigation are urging victims not to comply with the blackmailers’ demand and instead requesting that patients report these incidents to authorities and turn over incriminating emails. However, some data from patient records have already been released online.
“We deeply regret what happened and on behalf of our [patients] who have been compromised, we apologize for the shortcoming in data security, the consequences and human cost of which have been extremely heavy,” the center said in a statement. They added that the investigation into the situation is ongoing.
‘Sobering reminder’
In a comment, John Torous, MD, director of digital psychiatry at Beth Israel Deaconess Medical Center, Boston, Massachusetts, said this is “a sobering reminder that any digital data is subject to hacking.”
Torous is also chair of the American Psychiatric Association’s Health and Technology Committee.
“This is not the first time psychotherapy notes have been targeted and it actually happened, on a smaller scale, in the US in 2017,” he said.
In April of that year, confidential patient record information from a mental health center in Maine, including evaluations, session notes, and names of sex-abuse victims, was listed on the dark web.
Also in April, computer hackers released the WannaCry virus into the operating system of the United Kingdom’s National Health Service, which subsequently locked clinicians out of patient records and other digital tools for 3 days.
In addition, in 2016 hackers took Hollywood Presbyterian Medical Center in Los Angeles offline for more than a week after demanding a ransom of $3.6 million.
Criminal investigation
For Vastaamo, three of its employees were approached by the blackmailer via email at the end of September, the company reports. These incidents were immediately disclosed and the Central Criminal Police launched a criminal investigation.
In addition, several agencies were contacted, including the Finnish Cyber Security Center, the Data Protection Commission, and a cyber security company.
Investigators believe the breach, which led to the customer database theft, occurred back in November 2018. In addition, security “deficiencies” remained until March 2019.
“We do not know that the database was stolen after November 2018, but it is possible that individual data [have been] viewed or copied,” Vastaamo said in a press release. No additional “vulnerabilities were identified after March 2019.”
The center’s CEO, Ville Tapio, who did not disclose any of these incidents to the parent company and its board of directors, was subsequently fired.
Once the police investigation began, Vastaamo said it was not granted permission by the authorities to communicate the occurrence to its patients. However, after the blackmailer released some patient information online early on Oct. 21, permission to inform patients was granted.
The company noted that the blackmailer has started emailing victims, informing of the data breach, and demanding ransom. So far, the emails have not contained harmful digital content or “malware,” but authorities warn that any attachments should not be opened. The police have requested that such emails be kept so they can be used as evidence.
In a Q&A section on its website, Vastaamo noted that videos are never recorded during its centers’ telehealth sessions and patients should not be concerned about the possibility of leaked videos.
In addition, the cybercrime has not interrupted Vastaamo’s operations.
“The authorities and the response office will do their utmost to find out what happened, to prevent the dissemination of information, and to bring the perpetrators to justice,” the center said.
“The most important task ... is to support customers in the midst of an exceptionally serious and difficult situation,” it added.
“Worst-case scenario”
In a comment, Ipsit Vahia, MD, medical director at the Institute for Technology and Psychiatry at McLean Hospital, Belmont, Mass., said Vastaamo’s data breach “represents the worst-case scenario for digital health.”
He added that more information is needed about the specifics of the case, including exactly what happened, how the system was hacked, and what information was compromised.
Still, “it raises fundamental questions that healthcare systems, clinicians, and patients everywhere should be asking about what measures are in place to protect electronic medical records and other personal digital information,” said Dr. Vahia.
“This incident also serves as another reminder that the issue of data security and privacy is foundational to digital mental health. Ultimately, without a commitment from all stakeholders to maintaining the strictest levels of security, as well as transparency around how data are handled there will be little to no trust from clinicians or patients,” he said. All of that could prevent digital healthcare from achieving its full potential, he added.
In addition, Dr. Vahia noted that the rapid uptick of telemedicine because of the pandemic has accelerated the use of other forms of digital information in mental healthcare.
“This unfortunate incident should serve as a wake-up call and bring the issue of data protection back firmly into the spotlight,” said Dr. Vahia.
Now that telehealth has become a larger part of clinical practice, said Torous, it’s important for clinicians to be vigilant regarding security procedures.
“Telehealth and digital data are here to stay, and with them new benefits as well as risks. We can continue to work to minimize the risks and protect privacy while ensuring the benefits to patients expand,” he added.
This article first appeared on Medscape.com.
Hackers have accessed patient records at Finland’s largest private psychotherapy system, emailing some patients to pay up or face having their private medical records released online.
Vastaamo treats about 40,000 patients and runs 25 centers across the country. Hackers emailed some of the centers’ patients asking for a blackmail payment of 200 euro in bitcoin, The Guardian reports.
Agencies such as the country’s National Bureau of Investigation are urging victims not to comply with the blackmailers’ demand and instead requesting that patients report these incidents to authorities and turn over incriminating emails. However, some data from patient records have already been released online.
“We deeply regret what happened and on behalf of our [patients] who have been compromised, we apologize for the shortcoming in data security, the consequences and human cost of which have been extremely heavy,” the center said in a statement. They added that the investigation into the situation is ongoing.
‘Sobering reminder’
In a comment, John Torous, MD, director of digital psychiatry at Beth Israel Deaconess Medical Center, Boston, Massachusetts, said this is “a sobering reminder that any digital data is subject to hacking.”
Torous is also chair of the American Psychiatric Association’s Health and Technology Committee.
“This is not the first time psychotherapy notes have been targeted and it actually happened, on a smaller scale, in the US in 2017,” he said.
In April of that year, confidential patient record information from a mental health center in Maine, including evaluations, session notes, and names of sex-abuse victims, was listed on the dark web.
Also in April, computer hackers released the WannaCry virus into the operating system of the United Kingdom’s National Health Service, which subsequently locked clinicians out of patient records and other digital tools for 3 days.
In addition, in 2016 hackers took Hollywood Presbyterian Medical Center in Los Angeles offline for more than a week after demanding a ransom of $3.6 million.
Criminal investigation
For Vastaamo, three of its employees were approached by the blackmailer via email at the end of September, the company reports. These incidents were immediately disclosed and the Central Criminal Police launched a criminal investigation.
In addition, several agencies were contacted, including the Finnish Cyber Security Center, the Data Protection Commission, and a cyber security company.
Investigators believe the breach, which led to the customer database theft, occurred back in November 2018. In addition, security “deficiencies” remained until March 2019.
“We do not know that the database was stolen after November 2018, but it is possible that individual data [have been] viewed or copied,” Vastaamo said in a press release. No additional “vulnerabilities were identified after March 2019.”
The center’s CEO, Ville Tapio, who did not disclose any of these incidents to the parent company and its board of directors, was subsequently fired.
Once the police investigation began, Vastaamo said it was not granted permission by the authorities to communicate the occurrence to its patients. However, after the blackmailer released some patient information online early on Oct. 21, permission to inform patients was granted.
The company noted that the blackmailer has started emailing victims, informing of the data breach, and demanding ransom. So far, the emails have not contained harmful digital content or “malware,” but authorities warn that any attachments should not be opened. The police have requested that such emails be kept so they can be used as evidence.
In a Q&A section on its website, Vastaamo noted that videos are never recorded during its centers’ telehealth sessions and patients should not be concerned about the possibility of leaked videos.
In addition, the cybercrime has not interrupted Vastaamo’s operations.
“The authorities and the response office will do their utmost to find out what happened, to prevent the dissemination of information, and to bring the perpetrators to justice,” the center said.
“The most important task ... is to support customers in the midst of an exceptionally serious and difficult situation,” it added.
“Worst-case scenario”
In a comment, Ipsit Vahia, MD, medical director at the Institute for Technology and Psychiatry at McLean Hospital, Belmont, Mass., said Vastaamo’s data breach “represents the worst-case scenario for digital health.”
He added that more information is needed about the specifics of the case, including exactly what happened, how the system was hacked, and what information was compromised.
Still, “it raises fundamental questions that healthcare systems, clinicians, and patients everywhere should be asking about what measures are in place to protect electronic medical records and other personal digital information,” said Dr. Vahia.
“This incident also serves as another reminder that the issue of data security and privacy is foundational to digital mental health. Ultimately, without a commitment from all stakeholders to maintaining the strictest levels of security, as well as transparency around how data are handled there will be little to no trust from clinicians or patients,” he said. All of that could prevent digital healthcare from achieving its full potential, he added.
In addition, Dr. Vahia noted that the rapid uptick of telemedicine because of the pandemic has accelerated the use of other forms of digital information in mental healthcare.
“This unfortunate incident should serve as a wake-up call and bring the issue of data protection back firmly into the spotlight,” said Dr. Vahia.
Now that telehealth has become a larger part of clinical practice, said Torous, it’s important for clinicians to be vigilant regarding security procedures.
“Telehealth and digital data are here to stay, and with them new benefits as well as risks. We can continue to work to minimize the risks and protect privacy while ensuring the benefits to patients expand,” he added.
This article first appeared on Medscape.com.
Hackers have accessed patient records at Finland’s largest private psychotherapy system, emailing some patients to pay up or face having their private medical records released online.
Vastaamo treats about 40,000 patients and runs 25 centers across the country. Hackers emailed some of the centers’ patients asking for a blackmail payment of 200 euro in bitcoin, The Guardian reports.
Agencies such as the country’s National Bureau of Investigation are urging victims not to comply with the blackmailers’ demand and instead requesting that patients report these incidents to authorities and turn over incriminating emails. However, some data from patient records have already been released online.
“We deeply regret what happened and on behalf of our [patients] who have been compromised, we apologize for the shortcoming in data security, the consequences and human cost of which have been extremely heavy,” the center said in a statement. They added that the investigation into the situation is ongoing.
‘Sobering reminder’
In a comment, John Torous, MD, director of digital psychiatry at Beth Israel Deaconess Medical Center, Boston, Massachusetts, said this is “a sobering reminder that any digital data is subject to hacking.”
Torous is also chair of the American Psychiatric Association’s Health and Technology Committee.
“This is not the first time psychotherapy notes have been targeted and it actually happened, on a smaller scale, in the US in 2017,” he said.
In April of that year, confidential patient record information from a mental health center in Maine, including evaluations, session notes, and names of sex-abuse victims, was listed on the dark web.
Also in April, computer hackers released the WannaCry virus into the operating system of the United Kingdom’s National Health Service, which subsequently locked clinicians out of patient records and other digital tools for 3 days.
In addition, in 2016 hackers took Hollywood Presbyterian Medical Center in Los Angeles offline for more than a week after demanding a ransom of $3.6 million.
Criminal investigation
For Vastaamo, three of its employees were approached by the blackmailer via email at the end of September, the company reports. These incidents were immediately disclosed and the Central Criminal Police launched a criminal investigation.
In addition, several agencies were contacted, including the Finnish Cyber Security Center, the Data Protection Commission, and a cyber security company.
Investigators believe the breach, which led to the customer database theft, occurred back in November 2018. In addition, security “deficiencies” remained until March 2019.
“We do not know that the database was stolen after November 2018, but it is possible that individual data [have been] viewed or copied,” Vastaamo said in a press release. No additional “vulnerabilities were identified after March 2019.”
The center’s CEO, Ville Tapio, who did not disclose any of these incidents to the parent company and its board of directors, was subsequently fired.
Once the police investigation began, Vastaamo said it was not granted permission by the authorities to communicate the occurrence to its patients. However, after the blackmailer released some patient information online early on Oct. 21, permission to inform patients was granted.
The company noted that the blackmailer has started emailing victims, informing of the data breach, and demanding ransom. So far, the emails have not contained harmful digital content or “malware,” but authorities warn that any attachments should not be opened. The police have requested that such emails be kept so they can be used as evidence.
In a Q&A section on its website, Vastaamo noted that videos are never recorded during its centers’ telehealth sessions and patients should not be concerned about the possibility of leaked videos.
In addition, the cybercrime has not interrupted Vastaamo’s operations.
“The authorities and the response office will do their utmost to find out what happened, to prevent the dissemination of information, and to bring the perpetrators to justice,” the center said.
“The most important task ... is to support customers in the midst of an exceptionally serious and difficult situation,” it added.
“Worst-case scenario”
In a comment, Ipsit Vahia, MD, medical director at the Institute for Technology and Psychiatry at McLean Hospital, Belmont, Mass., said Vastaamo’s data breach “represents the worst-case scenario for digital health.”
He added that more information is needed about the specifics of the case, including exactly what happened, how the system was hacked, and what information was compromised.
Still, “it raises fundamental questions that healthcare systems, clinicians, and patients everywhere should be asking about what measures are in place to protect electronic medical records and other personal digital information,” said Dr. Vahia.
“This incident also serves as another reminder that the issue of data security and privacy is foundational to digital mental health. Ultimately, without a commitment from all stakeholders to maintaining the strictest levels of security, as well as transparency around how data are handled there will be little to no trust from clinicians or patients,” he said. All of that could prevent digital healthcare from achieving its full potential, he added.
In addition, Dr. Vahia noted that the rapid uptick of telemedicine because of the pandemic has accelerated the use of other forms of digital information in mental healthcare.
“This unfortunate incident should serve as a wake-up call and bring the issue of data protection back firmly into the spotlight,” said Dr. Vahia.
Now that telehealth has become a larger part of clinical practice, said Torous, it’s important for clinicians to be vigilant regarding security procedures.
“Telehealth and digital data are here to stay, and with them new benefits as well as risks. We can continue to work to minimize the risks and protect privacy while ensuring the benefits to patients expand,” he added.
This article first appeared on Medscape.com.
The new one-percenters: Children with COVID-19
according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
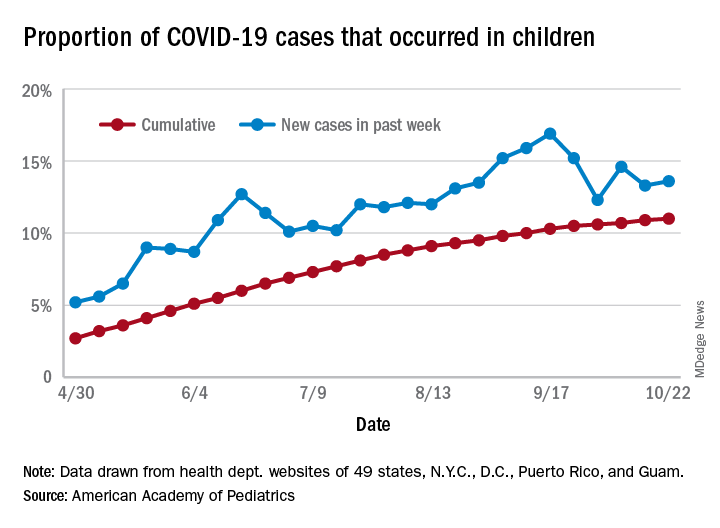
There have been 1,052 cases of COVID-19 per 100,000 children as of Oct. 22, and that works out to 1.05% of all children in the country. The cumulative number of pediatric cases is 792,188, and children now represent 11% of all COVID-19 cases, the AAP and the CHA reported Oct. 26.
There were just over 50,000 new child cases reported in the week ending Oct. 22, which was 13.6% of the national total of almost 370,000. That’s up slightly from the 13.3% the previous week but still down from the spike seen in mid-September, based on the data collected from the websites of 49 state health departments (New York does not report ages), along with the District of Columbia, New York City, Puerto Rico, and Guam.
The state-level data show that California has had more COVID-19 cases in children (92,864) than any other state, although Texas has reported ages for only 7% of its confirmed cases. Illinois is next with 46,006 cases, followed by Florida at 45,575, although Florida is using an age range of 0-14 years to define a child case, the AAP and CHA noted.
Other measures largely put small states at the extremes:
- North Dakota has the highest cumulative rate: 2,954 cases per 100,000 children.
- Vermont has the lowest cumulative rate: 190.5 per 100,000.
- Wyoming has the highest proportion of cases in children: 27.7%.
- New Jersey has the lowest proportion of child cases: 4.6%.
There were no COVID-19–related deaths in children reported the week ending Oct. 22, so the total number remains at 120, which is just 0.06% of the total for all ages, based on data from 42 states and New York City. Hospitalization figures put admissions at almost 5,600 in children, or 1.7% of all hospitalizations, although those data come from just 24 states and New York City, the AAP and CHA said.
according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
There have been 1,052 cases of COVID-19 per 100,000 children as of Oct. 22, and that works out to 1.05% of all children in the country. The cumulative number of pediatric cases is 792,188, and children now represent 11% of all COVID-19 cases, the AAP and the CHA reported Oct. 26.
There were just over 50,000 new child cases reported in the week ending Oct. 22, which was 13.6% of the national total of almost 370,000. That’s up slightly from the 13.3% the previous week but still down from the spike seen in mid-September, based on the data collected from the websites of 49 state health departments (New York does not report ages), along with the District of Columbia, New York City, Puerto Rico, and Guam.
The state-level data show that California has had more COVID-19 cases in children (92,864) than any other state, although Texas has reported ages for only 7% of its confirmed cases. Illinois is next with 46,006 cases, followed by Florida at 45,575, although Florida is using an age range of 0-14 years to define a child case, the AAP and CHA noted.
Other measures largely put small states at the extremes:
- North Dakota has the highest cumulative rate: 2,954 cases per 100,000 children.
- Vermont has the lowest cumulative rate: 190.5 per 100,000.
- Wyoming has the highest proportion of cases in children: 27.7%.
- New Jersey has the lowest proportion of child cases: 4.6%.
There were no COVID-19–related deaths in children reported the week ending Oct. 22, so the total number remains at 120, which is just 0.06% of the total for all ages, based on data from 42 states and New York City. Hospitalization figures put admissions at almost 5,600 in children, or 1.7% of all hospitalizations, although those data come from just 24 states and New York City, the AAP and CHA said.
according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
There have been 1,052 cases of COVID-19 per 100,000 children as of Oct. 22, and that works out to 1.05% of all children in the country. The cumulative number of pediatric cases is 792,188, and children now represent 11% of all COVID-19 cases, the AAP and the CHA reported Oct. 26.
There were just over 50,000 new child cases reported in the week ending Oct. 22, which was 13.6% of the national total of almost 370,000. That’s up slightly from the 13.3% the previous week but still down from the spike seen in mid-September, based on the data collected from the websites of 49 state health departments (New York does not report ages), along with the District of Columbia, New York City, Puerto Rico, and Guam.
The state-level data show that California has had more COVID-19 cases in children (92,864) than any other state, although Texas has reported ages for only 7% of its confirmed cases. Illinois is next with 46,006 cases, followed by Florida at 45,575, although Florida is using an age range of 0-14 years to define a child case, the AAP and CHA noted.
Other measures largely put small states at the extremes:
- North Dakota has the highest cumulative rate: 2,954 cases per 100,000 children.
- Vermont has the lowest cumulative rate: 190.5 per 100,000.
- Wyoming has the highest proportion of cases in children: 27.7%.
- New Jersey has the lowest proportion of child cases: 4.6%.
There were no COVID-19–related deaths in children reported the week ending Oct. 22, so the total number remains at 120, which is just 0.06% of the total for all ages, based on data from 42 states and New York City. Hospitalization figures put admissions at almost 5,600 in children, or 1.7% of all hospitalizations, although those data come from just 24 states and New York City, the AAP and CHA said.
COVID-19: Immunity from antibodies may decline rapidly
Antibody response to the SARS-CoV-2 virus wanes over time, latest research has suggested.
An ongoing study led by Imperial College London (ICL) found that the proportion of people testing positive for COVID-19 antibodies dropped by 26.5% over a 3-month period between June and September.
The findings from a non–peer reviewed preprint suggested that infection with SARS-CoV-2 confers only limited protection against reinfection.
Professor Paul Elliott, director of the REACT-2 programme at ICL, said: “Testing positive for antibodies does not mean you are immune to COVID-19.
“It remains unclear what level of immunity antibodies provide, or for how long this immunity lasts.”
Experts said that, while the findings suggested that immunity might fade over time, the severity of illness from further infections could be reduced.
Antibody prevalence declined in all adults
Results from cross-sectional studies over the 3-month period involved 365,104 adults who self-administered a lateral flow immunoassay test.
There were 17,576 positive tests over the three rounds.
Antibody prevalence, adjusted for test characteristics and weighted to the adult population of England, declined from 6.0% to 4.4%, a reduction of 26.5% over the 3 months.
The decline was seen in all age groups. However, the lowest prevalence of a positive test, and the largest fall, was seen in those aged 75 years and older.
No change was seen in positive antibody tests in health care workers over the 3 months.
The results suggested that people who did not show symptoms of COVID-19 were more likely to lose detectable antibodies sooner than those who did show symptoms.
Prof Helen Ward, one of the lead authors of the report said that, while it was clear that the proportion of people with antibodies was falling over time, “We don’t yet know whether this will leave these people at risk of reinfection with the virus that causes COVID-19, but it is essential that everyone continues to follow guidance to reduce the risk to themselves and others.”
Results ‘weaken argument for herd immunity’
Commenting on the results to the Science Media Centre, Rowland Kao, professor of veterinary epidemiology and data science at the University of Edinburgh, warned that, if the results were correct, “any strategy that relies on ‘herd immunity’ lacks credibility.”
However, he added that, “while the decline is substantial, nevertheless substantial proportions of the population do retain some immune response, over 4 months after the peak of the epidemic”.
Eleanor Riley, professor of immunology and infectious disease, also from the University of Edinburgh, said it was too early to assume that immunity to SARS-CoV-2 did not last because “the study does not look at antibody concentrations, antibody function, or other aspects of immunity such as T-cell immunity and does not look at the trajectory of antibody levels in the same individuals over time”.
However, she said the findings did not mean that a vaccine would be ineffective because vaccines contained adjuvants that could induce durable immune responses, particularly with multiple immunizations.
“What is not clear is how quickly antibody levels would rise again if a person encounters the SARS-CoV-2 virus a second time. It is possible they will still rapidly respond, and either have a milder illness, or remain protected through immune memory,” commented Dr. Alexander Edwards, associate professor in biomedical technology at the University of Reading.
Health Minister Lord Bethell said: “Regardless of the result of an antibody test, everyone must continue to comply with government guidelines including social distancing, self-isolating, and getting a test if you have symptoms, and always remember: hands, face, space.”
This article first appeared on Medscape.com.
Antibody response to the SARS-CoV-2 virus wanes over time, latest research has suggested.
An ongoing study led by Imperial College London (ICL) found that the proportion of people testing positive for COVID-19 antibodies dropped by 26.5% over a 3-month period between June and September.
The findings from a non–peer reviewed preprint suggested that infection with SARS-CoV-2 confers only limited protection against reinfection.
Professor Paul Elliott, director of the REACT-2 programme at ICL, said: “Testing positive for antibodies does not mean you are immune to COVID-19.
“It remains unclear what level of immunity antibodies provide, or for how long this immunity lasts.”
Experts said that, while the findings suggested that immunity might fade over time, the severity of illness from further infections could be reduced.
Antibody prevalence declined in all adults
Results from cross-sectional studies over the 3-month period involved 365,104 adults who self-administered a lateral flow immunoassay test.
There were 17,576 positive tests over the three rounds.
Antibody prevalence, adjusted for test characteristics and weighted to the adult population of England, declined from 6.0% to 4.4%, a reduction of 26.5% over the 3 months.
The decline was seen in all age groups. However, the lowest prevalence of a positive test, and the largest fall, was seen in those aged 75 years and older.
No change was seen in positive antibody tests in health care workers over the 3 months.
The results suggested that people who did not show symptoms of COVID-19 were more likely to lose detectable antibodies sooner than those who did show symptoms.
Prof Helen Ward, one of the lead authors of the report said that, while it was clear that the proportion of people with antibodies was falling over time, “We don’t yet know whether this will leave these people at risk of reinfection with the virus that causes COVID-19, but it is essential that everyone continues to follow guidance to reduce the risk to themselves and others.”
Results ‘weaken argument for herd immunity’
Commenting on the results to the Science Media Centre, Rowland Kao, professor of veterinary epidemiology and data science at the University of Edinburgh, warned that, if the results were correct, “any strategy that relies on ‘herd immunity’ lacks credibility.”
However, he added that, “while the decline is substantial, nevertheless substantial proportions of the population do retain some immune response, over 4 months after the peak of the epidemic”.
Eleanor Riley, professor of immunology and infectious disease, also from the University of Edinburgh, said it was too early to assume that immunity to SARS-CoV-2 did not last because “the study does not look at antibody concentrations, antibody function, or other aspects of immunity such as T-cell immunity and does not look at the trajectory of antibody levels in the same individuals over time”.
However, she said the findings did not mean that a vaccine would be ineffective because vaccines contained adjuvants that could induce durable immune responses, particularly with multiple immunizations.
“What is not clear is how quickly antibody levels would rise again if a person encounters the SARS-CoV-2 virus a second time. It is possible they will still rapidly respond, and either have a milder illness, or remain protected through immune memory,” commented Dr. Alexander Edwards, associate professor in biomedical technology at the University of Reading.
Health Minister Lord Bethell said: “Regardless of the result of an antibody test, everyone must continue to comply with government guidelines including social distancing, self-isolating, and getting a test if you have symptoms, and always remember: hands, face, space.”
This article first appeared on Medscape.com.
Antibody response to the SARS-CoV-2 virus wanes over time, latest research has suggested.
An ongoing study led by Imperial College London (ICL) found that the proportion of people testing positive for COVID-19 antibodies dropped by 26.5% over a 3-month period between June and September.
The findings from a non–peer reviewed preprint suggested that infection with SARS-CoV-2 confers only limited protection against reinfection.
Professor Paul Elliott, director of the REACT-2 programme at ICL, said: “Testing positive for antibodies does not mean you are immune to COVID-19.
“It remains unclear what level of immunity antibodies provide, or for how long this immunity lasts.”
Experts said that, while the findings suggested that immunity might fade over time, the severity of illness from further infections could be reduced.
Antibody prevalence declined in all adults
Results from cross-sectional studies over the 3-month period involved 365,104 adults who self-administered a lateral flow immunoassay test.
There were 17,576 positive tests over the three rounds.
Antibody prevalence, adjusted for test characteristics and weighted to the adult population of England, declined from 6.0% to 4.4%, a reduction of 26.5% over the 3 months.
The decline was seen in all age groups. However, the lowest prevalence of a positive test, and the largest fall, was seen in those aged 75 years and older.
No change was seen in positive antibody tests in health care workers over the 3 months.
The results suggested that people who did not show symptoms of COVID-19 were more likely to lose detectable antibodies sooner than those who did show symptoms.
Prof Helen Ward, one of the lead authors of the report said that, while it was clear that the proportion of people with antibodies was falling over time, “We don’t yet know whether this will leave these people at risk of reinfection with the virus that causes COVID-19, but it is essential that everyone continues to follow guidance to reduce the risk to themselves and others.”
Results ‘weaken argument for herd immunity’
Commenting on the results to the Science Media Centre, Rowland Kao, professor of veterinary epidemiology and data science at the University of Edinburgh, warned that, if the results were correct, “any strategy that relies on ‘herd immunity’ lacks credibility.”
However, he added that, “while the decline is substantial, nevertheless substantial proportions of the population do retain some immune response, over 4 months after the peak of the epidemic”.
Eleanor Riley, professor of immunology and infectious disease, also from the University of Edinburgh, said it was too early to assume that immunity to SARS-CoV-2 did not last because “the study does not look at antibody concentrations, antibody function, or other aspects of immunity such as T-cell immunity and does not look at the trajectory of antibody levels in the same individuals over time”.
However, she said the findings did not mean that a vaccine would be ineffective because vaccines contained adjuvants that could induce durable immune responses, particularly with multiple immunizations.
“What is not clear is how quickly antibody levels would rise again if a person encounters the SARS-CoV-2 virus a second time. It is possible they will still rapidly respond, and either have a milder illness, or remain protected through immune memory,” commented Dr. Alexander Edwards, associate professor in biomedical technology at the University of Reading.
Health Minister Lord Bethell said: “Regardless of the result of an antibody test, everyone must continue to comply with government guidelines including social distancing, self-isolating, and getting a test if you have symptoms, and always remember: hands, face, space.”
This article first appeared on Medscape.com.
Now USPSTF also suggests start CRC screening at age 45
that is open for public comment.
“This is the only change that was made,” said task force member Michael Barry, MD, director of the Informed Medical Decisions Program in the Health Decision Sciences Center at Massachusetts General Hospital, Boston.
The recommendation is that all adults aged 45-75 years be screened for CRC.
This is an “A” recommendation for adults aged 50-75 and a “B” recommendation for adults aged 45-49. Dr. Barry explained that the reason for this difference is that the benefit is smaller for the 45- to 49-years age group. “But there’s not much difference between A and B from a practical standpoint,” he explained.
For adults aged 76-85, the benefits and harms of screening need to be weighed against the individual’s overall health and personal circumstances. This is a “C” recommendation.
Barry emphasized that the USPSTF document is not final. The draft recommendation and supporting evidence is posted on the task force website and will be available for public comments until Nov. 23.
Mounting pressure
The move comes after mounting evidence of an increase in CRC among younger adults and mounting pressure to lower the starting age.
Two years ago, the American Cancer Society (ACS) revised its own screening guidelines and lowered the starting age to 45 years. Soon afterward, a coalition of 22 public health and patient advocacy groups joined the ACS in submitting a letter to the USPSTF asking that the task force reconsider its 2016 guidance (which recommends starting at age 50 years).
The starting age for screening is an important issue, commented Judy Yee, MD, chair of radiology at the Albert Einstein College of Medicine and the Montefiore Health System in New York and chair of the Colon Cancer Committee of the American College of Radiology.
“Right now it is very confusing to physicians and to the public,” Dr. Yee said in an interview at that time. “The USPSTF and the ACS differ as far as the age to begin screening, and insurers may not cover the cost of colorectal cancer screening before age 50.”
Dr. Barry said that the Task Force took notice of recent data showing an increase in the incidence of CRC among younger adults. “The risk now for age 45 to 49 is pretty similar to the risk for people in their early 50s. So in some ways, today’s late 40-year-olds are like yesterday’s 50-year-olds,” he commented.
The task force used simulation models that confirmed what the epidemiologic data suggested and “that we could prevent some additional colorectal cancer deaths by starting screening at age 45,” he said.
The rest of the new draft recommendation is similar to the 2016 guidelines, in which the task force says there is convincing evidence that CRC screening substantially reduces disease-related mortality. However, it does not recommend any one screening approach over another. It recommends both direct visualization, such as colonoscopy, as well as noninvasive stool-based tests. It does not recommend serum tests, urine tests, or capsule endoscopy because there is not yet enough evidence about the benefits and harms of these tests.
“The right test is the one a patient will do,” Dr. Barry commented.
Defining populations
CRC in young adults made the news in August 2020 when Chadwick Boseman, known for his role as King T’Challa in Marvel’s “Black Panther,” died of colon cancer. Diagnosed in 2016, he was only 43 years old.
“The recent passing of Chadwick Boseman is tragic, and our thoughts are with his loved ones during this difficult time,” said Dr. Barry. “As a Black man, the data show that Chadwick was at higher risk for developing colorectal cancer.”
Unfortunately, there is currently not enough evidence that screening Black men younger than 45 could help prevent tragic deaths such as Chadwick’s, he commented. “The task force is calling for more research on colorectal cancer screening in Black adults,” he added.
Limit screening to those at higher risk
In contrast to the USPSTF and ACS guidelines, which recommend screening for CRC for everyone over a certain age, a set of recommendations developed by an international panel of experts suggests screening only for individuals who are at higher risk for CRC.
As previously reported, these guidelines suggest restricting screening to adults whose cumulative cancer risk is 3% or more in the next 15 years, the point at which the balance between benefits and harms favors screening.
The authors, led by Lise Helsingen, MD, Clinical Effectiveness Research Group, University of Oslo, said “the optimal choice for each person requires shared decision-making.”
Such a risk-based approach is “increasingly regarded as the most appropriate way to discuss cancer screening.” That approach is already used in prostate and lung cancer screening, they noted.
A version of this article originally appeared on Medscape.com.
Clinicians and researchers have actively debated the pros and cons of lowering the screening age to 45 years since 2018, when the American Cancer Society released its colorectal cancer (CRC) screening guidelines. The most compelling argument in support of lowering the screening age is that recent data from Surveillance Epidemiology and End Results (SEER) show that the CRC incidence rates in 45- to 50-year-olds are similar to rates seen in 50- to 54-year-olds about 20 years ago, when the first guidelines to initiate screening at age 50 were widely established. Termed early-onset CRC (EOCRC), the underlying reasons for this increase are not completely understood, and while the absolute numbers of EOCRC cases are smaller than in older age groups, modeling studies show that screening this age group is both efficient and effective.

Over the last 20 years we have made major strides in reducing the incidence and mortality from CRC in ages 50 years and older, and now we must rise to the challenge of delivering CRC screening to this younger group in order to see similar dividends over time and curb the rising incidence curve of EOCRC. And we must do so without direct evidence to guide us as to the magnitude of the benefit of screening this younger group, the best modality to use, or tools to risk stratify who is likely to benefit from screening in this group. We must also be careful not to worsen racial and geographic disparities in CRC screening, which already exist for African Americans, Native Americans, and other minorities and rural residents. Finally, even though the goal posts are changing, our target remains to get to 80% screening rates for all age groups, and not neglect the currently underscreened 50- to 75-year-olds, who are at a much higher risk of CRC than their younger counterparts.
Aasma Shaukat, MD, MPH, is an investigator, Center for Care Delivery and Outcomes Research, section chief and staff physician, GI section, Minneapolis VA Health Care System; staff physician, Fairview University of Minnesota Medical Center, Minneapolis; and professor, University of Minnesota department of medicine, division of gastroenterology, Minneapolis. She has no conflicts of interest.
Clinicians and researchers have actively debated the pros and cons of lowering the screening age to 45 years since 2018, when the American Cancer Society released its colorectal cancer (CRC) screening guidelines. The most compelling argument in support of lowering the screening age is that recent data from Surveillance Epidemiology and End Results (SEER) show that the CRC incidence rates in 45- to 50-year-olds are similar to rates seen in 50- to 54-year-olds about 20 years ago, when the first guidelines to initiate screening at age 50 were widely established. Termed early-onset CRC (EOCRC), the underlying reasons for this increase are not completely understood, and while the absolute numbers of EOCRC cases are smaller than in older age groups, modeling studies show that screening this age group is both efficient and effective.
Over the last 20 years we have made major strides in reducing the incidence and mortality from CRC in ages 50 years and older, and now we must rise to the challenge of delivering CRC screening to this younger group in order to see similar dividends over time and curb the rising incidence curve of EOCRC. And we must do so without direct evidence to guide us as to the magnitude of the benefit of screening this younger group, the best modality to use, or tools to risk stratify who is likely to benefit from screening in this group. We must also be careful not to worsen racial and geographic disparities in CRC screening, which already exist for African Americans, Native Americans, and other minorities and rural residents. Finally, even though the goal posts are changing, our target remains to get to 80% screening rates for all age groups, and not neglect the currently underscreened 50- to 75-year-olds, who are at a much higher risk of CRC than their younger counterparts.
Aasma Shaukat, MD, MPH, is an investigator, Center for Care Delivery and Outcomes Research, section chief and staff physician, GI section, Minneapolis VA Health Care System; staff physician, Fairview University of Minnesota Medical Center, Minneapolis; and professor, University of Minnesota department of medicine, division of gastroenterology, Minneapolis. She has no conflicts of interest.
Clinicians and researchers have actively debated the pros and cons of lowering the screening age to 45 years since 2018, when the American Cancer Society released its colorectal cancer (CRC) screening guidelines. The most compelling argument in support of lowering the screening age is that recent data from Surveillance Epidemiology and End Results (SEER) show that the CRC incidence rates in 45- to 50-year-olds are similar to rates seen in 50- to 54-year-olds about 20 years ago, when the first guidelines to initiate screening at age 50 were widely established. Termed early-onset CRC (EOCRC), the underlying reasons for this increase are not completely understood, and while the absolute numbers of EOCRC cases are smaller than in older age groups, modeling studies show that screening this age group is both efficient and effective.
Over the last 20 years we have made major strides in reducing the incidence and mortality from CRC in ages 50 years and older, and now we must rise to the challenge of delivering CRC screening to this younger group in order to see similar dividends over time and curb the rising incidence curve of EOCRC. And we must do so without direct evidence to guide us as to the magnitude of the benefit of screening this younger group, the best modality to use, or tools to risk stratify who is likely to benefit from screening in this group. We must also be careful not to worsen racial and geographic disparities in CRC screening, which already exist for African Americans, Native Americans, and other minorities and rural residents. Finally, even though the goal posts are changing, our target remains to get to 80% screening rates for all age groups, and not neglect the currently underscreened 50- to 75-year-olds, who are at a much higher risk of CRC than their younger counterparts.
Aasma Shaukat, MD, MPH, is an investigator, Center for Care Delivery and Outcomes Research, section chief and staff physician, GI section, Minneapolis VA Health Care System; staff physician, Fairview University of Minnesota Medical Center, Minneapolis; and professor, University of Minnesota department of medicine, division of gastroenterology, Minneapolis. She has no conflicts of interest.
that is open for public comment.
“This is the only change that was made,” said task force member Michael Barry, MD, director of the Informed Medical Decisions Program in the Health Decision Sciences Center at Massachusetts General Hospital, Boston.
The recommendation is that all adults aged 45-75 years be screened for CRC.
This is an “A” recommendation for adults aged 50-75 and a “B” recommendation for adults aged 45-49. Dr. Barry explained that the reason for this difference is that the benefit is smaller for the 45- to 49-years age group. “But there’s not much difference between A and B from a practical standpoint,” he explained.
For adults aged 76-85, the benefits and harms of screening need to be weighed against the individual’s overall health and personal circumstances. This is a “C” recommendation.
Barry emphasized that the USPSTF document is not final. The draft recommendation and supporting evidence is posted on the task force website and will be available for public comments until Nov. 23.
Mounting pressure
The move comes after mounting evidence of an increase in CRC among younger adults and mounting pressure to lower the starting age.
Two years ago, the American Cancer Society (ACS) revised its own screening guidelines and lowered the starting age to 45 years. Soon afterward, a coalition of 22 public health and patient advocacy groups joined the ACS in submitting a letter to the USPSTF asking that the task force reconsider its 2016 guidance (which recommends starting at age 50 years).
The starting age for screening is an important issue, commented Judy Yee, MD, chair of radiology at the Albert Einstein College of Medicine and the Montefiore Health System in New York and chair of the Colon Cancer Committee of the American College of Radiology.
“Right now it is very confusing to physicians and to the public,” Dr. Yee said in an interview at that time. “The USPSTF and the ACS differ as far as the age to begin screening, and insurers may not cover the cost of colorectal cancer screening before age 50.”
Dr. Barry said that the Task Force took notice of recent data showing an increase in the incidence of CRC among younger adults. “The risk now for age 45 to 49 is pretty similar to the risk for people in their early 50s. So in some ways, today’s late 40-year-olds are like yesterday’s 50-year-olds,” he commented.
The task force used simulation models that confirmed what the epidemiologic data suggested and “that we could prevent some additional colorectal cancer deaths by starting screening at age 45,” he said.
The rest of the new draft recommendation is similar to the 2016 guidelines, in which the task force says there is convincing evidence that CRC screening substantially reduces disease-related mortality. However, it does not recommend any one screening approach over another. It recommends both direct visualization, such as colonoscopy, as well as noninvasive stool-based tests. It does not recommend serum tests, urine tests, or capsule endoscopy because there is not yet enough evidence about the benefits and harms of these tests.
“The right test is the one a patient will do,” Dr. Barry commented.
Defining populations
CRC in young adults made the news in August 2020 when Chadwick Boseman, known for his role as King T’Challa in Marvel’s “Black Panther,” died of colon cancer. Diagnosed in 2016, he was only 43 years old.
“The recent passing of Chadwick Boseman is tragic, and our thoughts are with his loved ones during this difficult time,” said Dr. Barry. “As a Black man, the data show that Chadwick was at higher risk for developing colorectal cancer.”
Unfortunately, there is currently not enough evidence that screening Black men younger than 45 could help prevent tragic deaths such as Chadwick’s, he commented. “The task force is calling for more research on colorectal cancer screening in Black adults,” he added.
Limit screening to those at higher risk
In contrast to the USPSTF and ACS guidelines, which recommend screening for CRC for everyone over a certain age, a set of recommendations developed by an international panel of experts suggests screening only for individuals who are at higher risk for CRC.
As previously reported, these guidelines suggest restricting screening to adults whose cumulative cancer risk is 3% or more in the next 15 years, the point at which the balance between benefits and harms favors screening.
The authors, led by Lise Helsingen, MD, Clinical Effectiveness Research Group, University of Oslo, said “the optimal choice for each person requires shared decision-making.”
Such a risk-based approach is “increasingly regarded as the most appropriate way to discuss cancer screening.” That approach is already used in prostate and lung cancer screening, they noted.
A version of this article originally appeared on Medscape.com.
that is open for public comment.
“This is the only change that was made,” said task force member Michael Barry, MD, director of the Informed Medical Decisions Program in the Health Decision Sciences Center at Massachusetts General Hospital, Boston.
The recommendation is that all adults aged 45-75 years be screened for CRC.
This is an “A” recommendation for adults aged 50-75 and a “B” recommendation for adults aged 45-49. Dr. Barry explained that the reason for this difference is that the benefit is smaller for the 45- to 49-years age group. “But there’s not much difference between A and B from a practical standpoint,” he explained.
For adults aged 76-85, the benefits and harms of screening need to be weighed against the individual’s overall health and personal circumstances. This is a “C” recommendation.
Barry emphasized that the USPSTF document is not final. The draft recommendation and supporting evidence is posted on the task force website and will be available for public comments until Nov. 23.
Mounting pressure
The move comes after mounting evidence of an increase in CRC among younger adults and mounting pressure to lower the starting age.
Two years ago, the American Cancer Society (ACS) revised its own screening guidelines and lowered the starting age to 45 years. Soon afterward, a coalition of 22 public health and patient advocacy groups joined the ACS in submitting a letter to the USPSTF asking that the task force reconsider its 2016 guidance (which recommends starting at age 50 years).
The starting age for screening is an important issue, commented Judy Yee, MD, chair of radiology at the Albert Einstein College of Medicine and the Montefiore Health System in New York and chair of the Colon Cancer Committee of the American College of Radiology.
“Right now it is very confusing to physicians and to the public,” Dr. Yee said in an interview at that time. “The USPSTF and the ACS differ as far as the age to begin screening, and insurers may not cover the cost of colorectal cancer screening before age 50.”
Dr. Barry said that the Task Force took notice of recent data showing an increase in the incidence of CRC among younger adults. “The risk now for age 45 to 49 is pretty similar to the risk for people in their early 50s. So in some ways, today’s late 40-year-olds are like yesterday’s 50-year-olds,” he commented.
The task force used simulation models that confirmed what the epidemiologic data suggested and “that we could prevent some additional colorectal cancer deaths by starting screening at age 45,” he said.
The rest of the new draft recommendation is similar to the 2016 guidelines, in which the task force says there is convincing evidence that CRC screening substantially reduces disease-related mortality. However, it does not recommend any one screening approach over another. It recommends both direct visualization, such as colonoscopy, as well as noninvasive stool-based tests. It does not recommend serum tests, urine tests, or capsule endoscopy because there is not yet enough evidence about the benefits and harms of these tests.
“The right test is the one a patient will do,” Dr. Barry commented.
Defining populations
CRC in young adults made the news in August 2020 when Chadwick Boseman, known for his role as King T’Challa in Marvel’s “Black Panther,” died of colon cancer. Diagnosed in 2016, he was only 43 years old.
“The recent passing of Chadwick Boseman is tragic, and our thoughts are with his loved ones during this difficult time,” said Dr. Barry. “As a Black man, the data show that Chadwick was at higher risk for developing colorectal cancer.”
Unfortunately, there is currently not enough evidence that screening Black men younger than 45 could help prevent tragic deaths such as Chadwick’s, he commented. “The task force is calling for more research on colorectal cancer screening in Black adults,” he added.
Limit screening to those at higher risk
In contrast to the USPSTF and ACS guidelines, which recommend screening for CRC for everyone over a certain age, a set of recommendations developed by an international panel of experts suggests screening only for individuals who are at higher risk for CRC.
As previously reported, these guidelines suggest restricting screening to adults whose cumulative cancer risk is 3% or more in the next 15 years, the point at which the balance between benefits and harms favors screening.
The authors, led by Lise Helsingen, MD, Clinical Effectiveness Research Group, University of Oslo, said “the optimal choice for each person requires shared decision-making.”
Such a risk-based approach is “increasingly regarded as the most appropriate way to discuss cancer screening.” That approach is already used in prostate and lung cancer screening, they noted.
A version of this article originally appeared on Medscape.com.
Trump signs CR with Medicare loan relief
President Trump on Oct. 1 signed a bill to keep the federal government running through Dec. 11. This “continuing resolution” (CR), which was approved by the House by a 359-57 vote and the Senate by a 84-10 vote, includes provisions to delay repayment by physicians of pandemic-related Medicare loans and to reduce the loans’ interest rate.
In an earlier news release, the American Medical Association reported that Congress and the White House had agreed to include the provisions on Medicare loans in the CR.
Under Medicare’s Accelerated and Advance Payments (AAP) Program, the Centers for Medicare & Medicaid Services (CMS) advanced funds to physicians who were financially impacted by the pandemic.
Revisions were made under the Coronavirus Aid, Relief, and Economic Security (CARES) Act to broaden the existing program to supply provider relief related to the public health emergency. The program was revised in March but suspended accepting new applications related to the pandemic in late April.
Physicians who received APP loans were required to begin repayment within 120 days after the loan disbursement. CMS planned to recoup the advances by offsetting them against Medicare claims payments due to physicians. Practices had up to 210 days (7 months) to repay the loans through this process before being asked to repay them directly with a 10.25 % interest rate.
For practices that received these advances, their Medicare cash flow was scheduled to dry up, starting in August. However, CMS quietly abstained from collecting these payments when they came due, according to Modern Healthcare.
New terms
Under the new loan repayment terms in the CR, repayment of the disbursed funds is postponed until 365 days after the date on which a practice received the money. The balance is due by September 2022.
The amount to be recouped from each claim is reduced from 100% to 25% of the claim for the first 11 months and to 50% of claims withheld for an additional 6 months. If the loan is not repaid in full by then, the provider must pay the balance with an interest rate of 4%.
More than 80% of the $100 billion that CMS loaned to health care providers through May 2 went to hospitals, Modern Healthcare calculated. Of the remainder, specialty or multispecialty practices received $3.5 billion, internal medicine specialists got $24 million, family physicians were loaned $15 million, and federally qualified health centers received $20 million.
In the AMA’s news release, AMA President Susan Bailey, MD, who assumed the post in June, called the original loan repayment plan an “economic sword hanging over physician practices.”
The American Gastroenterological Association has been advocating for more flexibility for the financial assistance programs, such as the Accelerated and Advanced Payment Program and the Paycheck Protection Program, that physicians have utilized. It is critical to give physicians leeway on these loans given that many practices are still not operating at full capacity.
Based on reporting from Medscape.com.
President Trump on Oct. 1 signed a bill to keep the federal government running through Dec. 11. This “continuing resolution” (CR), which was approved by the House by a 359-57 vote and the Senate by a 84-10 vote, includes provisions to delay repayment by physicians of pandemic-related Medicare loans and to reduce the loans’ interest rate.
In an earlier news release, the American Medical Association reported that Congress and the White House had agreed to include the provisions on Medicare loans in the CR.
Under Medicare’s Accelerated and Advance Payments (AAP) Program, the Centers for Medicare & Medicaid Services (CMS) advanced funds to physicians who were financially impacted by the pandemic.
Revisions were made under the Coronavirus Aid, Relief, and Economic Security (CARES) Act to broaden the existing program to supply provider relief related to the public health emergency. The program was revised in March but suspended accepting new applications related to the pandemic in late April.
Physicians who received APP loans were required to begin repayment within 120 days after the loan disbursement. CMS planned to recoup the advances by offsetting them against Medicare claims payments due to physicians. Practices had up to 210 days (7 months) to repay the loans through this process before being asked to repay them directly with a 10.25 % interest rate.
For practices that received these advances, their Medicare cash flow was scheduled to dry up, starting in August. However, CMS quietly abstained from collecting these payments when they came due, according to Modern Healthcare.
New terms
Under the new loan repayment terms in the CR, repayment of the disbursed funds is postponed until 365 days after the date on which a practice received the money. The balance is due by September 2022.
The amount to be recouped from each claim is reduced from 100% to 25% of the claim for the first 11 months and to 50% of claims withheld for an additional 6 months. If the loan is not repaid in full by then, the provider must pay the balance with an interest rate of 4%.
More than 80% of the $100 billion that CMS loaned to health care providers through May 2 went to hospitals, Modern Healthcare calculated. Of the remainder, specialty or multispecialty practices received $3.5 billion, internal medicine specialists got $24 million, family physicians were loaned $15 million, and federally qualified health centers received $20 million.
In the AMA’s news release, AMA President Susan Bailey, MD, who assumed the post in June, called the original loan repayment plan an “economic sword hanging over physician practices.”
The American Gastroenterological Association has been advocating for more flexibility for the financial assistance programs, such as the Accelerated and Advanced Payment Program and the Paycheck Protection Program, that physicians have utilized. It is critical to give physicians leeway on these loans given that many practices are still not operating at full capacity.
Based on reporting from Medscape.com.
President Trump on Oct. 1 signed a bill to keep the federal government running through Dec. 11. This “continuing resolution” (CR), which was approved by the House by a 359-57 vote and the Senate by a 84-10 vote, includes provisions to delay repayment by physicians of pandemic-related Medicare loans and to reduce the loans’ interest rate.
In an earlier news release, the American Medical Association reported that Congress and the White House had agreed to include the provisions on Medicare loans in the CR.
Under Medicare’s Accelerated and Advance Payments (AAP) Program, the Centers for Medicare & Medicaid Services (CMS) advanced funds to physicians who were financially impacted by the pandemic.
Revisions were made under the Coronavirus Aid, Relief, and Economic Security (CARES) Act to broaden the existing program to supply provider relief related to the public health emergency. The program was revised in March but suspended accepting new applications related to the pandemic in late April.
Physicians who received APP loans were required to begin repayment within 120 days after the loan disbursement. CMS planned to recoup the advances by offsetting them against Medicare claims payments due to physicians. Practices had up to 210 days (7 months) to repay the loans through this process before being asked to repay them directly with a 10.25 % interest rate.
For practices that received these advances, their Medicare cash flow was scheduled to dry up, starting in August. However, CMS quietly abstained from collecting these payments when they came due, according to Modern Healthcare.
New terms
Under the new loan repayment terms in the CR, repayment of the disbursed funds is postponed until 365 days after the date on which a practice received the money. The balance is due by September 2022.
The amount to be recouped from each claim is reduced from 100% to 25% of the claim for the first 11 months and to 50% of claims withheld for an additional 6 months. If the loan is not repaid in full by then, the provider must pay the balance with an interest rate of 4%.
More than 80% of the $100 billion that CMS loaned to health care providers through May 2 went to hospitals, Modern Healthcare calculated. Of the remainder, specialty or multispecialty practices received $3.5 billion, internal medicine specialists got $24 million, family physicians were loaned $15 million, and federally qualified health centers received $20 million.
In the AMA’s news release, AMA President Susan Bailey, MD, who assumed the post in June, called the original loan repayment plan an “economic sword hanging over physician practices.”
The American Gastroenterological Association has been advocating for more flexibility for the financial assistance programs, such as the Accelerated and Advanced Payment Program and the Paycheck Protection Program, that physicians have utilized. It is critical to give physicians leeway on these loans given that many practices are still not operating at full capacity.
Based on reporting from Medscape.com.
Health care workers implore OSHA for more oversight on COVID-19 safety
Last spring, when Cliff Willmeng, RN, was working at United Hospital in St. Paul, Minnesota, he’d take off his personal protective equipment (PPE) in the same hallway where children were transported from ambulances to the neighboring Children’s Hospital emergency department. Stretchers would roll across red tape on the floor that designated the area as a “hot zone.” The door from a break room was about 10 feet away.
Willmeng has been a union activist all his life, but he’d never filed a complaint with the Occupational Safety and Health Administration (OSHA) until the COVID-19 pandemic hit.
Concerned about the inadequate space for doffing PPE and other situations in which the spread of SARS-CoV-2 seemed possible, Willmeng and other colleagues filed multiple OSHA complaints with the Minnesota Department of Labor in March and April. Willmeng was also worried about bringing SARS-CoV-2 on his scrubs home to his wife and kids, and he started wearing hospital-supplied scrubs that were meant for doctors and that were washed on site, which was against hospital policy. The hospital fired Willmeng on May 8, citing code of conduct and respectful workplace violations arising from the uniform dispute.
In August, the state agency issued Willmeng’s hospital a $2,100 fine for failure to comply with guidance regarding “respiratory protection” in response to worker complaints over the fact that they were instructed to restaple elastic bands on N95 masks early in the pandemic. In a statement, United Hospital said it contested the citation, and it is in discussions with Minnesota OSHA. “We have and continue to instruct employees not to alter N95 respirators or reuse damaged or soiled N95 respirators,” such as when the straps are broken, the statement says.
Minnesota OSHA has received three times as many emails and phone calls from workers and employers requesting information and assistance during the pandemic, compared with last year, said spokesperson James Honerman. “If Minnesota OSHA is made aware of a workplace safety or health issue, it assesses the situation and determines how best to respond, including conducting a workplace investigation.”
But Willmeng, who has been out of work since he was fired, says that without a receipt or confirmation from OSHA, he has no way of knowing whether there has been any follow-up regarding his complaints. Minnesota OSHA said workers should receive a letter once a case is resolved.
Like Willmeng’s case, none of the more than 10,000 COVID-related complaints the federal OSHA office has received from across the country have resulted in meaningful sanctions. Unions have picketed local OSHA offices and publicized complaints on behalf of their members to protest what they see as a lack of oversight. Legislators have called on US Department of Labor Secretary Eugene Scalia to step up enforcement.
For many health care workers, complaining to OSHA is a last resort after failing to get satisfactory responses from supervisors and appealing to unions for help. But with such minimal oversight from OSHA, some union leaders and legislators say it’s actually more dangerous than not having workplace safety enforcement at all. Lack of directives from the Trump administration has left the agency without the teeth it has cut under previous administrations, and recent changes to the agency’s rules raise questions about whether companies are ever required to report workers’ hospitalizations due to COVID-19.
“It’s so ineffective that it’s more dangerous to workers,” said Kim Cordova, president of United Food and Commercial Workers (UFCW) Local 7, which represents 22,000 health care and other workers in Colorado and Wyoming. “Employers only do what they’re forced to do.” Instead of deterring a multi-billion-dollar company, she said, such low fines signal that a company doesn’t need to worry about COVID-related safety.
“OSHA is doing a lamentably poor job protecting workers during the pandemic,” said James Brudney, JD, a professor at Fordham Law School, in New York, and former chief counsel of the U.S. Senate Subcommittee on Labor. “I’m not alone in saying that the agency has performed so badly.”
Former government officials writing in JAMA were similarly critical: “In the face of the greatest worker health crisis in recent history, OSHA, the lead government agency responsible for worker health and safety, has not fulfilled its responsibilities.”
What could have been
There were early signs that the agency wouldn’t be heavy-handed about COVID-19 safety concerns, Brudney said.
The agency could have issued Emergency Temporary Standards, rules it can put in place during pandemics that address specific short-term concerns. These rules could have required employers to take infection-control measures to protect workers, including mask wearing, providing proper PPE, and screening for COVID-19 symptoms. “That’s what the agency is supposed to do. They’re supposed to respond to an emergency with emergency measures,” Brudney said.
But despite legislative pressure and a court case, Secretary of Labor Eugene Scalia has declined to do so, saying that the agency would instead rely on its regular general duty clause, which is always in place to keep workplaces free from hazards that “cause death or serious physical harm.” The agency invoked the general duty clause for COVID-19–related violations for the first time in September to levy modest fines.
In response to a request for an interview, a Department of Labor spokesperson said that preexisting OSHA requirements apply to workers during the pandemic, including providing PPE for workers and assessing sanitation and cleanliness standards. The agency has issued specific guidance to companies on pandemic preparedness, she said, and that it responds to all complaints. Additionally, she cited whistleblower laws that make it illegal for employers to retaliate against employees for making safety and health complaints.
The federal OSHA office received 10,868 COVID-related complaints from Feb. 1 through Oct. 20, citing issues ranging from failure to provide proper PPE to not informing workers about exposures. As of Oct. 22, a total of 2,349 of the complaints involved healthcare workers. This count doesn’t include the untold number of “informal” complaints handled by state OSHA offices.
In a recent JAMA opinion piece, two former government officials agreed that “the federal government has not fully utilized OSHA’s public safety authority” and called the issuing of an Emergency Temporary Standard that would require employers to develop and implement infection control plans “the most important action the federal government could take” to protect workers.
“Employers are more likely to implement these controls if they are mandated by a government agency that has adequate enforcement tools to ensure compliance,” wrote former Assistant Secretary of Labor David Michaels, PhD, MPH, now at the Milken Institute School of Public Health of the George Washington University, Washington, and Gregory Wagner, MD, a former senior adviser at the National Institute for Occupational Safety and Health at the Centers for Disease Control and Prevention, now at the Harvard T.H. Chan School of Public Health, Boston.
They cited the success of a standard that OSHA issued in 1991 in response to the HIV/AIDS crisis. “The bloodborne pathogens standard has contributed to a substantial decline in health care worker risk for bloodborne diseases like HIV and hepatitis B and C,” they wrote. In a new report for the Century Foundation, the pair offered recommendations to the federal government for controlling the spread of the disease by ramping up OSHA’s role.
OSHA did issue a response plan that requires employers to report in regard to employees who experienced workplace exposures to SARS-CoV-2 and who were hospitalized with COVID-19 or died of the disease within certain time frames, but recent changes to these rules make experts question whether companies are in fact required to report hospitalizations.
In its second revision of guidelines, added to its FAQ page on Sept. 30, the agency said that, in order to be reportable, “an in-patient hospitalization due to COVID-19 must occur within 24 hours of an exposure to SARS-CoV-2 at work” and that the employer must report the hospitalization within 24 hours of learning both that the employee has been hospitalized and that the reason for the hospitalization was a work-related case of COVID-19. Previously, the 24-hour hospitalization window started at the time of diagnosis of the disease, rather than the work-related exposure.
The agency subsequently dropped the first citation it had issued for a COVID-related violation, even though the company, a nursing home, had already agreed to pay $3,904 for reporting employee hospitalizations late.
“It’s a step backwards from an important workplace and public health function that OSHA should be doing,” said Wagner, coauthor of the JAMA opinion piece.
Even without issuing Emergency Temporary Standards, critics say OSHA could have acted much earlier. OSHA issued its first COVID-related federal citation, the one against the nursing home that was dropped, in May for events that occurred in mid-April. The second COVID-related federal citation came in July.
The agency could also charge much more substantial fines for the citations it has issued. If a medical facility was cited for a PPE violation, such as the Minnesota hospital where workers were told to restaple the elastic bands on N95s, the agency could have cited the hospital for one violation per employee. Such fines based on multiple violations could add up to the hundreds of thousands to millions of dollars.
“It would send a signal to the highest-risk employers that these are violations that need to be addressed immediately,” Brudney said.
Many of the 22 state OSHA offices appear to be more responsive to COVID-related complaints than the federal agency, creating a system in which health care workers have substantially different rights from one state to the next. The governor of California, for example, recently authorized California’s OSHA division to consider COVID-19 an imminent hazard, to prohibit workers from entering areas where the hazard exists, and to require employers to disclose exposures. The state also recently issued large fines for COVID safety issues: $222,075 to frozen food manufacturer Overhill Farms and $214,080 to employment agency Jobsource North America.
Elsewhere, state laws such as New Jersey’s Conscientious Employee Protection Act give workers the right to refuse to work in unsafe situations, Brudney said. “A lot more action is going on at the state level because so little is being done at the federal level,” he said. “Some of it is governors committed to protecting essential workers and their families.”
Unions call for sanctions
Unions are both decrying the lack of enforcement thus far and seeking more oversight going forward.
In August, the National Nurses’ United (NNU) union filed a complaint to implore OSHA to investigate the country’s biggest hospital systems, HCA Healthcare, which operates 184 hospitals and about 2,000 other care sites in 21 states and the United Kingdom. The union describes how, throughout HCA hospitals, there is an environment conducive to the spread of coronavirus. Nurses share space and equipment, such as computers, desks, phones, bathrooms, and break rooms, where staff take off masks to eat and drink. The complaint also describes how there is resistance to testing nurses and a lack of communication about infections among colleagues.
“When they have total disregard for safety, they should be punished to the utmost,” said Markowitz, noting that HCA Healthcare is worth $40 billion. “They can penalize them, but if it’s unsafe conditions for RNs and healthcare workers, we know it’s unsafe for the patients. There needs to be drastic measures to prevent hospital corporations from behaving that way.”
In a statement, HCA spokesman Harlow Sumerford said the company has followed CDC guidance for protecting frontline caregivers. “We’re proud of our response and the significant resources we’ve deployed to help protect our colleagues. Meanwhile, the NNU has chosen to use this pandemic as an opportunity to gain publicity by attacking hospitals across the country,” Sumerford said.
Members of the union recently protested in front of the federal OSHA offices in Denver.
After several months, OSHA finally penalized a meat packing plant where eight workers (six union members) had died of COVID-19 last spring. But the amount – $15,615 – was so low that Cordova worries it will actually have a worse impact than no fine.
“It’s more dangerous to workers because now employers know [they won’t be punished meaningfully],” she said. “During the pandemic, OSHA has been absolutely absent.”
Thus, the recent picketing outside the offices in Denver. But, Cordova noted, it’s unlikely OSHA employees saw them. Their own offices were deemed too risky to stay open during the pandemic. They were vacant.
A version of this article originally appeared on Medscape.com.
Last spring, when Cliff Willmeng, RN, was working at United Hospital in St. Paul, Minnesota, he’d take off his personal protective equipment (PPE) in the same hallway where children were transported from ambulances to the neighboring Children’s Hospital emergency department. Stretchers would roll across red tape on the floor that designated the area as a “hot zone.” The door from a break room was about 10 feet away.
Willmeng has been a union activist all his life, but he’d never filed a complaint with the Occupational Safety and Health Administration (OSHA) until the COVID-19 pandemic hit.
Concerned about the inadequate space for doffing PPE and other situations in which the spread of SARS-CoV-2 seemed possible, Willmeng and other colleagues filed multiple OSHA complaints with the Minnesota Department of Labor in March and April. Willmeng was also worried about bringing SARS-CoV-2 on his scrubs home to his wife and kids, and he started wearing hospital-supplied scrubs that were meant for doctors and that were washed on site, which was against hospital policy. The hospital fired Willmeng on May 8, citing code of conduct and respectful workplace violations arising from the uniform dispute.
In August, the state agency issued Willmeng’s hospital a $2,100 fine for failure to comply with guidance regarding “respiratory protection” in response to worker complaints over the fact that they were instructed to restaple elastic bands on N95 masks early in the pandemic. In a statement, United Hospital said it contested the citation, and it is in discussions with Minnesota OSHA. “We have and continue to instruct employees not to alter N95 respirators or reuse damaged or soiled N95 respirators,” such as when the straps are broken, the statement says.
Minnesota OSHA has received three times as many emails and phone calls from workers and employers requesting information and assistance during the pandemic, compared with last year, said spokesperson James Honerman. “If Minnesota OSHA is made aware of a workplace safety or health issue, it assesses the situation and determines how best to respond, including conducting a workplace investigation.”
But Willmeng, who has been out of work since he was fired, says that without a receipt or confirmation from OSHA, he has no way of knowing whether there has been any follow-up regarding his complaints. Minnesota OSHA said workers should receive a letter once a case is resolved.
Like Willmeng’s case, none of the more than 10,000 COVID-related complaints the federal OSHA office has received from across the country have resulted in meaningful sanctions. Unions have picketed local OSHA offices and publicized complaints on behalf of their members to protest what they see as a lack of oversight. Legislators have called on US Department of Labor Secretary Eugene Scalia to step up enforcement.
For many health care workers, complaining to OSHA is a last resort after failing to get satisfactory responses from supervisors and appealing to unions for help. But with such minimal oversight from OSHA, some union leaders and legislators say it’s actually more dangerous than not having workplace safety enforcement at all. Lack of directives from the Trump administration has left the agency without the teeth it has cut under previous administrations, and recent changes to the agency’s rules raise questions about whether companies are ever required to report workers’ hospitalizations due to COVID-19.
“It’s so ineffective that it’s more dangerous to workers,” said Kim Cordova, president of United Food and Commercial Workers (UFCW) Local 7, which represents 22,000 health care and other workers in Colorado and Wyoming. “Employers only do what they’re forced to do.” Instead of deterring a multi-billion-dollar company, she said, such low fines signal that a company doesn’t need to worry about COVID-related safety.
“OSHA is doing a lamentably poor job protecting workers during the pandemic,” said James Brudney, JD, a professor at Fordham Law School, in New York, and former chief counsel of the U.S. Senate Subcommittee on Labor. “I’m not alone in saying that the agency has performed so badly.”
Former government officials writing in JAMA were similarly critical: “In the face of the greatest worker health crisis in recent history, OSHA, the lead government agency responsible for worker health and safety, has not fulfilled its responsibilities.”
What could have been
There were early signs that the agency wouldn’t be heavy-handed about COVID-19 safety concerns, Brudney said.
The agency could have issued Emergency Temporary Standards, rules it can put in place during pandemics that address specific short-term concerns. These rules could have required employers to take infection-control measures to protect workers, including mask wearing, providing proper PPE, and screening for COVID-19 symptoms. “That’s what the agency is supposed to do. They’re supposed to respond to an emergency with emergency measures,” Brudney said.
But despite legislative pressure and a court case, Secretary of Labor Eugene Scalia has declined to do so, saying that the agency would instead rely on its regular general duty clause, which is always in place to keep workplaces free from hazards that “cause death or serious physical harm.” The agency invoked the general duty clause for COVID-19–related violations for the first time in September to levy modest fines.
In response to a request for an interview, a Department of Labor spokesperson said that preexisting OSHA requirements apply to workers during the pandemic, including providing PPE for workers and assessing sanitation and cleanliness standards. The agency has issued specific guidance to companies on pandemic preparedness, she said, and that it responds to all complaints. Additionally, she cited whistleblower laws that make it illegal for employers to retaliate against employees for making safety and health complaints.
The federal OSHA office received 10,868 COVID-related complaints from Feb. 1 through Oct. 20, citing issues ranging from failure to provide proper PPE to not informing workers about exposures. As of Oct. 22, a total of 2,349 of the complaints involved healthcare workers. This count doesn’t include the untold number of “informal” complaints handled by state OSHA offices.
In a recent JAMA opinion piece, two former government officials agreed that “the federal government has not fully utilized OSHA’s public safety authority” and called the issuing of an Emergency Temporary Standard that would require employers to develop and implement infection control plans “the most important action the federal government could take” to protect workers.
“Employers are more likely to implement these controls if they are mandated by a government agency that has adequate enforcement tools to ensure compliance,” wrote former Assistant Secretary of Labor David Michaels, PhD, MPH, now at the Milken Institute School of Public Health of the George Washington University, Washington, and Gregory Wagner, MD, a former senior adviser at the National Institute for Occupational Safety and Health at the Centers for Disease Control and Prevention, now at the Harvard T.H. Chan School of Public Health, Boston.
They cited the success of a standard that OSHA issued in 1991 in response to the HIV/AIDS crisis. “The bloodborne pathogens standard has contributed to a substantial decline in health care worker risk for bloodborne diseases like HIV and hepatitis B and C,” they wrote. In a new report for the Century Foundation, the pair offered recommendations to the federal government for controlling the spread of the disease by ramping up OSHA’s role.
OSHA did issue a response plan that requires employers to report in regard to employees who experienced workplace exposures to SARS-CoV-2 and who were hospitalized with COVID-19 or died of the disease within certain time frames, but recent changes to these rules make experts question whether companies are in fact required to report hospitalizations.
In its second revision of guidelines, added to its FAQ page on Sept. 30, the agency said that, in order to be reportable, “an in-patient hospitalization due to COVID-19 must occur within 24 hours of an exposure to SARS-CoV-2 at work” and that the employer must report the hospitalization within 24 hours of learning both that the employee has been hospitalized and that the reason for the hospitalization was a work-related case of COVID-19. Previously, the 24-hour hospitalization window started at the time of diagnosis of the disease, rather than the work-related exposure.
The agency subsequently dropped the first citation it had issued for a COVID-related violation, even though the company, a nursing home, had already agreed to pay $3,904 for reporting employee hospitalizations late.
“It’s a step backwards from an important workplace and public health function that OSHA should be doing,” said Wagner, coauthor of the JAMA opinion piece.
Even without issuing Emergency Temporary Standards, critics say OSHA could have acted much earlier. OSHA issued its first COVID-related federal citation, the one against the nursing home that was dropped, in May for events that occurred in mid-April. The second COVID-related federal citation came in July.
The agency could also charge much more substantial fines for the citations it has issued. If a medical facility was cited for a PPE violation, such as the Minnesota hospital where workers were told to restaple the elastic bands on N95s, the agency could have cited the hospital for one violation per employee. Such fines based on multiple violations could add up to the hundreds of thousands to millions of dollars.
“It would send a signal to the highest-risk employers that these are violations that need to be addressed immediately,” Brudney said.
Many of the 22 state OSHA offices appear to be more responsive to COVID-related complaints than the federal agency, creating a system in which health care workers have substantially different rights from one state to the next. The governor of California, for example, recently authorized California’s OSHA division to consider COVID-19 an imminent hazard, to prohibit workers from entering areas where the hazard exists, and to require employers to disclose exposures. The state also recently issued large fines for COVID safety issues: $222,075 to frozen food manufacturer Overhill Farms and $214,080 to employment agency Jobsource North America.
Elsewhere, state laws such as New Jersey’s Conscientious Employee Protection Act give workers the right to refuse to work in unsafe situations, Brudney said. “A lot more action is going on at the state level because so little is being done at the federal level,” he said. “Some of it is governors committed to protecting essential workers and their families.”
Unions call for sanctions
Unions are both decrying the lack of enforcement thus far and seeking more oversight going forward.
In August, the National Nurses’ United (NNU) union filed a complaint to implore OSHA to investigate the country’s biggest hospital systems, HCA Healthcare, which operates 184 hospitals and about 2,000 other care sites in 21 states and the United Kingdom. The union describes how, throughout HCA hospitals, there is an environment conducive to the spread of coronavirus. Nurses share space and equipment, such as computers, desks, phones, bathrooms, and break rooms, where staff take off masks to eat and drink. The complaint also describes how there is resistance to testing nurses and a lack of communication about infections among colleagues.
“When they have total disregard for safety, they should be punished to the utmost,” said Markowitz, noting that HCA Healthcare is worth $40 billion. “They can penalize them, but if it’s unsafe conditions for RNs and healthcare workers, we know it’s unsafe for the patients. There needs to be drastic measures to prevent hospital corporations from behaving that way.”
In a statement, HCA spokesman Harlow Sumerford said the company has followed CDC guidance for protecting frontline caregivers. “We’re proud of our response and the significant resources we’ve deployed to help protect our colleagues. Meanwhile, the NNU has chosen to use this pandemic as an opportunity to gain publicity by attacking hospitals across the country,” Sumerford said.
Members of the union recently protested in front of the federal OSHA offices in Denver.
After several months, OSHA finally penalized a meat packing plant where eight workers (six union members) had died of COVID-19 last spring. But the amount – $15,615 – was so low that Cordova worries it will actually have a worse impact than no fine.
“It’s more dangerous to workers because now employers know [they won’t be punished meaningfully],” she said. “During the pandemic, OSHA has been absolutely absent.”
Thus, the recent picketing outside the offices in Denver. But, Cordova noted, it’s unlikely OSHA employees saw them. Their own offices were deemed too risky to stay open during the pandemic. They were vacant.
A version of this article originally appeared on Medscape.com.
Last spring, when Cliff Willmeng, RN, was working at United Hospital in St. Paul, Minnesota, he’d take off his personal protective equipment (PPE) in the same hallway where children were transported from ambulances to the neighboring Children’s Hospital emergency department. Stretchers would roll across red tape on the floor that designated the area as a “hot zone.” The door from a break room was about 10 feet away.
Willmeng has been a union activist all his life, but he’d never filed a complaint with the Occupational Safety and Health Administration (OSHA) until the COVID-19 pandemic hit.
Concerned about the inadequate space for doffing PPE and other situations in which the spread of SARS-CoV-2 seemed possible, Willmeng and other colleagues filed multiple OSHA complaints with the Minnesota Department of Labor in March and April. Willmeng was also worried about bringing SARS-CoV-2 on his scrubs home to his wife and kids, and he started wearing hospital-supplied scrubs that were meant for doctors and that were washed on site, which was against hospital policy. The hospital fired Willmeng on May 8, citing code of conduct and respectful workplace violations arising from the uniform dispute.
In August, the state agency issued Willmeng’s hospital a $2,100 fine for failure to comply with guidance regarding “respiratory protection” in response to worker complaints over the fact that they were instructed to restaple elastic bands on N95 masks early in the pandemic. In a statement, United Hospital said it contested the citation, and it is in discussions with Minnesota OSHA. “We have and continue to instruct employees not to alter N95 respirators or reuse damaged or soiled N95 respirators,” such as when the straps are broken, the statement says.
Minnesota OSHA has received three times as many emails and phone calls from workers and employers requesting information and assistance during the pandemic, compared with last year, said spokesperson James Honerman. “If Minnesota OSHA is made aware of a workplace safety or health issue, it assesses the situation and determines how best to respond, including conducting a workplace investigation.”
But Willmeng, who has been out of work since he was fired, says that without a receipt or confirmation from OSHA, he has no way of knowing whether there has been any follow-up regarding his complaints. Minnesota OSHA said workers should receive a letter once a case is resolved.
Like Willmeng’s case, none of the more than 10,000 COVID-related complaints the federal OSHA office has received from across the country have resulted in meaningful sanctions. Unions have picketed local OSHA offices and publicized complaints on behalf of their members to protest what they see as a lack of oversight. Legislators have called on US Department of Labor Secretary Eugene Scalia to step up enforcement.
For many health care workers, complaining to OSHA is a last resort after failing to get satisfactory responses from supervisors and appealing to unions for help. But with such minimal oversight from OSHA, some union leaders and legislators say it’s actually more dangerous than not having workplace safety enforcement at all. Lack of directives from the Trump administration has left the agency without the teeth it has cut under previous administrations, and recent changes to the agency’s rules raise questions about whether companies are ever required to report workers’ hospitalizations due to COVID-19.
“It’s so ineffective that it’s more dangerous to workers,” said Kim Cordova, president of United Food and Commercial Workers (UFCW) Local 7, which represents 22,000 health care and other workers in Colorado and Wyoming. “Employers only do what they’re forced to do.” Instead of deterring a multi-billion-dollar company, she said, such low fines signal that a company doesn’t need to worry about COVID-related safety.
“OSHA is doing a lamentably poor job protecting workers during the pandemic,” said James Brudney, JD, a professor at Fordham Law School, in New York, and former chief counsel of the U.S. Senate Subcommittee on Labor. “I’m not alone in saying that the agency has performed so badly.”
Former government officials writing in JAMA were similarly critical: “In the face of the greatest worker health crisis in recent history, OSHA, the lead government agency responsible for worker health and safety, has not fulfilled its responsibilities.”
What could have been
There were early signs that the agency wouldn’t be heavy-handed about COVID-19 safety concerns, Brudney said.
The agency could have issued Emergency Temporary Standards, rules it can put in place during pandemics that address specific short-term concerns. These rules could have required employers to take infection-control measures to protect workers, including mask wearing, providing proper PPE, and screening for COVID-19 symptoms. “That’s what the agency is supposed to do. They’re supposed to respond to an emergency with emergency measures,” Brudney said.
But despite legislative pressure and a court case, Secretary of Labor Eugene Scalia has declined to do so, saying that the agency would instead rely on its regular general duty clause, which is always in place to keep workplaces free from hazards that “cause death or serious physical harm.” The agency invoked the general duty clause for COVID-19–related violations for the first time in September to levy modest fines.
In response to a request for an interview, a Department of Labor spokesperson said that preexisting OSHA requirements apply to workers during the pandemic, including providing PPE for workers and assessing sanitation and cleanliness standards. The agency has issued specific guidance to companies on pandemic preparedness, she said, and that it responds to all complaints. Additionally, she cited whistleblower laws that make it illegal for employers to retaliate against employees for making safety and health complaints.
The federal OSHA office received 10,868 COVID-related complaints from Feb. 1 through Oct. 20, citing issues ranging from failure to provide proper PPE to not informing workers about exposures. As of Oct. 22, a total of 2,349 of the complaints involved healthcare workers. This count doesn’t include the untold number of “informal” complaints handled by state OSHA offices.
In a recent JAMA opinion piece, two former government officials agreed that “the federal government has not fully utilized OSHA’s public safety authority” and called the issuing of an Emergency Temporary Standard that would require employers to develop and implement infection control plans “the most important action the federal government could take” to protect workers.
“Employers are more likely to implement these controls if they are mandated by a government agency that has adequate enforcement tools to ensure compliance,” wrote former Assistant Secretary of Labor David Michaels, PhD, MPH, now at the Milken Institute School of Public Health of the George Washington University, Washington, and Gregory Wagner, MD, a former senior adviser at the National Institute for Occupational Safety and Health at the Centers for Disease Control and Prevention, now at the Harvard T.H. Chan School of Public Health, Boston.
They cited the success of a standard that OSHA issued in 1991 in response to the HIV/AIDS crisis. “The bloodborne pathogens standard has contributed to a substantial decline in health care worker risk for bloodborne diseases like HIV and hepatitis B and C,” they wrote. In a new report for the Century Foundation, the pair offered recommendations to the federal government for controlling the spread of the disease by ramping up OSHA’s role.
OSHA did issue a response plan that requires employers to report in regard to employees who experienced workplace exposures to SARS-CoV-2 and who were hospitalized with COVID-19 or died of the disease within certain time frames, but recent changes to these rules make experts question whether companies are in fact required to report hospitalizations.
In its second revision of guidelines, added to its FAQ page on Sept. 30, the agency said that, in order to be reportable, “an in-patient hospitalization due to COVID-19 must occur within 24 hours of an exposure to SARS-CoV-2 at work” and that the employer must report the hospitalization within 24 hours of learning both that the employee has been hospitalized and that the reason for the hospitalization was a work-related case of COVID-19. Previously, the 24-hour hospitalization window started at the time of diagnosis of the disease, rather than the work-related exposure.
The agency subsequently dropped the first citation it had issued for a COVID-related violation, even though the company, a nursing home, had already agreed to pay $3,904 for reporting employee hospitalizations late.
“It’s a step backwards from an important workplace and public health function that OSHA should be doing,” said Wagner, coauthor of the JAMA opinion piece.
Even without issuing Emergency Temporary Standards, critics say OSHA could have acted much earlier. OSHA issued its first COVID-related federal citation, the one against the nursing home that was dropped, in May for events that occurred in mid-April. The second COVID-related federal citation came in July.
The agency could also charge much more substantial fines for the citations it has issued. If a medical facility was cited for a PPE violation, such as the Minnesota hospital where workers were told to restaple the elastic bands on N95s, the agency could have cited the hospital for one violation per employee. Such fines based on multiple violations could add up to the hundreds of thousands to millions of dollars.
“It would send a signal to the highest-risk employers that these are violations that need to be addressed immediately,” Brudney said.
Many of the 22 state OSHA offices appear to be more responsive to COVID-related complaints than the federal agency, creating a system in which health care workers have substantially different rights from one state to the next. The governor of California, for example, recently authorized California’s OSHA division to consider COVID-19 an imminent hazard, to prohibit workers from entering areas where the hazard exists, and to require employers to disclose exposures. The state also recently issued large fines for COVID safety issues: $222,075 to frozen food manufacturer Overhill Farms and $214,080 to employment agency Jobsource North America.
Elsewhere, state laws such as New Jersey’s Conscientious Employee Protection Act give workers the right to refuse to work in unsafe situations, Brudney said. “A lot more action is going on at the state level because so little is being done at the federal level,” he said. “Some of it is governors committed to protecting essential workers and their families.”
Unions call for sanctions
Unions are both decrying the lack of enforcement thus far and seeking more oversight going forward.
In August, the National Nurses’ United (NNU) union filed a complaint to implore OSHA to investigate the country’s biggest hospital systems, HCA Healthcare, which operates 184 hospitals and about 2,000 other care sites in 21 states and the United Kingdom. The union describes how, throughout HCA hospitals, there is an environment conducive to the spread of coronavirus. Nurses share space and equipment, such as computers, desks, phones, bathrooms, and break rooms, where staff take off masks to eat and drink. The complaint also describes how there is resistance to testing nurses and a lack of communication about infections among colleagues.
“When they have total disregard for safety, they should be punished to the utmost,” said Markowitz, noting that HCA Healthcare is worth $40 billion. “They can penalize them, but if it’s unsafe conditions for RNs and healthcare workers, we know it’s unsafe for the patients. There needs to be drastic measures to prevent hospital corporations from behaving that way.”
In a statement, HCA spokesman Harlow Sumerford said the company has followed CDC guidance for protecting frontline caregivers. “We’re proud of our response and the significant resources we’ve deployed to help protect our colleagues. Meanwhile, the NNU has chosen to use this pandemic as an opportunity to gain publicity by attacking hospitals across the country,” Sumerford said.
Members of the union recently protested in front of the federal OSHA offices in Denver.
After several months, OSHA finally penalized a meat packing plant where eight workers (six union members) had died of COVID-19 last spring. But the amount – $15,615 – was so low that Cordova worries it will actually have a worse impact than no fine.
“It’s more dangerous to workers because now employers know [they won’t be punished meaningfully],” she said. “During the pandemic, OSHA has been absolutely absent.”
Thus, the recent picketing outside the offices in Denver. But, Cordova noted, it’s unlikely OSHA employees saw them. Their own offices were deemed too risky to stay open during the pandemic. They were vacant.
A version of this article originally appeared on Medscape.com.
COVID spikes exacerbate health worker shortages in Rocky Mountains, Great Plains
In Montana, pandemic-induced staffing shortages have shuttered a clinic in the state’s capital, led a northwestern regional hospital to ask employees exposed to COVID-19 to continue to work and emptied a health department 400 miles to the east.
“Just one more person out and we wouldn’t be able to keep the surgeries going,” said Dr. Shelly Harkins, MD, chief medical officer of St. Peter’s Health in Helena, a city of roughly 32,000 where cases continue to spread. “When the virus is just all around you, it’s almost impossible to not be deemed a contact at some point. One case can take out a whole team of people in a blink of an eye.”
In North Dakota, where cases per resident are growing faster than any other state, hospitals may once again curtail elective surgeries and possibly seek government aid to hire more nurses if the situation gets worse, North Dakota Hospital Association President Tim Blasl said.
“How long can we run at this rate with the workforce that we have?” Blasl said. “You can have all the licensed beds you want, but if you don’t have anybody to staff those beds, it doesn’t do you any good.”
The northern Rocky Mountains, Great Plains and Upper Midwest are seeing the highest surge of COVID-19 cases in the nation, as some residents have ignored recommendations for curtailing the virus, such as wearing masks and avoiding large gatherings. Montana, Idaho, Utah, Wyoming, North Dakota, South Dakota, Nebraska, Iowa, and Wisconsin have recently ranked among the top 10 U.S. states in confirmed cases per 100,000 residents over a 7-day period, according to an analysis by the New York Times.
Such coronavirus infections – and the quarantines that occur because of them – are exacerbating the health care worker shortage that existed in these states well before the pandemic. Unlike in the nation’s metropolitan hubs, these outbreaks are scattered across hundreds of miles. And even in these states’ biggest cities, the ranks of medical professionals are in short supply. Specialists and registered nurses are sometimes harder to track down than ventilators, N95 masks or hospital beds. Without enough care providers, patients may not be able to get the medical attention they need.
Hospitals have asked staffers to cover extra shifts and learn new skills. They have brought in temporary workers from other parts of the country and transferred some patients to less-crowded hospitals. But, at St. Peter’s Health, if the hospital’s one kidney doctor gets sick or is told to quarantine, Dr. Harkins doesn’t expect to find a backup.
“We make a point to not have excessive staff because we have an obligation to keep the cost of health care down for a community – we just don’t have a lot of slack in our rope,” Dr. Harkins said. “What we don’t account for is a mass exodus of staff for 14 days.”
Some hospitals are already at patient capacity or are nearly there. That’s not just because of the growing number of COVID-19 patients. Elective surgeries have resumed, and medical emergencies don’t pause for a pandemic.
Some Montana hospitals formed agreements with local affiliates early in the pandemic to share staff if one came up short. But now that the disease is spreading fast – and widely – the hope is that their needs don’t peak all at once.
Montana state officials keep a list of primarily in-state volunteer workers ready to travel to towns with shortages of contact tracers, nurses and more. But during a press conference on Oct. 15, Democratic Gov. Steve Bullock said the state had exhausted that database, and its nationwide request for National Guard medical staffing hadn’t brought in new workers.
“If you are a registered nurse, licensed practical nurse, paramedic, EMT, CNA or contact tracer, and are able to join our workforce, please do consider joining our team,” Gov. Bullock said.
This month, Kalispell Regional Medical Center in northwestern Montana even stopped quarantining COVID-exposed staff who remain asymptomatic, a change allowed by Centers for Disease Control and Prevention guidelines for health facilities facing staffing shortages.
“That’s very telling for what staffing is going through right now,” said Andrea Lueck, a registered nurse at the center. “We’re so tight that employees are called off of quarantine.”
Financial pressure early in the pandemic led the hospital to furlough staff, but it had to bring most of them back to work because it needs those bodies more than ever. The regional hub is based in Flathead County, which has recorded the state’s second-highest number of active COVID-19 cases.
Mellody Sharpton, a hospital spokesperson, said hospital workers who are exposed to someone infected with the virus are tested within three to five days and monitored for symptoms. The hospital is also pulling in new workers, with 25 traveling health professionals on hand and another 25 temporary ones on the way.
But Ms. Sharpton said the best way to conserve the hospital’s workforce is to stop the disease surge in the community.
Earlier in the pandemic, Central Montana Medical Center in Lewistown, a town of fewer than 6,000, experienced an exodus of part-time workers or those close to retirement who decided their jobs weren’t worth the risk. The facility recently secured two traveling workers, but both backed out because they couldn’t find housing. And, so far, roughly 40 of the hospital’s 322 employees have missed work for reasons connected to COVID-19.
“We’re at a critical staffing shortage and have been since the beginning of COVID,” said Joanie Slaybaugh, Central Montana Medical Center’s director of human resources. “We’re small enough, everybody feels an obligation to protect themselves and to protect each other. But it doesn’t take much to take out our staff.”
Roosevelt County, where roughly 11,000 live on the northeastern edge of Montana, had one of the nation’s highest rates of new cases as of Oct. 15. But by the end of the month, the county health department will lose half of its registered nurses as one person is about to retire and another was hired through a grant that’s ending. That leaves only one registered nurse aside from its director, Patty Presser. The health department already had to close earlier during the pandemic because of COVID exposure and not enough staffers to cover the gap. Now, if Ms. Presser can’t find nurse replacements in time, she hopes volunteers will step in, though she added they typically stay for only a few weeks.
“I need someone to do immunizations for my community, and you don’t become an immunization nurse in 14 days,” she said. “We don’t have the workforce here to deal with this virus, not even right now, and then I’m going to have my best two people go.”
Back in Helena, Dr. Harkins said St. Peter’s Health had to close a specialty outpatient clinic that treats chronic diseases for two weeks at the end of September because the entire staff had to quarantine.
Now the hospital is considering having doctors take turns spending a week working from home, so that if another wave of quarantines hits in the hospital, at least one untainted person can be brought back to work. But that won’t help for some specialties, like the hospital’s sole kidney doctor.
Every time Dr. Harkins’ phone rings, she said, she takes a breath and hopes it’s not another case that will force a whole division to close.
“Because I think immediately of the hundreds of people that need that service and won’t have it for 14 days,” she said.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
In Montana, pandemic-induced staffing shortages have shuttered a clinic in the state’s capital, led a northwestern regional hospital to ask employees exposed to COVID-19 to continue to work and emptied a health department 400 miles to the east.
“Just one more person out and we wouldn’t be able to keep the surgeries going,” said Dr. Shelly Harkins, MD, chief medical officer of St. Peter’s Health in Helena, a city of roughly 32,000 where cases continue to spread. “When the virus is just all around you, it’s almost impossible to not be deemed a contact at some point. One case can take out a whole team of people in a blink of an eye.”
In North Dakota, where cases per resident are growing faster than any other state, hospitals may once again curtail elective surgeries and possibly seek government aid to hire more nurses if the situation gets worse, North Dakota Hospital Association President Tim Blasl said.
“How long can we run at this rate with the workforce that we have?” Blasl said. “You can have all the licensed beds you want, but if you don’t have anybody to staff those beds, it doesn’t do you any good.”
The northern Rocky Mountains, Great Plains and Upper Midwest are seeing the highest surge of COVID-19 cases in the nation, as some residents have ignored recommendations for curtailing the virus, such as wearing masks and avoiding large gatherings. Montana, Idaho, Utah, Wyoming, North Dakota, South Dakota, Nebraska, Iowa, and Wisconsin have recently ranked among the top 10 U.S. states in confirmed cases per 100,000 residents over a 7-day period, according to an analysis by the New York Times.
Such coronavirus infections – and the quarantines that occur because of them – are exacerbating the health care worker shortage that existed in these states well before the pandemic. Unlike in the nation’s metropolitan hubs, these outbreaks are scattered across hundreds of miles. And even in these states’ biggest cities, the ranks of medical professionals are in short supply. Specialists and registered nurses are sometimes harder to track down than ventilators, N95 masks or hospital beds. Without enough care providers, patients may not be able to get the medical attention they need.
Hospitals have asked staffers to cover extra shifts and learn new skills. They have brought in temporary workers from other parts of the country and transferred some patients to less-crowded hospitals. But, at St. Peter’s Health, if the hospital’s one kidney doctor gets sick or is told to quarantine, Dr. Harkins doesn’t expect to find a backup.
“We make a point to not have excessive staff because we have an obligation to keep the cost of health care down for a community – we just don’t have a lot of slack in our rope,” Dr. Harkins said. “What we don’t account for is a mass exodus of staff for 14 days.”
Some hospitals are already at patient capacity or are nearly there. That’s not just because of the growing number of COVID-19 patients. Elective surgeries have resumed, and medical emergencies don’t pause for a pandemic.
Some Montana hospitals formed agreements with local affiliates early in the pandemic to share staff if one came up short. But now that the disease is spreading fast – and widely – the hope is that their needs don’t peak all at once.
Montana state officials keep a list of primarily in-state volunteer workers ready to travel to towns with shortages of contact tracers, nurses and more. But during a press conference on Oct. 15, Democratic Gov. Steve Bullock said the state had exhausted that database, and its nationwide request for National Guard medical staffing hadn’t brought in new workers.
“If you are a registered nurse, licensed practical nurse, paramedic, EMT, CNA or contact tracer, and are able to join our workforce, please do consider joining our team,” Gov. Bullock said.
This month, Kalispell Regional Medical Center in northwestern Montana even stopped quarantining COVID-exposed staff who remain asymptomatic, a change allowed by Centers for Disease Control and Prevention guidelines for health facilities facing staffing shortages.
“That’s very telling for what staffing is going through right now,” said Andrea Lueck, a registered nurse at the center. “We’re so tight that employees are called off of quarantine.”
Financial pressure early in the pandemic led the hospital to furlough staff, but it had to bring most of them back to work because it needs those bodies more than ever. The regional hub is based in Flathead County, which has recorded the state’s second-highest number of active COVID-19 cases.
Mellody Sharpton, a hospital spokesperson, said hospital workers who are exposed to someone infected with the virus are tested within three to five days and monitored for symptoms. The hospital is also pulling in new workers, with 25 traveling health professionals on hand and another 25 temporary ones on the way.
But Ms. Sharpton said the best way to conserve the hospital’s workforce is to stop the disease surge in the community.
Earlier in the pandemic, Central Montana Medical Center in Lewistown, a town of fewer than 6,000, experienced an exodus of part-time workers or those close to retirement who decided their jobs weren’t worth the risk. The facility recently secured two traveling workers, but both backed out because they couldn’t find housing. And, so far, roughly 40 of the hospital’s 322 employees have missed work for reasons connected to COVID-19.
“We’re at a critical staffing shortage and have been since the beginning of COVID,” said Joanie Slaybaugh, Central Montana Medical Center’s director of human resources. “We’re small enough, everybody feels an obligation to protect themselves and to protect each other. But it doesn’t take much to take out our staff.”
Roosevelt County, where roughly 11,000 live on the northeastern edge of Montana, had one of the nation’s highest rates of new cases as of Oct. 15. But by the end of the month, the county health department will lose half of its registered nurses as one person is about to retire and another was hired through a grant that’s ending. That leaves only one registered nurse aside from its director, Patty Presser. The health department already had to close earlier during the pandemic because of COVID exposure and not enough staffers to cover the gap. Now, if Ms. Presser can’t find nurse replacements in time, she hopes volunteers will step in, though she added they typically stay for only a few weeks.
“I need someone to do immunizations for my community, and you don’t become an immunization nurse in 14 days,” she said. “We don’t have the workforce here to deal with this virus, not even right now, and then I’m going to have my best two people go.”
Back in Helena, Dr. Harkins said St. Peter’s Health had to close a specialty outpatient clinic that treats chronic diseases for two weeks at the end of September because the entire staff had to quarantine.
Now the hospital is considering having doctors take turns spending a week working from home, so that if another wave of quarantines hits in the hospital, at least one untainted person can be brought back to work. But that won’t help for some specialties, like the hospital’s sole kidney doctor.
Every time Dr. Harkins’ phone rings, she said, she takes a breath and hopes it’s not another case that will force a whole division to close.
“Because I think immediately of the hundreds of people that need that service and won’t have it for 14 days,” she said.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
In Montana, pandemic-induced staffing shortages have shuttered a clinic in the state’s capital, led a northwestern regional hospital to ask employees exposed to COVID-19 to continue to work and emptied a health department 400 miles to the east.
“Just one more person out and we wouldn’t be able to keep the surgeries going,” said Dr. Shelly Harkins, MD, chief medical officer of St. Peter’s Health in Helena, a city of roughly 32,000 where cases continue to spread. “When the virus is just all around you, it’s almost impossible to not be deemed a contact at some point. One case can take out a whole team of people in a blink of an eye.”
In North Dakota, where cases per resident are growing faster than any other state, hospitals may once again curtail elective surgeries and possibly seek government aid to hire more nurses if the situation gets worse, North Dakota Hospital Association President Tim Blasl said.
“How long can we run at this rate with the workforce that we have?” Blasl said. “You can have all the licensed beds you want, but if you don’t have anybody to staff those beds, it doesn’t do you any good.”
The northern Rocky Mountains, Great Plains and Upper Midwest are seeing the highest surge of COVID-19 cases in the nation, as some residents have ignored recommendations for curtailing the virus, such as wearing masks and avoiding large gatherings. Montana, Idaho, Utah, Wyoming, North Dakota, South Dakota, Nebraska, Iowa, and Wisconsin have recently ranked among the top 10 U.S. states in confirmed cases per 100,000 residents over a 7-day period, according to an analysis by the New York Times.
Such coronavirus infections – and the quarantines that occur because of them – are exacerbating the health care worker shortage that existed in these states well before the pandemic. Unlike in the nation’s metropolitan hubs, these outbreaks are scattered across hundreds of miles. And even in these states’ biggest cities, the ranks of medical professionals are in short supply. Specialists and registered nurses are sometimes harder to track down than ventilators, N95 masks or hospital beds. Without enough care providers, patients may not be able to get the medical attention they need.
Hospitals have asked staffers to cover extra shifts and learn new skills. They have brought in temporary workers from other parts of the country and transferred some patients to less-crowded hospitals. But, at St. Peter’s Health, if the hospital’s one kidney doctor gets sick or is told to quarantine, Dr. Harkins doesn’t expect to find a backup.
“We make a point to not have excessive staff because we have an obligation to keep the cost of health care down for a community – we just don’t have a lot of slack in our rope,” Dr. Harkins said. “What we don’t account for is a mass exodus of staff for 14 days.”
Some hospitals are already at patient capacity or are nearly there. That’s not just because of the growing number of COVID-19 patients. Elective surgeries have resumed, and medical emergencies don’t pause for a pandemic.
Some Montana hospitals formed agreements with local affiliates early in the pandemic to share staff if one came up short. But now that the disease is spreading fast – and widely – the hope is that their needs don’t peak all at once.
Montana state officials keep a list of primarily in-state volunteer workers ready to travel to towns with shortages of contact tracers, nurses and more. But during a press conference on Oct. 15, Democratic Gov. Steve Bullock said the state had exhausted that database, and its nationwide request for National Guard medical staffing hadn’t brought in new workers.
“If you are a registered nurse, licensed practical nurse, paramedic, EMT, CNA or contact tracer, and are able to join our workforce, please do consider joining our team,” Gov. Bullock said.
This month, Kalispell Regional Medical Center in northwestern Montana even stopped quarantining COVID-exposed staff who remain asymptomatic, a change allowed by Centers for Disease Control and Prevention guidelines for health facilities facing staffing shortages.
“That’s very telling for what staffing is going through right now,” said Andrea Lueck, a registered nurse at the center. “We’re so tight that employees are called off of quarantine.”
Financial pressure early in the pandemic led the hospital to furlough staff, but it had to bring most of them back to work because it needs those bodies more than ever. The regional hub is based in Flathead County, which has recorded the state’s second-highest number of active COVID-19 cases.
Mellody Sharpton, a hospital spokesperson, said hospital workers who are exposed to someone infected with the virus are tested within three to five days and monitored for symptoms. The hospital is also pulling in new workers, with 25 traveling health professionals on hand and another 25 temporary ones on the way.
But Ms. Sharpton said the best way to conserve the hospital’s workforce is to stop the disease surge in the community.
Earlier in the pandemic, Central Montana Medical Center in Lewistown, a town of fewer than 6,000, experienced an exodus of part-time workers or those close to retirement who decided their jobs weren’t worth the risk. The facility recently secured two traveling workers, but both backed out because they couldn’t find housing. And, so far, roughly 40 of the hospital’s 322 employees have missed work for reasons connected to COVID-19.
“We’re at a critical staffing shortage and have been since the beginning of COVID,” said Joanie Slaybaugh, Central Montana Medical Center’s director of human resources. “We’re small enough, everybody feels an obligation to protect themselves and to protect each other. But it doesn’t take much to take out our staff.”
Roosevelt County, where roughly 11,000 live on the northeastern edge of Montana, had one of the nation’s highest rates of new cases as of Oct. 15. But by the end of the month, the county health department will lose half of its registered nurses as one person is about to retire and another was hired through a grant that’s ending. That leaves only one registered nurse aside from its director, Patty Presser. The health department already had to close earlier during the pandemic because of COVID exposure and not enough staffers to cover the gap. Now, if Ms. Presser can’t find nurse replacements in time, she hopes volunteers will step in, though she added they typically stay for only a few weeks.
“I need someone to do immunizations for my community, and you don’t become an immunization nurse in 14 days,” she said. “We don’t have the workforce here to deal with this virus, not even right now, and then I’m going to have my best two people go.”
Back in Helena, Dr. Harkins said St. Peter’s Health had to close a specialty outpatient clinic that treats chronic diseases for two weeks at the end of September because the entire staff had to quarantine.
Now the hospital is considering having doctors take turns spending a week working from home, so that if another wave of quarantines hits in the hospital, at least one untainted person can be brought back to work. But that won’t help for some specialties, like the hospital’s sole kidney doctor.
Every time Dr. Harkins’ phone rings, she said, she takes a breath and hopes it’s not another case that will force a whole division to close.
“Because I think immediately of the hundreds of people that need that service and won’t have it for 14 days,” she said.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Twelve end-of-year tax tips: How COVID-19 could lower your tax bite
COVID-19 has had a huge impact on every aspect of physicians’ medical practice, incomes, and business. Although this will probably not end soon, there are some key tax strategies that can help your financial position if you take some important actions by the end of the year.
Some of the ways in which physicians were hard hit include:
- Physicians who are self-employed are facing increased costs for personal protective equipment, cleaning protocols, and new telehealth infrastructure. Many are also facing staffing shortages as employees fall to part-time work or take time off work to care for family members.
- Even physicians working for large hospitals are not isolated from the financial impact of the virus. A recent survey conducted by Medscape concluded that over 60% of physicians in the United States have experienced a decrease in income since the start of the pandemic.
- Saving and investing have been affected: Physicians may expect to see that companies in which they are invested are cutting dividends. Interest rates (CDs, bonds) are lower, and capital gains distributions are reduced this year. Overall, that makes for a fairly grim financial picture.
While taxable income this year has mostly declined, the applicable tax rates overall are low. However, federal, state, and local budget deficits have been skyrocketing owing to the demands of the pandemic. That means, in all likelihood, there will be tax increases in the coming years to cover spending. However, this year’s financial challenges could lend themselves to a unique tax planning scenario that could potentially benefit physicians as they make long-term plans for their investments.
Given these circumstances, these 12 tips can help you to lessen your tax bite this tax season. Many of these tips entail actions that you need to take before Dec. 31, 2020.
1. Coronavirus stimulus rebates
If you have significantly depressed income this year or have lost your job, you may find that you qualify for an Economic Impact Payment, a refundable tax credit on the 2020 tax return. The credit is $1,200 for individuals or $2,400 for joint filers, plus an additional $500 for each qualifying child aged 16 years or younger. You begin to phase out of the credit at an adjusted gross income (AGI) of $75,000 for individuals and $150,000 for joint filers. People who had AGI below these thresholds in 2019 already would have received the credit in advance, but those who now find themselves qualifying will receive the credit when they file their 2020 tax return. No action is needed on your part; your tax preparer will calculate whether you are eligible for the credit when filing your return.
2. Look to accelerate income at lower brackets
With reduced earned income, many physicians will find themselves in significantly lower tax brackets this year. Once you fall below $200,000 for individuals or $250,000 for joint filers, you no longer trigger two additional surcharge taxes. The first is the additional Medicare tax, which is a further 0.9% applied to earned income above those thresholds, on top of ordinary income tax brackets. The second is the Net Investment Income Tax (NIIT), which is an additional 3.8% applied to your investment income on top of capital gains tax brackets.
If you are someone to whom the additional Medicare tax or NIIT no longer applies for 2020, you might consider generating income this year in order to realize the lower tax rates. You could consider selling highly appreciated investments in your taxable portfolio and reinvest the proceeds by repurchasing the same securities, thereby receiving a step-up in cost basis. Remember, when you go to sell securities in retirement, you are only taxed on the gain on the security over your cost basis. By bringing the cost basis up to today’s fair market value, you could be greatly reducing the future tax applied on a sale.
For those with IRA or inherited IRA accounts who also have required minimum distributions (RMDs), you might consider making voluntary withdrawals this year and then reinvesting the proceeds into a savings or taxable account for when you need it. Keep in mind that under the CARES Act, you are no longer required to take RMDs for 2020. However, this action would help avoid being forced to withdraw the amount when you may be at a higher tax bracket. You would need to do this before Dec. 31.
3. Build Roth assets strategies
With reduced incomes and lower marginal tax rates applying to the last dollar of income this year, physicians should carefully consider how to take advantage of current tax rates by building Roth assets. There are a few strategies, including switching 401(k) or 457 contributions from pretax to Roth or performing a backdoor Roth IRA contribution. However, neither is as powerful as converting IRA assets to Roth assets because there is no restriction on conversion amount or income cutoffs.
The goal is to convert enough assets to fill up lower applicable marginal tax brackets while avoiding tax surcharges, where possible. Roth IRA conversions can get you in trouble if you don’t know what to expect, so it’s best to work with a financial advisor or tax professional to give you guidance. For example, Roth conversions can trigger some tax surprises, such as the phaseout for the 199A qualified business income deduction, increased taxation on your Social Security benefits, or higher Income-Related Monthly Adjustment Amount surcharges on Medicare Part B and Part D premiums.
Bear in mind that Roth conversions generate taxable income and cannot be undone once completed. However, paying the lower marginal tax rate today may be a big win when RMDs could push physicians into tax brackets as high as or higher than during their working years.
4. Coronavirus-related distributions
New this year is a penalty-free way to withdraw qualified retirement plan funds for those who are not yet eligible to make penalty-free withdrawals.
Congress introduced the Coronavirus-Related Distribution under the CARES Act. It allows individuals who have been affected by the pandemic to withdraw up to $100,000 before Dec. 31, 2020, without paying the 10% early withdrawal penalty. If you are considering an early retirement because of the pandemic, it may make sense to take this withdrawal while the option lasts and keep the cash available to help fund the gap before the remainder of your retirement plan assets are available penalty free. Keep in mind that this withdrawal generates taxable ordinary income, even though the early withdrawal penalty does not apply. Taking this withdrawal can boost your taxable income bracket, so calculate carefully before you do this.
5. Charitable donations for 2020
There is no shortage of people in need owing to the pandemic. For those who continue to be charitable-minded, a decrease in income may mean you have more opportunity for your regularly recurring charitable donations to decrease your taxes this year. Normally, charitable donations for itemizers are limited to 60% of AGI. However, the CARES Act increased the charitable deduction limit to 100% of AGI for 2020. Even those who claim the standard deduction can take advantage of a new “above-the-line” deduction worth $300 for individuals and $600 for joint filers by making qualified cash donations in 2020. Take special note that the contributions do not apply to donor-advised funds or nonoperating private foundations.
6. Noncash charitable donations
Many physicians are working longer and harder than ever, and for many, that means vacation plans have been placed on hold for the remainder of the year. Don’t let your paid-time-off days go to waste! The IRS now permits leave-based donation programs, which allow employers to make deductible charitable donations for the relief of victims of the COVID-19 pandemic on the basis of the value of the sick, vacation, or personal leave that employees voluntarily forgo. The value of the donation will not be treated as compensation for the employee and will be free of any otherwise applicable Federal Insurance Contributions Act (FICA) taxes, and the employer can deduct the donation as ordinary and necessary business expenses if they meet certain requirements.
7. Claiming 2020 losses on prior tax returns
For self-employed physicians, a wealth of tax planning strategies are available. One of the most significant may be the new provisions under the CARES Act that allow 100% of net operating losses (NOLs) for 3 calendar years of losses – namely 2018, 2019, and 2020 – to be carried back to the prior 5 tax years. Using these NOLs, you may be able to claim a refund for tax returns from prior tax years when there was otherwise a limit on NOLs at 80% of taxable income. If you think this applies to you, it’s wise to meet with your accountant or financial professional to discuss this.
8. Delay payroll taxes where possible
For physicians with employees looking for some cash flow relief, a new payroll tax deferral is available to you this year. Under the CARES Act, employers can delay payment of their 2020 employer payroll tax, namely the 6.2% Social Security tax, with 50% not due until Dec. 31, 2021, and the remainder due Dec. 31, 2022. The deferral will not incur any interest or penalties and is also available to those who are self-employed.
On top of that, a new payroll tax credit was created under the Families First Coronavirus Response Act. Eligible employers can receive this tax credit for the amount of wages they pay to eligible employees who are taking pandemic-related paid family leave or paid sick leave this year. The credit is also available to those who are self-employed. If you think this credit may be applicable to you, it’s worth speaking with your tax preparer about it.
9. Increased business property deductions
The nature of many physician business operations has drastically changed this year. For physicians who already have invested in and implemented new telehealth infrastructure, this can create valuable tax deductions to offset their ordinary income. Businesses may take 100% bonus depreciation on the cost of qualified property both acquired and placed in service after Sept. 27, 2017, and before Jan. 1, 2023. In general, during the last quarter of the year, you should look to decelerate business purchases until after Jan. 1, 2021, to get a deduction in 2021 at a higher marginal tax bracket.
10. Switch to cash accounting instead of accrual accounting
With higher expenses and lower profits, some large practice groups may take a second look to see whether they qualify to switch to cash accounting from accrual accounting to defer taxes. This rule change was adopted back in 2017 to allow small-business taxpayers with average annual gross receipts of $25 million or less in the prior 3 years to use the cash method of accounting. Ultimately, this switch should allow practices to owe the IRS money only after invoices were paid.
11. Physicians looking to sell their unprofitable practices
For physicians looking to make a quick exit from their practice in response to the pandemic, there is some tax relief in the event of a sale at a loss. Certain business owners who sell failed businesses will be able to use up to $50,000 of net losses as individuals or $100,000 as joint filers from the sale to offset ordinary income, current or future, under Internal Revenue Code (IRC) Section 1244. Remember that ordinary income tax rates are much higher than capital gains rates, so you could see some tax relief through a sale. The provision covers shareholders of domestic small-business corporations, both C or S corporations, but not partnerships. You would have to sell the business before Dec. 31 to get this deduction in 2020.
12. Physicians looking to sell their profitable practices
Even self-employed physicians who have managed to maintain profitable practices may be looking for early retirement after the exhaustion of the pandemic. If you own stock in a C corporation engaged in an active trade or business that has not had assets of more than $50 million at any time, you can take advantage of the IRC Section 1202 exemption. Section 1202 provides an exclusion from gain from the sale of stock of either $10 million or 10 times the adjusted basis of the stock, owned at least 5 years, in corporations regarded as “qualified small businesses.” This means you may be able to sell your practice at a gain with a handsome tax shield. Again, to get this tax benefit for April’s tax return, you’d have to engage in this activity before year end.
Regardless of whether the pandemic has placed financial constraints on you this year, tax-savvy opportunities are available to capitalize on your reduced income and lower tax rates. It’s always important to keep in mind not just your taxes in any one given year, but your lifetime tax obligations. Financial advisors and tax planners can perform multiyear tax calculations and recommend ways to manage your tax bracket and help lower your overall lifetime tax obligations.
A version of this article originally appeared on Medscape.com.
COVID-19 has had a huge impact on every aspect of physicians’ medical practice, incomes, and business. Although this will probably not end soon, there are some key tax strategies that can help your financial position if you take some important actions by the end of the year.
Some of the ways in which physicians were hard hit include:
- Physicians who are self-employed are facing increased costs for personal protective equipment, cleaning protocols, and new telehealth infrastructure. Many are also facing staffing shortages as employees fall to part-time work or take time off work to care for family members.
- Even physicians working for large hospitals are not isolated from the financial impact of the virus. A recent survey conducted by Medscape concluded that over 60% of physicians in the United States have experienced a decrease in income since the start of the pandemic.
- Saving and investing have been affected: Physicians may expect to see that companies in which they are invested are cutting dividends. Interest rates (CDs, bonds) are lower, and capital gains distributions are reduced this year. Overall, that makes for a fairly grim financial picture.
While taxable income this year has mostly declined, the applicable tax rates overall are low. However, federal, state, and local budget deficits have been skyrocketing owing to the demands of the pandemic. That means, in all likelihood, there will be tax increases in the coming years to cover spending. However, this year’s financial challenges could lend themselves to a unique tax planning scenario that could potentially benefit physicians as they make long-term plans for their investments.
Given these circumstances, these 12 tips can help you to lessen your tax bite this tax season. Many of these tips entail actions that you need to take before Dec. 31, 2020.
1. Coronavirus stimulus rebates
If you have significantly depressed income this year or have lost your job, you may find that you qualify for an Economic Impact Payment, a refundable tax credit on the 2020 tax return. The credit is $1,200 for individuals or $2,400 for joint filers, plus an additional $500 for each qualifying child aged 16 years or younger. You begin to phase out of the credit at an adjusted gross income (AGI) of $75,000 for individuals and $150,000 for joint filers. People who had AGI below these thresholds in 2019 already would have received the credit in advance, but those who now find themselves qualifying will receive the credit when they file their 2020 tax return. No action is needed on your part; your tax preparer will calculate whether you are eligible for the credit when filing your return.
2. Look to accelerate income at lower brackets
With reduced earned income, many physicians will find themselves in significantly lower tax brackets this year. Once you fall below $200,000 for individuals or $250,000 for joint filers, you no longer trigger two additional surcharge taxes. The first is the additional Medicare tax, which is a further 0.9% applied to earned income above those thresholds, on top of ordinary income tax brackets. The second is the Net Investment Income Tax (NIIT), which is an additional 3.8% applied to your investment income on top of capital gains tax brackets.
If you are someone to whom the additional Medicare tax or NIIT no longer applies for 2020, you might consider generating income this year in order to realize the lower tax rates. You could consider selling highly appreciated investments in your taxable portfolio and reinvest the proceeds by repurchasing the same securities, thereby receiving a step-up in cost basis. Remember, when you go to sell securities in retirement, you are only taxed on the gain on the security over your cost basis. By bringing the cost basis up to today’s fair market value, you could be greatly reducing the future tax applied on a sale.
For those with IRA or inherited IRA accounts who also have required minimum distributions (RMDs), you might consider making voluntary withdrawals this year and then reinvesting the proceeds into a savings or taxable account for when you need it. Keep in mind that under the CARES Act, you are no longer required to take RMDs for 2020. However, this action would help avoid being forced to withdraw the amount when you may be at a higher tax bracket. You would need to do this before Dec. 31.
3. Build Roth assets strategies
With reduced incomes and lower marginal tax rates applying to the last dollar of income this year, physicians should carefully consider how to take advantage of current tax rates by building Roth assets. There are a few strategies, including switching 401(k) or 457 contributions from pretax to Roth or performing a backdoor Roth IRA contribution. However, neither is as powerful as converting IRA assets to Roth assets because there is no restriction on conversion amount or income cutoffs.
The goal is to convert enough assets to fill up lower applicable marginal tax brackets while avoiding tax surcharges, where possible. Roth IRA conversions can get you in trouble if you don’t know what to expect, so it’s best to work with a financial advisor or tax professional to give you guidance. For example, Roth conversions can trigger some tax surprises, such as the phaseout for the 199A qualified business income deduction, increased taxation on your Social Security benefits, or higher Income-Related Monthly Adjustment Amount surcharges on Medicare Part B and Part D premiums.
Bear in mind that Roth conversions generate taxable income and cannot be undone once completed. However, paying the lower marginal tax rate today may be a big win when RMDs could push physicians into tax brackets as high as or higher than during their working years.
4. Coronavirus-related distributions
New this year is a penalty-free way to withdraw qualified retirement plan funds for those who are not yet eligible to make penalty-free withdrawals.
Congress introduced the Coronavirus-Related Distribution under the CARES Act. It allows individuals who have been affected by the pandemic to withdraw up to $100,000 before Dec. 31, 2020, without paying the 10% early withdrawal penalty. If you are considering an early retirement because of the pandemic, it may make sense to take this withdrawal while the option lasts and keep the cash available to help fund the gap before the remainder of your retirement plan assets are available penalty free. Keep in mind that this withdrawal generates taxable ordinary income, even though the early withdrawal penalty does not apply. Taking this withdrawal can boost your taxable income bracket, so calculate carefully before you do this.
5. Charitable donations for 2020
There is no shortage of people in need owing to the pandemic. For those who continue to be charitable-minded, a decrease in income may mean you have more opportunity for your regularly recurring charitable donations to decrease your taxes this year. Normally, charitable donations for itemizers are limited to 60% of AGI. However, the CARES Act increased the charitable deduction limit to 100% of AGI for 2020. Even those who claim the standard deduction can take advantage of a new “above-the-line” deduction worth $300 for individuals and $600 for joint filers by making qualified cash donations in 2020. Take special note that the contributions do not apply to donor-advised funds or nonoperating private foundations.
6. Noncash charitable donations
Many physicians are working longer and harder than ever, and for many, that means vacation plans have been placed on hold for the remainder of the year. Don’t let your paid-time-off days go to waste! The IRS now permits leave-based donation programs, which allow employers to make deductible charitable donations for the relief of victims of the COVID-19 pandemic on the basis of the value of the sick, vacation, or personal leave that employees voluntarily forgo. The value of the donation will not be treated as compensation for the employee and will be free of any otherwise applicable Federal Insurance Contributions Act (FICA) taxes, and the employer can deduct the donation as ordinary and necessary business expenses if they meet certain requirements.
7. Claiming 2020 losses on prior tax returns
For self-employed physicians, a wealth of tax planning strategies are available. One of the most significant may be the new provisions under the CARES Act that allow 100% of net operating losses (NOLs) for 3 calendar years of losses – namely 2018, 2019, and 2020 – to be carried back to the prior 5 tax years. Using these NOLs, you may be able to claim a refund for tax returns from prior tax years when there was otherwise a limit on NOLs at 80% of taxable income. If you think this applies to you, it’s wise to meet with your accountant or financial professional to discuss this.
8. Delay payroll taxes where possible
For physicians with employees looking for some cash flow relief, a new payroll tax deferral is available to you this year. Under the CARES Act, employers can delay payment of their 2020 employer payroll tax, namely the 6.2% Social Security tax, with 50% not due until Dec. 31, 2021, and the remainder due Dec. 31, 2022. The deferral will not incur any interest or penalties and is also available to those who are self-employed.
On top of that, a new payroll tax credit was created under the Families First Coronavirus Response Act. Eligible employers can receive this tax credit for the amount of wages they pay to eligible employees who are taking pandemic-related paid family leave or paid sick leave this year. The credit is also available to those who are self-employed. If you think this credit may be applicable to you, it’s worth speaking with your tax preparer about it.
9. Increased business property deductions
The nature of many physician business operations has drastically changed this year. For physicians who already have invested in and implemented new telehealth infrastructure, this can create valuable tax deductions to offset their ordinary income. Businesses may take 100% bonus depreciation on the cost of qualified property both acquired and placed in service after Sept. 27, 2017, and before Jan. 1, 2023. In general, during the last quarter of the year, you should look to decelerate business purchases until after Jan. 1, 2021, to get a deduction in 2021 at a higher marginal tax bracket.
10. Switch to cash accounting instead of accrual accounting
With higher expenses and lower profits, some large practice groups may take a second look to see whether they qualify to switch to cash accounting from accrual accounting to defer taxes. This rule change was adopted back in 2017 to allow small-business taxpayers with average annual gross receipts of $25 million or less in the prior 3 years to use the cash method of accounting. Ultimately, this switch should allow practices to owe the IRS money only after invoices were paid.
11. Physicians looking to sell their unprofitable practices
For physicians looking to make a quick exit from their practice in response to the pandemic, there is some tax relief in the event of a sale at a loss. Certain business owners who sell failed businesses will be able to use up to $50,000 of net losses as individuals or $100,000 as joint filers from the sale to offset ordinary income, current or future, under Internal Revenue Code (IRC) Section 1244. Remember that ordinary income tax rates are much higher than capital gains rates, so you could see some tax relief through a sale. The provision covers shareholders of domestic small-business corporations, both C or S corporations, but not partnerships. You would have to sell the business before Dec. 31 to get this deduction in 2020.
12. Physicians looking to sell their profitable practices
Even self-employed physicians who have managed to maintain profitable practices may be looking for early retirement after the exhaustion of the pandemic. If you own stock in a C corporation engaged in an active trade or business that has not had assets of more than $50 million at any time, you can take advantage of the IRC Section 1202 exemption. Section 1202 provides an exclusion from gain from the sale of stock of either $10 million or 10 times the adjusted basis of the stock, owned at least 5 years, in corporations regarded as “qualified small businesses.” This means you may be able to sell your practice at a gain with a handsome tax shield. Again, to get this tax benefit for April’s tax return, you’d have to engage in this activity before year end.
Regardless of whether the pandemic has placed financial constraints on you this year, tax-savvy opportunities are available to capitalize on your reduced income and lower tax rates. It’s always important to keep in mind not just your taxes in any one given year, but your lifetime tax obligations. Financial advisors and tax planners can perform multiyear tax calculations and recommend ways to manage your tax bracket and help lower your overall lifetime tax obligations.
A version of this article originally appeared on Medscape.com.
COVID-19 has had a huge impact on every aspect of physicians’ medical practice, incomes, and business. Although this will probably not end soon, there are some key tax strategies that can help your financial position if you take some important actions by the end of the year.
Some of the ways in which physicians were hard hit include:
- Physicians who are self-employed are facing increased costs for personal protective equipment, cleaning protocols, and new telehealth infrastructure. Many are also facing staffing shortages as employees fall to part-time work or take time off work to care for family members.
- Even physicians working for large hospitals are not isolated from the financial impact of the virus. A recent survey conducted by Medscape concluded that over 60% of physicians in the United States have experienced a decrease in income since the start of the pandemic.
- Saving and investing have been affected: Physicians may expect to see that companies in which they are invested are cutting dividends. Interest rates (CDs, bonds) are lower, and capital gains distributions are reduced this year. Overall, that makes for a fairly grim financial picture.
While taxable income this year has mostly declined, the applicable tax rates overall are low. However, federal, state, and local budget deficits have been skyrocketing owing to the demands of the pandemic. That means, in all likelihood, there will be tax increases in the coming years to cover spending. However, this year’s financial challenges could lend themselves to a unique tax planning scenario that could potentially benefit physicians as they make long-term plans for their investments.
Given these circumstances, these 12 tips can help you to lessen your tax bite this tax season. Many of these tips entail actions that you need to take before Dec. 31, 2020.
1. Coronavirus stimulus rebates
If you have significantly depressed income this year or have lost your job, you may find that you qualify for an Economic Impact Payment, a refundable tax credit on the 2020 tax return. The credit is $1,200 for individuals or $2,400 for joint filers, plus an additional $500 for each qualifying child aged 16 years or younger. You begin to phase out of the credit at an adjusted gross income (AGI) of $75,000 for individuals and $150,000 for joint filers. People who had AGI below these thresholds in 2019 already would have received the credit in advance, but those who now find themselves qualifying will receive the credit when they file their 2020 tax return. No action is needed on your part; your tax preparer will calculate whether you are eligible for the credit when filing your return.
2. Look to accelerate income at lower brackets
With reduced earned income, many physicians will find themselves in significantly lower tax brackets this year. Once you fall below $200,000 for individuals or $250,000 for joint filers, you no longer trigger two additional surcharge taxes. The first is the additional Medicare tax, which is a further 0.9% applied to earned income above those thresholds, on top of ordinary income tax brackets. The second is the Net Investment Income Tax (NIIT), which is an additional 3.8% applied to your investment income on top of capital gains tax brackets.
If you are someone to whom the additional Medicare tax or NIIT no longer applies for 2020, you might consider generating income this year in order to realize the lower tax rates. You could consider selling highly appreciated investments in your taxable portfolio and reinvest the proceeds by repurchasing the same securities, thereby receiving a step-up in cost basis. Remember, when you go to sell securities in retirement, you are only taxed on the gain on the security over your cost basis. By bringing the cost basis up to today’s fair market value, you could be greatly reducing the future tax applied on a sale.
For those with IRA or inherited IRA accounts who also have required minimum distributions (RMDs), you might consider making voluntary withdrawals this year and then reinvesting the proceeds into a savings or taxable account for when you need it. Keep in mind that under the CARES Act, you are no longer required to take RMDs for 2020. However, this action would help avoid being forced to withdraw the amount when you may be at a higher tax bracket. You would need to do this before Dec. 31.
3. Build Roth assets strategies
With reduced incomes and lower marginal tax rates applying to the last dollar of income this year, physicians should carefully consider how to take advantage of current tax rates by building Roth assets. There are a few strategies, including switching 401(k) or 457 contributions from pretax to Roth or performing a backdoor Roth IRA contribution. However, neither is as powerful as converting IRA assets to Roth assets because there is no restriction on conversion amount or income cutoffs.
The goal is to convert enough assets to fill up lower applicable marginal tax brackets while avoiding tax surcharges, where possible. Roth IRA conversions can get you in trouble if you don’t know what to expect, so it’s best to work with a financial advisor or tax professional to give you guidance. For example, Roth conversions can trigger some tax surprises, such as the phaseout for the 199A qualified business income deduction, increased taxation on your Social Security benefits, or higher Income-Related Monthly Adjustment Amount surcharges on Medicare Part B and Part D premiums.
Bear in mind that Roth conversions generate taxable income and cannot be undone once completed. However, paying the lower marginal tax rate today may be a big win when RMDs could push physicians into tax brackets as high as or higher than during their working years.
4. Coronavirus-related distributions
New this year is a penalty-free way to withdraw qualified retirement plan funds for those who are not yet eligible to make penalty-free withdrawals.
Congress introduced the Coronavirus-Related Distribution under the CARES Act. It allows individuals who have been affected by the pandemic to withdraw up to $100,000 before Dec. 31, 2020, without paying the 10% early withdrawal penalty. If you are considering an early retirement because of the pandemic, it may make sense to take this withdrawal while the option lasts and keep the cash available to help fund the gap before the remainder of your retirement plan assets are available penalty free. Keep in mind that this withdrawal generates taxable ordinary income, even though the early withdrawal penalty does not apply. Taking this withdrawal can boost your taxable income bracket, so calculate carefully before you do this.
5. Charitable donations for 2020
There is no shortage of people in need owing to the pandemic. For those who continue to be charitable-minded, a decrease in income may mean you have more opportunity for your regularly recurring charitable donations to decrease your taxes this year. Normally, charitable donations for itemizers are limited to 60% of AGI. However, the CARES Act increased the charitable deduction limit to 100% of AGI for 2020. Even those who claim the standard deduction can take advantage of a new “above-the-line” deduction worth $300 for individuals and $600 for joint filers by making qualified cash donations in 2020. Take special note that the contributions do not apply to donor-advised funds or nonoperating private foundations.
6. Noncash charitable donations
Many physicians are working longer and harder than ever, and for many, that means vacation plans have been placed on hold for the remainder of the year. Don’t let your paid-time-off days go to waste! The IRS now permits leave-based donation programs, which allow employers to make deductible charitable donations for the relief of victims of the COVID-19 pandemic on the basis of the value of the sick, vacation, or personal leave that employees voluntarily forgo. The value of the donation will not be treated as compensation for the employee and will be free of any otherwise applicable Federal Insurance Contributions Act (FICA) taxes, and the employer can deduct the donation as ordinary and necessary business expenses if they meet certain requirements.
7. Claiming 2020 losses on prior tax returns
For self-employed physicians, a wealth of tax planning strategies are available. One of the most significant may be the new provisions under the CARES Act that allow 100% of net operating losses (NOLs) for 3 calendar years of losses – namely 2018, 2019, and 2020 – to be carried back to the prior 5 tax years. Using these NOLs, you may be able to claim a refund for tax returns from prior tax years when there was otherwise a limit on NOLs at 80% of taxable income. If you think this applies to you, it’s wise to meet with your accountant or financial professional to discuss this.
8. Delay payroll taxes where possible
For physicians with employees looking for some cash flow relief, a new payroll tax deferral is available to you this year. Under the CARES Act, employers can delay payment of their 2020 employer payroll tax, namely the 6.2% Social Security tax, with 50% not due until Dec. 31, 2021, and the remainder due Dec. 31, 2022. The deferral will not incur any interest or penalties and is also available to those who are self-employed.
On top of that, a new payroll tax credit was created under the Families First Coronavirus Response Act. Eligible employers can receive this tax credit for the amount of wages they pay to eligible employees who are taking pandemic-related paid family leave or paid sick leave this year. The credit is also available to those who are self-employed. If you think this credit may be applicable to you, it’s worth speaking with your tax preparer about it.
9. Increased business property deductions
The nature of many physician business operations has drastically changed this year. For physicians who already have invested in and implemented new telehealth infrastructure, this can create valuable tax deductions to offset their ordinary income. Businesses may take 100% bonus depreciation on the cost of qualified property both acquired and placed in service after Sept. 27, 2017, and before Jan. 1, 2023. In general, during the last quarter of the year, you should look to decelerate business purchases until after Jan. 1, 2021, to get a deduction in 2021 at a higher marginal tax bracket.
10. Switch to cash accounting instead of accrual accounting
With higher expenses and lower profits, some large practice groups may take a second look to see whether they qualify to switch to cash accounting from accrual accounting to defer taxes. This rule change was adopted back in 2017 to allow small-business taxpayers with average annual gross receipts of $25 million or less in the prior 3 years to use the cash method of accounting. Ultimately, this switch should allow practices to owe the IRS money only after invoices were paid.
11. Physicians looking to sell their unprofitable practices
For physicians looking to make a quick exit from their practice in response to the pandemic, there is some tax relief in the event of a sale at a loss. Certain business owners who sell failed businesses will be able to use up to $50,000 of net losses as individuals or $100,000 as joint filers from the sale to offset ordinary income, current or future, under Internal Revenue Code (IRC) Section 1244. Remember that ordinary income tax rates are much higher than capital gains rates, so you could see some tax relief through a sale. The provision covers shareholders of domestic small-business corporations, both C or S corporations, but not partnerships. You would have to sell the business before Dec. 31 to get this deduction in 2020.
12. Physicians looking to sell their profitable practices
Even self-employed physicians who have managed to maintain profitable practices may be looking for early retirement after the exhaustion of the pandemic. If you own stock in a C corporation engaged in an active trade or business that has not had assets of more than $50 million at any time, you can take advantage of the IRC Section 1202 exemption. Section 1202 provides an exclusion from gain from the sale of stock of either $10 million or 10 times the adjusted basis of the stock, owned at least 5 years, in corporations regarded as “qualified small businesses.” This means you may be able to sell your practice at a gain with a handsome tax shield. Again, to get this tax benefit for April’s tax return, you’d have to engage in this activity before year end.
Regardless of whether the pandemic has placed financial constraints on you this year, tax-savvy opportunities are available to capitalize on your reduced income and lower tax rates. It’s always important to keep in mind not just your taxes in any one given year, but your lifetime tax obligations. Financial advisors and tax planners can perform multiyear tax calculations and recommend ways to manage your tax bracket and help lower your overall lifetime tax obligations.
A version of this article originally appeared on Medscape.com.