User login
A guide to the new agents reshaping ovarian cancer treatment
The treatment of ovarian cancer has evolved considerably in the last few years, with the approval of several PARP inhibitors, antiangiogenic agents, and other therapies for a multitude of indications. Additional treatments are likely to soon join this already diverse spectrum of available options, if their promising efficacy and safety continues to be borne out in ongoing research.
To better understand the individual merits and potential drawbacks of these treatments, Medscape recently spoke with Rebecca Stone, MD, an ovarian cancer expert and associate professor of gynecologic oncology at Johns Hopkins University, Baltimore. This interview has been edited for length and clarity.
Medscape: We’re starting to see preliminary data on pamiparib , an investigational inhibitor of PARP1 and PARP2, for the treatment of ovarian cancer. What is the evidence supporting this drug?
Dr. Stone: Currently, six different PARP inhibitors – olaparib, rucaparib, veliparib, niraparib, talazoparib, and pamiparib – have been in clinical development at different stages. In clinical applications, PARP inhibitors, including olaparib, rucaparib, niraparib, and talazoparib, have demonstrated sustained antitumor responses as single agents in patients with BRCA1 or BRCA2 mutations. Those with Food and Drug Administration indications in ovarian cancer include olaparib, rucaparib, and niraparib. The preclinical and clinical data with pamiparib is limited as of now. But, in a xenograft breast cancer model, it was found to be over 10 times more potent than olaparib.
If approved, where would pamiparib fit in the treatment paradigm for ovarian cancer?
It would potentially fit as monotherapy as well as in combination with agents other than standard chemotherapy for the treatment of BRCA mutated ovarian cancer. It could also be considered for maintenance therapy at the conclusion of chemotherapy treatment of newly diagnosed or recurrent BRCA-mutated ovarian cancer.
What adverse events are associated with pamiparib? How does the toxicity profile compare with other drugs for ovarian cancer?
With respect to PARP inhibitors, the differences in potency (PARP trapping) correlate with their toxicity profiles. The most common adverse events are gastrointestinal, hematologic, and constitutional (fatigue). Even though it is difficult to compare toxicities across different trials with heterogeneous patient populations, there are a few points worth noting.
Rucaparib leads to inhibition of renal transporter proteins involved in secretion of creatinine and can lead to increased creatinine (any grade: 15%; grade 3: ≤1%). Transaminitis is generally self-limiting and highest with rucaparib (any grade: 34%; grade 3: 10%). Hematologic toxicities are the highest with niraparib (any grade: thrombocytopenia 61%, anemia 50%, neutropenia 30%; grade ≥3: thrombocytopenia 34%, anemia 25%, neutropenia 20%).
Toxicities are more common in the first few cycles of treatment, warranting closer early monitoring. This differs somewhat from the gastrointestinal, hematological, and constitutional (fatigue) adverse events that we see with common chemotherapeutic agents used to treat ovarian cancer, which are generally cumulative.
PARP inhibitor treatment is also associated with an increased risk of developing myelodysplastic syndrome/acute myeloid leukemia (MDS/AML). That being said, therapy-related MDS/AML is a well-recognized complication of conventional chemotherapy used to treat a variety of primary malignancies, including ovarian cancer.
The expected toxicity profile for pamiparib is based on what we have seen with the other PARP inhibitors. This includes any grade nausea (50%), fatigue (33%), anemia (20%), vomiting (15%), and neutropenia (13%). Toxicity of grade 3 or higher includes anemia (13%), neutropenia (8%), and fatigue (5%).
Where do the newest drugs to be approved for ovarian cancer in recent years fit within the treatment paradigm? What do the research findings show about their efficacy and safety?
Data from phase 2/3 trials support the use of PARP inhibitors as monotherapy as well as in combination with other agents (most commonly agents other than standard chemotherapy) for the treatment of BRCA mutated or otherwise homologous recombination-deficient (HRD) ovarian cancer. They can also be considered for maintenance therapy at the conclusion of treatment of newly diagnosed or recurrent BRCA-mutated/HRD ovarian cancer.
Large phase 3 studies have resulted in the approval of the antiangiogenic agent bevacizumab in combination with chemotherapy for the treatment of newly diagnosed and recurrent ovarian cancer, as well as for maintenance therapy at the conclusion of combination chemotherapy plus bevacizumab treatment of newly diagnosed (GOG 218 and ICON 7 trials) or recurrent ovarian cancer (GOG 218, OCEANS, and AURELIA trials). The most common toxicity with antiangiogenic agents is hypertension. Women also commonly experience arthralgia/myalgia. There is an increased risk of proteinuria, blood clots, bleeding, and serious gastrointestinal events such as fistula and bowel perforation.
Data from the phase 2 KEYNOTE 158 trial support pembrolizumab for microsatellite high or mismatch repair-deficient ovarian cancers. Common side effects associated with the use of pembrolizumab include fatigue, itchy skin, diarrhea, nausea, decreased appetite, rash, fever, cough, difficulty breathing, musculoskeletal pain, constipation, and joint pain. Pembrolizumab can cause the immune system to attack normal organs and tissues in the body resulting in serious side effects, including inflammation of such organs as the lungs, colon, liver, endocrine glands, and kidneys.
Evidence for hormonal therapy (i.e., aromatase inhibitors like letrozole) for the treatment of newly diagnosed and recurrent low-grade serous/endometrioid epithelial ovarian cancer comes from largely retrospective cohort studies. A large phase 3 study, now enrolling, will examine if letrozole monotherapy/maintenance is non-inferior to intravenous paclitaxel/carboplatin and maintenance letrozole with respect to progression-free survival in women with stage II-IV primary low-grade serous carcinoma of the ovary or peritoneum after primary surgical cytoreduction.
Hormonal therapies are generally very well tolerated. Common side effects may include hot flashes, warmth or redness in the face or chest, headache, dizziness, weakness, bone pain, muscle or joint pain, swelling, weight gain, increased sweating, or increased cholesterol in the blood.
What other drugs are in development for ovarian cancer?
VEGF receptor tyrosine kinase inhibitors, such as cediranib, are in development. Anlotinib is another drug being investigated. It is a new multi-target tyrosine kinase inhibitor that targets VEGFR, PDGFR, and FGFR. Drugs targeting folate-alpha receptor, such as mirvetuximab, are under investigation, particularly for patients with high folate-alpha receptor membrane staining by immunohistochemistry. Drugs targeting cell cycle arrest, such as CDK4/6 inhibitors, are also being considered.
Can you provide some of the highlights of ovarian cancer research presented at this year’s American Society of Clinical Oncology meeting ?
My take is that we have gone from a monotonous landscape of platinum doublet chemotherapy to an exciting, diversified landscape over the past several years. All of this activity has driven median overall survival up from 3 years to 5 years and progression-free survival following first platinum sensitive recurrence to well beyond 6 months.
Since last year’s meeting, we have seen several new approvals, including niraparib for the treatment of BRCA mutated and HRD disease, as well as for first-line maintenance in all comers. In May, the FDA expanded the indication for olaparib to include its combination with bevacizumab as first-line maintenance for BRCA-mutated and HRD disease based on the results of PAOLA-1. With certainty, our treatment paradigms will continue to evolve in response to these and other new data.
At this year’s meeting, the SOLO-2 investigators revealed the first overall survival data for second-line PARP inhibitor maintenance, which is the first suggestion that PARP inhibitor maintenance improves overall survival.
We have a new understanding about the genetics of long-term responders to rucaparib on ARIEL-2.
We also understand how the role of secondary cytoreductive surgery and how nonchemotherapy options for the treatment of platinum sensitive relapse compare in terms of efficacy and toxicity (i.e., AVANOVA-2 and GY004 trials). We see again the importance of R0 cytoreduction when surgery is pursued. Achieving anything less than R0 cytoreduction for the treatment of first platinum sensitive recurrence may translate into shorter survival, compared with chemotherapy alone.
We are also becoming increasingly familiar with the limited therapeutic benefit of single-agent anti-PD-1/PD-L1, which is so different from our experience in mismatch repair-deficient endometrial cancer. In the small percentage of responders, there are some durable responses and a suggestion of particular efficacy among women with clear cell ovarian cancer.
What other recent findings in ovarian cancer research should oncologists be aware of?
Data supporting improved efficacy of a gastrointestinal-type chemotherapy regimen for mucinous epithelial ovarian cancers come from a retrospective cohort study of patients with ovarian mucinous carcinoma who received postoperative adjuvant chemotherapy at two academic centers.
Identification of inactivating SMARCA4 mutations as the driver of small cell carcinoma of the ovary, hypercalcemic type, and the idea that CDK4/6 inhibitors could be effectively repurposed to treat this rare but highly aggressive type of ovarian cancer is also new and exciting.
Dr. Stone has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The treatment of ovarian cancer has evolved considerably in the last few years, with the approval of several PARP inhibitors, antiangiogenic agents, and other therapies for a multitude of indications. Additional treatments are likely to soon join this already diverse spectrum of available options, if their promising efficacy and safety continues to be borne out in ongoing research.
To better understand the individual merits and potential drawbacks of these treatments, Medscape recently spoke with Rebecca Stone, MD, an ovarian cancer expert and associate professor of gynecologic oncology at Johns Hopkins University, Baltimore. This interview has been edited for length and clarity.
Medscape: We’re starting to see preliminary data on pamiparib , an investigational inhibitor of PARP1 and PARP2, for the treatment of ovarian cancer. What is the evidence supporting this drug?
Dr. Stone: Currently, six different PARP inhibitors – olaparib, rucaparib, veliparib, niraparib, talazoparib, and pamiparib – have been in clinical development at different stages. In clinical applications, PARP inhibitors, including olaparib, rucaparib, niraparib, and talazoparib, have demonstrated sustained antitumor responses as single agents in patients with BRCA1 or BRCA2 mutations. Those with Food and Drug Administration indications in ovarian cancer include olaparib, rucaparib, and niraparib. The preclinical and clinical data with pamiparib is limited as of now. But, in a xenograft breast cancer model, it was found to be over 10 times more potent than olaparib.
If approved, where would pamiparib fit in the treatment paradigm for ovarian cancer?
It would potentially fit as monotherapy as well as in combination with agents other than standard chemotherapy for the treatment of BRCA mutated ovarian cancer. It could also be considered for maintenance therapy at the conclusion of chemotherapy treatment of newly diagnosed or recurrent BRCA-mutated ovarian cancer.
What adverse events are associated with pamiparib? How does the toxicity profile compare with other drugs for ovarian cancer?
With respect to PARP inhibitors, the differences in potency (PARP trapping) correlate with their toxicity profiles. The most common adverse events are gastrointestinal, hematologic, and constitutional (fatigue). Even though it is difficult to compare toxicities across different trials with heterogeneous patient populations, there are a few points worth noting.
Rucaparib leads to inhibition of renal transporter proteins involved in secretion of creatinine and can lead to increased creatinine (any grade: 15%; grade 3: ≤1%). Transaminitis is generally self-limiting and highest with rucaparib (any grade: 34%; grade 3: 10%). Hematologic toxicities are the highest with niraparib (any grade: thrombocytopenia 61%, anemia 50%, neutropenia 30%; grade ≥3: thrombocytopenia 34%, anemia 25%, neutropenia 20%).
Toxicities are more common in the first few cycles of treatment, warranting closer early monitoring. This differs somewhat from the gastrointestinal, hematological, and constitutional (fatigue) adverse events that we see with common chemotherapeutic agents used to treat ovarian cancer, which are generally cumulative.
PARP inhibitor treatment is also associated with an increased risk of developing myelodysplastic syndrome/acute myeloid leukemia (MDS/AML). That being said, therapy-related MDS/AML is a well-recognized complication of conventional chemotherapy used to treat a variety of primary malignancies, including ovarian cancer.
The expected toxicity profile for pamiparib is based on what we have seen with the other PARP inhibitors. This includes any grade nausea (50%), fatigue (33%), anemia (20%), vomiting (15%), and neutropenia (13%). Toxicity of grade 3 or higher includes anemia (13%), neutropenia (8%), and fatigue (5%).
Where do the newest drugs to be approved for ovarian cancer in recent years fit within the treatment paradigm? What do the research findings show about their efficacy and safety?
Data from phase 2/3 trials support the use of PARP inhibitors as monotherapy as well as in combination with other agents (most commonly agents other than standard chemotherapy) for the treatment of BRCA mutated or otherwise homologous recombination-deficient (HRD) ovarian cancer. They can also be considered for maintenance therapy at the conclusion of treatment of newly diagnosed or recurrent BRCA-mutated/HRD ovarian cancer.
Large phase 3 studies have resulted in the approval of the antiangiogenic agent bevacizumab in combination with chemotherapy for the treatment of newly diagnosed and recurrent ovarian cancer, as well as for maintenance therapy at the conclusion of combination chemotherapy plus bevacizumab treatment of newly diagnosed (GOG 218 and ICON 7 trials) or recurrent ovarian cancer (GOG 218, OCEANS, and AURELIA trials). The most common toxicity with antiangiogenic agents is hypertension. Women also commonly experience arthralgia/myalgia. There is an increased risk of proteinuria, blood clots, bleeding, and serious gastrointestinal events such as fistula and bowel perforation.
Data from the phase 2 KEYNOTE 158 trial support pembrolizumab for microsatellite high or mismatch repair-deficient ovarian cancers. Common side effects associated with the use of pembrolizumab include fatigue, itchy skin, diarrhea, nausea, decreased appetite, rash, fever, cough, difficulty breathing, musculoskeletal pain, constipation, and joint pain. Pembrolizumab can cause the immune system to attack normal organs and tissues in the body resulting in serious side effects, including inflammation of such organs as the lungs, colon, liver, endocrine glands, and kidneys.
Evidence for hormonal therapy (i.e., aromatase inhibitors like letrozole) for the treatment of newly diagnosed and recurrent low-grade serous/endometrioid epithelial ovarian cancer comes from largely retrospective cohort studies. A large phase 3 study, now enrolling, will examine if letrozole monotherapy/maintenance is non-inferior to intravenous paclitaxel/carboplatin and maintenance letrozole with respect to progression-free survival in women with stage II-IV primary low-grade serous carcinoma of the ovary or peritoneum after primary surgical cytoreduction.
Hormonal therapies are generally very well tolerated. Common side effects may include hot flashes, warmth or redness in the face or chest, headache, dizziness, weakness, bone pain, muscle or joint pain, swelling, weight gain, increased sweating, or increased cholesterol in the blood.
What other drugs are in development for ovarian cancer?
VEGF receptor tyrosine kinase inhibitors, such as cediranib, are in development. Anlotinib is another drug being investigated. It is a new multi-target tyrosine kinase inhibitor that targets VEGFR, PDGFR, and FGFR. Drugs targeting folate-alpha receptor, such as mirvetuximab, are under investigation, particularly for patients with high folate-alpha receptor membrane staining by immunohistochemistry. Drugs targeting cell cycle arrest, such as CDK4/6 inhibitors, are also being considered.
Can you provide some of the highlights of ovarian cancer research presented at this year’s American Society of Clinical Oncology meeting ?
My take is that we have gone from a monotonous landscape of platinum doublet chemotherapy to an exciting, diversified landscape over the past several years. All of this activity has driven median overall survival up from 3 years to 5 years and progression-free survival following first platinum sensitive recurrence to well beyond 6 months.
Since last year’s meeting, we have seen several new approvals, including niraparib for the treatment of BRCA mutated and HRD disease, as well as for first-line maintenance in all comers. In May, the FDA expanded the indication for olaparib to include its combination with bevacizumab as first-line maintenance for BRCA-mutated and HRD disease based on the results of PAOLA-1. With certainty, our treatment paradigms will continue to evolve in response to these and other new data.
At this year’s meeting, the SOLO-2 investigators revealed the first overall survival data for second-line PARP inhibitor maintenance, which is the first suggestion that PARP inhibitor maintenance improves overall survival.
We have a new understanding about the genetics of long-term responders to rucaparib on ARIEL-2.
We also understand how the role of secondary cytoreductive surgery and how nonchemotherapy options for the treatment of platinum sensitive relapse compare in terms of efficacy and toxicity (i.e., AVANOVA-2 and GY004 trials). We see again the importance of R0 cytoreduction when surgery is pursued. Achieving anything less than R0 cytoreduction for the treatment of first platinum sensitive recurrence may translate into shorter survival, compared with chemotherapy alone.
We are also becoming increasingly familiar with the limited therapeutic benefit of single-agent anti-PD-1/PD-L1, which is so different from our experience in mismatch repair-deficient endometrial cancer. In the small percentage of responders, there are some durable responses and a suggestion of particular efficacy among women with clear cell ovarian cancer.
What other recent findings in ovarian cancer research should oncologists be aware of?
Data supporting improved efficacy of a gastrointestinal-type chemotherapy regimen for mucinous epithelial ovarian cancers come from a retrospective cohort study of patients with ovarian mucinous carcinoma who received postoperative adjuvant chemotherapy at two academic centers.
Identification of inactivating SMARCA4 mutations as the driver of small cell carcinoma of the ovary, hypercalcemic type, and the idea that CDK4/6 inhibitors could be effectively repurposed to treat this rare but highly aggressive type of ovarian cancer is also new and exciting.
Dr. Stone has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The treatment of ovarian cancer has evolved considerably in the last few years, with the approval of several PARP inhibitors, antiangiogenic agents, and other therapies for a multitude of indications. Additional treatments are likely to soon join this already diverse spectrum of available options, if their promising efficacy and safety continues to be borne out in ongoing research.
To better understand the individual merits and potential drawbacks of these treatments, Medscape recently spoke with Rebecca Stone, MD, an ovarian cancer expert and associate professor of gynecologic oncology at Johns Hopkins University, Baltimore. This interview has been edited for length and clarity.
Medscape: We’re starting to see preliminary data on pamiparib , an investigational inhibitor of PARP1 and PARP2, for the treatment of ovarian cancer. What is the evidence supporting this drug?
Dr. Stone: Currently, six different PARP inhibitors – olaparib, rucaparib, veliparib, niraparib, talazoparib, and pamiparib – have been in clinical development at different stages. In clinical applications, PARP inhibitors, including olaparib, rucaparib, niraparib, and talazoparib, have demonstrated sustained antitumor responses as single agents in patients with BRCA1 or BRCA2 mutations. Those with Food and Drug Administration indications in ovarian cancer include olaparib, rucaparib, and niraparib. The preclinical and clinical data with pamiparib is limited as of now. But, in a xenograft breast cancer model, it was found to be over 10 times more potent than olaparib.
If approved, where would pamiparib fit in the treatment paradigm for ovarian cancer?
It would potentially fit as monotherapy as well as in combination with agents other than standard chemotherapy for the treatment of BRCA mutated ovarian cancer. It could also be considered for maintenance therapy at the conclusion of chemotherapy treatment of newly diagnosed or recurrent BRCA-mutated ovarian cancer.
What adverse events are associated with pamiparib? How does the toxicity profile compare with other drugs for ovarian cancer?
With respect to PARP inhibitors, the differences in potency (PARP trapping) correlate with their toxicity profiles. The most common adverse events are gastrointestinal, hematologic, and constitutional (fatigue). Even though it is difficult to compare toxicities across different trials with heterogeneous patient populations, there are a few points worth noting.
Rucaparib leads to inhibition of renal transporter proteins involved in secretion of creatinine and can lead to increased creatinine (any grade: 15%; grade 3: ≤1%). Transaminitis is generally self-limiting and highest with rucaparib (any grade: 34%; grade 3: 10%). Hematologic toxicities are the highest with niraparib (any grade: thrombocytopenia 61%, anemia 50%, neutropenia 30%; grade ≥3: thrombocytopenia 34%, anemia 25%, neutropenia 20%).
Toxicities are more common in the first few cycles of treatment, warranting closer early monitoring. This differs somewhat from the gastrointestinal, hematological, and constitutional (fatigue) adverse events that we see with common chemotherapeutic agents used to treat ovarian cancer, which are generally cumulative.
PARP inhibitor treatment is also associated with an increased risk of developing myelodysplastic syndrome/acute myeloid leukemia (MDS/AML). That being said, therapy-related MDS/AML is a well-recognized complication of conventional chemotherapy used to treat a variety of primary malignancies, including ovarian cancer.
The expected toxicity profile for pamiparib is based on what we have seen with the other PARP inhibitors. This includes any grade nausea (50%), fatigue (33%), anemia (20%), vomiting (15%), and neutropenia (13%). Toxicity of grade 3 or higher includes anemia (13%), neutropenia (8%), and fatigue (5%).
Where do the newest drugs to be approved for ovarian cancer in recent years fit within the treatment paradigm? What do the research findings show about their efficacy and safety?
Data from phase 2/3 trials support the use of PARP inhibitors as monotherapy as well as in combination with other agents (most commonly agents other than standard chemotherapy) for the treatment of BRCA mutated or otherwise homologous recombination-deficient (HRD) ovarian cancer. They can also be considered for maintenance therapy at the conclusion of treatment of newly diagnosed or recurrent BRCA-mutated/HRD ovarian cancer.
Large phase 3 studies have resulted in the approval of the antiangiogenic agent bevacizumab in combination with chemotherapy for the treatment of newly diagnosed and recurrent ovarian cancer, as well as for maintenance therapy at the conclusion of combination chemotherapy plus bevacizumab treatment of newly diagnosed (GOG 218 and ICON 7 trials) or recurrent ovarian cancer (GOG 218, OCEANS, and AURELIA trials). The most common toxicity with antiangiogenic agents is hypertension. Women also commonly experience arthralgia/myalgia. There is an increased risk of proteinuria, blood clots, bleeding, and serious gastrointestinal events such as fistula and bowel perforation.
Data from the phase 2 KEYNOTE 158 trial support pembrolizumab for microsatellite high or mismatch repair-deficient ovarian cancers. Common side effects associated with the use of pembrolizumab include fatigue, itchy skin, diarrhea, nausea, decreased appetite, rash, fever, cough, difficulty breathing, musculoskeletal pain, constipation, and joint pain. Pembrolizumab can cause the immune system to attack normal organs and tissues in the body resulting in serious side effects, including inflammation of such organs as the lungs, colon, liver, endocrine glands, and kidneys.
Evidence for hormonal therapy (i.e., aromatase inhibitors like letrozole) for the treatment of newly diagnosed and recurrent low-grade serous/endometrioid epithelial ovarian cancer comes from largely retrospective cohort studies. A large phase 3 study, now enrolling, will examine if letrozole monotherapy/maintenance is non-inferior to intravenous paclitaxel/carboplatin and maintenance letrozole with respect to progression-free survival in women with stage II-IV primary low-grade serous carcinoma of the ovary or peritoneum after primary surgical cytoreduction.
Hormonal therapies are generally very well tolerated. Common side effects may include hot flashes, warmth or redness in the face or chest, headache, dizziness, weakness, bone pain, muscle or joint pain, swelling, weight gain, increased sweating, or increased cholesterol in the blood.
What other drugs are in development for ovarian cancer?
VEGF receptor tyrosine kinase inhibitors, such as cediranib, are in development. Anlotinib is another drug being investigated. It is a new multi-target tyrosine kinase inhibitor that targets VEGFR, PDGFR, and FGFR. Drugs targeting folate-alpha receptor, such as mirvetuximab, are under investigation, particularly for patients with high folate-alpha receptor membrane staining by immunohistochemistry. Drugs targeting cell cycle arrest, such as CDK4/6 inhibitors, are also being considered.
Can you provide some of the highlights of ovarian cancer research presented at this year’s American Society of Clinical Oncology meeting ?
My take is that we have gone from a monotonous landscape of platinum doublet chemotherapy to an exciting, diversified landscape over the past several years. All of this activity has driven median overall survival up from 3 years to 5 years and progression-free survival following first platinum sensitive recurrence to well beyond 6 months.
Since last year’s meeting, we have seen several new approvals, including niraparib for the treatment of BRCA mutated and HRD disease, as well as for first-line maintenance in all comers. In May, the FDA expanded the indication for olaparib to include its combination with bevacizumab as first-line maintenance for BRCA-mutated and HRD disease based on the results of PAOLA-1. With certainty, our treatment paradigms will continue to evolve in response to these and other new data.
At this year’s meeting, the SOLO-2 investigators revealed the first overall survival data for second-line PARP inhibitor maintenance, which is the first suggestion that PARP inhibitor maintenance improves overall survival.
We have a new understanding about the genetics of long-term responders to rucaparib on ARIEL-2.
We also understand how the role of secondary cytoreductive surgery and how nonchemotherapy options for the treatment of platinum sensitive relapse compare in terms of efficacy and toxicity (i.e., AVANOVA-2 and GY004 trials). We see again the importance of R0 cytoreduction when surgery is pursued. Achieving anything less than R0 cytoreduction for the treatment of first platinum sensitive recurrence may translate into shorter survival, compared with chemotherapy alone.
We are also becoming increasingly familiar with the limited therapeutic benefit of single-agent anti-PD-1/PD-L1, which is so different from our experience in mismatch repair-deficient endometrial cancer. In the small percentage of responders, there are some durable responses and a suggestion of particular efficacy among women with clear cell ovarian cancer.
What other recent findings in ovarian cancer research should oncologists be aware of?
Data supporting improved efficacy of a gastrointestinal-type chemotherapy regimen for mucinous epithelial ovarian cancers come from a retrospective cohort study of patients with ovarian mucinous carcinoma who received postoperative adjuvant chemotherapy at two academic centers.
Identification of inactivating SMARCA4 mutations as the driver of small cell carcinoma of the ovary, hypercalcemic type, and the idea that CDK4/6 inhibitors could be effectively repurposed to treat this rare but highly aggressive type of ovarian cancer is also new and exciting.
Dr. Stone has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Med student’s cardiac crisis a COVID-era medical mystery
Within minutes of her arrival at Community North Hospital in Indianapolis, Ramya Yeleti’s vital signs plummeted; her pulse was at 45 beats per minute and her ejection fraction was hovering near 10%. “I definitely thought there was a chance I would close my eyes and never open them again, but I only had a few seconds to process that,” she recalled. Then everything went black. Ramya fell unconscious as shock pads were positioned and a swarm of clinicians prepared to insert an Impella heart pump through a catheter into her aorta.
The third-year medical student and aspiring psychiatrist had been doing in-person neurology rotations in July when she began to experience fever and uncontrolled vomiting. Her initial thought was that she must have caught the flu from a patient.
After all, Ramya, along with her father Ram Yeleti, MD, mother Indira, and twin sister Divya, had all weathered COVID-19 in previous months and later tested positive for SARS-CoV-2 antibodies. The only family member who had been spared was her younger brother Rohith.
Indira suffered a severe case, requiring ICU care for 2 days but no ventilator; the others experienced mostly mild symptoms. Ramya — who was studying for her third-year board exams after classes at Marian University College of Osteopathic Medicine in Indianapolis went virtual in March — was left with lingering fatigue; however, her cough and muscle aches abated and her sense of taste and smell returned. When she started rotations, she thought her life was getting back to normal.
Ramya’s flu symptoms did not improve. A university-mandated rapid COVID test came back negative, but 2 more days of vomiting started to worry both her and her father, who is a cardiologist and chief physician executive at Community Health Network in Indianapolis. After Ramya felt some chest pain, she asked her father to listen to her heart. All sounded normal, and Ram prescribed ondansetron for her nausea.
But the antiemetic didn’t work, and by the next morning both father and daughter were convinced that they needed to head to the emergency department.
“I wanted to double-check if I was missing something about her being dehydrated,” Ram told Medscape Medical News. “Several things can cause protracted nausea, like hepatitis, appendicitis, or another infection. I feel terribly guilty I didn’t realize she had a heart condition.”
A surprising turn for the worst
Ramya’s subtle symptoms quickly gave way to the dramatic cardiac crisis that unfolded just after her arrival at Community North. “Her EKG looked absolutely horrendous, like a 75-year-old having a heart attack,” Ram said.
As a cardiologist, he knew his daughter’s situation was growing dire when he heard physicians shouting that the Impella wasn’t working and she needed extracorporeal membrane oxygenation (ECMO).
“At that point, I didn’t think she’d survive,” her father recalled. “We had 10 physicians in the room who worked on her for 5 hours to get her stabilized.”
“It was especially traumatic because, obviously, I knew exactly what was happening,” he added. “You can’t sugarcoat anything.”
After being connected to the heart–lung equipment, Ramya was transferred to IU Health Methodist Hospital, also in Indianapolis, where she was tested again for COVID-19. Unlike the rapid test administered just days earlier, the PCR assay came back positive.
“I knew she had acute myocarditis, but coronavirus never crossed my mind,” said Ram.
“As we were dealing with her heart, we were also dealing with this challenge: she was coming back positive for COVID-19 again,” said Roopa Rao, MD, the heart failure transplant cardiologist at IU Health who treated Ramya.
“We weren’t sure whether we were dealing with an active infection or dead virus” from her previous infection, Rao said, “so we started treating her like she had active COVID-19 and gave her remdesivir, convalescent plasma, and steroids, which was the protocol in our hospital.”
A biopsy of Ramya’s heart tissue, along with blood tests, indicated a past parvovirus infection. It’s possible that Ramya’s previous coronavirus infection made her susceptible to heart damage from a newer parvovirus infection, said Rao. Either virus, or both together, could have been responsible for the calamity.
Although it was unheard of during Ramya’s cardiac crisis in early August, evolving evidence now raises the possibility that she is one of a handful of people in the world to be reinfected with SARS-CoV-2. Also emerging are cases of COVID-related myocarditis and other extreme heart complications, particularly in young people.
“At the time, it wasn’t really clear if people could have another infection so quickly,” Rao told Medscape Medical News. “It is possible she is one of these rare individuals to have COVID-19 twice. I’m hoping at some point we will have some clarity.”
“I would favor a coinfection as probably the triggering factor for her sickness,” she said. “It may take some time, but like any other disease — and it doesn’t look like COVID will go away magically — I hope we’ll have some answers down the road.”
Another wrinkle
The next 48 hours brought astonishing news: Ramya’s heart function had rebounded to nearly normal, and her ejection fraction increased to about 45%. Heart transplantation wouldn’t be necessary, although Rao stood poised to follow through if ECMO only sustained, rather than improved, Ramya’s prognosis.
“Ramya was so sick that if she didn’t recover, the only option would be a heart transplant,” said Rao. “But we wanted to do everything to keep that heart.”
After steroid and COVID treatment, Ramya’s heart started to come back. “It didn’t make sense to me,” said Rao. “I don’t know what helped. If we hadn’t done ECMO, her heart probably wouldn’t have recovered, so I would say we have to support these patients and give them time for the heart to recover, even to the point of ECMO.”
Despite the good news, Ramya’s survival still hung in the balance. When she was disconnected from ECMO, clinicians discovered that the Impella device had caused a rare complication, damaging her mitral valve. The valve could be repaired surgically, but both Rao and Ram felt great trepidation at the prospect of cardiopulmonary bypass during the open-heart procedure.
“They would need to stop her heart and restart it, and I was concerned it would not restart,” Ram explained. “I didn’t like the idea of open-heart surgery, but my biggest fear was she was not going to survive it because of a really fresh, sick heart.”
The cardiologists’ fears did, in fact, come to pass: it took an hour to coax Ramya’s heart back at the end of surgery. But, just as the surgeon was preparing to reconnect Ramya to ECMO in desperation, “her heart recovered again,” Rao reported.
“Some things you never forget in life,” she said. “I can’t describe how everyone in the OR felt, all taking care of her. I told Ramya, ‘you are a fighter’.”
New strength
Six days would pass before Ramya woke up and learned of the astounding series of events that saved her. She knew “something was really wrong” because of the incision at the center of her chest, but learning she’d been on ECMO and the heart transplant list drove home how close to death she’d actually come.
“Most people don’t get off ECMO; they die on it,” she said. “And the chances of dying on the heart transplant list are very high. It was very strange to me that this was my story all of a sudden, when a week and a half earlier I was on rotation.”
Ongoing physical therapy over the past 3 months has transformed Ramya from a state of profound physical weakness to a place of relative strength. The now-fourth-year med student is turning 26 in November and is hungry to restart in-person rotations. Her downtime has been filled in part with researching myocarditis and collaborating with Rao on her own case study for journal publication.
But the mental trauma from her experience has girded her in ways she knows will make her stronger personally and professionally in the years ahead.
“It’s still very hard. I’m still recovering,” she acknowledged. “I described it to my therapist as an invisible wound on my brain.”
“When I came out of the hospital, I still had ECMO wounds, deep gashes on my legs that affected how fast and how long I could walk,” she said. “I felt like the same thing was going on my brain — a huge cut no one could see.”
Her intention to specialize in psychiatry has become more pressing now that Ramya has realized the impact of trauma on mental health.
“My body failing me was awful, but I could handle it,” she said. “Losing any part of my mind would have been way worse. I want to take care of that in my patients.”
This article first appeared on Medscape.com.
Within minutes of her arrival at Community North Hospital in Indianapolis, Ramya Yeleti’s vital signs plummeted; her pulse was at 45 beats per minute and her ejection fraction was hovering near 10%. “I definitely thought there was a chance I would close my eyes and never open them again, but I only had a few seconds to process that,” she recalled. Then everything went black. Ramya fell unconscious as shock pads were positioned and a swarm of clinicians prepared to insert an Impella heart pump through a catheter into her aorta.
The third-year medical student and aspiring psychiatrist had been doing in-person neurology rotations in July when she began to experience fever and uncontrolled vomiting. Her initial thought was that she must have caught the flu from a patient.
After all, Ramya, along with her father Ram Yeleti, MD, mother Indira, and twin sister Divya, had all weathered COVID-19 in previous months and later tested positive for SARS-CoV-2 antibodies. The only family member who had been spared was her younger brother Rohith.
Indira suffered a severe case, requiring ICU care for 2 days but no ventilator; the others experienced mostly mild symptoms. Ramya — who was studying for her third-year board exams after classes at Marian University College of Osteopathic Medicine in Indianapolis went virtual in March — was left with lingering fatigue; however, her cough and muscle aches abated and her sense of taste and smell returned. When she started rotations, she thought her life was getting back to normal.
Ramya’s flu symptoms did not improve. A university-mandated rapid COVID test came back negative, but 2 more days of vomiting started to worry both her and her father, who is a cardiologist and chief physician executive at Community Health Network in Indianapolis. After Ramya felt some chest pain, she asked her father to listen to her heart. All sounded normal, and Ram prescribed ondansetron for her nausea.
But the antiemetic didn’t work, and by the next morning both father and daughter were convinced that they needed to head to the emergency department.
“I wanted to double-check if I was missing something about her being dehydrated,” Ram told Medscape Medical News. “Several things can cause protracted nausea, like hepatitis, appendicitis, or another infection. I feel terribly guilty I didn’t realize she had a heart condition.”
A surprising turn for the worst
Ramya’s subtle symptoms quickly gave way to the dramatic cardiac crisis that unfolded just after her arrival at Community North. “Her EKG looked absolutely horrendous, like a 75-year-old having a heart attack,” Ram said.
As a cardiologist, he knew his daughter’s situation was growing dire when he heard physicians shouting that the Impella wasn’t working and she needed extracorporeal membrane oxygenation (ECMO).
“At that point, I didn’t think she’d survive,” her father recalled. “We had 10 physicians in the room who worked on her for 5 hours to get her stabilized.”
“It was especially traumatic because, obviously, I knew exactly what was happening,” he added. “You can’t sugarcoat anything.”
After being connected to the heart–lung equipment, Ramya was transferred to IU Health Methodist Hospital, also in Indianapolis, where she was tested again for COVID-19. Unlike the rapid test administered just days earlier, the PCR assay came back positive.
“I knew she had acute myocarditis, but coronavirus never crossed my mind,” said Ram.
“As we were dealing with her heart, we were also dealing with this challenge: she was coming back positive for COVID-19 again,” said Roopa Rao, MD, the heart failure transplant cardiologist at IU Health who treated Ramya.
“We weren’t sure whether we were dealing with an active infection or dead virus” from her previous infection, Rao said, “so we started treating her like she had active COVID-19 and gave her remdesivir, convalescent plasma, and steroids, which was the protocol in our hospital.”
A biopsy of Ramya’s heart tissue, along with blood tests, indicated a past parvovirus infection. It’s possible that Ramya’s previous coronavirus infection made her susceptible to heart damage from a newer parvovirus infection, said Rao. Either virus, or both together, could have been responsible for the calamity.
Although it was unheard of during Ramya’s cardiac crisis in early August, evolving evidence now raises the possibility that she is one of a handful of people in the world to be reinfected with SARS-CoV-2. Also emerging are cases of COVID-related myocarditis and other extreme heart complications, particularly in young people.
“At the time, it wasn’t really clear if people could have another infection so quickly,” Rao told Medscape Medical News. “It is possible she is one of these rare individuals to have COVID-19 twice. I’m hoping at some point we will have some clarity.”
“I would favor a coinfection as probably the triggering factor for her sickness,” she said. “It may take some time, but like any other disease — and it doesn’t look like COVID will go away magically — I hope we’ll have some answers down the road.”
Another wrinkle
The next 48 hours brought astonishing news: Ramya’s heart function had rebounded to nearly normal, and her ejection fraction increased to about 45%. Heart transplantation wouldn’t be necessary, although Rao stood poised to follow through if ECMO only sustained, rather than improved, Ramya’s prognosis.
“Ramya was so sick that if she didn’t recover, the only option would be a heart transplant,” said Rao. “But we wanted to do everything to keep that heart.”
After steroid and COVID treatment, Ramya’s heart started to come back. “It didn’t make sense to me,” said Rao. “I don’t know what helped. If we hadn’t done ECMO, her heart probably wouldn’t have recovered, so I would say we have to support these patients and give them time for the heart to recover, even to the point of ECMO.”
Despite the good news, Ramya’s survival still hung in the balance. When she was disconnected from ECMO, clinicians discovered that the Impella device had caused a rare complication, damaging her mitral valve. The valve could be repaired surgically, but both Rao and Ram felt great trepidation at the prospect of cardiopulmonary bypass during the open-heart procedure.
“They would need to stop her heart and restart it, and I was concerned it would not restart,” Ram explained. “I didn’t like the idea of open-heart surgery, but my biggest fear was she was not going to survive it because of a really fresh, sick heart.”
The cardiologists’ fears did, in fact, come to pass: it took an hour to coax Ramya’s heart back at the end of surgery. But, just as the surgeon was preparing to reconnect Ramya to ECMO in desperation, “her heart recovered again,” Rao reported.
“Some things you never forget in life,” she said. “I can’t describe how everyone in the OR felt, all taking care of her. I told Ramya, ‘you are a fighter’.”
New strength
Six days would pass before Ramya woke up and learned of the astounding series of events that saved her. She knew “something was really wrong” because of the incision at the center of her chest, but learning she’d been on ECMO and the heart transplant list drove home how close to death she’d actually come.
“Most people don’t get off ECMO; they die on it,” she said. “And the chances of dying on the heart transplant list are very high. It was very strange to me that this was my story all of a sudden, when a week and a half earlier I was on rotation.”
Ongoing physical therapy over the past 3 months has transformed Ramya from a state of profound physical weakness to a place of relative strength. The now-fourth-year med student is turning 26 in November and is hungry to restart in-person rotations. Her downtime has been filled in part with researching myocarditis and collaborating with Rao on her own case study for journal publication.
But the mental trauma from her experience has girded her in ways she knows will make her stronger personally and professionally in the years ahead.
“It’s still very hard. I’m still recovering,” she acknowledged. “I described it to my therapist as an invisible wound on my brain.”
“When I came out of the hospital, I still had ECMO wounds, deep gashes on my legs that affected how fast and how long I could walk,” she said. “I felt like the same thing was going on my brain — a huge cut no one could see.”
Her intention to specialize in psychiatry has become more pressing now that Ramya has realized the impact of trauma on mental health.
“My body failing me was awful, but I could handle it,” she said. “Losing any part of my mind would have been way worse. I want to take care of that in my patients.”
This article first appeared on Medscape.com.
Within minutes of her arrival at Community North Hospital in Indianapolis, Ramya Yeleti’s vital signs plummeted; her pulse was at 45 beats per minute and her ejection fraction was hovering near 10%. “I definitely thought there was a chance I would close my eyes and never open them again, but I only had a few seconds to process that,” she recalled. Then everything went black. Ramya fell unconscious as shock pads were positioned and a swarm of clinicians prepared to insert an Impella heart pump through a catheter into her aorta.
The third-year medical student and aspiring psychiatrist had been doing in-person neurology rotations in July when she began to experience fever and uncontrolled vomiting. Her initial thought was that she must have caught the flu from a patient.
After all, Ramya, along with her father Ram Yeleti, MD, mother Indira, and twin sister Divya, had all weathered COVID-19 in previous months and later tested positive for SARS-CoV-2 antibodies. The only family member who had been spared was her younger brother Rohith.
Indira suffered a severe case, requiring ICU care for 2 days but no ventilator; the others experienced mostly mild symptoms. Ramya — who was studying for her third-year board exams after classes at Marian University College of Osteopathic Medicine in Indianapolis went virtual in March — was left with lingering fatigue; however, her cough and muscle aches abated and her sense of taste and smell returned. When she started rotations, she thought her life was getting back to normal.
Ramya’s flu symptoms did not improve. A university-mandated rapid COVID test came back negative, but 2 more days of vomiting started to worry both her and her father, who is a cardiologist and chief physician executive at Community Health Network in Indianapolis. After Ramya felt some chest pain, she asked her father to listen to her heart. All sounded normal, and Ram prescribed ondansetron for her nausea.
But the antiemetic didn’t work, and by the next morning both father and daughter were convinced that they needed to head to the emergency department.
“I wanted to double-check if I was missing something about her being dehydrated,” Ram told Medscape Medical News. “Several things can cause protracted nausea, like hepatitis, appendicitis, or another infection. I feel terribly guilty I didn’t realize she had a heart condition.”
A surprising turn for the worst
Ramya’s subtle symptoms quickly gave way to the dramatic cardiac crisis that unfolded just after her arrival at Community North. “Her EKG looked absolutely horrendous, like a 75-year-old having a heart attack,” Ram said.
As a cardiologist, he knew his daughter’s situation was growing dire when he heard physicians shouting that the Impella wasn’t working and she needed extracorporeal membrane oxygenation (ECMO).
“At that point, I didn’t think she’d survive,” her father recalled. “We had 10 physicians in the room who worked on her for 5 hours to get her stabilized.”
“It was especially traumatic because, obviously, I knew exactly what was happening,” he added. “You can’t sugarcoat anything.”
After being connected to the heart–lung equipment, Ramya was transferred to IU Health Methodist Hospital, also in Indianapolis, where she was tested again for COVID-19. Unlike the rapid test administered just days earlier, the PCR assay came back positive.
“I knew she had acute myocarditis, but coronavirus never crossed my mind,” said Ram.
“As we were dealing with her heart, we were also dealing with this challenge: she was coming back positive for COVID-19 again,” said Roopa Rao, MD, the heart failure transplant cardiologist at IU Health who treated Ramya.
“We weren’t sure whether we were dealing with an active infection or dead virus” from her previous infection, Rao said, “so we started treating her like she had active COVID-19 and gave her remdesivir, convalescent plasma, and steroids, which was the protocol in our hospital.”
A biopsy of Ramya’s heart tissue, along with blood tests, indicated a past parvovirus infection. It’s possible that Ramya’s previous coronavirus infection made her susceptible to heart damage from a newer parvovirus infection, said Rao. Either virus, or both together, could have been responsible for the calamity.
Although it was unheard of during Ramya’s cardiac crisis in early August, evolving evidence now raises the possibility that she is one of a handful of people in the world to be reinfected with SARS-CoV-2. Also emerging are cases of COVID-related myocarditis and other extreme heart complications, particularly in young people.
“At the time, it wasn’t really clear if people could have another infection so quickly,” Rao told Medscape Medical News. “It is possible she is one of these rare individuals to have COVID-19 twice. I’m hoping at some point we will have some clarity.”
“I would favor a coinfection as probably the triggering factor for her sickness,” she said. “It may take some time, but like any other disease — and it doesn’t look like COVID will go away magically — I hope we’ll have some answers down the road.”
Another wrinkle
The next 48 hours brought astonishing news: Ramya’s heart function had rebounded to nearly normal, and her ejection fraction increased to about 45%. Heart transplantation wouldn’t be necessary, although Rao stood poised to follow through if ECMO only sustained, rather than improved, Ramya’s prognosis.
“Ramya was so sick that if she didn’t recover, the only option would be a heart transplant,” said Rao. “But we wanted to do everything to keep that heart.”
After steroid and COVID treatment, Ramya’s heart started to come back. “It didn’t make sense to me,” said Rao. “I don’t know what helped. If we hadn’t done ECMO, her heart probably wouldn’t have recovered, so I would say we have to support these patients and give them time for the heart to recover, even to the point of ECMO.”
Despite the good news, Ramya’s survival still hung in the balance. When she was disconnected from ECMO, clinicians discovered that the Impella device had caused a rare complication, damaging her mitral valve. The valve could be repaired surgically, but both Rao and Ram felt great trepidation at the prospect of cardiopulmonary bypass during the open-heart procedure.
“They would need to stop her heart and restart it, and I was concerned it would not restart,” Ram explained. “I didn’t like the idea of open-heart surgery, but my biggest fear was she was not going to survive it because of a really fresh, sick heart.”
The cardiologists’ fears did, in fact, come to pass: it took an hour to coax Ramya’s heart back at the end of surgery. But, just as the surgeon was preparing to reconnect Ramya to ECMO in desperation, “her heart recovered again,” Rao reported.
“Some things you never forget in life,” she said. “I can’t describe how everyone in the OR felt, all taking care of her. I told Ramya, ‘you are a fighter’.”
New strength
Six days would pass before Ramya woke up and learned of the astounding series of events that saved her. She knew “something was really wrong” because of the incision at the center of her chest, but learning she’d been on ECMO and the heart transplant list drove home how close to death she’d actually come.
“Most people don’t get off ECMO; they die on it,” she said. “And the chances of dying on the heart transplant list are very high. It was very strange to me that this was my story all of a sudden, when a week and a half earlier I was on rotation.”
Ongoing physical therapy over the past 3 months has transformed Ramya from a state of profound physical weakness to a place of relative strength. The now-fourth-year med student is turning 26 in November and is hungry to restart in-person rotations. Her downtime has been filled in part with researching myocarditis and collaborating with Rao on her own case study for journal publication.
But the mental trauma from her experience has girded her in ways she knows will make her stronger personally and professionally in the years ahead.
“It’s still very hard. I’m still recovering,” she acknowledged. “I described it to my therapist as an invisible wound on my brain.”
“When I came out of the hospital, I still had ECMO wounds, deep gashes on my legs that affected how fast and how long I could walk,” she said. “I felt like the same thing was going on my brain — a huge cut no one could see.”
Her intention to specialize in psychiatry has become more pressing now that Ramya has realized the impact of trauma on mental health.
“My body failing me was awful, but I could handle it,” she said. “Losing any part of my mind would have been way worse. I want to take care of that in my patients.”
This article first appeared on Medscape.com.
Is the tide turning on the ‘grubby’ affair of EXCEL and the European guidelines?
“I disapprove of what you say, but I will defend to the death your right to say it.” The choice of the secretary general of the European Association for Cardio-Thoracic Surgery to open with this quote was the first hint that the next presentation at the 2019 annual meeting would be anything but dull. The session chair followed with a reminder to keep the discussion polite and civil.
Presenter David Taggart, MD, PhD, did not disappoint. The professor of cardiovascular surgery at the University of Oxford (England) began with the announcement that he had withdrawn his name from a recent paper in the New England Journal of Medicine. He then proceeded to accuse his coinvestigators of misrepresenting the findings of a major clinical trial.
Dr. Taggart was chair of the surgical committee for the Abbott-sponsored EXCEL trial, which compared two procedures for patients who had blockages in their left main coronary artery: percutaneous coronary intervention (PCI) using coronary stents, and coronary artery bypass graft surgery (CABG). The investigators designed the trial to compare outcomes for the two treatments using a composite endpoint of death, stroke, and MI. The 3-year follow-up data had been published in NEJM without controversy – or, at least, without public controversy.
But when it came time to publish the 5-year follow-up, there was a significantly higher rate of death in the stent group, and both Dr. Taggart and the journal editors were concerned that this finding was being downplayed in the manuscript.
In their comments to the authors, the journal editors had recommended including the mortality difference (unless clearly trivial) ‘”in the concluding statement in the final paragraph.” Yet, the concluding statement of the published paper read that there “was no significant difference between PCI and CABG.”
In Dr. Taggart’s view, that claim was dangerous for patients, and so he was left with no choice but to remove himself as an author, a first for the academic with over 300 scientific papers to his name.
Earlier publications from the EXCEL trial had influenced European treatment guidelines. But subsequent allegations of misconduct and hidden data spurred the EACTS to repudiate those guidelines out of concern “that some results in the EXCEL trial appear to have been concealed and that some patients may therefore have received the wrong clinical advice.”
The controversy pitted cardiothoracic surgeons against interventional cardiologists, who were seen as increasingly encroaching on the surgeons’ turf. Dr. Taggart was a long-time critic of the subspecialty.
Surgeons demanded an independent analysis of the EXCEL trial data – a demand that the investigators have yet to satisfy. Dr. Taggart was the first to speak publicly, but others had major reservations about the trial reporting and conduct years earlier.
Mortality data held back
One such person was Lars Wallentin, MD, a professor of cardiology at Uppsala (Sweden) University Hospital, who chaired the independent committee that monitored the safety and scientific validity of the EXCEL trial.
The committee, known as the data and safety monitoring board (DSMB), received a report on March 23, 2016, that showed that increasingly more patients who had received stents were dying, compared with the group of patients that had undergone CABG. A graph of the survival curves showed the gap between the two groups widening after 3 years (Figure 1).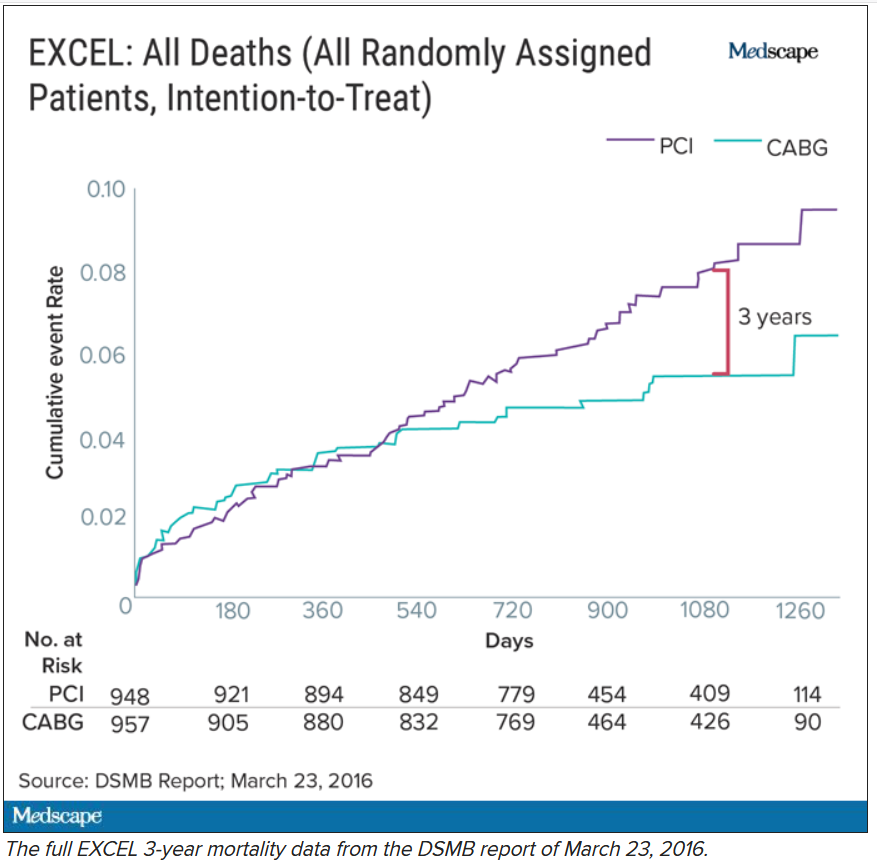
By September of that year, Dr. Wallentin and other members of the DSMB were anxious to share the concerning mortality difference with the broader medical community.
They were aware that EACTS and the European Society of Cardiology had started the process of updating their guidelines on myocardial revascularization, and were keen for the guideline writing committee to see all of the data.
Meanwhile, the trial investigators, led by principal investigator Gregg Stone, MD, then at New York–Presbyterian Hospital and Columbia University Medical Center, were preparing to publish a report of the 3-year outcomes. Recruitment for EXCEL started in September 2010, so at the time of the 3-year analysis in 2016, some patients had been followed up for over 5 years. But the data, published in NEJM in October 2016, were capped at 3 years (Figure 2). It didn’t show the widening gap in late mortality that Dr. Wallentin and the rest of the DSMB had seen.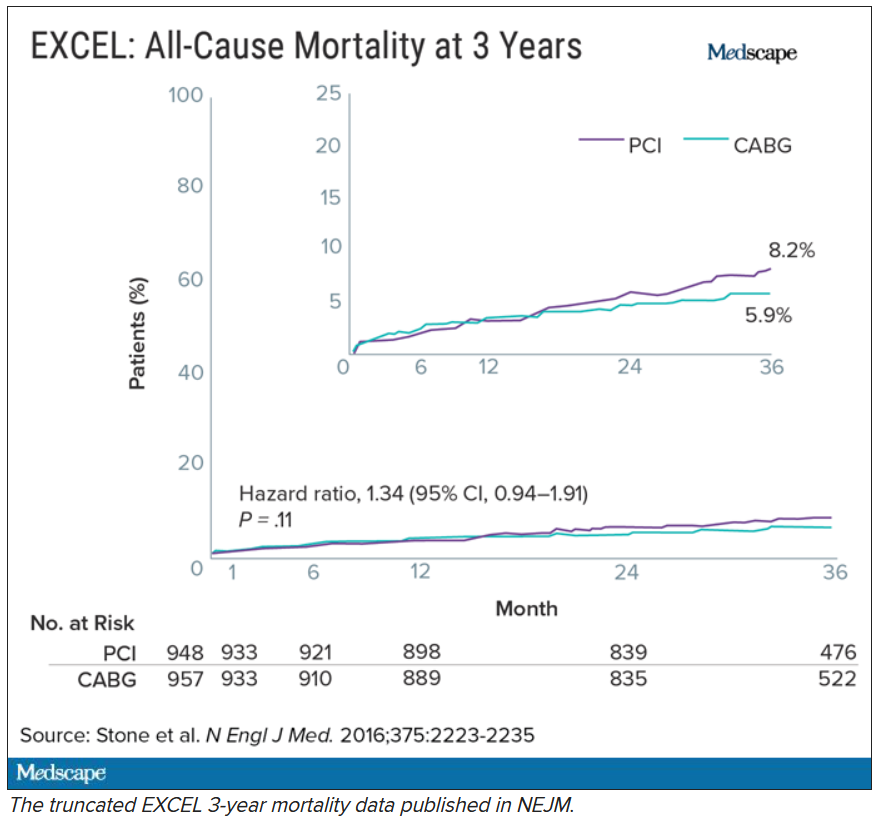
When asked about this, the investigators said they were transparent about their plans to cap the data at 3 years in an amendment to the study protocol. Stone’s coprincipal investigators were interventional cardiologist Patrick Serruys, MD, then of Imperial College London; and two surgeons: Joseph Sabik, MD, then of the Cleveland Clinic Foundation, and A. Pieter Kappetein, MD, PhD, then at Erasmus Medical Center, Rotterdam. The four principal investigators all declared financial payments from stent manufacturers either to themselves or their institutions.
Study sponsor Abbott has distanced itself from the decisions made and has referred all questions about the trial to the EXCEL investigators. Charles Simonton, chief medical officer at Abbott (now at Abiomed) was a coauthor on both the 3- and 5-year papers. Dr. Wallentin believes that the sponsor must have been aware of the DSMB’s concerns.
Continuing DSMB concerns
A year later, the DSMB was still troubled. Dr. Wallentin emailed Dr. Stone in September 2017 asking for an updated analysis of the mortality data without any capping in time.
Dr. Wallentin added that he didn’t think that unblinding the mortality results would be an issue at that stage because these were late deaths in a trial where the interventions were long completed. But, he warned, “it might be very concerning if, in the future, suspicions were raised that already available information on mortality was withheld from the cardiology and thoracic surgery community.”
The investigators took a month to respond. They declined the request, saying that the trial was not statistically powered to measure mortality. In his email to Dr. Wallentin, Dr. Stone stressed that they were committed to complete disclosure of all of the EXCEL data and that the responsible time point to unblind was after 4 years. His coprincipal investigators (Dr. Serruys, Dr. Sabik, and Dr. Kappetein) as well as EXCEL statistical committee chair Stuart Pocock, PhD, and Mr. Simonton were all copied on the email.
Dr. Wallentin deferred to the principal investigators’ arguments.
Missing MI data
Death was not the only outcome of the EXCEL trial to draw scrutiny.
The EXCEL investigators used a unique definition of MI that was almost exclusively based on a rise in the cardiac biomarker CK-MB. This protocol definition of MI was later adapted into the Society for Cardiovascular Angiography and Interventions definition in a paper coauthored by Dr. Stone. The investigators agreed to also measure MIs that met the more commonly used Third Universal Definition as a secondary endpoint. The Third Universal Definition of Myocardial Infarction uses a change in biomarkers – preferably troponin or alternatively CK-MB – coupled with other clinical signs.
It is standard practice to report secondary endpoints in any analysis of the main findings of a study. Yet, the EXCEL investigators did not report the universal definition of MI in either the 3-year or 5-year publications.
This is critical because MI according to one definition may not count according to the other, and the final tally could tip the trial results positive, negative, or neutral for coronary stents.
In Dr. Taggart’s opinion, the protocol definition puts CABG at a disadvantage because it uses the same biomarker threshold for procedural-related MI for both PCI and CABG. Because surgery involves more manipulation of the heart, cardiac enzyme levels will naturally be higher after CABG than PCI. These procedure-related enzyme elevations are not “true clinical MIs,” according to Dr. Taggart and others.
Late last year, a dataset containing the 3-year follow-up of EXCEL, including the information on the universal definition of MI, was leaked to the BBC. Working with biostatisticians, the BBC confirmed that according to this definition, there were more MIs in the stent group.
Originally, the investigators disputed the finding, calling the BBC data “imaginary.” They claimed that they were unable to calculate a rate of MI according to the universal definition because they lacked routine collection of troponins, although the universal definition also allows use of CK-MB. They have since published an analysis of 5-year MI data according to the universal definition, which showed twice the rate of MI in the PCI group.
From the leaked data, the BBC calculated the main composite endpoint of death, stroke, and MI using the universal definition of MI. Now the results swung in favor of CABG.
Impact on guidelines
None of this was known at the time the European cardiology societies convened a committee to write their new guidelines on myocardial revascularization. The writing panel disagreed about whether PCI and CABG were equivalent for patients with left main coronary artery disease (CAD).
Besides EXCEL, another study, the NOBLE trial, compared PCI and CABG in left main CAD and came to opposite conclusions – conclusions that matched the leaked data. In that trial, European investigators chose a slightly different primary endpoint: a composite of death, MI, stroke, and the need for a repeat procedure. They used the universal definition of MI exclusively, and notably, they omitted procedural MI from their clinical event count. The results, published at the same time as the EXCEL 3-year findings, suggested that CABG was better.
Given the discrepant findings of two large trials, the guideline committee considered all of the available data comparing the two methods of revascularization for left main CAD. But even then, things weren’t clear-cut. One draft meta-analysis, supported by the National Institute for Health Research, suggested that results were worse for first- and second-generation drug-eluting coronary stents – including those used in EXCEL – compared with surgery.
Another meta-analysis, later published in The Lancet, drew a different conclusion and found that PCI was just as good as surgery. The main author, Stuart Head, a cardiothoracic surgeon on the ESC/EACTS guideline committee, was a research fellow with EXCEL investigator Dr. Kappetein at Erasmus. EXCEL investigators Dr. Stone, Dr. Kappetein, and Dr. Serruys were coauthors of the Lancet meta-analysis.
There was heated discussion about the committee’s draft recommendations, which gave both CABG and PCI a Class IA recommendation in patients with left main CAD and low anatomical complexity. In October 2017, the ESC commissioned an anonymous external reviewer to weigh in. James Brophy, MD, PhD, a cardiologist and professor of medicine and epidemiology at McGill University, Montreal, confirmed that he was the reviewer after he published an updated version in June 2020.
Looking at all of the data available at the time comparing the procedures for left main CAD, Dr. Brophy’s analysis suggested a 73% chance that the excess in death, stroke, or MI represents at least two excess events per 100 patients treated with PCI rather than CABG.
Dr. Brophy thought that most patients would find these differences clinically meaningful and advised against giving both procedures the same class of recommendation. He was also concerned that many readers will skip to the summary recommendation table without reading the entire guideline document.
“I feel this is misleading in its present form,” he wrote in 2017.
Despite Dr. Brophy’s review, the guideline committee stuck with its original recommendations. The final 2018 ESC/EACTS Guidelines on myocardial revascularization gave equal weight to both CABG and PCI in patients with left main CAD and low anatomical complexity. In contrast, US guidelines do not put PCI and CABG on the same footing for any group of patients with left main CAD.
The lead author of the ESC/EACTS guidelines section on left main disease, and around a third of those on the writing task force, all declared financial payments from stent manufacturers either to themselves or their institutions. The EXCEL principal investigator, Dr. Kappetein, was secretary general of EACTS and oversaw the guidelines process for the surgical organization. He left to work for Medtronic midway through the process and was later joined there by his former research fellow, Stuart Head.
Dr. Brophy said in an interview that given the final guideline recommendations, he assumed that the committee had other reviews and went with the majority opinion.
But not everyone involved in the guidelines saw Dr. Brophy’s review. Nick Freemantle, a statistical reviewer appointed by EACTS, expected to see it but didn’t. This omission calls into question the neutrality of the whole process, in his view.
Mr. Freemantle believes that the deck was stacked so that he only saw the pieces of evidence that supported the conclusions that were already decided and that he was not shown “the bits that don’t fit that neatly.”
“And without that narrative, it all feels a bit grubby, to be honest,” he said.
Professor Barbara Casadei, ESC president, disputed this, saying that the guidelines were approved by all surgical members, including the EACTS council.
Missing from Dr. Brophy’s review were the later data from EXCEL. As he had told the DSMB in 2017, Stone presented the 4-year data from EXCEL at the TCT conference in September 2018. At this point, the analysis showed that 10.3% of people had died after PCI and 7.4% after CABG.
But this presentation was not given much prominence at the conference, which Dr. Stone organized, and occurred during a didactic session in a small room rather than on one of the main stages where the 3-year data from EXCEL were announced with much fanfare. The presentation also took place 3 weeks after the European guidelines were published.
Surgeons withdraw support
After the BBC report last year that the universal definition of MI data had been collected but not published in the 3-year follow-up manuscript, and showed more MI in the PCI group than the protocol definition, the EACTS withdrew its support for the guidelines. The ESC continued to uphold the guidelines «until there is robust scientific evidence (as opposed to allegations) indicating we should do otherwise,” said Ms. Casadei.
A spokesperson for NEJM said the journal stood by the EXCEL papers because “there is no credible harm to patients from the publication of the paper and accurate reporting of trial results.” NEJM has since conducted a review and published a series of letters in response. The letters have reinvigorated rather than appeased the dissenters, as reported by Medscape.
A number of cardiologists and researchers started a petition on change.org to revise the EACTS/ESC left main CAD guidelines, and surgical societies across the globe have written to the editor of NEJM asking him to retract or amend the EXCEL papers.
This has not happened. The journal’s editor maintains that the letters containing the analyses are “sufficient information” to allow readers and guideline authors to “evaluate the trial findings.”
Dr. Taggart was dismissive of that response. “There is still no recognition or acknowledgment that failure to publish these data in 2016 ‘misled’ the guideline writers for the ESC/EACTS guidelines, and there is still no formal correction of the 2016 and 2019 NEJM manuscripts.”
Over a year after the BBC received the leaked data, the EXCEL investigators published an analysis of the primary outcome using the universal definition of MI data in the Journal of the American College of Cardiology.
It shows 141 events in the PCI arm, compared with 102 in the CABG arm. The investigators acknowledge that the rates of procedural MI differ depending on the definition used. According to their analysis, the protocol definition was predictive of mortality after both treatments, whereas the universal definition of procedural MI was predictive of mortality only after CABG. Not everyone agrees with this interpretation, and an accompanying editorial questioned these conclusions.
For Dr. Wallentin, it’s a relief that these data are in the public domain so that their interpretation and clinical consequences can be “openly discussed.” He hoped that the whole experience will result in something constructive and useful for the future.
As for the guidelines, the tide may be turning.
In a joint statement with EACTS on Oct. 6, 2020, the ESC agreed to review its guidelines for left main disease in the light of emerging, longer-term outcome data from the trials of CABG versus PCI.
Dr. Taggart has no regrets about speaking out despite this being “an exceedingly painful and bruising experience.”
The saga, he said, “reflects very badly on our specialty, the investigators, industry, and the world’s ‘leading’ medical journal.”
This article first appeared on Medscape.com.
“I disapprove of what you say, but I will defend to the death your right to say it.” The choice of the secretary general of the European Association for Cardio-Thoracic Surgery to open with this quote was the first hint that the next presentation at the 2019 annual meeting would be anything but dull. The session chair followed with a reminder to keep the discussion polite and civil.
Presenter David Taggart, MD, PhD, did not disappoint. The professor of cardiovascular surgery at the University of Oxford (England) began with the announcement that he had withdrawn his name from a recent paper in the New England Journal of Medicine. He then proceeded to accuse his coinvestigators of misrepresenting the findings of a major clinical trial.
Dr. Taggart was chair of the surgical committee for the Abbott-sponsored EXCEL trial, which compared two procedures for patients who had blockages in their left main coronary artery: percutaneous coronary intervention (PCI) using coronary stents, and coronary artery bypass graft surgery (CABG). The investigators designed the trial to compare outcomes for the two treatments using a composite endpoint of death, stroke, and MI. The 3-year follow-up data had been published in NEJM without controversy – or, at least, without public controversy.
But when it came time to publish the 5-year follow-up, there was a significantly higher rate of death in the stent group, and both Dr. Taggart and the journal editors were concerned that this finding was being downplayed in the manuscript.
In their comments to the authors, the journal editors had recommended including the mortality difference (unless clearly trivial) ‘”in the concluding statement in the final paragraph.” Yet, the concluding statement of the published paper read that there “was no significant difference between PCI and CABG.”
In Dr. Taggart’s view, that claim was dangerous for patients, and so he was left with no choice but to remove himself as an author, a first for the academic with over 300 scientific papers to his name.
Earlier publications from the EXCEL trial had influenced European treatment guidelines. But subsequent allegations of misconduct and hidden data spurred the EACTS to repudiate those guidelines out of concern “that some results in the EXCEL trial appear to have been concealed and that some patients may therefore have received the wrong clinical advice.”
The controversy pitted cardiothoracic surgeons against interventional cardiologists, who were seen as increasingly encroaching on the surgeons’ turf. Dr. Taggart was a long-time critic of the subspecialty.
Surgeons demanded an independent analysis of the EXCEL trial data – a demand that the investigators have yet to satisfy. Dr. Taggart was the first to speak publicly, but others had major reservations about the trial reporting and conduct years earlier.
Mortality data held back
One such person was Lars Wallentin, MD, a professor of cardiology at Uppsala (Sweden) University Hospital, who chaired the independent committee that monitored the safety and scientific validity of the EXCEL trial.
The committee, known as the data and safety monitoring board (DSMB), received a report on March 23, 2016, that showed that increasingly more patients who had received stents were dying, compared with the group of patients that had undergone CABG. A graph of the survival curves showed the gap between the two groups widening after 3 years (Figure 1).
By September of that year, Dr. Wallentin and other members of the DSMB were anxious to share the concerning mortality difference with the broader medical community.
They were aware that EACTS and the European Society of Cardiology had started the process of updating their guidelines on myocardial revascularization, and were keen for the guideline writing committee to see all of the data.
Meanwhile, the trial investigators, led by principal investigator Gregg Stone, MD, then at New York–Presbyterian Hospital and Columbia University Medical Center, were preparing to publish a report of the 3-year outcomes. Recruitment for EXCEL started in September 2010, so at the time of the 3-year analysis in 2016, some patients had been followed up for over 5 years. But the data, published in NEJM in October 2016, were capped at 3 years (Figure 2). It didn’t show the widening gap in late mortality that Dr. Wallentin and the rest of the DSMB had seen.
When asked about this, the investigators said they were transparent about their plans to cap the data at 3 years in an amendment to the study protocol. Stone’s coprincipal investigators were interventional cardiologist Patrick Serruys, MD, then of Imperial College London; and two surgeons: Joseph Sabik, MD, then of the Cleveland Clinic Foundation, and A. Pieter Kappetein, MD, PhD, then at Erasmus Medical Center, Rotterdam. The four principal investigators all declared financial payments from stent manufacturers either to themselves or their institutions.
Study sponsor Abbott has distanced itself from the decisions made and has referred all questions about the trial to the EXCEL investigators. Charles Simonton, chief medical officer at Abbott (now at Abiomed) was a coauthor on both the 3- and 5-year papers. Dr. Wallentin believes that the sponsor must have been aware of the DSMB’s concerns.
Continuing DSMB concerns
A year later, the DSMB was still troubled. Dr. Wallentin emailed Dr. Stone in September 2017 asking for an updated analysis of the mortality data without any capping in time.
Dr. Wallentin added that he didn’t think that unblinding the mortality results would be an issue at that stage because these were late deaths in a trial where the interventions were long completed. But, he warned, “it might be very concerning if, in the future, suspicions were raised that already available information on mortality was withheld from the cardiology and thoracic surgery community.”
The investigators took a month to respond. They declined the request, saying that the trial was not statistically powered to measure mortality. In his email to Dr. Wallentin, Dr. Stone stressed that they were committed to complete disclosure of all of the EXCEL data and that the responsible time point to unblind was after 4 years. His coprincipal investigators (Dr. Serruys, Dr. Sabik, and Dr. Kappetein) as well as EXCEL statistical committee chair Stuart Pocock, PhD, and Mr. Simonton were all copied on the email.
Dr. Wallentin deferred to the principal investigators’ arguments.
Missing MI data
Death was not the only outcome of the EXCEL trial to draw scrutiny.
The EXCEL investigators used a unique definition of MI that was almost exclusively based on a rise in the cardiac biomarker CK-MB. This protocol definition of MI was later adapted into the Society for Cardiovascular Angiography and Interventions definition in a paper coauthored by Dr. Stone. The investigators agreed to also measure MIs that met the more commonly used Third Universal Definition as a secondary endpoint. The Third Universal Definition of Myocardial Infarction uses a change in biomarkers – preferably troponin or alternatively CK-MB – coupled with other clinical signs.
It is standard practice to report secondary endpoints in any analysis of the main findings of a study. Yet, the EXCEL investigators did not report the universal definition of MI in either the 3-year or 5-year publications.
This is critical because MI according to one definition may not count according to the other, and the final tally could tip the trial results positive, negative, or neutral for coronary stents.
In Dr. Taggart’s opinion, the protocol definition puts CABG at a disadvantage because it uses the same biomarker threshold for procedural-related MI for both PCI and CABG. Because surgery involves more manipulation of the heart, cardiac enzyme levels will naturally be higher after CABG than PCI. These procedure-related enzyme elevations are not “true clinical MIs,” according to Dr. Taggart and others.
Late last year, a dataset containing the 3-year follow-up of EXCEL, including the information on the universal definition of MI, was leaked to the BBC. Working with biostatisticians, the BBC confirmed that according to this definition, there were more MIs in the stent group.
Originally, the investigators disputed the finding, calling the BBC data “imaginary.” They claimed that they were unable to calculate a rate of MI according to the universal definition because they lacked routine collection of troponins, although the universal definition also allows use of CK-MB. They have since published an analysis of 5-year MI data according to the universal definition, which showed twice the rate of MI in the PCI group.
From the leaked data, the BBC calculated the main composite endpoint of death, stroke, and MI using the universal definition of MI. Now the results swung in favor of CABG.
Impact on guidelines
None of this was known at the time the European cardiology societies convened a committee to write their new guidelines on myocardial revascularization. The writing panel disagreed about whether PCI and CABG were equivalent for patients with left main coronary artery disease (CAD).
Besides EXCEL, another study, the NOBLE trial, compared PCI and CABG in left main CAD and came to opposite conclusions – conclusions that matched the leaked data. In that trial, European investigators chose a slightly different primary endpoint: a composite of death, MI, stroke, and the need for a repeat procedure. They used the universal definition of MI exclusively, and notably, they omitted procedural MI from their clinical event count. The results, published at the same time as the EXCEL 3-year findings, suggested that CABG was better.
Given the discrepant findings of two large trials, the guideline committee considered all of the available data comparing the two methods of revascularization for left main CAD. But even then, things weren’t clear-cut. One draft meta-analysis, supported by the National Institute for Health Research, suggested that results were worse for first- and second-generation drug-eluting coronary stents – including those used in EXCEL – compared with surgery.
Another meta-analysis, later published in The Lancet, drew a different conclusion and found that PCI was just as good as surgery. The main author, Stuart Head, a cardiothoracic surgeon on the ESC/EACTS guideline committee, was a research fellow with EXCEL investigator Dr. Kappetein at Erasmus. EXCEL investigators Dr. Stone, Dr. Kappetein, and Dr. Serruys were coauthors of the Lancet meta-analysis.
There was heated discussion about the committee’s draft recommendations, which gave both CABG and PCI a Class IA recommendation in patients with left main CAD and low anatomical complexity. In October 2017, the ESC commissioned an anonymous external reviewer to weigh in. James Brophy, MD, PhD, a cardiologist and professor of medicine and epidemiology at McGill University, Montreal, confirmed that he was the reviewer after he published an updated version in June 2020.
Looking at all of the data available at the time comparing the procedures for left main CAD, Dr. Brophy’s analysis suggested a 73% chance that the excess in death, stroke, or MI represents at least two excess events per 100 patients treated with PCI rather than CABG.
Dr. Brophy thought that most patients would find these differences clinically meaningful and advised against giving both procedures the same class of recommendation. He was also concerned that many readers will skip to the summary recommendation table without reading the entire guideline document.
“I feel this is misleading in its present form,” he wrote in 2017.
Despite Dr. Brophy’s review, the guideline committee stuck with its original recommendations. The final 2018 ESC/EACTS Guidelines on myocardial revascularization gave equal weight to both CABG and PCI in patients with left main CAD and low anatomical complexity. In contrast, US guidelines do not put PCI and CABG on the same footing for any group of patients with left main CAD.
The lead author of the ESC/EACTS guidelines section on left main disease, and around a third of those on the writing task force, all declared financial payments from stent manufacturers either to themselves or their institutions. The EXCEL principal investigator, Dr. Kappetein, was secretary general of EACTS and oversaw the guidelines process for the surgical organization. He left to work for Medtronic midway through the process and was later joined there by his former research fellow, Stuart Head.
Dr. Brophy said in an interview that given the final guideline recommendations, he assumed that the committee had other reviews and went with the majority opinion.
But not everyone involved in the guidelines saw Dr. Brophy’s review. Nick Freemantle, a statistical reviewer appointed by EACTS, expected to see it but didn’t. This omission calls into question the neutrality of the whole process, in his view.
Mr. Freemantle believes that the deck was stacked so that he only saw the pieces of evidence that supported the conclusions that were already decided and that he was not shown “the bits that don’t fit that neatly.”
“And without that narrative, it all feels a bit grubby, to be honest,” he said.
Professor Barbara Casadei, ESC president, disputed this, saying that the guidelines were approved by all surgical members, including the EACTS council.
Missing from Dr. Brophy’s review were the later data from EXCEL. As he had told the DSMB in 2017, Stone presented the 4-year data from EXCEL at the TCT conference in September 2018. At this point, the analysis showed that 10.3% of people had died after PCI and 7.4% after CABG.
But this presentation was not given much prominence at the conference, which Dr. Stone organized, and occurred during a didactic session in a small room rather than on one of the main stages where the 3-year data from EXCEL were announced with much fanfare. The presentation also took place 3 weeks after the European guidelines were published.
Surgeons withdraw support
After the BBC report last year that the universal definition of MI data had been collected but not published in the 3-year follow-up manuscript, and showed more MI in the PCI group than the protocol definition, the EACTS withdrew its support for the guidelines. The ESC continued to uphold the guidelines «until there is robust scientific evidence (as opposed to allegations) indicating we should do otherwise,” said Ms. Casadei.
A spokesperson for NEJM said the journal stood by the EXCEL papers because “there is no credible harm to patients from the publication of the paper and accurate reporting of trial results.” NEJM has since conducted a review and published a series of letters in response. The letters have reinvigorated rather than appeased the dissenters, as reported by Medscape.
A number of cardiologists and researchers started a petition on change.org to revise the EACTS/ESC left main CAD guidelines, and surgical societies across the globe have written to the editor of NEJM asking him to retract or amend the EXCEL papers.
This has not happened. The journal’s editor maintains that the letters containing the analyses are “sufficient information” to allow readers and guideline authors to “evaluate the trial findings.”
Dr. Taggart was dismissive of that response. “There is still no recognition or acknowledgment that failure to publish these data in 2016 ‘misled’ the guideline writers for the ESC/EACTS guidelines, and there is still no formal correction of the 2016 and 2019 NEJM manuscripts.”
Over a year after the BBC received the leaked data, the EXCEL investigators published an analysis of the primary outcome using the universal definition of MI data in the Journal of the American College of Cardiology.
It shows 141 events in the PCI arm, compared with 102 in the CABG arm. The investigators acknowledge that the rates of procedural MI differ depending on the definition used. According to their analysis, the protocol definition was predictive of mortality after both treatments, whereas the universal definition of procedural MI was predictive of mortality only after CABG. Not everyone agrees with this interpretation, and an accompanying editorial questioned these conclusions.
For Dr. Wallentin, it’s a relief that these data are in the public domain so that their interpretation and clinical consequences can be “openly discussed.” He hoped that the whole experience will result in something constructive and useful for the future.
As for the guidelines, the tide may be turning.
In a joint statement with EACTS on Oct. 6, 2020, the ESC agreed to review its guidelines for left main disease in the light of emerging, longer-term outcome data from the trials of CABG versus PCI.
Dr. Taggart has no regrets about speaking out despite this being “an exceedingly painful and bruising experience.”
The saga, he said, “reflects very badly on our specialty, the investigators, industry, and the world’s ‘leading’ medical journal.”
This article first appeared on Medscape.com.
“I disapprove of what you say, but I will defend to the death your right to say it.” The choice of the secretary general of the European Association for Cardio-Thoracic Surgery to open with this quote was the first hint that the next presentation at the 2019 annual meeting would be anything but dull. The session chair followed with a reminder to keep the discussion polite and civil.
Presenter David Taggart, MD, PhD, did not disappoint. The professor of cardiovascular surgery at the University of Oxford (England) began with the announcement that he had withdrawn his name from a recent paper in the New England Journal of Medicine. He then proceeded to accuse his coinvestigators of misrepresenting the findings of a major clinical trial.
Dr. Taggart was chair of the surgical committee for the Abbott-sponsored EXCEL trial, which compared two procedures for patients who had blockages in their left main coronary artery: percutaneous coronary intervention (PCI) using coronary stents, and coronary artery bypass graft surgery (CABG). The investigators designed the trial to compare outcomes for the two treatments using a composite endpoint of death, stroke, and MI. The 3-year follow-up data had been published in NEJM without controversy – or, at least, without public controversy.
But when it came time to publish the 5-year follow-up, there was a significantly higher rate of death in the stent group, and both Dr. Taggart and the journal editors were concerned that this finding was being downplayed in the manuscript.
In their comments to the authors, the journal editors had recommended including the mortality difference (unless clearly trivial) ‘”in the concluding statement in the final paragraph.” Yet, the concluding statement of the published paper read that there “was no significant difference between PCI and CABG.”
In Dr. Taggart’s view, that claim was dangerous for patients, and so he was left with no choice but to remove himself as an author, a first for the academic with over 300 scientific papers to his name.
Earlier publications from the EXCEL trial had influenced European treatment guidelines. But subsequent allegations of misconduct and hidden data spurred the EACTS to repudiate those guidelines out of concern “that some results in the EXCEL trial appear to have been concealed and that some patients may therefore have received the wrong clinical advice.”
The controversy pitted cardiothoracic surgeons against interventional cardiologists, who were seen as increasingly encroaching on the surgeons’ turf. Dr. Taggart was a long-time critic of the subspecialty.
Surgeons demanded an independent analysis of the EXCEL trial data – a demand that the investigators have yet to satisfy. Dr. Taggart was the first to speak publicly, but others had major reservations about the trial reporting and conduct years earlier.
Mortality data held back
One such person was Lars Wallentin, MD, a professor of cardiology at Uppsala (Sweden) University Hospital, who chaired the independent committee that monitored the safety and scientific validity of the EXCEL trial.
The committee, known as the data and safety monitoring board (DSMB), received a report on March 23, 2016, that showed that increasingly more patients who had received stents were dying, compared with the group of patients that had undergone CABG. A graph of the survival curves showed the gap between the two groups widening after 3 years (Figure 1).
By September of that year, Dr. Wallentin and other members of the DSMB were anxious to share the concerning mortality difference with the broader medical community.
They were aware that EACTS and the European Society of Cardiology had started the process of updating their guidelines on myocardial revascularization, and were keen for the guideline writing committee to see all of the data.
Meanwhile, the trial investigators, led by principal investigator Gregg Stone, MD, then at New York–Presbyterian Hospital and Columbia University Medical Center, were preparing to publish a report of the 3-year outcomes. Recruitment for EXCEL started in September 2010, so at the time of the 3-year analysis in 2016, some patients had been followed up for over 5 years. But the data, published in NEJM in October 2016, were capped at 3 years (Figure 2). It didn’t show the widening gap in late mortality that Dr. Wallentin and the rest of the DSMB had seen.
When asked about this, the investigators said they were transparent about their plans to cap the data at 3 years in an amendment to the study protocol. Stone’s coprincipal investigators were interventional cardiologist Patrick Serruys, MD, then of Imperial College London; and two surgeons: Joseph Sabik, MD, then of the Cleveland Clinic Foundation, and A. Pieter Kappetein, MD, PhD, then at Erasmus Medical Center, Rotterdam. The four principal investigators all declared financial payments from stent manufacturers either to themselves or their institutions.
Study sponsor Abbott has distanced itself from the decisions made and has referred all questions about the trial to the EXCEL investigators. Charles Simonton, chief medical officer at Abbott (now at Abiomed) was a coauthor on both the 3- and 5-year papers. Dr. Wallentin believes that the sponsor must have been aware of the DSMB’s concerns.
Continuing DSMB concerns
A year later, the DSMB was still troubled. Dr. Wallentin emailed Dr. Stone in September 2017 asking for an updated analysis of the mortality data without any capping in time.
Dr. Wallentin added that he didn’t think that unblinding the mortality results would be an issue at that stage because these were late deaths in a trial where the interventions were long completed. But, he warned, “it might be very concerning if, in the future, suspicions were raised that already available information on mortality was withheld from the cardiology and thoracic surgery community.”
The investigators took a month to respond. They declined the request, saying that the trial was not statistically powered to measure mortality. In his email to Dr. Wallentin, Dr. Stone stressed that they were committed to complete disclosure of all of the EXCEL data and that the responsible time point to unblind was after 4 years. His coprincipal investigators (Dr. Serruys, Dr. Sabik, and Dr. Kappetein) as well as EXCEL statistical committee chair Stuart Pocock, PhD, and Mr. Simonton were all copied on the email.
Dr. Wallentin deferred to the principal investigators’ arguments.
Missing MI data
Death was not the only outcome of the EXCEL trial to draw scrutiny.
The EXCEL investigators used a unique definition of MI that was almost exclusively based on a rise in the cardiac biomarker CK-MB. This protocol definition of MI was later adapted into the Society for Cardiovascular Angiography and Interventions definition in a paper coauthored by Dr. Stone. The investigators agreed to also measure MIs that met the more commonly used Third Universal Definition as a secondary endpoint. The Third Universal Definition of Myocardial Infarction uses a change in biomarkers – preferably troponin or alternatively CK-MB – coupled with other clinical signs.
It is standard practice to report secondary endpoints in any analysis of the main findings of a study. Yet, the EXCEL investigators did not report the universal definition of MI in either the 3-year or 5-year publications.
This is critical because MI according to one definition may not count according to the other, and the final tally could tip the trial results positive, negative, or neutral for coronary stents.
In Dr. Taggart’s opinion, the protocol definition puts CABG at a disadvantage because it uses the same biomarker threshold for procedural-related MI for both PCI and CABG. Because surgery involves more manipulation of the heart, cardiac enzyme levels will naturally be higher after CABG than PCI. These procedure-related enzyme elevations are not “true clinical MIs,” according to Dr. Taggart and others.
Late last year, a dataset containing the 3-year follow-up of EXCEL, including the information on the universal definition of MI, was leaked to the BBC. Working with biostatisticians, the BBC confirmed that according to this definition, there were more MIs in the stent group.
Originally, the investigators disputed the finding, calling the BBC data “imaginary.” They claimed that they were unable to calculate a rate of MI according to the universal definition because they lacked routine collection of troponins, although the universal definition also allows use of CK-MB. They have since published an analysis of 5-year MI data according to the universal definition, which showed twice the rate of MI in the PCI group.
From the leaked data, the BBC calculated the main composite endpoint of death, stroke, and MI using the universal definition of MI. Now the results swung in favor of CABG.
Impact on guidelines
None of this was known at the time the European cardiology societies convened a committee to write their new guidelines on myocardial revascularization. The writing panel disagreed about whether PCI and CABG were equivalent for patients with left main coronary artery disease (CAD).
Besides EXCEL, another study, the NOBLE trial, compared PCI and CABG in left main CAD and came to opposite conclusions – conclusions that matched the leaked data. In that trial, European investigators chose a slightly different primary endpoint: a composite of death, MI, stroke, and the need for a repeat procedure. They used the universal definition of MI exclusively, and notably, they omitted procedural MI from their clinical event count. The results, published at the same time as the EXCEL 3-year findings, suggested that CABG was better.
Given the discrepant findings of two large trials, the guideline committee considered all of the available data comparing the two methods of revascularization for left main CAD. But even then, things weren’t clear-cut. One draft meta-analysis, supported by the National Institute for Health Research, suggested that results were worse for first- and second-generation drug-eluting coronary stents – including those used in EXCEL – compared with surgery.
Another meta-analysis, later published in The Lancet, drew a different conclusion and found that PCI was just as good as surgery. The main author, Stuart Head, a cardiothoracic surgeon on the ESC/EACTS guideline committee, was a research fellow with EXCEL investigator Dr. Kappetein at Erasmus. EXCEL investigators Dr. Stone, Dr. Kappetein, and Dr. Serruys were coauthors of the Lancet meta-analysis.
There was heated discussion about the committee’s draft recommendations, which gave both CABG and PCI a Class IA recommendation in patients with left main CAD and low anatomical complexity. In October 2017, the ESC commissioned an anonymous external reviewer to weigh in. James Brophy, MD, PhD, a cardiologist and professor of medicine and epidemiology at McGill University, Montreal, confirmed that he was the reviewer after he published an updated version in June 2020.
Looking at all of the data available at the time comparing the procedures for left main CAD, Dr. Brophy’s analysis suggested a 73% chance that the excess in death, stroke, or MI represents at least two excess events per 100 patients treated with PCI rather than CABG.
Dr. Brophy thought that most patients would find these differences clinically meaningful and advised against giving both procedures the same class of recommendation. He was also concerned that many readers will skip to the summary recommendation table without reading the entire guideline document.
“I feel this is misleading in its present form,” he wrote in 2017.
Despite Dr. Brophy’s review, the guideline committee stuck with its original recommendations. The final 2018 ESC/EACTS Guidelines on myocardial revascularization gave equal weight to both CABG and PCI in patients with left main CAD and low anatomical complexity. In contrast, US guidelines do not put PCI and CABG on the same footing for any group of patients with left main CAD.
The lead author of the ESC/EACTS guidelines section on left main disease, and around a third of those on the writing task force, all declared financial payments from stent manufacturers either to themselves or their institutions. The EXCEL principal investigator, Dr. Kappetein, was secretary general of EACTS and oversaw the guidelines process for the surgical organization. He left to work for Medtronic midway through the process and was later joined there by his former research fellow, Stuart Head.
Dr. Brophy said in an interview that given the final guideline recommendations, he assumed that the committee had other reviews and went with the majority opinion.
But not everyone involved in the guidelines saw Dr. Brophy’s review. Nick Freemantle, a statistical reviewer appointed by EACTS, expected to see it but didn’t. This omission calls into question the neutrality of the whole process, in his view.
Mr. Freemantle believes that the deck was stacked so that he only saw the pieces of evidence that supported the conclusions that were already decided and that he was not shown “the bits that don’t fit that neatly.”
“And without that narrative, it all feels a bit grubby, to be honest,” he said.
Professor Barbara Casadei, ESC president, disputed this, saying that the guidelines were approved by all surgical members, including the EACTS council.
Missing from Dr. Brophy’s review were the later data from EXCEL. As he had told the DSMB in 2017, Stone presented the 4-year data from EXCEL at the TCT conference in September 2018. At this point, the analysis showed that 10.3% of people had died after PCI and 7.4% after CABG.
But this presentation was not given much prominence at the conference, which Dr. Stone organized, and occurred during a didactic session in a small room rather than on one of the main stages where the 3-year data from EXCEL were announced with much fanfare. The presentation also took place 3 weeks after the European guidelines were published.
Surgeons withdraw support
After the BBC report last year that the universal definition of MI data had been collected but not published in the 3-year follow-up manuscript, and showed more MI in the PCI group than the protocol definition, the EACTS withdrew its support for the guidelines. The ESC continued to uphold the guidelines «until there is robust scientific evidence (as opposed to allegations) indicating we should do otherwise,” said Ms. Casadei.
A spokesperson for NEJM said the journal stood by the EXCEL papers because “there is no credible harm to patients from the publication of the paper and accurate reporting of trial results.” NEJM has since conducted a review and published a series of letters in response. The letters have reinvigorated rather than appeased the dissenters, as reported by Medscape.
A number of cardiologists and researchers started a petition on change.org to revise the EACTS/ESC left main CAD guidelines, and surgical societies across the globe have written to the editor of NEJM asking him to retract or amend the EXCEL papers.
This has not happened. The journal’s editor maintains that the letters containing the analyses are “sufficient information” to allow readers and guideline authors to “evaluate the trial findings.”
Dr. Taggart was dismissive of that response. “There is still no recognition or acknowledgment that failure to publish these data in 2016 ‘misled’ the guideline writers for the ESC/EACTS guidelines, and there is still no formal correction of the 2016 and 2019 NEJM manuscripts.”
Over a year after the BBC received the leaked data, the EXCEL investigators published an analysis of the primary outcome using the universal definition of MI data in the Journal of the American College of Cardiology.
It shows 141 events in the PCI arm, compared with 102 in the CABG arm. The investigators acknowledge that the rates of procedural MI differ depending on the definition used. According to their analysis, the protocol definition was predictive of mortality after both treatments, whereas the universal definition of procedural MI was predictive of mortality only after CABG. Not everyone agrees with this interpretation, and an accompanying editorial questioned these conclusions.
For Dr. Wallentin, it’s a relief that these data are in the public domain so that their interpretation and clinical consequences can be “openly discussed.” He hoped that the whole experience will result in something constructive and useful for the future.
As for the guidelines, the tide may be turning.
In a joint statement with EACTS on Oct. 6, 2020, the ESC agreed to review its guidelines for left main disease in the light of emerging, longer-term outcome data from the trials of CABG versus PCI.
Dr. Taggart has no regrets about speaking out despite this being “an exceedingly painful and bruising experience.”
The saga, he said, “reflects very badly on our specialty, the investigators, industry, and the world’s ‘leading’ medical journal.”
This article first appeared on Medscape.com.
COVID and med ed cost: Are future docs paying more for less?
Like most medical students, Kaitlyn Thomas’s education was abruptly interrupted by the pandemic. Her school, an osteopathic medicine institution in the Midwest, followed guidelines issued by the American Association of Medical Colleges in March, shifting lectures online and suspending activities in which students interacted with patients. But even as Ms. Thomas’s learning opportunities dwindled for the sake of safety, the costs kept piling up.
Instead of going home to live with her family, she stayed in her apartment near school – and kept paying rent – so she could be nearby for the two licensing exams she was scheduled to take 3 months later. Both tests were canceled 9 days before she was scheduled to take them, one without any notification. This meant she had to travel to two different testing sites in two different states. All told, she said, the whole thing cost her around $2,000.
Ms. Thomas’s experience isn’t rare. Across the country, medical students find themselves paying substantial costs for a medical education now greatly altered by the pandemic. Despite restrictions on time spent in hospitals, hands-on learning, social events, and access to libraries, gyms, study spaces, and instructors, the price of tuition hasn’t dropped but has remained the same or has even risen.
In response, students have become vocal about the return on their pricey investment. “Am I just going to end up doing most of my year online, and what does that look like for my future patients?” Ms. Thomas asked. “It really doesn’t feel like a time to be limiting education.”
Medical schools and administrators are scrambling to find creative solutions for safely educating students. No matter what those solutions may be, experts say, the pandemic has drawn fresh attention to enduring questions about how the cost of medical education compares to its value. Although many are frustrated, some see the potential for COVID to open new opportunities for lasting innovation. At the very least, the pandemic has sparked conversations about what matters most in terms of producing qualified physicians.
“While this is a challenging time, we will get through it, and we will continue to educate doctors, and we will get them through to practice,” says Robert Cain, president and CEO of the American Association of Colleges of Osteopathic Medicine. Many in the midst of training still have one lingering question: Is the price future doctors are now paying still worth it?
COVID’s “hidden costs” for students
Tom is a third-year student at an allopathic medicine institution in the Caribbean. He asked not to be fully identified here, owing to concern about possible backlash. In March, Tom was doing clinical rotations in New York City when his training was put on hold. He returned home to Connecticut and resumed working 60-80 hours a week as a paramedic. As much as 75% of that income went to pay for the New York City apartment he was no longer living in – an apartment that cost more than $2,000 a month – and for student loans that suddenly came due when his enrollment status changed.
Tom has been able to take some online courses through his school. But he still doesn’t know whether state licensing boards will accept them, how residency programs will view them, or whether he will eventually have to retake those online classes in person. At the end of September, he was allowed to return to the hospital but was relocated to Chicago and was forced to move on short notice.
Like many students, Tom has worried that the pandemic may prevent him from acquiring crucial elements for his residency applications, things like letters of recommendation or key experiences. That could delay his next stage of training, which would mean lost future income, increasing student loan interest, and lost work experience. “This could also mean the difference between getting a residency and being able to practice medicine and not being able to practice my intended specialty,” he said. “This is the real hidden cost we may have to deal with.”
International medical students hoping to practice in the United States face additional costs. Michelle Warncke earned her bachelor’s degree in America but went to the United Kingdom for her master’s and her medical degree, which she completed in 2019. She then moved to North Carolina with her husband and saved money to take the exams she needed for residency in the states. But her scheduled Step 2 CS exam was canceled because of the pandemic. Now, like hundreds or even thousands of other students, she said she is unable to apply for residency, even as her student loans collect interest. An active Facebook group of international medical graduates includes about 1,500 people with comparable dilemmas.
The path to becoming a physician carries a well-known price tag, one that is already quite high. Now, for many, that price is substantially increasing. “The only way I can actually keep my medical credentials up to date and passable, to be able to ever get a shot at a residency in the following years,” she said, “is to move to another country and work for less pay, pay for a visa, pay for my exams, pay for my language test, and wait and hope that I might be able to as an older graduate then be able to apply for residency.”
Scaling back the price of med school?
Questions about the economics of medical education aren’t new, says David Asch, MD, MBA, an internal medicine physician and executive director of the Center for Health Care Innovation at the University of Pennsylvania, Philadelphia. But the changes forced by COVID could lead to innovations that may finally better balance the financial scales.
Such innovations are necessary, many say, given how medical education costs have skyrocketed over the past half century. In the 1960s, 4 years of medical school cost about $40,000 in today’s dollars, Dr. Asch and colleagues wrote in a 2020 analysis, which they conducted before the pandemic began. By 2018, the price of a medical education in the United States had ballooned to about $300,000. About 75% of students were taking out loans. Upon graduating, the average debt was $200,000.
Medical school is expensive for many tangible reasons, Dr. Asch said. Schools must pay for curriculum, faculty, technology, textbooks, lab materials, facilities, administrators, and more. But policy changes could decrease those costs.
He says one idea would be for medical schools to join forces and give students access to the same basic lectures in the early years, delivered online by top-notch instructors. Students could then participate in on-campus programs that might only require 3 years to complete instead of 4. By demonstrating what can be done via online platforms, he said, the pandemic might pave the way to permanent changes that could reduce costs.
“I’m not trying to pick on biochemistry professors and medical schools, but how many do we need in the country?” Dr. Asch asked. “We’re all watching the same episode of Seinfeld. Why can’t we all watch the same episode of the Krebs cycle?” If all 190 or so medical schools in the United States shared such preclinical courses, he says, each would require a fraction of the current cost to produce. “We could save 99.5% of the cost. So why don’t we do that?”
Pandemic as opportunity
Although the price of medical education has yet to decrease, schools are working to leverage the pandemic to provide increased educational value.
This generation of physicians will not only have to cope with the fallout of this pandemic, they will be the ones responsible for confronting the next pandemic as well, says Donald Brady, MD, senior associate dean for health sciences education at Vanderbilt University, Nashville, Tenn. “They will be the leaders in the future who will better be able to know how to handle it [a pandemic] because they were able to watch it and be part of it safely in the current circumstance.”
As much as possible, Vanderbilt is using the pandemic as an opportunity. As soon as it became clear that students couldn’t be involved in certain hands-on training, instructors developed a course about pandemics that included lectures on ethics, global health, systemic racism, and other topics. It also included experiential components of pandemic management, such as opportunities to work with patients through telehealth.
Students say they feel that they are getting less for their money and that they are paying for experiences that are no longer available, such as hands-on patient contact and community events. However, Dr. Brady said, schools have had to account for new expenses, including various now-required technologies and transitioning to courses online.
Some challenges can’t be solved with money alone. Medical schools across the country are working together to ensure that they are still adequately preparing students. Vanderbilt participates in an AAMC group that meets regularly and is also one of 37 institutions involved in an American Medical Association Consortium (AACOM). These groups discuss challenges, strategies, and opportunities for optimizing medical education during the pandemic.
Some institutions have come up with creative solutions. Ohio University’s Heritage College of Osteopathic Medicine, in Athens, Ohio, in collaboration with the Ohio Department of Health, launched a 4-week rotation for third-year students that focuses on public health. Harvard Medical School, Boston, was one of several schools that allowed students to graduate early in the spring. “We’re constantly talking to our colleagues and friends,” Dr. Brady said. “We learn from each other. There’s a lot of sharing going on.”
Other organizations are also working to make sure students ultimately get what they are paying for: a high-quality education. As soon as the pandemic began, the AACOM organized four working groups to address how schools could better use technology to deliver curricula and how students could participate in public health efforts, among other topics. “For the students, the part they don’t see and can’t really be aware of is all the things that happen behind the scenes,” Mr. Cain said. “People were working really hard to make sure that their education was still delivered, and delivered in a way that was going to assure a good product at the end.”
Ultimately, that product will be held to a rigid standard, said Geoffrey Young, the AAMC’s senior director for student affairs and programs. Medical schools must still meet standards of competency set by the liaison committee on medical education. Mr. Young says that even now those standards remain rigorous enough to ensure that medical students are learning what they need to know. “The core elements for competency may be slightly altered to address the realities that we’re experiencing because of COVID, but the core tenants of competencies will not change,” he said.
Even as conversations continue about what a medical education is worth, the pandemic is drawing new attention to the profession. No signs suggest that the value of tuition or a shift to more virtual offerings are scaring students away. Applications for medical schools were up 17% for the fall of 2021.
Brady expects the surge in interest to continue. “The increased focus and emphasis on public health, the increased focus and emphasis on health equity, the increased focus on the need for a more diverse physician workforce, the interest in basic science research around viruses, the interest in COVID itself – there are a lot of different elements that are setting us up for a potential boom in applications to medical school,” he said.
Beyond increasing interest, the pandemic may also finally force a reckoning on the disconnection between how schools think about costs and how students think about value, Dr. Asch said. “When students say: ‘I’m not getting as much from this,’ they’re saying, ‘you should price this according to its lower value.’ And when the medical schools are saying: ‘Oh, but it’s costing us so much more,’ they’re talking about pricing according to the cost. It’s like one group is speaking Latin and the other group is speaking Greek.” Perhaps, he said, COVID-related changes will finally get them speaking the same language.
This article first appeared on Medscape.com.
Like most medical students, Kaitlyn Thomas’s education was abruptly interrupted by the pandemic. Her school, an osteopathic medicine institution in the Midwest, followed guidelines issued by the American Association of Medical Colleges in March, shifting lectures online and suspending activities in which students interacted with patients. But even as Ms. Thomas’s learning opportunities dwindled for the sake of safety, the costs kept piling up.
Instead of going home to live with her family, she stayed in her apartment near school – and kept paying rent – so she could be nearby for the two licensing exams she was scheduled to take 3 months later. Both tests were canceled 9 days before she was scheduled to take them, one without any notification. This meant she had to travel to two different testing sites in two different states. All told, she said, the whole thing cost her around $2,000.
Ms. Thomas’s experience isn’t rare. Across the country, medical students find themselves paying substantial costs for a medical education now greatly altered by the pandemic. Despite restrictions on time spent in hospitals, hands-on learning, social events, and access to libraries, gyms, study spaces, and instructors, the price of tuition hasn’t dropped but has remained the same or has even risen.
In response, students have become vocal about the return on their pricey investment. “Am I just going to end up doing most of my year online, and what does that look like for my future patients?” Ms. Thomas asked. “It really doesn’t feel like a time to be limiting education.”
Medical schools and administrators are scrambling to find creative solutions for safely educating students. No matter what those solutions may be, experts say, the pandemic has drawn fresh attention to enduring questions about how the cost of medical education compares to its value. Although many are frustrated, some see the potential for COVID to open new opportunities for lasting innovation. At the very least, the pandemic has sparked conversations about what matters most in terms of producing qualified physicians.
“While this is a challenging time, we will get through it, and we will continue to educate doctors, and we will get them through to practice,” says Robert Cain, president and CEO of the American Association of Colleges of Osteopathic Medicine. Many in the midst of training still have one lingering question: Is the price future doctors are now paying still worth it?
COVID’s “hidden costs” for students
Tom is a third-year student at an allopathic medicine institution in the Caribbean. He asked not to be fully identified here, owing to concern about possible backlash. In March, Tom was doing clinical rotations in New York City when his training was put on hold. He returned home to Connecticut and resumed working 60-80 hours a week as a paramedic. As much as 75% of that income went to pay for the New York City apartment he was no longer living in – an apartment that cost more than $2,000 a month – and for student loans that suddenly came due when his enrollment status changed.
Tom has been able to take some online courses through his school. But he still doesn’t know whether state licensing boards will accept them, how residency programs will view them, or whether he will eventually have to retake those online classes in person. At the end of September, he was allowed to return to the hospital but was relocated to Chicago and was forced to move on short notice.
Like many students, Tom has worried that the pandemic may prevent him from acquiring crucial elements for his residency applications, things like letters of recommendation or key experiences. That could delay his next stage of training, which would mean lost future income, increasing student loan interest, and lost work experience. “This could also mean the difference between getting a residency and being able to practice medicine and not being able to practice my intended specialty,” he said. “This is the real hidden cost we may have to deal with.”
International medical students hoping to practice in the United States face additional costs. Michelle Warncke earned her bachelor’s degree in America but went to the United Kingdom for her master’s and her medical degree, which she completed in 2019. She then moved to North Carolina with her husband and saved money to take the exams she needed for residency in the states. But her scheduled Step 2 CS exam was canceled because of the pandemic. Now, like hundreds or even thousands of other students, she said she is unable to apply for residency, even as her student loans collect interest. An active Facebook group of international medical graduates includes about 1,500 people with comparable dilemmas.
The path to becoming a physician carries a well-known price tag, one that is already quite high. Now, for many, that price is substantially increasing. “The only way I can actually keep my medical credentials up to date and passable, to be able to ever get a shot at a residency in the following years,” she said, “is to move to another country and work for less pay, pay for a visa, pay for my exams, pay for my language test, and wait and hope that I might be able to as an older graduate then be able to apply for residency.”
Scaling back the price of med school?
Questions about the economics of medical education aren’t new, says David Asch, MD, MBA, an internal medicine physician and executive director of the Center for Health Care Innovation at the University of Pennsylvania, Philadelphia. But the changes forced by COVID could lead to innovations that may finally better balance the financial scales.
Such innovations are necessary, many say, given how medical education costs have skyrocketed over the past half century. In the 1960s, 4 years of medical school cost about $40,000 in today’s dollars, Dr. Asch and colleagues wrote in a 2020 analysis, which they conducted before the pandemic began. By 2018, the price of a medical education in the United States had ballooned to about $300,000. About 75% of students were taking out loans. Upon graduating, the average debt was $200,000.
Medical school is expensive for many tangible reasons, Dr. Asch said. Schools must pay for curriculum, faculty, technology, textbooks, lab materials, facilities, administrators, and more. But policy changes could decrease those costs.
He says one idea would be for medical schools to join forces and give students access to the same basic lectures in the early years, delivered online by top-notch instructors. Students could then participate in on-campus programs that might only require 3 years to complete instead of 4. By demonstrating what can be done via online platforms, he said, the pandemic might pave the way to permanent changes that could reduce costs.
“I’m not trying to pick on biochemistry professors and medical schools, but how many do we need in the country?” Dr. Asch asked. “We’re all watching the same episode of Seinfeld. Why can’t we all watch the same episode of the Krebs cycle?” If all 190 or so medical schools in the United States shared such preclinical courses, he says, each would require a fraction of the current cost to produce. “We could save 99.5% of the cost. So why don’t we do that?”
Pandemic as opportunity
Although the price of medical education has yet to decrease, schools are working to leverage the pandemic to provide increased educational value.
This generation of physicians will not only have to cope with the fallout of this pandemic, they will be the ones responsible for confronting the next pandemic as well, says Donald Brady, MD, senior associate dean for health sciences education at Vanderbilt University, Nashville, Tenn. “They will be the leaders in the future who will better be able to know how to handle it [a pandemic] because they were able to watch it and be part of it safely in the current circumstance.”
As much as possible, Vanderbilt is using the pandemic as an opportunity. As soon as it became clear that students couldn’t be involved in certain hands-on training, instructors developed a course about pandemics that included lectures on ethics, global health, systemic racism, and other topics. It also included experiential components of pandemic management, such as opportunities to work with patients through telehealth.
Students say they feel that they are getting less for their money and that they are paying for experiences that are no longer available, such as hands-on patient contact and community events. However, Dr. Brady said, schools have had to account for new expenses, including various now-required technologies and transitioning to courses online.
Some challenges can’t be solved with money alone. Medical schools across the country are working together to ensure that they are still adequately preparing students. Vanderbilt participates in an AAMC group that meets regularly and is also one of 37 institutions involved in an American Medical Association Consortium (AACOM). These groups discuss challenges, strategies, and opportunities for optimizing medical education during the pandemic.
Some institutions have come up with creative solutions. Ohio University’s Heritage College of Osteopathic Medicine, in Athens, Ohio, in collaboration with the Ohio Department of Health, launched a 4-week rotation for third-year students that focuses on public health. Harvard Medical School, Boston, was one of several schools that allowed students to graduate early in the spring. “We’re constantly talking to our colleagues and friends,” Dr. Brady said. “We learn from each other. There’s a lot of sharing going on.”
Other organizations are also working to make sure students ultimately get what they are paying for: a high-quality education. As soon as the pandemic began, the AACOM organized four working groups to address how schools could better use technology to deliver curricula and how students could participate in public health efforts, among other topics. “For the students, the part they don’t see and can’t really be aware of is all the things that happen behind the scenes,” Mr. Cain said. “People were working really hard to make sure that their education was still delivered, and delivered in a way that was going to assure a good product at the end.”
Ultimately, that product will be held to a rigid standard, said Geoffrey Young, the AAMC’s senior director for student affairs and programs. Medical schools must still meet standards of competency set by the liaison committee on medical education. Mr. Young says that even now those standards remain rigorous enough to ensure that medical students are learning what they need to know. “The core elements for competency may be slightly altered to address the realities that we’re experiencing because of COVID, but the core tenants of competencies will not change,” he said.
Even as conversations continue about what a medical education is worth, the pandemic is drawing new attention to the profession. No signs suggest that the value of tuition or a shift to more virtual offerings are scaring students away. Applications for medical schools were up 17% for the fall of 2021.
Brady expects the surge in interest to continue. “The increased focus and emphasis on public health, the increased focus and emphasis on health equity, the increased focus on the need for a more diverse physician workforce, the interest in basic science research around viruses, the interest in COVID itself – there are a lot of different elements that are setting us up for a potential boom in applications to medical school,” he said.
Beyond increasing interest, the pandemic may also finally force a reckoning on the disconnection between how schools think about costs and how students think about value, Dr. Asch said. “When students say: ‘I’m not getting as much from this,’ they’re saying, ‘you should price this according to its lower value.’ And when the medical schools are saying: ‘Oh, but it’s costing us so much more,’ they’re talking about pricing according to the cost. It’s like one group is speaking Latin and the other group is speaking Greek.” Perhaps, he said, COVID-related changes will finally get them speaking the same language.
This article first appeared on Medscape.com.
Like most medical students, Kaitlyn Thomas’s education was abruptly interrupted by the pandemic. Her school, an osteopathic medicine institution in the Midwest, followed guidelines issued by the American Association of Medical Colleges in March, shifting lectures online and suspending activities in which students interacted with patients. But even as Ms. Thomas’s learning opportunities dwindled for the sake of safety, the costs kept piling up.
Instead of going home to live with her family, she stayed in her apartment near school – and kept paying rent – so she could be nearby for the two licensing exams she was scheduled to take 3 months later. Both tests were canceled 9 days before she was scheduled to take them, one without any notification. This meant she had to travel to two different testing sites in two different states. All told, she said, the whole thing cost her around $2,000.
Ms. Thomas’s experience isn’t rare. Across the country, medical students find themselves paying substantial costs for a medical education now greatly altered by the pandemic. Despite restrictions on time spent in hospitals, hands-on learning, social events, and access to libraries, gyms, study spaces, and instructors, the price of tuition hasn’t dropped but has remained the same or has even risen.
In response, students have become vocal about the return on their pricey investment. “Am I just going to end up doing most of my year online, and what does that look like for my future patients?” Ms. Thomas asked. “It really doesn’t feel like a time to be limiting education.”
Medical schools and administrators are scrambling to find creative solutions for safely educating students. No matter what those solutions may be, experts say, the pandemic has drawn fresh attention to enduring questions about how the cost of medical education compares to its value. Although many are frustrated, some see the potential for COVID to open new opportunities for lasting innovation. At the very least, the pandemic has sparked conversations about what matters most in terms of producing qualified physicians.
“While this is a challenging time, we will get through it, and we will continue to educate doctors, and we will get them through to practice,” says Robert Cain, president and CEO of the American Association of Colleges of Osteopathic Medicine. Many in the midst of training still have one lingering question: Is the price future doctors are now paying still worth it?
COVID’s “hidden costs” for students
Tom is a third-year student at an allopathic medicine institution in the Caribbean. He asked not to be fully identified here, owing to concern about possible backlash. In March, Tom was doing clinical rotations in New York City when his training was put on hold. He returned home to Connecticut and resumed working 60-80 hours a week as a paramedic. As much as 75% of that income went to pay for the New York City apartment he was no longer living in – an apartment that cost more than $2,000 a month – and for student loans that suddenly came due when his enrollment status changed.
Tom has been able to take some online courses through his school. But he still doesn’t know whether state licensing boards will accept them, how residency programs will view them, or whether he will eventually have to retake those online classes in person. At the end of September, he was allowed to return to the hospital but was relocated to Chicago and was forced to move on short notice.
Like many students, Tom has worried that the pandemic may prevent him from acquiring crucial elements for his residency applications, things like letters of recommendation or key experiences. That could delay his next stage of training, which would mean lost future income, increasing student loan interest, and lost work experience. “This could also mean the difference between getting a residency and being able to practice medicine and not being able to practice my intended specialty,” he said. “This is the real hidden cost we may have to deal with.”
International medical students hoping to practice in the United States face additional costs. Michelle Warncke earned her bachelor’s degree in America but went to the United Kingdom for her master’s and her medical degree, which she completed in 2019. She then moved to North Carolina with her husband and saved money to take the exams she needed for residency in the states. But her scheduled Step 2 CS exam was canceled because of the pandemic. Now, like hundreds or even thousands of other students, she said she is unable to apply for residency, even as her student loans collect interest. An active Facebook group of international medical graduates includes about 1,500 people with comparable dilemmas.
The path to becoming a physician carries a well-known price tag, one that is already quite high. Now, for many, that price is substantially increasing. “The only way I can actually keep my medical credentials up to date and passable, to be able to ever get a shot at a residency in the following years,” she said, “is to move to another country and work for less pay, pay for a visa, pay for my exams, pay for my language test, and wait and hope that I might be able to as an older graduate then be able to apply for residency.”
Scaling back the price of med school?
Questions about the economics of medical education aren’t new, says David Asch, MD, MBA, an internal medicine physician and executive director of the Center for Health Care Innovation at the University of Pennsylvania, Philadelphia. But the changes forced by COVID could lead to innovations that may finally better balance the financial scales.
Such innovations are necessary, many say, given how medical education costs have skyrocketed over the past half century. In the 1960s, 4 years of medical school cost about $40,000 in today’s dollars, Dr. Asch and colleagues wrote in a 2020 analysis, which they conducted before the pandemic began. By 2018, the price of a medical education in the United States had ballooned to about $300,000. About 75% of students were taking out loans. Upon graduating, the average debt was $200,000.
Medical school is expensive for many tangible reasons, Dr. Asch said. Schools must pay for curriculum, faculty, technology, textbooks, lab materials, facilities, administrators, and more. But policy changes could decrease those costs.
He says one idea would be for medical schools to join forces and give students access to the same basic lectures in the early years, delivered online by top-notch instructors. Students could then participate in on-campus programs that might only require 3 years to complete instead of 4. By demonstrating what can be done via online platforms, he said, the pandemic might pave the way to permanent changes that could reduce costs.
“I’m not trying to pick on biochemistry professors and medical schools, but how many do we need in the country?” Dr. Asch asked. “We’re all watching the same episode of Seinfeld. Why can’t we all watch the same episode of the Krebs cycle?” If all 190 or so medical schools in the United States shared such preclinical courses, he says, each would require a fraction of the current cost to produce. “We could save 99.5% of the cost. So why don’t we do that?”
Pandemic as opportunity
Although the price of medical education has yet to decrease, schools are working to leverage the pandemic to provide increased educational value.
This generation of physicians will not only have to cope with the fallout of this pandemic, they will be the ones responsible for confronting the next pandemic as well, says Donald Brady, MD, senior associate dean for health sciences education at Vanderbilt University, Nashville, Tenn. “They will be the leaders in the future who will better be able to know how to handle it [a pandemic] because they were able to watch it and be part of it safely in the current circumstance.”
As much as possible, Vanderbilt is using the pandemic as an opportunity. As soon as it became clear that students couldn’t be involved in certain hands-on training, instructors developed a course about pandemics that included lectures on ethics, global health, systemic racism, and other topics. It also included experiential components of pandemic management, such as opportunities to work with patients through telehealth.
Students say they feel that they are getting less for their money and that they are paying for experiences that are no longer available, such as hands-on patient contact and community events. However, Dr. Brady said, schools have had to account for new expenses, including various now-required technologies and transitioning to courses online.
Some challenges can’t be solved with money alone. Medical schools across the country are working together to ensure that they are still adequately preparing students. Vanderbilt participates in an AAMC group that meets regularly and is also one of 37 institutions involved in an American Medical Association Consortium (AACOM). These groups discuss challenges, strategies, and opportunities for optimizing medical education during the pandemic.
Some institutions have come up with creative solutions. Ohio University’s Heritage College of Osteopathic Medicine, in Athens, Ohio, in collaboration with the Ohio Department of Health, launched a 4-week rotation for third-year students that focuses on public health. Harvard Medical School, Boston, was one of several schools that allowed students to graduate early in the spring. “We’re constantly talking to our colleagues and friends,” Dr. Brady said. “We learn from each other. There’s a lot of sharing going on.”
Other organizations are also working to make sure students ultimately get what they are paying for: a high-quality education. As soon as the pandemic began, the AACOM organized four working groups to address how schools could better use technology to deliver curricula and how students could participate in public health efforts, among other topics. “For the students, the part they don’t see and can’t really be aware of is all the things that happen behind the scenes,” Mr. Cain said. “People were working really hard to make sure that their education was still delivered, and delivered in a way that was going to assure a good product at the end.”
Ultimately, that product will be held to a rigid standard, said Geoffrey Young, the AAMC’s senior director for student affairs and programs. Medical schools must still meet standards of competency set by the liaison committee on medical education. Mr. Young says that even now those standards remain rigorous enough to ensure that medical students are learning what they need to know. “The core elements for competency may be slightly altered to address the realities that we’re experiencing because of COVID, but the core tenants of competencies will not change,” he said.
Even as conversations continue about what a medical education is worth, the pandemic is drawing new attention to the profession. No signs suggest that the value of tuition or a shift to more virtual offerings are scaring students away. Applications for medical schools were up 17% for the fall of 2021.
Brady expects the surge in interest to continue. “The increased focus and emphasis on public health, the increased focus and emphasis on health equity, the increased focus on the need for a more diverse physician workforce, the interest in basic science research around viruses, the interest in COVID itself – there are a lot of different elements that are setting us up for a potential boom in applications to medical school,” he said.
Beyond increasing interest, the pandemic may also finally force a reckoning on the disconnection between how schools think about costs and how students think about value, Dr. Asch said. “When students say: ‘I’m not getting as much from this,’ they’re saying, ‘you should price this according to its lower value.’ And when the medical schools are saying: ‘Oh, but it’s costing us so much more,’ they’re talking about pricing according to the cost. It’s like one group is speaking Latin and the other group is speaking Greek.” Perhaps, he said, COVID-related changes will finally get them speaking the same language.
This article first appeared on Medscape.com.
Two COVID-19 outpatient antibody drugs show encouraging results
Two COVID-19 antibody treatments, one developed by Regeneron and the other by Eli Lilly, show promise in the outpatient setting in results released on Oct. 28.
Regeneron, in a randomized, double-blind trial, is assessing the effect of adding its investigational antibody cocktail REGN-COV2 to usual standard of care in comparison with adding placebo to standard of care. A descriptive analysis from the first 275 patients was previously reported. The data described on Oct. 28, which involve an additional 524 patients, show that the trial met all of the first nine endpoints.
Regeneron announced prospective results from its phase 2/3 trial showing REGN-COV2 significantly reduced viral load and patient medical visits, which included hospitalizations, visits to an emergency department, visits for urgent care, and/or physician office/telemedicine visits.
Interest in the cocktail spiked after President Donald Trump extolled its benefits after it was used in his own COVID-19 treatment earlier in October.
Trump received the highest dose of the drug, 8 g, but, according to a Regeneron news release announcing the latest findings, “results showed no significant difference in virologic or clinical efficacy between the REGN-COV2 high dose (8 grams) and low dose (2.4 grams).”
The company described further results of the industry-funded study in the release: “On the primary endpoint, the average daily change in viral load through day 7 (mean time-weighted average change from baseline) in patients with high viral load (defined as greater than107 copies/mL) was a 0.68 log10 copies/mL greater reduction with REGN-COV2 compared to placebo (combined dose groups; P < .0001). There was a 1.08 log greater reduction with REGN-COV2 treatment by day 5, which corresponds to REGN-COV2 patients having, on average, a greater than 10-fold reduction in viral load, compared to placebo.”
The treatment appears to be most effective in patients most at risk, whether because of high viral load, ineffective baseline antibody immune response, or preexisting conditions, according to the researchers.
According to the press release, these results have not been peer reviewed but have been submitted to the US Food and Drug Administration, which is reviewing a potential emergency use authorization for the treatment in high-risk adults with mild to moderate COVID-19.
Operation Warp Speed, the Trump administration’s treatment and vaccine program, contracted in July with Regeneron for up to 300,000 doses of its antibody cocktail.
Lilly treatment shows drop in hospitalizations, symptoms
Another treatment, also given in the outpatient setting, shows promise as well.
Patients recently diagnosed with mild to moderate COVID-19 who received Eli Lilly’s antibody treatment LY-CoV555 had fewer hospitalizations and symptoms compared with a group that received placebo, an interim analysis of a phase 2 trial indicates.
Peter Chen, MD, with the Department of Medicine, Women’s Guild Lung Institute at Cedars-Sinai Medical Center, Los Angeles, California, and colleagues found that the most profound effects were in the high-risk groups.
The interim findings of the BLAZE-1 study, which was funded by Eli Lilly, were published online October 28 in The New England Journal of Medicine.
Researchers randomly assigned 452 patients to receive an intravenous infusion of LY-CoV555 in one of three doses (700 mg, 2800 mg, or 7000 mg) or placebo.
In the interim analysis, the researchers found that for the entire population, more than 99.97% of viral RNA was eliminated.
For patients who received the 2800-mg dose, the difference from placebo in the decrease from baseline was −0.53 (95% CI, −0.98 to −0.08; P = .02), for a log viral load that was lower by a factor of 3.4. Benefit over placebo was not significant with the other doses.
At day 29, according to the investigators, the percentage of patients hospitalized with COVID-19 was 1.6% (5 of 309 patients) in the treatment group compared with 6.3% (9 of 143 patients) in the placebo group.
Data indicate that the safety profile was similar whether patients received the active treatment or placebo.
“If these results are confirmed in additional analyses in this trial, LY-CoV555 could become a useful treatment for emergency use in patients with recently diagnosed Covid-19,” the authors write.
Deborah Fuller, PhD, professor in the Department of Microbiology at the University of Washington School of Medicine in Seattle, told Medscape Medical News the findings are «exciting» but only part of the treatment solution.
“What’s remarkable about these two studies and others I’ve seen,” she said, “is how consistent they are in terms of the window of time they will be effective, and that’s because they are just targeting the virus itself. They do not have an effect on the inflammation unless they stop the replication early enough.”
The treatments are effective when they are given near the time of diagnosis, she pointed out.
“Once the virus has started that inflammatory cascade in your body, then that train has left the station and you have to deal with the inflammation,” Fuller said.
She says future treatments will likely have to include both the antiviral and anti-inflammatory properties, and physicians will have to assess what’s best, given the stage of the the patient’s disease.
The trial of REGN-COV2 is funded by Regeneron. The BLAZE-1 study is funded by Eli Lilly. Many of the authors have financial ties to Eli Lilly. Fuller has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Two COVID-19 antibody treatments, one developed by Regeneron and the other by Eli Lilly, show promise in the outpatient setting in results released on Oct. 28.
Regeneron, in a randomized, double-blind trial, is assessing the effect of adding its investigational antibody cocktail REGN-COV2 to usual standard of care in comparison with adding placebo to standard of care. A descriptive analysis from the first 275 patients was previously reported. The data described on Oct. 28, which involve an additional 524 patients, show that the trial met all of the first nine endpoints.
Regeneron announced prospective results from its phase 2/3 trial showing REGN-COV2 significantly reduced viral load and patient medical visits, which included hospitalizations, visits to an emergency department, visits for urgent care, and/or physician office/telemedicine visits.
Interest in the cocktail spiked after President Donald Trump extolled its benefits after it was used in his own COVID-19 treatment earlier in October.
Trump received the highest dose of the drug, 8 g, but, according to a Regeneron news release announcing the latest findings, “results showed no significant difference in virologic or clinical efficacy between the REGN-COV2 high dose (8 grams) and low dose (2.4 grams).”
The company described further results of the industry-funded study in the release: “On the primary endpoint, the average daily change in viral load through day 7 (mean time-weighted average change from baseline) in patients with high viral load (defined as greater than107 copies/mL) was a 0.68 log10 copies/mL greater reduction with REGN-COV2 compared to placebo (combined dose groups; P < .0001). There was a 1.08 log greater reduction with REGN-COV2 treatment by day 5, which corresponds to REGN-COV2 patients having, on average, a greater than 10-fold reduction in viral load, compared to placebo.”
The treatment appears to be most effective in patients most at risk, whether because of high viral load, ineffective baseline antibody immune response, or preexisting conditions, according to the researchers.
According to the press release, these results have not been peer reviewed but have been submitted to the US Food and Drug Administration, which is reviewing a potential emergency use authorization for the treatment in high-risk adults with mild to moderate COVID-19.
Operation Warp Speed, the Trump administration’s treatment and vaccine program, contracted in July with Regeneron for up to 300,000 doses of its antibody cocktail.
Lilly treatment shows drop in hospitalizations, symptoms
Another treatment, also given in the outpatient setting, shows promise as well.
Patients recently diagnosed with mild to moderate COVID-19 who received Eli Lilly’s antibody treatment LY-CoV555 had fewer hospitalizations and symptoms compared with a group that received placebo, an interim analysis of a phase 2 trial indicates.
Peter Chen, MD, with the Department of Medicine, Women’s Guild Lung Institute at Cedars-Sinai Medical Center, Los Angeles, California, and colleagues found that the most profound effects were in the high-risk groups.
The interim findings of the BLAZE-1 study, which was funded by Eli Lilly, were published online October 28 in The New England Journal of Medicine.
Researchers randomly assigned 452 patients to receive an intravenous infusion of LY-CoV555 in one of three doses (700 mg, 2800 mg, or 7000 mg) or placebo.
In the interim analysis, the researchers found that for the entire population, more than 99.97% of viral RNA was eliminated.
For patients who received the 2800-mg dose, the difference from placebo in the decrease from baseline was −0.53 (95% CI, −0.98 to −0.08; P = .02), for a log viral load that was lower by a factor of 3.4. Benefit over placebo was not significant with the other doses.
At day 29, according to the investigators, the percentage of patients hospitalized with COVID-19 was 1.6% (5 of 309 patients) in the treatment group compared with 6.3% (9 of 143 patients) in the placebo group.
Data indicate that the safety profile was similar whether patients received the active treatment or placebo.
“If these results are confirmed in additional analyses in this trial, LY-CoV555 could become a useful treatment for emergency use in patients with recently diagnosed Covid-19,” the authors write.
Deborah Fuller, PhD, professor in the Department of Microbiology at the University of Washington School of Medicine in Seattle, told Medscape Medical News the findings are «exciting» but only part of the treatment solution.
“What’s remarkable about these two studies and others I’ve seen,” she said, “is how consistent they are in terms of the window of time they will be effective, and that’s because they are just targeting the virus itself. They do not have an effect on the inflammation unless they stop the replication early enough.”
The treatments are effective when they are given near the time of diagnosis, she pointed out.
“Once the virus has started that inflammatory cascade in your body, then that train has left the station and you have to deal with the inflammation,” Fuller said.
She says future treatments will likely have to include both the antiviral and anti-inflammatory properties, and physicians will have to assess what’s best, given the stage of the the patient’s disease.
The trial of REGN-COV2 is funded by Regeneron. The BLAZE-1 study is funded by Eli Lilly. Many of the authors have financial ties to Eli Lilly. Fuller has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Two COVID-19 antibody treatments, one developed by Regeneron and the other by Eli Lilly, show promise in the outpatient setting in results released on Oct. 28.
Regeneron, in a randomized, double-blind trial, is assessing the effect of adding its investigational antibody cocktail REGN-COV2 to usual standard of care in comparison with adding placebo to standard of care. A descriptive analysis from the first 275 patients was previously reported. The data described on Oct. 28, which involve an additional 524 patients, show that the trial met all of the first nine endpoints.
Regeneron announced prospective results from its phase 2/3 trial showing REGN-COV2 significantly reduced viral load and patient medical visits, which included hospitalizations, visits to an emergency department, visits for urgent care, and/or physician office/telemedicine visits.
Interest in the cocktail spiked after President Donald Trump extolled its benefits after it was used in his own COVID-19 treatment earlier in October.
Trump received the highest dose of the drug, 8 g, but, according to a Regeneron news release announcing the latest findings, “results showed no significant difference in virologic or clinical efficacy between the REGN-COV2 high dose (8 grams) and low dose (2.4 grams).”
The company described further results of the industry-funded study in the release: “On the primary endpoint, the average daily change in viral load through day 7 (mean time-weighted average change from baseline) in patients with high viral load (defined as greater than107 copies/mL) was a 0.68 log10 copies/mL greater reduction with REGN-COV2 compared to placebo (combined dose groups; P < .0001). There was a 1.08 log greater reduction with REGN-COV2 treatment by day 5, which corresponds to REGN-COV2 patients having, on average, a greater than 10-fold reduction in viral load, compared to placebo.”
The treatment appears to be most effective in patients most at risk, whether because of high viral load, ineffective baseline antibody immune response, or preexisting conditions, according to the researchers.
According to the press release, these results have not been peer reviewed but have been submitted to the US Food and Drug Administration, which is reviewing a potential emergency use authorization for the treatment in high-risk adults with mild to moderate COVID-19.
Operation Warp Speed, the Trump administration’s treatment and vaccine program, contracted in July with Regeneron for up to 300,000 doses of its antibody cocktail.
Lilly treatment shows drop in hospitalizations, symptoms
Another treatment, also given in the outpatient setting, shows promise as well.
Patients recently diagnosed with mild to moderate COVID-19 who received Eli Lilly’s antibody treatment LY-CoV555 had fewer hospitalizations and symptoms compared with a group that received placebo, an interim analysis of a phase 2 trial indicates.
Peter Chen, MD, with the Department of Medicine, Women’s Guild Lung Institute at Cedars-Sinai Medical Center, Los Angeles, California, and colleagues found that the most profound effects were in the high-risk groups.
The interim findings of the BLAZE-1 study, which was funded by Eli Lilly, were published online October 28 in The New England Journal of Medicine.
Researchers randomly assigned 452 patients to receive an intravenous infusion of LY-CoV555 in one of three doses (700 mg, 2800 mg, or 7000 mg) or placebo.
In the interim analysis, the researchers found that for the entire population, more than 99.97% of viral RNA was eliminated.
For patients who received the 2800-mg dose, the difference from placebo in the decrease from baseline was −0.53 (95% CI, −0.98 to −0.08; P = .02), for a log viral load that was lower by a factor of 3.4. Benefit over placebo was not significant with the other doses.
At day 29, according to the investigators, the percentage of patients hospitalized with COVID-19 was 1.6% (5 of 309 patients) in the treatment group compared with 6.3% (9 of 143 patients) in the placebo group.
Data indicate that the safety profile was similar whether patients received the active treatment or placebo.
“If these results are confirmed in additional analyses in this trial, LY-CoV555 could become a useful treatment for emergency use in patients with recently diagnosed Covid-19,” the authors write.
Deborah Fuller, PhD, professor in the Department of Microbiology at the University of Washington School of Medicine in Seattle, told Medscape Medical News the findings are «exciting» but only part of the treatment solution.
“What’s remarkable about these two studies and others I’ve seen,” she said, “is how consistent they are in terms of the window of time they will be effective, and that’s because they are just targeting the virus itself. They do not have an effect on the inflammation unless they stop the replication early enough.”
The treatments are effective when they are given near the time of diagnosis, she pointed out.
“Once the virus has started that inflammatory cascade in your body, then that train has left the station and you have to deal with the inflammation,” Fuller said.
She says future treatments will likely have to include both the antiviral and anti-inflammatory properties, and physicians will have to assess what’s best, given the stage of the the patient’s disease.
The trial of REGN-COV2 is funded by Regeneron. The BLAZE-1 study is funded by Eli Lilly. Many of the authors have financial ties to Eli Lilly. Fuller has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Diabetes screening program in optometry offices to expand

The program is sponsored by VSP Vision Care, a vision benefits company with over 40,000 network optometrists and nearly 90 million consumer members worldwide. “Optometrists are often the first to detect signs of diabetes by looking at the blood vessels in the eye during a comprehensive eye exam,” the company said in a statement.
In the pilot program, conducted from May 2019 to February 2020* in 12 VSP practices in five states, 818 patients who had come in for their annual vision exam were given the American Diabetes Association Risk Test for type 2 diabetes, and 287 identified at risk were offered an in-office fingerstick hemoglobin A1c test.
Materials were provided free to the optometrists, who were paid a professional fee to perform the HbA1c screenings.
Of the 287 eligible for the HbA1c test, 85% took it. Of those 244, 31% and 5% had levels in the prediabetes and diabetes range, respectively. None had been aware of their status previously, and 92% rated the screening as an extremely or very positive experience.
Now, VSP is expanding the pilot program for another year with two large clients in Ohio covering about 90,000 members.
“Coupled with the fact that VSP members are more likely to get their annual eye exam over their annual physical exam with their primary care physician, HbA1c screenings provided by eye doctors offer another critical way to detect the chronic condition earlier and help prevent eye disease and even vision loss caused by diabetes,” according to the statement.
In an interview, a VSP spokesperson explained that if the patient provides their primary care provider information to the optometrist, the optometrist will send a referral with exam information to that provider and also instruct the patient to make an appointment with the provider for follow-up testing and care.
The optometrist also educates the patient about the connection between eye health and overall health and provides them with a flier that gives tips on lifestyle changes they can make to help slow or prevent the progression to type 2 diabetes, the spokesperson said.
Thirty states, including Ohio, allow optometrists to perform in-office blood testing, including HbA1c screening, provided they obtain a Clinical Laboratory Improvement Amendments Certificate of Waiver. VSP is providing online training for participating optometrists on administering the HbA1c screening.
The pilot program is part of an alliance between VSP and the American Diabetes Association formed in November 2019 to raise awareness of eye health in people with diabetes and those at risk for it.
*Correction: The original article included the wrong end date for the pilot program.
The program is sponsored by VSP Vision Care, a vision benefits company with over 40,000 network optometrists and nearly 90 million consumer members worldwide. “Optometrists are often the first to detect signs of diabetes by looking at the blood vessels in the eye during a comprehensive eye exam,” the company said in a statement.
In the pilot program, conducted from May 2019 to February 2020* in 12 VSP practices in five states, 818 patients who had come in for their annual vision exam were given the American Diabetes Association Risk Test for type 2 diabetes, and 287 identified at risk were offered an in-office fingerstick hemoglobin A1c test.
Materials were provided free to the optometrists, who were paid a professional fee to perform the HbA1c screenings.
Of the 287 eligible for the HbA1c test, 85% took it. Of those 244, 31% and 5% had levels in the prediabetes and diabetes range, respectively. None had been aware of their status previously, and 92% rated the screening as an extremely or very positive experience.
Now, VSP is expanding the pilot program for another year with two large clients in Ohio covering about 90,000 members.
“Coupled with the fact that VSP members are more likely to get their annual eye exam over their annual physical exam with their primary care physician, HbA1c screenings provided by eye doctors offer another critical way to detect the chronic condition earlier and help prevent eye disease and even vision loss caused by diabetes,” according to the statement.
In an interview, a VSP spokesperson explained that if the patient provides their primary care provider information to the optometrist, the optometrist will send a referral with exam information to that provider and also instruct the patient to make an appointment with the provider for follow-up testing and care.
The optometrist also educates the patient about the connection between eye health and overall health and provides them with a flier that gives tips on lifestyle changes they can make to help slow or prevent the progression to type 2 diabetes, the spokesperson said.
Thirty states, including Ohio, allow optometrists to perform in-office blood testing, including HbA1c screening, provided they obtain a Clinical Laboratory Improvement Amendments Certificate of Waiver. VSP is providing online training for participating optometrists on administering the HbA1c screening.
The pilot program is part of an alliance between VSP and the American Diabetes Association formed in November 2019 to raise awareness of eye health in people with diabetes and those at risk for it.
*Correction: The original article included the wrong end date for the pilot program.
The program is sponsored by VSP Vision Care, a vision benefits company with over 40,000 network optometrists and nearly 90 million consumer members worldwide. “Optometrists are often the first to detect signs of diabetes by looking at the blood vessels in the eye during a comprehensive eye exam,” the company said in a statement.
In the pilot program, conducted from May 2019 to February 2020* in 12 VSP practices in five states, 818 patients who had come in for their annual vision exam were given the American Diabetes Association Risk Test for type 2 diabetes, and 287 identified at risk were offered an in-office fingerstick hemoglobin A1c test.
Materials were provided free to the optometrists, who were paid a professional fee to perform the HbA1c screenings.
Of the 287 eligible for the HbA1c test, 85% took it. Of those 244, 31% and 5% had levels in the prediabetes and diabetes range, respectively. None had been aware of their status previously, and 92% rated the screening as an extremely or very positive experience.
Now, VSP is expanding the pilot program for another year with two large clients in Ohio covering about 90,000 members.
“Coupled with the fact that VSP members are more likely to get their annual eye exam over their annual physical exam with their primary care physician, HbA1c screenings provided by eye doctors offer another critical way to detect the chronic condition earlier and help prevent eye disease and even vision loss caused by diabetes,” according to the statement.
In an interview, a VSP spokesperson explained that if the patient provides their primary care provider information to the optometrist, the optometrist will send a referral with exam information to that provider and also instruct the patient to make an appointment with the provider for follow-up testing and care.
The optometrist also educates the patient about the connection between eye health and overall health and provides them with a flier that gives tips on lifestyle changes they can make to help slow or prevent the progression to type 2 diabetes, the spokesperson said.
Thirty states, including Ohio, allow optometrists to perform in-office blood testing, including HbA1c screening, provided they obtain a Clinical Laboratory Improvement Amendments Certificate of Waiver. VSP is providing online training for participating optometrists on administering the HbA1c screening.
The pilot program is part of an alliance between VSP and the American Diabetes Association formed in November 2019 to raise awareness of eye health in people with diabetes and those at risk for it.
*Correction: The original article included the wrong end date for the pilot program.
Online tool offers diabetes device information free of industry funding
A new online tool aims to help patients with insulin-treated diabetes and their health care providers to identify the best diabetes technology based on individual needs and preferences.
The “Device Finder” tool is a new feature of the DiabetesWise website, www.diabeteswise.org, which is funded by the Leona M. and Harry B. Helmsley Charitable Trust with no industry contributions. It is intended for use by patients with either type 1 diabetes or insulin-treated type 2 diabetes and by endocrinologists and primary care clinicians in their discussions with patients.
The main DiabetesWise site was launched in June 2019 by a team led by Stanford (Calif.) University psychologist Korey K. Hood, PhD; this team included endocrinologists, psychologists, diabetes care and education specialists, nurses, and patients. The information provided in it was based on work from the past several years in examining human variables that influence diabetes technology uptake, Dr. Hood said in an interview.
“We realized there wasn’t really a great resource for people to actually compare different devices and understand what might fit their lifestyle and priorities. You had to go to a device manufacturer to get that information, and ... that’s probably a little bit biased,” said Dr. Hood, who is professor of pediatrics and psychiatry & behavioral sciences at Stanford.
The site offers a quick “Check Up” that asks patients about what devices they’re currently using, how they feel they’re handling their diabetes management, and about their priorities regarding devices. The new “Device Finder” tool provides information about different combinations of insulin pumps, continuous glucose monitors (CGMs), injections, and fingerstick glucose meters. The site also features resources for patients on speaking with their doctors, costs and health insurance, coping with COVID-19, and “wisdom” with patient narratives. Patients can download reports to share with their clinicians.
Asked to comment, diabetes technology expert David Ahn, MD, program director of the Allen Diabetes Center, Hoag Health, Newport Beach, Calif., said, “I love that DiabetesWise.org offers patients a way to compare and contrast different products all in one place that is not directly influenced or funded by a specific manufacturer or industry in general. I especially appreciate the patient stories and how they each arrived at their current devices.”
However, Dr. Ahn also noted, “when talking to my patients, I feel like having a personal discussion can lead to a better sense of their desires and preferences than a website that is just following an algorithm. ... The challenge with any resource like this is fully appreciating the nuances of each individual and device since choosing a device or combination of devices can be more of an art than a science.”
Nonetheless, he said that the site may be “a good starting place to learn key concepts and product details” for newly diagnosed patients and nonspecialist clinicians.
Indeed, Dr. Hood said, “It’s not perfect. We will revise it as we get more data.” The team is currently following about 500 patients with type 1 and type 2 diabetes, most of them not in specialty care and not initially using advanced devices (pumps/CGMs) to see how they’re engaging with the site and whether they adopt new technologies. “We were pretty encouraged that, in the first month, people were reaching out to their providers to get a prescription. I think we’re generating the awareness that we thought we would.”
Unfortunately, the COVID-19 pandemic has had a negative impact. “We queried people, [and] about half had lost some portion of employment and with that was tied their access to benefits and health insurance. We saw a dip in how much people could actually access. We’ll report that when we have all the data.”
Pending funding, Dr. Hood said the team also hopes to create a clinician-facing versions of the site. “We won’t forget about endocrinologists, but really we’re interested in making it a tool that primary care clinicians and even pharmacists can use to help with the engagement and uptake of diabetes devices, because the rate of use of these diabetes devices in adults with type 1 who aren’t in specialty care is pretty low. So we’re trying to reach the groups that will have a bigger impact.”
In addition to his work on DiabetesWise, Dr. Hood is a consultant for Cecelia Health. Dr. Ahn is a consultant for Senseonics and Eli Lilly and on the speaker’s bureau for Lilly.
A new online tool aims to help patients with insulin-treated diabetes and their health care providers to identify the best diabetes technology based on individual needs and preferences.
The “Device Finder” tool is a new feature of the DiabetesWise website, www.diabeteswise.org, which is funded by the Leona M. and Harry B. Helmsley Charitable Trust with no industry contributions. It is intended for use by patients with either type 1 diabetes or insulin-treated type 2 diabetes and by endocrinologists and primary care clinicians in their discussions with patients.
The main DiabetesWise site was launched in June 2019 by a team led by Stanford (Calif.) University psychologist Korey K. Hood, PhD; this team included endocrinologists, psychologists, diabetes care and education specialists, nurses, and patients. The information provided in it was based on work from the past several years in examining human variables that influence diabetes technology uptake, Dr. Hood said in an interview.
“We realized there wasn’t really a great resource for people to actually compare different devices and understand what might fit their lifestyle and priorities. You had to go to a device manufacturer to get that information, and ... that’s probably a little bit biased,” said Dr. Hood, who is professor of pediatrics and psychiatry & behavioral sciences at Stanford.
The site offers a quick “Check Up” that asks patients about what devices they’re currently using, how they feel they’re handling their diabetes management, and about their priorities regarding devices. The new “Device Finder” tool provides information about different combinations of insulin pumps, continuous glucose monitors (CGMs), injections, and fingerstick glucose meters. The site also features resources for patients on speaking with their doctors, costs and health insurance, coping with COVID-19, and “wisdom” with patient narratives. Patients can download reports to share with their clinicians.
Asked to comment, diabetes technology expert David Ahn, MD, program director of the Allen Diabetes Center, Hoag Health, Newport Beach, Calif., said, “I love that DiabetesWise.org offers patients a way to compare and contrast different products all in one place that is not directly influenced or funded by a specific manufacturer or industry in general. I especially appreciate the patient stories and how they each arrived at their current devices.”
However, Dr. Ahn also noted, “when talking to my patients, I feel like having a personal discussion can lead to a better sense of their desires and preferences than a website that is just following an algorithm. ... The challenge with any resource like this is fully appreciating the nuances of each individual and device since choosing a device or combination of devices can be more of an art than a science.”
Nonetheless, he said that the site may be “a good starting place to learn key concepts and product details” for newly diagnosed patients and nonspecialist clinicians.
Indeed, Dr. Hood said, “It’s not perfect. We will revise it as we get more data.” The team is currently following about 500 patients with type 1 and type 2 diabetes, most of them not in specialty care and not initially using advanced devices (pumps/CGMs) to see how they’re engaging with the site and whether they adopt new technologies. “We were pretty encouraged that, in the first month, people were reaching out to their providers to get a prescription. I think we’re generating the awareness that we thought we would.”
Unfortunately, the COVID-19 pandemic has had a negative impact. “We queried people, [and] about half had lost some portion of employment and with that was tied their access to benefits and health insurance. We saw a dip in how much people could actually access. We’ll report that when we have all the data.”
Pending funding, Dr. Hood said the team also hopes to create a clinician-facing versions of the site. “We won’t forget about endocrinologists, but really we’re interested in making it a tool that primary care clinicians and even pharmacists can use to help with the engagement and uptake of diabetes devices, because the rate of use of these diabetes devices in adults with type 1 who aren’t in specialty care is pretty low. So we’re trying to reach the groups that will have a bigger impact.”
In addition to his work on DiabetesWise, Dr. Hood is a consultant for Cecelia Health. Dr. Ahn is a consultant for Senseonics and Eli Lilly and on the speaker’s bureau for Lilly.
A new online tool aims to help patients with insulin-treated diabetes and their health care providers to identify the best diabetes technology based on individual needs and preferences.
The “Device Finder” tool is a new feature of the DiabetesWise website, www.diabeteswise.org, which is funded by the Leona M. and Harry B. Helmsley Charitable Trust with no industry contributions. It is intended for use by patients with either type 1 diabetes or insulin-treated type 2 diabetes and by endocrinologists and primary care clinicians in their discussions with patients.
The main DiabetesWise site was launched in June 2019 by a team led by Stanford (Calif.) University psychologist Korey K. Hood, PhD; this team included endocrinologists, psychologists, diabetes care and education specialists, nurses, and patients. The information provided in it was based on work from the past several years in examining human variables that influence diabetes technology uptake, Dr. Hood said in an interview.
“We realized there wasn’t really a great resource for people to actually compare different devices and understand what might fit their lifestyle and priorities. You had to go to a device manufacturer to get that information, and ... that’s probably a little bit biased,” said Dr. Hood, who is professor of pediatrics and psychiatry & behavioral sciences at Stanford.
The site offers a quick “Check Up” that asks patients about what devices they’re currently using, how they feel they’re handling their diabetes management, and about their priorities regarding devices. The new “Device Finder” tool provides information about different combinations of insulin pumps, continuous glucose monitors (CGMs), injections, and fingerstick glucose meters. The site also features resources for patients on speaking with their doctors, costs and health insurance, coping with COVID-19, and “wisdom” with patient narratives. Patients can download reports to share with their clinicians.
Asked to comment, diabetes technology expert David Ahn, MD, program director of the Allen Diabetes Center, Hoag Health, Newport Beach, Calif., said, “I love that DiabetesWise.org offers patients a way to compare and contrast different products all in one place that is not directly influenced or funded by a specific manufacturer or industry in general. I especially appreciate the patient stories and how they each arrived at their current devices.”
However, Dr. Ahn also noted, “when talking to my patients, I feel like having a personal discussion can lead to a better sense of their desires and preferences than a website that is just following an algorithm. ... The challenge with any resource like this is fully appreciating the nuances of each individual and device since choosing a device or combination of devices can be more of an art than a science.”
Nonetheless, he said that the site may be “a good starting place to learn key concepts and product details” for newly diagnosed patients and nonspecialist clinicians.
Indeed, Dr. Hood said, “It’s not perfect. We will revise it as we get more data.” The team is currently following about 500 patients with type 1 and type 2 diabetes, most of them not in specialty care and not initially using advanced devices (pumps/CGMs) to see how they’re engaging with the site and whether they adopt new technologies. “We were pretty encouraged that, in the first month, people were reaching out to their providers to get a prescription. I think we’re generating the awareness that we thought we would.”
Unfortunately, the COVID-19 pandemic has had a negative impact. “We queried people, [and] about half had lost some portion of employment and with that was tied their access to benefits and health insurance. We saw a dip in how much people could actually access. We’ll report that when we have all the data.”
Pending funding, Dr. Hood said the team also hopes to create a clinician-facing versions of the site. “We won’t forget about endocrinologists, but really we’re interested in making it a tool that primary care clinicians and even pharmacists can use to help with the engagement and uptake of diabetes devices, because the rate of use of these diabetes devices in adults with type 1 who aren’t in specialty care is pretty low. So we’re trying to reach the groups that will have a bigger impact.”
In addition to his work on DiabetesWise, Dr. Hood is a consultant for Cecelia Health. Dr. Ahn is a consultant for Senseonics and Eli Lilly and on the speaker’s bureau for Lilly.
Facebook $52M settlement flags need to screen for vicarious trauma
The images are graphic, disturbing, and endless, said a former Facebook employee. Her job as a content moderator required that she review and remove disturbing posts. That work, she claimed in a lawsuit, caused her to suffer serious psychological trauma.
In September 2018, she filed a complaint with the Superior Court of California.
“Every day, Facebook users post millions of videos, images, and livestream broadcasts of child sexual abuse, rape, torture, bestiality, beheadings, suicide, and murder,” reads the complaint. “By requiring its content moderators to work in dangerous conditions that cause debilitating physical and psychological harm, Facebook violates California law.”
In May, Facebook settled the case, agreeing to pay $52 million to content moderators to compensate them for the consequences their work had on their mental health. The settlement was the first to officially recognize the psychological toll of exposure to disturbing material resulting from online moderator jobs. It also highlights an emerging understanding of vicarious trauma.
Also known as secondary trauma, vicarious trauma can result from exposure to images, stories, or accounts that someone does not directly experience, said Françoise Mathieu, MEd, CCC, RP, a compassion fatigue specialist and executive director of TEND, a company in Kingston, Ont., that offers resources and training for people who work in high-stress, trauma-exposed workplaces.
Secondary trauma can affect people much as any other kind of intensely stressful experience. “What I can tell you as a specialist is that trauma is trauma,” Mathieu said. “Our brain doesn’t necessarily know the difference.”
The potential for vicarious trauma has long been recognized as a risk for journalists, health care providers, and anyone who watches television coverage of a disaster. Only recently, Mathieu said, have researchers started to investigate the psychological impact of jobs that require people to look at extreme, graphic, or disturbing images.
Physical fallout
In a 2017 study of digital forensic examiners, researchers found that examiners who worked on cases involving sexual crimes against children were at elevated risk of developing secondary trauma.
However, the exploratory study did not quantify the risks, and the study investigators concluded that more research is needed to understand how best to help people deal with PTSD resulting from working in the criminal justice system.
Content moderation requires sifting through upsetting images, and people can react in different ways to the task, says Anthony Ng, MD, a psychiatrist at Hartford (Conn.) Healthcare in Mansfield Center.
Dr. Ng says some individuals may become emotionally numb in order to protect themselves. Others might relate to what they are seeing, either because of their own life circumstances or because of experiences they have had in the past. For example, individuals might think: “I could see that kid being my son, I could see that woman who was assaulted as my wife who got beaten up”
that ramps up activity in an area of the brain called the locus coeruleus, Dr. Ng said.
Heart rate rises. Breathing rate goes up. Muscles become tense. If a threat occurs once and then dissipates, the body can often recover a state of calm. However, when that threat is part of the daily workday, it can cause chronic harm to mental and physical health. Unlike with direct, or primary, trauma, he adds, secondary trauma can take a while to become symptomatic.
“Your heart is not designed to be constantly pumping at a high rate,” Dr. Ng says. “We just can’t sustain that for long periods of time without starting to develop stress reactions.”
Under the radar
Some types of work appear to confer greater risk for trauma than others. Overall, estimates show that up to 8% of the U.S. population will develop PTSD at some point in their lives, Ms. Mathieu said.
For police officers, the rate is 15%. According to reporting by The Verge, lawyers in the Facebook lawsuit cited vicarious trauma rates of up to 50% among content moderators.
There are multiple reasons why content moderators suffer such high rates of mental health problems, Ms. Mathieu said. Content moderation is a low-paying, thankless, and solo job that can seem never-ending, she said.
Furthermore, content moderators are generally uninformed about the psychological risks associated with their occupation. They aren’t given the time to process what they are exposed to and generally don’t feel recognized or appreciated for the work they do.
That makes their jobs different from those of people such as law enforcement officers who investigate Internet crimes. For people pursuing justice, a sense of unity can counterbalance the exposure to tough imagery and information.
Going forward, Ms. Mathieu said, the only way to make content moderation safer is to institute changes such as better pay, more flexible schedules to allow breaks from exposure, and access to mental health professionals who can help employees process what they have seen.
Climate of fear
“This can’t be a climate of fear where people are afraid to ask for help,” Ms. Mathieu said. “They are really important jobs, but people need to feel that they are safe in expressing when it’s impacting them so that they’re not worried that they’re actually going to lose their work.”
It would help if content moderators received evidence-based guidance to help process their experiences, Ms. Mathieu added. However, to avoid doing more harm than good, debriefing has to be administered correctly.
For example, a method called “critical incident stress debriefing,” a longstanding approach that research has shown can do more harm than good, is still widely used in law enforcement agencies. The technique requires individuals to talk about their traumatic experience immediately after it happens, which can cause retraumatization.
Instead, Dr. Ng recommended a more self-aware approach called low-impact debriefing. The method involves strategies such as giving fair warning, asking for consent from listeners, and being selective about the details shared.
Employees should also be taught to recognize and report early signs and symptoms so that they can seek help before psychological distress becomes overwhelming, Dr. Ng says.
Plenty of moderators do not develop PTSD, he said, despite their exposure to upsetting imagery. This suggests an important avenue for research – understanding what makes some people resilient, even in the face of graphic and disturbing stressors.
A version of this story originally appeared on Medscape.com.
The images are graphic, disturbing, and endless, said a former Facebook employee. Her job as a content moderator required that she review and remove disturbing posts. That work, she claimed in a lawsuit, caused her to suffer serious psychological trauma.
In September 2018, she filed a complaint with the Superior Court of California.
“Every day, Facebook users post millions of videos, images, and livestream broadcasts of child sexual abuse, rape, torture, bestiality, beheadings, suicide, and murder,” reads the complaint. “By requiring its content moderators to work in dangerous conditions that cause debilitating physical and psychological harm, Facebook violates California law.”
In May, Facebook settled the case, agreeing to pay $52 million to content moderators to compensate them for the consequences their work had on their mental health. The settlement was the first to officially recognize the psychological toll of exposure to disturbing material resulting from online moderator jobs. It also highlights an emerging understanding of vicarious trauma.
Also known as secondary trauma, vicarious trauma can result from exposure to images, stories, or accounts that someone does not directly experience, said Françoise Mathieu, MEd, CCC, RP, a compassion fatigue specialist and executive director of TEND, a company in Kingston, Ont., that offers resources and training for people who work in high-stress, trauma-exposed workplaces.
Secondary trauma can affect people much as any other kind of intensely stressful experience. “What I can tell you as a specialist is that trauma is trauma,” Mathieu said. “Our brain doesn’t necessarily know the difference.”
The potential for vicarious trauma has long been recognized as a risk for journalists, health care providers, and anyone who watches television coverage of a disaster. Only recently, Mathieu said, have researchers started to investigate the psychological impact of jobs that require people to look at extreme, graphic, or disturbing images.
Physical fallout
In a 2017 study of digital forensic examiners, researchers found that examiners who worked on cases involving sexual crimes against children were at elevated risk of developing secondary trauma.
However, the exploratory study did not quantify the risks, and the study investigators concluded that more research is needed to understand how best to help people deal with PTSD resulting from working in the criminal justice system.
Content moderation requires sifting through upsetting images, and people can react in different ways to the task, says Anthony Ng, MD, a psychiatrist at Hartford (Conn.) Healthcare in Mansfield Center.
Dr. Ng says some individuals may become emotionally numb in order to protect themselves. Others might relate to what they are seeing, either because of their own life circumstances or because of experiences they have had in the past. For example, individuals might think: “I could see that kid being my son, I could see that woman who was assaulted as my wife who got beaten up”
that ramps up activity in an area of the brain called the locus coeruleus, Dr. Ng said.
Heart rate rises. Breathing rate goes up. Muscles become tense. If a threat occurs once and then dissipates, the body can often recover a state of calm. However, when that threat is part of the daily workday, it can cause chronic harm to mental and physical health. Unlike with direct, or primary, trauma, he adds, secondary trauma can take a while to become symptomatic.
“Your heart is not designed to be constantly pumping at a high rate,” Dr. Ng says. “We just can’t sustain that for long periods of time without starting to develop stress reactions.”
Under the radar
Some types of work appear to confer greater risk for trauma than others. Overall, estimates show that up to 8% of the U.S. population will develop PTSD at some point in their lives, Ms. Mathieu said.
For police officers, the rate is 15%. According to reporting by The Verge, lawyers in the Facebook lawsuit cited vicarious trauma rates of up to 50% among content moderators.
There are multiple reasons why content moderators suffer such high rates of mental health problems, Ms. Mathieu said. Content moderation is a low-paying, thankless, and solo job that can seem never-ending, she said.
Furthermore, content moderators are generally uninformed about the psychological risks associated with their occupation. They aren’t given the time to process what they are exposed to and generally don’t feel recognized or appreciated for the work they do.
That makes their jobs different from those of people such as law enforcement officers who investigate Internet crimes. For people pursuing justice, a sense of unity can counterbalance the exposure to tough imagery and information.
Going forward, Ms. Mathieu said, the only way to make content moderation safer is to institute changes such as better pay, more flexible schedules to allow breaks from exposure, and access to mental health professionals who can help employees process what they have seen.
Climate of fear
“This can’t be a climate of fear where people are afraid to ask for help,” Ms. Mathieu said. “They are really important jobs, but people need to feel that they are safe in expressing when it’s impacting them so that they’re not worried that they’re actually going to lose their work.”
It would help if content moderators received evidence-based guidance to help process their experiences, Ms. Mathieu added. However, to avoid doing more harm than good, debriefing has to be administered correctly.
For example, a method called “critical incident stress debriefing,” a longstanding approach that research has shown can do more harm than good, is still widely used in law enforcement agencies. The technique requires individuals to talk about their traumatic experience immediately after it happens, which can cause retraumatization.
Instead, Dr. Ng recommended a more self-aware approach called low-impact debriefing. The method involves strategies such as giving fair warning, asking for consent from listeners, and being selective about the details shared.
Employees should also be taught to recognize and report early signs and symptoms so that they can seek help before psychological distress becomes overwhelming, Dr. Ng says.
Plenty of moderators do not develop PTSD, he said, despite their exposure to upsetting imagery. This suggests an important avenue for research – understanding what makes some people resilient, even in the face of graphic and disturbing stressors.
A version of this story originally appeared on Medscape.com.
The images are graphic, disturbing, and endless, said a former Facebook employee. Her job as a content moderator required that she review and remove disturbing posts. That work, she claimed in a lawsuit, caused her to suffer serious psychological trauma.
In September 2018, she filed a complaint with the Superior Court of California.
“Every day, Facebook users post millions of videos, images, and livestream broadcasts of child sexual abuse, rape, torture, bestiality, beheadings, suicide, and murder,” reads the complaint. “By requiring its content moderators to work in dangerous conditions that cause debilitating physical and psychological harm, Facebook violates California law.”
In May, Facebook settled the case, agreeing to pay $52 million to content moderators to compensate them for the consequences their work had on their mental health. The settlement was the first to officially recognize the psychological toll of exposure to disturbing material resulting from online moderator jobs. It also highlights an emerging understanding of vicarious trauma.
Also known as secondary trauma, vicarious trauma can result from exposure to images, stories, or accounts that someone does not directly experience, said Françoise Mathieu, MEd, CCC, RP, a compassion fatigue specialist and executive director of TEND, a company in Kingston, Ont., that offers resources and training for people who work in high-stress, trauma-exposed workplaces.
Secondary trauma can affect people much as any other kind of intensely stressful experience. “What I can tell you as a specialist is that trauma is trauma,” Mathieu said. “Our brain doesn’t necessarily know the difference.”
The potential for vicarious trauma has long been recognized as a risk for journalists, health care providers, and anyone who watches television coverage of a disaster. Only recently, Mathieu said, have researchers started to investigate the psychological impact of jobs that require people to look at extreme, graphic, or disturbing images.
Physical fallout
In a 2017 study of digital forensic examiners, researchers found that examiners who worked on cases involving sexual crimes against children were at elevated risk of developing secondary trauma.
However, the exploratory study did not quantify the risks, and the study investigators concluded that more research is needed to understand how best to help people deal with PTSD resulting from working in the criminal justice system.
Content moderation requires sifting through upsetting images, and people can react in different ways to the task, says Anthony Ng, MD, a psychiatrist at Hartford (Conn.) Healthcare in Mansfield Center.
Dr. Ng says some individuals may become emotionally numb in order to protect themselves. Others might relate to what they are seeing, either because of their own life circumstances or because of experiences they have had in the past. For example, individuals might think: “I could see that kid being my son, I could see that woman who was assaulted as my wife who got beaten up”
that ramps up activity in an area of the brain called the locus coeruleus, Dr. Ng said.
Heart rate rises. Breathing rate goes up. Muscles become tense. If a threat occurs once and then dissipates, the body can often recover a state of calm. However, when that threat is part of the daily workday, it can cause chronic harm to mental and physical health. Unlike with direct, or primary, trauma, he adds, secondary trauma can take a while to become symptomatic.
“Your heart is not designed to be constantly pumping at a high rate,” Dr. Ng says. “We just can’t sustain that for long periods of time without starting to develop stress reactions.”
Under the radar
Some types of work appear to confer greater risk for trauma than others. Overall, estimates show that up to 8% of the U.S. population will develop PTSD at some point in their lives, Ms. Mathieu said.
For police officers, the rate is 15%. According to reporting by The Verge, lawyers in the Facebook lawsuit cited vicarious trauma rates of up to 50% among content moderators.
There are multiple reasons why content moderators suffer such high rates of mental health problems, Ms. Mathieu said. Content moderation is a low-paying, thankless, and solo job that can seem never-ending, she said.
Furthermore, content moderators are generally uninformed about the psychological risks associated with their occupation. They aren’t given the time to process what they are exposed to and generally don’t feel recognized or appreciated for the work they do.
That makes their jobs different from those of people such as law enforcement officers who investigate Internet crimes. For people pursuing justice, a sense of unity can counterbalance the exposure to tough imagery and information.
Going forward, Ms. Mathieu said, the only way to make content moderation safer is to institute changes such as better pay, more flexible schedules to allow breaks from exposure, and access to mental health professionals who can help employees process what they have seen.
Climate of fear
“This can’t be a climate of fear where people are afraid to ask for help,” Ms. Mathieu said. “They are really important jobs, but people need to feel that they are safe in expressing when it’s impacting them so that they’re not worried that they’re actually going to lose their work.”
It would help if content moderators received evidence-based guidance to help process their experiences, Ms. Mathieu added. However, to avoid doing more harm than good, debriefing has to be administered correctly.
For example, a method called “critical incident stress debriefing,” a longstanding approach that research has shown can do more harm than good, is still widely used in law enforcement agencies. The technique requires individuals to talk about their traumatic experience immediately after it happens, which can cause retraumatization.
Instead, Dr. Ng recommended a more self-aware approach called low-impact debriefing. The method involves strategies such as giving fair warning, asking for consent from listeners, and being selective about the details shared.
Employees should also be taught to recognize and report early signs and symptoms so that they can seek help before psychological distress becomes overwhelming, Dr. Ng says.
Plenty of moderators do not develop PTSD, he said, despite their exposure to upsetting imagery. This suggests an important avenue for research – understanding what makes some people resilient, even in the face of graphic and disturbing stressors.
A version of this story originally appeared on Medscape.com.
COVID-19 diagnosed on CTA scan in stroke patients
A routine scan used to evaluate some acute stroke patients can also detect SARS-CoV-2 infection in the upper lungs, a new study shows.
“As part of the stroke evaluation workup process, we were able to diagnose COVID-19 at the same time at no extra cost or additional workload,” lead author Charles Esenwa, MD, commented to Medscape Medical News. “This is an objective way to screen for COVID-19 in the acute stroke setting,” he added.
Esenwa is an assistant professor and a stroke neurologist at the Montefiore Medical Center/Albert Einstein College of Medicine in New York City.
He explained that, during the COVID-19 surge earlier this year, assessment of patients with severe acute stroke using computed tomography angiogram (CTA) scans – used to evaluate suitability for endovascular stroke therapy – also showed findings in the upper lung consistent with viral infection in some patients.
“We then assumed that these patients had COVID-19 and took extra precautions to keep them isolated and to protect staff involved in their care. It also allowed us to triage these patients more quickly than waiting for the COVID-19 swab test and arrange the most appropriate care for them,” Esenwa said.
The researchers have now gone back and analyzed their data on acute stroke patients who underwent CTA at their institution during the COVID-19 surge. They found that the changes identified in the lungs were highly specific for diagnosing SARS-CoV-2 infection.
The study was published online on Oct. 29 in Stroke.
“Stroke patients are normally screened for COVID-19 on hospitalization, but the swab test result can take several hours or longer to come back, and it is very useful for us to know if a patient could be infected,” Esenwa noted.
“When we do a CTA, we look at the blood vessels supplying the brain, but the scan also covers the top of the lung, as it starts at the aortic arch. We don’t normally look closely at that area, but we started to notice signs of active lung infection which could have been COVID-19,” he said. “For this paper, we went back to assess how accurate this approach actually was vs. the COVID-19 PCR test.”
The researchers report on 57 patients who presented to three Montefiore Health System hospitals in the Bronx, in New York City, with acute ischemic stroke and who underwent CTA of the head and neck in March and April 2020, the peak of the COVID-19 outbreak there. The patients also underwent PCR testing for COVID-19.
Results showed that 30 patients had a positive COVID-19 test result and that 27 had a negative result. Lung findings highly or very highly suspicious for COVID-19 pneumonia were identified during the CTA scan in 20 (67%) of the COVID-19–positive patients and in two (7%) of the COVID-19–negative patients.
These findings, when used in isolation, yielded a sensitivity of 0.67 and a specificity of 0.93. They had a positive predictive value of 0.19, a negative predictive value of 0.99, and accuracy of 0.92 for the diagnosis of COVID-19.
When apical lung assessment was combined with self-reported clinical symptoms of cough or dyspnea, sensitivity for the diagnosis of COVID-19 for patients presenting to the hospital for acute ischemic stroke increased to 0.83.
“We wondered whether looking at the whole lung would have found better results, but other studies which have done this actually found similar numbers to ours, so we think actually just looking at the top of the lungs, which can be seen in a stroke CTA, may be sufficient,” Esenwa said.
He emphasized the importance of establishing whether an acute stroke patient has COVID-19. “If we had a high suspicion of COVID-19 infection, we would take more precautions during any procedures, such as thrombectomy, and make sure to keep the patient isolated afterwards. It doesn’t necessarily affect the treatment given for stroke, but it affects the safety of the patients and everyone caring for them,” he commented.
Esenwa explained that intubation – which is sometime necessary during thrombectomy – can expose everyone in the room to aerosolized droplets. “So we would take much higher safety precautions if we thought the patient was COVID-19 positive,” he said.
“Early COVID-19 diagnosis also means patients can be given supportive treatment more quickly, admitted to ICU if appropriate, and we can all keep a close eye on pulmonary issues. So having that information is important in many ways,” he added.
Esenwa advises that any medical center that evaluates acute stroke patients for thrombectomy and is experiencing a COVID-19 surge can use this technique as a screening method for COVID-19.
He pointed out that the Montefiore Health System had a very high rate of COVID-19. That part of New York City was one of the worst hit areas of the world, and the CTA approach for identifying COVID-19 has been validated only in areas with such a high local incidence of COVID. If used in an area of lower prevalence, the accuracy would likely be less.
“We don’t know if this approach would work as well at times of low COVID-19 infection, where any lung findings would be more likely to be caused by other conditions, such as pneumonia due to other causes or congestive heart failure. So there would be more false positives,” Esenwa said.
“But when COVID-19 prevalence is high, the lung findings are much more likely to be a sign of COVID-19 infection. As COVID-19 numbers are now rising for a second time, it is likely to become a useful strategy again.”
The study was approved by the Albert Einstein College of Medicine/Montefiore Medical Center Institutional Review Board and had no external funding. Esenwa has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
A routine scan used to evaluate some acute stroke patients can also detect SARS-CoV-2 infection in the upper lungs, a new study shows.
“As part of the stroke evaluation workup process, we were able to diagnose COVID-19 at the same time at no extra cost or additional workload,” lead author Charles Esenwa, MD, commented to Medscape Medical News. “This is an objective way to screen for COVID-19 in the acute stroke setting,” he added.
Esenwa is an assistant professor and a stroke neurologist at the Montefiore Medical Center/Albert Einstein College of Medicine in New York City.
He explained that, during the COVID-19 surge earlier this year, assessment of patients with severe acute stroke using computed tomography angiogram (CTA) scans – used to evaluate suitability for endovascular stroke therapy – also showed findings in the upper lung consistent with viral infection in some patients.
“We then assumed that these patients had COVID-19 and took extra precautions to keep them isolated and to protect staff involved in their care. It also allowed us to triage these patients more quickly than waiting for the COVID-19 swab test and arrange the most appropriate care for them,” Esenwa said.
The researchers have now gone back and analyzed their data on acute stroke patients who underwent CTA at their institution during the COVID-19 surge. They found that the changes identified in the lungs were highly specific for diagnosing SARS-CoV-2 infection.
The study was published online on Oct. 29 in Stroke.
“Stroke patients are normally screened for COVID-19 on hospitalization, but the swab test result can take several hours or longer to come back, and it is very useful for us to know if a patient could be infected,” Esenwa noted.
“When we do a CTA, we look at the blood vessels supplying the brain, but the scan also covers the top of the lung, as it starts at the aortic arch. We don’t normally look closely at that area, but we started to notice signs of active lung infection which could have been COVID-19,” he said. “For this paper, we went back to assess how accurate this approach actually was vs. the COVID-19 PCR test.”
The researchers report on 57 patients who presented to three Montefiore Health System hospitals in the Bronx, in New York City, with acute ischemic stroke and who underwent CTA of the head and neck in March and April 2020, the peak of the COVID-19 outbreak there. The patients also underwent PCR testing for COVID-19.
Results showed that 30 patients had a positive COVID-19 test result and that 27 had a negative result. Lung findings highly or very highly suspicious for COVID-19 pneumonia were identified during the CTA scan in 20 (67%) of the COVID-19–positive patients and in two (7%) of the COVID-19–negative patients.
These findings, when used in isolation, yielded a sensitivity of 0.67 and a specificity of 0.93. They had a positive predictive value of 0.19, a negative predictive value of 0.99, and accuracy of 0.92 for the diagnosis of COVID-19.
When apical lung assessment was combined with self-reported clinical symptoms of cough or dyspnea, sensitivity for the diagnosis of COVID-19 for patients presenting to the hospital for acute ischemic stroke increased to 0.83.
“We wondered whether looking at the whole lung would have found better results, but other studies which have done this actually found similar numbers to ours, so we think actually just looking at the top of the lungs, which can be seen in a stroke CTA, may be sufficient,” Esenwa said.
He emphasized the importance of establishing whether an acute stroke patient has COVID-19. “If we had a high suspicion of COVID-19 infection, we would take more precautions during any procedures, such as thrombectomy, and make sure to keep the patient isolated afterwards. It doesn’t necessarily affect the treatment given for stroke, but it affects the safety of the patients and everyone caring for them,” he commented.
Esenwa explained that intubation – which is sometime necessary during thrombectomy – can expose everyone in the room to aerosolized droplets. “So we would take much higher safety precautions if we thought the patient was COVID-19 positive,” he said.
“Early COVID-19 diagnosis also means patients can be given supportive treatment more quickly, admitted to ICU if appropriate, and we can all keep a close eye on pulmonary issues. So having that information is important in many ways,” he added.
Esenwa advises that any medical center that evaluates acute stroke patients for thrombectomy and is experiencing a COVID-19 surge can use this technique as a screening method for COVID-19.
He pointed out that the Montefiore Health System had a very high rate of COVID-19. That part of New York City was one of the worst hit areas of the world, and the CTA approach for identifying COVID-19 has been validated only in areas with such a high local incidence of COVID. If used in an area of lower prevalence, the accuracy would likely be less.
“We don’t know if this approach would work as well at times of low COVID-19 infection, where any lung findings would be more likely to be caused by other conditions, such as pneumonia due to other causes or congestive heart failure. So there would be more false positives,” Esenwa said.
“But when COVID-19 prevalence is high, the lung findings are much more likely to be a sign of COVID-19 infection. As COVID-19 numbers are now rising for a second time, it is likely to become a useful strategy again.”
The study was approved by the Albert Einstein College of Medicine/Montefiore Medical Center Institutional Review Board and had no external funding. Esenwa has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
A routine scan used to evaluate some acute stroke patients can also detect SARS-CoV-2 infection in the upper lungs, a new study shows.
“As part of the stroke evaluation workup process, we were able to diagnose COVID-19 at the same time at no extra cost or additional workload,” lead author Charles Esenwa, MD, commented to Medscape Medical News. “This is an objective way to screen for COVID-19 in the acute stroke setting,” he added.
Esenwa is an assistant professor and a stroke neurologist at the Montefiore Medical Center/Albert Einstein College of Medicine in New York City.
He explained that, during the COVID-19 surge earlier this year, assessment of patients with severe acute stroke using computed tomography angiogram (CTA) scans – used to evaluate suitability for endovascular stroke therapy – also showed findings in the upper lung consistent with viral infection in some patients.
“We then assumed that these patients had COVID-19 and took extra precautions to keep them isolated and to protect staff involved in their care. It also allowed us to triage these patients more quickly than waiting for the COVID-19 swab test and arrange the most appropriate care for them,” Esenwa said.
The researchers have now gone back and analyzed their data on acute stroke patients who underwent CTA at their institution during the COVID-19 surge. They found that the changes identified in the lungs were highly specific for diagnosing SARS-CoV-2 infection.
The study was published online on Oct. 29 in Stroke.
“Stroke patients are normally screened for COVID-19 on hospitalization, but the swab test result can take several hours or longer to come back, and it is very useful for us to know if a patient could be infected,” Esenwa noted.
“When we do a CTA, we look at the blood vessels supplying the brain, but the scan also covers the top of the lung, as it starts at the aortic arch. We don’t normally look closely at that area, but we started to notice signs of active lung infection which could have been COVID-19,” he said. “For this paper, we went back to assess how accurate this approach actually was vs. the COVID-19 PCR test.”
The researchers report on 57 patients who presented to three Montefiore Health System hospitals in the Bronx, in New York City, with acute ischemic stroke and who underwent CTA of the head and neck in March and April 2020, the peak of the COVID-19 outbreak there. The patients also underwent PCR testing for COVID-19.
Results showed that 30 patients had a positive COVID-19 test result and that 27 had a negative result. Lung findings highly or very highly suspicious for COVID-19 pneumonia were identified during the CTA scan in 20 (67%) of the COVID-19–positive patients and in two (7%) of the COVID-19–negative patients.
These findings, when used in isolation, yielded a sensitivity of 0.67 and a specificity of 0.93. They had a positive predictive value of 0.19, a negative predictive value of 0.99, and accuracy of 0.92 for the diagnosis of COVID-19.
When apical lung assessment was combined with self-reported clinical symptoms of cough or dyspnea, sensitivity for the diagnosis of COVID-19 for patients presenting to the hospital for acute ischemic stroke increased to 0.83.
“We wondered whether looking at the whole lung would have found better results, but other studies which have done this actually found similar numbers to ours, so we think actually just looking at the top of the lungs, which can be seen in a stroke CTA, may be sufficient,” Esenwa said.
He emphasized the importance of establishing whether an acute stroke patient has COVID-19. “If we had a high suspicion of COVID-19 infection, we would take more precautions during any procedures, such as thrombectomy, and make sure to keep the patient isolated afterwards. It doesn’t necessarily affect the treatment given for stroke, but it affects the safety of the patients and everyone caring for them,” he commented.
Esenwa explained that intubation – which is sometime necessary during thrombectomy – can expose everyone in the room to aerosolized droplets. “So we would take much higher safety precautions if we thought the patient was COVID-19 positive,” he said.
“Early COVID-19 diagnosis also means patients can be given supportive treatment more quickly, admitted to ICU if appropriate, and we can all keep a close eye on pulmonary issues. So having that information is important in many ways,” he added.
Esenwa advises that any medical center that evaluates acute stroke patients for thrombectomy and is experiencing a COVID-19 surge can use this technique as a screening method for COVID-19.
He pointed out that the Montefiore Health System had a very high rate of COVID-19. That part of New York City was one of the worst hit areas of the world, and the CTA approach for identifying COVID-19 has been validated only in areas with such a high local incidence of COVID. If used in an area of lower prevalence, the accuracy would likely be less.
“We don’t know if this approach would work as well at times of low COVID-19 infection, where any lung findings would be more likely to be caused by other conditions, such as pneumonia due to other causes or congestive heart failure. So there would be more false positives,” Esenwa said.
“But when COVID-19 prevalence is high, the lung findings are much more likely to be a sign of COVID-19 infection. As COVID-19 numbers are now rising for a second time, it is likely to become a useful strategy again.”
The study was approved by the Albert Einstein College of Medicine/Montefiore Medical Center Institutional Review Board and had no external funding. Esenwa has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
More mask wearing could save 130,000 US lives by end of February
A cumulative 511,000 lives could be lost from COVID-19 in the United States by the end of February 2021, a new prediction study reveals.
However, if universal mask wearing is adopted — defined as 95% of Americans complying with the protective measure — along with social distancing mandates as warranted, nearly 130,000 of those lives could be saved.
And if even 85% of Americans comply, an additional 95,800 lives would be spared before March of next year, researchers at the University of Washington Institute for Health Metrics and Evaluation (IHME) report.
The study was published online October 23 in Nature Medicine.
“The study is sound and makes the case for mandatory mask policies,” said Arthur L. Caplan, PhD, a professor of bioethics at NYU Langone Health in New York City, who frequently provides commentary for Medscape.
Without mandatory mask requirements, he added, “we will see a pandemic slaughter and an overwhelmed healthcare system and workforce.”
The IHME team evaluated COVID-19 data for cases and related deaths between February 1 and September 21. Based on this data, they predicted the likely future of SARS-CoV-2 infections on a state level from September 22, 2020, to February 2021.
An Optimistic Projection
Lead author Robert C. Reiner Jr and colleagues looked at five scenarios. For example, they calculated likely deaths associated with COVID-19 if adoption of mask and social distancing recommendations were nearly universal. They note that Singapore achieved a 95% compliance rate with masks and used this as their “best-case scenario” model.
An estimated 129,574 (range, 85,284–170,867) additional lives could be saved if 95% of Americans wore masks in public, their research reveals. This optimistic scenario includes a “plausible reference” in which any US state reaching 8 COVID-19 deaths per 1 million residents would enact 6 weeks of social distancing mandates (SDMs).
Achieving this level of mask compliance in the United States “could be sufficient to ameliorate the worst effects of epidemic resurgences in many states,” the researchers note.
In contrast, the proportion of Americans wearing masks in public as of September 22 was 49%, according to IHME data.
Universal mask use unlikely
“I’m not a modeling expert, but it is an interesting, and as far as I can judge, well-conducted study which looks, state by state, at what might happen in various scenarios around masking policies going forward — and in particular the effect that mandated masking might have,” Trish Greenhalgh, MD, told Medscape Medical News.
“However, the scenario is a thought experiment. Near-universal mask use is not going to happen in the USA, nor indeed in any individual state, right now, given how emotive the issue has become,” added Greenhalgh, professor in the Nuffield Department of Primary Care Health Sciences at Oxford University, UK. She was not affiliated with the study.
“Hence, whilst I am broadly supportive of the science,” she said, “I’m not confident that this paper will be able to change policy.”
Other ‘What if?’ scenarios
The authors also predicted the mortality implications associated with lower adherence to masks, the presence or absence of SDMs, and what could happen if mandates continue to ease at their current rate.
For example, they considered a scenario with less-than-universal mask use in public, 85%, along with SDMs being reinstated based on the mortality rate threshold. In this instance, they found an additional 95,814 (range, 60,731–133,077) lives could be spared by February 28.
Another calculation looked at outcomes if 95% of Americans wore masks going forward without states instituting SDMs at any point. In this case, the researchers predict that 490,437 Americans would die from COVID-19 by February 2021.
A fourth analysis revealed what would happen without greater mask use if the mortality threshold triggered 6 weeks of SDMs as warranted. Under this ‘plausible reference’ calculation, a total 511,373 Americans would die from COVID-19 by the end of February.
A fifth scenario predicted potential mortality if states continue easing SDMs at the current pace. “This is an alternative scenario to the more probable situation where states are expected to respond to an impending health crisis by reinstating some SDMs,” the authors note. The predicted number of American deaths appears more dire in this calculation. The investigators predict cumulative total deaths could reach 1,053,206 (range, 759,693–1,452,397) by the end of February 2021.
The death toll would likely vary among states in this scenario. California, Florida, and Pennsylvania would like account for approximately one third of all deaths.
All the modeling scenarios considered other factors including pneumonia seasonality, mobility, testing rates, and mask use per capita.
“I have seen the IHME study and I agree with the broad conclusions,” Richard Stutt, PhD, of the Epidemiology and Modelling Group at the University of Cambridge, UK, told Medscape Medical News.
“Case numbers are climbing in the US, and without further intervention, there will be a significant number of deaths over the coming months,” he said.
Masks are low cost and widely available, Stutt said. “I am hopeful that even if masks are not widely adopted, we will not see as many deaths as predicted here, as these outbreaks can be significantly reduced by increased social distancing or lockdowns.”
“However this comes at a far higher economic cost than the use of masks, and still requires action,” added Stutt, who authored a study in June that modeled facemasks in combination with “lock-down” measures for managing the COVID-19 pandemic.
Modeling study results depend on the assumptions researchers make, and the IHME team rightly tested a number of different assumptions, Greenhalgh said.
“The key conclusion,” she added, “is here: ‘The implementation of SDMs as soon as individual states reach a threshold of 8 daily deaths per million could dramatically ameliorate the effects of the disease; achieving near-universal mask use could delay, or in many states, possibly prevent, this threshold from being reached and has the potential to save the most lives while minimizing damage to the economy.’ “
“This is a useful piece of information and I think is borne out by their data,” added Greenhalgh, lead author of an April study on face masks for the public during the pandemic.
You can visit the IHME website for the most current mortality projections.
Caplan, Greenhalgh, and Stutt have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
A cumulative 511,000 lives could be lost from COVID-19 in the United States by the end of February 2021, a new prediction study reveals.
However, if universal mask wearing is adopted — defined as 95% of Americans complying with the protective measure — along with social distancing mandates as warranted, nearly 130,000 of those lives could be saved.
And if even 85% of Americans comply, an additional 95,800 lives would be spared before March of next year, researchers at the University of Washington Institute for Health Metrics and Evaluation (IHME) report.
The study was published online October 23 in Nature Medicine.
“The study is sound and makes the case for mandatory mask policies,” said Arthur L. Caplan, PhD, a professor of bioethics at NYU Langone Health in New York City, who frequently provides commentary for Medscape.
Without mandatory mask requirements, he added, “we will see a pandemic slaughter and an overwhelmed healthcare system and workforce.”
The IHME team evaluated COVID-19 data for cases and related deaths between February 1 and September 21. Based on this data, they predicted the likely future of SARS-CoV-2 infections on a state level from September 22, 2020, to February 2021.
An Optimistic Projection
Lead author Robert C. Reiner Jr and colleagues looked at five scenarios. For example, they calculated likely deaths associated with COVID-19 if adoption of mask and social distancing recommendations were nearly universal. They note that Singapore achieved a 95% compliance rate with masks and used this as their “best-case scenario” model.
An estimated 129,574 (range, 85,284–170,867) additional lives could be saved if 95% of Americans wore masks in public, their research reveals. This optimistic scenario includes a “plausible reference” in which any US state reaching 8 COVID-19 deaths per 1 million residents would enact 6 weeks of social distancing mandates (SDMs).
Achieving this level of mask compliance in the United States “could be sufficient to ameliorate the worst effects of epidemic resurgences in many states,” the researchers note.
In contrast, the proportion of Americans wearing masks in public as of September 22 was 49%, according to IHME data.
Universal mask use unlikely
“I’m not a modeling expert, but it is an interesting, and as far as I can judge, well-conducted study which looks, state by state, at what might happen in various scenarios around masking policies going forward — and in particular the effect that mandated masking might have,” Trish Greenhalgh, MD, told Medscape Medical News.
“However, the scenario is a thought experiment. Near-universal mask use is not going to happen in the USA, nor indeed in any individual state, right now, given how emotive the issue has become,” added Greenhalgh, professor in the Nuffield Department of Primary Care Health Sciences at Oxford University, UK. She was not affiliated with the study.
“Hence, whilst I am broadly supportive of the science,” she said, “I’m not confident that this paper will be able to change policy.”
Other ‘What if?’ scenarios
The authors also predicted the mortality implications associated with lower adherence to masks, the presence or absence of SDMs, and what could happen if mandates continue to ease at their current rate.
For example, they considered a scenario with less-than-universal mask use in public, 85%, along with SDMs being reinstated based on the mortality rate threshold. In this instance, they found an additional 95,814 (range, 60,731–133,077) lives could be spared by February 28.
Another calculation looked at outcomes if 95% of Americans wore masks going forward without states instituting SDMs at any point. In this case, the researchers predict that 490,437 Americans would die from COVID-19 by February 2021.
A fourth analysis revealed what would happen without greater mask use if the mortality threshold triggered 6 weeks of SDMs as warranted. Under this ‘plausible reference’ calculation, a total 511,373 Americans would die from COVID-19 by the end of February.
A fifth scenario predicted potential mortality if states continue easing SDMs at the current pace. “This is an alternative scenario to the more probable situation where states are expected to respond to an impending health crisis by reinstating some SDMs,” the authors note. The predicted number of American deaths appears more dire in this calculation. The investigators predict cumulative total deaths could reach 1,053,206 (range, 759,693–1,452,397) by the end of February 2021.
The death toll would likely vary among states in this scenario. California, Florida, and Pennsylvania would like account for approximately one third of all deaths.
All the modeling scenarios considered other factors including pneumonia seasonality, mobility, testing rates, and mask use per capita.
“I have seen the IHME study and I agree with the broad conclusions,” Richard Stutt, PhD, of the Epidemiology and Modelling Group at the University of Cambridge, UK, told Medscape Medical News.
“Case numbers are climbing in the US, and without further intervention, there will be a significant number of deaths over the coming months,” he said.
Masks are low cost and widely available, Stutt said. “I am hopeful that even if masks are not widely adopted, we will not see as many deaths as predicted here, as these outbreaks can be significantly reduced by increased social distancing or lockdowns.”
“However this comes at a far higher economic cost than the use of masks, and still requires action,” added Stutt, who authored a study in June that modeled facemasks in combination with “lock-down” measures for managing the COVID-19 pandemic.
Modeling study results depend on the assumptions researchers make, and the IHME team rightly tested a number of different assumptions, Greenhalgh said.
“The key conclusion,” she added, “is here: ‘The implementation of SDMs as soon as individual states reach a threshold of 8 daily deaths per million could dramatically ameliorate the effects of the disease; achieving near-universal mask use could delay, or in many states, possibly prevent, this threshold from being reached and has the potential to save the most lives while minimizing damage to the economy.’ “
“This is a useful piece of information and I think is borne out by their data,” added Greenhalgh, lead author of an April study on face masks for the public during the pandemic.
You can visit the IHME website for the most current mortality projections.
Caplan, Greenhalgh, and Stutt have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
A cumulative 511,000 lives could be lost from COVID-19 in the United States by the end of February 2021, a new prediction study reveals.
However, if universal mask wearing is adopted — defined as 95% of Americans complying with the protective measure — along with social distancing mandates as warranted, nearly 130,000 of those lives could be saved.
And if even 85% of Americans comply, an additional 95,800 lives would be spared before March of next year, researchers at the University of Washington Institute for Health Metrics and Evaluation (IHME) report.
The study was published online October 23 in Nature Medicine.
“The study is sound and makes the case for mandatory mask policies,” said Arthur L. Caplan, PhD, a professor of bioethics at NYU Langone Health in New York City, who frequently provides commentary for Medscape.
Without mandatory mask requirements, he added, “we will see a pandemic slaughter and an overwhelmed healthcare system and workforce.”
The IHME team evaluated COVID-19 data for cases and related deaths between February 1 and September 21. Based on this data, they predicted the likely future of SARS-CoV-2 infections on a state level from September 22, 2020, to February 2021.
An Optimistic Projection
Lead author Robert C. Reiner Jr and colleagues looked at five scenarios. For example, they calculated likely deaths associated with COVID-19 if adoption of mask and social distancing recommendations were nearly universal. They note that Singapore achieved a 95% compliance rate with masks and used this as their “best-case scenario” model.
An estimated 129,574 (range, 85,284–170,867) additional lives could be saved if 95% of Americans wore masks in public, their research reveals. This optimistic scenario includes a “plausible reference” in which any US state reaching 8 COVID-19 deaths per 1 million residents would enact 6 weeks of social distancing mandates (SDMs).
Achieving this level of mask compliance in the United States “could be sufficient to ameliorate the worst effects of epidemic resurgences in many states,” the researchers note.
In contrast, the proportion of Americans wearing masks in public as of September 22 was 49%, according to IHME data.
Universal mask use unlikely
“I’m not a modeling expert, but it is an interesting, and as far as I can judge, well-conducted study which looks, state by state, at what might happen in various scenarios around masking policies going forward — and in particular the effect that mandated masking might have,” Trish Greenhalgh, MD, told Medscape Medical News.
“However, the scenario is a thought experiment. Near-universal mask use is not going to happen in the USA, nor indeed in any individual state, right now, given how emotive the issue has become,” added Greenhalgh, professor in the Nuffield Department of Primary Care Health Sciences at Oxford University, UK. She was not affiliated with the study.
“Hence, whilst I am broadly supportive of the science,” she said, “I’m not confident that this paper will be able to change policy.”
Other ‘What if?’ scenarios
The authors also predicted the mortality implications associated with lower adherence to masks, the presence or absence of SDMs, and what could happen if mandates continue to ease at their current rate.
For example, they considered a scenario with less-than-universal mask use in public, 85%, along with SDMs being reinstated based on the mortality rate threshold. In this instance, they found an additional 95,814 (range, 60,731–133,077) lives could be spared by February 28.
Another calculation looked at outcomes if 95% of Americans wore masks going forward without states instituting SDMs at any point. In this case, the researchers predict that 490,437 Americans would die from COVID-19 by February 2021.
A fourth analysis revealed what would happen without greater mask use if the mortality threshold triggered 6 weeks of SDMs as warranted. Under this ‘plausible reference’ calculation, a total 511,373 Americans would die from COVID-19 by the end of February.
A fifth scenario predicted potential mortality if states continue easing SDMs at the current pace. “This is an alternative scenario to the more probable situation where states are expected to respond to an impending health crisis by reinstating some SDMs,” the authors note. The predicted number of American deaths appears more dire in this calculation. The investigators predict cumulative total deaths could reach 1,053,206 (range, 759,693–1,452,397) by the end of February 2021.
The death toll would likely vary among states in this scenario. California, Florida, and Pennsylvania would like account for approximately one third of all deaths.
All the modeling scenarios considered other factors including pneumonia seasonality, mobility, testing rates, and mask use per capita.
“I have seen the IHME study and I agree with the broad conclusions,” Richard Stutt, PhD, of the Epidemiology and Modelling Group at the University of Cambridge, UK, told Medscape Medical News.
“Case numbers are climbing in the US, and without further intervention, there will be a significant number of deaths over the coming months,” he said.
Masks are low cost and widely available, Stutt said. “I am hopeful that even if masks are not widely adopted, we will not see as many deaths as predicted here, as these outbreaks can be significantly reduced by increased social distancing or lockdowns.”
“However this comes at a far higher economic cost than the use of masks, and still requires action,” added Stutt, who authored a study in June that modeled facemasks in combination with “lock-down” measures for managing the COVID-19 pandemic.
Modeling study results depend on the assumptions researchers make, and the IHME team rightly tested a number of different assumptions, Greenhalgh said.
“The key conclusion,” she added, “is here: ‘The implementation of SDMs as soon as individual states reach a threshold of 8 daily deaths per million could dramatically ameliorate the effects of the disease; achieving near-universal mask use could delay, or in many states, possibly prevent, this threshold from being reached and has the potential to save the most lives while minimizing damage to the economy.’ “
“This is a useful piece of information and I think is borne out by their data,” added Greenhalgh, lead author of an April study on face masks for the public during the pandemic.
You can visit the IHME website for the most current mortality projections.
Caplan, Greenhalgh, and Stutt have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.