User login
Newly approved tirzepatide’s retail price announced
Tirzepatide (Mounjaro) – the new twincretin approved by the Food and Drug Administration for glycemic control in patients with type 2 diabetes – was priced by Lilly, the company that will market the drug, at a list price of $974.33 for four weekly doses regardless of dose size, a cost that adds up to about $12,666 per year, according to a statement made on May 20 by a Lilly spokesperson.
This price puts tirzepatide, which combines the activity of two of the primary human incretins in one molecule, roughly in the same ballpark as what might be its main competitor, semaglutide (Ozempic) for type 2 diabetes, which retails at many U.S. pharmacies for about $925 for four weekly doses, or about $12,025 per year, although Ozempic’s posted retail price is about $100 higher for four doses.
According to the Lilly spokesperson, discount programs could reduce the monthly out-of-pocket cost for patients to as little as $25.
Tirzepatide, which received approval from the FDA on May 13, is a dual glucagonlike peptide–1 (GLP-1) receptor agonist and glucose-dependent insulinotropic polypeptide agonist. Several GLP-1 receptor agonists are already approved in the United States, including semaglutide, which is indicated as Wegovy for weight loss in patients with obesity regardless of diabetes status.
A version of this article first appeared on Medscape.com.
Tirzepatide (Mounjaro) – the new twincretin approved by the Food and Drug Administration for glycemic control in patients with type 2 diabetes – was priced by Lilly, the company that will market the drug, at a list price of $974.33 for four weekly doses regardless of dose size, a cost that adds up to about $12,666 per year, according to a statement made on May 20 by a Lilly spokesperson.
This price puts tirzepatide, which combines the activity of two of the primary human incretins in one molecule, roughly in the same ballpark as what might be its main competitor, semaglutide (Ozempic) for type 2 diabetes, which retails at many U.S. pharmacies for about $925 for four weekly doses, or about $12,025 per year, although Ozempic’s posted retail price is about $100 higher for four doses.
According to the Lilly spokesperson, discount programs could reduce the monthly out-of-pocket cost for patients to as little as $25.
Tirzepatide, which received approval from the FDA on May 13, is a dual glucagonlike peptide–1 (GLP-1) receptor agonist and glucose-dependent insulinotropic polypeptide agonist. Several GLP-1 receptor agonists are already approved in the United States, including semaglutide, which is indicated as Wegovy for weight loss in patients with obesity regardless of diabetes status.
A version of this article first appeared on Medscape.com.
Tirzepatide (Mounjaro) – the new twincretin approved by the Food and Drug Administration for glycemic control in patients with type 2 diabetes – was priced by Lilly, the company that will market the drug, at a list price of $974.33 for four weekly doses regardless of dose size, a cost that adds up to about $12,666 per year, according to a statement made on May 20 by a Lilly spokesperson.
This price puts tirzepatide, which combines the activity of two of the primary human incretins in one molecule, roughly in the same ballpark as what might be its main competitor, semaglutide (Ozempic) for type 2 diabetes, which retails at many U.S. pharmacies for about $925 for four weekly doses, or about $12,025 per year, although Ozempic’s posted retail price is about $100 higher for four doses.
According to the Lilly spokesperson, discount programs could reduce the monthly out-of-pocket cost for patients to as little as $25.
Tirzepatide, which received approval from the FDA on May 13, is a dual glucagonlike peptide–1 (GLP-1) receptor agonist and glucose-dependent insulinotropic polypeptide agonist. Several GLP-1 receptor agonists are already approved in the United States, including semaglutide, which is indicated as Wegovy for weight loss in patients with obesity regardless of diabetes status.
A version of this article first appeared on Medscape.com.
Third-generation Black woman physician makes cancer research history
When Jane Cooke Wright, MD, entered the medical profession in 1945, the notion that toxic drugs could target tumors struck many physicians and patients as outlandish. How could one poison be weaponized against another poison – a cancerous tumor – without creating more havoc? Let alone a combination of two or more chemicals?
Dr. Wright’s story would be extraordinary enough if she’d looked like most of her colleagues, but this surgeon and researcher stood apart. An African American woman at a time when medicine and science – like politics and law – were almost entirely the domain of White men, Dr. Wright had determination in her blood. Her father, once honored by a crowd of dignitaries that included a First Lady, persevered despite his horrific encounters with racism. She shared her father’s commitment to progress and added her own personal twists. She balanced elegance and beauty with scientific savvy, fierce ambition, and a refusal to be defined by anything other than her accomplishments.
“She didn’t focus on race, not at all,” her daughter Alison Jones, PhD, a psychologist in East Lansing, Mich., said in an interview. “Wherever she was, she wanted to be the best, not the best Black person. It was not about how she performed in a category, and she would get upset if someone said she was good as a Black physician.”
On the road to being the best, Dr. Jones said, her mother set a goal of curing cancer. National Cancer Research Month is a fitting opportunity to look back on a scientist dedicated to bringing humanity closer to that elusive achievement.
Medical legacy blazed in toil and trauma
A strong case could be made that Dr. Jane C. Wright and her father Louis Tompkins Wright, MD, are the most accomplished father-and-daughter team in all of medicine.
The elder Dr. Wright, son of a formerly enslaved man turned physician and a stepson of the first African American to graduate from Yale University, New Haven, Conn., himself graduated from Harvard Medical School in 1915. He earned a Purple Heart while serving in World War I, then went on to become the first Black surgeon to join the staff at Harlem Hospital.
Dr. Wright, who had witnessed mob violence and the aftermath of a lynching as a young man, became a supporter of the Harlem Renaissance and a prominent advocate for civil rights and integration. He served as chairman of the National Association for the Advancement of Colored People and was only the second Black member of the American College of Surgeons.
According to the 2009 book “Black Genius: Inspirational Portraits of African American Leaders,” he successfully treated the rare but devastating venereal disease lymphogranuloma venereum with a new antibiotic developed by his former colleague Yellapragada SubbaRow, MD. Dr. Wright even tried the drug himself, “as a lot of doctors in the olden days did,” according to another of his daughters, the late Barbara Wright Pierce, MD, who was quoted in “Black Genius.” She, too, was a physician.
In 1948, Dr. Jane C. Wright joined her father at Harlem Hospital’s Cancer Research Foundation. There the duo explored the cancer-fighting possibilities of a nitrogen mustard–like chemical agent that had been known since World War I to kill white blood cells. Ironically, Dr. Louis Wright himself suffered lifelong health problems because of an attack from the poisonous gas phosgene during his wartime service.
“Remissions were observed in patients with sarcoma, Hodgkin disease, and chronic myelogenous leukemia, mycosis fungoides, and lymphoma,” reported a 2013 obituary in the journal Oncology of the younger Dr. Wright. “They also performed early research into the clinical efficacy and toxicity of folic acid antagonists, documenting responses in 93 patients with various forms of incurable blood cancers and solid tumors.”
This research appears in a study that was authored by three Dr. Wrights – Dr. Louis T. Wright and his daughters Jane and Barbara.
“The elder Dr. Wright died in 1952, just months after 1,000 people – including Eleanor Roosevelt – honored him at a dinner to dedicate a Harlem Hospital library named after him. He was 61.
Scientific savvy mixed with modesty and elegance
After her father’s death, Dr. Janet C. Wright became director of the hospital’s cancer foundation. From the 1950s to the 1970s, she “worked out ways to use pieces of a patient’s own tumor, removed by surgery and grown in a nutrient culture medium in the laboratory, as a ‘guinea pig for testing drugs,’ ” according to the 1991 book “Black Scientists.” Previously, researchers had focused on mice as test subjects.
This approach also allowed Dr. Wright to determine if specific drugs such as methotrexate, a folic acid antagonist, would help specific patients. “She was looking for predictive activity for chemotherapeutic efficacy in vitro at a time when no one had good predictive tests,” wrote James F. Holland, MD, the late Mount Sinai School of Medicine oncologist, who was quoted in Dr. Wright’s 2013 Oncology obituary.
“Her strict attention to detail and concern for her patients helped determine effective dosing levels and establish treatment guidelines,” the Oncology obituary reported. “She treated patients that other physicians had given up on, and she was among the first small cadre of researchers to carefully test the effects of drugs against cancer in a clinical trial setting.”
Dr. Wright also focused on developing ways to administer chemotherapy, such using a catheter to reach difficult-to-access organs like the spleen without surgery, according to “Black Scientists.”
Along with her work, Dr. Wright’s appearance set her apart. According to “Black Genius,” a newspaper columnist dubbed her one of the 10 most beautiful Back woman in America, and Ebony Magazine in 1966 honored her as one of the best-dressed women in America. It featured a photograph of her in a stunning ivory and yellow brocade gown, noting that she was “in private life Mrs. David J. Jones.” (She’d married the Harvard University Law School graduate in 1946.)
Dr. Wright had a sense of modesty despite her accomplishments, according to her daughter Alison Jones. She even downplayed her own mental powers in a newspaper interview. “I know I’m a member of two minority groups,” she told The New York Post in 1967, “but I don’t think of myself that way. Sure, a woman has to try twice as hard. But – racial prejudice? I’ve met very little of it. It could be I met it – and wasn’t intelligent enough to recognize it.”
Sharp-eyed readers might have glimpsed her modesty nearly 2 decades later. In a 1984 article for the Journal of the National Medical Association, a society of African American physicians, she wrote about the past, present, and future of chemotherapy without noting her own prominent role in its development.
‘Global medical pioneer’ cofounds ASCO – and more
In the 1960s, Dr. Wright joined the influential President’s Commission on Heart Disease, Cancer, and Stroke and was named associate dean at New York Medical College, her alma mater, a first for a black woman at a prominent U.S. medical school. Even more importantly, Dr. Wright was the sole woman among seven physicians who founded the American Society of Clinical Oncology in Chicago in 1964. She served as ASCO’s first Secretary-Treasurer and was honored as its longest surviving founder when she passed away 9 years ago.
“Jane Wright had the vision to see that oncology was an important separate discipline within medicine with far-reaching implications for research and discovery,” Georgetown University Medical Center, Washington, oncologist Sandra M. Swain, MD, a former president of the ASCO and author of the 2013 Oncology obituary of Dr. Wright, said in an interview. “It is truly remarkable that, as a woman and an African American woman, she had a seat at the very small table for the formation of such an important group.”
As her friend and fellow oncologist Edith Mitchell, MD, said in a eulogy, “Dr. Wright led delegations of oncologists to China and the Soviet Union, and countries in Africa and Eastern Europe. She led medical teams providing medical and cancer care and education to other nurses and physicians in Ghana in 1957 and Kenya in 1961. From 1973 to 1984, she served as vice-president of the African Research and Medical foundation.”
Dr. Wright also raised two daughters. A 1968 Ebony article devoted to her career and family declared that neither of her teenagers was interested in medical careers. Their perspectives shifted, however – as had Dr. Wright’s. An undergraduate at Smith College, Dr. Wright majored in art, swam on the varsity team, and had a special affinity for German language studies before she switched to premed.
Like their mother, Dr. Wright’s daughters also changed paths, and they ultimately became the fourth generation of their family to enter the medical field. Dr. Alison Jones, the psychologist, currently works in a prison, while Jane Jones, MD, became a clinical psychiatrist. She’s now retired and lives in Guttenberg, N.J.
Both fondly remember their mother as a supportive force who insisted on excellence. “There couldn’t be any excuses for you not getting where you wanted to go,” Dr. Jane Jones recalled in an interview.
Nevertheless, Dr. Wright was still keenly aware of society’s limits. “She told me I had to be a doctor or lawyer,” Dr. Alison Jones said, “because that’s how you need to survive when you’re Black in America.”
Dr. Wright passed away in 2013 at age 93. “Dr. Jane C. Wright truly has made contributions that have changed the practice of medicine,” noted her friend Dr. Mitchell, an oncologist and a retired brigadier general with the U.S. Air Force who now teaches at Thomas Jefferson University, Philadelphia. “A true pioneer. A concerned mentor. A renowned researcher. A global teacher. A global medical pioneer. A talented researcher, beloved sister, wife, and mother, and a beautiful, kind, and loving human being.”
When Jane Cooke Wright, MD, entered the medical profession in 1945, the notion that toxic drugs could target tumors struck many physicians and patients as outlandish. How could one poison be weaponized against another poison – a cancerous tumor – without creating more havoc? Let alone a combination of two or more chemicals?
Dr. Wright’s story would be extraordinary enough if she’d looked like most of her colleagues, but this surgeon and researcher stood apart. An African American woman at a time when medicine and science – like politics and law – were almost entirely the domain of White men, Dr. Wright had determination in her blood. Her father, once honored by a crowd of dignitaries that included a First Lady, persevered despite his horrific encounters with racism. She shared her father’s commitment to progress and added her own personal twists. She balanced elegance and beauty with scientific savvy, fierce ambition, and a refusal to be defined by anything other than her accomplishments.
“She didn’t focus on race, not at all,” her daughter Alison Jones, PhD, a psychologist in East Lansing, Mich., said in an interview. “Wherever she was, she wanted to be the best, not the best Black person. It was not about how she performed in a category, and she would get upset if someone said she was good as a Black physician.”
On the road to being the best, Dr. Jones said, her mother set a goal of curing cancer. National Cancer Research Month is a fitting opportunity to look back on a scientist dedicated to bringing humanity closer to that elusive achievement.
Medical legacy blazed in toil and trauma
A strong case could be made that Dr. Jane C. Wright and her father Louis Tompkins Wright, MD, are the most accomplished father-and-daughter team in all of medicine.
The elder Dr. Wright, son of a formerly enslaved man turned physician and a stepson of the first African American to graduate from Yale University, New Haven, Conn., himself graduated from Harvard Medical School in 1915. He earned a Purple Heart while serving in World War I, then went on to become the first Black surgeon to join the staff at Harlem Hospital.
Dr. Wright, who had witnessed mob violence and the aftermath of a lynching as a young man, became a supporter of the Harlem Renaissance and a prominent advocate for civil rights and integration. He served as chairman of the National Association for the Advancement of Colored People and was only the second Black member of the American College of Surgeons.
According to the 2009 book “Black Genius: Inspirational Portraits of African American Leaders,” he successfully treated the rare but devastating venereal disease lymphogranuloma venereum with a new antibiotic developed by his former colleague Yellapragada SubbaRow, MD. Dr. Wright even tried the drug himself, “as a lot of doctors in the olden days did,” according to another of his daughters, the late Barbara Wright Pierce, MD, who was quoted in “Black Genius.” She, too, was a physician.
In 1948, Dr. Jane C. Wright joined her father at Harlem Hospital’s Cancer Research Foundation. There the duo explored the cancer-fighting possibilities of a nitrogen mustard–like chemical agent that had been known since World War I to kill white blood cells. Ironically, Dr. Louis Wright himself suffered lifelong health problems because of an attack from the poisonous gas phosgene during his wartime service.
“Remissions were observed in patients with sarcoma, Hodgkin disease, and chronic myelogenous leukemia, mycosis fungoides, and lymphoma,” reported a 2013 obituary in the journal Oncology of the younger Dr. Wright. “They also performed early research into the clinical efficacy and toxicity of folic acid antagonists, documenting responses in 93 patients with various forms of incurable blood cancers and solid tumors.”
This research appears in a study that was authored by three Dr. Wrights – Dr. Louis T. Wright and his daughters Jane and Barbara.
“The elder Dr. Wright died in 1952, just months after 1,000 people – including Eleanor Roosevelt – honored him at a dinner to dedicate a Harlem Hospital library named after him. He was 61.
Scientific savvy mixed with modesty and elegance
After her father’s death, Dr. Janet C. Wright became director of the hospital’s cancer foundation. From the 1950s to the 1970s, she “worked out ways to use pieces of a patient’s own tumor, removed by surgery and grown in a nutrient culture medium in the laboratory, as a ‘guinea pig for testing drugs,’ ” according to the 1991 book “Black Scientists.” Previously, researchers had focused on mice as test subjects.
This approach also allowed Dr. Wright to determine if specific drugs such as methotrexate, a folic acid antagonist, would help specific patients. “She was looking for predictive activity for chemotherapeutic efficacy in vitro at a time when no one had good predictive tests,” wrote James F. Holland, MD, the late Mount Sinai School of Medicine oncologist, who was quoted in Dr. Wright’s 2013 Oncology obituary.
“Her strict attention to detail and concern for her patients helped determine effective dosing levels and establish treatment guidelines,” the Oncology obituary reported. “She treated patients that other physicians had given up on, and she was among the first small cadre of researchers to carefully test the effects of drugs against cancer in a clinical trial setting.”
Dr. Wright also focused on developing ways to administer chemotherapy, such using a catheter to reach difficult-to-access organs like the spleen without surgery, according to “Black Scientists.”
Along with her work, Dr. Wright’s appearance set her apart. According to “Black Genius,” a newspaper columnist dubbed her one of the 10 most beautiful Back woman in America, and Ebony Magazine in 1966 honored her as one of the best-dressed women in America. It featured a photograph of her in a stunning ivory and yellow brocade gown, noting that she was “in private life Mrs. David J. Jones.” (She’d married the Harvard University Law School graduate in 1946.)
Dr. Wright had a sense of modesty despite her accomplishments, according to her daughter Alison Jones. She even downplayed her own mental powers in a newspaper interview. “I know I’m a member of two minority groups,” she told The New York Post in 1967, “but I don’t think of myself that way. Sure, a woman has to try twice as hard. But – racial prejudice? I’ve met very little of it. It could be I met it – and wasn’t intelligent enough to recognize it.”
Sharp-eyed readers might have glimpsed her modesty nearly 2 decades later. In a 1984 article for the Journal of the National Medical Association, a society of African American physicians, she wrote about the past, present, and future of chemotherapy without noting her own prominent role in its development.
‘Global medical pioneer’ cofounds ASCO – and more
In the 1960s, Dr. Wright joined the influential President’s Commission on Heart Disease, Cancer, and Stroke and was named associate dean at New York Medical College, her alma mater, a first for a black woman at a prominent U.S. medical school. Even more importantly, Dr. Wright was the sole woman among seven physicians who founded the American Society of Clinical Oncology in Chicago in 1964. She served as ASCO’s first Secretary-Treasurer and was honored as its longest surviving founder when she passed away 9 years ago.
“Jane Wright had the vision to see that oncology was an important separate discipline within medicine with far-reaching implications for research and discovery,” Georgetown University Medical Center, Washington, oncologist Sandra M. Swain, MD, a former president of the ASCO and author of the 2013 Oncology obituary of Dr. Wright, said in an interview. “It is truly remarkable that, as a woman and an African American woman, she had a seat at the very small table for the formation of such an important group.”
As her friend and fellow oncologist Edith Mitchell, MD, said in a eulogy, “Dr. Wright led delegations of oncologists to China and the Soviet Union, and countries in Africa and Eastern Europe. She led medical teams providing medical and cancer care and education to other nurses and physicians in Ghana in 1957 and Kenya in 1961. From 1973 to 1984, she served as vice-president of the African Research and Medical foundation.”
Dr. Wright also raised two daughters. A 1968 Ebony article devoted to her career and family declared that neither of her teenagers was interested in medical careers. Their perspectives shifted, however – as had Dr. Wright’s. An undergraduate at Smith College, Dr. Wright majored in art, swam on the varsity team, and had a special affinity for German language studies before she switched to premed.
Like their mother, Dr. Wright’s daughters also changed paths, and they ultimately became the fourth generation of their family to enter the medical field. Dr. Alison Jones, the psychologist, currently works in a prison, while Jane Jones, MD, became a clinical psychiatrist. She’s now retired and lives in Guttenberg, N.J.
Both fondly remember their mother as a supportive force who insisted on excellence. “There couldn’t be any excuses for you not getting where you wanted to go,” Dr. Jane Jones recalled in an interview.
Nevertheless, Dr. Wright was still keenly aware of society’s limits. “She told me I had to be a doctor or lawyer,” Dr. Alison Jones said, “because that’s how you need to survive when you’re Black in America.”
Dr. Wright passed away in 2013 at age 93. “Dr. Jane C. Wright truly has made contributions that have changed the practice of medicine,” noted her friend Dr. Mitchell, an oncologist and a retired brigadier general with the U.S. Air Force who now teaches at Thomas Jefferson University, Philadelphia. “A true pioneer. A concerned mentor. A renowned researcher. A global teacher. A global medical pioneer. A talented researcher, beloved sister, wife, and mother, and a beautiful, kind, and loving human being.”
When Jane Cooke Wright, MD, entered the medical profession in 1945, the notion that toxic drugs could target tumors struck many physicians and patients as outlandish. How could one poison be weaponized against another poison – a cancerous tumor – without creating more havoc? Let alone a combination of two or more chemicals?
Dr. Wright’s story would be extraordinary enough if she’d looked like most of her colleagues, but this surgeon and researcher stood apart. An African American woman at a time when medicine and science – like politics and law – were almost entirely the domain of White men, Dr. Wright had determination in her blood. Her father, once honored by a crowd of dignitaries that included a First Lady, persevered despite his horrific encounters with racism. She shared her father’s commitment to progress and added her own personal twists. She balanced elegance and beauty with scientific savvy, fierce ambition, and a refusal to be defined by anything other than her accomplishments.
“She didn’t focus on race, not at all,” her daughter Alison Jones, PhD, a psychologist in East Lansing, Mich., said in an interview. “Wherever she was, she wanted to be the best, not the best Black person. It was not about how she performed in a category, and she would get upset if someone said she was good as a Black physician.”
On the road to being the best, Dr. Jones said, her mother set a goal of curing cancer. National Cancer Research Month is a fitting opportunity to look back on a scientist dedicated to bringing humanity closer to that elusive achievement.
Medical legacy blazed in toil and trauma
A strong case could be made that Dr. Jane C. Wright and her father Louis Tompkins Wright, MD, are the most accomplished father-and-daughter team in all of medicine.
The elder Dr. Wright, son of a formerly enslaved man turned physician and a stepson of the first African American to graduate from Yale University, New Haven, Conn., himself graduated from Harvard Medical School in 1915. He earned a Purple Heart while serving in World War I, then went on to become the first Black surgeon to join the staff at Harlem Hospital.
Dr. Wright, who had witnessed mob violence and the aftermath of a lynching as a young man, became a supporter of the Harlem Renaissance and a prominent advocate for civil rights and integration. He served as chairman of the National Association for the Advancement of Colored People and was only the second Black member of the American College of Surgeons.
According to the 2009 book “Black Genius: Inspirational Portraits of African American Leaders,” he successfully treated the rare but devastating venereal disease lymphogranuloma venereum with a new antibiotic developed by his former colleague Yellapragada SubbaRow, MD. Dr. Wright even tried the drug himself, “as a lot of doctors in the olden days did,” according to another of his daughters, the late Barbara Wright Pierce, MD, who was quoted in “Black Genius.” She, too, was a physician.
In 1948, Dr. Jane C. Wright joined her father at Harlem Hospital’s Cancer Research Foundation. There the duo explored the cancer-fighting possibilities of a nitrogen mustard–like chemical agent that had been known since World War I to kill white blood cells. Ironically, Dr. Louis Wright himself suffered lifelong health problems because of an attack from the poisonous gas phosgene during his wartime service.
“Remissions were observed in patients with sarcoma, Hodgkin disease, and chronic myelogenous leukemia, mycosis fungoides, and lymphoma,” reported a 2013 obituary in the journal Oncology of the younger Dr. Wright. “They also performed early research into the clinical efficacy and toxicity of folic acid antagonists, documenting responses in 93 patients with various forms of incurable blood cancers and solid tumors.”
This research appears in a study that was authored by three Dr. Wrights – Dr. Louis T. Wright and his daughters Jane and Barbara.
“The elder Dr. Wright died in 1952, just months after 1,000 people – including Eleanor Roosevelt – honored him at a dinner to dedicate a Harlem Hospital library named after him. He was 61.
Scientific savvy mixed with modesty and elegance
After her father’s death, Dr. Janet C. Wright became director of the hospital’s cancer foundation. From the 1950s to the 1970s, she “worked out ways to use pieces of a patient’s own tumor, removed by surgery and grown in a nutrient culture medium in the laboratory, as a ‘guinea pig for testing drugs,’ ” according to the 1991 book “Black Scientists.” Previously, researchers had focused on mice as test subjects.
This approach also allowed Dr. Wright to determine if specific drugs such as methotrexate, a folic acid antagonist, would help specific patients. “She was looking for predictive activity for chemotherapeutic efficacy in vitro at a time when no one had good predictive tests,” wrote James F. Holland, MD, the late Mount Sinai School of Medicine oncologist, who was quoted in Dr. Wright’s 2013 Oncology obituary.
“Her strict attention to detail and concern for her patients helped determine effective dosing levels and establish treatment guidelines,” the Oncology obituary reported. “She treated patients that other physicians had given up on, and she was among the first small cadre of researchers to carefully test the effects of drugs against cancer in a clinical trial setting.”
Dr. Wright also focused on developing ways to administer chemotherapy, such using a catheter to reach difficult-to-access organs like the spleen without surgery, according to “Black Scientists.”
Along with her work, Dr. Wright’s appearance set her apart. According to “Black Genius,” a newspaper columnist dubbed her one of the 10 most beautiful Back woman in America, and Ebony Magazine in 1966 honored her as one of the best-dressed women in America. It featured a photograph of her in a stunning ivory and yellow brocade gown, noting that she was “in private life Mrs. David J. Jones.” (She’d married the Harvard University Law School graduate in 1946.)
Dr. Wright had a sense of modesty despite her accomplishments, according to her daughter Alison Jones. She even downplayed her own mental powers in a newspaper interview. “I know I’m a member of two minority groups,” she told The New York Post in 1967, “but I don’t think of myself that way. Sure, a woman has to try twice as hard. But – racial prejudice? I’ve met very little of it. It could be I met it – and wasn’t intelligent enough to recognize it.”
Sharp-eyed readers might have glimpsed her modesty nearly 2 decades later. In a 1984 article for the Journal of the National Medical Association, a society of African American physicians, she wrote about the past, present, and future of chemotherapy without noting her own prominent role in its development.
‘Global medical pioneer’ cofounds ASCO – and more
In the 1960s, Dr. Wright joined the influential President’s Commission on Heart Disease, Cancer, and Stroke and was named associate dean at New York Medical College, her alma mater, a first for a black woman at a prominent U.S. medical school. Even more importantly, Dr. Wright was the sole woman among seven physicians who founded the American Society of Clinical Oncology in Chicago in 1964. She served as ASCO’s first Secretary-Treasurer and was honored as its longest surviving founder when she passed away 9 years ago.
“Jane Wright had the vision to see that oncology was an important separate discipline within medicine with far-reaching implications for research and discovery,” Georgetown University Medical Center, Washington, oncologist Sandra M. Swain, MD, a former president of the ASCO and author of the 2013 Oncology obituary of Dr. Wright, said in an interview. “It is truly remarkable that, as a woman and an African American woman, she had a seat at the very small table for the formation of such an important group.”
As her friend and fellow oncologist Edith Mitchell, MD, said in a eulogy, “Dr. Wright led delegations of oncologists to China and the Soviet Union, and countries in Africa and Eastern Europe. She led medical teams providing medical and cancer care and education to other nurses and physicians in Ghana in 1957 and Kenya in 1961. From 1973 to 1984, she served as vice-president of the African Research and Medical foundation.”
Dr. Wright also raised two daughters. A 1968 Ebony article devoted to her career and family declared that neither of her teenagers was interested in medical careers. Their perspectives shifted, however – as had Dr. Wright’s. An undergraduate at Smith College, Dr. Wright majored in art, swam on the varsity team, and had a special affinity for German language studies before she switched to premed.
Like their mother, Dr. Wright’s daughters also changed paths, and they ultimately became the fourth generation of their family to enter the medical field. Dr. Alison Jones, the psychologist, currently works in a prison, while Jane Jones, MD, became a clinical psychiatrist. She’s now retired and lives in Guttenberg, N.J.
Both fondly remember their mother as a supportive force who insisted on excellence. “There couldn’t be any excuses for you not getting where you wanted to go,” Dr. Jane Jones recalled in an interview.
Nevertheless, Dr. Wright was still keenly aware of society’s limits. “She told me I had to be a doctor or lawyer,” Dr. Alison Jones said, “because that’s how you need to survive when you’re Black in America.”
Dr. Wright passed away in 2013 at age 93. “Dr. Jane C. Wright truly has made contributions that have changed the practice of medicine,” noted her friend Dr. Mitchell, an oncologist and a retired brigadier general with the U.S. Air Force who now teaches at Thomas Jefferson University, Philadelphia. “A true pioneer. A concerned mentor. A renowned researcher. A global teacher. A global medical pioneer. A talented researcher, beloved sister, wife, and mother, and a beautiful, kind, and loving human being.”
Fever after a tropical trip: A guide to differential diagnosis
After 2 years of a pandemic in which traveling was barely possible, tropical diseases are becoming important once more. At a 2022 conference for internal medicine specialists, tropical medicine specialist Fritz Holst, MD, of the Center for Tropical and Travel Medicine in Marburg, Germany, explained what questions you should be asking travelers with a fever at your practice and how to proceed with a suspected case.
The following article is based on the lecture: “Differential Diagnosis of Fever After a Trip to the Tropics,” which Dr. Holst gave at the 128th conference of the German Society of Internal Medicine.
A meta-analysis of studies concerning the topic, “returnee travelers from the tropics with fever,” was published in 2020. According to the analysis, purely tropical infections make up a third (33%) of fever diagnoses worldwide following an exotic trip. Malaria accounts for a fifth (22%), 5% are dengue fever, and 2.2% are typhoid (enteric fever).
In 26% of the returnee travelers investigated, nontropical infections were the cause of the fever. Acute gastroenteritis was responsible for 14%, and respiratory infections were responsible for 13%. In 18% of the cases, the cause of the fever remained unclear.
In Germany, the number of malaria cases has increased, said Dr. Holst. In Hessen, for example, there was recently a malaria fatality. “What we should do has been forgotten again,” he warned. More attention should also be paid once more to prophylaxis.
How to proceed
Dr. Holst described the following steps for treating recently returned travelers who are sick:
- Severely ill or not: If there are signs of a severe disease, such as dyspnea, signs of bleeding, hypotension, or central nervous system symptoms, the patient should be referred to a clinic. A diagnosis should be made within 1 day and treatment should be started.
- Transmissible or dangerous disease: This question should be quickly clarified to protect health care personnel, especially those treating patients. By using a thorough medical history (discussed below), a range of diseases may be clarified.
- Disease outbreak in destination country: Find out about possible disease outbreaks in the country that the traveler visited.
- Malaria? Immediate diagnostics: Malaria should always be excluded in patients at the practice on the same day by using a thick blood smear, even if no fever is present. If this is not possible because of time constraints, the affected person should be transferred directly to the clinic.
- Fever independent of the travel? Exclude other causes of the fever (for example, endocarditis).
- Involve tropical medicine specialists in a timely manner.
Nine mandatory questions
Dr. Holst also listed nine questions that clinicians should ask this patient population.
Where were you exactly?
Depending on the regional prevalence of tropical diseases, certain pathogens can be excluded quickly. Approximately 35% of travelers returning from Africa have malaria, whereas typhoid is much rarer. In contrast, typhoid and dengue fever are much more widespread in Southeast Asia. In Latin America, this is the case for both dengue fever and leptospirosis.
When did you travel?
By using the incubation time of the pathogen in question, as well as the time of return journey, you can determine which diseases are possible and which are not. In one patient who visited the practice 4 weeks after his return, dengue or typhoid were excluded.
Where did you stay overnight?
Whether in an unhygienic bed or under the stars, the question regarding how and where travelers stayed overnight provides important evidence of the following nocturnal vectors:
- Sandflies: Leishmaniasis
- Kissing bugs: Chagas disease
- Fleas: Spotted fever, bubonic plague
- Mosquitoes: Malaria, dengue, filariasis
What did you eat?
Many infections can be attributed to careless eating. For example, when eating fish, crabs, crawfish, or frogs, especially if raw, liver fluke, lung fluke, or ciguatera should be considered. Mussel toxins have been found on the coast of Kenya and even in the south of France. In North African countries, you should be cautious when eating nonpasteurized milk products (for example, camel milk). They can transmit the pathogens for brucellosis and tuberculosis. In beef or pork that has not been cooked thoroughly, there is the risk of trichinosis or of a tapeworm. Even vegetarians need to be careful. Infections with the common liver fluke are possible after eating watercress.
What have you been doing?
You can only get some diseases through certain activities, said Dr. Holst. If long-distance travelers tell you about the following excursions, prick up your ears:
- Freshwater contact: Schistosomiasis, leptospirosis
- Caving: Histoplasmosis, rabies
- Excavations: Anthrax, coccidioidomycosis
- Camel tour: MERS coronavirus (Do not mount a sniffling camel!)
- Walking around barefoot: Strongyloides, hookworm
Was there contact with animals?
Because of the risk of rabies following contact with cats or biting apes, Dr. Holst advised long-distance travelers to get vaccinated.
Were there new sexual partners?
In the event of new sexual contacts, tests for hepatitis A, B, C, and HIV should be performed.
Are you undergoing medical treatment?
The patient may already be under medical supervision because of having a disease.
What prophylactic measures did you take before traveling?
To progress in the differential diagnosis, questions should also be asked regarding prophylactic measures. Vaccination against hepatitis A provides very efficient infection protection, whereas vaccines against typhoid offer a much lower level of protection.
Diagnostic tests
As long as there are no abnormalities, such as meningism or heart murmurs, further diagnostics include routine infectiologic laboratory investigations (C-reactive protein, blood count, etc), blood culture (aerobic, anaerobic), a urine dipstick test, and rapid tests for malaria and dengue.
To exclude malaria, a thick blood smear should always be performed on the same day, said Dr. Holst. “The rapid test is occasionally negative. But you often only detect tertian malaria in the thick blood smear. And you have to repeat the diagnostics the following day.” For this, it is important to know that a single test result does not exclude malaria right away. In contrast, detecting malaria antibodies is obsolete. Depending on the result, further tests include serologies, antigen investigations, and polymerase chain reaction.
Treat early
A complete set of results is not always available promptly. Experts recommend that, “if you already have a hunch, then start the therapy, even without a definite diagnosis.” This applies in particular for the suspected diagnoses in the following table.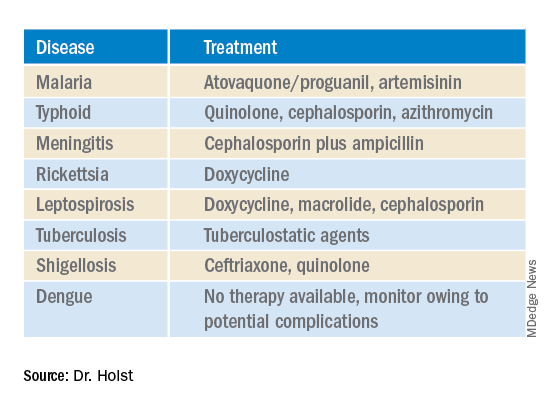
This article was translated from Coliquio. A version of this article appeared on Medscape.com.
After 2 years of a pandemic in which traveling was barely possible, tropical diseases are becoming important once more. At a 2022 conference for internal medicine specialists, tropical medicine specialist Fritz Holst, MD, of the Center for Tropical and Travel Medicine in Marburg, Germany, explained what questions you should be asking travelers with a fever at your practice and how to proceed with a suspected case.
The following article is based on the lecture: “Differential Diagnosis of Fever After a Trip to the Tropics,” which Dr. Holst gave at the 128th conference of the German Society of Internal Medicine.
A meta-analysis of studies concerning the topic, “returnee travelers from the tropics with fever,” was published in 2020. According to the analysis, purely tropical infections make up a third (33%) of fever diagnoses worldwide following an exotic trip. Malaria accounts for a fifth (22%), 5% are dengue fever, and 2.2% are typhoid (enteric fever).
In 26% of the returnee travelers investigated, nontropical infections were the cause of the fever. Acute gastroenteritis was responsible for 14%, and respiratory infections were responsible for 13%. In 18% of the cases, the cause of the fever remained unclear.
In Germany, the number of malaria cases has increased, said Dr. Holst. In Hessen, for example, there was recently a malaria fatality. “What we should do has been forgotten again,” he warned. More attention should also be paid once more to prophylaxis.
How to proceed
Dr. Holst described the following steps for treating recently returned travelers who are sick:
- Severely ill or not: If there are signs of a severe disease, such as dyspnea, signs of bleeding, hypotension, or central nervous system symptoms, the patient should be referred to a clinic. A diagnosis should be made within 1 day and treatment should be started.
- Transmissible or dangerous disease: This question should be quickly clarified to protect health care personnel, especially those treating patients. By using a thorough medical history (discussed below), a range of diseases may be clarified.
- Disease outbreak in destination country: Find out about possible disease outbreaks in the country that the traveler visited.
- Malaria? Immediate diagnostics: Malaria should always be excluded in patients at the practice on the same day by using a thick blood smear, even if no fever is present. If this is not possible because of time constraints, the affected person should be transferred directly to the clinic.
- Fever independent of the travel? Exclude other causes of the fever (for example, endocarditis).
- Involve tropical medicine specialists in a timely manner.
Nine mandatory questions
Dr. Holst also listed nine questions that clinicians should ask this patient population.
Where were you exactly?
Depending on the regional prevalence of tropical diseases, certain pathogens can be excluded quickly. Approximately 35% of travelers returning from Africa have malaria, whereas typhoid is much rarer. In contrast, typhoid and dengue fever are much more widespread in Southeast Asia. In Latin America, this is the case for both dengue fever and leptospirosis.
When did you travel?
By using the incubation time of the pathogen in question, as well as the time of return journey, you can determine which diseases are possible and which are not. In one patient who visited the practice 4 weeks after his return, dengue or typhoid were excluded.
Where did you stay overnight?
Whether in an unhygienic bed or under the stars, the question regarding how and where travelers stayed overnight provides important evidence of the following nocturnal vectors:
- Sandflies: Leishmaniasis
- Kissing bugs: Chagas disease
- Fleas: Spotted fever, bubonic plague
- Mosquitoes: Malaria, dengue, filariasis
What did you eat?
Many infections can be attributed to careless eating. For example, when eating fish, crabs, crawfish, or frogs, especially if raw, liver fluke, lung fluke, or ciguatera should be considered. Mussel toxins have been found on the coast of Kenya and even in the south of France. In North African countries, you should be cautious when eating nonpasteurized milk products (for example, camel milk). They can transmit the pathogens for brucellosis and tuberculosis. In beef or pork that has not been cooked thoroughly, there is the risk of trichinosis or of a tapeworm. Even vegetarians need to be careful. Infections with the common liver fluke are possible after eating watercress.
What have you been doing?
You can only get some diseases through certain activities, said Dr. Holst. If long-distance travelers tell you about the following excursions, prick up your ears:
- Freshwater contact: Schistosomiasis, leptospirosis
- Caving: Histoplasmosis, rabies
- Excavations: Anthrax, coccidioidomycosis
- Camel tour: MERS coronavirus (Do not mount a sniffling camel!)
- Walking around barefoot: Strongyloides, hookworm
Was there contact with animals?
Because of the risk of rabies following contact with cats or biting apes, Dr. Holst advised long-distance travelers to get vaccinated.
Were there new sexual partners?
In the event of new sexual contacts, tests for hepatitis A, B, C, and HIV should be performed.
Are you undergoing medical treatment?
The patient may already be under medical supervision because of having a disease.
What prophylactic measures did you take before traveling?
To progress in the differential diagnosis, questions should also be asked regarding prophylactic measures. Vaccination against hepatitis A provides very efficient infection protection, whereas vaccines against typhoid offer a much lower level of protection.
Diagnostic tests
As long as there are no abnormalities, such as meningism or heart murmurs, further diagnostics include routine infectiologic laboratory investigations (C-reactive protein, blood count, etc), blood culture (aerobic, anaerobic), a urine dipstick test, and rapid tests for malaria and dengue.
To exclude malaria, a thick blood smear should always be performed on the same day, said Dr. Holst. “The rapid test is occasionally negative. But you often only detect tertian malaria in the thick blood smear. And you have to repeat the diagnostics the following day.” For this, it is important to know that a single test result does not exclude malaria right away. In contrast, detecting malaria antibodies is obsolete. Depending on the result, further tests include serologies, antigen investigations, and polymerase chain reaction.
Treat early
A complete set of results is not always available promptly. Experts recommend that, “if you already have a hunch, then start the therapy, even without a definite diagnosis.” This applies in particular for the suspected diagnoses in the following table.
This article was translated from Coliquio. A version of this article appeared on Medscape.com.
After 2 years of a pandemic in which traveling was barely possible, tropical diseases are becoming important once more. At a 2022 conference for internal medicine specialists, tropical medicine specialist Fritz Holst, MD, of the Center for Tropical and Travel Medicine in Marburg, Germany, explained what questions you should be asking travelers with a fever at your practice and how to proceed with a suspected case.
The following article is based on the lecture: “Differential Diagnosis of Fever After a Trip to the Tropics,” which Dr. Holst gave at the 128th conference of the German Society of Internal Medicine.
A meta-analysis of studies concerning the topic, “returnee travelers from the tropics with fever,” was published in 2020. According to the analysis, purely tropical infections make up a third (33%) of fever diagnoses worldwide following an exotic trip. Malaria accounts for a fifth (22%), 5% are dengue fever, and 2.2% are typhoid (enteric fever).
In 26% of the returnee travelers investigated, nontropical infections were the cause of the fever. Acute gastroenteritis was responsible for 14%, and respiratory infections were responsible for 13%. In 18% of the cases, the cause of the fever remained unclear.
In Germany, the number of malaria cases has increased, said Dr. Holst. In Hessen, for example, there was recently a malaria fatality. “What we should do has been forgotten again,” he warned. More attention should also be paid once more to prophylaxis.
How to proceed
Dr. Holst described the following steps for treating recently returned travelers who are sick:
- Severely ill or not: If there are signs of a severe disease, such as dyspnea, signs of bleeding, hypotension, or central nervous system symptoms, the patient should be referred to a clinic. A diagnosis should be made within 1 day and treatment should be started.
- Transmissible or dangerous disease: This question should be quickly clarified to protect health care personnel, especially those treating patients. By using a thorough medical history (discussed below), a range of diseases may be clarified.
- Disease outbreak in destination country: Find out about possible disease outbreaks in the country that the traveler visited.
- Malaria? Immediate diagnostics: Malaria should always be excluded in patients at the practice on the same day by using a thick blood smear, even if no fever is present. If this is not possible because of time constraints, the affected person should be transferred directly to the clinic.
- Fever independent of the travel? Exclude other causes of the fever (for example, endocarditis).
- Involve tropical medicine specialists in a timely manner.
Nine mandatory questions
Dr. Holst also listed nine questions that clinicians should ask this patient population.
Where were you exactly?
Depending on the regional prevalence of tropical diseases, certain pathogens can be excluded quickly. Approximately 35% of travelers returning from Africa have malaria, whereas typhoid is much rarer. In contrast, typhoid and dengue fever are much more widespread in Southeast Asia. In Latin America, this is the case for both dengue fever and leptospirosis.
When did you travel?
By using the incubation time of the pathogen in question, as well as the time of return journey, you can determine which diseases are possible and which are not. In one patient who visited the practice 4 weeks after his return, dengue or typhoid were excluded.
Where did you stay overnight?
Whether in an unhygienic bed or under the stars, the question regarding how and where travelers stayed overnight provides important evidence of the following nocturnal vectors:
- Sandflies: Leishmaniasis
- Kissing bugs: Chagas disease
- Fleas: Spotted fever, bubonic plague
- Mosquitoes: Malaria, dengue, filariasis
What did you eat?
Many infections can be attributed to careless eating. For example, when eating fish, crabs, crawfish, or frogs, especially if raw, liver fluke, lung fluke, or ciguatera should be considered. Mussel toxins have been found on the coast of Kenya and even in the south of France. In North African countries, you should be cautious when eating nonpasteurized milk products (for example, camel milk). They can transmit the pathogens for brucellosis and tuberculosis. In beef or pork that has not been cooked thoroughly, there is the risk of trichinosis or of a tapeworm. Even vegetarians need to be careful. Infections with the common liver fluke are possible after eating watercress.
What have you been doing?
You can only get some diseases through certain activities, said Dr. Holst. If long-distance travelers tell you about the following excursions, prick up your ears:
- Freshwater contact: Schistosomiasis, leptospirosis
- Caving: Histoplasmosis, rabies
- Excavations: Anthrax, coccidioidomycosis
- Camel tour: MERS coronavirus (Do not mount a sniffling camel!)
- Walking around barefoot: Strongyloides, hookworm
Was there contact with animals?
Because of the risk of rabies following contact with cats or biting apes, Dr. Holst advised long-distance travelers to get vaccinated.
Were there new sexual partners?
In the event of new sexual contacts, tests for hepatitis A, B, C, and HIV should be performed.
Are you undergoing medical treatment?
The patient may already be under medical supervision because of having a disease.
What prophylactic measures did you take before traveling?
To progress in the differential diagnosis, questions should also be asked regarding prophylactic measures. Vaccination against hepatitis A provides very efficient infection protection, whereas vaccines against typhoid offer a much lower level of protection.
Diagnostic tests
As long as there are no abnormalities, such as meningism or heart murmurs, further diagnostics include routine infectiologic laboratory investigations (C-reactive protein, blood count, etc), blood culture (aerobic, anaerobic), a urine dipstick test, and rapid tests for malaria and dengue.
To exclude malaria, a thick blood smear should always be performed on the same day, said Dr. Holst. “The rapid test is occasionally negative. But you often only detect tertian malaria in the thick blood smear. And you have to repeat the diagnostics the following day.” For this, it is important to know that a single test result does not exclude malaria right away. In contrast, detecting malaria antibodies is obsolete. Depending on the result, further tests include serologies, antigen investigations, and polymerase chain reaction.
Treat early
A complete set of results is not always available promptly. Experts recommend that, “if you already have a hunch, then start the therapy, even without a definite diagnosis.” This applies in particular for the suspected diagnoses in the following table.
This article was translated from Coliquio. A version of this article appeared on Medscape.com.
Roe v. Wade’s pending fall raises privacy concerns
If Roe v. Wade is overturned, can criminal prosecutors or tech companies use smartphone data against someone?
Now that the future of U.S. abortion laws hangs in the balance, many women are questioning the degree of caution needed to keep their cyber activity confidential – especially period and fertility tracking apps, smartphone location data, and social media interactions.
Cybersecurity and legal experts say the answer largely boils down to one major issue: The right to privacy.
“There’s this notion of the expectation of privacy,” said Brad Malin, PhD, professor of biomedical informatics, biostatistics, and computer science at Vanderbilt University in Nashville, Tenn.
Dr. Malin said it’s directly related to bodily privacy that a person expects they have control of as part of their own environment.
According to Dr. Malin, this is “why this whole notion of Roe v. Wade at the present moment is really relevant. The right to privacy is mentioned about a dozen times within the law for the case.
“This is why we don’t know what’s going to happen with Roe v. Wade, but it worries a lot of privacy professionals,” he said. “It leads down this slippery slope of if you don’t even have control over your own body, then with electronic communications … we might as well not even start.”
Legal protections
The Fourth Amendment of the U.S. Constitution protects people against unreasonable searches and seizures.
To acquire cyber data that could be used as evidence in courts in states where abortion is deemed a crime, prosecutors would still have to go through standard criminal procedures, said Anthony Michael Kreis, JD, a constitutional law professor at Georgia State University, Atlanta.
But the data they do get could still be used in court against someone who is suspected of having had an abortion or who “miscarried under circumstances law enforcement officers found suspicious,” Mr. Kreis said.
And there’s another possibility, he noted: States holding women who end their pregnancies criminally or civilly responsible for “leaving their jurisdiction to obtain an abortion out-of-state.”
“That legal mechanism may abridge the constitutional right to travel, but it is not out of the realm of possibilities in a post-Roe America,” said Mr. Kreis.
But while many anti-abortion groups have said that criminalizing abortion or limiting access to contraception is not the end goal, “history is not promising here,” said Ellen Wright Clayton, MD, JD, professor of pediatrics and professor of law at Vanderbilt University.
She referred to a recent proposal from lawmakers in Louisiana to classify abortion as homicide.
The bill didn’t get far in the House of Representatives, but the concern is warranted, said Dr. Clayton.
Period and fertility tracking apps
Health information privacy laws, like the Health Insurance Portability and Accountability Act (HIPAA), do not protect information on period and fertility tracking apps.
Right now, there are no signs that people plan to use period and fertility tracking data to advance a prochoice agenda, according to Adam Levin, JD, a cybersecurity expert and founder of CyberScout, a global identity and data protection company.
Still, a cycle tracking app “created by a company owned by an antiabortion activist” is totally feasible, said Mr. Levin.
If you want to ensure your data is safe from such meddling, you may want to delete your app, he said, noting that using the notepad feature on your smartphone could be a safer alternative, as could using old-fashioned pen and paper.
You don’t have to stop with period and fertility tracking apps, either.
For any apps you share personal information with, set privacy settings “as tightly as possible” – and reconsider using apps if these options are unavailable, Mr. Levin advised.
“Make sure that company is not engaging in social or political activism that does not align with your politics.”
New York State Attorney General Letitia James recently spoke on the topic, noting on May 13 that “people use fertility tracking apps and location services every day, but if they’re not careful their personal information can end up in the wrong hands.
“With abortion rights in jeopardy, it’s more important than ever that everyone take their digital privacy seriously,” she said. “I urge everyone, especially those visiting abortion clinics or seeking abortion care, to follow the tips offered by my office and be more careful of the apps and websites they use.”
The New York State Attorney General’s Office recommends women use encrypted messaging when communicating about personal health information or behaviors, and to be careful about what they share on social media posts. The office also suggests turning off location and personalized advertising options on their smartphones.
Cellphone location data
Dr. Malin said there are several ways that location services could be used to track where a woman uses her smartphone. An app could track locations if someone grants permission through the app end user agreement, for example.
A second but less likely scenario would be the service provider tracking the pings coming off cellphone towers to find a smartphone.
So what recourse does a woman have if tracked by a third-party app?
“It’s a really tricky situation there because it depends on if the individual was put expressly in harm’s way,” Dr. Malin said. What’s more, tracking someone out in public is not prohibited in general.
“There’s a big difference between documenting what an individual does within a Planned Parenthood clinic versus what they do outside of it,” he said.
Dr. Malin said it’s better that regulations protect all smartphone users rather than requiring each person to remember to turn off the location tracker and then turn it back on again. Also, it should be more of an opt-in situation – where app developers must ask permission to track app usage or location services – versus making each woman opt out.
Think before you share
Vindictive or untrustworthy partners and family members of women in abusive relationships could also be a cause of concern, said Mr. Kreis.
“Individuals within a woman’s closest circles could hold abortions over their head or threaten reporting them for reproductive health care or miscarriages,” he said.
It’s not uncommon for women to experience domestic violence after having an abortion, particularly if their partners were unaware they had the procedure, according to Dr. Clayton.
She said women should also be mindful of what they share on social media.
Dr. Clayton gave the example of a woman seeking advice on where to get a safe abortion or how to order certain medications.
“If someone goes online to look for that, that’s potentially dangerous.”
A version of this article first appeared on WebMD.com.
If Roe v. Wade is overturned, can criminal prosecutors or tech companies use smartphone data against someone?
Now that the future of U.S. abortion laws hangs in the balance, many women are questioning the degree of caution needed to keep their cyber activity confidential – especially period and fertility tracking apps, smartphone location data, and social media interactions.
Cybersecurity and legal experts say the answer largely boils down to one major issue: The right to privacy.
“There’s this notion of the expectation of privacy,” said Brad Malin, PhD, professor of biomedical informatics, biostatistics, and computer science at Vanderbilt University in Nashville, Tenn.
Dr. Malin said it’s directly related to bodily privacy that a person expects they have control of as part of their own environment.
According to Dr. Malin, this is “why this whole notion of Roe v. Wade at the present moment is really relevant. The right to privacy is mentioned about a dozen times within the law for the case.
“This is why we don’t know what’s going to happen with Roe v. Wade, but it worries a lot of privacy professionals,” he said. “It leads down this slippery slope of if you don’t even have control over your own body, then with electronic communications … we might as well not even start.”
Legal protections
The Fourth Amendment of the U.S. Constitution protects people against unreasonable searches and seizures.
To acquire cyber data that could be used as evidence in courts in states where abortion is deemed a crime, prosecutors would still have to go through standard criminal procedures, said Anthony Michael Kreis, JD, a constitutional law professor at Georgia State University, Atlanta.
But the data they do get could still be used in court against someone who is suspected of having had an abortion or who “miscarried under circumstances law enforcement officers found suspicious,” Mr. Kreis said.
And there’s another possibility, he noted: States holding women who end their pregnancies criminally or civilly responsible for “leaving their jurisdiction to obtain an abortion out-of-state.”
“That legal mechanism may abridge the constitutional right to travel, but it is not out of the realm of possibilities in a post-Roe America,” said Mr. Kreis.
But while many anti-abortion groups have said that criminalizing abortion or limiting access to contraception is not the end goal, “history is not promising here,” said Ellen Wright Clayton, MD, JD, professor of pediatrics and professor of law at Vanderbilt University.
She referred to a recent proposal from lawmakers in Louisiana to classify abortion as homicide.
The bill didn’t get far in the House of Representatives, but the concern is warranted, said Dr. Clayton.
Period and fertility tracking apps
Health information privacy laws, like the Health Insurance Portability and Accountability Act (HIPAA), do not protect information on period and fertility tracking apps.
Right now, there are no signs that people plan to use period and fertility tracking data to advance a prochoice agenda, according to Adam Levin, JD, a cybersecurity expert and founder of CyberScout, a global identity and data protection company.
Still, a cycle tracking app “created by a company owned by an antiabortion activist” is totally feasible, said Mr. Levin.
If you want to ensure your data is safe from such meddling, you may want to delete your app, he said, noting that using the notepad feature on your smartphone could be a safer alternative, as could using old-fashioned pen and paper.
You don’t have to stop with period and fertility tracking apps, either.
For any apps you share personal information with, set privacy settings “as tightly as possible” – and reconsider using apps if these options are unavailable, Mr. Levin advised.
“Make sure that company is not engaging in social or political activism that does not align with your politics.”
New York State Attorney General Letitia James recently spoke on the topic, noting on May 13 that “people use fertility tracking apps and location services every day, but if they’re not careful their personal information can end up in the wrong hands.
“With abortion rights in jeopardy, it’s more important than ever that everyone take their digital privacy seriously,” she said. “I urge everyone, especially those visiting abortion clinics or seeking abortion care, to follow the tips offered by my office and be more careful of the apps and websites they use.”
The New York State Attorney General’s Office recommends women use encrypted messaging when communicating about personal health information or behaviors, and to be careful about what they share on social media posts. The office also suggests turning off location and personalized advertising options on their smartphones.
Cellphone location data
Dr. Malin said there are several ways that location services could be used to track where a woman uses her smartphone. An app could track locations if someone grants permission through the app end user agreement, for example.
A second but less likely scenario would be the service provider tracking the pings coming off cellphone towers to find a smartphone.
So what recourse does a woman have if tracked by a third-party app?
“It’s a really tricky situation there because it depends on if the individual was put expressly in harm’s way,” Dr. Malin said. What’s more, tracking someone out in public is not prohibited in general.
“There’s a big difference between documenting what an individual does within a Planned Parenthood clinic versus what they do outside of it,” he said.
Dr. Malin said it’s better that regulations protect all smartphone users rather than requiring each person to remember to turn off the location tracker and then turn it back on again. Also, it should be more of an opt-in situation – where app developers must ask permission to track app usage or location services – versus making each woman opt out.
Think before you share
Vindictive or untrustworthy partners and family members of women in abusive relationships could also be a cause of concern, said Mr. Kreis.
“Individuals within a woman’s closest circles could hold abortions over their head or threaten reporting them for reproductive health care or miscarriages,” he said.
It’s not uncommon for women to experience domestic violence after having an abortion, particularly if their partners were unaware they had the procedure, according to Dr. Clayton.
She said women should also be mindful of what they share on social media.
Dr. Clayton gave the example of a woman seeking advice on where to get a safe abortion or how to order certain medications.
“If someone goes online to look for that, that’s potentially dangerous.”
A version of this article first appeared on WebMD.com.
If Roe v. Wade is overturned, can criminal prosecutors or tech companies use smartphone data against someone?
Now that the future of U.S. abortion laws hangs in the balance, many women are questioning the degree of caution needed to keep their cyber activity confidential – especially period and fertility tracking apps, smartphone location data, and social media interactions.
Cybersecurity and legal experts say the answer largely boils down to one major issue: The right to privacy.
“There’s this notion of the expectation of privacy,” said Brad Malin, PhD, professor of biomedical informatics, biostatistics, and computer science at Vanderbilt University in Nashville, Tenn.
Dr. Malin said it’s directly related to bodily privacy that a person expects they have control of as part of their own environment.
According to Dr. Malin, this is “why this whole notion of Roe v. Wade at the present moment is really relevant. The right to privacy is mentioned about a dozen times within the law for the case.
“This is why we don’t know what’s going to happen with Roe v. Wade, but it worries a lot of privacy professionals,” he said. “It leads down this slippery slope of if you don’t even have control over your own body, then with electronic communications … we might as well not even start.”
Legal protections
The Fourth Amendment of the U.S. Constitution protects people against unreasonable searches and seizures.
To acquire cyber data that could be used as evidence in courts in states where abortion is deemed a crime, prosecutors would still have to go through standard criminal procedures, said Anthony Michael Kreis, JD, a constitutional law professor at Georgia State University, Atlanta.
But the data they do get could still be used in court against someone who is suspected of having had an abortion or who “miscarried under circumstances law enforcement officers found suspicious,” Mr. Kreis said.
And there’s another possibility, he noted: States holding women who end their pregnancies criminally or civilly responsible for “leaving their jurisdiction to obtain an abortion out-of-state.”
“That legal mechanism may abridge the constitutional right to travel, but it is not out of the realm of possibilities in a post-Roe America,” said Mr. Kreis.
But while many anti-abortion groups have said that criminalizing abortion or limiting access to contraception is not the end goal, “history is not promising here,” said Ellen Wright Clayton, MD, JD, professor of pediatrics and professor of law at Vanderbilt University.
She referred to a recent proposal from lawmakers in Louisiana to classify abortion as homicide.
The bill didn’t get far in the House of Representatives, but the concern is warranted, said Dr. Clayton.
Period and fertility tracking apps
Health information privacy laws, like the Health Insurance Portability and Accountability Act (HIPAA), do not protect information on period and fertility tracking apps.
Right now, there are no signs that people plan to use period and fertility tracking data to advance a prochoice agenda, according to Adam Levin, JD, a cybersecurity expert and founder of CyberScout, a global identity and data protection company.
Still, a cycle tracking app “created by a company owned by an antiabortion activist” is totally feasible, said Mr. Levin.
If you want to ensure your data is safe from such meddling, you may want to delete your app, he said, noting that using the notepad feature on your smartphone could be a safer alternative, as could using old-fashioned pen and paper.
You don’t have to stop with period and fertility tracking apps, either.
For any apps you share personal information with, set privacy settings “as tightly as possible” – and reconsider using apps if these options are unavailable, Mr. Levin advised.
“Make sure that company is not engaging in social or political activism that does not align with your politics.”
New York State Attorney General Letitia James recently spoke on the topic, noting on May 13 that “people use fertility tracking apps and location services every day, but if they’re not careful their personal information can end up in the wrong hands.
“With abortion rights in jeopardy, it’s more important than ever that everyone take their digital privacy seriously,” she said. “I urge everyone, especially those visiting abortion clinics or seeking abortion care, to follow the tips offered by my office and be more careful of the apps and websites they use.”
The New York State Attorney General’s Office recommends women use encrypted messaging when communicating about personal health information or behaviors, and to be careful about what they share on social media posts. The office also suggests turning off location and personalized advertising options on their smartphones.
Cellphone location data
Dr. Malin said there are several ways that location services could be used to track where a woman uses her smartphone. An app could track locations if someone grants permission through the app end user agreement, for example.
A second but less likely scenario would be the service provider tracking the pings coming off cellphone towers to find a smartphone.
So what recourse does a woman have if tracked by a third-party app?
“It’s a really tricky situation there because it depends on if the individual was put expressly in harm’s way,” Dr. Malin said. What’s more, tracking someone out in public is not prohibited in general.
“There’s a big difference between documenting what an individual does within a Planned Parenthood clinic versus what they do outside of it,” he said.
Dr. Malin said it’s better that regulations protect all smartphone users rather than requiring each person to remember to turn off the location tracker and then turn it back on again. Also, it should be more of an opt-in situation – where app developers must ask permission to track app usage or location services – versus making each woman opt out.
Think before you share
Vindictive or untrustworthy partners and family members of women in abusive relationships could also be a cause of concern, said Mr. Kreis.
“Individuals within a woman’s closest circles could hold abortions over their head or threaten reporting them for reproductive health care or miscarriages,” he said.
It’s not uncommon for women to experience domestic violence after having an abortion, particularly if their partners were unaware they had the procedure, according to Dr. Clayton.
She said women should also be mindful of what they share on social media.
Dr. Clayton gave the example of a woman seeking advice on where to get a safe abortion or how to order certain medications.
“If someone goes online to look for that, that’s potentially dangerous.”
A version of this article first appeared on WebMD.com.
Obesity and lung disease: Much more than BMI
The diverse effects of obesity on lung health and disease are increasingly being teased apart, with researchers honing in on the impact of metabolic dysfunction, circulating inflammatory factors produced by adipose tissue, lipid handling, and other factors – in addition to body mass index – that are associated with the obese state.
“The bird’s eye view is that obesity completely changes lung health. It’s something we’ve only recently begun to appreciate,” said Anne E. Dixon, MA, BM, BCh, director of the Vermont Lung Center at the University of Vermont, Burlington, who is focused on the research field of obesity and lung disease.

Structural, mechanical effects of obesity on lung function are better known and appreciated. Accumulation of fat in the mediastinum and abdominal and thoracic cavities causes reductions in lung volume, in functional residual capacity, and in the compliance of the lungs, chest wall, and entire respiratory system, for instance.
Yet obesity is more than a state of increased BMI, and “what we’ve begun to understand is that [its impact on the lungs and respiratory health] is much more complicated than just a mechanical problem,” said Dr. Dixon, also director of pulmonary and critical care medicine at the University of Vermont Medical Center and professor of medicine at the medical college.
With obesity, adipose tissue changes not only in quantity, but in function, producing proinflammatory cytokines and hormones – such as leptin, tumor necrosis factor-alpha (TNF-alpha), and interleukin-6 – that can have direct effects on the lung. Insulin resistance, which is common with obesity, is also seemingly deleterious. And obesity-associated changes in immune function, lipid handling, diet, and the gut microbiome may also impact lung health and disease, she said.
Dr. Dixon, who wrote about these changes in a 2018 review article in the journal CHEST and another 2019 piece in Expert Review of Respiratory Medicine, has developed a research program focused on obesity and lung disease and has edited a book and organized international conferences on the topic. (CHEST 2018;153[3]:702-9 and Exper Rev Respir Med. 2018;12[9]:755-67.)
“The more I do, the more I realize that there are multiple obesity-associated changes involved, and that [our current high level of] obesity is like a huge population-level natural experiment ... on lung health,” she told this news organization.
Associations between lung disease and the metabolic and other disturbances of obesity are most established in asthma research and have taken hold in the realm of sleep-disordered breathing. But as the prevalence of obesity continues to grow, its role in other lung diseases such as chronic obstructive pulmonary disorder (COPD) and, most recently, pulmonary arterial hypertension (PAH), is getting attention in academia.
And certainly, COVID-19 has highlighted an “urgent need” to better understand how obesity increases susceptibility to severe viral infections, Dr. Dixon added.
Here are some glimpses into current thinking and some examples of research that may have preventive and therapeutic implications in the future:
OSA and OHS
“With sleep apnea we tend to focus on anatomic considerations, but there may be relationships or interactions between obesity and neuromuscular function and neuroventilatory control,” Susheel P. Patil, MD, PhD, director of the sleep medicine program for University Hospitals and assistant professor at Case Western Reserve University, Cleveland, said in an interview.

Some studies suggest, for instance, that TNF-alpha can increase obstructive sleep apnea (OSA) susceptibility and severity through its neuroventilatory modulating properties during sleep. And the potential for additional proinflammatory cytokines produced by adipose tissue to similarly affect upper airway neuroventilatory control is an “intriguing line” of inquiry for researchers in the sleep apnea space, he said.
Leptin is of interest particularly in obesity hypoventilation syndrome (OHS), which is characterized by chronic daytime hypercapnia. Best known as a satiety hormone, leptin is produced by adipose tissue and suppresses appetite at the central nervous system level. But it has long been known that leptin also affects ventilation and the control of breathing.
When transported across the blood-brain barrier, leptin increases the hypercapnic ventilatory response, Babak Mokhlesi, MD, MSc, codirector of the Rush Lung Center and chief of pulmonary, critical care, and sleep medicine at Rush University Medical Center in Chicago, said in an interview.
Research suggests that patients with OHS may have resistance to leptin at the central nervous system level – with leptin not reaching the sites of ventilatory control. This is a “prevailing theory” and could explain why these patients “do not augment their ventilation to maintain homeostasis, normal levels of CO2,” Dr. Mokhlesi said.

“Why some patients with severe obesity develop CO2 retention while others do not is not fully understood,” he said, noting that patients with OHS can normalize their CO2 quickly when instructed to take deep breaths. “What we know is that the centers in the brain responsible for augmenting ventilation when CO2 goes up are somehow blunted.”
In a study of obese mice led by Vsevolod Y. Polotsky, MD, PhD, of Johns Hopkins University, Baltimore – and highlighted by Dr. Mokhlesi as an example of important, recent research – leptin delivered intranasally alleviated hypoventilation (and upper-airway obstruction), while intraperitoneally administered leptin did not, seemingly overcoming “central leptin deficiency.” (Am J Respir Crit Care Med. 2019;199[6]:773-83).
“This proved that there is some level of resistance in this animal model ... and has potential for therapeutics in the future,” Dr. Mokhlesi said.
Understanding the role of insulin resistance in OSA is another research focus. Some data suggest that insulin resistance, which is more common in obesity, is more prevalent in populations with OSA, Dr. Patil said. Researchers have discussed a bidirectional relationship for years, but it’s likely that insulin resistance is a precursor, he said.
In a mechanistic study published in 2016, Dr. Patil and his coinvestigators found that obese individuals with insulin resistance but without frank diabetes or sleep apnea demonstrated preclinical elevations in pharyngeal collapsibility during sleep. The findings suggest that insulin resistance could play a causal role in OSA pathogenesis by “generating requisite elevations in pharyngeal collapsibility,” they wrote (Eur. Respir J. 2016;47[6]:1718-26).
More recently, Dr. Patil noted in the interview, there is increasing appreciation in academia that the type of fat may be important to predicting OSA. “Visceral fat has a completely different cytokine-secretion profile than subcutaneous fat ... it is the more metabolically active fat that may secondarily impact upper airway function though a neuroinflammatory mechanism,” he said. “That is one of the working hypotheses today.”
Asthma
Research has so roundly suggested that metabolic dysfunction contributes to severe, poorly controlled asthma that there’s recent and growing interest in targeting metabolic dysfunction as part of the treatment of obese asthma, said Dr. Dixon, whose own research in obesity and lung disease has focused on asthma.
Data from animal models and some epidemiologic studies have suggested that drugs used to treat type 2 diabetes mellitus, such as glucagon-like peptide receptor-1 (GLPR-1) agonists and metformin, may help control asthma. In one recent study – cited by Dr. Dixon in a 2022 review of obesity and asthma – people with obesity and asthma who were prescribed GLPR-1 agonists for diabetes had fewer asthma exacerbations compared with those who took other medications for diabetes (Semin Respir Crit Care Med. 2022 Feb 17. doi: 10.1055/s-0042-1742384).
There is also research interest in targeting the pro-inflammatory adipokine interleukin 6 (IL-6), since increased circulating levels of IL-6 correlate with asthma severity, and in addressing oxidative stress in asthma through treatment with a mitochondrially targeted antioxidant, she said. Oxidative stress is increased in the airways of people with obesity, and researchers believe it may contribute to the pathophysiology of obese asthma through effects on airway nitric oxide levels.
(Her own research work at the University of Vermont has found associations between poor asthma control and high levels of leptin, and similar associations involving low levels of adiponectin, an anti-inflammatory adipokine that has been shown to downregulate eosinophil recruitment in the airways.)
Weight loss has been shown in mostly small, single-center studies to improve asthma control, but short of weight loss, researchers are also investigating the role of poor dietary quality. Thus far, data suggest that it’s the composition of the diet, and not just its contribution to weight gain, that could be impactful, Dr. Dixon said.
More basic research questions cited by Dr. Dixon include the extent to which adipose tissue inflammation causes inflammation in the lungs. “It’s a little unclear whether all the metabolic dysfunction associated with poor asthma control is causing inflammation in the lungs,” she said, though “we’ve done some work here that shows mediators produced by the adipose tissue could be impacting production of inflammatory mediators by the airway epithelium.”
Overall, she said, “the big questions [in asthma] are, how does adipose tissue affect the airway? Is it through direct effects? Through effects on the immune system? And obesity is affected by diet and the gut microbiome – how can these be [impacting] the airway?”
Obesity “is associated with so many changes – the gut, the immune system, and metabolic dysfunction, in addition to airway mechanics,” she said, “that I no longer think, as I did when I came to this, that it’s just one thing. It’s probably all of these things together.”
In the meantime, questions about potential shared pathways for the development of obesity and asthma remain. “Obesity is a risk factor for developing asthma, but it’s also entirely possible that asthma is a risk factor for developing obesity,” she said. (Some data from pediatric populations, she noted, suggest that nonobese children with asthma are at increased risk of developing obesity.)
Also important, Dr. Dixon said, is “emerging literature in the last 5-10 years” that suggests that people with obesity are more susceptible to the effects of air pollution. Research involving inner-city schoolchildren with asthma, for instance, has shown that those with obesity had worse symptoms with air pollution exposure than did those who were not obese.
Pulmonary arterial hypertension
Some research has looked at adipose tissue–produced substances in PAH, but the most well-established association in obesity and PAH involves insulin resistance.
“I don’t think we’re certain as a community that obesity [in general] is the problem – it’s not itself considered a risk factor for PAH,” Anna R. Hemnes, MD, associate professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn., said in an interview. She noted that it’s “hard to dissect obesity” apart.
Researchers are “more confident,” she said, “that insulin resistance – one feature of obesity [in some people] – is associated with worse outcomes in PAH.” Metabolic disease resembling insulin resistance is common in PAH and is believed to contribute to pulmonary vascular disease and right ventricular (RV) failure – the main cause of mortality in PAH – at least in part because of increased oxidative stress.
Dr. Hemnes led a mechanistic phase II clinical trial of metformin in PAH in which the drug was associated with improved RV fractional area change and reduced RV lipid deposition (J Am Heart Assoc. 2020;9[22]:e018349), and she’s now leading a National Institutes of Health–funded multicenter trial looking at the impact of metformin and an exercise intervention on 6-minute walk distance and World Health Organization functional class in PAH.
At the Rush Lung Center, in the meantime, Dr. Mokhlesi is utilizing animal models of OSA and OHS to explore the effect of hypoxia and nighttime hypercapnia on the development of PAH. “I think the jury is still out as to whether obesity itself is a major risk factor, but if so, by what mechanism?” he said. “Is it worsening [sleep-disordered breathing], which then worsens PAH?”
COPD
The focus in COPD has traditionally been on underweight, but the relationship between obesity and COPD has increasingly been recognized in the last 10-15 years, said Frits M. E. Franssen, MD, PhD, of CIRO, a research institute in Horn, the Netherlands, that treats COPD and other chronic lung diseases, and of the department of respiratory medicine at Maastricht University.
Researchers like Dr. Franssen are trying, for one, to understand obesity’s impact on COPD pathophysiology and to tease apart the impact of both conditions on disease severity and patient-related outcomes such as exercise capacity and exercise-related symptoms.
When Dr. Franssen’s group compared responses to weight-bearing exercise (6-min. walk test) and weight-supported exercise (cycling) in obese and normal weight COPD patients matched for age, gender, and degree of airflow limitation, the researchers found that walking capacity was significantly reduced while cycling capacity was preserved in the obese group (Respirology. 2016;21[3]:483-8).
Exercise-related symptoms (dyspnea and leg fatigue) were largely comparable between the obese and normal-weight COPD patients in both exercise modalities. However, in other studies, dyspnea ratings during cycling – at any given level of ventilation – have been lower in obese patients, indicating that “additional fat mass may have a beneficial effect on lung functioning [in non–weight-bearing exercise],” he said in an interview.
Dr. Franssen’s group also has assessed body composition in overweight and obese patients with COPD and found that a significant number have low muscle mass. These patients had worse lung function, exercise tolerance, and muscle strength compared to patients with comparable BMI and normal muscle mass (Respir Res. 2021 Mar 25. doi: 10.1186/s12931-021-01689-w).
“We’d always thought that obese patients have normal muscle mass ... but now we know it can be dramatically low,” he said. In assessing obesity and formulating any weight loss plans, “we’re now interested not only in weight but in the distribution of fat mass and fat-free mass ... and in maintaining muscle mass in patients who are [prescribed dietary interventions].”
Paradoxically, in patients with severe COPD, obesity is associated with prolonged survival, while in patients with mild to moderate COPD, obesity is associated with increased mortality risk, he noted.
The impact of adipose tissue and the chronic inflammation and metabolic disturbances that characterize obesity are currently largely unexplored, he said. Researchers have not yet studied what optimal weights may be for patients with COPD. “And we’re interested in the questions, are body weight and body composition the result of the disease, or [are they] determining the type of COPD one will get?” Dr. Franssen said.
Patients with COPD who are obese have “more of the phenotype of chronic bronchitis,” he noted, “while typical emphysema patients are normally underweight.”
The diverse effects of obesity on lung health and disease are increasingly being teased apart, with researchers honing in on the impact of metabolic dysfunction, circulating inflammatory factors produced by adipose tissue, lipid handling, and other factors – in addition to body mass index – that are associated with the obese state.
“The bird’s eye view is that obesity completely changes lung health. It’s something we’ve only recently begun to appreciate,” said Anne E. Dixon, MA, BM, BCh, director of the Vermont Lung Center at the University of Vermont, Burlington, who is focused on the research field of obesity and lung disease.
Structural, mechanical effects of obesity on lung function are better known and appreciated. Accumulation of fat in the mediastinum and abdominal and thoracic cavities causes reductions in lung volume, in functional residual capacity, and in the compliance of the lungs, chest wall, and entire respiratory system, for instance.
Yet obesity is more than a state of increased BMI, and “what we’ve begun to understand is that [its impact on the lungs and respiratory health] is much more complicated than just a mechanical problem,” said Dr. Dixon, also director of pulmonary and critical care medicine at the University of Vermont Medical Center and professor of medicine at the medical college.
With obesity, adipose tissue changes not only in quantity, but in function, producing proinflammatory cytokines and hormones – such as leptin, tumor necrosis factor-alpha (TNF-alpha), and interleukin-6 – that can have direct effects on the lung. Insulin resistance, which is common with obesity, is also seemingly deleterious. And obesity-associated changes in immune function, lipid handling, diet, and the gut microbiome may also impact lung health and disease, she said.
Dr. Dixon, who wrote about these changes in a 2018 review article in the journal CHEST and another 2019 piece in Expert Review of Respiratory Medicine, has developed a research program focused on obesity and lung disease and has edited a book and organized international conferences on the topic. (CHEST 2018;153[3]:702-9 and Exper Rev Respir Med. 2018;12[9]:755-67.)
“The more I do, the more I realize that there are multiple obesity-associated changes involved, and that [our current high level of] obesity is like a huge population-level natural experiment ... on lung health,” she told this news organization.
Associations between lung disease and the metabolic and other disturbances of obesity are most established in asthma research and have taken hold in the realm of sleep-disordered breathing. But as the prevalence of obesity continues to grow, its role in other lung diseases such as chronic obstructive pulmonary disorder (COPD) and, most recently, pulmonary arterial hypertension (PAH), is getting attention in academia.
And certainly, COVID-19 has highlighted an “urgent need” to better understand how obesity increases susceptibility to severe viral infections, Dr. Dixon added.
Here are some glimpses into current thinking and some examples of research that may have preventive and therapeutic implications in the future:
OSA and OHS
“With sleep apnea we tend to focus on anatomic considerations, but there may be relationships or interactions between obesity and neuromuscular function and neuroventilatory control,” Susheel P. Patil, MD, PhD, director of the sleep medicine program for University Hospitals and assistant professor at Case Western Reserve University, Cleveland, said in an interview.
Some studies suggest, for instance, that TNF-alpha can increase obstructive sleep apnea (OSA) susceptibility and severity through its neuroventilatory modulating properties during sleep. And the potential for additional proinflammatory cytokines produced by adipose tissue to similarly affect upper airway neuroventilatory control is an “intriguing line” of inquiry for researchers in the sleep apnea space, he said.
Leptin is of interest particularly in obesity hypoventilation syndrome (OHS), which is characterized by chronic daytime hypercapnia. Best known as a satiety hormone, leptin is produced by adipose tissue and suppresses appetite at the central nervous system level. But it has long been known that leptin also affects ventilation and the control of breathing.
When transported across the blood-brain barrier, leptin increases the hypercapnic ventilatory response, Babak Mokhlesi, MD, MSc, codirector of the Rush Lung Center and chief of pulmonary, critical care, and sleep medicine at Rush University Medical Center in Chicago, said in an interview.
Research suggests that patients with OHS may have resistance to leptin at the central nervous system level – with leptin not reaching the sites of ventilatory control. This is a “prevailing theory” and could explain why these patients “do not augment their ventilation to maintain homeostasis, normal levels of CO2,” Dr. Mokhlesi said.
“Why some patients with severe obesity develop CO2 retention while others do not is not fully understood,” he said, noting that patients with OHS can normalize their CO2 quickly when instructed to take deep breaths. “What we know is that the centers in the brain responsible for augmenting ventilation when CO2 goes up are somehow blunted.”
In a study of obese mice led by Vsevolod Y. Polotsky, MD, PhD, of Johns Hopkins University, Baltimore – and highlighted by Dr. Mokhlesi as an example of important, recent research – leptin delivered intranasally alleviated hypoventilation (and upper-airway obstruction), while intraperitoneally administered leptin did not, seemingly overcoming “central leptin deficiency.” (Am J Respir Crit Care Med. 2019;199[6]:773-83).
“This proved that there is some level of resistance in this animal model ... and has potential for therapeutics in the future,” Dr. Mokhlesi said.
Understanding the role of insulin resistance in OSA is another research focus. Some data suggest that insulin resistance, which is more common in obesity, is more prevalent in populations with OSA, Dr. Patil said. Researchers have discussed a bidirectional relationship for years, but it’s likely that insulin resistance is a precursor, he said.
In a mechanistic study published in 2016, Dr. Patil and his coinvestigators found that obese individuals with insulin resistance but without frank diabetes or sleep apnea demonstrated preclinical elevations in pharyngeal collapsibility during sleep. The findings suggest that insulin resistance could play a causal role in OSA pathogenesis by “generating requisite elevations in pharyngeal collapsibility,” they wrote (Eur. Respir J. 2016;47[6]:1718-26).
More recently, Dr. Patil noted in the interview, there is increasing appreciation in academia that the type of fat may be important to predicting OSA. “Visceral fat has a completely different cytokine-secretion profile than subcutaneous fat ... it is the more metabolically active fat that may secondarily impact upper airway function though a neuroinflammatory mechanism,” he said. “That is one of the working hypotheses today.”
Asthma
Research has so roundly suggested that metabolic dysfunction contributes to severe, poorly controlled asthma that there’s recent and growing interest in targeting metabolic dysfunction as part of the treatment of obese asthma, said Dr. Dixon, whose own research in obesity and lung disease has focused on asthma.
Data from animal models and some epidemiologic studies have suggested that drugs used to treat type 2 diabetes mellitus, such as glucagon-like peptide receptor-1 (GLPR-1) agonists and metformin, may help control asthma. In one recent study – cited by Dr. Dixon in a 2022 review of obesity and asthma – people with obesity and asthma who were prescribed GLPR-1 agonists for diabetes had fewer asthma exacerbations compared with those who took other medications for diabetes (Semin Respir Crit Care Med. 2022 Feb 17. doi: 10.1055/s-0042-1742384).
There is also research interest in targeting the pro-inflammatory adipokine interleukin 6 (IL-6), since increased circulating levels of IL-6 correlate with asthma severity, and in addressing oxidative stress in asthma through treatment with a mitochondrially targeted antioxidant, she said. Oxidative stress is increased in the airways of people with obesity, and researchers believe it may contribute to the pathophysiology of obese asthma through effects on airway nitric oxide levels.
(Her own research work at the University of Vermont has found associations between poor asthma control and high levels of leptin, and similar associations involving low levels of adiponectin, an anti-inflammatory adipokine that has been shown to downregulate eosinophil recruitment in the airways.)
Weight loss has been shown in mostly small, single-center studies to improve asthma control, but short of weight loss, researchers are also investigating the role of poor dietary quality. Thus far, data suggest that it’s the composition of the diet, and not just its contribution to weight gain, that could be impactful, Dr. Dixon said.
More basic research questions cited by Dr. Dixon include the extent to which adipose tissue inflammation causes inflammation in the lungs. “It’s a little unclear whether all the metabolic dysfunction associated with poor asthma control is causing inflammation in the lungs,” she said, though “we’ve done some work here that shows mediators produced by the adipose tissue could be impacting production of inflammatory mediators by the airway epithelium.”
Overall, she said, “the big questions [in asthma] are, how does adipose tissue affect the airway? Is it through direct effects? Through effects on the immune system? And obesity is affected by diet and the gut microbiome – how can these be [impacting] the airway?”
Obesity “is associated with so many changes – the gut, the immune system, and metabolic dysfunction, in addition to airway mechanics,” she said, “that I no longer think, as I did when I came to this, that it’s just one thing. It’s probably all of these things together.”
In the meantime, questions about potential shared pathways for the development of obesity and asthma remain. “Obesity is a risk factor for developing asthma, but it’s also entirely possible that asthma is a risk factor for developing obesity,” she said. (Some data from pediatric populations, she noted, suggest that nonobese children with asthma are at increased risk of developing obesity.)
Also important, Dr. Dixon said, is “emerging literature in the last 5-10 years” that suggests that people with obesity are more susceptible to the effects of air pollution. Research involving inner-city schoolchildren with asthma, for instance, has shown that those with obesity had worse symptoms with air pollution exposure than did those who were not obese.
Pulmonary arterial hypertension
Some research has looked at adipose tissue–produced substances in PAH, but the most well-established association in obesity and PAH involves insulin resistance.
“I don’t think we’re certain as a community that obesity [in general] is the problem – it’s not itself considered a risk factor for PAH,” Anna R. Hemnes, MD, associate professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn., said in an interview. She noted that it’s “hard to dissect obesity” apart.
Researchers are “more confident,” she said, “that insulin resistance – one feature of obesity [in some people] – is associated with worse outcomes in PAH.” Metabolic disease resembling insulin resistance is common in PAH and is believed to contribute to pulmonary vascular disease and right ventricular (RV) failure – the main cause of mortality in PAH – at least in part because of increased oxidative stress.
Dr. Hemnes led a mechanistic phase II clinical trial of metformin in PAH in which the drug was associated with improved RV fractional area change and reduced RV lipid deposition (J Am Heart Assoc. 2020;9[22]:e018349), and she’s now leading a National Institutes of Health–funded multicenter trial looking at the impact of metformin and an exercise intervention on 6-minute walk distance and World Health Organization functional class in PAH.
At the Rush Lung Center, in the meantime, Dr. Mokhlesi is utilizing animal models of OSA and OHS to explore the effect of hypoxia and nighttime hypercapnia on the development of PAH. “I think the jury is still out as to whether obesity itself is a major risk factor, but if so, by what mechanism?” he said. “Is it worsening [sleep-disordered breathing], which then worsens PAH?”
COPD
The focus in COPD has traditionally been on underweight, but the relationship between obesity and COPD has increasingly been recognized in the last 10-15 years, said Frits M. E. Franssen, MD, PhD, of CIRO, a research institute in Horn, the Netherlands, that treats COPD and other chronic lung diseases, and of the department of respiratory medicine at Maastricht University.
Researchers like Dr. Franssen are trying, for one, to understand obesity’s impact on COPD pathophysiology and to tease apart the impact of both conditions on disease severity and patient-related outcomes such as exercise capacity and exercise-related symptoms.
When Dr. Franssen’s group compared responses to weight-bearing exercise (6-min. walk test) and weight-supported exercise (cycling) in obese and normal weight COPD patients matched for age, gender, and degree of airflow limitation, the researchers found that walking capacity was significantly reduced while cycling capacity was preserved in the obese group (Respirology. 2016;21[3]:483-8).
Exercise-related symptoms (dyspnea and leg fatigue) were largely comparable between the obese and normal-weight COPD patients in both exercise modalities. However, in other studies, dyspnea ratings during cycling – at any given level of ventilation – have been lower in obese patients, indicating that “additional fat mass may have a beneficial effect on lung functioning [in non–weight-bearing exercise],” he said in an interview.
Dr. Franssen’s group also has assessed body composition in overweight and obese patients with COPD and found that a significant number have low muscle mass. These patients had worse lung function, exercise tolerance, and muscle strength compared to patients with comparable BMI and normal muscle mass (Respir Res. 2021 Mar 25. doi: 10.1186/s12931-021-01689-w).
“We’d always thought that obese patients have normal muscle mass ... but now we know it can be dramatically low,” he said. In assessing obesity and formulating any weight loss plans, “we’re now interested not only in weight but in the distribution of fat mass and fat-free mass ... and in maintaining muscle mass in patients who are [prescribed dietary interventions].”
Paradoxically, in patients with severe COPD, obesity is associated with prolonged survival, while in patients with mild to moderate COPD, obesity is associated with increased mortality risk, he noted.
The impact of adipose tissue and the chronic inflammation and metabolic disturbances that characterize obesity are currently largely unexplored, he said. Researchers have not yet studied what optimal weights may be for patients with COPD. “And we’re interested in the questions, are body weight and body composition the result of the disease, or [are they] determining the type of COPD one will get?” Dr. Franssen said.
Patients with COPD who are obese have “more of the phenotype of chronic bronchitis,” he noted, “while typical emphysema patients are normally underweight.”
The diverse effects of obesity on lung health and disease are increasingly being teased apart, with researchers honing in on the impact of metabolic dysfunction, circulating inflammatory factors produced by adipose tissue, lipid handling, and other factors – in addition to body mass index – that are associated with the obese state.
“The bird’s eye view is that obesity completely changes lung health. It’s something we’ve only recently begun to appreciate,” said Anne E. Dixon, MA, BM, BCh, director of the Vermont Lung Center at the University of Vermont, Burlington, who is focused on the research field of obesity and lung disease.
Structural, mechanical effects of obesity on lung function are better known and appreciated. Accumulation of fat in the mediastinum and abdominal and thoracic cavities causes reductions in lung volume, in functional residual capacity, and in the compliance of the lungs, chest wall, and entire respiratory system, for instance.
Yet obesity is more than a state of increased BMI, and “what we’ve begun to understand is that [its impact on the lungs and respiratory health] is much more complicated than just a mechanical problem,” said Dr. Dixon, also director of pulmonary and critical care medicine at the University of Vermont Medical Center and professor of medicine at the medical college.
With obesity, adipose tissue changes not only in quantity, but in function, producing proinflammatory cytokines and hormones – such as leptin, tumor necrosis factor-alpha (TNF-alpha), and interleukin-6 – that can have direct effects on the lung. Insulin resistance, which is common with obesity, is also seemingly deleterious. And obesity-associated changes in immune function, lipid handling, diet, and the gut microbiome may also impact lung health and disease, she said.
Dr. Dixon, who wrote about these changes in a 2018 review article in the journal CHEST and another 2019 piece in Expert Review of Respiratory Medicine, has developed a research program focused on obesity and lung disease and has edited a book and organized international conferences on the topic. (CHEST 2018;153[3]:702-9 and Exper Rev Respir Med. 2018;12[9]:755-67.)
“The more I do, the more I realize that there are multiple obesity-associated changes involved, and that [our current high level of] obesity is like a huge population-level natural experiment ... on lung health,” she told this news organization.
Associations between lung disease and the metabolic and other disturbances of obesity are most established in asthma research and have taken hold in the realm of sleep-disordered breathing. But as the prevalence of obesity continues to grow, its role in other lung diseases such as chronic obstructive pulmonary disorder (COPD) and, most recently, pulmonary arterial hypertension (PAH), is getting attention in academia.
And certainly, COVID-19 has highlighted an “urgent need” to better understand how obesity increases susceptibility to severe viral infections, Dr. Dixon added.
Here are some glimpses into current thinking and some examples of research that may have preventive and therapeutic implications in the future:
OSA and OHS
“With sleep apnea we tend to focus on anatomic considerations, but there may be relationships or interactions between obesity and neuromuscular function and neuroventilatory control,” Susheel P. Patil, MD, PhD, director of the sleep medicine program for University Hospitals and assistant professor at Case Western Reserve University, Cleveland, said in an interview.
Some studies suggest, for instance, that TNF-alpha can increase obstructive sleep apnea (OSA) susceptibility and severity through its neuroventilatory modulating properties during sleep. And the potential for additional proinflammatory cytokines produced by adipose tissue to similarly affect upper airway neuroventilatory control is an “intriguing line” of inquiry for researchers in the sleep apnea space, he said.
Leptin is of interest particularly in obesity hypoventilation syndrome (OHS), which is characterized by chronic daytime hypercapnia. Best known as a satiety hormone, leptin is produced by adipose tissue and suppresses appetite at the central nervous system level. But it has long been known that leptin also affects ventilation and the control of breathing.
When transported across the blood-brain barrier, leptin increases the hypercapnic ventilatory response, Babak Mokhlesi, MD, MSc, codirector of the Rush Lung Center and chief of pulmonary, critical care, and sleep medicine at Rush University Medical Center in Chicago, said in an interview.
Research suggests that patients with OHS may have resistance to leptin at the central nervous system level – with leptin not reaching the sites of ventilatory control. This is a “prevailing theory” and could explain why these patients “do not augment their ventilation to maintain homeostasis, normal levels of CO2,” Dr. Mokhlesi said.
“Why some patients with severe obesity develop CO2 retention while others do not is not fully understood,” he said, noting that patients with OHS can normalize their CO2 quickly when instructed to take deep breaths. “What we know is that the centers in the brain responsible for augmenting ventilation when CO2 goes up are somehow blunted.”
In a study of obese mice led by Vsevolod Y. Polotsky, MD, PhD, of Johns Hopkins University, Baltimore – and highlighted by Dr. Mokhlesi as an example of important, recent research – leptin delivered intranasally alleviated hypoventilation (and upper-airway obstruction), while intraperitoneally administered leptin did not, seemingly overcoming “central leptin deficiency.” (Am J Respir Crit Care Med. 2019;199[6]:773-83).
“This proved that there is some level of resistance in this animal model ... and has potential for therapeutics in the future,” Dr. Mokhlesi said.
Understanding the role of insulin resistance in OSA is another research focus. Some data suggest that insulin resistance, which is more common in obesity, is more prevalent in populations with OSA, Dr. Patil said. Researchers have discussed a bidirectional relationship for years, but it’s likely that insulin resistance is a precursor, he said.
In a mechanistic study published in 2016, Dr. Patil and his coinvestigators found that obese individuals with insulin resistance but without frank diabetes or sleep apnea demonstrated preclinical elevations in pharyngeal collapsibility during sleep. The findings suggest that insulin resistance could play a causal role in OSA pathogenesis by “generating requisite elevations in pharyngeal collapsibility,” they wrote (Eur. Respir J. 2016;47[6]:1718-26).
More recently, Dr. Patil noted in the interview, there is increasing appreciation in academia that the type of fat may be important to predicting OSA. “Visceral fat has a completely different cytokine-secretion profile than subcutaneous fat ... it is the more metabolically active fat that may secondarily impact upper airway function though a neuroinflammatory mechanism,” he said. “That is one of the working hypotheses today.”
Asthma
Research has so roundly suggested that metabolic dysfunction contributes to severe, poorly controlled asthma that there’s recent and growing interest in targeting metabolic dysfunction as part of the treatment of obese asthma, said Dr. Dixon, whose own research in obesity and lung disease has focused on asthma.
Data from animal models and some epidemiologic studies have suggested that drugs used to treat type 2 diabetes mellitus, such as glucagon-like peptide receptor-1 (GLPR-1) agonists and metformin, may help control asthma. In one recent study – cited by Dr. Dixon in a 2022 review of obesity and asthma – people with obesity and asthma who were prescribed GLPR-1 agonists for diabetes had fewer asthma exacerbations compared with those who took other medications for diabetes (Semin Respir Crit Care Med. 2022 Feb 17. doi: 10.1055/s-0042-1742384).
There is also research interest in targeting the pro-inflammatory adipokine interleukin 6 (IL-6), since increased circulating levels of IL-6 correlate with asthma severity, and in addressing oxidative stress in asthma through treatment with a mitochondrially targeted antioxidant, she said. Oxidative stress is increased in the airways of people with obesity, and researchers believe it may contribute to the pathophysiology of obese asthma through effects on airway nitric oxide levels.
(Her own research work at the University of Vermont has found associations between poor asthma control and high levels of leptin, and similar associations involving low levels of adiponectin, an anti-inflammatory adipokine that has been shown to downregulate eosinophil recruitment in the airways.)
Weight loss has been shown in mostly small, single-center studies to improve asthma control, but short of weight loss, researchers are also investigating the role of poor dietary quality. Thus far, data suggest that it’s the composition of the diet, and not just its contribution to weight gain, that could be impactful, Dr. Dixon said.
More basic research questions cited by Dr. Dixon include the extent to which adipose tissue inflammation causes inflammation in the lungs. “It’s a little unclear whether all the metabolic dysfunction associated with poor asthma control is causing inflammation in the lungs,” she said, though “we’ve done some work here that shows mediators produced by the adipose tissue could be impacting production of inflammatory mediators by the airway epithelium.”
Overall, she said, “the big questions [in asthma] are, how does adipose tissue affect the airway? Is it through direct effects? Through effects on the immune system? And obesity is affected by diet and the gut microbiome – how can these be [impacting] the airway?”
Obesity “is associated with so many changes – the gut, the immune system, and metabolic dysfunction, in addition to airway mechanics,” she said, “that I no longer think, as I did when I came to this, that it’s just one thing. It’s probably all of these things together.”
In the meantime, questions about potential shared pathways for the development of obesity and asthma remain. “Obesity is a risk factor for developing asthma, but it’s also entirely possible that asthma is a risk factor for developing obesity,” she said. (Some data from pediatric populations, she noted, suggest that nonobese children with asthma are at increased risk of developing obesity.)
Also important, Dr. Dixon said, is “emerging literature in the last 5-10 years” that suggests that people with obesity are more susceptible to the effects of air pollution. Research involving inner-city schoolchildren with asthma, for instance, has shown that those with obesity had worse symptoms with air pollution exposure than did those who were not obese.
Pulmonary arterial hypertension
Some research has looked at adipose tissue–produced substances in PAH, but the most well-established association in obesity and PAH involves insulin resistance.
“I don’t think we’re certain as a community that obesity [in general] is the problem – it’s not itself considered a risk factor for PAH,” Anna R. Hemnes, MD, associate professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn., said in an interview. She noted that it’s “hard to dissect obesity” apart.
Researchers are “more confident,” she said, “that insulin resistance – one feature of obesity [in some people] – is associated with worse outcomes in PAH.” Metabolic disease resembling insulin resistance is common in PAH and is believed to contribute to pulmonary vascular disease and right ventricular (RV) failure – the main cause of mortality in PAH – at least in part because of increased oxidative stress.
Dr. Hemnes led a mechanistic phase II clinical trial of metformin in PAH in which the drug was associated with improved RV fractional area change and reduced RV lipid deposition (J Am Heart Assoc. 2020;9[22]:e018349), and she’s now leading a National Institutes of Health–funded multicenter trial looking at the impact of metformin and an exercise intervention on 6-minute walk distance and World Health Organization functional class in PAH.
At the Rush Lung Center, in the meantime, Dr. Mokhlesi is utilizing animal models of OSA and OHS to explore the effect of hypoxia and nighttime hypercapnia on the development of PAH. “I think the jury is still out as to whether obesity itself is a major risk factor, but if so, by what mechanism?” he said. “Is it worsening [sleep-disordered breathing], which then worsens PAH?”
COPD
The focus in COPD has traditionally been on underweight, but the relationship between obesity and COPD has increasingly been recognized in the last 10-15 years, said Frits M. E. Franssen, MD, PhD, of CIRO, a research institute in Horn, the Netherlands, that treats COPD and other chronic lung diseases, and of the department of respiratory medicine at Maastricht University.
Researchers like Dr. Franssen are trying, for one, to understand obesity’s impact on COPD pathophysiology and to tease apart the impact of both conditions on disease severity and patient-related outcomes such as exercise capacity and exercise-related symptoms.
When Dr. Franssen’s group compared responses to weight-bearing exercise (6-min. walk test) and weight-supported exercise (cycling) in obese and normal weight COPD patients matched for age, gender, and degree of airflow limitation, the researchers found that walking capacity was significantly reduced while cycling capacity was preserved in the obese group (Respirology. 2016;21[3]:483-8).
Exercise-related symptoms (dyspnea and leg fatigue) were largely comparable between the obese and normal-weight COPD patients in both exercise modalities. However, in other studies, dyspnea ratings during cycling – at any given level of ventilation – have been lower in obese patients, indicating that “additional fat mass may have a beneficial effect on lung functioning [in non–weight-bearing exercise],” he said in an interview.
Dr. Franssen’s group also has assessed body composition in overweight and obese patients with COPD and found that a significant number have low muscle mass. These patients had worse lung function, exercise tolerance, and muscle strength compared to patients with comparable BMI and normal muscle mass (Respir Res. 2021 Mar 25. doi: 10.1186/s12931-021-01689-w).
“We’d always thought that obese patients have normal muscle mass ... but now we know it can be dramatically low,” he said. In assessing obesity and formulating any weight loss plans, “we’re now interested not only in weight but in the distribution of fat mass and fat-free mass ... and in maintaining muscle mass in patients who are [prescribed dietary interventions].”
Paradoxically, in patients with severe COPD, obesity is associated with prolonged survival, while in patients with mild to moderate COPD, obesity is associated with increased mortality risk, he noted.
The impact of adipose tissue and the chronic inflammation and metabolic disturbances that characterize obesity are currently largely unexplored, he said. Researchers have not yet studied what optimal weights may be for patients with COPD. “And we’re interested in the questions, are body weight and body composition the result of the disease, or [are they] determining the type of COPD one will get?” Dr. Franssen said.
Patients with COPD who are obese have “more of the phenotype of chronic bronchitis,” he noted, “while typical emphysema patients are normally underweight.”
Meet a miracle: Man with trisomy 13 to celebrate 20th birthday
Lloyd Tyler Rochez, born in 2002 with trisomy 13, a genetic disorder that can involve severe learning problems and health woes that affect nearly every organ.
Lloyd’s diagnosis was confirmed shortly after he was born, when his doctors noticed that his facial features weren’t measuring right for a baby of his size, he had an extra finger on his left hand, and his fingers were joined on the right. His heart was also on the right side of his chest instead of the left. When he had breathing issues, he was quickly rushed to the neonatal ICU (NICU) in the New York City hospital where he was born.
Ms. Nunez wasn’t sure exactly what was wrong with her newborn, but the next morning, a genetics expert came to her room to discuss her medical history and whether anyone in the family had Down syndrome. That same health care provider told her that the next step was to run some tests and do more bloodwork.
Four days later, when Ms. Nunez was told that Lloyd had trisomy 13 and was likely to live for only 2 weeks, she was unable to come to terms with the news.
“There was so much information being told to me at once,” recalls Ms. Nunez, now 42, who is also the mom of two daughters, ages 8 and 10. “I had just turned 22, and this was my first experience giving birth. I can’t even remember everything the doctors told me.”
But she does remember her doctor telling her something about faith.
“After he tried to explain trisomy 13 to me, the downside and the prognosis, at the end he said, ‘I don’t know if you believe in some supernatural being, but if you want to ask that someone for a miracle, I would advise you to do that. Pray for your miracle, and you may get it.’”
Prepared for the worst, Ms. Nunez, who now works from her Martinsburg, WV, home as a case manager for unaccompanied minors coming to the U.S., decided that she would commit to providing the best possible care for her new baby no matter how long he lived.
Thus began an incredible story of Lloyd defying all the odds. While he stayed in the hospital for 2 weeks, his breathing soon began to stabilize, and he could eat by mouth. With that, he was discharged and allowed to go home.
“I was this inexperienced first-time mom who had been told to watch for all sorts of things, like making sure he didn’t turn blue at night,” she says. “I spent so many sleepless nights, but I was dedicated to Lloyd.”
Then, when Lloyd was 6 months old, Ms. Nunez made another important choice.
“I decided that I wasn’t going to live each day as if he was going to die,” she says. “I decided, instead, to enjoy him every day.”
But many health complications still came about, including a serious intestine issue at 8 months, at which point Lloyd’s doctors suggested waiting until he was a year old to have surgery.
Lloyd was able to get through the procedure, but while he was in the recovery room, he stopped breathing.
“I started screaming ‘my son is dying,’” Ms. Nunez recalls. “The nurses put me in a room, and I think I was in there for 10 minutes, but it felt like an eternity of me screaming.”She soon learned that Lloyd had had a seizure. He spent the next 3 weeks in the hospital.
“That was our life,” she says. “He would have respiratory pneumonia, for example, and we would go back to the hospital. We were in and out and in and out.”
But she kept the faith, and since then, Lloyd’s health has mostly stabilized. Ms. Nunez can care for him at home on her own and with family members who help out from time to time.
And, while Lloyd is unable to speak, he smiles and laughs when he’s happy, he’s quiet when he feels ill, and, when he wants to be alone, he groans, Ms. Nunez says. He can stand up, and he crawls from place to place. He also can’t go to the bathroom on his own and is fed by a gastrostomy tube, or G-tube.
In December, when Lloyd was diagnosed with COVID-19, Ms. Nunez started worrying all over again.
“Seeing him in the ICU, all I could think of was ‘please don’t make my son suffer,’” she says. “If he goes, I want him to go in peace, and I don’t want to see him in a machine and suffering.”
But Lloyd once again defied the odds against him and came home again. He has since faced yet another health challenge: He recently had a pelvic fracture.
“When I saw the orthopedist, he told me that Lloyd has a bone deficiency and that his bones don’t have enough room to grow,” she says. “I’m afraid this will be the beginning of a new journey.”
How this mom finds strength
While Ms. Nunez doesn’t go to a support group or speak with a mental health professional about all that she’s juggling, she says she draws strength from Lloyd himself.
“I’m very private, and I come from a culture where you don’t want people feeling sorry for you,” she says. “But I want to give Lloyd everything – he goes to school, we go to church, he had a quinceañera when he was 15, we’ve been to Disney, and we’ve both gotten on a roller coaster. I haven’t limited his life.”
She also draws comfort from her daughters.
“Everyone calls him ‘Baby Lloyd,’” she says. “My girls come right home from school, wash their hands, and throw themselves on his bed and watch TV with him. They also worry about him a lot. When he goes to the hospital, they suffer more than I do.”
In the end, Ms. Nunez hopes her story inspires others to think beyond a prognosis.
“Don’t lose hope,” she says. “I want people to feel hopeful when they read about Lloyd. He’s going to be 20 years old, and no one ever believed he would be here today ... I feel blessed.”
A version of this article first appeared on WebMD.com.
Lloyd Tyler Rochez, born in 2002 with trisomy 13, a genetic disorder that can involve severe learning problems and health woes that affect nearly every organ.
Lloyd’s diagnosis was confirmed shortly after he was born, when his doctors noticed that his facial features weren’t measuring right for a baby of his size, he had an extra finger on his left hand, and his fingers were joined on the right. His heart was also on the right side of his chest instead of the left. When he had breathing issues, he was quickly rushed to the neonatal ICU (NICU) in the New York City hospital where he was born.
Ms. Nunez wasn’t sure exactly what was wrong with her newborn, but the next morning, a genetics expert came to her room to discuss her medical history and whether anyone in the family had Down syndrome. That same health care provider told her that the next step was to run some tests and do more bloodwork.
Four days later, when Ms. Nunez was told that Lloyd had trisomy 13 and was likely to live for only 2 weeks, she was unable to come to terms with the news.
“There was so much information being told to me at once,” recalls Ms. Nunez, now 42, who is also the mom of two daughters, ages 8 and 10. “I had just turned 22, and this was my first experience giving birth. I can’t even remember everything the doctors told me.”
But she does remember her doctor telling her something about faith.
“After he tried to explain trisomy 13 to me, the downside and the prognosis, at the end he said, ‘I don’t know if you believe in some supernatural being, but if you want to ask that someone for a miracle, I would advise you to do that. Pray for your miracle, and you may get it.’”
Prepared for the worst, Ms. Nunez, who now works from her Martinsburg, WV, home as a case manager for unaccompanied minors coming to the U.S., decided that she would commit to providing the best possible care for her new baby no matter how long he lived.
Thus began an incredible story of Lloyd defying all the odds. While he stayed in the hospital for 2 weeks, his breathing soon began to stabilize, and he could eat by mouth. With that, he was discharged and allowed to go home.
“I was this inexperienced first-time mom who had been told to watch for all sorts of things, like making sure he didn’t turn blue at night,” she says. “I spent so many sleepless nights, but I was dedicated to Lloyd.”
Then, when Lloyd was 6 months old, Ms. Nunez made another important choice.
“I decided that I wasn’t going to live each day as if he was going to die,” she says. “I decided, instead, to enjoy him every day.”
But many health complications still came about, including a serious intestine issue at 8 months, at which point Lloyd’s doctors suggested waiting until he was a year old to have surgery.
Lloyd was able to get through the procedure, but while he was in the recovery room, he stopped breathing.
“I started screaming ‘my son is dying,’” Ms. Nunez recalls. “The nurses put me in a room, and I think I was in there for 10 minutes, but it felt like an eternity of me screaming.”She soon learned that Lloyd had had a seizure. He spent the next 3 weeks in the hospital.
“That was our life,” she says. “He would have respiratory pneumonia, for example, and we would go back to the hospital. We were in and out and in and out.”
But she kept the faith, and since then, Lloyd’s health has mostly stabilized. Ms. Nunez can care for him at home on her own and with family members who help out from time to time.
And, while Lloyd is unable to speak, he smiles and laughs when he’s happy, he’s quiet when he feels ill, and, when he wants to be alone, he groans, Ms. Nunez says. He can stand up, and he crawls from place to place. He also can’t go to the bathroom on his own and is fed by a gastrostomy tube, or G-tube.
In December, when Lloyd was diagnosed with COVID-19, Ms. Nunez started worrying all over again.
“Seeing him in the ICU, all I could think of was ‘please don’t make my son suffer,’” she says. “If he goes, I want him to go in peace, and I don’t want to see him in a machine and suffering.”
But Lloyd once again defied the odds against him and came home again. He has since faced yet another health challenge: He recently had a pelvic fracture.
“When I saw the orthopedist, he told me that Lloyd has a bone deficiency and that his bones don’t have enough room to grow,” she says. “I’m afraid this will be the beginning of a new journey.”
How this mom finds strength
While Ms. Nunez doesn’t go to a support group or speak with a mental health professional about all that she’s juggling, she says she draws strength from Lloyd himself.
“I’m very private, and I come from a culture where you don’t want people feeling sorry for you,” she says. “But I want to give Lloyd everything – he goes to school, we go to church, he had a quinceañera when he was 15, we’ve been to Disney, and we’ve both gotten on a roller coaster. I haven’t limited his life.”
She also draws comfort from her daughters.
“Everyone calls him ‘Baby Lloyd,’” she says. “My girls come right home from school, wash their hands, and throw themselves on his bed and watch TV with him. They also worry about him a lot. When he goes to the hospital, they suffer more than I do.”
In the end, Ms. Nunez hopes her story inspires others to think beyond a prognosis.
“Don’t lose hope,” she says. “I want people to feel hopeful when they read about Lloyd. He’s going to be 20 years old, and no one ever believed he would be here today ... I feel blessed.”
A version of this article first appeared on WebMD.com.
Lloyd Tyler Rochez, born in 2002 with trisomy 13, a genetic disorder that can involve severe learning problems and health woes that affect nearly every organ.
Lloyd’s diagnosis was confirmed shortly after he was born, when his doctors noticed that his facial features weren’t measuring right for a baby of his size, he had an extra finger on his left hand, and his fingers were joined on the right. His heart was also on the right side of his chest instead of the left. When he had breathing issues, he was quickly rushed to the neonatal ICU (NICU) in the New York City hospital where he was born.
Ms. Nunez wasn’t sure exactly what was wrong with her newborn, but the next morning, a genetics expert came to her room to discuss her medical history and whether anyone in the family had Down syndrome. That same health care provider told her that the next step was to run some tests and do more bloodwork.
Four days later, when Ms. Nunez was told that Lloyd had trisomy 13 and was likely to live for only 2 weeks, she was unable to come to terms with the news.
“There was so much information being told to me at once,” recalls Ms. Nunez, now 42, who is also the mom of two daughters, ages 8 and 10. “I had just turned 22, and this was my first experience giving birth. I can’t even remember everything the doctors told me.”
But she does remember her doctor telling her something about faith.
“After he tried to explain trisomy 13 to me, the downside and the prognosis, at the end he said, ‘I don’t know if you believe in some supernatural being, but if you want to ask that someone for a miracle, I would advise you to do that. Pray for your miracle, and you may get it.’”
Prepared for the worst, Ms. Nunez, who now works from her Martinsburg, WV, home as a case manager for unaccompanied minors coming to the U.S., decided that she would commit to providing the best possible care for her new baby no matter how long he lived.
Thus began an incredible story of Lloyd defying all the odds. While he stayed in the hospital for 2 weeks, his breathing soon began to stabilize, and he could eat by mouth. With that, he was discharged and allowed to go home.
“I was this inexperienced first-time mom who had been told to watch for all sorts of things, like making sure he didn’t turn blue at night,” she says. “I spent so many sleepless nights, but I was dedicated to Lloyd.”
Then, when Lloyd was 6 months old, Ms. Nunez made another important choice.
“I decided that I wasn’t going to live each day as if he was going to die,” she says. “I decided, instead, to enjoy him every day.”
But many health complications still came about, including a serious intestine issue at 8 months, at which point Lloyd’s doctors suggested waiting until he was a year old to have surgery.
Lloyd was able to get through the procedure, but while he was in the recovery room, he stopped breathing.
“I started screaming ‘my son is dying,’” Ms. Nunez recalls. “The nurses put me in a room, and I think I was in there for 10 minutes, but it felt like an eternity of me screaming.”She soon learned that Lloyd had had a seizure. He spent the next 3 weeks in the hospital.
“That was our life,” she says. “He would have respiratory pneumonia, for example, and we would go back to the hospital. We were in and out and in and out.”
But she kept the faith, and since then, Lloyd’s health has mostly stabilized. Ms. Nunez can care for him at home on her own and with family members who help out from time to time.
And, while Lloyd is unable to speak, he smiles and laughs when he’s happy, he’s quiet when he feels ill, and, when he wants to be alone, he groans, Ms. Nunez says. He can stand up, and he crawls from place to place. He also can’t go to the bathroom on his own and is fed by a gastrostomy tube, or G-tube.
In December, when Lloyd was diagnosed with COVID-19, Ms. Nunez started worrying all over again.
“Seeing him in the ICU, all I could think of was ‘please don’t make my son suffer,’” she says. “If he goes, I want him to go in peace, and I don’t want to see him in a machine and suffering.”
But Lloyd once again defied the odds against him and came home again. He has since faced yet another health challenge: He recently had a pelvic fracture.
“When I saw the orthopedist, he told me that Lloyd has a bone deficiency and that his bones don’t have enough room to grow,” she says. “I’m afraid this will be the beginning of a new journey.”
How this mom finds strength
While Ms. Nunez doesn’t go to a support group or speak with a mental health professional about all that she’s juggling, she says she draws strength from Lloyd himself.
“I’m very private, and I come from a culture where you don’t want people feeling sorry for you,” she says. “But I want to give Lloyd everything – he goes to school, we go to church, he had a quinceañera when he was 15, we’ve been to Disney, and we’ve both gotten on a roller coaster. I haven’t limited his life.”
She also draws comfort from her daughters.
“Everyone calls him ‘Baby Lloyd,’” she says. “My girls come right home from school, wash their hands, and throw themselves on his bed and watch TV with him. They also worry about him a lot. When he goes to the hospital, they suffer more than I do.”
In the end, Ms. Nunez hopes her story inspires others to think beyond a prognosis.
“Don’t lose hope,” she says. “I want people to feel hopeful when they read about Lloyd. He’s going to be 20 years old, and no one ever believed he would be here today ... I feel blessed.”
A version of this article first appeared on WebMD.com.
AUA 2022: A report from the trenches
The annual meeting of the American Urological Association took place recently at the Ernest N. Morial Convention Center in New Orleans. Hundreds of talks and abstracts were presented over the 4 days in New Orleans; below is a summary of what I found to be the key scientific highlights.
1. Updates to the AUA’s guidelines for management of localized kidney cancer
The AUA’s recommendations for the treatment of localized kidney cancer have changed dramatically over the past few decades. Gone are the days of simply removing the entire kidney every time a mass is found. Today, a partial nephrectomy is preferred in most situations.
Our understanding that the prevalence of familial kidney cancer is much higher than previously thought has led to a change in the guidelines regarding which patients should receive genetic counseling. For the first time, the guidelines include the use of adjuvant medical treatment, such as pembrolizumab. A 2021 study in the New England Journal of Medicine showed a survival benefit for patients with high-risk disease who receive such therapies, so it›s not surprising that such treatments are now recommended.
The development of new second- and third-generation gadolinium contrast agents that spare the kidneys has dramatically increased the role for MRIs for patients with severe or even end-stage renal disease. As a result, the guidelines were updated to recommend the use of these agents. The role of a renal biopsy, which has always been limited, given the ability of cross-sectional imaging to diagnosis this disease, has further been constrained and should now be performed only when the results would clearly change a clinical decision, such as whether or not the lesion in question is a metastasis.
2. New and better ureteroscope technology
No one likes kidney stones, not the patient who deals with the incredible pain, nor the surgeon who has to remove them, given that these cases often present in the wee hours of the morning. The preferred surgical approach has changed dramatically over the past decade, moving away from extracorporeal shockwave lithotripsy toward flexible ureteroscope-based technology, which has a higher clearance rate and is more widely and more immediately available. Flexible ureteroscopy has been held back by technological barriers, including limited scope deflection and low laser power. The exceptionally high cost of repair and the tendency of the instruments to break haven’t helped, either. Although single-use ureteroscopes have been available for some time, it wasn’t until the recently introduced second-generation scopes became widely available that they have become popular. These new scopes have small external diameters, great optics, and can easily be used. Newer high-powered lasers and the change from holmium:YAG-based lasers to thulium technology is greatly increasing the size of stones that can be safely addressed ureteroscopically. The cost analysis of single-use technology versus reusable scopes tends to be site dependent but can be appealing in certain situations. Also, on the technology forefront, a new robotically assisted ureteroscope is being introduced that offers the chance for improved intrapelvic mobility and better ergonomics for the surgeon.
3. New options for the treatment of clinically localized prostate cancer
Since the guidelines were last updated in 2017, the definitive management of localized prostate cancer has changed dramatically. Although radical prostatectomy and radiotherapy remain the preferred options for men who choose treatment for their disease, the updated guidelines state that active surveillance is now the preferred approach for men with low-risk cancers.
Although the preferred surveillance protocol is still being debated, the consensus is that almost all men with low-risk disease can be safely monitored for some period. The imaging technology available to monitor patients is also radically changing with the rollout of prostate-specific membrane antigen–based PET technology. The increased sensitivity and specificity of this modality opens the door not only for better up-front staging of newly diagnosed patients with prostate cancer but also may allow clinicians to earlier identify and treat men with metastatic disease. The guidelines for the first time address the use of genetic markers to individualize treatment of men with advanced or metastatic prostate cancer. Exactly which treatments these patients need is still being debated, but the ability to use patient-specific genetic mutation information to customize treatment is potentially groundbreaking.
4. New treatment options for patients with high-grade non–muscle-invasive bladder cancer (NMIBC) refractory to bacille Calmette-Guérin (BCG) therapy
Patients with NMIBC who do not respond to BCG therapy are in a tough position. Cystectomy remains the preferred option as a second-line strategy, but the procedure has a complication rate approaching 30%. Further, many patients are not willing to have their bladder removed because of the life-altering changes that go along with having an urostomy or a neobladder. While intravesical treatments such as valrubicin, docetaxel, or gemcitabine have been available for many years, the success rates of those options are limited. The Food and Drug Administration recently approved the use of the immunotherapy-based treatment pembrolizumab. While none of these options is perfect, the fact that we now have at least some alternatives is a huge step in the right direction.
5. It’s all about the patient: Involving patients in designing the health care delivery system
Although it seems like an obvious concept, patients themselves have traditionally not been involved in designing the health care delivery system on which they rely. Research presented at the AUA shows that many health care outcomes improve when patients are actively involved in the process. For example, Angela Smith, MD, of the University of North Carolina at Chapel Hill, presented a study showing that including patients in the identification of possible research topics helps them feel engaged and more likely to participate in studies. Patients who are involved in advisory councils at the local hospital level are more likely to report having received high-quality care. And surveying patients on the goals of national health care policy helps them feel that the outcomes are more equitable.
As a small-town urologist who spends his days in the trenches of urology, I think the next time my group considers participating in new cancer research, I may talk to the local cancer support group first. If Dr. Smith’s data are correct, not only would our patients be better served, but we would also have an easier time filling the trial!
The 2023 AUA conference is going to be held in Chicago next spring. I hope to see you there!
A version of this article first appeared on Medscape.com.
The annual meeting of the American Urological Association took place recently at the Ernest N. Morial Convention Center in New Orleans. Hundreds of talks and abstracts were presented over the 4 days in New Orleans; below is a summary of what I found to be the key scientific highlights.
1. Updates to the AUA’s guidelines for management of localized kidney cancer
The AUA’s recommendations for the treatment of localized kidney cancer have changed dramatically over the past few decades. Gone are the days of simply removing the entire kidney every time a mass is found. Today, a partial nephrectomy is preferred in most situations.
Our understanding that the prevalence of familial kidney cancer is much higher than previously thought has led to a change in the guidelines regarding which patients should receive genetic counseling. For the first time, the guidelines include the use of adjuvant medical treatment, such as pembrolizumab. A 2021 study in the New England Journal of Medicine showed a survival benefit for patients with high-risk disease who receive such therapies, so it›s not surprising that such treatments are now recommended.
The development of new second- and third-generation gadolinium contrast agents that spare the kidneys has dramatically increased the role for MRIs for patients with severe or even end-stage renal disease. As a result, the guidelines were updated to recommend the use of these agents. The role of a renal biopsy, which has always been limited, given the ability of cross-sectional imaging to diagnosis this disease, has further been constrained and should now be performed only when the results would clearly change a clinical decision, such as whether or not the lesion in question is a metastasis.
2. New and better ureteroscope technology
No one likes kidney stones, not the patient who deals with the incredible pain, nor the surgeon who has to remove them, given that these cases often present in the wee hours of the morning. The preferred surgical approach has changed dramatically over the past decade, moving away from extracorporeal shockwave lithotripsy toward flexible ureteroscope-based technology, which has a higher clearance rate and is more widely and more immediately available. Flexible ureteroscopy has been held back by technological barriers, including limited scope deflection and low laser power. The exceptionally high cost of repair and the tendency of the instruments to break haven’t helped, either. Although single-use ureteroscopes have been available for some time, it wasn’t until the recently introduced second-generation scopes became widely available that they have become popular. These new scopes have small external diameters, great optics, and can easily be used. Newer high-powered lasers and the change from holmium:YAG-based lasers to thulium technology is greatly increasing the size of stones that can be safely addressed ureteroscopically. The cost analysis of single-use technology versus reusable scopes tends to be site dependent but can be appealing in certain situations. Also, on the technology forefront, a new robotically assisted ureteroscope is being introduced that offers the chance for improved intrapelvic mobility and better ergonomics for the surgeon.
3. New options for the treatment of clinically localized prostate cancer
Since the guidelines were last updated in 2017, the definitive management of localized prostate cancer has changed dramatically. Although radical prostatectomy and radiotherapy remain the preferred options for men who choose treatment for their disease, the updated guidelines state that active surveillance is now the preferred approach for men with low-risk cancers.
Although the preferred surveillance protocol is still being debated, the consensus is that almost all men with low-risk disease can be safely monitored for some period. The imaging technology available to monitor patients is also radically changing with the rollout of prostate-specific membrane antigen–based PET technology. The increased sensitivity and specificity of this modality opens the door not only for better up-front staging of newly diagnosed patients with prostate cancer but also may allow clinicians to earlier identify and treat men with metastatic disease. The guidelines for the first time address the use of genetic markers to individualize treatment of men with advanced or metastatic prostate cancer. Exactly which treatments these patients need is still being debated, but the ability to use patient-specific genetic mutation information to customize treatment is potentially groundbreaking.
4. New treatment options for patients with high-grade non–muscle-invasive bladder cancer (NMIBC) refractory to bacille Calmette-Guérin (BCG) therapy
Patients with NMIBC who do not respond to BCG therapy are in a tough position. Cystectomy remains the preferred option as a second-line strategy, but the procedure has a complication rate approaching 30%. Further, many patients are not willing to have their bladder removed because of the life-altering changes that go along with having an urostomy or a neobladder. While intravesical treatments such as valrubicin, docetaxel, or gemcitabine have been available for many years, the success rates of those options are limited. The Food and Drug Administration recently approved the use of the immunotherapy-based treatment pembrolizumab. While none of these options is perfect, the fact that we now have at least some alternatives is a huge step in the right direction.
5. It’s all about the patient: Involving patients in designing the health care delivery system
Although it seems like an obvious concept, patients themselves have traditionally not been involved in designing the health care delivery system on which they rely. Research presented at the AUA shows that many health care outcomes improve when patients are actively involved in the process. For example, Angela Smith, MD, of the University of North Carolina at Chapel Hill, presented a study showing that including patients in the identification of possible research topics helps them feel engaged and more likely to participate in studies. Patients who are involved in advisory councils at the local hospital level are more likely to report having received high-quality care. And surveying patients on the goals of national health care policy helps them feel that the outcomes are more equitable.
As a small-town urologist who spends his days in the trenches of urology, I think the next time my group considers participating in new cancer research, I may talk to the local cancer support group first. If Dr. Smith’s data are correct, not only would our patients be better served, but we would also have an easier time filling the trial!
The 2023 AUA conference is going to be held in Chicago next spring. I hope to see you there!
A version of this article first appeared on Medscape.com.
The annual meeting of the American Urological Association took place recently at the Ernest N. Morial Convention Center in New Orleans. Hundreds of talks and abstracts were presented over the 4 days in New Orleans; below is a summary of what I found to be the key scientific highlights.
1. Updates to the AUA’s guidelines for management of localized kidney cancer
The AUA’s recommendations for the treatment of localized kidney cancer have changed dramatically over the past few decades. Gone are the days of simply removing the entire kidney every time a mass is found. Today, a partial nephrectomy is preferred in most situations.
Our understanding that the prevalence of familial kidney cancer is much higher than previously thought has led to a change in the guidelines regarding which patients should receive genetic counseling. For the first time, the guidelines include the use of adjuvant medical treatment, such as pembrolizumab. A 2021 study in the New England Journal of Medicine showed a survival benefit for patients with high-risk disease who receive such therapies, so it›s not surprising that such treatments are now recommended.
The development of new second- and third-generation gadolinium contrast agents that spare the kidneys has dramatically increased the role for MRIs for patients with severe or even end-stage renal disease. As a result, the guidelines were updated to recommend the use of these agents. The role of a renal biopsy, which has always been limited, given the ability of cross-sectional imaging to diagnosis this disease, has further been constrained and should now be performed only when the results would clearly change a clinical decision, such as whether or not the lesion in question is a metastasis.
2. New and better ureteroscope technology
No one likes kidney stones, not the patient who deals with the incredible pain, nor the surgeon who has to remove them, given that these cases often present in the wee hours of the morning. The preferred surgical approach has changed dramatically over the past decade, moving away from extracorporeal shockwave lithotripsy toward flexible ureteroscope-based technology, which has a higher clearance rate and is more widely and more immediately available. Flexible ureteroscopy has been held back by technological barriers, including limited scope deflection and low laser power. The exceptionally high cost of repair and the tendency of the instruments to break haven’t helped, either. Although single-use ureteroscopes have been available for some time, it wasn’t until the recently introduced second-generation scopes became widely available that they have become popular. These new scopes have small external diameters, great optics, and can easily be used. Newer high-powered lasers and the change from holmium:YAG-based lasers to thulium technology is greatly increasing the size of stones that can be safely addressed ureteroscopically. The cost analysis of single-use technology versus reusable scopes tends to be site dependent but can be appealing in certain situations. Also, on the technology forefront, a new robotically assisted ureteroscope is being introduced that offers the chance for improved intrapelvic mobility and better ergonomics for the surgeon.
3. New options for the treatment of clinically localized prostate cancer
Since the guidelines were last updated in 2017, the definitive management of localized prostate cancer has changed dramatically. Although radical prostatectomy and radiotherapy remain the preferred options for men who choose treatment for their disease, the updated guidelines state that active surveillance is now the preferred approach for men with low-risk cancers.
Although the preferred surveillance protocol is still being debated, the consensus is that almost all men with low-risk disease can be safely monitored for some period. The imaging technology available to monitor patients is also radically changing with the rollout of prostate-specific membrane antigen–based PET technology. The increased sensitivity and specificity of this modality opens the door not only for better up-front staging of newly diagnosed patients with prostate cancer but also may allow clinicians to earlier identify and treat men with metastatic disease. The guidelines for the first time address the use of genetic markers to individualize treatment of men with advanced or metastatic prostate cancer. Exactly which treatments these patients need is still being debated, but the ability to use patient-specific genetic mutation information to customize treatment is potentially groundbreaking.
4. New treatment options for patients with high-grade non–muscle-invasive bladder cancer (NMIBC) refractory to bacille Calmette-Guérin (BCG) therapy
Patients with NMIBC who do not respond to BCG therapy are in a tough position. Cystectomy remains the preferred option as a second-line strategy, but the procedure has a complication rate approaching 30%. Further, many patients are not willing to have their bladder removed because of the life-altering changes that go along with having an urostomy or a neobladder. While intravesical treatments such as valrubicin, docetaxel, or gemcitabine have been available for many years, the success rates of those options are limited. The Food and Drug Administration recently approved the use of the immunotherapy-based treatment pembrolizumab. While none of these options is perfect, the fact that we now have at least some alternatives is a huge step in the right direction.
5. It’s all about the patient: Involving patients in designing the health care delivery system
Although it seems like an obvious concept, patients themselves have traditionally not been involved in designing the health care delivery system on which they rely. Research presented at the AUA shows that many health care outcomes improve when patients are actively involved in the process. For example, Angela Smith, MD, of the University of North Carolina at Chapel Hill, presented a study showing that including patients in the identification of possible research topics helps them feel engaged and more likely to participate in studies. Patients who are involved in advisory councils at the local hospital level are more likely to report having received high-quality care. And surveying patients on the goals of national health care policy helps them feel that the outcomes are more equitable.
As a small-town urologist who spends his days in the trenches of urology, I think the next time my group considers participating in new cancer research, I may talk to the local cancer support group first. If Dr. Smith’s data are correct, not only would our patients be better served, but we would also have an easier time filling the trial!
The 2023 AUA conference is going to be held in Chicago next spring. I hope to see you there!
A version of this article first appeared on Medscape.com.
FROM AUA 2022
New guideline gives active surveillance a boost
Experts hailed the new guidelines, released May 10 by the American Urological Association (AUA) and the American Society for Radiation Oncology (ASTRO) as a boon for patients with low-risk to favorable intermediate-risk prostate cancers.
“The guideline is unequivocal that AS is the preferred management option for the majority of men with low-risk prostate cancer,” panel chair James A. Eastham, MD, Peter T. Scardino Chair in Oncology and chief of urology at Memorial Sloan Kettering Cancer Center, New York, said in an interview.
The new guideline is the first guideline for localized prostate cancer since 2017.
In the new document, guideline writers merged low-risk patients and very-low-risk patients into a single category of “low-risk.” Dr. Eastham said a distinction between very-low-risk and low-risk is inconsequential since the treatment for the two groups of patients is identical.
The 2022 guideline for the first time makes AS the recommended treatment for select patients with favorable intermediate-risk Gleason 3+4 prostate cancer, he said. The document also provides guidance on how such patients should be selected for AS.
Most research suggests that as many as 40% of patients newly diagnosed with prostate cancer have low-risk disease. Favorable intermediate-risk cancer represents 10%-15% of newly diagnosed patients, said Todd Morgan, MD, the Jack Lapides, MD, Research Professor and chief of urologic oncology at Michigan Medicine, Ann Arbor.
Dr. Morgan, who was not on the AUA/ASTRO panel, called the new recommendations “a very strong update compared to the guideline from 5 years ago.”
The guideline has been pared back some from 2017 to include fewer statements, but it covers several key clinical trials that have appeared over the past 6 years to strengthen the evidence base for the document, he said.
“I would say that we still have to acknowledge that many statements are based on ‘expert opinion’ rather than high-level evidence, which highlights the continued need for well-conducted studies that prove or disprove some of these statements,” Dr. Morgan added.
Patients weighed in
This year, AUA’s advocacy group urged patients to comment on the proposed guideline.
Rick Davis, founder of the AnCan Foundation, a virtual support network for prostate cancer and other diseases, thanked the groups for acknowledging the value of peer support and virtual support groups.
“AnCan congratulates the AUA/ASTRO on endorsing the proper role for the Active Surveillance protocol to manage early low-risk and favorable intermediate-risk prostate cancer and also their qualified and well-supported warnings against focal therapy,” Mr. Davis, who reviewed the guideline, said in an email. “We are, however, disappointed at the lack of a recommendation to provide comprehensive counseling when hormone therapy is prescribed.”
James Schraidt, another patient reviewer for AnCan, said that on balance, the 2022 guideline was an improvement over 2017 and will benefit patients.
He praised AUA/ASTRO for, at the urging of patient reviewers, introducing the “cribriform” and “intraductal” pathology patterns into the guideline for the first time as risk factors.
But he criticized the doctor groups for “a less than fulsome and orderly discussion of the use of MRI. It is not mentioned as a tool that should be used prior to initial biopsy, leaving the door wide open to random biopsies. The recommended role of MRI in AS monitoring was unclear.” He also said the panel should have reviewed micro-ultrasound, an emerging technology, that can be used by itself or to complement MRIs.
Many of the AUA/ASTRO guideline changes involve semantic issues – but which experts said nevertheless were important nuances.
Dr. Eastham said the AUA/ASTRO panel debated and finally settled on the word “preferred” for AS rather than “recommended” or “strongly recommended.”
“This is a very strong statement from the AUA/ASTRO,” Dr. Morgan said. “The semantics are definitely important, but ... ’preferred’ is actually a strong word. For the AUA, what’s really important is the ‘strong recommendation’ and Grade A level of evidence.”
Dr. Morgan also observed that the AS recommendations for patients with low-risk prostate cancer are stronger in the new AUA guideline than those in the latest recommendations from the National Comprehensive Cancer Network (NCCN), which he helped write.
The AUA/ASTRO guideline states that AS is preferred for patients with low-risk cancer, whereas in the NCCN guideline the language is: “preferred for most patients with low-risk disease cancer,” Dr. Morgan said.
“All of these statements ultimately acknowledge what I think that the vast majority of experts agree on – a small proportion of patients with low-risk prostate cancer may appropriately be recommended to undergo primary therapy,” he said.
Dr. Eastham said the goal of the guideline is to persuade surgeons to emphasize that AS is the best choice for most patients with low-risk prostate cancer: “The hope is that surgeons read the guideline. The guideline is definitive in recommending AS in low-risk prostate cancer.”
Dr. Eastham said the new guideline also does the following:
- Further endorses shared decisionmaking, with the understanding that for a decision to be made, both patient and physician need appropriate information regarding the risk posed by the cancer and the risk posed by treatment;
- Endorses selective use of somatic genetic testing when the data are needed for shared decisionmaking;
- Updates a section on genetic testing in patients considered to be at high risk for a germline mutation;
- Updates pretreatment evaluation for patients opting for treatment, primarily the role of imaging and how the evolution of next-generation imaging – such as , a new type of nuclear medicine procedure, in clinically localized prostate cancer;
- Addresses aspects of both radiotherapy and surgery, including nerve sparing, pelvic lymph node dissection, and adjuvant/neoadjuvant therapy, such as chemotherapy or hormone therapy delivered before or after the primary treatment. Dr. Eastham said the “significant evolution” in how best to provide radiotherapy resulted in several changes to this section.
No relevant financial relationships have been reported.
A version of this article first appeared on Medscape.com.
Experts hailed the new guidelines, released May 10 by the American Urological Association (AUA) and the American Society for Radiation Oncology (ASTRO) as a boon for patients with low-risk to favorable intermediate-risk prostate cancers.
“The guideline is unequivocal that AS is the preferred management option for the majority of men with low-risk prostate cancer,” panel chair James A. Eastham, MD, Peter T. Scardino Chair in Oncology and chief of urology at Memorial Sloan Kettering Cancer Center, New York, said in an interview.
The new guideline is the first guideline for localized prostate cancer since 2017.
In the new document, guideline writers merged low-risk patients and very-low-risk patients into a single category of “low-risk.” Dr. Eastham said a distinction between very-low-risk and low-risk is inconsequential since the treatment for the two groups of patients is identical.
The 2022 guideline for the first time makes AS the recommended treatment for select patients with favorable intermediate-risk Gleason 3+4 prostate cancer, he said. The document also provides guidance on how such patients should be selected for AS.
Most research suggests that as many as 40% of patients newly diagnosed with prostate cancer have low-risk disease. Favorable intermediate-risk cancer represents 10%-15% of newly diagnosed patients, said Todd Morgan, MD, the Jack Lapides, MD, Research Professor and chief of urologic oncology at Michigan Medicine, Ann Arbor.
Dr. Morgan, who was not on the AUA/ASTRO panel, called the new recommendations “a very strong update compared to the guideline from 5 years ago.”
The guideline has been pared back some from 2017 to include fewer statements, but it covers several key clinical trials that have appeared over the past 6 years to strengthen the evidence base for the document, he said.
“I would say that we still have to acknowledge that many statements are based on ‘expert opinion’ rather than high-level evidence, which highlights the continued need for well-conducted studies that prove or disprove some of these statements,” Dr. Morgan added.
Patients weighed in
This year, AUA’s advocacy group urged patients to comment on the proposed guideline.
Rick Davis, founder of the AnCan Foundation, a virtual support network for prostate cancer and other diseases, thanked the groups for acknowledging the value of peer support and virtual support groups.
“AnCan congratulates the AUA/ASTRO on endorsing the proper role for the Active Surveillance protocol to manage early low-risk and favorable intermediate-risk prostate cancer and also their qualified and well-supported warnings against focal therapy,” Mr. Davis, who reviewed the guideline, said in an email. “We are, however, disappointed at the lack of a recommendation to provide comprehensive counseling when hormone therapy is prescribed.”
James Schraidt, another patient reviewer for AnCan, said that on balance, the 2022 guideline was an improvement over 2017 and will benefit patients.
He praised AUA/ASTRO for, at the urging of patient reviewers, introducing the “cribriform” and “intraductal” pathology patterns into the guideline for the first time as risk factors.
But he criticized the doctor groups for “a less than fulsome and orderly discussion of the use of MRI. It is not mentioned as a tool that should be used prior to initial biopsy, leaving the door wide open to random biopsies. The recommended role of MRI in AS monitoring was unclear.” He also said the panel should have reviewed micro-ultrasound, an emerging technology, that can be used by itself or to complement MRIs.
Many of the AUA/ASTRO guideline changes involve semantic issues – but which experts said nevertheless were important nuances.
Dr. Eastham said the AUA/ASTRO panel debated and finally settled on the word “preferred” for AS rather than “recommended” or “strongly recommended.”
“This is a very strong statement from the AUA/ASTRO,” Dr. Morgan said. “The semantics are definitely important, but ... ’preferred’ is actually a strong word. For the AUA, what’s really important is the ‘strong recommendation’ and Grade A level of evidence.”
Dr. Morgan also observed that the AS recommendations for patients with low-risk prostate cancer are stronger in the new AUA guideline than those in the latest recommendations from the National Comprehensive Cancer Network (NCCN), which he helped write.
The AUA/ASTRO guideline states that AS is preferred for patients with low-risk cancer, whereas in the NCCN guideline the language is: “preferred for most patients with low-risk disease cancer,” Dr. Morgan said.
“All of these statements ultimately acknowledge what I think that the vast majority of experts agree on – a small proportion of patients with low-risk prostate cancer may appropriately be recommended to undergo primary therapy,” he said.
Dr. Eastham said the goal of the guideline is to persuade surgeons to emphasize that AS is the best choice for most patients with low-risk prostate cancer: “The hope is that surgeons read the guideline. The guideline is definitive in recommending AS in low-risk prostate cancer.”
Dr. Eastham said the new guideline also does the following:
- Further endorses shared decisionmaking, with the understanding that for a decision to be made, both patient and physician need appropriate information regarding the risk posed by the cancer and the risk posed by treatment;
- Endorses selective use of somatic genetic testing when the data are needed for shared decisionmaking;
- Updates a section on genetic testing in patients considered to be at high risk for a germline mutation;
- Updates pretreatment evaluation for patients opting for treatment, primarily the role of imaging and how the evolution of next-generation imaging – such as , a new type of nuclear medicine procedure, in clinically localized prostate cancer;
- Addresses aspects of both radiotherapy and surgery, including nerve sparing, pelvic lymph node dissection, and adjuvant/neoadjuvant therapy, such as chemotherapy or hormone therapy delivered before or after the primary treatment. Dr. Eastham said the “significant evolution” in how best to provide radiotherapy resulted in several changes to this section.
No relevant financial relationships have been reported.
A version of this article first appeared on Medscape.com.
Experts hailed the new guidelines, released May 10 by the American Urological Association (AUA) and the American Society for Radiation Oncology (ASTRO) as a boon for patients with low-risk to favorable intermediate-risk prostate cancers.
“The guideline is unequivocal that AS is the preferred management option for the majority of men with low-risk prostate cancer,” panel chair James A. Eastham, MD, Peter T. Scardino Chair in Oncology and chief of urology at Memorial Sloan Kettering Cancer Center, New York, said in an interview.
The new guideline is the first guideline for localized prostate cancer since 2017.
In the new document, guideline writers merged low-risk patients and very-low-risk patients into a single category of “low-risk.” Dr. Eastham said a distinction between very-low-risk and low-risk is inconsequential since the treatment for the two groups of patients is identical.
The 2022 guideline for the first time makes AS the recommended treatment for select patients with favorable intermediate-risk Gleason 3+4 prostate cancer, he said. The document also provides guidance on how such patients should be selected for AS.
Most research suggests that as many as 40% of patients newly diagnosed with prostate cancer have low-risk disease. Favorable intermediate-risk cancer represents 10%-15% of newly diagnosed patients, said Todd Morgan, MD, the Jack Lapides, MD, Research Professor and chief of urologic oncology at Michigan Medicine, Ann Arbor.
Dr. Morgan, who was not on the AUA/ASTRO panel, called the new recommendations “a very strong update compared to the guideline from 5 years ago.”
The guideline has been pared back some from 2017 to include fewer statements, but it covers several key clinical trials that have appeared over the past 6 years to strengthen the evidence base for the document, he said.
“I would say that we still have to acknowledge that many statements are based on ‘expert opinion’ rather than high-level evidence, which highlights the continued need for well-conducted studies that prove or disprove some of these statements,” Dr. Morgan added.
Patients weighed in
This year, AUA’s advocacy group urged patients to comment on the proposed guideline.
Rick Davis, founder of the AnCan Foundation, a virtual support network for prostate cancer and other diseases, thanked the groups for acknowledging the value of peer support and virtual support groups.
“AnCan congratulates the AUA/ASTRO on endorsing the proper role for the Active Surveillance protocol to manage early low-risk and favorable intermediate-risk prostate cancer and also their qualified and well-supported warnings against focal therapy,” Mr. Davis, who reviewed the guideline, said in an email. “We are, however, disappointed at the lack of a recommendation to provide comprehensive counseling when hormone therapy is prescribed.”
James Schraidt, another patient reviewer for AnCan, said that on balance, the 2022 guideline was an improvement over 2017 and will benefit patients.
He praised AUA/ASTRO for, at the urging of patient reviewers, introducing the “cribriform” and “intraductal” pathology patterns into the guideline for the first time as risk factors.
But he criticized the doctor groups for “a less than fulsome and orderly discussion of the use of MRI. It is not mentioned as a tool that should be used prior to initial biopsy, leaving the door wide open to random biopsies. The recommended role of MRI in AS monitoring was unclear.” He also said the panel should have reviewed micro-ultrasound, an emerging technology, that can be used by itself or to complement MRIs.
Many of the AUA/ASTRO guideline changes involve semantic issues – but which experts said nevertheless were important nuances.
Dr. Eastham said the AUA/ASTRO panel debated and finally settled on the word “preferred” for AS rather than “recommended” or “strongly recommended.”
“This is a very strong statement from the AUA/ASTRO,” Dr. Morgan said. “The semantics are definitely important, but ... ’preferred’ is actually a strong word. For the AUA, what’s really important is the ‘strong recommendation’ and Grade A level of evidence.”
Dr. Morgan also observed that the AS recommendations for patients with low-risk prostate cancer are stronger in the new AUA guideline than those in the latest recommendations from the National Comprehensive Cancer Network (NCCN), which he helped write.
The AUA/ASTRO guideline states that AS is preferred for patients with low-risk cancer, whereas in the NCCN guideline the language is: “preferred for most patients with low-risk disease cancer,” Dr. Morgan said.
“All of these statements ultimately acknowledge what I think that the vast majority of experts agree on – a small proportion of patients with low-risk prostate cancer may appropriately be recommended to undergo primary therapy,” he said.
Dr. Eastham said the goal of the guideline is to persuade surgeons to emphasize that AS is the best choice for most patients with low-risk prostate cancer: “The hope is that surgeons read the guideline. The guideline is definitive in recommending AS in low-risk prostate cancer.”
Dr. Eastham said the new guideline also does the following:
- Further endorses shared decisionmaking, with the understanding that for a decision to be made, both patient and physician need appropriate information regarding the risk posed by the cancer and the risk posed by treatment;
- Endorses selective use of somatic genetic testing when the data are needed for shared decisionmaking;
- Updates a section on genetic testing in patients considered to be at high risk for a germline mutation;
- Updates pretreatment evaluation for patients opting for treatment, primarily the role of imaging and how the evolution of next-generation imaging – such as , a new type of nuclear medicine procedure, in clinically localized prostate cancer;
- Addresses aspects of both radiotherapy and surgery, including nerve sparing, pelvic lymph node dissection, and adjuvant/neoadjuvant therapy, such as chemotherapy or hormone therapy delivered before or after the primary treatment. Dr. Eastham said the “significant evolution” in how best to provide radiotherapy resulted in several changes to this section.
No relevant financial relationships have been reported.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF UROLOGY
Up in smoke: Cannabis-related ED visits increased 18-fold for older Californians
Researchers in California found an 18-fold increase in the rate of cannabis-related trips to the ED visits among adults over age 65 in the state from 2005 to 2019.
Addressing potential harms of cannabis use among older adults, who face heightened risk for adverse reactions to the substance, “is urgently required,” the researchers reported at the annual meeting of the American Geriatrics Society.
The researchers advised doctors to discuss cannabis use with older patients and screen older adults for cannabis use. Those living with multiple chronic conditions and taking multiple medications are especially likely to be at risk for harm, coinvestigator Benjamin Han, MD, MPH, a geriatrician at the University of California, San Diego, said in an interview.
Dr. Han added that “very little” is understood about the risks and benefits of cannabis use in the elderly, and more studies are needed “so that clinicians can have data-informed discussions with their patients.”
California legalized medical marijuana in 1996 and recreational marijuana in 2016.
The researchers used diagnostic code data from California’s nonmilitary acute care hospitals, collected by the state’s Department of Healthcare Access and Information, to calculate annual rates of cannabis-related visits per 10,000 ED visits.
ED trips up sharply among older adults
Rates of cannabis-related visits increased significantly for all older adult age ranges (P < .001), according to the researchers. Among those aged 65-74 years, the rate increased about 15-fold, from 44.9 per 10,000 visits in 2005 to 714.5 per 100,000 in 2019; for ages 75-84, the rate increased about 22-fold, from 8.4 to 193.9 per 10,000; and for those 85 and older the rate jumped nearly 18-fold, from 2.1 to 39.2 per 10,000.
The greatest increase occurred in visits categorized in diagnostic codes as cannabis abuse and unspecified use. Cannabis dependence and cannabis poisoning accounted for only a small fraction of cases, the investigators found.
The researchers did not have data on specific reasons for a visit, or whether patients had smoked or ingested marijuana products. They also could not discern whether patients had used delta-9-tetrahydrocannabinol, which has psychoactive properties, or cannabidiol, which typically does not have the same mind-altering effects.
Dr. Han said the data may not present a full picture of marijuana-related ED visits. “It is important to recognize that older adults have lived through the very putative language around drug use – including cannabis – as part of the racist war on drugs,” which could lead them to omit having used drugs during the intake process.
A 2017 study linked cannabis use among older adults with more injuries, which in turn led to greater emergency department use. Brian Kaskie, PhD, associate professor in health management and policy at the University of Iowa, Iowa City, said in an interview that the new findings show a state-specific, but alarming trend, and that more research is needed.
“Were these first-time users who were not familiar with anxiety-inducing aspects of cannabis use and took high potency products? Did they complete any education about how to use cannabis?” said Dr. Kaskie, who was not involved in the new study. “Were the ER visits for relatively benign, nonemergent reasons or were these ... visits an outcome of a tragic, harmful event like a car accident or overdose?”
Dr. Han and Dr. Kaskie disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Researchers in California found an 18-fold increase in the rate of cannabis-related trips to the ED visits among adults over age 65 in the state from 2005 to 2019.
Addressing potential harms of cannabis use among older adults, who face heightened risk for adverse reactions to the substance, “is urgently required,” the researchers reported at the annual meeting of the American Geriatrics Society.
The researchers advised doctors to discuss cannabis use with older patients and screen older adults for cannabis use. Those living with multiple chronic conditions and taking multiple medications are especially likely to be at risk for harm, coinvestigator Benjamin Han, MD, MPH, a geriatrician at the University of California, San Diego, said in an interview.
Dr. Han added that “very little” is understood about the risks and benefits of cannabis use in the elderly, and more studies are needed “so that clinicians can have data-informed discussions with their patients.”
California legalized medical marijuana in 1996 and recreational marijuana in 2016.
The researchers used diagnostic code data from California’s nonmilitary acute care hospitals, collected by the state’s Department of Healthcare Access and Information, to calculate annual rates of cannabis-related visits per 10,000 ED visits.
ED trips up sharply among older adults
Rates of cannabis-related visits increased significantly for all older adult age ranges (P < .001), according to the researchers. Among those aged 65-74 years, the rate increased about 15-fold, from 44.9 per 10,000 visits in 2005 to 714.5 per 100,000 in 2019; for ages 75-84, the rate increased about 22-fold, from 8.4 to 193.9 per 10,000; and for those 85 and older the rate jumped nearly 18-fold, from 2.1 to 39.2 per 10,000.
The greatest increase occurred in visits categorized in diagnostic codes as cannabis abuse and unspecified use. Cannabis dependence and cannabis poisoning accounted for only a small fraction of cases, the investigators found.
The researchers did not have data on specific reasons for a visit, or whether patients had smoked or ingested marijuana products. They also could not discern whether patients had used delta-9-tetrahydrocannabinol, which has psychoactive properties, or cannabidiol, which typically does not have the same mind-altering effects.
Dr. Han said the data may not present a full picture of marijuana-related ED visits. “It is important to recognize that older adults have lived through the very putative language around drug use – including cannabis – as part of the racist war on drugs,” which could lead them to omit having used drugs during the intake process.
A 2017 study linked cannabis use among older adults with more injuries, which in turn led to greater emergency department use. Brian Kaskie, PhD, associate professor in health management and policy at the University of Iowa, Iowa City, said in an interview that the new findings show a state-specific, but alarming trend, and that more research is needed.
“Were these first-time users who were not familiar with anxiety-inducing aspects of cannabis use and took high potency products? Did they complete any education about how to use cannabis?” said Dr. Kaskie, who was not involved in the new study. “Were the ER visits for relatively benign, nonemergent reasons or were these ... visits an outcome of a tragic, harmful event like a car accident or overdose?”
Dr. Han and Dr. Kaskie disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Researchers in California found an 18-fold increase in the rate of cannabis-related trips to the ED visits among adults over age 65 in the state from 2005 to 2019.
Addressing potential harms of cannabis use among older adults, who face heightened risk for adverse reactions to the substance, “is urgently required,” the researchers reported at the annual meeting of the American Geriatrics Society.
The researchers advised doctors to discuss cannabis use with older patients and screen older adults for cannabis use. Those living with multiple chronic conditions and taking multiple medications are especially likely to be at risk for harm, coinvestigator Benjamin Han, MD, MPH, a geriatrician at the University of California, San Diego, said in an interview.
Dr. Han added that “very little” is understood about the risks and benefits of cannabis use in the elderly, and more studies are needed “so that clinicians can have data-informed discussions with their patients.”
California legalized medical marijuana in 1996 and recreational marijuana in 2016.
The researchers used diagnostic code data from California’s nonmilitary acute care hospitals, collected by the state’s Department of Healthcare Access and Information, to calculate annual rates of cannabis-related visits per 10,000 ED visits.
ED trips up sharply among older adults
Rates of cannabis-related visits increased significantly for all older adult age ranges (P < .001), according to the researchers. Among those aged 65-74 years, the rate increased about 15-fold, from 44.9 per 10,000 visits in 2005 to 714.5 per 100,000 in 2019; for ages 75-84, the rate increased about 22-fold, from 8.4 to 193.9 per 10,000; and for those 85 and older the rate jumped nearly 18-fold, from 2.1 to 39.2 per 10,000.
The greatest increase occurred in visits categorized in diagnostic codes as cannabis abuse and unspecified use. Cannabis dependence and cannabis poisoning accounted for only a small fraction of cases, the investigators found.
The researchers did not have data on specific reasons for a visit, or whether patients had smoked or ingested marijuana products. They also could not discern whether patients had used delta-9-tetrahydrocannabinol, which has psychoactive properties, or cannabidiol, which typically does not have the same mind-altering effects.
Dr. Han said the data may not present a full picture of marijuana-related ED visits. “It is important to recognize that older adults have lived through the very putative language around drug use – including cannabis – as part of the racist war on drugs,” which could lead them to omit having used drugs during the intake process.
A 2017 study linked cannabis use among older adults with more injuries, which in turn led to greater emergency department use. Brian Kaskie, PhD, associate professor in health management and policy at the University of Iowa, Iowa City, said in an interview that the new findings show a state-specific, but alarming trend, and that more research is needed.
“Were these first-time users who were not familiar with anxiety-inducing aspects of cannabis use and took high potency products? Did they complete any education about how to use cannabis?” said Dr. Kaskie, who was not involved in the new study. “Were the ER visits for relatively benign, nonemergent reasons or were these ... visits an outcome of a tragic, harmful event like a car accident or overdose?”
Dr. Han and Dr. Kaskie disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AGS 2022
Tool helps health system cut risky scripts for older adults
In the largest implementation yet of the tool, designed by the U.S. Department of Veterans Affairs to decrease the use of potentially inappropriate medications (PIMs), Lifespan, a nonprofit system whose partners include Brown University, Providence, R.I., reported a significant drop in the number of such prescriptions to older adults on discharge from the emergency department (ED).
The number of PIMs among monthly prescriptions fell by roughly 26% at Lifespan’s three adult acute care EDs after the system adopted EQUiPPED – Enhancing Quality of Prescribing Practices for Older Adults Discharged from the Emergency Department. The VA deployed a version of the tool in 2013 to address the lack of training most emergency clinicians receive in the management of geriatric medications.
The model “should be implemented in other states and, with greater replication, could shape national policy regarding quality of care for older adults,” according to the researchers, who reported the results May 12 at the American Geriatrics Society (AGS) 2022 Annual Scientific Meeting, Orlando.
Older adults are three times as likely as younger patients to wind up in an ED because of medication-related harms. This is in part due to the greater number of prescriptions U.S. adults older than 65 years take daily.
A key quality measure
Although the Centers for Medicare & Medicaid Services and other groups have deemed minimizing PIMs an important quality measure, most EDs lack an expert in geriatric prescribing, Elizabeth Goldberg, MD, an associate professor of emergency medicine at Brown University, told this news organization.
With EQUiPPED, clinicians receive access to geriatric medication order sets embedded in electronic health records, individualized benchmark reports, and education about medication safety in older adults. PIMs are defined by the American Geriatrics Society Beers Criteria and include drugs such as proton-pump inhibitors and antipsychotics.
Lifespan’s program involved 362 clinicians who treat about 230,000 patients annually – 40,000 of them aged 65 and older. Dr. Goldberg said implementing the program in such a large population could “really move the needle for older adults” by reducing falls, improving cognitive function, and preventing harm from the use of medication.
She and fellow researchers examined ED prescribing 13 months before and 16 months after they had implemented EQUiPPED, in August and September of 2019. Of clinicians who participated, 48% were attending physicians, 37% were residents, and 34% were advanced practice providers.
PIM prescribing dropped from 8.93% prior to implementation (95% confidence interval: 8.5%-9.36%) to 6.59% after (95% CI: 6.2%-6.98%; P < .001). Before implementation, 1,495 of 16,681 prescribed medications were considered inappropriate, compared with 1,044 of 15,818 medications after, according to the researchers. The biggest declines in prescribing involved antihistamines, muscle relaxants, and benzodiazepines.
Despite the improvements, the system did not meet a goal of reducing PIMs to less than 5%. Dr. Goldberg said educating the large number of clinicians, some of whom rotated in and out of the ED, proved particularly challenging. The COVID-19 pandemic also potentially diverted attention from the quality improvement project, she said.
In addition to its size, the project was notable because it was supported by Blue Cross & Blue Shield of Rhode Island. Dr. Goldberg said obtaining private funding proved to be a quicker and less competitive process than obtaining a government grant. Other institutions interested in running similar studies may need to find insurers that are in the Medicare Advantage market or that have a significant number of younger enrollees with chronic conditions, such as kidney disease, who may benefit from more careful prescribing practices, she said.
The new study builds on previous research, such as a 2017 study that showed that EQUiPPED reduced PIM prescribing at four VA hospitals. Findings from a more recent rollout at three academic health systems suggested that the model might also be effective in targeting the overuse of specific drugs in facilities in which PIM prescribing is already low.
A researcher in those earlier studies, Susan Nicole Hastings, MD, a geriatric medicine specialist at Duke University, Durham, N.C., and the Durham VA Health Care System, told this news organization that Lifespan’s experience supports the idea that “with the right attention to balancing fidelity and tailoring for the new setting, there is tremendous potential for moving successful programs from the VA to other health systems.”
Ann E. Vandenberg, PhD, MPH, a gerontologist at Emory University, Atlanta, said the fragmented nature of the American health care system makes it difficult to disseminate EQUiPPED widely, but interoperability applications that pull data from different electronic health records could help hospital systems to adopt the program without undergoing site-specific customization.
Dr. Hastings and Dr. Vandenberg have received research funding to study EQUiPPED from the Agency for Healthcare Research and Quality. Dr. Hastings also received research funding from the VA.
A version of this article first appeared on Medscape.com.
In the largest implementation yet of the tool, designed by the U.S. Department of Veterans Affairs to decrease the use of potentially inappropriate medications (PIMs), Lifespan, a nonprofit system whose partners include Brown University, Providence, R.I., reported a significant drop in the number of such prescriptions to older adults on discharge from the emergency department (ED).
The number of PIMs among monthly prescriptions fell by roughly 26% at Lifespan’s three adult acute care EDs after the system adopted EQUiPPED – Enhancing Quality of Prescribing Practices for Older Adults Discharged from the Emergency Department. The VA deployed a version of the tool in 2013 to address the lack of training most emergency clinicians receive in the management of geriatric medications.
The model “should be implemented in other states and, with greater replication, could shape national policy regarding quality of care for older adults,” according to the researchers, who reported the results May 12 at the American Geriatrics Society (AGS) 2022 Annual Scientific Meeting, Orlando.
Older adults are three times as likely as younger patients to wind up in an ED because of medication-related harms. This is in part due to the greater number of prescriptions U.S. adults older than 65 years take daily.
A key quality measure
Although the Centers for Medicare & Medicaid Services and other groups have deemed minimizing PIMs an important quality measure, most EDs lack an expert in geriatric prescribing, Elizabeth Goldberg, MD, an associate professor of emergency medicine at Brown University, told this news organization.
With EQUiPPED, clinicians receive access to geriatric medication order sets embedded in electronic health records, individualized benchmark reports, and education about medication safety in older adults. PIMs are defined by the American Geriatrics Society Beers Criteria and include drugs such as proton-pump inhibitors and antipsychotics.
Lifespan’s program involved 362 clinicians who treat about 230,000 patients annually – 40,000 of them aged 65 and older. Dr. Goldberg said implementing the program in such a large population could “really move the needle for older adults” by reducing falls, improving cognitive function, and preventing harm from the use of medication.
She and fellow researchers examined ED prescribing 13 months before and 16 months after they had implemented EQUiPPED, in August and September of 2019. Of clinicians who participated, 48% were attending physicians, 37% were residents, and 34% were advanced practice providers.
PIM prescribing dropped from 8.93% prior to implementation (95% confidence interval: 8.5%-9.36%) to 6.59% after (95% CI: 6.2%-6.98%; P < .001). Before implementation, 1,495 of 16,681 prescribed medications were considered inappropriate, compared with 1,044 of 15,818 medications after, according to the researchers. The biggest declines in prescribing involved antihistamines, muscle relaxants, and benzodiazepines.
Despite the improvements, the system did not meet a goal of reducing PIMs to less than 5%. Dr. Goldberg said educating the large number of clinicians, some of whom rotated in and out of the ED, proved particularly challenging. The COVID-19 pandemic also potentially diverted attention from the quality improvement project, she said.
In addition to its size, the project was notable because it was supported by Blue Cross & Blue Shield of Rhode Island. Dr. Goldberg said obtaining private funding proved to be a quicker and less competitive process than obtaining a government grant. Other institutions interested in running similar studies may need to find insurers that are in the Medicare Advantage market or that have a significant number of younger enrollees with chronic conditions, such as kidney disease, who may benefit from more careful prescribing practices, she said.
The new study builds on previous research, such as a 2017 study that showed that EQUiPPED reduced PIM prescribing at four VA hospitals. Findings from a more recent rollout at three academic health systems suggested that the model might also be effective in targeting the overuse of specific drugs in facilities in which PIM prescribing is already low.
A researcher in those earlier studies, Susan Nicole Hastings, MD, a geriatric medicine specialist at Duke University, Durham, N.C., and the Durham VA Health Care System, told this news organization that Lifespan’s experience supports the idea that “with the right attention to balancing fidelity and tailoring for the new setting, there is tremendous potential for moving successful programs from the VA to other health systems.”
Ann E. Vandenberg, PhD, MPH, a gerontologist at Emory University, Atlanta, said the fragmented nature of the American health care system makes it difficult to disseminate EQUiPPED widely, but interoperability applications that pull data from different electronic health records could help hospital systems to adopt the program without undergoing site-specific customization.
Dr. Hastings and Dr. Vandenberg have received research funding to study EQUiPPED from the Agency for Healthcare Research and Quality. Dr. Hastings also received research funding from the VA.
A version of this article first appeared on Medscape.com.
In the largest implementation yet of the tool, designed by the U.S. Department of Veterans Affairs to decrease the use of potentially inappropriate medications (PIMs), Lifespan, a nonprofit system whose partners include Brown University, Providence, R.I., reported a significant drop in the number of such prescriptions to older adults on discharge from the emergency department (ED).
The number of PIMs among monthly prescriptions fell by roughly 26% at Lifespan’s three adult acute care EDs after the system adopted EQUiPPED – Enhancing Quality of Prescribing Practices for Older Adults Discharged from the Emergency Department. The VA deployed a version of the tool in 2013 to address the lack of training most emergency clinicians receive in the management of geriatric medications.
The model “should be implemented in other states and, with greater replication, could shape national policy regarding quality of care for older adults,” according to the researchers, who reported the results May 12 at the American Geriatrics Society (AGS) 2022 Annual Scientific Meeting, Orlando.
Older adults are three times as likely as younger patients to wind up in an ED because of medication-related harms. This is in part due to the greater number of prescriptions U.S. adults older than 65 years take daily.
A key quality measure
Although the Centers for Medicare & Medicaid Services and other groups have deemed minimizing PIMs an important quality measure, most EDs lack an expert in geriatric prescribing, Elizabeth Goldberg, MD, an associate professor of emergency medicine at Brown University, told this news organization.
With EQUiPPED, clinicians receive access to geriatric medication order sets embedded in electronic health records, individualized benchmark reports, and education about medication safety in older adults. PIMs are defined by the American Geriatrics Society Beers Criteria and include drugs such as proton-pump inhibitors and antipsychotics.
Lifespan’s program involved 362 clinicians who treat about 230,000 patients annually – 40,000 of them aged 65 and older. Dr. Goldberg said implementing the program in such a large population could “really move the needle for older adults” by reducing falls, improving cognitive function, and preventing harm from the use of medication.
She and fellow researchers examined ED prescribing 13 months before and 16 months after they had implemented EQUiPPED, in August and September of 2019. Of clinicians who participated, 48% were attending physicians, 37% were residents, and 34% were advanced practice providers.
PIM prescribing dropped from 8.93% prior to implementation (95% confidence interval: 8.5%-9.36%) to 6.59% after (95% CI: 6.2%-6.98%; P < .001). Before implementation, 1,495 of 16,681 prescribed medications were considered inappropriate, compared with 1,044 of 15,818 medications after, according to the researchers. The biggest declines in prescribing involved antihistamines, muscle relaxants, and benzodiazepines.
Despite the improvements, the system did not meet a goal of reducing PIMs to less than 5%. Dr. Goldberg said educating the large number of clinicians, some of whom rotated in and out of the ED, proved particularly challenging. The COVID-19 pandemic also potentially diverted attention from the quality improvement project, she said.
In addition to its size, the project was notable because it was supported by Blue Cross & Blue Shield of Rhode Island. Dr. Goldberg said obtaining private funding proved to be a quicker and less competitive process than obtaining a government grant. Other institutions interested in running similar studies may need to find insurers that are in the Medicare Advantage market or that have a significant number of younger enrollees with chronic conditions, such as kidney disease, who may benefit from more careful prescribing practices, she said.
The new study builds on previous research, such as a 2017 study that showed that EQUiPPED reduced PIM prescribing at four VA hospitals. Findings from a more recent rollout at three academic health systems suggested that the model might also be effective in targeting the overuse of specific drugs in facilities in which PIM prescribing is already low.
A researcher in those earlier studies, Susan Nicole Hastings, MD, a geriatric medicine specialist at Duke University, Durham, N.C., and the Durham VA Health Care System, told this news organization that Lifespan’s experience supports the idea that “with the right attention to balancing fidelity and tailoring for the new setting, there is tremendous potential for moving successful programs from the VA to other health systems.”
Ann E. Vandenberg, PhD, MPH, a gerontologist at Emory University, Atlanta, said the fragmented nature of the American health care system makes it difficult to disseminate EQUiPPED widely, but interoperability applications that pull data from different electronic health records could help hospital systems to adopt the program without undergoing site-specific customization.
Dr. Hastings and Dr. Vandenberg have received research funding to study EQUiPPED from the Agency for Healthcare Research and Quality. Dr. Hastings also received research funding from the VA.
A version of this article first appeared on Medscape.com.
FROM AGS 2022