User login
Children & COVID: Rise in new cases slows
New cases of COVID-19 in children climbed for the seventh consecutive week, but the latest increase was the smallest of the seven, according to the American Academy of Pediatrics and the Children’s Hospital Association.
Since the weekly total bottomed out at just under 26,000 in early April, the new-case count has risen by 28.0%, 11.8%, 43.5%, 17.4%, 50%, 14.6%, and 5.0%, based on data from the AAP/CHA weekly COVID-19 report.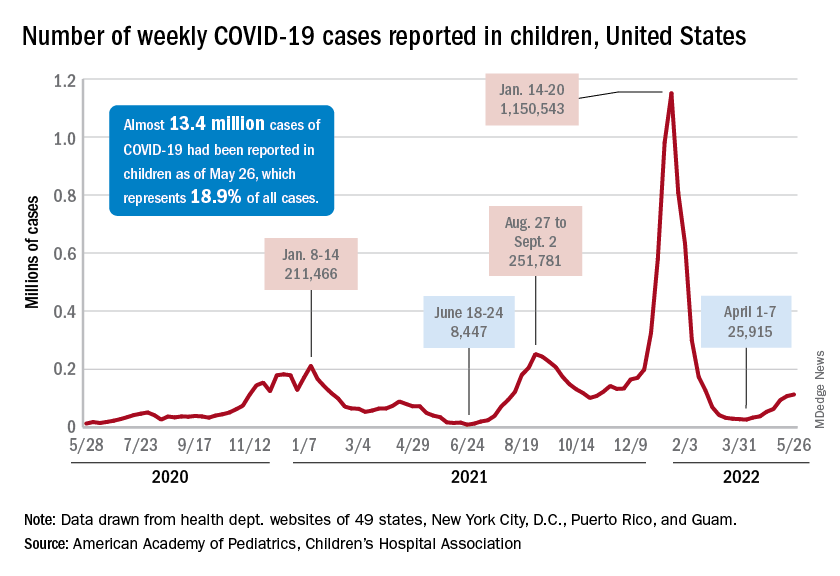
The cumulative number of pediatric cases is almost 13.4 million since the pandemic began, and those infected children represent 18.9% of all cases, the AAP and CHA said based on data from 49 states, New York City, the District of Columbia, Puerto Rico, and Guam.
That 18.9% is noteworthy because it marks the first decline in that particular measure since the AAP and CHA started keeping track in April of 2020. Children’s share of the overall COVID burden had been holding at 19.0% for 14 straight weeks, the AAP/CHA data show.
Regionally, new cases were up in the South and the West, where recent rising trends continued, and down in the Midwest and Northeast, where the recent rising trends were reversed for the first time. At the state/territory level, Puerto Rico had the largest percent increase over the last 2 weeks, followed by Maryland and Delaware, the organizations noted in their joint report.
Hospital admissions in children aged 0-17 have changed little in the last week, with the Centers for Disease Control and Prevention reporting rates of 0.25 per 100,000 population on May 23 and 0.25 per 100,000 on May 29, the latest date available. There was, however, a move up to 0.26 per 100,000 from May 24 to May 28, and the CDC acknowledges a possible reporting delay over the most recent 7-day period.
Emergency department visits have dipped slightly in recent days, with children aged 0-11 years at a 7-day average of 2.0% of ED visits with diagnosed COVID on May 28, down from a 5-day stretch at 2.2% from May 19 to May 23. Children aged 12-15 years were at 1.8% on May 28, compared with 2.0% on May 23-24, and 15- to 17-year-olds were at 2.0% on May 28, down from the 2.1% reached over the previous 2 days, the CDC reported on its COVID Data Tracker.
New cases of COVID-19 in children climbed for the seventh consecutive week, but the latest increase was the smallest of the seven, according to the American Academy of Pediatrics and the Children’s Hospital Association.
Since the weekly total bottomed out at just under 26,000 in early April, the new-case count has risen by 28.0%, 11.8%, 43.5%, 17.4%, 50%, 14.6%, and 5.0%, based on data from the AAP/CHA weekly COVID-19 report.
The cumulative number of pediatric cases is almost 13.4 million since the pandemic began, and those infected children represent 18.9% of all cases, the AAP and CHA said based on data from 49 states, New York City, the District of Columbia, Puerto Rico, and Guam.
That 18.9% is noteworthy because it marks the first decline in that particular measure since the AAP and CHA started keeping track in April of 2020. Children’s share of the overall COVID burden had been holding at 19.0% for 14 straight weeks, the AAP/CHA data show.
Regionally, new cases were up in the South and the West, where recent rising trends continued, and down in the Midwest and Northeast, where the recent rising trends were reversed for the first time. At the state/territory level, Puerto Rico had the largest percent increase over the last 2 weeks, followed by Maryland and Delaware, the organizations noted in their joint report.
Hospital admissions in children aged 0-17 have changed little in the last week, with the Centers for Disease Control and Prevention reporting rates of 0.25 per 100,000 population on May 23 and 0.25 per 100,000 on May 29, the latest date available. There was, however, a move up to 0.26 per 100,000 from May 24 to May 28, and the CDC acknowledges a possible reporting delay over the most recent 7-day period.
Emergency department visits have dipped slightly in recent days, with children aged 0-11 years at a 7-day average of 2.0% of ED visits with diagnosed COVID on May 28, down from a 5-day stretch at 2.2% from May 19 to May 23. Children aged 12-15 years were at 1.8% on May 28, compared with 2.0% on May 23-24, and 15- to 17-year-olds were at 2.0% on May 28, down from the 2.1% reached over the previous 2 days, the CDC reported on its COVID Data Tracker.
New cases of COVID-19 in children climbed for the seventh consecutive week, but the latest increase was the smallest of the seven, according to the American Academy of Pediatrics and the Children’s Hospital Association.
Since the weekly total bottomed out at just under 26,000 in early April, the new-case count has risen by 28.0%, 11.8%, 43.5%, 17.4%, 50%, 14.6%, and 5.0%, based on data from the AAP/CHA weekly COVID-19 report.
The cumulative number of pediatric cases is almost 13.4 million since the pandemic began, and those infected children represent 18.9% of all cases, the AAP and CHA said based on data from 49 states, New York City, the District of Columbia, Puerto Rico, and Guam.
That 18.9% is noteworthy because it marks the first decline in that particular measure since the AAP and CHA started keeping track in April of 2020. Children’s share of the overall COVID burden had been holding at 19.0% for 14 straight weeks, the AAP/CHA data show.
Regionally, new cases were up in the South and the West, where recent rising trends continued, and down in the Midwest and Northeast, where the recent rising trends were reversed for the first time. At the state/territory level, Puerto Rico had the largest percent increase over the last 2 weeks, followed by Maryland and Delaware, the organizations noted in their joint report.
Hospital admissions in children aged 0-17 have changed little in the last week, with the Centers for Disease Control and Prevention reporting rates of 0.25 per 100,000 population on May 23 and 0.25 per 100,000 on May 29, the latest date available. There was, however, a move up to 0.26 per 100,000 from May 24 to May 28, and the CDC acknowledges a possible reporting delay over the most recent 7-day period.
Emergency department visits have dipped slightly in recent days, with children aged 0-11 years at a 7-day average of 2.0% of ED visits with diagnosed COVID on May 28, down from a 5-day stretch at 2.2% from May 19 to May 23. Children aged 12-15 years were at 1.8% on May 28, compared with 2.0% on May 23-24, and 15- to 17-year-olds were at 2.0% on May 28, down from the 2.1% reached over the previous 2 days, the CDC reported on its COVID Data Tracker.
‘Smart inhalers’ may help diagnose and treat asthma – if used
After years going on and off medications for occasional asthma symptoms, things went downhill for Brian Blome in November 2020. The retired carpenter started feeling short of breath and wheezing during bike rides. At home, he struggled with chores.
“I was having a hard time climbing a flight of stairs, just doing laundry,” said Mr. Blome, who lives in the Chicago suburb of Palatine.
To get things under control, he saw an allergist and started regular medications – two tablets, two nasal sprays, and inhaled corticosteroids each day, plus an albuterol inhaler for flare-ups.
The inhalers have an extra feature: an electronic monitor that attaches to the device and automatically tracks where and when the medication is used. Bluetooth sends this information to an app on the patient’s mobile phone and to a dashboard where the medical team can see, at a glance, when symptoms are popping up and how regularly medications are taken – leading to the devices often being called “smart inhalers.”
At the 2022 American Academy of Allergy, Asthma, and Immunology conference in Phoenix, researchers explained how digital monitoring devices can help diagnose and treat hard-to-control asthma, potentially reducing the need for oral steroids or biologic therapies.
Even though electric monitors have been on the market for years, their use has been slow to catch on because of uncertainties around insurance coverage, liability, and how to manage and best use the data. One recent study said these devices cost $100-$500, but that price depends on many things, such as insurance.
About 17% of adult asthma patients have “difficult-to-control” asthma, meaning they limit their activity because of breathing symptoms and use reliever medications multiple times a week.
But research suggests that correcting inhaling technique and sticking to the use of the medications can cut that 17% down to just 3.7%, said Mr. Blome’s allergist, Giselle Mosnaim, MD, of NorthShore University HealthSystem in Glenview, Ill. Dr. Mosnaim spoke about digital monitoring at a conference session on digital technologies for asthma management.
A study of more than 5,000 asthma patients “showed that, if you have critical errors in inhaler technique, this leads to worse asthma outcomes and increased asthma exacerbations,” she said. It also shows that, despite new devices and new technologies, “we still have poor inhaler technique.”
Yet adherence is poorly gauged by doctors and patient self-reporting. “The ideal measure of adherence should be objective, accurate, and unobtrusive to minimize impact on patient behavior and allow reliable data collection in real-world settings,” Dr. Mosnaim said. “So electronic medication monitors are the gold standard.”
Improving use
Patients not following instructions or guidelines “is something we saw nonstop with kids,” said Caroline Moassessi, founder of the allergy and asthma blog Gratefulfoodie.com who formerly served on a regional board of the American Lung Association. She’s also the mother of two asthmatic children, now in college, who years ago used electronic medication monitors as part of a research trial.
They were “unimpressed – mostly since I think they thought their asthma was controlled,” she said. “When patients are not in crisis, they don’t manage their asthma well.”
Even in research studies such as the one Rachelle Ramsey, PhD, presented at the conference, it’s not only hard to determine if better adherence leads to improved health, but when.
“For example, does your adherence this week impact your asthma control this week, or does it impact your asthma control next week? Or is it even further out? Do you need to have some level of adherence over the course of a month in order to have better outcomes at the end of that month?” said Dr. Ramsey, a pediatric research psychologist at Cincinnati Children’s Hospital Medical Center. “I think it’s a little complicated.”
That said, results from several small studies do show a connection between remote monitoring and better clinical outcomes. One study enrolled asthma patients in the United Kingdom, and another was done by Dr. Mosnaim with Chicago-area patients.
In the U.K. quality improvement project, nurses asked patients with difficult-to-control asthma if they knew how to use their inhalers and were following treatment guidelines.
Those who said “yes” were invited to swap their steroid/inhalers for a controller fitted with a device that tracks use and measures acoustics to test inhaler technique. After 28 days of monitoring, many people in the study had better clinical outcomes.
And after 3 months of digital monitoring, patients didn’t use their rescue medication quite as often.
Mr. Blome has seen a marked improvement in his asthma since starting regular appointments and getting back on daily medications a year and a half ago. He says that now and then, he has wheezing and shortness of breath, usually while biking or exercising. But those symptoms aren’t as severe or frequent as before.
From a doctor’s perspective, “digital inhaler systems allow me to discern patterns in order to determine what triggers his asthma symptoms and to adjust medications at different times of the year,” Dr. Mosnaim said.
Electronic systems can monitor pollen counts and air quality as well as how often a patient uses a quick reliever medication. Thus, she said, tracking these measures year-round could raise attention to impending asthma attacks and suggest when to increase the dose of controller medications or add other treatments.
A version of this article first appeared on WebMD.com.
After years going on and off medications for occasional asthma symptoms, things went downhill for Brian Blome in November 2020. The retired carpenter started feeling short of breath and wheezing during bike rides. At home, he struggled with chores.
“I was having a hard time climbing a flight of stairs, just doing laundry,” said Mr. Blome, who lives in the Chicago suburb of Palatine.
To get things under control, he saw an allergist and started regular medications – two tablets, two nasal sprays, and inhaled corticosteroids each day, plus an albuterol inhaler for flare-ups.
The inhalers have an extra feature: an electronic monitor that attaches to the device and automatically tracks where and when the medication is used. Bluetooth sends this information to an app on the patient’s mobile phone and to a dashboard where the medical team can see, at a glance, when symptoms are popping up and how regularly medications are taken – leading to the devices often being called “smart inhalers.”
At the 2022 American Academy of Allergy, Asthma, and Immunology conference in Phoenix, researchers explained how digital monitoring devices can help diagnose and treat hard-to-control asthma, potentially reducing the need for oral steroids or biologic therapies.
Even though electric monitors have been on the market for years, their use has been slow to catch on because of uncertainties around insurance coverage, liability, and how to manage and best use the data. One recent study said these devices cost $100-$500, but that price depends on many things, such as insurance.
About 17% of adult asthma patients have “difficult-to-control” asthma, meaning they limit their activity because of breathing symptoms and use reliever medications multiple times a week.
But research suggests that correcting inhaling technique and sticking to the use of the medications can cut that 17% down to just 3.7%, said Mr. Blome’s allergist, Giselle Mosnaim, MD, of NorthShore University HealthSystem in Glenview, Ill. Dr. Mosnaim spoke about digital monitoring at a conference session on digital technologies for asthma management.
A study of more than 5,000 asthma patients “showed that, if you have critical errors in inhaler technique, this leads to worse asthma outcomes and increased asthma exacerbations,” she said. It also shows that, despite new devices and new technologies, “we still have poor inhaler technique.”
Yet adherence is poorly gauged by doctors and patient self-reporting. “The ideal measure of adherence should be objective, accurate, and unobtrusive to minimize impact on patient behavior and allow reliable data collection in real-world settings,” Dr. Mosnaim said. “So electronic medication monitors are the gold standard.”
Improving use
Patients not following instructions or guidelines “is something we saw nonstop with kids,” said Caroline Moassessi, founder of the allergy and asthma blog Gratefulfoodie.com who formerly served on a regional board of the American Lung Association. She’s also the mother of two asthmatic children, now in college, who years ago used electronic medication monitors as part of a research trial.
They were “unimpressed – mostly since I think they thought their asthma was controlled,” she said. “When patients are not in crisis, they don’t manage their asthma well.”
Even in research studies such as the one Rachelle Ramsey, PhD, presented at the conference, it’s not only hard to determine if better adherence leads to improved health, but when.
“For example, does your adherence this week impact your asthma control this week, or does it impact your asthma control next week? Or is it even further out? Do you need to have some level of adherence over the course of a month in order to have better outcomes at the end of that month?” said Dr. Ramsey, a pediatric research psychologist at Cincinnati Children’s Hospital Medical Center. “I think it’s a little complicated.”
That said, results from several small studies do show a connection between remote monitoring and better clinical outcomes. One study enrolled asthma patients in the United Kingdom, and another was done by Dr. Mosnaim with Chicago-area patients.
In the U.K. quality improvement project, nurses asked patients with difficult-to-control asthma if they knew how to use their inhalers and were following treatment guidelines.
Those who said “yes” were invited to swap their steroid/inhalers for a controller fitted with a device that tracks use and measures acoustics to test inhaler technique. After 28 days of monitoring, many people in the study had better clinical outcomes.
And after 3 months of digital monitoring, patients didn’t use their rescue medication quite as often.
Mr. Blome has seen a marked improvement in his asthma since starting regular appointments and getting back on daily medications a year and a half ago. He says that now and then, he has wheezing and shortness of breath, usually while biking or exercising. But those symptoms aren’t as severe or frequent as before.
From a doctor’s perspective, “digital inhaler systems allow me to discern patterns in order to determine what triggers his asthma symptoms and to adjust medications at different times of the year,” Dr. Mosnaim said.
Electronic systems can monitor pollen counts and air quality as well as how often a patient uses a quick reliever medication. Thus, she said, tracking these measures year-round could raise attention to impending asthma attacks and suggest when to increase the dose of controller medications or add other treatments.
A version of this article first appeared on WebMD.com.
After years going on and off medications for occasional asthma symptoms, things went downhill for Brian Blome in November 2020. The retired carpenter started feeling short of breath and wheezing during bike rides. At home, he struggled with chores.
“I was having a hard time climbing a flight of stairs, just doing laundry,” said Mr. Blome, who lives in the Chicago suburb of Palatine.
To get things under control, he saw an allergist and started regular medications – two tablets, two nasal sprays, and inhaled corticosteroids each day, plus an albuterol inhaler for flare-ups.
The inhalers have an extra feature: an electronic monitor that attaches to the device and automatically tracks where and when the medication is used. Bluetooth sends this information to an app on the patient’s mobile phone and to a dashboard where the medical team can see, at a glance, when symptoms are popping up and how regularly medications are taken – leading to the devices often being called “smart inhalers.”
At the 2022 American Academy of Allergy, Asthma, and Immunology conference in Phoenix, researchers explained how digital monitoring devices can help diagnose and treat hard-to-control asthma, potentially reducing the need for oral steroids or biologic therapies.
Even though electric monitors have been on the market for years, their use has been slow to catch on because of uncertainties around insurance coverage, liability, and how to manage and best use the data. One recent study said these devices cost $100-$500, but that price depends on many things, such as insurance.
About 17% of adult asthma patients have “difficult-to-control” asthma, meaning they limit their activity because of breathing symptoms and use reliever medications multiple times a week.
But research suggests that correcting inhaling technique and sticking to the use of the medications can cut that 17% down to just 3.7%, said Mr. Blome’s allergist, Giselle Mosnaim, MD, of NorthShore University HealthSystem in Glenview, Ill. Dr. Mosnaim spoke about digital monitoring at a conference session on digital technologies for asthma management.
A study of more than 5,000 asthma patients “showed that, if you have critical errors in inhaler technique, this leads to worse asthma outcomes and increased asthma exacerbations,” she said. It also shows that, despite new devices and new technologies, “we still have poor inhaler technique.”
Yet adherence is poorly gauged by doctors and patient self-reporting. “The ideal measure of adherence should be objective, accurate, and unobtrusive to minimize impact on patient behavior and allow reliable data collection in real-world settings,” Dr. Mosnaim said. “So electronic medication monitors are the gold standard.”
Improving use
Patients not following instructions or guidelines “is something we saw nonstop with kids,” said Caroline Moassessi, founder of the allergy and asthma blog Gratefulfoodie.com who formerly served on a regional board of the American Lung Association. She’s also the mother of two asthmatic children, now in college, who years ago used electronic medication monitors as part of a research trial.
They were “unimpressed – mostly since I think they thought their asthma was controlled,” she said. “When patients are not in crisis, they don’t manage their asthma well.”
Even in research studies such as the one Rachelle Ramsey, PhD, presented at the conference, it’s not only hard to determine if better adherence leads to improved health, but when.
“For example, does your adherence this week impact your asthma control this week, or does it impact your asthma control next week? Or is it even further out? Do you need to have some level of adherence over the course of a month in order to have better outcomes at the end of that month?” said Dr. Ramsey, a pediatric research psychologist at Cincinnati Children’s Hospital Medical Center. “I think it’s a little complicated.”
That said, results from several small studies do show a connection between remote monitoring and better clinical outcomes. One study enrolled asthma patients in the United Kingdom, and another was done by Dr. Mosnaim with Chicago-area patients.
In the U.K. quality improvement project, nurses asked patients with difficult-to-control asthma if they knew how to use their inhalers and were following treatment guidelines.
Those who said “yes” were invited to swap their steroid/inhalers for a controller fitted with a device that tracks use and measures acoustics to test inhaler technique. After 28 days of monitoring, many people in the study had better clinical outcomes.
And after 3 months of digital monitoring, patients didn’t use their rescue medication quite as often.
Mr. Blome has seen a marked improvement in his asthma since starting regular appointments and getting back on daily medications a year and a half ago. He says that now and then, he has wheezing and shortness of breath, usually while biking or exercising. But those symptoms aren’t as severe or frequent as before.
From a doctor’s perspective, “digital inhaler systems allow me to discern patterns in order to determine what triggers his asthma symptoms and to adjust medications at different times of the year,” Dr. Mosnaim said.
Electronic systems can monitor pollen counts and air quality as well as how often a patient uses a quick reliever medication. Thus, she said, tracking these measures year-round could raise attention to impending asthma attacks and suggest when to increase the dose of controller medications or add other treatments.
A version of this article first appeared on WebMD.com.
Abortion debate may affect Rx decisions for pregnant women
Obstetrician Beverly Gray, MD, is already seeing the effects of the Roe v. Wade abortion debate in her North Carolina practice.

The state allows abortion but requires that women get counseling with a qualified health professional 72 hours before the procedure. “Aside from that, we still have patients asking for more efficacious contraceptive methods just in case,” said Dr. Gray, residency director and division director for women’s community and population health and associate professor for obstetrics and gynecology at Duke University, Durham, N.C.
Patients and staff in her clinic have also been approaching her about tubal ligation. “They’re asking about additional birth control methods because they’re concerned about what’s going to happen” with the challenge to the historic Roe v. Wade decision in the Supreme Court and subsequent actions in the states to restrict or ban abortion, she said.
This has implications not just for abortion but for medications known to affect pregnancy. “What I’m really worried about is physicians will be withholding medicine because they’re concerned about teratogenic effects,” said Dr. Gray.
With more states issuing restrictions on abortion, doctors are worried that patients needing certain drugs to maintain their lupus flares, cancer, or other diseases may decide not to take them in the event they accidentally become pregnant. If the drug is known to affect the fetus, the fear is a patient who lives in a state with abortion restrictions will no longer have the option to terminate a pregnancy.

Instead, a scenario may arise in which the patient – and their physician – may opt not to treat at all with an otherwise lifesaving medication, experts told this news organization.
The U.S. landscape on abortion restrictions
A leaked draft of a U.S. Supreme Court opinion on Mississippi’s 15-week abortion ban has sent the medical community into a tailspin. The case, Dobbs v. Jackson Women’s Health Organization, challenges the 1973 Roe v. Wade decision that affirms the constitutional right to abortion. It’s anticipated the high court will decide on the case in June.
Although the upcoming decision is subject to change, the draft indicated the high court would uphold the Mississippi ban. This would essentially overturn the 1973 ruling. An earlier Supreme Court decision allowing a Texas law banning abortion at 6 weeks suggests the court may already be heading in this direction. At the state level, legislatures have been moving on divergent paths – some taking steps to preserve abortion rights, others initiating restrictions.
More than 100 abortion restrictions in 19 states took effect in 2021, according to the Guttmacher Institute, which tracks such metrics. In 2022, “two key themes are anti-abortion policymakers’ continued pursuit of various types of abortion bans and restrictions on medication abortion,” the institute reported.
Forty-six states and the District of Columbia have introduced 2,025 restrictions or proactive measures on sexual and reproductive health and rights so far this year. The latest tally from Guttmacher, updated in late May, revealed that 11 states so far have enacted 42 abortion restrictions. A total of 6 states (Arizona, Florida, Idaho, Kentucky, Oklahoma, and Wyoming) have issued nine bans on abortion.
Comparatively, 11 states have enacted 19 protective abortion measures.
Twenty-two states have introduced 117 restrictions on medication abortions, which account for 54% of U.S. abortions. This includes seven measures that would ban medication abortion outright, according to Guttmacher. Kentucky and South Dakota collectively have enacted 14 restrictions on medication abortion, as well as provisions that ban mailing of abortion pills.
Chilling effect on prescribing
Some physicians anticipate that drugs such as the “morning-after” pill (levonorgestrel) will become less available as restrictions go into effect, since these are medications designed to prevent pregnancy.*
However, the ongoing effort to put a lid on abortion measures has prompted concerns about a trickle-down effect on other medications that are otherwise life-changing or lifesaving to patients but pose a risk to the fetus.
Several drugs are well documented to affect fetal growth and development of the fetus, ranging from mild, transitory effects to severe, permanent birth defects, said Ronald G. Grifka, MD, chief medical officer of University of Michigan Health-West and clinical professor of pediatrics at the University of Michigan Medical School, Ann Arbor. “As new medications are developed, we will need heightened attention to make sure they are safe for the fetus,” he added.

Certain teratogenic medications are associated with a high risk of abortion even though this isn’t their primary use, noted Christina Chambers, PhD, MPH, co-director of the Center for Better Beginnings and associate director with the Altman Clinical & Translational Research Institute at the University of California, San Diego.

“I don’t think anyone would intentionally take these drugs to induce spontaneous abortion. But if the drugs pose a risk for it, I can see how the laws might be stretched” to include them, said Dr. Chambers.
Methotrexate, a medication for autoimmune disorders, has a high risk of spontaneous abortion. So do acne medications such as isotretinoin.
Patients are usually told they’re not supposed to get pregnant on these drugs because there’s a high risk of pregnancy loss and risk of malformations and potential learning problems in the fetus. But many pregnancies aren’t planned, said Dr. Chambers. “Patients may forget about the side effects or think their birth control will protect them. And the next time they refill the medication, they may not hear about the warnings again.”
With a restrictive abortion law or ban in effect, a woman might think: “I won’t take this drug because if there’s any potential that I might get pregnant, I won’t have the option to abort an at-risk pregnancy.” Women and their doctors, for that matter, don’t want to put themselves in this position, said Dr. Chambers.
Rheumatologist Megan Clowse, MD, who prescribes several medications that potentially cause major birth defects and pregnancy loss, worries about the ramifications of these accumulating bans.

“Methotrexate has been a leading drug for us for decades for rheumatoid arthritis. Mycophenolate is a vital drug for lupus,” said Dr. Clowse, associate professor of medicine at Duke University’s division of rheumatology and immunology.
Both methotrexate and mycophenolate pose about a 40% risk of pregnancy loss and significantly increase the risk for birth defects. “I’m definitely concerned that there might be doctors or women who elect not to use those medications in women of reproductive age because of the potential risk for pregnancy and absence of abortion rights,” said Dr. Clowse.
These situations might force women to use contraceptives they don’t want to use, such as hormonal implants or intrauterine devices, she added. Another side effect is that women and their partners may decide to abstain from sex.
The iPLEDGE factor
Some rheumatology drugs like lenalidomide (Revlimid) require a valid negative pregnancy test in a lab every month. Similarly, the iPLEDGE Risk Evaluation and Mitigation Strategy seeks to reduce the teratogenicity of isotretinoin by requiring two types of birth control and regular pregnancy tests by users.
For isotretinoin specifically, abortion restrictions “could lead to increased adherence to pregnancy prevention measures which are already stringent in iPLEDGE. But on the other hand, it could lead to reduced willingness of physicians to prescribe or patients to take the medication,” said Dr. Chambers.
With programs like iPLEDGE in effect, the rate of pregnancies and abortions that occur in dermatology are relatively low, said Jenny Murase, MD, associate clinical professor of dermatology at the University of California, San Francisco.

Nevertheless, as a physician who regularly prescribes medications like isotretinoin in women of childbearing age, “it’s terrifying to me that a woman wouldn’t have the option to terminate the pregnancy if a teratogenic effect from the medication caused a severe birth defect,” said Dr. Murase.
Dermatologists use other teratogenic medications such as thalidomide, mycophenolate mofetil, and methotrexate for chronic dermatologic disease like psoriasis and atopic dermatitis.
The situation is especially tricky for dermatologists since most patients – about 80% – never discuss their pregnancy with their specialist prior to pregnancy initiation. Dr. Murase recalls when a patient with chronic plaque psoriasis on methotrexate in her late 40s became pregnant and had an abortion even before Dr. Murase became aware of the pregnancy.
Because dermatologists routinely prescribe long-term medications for chronic diseases like acne, psoriasis, and atopic dermatitis, it is important to have a conversation regarding the risks and benefits of long-term medication should a pregnancy occur in any woman of childbearing age, she said.
Fewer women in clinical trials?
Abortion restrictions could possibly discourage women of reproductive age to participate in a clinical trial for a new medication, said Dr. Chambers.
A female patient with a chronic disease who’s randomized to receive a new medication may be required to use certain types of birth control because of unknown potential adverse effects the drug may have on the fetus. But in some cases, accidental pregnancies happen.
The participant in the trial may say, “I don’t know enough about the safety of this drug in pregnancy, and I’ve already taken it. I want to terminate the pregnancy,” said Dr. Chambers. Thinking ahead, a woman may decide not to do the trial to avoid the risk of getting pregnant and not having the option to terminate the pregnancy.
This could apply to new drugs such as antiviral treatments, or medications for severe chronic disease that typically have no clinical trial data in pregnancy prior to initial release into the market.
Women may start taking the drug without thinking about getting pregnant, then realize there are no safety data and become concerned about its effects on a future pregnancy.
The question is: Will abortion restrictions have a chilling effect on these new drugs as well? Patients and their doctors may decide not to try it until more data are available. “I can see where abortion restrictions would change the risk or benefit calculation in thinking about what you do or don’t prescribe or take during reproductive age,” said Dr. Chambers.
The upside of restrictions?
If there’s a positive side to these developments with abortion bans, it may encourage women taking new medications or joining clinical trials to think even more carefully about adherence to effective contraception, said Dr. Chambers.
Some methods are more effective than others, she emphasized. “When you have an unplanned pregnancy, it could mean that the method you used wasn’t optimal or you weren’t using it as recommended.” A goal moving forward is to encourage more thoughtful use of highly effective contraceptives, thus reducing the number of unplanned pregnancies, she added.
If patients are taking methotrexate, “the time to think about pregnancy is before getting pregnant so you can switch to a drug that’s compatible with pregnancy,” she said.
This whole thought process regarding pregnancy planning could work toward useful health goals, said Dr. Chambers. “Nobody thinks termination is the preferred method, but planning ahead should involve a discussion of what works best for the patient.”
Patients do have other choices, said Dr. Grifka. “Fortunately, there are many commonly prescribed medications which cross the placenta and have no ill effects on the fetus.”
Talking to patients about choices
Dr. Clowse, who spends a lot of time training rheumatologists, encourages them to have conversations with patients about pregnancy planning. It’s a lot to manage, getting the right drug to a female patient with chronic illness, especially in this current climate of abortion upheaval, she noted.
Her approach is to have an open and honest conversation with patients about their concerns and fears, what the realities are, and what the potential future options are for certain rheumatology drugs in the United States.
Some women who see what’s happening across the country may become so risk averse that they may choose to die rather than take a lifesaving drug that poses certain risks under new restrictions.
“I think that’s tragic,” said Dr. Clowse.
To help their patients, Dr. Gray believes physicians across specialties should better educate themselves about physiology in pregnancy and how to counsel patients on the impact of not taking medications in pregnancy.
In her view, it’s almost coercive to say to a patient, “You really need to have effective contraception if I’m going to give you this lifesaving or quality-of-life-improving medication.”
When confronting such scenarios, Dr. Gray doesn’t think physicians need to change how they counsel patients about contraception. “I don’t think we should be putting pressure on patients to consider other permanent methods just because there’s a lack of abortion options.”
Patients will eventually make those decisions for themselves, she said. “They’re going to want a more efficacious method because they’re worried about not having access to abortion if they get pregnant.”
Dr. Gray reports being a site principal investigator for a phase 3 trial for VeraCept IUD, funded by Sebela Pharmaceuticals. Dr. Clowse reports receiving research funding and doing consulting for GlaxoSmithKline.
*Correction, 6/2/2022: A previous version of this article misstated the intended use of drugs such as the “morning-after” pill (levonorgestrel). They are taken to prevent unintended pregnancy.
A version of this article first appeared on Medscape.com .
Obstetrician Beverly Gray, MD, is already seeing the effects of the Roe v. Wade abortion debate in her North Carolina practice.
The state allows abortion but requires that women get counseling with a qualified health professional 72 hours before the procedure. “Aside from that, we still have patients asking for more efficacious contraceptive methods just in case,” said Dr. Gray, residency director and division director for women’s community and population health and associate professor for obstetrics and gynecology at Duke University, Durham, N.C.
Patients and staff in her clinic have also been approaching her about tubal ligation. “They’re asking about additional birth control methods because they’re concerned about what’s going to happen” with the challenge to the historic Roe v. Wade decision in the Supreme Court and subsequent actions in the states to restrict or ban abortion, she said.
This has implications not just for abortion but for medications known to affect pregnancy. “What I’m really worried about is physicians will be withholding medicine because they’re concerned about teratogenic effects,” said Dr. Gray.
With more states issuing restrictions on abortion, doctors are worried that patients needing certain drugs to maintain their lupus flares, cancer, or other diseases may decide not to take them in the event they accidentally become pregnant. If the drug is known to affect the fetus, the fear is a patient who lives in a state with abortion restrictions will no longer have the option to terminate a pregnancy.
Instead, a scenario may arise in which the patient – and their physician – may opt not to treat at all with an otherwise lifesaving medication, experts told this news organization.
The U.S. landscape on abortion restrictions
A leaked draft of a U.S. Supreme Court opinion on Mississippi’s 15-week abortion ban has sent the medical community into a tailspin. The case, Dobbs v. Jackson Women’s Health Organization, challenges the 1973 Roe v. Wade decision that affirms the constitutional right to abortion. It’s anticipated the high court will decide on the case in June.
Although the upcoming decision is subject to change, the draft indicated the high court would uphold the Mississippi ban. This would essentially overturn the 1973 ruling. An earlier Supreme Court decision allowing a Texas law banning abortion at 6 weeks suggests the court may already be heading in this direction. At the state level, legislatures have been moving on divergent paths – some taking steps to preserve abortion rights, others initiating restrictions.
More than 100 abortion restrictions in 19 states took effect in 2021, according to the Guttmacher Institute, which tracks such metrics. In 2022, “two key themes are anti-abortion policymakers’ continued pursuit of various types of abortion bans and restrictions on medication abortion,” the institute reported.
Forty-six states and the District of Columbia have introduced 2,025 restrictions or proactive measures on sexual and reproductive health and rights so far this year. The latest tally from Guttmacher, updated in late May, revealed that 11 states so far have enacted 42 abortion restrictions. A total of 6 states (Arizona, Florida, Idaho, Kentucky, Oklahoma, and Wyoming) have issued nine bans on abortion.
Comparatively, 11 states have enacted 19 protective abortion measures.
Twenty-two states have introduced 117 restrictions on medication abortions, which account for 54% of U.S. abortions. This includes seven measures that would ban medication abortion outright, according to Guttmacher. Kentucky and South Dakota collectively have enacted 14 restrictions on medication abortion, as well as provisions that ban mailing of abortion pills.
Chilling effect on prescribing
Some physicians anticipate that drugs such as the “morning-after” pill (levonorgestrel) will become less available as restrictions go into effect, since these are medications designed to prevent pregnancy.*
However, the ongoing effort to put a lid on abortion measures has prompted concerns about a trickle-down effect on other medications that are otherwise life-changing or lifesaving to patients but pose a risk to the fetus.
Several drugs are well documented to affect fetal growth and development of the fetus, ranging from mild, transitory effects to severe, permanent birth defects, said Ronald G. Grifka, MD, chief medical officer of University of Michigan Health-West and clinical professor of pediatrics at the University of Michigan Medical School, Ann Arbor. “As new medications are developed, we will need heightened attention to make sure they are safe for the fetus,” he added.
Certain teratogenic medications are associated with a high risk of abortion even though this isn’t their primary use, noted Christina Chambers, PhD, MPH, co-director of the Center for Better Beginnings and associate director with the Altman Clinical & Translational Research Institute at the University of California, San Diego.
“I don’t think anyone would intentionally take these drugs to induce spontaneous abortion. But if the drugs pose a risk for it, I can see how the laws might be stretched” to include them, said Dr. Chambers.
Methotrexate, a medication for autoimmune disorders, has a high risk of spontaneous abortion. So do acne medications such as isotretinoin.
Patients are usually told they’re not supposed to get pregnant on these drugs because there’s a high risk of pregnancy loss and risk of malformations and potential learning problems in the fetus. But many pregnancies aren’t planned, said Dr. Chambers. “Patients may forget about the side effects or think their birth control will protect them. And the next time they refill the medication, they may not hear about the warnings again.”
With a restrictive abortion law or ban in effect, a woman might think: “I won’t take this drug because if there’s any potential that I might get pregnant, I won’t have the option to abort an at-risk pregnancy.” Women and their doctors, for that matter, don’t want to put themselves in this position, said Dr. Chambers.
Rheumatologist Megan Clowse, MD, who prescribes several medications that potentially cause major birth defects and pregnancy loss, worries about the ramifications of these accumulating bans.
“Methotrexate has been a leading drug for us for decades for rheumatoid arthritis. Mycophenolate is a vital drug for lupus,” said Dr. Clowse, associate professor of medicine at Duke University’s division of rheumatology and immunology.
Both methotrexate and mycophenolate pose about a 40% risk of pregnancy loss and significantly increase the risk for birth defects. “I’m definitely concerned that there might be doctors or women who elect not to use those medications in women of reproductive age because of the potential risk for pregnancy and absence of abortion rights,” said Dr. Clowse.
These situations might force women to use contraceptives they don’t want to use, such as hormonal implants or intrauterine devices, she added. Another side effect is that women and their partners may decide to abstain from sex.
The iPLEDGE factor
Some rheumatology drugs like lenalidomide (Revlimid) require a valid negative pregnancy test in a lab every month. Similarly, the iPLEDGE Risk Evaluation and Mitigation Strategy seeks to reduce the teratogenicity of isotretinoin by requiring two types of birth control and regular pregnancy tests by users.
For isotretinoin specifically, abortion restrictions “could lead to increased adherence to pregnancy prevention measures which are already stringent in iPLEDGE. But on the other hand, it could lead to reduced willingness of physicians to prescribe or patients to take the medication,” said Dr. Chambers.
With programs like iPLEDGE in effect, the rate of pregnancies and abortions that occur in dermatology are relatively low, said Jenny Murase, MD, associate clinical professor of dermatology at the University of California, San Francisco.
Nevertheless, as a physician who regularly prescribes medications like isotretinoin in women of childbearing age, “it’s terrifying to me that a woman wouldn’t have the option to terminate the pregnancy if a teratogenic effect from the medication caused a severe birth defect,” said Dr. Murase.
Dermatologists use other teratogenic medications such as thalidomide, mycophenolate mofetil, and methotrexate for chronic dermatologic disease like psoriasis and atopic dermatitis.
The situation is especially tricky for dermatologists since most patients – about 80% – never discuss their pregnancy with their specialist prior to pregnancy initiation. Dr. Murase recalls when a patient with chronic plaque psoriasis on methotrexate in her late 40s became pregnant and had an abortion even before Dr. Murase became aware of the pregnancy.
Because dermatologists routinely prescribe long-term medications for chronic diseases like acne, psoriasis, and atopic dermatitis, it is important to have a conversation regarding the risks and benefits of long-term medication should a pregnancy occur in any woman of childbearing age, she said.
Fewer women in clinical trials?
Abortion restrictions could possibly discourage women of reproductive age to participate in a clinical trial for a new medication, said Dr. Chambers.
A female patient with a chronic disease who’s randomized to receive a new medication may be required to use certain types of birth control because of unknown potential adverse effects the drug may have on the fetus. But in some cases, accidental pregnancies happen.
The participant in the trial may say, “I don’t know enough about the safety of this drug in pregnancy, and I’ve already taken it. I want to terminate the pregnancy,” said Dr. Chambers. Thinking ahead, a woman may decide not to do the trial to avoid the risk of getting pregnant and not having the option to terminate the pregnancy.
This could apply to new drugs such as antiviral treatments, or medications for severe chronic disease that typically have no clinical trial data in pregnancy prior to initial release into the market.
Women may start taking the drug without thinking about getting pregnant, then realize there are no safety data and become concerned about its effects on a future pregnancy.
The question is: Will abortion restrictions have a chilling effect on these new drugs as well? Patients and their doctors may decide not to try it until more data are available. “I can see where abortion restrictions would change the risk or benefit calculation in thinking about what you do or don’t prescribe or take during reproductive age,” said Dr. Chambers.
The upside of restrictions?
If there’s a positive side to these developments with abortion bans, it may encourage women taking new medications or joining clinical trials to think even more carefully about adherence to effective contraception, said Dr. Chambers.
Some methods are more effective than others, she emphasized. “When you have an unplanned pregnancy, it could mean that the method you used wasn’t optimal or you weren’t using it as recommended.” A goal moving forward is to encourage more thoughtful use of highly effective contraceptives, thus reducing the number of unplanned pregnancies, she added.
If patients are taking methotrexate, “the time to think about pregnancy is before getting pregnant so you can switch to a drug that’s compatible with pregnancy,” she said.
This whole thought process regarding pregnancy planning could work toward useful health goals, said Dr. Chambers. “Nobody thinks termination is the preferred method, but planning ahead should involve a discussion of what works best for the patient.”
Patients do have other choices, said Dr. Grifka. “Fortunately, there are many commonly prescribed medications which cross the placenta and have no ill effects on the fetus.”
Talking to patients about choices
Dr. Clowse, who spends a lot of time training rheumatologists, encourages them to have conversations with patients about pregnancy planning. It’s a lot to manage, getting the right drug to a female patient with chronic illness, especially in this current climate of abortion upheaval, she noted.
Her approach is to have an open and honest conversation with patients about their concerns and fears, what the realities are, and what the potential future options are for certain rheumatology drugs in the United States.
Some women who see what’s happening across the country may become so risk averse that they may choose to die rather than take a lifesaving drug that poses certain risks under new restrictions.
“I think that’s tragic,” said Dr. Clowse.
To help their patients, Dr. Gray believes physicians across specialties should better educate themselves about physiology in pregnancy and how to counsel patients on the impact of not taking medications in pregnancy.
In her view, it’s almost coercive to say to a patient, “You really need to have effective contraception if I’m going to give you this lifesaving or quality-of-life-improving medication.”
When confronting such scenarios, Dr. Gray doesn’t think physicians need to change how they counsel patients about contraception. “I don’t think we should be putting pressure on patients to consider other permanent methods just because there’s a lack of abortion options.”
Patients will eventually make those decisions for themselves, she said. “They’re going to want a more efficacious method because they’re worried about not having access to abortion if they get pregnant.”
Dr. Gray reports being a site principal investigator for a phase 3 trial for VeraCept IUD, funded by Sebela Pharmaceuticals. Dr. Clowse reports receiving research funding and doing consulting for GlaxoSmithKline.
*Correction, 6/2/2022: A previous version of this article misstated the intended use of drugs such as the “morning-after” pill (levonorgestrel). They are taken to prevent unintended pregnancy.
A version of this article first appeared on Medscape.com .
Obstetrician Beverly Gray, MD, is already seeing the effects of the Roe v. Wade abortion debate in her North Carolina practice.
The state allows abortion but requires that women get counseling with a qualified health professional 72 hours before the procedure. “Aside from that, we still have patients asking for more efficacious contraceptive methods just in case,” said Dr. Gray, residency director and division director for women’s community and population health and associate professor for obstetrics and gynecology at Duke University, Durham, N.C.
Patients and staff in her clinic have also been approaching her about tubal ligation. “They’re asking about additional birth control methods because they’re concerned about what’s going to happen” with the challenge to the historic Roe v. Wade decision in the Supreme Court and subsequent actions in the states to restrict or ban abortion, she said.
This has implications not just for abortion but for medications known to affect pregnancy. “What I’m really worried about is physicians will be withholding medicine because they’re concerned about teratogenic effects,” said Dr. Gray.
With more states issuing restrictions on abortion, doctors are worried that patients needing certain drugs to maintain their lupus flares, cancer, or other diseases may decide not to take them in the event they accidentally become pregnant. If the drug is known to affect the fetus, the fear is a patient who lives in a state with abortion restrictions will no longer have the option to terminate a pregnancy.
Instead, a scenario may arise in which the patient – and their physician – may opt not to treat at all with an otherwise lifesaving medication, experts told this news organization.
The U.S. landscape on abortion restrictions
A leaked draft of a U.S. Supreme Court opinion on Mississippi’s 15-week abortion ban has sent the medical community into a tailspin. The case, Dobbs v. Jackson Women’s Health Organization, challenges the 1973 Roe v. Wade decision that affirms the constitutional right to abortion. It’s anticipated the high court will decide on the case in June.
Although the upcoming decision is subject to change, the draft indicated the high court would uphold the Mississippi ban. This would essentially overturn the 1973 ruling. An earlier Supreme Court decision allowing a Texas law banning abortion at 6 weeks suggests the court may already be heading in this direction. At the state level, legislatures have been moving on divergent paths – some taking steps to preserve abortion rights, others initiating restrictions.
More than 100 abortion restrictions in 19 states took effect in 2021, according to the Guttmacher Institute, which tracks such metrics. In 2022, “two key themes are anti-abortion policymakers’ continued pursuit of various types of abortion bans and restrictions on medication abortion,” the institute reported.
Forty-six states and the District of Columbia have introduced 2,025 restrictions or proactive measures on sexual and reproductive health and rights so far this year. The latest tally from Guttmacher, updated in late May, revealed that 11 states so far have enacted 42 abortion restrictions. A total of 6 states (Arizona, Florida, Idaho, Kentucky, Oklahoma, and Wyoming) have issued nine bans on abortion.
Comparatively, 11 states have enacted 19 protective abortion measures.
Twenty-two states have introduced 117 restrictions on medication abortions, which account for 54% of U.S. abortions. This includes seven measures that would ban medication abortion outright, according to Guttmacher. Kentucky and South Dakota collectively have enacted 14 restrictions on medication abortion, as well as provisions that ban mailing of abortion pills.
Chilling effect on prescribing
Some physicians anticipate that drugs such as the “morning-after” pill (levonorgestrel) will become less available as restrictions go into effect, since these are medications designed to prevent pregnancy.*
However, the ongoing effort to put a lid on abortion measures has prompted concerns about a trickle-down effect on other medications that are otherwise life-changing or lifesaving to patients but pose a risk to the fetus.
Several drugs are well documented to affect fetal growth and development of the fetus, ranging from mild, transitory effects to severe, permanent birth defects, said Ronald G. Grifka, MD, chief medical officer of University of Michigan Health-West and clinical professor of pediatrics at the University of Michigan Medical School, Ann Arbor. “As new medications are developed, we will need heightened attention to make sure they are safe for the fetus,” he added.
Certain teratogenic medications are associated with a high risk of abortion even though this isn’t their primary use, noted Christina Chambers, PhD, MPH, co-director of the Center for Better Beginnings and associate director with the Altman Clinical & Translational Research Institute at the University of California, San Diego.
“I don’t think anyone would intentionally take these drugs to induce spontaneous abortion. But if the drugs pose a risk for it, I can see how the laws might be stretched” to include them, said Dr. Chambers.
Methotrexate, a medication for autoimmune disorders, has a high risk of spontaneous abortion. So do acne medications such as isotretinoin.
Patients are usually told they’re not supposed to get pregnant on these drugs because there’s a high risk of pregnancy loss and risk of malformations and potential learning problems in the fetus. But many pregnancies aren’t planned, said Dr. Chambers. “Patients may forget about the side effects or think their birth control will protect them. And the next time they refill the medication, they may not hear about the warnings again.”
With a restrictive abortion law or ban in effect, a woman might think: “I won’t take this drug because if there’s any potential that I might get pregnant, I won’t have the option to abort an at-risk pregnancy.” Women and their doctors, for that matter, don’t want to put themselves in this position, said Dr. Chambers.
Rheumatologist Megan Clowse, MD, who prescribes several medications that potentially cause major birth defects and pregnancy loss, worries about the ramifications of these accumulating bans.
“Methotrexate has been a leading drug for us for decades for rheumatoid arthritis. Mycophenolate is a vital drug for lupus,” said Dr. Clowse, associate professor of medicine at Duke University’s division of rheumatology and immunology.
Both methotrexate and mycophenolate pose about a 40% risk of pregnancy loss and significantly increase the risk for birth defects. “I’m definitely concerned that there might be doctors or women who elect not to use those medications in women of reproductive age because of the potential risk for pregnancy and absence of abortion rights,” said Dr. Clowse.
These situations might force women to use contraceptives they don’t want to use, such as hormonal implants or intrauterine devices, she added. Another side effect is that women and their partners may decide to abstain from sex.
The iPLEDGE factor
Some rheumatology drugs like lenalidomide (Revlimid) require a valid negative pregnancy test in a lab every month. Similarly, the iPLEDGE Risk Evaluation and Mitigation Strategy seeks to reduce the teratogenicity of isotretinoin by requiring two types of birth control and regular pregnancy tests by users.
For isotretinoin specifically, abortion restrictions “could lead to increased adherence to pregnancy prevention measures which are already stringent in iPLEDGE. But on the other hand, it could lead to reduced willingness of physicians to prescribe or patients to take the medication,” said Dr. Chambers.
With programs like iPLEDGE in effect, the rate of pregnancies and abortions that occur in dermatology are relatively low, said Jenny Murase, MD, associate clinical professor of dermatology at the University of California, San Francisco.
Nevertheless, as a physician who regularly prescribes medications like isotretinoin in women of childbearing age, “it’s terrifying to me that a woman wouldn’t have the option to terminate the pregnancy if a teratogenic effect from the medication caused a severe birth defect,” said Dr. Murase.
Dermatologists use other teratogenic medications such as thalidomide, mycophenolate mofetil, and methotrexate for chronic dermatologic disease like psoriasis and atopic dermatitis.
The situation is especially tricky for dermatologists since most patients – about 80% – never discuss their pregnancy with their specialist prior to pregnancy initiation. Dr. Murase recalls when a patient with chronic plaque psoriasis on methotrexate in her late 40s became pregnant and had an abortion even before Dr. Murase became aware of the pregnancy.
Because dermatologists routinely prescribe long-term medications for chronic diseases like acne, psoriasis, and atopic dermatitis, it is important to have a conversation regarding the risks and benefits of long-term medication should a pregnancy occur in any woman of childbearing age, she said.
Fewer women in clinical trials?
Abortion restrictions could possibly discourage women of reproductive age to participate in a clinical trial for a new medication, said Dr. Chambers.
A female patient with a chronic disease who’s randomized to receive a new medication may be required to use certain types of birth control because of unknown potential adverse effects the drug may have on the fetus. But in some cases, accidental pregnancies happen.
The participant in the trial may say, “I don’t know enough about the safety of this drug in pregnancy, and I’ve already taken it. I want to terminate the pregnancy,” said Dr. Chambers. Thinking ahead, a woman may decide not to do the trial to avoid the risk of getting pregnant and not having the option to terminate the pregnancy.
This could apply to new drugs such as antiviral treatments, or medications for severe chronic disease that typically have no clinical trial data in pregnancy prior to initial release into the market.
Women may start taking the drug without thinking about getting pregnant, then realize there are no safety data and become concerned about its effects on a future pregnancy.
The question is: Will abortion restrictions have a chilling effect on these new drugs as well? Patients and their doctors may decide not to try it until more data are available. “I can see where abortion restrictions would change the risk or benefit calculation in thinking about what you do or don’t prescribe or take during reproductive age,” said Dr. Chambers.
The upside of restrictions?
If there’s a positive side to these developments with abortion bans, it may encourage women taking new medications or joining clinical trials to think even more carefully about adherence to effective contraception, said Dr. Chambers.
Some methods are more effective than others, she emphasized. “When you have an unplanned pregnancy, it could mean that the method you used wasn’t optimal or you weren’t using it as recommended.” A goal moving forward is to encourage more thoughtful use of highly effective contraceptives, thus reducing the number of unplanned pregnancies, she added.
If patients are taking methotrexate, “the time to think about pregnancy is before getting pregnant so you can switch to a drug that’s compatible with pregnancy,” she said.
This whole thought process regarding pregnancy planning could work toward useful health goals, said Dr. Chambers. “Nobody thinks termination is the preferred method, but planning ahead should involve a discussion of what works best for the patient.”
Patients do have other choices, said Dr. Grifka. “Fortunately, there are many commonly prescribed medications which cross the placenta and have no ill effects on the fetus.”
Talking to patients about choices
Dr. Clowse, who spends a lot of time training rheumatologists, encourages them to have conversations with patients about pregnancy planning. It’s a lot to manage, getting the right drug to a female patient with chronic illness, especially in this current climate of abortion upheaval, she noted.
Her approach is to have an open and honest conversation with patients about their concerns and fears, what the realities are, and what the potential future options are for certain rheumatology drugs in the United States.
Some women who see what’s happening across the country may become so risk averse that they may choose to die rather than take a lifesaving drug that poses certain risks under new restrictions.
“I think that’s tragic,” said Dr. Clowse.
To help their patients, Dr. Gray believes physicians across specialties should better educate themselves about physiology in pregnancy and how to counsel patients on the impact of not taking medications in pregnancy.
In her view, it’s almost coercive to say to a patient, “You really need to have effective contraception if I’m going to give you this lifesaving or quality-of-life-improving medication.”
When confronting such scenarios, Dr. Gray doesn’t think physicians need to change how they counsel patients about contraception. “I don’t think we should be putting pressure on patients to consider other permanent methods just because there’s a lack of abortion options.”
Patients will eventually make those decisions for themselves, she said. “They’re going to want a more efficacious method because they’re worried about not having access to abortion if they get pregnant.”
Dr. Gray reports being a site principal investigator for a phase 3 trial for VeraCept IUD, funded by Sebela Pharmaceuticals. Dr. Clowse reports receiving research funding and doing consulting for GlaxoSmithKline.
*Correction, 6/2/2022: A previous version of this article misstated the intended use of drugs such as the “morning-after” pill (levonorgestrel). They are taken to prevent unintended pregnancy.
A version of this article first appeared on Medscape.com .
Focus on antivirals, vaccines as monkeypox continues
Since the first case of monkeypox on May 6, reports of outbreaks have come from multiple countries, with the United Kingdom, Spain, and Portugal in the lead, followed by Canada, Israel, and Australia, among others. The United States has reported cases in Boston and New York, and presumed cases have occurred in Utah and Florida. As of May 25, close to 350 cases, either suspected (83) or confirmed (265), have been reported globally.
Monkeypox outbreaks have previously been confined to Central and West Africa, except for an impressively large outbreak in the United States in 2003, during which 47 people were infected across six states. The epidemic was traced to a Gambian rat, rope squirrels, and dormice that had been imported from Ghana as pets and that had infected prairie dogs at a large wholesale pet store.
“It’s amazing how many of these viruses – COVID, now monkeypox and others – [exist]. They’re out there in the wild in the animal reservoir,” said Dennis Hruby, PhD, executive VP/chief scientific officer and scientific founder of SIGA Technologies.
“When it comes to the human population, they sometimes behave in ways we’re not expecting. That and a few mutations change those strains and pathogenicity and can be pandemic,” he told this news organization.
Now that the virus is pandemic, there is an urgent interest in medicines and vaccines that might halt its spread.
Smallpox drug tecovirimat
SIGA’s drug is tecovirimat, initially known as ST-246 and now branded as TPOXX. The U.S. Food and Drug Administration approved an oral formulation to treat smallpox in 2018. While smallpox was eradicated by 1980, there have been ongoing concerns about its potential use in a bioterrorism attack.
Tecovirimat is also approved for smallpox in Canada. In Europe, the approval includes treatment of monkeypox, cowpox, and complications from immunization with vaccinia. On May 19, the FDA approved an IV formulation of tecovirimat for those unable to tolerate oral medications.
In a press release, SIGA notes that tecovirimat was “developed through funding and collaboration with the Biomedical Advanced Research and Development Authority (BARDA) at the U.S. Department of Health & Human Services, as well as early-stage development supported by the National Institutes of Health, US Centers for Disease Control and Prevention, and the Department of Defense. Tecovirimat is stockpiled by the U.S. Government to mitigate the impact of a potential outbreak or bioterror attack.”
SIGA adds that, under Project Bioshield, “the United States maintains a stockpile of 1.7 million courses in the Strategic National Stockpile.” The drug is only available through the government’s stockpile.
Tecovirimat works by preventing the viruses from reproducing by interfering with a protein, VP37. The virus cannot escape the cell and so cannot infect other cells, Dr. Hruby explained.
Tecovirimat was developed under the FDA’s so-called Animal Rule, which allows approval on the basis of animal studies when human efficacy studies are unethical or impractical.
In a placebo-controlled human pharmacokinetic and safety study, only 2% of the 359 who received TPOXX had to have treatment stopped because of adverse reactions, a rate similar to placebo. The most common reactions (≥2%) were headache, nausea, and abdominal pain. Significant drug interactions were found with the coadministration of repaglinide and midazolam.
Of note is that tecovirimat’s efficacy may be reduced in immunocompromised patients. The smallpox vaccine is contraindicated for those who are immunocompromised. Those people should be offered vaccinia immune globulin.
With monkeypox, “the earlier the disease is recognized and you start treating, [the] more effective,” said Dr. Hruby. “In a monkey model which, much like humans, if we treat early on as the first lesions emerged or even several days after the lesions emerged, we see close to 100% protection.”
The other alternative drug for smallpox and (likely) monkeypox is Chimerix’s brincidofovir (BCV, Tembexa), a lipid conjugate of cidofovir, a drug for cytomegalovirus. Brincidofovir has a better safety profile than cidofovir and was also approved under the Animal Rule.
UpToDate suggests that tecovirimat is the drug of choice for monkeypox. They note that for severely infected patients, it can be combined with brincidofovir after consultation with the CDC or state health department officials.
Two vaccines available
Two vaccines are currently available. The oldest is ACAM2000, a replication-competent vaccine that replaced Dryvax, whose use was stopped in 1977, the last year in which naturally occurring cases of smallpox occurred. ACAM2000 is used to immunize military recruits. It was produced by Sanofi and is now produced by Emergent Biosolutions. Being a live vaccinia vaccine, it is contraindicated for people who are immunocompromised or pregnant, as well as for children and those with eczema, because serious and occasionally fatal reactions have occurred. Because of unexpected cardiac complications in first responders who received Dryvax, having a history of cardiac disease or significant risk factors is considered a contraindication to replication-competent (live) vaccination except in the setting of a bioterrorism event.
ACAM2000 is not FDA approved for monkeypox, but it is readily available. The United States stockpile has more than 100 million doses, according to the CDC.
“ACAM is not very different from Dryvax in terms of safety profile,” Melvin Sanicas, MD, a vaccinologist and health educator, told this news organization.
The newest option is a replication-deficient modified vaccinia Ankara vaccine called Jynneos in the United States (Imvanex in Europe; Imvamune in Canada). The vaccine is made by Denmark-based Bavarian Nordic. The FDA approved Jynneos in 2019. It, too, is available through BARDA’s stockpiles; 1,000 doses are available now and more are on order.
In the current monkeypox outbreak, Jynneos has been offered to higher-risk contacts in the United Kingdom. The CDC is planning to provide it to high-risk contacts of infected persons in the United States. This strategy is called “ring vaccination,” through which only close contacts are immunized initially. The rings are then enlarged to include more people as needed. Ring vaccination works well for easily identified diseases such as monkeypox and in situations in which there are few cases. It has been used very effectively for smallpox and Ebola.
Jynneos is not associated with the same risks as the live vaccine. In solicited reactions, injection-site reactions were common. Other reported systemic symptoms were muscle pain (42.8%), headache (34.8%), fatigue (30.4%), nausea (17.3%), and chills (10.4%).
Other vaccines are expected to be developed. Moderna has just thrown its hat into the ring, announcing it is beginning preclinical trials for monkeypox.
Prolonged close contact
Monkeypox is spread by large droplets or contact with infected lesions or body fluids. It’s thought to require prolonged close contact. In an email interview, Dr. Sanicas told this news organization that the “contact can be with (1) skin lesions of an infected person, (2) respiratory droplets in prolonged face-to-face contact, (3) fomites. The cases in the United Kingdom are in men having sex with men, but it does not mean the disease is now sexually transmitted. People do not need to have sex to be infected, but of course, sexual contact means there is prolonged contact.” The household transmission rate is less than 10%.
Dr. Sanicas confirmed that, as with smallpox, monkeypox could be transmitted by contact with clothing or bedding that has been contaminated through contact with the infected lesions, as smallpox was transmitted to Native Americans by colonizers. Airborne transmission is a theoretical possibility but is not considered likely. Being a DNA virus, monkeypox is less likely to mutate than COVID. “If it were as infectious as flu or coronavirus, there would be more infections and outbreaks in countries where MPX [monkeypox] is endemic in Western Africa or Congo Basin,” said Dr. Sanicas.
Fortunately, this clade of monkeypox, which appears to have originated in West Africa, is estimated to have a mortality rate of about 1%. In contrast, the Congo Basin clade has a death rate of up to 10%.
Dr. Sanicas concluded, “Be cautious, but there’s no need for further fear and panic on top of what we have for COVID-19. Monkeypox is not COVID and will not cause the same devastation/death/lockdowns as COVID-19.”
Dr. Hruby is an employee and stockholder of SIGA. Dr. Sanicas reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Since the first case of monkeypox on May 6, reports of outbreaks have come from multiple countries, with the United Kingdom, Spain, and Portugal in the lead, followed by Canada, Israel, and Australia, among others. The United States has reported cases in Boston and New York, and presumed cases have occurred in Utah and Florida. As of May 25, close to 350 cases, either suspected (83) or confirmed (265), have been reported globally.
Monkeypox outbreaks have previously been confined to Central and West Africa, except for an impressively large outbreak in the United States in 2003, during which 47 people were infected across six states. The epidemic was traced to a Gambian rat, rope squirrels, and dormice that had been imported from Ghana as pets and that had infected prairie dogs at a large wholesale pet store.
“It’s amazing how many of these viruses – COVID, now monkeypox and others – [exist]. They’re out there in the wild in the animal reservoir,” said Dennis Hruby, PhD, executive VP/chief scientific officer and scientific founder of SIGA Technologies.
“When it comes to the human population, they sometimes behave in ways we’re not expecting. That and a few mutations change those strains and pathogenicity and can be pandemic,” he told this news organization.
Now that the virus is pandemic, there is an urgent interest in medicines and vaccines that might halt its spread.
Smallpox drug tecovirimat
SIGA’s drug is tecovirimat, initially known as ST-246 and now branded as TPOXX. The U.S. Food and Drug Administration approved an oral formulation to treat smallpox in 2018. While smallpox was eradicated by 1980, there have been ongoing concerns about its potential use in a bioterrorism attack.
Tecovirimat is also approved for smallpox in Canada. In Europe, the approval includes treatment of monkeypox, cowpox, and complications from immunization with vaccinia. On May 19, the FDA approved an IV formulation of tecovirimat for those unable to tolerate oral medications.
In a press release, SIGA notes that tecovirimat was “developed through funding and collaboration with the Biomedical Advanced Research and Development Authority (BARDA) at the U.S. Department of Health & Human Services, as well as early-stage development supported by the National Institutes of Health, US Centers for Disease Control and Prevention, and the Department of Defense. Tecovirimat is stockpiled by the U.S. Government to mitigate the impact of a potential outbreak or bioterror attack.”
SIGA adds that, under Project Bioshield, “the United States maintains a stockpile of 1.7 million courses in the Strategic National Stockpile.” The drug is only available through the government’s stockpile.
Tecovirimat works by preventing the viruses from reproducing by interfering with a protein, VP37. The virus cannot escape the cell and so cannot infect other cells, Dr. Hruby explained.
Tecovirimat was developed under the FDA’s so-called Animal Rule, which allows approval on the basis of animal studies when human efficacy studies are unethical or impractical.
In a placebo-controlled human pharmacokinetic and safety study, only 2% of the 359 who received TPOXX had to have treatment stopped because of adverse reactions, a rate similar to placebo. The most common reactions (≥2%) were headache, nausea, and abdominal pain. Significant drug interactions were found with the coadministration of repaglinide and midazolam.
Of note is that tecovirimat’s efficacy may be reduced in immunocompromised patients. The smallpox vaccine is contraindicated for those who are immunocompromised. Those people should be offered vaccinia immune globulin.
With monkeypox, “the earlier the disease is recognized and you start treating, [the] more effective,” said Dr. Hruby. “In a monkey model which, much like humans, if we treat early on as the first lesions emerged or even several days after the lesions emerged, we see close to 100% protection.”
The other alternative drug for smallpox and (likely) monkeypox is Chimerix’s brincidofovir (BCV, Tembexa), a lipid conjugate of cidofovir, a drug for cytomegalovirus. Brincidofovir has a better safety profile than cidofovir and was also approved under the Animal Rule.
UpToDate suggests that tecovirimat is the drug of choice for monkeypox. They note that for severely infected patients, it can be combined with brincidofovir after consultation with the CDC or state health department officials.
Two vaccines available
Two vaccines are currently available. The oldest is ACAM2000, a replication-competent vaccine that replaced Dryvax, whose use was stopped in 1977, the last year in which naturally occurring cases of smallpox occurred. ACAM2000 is used to immunize military recruits. It was produced by Sanofi and is now produced by Emergent Biosolutions. Being a live vaccinia vaccine, it is contraindicated for people who are immunocompromised or pregnant, as well as for children and those with eczema, because serious and occasionally fatal reactions have occurred. Because of unexpected cardiac complications in first responders who received Dryvax, having a history of cardiac disease or significant risk factors is considered a contraindication to replication-competent (live) vaccination except in the setting of a bioterrorism event.
ACAM2000 is not FDA approved for monkeypox, but it is readily available. The United States stockpile has more than 100 million doses, according to the CDC.
“ACAM is not very different from Dryvax in terms of safety profile,” Melvin Sanicas, MD, a vaccinologist and health educator, told this news organization.
The newest option is a replication-deficient modified vaccinia Ankara vaccine called Jynneos in the United States (Imvanex in Europe; Imvamune in Canada). The vaccine is made by Denmark-based Bavarian Nordic. The FDA approved Jynneos in 2019. It, too, is available through BARDA’s stockpiles; 1,000 doses are available now and more are on order.
In the current monkeypox outbreak, Jynneos has been offered to higher-risk contacts in the United Kingdom. The CDC is planning to provide it to high-risk contacts of infected persons in the United States. This strategy is called “ring vaccination,” through which only close contacts are immunized initially. The rings are then enlarged to include more people as needed. Ring vaccination works well for easily identified diseases such as monkeypox and in situations in which there are few cases. It has been used very effectively for smallpox and Ebola.
Jynneos is not associated with the same risks as the live vaccine. In solicited reactions, injection-site reactions were common. Other reported systemic symptoms were muscle pain (42.8%), headache (34.8%), fatigue (30.4%), nausea (17.3%), and chills (10.4%).
Other vaccines are expected to be developed. Moderna has just thrown its hat into the ring, announcing it is beginning preclinical trials for monkeypox.
Prolonged close contact
Monkeypox is spread by large droplets or contact with infected lesions or body fluids. It’s thought to require prolonged close contact. In an email interview, Dr. Sanicas told this news organization that the “contact can be with (1) skin lesions of an infected person, (2) respiratory droplets in prolonged face-to-face contact, (3) fomites. The cases in the United Kingdom are in men having sex with men, but it does not mean the disease is now sexually transmitted. People do not need to have sex to be infected, but of course, sexual contact means there is prolonged contact.” The household transmission rate is less than 10%.
Dr. Sanicas confirmed that, as with smallpox, monkeypox could be transmitted by contact with clothing or bedding that has been contaminated through contact with the infected lesions, as smallpox was transmitted to Native Americans by colonizers. Airborne transmission is a theoretical possibility but is not considered likely. Being a DNA virus, monkeypox is less likely to mutate than COVID. “If it were as infectious as flu or coronavirus, there would be more infections and outbreaks in countries where MPX [monkeypox] is endemic in Western Africa or Congo Basin,” said Dr. Sanicas.
Fortunately, this clade of monkeypox, which appears to have originated in West Africa, is estimated to have a mortality rate of about 1%. In contrast, the Congo Basin clade has a death rate of up to 10%.
Dr. Sanicas concluded, “Be cautious, but there’s no need for further fear and panic on top of what we have for COVID-19. Monkeypox is not COVID and will not cause the same devastation/death/lockdowns as COVID-19.”
Dr. Hruby is an employee and stockholder of SIGA. Dr. Sanicas reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Since the first case of monkeypox on May 6, reports of outbreaks have come from multiple countries, with the United Kingdom, Spain, and Portugal in the lead, followed by Canada, Israel, and Australia, among others. The United States has reported cases in Boston and New York, and presumed cases have occurred in Utah and Florida. As of May 25, close to 350 cases, either suspected (83) or confirmed (265), have been reported globally.
Monkeypox outbreaks have previously been confined to Central and West Africa, except for an impressively large outbreak in the United States in 2003, during which 47 people were infected across six states. The epidemic was traced to a Gambian rat, rope squirrels, and dormice that had been imported from Ghana as pets and that had infected prairie dogs at a large wholesale pet store.
“It’s amazing how many of these viruses – COVID, now monkeypox and others – [exist]. They’re out there in the wild in the animal reservoir,” said Dennis Hruby, PhD, executive VP/chief scientific officer and scientific founder of SIGA Technologies.
“When it comes to the human population, they sometimes behave in ways we’re not expecting. That and a few mutations change those strains and pathogenicity and can be pandemic,” he told this news organization.
Now that the virus is pandemic, there is an urgent interest in medicines and vaccines that might halt its spread.
Smallpox drug tecovirimat
SIGA’s drug is tecovirimat, initially known as ST-246 and now branded as TPOXX. The U.S. Food and Drug Administration approved an oral formulation to treat smallpox in 2018. While smallpox was eradicated by 1980, there have been ongoing concerns about its potential use in a bioterrorism attack.
Tecovirimat is also approved for smallpox in Canada. In Europe, the approval includes treatment of monkeypox, cowpox, and complications from immunization with vaccinia. On May 19, the FDA approved an IV formulation of tecovirimat for those unable to tolerate oral medications.
In a press release, SIGA notes that tecovirimat was “developed through funding and collaboration with the Biomedical Advanced Research and Development Authority (BARDA) at the U.S. Department of Health & Human Services, as well as early-stage development supported by the National Institutes of Health, US Centers for Disease Control and Prevention, and the Department of Defense. Tecovirimat is stockpiled by the U.S. Government to mitigate the impact of a potential outbreak or bioterror attack.”
SIGA adds that, under Project Bioshield, “the United States maintains a stockpile of 1.7 million courses in the Strategic National Stockpile.” The drug is only available through the government’s stockpile.
Tecovirimat works by preventing the viruses from reproducing by interfering with a protein, VP37. The virus cannot escape the cell and so cannot infect other cells, Dr. Hruby explained.
Tecovirimat was developed under the FDA’s so-called Animal Rule, which allows approval on the basis of animal studies when human efficacy studies are unethical or impractical.
In a placebo-controlled human pharmacokinetic and safety study, only 2% of the 359 who received TPOXX had to have treatment stopped because of adverse reactions, a rate similar to placebo. The most common reactions (≥2%) were headache, nausea, and abdominal pain. Significant drug interactions were found with the coadministration of repaglinide and midazolam.
Of note is that tecovirimat’s efficacy may be reduced in immunocompromised patients. The smallpox vaccine is contraindicated for those who are immunocompromised. Those people should be offered vaccinia immune globulin.
With monkeypox, “the earlier the disease is recognized and you start treating, [the] more effective,” said Dr. Hruby. “In a monkey model which, much like humans, if we treat early on as the first lesions emerged or even several days after the lesions emerged, we see close to 100% protection.”
The other alternative drug for smallpox and (likely) monkeypox is Chimerix’s brincidofovir (BCV, Tembexa), a lipid conjugate of cidofovir, a drug for cytomegalovirus. Brincidofovir has a better safety profile than cidofovir and was also approved under the Animal Rule.
UpToDate suggests that tecovirimat is the drug of choice for monkeypox. They note that for severely infected patients, it can be combined with brincidofovir after consultation with the CDC or state health department officials.
Two vaccines available
Two vaccines are currently available. The oldest is ACAM2000, a replication-competent vaccine that replaced Dryvax, whose use was stopped in 1977, the last year in which naturally occurring cases of smallpox occurred. ACAM2000 is used to immunize military recruits. It was produced by Sanofi and is now produced by Emergent Biosolutions. Being a live vaccinia vaccine, it is contraindicated for people who are immunocompromised or pregnant, as well as for children and those with eczema, because serious and occasionally fatal reactions have occurred. Because of unexpected cardiac complications in first responders who received Dryvax, having a history of cardiac disease or significant risk factors is considered a contraindication to replication-competent (live) vaccination except in the setting of a bioterrorism event.
ACAM2000 is not FDA approved for monkeypox, but it is readily available. The United States stockpile has more than 100 million doses, according to the CDC.
“ACAM is not very different from Dryvax in terms of safety profile,” Melvin Sanicas, MD, a vaccinologist and health educator, told this news organization.
The newest option is a replication-deficient modified vaccinia Ankara vaccine called Jynneos in the United States (Imvanex in Europe; Imvamune in Canada). The vaccine is made by Denmark-based Bavarian Nordic. The FDA approved Jynneos in 2019. It, too, is available through BARDA’s stockpiles; 1,000 doses are available now and more are on order.
In the current monkeypox outbreak, Jynneos has been offered to higher-risk contacts in the United Kingdom. The CDC is planning to provide it to high-risk contacts of infected persons in the United States. This strategy is called “ring vaccination,” through which only close contacts are immunized initially. The rings are then enlarged to include more people as needed. Ring vaccination works well for easily identified diseases such as monkeypox and in situations in which there are few cases. It has been used very effectively for smallpox and Ebola.
Jynneos is not associated with the same risks as the live vaccine. In solicited reactions, injection-site reactions were common. Other reported systemic symptoms were muscle pain (42.8%), headache (34.8%), fatigue (30.4%), nausea (17.3%), and chills (10.4%).
Other vaccines are expected to be developed. Moderna has just thrown its hat into the ring, announcing it is beginning preclinical trials for monkeypox.
Prolonged close contact
Monkeypox is spread by large droplets or contact with infected lesions or body fluids. It’s thought to require prolonged close contact. In an email interview, Dr. Sanicas told this news organization that the “contact can be with (1) skin lesions of an infected person, (2) respiratory droplets in prolonged face-to-face contact, (3) fomites. The cases in the United Kingdom are in men having sex with men, but it does not mean the disease is now sexually transmitted. People do not need to have sex to be infected, but of course, sexual contact means there is prolonged contact.” The household transmission rate is less than 10%.
Dr. Sanicas confirmed that, as with smallpox, monkeypox could be transmitted by contact with clothing or bedding that has been contaminated through contact with the infected lesions, as smallpox was transmitted to Native Americans by colonizers. Airborne transmission is a theoretical possibility but is not considered likely. Being a DNA virus, monkeypox is less likely to mutate than COVID. “If it were as infectious as flu or coronavirus, there would be more infections and outbreaks in countries where MPX [monkeypox] is endemic in Western Africa or Congo Basin,” said Dr. Sanicas.
Fortunately, this clade of monkeypox, which appears to have originated in West Africa, is estimated to have a mortality rate of about 1%. In contrast, the Congo Basin clade has a death rate of up to 10%.
Dr. Sanicas concluded, “Be cautious, but there’s no need for further fear and panic on top of what we have for COVID-19. Monkeypox is not COVID and will not cause the same devastation/death/lockdowns as COVID-19.”
Dr. Hruby is an employee and stockholder of SIGA. Dr. Sanicas reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Childhood survivors of gun violence: What’s the long-term outlook?
As the parents of the 19 children shot dead Tuesday in Uvalde, Tex., by a teen gunman grapple with unspeakable grief and funeral preparations, the survivors and their families are dealing with their own angst and likely much more.
While the parents understandably feel lucky that their children made it out, what about the long-term effect on their children of witnessing that carnage, of seeing classmates, friends, and teachers die violently as they stood by helpless and fearful?
The outcome over the next few days, months, and years depends on many factors, but how parents address the trauma both immediately and long-term can make a huge difference, experts say.
Posttraumatic growth
Best long-term case scenario? Survivors can experience what experts call posttraumatic growth – reaching out to give back to society, to make the world a better place, and changing who they are and their view of the world.
A prime example of posttraumatic growth: A month after a teen gunman killed 17 students at Marjory Stoneman Douglas High School in Parkland, Fla., on Valentine’s Day 2018, an army of survivors from that day’s bloodbath headed to Washington, D.C., for the now-famous March for Our Lives. The student-led demonstration, with hundreds of thousands of supporters marching, called for gun control legislation and an end to gun violence. It remains a vibrant, nonprofit organization still advocating for universal background checks and increased support of mental health services.
No sign of future violence
While most children and teens who witness school violence won’t become high-profile activists, as survivors of Parkland and the numerous other school shootings have, neither will they become the next active shooter, mental health experts say. They can’t point to a study that follows the gun violence victims that shows who does OK and who doesn’t, but they know immediate support and therapy can go a long way to recovery.
“I can’t tell you how any particular child will do,” says Robin Gurwitch, PhD, psychologist and professor at Duke University Medical Center, Durham, N.C. “I can tell you the majority of kids will be OK.”
However, that doesn’t mean a surviving child won’t have behavior and other issues, she says. Research does suggest the next few days, weeks, or months will be rough.
What parents and other caretakers do in the days after the violence will help predict the long-term outcome. Dr. Gurwitch and other experts say it’s important to first focus on what they call “psychological first aid,” then phase in therapy such as trauma-focused cognitive behavioral therapy, if and when it’s needed.
First, ‘psychological first aid’
“Psychological first aid is designed to minimize the impact down the road,” Dr. Gurwitch says. “Validate that they are feeling scared or worried.”
Some may be angry, another understandable emotion. In the first few days of witnessing violence – or even just hearing about it – parents should expect clinginess, sleep problems, behavior meltdowns, and irritability, she says.
“Those kinds of changes are likely to last a few weeks,” she says.
If day-to-day functioning is very difficult, “don’t wait for those to pass,” Dr. Gurwitch says. “Reach out for help. Resources will be available. Check with your pediatrician or family physician.”
At home, parents can address specific problems related to the experience, Dr. Gurwitch says. If it’s sleep, she says, parents and kids can work together to figure out how to ease sleep, such as listening to their favorite music before bedtime.
While parents may be inclined to baby the kids after the violence, Dr. Gurwitch says it’s important to maintain routines. So it’s not cruel to insist they do their chores.
Expect change
Things won’t be the same.
“Anytime we go through a particular traumatic event, we are changed,” Dr. Gurwitch says. ‘’The question is, what do we do about it? How do we incorporate that change into who we are and have become?”
Also important is figuring out how to make meaning out of what happened.
“I am so impressed by the families at Sandy Hook (the Connecticut elementary school where a gunman killed 26 in 2012),” she says.
They set up foundations and did other advocacy work.
“These types of events are life-changing events,” agrees David Schonfeld, MD, a pediatrician and director of the National Center for Schools Crisis and Bereavement at Children’s Hospital Los Angeles, California. “They will change who children are as people, but it doesn’t mean they are damaged for life. They will remember it as long as they live, and it will also change who they are as a person.”
While people tend to stress the potential negative effects – and there certainly are some – ‘’some individuals actually emerge from these events with a renewed sense of purpose.’’
He tells parents: “Yes, your child has changed, and you can’t go back. But it doesn’t mean they are destined to never be able to cope [with trauma].”
Research
The effects of gun violence on children can be serious and dramatic, research shows.
- Exposure to neighborhood gun violence is linked with an increase in children’s mental health issues, have found. Children living within two or three blocks of gun violence had nearly twice the risk of going to the emergency department with a mental health complaint in the 14 days following the shooting.
- Exposure to gun violence should be classified, along with maltreatment, household dysfunction, and other issues known to impact children negatively, as an adverse childhood experience, other experts
- Direct gun violence exposure, witnessing it, and hearing gunshots are all associated with children being victimized in other ways, another found. And that poly-victimization, as it is called, was strongly associated with having posttraumatic symptoms.
Adverse Childhood Events, as these sorts of experiences are known, can have long-lasting effects on physical and mental health, as well as on even the economic future of a person, says Hansa Bhargava, MD, a pediatrician and chief medical officer of Medscape, WebMD’s sister site for medical professionals.
“Kids who have suffered through violent events can have brain development affected, as well as their immune systems,” she says. “They are more likely to have chronic disease, substance use disorder, sexually transmitted diseases, teen pregnancy, and lifelong depression. A high risk of [posttraumatic stress disorder] is likely for them and their families.”
The impact of family support
The gun violence and deaths are likely to remind children of other losses they have experienced, Dr. Schonfeld says, and that can make coping more difficult.
If the trauma from the Tuesday shootings is ‘’layered” on top of trauma from COVID-19 deaths or other trauma such as domestic violence, those children may have a more difficult time, says Allan Chrisman, MD, professor emeritus of psychiatry and behavioral sciences at Duke University Health System. However, protective factors such as the family response and the community response can build resilience in survivors, he says.
“The way in which parents handle it for themselves will have a huge impact on the kids,” Dr. Chrisman says. “The worst outcomes are linked with [parents saying], ‘We don’t want to talk about it.’ ”
The parents are understandably upset, Dr. Gurwitch says. It’s OK to show sadness, anger, and other emotions, but she tells parents: “It’s not OK to completely decompose.” It’s important for the children to see that parents can pull themselves together.
Longer-term effects
As time goes on, ‘’a very large percentage will have posttraumatic reactions,” Dr. Schonfeld says. “Those reactions tend to improve over time.”
While people talk about PTSD directly after an incident such as a school shooting, it isn’t officially diagnosed as PTSD until the symptoms describing PTSD have persisted for a month, Dr. Schonfeld says. However, ‘’that doesn’t mean you don’t have a problem” that needs attention from a mental health professional.
“As a country we are already struggling with a mental health crisis,” Dr. Bhargava says. “Events such as this serve to exacerbate even more crisis in a group of innocent children whose only crime was to attend school. We must address the ‘epidemic’ of gun violence and school shootings head on. For the sake of our children and their health. For all of us.”
Therapy that works
Cognitive behavioral therapy (CBT) approaches are effective in reducing the trauma, Dr. Gurwitch says.
She often recommends one type of CBT, called trauma-focused cognitive behavioral therapy. This approach involves children and parents and focuses on safety, coping skills, and gradual exposure. It’s a structured and short-term treatment of about eight to 25 sessions.
A version of this article first appeared on Medscape.com.
As the parents of the 19 children shot dead Tuesday in Uvalde, Tex., by a teen gunman grapple with unspeakable grief and funeral preparations, the survivors and their families are dealing with their own angst and likely much more.
While the parents understandably feel lucky that their children made it out, what about the long-term effect on their children of witnessing that carnage, of seeing classmates, friends, and teachers die violently as they stood by helpless and fearful?
The outcome over the next few days, months, and years depends on many factors, but how parents address the trauma both immediately and long-term can make a huge difference, experts say.
Posttraumatic growth
Best long-term case scenario? Survivors can experience what experts call posttraumatic growth – reaching out to give back to society, to make the world a better place, and changing who they are and their view of the world.
A prime example of posttraumatic growth: A month after a teen gunman killed 17 students at Marjory Stoneman Douglas High School in Parkland, Fla., on Valentine’s Day 2018, an army of survivors from that day’s bloodbath headed to Washington, D.C., for the now-famous March for Our Lives. The student-led demonstration, with hundreds of thousands of supporters marching, called for gun control legislation and an end to gun violence. It remains a vibrant, nonprofit organization still advocating for universal background checks and increased support of mental health services.
No sign of future violence
While most children and teens who witness school violence won’t become high-profile activists, as survivors of Parkland and the numerous other school shootings have, neither will they become the next active shooter, mental health experts say. They can’t point to a study that follows the gun violence victims that shows who does OK and who doesn’t, but they know immediate support and therapy can go a long way to recovery.
“I can’t tell you how any particular child will do,” says Robin Gurwitch, PhD, psychologist and professor at Duke University Medical Center, Durham, N.C. “I can tell you the majority of kids will be OK.”
However, that doesn’t mean a surviving child won’t have behavior and other issues, she says. Research does suggest the next few days, weeks, or months will be rough.
What parents and other caretakers do in the days after the violence will help predict the long-term outcome. Dr. Gurwitch and other experts say it’s important to first focus on what they call “psychological first aid,” then phase in therapy such as trauma-focused cognitive behavioral therapy, if and when it’s needed.
First, ‘psychological first aid’
“Psychological first aid is designed to minimize the impact down the road,” Dr. Gurwitch says. “Validate that they are feeling scared or worried.”
Some may be angry, another understandable emotion. In the first few days of witnessing violence – or even just hearing about it – parents should expect clinginess, sleep problems, behavior meltdowns, and irritability, she says.
“Those kinds of changes are likely to last a few weeks,” she says.
If day-to-day functioning is very difficult, “don’t wait for those to pass,” Dr. Gurwitch says. “Reach out for help. Resources will be available. Check with your pediatrician or family physician.”
At home, parents can address specific problems related to the experience, Dr. Gurwitch says. If it’s sleep, she says, parents and kids can work together to figure out how to ease sleep, such as listening to their favorite music before bedtime.
While parents may be inclined to baby the kids after the violence, Dr. Gurwitch says it’s important to maintain routines. So it’s not cruel to insist they do their chores.
Expect change
Things won’t be the same.
“Anytime we go through a particular traumatic event, we are changed,” Dr. Gurwitch says. ‘’The question is, what do we do about it? How do we incorporate that change into who we are and have become?”
Also important is figuring out how to make meaning out of what happened.
“I am so impressed by the families at Sandy Hook (the Connecticut elementary school where a gunman killed 26 in 2012),” she says.
They set up foundations and did other advocacy work.
“These types of events are life-changing events,” agrees David Schonfeld, MD, a pediatrician and director of the National Center for Schools Crisis and Bereavement at Children’s Hospital Los Angeles, California. “They will change who children are as people, but it doesn’t mean they are damaged for life. They will remember it as long as they live, and it will also change who they are as a person.”
While people tend to stress the potential negative effects – and there certainly are some – ‘’some individuals actually emerge from these events with a renewed sense of purpose.’’
He tells parents: “Yes, your child has changed, and you can’t go back. But it doesn’t mean they are destined to never be able to cope [with trauma].”
Research
The effects of gun violence on children can be serious and dramatic, research shows.
- Exposure to neighborhood gun violence is linked with an increase in children’s mental health issues, have found. Children living within two or three blocks of gun violence had nearly twice the risk of going to the emergency department with a mental health complaint in the 14 days following the shooting.
- Exposure to gun violence should be classified, along with maltreatment, household dysfunction, and other issues known to impact children negatively, as an adverse childhood experience, other experts
- Direct gun violence exposure, witnessing it, and hearing gunshots are all associated with children being victimized in other ways, another found. And that poly-victimization, as it is called, was strongly associated with having posttraumatic symptoms.
Adverse Childhood Events, as these sorts of experiences are known, can have long-lasting effects on physical and mental health, as well as on even the economic future of a person, says Hansa Bhargava, MD, a pediatrician and chief medical officer of Medscape, WebMD’s sister site for medical professionals.
“Kids who have suffered through violent events can have brain development affected, as well as their immune systems,” she says. “They are more likely to have chronic disease, substance use disorder, sexually transmitted diseases, teen pregnancy, and lifelong depression. A high risk of [posttraumatic stress disorder] is likely for them and their families.”
The impact of family support
The gun violence and deaths are likely to remind children of other losses they have experienced, Dr. Schonfeld says, and that can make coping more difficult.
If the trauma from the Tuesday shootings is ‘’layered” on top of trauma from COVID-19 deaths or other trauma such as domestic violence, those children may have a more difficult time, says Allan Chrisman, MD, professor emeritus of psychiatry and behavioral sciences at Duke University Health System. However, protective factors such as the family response and the community response can build resilience in survivors, he says.
“The way in which parents handle it for themselves will have a huge impact on the kids,” Dr. Chrisman says. “The worst outcomes are linked with [parents saying], ‘We don’t want to talk about it.’ ”
The parents are understandably upset, Dr. Gurwitch says. It’s OK to show sadness, anger, and other emotions, but she tells parents: “It’s not OK to completely decompose.” It’s important for the children to see that parents can pull themselves together.
Longer-term effects
As time goes on, ‘’a very large percentage will have posttraumatic reactions,” Dr. Schonfeld says. “Those reactions tend to improve over time.”
While people talk about PTSD directly after an incident such as a school shooting, it isn’t officially diagnosed as PTSD until the symptoms describing PTSD have persisted for a month, Dr. Schonfeld says. However, ‘’that doesn’t mean you don’t have a problem” that needs attention from a mental health professional.
“As a country we are already struggling with a mental health crisis,” Dr. Bhargava says. “Events such as this serve to exacerbate even more crisis in a group of innocent children whose only crime was to attend school. We must address the ‘epidemic’ of gun violence and school shootings head on. For the sake of our children and their health. For all of us.”
Therapy that works
Cognitive behavioral therapy (CBT) approaches are effective in reducing the trauma, Dr. Gurwitch says.
She often recommends one type of CBT, called trauma-focused cognitive behavioral therapy. This approach involves children and parents and focuses on safety, coping skills, and gradual exposure. It’s a structured and short-term treatment of about eight to 25 sessions.
A version of this article first appeared on Medscape.com.
As the parents of the 19 children shot dead Tuesday in Uvalde, Tex., by a teen gunman grapple with unspeakable grief and funeral preparations, the survivors and their families are dealing with their own angst and likely much more.
While the parents understandably feel lucky that their children made it out, what about the long-term effect on their children of witnessing that carnage, of seeing classmates, friends, and teachers die violently as they stood by helpless and fearful?
The outcome over the next few days, months, and years depends on many factors, but how parents address the trauma both immediately and long-term can make a huge difference, experts say.
Posttraumatic growth
Best long-term case scenario? Survivors can experience what experts call posttraumatic growth – reaching out to give back to society, to make the world a better place, and changing who they are and their view of the world.
A prime example of posttraumatic growth: A month after a teen gunman killed 17 students at Marjory Stoneman Douglas High School in Parkland, Fla., on Valentine’s Day 2018, an army of survivors from that day’s bloodbath headed to Washington, D.C., for the now-famous March for Our Lives. The student-led demonstration, with hundreds of thousands of supporters marching, called for gun control legislation and an end to gun violence. It remains a vibrant, nonprofit organization still advocating for universal background checks and increased support of mental health services.
No sign of future violence
While most children and teens who witness school violence won’t become high-profile activists, as survivors of Parkland and the numerous other school shootings have, neither will they become the next active shooter, mental health experts say. They can’t point to a study that follows the gun violence victims that shows who does OK and who doesn’t, but they know immediate support and therapy can go a long way to recovery.
“I can’t tell you how any particular child will do,” says Robin Gurwitch, PhD, psychologist and professor at Duke University Medical Center, Durham, N.C. “I can tell you the majority of kids will be OK.”
However, that doesn’t mean a surviving child won’t have behavior and other issues, she says. Research does suggest the next few days, weeks, or months will be rough.
What parents and other caretakers do in the days after the violence will help predict the long-term outcome. Dr. Gurwitch and other experts say it’s important to first focus on what they call “psychological first aid,” then phase in therapy such as trauma-focused cognitive behavioral therapy, if and when it’s needed.
First, ‘psychological first aid’
“Psychological first aid is designed to minimize the impact down the road,” Dr. Gurwitch says. “Validate that they are feeling scared or worried.”
Some may be angry, another understandable emotion. In the first few days of witnessing violence – or even just hearing about it – parents should expect clinginess, sleep problems, behavior meltdowns, and irritability, she says.
“Those kinds of changes are likely to last a few weeks,” she says.
If day-to-day functioning is very difficult, “don’t wait for those to pass,” Dr. Gurwitch says. “Reach out for help. Resources will be available. Check with your pediatrician or family physician.”
At home, parents can address specific problems related to the experience, Dr. Gurwitch says. If it’s sleep, she says, parents and kids can work together to figure out how to ease sleep, such as listening to their favorite music before bedtime.
While parents may be inclined to baby the kids after the violence, Dr. Gurwitch says it’s important to maintain routines. So it’s not cruel to insist they do their chores.
Expect change
Things won’t be the same.
“Anytime we go through a particular traumatic event, we are changed,” Dr. Gurwitch says. ‘’The question is, what do we do about it? How do we incorporate that change into who we are and have become?”
Also important is figuring out how to make meaning out of what happened.
“I am so impressed by the families at Sandy Hook (the Connecticut elementary school where a gunman killed 26 in 2012),” she says.
They set up foundations and did other advocacy work.
“These types of events are life-changing events,” agrees David Schonfeld, MD, a pediatrician and director of the National Center for Schools Crisis and Bereavement at Children’s Hospital Los Angeles, California. “They will change who children are as people, but it doesn’t mean they are damaged for life. They will remember it as long as they live, and it will also change who they are as a person.”
While people tend to stress the potential negative effects – and there certainly are some – ‘’some individuals actually emerge from these events with a renewed sense of purpose.’’
He tells parents: “Yes, your child has changed, and you can’t go back. But it doesn’t mean they are destined to never be able to cope [with trauma].”
Research
The effects of gun violence on children can be serious and dramatic, research shows.
- Exposure to neighborhood gun violence is linked with an increase in children’s mental health issues, have found. Children living within two or three blocks of gun violence had nearly twice the risk of going to the emergency department with a mental health complaint in the 14 days following the shooting.
- Exposure to gun violence should be classified, along with maltreatment, household dysfunction, and other issues known to impact children negatively, as an adverse childhood experience, other experts
- Direct gun violence exposure, witnessing it, and hearing gunshots are all associated with children being victimized in other ways, another found. And that poly-victimization, as it is called, was strongly associated with having posttraumatic symptoms.
Adverse Childhood Events, as these sorts of experiences are known, can have long-lasting effects on physical and mental health, as well as on even the economic future of a person, says Hansa Bhargava, MD, a pediatrician and chief medical officer of Medscape, WebMD’s sister site for medical professionals.
“Kids who have suffered through violent events can have brain development affected, as well as their immune systems,” she says. “They are more likely to have chronic disease, substance use disorder, sexually transmitted diseases, teen pregnancy, and lifelong depression. A high risk of [posttraumatic stress disorder] is likely for them and their families.”
The impact of family support
The gun violence and deaths are likely to remind children of other losses they have experienced, Dr. Schonfeld says, and that can make coping more difficult.
If the trauma from the Tuesday shootings is ‘’layered” on top of trauma from COVID-19 deaths or other trauma such as domestic violence, those children may have a more difficult time, says Allan Chrisman, MD, professor emeritus of psychiatry and behavioral sciences at Duke University Health System. However, protective factors such as the family response and the community response can build resilience in survivors, he says.
“The way in which parents handle it for themselves will have a huge impact on the kids,” Dr. Chrisman says. “The worst outcomes are linked with [parents saying], ‘We don’t want to talk about it.’ ”
The parents are understandably upset, Dr. Gurwitch says. It’s OK to show sadness, anger, and other emotions, but she tells parents: “It’s not OK to completely decompose.” It’s important for the children to see that parents can pull themselves together.
Longer-term effects
As time goes on, ‘’a very large percentage will have posttraumatic reactions,” Dr. Schonfeld says. “Those reactions tend to improve over time.”
While people talk about PTSD directly after an incident such as a school shooting, it isn’t officially diagnosed as PTSD until the symptoms describing PTSD have persisted for a month, Dr. Schonfeld says. However, ‘’that doesn’t mean you don’t have a problem” that needs attention from a mental health professional.
“As a country we are already struggling with a mental health crisis,” Dr. Bhargava says. “Events such as this serve to exacerbate even more crisis in a group of innocent children whose only crime was to attend school. We must address the ‘epidemic’ of gun violence and school shootings head on. For the sake of our children and their health. For all of us.”
Therapy that works
Cognitive behavioral therapy (CBT) approaches are effective in reducing the trauma, Dr. Gurwitch says.
She often recommends one type of CBT, called trauma-focused cognitive behavioral therapy. This approach involves children and parents and focuses on safety, coping skills, and gradual exposure. It’s a structured and short-term treatment of about eight to 25 sessions.
A version of this article first appeared on Medscape.com.
Crohn’s disease research goes to the dogs
Why it might be better to be a dog person
Here’s that old debate again: Dogs or cats? You probably have your own opinion, but research presented at this year’s Digestive Disease Week may have tipped the scale by showing that children who lived with dogs may be less likely to have Crohn’s disease as adults.
The research was done by having approximately 4,300 people closely related to patients with Crohn’s disease fill out an environmental questionnaire. Using these data, the research team looked into environmental factors such as size of the families, where the home was, how many bathrooms the homes had, and quality of drinking water.
The researchers found that those who had or were exposed to dogs between the ages of 5 and 15 years were more likely to have healthy gut permeability and balanced microbes, which increased their protection against Crohn’s disease.
“Our study seems to add to others that have explored the ‘hygiene hypothesis’ which suggests that the lack of exposure to microbes early in life may lead to lack of immune regulation toward environmental microbes,” senior author Williams Turpin, PhD, said in the written statement.
The researchers aren’t sure why they didn’t get the same findings with cats, but Dr. Turpin theorized that dog owners tend to be outside more with their dogs or live in places with more green space, which are good protectors against Crohn’s disease.
It’s all good for dog owners, but do their pets’ parasites make you more attractive? Just more fuel for the ongoing debate.
Come for the history, stay for the fossilized parasites
Another week, another analysis of old British poop. LOTME really is your one-stop shop for all the important, hard-hitting news about historic parasites. You’re welcome, Internet.

The news this week is from Stonehenge, which is apparently kind of a big deal. Rocks in a circle, celestial calendar, cultural significance, whatever. We’re not here to talk about rocks. We’re here to talk about, uh, rocks. Smaller rocks. Specifically, coprolites, which are essentially poop turned into a rock. (Though now we’re imagining Stonehenge made out of fossilized poop rocks. Would it still be a big tourist destination? We can see both sides of the argument on that one.)
Archaeologists from the University of Cambridge have conducted an analysis of coprolites from Durrington Walls, a Neolithic settlement just a few kilometers from Stonehenge. The town dates to the same time that Stonehenge was constructed, and it’s believed that the residents were responsible for building the landmark. These coprolites, depending on what’s inside, can tell us a lot about how the builders of Stonehenge lived and, more specifically, how they ate.
In this case, the coprolites of one human and three dogs contained capillariid worm eggs. These worms come from cows, and when a human is typically infected, the eggs embed in the liver and do not pass through the body. Finding them in excrement indicates that the people were eating raw cow organs and feeding leftovers to their dogs. This is interesting, because a preponderance of pottery and cooking implements also found at the site indicates that the residents of Durrington Walls were spit-roasting or boiling their beef and pork. So the meat was cooked, but not the organs. That is an interesting dietary decision, ancient British people. Then again, modern British cuisine exists. At least now we know where they got it from.
This new research raises one other very important question: When are we going to get a full-on guided tour of all the important coprolite sites in Britain? They’ve clearly got plenty of them, and the tourist demand for ancient parasites must be sky-high. Come on, capitalism, follow through on this. We’d go.
Everyone lies: Food intake edition
Do you have any patients on special diets? Do you ask them if they are following those diets? Don’t bother, because they’re lying. Everyone lies about the food they eat. Everyone. Obese people lie, and nonobese people lie.

Investigators at the University of Essex in England asked 221 adults to keep food diaries, and then they checked on energy consumption by analyzing radioactive water levels in the participants’ urine over a 10-day period.
Underreporting of food consumption was rampant, even among those who were not obese. The obese subjects did underreport by a greater extent (1,200 calories per day) than did those who were not obese, who were off by only 800 calories, but the obese participants burned about 400 calories more each day than did the nonobese, so the difference was a wash.
Everyone ended up underreporting their calorie consumption by an average of about 900 calories, and the investigators were good enough to provide some food equivalents, tops on the list being three MacDonald’s cheeseburgers.
“Public health recommendations have historically relied heavily on self-reported energy intake values,” senior author Gavin Sandercock, PhD, said in a EurekAlert statement, and “recognising that the measures of energy intake are incorrect might result in the setting of more realistic targets.”
Maybe you can be more realistic with your patients, too. Go ahead and ask Mr. Smith about the burger sticking out of his coat pocket, because there are probably two more you can’t see. We’ve each got 900 calories hiding on us somewhere. Ours is usually pizza.
The art of the gallbladder
Ever thought you would see a portrait of a gallbladder hanging up in a gallery? Not just an artist’s rendition, but an actual photo from an actual patient? Well, you can at the Soloway Gallery in Brooklyn, N.Y., at least until June 12.

The artist? K.C. Joseph, MD, a general surgeon from St. Marie, Pa., who died in 2015. His daughter Melissa is the curator of the show and told ARTnews about the interesting connection her father had with art and surgery.
In 2010, Dr. Joseph gave his daughter a box of photos and said “Make me a famous artist,” she recalled. At first, “I was like, ‘These are weird,’ and then I put them under my bed for 10 years.”
Apparently he had been making art with his patients’ organs for about 15 years and had a system in which he put each one together. Before a surgery Dr. Joseph would make a note card with the patient’s name handwritten in calligraphy with a couple of pages taken out of the magazine from the waiting room as the backdrop. Afterward, when the patient was in recovery, the removed organ would be placed among the pages and the name card. A photo was taken with the same endoscope that was used for the procedure.
After the show’s debut, people reached out expressing their love for their photos. “I wish, before he died, I had asked him more questions about it,” Ms. Joseph told ARTnews. “I’m regretting it so much now, kicking myself.”
Who gets to take home an artsy photo of their gallbladder after getting it removed? Not us, that’s who. Each collage is a one-of-a-kind piece. They definitely should be framed and shown in an art gallery. Oh, right. Never mind.
Why it might be better to be a dog person
Here’s that old debate again: Dogs or cats? You probably have your own opinion, but research presented at this year’s Digestive Disease Week may have tipped the scale by showing that children who lived with dogs may be less likely to have Crohn’s disease as adults.
The research was done by having approximately 4,300 people closely related to patients with Crohn’s disease fill out an environmental questionnaire. Using these data, the research team looked into environmental factors such as size of the families, where the home was, how many bathrooms the homes had, and quality of drinking water.
The researchers found that those who had or were exposed to dogs between the ages of 5 and 15 years were more likely to have healthy gut permeability and balanced microbes, which increased their protection against Crohn’s disease.
“Our study seems to add to others that have explored the ‘hygiene hypothesis’ which suggests that the lack of exposure to microbes early in life may lead to lack of immune regulation toward environmental microbes,” senior author Williams Turpin, PhD, said in the written statement.
The researchers aren’t sure why they didn’t get the same findings with cats, but Dr. Turpin theorized that dog owners tend to be outside more with their dogs or live in places with more green space, which are good protectors against Crohn’s disease.
It’s all good for dog owners, but do their pets’ parasites make you more attractive? Just more fuel for the ongoing debate.
Come for the history, stay for the fossilized parasites
Another week, another analysis of old British poop. LOTME really is your one-stop shop for all the important, hard-hitting news about historic parasites. You’re welcome, Internet.
The news this week is from Stonehenge, which is apparently kind of a big deal. Rocks in a circle, celestial calendar, cultural significance, whatever. We’re not here to talk about rocks. We’re here to talk about, uh, rocks. Smaller rocks. Specifically, coprolites, which are essentially poop turned into a rock. (Though now we’re imagining Stonehenge made out of fossilized poop rocks. Would it still be a big tourist destination? We can see both sides of the argument on that one.)
Archaeologists from the University of Cambridge have conducted an analysis of coprolites from Durrington Walls, a Neolithic settlement just a few kilometers from Stonehenge. The town dates to the same time that Stonehenge was constructed, and it’s believed that the residents were responsible for building the landmark. These coprolites, depending on what’s inside, can tell us a lot about how the builders of Stonehenge lived and, more specifically, how they ate.
In this case, the coprolites of one human and three dogs contained capillariid worm eggs. These worms come from cows, and when a human is typically infected, the eggs embed in the liver and do not pass through the body. Finding them in excrement indicates that the people were eating raw cow organs and feeding leftovers to their dogs. This is interesting, because a preponderance of pottery and cooking implements also found at the site indicates that the residents of Durrington Walls were spit-roasting or boiling their beef and pork. So the meat was cooked, but not the organs. That is an interesting dietary decision, ancient British people. Then again, modern British cuisine exists. At least now we know where they got it from.
This new research raises one other very important question: When are we going to get a full-on guided tour of all the important coprolite sites in Britain? They’ve clearly got plenty of them, and the tourist demand for ancient parasites must be sky-high. Come on, capitalism, follow through on this. We’d go.
Everyone lies: Food intake edition
Do you have any patients on special diets? Do you ask them if they are following those diets? Don’t bother, because they’re lying. Everyone lies about the food they eat. Everyone. Obese people lie, and nonobese people lie.
Investigators at the University of Essex in England asked 221 adults to keep food diaries, and then they checked on energy consumption by analyzing radioactive water levels in the participants’ urine over a 10-day period.
Underreporting of food consumption was rampant, even among those who were not obese. The obese subjects did underreport by a greater extent (1,200 calories per day) than did those who were not obese, who were off by only 800 calories, but the obese participants burned about 400 calories more each day than did the nonobese, so the difference was a wash.
Everyone ended up underreporting their calorie consumption by an average of about 900 calories, and the investigators were good enough to provide some food equivalents, tops on the list being three MacDonald’s cheeseburgers.
“Public health recommendations have historically relied heavily on self-reported energy intake values,” senior author Gavin Sandercock, PhD, said in a EurekAlert statement, and “recognising that the measures of energy intake are incorrect might result in the setting of more realistic targets.”
Maybe you can be more realistic with your patients, too. Go ahead and ask Mr. Smith about the burger sticking out of his coat pocket, because there are probably two more you can’t see. We’ve each got 900 calories hiding on us somewhere. Ours is usually pizza.
The art of the gallbladder
Ever thought you would see a portrait of a gallbladder hanging up in a gallery? Not just an artist’s rendition, but an actual photo from an actual patient? Well, you can at the Soloway Gallery in Brooklyn, N.Y., at least until June 12.
The artist? K.C. Joseph, MD, a general surgeon from St. Marie, Pa., who died in 2015. His daughter Melissa is the curator of the show and told ARTnews about the interesting connection her father had with art and surgery.
In 2010, Dr. Joseph gave his daughter a box of photos and said “Make me a famous artist,” she recalled. At first, “I was like, ‘These are weird,’ and then I put them under my bed for 10 years.”
Apparently he had been making art with his patients’ organs for about 15 years and had a system in which he put each one together. Before a surgery Dr. Joseph would make a note card with the patient’s name handwritten in calligraphy with a couple of pages taken out of the magazine from the waiting room as the backdrop. Afterward, when the patient was in recovery, the removed organ would be placed among the pages and the name card. A photo was taken with the same endoscope that was used for the procedure.
After the show’s debut, people reached out expressing their love for their photos. “I wish, before he died, I had asked him more questions about it,” Ms. Joseph told ARTnews. “I’m regretting it so much now, kicking myself.”
Who gets to take home an artsy photo of their gallbladder after getting it removed? Not us, that’s who. Each collage is a one-of-a-kind piece. They definitely should be framed and shown in an art gallery. Oh, right. Never mind.
Why it might be better to be a dog person
Here’s that old debate again: Dogs or cats? You probably have your own opinion, but research presented at this year’s Digestive Disease Week may have tipped the scale by showing that children who lived with dogs may be less likely to have Crohn’s disease as adults.
The research was done by having approximately 4,300 people closely related to patients with Crohn’s disease fill out an environmental questionnaire. Using these data, the research team looked into environmental factors such as size of the families, where the home was, how many bathrooms the homes had, and quality of drinking water.
The researchers found that those who had or were exposed to dogs between the ages of 5 and 15 years were more likely to have healthy gut permeability and balanced microbes, which increased their protection against Crohn’s disease.
“Our study seems to add to others that have explored the ‘hygiene hypothesis’ which suggests that the lack of exposure to microbes early in life may lead to lack of immune regulation toward environmental microbes,” senior author Williams Turpin, PhD, said in the written statement.
The researchers aren’t sure why they didn’t get the same findings with cats, but Dr. Turpin theorized that dog owners tend to be outside more with their dogs or live in places with more green space, which are good protectors against Crohn’s disease.
It’s all good for dog owners, but do their pets’ parasites make you more attractive? Just more fuel for the ongoing debate.
Come for the history, stay for the fossilized parasites
Another week, another analysis of old British poop. LOTME really is your one-stop shop for all the important, hard-hitting news about historic parasites. You’re welcome, Internet.
The news this week is from Stonehenge, which is apparently kind of a big deal. Rocks in a circle, celestial calendar, cultural significance, whatever. We’re not here to talk about rocks. We’re here to talk about, uh, rocks. Smaller rocks. Specifically, coprolites, which are essentially poop turned into a rock. (Though now we’re imagining Stonehenge made out of fossilized poop rocks. Would it still be a big tourist destination? We can see both sides of the argument on that one.)
Archaeologists from the University of Cambridge have conducted an analysis of coprolites from Durrington Walls, a Neolithic settlement just a few kilometers from Stonehenge. The town dates to the same time that Stonehenge was constructed, and it’s believed that the residents were responsible for building the landmark. These coprolites, depending on what’s inside, can tell us a lot about how the builders of Stonehenge lived and, more specifically, how they ate.
In this case, the coprolites of one human and three dogs contained capillariid worm eggs. These worms come from cows, and when a human is typically infected, the eggs embed in the liver and do not pass through the body. Finding them in excrement indicates that the people were eating raw cow organs and feeding leftovers to their dogs. This is interesting, because a preponderance of pottery and cooking implements also found at the site indicates that the residents of Durrington Walls were spit-roasting or boiling their beef and pork. So the meat was cooked, but not the organs. That is an interesting dietary decision, ancient British people. Then again, modern British cuisine exists. At least now we know where they got it from.
This new research raises one other very important question: When are we going to get a full-on guided tour of all the important coprolite sites in Britain? They’ve clearly got plenty of them, and the tourist demand for ancient parasites must be sky-high. Come on, capitalism, follow through on this. We’d go.
Everyone lies: Food intake edition
Do you have any patients on special diets? Do you ask them if they are following those diets? Don’t bother, because they’re lying. Everyone lies about the food they eat. Everyone. Obese people lie, and nonobese people lie.
Investigators at the University of Essex in England asked 221 adults to keep food diaries, and then they checked on energy consumption by analyzing radioactive water levels in the participants’ urine over a 10-day period.
Underreporting of food consumption was rampant, even among those who were not obese. The obese subjects did underreport by a greater extent (1,200 calories per day) than did those who were not obese, who were off by only 800 calories, but the obese participants burned about 400 calories more each day than did the nonobese, so the difference was a wash.
Everyone ended up underreporting their calorie consumption by an average of about 900 calories, and the investigators were good enough to provide some food equivalents, tops on the list being three MacDonald’s cheeseburgers.
“Public health recommendations have historically relied heavily on self-reported energy intake values,” senior author Gavin Sandercock, PhD, said in a EurekAlert statement, and “recognising that the measures of energy intake are incorrect might result in the setting of more realistic targets.”
Maybe you can be more realistic with your patients, too. Go ahead and ask Mr. Smith about the burger sticking out of his coat pocket, because there are probably two more you can’t see. We’ve each got 900 calories hiding on us somewhere. Ours is usually pizza.
The art of the gallbladder
Ever thought you would see a portrait of a gallbladder hanging up in a gallery? Not just an artist’s rendition, but an actual photo from an actual patient? Well, you can at the Soloway Gallery in Brooklyn, N.Y., at least until June 12.
The artist? K.C. Joseph, MD, a general surgeon from St. Marie, Pa., who died in 2015. His daughter Melissa is the curator of the show and told ARTnews about the interesting connection her father had with art and surgery.
In 2010, Dr. Joseph gave his daughter a box of photos and said “Make me a famous artist,” she recalled. At first, “I was like, ‘These are weird,’ and then I put them under my bed for 10 years.”
Apparently he had been making art with his patients’ organs for about 15 years and had a system in which he put each one together. Before a surgery Dr. Joseph would make a note card with the patient’s name handwritten in calligraphy with a couple of pages taken out of the magazine from the waiting room as the backdrop. Afterward, when the patient was in recovery, the removed organ would be placed among the pages and the name card. A photo was taken with the same endoscope that was used for the procedure.
After the show’s debut, people reached out expressing their love for their photos. “I wish, before he died, I had asked him more questions about it,” Ms. Joseph told ARTnews. “I’m regretting it so much now, kicking myself.”
Who gets to take home an artsy photo of their gallbladder after getting it removed? Not us, that’s who. Each collage is a one-of-a-kind piece. They definitely should be framed and shown in an art gallery. Oh, right. Never mind.
$7,000 for ‘flowers’: KY doc accused in murder plot against ex
A Kentucky pediatrician accused of hiring a hitman to kill her ex-husband – and type a fake suicide text on his cell phone to disguise the plot – initially hatched the scheme 4 years ago during a custody dispute, according to court documents.
On May 19, agents with the Federal Bureau of Investigation arrested Stephanie Russell, MD, on a charge of using interstate commerce facilities in the commission of murder-for-hire, which carries a maximum 10-year sentence in federal prison.
Dr. Russell, who prosecutors said is 52, vehemently denied the plot when it was first relayed to investigators in 2020. She also dismissed suspicion from a court-appointed guardian at the time that the doctor harmed her own son, then 2, in a way “to make it appear” as if his father had hurt the child.
According to an FBI agent’s affidavit, Dr. Russell tried to recruit a killer through employees and ex-employees of Kidz Life Pediatrics, in Prospect, an upscale suburb of Louisville, Ky. She allegedly planned to time the murder during a 2-hour visitation period with her two children on the last day of the school year.
On May 24, Magistrate Judge Regina Edwards, of the U.S. District Court for the Western District of Kentucky, ordered Dr. Russell to remain in custody. A future date for the next hearing has not been set.
‘No red flags’
The case has upended the Norton Commons development in Prospect, one of Kentucky’s wealthiest communities.
“There were no red flags,” said Lance Dooley, whose two daughters had been under Dr. Russell’s care at Kidz Life. “This neighborhood was like, ‘What the hell?’ Everybody went to her and trusted and respected her judgment.”
According to prosecutors, on May 15 – after having failed to have her ex-husband murdered during the holidays – Dr. Russell contacted a person she thought she had hired to murder her ex-husband in exchange for $7,000.
On May 18, Dr. Russell placed a $3,500 down payment in a specimen drop box outside her medical office. She agreed to pay the remaining half after the murder was done, according to prosecutors. The purported hit man was an undercover FBI agent.
While making plans, Dr. Russell used several burner phones and used the word “flowers” as a code word for killing her ex-husband, Ricky Crabtree, whom she had accused of sexually abusing their children. Mr. Crabtree, a financial planner, did not return phone messages left at his office.
Family Court Judge Denise Brown had earlier appointed a guardian to represent the children and an evaluator to monitor the couple’s custodial issues.
Dr. Russell sued the judge, saying Ms. Brown acted because of allegations that Dr. Russell was “coaching” her children and inflicting “emotional harm.” Dr. Russell also objected to what she called “a vague suggestion” that previously she “‘may’ have injured the older male child in a way to make it appear that [Mr.] Crabtree had done so.”
“There wasn’t any proof of it,” said David Mour, an attorney who represented Dr. Russell in that action. The state gave custody to the father in what Mr. Mour called a “Star Chamber” action based on unsubstantiated allegations. “I don’t believe a damned thing,” he said.
In her suit against Ms. Brown, which was dismissed in 2021, Dr. Russell criticized as “preposterous” allegations that, in May 2018, she “‘attempted to hire’ a ‘hitman’ to kill [Mr.] Crabtree.”
The FBI affidavit, however, displayed numerous text messages between Dr. Russell and a former nurse, whom she thought knew a hit man, and an FBI agent posing as the purported killer. When one witness initially agreed to find an assassin who would do the job over the 2021 holiday season, Dr. Russell texted, “I am hysterically crying tears of relief.”
The witness quit Kidz Life Pediatrics and ended contact with Dr. Russell when they realized Dr. Russell was “serious” about the plot, the affidavit stated. And when Dr. Russell found a willing contractor in May, she told the hitman to write a suicide text. The killer would have to unlock Mr. Crabtree’s cell phone by having the device recognize the face of his dead body.
Mr. Dooley said Kidz Life Pediatrics was closed during business hours when he tried to retrieve his children’s medical records. He has since found another pediatrician. Dr. Russell had cared for his children for more than 4 years, he said, betraying no clue of any darkness underneath. Kidz Life Pediatrics did not return phone calls seeking comment.
“It’s very close to home,” said Mr. Dooley, who runs an advertising agency with his wife. “Dr. Russell was really good.”
A version of this article first appeared on Medscape.com.
A Kentucky pediatrician accused of hiring a hitman to kill her ex-husband – and type a fake suicide text on his cell phone to disguise the plot – initially hatched the scheme 4 years ago during a custody dispute, according to court documents.
On May 19, agents with the Federal Bureau of Investigation arrested Stephanie Russell, MD, on a charge of using interstate commerce facilities in the commission of murder-for-hire, which carries a maximum 10-year sentence in federal prison.
Dr. Russell, who prosecutors said is 52, vehemently denied the plot when it was first relayed to investigators in 2020. She also dismissed suspicion from a court-appointed guardian at the time that the doctor harmed her own son, then 2, in a way “to make it appear” as if his father had hurt the child.
According to an FBI agent’s affidavit, Dr. Russell tried to recruit a killer through employees and ex-employees of Kidz Life Pediatrics, in Prospect, an upscale suburb of Louisville, Ky. She allegedly planned to time the murder during a 2-hour visitation period with her two children on the last day of the school year.
On May 24, Magistrate Judge Regina Edwards, of the U.S. District Court for the Western District of Kentucky, ordered Dr. Russell to remain in custody. A future date for the next hearing has not been set.
‘No red flags’
The case has upended the Norton Commons development in Prospect, one of Kentucky’s wealthiest communities.
“There were no red flags,” said Lance Dooley, whose two daughters had been under Dr. Russell’s care at Kidz Life. “This neighborhood was like, ‘What the hell?’ Everybody went to her and trusted and respected her judgment.”
According to prosecutors, on May 15 – after having failed to have her ex-husband murdered during the holidays – Dr. Russell contacted a person she thought she had hired to murder her ex-husband in exchange for $7,000.
On May 18, Dr. Russell placed a $3,500 down payment in a specimen drop box outside her medical office. She agreed to pay the remaining half after the murder was done, according to prosecutors. The purported hit man was an undercover FBI agent.
While making plans, Dr. Russell used several burner phones and used the word “flowers” as a code word for killing her ex-husband, Ricky Crabtree, whom she had accused of sexually abusing their children. Mr. Crabtree, a financial planner, did not return phone messages left at his office.
Family Court Judge Denise Brown had earlier appointed a guardian to represent the children and an evaluator to monitor the couple’s custodial issues.
Dr. Russell sued the judge, saying Ms. Brown acted because of allegations that Dr. Russell was “coaching” her children and inflicting “emotional harm.” Dr. Russell also objected to what she called “a vague suggestion” that previously she “‘may’ have injured the older male child in a way to make it appear that [Mr.] Crabtree had done so.”
“There wasn’t any proof of it,” said David Mour, an attorney who represented Dr. Russell in that action. The state gave custody to the father in what Mr. Mour called a “Star Chamber” action based on unsubstantiated allegations. “I don’t believe a damned thing,” he said.
In her suit against Ms. Brown, which was dismissed in 2021, Dr. Russell criticized as “preposterous” allegations that, in May 2018, she “‘attempted to hire’ a ‘hitman’ to kill [Mr.] Crabtree.”
The FBI affidavit, however, displayed numerous text messages between Dr. Russell and a former nurse, whom she thought knew a hit man, and an FBI agent posing as the purported killer. When one witness initially agreed to find an assassin who would do the job over the 2021 holiday season, Dr. Russell texted, “I am hysterically crying tears of relief.”
The witness quit Kidz Life Pediatrics and ended contact with Dr. Russell when they realized Dr. Russell was “serious” about the plot, the affidavit stated. And when Dr. Russell found a willing contractor in May, she told the hitman to write a suicide text. The killer would have to unlock Mr. Crabtree’s cell phone by having the device recognize the face of his dead body.
Mr. Dooley said Kidz Life Pediatrics was closed during business hours when he tried to retrieve his children’s medical records. He has since found another pediatrician. Dr. Russell had cared for his children for more than 4 years, he said, betraying no clue of any darkness underneath. Kidz Life Pediatrics did not return phone calls seeking comment.
“It’s very close to home,” said Mr. Dooley, who runs an advertising agency with his wife. “Dr. Russell was really good.”
A version of this article first appeared on Medscape.com.
A Kentucky pediatrician accused of hiring a hitman to kill her ex-husband – and type a fake suicide text on his cell phone to disguise the plot – initially hatched the scheme 4 years ago during a custody dispute, according to court documents.
On May 19, agents with the Federal Bureau of Investigation arrested Stephanie Russell, MD, on a charge of using interstate commerce facilities in the commission of murder-for-hire, which carries a maximum 10-year sentence in federal prison.
Dr. Russell, who prosecutors said is 52, vehemently denied the plot when it was first relayed to investigators in 2020. She also dismissed suspicion from a court-appointed guardian at the time that the doctor harmed her own son, then 2, in a way “to make it appear” as if his father had hurt the child.
According to an FBI agent’s affidavit, Dr. Russell tried to recruit a killer through employees and ex-employees of Kidz Life Pediatrics, in Prospect, an upscale suburb of Louisville, Ky. She allegedly planned to time the murder during a 2-hour visitation period with her two children on the last day of the school year.
On May 24, Magistrate Judge Regina Edwards, of the U.S. District Court for the Western District of Kentucky, ordered Dr. Russell to remain in custody. A future date for the next hearing has not been set.
‘No red flags’
The case has upended the Norton Commons development in Prospect, one of Kentucky’s wealthiest communities.
“There were no red flags,” said Lance Dooley, whose two daughters had been under Dr. Russell’s care at Kidz Life. “This neighborhood was like, ‘What the hell?’ Everybody went to her and trusted and respected her judgment.”
According to prosecutors, on May 15 – after having failed to have her ex-husband murdered during the holidays – Dr. Russell contacted a person she thought she had hired to murder her ex-husband in exchange for $7,000.
On May 18, Dr. Russell placed a $3,500 down payment in a specimen drop box outside her medical office. She agreed to pay the remaining half after the murder was done, according to prosecutors. The purported hit man was an undercover FBI agent.
While making plans, Dr. Russell used several burner phones and used the word “flowers” as a code word for killing her ex-husband, Ricky Crabtree, whom she had accused of sexually abusing their children. Mr. Crabtree, a financial planner, did not return phone messages left at his office.
Family Court Judge Denise Brown had earlier appointed a guardian to represent the children and an evaluator to monitor the couple’s custodial issues.
Dr. Russell sued the judge, saying Ms. Brown acted because of allegations that Dr. Russell was “coaching” her children and inflicting “emotional harm.” Dr. Russell also objected to what she called “a vague suggestion” that previously she “‘may’ have injured the older male child in a way to make it appear that [Mr.] Crabtree had done so.”
“There wasn’t any proof of it,” said David Mour, an attorney who represented Dr. Russell in that action. The state gave custody to the father in what Mr. Mour called a “Star Chamber” action based on unsubstantiated allegations. “I don’t believe a damned thing,” he said.
In her suit against Ms. Brown, which was dismissed in 2021, Dr. Russell criticized as “preposterous” allegations that, in May 2018, she “‘attempted to hire’ a ‘hitman’ to kill [Mr.] Crabtree.”
The FBI affidavit, however, displayed numerous text messages between Dr. Russell and a former nurse, whom she thought knew a hit man, and an FBI agent posing as the purported killer. When one witness initially agreed to find an assassin who would do the job over the 2021 holiday season, Dr. Russell texted, “I am hysterically crying tears of relief.”
The witness quit Kidz Life Pediatrics and ended contact with Dr. Russell when they realized Dr. Russell was “serious” about the plot, the affidavit stated. And when Dr. Russell found a willing contractor in May, she told the hitman to write a suicide text. The killer would have to unlock Mr. Crabtree’s cell phone by having the device recognize the face of his dead body.
Mr. Dooley said Kidz Life Pediatrics was closed during business hours when he tried to retrieve his children’s medical records. He has since found another pediatrician. Dr. Russell had cared for his children for more than 4 years, he said, betraying no clue of any darkness underneath. Kidz Life Pediatrics did not return phone calls seeking comment.
“It’s very close to home,” said Mr. Dooley, who runs an advertising agency with his wife. “Dr. Russell was really good.”
A version of this article first appeared on Medscape.com.
Specialists hail new era in hemophilia treatment
“It’s an amazing time to be a hemophilia provider,” Alice D. Ma, MD, University of North Carolina at Chapel Hill hematologist and bleeding disorder specialist, said in an interview. “There are real options, and it’s very exciting.”
But the drugs come with quirks that hematologists must understand, hemophilia specialists cautioned, and stubborn insurers pose significant obstacles to appropriate care. Also, new generations of medications in development offer both hope and more questions.
By far, the biggest game changer in hemophilia A is a monoclonal antibody called emicizumab (Hemlibra), first approved by the Food and Drug Administration for hemophilia A patients with factor VIII inhibitors and then in 2018 for those without factor VIII inhibitors.
“It’s just been getting a bigger and bigger slice of market share as patients and parents really buy in to how great that product is,” Dr. Ma said. “I do not have any hemophilia A patients with factor VIII inhibitors who aren’t on it. That’s just kind of a no-brainer, no ifs, ands, or buts.”
About 50%-60% of her noninhibitor patients with hemophilia A take the drug, she said.
According to its manufacturer, Genentech, the drug “acts like a bridge, bringing factor IXa and factor X together to allow the blood coagulation process to continue without needing to replace factor VIII.”
Since emicizumab is not a blood factor, Dr. Ma said, it doesn’t cross-react with antibodies or inhibitors. “The other thing that is pretty amazing is that it’s given subcutaneously as opposed to intravenously. It’s given under the skin, kind of like an insulin shot, rather than into a vein.”
Prophylaxis treatments did exist for patients with hemophilia A prior to emicizumab, University of North Carolina at Chapel Hill hematologist and blood disorder specialist Nigel S. Key, MB, ChB, said in an interview. But the treatments didn’t stop all bleeding. “We never really kept them under control,” he said, adding that patients needed to get infusions several times a week. “It was cumbersome and took a lot of compliance, a lot of effort to do it.
Thanks to emicizumab, adult patients don’t have to put on tourniquets and stick butterfly needles into their own veins anymore, and parents no longer need to regularly give factor infusions to their children every 2-3 days, Dr. Ma said. Instead, doses may be required just once a week.
Not every patient is eager to embrace emicizumab
Emicizumab isn’t necessarily an easy sell. Home-care company pharmacies don’t get reimbursed as much for providing emicizumab, compared with factor infusions, Dr. Ma said, and some of these companies are urging parents to not accept the drug for their kids.
Prior experience can also make people wary. According to Dr. Ma, one of her patients – a 62-year-old man – was reluctant to take factor because he’d gotten infected with HIV from an infusion. “For guys of that certain age, factor was death. It was poison, so you tried really hard not to take it.”
The patient now regrets not taking emicizumab earlier. He told Dr. Ma that his joints “do feel better than when I took factor regularly,” and “he really thinks that it has made his hemophilia recede into the background of his life, which is pretty, pretty nice.”
In fact, Dr. Ma said, he dropped a 7-pound rock on his foot but did not need to take factor or be hospitalized because of bleeding. Instead, he simply “watched a bruise form and then get better.”
As for challenges beyond convincing patients to take emicizumab, Dr. Ma said that insurers can may still refuse to pay for it in noninhibitor patients. “Some of them say you have to fail a regular clotting factor to be able to take Hemlibra,” she said, noting that she finds this viewpoint intolerable.
Hemlibra is remarkably expensive, but treatment of bleeds is also pricey. A 2021 study found that median 6-month hemostatic treatment costs in hemophilia A patients fell from more than $176,000 to barely $128,000 after they started taking the drug.
There’s another hitch. Some hematologists don’t realize that the drug can throw off certain coagulation readings. Dr. Ma recalled that a patient with hemophilia A went to a different healthcare facility for a gall bladder operation, and hematology fellows there failed to adjust his factor VIII level – an extraordinarily high 400%, suggesting high coagulation – to reflect his use of emicizumab.
“My patient bled severely and could have lost his life,” Dr. Ma said.
Despite gains, hemophilia B remains hard to treat
The much rarer hemophilia B (the type that affected members of European royal families who descended from Queen Victoria) has proved more difficult to treat than hemophilia A. An estimated 1 in 5,600 males in the United States are born with hemophilia A, compared with 1 in 19,300 males born with hemophilia B. The conditions rarely affect females.
Recombinant factor IX products that replace a missing protein have been improved and can now be given every 7 or 14 days, instead of twice a week, Dr. Key said. As for the future, so-called rebalancing therapies are in phase 3 trials and look promising: “Instead of trying to beef up the proclotting proteins, you’re trying to knock down the anticlotting proteins. ‘Rebalancing’ is a good way to think of it.”
These treatments are also agnostic – like Hemlibra – to the presence of inhibitors, he said.
These drugs could be available within a few years, Dr. Key said. “The major concern is always going to be a risk of thrombosis or clotting. Some of that has only become apparent through clinical trials and require a return to the drawing board to redesign the dosing to hit the safe, sweet spot that prevents bleeds but doesn’t cause clots.”
Dr. Ma agreed that clots are a significant risk from rebalancing agents. “I don’t know that I would put a factor IX patient without an inhibitor on a rebalancing therapy, because we already have pretty darn good therapies for them,” she said. However, factor IX patients with inhibitors do need better treatments, “and we’re all looking forward to the next approved drugs there.”
Hoopla for gene therapy, with questions, as well
The prospect of gene therapy for hemophilia, meanwhile, continues to draw attention as phase 3 trials continue. Potentially, gene therapy could be given just once to patients with hemophilia A or hemophilia B and provide bleeding control indefinitely, Dr. Ma said.
However, Dr. Key wondered whether gene therapy may be useful in hemophilia A, since emicizumab has worked so well. “I just don’t see the tsunami of patients who are wanting to undergo gene therapy in the first few years. I think there’ll be relatively slow uptake due to a lot of factors, including reimbursement.”
Hematologist Amar H. Kelkar, MD, of Dana-Farber Cancer Institute in Boston, is also skeptical that a groundswell of patients will embrace gene therapy, even if one-time treatment lasts for years. Current treatments are working well for many patients, Dr. Kelkar said in an interview, “and comfort with novel therapies may be slow within the community, especially if the treatment effect is expected to be transient. This is the same community that was hit hard by contaminated blood products during the HIV crisis, so it may be hard to convince a large number of patients to adopt a new type of therapy. There’s also the issue of the projected high upfront cost of gene therapies. Of course, I’d love to be wrong, especially if cost issues for the patients can be mitigated.”
Moving forward, both Dr. Ma and Dr. Key urged hematologists to send their hemophilia patients to Hemophilia Treatment Centers so they can get specialized care. There are about 140 of these federally funded centers around the country, according to the National Hemophilia Foundation. Many are located in children’s hospitals.
Hemophilia treatment now requires a subspecialty degree of knowledge that’s difficult for a hematologist in general practice to master, Dr. Ma said. “If you have a patient with hemophilia, and you’re in private practice for general hematology/oncology, please send them to a Hemophilia Treatment Center for something like a once-a-year check-in to make sure that the patient is getting comprehensive care.”
Dr. Ma discloses relationships with Takeda (research funding and consultation). Dr. Key discloses relationships with BioMarin and Takeda (advisory board), Novo Nordisk (grants review committee), and Uniqure (steering committee). Dr. Kelkar has no disclosures.
“It’s an amazing time to be a hemophilia provider,” Alice D. Ma, MD, University of North Carolina at Chapel Hill hematologist and bleeding disorder specialist, said in an interview. “There are real options, and it’s very exciting.”
But the drugs come with quirks that hematologists must understand, hemophilia specialists cautioned, and stubborn insurers pose significant obstacles to appropriate care. Also, new generations of medications in development offer both hope and more questions.
By far, the biggest game changer in hemophilia A is a monoclonal antibody called emicizumab (Hemlibra), first approved by the Food and Drug Administration for hemophilia A patients with factor VIII inhibitors and then in 2018 for those without factor VIII inhibitors.
“It’s just been getting a bigger and bigger slice of market share as patients and parents really buy in to how great that product is,” Dr. Ma said. “I do not have any hemophilia A patients with factor VIII inhibitors who aren’t on it. That’s just kind of a no-brainer, no ifs, ands, or buts.”
About 50%-60% of her noninhibitor patients with hemophilia A take the drug, she said.
According to its manufacturer, Genentech, the drug “acts like a bridge, bringing factor IXa and factor X together to allow the blood coagulation process to continue without needing to replace factor VIII.”
Since emicizumab is not a blood factor, Dr. Ma said, it doesn’t cross-react with antibodies or inhibitors. “The other thing that is pretty amazing is that it’s given subcutaneously as opposed to intravenously. It’s given under the skin, kind of like an insulin shot, rather than into a vein.”
Prophylaxis treatments did exist for patients with hemophilia A prior to emicizumab, University of North Carolina at Chapel Hill hematologist and blood disorder specialist Nigel S. Key, MB, ChB, said in an interview. But the treatments didn’t stop all bleeding. “We never really kept them under control,” he said, adding that patients needed to get infusions several times a week. “It was cumbersome and took a lot of compliance, a lot of effort to do it.
Thanks to emicizumab, adult patients don’t have to put on tourniquets and stick butterfly needles into their own veins anymore, and parents no longer need to regularly give factor infusions to their children every 2-3 days, Dr. Ma said. Instead, doses may be required just once a week.
Not every patient is eager to embrace emicizumab
Emicizumab isn’t necessarily an easy sell. Home-care company pharmacies don’t get reimbursed as much for providing emicizumab, compared with factor infusions, Dr. Ma said, and some of these companies are urging parents to not accept the drug for their kids.
Prior experience can also make people wary. According to Dr. Ma, one of her patients – a 62-year-old man – was reluctant to take factor because he’d gotten infected with HIV from an infusion. “For guys of that certain age, factor was death. It was poison, so you tried really hard not to take it.”
The patient now regrets not taking emicizumab earlier. He told Dr. Ma that his joints “do feel better than when I took factor regularly,” and “he really thinks that it has made his hemophilia recede into the background of his life, which is pretty, pretty nice.”
In fact, Dr. Ma said, he dropped a 7-pound rock on his foot but did not need to take factor or be hospitalized because of bleeding. Instead, he simply “watched a bruise form and then get better.”
As for challenges beyond convincing patients to take emicizumab, Dr. Ma said that insurers can may still refuse to pay for it in noninhibitor patients. “Some of them say you have to fail a regular clotting factor to be able to take Hemlibra,” she said, noting that she finds this viewpoint intolerable.
Hemlibra is remarkably expensive, but treatment of bleeds is also pricey. A 2021 study found that median 6-month hemostatic treatment costs in hemophilia A patients fell from more than $176,000 to barely $128,000 after they started taking the drug.
There’s another hitch. Some hematologists don’t realize that the drug can throw off certain coagulation readings. Dr. Ma recalled that a patient with hemophilia A went to a different healthcare facility for a gall bladder operation, and hematology fellows there failed to adjust his factor VIII level – an extraordinarily high 400%, suggesting high coagulation – to reflect his use of emicizumab.
“My patient bled severely and could have lost his life,” Dr. Ma said.
Despite gains, hemophilia B remains hard to treat
The much rarer hemophilia B (the type that affected members of European royal families who descended from Queen Victoria) has proved more difficult to treat than hemophilia A. An estimated 1 in 5,600 males in the United States are born with hemophilia A, compared with 1 in 19,300 males born with hemophilia B. The conditions rarely affect females.
Recombinant factor IX products that replace a missing protein have been improved and can now be given every 7 or 14 days, instead of twice a week, Dr. Key said. As for the future, so-called rebalancing therapies are in phase 3 trials and look promising: “Instead of trying to beef up the proclotting proteins, you’re trying to knock down the anticlotting proteins. ‘Rebalancing’ is a good way to think of it.”
These treatments are also agnostic – like Hemlibra – to the presence of inhibitors, he said.
These drugs could be available within a few years, Dr. Key said. “The major concern is always going to be a risk of thrombosis or clotting. Some of that has only become apparent through clinical trials and require a return to the drawing board to redesign the dosing to hit the safe, sweet spot that prevents bleeds but doesn’t cause clots.”
Dr. Ma agreed that clots are a significant risk from rebalancing agents. “I don’t know that I would put a factor IX patient without an inhibitor on a rebalancing therapy, because we already have pretty darn good therapies for them,” she said. However, factor IX patients with inhibitors do need better treatments, “and we’re all looking forward to the next approved drugs there.”
Hoopla for gene therapy, with questions, as well
The prospect of gene therapy for hemophilia, meanwhile, continues to draw attention as phase 3 trials continue. Potentially, gene therapy could be given just once to patients with hemophilia A or hemophilia B and provide bleeding control indefinitely, Dr. Ma said.
However, Dr. Key wondered whether gene therapy may be useful in hemophilia A, since emicizumab has worked so well. “I just don’t see the tsunami of patients who are wanting to undergo gene therapy in the first few years. I think there’ll be relatively slow uptake due to a lot of factors, including reimbursement.”
Hematologist Amar H. Kelkar, MD, of Dana-Farber Cancer Institute in Boston, is also skeptical that a groundswell of patients will embrace gene therapy, even if one-time treatment lasts for years. Current treatments are working well for many patients, Dr. Kelkar said in an interview, “and comfort with novel therapies may be slow within the community, especially if the treatment effect is expected to be transient. This is the same community that was hit hard by contaminated blood products during the HIV crisis, so it may be hard to convince a large number of patients to adopt a new type of therapy. There’s also the issue of the projected high upfront cost of gene therapies. Of course, I’d love to be wrong, especially if cost issues for the patients can be mitigated.”
Moving forward, both Dr. Ma and Dr. Key urged hematologists to send their hemophilia patients to Hemophilia Treatment Centers so they can get specialized care. There are about 140 of these federally funded centers around the country, according to the National Hemophilia Foundation. Many are located in children’s hospitals.
Hemophilia treatment now requires a subspecialty degree of knowledge that’s difficult for a hematologist in general practice to master, Dr. Ma said. “If you have a patient with hemophilia, and you’re in private practice for general hematology/oncology, please send them to a Hemophilia Treatment Center for something like a once-a-year check-in to make sure that the patient is getting comprehensive care.”
Dr. Ma discloses relationships with Takeda (research funding and consultation). Dr. Key discloses relationships with BioMarin and Takeda (advisory board), Novo Nordisk (grants review committee), and Uniqure (steering committee). Dr. Kelkar has no disclosures.
“It’s an amazing time to be a hemophilia provider,” Alice D. Ma, MD, University of North Carolina at Chapel Hill hematologist and bleeding disorder specialist, said in an interview. “There are real options, and it’s very exciting.”
But the drugs come with quirks that hematologists must understand, hemophilia specialists cautioned, and stubborn insurers pose significant obstacles to appropriate care. Also, new generations of medications in development offer both hope and more questions.
By far, the biggest game changer in hemophilia A is a monoclonal antibody called emicizumab (Hemlibra), first approved by the Food and Drug Administration for hemophilia A patients with factor VIII inhibitors and then in 2018 for those without factor VIII inhibitors.
“It’s just been getting a bigger and bigger slice of market share as patients and parents really buy in to how great that product is,” Dr. Ma said. “I do not have any hemophilia A patients with factor VIII inhibitors who aren’t on it. That’s just kind of a no-brainer, no ifs, ands, or buts.”
About 50%-60% of her noninhibitor patients with hemophilia A take the drug, she said.
According to its manufacturer, Genentech, the drug “acts like a bridge, bringing factor IXa and factor X together to allow the blood coagulation process to continue without needing to replace factor VIII.”
Since emicizumab is not a blood factor, Dr. Ma said, it doesn’t cross-react with antibodies or inhibitors. “The other thing that is pretty amazing is that it’s given subcutaneously as opposed to intravenously. It’s given under the skin, kind of like an insulin shot, rather than into a vein.”
Prophylaxis treatments did exist for patients with hemophilia A prior to emicizumab, University of North Carolina at Chapel Hill hematologist and blood disorder specialist Nigel S. Key, MB, ChB, said in an interview. But the treatments didn’t stop all bleeding. “We never really kept them under control,” he said, adding that patients needed to get infusions several times a week. “It was cumbersome and took a lot of compliance, a lot of effort to do it.
Thanks to emicizumab, adult patients don’t have to put on tourniquets and stick butterfly needles into their own veins anymore, and parents no longer need to regularly give factor infusions to their children every 2-3 days, Dr. Ma said. Instead, doses may be required just once a week.
Not every patient is eager to embrace emicizumab
Emicizumab isn’t necessarily an easy sell. Home-care company pharmacies don’t get reimbursed as much for providing emicizumab, compared with factor infusions, Dr. Ma said, and some of these companies are urging parents to not accept the drug for their kids.
Prior experience can also make people wary. According to Dr. Ma, one of her patients – a 62-year-old man – was reluctant to take factor because he’d gotten infected with HIV from an infusion. “For guys of that certain age, factor was death. It was poison, so you tried really hard not to take it.”
The patient now regrets not taking emicizumab earlier. He told Dr. Ma that his joints “do feel better than when I took factor regularly,” and “he really thinks that it has made his hemophilia recede into the background of his life, which is pretty, pretty nice.”
In fact, Dr. Ma said, he dropped a 7-pound rock on his foot but did not need to take factor or be hospitalized because of bleeding. Instead, he simply “watched a bruise form and then get better.”
As for challenges beyond convincing patients to take emicizumab, Dr. Ma said that insurers can may still refuse to pay for it in noninhibitor patients. “Some of them say you have to fail a regular clotting factor to be able to take Hemlibra,” she said, noting that she finds this viewpoint intolerable.
Hemlibra is remarkably expensive, but treatment of bleeds is also pricey. A 2021 study found that median 6-month hemostatic treatment costs in hemophilia A patients fell from more than $176,000 to barely $128,000 after they started taking the drug.
There’s another hitch. Some hematologists don’t realize that the drug can throw off certain coagulation readings. Dr. Ma recalled that a patient with hemophilia A went to a different healthcare facility for a gall bladder operation, and hematology fellows there failed to adjust his factor VIII level – an extraordinarily high 400%, suggesting high coagulation – to reflect his use of emicizumab.
“My patient bled severely and could have lost his life,” Dr. Ma said.
Despite gains, hemophilia B remains hard to treat
The much rarer hemophilia B (the type that affected members of European royal families who descended from Queen Victoria) has proved more difficult to treat than hemophilia A. An estimated 1 in 5,600 males in the United States are born with hemophilia A, compared with 1 in 19,300 males born with hemophilia B. The conditions rarely affect females.
Recombinant factor IX products that replace a missing protein have been improved and can now be given every 7 or 14 days, instead of twice a week, Dr. Key said. As for the future, so-called rebalancing therapies are in phase 3 trials and look promising: “Instead of trying to beef up the proclotting proteins, you’re trying to knock down the anticlotting proteins. ‘Rebalancing’ is a good way to think of it.”
These treatments are also agnostic – like Hemlibra – to the presence of inhibitors, he said.
These drugs could be available within a few years, Dr. Key said. “The major concern is always going to be a risk of thrombosis or clotting. Some of that has only become apparent through clinical trials and require a return to the drawing board to redesign the dosing to hit the safe, sweet spot that prevents bleeds but doesn’t cause clots.”
Dr. Ma agreed that clots are a significant risk from rebalancing agents. “I don’t know that I would put a factor IX patient without an inhibitor on a rebalancing therapy, because we already have pretty darn good therapies for them,” she said. However, factor IX patients with inhibitors do need better treatments, “and we’re all looking forward to the next approved drugs there.”
Hoopla for gene therapy, with questions, as well
The prospect of gene therapy for hemophilia, meanwhile, continues to draw attention as phase 3 trials continue. Potentially, gene therapy could be given just once to patients with hemophilia A or hemophilia B and provide bleeding control indefinitely, Dr. Ma said.
However, Dr. Key wondered whether gene therapy may be useful in hemophilia A, since emicizumab has worked so well. “I just don’t see the tsunami of patients who are wanting to undergo gene therapy in the first few years. I think there’ll be relatively slow uptake due to a lot of factors, including reimbursement.”
Hematologist Amar H. Kelkar, MD, of Dana-Farber Cancer Institute in Boston, is also skeptical that a groundswell of patients will embrace gene therapy, even if one-time treatment lasts for years. Current treatments are working well for many patients, Dr. Kelkar said in an interview, “and comfort with novel therapies may be slow within the community, especially if the treatment effect is expected to be transient. This is the same community that was hit hard by contaminated blood products during the HIV crisis, so it may be hard to convince a large number of patients to adopt a new type of therapy. There’s also the issue of the projected high upfront cost of gene therapies. Of course, I’d love to be wrong, especially if cost issues for the patients can be mitigated.”
Moving forward, both Dr. Ma and Dr. Key urged hematologists to send their hemophilia patients to Hemophilia Treatment Centers so they can get specialized care. There are about 140 of these federally funded centers around the country, according to the National Hemophilia Foundation. Many are located in children’s hospitals.
Hemophilia treatment now requires a subspecialty degree of knowledge that’s difficult for a hematologist in general practice to master, Dr. Ma said. “If you have a patient with hemophilia, and you’re in private practice for general hematology/oncology, please send them to a Hemophilia Treatment Center for something like a once-a-year check-in to make sure that the patient is getting comprehensive care.”
Dr. Ma discloses relationships with Takeda (research funding and consultation). Dr. Key discloses relationships with BioMarin and Takeda (advisory board), Novo Nordisk (grants review committee), and Uniqure (steering committee). Dr. Kelkar has no disclosures.
Children and COVID: Weekly cases keep rising past 100,000
, according to the American Academy of Pediatrics and the Children’s Hospital Association.
New cases were up by 14.6% over the previous week to just over 107,000 reported during May 13-16, marking the sixth straight increase since April 1-7, when the count was almost 26,000. Over that period, weekly cases rose 313%, based on data in the latest weekly COVID report from the AAP and CHA.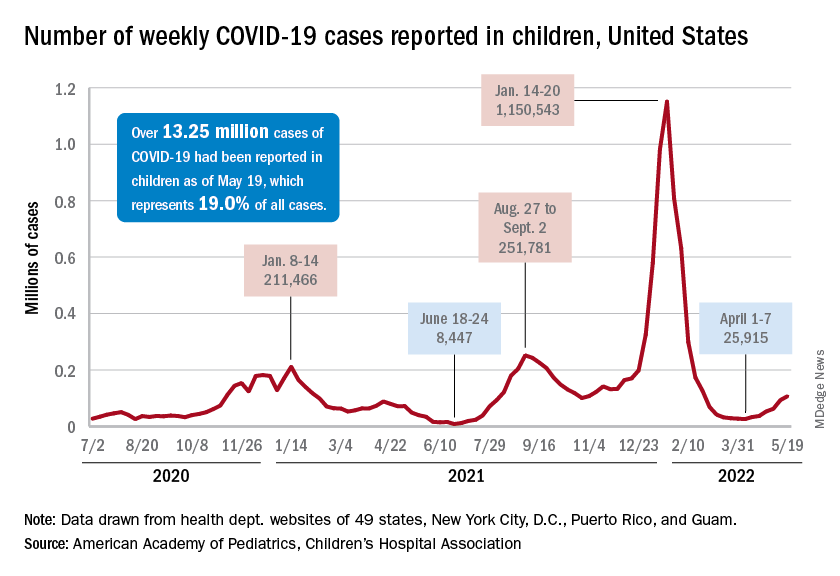
Rates reported by the Centers for Disease Control and Prevention show the same trend. Weekly cases per 100,000 population, which were down to 34.9 in children aged 0-4 years and 43.1 for those aged 5-11 on March 26, were up to 49.5 and 52.2, respectively, by April 16. The pace picked up right after that, and as of May 14, the rates of new cases were 125.4 per 100,000 in children aged 0-4 years and 143.1 in those aged 5-11, the CDC said.
Hospital admissions continue to rise as well. The rate of new admissions in children aged 0-17 was up to 0.25 per 100,000 population on May 18, nearly double the 0.13 per 100,000 recorded as late as April 13. The latest 7-day average count for new admissions, 163 per day from May 15-21, is down from the previous week’s 175 per day, but the CDC also acknowledges potential reporting delays in the most recent 7-day period.
Both of those weekly averages, however, are far below the peak rate for the pandemic, 914 per day, which occurred Jan. 10-16, 2022, during the Omicron surge. Since the CDC began keeping count at the beginning of August 2020, more than 125,000 children aged 0-17 years have been admitted with confirmed COVID-19, which is about 2.7% of all admissions over that period, the CDC’s data show.
Booster gets the green light
The week brought some positive news on the prevention side, though, as the CDC officially approved a COVID vaccine booster dose for children aged 5-11 years.
Even that good news came with a caveat, however. The vote by the CDC’s Advisory Committee on Immunization Practices was 11:1 in favor, with the negative vote cast by Helen Keipp Talbot, MD, of Vanderbilt University, Nashville, Tenn., who said that “boosters are great once we’ve gotten everyone their first round. That needs to be our priority in this.”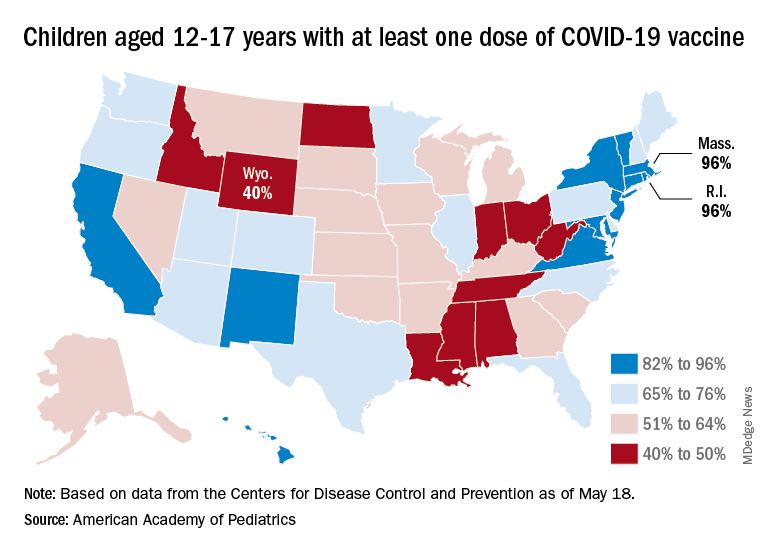
Nationally, in fact, just 35.7% of children aged 5-11 years have received at least one dose of the vaccine and only 29.0% are fully vaccinated. Those figures are nearly doubled among 12- to 17-year-olds: 69.3% have received at least one dose and 59.4% are fully vaccinated, the CDC said on its COVID Data Tracker.
Some states, meanwhile, are well below those national rates. In Wyoming, only 40% of children aged 12-17 have received an initial vaccine dose, and eight other states are below 50%. Among children aged 5-12, there are still five states below 20% in that measure, while the states on the other end of the spectrum – Vermont and Massachusetts – are above 60%, the AAP said in its separate vaccination report.
, according to the American Academy of Pediatrics and the Children’s Hospital Association.
New cases were up by 14.6% over the previous week to just over 107,000 reported during May 13-16, marking the sixth straight increase since April 1-7, when the count was almost 26,000. Over that period, weekly cases rose 313%, based on data in the latest weekly COVID report from the AAP and CHA.
Rates reported by the Centers for Disease Control and Prevention show the same trend. Weekly cases per 100,000 population, which were down to 34.9 in children aged 0-4 years and 43.1 for those aged 5-11 on March 26, were up to 49.5 and 52.2, respectively, by April 16. The pace picked up right after that, and as of May 14, the rates of new cases were 125.4 per 100,000 in children aged 0-4 years and 143.1 in those aged 5-11, the CDC said.
Hospital admissions continue to rise as well. The rate of new admissions in children aged 0-17 was up to 0.25 per 100,000 population on May 18, nearly double the 0.13 per 100,000 recorded as late as April 13. The latest 7-day average count for new admissions, 163 per day from May 15-21, is down from the previous week’s 175 per day, but the CDC also acknowledges potential reporting delays in the most recent 7-day period.
Both of those weekly averages, however, are far below the peak rate for the pandemic, 914 per day, which occurred Jan. 10-16, 2022, during the Omicron surge. Since the CDC began keeping count at the beginning of August 2020, more than 125,000 children aged 0-17 years have been admitted with confirmed COVID-19, which is about 2.7% of all admissions over that period, the CDC’s data show.
Booster gets the green light
The week brought some positive news on the prevention side, though, as the CDC officially approved a COVID vaccine booster dose for children aged 5-11 years.
Even that good news came with a caveat, however. The vote by the CDC’s Advisory Committee on Immunization Practices was 11:1 in favor, with the negative vote cast by Helen Keipp Talbot, MD, of Vanderbilt University, Nashville, Tenn., who said that “boosters are great once we’ve gotten everyone their first round. That needs to be our priority in this.”
Nationally, in fact, just 35.7% of children aged 5-11 years have received at least one dose of the vaccine and only 29.0% are fully vaccinated. Those figures are nearly doubled among 12- to 17-year-olds: 69.3% have received at least one dose and 59.4% are fully vaccinated, the CDC said on its COVID Data Tracker.
Some states, meanwhile, are well below those national rates. In Wyoming, only 40% of children aged 12-17 have received an initial vaccine dose, and eight other states are below 50%. Among children aged 5-12, there are still five states below 20% in that measure, while the states on the other end of the spectrum – Vermont and Massachusetts – are above 60%, the AAP said in its separate vaccination report.
, according to the American Academy of Pediatrics and the Children’s Hospital Association.
New cases were up by 14.6% over the previous week to just over 107,000 reported during May 13-16, marking the sixth straight increase since April 1-7, when the count was almost 26,000. Over that period, weekly cases rose 313%, based on data in the latest weekly COVID report from the AAP and CHA.
Rates reported by the Centers for Disease Control and Prevention show the same trend. Weekly cases per 100,000 population, which were down to 34.9 in children aged 0-4 years and 43.1 for those aged 5-11 on March 26, were up to 49.5 and 52.2, respectively, by April 16. The pace picked up right after that, and as of May 14, the rates of new cases were 125.4 per 100,000 in children aged 0-4 years and 143.1 in those aged 5-11, the CDC said.
Hospital admissions continue to rise as well. The rate of new admissions in children aged 0-17 was up to 0.25 per 100,000 population on May 18, nearly double the 0.13 per 100,000 recorded as late as April 13. The latest 7-day average count for new admissions, 163 per day from May 15-21, is down from the previous week’s 175 per day, but the CDC also acknowledges potential reporting delays in the most recent 7-day period.
Both of those weekly averages, however, are far below the peak rate for the pandemic, 914 per day, which occurred Jan. 10-16, 2022, during the Omicron surge. Since the CDC began keeping count at the beginning of August 2020, more than 125,000 children aged 0-17 years have been admitted with confirmed COVID-19, which is about 2.7% of all admissions over that period, the CDC’s data show.
Booster gets the green light
The week brought some positive news on the prevention side, though, as the CDC officially approved a COVID vaccine booster dose for children aged 5-11 years.
Even that good news came with a caveat, however. The vote by the CDC’s Advisory Committee on Immunization Practices was 11:1 in favor, with the negative vote cast by Helen Keipp Talbot, MD, of Vanderbilt University, Nashville, Tenn., who said that “boosters are great once we’ve gotten everyone their first round. That needs to be our priority in this.”
Nationally, in fact, just 35.7% of children aged 5-11 years have received at least one dose of the vaccine and only 29.0% are fully vaccinated. Those figures are nearly doubled among 12- to 17-year-olds: 69.3% have received at least one dose and 59.4% are fully vaccinated, the CDC said on its COVID Data Tracker.
Some states, meanwhile, are well below those national rates. In Wyoming, only 40% of children aged 12-17 have received an initial vaccine dose, and eight other states are below 50%. Among children aged 5-12, there are still five states below 20% in that measure, while the states on the other end of the spectrum – Vermont and Massachusetts – are above 60%, the AAP said in its separate vaccination report.
PA convicted of distributing more than 1.2 million opioid pills
A federal sting operation led to the recent conviction of a Texas physician assistant on charges of illegally prescribing a total of $3 million in drugs to patients at two “pill mill” clinics in Houston and helping others do the same.
The May 20 conviction of Charles Thompson, 76, of Houston, was based on charges of distributing more than 1.2 million opioid pills to thousands of individuals posing as patients at two pain management clinics, according to the U.S. Department of Justice.
Thompson’s conviction was the latest legal action in a string of cases involving the operation, including a doctor convicted in March who worked with Thompson at the West Parker Medical Clinic. Internist James Pierre, MD, 52, faces charges of unlawfully prescribing more than $1 million worth of opioid hydrocodone, according to federal officials.
Thompson also worked at Priority Wellness Clinic. Six people have pled guilty in connection with their conduct at West Parker or Priority Wellness, the justice department reported.
From June 2015 through July 2016, while Thompson was at West Parker, he helped Dr. Pierre unlawfully prescribe hydrocodone and the muscle relaxant carisoprodol, a combination of controlled substances for pain management known as the “Las Vegas cocktail,” to people in the sting operations pretending to be patients, authorities stated.
Thompson also distributed unlawful prescriptions for carisoprodol. So-called “runners” brought numerous people to pose as patients at West Parker and paid the clinic about $220 to $500 in cash for each visit that resulted in prescriptions for dangerous drugs. Throughout the scheme, West Parker pocketed about $1.75 million from prescriptions; Thompson was paid more than $208,000.
According to authorities, Thompson also helped others illegally prescribe controlled substances, including hydrocodone and oxycodone, from May to July 2017 at Priority Wellness, which opened in December 2016 after West Parker closed.
Priority Wellness reportedly operated as a pill mill similar to West Parker’s. Runners brought people posing as patients to Priority Wellness and paid the clinic between $300 and $600. The cost depended on whether the purported patient received a prescription for hydrocodone or oxycodone, almost always prescribed in combination with carisoprodol, authorities said. Throughout the scheme, Priority Wellness made about $1.1 million, and Thompson made between $700 and $900 a day.
He was convicted of one count of conspiracy to unlawfully distribute and dispense controlled substances and seven counts of unlawfully distributing and dispensing controlled substances in connection with his conduct at West Parker. For his conduct at Priority Wellness, he was convicted of one count of conspiracy to unlawfully distribute and dispense controlled substances and one count of unlawfully distributing and dispensing controlled substances.
He faces up to 20 years in prison for each count of conviction with sentencing scheduled for Oct. 3.
A version of this article first appeared on Medscape.com.
A federal sting operation led to the recent conviction of a Texas physician assistant on charges of illegally prescribing a total of $3 million in drugs to patients at two “pill mill” clinics in Houston and helping others do the same.
The May 20 conviction of Charles Thompson, 76, of Houston, was based on charges of distributing more than 1.2 million opioid pills to thousands of individuals posing as patients at two pain management clinics, according to the U.S. Department of Justice.
Thompson’s conviction was the latest legal action in a string of cases involving the operation, including a doctor convicted in March who worked with Thompson at the West Parker Medical Clinic. Internist James Pierre, MD, 52, faces charges of unlawfully prescribing more than $1 million worth of opioid hydrocodone, according to federal officials.
Thompson also worked at Priority Wellness Clinic. Six people have pled guilty in connection with their conduct at West Parker or Priority Wellness, the justice department reported.
From June 2015 through July 2016, while Thompson was at West Parker, he helped Dr. Pierre unlawfully prescribe hydrocodone and the muscle relaxant carisoprodol, a combination of controlled substances for pain management known as the “Las Vegas cocktail,” to people in the sting operations pretending to be patients, authorities stated.
Thompson also distributed unlawful prescriptions for carisoprodol. So-called “runners” brought numerous people to pose as patients at West Parker and paid the clinic about $220 to $500 in cash for each visit that resulted in prescriptions for dangerous drugs. Throughout the scheme, West Parker pocketed about $1.75 million from prescriptions; Thompson was paid more than $208,000.
According to authorities, Thompson also helped others illegally prescribe controlled substances, including hydrocodone and oxycodone, from May to July 2017 at Priority Wellness, which opened in December 2016 after West Parker closed.
Priority Wellness reportedly operated as a pill mill similar to West Parker’s. Runners brought people posing as patients to Priority Wellness and paid the clinic between $300 and $600. The cost depended on whether the purported patient received a prescription for hydrocodone or oxycodone, almost always prescribed in combination with carisoprodol, authorities said. Throughout the scheme, Priority Wellness made about $1.1 million, and Thompson made between $700 and $900 a day.
He was convicted of one count of conspiracy to unlawfully distribute and dispense controlled substances and seven counts of unlawfully distributing and dispensing controlled substances in connection with his conduct at West Parker. For his conduct at Priority Wellness, he was convicted of one count of conspiracy to unlawfully distribute and dispense controlled substances and one count of unlawfully distributing and dispensing controlled substances.
He faces up to 20 years in prison for each count of conviction with sentencing scheduled for Oct. 3.
A version of this article first appeared on Medscape.com.
A federal sting operation led to the recent conviction of a Texas physician assistant on charges of illegally prescribing a total of $3 million in drugs to patients at two “pill mill” clinics in Houston and helping others do the same.
The May 20 conviction of Charles Thompson, 76, of Houston, was based on charges of distributing more than 1.2 million opioid pills to thousands of individuals posing as patients at two pain management clinics, according to the U.S. Department of Justice.
Thompson’s conviction was the latest legal action in a string of cases involving the operation, including a doctor convicted in March who worked with Thompson at the West Parker Medical Clinic. Internist James Pierre, MD, 52, faces charges of unlawfully prescribing more than $1 million worth of opioid hydrocodone, according to federal officials.
Thompson also worked at Priority Wellness Clinic. Six people have pled guilty in connection with their conduct at West Parker or Priority Wellness, the justice department reported.
From June 2015 through July 2016, while Thompson was at West Parker, he helped Dr. Pierre unlawfully prescribe hydrocodone and the muscle relaxant carisoprodol, a combination of controlled substances for pain management known as the “Las Vegas cocktail,” to people in the sting operations pretending to be patients, authorities stated.
Thompson also distributed unlawful prescriptions for carisoprodol. So-called “runners” brought numerous people to pose as patients at West Parker and paid the clinic about $220 to $500 in cash for each visit that resulted in prescriptions for dangerous drugs. Throughout the scheme, West Parker pocketed about $1.75 million from prescriptions; Thompson was paid more than $208,000.
According to authorities, Thompson also helped others illegally prescribe controlled substances, including hydrocodone and oxycodone, from May to July 2017 at Priority Wellness, which opened in December 2016 after West Parker closed.
Priority Wellness reportedly operated as a pill mill similar to West Parker’s. Runners brought people posing as patients to Priority Wellness and paid the clinic between $300 and $600. The cost depended on whether the purported patient received a prescription for hydrocodone or oxycodone, almost always prescribed in combination with carisoprodol, authorities said. Throughout the scheme, Priority Wellness made about $1.1 million, and Thompson made between $700 and $900 a day.
He was convicted of one count of conspiracy to unlawfully distribute and dispense controlled substances and seven counts of unlawfully distributing and dispensing controlled substances in connection with his conduct at West Parker. For his conduct at Priority Wellness, he was convicted of one count of conspiracy to unlawfully distribute and dispense controlled substances and one count of unlawfully distributing and dispensing controlled substances.
He faces up to 20 years in prison for each count of conviction with sentencing scheduled for Oct. 3.
A version of this article first appeared on Medscape.com.