User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Sepsis mortality greater in Black than White children despite similar interventions
WASHINGTON – , according to research presented at the annual meeting of the American Academy of Pediatrics.
The only other difference between Black and White pediatric patients was the length of hospital stay and the length of time in the ICU among those who died. In both cases, Black children who died spent more time in the hospital and in the ICU, reported Michael H. Stroud, MD, a pediatric critical care physician at the University of Arkansas for Medical Sciences in Little Rock, and his colleagues.
“Further investigations are needed to identify biases, conscious and unconscious, potential socioeconomic factors, and genetic predispositions leading to racial disparities in outcomes of children with pediatric sepsis, severe sepsis, and septic shock,” Dr Stroud and his colleagues said.
Nathan T. Chomilo, MD, adjunct assistant professor of pediatrics at the University of Minnesota, Minneapolis, who was not involved in the study but reviewed it, said the research “builds upon existing evidence that our health care system has work to do to meet its goal of treating patients equitably and provide everyone the opportunity for health.” He found the racial disparity in death particularly striking in 2023. “In the U.S., with all our wealth, knowledge, and resources, very few children should die from this, let alone there be such a stark gap,” Dr. Chomilo wrote.
Racial disparities persist
Dr. Stroud noted that many institutions currently use “automated, real-time, algorithm-based detection of sepsis, severe sepsis, and septic shock incorporated into the electronic medical record,” which leads to earlier recognition and resuscitation and overall better outcomes. Yet racial disparities in sepsis mortality rates persist, and he and his colleagues wanted to explore whether they remained even with these EMR-incorporated systems.
The researchers analyzed data from all patients at Arkansas Children’s Hospital who had sepsis, severe sepsis, or septic shock between January 2018 and April 2022. The hospital uses a best practice advisory (BPA) in the EMR whose activation leads to a bedside huddle and clinical interventions. For this study, the researchers defined a sepsis episode as either a BPA activation or an EMR diagnosis of sepsis, severe sepsis, or septic shock.
Among the 3,514 patients who had a sepsis episode during the study, 60.5% were White (n = 2,126) and 20.9% were Black (n = 736). Overall mortality was 1.65%, but that included 3.13% of Black children versus 1.27% of White children (odds ratio [OR] 2.51, P = .001). No significant differences in mortality were seen in gender or age.
Clinical interventions in the two groups were also similar: Total IV antibiotic days were 23.8 days for Black children and 21.6 days for White children (P = .38); total vasoactive infusion days were 2.2 for Black children and 2.6 for White (P = .18); and extracorporeal membrane oxygenation was necessary for 26.1% of Black children and 18.5% of White children (P = .52).
Length of hospitalization stay, however, was an average 4 days longer for Black children (16.7 days) versus White children (12.7 days) who died (P = .03). ICU stay for Black children who died was also an average 1.9 days longer (7.57 vs. 5.7 days; P = .01). There were no significant differences in the EMR between Black and White patients, however, in the percent who were over the threshold for antibiotic administration and the percent who received an IV fluid bolus.
Contributing factors
Dr. Chomilo said that most BPA systems require staff – including rooming and triage staff, nurses. and physicians – to enter vital signs, order labs, enter the results into the system, and enter other data used by the algorithm. “So even though the time from when those BPA warnings flagged to when clinical interventions were documented didn’t show a significant difference, there are numerous other points along a child’s illness that may be contributing to these numbers,” Dr. Chomilo said.
For example, he pointed out that differences in health insurance coverage could have influenced whether their parent or caregiver was able to bring them in early enough to be diagnosed since studies have revealed disparate access to regular care due to structural racism in the health care system. Studies have also shown disparate rates of patients being triaged or having to wait longer in emergency departments, he added.
“When the child was brought in, how were they triaged? How long did they wait before they had vitals taken? How long until they were seen by a clinician?” Dr. Chomilo said. “Was their care on the inpatient ward the same or different? What was the source of sepsis? Was it all infectious or other issues [since] cancer and autoimmune illnesses can also trigger a sepsis evaluation, for example? Overall, I suspect answers to several of these questions would reveal a disparity due to structural racism that contributed to the ultimate disparity in deaths.”
Other social determinants of health that could have played a role in the outcome disparities here might include the family’s access to transportation options, parental employment or child care options, and nutrition access since baseline nutritional status can be a factor in the outcomes of severe illnesses like sepsis.
”I don’t think this study provided enough information about the potential causative factors to come to any strong conclusions,” Dr. Chomilo said. But it’s important for clinicians to be aware of how biases in the health care system put Black, Indigenous and other communities at higher risk for worse clinical outcomes.
“I would reiterate that clinicians in the hospital can help improve outcomes by being aware of structural racism and structural inequity and how that may contribute to their patient’s risk of severe illness as the decide how to approach their treatment and engaging the patient’s family,” Dr. Chomilo said. “We cannot rely solely on universal tools that don’t take this into account when we are looking to improve clinical outcomes for everyone. Otherwise we will see these gaps persist.”
No external funding sources were noted. Dr. Stroud and Dr. Chomilo had no disclosures.
WASHINGTON – , according to research presented at the annual meeting of the American Academy of Pediatrics.
The only other difference between Black and White pediatric patients was the length of hospital stay and the length of time in the ICU among those who died. In both cases, Black children who died spent more time in the hospital and in the ICU, reported Michael H. Stroud, MD, a pediatric critical care physician at the University of Arkansas for Medical Sciences in Little Rock, and his colleagues.
“Further investigations are needed to identify biases, conscious and unconscious, potential socioeconomic factors, and genetic predispositions leading to racial disparities in outcomes of children with pediatric sepsis, severe sepsis, and septic shock,” Dr Stroud and his colleagues said.
Nathan T. Chomilo, MD, adjunct assistant professor of pediatrics at the University of Minnesota, Minneapolis, who was not involved in the study but reviewed it, said the research “builds upon existing evidence that our health care system has work to do to meet its goal of treating patients equitably and provide everyone the opportunity for health.” He found the racial disparity in death particularly striking in 2023. “In the U.S., with all our wealth, knowledge, and resources, very few children should die from this, let alone there be such a stark gap,” Dr. Chomilo wrote.
Racial disparities persist
Dr. Stroud noted that many institutions currently use “automated, real-time, algorithm-based detection of sepsis, severe sepsis, and septic shock incorporated into the electronic medical record,” which leads to earlier recognition and resuscitation and overall better outcomes. Yet racial disparities in sepsis mortality rates persist, and he and his colleagues wanted to explore whether they remained even with these EMR-incorporated systems.
The researchers analyzed data from all patients at Arkansas Children’s Hospital who had sepsis, severe sepsis, or septic shock between January 2018 and April 2022. The hospital uses a best practice advisory (BPA) in the EMR whose activation leads to a bedside huddle and clinical interventions. For this study, the researchers defined a sepsis episode as either a BPA activation or an EMR diagnosis of sepsis, severe sepsis, or septic shock.
Among the 3,514 patients who had a sepsis episode during the study, 60.5% were White (n = 2,126) and 20.9% were Black (n = 736). Overall mortality was 1.65%, but that included 3.13% of Black children versus 1.27% of White children (odds ratio [OR] 2.51, P = .001). No significant differences in mortality were seen in gender or age.
Clinical interventions in the two groups were also similar: Total IV antibiotic days were 23.8 days for Black children and 21.6 days for White children (P = .38); total vasoactive infusion days were 2.2 for Black children and 2.6 for White (P = .18); and extracorporeal membrane oxygenation was necessary for 26.1% of Black children and 18.5% of White children (P = .52).
Length of hospitalization stay, however, was an average 4 days longer for Black children (16.7 days) versus White children (12.7 days) who died (P = .03). ICU stay for Black children who died was also an average 1.9 days longer (7.57 vs. 5.7 days; P = .01). There were no significant differences in the EMR between Black and White patients, however, in the percent who were over the threshold for antibiotic administration and the percent who received an IV fluid bolus.
Contributing factors
Dr. Chomilo said that most BPA systems require staff – including rooming and triage staff, nurses. and physicians – to enter vital signs, order labs, enter the results into the system, and enter other data used by the algorithm. “So even though the time from when those BPA warnings flagged to when clinical interventions were documented didn’t show a significant difference, there are numerous other points along a child’s illness that may be contributing to these numbers,” Dr. Chomilo said.
For example, he pointed out that differences in health insurance coverage could have influenced whether their parent or caregiver was able to bring them in early enough to be diagnosed since studies have revealed disparate access to regular care due to structural racism in the health care system. Studies have also shown disparate rates of patients being triaged or having to wait longer in emergency departments, he added.
“When the child was brought in, how were they triaged? How long did they wait before they had vitals taken? How long until they were seen by a clinician?” Dr. Chomilo said. “Was their care on the inpatient ward the same or different? What was the source of sepsis? Was it all infectious or other issues [since] cancer and autoimmune illnesses can also trigger a sepsis evaluation, for example? Overall, I suspect answers to several of these questions would reveal a disparity due to structural racism that contributed to the ultimate disparity in deaths.”
Other social determinants of health that could have played a role in the outcome disparities here might include the family’s access to transportation options, parental employment or child care options, and nutrition access since baseline nutritional status can be a factor in the outcomes of severe illnesses like sepsis.
”I don’t think this study provided enough information about the potential causative factors to come to any strong conclusions,” Dr. Chomilo said. But it’s important for clinicians to be aware of how biases in the health care system put Black, Indigenous and other communities at higher risk for worse clinical outcomes.
“I would reiterate that clinicians in the hospital can help improve outcomes by being aware of structural racism and structural inequity and how that may contribute to their patient’s risk of severe illness as the decide how to approach their treatment and engaging the patient’s family,” Dr. Chomilo said. “We cannot rely solely on universal tools that don’t take this into account when we are looking to improve clinical outcomes for everyone. Otherwise we will see these gaps persist.”
No external funding sources were noted. Dr. Stroud and Dr. Chomilo had no disclosures.
WASHINGTON – , according to research presented at the annual meeting of the American Academy of Pediatrics.
The only other difference between Black and White pediatric patients was the length of hospital stay and the length of time in the ICU among those who died. In both cases, Black children who died spent more time in the hospital and in the ICU, reported Michael H. Stroud, MD, a pediatric critical care physician at the University of Arkansas for Medical Sciences in Little Rock, and his colleagues.
“Further investigations are needed to identify biases, conscious and unconscious, potential socioeconomic factors, and genetic predispositions leading to racial disparities in outcomes of children with pediatric sepsis, severe sepsis, and septic shock,” Dr Stroud and his colleagues said.
Nathan T. Chomilo, MD, adjunct assistant professor of pediatrics at the University of Minnesota, Minneapolis, who was not involved in the study but reviewed it, said the research “builds upon existing evidence that our health care system has work to do to meet its goal of treating patients equitably and provide everyone the opportunity for health.” He found the racial disparity in death particularly striking in 2023. “In the U.S., with all our wealth, knowledge, and resources, very few children should die from this, let alone there be such a stark gap,” Dr. Chomilo wrote.
Racial disparities persist
Dr. Stroud noted that many institutions currently use “automated, real-time, algorithm-based detection of sepsis, severe sepsis, and septic shock incorporated into the electronic medical record,” which leads to earlier recognition and resuscitation and overall better outcomes. Yet racial disparities in sepsis mortality rates persist, and he and his colleagues wanted to explore whether they remained even with these EMR-incorporated systems.
The researchers analyzed data from all patients at Arkansas Children’s Hospital who had sepsis, severe sepsis, or septic shock between January 2018 and April 2022. The hospital uses a best practice advisory (BPA) in the EMR whose activation leads to a bedside huddle and clinical interventions. For this study, the researchers defined a sepsis episode as either a BPA activation or an EMR diagnosis of sepsis, severe sepsis, or septic shock.
Among the 3,514 patients who had a sepsis episode during the study, 60.5% were White (n = 2,126) and 20.9% were Black (n = 736). Overall mortality was 1.65%, but that included 3.13% of Black children versus 1.27% of White children (odds ratio [OR] 2.51, P = .001). No significant differences in mortality were seen in gender or age.
Clinical interventions in the two groups were also similar: Total IV antibiotic days were 23.8 days for Black children and 21.6 days for White children (P = .38); total vasoactive infusion days were 2.2 for Black children and 2.6 for White (P = .18); and extracorporeal membrane oxygenation was necessary for 26.1% of Black children and 18.5% of White children (P = .52).
Length of hospitalization stay, however, was an average 4 days longer for Black children (16.7 days) versus White children (12.7 days) who died (P = .03). ICU stay for Black children who died was also an average 1.9 days longer (7.57 vs. 5.7 days; P = .01). There were no significant differences in the EMR between Black and White patients, however, in the percent who were over the threshold for antibiotic administration and the percent who received an IV fluid bolus.
Contributing factors
Dr. Chomilo said that most BPA systems require staff – including rooming and triage staff, nurses. and physicians – to enter vital signs, order labs, enter the results into the system, and enter other data used by the algorithm. “So even though the time from when those BPA warnings flagged to when clinical interventions were documented didn’t show a significant difference, there are numerous other points along a child’s illness that may be contributing to these numbers,” Dr. Chomilo said.
For example, he pointed out that differences in health insurance coverage could have influenced whether their parent or caregiver was able to bring them in early enough to be diagnosed since studies have revealed disparate access to regular care due to structural racism in the health care system. Studies have also shown disparate rates of patients being triaged or having to wait longer in emergency departments, he added.
“When the child was brought in, how were they triaged? How long did they wait before they had vitals taken? How long until they were seen by a clinician?” Dr. Chomilo said. “Was their care on the inpatient ward the same or different? What was the source of sepsis? Was it all infectious or other issues [since] cancer and autoimmune illnesses can also trigger a sepsis evaluation, for example? Overall, I suspect answers to several of these questions would reveal a disparity due to structural racism that contributed to the ultimate disparity in deaths.”
Other social determinants of health that could have played a role in the outcome disparities here might include the family’s access to transportation options, parental employment or child care options, and nutrition access since baseline nutritional status can be a factor in the outcomes of severe illnesses like sepsis.
”I don’t think this study provided enough information about the potential causative factors to come to any strong conclusions,” Dr. Chomilo said. But it’s important for clinicians to be aware of how biases in the health care system put Black, Indigenous and other communities at higher risk for worse clinical outcomes.
“I would reiterate that clinicians in the hospital can help improve outcomes by being aware of structural racism and structural inequity and how that may contribute to their patient’s risk of severe illness as the decide how to approach their treatment and engaging the patient’s family,” Dr. Chomilo said. “We cannot rely solely on universal tools that don’t take this into account when we are looking to improve clinical outcomes for everyone. Otherwise we will see these gaps persist.”
No external funding sources were noted. Dr. Stroud and Dr. Chomilo had no disclosures.
AT AAP 2023
Low-dose aspirin reduces liver fat, inflammation markers
BOSTON – Patients with metabolic-associated steatotic liver disease (MASLD, formerly NAFLD) without cirrhosis who took daily low-dose aspirin in a double-blind randomized trial demonstrated significant reductions in liver fat content over 6 months compared with similar patients who took a placebo, study results show.
“In MASLD without cirrhosis, low-dose aspirin, 81 milligrams daily, led to decreases in liver fat and improved markers of hepatic inflammation and fibrosis,” reported Robert M. Wilechansky, MD, a transplant hepatology fellow at Massachusetts General Hospital in Boston.
“It was safe and well tolerated in this study, but we would like to see larger, longer-term clinical trials to test the efficacy of aspirin for improving histology and preventing adverse outcomes in MASLD,” he said at the annual meeting of the American Association for the Study of Liver Diseases.
“We don’t have current plans, to my knowledge, to test full-dose aspirin,” he said in an interview. “I’m encouraged by the results with low-dose aspirin, and I think that, given the risk profile, using a lower dose is preferable.”
Reduction in inflammation
Although promising therapies for MASLD are in development, none are currently approved by the Food and Drug Administration, prompting Dr. Wilechansky and colleagues to investigate aspirin, with its anti-inflammatory properties, as a potential treatment.
In preclinical studies, aspirin has been shown to have both anti-inflammatory and antitumor effects in the liver through inhibition of cycloxygenase-2 and platelet-derived growth factor signaling, as well as through modulation of bioactive lipids, Dr. Wilechansky said.
In observational studies, use of aspirin was associated with a reduction in the prevalence of hepatic steatosis and fibrosis progression in patients with MASLD, and there was a decrease in the incidence of hepatocellular carcinoma and liver-related mortality among patients with viral hepatitis, he noted.
As for the potential mechanism of action of aspirin for patients with MASLD, Dr. Wilechansky noted that there may be some reduction in steatosis, and “if there is a reduction in inflammation, we may see some reduction in steatohepatitis.”
Study details
To see whether the so-called “wonder drug” could work wonders for patients with MASLD without cirrhosis, the researchers recruited 80 adults with MASLD and randomly assigned them to receive either aspirin 81 mg once daily or placebo for 6 months.
Patients with baseline cirrhosis or other liver disease, heavy drinkers, those who had used aspirin within 6 months, or those who used other antiplatelet or anticoagulant agents were excluded, as were patients with severe renal or cardiovascular disease, active cancer, pregnancy, were breastfeeding, had thrombocytopenia, or had undergone bariatric surgery within the past 2 years.
At baseline, 36.3% of all patients had F2-F3 fibrosis, as determined by vibration-controlled transient elastography (VCTE), and of 44 patients who had previously undergone liver biopsy, 37 (84.1%) were confirmed to have steatohepatitis.
At 6 months, the absolute change in hepatic fat fraction (HFF) from baseline, the primary endpoint, was a decline of 6.1% for patients taking aspirin, compared with a 4.2% increase for patients taking placebo, which translates into a 10.3% difference in favor of aspirin (P = .009).
The relative change in HFF, a secondary endpoint, for aspirin versus placebo was –59.2% (P = .003).
In addition, the use of aspirin was associated with a relative reduction in HFF of at least 30% among 16 of the 40 patients who received it.
Aspirin was significantly better than placebo for the secondary endpoints of absolute change in hepatic fat by MRI proton-density fat fraction, with –2.9% versus placebo (P = .018), and the relative change in hepatic fat by MRI-PDFF, with a difference of –24.8% versus placebo (P = .009).
Aspirin was also associated with significantly greater reductions in liver transaminase levels and liver stiffness by VCTE.
About one-third of patients in each study arm had at least one adverse event. There was only one aspirin-related adverse event (heartburn) that led to discontinuation. There were no serious bleeding events in either arm.
“We’re going to have to consider stratifying by aspirin use now in our trials,” said Mark Hartman, MD, from Eli Lilly in Indianapolis.
Significant weight gain in placebo group
Mary E. McCarthy Rinella, MD, FAASLD, professor of medicine at the University of Chicago, commented that the 4% increase in liver fat in the control arm “is kind of a lot for a placebo, and I’m wondering how much that accounts for the [difference] that you saw.” Dr. Rinella served as a comoderator of the session.
Dr. Wilechansky said that there were a few outliers in the placebo group who experienced significant weight gain during the study, including one patient who gained 15 kg over 6 months.
A post hoc analysis suggested that most of the increase in hepatic fat among patients who took placebo could have been among that handful of patients, he added. When those patients were removed in an adjusted analysis, the difference between the aspirin and placebo groups was smaller but remained significant.
The trial was sponsored by Massachusetts General Hospital. Dr. Wilechansky, Dr. Rinella, and Dr. Hartman had no relevant disclosures.
A version of this article first appeared on Medscape.com.
BOSTON – Patients with metabolic-associated steatotic liver disease (MASLD, formerly NAFLD) without cirrhosis who took daily low-dose aspirin in a double-blind randomized trial demonstrated significant reductions in liver fat content over 6 months compared with similar patients who took a placebo, study results show.
“In MASLD without cirrhosis, low-dose aspirin, 81 milligrams daily, led to decreases in liver fat and improved markers of hepatic inflammation and fibrosis,” reported Robert M. Wilechansky, MD, a transplant hepatology fellow at Massachusetts General Hospital in Boston.
“It was safe and well tolerated in this study, but we would like to see larger, longer-term clinical trials to test the efficacy of aspirin for improving histology and preventing adverse outcomes in MASLD,” he said at the annual meeting of the American Association for the Study of Liver Diseases.
“We don’t have current plans, to my knowledge, to test full-dose aspirin,” he said in an interview. “I’m encouraged by the results with low-dose aspirin, and I think that, given the risk profile, using a lower dose is preferable.”
Reduction in inflammation
Although promising therapies for MASLD are in development, none are currently approved by the Food and Drug Administration, prompting Dr. Wilechansky and colleagues to investigate aspirin, with its anti-inflammatory properties, as a potential treatment.
In preclinical studies, aspirin has been shown to have both anti-inflammatory and antitumor effects in the liver through inhibition of cycloxygenase-2 and platelet-derived growth factor signaling, as well as through modulation of bioactive lipids, Dr. Wilechansky said.
In observational studies, use of aspirin was associated with a reduction in the prevalence of hepatic steatosis and fibrosis progression in patients with MASLD, and there was a decrease in the incidence of hepatocellular carcinoma and liver-related mortality among patients with viral hepatitis, he noted.
As for the potential mechanism of action of aspirin for patients with MASLD, Dr. Wilechansky noted that there may be some reduction in steatosis, and “if there is a reduction in inflammation, we may see some reduction in steatohepatitis.”
Study details
To see whether the so-called “wonder drug” could work wonders for patients with MASLD without cirrhosis, the researchers recruited 80 adults with MASLD and randomly assigned them to receive either aspirin 81 mg once daily or placebo for 6 months.
Patients with baseline cirrhosis or other liver disease, heavy drinkers, those who had used aspirin within 6 months, or those who used other antiplatelet or anticoagulant agents were excluded, as were patients with severe renal or cardiovascular disease, active cancer, pregnancy, were breastfeeding, had thrombocytopenia, or had undergone bariatric surgery within the past 2 years.
At baseline, 36.3% of all patients had F2-F3 fibrosis, as determined by vibration-controlled transient elastography (VCTE), and of 44 patients who had previously undergone liver biopsy, 37 (84.1%) were confirmed to have steatohepatitis.
At 6 months, the absolute change in hepatic fat fraction (HFF) from baseline, the primary endpoint, was a decline of 6.1% for patients taking aspirin, compared with a 4.2% increase for patients taking placebo, which translates into a 10.3% difference in favor of aspirin (P = .009).
The relative change in HFF, a secondary endpoint, for aspirin versus placebo was –59.2% (P = .003).
In addition, the use of aspirin was associated with a relative reduction in HFF of at least 30% among 16 of the 40 patients who received it.
Aspirin was significantly better than placebo for the secondary endpoints of absolute change in hepatic fat by MRI proton-density fat fraction, with –2.9% versus placebo (P = .018), and the relative change in hepatic fat by MRI-PDFF, with a difference of –24.8% versus placebo (P = .009).
Aspirin was also associated with significantly greater reductions in liver transaminase levels and liver stiffness by VCTE.
About one-third of patients in each study arm had at least one adverse event. There was only one aspirin-related adverse event (heartburn) that led to discontinuation. There were no serious bleeding events in either arm.
“We’re going to have to consider stratifying by aspirin use now in our trials,” said Mark Hartman, MD, from Eli Lilly in Indianapolis.
Significant weight gain in placebo group
Mary E. McCarthy Rinella, MD, FAASLD, professor of medicine at the University of Chicago, commented that the 4% increase in liver fat in the control arm “is kind of a lot for a placebo, and I’m wondering how much that accounts for the [difference] that you saw.” Dr. Rinella served as a comoderator of the session.
Dr. Wilechansky said that there were a few outliers in the placebo group who experienced significant weight gain during the study, including one patient who gained 15 kg over 6 months.
A post hoc analysis suggested that most of the increase in hepatic fat among patients who took placebo could have been among that handful of patients, he added. When those patients were removed in an adjusted analysis, the difference between the aspirin and placebo groups was smaller but remained significant.
The trial was sponsored by Massachusetts General Hospital. Dr. Wilechansky, Dr. Rinella, and Dr. Hartman had no relevant disclosures.
A version of this article first appeared on Medscape.com.
BOSTON – Patients with metabolic-associated steatotic liver disease (MASLD, formerly NAFLD) without cirrhosis who took daily low-dose aspirin in a double-blind randomized trial demonstrated significant reductions in liver fat content over 6 months compared with similar patients who took a placebo, study results show.
“In MASLD without cirrhosis, low-dose aspirin, 81 milligrams daily, led to decreases in liver fat and improved markers of hepatic inflammation and fibrosis,” reported Robert M. Wilechansky, MD, a transplant hepatology fellow at Massachusetts General Hospital in Boston.
“It was safe and well tolerated in this study, but we would like to see larger, longer-term clinical trials to test the efficacy of aspirin for improving histology and preventing adverse outcomes in MASLD,” he said at the annual meeting of the American Association for the Study of Liver Diseases.
“We don’t have current plans, to my knowledge, to test full-dose aspirin,” he said in an interview. “I’m encouraged by the results with low-dose aspirin, and I think that, given the risk profile, using a lower dose is preferable.”
Reduction in inflammation
Although promising therapies for MASLD are in development, none are currently approved by the Food and Drug Administration, prompting Dr. Wilechansky and colleagues to investigate aspirin, with its anti-inflammatory properties, as a potential treatment.
In preclinical studies, aspirin has been shown to have both anti-inflammatory and antitumor effects in the liver through inhibition of cycloxygenase-2 and platelet-derived growth factor signaling, as well as through modulation of bioactive lipids, Dr. Wilechansky said.
In observational studies, use of aspirin was associated with a reduction in the prevalence of hepatic steatosis and fibrosis progression in patients with MASLD, and there was a decrease in the incidence of hepatocellular carcinoma and liver-related mortality among patients with viral hepatitis, he noted.
As for the potential mechanism of action of aspirin for patients with MASLD, Dr. Wilechansky noted that there may be some reduction in steatosis, and “if there is a reduction in inflammation, we may see some reduction in steatohepatitis.”
Study details
To see whether the so-called “wonder drug” could work wonders for patients with MASLD without cirrhosis, the researchers recruited 80 adults with MASLD and randomly assigned them to receive either aspirin 81 mg once daily or placebo for 6 months.
Patients with baseline cirrhosis or other liver disease, heavy drinkers, those who had used aspirin within 6 months, or those who used other antiplatelet or anticoagulant agents were excluded, as were patients with severe renal or cardiovascular disease, active cancer, pregnancy, were breastfeeding, had thrombocytopenia, or had undergone bariatric surgery within the past 2 years.
At baseline, 36.3% of all patients had F2-F3 fibrosis, as determined by vibration-controlled transient elastography (VCTE), and of 44 patients who had previously undergone liver biopsy, 37 (84.1%) were confirmed to have steatohepatitis.
At 6 months, the absolute change in hepatic fat fraction (HFF) from baseline, the primary endpoint, was a decline of 6.1% for patients taking aspirin, compared with a 4.2% increase for patients taking placebo, which translates into a 10.3% difference in favor of aspirin (P = .009).
The relative change in HFF, a secondary endpoint, for aspirin versus placebo was –59.2% (P = .003).
In addition, the use of aspirin was associated with a relative reduction in HFF of at least 30% among 16 of the 40 patients who received it.
Aspirin was significantly better than placebo for the secondary endpoints of absolute change in hepatic fat by MRI proton-density fat fraction, with –2.9% versus placebo (P = .018), and the relative change in hepatic fat by MRI-PDFF, with a difference of –24.8% versus placebo (P = .009).
Aspirin was also associated with significantly greater reductions in liver transaminase levels and liver stiffness by VCTE.
About one-third of patients in each study arm had at least one adverse event. There was only one aspirin-related adverse event (heartburn) that led to discontinuation. There were no serious bleeding events in either arm.
“We’re going to have to consider stratifying by aspirin use now in our trials,” said Mark Hartman, MD, from Eli Lilly in Indianapolis.
Significant weight gain in placebo group
Mary E. McCarthy Rinella, MD, FAASLD, professor of medicine at the University of Chicago, commented that the 4% increase in liver fat in the control arm “is kind of a lot for a placebo, and I’m wondering how much that accounts for the [difference] that you saw.” Dr. Rinella served as a comoderator of the session.
Dr. Wilechansky said that there were a few outliers in the placebo group who experienced significant weight gain during the study, including one patient who gained 15 kg over 6 months.
A post hoc analysis suggested that most of the increase in hepatic fat among patients who took placebo could have been among that handful of patients, he added. When those patients were removed in an adjusted analysis, the difference between the aspirin and placebo groups was smaller but remained significant.
The trial was sponsored by Massachusetts General Hospital. Dr. Wilechansky, Dr. Rinella, and Dr. Hartman had no relevant disclosures.
A version of this article first appeared on Medscape.com.
AT THE LIVER MEETING 2023
Albuminuria reduction fuels finerenone’s kidney benefits
PHILADELPHIA – Reducing albuminuria is a key mediator of the way finerenone (Kerendia, Bayer) reduces adverse renal and cardiovascular events in people with type 2 diabetes and chronic kidney disease (CKD), based on findings from two novel mediation analyses run on data from more than 12,000 people included in the two finerenone pivotal trials.
Results from these analyses showed that that finerenone treatment produced in the FIDELIO-DKD and FIGARO-DKD phase 3 trials. FIDELIO-DKD, which had protection against adverse kidney outcomes as its primary endpoint, supplied the data that led to finerenone’s approval in 2021 by the U.S. Food and Drug Administration for treating people with type 2 diabetes and CKD.
The findings of the mediation analyses underscore the important role that albuminuria plays in the nephropathy and related comorbidities associated with type 2 diabetes and CKD and highlight the importance of ongoing monitoring of albuminuria to guide treatments aimed at minimizing this pathology, said Rajiv Agarwal, MD, who presented a poster on the mediation analyses at Kidney Week 2023, organized by the American Society of Nephrology.
“My hope is that this [report] heightens awareness of UACR” as an important marker of both CKD and of the response by patients with CKD to their treatment, said Dr. Agarwal, a nephrologist and professor at Indiana University in Indianapolis.
“Only about half of people with type 2 diabetes get their UACR measured even though every guideline says measure UACR in people with diabetes. Our findings say that UACR is important not just for CKD diagnosis but also to give feedback” on whether management is working, Dr. Agarwal said in an interview.
Incorporate UACR into clinical decision-making
“My hope is that clinicians will look at UACR as something they should incorporate into clinical decision-making. I measure UACR in my patients [with CKD and type 2 diabetes] at every visit; it’s so inexpensive. Albuminuria is not a good sign. If it’s not reduced in a patient by at least 30% [the recommended minimum reduction by the American Diabetes Association for people who start with a UACR of at least 300 mg/g] clinicians should think of what else they could do to lower albuminuria”: Reduce salt intake, improve blood pressure control, make sure the patient is adherent to treatments, and add additional treatments, Dr. Agarwal advised.

Multiple efforts are now underway or will soon start to boost the rate at which at-risk people get their UACR measured, noted Leslie A. Inker, MD, in a separate talk during Kidney Week. These efforts include the National Kidney Foundation’s CKD Learning Collaborative, which aims to improve clinician awareness of CKD and improve routine testing for CKD. Early results during 2023 from this program in Missouri showed a nearly 8–percentage point increase in the screening rate for UACR levels in at-risk people, said Dr. Inker, professor and director of the Kidney and Blood Pressure Center at Tufts Medical Center in Boston.
A second advance was introduction in 2018 of the “kidney profile” lab order by the American College of Clinical Pathology that allows clinicians to order as a single test both an estimated glomerular filtration rate (eGFR) and a UACR.
Also, the Centers for Medicare & Medicaid Services and the National Committee for Quality Assurance have both taken steps to encourage UACR ordering. The NCQA established a new Healthcare Effectiveness Data and Information Set performance measure for U.S. physicians starting in 2023 that will track measurement of UACR and eGFR in people with diabetes. CMS also has made assessment of kidney health a measure of care quality in programs effective in 2023 and 2024, Dr. Inker noted.
Most subjects had elevated UACRs
The study run by Dr. Agarwal and his associates used data from 12,512 of the more than 13,000 people enrolled in either FIDELITY-DKD or FIGARO-DKD who had UACR measurements recorded at baseline, at 4 months into either study, or both. Their median UACR at the time they began on finerenone or placebo was 514 mg/g, with 67% having a UACR of at least 300 mg/g (macroalbuminuria) and 31% having a UACR of 30-299 mg/g (microalbuminuria). By design, virtually all patients in these two trials were on a renin-angiotensin system inhibitor (either an angiotensin-converting enzyme inhibitor or an angiotensin-receptor blocker), but given the time period when the two trials enrolled participants (during 2015-2018) only 7% of those enrolled were on a sodium-glucose cotransporter 2 inhibitor and only 7% were on a glucagonlike peptide–1 receptor agonist.
Four months after treatment began, 53% of those randomized to finerenone treatment and 27% of those in the placebo arm had their UACR reduced by at least 30% from baseline, the cutpoint chosen by Dr. Agarwal based on the American Diabetes Association guideline.
Kaplan-Meier analyses showed that the incidence of the primary kidney outcome – kidney failure, a sustained ≥ 57% decrease in eGFR from baseline, or kidney death – showed close correlation with at least a 30% reduction in UACR regardless of whether the patients in this subgroup received finerenone or placebo.
A different correlation was found in those with a less than 30% reduction in their UACR from baseline to 4 months, regardless of whether this happened on finerenone or placebo. People in the two finerenone trials who had a lesser reduction from baseline in their UACR also had a significantly higher rate of adverse kidney outcomes whether they received finerenone or placebo.
84% of finerenone’s kidney benefit linked to lowering of UACR
The causal-mediation analysis run by Dr. Agarwal quantified this observation, showing that 84% of finerenone’s effect on the kidney outcome was mediated by the reduction in UACR.
“It seems like the kidney benefit [from finerenone] travels through the level of albuminuria. This has broad implications for treatment of people with type 2 diabetes and CKD,” he said.
The link with reduction in albuminuria was weaker for the primary cardiovascular disease outcome: CV death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure. The strongest effect on this outcome was only seen in Kaplan-Meier analysis in those on finerenone who had at least a 30% reduction in their UACR. Those on placebo and with a similarly robust 4-month reduction in UACR showed a much more modest cardiovascular benefit that resembled those on either finerenone or placebo who had a smaller, less than 30% UACR reduction. The mediation analysis of these data showed that UACR reduction accounted for about 37% of the observed cardiovascular benefit seen during the trials.
“The effect of UACR is much stronger for the kidney outcomes,” summed up Dr. Agarwal. The results suggest that for cardiovascular outcomes finerenone works through factors other than lowering of UACR, but he admitted that no one currently knows what those other factors might be.
Treat aggressively to lower UACR by 30%
“I wouldn’t stop finerenone treatment in people who do not get a 30% reduction in their UACR” because these analyses suggest that a portion of the overall benefits from finerenone occurs via other mechanisms, he said. But in patients whose UACR is not reduced by at least 30% “be more aggressive on other measures to reduce UACR,” he advised.
The mediation analyses he ran are “the first time this has been done in nephrology,” producing a “groundbreaking” analysis and finding, Dr. Agarwal said. He also highlighted that the findings primarily relate to the importance of controlling UACR rather than an endorsement of finerenone as the best way to achieve this.
“All I care about is that people think about UACR as a modifiable risk factor. It doesn’t have to be treated with finerenone. It could be a renin-angiotensin system inhibitor, it could be chlorthalidone [a thiazide diuretic]. It just happened that we had a large dataset of people treated with finerenone or placebo.”
He said that future mediation analyses should look at the link between outcomes and UACR reductions produced by agents from the classes of sodium-glucose cotransporter 2 inhibitors and the glucagonlike peptide–1 receptor agonists.
FIDELIO-DKD and FIGARO-DKD were both sponsored by Bayer, the company that markets finerenone. Dr. Agarwal has received personal fees and nonfinancial support from Bayer. He has also received personal fees and nonfinancial support from Akebia Therapeutics, AstraZeneca, Boehringer Ingelheim, Eli Lilly, and Vifor Pharma, and he is a member of data safety monitoring committees for Chinook and Vertex. Dr. Inker is a consultant to Diamtrix, and her department receives research funding from Chinook, Omeros, Reata, and Tricida.
PHILADELPHIA – Reducing albuminuria is a key mediator of the way finerenone (Kerendia, Bayer) reduces adverse renal and cardiovascular events in people with type 2 diabetes and chronic kidney disease (CKD), based on findings from two novel mediation analyses run on data from more than 12,000 people included in the two finerenone pivotal trials.
Results from these analyses showed that that finerenone treatment produced in the FIDELIO-DKD and FIGARO-DKD phase 3 trials. FIDELIO-DKD, which had protection against adverse kidney outcomes as its primary endpoint, supplied the data that led to finerenone’s approval in 2021 by the U.S. Food and Drug Administration for treating people with type 2 diabetes and CKD.
The findings of the mediation analyses underscore the important role that albuminuria plays in the nephropathy and related comorbidities associated with type 2 diabetes and CKD and highlight the importance of ongoing monitoring of albuminuria to guide treatments aimed at minimizing this pathology, said Rajiv Agarwal, MD, who presented a poster on the mediation analyses at Kidney Week 2023, organized by the American Society of Nephrology.
“My hope is that this [report] heightens awareness of UACR” as an important marker of both CKD and of the response by patients with CKD to their treatment, said Dr. Agarwal, a nephrologist and professor at Indiana University in Indianapolis.
“Only about half of people with type 2 diabetes get their UACR measured even though every guideline says measure UACR in people with diabetes. Our findings say that UACR is important not just for CKD diagnosis but also to give feedback” on whether management is working, Dr. Agarwal said in an interview.
Incorporate UACR into clinical decision-making
“My hope is that clinicians will look at UACR as something they should incorporate into clinical decision-making. I measure UACR in my patients [with CKD and type 2 diabetes] at every visit; it’s so inexpensive. Albuminuria is not a good sign. If it’s not reduced in a patient by at least 30% [the recommended minimum reduction by the American Diabetes Association for people who start with a UACR of at least 300 mg/g] clinicians should think of what else they could do to lower albuminuria”: Reduce salt intake, improve blood pressure control, make sure the patient is adherent to treatments, and add additional treatments, Dr. Agarwal advised.
Multiple efforts are now underway or will soon start to boost the rate at which at-risk people get their UACR measured, noted Leslie A. Inker, MD, in a separate talk during Kidney Week. These efforts include the National Kidney Foundation’s CKD Learning Collaborative, which aims to improve clinician awareness of CKD and improve routine testing for CKD. Early results during 2023 from this program in Missouri showed a nearly 8–percentage point increase in the screening rate for UACR levels in at-risk people, said Dr. Inker, professor and director of the Kidney and Blood Pressure Center at Tufts Medical Center in Boston.
A second advance was introduction in 2018 of the “kidney profile” lab order by the American College of Clinical Pathology that allows clinicians to order as a single test both an estimated glomerular filtration rate (eGFR) and a UACR.
Also, the Centers for Medicare & Medicaid Services and the National Committee for Quality Assurance have both taken steps to encourage UACR ordering. The NCQA established a new Healthcare Effectiveness Data and Information Set performance measure for U.S. physicians starting in 2023 that will track measurement of UACR and eGFR in people with diabetes. CMS also has made assessment of kidney health a measure of care quality in programs effective in 2023 and 2024, Dr. Inker noted.
Most subjects had elevated UACRs
The study run by Dr. Agarwal and his associates used data from 12,512 of the more than 13,000 people enrolled in either FIDELITY-DKD or FIGARO-DKD who had UACR measurements recorded at baseline, at 4 months into either study, or both. Their median UACR at the time they began on finerenone or placebo was 514 mg/g, with 67% having a UACR of at least 300 mg/g (macroalbuminuria) and 31% having a UACR of 30-299 mg/g (microalbuminuria). By design, virtually all patients in these two trials were on a renin-angiotensin system inhibitor (either an angiotensin-converting enzyme inhibitor or an angiotensin-receptor blocker), but given the time period when the two trials enrolled participants (during 2015-2018) only 7% of those enrolled were on a sodium-glucose cotransporter 2 inhibitor and only 7% were on a glucagonlike peptide–1 receptor agonist.
Four months after treatment began, 53% of those randomized to finerenone treatment and 27% of those in the placebo arm had their UACR reduced by at least 30% from baseline, the cutpoint chosen by Dr. Agarwal based on the American Diabetes Association guideline.
Kaplan-Meier analyses showed that the incidence of the primary kidney outcome – kidney failure, a sustained ≥ 57% decrease in eGFR from baseline, or kidney death – showed close correlation with at least a 30% reduction in UACR regardless of whether the patients in this subgroup received finerenone or placebo.
A different correlation was found in those with a less than 30% reduction in their UACR from baseline to 4 months, regardless of whether this happened on finerenone or placebo. People in the two finerenone trials who had a lesser reduction from baseline in their UACR also had a significantly higher rate of adverse kidney outcomes whether they received finerenone or placebo.
84% of finerenone’s kidney benefit linked to lowering of UACR
The causal-mediation analysis run by Dr. Agarwal quantified this observation, showing that 84% of finerenone’s effect on the kidney outcome was mediated by the reduction in UACR.
“It seems like the kidney benefit [from finerenone] travels through the level of albuminuria. This has broad implications for treatment of people with type 2 diabetes and CKD,” he said.
The link with reduction in albuminuria was weaker for the primary cardiovascular disease outcome: CV death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure. The strongest effect on this outcome was only seen in Kaplan-Meier analysis in those on finerenone who had at least a 30% reduction in their UACR. Those on placebo and with a similarly robust 4-month reduction in UACR showed a much more modest cardiovascular benefit that resembled those on either finerenone or placebo who had a smaller, less than 30% UACR reduction. The mediation analysis of these data showed that UACR reduction accounted for about 37% of the observed cardiovascular benefit seen during the trials.
“The effect of UACR is much stronger for the kidney outcomes,” summed up Dr. Agarwal. The results suggest that for cardiovascular outcomes finerenone works through factors other than lowering of UACR, but he admitted that no one currently knows what those other factors might be.
Treat aggressively to lower UACR by 30%
“I wouldn’t stop finerenone treatment in people who do not get a 30% reduction in their UACR” because these analyses suggest that a portion of the overall benefits from finerenone occurs via other mechanisms, he said. But in patients whose UACR is not reduced by at least 30% “be more aggressive on other measures to reduce UACR,” he advised.
The mediation analyses he ran are “the first time this has been done in nephrology,” producing a “groundbreaking” analysis and finding, Dr. Agarwal said. He also highlighted that the findings primarily relate to the importance of controlling UACR rather than an endorsement of finerenone as the best way to achieve this.
“All I care about is that people think about UACR as a modifiable risk factor. It doesn’t have to be treated with finerenone. It could be a renin-angiotensin system inhibitor, it could be chlorthalidone [a thiazide diuretic]. It just happened that we had a large dataset of people treated with finerenone or placebo.”
He said that future mediation analyses should look at the link between outcomes and UACR reductions produced by agents from the classes of sodium-glucose cotransporter 2 inhibitors and the glucagonlike peptide–1 receptor agonists.
FIDELIO-DKD and FIGARO-DKD were both sponsored by Bayer, the company that markets finerenone. Dr. Agarwal has received personal fees and nonfinancial support from Bayer. He has also received personal fees and nonfinancial support from Akebia Therapeutics, AstraZeneca, Boehringer Ingelheim, Eli Lilly, and Vifor Pharma, and he is a member of data safety monitoring committees for Chinook and Vertex. Dr. Inker is a consultant to Diamtrix, and her department receives research funding from Chinook, Omeros, Reata, and Tricida.
PHILADELPHIA – Reducing albuminuria is a key mediator of the way finerenone (Kerendia, Bayer) reduces adverse renal and cardiovascular events in people with type 2 diabetes and chronic kidney disease (CKD), based on findings from two novel mediation analyses run on data from more than 12,000 people included in the two finerenone pivotal trials.
Results from these analyses showed that that finerenone treatment produced in the FIDELIO-DKD and FIGARO-DKD phase 3 trials. FIDELIO-DKD, which had protection against adverse kidney outcomes as its primary endpoint, supplied the data that led to finerenone’s approval in 2021 by the U.S. Food and Drug Administration for treating people with type 2 diabetes and CKD.
The findings of the mediation analyses underscore the important role that albuminuria plays in the nephropathy and related comorbidities associated with type 2 diabetes and CKD and highlight the importance of ongoing monitoring of albuminuria to guide treatments aimed at minimizing this pathology, said Rajiv Agarwal, MD, who presented a poster on the mediation analyses at Kidney Week 2023, organized by the American Society of Nephrology.
“My hope is that this [report] heightens awareness of UACR” as an important marker of both CKD and of the response by patients with CKD to their treatment, said Dr. Agarwal, a nephrologist and professor at Indiana University in Indianapolis.
“Only about half of people with type 2 diabetes get their UACR measured even though every guideline says measure UACR in people with diabetes. Our findings say that UACR is important not just for CKD diagnosis but also to give feedback” on whether management is working, Dr. Agarwal said in an interview.
Incorporate UACR into clinical decision-making
“My hope is that clinicians will look at UACR as something they should incorporate into clinical decision-making. I measure UACR in my patients [with CKD and type 2 diabetes] at every visit; it’s so inexpensive. Albuminuria is not a good sign. If it’s not reduced in a patient by at least 30% [the recommended minimum reduction by the American Diabetes Association for people who start with a UACR of at least 300 mg/g] clinicians should think of what else they could do to lower albuminuria”: Reduce salt intake, improve blood pressure control, make sure the patient is adherent to treatments, and add additional treatments, Dr. Agarwal advised.
Multiple efforts are now underway or will soon start to boost the rate at which at-risk people get their UACR measured, noted Leslie A. Inker, MD, in a separate talk during Kidney Week. These efforts include the National Kidney Foundation’s CKD Learning Collaborative, which aims to improve clinician awareness of CKD and improve routine testing for CKD. Early results during 2023 from this program in Missouri showed a nearly 8–percentage point increase in the screening rate for UACR levels in at-risk people, said Dr. Inker, professor and director of the Kidney and Blood Pressure Center at Tufts Medical Center in Boston.
A second advance was introduction in 2018 of the “kidney profile” lab order by the American College of Clinical Pathology that allows clinicians to order as a single test both an estimated glomerular filtration rate (eGFR) and a UACR.
Also, the Centers for Medicare & Medicaid Services and the National Committee for Quality Assurance have both taken steps to encourage UACR ordering. The NCQA established a new Healthcare Effectiveness Data and Information Set performance measure for U.S. physicians starting in 2023 that will track measurement of UACR and eGFR in people with diabetes. CMS also has made assessment of kidney health a measure of care quality in programs effective in 2023 and 2024, Dr. Inker noted.
Most subjects had elevated UACRs
The study run by Dr. Agarwal and his associates used data from 12,512 of the more than 13,000 people enrolled in either FIDELITY-DKD or FIGARO-DKD who had UACR measurements recorded at baseline, at 4 months into either study, or both. Their median UACR at the time they began on finerenone or placebo was 514 mg/g, with 67% having a UACR of at least 300 mg/g (macroalbuminuria) and 31% having a UACR of 30-299 mg/g (microalbuminuria). By design, virtually all patients in these two trials were on a renin-angiotensin system inhibitor (either an angiotensin-converting enzyme inhibitor or an angiotensin-receptor blocker), but given the time period when the two trials enrolled participants (during 2015-2018) only 7% of those enrolled were on a sodium-glucose cotransporter 2 inhibitor and only 7% were on a glucagonlike peptide–1 receptor agonist.
Four months after treatment began, 53% of those randomized to finerenone treatment and 27% of those in the placebo arm had their UACR reduced by at least 30% from baseline, the cutpoint chosen by Dr. Agarwal based on the American Diabetes Association guideline.
Kaplan-Meier analyses showed that the incidence of the primary kidney outcome – kidney failure, a sustained ≥ 57% decrease in eGFR from baseline, or kidney death – showed close correlation with at least a 30% reduction in UACR regardless of whether the patients in this subgroup received finerenone or placebo.
A different correlation was found in those with a less than 30% reduction in their UACR from baseline to 4 months, regardless of whether this happened on finerenone or placebo. People in the two finerenone trials who had a lesser reduction from baseline in their UACR also had a significantly higher rate of adverse kidney outcomes whether they received finerenone or placebo.
84% of finerenone’s kidney benefit linked to lowering of UACR
The causal-mediation analysis run by Dr. Agarwal quantified this observation, showing that 84% of finerenone’s effect on the kidney outcome was mediated by the reduction in UACR.
“It seems like the kidney benefit [from finerenone] travels through the level of albuminuria. This has broad implications for treatment of people with type 2 diabetes and CKD,” he said.
The link with reduction in albuminuria was weaker for the primary cardiovascular disease outcome: CV death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure. The strongest effect on this outcome was only seen in Kaplan-Meier analysis in those on finerenone who had at least a 30% reduction in their UACR. Those on placebo and with a similarly robust 4-month reduction in UACR showed a much more modest cardiovascular benefit that resembled those on either finerenone or placebo who had a smaller, less than 30% UACR reduction. The mediation analysis of these data showed that UACR reduction accounted for about 37% of the observed cardiovascular benefit seen during the trials.
“The effect of UACR is much stronger for the kidney outcomes,” summed up Dr. Agarwal. The results suggest that for cardiovascular outcomes finerenone works through factors other than lowering of UACR, but he admitted that no one currently knows what those other factors might be.
Treat aggressively to lower UACR by 30%
“I wouldn’t stop finerenone treatment in people who do not get a 30% reduction in their UACR” because these analyses suggest that a portion of the overall benefits from finerenone occurs via other mechanisms, he said. But in patients whose UACR is not reduced by at least 30% “be more aggressive on other measures to reduce UACR,” he advised.
The mediation analyses he ran are “the first time this has been done in nephrology,” producing a “groundbreaking” analysis and finding, Dr. Agarwal said. He also highlighted that the findings primarily relate to the importance of controlling UACR rather than an endorsement of finerenone as the best way to achieve this.
“All I care about is that people think about UACR as a modifiable risk factor. It doesn’t have to be treated with finerenone. It could be a renin-angiotensin system inhibitor, it could be chlorthalidone [a thiazide diuretic]. It just happened that we had a large dataset of people treated with finerenone or placebo.”
He said that future mediation analyses should look at the link between outcomes and UACR reductions produced by agents from the classes of sodium-glucose cotransporter 2 inhibitors and the glucagonlike peptide–1 receptor agonists.
FIDELIO-DKD and FIGARO-DKD were both sponsored by Bayer, the company that markets finerenone. Dr. Agarwal has received personal fees and nonfinancial support from Bayer. He has also received personal fees and nonfinancial support from Akebia Therapeutics, AstraZeneca, Boehringer Ingelheim, Eli Lilly, and Vifor Pharma, and he is a member of data safety monitoring committees for Chinook and Vertex. Dr. Inker is a consultant to Diamtrix, and her department receives research funding from Chinook, Omeros, Reata, and Tricida.
AT KIDNEY WEEK 2023
AI-ECG gets STEMI patients to cath lab sooner
PHILADELPHIA – An artificial intelligence platform that sends alerts based on electrocardiography results enabled cardiologists and emergency department physicians at a major hospital in Taiwan to move patients with ST-elevation myocardial infarction (STEMI) into the catheterization laboratory 9 minutes sooner than the conventional protocol that did not use AI.
“This is the first randomized clinical trial to demonstrate the reduction of electrocardiography to coronary cath lab activation time" from 52.3 to 43.3 minutes (P = .003), Chin Sheng Lin, MD, PhD, director of cardiology at the National Defense Medical Center Tri-Service General Hospital in Taipei City, said in presenting the results at the American Heart Association scientific sessions.

Dr. Lin reported results from the Artificial Intelligence Enabled Rapid Identify of ST-Elevation Myocardial Infarction Using Electrocardiogram (ARISE) trial. The trial included 43,994 patients who came to the hospital’s emergency and inpatient departments with at least one ECG but no history of coronary angiography (CAG) in the previous 3 days between May 2022 and April 2023.
They were randomly assigned by date to either AI-ECG for rapid identification and triage of STEMI or standard care. Overall, 145 patients were finally diagnosed with STEMI based on CAG, 77 in the intervention group and 68 in the control group. All patients were seen by one of 20 cardiologists who participated in the study.
Dr. Lin and his group developed an AI algorithm that captures the ECG readout in the emergency department, analyzes the data and then sends a high-risk alarm to the front-line physician and on-duty cardiologist to activate the primary percutaneous coronary intervention (PCI).
Trial results
The differentiation between groups was even more pronounced in ED patients during regular working hours, Dr. Lin said, at 61.6 minutes for the intervention group vs. 33.1 minutes for controls (P = .001).*
He noted that the AI group showed a trend towards fewer cases of clinically suspected STEMI but not getting CAG, 6.5% vs. 15.8%, for an odds ratio of 0.37 (95% confidence interval, 0.14-0.94).
The AI-ECG model also demonstrated a high diagnostic accuracy. “With this AI-ECG system, because it has a very high accuracy and a high positive predictive variable that reach 88%, we can send a message to the on-duty cardiologists and also the emergency room physician and they can send the patients to receive the operation or the PCI as soon as possible,” Dr. Lin said in an interview.
The time differential is critical, Dr. Lin said. “For the patient with acute myocardial infarction, 1 minute is critical, because the patients can die within minutes,” he said. “If we can save 9 minutes I think we can save more lives, but it needs a larger study to evaluate that.”
Dr. Lin acknowledged a few limitations with the trial, among them its single-center nature, relatively small sample size of STEMI patients and the short-term of follow-up. Future study should involve multiple centers along with a prehospital, emergency medical services AI-ECG model.
‘Novel’ for an AI trial
“This is an incredible application of an AI technology in a real-world problem,” said Brahmajee K. Nallamothu, MD, MPH, an interventional cardiologist at the University of Michigan, Ann Arbor, who did not participate in the study. “What I really love about this study is it’s actually a clinical problem that has large implications, particularly for under-resourced areas.”

Using a randomized clinical trial to evaluate the AI platform is “very, very novel,” he said, and called the time improvement “enormous.” Referencing Dr. Lin’s next steps for studying the AI-ECG platform, Dr. Nallamothu said, “if we could push this up even earlier to paramedics and EMTs and prehospital systems, there would be a lot of excitement there.”
He noted the sensitivity analysis resulted in a rate of 88.8% along with the positive predictive value of 88%. “Missing 1 out of 10 ST-elevation MIs in my eyes can still be considered a big deal, so we need to know if this is happening in particular types of patients, for example women versus men, or other groups.”
However, some investigations reported false activation rates as high as 33%, he said. “So, to say that, the positive predictive value is at 88% is really exciting and I think it can make a real inroads,” Dr. Nallamothu said.
Dr. Lin and Dr. Nallamothu have no relevant disclosures.
*Correction, 11/20/23: An earlier version of this article misstated in both trial arms the time to coronary catheterization lab activation.
PHILADELPHIA – An artificial intelligence platform that sends alerts based on electrocardiography results enabled cardiologists and emergency department physicians at a major hospital in Taiwan to move patients with ST-elevation myocardial infarction (STEMI) into the catheterization laboratory 9 minutes sooner than the conventional protocol that did not use AI.
“This is the first randomized clinical trial to demonstrate the reduction of electrocardiography to coronary cath lab activation time" from 52.3 to 43.3 minutes (P = .003), Chin Sheng Lin, MD, PhD, director of cardiology at the National Defense Medical Center Tri-Service General Hospital in Taipei City, said in presenting the results at the American Heart Association scientific sessions.
Dr. Lin reported results from the Artificial Intelligence Enabled Rapid Identify of ST-Elevation Myocardial Infarction Using Electrocardiogram (ARISE) trial. The trial included 43,994 patients who came to the hospital’s emergency and inpatient departments with at least one ECG but no history of coronary angiography (CAG) in the previous 3 days between May 2022 and April 2023.
They were randomly assigned by date to either AI-ECG for rapid identification and triage of STEMI or standard care. Overall, 145 patients were finally diagnosed with STEMI based on CAG, 77 in the intervention group and 68 in the control group. All patients were seen by one of 20 cardiologists who participated in the study.
Dr. Lin and his group developed an AI algorithm that captures the ECG readout in the emergency department, analyzes the data and then sends a high-risk alarm to the front-line physician and on-duty cardiologist to activate the primary percutaneous coronary intervention (PCI).
Trial results
The differentiation between groups was even more pronounced in ED patients during regular working hours, Dr. Lin said, at 61.6 minutes for the intervention group vs. 33.1 minutes for controls (P = .001).*
He noted that the AI group showed a trend towards fewer cases of clinically suspected STEMI but not getting CAG, 6.5% vs. 15.8%, for an odds ratio of 0.37 (95% confidence interval, 0.14-0.94).
The AI-ECG model also demonstrated a high diagnostic accuracy. “With this AI-ECG system, because it has a very high accuracy and a high positive predictive variable that reach 88%, we can send a message to the on-duty cardiologists and also the emergency room physician and they can send the patients to receive the operation or the PCI as soon as possible,” Dr. Lin said in an interview.
The time differential is critical, Dr. Lin said. “For the patient with acute myocardial infarction, 1 minute is critical, because the patients can die within minutes,” he said. “If we can save 9 minutes I think we can save more lives, but it needs a larger study to evaluate that.”
Dr. Lin acknowledged a few limitations with the trial, among them its single-center nature, relatively small sample size of STEMI patients and the short-term of follow-up. Future study should involve multiple centers along with a prehospital, emergency medical services AI-ECG model.
‘Novel’ for an AI trial
“This is an incredible application of an AI technology in a real-world problem,” said Brahmajee K. Nallamothu, MD, MPH, an interventional cardiologist at the University of Michigan, Ann Arbor, who did not participate in the study. “What I really love about this study is it’s actually a clinical problem that has large implications, particularly for under-resourced areas.”
Using a randomized clinical trial to evaluate the AI platform is “very, very novel,” he said, and called the time improvement “enormous.” Referencing Dr. Lin’s next steps for studying the AI-ECG platform, Dr. Nallamothu said, “if we could push this up even earlier to paramedics and EMTs and prehospital systems, there would be a lot of excitement there.”
He noted the sensitivity analysis resulted in a rate of 88.8% along with the positive predictive value of 88%. “Missing 1 out of 10 ST-elevation MIs in my eyes can still be considered a big deal, so we need to know if this is happening in particular types of patients, for example women versus men, or other groups.”
However, some investigations reported false activation rates as high as 33%, he said. “So, to say that, the positive predictive value is at 88% is really exciting and I think it can make a real inroads,” Dr. Nallamothu said.
Dr. Lin and Dr. Nallamothu have no relevant disclosures.
*Correction, 11/20/23: An earlier version of this article misstated in both trial arms the time to coronary catheterization lab activation.
PHILADELPHIA – An artificial intelligence platform that sends alerts based on electrocardiography results enabled cardiologists and emergency department physicians at a major hospital in Taiwan to move patients with ST-elevation myocardial infarction (STEMI) into the catheterization laboratory 9 minutes sooner than the conventional protocol that did not use AI.
“This is the first randomized clinical trial to demonstrate the reduction of electrocardiography to coronary cath lab activation time" from 52.3 to 43.3 minutes (P = .003), Chin Sheng Lin, MD, PhD, director of cardiology at the National Defense Medical Center Tri-Service General Hospital in Taipei City, said in presenting the results at the American Heart Association scientific sessions.
Dr. Lin reported results from the Artificial Intelligence Enabled Rapid Identify of ST-Elevation Myocardial Infarction Using Electrocardiogram (ARISE) trial. The trial included 43,994 patients who came to the hospital’s emergency and inpatient departments with at least one ECG but no history of coronary angiography (CAG) in the previous 3 days between May 2022 and April 2023.
They were randomly assigned by date to either AI-ECG for rapid identification and triage of STEMI or standard care. Overall, 145 patients were finally diagnosed with STEMI based on CAG, 77 in the intervention group and 68 in the control group. All patients were seen by one of 20 cardiologists who participated in the study.
Dr. Lin and his group developed an AI algorithm that captures the ECG readout in the emergency department, analyzes the data and then sends a high-risk alarm to the front-line physician and on-duty cardiologist to activate the primary percutaneous coronary intervention (PCI).
Trial results
The differentiation between groups was even more pronounced in ED patients during regular working hours, Dr. Lin said, at 61.6 minutes for the intervention group vs. 33.1 minutes for controls (P = .001).*
He noted that the AI group showed a trend towards fewer cases of clinically suspected STEMI but not getting CAG, 6.5% vs. 15.8%, for an odds ratio of 0.37 (95% confidence interval, 0.14-0.94).
The AI-ECG model also demonstrated a high diagnostic accuracy. “With this AI-ECG system, because it has a very high accuracy and a high positive predictive variable that reach 88%, we can send a message to the on-duty cardiologists and also the emergency room physician and they can send the patients to receive the operation or the PCI as soon as possible,” Dr. Lin said in an interview.
The time differential is critical, Dr. Lin said. “For the patient with acute myocardial infarction, 1 minute is critical, because the patients can die within minutes,” he said. “If we can save 9 minutes I think we can save more lives, but it needs a larger study to evaluate that.”
Dr. Lin acknowledged a few limitations with the trial, among them its single-center nature, relatively small sample size of STEMI patients and the short-term of follow-up. Future study should involve multiple centers along with a prehospital, emergency medical services AI-ECG model.
‘Novel’ for an AI trial
“This is an incredible application of an AI technology in a real-world problem,” said Brahmajee K. Nallamothu, MD, MPH, an interventional cardiologist at the University of Michigan, Ann Arbor, who did not participate in the study. “What I really love about this study is it’s actually a clinical problem that has large implications, particularly for under-resourced areas.”
Using a randomized clinical trial to evaluate the AI platform is “very, very novel,” he said, and called the time improvement “enormous.” Referencing Dr. Lin’s next steps for studying the AI-ECG platform, Dr. Nallamothu said, “if we could push this up even earlier to paramedics and EMTs and prehospital systems, there would be a lot of excitement there.”
He noted the sensitivity analysis resulted in a rate of 88.8% along with the positive predictive value of 88%. “Missing 1 out of 10 ST-elevation MIs in my eyes can still be considered a big deal, so we need to know if this is happening in particular types of patients, for example women versus men, or other groups.”
However, some investigations reported false activation rates as high as 33%, he said. “So, to say that, the positive predictive value is at 88% is really exciting and I think it can make a real inroads,” Dr. Nallamothu said.
Dr. Lin and Dr. Nallamothu have no relevant disclosures.
*Correction, 11/20/23: An earlier version of this article misstated in both trial arms the time to coronary catheterization lab activation.
AT AHA 2023
‘Love more’: Why doctors should promote social connection
Those who embrace lifestyle medicine are familiar with the slogan Dean Ornish, MD, likes to use: Eat well, move more, stress less, love more.
That last one, love, was the renowned physician and author’s focus at the recent American College of Lifestyle Medicine Conference in Denver. That’s because love – essentially the support, connectedness, and caring that patients feel when they join a lifestyle-change program – is “where healing occurs at the deepest level.”
Indeed, social connectedness is emerging as a vital pillar in the burgeoning field of lifestyle medicine, a specialty that uses lifestyle interventions to treat chronic conditions. About 300 lifestyle medicine programs are now integrated into residencies in medical schools across the country, up from a handful just 5 years ago, said Meagan Grega, MD, the conference chair.
“The energy and growth in American lifestyle medicine is unparalleled by anything else I see in the health care world right now,” said Dr. Grega, a family physician for 25 years in eastern Pennsylvania.
The field applies volumes of research, from the 1990s to today, demonstrating the healing effects of lifestyle changes. Dr. Ornish’s Preventive Medicine Research Institute has published research on small changes (like pomegranate juice helping blood flow in the heart) and huge ones: Coronary heart patients reversed the narrowing of arteries without lipid-lowering drugs after 1 year of lifestyle changes, including a vegetarian diet, aerobic exercise, stress management, and group support.
Ranking alongside bedrocks such as healthy diet, sleep, exercise, and stress management is positive social connection. That part, the “love more” part, often draws skepticism but is vital, said Dr. Ornish, who is sometimes referred to as the father of lifestyle medicine.
It’s “invariably the part that’s the most meaningful – that sense of connection to community that can come when you bring total strangers together,” Dr. Ornish said. “The ‘love more’ part, in many ways, is not only as important, but in some ways even more because everything really flows from that.”
Patients in a support group, who can “let down their emotional defenses and talk openly and authentically,” are much more likely to make and maintain healthy changes, Dr. Ornish said.
Love as medicine
Mounting evidence links loneliness and isolation with a range of health issues, from mood disorders such as depression to chronic conditions such as cardiovascular disease. What’s more, data suggest that loneliness and social isolation in the United States are on the rise, and the COVID pandemic made that more clear. In May 2023, Surgeon General Vivek Murthy, MD, called loneliness, isolation, and lack of connection in the United States a “public health crisis.”
“Good relationships keep us happier and healthier,” said Robert Waldinger, MD, a psychiatrist at Massachusetts General Hospital, Boston.
Dr. Waldinger, who was not affiliated with the conference, is head of the Harvard Study of Adult Development, one of the longest studies of adult life. Beginning in 1938, the study has tracked 724 people plus more than 1,300 of their descendants and found that embracing community and close relationships helps us live longer and be happier.
In the study, the people who were most satisfied with their relationships at age 50 years were the healthiest at age 80 years. Knowing you have someone to rely on protects the brain: “Those people’s memories stay sharper longer,” Dr. Waldinger said.
He draws a distinction between connection and love. “Love is, I think, more of a feeling,” Dr. Waldinger noted. “Connection is a feeling, but it’s also an activity.”
One in five Americans say they’re lonely, he said, “and loneliness is a stressor.” People who are isolated don’t sleep as well, he added. Their health declines earlier in midlife, brain function slips sooner, and their lives are shorter.
“You don’t have anyone to complain to,” he said. If you do, “you can feel your body start to calm down.” Those without social connections may stay in a low-level “fight-or-flight mode.”
“What we think happens is that you have low levels of inflammation chronically, and those can gradually break down body systems.” Moreover, higher rates of cardiac reactivity, for instance, a racing heartbeat when upset, can lead to high blood pressure and lower immune function.
In his talk, Dr. Ornish said, “Anger is that one emotion that has consistently been shown to make heart disease worse.”
Helping people in those straits is gratifying, Dr. Ornish said. “If we can work with people as lifestyle medicine practitioners when they’re suffering, there’s an opportunity for transformation.”
Future
Of course, that can be easier said than done. Dr. Ornish relayed a patient’s typical reaction to a lifestyle program: “This is kind of weird stuff. Like, I get diet. But a plant-based diet, really? Meditation? Loving more? Really?”
He told the conference, “Part of our job as lifestyle medicine practitioners is to spend a little extra time with them. It doesn’t even take that much time. And to really help them understand what brings them a sense of hope and meaning and purpose.”
The results can be motivating. “Most people feel so much better so quickly,” Dr. Ornish said. “It reframes the reason for change from fear of dying to joy of living.”
Dr. Grega, for one, is optimistic for the future, citing survey results showing that 95% of medical students think that they›d be better counselors with lifestyle training. ‘They passionately want this type of thing,” she said.
A version of this article first appeared on Medscape.com.
Those who embrace lifestyle medicine are familiar with the slogan Dean Ornish, MD, likes to use: Eat well, move more, stress less, love more.
That last one, love, was the renowned physician and author’s focus at the recent American College of Lifestyle Medicine Conference in Denver. That’s because love – essentially the support, connectedness, and caring that patients feel when they join a lifestyle-change program – is “where healing occurs at the deepest level.”
Indeed, social connectedness is emerging as a vital pillar in the burgeoning field of lifestyle medicine, a specialty that uses lifestyle interventions to treat chronic conditions. About 300 lifestyle medicine programs are now integrated into residencies in medical schools across the country, up from a handful just 5 years ago, said Meagan Grega, MD, the conference chair.
“The energy and growth in American lifestyle medicine is unparalleled by anything else I see in the health care world right now,” said Dr. Grega, a family physician for 25 years in eastern Pennsylvania.
The field applies volumes of research, from the 1990s to today, demonstrating the healing effects of lifestyle changes. Dr. Ornish’s Preventive Medicine Research Institute has published research on small changes (like pomegranate juice helping blood flow in the heart) and huge ones: Coronary heart patients reversed the narrowing of arteries without lipid-lowering drugs after 1 year of lifestyle changes, including a vegetarian diet, aerobic exercise, stress management, and group support.
Ranking alongside bedrocks such as healthy diet, sleep, exercise, and stress management is positive social connection. That part, the “love more” part, often draws skepticism but is vital, said Dr. Ornish, who is sometimes referred to as the father of lifestyle medicine.
It’s “invariably the part that’s the most meaningful – that sense of connection to community that can come when you bring total strangers together,” Dr. Ornish said. “The ‘love more’ part, in many ways, is not only as important, but in some ways even more because everything really flows from that.”
Patients in a support group, who can “let down their emotional defenses and talk openly and authentically,” are much more likely to make and maintain healthy changes, Dr. Ornish said.
Love as medicine
Mounting evidence links loneliness and isolation with a range of health issues, from mood disorders such as depression to chronic conditions such as cardiovascular disease. What’s more, data suggest that loneliness and social isolation in the United States are on the rise, and the COVID pandemic made that more clear. In May 2023, Surgeon General Vivek Murthy, MD, called loneliness, isolation, and lack of connection in the United States a “public health crisis.”
“Good relationships keep us happier and healthier,” said Robert Waldinger, MD, a psychiatrist at Massachusetts General Hospital, Boston.
Dr. Waldinger, who was not affiliated with the conference, is head of the Harvard Study of Adult Development, one of the longest studies of adult life. Beginning in 1938, the study has tracked 724 people plus more than 1,300 of their descendants and found that embracing community and close relationships helps us live longer and be happier.
In the study, the people who were most satisfied with their relationships at age 50 years were the healthiest at age 80 years. Knowing you have someone to rely on protects the brain: “Those people’s memories stay sharper longer,” Dr. Waldinger said.
He draws a distinction between connection and love. “Love is, I think, more of a feeling,” Dr. Waldinger noted. “Connection is a feeling, but it’s also an activity.”
One in five Americans say they’re lonely, he said, “and loneliness is a stressor.” People who are isolated don’t sleep as well, he added. Their health declines earlier in midlife, brain function slips sooner, and their lives are shorter.
“You don’t have anyone to complain to,” he said. If you do, “you can feel your body start to calm down.” Those without social connections may stay in a low-level “fight-or-flight mode.”
“What we think happens is that you have low levels of inflammation chronically, and those can gradually break down body systems.” Moreover, higher rates of cardiac reactivity, for instance, a racing heartbeat when upset, can lead to high blood pressure and lower immune function.
In his talk, Dr. Ornish said, “Anger is that one emotion that has consistently been shown to make heart disease worse.”
Helping people in those straits is gratifying, Dr. Ornish said. “If we can work with people as lifestyle medicine practitioners when they’re suffering, there’s an opportunity for transformation.”
Future
Of course, that can be easier said than done. Dr. Ornish relayed a patient’s typical reaction to a lifestyle program: “This is kind of weird stuff. Like, I get diet. But a plant-based diet, really? Meditation? Loving more? Really?”
He told the conference, “Part of our job as lifestyle medicine practitioners is to spend a little extra time with them. It doesn’t even take that much time. And to really help them understand what brings them a sense of hope and meaning and purpose.”
The results can be motivating. “Most people feel so much better so quickly,” Dr. Ornish said. “It reframes the reason for change from fear of dying to joy of living.”
Dr. Grega, for one, is optimistic for the future, citing survey results showing that 95% of medical students think that they›d be better counselors with lifestyle training. ‘They passionately want this type of thing,” she said.
A version of this article first appeared on Medscape.com.
Those who embrace lifestyle medicine are familiar with the slogan Dean Ornish, MD, likes to use: Eat well, move more, stress less, love more.
That last one, love, was the renowned physician and author’s focus at the recent American College of Lifestyle Medicine Conference in Denver. That’s because love – essentially the support, connectedness, and caring that patients feel when they join a lifestyle-change program – is “where healing occurs at the deepest level.”
Indeed, social connectedness is emerging as a vital pillar in the burgeoning field of lifestyle medicine, a specialty that uses lifestyle interventions to treat chronic conditions. About 300 lifestyle medicine programs are now integrated into residencies in medical schools across the country, up from a handful just 5 years ago, said Meagan Grega, MD, the conference chair.
“The energy and growth in American lifestyle medicine is unparalleled by anything else I see in the health care world right now,” said Dr. Grega, a family physician for 25 years in eastern Pennsylvania.
The field applies volumes of research, from the 1990s to today, demonstrating the healing effects of lifestyle changes. Dr. Ornish’s Preventive Medicine Research Institute has published research on small changes (like pomegranate juice helping blood flow in the heart) and huge ones: Coronary heart patients reversed the narrowing of arteries without lipid-lowering drugs after 1 year of lifestyle changes, including a vegetarian diet, aerobic exercise, stress management, and group support.
Ranking alongside bedrocks such as healthy diet, sleep, exercise, and stress management is positive social connection. That part, the “love more” part, often draws skepticism but is vital, said Dr. Ornish, who is sometimes referred to as the father of lifestyle medicine.
It’s “invariably the part that’s the most meaningful – that sense of connection to community that can come when you bring total strangers together,” Dr. Ornish said. “The ‘love more’ part, in many ways, is not only as important, but in some ways even more because everything really flows from that.”
Patients in a support group, who can “let down their emotional defenses and talk openly and authentically,” are much more likely to make and maintain healthy changes, Dr. Ornish said.
Love as medicine
Mounting evidence links loneliness and isolation with a range of health issues, from mood disorders such as depression to chronic conditions such as cardiovascular disease. What’s more, data suggest that loneliness and social isolation in the United States are on the rise, and the COVID pandemic made that more clear. In May 2023, Surgeon General Vivek Murthy, MD, called loneliness, isolation, and lack of connection in the United States a “public health crisis.”
“Good relationships keep us happier and healthier,” said Robert Waldinger, MD, a psychiatrist at Massachusetts General Hospital, Boston.
Dr. Waldinger, who was not affiliated with the conference, is head of the Harvard Study of Adult Development, one of the longest studies of adult life. Beginning in 1938, the study has tracked 724 people plus more than 1,300 of their descendants and found that embracing community and close relationships helps us live longer and be happier.
In the study, the people who were most satisfied with their relationships at age 50 years were the healthiest at age 80 years. Knowing you have someone to rely on protects the brain: “Those people’s memories stay sharper longer,” Dr. Waldinger said.
He draws a distinction between connection and love. “Love is, I think, more of a feeling,” Dr. Waldinger noted. “Connection is a feeling, but it’s also an activity.”
One in five Americans say they’re lonely, he said, “and loneliness is a stressor.” People who are isolated don’t sleep as well, he added. Their health declines earlier in midlife, brain function slips sooner, and their lives are shorter.
“You don’t have anyone to complain to,” he said. If you do, “you can feel your body start to calm down.” Those without social connections may stay in a low-level “fight-or-flight mode.”
“What we think happens is that you have low levels of inflammation chronically, and those can gradually break down body systems.” Moreover, higher rates of cardiac reactivity, for instance, a racing heartbeat when upset, can lead to high blood pressure and lower immune function.
In his talk, Dr. Ornish said, “Anger is that one emotion that has consistently been shown to make heart disease worse.”
Helping people in those straits is gratifying, Dr. Ornish said. “If we can work with people as lifestyle medicine practitioners when they’re suffering, there’s an opportunity for transformation.”
Future
Of course, that can be easier said than done. Dr. Ornish relayed a patient’s typical reaction to a lifestyle program: “This is kind of weird stuff. Like, I get diet. But a plant-based diet, really? Meditation? Loving more? Really?”
He told the conference, “Part of our job as lifestyle medicine practitioners is to spend a little extra time with them. It doesn’t even take that much time. And to really help them understand what brings them a sense of hope and meaning and purpose.”
The results can be motivating. “Most people feel so much better so quickly,” Dr. Ornish said. “It reframes the reason for change from fear of dying to joy of living.”
Dr. Grega, for one, is optimistic for the future, citing survey results showing that 95% of medical students think that they›d be better counselors with lifestyle training. ‘They passionately want this type of thing,” she said.
A version of this article first appeared on Medscape.com.
First referral guide issued for axial spondyloarthritis
SAN DIEGO – The Spondyloarthritis Research and Treatment Network (SPARTAN) has created the first referral recommendations for axial spondyloarthritis (axSpA).
The draft recommendations use a points scoring system, with the goal that at least one in three patients referred would be diagnosed with axSpA, an inflammatory arthritis that affects the central skeleton and shares a genetic overlap with skin psoriasis, inflammatory bowel disease, and inflammatory eye disease.

Patients with axSpA can wait 10 years after symptom onset to be diagnosed with the condition. There are currently no guidelines to advise clinicians on when to refer to a rheumatologist, and with the rheumatology workforce shortage, “it is impossible for rheumatologists to evaluate the 20% of adults in the U.S. who have chronic back pain,” said Maureen Dubreuil, MD, a rheumatologist at Boston University. She presented the work at the annual meeting of the American College of Rheumatology.
To address this issue, Dr. Dubreuil and colleagues conducted a literature review to determine how predictive different spondyloarthritis features were of eventual axSpA diagnosis. The interdisciplinary team identified 38 studies published before March 2022, and uncovered 28 individual potential features associated with axSpA, including pain sites, family history of axSpA and related conditions, blood markers of inflammation, genetic testing, and imaging findings.
Inflammatory back pain elements had the lower predictive values, with positive likelihood ratios (LR+) ranging from 1.15 to 2.32, while imaging findings were the most predictive (LR+s from 6.40 to 10.02).
Using a Delphi exercise and discrete choice experiments, members narrowed the checklist down to 10 features. These 10 features were assigned points, with a score of 3 points qualifying for a referral of adults 45 years or younger with chronic pain (3 or more months) in the back, hip, or buttock.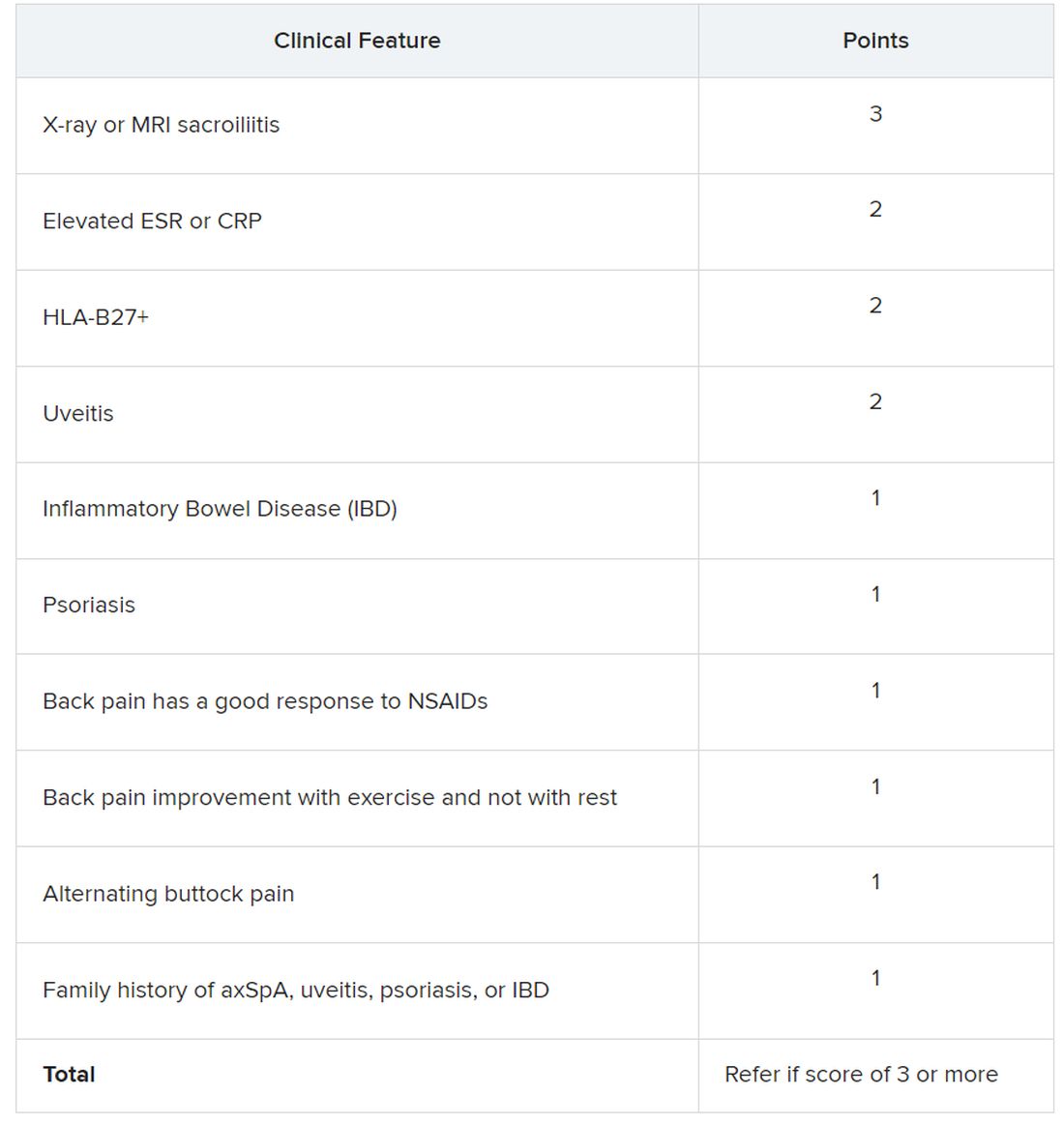
Sacroiliitis seen on imaging, either by x-ray or MRI, received the highest score of 3 points. Dr. Dubreuil emphasized that imaging was not required for a referral, but if a patient has received imaging “that shows sacroiliitis, that is sufficient for referral to a rheumatologist,” she said in her presentation.
Elevated erythrocyte sedimentation rate or C-reactive protein, HLA-B27 positivity, and uveitis score 2 points. Inflammatory bowel disease; psoriasis; back pain with good response to NSAIDs; back pain improvement with exercise and not with rest; alternating buttock pain; and family history of axial spondyloarthritis, uveitis, psoriasis, or IBD score 1 point.
Dr. Dubreuil and colleagues expect that these criteria for referral will result in about one in three referred adults aged 45 years or younger with chronic back pain being diagnosed with axSpA. They also say additional research is necessary to understand if these recommendations increase probability of axSpA diagnosis and reduce diagnostic delays.
“We’re now getting to the stage where we are creating this screening tool, but [testing the] performance of the screening tool is going to be the major next step,” said Mark Hwang, MD, of UTHealth Houston in an interview with this news organization. He is a member of SPARTAN but was not involved with authoring the recommendations. “Will the screening tool enhance the ability on the back end to identify axSpA? We don’t know yet.”
Jon Chan, MD, a rheumatologist at the University of British Columbia, Vancouver, agreed that these recommendations “are a good first step,” but that more awareness about axSpA from nonrheumatologists would also be helpful in identifying new axSpA patients. He is also a member of SPARTAN and comoderated with Dr. Hwang the session where the new recommendations were presented. “I think other diseases like rheumatoid arthritis or lupus have a lot more recognition in the nonrheumatology community,” he told this news organization.
Connecting with other health professionals who see a lot of patients with back pain – physiotherapists, chiropractors, and chronic pain physicians – could also be helpful, he added. “A lot of times, patients go straight to a physio and circumvent the doctor,” he said.
Dr. Chan reports success in educating other departments. “I put up a poster in the emergency department saying, ‘If you’re young with back pain and uveitis, you need to be seen by rheumatology,’ and we’ve identified a ton of axSpA patients that way,” he said. “Maybe their uveitis was very mild, but their back pain was quite severe, and no one really clued in.”
Dr. Dubreuil disclosed financial relationships with Amgen, Pfizer, and UCB Pharma. Her abstract coauthors disclosed financial relationships with multiple pharmaceutical companies. Dr. Hwang consults for UCB and has received research support from Janssen. Dr. Chan has relationships with AbbVie/Abbott, Eli Lilly, Janssen, Novartis, and UCB.
SAN DIEGO – The Spondyloarthritis Research and Treatment Network (SPARTAN) has created the first referral recommendations for axial spondyloarthritis (axSpA).
The draft recommendations use a points scoring system, with the goal that at least one in three patients referred would be diagnosed with axSpA, an inflammatory arthritis that affects the central skeleton and shares a genetic overlap with skin psoriasis, inflammatory bowel disease, and inflammatory eye disease.
Patients with axSpA can wait 10 years after symptom onset to be diagnosed with the condition. There are currently no guidelines to advise clinicians on when to refer to a rheumatologist, and with the rheumatology workforce shortage, “it is impossible for rheumatologists to evaluate the 20% of adults in the U.S. who have chronic back pain,” said Maureen Dubreuil, MD, a rheumatologist at Boston University. She presented the work at the annual meeting of the American College of Rheumatology.
To address this issue, Dr. Dubreuil and colleagues conducted a literature review to determine how predictive different spondyloarthritis features were of eventual axSpA diagnosis. The interdisciplinary team identified 38 studies published before March 2022, and uncovered 28 individual potential features associated with axSpA, including pain sites, family history of axSpA and related conditions, blood markers of inflammation, genetic testing, and imaging findings.
Inflammatory back pain elements had the lower predictive values, with positive likelihood ratios (LR+) ranging from 1.15 to 2.32, while imaging findings were the most predictive (LR+s from 6.40 to 10.02).
Using a Delphi exercise and discrete choice experiments, members narrowed the checklist down to 10 features. These 10 features were assigned points, with a score of 3 points qualifying for a referral of adults 45 years or younger with chronic pain (3 or more months) in the back, hip, or buttock.
Sacroiliitis seen on imaging, either by x-ray or MRI, received the highest score of 3 points. Dr. Dubreuil emphasized that imaging was not required for a referral, but if a patient has received imaging “that shows sacroiliitis, that is sufficient for referral to a rheumatologist,” she said in her presentation.
Elevated erythrocyte sedimentation rate or C-reactive protein, HLA-B27 positivity, and uveitis score 2 points. Inflammatory bowel disease; psoriasis; back pain with good response to NSAIDs; back pain improvement with exercise and not with rest; alternating buttock pain; and family history of axial spondyloarthritis, uveitis, psoriasis, or IBD score 1 point.
Dr. Dubreuil and colleagues expect that these criteria for referral will result in about one in three referred adults aged 45 years or younger with chronic back pain being diagnosed with axSpA. They also say additional research is necessary to understand if these recommendations increase probability of axSpA diagnosis and reduce diagnostic delays.
“We’re now getting to the stage where we are creating this screening tool, but [testing the] performance of the screening tool is going to be the major next step,” said Mark Hwang, MD, of UTHealth Houston in an interview with this news organization. He is a member of SPARTAN but was not involved with authoring the recommendations. “Will the screening tool enhance the ability on the back end to identify axSpA? We don’t know yet.”
Jon Chan, MD, a rheumatologist at the University of British Columbia, Vancouver, agreed that these recommendations “are a good first step,” but that more awareness about axSpA from nonrheumatologists would also be helpful in identifying new axSpA patients. He is also a member of SPARTAN and comoderated with Dr. Hwang the session where the new recommendations were presented. “I think other diseases like rheumatoid arthritis or lupus have a lot more recognition in the nonrheumatology community,” he told this news organization.
Connecting with other health professionals who see a lot of patients with back pain – physiotherapists, chiropractors, and chronic pain physicians – could also be helpful, he added. “A lot of times, patients go straight to a physio and circumvent the doctor,” he said.
Dr. Chan reports success in educating other departments. “I put up a poster in the emergency department saying, ‘If you’re young with back pain and uveitis, you need to be seen by rheumatology,’ and we’ve identified a ton of axSpA patients that way,” he said. “Maybe their uveitis was very mild, but their back pain was quite severe, and no one really clued in.”
Dr. Dubreuil disclosed financial relationships with Amgen, Pfizer, and UCB Pharma. Her abstract coauthors disclosed financial relationships with multiple pharmaceutical companies. Dr. Hwang consults for UCB and has received research support from Janssen. Dr. Chan has relationships with AbbVie/Abbott, Eli Lilly, Janssen, Novartis, and UCB.
SAN DIEGO – The Spondyloarthritis Research and Treatment Network (SPARTAN) has created the first referral recommendations for axial spondyloarthritis (axSpA).
The draft recommendations use a points scoring system, with the goal that at least one in three patients referred would be diagnosed with axSpA, an inflammatory arthritis that affects the central skeleton and shares a genetic overlap with skin psoriasis, inflammatory bowel disease, and inflammatory eye disease.
Patients with axSpA can wait 10 years after symptom onset to be diagnosed with the condition. There are currently no guidelines to advise clinicians on when to refer to a rheumatologist, and with the rheumatology workforce shortage, “it is impossible for rheumatologists to evaluate the 20% of adults in the U.S. who have chronic back pain,” said Maureen Dubreuil, MD, a rheumatologist at Boston University. She presented the work at the annual meeting of the American College of Rheumatology.
To address this issue, Dr. Dubreuil and colleagues conducted a literature review to determine how predictive different spondyloarthritis features were of eventual axSpA diagnosis. The interdisciplinary team identified 38 studies published before March 2022, and uncovered 28 individual potential features associated with axSpA, including pain sites, family history of axSpA and related conditions, blood markers of inflammation, genetic testing, and imaging findings.
Inflammatory back pain elements had the lower predictive values, with positive likelihood ratios (LR+) ranging from 1.15 to 2.32, while imaging findings were the most predictive (LR+s from 6.40 to 10.02).
Using a Delphi exercise and discrete choice experiments, members narrowed the checklist down to 10 features. These 10 features were assigned points, with a score of 3 points qualifying for a referral of adults 45 years or younger with chronic pain (3 or more months) in the back, hip, or buttock.
Sacroiliitis seen on imaging, either by x-ray or MRI, received the highest score of 3 points. Dr. Dubreuil emphasized that imaging was not required for a referral, but if a patient has received imaging “that shows sacroiliitis, that is sufficient for referral to a rheumatologist,” she said in her presentation.
Elevated erythrocyte sedimentation rate or C-reactive protein, HLA-B27 positivity, and uveitis score 2 points. Inflammatory bowel disease; psoriasis; back pain with good response to NSAIDs; back pain improvement with exercise and not with rest; alternating buttock pain; and family history of axial spondyloarthritis, uveitis, psoriasis, or IBD score 1 point.
Dr. Dubreuil and colleagues expect that these criteria for referral will result in about one in three referred adults aged 45 years or younger with chronic back pain being diagnosed with axSpA. They also say additional research is necessary to understand if these recommendations increase probability of axSpA diagnosis and reduce diagnostic delays.
“We’re now getting to the stage where we are creating this screening tool, but [testing the] performance of the screening tool is going to be the major next step,” said Mark Hwang, MD, of UTHealth Houston in an interview with this news organization. He is a member of SPARTAN but was not involved with authoring the recommendations. “Will the screening tool enhance the ability on the back end to identify axSpA? We don’t know yet.”
Jon Chan, MD, a rheumatologist at the University of British Columbia, Vancouver, agreed that these recommendations “are a good first step,” but that more awareness about axSpA from nonrheumatologists would also be helpful in identifying new axSpA patients. He is also a member of SPARTAN and comoderated with Dr. Hwang the session where the new recommendations were presented. “I think other diseases like rheumatoid arthritis or lupus have a lot more recognition in the nonrheumatology community,” he told this news organization.
Connecting with other health professionals who see a lot of patients with back pain – physiotherapists, chiropractors, and chronic pain physicians – could also be helpful, he added. “A lot of times, patients go straight to a physio and circumvent the doctor,” he said.
Dr. Chan reports success in educating other departments. “I put up a poster in the emergency department saying, ‘If you’re young with back pain and uveitis, you need to be seen by rheumatology,’ and we’ve identified a ton of axSpA patients that way,” he said. “Maybe their uveitis was very mild, but their back pain was quite severe, and no one really clued in.”
Dr. Dubreuil disclosed financial relationships with Amgen, Pfizer, and UCB Pharma. Her abstract coauthors disclosed financial relationships with multiple pharmaceutical companies. Dr. Hwang consults for UCB and has received research support from Janssen. Dr. Chan has relationships with AbbVie/Abbott, Eli Lilly, Janssen, Novartis, and UCB.
AT ACR 2023
Pharmacist-based strategy places more patients on statins
Visit-based strategy has more modest effect
PHILADELPHIA – In two studies run in parallel fashion to test different strategies, one that employed automatic referral to a pharmacist appeared to be superior to one using alerts from the electronic health record (EHR) in increasing the number of at-risk patients receiving a prescription for statins.
, reported Alexander C. Faranoff, MD, assistant professor of cardiovascular medicine at Penn Medicine, Philadelphia.
The parallel studies were part of the SUPER LIPID program, created to generate evidence-based strategies for increasing the proportion of at-risk patients on statins. Dr. Faranoff said current data show that at least 50% of patients indicated for high-intensity statins in the United States are not taking them.
The two studies were presented together in a late breaking presentation at the American Heart Association scientific sessions.
EHR algorithm identifies statin candidates
The candidates for statin therapy were identified through an EHR algorithm for both studies. Both compared the impact of the intervention against a baseline period of usual care, although the study of EHR alerts also randomized physicians to provide usual care for 3 months or 6 months prior to intervention.
Dr. Faranoff described these interventions as non–visit related and visit related.
In the study of the non–visit-related strategy, referrals were generated by EHR and sent directly to the pharmacist. Upon receipt, the pharmacist verified the order was appropriate and called the patient directly to discuss starting therapy. Patients agreeing to start a statin were provided with a prescription and followed by the pharmacist.
In the study of the patient-visit approach, physicians seeing EHR-identified candidates received interruptive pop-up alerts during patient encounters. The physicians were randomized to provide usual care for 3 or 6 months before they began receiving alerts. The alerts recommended referral to a pharmacist.
During usual care in the non–visit-related study, only 15.2% of the 975 candidates for statins received a prescription. During the intervention period, the rate climbed to 31.6%. Statistically, the intervention more than doubled the odds ratio (OR) of receiving a statin prescription relative to usual care (OR 2.22; 95% confidence interval [CI] 1.47-3.37).
In addition, the proportion of patients receiving an appropriate dose of statins climbed from 7.7% in the period of usual care to 24.8% in the intervention period (OR 6.79; 95% CI 4.00-11.53).
Visit-based study also randomized
In the study evaluating a visit-based intervention, 16 physicians were randomized to deliver usual care for 3 or 6 months. Of physicians randomized to 3 months, 970 candidates for statins were treated during the 6-month intervention period. The physicians randomized to usual care for 6 months treated 672 candidates for statins during a 3-month intervention period,
More than 3,000 alerts were sent to both groups of physicians over the intervention period. Only 165 (4.6%) were associated with a prescription.
For the group randomized to 3 months of usual care, the proportion of candidates for statins who received a prescription rose from 14.9% during the period of usual care to 17.6% in the first 3 months of intervention and then fell slightly to 15.5% in the second 3 months.
For the group randomized to usual care for 6 months, the proportion of candidates for statins who received a prescription rose from about 11% during the period of usual care to 14.6%. Combining data from both arms, the small gain in prescriptions was significant but modest (OR 1.43; 95% CI 1.02-2.00).
In addition, the visit-based EHR notifications failed to yield a significant gain in the proportion of patients on an appropriate statin dose. During the intervention period, this proportion was only about 9% of patients treated by either of the two groups of randomized physicians,
The SUPER LIPID program involved 11 internal medicine and family medicine clinics in rural Pennsylvania. In the visit-based intervention, 16 primary care physicians (PCPs) were randomized. In the asynchronous intervention, 10 primary care practices participated. The EHR identified a total of 1,950 candidates for a statin.
Although the gain in statin prescriptions was disappointing for the visit-based intervention, the strategy of using the EHR to refer statin-eligible patients to pharmacists “could be an effective adjunct to visit-based clinical interactions in increasing statin prescribing for high-risk patients,” Dr. Faranoff maintained.
Overcoming clinical inertia a challenge
The greater efficacy of a pharmacist-based approach did not surprise the AHA-invited discussant, Benjamin M. Scirica, MD, associate professor of medicine at Harvard Medical School, Boston.
Pointing out that the pharmacist-based strategy of increasing statin prescriptions is more complicated and more costly, he said, “You get what you pay for.” In his opinion, simple solutions are unlikely ever to be effective due to the complex reasons for clinical inertia. Overall, he thinks a multifaceted approach to placing more patients who need statins on therapy is essential.
“Implementation science is hard,” Dr. Scirica said. Even though the referral-to-a-pharmacist approach ended up putting more patients on statins and putting them on an appropriate dose, he said even this more effective strategy “is still not getting to the majority of patients.”
This does not mean that this approach is without merit or should not be one of many strategies employed, but Dr. Scirica said “there is so much more to be done,” and that it should be employed along with other initiatives.
Faranoff reports no potential conflicts of interest. Dr. Scirica reports financial relationships with AbbVie, Aktiia, AstraZeneca, Better Therapeutics, Boehringer-Ingelheim, Eisai, GlaxoSmithKline, Hanmi, Lexicon, Merck, Novartis, Novo Nordisk, Pfizer, and Sanofi.
Visit-based strategy has more modest effect
Visit-based strategy has more modest effect
PHILADELPHIA – In two studies run in parallel fashion to test different strategies, one that employed automatic referral to a pharmacist appeared to be superior to one using alerts from the electronic health record (EHR) in increasing the number of at-risk patients receiving a prescription for statins.
, reported Alexander C. Faranoff, MD, assistant professor of cardiovascular medicine at Penn Medicine, Philadelphia.
The parallel studies were part of the SUPER LIPID program, created to generate evidence-based strategies for increasing the proportion of at-risk patients on statins. Dr. Faranoff said current data show that at least 50% of patients indicated for high-intensity statins in the United States are not taking them.
The two studies were presented together in a late breaking presentation at the American Heart Association scientific sessions.
EHR algorithm identifies statin candidates
The candidates for statin therapy were identified through an EHR algorithm for both studies. Both compared the impact of the intervention against a baseline period of usual care, although the study of EHR alerts also randomized physicians to provide usual care for 3 months or 6 months prior to intervention.
Dr. Faranoff described these interventions as non–visit related and visit related.
In the study of the non–visit-related strategy, referrals were generated by EHR and sent directly to the pharmacist. Upon receipt, the pharmacist verified the order was appropriate and called the patient directly to discuss starting therapy. Patients agreeing to start a statin were provided with a prescription and followed by the pharmacist.
In the study of the patient-visit approach, physicians seeing EHR-identified candidates received interruptive pop-up alerts during patient encounters. The physicians were randomized to provide usual care for 3 or 6 months before they began receiving alerts. The alerts recommended referral to a pharmacist.
During usual care in the non–visit-related study, only 15.2% of the 975 candidates for statins received a prescription. During the intervention period, the rate climbed to 31.6%. Statistically, the intervention more than doubled the odds ratio (OR) of receiving a statin prescription relative to usual care (OR 2.22; 95% confidence interval [CI] 1.47-3.37).
In addition, the proportion of patients receiving an appropriate dose of statins climbed from 7.7% in the period of usual care to 24.8% in the intervention period (OR 6.79; 95% CI 4.00-11.53).
Visit-based study also randomized
In the study evaluating a visit-based intervention, 16 physicians were randomized to deliver usual care for 3 or 6 months. Of physicians randomized to 3 months, 970 candidates for statins were treated during the 6-month intervention period. The physicians randomized to usual care for 6 months treated 672 candidates for statins during a 3-month intervention period,
More than 3,000 alerts were sent to both groups of physicians over the intervention period. Only 165 (4.6%) were associated with a prescription.
For the group randomized to 3 months of usual care, the proportion of candidates for statins who received a prescription rose from 14.9% during the period of usual care to 17.6% in the first 3 months of intervention and then fell slightly to 15.5% in the second 3 months.
For the group randomized to usual care for 6 months, the proportion of candidates for statins who received a prescription rose from about 11% during the period of usual care to 14.6%. Combining data from both arms, the small gain in prescriptions was significant but modest (OR 1.43; 95% CI 1.02-2.00).
In addition, the visit-based EHR notifications failed to yield a significant gain in the proportion of patients on an appropriate statin dose. During the intervention period, this proportion was only about 9% of patients treated by either of the two groups of randomized physicians,
The SUPER LIPID program involved 11 internal medicine and family medicine clinics in rural Pennsylvania. In the visit-based intervention, 16 primary care physicians (PCPs) were randomized. In the asynchronous intervention, 10 primary care practices participated. The EHR identified a total of 1,950 candidates for a statin.
Although the gain in statin prescriptions was disappointing for the visit-based intervention, the strategy of using the EHR to refer statin-eligible patients to pharmacists “could be an effective adjunct to visit-based clinical interactions in increasing statin prescribing for high-risk patients,” Dr. Faranoff maintained.
Overcoming clinical inertia a challenge
The greater efficacy of a pharmacist-based approach did not surprise the AHA-invited discussant, Benjamin M. Scirica, MD, associate professor of medicine at Harvard Medical School, Boston.
Pointing out that the pharmacist-based strategy of increasing statin prescriptions is more complicated and more costly, he said, “You get what you pay for.” In his opinion, simple solutions are unlikely ever to be effective due to the complex reasons for clinical inertia. Overall, he thinks a multifaceted approach to placing more patients who need statins on therapy is essential.
“Implementation science is hard,” Dr. Scirica said. Even though the referral-to-a-pharmacist approach ended up putting more patients on statins and putting them on an appropriate dose, he said even this more effective strategy “is still not getting to the majority of patients.”
This does not mean that this approach is without merit or should not be one of many strategies employed, but Dr. Scirica said “there is so much more to be done,” and that it should be employed along with other initiatives.
Faranoff reports no potential conflicts of interest. Dr. Scirica reports financial relationships with AbbVie, Aktiia, AstraZeneca, Better Therapeutics, Boehringer-Ingelheim, Eisai, GlaxoSmithKline, Hanmi, Lexicon, Merck, Novartis, Novo Nordisk, Pfizer, and Sanofi.
PHILADELPHIA – In two studies run in parallel fashion to test different strategies, one that employed automatic referral to a pharmacist appeared to be superior to one using alerts from the electronic health record (EHR) in increasing the number of at-risk patients receiving a prescription for statins.
, reported Alexander C. Faranoff, MD, assistant professor of cardiovascular medicine at Penn Medicine, Philadelphia.
The parallel studies were part of the SUPER LIPID program, created to generate evidence-based strategies for increasing the proportion of at-risk patients on statins. Dr. Faranoff said current data show that at least 50% of patients indicated for high-intensity statins in the United States are not taking them.
The two studies were presented together in a late breaking presentation at the American Heart Association scientific sessions.
EHR algorithm identifies statin candidates
The candidates for statin therapy were identified through an EHR algorithm for both studies. Both compared the impact of the intervention against a baseline period of usual care, although the study of EHR alerts also randomized physicians to provide usual care for 3 months or 6 months prior to intervention.
Dr. Faranoff described these interventions as non–visit related and visit related.
In the study of the non–visit-related strategy, referrals were generated by EHR and sent directly to the pharmacist. Upon receipt, the pharmacist verified the order was appropriate and called the patient directly to discuss starting therapy. Patients agreeing to start a statin were provided with a prescription and followed by the pharmacist.
In the study of the patient-visit approach, physicians seeing EHR-identified candidates received interruptive pop-up alerts during patient encounters. The physicians were randomized to provide usual care for 3 or 6 months before they began receiving alerts. The alerts recommended referral to a pharmacist.
During usual care in the non–visit-related study, only 15.2% of the 975 candidates for statins received a prescription. During the intervention period, the rate climbed to 31.6%. Statistically, the intervention more than doubled the odds ratio (OR) of receiving a statin prescription relative to usual care (OR 2.22; 95% confidence interval [CI] 1.47-3.37).
In addition, the proportion of patients receiving an appropriate dose of statins climbed from 7.7% in the period of usual care to 24.8% in the intervention period (OR 6.79; 95% CI 4.00-11.53).
Visit-based study also randomized
In the study evaluating a visit-based intervention, 16 physicians were randomized to deliver usual care for 3 or 6 months. Of physicians randomized to 3 months, 970 candidates for statins were treated during the 6-month intervention period. The physicians randomized to usual care for 6 months treated 672 candidates for statins during a 3-month intervention period,
More than 3,000 alerts were sent to both groups of physicians over the intervention period. Only 165 (4.6%) were associated with a prescription.
For the group randomized to 3 months of usual care, the proportion of candidates for statins who received a prescription rose from 14.9% during the period of usual care to 17.6% in the first 3 months of intervention and then fell slightly to 15.5% in the second 3 months.
For the group randomized to usual care for 6 months, the proportion of candidates for statins who received a prescription rose from about 11% during the period of usual care to 14.6%. Combining data from both arms, the small gain in prescriptions was significant but modest (OR 1.43; 95% CI 1.02-2.00).
In addition, the visit-based EHR notifications failed to yield a significant gain in the proportion of patients on an appropriate statin dose. During the intervention period, this proportion was only about 9% of patients treated by either of the two groups of randomized physicians,
The SUPER LIPID program involved 11 internal medicine and family medicine clinics in rural Pennsylvania. In the visit-based intervention, 16 primary care physicians (PCPs) were randomized. In the asynchronous intervention, 10 primary care practices participated. The EHR identified a total of 1,950 candidates for a statin.
Although the gain in statin prescriptions was disappointing for the visit-based intervention, the strategy of using the EHR to refer statin-eligible patients to pharmacists “could be an effective adjunct to visit-based clinical interactions in increasing statin prescribing for high-risk patients,” Dr. Faranoff maintained.
Overcoming clinical inertia a challenge
The greater efficacy of a pharmacist-based approach did not surprise the AHA-invited discussant, Benjamin M. Scirica, MD, associate professor of medicine at Harvard Medical School, Boston.
Pointing out that the pharmacist-based strategy of increasing statin prescriptions is more complicated and more costly, he said, “You get what you pay for.” In his opinion, simple solutions are unlikely ever to be effective due to the complex reasons for clinical inertia. Overall, he thinks a multifaceted approach to placing more patients who need statins on therapy is essential.
“Implementation science is hard,” Dr. Scirica said. Even though the referral-to-a-pharmacist approach ended up putting more patients on statins and putting them on an appropriate dose, he said even this more effective strategy “is still not getting to the majority of patients.”
This does not mean that this approach is without merit or should not be one of many strategies employed, but Dr. Scirica said “there is so much more to be done,” and that it should be employed along with other initiatives.
Faranoff reports no potential conflicts of interest. Dr. Scirica reports financial relationships with AbbVie, Aktiia, AstraZeneca, Better Therapeutics, Boehringer-Ingelheim, Eisai, GlaxoSmithKline, Hanmi, Lexicon, Merck, Novartis, Novo Nordisk, Pfizer, and Sanofi.
AT AHA 2023
Low-salt diet cut BP by 6 mm Hg in 1 week: CARDIA-SSBP
The CARDIA-SSBP trial involved 213 individuals aged 50-75 years, including those with and those without hypertension, and showed that the decline in blood pressure brought about by a low-salt diet was independent of hypertension status and antihypertensive medication use. It was also generally consistent across subgroups and did not result in excess adverse events.
“The blood pressure reduction we see here is meaningful, and comparable to that produced by one antihypertensive medication,” lead investigator Deepak Gupta, MD, Vanderbilt University Medical Center, Nashville, Tenn., said in an interview.
Dr. Gupta presented the CARDIA-SSBP study on Nov. 11 at the American Heart Association scientific sessions, held in Philadelphia. The study was published online in JAMA. The exact menus used in the study are available in a supplement to the JAMA paper.
“In order to live a healthy lifestyle, understanding what we eat has important health effects. Raised blood pressure contributes to one out of every eight deaths worldwide,” Dr. Gupta noted. “If people want to lower their blood pressure, attention to dietary sodium is one part of that. If individuals can stick with a low sodium diet, they may be able to stop taking one of their antihypertensive medications, and those who are normotensive will be less likely to develop hypertension.”
Commentators said the study had significant implications for public health, but they pointed out that maintaining a low-sodium diet over the long term is challenging, given the high salt content of generally available foods.
Dr. Gupta noted that the study did use commercially available products in the low-sodium diets and the menus are available for people to follow, making it more accessible than some diets used in previous studies.
“What may also be attractive to people is that you don’t have to wait for months to see an effect. If you start to consume a low-sodium diet, you can see results on blood pressure rapidly, within a week,” he said.
The diet in this study brought about a large reduction in dietary sodium, but Dr. Gupta says any reduction in dietary sodium is likely to be beneficial.
“If you go to the level that we got to, you could expect to see a reduction of around 6 mm Hg. But it’s like walking – you don’t necessarily need to get to 10,000 steps every day. Any amount of walking or physical activity is of benefit. The same is probably true for salt: Any reduction that you can make is probably of benefit.”
For the study, participants had their blood pressure measured by 24-hour ambulatory monitoring while on their usual diets. They were then randomly assigned to either a high-sodium diet or a low-sodium diet for 1 week. Participants then crossed over to the opposite diet for 1 week, with blood pressure measured over a 24-hour period on the last day of each diet.
As assessed by 24-hour urine excretion, the usual diet of participants was found to already be high in sodium (median, 4.45 g/d). This increased to a median of 5.00 g/d when on the high-sodium diet in the study and decreased to 1.27 g/d while on the low-sodium diet.
Results found participants had a median systolic blood pressure of 125 mm Hg on their usual diets. This was raised to 126 mm Hg on the high-sodium diet and lowered to 119 mm Hg on the low-sodium diet.
The researchers also reported that 75% of individuals showed a blood pressure reduction on the low-sodium diet and are thus defined as “salt-sensitive.” This is a higher percentage than found in previous studies.
“Of those that didn’t show a blood pressure reduction with a low-sodium diet in this study, it appears that they may not have been so adherent to the diet as those who did show a blood pressure reduction,” Dr. Gupta said.
He noted that hypertension is the most common chronic disease condition worldwide, with about 1.3 billion people affected, and although it has been known for some time that dietary sodium affects blood pressure, there have been some gaps in previous studies.
For example, many studies have excluded individuals who were already taking antihypertensive medications and people with diabetes, and they have generally not included many older individuals. The current study found that all of these groups showed significant blood pressure reductions by reducing dietary sodium.
Large effect in people with diabetes
Subgroup analysis largely showed consistent results across the population, regardless of age, sex, race, and body mass index and whether participants were taking antihypertensive medication or not, but there were a couple of exceptions. Individuals with higher blood pressure at baseline seemed to have a greater effect of lowering dietary sodium, although those who were normotensive at baseline still showed significant blood pressure reduction, Dr. Gupta reported.
The researchers found a particularly large reduction in blood pressure from lowering sodium intake in people with diabetes, who made up about 21% of the overall cohort. Their average reduction in systolic blood pressure between the high and low sodium diet was close to 17 mm Hg rather than the 7-8 mm Hg in the whole cohort.
Dr. Gupta said that the results are applicable to most of the population.
“The people who will be most motivated to follow a low-sodium diet are those with hypertension. But even in normotensive individuals, there is likely to be benefit.”
To help people follow a low-sodium diet, Dr. Gupta says education campaigns are needed “to show people that they can do it and make it work.” But there are bigger structural issues that need to be addressed at policy and governmental levels.
“Most of our food available in grocery stores and restaurants is high in salt. We now have a preponderance of evidence showing us that we need to change what’s available in the food supply,” he said. “There is a push going on for this now, and the U.S. has introduced some guidelines for the food industry on sodium content of foods. These are voluntary at this point, but it’s a start.”
Difficult to maintain long term
Commenting on the study, Paul Whelton, MD, chair in global public health at Tulane University, New Orleans, noted that sodium reduction is known to reduce blood pressure, with greater sodium reductions giving greater blood pressure decreases, and that some people are more sensitive to the effects of sodium than others.
He described CARDIA-SSBP as a “well-done study.”
“They managed to get a very low sodium intake and a large difference between the two groups, which translated into a big reduction in systolic blood pressure,” Dr. Whelton said. “However, the problem with these sorts of trials where the diets are provided to the participants is that although they show proof of concept, it is difficult to generalize because we can’t normally provide patients with their meals. In this type of ‘feeding’ study, we find it difficult to maintain people on their behavioral intervention over the long term.”
Dr. Whelton said that he was more excited about this trial knowing that the food given was commercially available. “That makes it more practical, but you still have to be quite motivated to follow a diet like this. Buying low-sodium products in the supermarket does require quite a lot of work to read the labels, and sometimes the low-sodium foods are specialty products and are more expensive.”
He pointed out that older people in higher socioeconomic classes are more likely to attempt this and do better from behavioral interventions in general. “Unfortunately, people who don’t do well from behavioral interventions like this are those from lower socioeconomic groups, who are ones at most at risk for cardiovascular disease.”
Dr. Whelton noted that the food industry has been reluctant to lower sodium content because high-salt foods sell better. “Unfortunately, foods high in saturated fat and salt taste good to most people. We are generally attuned to a high salt intake. But when people have been following a low-salt diet for a while, they generally don’t like high-salt foods anymore. They become attuned to lower-sodium diet,” he added.
New U.S. sodium reduction guidelines
Discussant of the CARDIA-SSBP study at the AHA meeting, Cheryl Anderson, MD, University of California, San Diego, said that the findings were important and consistent with prior studies.
“These studies have global implications because salt is ubiquitous in the food supply in much of the world,” she noted, adding that, “Americans consume almost 50% more sodium than recommended, and there has been a persistent lack of adherence to healthy diet recommendations for reductions in salt, sugar, and fats.”
Dr. Anderson pointed out that in 2021, the Food and Drug Administration issued guidance for voluntary sodium reduction, which uses a gradual approach, with targets to reach a population goal of 3,000 mg/d of sodium by 2023 and 2,300 mg/d by 2031.
“These targets apply to 150 categories of food that are sales-weighted to focus on dominant sellers in each category. They apply to food manufacturers, restaurants and food service operations,” she concluded. “These targets serve as a basis for continued dialogue. The research community eagerly awaits the review of population-based data to help refine this approach and goals.”
This study was supported by grants from the National Heart, Lung, and Blood Institute, the National Institutes of Health, the American Heart Association, and the National Center for Advancing Translational Sciences. The authors report no disclosures.
A version of this article appeared on Medscape.com.
The CARDIA-SSBP trial involved 213 individuals aged 50-75 years, including those with and those without hypertension, and showed that the decline in blood pressure brought about by a low-salt diet was independent of hypertension status and antihypertensive medication use. It was also generally consistent across subgroups and did not result in excess adverse events.
“The blood pressure reduction we see here is meaningful, and comparable to that produced by one antihypertensive medication,” lead investigator Deepak Gupta, MD, Vanderbilt University Medical Center, Nashville, Tenn., said in an interview.
Dr. Gupta presented the CARDIA-SSBP study on Nov. 11 at the American Heart Association scientific sessions, held in Philadelphia. The study was published online in JAMA. The exact menus used in the study are available in a supplement to the JAMA paper.
“In order to live a healthy lifestyle, understanding what we eat has important health effects. Raised blood pressure contributes to one out of every eight deaths worldwide,” Dr. Gupta noted. “If people want to lower their blood pressure, attention to dietary sodium is one part of that. If individuals can stick with a low sodium diet, they may be able to stop taking one of their antihypertensive medications, and those who are normotensive will be less likely to develop hypertension.”
Commentators said the study had significant implications for public health, but they pointed out that maintaining a low-sodium diet over the long term is challenging, given the high salt content of generally available foods.
Dr. Gupta noted that the study did use commercially available products in the low-sodium diets and the menus are available for people to follow, making it more accessible than some diets used in previous studies.
“What may also be attractive to people is that you don’t have to wait for months to see an effect. If you start to consume a low-sodium diet, you can see results on blood pressure rapidly, within a week,” he said.
The diet in this study brought about a large reduction in dietary sodium, but Dr. Gupta says any reduction in dietary sodium is likely to be beneficial.
“If you go to the level that we got to, you could expect to see a reduction of around 6 mm Hg. But it’s like walking – you don’t necessarily need to get to 10,000 steps every day. Any amount of walking or physical activity is of benefit. The same is probably true for salt: Any reduction that you can make is probably of benefit.”
For the study, participants had their blood pressure measured by 24-hour ambulatory monitoring while on their usual diets. They were then randomly assigned to either a high-sodium diet or a low-sodium diet for 1 week. Participants then crossed over to the opposite diet for 1 week, with blood pressure measured over a 24-hour period on the last day of each diet.
As assessed by 24-hour urine excretion, the usual diet of participants was found to already be high in sodium (median, 4.45 g/d). This increased to a median of 5.00 g/d when on the high-sodium diet in the study and decreased to 1.27 g/d while on the low-sodium diet.
Results found participants had a median systolic blood pressure of 125 mm Hg on their usual diets. This was raised to 126 mm Hg on the high-sodium diet and lowered to 119 mm Hg on the low-sodium diet.
The researchers also reported that 75% of individuals showed a blood pressure reduction on the low-sodium diet and are thus defined as “salt-sensitive.” This is a higher percentage than found in previous studies.
“Of those that didn’t show a blood pressure reduction with a low-sodium diet in this study, it appears that they may not have been so adherent to the diet as those who did show a blood pressure reduction,” Dr. Gupta said.
He noted that hypertension is the most common chronic disease condition worldwide, with about 1.3 billion people affected, and although it has been known for some time that dietary sodium affects blood pressure, there have been some gaps in previous studies.
For example, many studies have excluded individuals who were already taking antihypertensive medications and people with diabetes, and they have generally not included many older individuals. The current study found that all of these groups showed significant blood pressure reductions by reducing dietary sodium.
Large effect in people with diabetes
Subgroup analysis largely showed consistent results across the population, regardless of age, sex, race, and body mass index and whether participants were taking antihypertensive medication or not, but there were a couple of exceptions. Individuals with higher blood pressure at baseline seemed to have a greater effect of lowering dietary sodium, although those who were normotensive at baseline still showed significant blood pressure reduction, Dr. Gupta reported.
The researchers found a particularly large reduction in blood pressure from lowering sodium intake in people with diabetes, who made up about 21% of the overall cohort. Their average reduction in systolic blood pressure between the high and low sodium diet was close to 17 mm Hg rather than the 7-8 mm Hg in the whole cohort.
Dr. Gupta said that the results are applicable to most of the population.
“The people who will be most motivated to follow a low-sodium diet are those with hypertension. But even in normotensive individuals, there is likely to be benefit.”
To help people follow a low-sodium diet, Dr. Gupta says education campaigns are needed “to show people that they can do it and make it work.” But there are bigger structural issues that need to be addressed at policy and governmental levels.
“Most of our food available in grocery stores and restaurants is high in salt. We now have a preponderance of evidence showing us that we need to change what’s available in the food supply,” he said. “There is a push going on for this now, and the U.S. has introduced some guidelines for the food industry on sodium content of foods. These are voluntary at this point, but it’s a start.”
Difficult to maintain long term
Commenting on the study, Paul Whelton, MD, chair in global public health at Tulane University, New Orleans, noted that sodium reduction is known to reduce blood pressure, with greater sodium reductions giving greater blood pressure decreases, and that some people are more sensitive to the effects of sodium than others.
He described CARDIA-SSBP as a “well-done study.”
“They managed to get a very low sodium intake and a large difference between the two groups, which translated into a big reduction in systolic blood pressure,” Dr. Whelton said. “However, the problem with these sorts of trials where the diets are provided to the participants is that although they show proof of concept, it is difficult to generalize because we can’t normally provide patients with their meals. In this type of ‘feeding’ study, we find it difficult to maintain people on their behavioral intervention over the long term.”
Dr. Whelton said that he was more excited about this trial knowing that the food given was commercially available. “That makes it more practical, but you still have to be quite motivated to follow a diet like this. Buying low-sodium products in the supermarket does require quite a lot of work to read the labels, and sometimes the low-sodium foods are specialty products and are more expensive.”
He pointed out that older people in higher socioeconomic classes are more likely to attempt this and do better from behavioral interventions in general. “Unfortunately, people who don’t do well from behavioral interventions like this are those from lower socioeconomic groups, who are ones at most at risk for cardiovascular disease.”
Dr. Whelton noted that the food industry has been reluctant to lower sodium content because high-salt foods sell better. “Unfortunately, foods high in saturated fat and salt taste good to most people. We are generally attuned to a high salt intake. But when people have been following a low-salt diet for a while, they generally don’t like high-salt foods anymore. They become attuned to lower-sodium diet,” he added.
New U.S. sodium reduction guidelines
Discussant of the CARDIA-SSBP study at the AHA meeting, Cheryl Anderson, MD, University of California, San Diego, said that the findings were important and consistent with prior studies.
“These studies have global implications because salt is ubiquitous in the food supply in much of the world,” she noted, adding that, “Americans consume almost 50% more sodium than recommended, and there has been a persistent lack of adherence to healthy diet recommendations for reductions in salt, sugar, and fats.”
Dr. Anderson pointed out that in 2021, the Food and Drug Administration issued guidance for voluntary sodium reduction, which uses a gradual approach, with targets to reach a population goal of 3,000 mg/d of sodium by 2023 and 2,300 mg/d by 2031.
“These targets apply to 150 categories of food that are sales-weighted to focus on dominant sellers in each category. They apply to food manufacturers, restaurants and food service operations,” she concluded. “These targets serve as a basis for continued dialogue. The research community eagerly awaits the review of population-based data to help refine this approach and goals.”
This study was supported by grants from the National Heart, Lung, and Blood Institute, the National Institutes of Health, the American Heart Association, and the National Center for Advancing Translational Sciences. The authors report no disclosures.
A version of this article appeared on Medscape.com.
The CARDIA-SSBP trial involved 213 individuals aged 50-75 years, including those with and those without hypertension, and showed that the decline in blood pressure brought about by a low-salt diet was independent of hypertension status and antihypertensive medication use. It was also generally consistent across subgroups and did not result in excess adverse events.
“The blood pressure reduction we see here is meaningful, and comparable to that produced by one antihypertensive medication,” lead investigator Deepak Gupta, MD, Vanderbilt University Medical Center, Nashville, Tenn., said in an interview.
Dr. Gupta presented the CARDIA-SSBP study on Nov. 11 at the American Heart Association scientific sessions, held in Philadelphia. The study was published online in JAMA. The exact menus used in the study are available in a supplement to the JAMA paper.
“In order to live a healthy lifestyle, understanding what we eat has important health effects. Raised blood pressure contributes to one out of every eight deaths worldwide,” Dr. Gupta noted. “If people want to lower their blood pressure, attention to dietary sodium is one part of that. If individuals can stick with a low sodium diet, they may be able to stop taking one of their antihypertensive medications, and those who are normotensive will be less likely to develop hypertension.”
Commentators said the study had significant implications for public health, but they pointed out that maintaining a low-sodium diet over the long term is challenging, given the high salt content of generally available foods.
Dr. Gupta noted that the study did use commercially available products in the low-sodium diets and the menus are available for people to follow, making it more accessible than some diets used in previous studies.
“What may also be attractive to people is that you don’t have to wait for months to see an effect. If you start to consume a low-sodium diet, you can see results on blood pressure rapidly, within a week,” he said.
The diet in this study brought about a large reduction in dietary sodium, but Dr. Gupta says any reduction in dietary sodium is likely to be beneficial.
“If you go to the level that we got to, you could expect to see a reduction of around 6 mm Hg. But it’s like walking – you don’t necessarily need to get to 10,000 steps every day. Any amount of walking or physical activity is of benefit. The same is probably true for salt: Any reduction that you can make is probably of benefit.”
For the study, participants had their blood pressure measured by 24-hour ambulatory monitoring while on their usual diets. They were then randomly assigned to either a high-sodium diet or a low-sodium diet for 1 week. Participants then crossed over to the opposite diet for 1 week, with blood pressure measured over a 24-hour period on the last day of each diet.
As assessed by 24-hour urine excretion, the usual diet of participants was found to already be high in sodium (median, 4.45 g/d). This increased to a median of 5.00 g/d when on the high-sodium diet in the study and decreased to 1.27 g/d while on the low-sodium diet.
Results found participants had a median systolic blood pressure of 125 mm Hg on their usual diets. This was raised to 126 mm Hg on the high-sodium diet and lowered to 119 mm Hg on the low-sodium diet.
The researchers also reported that 75% of individuals showed a blood pressure reduction on the low-sodium diet and are thus defined as “salt-sensitive.” This is a higher percentage than found in previous studies.
“Of those that didn’t show a blood pressure reduction with a low-sodium diet in this study, it appears that they may not have been so adherent to the diet as those who did show a blood pressure reduction,” Dr. Gupta said.
He noted that hypertension is the most common chronic disease condition worldwide, with about 1.3 billion people affected, and although it has been known for some time that dietary sodium affects blood pressure, there have been some gaps in previous studies.
For example, many studies have excluded individuals who were already taking antihypertensive medications and people with diabetes, and they have generally not included many older individuals. The current study found that all of these groups showed significant blood pressure reductions by reducing dietary sodium.
Large effect in people with diabetes
Subgroup analysis largely showed consistent results across the population, regardless of age, sex, race, and body mass index and whether participants were taking antihypertensive medication or not, but there were a couple of exceptions. Individuals with higher blood pressure at baseline seemed to have a greater effect of lowering dietary sodium, although those who were normotensive at baseline still showed significant blood pressure reduction, Dr. Gupta reported.
The researchers found a particularly large reduction in blood pressure from lowering sodium intake in people with diabetes, who made up about 21% of the overall cohort. Their average reduction in systolic blood pressure between the high and low sodium diet was close to 17 mm Hg rather than the 7-8 mm Hg in the whole cohort.
Dr. Gupta said that the results are applicable to most of the population.
“The people who will be most motivated to follow a low-sodium diet are those with hypertension. But even in normotensive individuals, there is likely to be benefit.”
To help people follow a low-sodium diet, Dr. Gupta says education campaigns are needed “to show people that they can do it and make it work.” But there are bigger structural issues that need to be addressed at policy and governmental levels.
“Most of our food available in grocery stores and restaurants is high in salt. We now have a preponderance of evidence showing us that we need to change what’s available in the food supply,” he said. “There is a push going on for this now, and the U.S. has introduced some guidelines for the food industry on sodium content of foods. These are voluntary at this point, but it’s a start.”
Difficult to maintain long term
Commenting on the study, Paul Whelton, MD, chair in global public health at Tulane University, New Orleans, noted that sodium reduction is known to reduce blood pressure, with greater sodium reductions giving greater blood pressure decreases, and that some people are more sensitive to the effects of sodium than others.
He described CARDIA-SSBP as a “well-done study.”
“They managed to get a very low sodium intake and a large difference between the two groups, which translated into a big reduction in systolic blood pressure,” Dr. Whelton said. “However, the problem with these sorts of trials where the diets are provided to the participants is that although they show proof of concept, it is difficult to generalize because we can’t normally provide patients with their meals. In this type of ‘feeding’ study, we find it difficult to maintain people on their behavioral intervention over the long term.”
Dr. Whelton said that he was more excited about this trial knowing that the food given was commercially available. “That makes it more practical, but you still have to be quite motivated to follow a diet like this. Buying low-sodium products in the supermarket does require quite a lot of work to read the labels, and sometimes the low-sodium foods are specialty products and are more expensive.”
He pointed out that older people in higher socioeconomic classes are more likely to attempt this and do better from behavioral interventions in general. “Unfortunately, people who don’t do well from behavioral interventions like this are those from lower socioeconomic groups, who are ones at most at risk for cardiovascular disease.”
Dr. Whelton noted that the food industry has been reluctant to lower sodium content because high-salt foods sell better. “Unfortunately, foods high in saturated fat and salt taste good to most people. We are generally attuned to a high salt intake. But when people have been following a low-salt diet for a while, they generally don’t like high-salt foods anymore. They become attuned to lower-sodium diet,” he added.
New U.S. sodium reduction guidelines
Discussant of the CARDIA-SSBP study at the AHA meeting, Cheryl Anderson, MD, University of California, San Diego, said that the findings were important and consistent with prior studies.
“These studies have global implications because salt is ubiquitous in the food supply in much of the world,” she noted, adding that, “Americans consume almost 50% more sodium than recommended, and there has been a persistent lack of adherence to healthy diet recommendations for reductions in salt, sugar, and fats.”
Dr. Anderson pointed out that in 2021, the Food and Drug Administration issued guidance for voluntary sodium reduction, which uses a gradual approach, with targets to reach a population goal of 3,000 mg/d of sodium by 2023 and 2,300 mg/d by 2031.
“These targets apply to 150 categories of food that are sales-weighted to focus on dominant sellers in each category. They apply to food manufacturers, restaurants and food service operations,” she concluded. “These targets serve as a basis for continued dialogue. The research community eagerly awaits the review of population-based data to help refine this approach and goals.”
This study was supported by grants from the National Heart, Lung, and Blood Institute, the National Institutes of Health, the American Heart Association, and the National Center for Advancing Translational Sciences. The authors report no disclosures.
A version of this article appeared on Medscape.com.
FROM AHA 2023
Study takes fine-grained look at MACE risk with glucocorticoids in RA
SAN DIEGO – Even when taken at low doses and over short periods, glucocorticoids (GCs) were linked to a higher risk of major adverse cardiovascular events (MACE) over the long term in a Veterans Affairs population of older, mostly male patients with rheumatoid arthritis, a new retrospective cohort study has found.
The analysis of nearly 19,000 patients, presented by rheumatologist Beth Wallace, MD, MSc, at the annual meeting of the American College of Rheumatology, showed that the level of risk for MACE rose with the dose, duration, and recency of GC use, in which risk increased significantly at prednisone-equivalent doses as low as 5 mg/day, durations as short as 30 days, and with last use as long as 1 year before MACE.

“Up to half of RA patients in the United States use long-term glucocorticoids despite previous work suggesting they increase MACE in a dose-dependent way,” said Dr. Wallace, assistant professor of medicine at the University of Michigan, Ann Arbor, and a rheumatologist at the VA Ann Arbor Healthcare Center. “Our group previously presented work suggesting that less than 14 days of glucocorticoid use in a 6-month period is associated with a two-thirds increase in odds of MACE over the following 6 months, with 90 days of use associated with more than twofold increase.”
In recent years, researchers such as Dr. Wallace have focused attention on the risks of GCs in RA. The American College of Rheumatology and the European Alliance of Associations for Rheumatology emphasize avoiding long-term use of GCs in RA and keeping doses as small and over the shortest amount of time as possible.
When Dr. Wallace and colleagues looked at the clinical pattern of GC use for patients with RA during the past 2 years, those who took 5 mg, 7.5 mg, and 10 mg daily doses for 30 days and had stopped at least a year before had risk for MACE that rose significantly by 3%, 5%, and 7%, respectively, compared with those who didn’t take GCs in the past 2 years.
While those increases were small, risk for MACE rose even more for those who took the same daily doses for 90 days, increasing 10%, 15%, and 21%, respectively. Researchers linked current ongoing use of GCs for the past 90 days to a 13%, 19%, and 27% higher risk for MACE at those respective doses.
The findings “add to the literature suggesting that there is some risk even with low-dose steroids,” said Michael George, MD, assistant professor of rheumatology and epidemiology at the University of Pennsylvania, Philadelphia, who did not take part in the research but is familiar with the findings.

“We can see that even glucocorticoids taken several years ago may affect cardiovascular risk but that recent use has a bigger effect on risk,” Dr. George said in an interview. “This study also suggests that very low-dose use affects risk.”
For the new study, Dr. Wallace and colleagues examined a Veterans Affairs database and identified 18,882 patients with RA (mean age, 62.5 years; 84% male; 66% GC users) who met the criteria of being > 40 and < 90 years old. The subjects had an initial VA rheumatology visit during 2010-2018 and were excluded if they had a non-RA rheumatologic disorder, prior MACE, or heart failure. MACE was defined as MI, stroke/TIA, cardiac arrest, coronary revascularization, or death from CV cause.
A total of 16% of the cohort had the largest exposure to GCs, defined as use for 90 days or more; 23% had exposure of 14-89 days, and 14% had exposure of 1-13 days.
The median 5-year MACE risk at baseline was 5.3%, and 3,754 patients (19.9%) had high baseline MACE risk. Incident MACE occurred in 4.1% of patients, and the median time to MACE was 2.67 years (interquartile ratio, 1.26-4.45 years).
Covariates included factors such as age, race, sex, body mass index, smoking status, adjusted Elixhauser index, VA risk score for cardiovascular disease, cancer, hospitalization for infection, number of rheumatology clinic visits, and use of lipid-lowering drugs, opioids, methotrexate, biologics, and hydroxychloroquine.
Dr. Wallace noted limitations including the possibility of residual confounding and the influence of background cardiovascular risk. The study didn’t examine the clinical value of taking GCs or compare that to the potential risk. Nor did it examine cost or the risks and benefits of alternative therapeutic options.
A study released earlier this year suggested that patients taking daily prednisolone doses under 5 mg do not have a higher risk of MACE. Previous studies had reached conflicting results.
“Glucocorticoids can provide major benefits to patients, but these benefits must be balanced with the potential risks,” Dr. George said. At low doses, these risks may be small, but they are present. In many cases, escalating DMARD [disease-modifying antirheumatic drug] therapy may be safer than continuing glucocorticoids.”
He added that the risks of GCs may be especially high in older patients and in those who have cardiovascular risk factors: “Often biologics are avoided in these higher-risk patients. But in fact, in many cases biologics may be the safer choice.”
No study funding was reported. Dr. Wallace reported no relevant financial relationships, and some of the other authors reported various ties with industry. Dr. George reported research funding from GlaxoSmithKline and Janssen and consulting fees from AbbVie.
SAN DIEGO – Even when taken at low doses and over short periods, glucocorticoids (GCs) were linked to a higher risk of major adverse cardiovascular events (MACE) over the long term in a Veterans Affairs population of older, mostly male patients with rheumatoid arthritis, a new retrospective cohort study has found.
The analysis of nearly 19,000 patients, presented by rheumatologist Beth Wallace, MD, MSc, at the annual meeting of the American College of Rheumatology, showed that the level of risk for MACE rose with the dose, duration, and recency of GC use, in which risk increased significantly at prednisone-equivalent doses as low as 5 mg/day, durations as short as 30 days, and with last use as long as 1 year before MACE.
“Up to half of RA patients in the United States use long-term glucocorticoids despite previous work suggesting they increase MACE in a dose-dependent way,” said Dr. Wallace, assistant professor of medicine at the University of Michigan, Ann Arbor, and a rheumatologist at the VA Ann Arbor Healthcare Center. “Our group previously presented work suggesting that less than 14 days of glucocorticoid use in a 6-month period is associated with a two-thirds increase in odds of MACE over the following 6 months, with 90 days of use associated with more than twofold increase.”
In recent years, researchers such as Dr. Wallace have focused attention on the risks of GCs in RA. The American College of Rheumatology and the European Alliance of Associations for Rheumatology emphasize avoiding long-term use of GCs in RA and keeping doses as small and over the shortest amount of time as possible.
When Dr. Wallace and colleagues looked at the clinical pattern of GC use for patients with RA during the past 2 years, those who took 5 mg, 7.5 mg, and 10 mg daily doses for 30 days and had stopped at least a year before had risk for MACE that rose significantly by 3%, 5%, and 7%, respectively, compared with those who didn’t take GCs in the past 2 years.
While those increases were small, risk for MACE rose even more for those who took the same daily doses for 90 days, increasing 10%, 15%, and 21%, respectively. Researchers linked current ongoing use of GCs for the past 90 days to a 13%, 19%, and 27% higher risk for MACE at those respective doses.
The findings “add to the literature suggesting that there is some risk even with low-dose steroids,” said Michael George, MD, assistant professor of rheumatology and epidemiology at the University of Pennsylvania, Philadelphia, who did not take part in the research but is familiar with the findings.
“We can see that even glucocorticoids taken several years ago may affect cardiovascular risk but that recent use has a bigger effect on risk,” Dr. George said in an interview. “This study also suggests that very low-dose use affects risk.”
For the new study, Dr. Wallace and colleagues examined a Veterans Affairs database and identified 18,882 patients with RA (mean age, 62.5 years; 84% male; 66% GC users) who met the criteria of being > 40 and < 90 years old. The subjects had an initial VA rheumatology visit during 2010-2018 and were excluded if they had a non-RA rheumatologic disorder, prior MACE, or heart failure. MACE was defined as MI, stroke/TIA, cardiac arrest, coronary revascularization, or death from CV cause.
A total of 16% of the cohort had the largest exposure to GCs, defined as use for 90 days or more; 23% had exposure of 14-89 days, and 14% had exposure of 1-13 days.
The median 5-year MACE risk at baseline was 5.3%, and 3,754 patients (19.9%) had high baseline MACE risk. Incident MACE occurred in 4.1% of patients, and the median time to MACE was 2.67 years (interquartile ratio, 1.26-4.45 years).
Covariates included factors such as age, race, sex, body mass index, smoking status, adjusted Elixhauser index, VA risk score for cardiovascular disease, cancer, hospitalization for infection, number of rheumatology clinic visits, and use of lipid-lowering drugs, opioids, methotrexate, biologics, and hydroxychloroquine.
Dr. Wallace noted limitations including the possibility of residual confounding and the influence of background cardiovascular risk. The study didn’t examine the clinical value of taking GCs or compare that to the potential risk. Nor did it examine cost or the risks and benefits of alternative therapeutic options.
A study released earlier this year suggested that patients taking daily prednisolone doses under 5 mg do not have a higher risk of MACE. Previous studies had reached conflicting results.
“Glucocorticoids can provide major benefits to patients, but these benefits must be balanced with the potential risks,” Dr. George said. At low doses, these risks may be small, but they are present. In many cases, escalating DMARD [disease-modifying antirheumatic drug] therapy may be safer than continuing glucocorticoids.”
He added that the risks of GCs may be especially high in older patients and in those who have cardiovascular risk factors: “Often biologics are avoided in these higher-risk patients. But in fact, in many cases biologics may be the safer choice.”
No study funding was reported. Dr. Wallace reported no relevant financial relationships, and some of the other authors reported various ties with industry. Dr. George reported research funding from GlaxoSmithKline and Janssen and consulting fees from AbbVie.
SAN DIEGO – Even when taken at low doses and over short periods, glucocorticoids (GCs) were linked to a higher risk of major adverse cardiovascular events (MACE) over the long term in a Veterans Affairs population of older, mostly male patients with rheumatoid arthritis, a new retrospective cohort study has found.
The analysis of nearly 19,000 patients, presented by rheumatologist Beth Wallace, MD, MSc, at the annual meeting of the American College of Rheumatology, showed that the level of risk for MACE rose with the dose, duration, and recency of GC use, in which risk increased significantly at prednisone-equivalent doses as low as 5 mg/day, durations as short as 30 days, and with last use as long as 1 year before MACE.
“Up to half of RA patients in the United States use long-term glucocorticoids despite previous work suggesting they increase MACE in a dose-dependent way,” said Dr. Wallace, assistant professor of medicine at the University of Michigan, Ann Arbor, and a rheumatologist at the VA Ann Arbor Healthcare Center. “Our group previously presented work suggesting that less than 14 days of glucocorticoid use in a 6-month period is associated with a two-thirds increase in odds of MACE over the following 6 months, with 90 days of use associated with more than twofold increase.”
In recent years, researchers such as Dr. Wallace have focused attention on the risks of GCs in RA. The American College of Rheumatology and the European Alliance of Associations for Rheumatology emphasize avoiding long-term use of GCs in RA and keeping doses as small and over the shortest amount of time as possible.
When Dr. Wallace and colleagues looked at the clinical pattern of GC use for patients with RA during the past 2 years, those who took 5 mg, 7.5 mg, and 10 mg daily doses for 30 days and had stopped at least a year before had risk for MACE that rose significantly by 3%, 5%, and 7%, respectively, compared with those who didn’t take GCs in the past 2 years.
While those increases were small, risk for MACE rose even more for those who took the same daily doses for 90 days, increasing 10%, 15%, and 21%, respectively. Researchers linked current ongoing use of GCs for the past 90 days to a 13%, 19%, and 27% higher risk for MACE at those respective doses.
The findings “add to the literature suggesting that there is some risk even with low-dose steroids,” said Michael George, MD, assistant professor of rheumatology and epidemiology at the University of Pennsylvania, Philadelphia, who did not take part in the research but is familiar with the findings.
“We can see that even glucocorticoids taken several years ago may affect cardiovascular risk but that recent use has a bigger effect on risk,” Dr. George said in an interview. “This study also suggests that very low-dose use affects risk.”
For the new study, Dr. Wallace and colleagues examined a Veterans Affairs database and identified 18,882 patients with RA (mean age, 62.5 years; 84% male; 66% GC users) who met the criteria of being > 40 and < 90 years old. The subjects had an initial VA rheumatology visit during 2010-2018 and were excluded if they had a non-RA rheumatologic disorder, prior MACE, or heart failure. MACE was defined as MI, stroke/TIA, cardiac arrest, coronary revascularization, or death from CV cause.
A total of 16% of the cohort had the largest exposure to GCs, defined as use for 90 days or more; 23% had exposure of 14-89 days, and 14% had exposure of 1-13 days.
The median 5-year MACE risk at baseline was 5.3%, and 3,754 patients (19.9%) had high baseline MACE risk. Incident MACE occurred in 4.1% of patients, and the median time to MACE was 2.67 years (interquartile ratio, 1.26-4.45 years).
Covariates included factors such as age, race, sex, body mass index, smoking status, adjusted Elixhauser index, VA risk score for cardiovascular disease, cancer, hospitalization for infection, number of rheumatology clinic visits, and use of lipid-lowering drugs, opioids, methotrexate, biologics, and hydroxychloroquine.
Dr. Wallace noted limitations including the possibility of residual confounding and the influence of background cardiovascular risk. The study didn’t examine the clinical value of taking GCs or compare that to the potential risk. Nor did it examine cost or the risks and benefits of alternative therapeutic options.
A study released earlier this year suggested that patients taking daily prednisolone doses under 5 mg do not have a higher risk of MACE. Previous studies had reached conflicting results.
“Glucocorticoids can provide major benefits to patients, but these benefits must be balanced with the potential risks,” Dr. George said. At low doses, these risks may be small, but they are present. In many cases, escalating DMARD [disease-modifying antirheumatic drug] therapy may be safer than continuing glucocorticoids.”
He added that the risks of GCs may be especially high in older patients and in those who have cardiovascular risk factors: “Often biologics are avoided in these higher-risk patients. But in fact, in many cases biologics may be the safer choice.”
No study funding was reported. Dr. Wallace reported no relevant financial relationships, and some of the other authors reported various ties with industry. Dr. George reported research funding from GlaxoSmithKline and Janssen and consulting fees from AbbVie.
AT ACR 2023
Saltwater gargling may help avoid COVID hospitalization
ANAHEIM, CALIF. –
“The hypothesis was that interventions that target the upper respiratory tract may reduce the frequency and duration of upper respiratory symptoms associated with COVID-19,” said Sebastian Espinoza, first author of the study; he is with Trinity University, San Antonio.
Adults aged 18-65 years who tested positive for SARS-CoV-2 on polymerase chain reaction (PCR) testing between 2020 and 2022 were randomly selected to use low- or high-dose saltwater regimens for 14 days at the Harris Health System, Houston. For patients to be included in the study, 14 days had to have elapsed since the onset of any symptoms associated with COVID.
The low dose was 2.13 grams of salt dissolved in 8 ounces of warm water, and the high dose was 6 grams. Participants gargled the saltwater and used it as a nasal rinse for 5 minutes four times a day.
Primary outcomes included frequency and duration of symptoms associated with SARS-CoV-2 infection; secondary outcomes included admission to the hospital or the intensive care unit, mechanical ventilatory support, or death.
The findings were presented in a poster at the annual meeting of the American College of Allergy, Asthma, and Immunology.
Fifty-eight people were randomly assigned to either the low-saline (n = 27) or the high-saline (n = 28) group; three patients were lost to follow-up in both these groups. The reference control population consisted of 9,398 people with confirmed SARS-CoV-2 infection. Rates of vaccination were similar for all participants.
Hospitalization rates in the low- (18.5%) and high- (21.4%) saline groups were significantly lower than in the reference control population (58.8%; P < .001). No significant differences were noted in other outcomes among these groups.
The average age of patients in the control population (n = 9,398) was 45 years. The average age was similar in the low- and high-saline groups. In the low-saline group (n = 27), the average age was 39, and in the high-saline group, the average age was 41.
In all three groups, body mass index was between 29.6 and 31.7.
Exclusion criteria included chronic hypertension or participation in another interventional study.
‘Low risk, small potential benefit’
Allergist Zach Rubin, MD, a spokesperson for the ACAAI, said in an interview that the findings are in line with other small studies that previously reported some benefit in using nasal saline irrigation and gargling to treat a SARS-CoV-2 infection.
“This is a type of intervention that is low risk with some small potential benefit,” he said.
The researchers did not evaluate the potential reason for the saline regimen’s association with fewer hospitalizations, but Dr. Rubin said, “It may be possible that nasal saline irrigation and gargling help improve viral clearance and reduce the risk of microaspiration into the lungs, so it may be possible that this intervention could reduce the risk of pneumonia, which is a major cause of hospitalization.”
Dr. Rubin, who is an allergist at Oak Brook Allergists, Ill., said, “I generally recommend nasal saline irrigation to my patients for allergic rhinitis and viral upper respiratory infections already. It can help reduce symptoms such as nasal congestion, rhinorrhea, postnasal drip, and sinus pain and pressure.”
The intervention may be reasonable beyond an adult population, he said.
“This could be used for pediatric patients as well, if they are developmentally ready to try this intervention,” he said.
Mr. Espinoza said further study is warranted, but he said that if confirmed in later trials, the simple intervention may be particularly helpful in low-resource settings.
Mr. Espinoza and Dr. Rubin have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
ANAHEIM, CALIF. –
“The hypothesis was that interventions that target the upper respiratory tract may reduce the frequency and duration of upper respiratory symptoms associated with COVID-19,” said Sebastian Espinoza, first author of the study; he is with Trinity University, San Antonio.
Adults aged 18-65 years who tested positive for SARS-CoV-2 on polymerase chain reaction (PCR) testing between 2020 and 2022 were randomly selected to use low- or high-dose saltwater regimens for 14 days at the Harris Health System, Houston. For patients to be included in the study, 14 days had to have elapsed since the onset of any symptoms associated with COVID.
The low dose was 2.13 grams of salt dissolved in 8 ounces of warm water, and the high dose was 6 grams. Participants gargled the saltwater and used it as a nasal rinse for 5 minutes four times a day.
Primary outcomes included frequency and duration of symptoms associated with SARS-CoV-2 infection; secondary outcomes included admission to the hospital or the intensive care unit, mechanical ventilatory support, or death.
The findings were presented in a poster at the annual meeting of the American College of Allergy, Asthma, and Immunology.
Fifty-eight people were randomly assigned to either the low-saline (n = 27) or the high-saline (n = 28) group; three patients were lost to follow-up in both these groups. The reference control population consisted of 9,398 people with confirmed SARS-CoV-2 infection. Rates of vaccination were similar for all participants.
Hospitalization rates in the low- (18.5%) and high- (21.4%) saline groups were significantly lower than in the reference control population (58.8%; P < .001). No significant differences were noted in other outcomes among these groups.
The average age of patients in the control population (n = 9,398) was 45 years. The average age was similar in the low- and high-saline groups. In the low-saline group (n = 27), the average age was 39, and in the high-saline group, the average age was 41.
In all three groups, body mass index was between 29.6 and 31.7.
Exclusion criteria included chronic hypertension or participation in another interventional study.
‘Low risk, small potential benefit’
Allergist Zach Rubin, MD, a spokesperson for the ACAAI, said in an interview that the findings are in line with other small studies that previously reported some benefit in using nasal saline irrigation and gargling to treat a SARS-CoV-2 infection.
“This is a type of intervention that is low risk with some small potential benefit,” he said.
The researchers did not evaluate the potential reason for the saline regimen’s association with fewer hospitalizations, but Dr. Rubin said, “It may be possible that nasal saline irrigation and gargling help improve viral clearance and reduce the risk of microaspiration into the lungs, so it may be possible that this intervention could reduce the risk of pneumonia, which is a major cause of hospitalization.”
Dr. Rubin, who is an allergist at Oak Brook Allergists, Ill., said, “I generally recommend nasal saline irrigation to my patients for allergic rhinitis and viral upper respiratory infections already. It can help reduce symptoms such as nasal congestion, rhinorrhea, postnasal drip, and sinus pain and pressure.”
The intervention may be reasonable beyond an adult population, he said.
“This could be used for pediatric patients as well, if they are developmentally ready to try this intervention,” he said.
Mr. Espinoza said further study is warranted, but he said that if confirmed in later trials, the simple intervention may be particularly helpful in low-resource settings.
Mr. Espinoza and Dr. Rubin have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
ANAHEIM, CALIF. –
“The hypothesis was that interventions that target the upper respiratory tract may reduce the frequency and duration of upper respiratory symptoms associated with COVID-19,” said Sebastian Espinoza, first author of the study; he is with Trinity University, San Antonio.
Adults aged 18-65 years who tested positive for SARS-CoV-2 on polymerase chain reaction (PCR) testing between 2020 and 2022 were randomly selected to use low- or high-dose saltwater regimens for 14 days at the Harris Health System, Houston. For patients to be included in the study, 14 days had to have elapsed since the onset of any symptoms associated with COVID.
The low dose was 2.13 grams of salt dissolved in 8 ounces of warm water, and the high dose was 6 grams. Participants gargled the saltwater and used it as a nasal rinse for 5 minutes four times a day.
Primary outcomes included frequency and duration of symptoms associated with SARS-CoV-2 infection; secondary outcomes included admission to the hospital or the intensive care unit, mechanical ventilatory support, or death.
The findings were presented in a poster at the annual meeting of the American College of Allergy, Asthma, and Immunology.
Fifty-eight people were randomly assigned to either the low-saline (n = 27) or the high-saline (n = 28) group; three patients were lost to follow-up in both these groups. The reference control population consisted of 9,398 people with confirmed SARS-CoV-2 infection. Rates of vaccination were similar for all participants.
Hospitalization rates in the low- (18.5%) and high- (21.4%) saline groups were significantly lower than in the reference control population (58.8%; P < .001). No significant differences were noted in other outcomes among these groups.
The average age of patients in the control population (n = 9,398) was 45 years. The average age was similar in the low- and high-saline groups. In the low-saline group (n = 27), the average age was 39, and in the high-saline group, the average age was 41.
In all three groups, body mass index was between 29.6 and 31.7.
Exclusion criteria included chronic hypertension or participation in another interventional study.
‘Low risk, small potential benefit’
Allergist Zach Rubin, MD, a spokesperson for the ACAAI, said in an interview that the findings are in line with other small studies that previously reported some benefit in using nasal saline irrigation and gargling to treat a SARS-CoV-2 infection.
“This is a type of intervention that is low risk with some small potential benefit,” he said.
The researchers did not evaluate the potential reason for the saline regimen’s association with fewer hospitalizations, but Dr. Rubin said, “It may be possible that nasal saline irrigation and gargling help improve viral clearance and reduce the risk of microaspiration into the lungs, so it may be possible that this intervention could reduce the risk of pneumonia, which is a major cause of hospitalization.”
Dr. Rubin, who is an allergist at Oak Brook Allergists, Ill., said, “I generally recommend nasal saline irrigation to my patients for allergic rhinitis and viral upper respiratory infections already. It can help reduce symptoms such as nasal congestion, rhinorrhea, postnasal drip, and sinus pain and pressure.”
The intervention may be reasonable beyond an adult population, he said.
“This could be used for pediatric patients as well, if they are developmentally ready to try this intervention,” he said.
Mr. Espinoza said further study is warranted, but he said that if confirmed in later trials, the simple intervention may be particularly helpful in low-resource settings.
Mr. Espinoza and Dr. Rubin have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM ACAAI 2023