User login
How might acknowledging a medical error promote patient safety?
Examination
- Patient looks well and is in no distress
- Weight 138 lbs; height 66 inches; body mass index 23; other vitals normal
- Normal heart, lung, and abdominal exam. No cervical or other adenopathy.
Medical history
- Has osteoporosis for which she takes alendronate weekly; also has diet-controlled hyperlipidemia, and is status post-remote hysterectomy for uterine bleeding
- Married, with 1 grown son who is healthy
- Nonsmoker; drinks 2 alcoholic beverages weekly; no illicit drugs
- Walks 40 minutes 4 times a week
- Mother died at age 93 from congestive heart failure; father alive, 92, has bladder cancer
- Review of systems negative for cough, fever, weight loss, or swollen glands
A Mantoux tuberculin skin test (TST) is administered per clinic protocol, and the patient is instructed to return in 48 to 72 hours for a reading of the test result.
The Mantoux TST is the most accurate test for determining tuberculosis (TB) infection.1 The standard procedure uses 0.1 cc (5 tuberculin units) of purified protein derivative (PPD) in a standard tuberculin syringe (3/8 inch, 26–27 gauge). This is administered on a flexor surface of the forearm, 2 to 4 inches below the elbow, and requires an intradermal injection (needle bevel upward) that raises a wheal 6 to 10 mm in diameter. A previously reported positive TST does not contraindicate repeated administration.1
A:
Interpreting TB test results
The definition of a positive tuberculin skin test result depends on a person’s risk factors as defined in the TABLE.1 Read a TST result 48 to 96 (ideally 72) hours after administration. Palpate and measure induration (not redness).
An alternative method is to use a ballpoint pen to draw a line starting at 1 cm from both sides of the skin reaction and moving toward its center. Where you encounter increased resistance, mark that as the border of induration. Then measure the distance between the 2 borders. This method has been reported to be slightly more precise than palpation.2
Another recently developed test for TB infection, the QuantiFERON, is based on quantification of interferon-gamma response in whole blood to TB infection. Its routine use is not recommended by the Centers for Disease Control and Prevention (CDC).3 It was unavailable in the county where the patient was tested.
TABLE
TST results regarded as positive for tuberculosis, given a patient’s specific risk factors
| 5 MM | INDURATION 10 MM | 15 MM |
|---|---|---|
| HIV infection Close contact of person with TB Previous TB on chest x-ray Intravenous drug use, or unknown HIV status | Native of country with endemic TB HIV-negative intravenous drug user Low income, inadequate healthcare Resident of long-term care facility Medical condition with increased TB risk Ages less than 4 years Likely exposure to TB | Patient has no risk factors |
The patient’s return 48 hours later
A nurse examines the patient’s arm and is uncertain how to interpret the test result. The patient’s primary physician is not in the clinic, and one of the other physicians is consulted. He reads the result as “20 mm induration, positive for TB infection.“
A chest X-ray shows no evidence of tuberculosis infection or other abnormality. The patient is referred to the local county health department. In accordance with CDC guidelines, she is diagnosed with latent tuberculosis infection and started on daily isoniazid therapy.4
The patient’s family physician learns of the patient’s diagnosis after she starts isoniazid therapy. Because of her low risk of tuberculosis, he wonders if the skin test result might have been misread. He discusses the issue with the physician who read the first skin test and discovers there was uncertainty regarding the redness (as opposed to the induration) of the skin reaction. The patient herself reports that she did not feel a hard “bump” on the skin where the test was administered.
The family physician informs the patient that the tuberculin skin test may have been incorrectly read as positive. He gives her the option of repeating the test at the county health department, whose personnel are experienced in administering and reading tuberculin skin tests. The patient chooses to repeat the TST, which is read as definitely negative. Isoniazid therapy is stopped. The patient is grateful that she does not have to continue unnecessary and potentially harmful therapy.
A:
Dealing responsibly with medical errors
A simple, straightforward explanation and apology is more likely to benefit both patient and physician than is silence or an explanation that is convoluted or places blame.
A growing consensus recommends that when a medical error is made, health care providers should tell patients about the error and apologize.5 In part this recommendation stems from accepted ethical principles of respect for patients as autonomous decision-makers, and from the obligation of providers to act with beneficence on the patient’s behalf. If a medical error impacts the patient’s care in some way, the patient is unable to make informed consent about subsequent care or trust the medical provider if the error is not divulged.
Furthermore, others have advocated that an apology after a medical error can reduce the cost or risk of tort litigation for medical malpractice.6
To encourage admissions of error, many states now prevent apologies from being used in court as evidence of guilt in malpractice cases.
Although organizations and liability insurance carriers may have specific requirements or guidelines about how to handle medical errors, practitioners may want to consider the following steps:
- Get the key facts of what happened, if possible from those who directly observed or who were involved in the care
- Report these facts to risk management or to the professional liability carrier, according to internal policies
- Apologize to the patient.
A:
Important features of an apology
- Make the apology promptly
- Be sincere
- Apologize in person
- Keep it simple—eg, “I am very sorry for any concern or inconvenience this event caused you.” Avoid blaming others, minimizing the event, or giving an involved explanation about how the problem occurred.
The purpose of the apology is simply that: to apologize. A patient may need to process feelings about what happened, so the apology should be viewed as an important opportunity for the patient to heal.
After apologizing, reassure the patient that you plan to learn from the mishap and prevent further events from happening. Stress that the trust the patient places in you and your team is not misplaced; that you take all mishaps, even minor ones, seriously and have an aggressive program of quality assurance.
Finally, though you cannot undo the event, offering to waive your professional fee for the visit that led to the mishap will help rebuild patient confidence and loyalty.
A:
Learning from errors is a vital way we prevent errors from occurring in the future. Others have described key steps to creating a culture and process of improvement.7 These include:
- Establish an atmosphere of quality improvement in your organization by emphasizing that errors are inevitable, are more often caused by faulty systems rather than faulty people, and are opportunities to learn and improve.
- Avoid blame—search for root causes.
- Create a mechanism to report all errors, mishaps, “near-misses,” and unhappy customers, and a method to systematically review these reports to identify areas to improve.
- Incorporate “lessons learned” into system changes designed to prevent recurrence of this and similar mishaps.
Openly acknowledging a mistake and apologizing to a patient, as the authors suggest, is sound advice increasingly followed in the United States and internationally. Disclosure of mistakes is a cornerstone of the safety work, as is being carried out in the United Kingdom by the National Patient Safety Agency (NPSA). They have prepared excellent online interactive educational materials to support health care professionals as they participate in the disclosure process.8
A second step the authors took was to learn about the inherent risks and potential failure points that are often deeply embedded in our care delivery processes. Mistakes are windows into the clinical work environment. If we peer through these windows regularly and systematically, we can learn a good deal about protecting our patients from harm. The mistake reported here—though of little or no harm to the patient (ie, possibly a near miss)—has potential as a rich information source about how care is delivered in the family practice clinic.9 In addition, because there was a recovery by the patient’s family physician, we have the added benefit of learning from that part of the narrative.
Learning from mistakes an intentional process, not an automatic one
First, an organization or setting must have a just culture to enable learning.10 Tools for assessing safety culture are available from the Agency for Healthcare Research and Quality (AHRQ)11 and from the Institute for Healthcare Improvement (IHI).12 A just culture is an essential attribute of a learning organization.13
Second, a systematic process must be available for inquiring about the root causes and contributing factors of events. Examples of such systems are those used by Veterans Health Administration (VHA)14 and the UK’s NPSA.15 The Medical Events Reporting System for transfusion medicine (MERS-TM) is a model reporting system in the US and is developed as a learning system.16,17
Third, we have learned that simply gathering information about the causes of events is not sufficient to prevent future events. Those involved in mistakes must be given an opportunity to come together to make sense of the causal information before they can make changes.
Fourth, a system-change method is needed to correct underlying causes. Such a method is the Plan-Do-Study Act (PDSA), which translates knowledge about causes into actions that can be implemented in the health care work environment.18
How might these processes apply to the case at hand
Two aspects of this case in particular bear scrutiny.
The clinic protocol. Protocols standardize care as well as complement the cognitive work required in clinical care. Understanding the contents and use of this protocol would shed light on this event. To what extent did the protocol support the interpretation of the TB test; how informative was it? Did it require obtaining a history from the patient as a component of the test interpretation? Did it detail the skills of the test interpreter? Did it spell out a contingency plan in the event those administering and reading the tests are unclear about the findings? Who had access to the protocol?
Handoffs, when things can get dropped. Another focus of this case is the 3 handoffs: the nurse reading the test handed the interpretation off to a physician; the physician handed the patient off to the public health clinic; and the clinic then handed the patient back to her primary care physician. Handoffs often lead to mistakes because they involve interpersonal communication and transfer of information, both of which are fraught with opportunities for errors.19
In the first handoff, we might well ask what information the nurse had about the patient’s history and what information she communicated to the physician? A full understanding of this handoff helps to make explicit hierarchical relationships in the clinic as well as information flow.
With the second handoff, we might ask what information regarding the uncertainty of the patient’s TB test interpretation and history were passed along to the TB clinic? How was the information communicated—on paper, electronically, by telephone? Each of these methods has unique constraints.
Finally, the fortunate third handoff—follow-up with the patient’s family practice physician that resulted in the discovery of the mistake and therefore recovery. It is particularly important to note that the recovery came because of an apparent system of feedback of information to the patient’s family physician. Such feedback loops contribute to safety. The family physician noticed something that did not make sense and investigated it. That is, the family physician was mindful.20 This attitude of mindfulness is a critical component in safe or reliable systems. Hubris is the enemy of safety.
Shirley Kellie, MD, MSc
Physician epidemiologist, American Medical Association
A:
In this particular case, a system-based approach to care might have anticipated and prevented this error through the following steps:
- Create specific written instructions for office procedures
- Have the written procedures handy and easily available for staff to reference, if needed, before performing the task
- Make sure during new staff orientation that personnel are trained and documented as proficient in each procedure
- Have regular updates or ”recertification,” particularly for procedures that are done infrequently
- A well-informed patient is often the first protection against mishaps. A patient education sheet given to the patient when the TST test was administered—describing the test, how it is interpreted, and implications of a “positive” test result—may have alerted the patient in the first place that her test had been misread
- Create documentation forms that have built in “decision support”—for instance, instead of having a blank that says: “TST_____,” the form instead could describe: “TST: date applied, date read, mm of induration measured in 2 dimensions.”
1. Tuberculosis control. North Carolina Tuberculosis Policy Manual (2nd rev, 2005). Available at: www.epi.state.nc.us/epi/gcdc/tb/manual.html. Accessed on July 27, 2006.
2. Pouchot J, Grassland A, et al. Reliability of tubercelin skin test measurement. Ann Int Med 1997;126:210-214.
3. Mazurek GH, Villarino ME. Guidelines for using the QuantiFERON-TB test for diagnosing latent Mycobacterium tuberculosis infection. MMWR Recomm Rep 2003;52(RR-02):15-18.Available at: www.cdc.gov/mmwr/preview/mmwrhtml/rr5202a2.htm. Accessed on July 27, 2006
4. American Thoracic Society, CDC, and Infectious Diseases Society of America. Treatment of tuberculosis. MMWR Recomm Rep 2003;52(RR-11):1-77.Available at: www.cdc.gov/mmwr/preview/mmwrhtml/rr5211a1.htm. Accessed on July 27, 2006.
5. Gallagher TH, Levinsen W. Disclosing harmful medical errors to patients: a time for professional action. Arch Int Med 2005;165:1819-1824.
6. Kraman SS, Ham G. Risk management: extreme honesty maybe the best policy. Ann Int Med 1999;131:963-967.
7. Vincent C. Patient safety: understanding and responding to adverse events. N Engl J Med 2003;348:1051-1056.
8. National Patient Safety Agency. Being open: Communicating patient safety incidents with patients and their carers [website]. Available at: www.npsa.nhs.uk/health/resources/beingopen. Accessed on July 27, 2006.
9. Kaplan HS. Benefiting from the “gift of failure”: essentials for an event reporting system. J Leg Med 2003;24:29-35.
10. Marx D. Patient safety and the “just culture”: a primer for health care executives. Available at: www.merstm.net/support/Marx_Primer.pdf. Accessed on July 27, 2006.
11. Agency for Healthcare Research and Quality. Hospital Survey on Patient Safety Culture [online database]. Available at: www.ahrq.gov/qual/hospculture. Accessed on July 27, 2006.
12. Institute for Healthcare Improvement. Safety climate survey 2005. Available at: www.ihi.org/IHI/Topics/PatientSafety/MedicationSystems/Tools/SafetyClimateSurvey2005IHITool.htm. Accessed on July 27, 2006.
13. Department of Health. An organisation with a memory: Report of an expert group on learning from adverse events in the NHS. London, 2000. Available at: www.dh.gov.uk/PublicationsAndStatistics/Publications/PublicationsPolicyAndGuidance/PublicationsPolicyAndGuidanceArticle/fs/en?CONTENT_ID=4065083&chk=PARoiF. Accessed on July 27, 2006.
14. Veterans Administration National Center for Patient Safety. Root cause analysis. Available at: www.va.gov/ncps/rca.html. Accessed on July 27, 2006.
15. National Patient Safety Agency. National Health Service, United Kingdom. Root cause analysis toolkit and e-learning. Available at: www.npsa.nhs.uk/health/resources/root_cause_analysis/conditions. Accessed on July 27, 2006.
16. Battles JB, Kaplan HS, Van der Schaaf TW, Shea CE. The attributes of medical event reporting systems: Experience with a prototype medical event reporting system for transfusion medicine. Arch Pathol Lab Med 1998;122:231-238.
17. Medical Event Reporting System (MERS)—transfusion medicine [website]. Available at: www.mers-tm.net. Accessed on July 27, 2006.
18. Institute for Healthcare Improvement. Improvement methods. Available at: www.ihi.org/IHI/Topics/Improvement/ImprovementMethods/Changes. Accessed on July 27, 2006.
19. Sutcliffe KM, Lewton E, Rosenthal MM. Communication failures: an insidious contributor to medical mishaps. Acad Med 2004;79:186-194.
20. Sutcliffe KM. A mindful infrastructure for increasing reliability. Ambul Outreach 2000;30-34.
CORRESPONDENCE: Wail Malaty, MD, Hendersonville Family Health Center & Residency Program, 741 6th Ave W, Hendersonville, NC 28739. E-mail: Wail.Malaty@pardeehospital.org
Examination
- Patient looks well and is in no distress
- Weight 138 lbs; height 66 inches; body mass index 23; other vitals normal
- Normal heart, lung, and abdominal exam. No cervical or other adenopathy.
Medical history
- Has osteoporosis for which she takes alendronate weekly; also has diet-controlled hyperlipidemia, and is status post-remote hysterectomy for uterine bleeding
- Married, with 1 grown son who is healthy
- Nonsmoker; drinks 2 alcoholic beverages weekly; no illicit drugs
- Walks 40 minutes 4 times a week
- Mother died at age 93 from congestive heart failure; father alive, 92, has bladder cancer
- Review of systems negative for cough, fever, weight loss, or swollen glands
A Mantoux tuberculin skin test (TST) is administered per clinic protocol, and the patient is instructed to return in 48 to 72 hours for a reading of the test result.
The Mantoux TST is the most accurate test for determining tuberculosis (TB) infection.1 The standard procedure uses 0.1 cc (5 tuberculin units) of purified protein derivative (PPD) in a standard tuberculin syringe (3/8 inch, 26–27 gauge). This is administered on a flexor surface of the forearm, 2 to 4 inches below the elbow, and requires an intradermal injection (needle bevel upward) that raises a wheal 6 to 10 mm in diameter. A previously reported positive TST does not contraindicate repeated administration.1
A:
Interpreting TB test results
The definition of a positive tuberculin skin test result depends on a person’s risk factors as defined in the TABLE.1 Read a TST result 48 to 96 (ideally 72) hours after administration. Palpate and measure induration (not redness).
An alternative method is to use a ballpoint pen to draw a line starting at 1 cm from both sides of the skin reaction and moving toward its center. Where you encounter increased resistance, mark that as the border of induration. Then measure the distance between the 2 borders. This method has been reported to be slightly more precise than palpation.2
Another recently developed test for TB infection, the QuantiFERON, is based on quantification of interferon-gamma response in whole blood to TB infection. Its routine use is not recommended by the Centers for Disease Control and Prevention (CDC).3 It was unavailable in the county where the patient was tested.
TABLE
TST results regarded as positive for tuberculosis, given a patient’s specific risk factors
| 5 MM | INDURATION 10 MM | 15 MM |
|---|---|---|
| HIV infection Close contact of person with TB Previous TB on chest x-ray Intravenous drug use, or unknown HIV status | Native of country with endemic TB HIV-negative intravenous drug user Low income, inadequate healthcare Resident of long-term care facility Medical condition with increased TB risk Ages less than 4 years Likely exposure to TB | Patient has no risk factors |
The patient’s return 48 hours later
A nurse examines the patient’s arm and is uncertain how to interpret the test result. The patient’s primary physician is not in the clinic, and one of the other physicians is consulted. He reads the result as “20 mm induration, positive for TB infection.“
A chest X-ray shows no evidence of tuberculosis infection or other abnormality. The patient is referred to the local county health department. In accordance with CDC guidelines, she is diagnosed with latent tuberculosis infection and started on daily isoniazid therapy.4
The patient’s family physician learns of the patient’s diagnosis after she starts isoniazid therapy. Because of her low risk of tuberculosis, he wonders if the skin test result might have been misread. He discusses the issue with the physician who read the first skin test and discovers there was uncertainty regarding the redness (as opposed to the induration) of the skin reaction. The patient herself reports that she did not feel a hard “bump” on the skin where the test was administered.
The family physician informs the patient that the tuberculin skin test may have been incorrectly read as positive. He gives her the option of repeating the test at the county health department, whose personnel are experienced in administering and reading tuberculin skin tests. The patient chooses to repeat the TST, which is read as definitely negative. Isoniazid therapy is stopped. The patient is grateful that she does not have to continue unnecessary and potentially harmful therapy.
A:
Dealing responsibly with medical errors
A simple, straightforward explanation and apology is more likely to benefit both patient and physician than is silence or an explanation that is convoluted or places blame.
A growing consensus recommends that when a medical error is made, health care providers should tell patients about the error and apologize.5 In part this recommendation stems from accepted ethical principles of respect for patients as autonomous decision-makers, and from the obligation of providers to act with beneficence on the patient’s behalf. If a medical error impacts the patient’s care in some way, the patient is unable to make informed consent about subsequent care or trust the medical provider if the error is not divulged.
Furthermore, others have advocated that an apology after a medical error can reduce the cost or risk of tort litigation for medical malpractice.6
To encourage admissions of error, many states now prevent apologies from being used in court as evidence of guilt in malpractice cases.
Although organizations and liability insurance carriers may have specific requirements or guidelines about how to handle medical errors, practitioners may want to consider the following steps:
- Get the key facts of what happened, if possible from those who directly observed or who were involved in the care
- Report these facts to risk management or to the professional liability carrier, according to internal policies
- Apologize to the patient.
A:
Important features of an apology
- Make the apology promptly
- Be sincere
- Apologize in person
- Keep it simple—eg, “I am very sorry for any concern or inconvenience this event caused you.” Avoid blaming others, minimizing the event, or giving an involved explanation about how the problem occurred.
The purpose of the apology is simply that: to apologize. A patient may need to process feelings about what happened, so the apology should be viewed as an important opportunity for the patient to heal.
After apologizing, reassure the patient that you plan to learn from the mishap and prevent further events from happening. Stress that the trust the patient places in you and your team is not misplaced; that you take all mishaps, even minor ones, seriously and have an aggressive program of quality assurance.
Finally, though you cannot undo the event, offering to waive your professional fee for the visit that led to the mishap will help rebuild patient confidence and loyalty.
A:
Learning from errors is a vital way we prevent errors from occurring in the future. Others have described key steps to creating a culture and process of improvement.7 These include:
- Establish an atmosphere of quality improvement in your organization by emphasizing that errors are inevitable, are more often caused by faulty systems rather than faulty people, and are opportunities to learn and improve.
- Avoid blame—search for root causes.
- Create a mechanism to report all errors, mishaps, “near-misses,” and unhappy customers, and a method to systematically review these reports to identify areas to improve.
- Incorporate “lessons learned” into system changes designed to prevent recurrence of this and similar mishaps.
Openly acknowledging a mistake and apologizing to a patient, as the authors suggest, is sound advice increasingly followed in the United States and internationally. Disclosure of mistakes is a cornerstone of the safety work, as is being carried out in the United Kingdom by the National Patient Safety Agency (NPSA). They have prepared excellent online interactive educational materials to support health care professionals as they participate in the disclosure process.8
A second step the authors took was to learn about the inherent risks and potential failure points that are often deeply embedded in our care delivery processes. Mistakes are windows into the clinical work environment. If we peer through these windows regularly and systematically, we can learn a good deal about protecting our patients from harm. The mistake reported here—though of little or no harm to the patient (ie, possibly a near miss)—has potential as a rich information source about how care is delivered in the family practice clinic.9 In addition, because there was a recovery by the patient’s family physician, we have the added benefit of learning from that part of the narrative.
Learning from mistakes an intentional process, not an automatic one
First, an organization or setting must have a just culture to enable learning.10 Tools for assessing safety culture are available from the Agency for Healthcare Research and Quality (AHRQ)11 and from the Institute for Healthcare Improvement (IHI).12 A just culture is an essential attribute of a learning organization.13
Second, a systematic process must be available for inquiring about the root causes and contributing factors of events. Examples of such systems are those used by Veterans Health Administration (VHA)14 and the UK’s NPSA.15 The Medical Events Reporting System for transfusion medicine (MERS-TM) is a model reporting system in the US and is developed as a learning system.16,17
Third, we have learned that simply gathering information about the causes of events is not sufficient to prevent future events. Those involved in mistakes must be given an opportunity to come together to make sense of the causal information before they can make changes.
Fourth, a system-change method is needed to correct underlying causes. Such a method is the Plan-Do-Study Act (PDSA), which translates knowledge about causes into actions that can be implemented in the health care work environment.18
How might these processes apply to the case at hand
Two aspects of this case in particular bear scrutiny.
The clinic protocol. Protocols standardize care as well as complement the cognitive work required in clinical care. Understanding the contents and use of this protocol would shed light on this event. To what extent did the protocol support the interpretation of the TB test; how informative was it? Did it require obtaining a history from the patient as a component of the test interpretation? Did it detail the skills of the test interpreter? Did it spell out a contingency plan in the event those administering and reading the tests are unclear about the findings? Who had access to the protocol?
Handoffs, when things can get dropped. Another focus of this case is the 3 handoffs: the nurse reading the test handed the interpretation off to a physician; the physician handed the patient off to the public health clinic; and the clinic then handed the patient back to her primary care physician. Handoffs often lead to mistakes because they involve interpersonal communication and transfer of information, both of which are fraught with opportunities for errors.19
In the first handoff, we might well ask what information the nurse had about the patient’s history and what information she communicated to the physician? A full understanding of this handoff helps to make explicit hierarchical relationships in the clinic as well as information flow.
With the second handoff, we might ask what information regarding the uncertainty of the patient’s TB test interpretation and history were passed along to the TB clinic? How was the information communicated—on paper, electronically, by telephone? Each of these methods has unique constraints.
Finally, the fortunate third handoff—follow-up with the patient’s family practice physician that resulted in the discovery of the mistake and therefore recovery. It is particularly important to note that the recovery came because of an apparent system of feedback of information to the patient’s family physician. Such feedback loops contribute to safety. The family physician noticed something that did not make sense and investigated it. That is, the family physician was mindful.20 This attitude of mindfulness is a critical component in safe or reliable systems. Hubris is the enemy of safety.
Shirley Kellie, MD, MSc
Physician epidemiologist, American Medical Association
A:
In this particular case, a system-based approach to care might have anticipated and prevented this error through the following steps:
- Create specific written instructions for office procedures
- Have the written procedures handy and easily available for staff to reference, if needed, before performing the task
- Make sure during new staff orientation that personnel are trained and documented as proficient in each procedure
- Have regular updates or ”recertification,” particularly for procedures that are done infrequently
- A well-informed patient is often the first protection against mishaps. A patient education sheet given to the patient when the TST test was administered—describing the test, how it is interpreted, and implications of a “positive” test result—may have alerted the patient in the first place that her test had been misread
- Create documentation forms that have built in “decision support”—for instance, instead of having a blank that says: “TST_____,” the form instead could describe: “TST: date applied, date read, mm of induration measured in 2 dimensions.”
Examination
- Patient looks well and is in no distress
- Weight 138 lbs; height 66 inches; body mass index 23; other vitals normal
- Normal heart, lung, and abdominal exam. No cervical or other adenopathy.
Medical history
- Has osteoporosis for which she takes alendronate weekly; also has diet-controlled hyperlipidemia, and is status post-remote hysterectomy for uterine bleeding
- Married, with 1 grown son who is healthy
- Nonsmoker; drinks 2 alcoholic beverages weekly; no illicit drugs
- Walks 40 minutes 4 times a week
- Mother died at age 93 from congestive heart failure; father alive, 92, has bladder cancer
- Review of systems negative for cough, fever, weight loss, or swollen glands
A Mantoux tuberculin skin test (TST) is administered per clinic protocol, and the patient is instructed to return in 48 to 72 hours for a reading of the test result.
The Mantoux TST is the most accurate test for determining tuberculosis (TB) infection.1 The standard procedure uses 0.1 cc (5 tuberculin units) of purified protein derivative (PPD) in a standard tuberculin syringe (3/8 inch, 26–27 gauge). This is administered on a flexor surface of the forearm, 2 to 4 inches below the elbow, and requires an intradermal injection (needle bevel upward) that raises a wheal 6 to 10 mm in diameter. A previously reported positive TST does not contraindicate repeated administration.1
A:
Interpreting TB test results
The definition of a positive tuberculin skin test result depends on a person’s risk factors as defined in the TABLE.1 Read a TST result 48 to 96 (ideally 72) hours after administration. Palpate and measure induration (not redness).
An alternative method is to use a ballpoint pen to draw a line starting at 1 cm from both sides of the skin reaction and moving toward its center. Where you encounter increased resistance, mark that as the border of induration. Then measure the distance between the 2 borders. This method has been reported to be slightly more precise than palpation.2
Another recently developed test for TB infection, the QuantiFERON, is based on quantification of interferon-gamma response in whole blood to TB infection. Its routine use is not recommended by the Centers for Disease Control and Prevention (CDC).3 It was unavailable in the county where the patient was tested.
TABLE
TST results regarded as positive for tuberculosis, given a patient’s specific risk factors
| 5 MM | INDURATION 10 MM | 15 MM |
|---|---|---|
| HIV infection Close contact of person with TB Previous TB on chest x-ray Intravenous drug use, or unknown HIV status | Native of country with endemic TB HIV-negative intravenous drug user Low income, inadequate healthcare Resident of long-term care facility Medical condition with increased TB risk Ages less than 4 years Likely exposure to TB | Patient has no risk factors |
The patient’s return 48 hours later
A nurse examines the patient’s arm and is uncertain how to interpret the test result. The patient’s primary physician is not in the clinic, and one of the other physicians is consulted. He reads the result as “20 mm induration, positive for TB infection.“
A chest X-ray shows no evidence of tuberculosis infection or other abnormality. The patient is referred to the local county health department. In accordance with CDC guidelines, she is diagnosed with latent tuberculosis infection and started on daily isoniazid therapy.4
The patient’s family physician learns of the patient’s diagnosis after she starts isoniazid therapy. Because of her low risk of tuberculosis, he wonders if the skin test result might have been misread. He discusses the issue with the physician who read the first skin test and discovers there was uncertainty regarding the redness (as opposed to the induration) of the skin reaction. The patient herself reports that she did not feel a hard “bump” on the skin where the test was administered.
The family physician informs the patient that the tuberculin skin test may have been incorrectly read as positive. He gives her the option of repeating the test at the county health department, whose personnel are experienced in administering and reading tuberculin skin tests. The patient chooses to repeat the TST, which is read as definitely negative. Isoniazid therapy is stopped. The patient is grateful that she does not have to continue unnecessary and potentially harmful therapy.
A:
Dealing responsibly with medical errors
A simple, straightforward explanation and apology is more likely to benefit both patient and physician than is silence or an explanation that is convoluted or places blame.
A growing consensus recommends that when a medical error is made, health care providers should tell patients about the error and apologize.5 In part this recommendation stems from accepted ethical principles of respect for patients as autonomous decision-makers, and from the obligation of providers to act with beneficence on the patient’s behalf. If a medical error impacts the patient’s care in some way, the patient is unable to make informed consent about subsequent care or trust the medical provider if the error is not divulged.
Furthermore, others have advocated that an apology after a medical error can reduce the cost or risk of tort litigation for medical malpractice.6
To encourage admissions of error, many states now prevent apologies from being used in court as evidence of guilt in malpractice cases.
Although organizations and liability insurance carriers may have specific requirements or guidelines about how to handle medical errors, practitioners may want to consider the following steps:
- Get the key facts of what happened, if possible from those who directly observed or who were involved in the care
- Report these facts to risk management or to the professional liability carrier, according to internal policies
- Apologize to the patient.
A:
Important features of an apology
- Make the apology promptly
- Be sincere
- Apologize in person
- Keep it simple—eg, “I am very sorry for any concern or inconvenience this event caused you.” Avoid blaming others, minimizing the event, or giving an involved explanation about how the problem occurred.
The purpose of the apology is simply that: to apologize. A patient may need to process feelings about what happened, so the apology should be viewed as an important opportunity for the patient to heal.
After apologizing, reassure the patient that you plan to learn from the mishap and prevent further events from happening. Stress that the trust the patient places in you and your team is not misplaced; that you take all mishaps, even minor ones, seriously and have an aggressive program of quality assurance.
Finally, though you cannot undo the event, offering to waive your professional fee for the visit that led to the mishap will help rebuild patient confidence and loyalty.
A:
Learning from errors is a vital way we prevent errors from occurring in the future. Others have described key steps to creating a culture and process of improvement.7 These include:
- Establish an atmosphere of quality improvement in your organization by emphasizing that errors are inevitable, are more often caused by faulty systems rather than faulty people, and are opportunities to learn and improve.
- Avoid blame—search for root causes.
- Create a mechanism to report all errors, mishaps, “near-misses,” and unhappy customers, and a method to systematically review these reports to identify areas to improve.
- Incorporate “lessons learned” into system changes designed to prevent recurrence of this and similar mishaps.
Openly acknowledging a mistake and apologizing to a patient, as the authors suggest, is sound advice increasingly followed in the United States and internationally. Disclosure of mistakes is a cornerstone of the safety work, as is being carried out in the United Kingdom by the National Patient Safety Agency (NPSA). They have prepared excellent online interactive educational materials to support health care professionals as they participate in the disclosure process.8
A second step the authors took was to learn about the inherent risks and potential failure points that are often deeply embedded in our care delivery processes. Mistakes are windows into the clinical work environment. If we peer through these windows regularly and systematically, we can learn a good deal about protecting our patients from harm. The mistake reported here—though of little or no harm to the patient (ie, possibly a near miss)—has potential as a rich information source about how care is delivered in the family practice clinic.9 In addition, because there was a recovery by the patient’s family physician, we have the added benefit of learning from that part of the narrative.
Learning from mistakes an intentional process, not an automatic one
First, an organization or setting must have a just culture to enable learning.10 Tools for assessing safety culture are available from the Agency for Healthcare Research and Quality (AHRQ)11 and from the Institute for Healthcare Improvement (IHI).12 A just culture is an essential attribute of a learning organization.13
Second, a systematic process must be available for inquiring about the root causes and contributing factors of events. Examples of such systems are those used by Veterans Health Administration (VHA)14 and the UK’s NPSA.15 The Medical Events Reporting System for transfusion medicine (MERS-TM) is a model reporting system in the US and is developed as a learning system.16,17
Third, we have learned that simply gathering information about the causes of events is not sufficient to prevent future events. Those involved in mistakes must be given an opportunity to come together to make sense of the causal information before they can make changes.
Fourth, a system-change method is needed to correct underlying causes. Such a method is the Plan-Do-Study Act (PDSA), which translates knowledge about causes into actions that can be implemented in the health care work environment.18
How might these processes apply to the case at hand
Two aspects of this case in particular bear scrutiny.
The clinic protocol. Protocols standardize care as well as complement the cognitive work required in clinical care. Understanding the contents and use of this protocol would shed light on this event. To what extent did the protocol support the interpretation of the TB test; how informative was it? Did it require obtaining a history from the patient as a component of the test interpretation? Did it detail the skills of the test interpreter? Did it spell out a contingency plan in the event those administering and reading the tests are unclear about the findings? Who had access to the protocol?
Handoffs, when things can get dropped. Another focus of this case is the 3 handoffs: the nurse reading the test handed the interpretation off to a physician; the physician handed the patient off to the public health clinic; and the clinic then handed the patient back to her primary care physician. Handoffs often lead to mistakes because they involve interpersonal communication and transfer of information, both of which are fraught with opportunities for errors.19
In the first handoff, we might well ask what information the nurse had about the patient’s history and what information she communicated to the physician? A full understanding of this handoff helps to make explicit hierarchical relationships in the clinic as well as information flow.
With the second handoff, we might ask what information regarding the uncertainty of the patient’s TB test interpretation and history were passed along to the TB clinic? How was the information communicated—on paper, electronically, by telephone? Each of these methods has unique constraints.
Finally, the fortunate third handoff—follow-up with the patient’s family practice physician that resulted in the discovery of the mistake and therefore recovery. It is particularly important to note that the recovery came because of an apparent system of feedback of information to the patient’s family physician. Such feedback loops contribute to safety. The family physician noticed something that did not make sense and investigated it. That is, the family physician was mindful.20 This attitude of mindfulness is a critical component in safe or reliable systems. Hubris is the enemy of safety.
Shirley Kellie, MD, MSc
Physician epidemiologist, American Medical Association
A:
In this particular case, a system-based approach to care might have anticipated and prevented this error through the following steps:
- Create specific written instructions for office procedures
- Have the written procedures handy and easily available for staff to reference, if needed, before performing the task
- Make sure during new staff orientation that personnel are trained and documented as proficient in each procedure
- Have regular updates or ”recertification,” particularly for procedures that are done infrequently
- A well-informed patient is often the first protection against mishaps. A patient education sheet given to the patient when the TST test was administered—describing the test, how it is interpreted, and implications of a “positive” test result—may have alerted the patient in the first place that her test had been misread
- Create documentation forms that have built in “decision support”—for instance, instead of having a blank that says: “TST_____,” the form instead could describe: “TST: date applied, date read, mm of induration measured in 2 dimensions.”
1. Tuberculosis control. North Carolina Tuberculosis Policy Manual (2nd rev, 2005). Available at: www.epi.state.nc.us/epi/gcdc/tb/manual.html. Accessed on July 27, 2006.
2. Pouchot J, Grassland A, et al. Reliability of tubercelin skin test measurement. Ann Int Med 1997;126:210-214.
3. Mazurek GH, Villarino ME. Guidelines for using the QuantiFERON-TB test for diagnosing latent Mycobacterium tuberculosis infection. MMWR Recomm Rep 2003;52(RR-02):15-18.Available at: www.cdc.gov/mmwr/preview/mmwrhtml/rr5202a2.htm. Accessed on July 27, 2006
4. American Thoracic Society, CDC, and Infectious Diseases Society of America. Treatment of tuberculosis. MMWR Recomm Rep 2003;52(RR-11):1-77.Available at: www.cdc.gov/mmwr/preview/mmwrhtml/rr5211a1.htm. Accessed on July 27, 2006.
5. Gallagher TH, Levinsen W. Disclosing harmful medical errors to patients: a time for professional action. Arch Int Med 2005;165:1819-1824.
6. Kraman SS, Ham G. Risk management: extreme honesty maybe the best policy. Ann Int Med 1999;131:963-967.
7. Vincent C. Patient safety: understanding and responding to adverse events. N Engl J Med 2003;348:1051-1056.
8. National Patient Safety Agency. Being open: Communicating patient safety incidents with patients and their carers [website]. Available at: www.npsa.nhs.uk/health/resources/beingopen. Accessed on July 27, 2006.
9. Kaplan HS. Benefiting from the “gift of failure”: essentials for an event reporting system. J Leg Med 2003;24:29-35.
10. Marx D. Patient safety and the “just culture”: a primer for health care executives. Available at: www.merstm.net/support/Marx_Primer.pdf. Accessed on July 27, 2006.
11. Agency for Healthcare Research and Quality. Hospital Survey on Patient Safety Culture [online database]. Available at: www.ahrq.gov/qual/hospculture. Accessed on July 27, 2006.
12. Institute for Healthcare Improvement. Safety climate survey 2005. Available at: www.ihi.org/IHI/Topics/PatientSafety/MedicationSystems/Tools/SafetyClimateSurvey2005IHITool.htm. Accessed on July 27, 2006.
13. Department of Health. An organisation with a memory: Report of an expert group on learning from adverse events in the NHS. London, 2000. Available at: www.dh.gov.uk/PublicationsAndStatistics/Publications/PublicationsPolicyAndGuidance/PublicationsPolicyAndGuidanceArticle/fs/en?CONTENT_ID=4065083&chk=PARoiF. Accessed on July 27, 2006.
14. Veterans Administration National Center for Patient Safety. Root cause analysis. Available at: www.va.gov/ncps/rca.html. Accessed on July 27, 2006.
15. National Patient Safety Agency. National Health Service, United Kingdom. Root cause analysis toolkit and e-learning. Available at: www.npsa.nhs.uk/health/resources/root_cause_analysis/conditions. Accessed on July 27, 2006.
16. Battles JB, Kaplan HS, Van der Schaaf TW, Shea CE. The attributes of medical event reporting systems: Experience with a prototype medical event reporting system for transfusion medicine. Arch Pathol Lab Med 1998;122:231-238.
17. Medical Event Reporting System (MERS)—transfusion medicine [website]. Available at: www.mers-tm.net. Accessed on July 27, 2006.
18. Institute for Healthcare Improvement. Improvement methods. Available at: www.ihi.org/IHI/Topics/Improvement/ImprovementMethods/Changes. Accessed on July 27, 2006.
19. Sutcliffe KM, Lewton E, Rosenthal MM. Communication failures: an insidious contributor to medical mishaps. Acad Med 2004;79:186-194.
20. Sutcliffe KM. A mindful infrastructure for increasing reliability. Ambul Outreach 2000;30-34.
CORRESPONDENCE: Wail Malaty, MD, Hendersonville Family Health Center & Residency Program, 741 6th Ave W, Hendersonville, NC 28739. E-mail: Wail.Malaty@pardeehospital.org
1. Tuberculosis control. North Carolina Tuberculosis Policy Manual (2nd rev, 2005). Available at: www.epi.state.nc.us/epi/gcdc/tb/manual.html. Accessed on July 27, 2006.
2. Pouchot J, Grassland A, et al. Reliability of tubercelin skin test measurement. Ann Int Med 1997;126:210-214.
3. Mazurek GH, Villarino ME. Guidelines for using the QuantiFERON-TB test for diagnosing latent Mycobacterium tuberculosis infection. MMWR Recomm Rep 2003;52(RR-02):15-18.Available at: www.cdc.gov/mmwr/preview/mmwrhtml/rr5202a2.htm. Accessed on July 27, 2006
4. American Thoracic Society, CDC, and Infectious Diseases Society of America. Treatment of tuberculosis. MMWR Recomm Rep 2003;52(RR-11):1-77.Available at: www.cdc.gov/mmwr/preview/mmwrhtml/rr5211a1.htm. Accessed on July 27, 2006.
5. Gallagher TH, Levinsen W. Disclosing harmful medical errors to patients: a time for professional action. Arch Int Med 2005;165:1819-1824.
6. Kraman SS, Ham G. Risk management: extreme honesty maybe the best policy. Ann Int Med 1999;131:963-967.
7. Vincent C. Patient safety: understanding and responding to adverse events. N Engl J Med 2003;348:1051-1056.
8. National Patient Safety Agency. Being open: Communicating patient safety incidents with patients and their carers [website]. Available at: www.npsa.nhs.uk/health/resources/beingopen. Accessed on July 27, 2006.
9. Kaplan HS. Benefiting from the “gift of failure”: essentials for an event reporting system. J Leg Med 2003;24:29-35.
10. Marx D. Patient safety and the “just culture”: a primer for health care executives. Available at: www.merstm.net/support/Marx_Primer.pdf. Accessed on July 27, 2006.
11. Agency for Healthcare Research and Quality. Hospital Survey on Patient Safety Culture [online database]. Available at: www.ahrq.gov/qual/hospculture. Accessed on July 27, 2006.
12. Institute for Healthcare Improvement. Safety climate survey 2005. Available at: www.ihi.org/IHI/Topics/PatientSafety/MedicationSystems/Tools/SafetyClimateSurvey2005IHITool.htm. Accessed on July 27, 2006.
13. Department of Health. An organisation with a memory: Report of an expert group on learning from adverse events in the NHS. London, 2000. Available at: www.dh.gov.uk/PublicationsAndStatistics/Publications/PublicationsPolicyAndGuidance/PublicationsPolicyAndGuidanceArticle/fs/en?CONTENT_ID=4065083&chk=PARoiF. Accessed on July 27, 2006.
14. Veterans Administration National Center for Patient Safety. Root cause analysis. Available at: www.va.gov/ncps/rca.html. Accessed on July 27, 2006.
15. National Patient Safety Agency. National Health Service, United Kingdom. Root cause analysis toolkit and e-learning. Available at: www.npsa.nhs.uk/health/resources/root_cause_analysis/conditions. Accessed on July 27, 2006.
16. Battles JB, Kaplan HS, Van der Schaaf TW, Shea CE. The attributes of medical event reporting systems: Experience with a prototype medical event reporting system for transfusion medicine. Arch Pathol Lab Med 1998;122:231-238.
17. Medical Event Reporting System (MERS)—transfusion medicine [website]. Available at: www.mers-tm.net. Accessed on July 27, 2006.
18. Institute for Healthcare Improvement. Improvement methods. Available at: www.ihi.org/IHI/Topics/Improvement/ImprovementMethods/Changes. Accessed on July 27, 2006.
19. Sutcliffe KM, Lewton E, Rosenthal MM. Communication failures: an insidious contributor to medical mishaps. Acad Med 2004;79:186-194.
20. Sutcliffe KM. A mindful infrastructure for increasing reliability. Ambul Outreach 2000;30-34.
CORRESPONDENCE: Wail Malaty, MD, Hendersonville Family Health Center & Residency Program, 741 6th Ave W, Hendersonville, NC 28739. E-mail: Wail.Malaty@pardeehospital.org
How a series of errors led to recurrent hypoglycemia
At about 4 P.M., while driving with his wife (she is at the wheel), he starts sweating, slurring his speech, and feeling drowsy. His wife heads to the emergency department (ED), where his glucose level by fingerstick is found to be 37 mg/dL. He receives an infusion of dextrose 50% and his symptoms promptly resolve. The patient says he has not missed any meals and that he has been taking his medications as prescribed. He was seen in the same ED yesterday after a brief syncopal attack that was also attributed to hypoglycemia. The patient is admitted to the hospital under the family medicine residency service for further monitoring and management of recurrent hypoglycemia. Since you are the primary doctor, the admitting resident calls you.
You pay the patient a visit and ask him about his medications. He shows you the list and says he is taking them all “faithfully.” You note that the list contains both glipizide (which he has misspelled as “glipizine”) and Glucotrol (a branded version of glipizide). When queried on this point, he insists these are different medicines your office prescribed for him, and he is taking both. This therapeutic duplication, you suspect, is the likely cause of his recurrent episodes of hypoglycemia.
You review your outpatient records (you do not have an EMR) and discuss events in more detail with the patient and his wife. One month ago, the patient came to your office for a routine follow-up visit. You were out of town, so he saw one of your colleagues. He recalls that the doctor told him his sugar levels were too high and gave him a prescription, instructing him to take it with-out fail. He already had enough Glucotrol XL at home and had not requested a refill, so he assumed this was a new medication. He does not recall reading the prescription. The outpatient record shows that the patient had admitted to missing doses of his Glucotrol XL and that the covering physician attributed the hyperglycemia to this poor compliance. The physician had therefore decided to keep the dose of Glucotrol XL the same, provided a refill of Glucotrol XL 10 mg daily, and counseled the patient to improve compliance.
The patient took the script to his usual pharmacy, but they had just closed. He went instead to another nearby pharmacy (part of another chain), where he had the prescription filled. The bottle was labeled by the pharmacy: Glipizide XL 10 mg. Since that date he has been taking both Glucotrol and glipizide and, following the physician’s advice, has not missed a dose.
Q: How could this duplication have occurred?
A:___________________________________________________________
Better monitoring systems needed
Therapeutic duplication (referring, in general, to the use of more than one medication from the same class) is a serious problem, as illustrated by this case. A study of 208 elderly patients on 5 or more medications at a general medical clinic in North Carolina found therapeutic duplication in 5.7% of patients.1 In a Canadian study involving 12,560 elderly patients in primary care settings, the rate was 4%.2 Rates in other settings have been found to be higher (21% of 1854 nursing home residents in Sweden,3 and 15% of 259 patients newly enrolled in a home healthcare pro-gram in New York and California.4) In this case we have a patient taking 2 different preparations of the same drug. The causes of therapeutic duplication have not been well studied, but potential reasons are outlined in TABLE 1.
Current systems go only so far. Practices that have well-maintained medication lists on paper or as part of an electronic medical record are in a good position to avoid duplicate prescribing. However, tracking systems restricted to an office practice will not prevent duplications made by consultants or hospital physicians.
Pharmacies generally have software that checks for therapeutic duplication, thereby allowing pharmacists to alert physicians of the potential problem. This works well if a patient uses one pharmacy exclusively. But in the case at hand, the patient elected to go to a different pharmacy instead of waiting for his usual pharmacy to reopen the next business day. This innocent action circumvented the safety system, which did not extend to the other pharmacy. Some pharmacy chains have databases integrated across multiple sites, which can help if patients stay loyal to one chain.
Similarly, third-party payers such as many state Medicaid systems have the opportunity to identify and alert physicians to therapeutic duplications. However, I could find no reports in the literature regarding the implementation or effectiveness of such systems.
TABLE 2 offers suggestions for reducing the risk of therapeutic duplication in your practice.
Medication reconciliation is key. As a step toward addressing the larger picture of medication errors, the Joint Commission for Accreditation of Healthcare Organizations (JCAHO) has introduced for the year 2006 the following Patient Safety Goal (Goal #8): “Accurately and completely reconcile medications across the continuum of care,” commonly referred to as “medication reconciliation.”5 JCAHO’s adoption of this goal acknowledges, first, that transitions between different parts of the system are a common source of error, and, second, that these transition points (eg, admission to the hospital, or transfer out of the ICU) are opportunities to detect and correct errors. Various tools have been reported in the literature for addressing this issue. 6-8 The strategies listed in TABLE 2 can also be seen as contributing to this JCAHO goal.
TABLE 1
Have you encountered these causes of therapeutic duplication?
| MISCOMMUNICATION |
| In this case, the patient misunderstood the prescription to be for a new medication rather than a refill of an existing one. Miscommunications can be caused by the patient, the doctor, nursing staff, pharmacy staff, or any combination of these. |
| KNOWLEDGE DEFICIT |
| For example, a physician who does not know that sulindac is an NSAID might prescribe another NSAID such as ibuprofen to a patient whose pain is not controlled with sulindac. |
| POOR MEDICATION TRACKING WITHIN A PRACTICE |
| The office in this case relied on paper-based medication lists that were poorly maintained. The covering physician did not have access to accurate information about the most recent prescription date and number of refills, and elected to give a refill on Glucotrol XL. It is important to note that the primary physician might also have made the same mistake given the ineffective tracking system. |
| POOR MEDICATION TRACKING DURING TRANSITIONS |
| When patients move between different parts of the healthcare system such as the primary physician’s office, a specialist’s office, emergency departments, hospitals, and nursing homes, there are opportunities for errors, including therapeutic duplication. Transitions into and out of the hospital are receiving increasing attention because of the trend towards use of hospitalists.25 Unless specific systems are put in place to ensure continuity (as exist in some integrated healthcare systems), hospitalists and residents who provide inpatient coverage often do not have immediate access to accurate information regarding a patient’s prior medications and refills. |
| FORMULARY ISSUES |
| The policies of some hospitals and health insurance carriers can lead to therapeutic substitutions that can in turn result in therapeutic duplication. For example, if a patient who takes ramipril at home for hypertension is changed to enalapril during hospitalization and is given a prescription for enalapril at discharge, he might take both. |
TABLE 2
Strategies for preventing or detecting therapeutic duplication
| Keep better medication records (preferably with an EMR). This includes keeping track of dosage changes, refill dates, and numbers of refills given. Consider including the indication for each drug so that it is easier to detect therapeutic duplication. |
| Communicate better with patients regarding medications, especially when changes are made. Ask patients to repeat your instructions to check their understanding. |
| Encourage patients to use the same pharmacy (or chain) consistently, explaining that the usual pharmacist will have much better access to their medication records. |
| For high-risk patients (such as cognitively impaired, those on multiple medications, those with multiple physicians), arrange for regular medication review, at which a patient brings all medications to the office. |
| If you use a hospitalist (or residency program) for inpatient coverage, ensure that you have adequate systems in place to provide continuity of care regarding medications and other issues. |
| At post-hospitalization follow-up visits, review medications carefully. You may detect a variety of errors. |
| Consider implementing patient-carried medication lists. These can be paper-based or electronic. |
The story unfolds
You now know the patient has been taking twice the intended dose of his sulphonylurea for about a month, and you ask how he has been feeling during this time. He says he did well initially and did not experience any symptoms of hypoglycemia or hyperglycemia. He has a glucometer at home but did not use it during this period.
Two days ago, his wife expressed concerned that he was seeing several doctors (urologist, medical oncologist, radiation oncologist) for the prostate cancer and wanted to make sure he told them about all his medications. She asked him to make a list of his medications and to keep it in his wallet. He did so (FIGURE 1). That night he went out drinking (in his words, “the whole night”) because he was worried about his upcoming prostate surgery.
The next morning he forgot to take his medications and at noon he experienced transient loss of consciousness. He went to the ED and was found to have a blood sugar of 55. The loss of consciousness was attributed to hypoglycemia secondary to an alcohol binge. The patient says he showed his medication list to one of the ED staff but was not given any advice, except to follow-up with his personal physician. Last night his wife insisted he take his medications since he had missed them in the morning. He did so. This morning he took his medication as prescribed and developed hypoglycemia at about 4 P.M. (while in the car), precipitating this admission.
Q: Why did the patient-carried medication list not seem to help in this case?
A:____________________________________________________________
Why didn’t the list help? A complete, accurate, up-to-date list of a patient’s medications, held by the patient and made available to all healthcare providers to review and update, should be an effective means of tracking medications within and across healthcare settings, thereby reducing risk of errors including duplication. However, in this case, the ED physician did not detect the error even though the patient did have a list that was complete, accurate (except for the misspelling of glipizide), and up-to-date.
The precise circumstances were unclear, but one might speculate that the ED staff were so busy they did not notice the duplication or were unfamiliar with the medications (confounded by the patient’s misspelling of glipizide), or did not take the list seriously because it was poorly written and in poor condition, or were convinced that the hypoglycemia was precipitated by alcohol. Though the ED staff’s failure to recognize the duplication was a missed opportunity, to blame them would be inappropriate and unproductive. Instead, as will be re-emphasized later, we should focus on the underlying system issues that precipitated the failure, including the presence or absence of protocols for medication reconciliation, and the characteristics of the medication list that the patient was using.
Improving patient-carried medication records. These records have been used with varying success.9-11 Studies show it is difficult to ensure that patients carry records consistently, and to ensure that prescribers update them. Optimal characteristics of such records have yet to be determined, and they will likely vary depending on circumstances. However, the published experiences9-11 together with review of the present case suggest simple strategies that might help improve the list our patient was carrying.
First, the list should be easy to read and update and be durable.
Second, it should be convenient to carry (wallet-size, for example).
Third, it should include the appropriate amount of information that helps busy practitioners detect errors easily. This issue requires further study, but we might consider using generic names and including information about drug class and indication.
What about electronic media? One proposed solution to paper records is the use of electronic media such as flash memory cards or web-based records.12-14 Two challenges to widespread implementation of this strategy are cost and compatibility. To deal with the latter issue, current legislative efforts (Wired for Health Care Quality Act S. 1418) are aiming to create standard formats for exchange of electronic health information. Obviously the ability to link to electronic prescribing systems from anywhere would greatly reduce the risk of duplicate prescribing.
In the meantime it may be reasonable, especially for high-risk patients, to provide or encourage the use of paper-based medication lists with the caveat that they need to be kept up to date and shared with all providers.
FIGURE 1 Patient’s medication list

The need for vigilance never ends
The patient is managed appropriately by the inpatient team. His diabetes medications are discontinued and he is placed on a 5% dextrose infusion. He does well. By the following evening, he is off intravenous fluids, is maintaining adequate glucose levels, and is ready for discharge home. The plan calls for him to stop the Glucotrol XL and continue the generic glipizide XL only.
You go to the hospital to check on him and find that he and his wife are about to leave. The nurse has reviewed discharge instructions with them and the patient is holding a copy. You ask to see the instructions. FIGURE 2 shows the medication section of the instruction sheet.
Glucotrol XL appears correctly in the section “Discontinued medications” with the clear instruction “Do NOT take these medications.” However, it is also listed under “Pre-hospital medications to be continued.” When you ask the patient what medications he intends to take at home, he admits that he and his wife are a little confused by the instructions. He says they decided he should continue the same medications he was on before since these are what you and your office colleague prescribed. He adds, by way of explanation, that he trusts you more than he trusts the hospital team because you know him best. You are surprised by his answer but then realize that neither you nor the house staff has explained the duplication error to him. He still believes Glucotrol and glipizide are different medications and does not understand that taking them together caused his symptoms.
Q: Why might you and the house staff have been vague about the cause of the hypoglycemia? What should you say now?
A:_____________________________________________________
Discussing prescribing errors is uncomfortable. In this instance, you the primary doctor may have been reluctant because your office appeared to be most responsible for the mistake. And the residents also may have been reluctant to say anything that might appear critical of the primary doctor’s office. Evidence suggests that most physicians prefer not to discuss the details of errors or even to use the term “error.” They prefer less emotive language.15 In contrast, there is some evidence to suggest that patients and families would like to be informed when an error occurs in their care.15,18
As the primary care physician discovered in this case, correcting a medication error often depends on informing the patient. The negative impacts of disclosure (including the possibility of litigation and other sanctions, and the potential for loss of trust) are the subject of much debate.19-21
Ultimately, the decision to disclose an error must be based on risks and benefits to both patient and physician. If you decide to disclose, choose words carefully. And be careful to avoid apportioning blame. As this case illustrates, adverse events can have many contributing factors, and, in most cases, further investigation is required before a full explanation can be given. Therefore it is generally recommended that when disclosure is made, you should limit the discussion to the known facts. Further disclosure can always be made at a later date if warranted, when more objective information is available.
FIGURE 2 Hospital discharge instructions

A closer examination of what went wrong
In this case, unusual situations, system problems, and errors by individuals combined to cause recurrent hypoglycemia and unnecessary hospitalization. James Reason has provided a framework in which a case such as this may be analyzed systematically. It is called the Adverse Event Trajectory,22 and its application to this case is depicted in FIGURE 3. Each contributing factor is categorized according to the framework and written onto the diagram in such a way as to provide a summary of the whole event. This format has been used successfully as a teaching tool for family medicine residents.23
The main advantage of this analysis is that it clearly separates human errors (Active Failures) and system problems (Latent Failures, and the lack of Safety Barriers). Often, human error is chiefly blamed for adverse events and little effort is made to look beyond this. However, if we accept that “to err is human”24 and that most errors have roots in systemic problems, then the Adverse Event Trajectory framework can focus our attention on areas more likely to yield workable solutions.
Preventing recurrent errors usually is best assured by (1) correcting latent failures and (2) creating effective safety barriers. The strategies in TABLE 2 that involve changing systems (such as implementing electronic prescribing as part of an electronic medical record) are more likely to be effective than those that change behavior only (such as encouraging patients to use one pharmacy exclusively). However, system strategies also tend to be more expensive and difficult to implement than the latter. Perhaps it is most appropriate to use a combination of approaches listed in TABLE 2.
As implied under “Safety Barriers” in FIGURE 3, an effective patient-carried medication list had the potential to protect this patient from harm. Possible strategies for implementing such a barrier have been discussed above.
Items 2 and 3 under “Latent Failures” apply to the pharmacy level, and solutions would likely require legislation. Restricting access to one pharmacy exclusively would probably have prevented the duplication in our case. However, if such restriction were enforced unilaterally by a payer, it could make that payer less competitive since patients may value the freedom of changing pharmacies at will.
A more realistic alternative is to give pharmacies access to one another’s databases or even to create a central database to which all pharmacies would have access, with the patient’s permission. Clearly confidentiality issues would need to be addressed before such a program was implemented. And there would likely be opposition from the large pharmacy chains who might see this approach as a threat.
FIGURE 3 Adverse event trajectory: Breaking down the process into revealing components
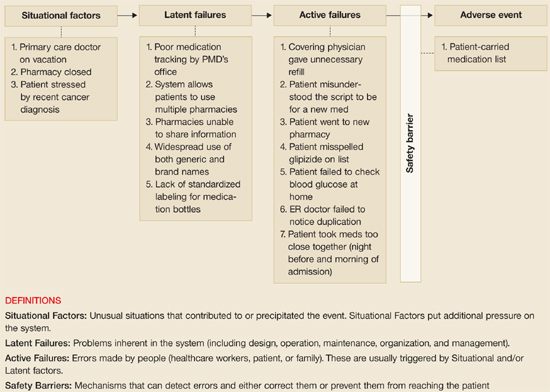
The value of this analytic technique is in identifying and categorizing all factors (not just human error) that potentially contribute to untoward events. Efforts aimed at correcting or improving factors under “Latent Failures” or “Safety Barriers” are usually most fruitful.
This case illustrates the complex interaction of hospital, physician’s office, pharmacy, and patient’s home in causing or preventing medication errors. Fostering better communication with patients and improving patient medication records become even more important in this day of internet website purchases and mail-order pharmacies.
However, creating the common medication record is insufficient to assuring patient safety. The medication record must be reconciled with the patient’s behavior, including actual use of prescribed, over the counter, herbal, homeopathic, home, and other alternative remedies.
Communication must be clear not only while the patient is being cared for, but also when care transitions occur. The patient’s health literacy, values about care, dependence on others, and cultural beliefs are known to influence how patients actually use medications.
Better technology systems would certainly help detect medication errors. But a non-technology solution is available now. In this case, the patient’s poor health literacy was certainly evident in his lack of knowledge of the names of medications and in not understanding the duplication of drugs he was prescribed. But what about the medication literacy of the physician and nurse professionals in this case? Explaining the unfamiliar (and misspelled) drug to the patient could have prevented the drug duplication.
This patient indicated his trust in his primary care physician. This is cornerstone to the therapeutic relationship. However, this trust was not adequate to prevent this error from occurring or from the patient experiencing harm. Patient advocate organizations, such as the National Council for Patient Information and Education, or the Agency for Healthcare Research and Quality, suggest that patients will best be protected from harm by becoming an active participant on the health care team. Safety is achieved through ongoing and appropriate communication with patients to prevent harm. Pharmacists do contribute to resolving many medication safety issues for patients. The practice of pharmacy includes comprehensive medication history taking and documentation to maintain a patients medication profile.
For many patients, the pharmacist is a primary provider who communicates with them fairly regularly about medicines, and maintains medication lists. Many pharmacists routinely provide patients with medication list wallet cards, conduct comprehensive “brown bag” medication reviews, and maintain an active medication profile, including the over the counter and alternative remedies that patients describe or purchase from the pharmacy.
With the Medicare Modernization Act of 2003 came the federal prescription drug benefit, covering some of the costs to elderly patients who elect a prescription drug benefit provider who chooses to provide drug therapy monitoring services. Many pharmacists are expanding medication management services to support the patient with needed communication and counseling to prevent harm and improve safety. These will be important additions to the health care safety needs of patients.
Even with the system improvements we have described above, medication safety remains a shared responsibility between health care providers, patients, and health care organizations. A few guides have been published and are available free of charge to assist patients in knowing what they can do to help themselves with proper medication use and safety. These guides offer some practical tools and advice for patients to build patient knowledge about what to expect. Patients who use these tools will better assure safe practices and minimize harm:
Your Medicine: Play It Safe. Patient Guide. AHRQ Publication No. 03-0019, February 2003. Rockville, Md: Agency for Healthcare Research and Quality; Bethesda, Md: National Council on Patient Information and Education; 2003. Available at: www.ahrq.gov/consumer/safemeds/safemeds.htm.
20 Tips to Help Prevent Medical Errors. Patient Fact Sheet. AHRQ Publication No. 00-PO38, February 2000. Rockville, Md: Agency for Healthcare Research and Quality; 2000. Available at: www.ahrq.gov/consumer/20tips.htm.
Quick Tips—When Getting a Prescription. AHRQ Publication No. 01-0040c, May 2002. Rockville, Md: Agency for Healthcare Research and Quality; 2002. Available at: www.ahrq.gov/consumer/quicktips/tipprescrip.htm.
Kimberly A. Galt, PharmD
Associate Dean for Research
Professor of Pharmacy Practice
Director, Creighton University Health Services Research Program (CHRP)
Creighton University
Omaha, Neb
The last two issues under “Latent Failures” regard medication name usage. In a free market system, multiple organizations are permitted to market the same active ingredient under their own brand name or under the generic name. If prescribers and pharmacies were permitted to use generic names only, this could have helped avoid the confusion that occurred in the present case. But, again, the legislation necessary to make this happen would likely be opposed by industry. A possible compromise would be to require prominent identification of the generic name on medication bottles and medication lists (whether in paper or electronic form), as well as the drug’s indication so that duplications are easier for both patients and health care workers to identify.
Change is possible. This case that initially seemed simple and could have been easily ignored was found on investigation to be complex. Multiple parties contributed to the problem, which raised issues in communications, information management, ethics, and policy. I hope you will be stimulated to re-examine your own systems and, when faced with errors, will look more deeply to the underlying issues and not be satisfied simply to blame “human error.”
Conflict of interest
The authors have no conflicts of interest to declare.
1. Schmader K, Hanlon JT, Weinberger M, et al. Appropriateness of medication prescribing in ambulatory elderly patients. J Am Geriatr Soc 1994;42:1241-1247.
2. Tamblyn R, Huang A, Perreault R, et al. The medical office of the 21st century (MOXXI): effectiveness of computerized decision-making support in reducing inappropriate prescribing in primary care. CMAJ 2003;169:549-556.
3. Schmidt I, Claesson CB, Westerholm B, Nilsson LG, Svarstad BL. The impact of regular multidisciplinary team interventions on psychotropic prescribing in Swedish nursing homes. J Am Geriatr Soc 1998;46:77-p82.
4. Meredith S, Feldman P, Frey D, et al. Improving medication use in newly admitted home healthcare patients: a randomized controlled trial. J Am Geriatr Soc 2002;50:1484-1491.
5. Joint Commission on Accreditation of Healthcare Organizations. 2006 Joint Commission National Patient Safety Goals. Available at: www.jcipatientsafety.org. Accessed on May 4, 2006.
6. Barnsteiner JH. Medication reconciliation: transfer of medication information across settings-keeping it free from error. J Infus Nurs 2005;28(2 Suppl):31-36.
7. Sullivan C, Gleason KM, Rooney D, Groszek JM, Barnard C. Medication reconciliation in the acute care setting: opportunity and challenge for nursing. J Nurs Care Qual 2005;20:95-98.
8. Pronovost P, Weast B, Schwarz M, et al. Medication reconciliation: a practical tool to reduce the risk of medication errors. J Crit Care 2003;18:201-205.
9. Atkin PA, Finnegan TP, Ogle SJ, Shenfield GM. Are medication record cards useful? Med J Aust 1995;162:300-301.
10. Atkin PA, Stringer RS, Duffy JB, et al. The influence of information provided by patients on the accuracy of medication records. Med J Aust 1998;169:85-88.
11. Whyte LA. Medication cards for elderly people: a study. Nurs Stand 1994;8(48):25-28.
12. Yang Y, Han X, Bao F, Deng RH. A smart-card-enabled privacy preserving E-prescription system. IEEE Trans Inf Technol Biomed 2004;8:47-58.
13. Naszlady A, Naszlady J. Patient health record on a smart card. International Journal of Medical Informatics. Int J Med Inform 1998;48:191-194.
14. Auber BA, Hamel G. Adoption of smart cards in the medical sector: the Canadian experience. Soc Sci Med 2001;53:879-894.
15. Gallagher TH, Waterman AD, Ebers AG, Fraser VJ, Levinson W. Patients’ and physicians’ attitudes regarding the disclosure of medical errors. JAMA 2003;289:1001-1007.
16. Witman AB, Park DM, Hardin SB. How do patients want physicians to handle mistakes? A survey of internal medicine patients in an academic setting. Arch Intern Med 1996;156:2565-2569.
17. Mazor KM, Simon SR, Yood RA, et al. Health plan members’ views about disclosure of medical errors. Ann Intern Med 2004;140:409-418.
18. Schwappach DL, Koeck CM. What makes an error unacceptable? A factorial survey on the disclosure of medical errors. Int J Qual Health Care 2004;16:317-326.
19. Finkelstein D, Wu AW, Holtzman NA, Smith MK. When a physician harms a patient by a medical error: ethical, legal, and risk-management considerations. J Clin Ethics 1997;8:330-335.
20. Wu AW, Cavanaugh TA, McPhee SJ, Lo B, Micco GP. To tell the truth: ethical and practical issues in disclosing medical mistakes to patients. J Gen Intern Med 1997;12:770-775.
21. Mazor KMS, Simon SR, Gurwitz JH. Communicating with patients about medical errors: a review of the literature. Arch Intern Med 2004;164:1690-1697.
22. Reason J. Human Error. New York, NY: Cambridge University Press; 1990.
23. Singh R, Naughton B, Taylor JS, et al. A comprehensive collaborative patient safety residency curriculum to address the ACGME core competencies. Med Educ 2005;39:1195-1204.
24. Kohn LT, Corrigan J, Donaldson MS, eds. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000.
25. Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA 2002;287:487-494.
26. Rooney WR. Maintaining a medication list in the chart. Fam Pract Management 2003;10:52-54.
CORRESPONDENCE: Ranjit Singh, MA, MBBChir(Cantab.), MBA, Associate Director, Patient Safety Research Center, Department of Family Medicine, Clinical Center, Room 155, 462 Grider Street, Buffalo NY 14215. E-mail: rs10@buffalo.edu
At about 4 P.M., while driving with his wife (she is at the wheel), he starts sweating, slurring his speech, and feeling drowsy. His wife heads to the emergency department (ED), where his glucose level by fingerstick is found to be 37 mg/dL. He receives an infusion of dextrose 50% and his symptoms promptly resolve. The patient says he has not missed any meals and that he has been taking his medications as prescribed. He was seen in the same ED yesterday after a brief syncopal attack that was also attributed to hypoglycemia. The patient is admitted to the hospital under the family medicine residency service for further monitoring and management of recurrent hypoglycemia. Since you are the primary doctor, the admitting resident calls you.
You pay the patient a visit and ask him about his medications. He shows you the list and says he is taking them all “faithfully.” You note that the list contains both glipizide (which he has misspelled as “glipizine”) and Glucotrol (a branded version of glipizide). When queried on this point, he insists these are different medicines your office prescribed for him, and he is taking both. This therapeutic duplication, you suspect, is the likely cause of his recurrent episodes of hypoglycemia.
You review your outpatient records (you do not have an EMR) and discuss events in more detail with the patient and his wife. One month ago, the patient came to your office for a routine follow-up visit. You were out of town, so he saw one of your colleagues. He recalls that the doctor told him his sugar levels were too high and gave him a prescription, instructing him to take it with-out fail. He already had enough Glucotrol XL at home and had not requested a refill, so he assumed this was a new medication. He does not recall reading the prescription. The outpatient record shows that the patient had admitted to missing doses of his Glucotrol XL and that the covering physician attributed the hyperglycemia to this poor compliance. The physician had therefore decided to keep the dose of Glucotrol XL the same, provided a refill of Glucotrol XL 10 mg daily, and counseled the patient to improve compliance.
The patient took the script to his usual pharmacy, but they had just closed. He went instead to another nearby pharmacy (part of another chain), where he had the prescription filled. The bottle was labeled by the pharmacy: Glipizide XL 10 mg. Since that date he has been taking both Glucotrol and glipizide and, following the physician’s advice, has not missed a dose.
Q: How could this duplication have occurred?
A:___________________________________________________________
Better monitoring systems needed
Therapeutic duplication (referring, in general, to the use of more than one medication from the same class) is a serious problem, as illustrated by this case. A study of 208 elderly patients on 5 or more medications at a general medical clinic in North Carolina found therapeutic duplication in 5.7% of patients.1 In a Canadian study involving 12,560 elderly patients in primary care settings, the rate was 4%.2 Rates in other settings have been found to be higher (21% of 1854 nursing home residents in Sweden,3 and 15% of 259 patients newly enrolled in a home healthcare pro-gram in New York and California.4) In this case we have a patient taking 2 different preparations of the same drug. The causes of therapeutic duplication have not been well studied, but potential reasons are outlined in TABLE 1.
Current systems go only so far. Practices that have well-maintained medication lists on paper or as part of an electronic medical record are in a good position to avoid duplicate prescribing. However, tracking systems restricted to an office practice will not prevent duplications made by consultants or hospital physicians.
Pharmacies generally have software that checks for therapeutic duplication, thereby allowing pharmacists to alert physicians of the potential problem. This works well if a patient uses one pharmacy exclusively. But in the case at hand, the patient elected to go to a different pharmacy instead of waiting for his usual pharmacy to reopen the next business day. This innocent action circumvented the safety system, which did not extend to the other pharmacy. Some pharmacy chains have databases integrated across multiple sites, which can help if patients stay loyal to one chain.
Similarly, third-party payers such as many state Medicaid systems have the opportunity to identify and alert physicians to therapeutic duplications. However, I could find no reports in the literature regarding the implementation or effectiveness of such systems.
TABLE 2 offers suggestions for reducing the risk of therapeutic duplication in your practice.
Medication reconciliation is key. As a step toward addressing the larger picture of medication errors, the Joint Commission for Accreditation of Healthcare Organizations (JCAHO) has introduced for the year 2006 the following Patient Safety Goal (Goal #8): “Accurately and completely reconcile medications across the continuum of care,” commonly referred to as “medication reconciliation.”5 JCAHO’s adoption of this goal acknowledges, first, that transitions between different parts of the system are a common source of error, and, second, that these transition points (eg, admission to the hospital, or transfer out of the ICU) are opportunities to detect and correct errors. Various tools have been reported in the literature for addressing this issue. 6-8 The strategies listed in TABLE 2 can also be seen as contributing to this JCAHO goal.
TABLE 1
Have you encountered these causes of therapeutic duplication?
| MISCOMMUNICATION |
| In this case, the patient misunderstood the prescription to be for a new medication rather than a refill of an existing one. Miscommunications can be caused by the patient, the doctor, nursing staff, pharmacy staff, or any combination of these. |
| KNOWLEDGE DEFICIT |
| For example, a physician who does not know that sulindac is an NSAID might prescribe another NSAID such as ibuprofen to a patient whose pain is not controlled with sulindac. |
| POOR MEDICATION TRACKING WITHIN A PRACTICE |
| The office in this case relied on paper-based medication lists that were poorly maintained. The covering physician did not have access to accurate information about the most recent prescription date and number of refills, and elected to give a refill on Glucotrol XL. It is important to note that the primary physician might also have made the same mistake given the ineffective tracking system. |
| POOR MEDICATION TRACKING DURING TRANSITIONS |
| When patients move between different parts of the healthcare system such as the primary physician’s office, a specialist’s office, emergency departments, hospitals, and nursing homes, there are opportunities for errors, including therapeutic duplication. Transitions into and out of the hospital are receiving increasing attention because of the trend towards use of hospitalists.25 Unless specific systems are put in place to ensure continuity (as exist in some integrated healthcare systems), hospitalists and residents who provide inpatient coverage often do not have immediate access to accurate information regarding a patient’s prior medications and refills. |
| FORMULARY ISSUES |
| The policies of some hospitals and health insurance carriers can lead to therapeutic substitutions that can in turn result in therapeutic duplication. For example, if a patient who takes ramipril at home for hypertension is changed to enalapril during hospitalization and is given a prescription for enalapril at discharge, he might take both. |
TABLE 2
Strategies for preventing or detecting therapeutic duplication
| Keep better medication records (preferably with an EMR). This includes keeping track of dosage changes, refill dates, and numbers of refills given. Consider including the indication for each drug so that it is easier to detect therapeutic duplication. |
| Communicate better with patients regarding medications, especially when changes are made. Ask patients to repeat your instructions to check their understanding. |
| Encourage patients to use the same pharmacy (or chain) consistently, explaining that the usual pharmacist will have much better access to their medication records. |
| For high-risk patients (such as cognitively impaired, those on multiple medications, those with multiple physicians), arrange for regular medication review, at which a patient brings all medications to the office. |
| If you use a hospitalist (or residency program) for inpatient coverage, ensure that you have adequate systems in place to provide continuity of care regarding medications and other issues. |
| At post-hospitalization follow-up visits, review medications carefully. You may detect a variety of errors. |
| Consider implementing patient-carried medication lists. These can be paper-based or electronic. |
The story unfolds
You now know the patient has been taking twice the intended dose of his sulphonylurea for about a month, and you ask how he has been feeling during this time. He says he did well initially and did not experience any symptoms of hypoglycemia or hyperglycemia. He has a glucometer at home but did not use it during this period.
Two days ago, his wife expressed concerned that he was seeing several doctors (urologist, medical oncologist, radiation oncologist) for the prostate cancer and wanted to make sure he told them about all his medications. She asked him to make a list of his medications and to keep it in his wallet. He did so (FIGURE 1). That night he went out drinking (in his words, “the whole night”) because he was worried about his upcoming prostate surgery.
The next morning he forgot to take his medications and at noon he experienced transient loss of consciousness. He went to the ED and was found to have a blood sugar of 55. The loss of consciousness was attributed to hypoglycemia secondary to an alcohol binge. The patient says he showed his medication list to one of the ED staff but was not given any advice, except to follow-up with his personal physician. Last night his wife insisted he take his medications since he had missed them in the morning. He did so. This morning he took his medication as prescribed and developed hypoglycemia at about 4 P.M. (while in the car), precipitating this admission.
Q: Why did the patient-carried medication list not seem to help in this case?
A:____________________________________________________________
Why didn’t the list help? A complete, accurate, up-to-date list of a patient’s medications, held by the patient and made available to all healthcare providers to review and update, should be an effective means of tracking medications within and across healthcare settings, thereby reducing risk of errors including duplication. However, in this case, the ED physician did not detect the error even though the patient did have a list that was complete, accurate (except for the misspelling of glipizide), and up-to-date.
The precise circumstances were unclear, but one might speculate that the ED staff were so busy they did not notice the duplication or were unfamiliar with the medications (confounded by the patient’s misspelling of glipizide), or did not take the list seriously because it was poorly written and in poor condition, or were convinced that the hypoglycemia was precipitated by alcohol. Though the ED staff’s failure to recognize the duplication was a missed opportunity, to blame them would be inappropriate and unproductive. Instead, as will be re-emphasized later, we should focus on the underlying system issues that precipitated the failure, including the presence or absence of protocols for medication reconciliation, and the characteristics of the medication list that the patient was using.
Improving patient-carried medication records. These records have been used with varying success.9-11 Studies show it is difficult to ensure that patients carry records consistently, and to ensure that prescribers update them. Optimal characteristics of such records have yet to be determined, and they will likely vary depending on circumstances. However, the published experiences9-11 together with review of the present case suggest simple strategies that might help improve the list our patient was carrying.
First, the list should be easy to read and update and be durable.
Second, it should be convenient to carry (wallet-size, for example).
Third, it should include the appropriate amount of information that helps busy practitioners detect errors easily. This issue requires further study, but we might consider using generic names and including information about drug class and indication.
What about electronic media? One proposed solution to paper records is the use of electronic media such as flash memory cards or web-based records.12-14 Two challenges to widespread implementation of this strategy are cost and compatibility. To deal with the latter issue, current legislative efforts (Wired for Health Care Quality Act S. 1418) are aiming to create standard formats for exchange of electronic health information. Obviously the ability to link to electronic prescribing systems from anywhere would greatly reduce the risk of duplicate prescribing.
In the meantime it may be reasonable, especially for high-risk patients, to provide or encourage the use of paper-based medication lists with the caveat that they need to be kept up to date and shared with all providers.
FIGURE 1 Patient’s medication list
The need for vigilance never ends
The patient is managed appropriately by the inpatient team. His diabetes medications are discontinued and he is placed on a 5% dextrose infusion. He does well. By the following evening, he is off intravenous fluids, is maintaining adequate glucose levels, and is ready for discharge home. The plan calls for him to stop the Glucotrol XL and continue the generic glipizide XL only.
You go to the hospital to check on him and find that he and his wife are about to leave. The nurse has reviewed discharge instructions with them and the patient is holding a copy. You ask to see the instructions. FIGURE 2 shows the medication section of the instruction sheet.
Glucotrol XL appears correctly in the section “Discontinued medications” with the clear instruction “Do NOT take these medications.” However, it is also listed under “Pre-hospital medications to be continued.” When you ask the patient what medications he intends to take at home, he admits that he and his wife are a little confused by the instructions. He says they decided he should continue the same medications he was on before since these are what you and your office colleague prescribed. He adds, by way of explanation, that he trusts you more than he trusts the hospital team because you know him best. You are surprised by his answer but then realize that neither you nor the house staff has explained the duplication error to him. He still believes Glucotrol and glipizide are different medications and does not understand that taking them together caused his symptoms.
Q: Why might you and the house staff have been vague about the cause of the hypoglycemia? What should you say now?
A:_____________________________________________________
Discussing prescribing errors is uncomfortable. In this instance, you the primary doctor may have been reluctant because your office appeared to be most responsible for the mistake. And the residents also may have been reluctant to say anything that might appear critical of the primary doctor’s office. Evidence suggests that most physicians prefer not to discuss the details of errors or even to use the term “error.” They prefer less emotive language.15 In contrast, there is some evidence to suggest that patients and families would like to be informed when an error occurs in their care.15,18
As the primary care physician discovered in this case, correcting a medication error often depends on informing the patient. The negative impacts of disclosure (including the possibility of litigation and other sanctions, and the potential for loss of trust) are the subject of much debate.19-21
Ultimately, the decision to disclose an error must be based on risks and benefits to both patient and physician. If you decide to disclose, choose words carefully. And be careful to avoid apportioning blame. As this case illustrates, adverse events can have many contributing factors, and, in most cases, further investigation is required before a full explanation can be given. Therefore it is generally recommended that when disclosure is made, you should limit the discussion to the known facts. Further disclosure can always be made at a later date if warranted, when more objective information is available.
FIGURE 2 Hospital discharge instructions
A closer examination of what went wrong
In this case, unusual situations, system problems, and errors by individuals combined to cause recurrent hypoglycemia and unnecessary hospitalization. James Reason has provided a framework in which a case such as this may be analyzed systematically. It is called the Adverse Event Trajectory,22 and its application to this case is depicted in FIGURE 3. Each contributing factor is categorized according to the framework and written onto the diagram in such a way as to provide a summary of the whole event. This format has been used successfully as a teaching tool for family medicine residents.23
The main advantage of this analysis is that it clearly separates human errors (Active Failures) and system problems (Latent Failures, and the lack of Safety Barriers). Often, human error is chiefly blamed for adverse events and little effort is made to look beyond this. However, if we accept that “to err is human”24 and that most errors have roots in systemic problems, then the Adverse Event Trajectory framework can focus our attention on areas more likely to yield workable solutions.
Preventing recurrent errors usually is best assured by (1) correcting latent failures and (2) creating effective safety barriers. The strategies in TABLE 2 that involve changing systems (such as implementing electronic prescribing as part of an electronic medical record) are more likely to be effective than those that change behavior only (such as encouraging patients to use one pharmacy exclusively). However, system strategies also tend to be more expensive and difficult to implement than the latter. Perhaps it is most appropriate to use a combination of approaches listed in TABLE 2.
As implied under “Safety Barriers” in FIGURE 3, an effective patient-carried medication list had the potential to protect this patient from harm. Possible strategies for implementing such a barrier have been discussed above.
Items 2 and 3 under “Latent Failures” apply to the pharmacy level, and solutions would likely require legislation. Restricting access to one pharmacy exclusively would probably have prevented the duplication in our case. However, if such restriction were enforced unilaterally by a payer, it could make that payer less competitive since patients may value the freedom of changing pharmacies at will.
A more realistic alternative is to give pharmacies access to one another’s databases or even to create a central database to which all pharmacies would have access, with the patient’s permission. Clearly confidentiality issues would need to be addressed before such a program was implemented. And there would likely be opposition from the large pharmacy chains who might see this approach as a threat.
FIGURE 3 Adverse event trajectory: Breaking down the process into revealing components
The value of this analytic technique is in identifying and categorizing all factors (not just human error) that potentially contribute to untoward events. Efforts aimed at correcting or improving factors under “Latent Failures” or “Safety Barriers” are usually most fruitful.
This case illustrates the complex interaction of hospital, physician’s office, pharmacy, and patient’s home in causing or preventing medication errors. Fostering better communication with patients and improving patient medication records become even more important in this day of internet website purchases and mail-order pharmacies.
However, creating the common medication record is insufficient to assuring patient safety. The medication record must be reconciled with the patient’s behavior, including actual use of prescribed, over the counter, herbal, homeopathic, home, and other alternative remedies.
Communication must be clear not only while the patient is being cared for, but also when care transitions occur. The patient’s health literacy, values about care, dependence on others, and cultural beliefs are known to influence how patients actually use medications.
Better technology systems would certainly help detect medication errors. But a non-technology solution is available now. In this case, the patient’s poor health literacy was certainly evident in his lack of knowledge of the names of medications and in not understanding the duplication of drugs he was prescribed. But what about the medication literacy of the physician and nurse professionals in this case? Explaining the unfamiliar (and misspelled) drug to the patient could have prevented the drug duplication.
This patient indicated his trust in his primary care physician. This is cornerstone to the therapeutic relationship. However, this trust was not adequate to prevent this error from occurring or from the patient experiencing harm. Patient advocate organizations, such as the National Council for Patient Information and Education, or the Agency for Healthcare Research and Quality, suggest that patients will best be protected from harm by becoming an active participant on the health care team. Safety is achieved through ongoing and appropriate communication with patients to prevent harm. Pharmacists do contribute to resolving many medication safety issues for patients. The practice of pharmacy includes comprehensive medication history taking and documentation to maintain a patients medication profile.
For many patients, the pharmacist is a primary provider who communicates with them fairly regularly about medicines, and maintains medication lists. Many pharmacists routinely provide patients with medication list wallet cards, conduct comprehensive “brown bag” medication reviews, and maintain an active medication profile, including the over the counter and alternative remedies that patients describe or purchase from the pharmacy.
With the Medicare Modernization Act of 2003 came the federal prescription drug benefit, covering some of the costs to elderly patients who elect a prescription drug benefit provider who chooses to provide drug therapy monitoring services. Many pharmacists are expanding medication management services to support the patient with needed communication and counseling to prevent harm and improve safety. These will be important additions to the health care safety needs of patients.
Even with the system improvements we have described above, medication safety remains a shared responsibility between health care providers, patients, and health care organizations. A few guides have been published and are available free of charge to assist patients in knowing what they can do to help themselves with proper medication use and safety. These guides offer some practical tools and advice for patients to build patient knowledge about what to expect. Patients who use these tools will better assure safe practices and minimize harm:
Your Medicine: Play It Safe. Patient Guide. AHRQ Publication No. 03-0019, February 2003. Rockville, Md: Agency for Healthcare Research and Quality; Bethesda, Md: National Council on Patient Information and Education; 2003. Available at: www.ahrq.gov/consumer/safemeds/safemeds.htm.
20 Tips to Help Prevent Medical Errors. Patient Fact Sheet. AHRQ Publication No. 00-PO38, February 2000. Rockville, Md: Agency for Healthcare Research and Quality; 2000. Available at: www.ahrq.gov/consumer/20tips.htm.
Quick Tips—When Getting a Prescription. AHRQ Publication No. 01-0040c, May 2002. Rockville, Md: Agency for Healthcare Research and Quality; 2002. Available at: www.ahrq.gov/consumer/quicktips/tipprescrip.htm.
Kimberly A. Galt, PharmD
Associate Dean for Research
Professor of Pharmacy Practice
Director, Creighton University Health Services Research Program (CHRP)
Creighton University
Omaha, Neb
The last two issues under “Latent Failures” regard medication name usage. In a free market system, multiple organizations are permitted to market the same active ingredient under their own brand name or under the generic name. If prescribers and pharmacies were permitted to use generic names only, this could have helped avoid the confusion that occurred in the present case. But, again, the legislation necessary to make this happen would likely be opposed by industry. A possible compromise would be to require prominent identification of the generic name on medication bottles and medication lists (whether in paper or electronic form), as well as the drug’s indication so that duplications are easier for both patients and health care workers to identify.
Change is possible. This case that initially seemed simple and could have been easily ignored was found on investigation to be complex. Multiple parties contributed to the problem, which raised issues in communications, information management, ethics, and policy. I hope you will be stimulated to re-examine your own systems and, when faced with errors, will look more deeply to the underlying issues and not be satisfied simply to blame “human error.”
Conflict of interest
The authors have no conflicts of interest to declare.
At about 4 P.M., while driving with his wife (she is at the wheel), he starts sweating, slurring his speech, and feeling drowsy. His wife heads to the emergency department (ED), where his glucose level by fingerstick is found to be 37 mg/dL. He receives an infusion of dextrose 50% and his symptoms promptly resolve. The patient says he has not missed any meals and that he has been taking his medications as prescribed. He was seen in the same ED yesterday after a brief syncopal attack that was also attributed to hypoglycemia. The patient is admitted to the hospital under the family medicine residency service for further monitoring and management of recurrent hypoglycemia. Since you are the primary doctor, the admitting resident calls you.
You pay the patient a visit and ask him about his medications. He shows you the list and says he is taking them all “faithfully.” You note that the list contains both glipizide (which he has misspelled as “glipizine”) and Glucotrol (a branded version of glipizide). When queried on this point, he insists these are different medicines your office prescribed for him, and he is taking both. This therapeutic duplication, you suspect, is the likely cause of his recurrent episodes of hypoglycemia.
You review your outpatient records (you do not have an EMR) and discuss events in more detail with the patient and his wife. One month ago, the patient came to your office for a routine follow-up visit. You were out of town, so he saw one of your colleagues. He recalls that the doctor told him his sugar levels were too high and gave him a prescription, instructing him to take it with-out fail. He already had enough Glucotrol XL at home and had not requested a refill, so he assumed this was a new medication. He does not recall reading the prescription. The outpatient record shows that the patient had admitted to missing doses of his Glucotrol XL and that the covering physician attributed the hyperglycemia to this poor compliance. The physician had therefore decided to keep the dose of Glucotrol XL the same, provided a refill of Glucotrol XL 10 mg daily, and counseled the patient to improve compliance.
The patient took the script to his usual pharmacy, but they had just closed. He went instead to another nearby pharmacy (part of another chain), where he had the prescription filled. The bottle was labeled by the pharmacy: Glipizide XL 10 mg. Since that date he has been taking both Glucotrol and glipizide and, following the physician’s advice, has not missed a dose.
Q: How could this duplication have occurred?
A:___________________________________________________________
Better monitoring systems needed
Therapeutic duplication (referring, in general, to the use of more than one medication from the same class) is a serious problem, as illustrated by this case. A study of 208 elderly patients on 5 or more medications at a general medical clinic in North Carolina found therapeutic duplication in 5.7% of patients.1 In a Canadian study involving 12,560 elderly patients in primary care settings, the rate was 4%.2 Rates in other settings have been found to be higher (21% of 1854 nursing home residents in Sweden,3 and 15% of 259 patients newly enrolled in a home healthcare pro-gram in New York and California.4) In this case we have a patient taking 2 different preparations of the same drug. The causes of therapeutic duplication have not been well studied, but potential reasons are outlined in TABLE 1.
Current systems go only so far. Practices that have well-maintained medication lists on paper or as part of an electronic medical record are in a good position to avoid duplicate prescribing. However, tracking systems restricted to an office practice will not prevent duplications made by consultants or hospital physicians.
Pharmacies generally have software that checks for therapeutic duplication, thereby allowing pharmacists to alert physicians of the potential problem. This works well if a patient uses one pharmacy exclusively. But in the case at hand, the patient elected to go to a different pharmacy instead of waiting for his usual pharmacy to reopen the next business day. This innocent action circumvented the safety system, which did not extend to the other pharmacy. Some pharmacy chains have databases integrated across multiple sites, which can help if patients stay loyal to one chain.
Similarly, third-party payers such as many state Medicaid systems have the opportunity to identify and alert physicians to therapeutic duplications. However, I could find no reports in the literature regarding the implementation or effectiveness of such systems.
TABLE 2 offers suggestions for reducing the risk of therapeutic duplication in your practice.
Medication reconciliation is key. As a step toward addressing the larger picture of medication errors, the Joint Commission for Accreditation of Healthcare Organizations (JCAHO) has introduced for the year 2006 the following Patient Safety Goal (Goal #8): “Accurately and completely reconcile medications across the continuum of care,” commonly referred to as “medication reconciliation.”5 JCAHO’s adoption of this goal acknowledges, first, that transitions between different parts of the system are a common source of error, and, second, that these transition points (eg, admission to the hospital, or transfer out of the ICU) are opportunities to detect and correct errors. Various tools have been reported in the literature for addressing this issue. 6-8 The strategies listed in TABLE 2 can also be seen as contributing to this JCAHO goal.
TABLE 1
Have you encountered these causes of therapeutic duplication?
| MISCOMMUNICATION |
| In this case, the patient misunderstood the prescription to be for a new medication rather than a refill of an existing one. Miscommunications can be caused by the patient, the doctor, nursing staff, pharmacy staff, or any combination of these. |
| KNOWLEDGE DEFICIT |
| For example, a physician who does not know that sulindac is an NSAID might prescribe another NSAID such as ibuprofen to a patient whose pain is not controlled with sulindac. |
| POOR MEDICATION TRACKING WITHIN A PRACTICE |
| The office in this case relied on paper-based medication lists that were poorly maintained. The covering physician did not have access to accurate information about the most recent prescription date and number of refills, and elected to give a refill on Glucotrol XL. It is important to note that the primary physician might also have made the same mistake given the ineffective tracking system. |
| POOR MEDICATION TRACKING DURING TRANSITIONS |
| When patients move between different parts of the healthcare system such as the primary physician’s office, a specialist’s office, emergency departments, hospitals, and nursing homes, there are opportunities for errors, including therapeutic duplication. Transitions into and out of the hospital are receiving increasing attention because of the trend towards use of hospitalists.25 Unless specific systems are put in place to ensure continuity (as exist in some integrated healthcare systems), hospitalists and residents who provide inpatient coverage often do not have immediate access to accurate information regarding a patient’s prior medications and refills. |
| FORMULARY ISSUES |
| The policies of some hospitals and health insurance carriers can lead to therapeutic substitutions that can in turn result in therapeutic duplication. For example, if a patient who takes ramipril at home for hypertension is changed to enalapril during hospitalization and is given a prescription for enalapril at discharge, he might take both. |
TABLE 2
Strategies for preventing or detecting therapeutic duplication
| Keep better medication records (preferably with an EMR). This includes keeping track of dosage changes, refill dates, and numbers of refills given. Consider including the indication for each drug so that it is easier to detect therapeutic duplication. |
| Communicate better with patients regarding medications, especially when changes are made. Ask patients to repeat your instructions to check their understanding. |
| Encourage patients to use the same pharmacy (or chain) consistently, explaining that the usual pharmacist will have much better access to their medication records. |
| For high-risk patients (such as cognitively impaired, those on multiple medications, those with multiple physicians), arrange for regular medication review, at which a patient brings all medications to the office. |
| If you use a hospitalist (or residency program) for inpatient coverage, ensure that you have adequate systems in place to provide continuity of care regarding medications and other issues. |
| At post-hospitalization follow-up visits, review medications carefully. You may detect a variety of errors. |
| Consider implementing patient-carried medication lists. These can be paper-based or electronic. |
The story unfolds
You now know the patient has been taking twice the intended dose of his sulphonylurea for about a month, and you ask how he has been feeling during this time. He says he did well initially and did not experience any symptoms of hypoglycemia or hyperglycemia. He has a glucometer at home but did not use it during this period.
Two days ago, his wife expressed concerned that he was seeing several doctors (urologist, medical oncologist, radiation oncologist) for the prostate cancer and wanted to make sure he told them about all his medications. She asked him to make a list of his medications and to keep it in his wallet. He did so (FIGURE 1). That night he went out drinking (in his words, “the whole night”) because he was worried about his upcoming prostate surgery.
The next morning he forgot to take his medications and at noon he experienced transient loss of consciousness. He went to the ED and was found to have a blood sugar of 55. The loss of consciousness was attributed to hypoglycemia secondary to an alcohol binge. The patient says he showed his medication list to one of the ED staff but was not given any advice, except to follow-up with his personal physician. Last night his wife insisted he take his medications since he had missed them in the morning. He did so. This morning he took his medication as prescribed and developed hypoglycemia at about 4 P.M. (while in the car), precipitating this admission.
Q: Why did the patient-carried medication list not seem to help in this case?
A:____________________________________________________________
Why didn’t the list help? A complete, accurate, up-to-date list of a patient’s medications, held by the patient and made available to all healthcare providers to review and update, should be an effective means of tracking medications within and across healthcare settings, thereby reducing risk of errors including duplication. However, in this case, the ED physician did not detect the error even though the patient did have a list that was complete, accurate (except for the misspelling of glipizide), and up-to-date.
The precise circumstances were unclear, but one might speculate that the ED staff were so busy they did not notice the duplication or were unfamiliar with the medications (confounded by the patient’s misspelling of glipizide), or did not take the list seriously because it was poorly written and in poor condition, or were convinced that the hypoglycemia was precipitated by alcohol. Though the ED staff’s failure to recognize the duplication was a missed opportunity, to blame them would be inappropriate and unproductive. Instead, as will be re-emphasized later, we should focus on the underlying system issues that precipitated the failure, including the presence or absence of protocols for medication reconciliation, and the characteristics of the medication list that the patient was using.
Improving patient-carried medication records. These records have been used with varying success.9-11 Studies show it is difficult to ensure that patients carry records consistently, and to ensure that prescribers update them. Optimal characteristics of such records have yet to be determined, and they will likely vary depending on circumstances. However, the published experiences9-11 together with review of the present case suggest simple strategies that might help improve the list our patient was carrying.
First, the list should be easy to read and update and be durable.
Second, it should be convenient to carry (wallet-size, for example).
Third, it should include the appropriate amount of information that helps busy practitioners detect errors easily. This issue requires further study, but we might consider using generic names and including information about drug class and indication.
What about electronic media? One proposed solution to paper records is the use of electronic media such as flash memory cards or web-based records.12-14 Two challenges to widespread implementation of this strategy are cost and compatibility. To deal with the latter issue, current legislative efforts (Wired for Health Care Quality Act S. 1418) are aiming to create standard formats for exchange of electronic health information. Obviously the ability to link to electronic prescribing systems from anywhere would greatly reduce the risk of duplicate prescribing.
In the meantime it may be reasonable, especially for high-risk patients, to provide or encourage the use of paper-based medication lists with the caveat that they need to be kept up to date and shared with all providers.
FIGURE 1 Patient’s medication list
The need for vigilance never ends
The patient is managed appropriately by the inpatient team. His diabetes medications are discontinued and he is placed on a 5% dextrose infusion. He does well. By the following evening, he is off intravenous fluids, is maintaining adequate glucose levels, and is ready for discharge home. The plan calls for him to stop the Glucotrol XL and continue the generic glipizide XL only.
You go to the hospital to check on him and find that he and his wife are about to leave. The nurse has reviewed discharge instructions with them and the patient is holding a copy. You ask to see the instructions. FIGURE 2 shows the medication section of the instruction sheet.
Glucotrol XL appears correctly in the section “Discontinued medications” with the clear instruction “Do NOT take these medications.” However, it is also listed under “Pre-hospital medications to be continued.” When you ask the patient what medications he intends to take at home, he admits that he and his wife are a little confused by the instructions. He says they decided he should continue the same medications he was on before since these are what you and your office colleague prescribed. He adds, by way of explanation, that he trusts you more than he trusts the hospital team because you know him best. You are surprised by his answer but then realize that neither you nor the house staff has explained the duplication error to him. He still believes Glucotrol and glipizide are different medications and does not understand that taking them together caused his symptoms.
Q: Why might you and the house staff have been vague about the cause of the hypoglycemia? What should you say now?
A:_____________________________________________________
Discussing prescribing errors is uncomfortable. In this instance, you the primary doctor may have been reluctant because your office appeared to be most responsible for the mistake. And the residents also may have been reluctant to say anything that might appear critical of the primary doctor’s office. Evidence suggests that most physicians prefer not to discuss the details of errors or even to use the term “error.” They prefer less emotive language.15 In contrast, there is some evidence to suggest that patients and families would like to be informed when an error occurs in their care.15,18
As the primary care physician discovered in this case, correcting a medication error often depends on informing the patient. The negative impacts of disclosure (including the possibility of litigation and other sanctions, and the potential for loss of trust) are the subject of much debate.19-21
Ultimately, the decision to disclose an error must be based on risks and benefits to both patient and physician. If you decide to disclose, choose words carefully. And be careful to avoid apportioning blame. As this case illustrates, adverse events can have many contributing factors, and, in most cases, further investigation is required before a full explanation can be given. Therefore it is generally recommended that when disclosure is made, you should limit the discussion to the known facts. Further disclosure can always be made at a later date if warranted, when more objective information is available.
FIGURE 2 Hospital discharge instructions
A closer examination of what went wrong
In this case, unusual situations, system problems, and errors by individuals combined to cause recurrent hypoglycemia and unnecessary hospitalization. James Reason has provided a framework in which a case such as this may be analyzed systematically. It is called the Adverse Event Trajectory,22 and its application to this case is depicted in FIGURE 3. Each contributing factor is categorized according to the framework and written onto the diagram in such a way as to provide a summary of the whole event. This format has been used successfully as a teaching tool for family medicine residents.23
The main advantage of this analysis is that it clearly separates human errors (Active Failures) and system problems (Latent Failures, and the lack of Safety Barriers). Often, human error is chiefly blamed for adverse events and little effort is made to look beyond this. However, if we accept that “to err is human”24 and that most errors have roots in systemic problems, then the Adverse Event Trajectory framework can focus our attention on areas more likely to yield workable solutions.
Preventing recurrent errors usually is best assured by (1) correcting latent failures and (2) creating effective safety barriers. The strategies in TABLE 2 that involve changing systems (such as implementing electronic prescribing as part of an electronic medical record) are more likely to be effective than those that change behavior only (such as encouraging patients to use one pharmacy exclusively). However, system strategies also tend to be more expensive and difficult to implement than the latter. Perhaps it is most appropriate to use a combination of approaches listed in TABLE 2.
As implied under “Safety Barriers” in FIGURE 3, an effective patient-carried medication list had the potential to protect this patient from harm. Possible strategies for implementing such a barrier have been discussed above.
Items 2 and 3 under “Latent Failures” apply to the pharmacy level, and solutions would likely require legislation. Restricting access to one pharmacy exclusively would probably have prevented the duplication in our case. However, if such restriction were enforced unilaterally by a payer, it could make that payer less competitive since patients may value the freedom of changing pharmacies at will.
A more realistic alternative is to give pharmacies access to one another’s databases or even to create a central database to which all pharmacies would have access, with the patient’s permission. Clearly confidentiality issues would need to be addressed before such a program was implemented. And there would likely be opposition from the large pharmacy chains who might see this approach as a threat.
FIGURE 3 Adverse event trajectory: Breaking down the process into revealing components
The value of this analytic technique is in identifying and categorizing all factors (not just human error) that potentially contribute to untoward events. Efforts aimed at correcting or improving factors under “Latent Failures” or “Safety Barriers” are usually most fruitful.
This case illustrates the complex interaction of hospital, physician’s office, pharmacy, and patient’s home in causing or preventing medication errors. Fostering better communication with patients and improving patient medication records become even more important in this day of internet website purchases and mail-order pharmacies.
However, creating the common medication record is insufficient to assuring patient safety. The medication record must be reconciled with the patient’s behavior, including actual use of prescribed, over the counter, herbal, homeopathic, home, and other alternative remedies.
Communication must be clear not only while the patient is being cared for, but also when care transitions occur. The patient’s health literacy, values about care, dependence on others, and cultural beliefs are known to influence how patients actually use medications.
Better technology systems would certainly help detect medication errors. But a non-technology solution is available now. In this case, the patient’s poor health literacy was certainly evident in his lack of knowledge of the names of medications and in not understanding the duplication of drugs he was prescribed. But what about the medication literacy of the physician and nurse professionals in this case? Explaining the unfamiliar (and misspelled) drug to the patient could have prevented the drug duplication.
This patient indicated his trust in his primary care physician. This is cornerstone to the therapeutic relationship. However, this trust was not adequate to prevent this error from occurring or from the patient experiencing harm. Patient advocate organizations, such as the National Council for Patient Information and Education, or the Agency for Healthcare Research and Quality, suggest that patients will best be protected from harm by becoming an active participant on the health care team. Safety is achieved through ongoing and appropriate communication with patients to prevent harm. Pharmacists do contribute to resolving many medication safety issues for patients. The practice of pharmacy includes comprehensive medication history taking and documentation to maintain a patients medication profile.
For many patients, the pharmacist is a primary provider who communicates with them fairly regularly about medicines, and maintains medication lists. Many pharmacists routinely provide patients with medication list wallet cards, conduct comprehensive “brown bag” medication reviews, and maintain an active medication profile, including the over the counter and alternative remedies that patients describe or purchase from the pharmacy.
With the Medicare Modernization Act of 2003 came the federal prescription drug benefit, covering some of the costs to elderly patients who elect a prescription drug benefit provider who chooses to provide drug therapy monitoring services. Many pharmacists are expanding medication management services to support the patient with needed communication and counseling to prevent harm and improve safety. These will be important additions to the health care safety needs of patients.
Even with the system improvements we have described above, medication safety remains a shared responsibility between health care providers, patients, and health care organizations. A few guides have been published and are available free of charge to assist patients in knowing what they can do to help themselves with proper medication use and safety. These guides offer some practical tools and advice for patients to build patient knowledge about what to expect. Patients who use these tools will better assure safe practices and minimize harm:
Your Medicine: Play It Safe. Patient Guide. AHRQ Publication No. 03-0019, February 2003. Rockville, Md: Agency for Healthcare Research and Quality; Bethesda, Md: National Council on Patient Information and Education; 2003. Available at: www.ahrq.gov/consumer/safemeds/safemeds.htm.
20 Tips to Help Prevent Medical Errors. Patient Fact Sheet. AHRQ Publication No. 00-PO38, February 2000. Rockville, Md: Agency for Healthcare Research and Quality; 2000. Available at: www.ahrq.gov/consumer/20tips.htm.
Quick Tips—When Getting a Prescription. AHRQ Publication No. 01-0040c, May 2002. Rockville, Md: Agency for Healthcare Research and Quality; 2002. Available at: www.ahrq.gov/consumer/quicktips/tipprescrip.htm.
Kimberly A. Galt, PharmD
Associate Dean for Research
Professor of Pharmacy Practice
Director, Creighton University Health Services Research Program (CHRP)
Creighton University
Omaha, Neb
The last two issues under “Latent Failures” regard medication name usage. In a free market system, multiple organizations are permitted to market the same active ingredient under their own brand name or under the generic name. If prescribers and pharmacies were permitted to use generic names only, this could have helped avoid the confusion that occurred in the present case. But, again, the legislation necessary to make this happen would likely be opposed by industry. A possible compromise would be to require prominent identification of the generic name on medication bottles and medication lists (whether in paper or electronic form), as well as the drug’s indication so that duplications are easier for both patients and health care workers to identify.
Change is possible. This case that initially seemed simple and could have been easily ignored was found on investigation to be complex. Multiple parties contributed to the problem, which raised issues in communications, information management, ethics, and policy. I hope you will be stimulated to re-examine your own systems and, when faced with errors, will look more deeply to the underlying issues and not be satisfied simply to blame “human error.”
Conflict of interest
The authors have no conflicts of interest to declare.
1. Schmader K, Hanlon JT, Weinberger M, et al. Appropriateness of medication prescribing in ambulatory elderly patients. J Am Geriatr Soc 1994;42:1241-1247.
2. Tamblyn R, Huang A, Perreault R, et al. The medical office of the 21st century (MOXXI): effectiveness of computerized decision-making support in reducing inappropriate prescribing in primary care. CMAJ 2003;169:549-556.
3. Schmidt I, Claesson CB, Westerholm B, Nilsson LG, Svarstad BL. The impact of regular multidisciplinary team interventions on psychotropic prescribing in Swedish nursing homes. J Am Geriatr Soc 1998;46:77-p82.
4. Meredith S, Feldman P, Frey D, et al. Improving medication use in newly admitted home healthcare patients: a randomized controlled trial. J Am Geriatr Soc 2002;50:1484-1491.
5. Joint Commission on Accreditation of Healthcare Organizations. 2006 Joint Commission National Patient Safety Goals. Available at: www.jcipatientsafety.org. Accessed on May 4, 2006.
6. Barnsteiner JH. Medication reconciliation: transfer of medication information across settings-keeping it free from error. J Infus Nurs 2005;28(2 Suppl):31-36.
7. Sullivan C, Gleason KM, Rooney D, Groszek JM, Barnard C. Medication reconciliation in the acute care setting: opportunity and challenge for nursing. J Nurs Care Qual 2005;20:95-98.
8. Pronovost P, Weast B, Schwarz M, et al. Medication reconciliation: a practical tool to reduce the risk of medication errors. J Crit Care 2003;18:201-205.
9. Atkin PA, Finnegan TP, Ogle SJ, Shenfield GM. Are medication record cards useful? Med J Aust 1995;162:300-301.
10. Atkin PA, Stringer RS, Duffy JB, et al. The influence of information provided by patients on the accuracy of medication records. Med J Aust 1998;169:85-88.
11. Whyte LA. Medication cards for elderly people: a study. Nurs Stand 1994;8(48):25-28.
12. Yang Y, Han X, Bao F, Deng RH. A smart-card-enabled privacy preserving E-prescription system. IEEE Trans Inf Technol Biomed 2004;8:47-58.
13. Naszlady A, Naszlady J. Patient health record on a smart card. International Journal of Medical Informatics. Int J Med Inform 1998;48:191-194.
14. Auber BA, Hamel G. Adoption of smart cards in the medical sector: the Canadian experience. Soc Sci Med 2001;53:879-894.
15. Gallagher TH, Waterman AD, Ebers AG, Fraser VJ, Levinson W. Patients’ and physicians’ attitudes regarding the disclosure of medical errors. JAMA 2003;289:1001-1007.
16. Witman AB, Park DM, Hardin SB. How do patients want physicians to handle mistakes? A survey of internal medicine patients in an academic setting. Arch Intern Med 1996;156:2565-2569.
17. Mazor KM, Simon SR, Yood RA, et al. Health plan members’ views about disclosure of medical errors. Ann Intern Med 2004;140:409-418.
18. Schwappach DL, Koeck CM. What makes an error unacceptable? A factorial survey on the disclosure of medical errors. Int J Qual Health Care 2004;16:317-326.
19. Finkelstein D, Wu AW, Holtzman NA, Smith MK. When a physician harms a patient by a medical error: ethical, legal, and risk-management considerations. J Clin Ethics 1997;8:330-335.
20. Wu AW, Cavanaugh TA, McPhee SJ, Lo B, Micco GP. To tell the truth: ethical and practical issues in disclosing medical mistakes to patients. J Gen Intern Med 1997;12:770-775.
21. Mazor KMS, Simon SR, Gurwitz JH. Communicating with patients about medical errors: a review of the literature. Arch Intern Med 2004;164:1690-1697.
22. Reason J. Human Error. New York, NY: Cambridge University Press; 1990.
23. Singh R, Naughton B, Taylor JS, et al. A comprehensive collaborative patient safety residency curriculum to address the ACGME core competencies. Med Educ 2005;39:1195-1204.
24. Kohn LT, Corrigan J, Donaldson MS, eds. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000.
25. Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA 2002;287:487-494.
26. Rooney WR. Maintaining a medication list in the chart. Fam Pract Management 2003;10:52-54.
CORRESPONDENCE: Ranjit Singh, MA, MBBChir(Cantab.), MBA, Associate Director, Patient Safety Research Center, Department of Family Medicine, Clinical Center, Room 155, 462 Grider Street, Buffalo NY 14215. E-mail: rs10@buffalo.edu
1. Schmader K, Hanlon JT, Weinberger M, et al. Appropriateness of medication prescribing in ambulatory elderly patients. J Am Geriatr Soc 1994;42:1241-1247.
2. Tamblyn R, Huang A, Perreault R, et al. The medical office of the 21st century (MOXXI): effectiveness of computerized decision-making support in reducing inappropriate prescribing in primary care. CMAJ 2003;169:549-556.
3. Schmidt I, Claesson CB, Westerholm B, Nilsson LG, Svarstad BL. The impact of regular multidisciplinary team interventions on psychotropic prescribing in Swedish nursing homes. J Am Geriatr Soc 1998;46:77-p82.
4. Meredith S, Feldman P, Frey D, et al. Improving medication use in newly admitted home healthcare patients: a randomized controlled trial. J Am Geriatr Soc 2002;50:1484-1491.
5. Joint Commission on Accreditation of Healthcare Organizations. 2006 Joint Commission National Patient Safety Goals. Available at: www.jcipatientsafety.org. Accessed on May 4, 2006.
6. Barnsteiner JH. Medication reconciliation: transfer of medication information across settings-keeping it free from error. J Infus Nurs 2005;28(2 Suppl):31-36.
7. Sullivan C, Gleason KM, Rooney D, Groszek JM, Barnard C. Medication reconciliation in the acute care setting: opportunity and challenge for nursing. J Nurs Care Qual 2005;20:95-98.
8. Pronovost P, Weast B, Schwarz M, et al. Medication reconciliation: a practical tool to reduce the risk of medication errors. J Crit Care 2003;18:201-205.
9. Atkin PA, Finnegan TP, Ogle SJ, Shenfield GM. Are medication record cards useful? Med J Aust 1995;162:300-301.
10. Atkin PA, Stringer RS, Duffy JB, et al. The influence of information provided by patients on the accuracy of medication records. Med J Aust 1998;169:85-88.
11. Whyte LA. Medication cards for elderly people: a study. Nurs Stand 1994;8(48):25-28.
12. Yang Y, Han X, Bao F, Deng RH. A smart-card-enabled privacy preserving E-prescription system. IEEE Trans Inf Technol Biomed 2004;8:47-58.
13. Naszlady A, Naszlady J. Patient health record on a smart card. International Journal of Medical Informatics. Int J Med Inform 1998;48:191-194.
14. Auber BA, Hamel G. Adoption of smart cards in the medical sector: the Canadian experience. Soc Sci Med 2001;53:879-894.
15. Gallagher TH, Waterman AD, Ebers AG, Fraser VJ, Levinson W. Patients’ and physicians’ attitudes regarding the disclosure of medical errors. JAMA 2003;289:1001-1007.
16. Witman AB, Park DM, Hardin SB. How do patients want physicians to handle mistakes? A survey of internal medicine patients in an academic setting. Arch Intern Med 1996;156:2565-2569.
17. Mazor KM, Simon SR, Yood RA, et al. Health plan members’ views about disclosure of medical errors. Ann Intern Med 2004;140:409-418.
18. Schwappach DL, Koeck CM. What makes an error unacceptable? A factorial survey on the disclosure of medical errors. Int J Qual Health Care 2004;16:317-326.
19. Finkelstein D, Wu AW, Holtzman NA, Smith MK. When a physician harms a patient by a medical error: ethical, legal, and risk-management considerations. J Clin Ethics 1997;8:330-335.
20. Wu AW, Cavanaugh TA, McPhee SJ, Lo B, Micco GP. To tell the truth: ethical and practical issues in disclosing medical mistakes to patients. J Gen Intern Med 1997;12:770-775.
21. Mazor KMS, Simon SR, Gurwitz JH. Communicating with patients about medical errors: a review of the literature. Arch Intern Med 2004;164:1690-1697.
22. Reason J. Human Error. New York, NY: Cambridge University Press; 1990.
23. Singh R, Naughton B, Taylor JS, et al. A comprehensive collaborative patient safety residency curriculum to address the ACGME core competencies. Med Educ 2005;39:1195-1204.
24. Kohn LT, Corrigan J, Donaldson MS, eds. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000.
25. Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA 2002;287:487-494.
26. Rooney WR. Maintaining a medication list in the chart. Fam Pract Management 2003;10:52-54.
CORRESPONDENCE: Ranjit Singh, MA, MBBChir(Cantab.), MBA, Associate Director, Patient Safety Research Center, Department of Family Medicine, Clinical Center, Room 155, 462 Grider Street, Buffalo NY 14215. E-mail: rs10@buffalo.edu
Chronic Invasive Sinus Aspergillosis in an Immunocompetent Patient
Chest pain, weakness, and elevated cardiac enzymes: How would you treat?
History of present illness
- Approximately 4 weeks of generalized extremity pain and weakness; left-sided, nonexertional chest pain, which is much less severe than his extremity pains
- Symptoms are most prominent in the proximal upper extremities, especially with movement; the right side is more effected than the left
- Dyspnea on exertion
- Seen twice in local urgent care facilities in the past 10 days; diagnosed with congestive heart failure; treated with furosemide, digoxin, and an unknown antibiotic without relief
- 20- to 30-pound weight loss over the past year
Other medical history
- No chronic medical problems or medications
- Until this past month, last seen by a physician about 3 or 4 years prior
Review of systems
- Up to the day of admission has been ambulatory and able to care for himself despite his weakness
- No fever, chills, or rash; but has night sweats
- Smokes; does not drink alcohol
- Retired; lives with his wife
Physical examination
- Alert, appears mildly uncomfortable
- Temperature 101°F, respirations 32, blood pressure 164/72, pulse 80
- 3/5 strength in proximal upper and lower extremities (can barely lift arms and legs off the bed; movement also limited by pain)
- Normal distal strength (hand grips and dorsi/plantar flexion of foot)
- Normal sensation, reflexes, cranial nerves, and mental status; no neck weakness
- No abnormal joint findings; has pink discoloration over extensor surface of MCP joint, which patient dismisses as scars from previous abrasions that have been present “for a long time”
- Heart, lungs unremarkable; no peripheral edema
Laboratory studies completed in the emergency department
- ECG: normal
- Chest x-ray: bibasilar peribronchial infiltrates
- Hemoglobin/hematocrit: normal
- White blood count: 27,000 with 92% neutrophils
- Erythrocyte sedimentation rate: normal
- Urinalysis: negative for blood
- Brain natriuretic peptide: normal
- Creatine kinase (CK): 2205 IU/L (normal range 35–232)
- Troponin-I: 0.6 ng/mL.
[Reference range:
<0.05=Negative
0.05–0.09=Equivocal
0.10–0.49=Suspicious
0.50=Consistent with myocardial injury]
A: ____________________________________________________________ ______________________________________________________________
Is this acute non-ST elevation myocardial infarction (NSTEMI)?
The American College of Cardiology and the American Heart Association define myocardial infarction primarily as elevated cardiac-specific enzymes troponin-I and troponin-T in the appropriate clinical setting.1,2 Elevated cardiac troponins have a sensitivity approaching 100% for myocardial damage. Specificity is much lower for acute ischemic cardiac disease, however, particularly for patients with a low pretest probability (45% false-positive rate in one series of 1000 consecutive patients presenting to a large urban emergency department with symptoms of acute coronary ischemia).3
Mechanisms other than atherosclerotic coronary artery disease that can elevate cardiac troponins:
- Increased cardiac demand (eg, sepsis, hypovolemia)
- Nonatherosclerotic ischemia (eg, cocaine or other sympathomimetic agents, coronary vasospasm)
- Direct myocardial injury (eg, cardiac contusion, myocarditis)
- Myocardial strain (eg, congestive heart failure, pulmonary embolus)
- Chronic renal insufficiency (mechanism unclear).4
In light of this patient’s history and physical exam findings, you doubt he’s having an acute cardiac event. The most remarkable features are his weakness, muscle pain, and markedly elevated CK.
Though you have ruled out anemia and several other possibilities, the differential diagnosis of weakness is still broad. You decide to explore the differential diagnosis of elevated CK, a more specific finding in this case.
Pursuing the differential
You consult UpToDate, searching under “creatine kinase,” and find an article entitled “Muscle enzymes in the evaluation of neuromuscular disease.”5 You conclude that the most likely cause of your patient’s problems is an idiopathic inflammatory myopathy: polymyositis, dermatomyositis, or inclusion-body myositis.6
Other possibilities include post-viral myositis and myositis associated with connective tissue disease, hypothyroidism, or drug reactions.
D-penicillamine, zidovudine (AZT), and viral or bacterial infection may produce inflammatory myopathy similar to polymyositis.7 A history of exposure to myotoxic drugs (such as statins) and toxins has been excluded.
The absence of a family history for neuromuscular disease and the relatively recent onset of symptoms rule out an inherited muscular dystrophy or congenital muscle enzyme deficiency.
Myasthenia gravis presents with extraocular muscle involvement. Guillain-Barré syndrome is characterized by ascending muscle weakness. Lyme disease may cause weakness secondary to peripheral neuropathy but it does not produce evidence of muscle inflammation such as elevation of the CK. West Nile virus encephalitis may present with muscle weakness and flaccid paralysis.8 Trichinellosis may also cause muscle inflammation with weakness and elevation of CK, but it is rare in the United States.
You repeat parts of your physical exam and confirm that his proximal upper extremity muscles are much weaker than his distal muscles.
In practice settings where specialty consultation is not always immediately available, your diagnostic skills may be challenged by uncommon presentations of disease. In this case, the challenge is “chest pain and positive cardiac enzymes” in a patient who does not appear to have a primary cardiac problem.
A: ____________________________________________________________ ______________________________________________________________
DTaP approach
When confronted with a difficult clinical problem, you may find it useful to organize the management plan according to the acronym “DTaP,” which for this patient would include:
- Diagnostic plan: serial ECGs and cardiac enzymes: an echocardiogram
- Therapeutic plan: pain control; antibiotics for possible pneumonia; consider steroids
- Assistance from consultants (who are you going to ask for help?): physiatrist consult for electromyography (EMG); cardiology consult; neurology consult
- Patient education (explain to the patient and his family the current diagnostic possibilities and your management plan)
- Provider education (learn more about myopathies!).
You request specialty consultations:
Neurology: possible polymyositis; recommends rheumatology consultation, multiple labs (most of which are sent out to a reference lab and return only several days later)
Cardiology: ECG normal; cardiologist does not see evidence for congestive heart failure or coronary artery disease
Physical medicine and rehabilitation: EMG performed; findings consistent with inflammatory myopathy
Rheumatology: recommends proceeding with muscle biopsy to differentiate polymyositis and inclusion-body myositis
Surgery: performs muscle biopsy which is sent to a regional neuropathologist; reveals inflammatory myopathy with prominent perivascular lymphocytic inflammation strongly suggestive of dermatomyositis.
Further case management and resolution
You administer solumedrol intravenously 1 g/d for 3 days, then change to prednisone orally 1 mg/kg/d.
The patient improves steadily with 3 months of oral steroid therapy. He tests positive for anti-Jo antibodies but his pulmonary symptoms resolve. He undergoes an outpatient evaluation for cancer screening. Colonoscopy, esophogastroduodenoscopy and chest/abdominal/pelvic computed tomography scans are negative for evidence of malignancy.
This case illustrates the importance of not letting dramatic laboratory abnormalities—for this patient, an elevated CK enzyme level—unduly influence your investigative focus. The patient’s history and physical exam findings provided a larger context in which the diagnosis of acute coronary insufficiency became unlikely. Balanced consideration of the patient’s muscle pain and weakness and elevated CK level narrowed the diagnostic possibilities appropriately.
Other ways in which you may encounter inflammatory myopathies
Dermatomyositis usually causes a characteristic rash that facilitates early diagnosis (though it did not appear in this case). As shown in FIGURES 1 AND 2, patients may have either a heliotrope rash (blue-purple to dusky erythematous discoloration on the upper eyelids, with or without edema), or Gottron’s papules (slightly raised violaceous papules and plaques overlying bony prominences, particularly the joints in the fingers and the knuckles).10
A variety of less specific skin and nail changes can occur. Dermatomyositis may present with skin lesions alone (dermatomyositis sine myositis) or rarely with myopathy alone (dermatomyositis sine dermatitis). In our case, multiple examiners failed to detect any classic dermatologic abnormalities, though the pinkish skin changes over the extensor aspect of the MCP joints were, in retrospect, suggestive of dermatomyositis. The weakness associated with this disease may be mild, moderate, or severe enough to result in quadriparesis. Dermatomyositis usually occurs alone but may be present with scleroderma and mixed connective tissue disease.
The main categories of idiopathic acquired inflammatory myopathy are polymyositis, dermatomyositis, and inclusion-body myositis. They cause moderate-to-severe weakness and inflammation of muscles.6 The prevalence of these disorders is unclear because diagnosis has not consistently been based on uniform, reliable criteria. But the incidence is believed to be 1 per 100,000 of the general population, with dermatomyositis being the most common and polymyositis the least common of these myopathies.9 Inclusion-body myositis is the most common form of inflammatory myopathy in patients older than 50 years. Polymyositis is generally seen after the second decade of life. Both children and adults may be affected by dermatomyositis. There have been rare familial occurrences.
Inclusion-body myositis is often misdiagnosed as polymyositis or dermatomyositis until identified by muscle biopsy findings (see How inflammatory myopathies develop), although suspicion is raised with a poor response to steroid therapy.9 Some patients report falling as a result of quadriceps weakness. On occasion the weakness can be asymmetric or distal (rare with dermatomyositis or polymyositis). Diagnosis is always made by muscle biopsy. Disease progression is slow but steady and most patients end up requiring a walker or assistive device.
Polymyositis is a sub-acute inflammatory myopathy affecting adults and, rarely, children. In most cases the actual onset of polymyositis is not easily determined as patients tend to delay seeking medical evaluation.
Other muscular disorders, as discussed in the case presentation, need to be excluded.
FIGURE 1 Heliotrope rash

Patients with dermatomyositis often have a characteristic rash on their face.
FIGURE 2 Gottron’s papules

Many patients also have papules and plaques on their hands, typically at the joints.
Evidence suggests the inflammatory myopathies are autoimmune disorders.6 They are often associated with connective tissue diseases and other systemic autoimmune conditions. Viral infections such as coxsackie, influenza, paramyxovirus, mumps, cytomegalovirus, and Epstein-Barr have been indirectly associated with chronic and acute myositis and may trigger the autoimmune process.
Specific muscle or capillary target antigens have not been identified, and the agents that initiate self-sensitization are still unknown. Other features of these disorders are their association with auto-antibodies, certain histocompatibility genes, T-cell–mediated myocytotoxicity, and complement-mediated microangiopathy.6
Dermatomyositis appears to be primarily a B-cell mediated microangiopathy. Antibodies directed against the endothelium of the endomysial capillaries lead to the primary histological changes in the blood vessels.9 The disease manifests when the complement system is activated to form the membrane attack complex (MAC).
Polymyositis and inclusion-body myositis appear to result from a cytotoxic T-cell response directed specifically against muscle fibers.9 CD-8+ cells are induced via T-cell activation to invade MHC-I antigen-expressing muscle cells.6 Usually most muscle cells do not express MHC Class I or II antigens. Histology demonstrates infiltration of individual muscle fibers by inflammatory cells. Inclusion-body myositis is differentiated from polymyositis by the presence of nuclear and cytoplasmic vacuoles.
Commonly associated clinical findings
Extramuscular manifestations of inflammatory myopathies. Dermatomyositis is a systemic inflammatory disorder that may extend beyond the dermatologic and muscular systems, and patients can exhibit such symptoms as fever, malaise, and weight loss.
Arthralgia and Raynaud’s phenomenon may occur with associated connective tissue disease.
Dysphagia indicates involvement of the oropharyngeal striated muscles and the upper esophagus.
Cardiac disturbances include atrioventricular conduction defects, tachyarrhythmias, myocarditis, heart failure, and possibly hypertension from long-term steroid use. The elevated troponin-I seen in our index case may have been evidence of a mild myocarditis, though the echocardiogram was normal.
Calcinosis (deposition of calcium in the skin or muscles) occurs in up to 40% of children with dermatomyositis but is unusual in adults.10
Pulmonary symptoms may be due to weakness of the thoracic muscles, interstitial lung disease, or aspiration. One retrospective study of 156 consecutive patients with dermatomyositis/polymyositis based on clinical criteria found a 23.1% incidence of interstitial lung disease.11
Malignant disorders. The frequency of cancer is increased in association with these diseases. Studies have placed the highest risk of concomitant malignancy with dermatomyositis and the least risk with polymyositis. (The relative risk for malignancy in dermatomyositis as compared with polymyositis was 2.4.) Malignancy associated with dermatomyositis or polymyositis is twice as likely in women than in men.12
Risk of associated malignancy was highest within the first year of diagnosis. Therefore, consider a diagnostic evaluation for malignancy at the time myopathy is diagnosed. The optimal diagnostic regimen in this setting is unknown. In one retrospective French study of 40 consecutive adult patients with inflammatory myopathy (33 with dermatomyositis and 7 with polymyositis) between the years 1981 and 2000, malignancy was present at the time of myopathy diagnosis in 16 patients (13 with dermatomyositis and 3 with polymyositis).12 An Australian population-based, retrospective cohort study of 537 individuals with biopsy-proven idiopathic inflammatory myopathy from 1981–1995 demonstrated 116 cases of malignancy in 104 patients.13 The risk was highest in dermatomyositis (standardized incidence ratio [SIR] 6.2), next highest in inclusion-body myositis (SIR 2.4), and lowest in polymyositis (SIR 2.0).
Diagnosis: What helps, what doesn’t
Suspect inflammatory myopathy by the constellation of clinical findings; confirm it by looking for elevated muscle enzymes and characteristic findings on EMG and muscle biopsy (see How inflammatory myopathies develop).
The most sensitive muscle enzyme for inflammatory myopathy is CK, levels of which usually parallel disease activity and may be used to assess response to therapy.6,10 Needle EMG demonstrates increased spontaneous activity with fibrillations; complex repetitive discharges; positive sharp waves; and voluntary motor units consisting of low-amplitude polyphasic units of short duration.6 EMG findings alone are not diagnostic.
Serologic tests are commonly done but their clinical usefulness is controversial.10 Antinuclear antibodies are found in about 80% of cases but are nonspecific and not clinically useful.14 Myositis-specific antibodies (MSAs) have been described in about 30% of idiopathic inflammatory myopathies but are also of uncertain diagnostic and pathogenic importance.14 The most prevalent MSA, anti-Jo, is present in only about 20% of cases and correlates with interstitial lung disease, but has uncertain usefulness in differentiating between dermatomyositis, polymyositis, and inclusion-body myositis.6,10,11,14,15
Differentiate between the inflammatory myopathies based on characteristic pathological findings on muscle biopsy (previously discussed). Muscle biopsy is the definitive test for establishing the diagnosis. In our case presentation, the regional neuropathologist thought the biopsy result was most consistent with dermatomyositis despite the clinical paucity of skin abnormalities, though our consulting neurologist favored a diagnosis of polymyositis on clinical grounds.
Treatment recommendations
Corticosteroids are the most efficacious treatment for dermatomyositis (strength of recommendation [SOR]: B).10 One empirical regimen is to give prednisone 1 mg/kg/d as initial therapy; maintain this therapy for 1 month after symptoms and CK have normalized; then slowly taper (SOR: C).10 Twenty-five percent of patients will not respond to steroids; others will not tolerate the side effects of steroid therapy.10
Immunosuppressive drugs such as azothioprine, methotrexate, cyclosporine, mycophenolate mofetil and cyclophosphamide may be used as second-line treatment (SOR: C).6 Intravenous immunoglobulin may have some efficacy (SOR: B).16 Plasmapheresis does not appear to be effective (SOR: B).17
Determinants of prognosis
Most patients will improve over several weeks or months with therapy, although a third or more are left with mild to severe muscle damage. Dermatomyositis responds better than polymyositis; inclusion-body myositis is the most difficult to treat.10 Poor prognostic factors include older age, association with cancer, pulmonary fibrosis, dysphagia with aspiration pneumonia, cardiac involvement, steroid-resistant disease, and calcinosis in dermatomyositis.6,10 Studies have demonstrated 5-year survival rates between 77% and 92%.18,19 The main causes of death were related to malignancy and cardiac or pulmonary complications.
1. Alpert JS, Thygesen K, Antman E, et al. Myocardial infarction redefined—a consensus document of the Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol 2000;36:959-969.
2. Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA 2002 guideline update for the management of patients with unstable angina and no-ST-segment elevation myocardial infarction—summary article: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on the Management of Patients With Unstable Angina). J Am Coll Cardiol 2002;40:1366-1374.
3. Ng SM, Krishnaswamy P, Morrisey R, et al. Mitigation of the clinical significance of spurious elevations of cardiac troponin I in settings of coronary ischemia using serial testing of multiple cardiac markers. Am J Cardiol 2001;87:994-999.
4. Jeremias A, Gibson C. Narrative review: Alternative causes for elevated cardiac troponin levels when acute coronary syndromes are excluded. Ann Intern Med 2005;142:786-791.
5. Miller M. Muscle enzymes in the evaluation of neuromuscular disease. In UpToDate [database]. Available at www.uptodate.com. Accessed on January 10, 2005.
6. Dalakas C, Hohlfeld R. Polymyositis and dermatomyositis. Lancet 2003;362:971-982.
7. Rowland LP. Polymyositis, inclusion body myositis, and related myopathies. In: Merritt’s Neurology. 10th ed. Philadelphia, Pa: Lippincott, Williams & Wilkins; 2000:765-769.
8. Peterson LZR, Marfin AA. West Nile virus: a primer for the clinician. Ann Intern Med 2002;137:173-179.
9. van der Meulen MFG, Bronner I, et al. Polymyositis: An overdiagnosed entity. Neurology 2003;61:316-321.
10. Callen J. Dermatomyositis. Lancet 2000;355:53-57.
11. Marie I, Hachulla E, Cherin P, et al. Interstitial lung disease in polymyositis and dermatomyositis. Arthritis Rheum 2002;47:614-622.
12. Sparsa A, Liozon E, Herrmann F, et al. Routine vs extensive malignancy search for adult dermatomyositis and polymyositis. Arch Dermatol 2002;138:885-890.
13. Buchbinder R, Forbes A, Hall S, Dennett X, Giles G. Incidence of malignant disease in biopsy-proven inflammatory myopathy. Ann Intern Med 2001;134:1087-1095.
14. Hengstman GJD, Brouwer, Egberts WT, et al. Clinical and serological characteristics of 125 Dutch myositis patients: Myositis specific antibodies aid in the differential diagnosis of the idiopathic inflammatory myopathies. J Neurol 2002;249:69-75.
15. Schmidt WA, Wetzel W, Friedlander R, et al. Clinical and serological aspects of patients with anti-Jo-1 antibodies—an evolving spectrum of disease manifestations. Clin Rheumatol 2000;19:371-377.
16. Dalakis M, Illa I. A controlled trial of high-dose intravenous immune globulin infusions as treatment for dermatomyositis. N Engl J Med 1993;329:1993-2000.
17. Miller FW, Leitman SF, Cronin M, et al. Controlled trial of plasma exchange and leukapheresis in polymyositis and dermatomyositis. N Engl J Med 1992;326:1380-1384.
18. Marie I, Hachulla E, Hatron PY, et al. Polymyositis and dermatomyositis: Short term and longterm outcome, and predictive factors of prognosis. J Rheumatol 2001;28:2230-2237.
19. Danko K, Ponyi A, Constantin T, Borgulya G, Szegedi G. Long-term survival of patients with idiopathic inflammatory myopathies according to clinical features: A longitudinal study of 162 cases. Medicine (Baltimore) 2004;83:35-42.
CORRESPONDENCE: Edward Onusko, MD, 825 West Locust Street, Wilmington OH 45177. edonusko@cmhregional.com
History of present illness
- Approximately 4 weeks of generalized extremity pain and weakness; left-sided, nonexertional chest pain, which is much less severe than his extremity pains
- Symptoms are most prominent in the proximal upper extremities, especially with movement; the right side is more effected than the left
- Dyspnea on exertion
- Seen twice in local urgent care facilities in the past 10 days; diagnosed with congestive heart failure; treated with furosemide, digoxin, and an unknown antibiotic without relief
- 20- to 30-pound weight loss over the past year
Other medical history
- No chronic medical problems or medications
- Until this past month, last seen by a physician about 3 or 4 years prior
Review of systems
- Up to the day of admission has been ambulatory and able to care for himself despite his weakness
- No fever, chills, or rash; but has night sweats
- Smokes; does not drink alcohol
- Retired; lives with his wife
Physical examination
- Alert, appears mildly uncomfortable
- Temperature 101°F, respirations 32, blood pressure 164/72, pulse 80
- 3/5 strength in proximal upper and lower extremities (can barely lift arms and legs off the bed; movement also limited by pain)
- Normal distal strength (hand grips and dorsi/plantar flexion of foot)
- Normal sensation, reflexes, cranial nerves, and mental status; no neck weakness
- No abnormal joint findings; has pink discoloration over extensor surface of MCP joint, which patient dismisses as scars from previous abrasions that have been present “for a long time”
- Heart, lungs unremarkable; no peripheral edema
Laboratory studies completed in the emergency department
- ECG: normal
- Chest x-ray: bibasilar peribronchial infiltrates
- Hemoglobin/hematocrit: normal
- White blood count: 27,000 with 92% neutrophils
- Erythrocyte sedimentation rate: normal
- Urinalysis: negative for blood
- Brain natriuretic peptide: normal
- Creatine kinase (CK): 2205 IU/L (normal range 35–232)
- Troponin-I: 0.6 ng/mL.
[Reference range:
<0.05=Negative
0.05–0.09=Equivocal
0.10–0.49=Suspicious
0.50=Consistent with myocardial injury]
A: ____________________________________________________________ ______________________________________________________________
Is this acute non-ST elevation myocardial infarction (NSTEMI)?
The American College of Cardiology and the American Heart Association define myocardial infarction primarily as elevated cardiac-specific enzymes troponin-I and troponin-T in the appropriate clinical setting.1,2 Elevated cardiac troponins have a sensitivity approaching 100% for myocardial damage. Specificity is much lower for acute ischemic cardiac disease, however, particularly for patients with a low pretest probability (45% false-positive rate in one series of 1000 consecutive patients presenting to a large urban emergency department with symptoms of acute coronary ischemia).3
Mechanisms other than atherosclerotic coronary artery disease that can elevate cardiac troponins:
- Increased cardiac demand (eg, sepsis, hypovolemia)
- Nonatherosclerotic ischemia (eg, cocaine or other sympathomimetic agents, coronary vasospasm)
- Direct myocardial injury (eg, cardiac contusion, myocarditis)
- Myocardial strain (eg, congestive heart failure, pulmonary embolus)
- Chronic renal insufficiency (mechanism unclear).4
In light of this patient’s history and physical exam findings, you doubt he’s having an acute cardiac event. The most remarkable features are his weakness, muscle pain, and markedly elevated CK.
Though you have ruled out anemia and several other possibilities, the differential diagnosis of weakness is still broad. You decide to explore the differential diagnosis of elevated CK, a more specific finding in this case.
Pursuing the differential
You consult UpToDate, searching under “creatine kinase,” and find an article entitled “Muscle enzymes in the evaluation of neuromuscular disease.”5 You conclude that the most likely cause of your patient’s problems is an idiopathic inflammatory myopathy: polymyositis, dermatomyositis, or inclusion-body myositis.6
Other possibilities include post-viral myositis and myositis associated with connective tissue disease, hypothyroidism, or drug reactions.
D-penicillamine, zidovudine (AZT), and viral or bacterial infection may produce inflammatory myopathy similar to polymyositis.7 A history of exposure to myotoxic drugs (such as statins) and toxins has been excluded.
The absence of a family history for neuromuscular disease and the relatively recent onset of symptoms rule out an inherited muscular dystrophy or congenital muscle enzyme deficiency.
Myasthenia gravis presents with extraocular muscle involvement. Guillain-Barré syndrome is characterized by ascending muscle weakness. Lyme disease may cause weakness secondary to peripheral neuropathy but it does not produce evidence of muscle inflammation such as elevation of the CK. West Nile virus encephalitis may present with muscle weakness and flaccid paralysis.8 Trichinellosis may also cause muscle inflammation with weakness and elevation of CK, but it is rare in the United States.
You repeat parts of your physical exam and confirm that his proximal upper extremity muscles are much weaker than his distal muscles.
In practice settings where specialty consultation is not always immediately available, your diagnostic skills may be challenged by uncommon presentations of disease. In this case, the challenge is “chest pain and positive cardiac enzymes” in a patient who does not appear to have a primary cardiac problem.
A: ____________________________________________________________ ______________________________________________________________
DTaP approach
When confronted with a difficult clinical problem, you may find it useful to organize the management plan according to the acronym “DTaP,” which for this patient would include:
- Diagnostic plan: serial ECGs and cardiac enzymes: an echocardiogram
- Therapeutic plan: pain control; antibiotics for possible pneumonia; consider steroids
- Assistance from consultants (who are you going to ask for help?): physiatrist consult for electromyography (EMG); cardiology consult; neurology consult
- Patient education (explain to the patient and his family the current diagnostic possibilities and your management plan)
- Provider education (learn more about myopathies!).
You request specialty consultations:
Neurology: possible polymyositis; recommends rheumatology consultation, multiple labs (most of which are sent out to a reference lab and return only several days later)
Cardiology: ECG normal; cardiologist does not see evidence for congestive heart failure or coronary artery disease
Physical medicine and rehabilitation: EMG performed; findings consistent with inflammatory myopathy
Rheumatology: recommends proceeding with muscle biopsy to differentiate polymyositis and inclusion-body myositis
Surgery: performs muscle biopsy which is sent to a regional neuropathologist; reveals inflammatory myopathy with prominent perivascular lymphocytic inflammation strongly suggestive of dermatomyositis.
Further case management and resolution
You administer solumedrol intravenously 1 g/d for 3 days, then change to prednisone orally 1 mg/kg/d.
The patient improves steadily with 3 months of oral steroid therapy. He tests positive for anti-Jo antibodies but his pulmonary symptoms resolve. He undergoes an outpatient evaluation for cancer screening. Colonoscopy, esophogastroduodenoscopy and chest/abdominal/pelvic computed tomography scans are negative for evidence of malignancy.
This case illustrates the importance of not letting dramatic laboratory abnormalities—for this patient, an elevated CK enzyme level—unduly influence your investigative focus. The patient’s history and physical exam findings provided a larger context in which the diagnosis of acute coronary insufficiency became unlikely. Balanced consideration of the patient’s muscle pain and weakness and elevated CK level narrowed the diagnostic possibilities appropriately.
Other ways in which you may encounter inflammatory myopathies
Dermatomyositis usually causes a characteristic rash that facilitates early diagnosis (though it did not appear in this case). As shown in FIGURES 1 AND 2, patients may have either a heliotrope rash (blue-purple to dusky erythematous discoloration on the upper eyelids, with or without edema), or Gottron’s papules (slightly raised violaceous papules and plaques overlying bony prominences, particularly the joints in the fingers and the knuckles).10
A variety of less specific skin and nail changes can occur. Dermatomyositis may present with skin lesions alone (dermatomyositis sine myositis) or rarely with myopathy alone (dermatomyositis sine dermatitis). In our case, multiple examiners failed to detect any classic dermatologic abnormalities, though the pinkish skin changes over the extensor aspect of the MCP joints were, in retrospect, suggestive of dermatomyositis. The weakness associated with this disease may be mild, moderate, or severe enough to result in quadriparesis. Dermatomyositis usually occurs alone but may be present with scleroderma and mixed connective tissue disease.
The main categories of idiopathic acquired inflammatory myopathy are polymyositis, dermatomyositis, and inclusion-body myositis. They cause moderate-to-severe weakness and inflammation of muscles.6 The prevalence of these disorders is unclear because diagnosis has not consistently been based on uniform, reliable criteria. But the incidence is believed to be 1 per 100,000 of the general population, with dermatomyositis being the most common and polymyositis the least common of these myopathies.9 Inclusion-body myositis is the most common form of inflammatory myopathy in patients older than 50 years. Polymyositis is generally seen after the second decade of life. Both children and adults may be affected by dermatomyositis. There have been rare familial occurrences.
Inclusion-body myositis is often misdiagnosed as polymyositis or dermatomyositis until identified by muscle biopsy findings (see How inflammatory myopathies develop), although suspicion is raised with a poor response to steroid therapy.9 Some patients report falling as a result of quadriceps weakness. On occasion the weakness can be asymmetric or distal (rare with dermatomyositis or polymyositis). Diagnosis is always made by muscle biopsy. Disease progression is slow but steady and most patients end up requiring a walker or assistive device.
Polymyositis is a sub-acute inflammatory myopathy affecting adults and, rarely, children. In most cases the actual onset of polymyositis is not easily determined as patients tend to delay seeking medical evaluation.
Other muscular disorders, as discussed in the case presentation, need to be excluded.
FIGURE 1 Heliotrope rash
Patients with dermatomyositis often have a characteristic rash on their face.
FIGURE 2 Gottron’s papules
Many patients also have papules and plaques on their hands, typically at the joints.
Evidence suggests the inflammatory myopathies are autoimmune disorders.6 They are often associated with connective tissue diseases and other systemic autoimmune conditions. Viral infections such as coxsackie, influenza, paramyxovirus, mumps, cytomegalovirus, and Epstein-Barr have been indirectly associated with chronic and acute myositis and may trigger the autoimmune process.
Specific muscle or capillary target antigens have not been identified, and the agents that initiate self-sensitization are still unknown. Other features of these disorders are their association with auto-antibodies, certain histocompatibility genes, T-cell–mediated myocytotoxicity, and complement-mediated microangiopathy.6
Dermatomyositis appears to be primarily a B-cell mediated microangiopathy. Antibodies directed against the endothelium of the endomysial capillaries lead to the primary histological changes in the blood vessels.9 The disease manifests when the complement system is activated to form the membrane attack complex (MAC).
Polymyositis and inclusion-body myositis appear to result from a cytotoxic T-cell response directed specifically against muscle fibers.9 CD-8+ cells are induced via T-cell activation to invade MHC-I antigen-expressing muscle cells.6 Usually most muscle cells do not express MHC Class I or II antigens. Histology demonstrates infiltration of individual muscle fibers by inflammatory cells. Inclusion-body myositis is differentiated from polymyositis by the presence of nuclear and cytoplasmic vacuoles.
Commonly associated clinical findings
Extramuscular manifestations of inflammatory myopathies. Dermatomyositis is a systemic inflammatory disorder that may extend beyond the dermatologic and muscular systems, and patients can exhibit such symptoms as fever, malaise, and weight loss.
Arthralgia and Raynaud’s phenomenon may occur with associated connective tissue disease.
Dysphagia indicates involvement of the oropharyngeal striated muscles and the upper esophagus.
Cardiac disturbances include atrioventricular conduction defects, tachyarrhythmias, myocarditis, heart failure, and possibly hypertension from long-term steroid use. The elevated troponin-I seen in our index case may have been evidence of a mild myocarditis, though the echocardiogram was normal.
Calcinosis (deposition of calcium in the skin or muscles) occurs in up to 40% of children with dermatomyositis but is unusual in adults.10
Pulmonary symptoms may be due to weakness of the thoracic muscles, interstitial lung disease, or aspiration. One retrospective study of 156 consecutive patients with dermatomyositis/polymyositis based on clinical criteria found a 23.1% incidence of interstitial lung disease.11
Malignant disorders. The frequency of cancer is increased in association with these diseases. Studies have placed the highest risk of concomitant malignancy with dermatomyositis and the least risk with polymyositis. (The relative risk for malignancy in dermatomyositis as compared with polymyositis was 2.4.) Malignancy associated with dermatomyositis or polymyositis is twice as likely in women than in men.12
Risk of associated malignancy was highest within the first year of diagnosis. Therefore, consider a diagnostic evaluation for malignancy at the time myopathy is diagnosed. The optimal diagnostic regimen in this setting is unknown. In one retrospective French study of 40 consecutive adult patients with inflammatory myopathy (33 with dermatomyositis and 7 with polymyositis) between the years 1981 and 2000, malignancy was present at the time of myopathy diagnosis in 16 patients (13 with dermatomyositis and 3 with polymyositis).12 An Australian population-based, retrospective cohort study of 537 individuals with biopsy-proven idiopathic inflammatory myopathy from 1981–1995 demonstrated 116 cases of malignancy in 104 patients.13 The risk was highest in dermatomyositis (standardized incidence ratio [SIR] 6.2), next highest in inclusion-body myositis (SIR 2.4), and lowest in polymyositis (SIR 2.0).
Diagnosis: What helps, what doesn’t
Suspect inflammatory myopathy by the constellation of clinical findings; confirm it by looking for elevated muscle enzymes and characteristic findings on EMG and muscle biopsy (see How inflammatory myopathies develop).
The most sensitive muscle enzyme for inflammatory myopathy is CK, levels of which usually parallel disease activity and may be used to assess response to therapy.6,10 Needle EMG demonstrates increased spontaneous activity with fibrillations; complex repetitive discharges; positive sharp waves; and voluntary motor units consisting of low-amplitude polyphasic units of short duration.6 EMG findings alone are not diagnostic.
Serologic tests are commonly done but their clinical usefulness is controversial.10 Antinuclear antibodies are found in about 80% of cases but are nonspecific and not clinically useful.14 Myositis-specific antibodies (MSAs) have been described in about 30% of idiopathic inflammatory myopathies but are also of uncertain diagnostic and pathogenic importance.14 The most prevalent MSA, anti-Jo, is present in only about 20% of cases and correlates with interstitial lung disease, but has uncertain usefulness in differentiating between dermatomyositis, polymyositis, and inclusion-body myositis.6,10,11,14,15
Differentiate between the inflammatory myopathies based on characteristic pathological findings on muscle biopsy (previously discussed). Muscle biopsy is the definitive test for establishing the diagnosis. In our case presentation, the regional neuropathologist thought the biopsy result was most consistent with dermatomyositis despite the clinical paucity of skin abnormalities, though our consulting neurologist favored a diagnosis of polymyositis on clinical grounds.
Treatment recommendations
Corticosteroids are the most efficacious treatment for dermatomyositis (strength of recommendation [SOR]: B).10 One empirical regimen is to give prednisone 1 mg/kg/d as initial therapy; maintain this therapy for 1 month after symptoms and CK have normalized; then slowly taper (SOR: C).10 Twenty-five percent of patients will not respond to steroids; others will not tolerate the side effects of steroid therapy.10
Immunosuppressive drugs such as azothioprine, methotrexate, cyclosporine, mycophenolate mofetil and cyclophosphamide may be used as second-line treatment (SOR: C).6 Intravenous immunoglobulin may have some efficacy (SOR: B).16 Plasmapheresis does not appear to be effective (SOR: B).17
Determinants of prognosis
Most patients will improve over several weeks or months with therapy, although a third or more are left with mild to severe muscle damage. Dermatomyositis responds better than polymyositis; inclusion-body myositis is the most difficult to treat.10 Poor prognostic factors include older age, association with cancer, pulmonary fibrosis, dysphagia with aspiration pneumonia, cardiac involvement, steroid-resistant disease, and calcinosis in dermatomyositis.6,10 Studies have demonstrated 5-year survival rates between 77% and 92%.18,19 The main causes of death were related to malignancy and cardiac or pulmonary complications.
History of present illness
- Approximately 4 weeks of generalized extremity pain and weakness; left-sided, nonexertional chest pain, which is much less severe than his extremity pains
- Symptoms are most prominent in the proximal upper extremities, especially with movement; the right side is more effected than the left
- Dyspnea on exertion
- Seen twice in local urgent care facilities in the past 10 days; diagnosed with congestive heart failure; treated with furosemide, digoxin, and an unknown antibiotic without relief
- 20- to 30-pound weight loss over the past year
Other medical history
- No chronic medical problems or medications
- Until this past month, last seen by a physician about 3 or 4 years prior
Review of systems
- Up to the day of admission has been ambulatory and able to care for himself despite his weakness
- No fever, chills, or rash; but has night sweats
- Smokes; does not drink alcohol
- Retired; lives with his wife
Physical examination
- Alert, appears mildly uncomfortable
- Temperature 101°F, respirations 32, blood pressure 164/72, pulse 80
- 3/5 strength in proximal upper and lower extremities (can barely lift arms and legs off the bed; movement also limited by pain)
- Normal distal strength (hand grips and dorsi/plantar flexion of foot)
- Normal sensation, reflexes, cranial nerves, and mental status; no neck weakness
- No abnormal joint findings; has pink discoloration over extensor surface of MCP joint, which patient dismisses as scars from previous abrasions that have been present “for a long time”
- Heart, lungs unremarkable; no peripheral edema
Laboratory studies completed in the emergency department
- ECG: normal
- Chest x-ray: bibasilar peribronchial infiltrates
- Hemoglobin/hematocrit: normal
- White blood count: 27,000 with 92% neutrophils
- Erythrocyte sedimentation rate: normal
- Urinalysis: negative for blood
- Brain natriuretic peptide: normal
- Creatine kinase (CK): 2205 IU/L (normal range 35–232)
- Troponin-I: 0.6 ng/mL.
[Reference range:
<0.05=Negative
0.05–0.09=Equivocal
0.10–0.49=Suspicious
0.50=Consistent with myocardial injury]
A: ____________________________________________________________ ______________________________________________________________
Is this acute non-ST elevation myocardial infarction (NSTEMI)?
The American College of Cardiology and the American Heart Association define myocardial infarction primarily as elevated cardiac-specific enzymes troponin-I and troponin-T in the appropriate clinical setting.1,2 Elevated cardiac troponins have a sensitivity approaching 100% for myocardial damage. Specificity is much lower for acute ischemic cardiac disease, however, particularly for patients with a low pretest probability (45% false-positive rate in one series of 1000 consecutive patients presenting to a large urban emergency department with symptoms of acute coronary ischemia).3
Mechanisms other than atherosclerotic coronary artery disease that can elevate cardiac troponins:
- Increased cardiac demand (eg, sepsis, hypovolemia)
- Nonatherosclerotic ischemia (eg, cocaine or other sympathomimetic agents, coronary vasospasm)
- Direct myocardial injury (eg, cardiac contusion, myocarditis)
- Myocardial strain (eg, congestive heart failure, pulmonary embolus)
- Chronic renal insufficiency (mechanism unclear).4
In light of this patient’s history and physical exam findings, you doubt he’s having an acute cardiac event. The most remarkable features are his weakness, muscle pain, and markedly elevated CK.
Though you have ruled out anemia and several other possibilities, the differential diagnosis of weakness is still broad. You decide to explore the differential diagnosis of elevated CK, a more specific finding in this case.
Pursuing the differential
You consult UpToDate, searching under “creatine kinase,” and find an article entitled “Muscle enzymes in the evaluation of neuromuscular disease.”5 You conclude that the most likely cause of your patient’s problems is an idiopathic inflammatory myopathy: polymyositis, dermatomyositis, or inclusion-body myositis.6
Other possibilities include post-viral myositis and myositis associated with connective tissue disease, hypothyroidism, or drug reactions.
D-penicillamine, zidovudine (AZT), and viral or bacterial infection may produce inflammatory myopathy similar to polymyositis.7 A history of exposure to myotoxic drugs (such as statins) and toxins has been excluded.
The absence of a family history for neuromuscular disease and the relatively recent onset of symptoms rule out an inherited muscular dystrophy or congenital muscle enzyme deficiency.
Myasthenia gravis presents with extraocular muscle involvement. Guillain-Barré syndrome is characterized by ascending muscle weakness. Lyme disease may cause weakness secondary to peripheral neuropathy but it does not produce evidence of muscle inflammation such as elevation of the CK. West Nile virus encephalitis may present with muscle weakness and flaccid paralysis.8 Trichinellosis may also cause muscle inflammation with weakness and elevation of CK, but it is rare in the United States.
You repeat parts of your physical exam and confirm that his proximal upper extremity muscles are much weaker than his distal muscles.
In practice settings where specialty consultation is not always immediately available, your diagnostic skills may be challenged by uncommon presentations of disease. In this case, the challenge is “chest pain and positive cardiac enzymes” in a patient who does not appear to have a primary cardiac problem.
A: ____________________________________________________________ ______________________________________________________________
DTaP approach
When confronted with a difficult clinical problem, you may find it useful to organize the management plan according to the acronym “DTaP,” which for this patient would include:
- Diagnostic plan: serial ECGs and cardiac enzymes: an echocardiogram
- Therapeutic plan: pain control; antibiotics for possible pneumonia; consider steroids
- Assistance from consultants (who are you going to ask for help?): physiatrist consult for electromyography (EMG); cardiology consult; neurology consult
- Patient education (explain to the patient and his family the current diagnostic possibilities and your management plan)
- Provider education (learn more about myopathies!).
You request specialty consultations:
Neurology: possible polymyositis; recommends rheumatology consultation, multiple labs (most of which are sent out to a reference lab and return only several days later)
Cardiology: ECG normal; cardiologist does not see evidence for congestive heart failure or coronary artery disease
Physical medicine and rehabilitation: EMG performed; findings consistent with inflammatory myopathy
Rheumatology: recommends proceeding with muscle biopsy to differentiate polymyositis and inclusion-body myositis
Surgery: performs muscle biopsy which is sent to a regional neuropathologist; reveals inflammatory myopathy with prominent perivascular lymphocytic inflammation strongly suggestive of dermatomyositis.
Further case management and resolution
You administer solumedrol intravenously 1 g/d for 3 days, then change to prednisone orally 1 mg/kg/d.
The patient improves steadily with 3 months of oral steroid therapy. He tests positive for anti-Jo antibodies but his pulmonary symptoms resolve. He undergoes an outpatient evaluation for cancer screening. Colonoscopy, esophogastroduodenoscopy and chest/abdominal/pelvic computed tomography scans are negative for evidence of malignancy.
This case illustrates the importance of not letting dramatic laboratory abnormalities—for this patient, an elevated CK enzyme level—unduly influence your investigative focus. The patient’s history and physical exam findings provided a larger context in which the diagnosis of acute coronary insufficiency became unlikely. Balanced consideration of the patient’s muscle pain and weakness and elevated CK level narrowed the diagnostic possibilities appropriately.
Other ways in which you may encounter inflammatory myopathies
Dermatomyositis usually causes a characteristic rash that facilitates early diagnosis (though it did not appear in this case). As shown in FIGURES 1 AND 2, patients may have either a heliotrope rash (blue-purple to dusky erythematous discoloration on the upper eyelids, with or without edema), or Gottron’s papules (slightly raised violaceous papules and plaques overlying bony prominences, particularly the joints in the fingers and the knuckles).10
A variety of less specific skin and nail changes can occur. Dermatomyositis may present with skin lesions alone (dermatomyositis sine myositis) or rarely with myopathy alone (dermatomyositis sine dermatitis). In our case, multiple examiners failed to detect any classic dermatologic abnormalities, though the pinkish skin changes over the extensor aspect of the MCP joints were, in retrospect, suggestive of dermatomyositis. The weakness associated with this disease may be mild, moderate, or severe enough to result in quadriparesis. Dermatomyositis usually occurs alone but may be present with scleroderma and mixed connective tissue disease.
The main categories of idiopathic acquired inflammatory myopathy are polymyositis, dermatomyositis, and inclusion-body myositis. They cause moderate-to-severe weakness and inflammation of muscles.6 The prevalence of these disorders is unclear because diagnosis has not consistently been based on uniform, reliable criteria. But the incidence is believed to be 1 per 100,000 of the general population, with dermatomyositis being the most common and polymyositis the least common of these myopathies.9 Inclusion-body myositis is the most common form of inflammatory myopathy in patients older than 50 years. Polymyositis is generally seen after the second decade of life. Both children and adults may be affected by dermatomyositis. There have been rare familial occurrences.
Inclusion-body myositis is often misdiagnosed as polymyositis or dermatomyositis until identified by muscle biopsy findings (see How inflammatory myopathies develop), although suspicion is raised with a poor response to steroid therapy.9 Some patients report falling as a result of quadriceps weakness. On occasion the weakness can be asymmetric or distal (rare with dermatomyositis or polymyositis). Diagnosis is always made by muscle biopsy. Disease progression is slow but steady and most patients end up requiring a walker or assistive device.
Polymyositis is a sub-acute inflammatory myopathy affecting adults and, rarely, children. In most cases the actual onset of polymyositis is not easily determined as patients tend to delay seeking medical evaluation.
Other muscular disorders, as discussed in the case presentation, need to be excluded.
FIGURE 1 Heliotrope rash
Patients with dermatomyositis often have a characteristic rash on their face.
FIGURE 2 Gottron’s papules
Many patients also have papules and plaques on their hands, typically at the joints.
Evidence suggests the inflammatory myopathies are autoimmune disorders.6 They are often associated with connective tissue diseases and other systemic autoimmune conditions. Viral infections such as coxsackie, influenza, paramyxovirus, mumps, cytomegalovirus, and Epstein-Barr have been indirectly associated with chronic and acute myositis and may trigger the autoimmune process.
Specific muscle or capillary target antigens have not been identified, and the agents that initiate self-sensitization are still unknown. Other features of these disorders are their association with auto-antibodies, certain histocompatibility genes, T-cell–mediated myocytotoxicity, and complement-mediated microangiopathy.6
Dermatomyositis appears to be primarily a B-cell mediated microangiopathy. Antibodies directed against the endothelium of the endomysial capillaries lead to the primary histological changes in the blood vessels.9 The disease manifests when the complement system is activated to form the membrane attack complex (MAC).
Polymyositis and inclusion-body myositis appear to result from a cytotoxic T-cell response directed specifically against muscle fibers.9 CD-8+ cells are induced via T-cell activation to invade MHC-I antigen-expressing muscle cells.6 Usually most muscle cells do not express MHC Class I or II antigens. Histology demonstrates infiltration of individual muscle fibers by inflammatory cells. Inclusion-body myositis is differentiated from polymyositis by the presence of nuclear and cytoplasmic vacuoles.
Commonly associated clinical findings
Extramuscular manifestations of inflammatory myopathies. Dermatomyositis is a systemic inflammatory disorder that may extend beyond the dermatologic and muscular systems, and patients can exhibit such symptoms as fever, malaise, and weight loss.
Arthralgia and Raynaud’s phenomenon may occur with associated connective tissue disease.
Dysphagia indicates involvement of the oropharyngeal striated muscles and the upper esophagus.
Cardiac disturbances include atrioventricular conduction defects, tachyarrhythmias, myocarditis, heart failure, and possibly hypertension from long-term steroid use. The elevated troponin-I seen in our index case may have been evidence of a mild myocarditis, though the echocardiogram was normal.
Calcinosis (deposition of calcium in the skin or muscles) occurs in up to 40% of children with dermatomyositis but is unusual in adults.10
Pulmonary symptoms may be due to weakness of the thoracic muscles, interstitial lung disease, or aspiration. One retrospective study of 156 consecutive patients with dermatomyositis/polymyositis based on clinical criteria found a 23.1% incidence of interstitial lung disease.11
Malignant disorders. The frequency of cancer is increased in association with these diseases. Studies have placed the highest risk of concomitant malignancy with dermatomyositis and the least risk with polymyositis. (The relative risk for malignancy in dermatomyositis as compared with polymyositis was 2.4.) Malignancy associated with dermatomyositis or polymyositis is twice as likely in women than in men.12
Risk of associated malignancy was highest within the first year of diagnosis. Therefore, consider a diagnostic evaluation for malignancy at the time myopathy is diagnosed. The optimal diagnostic regimen in this setting is unknown. In one retrospective French study of 40 consecutive adult patients with inflammatory myopathy (33 with dermatomyositis and 7 with polymyositis) between the years 1981 and 2000, malignancy was present at the time of myopathy diagnosis in 16 patients (13 with dermatomyositis and 3 with polymyositis).12 An Australian population-based, retrospective cohort study of 537 individuals with biopsy-proven idiopathic inflammatory myopathy from 1981–1995 demonstrated 116 cases of malignancy in 104 patients.13 The risk was highest in dermatomyositis (standardized incidence ratio [SIR] 6.2), next highest in inclusion-body myositis (SIR 2.4), and lowest in polymyositis (SIR 2.0).
Diagnosis: What helps, what doesn’t
Suspect inflammatory myopathy by the constellation of clinical findings; confirm it by looking for elevated muscle enzymes and characteristic findings on EMG and muscle biopsy (see How inflammatory myopathies develop).
The most sensitive muscle enzyme for inflammatory myopathy is CK, levels of which usually parallel disease activity and may be used to assess response to therapy.6,10 Needle EMG demonstrates increased spontaneous activity with fibrillations; complex repetitive discharges; positive sharp waves; and voluntary motor units consisting of low-amplitude polyphasic units of short duration.6 EMG findings alone are not diagnostic.
Serologic tests are commonly done but their clinical usefulness is controversial.10 Antinuclear antibodies are found in about 80% of cases but are nonspecific and not clinically useful.14 Myositis-specific antibodies (MSAs) have been described in about 30% of idiopathic inflammatory myopathies but are also of uncertain diagnostic and pathogenic importance.14 The most prevalent MSA, anti-Jo, is present in only about 20% of cases and correlates with interstitial lung disease, but has uncertain usefulness in differentiating between dermatomyositis, polymyositis, and inclusion-body myositis.6,10,11,14,15
Differentiate between the inflammatory myopathies based on characteristic pathological findings on muscle biopsy (previously discussed). Muscle biopsy is the definitive test for establishing the diagnosis. In our case presentation, the regional neuropathologist thought the biopsy result was most consistent with dermatomyositis despite the clinical paucity of skin abnormalities, though our consulting neurologist favored a diagnosis of polymyositis on clinical grounds.
Treatment recommendations
Corticosteroids are the most efficacious treatment for dermatomyositis (strength of recommendation [SOR]: B).10 One empirical regimen is to give prednisone 1 mg/kg/d as initial therapy; maintain this therapy for 1 month after symptoms and CK have normalized; then slowly taper (SOR: C).10 Twenty-five percent of patients will not respond to steroids; others will not tolerate the side effects of steroid therapy.10
Immunosuppressive drugs such as azothioprine, methotrexate, cyclosporine, mycophenolate mofetil and cyclophosphamide may be used as second-line treatment (SOR: C).6 Intravenous immunoglobulin may have some efficacy (SOR: B).16 Plasmapheresis does not appear to be effective (SOR: B).17
Determinants of prognosis
Most patients will improve over several weeks or months with therapy, although a third or more are left with mild to severe muscle damage. Dermatomyositis responds better than polymyositis; inclusion-body myositis is the most difficult to treat.10 Poor prognostic factors include older age, association with cancer, pulmonary fibrosis, dysphagia with aspiration pneumonia, cardiac involvement, steroid-resistant disease, and calcinosis in dermatomyositis.6,10 Studies have demonstrated 5-year survival rates between 77% and 92%.18,19 The main causes of death were related to malignancy and cardiac or pulmonary complications.
1. Alpert JS, Thygesen K, Antman E, et al. Myocardial infarction redefined—a consensus document of the Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol 2000;36:959-969.
2. Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA 2002 guideline update for the management of patients with unstable angina and no-ST-segment elevation myocardial infarction—summary article: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on the Management of Patients With Unstable Angina). J Am Coll Cardiol 2002;40:1366-1374.
3. Ng SM, Krishnaswamy P, Morrisey R, et al. Mitigation of the clinical significance of spurious elevations of cardiac troponin I in settings of coronary ischemia using serial testing of multiple cardiac markers. Am J Cardiol 2001;87:994-999.
4. Jeremias A, Gibson C. Narrative review: Alternative causes for elevated cardiac troponin levels when acute coronary syndromes are excluded. Ann Intern Med 2005;142:786-791.
5. Miller M. Muscle enzymes in the evaluation of neuromuscular disease. In UpToDate [database]. Available at www.uptodate.com. Accessed on January 10, 2005.
6. Dalakas C, Hohlfeld R. Polymyositis and dermatomyositis. Lancet 2003;362:971-982.
7. Rowland LP. Polymyositis, inclusion body myositis, and related myopathies. In: Merritt’s Neurology. 10th ed. Philadelphia, Pa: Lippincott, Williams & Wilkins; 2000:765-769.
8. Peterson LZR, Marfin AA. West Nile virus: a primer for the clinician. Ann Intern Med 2002;137:173-179.
9. van der Meulen MFG, Bronner I, et al. Polymyositis: An overdiagnosed entity. Neurology 2003;61:316-321.
10. Callen J. Dermatomyositis. Lancet 2000;355:53-57.
11. Marie I, Hachulla E, Cherin P, et al. Interstitial lung disease in polymyositis and dermatomyositis. Arthritis Rheum 2002;47:614-622.
12. Sparsa A, Liozon E, Herrmann F, et al. Routine vs extensive malignancy search for adult dermatomyositis and polymyositis. Arch Dermatol 2002;138:885-890.
13. Buchbinder R, Forbes A, Hall S, Dennett X, Giles G. Incidence of malignant disease in biopsy-proven inflammatory myopathy. Ann Intern Med 2001;134:1087-1095.
14. Hengstman GJD, Brouwer, Egberts WT, et al. Clinical and serological characteristics of 125 Dutch myositis patients: Myositis specific antibodies aid in the differential diagnosis of the idiopathic inflammatory myopathies. J Neurol 2002;249:69-75.
15. Schmidt WA, Wetzel W, Friedlander R, et al. Clinical and serological aspects of patients with anti-Jo-1 antibodies—an evolving spectrum of disease manifestations. Clin Rheumatol 2000;19:371-377.
16. Dalakis M, Illa I. A controlled trial of high-dose intravenous immune globulin infusions as treatment for dermatomyositis. N Engl J Med 1993;329:1993-2000.
17. Miller FW, Leitman SF, Cronin M, et al. Controlled trial of plasma exchange and leukapheresis in polymyositis and dermatomyositis. N Engl J Med 1992;326:1380-1384.
18. Marie I, Hachulla E, Hatron PY, et al. Polymyositis and dermatomyositis: Short term and longterm outcome, and predictive factors of prognosis. J Rheumatol 2001;28:2230-2237.
19. Danko K, Ponyi A, Constantin T, Borgulya G, Szegedi G. Long-term survival of patients with idiopathic inflammatory myopathies according to clinical features: A longitudinal study of 162 cases. Medicine (Baltimore) 2004;83:35-42.
CORRESPONDENCE: Edward Onusko, MD, 825 West Locust Street, Wilmington OH 45177. edonusko@cmhregional.com
1. Alpert JS, Thygesen K, Antman E, et al. Myocardial infarction redefined—a consensus document of the Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol 2000;36:959-969.
2. Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA 2002 guideline update for the management of patients with unstable angina and no-ST-segment elevation myocardial infarction—summary article: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on the Management of Patients With Unstable Angina). J Am Coll Cardiol 2002;40:1366-1374.
3. Ng SM, Krishnaswamy P, Morrisey R, et al. Mitigation of the clinical significance of spurious elevations of cardiac troponin I in settings of coronary ischemia using serial testing of multiple cardiac markers. Am J Cardiol 2001;87:994-999.
4. Jeremias A, Gibson C. Narrative review: Alternative causes for elevated cardiac troponin levels when acute coronary syndromes are excluded. Ann Intern Med 2005;142:786-791.
5. Miller M. Muscle enzymes in the evaluation of neuromuscular disease. In UpToDate [database]. Available at www.uptodate.com. Accessed on January 10, 2005.
6. Dalakas C, Hohlfeld R. Polymyositis and dermatomyositis. Lancet 2003;362:971-982.
7. Rowland LP. Polymyositis, inclusion body myositis, and related myopathies. In: Merritt’s Neurology. 10th ed. Philadelphia, Pa: Lippincott, Williams & Wilkins; 2000:765-769.
8. Peterson LZR, Marfin AA. West Nile virus: a primer for the clinician. Ann Intern Med 2002;137:173-179.
9. van der Meulen MFG, Bronner I, et al. Polymyositis: An overdiagnosed entity. Neurology 2003;61:316-321.
10. Callen J. Dermatomyositis. Lancet 2000;355:53-57.
11. Marie I, Hachulla E, Cherin P, et al. Interstitial lung disease in polymyositis and dermatomyositis. Arthritis Rheum 2002;47:614-622.
12. Sparsa A, Liozon E, Herrmann F, et al. Routine vs extensive malignancy search for adult dermatomyositis and polymyositis. Arch Dermatol 2002;138:885-890.
13. Buchbinder R, Forbes A, Hall S, Dennett X, Giles G. Incidence of malignant disease in biopsy-proven inflammatory myopathy. Ann Intern Med 2001;134:1087-1095.
14. Hengstman GJD, Brouwer, Egberts WT, et al. Clinical and serological characteristics of 125 Dutch myositis patients: Myositis specific antibodies aid in the differential diagnosis of the idiopathic inflammatory myopathies. J Neurol 2002;249:69-75.
15. Schmidt WA, Wetzel W, Friedlander R, et al. Clinical and serological aspects of patients with anti-Jo-1 antibodies—an evolving spectrum of disease manifestations. Clin Rheumatol 2000;19:371-377.
16. Dalakis M, Illa I. A controlled trial of high-dose intravenous immune globulin infusions as treatment for dermatomyositis. N Engl J Med 1993;329:1993-2000.
17. Miller FW, Leitman SF, Cronin M, et al. Controlled trial of plasma exchange and leukapheresis in polymyositis and dermatomyositis. N Engl J Med 1992;326:1380-1384.
18. Marie I, Hachulla E, Hatron PY, et al. Polymyositis and dermatomyositis: Short term and longterm outcome, and predictive factors of prognosis. J Rheumatol 2001;28:2230-2237.
19. Danko K, Ponyi A, Constantin T, Borgulya G, Szegedi G. Long-term survival of patients with idiopathic inflammatory myopathies according to clinical features: A longitudinal study of 162 cases. Medicine (Baltimore) 2004;83:35-42.
CORRESPONDENCE: Edward Onusko, MD, 825 West Locust Street, Wilmington OH 45177. edonusko@cmhregional.com
Vaginal pain and fever in a premenarchal girl: How would you treat?
Q: What are some causes of vaginal pain with fever? How would you proceed with the evaluation?
A: ______________________________________________________________ ______________________________________________________________
Other medical history
- Enuresis, recurrent perioral rash around age 7 with annual recurrences
- No chronic infections or illness
- Premenarchal
- Negative trauma history, including abuse
- Bike riding 2 days earlier but no falls
- Taking acyclovir as prescribed by ED; acetaminophen/ibuprofen for fever
- No known allergies
Family and social history
- Parents alive and well; no siblings
- Straight-A student
- Involved in JROTC (was on a retreat 2 weeks ago)
- No use of tobacco, alcohol, street drugs, or suspicious substances
- Denies any sexual activity
Physical examination
- Review of systems: Positive for chills, fever, dysuria, and perineal pain; otherwise negative
- Temperature 101.6°F, pulse 112, respiratory rate 22, blood pressure 110/70 mm Hg, weight 94 lb
- Alert female in no distress, normal neurologic exam
- HEENT: normal exam with clear oropharynx without lesions
- Skin/integument: no rashes, including arms, legs, hands, feet, and trunk
- Heart, lungs, and abdomen: tachycardia, otherwise normal
- Reproductive examination (chaperone present): Tanner stage III; perineal edema with marked purple ecchymoses located bilaterally at posterior introitus; multiple lacerations also noted as well as tenderness; some scabbed areas noted; no periurethral or perianal lesions or bruising; no vaginal discharge; speculum and bimanual exam were deferred due to pain.
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________ ______________________________________________________________
You are concerned about abuse. You interview the patient alone and she again denies any type of sexual encounter. She has never used tampons. She does report that she is a heavy sleeper and that she recently went on a retreat where she and a girlfriend slept in the same room. As far as she knows, there was no intruder. She tearfully says, “If anything happened, I can’t remember.”
You also interview the father alone. He says he and his wife “keep a tight rein” on their daughter. She has been out of their supervision only for the recent retreat. He is concerned that his daughter may have been given a “date-rape” drug and requests testing. His demeanor seems appropriate during the conversations both in the presence and absence of his daughter.
According to state law, you notify the Department of Social Services of unexplained perineal trauma. You also contact the local sexual abuse/rape experts in your area, who have arranged for an evaluation the following day. The father assists in making the arrangements for the evaluation while he is still in your office.
Department of Social Services forensic interview and medical examination
The next day, the patient and her family undergo a comprehensive evaluation by local medical and investigative professionals from the Department of Social Services.
The differential diagnosis for genital ulcers in a sexually inexperienced female includes sexual abuse, herpes simplex virus, Behçet’s disease, Epstein Barr infection, pilonidal disease, Crohn’s disease, and hidradenitis suppurativa. Definitive diagnosis can be difficult (TABLE 1).
One retrospective series reviewed the case of 9 adolescent females with vulvar ulcers and found that 6 had no formal diagnosis. Most important, the initial presentation should prompt healthcare professionals to take steps to ensure a patient’s safety.
After performing a physical examination, the abuse experts report that the patient’s presentation is consistent with Behçet’s disease. A genital culture was obtained, and the patient was given pain medication and azithromycin.
The expert also stated that the father’s reaction to the situation was appropriate and not that of an abusive father. Most perpetrators are very hostile and defensive, whereas this father was extremely concerned and cooperative. Still, a report to Child Protective Services had to be made because of the unexplained physical findings, especially in the genital area.
Further consideration
Additional information on Behçet’s disease is found in an article in the New England Journal of Medicine from 1999: “Behçet’s disease is an inflammatory disorder of unknown cause, characterized by recurrent oral aphthous ulcers, genital ulcers, uveitis, and skin lesions.”
You ponder this information and note that your patient has no oral lesions currently but apparently has a history of some oral lesions. You review your records indicating a history of recurrent perioral rash but do not find a history of oral lesions. However, the consultant remains constant in his diagnosis.
You review the results of the ED laboratory evaluation:
- Gonorrhea/chlamydia DNA probe negative
- Herpes culture and herpes immunoglobulin M (IgM) negative
- Rapid plasma reagin (RPR) nonreactive
- Serum pregnancy negative
- Urine drug screen negative for PCP, benzodiazepines, amphetamines, THC, opiates, barbiturates, methadone, tricyclic antidepressants
- Complete blood count normal; white blood count 9600 with a normal differential
As the family physician, you interpret these results and support the clinical plan for this patient, pending further changes in the clinical picture.
TABLE 1
Differential diagnosis of vulvar ulcers in sexually inexperienced females
| Sexual abuse |
| Herpes simplex virus infection |
| Behçet’s disease |
| Epstein-Barr viral infection |
| Crohn’s disease |
| Pilonidal disease |
| Hidradenitis suppurativa |
Next contact—ED visit 2 days later
The patient’s vaginal pain is worsening and she cannot void. Large ulcers with adhered pus are on the left labia; a smaller lesion is on the right labia. There are also questionable lacerations of the posterior fourchette. She is catheterized and 300 mL urine is emptied from the bladder. A gynecology consultation is obtained by the ED physician with your concurrence.
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________
Q: Is this Behçet’s disease?
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________
Details of Behçet’s disease
Behçet’s disease is most common in the third or fourth decade of life. It has an association with the human leukocyte antigen HLA-B51 and HLA-B5 allele. Vascular injuries, hyperfunction of neutrophils, and autoimmune responses lead to the clinical findings. Behçet’s disease is presumed to be an autoimmune disease, with the primary lesion being related to the vasculitis.
Clinical criteria of Behçet’s
Diagnosis of Behçet’s disease is based on clinical criteria. No single test can determine if a patient has Behçet’s.
An International Study Group of physicians was convened to develop a set of guidelines to diagnose Behçet’s disease. These criteria include recurrent, painful oral ulceration with at least 2 other symptoms (recurrent genital ulcers, eye lesions, skin lesions, and positive pathergy test) (TABLE 2). These diagnostic criteria may be accessed at the website of the American Behçet’s Disease Association, www.behcets.com.
Prevalence of signs
Oral ulcerations are the presenting signs in about 70% of cases. These ulcers may remain for as long as 3 weeks. In women, the genital lesions are often present in the vulvovaginal region; in men, they often appear in the scrotal area. Ocular complaints occur in about one-half of patients, sometimes with photophobia, watering, and blurred vision. The most common skin lesions are pseudofolliculitis and erythema nodosum.
The pathergy test uses a sterile needle to make a skin prick. The test result is positive if an aseptic erythematous nodule or pustule (>2 mm in diameter) occurs within 24 to 48 hours, indicating neutrophil hyperfunction.
Differential diagnosis
Skin, joint, gastrointestinal, vascular, and central nervous systems may also be involved. The differential diagnosis includes chronic oral aphthosis, herpes simplex virus infection, Sweet’s syndrome, ankylosing spondylitis, inflammatory bowel disease, and multiple sclerosis (TABLE 3).
Laboratory findings and treatment
Examination of the blood can reveal nonspecific findings consistent with inflammation, including elevated C-reactive protein, erythrocyte sedimentation rate, and positive markers for autoimmune diseases.
Treatmentdepends upon the particular symptoms and clinical findings and must be coordinated with the various specialists involved.
Topical steroids are used for oral and genital ulcers as well as ocular lesions.
Oral steroids are useful for gastrointestinal and neurological symptoms but may also help with skin, joint, vascular, and ocular symptoms.
Colchicine may help alleviate oral and genital ulcers as well as skin, ocular, and joint problems.
Topical tetracycline may be used to treat oral ulcers.
Anticoagulants may be indicated for vascular disturbances and progressive central nervous system lesions.
Cytotoxic and antirheumatic agents may treat vascular, ocular, neurological, and joint manifestations.
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________ ______________________________________________________________ ______________________________________________________________
TABLE 2
Diagnostic criteria of Behçet’s disease
| Recurrent oral ulceration |
|
| AND AT LEAST 2 OTHER SYMPTOMS: |
| Recurrent genital ulcers |
| Eye lesions |
|
| Skin lesions |
|
| Positive pathergy test |
|
| Adapted from Sakane et al, N Engl J Med 1999.1 |
TABLE 3
Differential diagnosis of Behçet’s disease
| Chronic oral aphthosis |
| Herpes simplex virus infection |
| Sweet’s syndrome |
| Ankylosing spondylitis |
| Inflammatory bowel disease (Crohn’s disease, ulcerative colitis) |
| Multiple sclerosis |
| Adapted from Sakane et al, N Engl J Med 1999.1 |
Gynecology consultation
The gynecologist recommends that the patient be admitted to the hospital for examination under anesthesia. This examination found an ulcerated area of perineum, cellulitis, and edema, without a palpable abscess. Necrotic tissue is debrided.
Biopsies are obtained for herpes, aerobic, and anaerobic cultures. Repeat gonorrhea and chlamydia polymerase chain reaction (PCR) probes are obtained as well. The patient is started on ampicillin/sulbactam (Unasyn) after the debridement.
Further laboratory testing is also done at admission, including a throat culture, cryoglobulin, hepatitis screen, antinuclear antibody (ANA), HIV, lupus anticoagulant, cardiolipin, herpes IgG, antithrombin III level, immune complex detection panel for C1q, and tissue transgluttin AB4 IgA. All results are negative. A possible rheumatology consultation is also discussed.
Culture results from the previous sexual abuse evaluation show strep and gramnegative rods. Initial cultures from exam under anesthesia reveal grampositive cocci, grampositive rods, and gramnegative rods on the Gram’s stain with final report pending. An infectious disease consultation is recommended. The family physician agreed.
Infectious disease consultation
The consultant believes streptococcal infection is the most likely culprit and recommends changing the IV antibiotic from ampicillin/sulbactam to piperacillin/tazobactam (Zosyn) with the addition of clindamycin for broad-spectrum coverage. Later, the final culture results from the sexual abuse evaluation show heavy Enterococcus colonization. Surgical culture results reveal moderate Escherichia coli, moderate Enterococcus, light Staphylococcus epidermidis, heavy bacteroides, and moderate Lactobacillus. All are susceptible to the piperacillin/tazobactam.
The patient does well and is successfully switched to oral amoxicillin/clavulanate (Augmentin) with no recurrent fever and continued healing of vaginal ulcers. She is sent home to continue to heal.
One week later, the patient is seen in follow-up with continued healing and no further lesions. A few months later, the patient has healed completely and no other lesions have occurred. Incidental discussions included recent menarche. The family physician, patient, and patient’s family do a final review of all clinical and pathological findings.
The pathology report shows inflammation and necrosis. In addition, the vulvar biopsy reveals “multiple hair follicles adjacent to the inflammation and necrosis, raising the possibility of infected hair follicles and pilonidal disease.”
Unlike the implications with the presumed Behçet’s, the patient’s localized disease process has no long-term health consequences. She is discharged with a diagnosis of labial ulcers with cellulitis, resolved urinary retention, and a pathological diagnosis of pilonidal disease.
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________ ______________________________________________________________ ______________________________________________________________
Pilonidal disease
Pilonidal disease, this patient’s final diagnosis, is more common than Behçet’s disease. Men are affected more often than women, and ages range from puberty to the third decade of life with decreased frequency after the age of 45.
Pilonidal disease becomes a problem when “nests of hair” become infected. It is mostly found in the natal cleft but can present in almost any hairy area, mostly in the midline. Other examples include the umbilicus and scalp. There are also reports of acquired pilonidal disease from trauma in the hands of barbers, hair dressers, sheep shearers, and animal groomers. It is important to distinguish pilonidal disease from other disorders in the same region, such as anal fistulas, perirectal abscesses, and hidradenitis suppurativa.
Recurrences of pilonidal disease are quite common, with painful inflamed masses, abscesses, or sinus tracts. An acute abscess must be incised and drained. Hair removal by laser may prevent the growth of hair temporarily. For recurring infections, the definitive treatment is surgical. Procedures range from simple incision and curettage to excision of the area with plastic flap reconstruction. Antibiotics are not routinely needed, but they may be appropriate when cultures indicate specific microbes, when significant cellulitis is present, or for perioperative prophylaxis.
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________
Could it be hidradenitis suppurativa?
Hidradenitis suppurativa is a possibility, but the clinical and pathological findings make pilonidal disease more likely. Hidradenitis suppurativa similar to pilonidal disease, but it usually is located in the axillary, perineal, or inguinal areas. Incidence is as high as 1 in 300, and it frequently begins with puberty.
Hidradenitis suppurativa differs from pilonidal disease in that the hair follicle becomes occluded due to a defect in the epithelium of the follicle’s terminal ends. This defect leads to trapping of bacteria and formation of firm, peasized nodules or cysts. Some associations between hidradenitis suppurativa and sex hormones have been proposed, but hormonal states of pregnancy, menstruation, and menopause have not shown clear association with hidradenitis suppurativa. Initial symptoms of hidradenitis suppurativa may be pruritus, erythema, and hyperhidrosis. Recurrences are common. Treatment includes medications such as antibiotics, antiandrogens, and retinoids, as well as surgical excision.
Although this case is unusual, several key points are worth noting.
- The family physician as case coordinator allows patients access to specialized medical care, particularly if problems are potentially difficult medically or socially. In this instance, multispecialty care with family physician support is what enabled the final diagnosis.
- The question remains: Why is a premenarchal female affected by pilonidal disease? The most reasonable explanation is that the patient began to experience other changes associated with puberty including secondary hair growth. The “nests of hair” in the deep intergluteal regions may also have been stimulated, leading to the inflammation, necrosis, and infection demonstrated by the pathology and culture findings.
- Fortunately, in follow up, the patient has done well and has continued to be followed by the family practitioner, who provided ongoing care and interpretation for this family.
Discussing sexual abuse. The approach to discussing possible sexual abuse is a difficult one. Many physicians do not feel comfortable dealing with such a sensitive situation. The physician cannot take away his or her human side when presented with this kind of situation. The key is clear, unbiased communication with both the parent and the child.
The child can initially be interviewed with the parent present. Then the child should be interviewed alone in a nonthreatening environment. When the family physician takes the time to sit and talk with the child, the child may reveal things otherwise not discussed. Any questions must be age-appropriate and openended, being careful not to lead the child. The parent should also be interviewed alone in a nonconfrontational manner, stating what is known at the present and what is the plan, including further evaluation and reports to appropriate agencies. Again, a calm demeanor is important. In all of these interviews, clear documentation is paramount.
Referral to child advocacy centers as this patient experienced can also be appropriate. Referral may allow the physician to serve as the case coordinator as done in this instance. The physician can also remain neutral, giving a unique perspective of the family as the situation is investigated.
Acknowledgements
The author would like to thank Jessie Junker, MD, Albert Meyer, MD, and Barbara Walker, DO, at New Hanover Regional Medical Center, Residency in Family Medicine, Wilmington, NC; and Beth Deaton, FNP, at Wilmington Health Access for Teens, Wilmington, NC.
Conflict Of Interest
The author has no conflicts of interest to declare.
1. Sakane T, Takeno M, Suzuki N, Inaba G. Behçet’s disease. N Engl J Med 1999;341:1284-1291.
2. Sullivan DJ. Pilonidal disease. UpToDate [database]. Dated October 28, 2003. Waltham, Mass: UpToDate; 2003.
3. Townsend CM, Beauchamp RD, Evers BM, Mattox K, eds. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice 17th ed. Philadelphia, Pa: Saunders; 2004.
4. Stewart EG. Hidradenitis suppurativa. UpToDate [data base]. Dated January 12, 2004. Waltham, Mass: UpToDate; 2004.
5. Deitch HR, Huppert J, Adams Hillard PJ. Unusual vulvar ulcerations in young adolescent females. J Pediatr Adolesc Gynecol 2004;17:13-16.
6. Lisse JR. Behçet disease. Emedicine [website]. Updated October 18, 2004. Available at: http://www.emedicine.com/med/topic218.htm. Accessed on September 23, 2005.
7. American Behçet’s Disease Association website. Available at: www.behcets.com. Accessed on September 25, 2005.
CORRESPONDING AUTHOR: Nadine Skinner, MD, Eastern North Carolina Medical Group, PLLC, 1041 Noell Lane, Suite 105, Rocky Mount, NC 27804. E-mail: jnskinner@earthlink.net
Q: What are some causes of vaginal pain with fever? How would you proceed with the evaluation?
A: ______________________________________________________________ ______________________________________________________________
Other medical history
- Enuresis, recurrent perioral rash around age 7 with annual recurrences
- No chronic infections or illness
- Premenarchal
- Negative trauma history, including abuse
- Bike riding 2 days earlier but no falls
- Taking acyclovir as prescribed by ED; acetaminophen/ibuprofen for fever
- No known allergies
Family and social history
- Parents alive and well; no siblings
- Straight-A student
- Involved in JROTC (was on a retreat 2 weeks ago)
- No use of tobacco, alcohol, street drugs, or suspicious substances
- Denies any sexual activity
Physical examination
- Review of systems: Positive for chills, fever, dysuria, and perineal pain; otherwise negative
- Temperature 101.6°F, pulse 112, respiratory rate 22, blood pressure 110/70 mm Hg, weight 94 lb
- Alert female in no distress, normal neurologic exam
- HEENT: normal exam with clear oropharynx without lesions
- Skin/integument: no rashes, including arms, legs, hands, feet, and trunk
- Heart, lungs, and abdomen: tachycardia, otherwise normal
- Reproductive examination (chaperone present): Tanner stage III; perineal edema with marked purple ecchymoses located bilaterally at posterior introitus; multiple lacerations also noted as well as tenderness; some scabbed areas noted; no periurethral or perianal lesions or bruising; no vaginal discharge; speculum and bimanual exam were deferred due to pain.
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________ ______________________________________________________________
You are concerned about abuse. You interview the patient alone and she again denies any type of sexual encounter. She has never used tampons. She does report that she is a heavy sleeper and that she recently went on a retreat where she and a girlfriend slept in the same room. As far as she knows, there was no intruder. She tearfully says, “If anything happened, I can’t remember.”
You also interview the father alone. He says he and his wife “keep a tight rein” on their daughter. She has been out of their supervision only for the recent retreat. He is concerned that his daughter may have been given a “date-rape” drug and requests testing. His demeanor seems appropriate during the conversations both in the presence and absence of his daughter.
According to state law, you notify the Department of Social Services of unexplained perineal trauma. You also contact the local sexual abuse/rape experts in your area, who have arranged for an evaluation the following day. The father assists in making the arrangements for the evaluation while he is still in your office.
Department of Social Services forensic interview and medical examination
The next day, the patient and her family undergo a comprehensive evaluation by local medical and investigative professionals from the Department of Social Services.
The differential diagnosis for genital ulcers in a sexually inexperienced female includes sexual abuse, herpes simplex virus, Behçet’s disease, Epstein Barr infection, pilonidal disease, Crohn’s disease, and hidradenitis suppurativa. Definitive diagnosis can be difficult (TABLE 1).
One retrospective series reviewed the case of 9 adolescent females with vulvar ulcers and found that 6 had no formal diagnosis. Most important, the initial presentation should prompt healthcare professionals to take steps to ensure a patient’s safety.
After performing a physical examination, the abuse experts report that the patient’s presentation is consistent with Behçet’s disease. A genital culture was obtained, and the patient was given pain medication and azithromycin.
The expert also stated that the father’s reaction to the situation was appropriate and not that of an abusive father. Most perpetrators are very hostile and defensive, whereas this father was extremely concerned and cooperative. Still, a report to Child Protective Services had to be made because of the unexplained physical findings, especially in the genital area.
Further consideration
Additional information on Behçet’s disease is found in an article in the New England Journal of Medicine from 1999: “Behçet’s disease is an inflammatory disorder of unknown cause, characterized by recurrent oral aphthous ulcers, genital ulcers, uveitis, and skin lesions.”
You ponder this information and note that your patient has no oral lesions currently but apparently has a history of some oral lesions. You review your records indicating a history of recurrent perioral rash but do not find a history of oral lesions. However, the consultant remains constant in his diagnosis.
You review the results of the ED laboratory evaluation:
- Gonorrhea/chlamydia DNA probe negative
- Herpes culture and herpes immunoglobulin M (IgM) negative
- Rapid plasma reagin (RPR) nonreactive
- Serum pregnancy negative
- Urine drug screen negative for PCP, benzodiazepines, amphetamines, THC, opiates, barbiturates, methadone, tricyclic antidepressants
- Complete blood count normal; white blood count 9600 with a normal differential
As the family physician, you interpret these results and support the clinical plan for this patient, pending further changes in the clinical picture.
TABLE 1
Differential diagnosis of vulvar ulcers in sexually inexperienced females
| Sexual abuse |
| Herpes simplex virus infection |
| Behçet’s disease |
| Epstein-Barr viral infection |
| Crohn’s disease |
| Pilonidal disease |
| Hidradenitis suppurativa |
Next contact—ED visit 2 days later
The patient’s vaginal pain is worsening and she cannot void. Large ulcers with adhered pus are on the left labia; a smaller lesion is on the right labia. There are also questionable lacerations of the posterior fourchette. She is catheterized and 300 mL urine is emptied from the bladder. A gynecology consultation is obtained by the ED physician with your concurrence.
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________
Q: Is this Behçet’s disease?
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________
Details of Behçet’s disease
Behçet’s disease is most common in the third or fourth decade of life. It has an association with the human leukocyte antigen HLA-B51 and HLA-B5 allele. Vascular injuries, hyperfunction of neutrophils, and autoimmune responses lead to the clinical findings. Behçet’s disease is presumed to be an autoimmune disease, with the primary lesion being related to the vasculitis.
Clinical criteria of Behçet’s
Diagnosis of Behçet’s disease is based on clinical criteria. No single test can determine if a patient has Behçet’s.
An International Study Group of physicians was convened to develop a set of guidelines to diagnose Behçet’s disease. These criteria include recurrent, painful oral ulceration with at least 2 other symptoms (recurrent genital ulcers, eye lesions, skin lesions, and positive pathergy test) (TABLE 2). These diagnostic criteria may be accessed at the website of the American Behçet’s Disease Association, www.behcets.com.
Prevalence of signs
Oral ulcerations are the presenting signs in about 70% of cases. These ulcers may remain for as long as 3 weeks. In women, the genital lesions are often present in the vulvovaginal region; in men, they often appear in the scrotal area. Ocular complaints occur in about one-half of patients, sometimes with photophobia, watering, and blurred vision. The most common skin lesions are pseudofolliculitis and erythema nodosum.
The pathergy test uses a sterile needle to make a skin prick. The test result is positive if an aseptic erythematous nodule or pustule (>2 mm in diameter) occurs within 24 to 48 hours, indicating neutrophil hyperfunction.
Differential diagnosis
Skin, joint, gastrointestinal, vascular, and central nervous systems may also be involved. The differential diagnosis includes chronic oral aphthosis, herpes simplex virus infection, Sweet’s syndrome, ankylosing spondylitis, inflammatory bowel disease, and multiple sclerosis (TABLE 3).
Laboratory findings and treatment
Examination of the blood can reveal nonspecific findings consistent with inflammation, including elevated C-reactive protein, erythrocyte sedimentation rate, and positive markers for autoimmune diseases.
Treatmentdepends upon the particular symptoms and clinical findings and must be coordinated with the various specialists involved.
Topical steroids are used for oral and genital ulcers as well as ocular lesions.
Oral steroids are useful for gastrointestinal and neurological symptoms but may also help with skin, joint, vascular, and ocular symptoms.
Colchicine may help alleviate oral and genital ulcers as well as skin, ocular, and joint problems.
Topical tetracycline may be used to treat oral ulcers.
Anticoagulants may be indicated for vascular disturbances and progressive central nervous system lesions.
Cytotoxic and antirheumatic agents may treat vascular, ocular, neurological, and joint manifestations.
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________ ______________________________________________________________ ______________________________________________________________
TABLE 2
Diagnostic criteria of Behçet’s disease
| Recurrent oral ulceration |
|
| AND AT LEAST 2 OTHER SYMPTOMS: |
| Recurrent genital ulcers |
| Eye lesions |
|
| Skin lesions |
|
| Positive pathergy test |
|
| Adapted from Sakane et al, N Engl J Med 1999.1 |
TABLE 3
Differential diagnosis of Behçet’s disease
| Chronic oral aphthosis |
| Herpes simplex virus infection |
| Sweet’s syndrome |
| Ankylosing spondylitis |
| Inflammatory bowel disease (Crohn’s disease, ulcerative colitis) |
| Multiple sclerosis |
| Adapted from Sakane et al, N Engl J Med 1999.1 |
Gynecology consultation
The gynecologist recommends that the patient be admitted to the hospital for examination under anesthesia. This examination found an ulcerated area of perineum, cellulitis, and edema, without a palpable abscess. Necrotic tissue is debrided.
Biopsies are obtained for herpes, aerobic, and anaerobic cultures. Repeat gonorrhea and chlamydia polymerase chain reaction (PCR) probes are obtained as well. The patient is started on ampicillin/sulbactam (Unasyn) after the debridement.
Further laboratory testing is also done at admission, including a throat culture, cryoglobulin, hepatitis screen, antinuclear antibody (ANA), HIV, lupus anticoagulant, cardiolipin, herpes IgG, antithrombin III level, immune complex detection panel for C1q, and tissue transgluttin AB4 IgA. All results are negative. A possible rheumatology consultation is also discussed.
Culture results from the previous sexual abuse evaluation show strep and gramnegative rods. Initial cultures from exam under anesthesia reveal grampositive cocci, grampositive rods, and gramnegative rods on the Gram’s stain with final report pending. An infectious disease consultation is recommended. The family physician agreed.
Infectious disease consultation
The consultant believes streptococcal infection is the most likely culprit and recommends changing the IV antibiotic from ampicillin/sulbactam to piperacillin/tazobactam (Zosyn) with the addition of clindamycin for broad-spectrum coverage. Later, the final culture results from the sexual abuse evaluation show heavy Enterococcus colonization. Surgical culture results reveal moderate Escherichia coli, moderate Enterococcus, light Staphylococcus epidermidis, heavy bacteroides, and moderate Lactobacillus. All are susceptible to the piperacillin/tazobactam.
The patient does well and is successfully switched to oral amoxicillin/clavulanate (Augmentin) with no recurrent fever and continued healing of vaginal ulcers. She is sent home to continue to heal.
One week later, the patient is seen in follow-up with continued healing and no further lesions. A few months later, the patient has healed completely and no other lesions have occurred. Incidental discussions included recent menarche. The family physician, patient, and patient’s family do a final review of all clinical and pathological findings.
The pathology report shows inflammation and necrosis. In addition, the vulvar biopsy reveals “multiple hair follicles adjacent to the inflammation and necrosis, raising the possibility of infected hair follicles and pilonidal disease.”
Unlike the implications with the presumed Behçet’s, the patient’s localized disease process has no long-term health consequences. She is discharged with a diagnosis of labial ulcers with cellulitis, resolved urinary retention, and a pathological diagnosis of pilonidal disease.
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________ ______________________________________________________________ ______________________________________________________________
Pilonidal disease
Pilonidal disease, this patient’s final diagnosis, is more common than Behçet’s disease. Men are affected more often than women, and ages range from puberty to the third decade of life with decreased frequency after the age of 45.
Pilonidal disease becomes a problem when “nests of hair” become infected. It is mostly found in the natal cleft but can present in almost any hairy area, mostly in the midline. Other examples include the umbilicus and scalp. There are also reports of acquired pilonidal disease from trauma in the hands of barbers, hair dressers, sheep shearers, and animal groomers. It is important to distinguish pilonidal disease from other disorders in the same region, such as anal fistulas, perirectal abscesses, and hidradenitis suppurativa.
Recurrences of pilonidal disease are quite common, with painful inflamed masses, abscesses, or sinus tracts. An acute abscess must be incised and drained. Hair removal by laser may prevent the growth of hair temporarily. For recurring infections, the definitive treatment is surgical. Procedures range from simple incision and curettage to excision of the area with plastic flap reconstruction. Antibiotics are not routinely needed, but they may be appropriate when cultures indicate specific microbes, when significant cellulitis is present, or for perioperative prophylaxis.
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________
Could it be hidradenitis suppurativa?
Hidradenitis suppurativa is a possibility, but the clinical and pathological findings make pilonidal disease more likely. Hidradenitis suppurativa similar to pilonidal disease, but it usually is located in the axillary, perineal, or inguinal areas. Incidence is as high as 1 in 300, and it frequently begins with puberty.
Hidradenitis suppurativa differs from pilonidal disease in that the hair follicle becomes occluded due to a defect in the epithelium of the follicle’s terminal ends. This defect leads to trapping of bacteria and formation of firm, peasized nodules or cysts. Some associations between hidradenitis suppurativa and sex hormones have been proposed, but hormonal states of pregnancy, menstruation, and menopause have not shown clear association with hidradenitis suppurativa. Initial symptoms of hidradenitis suppurativa may be pruritus, erythema, and hyperhidrosis. Recurrences are common. Treatment includes medications such as antibiotics, antiandrogens, and retinoids, as well as surgical excision.
Although this case is unusual, several key points are worth noting.
- The family physician as case coordinator allows patients access to specialized medical care, particularly if problems are potentially difficult medically or socially. In this instance, multispecialty care with family physician support is what enabled the final diagnosis.
- The question remains: Why is a premenarchal female affected by pilonidal disease? The most reasonable explanation is that the patient began to experience other changes associated with puberty including secondary hair growth. The “nests of hair” in the deep intergluteal regions may also have been stimulated, leading to the inflammation, necrosis, and infection demonstrated by the pathology and culture findings.
- Fortunately, in follow up, the patient has done well and has continued to be followed by the family practitioner, who provided ongoing care and interpretation for this family.
Discussing sexual abuse. The approach to discussing possible sexual abuse is a difficult one. Many physicians do not feel comfortable dealing with such a sensitive situation. The physician cannot take away his or her human side when presented with this kind of situation. The key is clear, unbiased communication with both the parent and the child.
The child can initially be interviewed with the parent present. Then the child should be interviewed alone in a nonthreatening environment. When the family physician takes the time to sit and talk with the child, the child may reveal things otherwise not discussed. Any questions must be age-appropriate and openended, being careful not to lead the child. The parent should also be interviewed alone in a nonconfrontational manner, stating what is known at the present and what is the plan, including further evaluation and reports to appropriate agencies. Again, a calm demeanor is important. In all of these interviews, clear documentation is paramount.
Referral to child advocacy centers as this patient experienced can also be appropriate. Referral may allow the physician to serve as the case coordinator as done in this instance. The physician can also remain neutral, giving a unique perspective of the family as the situation is investigated.
Acknowledgements
The author would like to thank Jessie Junker, MD, Albert Meyer, MD, and Barbara Walker, DO, at New Hanover Regional Medical Center, Residency in Family Medicine, Wilmington, NC; and Beth Deaton, FNP, at Wilmington Health Access for Teens, Wilmington, NC.
Conflict Of Interest
The author has no conflicts of interest to declare.
Q: What are some causes of vaginal pain with fever? How would you proceed with the evaluation?
A: ______________________________________________________________ ______________________________________________________________
Other medical history
- Enuresis, recurrent perioral rash around age 7 with annual recurrences
- No chronic infections or illness
- Premenarchal
- Negative trauma history, including abuse
- Bike riding 2 days earlier but no falls
- Taking acyclovir as prescribed by ED; acetaminophen/ibuprofen for fever
- No known allergies
Family and social history
- Parents alive and well; no siblings
- Straight-A student
- Involved in JROTC (was on a retreat 2 weeks ago)
- No use of tobacco, alcohol, street drugs, or suspicious substances
- Denies any sexual activity
Physical examination
- Review of systems: Positive for chills, fever, dysuria, and perineal pain; otherwise negative
- Temperature 101.6°F, pulse 112, respiratory rate 22, blood pressure 110/70 mm Hg, weight 94 lb
- Alert female in no distress, normal neurologic exam
- HEENT: normal exam with clear oropharynx without lesions
- Skin/integument: no rashes, including arms, legs, hands, feet, and trunk
- Heart, lungs, and abdomen: tachycardia, otherwise normal
- Reproductive examination (chaperone present): Tanner stage III; perineal edema with marked purple ecchymoses located bilaterally at posterior introitus; multiple lacerations also noted as well as tenderness; some scabbed areas noted; no periurethral or perianal lesions or bruising; no vaginal discharge; speculum and bimanual exam were deferred due to pain.
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________ ______________________________________________________________
You are concerned about abuse. You interview the patient alone and she again denies any type of sexual encounter. She has never used tampons. She does report that she is a heavy sleeper and that she recently went on a retreat where she and a girlfriend slept in the same room. As far as she knows, there was no intruder. She tearfully says, “If anything happened, I can’t remember.”
You also interview the father alone. He says he and his wife “keep a tight rein” on their daughter. She has been out of their supervision only for the recent retreat. He is concerned that his daughter may have been given a “date-rape” drug and requests testing. His demeanor seems appropriate during the conversations both in the presence and absence of his daughter.
According to state law, you notify the Department of Social Services of unexplained perineal trauma. You also contact the local sexual abuse/rape experts in your area, who have arranged for an evaluation the following day. The father assists in making the arrangements for the evaluation while he is still in your office.
Department of Social Services forensic interview and medical examination
The next day, the patient and her family undergo a comprehensive evaluation by local medical and investigative professionals from the Department of Social Services.
The differential diagnosis for genital ulcers in a sexually inexperienced female includes sexual abuse, herpes simplex virus, Behçet’s disease, Epstein Barr infection, pilonidal disease, Crohn’s disease, and hidradenitis suppurativa. Definitive diagnosis can be difficult (TABLE 1).
One retrospective series reviewed the case of 9 adolescent females with vulvar ulcers and found that 6 had no formal diagnosis. Most important, the initial presentation should prompt healthcare professionals to take steps to ensure a patient’s safety.
After performing a physical examination, the abuse experts report that the patient’s presentation is consistent with Behçet’s disease. A genital culture was obtained, and the patient was given pain medication and azithromycin.
The expert also stated that the father’s reaction to the situation was appropriate and not that of an abusive father. Most perpetrators are very hostile and defensive, whereas this father was extremely concerned and cooperative. Still, a report to Child Protective Services had to be made because of the unexplained physical findings, especially in the genital area.
Further consideration
Additional information on Behçet’s disease is found in an article in the New England Journal of Medicine from 1999: “Behçet’s disease is an inflammatory disorder of unknown cause, characterized by recurrent oral aphthous ulcers, genital ulcers, uveitis, and skin lesions.”
You ponder this information and note that your patient has no oral lesions currently but apparently has a history of some oral lesions. You review your records indicating a history of recurrent perioral rash but do not find a history of oral lesions. However, the consultant remains constant in his diagnosis.
You review the results of the ED laboratory evaluation:
- Gonorrhea/chlamydia DNA probe negative
- Herpes culture and herpes immunoglobulin M (IgM) negative
- Rapid plasma reagin (RPR) nonreactive
- Serum pregnancy negative
- Urine drug screen negative for PCP, benzodiazepines, amphetamines, THC, opiates, barbiturates, methadone, tricyclic antidepressants
- Complete blood count normal; white blood count 9600 with a normal differential
As the family physician, you interpret these results and support the clinical plan for this patient, pending further changes in the clinical picture.
TABLE 1
Differential diagnosis of vulvar ulcers in sexually inexperienced females
| Sexual abuse |
| Herpes simplex virus infection |
| Behçet’s disease |
| Epstein-Barr viral infection |
| Crohn’s disease |
| Pilonidal disease |
| Hidradenitis suppurativa |
Next contact—ED visit 2 days later
The patient’s vaginal pain is worsening and she cannot void. Large ulcers with adhered pus are on the left labia; a smaller lesion is on the right labia. There are also questionable lacerations of the posterior fourchette. She is catheterized and 300 mL urine is emptied from the bladder. A gynecology consultation is obtained by the ED physician with your concurrence.
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________
Q: Is this Behçet’s disease?
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________
Details of Behçet’s disease
Behçet’s disease is most common in the third or fourth decade of life. It has an association with the human leukocyte antigen HLA-B51 and HLA-B5 allele. Vascular injuries, hyperfunction of neutrophils, and autoimmune responses lead to the clinical findings. Behçet’s disease is presumed to be an autoimmune disease, with the primary lesion being related to the vasculitis.
Clinical criteria of Behçet’s
Diagnosis of Behçet’s disease is based on clinical criteria. No single test can determine if a patient has Behçet’s.
An International Study Group of physicians was convened to develop a set of guidelines to diagnose Behçet’s disease. These criteria include recurrent, painful oral ulceration with at least 2 other symptoms (recurrent genital ulcers, eye lesions, skin lesions, and positive pathergy test) (TABLE 2). These diagnostic criteria may be accessed at the website of the American Behçet’s Disease Association, www.behcets.com.
Prevalence of signs
Oral ulcerations are the presenting signs in about 70% of cases. These ulcers may remain for as long as 3 weeks. In women, the genital lesions are often present in the vulvovaginal region; in men, they often appear in the scrotal area. Ocular complaints occur in about one-half of patients, sometimes with photophobia, watering, and blurred vision. The most common skin lesions are pseudofolliculitis and erythema nodosum.
The pathergy test uses a sterile needle to make a skin prick. The test result is positive if an aseptic erythematous nodule or pustule (>2 mm in diameter) occurs within 24 to 48 hours, indicating neutrophil hyperfunction.
Differential diagnosis
Skin, joint, gastrointestinal, vascular, and central nervous systems may also be involved. The differential diagnosis includes chronic oral aphthosis, herpes simplex virus infection, Sweet’s syndrome, ankylosing spondylitis, inflammatory bowel disease, and multiple sclerosis (TABLE 3).
Laboratory findings and treatment
Examination of the blood can reveal nonspecific findings consistent with inflammation, including elevated C-reactive protein, erythrocyte sedimentation rate, and positive markers for autoimmune diseases.
Treatmentdepends upon the particular symptoms and clinical findings and must be coordinated with the various specialists involved.
Topical steroids are used for oral and genital ulcers as well as ocular lesions.
Oral steroids are useful for gastrointestinal and neurological symptoms but may also help with skin, joint, vascular, and ocular symptoms.
Colchicine may help alleviate oral and genital ulcers as well as skin, ocular, and joint problems.
Topical tetracycline may be used to treat oral ulcers.
Anticoagulants may be indicated for vascular disturbances and progressive central nervous system lesions.
Cytotoxic and antirheumatic agents may treat vascular, ocular, neurological, and joint manifestations.
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________ ______________________________________________________________ ______________________________________________________________
TABLE 2
Diagnostic criteria of Behçet’s disease
| Recurrent oral ulceration |
|
| AND AT LEAST 2 OTHER SYMPTOMS: |
| Recurrent genital ulcers |
| Eye lesions |
|
| Skin lesions |
|
| Positive pathergy test |
|
| Adapted from Sakane et al, N Engl J Med 1999.1 |
TABLE 3
Differential diagnosis of Behçet’s disease
| Chronic oral aphthosis |
| Herpes simplex virus infection |
| Sweet’s syndrome |
| Ankylosing spondylitis |
| Inflammatory bowel disease (Crohn’s disease, ulcerative colitis) |
| Multiple sclerosis |
| Adapted from Sakane et al, N Engl J Med 1999.1 |
Gynecology consultation
The gynecologist recommends that the patient be admitted to the hospital for examination under anesthesia. This examination found an ulcerated area of perineum, cellulitis, and edema, without a palpable abscess. Necrotic tissue is debrided.
Biopsies are obtained for herpes, aerobic, and anaerobic cultures. Repeat gonorrhea and chlamydia polymerase chain reaction (PCR) probes are obtained as well. The patient is started on ampicillin/sulbactam (Unasyn) after the debridement.
Further laboratory testing is also done at admission, including a throat culture, cryoglobulin, hepatitis screen, antinuclear antibody (ANA), HIV, lupus anticoagulant, cardiolipin, herpes IgG, antithrombin III level, immune complex detection panel for C1q, and tissue transgluttin AB4 IgA. All results are negative. A possible rheumatology consultation is also discussed.
Culture results from the previous sexual abuse evaluation show strep and gramnegative rods. Initial cultures from exam under anesthesia reveal grampositive cocci, grampositive rods, and gramnegative rods on the Gram’s stain with final report pending. An infectious disease consultation is recommended. The family physician agreed.
Infectious disease consultation
The consultant believes streptococcal infection is the most likely culprit and recommends changing the IV antibiotic from ampicillin/sulbactam to piperacillin/tazobactam (Zosyn) with the addition of clindamycin for broad-spectrum coverage. Later, the final culture results from the sexual abuse evaluation show heavy Enterococcus colonization. Surgical culture results reveal moderate Escherichia coli, moderate Enterococcus, light Staphylococcus epidermidis, heavy bacteroides, and moderate Lactobacillus. All are susceptible to the piperacillin/tazobactam.
The patient does well and is successfully switched to oral amoxicillin/clavulanate (Augmentin) with no recurrent fever and continued healing of vaginal ulcers. She is sent home to continue to heal.
One week later, the patient is seen in follow-up with continued healing and no further lesions. A few months later, the patient has healed completely and no other lesions have occurred. Incidental discussions included recent menarche. The family physician, patient, and patient’s family do a final review of all clinical and pathological findings.
The pathology report shows inflammation and necrosis. In addition, the vulvar biopsy reveals “multiple hair follicles adjacent to the inflammation and necrosis, raising the possibility of infected hair follicles and pilonidal disease.”
Unlike the implications with the presumed Behçet’s, the patient’s localized disease process has no long-term health consequences. She is discharged with a diagnosis of labial ulcers with cellulitis, resolved urinary retention, and a pathological diagnosis of pilonidal disease.
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________ ______________________________________________________________ ______________________________________________________________
Pilonidal disease
Pilonidal disease, this patient’s final diagnosis, is more common than Behçet’s disease. Men are affected more often than women, and ages range from puberty to the third decade of life with decreased frequency after the age of 45.
Pilonidal disease becomes a problem when “nests of hair” become infected. It is mostly found in the natal cleft but can present in almost any hairy area, mostly in the midline. Other examples include the umbilicus and scalp. There are also reports of acquired pilonidal disease from trauma in the hands of barbers, hair dressers, sheep shearers, and animal groomers. It is important to distinguish pilonidal disease from other disorders in the same region, such as anal fistulas, perirectal abscesses, and hidradenitis suppurativa.
Recurrences of pilonidal disease are quite common, with painful inflamed masses, abscesses, or sinus tracts. An acute abscess must be incised and drained. Hair removal by laser may prevent the growth of hair temporarily. For recurring infections, the definitive treatment is surgical. Procedures range from simple incision and curettage to excision of the area with plastic flap reconstruction. Antibiotics are not routinely needed, but they may be appropriate when cultures indicate specific microbes, when significant cellulitis is present, or for perioperative prophylaxis.
A: ____________________________________________________________ ______________________________________________________________ ______________________________________________________________
Could it be hidradenitis suppurativa?
Hidradenitis suppurativa is a possibility, but the clinical and pathological findings make pilonidal disease more likely. Hidradenitis suppurativa similar to pilonidal disease, but it usually is located in the axillary, perineal, or inguinal areas. Incidence is as high as 1 in 300, and it frequently begins with puberty.
Hidradenitis suppurativa differs from pilonidal disease in that the hair follicle becomes occluded due to a defect in the epithelium of the follicle’s terminal ends. This defect leads to trapping of bacteria and formation of firm, peasized nodules or cysts. Some associations between hidradenitis suppurativa and sex hormones have been proposed, but hormonal states of pregnancy, menstruation, and menopause have not shown clear association with hidradenitis suppurativa. Initial symptoms of hidradenitis suppurativa may be pruritus, erythema, and hyperhidrosis. Recurrences are common. Treatment includes medications such as antibiotics, antiandrogens, and retinoids, as well as surgical excision.
Although this case is unusual, several key points are worth noting.
- The family physician as case coordinator allows patients access to specialized medical care, particularly if problems are potentially difficult medically or socially. In this instance, multispecialty care with family physician support is what enabled the final diagnosis.
- The question remains: Why is a premenarchal female affected by pilonidal disease? The most reasonable explanation is that the patient began to experience other changes associated with puberty including secondary hair growth. The “nests of hair” in the deep intergluteal regions may also have been stimulated, leading to the inflammation, necrosis, and infection demonstrated by the pathology and culture findings.
- Fortunately, in follow up, the patient has done well and has continued to be followed by the family practitioner, who provided ongoing care and interpretation for this family.
Discussing sexual abuse. The approach to discussing possible sexual abuse is a difficult one. Many physicians do not feel comfortable dealing with such a sensitive situation. The physician cannot take away his or her human side when presented with this kind of situation. The key is clear, unbiased communication with both the parent and the child.
The child can initially be interviewed with the parent present. Then the child should be interviewed alone in a nonthreatening environment. When the family physician takes the time to sit and talk with the child, the child may reveal things otherwise not discussed. Any questions must be age-appropriate and openended, being careful not to lead the child. The parent should also be interviewed alone in a nonconfrontational manner, stating what is known at the present and what is the plan, including further evaluation and reports to appropriate agencies. Again, a calm demeanor is important. In all of these interviews, clear documentation is paramount.
Referral to child advocacy centers as this patient experienced can also be appropriate. Referral may allow the physician to serve as the case coordinator as done in this instance. The physician can also remain neutral, giving a unique perspective of the family as the situation is investigated.
Acknowledgements
The author would like to thank Jessie Junker, MD, Albert Meyer, MD, and Barbara Walker, DO, at New Hanover Regional Medical Center, Residency in Family Medicine, Wilmington, NC; and Beth Deaton, FNP, at Wilmington Health Access for Teens, Wilmington, NC.
Conflict Of Interest
The author has no conflicts of interest to declare.
1. Sakane T, Takeno M, Suzuki N, Inaba G. Behçet’s disease. N Engl J Med 1999;341:1284-1291.
2. Sullivan DJ. Pilonidal disease. UpToDate [database]. Dated October 28, 2003. Waltham, Mass: UpToDate; 2003.
3. Townsend CM, Beauchamp RD, Evers BM, Mattox K, eds. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice 17th ed. Philadelphia, Pa: Saunders; 2004.
4. Stewart EG. Hidradenitis suppurativa. UpToDate [data base]. Dated January 12, 2004. Waltham, Mass: UpToDate; 2004.
5. Deitch HR, Huppert J, Adams Hillard PJ. Unusual vulvar ulcerations in young adolescent females. J Pediatr Adolesc Gynecol 2004;17:13-16.
6. Lisse JR. Behçet disease. Emedicine [website]. Updated October 18, 2004. Available at: http://www.emedicine.com/med/topic218.htm. Accessed on September 23, 2005.
7. American Behçet’s Disease Association website. Available at: www.behcets.com. Accessed on September 25, 2005.
CORRESPONDING AUTHOR: Nadine Skinner, MD, Eastern North Carolina Medical Group, PLLC, 1041 Noell Lane, Suite 105, Rocky Mount, NC 27804. E-mail: jnskinner@earthlink.net
1. Sakane T, Takeno M, Suzuki N, Inaba G. Behçet’s disease. N Engl J Med 1999;341:1284-1291.
2. Sullivan DJ. Pilonidal disease. UpToDate [database]. Dated October 28, 2003. Waltham, Mass: UpToDate; 2003.
3. Townsend CM, Beauchamp RD, Evers BM, Mattox K, eds. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice 17th ed. Philadelphia, Pa: Saunders; 2004.
4. Stewart EG. Hidradenitis suppurativa. UpToDate [data base]. Dated January 12, 2004. Waltham, Mass: UpToDate; 2004.
5. Deitch HR, Huppert J, Adams Hillard PJ. Unusual vulvar ulcerations in young adolescent females. J Pediatr Adolesc Gynecol 2004;17:13-16.
6. Lisse JR. Behçet disease. Emedicine [website]. Updated October 18, 2004. Available at: http://www.emedicine.com/med/topic218.htm. Accessed on September 23, 2005.
7. American Behçet’s Disease Association website. Available at: www.behcets.com. Accessed on September 25, 2005.
CORRESPONDING AUTHOR: Nadine Skinner, MD, Eastern North Carolina Medical Group, PLLC, 1041 Noell Lane, Suite 105, Rocky Mount, NC 27804. E-mail: jnskinner@earthlink.net
Gastric Bypass in an Obese Patient with Paranoid Schizophrenia
Diabetic foot ulcer and poor compliance: How would you treat?
Other medical history
- Diabetes mellitus type II
- Diabetic retinopathy
- Hypertension
- Erectile dysfunction
- Obesity
- Pes planus
Family history
- Diabetes and hypertension in father and paternal grandmother. Father had 2 myocardial infarctions and died at age 62. Mother is healthy. Sister has borderline diabetes.
Social history
- Nonsmoker
- 4 to 5 beers per week
- Divorced
- Works as a baker
Review of systems
- Negative except for increased swelling of right foot
Physical exam
- Alert male in no distress
- Blood pressure 135/68 mm Hg, temperature 37.5 °C, respiratory rate 14, heart rate 80, weight 236 pounds
- Heart, lung, and abdominal exam unremarkable
- Right 3rd toe has erythema at the metatarsophalangeal joint, with a draining ulcer on the plantar surface. Foot is edematous with erythema spreading proximally toward lower extremity. Erythema is <2 cm from ulcer rim. Pedal pulses are 1+, and capillary refill is <2 seconds. Monofilament testing reveals insensitivity at more than 4 sites.
A:_______________________________________________________________
_________________________________________________________________
_________________________________________________________________
Important elements of the history and exam
Assess vascular integrity. Arterial insufficiency is suggested by a history of cardiac or cerebrovascular disease, leg claudication, impotence, or pain in the distal foot when the patient is supine. Exam may reveal diminished or absent pulses, pallor on elevation, redness of the foot on lowering the leg, delayed capillary refill in toes, and thickened nails or absence of toe hair. With diabetes or renal impairment, the pulse exam may be unreliable due to arterial calcification.
Helpful studies may include segmental limb pressures, pulse-volume wave form, transcutaneous oxygen pressure, and ankle brachial index (which can be normal with significant calcinosis). Obtain a vascular surgery consultation immediately if you suspect arterial insufficiency, as revascularization may be necessary.1
Evaluate for musculoskeletal problems. Examine gait, look for foot deformities, and test joint range of motion. If a mechanical basis of the ulceration is found, eliminate or reduce foot pressure with shoes, inserts, orthoses, etc. Reconstructive foot surgery may be an option for some patients.
Gauge neurologic status. Most foot ulcers develop because of loss of protective sensation; therefore, screen all patients with diabetes annually for loss of protective sensation, using a 10-g nylon monofilament. Press the monofilament against the plantar skin until it buckles, hold it there for 1 second, and remove it.2 The neurologic exam can also include testing for motor strength, deeptendon reflexes, and vibratory (128-Hz tuning fork), proprioceptive, and protective sensation.
Measure the wound, watch for infection. When examining an ulcer, assess location, size, and depth. When caring for wounds, document at each visit the length and width of the wound.3 Note any signs of infection (warmth, redness, pain, tenderness, induration, pus) or gangrene. Observe for fever, chills, and leukocytosis, but do not rely on systemic symptoms as indicators of infection. Assess the severity of infection, and explore the wound for foreign or necrotic material with a sterile metal instrument.
Examine toenails for fungal infection, as this may be a significant contributor to the initiation and continuation of a foot ulcer. Callus formation, especially with hemorrhage, may be evidence of an impending ulcer.3
M.N.’s physician was increasingly concerned about the lack of healing of his ulcer. The differential diagnosis for this patient’s swollen foot includes cellulitis, osteomyelitis, gout, foreign body, arthritis, trauma, deep venous thrombosis, pseudogout, and venous insufficiency. Many of these were excluded by the physical exam. A bone scan was ordered.
A:_______________________________________________________________
_________________________________________________________________
_________________________________________________________________
Referral to plastic surgeon
When M.N. returns to the clinic with worsening drainage, edema, and spreading erythema, the decision is made to admit him to the hospital, start intravenous ampicillin/sulbactam (Unasyn) and ciprofloxacin (Cipro), and consult with a plastic surgeon.
Following the examination and review of the bone scan results, which show osteomyelitis, the surgeon recommends surgical therapy of the affected toe. He advocates aggressive debridement, and also thinks that this wound could require a staged surgical approach or amputation.
A:_______________________________________________________________
_________________________________________________________________
_________________________________________________________________
Further primary care evaluation
Laboratory:
- Complete blood count, normal
- Erythrocyte sedimentation rate (ESR), 38
- C-reactive protein (CRP), 2.1
- Lipid panel: HDL 32 mg/dL, LDL 96 mg/dL, triglycerides 116 mg/dL
- Hemoglobin A1c, 6.0
Details of foot ulcers
Statistics
About 50% to 60% of serious foot infections are complicated by osteomyelitis, and 10% to 20% of mild to moderate infections likely involve the bone. Twenty-five percent of foot infections in persons with diabetes will spread to subcutaneous tissues or bone. Up to 50% of those with a foot infection will experience a recurrence within a few years.2 Approximately 10% to 30% with a diabetic foot ulcer will eventually require amputation. Infected foot ulcers precede 60% of amputations. Two thirds of patients with a diabetic foot ulcer have peripheral vascular disease, and 80% have lost protective sensation. Infections most commonly involve the forefoot, usually plantar surface.2
Pathophysiology
Ulcers develop from breaks in the dermal barrier with subsequent erosion of subcutaneous tissue. Healing is inhibited when wound-repair mechanisms are corrupted by impaired perfusion, infection, or repeated trauma. Ulceration progresses due to impaired arterial supply, neuropathy, or musculoskeletal deformities.1
Risk of ulceration correlates with number of risk factors. The risk is increased by 1.7 in persons with isolated peripheral neuropathy (TABLE 1), by 12 in those with neuropathy and foot deformity, and by 36 in those with peripheral neuropathy, deformity, and previous amputation.1
Pathology usually mixed. The feet have sensory and motor neuropathies that cause the patient to put abnormal stresses on them, resulting in trauma that may lead to infection. Immunologic impairment due to hyperglycemia also plays a role; this can include reduced function of neutrophils, monocytes, and complement. Skin and nail disorders are more common among persons with diabetes than in the general population, and these may also increase the rate of infection.2
TABLE 1
Risk factors predisposing to foot ulcers and inhibiting healing
| Vascular: arterial insufficiency or venous hypertension |
| Neurologic: sensory, motor, or autonomic neuropathy |
| Anatomical: altered biomechanics, limited joint mobility, bony deformity |
| Infections |
| Trauma |
| Diabetes |
A:_______________________________________________________________
_________________________________________________________________
_________________________________________________________________
Management of ulcers
Optimal management should involve a multidisciplinary group of consultants. Mechanical debridement, systemic antibiotic therapy, and measures to reduce weight bearing are the main elements of effective care. Foot soaks and whirlpool therapy may be detrimental and lead to further skin breakdown, but moist dressings on granulating wounds may help.
Debridement a must. Remove nonviable, infected tissue to achieve a border of healthy, bleeding soft tissue and uninfected bone. Debridement improves the outcome of foot ulcers.3
When hospitalization is indicated. Determine whether or not the patient requires hospitalization based on the presence of a severe infection (TABLE 2) and need for surgical intervention, fluid resuscitation, IV antibiotics, or control of metabolic derangements.2 Consider hospitalization also if there is concern about the patient’s ability or willingness to comply with wound care, antibiotic therapy, or off-loading of the affected area.
Consider need for off-loading. Most diabetic wounds develop because of unperceived trauma, and likely do not heal because of ongoing trauma. Total contact casting, whereby loading levels to a foot ulcer are drastically reduced, has been shown to be effective in healing ulcers in about 6 weeks.4 This suggests that healing of neuropathic ulcers must include mechanical off-loading of the ulcer. Total contact casting has several limitations, and new modalities are being investigated.5
Obtain cultures. Wound culture results can greatly assist in determining appropriate antimicrobials. Gram stain can help direct therapy, and culture results are consistent with Gram staining in 95% of cases. Gram-stained smear is 70% sensitive for identifying organisms that grow on culture, and is much better for gram-positive organisms than for gram-negative bacilli.
Deep tissue specimens collected aseptically at surgery contain the true pathogens more often than more superficial samples. Curettage, involving tissue scraping with a scalpel from the base of a debrided ulcer, is more accurate than a wound swab. Wound swabs are likely to miss key pathogens as well as include nonpathogenic bacteria that confuse the antibiotic choice.2
When antibiotics are needed. In gross infections and cellulitis, topical antibiotics may reduce bacterial loads, but there are few published data about their efficacy in diabetic foot infections. The Wagner ulcer grading system (TABLE 3) is most widely used for tracking diabetic foot ulcers, but it does not allow for identification of superficial infection and has not been validated as an effective tool.6 An alternate method of classifying foot ulcers, taken from Lipsky et al, is shown in TABLE 4.
Currently systemic antibiotics are recommended only for established infection, although one study suggested that antibiotic therapy in clinically uninfected foot ulcers may significantly improve healing.7
Optimal duration of antibiotic therapy has not been studied, but convention has found 1 to 2 weeks to be effective for mild to moderate infections, at least 2 weeks for serious infections, and at least 6 weeks for osteomyelitis.2
Oral antibiotics are indicated when the ulcer is believed to be infected, and they should cover the usual pathogens, streptococci or staphylococci7 (TABLE 5). Treat severe infections with intravenous broad-spectrum antibiotics, covering for gramnegative and gram-positive aerobes and anaerobes.
Studies have shown similar therapeutic outcomes between high-dose oral fluoroquinolones and intravenous cephalosporin therapy. Oral fluoroquinolones cause fewer side effects and reduce hospitalizationrelated costs compared with cephalosporins, penicillinase-resistant penicillins, and vancomycin.8 Clindamycin or metronidazole may be added to fluoroquinolones to cover anaerobic organisms in severe or limb-threatening infections.9 One study found that patients treated with vancomycin had a greater rate of recurrence.5
Staphylococcus aureus is the most important pathogen in diabetic foot infections and may cause disease in isolation or as part of a mixed infection. Gram-negative rods, usually Enterobacteriaceae, are found in patients with chronic or previously treated infections. Pseudomonas species may be isolated from wounds that have been soaked or treated with wet dressings. Enterococci are more likely to be cultured from patients previously treated with a cephalosporin. Suspect anaerobes in cases of ischemic necrosis or deep tissue infections.2
When a person with diabetes has peripheral vascular disease, therapeutic antibiotic concentrations are often not achieved in infected tissues even with adequate serum levels.2 Novel methods of antibiotic delivery are being experimented with in an effort to solve this problem.
Surgery. Surgical options may include plastic reconstruction involving debridement and either primary closure or flap coverage. Optimally, vascular-bypass is performed to allow either primary healing or surgical reconstruction. If revascularization is not possible, amputation may be required.
If osteomyelitis complicates the picture. No validated or well-accepted guidelines exist for diagnosing or treating diabetic foot osteomyelitis. Factors that may suggest osteomyelitis: long-standing ulcers (>4 weeks), large (>2 cm) or deep ulcers (>3 mm), elevated ESR (>70 mm/h).2
Laboratory assays for diagnosing osteomyelitis can include measurements of erythrocyte sedimentation rate or C-reactive protein, though there are insufficient studies to assess their usefulness. One study found that 100% of patients with an ESR >70 mm/hr had osteomyelitis, despite lack of physical signs of inflammation. In diabetic patients with noninflamed foot ulcers, ESR can have a specificity of 100% and sensitivity of 28%. With inflamed ulcers, the sensitivity decreases to 23%.8 Some believe that the ESR can be used to follow osteomyelitis, and a persistent elevation or rise after initial fall would suggest osteomyelitis. Studies are inadequate to support this, however.5
Imaging for osteomyelitis can begin with plain films, which may show softtissue swelling, disruption of the bone cortex, and periosteal elevation. The American College of Radiology suggests this in the guidelines.10 However, 50% of the bone may be destroyed before these changes are evident. Plain films have a sensitivity of 28% to 100% and a specificity of 69% to 92%. If initial films yield normal results, it may be useful to repeat them in 2 to 4 weeks.9
MRI is highly sensitive (>90%) and specific (>80%), and may be even better with gadolinium. MRI is more sensitive for forefoot osteomyelitis than a leukocyte scan.11 Positron-emission tomography (PET) scans and high-resolution ultrasound may be helpful in the future.
Some studies suggest probing of sinuses and deep ulcers may be more sensitive than imaging. Palpable bone found at the base of an ulcer, with no overlying soft tissue, is highly predictive of osteomyelitis.1 Visible bone in a nontraumatic wound suggests osteomyelitis, with a sensitivity of 32% and specificity of 100%.12 The gold standard for diagnosis of osteomyelitis is obtaining a specimen of bone for pathology and culture.9
This case highlights several functions of the family physician and illustrates some of the challenges faced by primary caregivers. The dilemma in this scenario is that the patient ignored medical advice from specialists who had been consulted because of his worsening condition. What is a family physician’s responsibility in this circumstance? If you place yourself in this physician’s situation, you may experience a variety of emotions and thoughts, including frustration. How do you to provide a high standard of care for a patient who will not accept your recommendations?
Patient autonomy is paramount
As physicians we always need to respect patient autonomy. Though we may need to perform many roles, we always are the patient’s advocate. This can be difficult when a patient deviates from what we consider appropriate medical care. We may fear complications arising from lack of cooperation with advised treatment. In this case, the physician was legitimately concerned about worsening bone and skin breakdown, which could ultimately lead to foot or limb loss.
We are trained to evaluate and treat patients within our scope of knowledge and then incorporate the help of specialists as necessary. We are less well trained to deal with patients who refuse recommended medical treatments. In these situations, we must first thoroughly review with patients their options and the risks and benefits of each. We must also assess whether patients are competent to make decisions. If they are competent, then we must allow our patients to choose to do nothing, though it may not be what we would choose. The physician must make a choice of continuing to care for the patient, or begin the process of transferring care. If the patient-physician relationship continues, physician and patient should negotiate responsibility for outcomes and document the patient’s understanding.
In the case presented here, the patient continued seeing his physician for follow-up of his ulcer, though he had not followed the physician’s treatment recommendation. This required the physician to continue his relationship with the patient despite a major difference of opinion. This is an example of respecting a patient’s autonomy while continuing a therapeutic relationship. This case demonstrates several family physician functions in addition to patient advocate:
Family physician as coordinator… The physician obtained appropriate specialty consultations, and facilitated the patient’s visits to the podiatrist, orthopedist, wound care specialist, and plastic surgeon. He remained the central point of contact for the patient and assured that the patient received adequate follow-up.
…as comprehensive caregiver… This patient required management of several chronic diseases, including diabetes, hypertension, and obesity. He also needed health care maintenance. To give good care, the physician had to understand the patient’s background, work situation, and personal values. To appropriately treat the patient’s foot ulcer, the physician needed to know the patient, his work situation, and his medical history. As family physicians, we are able to build relationships with our patients that allow them to communicate their values, their history, and their wishes to us.
…and as educator. M.N. needed adequate and accurate information to make a final, informed decision concerning the care of his foot ulcer and osteomyelitis. As family physicians, we should be able to summarize for our patients their medical problem and present them with an overall picture of the problem and recommended treatment. This relationship allows the patient to make educated choices with a trusted healthcare provider.
–Jessica Farnsworth, MD
Antibiotic choice should be based on bone culture, as soft-tissue or sinus tract cultures do not accurately predict bone pathogens. When empiric therapy is necessary, coverage should always include S aureus. Cure of osteomyelitis has traditionally been thought to require removal of infected bone, but studies are showing that antibiotics may be adequate in two thirds of cases, especially those with good bioavailability. When bone is removed, shorter antibiotic therapy may be sufficient.2
Additional treatment options may include revascularization in an ischemic foot, which has been shown to salvage up to 98% of limbs. Hyperbaric oxygen may provide benefit, but data are insufficient to document this measure. Edema control may be beneficial for wound healing. Promising adjuvant therapies include granulocyte colony-stimulating factor (G-CSF), antibiotic-impregnated beads or orthopedic implants, and “biosurgery” with fly larvae.2
TABLE 2
Clinical characteristics of a severe infection
| Acute or rapidly progressive |
| Penetrating to subcutaneous tissues or involving fascia, muscle, joint, bone |
| Extensive cellulitis (>2 cm around ulcer rim) |
| Signs of inflammation, crepitus, bullae, necrosis, gangrene |
| Systemic signs: fever, chills, hypotension, confusion, volume depletion, leukocytosis |
| Metabolic abnormalities: severe hyperglycemia, acidosis, azotemia, electrolyte abnormalities |
| Absent pulses |
TABLE 3
Wagner ulcer grading system
| WOUND GRADE | WOUND DEPTH |
|---|---|
| Grade 0 | Intact skin |
| Grade 1 | Superficial ulcer |
| Grade 2 | Deep ulcer to tendon, bone, or joint |
| Grade 3 | Deep ulcer with abscess or osteomyelitis |
| Grade 4 | Forefoot gangrene |
| Grade 5 | Whole foot gangrene |
| The Wagner ulcer grading system does not identify infectious processes except in Grade 3. Erythema, edema, and pain may be present in foot infections, and may manifest as paronychia, cellulitis, or superficial skin infection. | |
TABLE 4
Clinical classification of diabetic foot infections
| CLINICAL APPEARANCE | CLASSIFICATION |
|---|---|
| Wound lacking purulence or any manifestations of inflammation | Uninfected |
| Presence of 2 or more manifestations of inflammation (purulence, erythema, pain, tenderness, warmth, or induration). Any cellulitis/erythema extends 2 or more cm around the ulcer, and infection is limited to the skin or superficial subcutaneous tissues. No other local complications or systemic illness. | Mild |
| Infection (as above) in a patient who is systematically well and metabolically stable but which has 1 or more of the following characteristics: cellulites extending >2 cm, lymphagitic streaking, spread beneath the superficial fascia, deep-tissue abcess, gangrene, and involvement of muscle, tender, joint or bone | Moderate |
| Infection in a patient with systemic toxicity or metabolic instability (eg, fever, chills, tachycardia, hypotension, confusion, vomiting, leukocytosis, acidosis, severe hyperglycemia, or azotemia) | Severe |
| Source: Lipsky et al, 2004.2 | |
Case resolution
The family physician and M.N. discuss the options. The specialist recommends surgery, but the patient does not want to undergo this procedure. As his physician explains his concerns about the chronic, nonhealing ulcer and osteomyelitis, M.N. says he will negotiate a change in his work situation that would allow him to decrease the time spent on his feet and thus improve healing.
The patient has small clinical improvement of his ulcer while hospitalized, and a peripherally inserted central catheter (PICC) line is placed to administer long-term antibiotics on an outpatient basis. The ulcer heals gradually in coming weeks and months. Laboratory results show improvement as well, with normalization of the ESR and CRP. Given the clinical improvement and a steady decrease in inflammatory markers, a bone scan is not repeated. The patient now has a job that allows him to sit instead of being on his feet all day.
1. Sumpio BE. Primary care: foot ulcers. N Engl J Med 2000;343:787-793.
2. Lipsky BA. Medical treatment of diabetic foot infections. Clin Infect Dis 2004;39:S104-S114.
3. Brem, Harold, Sheehan P, Boulton AJM. Protocol for treatment of diabetic foot ulcers. Am J Surg 2004;187:1S-10S.
4. Ulbrecht JS, Cavanagh PR, Caputo GM. Foot problems in diabetes: an overview. Clin Infect Dis 2004;39:S73-S82.
5. Caputo GM, Cavanagh PR, Ulbrecht JS, et al. Assessment and management of foot disease in patients with diabetes. N Engl J Med 1994;331:854-860.
6. Smith RG. Validation of Wagner’s classification: a literature review. Ostomy Wound Manage 2003;49:54-62.
7. Foster AVM, Bates M, Doxford M, Edmonds ME. Should oral antibiotics be given to ‘clean’ foot ulcers with no cellulitis? Abstracts of the 3rd International Symposium of the Diabetic Foot (1998).
8. Tice AD, Hoaglund PA, Shoutlz DA. Outcomes of osteomyelitis among patients treated with outpatient parenteral antimicrobial therapy. Am J Med 2003;114:723-728.
9. Zimmerman J. Osteomyelitis. Am Acad Fam Pract Home Study 2005; Clinical Update 308.
10. Alazraki N, Dalinka MK, Berquist TH, et al. Imaging diagnosis of osteomyelitis in patients with diabetes mellitus. American College of Radiology. ACR Appropriateness Criteria. Radiology 2000;215:303-310.
11. Lipman BT, Collier BD, Carrera GF, et al. Detection of osteomyelitis in the neuropathic foot: nuclear medicine, MRI and conventional radiography. Clin Nucl Med 1998;23:77-82.
12. Newman LG, Waller J, Palestro CJ, et al. Unsuspected osteomyelitis in diabetic foot ulcers. Diagnosis and monitoring by leukocyte scanning with indium in 111 oxyquionolone. JAMA 1991;266:1246-1251.
CORRESPONDING AUTHOR: Paul M. Paulman, MD, University of Nebraska College of Medicine, Department of Family Medicine, 983075 Nebraska Medical Center, Omaha, NE 68198. E-mail: ppaulman@unmc.edu
Other medical history
- Diabetes mellitus type II
- Diabetic retinopathy
- Hypertension
- Erectile dysfunction
- Obesity
- Pes planus
Family history
- Diabetes and hypertension in father and paternal grandmother. Father had 2 myocardial infarctions and died at age 62. Mother is healthy. Sister has borderline diabetes.
Social history
- Nonsmoker
- 4 to 5 beers per week
- Divorced
- Works as a baker
Review of systems
- Negative except for increased swelling of right foot
Physical exam
- Alert male in no distress
- Blood pressure 135/68 mm Hg, temperature 37.5 °C, respiratory rate 14, heart rate 80, weight 236 pounds
- Heart, lung, and abdominal exam unremarkable
- Right 3rd toe has erythema at the metatarsophalangeal joint, with a draining ulcer on the plantar surface. Foot is edematous with erythema spreading proximally toward lower extremity. Erythema is <2 cm from ulcer rim. Pedal pulses are 1+, and capillary refill is <2 seconds. Monofilament testing reveals insensitivity at more than 4 sites.
A:_______________________________________________________________
_________________________________________________________________
_________________________________________________________________
Important elements of the history and exam
Assess vascular integrity. Arterial insufficiency is suggested by a history of cardiac or cerebrovascular disease, leg claudication, impotence, or pain in the distal foot when the patient is supine. Exam may reveal diminished or absent pulses, pallor on elevation, redness of the foot on lowering the leg, delayed capillary refill in toes, and thickened nails or absence of toe hair. With diabetes or renal impairment, the pulse exam may be unreliable due to arterial calcification.
Helpful studies may include segmental limb pressures, pulse-volume wave form, transcutaneous oxygen pressure, and ankle brachial index (which can be normal with significant calcinosis). Obtain a vascular surgery consultation immediately if you suspect arterial insufficiency, as revascularization may be necessary.1
Evaluate for musculoskeletal problems. Examine gait, look for foot deformities, and test joint range of motion. If a mechanical basis of the ulceration is found, eliminate or reduce foot pressure with shoes, inserts, orthoses, etc. Reconstructive foot surgery may be an option for some patients.
Gauge neurologic status. Most foot ulcers develop because of loss of protective sensation; therefore, screen all patients with diabetes annually for loss of protective sensation, using a 10-g nylon monofilament. Press the monofilament against the plantar skin until it buckles, hold it there for 1 second, and remove it.2 The neurologic exam can also include testing for motor strength, deeptendon reflexes, and vibratory (128-Hz tuning fork), proprioceptive, and protective sensation.
Measure the wound, watch for infection. When examining an ulcer, assess location, size, and depth. When caring for wounds, document at each visit the length and width of the wound.3 Note any signs of infection (warmth, redness, pain, tenderness, induration, pus) or gangrene. Observe for fever, chills, and leukocytosis, but do not rely on systemic symptoms as indicators of infection. Assess the severity of infection, and explore the wound for foreign or necrotic material with a sterile metal instrument.
Examine toenails for fungal infection, as this may be a significant contributor to the initiation and continuation of a foot ulcer. Callus formation, especially with hemorrhage, may be evidence of an impending ulcer.3
M.N.’s physician was increasingly concerned about the lack of healing of his ulcer. The differential diagnosis for this patient’s swollen foot includes cellulitis, osteomyelitis, gout, foreign body, arthritis, trauma, deep venous thrombosis, pseudogout, and venous insufficiency. Many of these were excluded by the physical exam. A bone scan was ordered.
A:_______________________________________________________________
_________________________________________________________________
_________________________________________________________________
Referral to plastic surgeon
When M.N. returns to the clinic with worsening drainage, edema, and spreading erythema, the decision is made to admit him to the hospital, start intravenous ampicillin/sulbactam (Unasyn) and ciprofloxacin (Cipro), and consult with a plastic surgeon.
Following the examination and review of the bone scan results, which show osteomyelitis, the surgeon recommends surgical therapy of the affected toe. He advocates aggressive debridement, and also thinks that this wound could require a staged surgical approach or amputation.
A:_______________________________________________________________
_________________________________________________________________
_________________________________________________________________
Further primary care evaluation
Laboratory:
- Complete blood count, normal
- Erythrocyte sedimentation rate (ESR), 38
- C-reactive protein (CRP), 2.1
- Lipid panel: HDL 32 mg/dL, LDL 96 mg/dL, triglycerides 116 mg/dL
- Hemoglobin A1c, 6.0
Details of foot ulcers
Statistics
About 50% to 60% of serious foot infections are complicated by osteomyelitis, and 10% to 20% of mild to moderate infections likely involve the bone. Twenty-five percent of foot infections in persons with diabetes will spread to subcutaneous tissues or bone. Up to 50% of those with a foot infection will experience a recurrence within a few years.2 Approximately 10% to 30% with a diabetic foot ulcer will eventually require amputation. Infected foot ulcers precede 60% of amputations. Two thirds of patients with a diabetic foot ulcer have peripheral vascular disease, and 80% have lost protective sensation. Infections most commonly involve the forefoot, usually plantar surface.2
Pathophysiology
Ulcers develop from breaks in the dermal barrier with subsequent erosion of subcutaneous tissue. Healing is inhibited when wound-repair mechanisms are corrupted by impaired perfusion, infection, or repeated trauma. Ulceration progresses due to impaired arterial supply, neuropathy, or musculoskeletal deformities.1
Risk of ulceration correlates with number of risk factors. The risk is increased by 1.7 in persons with isolated peripheral neuropathy (TABLE 1), by 12 in those with neuropathy and foot deformity, and by 36 in those with peripheral neuropathy, deformity, and previous amputation.1
Pathology usually mixed. The feet have sensory and motor neuropathies that cause the patient to put abnormal stresses on them, resulting in trauma that may lead to infection. Immunologic impairment due to hyperglycemia also plays a role; this can include reduced function of neutrophils, monocytes, and complement. Skin and nail disorders are more common among persons with diabetes than in the general population, and these may also increase the rate of infection.2
TABLE 1
Risk factors predisposing to foot ulcers and inhibiting healing
| Vascular: arterial insufficiency or venous hypertension |
| Neurologic: sensory, motor, or autonomic neuropathy |
| Anatomical: altered biomechanics, limited joint mobility, bony deformity |
| Infections |
| Trauma |
| Diabetes |
A:_______________________________________________________________
_________________________________________________________________
_________________________________________________________________
Management of ulcers
Optimal management should involve a multidisciplinary group of consultants. Mechanical debridement, systemic antibiotic therapy, and measures to reduce weight bearing are the main elements of effective care. Foot soaks and whirlpool therapy may be detrimental and lead to further skin breakdown, but moist dressings on granulating wounds may help.
Debridement a must. Remove nonviable, infected tissue to achieve a border of healthy, bleeding soft tissue and uninfected bone. Debridement improves the outcome of foot ulcers.3
When hospitalization is indicated. Determine whether or not the patient requires hospitalization based on the presence of a severe infection (TABLE 2) and need for surgical intervention, fluid resuscitation, IV antibiotics, or control of metabolic derangements.2 Consider hospitalization also if there is concern about the patient’s ability or willingness to comply with wound care, antibiotic therapy, or off-loading of the affected area.
Consider need for off-loading. Most diabetic wounds develop because of unperceived trauma, and likely do not heal because of ongoing trauma. Total contact casting, whereby loading levels to a foot ulcer are drastically reduced, has been shown to be effective in healing ulcers in about 6 weeks.4 This suggests that healing of neuropathic ulcers must include mechanical off-loading of the ulcer. Total contact casting has several limitations, and new modalities are being investigated.5
Obtain cultures. Wound culture results can greatly assist in determining appropriate antimicrobials. Gram stain can help direct therapy, and culture results are consistent with Gram staining in 95% of cases. Gram-stained smear is 70% sensitive for identifying organisms that grow on culture, and is much better for gram-positive organisms than for gram-negative bacilli.
Deep tissue specimens collected aseptically at surgery contain the true pathogens more often than more superficial samples. Curettage, involving tissue scraping with a scalpel from the base of a debrided ulcer, is more accurate than a wound swab. Wound swabs are likely to miss key pathogens as well as include nonpathogenic bacteria that confuse the antibiotic choice.2
When antibiotics are needed. In gross infections and cellulitis, topical antibiotics may reduce bacterial loads, but there are few published data about their efficacy in diabetic foot infections. The Wagner ulcer grading system (TABLE 3) is most widely used for tracking diabetic foot ulcers, but it does not allow for identification of superficial infection and has not been validated as an effective tool.6 An alternate method of classifying foot ulcers, taken from Lipsky et al, is shown in TABLE 4.
Currently systemic antibiotics are recommended only for established infection, although one study suggested that antibiotic therapy in clinically uninfected foot ulcers may significantly improve healing.7
Optimal duration of antibiotic therapy has not been studied, but convention has found 1 to 2 weeks to be effective for mild to moderate infections, at least 2 weeks for serious infections, and at least 6 weeks for osteomyelitis.2
Oral antibiotics are indicated when the ulcer is believed to be infected, and they should cover the usual pathogens, streptococci or staphylococci7 (TABLE 5). Treat severe infections with intravenous broad-spectrum antibiotics, covering for gramnegative and gram-positive aerobes and anaerobes.
Studies have shown similar therapeutic outcomes between high-dose oral fluoroquinolones and intravenous cephalosporin therapy. Oral fluoroquinolones cause fewer side effects and reduce hospitalizationrelated costs compared with cephalosporins, penicillinase-resistant penicillins, and vancomycin.8 Clindamycin or metronidazole may be added to fluoroquinolones to cover anaerobic organisms in severe or limb-threatening infections.9 One study found that patients treated with vancomycin had a greater rate of recurrence.5
Staphylococcus aureus is the most important pathogen in diabetic foot infections and may cause disease in isolation or as part of a mixed infection. Gram-negative rods, usually Enterobacteriaceae, are found in patients with chronic or previously treated infections. Pseudomonas species may be isolated from wounds that have been soaked or treated with wet dressings. Enterococci are more likely to be cultured from patients previously treated with a cephalosporin. Suspect anaerobes in cases of ischemic necrosis or deep tissue infections.2
When a person with diabetes has peripheral vascular disease, therapeutic antibiotic concentrations are often not achieved in infected tissues even with adequate serum levels.2 Novel methods of antibiotic delivery are being experimented with in an effort to solve this problem.
Surgery. Surgical options may include plastic reconstruction involving debridement and either primary closure or flap coverage. Optimally, vascular-bypass is performed to allow either primary healing or surgical reconstruction. If revascularization is not possible, amputation may be required.
If osteomyelitis complicates the picture. No validated or well-accepted guidelines exist for diagnosing or treating diabetic foot osteomyelitis. Factors that may suggest osteomyelitis: long-standing ulcers (>4 weeks), large (>2 cm) or deep ulcers (>3 mm), elevated ESR (>70 mm/h).2
Laboratory assays for diagnosing osteomyelitis can include measurements of erythrocyte sedimentation rate or C-reactive protein, though there are insufficient studies to assess their usefulness. One study found that 100% of patients with an ESR >70 mm/hr had osteomyelitis, despite lack of physical signs of inflammation. In diabetic patients with noninflamed foot ulcers, ESR can have a specificity of 100% and sensitivity of 28%. With inflamed ulcers, the sensitivity decreases to 23%.8 Some believe that the ESR can be used to follow osteomyelitis, and a persistent elevation or rise after initial fall would suggest osteomyelitis. Studies are inadequate to support this, however.5
Imaging for osteomyelitis can begin with plain films, which may show softtissue swelling, disruption of the bone cortex, and periosteal elevation. The American College of Radiology suggests this in the guidelines.10 However, 50% of the bone may be destroyed before these changes are evident. Plain films have a sensitivity of 28% to 100% and a specificity of 69% to 92%. If initial films yield normal results, it may be useful to repeat them in 2 to 4 weeks.9
MRI is highly sensitive (>90%) and specific (>80%), and may be even better with gadolinium. MRI is more sensitive for forefoot osteomyelitis than a leukocyte scan.11 Positron-emission tomography (PET) scans and high-resolution ultrasound may be helpful in the future.
Some studies suggest probing of sinuses and deep ulcers may be more sensitive than imaging. Palpable bone found at the base of an ulcer, with no overlying soft tissue, is highly predictive of osteomyelitis.1 Visible bone in a nontraumatic wound suggests osteomyelitis, with a sensitivity of 32% and specificity of 100%.12 The gold standard for diagnosis of osteomyelitis is obtaining a specimen of bone for pathology and culture.9
This case highlights several functions of the family physician and illustrates some of the challenges faced by primary caregivers. The dilemma in this scenario is that the patient ignored medical advice from specialists who had been consulted because of his worsening condition. What is a family physician’s responsibility in this circumstance? If you place yourself in this physician’s situation, you may experience a variety of emotions and thoughts, including frustration. How do you to provide a high standard of care for a patient who will not accept your recommendations?
Patient autonomy is paramount
As physicians we always need to respect patient autonomy. Though we may need to perform many roles, we always are the patient’s advocate. This can be difficult when a patient deviates from what we consider appropriate medical care. We may fear complications arising from lack of cooperation with advised treatment. In this case, the physician was legitimately concerned about worsening bone and skin breakdown, which could ultimately lead to foot or limb loss.
We are trained to evaluate and treat patients within our scope of knowledge and then incorporate the help of specialists as necessary. We are less well trained to deal with patients who refuse recommended medical treatments. In these situations, we must first thoroughly review with patients their options and the risks and benefits of each. We must also assess whether patients are competent to make decisions. If they are competent, then we must allow our patients to choose to do nothing, though it may not be what we would choose. The physician must make a choice of continuing to care for the patient, or begin the process of transferring care. If the patient-physician relationship continues, physician and patient should negotiate responsibility for outcomes and document the patient’s understanding.
In the case presented here, the patient continued seeing his physician for follow-up of his ulcer, though he had not followed the physician’s treatment recommendation. This required the physician to continue his relationship with the patient despite a major difference of opinion. This is an example of respecting a patient’s autonomy while continuing a therapeutic relationship. This case demonstrates several family physician functions in addition to patient advocate:
Family physician as coordinator… The physician obtained appropriate specialty consultations, and facilitated the patient’s visits to the podiatrist, orthopedist, wound care specialist, and plastic surgeon. He remained the central point of contact for the patient and assured that the patient received adequate follow-up.
…as comprehensive caregiver… This patient required management of several chronic diseases, including diabetes, hypertension, and obesity. He also needed health care maintenance. To give good care, the physician had to understand the patient’s background, work situation, and personal values. To appropriately treat the patient’s foot ulcer, the physician needed to know the patient, his work situation, and his medical history. As family physicians, we are able to build relationships with our patients that allow them to communicate their values, their history, and their wishes to us.
…and as educator. M.N. needed adequate and accurate information to make a final, informed decision concerning the care of his foot ulcer and osteomyelitis. As family physicians, we should be able to summarize for our patients their medical problem and present them with an overall picture of the problem and recommended treatment. This relationship allows the patient to make educated choices with a trusted healthcare provider.
–Jessica Farnsworth, MD
Antibiotic choice should be based on bone culture, as soft-tissue or sinus tract cultures do not accurately predict bone pathogens. When empiric therapy is necessary, coverage should always include S aureus. Cure of osteomyelitis has traditionally been thought to require removal of infected bone, but studies are showing that antibiotics may be adequate in two thirds of cases, especially those with good bioavailability. When bone is removed, shorter antibiotic therapy may be sufficient.2
Additional treatment options may include revascularization in an ischemic foot, which has been shown to salvage up to 98% of limbs. Hyperbaric oxygen may provide benefit, but data are insufficient to document this measure. Edema control may be beneficial for wound healing. Promising adjuvant therapies include granulocyte colony-stimulating factor (G-CSF), antibiotic-impregnated beads or orthopedic implants, and “biosurgery” with fly larvae.2
TABLE 2
Clinical characteristics of a severe infection
| Acute or rapidly progressive |
| Penetrating to subcutaneous tissues or involving fascia, muscle, joint, bone |
| Extensive cellulitis (>2 cm around ulcer rim) |
| Signs of inflammation, crepitus, bullae, necrosis, gangrene |
| Systemic signs: fever, chills, hypotension, confusion, volume depletion, leukocytosis |
| Metabolic abnormalities: severe hyperglycemia, acidosis, azotemia, electrolyte abnormalities |
| Absent pulses |
TABLE 3
Wagner ulcer grading system
| WOUND GRADE | WOUND DEPTH |
|---|---|
| Grade 0 | Intact skin |
| Grade 1 | Superficial ulcer |
| Grade 2 | Deep ulcer to tendon, bone, or joint |
| Grade 3 | Deep ulcer with abscess or osteomyelitis |
| Grade 4 | Forefoot gangrene |
| Grade 5 | Whole foot gangrene |
| The Wagner ulcer grading system does not identify infectious processes except in Grade 3. Erythema, edema, and pain may be present in foot infections, and may manifest as paronychia, cellulitis, or superficial skin infection. | |
TABLE 4
Clinical classification of diabetic foot infections
| CLINICAL APPEARANCE | CLASSIFICATION |
|---|---|
| Wound lacking purulence or any manifestations of inflammation | Uninfected |
| Presence of 2 or more manifestations of inflammation (purulence, erythema, pain, tenderness, warmth, or induration). Any cellulitis/erythema extends 2 or more cm around the ulcer, and infection is limited to the skin or superficial subcutaneous tissues. No other local complications or systemic illness. | Mild |
| Infection (as above) in a patient who is systematically well and metabolically stable but which has 1 or more of the following characteristics: cellulites extending >2 cm, lymphagitic streaking, spread beneath the superficial fascia, deep-tissue abcess, gangrene, and involvement of muscle, tender, joint or bone | Moderate |
| Infection in a patient with systemic toxicity or metabolic instability (eg, fever, chills, tachycardia, hypotension, confusion, vomiting, leukocytosis, acidosis, severe hyperglycemia, or azotemia) | Severe |
| Source: Lipsky et al, 2004.2 | |
Case resolution
The family physician and M.N. discuss the options. The specialist recommends surgery, but the patient does not want to undergo this procedure. As his physician explains his concerns about the chronic, nonhealing ulcer and osteomyelitis, M.N. says he will negotiate a change in his work situation that would allow him to decrease the time spent on his feet and thus improve healing.
The patient has small clinical improvement of his ulcer while hospitalized, and a peripherally inserted central catheter (PICC) line is placed to administer long-term antibiotics on an outpatient basis. The ulcer heals gradually in coming weeks and months. Laboratory results show improvement as well, with normalization of the ESR and CRP. Given the clinical improvement and a steady decrease in inflammatory markers, a bone scan is not repeated. The patient now has a job that allows him to sit instead of being on his feet all day.
Other medical history
- Diabetes mellitus type II
- Diabetic retinopathy
- Hypertension
- Erectile dysfunction
- Obesity
- Pes planus
Family history
- Diabetes and hypertension in father and paternal grandmother. Father had 2 myocardial infarctions and died at age 62. Mother is healthy. Sister has borderline diabetes.
Social history
- Nonsmoker
- 4 to 5 beers per week
- Divorced
- Works as a baker
Review of systems
- Negative except for increased swelling of right foot
Physical exam
- Alert male in no distress
- Blood pressure 135/68 mm Hg, temperature 37.5 °C, respiratory rate 14, heart rate 80, weight 236 pounds
- Heart, lung, and abdominal exam unremarkable
- Right 3rd toe has erythema at the metatarsophalangeal joint, with a draining ulcer on the plantar surface. Foot is edematous with erythema spreading proximally toward lower extremity. Erythema is <2 cm from ulcer rim. Pedal pulses are 1+, and capillary refill is <2 seconds. Monofilament testing reveals insensitivity at more than 4 sites.
A:_______________________________________________________________
_________________________________________________________________
_________________________________________________________________
Important elements of the history and exam
Assess vascular integrity. Arterial insufficiency is suggested by a history of cardiac or cerebrovascular disease, leg claudication, impotence, or pain in the distal foot when the patient is supine. Exam may reveal diminished or absent pulses, pallor on elevation, redness of the foot on lowering the leg, delayed capillary refill in toes, and thickened nails or absence of toe hair. With diabetes or renal impairment, the pulse exam may be unreliable due to arterial calcification.
Helpful studies may include segmental limb pressures, pulse-volume wave form, transcutaneous oxygen pressure, and ankle brachial index (which can be normal with significant calcinosis). Obtain a vascular surgery consultation immediately if you suspect arterial insufficiency, as revascularization may be necessary.1
Evaluate for musculoskeletal problems. Examine gait, look for foot deformities, and test joint range of motion. If a mechanical basis of the ulceration is found, eliminate or reduce foot pressure with shoes, inserts, orthoses, etc. Reconstructive foot surgery may be an option for some patients.
Gauge neurologic status. Most foot ulcers develop because of loss of protective sensation; therefore, screen all patients with diabetes annually for loss of protective sensation, using a 10-g nylon monofilament. Press the monofilament against the plantar skin until it buckles, hold it there for 1 second, and remove it.2 The neurologic exam can also include testing for motor strength, deeptendon reflexes, and vibratory (128-Hz tuning fork), proprioceptive, and protective sensation.
Measure the wound, watch for infection. When examining an ulcer, assess location, size, and depth. When caring for wounds, document at each visit the length and width of the wound.3 Note any signs of infection (warmth, redness, pain, tenderness, induration, pus) or gangrene. Observe for fever, chills, and leukocytosis, but do not rely on systemic symptoms as indicators of infection. Assess the severity of infection, and explore the wound for foreign or necrotic material with a sterile metal instrument.
Examine toenails for fungal infection, as this may be a significant contributor to the initiation and continuation of a foot ulcer. Callus formation, especially with hemorrhage, may be evidence of an impending ulcer.3
M.N.’s physician was increasingly concerned about the lack of healing of his ulcer. The differential diagnosis for this patient’s swollen foot includes cellulitis, osteomyelitis, gout, foreign body, arthritis, trauma, deep venous thrombosis, pseudogout, and venous insufficiency. Many of these were excluded by the physical exam. A bone scan was ordered.
A:_______________________________________________________________
_________________________________________________________________
_________________________________________________________________
Referral to plastic surgeon
When M.N. returns to the clinic with worsening drainage, edema, and spreading erythema, the decision is made to admit him to the hospital, start intravenous ampicillin/sulbactam (Unasyn) and ciprofloxacin (Cipro), and consult with a plastic surgeon.
Following the examination and review of the bone scan results, which show osteomyelitis, the surgeon recommends surgical therapy of the affected toe. He advocates aggressive debridement, and also thinks that this wound could require a staged surgical approach or amputation.
A:_______________________________________________________________
_________________________________________________________________
_________________________________________________________________
Further primary care evaluation
Laboratory:
- Complete blood count, normal
- Erythrocyte sedimentation rate (ESR), 38
- C-reactive protein (CRP), 2.1
- Lipid panel: HDL 32 mg/dL, LDL 96 mg/dL, triglycerides 116 mg/dL
- Hemoglobin A1c, 6.0
Details of foot ulcers
Statistics
About 50% to 60% of serious foot infections are complicated by osteomyelitis, and 10% to 20% of mild to moderate infections likely involve the bone. Twenty-five percent of foot infections in persons with diabetes will spread to subcutaneous tissues or bone. Up to 50% of those with a foot infection will experience a recurrence within a few years.2 Approximately 10% to 30% with a diabetic foot ulcer will eventually require amputation. Infected foot ulcers precede 60% of amputations. Two thirds of patients with a diabetic foot ulcer have peripheral vascular disease, and 80% have lost protective sensation. Infections most commonly involve the forefoot, usually plantar surface.2
Pathophysiology
Ulcers develop from breaks in the dermal barrier with subsequent erosion of subcutaneous tissue. Healing is inhibited when wound-repair mechanisms are corrupted by impaired perfusion, infection, or repeated trauma. Ulceration progresses due to impaired arterial supply, neuropathy, or musculoskeletal deformities.1
Risk of ulceration correlates with number of risk factors. The risk is increased by 1.7 in persons with isolated peripheral neuropathy (TABLE 1), by 12 in those with neuropathy and foot deformity, and by 36 in those with peripheral neuropathy, deformity, and previous amputation.1
Pathology usually mixed. The feet have sensory and motor neuropathies that cause the patient to put abnormal stresses on them, resulting in trauma that may lead to infection. Immunologic impairment due to hyperglycemia also plays a role; this can include reduced function of neutrophils, monocytes, and complement. Skin and nail disorders are more common among persons with diabetes than in the general population, and these may also increase the rate of infection.2
TABLE 1
Risk factors predisposing to foot ulcers and inhibiting healing
| Vascular: arterial insufficiency or venous hypertension |
| Neurologic: sensory, motor, or autonomic neuropathy |
| Anatomical: altered biomechanics, limited joint mobility, bony deformity |
| Infections |
| Trauma |
| Diabetes |
A:_______________________________________________________________
_________________________________________________________________
_________________________________________________________________
Management of ulcers
Optimal management should involve a multidisciplinary group of consultants. Mechanical debridement, systemic antibiotic therapy, and measures to reduce weight bearing are the main elements of effective care. Foot soaks and whirlpool therapy may be detrimental and lead to further skin breakdown, but moist dressings on granulating wounds may help.
Debridement a must. Remove nonviable, infected tissue to achieve a border of healthy, bleeding soft tissue and uninfected bone. Debridement improves the outcome of foot ulcers.3
When hospitalization is indicated. Determine whether or not the patient requires hospitalization based on the presence of a severe infection (TABLE 2) and need for surgical intervention, fluid resuscitation, IV antibiotics, or control of metabolic derangements.2 Consider hospitalization also if there is concern about the patient’s ability or willingness to comply with wound care, antibiotic therapy, or off-loading of the affected area.
Consider need for off-loading. Most diabetic wounds develop because of unperceived trauma, and likely do not heal because of ongoing trauma. Total contact casting, whereby loading levels to a foot ulcer are drastically reduced, has been shown to be effective in healing ulcers in about 6 weeks.4 This suggests that healing of neuropathic ulcers must include mechanical off-loading of the ulcer. Total contact casting has several limitations, and new modalities are being investigated.5
Obtain cultures. Wound culture results can greatly assist in determining appropriate antimicrobials. Gram stain can help direct therapy, and culture results are consistent with Gram staining in 95% of cases. Gram-stained smear is 70% sensitive for identifying organisms that grow on culture, and is much better for gram-positive organisms than for gram-negative bacilli.
Deep tissue specimens collected aseptically at surgery contain the true pathogens more often than more superficial samples. Curettage, involving tissue scraping with a scalpel from the base of a debrided ulcer, is more accurate than a wound swab. Wound swabs are likely to miss key pathogens as well as include nonpathogenic bacteria that confuse the antibiotic choice.2
When antibiotics are needed. In gross infections and cellulitis, topical antibiotics may reduce bacterial loads, but there are few published data about their efficacy in diabetic foot infections. The Wagner ulcer grading system (TABLE 3) is most widely used for tracking diabetic foot ulcers, but it does not allow for identification of superficial infection and has not been validated as an effective tool.6 An alternate method of classifying foot ulcers, taken from Lipsky et al, is shown in TABLE 4.
Currently systemic antibiotics are recommended only for established infection, although one study suggested that antibiotic therapy in clinically uninfected foot ulcers may significantly improve healing.7
Optimal duration of antibiotic therapy has not been studied, but convention has found 1 to 2 weeks to be effective for mild to moderate infections, at least 2 weeks for serious infections, and at least 6 weeks for osteomyelitis.2
Oral antibiotics are indicated when the ulcer is believed to be infected, and they should cover the usual pathogens, streptococci or staphylococci7 (TABLE 5). Treat severe infections with intravenous broad-spectrum antibiotics, covering for gramnegative and gram-positive aerobes and anaerobes.
Studies have shown similar therapeutic outcomes between high-dose oral fluoroquinolones and intravenous cephalosporin therapy. Oral fluoroquinolones cause fewer side effects and reduce hospitalizationrelated costs compared with cephalosporins, penicillinase-resistant penicillins, and vancomycin.8 Clindamycin or metronidazole may be added to fluoroquinolones to cover anaerobic organisms in severe or limb-threatening infections.9 One study found that patients treated with vancomycin had a greater rate of recurrence.5
Staphylococcus aureus is the most important pathogen in diabetic foot infections and may cause disease in isolation or as part of a mixed infection. Gram-negative rods, usually Enterobacteriaceae, are found in patients with chronic or previously treated infections. Pseudomonas species may be isolated from wounds that have been soaked or treated with wet dressings. Enterococci are more likely to be cultured from patients previously treated with a cephalosporin. Suspect anaerobes in cases of ischemic necrosis or deep tissue infections.2
When a person with diabetes has peripheral vascular disease, therapeutic antibiotic concentrations are often not achieved in infected tissues even with adequate serum levels.2 Novel methods of antibiotic delivery are being experimented with in an effort to solve this problem.
Surgery. Surgical options may include plastic reconstruction involving debridement and either primary closure or flap coverage. Optimally, vascular-bypass is performed to allow either primary healing or surgical reconstruction. If revascularization is not possible, amputation may be required.
If osteomyelitis complicates the picture. No validated or well-accepted guidelines exist for diagnosing or treating diabetic foot osteomyelitis. Factors that may suggest osteomyelitis: long-standing ulcers (>4 weeks), large (>2 cm) or deep ulcers (>3 mm), elevated ESR (>70 mm/h).2
Laboratory assays for diagnosing osteomyelitis can include measurements of erythrocyte sedimentation rate or C-reactive protein, though there are insufficient studies to assess their usefulness. One study found that 100% of patients with an ESR >70 mm/hr had osteomyelitis, despite lack of physical signs of inflammation. In diabetic patients with noninflamed foot ulcers, ESR can have a specificity of 100% and sensitivity of 28%. With inflamed ulcers, the sensitivity decreases to 23%.8 Some believe that the ESR can be used to follow osteomyelitis, and a persistent elevation or rise after initial fall would suggest osteomyelitis. Studies are inadequate to support this, however.5
Imaging for osteomyelitis can begin with plain films, which may show softtissue swelling, disruption of the bone cortex, and periosteal elevation. The American College of Radiology suggests this in the guidelines.10 However, 50% of the bone may be destroyed before these changes are evident. Plain films have a sensitivity of 28% to 100% and a specificity of 69% to 92%. If initial films yield normal results, it may be useful to repeat them in 2 to 4 weeks.9
MRI is highly sensitive (>90%) and specific (>80%), and may be even better with gadolinium. MRI is more sensitive for forefoot osteomyelitis than a leukocyte scan.11 Positron-emission tomography (PET) scans and high-resolution ultrasound may be helpful in the future.
Some studies suggest probing of sinuses and deep ulcers may be more sensitive than imaging. Palpable bone found at the base of an ulcer, with no overlying soft tissue, is highly predictive of osteomyelitis.1 Visible bone in a nontraumatic wound suggests osteomyelitis, with a sensitivity of 32% and specificity of 100%.12 The gold standard for diagnosis of osteomyelitis is obtaining a specimen of bone for pathology and culture.9
This case highlights several functions of the family physician and illustrates some of the challenges faced by primary caregivers. The dilemma in this scenario is that the patient ignored medical advice from specialists who had been consulted because of his worsening condition. What is a family physician’s responsibility in this circumstance? If you place yourself in this physician’s situation, you may experience a variety of emotions and thoughts, including frustration. How do you to provide a high standard of care for a patient who will not accept your recommendations?
Patient autonomy is paramount
As physicians we always need to respect patient autonomy. Though we may need to perform many roles, we always are the patient’s advocate. This can be difficult when a patient deviates from what we consider appropriate medical care. We may fear complications arising from lack of cooperation with advised treatment. In this case, the physician was legitimately concerned about worsening bone and skin breakdown, which could ultimately lead to foot or limb loss.
We are trained to evaluate and treat patients within our scope of knowledge and then incorporate the help of specialists as necessary. We are less well trained to deal with patients who refuse recommended medical treatments. In these situations, we must first thoroughly review with patients their options and the risks and benefits of each. We must also assess whether patients are competent to make decisions. If they are competent, then we must allow our patients to choose to do nothing, though it may not be what we would choose. The physician must make a choice of continuing to care for the patient, or begin the process of transferring care. If the patient-physician relationship continues, physician and patient should negotiate responsibility for outcomes and document the patient’s understanding.
In the case presented here, the patient continued seeing his physician for follow-up of his ulcer, though he had not followed the physician’s treatment recommendation. This required the physician to continue his relationship with the patient despite a major difference of opinion. This is an example of respecting a patient’s autonomy while continuing a therapeutic relationship. This case demonstrates several family physician functions in addition to patient advocate:
Family physician as coordinator… The physician obtained appropriate specialty consultations, and facilitated the patient’s visits to the podiatrist, orthopedist, wound care specialist, and plastic surgeon. He remained the central point of contact for the patient and assured that the patient received adequate follow-up.
…as comprehensive caregiver… This patient required management of several chronic diseases, including diabetes, hypertension, and obesity. He also needed health care maintenance. To give good care, the physician had to understand the patient’s background, work situation, and personal values. To appropriately treat the patient’s foot ulcer, the physician needed to know the patient, his work situation, and his medical history. As family physicians, we are able to build relationships with our patients that allow them to communicate their values, their history, and their wishes to us.
…and as educator. M.N. needed adequate and accurate information to make a final, informed decision concerning the care of his foot ulcer and osteomyelitis. As family physicians, we should be able to summarize for our patients their medical problem and present them with an overall picture of the problem and recommended treatment. This relationship allows the patient to make educated choices with a trusted healthcare provider.
–Jessica Farnsworth, MD
Antibiotic choice should be based on bone culture, as soft-tissue or sinus tract cultures do not accurately predict bone pathogens. When empiric therapy is necessary, coverage should always include S aureus. Cure of osteomyelitis has traditionally been thought to require removal of infected bone, but studies are showing that antibiotics may be adequate in two thirds of cases, especially those with good bioavailability. When bone is removed, shorter antibiotic therapy may be sufficient.2
Additional treatment options may include revascularization in an ischemic foot, which has been shown to salvage up to 98% of limbs. Hyperbaric oxygen may provide benefit, but data are insufficient to document this measure. Edema control may be beneficial for wound healing. Promising adjuvant therapies include granulocyte colony-stimulating factor (G-CSF), antibiotic-impregnated beads or orthopedic implants, and “biosurgery” with fly larvae.2
TABLE 2
Clinical characteristics of a severe infection
| Acute or rapidly progressive |
| Penetrating to subcutaneous tissues or involving fascia, muscle, joint, bone |
| Extensive cellulitis (>2 cm around ulcer rim) |
| Signs of inflammation, crepitus, bullae, necrosis, gangrene |
| Systemic signs: fever, chills, hypotension, confusion, volume depletion, leukocytosis |
| Metabolic abnormalities: severe hyperglycemia, acidosis, azotemia, electrolyte abnormalities |
| Absent pulses |
TABLE 3
Wagner ulcer grading system
| WOUND GRADE | WOUND DEPTH |
|---|---|
| Grade 0 | Intact skin |
| Grade 1 | Superficial ulcer |
| Grade 2 | Deep ulcer to tendon, bone, or joint |
| Grade 3 | Deep ulcer with abscess or osteomyelitis |
| Grade 4 | Forefoot gangrene |
| Grade 5 | Whole foot gangrene |
| The Wagner ulcer grading system does not identify infectious processes except in Grade 3. Erythema, edema, and pain may be present in foot infections, and may manifest as paronychia, cellulitis, or superficial skin infection. | |
TABLE 4
Clinical classification of diabetic foot infections
| CLINICAL APPEARANCE | CLASSIFICATION |
|---|---|
| Wound lacking purulence or any manifestations of inflammation | Uninfected |
| Presence of 2 or more manifestations of inflammation (purulence, erythema, pain, tenderness, warmth, or induration). Any cellulitis/erythema extends 2 or more cm around the ulcer, and infection is limited to the skin or superficial subcutaneous tissues. No other local complications or systemic illness. | Mild |
| Infection (as above) in a patient who is systematically well and metabolically stable but which has 1 or more of the following characteristics: cellulites extending >2 cm, lymphagitic streaking, spread beneath the superficial fascia, deep-tissue abcess, gangrene, and involvement of muscle, tender, joint or bone | Moderate |
| Infection in a patient with systemic toxicity or metabolic instability (eg, fever, chills, tachycardia, hypotension, confusion, vomiting, leukocytosis, acidosis, severe hyperglycemia, or azotemia) | Severe |
| Source: Lipsky et al, 2004.2 | |
Case resolution
The family physician and M.N. discuss the options. The specialist recommends surgery, but the patient does not want to undergo this procedure. As his physician explains his concerns about the chronic, nonhealing ulcer and osteomyelitis, M.N. says he will negotiate a change in his work situation that would allow him to decrease the time spent on his feet and thus improve healing.
The patient has small clinical improvement of his ulcer while hospitalized, and a peripherally inserted central catheter (PICC) line is placed to administer long-term antibiotics on an outpatient basis. The ulcer heals gradually in coming weeks and months. Laboratory results show improvement as well, with normalization of the ESR and CRP. Given the clinical improvement and a steady decrease in inflammatory markers, a bone scan is not repeated. The patient now has a job that allows him to sit instead of being on his feet all day.
1. Sumpio BE. Primary care: foot ulcers. N Engl J Med 2000;343:787-793.
2. Lipsky BA. Medical treatment of diabetic foot infections. Clin Infect Dis 2004;39:S104-S114.
3. Brem, Harold, Sheehan P, Boulton AJM. Protocol for treatment of diabetic foot ulcers. Am J Surg 2004;187:1S-10S.
4. Ulbrecht JS, Cavanagh PR, Caputo GM. Foot problems in diabetes: an overview. Clin Infect Dis 2004;39:S73-S82.
5. Caputo GM, Cavanagh PR, Ulbrecht JS, et al. Assessment and management of foot disease in patients with diabetes. N Engl J Med 1994;331:854-860.
6. Smith RG. Validation of Wagner’s classification: a literature review. Ostomy Wound Manage 2003;49:54-62.
7. Foster AVM, Bates M, Doxford M, Edmonds ME. Should oral antibiotics be given to ‘clean’ foot ulcers with no cellulitis? Abstracts of the 3rd International Symposium of the Diabetic Foot (1998).
8. Tice AD, Hoaglund PA, Shoutlz DA. Outcomes of osteomyelitis among patients treated with outpatient parenteral antimicrobial therapy. Am J Med 2003;114:723-728.
9. Zimmerman J. Osteomyelitis. Am Acad Fam Pract Home Study 2005; Clinical Update 308.
10. Alazraki N, Dalinka MK, Berquist TH, et al. Imaging diagnosis of osteomyelitis in patients with diabetes mellitus. American College of Radiology. ACR Appropriateness Criteria. Radiology 2000;215:303-310.
11. Lipman BT, Collier BD, Carrera GF, et al. Detection of osteomyelitis in the neuropathic foot: nuclear medicine, MRI and conventional radiography. Clin Nucl Med 1998;23:77-82.
12. Newman LG, Waller J, Palestro CJ, et al. Unsuspected osteomyelitis in diabetic foot ulcers. Diagnosis and monitoring by leukocyte scanning with indium in 111 oxyquionolone. JAMA 1991;266:1246-1251.
CORRESPONDING AUTHOR: Paul M. Paulman, MD, University of Nebraska College of Medicine, Department of Family Medicine, 983075 Nebraska Medical Center, Omaha, NE 68198. E-mail: ppaulman@unmc.edu
1. Sumpio BE. Primary care: foot ulcers. N Engl J Med 2000;343:787-793.
2. Lipsky BA. Medical treatment of diabetic foot infections. Clin Infect Dis 2004;39:S104-S114.
3. Brem, Harold, Sheehan P, Boulton AJM. Protocol for treatment of diabetic foot ulcers. Am J Surg 2004;187:1S-10S.
4. Ulbrecht JS, Cavanagh PR, Caputo GM. Foot problems in diabetes: an overview. Clin Infect Dis 2004;39:S73-S82.
5. Caputo GM, Cavanagh PR, Ulbrecht JS, et al. Assessment and management of foot disease in patients with diabetes. N Engl J Med 1994;331:854-860.
6. Smith RG. Validation of Wagner’s classification: a literature review. Ostomy Wound Manage 2003;49:54-62.
7. Foster AVM, Bates M, Doxford M, Edmonds ME. Should oral antibiotics be given to ‘clean’ foot ulcers with no cellulitis? Abstracts of the 3rd International Symposium of the Diabetic Foot (1998).
8. Tice AD, Hoaglund PA, Shoutlz DA. Outcomes of osteomyelitis among patients treated with outpatient parenteral antimicrobial therapy. Am J Med 2003;114:723-728.
9. Zimmerman J. Osteomyelitis. Am Acad Fam Pract Home Study 2005; Clinical Update 308.
10. Alazraki N, Dalinka MK, Berquist TH, et al. Imaging diagnosis of osteomyelitis in patients with diabetes mellitus. American College of Radiology. ACR Appropriateness Criteria. Radiology 2000;215:303-310.
11. Lipman BT, Collier BD, Carrera GF, et al. Detection of osteomyelitis in the neuropathic foot: nuclear medicine, MRI and conventional radiography. Clin Nucl Med 1998;23:77-82.
12. Newman LG, Waller J, Palestro CJ, et al. Unsuspected osteomyelitis in diabetic foot ulcers. Diagnosis and monitoring by leukocyte scanning with indium in 111 oxyquionolone. JAMA 1991;266:1246-1251.
CORRESPONDING AUTHOR: Paul M. Paulman, MD, University of Nebraska College of Medicine, Department of Family Medicine, 983075 Nebraska Medical Center, Omaha, NE 68198. E-mail: ppaulman@unmc.edu
Gastric Fundic Polyps or Cysts?
Craniocervical Neurenteric Cyst
Hormone replacement therapy: The right choice for your patient?
She did very well with estrogen. Her hot flashes and night sweats disappeared and she felt great. However, after hearing news reports about the danger of estrogen, she discontinued the hormone pills a few months ago. She is now feeling poorly with hot flashes, night sweats, vaginal dryness, and occasional stress incontinence. She has many questions and concerns and eagerly seeks your advice about what to do.
Medical history
- Borderline hypertension
- Hyperlipidemia
- Obesity: body-mass index of 32
Family history
- Mother, age 75, has hyperlipidemia, hypertension, myocardial infarction (MI) at age 60, and osteoporosis
- Father, died at age 55 of MI; had hypertension and diabetes
- Her grandparents also had history of stroke and heart disease, but she doesn’t know all the details about their health. She believes her maternal grandmother broke her hip when she was elderly.
Social history
- Married, 2 children, works as an attorney with the local government. Her job is fairly demanding
- Does not smoke, occasional alcohol consumption
- Does not exercise on a regular basis
Review of systems
Negative except for hot flashes, night sweats, vaginal dryness, and occasional stress incontinence.
Physical examination
- Alert female in no distress. Blood pressure, 145/90 mm Hg; weight, 165 lbs; pulse, 82; respiration, 18; temperature, 98.1°F
- HEENT exam, normal
- Neck, heart, lung, abdomen, breast, and pelvic exams are all normal except for mild atrophic changes of the vaginal and genital tracts.
You perform the gynecologic exam and order a mammogram. Mrs JC has not been seen for 2 years. Her lipid profile done 2 years ago was elevated, but Mrs JC did not repeat the tests as requested. You explain that you would like to further define her risk factors and would like to order a few tests. Making a well-informed decision on hormone replacement therapy (HRT) is complex and requires more information and adequate time for a full discussion. You would like to see her after her laboratory tests and will reserve time to address her concerns and questions.
Laboratory tests
Complete blood count, normal
Cholesterol, 250 mg/dL (LDL, 130 mg/dL; HDL, 45 mg/dL)
Triglyceride, 220 mg/dL
Electrolytes, blood urea nitrogen/creatine (BUN/Cr) ratio, normal; glucose, 85 mg/dL
Mrs JC has many symptoms of menopause:
- Vasomotor instability
- Urogenital symptoms She also has risk factors:
- Cardiac: hypertension, hyperlipidemia, obesity
- Osteoporosis: family history, sedentary lifestyle
Before addressing Mrs JC’s specific concerns, you review the findings of the Women’s Health Initiative (WHI) study,1,2 which probably prompted her concerns. You also have been asked to lead an upcoming geriatric grand round presentation on HRT, and you further prepare for both encounters by meeting with colleagues Dr Richard Pees, a gynecologist, and Dr Deborah Erickson, a urologist, to discuss practical applications of the WHI findings.
Findings of the WHI
WHI, sponsored by the National Institute of Health, comprised 2 multicentered clinical trials to determine if conjugated equine estrogen (CEE) given alone for women who had a hysterectomy or in combination with progestin (MPA, medroxyprogesterone acetate) would reduce the risk of cardiovascular events. The study also assessed the long-term risks and benefits of postmenopausal hormone therapy in other chronic disease prevention.
Exclusion criteria for the study included competing risks with survival <3 years, prior breast cancer, low hematocrit or platelets, severe menopausal symptoms, alcoholism, mental illness, and dementia. In this study, 27,000 women aged 50 to 79 years (mean age, 63) were randomized to take hormone or placebo.
The combined CEE/MPA (Prempro) trial, with 16,000 women enrolled, was discontinued at 5.2 years, on July 2002. The unopposed CEE (Premarin) trial, with 11,000 women, was discontinued at 6.8 years, on February 2004. The study was stopped earlier than planned (2005) because of increased adverse events in the group taking hormone.
TABLE 1 summarizes the absolute risks—number of events per 10,000 as compared with the control group—for both arms of the study. In the CEE/MPA arm, there were more cases per 10,000 of coronary heart disease (+7), breast cancer (+8), stroke (+8), and venous thromboembolic disease (VTE) including deep vein thrombosis/pulmonary embolism (DVT/PE) (+18). However, there were fewer cases per 10,000 of colorectal cancer (–6) and hip fracture (–5).
Recently published data2 on the unopposed estrogen arm showed an increase in stroke (+12) and VTE (+7). No significant increase was noted for coronary heart disease (CHD) (–5) or breast cancer (–7). While there is a reduction in osteoporotic fracture (–6) in the hormone arm, there is no significant difference in colorectal cancer (+1). The CEE arm demonstrated that CEE does not significantly affect the incidence of CHD, a difference compared with the CEE/MPA arm. Potential explanations for this include the role of progestin, differences in the study populations, and the role of chance. The reduction of breast cancer incidence was unanticipated and required further investigation.
A:_____________________________________________________________________
_______________________________________________________________________
Dr Pees: The WHI data do seem to confuse the issue of when to use hormonal therapy. The answer to your question lies in knowing how the WHI risks were calculated.
The WHI authors described 2 confidence indexes (CI). The first was calculated as if looking at a single outcome variable, a nominal CI; the second, an adjusted CI, took into account multiple outcomes.
For the CEE/MPA arm, when the nominal CI is used, CHD and breast cancer risks barely reached clinical significance; colon cancer and fracture reduction reached clinical significance; DVT and strokes were also clinically significant using both CIs. When the adjusted CI is used, DVT/strokes, and to a lesser degree fracture reduction, retain clinical significance.
In the CEE-only arm (February 2004 report), DVT/strokes were the only variable that reached clinical significance. CHD/breast cancer/colorectal cancer did not reach clinical significance, and fracture reduction only a slight decrease in risk.
The WHI study introduced a new term, the Global Index, which had not been tested for validity or significance of assigning weights to various outcomes. Additionally, there were certain biases in the construct of the study. Included were 1200 individuals who had prior MI, revascularization procedures, stroke, DVT, and PE. Excluded were those with severe menopausal symptoms, prior fracture/low bone mineral density (BMD), and cognitive function deficits. Also, only 10% of the group was in the 50- to 54-year-old group; 25% were in the 70- to 79-year-old group. The dropout rate was fairly high: 42% in the CEE/MPA arm, and 38% placebo arm; only 25% of the CEE/MPA arm remained at the study termination. Unblinding occurred in 40% of the CEE/MPA arm and 5.4% in the placebo arm.
It is worth noting that CHD increased in the first year of the study but decreased in subsequent years. VTE/DVT and total fractures were the only 2 items that achieved true clinical significance. Total fracture reduction was 1.6 times greater than the increases in CHD and breast cancer; and the fact that breast cancers double every 300 days and are present for 7 to 8 years before they are detected with current diagnostic testing.
Despite the biases and limitations of the data presented by the WHI report, the study does add to our knowledge and it should be included in our discussion with patients when addressing HRT.
A:____________________________________________________________________
______________________________________________________________________
Dr Pees: The WHI data have altered the way in which I counsel patients. I still prescribe hormone therapy within the American College of Obstetricians and Gynecologists (ACOG) guidelines, and, after a very thorough discussion, reference the WHI data. This is to ensure that patients make informed decisions about continuing or starting hormone therapy. Following ACOG recommendations, I evaluate each patient’s risk profile. I start treatment with the lowest effective dose to relieve symptoms. I discuss the use of alternative treatments for menopausal symptoms and osteoporosis prevention, as well as evaluation and treatment for quality of life issues. Most importantly I encourage periodic re-evaluation for hormone use.
After the WHI study was terminated, the North American Menopause Society (NAMS) convened an expert Hormone Therapy Advisory Panel to examine the data and prepare a report. A position statement on the recommendations for clinical practice was released in September 2003.2 The expert panel reached consensus on the following areas:
- The primary indication for systemic hormone therapy is moderate and severe menopausal symptoms: Hot flashes, night sweats/insomnia, mood swings.
- When treating moderate and severe urogenital atrophy (vaginal dryness, dyspareunia, urinary frequency, and incontinence), local estrogen preparations are preferred.
- The primary indication for progestogen is endometrial protection for all women with an intact uterus using systemic estrogen therapy (ET).
- Hormone therapy should not be used for primary or secondary prevention of CHD.
- Breast cancer risk is increased with ET and, to a greater extent, with estrogen progestogen therapy (EPT) used beyond 5 years.
- There is definitive evidence for EPT efficacy in reducing the risk of fracture. However, other effective alternate forms of therapy are readily available. Because of potential risk associated with long-term use of EPT, the risks and benefits of each option should be discussed with the patient.
- EPT is not recommended for primary prevention of dementia.
- Hormone therapy should be limited to the shortest duration to achieve treatment goals, taking into consideration the impact on quality of life.
- Lower-than-standard doses of EPT and ET should be considered (including 0.3 mg conjugated estrogen, 0.25–0.5 mg oral micronized 17 B-estradiol and 0.025 mg 17 B-estradiol patches). However, the long-term risk-benefit ratio has not been demonstrated.
- Extended use of ET/EPT is acceptable if the woman feels the benefits of symptom relief outweigh the risks, an attempt to withdraw ET has failed, or to prevent osteoporotic fracture when alternative therapies are not appropriate or usable.
TABLE 1
Absolute risks of HRT
| Differences between treatment and control groups; cases per 10,000 person-years | ||
|---|---|---|
| CEE/MPA | CEE | |
| Coronary heart disease | +7 | –5 |
| Breast cancer | +8 | –7 |
| Stroke | +8 | +12 |
| Venous thromboembolic disease | +18 | +7 |
| Colorectal cancer | –6 | +1 |
| Hip fracture | –5 | –6 |
| CEE/MPA, conjugated equine estrogen/medroxyprog-esterone acetate; CEE, conjugated equine estrogen. | ||
Menopausal symptoms
A:____________________________________________________________________
______________________________________________________________________
Dr. Leong: Because estrogen is the most effective treatment for menopausal symptoms, Mrs JC may yet consider taking it on a short-term basis, if her symptoms are debilitating. We should use the lowest dose required to control symptoms. She has already stopped her therapy, of course. But had she still been taking ET and told you she wished to discontinue it, you could have advised her that, often times, tapering estrogen over several months results in fewer symptoms than when quitting “cold turkey” (TABLES 2 AND 3).
If Mrs JC is absolutely against taking estrogen, several other drugs have been shown to reduce hot flashes. The selective serotonin reuptake inhibitors (SSRIs) were effective in several randomized trials using venlafaxine (Effexor),4 paroxetine (Paxil), and, less effectively, fluoxetine (Prozac).5 Clonidine (Catapres) was effective at reducing hot flushes in some, but not all, clinical trials.6Gabapentin (Neurontin) and megestrol acetate (Megace) are other possible choices.
Complementary and alternative therapies have been very popular among some postmenopausal women as they look for symptom relief. There are mixed data on soy compounds (phytoestrogen and isoflavone), with only 3 of 8 trials demonstrating a beneficial effect.7-9 Black cohosh showed modest benefits, but ginseng, dong quai, red clover, evening primrose oil, vitamin E, acupuncture, wild yam, and progesterone cream were ineffective. The main cautions with these products are that safety and efficacy are not well established and quality control of the products is often lacking.
Dr Erickson:Urinary problems most commonly associated with menopause are incontinence and recurrent urinary tract infections. Fortunately, both of these problems can be reduced with topical estrogen, which has minimal systemic absorption (TABLE 4). For example, a recent study of intravaginal estradiol (25 μg) vs placebo showed that the estrogen-treated group had significant reduction in symptoms (including dysuria, frequent voiding, and incontinence) and urodynamic findings, but no increase in serum estradiol levels or endometrial growth.10 Thus, a topical estrogen could provide the urologic benefits without the risks of systemic treatment. If she wants to avoid estrogen altogether, she has other options.
TABLE 2
Possible tapering schedules for estrogen regimens
| Current hormone regimen | CEE/MPA 0.625/2.5 mg daily |
| Month 1 | CEE/MPA 0.625/2.5 mg qod (x 1 mo) |
| Month 2 | CEE/MPA 0.3/1.5 mg daily (x 1 mo) |
| Month 3 | CEE/MPA 0.3/1.5 mg qod (x 1 mo) |
| Month 4 | CEE 0.3/1.5 mg 2/wk (x 1 mo) |
| Month 5 | Estrogen patch 0.025/wk if needed |
| CEE/MPA, conjugated equine estrogen/medroxyprogesterone acetate; qod, every other day | |
TABLE 3
HRT dosing options
| MEDICATION | DOSAGE |
|---|---|
| Conjugated estrogens (Premarin) | 0.3 mg, 0.45 mg, 0.625 mg, 0.9 mg |
| Estradiol (Estrace) | 0.5 mg, 1 mg, 2 mg(scored tablets) |
| Estradiol patches (Climara/Vivelle) | 0.025 mg/d, 0.0375, 0.05 mg/d |
Urinary tract symptoms
A:_________________________________________________________________
___________________________________________________________________
TABLE 4
Vaginal products for genitourinary atrophy
| PRODUCT | DOSAGE |
|---|---|
| Low-dose estrogen vaginal cream | 0.3 mg 2x/wk |
| Vaginal ring | |
| Estring | 6–9 μg of estrogen/d for 3 mo |
| Femring | 50 to 100 μg/d for vasomotor symptoms |
| Vaginal tablet (Vagifem) | 25 μg of estradiol 2x/wk or 10 μg 2x/wk may be effective for genitourinary atrophy |
Stress incontinence. For stress incontinence, pelvic floor muscle exercises are helpful. These can be done without any assistance if the patient is able to do the exercises and is motivated. For patients with marginal ability or motivation, options include biofeedback training, vaginal weights, electric stimulation, or magnetic stimulation.
Alpha-adrenergic agonists have also been used,11although treatment of stress incontinence is an off-label use for these drugs and they have risks including hypertension and tachycardia. Phenylpropa-nolamine (eg, Entex LA) is the alpha-adrenergic agent with the most reported studies for stress incontinence, but it was withdrawn from the market due to increased risk of cerebrovascular accident.12The alternative now contains pseudoephedrine (eg, Entex PSE) but there are no published trials of pseudoephedrine for stress incontinence.
More recent studies have shown duloxetine (Cymbalta) to be effective,13, 14 although incontinence is currently an offlabel use for it.
Fem-Soft urethral inserts are used by some patients and are covered by Medicare. These soft inserts are held in place by a unique balloon, which expands automatically after insertion and compresses when the patient pulls on the insert to remove it (ie, the balloon does not need to be inflated or deflated in the office). They are similar in width to Foley catheters (16 or 18 Fr) but are shorter, extending only about 1 cm out from the urethral meatus.
Surgical options for stress incontinence include periurethral injections and sling operations. The former involves injecting a bulking material (such as collagen paste) around the urethra to increase its coaptation (urethral closure). It is a simple, almost painless, outpatient procedure with minimal risks, but results vary. Several procedures may be required to achieve continence, and most patients have recurrent incontinence within 5 years.
In contrast, sling operations have a better success rate. Slings can be made from various materials including the patient’s own fascia, cadaveric fascia, animal materials such as porcine intestinal submucosa, or synthetic mesh. Most materials have good short-term results, with stress incontinence cured or significantly improved for over 90% of patients.15 Long-term success depends on the sling material used. The risks and duration of hospitalization depend on the specific materials and techniques, but most slings are inserted either as outpatient surgery or with overnight hospitalization.
Urge incontinence. For urge incontinence, pelvic floor muscle exercises are beneficial because contraction of the pelvic floor inhibits the detrusor by a reflex. This is well described in a book for lay people.16
Anticholinergic drugs are commonly used and are more effective than placebo.11, 17Side effects include dry mouth, constipation, and mental status changes.
Ways to reduce side effects:
- Sustained-release formulations of oxy-butynin (Ditropan XL) or tolterodine (Detrol LA)
- Anticholinergics that are more selective for the bladder, such as tolterodine (Detrol)
- Transdermal oxybutynin (Oxytrol), which decreases the first-pass liver metabolism and minimizes production of metabolites that have side effects of their own
- Trospium chloride (Sanctura), which does not cross the blood-brain barrier and therefore has less effect on the central nervous system.18
Interestingly, magnesium supplementation (MgOH, 350 mg twice daily) was effective for urge incontinence in a placebo controlled trial.19 If conservative treatments fail, the surgical options include sacral nerve stimulation or augmentation cystoplasty. The latter has high morbidity and should be considered only as a last resort for a person with incapacitating incontinence.
Recurrent UTI. For recurrent urinary tract infections, several options are available. Cranberries contain polymeric proanthocyanidins, which inhibit the binding of Escherichia coli to uroepithelial cells. Cranberry juice or cranberry extract tablets were more effective than placebo in the few studies available, but the optimum preparation and dose are unknown.20Also, since the P fimbriae on E coli bind to mannose residues on uroepithelial cells, it is expected that free mannose in the urine might competitively inhibit this binding.
Mannose is sold over the counter as a preventative for urinary tract infections. No published literature supports its use, but it appears harmless.
Another option is methenamine hippurate, which is a urinary tract antiseptic. Controlled trials to date have not proven its efficacy, but adverse events are infrequent.21
Antibiotics can also be used as chronic low-dose prophylaxis or intermittent self-start therapy when infection symptoms occur.22 Best for low-dose prophylaxis are antibiotics with minimal adverse effects on the fecal and vaginal flora, such as trimethoprim alone, trimethoprim/sulfamethoxazole, nitrofurantoin, cephalexin (in minimal doses), and fluoroquinolones.23
Cardiac risk factors
A:_____________________________________________________________________
_______________________________________________________________________
Dr Leong: Mrs JC’s risk factors for heart disease include hypertension, hyperlipidemia, obesity, and family history of CHD. While hormone therapy should not be used to prevent heart disease, there are well-established treatments for hyperlipidemia including diet, exercise, and lipid lowering medications, such as the statins. She should be advised to lose weight. If healthy lifestyle changes do not control her blood pressure, antihypertensive medication would be indicated.
For prevention of osteoporosis, Mrs JC should be advised to start weight-bearing exercise and to include adequate calcium and vitamin D in her diet. Besides estrogen, bisphosphonates, raloxifene, and calcitonin are effective medication for osteoporosis treatment and prevention.
Should the patient be treated with HRT?
A:_________________________________________________________________
___________________________________________________________________
Dr Pees: Mrs JC’s family history of CHD does not contraindicate hormonal therapy. But neither is hormonal therapy indicated to prevent CHD. Mrs JC should be strongly urged to begin an exercise program, diet modifications, and possibly the use of statins. Studies support exercise as a significant factor in reducing the risk of CHD and, to a lesser degree, the risk of breast cancer. If, after thorough counseling with reference to WHI risk findings, Mrs JC wishes to remain on or start hormone therapy, she should start on the lowest effective dosage to relieve her vasomotor symptoms. She should also be reevaluated periodically and be kept appraised of new data as they become available.
Hormone replacement therapy (HRT) has generated fear and confusion among many women. While the absolute risk for diseases associated with hormone use is low, the diseases are devastating. Breast cancer and stroke are 2 of the most feared illnesses, yet research studies often provided conflicting results on the risk of hormone replacement associated with these conditions.
Individualize every decision
The calculation of risks/benefits ratio has changed with the WHI data. All patients on HRT must be counseled on the new data, ideally in a face-to-face visit. Phone calls for medication refill, annual exam, and regular office visits are opportunities to revisit the subject of hormone therapy (HT). Given the mixed benefits and risks associated with HT, every decision should be individualized. A patient-centered counseling approach would allow a shared decision: the patient expresses her needs, goals, and preferences, and the physician applies medical knowledge to his and her values. In this dynamic approach, the physician can shift from a directive to a nondirective posture, taking the lead vs giving the patient full autonomy. The point in the continuum where the physician chooses to participate is determined by the patient, the physician, and the medical evidence.
The patient’s personal and family histories (breast/colon cancer, stroke, MI, osteoporosis) and risk factors (lipid profile, diet, exercise, body-mass index) play major roles in the decision. However, the patient’s philosophical approach to health often is the determining factor. The physician must provide the facts and ensure a patient is not taking HRT for reasons no longer valid. Questions such as, “What benefits do you hope to gain from HRT?” and “What are your major fears of HRT?” can help facilitate the discussion.
The patient’s philosophy
Patients often will select treatments most consistent with their philosophical approach to health. Patients with a holistic view of healthcare and an uneasiness with HRT are unlikely to have many questions. The patients who could benefit from your counsel are those who stopped HRT due to the findings of the WHI studies and those still on HRT who would like to continue. A recalculation of their individual risk/benefit ratio will help determine if HRT is still the right decision for them.
Considering symptoms
Menopausal symptoms are common and bothersome, often adversely impacting patients’ quality of life. Symptoms should be considered in calculating the risks/benefits ratio, but unfortunately, they are seldom included in research studies. In a UK qualitative study using a “time trade-off” method, participants were asked to make trade-offs between a shorter life span in “perfect health” compared with a longer life span with the condition under study.23 Women reported they might give up 3 months of their life to live the rest of the year without menopausal symptoms, underscoring the importance of menopausal symptoms.
Unanswered questions remain
Though national organizations such as ACOG, NAMS (The North American Menopause Society), and USPSTF (US Preventive Services Task Force) generally agree that estrogen and progestin should not be used routinely to prevent chronic conditions of menopause, such as CHD, there remain many unanswered questions. What are the risks associated with progestin? Is topical estrogen truly safe? Does the type of estrogen and delivery system have an impact on the safety profile? A recent systematic review and meta-analysis of the commonly used estrogen preparations showed that CEE and oral and transdermal 17 B-estradiol have consistent and comparable efficacy in the treatment of hot flashes and may have similar short-term adverse effects.24 But current clinical trials have many limitations, and further testing is needed to answer many remaining questions. Until clear strategies become available for HRT, the role of the physician continues to be that of a medical advisor helping patients make well-informed, personal, and thoughtful decisions.
—Shou Ling Leong, MD
1. Rossouw JE, Anderson GL, Prentice RL, et al. Writing Group for the Women’s Health Initiative Investigators Risks and benefits of estrogen and progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA 2002;288:321-333.
2. Anderson GL, Limacher M, Assaf AR, et al. Women’s Health Initiative Steering Committee Effects of conjugated equine estrogen in postmenopausal women with hysterectomy, the women’s health initiative randomized control trial. The Women’s Health Initiative Steering Committee. JAMA 2004;291:1701-1712.
3. The Hormone Therapy Advisory Panel of the North American Menopause Society position statement on hormone therapy. Available at: www.menopause.org. Accessed on April 1, 2005
4. Loprinzi CL, Kugler JW, Sloan JA, et al. Venlafaxine in management of hot flashes in survivors of breast cancer: a randomised controlled trial. Lancet 2000;356:2059-2063.
5. Stearns V, Beebe KL, Iyengar M, Dube E. Paroxetine controlled release in the treatment of menopausal hot flashes: a randomized controlled trial. JAMA 2003;289:2827-2834.
6. Nagamani M, Kelver ME, Smith ER. Treatment of menopausal hot flashes with transdermal administration of clonidine. Am J Obstet Gynecol 1987;156:561-565.
7. Upmalis DH, Lobo R, Bradley L, Warren M, Cone FL, Lamia CA. Vasomotor symptom relief by soy isoflavone extract tablets in postmenopausal women: a multicenter, double-blind, randomized, placebo-controlled study. Menopause 2000;7:236-242.
8. Tice JA, Ettinger B, Ensrud K, Wallace R, Blackwell T, Cummings SR. Phytoestrogen supplements for the treatment of hot flashes: the isoflavone clover extract (ICE) study: a randomized controlled trial. JAMA 2003;290:207-214.
9. Kronenberg F, Fugh-Berman A. Complementary and alternative medicine for menopausal symptoms: a review of randomized, controlled trials. Ann Intern Med 2002;137:805-813.
10. Simunic V, Banovic I, Ciglar S, Jeren L, Pavicic Baldani D, Sprem M. Local estrogen treatment in patients with urogenital symptoms. Int J Gynecol Obstet 2003;82:187-197.
11. Fantl JA, Newman DK, Colling J, et al. Urinary Incontinence in Adults: Acute and Chronic Management. Clinical Practice Guideline, No. 2; 1996 update. AHCPR Publication No. 96-0682. Rockville, Md: US Department of Health and Human Services, Public Health Services, Agency for Health Care Policy and Research 1996.
12. Kernan WN, Viscoli CM, Brass LM, et al. Phenylpropanolamine and the risk of hemorrhagic stroke. N Engl J Med 2000;343:1826-1832.
13. Millard RJ, Moore K, Rencken R, Yalcin I, Bump RC. Duloxetine UI Study Group Duloxetine vs. placebo in the treatment of stress urinary incontinence: a four-continent randomized clinical trial. BJU International 2004;93:311-318.
14. Dmochowski RR, Miklos JR, Norton PA, Zinner NR, Yalcin I, Bump RC. Duloxetine UI Study Group: Duloxetine versus placebo for the treatment of North American women with stress urinary incontinence J Urol 2003;170:1259-1263.
15. Leach GE, Dmochowski RR, Appell RA, et al. Female stress urinary incontinence clinical guidelines panel summary report on surgical management of female stress urinary incontinence. J Urol 1997;158:875-880.
16. Burgio KL, Pearce KL, Lucco AJ. Staying Dry: A Practical Guide to Bladder Control. Baltimore, Md: Johns Hopkins University Press; 1989.
17. Hay-Smith J, Herbison P, Ellis G, Moore K. Anticholinergic drugs versus placebo for overactive bladder syndrome in adults. Cochrane Database Syst Rev 2002;(3) CD003781.-
18. Halaska M, Ralph G, Weidemann A, et al. Controlled, double-blind, multicentre clinical trial to investigate long-term tolerability and efficacy of trospium chloride in patients with detrusor instability. World J Urol 2003;29:392-399.
19. Gordon D, Groutz A, Ascher-Landsberg J, Lessing JB, David MP, Razz O. Double-blind, placebo-controlled study of magnesium hydroxide for treatment of sensory urgency and detrusor instability: preliminary results. Br J Obstet Gynaecol 1998;105:667-669.
20. Jepson RG, Mihaljevic L, Craig J. Cranberries for preventing urinary tract infections. Cochrane Database Syst Rev 2004;(1) CD001321.-
21. Lee B, Bhuta T, Craig J, Simpson J. Methenamine hippurate for preventing urinary tract infections. Cochrane Database Syst Rev 2002;(1) CD003265.-
22. Schaeffer AJ. Infections of the urinary tract. In: Walsh PC, Retik AB, Vaughan ED, Wein AJ, eds. Campbell’s Urology 8th ed. Philadelphia, Pa: Saunders 2002;515-602.
23. Minelli C, Abrams KR, Sutton AJ, Cooper NJ. Benefits and harms associated with hormone replacement therapy: clinical decision analysis. BMJ 2004;328-371.
24. Nelson H. Commonly used types of postmenopausal estrogen for treatment of hot flashes: Scientific Review. JAMA 2004;292:1610-1619.
Drug brand names
- Calcitonin • Calcimar, Cibacalcin, Miacalcin
- Cephalexin • Biocef, Keflex, Keftab
- Clonidine • Catapres
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Megestrol acetate • Megace
- Nitrofurantoin • Furadantin, Macrobid, Macrodantin
- Oxybutynin • Ditropan, Oxytrol
- Paroxetine • Paxil
- Raloxifene • Evista
- Tolterodine • Detrol
- Trospium chloride • Sanctura
- Venlafaxine • Effexor
CORRESPONDING AUTHOR Shou Ling Leong, MD, Penn State College of Medicine, Penn State Milton S. Hershey Medical Center, P.O. Box 850, Hershey, PA 17033 -0850. E-mail: sleong@psu.edu
She did very well with estrogen. Her hot flashes and night sweats disappeared and she felt great. However, after hearing news reports about the danger of estrogen, she discontinued the hormone pills a few months ago. She is now feeling poorly with hot flashes, night sweats, vaginal dryness, and occasional stress incontinence. She has many questions and concerns and eagerly seeks your advice about what to do.
Medical history
- Borderline hypertension
- Hyperlipidemia
- Obesity: body-mass index of 32
Family history
- Mother, age 75, has hyperlipidemia, hypertension, myocardial infarction (MI) at age 60, and osteoporosis
- Father, died at age 55 of MI; had hypertension and diabetes
- Her grandparents also had history of stroke and heart disease, but she doesn’t know all the details about their health. She believes her maternal grandmother broke her hip when she was elderly.
Social history
- Married, 2 children, works as an attorney with the local government. Her job is fairly demanding
- Does not smoke, occasional alcohol consumption
- Does not exercise on a regular basis
Review of systems
Negative except for hot flashes, night sweats, vaginal dryness, and occasional stress incontinence.
Physical examination
- Alert female in no distress. Blood pressure, 145/90 mm Hg; weight, 165 lbs; pulse, 82; respiration, 18; temperature, 98.1°F
- HEENT exam, normal
- Neck, heart, lung, abdomen, breast, and pelvic exams are all normal except for mild atrophic changes of the vaginal and genital tracts.
You perform the gynecologic exam and order a mammogram. Mrs JC has not been seen for 2 years. Her lipid profile done 2 years ago was elevated, but Mrs JC did not repeat the tests as requested. You explain that you would like to further define her risk factors and would like to order a few tests. Making a well-informed decision on hormone replacement therapy (HRT) is complex and requires more information and adequate time for a full discussion. You would like to see her after her laboratory tests and will reserve time to address her concerns and questions.
Laboratory tests
Complete blood count, normal
Cholesterol, 250 mg/dL (LDL, 130 mg/dL; HDL, 45 mg/dL)
Triglyceride, 220 mg/dL
Electrolytes, blood urea nitrogen/creatine (BUN/Cr) ratio, normal; glucose, 85 mg/dL
Mrs JC has many symptoms of menopause:
- Vasomotor instability
- Urogenital symptoms She also has risk factors:
- Cardiac: hypertension, hyperlipidemia, obesity
- Osteoporosis: family history, sedentary lifestyle
Before addressing Mrs JC’s specific concerns, you review the findings of the Women’s Health Initiative (WHI) study,1,2 which probably prompted her concerns. You also have been asked to lead an upcoming geriatric grand round presentation on HRT, and you further prepare for both encounters by meeting with colleagues Dr Richard Pees, a gynecologist, and Dr Deborah Erickson, a urologist, to discuss practical applications of the WHI findings.
Findings of the WHI
WHI, sponsored by the National Institute of Health, comprised 2 multicentered clinical trials to determine if conjugated equine estrogen (CEE) given alone for women who had a hysterectomy or in combination with progestin (MPA, medroxyprogesterone acetate) would reduce the risk of cardiovascular events. The study also assessed the long-term risks and benefits of postmenopausal hormone therapy in other chronic disease prevention.
Exclusion criteria for the study included competing risks with survival <3 years, prior breast cancer, low hematocrit or platelets, severe menopausal symptoms, alcoholism, mental illness, and dementia. In this study, 27,000 women aged 50 to 79 years (mean age, 63) were randomized to take hormone or placebo.
The combined CEE/MPA (Prempro) trial, with 16,000 women enrolled, was discontinued at 5.2 years, on July 2002. The unopposed CEE (Premarin) trial, with 11,000 women, was discontinued at 6.8 years, on February 2004. The study was stopped earlier than planned (2005) because of increased adverse events in the group taking hormone.
TABLE 1 summarizes the absolute risks—number of events per 10,000 as compared with the control group—for both arms of the study. In the CEE/MPA arm, there were more cases per 10,000 of coronary heart disease (+7), breast cancer (+8), stroke (+8), and venous thromboembolic disease (VTE) including deep vein thrombosis/pulmonary embolism (DVT/PE) (+18). However, there were fewer cases per 10,000 of colorectal cancer (–6) and hip fracture (–5).
Recently published data2 on the unopposed estrogen arm showed an increase in stroke (+12) and VTE (+7). No significant increase was noted for coronary heart disease (CHD) (–5) or breast cancer (–7). While there is a reduction in osteoporotic fracture (–6) in the hormone arm, there is no significant difference in colorectal cancer (+1). The CEE arm demonstrated that CEE does not significantly affect the incidence of CHD, a difference compared with the CEE/MPA arm. Potential explanations for this include the role of progestin, differences in the study populations, and the role of chance. The reduction of breast cancer incidence was unanticipated and required further investigation.
A:_____________________________________________________________________
_______________________________________________________________________
Dr Pees: The WHI data do seem to confuse the issue of when to use hormonal therapy. The answer to your question lies in knowing how the WHI risks were calculated.
The WHI authors described 2 confidence indexes (CI). The first was calculated as if looking at a single outcome variable, a nominal CI; the second, an adjusted CI, took into account multiple outcomes.
For the CEE/MPA arm, when the nominal CI is used, CHD and breast cancer risks barely reached clinical significance; colon cancer and fracture reduction reached clinical significance; DVT and strokes were also clinically significant using both CIs. When the adjusted CI is used, DVT/strokes, and to a lesser degree fracture reduction, retain clinical significance.
In the CEE-only arm (February 2004 report), DVT/strokes were the only variable that reached clinical significance. CHD/breast cancer/colorectal cancer did not reach clinical significance, and fracture reduction only a slight decrease in risk.
The WHI study introduced a new term, the Global Index, which had not been tested for validity or significance of assigning weights to various outcomes. Additionally, there were certain biases in the construct of the study. Included were 1200 individuals who had prior MI, revascularization procedures, stroke, DVT, and PE. Excluded were those with severe menopausal symptoms, prior fracture/low bone mineral density (BMD), and cognitive function deficits. Also, only 10% of the group was in the 50- to 54-year-old group; 25% were in the 70- to 79-year-old group. The dropout rate was fairly high: 42% in the CEE/MPA arm, and 38% placebo arm; only 25% of the CEE/MPA arm remained at the study termination. Unblinding occurred in 40% of the CEE/MPA arm and 5.4% in the placebo arm.
It is worth noting that CHD increased in the first year of the study but decreased in subsequent years. VTE/DVT and total fractures were the only 2 items that achieved true clinical significance. Total fracture reduction was 1.6 times greater than the increases in CHD and breast cancer; and the fact that breast cancers double every 300 days and are present for 7 to 8 years before they are detected with current diagnostic testing.
Despite the biases and limitations of the data presented by the WHI report, the study does add to our knowledge and it should be included in our discussion with patients when addressing HRT.
A:____________________________________________________________________
______________________________________________________________________
Dr Pees: The WHI data have altered the way in which I counsel patients. I still prescribe hormone therapy within the American College of Obstetricians and Gynecologists (ACOG) guidelines, and, after a very thorough discussion, reference the WHI data. This is to ensure that patients make informed decisions about continuing or starting hormone therapy. Following ACOG recommendations, I evaluate each patient’s risk profile. I start treatment with the lowest effective dose to relieve symptoms. I discuss the use of alternative treatments for menopausal symptoms and osteoporosis prevention, as well as evaluation and treatment for quality of life issues. Most importantly I encourage periodic re-evaluation for hormone use.
After the WHI study was terminated, the North American Menopause Society (NAMS) convened an expert Hormone Therapy Advisory Panel to examine the data and prepare a report. A position statement on the recommendations for clinical practice was released in September 2003.2 The expert panel reached consensus on the following areas:
- The primary indication for systemic hormone therapy is moderate and severe menopausal symptoms: Hot flashes, night sweats/insomnia, mood swings.
- When treating moderate and severe urogenital atrophy (vaginal dryness, dyspareunia, urinary frequency, and incontinence), local estrogen preparations are preferred.
- The primary indication for progestogen is endometrial protection for all women with an intact uterus using systemic estrogen therapy (ET).
- Hormone therapy should not be used for primary or secondary prevention of CHD.
- Breast cancer risk is increased with ET and, to a greater extent, with estrogen progestogen therapy (EPT) used beyond 5 years.
- There is definitive evidence for EPT efficacy in reducing the risk of fracture. However, other effective alternate forms of therapy are readily available. Because of potential risk associated with long-term use of EPT, the risks and benefits of each option should be discussed with the patient.
- EPT is not recommended for primary prevention of dementia.
- Hormone therapy should be limited to the shortest duration to achieve treatment goals, taking into consideration the impact on quality of life.
- Lower-than-standard doses of EPT and ET should be considered (including 0.3 mg conjugated estrogen, 0.25–0.5 mg oral micronized 17 B-estradiol and 0.025 mg 17 B-estradiol patches). However, the long-term risk-benefit ratio has not been demonstrated.
- Extended use of ET/EPT is acceptable if the woman feels the benefits of symptom relief outweigh the risks, an attempt to withdraw ET has failed, or to prevent osteoporotic fracture when alternative therapies are not appropriate or usable.
TABLE 1
Absolute risks of HRT
| Differences between treatment and control groups; cases per 10,000 person-years | ||
|---|---|---|
| CEE/MPA | CEE | |
| Coronary heart disease | +7 | –5 |
| Breast cancer | +8 | –7 |
| Stroke | +8 | +12 |
| Venous thromboembolic disease | +18 | +7 |
| Colorectal cancer | –6 | +1 |
| Hip fracture | –5 | –6 |
| CEE/MPA, conjugated equine estrogen/medroxyprog-esterone acetate; CEE, conjugated equine estrogen. | ||
Menopausal symptoms
A:____________________________________________________________________
______________________________________________________________________
Dr. Leong: Because estrogen is the most effective treatment for menopausal symptoms, Mrs JC may yet consider taking it on a short-term basis, if her symptoms are debilitating. We should use the lowest dose required to control symptoms. She has already stopped her therapy, of course. But had she still been taking ET and told you she wished to discontinue it, you could have advised her that, often times, tapering estrogen over several months results in fewer symptoms than when quitting “cold turkey” (TABLES 2 AND 3).
If Mrs JC is absolutely against taking estrogen, several other drugs have been shown to reduce hot flashes. The selective serotonin reuptake inhibitors (SSRIs) were effective in several randomized trials using venlafaxine (Effexor),4 paroxetine (Paxil), and, less effectively, fluoxetine (Prozac).5 Clonidine (Catapres) was effective at reducing hot flushes in some, but not all, clinical trials.6Gabapentin (Neurontin) and megestrol acetate (Megace) are other possible choices.
Complementary and alternative therapies have been very popular among some postmenopausal women as they look for symptom relief. There are mixed data on soy compounds (phytoestrogen and isoflavone), with only 3 of 8 trials demonstrating a beneficial effect.7-9 Black cohosh showed modest benefits, but ginseng, dong quai, red clover, evening primrose oil, vitamin E, acupuncture, wild yam, and progesterone cream were ineffective. The main cautions with these products are that safety and efficacy are not well established and quality control of the products is often lacking.
Dr Erickson:Urinary problems most commonly associated with menopause are incontinence and recurrent urinary tract infections. Fortunately, both of these problems can be reduced with topical estrogen, which has minimal systemic absorption (TABLE 4). For example, a recent study of intravaginal estradiol (25 μg) vs placebo showed that the estrogen-treated group had significant reduction in symptoms (including dysuria, frequent voiding, and incontinence) and urodynamic findings, but no increase in serum estradiol levels or endometrial growth.10 Thus, a topical estrogen could provide the urologic benefits without the risks of systemic treatment. If she wants to avoid estrogen altogether, she has other options.
TABLE 2
Possible tapering schedules for estrogen regimens
| Current hormone regimen | CEE/MPA 0.625/2.5 mg daily |
| Month 1 | CEE/MPA 0.625/2.5 mg qod (x 1 mo) |
| Month 2 | CEE/MPA 0.3/1.5 mg daily (x 1 mo) |
| Month 3 | CEE/MPA 0.3/1.5 mg qod (x 1 mo) |
| Month 4 | CEE 0.3/1.5 mg 2/wk (x 1 mo) |
| Month 5 | Estrogen patch 0.025/wk if needed |
| CEE/MPA, conjugated equine estrogen/medroxyprogesterone acetate; qod, every other day | |
TABLE 3
HRT dosing options
| MEDICATION | DOSAGE |
|---|---|
| Conjugated estrogens (Premarin) | 0.3 mg, 0.45 mg, 0.625 mg, 0.9 mg |
| Estradiol (Estrace) | 0.5 mg, 1 mg, 2 mg(scored tablets) |
| Estradiol patches (Climara/Vivelle) | 0.025 mg/d, 0.0375, 0.05 mg/d |
Urinary tract symptoms
A:_________________________________________________________________
___________________________________________________________________
TABLE 4
Vaginal products for genitourinary atrophy
| PRODUCT | DOSAGE |
|---|---|
| Low-dose estrogen vaginal cream | 0.3 mg 2x/wk |
| Vaginal ring | |
| Estring | 6–9 μg of estrogen/d for 3 mo |
| Femring | 50 to 100 μg/d for vasomotor symptoms |
| Vaginal tablet (Vagifem) | 25 μg of estradiol 2x/wk or 10 μg 2x/wk may be effective for genitourinary atrophy |
Stress incontinence. For stress incontinence, pelvic floor muscle exercises are helpful. These can be done without any assistance if the patient is able to do the exercises and is motivated. For patients with marginal ability or motivation, options include biofeedback training, vaginal weights, electric stimulation, or magnetic stimulation.
Alpha-adrenergic agonists have also been used,11although treatment of stress incontinence is an off-label use for these drugs and they have risks including hypertension and tachycardia. Phenylpropa-nolamine (eg, Entex LA) is the alpha-adrenergic agent with the most reported studies for stress incontinence, but it was withdrawn from the market due to increased risk of cerebrovascular accident.12The alternative now contains pseudoephedrine (eg, Entex PSE) but there are no published trials of pseudoephedrine for stress incontinence.
More recent studies have shown duloxetine (Cymbalta) to be effective,13, 14 although incontinence is currently an offlabel use for it.
Fem-Soft urethral inserts are used by some patients and are covered by Medicare. These soft inserts are held in place by a unique balloon, which expands automatically after insertion and compresses when the patient pulls on the insert to remove it (ie, the balloon does not need to be inflated or deflated in the office). They are similar in width to Foley catheters (16 or 18 Fr) but are shorter, extending only about 1 cm out from the urethral meatus.
Surgical options for stress incontinence include periurethral injections and sling operations. The former involves injecting a bulking material (such as collagen paste) around the urethra to increase its coaptation (urethral closure). It is a simple, almost painless, outpatient procedure with minimal risks, but results vary. Several procedures may be required to achieve continence, and most patients have recurrent incontinence within 5 years.
In contrast, sling operations have a better success rate. Slings can be made from various materials including the patient’s own fascia, cadaveric fascia, animal materials such as porcine intestinal submucosa, or synthetic mesh. Most materials have good short-term results, with stress incontinence cured or significantly improved for over 90% of patients.15 Long-term success depends on the sling material used. The risks and duration of hospitalization depend on the specific materials and techniques, but most slings are inserted either as outpatient surgery or with overnight hospitalization.
Urge incontinence. For urge incontinence, pelvic floor muscle exercises are beneficial because contraction of the pelvic floor inhibits the detrusor by a reflex. This is well described in a book for lay people.16
Anticholinergic drugs are commonly used and are more effective than placebo.11, 17Side effects include dry mouth, constipation, and mental status changes.
Ways to reduce side effects:
- Sustained-release formulations of oxy-butynin (Ditropan XL) or tolterodine (Detrol LA)
- Anticholinergics that are more selective for the bladder, such as tolterodine (Detrol)
- Transdermal oxybutynin (Oxytrol), which decreases the first-pass liver metabolism and minimizes production of metabolites that have side effects of their own
- Trospium chloride (Sanctura), which does not cross the blood-brain barrier and therefore has less effect on the central nervous system.18
Interestingly, magnesium supplementation (MgOH, 350 mg twice daily) was effective for urge incontinence in a placebo controlled trial.19 If conservative treatments fail, the surgical options include sacral nerve stimulation or augmentation cystoplasty. The latter has high morbidity and should be considered only as a last resort for a person with incapacitating incontinence.
Recurrent UTI. For recurrent urinary tract infections, several options are available. Cranberries contain polymeric proanthocyanidins, which inhibit the binding of Escherichia coli to uroepithelial cells. Cranberry juice or cranberry extract tablets were more effective than placebo in the few studies available, but the optimum preparation and dose are unknown.20Also, since the P fimbriae on E coli bind to mannose residues on uroepithelial cells, it is expected that free mannose in the urine might competitively inhibit this binding.
Mannose is sold over the counter as a preventative for urinary tract infections. No published literature supports its use, but it appears harmless.
Another option is methenamine hippurate, which is a urinary tract antiseptic. Controlled trials to date have not proven its efficacy, but adverse events are infrequent.21
Antibiotics can also be used as chronic low-dose prophylaxis or intermittent self-start therapy when infection symptoms occur.22 Best for low-dose prophylaxis are antibiotics with minimal adverse effects on the fecal and vaginal flora, such as trimethoprim alone, trimethoprim/sulfamethoxazole, nitrofurantoin, cephalexin (in minimal doses), and fluoroquinolones.23
Cardiac risk factors
A:_____________________________________________________________________
_______________________________________________________________________
Dr Leong: Mrs JC’s risk factors for heart disease include hypertension, hyperlipidemia, obesity, and family history of CHD. While hormone therapy should not be used to prevent heart disease, there are well-established treatments for hyperlipidemia including diet, exercise, and lipid lowering medications, such as the statins. She should be advised to lose weight. If healthy lifestyle changes do not control her blood pressure, antihypertensive medication would be indicated.
For prevention of osteoporosis, Mrs JC should be advised to start weight-bearing exercise and to include adequate calcium and vitamin D in her diet. Besides estrogen, bisphosphonates, raloxifene, and calcitonin are effective medication for osteoporosis treatment and prevention.
Should the patient be treated with HRT?
A:_________________________________________________________________
___________________________________________________________________
Dr Pees: Mrs JC’s family history of CHD does not contraindicate hormonal therapy. But neither is hormonal therapy indicated to prevent CHD. Mrs JC should be strongly urged to begin an exercise program, diet modifications, and possibly the use of statins. Studies support exercise as a significant factor in reducing the risk of CHD and, to a lesser degree, the risk of breast cancer. If, after thorough counseling with reference to WHI risk findings, Mrs JC wishes to remain on or start hormone therapy, she should start on the lowest effective dosage to relieve her vasomotor symptoms. She should also be reevaluated periodically and be kept appraised of new data as they become available.
Hormone replacement therapy (HRT) has generated fear and confusion among many women. While the absolute risk for diseases associated with hormone use is low, the diseases are devastating. Breast cancer and stroke are 2 of the most feared illnesses, yet research studies often provided conflicting results on the risk of hormone replacement associated with these conditions.
Individualize every decision
The calculation of risks/benefits ratio has changed with the WHI data. All patients on HRT must be counseled on the new data, ideally in a face-to-face visit. Phone calls for medication refill, annual exam, and regular office visits are opportunities to revisit the subject of hormone therapy (HT). Given the mixed benefits and risks associated with HT, every decision should be individualized. A patient-centered counseling approach would allow a shared decision: the patient expresses her needs, goals, and preferences, and the physician applies medical knowledge to his and her values. In this dynamic approach, the physician can shift from a directive to a nondirective posture, taking the lead vs giving the patient full autonomy. The point in the continuum where the physician chooses to participate is determined by the patient, the physician, and the medical evidence.
The patient’s personal and family histories (breast/colon cancer, stroke, MI, osteoporosis) and risk factors (lipid profile, diet, exercise, body-mass index) play major roles in the decision. However, the patient’s philosophical approach to health often is the determining factor. The physician must provide the facts and ensure a patient is not taking HRT for reasons no longer valid. Questions such as, “What benefits do you hope to gain from HRT?” and “What are your major fears of HRT?” can help facilitate the discussion.
The patient’s philosophy
Patients often will select treatments most consistent with their philosophical approach to health. Patients with a holistic view of healthcare and an uneasiness with HRT are unlikely to have many questions. The patients who could benefit from your counsel are those who stopped HRT due to the findings of the WHI studies and those still on HRT who would like to continue. A recalculation of their individual risk/benefit ratio will help determine if HRT is still the right decision for them.
Considering symptoms
Menopausal symptoms are common and bothersome, often adversely impacting patients’ quality of life. Symptoms should be considered in calculating the risks/benefits ratio, but unfortunately, they are seldom included in research studies. In a UK qualitative study using a “time trade-off” method, participants were asked to make trade-offs between a shorter life span in “perfect health” compared with a longer life span with the condition under study.23 Women reported they might give up 3 months of their life to live the rest of the year without menopausal symptoms, underscoring the importance of menopausal symptoms.
Unanswered questions remain
Though national organizations such as ACOG, NAMS (The North American Menopause Society), and USPSTF (US Preventive Services Task Force) generally agree that estrogen and progestin should not be used routinely to prevent chronic conditions of menopause, such as CHD, there remain many unanswered questions. What are the risks associated with progestin? Is topical estrogen truly safe? Does the type of estrogen and delivery system have an impact on the safety profile? A recent systematic review and meta-analysis of the commonly used estrogen preparations showed that CEE and oral and transdermal 17 B-estradiol have consistent and comparable efficacy in the treatment of hot flashes and may have similar short-term adverse effects.24 But current clinical trials have many limitations, and further testing is needed to answer many remaining questions. Until clear strategies become available for HRT, the role of the physician continues to be that of a medical advisor helping patients make well-informed, personal, and thoughtful decisions.
—Shou Ling Leong, MD
She did very well with estrogen. Her hot flashes and night sweats disappeared and she felt great. However, after hearing news reports about the danger of estrogen, she discontinued the hormone pills a few months ago. She is now feeling poorly with hot flashes, night sweats, vaginal dryness, and occasional stress incontinence. She has many questions and concerns and eagerly seeks your advice about what to do.
Medical history
- Borderline hypertension
- Hyperlipidemia
- Obesity: body-mass index of 32
Family history
- Mother, age 75, has hyperlipidemia, hypertension, myocardial infarction (MI) at age 60, and osteoporosis
- Father, died at age 55 of MI; had hypertension and diabetes
- Her grandparents also had history of stroke and heart disease, but she doesn’t know all the details about their health. She believes her maternal grandmother broke her hip when she was elderly.
Social history
- Married, 2 children, works as an attorney with the local government. Her job is fairly demanding
- Does not smoke, occasional alcohol consumption
- Does not exercise on a regular basis
Review of systems
Negative except for hot flashes, night sweats, vaginal dryness, and occasional stress incontinence.
Physical examination
- Alert female in no distress. Blood pressure, 145/90 mm Hg; weight, 165 lbs; pulse, 82; respiration, 18; temperature, 98.1°F
- HEENT exam, normal
- Neck, heart, lung, abdomen, breast, and pelvic exams are all normal except for mild atrophic changes of the vaginal and genital tracts.
You perform the gynecologic exam and order a mammogram. Mrs JC has not been seen for 2 years. Her lipid profile done 2 years ago was elevated, but Mrs JC did not repeat the tests as requested. You explain that you would like to further define her risk factors and would like to order a few tests. Making a well-informed decision on hormone replacement therapy (HRT) is complex and requires more information and adequate time for a full discussion. You would like to see her after her laboratory tests and will reserve time to address her concerns and questions.
Laboratory tests
Complete blood count, normal
Cholesterol, 250 mg/dL (LDL, 130 mg/dL; HDL, 45 mg/dL)
Triglyceride, 220 mg/dL
Electrolytes, blood urea nitrogen/creatine (BUN/Cr) ratio, normal; glucose, 85 mg/dL
Mrs JC has many symptoms of menopause:
- Vasomotor instability
- Urogenital symptoms She also has risk factors:
- Cardiac: hypertension, hyperlipidemia, obesity
- Osteoporosis: family history, sedentary lifestyle
Before addressing Mrs JC’s specific concerns, you review the findings of the Women’s Health Initiative (WHI) study,1,2 which probably prompted her concerns. You also have been asked to lead an upcoming geriatric grand round presentation on HRT, and you further prepare for both encounters by meeting with colleagues Dr Richard Pees, a gynecologist, and Dr Deborah Erickson, a urologist, to discuss practical applications of the WHI findings.
Findings of the WHI
WHI, sponsored by the National Institute of Health, comprised 2 multicentered clinical trials to determine if conjugated equine estrogen (CEE) given alone for women who had a hysterectomy or in combination with progestin (MPA, medroxyprogesterone acetate) would reduce the risk of cardiovascular events. The study also assessed the long-term risks and benefits of postmenopausal hormone therapy in other chronic disease prevention.
Exclusion criteria for the study included competing risks with survival <3 years, prior breast cancer, low hematocrit or platelets, severe menopausal symptoms, alcoholism, mental illness, and dementia. In this study, 27,000 women aged 50 to 79 years (mean age, 63) were randomized to take hormone or placebo.
The combined CEE/MPA (Prempro) trial, with 16,000 women enrolled, was discontinued at 5.2 years, on July 2002. The unopposed CEE (Premarin) trial, with 11,000 women, was discontinued at 6.8 years, on February 2004. The study was stopped earlier than planned (2005) because of increased adverse events in the group taking hormone.
TABLE 1 summarizes the absolute risks—number of events per 10,000 as compared with the control group—for both arms of the study. In the CEE/MPA arm, there were more cases per 10,000 of coronary heart disease (+7), breast cancer (+8), stroke (+8), and venous thromboembolic disease (VTE) including deep vein thrombosis/pulmonary embolism (DVT/PE) (+18). However, there were fewer cases per 10,000 of colorectal cancer (–6) and hip fracture (–5).
Recently published data2 on the unopposed estrogen arm showed an increase in stroke (+12) and VTE (+7). No significant increase was noted for coronary heart disease (CHD) (–5) or breast cancer (–7). While there is a reduction in osteoporotic fracture (–6) in the hormone arm, there is no significant difference in colorectal cancer (+1). The CEE arm demonstrated that CEE does not significantly affect the incidence of CHD, a difference compared with the CEE/MPA arm. Potential explanations for this include the role of progestin, differences in the study populations, and the role of chance. The reduction of breast cancer incidence was unanticipated and required further investigation.
A:_____________________________________________________________________
_______________________________________________________________________
Dr Pees: The WHI data do seem to confuse the issue of when to use hormonal therapy. The answer to your question lies in knowing how the WHI risks were calculated.
The WHI authors described 2 confidence indexes (CI). The first was calculated as if looking at a single outcome variable, a nominal CI; the second, an adjusted CI, took into account multiple outcomes.
For the CEE/MPA arm, when the nominal CI is used, CHD and breast cancer risks barely reached clinical significance; colon cancer and fracture reduction reached clinical significance; DVT and strokes were also clinically significant using both CIs. When the adjusted CI is used, DVT/strokes, and to a lesser degree fracture reduction, retain clinical significance.
In the CEE-only arm (February 2004 report), DVT/strokes were the only variable that reached clinical significance. CHD/breast cancer/colorectal cancer did not reach clinical significance, and fracture reduction only a slight decrease in risk.
The WHI study introduced a new term, the Global Index, which had not been tested for validity or significance of assigning weights to various outcomes. Additionally, there were certain biases in the construct of the study. Included were 1200 individuals who had prior MI, revascularization procedures, stroke, DVT, and PE. Excluded were those with severe menopausal symptoms, prior fracture/low bone mineral density (BMD), and cognitive function deficits. Also, only 10% of the group was in the 50- to 54-year-old group; 25% were in the 70- to 79-year-old group. The dropout rate was fairly high: 42% in the CEE/MPA arm, and 38% placebo arm; only 25% of the CEE/MPA arm remained at the study termination. Unblinding occurred in 40% of the CEE/MPA arm and 5.4% in the placebo arm.
It is worth noting that CHD increased in the first year of the study but decreased in subsequent years. VTE/DVT and total fractures were the only 2 items that achieved true clinical significance. Total fracture reduction was 1.6 times greater than the increases in CHD and breast cancer; and the fact that breast cancers double every 300 days and are present for 7 to 8 years before they are detected with current diagnostic testing.
Despite the biases and limitations of the data presented by the WHI report, the study does add to our knowledge and it should be included in our discussion with patients when addressing HRT.
A:____________________________________________________________________
______________________________________________________________________
Dr Pees: The WHI data have altered the way in which I counsel patients. I still prescribe hormone therapy within the American College of Obstetricians and Gynecologists (ACOG) guidelines, and, after a very thorough discussion, reference the WHI data. This is to ensure that patients make informed decisions about continuing or starting hormone therapy. Following ACOG recommendations, I evaluate each patient’s risk profile. I start treatment with the lowest effective dose to relieve symptoms. I discuss the use of alternative treatments for menopausal symptoms and osteoporosis prevention, as well as evaluation and treatment for quality of life issues. Most importantly I encourage periodic re-evaluation for hormone use.
After the WHI study was terminated, the North American Menopause Society (NAMS) convened an expert Hormone Therapy Advisory Panel to examine the data and prepare a report. A position statement on the recommendations for clinical practice was released in September 2003.2 The expert panel reached consensus on the following areas:
- The primary indication for systemic hormone therapy is moderate and severe menopausal symptoms: Hot flashes, night sweats/insomnia, mood swings.
- When treating moderate and severe urogenital atrophy (vaginal dryness, dyspareunia, urinary frequency, and incontinence), local estrogen preparations are preferred.
- The primary indication for progestogen is endometrial protection for all women with an intact uterus using systemic estrogen therapy (ET).
- Hormone therapy should not be used for primary or secondary prevention of CHD.
- Breast cancer risk is increased with ET and, to a greater extent, with estrogen progestogen therapy (EPT) used beyond 5 years.
- There is definitive evidence for EPT efficacy in reducing the risk of fracture. However, other effective alternate forms of therapy are readily available. Because of potential risk associated with long-term use of EPT, the risks and benefits of each option should be discussed with the patient.
- EPT is not recommended for primary prevention of dementia.
- Hormone therapy should be limited to the shortest duration to achieve treatment goals, taking into consideration the impact on quality of life.
- Lower-than-standard doses of EPT and ET should be considered (including 0.3 mg conjugated estrogen, 0.25–0.5 mg oral micronized 17 B-estradiol and 0.025 mg 17 B-estradiol patches). However, the long-term risk-benefit ratio has not been demonstrated.
- Extended use of ET/EPT is acceptable if the woman feels the benefits of symptom relief outweigh the risks, an attempt to withdraw ET has failed, or to prevent osteoporotic fracture when alternative therapies are not appropriate or usable.
TABLE 1
Absolute risks of HRT
| Differences between treatment and control groups; cases per 10,000 person-years | ||
|---|---|---|
| CEE/MPA | CEE | |
| Coronary heart disease | +7 | –5 |
| Breast cancer | +8 | –7 |
| Stroke | +8 | +12 |
| Venous thromboembolic disease | +18 | +7 |
| Colorectal cancer | –6 | +1 |
| Hip fracture | –5 | –6 |
| CEE/MPA, conjugated equine estrogen/medroxyprog-esterone acetate; CEE, conjugated equine estrogen. | ||
Menopausal symptoms
A:____________________________________________________________________
______________________________________________________________________
Dr. Leong: Because estrogen is the most effective treatment for menopausal symptoms, Mrs JC may yet consider taking it on a short-term basis, if her symptoms are debilitating. We should use the lowest dose required to control symptoms. She has already stopped her therapy, of course. But had she still been taking ET and told you she wished to discontinue it, you could have advised her that, often times, tapering estrogen over several months results in fewer symptoms than when quitting “cold turkey” (TABLES 2 AND 3).
If Mrs JC is absolutely against taking estrogen, several other drugs have been shown to reduce hot flashes. The selective serotonin reuptake inhibitors (SSRIs) were effective in several randomized trials using venlafaxine (Effexor),4 paroxetine (Paxil), and, less effectively, fluoxetine (Prozac).5 Clonidine (Catapres) was effective at reducing hot flushes in some, but not all, clinical trials.6Gabapentin (Neurontin) and megestrol acetate (Megace) are other possible choices.
Complementary and alternative therapies have been very popular among some postmenopausal women as they look for symptom relief. There are mixed data on soy compounds (phytoestrogen and isoflavone), with only 3 of 8 trials demonstrating a beneficial effect.7-9 Black cohosh showed modest benefits, but ginseng, dong quai, red clover, evening primrose oil, vitamin E, acupuncture, wild yam, and progesterone cream were ineffective. The main cautions with these products are that safety and efficacy are not well established and quality control of the products is often lacking.
Dr Erickson:Urinary problems most commonly associated with menopause are incontinence and recurrent urinary tract infections. Fortunately, both of these problems can be reduced with topical estrogen, which has minimal systemic absorption (TABLE 4). For example, a recent study of intravaginal estradiol (25 μg) vs placebo showed that the estrogen-treated group had significant reduction in symptoms (including dysuria, frequent voiding, and incontinence) and urodynamic findings, but no increase in serum estradiol levels or endometrial growth.10 Thus, a topical estrogen could provide the urologic benefits without the risks of systemic treatment. If she wants to avoid estrogen altogether, she has other options.
TABLE 2
Possible tapering schedules for estrogen regimens
| Current hormone regimen | CEE/MPA 0.625/2.5 mg daily |
| Month 1 | CEE/MPA 0.625/2.5 mg qod (x 1 mo) |
| Month 2 | CEE/MPA 0.3/1.5 mg daily (x 1 mo) |
| Month 3 | CEE/MPA 0.3/1.5 mg qod (x 1 mo) |
| Month 4 | CEE 0.3/1.5 mg 2/wk (x 1 mo) |
| Month 5 | Estrogen patch 0.025/wk if needed |
| CEE/MPA, conjugated equine estrogen/medroxyprogesterone acetate; qod, every other day | |
TABLE 3
HRT dosing options
| MEDICATION | DOSAGE |
|---|---|
| Conjugated estrogens (Premarin) | 0.3 mg, 0.45 mg, 0.625 mg, 0.9 mg |
| Estradiol (Estrace) | 0.5 mg, 1 mg, 2 mg(scored tablets) |
| Estradiol patches (Climara/Vivelle) | 0.025 mg/d, 0.0375, 0.05 mg/d |
Urinary tract symptoms
A:_________________________________________________________________
___________________________________________________________________
TABLE 4
Vaginal products for genitourinary atrophy
| PRODUCT | DOSAGE |
|---|---|
| Low-dose estrogen vaginal cream | 0.3 mg 2x/wk |
| Vaginal ring | |
| Estring | 6–9 μg of estrogen/d for 3 mo |
| Femring | 50 to 100 μg/d for vasomotor symptoms |
| Vaginal tablet (Vagifem) | 25 μg of estradiol 2x/wk or 10 μg 2x/wk may be effective for genitourinary atrophy |
Stress incontinence. For stress incontinence, pelvic floor muscle exercises are helpful. These can be done without any assistance if the patient is able to do the exercises and is motivated. For patients with marginal ability or motivation, options include biofeedback training, vaginal weights, electric stimulation, or magnetic stimulation.
Alpha-adrenergic agonists have also been used,11although treatment of stress incontinence is an off-label use for these drugs and they have risks including hypertension and tachycardia. Phenylpropa-nolamine (eg, Entex LA) is the alpha-adrenergic agent with the most reported studies for stress incontinence, but it was withdrawn from the market due to increased risk of cerebrovascular accident.12The alternative now contains pseudoephedrine (eg, Entex PSE) but there are no published trials of pseudoephedrine for stress incontinence.
More recent studies have shown duloxetine (Cymbalta) to be effective,13, 14 although incontinence is currently an offlabel use for it.
Fem-Soft urethral inserts are used by some patients and are covered by Medicare. These soft inserts are held in place by a unique balloon, which expands automatically after insertion and compresses when the patient pulls on the insert to remove it (ie, the balloon does not need to be inflated or deflated in the office). They are similar in width to Foley catheters (16 or 18 Fr) but are shorter, extending only about 1 cm out from the urethral meatus.
Surgical options for stress incontinence include periurethral injections and sling operations. The former involves injecting a bulking material (such as collagen paste) around the urethra to increase its coaptation (urethral closure). It is a simple, almost painless, outpatient procedure with minimal risks, but results vary. Several procedures may be required to achieve continence, and most patients have recurrent incontinence within 5 years.
In contrast, sling operations have a better success rate. Slings can be made from various materials including the patient’s own fascia, cadaveric fascia, animal materials such as porcine intestinal submucosa, or synthetic mesh. Most materials have good short-term results, with stress incontinence cured or significantly improved for over 90% of patients.15 Long-term success depends on the sling material used. The risks and duration of hospitalization depend on the specific materials and techniques, but most slings are inserted either as outpatient surgery or with overnight hospitalization.
Urge incontinence. For urge incontinence, pelvic floor muscle exercises are beneficial because contraction of the pelvic floor inhibits the detrusor by a reflex. This is well described in a book for lay people.16
Anticholinergic drugs are commonly used and are more effective than placebo.11, 17Side effects include dry mouth, constipation, and mental status changes.
Ways to reduce side effects:
- Sustained-release formulations of oxy-butynin (Ditropan XL) or tolterodine (Detrol LA)
- Anticholinergics that are more selective for the bladder, such as tolterodine (Detrol)
- Transdermal oxybutynin (Oxytrol), which decreases the first-pass liver metabolism and minimizes production of metabolites that have side effects of their own
- Trospium chloride (Sanctura), which does not cross the blood-brain barrier and therefore has less effect on the central nervous system.18
Interestingly, magnesium supplementation (MgOH, 350 mg twice daily) was effective for urge incontinence in a placebo controlled trial.19 If conservative treatments fail, the surgical options include sacral nerve stimulation or augmentation cystoplasty. The latter has high morbidity and should be considered only as a last resort for a person with incapacitating incontinence.
Recurrent UTI. For recurrent urinary tract infections, several options are available. Cranberries contain polymeric proanthocyanidins, which inhibit the binding of Escherichia coli to uroepithelial cells. Cranberry juice or cranberry extract tablets were more effective than placebo in the few studies available, but the optimum preparation and dose are unknown.20Also, since the P fimbriae on E coli bind to mannose residues on uroepithelial cells, it is expected that free mannose in the urine might competitively inhibit this binding.
Mannose is sold over the counter as a preventative for urinary tract infections. No published literature supports its use, but it appears harmless.
Another option is methenamine hippurate, which is a urinary tract antiseptic. Controlled trials to date have not proven its efficacy, but adverse events are infrequent.21
Antibiotics can also be used as chronic low-dose prophylaxis or intermittent self-start therapy when infection symptoms occur.22 Best for low-dose prophylaxis are antibiotics with minimal adverse effects on the fecal and vaginal flora, such as trimethoprim alone, trimethoprim/sulfamethoxazole, nitrofurantoin, cephalexin (in minimal doses), and fluoroquinolones.23
Cardiac risk factors
A:_____________________________________________________________________
_______________________________________________________________________
Dr Leong: Mrs JC’s risk factors for heart disease include hypertension, hyperlipidemia, obesity, and family history of CHD. While hormone therapy should not be used to prevent heart disease, there are well-established treatments for hyperlipidemia including diet, exercise, and lipid lowering medications, such as the statins. She should be advised to lose weight. If healthy lifestyle changes do not control her blood pressure, antihypertensive medication would be indicated.
For prevention of osteoporosis, Mrs JC should be advised to start weight-bearing exercise and to include adequate calcium and vitamin D in her diet. Besides estrogen, bisphosphonates, raloxifene, and calcitonin are effective medication for osteoporosis treatment and prevention.
Should the patient be treated with HRT?
A:_________________________________________________________________
___________________________________________________________________
Dr Pees: Mrs JC’s family history of CHD does not contraindicate hormonal therapy. But neither is hormonal therapy indicated to prevent CHD. Mrs JC should be strongly urged to begin an exercise program, diet modifications, and possibly the use of statins. Studies support exercise as a significant factor in reducing the risk of CHD and, to a lesser degree, the risk of breast cancer. If, after thorough counseling with reference to WHI risk findings, Mrs JC wishes to remain on or start hormone therapy, she should start on the lowest effective dosage to relieve her vasomotor symptoms. She should also be reevaluated periodically and be kept appraised of new data as they become available.
Hormone replacement therapy (HRT) has generated fear and confusion among many women. While the absolute risk for diseases associated with hormone use is low, the diseases are devastating. Breast cancer and stroke are 2 of the most feared illnesses, yet research studies often provided conflicting results on the risk of hormone replacement associated with these conditions.
Individualize every decision
The calculation of risks/benefits ratio has changed with the WHI data. All patients on HRT must be counseled on the new data, ideally in a face-to-face visit. Phone calls for medication refill, annual exam, and regular office visits are opportunities to revisit the subject of hormone therapy (HT). Given the mixed benefits and risks associated with HT, every decision should be individualized. A patient-centered counseling approach would allow a shared decision: the patient expresses her needs, goals, and preferences, and the physician applies medical knowledge to his and her values. In this dynamic approach, the physician can shift from a directive to a nondirective posture, taking the lead vs giving the patient full autonomy. The point in the continuum where the physician chooses to participate is determined by the patient, the physician, and the medical evidence.
The patient’s personal and family histories (breast/colon cancer, stroke, MI, osteoporosis) and risk factors (lipid profile, diet, exercise, body-mass index) play major roles in the decision. However, the patient’s philosophical approach to health often is the determining factor. The physician must provide the facts and ensure a patient is not taking HRT for reasons no longer valid. Questions such as, “What benefits do you hope to gain from HRT?” and “What are your major fears of HRT?” can help facilitate the discussion.
The patient’s philosophy
Patients often will select treatments most consistent with their philosophical approach to health. Patients with a holistic view of healthcare and an uneasiness with HRT are unlikely to have many questions. The patients who could benefit from your counsel are those who stopped HRT due to the findings of the WHI studies and those still on HRT who would like to continue. A recalculation of their individual risk/benefit ratio will help determine if HRT is still the right decision for them.
Considering symptoms
Menopausal symptoms are common and bothersome, often adversely impacting patients’ quality of life. Symptoms should be considered in calculating the risks/benefits ratio, but unfortunately, they are seldom included in research studies. In a UK qualitative study using a “time trade-off” method, participants were asked to make trade-offs between a shorter life span in “perfect health” compared with a longer life span with the condition under study.23 Women reported they might give up 3 months of their life to live the rest of the year without menopausal symptoms, underscoring the importance of menopausal symptoms.
Unanswered questions remain
Though national organizations such as ACOG, NAMS (The North American Menopause Society), and USPSTF (US Preventive Services Task Force) generally agree that estrogen and progestin should not be used routinely to prevent chronic conditions of menopause, such as CHD, there remain many unanswered questions. What are the risks associated with progestin? Is topical estrogen truly safe? Does the type of estrogen and delivery system have an impact on the safety profile? A recent systematic review and meta-analysis of the commonly used estrogen preparations showed that CEE and oral and transdermal 17 B-estradiol have consistent and comparable efficacy in the treatment of hot flashes and may have similar short-term adverse effects.24 But current clinical trials have many limitations, and further testing is needed to answer many remaining questions. Until clear strategies become available for HRT, the role of the physician continues to be that of a medical advisor helping patients make well-informed, personal, and thoughtful decisions.
—Shou Ling Leong, MD
1. Rossouw JE, Anderson GL, Prentice RL, et al. Writing Group for the Women’s Health Initiative Investigators Risks and benefits of estrogen and progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA 2002;288:321-333.
2. Anderson GL, Limacher M, Assaf AR, et al. Women’s Health Initiative Steering Committee Effects of conjugated equine estrogen in postmenopausal women with hysterectomy, the women’s health initiative randomized control trial. The Women’s Health Initiative Steering Committee. JAMA 2004;291:1701-1712.
3. The Hormone Therapy Advisory Panel of the North American Menopause Society position statement on hormone therapy. Available at: www.menopause.org. Accessed on April 1, 2005
4. Loprinzi CL, Kugler JW, Sloan JA, et al. Venlafaxine in management of hot flashes in survivors of breast cancer: a randomised controlled trial. Lancet 2000;356:2059-2063.
5. Stearns V, Beebe KL, Iyengar M, Dube E. Paroxetine controlled release in the treatment of menopausal hot flashes: a randomized controlled trial. JAMA 2003;289:2827-2834.
6. Nagamani M, Kelver ME, Smith ER. Treatment of menopausal hot flashes with transdermal administration of clonidine. Am J Obstet Gynecol 1987;156:561-565.
7. Upmalis DH, Lobo R, Bradley L, Warren M, Cone FL, Lamia CA. Vasomotor symptom relief by soy isoflavone extract tablets in postmenopausal women: a multicenter, double-blind, randomized, placebo-controlled study. Menopause 2000;7:236-242.
8. Tice JA, Ettinger B, Ensrud K, Wallace R, Blackwell T, Cummings SR. Phytoestrogen supplements for the treatment of hot flashes: the isoflavone clover extract (ICE) study: a randomized controlled trial. JAMA 2003;290:207-214.
9. Kronenberg F, Fugh-Berman A. Complementary and alternative medicine for menopausal symptoms: a review of randomized, controlled trials. Ann Intern Med 2002;137:805-813.
10. Simunic V, Banovic I, Ciglar S, Jeren L, Pavicic Baldani D, Sprem M. Local estrogen treatment in patients with urogenital symptoms. Int J Gynecol Obstet 2003;82:187-197.
11. Fantl JA, Newman DK, Colling J, et al. Urinary Incontinence in Adults: Acute and Chronic Management. Clinical Practice Guideline, No. 2; 1996 update. AHCPR Publication No. 96-0682. Rockville, Md: US Department of Health and Human Services, Public Health Services, Agency for Health Care Policy and Research 1996.
12. Kernan WN, Viscoli CM, Brass LM, et al. Phenylpropanolamine and the risk of hemorrhagic stroke. N Engl J Med 2000;343:1826-1832.
13. Millard RJ, Moore K, Rencken R, Yalcin I, Bump RC. Duloxetine UI Study Group Duloxetine vs. placebo in the treatment of stress urinary incontinence: a four-continent randomized clinical trial. BJU International 2004;93:311-318.
14. Dmochowski RR, Miklos JR, Norton PA, Zinner NR, Yalcin I, Bump RC. Duloxetine UI Study Group: Duloxetine versus placebo for the treatment of North American women with stress urinary incontinence J Urol 2003;170:1259-1263.
15. Leach GE, Dmochowski RR, Appell RA, et al. Female stress urinary incontinence clinical guidelines panel summary report on surgical management of female stress urinary incontinence. J Urol 1997;158:875-880.
16. Burgio KL, Pearce KL, Lucco AJ. Staying Dry: A Practical Guide to Bladder Control. Baltimore, Md: Johns Hopkins University Press; 1989.
17. Hay-Smith J, Herbison P, Ellis G, Moore K. Anticholinergic drugs versus placebo for overactive bladder syndrome in adults. Cochrane Database Syst Rev 2002;(3) CD003781.-
18. Halaska M, Ralph G, Weidemann A, et al. Controlled, double-blind, multicentre clinical trial to investigate long-term tolerability and efficacy of trospium chloride in patients with detrusor instability. World J Urol 2003;29:392-399.
19. Gordon D, Groutz A, Ascher-Landsberg J, Lessing JB, David MP, Razz O. Double-blind, placebo-controlled study of magnesium hydroxide for treatment of sensory urgency and detrusor instability: preliminary results. Br J Obstet Gynaecol 1998;105:667-669.
20. Jepson RG, Mihaljevic L, Craig J. Cranberries for preventing urinary tract infections. Cochrane Database Syst Rev 2004;(1) CD001321.-
21. Lee B, Bhuta T, Craig J, Simpson J. Methenamine hippurate for preventing urinary tract infections. Cochrane Database Syst Rev 2002;(1) CD003265.-
22. Schaeffer AJ. Infections of the urinary tract. In: Walsh PC, Retik AB, Vaughan ED, Wein AJ, eds. Campbell’s Urology 8th ed. Philadelphia, Pa: Saunders 2002;515-602.
23. Minelli C, Abrams KR, Sutton AJ, Cooper NJ. Benefits and harms associated with hormone replacement therapy: clinical decision analysis. BMJ 2004;328-371.
24. Nelson H. Commonly used types of postmenopausal estrogen for treatment of hot flashes: Scientific Review. JAMA 2004;292:1610-1619.
Drug brand names
- Calcitonin • Calcimar, Cibacalcin, Miacalcin
- Cephalexin • Biocef, Keflex, Keftab
- Clonidine • Catapres
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Megestrol acetate • Megace
- Nitrofurantoin • Furadantin, Macrobid, Macrodantin
- Oxybutynin • Ditropan, Oxytrol
- Paroxetine • Paxil
- Raloxifene • Evista
- Tolterodine • Detrol
- Trospium chloride • Sanctura
- Venlafaxine • Effexor
CORRESPONDING AUTHOR Shou Ling Leong, MD, Penn State College of Medicine, Penn State Milton S. Hershey Medical Center, P.O. Box 850, Hershey, PA 17033 -0850. E-mail: sleong@psu.edu
1. Rossouw JE, Anderson GL, Prentice RL, et al. Writing Group for the Women’s Health Initiative Investigators Risks and benefits of estrogen and progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA 2002;288:321-333.
2. Anderson GL, Limacher M, Assaf AR, et al. Women’s Health Initiative Steering Committee Effects of conjugated equine estrogen in postmenopausal women with hysterectomy, the women’s health initiative randomized control trial. The Women’s Health Initiative Steering Committee. JAMA 2004;291:1701-1712.
3. The Hormone Therapy Advisory Panel of the North American Menopause Society position statement on hormone therapy. Available at: www.menopause.org. Accessed on April 1, 2005
4. Loprinzi CL, Kugler JW, Sloan JA, et al. Venlafaxine in management of hot flashes in survivors of breast cancer: a randomised controlled trial. Lancet 2000;356:2059-2063.
5. Stearns V, Beebe KL, Iyengar M, Dube E. Paroxetine controlled release in the treatment of menopausal hot flashes: a randomized controlled trial. JAMA 2003;289:2827-2834.
6. Nagamani M, Kelver ME, Smith ER. Treatment of menopausal hot flashes with transdermal administration of clonidine. Am J Obstet Gynecol 1987;156:561-565.
7. Upmalis DH, Lobo R, Bradley L, Warren M, Cone FL, Lamia CA. Vasomotor symptom relief by soy isoflavone extract tablets in postmenopausal women: a multicenter, double-blind, randomized, placebo-controlled study. Menopause 2000;7:236-242.
8. Tice JA, Ettinger B, Ensrud K, Wallace R, Blackwell T, Cummings SR. Phytoestrogen supplements for the treatment of hot flashes: the isoflavone clover extract (ICE) study: a randomized controlled trial. JAMA 2003;290:207-214.
9. Kronenberg F, Fugh-Berman A. Complementary and alternative medicine for menopausal symptoms: a review of randomized, controlled trials. Ann Intern Med 2002;137:805-813.
10. Simunic V, Banovic I, Ciglar S, Jeren L, Pavicic Baldani D, Sprem M. Local estrogen treatment in patients with urogenital symptoms. Int J Gynecol Obstet 2003;82:187-197.
11. Fantl JA, Newman DK, Colling J, et al. Urinary Incontinence in Adults: Acute and Chronic Management. Clinical Practice Guideline, No. 2; 1996 update. AHCPR Publication No. 96-0682. Rockville, Md: US Department of Health and Human Services, Public Health Services, Agency for Health Care Policy and Research 1996.
12. Kernan WN, Viscoli CM, Brass LM, et al. Phenylpropanolamine and the risk of hemorrhagic stroke. N Engl J Med 2000;343:1826-1832.
13. Millard RJ, Moore K, Rencken R, Yalcin I, Bump RC. Duloxetine UI Study Group Duloxetine vs. placebo in the treatment of stress urinary incontinence: a four-continent randomized clinical trial. BJU International 2004;93:311-318.
14. Dmochowski RR, Miklos JR, Norton PA, Zinner NR, Yalcin I, Bump RC. Duloxetine UI Study Group: Duloxetine versus placebo for the treatment of North American women with stress urinary incontinence J Urol 2003;170:1259-1263.
15. Leach GE, Dmochowski RR, Appell RA, et al. Female stress urinary incontinence clinical guidelines panel summary report on surgical management of female stress urinary incontinence. J Urol 1997;158:875-880.
16. Burgio KL, Pearce KL, Lucco AJ. Staying Dry: A Practical Guide to Bladder Control. Baltimore, Md: Johns Hopkins University Press; 1989.
17. Hay-Smith J, Herbison P, Ellis G, Moore K. Anticholinergic drugs versus placebo for overactive bladder syndrome in adults. Cochrane Database Syst Rev 2002;(3) CD003781.-
18. Halaska M, Ralph G, Weidemann A, et al. Controlled, double-blind, multicentre clinical trial to investigate long-term tolerability and efficacy of trospium chloride in patients with detrusor instability. World J Urol 2003;29:392-399.
19. Gordon D, Groutz A, Ascher-Landsberg J, Lessing JB, David MP, Razz O. Double-blind, placebo-controlled study of magnesium hydroxide for treatment of sensory urgency and detrusor instability: preliminary results. Br J Obstet Gynaecol 1998;105:667-669.
20. Jepson RG, Mihaljevic L, Craig J. Cranberries for preventing urinary tract infections. Cochrane Database Syst Rev 2004;(1) CD001321.-
21. Lee B, Bhuta T, Craig J, Simpson J. Methenamine hippurate for preventing urinary tract infections. Cochrane Database Syst Rev 2002;(1) CD003265.-
22. Schaeffer AJ. Infections of the urinary tract. In: Walsh PC, Retik AB, Vaughan ED, Wein AJ, eds. Campbell’s Urology 8th ed. Philadelphia, Pa: Saunders 2002;515-602.
23. Minelli C, Abrams KR, Sutton AJ, Cooper NJ. Benefits and harms associated with hormone replacement therapy: clinical decision analysis. BMJ 2004;328-371.
24. Nelson H. Commonly used types of postmenopausal estrogen for treatment of hot flashes: Scientific Review. JAMA 2004;292:1610-1619.
Drug brand names
- Calcitonin • Calcimar, Cibacalcin, Miacalcin
- Cephalexin • Biocef, Keflex, Keftab
- Clonidine • Catapres
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Megestrol acetate • Megace
- Nitrofurantoin • Furadantin, Macrobid, Macrodantin
- Oxybutynin • Ditropan, Oxytrol
- Paroxetine • Paxil
- Raloxifene • Evista
- Tolterodine • Detrol
- Trospium chloride • Sanctura
- Venlafaxine • Effexor
CORRESPONDING AUTHOR Shou Ling Leong, MD, Penn State College of Medicine, Penn State Milton S. Hershey Medical Center, P.O. Box 850, Hershey, PA 17033 -0850. E-mail: sleong@psu.edu