User login
Hyperbaric Oxygen for a U.S. Soldier with Oral Trauma
Milk-Alkali Syndrome [published correction appears in: Fed Pract. 2005;22(3):66.]
Newly diagnosed hypertension and depressive symptoms: How would you treat?
Medical history
- No other significant medical or psychiatric problems
- Married, with 2 teenaged children
- Employed as an administrator for an insurance company (>50 hrs/wk)
- Drinks 3 to 4 alcoholic beverages/wk
- Does not smoke
- Enjoys fishing and other outdoor activities
- Both parents had hypertension; father also had peripheral vascular disease
Examination
- Patient is in no acute distress
- Approximately 30 pounds over ideal body weight
- Other vital signs are normal
- Normal retinal examination, no carotid bruits, and clear lungs. Cardiac rate and rhythm are regular; no abdominal bruits
- Laboratory studies reveal normal renal function; cholesterol, 184 mg/dL; low-density lipoprotein (LDL) cholesterol, 129 mg/dL; high-density lipoprotein (HDL) cholesterol, 55 mg/dL; triglycerides, 163 mg/dL. Electrocardiogram shows no current or prior evidence of ischemia or left-ventricular strain.
Additional information is required in a number of domains. Blood pressure readings should be repeated to make an accurate diagnosis of hypertension. While the patient may have hypertension, only a single blood pressure reading is elevated. The Joint National Committee on Blood Pressure (JNC 7) specifications1 state that 2 such readings on different days are needed to confirm a diagnosis of hypertension. The symptoms of claudication should be investigated. Physical examination should focus on auscultation for bruits and on the examination of eye grounds to further investigate the possibility of peripheral vascular disease (PVD). In addition, a lipid profile should be drawn. While guidelines are conflicting, consideration should be given to assessing a fasting glucose, potassium, and renal function. Other tests, such as a C-reactive protein, are more controversial.2
The patient opts for drug treatment of his hypertension, and begins taking atenolol 50 mg/d (in addition to aspirin 81 mg/d). He is scheduled to follow-up by phone in 1 week to assure compliance and in 3 months in the office.
On a return visit to the office 3 months later, the patient reports the recent onset of fatigue.
Q: What is the differential diagnosis of the patient’s symptoms? What additional information might you like to know? A:__________________________________
____________________________________
On further questioning he reports that he initially tolerated the beta-blocker without problem, but more recently has experienced low energy and poor sleep (with early morning awakening); he acknowledges decreases in libido, interest in pleasurable activities (eg, hunting, fishing), and his ability to concentrate. He has gained 5 to 10 pounds in the last month.
Although he denies feeling “sad,” he says his emotions seem “flat.” He denies having thoughts of suicide, increased anxiety, symptoms of hypomania, or psychotic symptoms. He describes a mild increase in stress at work, and he feels that the process of preparing for his son to go to college had been “a big burden.” He says there are no other stressors.
The patient’s alcohol use has not changed significantly, and he reports being compliant with his new medication regimen.
When his father died 6 years earlier, he experienced similar symptoms; at no other time have such symptoms occurred. The patient reports no other new physical symptoms, and his physical examination is essentially unchanged from the exam conducted 3 months earlier. His vital signs are normal, including a blood pressure of 128/84 mm Hg.
Consider the differential diagnosis of the patient’s abnormal mood and neurovegetative symptoms. In the primary care setting, the differential diagnosis of depressed mood is broad (Table 1 ), including medical disorders and a variety of psychiatric syndromes.
Medical conditions to consider include a medication induced side effect, hypothyroidism (a metabolic masquerader of depression), anemia, sleep disorder (eg, sleep apnea), and alcohol abuse. PVD should also be considered—his symptoms may be secondary to poor perfusion of the cerebral cortex.
TABLE 1
Partial differential diagnosis of depressed mood and neurovegetative symptoms
| General medical conditions |
| Endocrine: hypothyroidism, Cushing’s syndrome |
| Hematologic: anemia |
| Nutritional: vitamin B12 deficiency |
| Neurologic: movement disorders (eg, Parkinson’s disease, Huntington’s disease), head trauma, seizure disorders |
| Vascular: peripheral vascular disease, cerebrovascular accident |
| Sleep disorders: sleep apnea, narcolepsy |
| Neoplastic: pancreatic, lung, central nervous system neoplasms |
| Substance abuse disorders |
| Alcohol, benzodiazepine, or barbiturate dependence |
| Cocaine or amphetamine withdrawal |
| Psychiatric disorders |
| Major depressive disorder |
| Dysthymia |
| Adjustment disorder with depressed mood |
| Bipolar disorder |
What effects might beta-blockers be having on his mood, energy level, and libido?
You call a psychiatrist colleague for an informal consultation.
Psychiatrist’s comments
It is important to distinguish major depression from other, less severe depressive syndromes. In major depression, 5 out of 9 symptoms (including depressed mood or anhedonia) are present most of the day nearly every day for 2 weeks.
With adjustment disorder and so-called minor depression, symptoms are fewer or less persistent (Table 2).
This distinction is important, as antidepressants are effective for major depression, but they have not yet been shown effective for adjustment disorders or minor depression. Major depression is the “hypertension of mental illness in primary care”—common, often undiagnosed, and associated with poor outcomes. Therefore, accurate diagnosis and appropriate treatment for major depression are essential.
Given the possibility of a depressive syndrome, gather further information to determine the duration of ongoing symptoms, and obtain answers to a short questionnaire (eg, the Beck Depression Inventory [BDI]3 or the PHQ-94). Elicit a family history of mood disorder, or personal history suggestive of thyroid dysfunction, a sleep disorder, or alcohol or drug abuse. Order a complete blood count (CBC) to evaluate for anemia, a thyroid-stimulating hormone (TSH) to evaluate for hypothyroidism, and, if indicated by history, a sleep study.
Beta-blockers and depression. The patient’s symptoms developed in the context of beta-blocker therapy. From the 1970s through the 1990s, the lore was that beta-blockers caused depression and should be avoided in patients with a history of depression. Because of this, many patients with myocardial infarction (MI) and congestive heart failure (CHF) have been denied treatment with beta-blockers when otherwise indicated.
Fortunately, a recent rigorous academic study of this issue was conducted by Ko and colleagues5 to rationally guide treatment. This study involved a meta-analysis of 15 randomized controlled trials of beta-blocker therapy in patients with MI, CHF, or hypertension; the authors found that beta-blockers were associated with a slight (though statistically significant) increase in fatigue and sexual dysfunction, and that their use was not associated with depressive symptoms. This is the best review to date of beta-blockers and depression, and it debunks the myth that beta-blockers cause depression—a myth that has prevented many post-MI patients from receiving much-needed beta-blocker therapy. In short, although idiosyncratic reactions are possible, it is unlikely the patient’s use of atenolol caused his apparent depressive symptoms.
TABLE 2
Major depression, minor depression, and adjustment disorder
| Major depressive disorder |
| Requires depressed mood or loss of interest/pleasure (anhedonia) most of the day, nearly every day for 2 weeks, with a total of 5 (out of 9) depressive symptoms, and resulting in functional impairment. |
| Minor depression (research criteria) |
| Requires depressed mood or loss of interest/pleasure (anhedonia) most of the day, nearly every day for 2 weeks, with a total of 2 to 4 depressive symptoms, and without history of major depressive disorder. |
| Adjustment disorder |
| Mood or anxiety symptoms occur within 3 months of a stressful life event. Such symptoms are in excess of the symptoms that would normally be expected as a result of the event or impair function. The symptoms do not meet criteria for major depressive disorder, bereavement, or another major psychiatric disorder. |
| Source: Adapted from DSM-IV.14 |
Further primary care evaluation
The patient has no cold intolerance or other symptoms of thyroid dysfunction. He does report a long history of snoring, confirmed by his wife. However, he did not notice feeling more fatigued after starting atenolol.Nonetheless, you switch his antihypertensive medication from atenolol to hydrochlorothiazide. In addition, you order a CBC, serum chemistries, a thyroid panel, and a sleep study. The patient is told to return for a follow-up appointment in 2 weeks and to call before that if symptoms worsen.
A:_______________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________
In this situation, the evidence (depressive symptoms in the context of good blood-pressure control) was insufficient to justify a switch from a beta-blocker to hydrochlorothiazide. One could argue that the switch was reasonable regardless of his depressive symptoms; the most recent guidelines from JNC 71 indicate that thiazide diuretics are first-line therapy for hypertension in patients without CAD, and that beta-blockers are not the first-line agent in the patient’s clinical situation.
But discontinuing atenolol because of ongoing depressive symptoms is not supported. The patient may well need a beta-blocker in the future (eg, if he were to develop CAD). By prematurely concluding that the beta-blocker caused adverse effects, we may be denying him an important treatment down the road.
Option 1: 2-week drug holiday
If there was concern that the patient was having an idiosyncratic reaction to atenolol, or if he developed substantial fatigue or sexual dysfunction, a 2-week drug holiday could be conducted while carefully monitoring blood pressure and depressive symptoms. Atenolol could then be restarted to identify a temporal relationship between the symptoms and the medication.
Option 2: Treat for depression
Another option would be to treat the patient as if his symptoms represented depression. Exhibiting 4 of the necessary diagnostic criteria, the patient nearly qualifies for a diagnosis of current major depression. An antidepressant could be started, exercise could be prescribed, or a referral could be made for psychotherapy. However, again there is insufficient evidence that his subsyndromal depression will respond to standard treatments designed for major depressive disorder.
The patient returns as scheduled 2 weeks later. He has tolerated the change in blood pressure medications without difficulty, but he is experiencing persistent anhedonia, terminal insomnia, and low levels of concentration, energy, and libido. He has felt increasingly hopeless and worthless over the past 2 weeks, though he denies having thoughts of suicide. Results on CBC, serum chemistries, thyroid panel, and sleep study are all unremarkable.
The patient now clearly meets criteria for a major depressive episode. As a first step, he should be educated about depression. An excellent self-help book is Getting Your Life Back by Wright and Basco.6 The patient should be taught to monitor his symptoms with the BDI3 or the PHQ-94 to better assess the severity of the current episode, to monitor changes in his symptoms, and to rapidly identify relapses.
Most physicians would start an antidepressant, unless the patient had significant objections. Other treatment options, alone or in concert with antidepressant treatment, include exercise or psychotherapy. The patient is an excellent candidate for exercise, given that he has 3 risk factors for CAD: hypertension, a sedentary lifestyle, and obesity (4, if you include depression). Exercising for at least 30 minutes, 2 to 3 times per week, would likely benefit his physical and mental health. In addition to its cardiac benefits, exercise 3 times weekly was found in at least one trial to be as effective as sertraline in treating major depression in outpatients.7
Choosing an antidepressant. A number of factors should be considered in choosing antidepressants, including efficacy, side effect profile, and cost. Table 3 outlines some of the main considerations in the choice of antidepressants for this patient. Note that tricyclic antidepressants are not listed, being contraindicated in CAD because of their tendency to contribute to arrhythmias in the post-MI period. In this patient’s case, mirtazapine should be avoided because of the possibility of weight gain; venlafaxine should be avoided because of hypertension. Sertraline would be an appropriate choice, given that it has been relatively well-studied in persons with CAD.
The patient begins treatment with fluoxetine (10 mg/d, which is then increased to 20 mg/d after several days). His depressive symptoms gradually diminish; he achieves a “50%” reduction of symptoms at follow-up visit 3 weeks later. Two months after fluoxetine was initiated, the patient is nearly euthymic, reporting only 2 depressive symptoms, and is again engaging in usual recreational activities.
TABLE 3
A comparison of antidepressants in the treatment of depressed patients in cardiac populations
| Medication | Class/mechanism | Risks/side effects | Benefits |
| Citalopram | SSRI | Low cost, minimal drug-drug interactions | |
| Escitalopram | SSRI | Newest/least studied agent | Low cost, minimal drug-drug interactions, possibly faster onset and fewer side effects |
| Fluoxetine | SSRI | Long half-life, more drug-drug interactions | |
| Paroxetine | SSRI | Sedation, mild anticholinergic effects | |
| Sertraline | SSRI | Sedation, mild | Best studied in CAD; few drug interactions |
| Mirtazapine | Atypical antidepressant (5HT2, 5HT3, and alpha2 refceptor blockade) | Sedation, weight gain, possible elevation of lipids | No sexual dysfunction |
| Venlafaxine | Selective serotonin and norepinephrine receptor blockade | Elevated blood pressure in 13% at doses of 300 mg or greater | |
| Bupropion | Increases noradrenergic and dopaminergic activity | Initial anxiety | No sexual dysfunction |
| SSRI, selective serotonin reuptake inhibitor; CAD, coronary artery disease | |||
Q: Is depression, like hypertension, a risk factor for the development of coronary artery disease (CAD)? A:____________________________________________________ _____________________________________________________ _____________________________________________________
Whether depression is a risk factor for CAD depends on how one defines a risk factor and whether one is discussing “major” or “minor” risk factors. At least 15 narrative reviews have been written on the relationship between depression and heart disease, but none has examined the epidemiologic evidence for depression as a major risk factor for CAD (Table 4).8
In looking at the 7 main epidemiologic criteria for a risk factor, depression does very well on 4: strength of association, consistency, dose-response effect, and predictability. Numerous studies have shown that depression is clearly and consistently associated with the development of CAD, and that clinical depression appears to predict CAD more robustly than does depressed mood alone.9-12
On 2 of the criteria, specificity and biological plausibility, there is fair evidence for depression as a CAD risk factor. We do not yet know the relative importance of recurrent major depression, dysthymia, BDI scores of 10 or greater, or some other marker of depression as predictors of CAD.
Because mild depressive symptoms may predict CAD, it is unclear what levels of depression increase the risk of CAD and require intervention. Excellent work exists regarding the development of plausible mechanisms by which depression may lead to CAD; however, these mechanisms have yet to be proven. Therefore, the evidence in this domain can only be rated as fair.
Finally, the evidence is incomplete for one important criterion: response to treatment. Only one study has been designed to examine the effect of depression treatments on cardiac risk reduction. This study (the ENRICHD trial13) was a treatment study of post-MI depression that found that cognitive-behavioral therapy did not have a significant impact on reducing recurrent cardiac events.
Based on the most stringent epidemiologic criteria, depression is almost, but not quite, a risk factor for CAD. However, depression is a minor risk factor for CAD, and may someday be considered a major risk factor. While the mechanisms by which depression may lead to CAD have not yet been established, the association between depression and subsequent CAD likely occurs via 2 pathways.
The first pathway is behavioral. Patients with depression have diminished self-care, possibly increasing other CAD risk factors such as smoking, poor diet/hyperlipidemia, diabetes, physical inactivity, and obesity.
The second pathway by which depression may lead to CAD is neuroendocrine. Hyperactivity of the hypothalamic-pituitary-adrenal (HPA) axis and hyperactive sympathomedullary activity may result in elevated cytokine levels, platelet activation, and vascular damage, thereby contributing to CAD.8
TABLE 4
Depression as a risk factor for CAD: a “report card”8
| Risk factor | Strength of evidence |
| Strength of association | Good |
| Predictability | Good |
| Specificity | Fair |
| Consistency | Good |
| Dose-response effect | Good |
| Biological plausibility | Fair |
| Response to treatment | Incomplete |
This case illustrates several important points in the management of depressive symptoms in the family practice setting.
First, patients may present with subsyndromal depressive illness; there is, as yet, no evidence that antidepressants are beneficial in this population, and they expose patients to side effects such as sexual dysfunction.
Second, practitioners in general should not shy away from using beta-blockers where indicated for patients with cardiovascular disease and depression; the link between beta-blockers and depression seems minimal at best.
Third, when patients do present with the syndrome of major depression, it is important to evaluate potential medical contributors (eg, obstructive sleep apnea) when appropriate, and to treat with adequate doses of antidepressants for an adequate duration.
Fourth, the potential effects of depression on the development of CAD give family physicians yet another reason to remain vigilant for the presence of depression in all patients.
Should the FP treat independently? This discussion then leads to the question of when an informal or formal psychiatric consultation is indicated for the treatment of a depressed patient, and when the FP may wish to handle the case independently. The short answer is, of course, “it depends.” As with all areas of medical specialty, FPs will have varying levels of comfort, knowledge, and experience in the treatment of psychiatric disorders, and this will often affect the threshold for obtaining consultation. Furthermore, the number of psychiatric consultants—and thus the opportunity for consultations—varies widely depending on practice location.
Value of informal consultations. In general, FPs are well-equipped to handle patients with uncomplicated major depressive disorder or dysthymia without suicidal ideation or psychotic features. Informal consultation may be useful in cases (as in this case) when it is difficult to distinguish whether the patient meets criteria for major depressive disorder (and therefore requires treatment) or has subthreshold depressive symptoms. In addition, informal consultation can be useful when there is a question about antidepressant agent selection in a specific clinical situation. Finally, informal consultation may be of benefit when there are comorbid psychiatric illnesses, for example, coexisting panic disorder, generalized anxiety disorder, and major depressive disorder.
Opting for formal consultation. Formal psychiatric consultation is often useful when there is a mood disorder with suicidal ideation or psychotic features, when the disorder has been refractory to 2 or more adequate trials of an antidepressant, when there is a question of bipolar disorder (for which monotherapy with antidepressants is contraindicated) or substance use disorder, or for progressively worsening depression despite treatment.
Billing and coding. The logistics of billing for the treatment of comorbid psychiatric disorders by primary care physicians vary with the type of payer and from state to state. Because it is often impractical to modify billing procedures with each patient, it is useful for each practice to develop general billing guidelines for psychiatric disorders billed to Medicaid, Medicare, and the most common managed care organizations in the practice. In general, the physician caring for the patient described in this report would bill for hypertension and depression and get paid under the primary diagnosis of hypertension. When in doubt about whether to bill for a psychiatric disorder, primary care clinicians may include the relevant physical symptom in the billing codes, such as fatigue, headache, insomnia and bill under that code.
· Acknowledgments ·
Portions of this article were presented at the Association of Medicine and Psychiatry Annual Meeting, San Diego, California, November 19, 2003.
1. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Detection, Evaluation, and Treatment of High Blood Report of the Joint National Committee on Prevention, Pressure: the JNC 7 report. JAMA. 2003;289:2560-2572.
2. Danesh J, Wheeler JG, Hirschfield GM, et al. C-reactive protein and other circulating markers of inflammation in the prediction of coronary heart disease. N Engl J Med 2004;350:1387-1397.
3. Beck AT. Beck Depression Inventory. In: Test Critiques, Vol II,. Deyser DJ, Sweetland RC (eds). Kansas City, Mo: Test Corporation of America; 1985;83-87.
4. Spitzer RL, Kroenke K, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001;16:606-613.
5. Ko DT, Hebert PR, Coffey CS, et al. Beta-blocker therapy and symptoms of depression, fatigue, and sexual dysfunction. JAMA. 2002;288:351-357.
6. Basco MR, Wright JH. Getting Your Life Back: The complete Guide to Recovery from Depression. New York: Touchstone; 2002;
7. Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older patients with major depression. Arch Intern Med. 1999;159:2349-2356.
8. Wulsin LR. Is depression a major risk factor for coronary disease? A systematic review of the epidemiologic evidence. Harv Rev Psychiatry. 2004;12:79-93.
9. Barefoot JC, Helms MJ, Mark DB, et al. Depression and long-term mortality risk in patients with coronary artery disease. Am J Cardiol. 1996;78:613-617.
10. Anda R, Williamson D, Jones D, et al. Depressed affect, hopelessness, and the risk of ischemic heart disease in a cohort of U.S. adults. Epidemiology 1993;4:285-294.
11. Ford DE, Mead LA, Chang PF, et al. Depression is a risk factor for coronary artery disease in men: the Precursors Study. Arch Intern Med. 1998;158:1422-1426.
12. Rugulies R. Depression as a predictor for coronary heart disease. a review and meta-analysis. Am J Prev Med 2002;23:51-61.
13. Berkman LF, Blumenthal J, Burg M, et al. Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) Randomized Trial. JAMA 2003;289:3106-3116.
14. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed.Washington, DC: American Psychiatric Press; 1994.
Drug brand names
- Atenolol • Tenormin
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Hydrochlorothiazide • Esidrix, HydroDIURIL, Oretic
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Medical history
- No other significant medical or psychiatric problems
- Married, with 2 teenaged children
- Employed as an administrator for an insurance company (>50 hrs/wk)
- Drinks 3 to 4 alcoholic beverages/wk
- Does not smoke
- Enjoys fishing and other outdoor activities
- Both parents had hypertension; father also had peripheral vascular disease
Examination
- Patient is in no acute distress
- Approximately 30 pounds over ideal body weight
- Other vital signs are normal
- Normal retinal examination, no carotid bruits, and clear lungs. Cardiac rate and rhythm are regular; no abdominal bruits
- Laboratory studies reveal normal renal function; cholesterol, 184 mg/dL; low-density lipoprotein (LDL) cholesterol, 129 mg/dL; high-density lipoprotein (HDL) cholesterol, 55 mg/dL; triglycerides, 163 mg/dL. Electrocardiogram shows no current or prior evidence of ischemia or left-ventricular strain.
Additional information is required in a number of domains. Blood pressure readings should be repeated to make an accurate diagnosis of hypertension. While the patient may have hypertension, only a single blood pressure reading is elevated. The Joint National Committee on Blood Pressure (JNC 7) specifications1 state that 2 such readings on different days are needed to confirm a diagnosis of hypertension. The symptoms of claudication should be investigated. Physical examination should focus on auscultation for bruits and on the examination of eye grounds to further investigate the possibility of peripheral vascular disease (PVD). In addition, a lipid profile should be drawn. While guidelines are conflicting, consideration should be given to assessing a fasting glucose, potassium, and renal function. Other tests, such as a C-reactive protein, are more controversial.2
The patient opts for drug treatment of his hypertension, and begins taking atenolol 50 mg/d (in addition to aspirin 81 mg/d). He is scheduled to follow-up by phone in 1 week to assure compliance and in 3 months in the office.
On a return visit to the office 3 months later, the patient reports the recent onset of fatigue.
Q: What is the differential diagnosis of the patient’s symptoms? What additional information might you like to know? A:__________________________________
____________________________________
On further questioning he reports that he initially tolerated the beta-blocker without problem, but more recently has experienced low energy and poor sleep (with early morning awakening); he acknowledges decreases in libido, interest in pleasurable activities (eg, hunting, fishing), and his ability to concentrate. He has gained 5 to 10 pounds in the last month.
Although he denies feeling “sad,” he says his emotions seem “flat.” He denies having thoughts of suicide, increased anxiety, symptoms of hypomania, or psychotic symptoms. He describes a mild increase in stress at work, and he feels that the process of preparing for his son to go to college had been “a big burden.” He says there are no other stressors.
The patient’s alcohol use has not changed significantly, and he reports being compliant with his new medication regimen.
When his father died 6 years earlier, he experienced similar symptoms; at no other time have such symptoms occurred. The patient reports no other new physical symptoms, and his physical examination is essentially unchanged from the exam conducted 3 months earlier. His vital signs are normal, including a blood pressure of 128/84 mm Hg.
Consider the differential diagnosis of the patient’s abnormal mood and neurovegetative symptoms. In the primary care setting, the differential diagnosis of depressed mood is broad (Table 1 ), including medical disorders and a variety of psychiatric syndromes.
Medical conditions to consider include a medication induced side effect, hypothyroidism (a metabolic masquerader of depression), anemia, sleep disorder (eg, sleep apnea), and alcohol abuse. PVD should also be considered—his symptoms may be secondary to poor perfusion of the cerebral cortex.
TABLE 1
Partial differential diagnosis of depressed mood and neurovegetative symptoms
| General medical conditions |
| Endocrine: hypothyroidism, Cushing’s syndrome |
| Hematologic: anemia |
| Nutritional: vitamin B12 deficiency |
| Neurologic: movement disorders (eg, Parkinson’s disease, Huntington’s disease), head trauma, seizure disorders |
| Vascular: peripheral vascular disease, cerebrovascular accident |
| Sleep disorders: sleep apnea, narcolepsy |
| Neoplastic: pancreatic, lung, central nervous system neoplasms |
| Substance abuse disorders |
| Alcohol, benzodiazepine, or barbiturate dependence |
| Cocaine or amphetamine withdrawal |
| Psychiatric disorders |
| Major depressive disorder |
| Dysthymia |
| Adjustment disorder with depressed mood |
| Bipolar disorder |
What effects might beta-blockers be having on his mood, energy level, and libido?
You call a psychiatrist colleague for an informal consultation.
Psychiatrist’s comments
It is important to distinguish major depression from other, less severe depressive syndromes. In major depression, 5 out of 9 symptoms (including depressed mood or anhedonia) are present most of the day nearly every day for 2 weeks.
With adjustment disorder and so-called minor depression, symptoms are fewer or less persistent (Table 2).
This distinction is important, as antidepressants are effective for major depression, but they have not yet been shown effective for adjustment disorders or minor depression. Major depression is the “hypertension of mental illness in primary care”—common, often undiagnosed, and associated with poor outcomes. Therefore, accurate diagnosis and appropriate treatment for major depression are essential.
Given the possibility of a depressive syndrome, gather further information to determine the duration of ongoing symptoms, and obtain answers to a short questionnaire (eg, the Beck Depression Inventory [BDI]3 or the PHQ-94). Elicit a family history of mood disorder, or personal history suggestive of thyroid dysfunction, a sleep disorder, or alcohol or drug abuse. Order a complete blood count (CBC) to evaluate for anemia, a thyroid-stimulating hormone (TSH) to evaluate for hypothyroidism, and, if indicated by history, a sleep study.
Beta-blockers and depression. The patient’s symptoms developed in the context of beta-blocker therapy. From the 1970s through the 1990s, the lore was that beta-blockers caused depression and should be avoided in patients with a history of depression. Because of this, many patients with myocardial infarction (MI) and congestive heart failure (CHF) have been denied treatment with beta-blockers when otherwise indicated.
Fortunately, a recent rigorous academic study of this issue was conducted by Ko and colleagues5 to rationally guide treatment. This study involved a meta-analysis of 15 randomized controlled trials of beta-blocker therapy in patients with MI, CHF, or hypertension; the authors found that beta-blockers were associated with a slight (though statistically significant) increase in fatigue and sexual dysfunction, and that their use was not associated with depressive symptoms. This is the best review to date of beta-blockers and depression, and it debunks the myth that beta-blockers cause depression—a myth that has prevented many post-MI patients from receiving much-needed beta-blocker therapy. In short, although idiosyncratic reactions are possible, it is unlikely the patient’s use of atenolol caused his apparent depressive symptoms.
TABLE 2
Major depression, minor depression, and adjustment disorder
| Major depressive disorder |
| Requires depressed mood or loss of interest/pleasure (anhedonia) most of the day, nearly every day for 2 weeks, with a total of 5 (out of 9) depressive symptoms, and resulting in functional impairment. |
| Minor depression (research criteria) |
| Requires depressed mood or loss of interest/pleasure (anhedonia) most of the day, nearly every day for 2 weeks, with a total of 2 to 4 depressive symptoms, and without history of major depressive disorder. |
| Adjustment disorder |
| Mood or anxiety symptoms occur within 3 months of a stressful life event. Such symptoms are in excess of the symptoms that would normally be expected as a result of the event or impair function. The symptoms do not meet criteria for major depressive disorder, bereavement, or another major psychiatric disorder. |
| Source: Adapted from DSM-IV.14 |
Further primary care evaluation
The patient has no cold intolerance or other symptoms of thyroid dysfunction. He does report a long history of snoring, confirmed by his wife. However, he did not notice feeling more fatigued after starting atenolol.Nonetheless, you switch his antihypertensive medication from atenolol to hydrochlorothiazide. In addition, you order a CBC, serum chemistries, a thyroid panel, and a sleep study. The patient is told to return for a follow-up appointment in 2 weeks and to call before that if symptoms worsen.
A:_______________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________
In this situation, the evidence (depressive symptoms in the context of good blood-pressure control) was insufficient to justify a switch from a beta-blocker to hydrochlorothiazide. One could argue that the switch was reasonable regardless of his depressive symptoms; the most recent guidelines from JNC 71 indicate that thiazide diuretics are first-line therapy for hypertension in patients without CAD, and that beta-blockers are not the first-line agent in the patient’s clinical situation.
But discontinuing atenolol because of ongoing depressive symptoms is not supported. The patient may well need a beta-blocker in the future (eg, if he were to develop CAD). By prematurely concluding that the beta-blocker caused adverse effects, we may be denying him an important treatment down the road.
Option 1: 2-week drug holiday
If there was concern that the patient was having an idiosyncratic reaction to atenolol, or if he developed substantial fatigue or sexual dysfunction, a 2-week drug holiday could be conducted while carefully monitoring blood pressure and depressive symptoms. Atenolol could then be restarted to identify a temporal relationship between the symptoms and the medication.
Option 2: Treat for depression
Another option would be to treat the patient as if his symptoms represented depression. Exhibiting 4 of the necessary diagnostic criteria, the patient nearly qualifies for a diagnosis of current major depression. An antidepressant could be started, exercise could be prescribed, or a referral could be made for psychotherapy. However, again there is insufficient evidence that his subsyndromal depression will respond to standard treatments designed for major depressive disorder.
The patient returns as scheduled 2 weeks later. He has tolerated the change in blood pressure medications without difficulty, but he is experiencing persistent anhedonia, terminal insomnia, and low levels of concentration, energy, and libido. He has felt increasingly hopeless and worthless over the past 2 weeks, though he denies having thoughts of suicide. Results on CBC, serum chemistries, thyroid panel, and sleep study are all unremarkable.
The patient now clearly meets criteria for a major depressive episode. As a first step, he should be educated about depression. An excellent self-help book is Getting Your Life Back by Wright and Basco.6 The patient should be taught to monitor his symptoms with the BDI3 or the PHQ-94 to better assess the severity of the current episode, to monitor changes in his symptoms, and to rapidly identify relapses.
Most physicians would start an antidepressant, unless the patient had significant objections. Other treatment options, alone or in concert with antidepressant treatment, include exercise or psychotherapy. The patient is an excellent candidate for exercise, given that he has 3 risk factors for CAD: hypertension, a sedentary lifestyle, and obesity (4, if you include depression). Exercising for at least 30 minutes, 2 to 3 times per week, would likely benefit his physical and mental health. In addition to its cardiac benefits, exercise 3 times weekly was found in at least one trial to be as effective as sertraline in treating major depression in outpatients.7
Choosing an antidepressant. A number of factors should be considered in choosing antidepressants, including efficacy, side effect profile, and cost. Table 3 outlines some of the main considerations in the choice of antidepressants for this patient. Note that tricyclic antidepressants are not listed, being contraindicated in CAD because of their tendency to contribute to arrhythmias in the post-MI period. In this patient’s case, mirtazapine should be avoided because of the possibility of weight gain; venlafaxine should be avoided because of hypertension. Sertraline would be an appropriate choice, given that it has been relatively well-studied in persons with CAD.
The patient begins treatment with fluoxetine (10 mg/d, which is then increased to 20 mg/d after several days). His depressive symptoms gradually diminish; he achieves a “50%” reduction of symptoms at follow-up visit 3 weeks later. Two months after fluoxetine was initiated, the patient is nearly euthymic, reporting only 2 depressive symptoms, and is again engaging in usual recreational activities.
TABLE 3
A comparison of antidepressants in the treatment of depressed patients in cardiac populations
| Medication | Class/mechanism | Risks/side effects | Benefits |
| Citalopram | SSRI | Low cost, minimal drug-drug interactions | |
| Escitalopram | SSRI | Newest/least studied agent | Low cost, minimal drug-drug interactions, possibly faster onset and fewer side effects |
| Fluoxetine | SSRI | Long half-life, more drug-drug interactions | |
| Paroxetine | SSRI | Sedation, mild anticholinergic effects | |
| Sertraline | SSRI | Sedation, mild | Best studied in CAD; few drug interactions |
| Mirtazapine | Atypical antidepressant (5HT2, 5HT3, and alpha2 refceptor blockade) | Sedation, weight gain, possible elevation of lipids | No sexual dysfunction |
| Venlafaxine | Selective serotonin and norepinephrine receptor blockade | Elevated blood pressure in 13% at doses of 300 mg or greater | |
| Bupropion | Increases noradrenergic and dopaminergic activity | Initial anxiety | No sexual dysfunction |
| SSRI, selective serotonin reuptake inhibitor; CAD, coronary artery disease | |||
Q: Is depression, like hypertension, a risk factor for the development of coronary artery disease (CAD)? A:____________________________________________________ _____________________________________________________ _____________________________________________________
Whether depression is a risk factor for CAD depends on how one defines a risk factor and whether one is discussing “major” or “minor” risk factors. At least 15 narrative reviews have been written on the relationship between depression and heart disease, but none has examined the epidemiologic evidence for depression as a major risk factor for CAD (Table 4).8
In looking at the 7 main epidemiologic criteria for a risk factor, depression does very well on 4: strength of association, consistency, dose-response effect, and predictability. Numerous studies have shown that depression is clearly and consistently associated with the development of CAD, and that clinical depression appears to predict CAD more robustly than does depressed mood alone.9-12
On 2 of the criteria, specificity and biological plausibility, there is fair evidence for depression as a CAD risk factor. We do not yet know the relative importance of recurrent major depression, dysthymia, BDI scores of 10 or greater, or some other marker of depression as predictors of CAD.
Because mild depressive symptoms may predict CAD, it is unclear what levels of depression increase the risk of CAD and require intervention. Excellent work exists regarding the development of plausible mechanisms by which depression may lead to CAD; however, these mechanisms have yet to be proven. Therefore, the evidence in this domain can only be rated as fair.
Finally, the evidence is incomplete for one important criterion: response to treatment. Only one study has been designed to examine the effect of depression treatments on cardiac risk reduction. This study (the ENRICHD trial13) was a treatment study of post-MI depression that found that cognitive-behavioral therapy did not have a significant impact on reducing recurrent cardiac events.
Based on the most stringent epidemiologic criteria, depression is almost, but not quite, a risk factor for CAD. However, depression is a minor risk factor for CAD, and may someday be considered a major risk factor. While the mechanisms by which depression may lead to CAD have not yet been established, the association between depression and subsequent CAD likely occurs via 2 pathways.
The first pathway is behavioral. Patients with depression have diminished self-care, possibly increasing other CAD risk factors such as smoking, poor diet/hyperlipidemia, diabetes, physical inactivity, and obesity.
The second pathway by which depression may lead to CAD is neuroendocrine. Hyperactivity of the hypothalamic-pituitary-adrenal (HPA) axis and hyperactive sympathomedullary activity may result in elevated cytokine levels, platelet activation, and vascular damage, thereby contributing to CAD.8
TABLE 4
Depression as a risk factor for CAD: a “report card”8
| Risk factor | Strength of evidence |
| Strength of association | Good |
| Predictability | Good |
| Specificity | Fair |
| Consistency | Good |
| Dose-response effect | Good |
| Biological plausibility | Fair |
| Response to treatment | Incomplete |
This case illustrates several important points in the management of depressive symptoms in the family practice setting.
First, patients may present with subsyndromal depressive illness; there is, as yet, no evidence that antidepressants are beneficial in this population, and they expose patients to side effects such as sexual dysfunction.
Second, practitioners in general should not shy away from using beta-blockers where indicated for patients with cardiovascular disease and depression; the link between beta-blockers and depression seems minimal at best.
Third, when patients do present with the syndrome of major depression, it is important to evaluate potential medical contributors (eg, obstructive sleep apnea) when appropriate, and to treat with adequate doses of antidepressants for an adequate duration.
Fourth, the potential effects of depression on the development of CAD give family physicians yet another reason to remain vigilant for the presence of depression in all patients.
Should the FP treat independently? This discussion then leads to the question of when an informal or formal psychiatric consultation is indicated for the treatment of a depressed patient, and when the FP may wish to handle the case independently. The short answer is, of course, “it depends.” As with all areas of medical specialty, FPs will have varying levels of comfort, knowledge, and experience in the treatment of psychiatric disorders, and this will often affect the threshold for obtaining consultation. Furthermore, the number of psychiatric consultants—and thus the opportunity for consultations—varies widely depending on practice location.
Value of informal consultations. In general, FPs are well-equipped to handle patients with uncomplicated major depressive disorder or dysthymia without suicidal ideation or psychotic features. Informal consultation may be useful in cases (as in this case) when it is difficult to distinguish whether the patient meets criteria for major depressive disorder (and therefore requires treatment) or has subthreshold depressive symptoms. In addition, informal consultation can be useful when there is a question about antidepressant agent selection in a specific clinical situation. Finally, informal consultation may be of benefit when there are comorbid psychiatric illnesses, for example, coexisting panic disorder, generalized anxiety disorder, and major depressive disorder.
Opting for formal consultation. Formal psychiatric consultation is often useful when there is a mood disorder with suicidal ideation or psychotic features, when the disorder has been refractory to 2 or more adequate trials of an antidepressant, when there is a question of bipolar disorder (for which monotherapy with antidepressants is contraindicated) or substance use disorder, or for progressively worsening depression despite treatment.
Billing and coding. The logistics of billing for the treatment of comorbid psychiatric disorders by primary care physicians vary with the type of payer and from state to state. Because it is often impractical to modify billing procedures with each patient, it is useful for each practice to develop general billing guidelines for psychiatric disorders billed to Medicaid, Medicare, and the most common managed care organizations in the practice. In general, the physician caring for the patient described in this report would bill for hypertension and depression and get paid under the primary diagnosis of hypertension. When in doubt about whether to bill for a psychiatric disorder, primary care clinicians may include the relevant physical symptom in the billing codes, such as fatigue, headache, insomnia and bill under that code.
· Acknowledgments ·
Portions of this article were presented at the Association of Medicine and Psychiatry Annual Meeting, San Diego, California, November 19, 2003.
Medical history
- No other significant medical or psychiatric problems
- Married, with 2 teenaged children
- Employed as an administrator for an insurance company (>50 hrs/wk)
- Drinks 3 to 4 alcoholic beverages/wk
- Does not smoke
- Enjoys fishing and other outdoor activities
- Both parents had hypertension; father also had peripheral vascular disease
Examination
- Patient is in no acute distress
- Approximately 30 pounds over ideal body weight
- Other vital signs are normal
- Normal retinal examination, no carotid bruits, and clear lungs. Cardiac rate and rhythm are regular; no abdominal bruits
- Laboratory studies reveal normal renal function; cholesterol, 184 mg/dL; low-density lipoprotein (LDL) cholesterol, 129 mg/dL; high-density lipoprotein (HDL) cholesterol, 55 mg/dL; triglycerides, 163 mg/dL. Electrocardiogram shows no current or prior evidence of ischemia or left-ventricular strain.
Additional information is required in a number of domains. Blood pressure readings should be repeated to make an accurate diagnosis of hypertension. While the patient may have hypertension, only a single blood pressure reading is elevated. The Joint National Committee on Blood Pressure (JNC 7) specifications1 state that 2 such readings on different days are needed to confirm a diagnosis of hypertension. The symptoms of claudication should be investigated. Physical examination should focus on auscultation for bruits and on the examination of eye grounds to further investigate the possibility of peripheral vascular disease (PVD). In addition, a lipid profile should be drawn. While guidelines are conflicting, consideration should be given to assessing a fasting glucose, potassium, and renal function. Other tests, such as a C-reactive protein, are more controversial.2
The patient opts for drug treatment of his hypertension, and begins taking atenolol 50 mg/d (in addition to aspirin 81 mg/d). He is scheduled to follow-up by phone in 1 week to assure compliance and in 3 months in the office.
On a return visit to the office 3 months later, the patient reports the recent onset of fatigue.
Q: What is the differential diagnosis of the patient’s symptoms? What additional information might you like to know? A:__________________________________
____________________________________
On further questioning he reports that he initially tolerated the beta-blocker without problem, but more recently has experienced low energy and poor sleep (with early morning awakening); he acknowledges decreases in libido, interest in pleasurable activities (eg, hunting, fishing), and his ability to concentrate. He has gained 5 to 10 pounds in the last month.
Although he denies feeling “sad,” he says his emotions seem “flat.” He denies having thoughts of suicide, increased anxiety, symptoms of hypomania, or psychotic symptoms. He describes a mild increase in stress at work, and he feels that the process of preparing for his son to go to college had been “a big burden.” He says there are no other stressors.
The patient’s alcohol use has not changed significantly, and he reports being compliant with his new medication regimen.
When his father died 6 years earlier, he experienced similar symptoms; at no other time have such symptoms occurred. The patient reports no other new physical symptoms, and his physical examination is essentially unchanged from the exam conducted 3 months earlier. His vital signs are normal, including a blood pressure of 128/84 mm Hg.
Consider the differential diagnosis of the patient’s abnormal mood and neurovegetative symptoms. In the primary care setting, the differential diagnosis of depressed mood is broad (Table 1 ), including medical disorders and a variety of psychiatric syndromes.
Medical conditions to consider include a medication induced side effect, hypothyroidism (a metabolic masquerader of depression), anemia, sleep disorder (eg, sleep apnea), and alcohol abuse. PVD should also be considered—his symptoms may be secondary to poor perfusion of the cerebral cortex.
TABLE 1
Partial differential diagnosis of depressed mood and neurovegetative symptoms
| General medical conditions |
| Endocrine: hypothyroidism, Cushing’s syndrome |
| Hematologic: anemia |
| Nutritional: vitamin B12 deficiency |
| Neurologic: movement disorders (eg, Parkinson’s disease, Huntington’s disease), head trauma, seizure disorders |
| Vascular: peripheral vascular disease, cerebrovascular accident |
| Sleep disorders: sleep apnea, narcolepsy |
| Neoplastic: pancreatic, lung, central nervous system neoplasms |
| Substance abuse disorders |
| Alcohol, benzodiazepine, or barbiturate dependence |
| Cocaine or amphetamine withdrawal |
| Psychiatric disorders |
| Major depressive disorder |
| Dysthymia |
| Adjustment disorder with depressed mood |
| Bipolar disorder |
What effects might beta-blockers be having on his mood, energy level, and libido?
You call a psychiatrist colleague for an informal consultation.
Psychiatrist’s comments
It is important to distinguish major depression from other, less severe depressive syndromes. In major depression, 5 out of 9 symptoms (including depressed mood or anhedonia) are present most of the day nearly every day for 2 weeks.
With adjustment disorder and so-called minor depression, symptoms are fewer or less persistent (Table 2).
This distinction is important, as antidepressants are effective for major depression, but they have not yet been shown effective for adjustment disorders or minor depression. Major depression is the “hypertension of mental illness in primary care”—common, often undiagnosed, and associated with poor outcomes. Therefore, accurate diagnosis and appropriate treatment for major depression are essential.
Given the possibility of a depressive syndrome, gather further information to determine the duration of ongoing symptoms, and obtain answers to a short questionnaire (eg, the Beck Depression Inventory [BDI]3 or the PHQ-94). Elicit a family history of mood disorder, or personal history suggestive of thyroid dysfunction, a sleep disorder, or alcohol or drug abuse. Order a complete blood count (CBC) to evaluate for anemia, a thyroid-stimulating hormone (TSH) to evaluate for hypothyroidism, and, if indicated by history, a sleep study.
Beta-blockers and depression. The patient’s symptoms developed in the context of beta-blocker therapy. From the 1970s through the 1990s, the lore was that beta-blockers caused depression and should be avoided in patients with a history of depression. Because of this, many patients with myocardial infarction (MI) and congestive heart failure (CHF) have been denied treatment with beta-blockers when otherwise indicated.
Fortunately, a recent rigorous academic study of this issue was conducted by Ko and colleagues5 to rationally guide treatment. This study involved a meta-analysis of 15 randomized controlled trials of beta-blocker therapy in patients with MI, CHF, or hypertension; the authors found that beta-blockers were associated with a slight (though statistically significant) increase in fatigue and sexual dysfunction, and that their use was not associated with depressive symptoms. This is the best review to date of beta-blockers and depression, and it debunks the myth that beta-blockers cause depression—a myth that has prevented many post-MI patients from receiving much-needed beta-blocker therapy. In short, although idiosyncratic reactions are possible, it is unlikely the patient’s use of atenolol caused his apparent depressive symptoms.
TABLE 2
Major depression, minor depression, and adjustment disorder
| Major depressive disorder |
| Requires depressed mood or loss of interest/pleasure (anhedonia) most of the day, nearly every day for 2 weeks, with a total of 5 (out of 9) depressive symptoms, and resulting in functional impairment. |
| Minor depression (research criteria) |
| Requires depressed mood or loss of interest/pleasure (anhedonia) most of the day, nearly every day for 2 weeks, with a total of 2 to 4 depressive symptoms, and without history of major depressive disorder. |
| Adjustment disorder |
| Mood or anxiety symptoms occur within 3 months of a stressful life event. Such symptoms are in excess of the symptoms that would normally be expected as a result of the event or impair function. The symptoms do not meet criteria for major depressive disorder, bereavement, or another major psychiatric disorder. |
| Source: Adapted from DSM-IV.14 |
Further primary care evaluation
The patient has no cold intolerance or other symptoms of thyroid dysfunction. He does report a long history of snoring, confirmed by his wife. However, he did not notice feeling more fatigued after starting atenolol.Nonetheless, you switch his antihypertensive medication from atenolol to hydrochlorothiazide. In addition, you order a CBC, serum chemistries, a thyroid panel, and a sleep study. The patient is told to return for a follow-up appointment in 2 weeks and to call before that if symptoms worsen.
A:_______________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________
In this situation, the evidence (depressive symptoms in the context of good blood-pressure control) was insufficient to justify a switch from a beta-blocker to hydrochlorothiazide. One could argue that the switch was reasonable regardless of his depressive symptoms; the most recent guidelines from JNC 71 indicate that thiazide diuretics are first-line therapy for hypertension in patients without CAD, and that beta-blockers are not the first-line agent in the patient’s clinical situation.
But discontinuing atenolol because of ongoing depressive symptoms is not supported. The patient may well need a beta-blocker in the future (eg, if he were to develop CAD). By prematurely concluding that the beta-blocker caused adverse effects, we may be denying him an important treatment down the road.
Option 1: 2-week drug holiday
If there was concern that the patient was having an idiosyncratic reaction to atenolol, or if he developed substantial fatigue or sexual dysfunction, a 2-week drug holiday could be conducted while carefully monitoring blood pressure and depressive symptoms. Atenolol could then be restarted to identify a temporal relationship between the symptoms and the medication.
Option 2: Treat for depression
Another option would be to treat the patient as if his symptoms represented depression. Exhibiting 4 of the necessary diagnostic criteria, the patient nearly qualifies for a diagnosis of current major depression. An antidepressant could be started, exercise could be prescribed, or a referral could be made for psychotherapy. However, again there is insufficient evidence that his subsyndromal depression will respond to standard treatments designed for major depressive disorder.
The patient returns as scheduled 2 weeks later. He has tolerated the change in blood pressure medications without difficulty, but he is experiencing persistent anhedonia, terminal insomnia, and low levels of concentration, energy, and libido. He has felt increasingly hopeless and worthless over the past 2 weeks, though he denies having thoughts of suicide. Results on CBC, serum chemistries, thyroid panel, and sleep study are all unremarkable.
The patient now clearly meets criteria for a major depressive episode. As a first step, he should be educated about depression. An excellent self-help book is Getting Your Life Back by Wright and Basco.6 The patient should be taught to monitor his symptoms with the BDI3 or the PHQ-94 to better assess the severity of the current episode, to monitor changes in his symptoms, and to rapidly identify relapses.
Most physicians would start an antidepressant, unless the patient had significant objections. Other treatment options, alone or in concert with antidepressant treatment, include exercise or psychotherapy. The patient is an excellent candidate for exercise, given that he has 3 risk factors for CAD: hypertension, a sedentary lifestyle, and obesity (4, if you include depression). Exercising for at least 30 minutes, 2 to 3 times per week, would likely benefit his physical and mental health. In addition to its cardiac benefits, exercise 3 times weekly was found in at least one trial to be as effective as sertraline in treating major depression in outpatients.7
Choosing an antidepressant. A number of factors should be considered in choosing antidepressants, including efficacy, side effect profile, and cost. Table 3 outlines some of the main considerations in the choice of antidepressants for this patient. Note that tricyclic antidepressants are not listed, being contraindicated in CAD because of their tendency to contribute to arrhythmias in the post-MI period. In this patient’s case, mirtazapine should be avoided because of the possibility of weight gain; venlafaxine should be avoided because of hypertension. Sertraline would be an appropriate choice, given that it has been relatively well-studied in persons with CAD.
The patient begins treatment with fluoxetine (10 mg/d, which is then increased to 20 mg/d after several days). His depressive symptoms gradually diminish; he achieves a “50%” reduction of symptoms at follow-up visit 3 weeks later. Two months after fluoxetine was initiated, the patient is nearly euthymic, reporting only 2 depressive symptoms, and is again engaging in usual recreational activities.
TABLE 3
A comparison of antidepressants in the treatment of depressed patients in cardiac populations
| Medication | Class/mechanism | Risks/side effects | Benefits |
| Citalopram | SSRI | Low cost, minimal drug-drug interactions | |
| Escitalopram | SSRI | Newest/least studied agent | Low cost, minimal drug-drug interactions, possibly faster onset and fewer side effects |
| Fluoxetine | SSRI | Long half-life, more drug-drug interactions | |
| Paroxetine | SSRI | Sedation, mild anticholinergic effects | |
| Sertraline | SSRI | Sedation, mild | Best studied in CAD; few drug interactions |
| Mirtazapine | Atypical antidepressant (5HT2, 5HT3, and alpha2 refceptor blockade) | Sedation, weight gain, possible elevation of lipids | No sexual dysfunction |
| Venlafaxine | Selective serotonin and norepinephrine receptor blockade | Elevated blood pressure in 13% at doses of 300 mg or greater | |
| Bupropion | Increases noradrenergic and dopaminergic activity | Initial anxiety | No sexual dysfunction |
| SSRI, selective serotonin reuptake inhibitor; CAD, coronary artery disease | |||
Q: Is depression, like hypertension, a risk factor for the development of coronary artery disease (CAD)? A:____________________________________________________ _____________________________________________________ _____________________________________________________
Whether depression is a risk factor for CAD depends on how one defines a risk factor and whether one is discussing “major” or “minor” risk factors. At least 15 narrative reviews have been written on the relationship between depression and heart disease, but none has examined the epidemiologic evidence for depression as a major risk factor for CAD (Table 4).8
In looking at the 7 main epidemiologic criteria for a risk factor, depression does very well on 4: strength of association, consistency, dose-response effect, and predictability. Numerous studies have shown that depression is clearly and consistently associated with the development of CAD, and that clinical depression appears to predict CAD more robustly than does depressed mood alone.9-12
On 2 of the criteria, specificity and biological plausibility, there is fair evidence for depression as a CAD risk factor. We do not yet know the relative importance of recurrent major depression, dysthymia, BDI scores of 10 or greater, or some other marker of depression as predictors of CAD.
Because mild depressive symptoms may predict CAD, it is unclear what levels of depression increase the risk of CAD and require intervention. Excellent work exists regarding the development of plausible mechanisms by which depression may lead to CAD; however, these mechanisms have yet to be proven. Therefore, the evidence in this domain can only be rated as fair.
Finally, the evidence is incomplete for one important criterion: response to treatment. Only one study has been designed to examine the effect of depression treatments on cardiac risk reduction. This study (the ENRICHD trial13) was a treatment study of post-MI depression that found that cognitive-behavioral therapy did not have a significant impact on reducing recurrent cardiac events.
Based on the most stringent epidemiologic criteria, depression is almost, but not quite, a risk factor for CAD. However, depression is a minor risk factor for CAD, and may someday be considered a major risk factor. While the mechanisms by which depression may lead to CAD have not yet been established, the association between depression and subsequent CAD likely occurs via 2 pathways.
The first pathway is behavioral. Patients with depression have diminished self-care, possibly increasing other CAD risk factors such as smoking, poor diet/hyperlipidemia, diabetes, physical inactivity, and obesity.
The second pathway by which depression may lead to CAD is neuroendocrine. Hyperactivity of the hypothalamic-pituitary-adrenal (HPA) axis and hyperactive sympathomedullary activity may result in elevated cytokine levels, platelet activation, and vascular damage, thereby contributing to CAD.8
TABLE 4
Depression as a risk factor for CAD: a “report card”8
| Risk factor | Strength of evidence |
| Strength of association | Good |
| Predictability | Good |
| Specificity | Fair |
| Consistency | Good |
| Dose-response effect | Good |
| Biological plausibility | Fair |
| Response to treatment | Incomplete |
This case illustrates several important points in the management of depressive symptoms in the family practice setting.
First, patients may present with subsyndromal depressive illness; there is, as yet, no evidence that antidepressants are beneficial in this population, and they expose patients to side effects such as sexual dysfunction.
Second, practitioners in general should not shy away from using beta-blockers where indicated for patients with cardiovascular disease and depression; the link between beta-blockers and depression seems minimal at best.
Third, when patients do present with the syndrome of major depression, it is important to evaluate potential medical contributors (eg, obstructive sleep apnea) when appropriate, and to treat with adequate doses of antidepressants for an adequate duration.
Fourth, the potential effects of depression on the development of CAD give family physicians yet another reason to remain vigilant for the presence of depression in all patients.
Should the FP treat independently? This discussion then leads to the question of when an informal or formal psychiatric consultation is indicated for the treatment of a depressed patient, and when the FP may wish to handle the case independently. The short answer is, of course, “it depends.” As with all areas of medical specialty, FPs will have varying levels of comfort, knowledge, and experience in the treatment of psychiatric disorders, and this will often affect the threshold for obtaining consultation. Furthermore, the number of psychiatric consultants—and thus the opportunity for consultations—varies widely depending on practice location.
Value of informal consultations. In general, FPs are well-equipped to handle patients with uncomplicated major depressive disorder or dysthymia without suicidal ideation or psychotic features. Informal consultation may be useful in cases (as in this case) when it is difficult to distinguish whether the patient meets criteria for major depressive disorder (and therefore requires treatment) or has subthreshold depressive symptoms. In addition, informal consultation can be useful when there is a question about antidepressant agent selection in a specific clinical situation. Finally, informal consultation may be of benefit when there are comorbid psychiatric illnesses, for example, coexisting panic disorder, generalized anxiety disorder, and major depressive disorder.
Opting for formal consultation. Formal psychiatric consultation is often useful when there is a mood disorder with suicidal ideation or psychotic features, when the disorder has been refractory to 2 or more adequate trials of an antidepressant, when there is a question of bipolar disorder (for which monotherapy with antidepressants is contraindicated) or substance use disorder, or for progressively worsening depression despite treatment.
Billing and coding. The logistics of billing for the treatment of comorbid psychiatric disorders by primary care physicians vary with the type of payer and from state to state. Because it is often impractical to modify billing procedures with each patient, it is useful for each practice to develop general billing guidelines for psychiatric disorders billed to Medicaid, Medicare, and the most common managed care organizations in the practice. In general, the physician caring for the patient described in this report would bill for hypertension and depression and get paid under the primary diagnosis of hypertension. When in doubt about whether to bill for a psychiatric disorder, primary care clinicians may include the relevant physical symptom in the billing codes, such as fatigue, headache, insomnia and bill under that code.
· Acknowledgments ·
Portions of this article were presented at the Association of Medicine and Psychiatry Annual Meeting, San Diego, California, November 19, 2003.
1. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Detection, Evaluation, and Treatment of High Blood Report of the Joint National Committee on Prevention, Pressure: the JNC 7 report. JAMA. 2003;289:2560-2572.
2. Danesh J, Wheeler JG, Hirschfield GM, et al. C-reactive protein and other circulating markers of inflammation in the prediction of coronary heart disease. N Engl J Med 2004;350:1387-1397.
3. Beck AT. Beck Depression Inventory. In: Test Critiques, Vol II,. Deyser DJ, Sweetland RC (eds). Kansas City, Mo: Test Corporation of America; 1985;83-87.
4. Spitzer RL, Kroenke K, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001;16:606-613.
5. Ko DT, Hebert PR, Coffey CS, et al. Beta-blocker therapy and symptoms of depression, fatigue, and sexual dysfunction. JAMA. 2002;288:351-357.
6. Basco MR, Wright JH. Getting Your Life Back: The complete Guide to Recovery from Depression. New York: Touchstone; 2002;
7. Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older patients with major depression. Arch Intern Med. 1999;159:2349-2356.
8. Wulsin LR. Is depression a major risk factor for coronary disease? A systematic review of the epidemiologic evidence. Harv Rev Psychiatry. 2004;12:79-93.
9. Barefoot JC, Helms MJ, Mark DB, et al. Depression and long-term mortality risk in patients with coronary artery disease. Am J Cardiol. 1996;78:613-617.
10. Anda R, Williamson D, Jones D, et al. Depressed affect, hopelessness, and the risk of ischemic heart disease in a cohort of U.S. adults. Epidemiology 1993;4:285-294.
11. Ford DE, Mead LA, Chang PF, et al. Depression is a risk factor for coronary artery disease in men: the Precursors Study. Arch Intern Med. 1998;158:1422-1426.
12. Rugulies R. Depression as a predictor for coronary heart disease. a review and meta-analysis. Am J Prev Med 2002;23:51-61.
13. Berkman LF, Blumenthal J, Burg M, et al. Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) Randomized Trial. JAMA 2003;289:3106-3116.
14. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed.Washington, DC: American Psychiatric Press; 1994.
Drug brand names
- Atenolol • Tenormin
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Hydrochlorothiazide • Esidrix, HydroDIURIL, Oretic
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
1. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Detection, Evaluation, and Treatment of High Blood Report of the Joint National Committee on Prevention, Pressure: the JNC 7 report. JAMA. 2003;289:2560-2572.
2. Danesh J, Wheeler JG, Hirschfield GM, et al. C-reactive protein and other circulating markers of inflammation in the prediction of coronary heart disease. N Engl J Med 2004;350:1387-1397.
3. Beck AT. Beck Depression Inventory. In: Test Critiques, Vol II,. Deyser DJ, Sweetland RC (eds). Kansas City, Mo: Test Corporation of America; 1985;83-87.
4. Spitzer RL, Kroenke K, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001;16:606-613.
5. Ko DT, Hebert PR, Coffey CS, et al. Beta-blocker therapy and symptoms of depression, fatigue, and sexual dysfunction. JAMA. 2002;288:351-357.
6. Basco MR, Wright JH. Getting Your Life Back: The complete Guide to Recovery from Depression. New York: Touchstone; 2002;
7. Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older patients with major depression. Arch Intern Med. 1999;159:2349-2356.
8. Wulsin LR. Is depression a major risk factor for coronary disease? A systematic review of the epidemiologic evidence. Harv Rev Psychiatry. 2004;12:79-93.
9. Barefoot JC, Helms MJ, Mark DB, et al. Depression and long-term mortality risk in patients with coronary artery disease. Am J Cardiol. 1996;78:613-617.
10. Anda R, Williamson D, Jones D, et al. Depressed affect, hopelessness, and the risk of ischemic heart disease in a cohort of U.S. adults. Epidemiology 1993;4:285-294.
11. Ford DE, Mead LA, Chang PF, et al. Depression is a risk factor for coronary artery disease in men: the Precursors Study. Arch Intern Med. 1998;158:1422-1426.
12. Rugulies R. Depression as a predictor for coronary heart disease. a review and meta-analysis. Am J Prev Med 2002;23:51-61.
13. Berkman LF, Blumenthal J, Burg M, et al. Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) Randomized Trial. JAMA 2003;289:3106-3116.
14. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed.Washington, DC: American Psychiatric Press; 1994.
Drug brand names
- Atenolol • Tenormin
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Hydrochlorothiazide • Esidrix, HydroDIURIL, Oretic
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Over 100 Unnecessary Psychiatric Admissions
Sudden loss of vision
Q: What causes of sudden unilateral vision loss would you consider? What would you do next?
Your examination yields the following:
Medical history
- Borderline hypertension
- Hyperlipidemia (was on a medication but discontinued it on his own)
- Smoking 25 pack-years; quit 2 years ago
- Occasional alcohol intake
- No medications
- Electrical contractor by trade
- Parents living and well; siblings have hypertension but no other illnesses.
Review of systems
Negative except for occasional nasal congestion and low back pain.
Physical examination
- Alert male in no distress. Blood pressure, 146/86 mm Hg; weight, 85 kg; heart rate, 80; respiratory rate, 20; temperature normal; skin warm and dry.
- Head, eyes, ears, nose, throat: pupils are equal, round, and reactive to light and accommodation; extraocular movement intact; retinal exam is depicted in the Figure. Tympanic membranes, throat, and neck normal; carotids normal.
- Heart and lung exam unremarkable. Spleen questionably palpable. Extremities normal. Neurologic exam normal, except for eye findings.
FIGURE
Retinal exam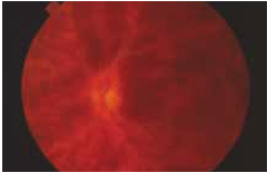
Referring to Harrison’s Textbook of Medicine, you find the following entry:
“Venous occlusion of the retina is often idiopathic, but hypertension, diabetes, and glaucoma are prominent risk factors. The benefit of treatment with anticoagulants is unproven and carries the risk of hemorrhage into the vitreous. Polycythemia, thrombocythemia, or other factors leading to an underlying hypercoagulable state should be corrected.”1
You also reviewed information from UpToDate, which revealed a British article linking retinal venous occlusion with an increased risk of cardiovascular disease. It recommends that clinicians use an algorithm to determine the appropriate treatment.2 Additional research noted various interventions for the venous occlusion itself, but none had sufficient numbers to be considered reliable in recommending treatment.
You have identified 3 problems, 2 of which you deal with regularly and a third that requires consultation:
- Hypertension
- Hyperlipidemia
- Central retinal venous occlusion (CRVO) (rule out underlying hypercoagulable state).
Ophthalmologist’s report
An ophthalmologist confirms a diagnosis of left retinal vein occlusion, and recommends a period of observation, to see if vision returns. The opthalmologist also asks the patient to return to you for an investigation of possible underlying medical conditions.
Further primary care evaluation
The patient’s history suggests nothing that would inhibit a return of vision. Findings on the physical examination are unchanged except for the left fundus. The patient is quite concerned about another “stroke,” particularly in the other eye. He wants a guarantee he will be okay.
Laboratory evaluation:
- Complete blood count, normal
- Urea nitrogen (BUN), 20 mg/dL
- Creatinine kinase, 1.2 mckat/L
- Liver functions within normal limits
- Glucose, 86 mg/dL
- Cholesterol, 230 mg/dL
- Triglycerides, 186 mg/dL
- HDL, 41 mg/dL; LDL, 136 mg/dL
- Total serum protein levels, normal.
Additional time was required by the family physician to coordinate care of this patient. A team management code (99361 for 30 minutes and 99362 for 60 minutes) may not be billed on the same day as an e/m code, as carriers bundle this into the e/m. In addition, most carriers do not pay for the 99361 or 99362 codes. Therefore, the conference should ideally occur the day of an e/m code and be documented with that service. In this instance, the care occurred over several days, so no additional billing was allowed for team management.
Details of central retinal venous occlusion
You assure the patient you will coordinate care with the ophthalmologist, who subsequently offers the following summary about CRVO:
- For most patients with CRVO, vision decreases to 20/100, 20/200, or worse, usually permanently if the occlusion is indeed venous and not arterial as well. If the condition is secondary to ischemia, vision is usually limited to 20/300 or worse, permanently.
- Most patients want their vision “fixed” right away, but that is usually not possible. Hypertension control is most important. Uncommon causes include polycythemia vera, emphysema, sickle cell disease, multiple myeloma, macroglobulinemia, hyperproteinemia, cystic fibrosis of the pancreas, and peritoneal dialysis. Occasionally, it can occur secondary to hypotension, as from a ruptured aortic aneurysm, delivery-associated blood loss, or surgical trauma.
- Hypertension and other atherosclerotic risk factors must be controlled. Treatment with platelet inhibitors is often recommended and glaucoma control is very important, especially for African American patients. Chronic open-angle glaucoma can present as CRVO, and results can be devastating. African Americans are about 100 times more likely than Caucasians to have glaucoma (1/7 vs 3/2000).
Management dos and don’ts
CRVO is entirely different than retinal hemorrhage or vitreous hemorrhage. The correct diagnosis must be confirmed by an ophthalmologist, to ensure proper evaluation and management.
Reduce blood pressure
You return to your patient and share your conversation with the consultant. According to the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) guidelines, the patient has Stage I hypertension. The goal for treatment is medical management to reduce pressure to below 120/80 mm Hg.3
The patient elects treatment with a beta-blocker rather than a thiazide diuretic; he wishes to avoid monitoring of electrolytes that would be necessary because he often becomes dehydrated on the job. He will have the nurse at his company monitor his blood pressure.
Reduce lipids
Also, according to the National Cholesterol Education Program, this patient meets criteria for treatment of hyperlipidemia.4 He is given dietary instruction, information about lipids, a prescription for a statin as he believes he has already been following a quite restrictive diet for over 4 months.
Use anticoagulant?
Finally, you consult a hematologist about the appropriate evaluation for a hypercoagulable state. Following is her report:
- The retinal vein is anatomically different from other veins, being tightly encased in a sheath with the retinal artery and optic nerve. Disorders of these structures can compress or inflame the vein, leading to thrombosis. Consequently, local factors may play a role in development of retinal vein thrombosis—a systemic disorder is not required for this process to occur. CVRO is seldom associated with an underlying hypercoagulable state.5,6
- The effectiveness of medical intervention is unproven. Acute anticoagulation is associated with retinal hemorrhage and is not recommended. Recurrent retinal venous occlusion in the contralateral eye occurs in approximately 12% of patients within 4 years. Because of the risks of anticoagulation and unproven benefits in CRVO, you both elect to avoid this treatment.
If the patient were to request anticoagulation, therapy should be withheld for 2 to 3 months, the time required for retinal perfusion to stabilize. Antiplatelet agents such as aspirin have no role in preventing recurrent venous thrombosis.
Confirmation of this controversy in treatment was obtained using a literature search. A review article in Eye discussed that while the role of thrombophilia is unclear, the need for a randomized study of anticoagulation in the patient with CRVO is needed.6
Final decisions
After considering your consultant’s suggestions, you realize that finding a prothrombotic state is unlikely and will be not change management. Moreover, medical intervention is unlikely to change the natural history of this condition, and it might lead inadvertently to insurance or employment discrimination. You review the previous complete blood count to make sure you have not missed erythrocytosis or thrombocytosis—both of which have well-defined treatments.
Follow-up monitoring was scheduled by the ophthalmologist and you continue to manage the patient’s hypertension and hyperlipidemia.
This patient had a relatively uncommon condition that necessitated consultation with 2 specialists. After weighing the evidence and likelihood of benefit of unproven therapies for CVRO, the patient elected to manage other clear risk factors for atherosclerotic vascular disease. Management of this patient melds issues of ethics and evidence, with core skills to foster a good doctor-patient relationship.
At the risk of sounding like a bad joke, I’d like to open my commentary with the question:
“Why did this patient go to the family physician?” This patient was seen in an urban setting with ample access to any medical specialist, and he had an insurance plan that allowed open access contact with most, if not all, of the physicians in the community. This patient also knew enough about his illness to know that the final answer or treatment for his presenting problem would likely not be found in the family physician’s office.
The value that the family physician brought to this patient can be described as follows:
Navigator/Coordinator: The family physician was able to help this patient through the maze of medical specialists to find the right physicians to evaluate and treat the presenting problem, and to arrange for ongoing evaluation and management after specialist consultations.
Interpreter/Translator: The family physician was able to take the information provided by the specialist physicians and translate that information into language the patient could understand. This process must occur if the patient is expected to comply with treatment, evaluation and lifestyle change recommendations.
Comprehensive caregiver: While supporting the patient in coping with his vision loss, the family physician used this unfortunate occurrence as motivation to address modifiable risk factors—hypertension, obesity, elevated blood glucose, and elevated lipids. Managing these conditions may not be glamorous, but addressing all facets of a patient’s well being is what we family physicians do best. Caring for patients, not just treating illnesses, is a core value of family medicine.
Imagine this patient’s thought process from his arrival with a loss of vision to his departure with a plan to deal with hypertension, obesity, elevated blood glucose, and elevated lipids, all in the context of his job and family and community life. The holistic management of this patient in the context of his life is the main value added by the family physician for this patient. This management also completely supports the patient’s wish to avoid “another stroke.”
One of my colleagues once asked me: “Wouldn’t you like to be the kind of physician whose patient comes in with a cold and leaves with an order for a mammogram?” Family physicians have the knowledge, skills, and perspective necessary to treat the patient, not just the illness. Let’s keep doing what we do best for our patients.
Paul Paulman, MD
1. Harrison’s Principles of Internal Medicine. 15th ed. Eds. Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL. New York, NY: McGraw-Hill; 2001.
2. Martin SC, Butcher A, Martin N, et al. Cardiovascular risk assessment in patients with retinal vein occlusion. Br J Ophthalmol 2002;86:774-776.
3. National Heart, Lung, and Blood Institute. National High Blood Pressure Education Program. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7). 2003. Available at: www.nhlbi.nih.gov/guidelines/hypertension/jncintro.htm. Accessed on March 16, 2004.
4. National Heart, Lung, and Blood Institute. National Cholesterol Education Program. Third Report of the Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Available at: www.nhlbi.nih.gov/guidelines/cholesterol/atp3_rpt.htm. Accessed on March 16, 2004.
5. Layey JM. Hypercoagulable states and central retinal vein occulsion. Curr Opin Pulm Med 2003;9:385-392.
6. Fegan CD. Central retinal vein occlusion and thrombophilia. Eye 2002;26:98-106.
Q: What causes of sudden unilateral vision loss would you consider? What would you do next?
Your examination yields the following:
Medical history
- Borderline hypertension
- Hyperlipidemia (was on a medication but discontinued it on his own)
- Smoking 25 pack-years; quit 2 years ago
- Occasional alcohol intake
- No medications
- Electrical contractor by trade
- Parents living and well; siblings have hypertension but no other illnesses.
Review of systems
Negative except for occasional nasal congestion and low back pain.
Physical examination
- Alert male in no distress. Blood pressure, 146/86 mm Hg; weight, 85 kg; heart rate, 80; respiratory rate, 20; temperature normal; skin warm and dry.
- Head, eyes, ears, nose, throat: pupils are equal, round, and reactive to light and accommodation; extraocular movement intact; retinal exam is depicted in the Figure. Tympanic membranes, throat, and neck normal; carotids normal.
- Heart and lung exam unremarkable. Spleen questionably palpable. Extremities normal. Neurologic exam normal, except for eye findings.
FIGURE
Retinal exam
Referring to Harrison’s Textbook of Medicine, you find the following entry:
“Venous occlusion of the retina is often idiopathic, but hypertension, diabetes, and glaucoma are prominent risk factors. The benefit of treatment with anticoagulants is unproven and carries the risk of hemorrhage into the vitreous. Polycythemia, thrombocythemia, or other factors leading to an underlying hypercoagulable state should be corrected.”1
You also reviewed information from UpToDate, which revealed a British article linking retinal venous occlusion with an increased risk of cardiovascular disease. It recommends that clinicians use an algorithm to determine the appropriate treatment.2 Additional research noted various interventions for the venous occlusion itself, but none had sufficient numbers to be considered reliable in recommending treatment.
You have identified 3 problems, 2 of which you deal with regularly and a third that requires consultation:
- Hypertension
- Hyperlipidemia
- Central retinal venous occlusion (CRVO) (rule out underlying hypercoagulable state).
Ophthalmologist’s report
An ophthalmologist confirms a diagnosis of left retinal vein occlusion, and recommends a period of observation, to see if vision returns. The opthalmologist also asks the patient to return to you for an investigation of possible underlying medical conditions.
Further primary care evaluation
The patient’s history suggests nothing that would inhibit a return of vision. Findings on the physical examination are unchanged except for the left fundus. The patient is quite concerned about another “stroke,” particularly in the other eye. He wants a guarantee he will be okay.
Laboratory evaluation:
- Complete blood count, normal
- Urea nitrogen (BUN), 20 mg/dL
- Creatinine kinase, 1.2 mckat/L
- Liver functions within normal limits
- Glucose, 86 mg/dL
- Cholesterol, 230 mg/dL
- Triglycerides, 186 mg/dL
- HDL, 41 mg/dL; LDL, 136 mg/dL
- Total serum protein levels, normal.
Additional time was required by the family physician to coordinate care of this patient. A team management code (99361 for 30 minutes and 99362 for 60 minutes) may not be billed on the same day as an e/m code, as carriers bundle this into the e/m. In addition, most carriers do not pay for the 99361 or 99362 codes. Therefore, the conference should ideally occur the day of an e/m code and be documented with that service. In this instance, the care occurred over several days, so no additional billing was allowed for team management.
Details of central retinal venous occlusion
You assure the patient you will coordinate care with the ophthalmologist, who subsequently offers the following summary about CRVO:
- For most patients with CRVO, vision decreases to 20/100, 20/200, or worse, usually permanently if the occlusion is indeed venous and not arterial as well. If the condition is secondary to ischemia, vision is usually limited to 20/300 or worse, permanently.
- Most patients want their vision “fixed” right away, but that is usually not possible. Hypertension control is most important. Uncommon causes include polycythemia vera, emphysema, sickle cell disease, multiple myeloma, macroglobulinemia, hyperproteinemia, cystic fibrosis of the pancreas, and peritoneal dialysis. Occasionally, it can occur secondary to hypotension, as from a ruptured aortic aneurysm, delivery-associated blood loss, or surgical trauma.
- Hypertension and other atherosclerotic risk factors must be controlled. Treatment with platelet inhibitors is often recommended and glaucoma control is very important, especially for African American patients. Chronic open-angle glaucoma can present as CRVO, and results can be devastating. African Americans are about 100 times more likely than Caucasians to have glaucoma (1/7 vs 3/2000).
Management dos and don’ts
CRVO is entirely different than retinal hemorrhage or vitreous hemorrhage. The correct diagnosis must be confirmed by an ophthalmologist, to ensure proper evaluation and management.
Reduce blood pressure
You return to your patient and share your conversation with the consultant. According to the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) guidelines, the patient has Stage I hypertension. The goal for treatment is medical management to reduce pressure to below 120/80 mm Hg.3
The patient elects treatment with a beta-blocker rather than a thiazide diuretic; he wishes to avoid monitoring of electrolytes that would be necessary because he often becomes dehydrated on the job. He will have the nurse at his company monitor his blood pressure.
Reduce lipids
Also, according to the National Cholesterol Education Program, this patient meets criteria for treatment of hyperlipidemia.4 He is given dietary instruction, information about lipids, a prescription for a statin as he believes he has already been following a quite restrictive diet for over 4 months.
Use anticoagulant?
Finally, you consult a hematologist about the appropriate evaluation for a hypercoagulable state. Following is her report:
- The retinal vein is anatomically different from other veins, being tightly encased in a sheath with the retinal artery and optic nerve. Disorders of these structures can compress or inflame the vein, leading to thrombosis. Consequently, local factors may play a role in development of retinal vein thrombosis—a systemic disorder is not required for this process to occur. CVRO is seldom associated with an underlying hypercoagulable state.5,6
- The effectiveness of medical intervention is unproven. Acute anticoagulation is associated with retinal hemorrhage and is not recommended. Recurrent retinal venous occlusion in the contralateral eye occurs in approximately 12% of patients within 4 years. Because of the risks of anticoagulation and unproven benefits in CRVO, you both elect to avoid this treatment.
If the patient were to request anticoagulation, therapy should be withheld for 2 to 3 months, the time required for retinal perfusion to stabilize. Antiplatelet agents such as aspirin have no role in preventing recurrent venous thrombosis.
Confirmation of this controversy in treatment was obtained using a literature search. A review article in Eye discussed that while the role of thrombophilia is unclear, the need for a randomized study of anticoagulation in the patient with CRVO is needed.6
Final decisions
After considering your consultant’s suggestions, you realize that finding a prothrombotic state is unlikely and will be not change management. Moreover, medical intervention is unlikely to change the natural history of this condition, and it might lead inadvertently to insurance or employment discrimination. You review the previous complete blood count to make sure you have not missed erythrocytosis or thrombocytosis—both of which have well-defined treatments.
Follow-up monitoring was scheduled by the ophthalmologist and you continue to manage the patient’s hypertension and hyperlipidemia.
This patient had a relatively uncommon condition that necessitated consultation with 2 specialists. After weighing the evidence and likelihood of benefit of unproven therapies for CVRO, the patient elected to manage other clear risk factors for atherosclerotic vascular disease. Management of this patient melds issues of ethics and evidence, with core skills to foster a good doctor-patient relationship.
At the risk of sounding like a bad joke, I’d like to open my commentary with the question:
“Why did this patient go to the family physician?” This patient was seen in an urban setting with ample access to any medical specialist, and he had an insurance plan that allowed open access contact with most, if not all, of the physicians in the community. This patient also knew enough about his illness to know that the final answer or treatment for his presenting problem would likely not be found in the family physician’s office.
The value that the family physician brought to this patient can be described as follows:
Navigator/Coordinator: The family physician was able to help this patient through the maze of medical specialists to find the right physicians to evaluate and treat the presenting problem, and to arrange for ongoing evaluation and management after specialist consultations.
Interpreter/Translator: The family physician was able to take the information provided by the specialist physicians and translate that information into language the patient could understand. This process must occur if the patient is expected to comply with treatment, evaluation and lifestyle change recommendations.
Comprehensive caregiver: While supporting the patient in coping with his vision loss, the family physician used this unfortunate occurrence as motivation to address modifiable risk factors—hypertension, obesity, elevated blood glucose, and elevated lipids. Managing these conditions may not be glamorous, but addressing all facets of a patient’s well being is what we family physicians do best. Caring for patients, not just treating illnesses, is a core value of family medicine.
Imagine this patient’s thought process from his arrival with a loss of vision to his departure with a plan to deal with hypertension, obesity, elevated blood glucose, and elevated lipids, all in the context of his job and family and community life. The holistic management of this patient in the context of his life is the main value added by the family physician for this patient. This management also completely supports the patient’s wish to avoid “another stroke.”
One of my colleagues once asked me: “Wouldn’t you like to be the kind of physician whose patient comes in with a cold and leaves with an order for a mammogram?” Family physicians have the knowledge, skills, and perspective necessary to treat the patient, not just the illness. Let’s keep doing what we do best for our patients.
Paul Paulman, MD
Q: What causes of sudden unilateral vision loss would you consider? What would you do next?
Your examination yields the following:
Medical history
- Borderline hypertension
- Hyperlipidemia (was on a medication but discontinued it on his own)
- Smoking 25 pack-years; quit 2 years ago
- Occasional alcohol intake
- No medications
- Electrical contractor by trade
- Parents living and well; siblings have hypertension but no other illnesses.
Review of systems
Negative except for occasional nasal congestion and low back pain.
Physical examination
- Alert male in no distress. Blood pressure, 146/86 mm Hg; weight, 85 kg; heart rate, 80; respiratory rate, 20; temperature normal; skin warm and dry.
- Head, eyes, ears, nose, throat: pupils are equal, round, and reactive to light and accommodation; extraocular movement intact; retinal exam is depicted in the Figure. Tympanic membranes, throat, and neck normal; carotids normal.
- Heart and lung exam unremarkable. Spleen questionably palpable. Extremities normal. Neurologic exam normal, except for eye findings.
FIGURE
Retinal exam
Referring to Harrison’s Textbook of Medicine, you find the following entry:
“Venous occlusion of the retina is often idiopathic, but hypertension, diabetes, and glaucoma are prominent risk factors. The benefit of treatment with anticoagulants is unproven and carries the risk of hemorrhage into the vitreous. Polycythemia, thrombocythemia, or other factors leading to an underlying hypercoagulable state should be corrected.”1
You also reviewed information from UpToDate, which revealed a British article linking retinal venous occlusion with an increased risk of cardiovascular disease. It recommends that clinicians use an algorithm to determine the appropriate treatment.2 Additional research noted various interventions for the venous occlusion itself, but none had sufficient numbers to be considered reliable in recommending treatment.
You have identified 3 problems, 2 of which you deal with regularly and a third that requires consultation:
- Hypertension
- Hyperlipidemia
- Central retinal venous occlusion (CRVO) (rule out underlying hypercoagulable state).
Ophthalmologist’s report
An ophthalmologist confirms a diagnosis of left retinal vein occlusion, and recommends a period of observation, to see if vision returns. The opthalmologist also asks the patient to return to you for an investigation of possible underlying medical conditions.
Further primary care evaluation
The patient’s history suggests nothing that would inhibit a return of vision. Findings on the physical examination are unchanged except for the left fundus. The patient is quite concerned about another “stroke,” particularly in the other eye. He wants a guarantee he will be okay.
Laboratory evaluation:
- Complete blood count, normal
- Urea nitrogen (BUN), 20 mg/dL
- Creatinine kinase, 1.2 mckat/L
- Liver functions within normal limits
- Glucose, 86 mg/dL
- Cholesterol, 230 mg/dL
- Triglycerides, 186 mg/dL
- HDL, 41 mg/dL; LDL, 136 mg/dL
- Total serum protein levels, normal.
Additional time was required by the family physician to coordinate care of this patient. A team management code (99361 for 30 minutes and 99362 for 60 minutes) may not be billed on the same day as an e/m code, as carriers bundle this into the e/m. In addition, most carriers do not pay for the 99361 or 99362 codes. Therefore, the conference should ideally occur the day of an e/m code and be documented with that service. In this instance, the care occurred over several days, so no additional billing was allowed for team management.
Details of central retinal venous occlusion
You assure the patient you will coordinate care with the ophthalmologist, who subsequently offers the following summary about CRVO:
- For most patients with CRVO, vision decreases to 20/100, 20/200, or worse, usually permanently if the occlusion is indeed venous and not arterial as well. If the condition is secondary to ischemia, vision is usually limited to 20/300 or worse, permanently.
- Most patients want their vision “fixed” right away, but that is usually not possible. Hypertension control is most important. Uncommon causes include polycythemia vera, emphysema, sickle cell disease, multiple myeloma, macroglobulinemia, hyperproteinemia, cystic fibrosis of the pancreas, and peritoneal dialysis. Occasionally, it can occur secondary to hypotension, as from a ruptured aortic aneurysm, delivery-associated blood loss, or surgical trauma.
- Hypertension and other atherosclerotic risk factors must be controlled. Treatment with platelet inhibitors is often recommended and glaucoma control is very important, especially for African American patients. Chronic open-angle glaucoma can present as CRVO, and results can be devastating. African Americans are about 100 times more likely than Caucasians to have glaucoma (1/7 vs 3/2000).
Management dos and don’ts
CRVO is entirely different than retinal hemorrhage or vitreous hemorrhage. The correct diagnosis must be confirmed by an ophthalmologist, to ensure proper evaluation and management.
Reduce blood pressure
You return to your patient and share your conversation with the consultant. According to the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) guidelines, the patient has Stage I hypertension. The goal for treatment is medical management to reduce pressure to below 120/80 mm Hg.3
The patient elects treatment with a beta-blocker rather than a thiazide diuretic; he wishes to avoid monitoring of electrolytes that would be necessary because he often becomes dehydrated on the job. He will have the nurse at his company monitor his blood pressure.
Reduce lipids
Also, according to the National Cholesterol Education Program, this patient meets criteria for treatment of hyperlipidemia.4 He is given dietary instruction, information about lipids, a prescription for a statin as he believes he has already been following a quite restrictive diet for over 4 months.
Use anticoagulant?
Finally, you consult a hematologist about the appropriate evaluation for a hypercoagulable state. Following is her report:
- The retinal vein is anatomically different from other veins, being tightly encased in a sheath with the retinal artery and optic nerve. Disorders of these structures can compress or inflame the vein, leading to thrombosis. Consequently, local factors may play a role in development of retinal vein thrombosis—a systemic disorder is not required for this process to occur. CVRO is seldom associated with an underlying hypercoagulable state.5,6
- The effectiveness of medical intervention is unproven. Acute anticoagulation is associated with retinal hemorrhage and is not recommended. Recurrent retinal venous occlusion in the contralateral eye occurs in approximately 12% of patients within 4 years. Because of the risks of anticoagulation and unproven benefits in CRVO, you both elect to avoid this treatment.
If the patient were to request anticoagulation, therapy should be withheld for 2 to 3 months, the time required for retinal perfusion to stabilize. Antiplatelet agents such as aspirin have no role in preventing recurrent venous thrombosis.
Confirmation of this controversy in treatment was obtained using a literature search. A review article in Eye discussed that while the role of thrombophilia is unclear, the need for a randomized study of anticoagulation in the patient with CRVO is needed.6
Final decisions
After considering your consultant’s suggestions, you realize that finding a prothrombotic state is unlikely and will be not change management. Moreover, medical intervention is unlikely to change the natural history of this condition, and it might lead inadvertently to insurance or employment discrimination. You review the previous complete blood count to make sure you have not missed erythrocytosis or thrombocytosis—both of which have well-defined treatments.
Follow-up monitoring was scheduled by the ophthalmologist and you continue to manage the patient’s hypertension and hyperlipidemia.
This patient had a relatively uncommon condition that necessitated consultation with 2 specialists. After weighing the evidence and likelihood of benefit of unproven therapies for CVRO, the patient elected to manage other clear risk factors for atherosclerotic vascular disease. Management of this patient melds issues of ethics and evidence, with core skills to foster a good doctor-patient relationship.
At the risk of sounding like a bad joke, I’d like to open my commentary with the question:
“Why did this patient go to the family physician?” This patient was seen in an urban setting with ample access to any medical specialist, and he had an insurance plan that allowed open access contact with most, if not all, of the physicians in the community. This patient also knew enough about his illness to know that the final answer or treatment for his presenting problem would likely not be found in the family physician’s office.
The value that the family physician brought to this patient can be described as follows:
Navigator/Coordinator: The family physician was able to help this patient through the maze of medical specialists to find the right physicians to evaluate and treat the presenting problem, and to arrange for ongoing evaluation and management after specialist consultations.
Interpreter/Translator: The family physician was able to take the information provided by the specialist physicians and translate that information into language the patient could understand. This process must occur if the patient is expected to comply with treatment, evaluation and lifestyle change recommendations.
Comprehensive caregiver: While supporting the patient in coping with his vision loss, the family physician used this unfortunate occurrence as motivation to address modifiable risk factors—hypertension, obesity, elevated blood glucose, and elevated lipids. Managing these conditions may not be glamorous, but addressing all facets of a patient’s well being is what we family physicians do best. Caring for patients, not just treating illnesses, is a core value of family medicine.
Imagine this patient’s thought process from his arrival with a loss of vision to his departure with a plan to deal with hypertension, obesity, elevated blood glucose, and elevated lipids, all in the context of his job and family and community life. The holistic management of this patient in the context of his life is the main value added by the family physician for this patient. This management also completely supports the patient’s wish to avoid “another stroke.”
One of my colleagues once asked me: “Wouldn’t you like to be the kind of physician whose patient comes in with a cold and leaves with an order for a mammogram?” Family physicians have the knowledge, skills, and perspective necessary to treat the patient, not just the illness. Let’s keep doing what we do best for our patients.
Paul Paulman, MD
1. Harrison’s Principles of Internal Medicine. 15th ed. Eds. Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL. New York, NY: McGraw-Hill; 2001.
2. Martin SC, Butcher A, Martin N, et al. Cardiovascular risk assessment in patients with retinal vein occlusion. Br J Ophthalmol 2002;86:774-776.
3. National Heart, Lung, and Blood Institute. National High Blood Pressure Education Program. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7). 2003. Available at: www.nhlbi.nih.gov/guidelines/hypertension/jncintro.htm. Accessed on March 16, 2004.
4. National Heart, Lung, and Blood Institute. National Cholesterol Education Program. Third Report of the Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Available at: www.nhlbi.nih.gov/guidelines/cholesterol/atp3_rpt.htm. Accessed on March 16, 2004.
5. Layey JM. Hypercoagulable states and central retinal vein occulsion. Curr Opin Pulm Med 2003;9:385-392.
6. Fegan CD. Central retinal vein occlusion and thrombophilia. Eye 2002;26:98-106.
1. Harrison’s Principles of Internal Medicine. 15th ed. Eds. Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL. New York, NY: McGraw-Hill; 2001.
2. Martin SC, Butcher A, Martin N, et al. Cardiovascular risk assessment in patients with retinal vein occlusion. Br J Ophthalmol 2002;86:774-776.
3. National Heart, Lung, and Blood Institute. National High Blood Pressure Education Program. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7). 2003. Available at: www.nhlbi.nih.gov/guidelines/hypertension/jncintro.htm. Accessed on March 16, 2004.
4. National Heart, Lung, and Blood Institute. National Cholesterol Education Program. Third Report of the Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Available at: www.nhlbi.nih.gov/guidelines/cholesterol/atp3_rpt.htm. Accessed on March 16, 2004.
5. Layey JM. Hypercoagulable states and central retinal vein occulsion. Curr Opin Pulm Med 2003;9:385-392.
6. Fegan CD. Central retinal vein occlusion and thrombophilia. Eye 2002;26:98-106.
Percutaneous Endovascular Treatment of Subclavian Steal Syndrome
Lichen Planus Actinicus
Lichen planus is a papulosquamous inflammatory dermatitis that affects less than 1% of the population. Classic lichen planus typically presents as erythematous to violaceous flat-topped papules that are pruritic and polygonal. The lesions usually involve the flexural areas of the arms, legs, trunk, and lower back.1 Multiple clinical variants of lichen planus have been described.1 We report a case of lichen planus actinicus, a subtype of lichen planus that characteristically affects sun-exposed areas of the face, forearms, and dorsa of the hands in individuals with dark complexions living in subtropical climates.2-8
Case Report
A 55-year-old Indian man presented with a 7-year history of asymptomatic hyperpigmentation on his face, neck, and forearms. The patient had tried treating the condition with hydroquinone preparations and topical steroids without improvement in the pigmentation. He had no other medical problems and was not taking any systemic medications.
On physical examination, there were hyperpigmented macules and patches on his forehead (Figure 1), nose, cheeks, and chin. He also had thin, flat-topped, hyperpigmented papules on the dorsal surfaces of his forearms and hands (Figure 2). All areas of hyperpigmentation were in areas of sun exposure. He had no associated mucous membrane or nail involvement. Histologic examination demonstrated an atrophic epidermis with mild hyperkeratosis and orthokeratosis (Figure 3). Basilar vacuolization, a bandlike lymphocytic infiltrate, and marked pigmentary incontinence were present. A diagnosis of lichen planus actinicus was made.
Please refer to the PDF to view the figures
The patient was treated with topical tacrolimus 0.1% ointment and oral acitretin 25 mg daily for 2 months. The acitretin was discontinued because of lack of improvement and unacceptable side effects (dryness of skin, peeling of hands, and scalp hair loss). He was then started on hydroxychloroquine 400 mg daily with improvement (decreased thickening and pigmentation) after one month of therapy.
Comment
Lichen planus actinicus is a photodistributed variant of lichen planus that most often occurs in dark-complexioned young adults of Middle Eastern descent.3,8-10 Other names for this disorder include: summertime actinic lichenoid eruption,2,6 lichen planus atrophicus annularis,2 lichen planus in subtropical countries,3,4 lichen planus subtropicus,5 lichen planus tropicus, and lichenoid melanodermatitis.7 Although the etiology of this disease has not been determined, sunlight appears to be the triggering factor in most cases.2-11 Lichen planus actinicus has been induced with artificial UV light sources. In one patient, repeated doses of UVB radiation induced lichen planus–like lesions, whereas UVA radiation did not invoke this cutaneous response.12 Subtropical climates and nutritional deficiencies also may be contributing factors.2
The lesions of lichen planus actinicus usually occur on the forehead, face, neck, and the extensor surfaces of the arms and hands. The lateral aspect of the forehead is the most common site of presentation.5 Several morphologic patterns have been reported including annular hyperpigmented plaques, melasmalike patches, dyschromic papules, and classic lichenoid papules/plaques (Table 1).2,3,10,11 The lesions often are exacerbated by sun exposure and may improve spontaneously in the winter months.3,4 Rarely, the nonexposed skin of the legs, trunk, genitals, and oral mucosa may be affected.3,4 Unlike classic lichen planus, lichen planus actinicus has an earlier age of onset, a longer course, a predilection for dark-complexioned females, and a seasonal occurrence.2-4 Additionally, pruritus, scaling, nail involvement, and the Köbner reaction frequently are absent (Table 2).2-4
Please refer to the PDF to view the tables
Differential diagnosis of lichen planus actinicus includes discoid lupus erythematosus, granuloma annulare, melasma, secondary syphilis, fixed drug eruption, polymorphous light eruption, and erythema dyschronicum perstans.5 The clinician also must exclude the possibility of a drug-induced photosensitive lichenoid eruption by taking a complete medication history.
The histologic features of lichen planus actinicus are consistent with findings in classic lichen planus.2-5 Hyperkeratosis of the stratum corneum, hypergranulosis, basal cell vacuolization, and Civatte bodies usually are present.10 The epidermis may demonstrate either sawtoothed hyperplasia or atrophy. Numerous melanophages, marked pigmentary incontinence, and a bandlike lymphocytic inflammatory infiltrate also are observed in the papillary dermis.2-4,7,10 Although clinically similar to cutaneous lupus and polymorphous light eruption, lichen planus actinicus can be distinguished histologically from these photodermatoses. Lichen planus actinicus lacks follicular plugging, thickening of the basement membrane, and the periadnexal inflammatory infiltrate seen in cutaneous lupus erythematosus.2 Papillary dermal edema, which is present in polymorphous light eruption, is not observed.2 The lupus erythematosus–lichen planus overlap syndrome and lichen planus actinicus may be similar histologically, but they can be easily distinguished clinically. Unlike lichen planus actinicus, the lupus erythematosus–lichen planus overlap syndrome features ulcerated, atrophic, violaceous plaques with telangiectasias on the palms and soles.1,2
Variable treatment responses have been reported with bismuth, grenz rays, arsenic compounds, and topical corticosteroids under occlusion.4,6 Hydroxychloroquine, intralesional corticosteroids, and topical sunscreens have been used with success.5,8 Acitretin, used in combination with topical steroids and sun avoidance, also has resulted in complete resolution of lesions without recurrence.13 Although psoralen-UVA, isotretinoin, systemic corticosteroids, cyclosporine, and dapsone have been used to treat classic lichen planus, there are currently no reports of their use in lichen planus actinicus.14 Some cases may remit spontaneously with sun avoidance and use of sunblock.6
- Boyd A, Neldner K. Lichen planus. J Am Acad Dermatol. 1991;25:593-619.
- Isaacson D, Turner ML, Elgart ML. Summertime actinic lichenoid eruption (lichen planus actinicus). J Am Acad Dermatol. 1981;4:404-411.
- Katzenellenbogen I. Lichen planus actinicus (lichen planus in subtropical countries). Dermatologica. 1962;124:10-20.
- Dostrovsky A, Sagher F. Lichen planus in subtropical countries. AMA Arch Derm Syphilol. 1942;59:308-328.
- Dilaimy M. Lichen planus subtropicus. Arch Dermatol. 1976;112:1251-1253.
- Bedi TR. Summertime actinic lichenoid eruption. Dermatologica. 1978;157:115-125.
- Verhagen AR, Koten JW. Lichenoid melanodermatitis. a clinicopathological study of fifty-one Kenyan patients with so-called tropical lichen planus. Brit J Dermatol. 1979;101:651-658.
- Zanca A, Zanca A. Lichen planus actinicus. Int J Dermatol. 1978;17:506-508.
- Baker H, Almeyda J. Lichen planus actinicus. Brit J Dermatol. 1970;82:426-427.
- Salman SM, Kibbi AG, Zaynoun S. Actinic lichen planus. J Am Acad Dermatol. 1989;20:226-231.
- Salman SM, Khallouf R, Zaynoun S. Actinic lichen planus mimicking melasma. J Am Acad Dermatol. 1988;18:275-278.
- van der Schroeff JG, Schothorst AA, Kanaar P. Induction of actinic lichen planus with artificial UV sources. Arch Dermatol. 1983;119:498-500.
- Jansen T, Gambichler T, von Kobyletzki L, et al. Lichen planus actinicus treated with acitretin and topical corticosteroids. J Eur Acad Dermatol Venereol. 2002;16:174-175.
- Cribier B, Frances C, Chosidow O. Treatment of lichen planus. an evidence-based medicine analysis of efficacy. Arch Dermatol. 1998;134:1521-1528.
Lichen planus is a papulosquamous inflammatory dermatitis that affects less than 1% of the population. Classic lichen planus typically presents as erythematous to violaceous flat-topped papules that are pruritic and polygonal. The lesions usually involve the flexural areas of the arms, legs, trunk, and lower back.1 Multiple clinical variants of lichen planus have been described.1 We report a case of lichen planus actinicus, a subtype of lichen planus that characteristically affects sun-exposed areas of the face, forearms, and dorsa of the hands in individuals with dark complexions living in subtropical climates.2-8
Case Report
A 55-year-old Indian man presented with a 7-year history of asymptomatic hyperpigmentation on his face, neck, and forearms. The patient had tried treating the condition with hydroquinone preparations and topical steroids without improvement in the pigmentation. He had no other medical problems and was not taking any systemic medications.
On physical examination, there were hyperpigmented macules and patches on his forehead (Figure 1), nose, cheeks, and chin. He also had thin, flat-topped, hyperpigmented papules on the dorsal surfaces of his forearms and hands (Figure 2). All areas of hyperpigmentation were in areas of sun exposure. He had no associated mucous membrane or nail involvement. Histologic examination demonstrated an atrophic epidermis with mild hyperkeratosis and orthokeratosis (Figure 3). Basilar vacuolization, a bandlike lymphocytic infiltrate, and marked pigmentary incontinence were present. A diagnosis of lichen planus actinicus was made.
Please refer to the PDF to view the figures
The patient was treated with topical tacrolimus 0.1% ointment and oral acitretin 25 mg daily for 2 months. The acitretin was discontinued because of lack of improvement and unacceptable side effects (dryness of skin, peeling of hands, and scalp hair loss). He was then started on hydroxychloroquine 400 mg daily with improvement (decreased thickening and pigmentation) after one month of therapy.
Comment
Lichen planus actinicus is a photodistributed variant of lichen planus that most often occurs in dark-complexioned young adults of Middle Eastern descent.3,8-10 Other names for this disorder include: summertime actinic lichenoid eruption,2,6 lichen planus atrophicus annularis,2 lichen planus in subtropical countries,3,4 lichen planus subtropicus,5 lichen planus tropicus, and lichenoid melanodermatitis.7 Although the etiology of this disease has not been determined, sunlight appears to be the triggering factor in most cases.2-11 Lichen planus actinicus has been induced with artificial UV light sources. In one patient, repeated doses of UVB radiation induced lichen planus–like lesions, whereas UVA radiation did not invoke this cutaneous response.12 Subtropical climates and nutritional deficiencies also may be contributing factors.2
The lesions of lichen planus actinicus usually occur on the forehead, face, neck, and the extensor surfaces of the arms and hands. The lateral aspect of the forehead is the most common site of presentation.5 Several morphologic patterns have been reported including annular hyperpigmented plaques, melasmalike patches, dyschromic papules, and classic lichenoid papules/plaques (Table 1).2,3,10,11 The lesions often are exacerbated by sun exposure and may improve spontaneously in the winter months.3,4 Rarely, the nonexposed skin of the legs, trunk, genitals, and oral mucosa may be affected.3,4 Unlike classic lichen planus, lichen planus actinicus has an earlier age of onset, a longer course, a predilection for dark-complexioned females, and a seasonal occurrence.2-4 Additionally, pruritus, scaling, nail involvement, and the Köbner reaction frequently are absent (Table 2).2-4
Please refer to the PDF to view the tables
Differential diagnosis of lichen planus actinicus includes discoid lupus erythematosus, granuloma annulare, melasma, secondary syphilis, fixed drug eruption, polymorphous light eruption, and erythema dyschronicum perstans.5 The clinician also must exclude the possibility of a drug-induced photosensitive lichenoid eruption by taking a complete medication history.
The histologic features of lichen planus actinicus are consistent with findings in classic lichen planus.2-5 Hyperkeratosis of the stratum corneum, hypergranulosis, basal cell vacuolization, and Civatte bodies usually are present.10 The epidermis may demonstrate either sawtoothed hyperplasia or atrophy. Numerous melanophages, marked pigmentary incontinence, and a bandlike lymphocytic inflammatory infiltrate also are observed in the papillary dermis.2-4,7,10 Although clinically similar to cutaneous lupus and polymorphous light eruption, lichen planus actinicus can be distinguished histologically from these photodermatoses. Lichen planus actinicus lacks follicular plugging, thickening of the basement membrane, and the periadnexal inflammatory infiltrate seen in cutaneous lupus erythematosus.2 Papillary dermal edema, which is present in polymorphous light eruption, is not observed.2 The lupus erythematosus–lichen planus overlap syndrome and lichen planus actinicus may be similar histologically, but they can be easily distinguished clinically. Unlike lichen planus actinicus, the lupus erythematosus–lichen planus overlap syndrome features ulcerated, atrophic, violaceous plaques with telangiectasias on the palms and soles.1,2
Variable treatment responses have been reported with bismuth, grenz rays, arsenic compounds, and topical corticosteroids under occlusion.4,6 Hydroxychloroquine, intralesional corticosteroids, and topical sunscreens have been used with success.5,8 Acitretin, used in combination with topical steroids and sun avoidance, also has resulted in complete resolution of lesions without recurrence.13 Although psoralen-UVA, isotretinoin, systemic corticosteroids, cyclosporine, and dapsone have been used to treat classic lichen planus, there are currently no reports of their use in lichen planus actinicus.14 Some cases may remit spontaneously with sun avoidance and use of sunblock.6
Lichen planus is a papulosquamous inflammatory dermatitis that affects less than 1% of the population. Classic lichen planus typically presents as erythematous to violaceous flat-topped papules that are pruritic and polygonal. The lesions usually involve the flexural areas of the arms, legs, trunk, and lower back.1 Multiple clinical variants of lichen planus have been described.1 We report a case of lichen planus actinicus, a subtype of lichen planus that characteristically affects sun-exposed areas of the face, forearms, and dorsa of the hands in individuals with dark complexions living in subtropical climates.2-8
Case Report
A 55-year-old Indian man presented with a 7-year history of asymptomatic hyperpigmentation on his face, neck, and forearms. The patient had tried treating the condition with hydroquinone preparations and topical steroids without improvement in the pigmentation. He had no other medical problems and was not taking any systemic medications.
On physical examination, there were hyperpigmented macules and patches on his forehead (Figure 1), nose, cheeks, and chin. He also had thin, flat-topped, hyperpigmented papules on the dorsal surfaces of his forearms and hands (Figure 2). All areas of hyperpigmentation were in areas of sun exposure. He had no associated mucous membrane or nail involvement. Histologic examination demonstrated an atrophic epidermis with mild hyperkeratosis and orthokeratosis (Figure 3). Basilar vacuolization, a bandlike lymphocytic infiltrate, and marked pigmentary incontinence were present. A diagnosis of lichen planus actinicus was made.
Please refer to the PDF to view the figures
The patient was treated with topical tacrolimus 0.1% ointment and oral acitretin 25 mg daily for 2 months. The acitretin was discontinued because of lack of improvement and unacceptable side effects (dryness of skin, peeling of hands, and scalp hair loss). He was then started on hydroxychloroquine 400 mg daily with improvement (decreased thickening and pigmentation) after one month of therapy.
Comment
Lichen planus actinicus is a photodistributed variant of lichen planus that most often occurs in dark-complexioned young adults of Middle Eastern descent.3,8-10 Other names for this disorder include: summertime actinic lichenoid eruption,2,6 lichen planus atrophicus annularis,2 lichen planus in subtropical countries,3,4 lichen planus subtropicus,5 lichen planus tropicus, and lichenoid melanodermatitis.7 Although the etiology of this disease has not been determined, sunlight appears to be the triggering factor in most cases.2-11 Lichen planus actinicus has been induced with artificial UV light sources. In one patient, repeated doses of UVB radiation induced lichen planus–like lesions, whereas UVA radiation did not invoke this cutaneous response.12 Subtropical climates and nutritional deficiencies also may be contributing factors.2
The lesions of lichen planus actinicus usually occur on the forehead, face, neck, and the extensor surfaces of the arms and hands. The lateral aspect of the forehead is the most common site of presentation.5 Several morphologic patterns have been reported including annular hyperpigmented plaques, melasmalike patches, dyschromic papules, and classic lichenoid papules/plaques (Table 1).2,3,10,11 The lesions often are exacerbated by sun exposure and may improve spontaneously in the winter months.3,4 Rarely, the nonexposed skin of the legs, trunk, genitals, and oral mucosa may be affected.3,4 Unlike classic lichen planus, lichen planus actinicus has an earlier age of onset, a longer course, a predilection for dark-complexioned females, and a seasonal occurrence.2-4 Additionally, pruritus, scaling, nail involvement, and the Köbner reaction frequently are absent (Table 2).2-4
Please refer to the PDF to view the tables
Differential diagnosis of lichen planus actinicus includes discoid lupus erythematosus, granuloma annulare, melasma, secondary syphilis, fixed drug eruption, polymorphous light eruption, and erythema dyschronicum perstans.5 The clinician also must exclude the possibility of a drug-induced photosensitive lichenoid eruption by taking a complete medication history.
The histologic features of lichen planus actinicus are consistent with findings in classic lichen planus.2-5 Hyperkeratosis of the stratum corneum, hypergranulosis, basal cell vacuolization, and Civatte bodies usually are present.10 The epidermis may demonstrate either sawtoothed hyperplasia or atrophy. Numerous melanophages, marked pigmentary incontinence, and a bandlike lymphocytic inflammatory infiltrate also are observed in the papillary dermis.2-4,7,10 Although clinically similar to cutaneous lupus and polymorphous light eruption, lichen planus actinicus can be distinguished histologically from these photodermatoses. Lichen planus actinicus lacks follicular plugging, thickening of the basement membrane, and the periadnexal inflammatory infiltrate seen in cutaneous lupus erythematosus.2 Papillary dermal edema, which is present in polymorphous light eruption, is not observed.2 The lupus erythematosus–lichen planus overlap syndrome and lichen planus actinicus may be similar histologically, but they can be easily distinguished clinically. Unlike lichen planus actinicus, the lupus erythematosus–lichen planus overlap syndrome features ulcerated, atrophic, violaceous plaques with telangiectasias on the palms and soles.1,2
Variable treatment responses have been reported with bismuth, grenz rays, arsenic compounds, and topical corticosteroids under occlusion.4,6 Hydroxychloroquine, intralesional corticosteroids, and topical sunscreens have been used with success.5,8 Acitretin, used in combination with topical steroids and sun avoidance, also has resulted in complete resolution of lesions without recurrence.13 Although psoralen-UVA, isotretinoin, systemic corticosteroids, cyclosporine, and dapsone have been used to treat classic lichen planus, there are currently no reports of their use in lichen planus actinicus.14 Some cases may remit spontaneously with sun avoidance and use of sunblock.6
- Boyd A, Neldner K. Lichen planus. J Am Acad Dermatol. 1991;25:593-619.
- Isaacson D, Turner ML, Elgart ML. Summertime actinic lichenoid eruption (lichen planus actinicus). J Am Acad Dermatol. 1981;4:404-411.
- Katzenellenbogen I. Lichen planus actinicus (lichen planus in subtropical countries). Dermatologica. 1962;124:10-20.
- Dostrovsky A, Sagher F. Lichen planus in subtropical countries. AMA Arch Derm Syphilol. 1942;59:308-328.
- Dilaimy M. Lichen planus subtropicus. Arch Dermatol. 1976;112:1251-1253.
- Bedi TR. Summertime actinic lichenoid eruption. Dermatologica. 1978;157:115-125.
- Verhagen AR, Koten JW. Lichenoid melanodermatitis. a clinicopathological study of fifty-one Kenyan patients with so-called tropical lichen planus. Brit J Dermatol. 1979;101:651-658.
- Zanca A, Zanca A. Lichen planus actinicus. Int J Dermatol. 1978;17:506-508.
- Baker H, Almeyda J. Lichen planus actinicus. Brit J Dermatol. 1970;82:426-427.
- Salman SM, Kibbi AG, Zaynoun S. Actinic lichen planus. J Am Acad Dermatol. 1989;20:226-231.
- Salman SM, Khallouf R, Zaynoun S. Actinic lichen planus mimicking melasma. J Am Acad Dermatol. 1988;18:275-278.
- van der Schroeff JG, Schothorst AA, Kanaar P. Induction of actinic lichen planus with artificial UV sources. Arch Dermatol. 1983;119:498-500.
- Jansen T, Gambichler T, von Kobyletzki L, et al. Lichen planus actinicus treated with acitretin and topical corticosteroids. J Eur Acad Dermatol Venereol. 2002;16:174-175.
- Cribier B, Frances C, Chosidow O. Treatment of lichen planus. an evidence-based medicine analysis of efficacy. Arch Dermatol. 1998;134:1521-1528.
- Boyd A, Neldner K. Lichen planus. J Am Acad Dermatol. 1991;25:593-619.
- Isaacson D, Turner ML, Elgart ML. Summertime actinic lichenoid eruption (lichen planus actinicus). J Am Acad Dermatol. 1981;4:404-411.
- Katzenellenbogen I. Lichen planus actinicus (lichen planus in subtropical countries). Dermatologica. 1962;124:10-20.
- Dostrovsky A, Sagher F. Lichen planus in subtropical countries. AMA Arch Derm Syphilol. 1942;59:308-328.
- Dilaimy M. Lichen planus subtropicus. Arch Dermatol. 1976;112:1251-1253.
- Bedi TR. Summertime actinic lichenoid eruption. Dermatologica. 1978;157:115-125.
- Verhagen AR, Koten JW. Lichenoid melanodermatitis. a clinicopathological study of fifty-one Kenyan patients with so-called tropical lichen planus. Brit J Dermatol. 1979;101:651-658.
- Zanca A, Zanca A. Lichen planus actinicus. Int J Dermatol. 1978;17:506-508.
- Baker H, Almeyda J. Lichen planus actinicus. Brit J Dermatol. 1970;82:426-427.
- Salman SM, Kibbi AG, Zaynoun S. Actinic lichen planus. J Am Acad Dermatol. 1989;20:226-231.
- Salman SM, Khallouf R, Zaynoun S. Actinic lichen planus mimicking melasma. J Am Acad Dermatol. 1988;18:275-278.
- van der Schroeff JG, Schothorst AA, Kanaar P. Induction of actinic lichen planus with artificial UV sources. Arch Dermatol. 1983;119:498-500.
- Jansen T, Gambichler T, von Kobyletzki L, et al. Lichen planus actinicus treated with acitretin and topical corticosteroids. J Eur Acad Dermatol Venereol. 2002;16:174-175.
- Cribier B, Frances C, Chosidow O. Treatment of lichen planus. an evidence-based medicine analysis of efficacy. Arch Dermatol. 1998;134:1521-1528.
A Case of Human Orf Contracted From a Deer
Orf, also known as contagious ecthyma, scabby mouth, soremouth, contagious pustular dermatitis, and ovine pustular dermatitis, is caused by a member of the genus Parapoxvirus in the family Poxviridae.1,2 The virus typically infects sheep or goats and produces papulovesicular lesions on non–wool-bearing areas (eg, gums, lips, nose, groin).3,4 The infection can be transmitted to humans either by direct contact with an infected animal or by indirect contact with contaminated fomites.4,5 After an incubation period of 3 to 7 days, an erythematous maculopapular lesion develops.1,4 Orf lesions are benign and progress to complete resolution in 6 weeks.4
Case Report
A 51-year-old woman presented to her primary care physician for evaluation of a lesion on the metacarpal-phalangeal joint of the left second digit. A raised annular lesion was identified, and the patient was started on dicloxacillin therapy. On reexamination 4 days later, an enlarging 2-cm nodule with signs of central necrosis was found. The lesion was incised, and a bacterial culture of purulent exudate was obtained. Gram stain and initial culture results were negative. The patient also complained of diarrhea, which was attributed to use of dicloxacillin; this antibiotic was replaced with clarithromycin. The patient was reevaluated the next day for signs of cellulitis and ascending lymphangitis. She denied constitutional symptoms or fever and chills. The lymphangitis was present on the dorsum of the left hand to the level of the wrist. Ceftriaxone was injected intramuscularly. Three days later, an enlarging lesion with serous discharge was identified. The patient was referred for further dermatologic evaluation.
On examining the patient, we found a 2.5-cm boggy fluctuant nodule over the metacarpal-phalangeal joint of the left second digit (Figure). The patient complained of pain, and the hand showed signs of lymphangitic spread. When her history was taken, the patient indicated that she worked at a deer station. Her job involved handling deer carcasses, and her bare hands had been exposed to blood from slaughtered deer. She denied having any contact with sheep, goats, cattle, and farm structures containing those animals. Results of bacterial cultures were negative, and a differential diagnosis of deep fungal infection, atypical mycobacterial infection, or contagious ecthyma was entertained. Two 3-mm punch biopsies were performed. Stains for acid-fast bacilli and fungi were negative. Results of microscopic examination showed vacuolation of cells in the upper third of the malpighian stratum, eosinophilic inclusion bodies, and massive dermal infiltrate.
PLEASE REFER TO THE PDF TO VIEW THE FIGURE
Because of the patient's clinical presentation, microscopic findings, and negative culture results, orf was diagnosed. Oral antibiotic therapy was discontinued, and daily cleansing and use of bacitracin ointment were started. The lesion resolved completely over the ensuing 3 to 4 weeks.
Comment
The diagnosis of orf is suggested by a characteristic skin lesion and a history of exposure. The typical lesion begins as a solitary papule on a finger, a hand,3 or the face.6 Orf lesions classically progress through a series of 6 clinical and histopathologic stages, each lasting approximately 1 week. In the initial maculopapular stage, an erythematous macule or papule erupts. In the target stage, the lesion becomes a papule with a red center, a white middle ring, and a red halo. In the acute stage, the lesion becomes a weeping nodule. In the regenerative stage, the lesion dries, a thin yellow crust develops, and small black dots form on the surface. In the papillomatous stage, tiny papillomas form on the surface. In the final, regressive stage, a dry crust forms.1,3,4,6 Uncomplicated lesions rarely leave a residual scar.4
The histopathology of an orf lesion evolves with the clinical stages and helps to secure the diagnosis. The maculopapular and target stages are characterized by vacuolated epidermal cells. In the maculopapular stage, cells have intracytoplasmic inclusions; in the target stage, they have both intracytoplasmic and intranuclear inclusions. The acute stage is marked by patchy areas of lost epidermis, reticular degeneration of the epidermis, and a dermal infiltrate composed primarily of lymphocytes. The regenerative stage involves epidermal regeneration and extrusion of pyknotic hair-follicle cells that form the small black dots on the surface of the lesion. In the papillomatous and regressive stages, fingerlike downward projections of epidermis are evident.1,4,6
The diagnosis of orf is further supported by a history of exposure to infected animals. The most compelling history involves exposure to sheep or goats, but the orf virus has infected other animals, including musk oxen7 and camels.8 Experimental inoculation has produced contagious ecthyma lesions in mule deer, white-tailed deer, pronghorn, and wapiti.9 That wild deer could contract orf and that the infection could be transmitted to humans through direct contact seem reasonable speculations. Our patient's clinical picture suggests that this mechanism may have been involved in her contracting the disease.
Electron microscopic views of characteristic viral particles in the cytoplasm of keratinocytes provide the definitive diagnosis of orf.1,10 Other diagnostic studies are tests of viral culture, complement fixation, and immunofluorescence.1,4,6 These tests are used mainly for epidemiology rather than clinical diagnosis.6
Complications of orf are generally rare but may include fever, chills, rigor, drenching sweat, malaise, lymphadenopathy, and lymphangitis.1,6,10 Secondary bacterial infection is the most common complication.1 Cases of erythema multiforme also have developed in the presence of orf.11
As a benign self-limited disease, orf requires no specific treatment. Antibiotics should be administered in cases of secondary bacterial infection but are otherwise unnecessary.1,2,6 Regression of the lesion may be accelerated by application of idoxuridine.10 Surgical excision also can bring about rapid resolution but is generally contraindicated because the lesion spontaneously regresses without leaving a scar.2 Corticosteroids and other immunosuppressive drugs should be avoided because they can exacerbate the lesion in its papillomatous stage.6,12 Use of topical cidofovir has been beneficial in treating patients who are immunocompromised.13
Although orf is a benign disease with a striking presentation that is easy to spot, early diagnosis can prevent unnecessary diagnostic workup and treatment.1 Orf should be considered in patients presenting with the characteristic skin lesion and a history of exposure to sheep or goats. As with our case, however, when a patient presents with a characteristic lesion and a history of exposure to other animals, orf should be kept in the differential diagnosis.
- Huerter CJ, Alvarez L, Stinson R. Orf: case report and literature review. Cleve Clin J Med. 1991;58:531-534.
- Chahidi N, de Fontaine S, Lacotte B. Human orf. Br J Plast Surg. 1993;46:532-534.
- Leavell UW, McNamara MJ, Muelling R, et al. Orf: report of 19 human cases with clinical and pathological observations. JAMA. 1968;204:109-116.
- Mendez B, Burnett JW. Orf. Cutis. 1989;44:286-287.
- Wilkinson JD. Orf: a family with unusual complications. Br J Dermatol. 1977;97:447-450.
- Bodnar MG, Miller OF, Tyler WB. Facial orf. J Am Acad Dermatol. 1999;40:815-817.
- Zarnke RL, Dieterich RA, Neiland KA, et al. Serologic and experimental investigations of contagious ecthyma in Alaska. J Wildl Dis. 1983;19:170-174.
- Azwai SM, Carter SD, Woldehiwet Z. Immune responses of the camel (Camelus dromedarius) to contagious ecthyma (orf) virus infection. Vet Microbiol. 1995;47:119-131.
- Lance WR, Hibler CP, DeMartini J. Experimental contagious ecthyma in mule deer, white-tailed deer, pronghorn and wapiti. J Wildl Dis. 1983;19:165-169.
- Lo C, Mathisen G. Human orf in Los Angeles County. West J Med. 1996;164:77-78.
- Agger WA, Webster SB. Human orf infection complicated by erythema multiforme. Cutis. 1983;31:334-338.
- Mohr BW, Katz D. Orf: a case report. Henry Ford Hosp Med J. 1989;37:79-80.
- Geerinck K, Lukito G, Snoeck R, et al. A case of human orf in an immunocompromised patient treated successfully with cidofovir cream. J Med Virol. 2001;64:543-549.
Orf, also known as contagious ecthyma, scabby mouth, soremouth, contagious pustular dermatitis, and ovine pustular dermatitis, is caused by a member of the genus Parapoxvirus in the family Poxviridae.1,2 The virus typically infects sheep or goats and produces papulovesicular lesions on non–wool-bearing areas (eg, gums, lips, nose, groin).3,4 The infection can be transmitted to humans either by direct contact with an infected animal or by indirect contact with contaminated fomites.4,5 After an incubation period of 3 to 7 days, an erythematous maculopapular lesion develops.1,4 Orf lesions are benign and progress to complete resolution in 6 weeks.4
Case Report
A 51-year-old woman presented to her primary care physician for evaluation of a lesion on the metacarpal-phalangeal joint of the left second digit. A raised annular lesion was identified, and the patient was started on dicloxacillin therapy. On reexamination 4 days later, an enlarging 2-cm nodule with signs of central necrosis was found. The lesion was incised, and a bacterial culture of purulent exudate was obtained. Gram stain and initial culture results were negative. The patient also complained of diarrhea, which was attributed to use of dicloxacillin; this antibiotic was replaced with clarithromycin. The patient was reevaluated the next day for signs of cellulitis and ascending lymphangitis. She denied constitutional symptoms or fever and chills. The lymphangitis was present on the dorsum of the left hand to the level of the wrist. Ceftriaxone was injected intramuscularly. Three days later, an enlarging lesion with serous discharge was identified. The patient was referred for further dermatologic evaluation.
On examining the patient, we found a 2.5-cm boggy fluctuant nodule over the metacarpal-phalangeal joint of the left second digit (Figure). The patient complained of pain, and the hand showed signs of lymphangitic spread. When her history was taken, the patient indicated that she worked at a deer station. Her job involved handling deer carcasses, and her bare hands had been exposed to blood from slaughtered deer. She denied having any contact with sheep, goats, cattle, and farm structures containing those animals. Results of bacterial cultures were negative, and a differential diagnosis of deep fungal infection, atypical mycobacterial infection, or contagious ecthyma was entertained. Two 3-mm punch biopsies were performed. Stains for acid-fast bacilli and fungi were negative. Results of microscopic examination showed vacuolation of cells in the upper third of the malpighian stratum, eosinophilic inclusion bodies, and massive dermal infiltrate.
PLEASE REFER TO THE PDF TO VIEW THE FIGURE
Because of the patient's clinical presentation, microscopic findings, and negative culture results, orf was diagnosed. Oral antibiotic therapy was discontinued, and daily cleansing and use of bacitracin ointment were started. The lesion resolved completely over the ensuing 3 to 4 weeks.
Comment
The diagnosis of orf is suggested by a characteristic skin lesion and a history of exposure. The typical lesion begins as a solitary papule on a finger, a hand,3 or the face.6 Orf lesions classically progress through a series of 6 clinical and histopathologic stages, each lasting approximately 1 week. In the initial maculopapular stage, an erythematous macule or papule erupts. In the target stage, the lesion becomes a papule with a red center, a white middle ring, and a red halo. In the acute stage, the lesion becomes a weeping nodule. In the regenerative stage, the lesion dries, a thin yellow crust develops, and small black dots form on the surface. In the papillomatous stage, tiny papillomas form on the surface. In the final, regressive stage, a dry crust forms.1,3,4,6 Uncomplicated lesions rarely leave a residual scar.4
The histopathology of an orf lesion evolves with the clinical stages and helps to secure the diagnosis. The maculopapular and target stages are characterized by vacuolated epidermal cells. In the maculopapular stage, cells have intracytoplasmic inclusions; in the target stage, they have both intracytoplasmic and intranuclear inclusions. The acute stage is marked by patchy areas of lost epidermis, reticular degeneration of the epidermis, and a dermal infiltrate composed primarily of lymphocytes. The regenerative stage involves epidermal regeneration and extrusion of pyknotic hair-follicle cells that form the small black dots on the surface of the lesion. In the papillomatous and regressive stages, fingerlike downward projections of epidermis are evident.1,4,6
The diagnosis of orf is further supported by a history of exposure to infected animals. The most compelling history involves exposure to sheep or goats, but the orf virus has infected other animals, including musk oxen7 and camels.8 Experimental inoculation has produced contagious ecthyma lesions in mule deer, white-tailed deer, pronghorn, and wapiti.9 That wild deer could contract orf and that the infection could be transmitted to humans through direct contact seem reasonable speculations. Our patient's clinical picture suggests that this mechanism may have been involved in her contracting the disease.
Electron microscopic views of characteristic viral particles in the cytoplasm of keratinocytes provide the definitive diagnosis of orf.1,10 Other diagnostic studies are tests of viral culture, complement fixation, and immunofluorescence.1,4,6 These tests are used mainly for epidemiology rather than clinical diagnosis.6
Complications of orf are generally rare but may include fever, chills, rigor, drenching sweat, malaise, lymphadenopathy, and lymphangitis.1,6,10 Secondary bacterial infection is the most common complication.1 Cases of erythema multiforme also have developed in the presence of orf.11
As a benign self-limited disease, orf requires no specific treatment. Antibiotics should be administered in cases of secondary bacterial infection but are otherwise unnecessary.1,2,6 Regression of the lesion may be accelerated by application of idoxuridine.10 Surgical excision also can bring about rapid resolution but is generally contraindicated because the lesion spontaneously regresses without leaving a scar.2 Corticosteroids and other immunosuppressive drugs should be avoided because they can exacerbate the lesion in its papillomatous stage.6,12 Use of topical cidofovir has been beneficial in treating patients who are immunocompromised.13
Although orf is a benign disease with a striking presentation that is easy to spot, early diagnosis can prevent unnecessary diagnostic workup and treatment.1 Orf should be considered in patients presenting with the characteristic skin lesion and a history of exposure to sheep or goats. As with our case, however, when a patient presents with a characteristic lesion and a history of exposure to other animals, orf should be kept in the differential diagnosis.
Orf, also known as contagious ecthyma, scabby mouth, soremouth, contagious pustular dermatitis, and ovine pustular dermatitis, is caused by a member of the genus Parapoxvirus in the family Poxviridae.1,2 The virus typically infects sheep or goats and produces papulovesicular lesions on non–wool-bearing areas (eg, gums, lips, nose, groin).3,4 The infection can be transmitted to humans either by direct contact with an infected animal or by indirect contact with contaminated fomites.4,5 After an incubation period of 3 to 7 days, an erythematous maculopapular lesion develops.1,4 Orf lesions are benign and progress to complete resolution in 6 weeks.4
Case Report
A 51-year-old woman presented to her primary care physician for evaluation of a lesion on the metacarpal-phalangeal joint of the left second digit. A raised annular lesion was identified, and the patient was started on dicloxacillin therapy. On reexamination 4 days later, an enlarging 2-cm nodule with signs of central necrosis was found. The lesion was incised, and a bacterial culture of purulent exudate was obtained. Gram stain and initial culture results were negative. The patient also complained of diarrhea, which was attributed to use of dicloxacillin; this antibiotic was replaced with clarithromycin. The patient was reevaluated the next day for signs of cellulitis and ascending lymphangitis. She denied constitutional symptoms or fever and chills. The lymphangitis was present on the dorsum of the left hand to the level of the wrist. Ceftriaxone was injected intramuscularly. Three days later, an enlarging lesion with serous discharge was identified. The patient was referred for further dermatologic evaluation.
On examining the patient, we found a 2.5-cm boggy fluctuant nodule over the metacarpal-phalangeal joint of the left second digit (Figure). The patient complained of pain, and the hand showed signs of lymphangitic spread. When her history was taken, the patient indicated that she worked at a deer station. Her job involved handling deer carcasses, and her bare hands had been exposed to blood from slaughtered deer. She denied having any contact with sheep, goats, cattle, and farm structures containing those animals. Results of bacterial cultures were negative, and a differential diagnosis of deep fungal infection, atypical mycobacterial infection, or contagious ecthyma was entertained. Two 3-mm punch biopsies were performed. Stains for acid-fast bacilli and fungi were negative. Results of microscopic examination showed vacuolation of cells in the upper third of the malpighian stratum, eosinophilic inclusion bodies, and massive dermal infiltrate.
PLEASE REFER TO THE PDF TO VIEW THE FIGURE
Because of the patient's clinical presentation, microscopic findings, and negative culture results, orf was diagnosed. Oral antibiotic therapy was discontinued, and daily cleansing and use of bacitracin ointment were started. The lesion resolved completely over the ensuing 3 to 4 weeks.
Comment
The diagnosis of orf is suggested by a characteristic skin lesion and a history of exposure. The typical lesion begins as a solitary papule on a finger, a hand,3 or the face.6 Orf lesions classically progress through a series of 6 clinical and histopathologic stages, each lasting approximately 1 week. In the initial maculopapular stage, an erythematous macule or papule erupts. In the target stage, the lesion becomes a papule with a red center, a white middle ring, and a red halo. In the acute stage, the lesion becomes a weeping nodule. In the regenerative stage, the lesion dries, a thin yellow crust develops, and small black dots form on the surface. In the papillomatous stage, tiny papillomas form on the surface. In the final, regressive stage, a dry crust forms.1,3,4,6 Uncomplicated lesions rarely leave a residual scar.4
The histopathology of an orf lesion evolves with the clinical stages and helps to secure the diagnosis. The maculopapular and target stages are characterized by vacuolated epidermal cells. In the maculopapular stage, cells have intracytoplasmic inclusions; in the target stage, they have both intracytoplasmic and intranuclear inclusions. The acute stage is marked by patchy areas of lost epidermis, reticular degeneration of the epidermis, and a dermal infiltrate composed primarily of lymphocytes. The regenerative stage involves epidermal regeneration and extrusion of pyknotic hair-follicle cells that form the small black dots on the surface of the lesion. In the papillomatous and regressive stages, fingerlike downward projections of epidermis are evident.1,4,6
The diagnosis of orf is further supported by a history of exposure to infected animals. The most compelling history involves exposure to sheep or goats, but the orf virus has infected other animals, including musk oxen7 and camels.8 Experimental inoculation has produced contagious ecthyma lesions in mule deer, white-tailed deer, pronghorn, and wapiti.9 That wild deer could contract orf and that the infection could be transmitted to humans through direct contact seem reasonable speculations. Our patient's clinical picture suggests that this mechanism may have been involved in her contracting the disease.
Electron microscopic views of characteristic viral particles in the cytoplasm of keratinocytes provide the definitive diagnosis of orf.1,10 Other diagnostic studies are tests of viral culture, complement fixation, and immunofluorescence.1,4,6 These tests are used mainly for epidemiology rather than clinical diagnosis.6
Complications of orf are generally rare but may include fever, chills, rigor, drenching sweat, malaise, lymphadenopathy, and lymphangitis.1,6,10 Secondary bacterial infection is the most common complication.1 Cases of erythema multiforme also have developed in the presence of orf.11
As a benign self-limited disease, orf requires no specific treatment. Antibiotics should be administered in cases of secondary bacterial infection but are otherwise unnecessary.1,2,6 Regression of the lesion may be accelerated by application of idoxuridine.10 Surgical excision also can bring about rapid resolution but is generally contraindicated because the lesion spontaneously regresses without leaving a scar.2 Corticosteroids and other immunosuppressive drugs should be avoided because they can exacerbate the lesion in its papillomatous stage.6,12 Use of topical cidofovir has been beneficial in treating patients who are immunocompromised.13
Although orf is a benign disease with a striking presentation that is easy to spot, early diagnosis can prevent unnecessary diagnostic workup and treatment.1 Orf should be considered in patients presenting with the characteristic skin lesion and a history of exposure to sheep or goats. As with our case, however, when a patient presents with a characteristic lesion and a history of exposure to other animals, orf should be kept in the differential diagnosis.
- Huerter CJ, Alvarez L, Stinson R. Orf: case report and literature review. Cleve Clin J Med. 1991;58:531-534.
- Chahidi N, de Fontaine S, Lacotte B. Human orf. Br J Plast Surg. 1993;46:532-534.
- Leavell UW, McNamara MJ, Muelling R, et al. Orf: report of 19 human cases with clinical and pathological observations. JAMA. 1968;204:109-116.
- Mendez B, Burnett JW. Orf. Cutis. 1989;44:286-287.
- Wilkinson JD. Orf: a family with unusual complications. Br J Dermatol. 1977;97:447-450.
- Bodnar MG, Miller OF, Tyler WB. Facial orf. J Am Acad Dermatol. 1999;40:815-817.
- Zarnke RL, Dieterich RA, Neiland KA, et al. Serologic and experimental investigations of contagious ecthyma in Alaska. J Wildl Dis. 1983;19:170-174.
- Azwai SM, Carter SD, Woldehiwet Z. Immune responses of the camel (Camelus dromedarius) to contagious ecthyma (orf) virus infection. Vet Microbiol. 1995;47:119-131.
- Lance WR, Hibler CP, DeMartini J. Experimental contagious ecthyma in mule deer, white-tailed deer, pronghorn and wapiti. J Wildl Dis. 1983;19:165-169.
- Lo C, Mathisen G. Human orf in Los Angeles County. West J Med. 1996;164:77-78.
- Agger WA, Webster SB. Human orf infection complicated by erythema multiforme. Cutis. 1983;31:334-338.
- Mohr BW, Katz D. Orf: a case report. Henry Ford Hosp Med J. 1989;37:79-80.
- Geerinck K, Lukito G, Snoeck R, et al. A case of human orf in an immunocompromised patient treated successfully with cidofovir cream. J Med Virol. 2001;64:543-549.
- Huerter CJ, Alvarez L, Stinson R. Orf: case report and literature review. Cleve Clin J Med. 1991;58:531-534.
- Chahidi N, de Fontaine S, Lacotte B. Human orf. Br J Plast Surg. 1993;46:532-534.
- Leavell UW, McNamara MJ, Muelling R, et al. Orf: report of 19 human cases with clinical and pathological observations. JAMA. 1968;204:109-116.
- Mendez B, Burnett JW. Orf. Cutis. 1989;44:286-287.
- Wilkinson JD. Orf: a family with unusual complications. Br J Dermatol. 1977;97:447-450.
- Bodnar MG, Miller OF, Tyler WB. Facial orf. J Am Acad Dermatol. 1999;40:815-817.
- Zarnke RL, Dieterich RA, Neiland KA, et al. Serologic and experimental investigations of contagious ecthyma in Alaska. J Wildl Dis. 1983;19:170-174.
- Azwai SM, Carter SD, Woldehiwet Z. Immune responses of the camel (Camelus dromedarius) to contagious ecthyma (orf) virus infection. Vet Microbiol. 1995;47:119-131.
- Lance WR, Hibler CP, DeMartini J. Experimental contagious ecthyma in mule deer, white-tailed deer, pronghorn and wapiti. J Wildl Dis. 1983;19:165-169.
- Lo C, Mathisen G. Human orf in Los Angeles County. West J Med. 1996;164:77-78.
- Agger WA, Webster SB. Human orf infection complicated by erythema multiforme. Cutis. 1983;31:334-338.
- Mohr BW, Katz D. Orf: a case report. Henry Ford Hosp Med J. 1989;37:79-80.
- Geerinck K, Lukito G, Snoeck R, et al. A case of human orf in an immunocompromised patient treated successfully with cidofovir cream. J Med Virol. 2001;64:543-549.
Case Report: Teledermatology and Epiluminescence Microscopy for the Diagnosis of Scabies
Fibro-Fatty Nodules and Low Back Pain
METHODS: We describe 2 patients with painful nodules in the lower back and lateral iliac crest areas. In both cases, the signs and symptoms were unusual and presented at locations distant from the nodule. One patient complained of severe acute lower abdominal pain, and the other had been treated for chronic recurrent trochanteric bursitis for several years.
RESULTS: In both patients, symptoms appeared to be relieved by multiple injection of the nodule.
DISCUSSION: There is agreement that back mice exist. Referred pain from the nodules might explain the distant symptoms and signs in these cases. Multiple puncture may be an effective treatment because it lessens the tension of a fibro-fatty nodule.
CONCLUSIONS: Randomized trials on this subject are needed. In the meantime, physicians should keep back mice in mind when presented with atypical and unaccountable symptoms in the lower abdomen, inguinal region, or legs.
A part from symptoms caused by vertebral disk injury, the scientific evidence for the specific causation and effective treatment of low back problems is relatively weak. Clinicians who wish to adhere to evidence-based practice when treating persistent low back pain are faced with a limited number of useful interventions: short-term therapy with muscle relaxants and analgesics, and encouragement to return to daily routines as quickly as possible.1-3
Though doubt has been cast on the real existence of subtypes or syndromes of low back pain, our clinical observation and experience suggest that a fibro-fatty nodule (“back mouse”) may be an identifiable and remediable cause of acute or chronic low back pain.4,5 Given the extent of the costs and suffering caused by low back pain, effective therapy for even a few cases of recurrent or chronic pain would be helpful. We describe 2 patients for whom back mice were the likely cause of low back pain and were associated with unusual symptoms and signs, masquerading as other clinical problems. In both cases, the full medical records from the Family Practice Center and University of North Carolina hospitals were available for evaluation.
Methods and results
Bilateral Trochanteric Bursitis
In 1985 Ms C, a 53-year-old nursing aide, developed typical signs and symptoms of trochanteric bursitis following a vaginal hysterectomy. She also suffered from mild hypertension and chronic depression. The hip pain was intermittent and would affect one side and then the other, often radiating down the legs and limiting her ability to walk. Examination revealed marked tenderness to palpation over the greater trochanter in either hip area. There were no clear precipitating factors.
She was first treated with a variety of nonsteroidal anti-inflammatory agents, with little effect. Subsequently, she received physical therapy including ultrasound, exercise, and cushioned shoes, all of which produced only temporary relief. Because of the chronic pain antidepressants were also tried, which improved her depression but provided minimal improvement for the hip problem.
In 1991, orthopedic evaluation confirmed the findings of relapsing bilateral trochanteric bursitis with an otherwise normal physical examination. Lumbosacral spine and hip radiographs showed only mild degeneration of the L4/5 vertebral disk. The greatest relief for the patient came from injections of lidocaine hydrochloride and methylprednisolone acetate directly into each bursa, but relief lasted only a few weeks after each injection. They had to be repeated on a regular basis. She also needed acetaminophen and oxycodone twice daily to help control the pain, and in 1995 she applied for disability.
At that time, the orthopedic specialist discharged her back to her family physician with a diagnosis of chronic trochanteric bursitis for which no other treatment could be offered. In 1997 another orthopedic consultation led to the same opinion, based on typical symptoms and clinical findings. In 1998, during a discussion of the lack of treatment options for this chronic problem, it was suggested that the symptoms could be secondary to a lower back problem and a careful soft tissue examination might be of value. Detailed examination revealed 2 long rubbery and tender fibro-fatty nodules, each one lying on an iliac crest (right side=3 cm by l cm; left side=6 cm by l cm) These findings correlated with previous descriptions of fibro-fatty nodules in the back region.4,7
Repeated testing using firm palpation of these nodules reproduced the pain over each greater trochanteric area where the patient had experienced pain in the past. Each nodule was treated with multiple puncture technique (6 to 8 punctures of the fibrous capsule of the nodule) and injected with 3 cc of lidocaine hydrochloride and 40 mg methylprednisolone acetate.4,5 There was immediate and complete relief of the clinical symptoms and signs. Five months after the injections there has been no recurrence of the clinical characteristics of trochanteric bursitis, though there have been other symptoms of lumbosacral pain.
An Abdominal Emergency
In 1997 Ms W, a 35-year-old with type 2 diabetes (controlled by diet and exercise) was working as a nurse on the pediatric ward. She came to the urgent care clinic at the Family Practice Center with symptoms of mild low back pain and right-sided lower abdominal pain which were associated with dysuria and frequency of urination during the previous 2 months. She had suffered an episode of low back pain 2 years earlier. Her urine showed a mildly positive leukocyte esterase test and a trace of protein, and she was given a course of trimethoprim.
Ten days later she returned reporting that the abdominal pain had become much worse, particularly when sitting and lying down, and it kept her awake at night. She complained of a feeling of fullness in the right lower quadrant of the abdomen. There were no changes in her bowel habit, and she had no fever, nausea, or anorexia. She was taking maximum doses of ibuprofen and acetaminophen for the pain. A repeat urinalysis was normal. She had previously had a hysterectomy and appendectomy, as well as polycystic ovaries, but the results of a pelvic examination were normal. Examination of the abdomen revealed normal bowel sounds and some tenderness in the right lower quadrant, close to the superior iliac spine. Because of her history of persistent back pain and a lack of explanation for her abdominal symptoms, x-rays of the lumbosacral spine and pelvis were ordered.
When she was seen again 2 days later, the abdominal pain had become much more severe. It was sharp, intermittent, not colicky, and traveled down into the groin and right anterior thigh. There was considerably less pain when she was standing. She had normal bowel sounds but was again acutely sensitive to palpation in the lower abdomen just above the anterior superior iliac crest. Assessment for acute abdominal pain included an electrolyte panel and complete blood count, which were normal except for a white blood count of 11,200. The lumbar and pelvic radiologic studies showed mild degeneration of the hip joints and some spurring of the inferior aspect of both sacroiliac joints.
With a working diagnosis of lower abdominal abscess, she was referred to the emergency department to be seen by the family medicine inpatient team. A computed tomography scan of the abdomen and pelvis was normal, showing only a small ovarian cyst on the left ovary. However, a repeat white blood count (several hours later) was 13,100. A surgical consultation was requested, but the surgeon found no evidence of an acute abdominal process, giving his opinion that this was a musculoskeletal problem.
At the suggestion of one of the family medicine faculty a more detailed examination of the sacroiliac joints was performed, and the resident found significant point tenderness over the right sacroiliac joint. Deep palpation of this joint area also produced pain radiating to the right inguinal region. It was felt that the acute abdominal problem might be caused by referred pain from the sacroiliac joint. The patient received an injection of 60 mg ketorolac tromethamine, which produced considerable relief, and she was sent home. However, there was no clear explanation for the 2 occasions of elevated white blood cell count.
At follow-up 10 days later the abdominal pain had subsided, but she was complaining of much more pain in the right lower back with referral down the front of her thighs. There was still tenderness over the right sacroiliac joint, and she was sent to a physical therapist for evaluation and treatment. During her first visit to the physical therapist, in addition to the low back symptoms she again reported increasing right lower abdominal pain that was worse when sitting, better when standing. Careful examination revealed an extremely tender 3 cm long, partly mobile, fibro-fatty nodule along the mid-region of the right iliac crest, approximately 4 inches lateral to the spinous process of the lumbar vertebra. Repeated firm, direct pressure on this nodule made the patient cry and reproduced the right lower abdominal symptoms.
Following injection with multiple puncture technique, lidocaine hydrochloride 3 cc and methyprednisolone acetate 40 mg, the patient experienced immediate pain relief with no more abdominal symptoms and no difficulty in sitting or lying down. Since that time (2 years ago), there has been no recurrence of these symptoms. Although the cause of the abdominal pain might have been a polycystic ovary, the workup did not support this conclusion and revealed no other obvious cause for the severe symptoms. Injecting a painful nodular swelling in the lower back that fitted the characteristics of previously described fibro-fatty nodules provided immediate relief of the pain, suggesting a possible association with the anterior abdominal symptoms.
Discussion
Do Back Mice Really Exist?
There is general agreement in a number of published case series from various rheumatologic and hospital populations that these nodules do exist, with an estimated prevalence of 15% in the general population.5,7 These studies all report characteristic locations and clinical findings of a rubbery, well-defined, often mobile, round or oval swelling in the deep subcutaneous tissues. Though these can be painful, they never show evidence of infection and are frequently asymptomatic. The only other frequently found nodules with a similar anatomical location are lipomas (more superficial and soft to palpation) and sebaceous cysts (more superficial and usually circular).
Why Would Back Mice Masquerade as Other Conditions?
It is difficult to postulate a direct mechanical effect in which a low back nodule would produce pain at a distant location, so it is more likely that this is some form of referred pain. The authors of previous studies have reported that these nodules may mimic sciatic nerve root compression and lead to a diagnosis of vertebral disk prolapse.6-8 The 2 cases we report appear to show a pattern different from that of the sciatic nerve. The first case is similar to data reported by Collee and colleagues9 in a study of hospital and primary care patients suffering from low back pain. They found that a substantial proportion of patients (45% and 25%, respectively) with low back pain also complained of greater trochanteric pain syndrome. There may be a specific referral pathway linking the 2 areas. It is more difficult to explain an association between a back mouse and the symptoms of abdominal pain in the second case. One possible mechanism could be a referral pattern, well reported in the literature, that comes from musculoskeletal structures (fascia, muscle, fibrous tissue, tendons) and follows sclerotomal distribution rather than the segmental dermatomes shown in most anatomical texts.10-12 There is ample evidence that anterior abdominal pain can be referred from musculoskeletal elements in the low back region and can be quite severe.13 Referred pain from the fibrous capsule surrounding fibro-fatty nodules might explain the distant symptoms and signs in our 2 cases.
Where Do Back Mice Come From?
Pathologic studies show that these nodules consist of a fibrous capsule containing fat divided by fibrous septa and some fine blood vessels and nerve fibers, and they usually have a stalk connecting them to the tissues below the deep fascial layers.8 It has been suggested that these nodules and their stalks are formed by extrusion through the neurovascular foramina in the deep fascia as a result of mechanical stresses.
Why Would Back Mice Cause Pain?
The answer to this is not known. Nodules that have been examined after surgery have not shown evidence of inflammation as a cause of pain, though nerve fibers are found in the fibrous capsule. In our experience, the immediate relief of pain frequently produced by multiple needle puncture, compared with poor relief with a single puncture, suggests that the pain might be caused by raised intranodular pressure.6
Why Would Injections Relieve Pain Caused by Back Mice?
A recent long-term follow-up study of 35 patients showed that 89% had lasting relief. Generally, placebo effects from injections do not exceed 50% improvement.6 If lidocaine hydrochloride is used, its possible beneficial effects may come from washing out irritant chemicals (substance P) from the area, from local vasodilation that facilitates the removal of metabolites, or from the interruption of the neural feedback mechanism.13 However, the local anesthetic effect is too short to explain lasting relief, and a randomized controlled study of injection therapy of the iliac crest syndrome showed no difference in pain outcome between lidocaine hydrochloride and saline.14 This would tend to support the possibility that multiple puncture, rather than the injected material, is effective because it lessens the tension of the innervated fibrous capsule. Does Injection Treatment of the Back Mouse Really Work? There have been no randomized controlled trials and, until recently, no published long-term follow-up studies of treatment. It is not clear if multiple puncture of the nodule followed by deep massage alone is effective or whether the addition of local anesthetic and steroid improves outcome.
Conclusions
Until a rigorous study demonstrates the reliability and reproducibility of the clinical diagnosis of the back mouse and the effectiveness of treatment in a randomized controlled trial, our best advice for physicians, based purely on clinical and biased observation, is to consider the back mouse when atypical and unaccountable symptoms and signs are found in the lower abdomen, inguinal region, or legs.
Acknowledgements
We are grateful to Barry R. Howes, PT, and Robert E. Gwyther for guidance in the preparation of this report.
1. Bigos S, Bowyer O, Braen G, et al. Acute low back problems in adults. Clinical practice guideline no.14. Rockville, Md: US Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1994. AHCPR publication no. 95-0643.
2. Cherkin DC, Deyo RA, Battie M, Street J, Barlow W. A comparison of physical therapy, chiropractic manipulation and provision of an educational booklet for the treatment of patients with low back pain. N Engl J Med 1998;339:1021-9.
3. Riddle DL. Classification and low back pain: a review of the literature and critical analysis of selected systems. Phys Therap 1998;78:708-37.
4. Curtis P. In search of the “back mouse”. J Fam Pract 1993;36:657-9.
5. Reis E. Episacroiliac lipoma. Am J Obstet Gynecol 1937;34:492-8.
6. Motyka TM, Howes BR, Gwyther R, Curtis P. Treatment of low back pain caused by “back mice”: a case series. In press.
7. Swezey RI. Non-fibrositic lumbar cutaneous nodules: prevalence and clinical significance. Br J Rheumatol 1991;30:376-8.
8. Copeman WSC, Ackerman WL. Edema or herniation of fat lobules as a cause for lumbar and gluteal “fibrositis”. Arch Intern Med 1947;79:22-35.
9. Collee G, Djikmans BAC, Vandenbroucke JP, Cats A. Greater trochanteric pain syndrome (trochanteric bursitis) in low back pain. Scan J Rheumatol 1991;20:262-6.
10. Kellgren JH. A preliminary account of referred pain arising from muscle. BMJ 1938;1:325-7.
11. Inman VT, Saunders JB, de CJM. Referred pain from skeletal structures. J Nerv Ment Dis 1944;99:660-7.
12. Wall P. Neurophysiological mechanisms of referred pain and hyperalgesia. In: Vecchiet L, Albe-Ferrard D, Lindblom U, eds. New trends in referred pain and hyperalgesia. Vol 7. Holland, Netherlands: Elsevier; 1993.
13. Travell JG, Simons DG. Myofascial pain and dysfunction: the trigger point manual. Vol 1, pp 638; Vol 2, pp 30. Baltimore, Md: Williams and Wilkins; 1983.
14. Collee G, Djikmans BAC, Vandenbroucke JP, Cats A. Iliac crest syndrome in low back pain: a double blind randomized study of local injection therapy. J Rheumatol 1991;18:1060-3.
METHODS: We describe 2 patients with painful nodules in the lower back and lateral iliac crest areas. In both cases, the signs and symptoms were unusual and presented at locations distant from the nodule. One patient complained of severe acute lower abdominal pain, and the other had been treated for chronic recurrent trochanteric bursitis for several years.
RESULTS: In both patients, symptoms appeared to be relieved by multiple injection of the nodule.
DISCUSSION: There is agreement that back mice exist. Referred pain from the nodules might explain the distant symptoms and signs in these cases. Multiple puncture may be an effective treatment because it lessens the tension of a fibro-fatty nodule.
CONCLUSIONS: Randomized trials on this subject are needed. In the meantime, physicians should keep back mice in mind when presented with atypical and unaccountable symptoms in the lower abdomen, inguinal region, or legs.
A part from symptoms caused by vertebral disk injury, the scientific evidence for the specific causation and effective treatment of low back problems is relatively weak. Clinicians who wish to adhere to evidence-based practice when treating persistent low back pain are faced with a limited number of useful interventions: short-term therapy with muscle relaxants and analgesics, and encouragement to return to daily routines as quickly as possible.1-3
Though doubt has been cast on the real existence of subtypes or syndromes of low back pain, our clinical observation and experience suggest that a fibro-fatty nodule (“back mouse”) may be an identifiable and remediable cause of acute or chronic low back pain.4,5 Given the extent of the costs and suffering caused by low back pain, effective therapy for even a few cases of recurrent or chronic pain would be helpful. We describe 2 patients for whom back mice were the likely cause of low back pain and were associated with unusual symptoms and signs, masquerading as other clinical problems. In both cases, the full medical records from the Family Practice Center and University of North Carolina hospitals were available for evaluation.
Methods and results
Bilateral Trochanteric Bursitis
In 1985 Ms C, a 53-year-old nursing aide, developed typical signs and symptoms of trochanteric bursitis following a vaginal hysterectomy. She also suffered from mild hypertension and chronic depression. The hip pain was intermittent and would affect one side and then the other, often radiating down the legs and limiting her ability to walk. Examination revealed marked tenderness to palpation over the greater trochanter in either hip area. There were no clear precipitating factors.
She was first treated with a variety of nonsteroidal anti-inflammatory agents, with little effect. Subsequently, she received physical therapy including ultrasound, exercise, and cushioned shoes, all of which produced only temporary relief. Because of the chronic pain antidepressants were also tried, which improved her depression but provided minimal improvement for the hip problem.
In 1991, orthopedic evaluation confirmed the findings of relapsing bilateral trochanteric bursitis with an otherwise normal physical examination. Lumbosacral spine and hip radiographs showed only mild degeneration of the L4/5 vertebral disk. The greatest relief for the patient came from injections of lidocaine hydrochloride and methylprednisolone acetate directly into each bursa, but relief lasted only a few weeks after each injection. They had to be repeated on a regular basis. She also needed acetaminophen and oxycodone twice daily to help control the pain, and in 1995 she applied for disability.
At that time, the orthopedic specialist discharged her back to her family physician with a diagnosis of chronic trochanteric bursitis for which no other treatment could be offered. In 1997 another orthopedic consultation led to the same opinion, based on typical symptoms and clinical findings. In 1998, during a discussion of the lack of treatment options for this chronic problem, it was suggested that the symptoms could be secondary to a lower back problem and a careful soft tissue examination might be of value. Detailed examination revealed 2 long rubbery and tender fibro-fatty nodules, each one lying on an iliac crest (right side=3 cm by l cm; left side=6 cm by l cm) These findings correlated with previous descriptions of fibro-fatty nodules in the back region.4,7
Repeated testing using firm palpation of these nodules reproduced the pain over each greater trochanteric area where the patient had experienced pain in the past. Each nodule was treated with multiple puncture technique (6 to 8 punctures of the fibrous capsule of the nodule) and injected with 3 cc of lidocaine hydrochloride and 40 mg methylprednisolone acetate.4,5 There was immediate and complete relief of the clinical symptoms and signs. Five months after the injections there has been no recurrence of the clinical characteristics of trochanteric bursitis, though there have been other symptoms of lumbosacral pain.
An Abdominal Emergency
In 1997 Ms W, a 35-year-old with type 2 diabetes (controlled by diet and exercise) was working as a nurse on the pediatric ward. She came to the urgent care clinic at the Family Practice Center with symptoms of mild low back pain and right-sided lower abdominal pain which were associated with dysuria and frequency of urination during the previous 2 months. She had suffered an episode of low back pain 2 years earlier. Her urine showed a mildly positive leukocyte esterase test and a trace of protein, and she was given a course of trimethoprim.
Ten days later she returned reporting that the abdominal pain had become much worse, particularly when sitting and lying down, and it kept her awake at night. She complained of a feeling of fullness in the right lower quadrant of the abdomen. There were no changes in her bowel habit, and she had no fever, nausea, or anorexia. She was taking maximum doses of ibuprofen and acetaminophen for the pain. A repeat urinalysis was normal. She had previously had a hysterectomy and appendectomy, as well as polycystic ovaries, but the results of a pelvic examination were normal. Examination of the abdomen revealed normal bowel sounds and some tenderness in the right lower quadrant, close to the superior iliac spine. Because of her history of persistent back pain and a lack of explanation for her abdominal symptoms, x-rays of the lumbosacral spine and pelvis were ordered.
When she was seen again 2 days later, the abdominal pain had become much more severe. It was sharp, intermittent, not colicky, and traveled down into the groin and right anterior thigh. There was considerably less pain when she was standing. She had normal bowel sounds but was again acutely sensitive to palpation in the lower abdomen just above the anterior superior iliac crest. Assessment for acute abdominal pain included an electrolyte panel and complete blood count, which were normal except for a white blood count of 11,200. The lumbar and pelvic radiologic studies showed mild degeneration of the hip joints and some spurring of the inferior aspect of both sacroiliac joints.
With a working diagnosis of lower abdominal abscess, she was referred to the emergency department to be seen by the family medicine inpatient team. A computed tomography scan of the abdomen and pelvis was normal, showing only a small ovarian cyst on the left ovary. However, a repeat white blood count (several hours later) was 13,100. A surgical consultation was requested, but the surgeon found no evidence of an acute abdominal process, giving his opinion that this was a musculoskeletal problem.
At the suggestion of one of the family medicine faculty a more detailed examination of the sacroiliac joints was performed, and the resident found significant point tenderness over the right sacroiliac joint. Deep palpation of this joint area also produced pain radiating to the right inguinal region. It was felt that the acute abdominal problem might be caused by referred pain from the sacroiliac joint. The patient received an injection of 60 mg ketorolac tromethamine, which produced considerable relief, and she was sent home. However, there was no clear explanation for the 2 occasions of elevated white blood cell count.
At follow-up 10 days later the abdominal pain had subsided, but she was complaining of much more pain in the right lower back with referral down the front of her thighs. There was still tenderness over the right sacroiliac joint, and she was sent to a physical therapist for evaluation and treatment. During her first visit to the physical therapist, in addition to the low back symptoms she again reported increasing right lower abdominal pain that was worse when sitting, better when standing. Careful examination revealed an extremely tender 3 cm long, partly mobile, fibro-fatty nodule along the mid-region of the right iliac crest, approximately 4 inches lateral to the spinous process of the lumbar vertebra. Repeated firm, direct pressure on this nodule made the patient cry and reproduced the right lower abdominal symptoms.
Following injection with multiple puncture technique, lidocaine hydrochloride 3 cc and methyprednisolone acetate 40 mg, the patient experienced immediate pain relief with no more abdominal symptoms and no difficulty in sitting or lying down. Since that time (2 years ago), there has been no recurrence of these symptoms. Although the cause of the abdominal pain might have been a polycystic ovary, the workup did not support this conclusion and revealed no other obvious cause for the severe symptoms. Injecting a painful nodular swelling in the lower back that fitted the characteristics of previously described fibro-fatty nodules provided immediate relief of the pain, suggesting a possible association with the anterior abdominal symptoms.
Discussion
Do Back Mice Really Exist?
There is general agreement in a number of published case series from various rheumatologic and hospital populations that these nodules do exist, with an estimated prevalence of 15% in the general population.5,7 These studies all report characteristic locations and clinical findings of a rubbery, well-defined, often mobile, round or oval swelling in the deep subcutaneous tissues. Though these can be painful, they never show evidence of infection and are frequently asymptomatic. The only other frequently found nodules with a similar anatomical location are lipomas (more superficial and soft to palpation) and sebaceous cysts (more superficial and usually circular).
Why Would Back Mice Masquerade as Other Conditions?
It is difficult to postulate a direct mechanical effect in which a low back nodule would produce pain at a distant location, so it is more likely that this is some form of referred pain. The authors of previous studies have reported that these nodules may mimic sciatic nerve root compression and lead to a diagnosis of vertebral disk prolapse.6-8 The 2 cases we report appear to show a pattern different from that of the sciatic nerve. The first case is similar to data reported by Collee and colleagues9 in a study of hospital and primary care patients suffering from low back pain. They found that a substantial proportion of patients (45% and 25%, respectively) with low back pain also complained of greater trochanteric pain syndrome. There may be a specific referral pathway linking the 2 areas. It is more difficult to explain an association between a back mouse and the symptoms of abdominal pain in the second case. One possible mechanism could be a referral pattern, well reported in the literature, that comes from musculoskeletal structures (fascia, muscle, fibrous tissue, tendons) and follows sclerotomal distribution rather than the segmental dermatomes shown in most anatomical texts.10-12 There is ample evidence that anterior abdominal pain can be referred from musculoskeletal elements in the low back region and can be quite severe.13 Referred pain from the fibrous capsule surrounding fibro-fatty nodules might explain the distant symptoms and signs in our 2 cases.
Where Do Back Mice Come From?
Pathologic studies show that these nodules consist of a fibrous capsule containing fat divided by fibrous septa and some fine blood vessels and nerve fibers, and they usually have a stalk connecting them to the tissues below the deep fascial layers.8 It has been suggested that these nodules and their stalks are formed by extrusion through the neurovascular foramina in the deep fascia as a result of mechanical stresses.
Why Would Back Mice Cause Pain?
The answer to this is not known. Nodules that have been examined after surgery have not shown evidence of inflammation as a cause of pain, though nerve fibers are found in the fibrous capsule. In our experience, the immediate relief of pain frequently produced by multiple needle puncture, compared with poor relief with a single puncture, suggests that the pain might be caused by raised intranodular pressure.6
Why Would Injections Relieve Pain Caused by Back Mice?
A recent long-term follow-up study of 35 patients showed that 89% had lasting relief. Generally, placebo effects from injections do not exceed 50% improvement.6 If lidocaine hydrochloride is used, its possible beneficial effects may come from washing out irritant chemicals (substance P) from the area, from local vasodilation that facilitates the removal of metabolites, or from the interruption of the neural feedback mechanism.13 However, the local anesthetic effect is too short to explain lasting relief, and a randomized controlled study of injection therapy of the iliac crest syndrome showed no difference in pain outcome between lidocaine hydrochloride and saline.14 This would tend to support the possibility that multiple puncture, rather than the injected material, is effective because it lessens the tension of the innervated fibrous capsule. Does Injection Treatment of the Back Mouse Really Work? There have been no randomized controlled trials and, until recently, no published long-term follow-up studies of treatment. It is not clear if multiple puncture of the nodule followed by deep massage alone is effective or whether the addition of local anesthetic and steroid improves outcome.
Conclusions
Until a rigorous study demonstrates the reliability and reproducibility of the clinical diagnosis of the back mouse and the effectiveness of treatment in a randomized controlled trial, our best advice for physicians, based purely on clinical and biased observation, is to consider the back mouse when atypical and unaccountable symptoms and signs are found in the lower abdomen, inguinal region, or legs.
Acknowledgements
We are grateful to Barry R. Howes, PT, and Robert E. Gwyther for guidance in the preparation of this report.
METHODS: We describe 2 patients with painful nodules in the lower back and lateral iliac crest areas. In both cases, the signs and symptoms were unusual and presented at locations distant from the nodule. One patient complained of severe acute lower abdominal pain, and the other had been treated for chronic recurrent trochanteric bursitis for several years.
RESULTS: In both patients, symptoms appeared to be relieved by multiple injection of the nodule.
DISCUSSION: There is agreement that back mice exist. Referred pain from the nodules might explain the distant symptoms and signs in these cases. Multiple puncture may be an effective treatment because it lessens the tension of a fibro-fatty nodule.
CONCLUSIONS: Randomized trials on this subject are needed. In the meantime, physicians should keep back mice in mind when presented with atypical and unaccountable symptoms in the lower abdomen, inguinal region, or legs.
A part from symptoms caused by vertebral disk injury, the scientific evidence for the specific causation and effective treatment of low back problems is relatively weak. Clinicians who wish to adhere to evidence-based practice when treating persistent low back pain are faced with a limited number of useful interventions: short-term therapy with muscle relaxants and analgesics, and encouragement to return to daily routines as quickly as possible.1-3
Though doubt has been cast on the real existence of subtypes or syndromes of low back pain, our clinical observation and experience suggest that a fibro-fatty nodule (“back mouse”) may be an identifiable and remediable cause of acute or chronic low back pain.4,5 Given the extent of the costs and suffering caused by low back pain, effective therapy for even a few cases of recurrent or chronic pain would be helpful. We describe 2 patients for whom back mice were the likely cause of low back pain and were associated with unusual symptoms and signs, masquerading as other clinical problems. In both cases, the full medical records from the Family Practice Center and University of North Carolina hospitals were available for evaluation.
Methods and results
Bilateral Trochanteric Bursitis
In 1985 Ms C, a 53-year-old nursing aide, developed typical signs and symptoms of trochanteric bursitis following a vaginal hysterectomy. She also suffered from mild hypertension and chronic depression. The hip pain was intermittent and would affect one side and then the other, often radiating down the legs and limiting her ability to walk. Examination revealed marked tenderness to palpation over the greater trochanter in either hip area. There were no clear precipitating factors.
She was first treated with a variety of nonsteroidal anti-inflammatory agents, with little effect. Subsequently, she received physical therapy including ultrasound, exercise, and cushioned shoes, all of which produced only temporary relief. Because of the chronic pain antidepressants were also tried, which improved her depression but provided minimal improvement for the hip problem.
In 1991, orthopedic evaluation confirmed the findings of relapsing bilateral trochanteric bursitis with an otherwise normal physical examination. Lumbosacral spine and hip radiographs showed only mild degeneration of the L4/5 vertebral disk. The greatest relief for the patient came from injections of lidocaine hydrochloride and methylprednisolone acetate directly into each bursa, but relief lasted only a few weeks after each injection. They had to be repeated on a regular basis. She also needed acetaminophen and oxycodone twice daily to help control the pain, and in 1995 she applied for disability.
At that time, the orthopedic specialist discharged her back to her family physician with a diagnosis of chronic trochanteric bursitis for which no other treatment could be offered. In 1997 another orthopedic consultation led to the same opinion, based on typical symptoms and clinical findings. In 1998, during a discussion of the lack of treatment options for this chronic problem, it was suggested that the symptoms could be secondary to a lower back problem and a careful soft tissue examination might be of value. Detailed examination revealed 2 long rubbery and tender fibro-fatty nodules, each one lying on an iliac crest (right side=3 cm by l cm; left side=6 cm by l cm) These findings correlated with previous descriptions of fibro-fatty nodules in the back region.4,7
Repeated testing using firm palpation of these nodules reproduced the pain over each greater trochanteric area where the patient had experienced pain in the past. Each nodule was treated with multiple puncture technique (6 to 8 punctures of the fibrous capsule of the nodule) and injected with 3 cc of lidocaine hydrochloride and 40 mg methylprednisolone acetate.4,5 There was immediate and complete relief of the clinical symptoms and signs. Five months after the injections there has been no recurrence of the clinical characteristics of trochanteric bursitis, though there have been other symptoms of lumbosacral pain.
An Abdominal Emergency
In 1997 Ms W, a 35-year-old with type 2 diabetes (controlled by diet and exercise) was working as a nurse on the pediatric ward. She came to the urgent care clinic at the Family Practice Center with symptoms of mild low back pain and right-sided lower abdominal pain which were associated with dysuria and frequency of urination during the previous 2 months. She had suffered an episode of low back pain 2 years earlier. Her urine showed a mildly positive leukocyte esterase test and a trace of protein, and she was given a course of trimethoprim.
Ten days later she returned reporting that the abdominal pain had become much worse, particularly when sitting and lying down, and it kept her awake at night. She complained of a feeling of fullness in the right lower quadrant of the abdomen. There were no changes in her bowel habit, and she had no fever, nausea, or anorexia. She was taking maximum doses of ibuprofen and acetaminophen for the pain. A repeat urinalysis was normal. She had previously had a hysterectomy and appendectomy, as well as polycystic ovaries, but the results of a pelvic examination were normal. Examination of the abdomen revealed normal bowel sounds and some tenderness in the right lower quadrant, close to the superior iliac spine. Because of her history of persistent back pain and a lack of explanation for her abdominal symptoms, x-rays of the lumbosacral spine and pelvis were ordered.
When she was seen again 2 days later, the abdominal pain had become much more severe. It was sharp, intermittent, not colicky, and traveled down into the groin and right anterior thigh. There was considerably less pain when she was standing. She had normal bowel sounds but was again acutely sensitive to palpation in the lower abdomen just above the anterior superior iliac crest. Assessment for acute abdominal pain included an electrolyte panel and complete blood count, which were normal except for a white blood count of 11,200. The lumbar and pelvic radiologic studies showed mild degeneration of the hip joints and some spurring of the inferior aspect of both sacroiliac joints.
With a working diagnosis of lower abdominal abscess, she was referred to the emergency department to be seen by the family medicine inpatient team. A computed tomography scan of the abdomen and pelvis was normal, showing only a small ovarian cyst on the left ovary. However, a repeat white blood count (several hours later) was 13,100. A surgical consultation was requested, but the surgeon found no evidence of an acute abdominal process, giving his opinion that this was a musculoskeletal problem.
At the suggestion of one of the family medicine faculty a more detailed examination of the sacroiliac joints was performed, and the resident found significant point tenderness over the right sacroiliac joint. Deep palpation of this joint area also produced pain radiating to the right inguinal region. It was felt that the acute abdominal problem might be caused by referred pain from the sacroiliac joint. The patient received an injection of 60 mg ketorolac tromethamine, which produced considerable relief, and she was sent home. However, there was no clear explanation for the 2 occasions of elevated white blood cell count.
At follow-up 10 days later the abdominal pain had subsided, but she was complaining of much more pain in the right lower back with referral down the front of her thighs. There was still tenderness over the right sacroiliac joint, and she was sent to a physical therapist for evaluation and treatment. During her first visit to the physical therapist, in addition to the low back symptoms she again reported increasing right lower abdominal pain that was worse when sitting, better when standing. Careful examination revealed an extremely tender 3 cm long, partly mobile, fibro-fatty nodule along the mid-region of the right iliac crest, approximately 4 inches lateral to the spinous process of the lumbar vertebra. Repeated firm, direct pressure on this nodule made the patient cry and reproduced the right lower abdominal symptoms.
Following injection with multiple puncture technique, lidocaine hydrochloride 3 cc and methyprednisolone acetate 40 mg, the patient experienced immediate pain relief with no more abdominal symptoms and no difficulty in sitting or lying down. Since that time (2 years ago), there has been no recurrence of these symptoms. Although the cause of the abdominal pain might have been a polycystic ovary, the workup did not support this conclusion and revealed no other obvious cause for the severe symptoms. Injecting a painful nodular swelling in the lower back that fitted the characteristics of previously described fibro-fatty nodules provided immediate relief of the pain, suggesting a possible association with the anterior abdominal symptoms.
Discussion
Do Back Mice Really Exist?
There is general agreement in a number of published case series from various rheumatologic and hospital populations that these nodules do exist, with an estimated prevalence of 15% in the general population.5,7 These studies all report characteristic locations and clinical findings of a rubbery, well-defined, often mobile, round or oval swelling in the deep subcutaneous tissues. Though these can be painful, they never show evidence of infection and are frequently asymptomatic. The only other frequently found nodules with a similar anatomical location are lipomas (more superficial and soft to palpation) and sebaceous cysts (more superficial and usually circular).
Why Would Back Mice Masquerade as Other Conditions?
It is difficult to postulate a direct mechanical effect in which a low back nodule would produce pain at a distant location, so it is more likely that this is some form of referred pain. The authors of previous studies have reported that these nodules may mimic sciatic nerve root compression and lead to a diagnosis of vertebral disk prolapse.6-8 The 2 cases we report appear to show a pattern different from that of the sciatic nerve. The first case is similar to data reported by Collee and colleagues9 in a study of hospital and primary care patients suffering from low back pain. They found that a substantial proportion of patients (45% and 25%, respectively) with low back pain also complained of greater trochanteric pain syndrome. There may be a specific referral pathway linking the 2 areas. It is more difficult to explain an association between a back mouse and the symptoms of abdominal pain in the second case. One possible mechanism could be a referral pattern, well reported in the literature, that comes from musculoskeletal structures (fascia, muscle, fibrous tissue, tendons) and follows sclerotomal distribution rather than the segmental dermatomes shown in most anatomical texts.10-12 There is ample evidence that anterior abdominal pain can be referred from musculoskeletal elements in the low back region and can be quite severe.13 Referred pain from the fibrous capsule surrounding fibro-fatty nodules might explain the distant symptoms and signs in our 2 cases.
Where Do Back Mice Come From?
Pathologic studies show that these nodules consist of a fibrous capsule containing fat divided by fibrous septa and some fine blood vessels and nerve fibers, and they usually have a stalk connecting them to the tissues below the deep fascial layers.8 It has been suggested that these nodules and their stalks are formed by extrusion through the neurovascular foramina in the deep fascia as a result of mechanical stresses.
Why Would Back Mice Cause Pain?
The answer to this is not known. Nodules that have been examined after surgery have not shown evidence of inflammation as a cause of pain, though nerve fibers are found in the fibrous capsule. In our experience, the immediate relief of pain frequently produced by multiple needle puncture, compared with poor relief with a single puncture, suggests that the pain might be caused by raised intranodular pressure.6
Why Would Injections Relieve Pain Caused by Back Mice?
A recent long-term follow-up study of 35 patients showed that 89% had lasting relief. Generally, placebo effects from injections do not exceed 50% improvement.6 If lidocaine hydrochloride is used, its possible beneficial effects may come from washing out irritant chemicals (substance P) from the area, from local vasodilation that facilitates the removal of metabolites, or from the interruption of the neural feedback mechanism.13 However, the local anesthetic effect is too short to explain lasting relief, and a randomized controlled study of injection therapy of the iliac crest syndrome showed no difference in pain outcome between lidocaine hydrochloride and saline.14 This would tend to support the possibility that multiple puncture, rather than the injected material, is effective because it lessens the tension of the innervated fibrous capsule. Does Injection Treatment of the Back Mouse Really Work? There have been no randomized controlled trials and, until recently, no published long-term follow-up studies of treatment. It is not clear if multiple puncture of the nodule followed by deep massage alone is effective or whether the addition of local anesthetic and steroid improves outcome.
Conclusions
Until a rigorous study demonstrates the reliability and reproducibility of the clinical diagnosis of the back mouse and the effectiveness of treatment in a randomized controlled trial, our best advice for physicians, based purely on clinical and biased observation, is to consider the back mouse when atypical and unaccountable symptoms and signs are found in the lower abdomen, inguinal region, or legs.
Acknowledgements
We are grateful to Barry R. Howes, PT, and Robert E. Gwyther for guidance in the preparation of this report.
1. Bigos S, Bowyer O, Braen G, et al. Acute low back problems in adults. Clinical practice guideline no.14. Rockville, Md: US Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1994. AHCPR publication no. 95-0643.
2. Cherkin DC, Deyo RA, Battie M, Street J, Barlow W. A comparison of physical therapy, chiropractic manipulation and provision of an educational booklet for the treatment of patients with low back pain. N Engl J Med 1998;339:1021-9.
3. Riddle DL. Classification and low back pain: a review of the literature and critical analysis of selected systems. Phys Therap 1998;78:708-37.
4. Curtis P. In search of the “back mouse”. J Fam Pract 1993;36:657-9.
5. Reis E. Episacroiliac lipoma. Am J Obstet Gynecol 1937;34:492-8.
6. Motyka TM, Howes BR, Gwyther R, Curtis P. Treatment of low back pain caused by “back mice”: a case series. In press.
7. Swezey RI. Non-fibrositic lumbar cutaneous nodules: prevalence and clinical significance. Br J Rheumatol 1991;30:376-8.
8. Copeman WSC, Ackerman WL. Edema or herniation of fat lobules as a cause for lumbar and gluteal “fibrositis”. Arch Intern Med 1947;79:22-35.
9. Collee G, Djikmans BAC, Vandenbroucke JP, Cats A. Greater trochanteric pain syndrome (trochanteric bursitis) in low back pain. Scan J Rheumatol 1991;20:262-6.
10. Kellgren JH. A preliminary account of referred pain arising from muscle. BMJ 1938;1:325-7.
11. Inman VT, Saunders JB, de CJM. Referred pain from skeletal structures. J Nerv Ment Dis 1944;99:660-7.
12. Wall P. Neurophysiological mechanisms of referred pain and hyperalgesia. In: Vecchiet L, Albe-Ferrard D, Lindblom U, eds. New trends in referred pain and hyperalgesia. Vol 7. Holland, Netherlands: Elsevier; 1993.
13. Travell JG, Simons DG. Myofascial pain and dysfunction: the trigger point manual. Vol 1, pp 638; Vol 2, pp 30. Baltimore, Md: Williams and Wilkins; 1983.
14. Collee G, Djikmans BAC, Vandenbroucke JP, Cats A. Iliac crest syndrome in low back pain: a double blind randomized study of local injection therapy. J Rheumatol 1991;18:1060-3.
1. Bigos S, Bowyer O, Braen G, et al. Acute low back problems in adults. Clinical practice guideline no.14. Rockville, Md: US Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1994. AHCPR publication no. 95-0643.
2. Cherkin DC, Deyo RA, Battie M, Street J, Barlow W. A comparison of physical therapy, chiropractic manipulation and provision of an educational booklet for the treatment of patients with low back pain. N Engl J Med 1998;339:1021-9.
3. Riddle DL. Classification and low back pain: a review of the literature and critical analysis of selected systems. Phys Therap 1998;78:708-37.
4. Curtis P. In search of the “back mouse”. J Fam Pract 1993;36:657-9.
5. Reis E. Episacroiliac lipoma. Am J Obstet Gynecol 1937;34:492-8.
6. Motyka TM, Howes BR, Gwyther R, Curtis P. Treatment of low back pain caused by “back mice”: a case series. In press.
7. Swezey RI. Non-fibrositic lumbar cutaneous nodules: prevalence and clinical significance. Br J Rheumatol 1991;30:376-8.
8. Copeman WSC, Ackerman WL. Edema or herniation of fat lobules as a cause for lumbar and gluteal “fibrositis”. Arch Intern Med 1947;79:22-35.
9. Collee G, Djikmans BAC, Vandenbroucke JP, Cats A. Greater trochanteric pain syndrome (trochanteric bursitis) in low back pain. Scan J Rheumatol 1991;20:262-6.
10. Kellgren JH. A preliminary account of referred pain arising from muscle. BMJ 1938;1:325-7.
11. Inman VT, Saunders JB, de CJM. Referred pain from skeletal structures. J Nerv Ment Dis 1944;99:660-7.
12. Wall P. Neurophysiological mechanisms of referred pain and hyperalgesia. In: Vecchiet L, Albe-Ferrard D, Lindblom U, eds. New trends in referred pain and hyperalgesia. Vol 7. Holland, Netherlands: Elsevier; 1993.
13. Travell JG, Simons DG. Myofascial pain and dysfunction: the trigger point manual. Vol 1, pp 638; Vol 2, pp 30. Baltimore, Md: Williams and Wilkins; 1983.
14. Collee G, Djikmans BAC, Vandenbroucke JP, Cats A. Iliac crest syndrome in low back pain: a double blind randomized study of local injection therapy. J Rheumatol 1991;18:1060-3.