User login
Piercing among adolescents: Body art as risk marker
- Without stigmatizing adolescents with piercing, use the topic of body piercing as a starting point for discussing unhealthy behaviors
Body piercing among young people has been linked with risk behaviors such as the abuse of legal and illegal substances, Perspicacity, profiling, and prejudice
Body art and, more specifically, piercing is becoming normative among adolescents, ("Perspicacity, profiling, and prejudice,”) Body art is more than just an indicator of deviancy.11 In other words, as all adolescents should be screened for risky behaviors, this specific population offers the advantage of piercing as a starting point for a discussion.
We found that body piercing is increasingly popular among adolescents in Switzerland, especially among females. Our prevalence rates are higher than those reported by Roberts,3 but (as they suggest) it may well be due to the societal trend, as their data were collected in 1996.
The pierced and the unpierced
Academic performance was the main sociodemographic difference between pierced and unpierced adolescents. As a marker of risk, piercing was negatively associated with academic performance, as found elsewhere regarding healthy behaviors.12 Like other studies, this sample exhibited increased drug use1,3,5 and risky sexual behavior,10 but no increase in suicide attempt.3
Since the late 1990s, estimates for body modification among US adolescents range from 10% to 25%.8,14 A 2002 study5 assessed tattoos and body piercing as markers of risk-taking in 484 adolescents presenting to an adolescent clinic in California; both were markers of greater instances of, and participation in, such behaviors as eating disorders, illegal drug use, sexual activity, and suicide. Tattooing was reported by 13.2% of respondents, with 5.2% having more than 1 tattoo. Excluding earlobes, 26.9% of adolescents had body piercings at some point during their lifetime, and 11.8% had a history of multiple piercings. Tattooing and body piercing were found to be more common in females than males, 16.6% vs 8.1% for tattoos and 36.7% vs 10.1% for body piercings, respectively. Index scores on 5 of 6 risk-taking indices—including the Disordered Eating Behavior Index, the Gateway Drug Index, the Hard Drug Index, the Sexual behavior Index, and the Suicide Index—were significantly higher in participants with at least 1 tattoo or body piercing compared with those with neither. Illegal drug use also increased with the number of piercings.
Another study15 looked at 14- to 18-year-olds presenting to an urban adolescent clinic in Massachusetts. Of 210 surveyed, 48% reported at least 1 body modification, with girls more likely than boys (59% vs 28%; P≥.0005). Forty-two percent reported piercings, 10% had tattoos, 4% had scarification; 21% had more than 1 type of modification. One third of the sample screened positive for problem substance use. Controlling for age, adolescents with body modification had 3.1 times greater odds of problem substance abuse with alcohol or drugs than those without (95% CI, 1.7–5.8).
Among females in our sample, more than 1 piercing is associated with having multiple sex partners and marijuana use. Carroll et al5 also found that having multiple piercings was associated with illegal drug use. For males in our study, the only association with multiple piercings was an increase in suicide attempts.
From our results, it could be hypothesized that more than 1 piercing is a cumulative marker for some risk behaviors, mainly among females. Though associations for males were similar to those for females, the differences between pierced and unpierced groups did not reach statistical significance. However, the relatively small sample of pierced males discourages definitive conclusions.
Pierced adolescents were less satisfied with their bodies than their unpierced counterparts, though the difference is significant only for females.
Young people indicate that the main reasons they obtain a piercing are a sense of uniqueness or self-expression, with only one fifth indicating that they obtain it for aesthetics only.2,8 As we did not assess the reasons to obtain a body piercing in this study, it could be that they had it done to increase their body satisfaction, that their body satisfaction was lower after having it done, or simply that they do not get pierced to increase their satisfaction with their body.
Methods
Population. Data were drawn from the 2002 Swiss Multicenter Adolescent Survey on Health database, a survey of 7548 students ages 16 to 20 years (3658 of whom were female). In Switzerland, school is mandatory up to age 16. Afterwards, about 30% of adolescents follow to further high school, 60% go to vocational school as an apprentice (1 or 2 days of class per week and the rest spent at work), and 10% do not continue their education.
Classroom survey. The survey was an anonymous classroom questionnaire approved by the ethical committee of the Medicine Faculty in Lausanne. The questionnaire and sampling method are described elsewhere.13 Ninety-one subjects (1%) did not answer the question referring to body piercing and were excluded. The final sample had 7457 subjects (3628 females).
(TABLE 1) lists selected characteristics and background variables analyzed. Analyses were performed separately by gender, as the literature indicates that females are more likely to have piercings.2-5 We conducted all analyses with Stata 8 (College Station, TX), which computes coefficient estimates taking into account sampling weights, clustering, and stratification procedure. All significant variables in the bivariate analysis were included in a logistic regression.
In a second step, adolescents having one piercing were compared with those having more than one piercing, using the same method.
TABLE 1
Selected characteristics of pierced and unpierced adolescents—females (N=3628) and males (N=3829)
| FEMALES | MALES | |||||||
|---|---|---|---|---|---|---|---|---|
| PIERCED (N=1225) | UNPIERCED (N=2403) | P VALUE | AOR (95% CI) | PIERCED (N=283) | UNPIERCED (N=3546) | P VALUE | AOR (95% CI) | |
| Age (years±SD) | 17.98±1.17 | 17.77±1.13 | <.001 | 0.94 (0.88–1.01) | 18.21±1.20 | 17.86±1.18 | <.001 | 0.90 (0.80–1.00) |
| Academic track (apprentice) | 73.1% | 53.1% | <.001 | 2.05 (1.75–2.41) | 91.5% | 71.0% | <.001 | 2.97 (1.92–4.62) |
| Body satisfaction (dissatisfied) | 67.4% | 71.2% | .02 | 0.96 (0.82–1.14) | 82.3% | 86.3% | .064 | — |
| Nationality (Swiss) | 10.9% | 13.5% | .027 | 0.72 (0.57–0.92) | 16.6% | 13.3% | .119 | — |
| Perceived puberty (advanced) | 36.6% | 30.2% | <.001 | 1.06 (0.91–1.25) | 39.6% | 23.3% | <.001 | 1.41 (1.07–1.86) |
| Parental status (not together) | 31.3% | 20.8% | <.001 | 1.30 (1.10–1.55) | 32.5% | 21.7% | <.001 | 1.35 (1.02–1.79) |
| Father’s education (low)* | 11.4% | 15.9% | <.001 | 0.67 (0.53–0.84) | 15.5% | 14.0% | .476 | — |
| Mother’s education (low)* | 21.2% | 22.9% | 0.24 | — | 23.0% | 20.8% | .379 | — |
| Sensation seeking (high) | 21.9% | 15.5% | <.001 | 1.14 (0.94–1.39) | 53.0% | 40.0% | <.001 | 1.13 (0.87–1.47) |
| Feeling depressed (yes) | 45.0% | 36.2% | <.001 | 1.16 (0.98–1.36) | 29.0% | 21.7% | .005 | 1.05 (0.78–1.42) |
| Number of sexual partners (≥4) | 20.6% | 8.3% | <.001 | 1.50 (1.20–1.87) | 45.6% | 17.9% | <.001 | 1.71 (1.29–2.28) |
| Condom use at last intercourse (no) | 46.9% | 27.5% | <.001 | 1.63 (1.39–1.92) | 39.6% | 19.5% | <.001 | 1.49 (1.12–1.98) |
| Regular smoker (yes) | 48.9% | 21.9% | <.001 | 2.06 (1.74–2.45) | 66.4% | 30.9% | <.001 | 2.28 (1.72–3.02) |
| Intoxication (last 30 days) | 26.9% | 15.7% | <.001 | 1.19 (0.98–1.44) | 60.8% | 39.0% | <.001 | 1.51 (1.15–1.97) |
| Cannabis use (last 30 days) | 40.9% | 20.6% | <.001 | 1.58 (1.32–1.89) | 67.5% | 39.1% | <.001 | 1.37 (1.05–1.79) |
| Illegal drug use (last 30 days) | 8.7% | 3.4% | <.001 | 1.67 (1.21–2.31) | 26.9% | 8.3% | <.001 | 2.17 (1.59–2.98) |
| Suicide ideation (last 12 months) | 26.8% | 21.2% | <.001 | 1.07 (0.88–1.29) | 22.6% | 15.5% | .002 | 1.22 (0.87–1.72) |
| Suicide attempt (last 12 months) | 5.3% | 2.7% | <.001 | 0.97 (0.65–1.45) | 3.2% | 1.4% | .02 | 1.02 (0.45–2.31) |
| AOR, adjusted odds ratio; CI, confidence interval. | ||||||||
| Statistically significant differences are in bold. | ||||||||
| *Low education=mandatory schooling or less. | ||||||||
Results
Overall, 20.2% (95% confidence interval [CI], 19.3–21.1) of our sample had a piercing, and it was significantly more prevalent among females than males: 33.8% (95% CI, 32.2–35.3) vs 7.4% (95% CI, 6.6–8.2); P<.001.
Single piercing
Bivariate analysis. Having a piercing was significantly associated with all the risk behavior variables both in males and females. In both genders, pierced adolescents were significantly older, more frequently on an apprentice academic track, perceived advanced puberty, not living with both parents, had felt depressed, and were sensation-seeking. Additionally, pierced females were less likely to be satisfied with their body, less likely to be foreign-born, and more likely to have a mother with low education (mandatory school or less).
Multivariate analysis. Controlling for all significant background variables, pierced females were more likely to have had multiple sexual partners, not to have used a condom at last intercourse, to be regular smokers, and to be current users of cannabis or other illegal drugs. Among males, all risk behavior variables remained significant, except suicide ideation and attempt (TABLE 1).
Multiple piercings
One third (34.1% [95% CI, 31.7–36.5]) of pierced subjects had more than 1 piercing, with similar rates for males (35.3% [95% CI, 29.8–40.9] and females (33.8% [95% CI, 31.1–36.4]).
Bivariate analysis. Among females, having more than one piercing was associated with being an apprentice, perceived advanced puberty, parents not living together, sensation seeking, and being depressed. With the exception of condom use at last intercourse, they were significantly more likely to engage in all risky behaviors.
For males, the only difference between single and multiple piercings was that the latter were more likely to have attempted suicide (TABLE 2).
Multivariate analysis. The only variables associated with females having more than one piercing were having multiple sexual partners (adjusted odds ratio [OR]=1.53 [95% CI, 1.13–2.09]) and using cannabis (adjusted OR=1.39 [95% CI, 1.06–1.82]).
TABLE 2
Characteristics of adolescents with more than 1 piercing
| FEMALES | MALES | |||||
|---|---|---|---|---|---|---|
| 1 PIERCING (N=811) | >1 PIERCING (N=414) | P VALUE | 1 PIERCING (N=183) | >1 PIERCING (N=100) | P VALUE | |
| Age (years±SD) | 17.97±1.16 | 18.01±1.18 | .55 | 18.15±1.23 | 18.34±1.15 | .190 |
| Academic track (apprentice) | 67.7% | 83.8% | <.001 | 91.3% | 92.0% | .830 |
| Body satisfaction (dissatisfied) | 67.7% | 66.9% | .781 | 81.4% | 84.0% | .587 |
| Nationality (Swiss) | 11.2 % | 10.4% | .658 | 16.9% | 16.0% | .839 |
| Perceived puberty (advanced) | 33.8% | 42.3% | .004 | 35.5% | 47.0% | .059 |
| Parental status (not together) | 28.1% | 37.4% | .001 | 29.0% | 39.0% | .085 |
| Father’s education (low)* | 11.6% | 11.1% | .803 | 15.3% | 16.0% | .877 |
| Mother’s education (low)* | 20.3% | 22.9% | .292 | 21.9% | 25.0% | .548 |
| Sensation seeking (high) | 81.5% | 72.0% | <.001 | 47.5% | 46.0% | .804 |
| Feeling depressed (yes) | 42.7% | 49.5% | .023 | 29.5% | 28.0% | .789 |
| Number of sexual partners (≥4) | 16.9% | 28.0% | <.001 | 47.0% | 43.0% | .519 |
| Condom use at last intercourse (no) | 45.2% | 50.0% | .115 | 36.6% | 45.0% | .168 |
| Regular smoker (yes) | 44.1% | 58.2% | <.001 | 65.0% | 69.0% | .499 |
| Intoxication (last 30 days) | 23.8% | 33.1% | .001 | 57.4% | 67.0% | .113 |
| Cannabis use (last 30 days) | 36.1% | 50.2% | <.001 | 67.2% | 68.0% | .893 |
| Illegal drug use (last 30 days) | 6.9% | 12.3% | .002 | 24.6% | 31.0% | .245 |
| Suicide ideation (last 12 mo) | 24.4% | 31.4% | .009 | 20.2% | 27.0% | .192 |
| Suicide attempt (last 12 mo) | 3.9% | 8.0% | .003 | 1.6% | 6.0% | .046 |
| Statistically significant differences are in bold. * Low education=mandatory school or less. | ||||||
Limitations of this study
The main strength of our study is that it is based on a nationally representative sample of adolescents. However, a few limitations need to be stressed.
Body piercing leads to medical complications in a non-negligible percentage of cases7,9,10 particularly if done by nonprofessionals.9 Given the high prevalence of adolescents, particularly females, who do body piercing, and their greater tendency to engage in risk-taking behaviors (and thus may be less careful about potential medical consequences), it seems important to make sure that they can do it under the safest conditions. Indeed, in Switzerland, new legislation regulating body piercing went into effect in 2006.
The cross-sectional nature of our survey does not allow us to assess causality. The questionnaire was filled in the classroom, which excludes absentees and dropouts, both known to be at higher risk.12 Additionally, we do not know the location or the size of the piercings; some locations (eg, nipples or genitalia) are more likely associated with risk behaviors.3,4
Can these results be generalized?
But to what extent can our results be generalized to other, non-European adolescent populations? The prevalence rate is similar to those found among North American adolescents4,5 and college students.2 All published studies seem to indicate that pierced adolescents are more likely to be risk-taking.
That would indicate that our results are on the right track. However, more population-based studies need to be done to fully confirm this.
Acknowledgments
The 2002 Swiss Multicenter adolescent Survey on Health survey was carried out with the financial support of the Swiss federal office of Public Health (contract 00.001721/2.24.02.-81) and the participating cantons.
CORRESPONDENCE
Joan-Carles Suris, MD, PhD, MPH Groupe de recherche sur la santé les adolescents, Institut universitaire de médecine sociale et préventive, Bugnon 17, 1005 Lausanne, Switzerland joan-carles.suris@chuv.ch
1. Braithwaite R, Robillard A, Woodring T, Stephens T, Arriola KJ. Tattooing and body piercing among adolescent detainees: relationship to alcohol and other drug use. J Substance Abuse 2001;13:5-16.
2. Armstrong ML, Roberts AE, Owen DC, Koch JR. Contemporary college students and body piercing. J Adol Health 2004;34:224-229.
3. Roberts TA, Auinger P, Ryan SA. Body piercing and high-risk behavior in adolescents. J Adol Health 2004;34:224-229.
4. Deschesnes M, Finès P, Demers S. Are tattooing and body piercing iindicators of risk-taking behaviours among high school students? J Adol 2006;29:379-379.
5. Carroll ST, Riffenburgh RH, Roberts TA, Myhre EB. Tattoos and body piercings as indicators of adolescent risk-taking behaviors. Pediatrics 2002;109:1021-1027.
6. Muldoon KA. Body piercing in adolescents. J Ped Health Care 1997;11:298-301.
7. Stirn A. Body piercing: medical consequences and psychological motivations. Lancet 2003;361:1205-1215.
8. Greif J, Hewitt W, Armstrong ML. Tattooing and body piercing. Clin Nursing Res 1999;8:368-385.
9. Gold MA, Scorzman CM, Murray PJ, Downs J, Tolentino G. Body piercing practices and attitudes among urban adolescents. J Adol Health 2005;36:352 e15-e21.
10. Mayers LB, Judelson DA, Moriarty BW, Rundell KW. Prevalence of body art (body piercing and tattooing) in university undergraduates and incidence of medical complications. Mayo Clin Proc 2002;77:29-34.
11. Armstrong ML, Roberts AE, Owen DC, Koch JR. Toward building a composite of college student influences with body art. Issues Comprehensive Ped Nursing 2004;27:277-295.
12. Mischaud PA, Delbos-Piot I, Narring F. Silent dropout in health surveys: are nonrespondent absent teenagers different from those who participate in school-based health surveys? J Adol Health 1998;22:326-333.
13. Jeannin A, Narring F, Tschumper A, et al. Self-reported health needs and use of primary health care services by adolescents enrolled in post-mandatory schools or vocational training programmes in Switzerland. Swiss Medical Weekly 2005;135(1-2):11-18.
14. Armstrong ML, Pace Murphy K. Tattooing: another adolescent risk behavior warranting health education. Applied Nurs Res 1997;10:181-189.
15. Brooks TL, Woods ER, Knight JR, Shrier LA. Body modification and substance use in adolescents: is there a link? J Adolesc Health 2003;32:44-49.
- Without stigmatizing adolescents with piercing, use the topic of body piercing as a starting point for discussing unhealthy behaviors
Body piercing among young people has been linked with risk behaviors such as the abuse of legal and illegal substances, Perspicacity, profiling, and prejudice
Body art and, more specifically, piercing is becoming normative among adolescents, ("Perspicacity, profiling, and prejudice,”) Body art is more than just an indicator of deviancy.11 In other words, as all adolescents should be screened for risky behaviors, this specific population offers the advantage of piercing as a starting point for a discussion.
We found that body piercing is increasingly popular among adolescents in Switzerland, especially among females. Our prevalence rates are higher than those reported by Roberts,3 but (as they suggest) it may well be due to the societal trend, as their data were collected in 1996.
The pierced and the unpierced
Academic performance was the main sociodemographic difference between pierced and unpierced adolescents. As a marker of risk, piercing was negatively associated with academic performance, as found elsewhere regarding healthy behaviors.12 Like other studies, this sample exhibited increased drug use1,3,5 and risky sexual behavior,10 but no increase in suicide attempt.3
Since the late 1990s, estimates for body modification among US adolescents range from 10% to 25%.8,14 A 2002 study5 assessed tattoos and body piercing as markers of risk-taking in 484 adolescents presenting to an adolescent clinic in California; both were markers of greater instances of, and participation in, such behaviors as eating disorders, illegal drug use, sexual activity, and suicide. Tattooing was reported by 13.2% of respondents, with 5.2% having more than 1 tattoo. Excluding earlobes, 26.9% of adolescents had body piercings at some point during their lifetime, and 11.8% had a history of multiple piercings. Tattooing and body piercing were found to be more common in females than males, 16.6% vs 8.1% for tattoos and 36.7% vs 10.1% for body piercings, respectively. Index scores on 5 of 6 risk-taking indices—including the Disordered Eating Behavior Index, the Gateway Drug Index, the Hard Drug Index, the Sexual behavior Index, and the Suicide Index—were significantly higher in participants with at least 1 tattoo or body piercing compared with those with neither. Illegal drug use also increased with the number of piercings.
Another study15 looked at 14- to 18-year-olds presenting to an urban adolescent clinic in Massachusetts. Of 210 surveyed, 48% reported at least 1 body modification, with girls more likely than boys (59% vs 28%; P≥.0005). Forty-two percent reported piercings, 10% had tattoos, 4% had scarification; 21% had more than 1 type of modification. One third of the sample screened positive for problem substance use. Controlling for age, adolescents with body modification had 3.1 times greater odds of problem substance abuse with alcohol or drugs than those without (95% CI, 1.7–5.8).
Among females in our sample, more than 1 piercing is associated with having multiple sex partners and marijuana use. Carroll et al5 also found that having multiple piercings was associated with illegal drug use. For males in our study, the only association with multiple piercings was an increase in suicide attempts.
From our results, it could be hypothesized that more than 1 piercing is a cumulative marker for some risk behaviors, mainly among females. Though associations for males were similar to those for females, the differences between pierced and unpierced groups did not reach statistical significance. However, the relatively small sample of pierced males discourages definitive conclusions.
Pierced adolescents were less satisfied with their bodies than their unpierced counterparts, though the difference is significant only for females.
Young people indicate that the main reasons they obtain a piercing are a sense of uniqueness or self-expression, with only one fifth indicating that they obtain it for aesthetics only.2,8 As we did not assess the reasons to obtain a body piercing in this study, it could be that they had it done to increase their body satisfaction, that their body satisfaction was lower after having it done, or simply that they do not get pierced to increase their satisfaction with their body.
Methods
Population. Data were drawn from the 2002 Swiss Multicenter Adolescent Survey on Health database, a survey of 7548 students ages 16 to 20 years (3658 of whom were female). In Switzerland, school is mandatory up to age 16. Afterwards, about 30% of adolescents follow to further high school, 60% go to vocational school as an apprentice (1 or 2 days of class per week and the rest spent at work), and 10% do not continue their education.
Classroom survey. The survey was an anonymous classroom questionnaire approved by the ethical committee of the Medicine Faculty in Lausanne. The questionnaire and sampling method are described elsewhere.13 Ninety-one subjects (1%) did not answer the question referring to body piercing and were excluded. The final sample had 7457 subjects (3628 females).
(TABLE 1) lists selected characteristics and background variables analyzed. Analyses were performed separately by gender, as the literature indicates that females are more likely to have piercings.2-5 We conducted all analyses with Stata 8 (College Station, TX), which computes coefficient estimates taking into account sampling weights, clustering, and stratification procedure. All significant variables in the bivariate analysis were included in a logistic regression.
In a second step, adolescents having one piercing were compared with those having more than one piercing, using the same method.
TABLE 1
Selected characteristics of pierced and unpierced adolescents—females (N=3628) and males (N=3829)
| FEMALES | MALES | |||||||
|---|---|---|---|---|---|---|---|---|
| PIERCED (N=1225) | UNPIERCED (N=2403) | P VALUE | AOR (95% CI) | PIERCED (N=283) | UNPIERCED (N=3546) | P VALUE | AOR (95% CI) | |
| Age (years±SD) | 17.98±1.17 | 17.77±1.13 | <.001 | 0.94 (0.88–1.01) | 18.21±1.20 | 17.86±1.18 | <.001 | 0.90 (0.80–1.00) |
| Academic track (apprentice) | 73.1% | 53.1% | <.001 | 2.05 (1.75–2.41) | 91.5% | 71.0% | <.001 | 2.97 (1.92–4.62) |
| Body satisfaction (dissatisfied) | 67.4% | 71.2% | .02 | 0.96 (0.82–1.14) | 82.3% | 86.3% | .064 | — |
| Nationality (Swiss) | 10.9% | 13.5% | .027 | 0.72 (0.57–0.92) | 16.6% | 13.3% | .119 | — |
| Perceived puberty (advanced) | 36.6% | 30.2% | <.001 | 1.06 (0.91–1.25) | 39.6% | 23.3% | <.001 | 1.41 (1.07–1.86) |
| Parental status (not together) | 31.3% | 20.8% | <.001 | 1.30 (1.10–1.55) | 32.5% | 21.7% | <.001 | 1.35 (1.02–1.79) |
| Father’s education (low)* | 11.4% | 15.9% | <.001 | 0.67 (0.53–0.84) | 15.5% | 14.0% | .476 | — |
| Mother’s education (low)* | 21.2% | 22.9% | 0.24 | — | 23.0% | 20.8% | .379 | — |
| Sensation seeking (high) | 21.9% | 15.5% | <.001 | 1.14 (0.94–1.39) | 53.0% | 40.0% | <.001 | 1.13 (0.87–1.47) |
| Feeling depressed (yes) | 45.0% | 36.2% | <.001 | 1.16 (0.98–1.36) | 29.0% | 21.7% | .005 | 1.05 (0.78–1.42) |
| Number of sexual partners (≥4) | 20.6% | 8.3% | <.001 | 1.50 (1.20–1.87) | 45.6% | 17.9% | <.001 | 1.71 (1.29–2.28) |
| Condom use at last intercourse (no) | 46.9% | 27.5% | <.001 | 1.63 (1.39–1.92) | 39.6% | 19.5% | <.001 | 1.49 (1.12–1.98) |
| Regular smoker (yes) | 48.9% | 21.9% | <.001 | 2.06 (1.74–2.45) | 66.4% | 30.9% | <.001 | 2.28 (1.72–3.02) |
| Intoxication (last 30 days) | 26.9% | 15.7% | <.001 | 1.19 (0.98–1.44) | 60.8% | 39.0% | <.001 | 1.51 (1.15–1.97) |
| Cannabis use (last 30 days) | 40.9% | 20.6% | <.001 | 1.58 (1.32–1.89) | 67.5% | 39.1% | <.001 | 1.37 (1.05–1.79) |
| Illegal drug use (last 30 days) | 8.7% | 3.4% | <.001 | 1.67 (1.21–2.31) | 26.9% | 8.3% | <.001 | 2.17 (1.59–2.98) |
| Suicide ideation (last 12 months) | 26.8% | 21.2% | <.001 | 1.07 (0.88–1.29) | 22.6% | 15.5% | .002 | 1.22 (0.87–1.72) |
| Suicide attempt (last 12 months) | 5.3% | 2.7% | <.001 | 0.97 (0.65–1.45) | 3.2% | 1.4% | .02 | 1.02 (0.45–2.31) |
| AOR, adjusted odds ratio; CI, confidence interval. | ||||||||
| Statistically significant differences are in bold. | ||||||||
| *Low education=mandatory schooling or less. | ||||||||
Results
Overall, 20.2% (95% confidence interval [CI], 19.3–21.1) of our sample had a piercing, and it was significantly more prevalent among females than males: 33.8% (95% CI, 32.2–35.3) vs 7.4% (95% CI, 6.6–8.2); P<.001.
Single piercing
Bivariate analysis. Having a piercing was significantly associated with all the risk behavior variables both in males and females. In both genders, pierced adolescents were significantly older, more frequently on an apprentice academic track, perceived advanced puberty, not living with both parents, had felt depressed, and were sensation-seeking. Additionally, pierced females were less likely to be satisfied with their body, less likely to be foreign-born, and more likely to have a mother with low education (mandatory school or less).
Multivariate analysis. Controlling for all significant background variables, pierced females were more likely to have had multiple sexual partners, not to have used a condom at last intercourse, to be regular smokers, and to be current users of cannabis or other illegal drugs. Among males, all risk behavior variables remained significant, except suicide ideation and attempt (TABLE 1).
Multiple piercings
One third (34.1% [95% CI, 31.7–36.5]) of pierced subjects had more than 1 piercing, with similar rates for males (35.3% [95% CI, 29.8–40.9] and females (33.8% [95% CI, 31.1–36.4]).
Bivariate analysis. Among females, having more than one piercing was associated with being an apprentice, perceived advanced puberty, parents not living together, sensation seeking, and being depressed. With the exception of condom use at last intercourse, they were significantly more likely to engage in all risky behaviors.
For males, the only difference between single and multiple piercings was that the latter were more likely to have attempted suicide (TABLE 2).
Multivariate analysis. The only variables associated with females having more than one piercing were having multiple sexual partners (adjusted odds ratio [OR]=1.53 [95% CI, 1.13–2.09]) and using cannabis (adjusted OR=1.39 [95% CI, 1.06–1.82]).
TABLE 2
Characteristics of adolescents with more than 1 piercing
| FEMALES | MALES | |||||
|---|---|---|---|---|---|---|
| 1 PIERCING (N=811) | >1 PIERCING (N=414) | P VALUE | 1 PIERCING (N=183) | >1 PIERCING (N=100) | P VALUE | |
| Age (years±SD) | 17.97±1.16 | 18.01±1.18 | .55 | 18.15±1.23 | 18.34±1.15 | .190 |
| Academic track (apprentice) | 67.7% | 83.8% | <.001 | 91.3% | 92.0% | .830 |
| Body satisfaction (dissatisfied) | 67.7% | 66.9% | .781 | 81.4% | 84.0% | .587 |
| Nationality (Swiss) | 11.2 % | 10.4% | .658 | 16.9% | 16.0% | .839 |
| Perceived puberty (advanced) | 33.8% | 42.3% | .004 | 35.5% | 47.0% | .059 |
| Parental status (not together) | 28.1% | 37.4% | .001 | 29.0% | 39.0% | .085 |
| Father’s education (low)* | 11.6% | 11.1% | .803 | 15.3% | 16.0% | .877 |
| Mother’s education (low)* | 20.3% | 22.9% | .292 | 21.9% | 25.0% | .548 |
| Sensation seeking (high) | 81.5% | 72.0% | <.001 | 47.5% | 46.0% | .804 |
| Feeling depressed (yes) | 42.7% | 49.5% | .023 | 29.5% | 28.0% | .789 |
| Number of sexual partners (≥4) | 16.9% | 28.0% | <.001 | 47.0% | 43.0% | .519 |
| Condom use at last intercourse (no) | 45.2% | 50.0% | .115 | 36.6% | 45.0% | .168 |
| Regular smoker (yes) | 44.1% | 58.2% | <.001 | 65.0% | 69.0% | .499 |
| Intoxication (last 30 days) | 23.8% | 33.1% | .001 | 57.4% | 67.0% | .113 |
| Cannabis use (last 30 days) | 36.1% | 50.2% | <.001 | 67.2% | 68.0% | .893 |
| Illegal drug use (last 30 days) | 6.9% | 12.3% | .002 | 24.6% | 31.0% | .245 |
| Suicide ideation (last 12 mo) | 24.4% | 31.4% | .009 | 20.2% | 27.0% | .192 |
| Suicide attempt (last 12 mo) | 3.9% | 8.0% | .003 | 1.6% | 6.0% | .046 |
| Statistically significant differences are in bold. * Low education=mandatory school or less. | ||||||
Limitations of this study
The main strength of our study is that it is based on a nationally representative sample of adolescents. However, a few limitations need to be stressed.
Body piercing leads to medical complications in a non-negligible percentage of cases7,9,10 particularly if done by nonprofessionals.9 Given the high prevalence of adolescents, particularly females, who do body piercing, and their greater tendency to engage in risk-taking behaviors (and thus may be less careful about potential medical consequences), it seems important to make sure that they can do it under the safest conditions. Indeed, in Switzerland, new legislation regulating body piercing went into effect in 2006.
The cross-sectional nature of our survey does not allow us to assess causality. The questionnaire was filled in the classroom, which excludes absentees and dropouts, both known to be at higher risk.12 Additionally, we do not know the location or the size of the piercings; some locations (eg, nipples or genitalia) are more likely associated with risk behaviors.3,4
Can these results be generalized?
But to what extent can our results be generalized to other, non-European adolescent populations? The prevalence rate is similar to those found among North American adolescents4,5 and college students.2 All published studies seem to indicate that pierced adolescents are more likely to be risk-taking.
That would indicate that our results are on the right track. However, more population-based studies need to be done to fully confirm this.
Acknowledgments
The 2002 Swiss Multicenter adolescent Survey on Health survey was carried out with the financial support of the Swiss federal office of Public Health (contract 00.001721/2.24.02.-81) and the participating cantons.
CORRESPONDENCE
Joan-Carles Suris, MD, PhD, MPH Groupe de recherche sur la santé les adolescents, Institut universitaire de médecine sociale et préventive, Bugnon 17, 1005 Lausanne, Switzerland joan-carles.suris@chuv.ch
- Without stigmatizing adolescents with piercing, use the topic of body piercing as a starting point for discussing unhealthy behaviors
Body piercing among young people has been linked with risk behaviors such as the abuse of legal and illegal substances, Perspicacity, profiling, and prejudice
Body art and, more specifically, piercing is becoming normative among adolescents, ("Perspicacity, profiling, and prejudice,”) Body art is more than just an indicator of deviancy.11 In other words, as all adolescents should be screened for risky behaviors, this specific population offers the advantage of piercing as a starting point for a discussion.
We found that body piercing is increasingly popular among adolescents in Switzerland, especially among females. Our prevalence rates are higher than those reported by Roberts,3 but (as they suggest) it may well be due to the societal trend, as their data were collected in 1996.
The pierced and the unpierced
Academic performance was the main sociodemographic difference between pierced and unpierced adolescents. As a marker of risk, piercing was negatively associated with academic performance, as found elsewhere regarding healthy behaviors.12 Like other studies, this sample exhibited increased drug use1,3,5 and risky sexual behavior,10 but no increase in suicide attempt.3
Since the late 1990s, estimates for body modification among US adolescents range from 10% to 25%.8,14 A 2002 study5 assessed tattoos and body piercing as markers of risk-taking in 484 adolescents presenting to an adolescent clinic in California; both were markers of greater instances of, and participation in, such behaviors as eating disorders, illegal drug use, sexual activity, and suicide. Tattooing was reported by 13.2% of respondents, with 5.2% having more than 1 tattoo. Excluding earlobes, 26.9% of adolescents had body piercings at some point during their lifetime, and 11.8% had a history of multiple piercings. Tattooing and body piercing were found to be more common in females than males, 16.6% vs 8.1% for tattoos and 36.7% vs 10.1% for body piercings, respectively. Index scores on 5 of 6 risk-taking indices—including the Disordered Eating Behavior Index, the Gateway Drug Index, the Hard Drug Index, the Sexual behavior Index, and the Suicide Index—were significantly higher in participants with at least 1 tattoo or body piercing compared with those with neither. Illegal drug use also increased with the number of piercings.
Another study15 looked at 14- to 18-year-olds presenting to an urban adolescent clinic in Massachusetts. Of 210 surveyed, 48% reported at least 1 body modification, with girls more likely than boys (59% vs 28%; P≥.0005). Forty-two percent reported piercings, 10% had tattoos, 4% had scarification; 21% had more than 1 type of modification. One third of the sample screened positive for problem substance use. Controlling for age, adolescents with body modification had 3.1 times greater odds of problem substance abuse with alcohol or drugs than those without (95% CI, 1.7–5.8).
Among females in our sample, more than 1 piercing is associated with having multiple sex partners and marijuana use. Carroll et al5 also found that having multiple piercings was associated with illegal drug use. For males in our study, the only association with multiple piercings was an increase in suicide attempts.
From our results, it could be hypothesized that more than 1 piercing is a cumulative marker for some risk behaviors, mainly among females. Though associations for males were similar to those for females, the differences between pierced and unpierced groups did not reach statistical significance. However, the relatively small sample of pierced males discourages definitive conclusions.
Pierced adolescents were less satisfied with their bodies than their unpierced counterparts, though the difference is significant only for females.
Young people indicate that the main reasons they obtain a piercing are a sense of uniqueness or self-expression, with only one fifth indicating that they obtain it for aesthetics only.2,8 As we did not assess the reasons to obtain a body piercing in this study, it could be that they had it done to increase their body satisfaction, that their body satisfaction was lower after having it done, or simply that they do not get pierced to increase their satisfaction with their body.
Methods
Population. Data were drawn from the 2002 Swiss Multicenter Adolescent Survey on Health database, a survey of 7548 students ages 16 to 20 years (3658 of whom were female). In Switzerland, school is mandatory up to age 16. Afterwards, about 30% of adolescents follow to further high school, 60% go to vocational school as an apprentice (1 or 2 days of class per week and the rest spent at work), and 10% do not continue their education.
Classroom survey. The survey was an anonymous classroom questionnaire approved by the ethical committee of the Medicine Faculty in Lausanne. The questionnaire and sampling method are described elsewhere.13 Ninety-one subjects (1%) did not answer the question referring to body piercing and were excluded. The final sample had 7457 subjects (3628 females).
(TABLE 1) lists selected characteristics and background variables analyzed. Analyses were performed separately by gender, as the literature indicates that females are more likely to have piercings.2-5 We conducted all analyses with Stata 8 (College Station, TX), which computes coefficient estimates taking into account sampling weights, clustering, and stratification procedure. All significant variables in the bivariate analysis were included in a logistic regression.
In a second step, adolescents having one piercing were compared with those having more than one piercing, using the same method.
TABLE 1
Selected characteristics of pierced and unpierced adolescents—females (N=3628) and males (N=3829)
| FEMALES | MALES | |||||||
|---|---|---|---|---|---|---|---|---|
| PIERCED (N=1225) | UNPIERCED (N=2403) | P VALUE | AOR (95% CI) | PIERCED (N=283) | UNPIERCED (N=3546) | P VALUE | AOR (95% CI) | |
| Age (years±SD) | 17.98±1.17 | 17.77±1.13 | <.001 | 0.94 (0.88–1.01) | 18.21±1.20 | 17.86±1.18 | <.001 | 0.90 (0.80–1.00) |
| Academic track (apprentice) | 73.1% | 53.1% | <.001 | 2.05 (1.75–2.41) | 91.5% | 71.0% | <.001 | 2.97 (1.92–4.62) |
| Body satisfaction (dissatisfied) | 67.4% | 71.2% | .02 | 0.96 (0.82–1.14) | 82.3% | 86.3% | .064 | — |
| Nationality (Swiss) | 10.9% | 13.5% | .027 | 0.72 (0.57–0.92) | 16.6% | 13.3% | .119 | — |
| Perceived puberty (advanced) | 36.6% | 30.2% | <.001 | 1.06 (0.91–1.25) | 39.6% | 23.3% | <.001 | 1.41 (1.07–1.86) |
| Parental status (not together) | 31.3% | 20.8% | <.001 | 1.30 (1.10–1.55) | 32.5% | 21.7% | <.001 | 1.35 (1.02–1.79) |
| Father’s education (low)* | 11.4% | 15.9% | <.001 | 0.67 (0.53–0.84) | 15.5% | 14.0% | .476 | — |
| Mother’s education (low)* | 21.2% | 22.9% | 0.24 | — | 23.0% | 20.8% | .379 | — |
| Sensation seeking (high) | 21.9% | 15.5% | <.001 | 1.14 (0.94–1.39) | 53.0% | 40.0% | <.001 | 1.13 (0.87–1.47) |
| Feeling depressed (yes) | 45.0% | 36.2% | <.001 | 1.16 (0.98–1.36) | 29.0% | 21.7% | .005 | 1.05 (0.78–1.42) |
| Number of sexual partners (≥4) | 20.6% | 8.3% | <.001 | 1.50 (1.20–1.87) | 45.6% | 17.9% | <.001 | 1.71 (1.29–2.28) |
| Condom use at last intercourse (no) | 46.9% | 27.5% | <.001 | 1.63 (1.39–1.92) | 39.6% | 19.5% | <.001 | 1.49 (1.12–1.98) |
| Regular smoker (yes) | 48.9% | 21.9% | <.001 | 2.06 (1.74–2.45) | 66.4% | 30.9% | <.001 | 2.28 (1.72–3.02) |
| Intoxication (last 30 days) | 26.9% | 15.7% | <.001 | 1.19 (0.98–1.44) | 60.8% | 39.0% | <.001 | 1.51 (1.15–1.97) |
| Cannabis use (last 30 days) | 40.9% | 20.6% | <.001 | 1.58 (1.32–1.89) | 67.5% | 39.1% | <.001 | 1.37 (1.05–1.79) |
| Illegal drug use (last 30 days) | 8.7% | 3.4% | <.001 | 1.67 (1.21–2.31) | 26.9% | 8.3% | <.001 | 2.17 (1.59–2.98) |
| Suicide ideation (last 12 months) | 26.8% | 21.2% | <.001 | 1.07 (0.88–1.29) | 22.6% | 15.5% | .002 | 1.22 (0.87–1.72) |
| Suicide attempt (last 12 months) | 5.3% | 2.7% | <.001 | 0.97 (0.65–1.45) | 3.2% | 1.4% | .02 | 1.02 (0.45–2.31) |
| AOR, adjusted odds ratio; CI, confidence interval. | ||||||||
| Statistically significant differences are in bold. | ||||||||
| *Low education=mandatory schooling or less. | ||||||||
Results
Overall, 20.2% (95% confidence interval [CI], 19.3–21.1) of our sample had a piercing, and it was significantly more prevalent among females than males: 33.8% (95% CI, 32.2–35.3) vs 7.4% (95% CI, 6.6–8.2); P<.001.
Single piercing
Bivariate analysis. Having a piercing was significantly associated with all the risk behavior variables both in males and females. In both genders, pierced adolescents were significantly older, more frequently on an apprentice academic track, perceived advanced puberty, not living with both parents, had felt depressed, and were sensation-seeking. Additionally, pierced females were less likely to be satisfied with their body, less likely to be foreign-born, and more likely to have a mother with low education (mandatory school or less).
Multivariate analysis. Controlling for all significant background variables, pierced females were more likely to have had multiple sexual partners, not to have used a condom at last intercourse, to be regular smokers, and to be current users of cannabis or other illegal drugs. Among males, all risk behavior variables remained significant, except suicide ideation and attempt (TABLE 1).
Multiple piercings
One third (34.1% [95% CI, 31.7–36.5]) of pierced subjects had more than 1 piercing, with similar rates for males (35.3% [95% CI, 29.8–40.9] and females (33.8% [95% CI, 31.1–36.4]).
Bivariate analysis. Among females, having more than one piercing was associated with being an apprentice, perceived advanced puberty, parents not living together, sensation seeking, and being depressed. With the exception of condom use at last intercourse, they were significantly more likely to engage in all risky behaviors.
For males, the only difference between single and multiple piercings was that the latter were more likely to have attempted suicide (TABLE 2).
Multivariate analysis. The only variables associated with females having more than one piercing were having multiple sexual partners (adjusted odds ratio [OR]=1.53 [95% CI, 1.13–2.09]) and using cannabis (adjusted OR=1.39 [95% CI, 1.06–1.82]).
TABLE 2
Characteristics of adolescents with more than 1 piercing
| FEMALES | MALES | |||||
|---|---|---|---|---|---|---|
| 1 PIERCING (N=811) | >1 PIERCING (N=414) | P VALUE | 1 PIERCING (N=183) | >1 PIERCING (N=100) | P VALUE | |
| Age (years±SD) | 17.97±1.16 | 18.01±1.18 | .55 | 18.15±1.23 | 18.34±1.15 | .190 |
| Academic track (apprentice) | 67.7% | 83.8% | <.001 | 91.3% | 92.0% | .830 |
| Body satisfaction (dissatisfied) | 67.7% | 66.9% | .781 | 81.4% | 84.0% | .587 |
| Nationality (Swiss) | 11.2 % | 10.4% | .658 | 16.9% | 16.0% | .839 |
| Perceived puberty (advanced) | 33.8% | 42.3% | .004 | 35.5% | 47.0% | .059 |
| Parental status (not together) | 28.1% | 37.4% | .001 | 29.0% | 39.0% | .085 |
| Father’s education (low)* | 11.6% | 11.1% | .803 | 15.3% | 16.0% | .877 |
| Mother’s education (low)* | 20.3% | 22.9% | .292 | 21.9% | 25.0% | .548 |
| Sensation seeking (high) | 81.5% | 72.0% | <.001 | 47.5% | 46.0% | .804 |
| Feeling depressed (yes) | 42.7% | 49.5% | .023 | 29.5% | 28.0% | .789 |
| Number of sexual partners (≥4) | 16.9% | 28.0% | <.001 | 47.0% | 43.0% | .519 |
| Condom use at last intercourse (no) | 45.2% | 50.0% | .115 | 36.6% | 45.0% | .168 |
| Regular smoker (yes) | 44.1% | 58.2% | <.001 | 65.0% | 69.0% | .499 |
| Intoxication (last 30 days) | 23.8% | 33.1% | .001 | 57.4% | 67.0% | .113 |
| Cannabis use (last 30 days) | 36.1% | 50.2% | <.001 | 67.2% | 68.0% | .893 |
| Illegal drug use (last 30 days) | 6.9% | 12.3% | .002 | 24.6% | 31.0% | .245 |
| Suicide ideation (last 12 mo) | 24.4% | 31.4% | .009 | 20.2% | 27.0% | .192 |
| Suicide attempt (last 12 mo) | 3.9% | 8.0% | .003 | 1.6% | 6.0% | .046 |
| Statistically significant differences are in bold. * Low education=mandatory school or less. | ||||||
Limitations of this study
The main strength of our study is that it is based on a nationally representative sample of adolescents. However, a few limitations need to be stressed.
Body piercing leads to medical complications in a non-negligible percentage of cases7,9,10 particularly if done by nonprofessionals.9 Given the high prevalence of adolescents, particularly females, who do body piercing, and their greater tendency to engage in risk-taking behaviors (and thus may be less careful about potential medical consequences), it seems important to make sure that they can do it under the safest conditions. Indeed, in Switzerland, new legislation regulating body piercing went into effect in 2006.
The cross-sectional nature of our survey does not allow us to assess causality. The questionnaire was filled in the classroom, which excludes absentees and dropouts, both known to be at higher risk.12 Additionally, we do not know the location or the size of the piercings; some locations (eg, nipples or genitalia) are more likely associated with risk behaviors.3,4
Can these results be generalized?
But to what extent can our results be generalized to other, non-European adolescent populations? The prevalence rate is similar to those found among North American adolescents4,5 and college students.2 All published studies seem to indicate that pierced adolescents are more likely to be risk-taking.
That would indicate that our results are on the right track. However, more population-based studies need to be done to fully confirm this.
Acknowledgments
The 2002 Swiss Multicenter adolescent Survey on Health survey was carried out with the financial support of the Swiss federal office of Public Health (contract 00.001721/2.24.02.-81) and the participating cantons.
CORRESPONDENCE
Joan-Carles Suris, MD, PhD, MPH Groupe de recherche sur la santé les adolescents, Institut universitaire de médecine sociale et préventive, Bugnon 17, 1005 Lausanne, Switzerland joan-carles.suris@chuv.ch
1. Braithwaite R, Robillard A, Woodring T, Stephens T, Arriola KJ. Tattooing and body piercing among adolescent detainees: relationship to alcohol and other drug use. J Substance Abuse 2001;13:5-16.
2. Armstrong ML, Roberts AE, Owen DC, Koch JR. Contemporary college students and body piercing. J Adol Health 2004;34:224-229.
3. Roberts TA, Auinger P, Ryan SA. Body piercing and high-risk behavior in adolescents. J Adol Health 2004;34:224-229.
4. Deschesnes M, Finès P, Demers S. Are tattooing and body piercing iindicators of risk-taking behaviours among high school students? J Adol 2006;29:379-379.
5. Carroll ST, Riffenburgh RH, Roberts TA, Myhre EB. Tattoos and body piercings as indicators of adolescent risk-taking behaviors. Pediatrics 2002;109:1021-1027.
6. Muldoon KA. Body piercing in adolescents. J Ped Health Care 1997;11:298-301.
7. Stirn A. Body piercing: medical consequences and psychological motivations. Lancet 2003;361:1205-1215.
8. Greif J, Hewitt W, Armstrong ML. Tattooing and body piercing. Clin Nursing Res 1999;8:368-385.
9. Gold MA, Scorzman CM, Murray PJ, Downs J, Tolentino G. Body piercing practices and attitudes among urban adolescents. J Adol Health 2005;36:352 e15-e21.
10. Mayers LB, Judelson DA, Moriarty BW, Rundell KW. Prevalence of body art (body piercing and tattooing) in university undergraduates and incidence of medical complications. Mayo Clin Proc 2002;77:29-34.
11. Armstrong ML, Roberts AE, Owen DC, Koch JR. Toward building a composite of college student influences with body art. Issues Comprehensive Ped Nursing 2004;27:277-295.
12. Mischaud PA, Delbos-Piot I, Narring F. Silent dropout in health surveys: are nonrespondent absent teenagers different from those who participate in school-based health surveys? J Adol Health 1998;22:326-333.
13. Jeannin A, Narring F, Tschumper A, et al. Self-reported health needs and use of primary health care services by adolescents enrolled in post-mandatory schools or vocational training programmes in Switzerland. Swiss Medical Weekly 2005;135(1-2):11-18.
14. Armstrong ML, Pace Murphy K. Tattooing: another adolescent risk behavior warranting health education. Applied Nurs Res 1997;10:181-189.
15. Brooks TL, Woods ER, Knight JR, Shrier LA. Body modification and substance use in adolescents: is there a link? J Adolesc Health 2003;32:44-49.
1. Braithwaite R, Robillard A, Woodring T, Stephens T, Arriola KJ. Tattooing and body piercing among adolescent detainees: relationship to alcohol and other drug use. J Substance Abuse 2001;13:5-16.
2. Armstrong ML, Roberts AE, Owen DC, Koch JR. Contemporary college students and body piercing. J Adol Health 2004;34:224-229.
3. Roberts TA, Auinger P, Ryan SA. Body piercing and high-risk behavior in adolescents. J Adol Health 2004;34:224-229.
4. Deschesnes M, Finès P, Demers S. Are tattooing and body piercing iindicators of risk-taking behaviours among high school students? J Adol 2006;29:379-379.
5. Carroll ST, Riffenburgh RH, Roberts TA, Myhre EB. Tattoos and body piercings as indicators of adolescent risk-taking behaviors. Pediatrics 2002;109:1021-1027.
6. Muldoon KA. Body piercing in adolescents. J Ped Health Care 1997;11:298-301.
7. Stirn A. Body piercing: medical consequences and psychological motivations. Lancet 2003;361:1205-1215.
8. Greif J, Hewitt W, Armstrong ML. Tattooing and body piercing. Clin Nursing Res 1999;8:368-385.
9. Gold MA, Scorzman CM, Murray PJ, Downs J, Tolentino G. Body piercing practices and attitudes among urban adolescents. J Adol Health 2005;36:352 e15-e21.
10. Mayers LB, Judelson DA, Moriarty BW, Rundell KW. Prevalence of body art (body piercing and tattooing) in university undergraduates and incidence of medical complications. Mayo Clin Proc 2002;77:29-34.
11. Armstrong ML, Roberts AE, Owen DC, Koch JR. Toward building a composite of college student influences with body art. Issues Comprehensive Ped Nursing 2004;27:277-295.
12. Mischaud PA, Delbos-Piot I, Narring F. Silent dropout in health surveys: are nonrespondent absent teenagers different from those who participate in school-based health surveys? J Adol Health 1998;22:326-333.
13. Jeannin A, Narring F, Tschumper A, et al. Self-reported health needs and use of primary health care services by adolescents enrolled in post-mandatory schools or vocational training programmes in Switzerland. Swiss Medical Weekly 2005;135(1-2):11-18.
14. Armstrong ML, Pace Murphy K. Tattooing: another adolescent risk behavior warranting health education. Applied Nurs Res 1997;10:181-189.
15. Brooks TL, Woods ER, Knight JR, Shrier LA. Body modification and substance use in adolescents: is there a link? J Adolesc Health 2003;32:44-49.
Neck mass: How would you treat?
A 57-year-old woman with a history of breast cancer comes to your office complaining of pain and swelling on the left side of her neck. She has recently had a mastectomy and chemotherapy; her port was removed in the past week. She has no chills, cough, dyspnea, palpitations, chest pain, nausea, weight gain, edema, or urinary complaints. She is, however, experiencing mild, general fatigue and a “scratchy throat”; otherwise there are no systemic symptoms. She is worried that her “cancer has come back.”
A:
Other medical history
- Hypothyroidism and hypertension
- History of deep venous thrombosis (DVT) attributed to her cancer; was on warfarin but “held” last week for her port removal surgery.
- Remote history of cholecystectomy
- No known drug allergies
- No history of myocardial infarction, congestive heart failure, stroke, or diabetes
- No recent international travel
- Current medications: anastrozole, hydrochlorothiazide, levothyroxine, calcium, warfarin, epoetin alfa, and acetaminophen
Family and social history
- Family history is significant for coronary artery disease late in life in her parents
- No family history of cancer, blood dyscrasia, or immunocompromise
- Formerly a smoker, only recently quit
- Moderate caffeine intake (coffee)
- Employed as a banker
Physical examination
- Temperature 99.7°F, pulse 92, respirations 20, blood pressure 122/74 mm Hg, weight 130 lbs
- Alert, oriented, no distress, full affect
- PERRLA (pupils equal, round, reactive to light and accommodation), extraocular motions intact, cranial nerves II–XII intact, mucous membranes moist, pharynx clear, no carotid bruits, minimal cervical adenopathy
- There is a tender, ill-defined mass on the left side of the neck, extending from angle of the mandible to the clavicle behind which it disappears
- Heart regular without murmurs or enlargement
- Lungs clear to auscultation in all fields
- Operative site on the left anterior thorax (port removal) is clean, dry, nonerythematous, healing well
- Abdomen is soft, nontender, nondistended, no organomegaly, normal bowel sounds
- Extremities show no significant edema or venous distention
A:
Lab results
- White bloods cell count elevated at 13 (3.9–10.9), 76% neutrophils with no bands
- Mild anemia of 11.3 (11.7–16.0)
- International normalized ratio (INR)= 0.94
- Blood cultures are pending
- Rapid strep test is negative
Next step: Order imaging studies
This particular presentation prompts you to order a computed tomography (CT) scan of her neck and chest, looking for a specific pathology (FIGURE 1).
When the scan is complete, the radiologist calls and confirms that there is occlusion of the left internal jugular vein, brachiocephalic vein, and a portion of the left subclavian vein with thrombosis.
A second CT of the chest again reveals the thrombosed veins, but there are no filling defects suggestive of pulmonary emboli or peripheral infiltrates or cavitary lesions suggestive of septic emboli (FIGURE 2).
The details. Thrombosis of the left internal jugular vein extends from the jugular siphon to the left subclavian vein. A portion of the left subclavian vein and probably the left brachiocephalic vein are also thrombosed. Numerous collaterals appear in the neck base. The left internal jugular vein measures 2.0 cm in diameter; the right measures 1.5 × 1.1 cm. There is also mild wall thickening of the internal jugular vein and infiltration of the surrounding fat—suggestive of septic thrombosis. No soft-tissue abscess is seen in the neck. The right internal jugular vein is normal. No definite thrombus is seen in the left jugular siphon or sigmoid sinus.
The parapharyngeal spaces are symmetric, though the infiltration of the fat around the left internal jugular vein is causing soft-tissue swelling and possibly mild tracheal deviation. The airway is not compromised. The superior mediastinum is grossly unremarkable. The upper lungs are clear.
A:
You vaguely recall that jugular thrombophlebitis is associated with some syndrome, so you turn to UpToDate and do a search on “jugular thrombophlebitis.”
There you learn that Lemierre’s syndrome, also known as necrobacillosis, is septic thrombophlebitis of the jugular vein. It most commonly develops following pharyngitis, and has been associated with dental microbes.1,2
Similar syndromes of suppurative thrombophlebitis may also occur in peripheral veins, associated with intravenous catheterization (especially PICC lines3), the superior and inferior vena cava, always associated with central lines,4 and the ovarian veins.5
FIGURE 1 Thrombosed veins
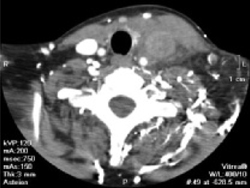
CT image with IV contrast of the base of the neck showing thrombosed veins.
FIGURE 2 Collateral circulation

This 3D reconstruction of CT images shows the extensive collateral circulation on the left, compared with the right.
You caught it early
Suppurative thrombophlebitis. This problem often presents with fever and rigorous chills. Swelling and tenderness is noted over the affected vein in about half the cases. Obviously, though, inspection and palpation of the vena cava is challenging and such signs do not apply when these vessels are involved.
Respiratory distress due to septic pulmonary emboli and secondary pneumonia is common. Metastatic abscess formation at other sites, such as joint and bone, have been reported.1,6
You realize that most patients with suppurative thrombophlebitis present in a much more toxic state than yours did. Perhaps you caught it early. She certainly has risk factors, including her recent pharyngitis and central venous catheterization. The prominent collateral circulation raises the possibility that this may have developed subacutely, following a more indolent course than is generally reported.
The organisms responsible for suppurative thrombophlebitis depend on the infection’s site of origin. Most of the time in the peripheral veins or vena cava, Staphylococcus, a member of normal skin flora, is the pathogen. Streptococcus, Enterobacteriaceae, Candida, and even cytomegalovirus have been documented.4,7,8 Jugular septic thrombophlebitis draws from the oral flora, with the most common causative agent being the anaerobic Fusobacterium.
A thrombus provides an excellent source of nutrients for the microbes, which colonize it and establish what is essentially a biofilm. These complex microbial architectures are extraordinarily resistant to antibiotic therapy, especially when compared with plantonic bacteria.9 Not only does the thrombus facilitate the infection, but the bacteria facilitate thrombus formation by promoting platelet aggregation.10
A:
Chemotherapy is only one of the many circumstances in which central venous access is required. Central venous access devices (CVADs) are also used for administration of antibiotics, hydration, total parenteral nutrition, or long-term blood sampling.
The central lines that most family physicians learned to insert during residency are only one of a dizzying array of CVADs in use. The triple-lumen lines are inserted transcutaneously by the resident into either the jugular or subclavian veins and are good for short-to-medium duration therapies. They require diligent care to prevent occlusion or infection, including daily flushing.
For longer-duration therapies, tunneled catheters may be placed, typically by surgical consultants. These are less prone to bleeding or infection but still require diligent attention and regular flushing. Some models do permit weekly flushing.
Peripherally-inserted central venous catheters (PICCs) may be used for up to a year. Generally inserted by nursing staff, they are still fairly high-maintenance and require daily flushes.

Representative venous access devices. Clockwise from upper left: triple lumen catheter, tunneled catheter, subcutaneous port, PICC.
Your patient had a subcutaneous CVAD, which is often called a “port.” It is surgically implanted, not unlike a pacemaker, and is ideal for long-term use, especially when required access is intermittent. It requires flushing only monthly (weekly when being accessed).
Medication or surgery?
Because of its resistance to antibiotic treatment, peripheral venous suppurative thrombophlebitis is a surgical disease, not unlike an abscess, and requires excision or incision and drainage of the affected vessel. Antibiotics alone are inadequate. Excision of thrombophlebitis of the central veins affected is not feasible (though thrombectomies are occasionally undertaken). In this case, prolonged antibiotic therapy is indicated.
Anticoagulation may also be considered, though no strong evidence supports that addition. Given the effect of Fusobacterium on platelet aggregation, aspirin might be expected to provide benefit. In vitro studies show inhibition of this aggregation with aspirin,10 but no clinical studies or even case reports indicate improved outcomes with its use.
A hospital stay
Prolonged antibiotics
You admit the patient to the hospital with a presumptive diagnosis of Lemierre’s syndrome and begin piperacillin/tazobactam intravenously, covering both Fusobacterium and Staphlococcus. You also opt to begin heparin and resume her warfarin, more for her history of DVT than because of documented benefit of anticoagulation in the management of suppurative thrombophlebitis.
An awareness of potential complications is vital before undertaking any medical intervention. Although it would be unusual for a family physician to place a port, insertion of central venous lines is a commonly performed procedure that shares many of the same risks. fortunately, septic thrombophlebitis is a rare complication; unfortunately, a variety of other complications may occur. These include hemorrhage, venous thrombosis (uninfected), extravascular hematoma, local or systemic infection, pneumo- hydro- hemo- or chylo-thorax, air embolus, catheter fragment embolus, nerve injury, arteriovenous fistula, and cardiac arrhythmias or tamponade. The likelihood of complications from this procedure can be diminished by strict adherence to aseptic technique, and a thorough knowledge of the surrounding anatomy. Contraindications include distorted anatomy, suspected superior vena cava injury, compromise (such as pneumothorax on the side contralateral to the planned insertion site), infection or full-thickness burns at the planned insertion site, and coagulopathy.
—Mark Huntington, MD
Anticoagulation
Over the course of her hospital stay, she spikes a fever (≥100°F) every 24 hours for the first 5 days, after which the peak temperatures slowly drop to normal. She reaches therapeutic levels on warfarin and the heparin is discontinued. At no point do any respiratory symptoms develop. Aerobic blood cultures show no growth; to your chagrin, you find out that anaerobic cultures were not obtained. After 8 days, the patient’s neck is no longer tender, the swelling has gone down, she’s adequately anticoagulated, has been afebrile for 48 hours, and is extremely eager to go home.
She is discharged with a prescription of amoxicillin/clavulanate 3 times daily for 4 weeks, as the literature suggests that most Fusobacterium are sensitive to this agent.11 She is instructed to return if any recurrent fevers, chest pain, or respiratory symptoms develop. At a routine follow-up appointment in a month, she remains asymptomatic.
1. Sinave CP, Hardy GJ, Fardy PW. The lemierre Syndrome: suppurative thrombophlebitis of the internal jugular vein secondary to oropharyngeal infection. Medicine (Baltimore) 1989;68:85-94.
2. Ely EW, Stump TE, Hudspeth AS, Haponik EF. Thoracic complications of dental surgical procedures: hazards of the dental drill. Am J Med 1993;95:456-465.
3. Andres DR, Urban AW, Acher CW, Maki DG. Septic thrombosis of the basilic, axillary, and subclavian veins caused by a peripherally inserted central venous catheter. Am J Med 1998;105:446-450.
4. Strinden WD, Helgerson RB, Maki DG. Candida septic thrombosis of the great central veins associated with central catheters. Clinical features and management. Ann Surg 1985;202:653-658.
5. Garcia J, Aboujaoude R, Apuzzio J, Alvares JR. Septic pelvic thrombophlebitis: diagnosis and management. Infect Dis Obstetr Gynecol 2006;2006:1-4.
6. Pruitt BA, Jr, McManus WF, Kim SH, Treat RC. Diagnosis and treatment of cannula-related intravenous sepsis in burn patients. Ann Surg 1980;191:546-554.
7. Baker CC, Petersen SR, Sheldon GF. Septic phlebitis: a neglected disease. Am J Surg 1979;138:97-103.
8. Peterson P, Stahl-Bayliss CM. Cytomegalovirus thrombophlebitis after successful DHPG therapy [letter]. Ann Intern Med 1987;106:632-633.
9. Parsek MR, Singh PK. Bacterial biofilms: an emerging link to disease pathogenesis. Ann Rev Microbiol 2003;57:677-701.
10. Forrester LJ, Campbell BJ, Berg JN, Barrett JT. Aggregation of platelets by Fusobacterium necrophorum. J Clin Micro 1985;22:245-249.
11. Kuriyama T, Karasawa T, Nakagawa K, Yamamoto E, Nakamura S. Incidence of beta-lactamase production and antimicrobial susceptibility of anaerobic gram-negative rods isolated from pus specimens of orofacial odontogenic infections. Oral Microbiol Immunol 2001;16:10-15.
CORRESPONDENCE: Mark K. Huntington, MD, PhD, Center for Family Medicine, 1115 East 20th Street, Sioux Falls, SD 57105. E-mail: mark.huntington@usd.edu
A 57-year-old woman with a history of breast cancer comes to your office complaining of pain and swelling on the left side of her neck. She has recently had a mastectomy and chemotherapy; her port was removed in the past week. She has no chills, cough, dyspnea, palpitations, chest pain, nausea, weight gain, edema, or urinary complaints. She is, however, experiencing mild, general fatigue and a “scratchy throat”; otherwise there are no systemic symptoms. She is worried that her “cancer has come back.”
A:
Other medical history
- Hypothyroidism and hypertension
- History of deep venous thrombosis (DVT) attributed to her cancer; was on warfarin but “held” last week for her port removal surgery.
- Remote history of cholecystectomy
- No known drug allergies
- No history of myocardial infarction, congestive heart failure, stroke, or diabetes
- No recent international travel
- Current medications: anastrozole, hydrochlorothiazide, levothyroxine, calcium, warfarin, epoetin alfa, and acetaminophen
Family and social history
- Family history is significant for coronary artery disease late in life in her parents
- No family history of cancer, blood dyscrasia, or immunocompromise
- Formerly a smoker, only recently quit
- Moderate caffeine intake (coffee)
- Employed as a banker
Physical examination
- Temperature 99.7°F, pulse 92, respirations 20, blood pressure 122/74 mm Hg, weight 130 lbs
- Alert, oriented, no distress, full affect
- PERRLA (pupils equal, round, reactive to light and accommodation), extraocular motions intact, cranial nerves II–XII intact, mucous membranes moist, pharynx clear, no carotid bruits, minimal cervical adenopathy
- There is a tender, ill-defined mass on the left side of the neck, extending from angle of the mandible to the clavicle behind which it disappears
- Heart regular without murmurs or enlargement
- Lungs clear to auscultation in all fields
- Operative site on the left anterior thorax (port removal) is clean, dry, nonerythematous, healing well
- Abdomen is soft, nontender, nondistended, no organomegaly, normal bowel sounds
- Extremities show no significant edema or venous distention
A:
Lab results
- White bloods cell count elevated at 13 (3.9–10.9), 76% neutrophils with no bands
- Mild anemia of 11.3 (11.7–16.0)
- International normalized ratio (INR)= 0.94
- Blood cultures are pending
- Rapid strep test is negative
Next step: Order imaging studies
This particular presentation prompts you to order a computed tomography (CT) scan of her neck and chest, looking for a specific pathology (FIGURE 1).
When the scan is complete, the radiologist calls and confirms that there is occlusion of the left internal jugular vein, brachiocephalic vein, and a portion of the left subclavian vein with thrombosis.
A second CT of the chest again reveals the thrombosed veins, but there are no filling defects suggestive of pulmonary emboli or peripheral infiltrates or cavitary lesions suggestive of septic emboli (FIGURE 2).
The details. Thrombosis of the left internal jugular vein extends from the jugular siphon to the left subclavian vein. A portion of the left subclavian vein and probably the left brachiocephalic vein are also thrombosed. Numerous collaterals appear in the neck base. The left internal jugular vein measures 2.0 cm in diameter; the right measures 1.5 × 1.1 cm. There is also mild wall thickening of the internal jugular vein and infiltration of the surrounding fat—suggestive of septic thrombosis. No soft-tissue abscess is seen in the neck. The right internal jugular vein is normal. No definite thrombus is seen in the left jugular siphon or sigmoid sinus.
The parapharyngeal spaces are symmetric, though the infiltration of the fat around the left internal jugular vein is causing soft-tissue swelling and possibly mild tracheal deviation. The airway is not compromised. The superior mediastinum is grossly unremarkable. The upper lungs are clear.
A:
You vaguely recall that jugular thrombophlebitis is associated with some syndrome, so you turn to UpToDate and do a search on “jugular thrombophlebitis.”
There you learn that Lemierre’s syndrome, also known as necrobacillosis, is septic thrombophlebitis of the jugular vein. It most commonly develops following pharyngitis, and has been associated with dental microbes.1,2
Similar syndromes of suppurative thrombophlebitis may also occur in peripheral veins, associated with intravenous catheterization (especially PICC lines3), the superior and inferior vena cava, always associated with central lines,4 and the ovarian veins.5
FIGURE 1 Thrombosed veins
CT image with IV contrast of the base of the neck showing thrombosed veins.
FIGURE 2 Collateral circulation
This 3D reconstruction of CT images shows the extensive collateral circulation on the left, compared with the right.
You caught it early
Suppurative thrombophlebitis. This problem often presents with fever and rigorous chills. Swelling and tenderness is noted over the affected vein in about half the cases. Obviously, though, inspection and palpation of the vena cava is challenging and such signs do not apply when these vessels are involved.
Respiratory distress due to septic pulmonary emboli and secondary pneumonia is common. Metastatic abscess formation at other sites, such as joint and bone, have been reported.1,6
You realize that most patients with suppurative thrombophlebitis present in a much more toxic state than yours did. Perhaps you caught it early. She certainly has risk factors, including her recent pharyngitis and central venous catheterization. The prominent collateral circulation raises the possibility that this may have developed subacutely, following a more indolent course than is generally reported.
The organisms responsible for suppurative thrombophlebitis depend on the infection’s site of origin. Most of the time in the peripheral veins or vena cava, Staphylococcus, a member of normal skin flora, is the pathogen. Streptococcus, Enterobacteriaceae, Candida, and even cytomegalovirus have been documented.4,7,8 Jugular septic thrombophlebitis draws from the oral flora, with the most common causative agent being the anaerobic Fusobacterium.
A thrombus provides an excellent source of nutrients for the microbes, which colonize it and establish what is essentially a biofilm. These complex microbial architectures are extraordinarily resistant to antibiotic therapy, especially when compared with plantonic bacteria.9 Not only does the thrombus facilitate the infection, but the bacteria facilitate thrombus formation by promoting platelet aggregation.10
A:
Chemotherapy is only one of the many circumstances in which central venous access is required. Central venous access devices (CVADs) are also used for administration of antibiotics, hydration, total parenteral nutrition, or long-term blood sampling.
The central lines that most family physicians learned to insert during residency are only one of a dizzying array of CVADs in use. The triple-lumen lines are inserted transcutaneously by the resident into either the jugular or subclavian veins and are good for short-to-medium duration therapies. They require diligent care to prevent occlusion or infection, including daily flushing.
For longer-duration therapies, tunneled catheters may be placed, typically by surgical consultants. These are less prone to bleeding or infection but still require diligent attention and regular flushing. Some models do permit weekly flushing.
Peripherally-inserted central venous catheters (PICCs) may be used for up to a year. Generally inserted by nursing staff, they are still fairly high-maintenance and require daily flushes.
Representative venous access devices. Clockwise from upper left: triple lumen catheter, tunneled catheter, subcutaneous port, PICC.
Your patient had a subcutaneous CVAD, which is often called a “port.” It is surgically implanted, not unlike a pacemaker, and is ideal for long-term use, especially when required access is intermittent. It requires flushing only monthly (weekly when being accessed).
Medication or surgery?
Because of its resistance to antibiotic treatment, peripheral venous suppurative thrombophlebitis is a surgical disease, not unlike an abscess, and requires excision or incision and drainage of the affected vessel. Antibiotics alone are inadequate. Excision of thrombophlebitis of the central veins affected is not feasible (though thrombectomies are occasionally undertaken). In this case, prolonged antibiotic therapy is indicated.
Anticoagulation may also be considered, though no strong evidence supports that addition. Given the effect of Fusobacterium on platelet aggregation, aspirin might be expected to provide benefit. In vitro studies show inhibition of this aggregation with aspirin,10 but no clinical studies or even case reports indicate improved outcomes with its use.
A hospital stay
Prolonged antibiotics
You admit the patient to the hospital with a presumptive diagnosis of Lemierre’s syndrome and begin piperacillin/tazobactam intravenously, covering both Fusobacterium and Staphlococcus. You also opt to begin heparin and resume her warfarin, more for her history of DVT than because of documented benefit of anticoagulation in the management of suppurative thrombophlebitis.
An awareness of potential complications is vital before undertaking any medical intervention. Although it would be unusual for a family physician to place a port, insertion of central venous lines is a commonly performed procedure that shares many of the same risks. fortunately, septic thrombophlebitis is a rare complication; unfortunately, a variety of other complications may occur. These include hemorrhage, venous thrombosis (uninfected), extravascular hematoma, local or systemic infection, pneumo- hydro- hemo- or chylo-thorax, air embolus, catheter fragment embolus, nerve injury, arteriovenous fistula, and cardiac arrhythmias or tamponade. The likelihood of complications from this procedure can be diminished by strict adherence to aseptic technique, and a thorough knowledge of the surrounding anatomy. Contraindications include distorted anatomy, suspected superior vena cava injury, compromise (such as pneumothorax on the side contralateral to the planned insertion site), infection or full-thickness burns at the planned insertion site, and coagulopathy.
—Mark Huntington, MD
Anticoagulation
Over the course of her hospital stay, she spikes a fever (≥100°F) every 24 hours for the first 5 days, after which the peak temperatures slowly drop to normal. She reaches therapeutic levels on warfarin and the heparin is discontinued. At no point do any respiratory symptoms develop. Aerobic blood cultures show no growth; to your chagrin, you find out that anaerobic cultures were not obtained. After 8 days, the patient’s neck is no longer tender, the swelling has gone down, she’s adequately anticoagulated, has been afebrile for 48 hours, and is extremely eager to go home.
She is discharged with a prescription of amoxicillin/clavulanate 3 times daily for 4 weeks, as the literature suggests that most Fusobacterium are sensitive to this agent.11 She is instructed to return if any recurrent fevers, chest pain, or respiratory symptoms develop. At a routine follow-up appointment in a month, she remains asymptomatic.
A 57-year-old woman with a history of breast cancer comes to your office complaining of pain and swelling on the left side of her neck. She has recently had a mastectomy and chemotherapy; her port was removed in the past week. She has no chills, cough, dyspnea, palpitations, chest pain, nausea, weight gain, edema, or urinary complaints. She is, however, experiencing mild, general fatigue and a “scratchy throat”; otherwise there are no systemic symptoms. She is worried that her “cancer has come back.”
A:
Other medical history
- Hypothyroidism and hypertension
- History of deep venous thrombosis (DVT) attributed to her cancer; was on warfarin but “held” last week for her port removal surgery.
- Remote history of cholecystectomy
- No known drug allergies
- No history of myocardial infarction, congestive heart failure, stroke, or diabetes
- No recent international travel
- Current medications: anastrozole, hydrochlorothiazide, levothyroxine, calcium, warfarin, epoetin alfa, and acetaminophen
Family and social history
- Family history is significant for coronary artery disease late in life in her parents
- No family history of cancer, blood dyscrasia, or immunocompromise
- Formerly a smoker, only recently quit
- Moderate caffeine intake (coffee)
- Employed as a banker
Physical examination
- Temperature 99.7°F, pulse 92, respirations 20, blood pressure 122/74 mm Hg, weight 130 lbs
- Alert, oriented, no distress, full affect
- PERRLA (pupils equal, round, reactive to light and accommodation), extraocular motions intact, cranial nerves II–XII intact, mucous membranes moist, pharynx clear, no carotid bruits, minimal cervical adenopathy
- There is a tender, ill-defined mass on the left side of the neck, extending from angle of the mandible to the clavicle behind which it disappears
- Heart regular without murmurs or enlargement
- Lungs clear to auscultation in all fields
- Operative site on the left anterior thorax (port removal) is clean, dry, nonerythematous, healing well
- Abdomen is soft, nontender, nondistended, no organomegaly, normal bowel sounds
- Extremities show no significant edema or venous distention
A:
Lab results
- White bloods cell count elevated at 13 (3.9–10.9), 76% neutrophils with no bands
- Mild anemia of 11.3 (11.7–16.0)
- International normalized ratio (INR)= 0.94
- Blood cultures are pending
- Rapid strep test is negative
Next step: Order imaging studies
This particular presentation prompts you to order a computed tomography (CT) scan of her neck and chest, looking for a specific pathology (FIGURE 1).
When the scan is complete, the radiologist calls and confirms that there is occlusion of the left internal jugular vein, brachiocephalic vein, and a portion of the left subclavian vein with thrombosis.
A second CT of the chest again reveals the thrombosed veins, but there are no filling defects suggestive of pulmonary emboli or peripheral infiltrates or cavitary lesions suggestive of septic emboli (FIGURE 2).
The details. Thrombosis of the left internal jugular vein extends from the jugular siphon to the left subclavian vein. A portion of the left subclavian vein and probably the left brachiocephalic vein are also thrombosed. Numerous collaterals appear in the neck base. The left internal jugular vein measures 2.0 cm in diameter; the right measures 1.5 × 1.1 cm. There is also mild wall thickening of the internal jugular vein and infiltration of the surrounding fat—suggestive of septic thrombosis. No soft-tissue abscess is seen in the neck. The right internal jugular vein is normal. No definite thrombus is seen in the left jugular siphon or sigmoid sinus.
The parapharyngeal spaces are symmetric, though the infiltration of the fat around the left internal jugular vein is causing soft-tissue swelling and possibly mild tracheal deviation. The airway is not compromised. The superior mediastinum is grossly unremarkable. The upper lungs are clear.
A:
You vaguely recall that jugular thrombophlebitis is associated with some syndrome, so you turn to UpToDate and do a search on “jugular thrombophlebitis.”
There you learn that Lemierre’s syndrome, also known as necrobacillosis, is septic thrombophlebitis of the jugular vein. It most commonly develops following pharyngitis, and has been associated with dental microbes.1,2
Similar syndromes of suppurative thrombophlebitis may also occur in peripheral veins, associated with intravenous catheterization (especially PICC lines3), the superior and inferior vena cava, always associated with central lines,4 and the ovarian veins.5
FIGURE 1 Thrombosed veins
CT image with IV contrast of the base of the neck showing thrombosed veins.
FIGURE 2 Collateral circulation
This 3D reconstruction of CT images shows the extensive collateral circulation on the left, compared with the right.
You caught it early
Suppurative thrombophlebitis. This problem often presents with fever and rigorous chills. Swelling and tenderness is noted over the affected vein in about half the cases. Obviously, though, inspection and palpation of the vena cava is challenging and such signs do not apply when these vessels are involved.
Respiratory distress due to septic pulmonary emboli and secondary pneumonia is common. Metastatic abscess formation at other sites, such as joint and bone, have been reported.1,6
You realize that most patients with suppurative thrombophlebitis present in a much more toxic state than yours did. Perhaps you caught it early. She certainly has risk factors, including her recent pharyngitis and central venous catheterization. The prominent collateral circulation raises the possibility that this may have developed subacutely, following a more indolent course than is generally reported.
The organisms responsible for suppurative thrombophlebitis depend on the infection’s site of origin. Most of the time in the peripheral veins or vena cava, Staphylococcus, a member of normal skin flora, is the pathogen. Streptococcus, Enterobacteriaceae, Candida, and even cytomegalovirus have been documented.4,7,8 Jugular septic thrombophlebitis draws from the oral flora, with the most common causative agent being the anaerobic Fusobacterium.
A thrombus provides an excellent source of nutrients for the microbes, which colonize it and establish what is essentially a biofilm. These complex microbial architectures are extraordinarily resistant to antibiotic therapy, especially when compared with plantonic bacteria.9 Not only does the thrombus facilitate the infection, but the bacteria facilitate thrombus formation by promoting platelet aggregation.10
A:
Chemotherapy is only one of the many circumstances in which central venous access is required. Central venous access devices (CVADs) are also used for administration of antibiotics, hydration, total parenteral nutrition, or long-term blood sampling.
The central lines that most family physicians learned to insert during residency are only one of a dizzying array of CVADs in use. The triple-lumen lines are inserted transcutaneously by the resident into either the jugular or subclavian veins and are good for short-to-medium duration therapies. They require diligent care to prevent occlusion or infection, including daily flushing.
For longer-duration therapies, tunneled catheters may be placed, typically by surgical consultants. These are less prone to bleeding or infection but still require diligent attention and regular flushing. Some models do permit weekly flushing.
Peripherally-inserted central venous catheters (PICCs) may be used for up to a year. Generally inserted by nursing staff, they are still fairly high-maintenance and require daily flushes.
Representative venous access devices. Clockwise from upper left: triple lumen catheter, tunneled catheter, subcutaneous port, PICC.
Your patient had a subcutaneous CVAD, which is often called a “port.” It is surgically implanted, not unlike a pacemaker, and is ideal for long-term use, especially when required access is intermittent. It requires flushing only monthly (weekly when being accessed).
Medication or surgery?
Because of its resistance to antibiotic treatment, peripheral venous suppurative thrombophlebitis is a surgical disease, not unlike an abscess, and requires excision or incision and drainage of the affected vessel. Antibiotics alone are inadequate. Excision of thrombophlebitis of the central veins affected is not feasible (though thrombectomies are occasionally undertaken). In this case, prolonged antibiotic therapy is indicated.
Anticoagulation may also be considered, though no strong evidence supports that addition. Given the effect of Fusobacterium on platelet aggregation, aspirin might be expected to provide benefit. In vitro studies show inhibition of this aggregation with aspirin,10 but no clinical studies or even case reports indicate improved outcomes with its use.
A hospital stay
Prolonged antibiotics
You admit the patient to the hospital with a presumptive diagnosis of Lemierre’s syndrome and begin piperacillin/tazobactam intravenously, covering both Fusobacterium and Staphlococcus. You also opt to begin heparin and resume her warfarin, more for her history of DVT than because of documented benefit of anticoagulation in the management of suppurative thrombophlebitis.
An awareness of potential complications is vital before undertaking any medical intervention. Although it would be unusual for a family physician to place a port, insertion of central venous lines is a commonly performed procedure that shares many of the same risks. fortunately, septic thrombophlebitis is a rare complication; unfortunately, a variety of other complications may occur. These include hemorrhage, venous thrombosis (uninfected), extravascular hematoma, local or systemic infection, pneumo- hydro- hemo- or chylo-thorax, air embolus, catheter fragment embolus, nerve injury, arteriovenous fistula, and cardiac arrhythmias or tamponade. The likelihood of complications from this procedure can be diminished by strict adherence to aseptic technique, and a thorough knowledge of the surrounding anatomy. Contraindications include distorted anatomy, suspected superior vena cava injury, compromise (such as pneumothorax on the side contralateral to the planned insertion site), infection or full-thickness burns at the planned insertion site, and coagulopathy.
—Mark Huntington, MD
Anticoagulation
Over the course of her hospital stay, she spikes a fever (≥100°F) every 24 hours for the first 5 days, after which the peak temperatures slowly drop to normal. She reaches therapeutic levels on warfarin and the heparin is discontinued. At no point do any respiratory symptoms develop. Aerobic blood cultures show no growth; to your chagrin, you find out that anaerobic cultures were not obtained. After 8 days, the patient’s neck is no longer tender, the swelling has gone down, she’s adequately anticoagulated, has been afebrile for 48 hours, and is extremely eager to go home.
She is discharged with a prescription of amoxicillin/clavulanate 3 times daily for 4 weeks, as the literature suggests that most Fusobacterium are sensitive to this agent.11 She is instructed to return if any recurrent fevers, chest pain, or respiratory symptoms develop. At a routine follow-up appointment in a month, she remains asymptomatic.
1. Sinave CP, Hardy GJ, Fardy PW. The lemierre Syndrome: suppurative thrombophlebitis of the internal jugular vein secondary to oropharyngeal infection. Medicine (Baltimore) 1989;68:85-94.
2. Ely EW, Stump TE, Hudspeth AS, Haponik EF. Thoracic complications of dental surgical procedures: hazards of the dental drill. Am J Med 1993;95:456-465.
3. Andres DR, Urban AW, Acher CW, Maki DG. Septic thrombosis of the basilic, axillary, and subclavian veins caused by a peripherally inserted central venous catheter. Am J Med 1998;105:446-450.
4. Strinden WD, Helgerson RB, Maki DG. Candida septic thrombosis of the great central veins associated with central catheters. Clinical features and management. Ann Surg 1985;202:653-658.
5. Garcia J, Aboujaoude R, Apuzzio J, Alvares JR. Septic pelvic thrombophlebitis: diagnosis and management. Infect Dis Obstetr Gynecol 2006;2006:1-4.
6. Pruitt BA, Jr, McManus WF, Kim SH, Treat RC. Diagnosis and treatment of cannula-related intravenous sepsis in burn patients. Ann Surg 1980;191:546-554.
7. Baker CC, Petersen SR, Sheldon GF. Septic phlebitis: a neglected disease. Am J Surg 1979;138:97-103.
8. Peterson P, Stahl-Bayliss CM. Cytomegalovirus thrombophlebitis after successful DHPG therapy [letter]. Ann Intern Med 1987;106:632-633.
9. Parsek MR, Singh PK. Bacterial biofilms: an emerging link to disease pathogenesis. Ann Rev Microbiol 2003;57:677-701.
10. Forrester LJ, Campbell BJ, Berg JN, Barrett JT. Aggregation of platelets by Fusobacterium necrophorum. J Clin Micro 1985;22:245-249.
11. Kuriyama T, Karasawa T, Nakagawa K, Yamamoto E, Nakamura S. Incidence of beta-lactamase production and antimicrobial susceptibility of anaerobic gram-negative rods isolated from pus specimens of orofacial odontogenic infections. Oral Microbiol Immunol 2001;16:10-15.
CORRESPONDENCE: Mark K. Huntington, MD, PhD, Center for Family Medicine, 1115 East 20th Street, Sioux Falls, SD 57105. E-mail: mark.huntington@usd.edu
1. Sinave CP, Hardy GJ, Fardy PW. The lemierre Syndrome: suppurative thrombophlebitis of the internal jugular vein secondary to oropharyngeal infection. Medicine (Baltimore) 1989;68:85-94.
2. Ely EW, Stump TE, Hudspeth AS, Haponik EF. Thoracic complications of dental surgical procedures: hazards of the dental drill. Am J Med 1993;95:456-465.
3. Andres DR, Urban AW, Acher CW, Maki DG. Septic thrombosis of the basilic, axillary, and subclavian veins caused by a peripherally inserted central venous catheter. Am J Med 1998;105:446-450.
4. Strinden WD, Helgerson RB, Maki DG. Candida septic thrombosis of the great central veins associated with central catheters. Clinical features and management. Ann Surg 1985;202:653-658.
5. Garcia J, Aboujaoude R, Apuzzio J, Alvares JR. Septic pelvic thrombophlebitis: diagnosis and management. Infect Dis Obstetr Gynecol 2006;2006:1-4.
6. Pruitt BA, Jr, McManus WF, Kim SH, Treat RC. Diagnosis and treatment of cannula-related intravenous sepsis in burn patients. Ann Surg 1980;191:546-554.
7. Baker CC, Petersen SR, Sheldon GF. Septic phlebitis: a neglected disease. Am J Surg 1979;138:97-103.
8. Peterson P, Stahl-Bayliss CM. Cytomegalovirus thrombophlebitis after successful DHPG therapy [letter]. Ann Intern Med 1987;106:632-633.
9. Parsek MR, Singh PK. Bacterial biofilms: an emerging link to disease pathogenesis. Ann Rev Microbiol 2003;57:677-701.
10. Forrester LJ, Campbell BJ, Berg JN, Barrett JT. Aggregation of platelets by Fusobacterium necrophorum. J Clin Micro 1985;22:245-249.
11. Kuriyama T, Karasawa T, Nakagawa K, Yamamoto E, Nakamura S. Incidence of beta-lactamase production and antimicrobial susceptibility of anaerobic gram-negative rods isolated from pus specimens of orofacial odontogenic infections. Oral Microbiol Immunol 2001;16:10-15.
CORRESPONDENCE: Mark K. Huntington, MD, PhD, Center for Family Medicine, 1115 East 20th Street, Sioux Falls, SD 57105. E-mail: mark.huntington@usd.edu
Blastomyces dermatitidis Osteomyelitis of the Tibia
Flexible Intramedullary Nailing for a Segmental Radial Fracture of the Neck and Shaft in a Child
Hydatid Disease of the Lumbar Spine: Combined Surgical and Medical Treatment—A Case Report
Chronic Septic Bursitis Caused by Dematiaceous Fungi
Gemella morbillorum Septic Arthritis of the Knee and Infective Endocarditis
Late Recurrent Salmonella Sacroiliac Osteomyelitis With Psoas Abscess in a Non-Sickle Cell Adult: Case Report
Staphylococcus lugdunensis Osteomyelitis: A Case Report
Octreotide Scan for Carcinoids
Bronchopulmonary carcinoids are relatively rare endocrine tumors. They can present with Cushing's syndrome secondary to ectopic adrenocorticotropic hormone (ACTH) secretion. They were first described in 1957, and by 1990, only 72 cases had been reported in the literature worldwide.1 The largest series reported had 7 patients seen over a 16‐year period.2 Curative resection is possible only after adequate localization of the ectopic source. In this article, we describe a case illustrating the role of octreotide scanning in the management of bronchopulmonary carcinoid.
Case
A 23‐year‐old male presented with features of Cushing's syndrome. He had a 2‐year history of abdominal striae associated with progressive fatigue, adiposity, mood swings, a 10‐kg weight gain over 6 months, and recent onset of recurrent stones in his left kidney. His past medical history was significant for delayed puberty and juvenile rheumatoid arthritis. Family history also was remarkable for rheumatoid arthritis. Physical examination of the patient at the time of presentation revealed elevated blood pressure (150‐180 mm Hg systolic and 90‐120 mm Hg diastolic) and classic cushingoid features including moon facies and abdominal and axillary striae.
Blood work performed at this time revealed elevated morning and afternoon cortisol of 841 and 918 nmol/L (30.5 and 33.3 g/dL), respectively. Thyroid‐stimulating hormone was low at 0.17 mU/L (normal 0.35‐5.5 mU/L), and free triiodothyronine (T3) and thyroxine (T4) were normal. ACTH was elevated at 70.21 pmol/L (normal 1.98‐11.6 pmol/L). Cortisol levels failed to suppress in response to our dexamethasone suppression test, as shown by the absence of suppression of urinary and serum cortisol despite administration of 0.5 mg of dexamethasone intramuscularly every 6 hours for 2 days, followed by high‐dose dexamethasone (2.0 mg) every 6 hours for 2 additional days. The chest radiograph was normal. Computed tomography (CT) could not confirm a mass but suggested a possible 1.5‐cm lesion in the superior segment of the right lower lobe of the lung. The liver, spleen, pancreas, kidneys, and adrenals were normal. There was no lymphadenopathy.
Octreotide scanning was done following intravenous administration of indium 111 Octreotide at a dose of 119 MBq. It showed a solitary focus in the superior segment of the right lower lobe, confirming the neuroendocrine nature of the suspicious lesion initially suspected on CT scan (Fig. 1). No other foci were found. The patient was diagnosed with ectopic adrenocorticotropic hormone (ACTH) secretion secondary to a bronchopulmonary carcinoid in the superior segment of the right lower lobe.
The patient was brought to the operating room for resection. Intraoperative bronchoscopy revealed no evidence of endotracheal lesions. At thoracotomy the mass was difficult to appreciate on palpation. On the basis of what preoperative imaging showed, the patient underwent a right lower lobe superior segmentectomy. Local nodes dissected at the time of the operation were negative for malignancy. To confirm adequate surgical resection, postoperative ACTH levels and octreotide scanning were performed. The ACTH level was 1.21 pmol/L (normal). A second octreotide scan showed no evidence of residual tumor (Fig. 2). The patient's blood pressure normalized, and his cushingoid features had declined by his first follow‐up visit. The final pathology confirmed carcinoid tumor, and the tumor stained with ACTH.
DISCUSSION
Ectopic ACTH secretion is responsible for 10%‐15% of the cases of Cushing's syndrome.3 Sources of the ectopic ACTH include small cell carcinoma of the lung, bronchopulmonary carcinoid, islet cell tumors, medullary carcinoma of the thyroid, and pheochromocytoma. The diagnosis of Cushing's syndrome is established by the nonsuppressibility of the serum and urinary cortisol levels. The etiology may be ACTH dependent (eg, Cushing's disease or ectopic ACTH syndrome) or ACTH independent (eg, adrenal tumor). A pituitary source is usually excluded by lack of cortisol suppression with high‐dose dexamethasone, which supports a diagnosis of ectopic ACTH. The CRH‐stimulation test can also be used to differentiate patients with Cushing's disease from those with ectopic ACTH secretion. Typically, 1 g/kg of intravenous CRH is administered to the patient, which elicits a rise in plasma ACTH or cortisol levels in a patient with Cushing's disease. However, only 5% of patients with ectopic ACTH secretion will demonstrate a plasma response,18, 19 thereby helping these 2 groups of patients. Following this differentiation, the source of ACTH can sometimes be located with traditional investigations including computed tomography of the thorax and abdomen. Finally, some authors have also advocated the use of bilateral petrosal sinus catheterization for diagnosing Cushing's syndrome if this diagnosis remains uncertain. Performed since 1982, this procedure involves the simultaneous sampling of petrosal sinuses and peripheral veins for ACTH levels both prior to and following administration of CRH. A diagnosis of ectopic ACTH secretion is strongly suggested by lack of a gradient between central and peripheral ACTH levels.
Carcinoid tumors account for 5% of lung tumors, and only a minority of these secrete ACTH. Only 1% of cases of Cushing's syndrome are accounted for by bronchial carcinoids,4 and as of 2004, only 100 cases had been reviewed in the literature worldwide.23 Pathologically, carcinoids tumors represent a low‐grade neuroendocrine malignancy arising from enterochromaffin or Kulchitsky cells, which are in the mucosa of the bronchi. There is a single line of derivation between bronchial carcinoid and small cell lung carcinoma, which was first demonstrated by Arrigoni.5
It is known that most carcinoid and other types of neuroendocrine tumors express somatostatin receptors,7, 11 and as such, a number of authors have recently described the ability to localize tumors of this type with radiolabeled somatostatin analogues.7, 1116 The sensitivity of somatostatin‐analogue scanning has been well described in the workup of gastropancreatic neuroendocrine malignancies.3, 17 although some false‐positive results do occur and have been attributed to inflammatory conditions such as sarcoidosis. Some work has been documented with this technique in other neuroendocrine malignancies.11, 14 Specifically, this technique was used by Rodriguez et al.12 to intraoperatively scan a patient's resection bed following primary removal of a bronchial carcinoid. This scan was able to identify residual disease despite gross tumor‐free margins of the primary resection specimen and thus enable complete removal of the disease.
In the past, authors have suggested that somatostatin‐analogue scanning is a useful tool in the localization of ectopic ACTH sources only after traditional modalities like CT have yielded equivocal results.3, 9, 10 Indeed, many studies have demonstrated the usefulness of octreotide scanning in localizing tumors with ectopic ACTH secretion. However, 2 recent studies have raised doubts about the clinical utility of octreotide scanning.20, 21 The study by Torpy et al. reported a significantly high false‐positive rate with octreotide scans. However, they also had false positives with conventional imaging in their series. Perhaps the best synthesis of the literature on the subject comes from Pacak et al., who looked at 17 patients with ectopic ACTH syndrome.22 They demonstrated that low‐dose octreotide scanning (L‐OCT) worked just as well as CT and better than MRI in visualizing ACTH‐secreting tumors. Moreover, they demonstrated that L‐OCT highlighted involvement of lymph nodes that was missed by CT and MRI and identified 2 abdominal lesions missed by conventional imaging. Finally, high‐dose octreotide scanning (H‐OCT) was able to pick up an intrathoracic ACTH‐secreting tumor that was not seen on CT, MRI, or L‐OCT. Although in the article the authors advocated L‐OCT as complimentary to CT and MRI, they did acknowledge that it provided additional diagnostic information, at least in their series. They advocated the use of all 3 modalities in order to provide the most comprehensive information on the location and extent of a tumor.
In this case report, we document the use of pre‐ and postoperative octreotide scanning in a patient whose CT scan was equivocal and for whom adequate surgical excision of an indistinct lesion was questionable. The use of octreotide scanning also permitted a limited resection, allowing preservation of lung parenchyma. Furthermore, it allowed us to avoid petrosal sinus catheterization. We propose that octreotide scanning can be a very important and informative test in the management of carcinoid tumors. In situations when conventional imaging is not conclusive, octreotide scanning may be of help in determining the source of ectopic ACTH syndrome. Certainly, CT scanning, currently the modality of first choice, is presently more practical and cost effective. However, octreotide scanning has been shown to be at least as sensitive in localizing ectopic ACTH‐secreting tumors and often can provide additional diagnostic information that can influence surgical management. Somatostatin‐analogue scanning, if performed initially, can guide a diagnostician about where to perform further imaging, so that limited but complete resections of this rare but curable tumor can be planned. Somatostatin‐analogue scanning also may have a role intraoperatively in ensuring complete resection despite pathologically clear tumor margins of the primary specimen, as well as an effective modality in following patients after their primary surgery for disease recurrence. These points all support the idea that octreotide scanning should play a vital and perhaps more central role in the diagnostic workup for ectopic ACTH‐secreting tumors.
CONCLUSIONS
Accurate localization of an ectopic source of ACTH in Cushing's syndrome is important for surgical cure. Octreotide scanning has been shown to be an excellent modality for both the diagnosis and the follow‐up of neuroendocrine tumors. Although computed tomography scanning of the chest and abdomen is currently used as the initial adjuncts in an attempt to localize such tumors, in the case we have presented, in which the initial CT scan was equivocal, subsequent octreotide scanning provided excellent localization of the ectopic ACTH source. We also believe that postoperative surveillance with octreotide scanning offers an excellent means of detecting residual or metastatic tumor. Indeed, somatostatin‐analogue scanning is a very useful modality for the detection, perioperative planning, and postoperative follow‐up of ectopic ACTH‐secreting tumors and neuroendocrine tumors in general and should be considered in surgical workups of such malignancies.
- ,,, et al.Management of the ectopic ACTH syndrome due to thoracic carcinoids.Ann Thorac Surg.1990;50(1):52–57.
- ,,,,,.Bronchopulmonary cacinoid tumors associated with Cushing's syndrome: a more aggressive variant of the typical carcinoid.J Thorac Cardiovasc Surg.1997;114:367–375.
- ,,,,.Ectopic ACTH secretion due to a bronchopulmonary carcinoid localized by somatostatin receptor scintigraphy.Clin Investig.1994;72:887–891.
- .Diagnostic evaluation of Cushing's syndrome.Endocrinol Metab Clin North Am.1988;17:445–472.
- ,,.Atypical carcinoid tumors of the lung.J Thorac Cardiovasc Surg.1972;64:413–421.
- ,,, et al.Somatostatin receptor scintigraphy. In:Freeman LM, ed.Nuclear Medicine Annual 1995.New York:Raven Press,1995:1–21.
- ,,.The role of somatostatin and its analogues in the diagnosis and treatment of tumors.Endocr Rev.1991;12:450–482.
- ,,.Somatostatin analogue treatment of neuroendocrine tumours.Postgrad Med J.1996;72:403–408.
- ,,, et al.Bronchial carcinoid associated with Cushing's syndrome.J Cardiovasc Surg (Torino).1995;36:511–514.
- ,,, et al.Somatostatin analogs for the localization and preoperative treatment of an adrenocorticotropin‐secreting bronchial carcinoid tumor.J Clin Endocrinol Metab.1994;78(1):20–24.
- ,,, et al.In vitro detection of somatostatin receptors in human tumors.Digestion.1993;54(suppl.):68–71.
- ,,, et al.Intraoperative detection of a bronchial carcinoid with a radiolabeled somatostatin analog.Chest.2002;121:985–988.
- ,,, et al.Localization of endocrine‐related tumours with a radioiodinated analogue of somatostatin.Lancet.1989;1:242–244.
- ,,, et al.Somatostatin receptor scintigraphy with [111In‐DTPA‐D‐Phe1]‐octreotide and [123I‐Tyr3]‐octreotide: the Rotterdam experience with more that 1,000 patients.Eur J Nucl Med.1993;20:716–731.
- ,,, et al.Comparison of somatostatin analog and meta‐iodobenzylguanidine radionuclides in the diagnosis and localization of advanced neuroendocrine tumors.J Clin Endocr Metab.2001;86:895–902.
- .MIBG and radiolabeled octreotide in neuroendocrine tumors.Q J Nucl Med.1995;39(suppl 1‐4):137–139.
- ,,, et al.Recent advances in radiological and radionuclide imaging and therapy of neuroendocrine tumours.Eur J Endocrinol2004;151:15–27.
- ,,, et al.Cushing's syndrome in children and adolescents. Presentation, diagnosis, and therapy.N Engl J Med.1994;331:629–636.
- ,,, et al.A simplified morning ovine corticotropin‐releasing hormone stimulation test for the differential diagnosis of adrenocorticotropin‐dependent Cushing's syndrome.J Clin Endocrinol Metab.1993;77:1308–1312.
- ,,, et al.Lack of utility of 111In‐pentreotide scintigraphy in localizing ectopic ACTH producing tumors: follow‐up of 18 patients.J Clin Endocrinol Metab.1999;84:1186–1192.
- ,,, et al.Usefulness of somatostatin receptor scintigraphy in patients with occult ectopic adrenocorticotropin syndrome.J Clin Endocrinol Metab.1999;84:1193–1202.
- ,,,,,.The role of [18F]fluorodeoxyglucose positron emission tomography and [111In]‐diethylenetriaminepentaacetate‐D‐Phe‐pentetreotide scintigraphy in the localization of ectopic adrenocorticotropin‐secreting tumors causing Cushing's syndrome.J Clin Endocrin Metab.2004;89:2214–2221.
- ,,, et al.Cushing's syndrome induced by bronchopulmonary carcinoid tumours: a review of 98 cases and our experience of two cases.Chir Ita.2004;56(1):63–70.
Bronchopulmonary carcinoids are relatively rare endocrine tumors. They can present with Cushing's syndrome secondary to ectopic adrenocorticotropic hormone (ACTH) secretion. They were first described in 1957, and by 1990, only 72 cases had been reported in the literature worldwide.1 The largest series reported had 7 patients seen over a 16‐year period.2 Curative resection is possible only after adequate localization of the ectopic source. In this article, we describe a case illustrating the role of octreotide scanning in the management of bronchopulmonary carcinoid.
Case
A 23‐year‐old male presented with features of Cushing's syndrome. He had a 2‐year history of abdominal striae associated with progressive fatigue, adiposity, mood swings, a 10‐kg weight gain over 6 months, and recent onset of recurrent stones in his left kidney. His past medical history was significant for delayed puberty and juvenile rheumatoid arthritis. Family history also was remarkable for rheumatoid arthritis. Physical examination of the patient at the time of presentation revealed elevated blood pressure (150‐180 mm Hg systolic and 90‐120 mm Hg diastolic) and classic cushingoid features including moon facies and abdominal and axillary striae.
Blood work performed at this time revealed elevated morning and afternoon cortisol of 841 and 918 nmol/L (30.5 and 33.3 g/dL), respectively. Thyroid‐stimulating hormone was low at 0.17 mU/L (normal 0.35‐5.5 mU/L), and free triiodothyronine (T3) and thyroxine (T4) were normal. ACTH was elevated at 70.21 pmol/L (normal 1.98‐11.6 pmol/L). Cortisol levels failed to suppress in response to our dexamethasone suppression test, as shown by the absence of suppression of urinary and serum cortisol despite administration of 0.5 mg of dexamethasone intramuscularly every 6 hours for 2 days, followed by high‐dose dexamethasone (2.0 mg) every 6 hours for 2 additional days. The chest radiograph was normal. Computed tomography (CT) could not confirm a mass but suggested a possible 1.5‐cm lesion in the superior segment of the right lower lobe of the lung. The liver, spleen, pancreas, kidneys, and adrenals were normal. There was no lymphadenopathy.
Octreotide scanning was done following intravenous administration of indium 111 Octreotide at a dose of 119 MBq. It showed a solitary focus in the superior segment of the right lower lobe, confirming the neuroendocrine nature of the suspicious lesion initially suspected on CT scan (Fig. 1). No other foci were found. The patient was diagnosed with ectopic adrenocorticotropic hormone (ACTH) secretion secondary to a bronchopulmonary carcinoid in the superior segment of the right lower lobe.
The patient was brought to the operating room for resection. Intraoperative bronchoscopy revealed no evidence of endotracheal lesions. At thoracotomy the mass was difficult to appreciate on palpation. On the basis of what preoperative imaging showed, the patient underwent a right lower lobe superior segmentectomy. Local nodes dissected at the time of the operation were negative for malignancy. To confirm adequate surgical resection, postoperative ACTH levels and octreotide scanning were performed. The ACTH level was 1.21 pmol/L (normal). A second octreotide scan showed no evidence of residual tumor (Fig. 2). The patient's blood pressure normalized, and his cushingoid features had declined by his first follow‐up visit. The final pathology confirmed carcinoid tumor, and the tumor stained with ACTH.
DISCUSSION
Ectopic ACTH secretion is responsible for 10%‐15% of the cases of Cushing's syndrome.3 Sources of the ectopic ACTH include small cell carcinoma of the lung, bronchopulmonary carcinoid, islet cell tumors, medullary carcinoma of the thyroid, and pheochromocytoma. The diagnosis of Cushing's syndrome is established by the nonsuppressibility of the serum and urinary cortisol levels. The etiology may be ACTH dependent (eg, Cushing's disease or ectopic ACTH syndrome) or ACTH independent (eg, adrenal tumor). A pituitary source is usually excluded by lack of cortisol suppression with high‐dose dexamethasone, which supports a diagnosis of ectopic ACTH. The CRH‐stimulation test can also be used to differentiate patients with Cushing's disease from those with ectopic ACTH secretion. Typically, 1 g/kg of intravenous CRH is administered to the patient, which elicits a rise in plasma ACTH or cortisol levels in a patient with Cushing's disease. However, only 5% of patients with ectopic ACTH secretion will demonstrate a plasma response,18, 19 thereby helping these 2 groups of patients. Following this differentiation, the source of ACTH can sometimes be located with traditional investigations including computed tomography of the thorax and abdomen. Finally, some authors have also advocated the use of bilateral petrosal sinus catheterization for diagnosing Cushing's syndrome if this diagnosis remains uncertain. Performed since 1982, this procedure involves the simultaneous sampling of petrosal sinuses and peripheral veins for ACTH levels both prior to and following administration of CRH. A diagnosis of ectopic ACTH secretion is strongly suggested by lack of a gradient between central and peripheral ACTH levels.
Carcinoid tumors account for 5% of lung tumors, and only a minority of these secrete ACTH. Only 1% of cases of Cushing's syndrome are accounted for by bronchial carcinoids,4 and as of 2004, only 100 cases had been reviewed in the literature worldwide.23 Pathologically, carcinoids tumors represent a low‐grade neuroendocrine malignancy arising from enterochromaffin or Kulchitsky cells, which are in the mucosa of the bronchi. There is a single line of derivation between bronchial carcinoid and small cell lung carcinoma, which was first demonstrated by Arrigoni.5
It is known that most carcinoid and other types of neuroendocrine tumors express somatostatin receptors,7, 11 and as such, a number of authors have recently described the ability to localize tumors of this type with radiolabeled somatostatin analogues.7, 1116 The sensitivity of somatostatin‐analogue scanning has been well described in the workup of gastropancreatic neuroendocrine malignancies.3, 17 although some false‐positive results do occur and have been attributed to inflammatory conditions such as sarcoidosis. Some work has been documented with this technique in other neuroendocrine malignancies.11, 14 Specifically, this technique was used by Rodriguez et al.12 to intraoperatively scan a patient's resection bed following primary removal of a bronchial carcinoid. This scan was able to identify residual disease despite gross tumor‐free margins of the primary resection specimen and thus enable complete removal of the disease.
In the past, authors have suggested that somatostatin‐analogue scanning is a useful tool in the localization of ectopic ACTH sources only after traditional modalities like CT have yielded equivocal results.3, 9, 10 Indeed, many studies have demonstrated the usefulness of octreotide scanning in localizing tumors with ectopic ACTH secretion. However, 2 recent studies have raised doubts about the clinical utility of octreotide scanning.20, 21 The study by Torpy et al. reported a significantly high false‐positive rate with octreotide scans. However, they also had false positives with conventional imaging in their series. Perhaps the best synthesis of the literature on the subject comes from Pacak et al., who looked at 17 patients with ectopic ACTH syndrome.22 They demonstrated that low‐dose octreotide scanning (L‐OCT) worked just as well as CT and better than MRI in visualizing ACTH‐secreting tumors. Moreover, they demonstrated that L‐OCT highlighted involvement of lymph nodes that was missed by CT and MRI and identified 2 abdominal lesions missed by conventional imaging. Finally, high‐dose octreotide scanning (H‐OCT) was able to pick up an intrathoracic ACTH‐secreting tumor that was not seen on CT, MRI, or L‐OCT. Although in the article the authors advocated L‐OCT as complimentary to CT and MRI, they did acknowledge that it provided additional diagnostic information, at least in their series. They advocated the use of all 3 modalities in order to provide the most comprehensive information on the location and extent of a tumor.
In this case report, we document the use of pre‐ and postoperative octreotide scanning in a patient whose CT scan was equivocal and for whom adequate surgical excision of an indistinct lesion was questionable. The use of octreotide scanning also permitted a limited resection, allowing preservation of lung parenchyma. Furthermore, it allowed us to avoid petrosal sinus catheterization. We propose that octreotide scanning can be a very important and informative test in the management of carcinoid tumors. In situations when conventional imaging is not conclusive, octreotide scanning may be of help in determining the source of ectopic ACTH syndrome. Certainly, CT scanning, currently the modality of first choice, is presently more practical and cost effective. However, octreotide scanning has been shown to be at least as sensitive in localizing ectopic ACTH‐secreting tumors and often can provide additional diagnostic information that can influence surgical management. Somatostatin‐analogue scanning, if performed initially, can guide a diagnostician about where to perform further imaging, so that limited but complete resections of this rare but curable tumor can be planned. Somatostatin‐analogue scanning also may have a role intraoperatively in ensuring complete resection despite pathologically clear tumor margins of the primary specimen, as well as an effective modality in following patients after their primary surgery for disease recurrence. These points all support the idea that octreotide scanning should play a vital and perhaps more central role in the diagnostic workup for ectopic ACTH‐secreting tumors.
CONCLUSIONS
Accurate localization of an ectopic source of ACTH in Cushing's syndrome is important for surgical cure. Octreotide scanning has been shown to be an excellent modality for both the diagnosis and the follow‐up of neuroendocrine tumors. Although computed tomography scanning of the chest and abdomen is currently used as the initial adjuncts in an attempt to localize such tumors, in the case we have presented, in which the initial CT scan was equivocal, subsequent octreotide scanning provided excellent localization of the ectopic ACTH source. We also believe that postoperative surveillance with octreotide scanning offers an excellent means of detecting residual or metastatic tumor. Indeed, somatostatin‐analogue scanning is a very useful modality for the detection, perioperative planning, and postoperative follow‐up of ectopic ACTH‐secreting tumors and neuroendocrine tumors in general and should be considered in surgical workups of such malignancies.
Bronchopulmonary carcinoids are relatively rare endocrine tumors. They can present with Cushing's syndrome secondary to ectopic adrenocorticotropic hormone (ACTH) secretion. They were first described in 1957, and by 1990, only 72 cases had been reported in the literature worldwide.1 The largest series reported had 7 patients seen over a 16‐year period.2 Curative resection is possible only after adequate localization of the ectopic source. In this article, we describe a case illustrating the role of octreotide scanning in the management of bronchopulmonary carcinoid.
Case
A 23‐year‐old male presented with features of Cushing's syndrome. He had a 2‐year history of abdominal striae associated with progressive fatigue, adiposity, mood swings, a 10‐kg weight gain over 6 months, and recent onset of recurrent stones in his left kidney. His past medical history was significant for delayed puberty and juvenile rheumatoid arthritis. Family history also was remarkable for rheumatoid arthritis. Physical examination of the patient at the time of presentation revealed elevated blood pressure (150‐180 mm Hg systolic and 90‐120 mm Hg diastolic) and classic cushingoid features including moon facies and abdominal and axillary striae.
Blood work performed at this time revealed elevated morning and afternoon cortisol of 841 and 918 nmol/L (30.5 and 33.3 g/dL), respectively. Thyroid‐stimulating hormone was low at 0.17 mU/L (normal 0.35‐5.5 mU/L), and free triiodothyronine (T3) and thyroxine (T4) were normal. ACTH was elevated at 70.21 pmol/L (normal 1.98‐11.6 pmol/L). Cortisol levels failed to suppress in response to our dexamethasone suppression test, as shown by the absence of suppression of urinary and serum cortisol despite administration of 0.5 mg of dexamethasone intramuscularly every 6 hours for 2 days, followed by high‐dose dexamethasone (2.0 mg) every 6 hours for 2 additional days. The chest radiograph was normal. Computed tomography (CT) could not confirm a mass but suggested a possible 1.5‐cm lesion in the superior segment of the right lower lobe of the lung. The liver, spleen, pancreas, kidneys, and adrenals were normal. There was no lymphadenopathy.
Octreotide scanning was done following intravenous administration of indium 111 Octreotide at a dose of 119 MBq. It showed a solitary focus in the superior segment of the right lower lobe, confirming the neuroendocrine nature of the suspicious lesion initially suspected on CT scan (Fig. 1). No other foci were found. The patient was diagnosed with ectopic adrenocorticotropic hormone (ACTH) secretion secondary to a bronchopulmonary carcinoid in the superior segment of the right lower lobe.
The patient was brought to the operating room for resection. Intraoperative bronchoscopy revealed no evidence of endotracheal lesions. At thoracotomy the mass was difficult to appreciate on palpation. On the basis of what preoperative imaging showed, the patient underwent a right lower lobe superior segmentectomy. Local nodes dissected at the time of the operation were negative for malignancy. To confirm adequate surgical resection, postoperative ACTH levels and octreotide scanning were performed. The ACTH level was 1.21 pmol/L (normal). A second octreotide scan showed no evidence of residual tumor (Fig. 2). The patient's blood pressure normalized, and his cushingoid features had declined by his first follow‐up visit. The final pathology confirmed carcinoid tumor, and the tumor stained with ACTH.
DISCUSSION
Ectopic ACTH secretion is responsible for 10%‐15% of the cases of Cushing's syndrome.3 Sources of the ectopic ACTH include small cell carcinoma of the lung, bronchopulmonary carcinoid, islet cell tumors, medullary carcinoma of the thyroid, and pheochromocytoma. The diagnosis of Cushing's syndrome is established by the nonsuppressibility of the serum and urinary cortisol levels. The etiology may be ACTH dependent (eg, Cushing's disease or ectopic ACTH syndrome) or ACTH independent (eg, adrenal tumor). A pituitary source is usually excluded by lack of cortisol suppression with high‐dose dexamethasone, which supports a diagnosis of ectopic ACTH. The CRH‐stimulation test can also be used to differentiate patients with Cushing's disease from those with ectopic ACTH secretion. Typically, 1 g/kg of intravenous CRH is administered to the patient, which elicits a rise in plasma ACTH or cortisol levels in a patient with Cushing's disease. However, only 5% of patients with ectopic ACTH secretion will demonstrate a plasma response,18, 19 thereby helping these 2 groups of patients. Following this differentiation, the source of ACTH can sometimes be located with traditional investigations including computed tomography of the thorax and abdomen. Finally, some authors have also advocated the use of bilateral petrosal sinus catheterization for diagnosing Cushing's syndrome if this diagnosis remains uncertain. Performed since 1982, this procedure involves the simultaneous sampling of petrosal sinuses and peripheral veins for ACTH levels both prior to and following administration of CRH. A diagnosis of ectopic ACTH secretion is strongly suggested by lack of a gradient between central and peripheral ACTH levels.
Carcinoid tumors account for 5% of lung tumors, and only a minority of these secrete ACTH. Only 1% of cases of Cushing's syndrome are accounted for by bronchial carcinoids,4 and as of 2004, only 100 cases had been reviewed in the literature worldwide.23 Pathologically, carcinoids tumors represent a low‐grade neuroendocrine malignancy arising from enterochromaffin or Kulchitsky cells, which are in the mucosa of the bronchi. There is a single line of derivation between bronchial carcinoid and small cell lung carcinoma, which was first demonstrated by Arrigoni.5
It is known that most carcinoid and other types of neuroendocrine tumors express somatostatin receptors,7, 11 and as such, a number of authors have recently described the ability to localize tumors of this type with radiolabeled somatostatin analogues.7, 1116 The sensitivity of somatostatin‐analogue scanning has been well described in the workup of gastropancreatic neuroendocrine malignancies.3, 17 although some false‐positive results do occur and have been attributed to inflammatory conditions such as sarcoidosis. Some work has been documented with this technique in other neuroendocrine malignancies.11, 14 Specifically, this technique was used by Rodriguez et al.12 to intraoperatively scan a patient's resection bed following primary removal of a bronchial carcinoid. This scan was able to identify residual disease despite gross tumor‐free margins of the primary resection specimen and thus enable complete removal of the disease.
In the past, authors have suggested that somatostatin‐analogue scanning is a useful tool in the localization of ectopic ACTH sources only after traditional modalities like CT have yielded equivocal results.3, 9, 10 Indeed, many studies have demonstrated the usefulness of octreotide scanning in localizing tumors with ectopic ACTH secretion. However, 2 recent studies have raised doubts about the clinical utility of octreotide scanning.20, 21 The study by Torpy et al. reported a significantly high false‐positive rate with octreotide scans. However, they also had false positives with conventional imaging in their series. Perhaps the best synthesis of the literature on the subject comes from Pacak et al., who looked at 17 patients with ectopic ACTH syndrome.22 They demonstrated that low‐dose octreotide scanning (L‐OCT) worked just as well as CT and better than MRI in visualizing ACTH‐secreting tumors. Moreover, they demonstrated that L‐OCT highlighted involvement of lymph nodes that was missed by CT and MRI and identified 2 abdominal lesions missed by conventional imaging. Finally, high‐dose octreotide scanning (H‐OCT) was able to pick up an intrathoracic ACTH‐secreting tumor that was not seen on CT, MRI, or L‐OCT. Although in the article the authors advocated L‐OCT as complimentary to CT and MRI, they did acknowledge that it provided additional diagnostic information, at least in their series. They advocated the use of all 3 modalities in order to provide the most comprehensive information on the location and extent of a tumor.
In this case report, we document the use of pre‐ and postoperative octreotide scanning in a patient whose CT scan was equivocal and for whom adequate surgical excision of an indistinct lesion was questionable. The use of octreotide scanning also permitted a limited resection, allowing preservation of lung parenchyma. Furthermore, it allowed us to avoid petrosal sinus catheterization. We propose that octreotide scanning can be a very important and informative test in the management of carcinoid tumors. In situations when conventional imaging is not conclusive, octreotide scanning may be of help in determining the source of ectopic ACTH syndrome. Certainly, CT scanning, currently the modality of first choice, is presently more practical and cost effective. However, octreotide scanning has been shown to be at least as sensitive in localizing ectopic ACTH‐secreting tumors and often can provide additional diagnostic information that can influence surgical management. Somatostatin‐analogue scanning, if performed initially, can guide a diagnostician about where to perform further imaging, so that limited but complete resections of this rare but curable tumor can be planned. Somatostatin‐analogue scanning also may have a role intraoperatively in ensuring complete resection despite pathologically clear tumor margins of the primary specimen, as well as an effective modality in following patients after their primary surgery for disease recurrence. These points all support the idea that octreotide scanning should play a vital and perhaps more central role in the diagnostic workup for ectopic ACTH‐secreting tumors.
CONCLUSIONS
Accurate localization of an ectopic source of ACTH in Cushing's syndrome is important for surgical cure. Octreotide scanning has been shown to be an excellent modality for both the diagnosis and the follow‐up of neuroendocrine tumors. Although computed tomography scanning of the chest and abdomen is currently used as the initial adjuncts in an attempt to localize such tumors, in the case we have presented, in which the initial CT scan was equivocal, subsequent octreotide scanning provided excellent localization of the ectopic ACTH source. We also believe that postoperative surveillance with octreotide scanning offers an excellent means of detecting residual or metastatic tumor. Indeed, somatostatin‐analogue scanning is a very useful modality for the detection, perioperative planning, and postoperative follow‐up of ectopic ACTH‐secreting tumors and neuroendocrine tumors in general and should be considered in surgical workups of such malignancies.
- ,,, et al.Management of the ectopic ACTH syndrome due to thoracic carcinoids.Ann Thorac Surg.1990;50(1):52–57.
- ,,,,,.Bronchopulmonary cacinoid tumors associated with Cushing's syndrome: a more aggressive variant of the typical carcinoid.J Thorac Cardiovasc Surg.1997;114:367–375.
- ,,,,.Ectopic ACTH secretion due to a bronchopulmonary carcinoid localized by somatostatin receptor scintigraphy.Clin Investig.1994;72:887–891.
- .Diagnostic evaluation of Cushing's syndrome.Endocrinol Metab Clin North Am.1988;17:445–472.
- ,,.Atypical carcinoid tumors of the lung.J Thorac Cardiovasc Surg.1972;64:413–421.
- ,,, et al.Somatostatin receptor scintigraphy. In:Freeman LM, ed.Nuclear Medicine Annual 1995.New York:Raven Press,1995:1–21.
- ,,.The role of somatostatin and its analogues in the diagnosis and treatment of tumors.Endocr Rev.1991;12:450–482.
- ,,.Somatostatin analogue treatment of neuroendocrine tumours.Postgrad Med J.1996;72:403–408.
- ,,, et al.Bronchial carcinoid associated with Cushing's syndrome.J Cardiovasc Surg (Torino).1995;36:511–514.
- ,,, et al.Somatostatin analogs for the localization and preoperative treatment of an adrenocorticotropin‐secreting bronchial carcinoid tumor.J Clin Endocrinol Metab.1994;78(1):20–24.
- ,,, et al.In vitro detection of somatostatin receptors in human tumors.Digestion.1993;54(suppl.):68–71.
- ,,, et al.Intraoperative detection of a bronchial carcinoid with a radiolabeled somatostatin analog.Chest.2002;121:985–988.
- ,,, et al.Localization of endocrine‐related tumours with a radioiodinated analogue of somatostatin.Lancet.1989;1:242–244.
- ,,, et al.Somatostatin receptor scintigraphy with [111In‐DTPA‐D‐Phe1]‐octreotide and [123I‐Tyr3]‐octreotide: the Rotterdam experience with more that 1,000 patients.Eur J Nucl Med.1993;20:716–731.
- ,,, et al.Comparison of somatostatin analog and meta‐iodobenzylguanidine radionuclides in the diagnosis and localization of advanced neuroendocrine tumors.J Clin Endocr Metab.2001;86:895–902.
- .MIBG and radiolabeled octreotide in neuroendocrine tumors.Q J Nucl Med.1995;39(suppl 1‐4):137–139.
- ,,, et al.Recent advances in radiological and radionuclide imaging and therapy of neuroendocrine tumours.Eur J Endocrinol2004;151:15–27.
- ,,, et al.Cushing's syndrome in children and adolescents. Presentation, diagnosis, and therapy.N Engl J Med.1994;331:629–636.
- ,,, et al.A simplified morning ovine corticotropin‐releasing hormone stimulation test for the differential diagnosis of adrenocorticotropin‐dependent Cushing's syndrome.J Clin Endocrinol Metab.1993;77:1308–1312.
- ,,, et al.Lack of utility of 111In‐pentreotide scintigraphy in localizing ectopic ACTH producing tumors: follow‐up of 18 patients.J Clin Endocrinol Metab.1999;84:1186–1192.
- ,,, et al.Usefulness of somatostatin receptor scintigraphy in patients with occult ectopic adrenocorticotropin syndrome.J Clin Endocrinol Metab.1999;84:1193–1202.
- ,,,,,.The role of [18F]fluorodeoxyglucose positron emission tomography and [111In]‐diethylenetriaminepentaacetate‐D‐Phe‐pentetreotide scintigraphy in the localization of ectopic adrenocorticotropin‐secreting tumors causing Cushing's syndrome.J Clin Endocrin Metab.2004;89:2214–2221.
- ,,, et al.Cushing's syndrome induced by bronchopulmonary carcinoid tumours: a review of 98 cases and our experience of two cases.Chir Ita.2004;56(1):63–70.
- ,,, et al.Management of the ectopic ACTH syndrome due to thoracic carcinoids.Ann Thorac Surg.1990;50(1):52–57.
- ,,,,,.Bronchopulmonary cacinoid tumors associated with Cushing's syndrome: a more aggressive variant of the typical carcinoid.J Thorac Cardiovasc Surg.1997;114:367–375.
- ,,,,.Ectopic ACTH secretion due to a bronchopulmonary carcinoid localized by somatostatin receptor scintigraphy.Clin Investig.1994;72:887–891.
- .Diagnostic evaluation of Cushing's syndrome.Endocrinol Metab Clin North Am.1988;17:445–472.
- ,,.Atypical carcinoid tumors of the lung.J Thorac Cardiovasc Surg.1972;64:413–421.
- ,,, et al.Somatostatin receptor scintigraphy. In:Freeman LM, ed.Nuclear Medicine Annual 1995.New York:Raven Press,1995:1–21.
- ,,.The role of somatostatin and its analogues in the diagnosis and treatment of tumors.Endocr Rev.1991;12:450–482.
- ,,.Somatostatin analogue treatment of neuroendocrine tumours.Postgrad Med J.1996;72:403–408.
- ,,, et al.Bronchial carcinoid associated with Cushing's syndrome.J Cardiovasc Surg (Torino).1995;36:511–514.
- ,,, et al.Somatostatin analogs for the localization and preoperative treatment of an adrenocorticotropin‐secreting bronchial carcinoid tumor.J Clin Endocrinol Metab.1994;78(1):20–24.
- ,,, et al.In vitro detection of somatostatin receptors in human tumors.Digestion.1993;54(suppl.):68–71.
- ,,, et al.Intraoperative detection of a bronchial carcinoid with a radiolabeled somatostatin analog.Chest.2002;121:985–988.
- ,,, et al.Localization of endocrine‐related tumours with a radioiodinated analogue of somatostatin.Lancet.1989;1:242–244.
- ,,, et al.Somatostatin receptor scintigraphy with [111In‐DTPA‐D‐Phe1]‐octreotide and [123I‐Tyr3]‐octreotide: the Rotterdam experience with more that 1,000 patients.Eur J Nucl Med.1993;20:716–731.
- ,,, et al.Comparison of somatostatin analog and meta‐iodobenzylguanidine radionuclides in the diagnosis and localization of advanced neuroendocrine tumors.J Clin Endocr Metab.2001;86:895–902.
- .MIBG and radiolabeled octreotide in neuroendocrine tumors.Q J Nucl Med.1995;39(suppl 1‐4):137–139.
- ,,, et al.Recent advances in radiological and radionuclide imaging and therapy of neuroendocrine tumours.Eur J Endocrinol2004;151:15–27.
- ,,, et al.Cushing's syndrome in children and adolescents. Presentation, diagnosis, and therapy.N Engl J Med.1994;331:629–636.
- ,,, et al.A simplified morning ovine corticotropin‐releasing hormone stimulation test for the differential diagnosis of adrenocorticotropin‐dependent Cushing's syndrome.J Clin Endocrinol Metab.1993;77:1308–1312.
- ,,, et al.Lack of utility of 111In‐pentreotide scintigraphy in localizing ectopic ACTH producing tumors: follow‐up of 18 patients.J Clin Endocrinol Metab.1999;84:1186–1192.
- ,,, et al.Usefulness of somatostatin receptor scintigraphy in patients with occult ectopic adrenocorticotropin syndrome.J Clin Endocrinol Metab.1999;84:1193–1202.
- ,,,,,.The role of [18F]fluorodeoxyglucose positron emission tomography and [111In]‐diethylenetriaminepentaacetate‐D‐Phe‐pentetreotide scintigraphy in the localization of ectopic adrenocorticotropin‐secreting tumors causing Cushing's syndrome.J Clin Endocrin Metab.2004;89:2214–2221.
- ,,, et al.Cushing's syndrome induced by bronchopulmonary carcinoid tumours: a review of 98 cases and our experience of two cases.Chir Ita.2004;56(1):63–70.