User login
ICD for Vasospasm‐Induced Polymorphic VT
Arrhythmias are well‐described in patients with vasospastic angina. Coronary vasospasm may occur in the setting of angiographically normal or diseased coronary arteries. Patients with vasospastic angina are at increased risk of sudden death. However, it is unclear which of these patients would benefit from implantable cardioverter defibrillator (ICD) insertion.
We report a case of a young woman who presented with atypical angina. During an episode of chest pain she had a documented run of sustained polymorphic ventricular tachycardia (VT). In addition to medical therapy, she received an ICD to prevent future episodes of sudden cardiac death.
Case Report
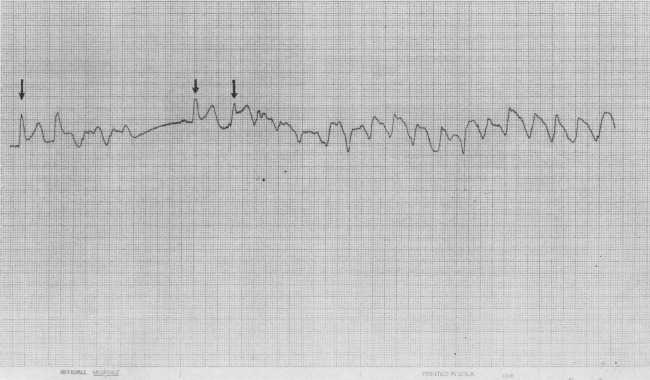
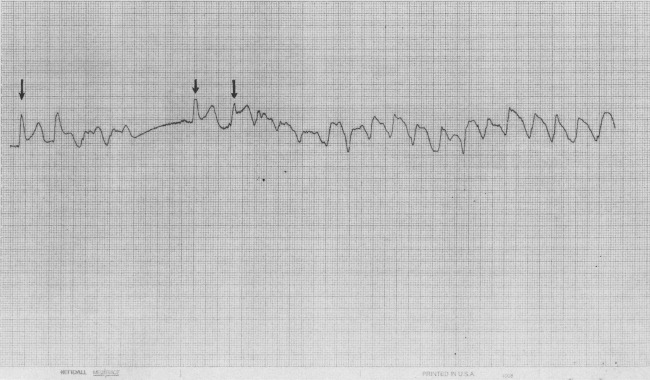
A 38‐year‐old woman was admitted with an episode of severe central chest pain. The pain was sharp, localized, occurred at rest, and resolved spontaneously after about 2 hours. She reported intermittent but shorter episodes of similar chest pain for the preceding 5 months. These episodes were associated with palpitation and lightheadedness. She was a smoker with past medical history of hyperlipidemia, asthma, and psoriasis. There was no family history of sudden cardiac death or premature coronary artery disease. On presentation, she was pain‐free, and vitals were stable. Electrocardiogram revealed normal sinus rhythm, no ischemic ST segment changes, and a QTc interval of 479 msec. Serum troponins were normal, serum potassium was 3.5 mmol/L, and serum magnesium was 1.9 mg/dL. While she was being monitored on telemetry, she suddenly experienced chest pain with palpitation. The telemetry recording of the event showed transient ST segment elevation followed by an episode of sustained polymorphic ventricular tachycardia (VT) (Figure 1). She remained hemodynamically stable and did not lose consciousness. The VT was self‐terminating.
Coronary angiogram revealed moderate 2‐vessel disease and spontaneous spasm of the dominant left circumflex artery. Therapy was initiated using both an oral nitrate and calcium channel antagonist. Potassium and magnesium levels were corrected with supplementation. On further questioning, she reported 1 episode of near‐syncope in the past. In view of the above history and a documented episode of spontaneous sustained polymorphic VT, an implantable cardioverter defibrillator (ICD) was implanted. She was strongly advised to quit smoking and was discharged home in stable condition. Three months later, she was admitted with recurrence of similar episodes of chest pain and dizziness, and multiple shocks from her ICD. Interrogation of the ICD revealed 5 episodes of polymorphic VT that were appropriately terminated with ICD discharges. The doses of calcium channel antagonist and oral nitrate were maximized, and she was discharged home in stable condition.
Discussion
Our case highlights an important management dilemma in patients with vasospastic angina. ICD implantation in this group has been reported in patients resuscitated from cardiac arrest. Our patient was recognized to be at high risk of sudden death but had never experienced cardiac arrest.
An increased incidence of sudden cardiac death, VT, and ventricular fibrillation has been observed during episodes of vasospastic angina. In a retrospective multicenter study of 349 patients with vasospastic angina, VT or ventricular fibrillation was noted in 6.5% of patients.1 Sudden death was reported in 2% of the patients (mean follow‐up period, 3.4 years), of whom the majority had ST segment elevation during anginal attacks. Increased ventricular vulnerability has been noted even during symptom‐free periods.2 Some cases of unexplained out‐of‐hospital cardiac arrest and sudden deaths may be secondary to coronary artery spasm.3 In a prospective study of 356 survivors of out‐of‐hospital cardiac arrest, Myerburg et al.4 reported 5 patients with coronary artery spasm who had silent ischemic events associated with life‐threatening ventricular arrhythmias. Interestingly, in 2 of the 5 patients, onset of ventricular arrhythmia correlated with reperfusion, rather than ischemia.
Calcium‐channel antagonists and nitrates are accepted as the first‐line treatment for vasospastic angina. Although this therapy improves prognosis, the risk of ventricular arrhythmia and sudden death is not eliminated.1 The data regarding use of ICDs in patients with coronary vasospasm are limited to case reports. Lacroix et al.5 reported 2 patients with vasospastic angina resuscitated from out‐of‐hospital cardiac arrest who received ICDs. Postimplantation, at 4 months and 11 months, respectively, each of the 2 patients had appropriate ICD discharges. Fuertes et al.6 reported a patient resuscitated from cardiac arrest due to ventricular fibrillation related to an episode of angina. The patient had vasospasm despite intensive medical therapy and had an ICD implanted. The above previously published cases describe ICD implantation for patients resuscitated from cardiac arrest.
However, in patients with coronary vasospasm who have never experienced cardiac arrest, it is unclear which subset would benefit from an ICD. Electrophysiological studies are not always helpful in identifying these patients. In the study by Myerburg et al.,4 only 1 out of the 5 patients with coronary artery spasm had inducible arrhythmia during electrophysiological testing. Clinical features associated with increased risk of sudden death were reported by McAlpin3 in a study of 81 patients with vasospastic angina. The risk of sudden death was tripled by the presence of either a history of angina‐linked syncope or documentation of serious arrhythmia complicating attacks. Paradoxically, the risk was increased by the absence of high‐grade coronary artery stenosis. Some researchers have reported a strong association between cigarette smoking and coronary spasm.7 Patients with known or suspected coronary artery spasm should be strongly discouraged from smoking. Our patient, in addition to being a smoker, had 2 of the 3 risk factors described by McAlpin,3 namely, documented serious arrhythmia and absence of high‐grade coronary stenosis. Considering these risk factors, an ICD was implanted. To our knowledge this is the first reported case of ICD insertion in a patient with vasospasm‐induced VT who had never experienced cardiac arrest.
Conclusions
In summary, patients with vasospastic angina are at increased risk of sudden death, especially during an episode of angina. Some cases of unexplained sudden death and malignant ventricular arrhythmia are probably a consequence of acute myocardial ischemia resulting from coronary arterial spasm. Early recognition and treatment of polymorphic VT is critical in preventing sudden cardiac death. In the absence of myocardial infarction, ST segment elevation preceding an episode of syncope or arrhythmia should raise the suspicion of coronary vasospasm as the underlying etiology. ICD placement is potentially beneficial in patients with coronary spasm who are at high risk of sudden cardiac death. Larger trials with longer follow‐up periods would help clinicians make this decision with greater confidence.
- ,,.Clinical characteristics associated with myocardial infarction, arrhythmias, and sudden death in patients with vasospastic angina.Circulation.1987;75:1110–1116.
- ,,, et al.Induction of polymorphic ventricular tachycardia by programmed ventricular stimulation in vasospastic angina pectoris.Am J Cardiol.1996;77:355–360.
- .Cardiac arrest and sudden unexpected death in variant angina: complications of coronary spasm that can occur in the absence of severe organic coronary stenosis.Am Heart J.1993;125:1011–1017.
- ,,, et al.Life‐threatening ventricular arrhythmias in patients with silent myocardial ischemia due to coronary‐artery spasm.N Engl J Med.1992;326(22):1451–1455.
- ,,.Vasospastic angina without flow‐limiting coronary lesion as a cause for aborted sudden death.Int J Cardiol (Ireland).1994;43:247–249.
- ,,,.Implantable cardioverter defibrillator as a therapeutic option for sudden cardiac death secondary to severe coronary vasospasm.Int J Cardiol.1998;63:181–183.
- ,.Cigarette smoking is a major risk factor for coronary spasm.Circulation.1993;87:76–79.
Arrhythmias are well‐described in patients with vasospastic angina. Coronary vasospasm may occur in the setting of angiographically normal or diseased coronary arteries. Patients with vasospastic angina are at increased risk of sudden death. However, it is unclear which of these patients would benefit from implantable cardioverter defibrillator (ICD) insertion.
We report a case of a young woman who presented with atypical angina. During an episode of chest pain she had a documented run of sustained polymorphic ventricular tachycardia (VT). In addition to medical therapy, she received an ICD to prevent future episodes of sudden cardiac death.
Case Report
A 38‐year‐old woman was admitted with an episode of severe central chest pain. The pain was sharp, localized, occurred at rest, and resolved spontaneously after about 2 hours. She reported intermittent but shorter episodes of similar chest pain for the preceding 5 months. These episodes were associated with palpitation and lightheadedness. She was a smoker with past medical history of hyperlipidemia, asthma, and psoriasis. There was no family history of sudden cardiac death or premature coronary artery disease. On presentation, she was pain‐free, and vitals were stable. Electrocardiogram revealed normal sinus rhythm, no ischemic ST segment changes, and a QTc interval of 479 msec. Serum troponins were normal, serum potassium was 3.5 mmol/L, and serum magnesium was 1.9 mg/dL. While she was being monitored on telemetry, she suddenly experienced chest pain with palpitation. The telemetry recording of the event showed transient ST segment elevation followed by an episode of sustained polymorphic ventricular tachycardia (VT) (Figure 1). She remained hemodynamically stable and did not lose consciousness. The VT was self‐terminating.
Coronary angiogram revealed moderate 2‐vessel disease and spontaneous spasm of the dominant left circumflex artery. Therapy was initiated using both an oral nitrate and calcium channel antagonist. Potassium and magnesium levels were corrected with supplementation. On further questioning, she reported 1 episode of near‐syncope in the past. In view of the above history and a documented episode of spontaneous sustained polymorphic VT, an implantable cardioverter defibrillator (ICD) was implanted. She was strongly advised to quit smoking and was discharged home in stable condition. Three months later, she was admitted with recurrence of similar episodes of chest pain and dizziness, and multiple shocks from her ICD. Interrogation of the ICD revealed 5 episodes of polymorphic VT that were appropriately terminated with ICD discharges. The doses of calcium channel antagonist and oral nitrate were maximized, and she was discharged home in stable condition.
Discussion
Our case highlights an important management dilemma in patients with vasospastic angina. ICD implantation in this group has been reported in patients resuscitated from cardiac arrest. Our patient was recognized to be at high risk of sudden death but had never experienced cardiac arrest.
An increased incidence of sudden cardiac death, VT, and ventricular fibrillation has been observed during episodes of vasospastic angina. In a retrospective multicenter study of 349 patients with vasospastic angina, VT or ventricular fibrillation was noted in 6.5% of patients.1 Sudden death was reported in 2% of the patients (mean follow‐up period, 3.4 years), of whom the majority had ST segment elevation during anginal attacks. Increased ventricular vulnerability has been noted even during symptom‐free periods.2 Some cases of unexplained out‐of‐hospital cardiac arrest and sudden deaths may be secondary to coronary artery spasm.3 In a prospective study of 356 survivors of out‐of‐hospital cardiac arrest, Myerburg et al.4 reported 5 patients with coronary artery spasm who had silent ischemic events associated with life‐threatening ventricular arrhythmias. Interestingly, in 2 of the 5 patients, onset of ventricular arrhythmia correlated with reperfusion, rather than ischemia.
Calcium‐channel antagonists and nitrates are accepted as the first‐line treatment for vasospastic angina. Although this therapy improves prognosis, the risk of ventricular arrhythmia and sudden death is not eliminated.1 The data regarding use of ICDs in patients with coronary vasospasm are limited to case reports. Lacroix et al.5 reported 2 patients with vasospastic angina resuscitated from out‐of‐hospital cardiac arrest who received ICDs. Postimplantation, at 4 months and 11 months, respectively, each of the 2 patients had appropriate ICD discharges. Fuertes et al.6 reported a patient resuscitated from cardiac arrest due to ventricular fibrillation related to an episode of angina. The patient had vasospasm despite intensive medical therapy and had an ICD implanted. The above previously published cases describe ICD implantation for patients resuscitated from cardiac arrest.
However, in patients with coronary vasospasm who have never experienced cardiac arrest, it is unclear which subset would benefit from an ICD. Electrophysiological studies are not always helpful in identifying these patients. In the study by Myerburg et al.,4 only 1 out of the 5 patients with coronary artery spasm had inducible arrhythmia during electrophysiological testing. Clinical features associated with increased risk of sudden death were reported by McAlpin3 in a study of 81 patients with vasospastic angina. The risk of sudden death was tripled by the presence of either a history of angina‐linked syncope or documentation of serious arrhythmia complicating attacks. Paradoxically, the risk was increased by the absence of high‐grade coronary artery stenosis. Some researchers have reported a strong association between cigarette smoking and coronary spasm.7 Patients with known or suspected coronary artery spasm should be strongly discouraged from smoking. Our patient, in addition to being a smoker, had 2 of the 3 risk factors described by McAlpin,3 namely, documented serious arrhythmia and absence of high‐grade coronary stenosis. Considering these risk factors, an ICD was implanted. To our knowledge this is the first reported case of ICD insertion in a patient with vasospasm‐induced VT who had never experienced cardiac arrest.
Conclusions
In summary, patients with vasospastic angina are at increased risk of sudden death, especially during an episode of angina. Some cases of unexplained sudden death and malignant ventricular arrhythmia are probably a consequence of acute myocardial ischemia resulting from coronary arterial spasm. Early recognition and treatment of polymorphic VT is critical in preventing sudden cardiac death. In the absence of myocardial infarction, ST segment elevation preceding an episode of syncope or arrhythmia should raise the suspicion of coronary vasospasm as the underlying etiology. ICD placement is potentially beneficial in patients with coronary spasm who are at high risk of sudden cardiac death. Larger trials with longer follow‐up periods would help clinicians make this decision with greater confidence.
Arrhythmias are well‐described in patients with vasospastic angina. Coronary vasospasm may occur in the setting of angiographically normal or diseased coronary arteries. Patients with vasospastic angina are at increased risk of sudden death. However, it is unclear which of these patients would benefit from implantable cardioverter defibrillator (ICD) insertion.
We report a case of a young woman who presented with atypical angina. During an episode of chest pain she had a documented run of sustained polymorphic ventricular tachycardia (VT). In addition to medical therapy, she received an ICD to prevent future episodes of sudden cardiac death.
Case Report
A 38‐year‐old woman was admitted with an episode of severe central chest pain. The pain was sharp, localized, occurred at rest, and resolved spontaneously after about 2 hours. She reported intermittent but shorter episodes of similar chest pain for the preceding 5 months. These episodes were associated with palpitation and lightheadedness. She was a smoker with past medical history of hyperlipidemia, asthma, and psoriasis. There was no family history of sudden cardiac death or premature coronary artery disease. On presentation, she was pain‐free, and vitals were stable. Electrocardiogram revealed normal sinus rhythm, no ischemic ST segment changes, and a QTc interval of 479 msec. Serum troponins were normal, serum potassium was 3.5 mmol/L, and serum magnesium was 1.9 mg/dL. While she was being monitored on telemetry, she suddenly experienced chest pain with palpitation. The telemetry recording of the event showed transient ST segment elevation followed by an episode of sustained polymorphic ventricular tachycardia (VT) (Figure 1). She remained hemodynamically stable and did not lose consciousness. The VT was self‐terminating.
Coronary angiogram revealed moderate 2‐vessel disease and spontaneous spasm of the dominant left circumflex artery. Therapy was initiated using both an oral nitrate and calcium channel antagonist. Potassium and magnesium levels were corrected with supplementation. On further questioning, she reported 1 episode of near‐syncope in the past. In view of the above history and a documented episode of spontaneous sustained polymorphic VT, an implantable cardioverter defibrillator (ICD) was implanted. She was strongly advised to quit smoking and was discharged home in stable condition. Three months later, she was admitted with recurrence of similar episodes of chest pain and dizziness, and multiple shocks from her ICD. Interrogation of the ICD revealed 5 episodes of polymorphic VT that were appropriately terminated with ICD discharges. The doses of calcium channel antagonist and oral nitrate were maximized, and she was discharged home in stable condition.
Discussion
Our case highlights an important management dilemma in patients with vasospastic angina. ICD implantation in this group has been reported in patients resuscitated from cardiac arrest. Our patient was recognized to be at high risk of sudden death but had never experienced cardiac arrest.
An increased incidence of sudden cardiac death, VT, and ventricular fibrillation has been observed during episodes of vasospastic angina. In a retrospective multicenter study of 349 patients with vasospastic angina, VT or ventricular fibrillation was noted in 6.5% of patients.1 Sudden death was reported in 2% of the patients (mean follow‐up period, 3.4 years), of whom the majority had ST segment elevation during anginal attacks. Increased ventricular vulnerability has been noted even during symptom‐free periods.2 Some cases of unexplained out‐of‐hospital cardiac arrest and sudden deaths may be secondary to coronary artery spasm.3 In a prospective study of 356 survivors of out‐of‐hospital cardiac arrest, Myerburg et al.4 reported 5 patients with coronary artery spasm who had silent ischemic events associated with life‐threatening ventricular arrhythmias. Interestingly, in 2 of the 5 patients, onset of ventricular arrhythmia correlated with reperfusion, rather than ischemia.
Calcium‐channel antagonists and nitrates are accepted as the first‐line treatment for vasospastic angina. Although this therapy improves prognosis, the risk of ventricular arrhythmia and sudden death is not eliminated.1 The data regarding use of ICDs in patients with coronary vasospasm are limited to case reports. Lacroix et al.5 reported 2 patients with vasospastic angina resuscitated from out‐of‐hospital cardiac arrest who received ICDs. Postimplantation, at 4 months and 11 months, respectively, each of the 2 patients had appropriate ICD discharges. Fuertes et al.6 reported a patient resuscitated from cardiac arrest due to ventricular fibrillation related to an episode of angina. The patient had vasospasm despite intensive medical therapy and had an ICD implanted. The above previously published cases describe ICD implantation for patients resuscitated from cardiac arrest.
However, in patients with coronary vasospasm who have never experienced cardiac arrest, it is unclear which subset would benefit from an ICD. Electrophysiological studies are not always helpful in identifying these patients. In the study by Myerburg et al.,4 only 1 out of the 5 patients with coronary artery spasm had inducible arrhythmia during electrophysiological testing. Clinical features associated with increased risk of sudden death were reported by McAlpin3 in a study of 81 patients with vasospastic angina. The risk of sudden death was tripled by the presence of either a history of angina‐linked syncope or documentation of serious arrhythmia complicating attacks. Paradoxically, the risk was increased by the absence of high‐grade coronary artery stenosis. Some researchers have reported a strong association between cigarette smoking and coronary spasm.7 Patients with known or suspected coronary artery spasm should be strongly discouraged from smoking. Our patient, in addition to being a smoker, had 2 of the 3 risk factors described by McAlpin,3 namely, documented serious arrhythmia and absence of high‐grade coronary stenosis. Considering these risk factors, an ICD was implanted. To our knowledge this is the first reported case of ICD insertion in a patient with vasospasm‐induced VT who had never experienced cardiac arrest.
Conclusions
In summary, patients with vasospastic angina are at increased risk of sudden death, especially during an episode of angina. Some cases of unexplained sudden death and malignant ventricular arrhythmia are probably a consequence of acute myocardial ischemia resulting from coronary arterial spasm. Early recognition and treatment of polymorphic VT is critical in preventing sudden cardiac death. In the absence of myocardial infarction, ST segment elevation preceding an episode of syncope or arrhythmia should raise the suspicion of coronary vasospasm as the underlying etiology. ICD placement is potentially beneficial in patients with coronary spasm who are at high risk of sudden cardiac death. Larger trials with longer follow‐up periods would help clinicians make this decision with greater confidence.
- ,,.Clinical characteristics associated with myocardial infarction, arrhythmias, and sudden death in patients with vasospastic angina.Circulation.1987;75:1110–1116.
- ,,, et al.Induction of polymorphic ventricular tachycardia by programmed ventricular stimulation in vasospastic angina pectoris.Am J Cardiol.1996;77:355–360.
- .Cardiac arrest and sudden unexpected death in variant angina: complications of coronary spasm that can occur in the absence of severe organic coronary stenosis.Am Heart J.1993;125:1011–1017.
- ,,, et al.Life‐threatening ventricular arrhythmias in patients with silent myocardial ischemia due to coronary‐artery spasm.N Engl J Med.1992;326(22):1451–1455.
- ,,.Vasospastic angina without flow‐limiting coronary lesion as a cause for aborted sudden death.Int J Cardiol (Ireland).1994;43:247–249.
- ,,,.Implantable cardioverter defibrillator as a therapeutic option for sudden cardiac death secondary to severe coronary vasospasm.Int J Cardiol.1998;63:181–183.
- ,.Cigarette smoking is a major risk factor for coronary spasm.Circulation.1993;87:76–79.
- ,,.Clinical characteristics associated with myocardial infarction, arrhythmias, and sudden death in patients with vasospastic angina.Circulation.1987;75:1110–1116.
- ,,, et al.Induction of polymorphic ventricular tachycardia by programmed ventricular stimulation in vasospastic angina pectoris.Am J Cardiol.1996;77:355–360.
- .Cardiac arrest and sudden unexpected death in variant angina: complications of coronary spasm that can occur in the absence of severe organic coronary stenosis.Am Heart J.1993;125:1011–1017.
- ,,, et al.Life‐threatening ventricular arrhythmias in patients with silent myocardial ischemia due to coronary‐artery spasm.N Engl J Med.1992;326(22):1451–1455.
- ,,.Vasospastic angina without flow‐limiting coronary lesion as a cause for aborted sudden death.Int J Cardiol (Ireland).1994;43:247–249.
- ,,,.Implantable cardioverter defibrillator as a therapeutic option for sudden cardiac death secondary to severe coronary vasospasm.Int J Cardiol.1998;63:181–183.
- ,.Cigarette smoking is a major risk factor for coronary spasm.Circulation.1993;87:76–79.
VZV Meningoencephalitis
Case Report
A 66‐year‐old woman with a history of breast cancer treated with lumpectomy, chemotherapy, and radiation presented to the emergency department with a 1‐week history of left eye pain, progressive fatigue, and numbness and tingling on the left upper face. One week prior to presentation, she experienced dull pain in her left eye, anorexia, vomiting, and numbness and tingling in her upper left face. She was diagnosed with sinusitis by a local physician and prescribed a nasal spray and an unknown antibiotic. She became progressively weaker and fatigued and then 2 days prior to admission she noticed red papules on her forehead. She presented to the emergency department 1 day prior to admission. In the emergency department, she was diagnosed with herpes zoster ophthalmicus, placed on acyclovir, acetaminophen/hydrocodone, ondansetron, and trifluridine eye drops, and discharged. Her symptoms worsened throughout the night and she became progressively more somnolent. She was brought to the emergency department again the following day and was found to be extremely somnolent and oriented only to person. The patient's past medical history was significant for lobular carcinoma in situ of the breast, which was diagnosed 22 years ago and treated with a lumpectomy. She had a recurrence of ductal and lobular carcinoma in‐situ 20 years after her initial diagnosis and was treated with 3 months of chemotherapy, completed 13 months prior to admission, and 6 months of radiation therapy, completed 6 months prior to admission. Her physical examination was remarkable for an erythematous maculopapular rash in the distribution of the ophthalmic division of the trigeminal nerve, swelling of the left orbit such that she could not open her eye without assistance, and white mucus‐like drainage from the left eye. The area around the eyelid was tender and the left sclera was pink. Extraocular movements were intact and the pupils were equal, round, and reactive to light and accommodation. Cranial nerves III to XII were intact bilaterally; cerebellar function, sensation, proprioception, and deep tendon reflexes were also intact. The patient did not have any meningismus.
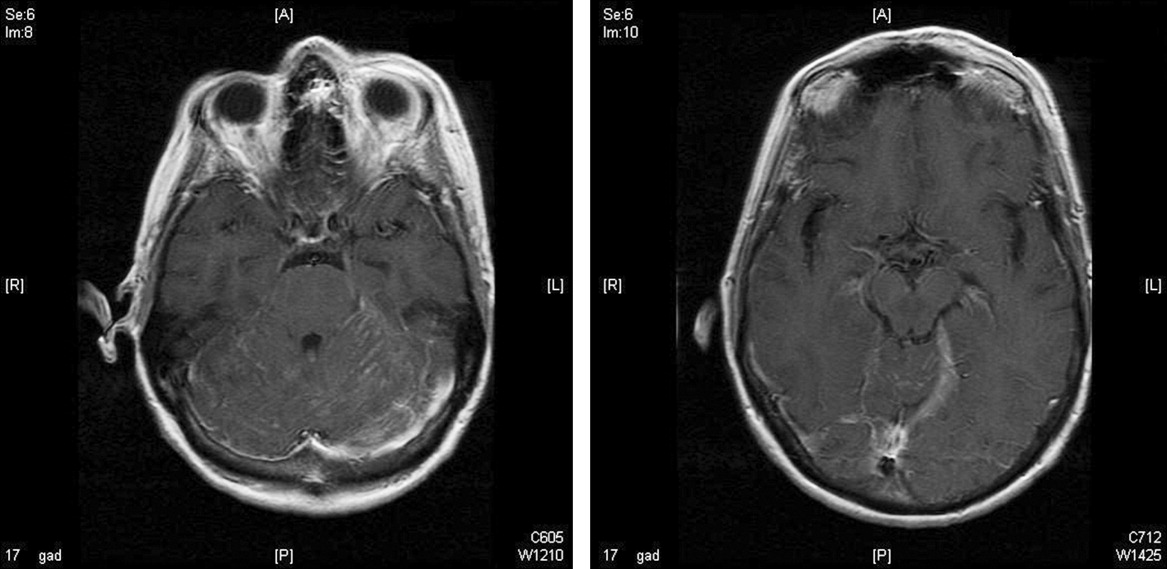
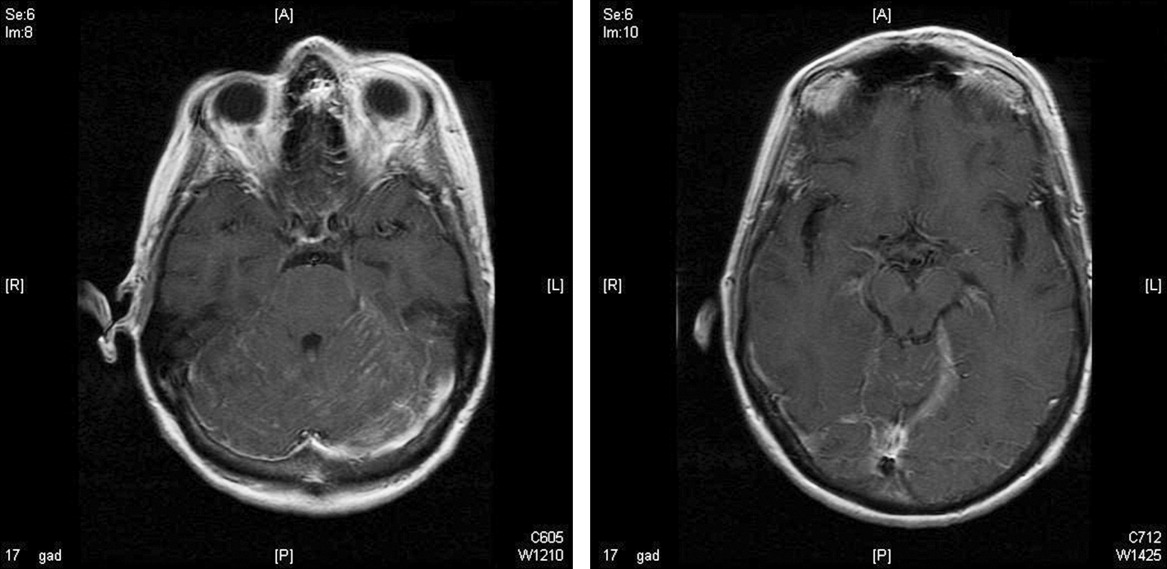
On lumbar puncture in the emergency department (ED), the cerebrospinal fluid (CSF) from tube 4 was found to have a glucose concentration of 52 mg/dL (blood glucose of 111 mg/dL), a protein concentration of 90 mg/dL, a red blood cell (RBC) count of 70 cells/mL, and 16 nucleated cells/mL with 67% lymphocytes and 20% monocytes. Viral cultures and polymerase chain reaction (PCR) for herpes simplex virus (HSV)‐1, HSV‐2, and varicella zoster virus (VZV) were sent to the laboratory. Therapy with acyclovir, vancomycin, and cefotaxime was initiated. Magnetic resonance imaging (MRI) revealed leptomeningeal and dural enhancement involving the posterior fossa, which was read to be consistent with infectious meningitis; temporal lobe involvement was not seen (Figure 1).
Additional results from the lumbar puncture were received the following day. PCR for HSV‐1 and HSV‐2 was found to be negative, while PCR for VZV was found to be positive. Treatment with intravenous (IV) acyclovir was continued. The patient's clinical condition improved significantly by the morning after admission and she was found to be less somnolent and alert and oriented to person, place, and time. Her condition continued to improve and she was discharged 4 days after admission after her mental status returned to baseline; the patient subsequently completed a 21‐day course of 540 mg twice a day IV acyclovir.
In the 9 months following her initial hospitalization, the patient was admitted multiple times to an outside hospital for varicella zoster meningitis and herpes zoster ophthalmicus, with complete resolution of her symptoms after each hospitalization. However, 10 months after her initial hospitalization, the patient presented to our hospital with lethargy and was found to have a recurrence of her breast cancer with metastatic disease. She was subsequently diagnosed with carcinomatous meningitis and passed away shortly after this diagnosis.
Discussion
The development of clinically significant varicella zosterassociated meningoencephalitis after herpes zoster ophthalmicus is rare. Cerebrospinal fluid PCR has been shown to have a sensitivity and specificity >95% for diagnosing VZV encephalitis.3 The interpretation of the MRI was consistent with several case reports in the literature that also described enhancing meningeal lesions on MRI in patients with varicella encephalitis.3
While subclinical invasion of VZV into the central nervous system (CNS) is relatively common, with approximately one‐third of asymptomatic immunocompetent patients having a CSF PCR positive for VZV and 46% of patients demonstrating CSF leukocytosis, it is rare for patients to present with the serious clinical manifestations seen in this case.4 It is hypothesized that herpes zosterassociated meningoencephalitis most likely occurs when the zoster involves the ophthalmic branch of the trigeminal nerve, allowing for the spread of the virus to the tentorium through the recurrent nerve of Arnold, which branches off the ophthalmic division of the trigeminal nerve.5 On review of the literature, there are very few studies and no controlled trials on the optimal treatment of this complication, although an empirical treatment of 15 to 30 mg of acyclovir per kilogram of body weight for 10 days has been suggested.3 There have been several reports of rapid responses to IV acyclovir but, due to the rarity of this complication, to our knowledge, no studies have been conducted to determine the optimal treatment of herpes zosterassociated meningoencephalitis.3, 6 A similar case of meningoencephalitis has been described in a 5‐year‐old boy whose presentation was similar to that of our patient, with periorbital vesicular lesions and mental status changes including somnolence. This child was treated with acyclovir and made a full recovery.7
Several other CNS‐related manifestations of CN zoster have been reported, including development of the syndrome of inappropriate antidiuretic hormone, development of contralateral hemiparesis, and the coexistence of Ramsay‐Hunt syndrome and zoster encephalitis (Table 1). It is hypothesized that stimulation of the ophthalmic division of the trigeminal nerve by the zoster virus leads to excess antidiuretic hormone (ADH) secretion from the posterior pituitary, which results in the development of syndrome of inappropriate secretion of antidiuretic hormone (SIADH). To date, 2 cases of SIADH following a herpes zoster ophthalmicus infection have been reported.8, 9 Several cases of coexisting varicella zoster encephalitis and Ramsay‐Hunt syndrome have been reported. Ramsay‐Hunt syndrome, which is characterized by zoster oticus and peripheral facial nerve involvement, is a known complication of varicella zoster infection; however, coexistence of Ramsay‐Hunt syndrome and varicella encephalitis is rare and has only been reported in 9 patients.3, 10 To our knowledge, the coexistence of these 2 complications has not been reported in a patient with herpes zoster ophthalmicus. Contralateral hemiparesis following herpes zoster infection has been reported in 2 patients, both of whom were treated with acyclovir, resulting in partial recovery. Other CNS complications of herpes zoster include myelitis, large‐vessel encephalitis, and small‐vessel encephalitis.3
| Report (year) | Age (years), Gender | Presenting Symptom | CNS Complication | Treatment | Outcome |
|---|---|---|---|---|---|
| |||||
| This case | 66, female | Vesicles on the left forehead, altered mental status | Varicella zoster meningoencephalitis | IV acyclovir, 540 mg IV q12h, 21‐day course | Resolved without complications |
| Haargaard et al.2 (2008) | 68, female; 82, female; 90, female; 72, male | Unknown | CN III and IV palsies | Systemic acyclovir | Complete recovery in 3 patients, 1 patient with no clinical recovery at 1 month follow‐up |
| 64, female | Unknown | Clinical meningitis (headache, photophobia, neck stiffness) with CSF negative for VZV PCR | IV acyclovir | Complete recovery | |
| 62, female | Unknown | CN III palsy and facial nerve palsy followed by encephalitis | Oral acyclovir 1000 mg Q day followed by IV acyclovir 10 mg/kg TID 10 days | Minimal recovery with severe neurological and cognitive impairment | |
| Kucukardali et al.9 (2007) | 76, female | Vesicles on left side of forehead | Syndrome of inappropriate antidiuretic hormone | IV acyclovir, 10‐12 mg/kg TID for 7 days | Resolved without complications |
| Dhawan8 (2006) | 71, female | Vesicles on left side of forehead | Syndrome of inappropriate antidiuretic hormone | IV acyclovir, dose unknown | Resolved without complications |
| Ofek‐Shlomai et al.7 (2005) | 5, male | Vesicles on right side of forehead, altered mental status | Varicella zoster meningoencephalitis | IV acyclovir, 1500 mg/m2/day for 10 days, followed by 14 days of oral acyclovir | Resolved without complications |
| Ngoueira et al.13 (2002) | 71, male | Recurrent facial rash on right forehead, altered mental status, left hemiparesis | Left hemiparesis, partial palsy of right third CN, complete palsy of left seventh CN with upper motor neuron distribution | IV acyclovir, 21‐day course, prednisone short course | Treatment course complicated by renal failure, partial improvement of symptoms with steroids |
| Hughes et al.11 (1993) | 76, female | Headache, confusion, somnolence, left complete ophthalmoplegia | Meningoencephalitis | Of the 9 patients diagnosed with meningoencephalitis, 5 patients were treated with acyclovir, 3 patients were treated with cytarabine, and 1 patient did not receive any antiviral treatment | 4 of the 5 patients treated with acyclovir and the 1 patient who did not receive any antiviral treatment returned to their baseline mental status within 2 weeks. All 3 patients treated with cytarabine and 1 patient treated with acyclovir remained confused and disoriented at 2 weeks and were discharged to care facilities |
| 74, male | Somnolence, confusion, bilateral Babinski reflexes | Meningoencephalitis | |||
| 69, male | Headache, photophobia, confusion, somnolence | Meningoencephalitis | |||
| 63, female | Headache, blurring of vision, nausea, vomiting, confusion, somnolence | Meningoencephalitis | |||
| McNeil et al.14 (1991) | 51, male | Right hemiparesis, dysphasia | Moderate global dysphasia, right upper motor neuron facial weakness, mild right hemiparesis | Unknown | Progressive improvement of speech, impaired right hand motor function, persistent global weakness |
It has also been shown that patients with compromised immune systems are at a greater risk for recurrence of the herpes zoster infection and for development of zoster encephalitis. It is estimated that mortality rates from zoster encephalitis are as high as 25%, with an average rate of 10%, and are determined by the patient's immune status.3, 4 Our particular patient was immunosuppressed, given that she had been treated for breast cancer with radiation 6 months prior to admission and chemotherapy 13 months prior to admission, putting her at an increased risk of developing encephalitis. There have been reports of herpes‐associated meningoencephalitis in patients with systemic cancers, including adenocarcinoma of the lung, prostate cancer, chronic lymphocytic leukemia, and lymphoma; the response to treatment with acyclovir was favorable in these cases.11 It has also been established that patients with human immunodeficiency virus (HIV) are at increased risk for developing meningoencephalitis after herpes zoster infection as a result of their compromised immune systems.12 In addition to having a higher mortality rate, patients with compromised immune systems are at a greater risk for recurrence of herpes zoster, which leads to an additional increase in mortality, as was seen in the case of this particular patient.
- .Herpes zoster ophthalmicus.Neurology.1995;45(12 Suppl 8):S50–S51.
- ,,.Central Nervous System involvement after herpes zoster ophthalmicus.Acta Ophthalmologica.2008. E‐pub January 2008.
- ,,, et al.Neurologic complications of the reactivation of varicella‐zoster virus.N Engl J Med.2000;342(9):635–645.
- ,,, et al.Recommendations for the management of herpes zoster.Clin Infect Dis.2007;44(suppl 1):S1–S26.
- ,.Herpes zoster encephalitis: 2 case reports and review of literature.Infect Dis Clin Pract.2007;15(4):284–288.
- ,.Rapid response to acyclovir in herpes zoster‐associated encephalitis.Am J Med.1987;82(3):560–562.
- ,,, et al.Varicella zoster virus encephalitis in a previously healthy five‐year‐old child with herpes zoster ophthalmicus.Pediatr Infect Dis J.2005;24(5):476–477.
- .Herpes zoster ophthalmicus and syndrome of inappropriate antidiuretic hormone secretion.Am J Med Sci.2007;333(1):56–57.
- ,,, et al.Herpes zoster ophthalmicus and syndrome of inappropriate antidiuretic hormone secretion.Intern Med.2008;47(5):463–465.
- ,,,.Coexistence of Ramsay‐Hunt syndrome and varicella‐zoster virus encephalitis.Infection.2006;34(6):352–354.
- ,,.Herpes zoster‐associated meningoencephalitis in patients with systemic cancer.Mayo Clin Proc.1993;68(7):652–655.
- ,,, et al.Herpes zoster ophthalmicus in patients with human immunodeficiency virus infection.Am J Ophthalmol.1998;125(3):285–291.
- ,.Images in clinical medicine. Herpes zoster ophthalmicus followed by contralateral hemiparesis.N Engl J Med.2002;346(15):1127.
- ,.Contralateral hemiplegia complicating herpes zoster ophthalmicus.J R Soc Med.1991;84(8):501–502.
Case Report
A 66‐year‐old woman with a history of breast cancer treated with lumpectomy, chemotherapy, and radiation presented to the emergency department with a 1‐week history of left eye pain, progressive fatigue, and numbness and tingling on the left upper face. One week prior to presentation, she experienced dull pain in her left eye, anorexia, vomiting, and numbness and tingling in her upper left face. She was diagnosed with sinusitis by a local physician and prescribed a nasal spray and an unknown antibiotic. She became progressively weaker and fatigued and then 2 days prior to admission she noticed red papules on her forehead. She presented to the emergency department 1 day prior to admission. In the emergency department, she was diagnosed with herpes zoster ophthalmicus, placed on acyclovir, acetaminophen/hydrocodone, ondansetron, and trifluridine eye drops, and discharged. Her symptoms worsened throughout the night and she became progressively more somnolent. She was brought to the emergency department again the following day and was found to be extremely somnolent and oriented only to person. The patient's past medical history was significant for lobular carcinoma in situ of the breast, which was diagnosed 22 years ago and treated with a lumpectomy. She had a recurrence of ductal and lobular carcinoma in‐situ 20 years after her initial diagnosis and was treated with 3 months of chemotherapy, completed 13 months prior to admission, and 6 months of radiation therapy, completed 6 months prior to admission. Her physical examination was remarkable for an erythematous maculopapular rash in the distribution of the ophthalmic division of the trigeminal nerve, swelling of the left orbit such that she could not open her eye without assistance, and white mucus‐like drainage from the left eye. The area around the eyelid was tender and the left sclera was pink. Extraocular movements were intact and the pupils were equal, round, and reactive to light and accommodation. Cranial nerves III to XII were intact bilaterally; cerebellar function, sensation, proprioception, and deep tendon reflexes were also intact. The patient did not have any meningismus.
On lumbar puncture in the emergency department (ED), the cerebrospinal fluid (CSF) from tube 4 was found to have a glucose concentration of 52 mg/dL (blood glucose of 111 mg/dL), a protein concentration of 90 mg/dL, a red blood cell (RBC) count of 70 cells/mL, and 16 nucleated cells/mL with 67% lymphocytes and 20% monocytes. Viral cultures and polymerase chain reaction (PCR) for herpes simplex virus (HSV)‐1, HSV‐2, and varicella zoster virus (VZV) were sent to the laboratory. Therapy with acyclovir, vancomycin, and cefotaxime was initiated. Magnetic resonance imaging (MRI) revealed leptomeningeal and dural enhancement involving the posterior fossa, which was read to be consistent with infectious meningitis; temporal lobe involvement was not seen (Figure 1).
Additional results from the lumbar puncture were received the following day. PCR for HSV‐1 and HSV‐2 was found to be negative, while PCR for VZV was found to be positive. Treatment with intravenous (IV) acyclovir was continued. The patient's clinical condition improved significantly by the morning after admission and she was found to be less somnolent and alert and oriented to person, place, and time. Her condition continued to improve and she was discharged 4 days after admission after her mental status returned to baseline; the patient subsequently completed a 21‐day course of 540 mg twice a day IV acyclovir.
In the 9 months following her initial hospitalization, the patient was admitted multiple times to an outside hospital for varicella zoster meningitis and herpes zoster ophthalmicus, with complete resolution of her symptoms after each hospitalization. However, 10 months after her initial hospitalization, the patient presented to our hospital with lethargy and was found to have a recurrence of her breast cancer with metastatic disease. She was subsequently diagnosed with carcinomatous meningitis and passed away shortly after this diagnosis.
Discussion
The development of clinically significant varicella zosterassociated meningoencephalitis after herpes zoster ophthalmicus is rare. Cerebrospinal fluid PCR has been shown to have a sensitivity and specificity >95% for diagnosing VZV encephalitis.3 The interpretation of the MRI was consistent with several case reports in the literature that also described enhancing meningeal lesions on MRI in patients with varicella encephalitis.3
While subclinical invasion of VZV into the central nervous system (CNS) is relatively common, with approximately one‐third of asymptomatic immunocompetent patients having a CSF PCR positive for VZV and 46% of patients demonstrating CSF leukocytosis, it is rare for patients to present with the serious clinical manifestations seen in this case.4 It is hypothesized that herpes zosterassociated meningoencephalitis most likely occurs when the zoster involves the ophthalmic branch of the trigeminal nerve, allowing for the spread of the virus to the tentorium through the recurrent nerve of Arnold, which branches off the ophthalmic division of the trigeminal nerve.5 On review of the literature, there are very few studies and no controlled trials on the optimal treatment of this complication, although an empirical treatment of 15 to 30 mg of acyclovir per kilogram of body weight for 10 days has been suggested.3 There have been several reports of rapid responses to IV acyclovir but, due to the rarity of this complication, to our knowledge, no studies have been conducted to determine the optimal treatment of herpes zosterassociated meningoencephalitis.3, 6 A similar case of meningoencephalitis has been described in a 5‐year‐old boy whose presentation was similar to that of our patient, with periorbital vesicular lesions and mental status changes including somnolence. This child was treated with acyclovir and made a full recovery.7
Several other CNS‐related manifestations of CN zoster have been reported, including development of the syndrome of inappropriate antidiuretic hormone, development of contralateral hemiparesis, and the coexistence of Ramsay‐Hunt syndrome and zoster encephalitis (Table 1). It is hypothesized that stimulation of the ophthalmic division of the trigeminal nerve by the zoster virus leads to excess antidiuretic hormone (ADH) secretion from the posterior pituitary, which results in the development of syndrome of inappropriate secretion of antidiuretic hormone (SIADH). To date, 2 cases of SIADH following a herpes zoster ophthalmicus infection have been reported.8, 9 Several cases of coexisting varicella zoster encephalitis and Ramsay‐Hunt syndrome have been reported. Ramsay‐Hunt syndrome, which is characterized by zoster oticus and peripheral facial nerve involvement, is a known complication of varicella zoster infection; however, coexistence of Ramsay‐Hunt syndrome and varicella encephalitis is rare and has only been reported in 9 patients.3, 10 To our knowledge, the coexistence of these 2 complications has not been reported in a patient with herpes zoster ophthalmicus. Contralateral hemiparesis following herpes zoster infection has been reported in 2 patients, both of whom were treated with acyclovir, resulting in partial recovery. Other CNS complications of herpes zoster include myelitis, large‐vessel encephalitis, and small‐vessel encephalitis.3
| Report (year) | Age (years), Gender | Presenting Symptom | CNS Complication | Treatment | Outcome |
|---|---|---|---|---|---|
| |||||
| This case | 66, female | Vesicles on the left forehead, altered mental status | Varicella zoster meningoencephalitis | IV acyclovir, 540 mg IV q12h, 21‐day course | Resolved without complications |
| Haargaard et al.2 (2008) | 68, female; 82, female; 90, female; 72, male | Unknown | CN III and IV palsies | Systemic acyclovir | Complete recovery in 3 patients, 1 patient with no clinical recovery at 1 month follow‐up |
| 64, female | Unknown | Clinical meningitis (headache, photophobia, neck stiffness) with CSF negative for VZV PCR | IV acyclovir | Complete recovery | |
| 62, female | Unknown | CN III palsy and facial nerve palsy followed by encephalitis | Oral acyclovir 1000 mg Q day followed by IV acyclovir 10 mg/kg TID 10 days | Minimal recovery with severe neurological and cognitive impairment | |
| Kucukardali et al.9 (2007) | 76, female | Vesicles on left side of forehead | Syndrome of inappropriate antidiuretic hormone | IV acyclovir, 10‐12 mg/kg TID for 7 days | Resolved without complications |
| Dhawan8 (2006) | 71, female | Vesicles on left side of forehead | Syndrome of inappropriate antidiuretic hormone | IV acyclovir, dose unknown | Resolved without complications |
| Ofek‐Shlomai et al.7 (2005) | 5, male | Vesicles on right side of forehead, altered mental status | Varicella zoster meningoencephalitis | IV acyclovir, 1500 mg/m2/day for 10 days, followed by 14 days of oral acyclovir | Resolved without complications |
| Ngoueira et al.13 (2002) | 71, male | Recurrent facial rash on right forehead, altered mental status, left hemiparesis | Left hemiparesis, partial palsy of right third CN, complete palsy of left seventh CN with upper motor neuron distribution | IV acyclovir, 21‐day course, prednisone short course | Treatment course complicated by renal failure, partial improvement of symptoms with steroids |
| Hughes et al.11 (1993) | 76, female | Headache, confusion, somnolence, left complete ophthalmoplegia | Meningoencephalitis | Of the 9 patients diagnosed with meningoencephalitis, 5 patients were treated with acyclovir, 3 patients were treated with cytarabine, and 1 patient did not receive any antiviral treatment | 4 of the 5 patients treated with acyclovir and the 1 patient who did not receive any antiviral treatment returned to their baseline mental status within 2 weeks. All 3 patients treated with cytarabine and 1 patient treated with acyclovir remained confused and disoriented at 2 weeks and were discharged to care facilities |
| 74, male | Somnolence, confusion, bilateral Babinski reflexes | Meningoencephalitis | |||
| 69, male | Headache, photophobia, confusion, somnolence | Meningoencephalitis | |||
| 63, female | Headache, blurring of vision, nausea, vomiting, confusion, somnolence | Meningoencephalitis | |||
| McNeil et al.14 (1991) | 51, male | Right hemiparesis, dysphasia | Moderate global dysphasia, right upper motor neuron facial weakness, mild right hemiparesis | Unknown | Progressive improvement of speech, impaired right hand motor function, persistent global weakness |
It has also been shown that patients with compromised immune systems are at a greater risk for recurrence of the herpes zoster infection and for development of zoster encephalitis. It is estimated that mortality rates from zoster encephalitis are as high as 25%, with an average rate of 10%, and are determined by the patient's immune status.3, 4 Our particular patient was immunosuppressed, given that she had been treated for breast cancer with radiation 6 months prior to admission and chemotherapy 13 months prior to admission, putting her at an increased risk of developing encephalitis. There have been reports of herpes‐associated meningoencephalitis in patients with systemic cancers, including adenocarcinoma of the lung, prostate cancer, chronic lymphocytic leukemia, and lymphoma; the response to treatment with acyclovir was favorable in these cases.11 It has also been established that patients with human immunodeficiency virus (HIV) are at increased risk for developing meningoencephalitis after herpes zoster infection as a result of their compromised immune systems.12 In addition to having a higher mortality rate, patients with compromised immune systems are at a greater risk for recurrence of herpes zoster, which leads to an additional increase in mortality, as was seen in the case of this particular patient.
Case Report
A 66‐year‐old woman with a history of breast cancer treated with lumpectomy, chemotherapy, and radiation presented to the emergency department with a 1‐week history of left eye pain, progressive fatigue, and numbness and tingling on the left upper face. One week prior to presentation, she experienced dull pain in her left eye, anorexia, vomiting, and numbness and tingling in her upper left face. She was diagnosed with sinusitis by a local physician and prescribed a nasal spray and an unknown antibiotic. She became progressively weaker and fatigued and then 2 days prior to admission she noticed red papules on her forehead. She presented to the emergency department 1 day prior to admission. In the emergency department, she was diagnosed with herpes zoster ophthalmicus, placed on acyclovir, acetaminophen/hydrocodone, ondansetron, and trifluridine eye drops, and discharged. Her symptoms worsened throughout the night and she became progressively more somnolent. She was brought to the emergency department again the following day and was found to be extremely somnolent and oriented only to person. The patient's past medical history was significant for lobular carcinoma in situ of the breast, which was diagnosed 22 years ago and treated with a lumpectomy. She had a recurrence of ductal and lobular carcinoma in‐situ 20 years after her initial diagnosis and was treated with 3 months of chemotherapy, completed 13 months prior to admission, and 6 months of radiation therapy, completed 6 months prior to admission. Her physical examination was remarkable for an erythematous maculopapular rash in the distribution of the ophthalmic division of the trigeminal nerve, swelling of the left orbit such that she could not open her eye without assistance, and white mucus‐like drainage from the left eye. The area around the eyelid was tender and the left sclera was pink. Extraocular movements were intact and the pupils were equal, round, and reactive to light and accommodation. Cranial nerves III to XII were intact bilaterally; cerebellar function, sensation, proprioception, and deep tendon reflexes were also intact. The patient did not have any meningismus.
On lumbar puncture in the emergency department (ED), the cerebrospinal fluid (CSF) from tube 4 was found to have a glucose concentration of 52 mg/dL (blood glucose of 111 mg/dL), a protein concentration of 90 mg/dL, a red blood cell (RBC) count of 70 cells/mL, and 16 nucleated cells/mL with 67% lymphocytes and 20% monocytes. Viral cultures and polymerase chain reaction (PCR) for herpes simplex virus (HSV)‐1, HSV‐2, and varicella zoster virus (VZV) were sent to the laboratory. Therapy with acyclovir, vancomycin, and cefotaxime was initiated. Magnetic resonance imaging (MRI) revealed leptomeningeal and dural enhancement involving the posterior fossa, which was read to be consistent with infectious meningitis; temporal lobe involvement was not seen (Figure 1).
Additional results from the lumbar puncture were received the following day. PCR for HSV‐1 and HSV‐2 was found to be negative, while PCR for VZV was found to be positive. Treatment with intravenous (IV) acyclovir was continued. The patient's clinical condition improved significantly by the morning after admission and she was found to be less somnolent and alert and oriented to person, place, and time. Her condition continued to improve and she was discharged 4 days after admission after her mental status returned to baseline; the patient subsequently completed a 21‐day course of 540 mg twice a day IV acyclovir.
In the 9 months following her initial hospitalization, the patient was admitted multiple times to an outside hospital for varicella zoster meningitis and herpes zoster ophthalmicus, with complete resolution of her symptoms after each hospitalization. However, 10 months after her initial hospitalization, the patient presented to our hospital with lethargy and was found to have a recurrence of her breast cancer with metastatic disease. She was subsequently diagnosed with carcinomatous meningitis and passed away shortly after this diagnosis.
Discussion
The development of clinically significant varicella zosterassociated meningoencephalitis after herpes zoster ophthalmicus is rare. Cerebrospinal fluid PCR has been shown to have a sensitivity and specificity >95% for diagnosing VZV encephalitis.3 The interpretation of the MRI was consistent with several case reports in the literature that also described enhancing meningeal lesions on MRI in patients with varicella encephalitis.3
While subclinical invasion of VZV into the central nervous system (CNS) is relatively common, with approximately one‐third of asymptomatic immunocompetent patients having a CSF PCR positive for VZV and 46% of patients demonstrating CSF leukocytosis, it is rare for patients to present with the serious clinical manifestations seen in this case.4 It is hypothesized that herpes zosterassociated meningoencephalitis most likely occurs when the zoster involves the ophthalmic branch of the trigeminal nerve, allowing for the spread of the virus to the tentorium through the recurrent nerve of Arnold, which branches off the ophthalmic division of the trigeminal nerve.5 On review of the literature, there are very few studies and no controlled trials on the optimal treatment of this complication, although an empirical treatment of 15 to 30 mg of acyclovir per kilogram of body weight for 10 days has been suggested.3 There have been several reports of rapid responses to IV acyclovir but, due to the rarity of this complication, to our knowledge, no studies have been conducted to determine the optimal treatment of herpes zosterassociated meningoencephalitis.3, 6 A similar case of meningoencephalitis has been described in a 5‐year‐old boy whose presentation was similar to that of our patient, with periorbital vesicular lesions and mental status changes including somnolence. This child was treated with acyclovir and made a full recovery.7
Several other CNS‐related manifestations of CN zoster have been reported, including development of the syndrome of inappropriate antidiuretic hormone, development of contralateral hemiparesis, and the coexistence of Ramsay‐Hunt syndrome and zoster encephalitis (Table 1). It is hypothesized that stimulation of the ophthalmic division of the trigeminal nerve by the zoster virus leads to excess antidiuretic hormone (ADH) secretion from the posterior pituitary, which results in the development of syndrome of inappropriate secretion of antidiuretic hormone (SIADH). To date, 2 cases of SIADH following a herpes zoster ophthalmicus infection have been reported.8, 9 Several cases of coexisting varicella zoster encephalitis and Ramsay‐Hunt syndrome have been reported. Ramsay‐Hunt syndrome, which is characterized by zoster oticus and peripheral facial nerve involvement, is a known complication of varicella zoster infection; however, coexistence of Ramsay‐Hunt syndrome and varicella encephalitis is rare and has only been reported in 9 patients.3, 10 To our knowledge, the coexistence of these 2 complications has not been reported in a patient with herpes zoster ophthalmicus. Contralateral hemiparesis following herpes zoster infection has been reported in 2 patients, both of whom were treated with acyclovir, resulting in partial recovery. Other CNS complications of herpes zoster include myelitis, large‐vessel encephalitis, and small‐vessel encephalitis.3
| Report (year) | Age (years), Gender | Presenting Symptom | CNS Complication | Treatment | Outcome |
|---|---|---|---|---|---|
| |||||
| This case | 66, female | Vesicles on the left forehead, altered mental status | Varicella zoster meningoencephalitis | IV acyclovir, 540 mg IV q12h, 21‐day course | Resolved without complications |
| Haargaard et al.2 (2008) | 68, female; 82, female; 90, female; 72, male | Unknown | CN III and IV palsies | Systemic acyclovir | Complete recovery in 3 patients, 1 patient with no clinical recovery at 1 month follow‐up |
| 64, female | Unknown | Clinical meningitis (headache, photophobia, neck stiffness) with CSF negative for VZV PCR | IV acyclovir | Complete recovery | |
| 62, female | Unknown | CN III palsy and facial nerve palsy followed by encephalitis | Oral acyclovir 1000 mg Q day followed by IV acyclovir 10 mg/kg TID 10 days | Minimal recovery with severe neurological and cognitive impairment | |
| Kucukardali et al.9 (2007) | 76, female | Vesicles on left side of forehead | Syndrome of inappropriate antidiuretic hormone | IV acyclovir, 10‐12 mg/kg TID for 7 days | Resolved without complications |
| Dhawan8 (2006) | 71, female | Vesicles on left side of forehead | Syndrome of inappropriate antidiuretic hormone | IV acyclovir, dose unknown | Resolved without complications |
| Ofek‐Shlomai et al.7 (2005) | 5, male | Vesicles on right side of forehead, altered mental status | Varicella zoster meningoencephalitis | IV acyclovir, 1500 mg/m2/day for 10 days, followed by 14 days of oral acyclovir | Resolved without complications |
| Ngoueira et al.13 (2002) | 71, male | Recurrent facial rash on right forehead, altered mental status, left hemiparesis | Left hemiparesis, partial palsy of right third CN, complete palsy of left seventh CN with upper motor neuron distribution | IV acyclovir, 21‐day course, prednisone short course | Treatment course complicated by renal failure, partial improvement of symptoms with steroids |
| Hughes et al.11 (1993) | 76, female | Headache, confusion, somnolence, left complete ophthalmoplegia | Meningoencephalitis | Of the 9 patients diagnosed with meningoencephalitis, 5 patients were treated with acyclovir, 3 patients were treated with cytarabine, and 1 patient did not receive any antiviral treatment | 4 of the 5 patients treated with acyclovir and the 1 patient who did not receive any antiviral treatment returned to their baseline mental status within 2 weeks. All 3 patients treated with cytarabine and 1 patient treated with acyclovir remained confused and disoriented at 2 weeks and were discharged to care facilities |
| 74, male | Somnolence, confusion, bilateral Babinski reflexes | Meningoencephalitis | |||
| 69, male | Headache, photophobia, confusion, somnolence | Meningoencephalitis | |||
| 63, female | Headache, blurring of vision, nausea, vomiting, confusion, somnolence | Meningoencephalitis | |||
| McNeil et al.14 (1991) | 51, male | Right hemiparesis, dysphasia | Moderate global dysphasia, right upper motor neuron facial weakness, mild right hemiparesis | Unknown | Progressive improvement of speech, impaired right hand motor function, persistent global weakness |
It has also been shown that patients with compromised immune systems are at a greater risk for recurrence of the herpes zoster infection and for development of zoster encephalitis. It is estimated that mortality rates from zoster encephalitis are as high as 25%, with an average rate of 10%, and are determined by the patient's immune status.3, 4 Our particular patient was immunosuppressed, given that she had been treated for breast cancer with radiation 6 months prior to admission and chemotherapy 13 months prior to admission, putting her at an increased risk of developing encephalitis. There have been reports of herpes‐associated meningoencephalitis in patients with systemic cancers, including adenocarcinoma of the lung, prostate cancer, chronic lymphocytic leukemia, and lymphoma; the response to treatment with acyclovir was favorable in these cases.11 It has also been established that patients with human immunodeficiency virus (HIV) are at increased risk for developing meningoencephalitis after herpes zoster infection as a result of their compromised immune systems.12 In addition to having a higher mortality rate, patients with compromised immune systems are at a greater risk for recurrence of herpes zoster, which leads to an additional increase in mortality, as was seen in the case of this particular patient.
- .Herpes zoster ophthalmicus.Neurology.1995;45(12 Suppl 8):S50–S51.
- ,,.Central Nervous System involvement after herpes zoster ophthalmicus.Acta Ophthalmologica.2008. E‐pub January 2008.
- ,,, et al.Neurologic complications of the reactivation of varicella‐zoster virus.N Engl J Med.2000;342(9):635–645.
- ,,, et al.Recommendations for the management of herpes zoster.Clin Infect Dis.2007;44(suppl 1):S1–S26.
- ,.Herpes zoster encephalitis: 2 case reports and review of literature.Infect Dis Clin Pract.2007;15(4):284–288.
- ,.Rapid response to acyclovir in herpes zoster‐associated encephalitis.Am J Med.1987;82(3):560–562.
- ,,, et al.Varicella zoster virus encephalitis in a previously healthy five‐year‐old child with herpes zoster ophthalmicus.Pediatr Infect Dis J.2005;24(5):476–477.
- .Herpes zoster ophthalmicus and syndrome of inappropriate antidiuretic hormone secretion.Am J Med Sci.2007;333(1):56–57.
- ,,, et al.Herpes zoster ophthalmicus and syndrome of inappropriate antidiuretic hormone secretion.Intern Med.2008;47(5):463–465.
- ,,,.Coexistence of Ramsay‐Hunt syndrome and varicella‐zoster virus encephalitis.Infection.2006;34(6):352–354.
- ,,.Herpes zoster‐associated meningoencephalitis in patients with systemic cancer.Mayo Clin Proc.1993;68(7):652–655.
- ,,, et al.Herpes zoster ophthalmicus in patients with human immunodeficiency virus infection.Am J Ophthalmol.1998;125(3):285–291.
- ,.Images in clinical medicine. Herpes zoster ophthalmicus followed by contralateral hemiparesis.N Engl J Med.2002;346(15):1127.
- ,.Contralateral hemiplegia complicating herpes zoster ophthalmicus.J R Soc Med.1991;84(8):501–502.
- .Herpes zoster ophthalmicus.Neurology.1995;45(12 Suppl 8):S50–S51.
- ,,.Central Nervous System involvement after herpes zoster ophthalmicus.Acta Ophthalmologica.2008. E‐pub January 2008.
- ,,, et al.Neurologic complications of the reactivation of varicella‐zoster virus.N Engl J Med.2000;342(9):635–645.
- ,,, et al.Recommendations for the management of herpes zoster.Clin Infect Dis.2007;44(suppl 1):S1–S26.
- ,.Herpes zoster encephalitis: 2 case reports and review of literature.Infect Dis Clin Pract.2007;15(4):284–288.
- ,.Rapid response to acyclovir in herpes zoster‐associated encephalitis.Am J Med.1987;82(3):560–562.
- ,,, et al.Varicella zoster virus encephalitis in a previously healthy five‐year‐old child with herpes zoster ophthalmicus.Pediatr Infect Dis J.2005;24(5):476–477.
- .Herpes zoster ophthalmicus and syndrome of inappropriate antidiuretic hormone secretion.Am J Med Sci.2007;333(1):56–57.
- ,,, et al.Herpes zoster ophthalmicus and syndrome of inappropriate antidiuretic hormone secretion.Intern Med.2008;47(5):463–465.
- ,,,.Coexistence of Ramsay‐Hunt syndrome and varicella‐zoster virus encephalitis.Infection.2006;34(6):352–354.
- ,,.Herpes zoster‐associated meningoencephalitis in patients with systemic cancer.Mayo Clin Proc.1993;68(7):652–655.
- ,,, et al.Herpes zoster ophthalmicus in patients with human immunodeficiency virus infection.Am J Ophthalmol.1998;125(3):285–291.
- ,.Images in clinical medicine. Herpes zoster ophthalmicus followed by contralateral hemiparesis.N Engl J Med.2002;346(15):1127.
- ,.Contralateral hemiplegia complicating herpes zoster ophthalmicus.J R Soc Med.1991;84(8):501–502.
Case of Sudden Desaturation and Cyanosis
A 38‐year‐old Hispanic man was admitted to the telemetry floor with diagnosis of pericarditis. Blood cultures revealed methicillin‐sensitive Staphylococcus aureus and the patient was started on nafcillin. Despite appropriate antibiotic therapy, the patient remained febrile. Transesophageal echocardiogram (TEE) was performed to evaluate for endocarditis. An hour after the TEE, patient started to desaturate and complained of shortness of breath. At this point, the patient was afebrile, with a pulse rate of 110 beats/minute and blood pressure of 97/63 mm Hg. Oxygen saturation by pulse oximetry of 82% on room air progressively declined even with administration of supplemental oxygen to 77%, necessitating intubation. Despite mechanical ventilation with 100% oxygen delivery, the patient remained cyanotic, with pulse oximetry reading of 69%, and with the arterial blood obtained from the patient at this time for laboratory analysis appearing brown in color.
Based on the temporal correlation of benzocaine spray used during TEE and the symptomscyanosis, hypoxia despite 100% fraction of inspired oxygen (FiO2), and chocolate‐brown arterial blooda diagnosis of methemoglobinemia was made. The patient's methemoglobin level was reported at 41% (normal range, 0‐3%). The patient received methylene blue, recovered rapidly, and was extubated the next day. Subsequent methemoglobin level obtained less than 24 hours later was reduced to 0.8%. Two days later the patient was discharged to home.
Discussion
Methemoglobin is the state in which ferrous (Fe2+) ions of heme are oxidized to the ferric state (Fe3+). Because red blood cells are continuously exposed to various oxidative stresses, a methemoglobinemia level of approximately 1% is present in normal individuals at baseline. This low level is maintained through reduction by enzyme systems within the erythrocyte. The most important is the reduced nicotinamide adenine dinucleotide (NADH)‐cytochrome‐b5 reductase system.1 Others, functioning mainly as reserve systems, are ascorbic acid, reduced glutathione, and reduced nicotinamide adenine dinucleotide phosphate (NADPH)‐methemoglobin reductase. The latter requires a natural cofactor or an autooxidizable dye such as methylene blue for activity.
Methemoglobinemia can be congenital or acquired. Congenital methemoglobinemia is very rare and is due to a cytochrome‐b5 reductase deficiency or presence of an abnormal hemoglobin M molecule.2 Acquired methemoglobinemia, the more common type, results from exposure to chemicals that cause more rapid accumulation of methemoglobin than the rate at which methemoglobin can be reduced. Many chemical and environmental agents can cause acquired methemoglobinemia (Table 1). Local anesthetics are the most common hospital‐based pharmacologic agents to cause methemoglobinemia. Prilocaine has been implicated most frequently, especially in newborns. Prilocaine‐induced methemoglobinemia is dose‐dependent and occurs when doses used exceed 600 mg in a 24‐hour period. Lidocaine is a rare cause of methemoglobinemia, but comorbidities like renal failure and use of other local anesthetics like benzocaine will increase the chances of methemoglobinemia. Benzocaine has been reported to cause methemoglobinemia after its use as a lubricant on endotracheal, bronchoscopic, and nasogastric or orogastric tubes, but more commonly after its use as a spray. Benzocaine is lipophilic and may continue to enter the bloodstream from adipose tissue after methylene blue concentrations are no longer therapeutic.
| Name | Key Features |
|---|---|
| Industrial agents | |
| Naphthalene | Coal tar, mothballs. Newborns are at increased risk for methemoglobinemia |
| Inorganic nitrates/nitrites | Meat preservatives; vegetablescarrot juice, spinach. Nitrates are converted to nitrite by the bacteria in the gut. Most commonly acquired from ground water contaminated with pesticides and fertilizers |
| Aniline/aminophenols | Laundry ink. Aniline‐induced methemoglobinemia is less responsive to methylene blue |
| Chlorates | Matches, explosives, pyrotechnics, weed killers. Also cause intravascular hemolysis and toxic nephritis |
| Pharmaceutical agents | |
| Local anesthetics: benzocaine, lidocaine, prilocaine | Benzocaine: It is lipophilic and may continue to enter the blood stream from adipose tissue even after methylene blue concentrations are no longer therapeutic. |
| Lidocaine: Very rarely causes methemoglobinemia alone. Comorbidities like renal failure and use of other local anesthetics will increase the chances of methemoglobinemia. Prilocaine: Dose‐dependent. Occurs when doses used exceed 600 mg. Newborns are at higher risk | |
| Primaquine | Primaquine‐induced methemoglobinemia, although almost universal with clinical doses, seems to be mild, self‐limited, and tolerated without symptoms or signs of cyanosis in otherwise healthy people |
| Dapsone | Can cause methemoglobinemia both in acute intoxication as well as chronic use. May precipitate acute hemolytic anemia. Metabolites that cause methemoglobinemia may last in the circulation for about 35 days |
| Phenacetin | Phenacetin is generally metabolized to acetaminophen. In patients unable to metabolize phenacetin to acetaminophen, alternate metabolites are produced that cause methemoglobinemia |
| Sulfonamides | Does not respond well to methylene blue. Alternative therapies include ascorbic acid, riboflavin, or exchange transfusion |
| Nitrites (amyl and butyl) | Amyl nitrite: Used in treating angina. Butyl nitrite: Used in room deodorizers. Both drugs are used for their alleged sexual enhancing properties |
| Nitroprusside | Methemoglobinemia occurs in patients who have received a dose larger than 10 mg/kg in 1 day. It takes 16 hours of continuous infusion at the maximum rate of 10 g/kg/minute to reach the total accumulated dose |
| Phenazopyridine | Increased incidence of methemoglobinemia in patients with renal failure. Drug also causes hemolytic anemia and turns the urine orange‐yellow in color. One of its metabolites is aniline |
| Metoclopromide | Overdose in infants causes methemoglobinemia |
| Trimethoprim | Methemoglobinemia usually occurs after prolonged periods of administration. Caution when used with dapsone |
Clinical presentation varies based on methemoglobin levels. Early symptoms of methemoglobinemia, when the blood contains 15% to 50% methemoglobin, include nonspecific headache, fatigues, dyspnea, and lethargy. As the amount of methemoglobin in the blood exceeds 50%, the patients develop more serious neurological symptoms, ranging from confusion to seizures, respiratory depression, and death (Table 2). Clinical interpretation of methemoglobin levels must take into account the total hemoglobin value because anemic patients will have proportionately less functional hemoglobin.3 Methemoglobinemia that develops rapidly will be clinically more severe than a similar degree that develops gradually. The acute accumulation of 30% methemoglobinemia is usually well tolerated in the nonanemic patient.
| Level of methemoglobinemia | Symptoms |
|---|---|
| 0‐15% | No signs or symptoms |
| 15‐20% | Cyanosis and chocolate brown blood |
| 20‐50% | Headache, fatigues, dyspnea, and lethargy |
| >50% | Serious neurological symptoms ranging from confusion to seizures; respiratory depression and death |
The suspicion for methemoglobinemia should be raised in the presence of dark or chocolate‐brown arterial blood that does not become red with exposure to air.4 Dark‐colored blood from patients with hypoxia should redden with exposure to air; blood darkened by methemoglobin does not. The suspicion for methemoglobinemia should also be raised in the presence of a saturation gap, when the measured oxygen saturation of blood by pulse oximetry is less than the oxygen saturation calculated by routine blood gas analysis by more than 5%.5 The oxygen saturation on arterial blood gas is calculated from partial pressure of arterial oxygen (PaO2) and pH. Since PaO2 is within normal limits in methemoglobinemia, it leads to a normal, though inaccurate, calculated oxygen saturation. Multiple‐wavelength cooximetry is the accepted standard for confirming and quantifying methemoglobinemia.6 This assay involves measuring methemoglobin at its peak absorbance of 630 nm and requires the addition of cyanide to convert methemoglobin to cyanomethemoglobin, which absorbs at shorter wavelengths, resulting in an absorbance decrease at 630 nm due to the disappearance of methemoglobin. Hyperlipidemia and intravenous administration of methylene blue or other dyes may interfere with cooximetry measurements.
In asymptomatic patients with acute methemoglobinemia, discontinuation of the offending drug and proper monitoring is sufficient. In patients who are symptomatic, in addition to supplemental oxygen, methylene blue should be used to enhance the reducing capacity of erythrocytes. Methylene blue, given intravenously in a dose of 1 mg/kg over 5 minutes, acts as an electron acceptor, enhances the NADPH pathway, and rapidly reduces methemoglobin to hemoglobin.7 However, methylene blue should not be used in patients with glucose‐6‐phosphate dehydrogenase deficiency as it can cause life‐threatening hemolysis. In these patients, ascorbic acid should be used. Hyperbaric oxygen or exchange transfusion can also be used. In patients who are in shock secondary to the methemoglobinemia, blood transfusion or exchange transfusion is helpful.
Summary
Agents that inflict large oxidative stress, such as topical anesthetics, can cause methemoglobinemia. A frequently‐used topical anesthetic agent like benzocaine is a common cause of methemoglobinemia. The most characteristic findings of methemoglobinemia are blue‐gray or brown‐gray cyanosis of the skin, lips, and nail beds, dark brown color of the blood, and saturation gap. Symptomatic patients should be given methylene blue intravenously.
- .Methemoglobin—it's not just blue: a concise review.Am J Hematol.2007;82(2):134–144.
- ,,.Cyanosis.J Emerg Med.2000;18(3):369–371.
- ,,,.Benzocaine‐induced methemoglobinemia based on the Mayo Clinic experience from 28,478 transesophageal echocardiograms: incidence, outcomes, and predisposing factors.Arch Intern Med.2007;167(18):1977–1982.
- ,,.Methemoglobinemia: etiology, pharmacology, and clinical management.Ann Emerg Med.1999;34(5):646–656.
- ,,.Mind the gap.J Emerg Med.2007;33(2):131–132.
- ,.A 74‐year‐old woman with desaturation following surgery. Co‐oximetry is the first step in making the diagnosis of dyshemoglobinemia.Chest.2003;123(2):613–616.
- ,.Methylene blue.Am J Ther.2003;10(4):289–291.
A 38‐year‐old Hispanic man was admitted to the telemetry floor with diagnosis of pericarditis. Blood cultures revealed methicillin‐sensitive Staphylococcus aureus and the patient was started on nafcillin. Despite appropriate antibiotic therapy, the patient remained febrile. Transesophageal echocardiogram (TEE) was performed to evaluate for endocarditis. An hour after the TEE, patient started to desaturate and complained of shortness of breath. At this point, the patient was afebrile, with a pulse rate of 110 beats/minute and blood pressure of 97/63 mm Hg. Oxygen saturation by pulse oximetry of 82% on room air progressively declined even with administration of supplemental oxygen to 77%, necessitating intubation. Despite mechanical ventilation with 100% oxygen delivery, the patient remained cyanotic, with pulse oximetry reading of 69%, and with the arterial blood obtained from the patient at this time for laboratory analysis appearing brown in color.
Based on the temporal correlation of benzocaine spray used during TEE and the symptomscyanosis, hypoxia despite 100% fraction of inspired oxygen (FiO2), and chocolate‐brown arterial blooda diagnosis of methemoglobinemia was made. The patient's methemoglobin level was reported at 41% (normal range, 0‐3%). The patient received methylene blue, recovered rapidly, and was extubated the next day. Subsequent methemoglobin level obtained less than 24 hours later was reduced to 0.8%. Two days later the patient was discharged to home.
Discussion
Methemoglobin is the state in which ferrous (Fe2+) ions of heme are oxidized to the ferric state (Fe3+). Because red blood cells are continuously exposed to various oxidative stresses, a methemoglobinemia level of approximately 1% is present in normal individuals at baseline. This low level is maintained through reduction by enzyme systems within the erythrocyte. The most important is the reduced nicotinamide adenine dinucleotide (NADH)‐cytochrome‐b5 reductase system.1 Others, functioning mainly as reserve systems, are ascorbic acid, reduced glutathione, and reduced nicotinamide adenine dinucleotide phosphate (NADPH)‐methemoglobin reductase. The latter requires a natural cofactor or an autooxidizable dye such as methylene blue for activity.
Methemoglobinemia can be congenital or acquired. Congenital methemoglobinemia is very rare and is due to a cytochrome‐b5 reductase deficiency or presence of an abnormal hemoglobin M molecule.2 Acquired methemoglobinemia, the more common type, results from exposure to chemicals that cause more rapid accumulation of methemoglobin than the rate at which methemoglobin can be reduced. Many chemical and environmental agents can cause acquired methemoglobinemia (Table 1). Local anesthetics are the most common hospital‐based pharmacologic agents to cause methemoglobinemia. Prilocaine has been implicated most frequently, especially in newborns. Prilocaine‐induced methemoglobinemia is dose‐dependent and occurs when doses used exceed 600 mg in a 24‐hour period. Lidocaine is a rare cause of methemoglobinemia, but comorbidities like renal failure and use of other local anesthetics like benzocaine will increase the chances of methemoglobinemia. Benzocaine has been reported to cause methemoglobinemia after its use as a lubricant on endotracheal, bronchoscopic, and nasogastric or orogastric tubes, but more commonly after its use as a spray. Benzocaine is lipophilic and may continue to enter the bloodstream from adipose tissue after methylene blue concentrations are no longer therapeutic.
| Name | Key Features |
|---|---|
| Industrial agents | |
| Naphthalene | Coal tar, mothballs. Newborns are at increased risk for methemoglobinemia |
| Inorganic nitrates/nitrites | Meat preservatives; vegetablescarrot juice, spinach. Nitrates are converted to nitrite by the bacteria in the gut. Most commonly acquired from ground water contaminated with pesticides and fertilizers |
| Aniline/aminophenols | Laundry ink. Aniline‐induced methemoglobinemia is less responsive to methylene blue |
| Chlorates | Matches, explosives, pyrotechnics, weed killers. Also cause intravascular hemolysis and toxic nephritis |
| Pharmaceutical agents | |
| Local anesthetics: benzocaine, lidocaine, prilocaine | Benzocaine: It is lipophilic and may continue to enter the blood stream from adipose tissue even after methylene blue concentrations are no longer therapeutic. |
| Lidocaine: Very rarely causes methemoglobinemia alone. Comorbidities like renal failure and use of other local anesthetics will increase the chances of methemoglobinemia. Prilocaine: Dose‐dependent. Occurs when doses used exceed 600 mg. Newborns are at higher risk | |
| Primaquine | Primaquine‐induced methemoglobinemia, although almost universal with clinical doses, seems to be mild, self‐limited, and tolerated without symptoms or signs of cyanosis in otherwise healthy people |
| Dapsone | Can cause methemoglobinemia both in acute intoxication as well as chronic use. May precipitate acute hemolytic anemia. Metabolites that cause methemoglobinemia may last in the circulation for about 35 days |
| Phenacetin | Phenacetin is generally metabolized to acetaminophen. In patients unable to metabolize phenacetin to acetaminophen, alternate metabolites are produced that cause methemoglobinemia |
| Sulfonamides | Does not respond well to methylene blue. Alternative therapies include ascorbic acid, riboflavin, or exchange transfusion |
| Nitrites (amyl and butyl) | Amyl nitrite: Used in treating angina. Butyl nitrite: Used in room deodorizers. Both drugs are used for their alleged sexual enhancing properties |
| Nitroprusside | Methemoglobinemia occurs in patients who have received a dose larger than 10 mg/kg in 1 day. It takes 16 hours of continuous infusion at the maximum rate of 10 g/kg/minute to reach the total accumulated dose |
| Phenazopyridine | Increased incidence of methemoglobinemia in patients with renal failure. Drug also causes hemolytic anemia and turns the urine orange‐yellow in color. One of its metabolites is aniline |
| Metoclopromide | Overdose in infants causes methemoglobinemia |
| Trimethoprim | Methemoglobinemia usually occurs after prolonged periods of administration. Caution when used with dapsone |
Clinical presentation varies based on methemoglobin levels. Early symptoms of methemoglobinemia, when the blood contains 15% to 50% methemoglobin, include nonspecific headache, fatigues, dyspnea, and lethargy. As the amount of methemoglobin in the blood exceeds 50%, the patients develop more serious neurological symptoms, ranging from confusion to seizures, respiratory depression, and death (Table 2). Clinical interpretation of methemoglobin levels must take into account the total hemoglobin value because anemic patients will have proportionately less functional hemoglobin.3 Methemoglobinemia that develops rapidly will be clinically more severe than a similar degree that develops gradually. The acute accumulation of 30% methemoglobinemia is usually well tolerated in the nonanemic patient.
| Level of methemoglobinemia | Symptoms |
|---|---|
| 0‐15% | No signs or symptoms |
| 15‐20% | Cyanosis and chocolate brown blood |
| 20‐50% | Headache, fatigues, dyspnea, and lethargy |
| >50% | Serious neurological symptoms ranging from confusion to seizures; respiratory depression and death |
The suspicion for methemoglobinemia should be raised in the presence of dark or chocolate‐brown arterial blood that does not become red with exposure to air.4 Dark‐colored blood from patients with hypoxia should redden with exposure to air; blood darkened by methemoglobin does not. The suspicion for methemoglobinemia should also be raised in the presence of a saturation gap, when the measured oxygen saturation of blood by pulse oximetry is less than the oxygen saturation calculated by routine blood gas analysis by more than 5%.5 The oxygen saturation on arterial blood gas is calculated from partial pressure of arterial oxygen (PaO2) and pH. Since PaO2 is within normal limits in methemoglobinemia, it leads to a normal, though inaccurate, calculated oxygen saturation. Multiple‐wavelength cooximetry is the accepted standard for confirming and quantifying methemoglobinemia.6 This assay involves measuring methemoglobin at its peak absorbance of 630 nm and requires the addition of cyanide to convert methemoglobin to cyanomethemoglobin, which absorbs at shorter wavelengths, resulting in an absorbance decrease at 630 nm due to the disappearance of methemoglobin. Hyperlipidemia and intravenous administration of methylene blue or other dyes may interfere with cooximetry measurements.
In asymptomatic patients with acute methemoglobinemia, discontinuation of the offending drug and proper monitoring is sufficient. In patients who are symptomatic, in addition to supplemental oxygen, methylene blue should be used to enhance the reducing capacity of erythrocytes. Methylene blue, given intravenously in a dose of 1 mg/kg over 5 minutes, acts as an electron acceptor, enhances the NADPH pathway, and rapidly reduces methemoglobin to hemoglobin.7 However, methylene blue should not be used in patients with glucose‐6‐phosphate dehydrogenase deficiency as it can cause life‐threatening hemolysis. In these patients, ascorbic acid should be used. Hyperbaric oxygen or exchange transfusion can also be used. In patients who are in shock secondary to the methemoglobinemia, blood transfusion or exchange transfusion is helpful.
Summary
Agents that inflict large oxidative stress, such as topical anesthetics, can cause methemoglobinemia. A frequently‐used topical anesthetic agent like benzocaine is a common cause of methemoglobinemia. The most characteristic findings of methemoglobinemia are blue‐gray or brown‐gray cyanosis of the skin, lips, and nail beds, dark brown color of the blood, and saturation gap. Symptomatic patients should be given methylene blue intravenously.
A 38‐year‐old Hispanic man was admitted to the telemetry floor with diagnosis of pericarditis. Blood cultures revealed methicillin‐sensitive Staphylococcus aureus and the patient was started on nafcillin. Despite appropriate antibiotic therapy, the patient remained febrile. Transesophageal echocardiogram (TEE) was performed to evaluate for endocarditis. An hour after the TEE, patient started to desaturate and complained of shortness of breath. At this point, the patient was afebrile, with a pulse rate of 110 beats/minute and blood pressure of 97/63 mm Hg. Oxygen saturation by pulse oximetry of 82% on room air progressively declined even with administration of supplemental oxygen to 77%, necessitating intubation. Despite mechanical ventilation with 100% oxygen delivery, the patient remained cyanotic, with pulse oximetry reading of 69%, and with the arterial blood obtained from the patient at this time for laboratory analysis appearing brown in color.
Based on the temporal correlation of benzocaine spray used during TEE and the symptomscyanosis, hypoxia despite 100% fraction of inspired oxygen (FiO2), and chocolate‐brown arterial blooda diagnosis of methemoglobinemia was made. The patient's methemoglobin level was reported at 41% (normal range, 0‐3%). The patient received methylene blue, recovered rapidly, and was extubated the next day. Subsequent methemoglobin level obtained less than 24 hours later was reduced to 0.8%. Two days later the patient was discharged to home.
Discussion
Methemoglobin is the state in which ferrous (Fe2+) ions of heme are oxidized to the ferric state (Fe3+). Because red blood cells are continuously exposed to various oxidative stresses, a methemoglobinemia level of approximately 1% is present in normal individuals at baseline. This low level is maintained through reduction by enzyme systems within the erythrocyte. The most important is the reduced nicotinamide adenine dinucleotide (NADH)‐cytochrome‐b5 reductase system.1 Others, functioning mainly as reserve systems, are ascorbic acid, reduced glutathione, and reduced nicotinamide adenine dinucleotide phosphate (NADPH)‐methemoglobin reductase. The latter requires a natural cofactor or an autooxidizable dye such as methylene blue for activity.
Methemoglobinemia can be congenital or acquired. Congenital methemoglobinemia is very rare and is due to a cytochrome‐b5 reductase deficiency or presence of an abnormal hemoglobin M molecule.2 Acquired methemoglobinemia, the more common type, results from exposure to chemicals that cause more rapid accumulation of methemoglobin than the rate at which methemoglobin can be reduced. Many chemical and environmental agents can cause acquired methemoglobinemia (Table 1). Local anesthetics are the most common hospital‐based pharmacologic agents to cause methemoglobinemia. Prilocaine has been implicated most frequently, especially in newborns. Prilocaine‐induced methemoglobinemia is dose‐dependent and occurs when doses used exceed 600 mg in a 24‐hour period. Lidocaine is a rare cause of methemoglobinemia, but comorbidities like renal failure and use of other local anesthetics like benzocaine will increase the chances of methemoglobinemia. Benzocaine has been reported to cause methemoglobinemia after its use as a lubricant on endotracheal, bronchoscopic, and nasogastric or orogastric tubes, but more commonly after its use as a spray. Benzocaine is lipophilic and may continue to enter the bloodstream from adipose tissue after methylene blue concentrations are no longer therapeutic.
| Name | Key Features |
|---|---|
| Industrial agents | |
| Naphthalene | Coal tar, mothballs. Newborns are at increased risk for methemoglobinemia |
| Inorganic nitrates/nitrites | Meat preservatives; vegetablescarrot juice, spinach. Nitrates are converted to nitrite by the bacteria in the gut. Most commonly acquired from ground water contaminated with pesticides and fertilizers |
| Aniline/aminophenols | Laundry ink. Aniline‐induced methemoglobinemia is less responsive to methylene blue |
| Chlorates | Matches, explosives, pyrotechnics, weed killers. Also cause intravascular hemolysis and toxic nephritis |
| Pharmaceutical agents | |
| Local anesthetics: benzocaine, lidocaine, prilocaine | Benzocaine: It is lipophilic and may continue to enter the blood stream from adipose tissue even after methylene blue concentrations are no longer therapeutic. |
| Lidocaine: Very rarely causes methemoglobinemia alone. Comorbidities like renal failure and use of other local anesthetics will increase the chances of methemoglobinemia. Prilocaine: Dose‐dependent. Occurs when doses used exceed 600 mg. Newborns are at higher risk | |
| Primaquine | Primaquine‐induced methemoglobinemia, although almost universal with clinical doses, seems to be mild, self‐limited, and tolerated without symptoms or signs of cyanosis in otherwise healthy people |
| Dapsone | Can cause methemoglobinemia both in acute intoxication as well as chronic use. May precipitate acute hemolytic anemia. Metabolites that cause methemoglobinemia may last in the circulation for about 35 days |
| Phenacetin | Phenacetin is generally metabolized to acetaminophen. In patients unable to metabolize phenacetin to acetaminophen, alternate metabolites are produced that cause methemoglobinemia |
| Sulfonamides | Does not respond well to methylene blue. Alternative therapies include ascorbic acid, riboflavin, or exchange transfusion |
| Nitrites (amyl and butyl) | Amyl nitrite: Used in treating angina. Butyl nitrite: Used in room deodorizers. Both drugs are used for their alleged sexual enhancing properties |
| Nitroprusside | Methemoglobinemia occurs in patients who have received a dose larger than 10 mg/kg in 1 day. It takes 16 hours of continuous infusion at the maximum rate of 10 g/kg/minute to reach the total accumulated dose |
| Phenazopyridine | Increased incidence of methemoglobinemia in patients with renal failure. Drug also causes hemolytic anemia and turns the urine orange‐yellow in color. One of its metabolites is aniline |
| Metoclopromide | Overdose in infants causes methemoglobinemia |
| Trimethoprim | Methemoglobinemia usually occurs after prolonged periods of administration. Caution when used with dapsone |
Clinical presentation varies based on methemoglobin levels. Early symptoms of methemoglobinemia, when the blood contains 15% to 50% methemoglobin, include nonspecific headache, fatigues, dyspnea, and lethargy. As the amount of methemoglobin in the blood exceeds 50%, the patients develop more serious neurological symptoms, ranging from confusion to seizures, respiratory depression, and death (Table 2). Clinical interpretation of methemoglobin levels must take into account the total hemoglobin value because anemic patients will have proportionately less functional hemoglobin.3 Methemoglobinemia that develops rapidly will be clinically more severe than a similar degree that develops gradually. The acute accumulation of 30% methemoglobinemia is usually well tolerated in the nonanemic patient.
| Level of methemoglobinemia | Symptoms |
|---|---|
| 0‐15% | No signs or symptoms |
| 15‐20% | Cyanosis and chocolate brown blood |
| 20‐50% | Headache, fatigues, dyspnea, and lethargy |
| >50% | Serious neurological symptoms ranging from confusion to seizures; respiratory depression and death |
The suspicion for methemoglobinemia should be raised in the presence of dark or chocolate‐brown arterial blood that does not become red with exposure to air.4 Dark‐colored blood from patients with hypoxia should redden with exposure to air; blood darkened by methemoglobin does not. The suspicion for methemoglobinemia should also be raised in the presence of a saturation gap, when the measured oxygen saturation of blood by pulse oximetry is less than the oxygen saturation calculated by routine blood gas analysis by more than 5%.5 The oxygen saturation on arterial blood gas is calculated from partial pressure of arterial oxygen (PaO2) and pH. Since PaO2 is within normal limits in methemoglobinemia, it leads to a normal, though inaccurate, calculated oxygen saturation. Multiple‐wavelength cooximetry is the accepted standard for confirming and quantifying methemoglobinemia.6 This assay involves measuring methemoglobin at its peak absorbance of 630 nm and requires the addition of cyanide to convert methemoglobin to cyanomethemoglobin, which absorbs at shorter wavelengths, resulting in an absorbance decrease at 630 nm due to the disappearance of methemoglobin. Hyperlipidemia and intravenous administration of methylene blue or other dyes may interfere with cooximetry measurements.
In asymptomatic patients with acute methemoglobinemia, discontinuation of the offending drug and proper monitoring is sufficient. In patients who are symptomatic, in addition to supplemental oxygen, methylene blue should be used to enhance the reducing capacity of erythrocytes. Methylene blue, given intravenously in a dose of 1 mg/kg over 5 minutes, acts as an electron acceptor, enhances the NADPH pathway, and rapidly reduces methemoglobin to hemoglobin.7 However, methylene blue should not be used in patients with glucose‐6‐phosphate dehydrogenase deficiency as it can cause life‐threatening hemolysis. In these patients, ascorbic acid should be used. Hyperbaric oxygen or exchange transfusion can also be used. In patients who are in shock secondary to the methemoglobinemia, blood transfusion or exchange transfusion is helpful.
Summary
Agents that inflict large oxidative stress, such as topical anesthetics, can cause methemoglobinemia. A frequently‐used topical anesthetic agent like benzocaine is a common cause of methemoglobinemia. The most characteristic findings of methemoglobinemia are blue‐gray or brown‐gray cyanosis of the skin, lips, and nail beds, dark brown color of the blood, and saturation gap. Symptomatic patients should be given methylene blue intravenously.
- .Methemoglobin—it's not just blue: a concise review.Am J Hematol.2007;82(2):134–144.
- ,,.Cyanosis.J Emerg Med.2000;18(3):369–371.
- ,,,.Benzocaine‐induced methemoglobinemia based on the Mayo Clinic experience from 28,478 transesophageal echocardiograms: incidence, outcomes, and predisposing factors.Arch Intern Med.2007;167(18):1977–1982.
- ,,.Methemoglobinemia: etiology, pharmacology, and clinical management.Ann Emerg Med.1999;34(5):646–656.
- ,,.Mind the gap.J Emerg Med.2007;33(2):131–132.
- ,.A 74‐year‐old woman with desaturation following surgery. Co‐oximetry is the first step in making the diagnosis of dyshemoglobinemia.Chest.2003;123(2):613–616.
- ,.Methylene blue.Am J Ther.2003;10(4):289–291.
- .Methemoglobin—it's not just blue: a concise review.Am J Hematol.2007;82(2):134–144.
- ,,.Cyanosis.J Emerg Med.2000;18(3):369–371.
- ,,,.Benzocaine‐induced methemoglobinemia based on the Mayo Clinic experience from 28,478 transesophageal echocardiograms: incidence, outcomes, and predisposing factors.Arch Intern Med.2007;167(18):1977–1982.
- ,,.Methemoglobinemia: etiology, pharmacology, and clinical management.Ann Emerg Med.1999;34(5):646–656.
- ,,.Mind the gap.J Emerg Med.2007;33(2):131–132.
- ,.A 74‐year‐old woman with desaturation following surgery. Co‐oximetry is the first step in making the diagnosis of dyshemoglobinemia.Chest.2003;123(2):613–616.
- ,.Methylene blue.Am J Ther.2003;10(4):289–291.