User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Primary Care Offices Unprepared for Allergen Therapy Emergencies
ORLANDO – A survey of primary care offices revealed that the majority were not fully equipped to handle adverse reactions to allergen immunotherapy.
"Primary care offices require further education on administration of allergen immunotherapy to ensure adherence to the updated practice parameter, as well as to ensure safety," Dr. Vinitha Reddy said at the annual meeting of the American Academy of Allergy, Asthma and Immunology.
The telephone survey involved a questionnaire administered to nurses at 43 primary care offices (35 family medicine, 4 pediatric, and 4 internal medicine) that administer allergen immunotherapy (AIT). The practices employed a total 194 physicians, and administered AIT to approximately 500 patients.
The survey assessed adherence to the recommendations in "Allergen immunotherapy: a practice parameter third update," a joint guideline issued by the American Academy of Allergy, Asthma, and Immunology and the American College of Allergy, Asthma, and Immunology (J. Allergy Clin. Immunol. 2011;127:S1-55).
The guideline states that allergists’ offices are the preferred setting, but that primary care offices can perform AIT if the appropriate personnel and equipment are available to identify and treat anaphylaxis or other emergencies. The risk is low – approximately 0.2% of patients experience systemic reactions per injection, and deaths occur in just 1 per 2.5 million injections. However, the risk is not nonexistent, said Dr. Reddy, a second-year postgraduate fellow at Pennsylvania State University, Hershey.
Only 53% of the offices reported performing the recommended preinjection health assessment, which should include a determination of the presence of asthma and the degree of asthma control. Only 23% reported measuring peak flow, which is suggested as a method for assessing lung function in asthma patients.
Just 33% of the practices reported routinely having patients wait the recommended 30 minutes following AIT before leaving the office. Another 42% had patients wait just 20 minutes, and the other 25% had patients wait only 10 minutes.
Adverse reactions in the past 6 months, including hives, wheezing, or shortness of breath, were reported by 30% of the offices. None of the nurses reported having had a case of anaphylaxis, Dr. Reddy said.
All of the offices’ nurses said that they felt prepared to handle adverse reactions, and all said that they stock epinephrine, oxygen, and needles. The ability to administer antihistamines, corticosteroids, airway maintenance, and intravenous fluids was reported by 91%, 93%, 93%, and 70% of offices, respectively.
When offered in-service education on the AIT practice parameter, only 42% expressed interest. The other 58% stated that they did not have the time, Dr. Reddy reported.
During the question and answer period, an audience member commented that "it would be interesting" to conduct the same assessment in allergy practices, noting that "it may be about equal."
Dr. Reddy stated that she had no financial disclosures.
ORLANDO – A survey of primary care offices revealed that the majority were not fully equipped to handle adverse reactions to allergen immunotherapy.
"Primary care offices require further education on administration of allergen immunotherapy to ensure adherence to the updated practice parameter, as well as to ensure safety," Dr. Vinitha Reddy said at the annual meeting of the American Academy of Allergy, Asthma and Immunology.
The telephone survey involved a questionnaire administered to nurses at 43 primary care offices (35 family medicine, 4 pediatric, and 4 internal medicine) that administer allergen immunotherapy (AIT). The practices employed a total 194 physicians, and administered AIT to approximately 500 patients.
The survey assessed adherence to the recommendations in "Allergen immunotherapy: a practice parameter third update," a joint guideline issued by the American Academy of Allergy, Asthma, and Immunology and the American College of Allergy, Asthma, and Immunology (J. Allergy Clin. Immunol. 2011;127:S1-55).
The guideline states that allergists’ offices are the preferred setting, but that primary care offices can perform AIT if the appropriate personnel and equipment are available to identify and treat anaphylaxis or other emergencies. The risk is low – approximately 0.2% of patients experience systemic reactions per injection, and deaths occur in just 1 per 2.5 million injections. However, the risk is not nonexistent, said Dr. Reddy, a second-year postgraduate fellow at Pennsylvania State University, Hershey.
Only 53% of the offices reported performing the recommended preinjection health assessment, which should include a determination of the presence of asthma and the degree of asthma control. Only 23% reported measuring peak flow, which is suggested as a method for assessing lung function in asthma patients.
Just 33% of the practices reported routinely having patients wait the recommended 30 minutes following AIT before leaving the office. Another 42% had patients wait just 20 minutes, and the other 25% had patients wait only 10 minutes.
Adverse reactions in the past 6 months, including hives, wheezing, or shortness of breath, were reported by 30% of the offices. None of the nurses reported having had a case of anaphylaxis, Dr. Reddy said.
All of the offices’ nurses said that they felt prepared to handle adverse reactions, and all said that they stock epinephrine, oxygen, and needles. The ability to administer antihistamines, corticosteroids, airway maintenance, and intravenous fluids was reported by 91%, 93%, 93%, and 70% of offices, respectively.
When offered in-service education on the AIT practice parameter, only 42% expressed interest. The other 58% stated that they did not have the time, Dr. Reddy reported.
During the question and answer period, an audience member commented that "it would be interesting" to conduct the same assessment in allergy practices, noting that "it may be about equal."
Dr. Reddy stated that she had no financial disclosures.
ORLANDO – A survey of primary care offices revealed that the majority were not fully equipped to handle adverse reactions to allergen immunotherapy.
"Primary care offices require further education on administration of allergen immunotherapy to ensure adherence to the updated practice parameter, as well as to ensure safety," Dr. Vinitha Reddy said at the annual meeting of the American Academy of Allergy, Asthma and Immunology.
The telephone survey involved a questionnaire administered to nurses at 43 primary care offices (35 family medicine, 4 pediatric, and 4 internal medicine) that administer allergen immunotherapy (AIT). The practices employed a total 194 physicians, and administered AIT to approximately 500 patients.
The survey assessed adherence to the recommendations in "Allergen immunotherapy: a practice parameter third update," a joint guideline issued by the American Academy of Allergy, Asthma, and Immunology and the American College of Allergy, Asthma, and Immunology (J. Allergy Clin. Immunol. 2011;127:S1-55).
The guideline states that allergists’ offices are the preferred setting, but that primary care offices can perform AIT if the appropriate personnel and equipment are available to identify and treat anaphylaxis or other emergencies. The risk is low – approximately 0.2% of patients experience systemic reactions per injection, and deaths occur in just 1 per 2.5 million injections. However, the risk is not nonexistent, said Dr. Reddy, a second-year postgraduate fellow at Pennsylvania State University, Hershey.
Only 53% of the offices reported performing the recommended preinjection health assessment, which should include a determination of the presence of asthma and the degree of asthma control. Only 23% reported measuring peak flow, which is suggested as a method for assessing lung function in asthma patients.
Just 33% of the practices reported routinely having patients wait the recommended 30 minutes following AIT before leaving the office. Another 42% had patients wait just 20 minutes, and the other 25% had patients wait only 10 minutes.
Adverse reactions in the past 6 months, including hives, wheezing, or shortness of breath, were reported by 30% of the offices. None of the nurses reported having had a case of anaphylaxis, Dr. Reddy said.
All of the offices’ nurses said that they felt prepared to handle adverse reactions, and all said that they stock epinephrine, oxygen, and needles. The ability to administer antihistamines, corticosteroids, airway maintenance, and intravenous fluids was reported by 91%, 93%, 93%, and 70% of offices, respectively.
When offered in-service education on the AIT practice parameter, only 42% expressed interest. The other 58% stated that they did not have the time, Dr. Reddy reported.
During the question and answer period, an audience member commented that "it would be interesting" to conduct the same assessment in allergy practices, noting that "it may be about equal."
Dr. Reddy stated that she had no financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF ALLERGY, ASTHMA AND IMMUNOLOGY
Surgeon General: Decline in Tobacco Use Stalls
Approximately 3,800 children smoke their first cigarette every day and the rates of tobacco initiation are no longer declining, according to the Surgeon General’s report, "Preventing Tobacco Use Among Youth and Young Adults."
"Every day, 1,200 Americans die from smoking and each of those people are replaced by two young smokers," Surgeon General Regina Benjamin said at a press conference. "We know that prevention is the key ... If we can just get [young people] to remain smoke free until they’re 26, then less than 1% of them will ever start."

Among adults who smoke daily, 88% smoked their first cigarette before their 18th birthday; nearly all (99%) did so before their 26th.
According to the report, nearly 25% of high school seniors are current smokers, compared with about 33% of young adults, and about 20% of adults. And it’s not all cigarettes: About 1 in 10 male high school seniors currently uses smokeless tobacco and about 1 in 5 smokes cigars, according to the report.
The report, which updates the 1994 Surgeon General report on tobacco use in youth, highlights the immediate and long-term health consequences to which children and young adults are most vulnerable. These include cardiovascular damage, reduced lung function and growth, and risk of chronic obstructive pulmonary disease.
Because they’re impressionable, young adults and children also are vulnerable to tobacco advertising and targeted products. Even though the landmark 1998 Master Settlement Agreement drastically restricted the way tobacco can be marketed, one-third of the top grossing children’s movies in 2010 contained images of smoking, according to the report.
"Far too many kids still see smoking images and messages every day that normalize this dependence," said Dr. Howard Koh, assistant secretary for health in the Health and Human Services department. "Kids see smoking in the movies they watch, the video games they play, the websites they visit, and in the communities where they live."
Physician organizations voiced support of the report and recommended that it be used to help protect young people from using tobacco products.
"As pediatricians, and parents, we need to send a clear message to the studios that this must stop now," Dr. Robert W. Block, AAP president, said in a statement. Dr. Block added that the Surgeon General’s report should be used to help overturn a recent federal court decision that called graphic cigarette warning labels unconstitutional.
"Warning labels play a critical role in educating children, teens, and parents about the negative health impacts of tobacco. By ignoring health harms from tobacco, we are not only sustaining incredible costs in health care, but we are also risking the lives of youth and young adults. This is simply irresponsible," he said.
"If we can just get [young people] to remain smoke free until they’re 26, then less than 1% of them will ever start."
In a statement, Dr. Jack Lewin, chief executive officer of the American College of Cardiology said, "the Surgeon General’s decision to reinvigorate efforts to keep children and young adults from smoking and to encourage smoking cessation will help us continue downward the trend of mortality due to heart disease and save millions in spending on health care."
The American Medical Association called for better funding of smoking cessation programs. The AMA "is concerned that these smokers will not get the support and assistance needed to combat their addiction," Dr. Peter Carmel, the association’s president, said in a statement. "Increasing the price of tobacco and adopting comprehensive smoke-free laws throughout the entire nation would also help reduce the health, social, and economic consequences associated with tobacco use among our youth."
The American Heart Association called the report a wake-up call. "This insightful new report makes it clear that we cannot let our guard down for a minute when it comes to tobacco addiction," CEO Nancy Brown said in a statement. While many Americans may think tobacco use is fading away, the evidence in this report tells a dramatically different story."
Approximately 3,800 children smoke their first cigarette every day and the rates of tobacco initiation are no longer declining, according to the Surgeon General’s report, "Preventing Tobacco Use Among Youth and Young Adults."
"Every day, 1,200 Americans die from smoking and each of those people are replaced by two young smokers," Surgeon General Regina Benjamin said at a press conference. "We know that prevention is the key ... If we can just get [young people] to remain smoke free until they’re 26, then less than 1% of them will ever start."
Among adults who smoke daily, 88% smoked their first cigarette before their 18th birthday; nearly all (99%) did so before their 26th.
According to the report, nearly 25% of high school seniors are current smokers, compared with about 33% of young adults, and about 20% of adults. And it’s not all cigarettes: About 1 in 10 male high school seniors currently uses smokeless tobacco and about 1 in 5 smokes cigars, according to the report.
The report, which updates the 1994 Surgeon General report on tobacco use in youth, highlights the immediate and long-term health consequences to which children and young adults are most vulnerable. These include cardiovascular damage, reduced lung function and growth, and risk of chronic obstructive pulmonary disease.
Because they’re impressionable, young adults and children also are vulnerable to tobacco advertising and targeted products. Even though the landmark 1998 Master Settlement Agreement drastically restricted the way tobacco can be marketed, one-third of the top grossing children’s movies in 2010 contained images of smoking, according to the report.
"Far too many kids still see smoking images and messages every day that normalize this dependence," said Dr. Howard Koh, assistant secretary for health in the Health and Human Services department. "Kids see smoking in the movies they watch, the video games they play, the websites they visit, and in the communities where they live."
Physician organizations voiced support of the report and recommended that it be used to help protect young people from using tobacco products.
"As pediatricians, and parents, we need to send a clear message to the studios that this must stop now," Dr. Robert W. Block, AAP president, said in a statement. Dr. Block added that the Surgeon General’s report should be used to help overturn a recent federal court decision that called graphic cigarette warning labels unconstitutional.
"Warning labels play a critical role in educating children, teens, and parents about the negative health impacts of tobacco. By ignoring health harms from tobacco, we are not only sustaining incredible costs in health care, but we are also risking the lives of youth and young adults. This is simply irresponsible," he said.
"If we can just get [young people] to remain smoke free until they’re 26, then less than 1% of them will ever start."
In a statement, Dr. Jack Lewin, chief executive officer of the American College of Cardiology said, "the Surgeon General’s decision to reinvigorate efforts to keep children and young adults from smoking and to encourage smoking cessation will help us continue downward the trend of mortality due to heart disease and save millions in spending on health care."
The American Medical Association called for better funding of smoking cessation programs. The AMA "is concerned that these smokers will not get the support and assistance needed to combat their addiction," Dr. Peter Carmel, the association’s president, said in a statement. "Increasing the price of tobacco and adopting comprehensive smoke-free laws throughout the entire nation would also help reduce the health, social, and economic consequences associated with tobacco use among our youth."
The American Heart Association called the report a wake-up call. "This insightful new report makes it clear that we cannot let our guard down for a minute when it comes to tobacco addiction," CEO Nancy Brown said in a statement. While many Americans may think tobacco use is fading away, the evidence in this report tells a dramatically different story."
Approximately 3,800 children smoke their first cigarette every day and the rates of tobacco initiation are no longer declining, according to the Surgeon General’s report, "Preventing Tobacco Use Among Youth and Young Adults."
"Every day, 1,200 Americans die from smoking and each of those people are replaced by two young smokers," Surgeon General Regina Benjamin said at a press conference. "We know that prevention is the key ... If we can just get [young people] to remain smoke free until they’re 26, then less than 1% of them will ever start."
Among adults who smoke daily, 88% smoked their first cigarette before their 18th birthday; nearly all (99%) did so before their 26th.
According to the report, nearly 25% of high school seniors are current smokers, compared with about 33% of young adults, and about 20% of adults. And it’s not all cigarettes: About 1 in 10 male high school seniors currently uses smokeless tobacco and about 1 in 5 smokes cigars, according to the report.
The report, which updates the 1994 Surgeon General report on tobacco use in youth, highlights the immediate and long-term health consequences to which children and young adults are most vulnerable. These include cardiovascular damage, reduced lung function and growth, and risk of chronic obstructive pulmonary disease.
Because they’re impressionable, young adults and children also are vulnerable to tobacco advertising and targeted products. Even though the landmark 1998 Master Settlement Agreement drastically restricted the way tobacco can be marketed, one-third of the top grossing children’s movies in 2010 contained images of smoking, according to the report.
"Far too many kids still see smoking images and messages every day that normalize this dependence," said Dr. Howard Koh, assistant secretary for health in the Health and Human Services department. "Kids see smoking in the movies they watch, the video games they play, the websites they visit, and in the communities where they live."
Physician organizations voiced support of the report and recommended that it be used to help protect young people from using tobacco products.
"As pediatricians, and parents, we need to send a clear message to the studios that this must stop now," Dr. Robert W. Block, AAP president, said in a statement. Dr. Block added that the Surgeon General’s report should be used to help overturn a recent federal court decision that called graphic cigarette warning labels unconstitutional.
"Warning labels play a critical role in educating children, teens, and parents about the negative health impacts of tobacco. By ignoring health harms from tobacco, we are not only sustaining incredible costs in health care, but we are also risking the lives of youth and young adults. This is simply irresponsible," he said.
"If we can just get [young people] to remain smoke free until they’re 26, then less than 1% of them will ever start."
In a statement, Dr. Jack Lewin, chief executive officer of the American College of Cardiology said, "the Surgeon General’s decision to reinvigorate efforts to keep children and young adults from smoking and to encourage smoking cessation will help us continue downward the trend of mortality due to heart disease and save millions in spending on health care."
The American Medical Association called for better funding of smoking cessation programs. The AMA "is concerned that these smokers will not get the support and assistance needed to combat their addiction," Dr. Peter Carmel, the association’s president, said in a statement. "Increasing the price of tobacco and adopting comprehensive smoke-free laws throughout the entire nation would also help reduce the health, social, and economic consequences associated with tobacco use among our youth."
The American Heart Association called the report a wake-up call. "This insightful new report makes it clear that we cannot let our guard down for a minute when it comes to tobacco addiction," CEO Nancy Brown said in a statement. While many Americans may think tobacco use is fading away, the evidence in this report tells a dramatically different story."
Asthma Meds: Men Prefer to Inhale, Women to Take Pills
ORLANDO – Men may be more adherent than women are in their use of asthma controller medications, but adherence overall is poor, according to an analysis of claims from a large database.
Older adults were also more adherent than were younger adults in the retrospective cohort study, which included medical and pharmacy claims for 145,950 patients aged 18-65 years who were seen from January 2006 to December 2008.
To be included, patients included had to have 12 months or more of continuous medical and pharmacy eligibility following the index date (6 months after first medical claim for asthma), said Leslie J. Hinyard, Ph.D. at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Mean age at enrollment was 41 years for the 53,532 men, and 43 years for the 92,418 women. Adherence was defined by the Medication Possession Ratio (MPR), calculated as the number of days for which the medication is supplied divided by the number of days from first fill through the end of study eligibility.
Overall adherence, stratified by gender, ranged from a low MPR of 0.246 for inhaled corticosteroid use among women to a high of 0.597 for omalizumab use in women.
"I was actually surprised by how poor adherence was across the board. It’s actually consistent with what you find throughout the literature; but the adherence to what should be medicines taken daily over a long period of time is rather poor," said Dr. Hinyard, who is with the St. Louis University Center for Outcomes Research and also the university’s department of internal medicine, division of allergy.
Men had significantly greater adherence than did women for inhaled corticosteroid (MPR, 0.259 vs. 0.246), long-acting beta-agonists (0.384 vs. 0.345), combinations of the two (0.388 vs. 0.352), and for mast cell–stabilizing agents (0.238 vs. 0.205). On the other hand, women were significantly more adherent than men were for leukotriene modifiers (0.499 vs. 0.472).
"I was intrigued by the fact that, across the board, men seemed to have slightly higher adherence than women, except for leukotriene modifiers, which are pills. The rest are all inhaled," Dr. Hinyard said in an interview.
She noted that the explanation could be that women are more accustomed than are men to taking pills, rather than that men are more apt to use inhalers. However, she emphasized, "I’m completely speculating."
There was no statistically significant difference between men and women for oral steroid use, monoclonal antibodies, or theophylline.
Examined by age tertiles of 18-34 years, 35-49 years, and 50-65 years, there was a positive linear association between age and adherence for all drug categories except for chronic oral steroids.
For example, with inhaled corticosteroids, 45% of those aged 50-65 years fell into the top tertile for adherence, compared with 16% of the 18- to 34-year-olds. "Older adults were more adherent, especially compared to the younger adults," she noted.
"We need to understand if there’s a minimal threshold for adherence that will keep people from having exacerbations," Dr. Hinyard said. "We’re never going to get perfect adherence, but perhaps we can set a more realistic goal for people to strive for."
Dr. Hinyard had no relevant disclosures.
ORLANDO – Men may be more adherent than women are in their use of asthma controller medications, but adherence overall is poor, according to an analysis of claims from a large database.
Older adults were also more adherent than were younger adults in the retrospective cohort study, which included medical and pharmacy claims for 145,950 patients aged 18-65 years who were seen from January 2006 to December 2008.
To be included, patients included had to have 12 months or more of continuous medical and pharmacy eligibility following the index date (6 months after first medical claim for asthma), said Leslie J. Hinyard, Ph.D. at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Mean age at enrollment was 41 years for the 53,532 men, and 43 years for the 92,418 women. Adherence was defined by the Medication Possession Ratio (MPR), calculated as the number of days for which the medication is supplied divided by the number of days from first fill through the end of study eligibility.
Overall adherence, stratified by gender, ranged from a low MPR of 0.246 for inhaled corticosteroid use among women to a high of 0.597 for omalizumab use in women.
"I was actually surprised by how poor adherence was across the board. It’s actually consistent with what you find throughout the literature; but the adherence to what should be medicines taken daily over a long period of time is rather poor," said Dr. Hinyard, who is with the St. Louis University Center for Outcomes Research and also the university’s department of internal medicine, division of allergy.
Men had significantly greater adherence than did women for inhaled corticosteroid (MPR, 0.259 vs. 0.246), long-acting beta-agonists (0.384 vs. 0.345), combinations of the two (0.388 vs. 0.352), and for mast cell–stabilizing agents (0.238 vs. 0.205). On the other hand, women were significantly more adherent than men were for leukotriene modifiers (0.499 vs. 0.472).
"I was intrigued by the fact that, across the board, men seemed to have slightly higher adherence than women, except for leukotriene modifiers, which are pills. The rest are all inhaled," Dr. Hinyard said in an interview.
She noted that the explanation could be that women are more accustomed than are men to taking pills, rather than that men are more apt to use inhalers. However, she emphasized, "I’m completely speculating."
There was no statistically significant difference between men and women for oral steroid use, monoclonal antibodies, or theophylline.
Examined by age tertiles of 18-34 years, 35-49 years, and 50-65 years, there was a positive linear association between age and adherence for all drug categories except for chronic oral steroids.
For example, with inhaled corticosteroids, 45% of those aged 50-65 years fell into the top tertile for adherence, compared with 16% of the 18- to 34-year-olds. "Older adults were more adherent, especially compared to the younger adults," she noted.
"We need to understand if there’s a minimal threshold for adherence that will keep people from having exacerbations," Dr. Hinyard said. "We’re never going to get perfect adherence, but perhaps we can set a more realistic goal for people to strive for."
Dr. Hinyard had no relevant disclosures.
ORLANDO – Men may be more adherent than women are in their use of asthma controller medications, but adherence overall is poor, according to an analysis of claims from a large database.
Older adults were also more adherent than were younger adults in the retrospective cohort study, which included medical and pharmacy claims for 145,950 patients aged 18-65 years who were seen from January 2006 to December 2008.
To be included, patients included had to have 12 months or more of continuous medical and pharmacy eligibility following the index date (6 months after first medical claim for asthma), said Leslie J. Hinyard, Ph.D. at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Mean age at enrollment was 41 years for the 53,532 men, and 43 years for the 92,418 women. Adherence was defined by the Medication Possession Ratio (MPR), calculated as the number of days for which the medication is supplied divided by the number of days from first fill through the end of study eligibility.
Overall adherence, stratified by gender, ranged from a low MPR of 0.246 for inhaled corticosteroid use among women to a high of 0.597 for omalizumab use in women.
"I was actually surprised by how poor adherence was across the board. It’s actually consistent with what you find throughout the literature; but the adherence to what should be medicines taken daily over a long period of time is rather poor," said Dr. Hinyard, who is with the St. Louis University Center for Outcomes Research and also the university’s department of internal medicine, division of allergy.
Men had significantly greater adherence than did women for inhaled corticosteroid (MPR, 0.259 vs. 0.246), long-acting beta-agonists (0.384 vs. 0.345), combinations of the two (0.388 vs. 0.352), and for mast cell–stabilizing agents (0.238 vs. 0.205). On the other hand, women were significantly more adherent than men were for leukotriene modifiers (0.499 vs. 0.472).
"I was intrigued by the fact that, across the board, men seemed to have slightly higher adherence than women, except for leukotriene modifiers, which are pills. The rest are all inhaled," Dr. Hinyard said in an interview.
She noted that the explanation could be that women are more accustomed than are men to taking pills, rather than that men are more apt to use inhalers. However, she emphasized, "I’m completely speculating."
There was no statistically significant difference between men and women for oral steroid use, monoclonal antibodies, or theophylline.
Examined by age tertiles of 18-34 years, 35-49 years, and 50-65 years, there was a positive linear association between age and adherence for all drug categories except for chronic oral steroids.
For example, with inhaled corticosteroids, 45% of those aged 50-65 years fell into the top tertile for adherence, compared with 16% of the 18- to 34-year-olds. "Older adults were more adherent, especially compared to the younger adults," she noted.
"We need to understand if there’s a minimal threshold for adherence that will keep people from having exacerbations," Dr. Hinyard said. "We’re never going to get perfect adherence, but perhaps we can set a more realistic goal for people to strive for."
Dr. Hinyard had no relevant disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF ALLERGY, ASTHMA, AND IMMUNOLOGY
Asthma Guidelines Are Not Always Followed
ORLANDO – The 2007 National Asthma Education and Prevention Program guidelines are viewed as cumbersome and too time-consuming by some primary care physicians caring for children.
That finding, from a 23-question survey sent to 80 pediatricians, suggests that "there is room for improvement. I think the allergist can play a big role in helping co-manage severe asthmatic patients," Dr. Nabeel Farooqui of Ohio State University and Nationwide Children’s Hospital, Columbus, Ohio, said in an interview at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The Expert Panel Report 3 (EPR3): Guidelines for the Diagnosis and Management of Asthma, published by the National Heart, Lung, and Blood Institute, recommend referral to an asthma subspecialist for patients with difficult-to-manage moderate to severe persistent asthma, when a diagnosis is in question, or for patients who need additional testing. Such a subspecialist could be either an allergist or a pulmonologist, but only the allergist can do an allergy assessment, Dr. Farooqui noted.
"Many children with asthma also have allergic rhinitis. These children should be skin-tested. Allergists can help diagnose and treat some of the allergic comorbidities associated with asthma such as allergic rhinitis, and thereby get better control of the asthma," he said.
Of the 28 pediatricians who responded to the anonymous survey, 13 (46%) said that they "always" follow the NAEPP EPR 3 guidelines. Another 8 (29%) said they follow the guidelines "most of the time." Among those who didn’t always follow the guidelines, the most common reason, given by 11 respondents (39% of the total), was that they are "too cumbersome."
Nearly two-thirds of the respondents (17) reported always initiating inhaled steroids for patients with persistent asthma, whereas the other 11 expressed at least some hesitation. "Concern about nonadherence" to inhaled steroids was listed most often as the reason.
Just 15 of the 28 respondents (54%) reported reviewing a written asthma action plan with their patients at every visit as recommended, whereas another 12 (43%) did so only when they made a change in the patient’s care. Lack of time was listed by eight respondents as the reason not to review the plan at every visit, while another six said they did not think that such plans improve management or outcomes.
While all of the respondents endorsed influenza immunization for all asthma patients, nine mistakenly believed that egg allergy is a contraindication to receipt of the vaccine. (The contraindication was lifted in June 2011.)
While all but one respondent said that they refer difficult-to-manage asthma patients to subspecialists, only half referred for additional testing and less than half for a questionable diagnosis. The majority (69%) refer to pulmonologists, while the other 31% referred patients to both a pulmonologist and an allergist/immunologist. "The only time referral to allergist is made is when the patient is sent to pulmonary as well," Dr. Farooqui commented.
"Lack of timely appointment" was the most common reason given for not referring to a subspecialist.
For patients with well-controlled asthma who are on a daily controller medication, half of the respondents endorsed the recommended evaluation at 3-6 months for consideration of step-down therapy. However, the other half reported waiting a year or never stepping down therapy.
"Allergists should continue to promote their role, both in the community and academic centers, as specialists in the evaluation and management of asthma," Dr. Farooqui advised his colleagues.
Dr. Farooqui said he had no relevant financial disclosures.
ORLANDO – The 2007 National Asthma Education and Prevention Program guidelines are viewed as cumbersome and too time-consuming by some primary care physicians caring for children.
That finding, from a 23-question survey sent to 80 pediatricians, suggests that "there is room for improvement. I think the allergist can play a big role in helping co-manage severe asthmatic patients," Dr. Nabeel Farooqui of Ohio State University and Nationwide Children’s Hospital, Columbus, Ohio, said in an interview at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The Expert Panel Report 3 (EPR3): Guidelines for the Diagnosis and Management of Asthma, published by the National Heart, Lung, and Blood Institute, recommend referral to an asthma subspecialist for patients with difficult-to-manage moderate to severe persistent asthma, when a diagnosis is in question, or for patients who need additional testing. Such a subspecialist could be either an allergist or a pulmonologist, but only the allergist can do an allergy assessment, Dr. Farooqui noted.
"Many children with asthma also have allergic rhinitis. These children should be skin-tested. Allergists can help diagnose and treat some of the allergic comorbidities associated with asthma such as allergic rhinitis, and thereby get better control of the asthma," he said.
Of the 28 pediatricians who responded to the anonymous survey, 13 (46%) said that they "always" follow the NAEPP EPR 3 guidelines. Another 8 (29%) said they follow the guidelines "most of the time." Among those who didn’t always follow the guidelines, the most common reason, given by 11 respondents (39% of the total), was that they are "too cumbersome."
Nearly two-thirds of the respondents (17) reported always initiating inhaled steroids for patients with persistent asthma, whereas the other 11 expressed at least some hesitation. "Concern about nonadherence" to inhaled steroids was listed most often as the reason.
Just 15 of the 28 respondents (54%) reported reviewing a written asthma action plan with their patients at every visit as recommended, whereas another 12 (43%) did so only when they made a change in the patient’s care. Lack of time was listed by eight respondents as the reason not to review the plan at every visit, while another six said they did not think that such plans improve management or outcomes.
While all of the respondents endorsed influenza immunization for all asthma patients, nine mistakenly believed that egg allergy is a contraindication to receipt of the vaccine. (The contraindication was lifted in June 2011.)
While all but one respondent said that they refer difficult-to-manage asthma patients to subspecialists, only half referred for additional testing and less than half for a questionable diagnosis. The majority (69%) refer to pulmonologists, while the other 31% referred patients to both a pulmonologist and an allergist/immunologist. "The only time referral to allergist is made is when the patient is sent to pulmonary as well," Dr. Farooqui commented.
"Lack of timely appointment" was the most common reason given for not referring to a subspecialist.
For patients with well-controlled asthma who are on a daily controller medication, half of the respondents endorsed the recommended evaluation at 3-6 months for consideration of step-down therapy. However, the other half reported waiting a year or never stepping down therapy.
"Allergists should continue to promote their role, both in the community and academic centers, as specialists in the evaluation and management of asthma," Dr. Farooqui advised his colleagues.
Dr. Farooqui said he had no relevant financial disclosures.
ORLANDO – The 2007 National Asthma Education and Prevention Program guidelines are viewed as cumbersome and too time-consuming by some primary care physicians caring for children.
That finding, from a 23-question survey sent to 80 pediatricians, suggests that "there is room for improvement. I think the allergist can play a big role in helping co-manage severe asthmatic patients," Dr. Nabeel Farooqui of Ohio State University and Nationwide Children’s Hospital, Columbus, Ohio, said in an interview at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The Expert Panel Report 3 (EPR3): Guidelines for the Diagnosis and Management of Asthma, published by the National Heart, Lung, and Blood Institute, recommend referral to an asthma subspecialist for patients with difficult-to-manage moderate to severe persistent asthma, when a diagnosis is in question, or for patients who need additional testing. Such a subspecialist could be either an allergist or a pulmonologist, but only the allergist can do an allergy assessment, Dr. Farooqui noted.
"Many children with asthma also have allergic rhinitis. These children should be skin-tested. Allergists can help diagnose and treat some of the allergic comorbidities associated with asthma such as allergic rhinitis, and thereby get better control of the asthma," he said.
Of the 28 pediatricians who responded to the anonymous survey, 13 (46%) said that they "always" follow the NAEPP EPR 3 guidelines. Another 8 (29%) said they follow the guidelines "most of the time." Among those who didn’t always follow the guidelines, the most common reason, given by 11 respondents (39% of the total), was that they are "too cumbersome."
Nearly two-thirds of the respondents (17) reported always initiating inhaled steroids for patients with persistent asthma, whereas the other 11 expressed at least some hesitation. "Concern about nonadherence" to inhaled steroids was listed most often as the reason.
Just 15 of the 28 respondents (54%) reported reviewing a written asthma action plan with their patients at every visit as recommended, whereas another 12 (43%) did so only when they made a change in the patient’s care. Lack of time was listed by eight respondents as the reason not to review the plan at every visit, while another six said they did not think that such plans improve management or outcomes.
While all of the respondents endorsed influenza immunization for all asthma patients, nine mistakenly believed that egg allergy is a contraindication to receipt of the vaccine. (The contraindication was lifted in June 2011.)
While all but one respondent said that they refer difficult-to-manage asthma patients to subspecialists, only half referred for additional testing and less than half for a questionable diagnosis. The majority (69%) refer to pulmonologists, while the other 31% referred patients to both a pulmonologist and an allergist/immunologist. "The only time referral to allergist is made is when the patient is sent to pulmonary as well," Dr. Farooqui commented.
"Lack of timely appointment" was the most common reason given for not referring to a subspecialist.
For patients with well-controlled asthma who are on a daily controller medication, half of the respondents endorsed the recommended evaluation at 3-6 months for consideration of step-down therapy. However, the other half reported waiting a year or never stepping down therapy.
"Allergists should continue to promote their role, both in the community and academic centers, as specialists in the evaluation and management of asthma," Dr. Farooqui advised his colleagues.
Dr. Farooqui said he had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF ALLERGY, ASTHMA, AND IMMUNOLOGY
Major Finding: Forty-six percent of pediatricians responded that they "always" follow the NAEPP EPR 3 guidelines. Another 29% said they follow the guidelines "most of the time." Among those who didn’t always follow the guidelines, the most common reason, given by 11 respondents (39% of the total), was that they are "too cumbersome."
Data Source: These were results of a 23-question survey sent to 80 pediatricians, of whom 28 responded.
Disclosures: Dr. Farooqui said he had no relevant financial disclosures.
Working Out Works Well in Asthma
ORLANDO – People with asthma who engaged in a structured exercise program had sustained quality-of-life improvements, a small study has shown.
Although exercise is often anathema to people with asthma, previously sedentary people with asthma who were randomized in a small study to engage in three exercise sessions per week reported a twofold greater improvement in their symptom-related quality of life, compared with those who did not increase their routine exercise, reported Dr. Thomas Platts-Mills, professor of medicine, allergy, and clinical immunology at the University of Virginia in Charlottesville.

The preliminary study was designed to convince health insurers to fund structured exercise programs in commercial gyms for patients with asthma, Dr. Platts-Mills said.
"You’ve got three obstacles to overcome: one is that the patients think that it’s a problem having to do exercise, because it will make their asthma worse," he noted. "Secondly, the gym may be resistant, because they think they’ll have asthma attacks to deal with; and third, the insurance companies are resistant, period."
The investigators recruited from a local commercial health plan 13 patients with persistent asthma as defined by National Asthma Education and Prevention Program guidelines. The participants were all treated with inhaled corticosteroids (ICS) and leukotriene agents that were on the health plan’s formulary.
All 13 patients were identified as engaging in no or little exercise (fewer than two sessions of aerobic activity per week over the past 6 months). Patients who participated more than 3 hours per week in any kind of moderate-level physical activity were excluded, as were patients with active pulmonary infections, cardiovascular disease, musculoskeletal disease, or other conditions that might impair their ability to exercise.
The authors convinced the insurer to pay a gym to enroll plan members with asthma, and they helped gym staff establish an asthma protocol that included monitoring asthmatics for symptoms and providing access to nebulizers.
"The gyms, we hope, will want to do this, and it’s very much in the insurance company’s favor to do it," Dr. Platts-Mills said. "But it’s still very difficult to get people to do regular exercise."
The seven participants assigned to the exercise group kept an exercise log recording the duration, type, and perceived exertion of all physical activities, including the three assigned exercise sessions each week. They also kept a log of medication use, asthma symptoms, unplanned medical visits, and unplanned asthma-related absences from work or school. Participants also answered a telephone-based asthma quality of life questionnaire at the end of weeks 4, 8, 12 and 16 (the study’s end).
Six participants assigned to be controls were given educational materials on exercise, participated in the telephone survey, and kept logs recording the same information as that of the exercise group. Researchers crossed over those participants to the exercise arm at 4 months.
At week 8, scores on the symptom domain of the quality-of-life questionnaire were significantly higher among exercisers, with 78.3% of responses indicating improvement, compared with 39.5% of responses by participants in the delayed-exercise group (P = .05).
Similarly, on the activity limitations domain, 78.3% of responding exercisers said they saw improvement, compared with 37.2% of delayed exercisers (P = .036). There were trends favoring exercise, but no significant differences, in the emotional function and environmental stimuli domains of the quality-of-life questionnaire.
"We have established that you can get an insurance company to pay a gym to enroll people and establish a protocol in the gym for asthmatics," Dr. Platts-Mills said. "I think this would be far more important for children with asthma if this could be achieved."
The study was supported by Southern Health Services Inc. Dr. Platts-Mills and colleagues reported that they had no conflicts of interest.
ORLANDO – People with asthma who engaged in a structured exercise program had sustained quality-of-life improvements, a small study has shown.
Although exercise is often anathema to people with asthma, previously sedentary people with asthma who were randomized in a small study to engage in three exercise sessions per week reported a twofold greater improvement in their symptom-related quality of life, compared with those who did not increase their routine exercise, reported Dr. Thomas Platts-Mills, professor of medicine, allergy, and clinical immunology at the University of Virginia in Charlottesville.
The preliminary study was designed to convince health insurers to fund structured exercise programs in commercial gyms for patients with asthma, Dr. Platts-Mills said.
"You’ve got three obstacles to overcome: one is that the patients think that it’s a problem having to do exercise, because it will make their asthma worse," he noted. "Secondly, the gym may be resistant, because they think they’ll have asthma attacks to deal with; and third, the insurance companies are resistant, period."
The investigators recruited from a local commercial health plan 13 patients with persistent asthma as defined by National Asthma Education and Prevention Program guidelines. The participants were all treated with inhaled corticosteroids (ICS) and leukotriene agents that were on the health plan’s formulary.
All 13 patients were identified as engaging in no or little exercise (fewer than two sessions of aerobic activity per week over the past 6 months). Patients who participated more than 3 hours per week in any kind of moderate-level physical activity were excluded, as were patients with active pulmonary infections, cardiovascular disease, musculoskeletal disease, or other conditions that might impair their ability to exercise.
The authors convinced the insurer to pay a gym to enroll plan members with asthma, and they helped gym staff establish an asthma protocol that included monitoring asthmatics for symptoms and providing access to nebulizers.
"The gyms, we hope, will want to do this, and it’s very much in the insurance company’s favor to do it," Dr. Platts-Mills said. "But it’s still very difficult to get people to do regular exercise."
The seven participants assigned to the exercise group kept an exercise log recording the duration, type, and perceived exertion of all physical activities, including the three assigned exercise sessions each week. They also kept a log of medication use, asthma symptoms, unplanned medical visits, and unplanned asthma-related absences from work or school. Participants also answered a telephone-based asthma quality of life questionnaire at the end of weeks 4, 8, 12 and 16 (the study’s end).
Six participants assigned to be controls were given educational materials on exercise, participated in the telephone survey, and kept logs recording the same information as that of the exercise group. Researchers crossed over those participants to the exercise arm at 4 months.
At week 8, scores on the symptom domain of the quality-of-life questionnaire were significantly higher among exercisers, with 78.3% of responses indicating improvement, compared with 39.5% of responses by participants in the delayed-exercise group (P = .05).
Similarly, on the activity limitations domain, 78.3% of responding exercisers said they saw improvement, compared with 37.2% of delayed exercisers (P = .036). There were trends favoring exercise, but no significant differences, in the emotional function and environmental stimuli domains of the quality-of-life questionnaire.
"We have established that you can get an insurance company to pay a gym to enroll people and establish a protocol in the gym for asthmatics," Dr. Platts-Mills said. "I think this would be far more important for children with asthma if this could be achieved."
The study was supported by Southern Health Services Inc. Dr. Platts-Mills and colleagues reported that they had no conflicts of interest.
ORLANDO – People with asthma who engaged in a structured exercise program had sustained quality-of-life improvements, a small study has shown.
Although exercise is often anathema to people with asthma, previously sedentary people with asthma who were randomized in a small study to engage in three exercise sessions per week reported a twofold greater improvement in their symptom-related quality of life, compared with those who did not increase their routine exercise, reported Dr. Thomas Platts-Mills, professor of medicine, allergy, and clinical immunology at the University of Virginia in Charlottesville.
The preliminary study was designed to convince health insurers to fund structured exercise programs in commercial gyms for patients with asthma, Dr. Platts-Mills said.
"You’ve got three obstacles to overcome: one is that the patients think that it’s a problem having to do exercise, because it will make their asthma worse," he noted. "Secondly, the gym may be resistant, because they think they’ll have asthma attacks to deal with; and third, the insurance companies are resistant, period."
The investigators recruited from a local commercial health plan 13 patients with persistent asthma as defined by National Asthma Education and Prevention Program guidelines. The participants were all treated with inhaled corticosteroids (ICS) and leukotriene agents that were on the health plan’s formulary.
All 13 patients were identified as engaging in no or little exercise (fewer than two sessions of aerobic activity per week over the past 6 months). Patients who participated more than 3 hours per week in any kind of moderate-level physical activity were excluded, as were patients with active pulmonary infections, cardiovascular disease, musculoskeletal disease, or other conditions that might impair their ability to exercise.
The authors convinced the insurer to pay a gym to enroll plan members with asthma, and they helped gym staff establish an asthma protocol that included monitoring asthmatics for symptoms and providing access to nebulizers.
"The gyms, we hope, will want to do this, and it’s very much in the insurance company’s favor to do it," Dr. Platts-Mills said. "But it’s still very difficult to get people to do regular exercise."
The seven participants assigned to the exercise group kept an exercise log recording the duration, type, and perceived exertion of all physical activities, including the three assigned exercise sessions each week. They also kept a log of medication use, asthma symptoms, unplanned medical visits, and unplanned asthma-related absences from work or school. Participants also answered a telephone-based asthma quality of life questionnaire at the end of weeks 4, 8, 12 and 16 (the study’s end).
Six participants assigned to be controls were given educational materials on exercise, participated in the telephone survey, and kept logs recording the same information as that of the exercise group. Researchers crossed over those participants to the exercise arm at 4 months.
At week 8, scores on the symptom domain of the quality-of-life questionnaire were significantly higher among exercisers, with 78.3% of responses indicating improvement, compared with 39.5% of responses by participants in the delayed-exercise group (P = .05).
Similarly, on the activity limitations domain, 78.3% of responding exercisers said they saw improvement, compared with 37.2% of delayed exercisers (P = .036). There were trends favoring exercise, but no significant differences, in the emotional function and environmental stimuli domains of the quality-of-life questionnaire.
"We have established that you can get an insurance company to pay a gym to enroll people and establish a protocol in the gym for asthmatics," Dr. Platts-Mills said. "I think this would be far more important for children with asthma if this could be achieved."
The study was supported by Southern Health Services Inc. Dr. Platts-Mills and colleagues reported that they had no conflicts of interest.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF ALLERGY, ASTHMA, AND IMMUNOLOGY
Major Finding: At week 8, scores on the symptom domain of an asthma quality-of-life questionnaire were significantly higher among exercisers, with 78.3% of responses indicating improvement, compared with 39.5% of responses by nonexercising controls (P = .05).
Data Source: This was a randomized study.
Disclosures: The study was supported by Southern Health Services Inc. Dr. Platts-Mills and colleagues reported that they had no conflicts of interest.
Schools Tackle Socioeconomic Gap in Asthma Control
ORLANDO – Adding asthma education to reading, writing, and arithmetic in public schools resulted in significant improvements in asthma control measures among at-risk children, researchers reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Children in the intervention group also had fewer urgent-care visits, suggesting better asthma control, the authors found.
In a pilot study aimed at reducing socioeconomic disparities in asthma control, at-risk children from schools assigned to implement the American Lung Association’s Open Airways for Schools (OAS) program had significantly better activity quality-of-life (QoL) scores and demonstrated significantly greater improvements in the use of metered-dose inhalers (MDI) than did their peers in schools that did not receive the intervention, reported Dr. Summer Monforte, a second-year fellow at National Jewish Health in Denver.
The study’s senior author was Dr. Stanley J. Szefler, head of pediatric clinical pharmacology at National Jewish Health.
The improvement in MDI use is an indicator that such programs can help to improve the health of children who are at risk for poor asthma outcomes, Dr. Monforte said in an interview.
"Every single time a child comes in, you have to make sure that they take their inhaler correctly; so it’s nice when the medicine gets where it’s supposed to go," she said.
The overall asthma prevalence rate in Colorado is 8.5% – but in some inner-city schools, the rate is nearly three times higher (22.8%). School-based asthma-education programs can help children improve their asthma control and avoid or reduce exacerbations, but such programs are not always available in poorer urban districts, the investigators noted.
They conducted a randomized, controlled study to see whether the evidence-based OAS intervention would work in schools where children were at risk for health care disparities. At-risk schools were defined as those in which more than 75% of children qualified for free lunch programs, or those with a greater than 50% Hispanic or African American student population.
Four of the schools (with a total of 49 children with asthma, plus their parents or guardians) were randomized to receive the intervention, and four other schools (total of 43 asthmatic children) were assigned as controls. All participants had a visit at baseline and at 3 months’ follow-up.
The children in the intervention groups attended a 40-minute OAS session once weekly for 6 weeks, while controls received their usual care.
At baseline, children in both groups were evaluated with the Health Risk Assessment instrument. Children in both groups also were assessed at baseline and follow-up with the Asthma Control Test (ACT) or Childhood ACT, asthma history questionnaires, Juniper’s Pediatric Asthma Quality of Life Questionnaire and Caregiver Quality of Life tools, spirometry, and observation and assessment of inhaler technique.
At 3-month follow-up, children in the intervention group had a mean improvement of 0.8 (plus or minus .22) points on the activity subscale of the QoL scale, which is scored from 1 (worst) to 7 (best). In comparison, controls had a mean improvement of only 0.2 (plus or minus 1.7) points (P = .05).
Assessments of MDI technique showed that children in the intervention group improved by a mean of 2.3 points on a 5-point scale, compared with just 0.7 for controls (P less than .0001).
The authors noted that this was a pilot study of short duration, with limited enrollment attributable to insufficient funding.
Nonetheless, the results indicate that a proven intervention "can be implemented with minor modifications in populations, such as the Denver Public Schools, that differ from the population where it was originally developed," the researchers noted in a poster presentation at the meeting.
The Step Up asthma program, a collaboration between National Jewish Health and the Denver Public Schools, was designed based on the needs identified in the pilot study, and is currently in place. The investigators plan to evaluate its ability to improve asthma control over a 5-year period.
GlaxoSmithKline supported the study. Dr. Monforte reported that she had no relevant disclosures.
ORLANDO – Adding asthma education to reading, writing, and arithmetic in public schools resulted in significant improvements in asthma control measures among at-risk children, researchers reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Children in the intervention group also had fewer urgent-care visits, suggesting better asthma control, the authors found.
In a pilot study aimed at reducing socioeconomic disparities in asthma control, at-risk children from schools assigned to implement the American Lung Association’s Open Airways for Schools (OAS) program had significantly better activity quality-of-life (QoL) scores and demonstrated significantly greater improvements in the use of metered-dose inhalers (MDI) than did their peers in schools that did not receive the intervention, reported Dr. Summer Monforte, a second-year fellow at National Jewish Health in Denver.
The study’s senior author was Dr. Stanley J. Szefler, head of pediatric clinical pharmacology at National Jewish Health.
The improvement in MDI use is an indicator that such programs can help to improve the health of children who are at risk for poor asthma outcomes, Dr. Monforte said in an interview.
"Every single time a child comes in, you have to make sure that they take their inhaler correctly; so it’s nice when the medicine gets where it’s supposed to go," she said.
The overall asthma prevalence rate in Colorado is 8.5% – but in some inner-city schools, the rate is nearly three times higher (22.8%). School-based asthma-education programs can help children improve their asthma control and avoid or reduce exacerbations, but such programs are not always available in poorer urban districts, the investigators noted.
They conducted a randomized, controlled study to see whether the evidence-based OAS intervention would work in schools where children were at risk for health care disparities. At-risk schools were defined as those in which more than 75% of children qualified for free lunch programs, or those with a greater than 50% Hispanic or African American student population.
Four of the schools (with a total of 49 children with asthma, plus their parents or guardians) were randomized to receive the intervention, and four other schools (total of 43 asthmatic children) were assigned as controls. All participants had a visit at baseline and at 3 months’ follow-up.
The children in the intervention groups attended a 40-minute OAS session once weekly for 6 weeks, while controls received their usual care.
At baseline, children in both groups were evaluated with the Health Risk Assessment instrument. Children in both groups also were assessed at baseline and follow-up with the Asthma Control Test (ACT) or Childhood ACT, asthma history questionnaires, Juniper’s Pediatric Asthma Quality of Life Questionnaire and Caregiver Quality of Life tools, spirometry, and observation and assessment of inhaler technique.
At 3-month follow-up, children in the intervention group had a mean improvement of 0.8 (plus or minus .22) points on the activity subscale of the QoL scale, which is scored from 1 (worst) to 7 (best). In comparison, controls had a mean improvement of only 0.2 (plus or minus 1.7) points (P = .05).
Assessments of MDI technique showed that children in the intervention group improved by a mean of 2.3 points on a 5-point scale, compared with just 0.7 for controls (P less than .0001).
The authors noted that this was a pilot study of short duration, with limited enrollment attributable to insufficient funding.
Nonetheless, the results indicate that a proven intervention "can be implemented with minor modifications in populations, such as the Denver Public Schools, that differ from the population where it was originally developed," the researchers noted in a poster presentation at the meeting.
The Step Up asthma program, a collaboration between National Jewish Health and the Denver Public Schools, was designed based on the needs identified in the pilot study, and is currently in place. The investigators plan to evaluate its ability to improve asthma control over a 5-year period.
GlaxoSmithKline supported the study. Dr. Monforte reported that she had no relevant disclosures.
ORLANDO – Adding asthma education to reading, writing, and arithmetic in public schools resulted in significant improvements in asthma control measures among at-risk children, researchers reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Children in the intervention group also had fewer urgent-care visits, suggesting better asthma control, the authors found.
In a pilot study aimed at reducing socioeconomic disparities in asthma control, at-risk children from schools assigned to implement the American Lung Association’s Open Airways for Schools (OAS) program had significantly better activity quality-of-life (QoL) scores and demonstrated significantly greater improvements in the use of metered-dose inhalers (MDI) than did their peers in schools that did not receive the intervention, reported Dr. Summer Monforte, a second-year fellow at National Jewish Health in Denver.
The study’s senior author was Dr. Stanley J. Szefler, head of pediatric clinical pharmacology at National Jewish Health.
The improvement in MDI use is an indicator that such programs can help to improve the health of children who are at risk for poor asthma outcomes, Dr. Monforte said in an interview.
"Every single time a child comes in, you have to make sure that they take their inhaler correctly; so it’s nice when the medicine gets where it’s supposed to go," she said.
The overall asthma prevalence rate in Colorado is 8.5% – but in some inner-city schools, the rate is nearly three times higher (22.8%). School-based asthma-education programs can help children improve their asthma control and avoid or reduce exacerbations, but such programs are not always available in poorer urban districts, the investigators noted.
They conducted a randomized, controlled study to see whether the evidence-based OAS intervention would work in schools where children were at risk for health care disparities. At-risk schools were defined as those in which more than 75% of children qualified for free lunch programs, or those with a greater than 50% Hispanic or African American student population.
Four of the schools (with a total of 49 children with asthma, plus their parents or guardians) were randomized to receive the intervention, and four other schools (total of 43 asthmatic children) were assigned as controls. All participants had a visit at baseline and at 3 months’ follow-up.
The children in the intervention groups attended a 40-minute OAS session once weekly for 6 weeks, while controls received their usual care.
At baseline, children in both groups were evaluated with the Health Risk Assessment instrument. Children in both groups also were assessed at baseline and follow-up with the Asthma Control Test (ACT) or Childhood ACT, asthma history questionnaires, Juniper’s Pediatric Asthma Quality of Life Questionnaire and Caregiver Quality of Life tools, spirometry, and observation and assessment of inhaler technique.
At 3-month follow-up, children in the intervention group had a mean improvement of 0.8 (plus or minus .22) points on the activity subscale of the QoL scale, which is scored from 1 (worst) to 7 (best). In comparison, controls had a mean improvement of only 0.2 (plus or minus 1.7) points (P = .05).
Assessments of MDI technique showed that children in the intervention group improved by a mean of 2.3 points on a 5-point scale, compared with just 0.7 for controls (P less than .0001).
The authors noted that this was a pilot study of short duration, with limited enrollment attributable to insufficient funding.
Nonetheless, the results indicate that a proven intervention "can be implemented with minor modifications in populations, such as the Denver Public Schools, that differ from the population where it was originally developed," the researchers noted in a poster presentation at the meeting.
The Step Up asthma program, a collaboration between National Jewish Health and the Denver Public Schools, was designed based on the needs identified in the pilot study, and is currently in place. The investigators plan to evaluate its ability to improve asthma control over a 5-year period.
GlaxoSmithKline supported the study. Dr. Monforte reported that she had no relevant disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF ALLERGY, ASTHMA, AND IMMUNOLOGY
Major Finding: Children assigned to a school-based asthma education program had significant improvements compared with controls in activity-related quality of life scores (0.8 vs. 0.2 on a 7-point scale, P = .05), and in metered-dose inhaler use (2.3 vs. 0.7 points on a 5-point scale, P less than .0001)
Data Source: This was a randomized, controlled study of an asthma education program.
Disclosures: The study was supported by GlaxoSmithKline. Dr. Monforte reported that she had no relevant disclosures.
Repeat BAL Advised With Prolonged Therapy for Ventilator-Associated Pneumonia
HOUSTON – Repeat bronchoalveolar lavage should be considered for tailoring the duration of antibiotic therapy and for reassessing resistance profiles in patients with ventilator-associated pneumonia from infection with non–lactose fermenting gram-negative bacilli.
New clinical evidence endorses prolonged antibiotic therapy in these patients. Importantly, the findings also indicate that these patients have persistent primary infections, rather than recurrent infections, as has been previously suggested, Dr. Gina R. Shirah reported at Annual Congress of the Society for Critical Care Medicine.
The distinction between persistent and recurrent infection is important, she emphasized, as the former may signal drug resistance in some patients. For this reason, repeat bronchoalveolar lavage (BAL) should be considered during therapy, both to tailor duration of antibiotics and reassess for changes in resistance profiles.
The American Thoracic Society recommends an 8-day antimicrobial treatment protocol for ventilator-associated pneumonia (VAP) but advises a longer course of therapy in patients with non–lactose fermenting gram-negative rods (NLF-GNR), which include Pseudomonas aeruginosa, Acinetobacter baumannii, and Stenotrophomonas maltophilia (Am. J. Respir. Crit. Care Med. 2005;171:388-416). The recommendation is based on the findings of a pioneering randomized study by the PneumA Trial Group that showed 8-day treatment to be as effective as 15-day treatment except in a subgroup of patients with NLF-GNR, in whom they observed higher recurrence rates (JAMA 2003;290:2588-98).
Dr. Shirah and her fellow researchers at the Maricopa Integrated Health System in Phoenix, including lead investigator Dr. Tammy Kopelman, conducted a study that indicates 8-day antibiotic regimens were associated with persistent primary infections, not recurrent infections, in patients with gram-negative bacilli.
The researchers retrospectively studied patients at a level I trauma center admitted over a 4½-year time period. They examined data for all ventilator-associated pneumonia patients who were diagnosed via bronchoalveolar lavage – and who underwent subsequent BAL during the antimicrobial treatment course. Based upon initial BAL pathogen, the patients were classified into two groups: those with NLF-GNR and those with all other pathogens, including Enterobacteriaceae, methicillin-resistant Staphylococcus aureus, and community-acquired Haemophilus spp, methicillin-sensitive S. aureus, and Streptococcus spp. They were then further divided based on whether the repeat BAL was conducted within fewer than 8 days of appropriate antibiotic therapy or at day 8 or later, Dr. Shirah said. "Persistent primary infection was defined as a less than 2-log 10 decrease of the initial species on subsequent bronchoalveolar lavage," she explained.
Of the 77 surgical intensive care unit patients who met the study criteria, 99% received appropriate empiric therapy, said Dr. Shirah. The average subsequent BAL performance was on day 7 (range, 3-14 days), with 37 patients undergoing the procedure after 8 days of therapy; of those, 13 patients were in the NLF-GNR group. Within that group, persistent primary infection after more than 8 days of appropriate antimicrobial therapy was reported in nine of the patients (69%) – seven with P. aeruginosa and two with A. baumannii.
By comparison, only two patients in the second group (8%) – both with Enterobacteriaceae – had evidence of persistent primary infection, representing a statistically significant difference, she said. "Importantly, in the [NLF-GNB] group, 56% of the pathogens obtained on repeat BAL remained sensitive to the treatment antibiotics, so nearly half of the patients required alternative antibiotic treatment."
The investigators also sought to determine whether persistent infection could have been predicted. They separated patients into three groups based on treatment status: treated (microbiologic cure on subsequent BAL); persistently infected antimicrobial sensitive; and persistently infected antimicrobial resistant. A comparison of clinical parameters across the groups showed that although there was some variation in white blood cell count, temperature, and ventilator needs "none of the differences were statistically significant," and thus not predictive of short-course treatment success or persistent infection, Dr. Shirah said.
The data strongly support the conclusion that a shortened course of antibiotics in patients with VAP caused by NLF-GNR will frequently lead to a persistent primary infection, said Dr. Shirah, noting that, in the case of NLF-GNR, "changes in antibiotic profiles are common and without reliable clinical indicators." For this reason, she stressed, repeat BAL should be considered during therapy, both to tailor duration of antibiotics and to reassess for changes in resistance profiles.
"Eight days is simply not enough," Dr. Shirah said.
On behalf of her coinvestigators and herself, Dr. Shirah reported no conflicts of interest with respect to this study.
HOUSTON – Repeat bronchoalveolar lavage should be considered for tailoring the duration of antibiotic therapy and for reassessing resistance profiles in patients with ventilator-associated pneumonia from infection with non–lactose fermenting gram-negative bacilli.
New clinical evidence endorses prolonged antibiotic therapy in these patients. Importantly, the findings also indicate that these patients have persistent primary infections, rather than recurrent infections, as has been previously suggested, Dr. Gina R. Shirah reported at Annual Congress of the Society for Critical Care Medicine.
The distinction between persistent and recurrent infection is important, she emphasized, as the former may signal drug resistance in some patients. For this reason, repeat bronchoalveolar lavage (BAL) should be considered during therapy, both to tailor duration of antibiotics and reassess for changes in resistance profiles.
The American Thoracic Society recommends an 8-day antimicrobial treatment protocol for ventilator-associated pneumonia (VAP) but advises a longer course of therapy in patients with non–lactose fermenting gram-negative rods (NLF-GNR), which include Pseudomonas aeruginosa, Acinetobacter baumannii, and Stenotrophomonas maltophilia (Am. J. Respir. Crit. Care Med. 2005;171:388-416). The recommendation is based on the findings of a pioneering randomized study by the PneumA Trial Group that showed 8-day treatment to be as effective as 15-day treatment except in a subgroup of patients with NLF-GNR, in whom they observed higher recurrence rates (JAMA 2003;290:2588-98).
Dr. Shirah and her fellow researchers at the Maricopa Integrated Health System in Phoenix, including lead investigator Dr. Tammy Kopelman, conducted a study that indicates 8-day antibiotic regimens were associated with persistent primary infections, not recurrent infections, in patients with gram-negative bacilli.
The researchers retrospectively studied patients at a level I trauma center admitted over a 4½-year time period. They examined data for all ventilator-associated pneumonia patients who were diagnosed via bronchoalveolar lavage – and who underwent subsequent BAL during the antimicrobial treatment course. Based upon initial BAL pathogen, the patients were classified into two groups: those with NLF-GNR and those with all other pathogens, including Enterobacteriaceae, methicillin-resistant Staphylococcus aureus, and community-acquired Haemophilus spp, methicillin-sensitive S. aureus, and Streptococcus spp. They were then further divided based on whether the repeat BAL was conducted within fewer than 8 days of appropriate antibiotic therapy or at day 8 or later, Dr. Shirah said. "Persistent primary infection was defined as a less than 2-log 10 decrease of the initial species on subsequent bronchoalveolar lavage," she explained.
Of the 77 surgical intensive care unit patients who met the study criteria, 99% received appropriate empiric therapy, said Dr. Shirah. The average subsequent BAL performance was on day 7 (range, 3-14 days), with 37 patients undergoing the procedure after 8 days of therapy; of those, 13 patients were in the NLF-GNR group. Within that group, persistent primary infection after more than 8 days of appropriate antimicrobial therapy was reported in nine of the patients (69%) – seven with P. aeruginosa and two with A. baumannii.
By comparison, only two patients in the second group (8%) – both with Enterobacteriaceae – had evidence of persistent primary infection, representing a statistically significant difference, she said. "Importantly, in the [NLF-GNB] group, 56% of the pathogens obtained on repeat BAL remained sensitive to the treatment antibiotics, so nearly half of the patients required alternative antibiotic treatment."
The investigators also sought to determine whether persistent infection could have been predicted. They separated patients into three groups based on treatment status: treated (microbiologic cure on subsequent BAL); persistently infected antimicrobial sensitive; and persistently infected antimicrobial resistant. A comparison of clinical parameters across the groups showed that although there was some variation in white blood cell count, temperature, and ventilator needs "none of the differences were statistically significant," and thus not predictive of short-course treatment success or persistent infection, Dr. Shirah said.
The data strongly support the conclusion that a shortened course of antibiotics in patients with VAP caused by NLF-GNR will frequently lead to a persistent primary infection, said Dr. Shirah, noting that, in the case of NLF-GNR, "changes in antibiotic profiles are common and without reliable clinical indicators." For this reason, she stressed, repeat BAL should be considered during therapy, both to tailor duration of antibiotics and to reassess for changes in resistance profiles.
"Eight days is simply not enough," Dr. Shirah said.
On behalf of her coinvestigators and herself, Dr. Shirah reported no conflicts of interest with respect to this study.
HOUSTON – Repeat bronchoalveolar lavage should be considered for tailoring the duration of antibiotic therapy and for reassessing resistance profiles in patients with ventilator-associated pneumonia from infection with non–lactose fermenting gram-negative bacilli.
New clinical evidence endorses prolonged antibiotic therapy in these patients. Importantly, the findings also indicate that these patients have persistent primary infections, rather than recurrent infections, as has been previously suggested, Dr. Gina R. Shirah reported at Annual Congress of the Society for Critical Care Medicine.
The distinction between persistent and recurrent infection is important, she emphasized, as the former may signal drug resistance in some patients. For this reason, repeat bronchoalveolar lavage (BAL) should be considered during therapy, both to tailor duration of antibiotics and reassess for changes in resistance profiles.
The American Thoracic Society recommends an 8-day antimicrobial treatment protocol for ventilator-associated pneumonia (VAP) but advises a longer course of therapy in patients with non–lactose fermenting gram-negative rods (NLF-GNR), which include Pseudomonas aeruginosa, Acinetobacter baumannii, and Stenotrophomonas maltophilia (Am. J. Respir. Crit. Care Med. 2005;171:388-416). The recommendation is based on the findings of a pioneering randomized study by the PneumA Trial Group that showed 8-day treatment to be as effective as 15-day treatment except in a subgroup of patients with NLF-GNR, in whom they observed higher recurrence rates (JAMA 2003;290:2588-98).
Dr. Shirah and her fellow researchers at the Maricopa Integrated Health System in Phoenix, including lead investigator Dr. Tammy Kopelman, conducted a study that indicates 8-day antibiotic regimens were associated with persistent primary infections, not recurrent infections, in patients with gram-negative bacilli.
The researchers retrospectively studied patients at a level I trauma center admitted over a 4½-year time period. They examined data for all ventilator-associated pneumonia patients who were diagnosed via bronchoalveolar lavage – and who underwent subsequent BAL during the antimicrobial treatment course. Based upon initial BAL pathogen, the patients were classified into two groups: those with NLF-GNR and those with all other pathogens, including Enterobacteriaceae, methicillin-resistant Staphylococcus aureus, and community-acquired Haemophilus spp, methicillin-sensitive S. aureus, and Streptococcus spp. They were then further divided based on whether the repeat BAL was conducted within fewer than 8 days of appropriate antibiotic therapy or at day 8 or later, Dr. Shirah said. "Persistent primary infection was defined as a less than 2-log 10 decrease of the initial species on subsequent bronchoalveolar lavage," she explained.
Of the 77 surgical intensive care unit patients who met the study criteria, 99% received appropriate empiric therapy, said Dr. Shirah. The average subsequent BAL performance was on day 7 (range, 3-14 days), with 37 patients undergoing the procedure after 8 days of therapy; of those, 13 patients were in the NLF-GNR group. Within that group, persistent primary infection after more than 8 days of appropriate antimicrobial therapy was reported in nine of the patients (69%) – seven with P. aeruginosa and two with A. baumannii.
By comparison, only two patients in the second group (8%) – both with Enterobacteriaceae – had evidence of persistent primary infection, representing a statistically significant difference, she said. "Importantly, in the [NLF-GNB] group, 56% of the pathogens obtained on repeat BAL remained sensitive to the treatment antibiotics, so nearly half of the patients required alternative antibiotic treatment."
The investigators also sought to determine whether persistent infection could have been predicted. They separated patients into three groups based on treatment status: treated (microbiologic cure on subsequent BAL); persistently infected antimicrobial sensitive; and persistently infected antimicrobial resistant. A comparison of clinical parameters across the groups showed that although there was some variation in white blood cell count, temperature, and ventilator needs "none of the differences were statistically significant," and thus not predictive of short-course treatment success or persistent infection, Dr. Shirah said.
The data strongly support the conclusion that a shortened course of antibiotics in patients with VAP caused by NLF-GNR will frequently lead to a persistent primary infection, said Dr. Shirah, noting that, in the case of NLF-GNR, "changes in antibiotic profiles are common and without reliable clinical indicators." For this reason, she stressed, repeat BAL should be considered during therapy, both to tailor duration of antibiotics and to reassess for changes in resistance profiles.
"Eight days is simply not enough," Dr. Shirah said.
On behalf of her coinvestigators and herself, Dr. Shirah reported no conflicts of interest with respect to this study.
FROM THE ANNUAL CONGRESS OF THE SOCIETY FOR CRITICAL CARE MEDICINE
Major Finding: Repeat bronchoalveolar lavage (BAL) of 37 patients after 8 days of appropriate antimicrobial therapy indicated that 69% patients with non–lactose fermenting gram-negative rods had persistent primary infection, compared with 8% patients with all other pathogens.
Data Source: Results came from a retrospective study of 77 patients with BAL-diagnosed ventilator-associated pneumonia who underwent repeat BAL while on antibiotic therapy at a level 1 trauma center.
Disclosures: The investigators reported having no relevant financial disclosures.
Farm Living Linked to Low Asthma Prevalence
ORLANDO – Amish farms appear to be havens of peace and contentment, free from the insults of modern life – including, it appears, inhalant allergies and asthma, researchers reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
A study comparing asthma and allergic rhinitis prevalence among Amish children in the United States with those of Swiss children living both on and off farms shows that asthma prevalence among the Amish is low and similar to that of children living on Swiss farms, lending further support to the hygiene hypothesis of allergy and asthma, said Dr. Mark Holbreich of Allergy & Asthma Consultants in Indianapolis.

Only 8 (5%) of 157 in a sample of Amish children had ever received a diagnosis of asthma, and only 1 (0.6%) had ever been diagnosed with hay fever. Swiss farm children had similarly low prevalence levels, with 202 (6.7%) of 3,006 having ever been diagnosed with asthma, and 94 (3.1%) with allergy. In contrast, 1,218 (11.2%) of 10,912 Swiss non–farm dwelling children had been diagnosed with asthma, and 1,259 (11.6%) had a hay fever diagnosis at some point in their lives.
"This study clearly supports the effect of early farm exposures in reducing allergic sensitization," said Dr. Holbreich.
Although the sample of Amish children was too small to determine whether specific factors were protective in farm dwellers both in the United States and Europe, multivariate analyses from other studies suggest that drinking raw, unpasteurized milk, and child and maternal exposure to large animals (especially cows) during pregnancy may confer immune tolerance on the child, Dr. Holbreich said in an interview.
The investigators chose for their comparison group Swiss children aged 6-12 years enrolled in the phase I GABRIEL study, which looked at genetic and environmental causes of asthma in Europe. A stratified sample of these children had undergone serum specific immunoglobulin E (IgE) testing to inhalant allergens, including house dust mites (Dermatophagoides pteronyssinus), cat, birch, mixed trees, and grasses. The GABRIEL investigators defined atopy as any positive IgE level of 0.7 kU/L or greater.
Dr. Holbreich and his colleagues distributed to the families of Amish school children a modified GABRIEL questionnaire, and invited consenting children to a skin test session at the school. The children were tested for skin-prick response to D. pteronyssinus, D. farinae, grass mix, tree mix, ragweed, cat, horse, and Alternaria. They considered a skin prick test positive if it induced a 3-mm or greater wheal after subtraction of the negative control.
Although the testing methods were different between the groups (skin-prick testing for the Amish children, and IgE for the Swiss children), the investigators are confident that the prevalence results are valid, Dr. Holbreich said.
Dust mites were the common offenders in causing atopy among the Amish children (5.8%), with sensitivity to mixed grasses occurring in 2.9%. In contrast, 20.1% of Swiss farm dwelling children, and 39.8% of children who did not live on farms had grass sensitivity, with dust mite sensitivity coming in second (9.3% and 16.4%, respectively), and with birch being the third most common allergen (80% and 19.6%, respectively).
Asked in the question-and-response portion of his presentation whether helminth infections might play a role in allergic desensitization of the Amish children, Dr. Holbreich noted that the Amish people "live a very traditional lifestyle, but they see doctors, they get all their immunizations, and they’re cleanly, and I’m not aware of data [showing] that Amish get helminth infections, so I don’t think that is a factor."
The study was supported by the St. Vincent Foundation, AAAAI, and the European Commission. Dr. Holbreich reported having no conflicts of interest.
ORLANDO – Amish farms appear to be havens of peace and contentment, free from the insults of modern life – including, it appears, inhalant allergies and asthma, researchers reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
A study comparing asthma and allergic rhinitis prevalence among Amish children in the United States with those of Swiss children living both on and off farms shows that asthma prevalence among the Amish is low and similar to that of children living on Swiss farms, lending further support to the hygiene hypothesis of allergy and asthma, said Dr. Mark Holbreich of Allergy & Asthma Consultants in Indianapolis.
Only 8 (5%) of 157 in a sample of Amish children had ever received a diagnosis of asthma, and only 1 (0.6%) had ever been diagnosed with hay fever. Swiss farm children had similarly low prevalence levels, with 202 (6.7%) of 3,006 having ever been diagnosed with asthma, and 94 (3.1%) with allergy. In contrast, 1,218 (11.2%) of 10,912 Swiss non–farm dwelling children had been diagnosed with asthma, and 1,259 (11.6%) had a hay fever diagnosis at some point in their lives.
"This study clearly supports the effect of early farm exposures in reducing allergic sensitization," said Dr. Holbreich.
Although the sample of Amish children was too small to determine whether specific factors were protective in farm dwellers both in the United States and Europe, multivariate analyses from other studies suggest that drinking raw, unpasteurized milk, and child and maternal exposure to large animals (especially cows) during pregnancy may confer immune tolerance on the child, Dr. Holbreich said in an interview.
The investigators chose for their comparison group Swiss children aged 6-12 years enrolled in the phase I GABRIEL study, which looked at genetic and environmental causes of asthma in Europe. A stratified sample of these children had undergone serum specific immunoglobulin E (IgE) testing to inhalant allergens, including house dust mites (Dermatophagoides pteronyssinus), cat, birch, mixed trees, and grasses. The GABRIEL investigators defined atopy as any positive IgE level of 0.7 kU/L or greater.
Dr. Holbreich and his colleagues distributed to the families of Amish school children a modified GABRIEL questionnaire, and invited consenting children to a skin test session at the school. The children were tested for skin-prick response to D. pteronyssinus, D. farinae, grass mix, tree mix, ragweed, cat, horse, and Alternaria. They considered a skin prick test positive if it induced a 3-mm or greater wheal after subtraction of the negative control.
Although the testing methods were different between the groups (skin-prick testing for the Amish children, and IgE for the Swiss children), the investigators are confident that the prevalence results are valid, Dr. Holbreich said.
Dust mites were the common offenders in causing atopy among the Amish children (5.8%), with sensitivity to mixed grasses occurring in 2.9%. In contrast, 20.1% of Swiss farm dwelling children, and 39.8% of children who did not live on farms had grass sensitivity, with dust mite sensitivity coming in second (9.3% and 16.4%, respectively), and with birch being the third most common allergen (80% and 19.6%, respectively).
Asked in the question-and-response portion of his presentation whether helminth infections might play a role in allergic desensitization of the Amish children, Dr. Holbreich noted that the Amish people "live a very traditional lifestyle, but they see doctors, they get all their immunizations, and they’re cleanly, and I’m not aware of data [showing] that Amish get helminth infections, so I don’t think that is a factor."
The study was supported by the St. Vincent Foundation, AAAAI, and the European Commission. Dr. Holbreich reported having no conflicts of interest.
ORLANDO – Amish farms appear to be havens of peace and contentment, free from the insults of modern life – including, it appears, inhalant allergies and asthma, researchers reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
A study comparing asthma and allergic rhinitis prevalence among Amish children in the United States with those of Swiss children living both on and off farms shows that asthma prevalence among the Amish is low and similar to that of children living on Swiss farms, lending further support to the hygiene hypothesis of allergy and asthma, said Dr. Mark Holbreich of Allergy & Asthma Consultants in Indianapolis.
Only 8 (5%) of 157 in a sample of Amish children had ever received a diagnosis of asthma, and only 1 (0.6%) had ever been diagnosed with hay fever. Swiss farm children had similarly low prevalence levels, with 202 (6.7%) of 3,006 having ever been diagnosed with asthma, and 94 (3.1%) with allergy. In contrast, 1,218 (11.2%) of 10,912 Swiss non–farm dwelling children had been diagnosed with asthma, and 1,259 (11.6%) had a hay fever diagnosis at some point in their lives.
"This study clearly supports the effect of early farm exposures in reducing allergic sensitization," said Dr. Holbreich.
Although the sample of Amish children was too small to determine whether specific factors were protective in farm dwellers both in the United States and Europe, multivariate analyses from other studies suggest that drinking raw, unpasteurized milk, and child and maternal exposure to large animals (especially cows) during pregnancy may confer immune tolerance on the child, Dr. Holbreich said in an interview.
The investigators chose for their comparison group Swiss children aged 6-12 years enrolled in the phase I GABRIEL study, which looked at genetic and environmental causes of asthma in Europe. A stratified sample of these children had undergone serum specific immunoglobulin E (IgE) testing to inhalant allergens, including house dust mites (Dermatophagoides pteronyssinus), cat, birch, mixed trees, and grasses. The GABRIEL investigators defined atopy as any positive IgE level of 0.7 kU/L or greater.
Dr. Holbreich and his colleagues distributed to the families of Amish school children a modified GABRIEL questionnaire, and invited consenting children to a skin test session at the school. The children were tested for skin-prick response to D. pteronyssinus, D. farinae, grass mix, tree mix, ragweed, cat, horse, and Alternaria. They considered a skin prick test positive if it induced a 3-mm or greater wheal after subtraction of the negative control.
Although the testing methods were different between the groups (skin-prick testing for the Amish children, and IgE for the Swiss children), the investigators are confident that the prevalence results are valid, Dr. Holbreich said.
Dust mites were the common offenders in causing atopy among the Amish children (5.8%), with sensitivity to mixed grasses occurring in 2.9%. In contrast, 20.1% of Swiss farm dwelling children, and 39.8% of children who did not live on farms had grass sensitivity, with dust mite sensitivity coming in second (9.3% and 16.4%, respectively), and with birch being the third most common allergen (80% and 19.6%, respectively).
Asked in the question-and-response portion of his presentation whether helminth infections might play a role in allergic desensitization of the Amish children, Dr. Holbreich noted that the Amish people "live a very traditional lifestyle, but they see doctors, they get all their immunizations, and they’re cleanly, and I’m not aware of data [showing] that Amish get helminth infections, so I don’t think that is a factor."
The study was supported by the St. Vincent Foundation, AAAAI, and the European Commission. Dr. Holbreich reported having no conflicts of interest.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF ALLERGY, ASTHMA, AND IMMUNOLOGY
Major Finding: Only 5.2% of a sample of Amish children had ever received a diagnosis of asthma, and only 0.6% had ever been diagnosed with hay fever. The levels were similar to those of Swiss children living on a farm (6.8% and 3.1%, respectively), and much lower than those of Swiss children not living on a farm (11.2% and 11.6%, respectively).
Data Source: This was a comparison cohort study.
Disclosures: The study was supported by the St. Vincent Foundation of Indianapolis, AAAAI, and the European Commission. Dr. Holbreich reported having no conflicts of interest.
A Late and Light Flu Season
The 2011-2012 influenza season is late and likely to be light.
The season only officially began at the end of February, marked by the point at which the third consecutive weekly percent of respiratory specimens testing positive for influenza surpassed 10%. This is the latest start to the U.S. flu season in 24 years. According to the Centers for Disease Control and Prevention, the percentage of respiratory samples testing positive for flu has remained below the 10% mark until February only once before, during the 1987-1988 season.

Clinicians around the country have been seeing essentially no flu among our pediatric patients. But at the same time, we are seeing a prolonged respiratory syncytial virus (RSV) season. Usually we see RSV in the northeast from about December through January, when it’s replaced by flu. This year, RSV has continued through all of February and into March. Because RSV is predominantly a more severe and symptomatic illness in younger children, our population of respiratory illness patients mostly involved visits by children less than 3 years old. Flu, in contrast, results in significant symptomatic illness in all ages of pediatric practice.
The CDC is still recommending that people get vaccinated, but many primary care providers have administered all of the influenza vaccine they ordered months ago. Unless there’s a serious resurgence, it would be unlikely many would order more at this late point in the winter season with spring just around the corner.
We don’t really know why the 1987-1988 season was late, but this time around we have several possible explanations. There was no change in vaccine strains circulating in the 2011-2012 winter season compared to the 2010-2011 season. Since there was no change in influenza strains, patients who were vaccinated last year are still protected this year. In fact, the H1N1 component from the 2009 pandemic has remained the same for three consecutive seasons now, so I think we’re seeing much wider persisting immunity throughout the population.
Add to that patients who missed their vaccine last year but got their flu vaccine this year are protected too, as are patients who were vaccinated last year and this year. The vaccine given this year really boosted their immunity to sky-high levels. Together, it seems we have achieved very high herd immunity. Recall that herd immunity occurs with many vaccines. Herd immunity occurs because vaccinated persons are unable to contract and transmit an infectious disease, so even those who are not vaccinated get protection because there is less circulation of the infectious agent and thereby less transmission (contagion).
There has long been a mistaken belief that immunity to the flu vaccine wanes toward the end of the season. This is not true. The reason that flu vaccines are recommended for annual administration is because the flu strains "drift," resulting in a loss of protection afforded by the vaccine strains included in the previous year’s vaccine. I have been asked by parents whether they should postpone flu vaccination until early winter rather than receive the vaccine in the fall when it becomes available. They think the protection from flu vaccine is short-lived and may not last through the flu season. I explain that there is no need to delay vaccination. Immunity induced by vaccination lasts for years, not months.
A second factor that may be contributing to the late and light flu season could well be the uptake of the influenza vaccine among all pediatric age groups. Since the CDC and American Academy of Pediatrics recommended universal vaccination for all children down to 6 months of age, the number of vaccinated patients has been steadily rising. This too adds to the herd immunity effect. We don’t have national data yet, but our pediatric practice has been purchasing more vaccine each year since 2009. I suspect this is a national trend of increasing use among all pediatric age groups.
A third factor that influences the flu season is the weather – colder weather. We had a mild winter. Influenza is transmitted through respiratory droplets, mainly by sneezes and coughing. When people remain indoors due to colder weather there is more opportunity for sneezing and coughing to result in respiratory virus transmission. With less indoor crowding, we would expect to see less transmission.
The benefits of a light flu season are many. Fewer flu cases result in fewer cases of otitis media. Part of this could be due to the impact of the new 13-valent pneumococcal conjugate vaccine. However, there is ample evidence that kids get ear infections with flu. I think the decline this year in ear infections is due to both factors.
Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Rochester (N.Y.) General Research Institute. He is also a pediatrician at Legacy Pediatrics in Rochester. He said he had no relevant financial disclosures.
The 2011-2012 influenza season is late and likely to be light.
The season only officially began at the end of February, marked by the point at which the third consecutive weekly percent of respiratory specimens testing positive for influenza surpassed 10%. This is the latest start to the U.S. flu season in 24 years. According to the Centers for Disease Control and Prevention, the percentage of respiratory samples testing positive for flu has remained below the 10% mark until February only once before, during the 1987-1988 season.
Clinicians around the country have been seeing essentially no flu among our pediatric patients. But at the same time, we are seeing a prolonged respiratory syncytial virus (RSV) season. Usually we see RSV in the northeast from about December through January, when it’s replaced by flu. This year, RSV has continued through all of February and into March. Because RSV is predominantly a more severe and symptomatic illness in younger children, our population of respiratory illness patients mostly involved visits by children less than 3 years old. Flu, in contrast, results in significant symptomatic illness in all ages of pediatric practice.
The CDC is still recommending that people get vaccinated, but many primary care providers have administered all of the influenza vaccine they ordered months ago. Unless there’s a serious resurgence, it would be unlikely many would order more at this late point in the winter season with spring just around the corner.
We don’t really know why the 1987-1988 season was late, but this time around we have several possible explanations. There was no change in vaccine strains circulating in the 2011-2012 winter season compared to the 2010-2011 season. Since there was no change in influenza strains, patients who were vaccinated last year are still protected this year. In fact, the H1N1 component from the 2009 pandemic has remained the same for three consecutive seasons now, so I think we’re seeing much wider persisting immunity throughout the population.
Add to that patients who missed their vaccine last year but got their flu vaccine this year are protected too, as are patients who were vaccinated last year and this year. The vaccine given this year really boosted their immunity to sky-high levels. Together, it seems we have achieved very high herd immunity. Recall that herd immunity occurs with many vaccines. Herd immunity occurs because vaccinated persons are unable to contract and transmit an infectious disease, so even those who are not vaccinated get protection because there is less circulation of the infectious agent and thereby less transmission (contagion).
There has long been a mistaken belief that immunity to the flu vaccine wanes toward the end of the season. This is not true. The reason that flu vaccines are recommended for annual administration is because the flu strains "drift," resulting in a loss of protection afforded by the vaccine strains included in the previous year’s vaccine. I have been asked by parents whether they should postpone flu vaccination until early winter rather than receive the vaccine in the fall when it becomes available. They think the protection from flu vaccine is short-lived and may not last through the flu season. I explain that there is no need to delay vaccination. Immunity induced by vaccination lasts for years, not months.
A second factor that may be contributing to the late and light flu season could well be the uptake of the influenza vaccine among all pediatric age groups. Since the CDC and American Academy of Pediatrics recommended universal vaccination for all children down to 6 months of age, the number of vaccinated patients has been steadily rising. This too adds to the herd immunity effect. We don’t have national data yet, but our pediatric practice has been purchasing more vaccine each year since 2009. I suspect this is a national trend of increasing use among all pediatric age groups.
A third factor that influences the flu season is the weather – colder weather. We had a mild winter. Influenza is transmitted through respiratory droplets, mainly by sneezes and coughing. When people remain indoors due to colder weather there is more opportunity for sneezing and coughing to result in respiratory virus transmission. With less indoor crowding, we would expect to see less transmission.
The benefits of a light flu season are many. Fewer flu cases result in fewer cases of otitis media. Part of this could be due to the impact of the new 13-valent pneumococcal conjugate vaccine. However, there is ample evidence that kids get ear infections with flu. I think the decline this year in ear infections is due to both factors.
Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Rochester (N.Y.) General Research Institute. He is also a pediatrician at Legacy Pediatrics in Rochester. He said he had no relevant financial disclosures.
The 2011-2012 influenza season is late and likely to be light.
The season only officially began at the end of February, marked by the point at which the third consecutive weekly percent of respiratory specimens testing positive for influenza surpassed 10%. This is the latest start to the U.S. flu season in 24 years. According to the Centers for Disease Control and Prevention, the percentage of respiratory samples testing positive for flu has remained below the 10% mark until February only once before, during the 1987-1988 season.
Clinicians around the country have been seeing essentially no flu among our pediatric patients. But at the same time, we are seeing a prolonged respiratory syncytial virus (RSV) season. Usually we see RSV in the northeast from about December through January, when it’s replaced by flu. This year, RSV has continued through all of February and into March. Because RSV is predominantly a more severe and symptomatic illness in younger children, our population of respiratory illness patients mostly involved visits by children less than 3 years old. Flu, in contrast, results in significant symptomatic illness in all ages of pediatric practice.
The CDC is still recommending that people get vaccinated, but many primary care providers have administered all of the influenza vaccine they ordered months ago. Unless there’s a serious resurgence, it would be unlikely many would order more at this late point in the winter season with spring just around the corner.
We don’t really know why the 1987-1988 season was late, but this time around we have several possible explanations. There was no change in vaccine strains circulating in the 2011-2012 winter season compared to the 2010-2011 season. Since there was no change in influenza strains, patients who were vaccinated last year are still protected this year. In fact, the H1N1 component from the 2009 pandemic has remained the same for three consecutive seasons now, so I think we’re seeing much wider persisting immunity throughout the population.
Add to that patients who missed their vaccine last year but got their flu vaccine this year are protected too, as are patients who were vaccinated last year and this year. The vaccine given this year really boosted their immunity to sky-high levels. Together, it seems we have achieved very high herd immunity. Recall that herd immunity occurs with many vaccines. Herd immunity occurs because vaccinated persons are unable to contract and transmit an infectious disease, so even those who are not vaccinated get protection because there is less circulation of the infectious agent and thereby less transmission (contagion).
There has long been a mistaken belief that immunity to the flu vaccine wanes toward the end of the season. This is not true. The reason that flu vaccines are recommended for annual administration is because the flu strains "drift," resulting in a loss of protection afforded by the vaccine strains included in the previous year’s vaccine. I have been asked by parents whether they should postpone flu vaccination until early winter rather than receive the vaccine in the fall when it becomes available. They think the protection from flu vaccine is short-lived and may not last through the flu season. I explain that there is no need to delay vaccination. Immunity induced by vaccination lasts for years, not months.
A second factor that may be contributing to the late and light flu season could well be the uptake of the influenza vaccine among all pediatric age groups. Since the CDC and American Academy of Pediatrics recommended universal vaccination for all children down to 6 months of age, the number of vaccinated patients has been steadily rising. This too adds to the herd immunity effect. We don’t have national data yet, but our pediatric practice has been purchasing more vaccine each year since 2009. I suspect this is a national trend of increasing use among all pediatric age groups.
A third factor that influences the flu season is the weather – colder weather. We had a mild winter. Influenza is transmitted through respiratory droplets, mainly by sneezes and coughing. When people remain indoors due to colder weather there is more opportunity for sneezing and coughing to result in respiratory virus transmission. With less indoor crowding, we would expect to see less transmission.
The benefits of a light flu season are many. Fewer flu cases result in fewer cases of otitis media. Part of this could be due to the impact of the new 13-valent pneumococcal conjugate vaccine. However, there is ample evidence that kids get ear infections with flu. I think the decline this year in ear infections is due to both factors.
Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Rochester (N.Y.) General Research Institute. He is also a pediatrician at Legacy Pediatrics in Rochester. He said he had no relevant financial disclosures.
Sublingual Pollen Pill Delivered Durable Allergy Relief
ORLANDO – Patients who underwent 3 consecutive years of desensitization to grass pollen with seasonal use of a daily, sublingual pill maintained their reduced level of grass pollen allergy during the following fourth season despite stopping pill treatment, according to results from a study of 432 patients who stayed in the study for 4 years.
The findings provide the first evidence that sublingual desensitization produces allergy disease modification similar to subcutaneous desensitization, Dr. Hans-Jørgen Malling said during a poster presentation March 4 at the meeting.
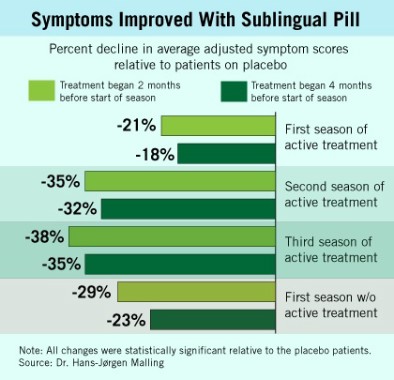
"The data show sustained clinical efficacy when you stop treatment," said Dr. Malling, professor of medicine at the University of Copenhagen and chief of the allergy clinic at Gentofte Hospital in nearby Hellerup. "That is disease modifying. If there is no efficacy after you stop treatment, then this treatment will not be viable."
Although long-term efficacy is crucial, "up to now, it seems like sublingual is equivalent to subcutaneous," he said in an interview.
But Dr. Malling also cautioned that a major test will be the ability of sublingual desensitization to maintain allergy desensitization during a second year off treatment – results that will come during the fifth and final year of the study and will be available a year from now.
Prior reports from the current study documented the ability of the sublingual grass pollen pill to produce desensitization in adult patients during each of the 3 years of active treatment (J. Allergy Clin. Immunol. 2011;128:559-66).
During the first 3 years, the oral desensitization regimen led to progressively higher levels of symptom reduction each year, compared with placebo, a pattern that mimicked what typically occurs with subcutaneous desensitization.
The new results showed that during patients’ first year off active treatment, symptom relief showed a trend toward a small dip in efficacy (see box), compared with placebo, although patients also self reported a maintained, positive effect on their total quality of life scores.
During the first year off treatment, the average adjusted symptom score (the study’s primary end point) was 29% below the placebo level among 136 patients who both took the pill starting 2 months before the start of their allergy season and remained in the study. The symptom score was 23% below placebo among the 142 patients who took the pill starting 4 months before the start of their allergy season and remained in the study.
The study initially randomized 633 adult patients with grass pollen allergy at several European centers. Patients began receiving either the active desensitization tablet or placebo at 2 months or 4 months before the onset of their local grass pollen season, and continued daily treatment through the end of the local pollen season. They then resumed the same treatment schedule during the subsequent 2 years. By the end of the fourth year of the study, roughly two-thirds of the initially enrolled patients remained in the study.
The most common adverse effect during treatment was mouth pruritus, followed by throat irritation. All of the adverse effects were mild or moderate, and their incidence and severity steadily declined during the 3 years of active treatment.
No patients in the study had an anaphylactic reaction, unlike what occurs with subcutaneous injections, which are know to cause anaphylaxis occasionally. The entire worldwide experience with the sublingual grass pollen tablet has so far resulted in six episodes of "doubtful" anaphylaxis, an experience that led Dr. Malling to declare that the sublingual tablet "is safer" than subcutaneous injections.
"For some patients, [sublingual] is probably optimal, while for others subcutaneous will be better," Dr. Malling said. Having both options available gives patients a choice of disease-modifying therapy. One advantage of the sublingual tablet is that it precludes the need for patients to travel to a physician’s office for regular injections, he noted, although being on a schedule of regular injections helps ensure compliance.
Stallergenes developed the sublingual tablet, and has marketed it as Oralair in Europe since 2009. The tablet contains pollen extracts from five grass types that are common throughout Europe.
A pivotal trial of the formulation is in progress in the United States, but has not yet progressed to the stage where patients have stopped active, seasonal treatment. Other companies are also conducting clinical trials to test the efficacy and safety of sublingual desensitization tablets for grass pollen and for other allergens. The new results reported by Dr. Malling and his associates are the first to report what happens once patients stop active, annual treatment.
The study was sponsored by Stallergenes, the company that markets the sublingual grass pollen tablet as Oralair. Dr. Malling said that he is a consultant to and has received research support from Stallergenes and from several other drug companies.
ORLANDO – Patients who underwent 3 consecutive years of desensitization to grass pollen with seasonal use of a daily, sublingual pill maintained their reduced level of grass pollen allergy during the following fourth season despite stopping pill treatment, according to results from a study of 432 patients who stayed in the study for 4 years.
The findings provide the first evidence that sublingual desensitization produces allergy disease modification similar to subcutaneous desensitization, Dr. Hans-Jørgen Malling said during a poster presentation March 4 at the meeting.
"The data show sustained clinical efficacy when you stop treatment," said Dr. Malling, professor of medicine at the University of Copenhagen and chief of the allergy clinic at Gentofte Hospital in nearby Hellerup. "That is disease modifying. If there is no efficacy after you stop treatment, then this treatment will not be viable."
Although long-term efficacy is crucial, "up to now, it seems like sublingual is equivalent to subcutaneous," he said in an interview.
But Dr. Malling also cautioned that a major test will be the ability of sublingual desensitization to maintain allergy desensitization during a second year off treatment – results that will come during the fifth and final year of the study and will be available a year from now.
Prior reports from the current study documented the ability of the sublingual grass pollen pill to produce desensitization in adult patients during each of the 3 years of active treatment (J. Allergy Clin. Immunol. 2011;128:559-66).
During the first 3 years, the oral desensitization regimen led to progressively higher levels of symptom reduction each year, compared with placebo, a pattern that mimicked what typically occurs with subcutaneous desensitization.
The new results showed that during patients’ first year off active treatment, symptom relief showed a trend toward a small dip in efficacy (see box), compared with placebo, although patients also self reported a maintained, positive effect on their total quality of life scores.
During the first year off treatment, the average adjusted symptom score (the study’s primary end point) was 29% below the placebo level among 136 patients who both took the pill starting 2 months before the start of their allergy season and remained in the study. The symptom score was 23% below placebo among the 142 patients who took the pill starting 4 months before the start of their allergy season and remained in the study.
The study initially randomized 633 adult patients with grass pollen allergy at several European centers. Patients began receiving either the active desensitization tablet or placebo at 2 months or 4 months before the onset of their local grass pollen season, and continued daily treatment through the end of the local pollen season. They then resumed the same treatment schedule during the subsequent 2 years. By the end of the fourth year of the study, roughly two-thirds of the initially enrolled patients remained in the study.
The most common adverse effect during treatment was mouth pruritus, followed by throat irritation. All of the adverse effects were mild or moderate, and their incidence and severity steadily declined during the 3 years of active treatment.
No patients in the study had an anaphylactic reaction, unlike what occurs with subcutaneous injections, which are know to cause anaphylaxis occasionally. The entire worldwide experience with the sublingual grass pollen tablet has so far resulted in six episodes of "doubtful" anaphylaxis, an experience that led Dr. Malling to declare that the sublingual tablet "is safer" than subcutaneous injections.
"For some patients, [sublingual] is probably optimal, while for others subcutaneous will be better," Dr. Malling said. Having both options available gives patients a choice of disease-modifying therapy. One advantage of the sublingual tablet is that it precludes the need for patients to travel to a physician’s office for regular injections, he noted, although being on a schedule of regular injections helps ensure compliance.
Stallergenes developed the sublingual tablet, and has marketed it as Oralair in Europe since 2009. The tablet contains pollen extracts from five grass types that are common throughout Europe.
A pivotal trial of the formulation is in progress in the United States, but has not yet progressed to the stage where patients have stopped active, seasonal treatment. Other companies are also conducting clinical trials to test the efficacy and safety of sublingual desensitization tablets for grass pollen and for other allergens. The new results reported by Dr. Malling and his associates are the first to report what happens once patients stop active, annual treatment.
The study was sponsored by Stallergenes, the company that markets the sublingual grass pollen tablet as Oralair. Dr. Malling said that he is a consultant to and has received research support from Stallergenes and from several other drug companies.
ORLANDO – Patients who underwent 3 consecutive years of desensitization to grass pollen with seasonal use of a daily, sublingual pill maintained their reduced level of grass pollen allergy during the following fourth season despite stopping pill treatment, according to results from a study of 432 patients who stayed in the study for 4 years.
The findings provide the first evidence that sublingual desensitization produces allergy disease modification similar to subcutaneous desensitization, Dr. Hans-Jørgen Malling said during a poster presentation March 4 at the meeting.
"The data show sustained clinical efficacy when you stop treatment," said Dr. Malling, professor of medicine at the University of Copenhagen and chief of the allergy clinic at Gentofte Hospital in nearby Hellerup. "That is disease modifying. If there is no efficacy after you stop treatment, then this treatment will not be viable."
Although long-term efficacy is crucial, "up to now, it seems like sublingual is equivalent to subcutaneous," he said in an interview.
But Dr. Malling also cautioned that a major test will be the ability of sublingual desensitization to maintain allergy desensitization during a second year off treatment – results that will come during the fifth and final year of the study and will be available a year from now.
Prior reports from the current study documented the ability of the sublingual grass pollen pill to produce desensitization in adult patients during each of the 3 years of active treatment (J. Allergy Clin. Immunol. 2011;128:559-66).
During the first 3 years, the oral desensitization regimen led to progressively higher levels of symptom reduction each year, compared with placebo, a pattern that mimicked what typically occurs with subcutaneous desensitization.
The new results showed that during patients’ first year off active treatment, symptom relief showed a trend toward a small dip in efficacy (see box), compared with placebo, although patients also self reported a maintained, positive effect on their total quality of life scores.
During the first year off treatment, the average adjusted symptom score (the study’s primary end point) was 29% below the placebo level among 136 patients who both took the pill starting 2 months before the start of their allergy season and remained in the study. The symptom score was 23% below placebo among the 142 patients who took the pill starting 4 months before the start of their allergy season and remained in the study.
The study initially randomized 633 adult patients with grass pollen allergy at several European centers. Patients began receiving either the active desensitization tablet or placebo at 2 months or 4 months before the onset of their local grass pollen season, and continued daily treatment through the end of the local pollen season. They then resumed the same treatment schedule during the subsequent 2 years. By the end of the fourth year of the study, roughly two-thirds of the initially enrolled patients remained in the study.
The most common adverse effect during treatment was mouth pruritus, followed by throat irritation. All of the adverse effects were mild or moderate, and their incidence and severity steadily declined during the 3 years of active treatment.
No patients in the study had an anaphylactic reaction, unlike what occurs with subcutaneous injections, which are know to cause anaphylaxis occasionally. The entire worldwide experience with the sublingual grass pollen tablet has so far resulted in six episodes of "doubtful" anaphylaxis, an experience that led Dr. Malling to declare that the sublingual tablet "is safer" than subcutaneous injections.
"For some patients, [sublingual] is probably optimal, while for others subcutaneous will be better," Dr. Malling said. Having both options available gives patients a choice of disease-modifying therapy. One advantage of the sublingual tablet is that it precludes the need for patients to travel to a physician’s office for regular injections, he noted, although being on a schedule of regular injections helps ensure compliance.
Stallergenes developed the sublingual tablet, and has marketed it as Oralair in Europe since 2009. The tablet contains pollen extracts from five grass types that are common throughout Europe.
A pivotal trial of the formulation is in progress in the United States, but has not yet progressed to the stage where patients have stopped active, seasonal treatment. Other companies are also conducting clinical trials to test the efficacy and safety of sublingual desensitization tablets for grass pollen and for other allergens. The new results reported by Dr. Malling and his associates are the first to report what happens once patients stop active, annual treatment.
The study was sponsored by Stallergenes, the company that markets the sublingual grass pollen tablet as Oralair. Dr. Malling said that he is a consultant to and has received research support from Stallergenes and from several other drug companies.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF ALLERGY, ASTHMA, AND IMMUNOLOGY
Major Finding: Grass-allergy patients with 3 years of desensitization with a sublingual tablet maintained desensitization in their first season without treatment.
Data Source: A multicenter, randomized, placebo-controlled study that initially enrolled 633 adult patients with grass pollen allergy.
Disclosures: The study was sponsored by Stallergenes, the company that markets the sublingual grass pollen tablet as Oralair. Dr. Malling said that he is a consultant to and has received research support from Stallergenes and from several other drug companies.