User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
'But I'm vaccinated!': Why chemoprophylaxis is needed after pertussis exposure
VAIL, COLO. – It’s a question hospital infection control officers field from physicians and other health care personnel every time a pertussis exposure occurs: "I’ve been vaccinated, so why do I have to get a course of azithromycin for postexposure prophylaxis?"
The Advisory Committee on Immunization Practices (ACIP) based its updated recommendation for antibiotic postexposure prophylaxis on the findings of a randomized trial known as the Vanderbilt Study. The results, while nondefinitive, suggested that a policy of watchful waiting with daily symptom monitoring for 21 days post exposure may not be as effective as azithromycin postexposure prophylaxis in preventing pertussis infection, Dr. Ann-Christine Nyquist explained at a conference on pediatric infectious diseases sponsored by the Children’s Hospital Colorado.

The ACIP recommendation is for antibiotic prophylaxis for all pertussis-exposed health care workers likely to secondarily expose high-risk patients, such as neonates and pregnant women. Other vaccinated health care workers could receive either postexposure prophylaxis or 21 days of symptom monitoring with prompt antimicrobial therapy to be started should pertussis symptoms arise.
For Dr. Nyquist, the issue is a no-brainer. The vaccine is not 100% protective, the duration of protection is uncertain, and the adverse impact of a pertussis outbreak in a health care facility is enormous.
"When I put on my hospital epidemiologist hat and I think about pertussis in my hospital, it scares me to death. I would give everyone I was concerned about 5 days of azithromycin at $60 a pop," said Dr. Nyquist, professor of pediatrics at the University of Colorado, Denver.
The children’s hospital affiliated with Vanderbilt University, Nashville, Tenn., has a universal tetanus-diphtheria-acellular pertussis (Tdap) vaccine immunization policy for all health care personnel. So it was an ideal location for a randomized comparison of two strategies to prevent infection following pertussis exposure in vaccinated physicians, nurses, and other health care personnel.
Following a pertussis exposure, health care personnel were randomized to 5 days of azithromycin or 21 days of watchful waiting. A bona fide exposure typically involved face-to-face exposure within a few feet when the health care provider wasn’t wearing a mask, or ungloved contact with a patient’s secretions.
Although 1,091 health care personnel enrolled in the trial, during a 30-month period only 86 subjects were randomized, limiting the statistical power of the findings. The key result: Only 1 of 42 patients who received postexposure prophylaxis met the prespecified definition of pertussis, compared with 6 of 44 in the watchful waiting group.
However, pertussis infection was defined quite strictly as a positive culture or PCR, a twofold increase in anti–pertussis toxin titer, or a single anti–pertussis toxin titer of at least 94 enzyme-linked immunosorbent assay units per milliliter. In fact, not a single study participant developed symptomatic pertussis, and the investigators concluded that "it is likely that none of the health care personnel who met the predefined serologic or PCR for infection were truly infected with pertussis" (Clin. Infect. Dis. 2012;54:938-45).
Dr. Nyquist noted that the Centers for Disease Control and Prevention (CDC) has identified health care workers as being at the epicenter of numerous pertussis outbreaks in hospitals. Health care personnel have regular contact with infected patients, and as adults they have waning immunity. The cost per hospital outbreak was calculated by the CDC at $44,000-$75,000.
"But that figure doesn’t include the human pain and suffering, which I would multiply maybe times five," she added.
ACIP recommends that all health care personnel with direct patient contact in hospitals or ambulatory settings receive a single dose of Tdap. In addition, at its June meeting ACIP directed the Pertussis Vaccines Work Group to explore the possibility of giving a booster dose of Tdap to health care workers in order to beef up their protection.
Dr. Nyquist reported having no relevant financial relationships with any commercial interests.
VAIL, COLO. – It’s a question hospital infection control officers field from physicians and other health care personnel every time a pertussis exposure occurs: "I’ve been vaccinated, so why do I have to get a course of azithromycin for postexposure prophylaxis?"
The Advisory Committee on Immunization Practices (ACIP) based its updated recommendation for antibiotic postexposure prophylaxis on the findings of a randomized trial known as the Vanderbilt Study. The results, while nondefinitive, suggested that a policy of watchful waiting with daily symptom monitoring for 21 days post exposure may not be as effective as azithromycin postexposure prophylaxis in preventing pertussis infection, Dr. Ann-Christine Nyquist explained at a conference on pediatric infectious diseases sponsored by the Children’s Hospital Colorado.
The ACIP recommendation is for antibiotic prophylaxis for all pertussis-exposed health care workers likely to secondarily expose high-risk patients, such as neonates and pregnant women. Other vaccinated health care workers could receive either postexposure prophylaxis or 21 days of symptom monitoring with prompt antimicrobial therapy to be started should pertussis symptoms arise.
For Dr. Nyquist, the issue is a no-brainer. The vaccine is not 100% protective, the duration of protection is uncertain, and the adverse impact of a pertussis outbreak in a health care facility is enormous.
"When I put on my hospital epidemiologist hat and I think about pertussis in my hospital, it scares me to death. I would give everyone I was concerned about 5 days of azithromycin at $60 a pop," said Dr. Nyquist, professor of pediatrics at the University of Colorado, Denver.
The children’s hospital affiliated with Vanderbilt University, Nashville, Tenn., has a universal tetanus-diphtheria-acellular pertussis (Tdap) vaccine immunization policy for all health care personnel. So it was an ideal location for a randomized comparison of two strategies to prevent infection following pertussis exposure in vaccinated physicians, nurses, and other health care personnel.
Following a pertussis exposure, health care personnel were randomized to 5 days of azithromycin or 21 days of watchful waiting. A bona fide exposure typically involved face-to-face exposure within a few feet when the health care provider wasn’t wearing a mask, or ungloved contact with a patient’s secretions.
Although 1,091 health care personnel enrolled in the trial, during a 30-month period only 86 subjects were randomized, limiting the statistical power of the findings. The key result: Only 1 of 42 patients who received postexposure prophylaxis met the prespecified definition of pertussis, compared with 6 of 44 in the watchful waiting group.
However, pertussis infection was defined quite strictly as a positive culture or PCR, a twofold increase in anti–pertussis toxin titer, or a single anti–pertussis toxin titer of at least 94 enzyme-linked immunosorbent assay units per milliliter. In fact, not a single study participant developed symptomatic pertussis, and the investigators concluded that "it is likely that none of the health care personnel who met the predefined serologic or PCR for infection were truly infected with pertussis" (Clin. Infect. Dis. 2012;54:938-45).
Dr. Nyquist noted that the Centers for Disease Control and Prevention (CDC) has identified health care workers as being at the epicenter of numerous pertussis outbreaks in hospitals. Health care personnel have regular contact with infected patients, and as adults they have waning immunity. The cost per hospital outbreak was calculated by the CDC at $44,000-$75,000.
"But that figure doesn’t include the human pain and suffering, which I would multiply maybe times five," she added.
ACIP recommends that all health care personnel with direct patient contact in hospitals or ambulatory settings receive a single dose of Tdap. In addition, at its June meeting ACIP directed the Pertussis Vaccines Work Group to explore the possibility of giving a booster dose of Tdap to health care workers in order to beef up their protection.
Dr. Nyquist reported having no relevant financial relationships with any commercial interests.
VAIL, COLO. – It’s a question hospital infection control officers field from physicians and other health care personnel every time a pertussis exposure occurs: "I’ve been vaccinated, so why do I have to get a course of azithromycin for postexposure prophylaxis?"
The Advisory Committee on Immunization Practices (ACIP) based its updated recommendation for antibiotic postexposure prophylaxis on the findings of a randomized trial known as the Vanderbilt Study. The results, while nondefinitive, suggested that a policy of watchful waiting with daily symptom monitoring for 21 days post exposure may not be as effective as azithromycin postexposure prophylaxis in preventing pertussis infection, Dr. Ann-Christine Nyquist explained at a conference on pediatric infectious diseases sponsored by the Children’s Hospital Colorado.
The ACIP recommendation is for antibiotic prophylaxis for all pertussis-exposed health care workers likely to secondarily expose high-risk patients, such as neonates and pregnant women. Other vaccinated health care workers could receive either postexposure prophylaxis or 21 days of symptom monitoring with prompt antimicrobial therapy to be started should pertussis symptoms arise.
For Dr. Nyquist, the issue is a no-brainer. The vaccine is not 100% protective, the duration of protection is uncertain, and the adverse impact of a pertussis outbreak in a health care facility is enormous.
"When I put on my hospital epidemiologist hat and I think about pertussis in my hospital, it scares me to death. I would give everyone I was concerned about 5 days of azithromycin at $60 a pop," said Dr. Nyquist, professor of pediatrics at the University of Colorado, Denver.
The children’s hospital affiliated with Vanderbilt University, Nashville, Tenn., has a universal tetanus-diphtheria-acellular pertussis (Tdap) vaccine immunization policy for all health care personnel. So it was an ideal location for a randomized comparison of two strategies to prevent infection following pertussis exposure in vaccinated physicians, nurses, and other health care personnel.
Following a pertussis exposure, health care personnel were randomized to 5 days of azithromycin or 21 days of watchful waiting. A bona fide exposure typically involved face-to-face exposure within a few feet when the health care provider wasn’t wearing a mask, or ungloved contact with a patient’s secretions.
Although 1,091 health care personnel enrolled in the trial, during a 30-month period only 86 subjects were randomized, limiting the statistical power of the findings. The key result: Only 1 of 42 patients who received postexposure prophylaxis met the prespecified definition of pertussis, compared with 6 of 44 in the watchful waiting group.
However, pertussis infection was defined quite strictly as a positive culture or PCR, a twofold increase in anti–pertussis toxin titer, or a single anti–pertussis toxin titer of at least 94 enzyme-linked immunosorbent assay units per milliliter. In fact, not a single study participant developed symptomatic pertussis, and the investigators concluded that "it is likely that none of the health care personnel who met the predefined serologic or PCR for infection were truly infected with pertussis" (Clin. Infect. Dis. 2012;54:938-45).
Dr. Nyquist noted that the Centers for Disease Control and Prevention (CDC) has identified health care workers as being at the epicenter of numerous pertussis outbreaks in hospitals. Health care personnel have regular contact with infected patients, and as adults they have waning immunity. The cost per hospital outbreak was calculated by the CDC at $44,000-$75,000.
"But that figure doesn’t include the human pain and suffering, which I would multiply maybe times five," she added.
ACIP recommends that all health care personnel with direct patient contact in hospitals or ambulatory settings receive a single dose of Tdap. In addition, at its June meeting ACIP directed the Pertussis Vaccines Work Group to explore the possibility of giving a booster dose of Tdap to health care workers in order to beef up their protection.
Dr. Nyquist reported having no relevant financial relationships with any commercial interests.
EXPERT OPINION FROM THE ANNUAL PEDIATRIC INFECTIOUS DISEASES CONFERENCE

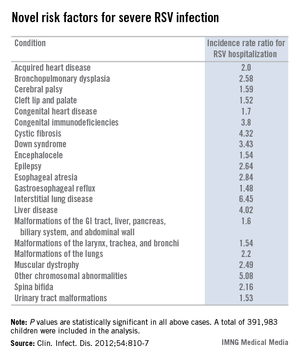
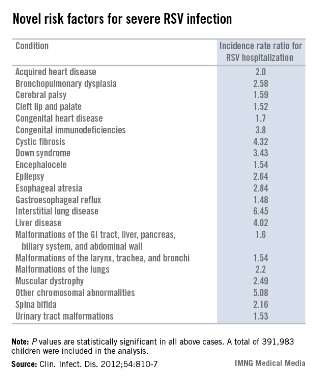
Novel risk factors for serious RSV identified
VAIL, COLO. – Children with congenital malformations or a variety of chronic diseases are at a previously undescribed, sharply increased risk for serious respiratory syncytial virus infection, according to a landmark Danish study.
Among the newly identified risk factors for hospitalization for RSV infection are neuromuscular disease, interstitial lung disease, liver disease, congenital malformations, liver disease, and congenital immunodeficiencies, Dr. Eric A.F. Simões said at a conference on pediatric infectious diseases sponsored by the Children’s Hospital Colorado.
"When you are fighting with an insurance company over whether treatment with palivizumab is appropriate, you can show them this study. It’s the only one of its kind," said Dr. Simões, a coauthor of the Danish study and professor of pediatrics at the University of Colorado, Denver.
This was a population-based cohort study including 391,983 children born in Denmark during 1997-2003. Dr. Simões and his coinvestigators utilized the comprehensive Danish National Patient Registry to determine that 2.7% of the children carried a diagnosis for one or more chronic diseases, a broad heading which included congenital malformations, chromosomal abnormalities, and acquired chronic disorders.
During their first 23 months of life, 2.8% of the study population was hospitalized for an RSV infection. Of those hospitalized children, 8.8% had at least one diagnosis of chronic disease. In a multivariate analysis adjusted for maternal smoking, prematurity, hospitalization within the last 30 days, and other potential confounding factors, the incidence rate ratio for RSV hospitalization in children with any congenital chronic condition was 2.18. For children with any acquired chronic condition, it was 2.25. (See chart.)
Dr. Simoes and his colleagues put forth biologically plausible mechanistic explanations for the increased risks of severe RSV in many of the newly identified at-risk subgroups. For example, they argued that children with cleft lip and palate are known to have a high incidence of middle ear disease, and it’s possible that difficulties in swallowing could result in aspiration of infected nasal secretions, with resultant lower respiratory tract RSV infection.
Children with various neuromuscular diseases were found to be at increased risk for RSV hospitalization. These included children with epilepsy, cerebral palsy, muscular dystrophy, and spina bifida or other congenital malformations of the nervous system. Moreover, children with neuromuscular disease also had significantly longer-than-average RSV hospitalizations. It’s possible that the increased RSV morbidity seen in these patients was due at least in part to diminished vital capacity secondary to muscular dysfunction, coupled with disrupted clearance of respiratory secretions, the investigators speculated.
The finding of an elevated risk of RSV hospitalization among children with malformations of the urinary system might be explained as follows: Lower urinary tract obstruction results in oligohydramnios, in turn resulting in pulmonary hypoplasia.
The 4.32-fold increased risk of severe RSV infection documented in this study in children with cystic fibrosis may be related to the reduced levels of surfactant proteins A and D, which characterize this disease. Those proteins are key components of the pulmonary innate immune system, Dr. Simões and his coworkers noted (Clin. Infect. Dis. 2012;54:810-7).
In contrast, the finding of a fourfold increased risk of RSV hospitalization in children with liver disease was unexpected, and the investigators had no explanation for it.
The Danish study was supported by Abbott Laboratories. Dr. Simões has received research grants from and served as a consultant to Abbott and half a dozen other companies, as well as UNICEF, the Bill & Melinda Gates Foundation, and the World Health Organization.
VAIL, COLO. – Children with congenital malformations or a variety of chronic diseases are at a previously undescribed, sharply increased risk for serious respiratory syncytial virus infection, according to a landmark Danish study.
Among the newly identified risk factors for hospitalization for RSV infection are neuromuscular disease, interstitial lung disease, liver disease, congenital malformations, liver disease, and congenital immunodeficiencies, Dr. Eric A.F. Simões said at a conference on pediatric infectious diseases sponsored by the Children’s Hospital Colorado.
"When you are fighting with an insurance company over whether treatment with palivizumab is appropriate, you can show them this study. It’s the only one of its kind," said Dr. Simões, a coauthor of the Danish study and professor of pediatrics at the University of Colorado, Denver.
This was a population-based cohort study including 391,983 children born in Denmark during 1997-2003. Dr. Simões and his coinvestigators utilized the comprehensive Danish National Patient Registry to determine that 2.7% of the children carried a diagnosis for one or more chronic diseases, a broad heading which included congenital malformations, chromosomal abnormalities, and acquired chronic disorders.
During their first 23 months of life, 2.8% of the study population was hospitalized for an RSV infection. Of those hospitalized children, 8.8% had at least one diagnosis of chronic disease. In a multivariate analysis adjusted for maternal smoking, prematurity, hospitalization within the last 30 days, and other potential confounding factors, the incidence rate ratio for RSV hospitalization in children with any congenital chronic condition was 2.18. For children with any acquired chronic condition, it was 2.25. (See chart.)
Dr. Simoes and his colleagues put forth biologically plausible mechanistic explanations for the increased risks of severe RSV in many of the newly identified at-risk subgroups. For example, they argued that children with cleft lip and palate are known to have a high incidence of middle ear disease, and it’s possible that difficulties in swallowing could result in aspiration of infected nasal secretions, with resultant lower respiratory tract RSV infection.
Children with various neuromuscular diseases were found to be at increased risk for RSV hospitalization. These included children with epilepsy, cerebral palsy, muscular dystrophy, and spina bifida or other congenital malformations of the nervous system. Moreover, children with neuromuscular disease also had significantly longer-than-average RSV hospitalizations. It’s possible that the increased RSV morbidity seen in these patients was due at least in part to diminished vital capacity secondary to muscular dysfunction, coupled with disrupted clearance of respiratory secretions, the investigators speculated.
The finding of an elevated risk of RSV hospitalization among children with malformations of the urinary system might be explained as follows: Lower urinary tract obstruction results in oligohydramnios, in turn resulting in pulmonary hypoplasia.
The 4.32-fold increased risk of severe RSV infection documented in this study in children with cystic fibrosis may be related to the reduced levels of surfactant proteins A and D, which characterize this disease. Those proteins are key components of the pulmonary innate immune system, Dr. Simões and his coworkers noted (Clin. Infect. Dis. 2012;54:810-7).
In contrast, the finding of a fourfold increased risk of RSV hospitalization in children with liver disease was unexpected, and the investigators had no explanation for it.
The Danish study was supported by Abbott Laboratories. Dr. Simões has received research grants from and served as a consultant to Abbott and half a dozen other companies, as well as UNICEF, the Bill & Melinda Gates Foundation, and the World Health Organization.
VAIL, COLO. – Children with congenital malformations or a variety of chronic diseases are at a previously undescribed, sharply increased risk for serious respiratory syncytial virus infection, according to a landmark Danish study.
Among the newly identified risk factors for hospitalization for RSV infection are neuromuscular disease, interstitial lung disease, liver disease, congenital malformations, liver disease, and congenital immunodeficiencies, Dr. Eric A.F. Simões said at a conference on pediatric infectious diseases sponsored by the Children’s Hospital Colorado.
"When you are fighting with an insurance company over whether treatment with palivizumab is appropriate, you can show them this study. It’s the only one of its kind," said Dr. Simões, a coauthor of the Danish study and professor of pediatrics at the University of Colorado, Denver.
This was a population-based cohort study including 391,983 children born in Denmark during 1997-2003. Dr. Simões and his coinvestigators utilized the comprehensive Danish National Patient Registry to determine that 2.7% of the children carried a diagnosis for one or more chronic diseases, a broad heading which included congenital malformations, chromosomal abnormalities, and acquired chronic disorders.
During their first 23 months of life, 2.8% of the study population was hospitalized for an RSV infection. Of those hospitalized children, 8.8% had at least one diagnosis of chronic disease. In a multivariate analysis adjusted for maternal smoking, prematurity, hospitalization within the last 30 days, and other potential confounding factors, the incidence rate ratio for RSV hospitalization in children with any congenital chronic condition was 2.18. For children with any acquired chronic condition, it was 2.25. (See chart.)
Dr. Simoes and his colleagues put forth biologically plausible mechanistic explanations for the increased risks of severe RSV in many of the newly identified at-risk subgroups. For example, they argued that children with cleft lip and palate are known to have a high incidence of middle ear disease, and it’s possible that difficulties in swallowing could result in aspiration of infected nasal secretions, with resultant lower respiratory tract RSV infection.
Children with various neuromuscular diseases were found to be at increased risk for RSV hospitalization. These included children with epilepsy, cerebral palsy, muscular dystrophy, and spina bifida or other congenital malformations of the nervous system. Moreover, children with neuromuscular disease also had significantly longer-than-average RSV hospitalizations. It’s possible that the increased RSV morbidity seen in these patients was due at least in part to diminished vital capacity secondary to muscular dysfunction, coupled with disrupted clearance of respiratory secretions, the investigators speculated.
The finding of an elevated risk of RSV hospitalization among children with malformations of the urinary system might be explained as follows: Lower urinary tract obstruction results in oligohydramnios, in turn resulting in pulmonary hypoplasia.
The 4.32-fold increased risk of severe RSV infection documented in this study in children with cystic fibrosis may be related to the reduced levels of surfactant proteins A and D, which characterize this disease. Those proteins are key components of the pulmonary innate immune system, Dr. Simões and his coworkers noted (Clin. Infect. Dis. 2012;54:810-7).
In contrast, the finding of a fourfold increased risk of RSV hospitalization in children with liver disease was unexpected, and the investigators had no explanation for it.
The Danish study was supported by Abbott Laboratories. Dr. Simões has received research grants from and served as a consultant to Abbott and half a dozen other companies, as well as UNICEF, the Bill & Melinda Gates Foundation, and the World Health Organization.
AT THE ANNUAL PEDIATRIC INFECTIOUS DISEASES CONFERENCE
Major finding: Children with congenital malformations, neuromuscular disease, interstitial lung disease, a variety of chromosomal abnormalities, acquired heart disease, and other chronic conditions are newly recognized as being at significantly increased risk for severe respiratory syncytial virus infection.
Data source: This was a Danish national population-based cohort study involving nearly 400,000 children born in Denmark during 1997-2003, of whom 2.8% were hospitalized for RSV before 24 months of age.
Disclosures: The Danish study was supported by Abbott Laboratories. Dr. Simões has received research grants from and served as a consultant to Abbott and half a dozen other companies, as well as UNICEF, the Bill & Melinda Gates Foundation, and the World Health Organization.
Acute pulmonary embolism doesn’t always require hospitalization
AMSTERDAM – Two-thirds of patients who presented to the emergency department of a U.S. tertiary care hospital with an acute pulmonary embolism had no acute deterioration and required no short-term hospital-based interventions, in an analysis of 298 patients seen over a 2-year period.
The finding "supports the assertion that outpatient treatment of patients with pulmonary embolism [PE] is safe," said Dr. Christopher Kabrhel at the 24th Congress of the International Society on Thrombosis and Haemostasis.
"We want to identify patients for whom nothing bad will happen. We showed that two-thirds of patients did well and didn’t need anything from the hospital and didn’t benefit from being in the hospital. We need to identify some of these patients," soon after they present in the emergency department, said Dr. Kabrhel, a surgeon and emergency-medicine physician at Massachusetts General Hospital and Harvard Medical School in Boston. If reliable risk markers can be found with further research, "perhaps we can identify half of the two-thirds—a third of all patients who come to the emergency department with a PE—who we know will be safe with outpatient treatment so we can send those patients home from the emergency department and not admit them."

Most symptomatic U.S. patients who come to an emergency department, and are diagnosed with a PE are immediately admitted to the hospital. In the current study, the hospitalization rate was 92% with a median length of stay of 3 days. "We need a better rule to decide whether a patient needs hospitalization. We need to find which patients benefit from hospitalization," Dr. Kabrhel said in an interview.
He and his associates reviewed 298 adults 18 years or older who presented to the Massachusetts General Hospital emergency department during October 2009 through December 2011 with a radiographically proven PE diagnosed within 24 hours of arrival. They averaged 59 years old, half were women, and the most common comorbidity was malignancy in 107 patients (36%).
The study’s primary outcome was any clinical deterioration or need for hospital-based intervention during the 5 days following presentation at the emergency department, including the need for advanced cardiac life support, the development of a new cardiac dysrhythmia, the development of hypoxia or hypotension, the need for thrombolysis or thrombectomy, recurrent PE, or death. These events occurred in 99 patients (33%); of these, 28 patients (9% of the total group) had "severe" deterioration or required a "major" intervention. Twelve patients (4%) died within 30 days of their initial emergency presentation. The most common acute complication was the need for respiratory support, in about 55 patients, followed by hypotension, in about 34.
A multivariate analysis identified five baseline factors that significantly correlated with the primary outcome. Patients who had normal vital signs at baseline had a 79% reduced rate of significant deterioration or need for hospital-based intervention. The other four factors were linked with increased rates of deterioration and need for intervention: Right heart strain caused by the PE and identified by an echocardiogram boosted the risk of a bad outcome more than fourfold, coronary disease and cerebrovascular disease each were tied to a more than threefold increased rate, and residual deep vein thrombosis was linked with a more than doubled rate of bad outcomes.
The subset of patients with the most severe outcomes had only one direct correlation with bad outcomes, right heart strain on echo. This subset of patients also showed a protective link against bad outcomes when their systolic blood pressure never fell below 90 mm Hg.
In contrast to these factors linked to 5-day outcomes, two different types of patient factors were significantly linked with 30-day mortality: having a malignancy and having chronic lung disease.
"Previously validated clinical prediction rules that looked at outcomes after PE were primarily validated based on 30-day mortality or recurrent PE, and included factors like having cancer, heart failure, or chronic lung disease. But these scores are only able to predict the outcomes we examined with 70% sensitivity," Dr. Kabrhel said. He found this out by running the numbers he collected through three validated scores for predicting PE outcome: the Geneva Prediction Score (Ann. Intern. Med. 2006;144:165-71), the Severity Index (Am. J. Respir. Crit. Care Med. 2005; 172:1041-6), and the Simplified Pulmonary Embolism Severity Index (Arch. Intern. Med. 2010;170:1383-9). "Predictors of all-cause 30-day mortality are different than predictors of short-term outcomes" in PE patients, he said.
"We found that echo is a very good predictor of short-term outcomes, and also abnormal vital signs. The key point is we need to look at outcomes that are relevant to the decisions made" in the emergency department, Dr. Kabrhel said. "Looking at 30-day mortality in patients who are only hospitalized for 3 days doesn’t really inform the decision on who should be in the hospital. I would suggest caution on using [prediction] tools validated against 30-day mortality and recurrent PE to determine what to do acutely. We need better rules to decide which PE patients need hospitalization."
Dr. Kabrhel said he has been a consultant to Diagnostica Stago, and is an officer for LitPulse.
On Twitter @mitchelzoler
AMSTERDAM – Two-thirds of patients who presented to the emergency department of a U.S. tertiary care hospital with an acute pulmonary embolism had no acute deterioration and required no short-term hospital-based interventions, in an analysis of 298 patients seen over a 2-year period.
The finding "supports the assertion that outpatient treatment of patients with pulmonary embolism [PE] is safe," said Dr. Christopher Kabrhel at the 24th Congress of the International Society on Thrombosis and Haemostasis.
"We want to identify patients for whom nothing bad will happen. We showed that two-thirds of patients did well and didn’t need anything from the hospital and didn’t benefit from being in the hospital. We need to identify some of these patients," soon after they present in the emergency department, said Dr. Kabrhel, a surgeon and emergency-medicine physician at Massachusetts General Hospital and Harvard Medical School in Boston. If reliable risk markers can be found with further research, "perhaps we can identify half of the two-thirds—a third of all patients who come to the emergency department with a PE—who we know will be safe with outpatient treatment so we can send those patients home from the emergency department and not admit them."
Most symptomatic U.S. patients who come to an emergency department, and are diagnosed with a PE are immediately admitted to the hospital. In the current study, the hospitalization rate was 92% with a median length of stay of 3 days. "We need a better rule to decide whether a patient needs hospitalization. We need to find which patients benefit from hospitalization," Dr. Kabrhel said in an interview.
He and his associates reviewed 298 adults 18 years or older who presented to the Massachusetts General Hospital emergency department during October 2009 through December 2011 with a radiographically proven PE diagnosed within 24 hours of arrival. They averaged 59 years old, half were women, and the most common comorbidity was malignancy in 107 patients (36%).
The study’s primary outcome was any clinical deterioration or need for hospital-based intervention during the 5 days following presentation at the emergency department, including the need for advanced cardiac life support, the development of a new cardiac dysrhythmia, the development of hypoxia or hypotension, the need for thrombolysis or thrombectomy, recurrent PE, or death. These events occurred in 99 patients (33%); of these, 28 patients (9% of the total group) had "severe" deterioration or required a "major" intervention. Twelve patients (4%) died within 30 days of their initial emergency presentation. The most common acute complication was the need for respiratory support, in about 55 patients, followed by hypotension, in about 34.
A multivariate analysis identified five baseline factors that significantly correlated with the primary outcome. Patients who had normal vital signs at baseline had a 79% reduced rate of significant deterioration or need for hospital-based intervention. The other four factors were linked with increased rates of deterioration and need for intervention: Right heart strain caused by the PE and identified by an echocardiogram boosted the risk of a bad outcome more than fourfold, coronary disease and cerebrovascular disease each were tied to a more than threefold increased rate, and residual deep vein thrombosis was linked with a more than doubled rate of bad outcomes.
The subset of patients with the most severe outcomes had only one direct correlation with bad outcomes, right heart strain on echo. This subset of patients also showed a protective link against bad outcomes when their systolic blood pressure never fell below 90 mm Hg.
In contrast to these factors linked to 5-day outcomes, two different types of patient factors were significantly linked with 30-day mortality: having a malignancy and having chronic lung disease.
"Previously validated clinical prediction rules that looked at outcomes after PE were primarily validated based on 30-day mortality or recurrent PE, and included factors like having cancer, heart failure, or chronic lung disease. But these scores are only able to predict the outcomes we examined with 70% sensitivity," Dr. Kabrhel said. He found this out by running the numbers he collected through three validated scores for predicting PE outcome: the Geneva Prediction Score (Ann. Intern. Med. 2006;144:165-71), the Severity Index (Am. J. Respir. Crit. Care Med. 2005; 172:1041-6), and the Simplified Pulmonary Embolism Severity Index (Arch. Intern. Med. 2010;170:1383-9). "Predictors of all-cause 30-day mortality are different than predictors of short-term outcomes" in PE patients, he said.
"We found that echo is a very good predictor of short-term outcomes, and also abnormal vital signs. The key point is we need to look at outcomes that are relevant to the decisions made" in the emergency department, Dr. Kabrhel said. "Looking at 30-day mortality in patients who are only hospitalized for 3 days doesn’t really inform the decision on who should be in the hospital. I would suggest caution on using [prediction] tools validated against 30-day mortality and recurrent PE to determine what to do acutely. We need better rules to decide which PE patients need hospitalization."
Dr. Kabrhel said he has been a consultant to Diagnostica Stago, and is an officer for LitPulse.
On Twitter @mitchelzoler
AMSTERDAM – Two-thirds of patients who presented to the emergency department of a U.S. tertiary care hospital with an acute pulmonary embolism had no acute deterioration and required no short-term hospital-based interventions, in an analysis of 298 patients seen over a 2-year period.
The finding "supports the assertion that outpatient treatment of patients with pulmonary embolism [PE] is safe," said Dr. Christopher Kabrhel at the 24th Congress of the International Society on Thrombosis and Haemostasis.
"We want to identify patients for whom nothing bad will happen. We showed that two-thirds of patients did well and didn’t need anything from the hospital and didn’t benefit from being in the hospital. We need to identify some of these patients," soon after they present in the emergency department, said Dr. Kabrhel, a surgeon and emergency-medicine physician at Massachusetts General Hospital and Harvard Medical School in Boston. If reliable risk markers can be found with further research, "perhaps we can identify half of the two-thirds—a third of all patients who come to the emergency department with a PE—who we know will be safe with outpatient treatment so we can send those patients home from the emergency department and not admit them."
Most symptomatic U.S. patients who come to an emergency department, and are diagnosed with a PE are immediately admitted to the hospital. In the current study, the hospitalization rate was 92% with a median length of stay of 3 days. "We need a better rule to decide whether a patient needs hospitalization. We need to find which patients benefit from hospitalization," Dr. Kabrhel said in an interview.
He and his associates reviewed 298 adults 18 years or older who presented to the Massachusetts General Hospital emergency department during October 2009 through December 2011 with a radiographically proven PE diagnosed within 24 hours of arrival. They averaged 59 years old, half were women, and the most common comorbidity was malignancy in 107 patients (36%).
The study’s primary outcome was any clinical deterioration or need for hospital-based intervention during the 5 days following presentation at the emergency department, including the need for advanced cardiac life support, the development of a new cardiac dysrhythmia, the development of hypoxia or hypotension, the need for thrombolysis or thrombectomy, recurrent PE, or death. These events occurred in 99 patients (33%); of these, 28 patients (9% of the total group) had "severe" deterioration or required a "major" intervention. Twelve patients (4%) died within 30 days of their initial emergency presentation. The most common acute complication was the need for respiratory support, in about 55 patients, followed by hypotension, in about 34.
A multivariate analysis identified five baseline factors that significantly correlated with the primary outcome. Patients who had normal vital signs at baseline had a 79% reduced rate of significant deterioration or need for hospital-based intervention. The other four factors were linked with increased rates of deterioration and need for intervention: Right heart strain caused by the PE and identified by an echocardiogram boosted the risk of a bad outcome more than fourfold, coronary disease and cerebrovascular disease each were tied to a more than threefold increased rate, and residual deep vein thrombosis was linked with a more than doubled rate of bad outcomes.
The subset of patients with the most severe outcomes had only one direct correlation with bad outcomes, right heart strain on echo. This subset of patients also showed a protective link against bad outcomes when their systolic blood pressure never fell below 90 mm Hg.
In contrast to these factors linked to 5-day outcomes, two different types of patient factors were significantly linked with 30-day mortality: having a malignancy and having chronic lung disease.
"Previously validated clinical prediction rules that looked at outcomes after PE were primarily validated based on 30-day mortality or recurrent PE, and included factors like having cancer, heart failure, or chronic lung disease. But these scores are only able to predict the outcomes we examined with 70% sensitivity," Dr. Kabrhel said. He found this out by running the numbers he collected through three validated scores for predicting PE outcome: the Geneva Prediction Score (Ann. Intern. Med. 2006;144:165-71), the Severity Index (Am. J. Respir. Crit. Care Med. 2005; 172:1041-6), and the Simplified Pulmonary Embolism Severity Index (Arch. Intern. Med. 2010;170:1383-9). "Predictors of all-cause 30-day mortality are different than predictors of short-term outcomes" in PE patients, he said.
"We found that echo is a very good predictor of short-term outcomes, and also abnormal vital signs. The key point is we need to look at outcomes that are relevant to the decisions made" in the emergency department, Dr. Kabrhel said. "Looking at 30-day mortality in patients who are only hospitalized for 3 days doesn’t really inform the decision on who should be in the hospital. I would suggest caution on using [prediction] tools validated against 30-day mortality and recurrent PE to determine what to do acutely. We need better rules to decide which PE patients need hospitalization."
Dr. Kabrhel said he has been a consultant to Diagnostica Stago, and is an officer for LitPulse.
On Twitter @mitchelzoler
AT ISTH 2013
Major finding: Among patients newly diagnosed with acute pulmonary embolism, 67% had no acute complication and didn’t require a hospital-based intervention.
Data source: A review of 298 patients diagnosed in the emergency department with acute pulmonary embolism at one U.S. center during 2009-2011.
Disclosures: Dr. Kabrhel said that he has been a consultant to Diagnostica Stago, and is an officer for LitPulse.

Macitentan cuts morbidity, mortality in PAH
Macitentan reduced morbidity and mortality in patients who had pulmonary arterial hypertension in an industry-sponsored phase III clinical trial, chiefly by slowing progression of the disease, according to a report published online Aug. 29 in the New England Journal of Medicine.
Two doses of macitentan, a dual endothelin receptor antagonist developed by altering the structure of bosentan to enhance efficacy and safety, were tested against placebo in 742 patients treated at 151 medical centers in 39 countries. The study subjects were patients aged 12 and older who had idiopathic or heritable pulmonary arterial hypertension (PAH), or PAH related to connective tissue disease, repaired congenital systemic-to-pulmonary shunts, HIV infection, drug use, or toxin exposure, said Dr. Tomás Pulido of Ignacio Chavez National Heart Institute, Mexico City, and his associates in SERAPHIN (Study With an Endothelin Receptor Antagonist in Pulmonary Arterial Hypertension to Improve Clinical Outcome).
The study subjects were randomly assigned to receive 3-mg macitentan (250 patients), 10-mg macitentan (242 patients), or placebo (250 patients) once daily for a median treatment period of 115 weeks. The primary end point, a composite of a PAH event or death from any cause, was reached by 38% of patients receiving 3-mg macitentan and 31% of those receiving 10-mg macitentan, compared with 46% of patients receiving placebo.
Rates of hospitalization or death due to PAH also were significantly lower in patients who received active treatment, at 26% for 3-mg macitentan and 21% for 10-mg macitentan, compared with 34% for placebo. Six-minute walk distance increased by 7.4 m with 3-mg macitentan and by 12.5 m with 10-mg macitentan, but decreased by 9.4 m with placebo, the investigators said (N. Engl. J. Med. 2013 Aug. 29 [doi:10.1056/NEJMoa1213917]).
Similarly, WHO heart failure functional class improved in 20% of patients receiving 3-mg macitentan and 22% of those receiving 10-mg macitentan, compared with only 13% of those receiving placebo. And patients in both active treatment groups showed significant reductions in pulmonary vascular resistance as well as significant increases in the cardiac index, compared with those in the placebo group.
SERAPHIN was funded by Actelion Pharmaceuticals. Dr. Pulido reported ties to Actelion, Pfizer, Eli Lilly, Bayer, United Therapeutics, and Gilead, and his associates reported ties to numerous industry sources.
Macitentan reduced morbidity and mortality in patients who had pulmonary arterial hypertension in an industry-sponsored phase III clinical trial, chiefly by slowing progression of the disease, according to a report published online Aug. 29 in the New England Journal of Medicine.
Two doses of macitentan, a dual endothelin receptor antagonist developed by altering the structure of bosentan to enhance efficacy and safety, were tested against placebo in 742 patients treated at 151 medical centers in 39 countries. The study subjects were patients aged 12 and older who had idiopathic or heritable pulmonary arterial hypertension (PAH), or PAH related to connective tissue disease, repaired congenital systemic-to-pulmonary shunts, HIV infection, drug use, or toxin exposure, said Dr. Tomás Pulido of Ignacio Chavez National Heart Institute, Mexico City, and his associates in SERAPHIN (Study With an Endothelin Receptor Antagonist in Pulmonary Arterial Hypertension to Improve Clinical Outcome).
The study subjects were randomly assigned to receive 3-mg macitentan (250 patients), 10-mg macitentan (242 patients), or placebo (250 patients) once daily for a median treatment period of 115 weeks. The primary end point, a composite of a PAH event or death from any cause, was reached by 38% of patients receiving 3-mg macitentan and 31% of those receiving 10-mg macitentan, compared with 46% of patients receiving placebo.
Rates of hospitalization or death due to PAH also were significantly lower in patients who received active treatment, at 26% for 3-mg macitentan and 21% for 10-mg macitentan, compared with 34% for placebo. Six-minute walk distance increased by 7.4 m with 3-mg macitentan and by 12.5 m with 10-mg macitentan, but decreased by 9.4 m with placebo, the investigators said (N. Engl. J. Med. 2013 Aug. 29 [doi:10.1056/NEJMoa1213917]).
Similarly, WHO heart failure functional class improved in 20% of patients receiving 3-mg macitentan and 22% of those receiving 10-mg macitentan, compared with only 13% of those receiving placebo. And patients in both active treatment groups showed significant reductions in pulmonary vascular resistance as well as significant increases in the cardiac index, compared with those in the placebo group.
SERAPHIN was funded by Actelion Pharmaceuticals. Dr. Pulido reported ties to Actelion, Pfizer, Eli Lilly, Bayer, United Therapeutics, and Gilead, and his associates reported ties to numerous industry sources.
Macitentan reduced morbidity and mortality in patients who had pulmonary arterial hypertension in an industry-sponsored phase III clinical trial, chiefly by slowing progression of the disease, according to a report published online Aug. 29 in the New England Journal of Medicine.
Two doses of macitentan, a dual endothelin receptor antagonist developed by altering the structure of bosentan to enhance efficacy and safety, were tested against placebo in 742 patients treated at 151 medical centers in 39 countries. The study subjects were patients aged 12 and older who had idiopathic or heritable pulmonary arterial hypertension (PAH), or PAH related to connective tissue disease, repaired congenital systemic-to-pulmonary shunts, HIV infection, drug use, or toxin exposure, said Dr. Tomás Pulido of Ignacio Chavez National Heart Institute, Mexico City, and his associates in SERAPHIN (Study With an Endothelin Receptor Antagonist in Pulmonary Arterial Hypertension to Improve Clinical Outcome).
The study subjects were randomly assigned to receive 3-mg macitentan (250 patients), 10-mg macitentan (242 patients), or placebo (250 patients) once daily for a median treatment period of 115 weeks. The primary end point, a composite of a PAH event or death from any cause, was reached by 38% of patients receiving 3-mg macitentan and 31% of those receiving 10-mg macitentan, compared with 46% of patients receiving placebo.
Rates of hospitalization or death due to PAH also were significantly lower in patients who received active treatment, at 26% for 3-mg macitentan and 21% for 10-mg macitentan, compared with 34% for placebo. Six-minute walk distance increased by 7.4 m with 3-mg macitentan and by 12.5 m with 10-mg macitentan, but decreased by 9.4 m with placebo, the investigators said (N. Engl. J. Med. 2013 Aug. 29 [doi:10.1056/NEJMoa1213917]).
Similarly, WHO heart failure functional class improved in 20% of patients receiving 3-mg macitentan and 22% of those receiving 10-mg macitentan, compared with only 13% of those receiving placebo. And patients in both active treatment groups showed significant reductions in pulmonary vascular resistance as well as significant increases in the cardiac index, compared with those in the placebo group.
SERAPHIN was funded by Actelion Pharmaceuticals. Dr. Pulido reported ties to Actelion, Pfizer, Eli Lilly, Bayer, United Therapeutics, and Gilead, and his associates reported ties to numerous industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: Composite rates of a PAH event or death from any cause were only 38% for 3-mg macitentan and 31% for 10-mg macitentan, compared with 46% for placebo.
Data Source: A phase III randomized, double-blind clinical trial involving patients with PAH who were treated for a median of 115 weeks using daily oral 3-mg macitentan (250 subjects), 10-mg macitentan (242 subjects), or placebo (250 subjects).
Disclosures: SERAPHIN was funded by Actelion Pharmaceuticals. Dr. Pulido reported ties to Actelion, Pfizer, Eli Lilly, Bayer, United Therapeutics, and Gilead, and his associates reported ties to numerous industry sources.
Slap an ‘app’ on these five tough clinical decisions
ESTES PARK, COLO. – These days there’s a smartphone app for everything. But not all apps for clinical decision rules are truly helpful in making better patient care decisions in frontline primary care medicine, Dr. Robert E. Burke cautioned at a conference on internal medicine sponsored by the University of Colorado.
Five clinical decision rules have proven merit, each accessible via app as well as by an online website, he said. All five address medical issues that are common, important, and complex. What these rules have in common is excellent – not merely good – predictive value, thorough validation in multiple populations, a high likelihood that their use will influence patient management in individual cases, and an enthusiastic thumbs-up vote by physician-users.

These top-tier clinical decision rules address the following situations: determining which patients with community-acquired pneumonia can safely be managed at home, assessing whether a patient with chronic liver disease is likely to have advanced fibrosis or cirrhosis without resorting to liver biopsy, identifying who can be sent home safely after an episode of syncope, determining whether to prescribe oral anticoagulation for atrial fibrillation, and stratifying risk after a transient ischemic attack (TIA) or stroke.
These clinical decision rules are not a replacement for clinical judgment, but they do make risk/benefit calculations a lot easier, said Dr. Burke, a hospitalist at the Denver VA Medical Center and the university.
Triage of pneumonia patients. Pneumonia is the third most common reason for hospital admission as well as early readmission in the United States. So lots of different pneumonia severity scores have been developed. But few of them are any good, according to Dr. Burke.
Many of these subpar scores measure the likelihood that a patient with pneumonia will be admitted to the intensive care unit. That’s not what primary care physicians really want to know.
"Unfortunately, ICU admission rates vary widely in the U.S. and have nothing to do with how sick patients are or their comorbid conditions. It’s really not clear why the rates vary so much, but the predictive value of those scores is pretty poor, since ICU admission is a subjective thing," he explained.
The score he recommends is the Pneumonia Severity Index. It has been validated as an admission rule in several randomized trials totaling more than 4,000 patients. The score places patients into one of five risk categories. In the randomized trials, patients in the three lowest-risk categories had no negative outcomes when treated as outpatients. Plus, the use of the Pneumonia Severity Index reduced hospital admissions by up to 20%.
The score is calculated using 20 factors readily obtainable from the patient history, physical exam, and lab work. It’s a laborious calculation that’s perfect for an app. And the app exists: It’s called Simpli PSI.
Assessing fibrosis/cirrhosis risk in patients with chronic liver disease. Liver biopsy is painful, costly, decidedly not risk free, and often misleading due to the small tissue sample obtained. Transient elastography, a noninvasive ultrasound-based alternative, is promising but not ready for prime time. Yet knowing whether a patient has advanced fibrosis or cirrhosis is important in terms of prognosis, treatment, and surveillance strategy.
This is where the FIB-4 Index, a serum score for fibrosis, is of value. The FIB-4 Index is easily calculated from basic laboratory data. Findings from multiple studies have shown excellent discrimination regardless of whether patients had hepatitis C, hepatitis B, or nonalcoholic fatty liver disease.
"It has a c-statistic [equivalent to the area under the receiver operating characteristic curve] of 0.84. That’s about as good as it gets," according to the hospitalist.
The app is called Liver Calc. Like all the other apps Dr. Burke highlighted, it is available to iPhone users at the App Store.
"Or if you were to type in ‘FIB-4 Index’ on Google, you’ll find a website that will actually calculate the score online," he noted.
Whom to hospitalize for syncope. "Syncope is one of the most common things I see as a physician of in-patients," Dr. Burke said. "It accounts for maybe 1%-3% of emergency department visits and 6% of hospitalizations in the United States."
The San Francisco Syncope Rule is of proven value in helping to identify patients at low risk of serious outcomes in the 30 days following a syncopal episode. These are the patients who don’t need to undergo emergency department evaluation. The rule has been prospectively validated in tens of thousands of patients. It had a negative predictive value of 97% in a systematic review. The rule works less well in patients over age 65, where the likelihood of arrhythmia as the cause of syncope increases sharply. And the rule works best when applied only after a thorough history and physical exam aimed at finding a cause for the patient’s syncope.
"For example, the rule assumes you’ve already checked for hypoglycemia, a common cause of syncope," the hospitalist explained.
The San Francisco Syncope Rule is available in app form as Doctor Tools of the Trade.
Atrial fibrillation: To anticoagulate or not? This is a decision that entails balancing the reduction in stroke risk obtained with anticoagulation against the potential harm in the form of bleeding. The best tool for assessing the potential stroke-risk benefit is the CHA2DS2-VASc score, which represents a significant advance over the CHADS2 score, in Dr. Burke’s view.
"What the CHA2DS2-VASc score is really useful for, I think, is in putting people into low- or high-risk buckets. It takes people out of that intermediate-risk category in CHADS2," he explained.
It turns out that when physicians rely upon clinical intuition to estimate the risk of clinically important bleeding in patients on oral anticoagulation, they tend to overestimate the true risk. This observation has led to a proliferation of scales aimed at predicting who is likely to bleed when placed on warfarin. The best performer among them, regardless of whether the endpoint is any clinically relevant bleeding, major bleeding, or all-cause mortality, is the HAS-BLED score.
"I would encourage you to use both the CHA2DS2-VASc and HAS-BLED, and to use them at the same time. In some cases you’ll find the numbers are really discordant; there may be much more benefit than you thought, or much more risk," Dr. Burke said.
The focus-AF calculator is the app that will do the work.
Risk stratification after TIA or stroke. The ABCD2 score provides an estimate of stroke risk within 7 or 90 days after a TIA. This information helps establish the urgency of patient evaluation and risk factor management. A patient with an ABCD2 score of 4 or more should go straight to the emergency department, while a score of 3 or less indicates outpatient evaluation is appropriate. The Neuro Toolkit app will run the numbers.
Dr. Burke is keeping a watchful eye on a number of other clinical decision rules that, while promising, aren’t quite ready for prime time in his view. These include the FRAX score, the TIMI score, and the Marburg Heart Score. The Marburg score, for example, has been extensively validated as a tool to help primary care physicians decide whether chest pain is cardiac or noncardiac. But in the clinical trials, the score wasn’t compared to clinical intuition. That’s a problem.
"I think our clinical intuition here is relatively good. So I’d like to see data showing the rule adds something to clinical intuition before I recommend it," he said.
In a head-to-head comparative trial, the Pittsburgh Knee Rule outperformed the older Ottawa Knee Rule as an aid in figuring out who needs imaging after a knee injury. Impressive, in Dr. Burke’s view, but he’d like to see the results confirmed in a second study.
He reported having no financial conflicts.
ESTES PARK, COLO. – These days there’s a smartphone app for everything. But not all apps for clinical decision rules are truly helpful in making better patient care decisions in frontline primary care medicine, Dr. Robert E. Burke cautioned at a conference on internal medicine sponsored by the University of Colorado.
Five clinical decision rules have proven merit, each accessible via app as well as by an online website, he said. All five address medical issues that are common, important, and complex. What these rules have in common is excellent – not merely good – predictive value, thorough validation in multiple populations, a high likelihood that their use will influence patient management in individual cases, and an enthusiastic thumbs-up vote by physician-users.
These top-tier clinical decision rules address the following situations: determining which patients with community-acquired pneumonia can safely be managed at home, assessing whether a patient with chronic liver disease is likely to have advanced fibrosis or cirrhosis without resorting to liver biopsy, identifying who can be sent home safely after an episode of syncope, determining whether to prescribe oral anticoagulation for atrial fibrillation, and stratifying risk after a transient ischemic attack (TIA) or stroke.
These clinical decision rules are not a replacement for clinical judgment, but they do make risk/benefit calculations a lot easier, said Dr. Burke, a hospitalist at the Denver VA Medical Center and the university.
Triage of pneumonia patients. Pneumonia is the third most common reason for hospital admission as well as early readmission in the United States. So lots of different pneumonia severity scores have been developed. But few of them are any good, according to Dr. Burke.
Many of these subpar scores measure the likelihood that a patient with pneumonia will be admitted to the intensive care unit. That’s not what primary care physicians really want to know.
"Unfortunately, ICU admission rates vary widely in the U.S. and have nothing to do with how sick patients are or their comorbid conditions. It’s really not clear why the rates vary so much, but the predictive value of those scores is pretty poor, since ICU admission is a subjective thing," he explained.
The score he recommends is the Pneumonia Severity Index. It has been validated as an admission rule in several randomized trials totaling more than 4,000 patients. The score places patients into one of five risk categories. In the randomized trials, patients in the three lowest-risk categories had no negative outcomes when treated as outpatients. Plus, the use of the Pneumonia Severity Index reduced hospital admissions by up to 20%.
The score is calculated using 20 factors readily obtainable from the patient history, physical exam, and lab work. It’s a laborious calculation that’s perfect for an app. And the app exists: It’s called Simpli PSI.
Assessing fibrosis/cirrhosis risk in patients with chronic liver disease. Liver biopsy is painful, costly, decidedly not risk free, and often misleading due to the small tissue sample obtained. Transient elastography, a noninvasive ultrasound-based alternative, is promising but not ready for prime time. Yet knowing whether a patient has advanced fibrosis or cirrhosis is important in terms of prognosis, treatment, and surveillance strategy.
This is where the FIB-4 Index, a serum score for fibrosis, is of value. The FIB-4 Index is easily calculated from basic laboratory data. Findings from multiple studies have shown excellent discrimination regardless of whether patients had hepatitis C, hepatitis B, or nonalcoholic fatty liver disease.
"It has a c-statistic [equivalent to the area under the receiver operating characteristic curve] of 0.84. That’s about as good as it gets," according to the hospitalist.
The app is called Liver Calc. Like all the other apps Dr. Burke highlighted, it is available to iPhone users at the App Store.
"Or if you were to type in ‘FIB-4 Index’ on Google, you’ll find a website that will actually calculate the score online," he noted.
Whom to hospitalize for syncope. "Syncope is one of the most common things I see as a physician of in-patients," Dr. Burke said. "It accounts for maybe 1%-3% of emergency department visits and 6% of hospitalizations in the United States."
The San Francisco Syncope Rule is of proven value in helping to identify patients at low risk of serious outcomes in the 30 days following a syncopal episode. These are the patients who don’t need to undergo emergency department evaluation. The rule has been prospectively validated in tens of thousands of patients. It had a negative predictive value of 97% in a systematic review. The rule works less well in patients over age 65, where the likelihood of arrhythmia as the cause of syncope increases sharply. And the rule works best when applied only after a thorough history and physical exam aimed at finding a cause for the patient’s syncope.
"For example, the rule assumes you’ve already checked for hypoglycemia, a common cause of syncope," the hospitalist explained.
The San Francisco Syncope Rule is available in app form as Doctor Tools of the Trade.
Atrial fibrillation: To anticoagulate or not? This is a decision that entails balancing the reduction in stroke risk obtained with anticoagulation against the potential harm in the form of bleeding. The best tool for assessing the potential stroke-risk benefit is the CHA2DS2-VASc score, which represents a significant advance over the CHADS2 score, in Dr. Burke’s view.
"What the CHA2DS2-VASc score is really useful for, I think, is in putting people into low- or high-risk buckets. It takes people out of that intermediate-risk category in CHADS2," he explained.
It turns out that when physicians rely upon clinical intuition to estimate the risk of clinically important bleeding in patients on oral anticoagulation, they tend to overestimate the true risk. This observation has led to a proliferation of scales aimed at predicting who is likely to bleed when placed on warfarin. The best performer among them, regardless of whether the endpoint is any clinically relevant bleeding, major bleeding, or all-cause mortality, is the HAS-BLED score.
"I would encourage you to use both the CHA2DS2-VASc and HAS-BLED, and to use them at the same time. In some cases you’ll find the numbers are really discordant; there may be much more benefit than you thought, or much more risk," Dr. Burke said.
The focus-AF calculator is the app that will do the work.
Risk stratification after TIA or stroke. The ABCD2 score provides an estimate of stroke risk within 7 or 90 days after a TIA. This information helps establish the urgency of patient evaluation and risk factor management. A patient with an ABCD2 score of 4 or more should go straight to the emergency department, while a score of 3 or less indicates outpatient evaluation is appropriate. The Neuro Toolkit app will run the numbers.
Dr. Burke is keeping a watchful eye on a number of other clinical decision rules that, while promising, aren’t quite ready for prime time in his view. These include the FRAX score, the TIMI score, and the Marburg Heart Score. The Marburg score, for example, has been extensively validated as a tool to help primary care physicians decide whether chest pain is cardiac or noncardiac. But in the clinical trials, the score wasn’t compared to clinical intuition. That’s a problem.
"I think our clinical intuition here is relatively good. So I’d like to see data showing the rule adds something to clinical intuition before I recommend it," he said.
In a head-to-head comparative trial, the Pittsburgh Knee Rule outperformed the older Ottawa Knee Rule as an aid in figuring out who needs imaging after a knee injury. Impressive, in Dr. Burke’s view, but he’d like to see the results confirmed in a second study.
He reported having no financial conflicts.
ESTES PARK, COLO. – These days there’s a smartphone app for everything. But not all apps for clinical decision rules are truly helpful in making better patient care decisions in frontline primary care medicine, Dr. Robert E. Burke cautioned at a conference on internal medicine sponsored by the University of Colorado.
Five clinical decision rules have proven merit, each accessible via app as well as by an online website, he said. All five address medical issues that are common, important, and complex. What these rules have in common is excellent – not merely good – predictive value, thorough validation in multiple populations, a high likelihood that their use will influence patient management in individual cases, and an enthusiastic thumbs-up vote by physician-users.
These top-tier clinical decision rules address the following situations: determining which patients with community-acquired pneumonia can safely be managed at home, assessing whether a patient with chronic liver disease is likely to have advanced fibrosis or cirrhosis without resorting to liver biopsy, identifying who can be sent home safely after an episode of syncope, determining whether to prescribe oral anticoagulation for atrial fibrillation, and stratifying risk after a transient ischemic attack (TIA) or stroke.
These clinical decision rules are not a replacement for clinical judgment, but they do make risk/benefit calculations a lot easier, said Dr. Burke, a hospitalist at the Denver VA Medical Center and the university.
Triage of pneumonia patients. Pneumonia is the third most common reason for hospital admission as well as early readmission in the United States. So lots of different pneumonia severity scores have been developed. But few of them are any good, according to Dr. Burke.
Many of these subpar scores measure the likelihood that a patient with pneumonia will be admitted to the intensive care unit. That’s not what primary care physicians really want to know.
"Unfortunately, ICU admission rates vary widely in the U.S. and have nothing to do with how sick patients are or their comorbid conditions. It’s really not clear why the rates vary so much, but the predictive value of those scores is pretty poor, since ICU admission is a subjective thing," he explained.
The score he recommends is the Pneumonia Severity Index. It has been validated as an admission rule in several randomized trials totaling more than 4,000 patients. The score places patients into one of five risk categories. In the randomized trials, patients in the three lowest-risk categories had no negative outcomes when treated as outpatients. Plus, the use of the Pneumonia Severity Index reduced hospital admissions by up to 20%.
The score is calculated using 20 factors readily obtainable from the patient history, physical exam, and lab work. It’s a laborious calculation that’s perfect for an app. And the app exists: It’s called Simpli PSI.
Assessing fibrosis/cirrhosis risk in patients with chronic liver disease. Liver biopsy is painful, costly, decidedly not risk free, and often misleading due to the small tissue sample obtained. Transient elastography, a noninvasive ultrasound-based alternative, is promising but not ready for prime time. Yet knowing whether a patient has advanced fibrosis or cirrhosis is important in terms of prognosis, treatment, and surveillance strategy.
This is where the FIB-4 Index, a serum score for fibrosis, is of value. The FIB-4 Index is easily calculated from basic laboratory data. Findings from multiple studies have shown excellent discrimination regardless of whether patients had hepatitis C, hepatitis B, or nonalcoholic fatty liver disease.
"It has a c-statistic [equivalent to the area under the receiver operating characteristic curve] of 0.84. That’s about as good as it gets," according to the hospitalist.
The app is called Liver Calc. Like all the other apps Dr. Burke highlighted, it is available to iPhone users at the App Store.
"Or if you were to type in ‘FIB-4 Index’ on Google, you’ll find a website that will actually calculate the score online," he noted.
Whom to hospitalize for syncope. "Syncope is one of the most common things I see as a physician of in-patients," Dr. Burke said. "It accounts for maybe 1%-3% of emergency department visits and 6% of hospitalizations in the United States."
The San Francisco Syncope Rule is of proven value in helping to identify patients at low risk of serious outcomes in the 30 days following a syncopal episode. These are the patients who don’t need to undergo emergency department evaluation. The rule has been prospectively validated in tens of thousands of patients. It had a negative predictive value of 97% in a systematic review. The rule works less well in patients over age 65, where the likelihood of arrhythmia as the cause of syncope increases sharply. And the rule works best when applied only after a thorough history and physical exam aimed at finding a cause for the patient’s syncope.
"For example, the rule assumes you’ve already checked for hypoglycemia, a common cause of syncope," the hospitalist explained.
The San Francisco Syncope Rule is available in app form as Doctor Tools of the Trade.
Atrial fibrillation: To anticoagulate or not? This is a decision that entails balancing the reduction in stroke risk obtained with anticoagulation against the potential harm in the form of bleeding. The best tool for assessing the potential stroke-risk benefit is the CHA2DS2-VASc score, which represents a significant advance over the CHADS2 score, in Dr. Burke’s view.
"What the CHA2DS2-VASc score is really useful for, I think, is in putting people into low- or high-risk buckets. It takes people out of that intermediate-risk category in CHADS2," he explained.
It turns out that when physicians rely upon clinical intuition to estimate the risk of clinically important bleeding in patients on oral anticoagulation, they tend to overestimate the true risk. This observation has led to a proliferation of scales aimed at predicting who is likely to bleed when placed on warfarin. The best performer among them, regardless of whether the endpoint is any clinically relevant bleeding, major bleeding, or all-cause mortality, is the HAS-BLED score.
"I would encourage you to use both the CHA2DS2-VASc and HAS-BLED, and to use them at the same time. In some cases you’ll find the numbers are really discordant; there may be much more benefit than you thought, or much more risk," Dr. Burke said.
The focus-AF calculator is the app that will do the work.
Risk stratification after TIA or stroke. The ABCD2 score provides an estimate of stroke risk within 7 or 90 days after a TIA. This information helps establish the urgency of patient evaluation and risk factor management. A patient with an ABCD2 score of 4 or more should go straight to the emergency department, while a score of 3 or less indicates outpatient evaluation is appropriate. The Neuro Toolkit app will run the numbers.
Dr. Burke is keeping a watchful eye on a number of other clinical decision rules that, while promising, aren’t quite ready for prime time in his view. These include the FRAX score, the TIMI score, and the Marburg Heart Score. The Marburg score, for example, has been extensively validated as a tool to help primary care physicians decide whether chest pain is cardiac or noncardiac. But in the clinical trials, the score wasn’t compared to clinical intuition. That’s a problem.
"I think our clinical intuition here is relatively good. So I’d like to see data showing the rule adds something to clinical intuition before I recommend it," he said.
In a head-to-head comparative trial, the Pittsburgh Knee Rule outperformed the older Ottawa Knee Rule as an aid in figuring out who needs imaging after a knee injury. Impressive, in Dr. Burke’s view, but he’d like to see the results confirmed in a second study.
He reported having no financial conflicts.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM

Exercise-induced bronchoconstriction
Exercise-induced bronchoconstriction is defined as acute, reversible airway narrowing that occurs during or after strenuous exercise. It is a very common problem, especially in physically active people, and can occur with or without underlying asthma. It is estimated that 10%-20% of the general population and up to 90% of people previously diagnosed with asthma have exercise-induced bronchoconstriction. Some studies suggest that exercise-induced bronchoconstriction can occur in as many as 30-70% of Olympic or elite-level athletes.
The following evidence-based guidelines were developed by the American Thoracic Society (ATS) to provide clinicians with practical guidance for the diagnosis and treatment of exercise-induced bronchoconstriction (EIB).
Diagnosis
Diagnosing EIB can be difficult as symptoms tend to be nonspecific and variable. Further, the presence or absence of common respiratory symptoms (such as chest tightness, cough, wheezing, and dyspnea) has very poor predictive value for the confirmation of EIB. Symptom severity ranges from mild to moderate – defined as causing impairment of athletic performance but rarely significant respiratory distress – and can be provoked by exercise or specific environments such as snowy mountains, ice rinks, or indoor swimming pools. An official EIB diagnosis should be established by monitoring changes in lung function provoked by exercise, not simply on the basis of symptoms.
Testing
To determine if EIB is present and to quantify the severity of the disorder, providers should conduct serial lung function measurements after a specific exercise or hyperpnea challenge. An example of an exercise challenge protocol is 5-8 minutes of exercise at 85% of maximum heart rate or 80% of maximal oxygen uptake (80% VO2 max). The type, duration, and intensity of exercise and the temperature and water content of the air are variables that should be considered. According to ATS and the European Respiratory Society guidelines, at least two reproducible FEV1 (forced expiratory volume in 1 second) values should be measured after the exercise challenge, with the highest value recorded at each interval – usually 5, 10, 15, and 30 minutes after exercise. Experts prefer measuring FEV1 because it is more discriminating and has better repeatability than peak expiratory flow rate.
There are a number of alternatives for testing, described in detail in ATS’s online supplement, which may be easier to implement than exercise challenges. These alternatives include eucapnic voluntary hyperpnea of dry air and inhalation of hyperosmolar aerosols of 4.5% saline or dry powder mannitol.
Interpreting results
Airway response is first calculated by finding the difference between the pre-exercise FEV1 value and the lowest FEV1 value recorded within 30 minutes after exercise. The percent fall in FEV1 from the baseline value is used to diagnose EIB, requiring a percentage fall of greater than 10% for official diagnosis. The severity of EIB can be graded as mild (more than 10% but less than 25% fall in FEV1), moderate (more than 25% but less than 50%), or severe (more than 50%).
Treatment
To prevent EIB, ATS recommends that patients use an inhaled short-acting beta2-agonist (SABA) 15 minutes prior to exercise and perform "interval or combination warm-up exercises" when possible. Use of a SABA prior to exercise provides 2-4 hours of attenuation of exercise-induced bronchospasm. Because of the potential for environmental triggers, ATS also recommends routine use of an air-warming and humidifying mask during exercise in cold weather. Daily use of a SABA may result in the development of tolerance, with reduction in the amount and duration of protection from EIB. This is thought to be due to desensitization of the beta2-receptors on mast cells.
For patients who have an inadequate response to an inhaled SABA before exercise and/or patients who require an inhaled SABA daily or more frequently, a controller agent such as an inhaled corticosteroid or a leukotriene receptor antagonist is recommended. Patients should be informed that maximal therapeutic benefit may take 2-4 treatment weeks.
In addition to the daily regime, ATS suggests the addition of a mast cell stabilizing agent or an inhaled anticholinergic agent before exercise if needed (both are relatively weaker recommendations). And finally, they recommend against daily use of an inhaled long-acting beta2-agonist (LABA) as a single therapy because of the strong concern for adverse side effects.
Special provisions
ATS recommends antihistamine use for patients with EIB and allergies who continue to be symptomatic despite daily or more frequent inhaled SABA use. They recommend against using antihistamines for patients who have EIB but who do not have allergies.
ATS also provides some weaker recommendations for those who want to control EIB symptoms with dietary modification. A low-salt diet supplemented with fish oils and ascorbic acid may increase symptom control.
Bottom line
EIB is an acute, reversible airway narrowing that occurs during or after strenuous exercise. A high percentage of physically active patients have EIB, regardless of whether they have underlying asthma conditions. Administration of an inhaled SABA 15 minutes prior to exercise and a variety of warm-up exercises act as a first-line treatment, with an inhaled corticosteroid or a leukotriene receptor antagonist effective for those who do not respond to the SABA alone.
Reference
J. P. Parsons et al. "An Official American Thoracic Society Clinical Practice Guideline: Exercise-induced Bronchoconstriction," Am. J. Respir. Crit. Care Med. 2013;187:1016-27.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. Dr. Beddis is an attending physician in the Abington Health Network at Wyncote Family Medicine.
Exercise-induced bronchoconstriction is defined as acute, reversible airway narrowing that occurs during or after strenuous exercise. It is a very common problem, especially in physically active people, and can occur with or without underlying asthma. It is estimated that 10%-20% of the general population and up to 90% of people previously diagnosed with asthma have exercise-induced bronchoconstriction. Some studies suggest that exercise-induced bronchoconstriction can occur in as many as 30-70% of Olympic or elite-level athletes.
The following evidence-based guidelines were developed by the American Thoracic Society (ATS) to provide clinicians with practical guidance for the diagnosis and treatment of exercise-induced bronchoconstriction (EIB).
Diagnosis
Diagnosing EIB can be difficult as symptoms tend to be nonspecific and variable. Further, the presence or absence of common respiratory symptoms (such as chest tightness, cough, wheezing, and dyspnea) has very poor predictive value for the confirmation of EIB. Symptom severity ranges from mild to moderate – defined as causing impairment of athletic performance but rarely significant respiratory distress – and can be provoked by exercise or specific environments such as snowy mountains, ice rinks, or indoor swimming pools. An official EIB diagnosis should be established by monitoring changes in lung function provoked by exercise, not simply on the basis of symptoms.
Testing
To determine if EIB is present and to quantify the severity of the disorder, providers should conduct serial lung function measurements after a specific exercise or hyperpnea challenge. An example of an exercise challenge protocol is 5-8 minutes of exercise at 85% of maximum heart rate or 80% of maximal oxygen uptake (80% VO2 max). The type, duration, and intensity of exercise and the temperature and water content of the air are variables that should be considered. According to ATS and the European Respiratory Society guidelines, at least two reproducible FEV1 (forced expiratory volume in 1 second) values should be measured after the exercise challenge, with the highest value recorded at each interval – usually 5, 10, 15, and 30 minutes after exercise. Experts prefer measuring FEV1 because it is more discriminating and has better repeatability than peak expiratory flow rate.
There are a number of alternatives for testing, described in detail in ATS’s online supplement, which may be easier to implement than exercise challenges. These alternatives include eucapnic voluntary hyperpnea of dry air and inhalation of hyperosmolar aerosols of 4.5% saline or dry powder mannitol.
Interpreting results
Airway response is first calculated by finding the difference between the pre-exercise FEV1 value and the lowest FEV1 value recorded within 30 minutes after exercise. The percent fall in FEV1 from the baseline value is used to diagnose EIB, requiring a percentage fall of greater than 10% for official diagnosis. The severity of EIB can be graded as mild (more than 10% but less than 25% fall in FEV1), moderate (more than 25% but less than 50%), or severe (more than 50%).
Treatment
To prevent EIB, ATS recommends that patients use an inhaled short-acting beta2-agonist (SABA) 15 minutes prior to exercise and perform "interval or combination warm-up exercises" when possible. Use of a SABA prior to exercise provides 2-4 hours of attenuation of exercise-induced bronchospasm. Because of the potential for environmental triggers, ATS also recommends routine use of an air-warming and humidifying mask during exercise in cold weather. Daily use of a SABA may result in the development of tolerance, with reduction in the amount and duration of protection from EIB. This is thought to be due to desensitization of the beta2-receptors on mast cells.
For patients who have an inadequate response to an inhaled SABA before exercise and/or patients who require an inhaled SABA daily or more frequently, a controller agent such as an inhaled corticosteroid or a leukotriene receptor antagonist is recommended. Patients should be informed that maximal therapeutic benefit may take 2-4 treatment weeks.
In addition to the daily regime, ATS suggests the addition of a mast cell stabilizing agent or an inhaled anticholinergic agent before exercise if needed (both are relatively weaker recommendations). And finally, they recommend against daily use of an inhaled long-acting beta2-agonist (LABA) as a single therapy because of the strong concern for adverse side effects.
Special provisions
ATS recommends antihistamine use for patients with EIB and allergies who continue to be symptomatic despite daily or more frequent inhaled SABA use. They recommend against using antihistamines for patients who have EIB but who do not have allergies.
ATS also provides some weaker recommendations for those who want to control EIB symptoms with dietary modification. A low-salt diet supplemented with fish oils and ascorbic acid may increase symptom control.
Bottom line
EIB is an acute, reversible airway narrowing that occurs during or after strenuous exercise. A high percentage of physically active patients have EIB, regardless of whether they have underlying asthma conditions. Administration of an inhaled SABA 15 minutes prior to exercise and a variety of warm-up exercises act as a first-line treatment, with an inhaled corticosteroid or a leukotriene receptor antagonist effective for those who do not respond to the SABA alone.
Reference
J. P. Parsons et al. "An Official American Thoracic Society Clinical Practice Guideline: Exercise-induced Bronchoconstriction," Am. J. Respir. Crit. Care Med. 2013;187:1016-27.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. Dr. Beddis is an attending physician in the Abington Health Network at Wyncote Family Medicine.
Exercise-induced bronchoconstriction is defined as acute, reversible airway narrowing that occurs during or after strenuous exercise. It is a very common problem, especially in physically active people, and can occur with or without underlying asthma. It is estimated that 10%-20% of the general population and up to 90% of people previously diagnosed with asthma have exercise-induced bronchoconstriction. Some studies suggest that exercise-induced bronchoconstriction can occur in as many as 30-70% of Olympic or elite-level athletes.
The following evidence-based guidelines were developed by the American Thoracic Society (ATS) to provide clinicians with practical guidance for the diagnosis and treatment of exercise-induced bronchoconstriction (EIB).
Diagnosis
Diagnosing EIB can be difficult as symptoms tend to be nonspecific and variable. Further, the presence or absence of common respiratory symptoms (such as chest tightness, cough, wheezing, and dyspnea) has very poor predictive value for the confirmation of EIB. Symptom severity ranges from mild to moderate – defined as causing impairment of athletic performance but rarely significant respiratory distress – and can be provoked by exercise or specific environments such as snowy mountains, ice rinks, or indoor swimming pools. An official EIB diagnosis should be established by monitoring changes in lung function provoked by exercise, not simply on the basis of symptoms.
Testing
To determine if EIB is present and to quantify the severity of the disorder, providers should conduct serial lung function measurements after a specific exercise or hyperpnea challenge. An example of an exercise challenge protocol is 5-8 minutes of exercise at 85% of maximum heart rate or 80% of maximal oxygen uptake (80% VO2 max). The type, duration, and intensity of exercise and the temperature and water content of the air are variables that should be considered. According to ATS and the European Respiratory Society guidelines, at least two reproducible FEV1 (forced expiratory volume in 1 second) values should be measured after the exercise challenge, with the highest value recorded at each interval – usually 5, 10, 15, and 30 minutes after exercise. Experts prefer measuring FEV1 because it is more discriminating and has better repeatability than peak expiratory flow rate.
There are a number of alternatives for testing, described in detail in ATS’s online supplement, which may be easier to implement than exercise challenges. These alternatives include eucapnic voluntary hyperpnea of dry air and inhalation of hyperosmolar aerosols of 4.5% saline or dry powder mannitol.
Interpreting results
Airway response is first calculated by finding the difference between the pre-exercise FEV1 value and the lowest FEV1 value recorded within 30 minutes after exercise. The percent fall in FEV1 from the baseline value is used to diagnose EIB, requiring a percentage fall of greater than 10% for official diagnosis. The severity of EIB can be graded as mild (more than 10% but less than 25% fall in FEV1), moderate (more than 25% but less than 50%), or severe (more than 50%).
Treatment
To prevent EIB, ATS recommends that patients use an inhaled short-acting beta2-agonist (SABA) 15 minutes prior to exercise and perform "interval or combination warm-up exercises" when possible. Use of a SABA prior to exercise provides 2-4 hours of attenuation of exercise-induced bronchospasm. Because of the potential for environmental triggers, ATS also recommends routine use of an air-warming and humidifying mask during exercise in cold weather. Daily use of a SABA may result in the development of tolerance, with reduction in the amount and duration of protection from EIB. This is thought to be due to desensitization of the beta2-receptors on mast cells.
For patients who have an inadequate response to an inhaled SABA before exercise and/or patients who require an inhaled SABA daily or more frequently, a controller agent such as an inhaled corticosteroid or a leukotriene receptor antagonist is recommended. Patients should be informed that maximal therapeutic benefit may take 2-4 treatment weeks.
In addition to the daily regime, ATS suggests the addition of a mast cell stabilizing agent or an inhaled anticholinergic agent before exercise if needed (both are relatively weaker recommendations). And finally, they recommend against daily use of an inhaled long-acting beta2-agonist (LABA) as a single therapy because of the strong concern for adverse side effects.
Special provisions
ATS recommends antihistamine use for patients with EIB and allergies who continue to be symptomatic despite daily or more frequent inhaled SABA use. They recommend against using antihistamines for patients who have EIB but who do not have allergies.
ATS also provides some weaker recommendations for those who want to control EIB symptoms with dietary modification. A low-salt diet supplemented with fish oils and ascorbic acid may increase symptom control.
Bottom line
EIB is an acute, reversible airway narrowing that occurs during or after strenuous exercise. A high percentage of physically active patients have EIB, regardless of whether they have underlying asthma conditions. Administration of an inhaled SABA 15 minutes prior to exercise and a variety of warm-up exercises act as a first-line treatment, with an inhaled corticosteroid or a leukotriene receptor antagonist effective for those who do not respond to the SABA alone.
Reference
J. P. Parsons et al. "An Official American Thoracic Society Clinical Practice Guideline: Exercise-induced Bronchoconstriction," Am. J. Respir. Crit. Care Med. 2013;187:1016-27.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. Dr. Beddis is an attending physician in the Abington Health Network at Wyncote Family Medicine.
Estrogen-related VTE shows low recurrence rate
AMSTERDAM – Women with an unprovoked index venous thromboembolism while they are on estrogen treatment have a low recurrence risk as long as they stop estrogen, and therefore don’t need prolonged anticoagulant treatment, based on a review of 630 cases.
Women whose index venous thromboembolism (VTE) occurred while on estrogen had 4 recurrences for every 10 among the women who had unprovoked VTE and were not on estrogen during an average follow-up of more than 6 years, Dr. Lisbeth Eischer said at the 24th Congress of the International Society on Thrombosis and Haemostasis.
"We propose that these women [whose index VTE occurred while on estrogen] should receive anticoagulant treatment for no longer than 3 months," said Dr. Eischer of the division of hematology and hemostasis at the Medical University of Vienna.
"I think the recommendation [for duration of anticoagulation] should be comparable to women who have undergone surgery, not more than 3 months," she said. In the review she presented, which included 630 women treated for a VTE since 1992, the average duration of anticoagulant treatment was 7 months among women whose VTE occurred when on estrogen as well as those not on estrogen at the time of their VTE.
Dr. Eischer and her associates studied women enrolled in the prospective Austrian Study on Recurrent Venous Thromboembolism (AUREC). The group of 630 included women aged 18 years or older who had a first VTE and received at least 3 months of anticoagulant treatment. The study excluded women with another identifiable cause of VTE, such as surgery, trauma, pregnancy, cancer, or significant thrombophilia. Women were not excluded if they were heterozygous for a factor V Leiden mutation. They averaged 46 years old; 361 (57%) had deep vein thrombosis as their index case, and 269 (43%) had pulmonary embolism as their index case. The average length of follow-up was 76 months (6.3 years).
Three hundred thirty-three (53%) women were on estrogen treatment at the time of their VTE. These women were significantly younger, averaging 38 years compared with an average of 55 among the women not receiving estrogen at the time of their VTE. The prevalence of women with a single factor V Leiden mutation was 48 (16%) among those not on estrogen and 98 (28%) among those on estrogen, a statistically significant difference.
During follow-up, the incidence of recurrent VTE was 22 (7%) among the 333 women whose index VTE occurred while on estrogen, and 49 (16%) among the 297 with an unprovoked index VTE. In a multivariate analysis that adjusted for age, location of the VTE (pulmonary or deep vein), and presence of a factor V Leiden mutation, women whose index VTE occurred while they were taking estrogen had a statistically significant 60% reduced rate of having a recurrent VTE during follow-up compared with the women whose index VTE occurred when they were not on estrogen.
Dr. Eischer said she had no relevant financial disclosures.
On Twitter @mitchelzoler
AMSTERDAM – Women with an unprovoked index venous thromboembolism while they are on estrogen treatment have a low recurrence risk as long as they stop estrogen, and therefore don’t need prolonged anticoagulant treatment, based on a review of 630 cases.
Women whose index venous thromboembolism (VTE) occurred while on estrogen had 4 recurrences for every 10 among the women who had unprovoked VTE and were not on estrogen during an average follow-up of more than 6 years, Dr. Lisbeth Eischer said at the 24th Congress of the International Society on Thrombosis and Haemostasis.
"We propose that these women [whose index VTE occurred while on estrogen] should receive anticoagulant treatment for no longer than 3 months," said Dr. Eischer of the division of hematology and hemostasis at the Medical University of Vienna.
"I think the recommendation [for duration of anticoagulation] should be comparable to women who have undergone surgery, not more than 3 months," she said. In the review she presented, which included 630 women treated for a VTE since 1992, the average duration of anticoagulant treatment was 7 months among women whose VTE occurred when on estrogen as well as those not on estrogen at the time of their VTE.
Dr. Eischer and her associates studied women enrolled in the prospective Austrian Study on Recurrent Venous Thromboembolism (AUREC). The group of 630 included women aged 18 years or older who had a first VTE and received at least 3 months of anticoagulant treatment. The study excluded women with another identifiable cause of VTE, such as surgery, trauma, pregnancy, cancer, or significant thrombophilia. Women were not excluded if they were heterozygous for a factor V Leiden mutation. They averaged 46 years old; 361 (57%) had deep vein thrombosis as their index case, and 269 (43%) had pulmonary embolism as their index case. The average length of follow-up was 76 months (6.3 years).
Three hundred thirty-three (53%) women were on estrogen treatment at the time of their VTE. These women were significantly younger, averaging 38 years compared with an average of 55 among the women not receiving estrogen at the time of their VTE. The prevalence of women with a single factor V Leiden mutation was 48 (16%) among those not on estrogen and 98 (28%) among those on estrogen, a statistically significant difference.
During follow-up, the incidence of recurrent VTE was 22 (7%) among the 333 women whose index VTE occurred while on estrogen, and 49 (16%) among the 297 with an unprovoked index VTE. In a multivariate analysis that adjusted for age, location of the VTE (pulmonary or deep vein), and presence of a factor V Leiden mutation, women whose index VTE occurred while they were taking estrogen had a statistically significant 60% reduced rate of having a recurrent VTE during follow-up compared with the women whose index VTE occurred when they were not on estrogen.
Dr. Eischer said she had no relevant financial disclosures.
On Twitter @mitchelzoler
AMSTERDAM – Women with an unprovoked index venous thromboembolism while they are on estrogen treatment have a low recurrence risk as long as they stop estrogen, and therefore don’t need prolonged anticoagulant treatment, based on a review of 630 cases.
Women whose index venous thromboembolism (VTE) occurred while on estrogen had 4 recurrences for every 10 among the women who had unprovoked VTE and were not on estrogen during an average follow-up of more than 6 years, Dr. Lisbeth Eischer said at the 24th Congress of the International Society on Thrombosis and Haemostasis.
"We propose that these women [whose index VTE occurred while on estrogen] should receive anticoagulant treatment for no longer than 3 months," said Dr. Eischer of the division of hematology and hemostasis at the Medical University of Vienna.
"I think the recommendation [for duration of anticoagulation] should be comparable to women who have undergone surgery, not more than 3 months," she said. In the review she presented, which included 630 women treated for a VTE since 1992, the average duration of anticoagulant treatment was 7 months among women whose VTE occurred when on estrogen as well as those not on estrogen at the time of their VTE.
Dr. Eischer and her associates studied women enrolled in the prospective Austrian Study on Recurrent Venous Thromboembolism (AUREC). The group of 630 included women aged 18 years or older who had a first VTE and received at least 3 months of anticoagulant treatment. The study excluded women with another identifiable cause of VTE, such as surgery, trauma, pregnancy, cancer, or significant thrombophilia. Women were not excluded if they were heterozygous for a factor V Leiden mutation. They averaged 46 years old; 361 (57%) had deep vein thrombosis as their index case, and 269 (43%) had pulmonary embolism as their index case. The average length of follow-up was 76 months (6.3 years).
Three hundred thirty-three (53%) women were on estrogen treatment at the time of their VTE. These women were significantly younger, averaging 38 years compared with an average of 55 among the women not receiving estrogen at the time of their VTE. The prevalence of women with a single factor V Leiden mutation was 48 (16%) among those not on estrogen and 98 (28%) among those on estrogen, a statistically significant difference.
During follow-up, the incidence of recurrent VTE was 22 (7%) among the 333 women whose index VTE occurred while on estrogen, and 49 (16%) among the 297 with an unprovoked index VTE. In a multivariate analysis that adjusted for age, location of the VTE (pulmonary or deep vein), and presence of a factor V Leiden mutation, women whose index VTE occurred while they were taking estrogen had a statistically significant 60% reduced rate of having a recurrent VTE during follow-up compared with the women whose index VTE occurred when they were not on estrogen.
Dr. Eischer said she had no relevant financial disclosures.
On Twitter @mitchelzoler
AT ISTH 2013

Estrogen-related VTE shows low recurrence rate
AMSTERDAM – Women with an unprovoked index venous thromboembolism while they are on estrogen treatment have a low recurrence risk as long as they stop estrogen, and therefore don’t need prolonged anticoagulant treatment, based on a review of 630 cases.
Women whose index venous thromboembolism (VTE) occurred while on estrogen had 4 recurrences for every 10 among the women who had unprovoked VTE and were not on estrogen during an average follow-up of more than 6 years, Dr. Lisbeth Eischer said at the 24th Congress of the International Society on Thrombosis and Haemostasis.
"We propose that these women [whose index VTE occurred while on estrogen] should receive anticoagulant treatment for no longer than 3 months," said Dr. Eischer of the division of hematology and hemostasis at the Medical University of Vienna.

"I think the recommendation [for duration of anticoagulation] should be comparable to women who have undergone surgery, not more than 3 months," she said. In the review she presented, which included 630 women treated for a VTE since 1992, the average duration of anticoagulant treatment was 7 months among women whose VTE occurred when on estrogen as well as those not on estrogen at the time of their VTE.
Dr. Eischer and her associates studied women enrolled in the prospective Austrian Study on Recurrent Venous Thromboembolism (AUREC). The group of 630 included women aged 18 years or older who had a first VTE and received at least 3 months of anticoagulant treatment. The study excluded women with another identifiable cause of VTE, such as surgery, trauma, pregnancy, cancer, or significant thrombophilia. Women were not excluded if they were heterozygous for a factor V Leiden mutation. They averaged 46 years old; 361 (57%) had deep vein thrombosis as their index case, and 269 (43%) had pulmonary embolism as their index case. The average length of follow-up was 76 months (6.3 years).
Three hundred thirty-three (53%) women were on estrogen treatment at the time of their VTE. These women were significantly younger, averaging 38 years compared with an average of 55 among the women not receiving estrogen at the time of their VTE. The prevalence of women with a single factor V Leiden mutation was 48 (16%) among those not on estrogen and 98 (28%) among those on estrogen, a statistically significant difference.
During follow-up, the incidence of recurrent VTE was 22 (7%) among the 333 women whose index VTE occurred while on estrogen, and 49 (16%) among the 297 with an unprovoked index VTE. In a multivariate analysis that adjusted for age, location of the VTE (pulmonary or deep vein), and presence of a factor V Leiden mutation, women whose index VTE occurred while they were taking estrogen had a statistically significant 60% reduced rate of having a recurrent VTE during follow-up compared with the women whose index VTE occurred when they were not on estrogen.
Dr. Eischer said she had no relevant financial disclosures.
On Twitter @mitchelzoler
AMSTERDAM – Women with an unprovoked index venous thromboembolism while they are on estrogen treatment have a low recurrence risk as long as they stop estrogen, and therefore don’t need prolonged anticoagulant treatment, based on a review of 630 cases.
Women whose index venous thromboembolism (VTE) occurred while on estrogen had 4 recurrences for every 10 among the women who had unprovoked VTE and were not on estrogen during an average follow-up of more than 6 years, Dr. Lisbeth Eischer said at the 24th Congress of the International Society on Thrombosis and Haemostasis.
"We propose that these women [whose index VTE occurred while on estrogen] should receive anticoagulant treatment for no longer than 3 months," said Dr. Eischer of the division of hematology and hemostasis at the Medical University of Vienna.
"I think the recommendation [for duration of anticoagulation] should be comparable to women who have undergone surgery, not more than 3 months," she said. In the review she presented, which included 630 women treated for a VTE since 1992, the average duration of anticoagulant treatment was 7 months among women whose VTE occurred when on estrogen as well as those not on estrogen at the time of their VTE.
Dr. Eischer and her associates studied women enrolled in the prospective Austrian Study on Recurrent Venous Thromboembolism (AUREC). The group of 630 included women aged 18 years or older who had a first VTE and received at least 3 months of anticoagulant treatment. The study excluded women with another identifiable cause of VTE, such as surgery, trauma, pregnancy, cancer, or significant thrombophilia. Women were not excluded if they were heterozygous for a factor V Leiden mutation. They averaged 46 years old; 361 (57%) had deep vein thrombosis as their index case, and 269 (43%) had pulmonary embolism as their index case. The average length of follow-up was 76 months (6.3 years).
Three hundred thirty-three (53%) women were on estrogen treatment at the time of their VTE. These women were significantly younger, averaging 38 years compared with an average of 55 among the women not receiving estrogen at the time of their VTE. The prevalence of women with a single factor V Leiden mutation was 48 (16%) among those not on estrogen and 98 (28%) among those on estrogen, a statistically significant difference.
During follow-up, the incidence of recurrent VTE was 22 (7%) among the 333 women whose index VTE occurred while on estrogen, and 49 (16%) among the 297 with an unprovoked index VTE. In a multivariate analysis that adjusted for age, location of the VTE (pulmonary or deep vein), and presence of a factor V Leiden mutation, women whose index VTE occurred while they were taking estrogen had a statistically significant 60% reduced rate of having a recurrent VTE during follow-up compared with the women whose index VTE occurred when they were not on estrogen.
Dr. Eischer said she had no relevant financial disclosures.
On Twitter @mitchelzoler
AMSTERDAM – Women with an unprovoked index venous thromboembolism while they are on estrogen treatment have a low recurrence risk as long as they stop estrogen, and therefore don’t need prolonged anticoagulant treatment, based on a review of 630 cases.
Women whose index venous thromboembolism (VTE) occurred while on estrogen had 4 recurrences for every 10 among the women who had unprovoked VTE and were not on estrogen during an average follow-up of more than 6 years, Dr. Lisbeth Eischer said at the 24th Congress of the International Society on Thrombosis and Haemostasis.
"We propose that these women [whose index VTE occurred while on estrogen] should receive anticoagulant treatment for no longer than 3 months," said Dr. Eischer of the division of hematology and hemostasis at the Medical University of Vienna.
"I think the recommendation [for duration of anticoagulation] should be comparable to women who have undergone surgery, not more than 3 months," she said. In the review she presented, which included 630 women treated for a VTE since 1992, the average duration of anticoagulant treatment was 7 months among women whose VTE occurred when on estrogen as well as those not on estrogen at the time of their VTE.
Dr. Eischer and her associates studied women enrolled in the prospective Austrian Study on Recurrent Venous Thromboembolism (AUREC). The group of 630 included women aged 18 years or older who had a first VTE and received at least 3 months of anticoagulant treatment. The study excluded women with another identifiable cause of VTE, such as surgery, trauma, pregnancy, cancer, or significant thrombophilia. Women were not excluded if they were heterozygous for a factor V Leiden mutation. They averaged 46 years old; 361 (57%) had deep vein thrombosis as their index case, and 269 (43%) had pulmonary embolism as their index case. The average length of follow-up was 76 months (6.3 years).
Three hundred thirty-three (53%) women were on estrogen treatment at the time of their VTE. These women were significantly younger, averaging 38 years compared with an average of 55 among the women not receiving estrogen at the time of their VTE. The prevalence of women with a single factor V Leiden mutation was 48 (16%) among those not on estrogen and 98 (28%) among those on estrogen, a statistically significant difference.
During follow-up, the incidence of recurrent VTE was 22 (7%) among the 333 women whose index VTE occurred while on estrogen, and 49 (16%) among the 297 with an unprovoked index VTE. In a multivariate analysis that adjusted for age, location of the VTE (pulmonary or deep vein), and presence of a factor V Leiden mutation, women whose index VTE occurred while they were taking estrogen had a statistically significant 60% reduced rate of having a recurrent VTE during follow-up compared with the women whose index VTE occurred when they were not on estrogen.
Dr. Eischer said she had no relevant financial disclosures.
On Twitter @mitchelzoler
AT ISTH 2013
Major finding: Women whose otherwise unprovoked venous thromboembolism occurred while they were on estrogen had 60% fewer recurrences than did women not on estrogen.
Data source: A review of 630 women followed after a first-time VTE at one Austrian center.
Disclosures: Dr. Eischer said she had no relevant financial disclosures.

This asthma treatment has a lasting side effect in children
Before prescribing inhaled corticosteroids (ICS) for a child with asthma, tell the patient—and parents—that their use could lead to a small but permanent effect on adult height.1
STRENGTH OF RECOMMENDATIONS
B: Based on one prospective study.
Kelly HW, Sternberg AL, Lescher R, et al; CAMP Research Group. Effect of inhaled glucocorticoids in childhood on adult height. N Engl J Med. 2012;367:904-912.
Illustrative case
A 10-year-old boy is brought in by his father for asthma follow-up. The child uses an albuterol inhaler, but has had increased coughing and wheezing recently. You are ready to step up his asthma therapy to include ICS. But the patient’s father questions this, noting that he recently read that steroids may reduce a child’s growth. How should you respond?
Inhaled corticosteroids (ICS) are a mainstay in the treatment of asthma ranging from mild persistent to severe. Standards of care for asthma treatment involve a stepwise approach, with ICS added if symptoms are not controlled with short-acting beta antagonists alone.2 In addition, monotherapy with ICS is more effective for controlling symptoms than leukotriene inhibitors or other controller medications, while also decreasing hospitalizations and nocturnal awakenings and improving quality of life—with few side effects.3
What we know about ICS and children’s growth
One adverse effect of ICS, however, is that of “decreased linear growth velocity”4—ie, slowing the rate at which children grow. Until recently, children were thought to “catch up” later in life, either by growing for a longer period of time than they would had they not taken ICS or by growing at an increased velocity after ICS medications are discontinued.4-6
Study summary: The effect on growth is small, but long-lasting
Kelly et al conducted a prospective observational cohort study that followed 943 (90.7%) participants in the Childhood Asthma Management Program (CAMP) in the years after the randomized controlled trial (RCT) ended.
A double-blind, placebo-controlled RCT, CAMP studied the linear growth of 1041 children with mild-to-moderate persistent asthma who were divided into 3 treatment groups: One group received 200 mcg inhaled budesonide twice daily; a second group received 8 mg inhaled nedocromil twice daily; and a third group received placebo. Albuterol was used symptomatically by all 3 groups.7 The children ranged in age from 5 to 13 years at the start of the study; 98 patients—split evenly among the 3 treatment arms—were lost to follow-up.
During the 4 to 6 years of the CAMP trial, the budesonide group received a mean total of 636 mg ICS, whereas the nedocromil and placebo groups received an average of 88.5 and 109.4 mg ICS, respectively. After the RCT ended, all participants had standardized asthma treatment, receiving mean adjusted total doses of ICS of 381 mg for the budesonide group, 347.9 mg for the nedocromil group, and 355 mg for the placebo group.
Patients’ height was measured every 6 months for the next 4.5 years, and once or twice a year thereafter until they reached adult height (at a mean age of 24.9±2.7 years).
ICS users were a half inch shorter
Long-term ICS use was linked to a lower adult height. The adjusted mean height was 171.1 cm for the budesonide group vs 172.3 cm for those on placebo, a difference of 1.2 cm, or 0.47 inch (95% confidence interval [CI], −1.9 to −0.5; P=.001); the mean adult height in the nedocromil group (172.1 cm) was similar to that of the placebo group (−0.2 cm; 95% CI, −0.9 to 0.5; P=.61).
The lower adult height in the ICS group did not vary significantly based on sex, age at trial entry, race, or duration of asthma prior to trial entry; however, dose was a key factor. A larger daily dose of budesonide—particularly in the first 2 years of the RCT—was associated with a lower adult height (about −0.1 cm for each mcg/kg in that 2-year time frame). This was consistent with results from studies that looked at other types of ICS (beclomethasone, fluticasone, and mometasone).8-11
The study also showed that growth velocity was reduced in the first 2 years of assigned treatment with budesonide, and this was primarily among prepubertal participants. After the initial 2-year slowing in growth rate, the children resumed growing at normal speeds.
What’s new: Now we know: Children don’t “catch up"
Retrospective studies have reported that children on ICS for mild persistent to moderate asthma would have an initial slowing in growth velocity but then “catch up” by growing for a longer period of time.3-5 This is the first prospective study with good follow-up to show that ICS use affects long-term growth and adult height. While the effect is not large, some children and their families might be concerned about it.
Caveats: ICS use was atypical
The randomized controlled portion of the study used a prescribed dose of budesonide without regard to symptoms. This is not the typical pattern of ICS use. In addition, compliance with ICS varies significantly.12 Because the effect on adult height appears to be dose dependent, however, we think the results of this study are valid.
In addition, there was a placebo control group (and big differences in exposure to ICS) only for the duration of the RCT. During the subsequent study, all patients received equivalent doses of ICS. This means that the variation in mean adult height achieved can be primarily ascribed to participants’ use of ICS during the 4- to 6-year CAMP trial. Of note, the effect of ICS was greatest in prepubertal participants, so there may be a diminished effect as teens approach their final height.
The study did not look at the effect of ICS use in patients with severe asthma—the group most likely to use ICS. However, the benefits of ICS for those with severe asthma likely outweigh any negative effects on adult height.
Challenges to implementation: What to tell patients
The message we convey to patients (and parents) about ICS use is a nuanced one. We can stress that ICS remain very important in the treatment of asthma and, while it appears that their use causes a slight decrease in adult height, most children with persistent asthma benefit from ICS.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
1. Kelly HW, Sternberg AL, Lescher R, et al; CAMP Research Group. Effect of inhaled glucocorticoids in childhood on adult height. N Engl J Med. 2012;367:904-912.
2. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. National Institutes of Health National Heart, Lung and Blood Institute: National Asthma Education and Prevention Program, 2007. Available at: http://www.nhlbi. nih.gov/guidelines/asthma/asthgdln.pdf. Accessed August 15, 2013.
3. Chauhan BF, Ducharme FM. Anti-leukotriene agents compared to inhaled corticosteroids in the management of recurrent and/ or chronic asthma in adults and children. Cochrane Database Syst Rev. 2012;(5):CD002314.
4. Agertoft L, Pedersen S. Effect of long- term treatment with budesonide on adult height in children with asthma. N Engl J Med. 2000;343:1064-1069.
5. Van Bever HP, Desager KN, Lijssens N, et al. Does treatment of asthmatic children with inhaled corticosteroids affect their adult height? Pediatr Pulmonol. 1999;27:369-375.
6. Silverstein MD, Yunginger JW, Reed CE, et al. Attained adult height after childhood asthma: effect of glucocorticoid therapy. J Allergy Clin Immunol. 1997;99:466-474.
7. The Childhood Asthma Management Program Research Group. Long-term effects of budesonide or nedocromil in children with asthma. N Engl J Med. 2000;343:1054-1063.
8. Tinkelman DG, Reed CE, Nelson HS, et al. Aerosol beclomethasone dipropionate compared with theophylline as primary treatment of chronic, mild to moderately severe asthma in children. Pediatrics. 1993;92:64-77.
9. Verberne AA, Frost C, Roorda RJ, et al. One year treatment with salmeterol compared with beclomethasone in children with asthma. Am J Respir Crit Care Med. 1997;156:688-695.
10. Allen DB, Bronsky EA, LaForce CF, et al. Growth in asthmatic children treated with fluticasone propionate. J Pediatr 1998;132: 472-477.
11. Skoner DP, Meltzer EO, Milgrom H, et al. Effects of inhaled mometasone furoate on growth velocity and adrenal function: a placebo-controlled trial in children 4-9 years old with mild persistent asthma. J Asthma. 2011;48:848-859.
12. Cochrane MG, Bala MV, Downs KE, et al. Inhaled corticosteroids for asthma therapy: patient compliance, devices, and inhalation technique. Chest. 2000;117:542-550.
Before prescribing inhaled corticosteroids (ICS) for a child with asthma, tell the patient—and parents—that their use could lead to a small but permanent effect on adult height.1
STRENGTH OF RECOMMENDATIONS
B: Based on one prospective study.
Kelly HW, Sternberg AL, Lescher R, et al; CAMP Research Group. Effect of inhaled glucocorticoids in childhood on adult height. N Engl J Med. 2012;367:904-912.
Illustrative case
A 10-year-old boy is brought in by his father for asthma follow-up. The child uses an albuterol inhaler, but has had increased coughing and wheezing recently. You are ready to step up his asthma therapy to include ICS. But the patient’s father questions this, noting that he recently read that steroids may reduce a child’s growth. How should you respond?
Inhaled corticosteroids (ICS) are a mainstay in the treatment of asthma ranging from mild persistent to severe. Standards of care for asthma treatment involve a stepwise approach, with ICS added if symptoms are not controlled with short-acting beta antagonists alone.2 In addition, monotherapy with ICS is more effective for controlling symptoms than leukotriene inhibitors or other controller medications, while also decreasing hospitalizations and nocturnal awakenings and improving quality of life—with few side effects.3
What we know about ICS and children’s growth
One adverse effect of ICS, however, is that of “decreased linear growth velocity”4—ie, slowing the rate at which children grow. Until recently, children were thought to “catch up” later in life, either by growing for a longer period of time than they would had they not taken ICS or by growing at an increased velocity after ICS medications are discontinued.4-6
Study summary: The effect on growth is small, but long-lasting
Kelly et al conducted a prospective observational cohort study that followed 943 (90.7%) participants in the Childhood Asthma Management Program (CAMP) in the years after the randomized controlled trial (RCT) ended.
A double-blind, placebo-controlled RCT, CAMP studied the linear growth of 1041 children with mild-to-moderate persistent asthma who were divided into 3 treatment groups: One group received 200 mcg inhaled budesonide twice daily; a second group received 8 mg inhaled nedocromil twice daily; and a third group received placebo. Albuterol was used symptomatically by all 3 groups.7 The children ranged in age from 5 to 13 years at the start of the study; 98 patients—split evenly among the 3 treatment arms—were lost to follow-up.
During the 4 to 6 years of the CAMP trial, the budesonide group received a mean total of 636 mg ICS, whereas the nedocromil and placebo groups received an average of 88.5 and 109.4 mg ICS, respectively. After the RCT ended, all participants had standardized asthma treatment, receiving mean adjusted total doses of ICS of 381 mg for the budesonide group, 347.9 mg for the nedocromil group, and 355 mg for the placebo group.
Patients’ height was measured every 6 months for the next 4.5 years, and once or twice a year thereafter until they reached adult height (at a mean age of 24.9±2.7 years).
ICS users were a half inch shorter
Long-term ICS use was linked to a lower adult height. The adjusted mean height was 171.1 cm for the budesonide group vs 172.3 cm for those on placebo, a difference of 1.2 cm, or 0.47 inch (95% confidence interval [CI], −1.9 to −0.5; P=.001); the mean adult height in the nedocromil group (172.1 cm) was similar to that of the placebo group (−0.2 cm; 95% CI, −0.9 to 0.5; P=.61).
The lower adult height in the ICS group did not vary significantly based on sex, age at trial entry, race, or duration of asthma prior to trial entry; however, dose was a key factor. A larger daily dose of budesonide—particularly in the first 2 years of the RCT—was associated with a lower adult height (about −0.1 cm for each mcg/kg in that 2-year time frame). This was consistent with results from studies that looked at other types of ICS (beclomethasone, fluticasone, and mometasone).8-11
The study also showed that growth velocity was reduced in the first 2 years of assigned treatment with budesonide, and this was primarily among prepubertal participants. After the initial 2-year slowing in growth rate, the children resumed growing at normal speeds.
What’s new: Now we know: Children don’t “catch up"
Retrospective studies have reported that children on ICS for mild persistent to moderate asthma would have an initial slowing in growth velocity but then “catch up” by growing for a longer period of time.3-5 This is the first prospective study with good follow-up to show that ICS use affects long-term growth and adult height. While the effect is not large, some children and their families might be concerned about it.
Caveats: ICS use was atypical
The randomized controlled portion of the study used a prescribed dose of budesonide without regard to symptoms. This is not the typical pattern of ICS use. In addition, compliance with ICS varies significantly.12 Because the effect on adult height appears to be dose dependent, however, we think the results of this study are valid.
In addition, there was a placebo control group (and big differences in exposure to ICS) only for the duration of the RCT. During the subsequent study, all patients received equivalent doses of ICS. This means that the variation in mean adult height achieved can be primarily ascribed to participants’ use of ICS during the 4- to 6-year CAMP trial. Of note, the effect of ICS was greatest in prepubertal participants, so there may be a diminished effect as teens approach their final height.
The study did not look at the effect of ICS use in patients with severe asthma—the group most likely to use ICS. However, the benefits of ICS for those with severe asthma likely outweigh any negative effects on adult height.
Challenges to implementation: What to tell patients
The message we convey to patients (and parents) about ICS use is a nuanced one. We can stress that ICS remain very important in the treatment of asthma and, while it appears that their use causes a slight decrease in adult height, most children with persistent asthma benefit from ICS.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Before prescribing inhaled corticosteroids (ICS) for a child with asthma, tell the patient—and parents—that their use could lead to a small but permanent effect on adult height.1
STRENGTH OF RECOMMENDATIONS
B: Based on one prospective study.
Kelly HW, Sternberg AL, Lescher R, et al; CAMP Research Group. Effect of inhaled glucocorticoids in childhood on adult height. N Engl J Med. 2012;367:904-912.
Illustrative case
A 10-year-old boy is brought in by his father for asthma follow-up. The child uses an albuterol inhaler, but has had increased coughing and wheezing recently. You are ready to step up his asthma therapy to include ICS. But the patient’s father questions this, noting that he recently read that steroids may reduce a child’s growth. How should you respond?
Inhaled corticosteroids (ICS) are a mainstay in the treatment of asthma ranging from mild persistent to severe. Standards of care for asthma treatment involve a stepwise approach, with ICS added if symptoms are not controlled with short-acting beta antagonists alone.2 In addition, monotherapy with ICS is more effective for controlling symptoms than leukotriene inhibitors or other controller medications, while also decreasing hospitalizations and nocturnal awakenings and improving quality of life—with few side effects.3
What we know about ICS and children’s growth
One adverse effect of ICS, however, is that of “decreased linear growth velocity”4—ie, slowing the rate at which children grow. Until recently, children were thought to “catch up” later in life, either by growing for a longer period of time than they would had they not taken ICS or by growing at an increased velocity after ICS medications are discontinued.4-6
Study summary: The effect on growth is small, but long-lasting
Kelly et al conducted a prospective observational cohort study that followed 943 (90.7%) participants in the Childhood Asthma Management Program (CAMP) in the years after the randomized controlled trial (RCT) ended.
A double-blind, placebo-controlled RCT, CAMP studied the linear growth of 1041 children with mild-to-moderate persistent asthma who were divided into 3 treatment groups: One group received 200 mcg inhaled budesonide twice daily; a second group received 8 mg inhaled nedocromil twice daily; and a third group received placebo. Albuterol was used symptomatically by all 3 groups.7 The children ranged in age from 5 to 13 years at the start of the study; 98 patients—split evenly among the 3 treatment arms—were lost to follow-up.
During the 4 to 6 years of the CAMP trial, the budesonide group received a mean total of 636 mg ICS, whereas the nedocromil and placebo groups received an average of 88.5 and 109.4 mg ICS, respectively. After the RCT ended, all participants had standardized asthma treatment, receiving mean adjusted total doses of ICS of 381 mg for the budesonide group, 347.9 mg for the nedocromil group, and 355 mg for the placebo group.
Patients’ height was measured every 6 months for the next 4.5 years, and once or twice a year thereafter until they reached adult height (at a mean age of 24.9±2.7 years).
ICS users were a half inch shorter
Long-term ICS use was linked to a lower adult height. The adjusted mean height was 171.1 cm for the budesonide group vs 172.3 cm for those on placebo, a difference of 1.2 cm, or 0.47 inch (95% confidence interval [CI], −1.9 to −0.5; P=.001); the mean adult height in the nedocromil group (172.1 cm) was similar to that of the placebo group (−0.2 cm; 95% CI, −0.9 to 0.5; P=.61).
The lower adult height in the ICS group did not vary significantly based on sex, age at trial entry, race, or duration of asthma prior to trial entry; however, dose was a key factor. A larger daily dose of budesonide—particularly in the first 2 years of the RCT—was associated with a lower adult height (about −0.1 cm for each mcg/kg in that 2-year time frame). This was consistent with results from studies that looked at other types of ICS (beclomethasone, fluticasone, and mometasone).8-11
The study also showed that growth velocity was reduced in the first 2 years of assigned treatment with budesonide, and this was primarily among prepubertal participants. After the initial 2-year slowing in growth rate, the children resumed growing at normal speeds.
What’s new: Now we know: Children don’t “catch up"
Retrospective studies have reported that children on ICS for mild persistent to moderate asthma would have an initial slowing in growth velocity but then “catch up” by growing for a longer period of time.3-5 This is the first prospective study with good follow-up to show that ICS use affects long-term growth and adult height. While the effect is not large, some children and their families might be concerned about it.
Caveats: ICS use was atypical
The randomized controlled portion of the study used a prescribed dose of budesonide without regard to symptoms. This is not the typical pattern of ICS use. In addition, compliance with ICS varies significantly.12 Because the effect on adult height appears to be dose dependent, however, we think the results of this study are valid.
In addition, there was a placebo control group (and big differences in exposure to ICS) only for the duration of the RCT. During the subsequent study, all patients received equivalent doses of ICS. This means that the variation in mean adult height achieved can be primarily ascribed to participants’ use of ICS during the 4- to 6-year CAMP trial. Of note, the effect of ICS was greatest in prepubertal participants, so there may be a diminished effect as teens approach their final height.
The study did not look at the effect of ICS use in patients with severe asthma—the group most likely to use ICS. However, the benefits of ICS for those with severe asthma likely outweigh any negative effects on adult height.
Challenges to implementation: What to tell patients
The message we convey to patients (and parents) about ICS use is a nuanced one. We can stress that ICS remain very important in the treatment of asthma and, while it appears that their use causes a slight decrease in adult height, most children with persistent asthma benefit from ICS.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
1. Kelly HW, Sternberg AL, Lescher R, et al; CAMP Research Group. Effect of inhaled glucocorticoids in childhood on adult height. N Engl J Med. 2012;367:904-912.
2. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. National Institutes of Health National Heart, Lung and Blood Institute: National Asthma Education and Prevention Program, 2007. Available at: http://www.nhlbi. nih.gov/guidelines/asthma/asthgdln.pdf. Accessed August 15, 2013.
3. Chauhan BF, Ducharme FM. Anti-leukotriene agents compared to inhaled corticosteroids in the management of recurrent and/ or chronic asthma in adults and children. Cochrane Database Syst Rev. 2012;(5):CD002314.
4. Agertoft L, Pedersen S. Effect of long- term treatment with budesonide on adult height in children with asthma. N Engl J Med. 2000;343:1064-1069.
5. Van Bever HP, Desager KN, Lijssens N, et al. Does treatment of asthmatic children with inhaled corticosteroids affect their adult height? Pediatr Pulmonol. 1999;27:369-375.
6. Silverstein MD, Yunginger JW, Reed CE, et al. Attained adult height after childhood asthma: effect of glucocorticoid therapy. J Allergy Clin Immunol. 1997;99:466-474.
7. The Childhood Asthma Management Program Research Group. Long-term effects of budesonide or nedocromil in children with asthma. N Engl J Med. 2000;343:1054-1063.
8. Tinkelman DG, Reed CE, Nelson HS, et al. Aerosol beclomethasone dipropionate compared with theophylline as primary treatment of chronic, mild to moderately severe asthma in children. Pediatrics. 1993;92:64-77.
9. Verberne AA, Frost C, Roorda RJ, et al. One year treatment with salmeterol compared with beclomethasone in children with asthma. Am J Respir Crit Care Med. 1997;156:688-695.
10. Allen DB, Bronsky EA, LaForce CF, et al. Growth in asthmatic children treated with fluticasone propionate. J Pediatr 1998;132: 472-477.
11. Skoner DP, Meltzer EO, Milgrom H, et al. Effects of inhaled mometasone furoate on growth velocity and adrenal function: a placebo-controlled trial in children 4-9 years old with mild persistent asthma. J Asthma. 2011;48:848-859.
12. Cochrane MG, Bala MV, Downs KE, et al. Inhaled corticosteroids for asthma therapy: patient compliance, devices, and inhalation technique. Chest. 2000;117:542-550.
1. Kelly HW, Sternberg AL, Lescher R, et al; CAMP Research Group. Effect of inhaled glucocorticoids in childhood on adult height. N Engl J Med. 2012;367:904-912.
2. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. National Institutes of Health National Heart, Lung and Blood Institute: National Asthma Education and Prevention Program, 2007. Available at: http://www.nhlbi. nih.gov/guidelines/asthma/asthgdln.pdf. Accessed August 15, 2013.
3. Chauhan BF, Ducharme FM. Anti-leukotriene agents compared to inhaled corticosteroids in the management of recurrent and/ or chronic asthma in adults and children. Cochrane Database Syst Rev. 2012;(5):CD002314.
4. Agertoft L, Pedersen S. Effect of long- term treatment with budesonide on adult height in children with asthma. N Engl J Med. 2000;343:1064-1069.
5. Van Bever HP, Desager KN, Lijssens N, et al. Does treatment of asthmatic children with inhaled corticosteroids affect their adult height? Pediatr Pulmonol. 1999;27:369-375.
6. Silverstein MD, Yunginger JW, Reed CE, et al. Attained adult height after childhood asthma: effect of glucocorticoid therapy. J Allergy Clin Immunol. 1997;99:466-474.
7. The Childhood Asthma Management Program Research Group. Long-term effects of budesonide or nedocromil in children with asthma. N Engl J Med. 2000;343:1054-1063.
8. Tinkelman DG, Reed CE, Nelson HS, et al. Aerosol beclomethasone dipropionate compared with theophylline as primary treatment of chronic, mild to moderately severe asthma in children. Pediatrics. 1993;92:64-77.
9. Verberne AA, Frost C, Roorda RJ, et al. One year treatment with salmeterol compared with beclomethasone in children with asthma. Am J Respir Crit Care Med. 1997;156:688-695.
10. Allen DB, Bronsky EA, LaForce CF, et al. Growth in asthmatic children treated with fluticasone propionate. J Pediatr 1998;132: 472-477.
11. Skoner DP, Meltzer EO, Milgrom H, et al. Effects of inhaled mometasone furoate on growth velocity and adrenal function: a placebo-controlled trial in children 4-9 years old with mild persistent asthma. J Asthma. 2011;48:848-859.
12. Cochrane MG, Bala MV, Downs KE, et al. Inhaled corticosteroids for asthma therapy: patient compliance, devices, and inhalation technique. Chest. 2000;117:542-550.
Copyright © 2013 Family Physicians Inquiries Network. All rights reserved.

High dependency predicts BMI increase during smoking cessation
Smokers who are heavily addicted to nicotine are significantly more likely to gain weight when they try to quit, researchers report.
Investigators studying 186 patients who successfully quit smoking after receiving nicotine replacement therapy at an outpatient clinic found that mean body mass index increased significantly from 23.5 kg/m2 at an initial consultation to 23.9 kg/m2 at 3 months after the start of therapy. A high Fagerstrom Test for Nicotine Dependence (FTND) score, indicating severe dependency, was found on multivariate analysis to be the strongest predictor of increase (using a gender-adjusted standardized coefficient).
Dr. Maki Komiyama of Kyoto (Japan) Medical Center and colleagues reported their findings online Aug. 21 in the open access journal PLoS One (PLoS One 2013 Aug. 21 [doi:10.1371/journal.pone.0072010]).
The findings are important because, while smoking cessation is known to reduce cardiovascular and cancer risk and to reduce all-cause mortality, associated weight gain is linked with greater risk of glucose intolerance and a reduction in the beneficial effects that quitting has on pulmonary function. Concerns about weight gain also can lead to a failure to quit smoking, they said.
"Even if one is expected to experience post-cessation weight gain, quitting smoking still leads to a reduced cardiovascular risk. However, there is also a possibility that if one can prevent post-cessation weight gain, then this will further reduce the cardiovascular risk due to having ceased smoking," they wrote.
"Even if one is expected to experience post-cessation weight gain, quitting smoking still leads to a reduced cardiovascular risk"
Thus, they continued, the ability to predict which patients are likely to gain weight during smoking cessation therapy – and performing weight control accordingly at the outset – could lead to improved outcomes, and the findings of this study may be useful for discriminating such patient groups.
Study participants were 132 men and 54 women with a mean age of 59.6 years who visited the smoking cessation clinic at the National Hospital Organization Kyoto Medical Center between July 2007 and November 2011 and successfully quit smoking.
Other factors found on univariate analysis to be significantly associated with BMI increase included triglyceride level, high-density lipoprotein cholesterol, and daily cigarette consumption. "To further investigate ... we performed multivariate analysis. The results demonstrated that the triglyceride level and FTND score were factors determining the post-cessation BMI increase, and that the FTND score was the strongest one," the investigators wrote.
An FTND score of 8 or more (on a scale of 1-10) was associated with larger postcessation BMI increase, and the increase was statistically significant when compared with the level of BMI increase in those with a score of 7 or less, they noted.
"The result that a high FTND score was the most important determinant of a BMI increase supports the hypothesis that post-cessation weight gain is one of the nicotine withdrawal symptoms," they said.
As for the association between triglyceride elevation and weight gain, the mechanism is not clearly understood and requires further study, they noted.
With the exception of two patients who did not receive medical treatment, study participants were treated with either oral varenicline (95 patients) or nicotine patch (89 patients). No difference was seen between the varenicline and nicotine patch groups with respect to BMI increase, but the varenicline group had higher nicotine dependency.
They also noted that, in their study, "although a significant increase in BMI was confirmed after smoking-cessation therapy, the BMI increase was only 0.4 kg/m2 (1.1 kg), which is much smaller than reported in previous studies for people who quit smoking on their own initiative (2.8-3.8 kg)."
Additional study is needed to determine the appropriate timing for initiating interventions against post–smoking cessation weight gain, they noted.
This study was supported by a grant-in-aid for clinical research from the National Hospital Organization and the Pfizer Health Research Foundation. The authors reported that one study drug (varenicline) is manufactured by Pfizer but confirmed "that this does not alter their adherence to all the PLoS One policies on sharing data and materials."
Smokers who are heavily addicted to nicotine are significantly more likely to gain weight when they try to quit, researchers report.
Investigators studying 186 patients who successfully quit smoking after receiving nicotine replacement therapy at an outpatient clinic found that mean body mass index increased significantly from 23.5 kg/m2 at an initial consultation to 23.9 kg/m2 at 3 months after the start of therapy. A high Fagerstrom Test for Nicotine Dependence (FTND) score, indicating severe dependency, was found on multivariate analysis to be the strongest predictor of increase (using a gender-adjusted standardized coefficient).
Dr. Maki Komiyama of Kyoto (Japan) Medical Center and colleagues reported their findings online Aug. 21 in the open access journal PLoS One (PLoS One 2013 Aug. 21 [doi:10.1371/journal.pone.0072010]).
The findings are important because, while smoking cessation is known to reduce cardiovascular and cancer risk and to reduce all-cause mortality, associated weight gain is linked with greater risk of glucose intolerance and a reduction in the beneficial effects that quitting has on pulmonary function. Concerns about weight gain also can lead to a failure to quit smoking, they said.
"Even if one is expected to experience post-cessation weight gain, quitting smoking still leads to a reduced cardiovascular risk. However, there is also a possibility that if one can prevent post-cessation weight gain, then this will further reduce the cardiovascular risk due to having ceased smoking," they wrote.
"Even if one is expected to experience post-cessation weight gain, quitting smoking still leads to a reduced cardiovascular risk"
Thus, they continued, the ability to predict which patients are likely to gain weight during smoking cessation therapy – and performing weight control accordingly at the outset – could lead to improved outcomes, and the findings of this study may be useful for discriminating such patient groups.
Study participants were 132 men and 54 women with a mean age of 59.6 years who visited the smoking cessation clinic at the National Hospital Organization Kyoto Medical Center between July 2007 and November 2011 and successfully quit smoking.
Other factors found on univariate analysis to be significantly associated with BMI increase included triglyceride level, high-density lipoprotein cholesterol, and daily cigarette consumption. "To further investigate ... we performed multivariate analysis. The results demonstrated that the triglyceride level and FTND score were factors determining the post-cessation BMI increase, and that the FTND score was the strongest one," the investigators wrote.
An FTND score of 8 or more (on a scale of 1-10) was associated with larger postcessation BMI increase, and the increase was statistically significant when compared with the level of BMI increase in those with a score of 7 or less, they noted.
"The result that a high FTND score was the most important determinant of a BMI increase supports the hypothesis that post-cessation weight gain is one of the nicotine withdrawal symptoms," they said.
As for the association between triglyceride elevation and weight gain, the mechanism is not clearly understood and requires further study, they noted.
With the exception of two patients who did not receive medical treatment, study participants were treated with either oral varenicline (95 patients) or nicotine patch (89 patients). No difference was seen between the varenicline and nicotine patch groups with respect to BMI increase, but the varenicline group had higher nicotine dependency.
They also noted that, in their study, "although a significant increase in BMI was confirmed after smoking-cessation therapy, the BMI increase was only 0.4 kg/m2 (1.1 kg), which is much smaller than reported in previous studies for people who quit smoking on their own initiative (2.8-3.8 kg)."
Additional study is needed to determine the appropriate timing for initiating interventions against post–smoking cessation weight gain, they noted.
This study was supported by a grant-in-aid for clinical research from the National Hospital Organization and the Pfizer Health Research Foundation. The authors reported that one study drug (varenicline) is manufactured by Pfizer but confirmed "that this does not alter their adherence to all the PLoS One policies on sharing data and materials."
Smokers who are heavily addicted to nicotine are significantly more likely to gain weight when they try to quit, researchers report.
Investigators studying 186 patients who successfully quit smoking after receiving nicotine replacement therapy at an outpatient clinic found that mean body mass index increased significantly from 23.5 kg/m2 at an initial consultation to 23.9 kg/m2 at 3 months after the start of therapy. A high Fagerstrom Test for Nicotine Dependence (FTND) score, indicating severe dependency, was found on multivariate analysis to be the strongest predictor of increase (using a gender-adjusted standardized coefficient).
Dr. Maki Komiyama of Kyoto (Japan) Medical Center and colleagues reported their findings online Aug. 21 in the open access journal PLoS One (PLoS One 2013 Aug. 21 [doi:10.1371/journal.pone.0072010]).
The findings are important because, while smoking cessation is known to reduce cardiovascular and cancer risk and to reduce all-cause mortality, associated weight gain is linked with greater risk of glucose intolerance and a reduction in the beneficial effects that quitting has on pulmonary function. Concerns about weight gain also can lead to a failure to quit smoking, they said.
"Even if one is expected to experience post-cessation weight gain, quitting smoking still leads to a reduced cardiovascular risk. However, there is also a possibility that if one can prevent post-cessation weight gain, then this will further reduce the cardiovascular risk due to having ceased smoking," they wrote.
"Even if one is expected to experience post-cessation weight gain, quitting smoking still leads to a reduced cardiovascular risk"
Thus, they continued, the ability to predict which patients are likely to gain weight during smoking cessation therapy – and performing weight control accordingly at the outset – could lead to improved outcomes, and the findings of this study may be useful for discriminating such patient groups.
Study participants were 132 men and 54 women with a mean age of 59.6 years who visited the smoking cessation clinic at the National Hospital Organization Kyoto Medical Center between July 2007 and November 2011 and successfully quit smoking.
Other factors found on univariate analysis to be significantly associated with BMI increase included triglyceride level, high-density lipoprotein cholesterol, and daily cigarette consumption. "To further investigate ... we performed multivariate analysis. The results demonstrated that the triglyceride level and FTND score were factors determining the post-cessation BMI increase, and that the FTND score was the strongest one," the investigators wrote.
An FTND score of 8 or more (on a scale of 1-10) was associated with larger postcessation BMI increase, and the increase was statistically significant when compared with the level of BMI increase in those with a score of 7 or less, they noted.
"The result that a high FTND score was the most important determinant of a BMI increase supports the hypothesis that post-cessation weight gain is one of the nicotine withdrawal symptoms," they said.
As for the association between triglyceride elevation and weight gain, the mechanism is not clearly understood and requires further study, they noted.
With the exception of two patients who did not receive medical treatment, study participants were treated with either oral varenicline (95 patients) or nicotine patch (89 patients). No difference was seen between the varenicline and nicotine patch groups with respect to BMI increase, but the varenicline group had higher nicotine dependency.
They also noted that, in their study, "although a significant increase in BMI was confirmed after smoking-cessation therapy, the BMI increase was only 0.4 kg/m2 (1.1 kg), which is much smaller than reported in previous studies for people who quit smoking on their own initiative (2.8-3.8 kg)."
Additional study is needed to determine the appropriate timing for initiating interventions against post–smoking cessation weight gain, they noted.
This study was supported by a grant-in-aid for clinical research from the National Hospital Organization and the Pfizer Health Research Foundation. The authors reported that one study drug (varenicline) is manufactured by Pfizer but confirmed "that this does not alter their adherence to all the PLoS One policies on sharing data and materials."
FROM PLOS ONE
Major finding: FTND score was a strong predictor of BMI increase (gender-adjusted standardized coefficient, 0.236). BMI increased significantly from 23.5 kg/m2 at an initial consultation to 23.9 kg/m2 at 3 months after the start of smoking cessation therapy.
Data source: A study of 186 adults who successfully completed smoking cessation therapy.
Disclosures: This study was supported by a grant-in-aid for clinical research from the National Hospital Organization and the Pfizer Health Research Foundation. The authors reported that one study drug (varenicline) is manufactured by Pfizer but confirmed "that this does not alter their adherence to all the PLOS ONE policies on sharing data and materials."