User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
International AIDS conference pays tribute to colleagues on flight MH17
MELBOURNE – Speakers at the opening plenary of the 20th International AIDS Conference struggled with their emotions as they paid tribute to colleagues – including former International AIDS Society President Dr. Joep Lange – who were killed when Malaysian Airlines flight MH17 crashed in Ukraine.
Dr. Lange was instrumental in research and implementation of mother-to-child transmission therapy, and as president of the society, showed a rare combination of enthusiasm, commitment, and perseverance, Lambert Grijns, Dutch Ambassador for Sexual and Reproductive Health and Rights and HIV/AIDS, said July 20.

Dr. Lange’s partner, Jacqueline van Tongeren, of the Amsterdam Institute for Global Health and Development, also was killed in the incident, along with Lucie van Mens, who Mr. Grijns said had advocated the cause of sex workers at a time when few other were doing so.
"She was a driving force in advocacy for the female condom, she gave the product its rightful place in the field of sexual reproductive health and rights, and her impact will continue to be felt," Mr Grijns told the packed auditorium.
Other high-profile researchers on the flight included Martine de Schutter, program manager for Bridging The Gap, who Mr. Grijns said had been a staunch defender of human rights and the right to good health; Glenn Thomas from the World Health Organization’s communications team; and Pim de Kuijer, a prominent AIDS campaigner and lobbyist for Stop AIDS Now!
Prof. Françoise Barré-Sinoussi, IAS president and the director of the regulation of retroviral infections unit at the Institut Pasteur in Paris, called for a moment’s silence in their memory, during which the audience spontaneously rose to its feet.
"Our colleagues were traveling because of their dedication to bringing an end to AIDS, and our determination to continue their work honors their commitment," she said.
MELBOURNE – Speakers at the opening plenary of the 20th International AIDS Conference struggled with their emotions as they paid tribute to colleagues – including former International AIDS Society President Dr. Joep Lange – who were killed when Malaysian Airlines flight MH17 crashed in Ukraine.
Dr. Lange was instrumental in research and implementation of mother-to-child transmission therapy, and as president of the society, showed a rare combination of enthusiasm, commitment, and perseverance, Lambert Grijns, Dutch Ambassador for Sexual and Reproductive Health and Rights and HIV/AIDS, said July 20.
Dr. Lange’s partner, Jacqueline van Tongeren, of the Amsterdam Institute for Global Health and Development, also was killed in the incident, along with Lucie van Mens, who Mr. Grijns said had advocated the cause of sex workers at a time when few other were doing so.
"She was a driving force in advocacy for the female condom, she gave the product its rightful place in the field of sexual reproductive health and rights, and her impact will continue to be felt," Mr Grijns told the packed auditorium.
Other high-profile researchers on the flight included Martine de Schutter, program manager for Bridging The Gap, who Mr. Grijns said had been a staunch defender of human rights and the right to good health; Glenn Thomas from the World Health Organization’s communications team; and Pim de Kuijer, a prominent AIDS campaigner and lobbyist for Stop AIDS Now!
Prof. Françoise Barré-Sinoussi, IAS president and the director of the regulation of retroviral infections unit at the Institut Pasteur in Paris, called for a moment’s silence in their memory, during which the audience spontaneously rose to its feet.
"Our colleagues were traveling because of their dedication to bringing an end to AIDS, and our determination to continue their work honors their commitment," she said.
MELBOURNE – Speakers at the opening plenary of the 20th International AIDS Conference struggled with their emotions as they paid tribute to colleagues – including former International AIDS Society President Dr. Joep Lange – who were killed when Malaysian Airlines flight MH17 crashed in Ukraine.
Dr. Lange was instrumental in research and implementation of mother-to-child transmission therapy, and as president of the society, showed a rare combination of enthusiasm, commitment, and perseverance, Lambert Grijns, Dutch Ambassador for Sexual and Reproductive Health and Rights and HIV/AIDS, said July 20.
Dr. Lange’s partner, Jacqueline van Tongeren, of the Amsterdam Institute for Global Health and Development, also was killed in the incident, along with Lucie van Mens, who Mr. Grijns said had advocated the cause of sex workers at a time when few other were doing so.
"She was a driving force in advocacy for the female condom, she gave the product its rightful place in the field of sexual reproductive health and rights, and her impact will continue to be felt," Mr Grijns told the packed auditorium.
Other high-profile researchers on the flight included Martine de Schutter, program manager for Bridging The Gap, who Mr. Grijns said had been a staunch defender of human rights and the right to good health; Glenn Thomas from the World Health Organization’s communications team; and Pim de Kuijer, a prominent AIDS campaigner and lobbyist for Stop AIDS Now!
Prof. Françoise Barré-Sinoussi, IAS president and the director of the regulation of retroviral infections unit at the Institut Pasteur in Paris, called for a moment’s silence in their memory, during which the audience spontaneously rose to its feet.
"Our colleagues were traveling because of their dedication to bringing an end to AIDS, and our determination to continue their work honors their commitment," she said.
AT AIDS 2014

Oncology hospitalist field is small, but growing
Have you met an oncology hospitalist yet? If you haven’t, you probably will soon.
The latest offshoot of hospital medicine aims to take all the strengths of the hospitalist movement – increased efficiency and improved quality and safety – and apply them to inpatient cancer care.
While there is no typical oncology-hospitalist program, most manage the complications of a patient’s cancer and treatment, as well as providing some type of end-of-life services. Oncology hospitalists may be oncologists with an interest in taking care of hospitalized patients. Or they could be hospitalists trained in internal or family medicine, who have an interest in caring for cancer patients.
"People are very interested in this, and we really want to grow it," said Dr. Maria-Claudia Campagna, an oncology-hospitalist at the University of Texas MD Anderson Cancer Center in Houston.
Dr. Campagna is part of a nine-physician oncology-hospitalist program at MD Anderson. The program was launched in 2006 with just one hospitalist, but has grown to nine hospitalists over the last several years. And the program is in the process of recruiting three more physicians.
They are also piloting an observation unit geared toward oncology patients, she said.
Much like in the early days of hospital medicine, Dr. Campagna said the program initially got pushback from oncologists who didn’t want to give up care of their patients in the hospital. But over time, the hospitalists have proven their competence and oncologists have gotten even busier with their outpatient practices.

"They know we take good care of their patients, so ultimately they trust our criteria. And when we don’t know, we tell them," Dr. Campagna said. "So we have a very symbiotic relationship."
The experience at MD Anderson is being replicated at cancer centers and academic medical centers around the country. Even some community hospitals are exploring the idea.
The reason is simple, said Dr. Eddy Chen, an oncology hospitalist at Dana-Farber/Brigham and Women’s Cancer Center in Boston. The combination of a coming shortage of oncologists combined with an expected surge in cancer patients among aging baby boomers means that virtually every hospital will see a marked increase in cancer patients over the next several years.
"In the future, there are going to be a lot more patients with cancer who are going to be coming into the hospital," Dr. Chen said. "And who is going to take care of these patients?"
But I’m not an oncologist ...
At Dana-Farber/Brigham and Women’s, they have three oncology hospitalists, including Dr. Chen. Along with the regular cadre of oncologists, they manage all of the hospitalized cancer patients. What makes hospitalist management different from that of the oncologists, who are treating both inpatients and outpatients, is the focus on quality improvement, patient safety, and research, said Dr. Chen.
Dr. Chen, who is trained as an oncologist, said hospitalists don’t need to be oncologists to do this job. But as the field develops, there are likely to be some training or prerequisites that will develop. For now, Dr. Chen said hospitalists need to have an interest in treating complex patients and be willing to develop a deeper understanding of the principles of cancer medicine.
"We are now at a point in the road of this endeavor where best practices, and understanding these issues, can be further defined," Dr. Chen said.
As Dr. Chen proves, oncology hospitalists can be oncologists or traditional hospitalists trained in internal medicine or family medicine. But they must all be prepared to handle complex patients and take on end-of-life discussions.

At Memorial Sloan-Kettering Cancer Center in New York, where the oncology-hospitalist team works mainly with GI oncology and lymphoma patients, they treat patients with very advanced disease, many of whom are in the last 6 months of life.
"We’ve attained a lot of experience and expertise in end-of-life care, but it’s all been on-the-job training," said Dr. Barbara C. Egan, chief of the hospital medicine service at Sloan-Kettering.
Because of the heavy focus on end-of-life care, Dr. Egan and some of the other hospitalists in her group were recently board certified in hospice and palliative medicine based in part on their clinical experience working with cancer patients.
Emotional days
The work is very different from a general medicine hospitalist service. For oncology hospitalists, all of the patients have multisystem organ disease and also typically have complicated psychosocial dynamics end-of-life care. The result is a time-consuming, emotionally charged day that isn’t accurately measured by RVUs (relative value units) or the number of encounters per day, Dr. Egan said.
"It’s very different to round on a 25-year-old who’s dying of colon cancer, than in a general medicine hospital where you might have several patients on the service who are there for single issue, uncomplicated soft rule-out MI." she said. "It’s definitely very emotionally draining on the physicians."
To try to prevent burnout among their physicians, Sloan-Kettering’s program consists of seven daytime hospitalists who work a typical 2-week on/2-week off schedule. The other 10 hospitalists are dedicated nocturnalists. The model has resulted in virtually no turnover among the daytime hospitalists. The nocturnal group has high turnover, which is typical of most night-shift work. At this point, there’s no definitive count of the number of oncology hospitalists working in the United States today. But what is clear, is that the small niche is growing.

Dr. A. Charlotta Weaver, medical director of oncology hospitalists at Northwestern Memorial Hospital in Chicago, epitomizes the appeal for some young physicians.
Dr. Weaver graduated from residency in 2008, a year after Northwestern launched its oncology-hospitalist program. She had been considering a fellowship in hematology/oncology when she heard about the new program. "This little light went off in my head that that’s what I wanted to do," she said.
Initially, she thought about working as an oncology hospitalist for a few years as a bridge to fellowship, but ultimately decided to stay on with the program. The appeals, she said, was a combination of the hospitalist schedule and taking care of hematology/oncology patients.
"I think of it as real medicine. They are really sick," Dr. Weaver said. "There is something legitimately wrong with them and I can help; whereas in general medicine, you don’t always have that sense."
mschneider@frontlinemedcom.com
On Twitter @maryellenny
Have you met an oncology hospitalist yet? If you haven’t, you probably will soon.
The latest offshoot of hospital medicine aims to take all the strengths of the hospitalist movement – increased efficiency and improved quality and safety – and apply them to inpatient cancer care.
While there is no typical oncology-hospitalist program, most manage the complications of a patient’s cancer and treatment, as well as providing some type of end-of-life services. Oncology hospitalists may be oncologists with an interest in taking care of hospitalized patients. Or they could be hospitalists trained in internal or family medicine, who have an interest in caring for cancer patients.
"People are very interested in this, and we really want to grow it," said Dr. Maria-Claudia Campagna, an oncology-hospitalist at the University of Texas MD Anderson Cancer Center in Houston.
Dr. Campagna is part of a nine-physician oncology-hospitalist program at MD Anderson. The program was launched in 2006 with just one hospitalist, but has grown to nine hospitalists over the last several years. And the program is in the process of recruiting three more physicians.
They are also piloting an observation unit geared toward oncology patients, she said.
Much like in the early days of hospital medicine, Dr. Campagna said the program initially got pushback from oncologists who didn’t want to give up care of their patients in the hospital. But over time, the hospitalists have proven their competence and oncologists have gotten even busier with their outpatient practices.
"They know we take good care of their patients, so ultimately they trust our criteria. And when we don’t know, we tell them," Dr. Campagna said. "So we have a very symbiotic relationship."
The experience at MD Anderson is being replicated at cancer centers and academic medical centers around the country. Even some community hospitals are exploring the idea.
The reason is simple, said Dr. Eddy Chen, an oncology hospitalist at Dana-Farber/Brigham and Women’s Cancer Center in Boston. The combination of a coming shortage of oncologists combined with an expected surge in cancer patients among aging baby boomers means that virtually every hospital will see a marked increase in cancer patients over the next several years.
"In the future, there are going to be a lot more patients with cancer who are going to be coming into the hospital," Dr. Chen said. "And who is going to take care of these patients?"
But I’m not an oncologist ...
At Dana-Farber/Brigham and Women’s, they have three oncology hospitalists, including Dr. Chen. Along with the regular cadre of oncologists, they manage all of the hospitalized cancer patients. What makes hospitalist management different from that of the oncologists, who are treating both inpatients and outpatients, is the focus on quality improvement, patient safety, and research, said Dr. Chen.
Dr. Chen, who is trained as an oncologist, said hospitalists don’t need to be oncologists to do this job. But as the field develops, there are likely to be some training or prerequisites that will develop. For now, Dr. Chen said hospitalists need to have an interest in treating complex patients and be willing to develop a deeper understanding of the principles of cancer medicine.
"We are now at a point in the road of this endeavor where best practices, and understanding these issues, can be further defined," Dr. Chen said.
As Dr. Chen proves, oncology hospitalists can be oncologists or traditional hospitalists trained in internal medicine or family medicine. But they must all be prepared to handle complex patients and take on end-of-life discussions.
At Memorial Sloan-Kettering Cancer Center in New York, where the oncology-hospitalist team works mainly with GI oncology and lymphoma patients, they treat patients with very advanced disease, many of whom are in the last 6 months of life.
"We’ve attained a lot of experience and expertise in end-of-life care, but it’s all been on-the-job training," said Dr. Barbara C. Egan, chief of the hospital medicine service at Sloan-Kettering.
Because of the heavy focus on end-of-life care, Dr. Egan and some of the other hospitalists in her group were recently board certified in hospice and palliative medicine based in part on their clinical experience working with cancer patients.
Emotional days
The work is very different from a general medicine hospitalist service. For oncology hospitalists, all of the patients have multisystem organ disease and also typically have complicated psychosocial dynamics end-of-life care. The result is a time-consuming, emotionally charged day that isn’t accurately measured by RVUs (relative value units) or the number of encounters per day, Dr. Egan said.
"It’s very different to round on a 25-year-old who’s dying of colon cancer, than in a general medicine hospital where you might have several patients on the service who are there for single issue, uncomplicated soft rule-out MI." she said. "It’s definitely very emotionally draining on the physicians."
To try to prevent burnout among their physicians, Sloan-Kettering’s program consists of seven daytime hospitalists who work a typical 2-week on/2-week off schedule. The other 10 hospitalists are dedicated nocturnalists. The model has resulted in virtually no turnover among the daytime hospitalists. The nocturnal group has high turnover, which is typical of most night-shift work. At this point, there’s no definitive count of the number of oncology hospitalists working in the United States today. But what is clear, is that the small niche is growing.
Dr. A. Charlotta Weaver, medical director of oncology hospitalists at Northwestern Memorial Hospital in Chicago, epitomizes the appeal for some young physicians.
Dr. Weaver graduated from residency in 2008, a year after Northwestern launched its oncology-hospitalist program. She had been considering a fellowship in hematology/oncology when she heard about the new program. "This little light went off in my head that that’s what I wanted to do," she said.
Initially, she thought about working as an oncology hospitalist for a few years as a bridge to fellowship, but ultimately decided to stay on with the program. The appeals, she said, was a combination of the hospitalist schedule and taking care of hematology/oncology patients.
"I think of it as real medicine. They are really sick," Dr. Weaver said. "There is something legitimately wrong with them and I can help; whereas in general medicine, you don’t always have that sense."
mschneider@frontlinemedcom.com
On Twitter @maryellenny
Have you met an oncology hospitalist yet? If you haven’t, you probably will soon.
The latest offshoot of hospital medicine aims to take all the strengths of the hospitalist movement – increased efficiency and improved quality and safety – and apply them to inpatient cancer care.
While there is no typical oncology-hospitalist program, most manage the complications of a patient’s cancer and treatment, as well as providing some type of end-of-life services. Oncology hospitalists may be oncologists with an interest in taking care of hospitalized patients. Or they could be hospitalists trained in internal or family medicine, who have an interest in caring for cancer patients.
"People are very interested in this, and we really want to grow it," said Dr. Maria-Claudia Campagna, an oncology-hospitalist at the University of Texas MD Anderson Cancer Center in Houston.
Dr. Campagna is part of a nine-physician oncology-hospitalist program at MD Anderson. The program was launched in 2006 with just one hospitalist, but has grown to nine hospitalists over the last several years. And the program is in the process of recruiting three more physicians.
They are also piloting an observation unit geared toward oncology patients, she said.
Much like in the early days of hospital medicine, Dr. Campagna said the program initially got pushback from oncologists who didn’t want to give up care of their patients in the hospital. But over time, the hospitalists have proven their competence and oncologists have gotten even busier with their outpatient practices.
"They know we take good care of their patients, so ultimately they trust our criteria. And when we don’t know, we tell them," Dr. Campagna said. "So we have a very symbiotic relationship."
The experience at MD Anderson is being replicated at cancer centers and academic medical centers around the country. Even some community hospitals are exploring the idea.
The reason is simple, said Dr. Eddy Chen, an oncology hospitalist at Dana-Farber/Brigham and Women’s Cancer Center in Boston. The combination of a coming shortage of oncologists combined with an expected surge in cancer patients among aging baby boomers means that virtually every hospital will see a marked increase in cancer patients over the next several years.
"In the future, there are going to be a lot more patients with cancer who are going to be coming into the hospital," Dr. Chen said. "And who is going to take care of these patients?"
But I’m not an oncologist ...
At Dana-Farber/Brigham and Women’s, they have three oncology hospitalists, including Dr. Chen. Along with the regular cadre of oncologists, they manage all of the hospitalized cancer patients. What makes hospitalist management different from that of the oncologists, who are treating both inpatients and outpatients, is the focus on quality improvement, patient safety, and research, said Dr. Chen.
Dr. Chen, who is trained as an oncologist, said hospitalists don’t need to be oncologists to do this job. But as the field develops, there are likely to be some training or prerequisites that will develop. For now, Dr. Chen said hospitalists need to have an interest in treating complex patients and be willing to develop a deeper understanding of the principles of cancer medicine.
"We are now at a point in the road of this endeavor where best practices, and understanding these issues, can be further defined," Dr. Chen said.
As Dr. Chen proves, oncology hospitalists can be oncologists or traditional hospitalists trained in internal medicine or family medicine. But they must all be prepared to handle complex patients and take on end-of-life discussions.
At Memorial Sloan-Kettering Cancer Center in New York, where the oncology-hospitalist team works mainly with GI oncology and lymphoma patients, they treat patients with very advanced disease, many of whom are in the last 6 months of life.
"We’ve attained a lot of experience and expertise in end-of-life care, but it’s all been on-the-job training," said Dr. Barbara C. Egan, chief of the hospital medicine service at Sloan-Kettering.
Because of the heavy focus on end-of-life care, Dr. Egan and some of the other hospitalists in her group were recently board certified in hospice and palliative medicine based in part on their clinical experience working with cancer patients.
Emotional days
The work is very different from a general medicine hospitalist service. For oncology hospitalists, all of the patients have multisystem organ disease and also typically have complicated psychosocial dynamics end-of-life care. The result is a time-consuming, emotionally charged day that isn’t accurately measured by RVUs (relative value units) or the number of encounters per day, Dr. Egan said.
"It’s very different to round on a 25-year-old who’s dying of colon cancer, than in a general medicine hospital where you might have several patients on the service who are there for single issue, uncomplicated soft rule-out MI." she said. "It’s definitely very emotionally draining on the physicians."
To try to prevent burnout among their physicians, Sloan-Kettering’s program consists of seven daytime hospitalists who work a typical 2-week on/2-week off schedule. The other 10 hospitalists are dedicated nocturnalists. The model has resulted in virtually no turnover among the daytime hospitalists. The nocturnal group has high turnover, which is typical of most night-shift work. At this point, there’s no definitive count of the number of oncology hospitalists working in the United States today. But what is clear, is that the small niche is growing.
Dr. A. Charlotta Weaver, medical director of oncology hospitalists at Northwestern Memorial Hospital in Chicago, epitomizes the appeal for some young physicians.
Dr. Weaver graduated from residency in 2008, a year after Northwestern launched its oncology-hospitalist program. She had been considering a fellowship in hematology/oncology when she heard about the new program. "This little light went off in my head that that’s what I wanted to do," she said.
Initially, she thought about working as an oncology hospitalist for a few years as a bridge to fellowship, but ultimately decided to stay on with the program. The appeals, she said, was a combination of the hospitalist schedule and taking care of hematology/oncology patients.
"I think of it as real medicine. They are really sick," Dr. Weaver said. "There is something legitimately wrong with them and I can help; whereas in general medicine, you don’t always have that sense."
mschneider@frontlinemedcom.com
On Twitter @maryellenny

VIDEO: Dementia risk spikes in older veterans with sleep disorders, PTSD
COPENHAGEN – Older veterans who had sleep disturbances were at a 30% greater risk of developing dementia, according to a retrospective analysis of 200,000 medical records presented at the Alzheimer’s Association International Conference 2014.
And having posttraumatic stress disorder (PTSD) in addition to sleep disturbances put veterans at an 80% greater risk.
"As veterans are turning 65 and older, it’s important for us to understand who in that population is at an increased risk of developing dementia, so when we have that therapy or lifestyle intervention, we can intervene at that point," said Heather M. Snyder, Ph.D., director of medical and scientific operations at the Alzheimer’s Association. Dr. Snyder was not involved in the study.
For the study, researchers studied the records of veterans 55 years and older for 8 years. They found that almost 11% of the veterans with sleep disturbance developed dementia, compared with 9% of those without sleep disturbance, almost a 30% risk increase. The results were similar for veterans who had sleep apnea and nonapnea insomnia.
Meanwhile, researchers found no significant interaction between sleep disturbance and traumatic brain injury or PTSD, with regard to increased risk of dementia. However, veterans who had both PTSD and sleep disturbance had an 80% increased risk of developing dementia.
In a video interview, Dr. Kristine Yaffe, professor of psychiatry and neurology at the University of California, San Francisco, explains the study’s findings, shares practice pearls, and discusses the implications for younger veterans.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @naseemmiller
COPENHAGEN – Older veterans who had sleep disturbances were at a 30% greater risk of developing dementia, according to a retrospective analysis of 200,000 medical records presented at the Alzheimer’s Association International Conference 2014.
And having posttraumatic stress disorder (PTSD) in addition to sleep disturbances put veterans at an 80% greater risk.
"As veterans are turning 65 and older, it’s important for us to understand who in that population is at an increased risk of developing dementia, so when we have that therapy or lifestyle intervention, we can intervene at that point," said Heather M. Snyder, Ph.D., director of medical and scientific operations at the Alzheimer’s Association. Dr. Snyder was not involved in the study.
For the study, researchers studied the records of veterans 55 years and older for 8 years. They found that almost 11% of the veterans with sleep disturbance developed dementia, compared with 9% of those without sleep disturbance, almost a 30% risk increase. The results were similar for veterans who had sleep apnea and nonapnea insomnia.
Meanwhile, researchers found no significant interaction between sleep disturbance and traumatic brain injury or PTSD, with regard to increased risk of dementia. However, veterans who had both PTSD and sleep disturbance had an 80% increased risk of developing dementia.
In a video interview, Dr. Kristine Yaffe, professor of psychiatry and neurology at the University of California, San Francisco, explains the study’s findings, shares practice pearls, and discusses the implications for younger veterans.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @naseemmiller
COPENHAGEN – Older veterans who had sleep disturbances were at a 30% greater risk of developing dementia, according to a retrospective analysis of 200,000 medical records presented at the Alzheimer’s Association International Conference 2014.
And having posttraumatic stress disorder (PTSD) in addition to sleep disturbances put veterans at an 80% greater risk.
"As veterans are turning 65 and older, it’s important for us to understand who in that population is at an increased risk of developing dementia, so when we have that therapy or lifestyle intervention, we can intervene at that point," said Heather M. Snyder, Ph.D., director of medical and scientific operations at the Alzheimer’s Association. Dr. Snyder was not involved in the study.
For the study, researchers studied the records of veterans 55 years and older for 8 years. They found that almost 11% of the veterans with sleep disturbance developed dementia, compared with 9% of those without sleep disturbance, almost a 30% risk increase. The results were similar for veterans who had sleep apnea and nonapnea insomnia.
Meanwhile, researchers found no significant interaction between sleep disturbance and traumatic brain injury or PTSD, with regard to increased risk of dementia. However, veterans who had both PTSD and sleep disturbance had an 80% increased risk of developing dementia.
In a video interview, Dr. Kristine Yaffe, professor of psychiatry and neurology at the University of California, San Francisco, explains the study’s findings, shares practice pearls, and discusses the implications for younger veterans.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @naseemmiller
AT AAIC 2014

Daily inhaled corticosteroids marginally suppress children’s growth
Daily use of low- to medium-dose inhaled corticosteroids for mild to moderate persistent asthma suppresses growth to a "small" degree in children of all ages, according to a Cochrane review published online July 16 in the Cochrane Database of Systematic Reviews.
This level of use was associated with a mean reduction of 0.48 cm per year in linear growth velocity during the first year of treatment, against a background average growth rate of 6-9 cm per year. The growth suppression was less pronounced in subsequent years of treatment, and the magnitude of growth suppression was more strongly related to the particular drug used than to the dose or delivery device, said Dr. Linjie Zhang of the Federal University of Rio Grande (Brazil) and his associates.

"The evidence we reviewed suggests that children treated daily with inhaled corticosteroids may grow approximately half a centimeter less during the first year of treatment. But this effect is less pronounced in subsequent years, is not cumulative, and seems minor compared with the known benefits of the drugs for controlling asthma and ensuring full lung growth," Dr. Zhang said in a press statement accompanying the report.
The investigators undertook this comprehensive review of the literature and metaanalysis because of persistent concerns about possible adverse effects of inhaled corticosteroids on children’s growth and because several recent randomized trials have examined the issue and have assessed newly available agents and modes of delivery. They identified 25 good-quality, parallel-group, randomized clinical trials involving 8,471 children up to age 18, of whom 5,128 were treated with inhaled corticosteroids and 3,343 were treated with nonsteroidal anti-inflammatory drugs or placebo and served as controls.
Most of the trials were blinded, and most were multicenter. Seventeen of the 25 were funded by pharmaceutical companies.
The participating children used beclomethasone, budesonide, ciclesonide, flunisolide, fluticasone, or mometasone, delivered by any type of inhalation device, and were followed for 3 months to 6 years.
All six inhaled corticosteroids were found to suppress linear growth velocity during 1 year of treatment, which was the primary outcome of interest. They all also suppressed growth as measured by the secondary outcomes of change in height standard deviation score over time and change from baseline in height over time. These effects were less pronounced in subsequent years of treatment, but persisted until patients reached their adult height.
The one study that followed prepubescent participants into adulthood showed that those who used inhaled corticosteroids had a mean reduction of 1.2 cm in adult height, compared with those who did not.
Daily dose, delivery device, and patient age had had no significant impact on the magnitude of growth suppression. A small number of studies that compared the various corticosteroids against each other showed that beclomethasone and budesonide were somewhat more potent growth suppressors, compared with the other four agents. However, a meta-analysis is not the best method for exploring these issues, and data from more head-to-head randomized trials are required to confirm these findings, Dr. Zhang and his associates noted (Cochrane Database Systematic Rev. 2014 July 16 [doi:10.1002/I4651858.CD009471.pub2]).
Their findings indicate that inhaled corticosteroids should be prescribed at the lowest effective dose. "Moreover, it is prudent to monitor linear growth in children treated with inhaled corticosteroids, given that individual susceptibility to these drugs may vary considerably," the investigators added.
Daily use of low- to medium-dose inhaled corticosteroids for mild to moderate persistent asthma suppresses growth to a "small" degree in children of all ages, according to a Cochrane review published online July 16 in the Cochrane Database of Systematic Reviews.
This level of use was associated with a mean reduction of 0.48 cm per year in linear growth velocity during the first year of treatment, against a background average growth rate of 6-9 cm per year. The growth suppression was less pronounced in subsequent years of treatment, and the magnitude of growth suppression was more strongly related to the particular drug used than to the dose or delivery device, said Dr. Linjie Zhang of the Federal University of Rio Grande (Brazil) and his associates.
"The evidence we reviewed suggests that children treated daily with inhaled corticosteroids may grow approximately half a centimeter less during the first year of treatment. But this effect is less pronounced in subsequent years, is not cumulative, and seems minor compared with the known benefits of the drugs for controlling asthma and ensuring full lung growth," Dr. Zhang said in a press statement accompanying the report.
The investigators undertook this comprehensive review of the literature and metaanalysis because of persistent concerns about possible adverse effects of inhaled corticosteroids on children’s growth and because several recent randomized trials have examined the issue and have assessed newly available agents and modes of delivery. They identified 25 good-quality, parallel-group, randomized clinical trials involving 8,471 children up to age 18, of whom 5,128 were treated with inhaled corticosteroids and 3,343 were treated with nonsteroidal anti-inflammatory drugs or placebo and served as controls.
Most of the trials were blinded, and most were multicenter. Seventeen of the 25 were funded by pharmaceutical companies.
The participating children used beclomethasone, budesonide, ciclesonide, flunisolide, fluticasone, or mometasone, delivered by any type of inhalation device, and were followed for 3 months to 6 years.
All six inhaled corticosteroids were found to suppress linear growth velocity during 1 year of treatment, which was the primary outcome of interest. They all also suppressed growth as measured by the secondary outcomes of change in height standard deviation score over time and change from baseline in height over time. These effects were less pronounced in subsequent years of treatment, but persisted until patients reached their adult height.
The one study that followed prepubescent participants into adulthood showed that those who used inhaled corticosteroids had a mean reduction of 1.2 cm in adult height, compared with those who did not.
Daily dose, delivery device, and patient age had had no significant impact on the magnitude of growth suppression. A small number of studies that compared the various corticosteroids against each other showed that beclomethasone and budesonide were somewhat more potent growth suppressors, compared with the other four agents. However, a meta-analysis is not the best method for exploring these issues, and data from more head-to-head randomized trials are required to confirm these findings, Dr. Zhang and his associates noted (Cochrane Database Systematic Rev. 2014 July 16 [doi:10.1002/I4651858.CD009471.pub2]).
Their findings indicate that inhaled corticosteroids should be prescribed at the lowest effective dose. "Moreover, it is prudent to monitor linear growth in children treated with inhaled corticosteroids, given that individual susceptibility to these drugs may vary considerably," the investigators added.
Daily use of low- to medium-dose inhaled corticosteroids for mild to moderate persistent asthma suppresses growth to a "small" degree in children of all ages, according to a Cochrane review published online July 16 in the Cochrane Database of Systematic Reviews.
This level of use was associated with a mean reduction of 0.48 cm per year in linear growth velocity during the first year of treatment, against a background average growth rate of 6-9 cm per year. The growth suppression was less pronounced in subsequent years of treatment, and the magnitude of growth suppression was more strongly related to the particular drug used than to the dose or delivery device, said Dr. Linjie Zhang of the Federal University of Rio Grande (Brazil) and his associates.
"The evidence we reviewed suggests that children treated daily with inhaled corticosteroids may grow approximately half a centimeter less during the first year of treatment. But this effect is less pronounced in subsequent years, is not cumulative, and seems minor compared with the known benefits of the drugs for controlling asthma and ensuring full lung growth," Dr. Zhang said in a press statement accompanying the report.
The investigators undertook this comprehensive review of the literature and metaanalysis because of persistent concerns about possible adverse effects of inhaled corticosteroids on children’s growth and because several recent randomized trials have examined the issue and have assessed newly available agents and modes of delivery. They identified 25 good-quality, parallel-group, randomized clinical trials involving 8,471 children up to age 18, of whom 5,128 were treated with inhaled corticosteroids and 3,343 were treated with nonsteroidal anti-inflammatory drugs or placebo and served as controls.
Most of the trials were blinded, and most were multicenter. Seventeen of the 25 were funded by pharmaceutical companies.
The participating children used beclomethasone, budesonide, ciclesonide, flunisolide, fluticasone, or mometasone, delivered by any type of inhalation device, and were followed for 3 months to 6 years.
All six inhaled corticosteroids were found to suppress linear growth velocity during 1 year of treatment, which was the primary outcome of interest. They all also suppressed growth as measured by the secondary outcomes of change in height standard deviation score over time and change from baseline in height over time. These effects were less pronounced in subsequent years of treatment, but persisted until patients reached their adult height.
The one study that followed prepubescent participants into adulthood showed that those who used inhaled corticosteroids had a mean reduction of 1.2 cm in adult height, compared with those who did not.
Daily dose, delivery device, and patient age had had no significant impact on the magnitude of growth suppression. A small number of studies that compared the various corticosteroids against each other showed that beclomethasone and budesonide were somewhat more potent growth suppressors, compared with the other four agents. However, a meta-analysis is not the best method for exploring these issues, and data from more head-to-head randomized trials are required to confirm these findings, Dr. Zhang and his associates noted (Cochrane Database Systematic Rev. 2014 July 16 [doi:10.1002/I4651858.CD009471.pub2]).
Their findings indicate that inhaled corticosteroids should be prescribed at the lowest effective dose. "Moreover, it is prudent to monitor linear growth in children treated with inhaled corticosteroids, given that individual susceptibility to these drugs may vary considerably," the investigators added.
FROM THE COCHRANE DATABASE OF SYSTEMATIC REVIEWS
Major finding: All six inhaled corticosteroids in this review were found to suppress linear growth velocity during 1 year of treatment; they all also suppressed growth as measured by the secondary outcomes of change in height standard deviation score over time and change from baseline in height over time.
Data source: A comprehensive meta-analysis of 25 good-quality, parallel-group, randomized clinical trials involving 8,471 children of all ages with mild to moderate persistent asthma whose growth was assessed for up to 6 years of follow-up.
Disclosures: Dr. Zhang and his associates reported no financial conflicts of interest.

Sleep Strategies: Choosing the right CPAP equipment
Continuous positive airway pressure (CPAP) has long been considered the gold standard treatment for OSA. Recently, a variety of new treatment approaches have become available for mild and moderate OSA, including nasal resistance valves, nerve stimulators, and negative pressure devices. Nonetheless, CPAP remains unmatched in efficacy, as well as the frequency and severity of side effects associated with treatment. The main drawback of CPAP is the required use of a mask interface and pressurized air during sleep, which is uncomfortable for some patients.
This article will highlight recent work investigating issues associated with equipment choice for practitioners treating OSA patients with CPAP and discuss how proper equipment choices and educational programs can reduce common complaints associated with CPAP use.
Mask choice
Finding a suitable mask interface is one of the most critical aspects of achieving adequate treatment compliance. The four general styles to choose from are oronasal (full-mask), standard nasal (over the nose), nasal pillows (in the nose), and the rarely-used oral.
Most clinicians choose an initial mask after CPAP titration based on a combination of patient feedback and air leakage rates but may change the mask style after home implementation in order to improve patient tolerance. Unfortunately, many clinicians are unaware that CPAP levels may need to be adjusted after changing masks. Two studies have shown that oronasal masks require significantly more pressure to ensure adequate OSA treatment during CPAP titration compared with standard nasal and nasal pillows masks (Ebben et al. Sleep Med. 2012;13[6]:645; Borel et al. PLoS ONE. 2013;8[5]:e64382).
In a separate study in which nasal masks were replaced with oronasal masks, the apnea-hypopnea index (AHI) increased to greater than 10 events per hour in half of patients who had been previously titrated to less than five per hour with the nasal mask (Ebben et al. Sleep Med. 2014;15[6]:619). Caution should be used when making a mask change to ensure that adequate disease control is maintained.
Humidification
In the past few years, humidification has been routinely added to most CPAP machines in order to improve comfort. The benefit appears to come from a reduction in dryness related to regular CPAP use (Ruhle et al. Sleep Breath. 2011;15[3]:479). Some patients report that humidification is particularly helpful in the winter months, when indoor humidity is low. Heated humidification has been found to produce significantly more humidity and causes less insensible water loss from the respiratory tract compared with unheated units (Randerath et al. Eur J Respir. 2002;20[1]:183). Unfortunately, the humidifier significantly increases the size and weight of the treatment machine, though it can be removed for travel if desired. In addition, the humidifier requires additional maintenance; if not cleaned regularly, there is a risk of bacterial colonization of the humidification chamber (Chin et al. J Clin Sleep Med. 2013; 9[8]:747).
In some instances, patients may complain of excess water condensation in the hose, particularly in the presence of a cool sleeping environment. Some CPAP manufacturers now offer heated hoses, which can significantly reduce this condensation. A second option is to add an insulating hose cover to help maintain a higher internal temperature. Generally, these covers are a good choice if the cost of a heated hose is not covered by a patient’s insurance.
Pressure relief

A common complaint often heard from patients using CPAP is that the pressure feels too high, particularly when exhaling. In response, some equipment makers have developed pressure relief systems that allow an adjustable pressure drop during exhalation with standard CPAP units. These systems work by transiently reducing pressure during exhalation by a set amount, according to their proprietary algorithm (Dolan et al. Sleep and Breath. 2009;13:73). However, not all patients find this pressure relief effective at making CPAP easier to use. When tested empirically, pressure relief has not been consistently shown to improve CPAP compliance (Dolan et al. Sleep Breath. 2009;13[1]:73).
Compliance data monitoring
Many patients benefit from discussing and reviewing treatment efficacy at their follow-up visits. Most modern CPAP equipment allows for such data monitoring, that may include duration and specific times of machine use, leak rate, snoring periods, and residual respiratory events, subdivided into hypopneas and apneas. In some cases, the software can distinguish between central ("clear airway") and obstructive events using forced oscillation techniques to measure upper airway resistance. This information allows the clinician to adjust settings and ensure that treatment is optimized and used as prescribed.
Clinicians should familiarize themselves with the different reporting systems that provide these data, and train their office staff on using software to capture information for all CPAP users. Notably, the algorithms used to capture residual respiratory events are not completely accurate; identification of such events is based only on measures of flow.
While it is probably acceptable to take extreme values at face value, whether low or very high, the imprecision of the methodology makes it more difficult to reliably use middling values in a clinical setting. (Schwab et al. Am J Respir Crit Care Med. 2013;188[5]:613). If a patient remains symptomatic despite no evidence of residual respiratory events from the adherence data download, a retitration study should still be considered.
Educational programs
Adherence to CPAP has been shown to increase when providers engage patients in educational programs to enhance compliance and understanding of the potential health-care consequences of untreated OSA (Lai et al. Chest. 2014 May 8. doi: 10.1378/ chest.13-2228. [Epub ahead of print]).
Early education and continuous support provide reinforcement of the need for adherence to therapy, as well as an opportunity to personalize the treatment and adjust settings and equipment as needed for each individual patient. Although specific guidelines for the best timing of the educational intervention are still lacking, evidence suggests that long-term compliance with CPAP might be determined as early as 2 weeks after therapy is initiated (Aloia et al. J Clin Sleep Med. 2005;1[4]:346). Therefore, educational programs should be readily available for prospective and new CPAP users in order to enhance their understanding of OSA and knowledge about CPAP treatment and to provide them with a venue for reviewing and managing compliance-related issues. Such programs can be run by dedicated sleep technologists, respiratory therapists, or nurses in clinics where physician availability is more limited.
Summary
CPAP remains the most effective treatment for OSA, though adherence is a struggle for many patients. Identifying the best mask for a given patient, determining whether humidification or an expiratory pressure drop should be added and making early and frequent contact after prescription can all assist in improving long-term CPAP use. Regular review of adherence data with the patient is also important, modifying the therapy as necessary to optimize comfort, understanding that such changes may necessitate a subsequent pressure adjustment to maintain disease control.
Implementing a comprehensive approach to managing patients using CPAP therapy can impact compliance by reducing treatment-related complaints and improving comfort.
Dr. Ebben is Assistant Professor of Psychology in Clinical Neurology, Department of Neurology; and Dr. Krieger is Associate Clinical Professor, Departments of Medicine, Neurology, and Genetic Medicine; Weill Cornell Medical College of Cornell University, New York, New York.

|
|
Dr. David Schulman, FCCP comments: The provision of positive airway pressure therapy to patients with sleep-disordered breathing is a daily practice for sleep medicine providers. Though the suboptimal adherence data are long-known and well-published, are there opportunities for us to help our patients do better? Has the limited time we allow in our clinic schedules for a routine sleep apnea follow-up impaired our patients’ ability to master the art of using CPAP?
Drs. Ebben and Krieger use this month’s Sleep Strategies to review important considerations of which providers should remain mindful when prescribing and monitoring this treatment. Recognizing that CPAP is a difficult therapy to reliably use is an important part of being a sleep medicine provider. Partnering with our patients to improve their acceptance and long-term use of this vitally important intervention is an underemphasized, but no less critical, part of the job.
|
|
|
Dr. David Schulman, FCCP comments: The provision of positive airway pressure therapy to patients with sleep-disordered breathing is a daily practice for sleep medicine providers. Though the suboptimal adherence data are long-known and well-published, are there opportunities for us to help our patients do better? Has the limited time we allow in our clinic schedules for a routine sleep apnea follow-up impaired our patients’ ability to master the art of using CPAP?
Drs. Ebben and Krieger use this month’s Sleep Strategies to review important considerations of which providers should remain mindful when prescribing and monitoring this treatment. Recognizing that CPAP is a difficult therapy to reliably use is an important part of being a sleep medicine provider. Partnering with our patients to improve their acceptance and long-term use of this vitally important intervention is an underemphasized, but no less critical, part of the job.
|
|
|
Dr. David Schulman, FCCP comments: The provision of positive airway pressure therapy to patients with sleep-disordered breathing is a daily practice for sleep medicine providers. Though the suboptimal adherence data are long-known and well-published, are there opportunities for us to help our patients do better? Has the limited time we allow in our clinic schedules for a routine sleep apnea follow-up impaired our patients’ ability to master the art of using CPAP?
Drs. Ebben and Krieger use this month’s Sleep Strategies to review important considerations of which providers should remain mindful when prescribing and monitoring this treatment. Recognizing that CPAP is a difficult therapy to reliably use is an important part of being a sleep medicine provider. Partnering with our patients to improve their acceptance and long-term use of this vitally important intervention is an underemphasized, but no less critical, part of the job.
Continuous positive airway pressure (CPAP) has long been considered the gold standard treatment for OSA. Recently, a variety of new treatment approaches have become available for mild and moderate OSA, including nasal resistance valves, nerve stimulators, and negative pressure devices. Nonetheless, CPAP remains unmatched in efficacy, as well as the frequency and severity of side effects associated with treatment. The main drawback of CPAP is the required use of a mask interface and pressurized air during sleep, which is uncomfortable for some patients.
This article will highlight recent work investigating issues associated with equipment choice for practitioners treating OSA patients with CPAP and discuss how proper equipment choices and educational programs can reduce common complaints associated with CPAP use.
Mask choice
Finding a suitable mask interface is one of the most critical aspects of achieving adequate treatment compliance. The four general styles to choose from are oronasal (full-mask), standard nasal (over the nose), nasal pillows (in the nose), and the rarely-used oral.
Most clinicians choose an initial mask after CPAP titration based on a combination of patient feedback and air leakage rates but may change the mask style after home implementation in order to improve patient tolerance. Unfortunately, many clinicians are unaware that CPAP levels may need to be adjusted after changing masks. Two studies have shown that oronasal masks require significantly more pressure to ensure adequate OSA treatment during CPAP titration compared with standard nasal and nasal pillows masks (Ebben et al. Sleep Med. 2012;13[6]:645; Borel et al. PLoS ONE. 2013;8[5]:e64382).
In a separate study in which nasal masks were replaced with oronasal masks, the apnea-hypopnea index (AHI) increased to greater than 10 events per hour in half of patients who had been previously titrated to less than five per hour with the nasal mask (Ebben et al. Sleep Med. 2014;15[6]:619). Caution should be used when making a mask change to ensure that adequate disease control is maintained.
Humidification
In the past few years, humidification has been routinely added to most CPAP machines in order to improve comfort. The benefit appears to come from a reduction in dryness related to regular CPAP use (Ruhle et al. Sleep Breath. 2011;15[3]:479). Some patients report that humidification is particularly helpful in the winter months, when indoor humidity is low. Heated humidification has been found to produce significantly more humidity and causes less insensible water loss from the respiratory tract compared with unheated units (Randerath et al. Eur J Respir. 2002;20[1]:183). Unfortunately, the humidifier significantly increases the size and weight of the treatment machine, though it can be removed for travel if desired. In addition, the humidifier requires additional maintenance; if not cleaned regularly, there is a risk of bacterial colonization of the humidification chamber (Chin et al. J Clin Sleep Med. 2013; 9[8]:747).
In some instances, patients may complain of excess water condensation in the hose, particularly in the presence of a cool sleeping environment. Some CPAP manufacturers now offer heated hoses, which can significantly reduce this condensation. A second option is to add an insulating hose cover to help maintain a higher internal temperature. Generally, these covers are a good choice if the cost of a heated hose is not covered by a patient’s insurance.
Pressure relief
A common complaint often heard from patients using CPAP is that the pressure feels too high, particularly when exhaling. In response, some equipment makers have developed pressure relief systems that allow an adjustable pressure drop during exhalation with standard CPAP units. These systems work by transiently reducing pressure during exhalation by a set amount, according to their proprietary algorithm (Dolan et al. Sleep and Breath. 2009;13:73). However, not all patients find this pressure relief effective at making CPAP easier to use. When tested empirically, pressure relief has not been consistently shown to improve CPAP compliance (Dolan et al. Sleep Breath. 2009;13[1]:73).
Compliance data monitoring
Many patients benefit from discussing and reviewing treatment efficacy at their follow-up visits. Most modern CPAP equipment allows for such data monitoring, that may include duration and specific times of machine use, leak rate, snoring periods, and residual respiratory events, subdivided into hypopneas and apneas. In some cases, the software can distinguish between central ("clear airway") and obstructive events using forced oscillation techniques to measure upper airway resistance. This information allows the clinician to adjust settings and ensure that treatment is optimized and used as prescribed.
Clinicians should familiarize themselves with the different reporting systems that provide these data, and train their office staff on using software to capture information for all CPAP users. Notably, the algorithms used to capture residual respiratory events are not completely accurate; identification of such events is based only on measures of flow.
While it is probably acceptable to take extreme values at face value, whether low or very high, the imprecision of the methodology makes it more difficult to reliably use middling values in a clinical setting. (Schwab et al. Am J Respir Crit Care Med. 2013;188[5]:613). If a patient remains symptomatic despite no evidence of residual respiratory events from the adherence data download, a retitration study should still be considered.
Educational programs
Adherence to CPAP has been shown to increase when providers engage patients in educational programs to enhance compliance and understanding of the potential health-care consequences of untreated OSA (Lai et al. Chest. 2014 May 8. doi: 10.1378/ chest.13-2228. [Epub ahead of print]).
Early education and continuous support provide reinforcement of the need for adherence to therapy, as well as an opportunity to personalize the treatment and adjust settings and equipment as needed for each individual patient. Although specific guidelines for the best timing of the educational intervention are still lacking, evidence suggests that long-term compliance with CPAP might be determined as early as 2 weeks after therapy is initiated (Aloia et al. J Clin Sleep Med. 2005;1[4]:346). Therefore, educational programs should be readily available for prospective and new CPAP users in order to enhance their understanding of OSA and knowledge about CPAP treatment and to provide them with a venue for reviewing and managing compliance-related issues. Such programs can be run by dedicated sleep technologists, respiratory therapists, or nurses in clinics where physician availability is more limited.
Summary
CPAP remains the most effective treatment for OSA, though adherence is a struggle for many patients. Identifying the best mask for a given patient, determining whether humidification or an expiratory pressure drop should be added and making early and frequent contact after prescription can all assist in improving long-term CPAP use. Regular review of adherence data with the patient is also important, modifying the therapy as necessary to optimize comfort, understanding that such changes may necessitate a subsequent pressure adjustment to maintain disease control.
Implementing a comprehensive approach to managing patients using CPAP therapy can impact compliance by reducing treatment-related complaints and improving comfort.
Dr. Ebben is Assistant Professor of Psychology in Clinical Neurology, Department of Neurology; and Dr. Krieger is Associate Clinical Professor, Departments of Medicine, Neurology, and Genetic Medicine; Weill Cornell Medical College of Cornell University, New York, New York.
Continuous positive airway pressure (CPAP) has long been considered the gold standard treatment for OSA. Recently, a variety of new treatment approaches have become available for mild and moderate OSA, including nasal resistance valves, nerve stimulators, and negative pressure devices. Nonetheless, CPAP remains unmatched in efficacy, as well as the frequency and severity of side effects associated with treatment. The main drawback of CPAP is the required use of a mask interface and pressurized air during sleep, which is uncomfortable for some patients.
This article will highlight recent work investigating issues associated with equipment choice for practitioners treating OSA patients with CPAP and discuss how proper equipment choices and educational programs can reduce common complaints associated with CPAP use.
Mask choice
Finding a suitable mask interface is one of the most critical aspects of achieving adequate treatment compliance. The four general styles to choose from are oronasal (full-mask), standard nasal (over the nose), nasal pillows (in the nose), and the rarely-used oral.
Most clinicians choose an initial mask after CPAP titration based on a combination of patient feedback and air leakage rates but may change the mask style after home implementation in order to improve patient tolerance. Unfortunately, many clinicians are unaware that CPAP levels may need to be adjusted after changing masks. Two studies have shown that oronasal masks require significantly more pressure to ensure adequate OSA treatment during CPAP titration compared with standard nasal and nasal pillows masks (Ebben et al. Sleep Med. 2012;13[6]:645; Borel et al. PLoS ONE. 2013;8[5]:e64382).
In a separate study in which nasal masks were replaced with oronasal masks, the apnea-hypopnea index (AHI) increased to greater than 10 events per hour in half of patients who had been previously titrated to less than five per hour with the nasal mask (Ebben et al. Sleep Med. 2014;15[6]:619). Caution should be used when making a mask change to ensure that adequate disease control is maintained.
Humidification
In the past few years, humidification has been routinely added to most CPAP machines in order to improve comfort. The benefit appears to come from a reduction in dryness related to regular CPAP use (Ruhle et al. Sleep Breath. 2011;15[3]:479). Some patients report that humidification is particularly helpful in the winter months, when indoor humidity is low. Heated humidification has been found to produce significantly more humidity and causes less insensible water loss from the respiratory tract compared with unheated units (Randerath et al. Eur J Respir. 2002;20[1]:183). Unfortunately, the humidifier significantly increases the size and weight of the treatment machine, though it can be removed for travel if desired. In addition, the humidifier requires additional maintenance; if not cleaned regularly, there is a risk of bacterial colonization of the humidification chamber (Chin et al. J Clin Sleep Med. 2013; 9[8]:747).
In some instances, patients may complain of excess water condensation in the hose, particularly in the presence of a cool sleeping environment. Some CPAP manufacturers now offer heated hoses, which can significantly reduce this condensation. A second option is to add an insulating hose cover to help maintain a higher internal temperature. Generally, these covers are a good choice if the cost of a heated hose is not covered by a patient’s insurance.
Pressure relief
A common complaint often heard from patients using CPAP is that the pressure feels too high, particularly when exhaling. In response, some equipment makers have developed pressure relief systems that allow an adjustable pressure drop during exhalation with standard CPAP units. These systems work by transiently reducing pressure during exhalation by a set amount, according to their proprietary algorithm (Dolan et al. Sleep and Breath. 2009;13:73). However, not all patients find this pressure relief effective at making CPAP easier to use. When tested empirically, pressure relief has not been consistently shown to improve CPAP compliance (Dolan et al. Sleep Breath. 2009;13[1]:73).
Compliance data monitoring
Many patients benefit from discussing and reviewing treatment efficacy at their follow-up visits. Most modern CPAP equipment allows for such data monitoring, that may include duration and specific times of machine use, leak rate, snoring periods, and residual respiratory events, subdivided into hypopneas and apneas. In some cases, the software can distinguish between central ("clear airway") and obstructive events using forced oscillation techniques to measure upper airway resistance. This information allows the clinician to adjust settings and ensure that treatment is optimized and used as prescribed.
Clinicians should familiarize themselves with the different reporting systems that provide these data, and train their office staff on using software to capture information for all CPAP users. Notably, the algorithms used to capture residual respiratory events are not completely accurate; identification of such events is based only on measures of flow.
While it is probably acceptable to take extreme values at face value, whether low or very high, the imprecision of the methodology makes it more difficult to reliably use middling values in a clinical setting. (Schwab et al. Am J Respir Crit Care Med. 2013;188[5]:613). If a patient remains symptomatic despite no evidence of residual respiratory events from the adherence data download, a retitration study should still be considered.
Educational programs
Adherence to CPAP has been shown to increase when providers engage patients in educational programs to enhance compliance and understanding of the potential health-care consequences of untreated OSA (Lai et al. Chest. 2014 May 8. doi: 10.1378/ chest.13-2228. [Epub ahead of print]).
Early education and continuous support provide reinforcement of the need for adherence to therapy, as well as an opportunity to personalize the treatment and adjust settings and equipment as needed for each individual patient. Although specific guidelines for the best timing of the educational intervention are still lacking, evidence suggests that long-term compliance with CPAP might be determined as early as 2 weeks after therapy is initiated (Aloia et al. J Clin Sleep Med. 2005;1[4]:346). Therefore, educational programs should be readily available for prospective and new CPAP users in order to enhance their understanding of OSA and knowledge about CPAP treatment and to provide them with a venue for reviewing and managing compliance-related issues. Such programs can be run by dedicated sleep technologists, respiratory therapists, or nurses in clinics where physician availability is more limited.
Summary
CPAP remains the most effective treatment for OSA, though adherence is a struggle for many patients. Identifying the best mask for a given patient, determining whether humidification or an expiratory pressure drop should be added and making early and frequent contact after prescription can all assist in improving long-term CPAP use. Regular review of adherence data with the patient is also important, modifying the therapy as necessary to optimize comfort, understanding that such changes may necessitate a subsequent pressure adjustment to maintain disease control.
Implementing a comprehensive approach to managing patients using CPAP therapy can impact compliance by reducing treatment-related complaints and improving comfort.
Dr. Ebben is Assistant Professor of Psychology in Clinical Neurology, Department of Neurology; and Dr. Krieger is Associate Clinical Professor, Departments of Medicine, Neurology, and Genetic Medicine; Weill Cornell Medical College of Cornell University, New York, New York.

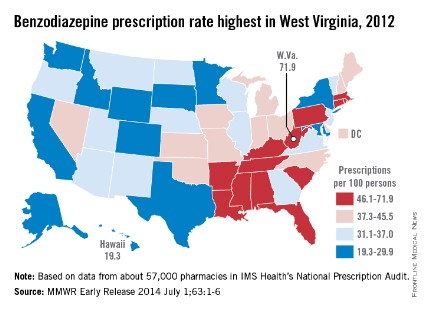
Sleep apnea raises cardiomyopathy risk ninefold in pregnancy
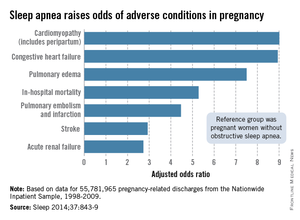
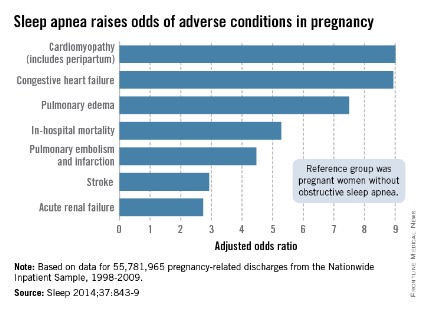
Pregnant women with obstructive sleep apnea are more likely to experience adverse clinical conditions than are pregnant women who do not have sleep apnea, according to an analysis of over 55 million pregnancy-related hospital discharges from 1998 to 2009.
Women with obstructive sleep apnea (OSA) were nine times more likely to have cardiomyopathy and 8.9 times more likely to have congestive heart failure during pregnancy than were women without OSA, after adjustment for numerous factors, including maternal age and obesity, race/ethnicity, household income, heart disease, hyperlipidemia, and prepregnancy diabetes, reported Dr. Judette M. Louis of the University of South Florida, Tampa, and her associates.
Women with OSA also were more likely to have pulmonary edema (adjusted odds ratio, 7.5), in-hospital mortality (AOR, 5.3), pulmonary embolism and infarction (AOR, 4.5), stroke (AOR, 2.9), and acute renal failure (AOR, 2.7), Dr. Louis and her associates said (Sleep 2014;37:843-9).
The investigators analyzed data on 55,781,965 maternal hospital discharges from 1998 to 2009 in the Agency for Healthcare Research and Quality’s Nationwide Inpatient Sample. The institution of one investigator received a grant from ResMed Inc. and equipment from ResMed and Philips Respironics for use in clinical trials.
Pregnant women with obstructive sleep apnea are more likely to experience adverse clinical conditions than are pregnant women who do not have sleep apnea, according to an analysis of over 55 million pregnancy-related hospital discharges from 1998 to 2009.
Women with obstructive sleep apnea (OSA) were nine times more likely to have cardiomyopathy and 8.9 times more likely to have congestive heart failure during pregnancy than were women without OSA, after adjustment for numerous factors, including maternal age and obesity, race/ethnicity, household income, heart disease, hyperlipidemia, and prepregnancy diabetes, reported Dr. Judette M. Louis of the University of South Florida, Tampa, and her associates.
Women with OSA also were more likely to have pulmonary edema (adjusted odds ratio, 7.5), in-hospital mortality (AOR, 5.3), pulmonary embolism and infarction (AOR, 4.5), stroke (AOR, 2.9), and acute renal failure (AOR, 2.7), Dr. Louis and her associates said (Sleep 2014;37:843-9).
The investigators analyzed data on 55,781,965 maternal hospital discharges from 1998 to 2009 in the Agency for Healthcare Research and Quality’s Nationwide Inpatient Sample. The institution of one investigator received a grant from ResMed Inc. and equipment from ResMed and Philips Respironics for use in clinical trials.
Pregnant women with obstructive sleep apnea are more likely to experience adverse clinical conditions than are pregnant women who do not have sleep apnea, according to an analysis of over 55 million pregnancy-related hospital discharges from 1998 to 2009.
Women with obstructive sleep apnea (OSA) were nine times more likely to have cardiomyopathy and 8.9 times more likely to have congestive heart failure during pregnancy than were women without OSA, after adjustment for numerous factors, including maternal age and obesity, race/ethnicity, household income, heart disease, hyperlipidemia, and prepregnancy diabetes, reported Dr. Judette M. Louis of the University of South Florida, Tampa, and her associates.
Women with OSA also were more likely to have pulmonary edema (adjusted odds ratio, 7.5), in-hospital mortality (AOR, 5.3), pulmonary embolism and infarction (AOR, 4.5), stroke (AOR, 2.9), and acute renal failure (AOR, 2.7), Dr. Louis and her associates said (Sleep 2014;37:843-9).
The investigators analyzed data on 55,781,965 maternal hospital discharges from 1998 to 2009 in the Agency for Healthcare Research and Quality’s Nationwide Inpatient Sample. The institution of one investigator received a grant from ResMed Inc. and equipment from ResMed and Philips Respironics for use in clinical trials.
FROM SLEEP
Novel antimetabolite strategy slows progression of deadly mesothelioma
CHICAGO – The arginine depletor ADI-PEG 20 cut the risk of progression in half for patients with malignant pleural mesothelioma in the randomized ADAM trial.
Median progression-free survival improved from 1.9 months with best supportive care (BSC) to 3.2 months with the addition of ADI-PEG 20 (hazard ratio, 0.51; P = .012).
The study was not powered for overall survival, but five patients have lived beyond 2 years, all on the ADI-PEG 20 plus BSC arm, Dr. Peter Szlosarek said at the annual meeting of the American Society of Clinical Oncology.
Mean overall survival was 12.8 months for patients assigned BSC and 14.5 months for those also given ADI-PEG 20 (P = .53). Median survival with this invariably fatal disease is typically 9-12 months.
"Arginine deprivation may have a role in the future management of mesothelioma," said Dr. Szlosarek, a medical oncology consultant at the Barts Cancer Institute and St. Bartholomew’s Hospital in London.
ADI-PEG 20 is one of several arginine-depleting agents in development and has been granted orphan drug status in the U.S. for hepatocellular carcinoma and melanoma.
ADI-PEG 20 is a pegylated arginine deiminase that exerts antitumor activity by depletion of serum arginine, an essential amino acid. Normal cells synthesize arginine from citrulline via the urea cycle enzyme argininosuccinate synthase 1 (ASS1), he explained.
Studies have shown that many malignancies including mesothelial and urological cancers, melanoma, and sarcomas lack ASS1 and therefore obtain arginine from the blood for tumor growth and survival. Recent evidence suggests that expression of argininosuccinate lyase, an enzyme immediately downstream of ASS1, may also play a role in tumor survival.
ADAM (ADI-PEG 20 in Patients with Malignant Pleural Mesothelioma) screened 214 patients with malignant pleural mesothelioma, roughly half of whom who were chemotherapy naive and half of whom were previously treated with platinum combination chemotherapy. Of these, 68 patients had tumors with negative or low ASS1 expression by immunohistochemistry including 24 who were randomly assigned to BSC and 44 assigned to BSC plus weekly intramuscular injections of ADI-PEG 20 36.8 mg/m2. Median follow-up was 25.3 months.
No complete or partial responses were seen on computed tomography scan, but 58% of patients had stable disease at 6 months with ADI-PEG 20 versus none given BSC alone, Dr. Szlosarek said.
Among 39 patients with ASS1-low mesothelioma, 46% had a partial response and 31% had stable disease on positron emission tomography/CT.
A post hoc analysis suggested a much greater benefit with ADI-PEG 20 in patients with an ASS1 loss of more than 75% (HR, 0.27), compared with those with an ASS1 loss of 50-75% (HR, 0.60).
The data support use of a cutoff of at least 50% ASS1 activity to select patients with mesothelioma for ADI-PEG 20 therapy, he said. Notably, this is lower than the cut point of at least 95% ASS1-negative cells used in previous trials in melanoma and small-cell lung cancer.
"Some patients with ASS1 low 50%-75% tumors still benefitted from the drug since the hazard ratio of 0.60 was met and was the target HR for the study," Dr. Szlosarek explained in an interview. "Indeed, the remaining nonprogressing patient, for 18 months so far, was in the 50%-75% group."
Invited discussant Dr. Lee M. Krug, a thoracic oncologist at Memorial Sloan-Kettering Cancer Center, New York, commended the investigators for using "a completely novel strategy in this disease," but said it was unclear whether the 1.3-month gain in progression-free survival was clinically meaningful. It might be interesting to consider combinations with chemotherapy and better selection of patients with the more stringent (ASS1 75%-100%) biomarker, Dr. Krug said.
He described this as an exciting time in mesothelioma, with new insights into the genomics of the disease and more randomized trials than ever before, including a pilot study showing dramatic responses in several patients with the immunoconjugate SS1P in combination with pentostatin and cyclophosphamide.
ADI-PEG 20 monotherapy trials are currently under discussion for patients with ASS1 75%-100% tumors. To improve disease control in the ASS1 low 50%-75% tumors, the investigators plan to move forward with the TRAP (Tumors Requiring Arginine to Assess ADI-PEG 20 with Pemetrexed and Cisplatin) trial due to open in July in the United Kingdom, Dr. Szlosarek said.
Further study is also needed to tackle drug resistance, a known challenge with arginine depletors, he added.
"Several of the patients who had early partial metabolic responses at 3 weeks by PET imaging progressed very quickly at 8 weeks by CT (modified RECIST) criteria, indicating onset of early resistance," Dr. Szlosarek said in the interview. "We are currently exploring a novel mechanism of resistance and will submit a paper later this year addressing this question."
The most common grade 3/4 adverse events with ADI-PEG 20 were neutropenia (11%), fatigue (7%), anaphylactoid/anaphylaxis (7%), rash (2%), and serum sickness (2%).
ADAM was funded by Cancer Research UK. Polaris Pharmaceuticals provided the study drug. Dr. Szlosarek disclosed ties with Roche and BMS. A coauthor reported ties with Polaris Group.
CHICAGO – The arginine depletor ADI-PEG 20 cut the risk of progression in half for patients with malignant pleural mesothelioma in the randomized ADAM trial.
Median progression-free survival improved from 1.9 months with best supportive care (BSC) to 3.2 months with the addition of ADI-PEG 20 (hazard ratio, 0.51; P = .012).
The study was not powered for overall survival, but five patients have lived beyond 2 years, all on the ADI-PEG 20 plus BSC arm, Dr. Peter Szlosarek said at the annual meeting of the American Society of Clinical Oncology.
Mean overall survival was 12.8 months for patients assigned BSC and 14.5 months for those also given ADI-PEG 20 (P = .53). Median survival with this invariably fatal disease is typically 9-12 months.
"Arginine deprivation may have a role in the future management of mesothelioma," said Dr. Szlosarek, a medical oncology consultant at the Barts Cancer Institute and St. Bartholomew’s Hospital in London.
ADI-PEG 20 is one of several arginine-depleting agents in development and has been granted orphan drug status in the U.S. for hepatocellular carcinoma and melanoma.
ADI-PEG 20 is a pegylated arginine deiminase that exerts antitumor activity by depletion of serum arginine, an essential amino acid. Normal cells synthesize arginine from citrulline via the urea cycle enzyme argininosuccinate synthase 1 (ASS1), he explained.
Studies have shown that many malignancies including mesothelial and urological cancers, melanoma, and sarcomas lack ASS1 and therefore obtain arginine from the blood for tumor growth and survival. Recent evidence suggests that expression of argininosuccinate lyase, an enzyme immediately downstream of ASS1, may also play a role in tumor survival.
ADAM (ADI-PEG 20 in Patients with Malignant Pleural Mesothelioma) screened 214 patients with malignant pleural mesothelioma, roughly half of whom who were chemotherapy naive and half of whom were previously treated with platinum combination chemotherapy. Of these, 68 patients had tumors with negative or low ASS1 expression by immunohistochemistry including 24 who were randomly assigned to BSC and 44 assigned to BSC plus weekly intramuscular injections of ADI-PEG 20 36.8 mg/m2. Median follow-up was 25.3 months.
No complete or partial responses were seen on computed tomography scan, but 58% of patients had stable disease at 6 months with ADI-PEG 20 versus none given BSC alone, Dr. Szlosarek said.
Among 39 patients with ASS1-low mesothelioma, 46% had a partial response and 31% had stable disease on positron emission tomography/CT.
A post hoc analysis suggested a much greater benefit with ADI-PEG 20 in patients with an ASS1 loss of more than 75% (HR, 0.27), compared with those with an ASS1 loss of 50-75% (HR, 0.60).
The data support use of a cutoff of at least 50% ASS1 activity to select patients with mesothelioma for ADI-PEG 20 therapy, he said. Notably, this is lower than the cut point of at least 95% ASS1-negative cells used in previous trials in melanoma and small-cell lung cancer.
"Some patients with ASS1 low 50%-75% tumors still benefitted from the drug since the hazard ratio of 0.60 was met and was the target HR for the study," Dr. Szlosarek explained in an interview. "Indeed, the remaining nonprogressing patient, for 18 months so far, was in the 50%-75% group."
Invited discussant Dr. Lee M. Krug, a thoracic oncologist at Memorial Sloan-Kettering Cancer Center, New York, commended the investigators for using "a completely novel strategy in this disease," but said it was unclear whether the 1.3-month gain in progression-free survival was clinically meaningful. It might be interesting to consider combinations with chemotherapy and better selection of patients with the more stringent (ASS1 75%-100%) biomarker, Dr. Krug said.
He described this as an exciting time in mesothelioma, with new insights into the genomics of the disease and more randomized trials than ever before, including a pilot study showing dramatic responses in several patients with the immunoconjugate SS1P in combination with pentostatin and cyclophosphamide.
ADI-PEG 20 monotherapy trials are currently under discussion for patients with ASS1 75%-100% tumors. To improve disease control in the ASS1 low 50%-75% tumors, the investigators plan to move forward with the TRAP (Tumors Requiring Arginine to Assess ADI-PEG 20 with Pemetrexed and Cisplatin) trial due to open in July in the United Kingdom, Dr. Szlosarek said.
Further study is also needed to tackle drug resistance, a known challenge with arginine depletors, he added.
"Several of the patients who had early partial metabolic responses at 3 weeks by PET imaging progressed very quickly at 8 weeks by CT (modified RECIST) criteria, indicating onset of early resistance," Dr. Szlosarek said in the interview. "We are currently exploring a novel mechanism of resistance and will submit a paper later this year addressing this question."
The most common grade 3/4 adverse events with ADI-PEG 20 were neutropenia (11%), fatigue (7%), anaphylactoid/anaphylaxis (7%), rash (2%), and serum sickness (2%).
ADAM was funded by Cancer Research UK. Polaris Pharmaceuticals provided the study drug. Dr. Szlosarek disclosed ties with Roche and BMS. A coauthor reported ties with Polaris Group.
CHICAGO – The arginine depletor ADI-PEG 20 cut the risk of progression in half for patients with malignant pleural mesothelioma in the randomized ADAM trial.
Median progression-free survival improved from 1.9 months with best supportive care (BSC) to 3.2 months with the addition of ADI-PEG 20 (hazard ratio, 0.51; P = .012).
The study was not powered for overall survival, but five patients have lived beyond 2 years, all on the ADI-PEG 20 plus BSC arm, Dr. Peter Szlosarek said at the annual meeting of the American Society of Clinical Oncology.
Mean overall survival was 12.8 months for patients assigned BSC and 14.5 months for those also given ADI-PEG 20 (P = .53). Median survival with this invariably fatal disease is typically 9-12 months.
"Arginine deprivation may have a role in the future management of mesothelioma," said Dr. Szlosarek, a medical oncology consultant at the Barts Cancer Institute and St. Bartholomew’s Hospital in London.
ADI-PEG 20 is one of several arginine-depleting agents in development and has been granted orphan drug status in the U.S. for hepatocellular carcinoma and melanoma.
ADI-PEG 20 is a pegylated arginine deiminase that exerts antitumor activity by depletion of serum arginine, an essential amino acid. Normal cells synthesize arginine from citrulline via the urea cycle enzyme argininosuccinate synthase 1 (ASS1), he explained.
Studies have shown that many malignancies including mesothelial and urological cancers, melanoma, and sarcomas lack ASS1 and therefore obtain arginine from the blood for tumor growth and survival. Recent evidence suggests that expression of argininosuccinate lyase, an enzyme immediately downstream of ASS1, may also play a role in tumor survival.
ADAM (ADI-PEG 20 in Patients with Malignant Pleural Mesothelioma) screened 214 patients with malignant pleural mesothelioma, roughly half of whom who were chemotherapy naive and half of whom were previously treated with platinum combination chemotherapy. Of these, 68 patients had tumors with negative or low ASS1 expression by immunohistochemistry including 24 who were randomly assigned to BSC and 44 assigned to BSC plus weekly intramuscular injections of ADI-PEG 20 36.8 mg/m2. Median follow-up was 25.3 months.
No complete or partial responses were seen on computed tomography scan, but 58% of patients had stable disease at 6 months with ADI-PEG 20 versus none given BSC alone, Dr. Szlosarek said.
Among 39 patients with ASS1-low mesothelioma, 46% had a partial response and 31% had stable disease on positron emission tomography/CT.
A post hoc analysis suggested a much greater benefit with ADI-PEG 20 in patients with an ASS1 loss of more than 75% (HR, 0.27), compared with those with an ASS1 loss of 50-75% (HR, 0.60).
The data support use of a cutoff of at least 50% ASS1 activity to select patients with mesothelioma for ADI-PEG 20 therapy, he said. Notably, this is lower than the cut point of at least 95% ASS1-negative cells used in previous trials in melanoma and small-cell lung cancer.
"Some patients with ASS1 low 50%-75% tumors still benefitted from the drug since the hazard ratio of 0.60 was met and was the target HR for the study," Dr. Szlosarek explained in an interview. "Indeed, the remaining nonprogressing patient, for 18 months so far, was in the 50%-75% group."
Invited discussant Dr. Lee M. Krug, a thoracic oncologist at Memorial Sloan-Kettering Cancer Center, New York, commended the investigators for using "a completely novel strategy in this disease," but said it was unclear whether the 1.3-month gain in progression-free survival was clinically meaningful. It might be interesting to consider combinations with chemotherapy and better selection of patients with the more stringent (ASS1 75%-100%) biomarker, Dr. Krug said.
He described this as an exciting time in mesothelioma, with new insights into the genomics of the disease and more randomized trials than ever before, including a pilot study showing dramatic responses in several patients with the immunoconjugate SS1P in combination with pentostatin and cyclophosphamide.
ADI-PEG 20 monotherapy trials are currently under discussion for patients with ASS1 75%-100% tumors. To improve disease control in the ASS1 low 50%-75% tumors, the investigators plan to move forward with the TRAP (Tumors Requiring Arginine to Assess ADI-PEG 20 with Pemetrexed and Cisplatin) trial due to open in July in the United Kingdom, Dr. Szlosarek said.
Further study is also needed to tackle drug resistance, a known challenge with arginine depletors, he added.
"Several of the patients who had early partial metabolic responses at 3 weeks by PET imaging progressed very quickly at 8 weeks by CT (modified RECIST) criteria, indicating onset of early resistance," Dr. Szlosarek said in the interview. "We are currently exploring a novel mechanism of resistance and will submit a paper later this year addressing this question."
The most common grade 3/4 adverse events with ADI-PEG 20 were neutropenia (11%), fatigue (7%), anaphylactoid/anaphylaxis (7%), rash (2%), and serum sickness (2%).
ADAM was funded by Cancer Research UK. Polaris Pharmaceuticals provided the study drug. Dr. Szlosarek disclosed ties with Roche and BMS. A coauthor reported ties with Polaris Group.
AT THE ASCO ANNUAL MEETING 2014
Key clinical point: An antimetabolite strategy that cuts off the supply of arginine to tumors may benefit patients with mesothelioma.
Major finding: Median progression-free survival was 1.9 months with best supportive care and 3.2 months with the addition of ADI-PEG 20 (HR, 0.51; P = .012).
Data source: A randomized trial of 68 patients with malignant pleural mesothelioma.
Disclosures: ADAM was funded by Cancer Research UK. Polaris Pharmaceuticals provided the study drug. Dr. Szlosarek disclosed ties with Roche and BMS. A coauthor reported ties with Polaris Group.
No blood clot risk found with HPV vaccination
The quadrivalent human papillomavirus vaccine does not increase the risk of venous thromboembolism, a study showed.
Two previous studies finding an association, one based on the Vaccine Adverse Event Reporting System and the other on the Vaccine Safety Datalink, reported few vaccinated cases, many of whom had known venous thromboembolism (VTE) risk factors, Nikolai Madrid Scheller and his colleagues at Statens Serum Institut in Copenhagen reported in a research letter (JAMA 2014;312:187-8).

The team used the self-controlled case series method with the main risk period for a first diagnosis of VTE set at 1-42 days after vaccination. They excluded women who were likely pregnant at the time of the VTE or had undergone major surgery in the previous 4 weeks or had a cancer diagnosis in the previous year from the VTE.
Women with VTE aged 10-44 years were followed until the end of the study or until emigration, death, or age 45 years during the study period from Oct. 1, 2006, to July 31, 2013. Among the 1.6 million women in the population cohort, 31% had received the quadrivalent HPV vaccine, and 4,375 women had VTE, 20% of whom had been vaccinated and served as the self-controlled cases.
The researchers found no association between the quadrivalent HPV vaccine and VTE (incidence ratio, 0.77). The lack of association remained in subsequent analyses adjusting for age and oral contraceptive use, and using only cases of VTE in which the women were receiving anticoagulants 4 weeks after diagnosis.
The study did not report external funding. The authors reported no disclosures.
The quadrivalent human papillomavirus vaccine does not increase the risk of venous thromboembolism, a study showed.
Two previous studies finding an association, one based on the Vaccine Adverse Event Reporting System and the other on the Vaccine Safety Datalink, reported few vaccinated cases, many of whom had known venous thromboembolism (VTE) risk factors, Nikolai Madrid Scheller and his colleagues at Statens Serum Institut in Copenhagen reported in a research letter (JAMA 2014;312:187-8).
The team used the self-controlled case series method with the main risk period for a first diagnosis of VTE set at 1-42 days after vaccination. They excluded women who were likely pregnant at the time of the VTE or had undergone major surgery in the previous 4 weeks or had a cancer diagnosis in the previous year from the VTE.
Women with VTE aged 10-44 years were followed until the end of the study or until emigration, death, or age 45 years during the study period from Oct. 1, 2006, to July 31, 2013. Among the 1.6 million women in the population cohort, 31% had received the quadrivalent HPV vaccine, and 4,375 women had VTE, 20% of whom had been vaccinated and served as the self-controlled cases.
The researchers found no association between the quadrivalent HPV vaccine and VTE (incidence ratio, 0.77). The lack of association remained in subsequent analyses adjusting for age and oral contraceptive use, and using only cases of VTE in which the women were receiving anticoagulants 4 weeks after diagnosis.
The study did not report external funding. The authors reported no disclosures.
The quadrivalent human papillomavirus vaccine does not increase the risk of venous thromboembolism, a study showed.
Two previous studies finding an association, one based on the Vaccine Adverse Event Reporting System and the other on the Vaccine Safety Datalink, reported few vaccinated cases, many of whom had known venous thromboembolism (VTE) risk factors, Nikolai Madrid Scheller and his colleagues at Statens Serum Institut in Copenhagen reported in a research letter (JAMA 2014;312:187-8).
The team used the self-controlled case series method with the main risk period for a first diagnosis of VTE set at 1-42 days after vaccination. They excluded women who were likely pregnant at the time of the VTE or had undergone major surgery in the previous 4 weeks or had a cancer diagnosis in the previous year from the VTE.
Women with VTE aged 10-44 years were followed until the end of the study or until emigration, death, or age 45 years during the study period from Oct. 1, 2006, to July 31, 2013. Among the 1.6 million women in the population cohort, 31% had received the quadrivalent HPV vaccine, and 4,375 women had VTE, 20% of whom had been vaccinated and served as the self-controlled cases.
The researchers found no association between the quadrivalent HPV vaccine and VTE (incidence ratio, 0.77). The lack of association remained in subsequent analyses adjusting for age and oral contraceptive use, and using only cases of VTE in which the women were receiving anticoagulants 4 weeks after diagnosis.
The study did not report external funding. The authors reported no disclosures.
FROM JAMA
Key clinical point: There appears to be no increased risk of VTE linked with HPV vaccination.
Major finding: The quadrivalent HPV vaccine is not associated with venous thromboembolism (incidence ratio, 0.77).
Data source: The findings are based on a self-controlled case series analysis of 4,375 Danish women from a population cohort of 1.6 million women, aged 10-44 years, who had a venous thromboembolism during Oct. 1, 2006, to July 31, 2013.
Disclosures: The study did not report external funding. The authors reported no disclosures.

No blood clot risk found with HPV vaccination
The quadrivalent human papillomavirus vaccine does not increase the risk of venous thromboembolism, a study showed.
Two previous studies finding an association, one based on the Vaccine Adverse Event Reporting System and the other on the Vaccine Safety Datalink, reported few vaccinated cases, many of whom had known venous thromboembolism (VTE) risk factors, Nikolai Madrid Scheller and his colleagues at Statens Serum Institut in Copenhagen reported in a research letter (JAMA 2014;312:187-8).
The team used the self-controlled case series method with the main risk period for a first diagnosis of VTE set at 1-42 days after vaccination. They excluded women who were likely pregnant at the time of the VTE or had undergone major surgery in the previous 4 weeks or had a cancer diagnosis in the previous year from the VTE.
Women with VTE aged 10-44 years were followed until the end of the study or until emigration, death, or age 45 years during the study period from Oct. 1, 2006, to July 31, 2013. Among the 1.6 million women in the population cohort, 31% had received the quadrivalent HPV vaccine, and 4,375 women had VTE, 20% of whom had been vaccinated and served as the self-controlled cases.
The researchers found no association between the quadrivalent HPV vaccine and VTE (incidence ratio, 0.77). The lack of association remained in subsequent analyses adjusting for age and oral contraceptive use, and using only cases of VTE in which the women were receiving anticoagulants 4 weeks after diagnosis.
The study did not report external funding. The authors reported no disclosures.
The quadrivalent human papillomavirus vaccine does not increase the risk of venous thromboembolism, a study showed.
Two previous studies finding an association, one based on the Vaccine Adverse Event Reporting System and the other on the Vaccine Safety Datalink, reported few vaccinated cases, many of whom had known venous thromboembolism (VTE) risk factors, Nikolai Madrid Scheller and his colleagues at Statens Serum Institut in Copenhagen reported in a research letter (JAMA 2014;312:187-8).
The team used the self-controlled case series method with the main risk period for a first diagnosis of VTE set at 1-42 days after vaccination. They excluded women who were likely pregnant at the time of the VTE or had undergone major surgery in the previous 4 weeks or had a cancer diagnosis in the previous year from the VTE.
Women with VTE aged 10-44 years were followed until the end of the study or until emigration, death, or age 45 years during the study period from Oct. 1, 2006, to July 31, 2013. Among the 1.6 million women in the population cohort, 31% had received the quadrivalent HPV vaccine, and 4,375 women had VTE, 20% of whom had been vaccinated and served as the self-controlled cases.
The researchers found no association between the quadrivalent HPV vaccine and VTE (incidence ratio, 0.77). The lack of association remained in subsequent analyses adjusting for age and oral contraceptive use, and using only cases of VTE in which the women were receiving anticoagulants 4 weeks after diagnosis.
The study did not report external funding. The authors reported no disclosures.
The quadrivalent human papillomavirus vaccine does not increase the risk of venous thromboembolism, a study showed.
Two previous studies finding an association, one based on the Vaccine Adverse Event Reporting System and the other on the Vaccine Safety Datalink, reported few vaccinated cases, many of whom had known venous thromboembolism (VTE) risk factors, Nikolai Madrid Scheller and his colleagues at Statens Serum Institut in Copenhagen reported in a research letter (JAMA 2014;312:187-8).
The team used the self-controlled case series method with the main risk period for a first diagnosis of VTE set at 1-42 days after vaccination. They excluded women who were likely pregnant at the time of the VTE or had undergone major surgery in the previous 4 weeks or had a cancer diagnosis in the previous year from the VTE.
Women with VTE aged 10-44 years were followed until the end of the study or until emigration, death, or age 45 years during the study period from Oct. 1, 2006, to July 31, 2013. Among the 1.6 million women in the population cohort, 31% had received the quadrivalent HPV vaccine, and 4,375 women had VTE, 20% of whom had been vaccinated and served as the self-controlled cases.
The researchers found no association between the quadrivalent HPV vaccine and VTE (incidence ratio, 0.77). The lack of association remained in subsequent analyses adjusting for age and oral contraceptive use, and using only cases of VTE in which the women were receiving anticoagulants 4 weeks after diagnosis.
The study did not report external funding. The authors reported no disclosures.
FROM JAMA
Key clinical point: There appears to be no increased risk of VTE linked with HPV vaccination.
Major finding: The quadrivalent HPV vaccine is not associated with venous thromboembolism (incidence ratio, 0.77).
Data source: The findings are based on a self-controlled case series analysis of 4,375 Danish women from a population cohort of 1.6 million women, aged 10-44 years, who had a venous thromboembolism during Oct. 1, 2006, to July 31, 2013.
Disclosures: The study did not report external funding. The authors reported no disclosures.

Benzodiazepine prescribing rates highest in the South
There is wide variation between states in the prescription of benzodiazepines, with rates highest in the South and lowest in the West, the Centers for Disease Control and Prevention reported.
The overall prescribing rate for benzodiazepines in the South for 2012 was 43.1/100 persons – 54% higher than the West’s 27.9/100. Like the South, prescribing rates in the Midwest (38.2/100) and the Northeast (38.1/100) were both above the national rate of 37.6/100 persons, according to the CDC (MMWR 2014 July 1;63:1-6).
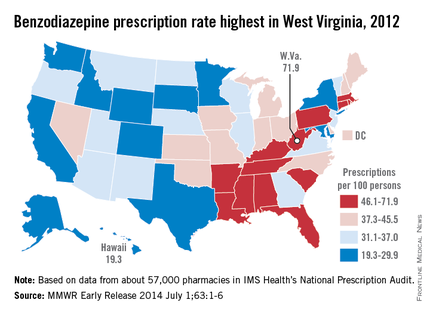
Among individual states, West Virginia’s U.S.-high rate of 71.9/100 was 3.7-fold higher than Hawaii’s low of 19.3/100. West Virginia was even one standard deviation above the states with the next-highest rates: Alabama (61.9), Tennessee (61.4), and Rhode Island (60.2), the analysis showed.
"Previous studies have found that regional prescribing variation cannot be explained by variation in the prevalence of the conditions treated by these drugs," the investigators noted.
The analysis was based on a sample of approximately 57,000 pharmacies from IMS Health’s National Prescription Audit that "dispense nearly 80% of the retail prescriptions in the United States," they wrote.
There is wide variation between states in the prescription of benzodiazepines, with rates highest in the South and lowest in the West, the Centers for Disease Control and Prevention reported.
The overall prescribing rate for benzodiazepines in the South for 2012 was 43.1/100 persons – 54% higher than the West’s 27.9/100. Like the South, prescribing rates in the Midwest (38.2/100) and the Northeast (38.1/100) were both above the national rate of 37.6/100 persons, according to the CDC (MMWR 2014 July 1;63:1-6).
Among individual states, West Virginia’s U.S.-high rate of 71.9/100 was 3.7-fold higher than Hawaii’s low of 19.3/100. West Virginia was even one standard deviation above the states with the next-highest rates: Alabama (61.9), Tennessee (61.4), and Rhode Island (60.2), the analysis showed.
"Previous studies have found that regional prescribing variation cannot be explained by variation in the prevalence of the conditions treated by these drugs," the investigators noted.
The analysis was based on a sample of approximately 57,000 pharmacies from IMS Health’s National Prescription Audit that "dispense nearly 80% of the retail prescriptions in the United States," they wrote.
There is wide variation between states in the prescription of benzodiazepines, with rates highest in the South and lowest in the West, the Centers for Disease Control and Prevention reported.
The overall prescribing rate for benzodiazepines in the South for 2012 was 43.1/100 persons – 54% higher than the West’s 27.9/100. Like the South, prescribing rates in the Midwest (38.2/100) and the Northeast (38.1/100) were both above the national rate of 37.6/100 persons, according to the CDC (MMWR 2014 July 1;63:1-6).
Among individual states, West Virginia’s U.S.-high rate of 71.9/100 was 3.7-fold higher than Hawaii’s low of 19.3/100. West Virginia was even one standard deviation above the states with the next-highest rates: Alabama (61.9), Tennessee (61.4), and Rhode Island (60.2), the analysis showed.
"Previous studies have found that regional prescribing variation cannot be explained by variation in the prevalence of the conditions treated by these drugs," the investigators noted.
The analysis was based on a sample of approximately 57,000 pharmacies from IMS Health’s National Prescription Audit that "dispense nearly 80% of the retail prescriptions in the United States," they wrote.
FROM MORBIDITY AND MORTALITY WEEKLY REPORT