User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Benzodiazepine prescribing rates highest in the South
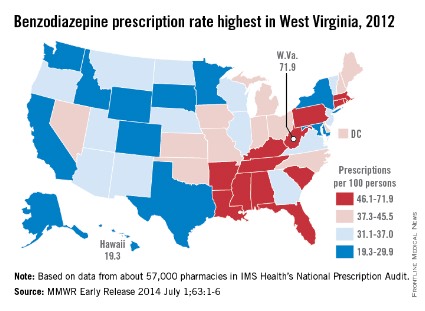
There is wide variation between states in the prescription of benzodiazepines, with rates highest in the South and lowest in the West, the Centers for Disease Control and Prevention reported.
The overall prescribing rate for benzodiazepines in the South for 2012 was 43.1/100 persons – 54% higher than the West’s 27.9/100. Like the South, prescribing rates in the Midwest (38.2/100) and the Northeast (38.1/100) were both above the national rate of 37.6/100 persons, according to the CDC (MMWR 2014 July 1;63:1-6).
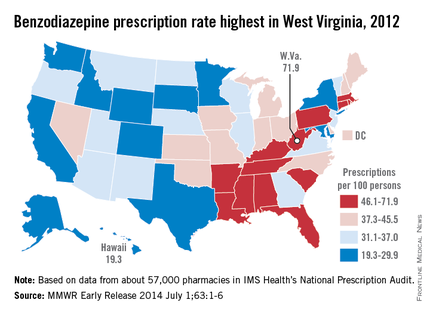
Among individual states, West Virginia’s U.S.-high rate of 71.9/100 was 3.7-fold higher than Hawaii’s low of 19.3/100. West Virginia was even one standard deviation above the states with the next-highest rates: Alabama (61.9), Tennessee (61.4), and Rhode Island (60.2), the analysis showed.
"Previous studies have found that regional prescribing variation cannot be explained by variation in the prevalence of the conditions treated by these drugs," the investigators noted.
The analysis was based on a sample of approximately 57,000 pharmacies from IMS Health’s National Prescription Audit that "dispense nearly 80% of the retail prescriptions in the United States," they wrote.
There is wide variation between states in the prescription of benzodiazepines, with rates highest in the South and lowest in the West, the Centers for Disease Control and Prevention reported.
The overall prescribing rate for benzodiazepines in the South for 2012 was 43.1/100 persons – 54% higher than the West’s 27.9/100. Like the South, prescribing rates in the Midwest (38.2/100) and the Northeast (38.1/100) were both above the national rate of 37.6/100 persons, according to the CDC (MMWR 2014 July 1;63:1-6).
Among individual states, West Virginia’s U.S.-high rate of 71.9/100 was 3.7-fold higher than Hawaii’s low of 19.3/100. West Virginia was even one standard deviation above the states with the next-highest rates: Alabama (61.9), Tennessee (61.4), and Rhode Island (60.2), the analysis showed.
"Previous studies have found that regional prescribing variation cannot be explained by variation in the prevalence of the conditions treated by these drugs," the investigators noted.
The analysis was based on a sample of approximately 57,000 pharmacies from IMS Health’s National Prescription Audit that "dispense nearly 80% of the retail prescriptions in the United States," they wrote.
There is wide variation between states in the prescription of benzodiazepines, with rates highest in the South and lowest in the West, the Centers for Disease Control and Prevention reported.
The overall prescribing rate for benzodiazepines in the South for 2012 was 43.1/100 persons – 54% higher than the West’s 27.9/100. Like the South, prescribing rates in the Midwest (38.2/100) and the Northeast (38.1/100) were both above the national rate of 37.6/100 persons, according to the CDC (MMWR 2014 July 1;63:1-6).
Among individual states, West Virginia’s U.S.-high rate of 71.9/100 was 3.7-fold higher than Hawaii’s low of 19.3/100. West Virginia was even one standard deviation above the states with the next-highest rates: Alabama (61.9), Tennessee (61.4), and Rhode Island (60.2), the analysis showed.
"Previous studies have found that regional prescribing variation cannot be explained by variation in the prevalence of the conditions treated by these drugs," the investigators noted.
The analysis was based on a sample of approximately 57,000 pharmacies from IMS Health’s National Prescription Audit that "dispense nearly 80% of the retail prescriptions in the United States," they wrote.
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
Individualized program improves sleep in preschoolers
MINNEAPOLIS – Tailoring an intervention to the particular needs of a child and his or her family can markedly improve the child’s ability to go to sleep and stay asleep, a pilot study shows.
The trial was successful enough that the National Institute of Child Health and Development has given the lead researcher, Michelle M. Garrison, Ph.D., of the Seattle Children’s Research Institute, funding to enroll 500 children in a randomized, controlled trial to validate the intervention.
Dr. Garrison undertook the pilot in part to see what would help sleep-deprived and frustrated parents, and pediatricians, who might not have a ready solution for a preschooler who persistently won’t go to bed or won’t stay in bed.

To recruit children for the study, Dr. Garrison sent the CSHQ (Children’s Sleep Habits Questionnaire) to parents of all children aged 2.5-5 years who had been seen at local pediatric clinics. If parents were interested, they returned the survey. If the children met the eligibility criteria for having a behavioral sleep problem, they were included. Not every parent agreed that their child had an issue, which created an initial hurdle for making the intervention work, said Dr. Garrison.
The program started with a home visit, in which parents received education and a kit that included a binder with educational handouts, the book
Take Charge of Your Child's Sleep (New York: Marlowe and Co., 2005), a bedtime routine chart with cards that can be individualized to the child, laminated passes that allow the child to step outside the routine occasionally, and a clock that glows green when it is okay to get out of bed in the morning.
Parents received three follow-up phone calls for education, to set goals, and to engage in preemptive problem solving. Parents were coached on setting bedtime routines, creating a consistent bedtime, eliminating screen time in the hour or two before bed, setting limits, and working on night waking.
The pilot enrolled 36 children with a mean age of about 4 years. Forty-four percent were female and 72% were white, 19% were Asian, 8% were black, and 6% were Hispanic. The race and ethnicity categories were not mutually exclusive, said Dr. Garrison. A total of 22% of children had been adopted after 1 year of age. The mean age of the parents was 38 years. Only 11% of children lived in a one-adult home, and 11% lived in a multigenerational home.
Sleep habits and issues were assessed at baseline and at 3 months through 7-day diaries, actigraphy, and several sleep scales. The researchers were able to perform actigraphy on only 15 children, but there was good concordance between those measures and the diaries, said Dr. Garrison.
Overall, on average, children slept an additional 36 minutes a night. According to the diaries, 14% slept 10-30 minutes more, a third slept 30-60 minutes more, and 25% slept an additional hour. The actigraphy showed that 14% of children gained 10-30 minutes sleep, 36% gained 30-60 minutes, and 7% gained more than an hour. The average onset latency decreased by 10 minutes.
Dr. Garrison said the intervention could be tailored to children and parents with varying needs. For instance, adopted and nonadopted children did equally well with the program. She and her colleagues also worked with co-sleepers. She split them into "reactive" co-sleepers – that is, parents who felt like they had no choice – and "lifestyle" co-sleepers, who saw it as a way to bond. Reactive co-sleepers were coached on getting children to sleep in their own beds. Lifestyle parents were taught how to get children to get to sleep first, before the adults joined them in bed. There was a significant increase in sleep duration in those children of lifestyle co-sleepers, said Dr. Garrison.
Overall, there were no differences observed by age, sex, or comorbid conditions such as asthma.
The things that seemed to help the most included the number of contacts with the families, the tailored bedtime routine, and anticipatory problem solving around bedtime consistency. Parents who were the most skeptical about the benefits of sleep benefited the most from the program, said Dr. Garrison.
She will now take her methods into a larger trial that is being funded by the NICHD and has begun enrolling children. It will include 500 children and families will get monthly phone follow-ups for 9 months. Children will be analyzed for 3 years, in part to see if improving sleep has any impact on body mass index, learning, and cognitive function, she said.
The study was funded by the Sleep Research Society Foundation’s J. Christian Gillin, M.D., Research Grant; the Institution of Translational Health Sciences; and Seattle Children’s Research Institute. Dr. Garrison reported no conflicts.
On Twitter @aliciaault
MINNEAPOLIS – Tailoring an intervention to the particular needs of a child and his or her family can markedly improve the child’s ability to go to sleep and stay asleep, a pilot study shows.
The trial was successful enough that the National Institute of Child Health and Development has given the lead researcher, Michelle M. Garrison, Ph.D., of the Seattle Children’s Research Institute, funding to enroll 500 children in a randomized, controlled trial to validate the intervention.
Dr. Garrison undertook the pilot in part to see what would help sleep-deprived and frustrated parents, and pediatricians, who might not have a ready solution for a preschooler who persistently won’t go to bed or won’t stay in bed.
To recruit children for the study, Dr. Garrison sent the CSHQ (Children’s Sleep Habits Questionnaire) to parents of all children aged 2.5-5 years who had been seen at local pediatric clinics. If parents were interested, they returned the survey. If the children met the eligibility criteria for having a behavioral sleep problem, they were included. Not every parent agreed that their child had an issue, which created an initial hurdle for making the intervention work, said Dr. Garrison.
The program started with a home visit, in which parents received education and a kit that included a binder with educational handouts, the book
Take Charge of Your Child's Sleep (New York: Marlowe and Co., 2005), a bedtime routine chart with cards that can be individualized to the child, laminated passes that allow the child to step outside the routine occasionally, and a clock that glows green when it is okay to get out of bed in the morning.
Parents received three follow-up phone calls for education, to set goals, and to engage in preemptive problem solving. Parents were coached on setting bedtime routines, creating a consistent bedtime, eliminating screen time in the hour or two before bed, setting limits, and working on night waking.
The pilot enrolled 36 children with a mean age of about 4 years. Forty-four percent were female and 72% were white, 19% were Asian, 8% were black, and 6% were Hispanic. The race and ethnicity categories were not mutually exclusive, said Dr. Garrison. A total of 22% of children had been adopted after 1 year of age. The mean age of the parents was 38 years. Only 11% of children lived in a one-adult home, and 11% lived in a multigenerational home.
Sleep habits and issues were assessed at baseline and at 3 months through 7-day diaries, actigraphy, and several sleep scales. The researchers were able to perform actigraphy on only 15 children, but there was good concordance between those measures and the diaries, said Dr. Garrison.
Overall, on average, children slept an additional 36 minutes a night. According to the diaries, 14% slept 10-30 minutes more, a third slept 30-60 minutes more, and 25% slept an additional hour. The actigraphy showed that 14% of children gained 10-30 minutes sleep, 36% gained 30-60 minutes, and 7% gained more than an hour. The average onset latency decreased by 10 minutes.
Dr. Garrison said the intervention could be tailored to children and parents with varying needs. For instance, adopted and nonadopted children did equally well with the program. She and her colleagues also worked with co-sleepers. She split them into "reactive" co-sleepers – that is, parents who felt like they had no choice – and "lifestyle" co-sleepers, who saw it as a way to bond. Reactive co-sleepers were coached on getting children to sleep in their own beds. Lifestyle parents were taught how to get children to get to sleep first, before the adults joined them in bed. There was a significant increase in sleep duration in those children of lifestyle co-sleepers, said Dr. Garrison.
Overall, there were no differences observed by age, sex, or comorbid conditions such as asthma.
The things that seemed to help the most included the number of contacts with the families, the tailored bedtime routine, and anticipatory problem solving around bedtime consistency. Parents who were the most skeptical about the benefits of sleep benefited the most from the program, said Dr. Garrison.
She will now take her methods into a larger trial that is being funded by the NICHD and has begun enrolling children. It will include 500 children and families will get monthly phone follow-ups for 9 months. Children will be analyzed for 3 years, in part to see if improving sleep has any impact on body mass index, learning, and cognitive function, she said.
The study was funded by the Sleep Research Society Foundation’s J. Christian Gillin, M.D., Research Grant; the Institution of Translational Health Sciences; and Seattle Children’s Research Institute. Dr. Garrison reported no conflicts.
On Twitter @aliciaault
MINNEAPOLIS – Tailoring an intervention to the particular needs of a child and his or her family can markedly improve the child’s ability to go to sleep and stay asleep, a pilot study shows.
The trial was successful enough that the National Institute of Child Health and Development has given the lead researcher, Michelle M. Garrison, Ph.D., of the Seattle Children’s Research Institute, funding to enroll 500 children in a randomized, controlled trial to validate the intervention.
Dr. Garrison undertook the pilot in part to see what would help sleep-deprived and frustrated parents, and pediatricians, who might not have a ready solution for a preschooler who persistently won’t go to bed or won’t stay in bed.
To recruit children for the study, Dr. Garrison sent the CSHQ (Children’s Sleep Habits Questionnaire) to parents of all children aged 2.5-5 years who had been seen at local pediatric clinics. If parents were interested, they returned the survey. If the children met the eligibility criteria for having a behavioral sleep problem, they were included. Not every parent agreed that their child had an issue, which created an initial hurdle for making the intervention work, said Dr. Garrison.
The program started with a home visit, in which parents received education and a kit that included a binder with educational handouts, the book
Take Charge of Your Child's Sleep (New York: Marlowe and Co., 2005), a bedtime routine chart with cards that can be individualized to the child, laminated passes that allow the child to step outside the routine occasionally, and a clock that glows green when it is okay to get out of bed in the morning.
Parents received three follow-up phone calls for education, to set goals, and to engage in preemptive problem solving. Parents were coached on setting bedtime routines, creating a consistent bedtime, eliminating screen time in the hour or two before bed, setting limits, and working on night waking.
The pilot enrolled 36 children with a mean age of about 4 years. Forty-four percent were female and 72% were white, 19% were Asian, 8% were black, and 6% were Hispanic. The race and ethnicity categories were not mutually exclusive, said Dr. Garrison. A total of 22% of children had been adopted after 1 year of age. The mean age of the parents was 38 years. Only 11% of children lived in a one-adult home, and 11% lived in a multigenerational home.
Sleep habits and issues were assessed at baseline and at 3 months through 7-day diaries, actigraphy, and several sleep scales. The researchers were able to perform actigraphy on only 15 children, but there was good concordance between those measures and the diaries, said Dr. Garrison.
Overall, on average, children slept an additional 36 minutes a night. According to the diaries, 14% slept 10-30 minutes more, a third slept 30-60 minutes more, and 25% slept an additional hour. The actigraphy showed that 14% of children gained 10-30 minutes sleep, 36% gained 30-60 minutes, and 7% gained more than an hour. The average onset latency decreased by 10 minutes.
Dr. Garrison said the intervention could be tailored to children and parents with varying needs. For instance, adopted and nonadopted children did equally well with the program. She and her colleagues also worked with co-sleepers. She split them into "reactive" co-sleepers – that is, parents who felt like they had no choice – and "lifestyle" co-sleepers, who saw it as a way to bond. Reactive co-sleepers were coached on getting children to sleep in their own beds. Lifestyle parents were taught how to get children to get to sleep first, before the adults joined them in bed. There was a significant increase in sleep duration in those children of lifestyle co-sleepers, said Dr. Garrison.
Overall, there were no differences observed by age, sex, or comorbid conditions such as asthma.
The things that seemed to help the most included the number of contacts with the families, the tailored bedtime routine, and anticipatory problem solving around bedtime consistency. Parents who were the most skeptical about the benefits of sleep benefited the most from the program, said Dr. Garrison.
She will now take her methods into a larger trial that is being funded by the NICHD and has begun enrolling children. It will include 500 children and families will get monthly phone follow-ups for 9 months. Children will be analyzed for 3 years, in part to see if improving sleep has any impact on body mass index, learning, and cognitive function, she said.
The study was funded by the Sleep Research Society Foundation’s J. Christian Gillin, M.D., Research Grant; the Institution of Translational Health Sciences; and Seattle Children’s Research Institute. Dr. Garrison reported no conflicts.
On Twitter @aliciaault
FROM SLEEP 2014
Key clinical point: A focused, individualized program can help recalcitrant preschoolers get to sleep and stay asleep.
Major finding: In a pilot study with 36 children, they slept an additional 36 minutes a night with the program.
Data source: The Sleep Health in Preschoolers intervention program, which was conducted in children aged 2.5-5 years over 3 months.
Disclosures: The study was funded by the Sleep Research Society Foundation’s J. Christian Gillin, M.D., Research Grant; the Institution of Translational Health Sciences; and Seattle Children’s Research Institute. Dr. Garrison reported no conflicts.

Acromegaly: Look closely for sleep-disordered breathing
CHICAGO – Roughly 80% of patients with newly diagnosed and as-yet untreated acromegaly already have obstructive sleep apnea, according to the findings of what’s believed to be the largest-ever polysomnography study in such subjects.
Importantly, this study showed that the common practice of screening for sleep-disordered breathing with the Epworth Sleepiness Scale (ESS) and overnight oximetry to measure the desaturation index will greatly underdiagnose this important condition in patients with acromegaly. These are poor screening tools in this setting. They need to be supplemented by polysomnography, with the diagnosis of obstructive sleep apnea (OSA) hinging upon the finding of an abnormal apnea-hypopnea index, Dr. Andrew S. Powlson asserted at the joint meeting of the International Congress of Endocrinology and the Endocrine Society.
Dr. Powlson of the University of Cambridge (U.K.), reported on 40 consecutive patients with newly diagnosed, treatment-naive acromegaly who were evaluated by the ESS, desaturation index, and polysomnography. The study’s purpose was to shed light on a controversy: Is sleep-disordered breathing an inherent feature of acromegaly or a secondary side effect of its treatment? The question takes on added clinical relevance in light of OSA’s known predisposition to premature cardiovascular and metabolic disease, motor vehicle accidents, and impaired quality of life.
Of the 40 patients, 31 (78%) met diagnostic criteria for OSA by polysomnography. The OSA was defined on the basis of the apnea-hypopnea index as mild in 12, moderate in 5, and severe in 14.
In contrast, the ESS performed dismally as a screening instrument: Only 12 of the 31 patients with OSA had an ESS score greater than 11, which is the standard threshold for further investigation. Moreover, measurement of the diffusion index during overnight oximetry identified only 21 patients as having OSA: 11 rated mild, 7 moderate, and 3 severe, as compared to 14 patients classified as having severe OSA by polysomnography.
Patients with acromegaly displayed an increased sleep arousal index and more periodic limb movements during sleep than in reference norms, which translates into marked disruption of the normal sleep cycle. Of note, however, polysomnography showed that sleep latency – that is, the time it takes to fall asleep – and total sleep time were normal in the acromegaly patients with OSA.
Instead, the predominant pattern was one of disrupted sleep architecture. Twenty-seven acromegaly patients spent longer than expected in stage-1 sleep, while the deeper sleep stages were dramatically diminished. Indeed, 26 patients had reduced stage-2 sleep, 31 had reduced REM sleep, and 26 had shortened slow wave sleep.
Dr. Powlson reported having no financial disclosures in connection with this study, conducted with institutional funds.
CHICAGO – Roughly 80% of patients with newly diagnosed and as-yet untreated acromegaly already have obstructive sleep apnea, according to the findings of what’s believed to be the largest-ever polysomnography study in such subjects.
Importantly, this study showed that the common practice of screening for sleep-disordered breathing with the Epworth Sleepiness Scale (ESS) and overnight oximetry to measure the desaturation index will greatly underdiagnose this important condition in patients with acromegaly. These are poor screening tools in this setting. They need to be supplemented by polysomnography, with the diagnosis of obstructive sleep apnea (OSA) hinging upon the finding of an abnormal apnea-hypopnea index, Dr. Andrew S. Powlson asserted at the joint meeting of the International Congress of Endocrinology and the Endocrine Society.
Dr. Powlson of the University of Cambridge (U.K.), reported on 40 consecutive patients with newly diagnosed, treatment-naive acromegaly who were evaluated by the ESS, desaturation index, and polysomnography. The study’s purpose was to shed light on a controversy: Is sleep-disordered breathing an inherent feature of acromegaly or a secondary side effect of its treatment? The question takes on added clinical relevance in light of OSA’s known predisposition to premature cardiovascular and metabolic disease, motor vehicle accidents, and impaired quality of life.
Of the 40 patients, 31 (78%) met diagnostic criteria for OSA by polysomnography. The OSA was defined on the basis of the apnea-hypopnea index as mild in 12, moderate in 5, and severe in 14.
In contrast, the ESS performed dismally as a screening instrument: Only 12 of the 31 patients with OSA had an ESS score greater than 11, which is the standard threshold for further investigation. Moreover, measurement of the diffusion index during overnight oximetry identified only 21 patients as having OSA: 11 rated mild, 7 moderate, and 3 severe, as compared to 14 patients classified as having severe OSA by polysomnography.
Patients with acromegaly displayed an increased sleep arousal index and more periodic limb movements during sleep than in reference norms, which translates into marked disruption of the normal sleep cycle. Of note, however, polysomnography showed that sleep latency – that is, the time it takes to fall asleep – and total sleep time were normal in the acromegaly patients with OSA.
Instead, the predominant pattern was one of disrupted sleep architecture. Twenty-seven acromegaly patients spent longer than expected in stage-1 sleep, while the deeper sleep stages were dramatically diminished. Indeed, 26 patients had reduced stage-2 sleep, 31 had reduced REM sleep, and 26 had shortened slow wave sleep.
Dr. Powlson reported having no financial disclosures in connection with this study, conducted with institutional funds.
CHICAGO – Roughly 80% of patients with newly diagnosed and as-yet untreated acromegaly already have obstructive sleep apnea, according to the findings of what’s believed to be the largest-ever polysomnography study in such subjects.
Importantly, this study showed that the common practice of screening for sleep-disordered breathing with the Epworth Sleepiness Scale (ESS) and overnight oximetry to measure the desaturation index will greatly underdiagnose this important condition in patients with acromegaly. These are poor screening tools in this setting. They need to be supplemented by polysomnography, with the diagnosis of obstructive sleep apnea (OSA) hinging upon the finding of an abnormal apnea-hypopnea index, Dr. Andrew S. Powlson asserted at the joint meeting of the International Congress of Endocrinology and the Endocrine Society.
Dr. Powlson of the University of Cambridge (U.K.), reported on 40 consecutive patients with newly diagnosed, treatment-naive acromegaly who were evaluated by the ESS, desaturation index, and polysomnography. The study’s purpose was to shed light on a controversy: Is sleep-disordered breathing an inherent feature of acromegaly or a secondary side effect of its treatment? The question takes on added clinical relevance in light of OSA’s known predisposition to premature cardiovascular and metabolic disease, motor vehicle accidents, and impaired quality of life.
Of the 40 patients, 31 (78%) met diagnostic criteria for OSA by polysomnography. The OSA was defined on the basis of the apnea-hypopnea index as mild in 12, moderate in 5, and severe in 14.
In contrast, the ESS performed dismally as a screening instrument: Only 12 of the 31 patients with OSA had an ESS score greater than 11, which is the standard threshold for further investigation. Moreover, measurement of the diffusion index during overnight oximetry identified only 21 patients as having OSA: 11 rated mild, 7 moderate, and 3 severe, as compared to 14 patients classified as having severe OSA by polysomnography.
Patients with acromegaly displayed an increased sleep arousal index and more periodic limb movements during sleep than in reference norms, which translates into marked disruption of the normal sleep cycle. Of note, however, polysomnography showed that sleep latency – that is, the time it takes to fall asleep – and total sleep time were normal in the acromegaly patients with OSA.
Instead, the predominant pattern was one of disrupted sleep architecture. Twenty-seven acromegaly patients spent longer than expected in stage-1 sleep, while the deeper sleep stages were dramatically diminished. Indeed, 26 patients had reduced stage-2 sleep, 31 had reduced REM sleep, and 26 had shortened slow wave sleep.
Dr. Powlson reported having no financial disclosures in connection with this study, conducted with institutional funds.
AT ICE/ENDO 2014
Key clinical point: Reliance on the Epworth Sleepiness Scale and desaturation index on overnight oximetry to screen for OSA in patients with newly diagnosed acromegaly results in an unacceptable underdiagnosis rate.
Major finding: Thirty-one of 40 consecutive patients with de novo acromegaly had OSA on polysomnography.
Data source: Forty consecutive patients with newly diagnosed acromegaly underwent evaluation via the Epworth Sleepiness Scale, desaturation index, and polysomnography.
Disclosures: The presenter reported having no financial conflicts regarding this study, carried out with institutional funds.
CDC panel: For children, live attenuated intranasal flu vaccine is best
The live attenuated intranasal flu vaccine is the preferred method of immunizing healthy children aged 2-8 years against seasonal influenza, a federal panel has recommended.
At a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, committee members unanimously agreed that healthy children with no contraindications should receive the quadrivalent live attenuated vaccine (LAIV) rather than an inactivated vaccine, provided that the LAIV is readily available.
"If the LAIV is not immediately available, [inactivated influenza vaccine (IIV)] should be used," the recommendation reads. "Vaccination should not be delayed in order to procure LAIV."

All children aged 6 months or older should receive influenza vaccine, according to the recommendation. "Influenza vaccine should not be delayed to procure a specific vaccine preparation if an appropriate one is already available."
The committee approved the recommendation after hearing an evidence review that found the LAIV to be "moderately" more effective for this age group than the inactivated vaccine was. Although the data are not plentiful, they suggest that it would probably prevent about 47 more lab-confirmed cases of flu per 1,000 children than the IIV, Dr. Lisa Grohskopf said
"The benefits appear to outweigh the potential harms, with modestly better efficacy," and no appreciable increase in adverse events associated with the live vaccine, said Dr. Grohskopf, who is a medical officer in the influenza division of the Centers for Disease Control and Prevention in Atlanta.
Her review was based on two studies – one published in 2006 and one in 2007. The earlier study was an open-label trial that randomized about 2,300 children aged 6-71 months to either the LAIV or an IIV. The much larger 2007 study randomized about 16,000 children aged 6-59 months to the two vaccine types or to matching placebos.
The pooled analysis was limited to healthy children aged 24-59 months who were without a history of asthma or wheezing. The primary endpoint of lab-confirmed influenza infection was significantly less likely among children who had received the LAIV (hazard ratio, 0.47). The secondary endpoint of influenza-associated otitis media was also significantly less likely to occur among those who got the LAIV (HR, 0.47).
Neither of the vaccines was associated with any medically significant wheezing or fever, Dr. Grohskopf said.
She also examined these same endpoints in children who had a history of wheezing or asthma. The LAIV significantly reduced the risk of lab-confirmed influenza in this group (HR, 0.53). There were no significantly increased risks of medically significant wheezing in the children, regardless of whether or not they had experienced wheezing within the past 12 months.
However, Dr. Grohskopf said, she and her colleagues didn’t feel that the studies were strong enough to make any initial recommendations to the committee about whether the LAIV could safely be used in children with a history of wheezing or asthma. The studies didn’t drill down into data on this group enough, and the data are now too old to be completely reliable for this population.
Asthma and wheezing are not strict contraindications to the LAIV, she said, but ACIP does not recommend it for children with those issues or for those with any chronic conditions that might predispose them to complications from the flu.
The committee also heard that the strains included in the 2014-2015 vaccine will be the same as last season’s. Because of this, children who received at least one dose of the 2013-2014 vaccine will only need one dose of this year’s vaccine to ensure immunity. "This is analogous to what happened in the 2011-2012 season, when the vaccine strains were unchanged from the previous season," Dr. Grohskopf said.
She also touched on the issue of cost. "We haven’t done a formal cost-effectiveness analysis," she said.
"It’s likely to be a very complex undertaking because of the large number of products out there. It will probably be a few years before that could be done."
The best estimates available now can be drawn from the 2013-2014 private sector costs associated with CDC’s Vaccines for Children program. "The cost of the LAIV intranasal vaccine is $22.70/dose, and for the inactivated vaccine, there is a broad range of variability, from $7.65-$14.81/dose for the trivalent to $14.90-$21.09/dose for the quadrivalent."
On Twitter @alz_gal
The live attenuated intranasal flu vaccine is the preferred method of immunizing healthy children aged 2-8 years against seasonal influenza, a federal panel has recommended.
At a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, committee members unanimously agreed that healthy children with no contraindications should receive the quadrivalent live attenuated vaccine (LAIV) rather than an inactivated vaccine, provided that the LAIV is readily available.
"If the LAIV is not immediately available, [inactivated influenza vaccine (IIV)] should be used," the recommendation reads. "Vaccination should not be delayed in order to procure LAIV."
All children aged 6 months or older should receive influenza vaccine, according to the recommendation. "Influenza vaccine should not be delayed to procure a specific vaccine preparation if an appropriate one is already available."
The committee approved the recommendation after hearing an evidence review that found the LAIV to be "moderately" more effective for this age group than the inactivated vaccine was. Although the data are not plentiful, they suggest that it would probably prevent about 47 more lab-confirmed cases of flu per 1,000 children than the IIV, Dr. Lisa Grohskopf said
"The benefits appear to outweigh the potential harms, with modestly better efficacy," and no appreciable increase in adverse events associated with the live vaccine, said Dr. Grohskopf, who is a medical officer in the influenza division of the Centers for Disease Control and Prevention in Atlanta.
Her review was based on two studies – one published in 2006 and one in 2007. The earlier study was an open-label trial that randomized about 2,300 children aged 6-71 months to either the LAIV or an IIV. The much larger 2007 study randomized about 16,000 children aged 6-59 months to the two vaccine types or to matching placebos.
The pooled analysis was limited to healthy children aged 24-59 months who were without a history of asthma or wheezing. The primary endpoint of lab-confirmed influenza infection was significantly less likely among children who had received the LAIV (hazard ratio, 0.47). The secondary endpoint of influenza-associated otitis media was also significantly less likely to occur among those who got the LAIV (HR, 0.47).
Neither of the vaccines was associated with any medically significant wheezing or fever, Dr. Grohskopf said.
She also examined these same endpoints in children who had a history of wheezing or asthma. The LAIV significantly reduced the risk of lab-confirmed influenza in this group (HR, 0.53). There were no significantly increased risks of medically significant wheezing in the children, regardless of whether or not they had experienced wheezing within the past 12 months.
However, Dr. Grohskopf said, she and her colleagues didn’t feel that the studies were strong enough to make any initial recommendations to the committee about whether the LAIV could safely be used in children with a history of wheezing or asthma. The studies didn’t drill down into data on this group enough, and the data are now too old to be completely reliable for this population.
Asthma and wheezing are not strict contraindications to the LAIV, she said, but ACIP does not recommend it for children with those issues or for those with any chronic conditions that might predispose them to complications from the flu.
The committee also heard that the strains included in the 2014-2015 vaccine will be the same as last season’s. Because of this, children who received at least one dose of the 2013-2014 vaccine will only need one dose of this year’s vaccine to ensure immunity. "This is analogous to what happened in the 2011-2012 season, when the vaccine strains were unchanged from the previous season," Dr. Grohskopf said.
She also touched on the issue of cost. "We haven’t done a formal cost-effectiveness analysis," she said.
"It’s likely to be a very complex undertaking because of the large number of products out there. It will probably be a few years before that could be done."
The best estimates available now can be drawn from the 2013-2014 private sector costs associated with CDC’s Vaccines for Children program. "The cost of the LAIV intranasal vaccine is $22.70/dose, and for the inactivated vaccine, there is a broad range of variability, from $7.65-$14.81/dose for the trivalent to $14.90-$21.09/dose for the quadrivalent."
On Twitter @alz_gal
The live attenuated intranasal flu vaccine is the preferred method of immunizing healthy children aged 2-8 years against seasonal influenza, a federal panel has recommended.
At a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, committee members unanimously agreed that healthy children with no contraindications should receive the quadrivalent live attenuated vaccine (LAIV) rather than an inactivated vaccine, provided that the LAIV is readily available.
"If the LAIV is not immediately available, [inactivated influenza vaccine (IIV)] should be used," the recommendation reads. "Vaccination should not be delayed in order to procure LAIV."
All children aged 6 months or older should receive influenza vaccine, according to the recommendation. "Influenza vaccine should not be delayed to procure a specific vaccine preparation if an appropriate one is already available."
The committee approved the recommendation after hearing an evidence review that found the LAIV to be "moderately" more effective for this age group than the inactivated vaccine was. Although the data are not plentiful, they suggest that it would probably prevent about 47 more lab-confirmed cases of flu per 1,000 children than the IIV, Dr. Lisa Grohskopf said
"The benefits appear to outweigh the potential harms, with modestly better efficacy," and no appreciable increase in adverse events associated with the live vaccine, said Dr. Grohskopf, who is a medical officer in the influenza division of the Centers for Disease Control and Prevention in Atlanta.
Her review was based on two studies – one published in 2006 and one in 2007. The earlier study was an open-label trial that randomized about 2,300 children aged 6-71 months to either the LAIV or an IIV. The much larger 2007 study randomized about 16,000 children aged 6-59 months to the two vaccine types or to matching placebos.
The pooled analysis was limited to healthy children aged 24-59 months who were without a history of asthma or wheezing. The primary endpoint of lab-confirmed influenza infection was significantly less likely among children who had received the LAIV (hazard ratio, 0.47). The secondary endpoint of influenza-associated otitis media was also significantly less likely to occur among those who got the LAIV (HR, 0.47).
Neither of the vaccines was associated with any medically significant wheezing or fever, Dr. Grohskopf said.
She also examined these same endpoints in children who had a history of wheezing or asthma. The LAIV significantly reduced the risk of lab-confirmed influenza in this group (HR, 0.53). There were no significantly increased risks of medically significant wheezing in the children, regardless of whether or not they had experienced wheezing within the past 12 months.
However, Dr. Grohskopf said, she and her colleagues didn’t feel that the studies were strong enough to make any initial recommendations to the committee about whether the LAIV could safely be used in children with a history of wheezing or asthma. The studies didn’t drill down into data on this group enough, and the data are now too old to be completely reliable for this population.
Asthma and wheezing are not strict contraindications to the LAIV, she said, but ACIP does not recommend it for children with those issues or for those with any chronic conditions that might predispose them to complications from the flu.
The committee also heard that the strains included in the 2014-2015 vaccine will be the same as last season’s. Because of this, children who received at least one dose of the 2013-2014 vaccine will only need one dose of this year’s vaccine to ensure immunity. "This is analogous to what happened in the 2011-2012 season, when the vaccine strains were unchanged from the previous season," Dr. Grohskopf said.
She also touched on the issue of cost. "We haven’t done a formal cost-effectiveness analysis," she said.
"It’s likely to be a very complex undertaking because of the large number of products out there. It will probably be a few years before that could be done."
The best estimates available now can be drawn from the 2013-2014 private sector costs associated with CDC’s Vaccines for Children program. "The cost of the LAIV intranasal vaccine is $22.70/dose, and for the inactivated vaccine, there is a broad range of variability, from $7.65-$14.81/dose for the trivalent to $14.90-$21.09/dose for the quadrivalent."
On Twitter @alz_gal
FROM AN ACIP MEETING

OTC topical acne meds can cause severe reactions
The Food and Drug Administration says that some over-the-counter acne products can cause severe hypersensitivity or allergic reactions and is warning consumers to discontinue use immediately and seek emergency medical attention if they experience such symptoms.
The reactions seem to be on the upswing, according to the agency’s review of reports from 1969 to early 2013.
The agency said in safety announcement that it has not determined whether the reactions are being triggered by the active ingredients in the products – benzoyl peroxide or salicylic acid – or by the inactive ingredients or a combination of the inactive and active ingredients.
The products include Proactiv, Neutrogena, MaxClarity, Oxy, Ambi, Aveeno, Clean & Clear, and private label store brands, and are sold as gels, lotions, face washes, solutions, cleansing pads, toners, and face scrubs, among other products, according to the agency.
The FDA has received reports stating that – within minutes to a day or longer of use – consumers have had hypersensitivity reactions that include throat tightness, difficulty breathing, or swelling of the eyes, face, lips, or tongue. Hives and itching are also indications of an allergic reaction.
From 1969 to January 2013, the agency identified 131 cases of hypersensitivity reactions, with the majority reported in 2012-2013. A total of 86% (113) of the cases were in women, and the reactions were reported in people aged 11-78 years.
There were no deaths, but 58 of the consumers were hospitalized. A total of 38 of the 131 cases (29%) were categorized as anaphylactic reactions, and the remainder were categorized as nonanaphylactic hypersensitivity. Almost half of the consumers said they had discontinued use after the reaction, the majority of whom reported some degree of recovery after discontinuing product use, with final outcomes unavailable for the rest. Four of the patients who used the product again reported a recurrence of the reaction.
The agency is encouraging manufacturers to add directions on testing for hypersensitivity to the labels of all OTC topical acne products. Some labels already include those instructions, which direct users to apply a small amount to one or two small affected areas of the skin for 3 days. If there is no reaction – topical or otherwise – then the product can be used according to the directions.
Consumers are also being urged to avoid using a product if they have previously experienced a hypersensitivity reaction with its use.
The FDA says that physicians should be aware that some topical prescription acne drug products also contain warnings about allergic reactions, including anaphylaxis.
Physicians can report adverse events involving OTC topical acne products to the FDA MedWatch program.
On Twitter @aliciaault
The Food and Drug Administration says that some over-the-counter acne products can cause severe hypersensitivity or allergic reactions and is warning consumers to discontinue use immediately and seek emergency medical attention if they experience such symptoms.
The reactions seem to be on the upswing, according to the agency’s review of reports from 1969 to early 2013.
The agency said in safety announcement that it has not determined whether the reactions are being triggered by the active ingredients in the products – benzoyl peroxide or salicylic acid – or by the inactive ingredients or a combination of the inactive and active ingredients.
The products include Proactiv, Neutrogena, MaxClarity, Oxy, Ambi, Aveeno, Clean & Clear, and private label store brands, and are sold as gels, lotions, face washes, solutions, cleansing pads, toners, and face scrubs, among other products, according to the agency.
The FDA has received reports stating that – within minutes to a day or longer of use – consumers have had hypersensitivity reactions that include throat tightness, difficulty breathing, or swelling of the eyes, face, lips, or tongue. Hives and itching are also indications of an allergic reaction.
From 1969 to January 2013, the agency identified 131 cases of hypersensitivity reactions, with the majority reported in 2012-2013. A total of 86% (113) of the cases were in women, and the reactions were reported in people aged 11-78 years.
There were no deaths, but 58 of the consumers were hospitalized. A total of 38 of the 131 cases (29%) were categorized as anaphylactic reactions, and the remainder were categorized as nonanaphylactic hypersensitivity. Almost half of the consumers said they had discontinued use after the reaction, the majority of whom reported some degree of recovery after discontinuing product use, with final outcomes unavailable for the rest. Four of the patients who used the product again reported a recurrence of the reaction.
The agency is encouraging manufacturers to add directions on testing for hypersensitivity to the labels of all OTC topical acne products. Some labels already include those instructions, which direct users to apply a small amount to one or two small affected areas of the skin for 3 days. If there is no reaction – topical or otherwise – then the product can be used according to the directions.
Consumers are also being urged to avoid using a product if they have previously experienced a hypersensitivity reaction with its use.
The FDA says that physicians should be aware that some topical prescription acne drug products also contain warnings about allergic reactions, including anaphylaxis.
Physicians can report adverse events involving OTC topical acne products to the FDA MedWatch program.
On Twitter @aliciaault
The Food and Drug Administration says that some over-the-counter acne products can cause severe hypersensitivity or allergic reactions and is warning consumers to discontinue use immediately and seek emergency medical attention if they experience such symptoms.
The reactions seem to be on the upswing, according to the agency’s review of reports from 1969 to early 2013.
The agency said in safety announcement that it has not determined whether the reactions are being triggered by the active ingredients in the products – benzoyl peroxide or salicylic acid – or by the inactive ingredients or a combination of the inactive and active ingredients.
The products include Proactiv, Neutrogena, MaxClarity, Oxy, Ambi, Aveeno, Clean & Clear, and private label store brands, and are sold as gels, lotions, face washes, solutions, cleansing pads, toners, and face scrubs, among other products, according to the agency.
The FDA has received reports stating that – within minutes to a day or longer of use – consumers have had hypersensitivity reactions that include throat tightness, difficulty breathing, or swelling of the eyes, face, lips, or tongue. Hives and itching are also indications of an allergic reaction.
From 1969 to January 2013, the agency identified 131 cases of hypersensitivity reactions, with the majority reported in 2012-2013. A total of 86% (113) of the cases were in women, and the reactions were reported in people aged 11-78 years.
There were no deaths, but 58 of the consumers were hospitalized. A total of 38 of the 131 cases (29%) were categorized as anaphylactic reactions, and the remainder were categorized as nonanaphylactic hypersensitivity. Almost half of the consumers said they had discontinued use after the reaction, the majority of whom reported some degree of recovery after discontinuing product use, with final outcomes unavailable for the rest. Four of the patients who used the product again reported a recurrence of the reaction.
The agency is encouraging manufacturers to add directions on testing for hypersensitivity to the labels of all OTC topical acne products. Some labels already include those instructions, which direct users to apply a small amount to one or two small affected areas of the skin for 3 days. If there is no reaction – topical or otherwise – then the product can be used according to the directions.
Consumers are also being urged to avoid using a product if they have previously experienced a hypersensitivity reaction with its use.
The FDA says that physicians should be aware that some topical prescription acne drug products also contain warnings about allergic reactions, including anaphylaxis.
Physicians can report adverse events involving OTC topical acne products to the FDA MedWatch program.
On Twitter @aliciaault
LGBT adults more likely to use tobacco
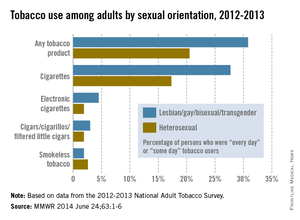
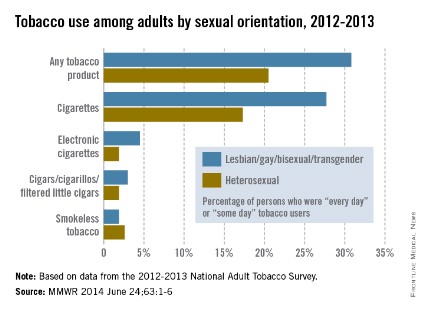
LGBT adults are considerably more likely to use tobacco products than are heterosexual adults, according to a Centers for Disease Control and Prevention report published June 24.
In 2012-2013, the prevalence of "every day" or "some day" use of any tobacco product among lesbian, gay, bisexual, or transgender adults was 30.8%, compared with 20.5% for heterosexual adults. "Every day" or "some day" cigarette use was reported by 27.7% of LGBT adults and 17.3% of heterosexual adults, according to the CDC (MMWR 2014 June 24;63:1-6).
The data from the National Adult Tobacco Survey show that LGBT adults also were more likely to use cigars/cigarillos/filtered small cigarettes (3.0% vs. 1.9%) and electronic cigarettes (4.5% vs. 1.9%), while heterosexual adults were more likely to use smokeless tobacco (2.6% vs. 1.9%), according to the CDC report.
In 2012-2013, the prevalence of "every day" or "some day" use of any tobacco product among lesbian, gay, bisexual, or transgender adults was 30.8%, compared with 20.5% for heterosexual adults. "Every day" or "some day" cigarette use was reported by 27.7% of LGBT adults and 17.3% of heterosexual adults, according to the CDC (MMWR 2014 June 24;63:1-6).
The data from the National Adult Tobacco Survey show that LGBT adults also were more likely to use cigars/cigarillos/filtered small cigarettes (3.0% vs. 1.9%) and electronic cigarettes (4.5% vs. 1.9%), while he
LGBT adults are considerably more likely to use tobacco products than are heterosexual adults, according to a Centers for Disease Control and Prevention report published June 24.
In 2012-2013, the prevalence of "every day" or "some day" use of any tobacco product among lesbian, gay, bisexual, or transgender adults was 30.8%, compared with 20.5% for heterosexual adults. "Every day" or "some day" cigarette use was reported by 27.7% of LGBT adults and 17.3% of heterosexual adults, according to the CDC (MMWR 2014 June 24;63:1-6).
The data from the National Adult Tobacco Survey show that LGBT adults also were more likely to use cigars/cigarillos/filtered small cigarettes (3.0% vs. 1.9%) and electronic cigarettes (4.5% vs. 1.9%), while heterosexual adults were more likely to use smokeless tobacco (2.6% vs. 1.9%), according to the CDC report.
LGBT adults are considerably more likely to use tobacco products than are heterosexual adults, according to a Centers for Disease Control and Prevention report published June 24.
In 2012-2013, the prevalence of "every day" or "some day" use of any tobacco product among lesbian, gay, bisexual, or transgender adults was 30.8%, compared with 20.5% for heterosexual adults. "Every day" or "some day" cigarette use was reported by 27.7% of LGBT adults and 17.3% of heterosexual adults, according to the CDC (MMWR 2014 June 24;63:1-6).
The data from the National Adult Tobacco Survey show that LGBT adults also were more likely to use cigars/cigarillos/filtered small cigarettes (3.0% vs. 1.9%) and electronic cigarettes (4.5% vs. 1.9%), while heterosexual adults were more likely to use smokeless tobacco (2.6% vs. 1.9%), according to the CDC report.
In 2012-2013, the prevalence of "every day" or "some day" use of any tobacco product among lesbian, gay, bisexual, or transgender adults was 30.8%, compared with 20.5% for heterosexual adults. "Every day" or "some day" cigarette use was reported by 27.7% of LGBT adults and 17.3% of heterosexual adults, according to the CDC (MMWR 2014 June 24;63:1-6).
The data from the National Adult Tobacco Survey show that LGBT adults also were more likely to use cigars/cigarillos/filtered small cigarettes (3.0% vs. 1.9%) and electronic cigarettes (4.5% vs. 1.9%), while he
In 2012-2013, the prevalence of "every day" or "some day" use of any tobacco product among lesbian, gay, bisexual, or transgender adults was 30.8%, compared with 20.5% for heterosexual adults. "Every day" or "some day" cigarette use was reported by 27.7% of LGBT adults and 17.3% of heterosexual adults, according to the CDC (MMWR 2014 June 24;63:1-6).
The data from the National Adult Tobacco Survey show that LGBT adults also were more likely to use cigars/cigarillos/filtered small cigarettes (3.0% vs. 1.9%) and electronic cigarettes (4.5% vs. 1.9%), while he
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
Think Twice About Nebulizers for Asthma Attacks
PRACTICE CHANGER
Stop ordering nebulizers to deliver β-agonists to patients older than 2 who have mild or moderate asthma exacerbations. A metered-dose inhaler (MDI) with a spacer produces the same benefits with fewer adverse effects.1

STRENGTH OF RECOMMENDATION
A: Based on an updated Cochrane meta-analysis of 39 randomized controlled trials (RCTs). 1
ILLUSTRATIVE CASE
A 6-year-old girl with a history of reactive airway disease comes to your office complaining of cough and wheezing. On exam, she has mild retractions, a respiratory rate of 35 breaths/min, and an O2 saturation of 96% on room air. Her lung fields are diffusely wheezy. Her parents would like to keep her out of the hospital. How should you order her albuterol to decrease her wheezing and minimize adverse effects?
Asthma affects nearly 19 million adults and 7 million children in the United States.2 Asthma exacerbations are the third most common reason for hospitalization in children.2,3 Treatment usually requires multiple agents, including inhaled β-agonists. These are most effective when delivered to the peripheral airways, which is a challenge during an asthma exacerbation because of airway swelling and rapid breathing. Two devices have been developed to effectively deliver medication to the peripheral airways: nebulizers and MDIs with a holding chamber (spacer).1
Several studies have demonstrated that for mild to moderate asthma exacerbations, administering a β-agonist via an MDI with a spacer is as effective as using a nebulizer.4,5 Asthma treatment guidelines also state that spacers are either comparable or preferable to nebulizers for β-agonist administration in children and adults.6,7 However, based on our experience, clinicians still frequently order nebulizer treatments for patients with asthma exacerbations, despite several advantages of MDIs with spacers. Notably, they cost less and don’t require maintenance or a power source. Clinicians administered nebulizer therapy at more than 3.6 million emergency department (ED) visits in 2006.8
In this latest Cochrane review, Cates et al1 added four new studies to those included in their earlier Cochrane meta-analysis and evaluated what, if any, effect these studies had on our understanding of nebulizers versus MDIs with spacers.
STUDY SUMMARY
Outcomes with nebulizers are no better than those with spacers
This systematic review and meta-analysis pooled the results of RCTs comparing spacers to nebulizers for administering β-agonists during acute, non–life-threatening asthma exacerbations.1 The authors reviewed studies conducted in EDs, hospitals, and outpatient settings that included children and adults. The primary outcomes were hospital admission rates and duration of hospital stay. Secondary outcomes included time spent in the ED, change in pulse rate, and incidence of tremor.
Cates et al1 analyzed 39 trials that included 1,897 children and 729 adults and were conducted primarily in an ED or outpatient setting. The four new studies added 295 children and 58 adults to the researchers’ earlier meta-analysis. Studies involving adults and children were pooled separately. Most patients received multiple treatments with β-agonists titrated to the individual’s response.
No differences in hospitalizations. Rates of hospital admissions did not differ between patients receiving β-agonists via a spacer compared to a nebulizer in both adults (relative risk [RR] = 0.94) and children (RR = 0.71). Duration of hospital stay did not differ between the two delivery methods in adults (mean difference [MD] = –0.60 d) and children (MD = 0.33 d).
For kids, spacers meant less time in the ED. Duration in the ED was approximately half an hour shorter for children using spacers (MD = –33.48 min). There was no difference observed in adults (MD = 1.75 min). The rate of tremor was lower in children using spacers (RR = 0.64) and was similar in adults (RR = 1.12). The rise in pulse rate was lower in children using spacers
(MD = –5.41% change from baseline) and was similar in adults (MD = –1.23%).
On the next page: What's new and challenges to implementation >>
WHAT’S NEW
Additional evidence that spacers are as effective as nebulizers
This meta-analysis, which included four new studies, should finally dispel the myth that nebulizers deliver β-agonists more effectively than MDIs with spacers. Additionally, in children, spacers are associated with lower rates of adverse effects, including tremor and elevated pulse rate.
CAVEATS
Most studies involving children were open label
Although most of the adult trials in this meta-analysis involved a double-dummy design, which allows for effective participant blinding, most of the studies involving children were open label. This open-label design might have been a source of reporting bias for symptom-related outcomes but should not have affected hospital admission rates or duration of hospital stay.
In the double-dummy studies, adults received both a nebulizer and a spacer, which likely explains the similar time spent in the ED by the treatment and control groups.
CHALLENGES TO IMPLEMENTATION
Old habits are hard to break
Clinicians may think that patients view nebulizers as more potent or more effective than spacers and thus be more likely to order them. Some patients may prefer nebulizers because of convenience or other factors.
REFERENCES
1. Cates CJ, Welsh EJ, Rowe BH. Holding chambers (spacers) versus nebulisers for beta-agonist treatment of acute asthma. Cochrane Database Syst Rev. 2013;9: CD000052.
2. Barrett ML, Wier LM, Washington R. Trends in pediatric and adult hospital stays for asthma, 2000-2010. HCUP Statistical Brief #169. www.hcup-us.ahrq.gov/reports/stat briefs/sb169-Asthma-Trends-Hospital-Stays.pdf. Accessed June 16, 2014.
3. Pfuntner A, Wier LM, Stocks C. Most frequent conditions in US hospitals, 2011. HCUP Statistical Brief #162. www.hcup-us.ahrq.gov/reports/statbriefs/sb162.pdf. Accessed June 16, 2014.
4. Cates CJ, Crilly JA, Rowe BH. Holding chambers (spacers) versus nebulisers for beta-agonist treatment of acute asthma. Cochrane Database Syst Rev. 2006;(2): CD000052.
5. Turner MO, Patel A, Ginsburg S, et al. Bronchodilator delivery in acute airflow obstruction: a meta-analysis. Arch Intern Med. 1997;157:1736-1744.
6. National Heart, Lung, and Blood Institute Expert Panel Report 3 (EPR3): Guidelines for the diagnosis and management of asthma. www.nhlbi.nih.gov/guidelines/asthma/asth gdln.htm. Accessed June 16, 2014.
7. British Thoracic Society. British guideline of the management of asthma: a national clinical guideline. www.brit-thoracic.org.uk/document-library/clinical-information/asth ma/btssign-guideline-on-the-management-of-asthma/. Accessed June 16, 2014.
8. Pitts SR, Niska RW, Xu J, et al. National Hospital Ambulatory Medical Care Survey: 2006 emergency department summary. www.cdc.gov/nchs/data/nhsr/nhsr007.pdf. Accessed June 16, 2014.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(6):321-322, 346.
PRACTICE CHANGER
Stop ordering nebulizers to deliver β-agonists to patients older than 2 who have mild or moderate asthma exacerbations. A metered-dose inhaler (MDI) with a spacer produces the same benefits with fewer adverse effects.1
STRENGTH OF RECOMMENDATION
A: Based on an updated Cochrane meta-analysis of 39 randomized controlled trials (RCTs). 1
ILLUSTRATIVE CASE
A 6-year-old girl with a history of reactive airway disease comes to your office complaining of cough and wheezing. On exam, she has mild retractions, a respiratory rate of 35 breaths/min, and an O2 saturation of 96% on room air. Her lung fields are diffusely wheezy. Her parents would like to keep her out of the hospital. How should you order her albuterol to decrease her wheezing and minimize adverse effects?
Asthma affects nearly 19 million adults and 7 million children in the United States.2 Asthma exacerbations are the third most common reason for hospitalization in children.2,3 Treatment usually requires multiple agents, including inhaled β-agonists. These are most effective when delivered to the peripheral airways, which is a challenge during an asthma exacerbation because of airway swelling and rapid breathing. Two devices have been developed to effectively deliver medication to the peripheral airways: nebulizers and MDIs with a holding chamber (spacer).1
Several studies have demonstrated that for mild to moderate asthma exacerbations, administering a β-agonist via an MDI with a spacer is as effective as using a nebulizer.4,5 Asthma treatment guidelines also state that spacers are either comparable or preferable to nebulizers for β-agonist administration in children and adults.6,7 However, based on our experience, clinicians still frequently order nebulizer treatments for patients with asthma exacerbations, despite several advantages of MDIs with spacers. Notably, they cost less and don’t require maintenance or a power source. Clinicians administered nebulizer therapy at more than 3.6 million emergency department (ED) visits in 2006.8
In this latest Cochrane review, Cates et al1 added four new studies to those included in their earlier Cochrane meta-analysis and evaluated what, if any, effect these studies had on our understanding of nebulizers versus MDIs with spacers.
STUDY SUMMARY
Outcomes with nebulizers are no better than those with spacers
This systematic review and meta-analysis pooled the results of RCTs comparing spacers to nebulizers for administering β-agonists during acute, non–life-threatening asthma exacerbations.1 The authors reviewed studies conducted in EDs, hospitals, and outpatient settings that included children and adults. The primary outcomes were hospital admission rates and duration of hospital stay. Secondary outcomes included time spent in the ED, change in pulse rate, and incidence of tremor.
Cates et al1 analyzed 39 trials that included 1,897 children and 729 adults and were conducted primarily in an ED or outpatient setting. The four new studies added 295 children and 58 adults to the researchers’ earlier meta-analysis. Studies involving adults and children were pooled separately. Most patients received multiple treatments with β-agonists titrated to the individual’s response.
No differences in hospitalizations. Rates of hospital admissions did not differ between patients receiving β-agonists via a spacer compared to a nebulizer in both adults (relative risk [RR] = 0.94) and children (RR = 0.71). Duration of hospital stay did not differ between the two delivery methods in adults (mean difference [MD] = –0.60 d) and children (MD = 0.33 d).
For kids, spacers meant less time in the ED. Duration in the ED was approximately half an hour shorter for children using spacers (MD = –33.48 min). There was no difference observed in adults (MD = 1.75 min). The rate of tremor was lower in children using spacers (RR = 0.64) and was similar in adults (RR = 1.12). The rise in pulse rate was lower in children using spacers
(MD = –5.41% change from baseline) and was similar in adults (MD = –1.23%).
On the next page: What's new and challenges to implementation >>
WHAT’S NEW
Additional evidence that spacers are as effective as nebulizers
This meta-analysis, which included four new studies, should finally dispel the myth that nebulizers deliver β-agonists more effectively than MDIs with spacers. Additionally, in children, spacers are associated with lower rates of adverse effects, including tremor and elevated pulse rate.
CAVEATS
Most studies involving children were open label
Although most of the adult trials in this meta-analysis involved a double-dummy design, which allows for effective participant blinding, most of the studies involving children were open label. This open-label design might have been a source of reporting bias for symptom-related outcomes but should not have affected hospital admission rates or duration of hospital stay.
In the double-dummy studies, adults received both a nebulizer and a spacer, which likely explains the similar time spent in the ED by the treatment and control groups.
CHALLENGES TO IMPLEMENTATION
Old habits are hard to break
Clinicians may think that patients view nebulizers as more potent or more effective than spacers and thus be more likely to order them. Some patients may prefer nebulizers because of convenience or other factors.
REFERENCES
1. Cates CJ, Welsh EJ, Rowe BH. Holding chambers (spacers) versus nebulisers for beta-agonist treatment of acute asthma. Cochrane Database Syst Rev. 2013;9: CD000052.
2. Barrett ML, Wier LM, Washington R. Trends in pediatric and adult hospital stays for asthma, 2000-2010. HCUP Statistical Brief #169. www.hcup-us.ahrq.gov/reports/stat briefs/sb169-Asthma-Trends-Hospital-Stays.pdf. Accessed June 16, 2014.
3. Pfuntner A, Wier LM, Stocks C. Most frequent conditions in US hospitals, 2011. HCUP Statistical Brief #162. www.hcup-us.ahrq.gov/reports/statbriefs/sb162.pdf. Accessed June 16, 2014.
4. Cates CJ, Crilly JA, Rowe BH. Holding chambers (spacers) versus nebulisers for beta-agonist treatment of acute asthma. Cochrane Database Syst Rev. 2006;(2): CD000052.
5. Turner MO, Patel A, Ginsburg S, et al. Bronchodilator delivery in acute airflow obstruction: a meta-analysis. Arch Intern Med. 1997;157:1736-1744.
6. National Heart, Lung, and Blood Institute Expert Panel Report 3 (EPR3): Guidelines for the diagnosis and management of asthma. www.nhlbi.nih.gov/guidelines/asthma/asth gdln.htm. Accessed June 16, 2014.
7. British Thoracic Society. British guideline of the management of asthma: a national clinical guideline. www.brit-thoracic.org.uk/document-library/clinical-information/asth ma/btssign-guideline-on-the-management-of-asthma/. Accessed June 16, 2014.
8. Pitts SR, Niska RW, Xu J, et al. National Hospital Ambulatory Medical Care Survey: 2006 emergency department summary. www.cdc.gov/nchs/data/nhsr/nhsr007.pdf. Accessed June 16, 2014.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(6):321-322, 346.
PRACTICE CHANGER
Stop ordering nebulizers to deliver β-agonists to patients older than 2 who have mild or moderate asthma exacerbations. A metered-dose inhaler (MDI) with a spacer produces the same benefits with fewer adverse effects.1
STRENGTH OF RECOMMENDATION
A: Based on an updated Cochrane meta-analysis of 39 randomized controlled trials (RCTs). 1
ILLUSTRATIVE CASE
A 6-year-old girl with a history of reactive airway disease comes to your office complaining of cough and wheezing. On exam, she has mild retractions, a respiratory rate of 35 breaths/min, and an O2 saturation of 96% on room air. Her lung fields are diffusely wheezy. Her parents would like to keep her out of the hospital. How should you order her albuterol to decrease her wheezing and minimize adverse effects?
Asthma affects nearly 19 million adults and 7 million children in the United States.2 Asthma exacerbations are the third most common reason for hospitalization in children.2,3 Treatment usually requires multiple agents, including inhaled β-agonists. These are most effective when delivered to the peripheral airways, which is a challenge during an asthma exacerbation because of airway swelling and rapid breathing. Two devices have been developed to effectively deliver medication to the peripheral airways: nebulizers and MDIs with a holding chamber (spacer).1
Several studies have demonstrated that for mild to moderate asthma exacerbations, administering a β-agonist via an MDI with a spacer is as effective as using a nebulizer.4,5 Asthma treatment guidelines also state that spacers are either comparable or preferable to nebulizers for β-agonist administration in children and adults.6,7 However, based on our experience, clinicians still frequently order nebulizer treatments for patients with asthma exacerbations, despite several advantages of MDIs with spacers. Notably, they cost less and don’t require maintenance or a power source. Clinicians administered nebulizer therapy at more than 3.6 million emergency department (ED) visits in 2006.8
In this latest Cochrane review, Cates et al1 added four new studies to those included in their earlier Cochrane meta-analysis and evaluated what, if any, effect these studies had on our understanding of nebulizers versus MDIs with spacers.
STUDY SUMMARY
Outcomes with nebulizers are no better than those with spacers
This systematic review and meta-analysis pooled the results of RCTs comparing spacers to nebulizers for administering β-agonists during acute, non–life-threatening asthma exacerbations.1 The authors reviewed studies conducted in EDs, hospitals, and outpatient settings that included children and adults. The primary outcomes were hospital admission rates and duration of hospital stay. Secondary outcomes included time spent in the ED, change in pulse rate, and incidence of tremor.
Cates et al1 analyzed 39 trials that included 1,897 children and 729 adults and were conducted primarily in an ED or outpatient setting. The four new studies added 295 children and 58 adults to the researchers’ earlier meta-analysis. Studies involving adults and children were pooled separately. Most patients received multiple treatments with β-agonists titrated to the individual’s response.
No differences in hospitalizations. Rates of hospital admissions did not differ between patients receiving β-agonists via a spacer compared to a nebulizer in both adults (relative risk [RR] = 0.94) and children (RR = 0.71). Duration of hospital stay did not differ between the two delivery methods in adults (mean difference [MD] = –0.60 d) and children (MD = 0.33 d).
For kids, spacers meant less time in the ED. Duration in the ED was approximately half an hour shorter for children using spacers (MD = –33.48 min). There was no difference observed in adults (MD = 1.75 min). The rate of tremor was lower in children using spacers (RR = 0.64) and was similar in adults (RR = 1.12). The rise in pulse rate was lower in children using spacers
(MD = –5.41% change from baseline) and was similar in adults (MD = –1.23%).
On the next page: What's new and challenges to implementation >>
WHAT’S NEW
Additional evidence that spacers are as effective as nebulizers
This meta-analysis, which included four new studies, should finally dispel the myth that nebulizers deliver β-agonists more effectively than MDIs with spacers. Additionally, in children, spacers are associated with lower rates of adverse effects, including tremor and elevated pulse rate.
CAVEATS
Most studies involving children were open label
Although most of the adult trials in this meta-analysis involved a double-dummy design, which allows for effective participant blinding, most of the studies involving children were open label. This open-label design might have been a source of reporting bias for symptom-related outcomes but should not have affected hospital admission rates or duration of hospital stay.
In the double-dummy studies, adults received both a nebulizer and a spacer, which likely explains the similar time spent in the ED by the treatment and control groups.
CHALLENGES TO IMPLEMENTATION
Old habits are hard to break
Clinicians may think that patients view nebulizers as more potent or more effective than spacers and thus be more likely to order them. Some patients may prefer nebulizers because of convenience or other factors.
REFERENCES
1. Cates CJ, Welsh EJ, Rowe BH. Holding chambers (spacers) versus nebulisers for beta-agonist treatment of acute asthma. Cochrane Database Syst Rev. 2013;9: CD000052.
2. Barrett ML, Wier LM, Washington R. Trends in pediatric and adult hospital stays for asthma, 2000-2010. HCUP Statistical Brief #169. www.hcup-us.ahrq.gov/reports/stat briefs/sb169-Asthma-Trends-Hospital-Stays.pdf. Accessed June 16, 2014.
3. Pfuntner A, Wier LM, Stocks C. Most frequent conditions in US hospitals, 2011. HCUP Statistical Brief #162. www.hcup-us.ahrq.gov/reports/statbriefs/sb162.pdf. Accessed June 16, 2014.
4. Cates CJ, Crilly JA, Rowe BH. Holding chambers (spacers) versus nebulisers for beta-agonist treatment of acute asthma. Cochrane Database Syst Rev. 2006;(2): CD000052.
5. Turner MO, Patel A, Ginsburg S, et al. Bronchodilator delivery in acute airflow obstruction: a meta-analysis. Arch Intern Med. 1997;157:1736-1744.
6. National Heart, Lung, and Blood Institute Expert Panel Report 3 (EPR3): Guidelines for the diagnosis and management of asthma. www.nhlbi.nih.gov/guidelines/asthma/asth gdln.htm. Accessed June 16, 2014.
7. British Thoracic Society. British guideline of the management of asthma: a national clinical guideline. www.brit-thoracic.org.uk/document-library/clinical-information/asth ma/btssign-guideline-on-the-management-of-asthma/. Accessed June 16, 2014.
8. Pitts SR, Niska RW, Xu J, et al. National Hospital Ambulatory Medical Care Survey: 2006 emergency department summary. www.cdc.gov/nchs/data/nhsr/nhsr007.pdf. Accessed June 16, 2014.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(6):321-322, 346.
Immunological testing alone missed TB cases in HIV population
SAN DIEGO – Mycobacterium tuberculosis can still be grown in the sputum of people living with HIV who have negative TB immunological testing, and in people who have been treated with TB previously, results from a study of nearly 200 patients demonstrated.
"Previous studies in low TB incidence areas have tested people with positive tuberculin skin tests or interferon release assays for active TB, but we have tested people for TB irrespective of this – and found a case of active tuberculosis and someone with TB in their sputum who would otherwise not have been tested using previous guidelines," lead author Dr. Santino Capocci, a research registrar in respiratory medicine at Royal Free Hospital, London, said in an interview in advance of an international conference of the American Thoracic Society, where the research was presented.

Guidelines from the United Kingdom recommend using blood interferon-gamma release assay with or without tuberculin skin testing for latent TB diagnosis, but it does not cover screening for active TB. "Implementation is patchy with little robust evidence for effectiveness," the researchers wrote in their abstract.
In an effort to determine the impact of comprehensive assessment for TB disease and infection in an ambulatory HIV clinic population with high antiretroviral usage, Dr. Capocci and his associates tested 194 patients, mean age 46 years, who had no clinical suspicion of active tuberculosis. Testing consisted of tuberculin skin testing (TST), interferon-gamma release assay (IGRA), frontal chest radiograph (CXR), and sputum induction for TB culture. Latent TB was defined as a positive IGRA and/or TST of 5 mm or greater in the absence of previously active TB disease.
Nearly one-quarter of patients (24%) were black African, 81% had received a previous Bacillus Calmette-Guerin vaccination, 94% were on antiretroviral medication, and 8% had previous TB disease. Dr. Capocci reported that latent TB infection was detected in 12 (6%) of the 194 patients. Of these, four were diagnosed by positive IGRA and TST of 5 mm or greater; one was diagnosed by positive IGRA and negative TST; five were diagnosed by TST of 10 mm or greater (with negative or borderline IGRA), and two were diagnosed by TST 5-9 mm (with negative IGRA). Two subjects had a positive sputum culture.
"One subject had evidence of tuberculosis in his sputum but no symptoms, normal blood tests and x-rays, and negative immunological testing (tuberculin skin test and IGRA)," Dr. Capocci said. "This has been seen in Africa in people living with HIV, but is not reported as far as we know in low TB incidence areas such as the UK. The case of active TB that we saw was in someone who has had tuberculosis previously, but without persistent symptoms. He may not have been tested using national testing guidelines."
Dr. Capocci acknowledged certain limitations of the study, including the fact that the sample size is "fairly small compared to studies that have used IGRAs or tuberculin skin testing. "It is also important to evaluate the cost effectiveness of this approach [for] future health care policy."
Dr. Capocci said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Mycobacterium tuberculosis can still be grown in the sputum of people living with HIV who have negative TB immunological testing, and in people who have been treated with TB previously, results from a study of nearly 200 patients demonstrated.
"Previous studies in low TB incidence areas have tested people with positive tuberculin skin tests or interferon release assays for active TB, but we have tested people for TB irrespective of this – and found a case of active tuberculosis and someone with TB in their sputum who would otherwise not have been tested using previous guidelines," lead author Dr. Santino Capocci, a research registrar in respiratory medicine at Royal Free Hospital, London, said in an interview in advance of an international conference of the American Thoracic Society, where the research was presented.
Guidelines from the United Kingdom recommend using blood interferon-gamma release assay with or without tuberculin skin testing for latent TB diagnosis, but it does not cover screening for active TB. "Implementation is patchy with little robust evidence for effectiveness," the researchers wrote in their abstract.
In an effort to determine the impact of comprehensive assessment for TB disease and infection in an ambulatory HIV clinic population with high antiretroviral usage, Dr. Capocci and his associates tested 194 patients, mean age 46 years, who had no clinical suspicion of active tuberculosis. Testing consisted of tuberculin skin testing (TST), interferon-gamma release assay (IGRA), frontal chest radiograph (CXR), and sputum induction for TB culture. Latent TB was defined as a positive IGRA and/or TST of 5 mm or greater in the absence of previously active TB disease.
Nearly one-quarter of patients (24%) were black African, 81% had received a previous Bacillus Calmette-Guerin vaccination, 94% were on antiretroviral medication, and 8% had previous TB disease. Dr. Capocci reported that latent TB infection was detected in 12 (6%) of the 194 patients. Of these, four were diagnosed by positive IGRA and TST of 5 mm or greater; one was diagnosed by positive IGRA and negative TST; five were diagnosed by TST of 10 mm or greater (with negative or borderline IGRA), and two were diagnosed by TST 5-9 mm (with negative IGRA). Two subjects had a positive sputum culture.
"One subject had evidence of tuberculosis in his sputum but no symptoms, normal blood tests and x-rays, and negative immunological testing (tuberculin skin test and IGRA)," Dr. Capocci said. "This has been seen in Africa in people living with HIV, but is not reported as far as we know in low TB incidence areas such as the UK. The case of active TB that we saw was in someone who has had tuberculosis previously, but without persistent symptoms. He may not have been tested using national testing guidelines."
Dr. Capocci acknowledged certain limitations of the study, including the fact that the sample size is "fairly small compared to studies that have used IGRAs or tuberculin skin testing. "It is also important to evaluate the cost effectiveness of this approach [for] future health care policy."
Dr. Capocci said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Mycobacterium tuberculosis can still be grown in the sputum of people living with HIV who have negative TB immunological testing, and in people who have been treated with TB previously, results from a study of nearly 200 patients demonstrated.
"Previous studies in low TB incidence areas have tested people with positive tuberculin skin tests or interferon release assays for active TB, but we have tested people for TB irrespective of this – and found a case of active tuberculosis and someone with TB in their sputum who would otherwise not have been tested using previous guidelines," lead author Dr. Santino Capocci, a research registrar in respiratory medicine at Royal Free Hospital, London, said in an interview in advance of an international conference of the American Thoracic Society, where the research was presented.
Guidelines from the United Kingdom recommend using blood interferon-gamma release assay with or without tuberculin skin testing for latent TB diagnosis, but it does not cover screening for active TB. "Implementation is patchy with little robust evidence for effectiveness," the researchers wrote in their abstract.
In an effort to determine the impact of comprehensive assessment for TB disease and infection in an ambulatory HIV clinic population with high antiretroviral usage, Dr. Capocci and his associates tested 194 patients, mean age 46 years, who had no clinical suspicion of active tuberculosis. Testing consisted of tuberculin skin testing (TST), interferon-gamma release assay (IGRA), frontal chest radiograph (CXR), and sputum induction for TB culture. Latent TB was defined as a positive IGRA and/or TST of 5 mm or greater in the absence of previously active TB disease.
Nearly one-quarter of patients (24%) were black African, 81% had received a previous Bacillus Calmette-Guerin vaccination, 94% were on antiretroviral medication, and 8% had previous TB disease. Dr. Capocci reported that latent TB infection was detected in 12 (6%) of the 194 patients. Of these, four were diagnosed by positive IGRA and TST of 5 mm or greater; one was diagnosed by positive IGRA and negative TST; five were diagnosed by TST of 10 mm or greater (with negative or borderline IGRA), and two were diagnosed by TST 5-9 mm (with negative IGRA). Two subjects had a positive sputum culture.
"One subject had evidence of tuberculosis in his sputum but no symptoms, normal blood tests and x-rays, and negative immunological testing (tuberculin skin test and IGRA)," Dr. Capocci said. "This has been seen in Africa in people living with HIV, but is not reported as far as we know in low TB incidence areas such as the UK. The case of active TB that we saw was in someone who has had tuberculosis previously, but without persistent symptoms. He may not have been tested using national testing guidelines."
Dr. Capocci acknowledged certain limitations of the study, including the fact that the sample size is "fairly small compared to studies that have used IGRAs or tuberculin skin testing. "It is also important to evaluate the cost effectiveness of this approach [for] future health care policy."
Dr. Capocci said that he had no relevant financial conflicts to disclose.
AT ATS 2014
Key clinical point: Use of immunological testing alone to detect TB in people with HIV missed cases of subclinical disease.
Major finding: Despite the convenience of immunological tests to screen for TB in people with HIV, the use of comprehensive assessments detected 12 cases of latent TB in 194 patients with HIV, even in those with good CD4 and no symptoms.
Data source: A study of 194 HIV patients, mean age 46 years, who had no clinical suspicion of active tuberculosis.
Disclosures: Dr. Capocci had financial conflicts.

Technique identifies when oxygen will benefit apnea
SAN DIEGO – Obstructive sleep apnea mechanisms may be quantified by polysomnography to select patients who are likely to respond to supplemental oxygen therapy if they can’t tolerate continuous positive airway pressure therapy, a study of 19 patients suggested.
"When [continuous positive airway pressure] isn’t enough, we’ve turned to supplemental oxygen," which can greatly reduce the severity of obstructive sleep apnea [OSA] in some patients but is ineffective in others, Scott A. Sands, Ph.D., said at an international conference of the American Thoracic Society.
He and his associates applied their recently validated technique to quantify "loop gain" or breathing control from routine polysomnography in an attempt to identify patients with increased peripheral chemosensitivity, thinking they might be more responsive to oxygen therapy. An elevated loop gain represents an exaggerated ventilatory effort – a sensitive and fast ventilatory drive – in response to apnea or hypopnea, he explained.
The investigators randomized patients with OSA and an apnea-hypopnea index of at least 20 events per hour in a single-blind, sham-controlled crossover study. Patients underwent full polysomnography with either supplemental oxygen or air (the sham treatment), which was repeated with the other treatment 1 week later.
The results showed that OSA improved substantially in patients with high loop gain but not in those with low loop gain, reported Dr. Sands of Brigham and Women’s Hospital, Boston.
The apnea-hypopnea index improved significantly in patients with high loop gain when they got oxygen but not in patients with low loop gain. Apnea-hypopnea events ranged from approximately 20 to 90 per hour in patients with high loop gain while on air and from approximately 0 to 45 per hour on oxygen. In patients with low loop gain, apnea-hypopnea events ranged from approximately 25 to 110 per hour while on air and from 10 to 80 per hour on oxygen.
The percentage of sleep with stable breathing improved significantly from less than 20% while on air to approximately 35% on oxygen in patients with high loop gain but hovered just under 15% with either treatment in patients with low loop gain.
The arousal index improved significantly from nearly 50 events per hour while on air to 20 events per hour on oxygen in patients with high loop gain but hovered around 50 events per hour on either treatment in patients with low loop gain. The percentage of sleep spent in stage 1 sleep improved significantly from approximately 16% while on air to approximately 6% on oxygen in patients with high loop gain and increased in patients with low loop gain from approximately 15% on air to nearly 20% on oxygen, an increase that was not statistically significant, he said.
"These are promising findings so far," Dr. Sands said. He and his associates are working to fully automate the method of assessing loop gain and to measure additional traits from polysomnography.
Dr. Sands reported having no financial disclosures.
On Twitter @sherryboschert
SAN DIEGO – Obstructive sleep apnea mechanisms may be quantified by polysomnography to select patients who are likely to respond to supplemental oxygen therapy if they can’t tolerate continuous positive airway pressure therapy, a study of 19 patients suggested.
"When [continuous positive airway pressure] isn’t enough, we’ve turned to supplemental oxygen," which can greatly reduce the severity of obstructive sleep apnea [OSA] in some patients but is ineffective in others, Scott A. Sands, Ph.D., said at an international conference of the American Thoracic Society.
He and his associates applied their recently validated technique to quantify "loop gain" or breathing control from routine polysomnography in an attempt to identify patients with increased peripheral chemosensitivity, thinking they might be more responsive to oxygen therapy. An elevated loop gain represents an exaggerated ventilatory effort – a sensitive and fast ventilatory drive – in response to apnea or hypopnea, he explained.
The investigators randomized patients with OSA and an apnea-hypopnea index of at least 20 events per hour in a single-blind, sham-controlled crossover study. Patients underwent full polysomnography with either supplemental oxygen or air (the sham treatment), which was repeated with the other treatment 1 week later.
The results showed that OSA improved substantially in patients with high loop gain but not in those with low loop gain, reported Dr. Sands of Brigham and Women’s Hospital, Boston.
The apnea-hypopnea index improved significantly in patients with high loop gain when they got oxygen but not in patients with low loop gain. Apnea-hypopnea events ranged from approximately 20 to 90 per hour in patients with high loop gain while on air and from approximately 0 to 45 per hour on oxygen. In patients with low loop gain, apnea-hypopnea events ranged from approximately 25 to 110 per hour while on air and from 10 to 80 per hour on oxygen.
The percentage of sleep with stable breathing improved significantly from less than 20% while on air to approximately 35% on oxygen in patients with high loop gain but hovered just under 15% with either treatment in patients with low loop gain.
The arousal index improved significantly from nearly 50 events per hour while on air to 20 events per hour on oxygen in patients with high loop gain but hovered around 50 events per hour on either treatment in patients with low loop gain. The percentage of sleep spent in stage 1 sleep improved significantly from approximately 16% while on air to approximately 6% on oxygen in patients with high loop gain and increased in patients with low loop gain from approximately 15% on air to nearly 20% on oxygen, an increase that was not statistically significant, he said.
"These are promising findings so far," Dr. Sands said. He and his associates are working to fully automate the method of assessing loop gain and to measure additional traits from polysomnography.
Dr. Sands reported having no financial disclosures.
On Twitter @sherryboschert
SAN DIEGO – Obstructive sleep apnea mechanisms may be quantified by polysomnography to select patients who are likely to respond to supplemental oxygen therapy if they can’t tolerate continuous positive airway pressure therapy, a study of 19 patients suggested.
"When [continuous positive airway pressure] isn’t enough, we’ve turned to supplemental oxygen," which can greatly reduce the severity of obstructive sleep apnea [OSA] in some patients but is ineffective in others, Scott A. Sands, Ph.D., said at an international conference of the American Thoracic Society.
He and his associates applied their recently validated technique to quantify "loop gain" or breathing control from routine polysomnography in an attempt to identify patients with increased peripheral chemosensitivity, thinking they might be more responsive to oxygen therapy. An elevated loop gain represents an exaggerated ventilatory effort – a sensitive and fast ventilatory drive – in response to apnea or hypopnea, he explained.
The investigators randomized patients with OSA and an apnea-hypopnea index of at least 20 events per hour in a single-blind, sham-controlled crossover study. Patients underwent full polysomnography with either supplemental oxygen or air (the sham treatment), which was repeated with the other treatment 1 week later.
The results showed that OSA improved substantially in patients with high loop gain but not in those with low loop gain, reported Dr. Sands of Brigham and Women’s Hospital, Boston.
The apnea-hypopnea index improved significantly in patients with high loop gain when they got oxygen but not in patients with low loop gain. Apnea-hypopnea events ranged from approximately 20 to 90 per hour in patients with high loop gain while on air and from approximately 0 to 45 per hour on oxygen. In patients with low loop gain, apnea-hypopnea events ranged from approximately 25 to 110 per hour while on air and from 10 to 80 per hour on oxygen.
The percentage of sleep with stable breathing improved significantly from less than 20% while on air to approximately 35% on oxygen in patients with high loop gain but hovered just under 15% with either treatment in patients with low loop gain.
The arousal index improved significantly from nearly 50 events per hour while on air to 20 events per hour on oxygen in patients with high loop gain but hovered around 50 events per hour on either treatment in patients with low loop gain. The percentage of sleep spent in stage 1 sleep improved significantly from approximately 16% while on air to approximately 6% on oxygen in patients with high loop gain and increased in patients with low loop gain from approximately 15% on air to nearly 20% on oxygen, an increase that was not statistically significant, he said.
"These are promising findings so far," Dr. Sands said. He and his associates are working to fully automate the method of assessing loop gain and to measure additional traits from polysomnography.
Dr. Sands reported having no financial disclosures.
On Twitter @sherryboschert
AT ATS 2014
Key clinical point: A new polysomnography technique can identify which patients with obstructive sleep apnea will benefit from supplemental oxygen.
Major finding: Patients with high loop gain but not those with low loop gain on polysomnography showed significant improvements on oxygen in the apnea-hypopnea index, percentage of sleep in stable breathing or stage 1 sleep, and arousal index.
Data source: A single-blind, randomized, sham-controlled crossover trial of supplemental oxygen or air for 19 patients with obstructive sleep apnea.
Disclosures: Dr. Sands reported having no financial disclosures.

Higher risk of death seen with oral steroids in RA interstitial lung disease
The use of prednisone for 3 or more months at a time was associated with a significantly elevated risk of death in patients with rheumatoid arthritis and interstitial lung disease in a retrospective cohort study.
Interstitial lung disease is present in about 5% of patients with rheumatoid arthritis. For years, oral steroids were commonly used in patients with the disease, but today’s rheumatologists "no longer view oral steroids as optimal treatment in RA-ILD [rheumatoid arthritis–associated interstitial lung disease], and our data now confirm that," said Dr. Clive Kelly of Queen Elizabeth Hospital in Gateshead, England, senior investigator of the study. He added that clinicians should avoid long-term treatment with steroids in this patient group whenever possible.
Dr. Kelly led the British Rheumatoid Interstitial Lung (BRILL) Network’s cohort study of 260 patients with RA-ILD diagnosed over a 25-year period. The BRILL study compared patients with RA-ILD and an equal number of RA controls without lung involvement who were matched for age, sex, and time of diagnosis.
At the annual European Congress of Rheumatology, Dr. Kelly reported that steroid-treated RA-ILD patients, who represented nearly 60% of the cohort, had an elevated relative risk of all-cause death, compared with those who had never been treated with steroids (RR, 1.65; 95% confidence interval, 1.2-2.3; P = .002). Although the relative risk of respiratory death was significantly increased for RA-ILD patients, regardless of treatment, when compared with RA patients without ILD, the risk was higher in those who had been on steroids (RR, 2.75; 95% CI, 1.6-4.7; P = .0002) than in those who had not received steroids (RR, 2.06; 95% CI, 1.1-3.8; P = .02), the investigators found.
The comparison also revealed other important findings related to RA-ILD. Patients with RA-ILD had significantly higher mortality than did those with RA alone. Over the course of the 25-year study period, however, mortality progressively improved among the RA-ILD patients, with median age at death rising from 63 to 76 years. This steady improvement, Dr. Kelly said, is partly the result of better and earlier diagnosis of lung involvement.
"It’s one of my many missions in life to get rheumatologists to listen to the lungs when they examine the joints in patients with rheumatoid arthritis," he said. "I think we are getting better. We’ve persuaded the British Society for Rheumatology to incorporate lung function testing and clinical examination of the chest into their basic assessment of a rheumatoid patient."
Also likely affecting the improved mortality seen over the cohort’s study period is a change in therapeutic approach. While RA-ILD patients diagnosed in the first half of the study period were likely to have been treated with only prednisone and azathioprine, in the latter half they were more likely to have received cyclophosphamide and methylprednisolone or mycophenolate. Over the last 12 years, more were treated with biologics, and in the final 6 years of the cohort, patients requiring biologics tended to be treated with rituximab, a B-cell inhibitor, rather than anti–tumor necrosis factor (anti-TNF) agents, the BRILL investigators found.
Mortality was lower among RA-ILD patients treated with mycophenolate than in those treated with other immunosuppressive agents. Among biologic agents used in the cohort, rituximab treatment was associated with improved mortality, but anti-TNF inhibitors were seen to be associated with elevated risk of death.
About 95% of RA-ILD patients are anticyclic citrullinated peptide (anti-CCP) antibody positive, compared with 55%-60% of the RA population as a whole, Dr. Kelly said, "so there’s a strong statistical association of seropositivity, and in those who are seropositive, rituximab works well."
The finding that rituximab was associated with improved survival in the cohort not only has implications for RA-ILD, he said, but also, potentially, for people with idiopathic pulmonary fibrosis (IPF) who are anti-CCP antibody positive. "What [rheumatologists] have, and chest physicians traditionally don’t, is access to rituximab and mycophenolate. But these might be worth trying in IPF as well," he said.
Dr. Kelly noted that prospective trials in RA-ILD are beginning to enroll patients with progressive disease to compare azathioprine and mycophenolate, allowing for the use of oral steroids, as well as patients with active RA and ILD to compare anti-TNF inhibitors against rituximab, also allowing oral steroids.
Dr. Kelly reported that he had no conflicts of interest related to his findings and that none of his fellow BRILL investigators had conflicts.
The use of prednisone for 3 or more months at a time was associated with a significantly elevated risk of death in patients with rheumatoid arthritis and interstitial lung disease in a retrospective cohort study.
Interstitial lung disease is present in about 5% of patients with rheumatoid arthritis. For years, oral steroids were commonly used in patients with the disease, but today’s rheumatologists "no longer view oral steroids as optimal treatment in RA-ILD [rheumatoid arthritis–associated interstitial lung disease], and our data now confirm that," said Dr. Clive Kelly of Queen Elizabeth Hospital in Gateshead, England, senior investigator of the study. He added that clinicians should avoid long-term treatment with steroids in this patient group whenever possible.
Dr. Kelly led the British Rheumatoid Interstitial Lung (BRILL) Network’s cohort study of 260 patients with RA-ILD diagnosed over a 25-year period. The BRILL study compared patients with RA-ILD and an equal number of RA controls without lung involvement who were matched for age, sex, and time of diagnosis.
At the annual European Congress of Rheumatology, Dr. Kelly reported that steroid-treated RA-ILD patients, who represented nearly 60% of the cohort, had an elevated relative risk of all-cause death, compared with those who had never been treated with steroids (RR, 1.65; 95% confidence interval, 1.2-2.3; P = .002). Although the relative risk of respiratory death was significantly increased for RA-ILD patients, regardless of treatment, when compared with RA patients without ILD, the risk was higher in those who had been on steroids (RR, 2.75; 95% CI, 1.6-4.7; P = .0002) than in those who had not received steroids (RR, 2.06; 95% CI, 1.1-3.8; P = .02), the investigators found.
The comparison also revealed other important findings related to RA-ILD. Patients with RA-ILD had significantly higher mortality than did those with RA alone. Over the course of the 25-year study period, however, mortality progressively improved among the RA-ILD patients, with median age at death rising from 63 to 76 years. This steady improvement, Dr. Kelly said, is partly the result of better and earlier diagnosis of lung involvement.
"It’s one of my many missions in life to get rheumatologists to listen to the lungs when they examine the joints in patients with rheumatoid arthritis," he said. "I think we are getting better. We’ve persuaded the British Society for Rheumatology to incorporate lung function testing and clinical examination of the chest into their basic assessment of a rheumatoid patient."
Also likely affecting the improved mortality seen over the cohort’s study period is a change in therapeutic approach. While RA-ILD patients diagnosed in the first half of the study period were likely to have been treated with only prednisone and azathioprine, in the latter half they were more likely to have received cyclophosphamide and methylprednisolone or mycophenolate. Over the last 12 years, more were treated with biologics, and in the final 6 years of the cohort, patients requiring biologics tended to be treated with rituximab, a B-cell inhibitor, rather than anti–tumor necrosis factor (anti-TNF) agents, the BRILL investigators found.
Mortality was lower among RA-ILD patients treated with mycophenolate than in those treated with other immunosuppressive agents. Among biologic agents used in the cohort, rituximab treatment was associated with improved mortality, but anti-TNF inhibitors were seen to be associated with elevated risk of death.
About 95% of RA-ILD patients are anticyclic citrullinated peptide (anti-CCP) antibody positive, compared with 55%-60% of the RA population as a whole, Dr. Kelly said, "so there’s a strong statistical association of seropositivity, and in those who are seropositive, rituximab works well."
The finding that rituximab was associated with improved survival in the cohort not only has implications for RA-ILD, he said, but also, potentially, for people with idiopathic pulmonary fibrosis (IPF) who are anti-CCP antibody positive. "What [rheumatologists] have, and chest physicians traditionally don’t, is access to rituximab and mycophenolate. But these might be worth trying in IPF as well," he said.
Dr. Kelly noted that prospective trials in RA-ILD are beginning to enroll patients with progressive disease to compare azathioprine and mycophenolate, allowing for the use of oral steroids, as well as patients with active RA and ILD to compare anti-TNF inhibitors against rituximab, also allowing oral steroids.
Dr. Kelly reported that he had no conflicts of interest related to his findings and that none of his fellow BRILL investigators had conflicts.
The use of prednisone for 3 or more months at a time was associated with a significantly elevated risk of death in patients with rheumatoid arthritis and interstitial lung disease in a retrospective cohort study.
Interstitial lung disease is present in about 5% of patients with rheumatoid arthritis. For years, oral steroids were commonly used in patients with the disease, but today’s rheumatologists "no longer view oral steroids as optimal treatment in RA-ILD [rheumatoid arthritis–associated interstitial lung disease], and our data now confirm that," said Dr. Clive Kelly of Queen Elizabeth Hospital in Gateshead, England, senior investigator of the study. He added that clinicians should avoid long-term treatment with steroids in this patient group whenever possible.
Dr. Kelly led the British Rheumatoid Interstitial Lung (BRILL) Network’s cohort study of 260 patients with RA-ILD diagnosed over a 25-year period. The BRILL study compared patients with RA-ILD and an equal number of RA controls without lung involvement who were matched for age, sex, and time of diagnosis.
At the annual European Congress of Rheumatology, Dr. Kelly reported that steroid-treated RA-ILD patients, who represented nearly 60% of the cohort, had an elevated relative risk of all-cause death, compared with those who had never been treated with steroids (RR, 1.65; 95% confidence interval, 1.2-2.3; P = .002). Although the relative risk of respiratory death was significantly increased for RA-ILD patients, regardless of treatment, when compared with RA patients without ILD, the risk was higher in those who had been on steroids (RR, 2.75; 95% CI, 1.6-4.7; P = .0002) than in those who had not received steroids (RR, 2.06; 95% CI, 1.1-3.8; P = .02), the investigators found.
The comparison also revealed other important findings related to RA-ILD. Patients with RA-ILD had significantly higher mortality than did those with RA alone. Over the course of the 25-year study period, however, mortality progressively improved among the RA-ILD patients, with median age at death rising from 63 to 76 years. This steady improvement, Dr. Kelly said, is partly the result of better and earlier diagnosis of lung involvement.
"It’s one of my many missions in life to get rheumatologists to listen to the lungs when they examine the joints in patients with rheumatoid arthritis," he said. "I think we are getting better. We’ve persuaded the British Society for Rheumatology to incorporate lung function testing and clinical examination of the chest into their basic assessment of a rheumatoid patient."
Also likely affecting the improved mortality seen over the cohort’s study period is a change in therapeutic approach. While RA-ILD patients diagnosed in the first half of the study period were likely to have been treated with only prednisone and azathioprine, in the latter half they were more likely to have received cyclophosphamide and methylprednisolone or mycophenolate. Over the last 12 years, more were treated with biologics, and in the final 6 years of the cohort, patients requiring biologics tended to be treated with rituximab, a B-cell inhibitor, rather than anti–tumor necrosis factor (anti-TNF) agents, the BRILL investigators found.
Mortality was lower among RA-ILD patients treated with mycophenolate than in those treated with other immunosuppressive agents. Among biologic agents used in the cohort, rituximab treatment was associated with improved mortality, but anti-TNF inhibitors were seen to be associated with elevated risk of death.
About 95% of RA-ILD patients are anticyclic citrullinated peptide (anti-CCP) antibody positive, compared with 55%-60% of the RA population as a whole, Dr. Kelly said, "so there’s a strong statistical association of seropositivity, and in those who are seropositive, rituximab works well."
The finding that rituximab was associated with improved survival in the cohort not only has implications for RA-ILD, he said, but also, potentially, for people with idiopathic pulmonary fibrosis (IPF) who are anti-CCP antibody positive. "What [rheumatologists] have, and chest physicians traditionally don’t, is access to rituximab and mycophenolate. But these might be worth trying in IPF as well," he said.
Dr. Kelly noted that prospective trials in RA-ILD are beginning to enroll patients with progressive disease to compare azathioprine and mycophenolate, allowing for the use of oral steroids, as well as patients with active RA and ILD to compare anti-TNF inhibitors against rituximab, also allowing oral steroids.
Dr. Kelly reported that he had no conflicts of interest related to his findings and that none of his fellow BRILL investigators had conflicts.
FROM THE EULAR CONGRESS 2014
Key clinical point: Rather than corticosteroids, consider using mycophenolate or rituximab in patients with RA-ILD.
Major finding: Steroid-treated RA-ILD patients had an elevated relative risk of all-cause death, compared with those who had never been treated with steroids (RR, 1.65; 95% confidence interval, 1.2-2.3; P = .002).
Data source: A retrospective study of 260 patients with RA-ILD in the British Rheumatoid Interstitial Lung Network.
Disclosures: Dr. Kelly reported that he had no conflicts of interest related to his findings and that none of his fellow BRILL investigators had conflicts.