User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Bathroom wisdom: Simple strategies boost compliance in older asthma patients
Two simple recommendations for older patients with asthma – keeping medication in the bathroom and integrating its use into a daily routine – can significantly improve adherence to inhaled corticosteroids.
When patients consistently did either of those, adherence rose threefold, compared with patients who didn’t, Dr. Alex Federman and his associates wrote in the August issue of the Journal of Internal Medicine.
The findings suggest that clinicians might help improve adherence by suggesting that their patients store the medication in their bathroom cabinet, and take it, for example, when they brush their teeth every day.

"Because adherence strategies are modifiable, the findings in this study may provide clinicians and care coaches with straightforward and useful messages to help older patients improve their medication adherence," wrote Dr. Federman of Icahn School of Medicine at Mount Sinai, New York, and his coauthors (J. Intern. Med. 2014 Aug. 5 [doi:10.1007/s11606-014-2940-8]).
The team investigated adherence to inhaled corticosteroids among 358 elderly patients with asthma. They were a mean of 67 years old, with 31% older than 70 years. Most (84%) were women and many were Latino (38%). Black patients comprised 31% of the cohort and the others were non-Hispanic whites.
The majority had a low monthly income ($1,350 or less), and 25% were not fully literate in English. Many had comorbid psychological conditions, including depression (20%) and anxiety (21%).
Low health literacy was common (34%), although most (71%) did understand that they would always have asthma and that it could not be cured (81%) But half believed that they only had the disease when they were symptomatic. In a survey of medication beliefs, most did believe that the steroids were good for them and that their benefits outweighed the risks.
However, only 37% of the cohort reported good medication adherence. This proportion was significantly worse among blacks and Hispanics; those with lower incomes and lower education; those born in Puerto Rico and the Dominican Republic; and those with poor physical health, anxiety, or depression.
The authors identified six medication adherence strategies among the group: keeping the medication in a usual location (44%); integrating it into their daily routine (33%); taking it at a specific time of day (22%); taking it with other medications (13%); using it only when needed; (13%) and using other reminders (12%). Less than 2% reported using written notes as a reminder or having someone else remind them; 4% had no specific strategy.
The most common places to keep medicine were at the bedside (20%) and in the bathroom (9%). Those who integrated taking it with other daily routines did in the morning (12%) and at bedtime (8%).
Only three of the strategies were significantly associated with good adherence: keeping medication in the bathroom (16% adherent vs. 5% nonadherent); integrating it into a daily routine (morning 25% vs. 5%; evening 13% vs. 6%); and taking it at a specific time of day (29% vs. 17%).

Taking the medication only when needed was associated with significantly worse adherence.
After controlling for other variables, only leaving the medication in the bathroom significantly predicted good adherence (odds ratio 3), compared with those who kept it somewhere else).
Those who integrated medication into other daily routines were also significantly more likely to be adherent (OR 3.7) in a partially adjusted model, but not in a fully adjusted model. Still, the authors noted, this recommendation would be a good suggestion toward improving adherence.
Patients who used these two strategies were more likely to be white, have at least a partial education, and to have been born in the United States. Low income, limited English proficiency, low health literacy, poor physical and psychological health, and erroneous beliefs about asthma predicted poor adherence.
The team postulated that there are two types of nonadherence: simple forgetfulness or lack of understanding about its importance and deliberate nonadherence.
"The bathroom and daily routine strategies may address forgetful nonadherence. ... Taking the medication only as needed, on the other hand, may indicate faulty disease or medication beliefs. ... Taken together, these findings provide further evidence of the value of patient-centered care: Clinicians need to understand why patients do not use their medications appropriately before counseling patients on ways to improve adherence."
The study was supported by a grant from the National Heart, Lung, and Blood Institute. None of the authors had any financial disclosures.
Two simple recommendations for older patients with asthma – keeping medication in the bathroom and integrating its use into a daily routine – can significantly improve adherence to inhaled corticosteroids.
When patients consistently did either of those, adherence rose threefold, compared with patients who didn’t, Dr. Alex Federman and his associates wrote in the August issue of the Journal of Internal Medicine.
The findings suggest that clinicians might help improve adherence by suggesting that their patients store the medication in their bathroom cabinet, and take it, for example, when they brush their teeth every day.
"Because adherence strategies are modifiable, the findings in this study may provide clinicians and care coaches with straightforward and useful messages to help older patients improve their medication adherence," wrote Dr. Federman of Icahn School of Medicine at Mount Sinai, New York, and his coauthors (J. Intern. Med. 2014 Aug. 5 [doi:10.1007/s11606-014-2940-8]).
The team investigated adherence to inhaled corticosteroids among 358 elderly patients with asthma. They were a mean of 67 years old, with 31% older than 70 years. Most (84%) were women and many were Latino (38%). Black patients comprised 31% of the cohort and the others were non-Hispanic whites.
The majority had a low monthly income ($1,350 or less), and 25% were not fully literate in English. Many had comorbid psychological conditions, including depression (20%) and anxiety (21%).
Low health literacy was common (34%), although most (71%) did understand that they would always have asthma and that it could not be cured (81%) But half believed that they only had the disease when they were symptomatic. In a survey of medication beliefs, most did believe that the steroids were good for them and that their benefits outweighed the risks.
However, only 37% of the cohort reported good medication adherence. This proportion was significantly worse among blacks and Hispanics; those with lower incomes and lower education; those born in Puerto Rico and the Dominican Republic; and those with poor physical health, anxiety, or depression.
The authors identified six medication adherence strategies among the group: keeping the medication in a usual location (44%); integrating it into their daily routine (33%); taking it at a specific time of day (22%); taking it with other medications (13%); using it only when needed; (13%) and using other reminders (12%). Less than 2% reported using written notes as a reminder or having someone else remind them; 4% had no specific strategy.
The most common places to keep medicine were at the bedside (20%) and in the bathroom (9%). Those who integrated taking it with other daily routines did in the morning (12%) and at bedtime (8%).
Only three of the strategies were significantly associated with good adherence: keeping medication in the bathroom (16% adherent vs. 5% nonadherent); integrating it into a daily routine (morning 25% vs. 5%; evening 13% vs. 6%); and taking it at a specific time of day (29% vs. 17%).
Taking the medication only when needed was associated with significantly worse adherence.
After controlling for other variables, only leaving the medication in the bathroom significantly predicted good adherence (odds ratio 3), compared with those who kept it somewhere else).
Those who integrated medication into other daily routines were also significantly more likely to be adherent (OR 3.7) in a partially adjusted model, but not in a fully adjusted model. Still, the authors noted, this recommendation would be a good suggestion toward improving adherence.
Patients who used these two strategies were more likely to be white, have at least a partial education, and to have been born in the United States. Low income, limited English proficiency, low health literacy, poor physical and psychological health, and erroneous beliefs about asthma predicted poor adherence.
The team postulated that there are two types of nonadherence: simple forgetfulness or lack of understanding about its importance and deliberate nonadherence.
"The bathroom and daily routine strategies may address forgetful nonadherence. ... Taking the medication only as needed, on the other hand, may indicate faulty disease or medication beliefs. ... Taken together, these findings provide further evidence of the value of patient-centered care: Clinicians need to understand why patients do not use their medications appropriately before counseling patients on ways to improve adherence."
The study was supported by a grant from the National Heart, Lung, and Blood Institute. None of the authors had any financial disclosures.
Two simple recommendations for older patients with asthma – keeping medication in the bathroom and integrating its use into a daily routine – can significantly improve adherence to inhaled corticosteroids.
When patients consistently did either of those, adherence rose threefold, compared with patients who didn’t, Dr. Alex Federman and his associates wrote in the August issue of the Journal of Internal Medicine.
The findings suggest that clinicians might help improve adherence by suggesting that their patients store the medication in their bathroom cabinet, and take it, for example, when they brush their teeth every day.
"Because adherence strategies are modifiable, the findings in this study may provide clinicians and care coaches with straightforward and useful messages to help older patients improve their medication adherence," wrote Dr. Federman of Icahn School of Medicine at Mount Sinai, New York, and his coauthors (J. Intern. Med. 2014 Aug. 5 [doi:10.1007/s11606-014-2940-8]).
The team investigated adherence to inhaled corticosteroids among 358 elderly patients with asthma. They were a mean of 67 years old, with 31% older than 70 years. Most (84%) were women and many were Latino (38%). Black patients comprised 31% of the cohort and the others were non-Hispanic whites.
The majority had a low monthly income ($1,350 or less), and 25% were not fully literate in English. Many had comorbid psychological conditions, including depression (20%) and anxiety (21%).
Low health literacy was common (34%), although most (71%) did understand that they would always have asthma and that it could not be cured (81%) But half believed that they only had the disease when they were symptomatic. In a survey of medication beliefs, most did believe that the steroids were good for them and that their benefits outweighed the risks.
However, only 37% of the cohort reported good medication adherence. This proportion was significantly worse among blacks and Hispanics; those with lower incomes and lower education; those born in Puerto Rico and the Dominican Republic; and those with poor physical health, anxiety, or depression.
The authors identified six medication adherence strategies among the group: keeping the medication in a usual location (44%); integrating it into their daily routine (33%); taking it at a specific time of day (22%); taking it with other medications (13%); using it only when needed; (13%) and using other reminders (12%). Less than 2% reported using written notes as a reminder or having someone else remind them; 4% had no specific strategy.
The most common places to keep medicine were at the bedside (20%) and in the bathroom (9%). Those who integrated taking it with other daily routines did in the morning (12%) and at bedtime (8%).
Only three of the strategies were significantly associated with good adherence: keeping medication in the bathroom (16% adherent vs. 5% nonadherent); integrating it into a daily routine (morning 25% vs. 5%; evening 13% vs. 6%); and taking it at a specific time of day (29% vs. 17%).
Taking the medication only when needed was associated with significantly worse adherence.
After controlling for other variables, only leaving the medication in the bathroom significantly predicted good adherence (odds ratio 3), compared with those who kept it somewhere else).
Those who integrated medication into other daily routines were also significantly more likely to be adherent (OR 3.7) in a partially adjusted model, but not in a fully adjusted model. Still, the authors noted, this recommendation would be a good suggestion toward improving adherence.
Patients who used these two strategies were more likely to be white, have at least a partial education, and to have been born in the United States. Low income, limited English proficiency, low health literacy, poor physical and psychological health, and erroneous beliefs about asthma predicted poor adherence.
The team postulated that there are two types of nonadherence: simple forgetfulness or lack of understanding about its importance and deliberate nonadherence.
"The bathroom and daily routine strategies may address forgetful nonadherence. ... Taking the medication only as needed, on the other hand, may indicate faulty disease or medication beliefs. ... Taken together, these findings provide further evidence of the value of patient-centered care: Clinicians need to understand why patients do not use their medications appropriately before counseling patients on ways to improve adherence."
The study was supported by a grant from the National Heart, Lung, and Blood Institute. None of the authors had any financial disclosures.
FROM THE JOURNAL OF INTERNAL MEDICINE
Key clinical point: Specific advice on how and when to take medication helps older asthma patients take inhaled corticosteroids consistently.
Major finding: Keeping inhaled corticosteroids in the bathroom or incorporating them into a daily routine increased the likelihood of compliance by threefold (16% adherent vs. 5% nonadherent).
Data source: The prospective study comprised 358 elderly patients with asthma.
Disclosures: The National Heart, Lung, and Blood Institute sponsored the study. None of the authors had any financial disclosures,

Suicide linked to poor sleep in older patients
Elderly patients who report poor sleep quality face a significantly increased risk of suicide for up to a decade, whether or not depression is also present.
Even after controlling for comorbid depression, investigators found that impaired sleep was associated with a 20% increased risk of suicide in these patients.
Results of the prospective observational study suggest that regularly asking about sleep quality might help improve suicide risk assessment, Rebecca A. Bernert, Ph.D., and her colleagues reported online Aug. 13 in JAMA Psychiatry (doi: 10.1001/jamapsychiatry.2014.1126).
Older adults tend to seek more physician care in the final weeks and months before a suicide than do other at-risk populations (73% and 45%, respectively).
"Furthermore, at least one psychological autopsy study indicates that disturbed sleep is visible to friends and family members in the weeks and months preceding death," wrote Dr. Bernert of Stanford (Calif.) University and her coauthors. "Targeting disturbed sleep as a visible warning sign of suicide may, in this way, constitute a novel opportunity for improved risk detection; this more narrowed, demographic focus may specifically inform intervention among a group at heightened risk for suicide."
The cohort comprised 420 subjects who were a subpopulation of the Established Populations for Epidemiologic Studies of the Elderly study. This project followed 14,500 older adults from 1981 to 1993; its purpose was to identify predictors of mortality, hospitalization, and placement in long-term care facilities and to investigate risk factors for chronic diseases and loss of function.
From this group, 400 controls were matched to 20 subjects who had committed suicide.
Sleep was evaluated with a five-item Sleep Quality Index (SQI) constructed by the investigators. Other measures included assessments of depression, cognition, and physical function.
Subjects were a mean of 75 years old at baseline; 60% were white, 19% were African American, and 1% were Asian, American Indian, or Hispanic. The methods of suicide included firearm (62%), cutting (10%), hanging (9%), poisoning (5%), drowning (5%), lethal jump (5%), and suffocation (5%).
The mean SQI scores were significantly higher among those who committed suicide than among the controls (10 vs. 8). Individuals who committed suicide also reported higher scores on all of the SQI subsets: difficulty falling asleep, difficulty staying asleep, early morning awakening, daytime sleepiness, and nonrestorative sleep.
In the univariate analysis, the total sleep score was a significant predictor of suicide (higher score odds ratio, 1.39) over the 10-year follow-up period. Difficulty falling asleep and nonrestorative sleep also were significant predictors (OR, 2.24 and 2.17, respectively).
After controlling for the presence of baseline comorbid depression, the investigators found that the relationship between overall sleep quality and suicide remained significant (OR, 1.2). Difficulty falling asleep and nonrestorative sleep lost their significance in the multivariate analysis.
The authors proposed that sleep-related deficits in cognitive and emotional processing might be a key factor in suicide among such patients.
"Research indicates that sleep fragmentation results in increased emotional reactivity, intensifying negative emotional responses while blunting positive affect," they noted. "Similarly, sleep deprivation among healthy adults is associated with amplification of amygdala activation, as well as increased reactivity to negative emotions such as anger and fear. Notably, a night of recovery sleep following sleep deprivation reverses this effect, decreasing amygdala activation and reducing such emotional reactivity.
"We propose that such deficits may lower the threshold for suicidal behaviors by impairing the processing of emotionally salient information and associated neural circuitry."
The authors cited several limitations of their study. For example, the measures of sleep quality were self-reported rather than measured objectively. Also, diagnostic information that might influence sleep quality, such as chronic pain and substance use, was not included. Finally, the results are not generalizable to the larger population because 19 of the 20 decedents in the current study were male. "Although this reflects national rates and statistics, the present results should be interpreted as primarily applicable to men and chiefly white men," Dr. Bernert and her associates wrote.
The study was sponsored by the National Institutes of Health and the Centers for Disease Control and Prevention. Neither Dr. Bernert nor her coauthors reported any financial conflicts.
Elderly patients who report poor sleep quality face a significantly increased risk of suicide for up to a decade, whether or not depression is also present.
Even after controlling for comorbid depression, investigators found that impaired sleep was associated with a 20% increased risk of suicide in these patients.
Results of the prospective observational study suggest that regularly asking about sleep quality might help improve suicide risk assessment, Rebecca A. Bernert, Ph.D., and her colleagues reported online Aug. 13 in JAMA Psychiatry (doi: 10.1001/jamapsychiatry.2014.1126).
Older adults tend to seek more physician care in the final weeks and months before a suicide than do other at-risk populations (73% and 45%, respectively).
"Furthermore, at least one psychological autopsy study indicates that disturbed sleep is visible to friends and family members in the weeks and months preceding death," wrote Dr. Bernert of Stanford (Calif.) University and her coauthors. "Targeting disturbed sleep as a visible warning sign of suicide may, in this way, constitute a novel opportunity for improved risk detection; this more narrowed, demographic focus may specifically inform intervention among a group at heightened risk for suicide."
The cohort comprised 420 subjects who were a subpopulation of the Established Populations for Epidemiologic Studies of the Elderly study. This project followed 14,500 older adults from 1981 to 1993; its purpose was to identify predictors of mortality, hospitalization, and placement in long-term care facilities and to investigate risk factors for chronic diseases and loss of function.
From this group, 400 controls were matched to 20 subjects who had committed suicide.
Sleep was evaluated with a five-item Sleep Quality Index (SQI) constructed by the investigators. Other measures included assessments of depression, cognition, and physical function.
Subjects were a mean of 75 years old at baseline; 60% were white, 19% were African American, and 1% were Asian, American Indian, or Hispanic. The methods of suicide included firearm (62%), cutting (10%), hanging (9%), poisoning (5%), drowning (5%), lethal jump (5%), and suffocation (5%).
The mean SQI scores were significantly higher among those who committed suicide than among the controls (10 vs. 8). Individuals who committed suicide also reported higher scores on all of the SQI subsets: difficulty falling asleep, difficulty staying asleep, early morning awakening, daytime sleepiness, and nonrestorative sleep.
In the univariate analysis, the total sleep score was a significant predictor of suicide (higher score odds ratio, 1.39) over the 10-year follow-up period. Difficulty falling asleep and nonrestorative sleep also were significant predictors (OR, 2.24 and 2.17, respectively).
After controlling for the presence of baseline comorbid depression, the investigators found that the relationship between overall sleep quality and suicide remained significant (OR, 1.2). Difficulty falling asleep and nonrestorative sleep lost their significance in the multivariate analysis.
The authors proposed that sleep-related deficits in cognitive and emotional processing might be a key factor in suicide among such patients.
"Research indicates that sleep fragmentation results in increased emotional reactivity, intensifying negative emotional responses while blunting positive affect," they noted. "Similarly, sleep deprivation among healthy adults is associated with amplification of amygdala activation, as well as increased reactivity to negative emotions such as anger and fear. Notably, a night of recovery sleep following sleep deprivation reverses this effect, decreasing amygdala activation and reducing such emotional reactivity.
"We propose that such deficits may lower the threshold for suicidal behaviors by impairing the processing of emotionally salient information and associated neural circuitry."
The authors cited several limitations of their study. For example, the measures of sleep quality were self-reported rather than measured objectively. Also, diagnostic information that might influence sleep quality, such as chronic pain and substance use, was not included. Finally, the results are not generalizable to the larger population because 19 of the 20 decedents in the current study were male. "Although this reflects national rates and statistics, the present results should be interpreted as primarily applicable to men and chiefly white men," Dr. Bernert and her associates wrote.
The study was sponsored by the National Institutes of Health and the Centers for Disease Control and Prevention. Neither Dr. Bernert nor her coauthors reported any financial conflicts.
Elderly patients who report poor sleep quality face a significantly increased risk of suicide for up to a decade, whether or not depression is also present.
Even after controlling for comorbid depression, investigators found that impaired sleep was associated with a 20% increased risk of suicide in these patients.
Results of the prospective observational study suggest that regularly asking about sleep quality might help improve suicide risk assessment, Rebecca A. Bernert, Ph.D., and her colleagues reported online Aug. 13 in JAMA Psychiatry (doi: 10.1001/jamapsychiatry.2014.1126).
Older adults tend to seek more physician care in the final weeks and months before a suicide than do other at-risk populations (73% and 45%, respectively).
"Furthermore, at least one psychological autopsy study indicates that disturbed sleep is visible to friends and family members in the weeks and months preceding death," wrote Dr. Bernert of Stanford (Calif.) University and her coauthors. "Targeting disturbed sleep as a visible warning sign of suicide may, in this way, constitute a novel opportunity for improved risk detection; this more narrowed, demographic focus may specifically inform intervention among a group at heightened risk for suicide."
The cohort comprised 420 subjects who were a subpopulation of the Established Populations for Epidemiologic Studies of the Elderly study. This project followed 14,500 older adults from 1981 to 1993; its purpose was to identify predictors of mortality, hospitalization, and placement in long-term care facilities and to investigate risk factors for chronic diseases and loss of function.
From this group, 400 controls were matched to 20 subjects who had committed suicide.
Sleep was evaluated with a five-item Sleep Quality Index (SQI) constructed by the investigators. Other measures included assessments of depression, cognition, and physical function.
Subjects were a mean of 75 years old at baseline; 60% were white, 19% were African American, and 1% were Asian, American Indian, or Hispanic. The methods of suicide included firearm (62%), cutting (10%), hanging (9%), poisoning (5%), drowning (5%), lethal jump (5%), and suffocation (5%).
The mean SQI scores were significantly higher among those who committed suicide than among the controls (10 vs. 8). Individuals who committed suicide also reported higher scores on all of the SQI subsets: difficulty falling asleep, difficulty staying asleep, early morning awakening, daytime sleepiness, and nonrestorative sleep.
In the univariate analysis, the total sleep score was a significant predictor of suicide (higher score odds ratio, 1.39) over the 10-year follow-up period. Difficulty falling asleep and nonrestorative sleep also were significant predictors (OR, 2.24 and 2.17, respectively).
After controlling for the presence of baseline comorbid depression, the investigators found that the relationship between overall sleep quality and suicide remained significant (OR, 1.2). Difficulty falling asleep and nonrestorative sleep lost their significance in the multivariate analysis.
The authors proposed that sleep-related deficits in cognitive and emotional processing might be a key factor in suicide among such patients.
"Research indicates that sleep fragmentation results in increased emotional reactivity, intensifying negative emotional responses while blunting positive affect," they noted. "Similarly, sleep deprivation among healthy adults is associated with amplification of amygdala activation, as well as increased reactivity to negative emotions such as anger and fear. Notably, a night of recovery sleep following sleep deprivation reverses this effect, decreasing amygdala activation and reducing such emotional reactivity.
"We propose that such deficits may lower the threshold for suicidal behaviors by impairing the processing of emotionally salient information and associated neural circuitry."
The authors cited several limitations of their study. For example, the measures of sleep quality were self-reported rather than measured objectively. Also, diagnostic information that might influence sleep quality, such as chronic pain and substance use, was not included. Finally, the results are not generalizable to the larger population because 19 of the 20 decedents in the current study were male. "Although this reflects national rates and statistics, the present results should be interpreted as primarily applicable to men and chiefly white men," Dr. Bernert and her associates wrote.
The study was sponsored by the National Institutes of Health and the Centers for Disease Control and Prevention. Neither Dr. Bernert nor her coauthors reported any financial conflicts.
FROM JAMA PSYCHIATRY
Key clinical point: Assessing the sleep quality of older patients might be a "useful screening tool and a novel therapeutic target for suicide prevention in late life."
Major findings: Elderly subjects who reported poor sleep quality were 20% more likely to commit suicide over a 10-year period.
Data source: The prospective, observational study comprised 420 subjects.
Disclosures: The study was sponsored by the National Institutes of Health and the Centers for Disease Control and Prevention. Neither Dr. Bernert nor her coauthors reported any financial conflicts.
Varenicline combined with nicotine replacement therapy ups smoking quit rates
An estimated 42 million (18.1%) of the U.S. adult population continues to smoke cigarettes. Effective treatments exist for patients who are willing to avail themselves of such assistance. Varenicline is one of the most effective medications that we have to combat tobacco dependence. However, it doesn’t work for everybody, and questions have remained about how safe and effective it is to combine varenicline with other smoking cessation therapies such as nicotine replacement therapy.
Varenicline binds to a specific nicotine receptor, thereby partially agonizing and blocking it. The result is decreased cravings for tobacco and increased smoking quit rates. Data from early studies conducted by our group suggested that nicotine replacement therapy (NRT) combined with varenicline was safe, but questions remained about its efficacy.
One group of researchers conducted a multicenter clinical trial evaluating the efficacy of combining varenicline and the nicotine patch for increasing smoking cessation rates. Smokers were eligible if they smoked at least 10 cigarettes per day, reported F.N. Coenraad, from the Stellenbosch University, Cape Town, South Africa, and associates. Participants were randomized to active 15-mg nicotine patches or placebo patches started 2 weeks before the target quit date. All participants received varenicline for a total of 14 weeks with a 1-week ramp-up and a 1-week taper. Use of the varenicline in combination with the nicotine patch resulted in increased rates of continuous abstinence from smoking at 12 weeks (no smoking from weeks 9 to 12: 55.4% vs. 40.9%; odds ratio, 1.85; 95% confidence interval, 1.19-2.89; P = .007) and at 24 weeks (no smoking from weeks 9 to 24: 49% vs. 32.6%; OR, 1.98; 95% CI, 1.25-3.14; P = .004) (JAMA 2014;312:155-61).
This is a fantastic study answering a lingering question in tobacco control. But what is the theoretical underpinning by which this combination works? Isn’t the NRT blocked by the varenicline? It is possible that the varenicline incompletely saturates the nicotine receptors, which are additionally saturated by the supplemented nicotine. The varenicline effect is mediated through the alpha-4 beta-2 nicotinic receptor, and it is also possible that nicotine binds to nicotine receptor types that varenicline does not bind to, which decreases withdrawal symptoms.
We aren’t exactly sure how this might be working, but a near doubling of the odds of quitting is not to be disregarded. We are also not sure whether the effect holds when one uses other types of NRT such as the nicotine inhaler, nicotine lozenge, nicotine nasal spray, and nicotine gum. In practice, I tend to lean toward a combination of varenicline with the nicotine inhaler since the inhaler can help with some of the behavioral aspects of smoking while the varenicline does its heavy lifting.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. Dr. Ebbert reports receiving research support from Pfizer, manufacturer of varenicline and the nicotine inhaler, and consulting fees from GlaxoSmithKline, manufacturer of the nicotine patch. The opinions expressed in this article should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician.
An estimated 42 million (18.1%) of the U.S. adult population continues to smoke cigarettes. Effective treatments exist for patients who are willing to avail themselves of such assistance. Varenicline is one of the most effective medications that we have to combat tobacco dependence. However, it doesn’t work for everybody, and questions have remained about how safe and effective it is to combine varenicline with other smoking cessation therapies such as nicotine replacement therapy.
Varenicline binds to a specific nicotine receptor, thereby partially agonizing and blocking it. The result is decreased cravings for tobacco and increased smoking quit rates. Data from early studies conducted by our group suggested that nicotine replacement therapy (NRT) combined with varenicline was safe, but questions remained about its efficacy.
One group of researchers conducted a multicenter clinical trial evaluating the efficacy of combining varenicline and the nicotine patch for increasing smoking cessation rates. Smokers were eligible if they smoked at least 10 cigarettes per day, reported F.N. Coenraad, from the Stellenbosch University, Cape Town, South Africa, and associates. Participants were randomized to active 15-mg nicotine patches or placebo patches started 2 weeks before the target quit date. All participants received varenicline for a total of 14 weeks with a 1-week ramp-up and a 1-week taper. Use of the varenicline in combination with the nicotine patch resulted in increased rates of continuous abstinence from smoking at 12 weeks (no smoking from weeks 9 to 12: 55.4% vs. 40.9%; odds ratio, 1.85; 95% confidence interval, 1.19-2.89; P = .007) and at 24 weeks (no smoking from weeks 9 to 24: 49% vs. 32.6%; OR, 1.98; 95% CI, 1.25-3.14; P = .004) (JAMA 2014;312:155-61).
This is a fantastic study answering a lingering question in tobacco control. But what is the theoretical underpinning by which this combination works? Isn’t the NRT blocked by the varenicline? It is possible that the varenicline incompletely saturates the nicotine receptors, which are additionally saturated by the supplemented nicotine. The varenicline effect is mediated through the alpha-4 beta-2 nicotinic receptor, and it is also possible that nicotine binds to nicotine receptor types that varenicline does not bind to, which decreases withdrawal symptoms.
We aren’t exactly sure how this might be working, but a near doubling of the odds of quitting is not to be disregarded. We are also not sure whether the effect holds when one uses other types of NRT such as the nicotine inhaler, nicotine lozenge, nicotine nasal spray, and nicotine gum. In practice, I tend to lean toward a combination of varenicline with the nicotine inhaler since the inhaler can help with some of the behavioral aspects of smoking while the varenicline does its heavy lifting.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. Dr. Ebbert reports receiving research support from Pfizer, manufacturer of varenicline and the nicotine inhaler, and consulting fees from GlaxoSmithKline, manufacturer of the nicotine patch. The opinions expressed in this article should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician.
An estimated 42 million (18.1%) of the U.S. adult population continues to smoke cigarettes. Effective treatments exist for patients who are willing to avail themselves of such assistance. Varenicline is one of the most effective medications that we have to combat tobacco dependence. However, it doesn’t work for everybody, and questions have remained about how safe and effective it is to combine varenicline with other smoking cessation therapies such as nicotine replacement therapy.
Varenicline binds to a specific nicotine receptor, thereby partially agonizing and blocking it. The result is decreased cravings for tobacco and increased smoking quit rates. Data from early studies conducted by our group suggested that nicotine replacement therapy (NRT) combined with varenicline was safe, but questions remained about its efficacy.
One group of researchers conducted a multicenter clinical trial evaluating the efficacy of combining varenicline and the nicotine patch for increasing smoking cessation rates. Smokers were eligible if they smoked at least 10 cigarettes per day, reported F.N. Coenraad, from the Stellenbosch University, Cape Town, South Africa, and associates. Participants were randomized to active 15-mg nicotine patches or placebo patches started 2 weeks before the target quit date. All participants received varenicline for a total of 14 weeks with a 1-week ramp-up and a 1-week taper. Use of the varenicline in combination with the nicotine patch resulted in increased rates of continuous abstinence from smoking at 12 weeks (no smoking from weeks 9 to 12: 55.4% vs. 40.9%; odds ratio, 1.85; 95% confidence interval, 1.19-2.89; P = .007) and at 24 weeks (no smoking from weeks 9 to 24: 49% vs. 32.6%; OR, 1.98; 95% CI, 1.25-3.14; P = .004) (JAMA 2014;312:155-61).
This is a fantastic study answering a lingering question in tobacco control. But what is the theoretical underpinning by which this combination works? Isn’t the NRT blocked by the varenicline? It is possible that the varenicline incompletely saturates the nicotine receptors, which are additionally saturated by the supplemented nicotine. The varenicline effect is mediated through the alpha-4 beta-2 nicotinic receptor, and it is also possible that nicotine binds to nicotine receptor types that varenicline does not bind to, which decreases withdrawal symptoms.
We aren’t exactly sure how this might be working, but a near doubling of the odds of quitting is not to be disregarded. We are also not sure whether the effect holds when one uses other types of NRT such as the nicotine inhaler, nicotine lozenge, nicotine nasal spray, and nicotine gum. In practice, I tend to lean toward a combination of varenicline with the nicotine inhaler since the inhaler can help with some of the behavioral aspects of smoking while the varenicline does its heavy lifting.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. Dr. Ebbert reports receiving research support from Pfizer, manufacturer of varenicline and the nicotine inhaler, and consulting fees from GlaxoSmithKline, manufacturer of the nicotine patch. The opinions expressed in this article should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician.

Medical consultation rates for surgical cases vary
The use of inpatient medical consultations for hospitalized surgical patients was found to vary by hospital, but consultations didn’t appear to have much of an impact on risk-adjusted 30-day mortality rates, a study found.
Rates of medical consultations varied from 50% to 91% among 91,684 patients undergoing colectomy and from 36% to 90% among 339,319 patients undergoing total hip replacements, a retrospective study found.

The variation was most dramatic for patients undergoing colectomy who did not have complications, among whom rates of inpatient medical consultation ranged from 47% to 79% between hospitals, Dr. Lena M. Chen and her associates reported. For patients undergoing colectomy who did have complications, 90%-95% received medical consultations.
Similarly, variation in the use of medical consultation for patients getting total hip replacement was wider for those without complications (36%-87%), compared with patients with complications (89%-94%).
The results highlight the fact that there’s no consensus on when and how to best provide medical consultation for hospitalized surgical patients. "Wide variation in medical consultation use – particularly among patients without complications – suggests that understanding when medical consultations provide value will be important as hospitals seek to increase their efficiency under bundled payments," wrote Dr. Chen of the University of Michigan, Ann Arbor (JAMA Intern. Med. 2014 Aug. 4 [doi:10.1001/jamainternmed.2014.3376]).
She and her associates analyzed Medicare claims data and American Hospital Association data on patients aged 65-99 years who underwent colectomy at 930 hospitals or total hip replacement at 1,589 hospitals in 2007-2010. These are 2 of the top 10 procedures performed on Medicare patients, and total hip replacement is included in the Centers for Medicare & Medicaid Services bundled payment demonstration project, the authors noted.
At least one medical consultant saw 69% of patients undergoing colectomy and 63% of patients getting a total hip replacement. Among patients who got consultations, colectomy patients saw consultants a median of nine times, and hip replacement patients saw consultants a median of three times.
Colectomy patients most often saw general medicine consultants (50%), followed by cardiologists (28%), oncologists (25%), or gastroenterologists (22%). Among patients receiving total hip replacement, 53% had a general medicine consultation, and the most common specialist consultations were for physical medicine and rehabilitation (11%) or cardiology (8%).
Approximately a third of hip replacement patients were "comanaged" by surgeons and medical consultants, defined by records of a claim for evaluation and management by a medicine physician on at least 70% of inpatient days.
It seems logical to assume that extra care from nonsurgical physicians should improve outcomes for some surgical patients, but an exploratory analysis of the data found that risk-adjusted 30-day mortality rates were not significantly different between hospitals with the greatest or least use of medical consultations, Dr. Chen reported. The 30-day mortality rate for colectomy patients was 5% at hospitals in the lowest quintile of medical consultations and 6% at hospitals in the highest quintile. The results for total hip replacement were similar.
Greater use of medical consultation was associated with a significantly greater likelihood of having at least one postoperative complication, affecting 24% of colectomy patients at hospitals in the lowest quintile of consultations and 28% at hospitals in the highest quintile. The results for total hip replacement were similar.
The National Institute of Aging and a University of Michigan McCubed grant funded the study. Dr. Chen reported having no relevant financial disclosures. One of her coinvestigators owns stock in ArborMetrix, a company that analyzes hospital quality and cost efficiency.
On Twitter @sherryboschert
Dr. Chen’s findings that rates of medical consultation varied widely for surgical patients without complications complement a 2010 study by Dr. Gulshan Sharma and his associates that found 35% of patients hospitalized for a common surgical procedure were comanaged by medicine physicians (Arch. Intern. Med. 2010;170:363-8).
"I agree [with Dr. Chen] that understanding the ‘value’ of medical consultation is an important next step, especially in low-risk patients undergoing elective surgery," Dr. Sharma commented in an article accompanying Dr. Chen’s study (JAMA Intern. Med. 2014 Aug. 4 [doi:10.1001/jamainternmed.2014.1499]).
Comanagement may benefit patients by increasing the use of evidence-based treatments or reducing the time to surgery, postoperative complications, the need for ICU care, the length of stay, and readmission rates, among other possibilities. But there are possible downsides, too, including potential confusion among caregivers, more complicated decision making, lack of "ownership" of problems, or added costs, he noted.
Hospitals with the greatest use of medical consultation in Dr. Chen’s study had higher risk-adjusted rates of 30-day mortality and complications, compared with hospitals with the least use of medical consultation (though the difference in mortality was not statistically significant). "Is there a potential harm associated with medical consultation?" Dr. Sharma asked.
"There is no one fit for all" hospitals, he wrote. Institutional data on quality and cost should drive decisions on the routine use of medical consultation. The practice of mandating comanagement of all surgical patients "should be discouraged," Dr. Sharma said. "During preoperative evaluation, patients with comorbid conditions and those at significant risk of postoperative complications should be considered for medical comanagement."
Dr. Sharma is director of the division of pulmonary critical care and sleep medicine at the University of Texas Medical Branch, Galveston. He reported having no relevant financial disclosures.
Dr. Chen’s findings that rates of medical consultation varied widely for surgical patients without complications complement a 2010 study by Dr. Gulshan Sharma and his associates that found 35% of patients hospitalized for a common surgical procedure were comanaged by medicine physicians (Arch. Intern. Med. 2010;170:363-8).
"I agree [with Dr. Chen] that understanding the ‘value’ of medical consultation is an important next step, especially in low-risk patients undergoing elective surgery," Dr. Sharma commented in an article accompanying Dr. Chen’s study (JAMA Intern. Med. 2014 Aug. 4 [doi:10.1001/jamainternmed.2014.1499]).
Comanagement may benefit patients by increasing the use of evidence-based treatments or reducing the time to surgery, postoperative complications, the need for ICU care, the length of stay, and readmission rates, among other possibilities. But there are possible downsides, too, including potential confusion among caregivers, more complicated decision making, lack of "ownership" of problems, or added costs, he noted.
Hospitals with the greatest use of medical consultation in Dr. Chen’s study had higher risk-adjusted rates of 30-day mortality and complications, compared with hospitals with the least use of medical consultation (though the difference in mortality was not statistically significant). "Is there a potential harm associated with medical consultation?" Dr. Sharma asked.
"There is no one fit for all" hospitals, he wrote. Institutional data on quality and cost should drive decisions on the routine use of medical consultation. The practice of mandating comanagement of all surgical patients "should be discouraged," Dr. Sharma said. "During preoperative evaluation, patients with comorbid conditions and those at significant risk of postoperative complications should be considered for medical comanagement."
Dr. Sharma is director of the division of pulmonary critical care and sleep medicine at the University of Texas Medical Branch, Galveston. He reported having no relevant financial disclosures.
Dr. Chen’s findings that rates of medical consultation varied widely for surgical patients without complications complement a 2010 study by Dr. Gulshan Sharma and his associates that found 35% of patients hospitalized for a common surgical procedure were comanaged by medicine physicians (Arch. Intern. Med. 2010;170:363-8).
"I agree [with Dr. Chen] that understanding the ‘value’ of medical consultation is an important next step, especially in low-risk patients undergoing elective surgery," Dr. Sharma commented in an article accompanying Dr. Chen’s study (JAMA Intern. Med. 2014 Aug. 4 [doi:10.1001/jamainternmed.2014.1499]).
Comanagement may benefit patients by increasing the use of evidence-based treatments or reducing the time to surgery, postoperative complications, the need for ICU care, the length of stay, and readmission rates, among other possibilities. But there are possible downsides, too, including potential confusion among caregivers, more complicated decision making, lack of "ownership" of problems, or added costs, he noted.
Hospitals with the greatest use of medical consultation in Dr. Chen’s study had higher risk-adjusted rates of 30-day mortality and complications, compared with hospitals with the least use of medical consultation (though the difference in mortality was not statistically significant). "Is there a potential harm associated with medical consultation?" Dr. Sharma asked.
"There is no one fit for all" hospitals, he wrote. Institutional data on quality and cost should drive decisions on the routine use of medical consultation. The practice of mandating comanagement of all surgical patients "should be discouraged," Dr. Sharma said. "During preoperative evaluation, patients with comorbid conditions and those at significant risk of postoperative complications should be considered for medical comanagement."
Dr. Sharma is director of the division of pulmonary critical care and sleep medicine at the University of Texas Medical Branch, Galveston. He reported having no relevant financial disclosures.
The use of inpatient medical consultations for hospitalized surgical patients was found to vary by hospital, but consultations didn’t appear to have much of an impact on risk-adjusted 30-day mortality rates, a study found.
Rates of medical consultations varied from 50% to 91% among 91,684 patients undergoing colectomy and from 36% to 90% among 339,319 patients undergoing total hip replacements, a retrospective study found.
The variation was most dramatic for patients undergoing colectomy who did not have complications, among whom rates of inpatient medical consultation ranged from 47% to 79% between hospitals, Dr. Lena M. Chen and her associates reported. For patients undergoing colectomy who did have complications, 90%-95% received medical consultations.
Similarly, variation in the use of medical consultation for patients getting total hip replacement was wider for those without complications (36%-87%), compared with patients with complications (89%-94%).
The results highlight the fact that there’s no consensus on when and how to best provide medical consultation for hospitalized surgical patients. "Wide variation in medical consultation use – particularly among patients without complications – suggests that understanding when medical consultations provide value will be important as hospitals seek to increase their efficiency under bundled payments," wrote Dr. Chen of the University of Michigan, Ann Arbor (JAMA Intern. Med. 2014 Aug. 4 [doi:10.1001/jamainternmed.2014.3376]).
She and her associates analyzed Medicare claims data and American Hospital Association data on patients aged 65-99 years who underwent colectomy at 930 hospitals or total hip replacement at 1,589 hospitals in 2007-2010. These are 2 of the top 10 procedures performed on Medicare patients, and total hip replacement is included in the Centers for Medicare & Medicaid Services bundled payment demonstration project, the authors noted.
At least one medical consultant saw 69% of patients undergoing colectomy and 63% of patients getting a total hip replacement. Among patients who got consultations, colectomy patients saw consultants a median of nine times, and hip replacement patients saw consultants a median of three times.
Colectomy patients most often saw general medicine consultants (50%), followed by cardiologists (28%), oncologists (25%), or gastroenterologists (22%). Among patients receiving total hip replacement, 53% had a general medicine consultation, and the most common specialist consultations were for physical medicine and rehabilitation (11%) or cardiology (8%).
Approximately a third of hip replacement patients were "comanaged" by surgeons and medical consultants, defined by records of a claim for evaluation and management by a medicine physician on at least 70% of inpatient days.
It seems logical to assume that extra care from nonsurgical physicians should improve outcomes for some surgical patients, but an exploratory analysis of the data found that risk-adjusted 30-day mortality rates were not significantly different between hospitals with the greatest or least use of medical consultations, Dr. Chen reported. The 30-day mortality rate for colectomy patients was 5% at hospitals in the lowest quintile of medical consultations and 6% at hospitals in the highest quintile. The results for total hip replacement were similar.
Greater use of medical consultation was associated with a significantly greater likelihood of having at least one postoperative complication, affecting 24% of colectomy patients at hospitals in the lowest quintile of consultations and 28% at hospitals in the highest quintile. The results for total hip replacement were similar.
The National Institute of Aging and a University of Michigan McCubed grant funded the study. Dr. Chen reported having no relevant financial disclosures. One of her coinvestigators owns stock in ArborMetrix, a company that analyzes hospital quality and cost efficiency.
On Twitter @sherryboschert
The use of inpatient medical consultations for hospitalized surgical patients was found to vary by hospital, but consultations didn’t appear to have much of an impact on risk-adjusted 30-day mortality rates, a study found.
Rates of medical consultations varied from 50% to 91% among 91,684 patients undergoing colectomy and from 36% to 90% among 339,319 patients undergoing total hip replacements, a retrospective study found.
The variation was most dramatic for patients undergoing colectomy who did not have complications, among whom rates of inpatient medical consultation ranged from 47% to 79% between hospitals, Dr. Lena M. Chen and her associates reported. For patients undergoing colectomy who did have complications, 90%-95% received medical consultations.
Similarly, variation in the use of medical consultation for patients getting total hip replacement was wider for those without complications (36%-87%), compared with patients with complications (89%-94%).
The results highlight the fact that there’s no consensus on when and how to best provide medical consultation for hospitalized surgical patients. "Wide variation in medical consultation use – particularly among patients without complications – suggests that understanding when medical consultations provide value will be important as hospitals seek to increase their efficiency under bundled payments," wrote Dr. Chen of the University of Michigan, Ann Arbor (JAMA Intern. Med. 2014 Aug. 4 [doi:10.1001/jamainternmed.2014.3376]).
She and her associates analyzed Medicare claims data and American Hospital Association data on patients aged 65-99 years who underwent colectomy at 930 hospitals or total hip replacement at 1,589 hospitals in 2007-2010. These are 2 of the top 10 procedures performed on Medicare patients, and total hip replacement is included in the Centers for Medicare & Medicaid Services bundled payment demonstration project, the authors noted.
At least one medical consultant saw 69% of patients undergoing colectomy and 63% of patients getting a total hip replacement. Among patients who got consultations, colectomy patients saw consultants a median of nine times, and hip replacement patients saw consultants a median of three times.
Colectomy patients most often saw general medicine consultants (50%), followed by cardiologists (28%), oncologists (25%), or gastroenterologists (22%). Among patients receiving total hip replacement, 53% had a general medicine consultation, and the most common specialist consultations were for physical medicine and rehabilitation (11%) or cardiology (8%).
Approximately a third of hip replacement patients were "comanaged" by surgeons and medical consultants, defined by records of a claim for evaluation and management by a medicine physician on at least 70% of inpatient days.
It seems logical to assume that extra care from nonsurgical physicians should improve outcomes for some surgical patients, but an exploratory analysis of the data found that risk-adjusted 30-day mortality rates were not significantly different between hospitals with the greatest or least use of medical consultations, Dr. Chen reported. The 30-day mortality rate for colectomy patients was 5% at hospitals in the lowest quintile of medical consultations and 6% at hospitals in the highest quintile. The results for total hip replacement were similar.
Greater use of medical consultation was associated with a significantly greater likelihood of having at least one postoperative complication, affecting 24% of colectomy patients at hospitals in the lowest quintile of consultations and 28% at hospitals in the highest quintile. The results for total hip replacement were similar.
The National Institute of Aging and a University of Michigan McCubed grant funded the study. Dr. Chen reported having no relevant financial disclosures. One of her coinvestigators owns stock in ArborMetrix, a company that analyzes hospital quality and cost efficiency.
On Twitter @sherryboschert
FROM JAMA INTERNAL MEDICINE
Key clinical point: In the era of bundled payments for episodes of care, consider when and how medical consultation for surgical patients is helpful.
Major finding: Use of medical consultations ranged from 50%-91% for colectomies and 36%-90% for total hip replacements.
Data source: A retrospective study of Medicare data on 431,003 older adults undergoing colectomy or total hip replacement in 2007-2010.
Disclosures: Dr. Chen reported having no financial disclosures. One of her associates owns stock in ArborMetrix, a company that analyzes hospital quality and cost efficiency.

Texting intervention helped smokers quit
Text-messaging programs on phones seem to help smokers quit. The jury’s still out on smartphone apps for smoking cessation when used by patients, but they may help nurses improve screening, several separate studies suggest.
The interactive text-messaging program Text2Quit helped U.S. smokers quit and stay off cigarettes in a 6-month randomized, controlled trial in 503 adults who smoked at least five cigarettes a day, owned a cell phone with an unlimited service plan for short text messaging, and had expressed an interest in quitting cigarettes. Participants already were avid texters, sending or receiving an average of 29 text messages per day before they enrolled in the study.

At the 6-month follow-up, 20% of 241 people in the Text2Quit group said they had not smoked in the prior 7 days, compared with 10% of 262 people in the control group, reported Lorien C. Abroms, Sc.D., and her associates.
Laboratory analyses of saliva from 54 members of the intervention group and 32 in the control group showed that nearly a quarter of participants had lied about quitting. Text2Quit still was effective, however, with biochemically confirmed abstinence from smoking in 11% of the intervention group and 5% of the control group (Am. J. Prev. Med. 2014 June 5 [doi: 10.1016/j.amepre.2014.04.010]). Those biochemical quit rates are similar to rates reported in studies of other text-messaging programs for smoking cessation or of telephone quit-line counseling, she said.
The results support a meta-analysis of five studies that found mobile phone–based interventions (predominantly text messaging) for smoking cessation increased 6-month quit rates (Cochrane Database Syst. Rev. 2012;11:CD006611 [doi: 10.1002/14651858]). Most U.S. studies, however, have been small, uncontrolled pilot trials with shorter follow-up and no biochemical verification of quit rates, Dr. Abroms said.
Text2Quit costs $30 for a 4-month subscription unless you have a code from a sponsoring organization. When U.S. smokers call the national quit-line number (1-800-QUIT-NOW), residents of some states get offered Text2Quit. More than 50,000 smokers have enrolled since the program became available in 2011, reported Dr. Abroms of George Washington University, Washington. Other text-messaging programs are available, such as the free SmokefreeTXT program from the National Cancer Institute’s smokefree.gov site.
People randomized to the control group in Dr. Abroms’ trial initially were given a link to smokefree.gov, but after the launch of SmokefreeTXT in 2011, new control group members instead were given a link to the National Cancer Institute’s "Clearing the Air" guidebook on quitting smoking.
Text2Quit consists of automated, bidirectional text messages, with extra support from e-mails and a web portal. The texts prompt users to track their smoking and report on their cravings and smoking status, with the messages to participants tailored by the reasons for quitting, money saved, and use of medications for smoking cessation. The frequency of texts peaked around the smoker’s chosen quit date, with five texts on that date, approximately two per day in the following week, three per week in the next 2 months, and less than one per week after that.
Considering that an estimated 75% of adults around the world have access to cell phones, text-messaging interventions potentially could puff up the number of quitters, she suggested.
Smartphones aren’t yet as ubiquitous but, still, an estimated 11 million U.S. smokers own a smartphone, Dr. Abroms wrote in a separate study of apps for smoking cessation. We don’t yet know if any of the 400 smoking cessation apps that were available in 2012 work, but her analysis of 98 of the most popular smoking cessation apps found that they seldom include information and strategies that have been proven to help smokers quit.
She and her associates rated 47 apps for iPhones and 51 for Android phones on a 42-point scale, with a top score indicating adherence to the U.S. Public Health Service’s Clinical Practice Guidelines for Treating Tobacco Use and Dependence. The average score was 13. No apps recommended calling a quit line, for example. Only 4% recommended using medications approved for smoking cessation. Only 19% offered practical counseling or advice on how to quit or stay quit (Am. J. Prev. Med. 2013;45:732-36).
On the other hand, it’s possible that national guidelines that were developed for clinical settings don’t apply to mobile apps. If the apps somehow are effective, their reach could magnify any impact, Dr. Abroms suggested. Approximately 779,400 English-language apps for smoking cessation were downloaded per month for Android phones alone during the study period. (The iTunes App Store does not provide numbers for downloads.) That’s more than the approximately 100,000 calls per month to the national quit line in the same time period and 200,000 unique visitors per month to a leading website for smoking cessation, she reported.
"Text messaging programs for smoking cessation have a reasonably good evidence base," according to Dr. Abroms. "The evidence for smartphone apps is still in its early stages. I would not recommend them as a stand-alone intervention, though many with tracking elements may be useful as part of a comprehensive program. Apps that include games could be good as a distraction from smoking."
A separate study found that an experimental "decision support system" app, created for use by nurses on smartphones and tablets, improved rates of screening and counseling for tobacco use by prompting nurses to screen for tobacco use and offered guideline-based treatment recommendations, reported Kenrick Cato, Ph.D. of Columbia University, New York, and his associates.
The 185 registered nurses who were enrolled in advanced practice degree programs handled 14,115 clinic visits, in which they asked patients about smoking status in 84% of visits and offered cessation counseling to 90% of those who expressed a willingness to stop smoking (Oncol. Nurs. Forum 2014;41:145-52).
That compares favorably with federal U.S. data suggesting that tobacco screening happens in approximately 60% of clinic visits, and fewer than 20% of patients get counseling on quitting, Dr. Cato said in a prepared statement released by the university. The federal Healthy People 2020 program aims for tobacco screening in 69% of office visits and counseling rates of 21%, he said.
If further development of the app confirms that it’s useful, it could light a fire under tobacco screening.
Dr. Abroms designed Text2Quit and receives royalties from sales. Dr. Cato reported having no financial disclosures.
On Twitter @sherryboschert
Text-messaging programs on phones seem to help smokers quit. The jury’s still out on smartphone apps for smoking cessation when used by patients, but they may help nurses improve screening, several separate studies suggest.
The interactive text-messaging program Text2Quit helped U.S. smokers quit and stay off cigarettes in a 6-month randomized, controlled trial in 503 adults who smoked at least five cigarettes a day, owned a cell phone with an unlimited service plan for short text messaging, and had expressed an interest in quitting cigarettes. Participants already were avid texters, sending or receiving an average of 29 text messages per day before they enrolled in the study.
At the 6-month follow-up, 20% of 241 people in the Text2Quit group said they had not smoked in the prior 7 days, compared with 10% of 262 people in the control group, reported Lorien C. Abroms, Sc.D., and her associates.
Laboratory analyses of saliva from 54 members of the intervention group and 32 in the control group showed that nearly a quarter of participants had lied about quitting. Text2Quit still was effective, however, with biochemically confirmed abstinence from smoking in 11% of the intervention group and 5% of the control group (Am. J. Prev. Med. 2014 June 5 [doi: 10.1016/j.amepre.2014.04.010]). Those biochemical quit rates are similar to rates reported in studies of other text-messaging programs for smoking cessation or of telephone quit-line counseling, she said.
The results support a meta-analysis of five studies that found mobile phone–based interventions (predominantly text messaging) for smoking cessation increased 6-month quit rates (Cochrane Database Syst. Rev. 2012;11:CD006611 [doi: 10.1002/14651858]). Most U.S. studies, however, have been small, uncontrolled pilot trials with shorter follow-up and no biochemical verification of quit rates, Dr. Abroms said.
Text2Quit costs $30 for a 4-month subscription unless you have a code from a sponsoring organization. When U.S. smokers call the national quit-line number (1-800-QUIT-NOW), residents of some states get offered Text2Quit. More than 50,000 smokers have enrolled since the program became available in 2011, reported Dr. Abroms of George Washington University, Washington. Other text-messaging programs are available, such as the free SmokefreeTXT program from the National Cancer Institute’s smokefree.gov site.
People randomized to the control group in Dr. Abroms’ trial initially were given a link to smokefree.gov, but after the launch of SmokefreeTXT in 2011, new control group members instead were given a link to the National Cancer Institute’s "Clearing the Air" guidebook on quitting smoking.
Text2Quit consists of automated, bidirectional text messages, with extra support from e-mails and a web portal. The texts prompt users to track their smoking and report on their cravings and smoking status, with the messages to participants tailored by the reasons for quitting, money saved, and use of medications for smoking cessation. The frequency of texts peaked around the smoker’s chosen quit date, with five texts on that date, approximately two per day in the following week, three per week in the next 2 months, and less than one per week after that.
Considering that an estimated 75% of adults around the world have access to cell phones, text-messaging interventions potentially could puff up the number of quitters, she suggested.
Smartphones aren’t yet as ubiquitous but, still, an estimated 11 million U.S. smokers own a smartphone, Dr. Abroms wrote in a separate study of apps for smoking cessation. We don’t yet know if any of the 400 smoking cessation apps that were available in 2012 work, but her analysis of 98 of the most popular smoking cessation apps found that they seldom include information and strategies that have been proven to help smokers quit.
She and her associates rated 47 apps for iPhones and 51 for Android phones on a 42-point scale, with a top score indicating adherence to the U.S. Public Health Service’s Clinical Practice Guidelines for Treating Tobacco Use and Dependence. The average score was 13. No apps recommended calling a quit line, for example. Only 4% recommended using medications approved for smoking cessation. Only 19% offered practical counseling or advice on how to quit or stay quit (Am. J. Prev. Med. 2013;45:732-36).
On the other hand, it’s possible that national guidelines that were developed for clinical settings don’t apply to mobile apps. If the apps somehow are effective, their reach could magnify any impact, Dr. Abroms suggested. Approximately 779,400 English-language apps for smoking cessation were downloaded per month for Android phones alone during the study period. (The iTunes App Store does not provide numbers for downloads.) That’s more than the approximately 100,000 calls per month to the national quit line in the same time period and 200,000 unique visitors per month to a leading website for smoking cessation, she reported.
"Text messaging programs for smoking cessation have a reasonably good evidence base," according to Dr. Abroms. "The evidence for smartphone apps is still in its early stages. I would not recommend them as a stand-alone intervention, though many with tracking elements may be useful as part of a comprehensive program. Apps that include games could be good as a distraction from smoking."
A separate study found that an experimental "decision support system" app, created for use by nurses on smartphones and tablets, improved rates of screening and counseling for tobacco use by prompting nurses to screen for tobacco use and offered guideline-based treatment recommendations, reported Kenrick Cato, Ph.D. of Columbia University, New York, and his associates.
The 185 registered nurses who were enrolled in advanced practice degree programs handled 14,115 clinic visits, in which they asked patients about smoking status in 84% of visits and offered cessation counseling to 90% of those who expressed a willingness to stop smoking (Oncol. Nurs. Forum 2014;41:145-52).
That compares favorably with federal U.S. data suggesting that tobacco screening happens in approximately 60% of clinic visits, and fewer than 20% of patients get counseling on quitting, Dr. Cato said in a prepared statement released by the university. The federal Healthy People 2020 program aims for tobacco screening in 69% of office visits and counseling rates of 21%, he said.
If further development of the app confirms that it’s useful, it could light a fire under tobacco screening.
Dr. Abroms designed Text2Quit and receives royalties from sales. Dr. Cato reported having no financial disclosures.
On Twitter @sherryboschert
Text-messaging programs on phones seem to help smokers quit. The jury’s still out on smartphone apps for smoking cessation when used by patients, but they may help nurses improve screening, several separate studies suggest.
The interactive text-messaging program Text2Quit helped U.S. smokers quit and stay off cigarettes in a 6-month randomized, controlled trial in 503 adults who smoked at least five cigarettes a day, owned a cell phone with an unlimited service plan for short text messaging, and had expressed an interest in quitting cigarettes. Participants already were avid texters, sending or receiving an average of 29 text messages per day before they enrolled in the study.
At the 6-month follow-up, 20% of 241 people in the Text2Quit group said they had not smoked in the prior 7 days, compared with 10% of 262 people in the control group, reported Lorien C. Abroms, Sc.D., and her associates.
Laboratory analyses of saliva from 54 members of the intervention group and 32 in the control group showed that nearly a quarter of participants had lied about quitting. Text2Quit still was effective, however, with biochemically confirmed abstinence from smoking in 11% of the intervention group and 5% of the control group (Am. J. Prev. Med. 2014 June 5 [doi: 10.1016/j.amepre.2014.04.010]). Those biochemical quit rates are similar to rates reported in studies of other text-messaging programs for smoking cessation or of telephone quit-line counseling, she said.
The results support a meta-analysis of five studies that found mobile phone–based interventions (predominantly text messaging) for smoking cessation increased 6-month quit rates (Cochrane Database Syst. Rev. 2012;11:CD006611 [doi: 10.1002/14651858]). Most U.S. studies, however, have been small, uncontrolled pilot trials with shorter follow-up and no biochemical verification of quit rates, Dr. Abroms said.
Text2Quit costs $30 for a 4-month subscription unless you have a code from a sponsoring organization. When U.S. smokers call the national quit-line number (1-800-QUIT-NOW), residents of some states get offered Text2Quit. More than 50,000 smokers have enrolled since the program became available in 2011, reported Dr. Abroms of George Washington University, Washington. Other text-messaging programs are available, such as the free SmokefreeTXT program from the National Cancer Institute’s smokefree.gov site.
People randomized to the control group in Dr. Abroms’ trial initially were given a link to smokefree.gov, but after the launch of SmokefreeTXT in 2011, new control group members instead were given a link to the National Cancer Institute’s "Clearing the Air" guidebook on quitting smoking.
Text2Quit consists of automated, bidirectional text messages, with extra support from e-mails and a web portal. The texts prompt users to track their smoking and report on their cravings and smoking status, with the messages to participants tailored by the reasons for quitting, money saved, and use of medications for smoking cessation. The frequency of texts peaked around the smoker’s chosen quit date, with five texts on that date, approximately two per day in the following week, three per week in the next 2 months, and less than one per week after that.
Considering that an estimated 75% of adults around the world have access to cell phones, text-messaging interventions potentially could puff up the number of quitters, she suggested.
Smartphones aren’t yet as ubiquitous but, still, an estimated 11 million U.S. smokers own a smartphone, Dr. Abroms wrote in a separate study of apps for smoking cessation. We don’t yet know if any of the 400 smoking cessation apps that were available in 2012 work, but her analysis of 98 of the most popular smoking cessation apps found that they seldom include information and strategies that have been proven to help smokers quit.
She and her associates rated 47 apps for iPhones and 51 for Android phones on a 42-point scale, with a top score indicating adherence to the U.S. Public Health Service’s Clinical Practice Guidelines for Treating Tobacco Use and Dependence. The average score was 13. No apps recommended calling a quit line, for example. Only 4% recommended using medications approved for smoking cessation. Only 19% offered practical counseling or advice on how to quit or stay quit (Am. J. Prev. Med. 2013;45:732-36).
On the other hand, it’s possible that national guidelines that were developed for clinical settings don’t apply to mobile apps. If the apps somehow are effective, their reach could magnify any impact, Dr. Abroms suggested. Approximately 779,400 English-language apps for smoking cessation were downloaded per month for Android phones alone during the study period. (The iTunes App Store does not provide numbers for downloads.) That’s more than the approximately 100,000 calls per month to the national quit line in the same time period and 200,000 unique visitors per month to a leading website for smoking cessation, she reported.
"Text messaging programs for smoking cessation have a reasonably good evidence base," according to Dr. Abroms. "The evidence for smartphone apps is still in its early stages. I would not recommend them as a stand-alone intervention, though many with tracking elements may be useful as part of a comprehensive program. Apps that include games could be good as a distraction from smoking."
A separate study found that an experimental "decision support system" app, created for use by nurses on smartphones and tablets, improved rates of screening and counseling for tobacco use by prompting nurses to screen for tobacco use and offered guideline-based treatment recommendations, reported Kenrick Cato, Ph.D. of Columbia University, New York, and his associates.
The 185 registered nurses who were enrolled in advanced practice degree programs handled 14,115 clinic visits, in which they asked patients about smoking status in 84% of visits and offered cessation counseling to 90% of those who expressed a willingness to stop smoking (Oncol. Nurs. Forum 2014;41:145-52).
That compares favorably with federal U.S. data suggesting that tobacco screening happens in approximately 60% of clinic visits, and fewer than 20% of patients get counseling on quitting, Dr. Cato said in a prepared statement released by the university. The federal Healthy People 2020 program aims for tobacco screening in 69% of office visits and counseling rates of 21%, he said.
If further development of the app confirms that it’s useful, it could light a fire under tobacco screening.
Dr. Abroms designed Text2Quit and receives royalties from sales. Dr. Cato reported having no financial disclosures.
On Twitter @sherryboschert

Be alert to less common, but dangerous, thoracic injuries in children
SAN DIEGO – Many thoracic injuries sustained by children and adolescents can be diagnosed with clinical assessment and chest x-ray, and many heal without surgical intervention, according to Dr. Timothy Fairbanks.
"When the pager goes off and says ‘3-year-old involved in a accident,’ that kid may be going home with a physical exam, stickers, and a high five; or he may require a life-saving procedure" in the emergency department. Dr. Fairbanks, of the division of pediatric surgery at Rady Children’s Hospital of San Diego, said at the University of California, San Diego, Critical Care Summer Session. "There’s complete variability in what we see and how serious the injuries can be."

According to data from the National Pediatric Trauma Registry, 86% of injuries are blunt and 14% are penetrating. Chest injuries "are the second leading cause of death to central nervous system injuries," Dr. Fairbanks said. "Mortality rates for blunt and penetrating injuries are similar. In blunt traumas, most kids don’t die from their blunt thoracic injury, but from a CNS injury that they acquired at the same time. Most of the kids who die from penetrating injuries die in the field before reaching the hospital."
Thoracic injuries occur in about 25% of patients who present to a Level I trauma center. While thoracic injuries are less common than abdominal and extremity injuries are, "they are of potentially higher risk and more lethal," he said. "Most can be treated successfully. Male to female injury rate is 2:1 to 3:1 in favor of males having more traumas."
He classifies thoracic trauma injuries by anatomy (rib, pulmonary, bronchial), blunt vs. penetrating, and threat to life (immediate or potentially life threatening). Motor vehicles are the most common mechanism of thoracic injury, and children have an increased risk in all traumas of auto vs. pedestrian, compared with adults. "When children become teenagers, their mechanisms of injuries approach those of the data for adults," Dr. Fairbanks explained. "We see more penetrating knife and gunshot wounds to the chest, although they are rare in our younger patient population. Tracheobronchial lacerations are more common in children, compared with adults. Aortic disruptions are less likely in children."
Common thoracic injuries that he and his associates see at Rady Children’s Hospital are lung contusion, pneumothorax, hemothorax, and fractures to the ribs, sternum, or scapula. Less common "but perhaps more dangerous injuries" are those to the heart, aorta, trachea, bronchi, and diaphragm. "The most common immediately life-threatening thoracic injuries in children are airway obstruction, pneumothorax, hemothorax, and cardiac tamponade," he said. "A large percentage of thoracic injuries have stable vital signs at presentation. Rib fractures are less common in children and are a marker for a significant mechanism of injury or force. Mediastinal structures are more mobile, making tension pneumothorax a bigger problem."
Diagnosis and treatment of thoracic injuries proceeds simultaneously, with an initial goal to rule out life-threatening injuries, which should be identified and treated during the initial resuscitation phase. This includes making sure the airway is clear and secure and providing supplemental oxygen. "If endotracheal intubation is needed, check the position," he advised. "You want to see bilateral chest rise and CO2 waveform on your monitor. It’s very common for a child to have a right mainstem intubation and no breath sounds on the left side." He also makes it a point to assess their ventilation and treat their pneumothorax. "Don’t wait for the chest x-ray if you have a good clinical suspicion," he said.
A chest x-ray can often guide your management decisions in cases of thoracic trauma, while a FAST scan – specifically an ultrasound – is good for seeing a cardiac tamponade.
Sometimes thoracic injuries require an immediate thoracotomy in the emergency department, but its indications "are controversial," Dr. Fairbanks said. "It’s a potentially life-threatening maneuver, especially with penetrating cardiac injuries." The indications for emergency department thoracotomy are post-traumatic arrest or near arrest in all cases of penetrating thoracic injuries; in blunt trauma with loss of vital signs in the ED; or in blunt trauma with loss of vital signs in route to the ED.
"One of the things we struggle with in pediatric trauma is the timing at which they lost the vital signs in the field," he said. "After 20 minutes the chance of survival is almost nil. However, the family is going to want to know that you did everything possible to save their 3- or 4-year-old child."
If the patient is stable, complete the physical exam. "You’re looking for tachypnea, tenderness to the chest wall and abrasions, or signs of thoracic trauma that require further investigation," he said. Important signs include cyanosis, dyspnea, tracheal deviation, hoarseness, jugular engagement, and subcutaneous emphysema.
Chest auscultation is recommended and an anteroposterior (AP) chest x-ray becomes valuable, "because it’s quick, simple, and yields a lot of information," he said. He characterized a thoracic CT scan as "an excellent study" that can help with the diagnosis of aortic and diaphragmatic injuries which can be missed on chest x-ray. "However, there is a lot more radiation with a chest CT," Dr. Fairbanks noted. "Only 1 in 200 chest CTs for trauma yields a new diagnosis." Other studies to consider include EKG, echocardiogram, bronchoscopy, video-assisted thoracic surgery, radionuclide bone scan, and MRI.
A thoracotomy is indicated when the patient is coding or near coding. The other indications are penetrating wound of the heart or great vessels; massive or continuous intrathoracic bleeding; open pneumothorax with major chest wall defect; aortogram indicating injury to the aorta or major branch; massive or continuing air leak, indicating injury to a major airway; cardiac tamponade; esophageal perforation, or diaphragmatic rupture.
Chest wall soft-tissue injuries are usually not clinically significant, "but they’re a marker for a more serious injury under a bruise," he said. "Rib fractures are less common in children. It’s an indicator of significant force. Treatment is pain control and prevention of atelectasis, which is not as big of a problem in kids as it is in adults. They will heal in 6 weeks. Consider child abuse, specifically in cases of multiple rib fractures and those that don’t make sense with the mechanism of reported injury, or rib fractures that are at different stages of healing."
Dr. Fairbanks said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Many thoracic injuries sustained by children and adolescents can be diagnosed with clinical assessment and chest x-ray, and many heal without surgical intervention, according to Dr. Timothy Fairbanks.
"When the pager goes off and says ‘3-year-old involved in a accident,’ that kid may be going home with a physical exam, stickers, and a high five; or he may require a life-saving procedure" in the emergency department. Dr. Fairbanks, of the division of pediatric surgery at Rady Children’s Hospital of San Diego, said at the University of California, San Diego, Critical Care Summer Session. "There’s complete variability in what we see and how serious the injuries can be."
According to data from the National Pediatric Trauma Registry, 86% of injuries are blunt and 14% are penetrating. Chest injuries "are the second leading cause of death to central nervous system injuries," Dr. Fairbanks said. "Mortality rates for blunt and penetrating injuries are similar. In blunt traumas, most kids don’t die from their blunt thoracic injury, but from a CNS injury that they acquired at the same time. Most of the kids who die from penetrating injuries die in the field before reaching the hospital."
Thoracic injuries occur in about 25% of patients who present to a Level I trauma center. While thoracic injuries are less common than abdominal and extremity injuries are, "they are of potentially higher risk and more lethal," he said. "Most can be treated successfully. Male to female injury rate is 2:1 to 3:1 in favor of males having more traumas."
He classifies thoracic trauma injuries by anatomy (rib, pulmonary, bronchial), blunt vs. penetrating, and threat to life (immediate or potentially life threatening). Motor vehicles are the most common mechanism of thoracic injury, and children have an increased risk in all traumas of auto vs. pedestrian, compared with adults. "When children become teenagers, their mechanisms of injuries approach those of the data for adults," Dr. Fairbanks explained. "We see more penetrating knife and gunshot wounds to the chest, although they are rare in our younger patient population. Tracheobronchial lacerations are more common in children, compared with adults. Aortic disruptions are less likely in children."
Common thoracic injuries that he and his associates see at Rady Children’s Hospital are lung contusion, pneumothorax, hemothorax, and fractures to the ribs, sternum, or scapula. Less common "but perhaps more dangerous injuries" are those to the heart, aorta, trachea, bronchi, and diaphragm. "The most common immediately life-threatening thoracic injuries in children are airway obstruction, pneumothorax, hemothorax, and cardiac tamponade," he said. "A large percentage of thoracic injuries have stable vital signs at presentation. Rib fractures are less common in children and are a marker for a significant mechanism of injury or force. Mediastinal structures are more mobile, making tension pneumothorax a bigger problem."
Diagnosis and treatment of thoracic injuries proceeds simultaneously, with an initial goal to rule out life-threatening injuries, which should be identified and treated during the initial resuscitation phase. This includes making sure the airway is clear and secure and providing supplemental oxygen. "If endotracheal intubation is needed, check the position," he advised. "You want to see bilateral chest rise and CO2 waveform on your monitor. It’s very common for a child to have a right mainstem intubation and no breath sounds on the left side." He also makes it a point to assess their ventilation and treat their pneumothorax. "Don’t wait for the chest x-ray if you have a good clinical suspicion," he said.
A chest x-ray can often guide your management decisions in cases of thoracic trauma, while a FAST scan – specifically an ultrasound – is good for seeing a cardiac tamponade.
Sometimes thoracic injuries require an immediate thoracotomy in the emergency department, but its indications "are controversial," Dr. Fairbanks said. "It’s a potentially life-threatening maneuver, especially with penetrating cardiac injuries." The indications for emergency department thoracotomy are post-traumatic arrest or near arrest in all cases of penetrating thoracic injuries; in blunt trauma with loss of vital signs in the ED; or in blunt trauma with loss of vital signs in route to the ED.
"One of the things we struggle with in pediatric trauma is the timing at which they lost the vital signs in the field," he said. "After 20 minutes the chance of survival is almost nil. However, the family is going to want to know that you did everything possible to save their 3- or 4-year-old child."
If the patient is stable, complete the physical exam. "You’re looking for tachypnea, tenderness to the chest wall and abrasions, or signs of thoracic trauma that require further investigation," he said. Important signs include cyanosis, dyspnea, tracheal deviation, hoarseness, jugular engagement, and subcutaneous emphysema.
Chest auscultation is recommended and an anteroposterior (AP) chest x-ray becomes valuable, "because it’s quick, simple, and yields a lot of information," he said. He characterized a thoracic CT scan as "an excellent study" that can help with the diagnosis of aortic and diaphragmatic injuries which can be missed on chest x-ray. "However, there is a lot more radiation with a chest CT," Dr. Fairbanks noted. "Only 1 in 200 chest CTs for trauma yields a new diagnosis." Other studies to consider include EKG, echocardiogram, bronchoscopy, video-assisted thoracic surgery, radionuclide bone scan, and MRI.
A thoracotomy is indicated when the patient is coding or near coding. The other indications are penetrating wound of the heart or great vessels; massive or continuous intrathoracic bleeding; open pneumothorax with major chest wall defect; aortogram indicating injury to the aorta or major branch; massive or continuing air leak, indicating injury to a major airway; cardiac tamponade; esophageal perforation, or diaphragmatic rupture.
Chest wall soft-tissue injuries are usually not clinically significant, "but they’re a marker for a more serious injury under a bruise," he said. "Rib fractures are less common in children. It’s an indicator of significant force. Treatment is pain control and prevention of atelectasis, which is not as big of a problem in kids as it is in adults. They will heal in 6 weeks. Consider child abuse, specifically in cases of multiple rib fractures and those that don’t make sense with the mechanism of reported injury, or rib fractures that are at different stages of healing."
Dr. Fairbanks said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Many thoracic injuries sustained by children and adolescents can be diagnosed with clinical assessment and chest x-ray, and many heal without surgical intervention, according to Dr. Timothy Fairbanks.
"When the pager goes off and says ‘3-year-old involved in a accident,’ that kid may be going home with a physical exam, stickers, and a high five; or he may require a life-saving procedure" in the emergency department. Dr. Fairbanks, of the division of pediatric surgery at Rady Children’s Hospital of San Diego, said at the University of California, San Diego, Critical Care Summer Session. "There’s complete variability in what we see and how serious the injuries can be."
According to data from the National Pediatric Trauma Registry, 86% of injuries are blunt and 14% are penetrating. Chest injuries "are the second leading cause of death to central nervous system injuries," Dr. Fairbanks said. "Mortality rates for blunt and penetrating injuries are similar. In blunt traumas, most kids don’t die from their blunt thoracic injury, but from a CNS injury that they acquired at the same time. Most of the kids who die from penetrating injuries die in the field before reaching the hospital."
Thoracic injuries occur in about 25% of patients who present to a Level I trauma center. While thoracic injuries are less common than abdominal and extremity injuries are, "they are of potentially higher risk and more lethal," he said. "Most can be treated successfully. Male to female injury rate is 2:1 to 3:1 in favor of males having more traumas."
He classifies thoracic trauma injuries by anatomy (rib, pulmonary, bronchial), blunt vs. penetrating, and threat to life (immediate or potentially life threatening). Motor vehicles are the most common mechanism of thoracic injury, and children have an increased risk in all traumas of auto vs. pedestrian, compared with adults. "When children become teenagers, their mechanisms of injuries approach those of the data for adults," Dr. Fairbanks explained. "We see more penetrating knife and gunshot wounds to the chest, although they are rare in our younger patient population. Tracheobronchial lacerations are more common in children, compared with adults. Aortic disruptions are less likely in children."
Common thoracic injuries that he and his associates see at Rady Children’s Hospital are lung contusion, pneumothorax, hemothorax, and fractures to the ribs, sternum, or scapula. Less common "but perhaps more dangerous injuries" are those to the heart, aorta, trachea, bronchi, and diaphragm. "The most common immediately life-threatening thoracic injuries in children are airway obstruction, pneumothorax, hemothorax, and cardiac tamponade," he said. "A large percentage of thoracic injuries have stable vital signs at presentation. Rib fractures are less common in children and are a marker for a significant mechanism of injury or force. Mediastinal structures are more mobile, making tension pneumothorax a bigger problem."
Diagnosis and treatment of thoracic injuries proceeds simultaneously, with an initial goal to rule out life-threatening injuries, which should be identified and treated during the initial resuscitation phase. This includes making sure the airway is clear and secure and providing supplemental oxygen. "If endotracheal intubation is needed, check the position," he advised. "You want to see bilateral chest rise and CO2 waveform on your monitor. It’s very common for a child to have a right mainstem intubation and no breath sounds on the left side." He also makes it a point to assess their ventilation and treat their pneumothorax. "Don’t wait for the chest x-ray if you have a good clinical suspicion," he said.
A chest x-ray can often guide your management decisions in cases of thoracic trauma, while a FAST scan – specifically an ultrasound – is good for seeing a cardiac tamponade.
Sometimes thoracic injuries require an immediate thoracotomy in the emergency department, but its indications "are controversial," Dr. Fairbanks said. "It’s a potentially life-threatening maneuver, especially with penetrating cardiac injuries." The indications for emergency department thoracotomy are post-traumatic arrest or near arrest in all cases of penetrating thoracic injuries; in blunt trauma with loss of vital signs in the ED; or in blunt trauma with loss of vital signs in route to the ED.
"One of the things we struggle with in pediatric trauma is the timing at which they lost the vital signs in the field," he said. "After 20 minutes the chance of survival is almost nil. However, the family is going to want to know that you did everything possible to save their 3- or 4-year-old child."
If the patient is stable, complete the physical exam. "You’re looking for tachypnea, tenderness to the chest wall and abrasions, or signs of thoracic trauma that require further investigation," he said. Important signs include cyanosis, dyspnea, tracheal deviation, hoarseness, jugular engagement, and subcutaneous emphysema.
Chest auscultation is recommended and an anteroposterior (AP) chest x-ray becomes valuable, "because it’s quick, simple, and yields a lot of information," he said. He characterized a thoracic CT scan as "an excellent study" that can help with the diagnosis of aortic and diaphragmatic injuries which can be missed on chest x-ray. "However, there is a lot more radiation with a chest CT," Dr. Fairbanks noted. "Only 1 in 200 chest CTs for trauma yields a new diagnosis." Other studies to consider include EKG, echocardiogram, bronchoscopy, video-assisted thoracic surgery, radionuclide bone scan, and MRI.
A thoracotomy is indicated when the patient is coding or near coding. The other indications are penetrating wound of the heart or great vessels; massive or continuous intrathoracic bleeding; open pneumothorax with major chest wall defect; aortogram indicating injury to the aorta or major branch; massive or continuing air leak, indicating injury to a major airway; cardiac tamponade; esophageal perforation, or diaphragmatic rupture.
Chest wall soft-tissue injuries are usually not clinically significant, "but they’re a marker for a more serious injury under a bruise," he said. "Rib fractures are less common in children. It’s an indicator of significant force. Treatment is pain control and prevention of atelectasis, which is not as big of a problem in kids as it is in adults. They will heal in 6 weeks. Consider child abuse, specifically in cases of multiple rib fractures and those that don’t make sense with the mechanism of reported injury, or rib fractures that are at different stages of healing."
Dr. Fairbanks said that he had no relevant financial conflicts to disclose.
EXPERT ANALYSIS AT THE UCSD CRITICAL CARE SUMMER SESSION

Additional chronic conditions seen in 87% of diabetes patients
In 2010, 87% of diabetes patients who visited an office-based physician had at least one additional chronic condition, the National Center for Health Statistics reported.
For diabetes patients under the age of 25 years, just over half (51%) of their visits involved patients who had two or more additional chronic conditions, and the number of conditions increased with age. Among those aged 25-44 years, 72% of visits in 2010 involved patients with two or more chronic conditions, according to the NCHS.
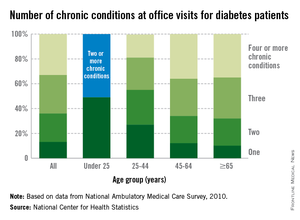
In the 45- to 64-year age group, 88% of visits were made by patients with two or more chronic conditions, with 36% involving patients who had four or more such conditions. Among those aged 65 years and over, 90% of visits by patients with diabetes were made by those with two or more additional chronic conditions, the NCHS report said.
The analysis was based on data from the National Ambulatory Medical Care Survey. Information was collected on 13 other chronic conditions besides diabetes: arthritis, asthma, cancer, chronic kidney disease, chronic obstructive pulmonary disease, heart failure, coronary heart disease, depression, hyperlipidemia, hypertension, obesity, osteoporosis, and stroke.
In 2010, 87% of diabetes patients who visited an office-based physician had at least one additional chronic condition, the National Center for Health Statistics reported.
For diabetes patients under the age of 25 years, just over half (51%) of their visits involved patients who had two or more additional chronic conditions, and the number of conditions increased with age. Among those aged 25-44 years, 72% of visits in 2010 involved patients with two or more chronic conditions, according to the NCHS.
In the 45- to 64-year age group, 88% of visits were made by patients with two or more chronic conditions, with 36% involving patients who had four or more such conditions. Among those aged 65 years and over, 90% of visits by patients with diabetes were made by those with two or more additional chronic conditions, the NCHS report said.
The analysis was based on data from the National Ambulatory Medical Care Survey. Information was collected on 13 other chronic conditions besides diabetes: arthritis, asthma, cancer, chronic kidney disease, chronic obstructive pulmonary disease, heart failure, coronary heart disease, depression, hyperlipidemia, hypertension, obesity, osteoporosis, and stroke.
In 2010, 87% of diabetes patients who visited an office-based physician had at least one additional chronic condition, the National Center for Health Statistics reported.
For diabetes patients under the age of 25 years, just over half (51%) of their visits involved patients who had two or more additional chronic conditions, and the number of conditions increased with age. Among those aged 25-44 years, 72% of visits in 2010 involved patients with two or more chronic conditions, according to the NCHS.
In the 45- to 64-year age group, 88% of visits were made by patients with two or more chronic conditions, with 36% involving patients who had four or more such conditions. Among those aged 65 years and over, 90% of visits by patients with diabetes were made by those with two or more additional chronic conditions, the NCHS report said.
The analysis was based on data from the National Ambulatory Medical Care Survey. Information was collected on 13 other chronic conditions besides diabetes: arthritis, asthma, cancer, chronic kidney disease, chronic obstructive pulmonary disease, heart failure, coronary heart disease, depression, hyperlipidemia, hypertension, obesity, osteoporosis, and stroke.
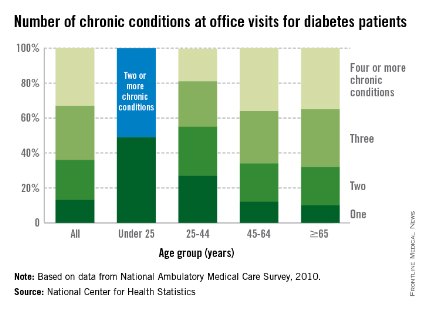
Combined hormonal contraception raises VTE risk fivefold
Combined hormonal contraception raises the risk for venous thromboembolism fivefold overall, with certain formulations increasing that risk even further and with thrombophilic genotypes raising it further still, according to a report published online Aug. 5 in Obstetrics & Gynecology.
To assess the association between various types of hormonal contraception and venous thromboembolism (VTE) risk, Swedish investigators performed a nationwide case-control study involving 948 women aged 18-54 years who were treated for deep vein thrombosis of the leg or pelvis, pulmonary embolism, or both conditions during a 6-year period and 902 healthy control subjects from the general population. All the women provided a blood sample for genetic analysis and provided detailed information regarding their contraceptive use, body mass index (BMI), smoking status, and recent history of immobilization, said Dr. Annica Bergendal of the Centre for Pharmacoepidemiology, Karolinska Institutet, Stockholm, and her associates.

A total of 32.8% of the case group reported current use of combined hormonal contraception, compared with only 11.9% of the control group. Overall, current use of combined hormonal contraception was associated with a fivefold increased risk of VTE, with an adjusted OR of 5.3. "Combinations with the progestogen desogestrel yielded the highest risk estimate (adjusted OR, 11.4), followed by drospirenone (adjusted OR, 8.4). The adjusted OR could not be calculated for lynestrenol because there were no exposed women in the control group," the investigators wrote (Obstet. Gynecol. 2014;124:600-9).
In contrast, progestogen-only contraception did not increase the risk of VTE, except at the highest dose level.
Women who used combination contraception and were carriers of factor V Leiden or of the prothrombin gene mutation were at extremely high risk for VTE, nearly 20-fold for either, compared with nonusers and noncarriers. Women who used combination contraception and were carriers of factor XIII had a much lower, but still elevated, risk for VTE (OR, 2.8).
All of these differences in risk appeared to be independent of BMI, smoking status, and recent history of immobilization, Dr. Bergendal and her associates added.
This study was supported by unrestricted grants from Janssen-Cilag, Novartis, Organon, Schering, Wyeth, AFA Insurance, and the Medical Products Agency. Dr. Bergendal and her associates reported no relevant financial conflicts.
Combined hormonal contraception raises the risk for venous thromboembolism fivefold overall, with certain formulations increasing that risk even further and with thrombophilic genotypes raising it further still, according to a report published online Aug. 5 in Obstetrics & Gynecology.
To assess the association between various types of hormonal contraception and venous thromboembolism (VTE) risk, Swedish investigators performed a nationwide case-control study involving 948 women aged 18-54 years who were treated for deep vein thrombosis of the leg or pelvis, pulmonary embolism, or both conditions during a 6-year period and 902 healthy control subjects from the general population. All the women provided a blood sample for genetic analysis and provided detailed information regarding their contraceptive use, body mass index (BMI), smoking status, and recent history of immobilization, said Dr. Annica Bergendal of the Centre for Pharmacoepidemiology, Karolinska Institutet, Stockholm, and her associates.
A total of 32.8% of the case group reported current use of combined hormonal contraception, compared with only 11.9% of the control group. Overall, current use of combined hormonal contraception was associated with a fivefold increased risk of VTE, with an adjusted OR of 5.3. "Combinations with the progestogen desogestrel yielded the highest risk estimate (adjusted OR, 11.4), followed by drospirenone (adjusted OR, 8.4). The adjusted OR could not be calculated for lynestrenol because there were no exposed women in the control group," the investigators wrote (Obstet. Gynecol. 2014;124:600-9).
In contrast, progestogen-only contraception did not increase the risk of VTE, except at the highest dose level.
Women who used combination contraception and were carriers of factor V Leiden or of the prothrombin gene mutation were at extremely high risk for VTE, nearly 20-fold for either, compared with nonusers and noncarriers. Women who used combination contraception and were carriers of factor XIII had a much lower, but still elevated, risk for VTE (OR, 2.8).
All of these differences in risk appeared to be independent of BMI, smoking status, and recent history of immobilization, Dr. Bergendal and her associates added.
This study was supported by unrestricted grants from Janssen-Cilag, Novartis, Organon, Schering, Wyeth, AFA Insurance, and the Medical Products Agency. Dr. Bergendal and her associates reported no relevant financial conflicts.
Combined hormonal contraception raises the risk for venous thromboembolism fivefold overall, with certain formulations increasing that risk even further and with thrombophilic genotypes raising it further still, according to a report published online Aug. 5 in Obstetrics & Gynecology.
To assess the association between various types of hormonal contraception and venous thromboembolism (VTE) risk, Swedish investigators performed a nationwide case-control study involving 948 women aged 18-54 years who were treated for deep vein thrombosis of the leg or pelvis, pulmonary embolism, or both conditions during a 6-year period and 902 healthy control subjects from the general population. All the women provided a blood sample for genetic analysis and provided detailed information regarding their contraceptive use, body mass index (BMI), smoking status, and recent history of immobilization, said Dr. Annica Bergendal of the Centre for Pharmacoepidemiology, Karolinska Institutet, Stockholm, and her associates.
A total of 32.8% of the case group reported current use of combined hormonal contraception, compared with only 11.9% of the control group. Overall, current use of combined hormonal contraception was associated with a fivefold increased risk of VTE, with an adjusted OR of 5.3. "Combinations with the progestogen desogestrel yielded the highest risk estimate (adjusted OR, 11.4), followed by drospirenone (adjusted OR, 8.4). The adjusted OR could not be calculated for lynestrenol because there were no exposed women in the control group," the investigators wrote (Obstet. Gynecol. 2014;124:600-9).
In contrast, progestogen-only contraception did not increase the risk of VTE, except at the highest dose level.
Women who used combination contraception and were carriers of factor V Leiden or of the prothrombin gene mutation were at extremely high risk for VTE, nearly 20-fold for either, compared with nonusers and noncarriers. Women who used combination contraception and were carriers of factor XIII had a much lower, but still elevated, risk for VTE (OR, 2.8).
All of these differences in risk appeared to be independent of BMI, smoking status, and recent history of immobilization, Dr. Bergendal and her associates added.
This study was supported by unrestricted grants from Janssen-Cilag, Novartis, Organon, Schering, Wyeth, AFA Insurance, and the Medical Products Agency. Dr. Bergendal and her associates reported no relevant financial conflicts.
FROM OBSTETRICS & GYNECOLOGY
Key clinical point: Combined hormonal contraception increases the risk of VTE, especially in women with certain thrombophilic genotypes.
Major finding: Current use of combined hormonal contraception was associated with a fivefold increased risk of VTE (adjusted OR, 5.3); combinations with the progestogen desogestrel yielded the highest risk estimate (adjusted OR, 11.4), followed by those containing drospirenone (adjusted OR, 8.4).
Data source: A nationwide Swedish case-control study involving 948 women aged 18-54 years treated for deep vein thrombosis or pulmonary embolism over the course of 6 years and 902 control subjects.
Disclosures: This study was supported by unrestricted grants from Janssen-Cilag, Novartis, Organon, Schering, Wyeth, AFA Insurance, and the Medical Products Agency. Dr. Bergendal and her associates reported no financial conflicts.

Guideline recommends study for unexplained daytime sleepiness
Clinicians should recommend a sleep study using polysomnography for adults who have unexplained daytime sleepiness, according to a clinical practice guideline on diagnosing obstructive sleep apnea.
The guideline was published online Aug. 4 in Annals of Internal Medicine.
There is still "considerable" controversy concerning the type and level of respiratory abnormality that defines obstructive sleep apnea (OSA), as well as the presence and type of signs or symptoms that are diagnostic of the disorder, said Dr. Amir Qaseem, director of clinical policy at the American College of Physicians, Philadelphia.
To formulate a clinical practice guideline, Dr. Qaseem and his associates performed a comprehensive review of the literature through May 2013, which included a comparative effectiveness technology review of portable sleep monitors sponsored by the Agency for Healthcare Research and Quality.
The guideline recommends that internists, family physicians, and other clinicians focus assessment of OSA on their adult patients who have unexplained daytime sleepiness. To do so, they must rule out other potential causes such as thyroid disease or gastroesophageal reflux disease.
Then, clinicians should evaluate patients for risk factors and common presenting symptoms of the disorder. Chief among risk factors is obesity, and frequent symptoms include unintentionally falling asleep during waking hours, unrefreshing sleep, fatigue, insomnia, and snoring (Ann. Intern. Med. 2014;161:210-20).
Once OSA is suspected, the guideline recommends full-night, in-laboratory polysomnography to establish the diagnosis. This requires specialized facilities, is expensive, and demands that patients "spend the night under observation in a foreign environment," but yields the most accurate diagnostic information.
Portable sleep monitors for home use are an alternative if a sleep laboratory is not available, but these can yield substantially different scores on the apnea-hypopnea index, usually because of data loss that limits interpretation of the results.
In addition, the ability of portable sleep monitors to diagnose OSA is questionable in the subset of patients who have comorbid conditions such as chronic lung disease, heart failure, or neurologic disorders.
Development of this clinical practice guideline was supported solely by the American College of Physicians. Dr. Qaseem and his associates reported no relevant financial conflicts of interest.
Clinicians should recommend a sleep study using polysomnography for adults who have unexplained daytime sleepiness, according to a clinical practice guideline on diagnosing obstructive sleep apnea.
The guideline was published online Aug. 4 in Annals of Internal Medicine.
There is still "considerable" controversy concerning the type and level of respiratory abnormality that defines obstructive sleep apnea (OSA), as well as the presence and type of signs or symptoms that are diagnostic of the disorder, said Dr. Amir Qaseem, director of clinical policy at the American College of Physicians, Philadelphia.
To formulate a clinical practice guideline, Dr. Qaseem and his associates performed a comprehensive review of the literature through May 2013, which included a comparative effectiveness technology review of portable sleep monitors sponsored by the Agency for Healthcare Research and Quality.
The guideline recommends that internists, family physicians, and other clinicians focus assessment of OSA on their adult patients who have unexplained daytime sleepiness. To do so, they must rule out other potential causes such as thyroid disease or gastroesophageal reflux disease.
Then, clinicians should evaluate patients for risk factors and common presenting symptoms of the disorder. Chief among risk factors is obesity, and frequent symptoms include unintentionally falling asleep during waking hours, unrefreshing sleep, fatigue, insomnia, and snoring (Ann. Intern. Med. 2014;161:210-20).
Once OSA is suspected, the guideline recommends full-night, in-laboratory polysomnography to establish the diagnosis. This requires specialized facilities, is expensive, and demands that patients "spend the night under observation in a foreign environment," but yields the most accurate diagnostic information.
Portable sleep monitors for home use are an alternative if a sleep laboratory is not available, but these can yield substantially different scores on the apnea-hypopnea index, usually because of data loss that limits interpretation of the results.
In addition, the ability of portable sleep monitors to diagnose OSA is questionable in the subset of patients who have comorbid conditions such as chronic lung disease, heart failure, or neurologic disorders.
Development of this clinical practice guideline was supported solely by the American College of Physicians. Dr. Qaseem and his associates reported no relevant financial conflicts of interest.
Clinicians should recommend a sleep study using polysomnography for adults who have unexplained daytime sleepiness, according to a clinical practice guideline on diagnosing obstructive sleep apnea.
The guideline was published online Aug. 4 in Annals of Internal Medicine.
There is still "considerable" controversy concerning the type and level of respiratory abnormality that defines obstructive sleep apnea (OSA), as well as the presence and type of signs or symptoms that are diagnostic of the disorder, said Dr. Amir Qaseem, director of clinical policy at the American College of Physicians, Philadelphia.
To formulate a clinical practice guideline, Dr. Qaseem and his associates performed a comprehensive review of the literature through May 2013, which included a comparative effectiveness technology review of portable sleep monitors sponsored by the Agency for Healthcare Research and Quality.
The guideline recommends that internists, family physicians, and other clinicians focus assessment of OSA on their adult patients who have unexplained daytime sleepiness. To do so, they must rule out other potential causes such as thyroid disease or gastroesophageal reflux disease.
Then, clinicians should evaluate patients for risk factors and common presenting symptoms of the disorder. Chief among risk factors is obesity, and frequent symptoms include unintentionally falling asleep during waking hours, unrefreshing sleep, fatigue, insomnia, and snoring (Ann. Intern. Med. 2014;161:210-20).
Once OSA is suspected, the guideline recommends full-night, in-laboratory polysomnography to establish the diagnosis. This requires specialized facilities, is expensive, and demands that patients "spend the night under observation in a foreign environment," but yields the most accurate diagnostic information.
Portable sleep monitors for home use are an alternative if a sleep laboratory is not available, but these can yield substantially different scores on the apnea-hypopnea index, usually because of data loss that limits interpretation of the results.
In addition, the ability of portable sleep monitors to diagnose OSA is questionable in the subset of patients who have comorbid conditions such as chronic lung disease, heart failure, or neurologic disorders.
Development of this clinical practice guideline was supported solely by the American College of Physicians. Dr. Qaseem and his associates reported no relevant financial conflicts of interest.
FROM ANNALS OF INTERNAL MEDICINE
Complications from influenzalike illnesses occur in one-third of children
One in three (35.3%) children developed complications with influenzalike illnesses, and children with neurologic or neuromuscular conditions were at highest risk for complications, according to a recent study.
The most commonly developed complication was pneumonia (26.1% of the participants), but the overall rate of complications did not vary among those who had influenza, compared with those with a different virus, Dr. Rakesh D. Mistry of the University of Colorado in Aurora, and his colleagues reported online (Pediatrics 2014 Aug. 4 [doi:10.1542/peds.2014-0505]). The next most common complications were respiratory failure (7.1%) and seizures (5.8%).
The researchers prospectively assessed 241 children aged 0-19 years who presented to a children’s hospital emergency department with influenzalike illness – fever plus a cough or sore throat without another cause – from early winter 2008 to late spring 2010. The study included only children with moderate to severe symptoms (defined by physicians’ decision to do venipuncture and respiratory viral testing) who did not already have severe complications. Severe complications included seizures, encephalopathy, pneumonia, bacteremia, bacterial tracheitis, respiratory failure, myocarditis, or death.
Overall, 24.9% of the children had influenza, 28.2% had no virus detected, 14.5% had rhinovirus, 11.6% had respiratory syncytial virus, and the remainder had human metapneumovirus, adenovirus or parainfluenza viruses. Among children with influenza, the risk of developing pneumonia was 7.6 times higher with the H1N1 strain than with other strains.
Asthma was the most common chronic medical condition among the 53.5% of children who had one. Although children with neurologic or neuromuscular conditions were four times more likely to develop complications, no other high-risk conditions were linked to complications, and 41.2% of children developing complications had no underlying conditions.
The authors wrote that their findings regarding children with underlying conditions "support the need for increased preventive measures in this subgroup of children, including influenza vaccination and early institution of antiviral treatment."
The study was supported in part by the Commonwealth of Pennsylvania Department of Health. The authors reported no disclosures.
In an attempt to identify those at risk for serious complications of influenza, investigators analyzed outcomes for 241 children who presented to the emergency department, met the CDC definition of influenzalike illness (ILI) – fever and sore throat or cough – and had moderate to severe illness based on a medical decision to obtain a venipuncture and multiplex polymerase chain reaction (PCR) respiratory viral testing at the time of the visit. While influenza was confirmed in 25% (80% with influenza A), many other viral respiratory pathogens also were identified, confirming that ILI is not specific for influenza in children. More than one virus was detected in 12%. A chronic medical condition was noted in about one-half, most commonly neurologic and neuromuscular diseases or asthma, and complications including pneumonia and respiratory failure occurred in 30% of those with influenza and 35% with non-influenza viral infection.
Consistent with American Academy of Pediatrics and the Centers for Disease Control and Prevention guidelines, the authors recommend empiric oseltamivir for a child with influenzalike illness who has a condition that places them at risk for influenza complications, particularly if the suspected agent is the pandemic H1N1 virus. However, the data highlight the difficulty in identifying all children who may benefit from oseltamivir therapy, especially given that the majority of children with ILI don’t have influenza, oseltamivir therapy is best initiated within 48 hours of onset of symptoms, the most readily available test (rapid influenza testing) generally lacks sensitivity to identify those with influenza, and PCR testing is expensive and not available in many hospital emergency rooms.
Approximately half of the study patients had a history of influenza vaccine, and it is unclear whether this represented one or two doses in the younger patients. The results underscore the importance of influenza vaccine, and this year the AAP has issued a preference for the nasal live attenuated vaccine for any child aged 2-8 years who doesn’t have an underlying contraindication – emphasizing that vaccination should not be delayed in order to obtain a specific product for either dose.
Dr. Mary Anne Jackson is director of the division of infectious diseases and associate chair of community and regional pediatric collaboration at Children’s Mercy Hospital & Clinics, and professor of pediatrics at University of Missouri–Kansas City. She has no disclosures.
In an attempt to identify those at risk for serious complications of influenza, investigators analyzed outcomes for 241 children who presented to the emergency department, met the CDC definition of influenzalike illness (ILI) – fever and sore throat or cough – and had moderate to severe illness based on a medical decision to obtain a venipuncture and multiplex polymerase chain reaction (PCR) respiratory viral testing at the time of the visit. While influenza was confirmed in 25% (80% with influenza A), many other viral respiratory pathogens also were identified, confirming that ILI is not specific for influenza in children. More than one virus was detected in 12%. A chronic medical condition was noted in about one-half, most commonly neurologic and neuromuscular diseases or asthma, and complications including pneumonia and respiratory failure occurred in 30% of those with influenza and 35% with non-influenza viral infection.
Consistent with American Academy of Pediatrics and the Centers for Disease Control and Prevention guidelines, the authors recommend empiric oseltamivir for a child with influenzalike illness who has a condition that places them at risk for influenza complications, particularly if the suspected agent is the pandemic H1N1 virus. However, the data highlight the difficulty in identifying all children who may benefit from oseltamivir therapy, especially given that the majority of children with ILI don’t have influenza, oseltamivir therapy is best initiated within 48 hours of onset of symptoms, the most readily available test (rapid influenza testing) generally lacks sensitivity to identify those with influenza, and PCR testing is expensive and not available in many hospital emergency rooms.
Approximately half of the study patients had a history of influenza vaccine, and it is unclear whether this represented one or two doses in the younger patients. The results underscore the importance of influenza vaccine, and this year the AAP has issued a preference for the nasal live attenuated vaccine for any child aged 2-8 years who doesn’t have an underlying contraindication – emphasizing that vaccination should not be delayed in order to obtain a specific product for either dose.
Dr. Mary Anne Jackson is director of the division of infectious diseases and associate chair of community and regional pediatric collaboration at Children’s Mercy Hospital & Clinics, and professor of pediatrics at University of Missouri–Kansas City. She has no disclosures.
In an attempt to identify those at risk for serious complications of influenza, investigators analyzed outcomes for 241 children who presented to the emergency department, met the CDC definition of influenzalike illness (ILI) – fever and sore throat or cough – and had moderate to severe illness based on a medical decision to obtain a venipuncture and multiplex polymerase chain reaction (PCR) respiratory viral testing at the time of the visit. While influenza was confirmed in 25% (80% with influenza A), many other viral respiratory pathogens also were identified, confirming that ILI is not specific for influenza in children. More than one virus was detected in 12%. A chronic medical condition was noted in about one-half, most commonly neurologic and neuromuscular diseases or asthma, and complications including pneumonia and respiratory failure occurred in 30% of those with influenza and 35% with non-influenza viral infection.
Consistent with American Academy of Pediatrics and the Centers for Disease Control and Prevention guidelines, the authors recommend empiric oseltamivir for a child with influenzalike illness who has a condition that places them at risk for influenza complications, particularly if the suspected agent is the pandemic H1N1 virus. However, the data highlight the difficulty in identifying all children who may benefit from oseltamivir therapy, especially given that the majority of children with ILI don’t have influenza, oseltamivir therapy is best initiated within 48 hours of onset of symptoms, the most readily available test (rapid influenza testing) generally lacks sensitivity to identify those with influenza, and PCR testing is expensive and not available in many hospital emergency rooms.
Approximately half of the study patients had a history of influenza vaccine, and it is unclear whether this represented one or two doses in the younger patients. The results underscore the importance of influenza vaccine, and this year the AAP has issued a preference for the nasal live attenuated vaccine for any child aged 2-8 years who doesn’t have an underlying contraindication – emphasizing that vaccination should not be delayed in order to obtain a specific product for either dose.
Dr. Mary Anne Jackson is director of the division of infectious diseases and associate chair of community and regional pediatric collaboration at Children’s Mercy Hospital & Clinics, and professor of pediatrics at University of Missouri–Kansas City. She has no disclosures.
One in three (35.3%) children developed complications with influenzalike illnesses, and children with neurologic or neuromuscular conditions were at highest risk for complications, according to a recent study.
The most commonly developed complication was pneumonia (26.1% of the participants), but the overall rate of complications did not vary among those who had influenza, compared with those with a different virus, Dr. Rakesh D. Mistry of the University of Colorado in Aurora, and his colleagues reported online (Pediatrics 2014 Aug. 4 [doi:10.1542/peds.2014-0505]). The next most common complications were respiratory failure (7.1%) and seizures (5.8%).
The researchers prospectively assessed 241 children aged 0-19 years who presented to a children’s hospital emergency department with influenzalike illness – fever plus a cough or sore throat without another cause – from early winter 2008 to late spring 2010. The study included only children with moderate to severe symptoms (defined by physicians’ decision to do venipuncture and respiratory viral testing) who did not already have severe complications. Severe complications included seizures, encephalopathy, pneumonia, bacteremia, bacterial tracheitis, respiratory failure, myocarditis, or death.
Overall, 24.9% of the children had influenza, 28.2% had no virus detected, 14.5% had rhinovirus, 11.6% had respiratory syncytial virus, and the remainder had human metapneumovirus, adenovirus or parainfluenza viruses. Among children with influenza, the risk of developing pneumonia was 7.6 times higher with the H1N1 strain than with other strains.
Asthma was the most common chronic medical condition among the 53.5% of children who had one. Although children with neurologic or neuromuscular conditions were four times more likely to develop complications, no other high-risk conditions were linked to complications, and 41.2% of children developing complications had no underlying conditions.
The authors wrote that their findings regarding children with underlying conditions "support the need for increased preventive measures in this subgroup of children, including influenza vaccination and early institution of antiviral treatment."
The study was supported in part by the Commonwealth of Pennsylvania Department of Health. The authors reported no disclosures.
One in three (35.3%) children developed complications with influenzalike illnesses, and children with neurologic or neuromuscular conditions were at highest risk for complications, according to a recent study.
The most commonly developed complication was pneumonia (26.1% of the participants), but the overall rate of complications did not vary among those who had influenza, compared with those with a different virus, Dr. Rakesh D. Mistry of the University of Colorado in Aurora, and his colleagues reported online (Pediatrics 2014 Aug. 4 [doi:10.1542/peds.2014-0505]). The next most common complications were respiratory failure (7.1%) and seizures (5.8%).
The researchers prospectively assessed 241 children aged 0-19 years who presented to a children’s hospital emergency department with influenzalike illness – fever plus a cough or sore throat without another cause – from early winter 2008 to late spring 2010. The study included only children with moderate to severe symptoms (defined by physicians’ decision to do venipuncture and respiratory viral testing) who did not already have severe complications. Severe complications included seizures, encephalopathy, pneumonia, bacteremia, bacterial tracheitis, respiratory failure, myocarditis, or death.
Overall, 24.9% of the children had influenza, 28.2% had no virus detected, 14.5% had rhinovirus, 11.6% had respiratory syncytial virus, and the remainder had human metapneumovirus, adenovirus or parainfluenza viruses. Among children with influenza, the risk of developing pneumonia was 7.6 times higher with the H1N1 strain than with other strains.
Asthma was the most common chronic medical condition among the 53.5% of children who had one. Although children with neurologic or neuromuscular conditions were four times more likely to develop complications, no other high-risk conditions were linked to complications, and 41.2% of children developing complications had no underlying conditions.
The authors wrote that their findings regarding children with underlying conditions "support the need for increased preventive measures in this subgroup of children, including influenza vaccination and early institution of antiviral treatment."
The study was supported in part by the Commonwealth of Pennsylvania Department of Health. The authors reported no disclosures.
FROM PEDIATRICS
Key clinical point: Keep an eye out for severe complications of influenzalike illness, whether or not children have underlying conditions
Major finding: Severe complications from complications of influenzalike illness occurred in 35.3% of children, and those with neurologic or neuromuscular conditions were four times more likely to develop complications.
Data source: The findings are based on a prospective cohort study of 241 children, aged 0 to 19 years, presenting to an emergency department during respiratory viral seasons during 2008-2010.
Disclosures: The study was supported by the Commonwealth of Pennsylvania Department of Health. The authors reported no disclosures.