User login
Managing menopausal symptoms after risk-reducing salpingo-oophorectomy
Compared to the general population, women with mutations in the BRCA1 or BRCA2 genes have a significantly higher lifetime risk of ovarian and breast cancers (Science. 2003 Oct 24;302[5645]:643-6). Since the occurrence of ovarian and breast cancer in BRCA carriers is often prior to menopause, and because we have no screening test to detect early stage ovarian cancer, risk-reducing salpingo-oophorectomy has been recommended around age 40.
It has been shown that risk-reducing salpingo-oophorectomy significantly reduces ovarian cancer risk by 85%-95% in BRCA-affected women. Also, this surgery can reduce breast cancer risk by 53%-68% (N Engl J Med. 2002 May 23;346[21]:1609-15). The 2008 Practice Bulletin from the American College of Obstetricians and Gynecologists recommends that risk-reducing salpingo-oophorectomy should be performed in women with BRCA1 or BRCA2 mutations after the completion of childbearing or age 40 (Obstet Gynecol. 2008 Jan;111[1]:231-41).
Health implications

Nearly 60% of women who have a BRCA1 or BRCA2 mutation will elect to undergo risk-reducing salpingo-oophorectomy between the ages of 35 and 40 years (Open Med. 2007 Aug 13;1[2]:e92-8). As such, surgical menopause can result in hot flashes, vaginal dryness, sexual dysfunction, sleep disturbances, and cognitive changes, which may significantly impact a woman’s quality of life. In addition, increased risk of cardiovascular disease and osteoporosis following bilateral salpingo-oophorectomy may have a significant impact on a woman’s health.
Since these women undergo surgical menopause as opposed to natural menopause, they have an abrupt loss in hormones, and due to their younger age at the time of surgery, they may also have a longer exposure period to the detrimental effects of hypoestrogenism.
Symptom management
Various treatment options exist for relief of menopausal symptoms, including nonhormonal therapies and hormone replacement therapies (HT).
Nonhormonal therapies include serotonin receptor inhibitors (venlafaxine and paroxetine) and alpha-2 adrenergic agonists (clonidine), which are most appropriate for the treatment of vasomotor symptoms. Unfortunately, these options have proved to be as effective as HT. Also, women should be adequately counseled regarding the various side effects of these nonhormonal medications. Alternative approaches such as phytoestrogens are unproven and are still undergoing investigation. As such, HT remains the standard for treatment of menopausal symptoms, and many trials have confirmed that HT can effectively treat menopausal symptoms following risk-reducing salpingo-oophorectomy.
This then raises the question of safety regarding use of HT in this patient population; especially the possibility of increased risk of breast cancer. Interestingly, only 10%-25% of BRCA1 carriers will have estrogen receptor–positive breast cancer, while 65%-79% of BRCA2-associated breast cancers will be positive for the receptor (Clin Cancer Res. 2004 Mar 15;10[6]:2029-34).

Unfortunately, we do not have adequate trials or studies with sufficient long-term follow-up to validate whether HT increases the risk of breast cancer or recurrence. However, the PROSE Study Group did report on a prospective cohort of 462 women with BRCA1 or BRCA2 mutations. In this study, HT did not alter the reduction in breast cancer risk from risk-reducing salpingo-oophorectomy (J Clin Oncol. 2005 Nov 1;23[31]:7804-10). In addition to a paucity of data regarding systemic HT, there is little data in the BRCA-positive population to confirm the safety of local vaginal estrogen for treatment of vaginal atrophy (J Clin Oncol. 2004 Mar 15;22[6]:1045-54).
Understanding the options
Use of HT in women with BRCA1 and BRCA2 mutations requires further investigation. There should be shared decision making between the patient and provider when counseling on the management of menopausal symptoms following risk-reducing salpingo-oophorectomy. Most importantly, women should understand the options of nonhormonal therapies and their specific side effects. They should also understand the lack of significant data regarding use of systemic HT, and that if use is elected, there may be an increased risk of breast cancer.
Women who do elect to use systemic HT following risk-reducing salpingo-oophorectomy have options that can help reduce the risk of HT-associated breast cancer, including a shorter duration of systemic HT or concurrent hysterectomy to allow for estrogen-only HT, which has a decreased risk of breast cancer compared with combined therapies that include progestins. These women may also be considering prophylactic mastectomy, which would change the concerns regarding HT and an increased risk of breast cancer.
Increased awareness of these options among physicians and patients alike can help to decrease unsatisfactory symptoms and improve quality of life in women undergoing risk-reducing salpingo-oophorectomy.
Dr. Staley is a resident physician in the department of obstetrics and gynecology at the University of North Carolina at Chapel Hill. Dr. Gehrig is professor and director of gynecologic oncology at the university. They reported having no relevant financial disclosures. Email them at obnews@frontlinemedcom.com.
Compared to the general population, women with mutations in the BRCA1 or BRCA2 genes have a significantly higher lifetime risk of ovarian and breast cancers (Science. 2003 Oct 24;302[5645]:643-6). Since the occurrence of ovarian and breast cancer in BRCA carriers is often prior to menopause, and because we have no screening test to detect early stage ovarian cancer, risk-reducing salpingo-oophorectomy has been recommended around age 40.
It has been shown that risk-reducing salpingo-oophorectomy significantly reduces ovarian cancer risk by 85%-95% in BRCA-affected women. Also, this surgery can reduce breast cancer risk by 53%-68% (N Engl J Med. 2002 May 23;346[21]:1609-15). The 2008 Practice Bulletin from the American College of Obstetricians and Gynecologists recommends that risk-reducing salpingo-oophorectomy should be performed in women with BRCA1 or BRCA2 mutations after the completion of childbearing or age 40 (Obstet Gynecol. 2008 Jan;111[1]:231-41).
Health implications
Nearly 60% of women who have a BRCA1 or BRCA2 mutation will elect to undergo risk-reducing salpingo-oophorectomy between the ages of 35 and 40 years (Open Med. 2007 Aug 13;1[2]:e92-8). As such, surgical menopause can result in hot flashes, vaginal dryness, sexual dysfunction, sleep disturbances, and cognitive changes, which may significantly impact a woman’s quality of life. In addition, increased risk of cardiovascular disease and osteoporosis following bilateral salpingo-oophorectomy may have a significant impact on a woman’s health.
Since these women undergo surgical menopause as opposed to natural menopause, they have an abrupt loss in hormones, and due to their younger age at the time of surgery, they may also have a longer exposure period to the detrimental effects of hypoestrogenism.
Symptom management
Various treatment options exist for relief of menopausal symptoms, including nonhormonal therapies and hormone replacement therapies (HT).
Nonhormonal therapies include serotonin receptor inhibitors (venlafaxine and paroxetine) and alpha-2 adrenergic agonists (clonidine), which are most appropriate for the treatment of vasomotor symptoms. Unfortunately, these options have proved to be as effective as HT. Also, women should be adequately counseled regarding the various side effects of these nonhormonal medications. Alternative approaches such as phytoestrogens are unproven and are still undergoing investigation. As such, HT remains the standard for treatment of menopausal symptoms, and many trials have confirmed that HT can effectively treat menopausal symptoms following risk-reducing salpingo-oophorectomy.
This then raises the question of safety regarding use of HT in this patient population; especially the possibility of increased risk of breast cancer. Interestingly, only 10%-25% of BRCA1 carriers will have estrogen receptor–positive breast cancer, while 65%-79% of BRCA2-associated breast cancers will be positive for the receptor (Clin Cancer Res. 2004 Mar 15;10[6]:2029-34).
Unfortunately, we do not have adequate trials or studies with sufficient long-term follow-up to validate whether HT increases the risk of breast cancer or recurrence. However, the PROSE Study Group did report on a prospective cohort of 462 women with BRCA1 or BRCA2 mutations. In this study, HT did not alter the reduction in breast cancer risk from risk-reducing salpingo-oophorectomy (J Clin Oncol. 2005 Nov 1;23[31]:7804-10). In addition to a paucity of data regarding systemic HT, there is little data in the BRCA-positive population to confirm the safety of local vaginal estrogen for treatment of vaginal atrophy (J Clin Oncol. 2004 Mar 15;22[6]:1045-54).
Understanding the options
Use of HT in women with BRCA1 and BRCA2 mutations requires further investigation. There should be shared decision making between the patient and provider when counseling on the management of menopausal symptoms following risk-reducing salpingo-oophorectomy. Most importantly, women should understand the options of nonhormonal therapies and their specific side effects. They should also understand the lack of significant data regarding use of systemic HT, and that if use is elected, there may be an increased risk of breast cancer.
Women who do elect to use systemic HT following risk-reducing salpingo-oophorectomy have options that can help reduce the risk of HT-associated breast cancer, including a shorter duration of systemic HT or concurrent hysterectomy to allow for estrogen-only HT, which has a decreased risk of breast cancer compared with combined therapies that include progestins. These women may also be considering prophylactic mastectomy, which would change the concerns regarding HT and an increased risk of breast cancer.
Increased awareness of these options among physicians and patients alike can help to decrease unsatisfactory symptoms and improve quality of life in women undergoing risk-reducing salpingo-oophorectomy.
Dr. Staley is a resident physician in the department of obstetrics and gynecology at the University of North Carolina at Chapel Hill. Dr. Gehrig is professor and director of gynecologic oncology at the university. They reported having no relevant financial disclosures. Email them at obnews@frontlinemedcom.com.
Compared to the general population, women with mutations in the BRCA1 or BRCA2 genes have a significantly higher lifetime risk of ovarian and breast cancers (Science. 2003 Oct 24;302[5645]:643-6). Since the occurrence of ovarian and breast cancer in BRCA carriers is often prior to menopause, and because we have no screening test to detect early stage ovarian cancer, risk-reducing salpingo-oophorectomy has been recommended around age 40.
It has been shown that risk-reducing salpingo-oophorectomy significantly reduces ovarian cancer risk by 85%-95% in BRCA-affected women. Also, this surgery can reduce breast cancer risk by 53%-68% (N Engl J Med. 2002 May 23;346[21]:1609-15). The 2008 Practice Bulletin from the American College of Obstetricians and Gynecologists recommends that risk-reducing salpingo-oophorectomy should be performed in women with BRCA1 or BRCA2 mutations after the completion of childbearing or age 40 (Obstet Gynecol. 2008 Jan;111[1]:231-41).
Health implications
Nearly 60% of women who have a BRCA1 or BRCA2 mutation will elect to undergo risk-reducing salpingo-oophorectomy between the ages of 35 and 40 years (Open Med. 2007 Aug 13;1[2]:e92-8). As such, surgical menopause can result in hot flashes, vaginal dryness, sexual dysfunction, sleep disturbances, and cognitive changes, which may significantly impact a woman’s quality of life. In addition, increased risk of cardiovascular disease and osteoporosis following bilateral salpingo-oophorectomy may have a significant impact on a woman’s health.
Since these women undergo surgical menopause as opposed to natural menopause, they have an abrupt loss in hormones, and due to their younger age at the time of surgery, they may also have a longer exposure period to the detrimental effects of hypoestrogenism.
Symptom management
Various treatment options exist for relief of menopausal symptoms, including nonhormonal therapies and hormone replacement therapies (HT).
Nonhormonal therapies include serotonin receptor inhibitors (venlafaxine and paroxetine) and alpha-2 adrenergic agonists (clonidine), which are most appropriate for the treatment of vasomotor symptoms. Unfortunately, these options have proved to be as effective as HT. Also, women should be adequately counseled regarding the various side effects of these nonhormonal medications. Alternative approaches such as phytoestrogens are unproven and are still undergoing investigation. As such, HT remains the standard for treatment of menopausal symptoms, and many trials have confirmed that HT can effectively treat menopausal symptoms following risk-reducing salpingo-oophorectomy.
This then raises the question of safety regarding use of HT in this patient population; especially the possibility of increased risk of breast cancer. Interestingly, only 10%-25% of BRCA1 carriers will have estrogen receptor–positive breast cancer, while 65%-79% of BRCA2-associated breast cancers will be positive for the receptor (Clin Cancer Res. 2004 Mar 15;10[6]:2029-34).
Unfortunately, we do not have adequate trials or studies with sufficient long-term follow-up to validate whether HT increases the risk of breast cancer or recurrence. However, the PROSE Study Group did report on a prospective cohort of 462 women with BRCA1 or BRCA2 mutations. In this study, HT did not alter the reduction in breast cancer risk from risk-reducing salpingo-oophorectomy (J Clin Oncol. 2005 Nov 1;23[31]:7804-10). In addition to a paucity of data regarding systemic HT, there is little data in the BRCA-positive population to confirm the safety of local vaginal estrogen for treatment of vaginal atrophy (J Clin Oncol. 2004 Mar 15;22[6]:1045-54).
Understanding the options
Use of HT in women with BRCA1 and BRCA2 mutations requires further investigation. There should be shared decision making between the patient and provider when counseling on the management of menopausal symptoms following risk-reducing salpingo-oophorectomy. Most importantly, women should understand the options of nonhormonal therapies and their specific side effects. They should also understand the lack of significant data regarding use of systemic HT, and that if use is elected, there may be an increased risk of breast cancer.
Women who do elect to use systemic HT following risk-reducing salpingo-oophorectomy have options that can help reduce the risk of HT-associated breast cancer, including a shorter duration of systemic HT or concurrent hysterectomy to allow for estrogen-only HT, which has a decreased risk of breast cancer compared with combined therapies that include progestins. These women may also be considering prophylactic mastectomy, which would change the concerns regarding HT and an increased risk of breast cancer.
Increased awareness of these options among physicians and patients alike can help to decrease unsatisfactory symptoms and improve quality of life in women undergoing risk-reducing salpingo-oophorectomy.
Dr. Staley is a resident physician in the department of obstetrics and gynecology at the University of North Carolina at Chapel Hill. Dr. Gehrig is professor and director of gynecologic oncology at the university. They reported having no relevant financial disclosures. Email them at obnews@frontlinemedcom.com.

Low incidence of DVT reported after percutaneous EVAR
Completely percutaneous endovascular aortic aneurysm repair (PEVAR) has become more common, using the suture-mediated “preclose” technique. The rate of periprocedural, iatrogenic, acute deep vein thrombosis (DVT), hitherto unknown, was found to be low for this approach, according to a study reported by Dr. Courtney E. Morgan and her colleagues at the Northwestern University, Chicago.
The researchers assessed 52 consecutive patients (44 men) with a mean age of 73 years, who underwent PEVAR at their center. Only 6% had a prior history of DVT (J Vasc Surg. 2015 Aug; 62:351-4).

Acute DVT was seen in four patients on postoperative day 1. These four DVTs comprised one femoropopliteal, and three calf DVTs. Three of these patients had associated risk factors: history of DVT (two patients); active smokers (one patient); and obesity (body mass index greater than 30 kg/m2 in all three patients).
At 2 weeks postoperatively, 75% of the DVTs had resolved.
“We found an overall rate of proximal DVT of 4% after PEVAR, which increased to 13% when calf-vein DVTs were included. Most patients with postoperative DVT had preexisting risk factors, which suggests that routine duplex ultrasound screening after PEVAR is not necessary unless there exist preclinical risk factors or postprocedural clinical indications suggestive of DVT,” the authors concluded.
Two of the researchers have received funding and/or served as speakers/consultants for device companies involved in EVAR.
Read the full study online in the Journal of Vascular Surgery.
Completely percutaneous endovascular aortic aneurysm repair (PEVAR) has become more common, using the suture-mediated “preclose” technique. The rate of periprocedural, iatrogenic, acute deep vein thrombosis (DVT), hitherto unknown, was found to be low for this approach, according to a study reported by Dr. Courtney E. Morgan and her colleagues at the Northwestern University, Chicago.
The researchers assessed 52 consecutive patients (44 men) with a mean age of 73 years, who underwent PEVAR at their center. Only 6% had a prior history of DVT (J Vasc Surg. 2015 Aug; 62:351-4).
Acute DVT was seen in four patients on postoperative day 1. These four DVTs comprised one femoropopliteal, and three calf DVTs. Three of these patients had associated risk factors: history of DVT (two patients); active smokers (one patient); and obesity (body mass index greater than 30 kg/m2 in all three patients).
At 2 weeks postoperatively, 75% of the DVTs had resolved.
“We found an overall rate of proximal DVT of 4% after PEVAR, which increased to 13% when calf-vein DVTs were included. Most patients with postoperative DVT had preexisting risk factors, which suggests that routine duplex ultrasound screening after PEVAR is not necessary unless there exist preclinical risk factors or postprocedural clinical indications suggestive of DVT,” the authors concluded.
Two of the researchers have received funding and/or served as speakers/consultants for device companies involved in EVAR.
Read the full study online in the Journal of Vascular Surgery.
Completely percutaneous endovascular aortic aneurysm repair (PEVAR) has become more common, using the suture-mediated “preclose” technique. The rate of periprocedural, iatrogenic, acute deep vein thrombosis (DVT), hitherto unknown, was found to be low for this approach, according to a study reported by Dr. Courtney E. Morgan and her colleagues at the Northwestern University, Chicago.
The researchers assessed 52 consecutive patients (44 men) with a mean age of 73 years, who underwent PEVAR at their center. Only 6% had a prior history of DVT (J Vasc Surg. 2015 Aug; 62:351-4).
Acute DVT was seen in four patients on postoperative day 1. These four DVTs comprised one femoropopliteal, and three calf DVTs. Three of these patients had associated risk factors: history of DVT (two patients); active smokers (one patient); and obesity (body mass index greater than 30 kg/m2 in all three patients).
At 2 weeks postoperatively, 75% of the DVTs had resolved.
“We found an overall rate of proximal DVT of 4% after PEVAR, which increased to 13% when calf-vein DVTs were included. Most patients with postoperative DVT had preexisting risk factors, which suggests that routine duplex ultrasound screening after PEVAR is not necessary unless there exist preclinical risk factors or postprocedural clinical indications suggestive of DVT,” the authors concluded.
Two of the researchers have received funding and/or served as speakers/consultants for device companies involved in EVAR.
Read the full study online in the Journal of Vascular Surgery.
FROM THE JOURNAL OF VASCULAR SURGERY

Will New American Cancer Society Mammography Policy Change VHA Practice?
The new American Cancer Society (ACS) policy for mammography screening now recommends annual mammograms from age 45 until age 54, suggesting a less aggressive approach to screening than in the 2003 guidelines. The recommendation is for asymptomatic women at average risk of developing breast cancer.
Related: How Much Is Too Much Cancer Screening?
“These recommendations are made with the intent of maximizing reductions in breast cancer mortality and years of life saved while being attentive to the need to minimize harms associated with screening,” said Dr. Kevin C. Oeffinger, chairman of the breast cancer guideline panel.
Related: Advances in Targeted Therapy for Breast Cancer
The guideline, developed by a panel of outside experts, was published October 20, 2015, in The Journal of the American Medical Association.
Other important recommendation changes include:
- ŸWomen aged 45 to 54 years should receive annual screening mammography and at age 55 women should transition to biennial screening.
- ŸWomen should continue screening mammography as long as their overall health is good and they have a life expectancy of 10 years or longer.
- ŸClinical breast examination is no longer recommended at any age.
- ŸThe panel noted that the recommendations are an effort to avoid false positive findings, which can take an emotional toll.
The current VHA recommendations state:
- Mammography is not recommended for women aged 13 to 39 years.
- Women aged 40 to 49 years should talk with their health care providers about screening.
- ŸMammograms are recommended every 2 years for women aged 50 to 74 years.
- ŸWomen aged > 75 years should talk with their health care providers.
According to Anita Aggarwal, DO, PhD, president of the Association of VA Hematology and Oncology (AVAHO), the VHA recommendations leave a lot of wiggle room; every year starting at age 40 is still acceptable practice at the VA.
Related: Breast Cancer Research Group Aims to Improve Veteran Survival Rates
“Keep in mind that recommendations are just recommendations,” Dr. Aggarwal told Federal Practitioner. “One size may not fit all. I believe we should use our sound judgment based on valid research to recommend what is best for the patient. Based on my literature search, annual screening starting at 40 saves the most lives via early detection.”
The new American Cancer Society (ACS) policy for mammography screening now recommends annual mammograms from age 45 until age 54, suggesting a less aggressive approach to screening than in the 2003 guidelines. The recommendation is for asymptomatic women at average risk of developing breast cancer.
Related: How Much Is Too Much Cancer Screening?
“These recommendations are made with the intent of maximizing reductions in breast cancer mortality and years of life saved while being attentive to the need to minimize harms associated with screening,” said Dr. Kevin C. Oeffinger, chairman of the breast cancer guideline panel.
Related: Advances in Targeted Therapy for Breast Cancer
The guideline, developed by a panel of outside experts, was published October 20, 2015, in The Journal of the American Medical Association.
Other important recommendation changes include:
- ŸWomen aged 45 to 54 years should receive annual screening mammography and at age 55 women should transition to biennial screening.
- ŸWomen should continue screening mammography as long as their overall health is good and they have a life expectancy of 10 years or longer.
- ŸClinical breast examination is no longer recommended at any age.
- ŸThe panel noted that the recommendations are an effort to avoid false positive findings, which can take an emotional toll.
The current VHA recommendations state:
- Mammography is not recommended for women aged 13 to 39 years.
- Women aged 40 to 49 years should talk with their health care providers about screening.
- ŸMammograms are recommended every 2 years for women aged 50 to 74 years.
- ŸWomen aged > 75 years should talk with their health care providers.
According to Anita Aggarwal, DO, PhD, president of the Association of VA Hematology and Oncology (AVAHO), the VHA recommendations leave a lot of wiggle room; every year starting at age 40 is still acceptable practice at the VA.
Related: Breast Cancer Research Group Aims to Improve Veteran Survival Rates
“Keep in mind that recommendations are just recommendations,” Dr. Aggarwal told Federal Practitioner. “One size may not fit all. I believe we should use our sound judgment based on valid research to recommend what is best for the patient. Based on my literature search, annual screening starting at 40 saves the most lives via early detection.”
The new American Cancer Society (ACS) policy for mammography screening now recommends annual mammograms from age 45 until age 54, suggesting a less aggressive approach to screening than in the 2003 guidelines. The recommendation is for asymptomatic women at average risk of developing breast cancer.
Related: How Much Is Too Much Cancer Screening?
“These recommendations are made with the intent of maximizing reductions in breast cancer mortality and years of life saved while being attentive to the need to minimize harms associated with screening,” said Dr. Kevin C. Oeffinger, chairman of the breast cancer guideline panel.
Related: Advances in Targeted Therapy for Breast Cancer
The guideline, developed by a panel of outside experts, was published October 20, 2015, in The Journal of the American Medical Association.
Other important recommendation changes include:
- ŸWomen aged 45 to 54 years should receive annual screening mammography and at age 55 women should transition to biennial screening.
- ŸWomen should continue screening mammography as long as their overall health is good and they have a life expectancy of 10 years or longer.
- ŸClinical breast examination is no longer recommended at any age.
- ŸThe panel noted that the recommendations are an effort to avoid false positive findings, which can take an emotional toll.
The current VHA recommendations state:
- Mammography is not recommended for women aged 13 to 39 years.
- Women aged 40 to 49 years should talk with their health care providers about screening.
- ŸMammograms are recommended every 2 years for women aged 50 to 74 years.
- ŸWomen aged > 75 years should talk with their health care providers.
According to Anita Aggarwal, DO, PhD, president of the Association of VA Hematology and Oncology (AVAHO), the VHA recommendations leave a lot of wiggle room; every year starting at age 40 is still acceptable practice at the VA.
Related: Breast Cancer Research Group Aims to Improve Veteran Survival Rates
“Keep in mind that recommendations are just recommendations,” Dr. Aggarwal told Federal Practitioner. “One size may not fit all. I believe we should use our sound judgment based on valid research to recommend what is best for the patient. Based on my literature search, annual screening starting at 40 saves the most lives via early detection.”
No flu vaccine for patients with egg allergy?
A 35-year-old woman with asthma presents for a follow-up visit in October. You recommend that she receive the influenza vaccine. She tells you that she cannot take the influenza vaccine because she is allergic to eggs.

What do you recommend?
A. Give her the influenza vaccine.
B. Give her an oseltamivir prescription, and have her start it if any flu-like symptoms appear.
C. Give her the nasal influenza vaccine.
D. Give her the cell-based influenza vaccine.
The clinic I work in asks all patients if they have allergy to eggs before giving the influenza vaccine. If the patient replies yes, then the vaccine is not given and the physician is consulted.
For many years, allergy to egg was considered a contraindication to receiving the influenza vaccine. This contraindication was based on the fear that administering a vaccine that was grown in eggs and could contain egg protein might cause anaphylaxis in patients with immunoglobulin E antibodies against egg proteins.
Fortunately, there is a good evidence base that shows that administering influenza vaccine to patients with egg allergy is safe.
This is extremely important information, because it is estimated that there are about 200,000-300,000 hospitalizations annually because of influenza. For the 2012-2013 influenza season, the CDC estimated that the flu vaccine prevented 6.6 million cases of influenza, 3.2 million doctor visits, and 79,000 hospitalizations. There were 170 pediatric deaths from the flu during the 2012-2013 influenza season (MMWR Morb Mortal Wkly Rep. 2013 Dec 13;62[49]:997-1000). The need for widespread vaccination is great, and decreasing the number of people unable to receive the vaccine is an important goal.

There are many studies in children and adults that show that those with egg allergy can be safely vaccinated with influenza vaccine. Dr. John M. James and colleagues reported a study of mostly children with egg allergy confirmed with skin testing (average age of the study group was 3 years) receiving influenza vaccine (J Pediatr. 1998 Nov;133[5]:624-8). A total of 83 patients with egg allergy received the vaccine (including 27 patients with a history of anaphylaxis or severe reactions after egg ingestion). No patients suffered severe reactions with the vaccine, with only four patients having mild, self-limited symptoms.
In another study, Dr. Anne Des Roches and colleagues performed a prospective, cohort study recruiting and vaccinating egg-allergic patients with trivalent inactivated influenza vaccine between 2010 and 2012 (J Allergy Clin Immunol. 2012 Nov;130[5]:1213-1216.e1). In the second year of the study, the focus was on recruiting patients with a history of anaphylaxis or severe cardiopulmonary symptoms upon egg ingestion. In addition, a retrospective study of all egg-allergic patients who had received an influenza vaccine between 2007 and 2010 was included.
A total of 457 doses of vaccine were administered to 367 patients with egg allergy, of whom 132 had a history of severe allergy. No patients developed anaphylaxis, and 13 patients developed mild allergiclike symptoms in the 24 hours after vaccination.
In an authoritative review on the subject of influenza vaccination in egg-allergic patients, Dr. John Kelso reported on 28 studies with a total of 4,315 patients with egg allergy, including 656 with history of anaphylaxis with egg ingestion (Expert Rev Vaccines. 2014 Aug;13[8]:1049-57). None of these patients developed a serious reaction when they received influenza vaccine.
Dr. Des Roches and colleagues reported on a prospective, cohort study in which 68 children with previous egg allergy received intranasal live attenuated influenza vaccine (J Allergy Clin Immunol Pract. 2015 Jan-Feb;3[1]:138-9). No patients had anaphylaxis or a severe allergic reaction. There were more adverse reactions in the patients with egg (7 patients) than in the control group (1 patient), but these were mild and nonspecific (abdominal pain, nasal congestion, headache, and cough).
The 2012 adverse reactions to vaccines practice parameter update recommended that patients with egg allergy should receive influenza vaccinations (trivalent influenza vaccine), because the risks of vaccinating are outweighed by the risks of not vaccinating (J Allergy Clin Immunol. 2012 Jul;130[1]:25-43).
A subsequent recommendation takes this a step further, recommending that all patients with egg allergy of any severity should receive inactivated influenza vaccine annually, using any age-approved brand (Ann Allergy Asthma Immunol. 2013 Oct;111[4]:301-2). In addition, there are no special waiting periods after vaccination of egg allergic patients beyond what is standard practice for any vaccine.
I think that we have plenty of evidence now to immunize all patients who report egg allergy, and to do so in the primary care setting.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at dpaauw@uw.edu.
A 35-year-old woman with asthma presents for a follow-up visit in October. You recommend that she receive the influenza vaccine. She tells you that she cannot take the influenza vaccine because she is allergic to eggs.
What do you recommend?
A. Give her the influenza vaccine.
B. Give her an oseltamivir prescription, and have her start it if any flu-like symptoms appear.
C. Give her the nasal influenza vaccine.
D. Give her the cell-based influenza vaccine.
The clinic I work in asks all patients if they have allergy to eggs before giving the influenza vaccine. If the patient replies yes, then the vaccine is not given and the physician is consulted.
For many years, allergy to egg was considered a contraindication to receiving the influenza vaccine. This contraindication was based on the fear that administering a vaccine that was grown in eggs and could contain egg protein might cause anaphylaxis in patients with immunoglobulin E antibodies against egg proteins.
Fortunately, there is a good evidence base that shows that administering influenza vaccine to patients with egg allergy is safe.
This is extremely important information, because it is estimated that there are about 200,000-300,000 hospitalizations annually because of influenza. For the 2012-2013 influenza season, the CDC estimated that the flu vaccine prevented 6.6 million cases of influenza, 3.2 million doctor visits, and 79,000 hospitalizations. There were 170 pediatric deaths from the flu during the 2012-2013 influenza season (MMWR Morb Mortal Wkly Rep. 2013 Dec 13;62[49]:997-1000). The need for widespread vaccination is great, and decreasing the number of people unable to receive the vaccine is an important goal.
There are many studies in children and adults that show that those with egg allergy can be safely vaccinated with influenza vaccine. Dr. John M. James and colleagues reported a study of mostly children with egg allergy confirmed with skin testing (average age of the study group was 3 years) receiving influenza vaccine (J Pediatr. 1998 Nov;133[5]:624-8). A total of 83 patients with egg allergy received the vaccine (including 27 patients with a history of anaphylaxis or severe reactions after egg ingestion). No patients suffered severe reactions with the vaccine, with only four patients having mild, self-limited symptoms.
In another study, Dr. Anne Des Roches and colleagues performed a prospective, cohort study recruiting and vaccinating egg-allergic patients with trivalent inactivated influenza vaccine between 2010 and 2012 (J Allergy Clin Immunol. 2012 Nov;130[5]:1213-1216.e1). In the second year of the study, the focus was on recruiting patients with a history of anaphylaxis or severe cardiopulmonary symptoms upon egg ingestion. In addition, a retrospective study of all egg-allergic patients who had received an influenza vaccine between 2007 and 2010 was included.
A total of 457 doses of vaccine were administered to 367 patients with egg allergy, of whom 132 had a history of severe allergy. No patients developed anaphylaxis, and 13 patients developed mild allergiclike symptoms in the 24 hours after vaccination.
In an authoritative review on the subject of influenza vaccination in egg-allergic patients, Dr. John Kelso reported on 28 studies with a total of 4,315 patients with egg allergy, including 656 with history of anaphylaxis with egg ingestion (Expert Rev Vaccines. 2014 Aug;13[8]:1049-57). None of these patients developed a serious reaction when they received influenza vaccine.
Dr. Des Roches and colleagues reported on a prospective, cohort study in which 68 children with previous egg allergy received intranasal live attenuated influenza vaccine (J Allergy Clin Immunol Pract. 2015 Jan-Feb;3[1]:138-9). No patients had anaphylaxis or a severe allergic reaction. There were more adverse reactions in the patients with egg (7 patients) than in the control group (1 patient), but these were mild and nonspecific (abdominal pain, nasal congestion, headache, and cough).
The 2012 adverse reactions to vaccines practice parameter update recommended that patients with egg allergy should receive influenza vaccinations (trivalent influenza vaccine), because the risks of vaccinating are outweighed by the risks of not vaccinating (J Allergy Clin Immunol. 2012 Jul;130[1]:25-43).
A subsequent recommendation takes this a step further, recommending that all patients with egg allergy of any severity should receive inactivated influenza vaccine annually, using any age-approved brand (Ann Allergy Asthma Immunol. 2013 Oct;111[4]:301-2). In addition, there are no special waiting periods after vaccination of egg allergic patients beyond what is standard practice for any vaccine.
I think that we have plenty of evidence now to immunize all patients who report egg allergy, and to do so in the primary care setting.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at dpaauw@uw.edu.
A 35-year-old woman with asthma presents for a follow-up visit in October. You recommend that she receive the influenza vaccine. She tells you that she cannot take the influenza vaccine because she is allergic to eggs.
What do you recommend?
A. Give her the influenza vaccine.
B. Give her an oseltamivir prescription, and have her start it if any flu-like symptoms appear.
C. Give her the nasal influenza vaccine.
D. Give her the cell-based influenza vaccine.
The clinic I work in asks all patients if they have allergy to eggs before giving the influenza vaccine. If the patient replies yes, then the vaccine is not given and the physician is consulted.
For many years, allergy to egg was considered a contraindication to receiving the influenza vaccine. This contraindication was based on the fear that administering a vaccine that was grown in eggs and could contain egg protein might cause anaphylaxis in patients with immunoglobulin E antibodies against egg proteins.
Fortunately, there is a good evidence base that shows that administering influenza vaccine to patients with egg allergy is safe.
This is extremely important information, because it is estimated that there are about 200,000-300,000 hospitalizations annually because of influenza. For the 2012-2013 influenza season, the CDC estimated that the flu vaccine prevented 6.6 million cases of influenza, 3.2 million doctor visits, and 79,000 hospitalizations. There were 170 pediatric deaths from the flu during the 2012-2013 influenza season (MMWR Morb Mortal Wkly Rep. 2013 Dec 13;62[49]:997-1000). The need for widespread vaccination is great, and decreasing the number of people unable to receive the vaccine is an important goal.
There are many studies in children and adults that show that those with egg allergy can be safely vaccinated with influenza vaccine. Dr. John M. James and colleagues reported a study of mostly children with egg allergy confirmed with skin testing (average age of the study group was 3 years) receiving influenza vaccine (J Pediatr. 1998 Nov;133[5]:624-8). A total of 83 patients with egg allergy received the vaccine (including 27 patients with a history of anaphylaxis or severe reactions after egg ingestion). No patients suffered severe reactions with the vaccine, with only four patients having mild, self-limited symptoms.
In another study, Dr. Anne Des Roches and colleagues performed a prospective, cohort study recruiting and vaccinating egg-allergic patients with trivalent inactivated influenza vaccine between 2010 and 2012 (J Allergy Clin Immunol. 2012 Nov;130[5]:1213-1216.e1). In the second year of the study, the focus was on recruiting patients with a history of anaphylaxis or severe cardiopulmonary symptoms upon egg ingestion. In addition, a retrospective study of all egg-allergic patients who had received an influenza vaccine between 2007 and 2010 was included.
A total of 457 doses of vaccine were administered to 367 patients with egg allergy, of whom 132 had a history of severe allergy. No patients developed anaphylaxis, and 13 patients developed mild allergiclike symptoms in the 24 hours after vaccination.
In an authoritative review on the subject of influenza vaccination in egg-allergic patients, Dr. John Kelso reported on 28 studies with a total of 4,315 patients with egg allergy, including 656 with history of anaphylaxis with egg ingestion (Expert Rev Vaccines. 2014 Aug;13[8]:1049-57). None of these patients developed a serious reaction when they received influenza vaccine.
Dr. Des Roches and colleagues reported on a prospective, cohort study in which 68 children with previous egg allergy received intranasal live attenuated influenza vaccine (J Allergy Clin Immunol Pract. 2015 Jan-Feb;3[1]:138-9). No patients had anaphylaxis or a severe allergic reaction. There were more adverse reactions in the patients with egg (7 patients) than in the control group (1 patient), but these were mild and nonspecific (abdominal pain, nasal congestion, headache, and cough).
The 2012 adverse reactions to vaccines practice parameter update recommended that patients with egg allergy should receive influenza vaccinations (trivalent influenza vaccine), because the risks of vaccinating are outweighed by the risks of not vaccinating (J Allergy Clin Immunol. 2012 Jul;130[1]:25-43).
A subsequent recommendation takes this a step further, recommending that all patients with egg allergy of any severity should receive inactivated influenza vaccine annually, using any age-approved brand (Ann Allergy Asthma Immunol. 2013 Oct;111[4]:301-2). In addition, there are no special waiting periods after vaccination of egg allergic patients beyond what is standard practice for any vaccine.
I think that we have plenty of evidence now to immunize all patients who report egg allergy, and to do so in the primary care setting.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at dpaauw@uw.edu.

Percutaneous ethanol effective for small papillary thyroid cancers
LAKE BUENA VISTA, FLA. – An outpatient procedure may represent an efficacious and safe alternative to surgery for those patients with small papillary thyroid cancers who prefer definitive treatment over the “wait and watch” approach. Further, at one institution, the cost-effective alternative to surgery saved almost $40,000 per patient.
Ultrasound-guided percutaneous ethanol injection (UPEA) of small (cT1N0) intrathyroidal papillary thyroid cancer (SIPC) successfully reduced tumor volume by a median of 92%, eliminated tumor blood flow, and was very well tolerated by a series of 13 patients who received UPEA at the Mayo Clinic, Rochester, Minn.
Dr. Ian D. Hay, a consultant in Mayo’s division of endocrinology, diabetes, metabolism, and nutrition, presented the findings during a poster session at the International Thyroid Congress.
Dr. Hay and his colleagues treated 13 patients with a total of 15 tumors with injections of percutaneous ethanol. The first patient received just one injection; the remaining patients received one injection to each tumor site on each of 2 consecutive days. Five of the tumor foci had less than a 50% reduction in tumor volume at the first follow-up visit, so those tumors were injected a third time.
Patients in the series ranged from 38 to 86 years old (median 45), and five patients had significant comorbidities: one had congestive heart failure and the other four had concomitant unrelated cancers. Tumors were a median 8 mm in size, with volumes ranging from 25 to 676 mm3 (median 140 mm3).
All of the injections were performed under ultrasound guidance, and a median of 0.9 cc of ethanol was injected into each tumor. Ultrasound examination was performed at each follow-up visit to evaluate tumor volume and blood flow. Dr. Hay reported that the procedure was well tolerated: Local neck tenderness resolved within a day or two, and there were no reports of hoarseness or laryngeal nerve palsy.
Patients were followed for a mean 2.0 years (range, 0.4-5.7 years), with a median tumor reduction of 92% (range 46%-100%). For the nine tumors that were still identifiable on ultrasound at the time of reporting, the mean volume had decreased by 73%. Six tumor foci had completely disappeared, and no tumor had detectable blood flow on Doppler exam. Tumor thyroglobulin levels remained stable in all patients, and no nodal metastases were identified, Dr. Hay reported at the meeting, which was held by the American Thyroid Association, Asia-Oceania Thyroid Association, European Thyroid Association, and Latin American Thyroid Society.
Internationally, the approach to managing SIPC varies from lobectomy to near-total thyroidectomy to active surveillance. For patients who prefer definitive management of their tumors but are reluctant to have surgery or who may have significant comorbidities, UPEA may represent a safe alternative, and at significant cost savings compared to surgery: Dr. Hay and his colleagues reported that they estimated the average cost savings at their institution to be over $38,000 per patient. “If prospective trials of observation vs. surgery for SIPC are to occur in the USA, perhaps it could be included as a ‘third arm’ in such trials,” Dr. Hay and his colleagues said.
On Twitter @karioakes
LAKE BUENA VISTA, FLA. – An outpatient procedure may represent an efficacious and safe alternative to surgery for those patients with small papillary thyroid cancers who prefer definitive treatment over the “wait and watch” approach. Further, at one institution, the cost-effective alternative to surgery saved almost $40,000 per patient.
Ultrasound-guided percutaneous ethanol injection (UPEA) of small (cT1N0) intrathyroidal papillary thyroid cancer (SIPC) successfully reduced tumor volume by a median of 92%, eliminated tumor blood flow, and was very well tolerated by a series of 13 patients who received UPEA at the Mayo Clinic, Rochester, Minn.
Dr. Ian D. Hay, a consultant in Mayo’s division of endocrinology, diabetes, metabolism, and nutrition, presented the findings during a poster session at the International Thyroid Congress.
Dr. Hay and his colleagues treated 13 patients with a total of 15 tumors with injections of percutaneous ethanol. The first patient received just one injection; the remaining patients received one injection to each tumor site on each of 2 consecutive days. Five of the tumor foci had less than a 50% reduction in tumor volume at the first follow-up visit, so those tumors were injected a third time.
Patients in the series ranged from 38 to 86 years old (median 45), and five patients had significant comorbidities: one had congestive heart failure and the other four had concomitant unrelated cancers. Tumors were a median 8 mm in size, with volumes ranging from 25 to 676 mm3 (median 140 mm3).
All of the injections were performed under ultrasound guidance, and a median of 0.9 cc of ethanol was injected into each tumor. Ultrasound examination was performed at each follow-up visit to evaluate tumor volume and blood flow. Dr. Hay reported that the procedure was well tolerated: Local neck tenderness resolved within a day or two, and there were no reports of hoarseness or laryngeal nerve palsy.
Patients were followed for a mean 2.0 years (range, 0.4-5.7 years), with a median tumor reduction of 92% (range 46%-100%). For the nine tumors that were still identifiable on ultrasound at the time of reporting, the mean volume had decreased by 73%. Six tumor foci had completely disappeared, and no tumor had detectable blood flow on Doppler exam. Tumor thyroglobulin levels remained stable in all patients, and no nodal metastases were identified, Dr. Hay reported at the meeting, which was held by the American Thyroid Association, Asia-Oceania Thyroid Association, European Thyroid Association, and Latin American Thyroid Society.
Internationally, the approach to managing SIPC varies from lobectomy to near-total thyroidectomy to active surveillance. For patients who prefer definitive management of their tumors but are reluctant to have surgery or who may have significant comorbidities, UPEA may represent a safe alternative, and at significant cost savings compared to surgery: Dr. Hay and his colleagues reported that they estimated the average cost savings at their institution to be over $38,000 per patient. “If prospective trials of observation vs. surgery for SIPC are to occur in the USA, perhaps it could be included as a ‘third arm’ in such trials,” Dr. Hay and his colleagues said.
On Twitter @karioakes
LAKE BUENA VISTA, FLA. – An outpatient procedure may represent an efficacious and safe alternative to surgery for those patients with small papillary thyroid cancers who prefer definitive treatment over the “wait and watch” approach. Further, at one institution, the cost-effective alternative to surgery saved almost $40,000 per patient.
Ultrasound-guided percutaneous ethanol injection (UPEA) of small (cT1N0) intrathyroidal papillary thyroid cancer (SIPC) successfully reduced tumor volume by a median of 92%, eliminated tumor blood flow, and was very well tolerated by a series of 13 patients who received UPEA at the Mayo Clinic, Rochester, Minn.
Dr. Ian D. Hay, a consultant in Mayo’s division of endocrinology, diabetes, metabolism, and nutrition, presented the findings during a poster session at the International Thyroid Congress.
Dr. Hay and his colleagues treated 13 patients with a total of 15 tumors with injections of percutaneous ethanol. The first patient received just one injection; the remaining patients received one injection to each tumor site on each of 2 consecutive days. Five of the tumor foci had less than a 50% reduction in tumor volume at the first follow-up visit, so those tumors were injected a third time.
Patients in the series ranged from 38 to 86 years old (median 45), and five patients had significant comorbidities: one had congestive heart failure and the other four had concomitant unrelated cancers. Tumors were a median 8 mm in size, with volumes ranging from 25 to 676 mm3 (median 140 mm3).
All of the injections were performed under ultrasound guidance, and a median of 0.9 cc of ethanol was injected into each tumor. Ultrasound examination was performed at each follow-up visit to evaluate tumor volume and blood flow. Dr. Hay reported that the procedure was well tolerated: Local neck tenderness resolved within a day or two, and there were no reports of hoarseness or laryngeal nerve palsy.
Patients were followed for a mean 2.0 years (range, 0.4-5.7 years), with a median tumor reduction of 92% (range 46%-100%). For the nine tumors that were still identifiable on ultrasound at the time of reporting, the mean volume had decreased by 73%. Six tumor foci had completely disappeared, and no tumor had detectable blood flow on Doppler exam. Tumor thyroglobulin levels remained stable in all patients, and no nodal metastases were identified, Dr. Hay reported at the meeting, which was held by the American Thyroid Association, Asia-Oceania Thyroid Association, European Thyroid Association, and Latin American Thyroid Society.
Internationally, the approach to managing SIPC varies from lobectomy to near-total thyroidectomy to active surveillance. For patients who prefer definitive management of their tumors but are reluctant to have surgery or who may have significant comorbidities, UPEA may represent a safe alternative, and at significant cost savings compared to surgery: Dr. Hay and his colleagues reported that they estimated the average cost savings at their institution to be over $38,000 per patient. “If prospective trials of observation vs. surgery for SIPC are to occur in the USA, perhaps it could be included as a ‘third arm’ in such trials,” Dr. Hay and his colleagues said.
On Twitter @karioakes
AT ITC 2015
Key clinical point: Ultrasound-guided percutaneous ethanol ablation (UPEA) is an efficacious, cost-effective, and noninvasive definitive treatment for small papillary thyroid cancers.
Major finding: Fifteen tumors in 13 patients were successfully treated with UPEA with a mean 92% reduction in tumor volume and no complications or metastasis at a mean 2-year follow-up.
Data source: Series of 13 patients with 15 tumors treated at the Mayo Clinic for small intrathyroidal papillary cancers.
Disclosures: No disclosures were identified.
RFA, ethanol ablation equally effective for thyroid nodules
LAKE BUENA VISTA, FLA. – Ethanol ablation is just as effective as radiofrequency ablation for cystic thyroid nodules, resulting in similar volume reduction and similarly improving symptomatic and cosmetic outcomes at 6 months.
Radiofrequnecy ablation (RFA) did have a slight edge over ethanol injection (EA) in therapeutic response, Dr. Hye Sun Park said at the International Thyroid Conference. But because ethanol ablation is easier and less expensive, she recommended that it be considered as first-line therapy for these lesions.

Dr. Park of the University of Ulsan, Asan Medical Center in Seoul, South Korea, reported a trial of 46 patients, mean age 50 years old, with benign cystic thyroid nodules who were randomized to the two treatments. Patients randomized to ethanol, however, had significantly larger-volume lesions (14.7 vs. 8.6 mL), and symptom scores. Cosmetic scores and nodule vascularity were similar.
RFA was performed with an 18-gauge monopolar, internally cooled electrode with a 1-cm active tip, using the moving shot technique. Patients undergoing EA first had fluid removed from the nodules using a 16-gauge needle. Ablation consisted of an injection of 99% ethanol into the cystic space, which was removed after 2 minutes.
The primary outcome was nodule volume at 6 months. Secondary outcomes were postprocedural pain and complications, Dr. Park said at the meeting held by the American Thyroid Association, Asia-Oceania Thyroid Association , European Thyroid Association, and Latin American Thyroid Society.
At follow-up, the volume reductions were similar in RFA and EA (87.5 vs. 82.4 ml). The therapeutic success rate was 100% for patients who had RFA and 92% for those who had EA. Two patients in the EA group had major bleeding from the nodule, which interrupted the procedure; they later had a successful RFA. There were no complications in the RFA group.
There was only one major complication during follow-up: One patient who received EA complained of voice change, which resolved spontaneously by 2 months after ablation.
Dr. Park had no financial disclosures.
LAKE BUENA VISTA, FLA. – Ethanol ablation is just as effective as radiofrequency ablation for cystic thyroid nodules, resulting in similar volume reduction and similarly improving symptomatic and cosmetic outcomes at 6 months.
Radiofrequnecy ablation (RFA) did have a slight edge over ethanol injection (EA) in therapeutic response, Dr. Hye Sun Park said at the International Thyroid Conference. But because ethanol ablation is easier and less expensive, she recommended that it be considered as first-line therapy for these lesions.
Dr. Park of the University of Ulsan, Asan Medical Center in Seoul, South Korea, reported a trial of 46 patients, mean age 50 years old, with benign cystic thyroid nodules who were randomized to the two treatments. Patients randomized to ethanol, however, had significantly larger-volume lesions (14.7 vs. 8.6 mL), and symptom scores. Cosmetic scores and nodule vascularity were similar.
RFA was performed with an 18-gauge monopolar, internally cooled electrode with a 1-cm active tip, using the moving shot technique. Patients undergoing EA first had fluid removed from the nodules using a 16-gauge needle. Ablation consisted of an injection of 99% ethanol into the cystic space, which was removed after 2 minutes.
The primary outcome was nodule volume at 6 months. Secondary outcomes were postprocedural pain and complications, Dr. Park said at the meeting held by the American Thyroid Association, Asia-Oceania Thyroid Association , European Thyroid Association, and Latin American Thyroid Society.
At follow-up, the volume reductions were similar in RFA and EA (87.5 vs. 82.4 ml). The therapeutic success rate was 100% for patients who had RFA and 92% for those who had EA. Two patients in the EA group had major bleeding from the nodule, which interrupted the procedure; they later had a successful RFA. There were no complications in the RFA group.
There was only one major complication during follow-up: One patient who received EA complained of voice change, which resolved spontaneously by 2 months after ablation.
Dr. Park had no financial disclosures.
LAKE BUENA VISTA, FLA. – Ethanol ablation is just as effective as radiofrequency ablation for cystic thyroid nodules, resulting in similar volume reduction and similarly improving symptomatic and cosmetic outcomes at 6 months.
Radiofrequnecy ablation (RFA) did have a slight edge over ethanol injection (EA) in therapeutic response, Dr. Hye Sun Park said at the International Thyroid Conference. But because ethanol ablation is easier and less expensive, she recommended that it be considered as first-line therapy for these lesions.
Dr. Park of the University of Ulsan, Asan Medical Center in Seoul, South Korea, reported a trial of 46 patients, mean age 50 years old, with benign cystic thyroid nodules who were randomized to the two treatments. Patients randomized to ethanol, however, had significantly larger-volume lesions (14.7 vs. 8.6 mL), and symptom scores. Cosmetic scores and nodule vascularity were similar.
RFA was performed with an 18-gauge monopolar, internally cooled electrode with a 1-cm active tip, using the moving shot technique. Patients undergoing EA first had fluid removed from the nodules using a 16-gauge needle. Ablation consisted of an injection of 99% ethanol into the cystic space, which was removed after 2 minutes.
The primary outcome was nodule volume at 6 months. Secondary outcomes were postprocedural pain and complications, Dr. Park said at the meeting held by the American Thyroid Association, Asia-Oceania Thyroid Association , European Thyroid Association, and Latin American Thyroid Society.
At follow-up, the volume reductions were similar in RFA and EA (87.5 vs. 82.4 ml). The therapeutic success rate was 100% for patients who had RFA and 92% for those who had EA. Two patients in the EA group had major bleeding from the nodule, which interrupted the procedure; they later had a successful RFA. There were no complications in the RFA group.
There was only one major complication during follow-up: One patient who received EA complained of voice change, which resolved spontaneously by 2 months after ablation.
Dr. Park had no financial disclosures.
AT ITC 2015
Key clinical point: Radiofrequency ablation and ethanol ablation were similarly effective in treating cystic thyroid nodules.
Major finding: At 6 months, radiofrequency ablation and ethanol ablation achieved similar reductions in the volume of benign cystic thyroid nodules (87.5 vs. 82.4 mL).
Data source: The randomized study comprised 46 patients.
Disclosures: Dr Hye Sun Park had no financial disclosures.

Mean platelet volume higher in DVT patients with PE than without
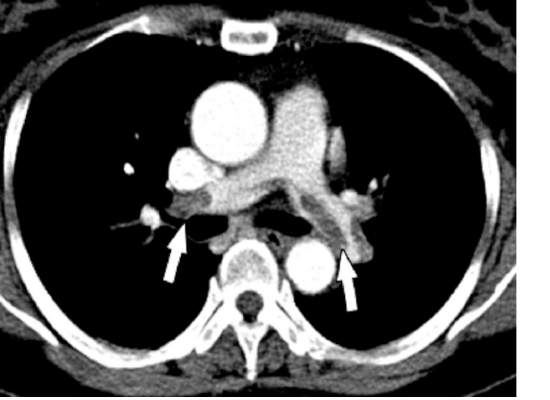
Mean platelet volume (MPV) has been associated with deep vein thrombosis (DVT), but it also appears to be a potential predictor of the presence of pulmonary embolism (PE), according to a retrospective analysis of patients reported by Dr. Atilla Icli of Ahi Evran University, Kirsehir, Turkey, and his colleagues.
The researchers assessed three groups of patients among those admitted to the emergency department or outpatient clinic of two university hospitals during 2005-2014. The patient study groups consisted of 98 patients with DVT and PE (48 men; mean age, 56.8 years); 97 patients with DVT without PE (48 men; mean age, 54.2 years); and 98 patients admitted with suspicion of DVT, but confirmed to be free of DVT and PE (45 men; mean age, 55.0 years) (Heart Lung Circulation. 2015 Nov;24[11]:1081-6).

There were no statistically significant differences between the groups with regard to sex, age, body mass index, or comorbidities such as hypertension or diabetes. Blood samples were drawn from all patients and assessed for MPV.
MPV was significantly higher in all DVT patients than controls (9.3 femtoliter vs. 7.9 fL; P less than .001) and in DVT patients with PE as compared to DVT patients without PE (9.9 fL vs. 8.7 fL, respectively; P less than .001). A cut-off point was seen where the rate of PE was significantly higher in patients with MPV greater than 9.15 fL, as compared with those with MPV equal to or below 9.15 fL. In addition, the presence of PE in patients with DVT was independently associated with MPV (odds ratio, 22.2; P less than .001).
“Our findings suggest that MPVs are elevated in patients with DVT, and higher MPVs may be associated with this group of patients,” Dr. Icli and his colleagues concluded.
The authors indicated that they had no relevant conflicts.
Read the full study online in Heart, Lung and Circulation.
Mean platelet volume (MPV) has been associated with deep vein thrombosis (DVT), but it also appears to be a potential predictor of the presence of pulmonary embolism (PE), according to a retrospective analysis of patients reported by Dr. Atilla Icli of Ahi Evran University, Kirsehir, Turkey, and his colleagues.
The researchers assessed three groups of patients among those admitted to the emergency department or outpatient clinic of two university hospitals during 2005-2014. The patient study groups consisted of 98 patients with DVT and PE (48 men; mean age, 56.8 years); 97 patients with DVT without PE (48 men; mean age, 54.2 years); and 98 patients admitted with suspicion of DVT, but confirmed to be free of DVT and PE (45 men; mean age, 55.0 years) (Heart Lung Circulation. 2015 Nov;24[11]:1081-6).
There were no statistically significant differences between the groups with regard to sex, age, body mass index, or comorbidities such as hypertension or diabetes. Blood samples were drawn from all patients and assessed for MPV.
MPV was significantly higher in all DVT patients than controls (9.3 femtoliter vs. 7.9 fL; P less than .001) and in DVT patients with PE as compared to DVT patients without PE (9.9 fL vs. 8.7 fL, respectively; P less than .001). A cut-off point was seen where the rate of PE was significantly higher in patients with MPV greater than 9.15 fL, as compared with those with MPV equal to or below 9.15 fL. In addition, the presence of PE in patients with DVT was independently associated with MPV (odds ratio, 22.2; P less than .001).
“Our findings suggest that MPVs are elevated in patients with DVT, and higher MPVs may be associated with this group of patients,” Dr. Icli and his colleagues concluded.
The authors indicated that they had no relevant conflicts.
Read the full study online in Heart, Lung and Circulation.
Mean platelet volume (MPV) has been associated with deep vein thrombosis (DVT), but it also appears to be a potential predictor of the presence of pulmonary embolism (PE), according to a retrospective analysis of patients reported by Dr. Atilla Icli of Ahi Evran University, Kirsehir, Turkey, and his colleagues.
The researchers assessed three groups of patients among those admitted to the emergency department or outpatient clinic of two university hospitals during 2005-2014. The patient study groups consisted of 98 patients with DVT and PE (48 men; mean age, 56.8 years); 97 patients with DVT without PE (48 men; mean age, 54.2 years); and 98 patients admitted with suspicion of DVT, but confirmed to be free of DVT and PE (45 men; mean age, 55.0 years) (Heart Lung Circulation. 2015 Nov;24[11]:1081-6).
There were no statistically significant differences between the groups with regard to sex, age, body mass index, or comorbidities such as hypertension or diabetes. Blood samples were drawn from all patients and assessed for MPV.
MPV was significantly higher in all DVT patients than controls (9.3 femtoliter vs. 7.9 fL; P less than .001) and in DVT patients with PE as compared to DVT patients without PE (9.9 fL vs. 8.7 fL, respectively; P less than .001). A cut-off point was seen where the rate of PE was significantly higher in patients with MPV greater than 9.15 fL, as compared with those with MPV equal to or below 9.15 fL. In addition, the presence of PE in patients with DVT was independently associated with MPV (odds ratio, 22.2; P less than .001).
“Our findings suggest that MPVs are elevated in patients with DVT, and higher MPVs may be associated with this group of patients,” Dr. Icli and his colleagues concluded.
The authors indicated that they had no relevant conflicts.
Read the full study online in Heart, Lung and Circulation.
FROM HEART, LUNG AND CIRCULATION
Hybrid approach tackles critical limb ischemia
CHICAGO – A hybrid approach combining external iliac endarterectomy with stenting may offer vascular surgeons a more robust option to stenting alone or aortofemoral bypass in patients with critical limb ischemia.
“Hybrid-based iliofemoral endarterectomy provides a minimally invasive option for revascularization, producing robust inflow restoration and low perioperative morbidity,” study author Dr. Crystal Kavanagh of St. Joseph Mercy Health Center in Ann Arbor, Mich., said.

The 5-year retrospective series, presented here at the annual meeting of the Midwestern Vascular Surgical Society, earned the prestigious Szilagyi Award for best clinical research.
Dr. Kavanagh and her colleagues crafted the hybrid technique because conventional open approaches in managing external iliac occlusive disease are associated with considerable morbidity. At the same time, long or multisegmental external iliac-to-femoral arterial lesions treated with stenting alone have produced poor patency and typically require additional outflow procedures, she explained.
The technique uses external iliac endarterectomy, aided with a traditional moll-ring stripper. A longitudinal, femoral cut-down is completed. A wire is advanced through the ipsilateral external iliac artery into the aorta after heparinization and obtaining access via an 18-gauge micropuncture in the common femoral artery. Intraluminal positioning is confirmed and a moll-ring endarterectomy is completed over the wire using a balloon to create the distal transection point, Dr. Kavanagh explained. The moll-ring is sized to the maximum diameter that will be accommodated by the ring.
After partially deflating the balloon, the plaque is extracted. A long-segment endarterectomy is typically completed, leaving a widely patent external iliac artery, she said.
In cases where adjunct iliac stenting is required, such as a proximal dissection flap, the stent size is larger than what is typically placed with stenting alone, Dr. Kavanagh observed.
The 2007 TASC (TransAtlantic InterSociety Consensus) recommendations suggest that TASC A lesions should undergo endovascular treatment as first-line therapy, while TASC D lesions should undergo traditional open surgical bypass.
Consensus has been slow to form for TASC B and C lesions, although most TASC B lesions undergo endovascular treatment and most TASC C lesions undergo open bypass.
Among the 40 limbs in the series, a common iliac (CI) artery stent (mean diameter, 8 mm: mean length, 59 mm) was placed in 19 limbs; a CI-to-external iliac (EI) stent (mean diameter, 10 mm; mean length, 100 mm) in 7 limbs; and an EI stent (mean diameter, 10 mm; mean length, 100 mm) in 21 limbs.
None of the iliac lesions were TASC category A or B, 17% were TASC C, and 83% TASC D. Concomitant infrainguinal disease of these patients had femoral/popliteal lesions, of which 16% were type A, 33% type B, 19% type C, and 32% type D.
Half of the 33 patients had three-vessel runoff, 33% two-vessel runoff, and 17% single-vessel runoff.
The hybrid procedure was completed as planned in all 40 limbs, Dr. Kavanagh said. There was no intraoperative or 90-day mortality.
Perioperative complications were minimal, with a 30-day readmission rate of only 12%, she said. This included one patient with one-vessel run-off who re-presented with ischemia requiring common femoral-to-below-the-knee popliteal bypass.
A second patient was admitted at postoperative day 47 with an infected pseudoaneurysm requiring patch angioplasty revision, for a 90-day readmission rate of 15%.
“Concerns about potential plaque rupture or hemorrhage can easily be dealt with via a covered stent graft, given intraluminal wire access throughout the procedure,” senior author Dr. Abdulhameed Aziz said in an interview.
Significant gains were made from baseline in postoperative ankle-brachial index (mean, 0.4 vs. 076; P less than .001), as well as in toe pressures (mean, 32 mm Hg vs. 60 mm Hg; P less than .001), Dr. Kavanagh said.
After a median follow-up of 13 months, primary patency was 100%.
“Combined common femoral endarterectomy with iliac stenting has demonstrated comparable patency to operative bypass in the short term,” she said.
“We theorize that the longer-segment endarterectomy, in our case essentially going from the iliac bifurcation to the common femoral, may produce a more durable result ... Stenting the proximal transection point may prevent restenosis.”
The authors reported no financial disclosures.
The combination of open surgical procedures with endovascular interventions has enriched the spectrum of vascular reconstructions significantly. These so-called hybrid procedures are especially worthwhile if pros and cons of both approaches could be combined and the groin could be considered as the hub. Technically spoken, the groin is the ideal hub for these kind of procedures. Why is that the case? Usually the surgical access to the common femoral artery (CFA) is easy. Furthermore the long-term results of femoral/retrograde iliac endarterectomy (often in combination with profundoplasty) are undoubtedly excellent. For the endovascular world, the (almost) NO-GO for any metal in the groin is still valid, and balloon dilatation of the femoral arteries is hemodynamically insufficient in most cases. However, PTA [percutaneous transluminal angioplasty] and stenting of the iliac arteries comes with good long-term results and avoids the sometimes-extended surgical access via the abdomen or the retroperitoneum.
Technically, it is advisable to perform the procedure in the following way: exposure of the CFA up to the inguinal ligament and down to the proximal superficial and deep femoral artery; puncture of the CFA in a noncalcified area and retrograde guide-wire access to the distal aorta (confirmation by angiography); balloon blockage of the proximal iliac artery (if technically possible; open endarterectomy of the CFA (including the proximal superficial and deep femoral artery; and retrograde ring-stripper endarterectomy of the iliac arteries and reconstruction of the femoral arteries (patchplasty, femoral transposition, profundoplasty). Balloon dilatation and stenting will be performed at the end of the procedure via a 7F or 9F sheath. We prefer balloon-expandable stents for the common and self-expandable stents for the external iliac artery, respectively. The contralateral groin should also be prepared for kissing stenting of both iliac arteries. Very rarely, an antegrade iliac access (via contralateral or brachial) access) is necessary. Whether or not covered stents have better long-term results is an open issue, however, covered stents should always be available to treat rare complications like an iatrogenic iliac rupture.
Especially Rutherford stage 5 or 6 patients very often present with multisegment disease including the femoropopliteal and the crural arteries. Since an even perfect inguinal inflow might not be sufficient in CLI [critical limb ischemia], these patients often need additional open or endovascular procedures. Again, the latter can be performed simultaneously via the hub femoral artery.
Even though hybrid procedures have been an essential part of vascular surgical practice for some years now, the Midwestern Vascular Surgical Society and Dr. Kavanagh have to be congratulated for raising this clinically very important topic again.
Dr. Hans-Henning Eckstein is a Professor at the Department for Vascular and Endovascular Surgery, Klinikum rechts der Isar, Technical University Munich, and is an associate medical editor for Vascular Specialist.
The combination of open surgical procedures with endovascular interventions has enriched the spectrum of vascular reconstructions significantly. These so-called hybrid procedures are especially worthwhile if pros and cons of both approaches could be combined and the groin could be considered as the hub. Technically spoken, the groin is the ideal hub for these kind of procedures. Why is that the case? Usually the surgical access to the common femoral artery (CFA) is easy. Furthermore the long-term results of femoral/retrograde iliac endarterectomy (often in combination with profundoplasty) are undoubtedly excellent. For the endovascular world, the (almost) NO-GO for any metal in the groin is still valid, and balloon dilatation of the femoral arteries is hemodynamically insufficient in most cases. However, PTA [percutaneous transluminal angioplasty] and stenting of the iliac arteries comes with good long-term results and avoids the sometimes-extended surgical access via the abdomen or the retroperitoneum.
Technically, it is advisable to perform the procedure in the following way: exposure of the CFA up to the inguinal ligament and down to the proximal superficial and deep femoral artery; puncture of the CFA in a noncalcified area and retrograde guide-wire access to the distal aorta (confirmation by angiography); balloon blockage of the proximal iliac artery (if technically possible; open endarterectomy of the CFA (including the proximal superficial and deep femoral artery; and retrograde ring-stripper endarterectomy of the iliac arteries and reconstruction of the femoral arteries (patchplasty, femoral transposition, profundoplasty). Balloon dilatation and stenting will be performed at the end of the procedure via a 7F or 9F sheath. We prefer balloon-expandable stents for the common and self-expandable stents for the external iliac artery, respectively. The contralateral groin should also be prepared for kissing stenting of both iliac arteries. Very rarely, an antegrade iliac access (via contralateral or brachial) access) is necessary. Whether or not covered stents have better long-term results is an open issue, however, covered stents should always be available to treat rare complications like an iatrogenic iliac rupture.
Especially Rutherford stage 5 or 6 patients very often present with multisegment disease including the femoropopliteal and the crural arteries. Since an even perfect inguinal inflow might not be sufficient in CLI [critical limb ischemia], these patients often need additional open or endovascular procedures. Again, the latter can be performed simultaneously via the hub femoral artery.
Even though hybrid procedures have been an essential part of vascular surgical practice for some years now, the Midwestern Vascular Surgical Society and Dr. Kavanagh have to be congratulated for raising this clinically very important topic again.
Dr. Hans-Henning Eckstein is a Professor at the Department for Vascular and Endovascular Surgery, Klinikum rechts der Isar, Technical University Munich, and is an associate medical editor for Vascular Specialist.
The combination of open surgical procedures with endovascular interventions has enriched the spectrum of vascular reconstructions significantly. These so-called hybrid procedures are especially worthwhile if pros and cons of both approaches could be combined and the groin could be considered as the hub. Technically spoken, the groin is the ideal hub for these kind of procedures. Why is that the case? Usually the surgical access to the common femoral artery (CFA) is easy. Furthermore the long-term results of femoral/retrograde iliac endarterectomy (often in combination with profundoplasty) are undoubtedly excellent. For the endovascular world, the (almost) NO-GO for any metal in the groin is still valid, and balloon dilatation of the femoral arteries is hemodynamically insufficient in most cases. However, PTA [percutaneous transluminal angioplasty] and stenting of the iliac arteries comes with good long-term results and avoids the sometimes-extended surgical access via the abdomen or the retroperitoneum.
Technically, it is advisable to perform the procedure in the following way: exposure of the CFA up to the inguinal ligament and down to the proximal superficial and deep femoral artery; puncture of the CFA in a noncalcified area and retrograde guide-wire access to the distal aorta (confirmation by angiography); balloon blockage of the proximal iliac artery (if technically possible; open endarterectomy of the CFA (including the proximal superficial and deep femoral artery; and retrograde ring-stripper endarterectomy of the iliac arteries and reconstruction of the femoral arteries (patchplasty, femoral transposition, profundoplasty). Balloon dilatation and stenting will be performed at the end of the procedure via a 7F or 9F sheath. We prefer balloon-expandable stents for the common and self-expandable stents for the external iliac artery, respectively. The contralateral groin should also be prepared for kissing stenting of both iliac arteries. Very rarely, an antegrade iliac access (via contralateral or brachial) access) is necessary. Whether or not covered stents have better long-term results is an open issue, however, covered stents should always be available to treat rare complications like an iatrogenic iliac rupture.
Especially Rutherford stage 5 or 6 patients very often present with multisegment disease including the femoropopliteal and the crural arteries. Since an even perfect inguinal inflow might not be sufficient in CLI [critical limb ischemia], these patients often need additional open or endovascular procedures. Again, the latter can be performed simultaneously via the hub femoral artery.
Even though hybrid procedures have been an essential part of vascular surgical practice for some years now, the Midwestern Vascular Surgical Society and Dr. Kavanagh have to be congratulated for raising this clinically very important topic again.
Dr. Hans-Henning Eckstein is a Professor at the Department for Vascular and Endovascular Surgery, Klinikum rechts der Isar, Technical University Munich, and is an associate medical editor for Vascular Specialist.
CHICAGO – A hybrid approach combining external iliac endarterectomy with stenting may offer vascular surgeons a more robust option to stenting alone or aortofemoral bypass in patients with critical limb ischemia.
“Hybrid-based iliofemoral endarterectomy provides a minimally invasive option for revascularization, producing robust inflow restoration and low perioperative morbidity,” study author Dr. Crystal Kavanagh of St. Joseph Mercy Health Center in Ann Arbor, Mich., said.
The 5-year retrospective series, presented here at the annual meeting of the Midwestern Vascular Surgical Society, earned the prestigious Szilagyi Award for best clinical research.
Dr. Kavanagh and her colleagues crafted the hybrid technique because conventional open approaches in managing external iliac occlusive disease are associated with considerable morbidity. At the same time, long or multisegmental external iliac-to-femoral arterial lesions treated with stenting alone have produced poor patency and typically require additional outflow procedures, she explained.
The technique uses external iliac endarterectomy, aided with a traditional moll-ring stripper. A longitudinal, femoral cut-down is completed. A wire is advanced through the ipsilateral external iliac artery into the aorta after heparinization and obtaining access via an 18-gauge micropuncture in the common femoral artery. Intraluminal positioning is confirmed and a moll-ring endarterectomy is completed over the wire using a balloon to create the distal transection point, Dr. Kavanagh explained. The moll-ring is sized to the maximum diameter that will be accommodated by the ring.
After partially deflating the balloon, the plaque is extracted. A long-segment endarterectomy is typically completed, leaving a widely patent external iliac artery, she said.
In cases where adjunct iliac stenting is required, such as a proximal dissection flap, the stent size is larger than what is typically placed with stenting alone, Dr. Kavanagh observed.
The 2007 TASC (TransAtlantic InterSociety Consensus) recommendations suggest that TASC A lesions should undergo endovascular treatment as first-line therapy, while TASC D lesions should undergo traditional open surgical bypass.
Consensus has been slow to form for TASC B and C lesions, although most TASC B lesions undergo endovascular treatment and most TASC C lesions undergo open bypass.
Among the 40 limbs in the series, a common iliac (CI) artery stent (mean diameter, 8 mm: mean length, 59 mm) was placed in 19 limbs; a CI-to-external iliac (EI) stent (mean diameter, 10 mm; mean length, 100 mm) in 7 limbs; and an EI stent (mean diameter, 10 mm; mean length, 100 mm) in 21 limbs.
None of the iliac lesions were TASC category A or B, 17% were TASC C, and 83% TASC D. Concomitant infrainguinal disease of these patients had femoral/popliteal lesions, of which 16% were type A, 33% type B, 19% type C, and 32% type D.
Half of the 33 patients had three-vessel runoff, 33% two-vessel runoff, and 17% single-vessel runoff.
The hybrid procedure was completed as planned in all 40 limbs, Dr. Kavanagh said. There was no intraoperative or 90-day mortality.
Perioperative complications were minimal, with a 30-day readmission rate of only 12%, she said. This included one patient with one-vessel run-off who re-presented with ischemia requiring common femoral-to-below-the-knee popliteal bypass.
A second patient was admitted at postoperative day 47 with an infected pseudoaneurysm requiring patch angioplasty revision, for a 90-day readmission rate of 15%.
“Concerns about potential plaque rupture or hemorrhage can easily be dealt with via a covered stent graft, given intraluminal wire access throughout the procedure,” senior author Dr. Abdulhameed Aziz said in an interview.
Significant gains were made from baseline in postoperative ankle-brachial index (mean, 0.4 vs. 076; P less than .001), as well as in toe pressures (mean, 32 mm Hg vs. 60 mm Hg; P less than .001), Dr. Kavanagh said.
After a median follow-up of 13 months, primary patency was 100%.
“Combined common femoral endarterectomy with iliac stenting has demonstrated comparable patency to operative bypass in the short term,” she said.
“We theorize that the longer-segment endarterectomy, in our case essentially going from the iliac bifurcation to the common femoral, may produce a more durable result ... Stenting the proximal transection point may prevent restenosis.”
The authors reported no financial disclosures.
CHICAGO – A hybrid approach combining external iliac endarterectomy with stenting may offer vascular surgeons a more robust option to stenting alone or aortofemoral bypass in patients with critical limb ischemia.
“Hybrid-based iliofemoral endarterectomy provides a minimally invasive option for revascularization, producing robust inflow restoration and low perioperative morbidity,” study author Dr. Crystal Kavanagh of St. Joseph Mercy Health Center in Ann Arbor, Mich., said.
The 5-year retrospective series, presented here at the annual meeting of the Midwestern Vascular Surgical Society, earned the prestigious Szilagyi Award for best clinical research.
Dr. Kavanagh and her colleagues crafted the hybrid technique because conventional open approaches in managing external iliac occlusive disease are associated with considerable morbidity. At the same time, long or multisegmental external iliac-to-femoral arterial lesions treated with stenting alone have produced poor patency and typically require additional outflow procedures, she explained.
The technique uses external iliac endarterectomy, aided with a traditional moll-ring stripper. A longitudinal, femoral cut-down is completed. A wire is advanced through the ipsilateral external iliac artery into the aorta after heparinization and obtaining access via an 18-gauge micropuncture in the common femoral artery. Intraluminal positioning is confirmed and a moll-ring endarterectomy is completed over the wire using a balloon to create the distal transection point, Dr. Kavanagh explained. The moll-ring is sized to the maximum diameter that will be accommodated by the ring.
After partially deflating the balloon, the plaque is extracted. A long-segment endarterectomy is typically completed, leaving a widely patent external iliac artery, she said.
In cases where adjunct iliac stenting is required, such as a proximal dissection flap, the stent size is larger than what is typically placed with stenting alone, Dr. Kavanagh observed.
The 2007 TASC (TransAtlantic InterSociety Consensus) recommendations suggest that TASC A lesions should undergo endovascular treatment as first-line therapy, while TASC D lesions should undergo traditional open surgical bypass.
Consensus has been slow to form for TASC B and C lesions, although most TASC B lesions undergo endovascular treatment and most TASC C lesions undergo open bypass.
Among the 40 limbs in the series, a common iliac (CI) artery stent (mean diameter, 8 mm: mean length, 59 mm) was placed in 19 limbs; a CI-to-external iliac (EI) stent (mean diameter, 10 mm; mean length, 100 mm) in 7 limbs; and an EI stent (mean diameter, 10 mm; mean length, 100 mm) in 21 limbs.
None of the iliac lesions were TASC category A or B, 17% were TASC C, and 83% TASC D. Concomitant infrainguinal disease of these patients had femoral/popliteal lesions, of which 16% were type A, 33% type B, 19% type C, and 32% type D.
Half of the 33 patients had three-vessel runoff, 33% two-vessel runoff, and 17% single-vessel runoff.
The hybrid procedure was completed as planned in all 40 limbs, Dr. Kavanagh said. There was no intraoperative or 90-day mortality.
Perioperative complications were minimal, with a 30-day readmission rate of only 12%, she said. This included one patient with one-vessel run-off who re-presented with ischemia requiring common femoral-to-below-the-knee popliteal bypass.
A second patient was admitted at postoperative day 47 with an infected pseudoaneurysm requiring patch angioplasty revision, for a 90-day readmission rate of 15%.
“Concerns about potential plaque rupture or hemorrhage can easily be dealt with via a covered stent graft, given intraluminal wire access throughout the procedure,” senior author Dr. Abdulhameed Aziz said in an interview.
Significant gains were made from baseline in postoperative ankle-brachial index (mean, 0.4 vs. 076; P less than .001), as well as in toe pressures (mean, 32 mm Hg vs. 60 mm Hg; P less than .001), Dr. Kavanagh said.
After a median follow-up of 13 months, primary patency was 100%.
“Combined common femoral endarterectomy with iliac stenting has demonstrated comparable patency to operative bypass in the short term,” she said.
“We theorize that the longer-segment endarterectomy, in our case essentially going from the iliac bifurcation to the common femoral, may produce a more durable result ... Stenting the proximal transection point may prevent restenosis.”
The authors reported no financial disclosures.
AT MIDWESTERN VASCULAR 2015
Key clinical point: Hybrid-based iliofemoral endarterectomy provides robust inflow restoration comparable to aortofemoral bypass, with minimal perioperative morbidity.
Major finding: Primary patency was 100% with a mean follow-up of 13 months.
Data source: Five-year retrospective study in 40 limbs in 33 patients with critical limb ischemia.
Disclosures: The authors reported having no financial disclosures.

BEST PRACTICES: An Oral Treatment for Moderate to Severe Plaque Psoriasis
A Best Practices Supplement to Dermatology News. This supplement was sponsored by Celgene Corporation.

Faculty/Faculty Disclosures
Alan Menter, MD
Baylor University Medical Center
Dallas, TX
Dr Menter is on the advisory board for AbbVie, Allergan, Amgen, Boehringer Ingelheim, Eli Lilly, Genentech Inc., Janssen Biotech, Inc., LEO Pharma and Pfizer; is a consultant for AbbVie, Allergan, Amgen, Convoy Therapeutics, Inc., Eli Lilly, Janssen Biotech, Inc., LEO Pharma, Novartis, Pfizer, Syntrix, Vitae, Wyeth and XenoPort; is an investigator for AbbVie, Allergan, Amgen, Boehringer Ingelheim, Celgene, Eli Lilly, Genentech, Janssen Biotech, Inc., LEO Pharma, Merck, Novartis, Pfizer, Symbio/Maruho, Syntrix and Wyeth; is a speaker for AbbVie, Amgen, Janssen Biotech, Inc., LEO Pharma and Wyeth; has received grant funds from AbbVie, Allergan, Amgen, Boehringer Ingelheim, Celgene, Genentech, Janssen Biotech, Inc., LEO Pharma, Merck, Novartis, Pfizer, Symbio/Maruho and Syntrix; and has received honoraria from AbbVie, Allergan, Amgen, Boehringer Ingelheim, Convoy Therapeutics, Inc., Eli Lilly, Genentech, Janssen Biotech, Inc., LEO Pharma, Novartis, Pfizer, Syntrix, Vitae, Wyeth and XenoPort.
Copyright © by Frontline Medical Communications Inc.
A Best Practices Supplement to Dermatology News. This supplement was sponsored by Celgene Corporation.
Faculty/Faculty Disclosures
Alan Menter, MD
Baylor University Medical Center
Dallas, TX
Dr Menter is on the advisory board for AbbVie, Allergan, Amgen, Boehringer Ingelheim, Eli Lilly, Genentech Inc., Janssen Biotech, Inc., LEO Pharma and Pfizer; is a consultant for AbbVie, Allergan, Amgen, Convoy Therapeutics, Inc., Eli Lilly, Janssen Biotech, Inc., LEO Pharma, Novartis, Pfizer, Syntrix, Vitae, Wyeth and XenoPort; is an investigator for AbbVie, Allergan, Amgen, Boehringer Ingelheim, Celgene, Eli Lilly, Genentech, Janssen Biotech, Inc., LEO Pharma, Merck, Novartis, Pfizer, Symbio/Maruho, Syntrix and Wyeth; is a speaker for AbbVie, Amgen, Janssen Biotech, Inc., LEO Pharma and Wyeth; has received grant funds from AbbVie, Allergan, Amgen, Boehringer Ingelheim, Celgene, Genentech, Janssen Biotech, Inc., LEO Pharma, Merck, Novartis, Pfizer, Symbio/Maruho and Syntrix; and has received honoraria from AbbVie, Allergan, Amgen, Boehringer Ingelheim, Convoy Therapeutics, Inc., Eli Lilly, Genentech, Janssen Biotech, Inc., LEO Pharma, Novartis, Pfizer, Syntrix, Vitae, Wyeth and XenoPort.
Copyright © by Frontline Medical Communications Inc.
A Best Practices Supplement to Dermatology News. This supplement was sponsored by Celgene Corporation.
Faculty/Faculty Disclosures
Alan Menter, MD
Baylor University Medical Center
Dallas, TX
Dr Menter is on the advisory board for AbbVie, Allergan, Amgen, Boehringer Ingelheim, Eli Lilly, Genentech Inc., Janssen Biotech, Inc., LEO Pharma and Pfizer; is a consultant for AbbVie, Allergan, Amgen, Convoy Therapeutics, Inc., Eli Lilly, Janssen Biotech, Inc., LEO Pharma, Novartis, Pfizer, Syntrix, Vitae, Wyeth and XenoPort; is an investigator for AbbVie, Allergan, Amgen, Boehringer Ingelheim, Celgene, Eli Lilly, Genentech, Janssen Biotech, Inc., LEO Pharma, Merck, Novartis, Pfizer, Symbio/Maruho, Syntrix and Wyeth; is a speaker for AbbVie, Amgen, Janssen Biotech, Inc., LEO Pharma and Wyeth; has received grant funds from AbbVie, Allergan, Amgen, Boehringer Ingelheim, Celgene, Genentech, Janssen Biotech, Inc., LEO Pharma, Merck, Novartis, Pfizer, Symbio/Maruho and Syntrix; and has received honoraria from AbbVie, Allergan, Amgen, Boehringer Ingelheim, Convoy Therapeutics, Inc., Eli Lilly, Genentech, Janssen Biotech, Inc., LEO Pharma, Novartis, Pfizer, Syntrix, Vitae, Wyeth and XenoPort.
Copyright © by Frontline Medical Communications Inc.

Reality check about IUDs
The Centers for Disease Control and Prevention recently released data regarding the use of long-acting reversible contraception (LARC), specifically intrauterine devices (IUDs), in adolescents, and suggested ways to increase their use. The American Congress of Obstetricians and Gynecologists then reiterated its recommendation promoting the use of LARC in adolescents (Obstet Gynecol. 2012;120:983-8). Historically, the use of IUDs in nulliparous females was concerning because of the risk of pelvic inflammatory disease (which could lead to infertility), pain at insertion, and the cost. But more recent research has dispelled many of those concerns, and new legislation has made access and affordability a reality; hence, the use of IUDs in teens was recommended. Despite these advances, physicians still are not making teens aware of this method of contraception.
In 2013, two important things occurred. First, emergency contraception was made available over the counter without age restriction. Second, the Affordable Care Act required most private insurance plans to cover at least one type of all 18 Food and Drug Administration–approved contraceptive methods for women as prescribed without cost sharing; this reduced the barrier of cost for IUDs. For patients covered by Medicaid, details vary, but in many cases some type of IUD is covered. In considering the best method of contraception in teens, we can all agree contraception is only as good as its proper use. If we remove the concern of infertility secondary to pelvic inflammatory disease and the barrier of cost, we can make the argument that LARC is an ideal choice for young women.
Birth rates for teenagers fell 9% from 2013 to 2014, to 24.2 births per 1,000 females aged 15-19 years – a record low according to CDC data. The rate has declined 42% since 2007 and 61% since 1991. Considering that the percent of teens who engage in sexual activity has not changed, the cause of the decline has to be related to increased contraception use and education. Although rates have declined significantly, there is much work to be done to protect our teens from unintended pregnancies.
The Contraceptive Choice Project was designed to give teens the option of birth control with the barrier of cost removed. Sixty-nine percent of 10,000 girls aged 14-17 years chose the IUD (Am J Obstet Gynecol. 2010;203[2]:115.e1-e7). The Contraceptive Choice Project also stated that the teens in this study were 20 times more likely to become pregnant using oral contraceptives, the patch, or a vaginal ring, compared with LARC or an injectable contraceptive. That is a significant statistic given that the choice of birth control used is heavily dependent on the options available. As primary care physicians, we are likely the first line of intervention, so it is important that we do not exclude the options most likely to prevent unintended pregnancies.
The rate of adolescents using IUDs increased from 0.2 to 2.5 in the 2002 and 2006-2010 National Surveys of Family Growth (J Adolesc Health. 2013;53:401-6).
There are choices when it comes to IUDs. ParaGard and Mirena are most well known. ParaGard contains copper and is hormone free; it can be used as emergency contraception and can remain in place for 12 years. Mirena releases levonorgestrel, and can be left in place for 5 years; there now is a generic form. There has been hesitation in using this product in teens because of a marketing decision made when Mirena was brought to the U.S. market. The company sought FDA approval only for women who already had children to avoid concerns about fertility. But research shows IUDS are safe and effective in women of all ages.
Unlike birth control pills, Mirena and Paragard do not reduce acne. But Mirena does reduce bloating and cramping associated with periods. Paragard has unpredictable bleeding and, therefore, is a less favorable choice in women who are not restricted to hormone-free contraception.
Newer brands on the market are Skyla and Liletta. Both are comparable to Mirena but have lower amounts of hormone, so these IUDs will be less effective in controlling the cramping and bloating. Skyla, unlike Mirena, is marketed to teens.
Implementing birth control options in your practice is imperative in caring for adolescents. Bedsider.org is a wonderful website that reviews all forms of birth control, and the pros and cons associated with each; it also compares the different types to help young women make the best choice. Another useful website is thenationalcampaign.org; this website is dedicated to educating physicians, parents, and adolescents in birth control choices to reduce unplanned pregnancies.
Dr. Pearce is a pediatrician in Frankfort, Ill.
The Centers for Disease Control and Prevention recently released data regarding the use of long-acting reversible contraception (LARC), specifically intrauterine devices (IUDs), in adolescents, and suggested ways to increase their use. The American Congress of Obstetricians and Gynecologists then reiterated its recommendation promoting the use of LARC in adolescents (Obstet Gynecol. 2012;120:983-8). Historically, the use of IUDs in nulliparous females was concerning because of the risk of pelvic inflammatory disease (which could lead to infertility), pain at insertion, and the cost. But more recent research has dispelled many of those concerns, and new legislation has made access and affordability a reality; hence, the use of IUDs in teens was recommended. Despite these advances, physicians still are not making teens aware of this method of contraception.
In 2013, two important things occurred. First, emergency contraception was made available over the counter without age restriction. Second, the Affordable Care Act required most private insurance plans to cover at least one type of all 18 Food and Drug Administration–approved contraceptive methods for women as prescribed without cost sharing; this reduced the barrier of cost for IUDs. For patients covered by Medicaid, details vary, but in many cases some type of IUD is covered. In considering the best method of contraception in teens, we can all agree contraception is only as good as its proper use. If we remove the concern of infertility secondary to pelvic inflammatory disease and the barrier of cost, we can make the argument that LARC is an ideal choice for young women.
Birth rates for teenagers fell 9% from 2013 to 2014, to 24.2 births per 1,000 females aged 15-19 years – a record low according to CDC data. The rate has declined 42% since 2007 and 61% since 1991. Considering that the percent of teens who engage in sexual activity has not changed, the cause of the decline has to be related to increased contraception use and education. Although rates have declined significantly, there is much work to be done to protect our teens from unintended pregnancies.
The Contraceptive Choice Project was designed to give teens the option of birth control with the barrier of cost removed. Sixty-nine percent of 10,000 girls aged 14-17 years chose the IUD (Am J Obstet Gynecol. 2010;203[2]:115.e1-e7). The Contraceptive Choice Project also stated that the teens in this study were 20 times more likely to become pregnant using oral contraceptives, the patch, or a vaginal ring, compared with LARC or an injectable contraceptive. That is a significant statistic given that the choice of birth control used is heavily dependent on the options available. As primary care physicians, we are likely the first line of intervention, so it is important that we do not exclude the options most likely to prevent unintended pregnancies.
The rate of adolescents using IUDs increased from 0.2 to 2.5 in the 2002 and 2006-2010 National Surveys of Family Growth (J Adolesc Health. 2013;53:401-6).
There are choices when it comes to IUDs. ParaGard and Mirena are most well known. ParaGard contains copper and is hormone free; it can be used as emergency contraception and can remain in place for 12 years. Mirena releases levonorgestrel, and can be left in place for 5 years; there now is a generic form. There has been hesitation in using this product in teens because of a marketing decision made when Mirena was brought to the U.S. market. The company sought FDA approval only for women who already had children to avoid concerns about fertility. But research shows IUDS are safe and effective in women of all ages.
Unlike birth control pills, Mirena and Paragard do not reduce acne. But Mirena does reduce bloating and cramping associated with periods. Paragard has unpredictable bleeding and, therefore, is a less favorable choice in women who are not restricted to hormone-free contraception.
Newer brands on the market are Skyla and Liletta. Both are comparable to Mirena but have lower amounts of hormone, so these IUDs will be less effective in controlling the cramping and bloating. Skyla, unlike Mirena, is marketed to teens.
Implementing birth control options in your practice is imperative in caring for adolescents. Bedsider.org is a wonderful website that reviews all forms of birth control, and the pros and cons associated with each; it also compares the different types to help young women make the best choice. Another useful website is thenationalcampaign.org; this website is dedicated to educating physicians, parents, and adolescents in birth control choices to reduce unplanned pregnancies.
Dr. Pearce is a pediatrician in Frankfort, Ill.
The Centers for Disease Control and Prevention recently released data regarding the use of long-acting reversible contraception (LARC), specifically intrauterine devices (IUDs), in adolescents, and suggested ways to increase their use. The American Congress of Obstetricians and Gynecologists then reiterated its recommendation promoting the use of LARC in adolescents (Obstet Gynecol. 2012;120:983-8). Historically, the use of IUDs in nulliparous females was concerning because of the risk of pelvic inflammatory disease (which could lead to infertility), pain at insertion, and the cost. But more recent research has dispelled many of those concerns, and new legislation has made access and affordability a reality; hence, the use of IUDs in teens was recommended. Despite these advances, physicians still are not making teens aware of this method of contraception.
In 2013, two important things occurred. First, emergency contraception was made available over the counter without age restriction. Second, the Affordable Care Act required most private insurance plans to cover at least one type of all 18 Food and Drug Administration–approved contraceptive methods for women as prescribed without cost sharing; this reduced the barrier of cost for IUDs. For patients covered by Medicaid, details vary, but in many cases some type of IUD is covered. In considering the best method of contraception in teens, we can all agree contraception is only as good as its proper use. If we remove the concern of infertility secondary to pelvic inflammatory disease and the barrier of cost, we can make the argument that LARC is an ideal choice for young women.
Birth rates for teenagers fell 9% from 2013 to 2014, to 24.2 births per 1,000 females aged 15-19 years – a record low according to CDC data. The rate has declined 42% since 2007 and 61% since 1991. Considering that the percent of teens who engage in sexual activity has not changed, the cause of the decline has to be related to increased contraception use and education. Although rates have declined significantly, there is much work to be done to protect our teens from unintended pregnancies.
The Contraceptive Choice Project was designed to give teens the option of birth control with the barrier of cost removed. Sixty-nine percent of 10,000 girls aged 14-17 years chose the IUD (Am J Obstet Gynecol. 2010;203[2]:115.e1-e7). The Contraceptive Choice Project also stated that the teens in this study were 20 times more likely to become pregnant using oral contraceptives, the patch, or a vaginal ring, compared with LARC or an injectable contraceptive. That is a significant statistic given that the choice of birth control used is heavily dependent on the options available. As primary care physicians, we are likely the first line of intervention, so it is important that we do not exclude the options most likely to prevent unintended pregnancies.
The rate of adolescents using IUDs increased from 0.2 to 2.5 in the 2002 and 2006-2010 National Surveys of Family Growth (J Adolesc Health. 2013;53:401-6).
There are choices when it comes to IUDs. ParaGard and Mirena are most well known. ParaGard contains copper and is hormone free; it can be used as emergency contraception and can remain in place for 12 years. Mirena releases levonorgestrel, and can be left in place for 5 years; there now is a generic form. There has been hesitation in using this product in teens because of a marketing decision made when Mirena was brought to the U.S. market. The company sought FDA approval only for women who already had children to avoid concerns about fertility. But research shows IUDS are safe and effective in women of all ages.
Unlike birth control pills, Mirena and Paragard do not reduce acne. But Mirena does reduce bloating and cramping associated with periods. Paragard has unpredictable bleeding and, therefore, is a less favorable choice in women who are not restricted to hormone-free contraception.
Newer brands on the market are Skyla and Liletta. Both are comparable to Mirena but have lower amounts of hormone, so these IUDs will be less effective in controlling the cramping and bloating. Skyla, unlike Mirena, is marketed to teens.
Implementing birth control options in your practice is imperative in caring for adolescents. Bedsider.org is a wonderful website that reviews all forms of birth control, and the pros and cons associated with each; it also compares the different types to help young women make the best choice. Another useful website is thenationalcampaign.org; this website is dedicated to educating physicians, parents, and adolescents in birth control choices to reduce unplanned pregnancies.
Dr. Pearce is a pediatrician in Frankfort, Ill.
