User login
Group uses lettuce to produce clotting factor on large scale

Photo by Daniel Ventura
Investigators have shown they can use lettuce to produce a factor IX product on a large scale.
The product successfully delivered factor IX to mice with hemophilia B while preventing the formation of inhibitors.
“This is a milestone in our field—to make a fully functional drug in plants, produce it at a large scale and in quantities sufficient for human clinical trials,” said Henry Daniell, PhD, of the University of Pennsylvania School of Dental Medicine in Philadelphia.
Dr Daniell and his colleagues described this work in Biomaterials.
This research builds on Dr Daniell’s previous work using genetically modified plants to introduce a protein into the body that would teach the immune system to tolerate clotting factors given as a treatment for hemophilia.
In that study, Dr Daniell and his colleagues successfully stopped and even reversed the production of inhibitors by feeding the plant-based drug to mice with hemophilia A. At that time, the investigators used a tobacco plant platform to “grow” the drug.
To take this approach to humans, Dr Daniell’s team turned to lettuce. They identified the genetic vector to introduce the therapeutic gene into the plant cells’ DNA and grow the drug within the lettuce leaves, which are then freeze-dried and encapsulated.
Two different growing systems were used. One was in Dr Daniell’s greenhouse, a high-tech facility that grows the plants in soil, using natural light.
The second system was used in the Fraunhofer USA facility, which more closely replicates how a commercial pharmaceutical production facility would run, using a hydroponic system and artificial lighting.
The investigators determined they could produce 36,000 doses in just 1000 square feet and harvest a new batch of pharmaceutical-containing lettuce every 4 to 6 weeks.
“This changes the way we think about delivering protein-based drugs and making them affordable to the global population,” Dr Daniell said.
“Over 90% of the global population can’t afford protein drugs, like insulin, due to the expense of production and the required refrigeration for storage or transportation. I am determined to challenge this scenario.” ![]()
Photo by Daniel Ventura
Investigators have shown they can use lettuce to produce a factor IX product on a large scale.
The product successfully delivered factor IX to mice with hemophilia B while preventing the formation of inhibitors.
“This is a milestone in our field—to make a fully functional drug in plants, produce it at a large scale and in quantities sufficient for human clinical trials,” said Henry Daniell, PhD, of the University of Pennsylvania School of Dental Medicine in Philadelphia.
Dr Daniell and his colleagues described this work in Biomaterials.
This research builds on Dr Daniell’s previous work using genetically modified plants to introduce a protein into the body that would teach the immune system to tolerate clotting factors given as a treatment for hemophilia.
In that study, Dr Daniell and his colleagues successfully stopped and even reversed the production of inhibitors by feeding the plant-based drug to mice with hemophilia A. At that time, the investigators used a tobacco plant platform to “grow” the drug.
To take this approach to humans, Dr Daniell’s team turned to lettuce. They identified the genetic vector to introduce the therapeutic gene into the plant cells’ DNA and grow the drug within the lettuce leaves, which are then freeze-dried and encapsulated.
Two different growing systems were used. One was in Dr Daniell’s greenhouse, a high-tech facility that grows the plants in soil, using natural light.
The second system was used in the Fraunhofer USA facility, which more closely replicates how a commercial pharmaceutical production facility would run, using a hydroponic system and artificial lighting.
The investigators determined they could produce 36,000 doses in just 1000 square feet and harvest a new batch of pharmaceutical-containing lettuce every 4 to 6 weeks.
“This changes the way we think about delivering protein-based drugs and making them affordable to the global population,” Dr Daniell said.
“Over 90% of the global population can’t afford protein drugs, like insulin, due to the expense of production and the required refrigeration for storage or transportation. I am determined to challenge this scenario.” ![]()
Photo by Daniel Ventura
Investigators have shown they can use lettuce to produce a factor IX product on a large scale.
The product successfully delivered factor IX to mice with hemophilia B while preventing the formation of inhibitors.
“This is a milestone in our field—to make a fully functional drug in plants, produce it at a large scale and in quantities sufficient for human clinical trials,” said Henry Daniell, PhD, of the University of Pennsylvania School of Dental Medicine in Philadelphia.
Dr Daniell and his colleagues described this work in Biomaterials.
This research builds on Dr Daniell’s previous work using genetically modified plants to introduce a protein into the body that would teach the immune system to tolerate clotting factors given as a treatment for hemophilia.
In that study, Dr Daniell and his colleagues successfully stopped and even reversed the production of inhibitors by feeding the plant-based drug to mice with hemophilia A. At that time, the investigators used a tobacco plant platform to “grow” the drug.
To take this approach to humans, Dr Daniell’s team turned to lettuce. They identified the genetic vector to introduce the therapeutic gene into the plant cells’ DNA and grow the drug within the lettuce leaves, which are then freeze-dried and encapsulated.
Two different growing systems were used. One was in Dr Daniell’s greenhouse, a high-tech facility that grows the plants in soil, using natural light.
The second system was used in the Fraunhofer USA facility, which more closely replicates how a commercial pharmaceutical production facility would run, using a hydroponic system and artificial lighting.
The investigators determined they could produce 36,000 doses in just 1000 square feet and harvest a new batch of pharmaceutical-containing lettuce every 4 to 6 weeks.
“This changes the way we think about delivering protein-based drugs and making them affordable to the global population,” Dr Daniell said.
“Over 90% of the global population can’t afford protein drugs, like insulin, due to the expense of production and the required refrigeration for storage or transportation. I am determined to challenge this scenario.” ![]()
FDA approves ixazomib for MM

The US Food and Drug Administration (FDA) has approved ixazomib (Ninlaro), the first oral proteasome inhibitor, for use in combination with lenalidomide and dexamethasone to treat multiple myeloma (MM) patients who have received at least 1 prior therapy.
The FDA previously granted ixazomib priority review and orphan designation.
The regulatory submission for ixazomib was primarily based on results from the first interim analysis of the phase 3 TOURMALINE-MM1 trial.
In this trial, patients with relapsed and/or refractory MM who received ixazomib plus lenalidomide and dexamethasone had superior progression-free survival when compared to patients who received placebo plus lenalidomide and dexamethasone.
Results from TOURMALINE-MM1 are scheduled to be presented at the 2015 ASH Annual Meeting (abstract 727) in December.
Ixazomib is currently under investigation in 3 other phase 3 trials of MM patients:
- TOURMALINE-MM2, investigating ixazomib vs placebo, both in combination with lenalidomide and dexamethasone in patients with newly diagnosed MM
- TOURMALINE-MM3, investigating ixazomib vs placebo as maintenance therapy in patients with newly diagnosed MM following induction therapy and autologous stem cell transplant
- TOURMALINE-MM4, investigating ixazomib vs placebo as maintenance therapy in patients with newly diagnosed MM who have not undergone autologous stem cell transplant.
Ixazomib is marketed by Takeda Pharmaceuticals. ![]()
The US Food and Drug Administration (FDA) has approved ixazomib (Ninlaro), the first oral proteasome inhibitor, for use in combination with lenalidomide and dexamethasone to treat multiple myeloma (MM) patients who have received at least 1 prior therapy.
The FDA previously granted ixazomib priority review and orphan designation.
The regulatory submission for ixazomib was primarily based on results from the first interim analysis of the phase 3 TOURMALINE-MM1 trial.
In this trial, patients with relapsed and/or refractory MM who received ixazomib plus lenalidomide and dexamethasone had superior progression-free survival when compared to patients who received placebo plus lenalidomide and dexamethasone.
Results from TOURMALINE-MM1 are scheduled to be presented at the 2015 ASH Annual Meeting (abstract 727) in December.
Ixazomib is currently under investigation in 3 other phase 3 trials of MM patients:
- TOURMALINE-MM2, investigating ixazomib vs placebo, both in combination with lenalidomide and dexamethasone in patients with newly diagnosed MM
- TOURMALINE-MM3, investigating ixazomib vs placebo as maintenance therapy in patients with newly diagnosed MM following induction therapy and autologous stem cell transplant
- TOURMALINE-MM4, investigating ixazomib vs placebo as maintenance therapy in patients with newly diagnosed MM who have not undergone autologous stem cell transplant.
Ixazomib is marketed by Takeda Pharmaceuticals. ![]()
The US Food and Drug Administration (FDA) has approved ixazomib (Ninlaro), the first oral proteasome inhibitor, for use in combination with lenalidomide and dexamethasone to treat multiple myeloma (MM) patients who have received at least 1 prior therapy.
The FDA previously granted ixazomib priority review and orphan designation.
The regulatory submission for ixazomib was primarily based on results from the first interim analysis of the phase 3 TOURMALINE-MM1 trial.
In this trial, patients with relapsed and/or refractory MM who received ixazomib plus lenalidomide and dexamethasone had superior progression-free survival when compared to patients who received placebo plus lenalidomide and dexamethasone.
Results from TOURMALINE-MM1 are scheduled to be presented at the 2015 ASH Annual Meeting (abstract 727) in December.
Ixazomib is currently under investigation in 3 other phase 3 trials of MM patients:
- TOURMALINE-MM2, investigating ixazomib vs placebo, both in combination with lenalidomide and dexamethasone in patients with newly diagnosed MM
- TOURMALINE-MM3, investigating ixazomib vs placebo as maintenance therapy in patients with newly diagnosed MM following induction therapy and autologous stem cell transplant
- TOURMALINE-MM4, investigating ixazomib vs placebo as maintenance therapy in patients with newly diagnosed MM who have not undergone autologous stem cell transplant.
Ixazomib is marketed by Takeda Pharmaceuticals. ![]()
EC approves carfilzomib for relapsed MM

Photo courtesy of Amgen
The European Commission (EC) has granted marketing authorization for carfilzomib (Kyprolis) to be used in combination with lenalidomide and dexamethasone to treat adults with multiple myeloma (MM) who have received at least 1 prior therapy.
Carfilzomib is the first irreversible proteasome inhibitor approved in the European Union (EU) as part of combination treatment for patients with relapsed MM.
Carfilzomib was granted orphan designation in the EU in 2008. The drug also received accelerated assessment, which shortened the review period from 210 days to 150 days.
Carfilzomib is a product of Onyx Pharmaceuticals, Inc., a subsidiary of Amgen that holds development and commercialization rights to the drug globally, excluding Japan.
ASPIRE trial
The EC approved carfilzomib based on data from the phase 3 ASPIRE trial, which were presented at ASH 2014 and published in NEJM.
The trial enrolled 792 patients with relapsed or refractory MM who had received 1 to 3 prior lines of therapy. The patients were randomized (1:1) to receive carfilzomib plus lenalidomide and dexamethasone (KRd) or just lenalidomide and dexamethasone (Rd) for 18 cycles.
Lenalidomide and dexamethasone were continued thereafter until disease progression. There was no planned cross-over from the control arm to treatment with carfilzomib.
The study’s primary endpoint was progression-free survival. The median progression-free survival was significantly longer in the KRd arm than the Rd arm—26.3 months and 17.6 months, respectively (hazard ratio=0.69, P=0.0001).
At the time of analysis, the difference in overall survival did not reach the prespecified boundary for statistical significance.
The overall response rate was 87% in the KRd arm and 67% in the Rd arm. The median duration of response was 28.6 months and 21.2 months, respectively.
The rates of death due to adverse events (AEs) within 30 days of the last dose were similar between the treatment arms.
The most common causes of death not due to progressive disease occurring in patients in the KRd arm and the Rd arm, respectively, were cardiac disorders (3% vs 2%), infection (2% vs 3%), renal events (0% vs less than 1%), and other AEs (2% vs 3%).
Serious AEs were reported in 60% of patients in the KRd arm and 54% in the Rd arm. The most common serious AEs reported in the KRd arm and the Rd arm, respectively, were pneumonia (14% vs 11%), respiratory tract infection (4% vs 2%), pyrexia (4% vs 2%), and pulmonary embolism (3% vs 2%).
Global development
In the US, carfilzomib is approved for use in combination with lenalidomide and dexamethasone to treat MM patients who have received 1 to 3 prior lines of therapy.
Carfilzomib also has accelerated approval in the US as a single agent to treat MM patients who have received at least 2 prior therapies, including bortezomib and an immunomodulatory agent, and have demonstrated disease progression on or within 60 days of the completion of last therapy.
Amgen plans to submit data from the phase 3 ENDEAVOR trial for potential authorization of carfilzomib in combination with dexamethasone in the EU.
This data serves as the basis of the supplemental new drug application of carfilzomib in combination with dexamethasone for patients with relapsed MM, which has been accepted for priority review in the US.
In addition to the US and EU, carfilzomib is approved for use in Argentina, Israel, Kuwait, Mexico, Thailand, and Colombia. Additional regulatory applications for the drug have been submitted to health authorities worldwide. ![]()
Photo courtesy of Amgen
The European Commission (EC) has granted marketing authorization for carfilzomib (Kyprolis) to be used in combination with lenalidomide and dexamethasone to treat adults with multiple myeloma (MM) who have received at least 1 prior therapy.
Carfilzomib is the first irreversible proteasome inhibitor approved in the European Union (EU) as part of combination treatment for patients with relapsed MM.
Carfilzomib was granted orphan designation in the EU in 2008. The drug also received accelerated assessment, which shortened the review period from 210 days to 150 days.
Carfilzomib is a product of Onyx Pharmaceuticals, Inc., a subsidiary of Amgen that holds development and commercialization rights to the drug globally, excluding Japan.
ASPIRE trial
The EC approved carfilzomib based on data from the phase 3 ASPIRE trial, which were presented at ASH 2014 and published in NEJM.
The trial enrolled 792 patients with relapsed or refractory MM who had received 1 to 3 prior lines of therapy. The patients were randomized (1:1) to receive carfilzomib plus lenalidomide and dexamethasone (KRd) or just lenalidomide and dexamethasone (Rd) for 18 cycles.
Lenalidomide and dexamethasone were continued thereafter until disease progression. There was no planned cross-over from the control arm to treatment with carfilzomib.
The study’s primary endpoint was progression-free survival. The median progression-free survival was significantly longer in the KRd arm than the Rd arm—26.3 months and 17.6 months, respectively (hazard ratio=0.69, P=0.0001).
At the time of analysis, the difference in overall survival did not reach the prespecified boundary for statistical significance.
The overall response rate was 87% in the KRd arm and 67% in the Rd arm. The median duration of response was 28.6 months and 21.2 months, respectively.
The rates of death due to adverse events (AEs) within 30 days of the last dose were similar between the treatment arms.
The most common causes of death not due to progressive disease occurring in patients in the KRd arm and the Rd arm, respectively, were cardiac disorders (3% vs 2%), infection (2% vs 3%), renal events (0% vs less than 1%), and other AEs (2% vs 3%).
Serious AEs were reported in 60% of patients in the KRd arm and 54% in the Rd arm. The most common serious AEs reported in the KRd arm and the Rd arm, respectively, were pneumonia (14% vs 11%), respiratory tract infection (4% vs 2%), pyrexia (4% vs 2%), and pulmonary embolism (3% vs 2%).
Global development
In the US, carfilzomib is approved for use in combination with lenalidomide and dexamethasone to treat MM patients who have received 1 to 3 prior lines of therapy.
Carfilzomib also has accelerated approval in the US as a single agent to treat MM patients who have received at least 2 prior therapies, including bortezomib and an immunomodulatory agent, and have demonstrated disease progression on or within 60 days of the completion of last therapy.
Amgen plans to submit data from the phase 3 ENDEAVOR trial for potential authorization of carfilzomib in combination with dexamethasone in the EU.
This data serves as the basis of the supplemental new drug application of carfilzomib in combination with dexamethasone for patients with relapsed MM, which has been accepted for priority review in the US.
In addition to the US and EU, carfilzomib is approved for use in Argentina, Israel, Kuwait, Mexico, Thailand, and Colombia. Additional regulatory applications for the drug have been submitted to health authorities worldwide. ![]()
Photo courtesy of Amgen
The European Commission (EC) has granted marketing authorization for carfilzomib (Kyprolis) to be used in combination with lenalidomide and dexamethasone to treat adults with multiple myeloma (MM) who have received at least 1 prior therapy.
Carfilzomib is the first irreversible proteasome inhibitor approved in the European Union (EU) as part of combination treatment for patients with relapsed MM.
Carfilzomib was granted orphan designation in the EU in 2008. The drug also received accelerated assessment, which shortened the review period from 210 days to 150 days.
Carfilzomib is a product of Onyx Pharmaceuticals, Inc., a subsidiary of Amgen that holds development and commercialization rights to the drug globally, excluding Japan.
ASPIRE trial
The EC approved carfilzomib based on data from the phase 3 ASPIRE trial, which were presented at ASH 2014 and published in NEJM.
The trial enrolled 792 patients with relapsed or refractory MM who had received 1 to 3 prior lines of therapy. The patients were randomized (1:1) to receive carfilzomib plus lenalidomide and dexamethasone (KRd) or just lenalidomide and dexamethasone (Rd) for 18 cycles.
Lenalidomide and dexamethasone were continued thereafter until disease progression. There was no planned cross-over from the control arm to treatment with carfilzomib.
The study’s primary endpoint was progression-free survival. The median progression-free survival was significantly longer in the KRd arm than the Rd arm—26.3 months and 17.6 months, respectively (hazard ratio=0.69, P=0.0001).
At the time of analysis, the difference in overall survival did not reach the prespecified boundary for statistical significance.
The overall response rate was 87% in the KRd arm and 67% in the Rd arm. The median duration of response was 28.6 months and 21.2 months, respectively.
The rates of death due to adverse events (AEs) within 30 days of the last dose were similar between the treatment arms.
The most common causes of death not due to progressive disease occurring in patients in the KRd arm and the Rd arm, respectively, were cardiac disorders (3% vs 2%), infection (2% vs 3%), renal events (0% vs less than 1%), and other AEs (2% vs 3%).
Serious AEs were reported in 60% of patients in the KRd arm and 54% in the Rd arm. The most common serious AEs reported in the KRd arm and the Rd arm, respectively, were pneumonia (14% vs 11%), respiratory tract infection (4% vs 2%), pyrexia (4% vs 2%), and pulmonary embolism (3% vs 2%).
Global development
In the US, carfilzomib is approved for use in combination with lenalidomide and dexamethasone to treat MM patients who have received 1 to 3 prior lines of therapy.
Carfilzomib also has accelerated approval in the US as a single agent to treat MM patients who have received at least 2 prior therapies, including bortezomib and an immunomodulatory agent, and have demonstrated disease progression on or within 60 days of the completion of last therapy.
Amgen plans to submit data from the phase 3 ENDEAVOR trial for potential authorization of carfilzomib in combination with dexamethasone in the EU.
This data serves as the basis of the supplemental new drug application of carfilzomib in combination with dexamethasone for patients with relapsed MM, which has been accepted for priority review in the US.
In addition to the US and EU, carfilzomib is approved for use in Argentina, Israel, Kuwait, Mexico, Thailand, and Colombia. Additional regulatory applications for the drug have been submitted to health authorities worldwide. ![]()
Do Heavier Patients Require Fewer Blood Transfusions In Hip, Knee Replacement Surgery?
VIENNA—Blood transfusion rates in hip and knee replacement surgery are lower in overweight or obese patients than in patients with a normal weight, according to a study presented at the 2015 International Society for Technology in Arthroplasty conference.
In this retrospective study, which included 2,399 participants, researchers sought to evaluate the impact of BMI on blood transfusions and postsurgical complications in hip and knee replacement surgery. In all, 1,503 patients underwent knee replacement and 896 patients underwent hip surgery between January 1, 2011, and November 1, 2013.

Patients were classified into groups according to BMI—normal (< 25 BMI), overweight (25 to 29.9 BMI), and obese (> 30 BMI).
Among the study’s findings were:
• A 34.8% blood transfusion rate for normal BMI patients compared with 21.9% for obese BMI patients for hip replacement.
• A 17.3% blood transfusion rate for normal BMI patients compared with 8.3% for obese BMI patients for knee replacement.
• A trend towards increased rates of deep surgical site infections in obese BMI patients.
“The results were surprising to us. It goes against the normal thought process,” said Craig Silverton, DO, a joint replacement surgeon at Henry Ford Hospital in Detroit and the study’s lead author. “It’s hard to explain but one theory could be that heavier patients have larger blood volume than patients of normal weight.”
Researchers also found no correlation between the heavier patients and post-surgical complications such as blood clots and heart attacks.
An estimated 78.6 million adult Americans are obese, and their weight problems are closely linked with an increased demand for hip and knee replacement surgery, according to government and research figures.
Patients who undergo a hip replacement typically lose about 2 pints of blood during surgery. For a knee replacement, patients usually lose about 1 pint of blood.
VIENNA—Blood transfusion rates in hip and knee replacement surgery are lower in overweight or obese patients than in patients with a normal weight, according to a study presented at the 2015 International Society for Technology in Arthroplasty conference.
In this retrospective study, which included 2,399 participants, researchers sought to evaluate the impact of BMI on blood transfusions and postsurgical complications in hip and knee replacement surgery. In all, 1,503 patients underwent knee replacement and 896 patients underwent hip surgery between January 1, 2011, and November 1, 2013.
Patients were classified into groups according to BMI—normal (< 25 BMI), overweight (25 to 29.9 BMI), and obese (> 30 BMI).
Among the study’s findings were:
• A 34.8% blood transfusion rate for normal BMI patients compared with 21.9% for obese BMI patients for hip replacement.
• A 17.3% blood transfusion rate for normal BMI patients compared with 8.3% for obese BMI patients for knee replacement.
• A trend towards increased rates of deep surgical site infections in obese BMI patients.
“The results were surprising to us. It goes against the normal thought process,” said Craig Silverton, DO, a joint replacement surgeon at Henry Ford Hospital in Detroit and the study’s lead author. “It’s hard to explain but one theory could be that heavier patients have larger blood volume than patients of normal weight.”
Researchers also found no correlation between the heavier patients and post-surgical complications such as blood clots and heart attacks.
An estimated 78.6 million adult Americans are obese, and their weight problems are closely linked with an increased demand for hip and knee replacement surgery, according to government and research figures.
Patients who undergo a hip replacement typically lose about 2 pints of blood during surgery. For a knee replacement, patients usually lose about 1 pint of blood.
VIENNA—Blood transfusion rates in hip and knee replacement surgery are lower in overweight or obese patients than in patients with a normal weight, according to a study presented at the 2015 International Society for Technology in Arthroplasty conference.
In this retrospective study, which included 2,399 participants, researchers sought to evaluate the impact of BMI on blood transfusions and postsurgical complications in hip and knee replacement surgery. In all, 1,503 patients underwent knee replacement and 896 patients underwent hip surgery between January 1, 2011, and November 1, 2013.
Patients were classified into groups according to BMI—normal (< 25 BMI), overweight (25 to 29.9 BMI), and obese (> 30 BMI).
Among the study’s findings were:
• A 34.8% blood transfusion rate for normal BMI patients compared with 21.9% for obese BMI patients for hip replacement.
• A 17.3% blood transfusion rate for normal BMI patients compared with 8.3% for obese BMI patients for knee replacement.
• A trend towards increased rates of deep surgical site infections in obese BMI patients.
“The results were surprising to us. It goes against the normal thought process,” said Craig Silverton, DO, a joint replacement surgeon at Henry Ford Hospital in Detroit and the study’s lead author. “It’s hard to explain but one theory could be that heavier patients have larger blood volume than patients of normal weight.”
Researchers also found no correlation between the heavier patients and post-surgical complications such as blood clots and heart attacks.
An estimated 78.6 million adult Americans are obese, and their weight problems are closely linked with an increased demand for hip and knee replacement surgery, according to government and research figures.
Patients who undergo a hip replacement typically lose about 2 pints of blood during surgery. For a knee replacement, patients usually lose about 1 pint of blood.

Transient Reactive Papulotranslucent Acrokeratoderma: A Report of 3 Cases Showing Excellent Response to Topical Calcipotriene
To the Editor:
Transient reactive papulotranslucent acrokeratoderma (TRPA) is a rare disorder that also has been described using the terms aquagenic syringeal acrokeratoderma, aquagenic palmoplantar keratoderma, aquagenic acrokeratoderma, aquagenic papulotranslucent acrokeratoderma, and aquagenic wrinkling of the palms.1 It was initially described in 1996 by English and McCollough,2 and since then fewer than 100 cases have been reported.1-12
A 38-year-old man presented with prominent palmar hyperhidrosis with whitish papules on the palms of 10 days’ duration. The lesions were exacerbated following exposure to water but were asymptomatic aside from their unsightly cosmetic appearance. Dermatologic examination revealed translucent, whitish, pebbly papules confined to the central palmar creases (Figure 1) that were intensified following a 5-minute water immersion test.
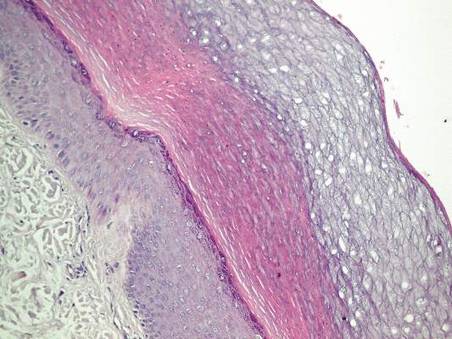
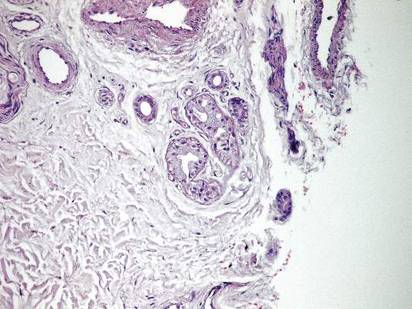
Histopathologic examination of a punch biopsy specimen from the right palm revealed orthokeratotic hyperkeratosis and slight hypergranulosis in the epidermis (Figure 2). Subtle eccrine glandular hyperplasia was evident in the dermis (Figure 3). Periodic acid–Schiff staining was negative. Based on the clinical findings and results of the water immersion test, a diagnosis of TRPA was made. A therapeutic trial of calcipotriene ointment 0.005% twice daily was initiated and resulted in dramatic clearance of the lesions within 2 weeks (Figure 4). At 1-month follow-up, the patient was virtually free of all symptoms and no disease recurrence was noted at 5-year follow-up.

| 
| ||
Figure 1. Whitish, pebbly papules confined to the central palmar creases in a 38-year-old man. | Figure 2. Orthokeratotic hyperkeratosis and mild hypergranulosis was noted in the epidermis (H&E, original magnification ×100). | ||
| 
| ||
| Figure 3. Luminal dilatation in the eccrine glands with a prominence of glandular epithelial cells, which displayed abundant cytoplasm with a granular appearance (H&E, original magnification ×100). | Figure 4. Remarkable response to calcipotriene ointment 0.005%. The white punctuate scar indicates the previous punch biopsy site. |
A 25-year-old woman presented with whitish plaques on the palms of 7 days’ duration. She reported frequent use of household cleansers in the month prior to presentation. The lesions were associated with prominent hyperhidrosis, pruritus, and a tingling sensation in the palms. Dermatologic examination revealed confluent, macerated, white, pavement stone–like papules with prominent puncta around the palmar flexures on both palms. Lesions were exacerbated after a 5-minute water immersion test (Figure 5).

The patient refused skin biopsy, and conservative treatment with a barrier cream and limited water exposure were of no benefit. Based on the clinical findings and results of the water immersion test, a diagnosis of TRPA was made. Due to the excellent outcome experienced in treating the previous patient, a trial of calcipotriene ointment 0.005% twice daily was initiated, and the patient reported complete resolution of signs and symptoms within the initial 2 weeks of treatment. Treatment was terminated at 1-month follow-up.
A 6-year-old boy presented with swollen, itchy palms of 2 months’ duration that the patient described as “wet” and “white.” Due to a recent epidemic of bird flu, the patient’s mother had advised him to use liquid cleansers and antiseptic gels on the hands for the past 2 months, which is when the symptoms on the palms started to develop. On dermatologic examination, whitish, cobblestonelike papules were noted near the palmar creases in association with profuse hyperhidrosis (Figure 6). Based on the clinical findings, a diagnosis of TRPA was made. Biopsy was not attempted and the patient was treated with calcipotriene ointment 0.005% twice daily. At 1-month follow-up, complete clearance of the lesions was noted.
Transient reactive papulotranslucent acrokeratoderma is an acquired and sporadic disorder that can occur in both sexes.2,4,6,8-11 Onset generally occurs during adolescence or young adulthood.1,3,8,9 Clinically, TRPA is characterized by edema and wrinkling of the palms following 5 to 10 minutes of contact with water that typically resolves within 1 hour after cessation of exposure.2,3,6-8,10 The “hand-in-the-bucket” sign refers to accentuation of physical findings upon immersion of the hand in water.6,10,11 Patients frequently report itching, burning, or tingling sensations in the affected areas.2,4,6,7,9,11 Transient reactive papulotranslucent acrokeratoderma usually affects the palms in a diffuse, bilateral, and symmetrical pattern,2,4,6-10 but cases showing involvement of the soles,6,7 marginal distribution of lesions,3 unilateral involvement,1 and prominence on the dorsal fingers5 also have been reported. The natural disease course involves reactive episodes and quiescent intervals.2,7,9 Spontaneous resolution of TRPA has been reported.4,6,8

The histological characteristics described in previous reports involve compact orthohyperkeratosis with dilated acrosyringia,2-6,9,11 hyperkeratosis and hypergranulosis in the epidermis,4,8,12 and eccrine glandular hyperplasia.5,12 Alternatively, the skin may appear completely normal on histology.1,7
Originally, it was proposed that TRPA is a variant of punctate keratoderma or hereditary papulotranslucent acrokeratoderma.2,3 However, its position within the keratoderma spectrum is unclear and the etiopathogenesis has not been fully elucidated. Some investigators believe that transient structural and functional alterations in the epidermal milieu prompt epidermal swelling and compensatory dilation of eccrine ducts.3,4,7,8,10 Other reports implicate the inherent structural weakness of eccrine duct walls3,4,11 or aberrations in eccrine glands.5,12 Whether the fundamental pathology lies within the epidermis, eccrine ducts, or the eccrine glands remains to be determined. Nevertheless, reports of TRPA in the setting of cystic fibrosis and its carrier state3,11 as well as the presence of hyperhidrosis in most affected patients and the accumulation of lesions along the palmar creases may implicate oversaturation of the epidermis (due to salt retention or abnormal water absorption by the stratum corneum) as the pivotal event in TRPA pathogenesis.1,10 Once the disease is expressed in susceptible individuals, episodes might be provoked by external factors such as friction, occlusion, sweating, liquid cleansers, antiseptic gels, gloves, topical preparations, and oral medications (eg, salicylic acid, cyclooxygenase 2 inhibitors).1,4
Treatment alternatives such as hydrophilic petrolatum and glycerin, ammonium lactate, salicylic acid (with or without urea), aluminum chloride hexahydrate, and topical corticosteroids are limited by unsuccessful or temporary outcomes.1,4,6,8-10 Botulinum toxin injections were effective in a patient with TRPA associated with hyperhidrosis.7 In the cases reported here, topical calcipotriene accomplished dramatic clearance of the lesions within the initial weeks of therapy. Spontaneous resolution was unlikely in these cases, as conservative therapies had not alleviated the signs and symptoms in any of the patients. However, we cannot exclude the possibility that improvement of the skin barrier function associated with other ingredients in the calcipotriene ointment (eg, petrolatum, mineral oil, α-tocopherol) may have led to the resolution of the lesions.
Calcipotriene has demonstrated efficacy in treating cutaneous disorders characterized by epidermal hyperproliferation and impaired terminal differentiation. Immunohistochemical and molecular biological evidence has indicated that topical calcipotriene exerts more pronounced inhibitory effects on epidermal proliferation than on dermal inflammation. It has been proposed that the bioavailability of calcipotriene in the dermal compartment may be markedly reduced compared to its availability in the epidermal compartment13; therefore it can be deduced that its penetration into the dermis is low in the thick skin of palms and its effect on eccrine sweat glands is negligible. Based on these factors, the clinical benefit of calcipotriene in TRPA could be ascribed directly to its antiproliferative and prodifferentiating effects on epidermal keratinocytes. We believe the primary pathology of TRPA lies in the epidermis and that changes in eccrine ducts and glands are secondary to the epidermal changes.
It is difficult to conduct large-scale studies of TRPA due to its rare presentation. Based on our encouraging preliminary observations in 3 patients, we recommend further therapeutic trials of topical calcipotriene in the treatment of TRPA.
1. Erkek E. Unilateral transient reactive papulotranslucent acrokeratoderma in a child. Pediatr Dermatol. 2007;24:564-566.
2. English JC 3rd, McCollough ML. Transient reactive papulotranslucent acrokeratoderma. J Am Acad Dermatol. 1996;34:686-687.
3. Lowes MA, Khaira GS, Holt D. Transient reactive papulotranslucent acrokeratoderma associated with cystic fibrosis. Australas J Dermatol. 2000;41:172-174.
4. MacCormack MA, Wiss K, Malhotra R. Aquagenic syringeal acrokeratoderma: report of two teenage cases. J Am Acad Dermatol. 2001;45:124-126.
5. Yoon TY, Kim KR, Lee JY, et al. Aquagenic syringeal acrokeratoderma: unusual prominence on the dorsal aspect of fingers [published online ahead of print May 22, 2008]. Br J Dermatol. 2008;159:486-488.
6. Yan AC, Aasi SZ, Alms WJ, et al. Aquagenic palmoplantar keratoderma. J Am Acad Dermatol. 2001;44:696-699.
7. Diba VC, Cormack GC, Burrows NP. Botulinum toxin is helpful in aquagenic palmoplantar keratoderma. Br J Dermatol. 2005;152:394-395.
8. Saray Y, Seckin D. Familial aquagenic acrokeratoderma: case reports and review of the literature. Int J Dermatol. 2005;44:906-909.
9. Yalcin B, Artuz F, Toy GG, et al. Acquired aquagenic papulotranslucent acrokeratoderma. J Eur Acad Dermatol Venereol. 2005;19:654-656.
10. Neri I, Bianchi F, Patrizi A. Transient aquagenic palmar hyperwrinkling: the first instance reported in a young boy. Pediatr Dermatol. 2006;23:39-42.
11. Katz KA, Yan AC, Turner ML. Aquagenic wrinkling of the palms in patients with cystic fibrosis homozygous for the delta F508 CFTR mutation. Arch Dermatol. 2005;141:621-624.
12. Kabashima K, Shimauchi T, Kobayashi M, et al. Aberrant aquaporin 5 expression in the sweat gland in aquagenic wrinkling of the palms. J Am Acad Dermatol. 2008;59(suppl 1):S28-S32.
13. Lehmann B, Querings K, Reichrath J. Vitamin D and skin: new aspects for dermatology. Exp Dermatol. 2004;13:11-15.
To the Editor:
Transient reactive papulotranslucent acrokeratoderma (TRPA) is a rare disorder that also has been described using the terms aquagenic syringeal acrokeratoderma, aquagenic palmoplantar keratoderma, aquagenic acrokeratoderma, aquagenic papulotranslucent acrokeratoderma, and aquagenic wrinkling of the palms.1 It was initially described in 1996 by English and McCollough,2 and since then fewer than 100 cases have been reported.1-12
A 38-year-old man presented with prominent palmar hyperhidrosis with whitish papules on the palms of 10 days’ duration. The lesions were exacerbated following exposure to water but were asymptomatic aside from their unsightly cosmetic appearance. Dermatologic examination revealed translucent, whitish, pebbly papules confined to the central palmar creases (Figure 1) that were intensified following a 5-minute water immersion test.
Histopathologic examination of a punch biopsy specimen from the right palm revealed orthokeratotic hyperkeratosis and slight hypergranulosis in the epidermis (Figure 2). Subtle eccrine glandular hyperplasia was evident in the dermis (Figure 3). Periodic acid–Schiff staining was negative. Based on the clinical findings and results of the water immersion test, a diagnosis of TRPA was made. A therapeutic trial of calcipotriene ointment 0.005% twice daily was initiated and resulted in dramatic clearance of the lesions within 2 weeks (Figure 4). At 1-month follow-up, the patient was virtually free of all symptoms and no disease recurrence was noted at 5-year follow-up.
|
|
| ||
Figure 1. Whitish, pebbly papules confined to the central palmar creases in a 38-year-old man. | Figure 2. Orthokeratotic hyperkeratosis and mild hypergranulosis was noted in the epidermis (H&E, original magnification ×100). | ||
|
|
| ||
| Figure 3. Luminal dilatation in the eccrine glands with a prominence of glandular epithelial cells, which displayed abundant cytoplasm with a granular appearance (H&E, original magnification ×100). | Figure 4. Remarkable response to calcipotriene ointment 0.005%. The white punctuate scar indicates the previous punch biopsy site. |
A 25-year-old woman presented with whitish plaques on the palms of 7 days’ duration. She reported frequent use of household cleansers in the month prior to presentation. The lesions were associated with prominent hyperhidrosis, pruritus, and a tingling sensation in the palms. Dermatologic examination revealed confluent, macerated, white, pavement stone–like papules with prominent puncta around the palmar flexures on both palms. Lesions were exacerbated after a 5-minute water immersion test (Figure 5).
The patient refused skin biopsy, and conservative treatment with a barrier cream and limited water exposure were of no benefit. Based on the clinical findings and results of the water immersion test, a diagnosis of TRPA was made. Due to the excellent outcome experienced in treating the previous patient, a trial of calcipotriene ointment 0.005% twice daily was initiated, and the patient reported complete resolution of signs and symptoms within the initial 2 weeks of treatment. Treatment was terminated at 1-month follow-up.
A 6-year-old boy presented with swollen, itchy palms of 2 months’ duration that the patient described as “wet” and “white.” Due to a recent epidemic of bird flu, the patient’s mother had advised him to use liquid cleansers and antiseptic gels on the hands for the past 2 months, which is when the symptoms on the palms started to develop. On dermatologic examination, whitish, cobblestonelike papules were noted near the palmar creases in association with profuse hyperhidrosis (Figure 6). Based on the clinical findings, a diagnosis of TRPA was made. Biopsy was not attempted and the patient was treated with calcipotriene ointment 0.005% twice daily. At 1-month follow-up, complete clearance of the lesions was noted.
Transient reactive papulotranslucent acrokeratoderma is an acquired and sporadic disorder that can occur in both sexes.2,4,6,8-11 Onset generally occurs during adolescence or young adulthood.1,3,8,9 Clinically, TRPA is characterized by edema and wrinkling of the palms following 5 to 10 minutes of contact with water that typically resolves within 1 hour after cessation of exposure.2,3,6-8,10 The “hand-in-the-bucket” sign refers to accentuation of physical findings upon immersion of the hand in water.6,10,11 Patients frequently report itching, burning, or tingling sensations in the affected areas.2,4,6,7,9,11 Transient reactive papulotranslucent acrokeratoderma usually affects the palms in a diffuse, bilateral, and symmetrical pattern,2,4,6-10 but cases showing involvement of the soles,6,7 marginal distribution of lesions,3 unilateral involvement,1 and prominence on the dorsal fingers5 also have been reported. The natural disease course involves reactive episodes and quiescent intervals.2,7,9 Spontaneous resolution of TRPA has been reported.4,6,8
The histological characteristics described in previous reports involve compact orthohyperkeratosis with dilated acrosyringia,2-6,9,11 hyperkeratosis and hypergranulosis in the epidermis,4,8,12 and eccrine glandular hyperplasia.5,12 Alternatively, the skin may appear completely normal on histology.1,7
Originally, it was proposed that TRPA is a variant of punctate keratoderma or hereditary papulotranslucent acrokeratoderma.2,3 However, its position within the keratoderma spectrum is unclear and the etiopathogenesis has not been fully elucidated. Some investigators believe that transient structural and functional alterations in the epidermal milieu prompt epidermal swelling and compensatory dilation of eccrine ducts.3,4,7,8,10 Other reports implicate the inherent structural weakness of eccrine duct walls3,4,11 or aberrations in eccrine glands.5,12 Whether the fundamental pathology lies within the epidermis, eccrine ducts, or the eccrine glands remains to be determined. Nevertheless, reports of TRPA in the setting of cystic fibrosis and its carrier state3,11 as well as the presence of hyperhidrosis in most affected patients and the accumulation of lesions along the palmar creases may implicate oversaturation of the epidermis (due to salt retention or abnormal water absorption by the stratum corneum) as the pivotal event in TRPA pathogenesis.1,10 Once the disease is expressed in susceptible individuals, episodes might be provoked by external factors such as friction, occlusion, sweating, liquid cleansers, antiseptic gels, gloves, topical preparations, and oral medications (eg, salicylic acid, cyclooxygenase 2 inhibitors).1,4
Treatment alternatives such as hydrophilic petrolatum and glycerin, ammonium lactate, salicylic acid (with or without urea), aluminum chloride hexahydrate, and topical corticosteroids are limited by unsuccessful or temporary outcomes.1,4,6,8-10 Botulinum toxin injections were effective in a patient with TRPA associated with hyperhidrosis.7 In the cases reported here, topical calcipotriene accomplished dramatic clearance of the lesions within the initial weeks of therapy. Spontaneous resolution was unlikely in these cases, as conservative therapies had not alleviated the signs and symptoms in any of the patients. However, we cannot exclude the possibility that improvement of the skin barrier function associated with other ingredients in the calcipotriene ointment (eg, petrolatum, mineral oil, α-tocopherol) may have led to the resolution of the lesions.
Calcipotriene has demonstrated efficacy in treating cutaneous disorders characterized by epidermal hyperproliferation and impaired terminal differentiation. Immunohistochemical and molecular biological evidence has indicated that topical calcipotriene exerts more pronounced inhibitory effects on epidermal proliferation than on dermal inflammation. It has been proposed that the bioavailability of calcipotriene in the dermal compartment may be markedly reduced compared to its availability in the epidermal compartment13; therefore it can be deduced that its penetration into the dermis is low in the thick skin of palms and its effect on eccrine sweat glands is negligible. Based on these factors, the clinical benefit of calcipotriene in TRPA could be ascribed directly to its antiproliferative and prodifferentiating effects on epidermal keratinocytes. We believe the primary pathology of TRPA lies in the epidermis and that changes in eccrine ducts and glands are secondary to the epidermal changes.
It is difficult to conduct large-scale studies of TRPA due to its rare presentation. Based on our encouraging preliminary observations in 3 patients, we recommend further therapeutic trials of topical calcipotriene in the treatment of TRPA.
To the Editor:
Transient reactive papulotranslucent acrokeratoderma (TRPA) is a rare disorder that also has been described using the terms aquagenic syringeal acrokeratoderma, aquagenic palmoplantar keratoderma, aquagenic acrokeratoderma, aquagenic papulotranslucent acrokeratoderma, and aquagenic wrinkling of the palms.1 It was initially described in 1996 by English and McCollough,2 and since then fewer than 100 cases have been reported.1-12
A 38-year-old man presented with prominent palmar hyperhidrosis with whitish papules on the palms of 10 days’ duration. The lesions were exacerbated following exposure to water but were asymptomatic aside from their unsightly cosmetic appearance. Dermatologic examination revealed translucent, whitish, pebbly papules confined to the central palmar creases (Figure 1) that were intensified following a 5-minute water immersion test.
Histopathologic examination of a punch biopsy specimen from the right palm revealed orthokeratotic hyperkeratosis and slight hypergranulosis in the epidermis (Figure 2). Subtle eccrine glandular hyperplasia was evident in the dermis (Figure 3). Periodic acid–Schiff staining was negative. Based on the clinical findings and results of the water immersion test, a diagnosis of TRPA was made. A therapeutic trial of calcipotriene ointment 0.005% twice daily was initiated and resulted in dramatic clearance of the lesions within 2 weeks (Figure 4). At 1-month follow-up, the patient was virtually free of all symptoms and no disease recurrence was noted at 5-year follow-up.
|
|
| ||
Figure 1. Whitish, pebbly papules confined to the central palmar creases in a 38-year-old man. | Figure 2. Orthokeratotic hyperkeratosis and mild hypergranulosis was noted in the epidermis (H&E, original magnification ×100). | ||
|
|
| ||
| Figure 3. Luminal dilatation in the eccrine glands with a prominence of glandular epithelial cells, which displayed abundant cytoplasm with a granular appearance (H&E, original magnification ×100). | Figure 4. Remarkable response to calcipotriene ointment 0.005%. The white punctuate scar indicates the previous punch biopsy site. |
A 25-year-old woman presented with whitish plaques on the palms of 7 days’ duration. She reported frequent use of household cleansers in the month prior to presentation. The lesions were associated with prominent hyperhidrosis, pruritus, and a tingling sensation in the palms. Dermatologic examination revealed confluent, macerated, white, pavement stone–like papules with prominent puncta around the palmar flexures on both palms. Lesions were exacerbated after a 5-minute water immersion test (Figure 5).
The patient refused skin biopsy, and conservative treatment with a barrier cream and limited water exposure were of no benefit. Based on the clinical findings and results of the water immersion test, a diagnosis of TRPA was made. Due to the excellent outcome experienced in treating the previous patient, a trial of calcipotriene ointment 0.005% twice daily was initiated, and the patient reported complete resolution of signs and symptoms within the initial 2 weeks of treatment. Treatment was terminated at 1-month follow-up.
A 6-year-old boy presented with swollen, itchy palms of 2 months’ duration that the patient described as “wet” and “white.” Due to a recent epidemic of bird flu, the patient’s mother had advised him to use liquid cleansers and antiseptic gels on the hands for the past 2 months, which is when the symptoms on the palms started to develop. On dermatologic examination, whitish, cobblestonelike papules were noted near the palmar creases in association with profuse hyperhidrosis (Figure 6). Based on the clinical findings, a diagnosis of TRPA was made. Biopsy was not attempted and the patient was treated with calcipotriene ointment 0.005% twice daily. At 1-month follow-up, complete clearance of the lesions was noted.
Transient reactive papulotranslucent acrokeratoderma is an acquired and sporadic disorder that can occur in both sexes.2,4,6,8-11 Onset generally occurs during adolescence or young adulthood.1,3,8,9 Clinically, TRPA is characterized by edema and wrinkling of the palms following 5 to 10 minutes of contact with water that typically resolves within 1 hour after cessation of exposure.2,3,6-8,10 The “hand-in-the-bucket” sign refers to accentuation of physical findings upon immersion of the hand in water.6,10,11 Patients frequently report itching, burning, or tingling sensations in the affected areas.2,4,6,7,9,11 Transient reactive papulotranslucent acrokeratoderma usually affects the palms in a diffuse, bilateral, and symmetrical pattern,2,4,6-10 but cases showing involvement of the soles,6,7 marginal distribution of lesions,3 unilateral involvement,1 and prominence on the dorsal fingers5 also have been reported. The natural disease course involves reactive episodes and quiescent intervals.2,7,9 Spontaneous resolution of TRPA has been reported.4,6,8
The histological characteristics described in previous reports involve compact orthohyperkeratosis with dilated acrosyringia,2-6,9,11 hyperkeratosis and hypergranulosis in the epidermis,4,8,12 and eccrine glandular hyperplasia.5,12 Alternatively, the skin may appear completely normal on histology.1,7
Originally, it was proposed that TRPA is a variant of punctate keratoderma or hereditary papulotranslucent acrokeratoderma.2,3 However, its position within the keratoderma spectrum is unclear and the etiopathogenesis has not been fully elucidated. Some investigators believe that transient structural and functional alterations in the epidermal milieu prompt epidermal swelling and compensatory dilation of eccrine ducts.3,4,7,8,10 Other reports implicate the inherent structural weakness of eccrine duct walls3,4,11 or aberrations in eccrine glands.5,12 Whether the fundamental pathology lies within the epidermis, eccrine ducts, or the eccrine glands remains to be determined. Nevertheless, reports of TRPA in the setting of cystic fibrosis and its carrier state3,11 as well as the presence of hyperhidrosis in most affected patients and the accumulation of lesions along the palmar creases may implicate oversaturation of the epidermis (due to salt retention or abnormal water absorption by the stratum corneum) as the pivotal event in TRPA pathogenesis.1,10 Once the disease is expressed in susceptible individuals, episodes might be provoked by external factors such as friction, occlusion, sweating, liquid cleansers, antiseptic gels, gloves, topical preparations, and oral medications (eg, salicylic acid, cyclooxygenase 2 inhibitors).1,4
Treatment alternatives such as hydrophilic petrolatum and glycerin, ammonium lactate, salicylic acid (with or without urea), aluminum chloride hexahydrate, and topical corticosteroids are limited by unsuccessful or temporary outcomes.1,4,6,8-10 Botulinum toxin injections were effective in a patient with TRPA associated with hyperhidrosis.7 In the cases reported here, topical calcipotriene accomplished dramatic clearance of the lesions within the initial weeks of therapy. Spontaneous resolution was unlikely in these cases, as conservative therapies had not alleviated the signs and symptoms in any of the patients. However, we cannot exclude the possibility that improvement of the skin barrier function associated with other ingredients in the calcipotriene ointment (eg, petrolatum, mineral oil, α-tocopherol) may have led to the resolution of the lesions.
Calcipotriene has demonstrated efficacy in treating cutaneous disorders characterized by epidermal hyperproliferation and impaired terminal differentiation. Immunohistochemical and molecular biological evidence has indicated that topical calcipotriene exerts more pronounced inhibitory effects on epidermal proliferation than on dermal inflammation. It has been proposed that the bioavailability of calcipotriene in the dermal compartment may be markedly reduced compared to its availability in the epidermal compartment13; therefore it can be deduced that its penetration into the dermis is low in the thick skin of palms and its effect on eccrine sweat glands is negligible. Based on these factors, the clinical benefit of calcipotriene in TRPA could be ascribed directly to its antiproliferative and prodifferentiating effects on epidermal keratinocytes. We believe the primary pathology of TRPA lies in the epidermis and that changes in eccrine ducts and glands are secondary to the epidermal changes.
It is difficult to conduct large-scale studies of TRPA due to its rare presentation. Based on our encouraging preliminary observations in 3 patients, we recommend further therapeutic trials of topical calcipotriene in the treatment of TRPA.
1. Erkek E. Unilateral transient reactive papulotranslucent acrokeratoderma in a child. Pediatr Dermatol. 2007;24:564-566.
2. English JC 3rd, McCollough ML. Transient reactive papulotranslucent acrokeratoderma. J Am Acad Dermatol. 1996;34:686-687.
3. Lowes MA, Khaira GS, Holt D. Transient reactive papulotranslucent acrokeratoderma associated with cystic fibrosis. Australas J Dermatol. 2000;41:172-174.
4. MacCormack MA, Wiss K, Malhotra R. Aquagenic syringeal acrokeratoderma: report of two teenage cases. J Am Acad Dermatol. 2001;45:124-126.
5. Yoon TY, Kim KR, Lee JY, et al. Aquagenic syringeal acrokeratoderma: unusual prominence on the dorsal aspect of fingers [published online ahead of print May 22, 2008]. Br J Dermatol. 2008;159:486-488.
6. Yan AC, Aasi SZ, Alms WJ, et al. Aquagenic palmoplantar keratoderma. J Am Acad Dermatol. 2001;44:696-699.
7. Diba VC, Cormack GC, Burrows NP. Botulinum toxin is helpful in aquagenic palmoplantar keratoderma. Br J Dermatol. 2005;152:394-395.
8. Saray Y, Seckin D. Familial aquagenic acrokeratoderma: case reports and review of the literature. Int J Dermatol. 2005;44:906-909.
9. Yalcin B, Artuz F, Toy GG, et al. Acquired aquagenic papulotranslucent acrokeratoderma. J Eur Acad Dermatol Venereol. 2005;19:654-656.
10. Neri I, Bianchi F, Patrizi A. Transient aquagenic palmar hyperwrinkling: the first instance reported in a young boy. Pediatr Dermatol. 2006;23:39-42.
11. Katz KA, Yan AC, Turner ML. Aquagenic wrinkling of the palms in patients with cystic fibrosis homozygous for the delta F508 CFTR mutation. Arch Dermatol. 2005;141:621-624.
12. Kabashima K, Shimauchi T, Kobayashi M, et al. Aberrant aquaporin 5 expression in the sweat gland in aquagenic wrinkling of the palms. J Am Acad Dermatol. 2008;59(suppl 1):S28-S32.
13. Lehmann B, Querings K, Reichrath J. Vitamin D and skin: new aspects for dermatology. Exp Dermatol. 2004;13:11-15.
1. Erkek E. Unilateral transient reactive papulotranslucent acrokeratoderma in a child. Pediatr Dermatol. 2007;24:564-566.
2. English JC 3rd, McCollough ML. Transient reactive papulotranslucent acrokeratoderma. J Am Acad Dermatol. 1996;34:686-687.
3. Lowes MA, Khaira GS, Holt D. Transient reactive papulotranslucent acrokeratoderma associated with cystic fibrosis. Australas J Dermatol. 2000;41:172-174.
4. MacCormack MA, Wiss K, Malhotra R. Aquagenic syringeal acrokeratoderma: report of two teenage cases. J Am Acad Dermatol. 2001;45:124-126.
5. Yoon TY, Kim KR, Lee JY, et al. Aquagenic syringeal acrokeratoderma: unusual prominence on the dorsal aspect of fingers [published online ahead of print May 22, 2008]. Br J Dermatol. 2008;159:486-488.
6. Yan AC, Aasi SZ, Alms WJ, et al. Aquagenic palmoplantar keratoderma. J Am Acad Dermatol. 2001;44:696-699.
7. Diba VC, Cormack GC, Burrows NP. Botulinum toxin is helpful in aquagenic palmoplantar keratoderma. Br J Dermatol. 2005;152:394-395.
8. Saray Y, Seckin D. Familial aquagenic acrokeratoderma: case reports and review of the literature. Int J Dermatol. 2005;44:906-909.
9. Yalcin B, Artuz F, Toy GG, et al. Acquired aquagenic papulotranslucent acrokeratoderma. J Eur Acad Dermatol Venereol. 2005;19:654-656.
10. Neri I, Bianchi F, Patrizi A. Transient aquagenic palmar hyperwrinkling: the first instance reported in a young boy. Pediatr Dermatol. 2006;23:39-42.
11. Katz KA, Yan AC, Turner ML. Aquagenic wrinkling of the palms in patients with cystic fibrosis homozygous for the delta F508 CFTR mutation. Arch Dermatol. 2005;141:621-624.
12. Kabashima K, Shimauchi T, Kobayashi M, et al. Aberrant aquaporin 5 expression in the sweat gland in aquagenic wrinkling of the palms. J Am Acad Dermatol. 2008;59(suppl 1):S28-S32.
13. Lehmann B, Querings K, Reichrath J. Vitamin D and skin: new aspects for dermatology. Exp Dermatol. 2004;13:11-15.

Sleep medicine specialists issue statement on drowsy driving
In an effort to combat drowsy driving, the American Academy of Sleep Medicine is calling for better education on the symptoms.
The organization also is calling for more research to understand the thresholds for when sleepiness while driving becomes dangerous.

“Driving while drowsy can have the same consequences as driving while under the influence of drugs and alcohol: drowsiness is similar to alcohol in how it compromises driving ability by reducing alertness and attentiveness, delaying reaction times, and hindering decision-making skills,” the American Academy of Sleep Medicine (AASM) said in a policy statement published Nov. 11, 2015, in the Journal of Clinical Sleep Medicine (doi: 10.5664/jcsm.5200).
AASM is incorporating drowsy driving education online as part of its broader National Healthy Sleep Awareness Project.
The group identified a number of symptoms of drowsy driving, including frequent yawning or difficulty keeping eyes open, “nodding off” or difficulty keeping your head up, inability to remember driving the last few miles, missing road signs or turns, difficulty maintaining speed, and drifting out of your driving lane.
AASM is calling for collaboration among sleep physicians, state departments of motor vehicles and licensing, highway patrol, and the insurance industry to develop policies and procedures that reduce drowsy driving, educational material to be used in driver’s education and licensing examination, drowsy driving educational insurance discount programs, and manufacturing and infrastructure technologies that mitigate drowsy driving.
In addition, AASM “encourages more research that better defines indicators of drowsy driving, identifies the threshold at which sleepiness while driving becomes dangerous, and provides the public with simple methods to determine when they might be too tired to drive safely.”
It also warned that consumption of caffeine can temporarily increase alertness but is not a substitute for healthy sleep, and things like turning on the radio, opening the window, or turning on the air conditioner “are not effective techniques for staying awake while driving.”
In an effort to combat drowsy driving, the American Academy of Sleep Medicine is calling for better education on the symptoms.
The organization also is calling for more research to understand the thresholds for when sleepiness while driving becomes dangerous.
“Driving while drowsy can have the same consequences as driving while under the influence of drugs and alcohol: drowsiness is similar to alcohol in how it compromises driving ability by reducing alertness and attentiveness, delaying reaction times, and hindering decision-making skills,” the American Academy of Sleep Medicine (AASM) said in a policy statement published Nov. 11, 2015, in the Journal of Clinical Sleep Medicine (doi: 10.5664/jcsm.5200).
AASM is incorporating drowsy driving education online as part of its broader National Healthy Sleep Awareness Project.
The group identified a number of symptoms of drowsy driving, including frequent yawning or difficulty keeping eyes open, “nodding off” or difficulty keeping your head up, inability to remember driving the last few miles, missing road signs or turns, difficulty maintaining speed, and drifting out of your driving lane.
AASM is calling for collaboration among sleep physicians, state departments of motor vehicles and licensing, highway patrol, and the insurance industry to develop policies and procedures that reduce drowsy driving, educational material to be used in driver’s education and licensing examination, drowsy driving educational insurance discount programs, and manufacturing and infrastructure technologies that mitigate drowsy driving.
In addition, AASM “encourages more research that better defines indicators of drowsy driving, identifies the threshold at which sleepiness while driving becomes dangerous, and provides the public with simple methods to determine when they might be too tired to drive safely.”
It also warned that consumption of caffeine can temporarily increase alertness but is not a substitute for healthy sleep, and things like turning on the radio, opening the window, or turning on the air conditioner “are not effective techniques for staying awake while driving.”
In an effort to combat drowsy driving, the American Academy of Sleep Medicine is calling for better education on the symptoms.
The organization also is calling for more research to understand the thresholds for when sleepiness while driving becomes dangerous.
“Driving while drowsy can have the same consequences as driving while under the influence of drugs and alcohol: drowsiness is similar to alcohol in how it compromises driving ability by reducing alertness and attentiveness, delaying reaction times, and hindering decision-making skills,” the American Academy of Sleep Medicine (AASM) said in a policy statement published Nov. 11, 2015, in the Journal of Clinical Sleep Medicine (doi: 10.5664/jcsm.5200).
AASM is incorporating drowsy driving education online as part of its broader National Healthy Sleep Awareness Project.
The group identified a number of symptoms of drowsy driving, including frequent yawning or difficulty keeping eyes open, “nodding off” or difficulty keeping your head up, inability to remember driving the last few miles, missing road signs or turns, difficulty maintaining speed, and drifting out of your driving lane.
AASM is calling for collaboration among sleep physicians, state departments of motor vehicles and licensing, highway patrol, and the insurance industry to develop policies and procedures that reduce drowsy driving, educational material to be used in driver’s education and licensing examination, drowsy driving educational insurance discount programs, and manufacturing and infrastructure technologies that mitigate drowsy driving.
In addition, AASM “encourages more research that better defines indicators of drowsy driving, identifies the threshold at which sleepiness while driving becomes dangerous, and provides the public with simple methods to determine when they might be too tired to drive safely.”
It also warned that consumption of caffeine can temporarily increase alertness but is not a substitute for healthy sleep, and things like turning on the radio, opening the window, or turning on the air conditioner “are not effective techniques for staying awake while driving.”
FROM JOURNAL OF CLINICAL SLEEP MEDICINE

Patients Dissatisfied with Medicare Advantage Plans
NEW YORK - Medicare Advantage plans might not be meeting the needs of patients requiring the costliest and most complex levels of care, a new study suggests.
Between 2010 and 2011, such patients were more likely to switch from Medicare Advantage plans to traditional Medicare, rather than vice versa, researchers found.
The results suggest people should carefully consider all the benefits, payments, and quality measures before enrolling in Medicare Advantage plans, said lead author Dr. Momotazur Rahman of Brown University in Providence, R.I.
Unlike traditional Medicare, which is the U.S. health insurance program for the elderly and disabled, Medicare Advantage is offered by private insurance companies. While the plans cover all services provided under traditional Medicare, Advantage plans may also include added services like eye and dental coverage. They may also charge different out-of pocket costs and offer access to different sets of providers.
At the beginning of each month, the government pays Medicare Advantage companies a lump sum to cover enrollees' expenses - with higher sums for high-risk patients.
Rahman and his colleagues write in Health Affairs that lump sums encourage companies to keep healthcare costs low. But there's been some concern that companies were maximizing profits by enrolling healthier people, whereas traditional Medicare is obligated to enroll all comers.
According to the authors of the new study, legislation in 2003 aimed to address those concerns, and research suggests it helped close the gap in deaths and healthcare use and spending between people in the two types of plans.
Other studies, however, have suggested Advantage plans were still overpaid under the new system and switching between plans was limited to those needing the most care.
The researchers analyzed data on more than 36,000 Medicare beneficiaries, about a quarter of whom were enrolled in Medicare Advantage plans, to see how many switched from one type of plan to the other over the course of the year.
Overall, there was little difference, with 4 percent of traditional Medicare beneficiaries switching, compared to 5 percent of those in Medicare Advantage plans.
But there was a difference when the researchers looked at people requiring complex care - with more switching away from Medicare Advantage plans than from traditional Medicare.
For example, 17 percent of people in nursing homes for long stays switched from Medicare Advantage to traditional Medicare between 2010 and 2011, while only 3 percent moved in the opposite direction.
Also, 8 percent of people receiving home healthcare switched from Medicare Advantage during that time, compared to 3 percent switching from traditional Medicare.
The results were more exaggerated for people enrolled in both Medicare and Medicaid. Those people are allowed to switch anytime and usually use increasingly expensive care, Dr. Rahman said.
It's not clear why people needing higher levels of care are more likely to switch out of Medicare Advantage plans, said Dr. Gretchen Jacobson, associate director with the Kaiser Family Foundation's Program on Medicare Policy in Washington, D.C.
For example, it could be due to limited provider networks, unused extra benefits, or prescription drug needs, said Dr. Jacobson, who wasn't involved with the new study.
However, she said, it's important to point out that the vast majority of people remain in their chosen programs.
"Most people are not changing when they make an initial decision about their coverage, but this is an area that's ripe for more research," she said.
A representative of America's Health Insurance Plans (AHIP) also stressed that the study only looked at one point in time, and changes for Medicare Advantage plans were adopted since that period.
"More specifically, enrollment in Medicare Advantage has continued to increase year after year as program continues to offer coordinated care that leads to better outcomes for seniors and those with chronic conditions," said AHIP's Clare Krusing.
"If the type of disenrollment that was highlighted in this study was as pervasive as the authors suggest, there would be much greater evidence that beneficiaries were leaving the program in significant numbers," she said.
NEW YORK - Medicare Advantage plans might not be meeting the needs of patients requiring the costliest and most complex levels of care, a new study suggests.
Between 2010 and 2011, such patients were more likely to switch from Medicare Advantage plans to traditional Medicare, rather than vice versa, researchers found.
The results suggest people should carefully consider all the benefits, payments, and quality measures before enrolling in Medicare Advantage plans, said lead author Dr. Momotazur Rahman of Brown University in Providence, R.I.
Unlike traditional Medicare, which is the U.S. health insurance program for the elderly and disabled, Medicare Advantage is offered by private insurance companies. While the plans cover all services provided under traditional Medicare, Advantage plans may also include added services like eye and dental coverage. They may also charge different out-of pocket costs and offer access to different sets of providers.
At the beginning of each month, the government pays Medicare Advantage companies a lump sum to cover enrollees' expenses - with higher sums for high-risk patients.
Rahman and his colleagues write in Health Affairs that lump sums encourage companies to keep healthcare costs low. But there's been some concern that companies were maximizing profits by enrolling healthier people, whereas traditional Medicare is obligated to enroll all comers.
According to the authors of the new study, legislation in 2003 aimed to address those concerns, and research suggests it helped close the gap in deaths and healthcare use and spending between people in the two types of plans.
Other studies, however, have suggested Advantage plans were still overpaid under the new system and switching between plans was limited to those needing the most care.
The researchers analyzed data on more than 36,000 Medicare beneficiaries, about a quarter of whom were enrolled in Medicare Advantage plans, to see how many switched from one type of plan to the other over the course of the year.
Overall, there was little difference, with 4 percent of traditional Medicare beneficiaries switching, compared to 5 percent of those in Medicare Advantage plans.
But there was a difference when the researchers looked at people requiring complex care - with more switching away from Medicare Advantage plans than from traditional Medicare.
For example, 17 percent of people in nursing homes for long stays switched from Medicare Advantage to traditional Medicare between 2010 and 2011, while only 3 percent moved in the opposite direction.
Also, 8 percent of people receiving home healthcare switched from Medicare Advantage during that time, compared to 3 percent switching from traditional Medicare.
The results were more exaggerated for people enrolled in both Medicare and Medicaid. Those people are allowed to switch anytime and usually use increasingly expensive care, Dr. Rahman said.
It's not clear why people needing higher levels of care are more likely to switch out of Medicare Advantage plans, said Dr. Gretchen Jacobson, associate director with the Kaiser Family Foundation's Program on Medicare Policy in Washington, D.C.
For example, it could be due to limited provider networks, unused extra benefits, or prescription drug needs, said Dr. Jacobson, who wasn't involved with the new study.
However, she said, it's important to point out that the vast majority of people remain in their chosen programs.
"Most people are not changing when they make an initial decision about their coverage, but this is an area that's ripe for more research," she said.
A representative of America's Health Insurance Plans (AHIP) also stressed that the study only looked at one point in time, and changes for Medicare Advantage plans were adopted since that period.
"More specifically, enrollment in Medicare Advantage has continued to increase year after year as program continues to offer coordinated care that leads to better outcomes for seniors and those with chronic conditions," said AHIP's Clare Krusing.
"If the type of disenrollment that was highlighted in this study was as pervasive as the authors suggest, there would be much greater evidence that beneficiaries were leaving the program in significant numbers," she said.
NEW YORK - Medicare Advantage plans might not be meeting the needs of patients requiring the costliest and most complex levels of care, a new study suggests.
Between 2010 and 2011, such patients were more likely to switch from Medicare Advantage plans to traditional Medicare, rather than vice versa, researchers found.
The results suggest people should carefully consider all the benefits, payments, and quality measures before enrolling in Medicare Advantage plans, said lead author Dr. Momotazur Rahman of Brown University in Providence, R.I.
Unlike traditional Medicare, which is the U.S. health insurance program for the elderly and disabled, Medicare Advantage is offered by private insurance companies. While the plans cover all services provided under traditional Medicare, Advantage plans may also include added services like eye and dental coverage. They may also charge different out-of pocket costs and offer access to different sets of providers.
At the beginning of each month, the government pays Medicare Advantage companies a lump sum to cover enrollees' expenses - with higher sums for high-risk patients.
Rahman and his colleagues write in Health Affairs that lump sums encourage companies to keep healthcare costs low. But there's been some concern that companies were maximizing profits by enrolling healthier people, whereas traditional Medicare is obligated to enroll all comers.
According to the authors of the new study, legislation in 2003 aimed to address those concerns, and research suggests it helped close the gap in deaths and healthcare use and spending between people in the two types of plans.
Other studies, however, have suggested Advantage plans were still overpaid under the new system and switching between plans was limited to those needing the most care.
The researchers analyzed data on more than 36,000 Medicare beneficiaries, about a quarter of whom were enrolled in Medicare Advantage plans, to see how many switched from one type of plan to the other over the course of the year.
Overall, there was little difference, with 4 percent of traditional Medicare beneficiaries switching, compared to 5 percent of those in Medicare Advantage plans.
But there was a difference when the researchers looked at people requiring complex care - with more switching away from Medicare Advantage plans than from traditional Medicare.
For example, 17 percent of people in nursing homes for long stays switched from Medicare Advantage to traditional Medicare between 2010 and 2011, while only 3 percent moved in the opposite direction.
Also, 8 percent of people receiving home healthcare switched from Medicare Advantage during that time, compared to 3 percent switching from traditional Medicare.
The results were more exaggerated for people enrolled in both Medicare and Medicaid. Those people are allowed to switch anytime and usually use increasingly expensive care, Dr. Rahman said.
It's not clear why people needing higher levels of care are more likely to switch out of Medicare Advantage plans, said Dr. Gretchen Jacobson, associate director with the Kaiser Family Foundation's Program on Medicare Policy in Washington, D.C.
For example, it could be due to limited provider networks, unused extra benefits, or prescription drug needs, said Dr. Jacobson, who wasn't involved with the new study.
However, she said, it's important to point out that the vast majority of people remain in their chosen programs.
"Most people are not changing when they make an initial decision about their coverage, but this is an area that's ripe for more research," she said.
A representative of America's Health Insurance Plans (AHIP) also stressed that the study only looked at one point in time, and changes for Medicare Advantage plans were adopted since that period.
"More specifically, enrollment in Medicare Advantage has continued to increase year after year as program continues to offer coordinated care that leads to better outcomes for seniors and those with chronic conditions," said AHIP's Clare Krusing.
"If the type of disenrollment that was highlighted in this study was as pervasive as the authors suggest, there would be much greater evidence that beneficiaries were leaving the program in significant numbers," she said.
Practical tips help quell pseudofolliculitis barbae
LAS VEGAS – Stubble is okay, and not just because it’s trendy to sport a beard. This was a key message during a presentation on pseudofolliculitis barbae at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
Changing up personal grooming habits is an important tactic for men who are plagued with pseudofolliculitis barbae, according to Dr. Andrew F. Alexis, chair of the department of dermatology and director of The Skin of Color Center, Mount Sinai St. Luke’s and Mount Sinai Roosevelt, New York.

This very common skin condition, affecting 45%-83% of men of African ancestry, is best managed by avoiding close shaving and preventing a sharp hair shaft tip. For those who don’t want a full beard for personal or professional reasons, using single blade razors, electric clippers, and even depilatories can help, he said.
All of these techniques prevent curly beard hairs from repenetrating or recurving before emergence – the underpinning of the pathology of pseudofolliculitis barbae. The embedded hairs eventually form a papular or pustular lesion that mimics infectious folliculitis. The inflammatory process can also prompt keloid formation in susceptible individuals.
Providing treatment options is important because the condition can be disfiguring, with such long-term physical sequelae as scarring beard alopecia and postinflammatory hyperpigmentation – changes in appearance that can have a significant psychosocial impact on affected men, Dr. Alexis said.
Therapies are centered around avoiding close shaving and/or preventing a sharp hair shaft tip.

One primary treatment is to stop shaving. “Embedded hairs spontaneously release after about one centimeter of growth,” Dr. Alexis said. This process can take up to 2 months, he said, but military studies dating back to the 1970s showed that the vast majority of pseudofolliculitis barbae cases resolved when service members stopped close shaving practices.
However, many patients want a clean-shaven appearance. “We can work with them to modify their shaving practices. Historically, we have recommended single-blade razors over multiple blade razors” because they shave less closely, he said, pointing out that razor manufacturers have funded studies that challenge this finding.
“Electric clippers are a very good alternative” to razors, Dr. Alexis said. A blade setting that allows at least 0.5-1 mm stubble is desirable.
Chemical depilatories, which act by weakening keratin disulfide bonds, can be effective, since depilated hair does not have a sharp, beveled tip on regrowth and is therefore less likely to repuncture the skin. Patients should be aware, though, that these substances can cause irritant contact dermatitis, he pointed out. Newer formulations are less caustic, but also less efficacious, he said.
In terms of practical tips, shaving technique is important. “Don’t assume the patient knows. There are all sorts of varying techniques out there,” some of which can exacerbate pseudofolliculitis barbae, Dr. Alexis said.
Before shaving, men should wash with a mild cleanser, using a gentle circular technique to free any entrapped hairs, then a moisturizing shaving cream. Razors should be changed every five to seven shaves, and shaving should always be done in the direction of beard growth without pulling on the skin.

Post shave, topical benzoyl peroxide 5%/clindamycin 1% can significantly reduce papules and pustules. Topical retinoids are another effective option. A low-potency steroid can be helpful for inflammatory symptoms.
For cases that just don’t respond to conservative and medical management, laser hair removal is an option. A recent military-funded split-face study found further improvement when topical eflornithine was added to long-pulse Nd:Yag laser therapy, Dr. Alexis said.
Affected individuals may find it difficult to modify shaving practices when uniformed service regulations or office dress codes require men to be close shaven; a note from a physician can be helpful. Dr. Alexis provides patients with a form letter to show their employers, explaining that the patient has a skin disorder that is exacerbated by shaving, and that the patient should be permitted to maintain a well-groomed beard. “I end up writing a lot of these for New York police officers,” he said.
Dr. Alexis disclosed that he has received grants and research support from Allergan and Novartis, and speaker honoraria from Cipla. He has received consulting fees from Aclaris, Allergan, Amgen, Anacor, Bayer, Galderma, Johnson & Johnson, Leo, L’Oreal, Roche, Schick, Suneva, and Valeant.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – Stubble is okay, and not just because it’s trendy to sport a beard. This was a key message during a presentation on pseudofolliculitis barbae at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
Changing up personal grooming habits is an important tactic for men who are plagued with pseudofolliculitis barbae, according to Dr. Andrew F. Alexis, chair of the department of dermatology and director of The Skin of Color Center, Mount Sinai St. Luke’s and Mount Sinai Roosevelt, New York.
This very common skin condition, affecting 45%-83% of men of African ancestry, is best managed by avoiding close shaving and preventing a sharp hair shaft tip. For those who don’t want a full beard for personal or professional reasons, using single blade razors, electric clippers, and even depilatories can help, he said.
All of these techniques prevent curly beard hairs from repenetrating or recurving before emergence – the underpinning of the pathology of pseudofolliculitis barbae. The embedded hairs eventually form a papular or pustular lesion that mimics infectious folliculitis. The inflammatory process can also prompt keloid formation in susceptible individuals.
Providing treatment options is important because the condition can be disfiguring, with such long-term physical sequelae as scarring beard alopecia and postinflammatory hyperpigmentation – changes in appearance that can have a significant psychosocial impact on affected men, Dr. Alexis said.
Therapies are centered around avoiding close shaving and/or preventing a sharp hair shaft tip.
One primary treatment is to stop shaving. “Embedded hairs spontaneously release after about one centimeter of growth,” Dr. Alexis said. This process can take up to 2 months, he said, but military studies dating back to the 1970s showed that the vast majority of pseudofolliculitis barbae cases resolved when service members stopped close shaving practices.
However, many patients want a clean-shaven appearance. “We can work with them to modify their shaving practices. Historically, we have recommended single-blade razors over multiple blade razors” because they shave less closely, he said, pointing out that razor manufacturers have funded studies that challenge this finding.
“Electric clippers are a very good alternative” to razors, Dr. Alexis said. A blade setting that allows at least 0.5-1 mm stubble is desirable.
Chemical depilatories, which act by weakening keratin disulfide bonds, can be effective, since depilated hair does not have a sharp, beveled tip on regrowth and is therefore less likely to repuncture the skin. Patients should be aware, though, that these substances can cause irritant contact dermatitis, he pointed out. Newer formulations are less caustic, but also less efficacious, he said.
In terms of practical tips, shaving technique is important. “Don’t assume the patient knows. There are all sorts of varying techniques out there,” some of which can exacerbate pseudofolliculitis barbae, Dr. Alexis said.
Before shaving, men should wash with a mild cleanser, using a gentle circular technique to free any entrapped hairs, then a moisturizing shaving cream. Razors should be changed every five to seven shaves, and shaving should always be done in the direction of beard growth without pulling on the skin.
Post shave, topical benzoyl peroxide 5%/clindamycin 1% can significantly reduce papules and pustules. Topical retinoids are another effective option. A low-potency steroid can be helpful for inflammatory symptoms.
For cases that just don’t respond to conservative and medical management, laser hair removal is an option. A recent military-funded split-face study found further improvement when topical eflornithine was added to long-pulse Nd:Yag laser therapy, Dr. Alexis said.
Affected individuals may find it difficult to modify shaving practices when uniformed service regulations or office dress codes require men to be close shaven; a note from a physician can be helpful. Dr. Alexis provides patients with a form letter to show their employers, explaining that the patient has a skin disorder that is exacerbated by shaving, and that the patient should be permitted to maintain a well-groomed beard. “I end up writing a lot of these for New York police officers,” he said.
Dr. Alexis disclosed that he has received grants and research support from Allergan and Novartis, and speaker honoraria from Cipla. He has received consulting fees from Aclaris, Allergan, Amgen, Anacor, Bayer, Galderma, Johnson & Johnson, Leo, L’Oreal, Roche, Schick, Suneva, and Valeant.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – Stubble is okay, and not just because it’s trendy to sport a beard. This was a key message during a presentation on pseudofolliculitis barbae at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
Changing up personal grooming habits is an important tactic for men who are plagued with pseudofolliculitis barbae, according to Dr. Andrew F. Alexis, chair of the department of dermatology and director of The Skin of Color Center, Mount Sinai St. Luke’s and Mount Sinai Roosevelt, New York.
This very common skin condition, affecting 45%-83% of men of African ancestry, is best managed by avoiding close shaving and preventing a sharp hair shaft tip. For those who don’t want a full beard for personal or professional reasons, using single blade razors, electric clippers, and even depilatories can help, he said.
All of these techniques prevent curly beard hairs from repenetrating or recurving before emergence – the underpinning of the pathology of pseudofolliculitis barbae. The embedded hairs eventually form a papular or pustular lesion that mimics infectious folliculitis. The inflammatory process can also prompt keloid formation in susceptible individuals.
Providing treatment options is important because the condition can be disfiguring, with such long-term physical sequelae as scarring beard alopecia and postinflammatory hyperpigmentation – changes in appearance that can have a significant psychosocial impact on affected men, Dr. Alexis said.
Therapies are centered around avoiding close shaving and/or preventing a sharp hair shaft tip.
One primary treatment is to stop shaving. “Embedded hairs spontaneously release after about one centimeter of growth,” Dr. Alexis said. This process can take up to 2 months, he said, but military studies dating back to the 1970s showed that the vast majority of pseudofolliculitis barbae cases resolved when service members stopped close shaving practices.
However, many patients want a clean-shaven appearance. “We can work with them to modify their shaving practices. Historically, we have recommended single-blade razors over multiple blade razors” because they shave less closely, he said, pointing out that razor manufacturers have funded studies that challenge this finding.
“Electric clippers are a very good alternative” to razors, Dr. Alexis said. A blade setting that allows at least 0.5-1 mm stubble is desirable.
Chemical depilatories, which act by weakening keratin disulfide bonds, can be effective, since depilated hair does not have a sharp, beveled tip on regrowth and is therefore less likely to repuncture the skin. Patients should be aware, though, that these substances can cause irritant contact dermatitis, he pointed out. Newer formulations are less caustic, but also less efficacious, he said.
In terms of practical tips, shaving technique is important. “Don’t assume the patient knows. There are all sorts of varying techniques out there,” some of which can exacerbate pseudofolliculitis barbae, Dr. Alexis said.
Before shaving, men should wash with a mild cleanser, using a gentle circular technique to free any entrapped hairs, then a moisturizing shaving cream. Razors should be changed every five to seven shaves, and shaving should always be done in the direction of beard growth without pulling on the skin.
Post shave, topical benzoyl peroxide 5%/clindamycin 1% can significantly reduce papules and pustules. Topical retinoids are another effective option. A low-potency steroid can be helpful for inflammatory symptoms.
For cases that just don’t respond to conservative and medical management, laser hair removal is an option. A recent military-funded split-face study found further improvement when topical eflornithine was added to long-pulse Nd:Yag laser therapy, Dr. Alexis said.
Affected individuals may find it difficult to modify shaving practices when uniformed service regulations or office dress codes require men to be close shaven; a note from a physician can be helpful. Dr. Alexis provides patients with a form letter to show their employers, explaining that the patient has a skin disorder that is exacerbated by shaving, and that the patient should be permitted to maintain a well-groomed beard. “I end up writing a lot of these for New York police officers,” he said.
Dr. Alexis disclosed that he has received grants and research support from Allergan and Novartis, and speaker honoraria from Cipla. He has received consulting fees from Aclaris, Allergan, Amgen, Anacor, Bayer, Galderma, Johnson & Johnson, Leo, L’Oreal, Roche, Schick, Suneva, and Valeant.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
EXPERT ANALYSIS FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR

Long-term risk of hospitalization in cancer survivors

patient and her father
Photo by Rhoda Baer
Results of a large study suggest that adolescent and young adult cancer survivors have an increased risk of hospitalization up to 34 years after their diagnosis.
Cancer survivors with the highest risk of hospitalization were those who had been diagnosed with leukemia, brain cancer, or Hodgkin lymphoma.
Kathrine Rugbjerg, PhD, and Jørgen H. Olsen, MD, of the Danish Cancer Society Research Center in Copenhagen, Denmark, reported these results in JAMA Oncology.
The pair examined the risk of hospitalization in 33,555 subjects who had cancer as adolescents or young adults and survived at least 5 years. The subjects were diagnosed from 1943 through 2004, when they were 15 to 39 years of age.
The researchers compared the cancer survivors to a cohort of 228,447 subjects from the general population who were matched to the cancer survivors by sex and year of birth.
All study subjects were followed up for hospitalizations in the Danish Patient Register through December 2010. The median follow-up was 14 years.
There were 53,032 hospitalizations among the cancer survivors, but only 38,423 were expected. So the standardized hospitalization rate ratio (RR) was 1.38.
The highest risks of hospitalization were for diseases of blood and blood-forming organs (RR=2.00), infectious and parasitic diseases (RR=1.69), and malignant neoplasms (RR=1.63).
The overall absolute excess risk of hospitalization for the cancer survivors was 2803 per 100,000 person-years. The highest absolute excess risks were for malignant neoplasms (18%), diseases of digestive organs (15%), and diseases of the circulatory system (14%).
The researchers said these results suggest that survivors of adolescent and young adult cancers face persistent risks for a broad range of somatic diseases that require hospitalization. And the morbidity pattern is highly dependent on the type of cancer being treated. ![]()
patient and her father
Photo by Rhoda Baer
Results of a large study suggest that adolescent and young adult cancer survivors have an increased risk of hospitalization up to 34 years after their diagnosis.
Cancer survivors with the highest risk of hospitalization were those who had been diagnosed with leukemia, brain cancer, or Hodgkin lymphoma.
Kathrine Rugbjerg, PhD, and Jørgen H. Olsen, MD, of the Danish Cancer Society Research Center in Copenhagen, Denmark, reported these results in JAMA Oncology.
The pair examined the risk of hospitalization in 33,555 subjects who had cancer as adolescents or young adults and survived at least 5 years. The subjects were diagnosed from 1943 through 2004, when they were 15 to 39 years of age.
The researchers compared the cancer survivors to a cohort of 228,447 subjects from the general population who were matched to the cancer survivors by sex and year of birth.
All study subjects were followed up for hospitalizations in the Danish Patient Register through December 2010. The median follow-up was 14 years.
There were 53,032 hospitalizations among the cancer survivors, but only 38,423 were expected. So the standardized hospitalization rate ratio (RR) was 1.38.
The highest risks of hospitalization were for diseases of blood and blood-forming organs (RR=2.00), infectious and parasitic diseases (RR=1.69), and malignant neoplasms (RR=1.63).
The overall absolute excess risk of hospitalization for the cancer survivors was 2803 per 100,000 person-years. The highest absolute excess risks were for malignant neoplasms (18%), diseases of digestive organs (15%), and diseases of the circulatory system (14%).
The researchers said these results suggest that survivors of adolescent and young adult cancers face persistent risks for a broad range of somatic diseases that require hospitalization. And the morbidity pattern is highly dependent on the type of cancer being treated. ![]()
patient and her father
Photo by Rhoda Baer
Results of a large study suggest that adolescent and young adult cancer survivors have an increased risk of hospitalization up to 34 years after their diagnosis.
Cancer survivors with the highest risk of hospitalization were those who had been diagnosed with leukemia, brain cancer, or Hodgkin lymphoma.
Kathrine Rugbjerg, PhD, and Jørgen H. Olsen, MD, of the Danish Cancer Society Research Center in Copenhagen, Denmark, reported these results in JAMA Oncology.
The pair examined the risk of hospitalization in 33,555 subjects who had cancer as adolescents or young adults and survived at least 5 years. The subjects were diagnosed from 1943 through 2004, when they were 15 to 39 years of age.
The researchers compared the cancer survivors to a cohort of 228,447 subjects from the general population who were matched to the cancer survivors by sex and year of birth.
All study subjects were followed up for hospitalizations in the Danish Patient Register through December 2010. The median follow-up was 14 years.
There were 53,032 hospitalizations among the cancer survivors, but only 38,423 were expected. So the standardized hospitalization rate ratio (RR) was 1.38.
The highest risks of hospitalization were for diseases of blood and blood-forming organs (RR=2.00), infectious and parasitic diseases (RR=1.69), and malignant neoplasms (RR=1.63).
The overall absolute excess risk of hospitalization for the cancer survivors was 2803 per 100,000 person-years. The highest absolute excess risks were for malignant neoplasms (18%), diseases of digestive organs (15%), and diseases of the circulatory system (14%).
The researchers said these results suggest that survivors of adolescent and young adult cancers face persistent risks for a broad range of somatic diseases that require hospitalization. And the morbidity pattern is highly dependent on the type of cancer being treated. ![]()
Unexpected findings in young cancer patients

Photo by Bill Branson
Many young cancer patients—not just those with a family history of cancer—may benefit from comprehensive genomic screening, according to a study published in NEJM.
The research revealed germline mutations in cancer-predisposing genes in 8.5% of the children and adolescents studied.
Information on family history was available for roughly 60% of these cancer patients, and, in this group, only 40% of patients had a family history of cancer.
Prior to this study, the presence of such germline mutations was thought to be extremely rare and restricted to children in families with strong histories of cancer.
“This paper marks an important turning point in our understanding of pediatric cancer risk and will likely change how patients are evaluated,” said James R. Downing, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“For many pediatric cancer patients, comprehensive next-generation DNA sequencing of both their tumor and normal tissue may provide valuable information that will not only influence their clinical management but also lead to genetic counseling and testing of their parents and siblings who may be at risk and would benefit from ongoing surveillance.”
To conduct this research, Dr Downing and his colleagues performed next-generation sequencing of both the tumor and normal tissues of 1120 cancer patients younger than 20 years of age.
The investigators sequenced the whole genome in 595 patients, the whole exome in 456 patients, and both in 69 patients.
The team analyzed the DNA sequences of 565 genes, including 60 that have been associated with autosomal dominant cancer-predisposition syndromes, for the presence of germline mutations.
A total of 95 patients, or 8.5%, had germline mutations in 21 of the 60 genes. In comparison, only 1.1% of individuals in a non-cancer cohort had alterations in the same genes.
Fifty-eight of the cancer patients who had a cancer-predisposing mutation also had available information on their family history. Forty percent (n=23) of these patients had a family history of cancer.
The frequency of germline mutations in cancer-predisposition genes varied by the type of cancer a patient had. The highest frequency, 16.7%, was in patients with non-central nervous system (CNS) solid tumors, followed by CNS tumors, at 9%, and leukemia, at 4.4%.
The most commonly mutated genes were TP53 (n=50), APC (n=6), BRCA2 (n=6), NF1 (n=4), PMS2 (n=4), RB1 (n=3), and RUNX1 (n=3).
The investigators were surprised to find mutations in the breast and ovarian cancer genes BRCA1 and BRCA2 in a number of the patients. These genes are not currently included in pediatric cancer genetic screening.
“Another surprising finding to emerge from this study was the prevalence of germline mutations in 6 patients with Ewing sarcoma,” said study author Kim Nichols, MD, also of St. Jude. “[This cancer] was not previously thought to be part of any cancer-predisposition syndrome.” ![]()
Photo by Bill Branson
Many young cancer patients—not just those with a family history of cancer—may benefit from comprehensive genomic screening, according to a study published in NEJM.
The research revealed germline mutations in cancer-predisposing genes in 8.5% of the children and adolescents studied.
Information on family history was available for roughly 60% of these cancer patients, and, in this group, only 40% of patients had a family history of cancer.
Prior to this study, the presence of such germline mutations was thought to be extremely rare and restricted to children in families with strong histories of cancer.
“This paper marks an important turning point in our understanding of pediatric cancer risk and will likely change how patients are evaluated,” said James R. Downing, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“For many pediatric cancer patients, comprehensive next-generation DNA sequencing of both their tumor and normal tissue may provide valuable information that will not only influence their clinical management but also lead to genetic counseling and testing of their parents and siblings who may be at risk and would benefit from ongoing surveillance.”
To conduct this research, Dr Downing and his colleagues performed next-generation sequencing of both the tumor and normal tissues of 1120 cancer patients younger than 20 years of age.
The investigators sequenced the whole genome in 595 patients, the whole exome in 456 patients, and both in 69 patients.
The team analyzed the DNA sequences of 565 genes, including 60 that have been associated with autosomal dominant cancer-predisposition syndromes, for the presence of germline mutations.
A total of 95 patients, or 8.5%, had germline mutations in 21 of the 60 genes. In comparison, only 1.1% of individuals in a non-cancer cohort had alterations in the same genes.
Fifty-eight of the cancer patients who had a cancer-predisposing mutation also had available information on their family history. Forty percent (n=23) of these patients had a family history of cancer.
The frequency of germline mutations in cancer-predisposition genes varied by the type of cancer a patient had. The highest frequency, 16.7%, was in patients with non-central nervous system (CNS) solid tumors, followed by CNS tumors, at 9%, and leukemia, at 4.4%.
The most commonly mutated genes were TP53 (n=50), APC (n=6), BRCA2 (n=6), NF1 (n=4), PMS2 (n=4), RB1 (n=3), and RUNX1 (n=3).
The investigators were surprised to find mutations in the breast and ovarian cancer genes BRCA1 and BRCA2 in a number of the patients. These genes are not currently included in pediatric cancer genetic screening.
“Another surprising finding to emerge from this study was the prevalence of germline mutations in 6 patients with Ewing sarcoma,” said study author Kim Nichols, MD, also of St. Jude. “[This cancer] was not previously thought to be part of any cancer-predisposition syndrome.” ![]()
Photo by Bill Branson
Many young cancer patients—not just those with a family history of cancer—may benefit from comprehensive genomic screening, according to a study published in NEJM.
The research revealed germline mutations in cancer-predisposing genes in 8.5% of the children and adolescents studied.
Information on family history was available for roughly 60% of these cancer patients, and, in this group, only 40% of patients had a family history of cancer.
Prior to this study, the presence of such germline mutations was thought to be extremely rare and restricted to children in families with strong histories of cancer.
“This paper marks an important turning point in our understanding of pediatric cancer risk and will likely change how patients are evaluated,” said James R. Downing, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“For many pediatric cancer patients, comprehensive next-generation DNA sequencing of both their tumor and normal tissue may provide valuable information that will not only influence their clinical management but also lead to genetic counseling and testing of their parents and siblings who may be at risk and would benefit from ongoing surveillance.”
To conduct this research, Dr Downing and his colleagues performed next-generation sequencing of both the tumor and normal tissues of 1120 cancer patients younger than 20 years of age.
The investigators sequenced the whole genome in 595 patients, the whole exome in 456 patients, and both in 69 patients.
The team analyzed the DNA sequences of 565 genes, including 60 that have been associated with autosomal dominant cancer-predisposition syndromes, for the presence of germline mutations.
A total of 95 patients, or 8.5%, had germline mutations in 21 of the 60 genes. In comparison, only 1.1% of individuals in a non-cancer cohort had alterations in the same genes.
Fifty-eight of the cancer patients who had a cancer-predisposing mutation also had available information on their family history. Forty percent (n=23) of these patients had a family history of cancer.
The frequency of germline mutations in cancer-predisposition genes varied by the type of cancer a patient had. The highest frequency, 16.7%, was in patients with non-central nervous system (CNS) solid tumors, followed by CNS tumors, at 9%, and leukemia, at 4.4%.
The most commonly mutated genes were TP53 (n=50), APC (n=6), BRCA2 (n=6), NF1 (n=4), PMS2 (n=4), RB1 (n=3), and RUNX1 (n=3).
The investigators were surprised to find mutations in the breast and ovarian cancer genes BRCA1 and BRCA2 in a number of the patients. These genes are not currently included in pediatric cancer genetic screening.
“Another surprising finding to emerge from this study was the prevalence of germline mutations in 6 patients with Ewing sarcoma,” said study author Kim Nichols, MD, also of St. Jude. “[This cancer] was not previously thought to be part of any cancer-predisposition syndrome.” ![]()