User login
Tool may help predict persistent postconcussion symptoms
A new tool – a clinical risk score – may help identify which children and adolescents who recently sustained a head injury are at risk for persistent postconcussion symptoms, according to a report published online March 7 in JAMA.
Approximately one-third of pediatric patients with concussion will have ongoing somatic, cognitive, psychological, and/or behavioral symptoms at 28 days, and at present, there are no tools to help predict which patients will be affected. The 5P (Preventing Postconcussive Problems in Pediatrics) study was performed to develop and validate a clinical risk score for this purpose, said Dr. Roger Zemek of Children’s Hospital of Eastern Ontario Research Institute, Ottawa, and his associates (JAMA 2016 Mar 8;315[10]:1014-25).

This prospective cohort study involved patients aged 5-17 years (median age, 12 years) who presented to one of nine Canadian pediatric emergency departments within 48 hours of sustaining a concussion.
In the derivation cohort, 510 of 1,701 participants (30%) met the criteria for persistent postconcussion symptoms (PPCS). A total of 47 possible predictive variables were assessed for their usefulness in predicting PPCS in this cohort. They were collected from demographic data, patient history, injury characteristics, physical examination, results on the Acute Concussion Evaluation Inventory and the Postconcussion Symptom Inventory, and patient/parent responses to weekly follow-up surveys during the month following the injury.
The investigators devised a clinical risk score using the nine predictors they found to be most accurate: patient age, patient gender, the presence or absence of prior concussion, migraine history, the presence or absence of current headache, sensitivity to noise, fatigue, slow responses to questions, and an abnormal tandem stance. They then selected three cutoff points to delineate PPCS risk: 0-3 points indicated low risk, 4-8 points indicated intermediate risk, and 9 or more points indicated high risk.
Treating physicians also were asked to predict the likelihood of PPCS.
In the validation cohort, 291 of 883 participants (33%) met the criteria for PPCS.
For low-risk patients, the sensitivity of the clinical risk score was 94%, the specificity was 18%, the negative predictive value was 85%, and the positive predictive value was 36%. For high-risk patients, the sensitivity of the clinical risk score was 20%, the specificity was 94%, the negative predictive value was 70%, and the positive predictive value was 60%.
In both sets of patients, the clinical risk score was significantly better than physician judgment in predicting PPCS. However, in its present form, it is only modestly accurate at distinguishing who will and who will not have the disorder. This tool could be further refined, perhaps by adding information regarding biomarkers, genetic susceptibility, or advanced neuroimaging, Dr. Zemek and his associates wrote.
“Before this score is adopted in clinical practice, further research is needed for external validation, assessment of accuracy in an office setting, and determination of clinical utility,” they concluded.
This work was supported by the Canadian Institutes of Health Research, the Ontario Neurotrauma Foundation Mild Traumatic Brain Injury Team, and the Alberta Children’s Hospital Foundation. Dr. Zemek and his associates reported having no relevant financial disclosures.
The clinical risk score devised by Zemek et al. may facilitate selection of patients who are at highest risk of long-term impairment, both for more intensive monitoring and treatment in the clinical setting and for inclusion in much-needed interventional trials in the research setting. It also may support clinicians in reassuring low-risk patients and their families of the likelihood of full recovery.
However, this tool first must be validated in other settings where children and adolescents are assessed for head injury, including general emergency departments; urgent care centers; and primary care, orthopedic, and sports medicine practices. Its performance should also be evaluated when used in conjunction with bedside vestibular ocular measures, serum biomarkers, genetic factors, and advanced neuroimaging measures. And determining its usefulness in other patient groups excluded from this trial also is warranted, including children younger than age 5, those with multiple trauma, and those found to have structural abnormalities on neuroimaging tests.
Dr. Lynn Babcock is in the division of pediatric emergency medicine at the University of Cincinnati and at the Cincinnati Children’s Hospital Medical Center. Dr. Brad G. Kurowski is in the division of physical medicine and rehabilitation in the department of pediatrics at Cincinnati Children’s Hospital Medical Center. Dr. Kurowski reported receiving grants from the National Institutes of Health and the Centers for Disease Control and Prevention. Dr. Babcock and Dr. Kurowski made these remarks in an editorial accompanying Dr. Zemek’s report (JAMA 2016 Mar 8;315[10]:987-8).
The clinical risk score devised by Zemek et al. may facilitate selection of patients who are at highest risk of long-term impairment, both for more intensive monitoring and treatment in the clinical setting and for inclusion in much-needed interventional trials in the research setting. It also may support clinicians in reassuring low-risk patients and their families of the likelihood of full recovery.
However, this tool first must be validated in other settings where children and adolescents are assessed for head injury, including general emergency departments; urgent care centers; and primary care, orthopedic, and sports medicine practices. Its performance should also be evaluated when used in conjunction with bedside vestibular ocular measures, serum biomarkers, genetic factors, and advanced neuroimaging measures. And determining its usefulness in other patient groups excluded from this trial also is warranted, including children younger than age 5, those with multiple trauma, and those found to have structural abnormalities on neuroimaging tests.
Dr. Lynn Babcock is in the division of pediatric emergency medicine at the University of Cincinnati and at the Cincinnati Children’s Hospital Medical Center. Dr. Brad G. Kurowski is in the division of physical medicine and rehabilitation in the department of pediatrics at Cincinnati Children’s Hospital Medical Center. Dr. Kurowski reported receiving grants from the National Institutes of Health and the Centers for Disease Control and Prevention. Dr. Babcock and Dr. Kurowski made these remarks in an editorial accompanying Dr. Zemek’s report (JAMA 2016 Mar 8;315[10]:987-8).
The clinical risk score devised by Zemek et al. may facilitate selection of patients who are at highest risk of long-term impairment, both for more intensive monitoring and treatment in the clinical setting and for inclusion in much-needed interventional trials in the research setting. It also may support clinicians in reassuring low-risk patients and their families of the likelihood of full recovery.
However, this tool first must be validated in other settings where children and adolescents are assessed for head injury, including general emergency departments; urgent care centers; and primary care, orthopedic, and sports medicine practices. Its performance should also be evaluated when used in conjunction with bedside vestibular ocular measures, serum biomarkers, genetic factors, and advanced neuroimaging measures. And determining its usefulness in other patient groups excluded from this trial also is warranted, including children younger than age 5, those with multiple trauma, and those found to have structural abnormalities on neuroimaging tests.
Dr. Lynn Babcock is in the division of pediatric emergency medicine at the University of Cincinnati and at the Cincinnati Children’s Hospital Medical Center. Dr. Brad G. Kurowski is in the division of physical medicine and rehabilitation in the department of pediatrics at Cincinnati Children’s Hospital Medical Center. Dr. Kurowski reported receiving grants from the National Institutes of Health and the Centers for Disease Control and Prevention. Dr. Babcock and Dr. Kurowski made these remarks in an editorial accompanying Dr. Zemek’s report (JAMA 2016 Mar 8;315[10]:987-8).
A new tool – a clinical risk score – may help identify which children and adolescents who recently sustained a head injury are at risk for persistent postconcussion symptoms, according to a report published online March 7 in JAMA.
Approximately one-third of pediatric patients with concussion will have ongoing somatic, cognitive, psychological, and/or behavioral symptoms at 28 days, and at present, there are no tools to help predict which patients will be affected. The 5P (Preventing Postconcussive Problems in Pediatrics) study was performed to develop and validate a clinical risk score for this purpose, said Dr. Roger Zemek of Children’s Hospital of Eastern Ontario Research Institute, Ottawa, and his associates (JAMA 2016 Mar 8;315[10]:1014-25).
This prospective cohort study involved patients aged 5-17 years (median age, 12 years) who presented to one of nine Canadian pediatric emergency departments within 48 hours of sustaining a concussion.
In the derivation cohort, 510 of 1,701 participants (30%) met the criteria for persistent postconcussion symptoms (PPCS). A total of 47 possible predictive variables were assessed for their usefulness in predicting PPCS in this cohort. They were collected from demographic data, patient history, injury characteristics, physical examination, results on the Acute Concussion Evaluation Inventory and the Postconcussion Symptom Inventory, and patient/parent responses to weekly follow-up surveys during the month following the injury.
The investigators devised a clinical risk score using the nine predictors they found to be most accurate: patient age, patient gender, the presence or absence of prior concussion, migraine history, the presence or absence of current headache, sensitivity to noise, fatigue, slow responses to questions, and an abnormal tandem stance. They then selected three cutoff points to delineate PPCS risk: 0-3 points indicated low risk, 4-8 points indicated intermediate risk, and 9 or more points indicated high risk.
Treating physicians also were asked to predict the likelihood of PPCS.
In the validation cohort, 291 of 883 participants (33%) met the criteria for PPCS.
For low-risk patients, the sensitivity of the clinical risk score was 94%, the specificity was 18%, the negative predictive value was 85%, and the positive predictive value was 36%. For high-risk patients, the sensitivity of the clinical risk score was 20%, the specificity was 94%, the negative predictive value was 70%, and the positive predictive value was 60%.
In both sets of patients, the clinical risk score was significantly better than physician judgment in predicting PPCS. However, in its present form, it is only modestly accurate at distinguishing who will and who will not have the disorder. This tool could be further refined, perhaps by adding information regarding biomarkers, genetic susceptibility, or advanced neuroimaging, Dr. Zemek and his associates wrote.
“Before this score is adopted in clinical practice, further research is needed for external validation, assessment of accuracy in an office setting, and determination of clinical utility,” they concluded.
This work was supported by the Canadian Institutes of Health Research, the Ontario Neurotrauma Foundation Mild Traumatic Brain Injury Team, and the Alberta Children’s Hospital Foundation. Dr. Zemek and his associates reported having no relevant financial disclosures.
A new tool – a clinical risk score – may help identify which children and adolescents who recently sustained a head injury are at risk for persistent postconcussion symptoms, according to a report published online March 7 in JAMA.
Approximately one-third of pediatric patients with concussion will have ongoing somatic, cognitive, psychological, and/or behavioral symptoms at 28 days, and at present, there are no tools to help predict which patients will be affected. The 5P (Preventing Postconcussive Problems in Pediatrics) study was performed to develop and validate a clinical risk score for this purpose, said Dr. Roger Zemek of Children’s Hospital of Eastern Ontario Research Institute, Ottawa, and his associates (JAMA 2016 Mar 8;315[10]:1014-25).
This prospective cohort study involved patients aged 5-17 years (median age, 12 years) who presented to one of nine Canadian pediatric emergency departments within 48 hours of sustaining a concussion.
In the derivation cohort, 510 of 1,701 participants (30%) met the criteria for persistent postconcussion symptoms (PPCS). A total of 47 possible predictive variables were assessed for their usefulness in predicting PPCS in this cohort. They were collected from demographic data, patient history, injury characteristics, physical examination, results on the Acute Concussion Evaluation Inventory and the Postconcussion Symptom Inventory, and patient/parent responses to weekly follow-up surveys during the month following the injury.
The investigators devised a clinical risk score using the nine predictors they found to be most accurate: patient age, patient gender, the presence or absence of prior concussion, migraine history, the presence or absence of current headache, sensitivity to noise, fatigue, slow responses to questions, and an abnormal tandem stance. They then selected three cutoff points to delineate PPCS risk: 0-3 points indicated low risk, 4-8 points indicated intermediate risk, and 9 or more points indicated high risk.
Treating physicians also were asked to predict the likelihood of PPCS.
In the validation cohort, 291 of 883 participants (33%) met the criteria for PPCS.
For low-risk patients, the sensitivity of the clinical risk score was 94%, the specificity was 18%, the negative predictive value was 85%, and the positive predictive value was 36%. For high-risk patients, the sensitivity of the clinical risk score was 20%, the specificity was 94%, the negative predictive value was 70%, and the positive predictive value was 60%.
In both sets of patients, the clinical risk score was significantly better than physician judgment in predicting PPCS. However, in its present form, it is only modestly accurate at distinguishing who will and who will not have the disorder. This tool could be further refined, perhaps by adding information regarding biomarkers, genetic susceptibility, or advanced neuroimaging, Dr. Zemek and his associates wrote.
“Before this score is adopted in clinical practice, further research is needed for external validation, assessment of accuracy in an office setting, and determination of clinical utility,” they concluded.
This work was supported by the Canadian Institutes of Health Research, the Ontario Neurotrauma Foundation Mild Traumatic Brain Injury Team, and the Alberta Children’s Hospital Foundation. Dr. Zemek and his associates reported having no relevant financial disclosures.
FROM JAMA
Key clinical point: A new tool has been developed to help identify children and adolescents at risk for persistent postconcussion symptoms.
Major finding: For high-risk patients, the sensitivity of the clinical risk score was 20%, the specificity was 93%, the negative predictive value was 70%, and the positive predictive value was 60%.
Data source: A prospective, multicenter cohort study involving 1,701 pediatric patients to develop a clinical risk score, and a validation study involving 883 to test the performance of that tool.
Disclosures: This work was supported by the Canadian Institutes of Health Research, the Ontario Neurotrauma Foundation Mild Traumatic Brain Injury Team, and the Alberta Children’s Hospital Foundation. Dr. Zemek and his associates reported having no relevant financial disclosures.

No LIGHT shed on CV safety of naltrexone-bupropion
The cardiovascular risks of the weight-loss combination drug naltrexone-bupropion are still uncertain, because the FDA-mandated safety trial, LIGHT, was terminated prematurely due to the sponsoring drug company’s breach of confidentiality. Other irregularities also were discovered, according to a report published online March 8 in JAMA.
Orexigen violated its agreement with FDA not to disclose the findings of an interim analysis performed after only 25% of expected CV events accrued. These findings appeared highly favorable for the drug, prompting the sponsor to publicly, and prematurely, claim naltrexone-bupropion reduced CV risk by 41% independently of its weight-loss effect. This favorable outcome was later found to be “driven almost exclusively by a 12-to-1 imbalance in death favoring naltrexone-bupropion among patients who were no longer taking the study drug,” said Dr. Steven E. Nissen of the Cleveland Clinic Center for Cardiovascular Research and his associates.

They now report the results of a second interim analysis of LIGHT (Cardiovascular Outcomes Study of Naltrexone SR/Bupropion SR in Overweight and Obese Subjects With Cardiovascular Risk Factors) performed after 50% of expected CV events accrued, as well as those of a final analysis performed when the trial was halted and 64% of expected CV events accrued. These findings are much less favorable, showing no significant difference between naltrexone-bupropion and placebo in the rate of major adverse cardiovascular events (MACE). In addition, extremely poor adherence to both active treatment and placebo over time, together with the complex statistical issues involved, call into question any interpretation of the results and preclude “any reliable conclusions about the long-term safety of naltrexone-bupropion,” the investigators said.
“The cardiovascular safety of this treatment remains uncertain and will require evaluation in a new, adequately powered outcome trial.” The results of such a study, should it be undertaken, wouldn’t be available for at least 3-4 years, they noted.
In their report, the investigators described in detail why the FDA required a CV safety study even though the agency had already approved naltrexone-bupropion as a weight-loss treatment.
The study was a phase IIIb randomized, double-blind, placebo-controlled trial involving 8,910 overweight/obese patients aged 45 or older (mean age, 61 years) who were at risk of adverse CV outcomes due to preexisting CV disease; exercise-induced angina; an unfavorable ankle/brachial index; stenosis of coronary, carotid, or lower extremity arteries; type 2 diabetes; hypertension; dyslipidemia; or smoking. These participants received daily tablets of either 32 mg naltrexone plus 360 mg bupropion or a matching placebo and were to be followed for 4 years at 266 U.S. medical centers.
The analysis performed after 50% of expected CV events accrued showed that MACE – the primary safety outcome – occurred in 2.0% of the naltrexone-bupropion group and 2.3% of the placebo group, a nonsignificant difference. Differences between the two study groups also were nonsignificant for the individual components of the primary outcome, including cardiovascular death (0.4% vs. 0.8%), nonfatal stroke (0.5% vs. 0.4%), and nonfatal MI (1.2% vs. 1.2%). These results were confirmed in a sensitivity analysis based on the final data collection, when 64% of expected CV events accrued: MACE occurred in 2.7% of the naltrexone-bupropion group and 2.8% of the placebo group, another nonsignificant difference.
The active treatment also was no better than placebo regarding all secondary outcomes, including all-cause mortality, CV hospitalization, and coronary revascularization, Dr. Nissen and his associates said (JAMA. 2016 Mar 8. doi: 10.1001/jama.2016.1558). Treatment adherence was low. At 16 weeks, only 64% of the naltrexone-bupropion group and 72% of the placebo group were still taking the study treatment. By 2 years, only 27% of the naltrexone-bupropion group and 17% of the placebo group were. The mean duration of treatment was only 18.4 weeks for naltrexone-bupropion and 16.3 weeks for placebo. Most treatment discontinuations were due to a failure to lose weight, but a substantial proportion occurred because of treatment-related increases in blood pressure or heart rate.
The active treatment’s ability to reduce body weight was deemed “modest.” When the trial was halted, the mean decrease in weight was 3.9 kg with naltrexone-bupropion, representing a 3.6% reduction in total weight, and was 1.2 kg with placebo, representing a 1.1% reduction.
Adverse effects developed in 28.1% of patients taking naltrexone-bupropion, which was a significantly greater proportion than the 8.7% rate in the placebo group. The most common adverse events leading to discontinuation of the study drug affected the gastrointestinal system (nausea, constipation, vomiting), the CNS (tremor, dizziness, headache), and mental/emotional problems (insomnia, anxiety, hallucinations, depression).
The sponsor of this trial, Orexigen Therapeutics, disregarded the multiple harms caused by breaches of confidentiality, treated the academic investigators unfairly, ignored the trial’s data monitoring committee, and defied the FDA. Their statements about the naltrexone-bupropion’s cardiovascular efficacy were highly misleading, and there were obvious signs that the supporting data were not reliable. For example, nearly all of the CV mortality in the first interim analysis occurred well after participants had stopped taking their medication.
Yet the drug company was not sanctioned, and the naltrexone-bupropion retains FDA approval. At a minimum, the FDA should withhold approval until a viable replacement study is conducted, or it should require Risk Evaluation and Mitigation Strategies to counter the misinformation disseminated by the study sponsor, or it should restrict use of the drug outright.
Clinicians should be aware of these research improprieties and should know that the purported weight-loss benefit of naltrexone-bupropion is only 2.7 kg more than that achieved with placebo. How does this modest benefit balance against an unknown cardiovascular risk? In addition, the drug’s lack of efficacy clearly contributed to the very poor adherence rate in this trial: At 1 year, only 37.5% were still taking naltrexone-bupropion and 26.3% were still taking placebo.
Dr. Joshua M. Sharfstein is in the department of health policy and management at Johns Hopkins Bloomberg School of Public Health, Baltimore. Dr. Bruce M. Psaty is in the Cardiovascular Health Research Unit and the departments of medicine, epidemiology, and health services at the University of Washington, Seattle. They reported that this work was supported by the National Heart, Lung, and Blood Institute. Dr. Sharfstein reported serving as principal deputy commissioner of the FDA in 2009-2011. Dr. Psaty reported serving on the data monitoring committee of a clinical trial funded by Zoll LifeCor, on the steering committee of the Yale Open Data Access Project funded by Johnson & Johnson, and on the FDA Science Board. Dr. Sharfstein and Dr. Psaty made these remarks in an editorial accompanying Dr. Nissen’s report (JAMA. 2016;315:984-6).
The sponsor of this trial, Orexigen Therapeutics, disregarded the multiple harms caused by breaches of confidentiality, treated the academic investigators unfairly, ignored the trial’s data monitoring committee, and defied the FDA. Their statements about the naltrexone-bupropion’s cardiovascular efficacy were highly misleading, and there were obvious signs that the supporting data were not reliable. For example, nearly all of the CV mortality in the first interim analysis occurred well after participants had stopped taking their medication.
Yet the drug company was not sanctioned, and the naltrexone-bupropion retains FDA approval. At a minimum, the FDA should withhold approval until a viable replacement study is conducted, or it should require Risk Evaluation and Mitigation Strategies to counter the misinformation disseminated by the study sponsor, or it should restrict use of the drug outright.
Clinicians should be aware of these research improprieties and should know that the purported weight-loss benefit of naltrexone-bupropion is only 2.7 kg more than that achieved with placebo. How does this modest benefit balance against an unknown cardiovascular risk? In addition, the drug’s lack of efficacy clearly contributed to the very poor adherence rate in this trial: At 1 year, only 37.5% were still taking naltrexone-bupropion and 26.3% were still taking placebo.
Dr. Joshua M. Sharfstein is in the department of health policy and management at Johns Hopkins Bloomberg School of Public Health, Baltimore. Dr. Bruce M. Psaty is in the Cardiovascular Health Research Unit and the departments of medicine, epidemiology, and health services at the University of Washington, Seattle. They reported that this work was supported by the National Heart, Lung, and Blood Institute. Dr. Sharfstein reported serving as principal deputy commissioner of the FDA in 2009-2011. Dr. Psaty reported serving on the data monitoring committee of a clinical trial funded by Zoll LifeCor, on the steering committee of the Yale Open Data Access Project funded by Johnson & Johnson, and on the FDA Science Board. Dr. Sharfstein and Dr. Psaty made these remarks in an editorial accompanying Dr. Nissen’s report (JAMA. 2016;315:984-6).
The sponsor of this trial, Orexigen Therapeutics, disregarded the multiple harms caused by breaches of confidentiality, treated the academic investigators unfairly, ignored the trial’s data monitoring committee, and defied the FDA. Their statements about the naltrexone-bupropion’s cardiovascular efficacy were highly misleading, and there were obvious signs that the supporting data were not reliable. For example, nearly all of the CV mortality in the first interim analysis occurred well after participants had stopped taking their medication.
Yet the drug company was not sanctioned, and the naltrexone-bupropion retains FDA approval. At a minimum, the FDA should withhold approval until a viable replacement study is conducted, or it should require Risk Evaluation and Mitigation Strategies to counter the misinformation disseminated by the study sponsor, or it should restrict use of the drug outright.
Clinicians should be aware of these research improprieties and should know that the purported weight-loss benefit of naltrexone-bupropion is only 2.7 kg more than that achieved with placebo. How does this modest benefit balance against an unknown cardiovascular risk? In addition, the drug’s lack of efficacy clearly contributed to the very poor adherence rate in this trial: At 1 year, only 37.5% were still taking naltrexone-bupropion and 26.3% were still taking placebo.
Dr. Joshua M. Sharfstein is in the department of health policy and management at Johns Hopkins Bloomberg School of Public Health, Baltimore. Dr. Bruce M. Psaty is in the Cardiovascular Health Research Unit and the departments of medicine, epidemiology, and health services at the University of Washington, Seattle. They reported that this work was supported by the National Heart, Lung, and Blood Institute. Dr. Sharfstein reported serving as principal deputy commissioner of the FDA in 2009-2011. Dr. Psaty reported serving on the data monitoring committee of a clinical trial funded by Zoll LifeCor, on the steering committee of the Yale Open Data Access Project funded by Johnson & Johnson, and on the FDA Science Board. Dr. Sharfstein and Dr. Psaty made these remarks in an editorial accompanying Dr. Nissen’s report (JAMA. 2016;315:984-6).
The cardiovascular risks of the weight-loss combination drug naltrexone-bupropion are still uncertain, because the FDA-mandated safety trial, LIGHT, was terminated prematurely due to the sponsoring drug company’s breach of confidentiality. Other irregularities also were discovered, according to a report published online March 8 in JAMA.
Orexigen violated its agreement with FDA not to disclose the findings of an interim analysis performed after only 25% of expected CV events accrued. These findings appeared highly favorable for the drug, prompting the sponsor to publicly, and prematurely, claim naltrexone-bupropion reduced CV risk by 41% independently of its weight-loss effect. This favorable outcome was later found to be “driven almost exclusively by a 12-to-1 imbalance in death favoring naltrexone-bupropion among patients who were no longer taking the study drug,” said Dr. Steven E. Nissen of the Cleveland Clinic Center for Cardiovascular Research and his associates.
They now report the results of a second interim analysis of LIGHT (Cardiovascular Outcomes Study of Naltrexone SR/Bupropion SR in Overweight and Obese Subjects With Cardiovascular Risk Factors) performed after 50% of expected CV events accrued, as well as those of a final analysis performed when the trial was halted and 64% of expected CV events accrued. These findings are much less favorable, showing no significant difference between naltrexone-bupropion and placebo in the rate of major adverse cardiovascular events (MACE). In addition, extremely poor adherence to both active treatment and placebo over time, together with the complex statistical issues involved, call into question any interpretation of the results and preclude “any reliable conclusions about the long-term safety of naltrexone-bupropion,” the investigators said.
“The cardiovascular safety of this treatment remains uncertain and will require evaluation in a new, adequately powered outcome trial.” The results of such a study, should it be undertaken, wouldn’t be available for at least 3-4 years, they noted.
In their report, the investigators described in detail why the FDA required a CV safety study even though the agency had already approved naltrexone-bupropion as a weight-loss treatment.
The study was a phase IIIb randomized, double-blind, placebo-controlled trial involving 8,910 overweight/obese patients aged 45 or older (mean age, 61 years) who were at risk of adverse CV outcomes due to preexisting CV disease; exercise-induced angina; an unfavorable ankle/brachial index; stenosis of coronary, carotid, or lower extremity arteries; type 2 diabetes; hypertension; dyslipidemia; or smoking. These participants received daily tablets of either 32 mg naltrexone plus 360 mg bupropion or a matching placebo and were to be followed for 4 years at 266 U.S. medical centers.
The analysis performed after 50% of expected CV events accrued showed that MACE – the primary safety outcome – occurred in 2.0% of the naltrexone-bupropion group and 2.3% of the placebo group, a nonsignificant difference. Differences between the two study groups also were nonsignificant for the individual components of the primary outcome, including cardiovascular death (0.4% vs. 0.8%), nonfatal stroke (0.5% vs. 0.4%), and nonfatal MI (1.2% vs. 1.2%). These results were confirmed in a sensitivity analysis based on the final data collection, when 64% of expected CV events accrued: MACE occurred in 2.7% of the naltrexone-bupropion group and 2.8% of the placebo group, another nonsignificant difference.
The active treatment also was no better than placebo regarding all secondary outcomes, including all-cause mortality, CV hospitalization, and coronary revascularization, Dr. Nissen and his associates said (JAMA. 2016 Mar 8. doi: 10.1001/jama.2016.1558). Treatment adherence was low. At 16 weeks, only 64% of the naltrexone-bupropion group and 72% of the placebo group were still taking the study treatment. By 2 years, only 27% of the naltrexone-bupropion group and 17% of the placebo group were. The mean duration of treatment was only 18.4 weeks for naltrexone-bupropion and 16.3 weeks for placebo. Most treatment discontinuations were due to a failure to lose weight, but a substantial proportion occurred because of treatment-related increases in blood pressure or heart rate.
The active treatment’s ability to reduce body weight was deemed “modest.” When the trial was halted, the mean decrease in weight was 3.9 kg with naltrexone-bupropion, representing a 3.6% reduction in total weight, and was 1.2 kg with placebo, representing a 1.1% reduction.
Adverse effects developed in 28.1% of patients taking naltrexone-bupropion, which was a significantly greater proportion than the 8.7% rate in the placebo group. The most common adverse events leading to discontinuation of the study drug affected the gastrointestinal system (nausea, constipation, vomiting), the CNS (tremor, dizziness, headache), and mental/emotional problems (insomnia, anxiety, hallucinations, depression).
The cardiovascular risks of the weight-loss combination drug naltrexone-bupropion are still uncertain, because the FDA-mandated safety trial, LIGHT, was terminated prematurely due to the sponsoring drug company’s breach of confidentiality. Other irregularities also were discovered, according to a report published online March 8 in JAMA.
Orexigen violated its agreement with FDA not to disclose the findings of an interim analysis performed after only 25% of expected CV events accrued. These findings appeared highly favorable for the drug, prompting the sponsor to publicly, and prematurely, claim naltrexone-bupropion reduced CV risk by 41% independently of its weight-loss effect. This favorable outcome was later found to be “driven almost exclusively by a 12-to-1 imbalance in death favoring naltrexone-bupropion among patients who were no longer taking the study drug,” said Dr. Steven E. Nissen of the Cleveland Clinic Center for Cardiovascular Research and his associates.
They now report the results of a second interim analysis of LIGHT (Cardiovascular Outcomes Study of Naltrexone SR/Bupropion SR in Overweight and Obese Subjects With Cardiovascular Risk Factors) performed after 50% of expected CV events accrued, as well as those of a final analysis performed when the trial was halted and 64% of expected CV events accrued. These findings are much less favorable, showing no significant difference between naltrexone-bupropion and placebo in the rate of major adverse cardiovascular events (MACE). In addition, extremely poor adherence to both active treatment and placebo over time, together with the complex statistical issues involved, call into question any interpretation of the results and preclude “any reliable conclusions about the long-term safety of naltrexone-bupropion,” the investigators said.
“The cardiovascular safety of this treatment remains uncertain and will require evaluation in a new, adequately powered outcome trial.” The results of such a study, should it be undertaken, wouldn’t be available for at least 3-4 years, they noted.
In their report, the investigators described in detail why the FDA required a CV safety study even though the agency had already approved naltrexone-bupropion as a weight-loss treatment.
The study was a phase IIIb randomized, double-blind, placebo-controlled trial involving 8,910 overweight/obese patients aged 45 or older (mean age, 61 years) who were at risk of adverse CV outcomes due to preexisting CV disease; exercise-induced angina; an unfavorable ankle/brachial index; stenosis of coronary, carotid, or lower extremity arteries; type 2 diabetes; hypertension; dyslipidemia; or smoking. These participants received daily tablets of either 32 mg naltrexone plus 360 mg bupropion or a matching placebo and were to be followed for 4 years at 266 U.S. medical centers.
The analysis performed after 50% of expected CV events accrued showed that MACE – the primary safety outcome – occurred in 2.0% of the naltrexone-bupropion group and 2.3% of the placebo group, a nonsignificant difference. Differences between the two study groups also were nonsignificant for the individual components of the primary outcome, including cardiovascular death (0.4% vs. 0.8%), nonfatal stroke (0.5% vs. 0.4%), and nonfatal MI (1.2% vs. 1.2%). These results were confirmed in a sensitivity analysis based on the final data collection, when 64% of expected CV events accrued: MACE occurred in 2.7% of the naltrexone-bupropion group and 2.8% of the placebo group, another nonsignificant difference.
The active treatment also was no better than placebo regarding all secondary outcomes, including all-cause mortality, CV hospitalization, and coronary revascularization, Dr. Nissen and his associates said (JAMA. 2016 Mar 8. doi: 10.1001/jama.2016.1558). Treatment adherence was low. At 16 weeks, only 64% of the naltrexone-bupropion group and 72% of the placebo group were still taking the study treatment. By 2 years, only 27% of the naltrexone-bupropion group and 17% of the placebo group were. The mean duration of treatment was only 18.4 weeks for naltrexone-bupropion and 16.3 weeks for placebo. Most treatment discontinuations were due to a failure to lose weight, but a substantial proportion occurred because of treatment-related increases in blood pressure or heart rate.
The active treatment’s ability to reduce body weight was deemed “modest.” When the trial was halted, the mean decrease in weight was 3.9 kg with naltrexone-bupropion, representing a 3.6% reduction in total weight, and was 1.2 kg with placebo, representing a 1.1% reduction.
Adverse effects developed in 28.1% of patients taking naltrexone-bupropion, which was a significantly greater proportion than the 8.7% rate in the placebo group. The most common adverse events leading to discontinuation of the study drug affected the gastrointestinal system (nausea, constipation, vomiting), the CNS (tremor, dizziness, headache), and mental/emotional problems (insomnia, anxiety, hallucinations, depression).
FROM JAMA
Key clinical point: The cardiovascular risks of the weight-loss combination drug naltrexone-bupropion are still uncertain.
Major finding: The primary safety outcome, major adverse cardiovascular events, occurred in 2.0% of the naltrexone-bupropion group and 2.3% of the placebo group, a nonsignificant difference.
Data source: LIGHT, a multicenter randomized placebo-controlled double-blind noninferiority trial involving 8,910 overweight/obese patients.
Disclosures: This trial was sponsored by Orexigen Therapeutics and Takeda Pharmaceuticals. Dr. Nissen reported receiving grants from The Medicines Company, Amgen, Pfizer, AstraZeneca, Esperion Therapeutics, Eli Lilly, and Cerenis, and consulting for numerous drug companies that pay his fees directly to charities. His associates reported ties to numerous industry sources.

HM16 Session Analysis: Hospital Quality, Patient Safety Update for 2015
HM16 Presenters: Mangla Gulati, MD, FACP, FHM, and Ian Jenkins, MD
Summary: There is some evidence that hospital adverse events may be decreasing. The Agency for Healthcare Research and Quality (AHRQ) report of Partnership for Patients data found that there were 1.3 million hospital-acquired conditions prevented from 2011-2013, translating to 50,000 lives saved and $12 billion in savings. However, there is still much work to be done. Here are some major themes from the recent literature that may inform your own QI projects:
- Electronic medical records (EMR): Increased adoption raises concerns for unintended consequences which could detract from patient safety. These are derived from case reports, claims databases, reports through patient safety organizations. Consider reviewing alerts, advisories, and hard-stops within your hospital’s EMR.
- Improving diagnosis: Misdiagnosis affects 10% of Americans but measurement of this phenomenon remains difficult. Strategies to improve diagnosis include: focus on collaboration, teaching diagnostic skills, IT and algorithmic support, feedback and blame reduction, and reimbursement reform. There is growing recognition that hospitalists are well positioned to engage in these efforts.
- Hand hygiene: Multiple culture and environmental contributors to poor compliance (i.e., 40% compliance rate) and few good intervention studies. Recent studies have focused on the development of cause-specific plans and targeted interventions. Consider applying a targeted solutions tool to a project at your hospital.
- “Second victim”: Healthcare providers frequently experience emotional distress following patient safety events but there is a lack of resources to support providers after such an event. Consider implementing a “care for the caregiver” program at your hospital.
- Sepsis: North Shore-LIJ hospital system (in collaboration with the IHI) received the 2014 Eisenberg Award for developing and implementing a Sepsis Recognition Program and tool-kit. Such collaborations may be useful for driving and magnifying your QI initiatives.
- Patient experience: Recent studies emphasize the importance of patients being actively involved in their medical decisions and providing meaningful feedback. Consider implementing a patient/family council and getting involved with local patient experience initiatives.
- Incident reporting systems (IRS): Widespread under-reporting raises concerns over the value of IRS. Consider modifying or minimizing IRS and/or giving reports to local units to ignite safety culture.
- Discharge before noon (DBN): Delayed discharges may result in lost revenue and poor patient satisfaction. Wertheimer et al. reported on a successful intervention to increase DBN in the Journal of Hospital Medicine. Check out their intervention and consider something similar at your hospital.
- Patient monitoring: Vital sign measurements are often poorly timed, integrated and/or communicated. Recent studies of wireless Electronic Physiologic Surveillance System devices in hospitals have shown positive outcomes.TH
HM16 Presenters: Mangla Gulati, MD, FACP, FHM, and Ian Jenkins, MD
Summary: There is some evidence that hospital adverse events may be decreasing. The Agency for Healthcare Research and Quality (AHRQ) report of Partnership for Patients data found that there were 1.3 million hospital-acquired conditions prevented from 2011-2013, translating to 50,000 lives saved and $12 billion in savings. However, there is still much work to be done. Here are some major themes from the recent literature that may inform your own QI projects:
- Electronic medical records (EMR): Increased adoption raises concerns for unintended consequences which could detract from patient safety. These are derived from case reports, claims databases, reports through patient safety organizations. Consider reviewing alerts, advisories, and hard-stops within your hospital’s EMR.
- Improving diagnosis: Misdiagnosis affects 10% of Americans but measurement of this phenomenon remains difficult. Strategies to improve diagnosis include: focus on collaboration, teaching diagnostic skills, IT and algorithmic support, feedback and blame reduction, and reimbursement reform. There is growing recognition that hospitalists are well positioned to engage in these efforts.
- Hand hygiene: Multiple culture and environmental contributors to poor compliance (i.e., 40% compliance rate) and few good intervention studies. Recent studies have focused on the development of cause-specific plans and targeted interventions. Consider applying a targeted solutions tool to a project at your hospital.
- “Second victim”: Healthcare providers frequently experience emotional distress following patient safety events but there is a lack of resources to support providers after such an event. Consider implementing a “care for the caregiver” program at your hospital.
- Sepsis: North Shore-LIJ hospital system (in collaboration with the IHI) received the 2014 Eisenberg Award for developing and implementing a Sepsis Recognition Program and tool-kit. Such collaborations may be useful for driving and magnifying your QI initiatives.
- Patient experience: Recent studies emphasize the importance of patients being actively involved in their medical decisions and providing meaningful feedback. Consider implementing a patient/family council and getting involved with local patient experience initiatives.
- Incident reporting systems (IRS): Widespread under-reporting raises concerns over the value of IRS. Consider modifying or minimizing IRS and/or giving reports to local units to ignite safety culture.
- Discharge before noon (DBN): Delayed discharges may result in lost revenue and poor patient satisfaction. Wertheimer et al. reported on a successful intervention to increase DBN in the Journal of Hospital Medicine. Check out their intervention and consider something similar at your hospital.
- Patient monitoring: Vital sign measurements are often poorly timed, integrated and/or communicated. Recent studies of wireless Electronic Physiologic Surveillance System devices in hospitals have shown positive outcomes.TH
HM16 Presenters: Mangla Gulati, MD, FACP, FHM, and Ian Jenkins, MD
Summary: There is some evidence that hospital adverse events may be decreasing. The Agency for Healthcare Research and Quality (AHRQ) report of Partnership for Patients data found that there were 1.3 million hospital-acquired conditions prevented from 2011-2013, translating to 50,000 lives saved and $12 billion in savings. However, there is still much work to be done. Here are some major themes from the recent literature that may inform your own QI projects:
- Electronic medical records (EMR): Increased adoption raises concerns for unintended consequences which could detract from patient safety. These are derived from case reports, claims databases, reports through patient safety organizations. Consider reviewing alerts, advisories, and hard-stops within your hospital’s EMR.
- Improving diagnosis: Misdiagnosis affects 10% of Americans but measurement of this phenomenon remains difficult. Strategies to improve diagnosis include: focus on collaboration, teaching diagnostic skills, IT and algorithmic support, feedback and blame reduction, and reimbursement reform. There is growing recognition that hospitalists are well positioned to engage in these efforts.
- Hand hygiene: Multiple culture and environmental contributors to poor compliance (i.e., 40% compliance rate) and few good intervention studies. Recent studies have focused on the development of cause-specific plans and targeted interventions. Consider applying a targeted solutions tool to a project at your hospital.
- “Second victim”: Healthcare providers frequently experience emotional distress following patient safety events but there is a lack of resources to support providers after such an event. Consider implementing a “care for the caregiver” program at your hospital.
- Sepsis: North Shore-LIJ hospital system (in collaboration with the IHI) received the 2014 Eisenberg Award for developing and implementing a Sepsis Recognition Program and tool-kit. Such collaborations may be useful for driving and magnifying your QI initiatives.
- Patient experience: Recent studies emphasize the importance of patients being actively involved in their medical decisions and providing meaningful feedback. Consider implementing a patient/family council and getting involved with local patient experience initiatives.
- Incident reporting systems (IRS): Widespread under-reporting raises concerns over the value of IRS. Consider modifying or minimizing IRS and/or giving reports to local units to ignite safety culture.
- Discharge before noon (DBN): Delayed discharges may result in lost revenue and poor patient satisfaction. Wertheimer et al. reported on a successful intervention to increase DBN in the Journal of Hospital Medicine. Check out their intervention and consider something similar at your hospital.
- Patient monitoring: Vital sign measurements are often poorly timed, integrated and/or communicated. Recent studies of wireless Electronic Physiologic Surveillance System devices in hospitals have shown positive outcomes.TH
Start Thinking about Hospital Medicine 2017
Thanks to all who attended HM16 in San Diego! From the featured speakers—Acting Assistant Secretary for Health in the U.S. Department of Health and Human Services Karen DeSalvo, MD, MPH, MSc, and faculty—to the attendees and staff, it would not have been such a success without you and your enthusiasm.
Join us again in 2017! Save the dates for another premier networking and educational event in Las Vegas. HM17 is slated for May 1–4, 2017, at Mandalay Bay Resort and Casino. More details will be coming soon.
Thanks to all who attended HM16 in San Diego! From the featured speakers—Acting Assistant Secretary for Health in the U.S. Department of Health and Human Services Karen DeSalvo, MD, MPH, MSc, and faculty—to the attendees and staff, it would not have been such a success without you and your enthusiasm.
Join us again in 2017! Save the dates for another premier networking and educational event in Las Vegas. HM17 is slated for May 1–4, 2017, at Mandalay Bay Resort and Casino. More details will be coming soon.
Thanks to all who attended HM16 in San Diego! From the featured speakers—Acting Assistant Secretary for Health in the U.S. Department of Health and Human Services Karen DeSalvo, MD, MPH, MSc, and faculty—to the attendees and staff, it would not have been such a success without you and your enthusiasm.
Join us again in 2017! Save the dates for another premier networking and educational event in Las Vegas. HM17 is slated for May 1–4, 2017, at Mandalay Bay Resort and Casino. More details will be coming soon.
Defining Sepsis and Septic Shock
NEW YORK (Reuters Health) - The Sepsis Definitions Task Force, using expanded quantitative information, has updated its definitions for sepsis and septic shock and the clinical criteria underlying them.
Two reports and one summary communication published in JAMA February 23 detail the processes used to reach the consensus
definitions that have remained largely unchanged for more than two decades.
"The new definitions and clinical criteria of sepsis and septic shock are aimed to help clinicians at the bedside recognize these deadly syndromes and start therapy promptly," Dr. Christopher W. Seymour, from the University of Pittsburgh School of Medicine in Pennsylvania, told Reuters Health by email.
"After two years of deliberations and research, we were surprised to uncover the broad differences in how clinicians approach sepsis, and variety of criteria used in septic shock trials in the past decade. This mandated a re-examination of the criteria, strong efforts to speak a common language, and generate simple, easy to use criteria," Dr. Seymour said.
Dr. Seymour and colleagues recommended elimination of the terms sepsis syndrome, septicemia, and severe sepsis and settled on the definition of sepsis as "life-threatening organ dysfunction due to a dysregulated host response to infection."
They explored several sets of clinical criteria and their predictive validity for hospital mortality, including the Sequential Organ Function Assessment (SOFA), Logistic Organ Dysfunction System (LODS), systemic inflammatory response syndrome (SIRS), and a simplified qSOFA model that included Glasgow Coma Scale (GCS) score of 13 or less, systolic blood pressure of 100 mm Hg or less, and respiratory rate of 22/min or more (1 point each; score range, 0-3).
For intensive care unit encounters with suspected infection, SOFA came out on top, whereas for encounters with suspected infection outside of the ICU, qSOFA offered the best predictive validity for in-hospital mortality.
"Sepsis has no gold standard for diagnosis," Dr. Seymour said. "Given its complex pathophysiology and our evolving knowledge base, the current definition and criteria for sepsis represent a first step. Our field will need to continue to embark on improvements in the practicality, validity, and scientific rationale for sepsis definitions/criteria in future iterations."
He added,"We also hope that physicians recognize that, for the first time, these criteria derive from new data analyses in real patients. More than 700,000 encounters in 170 hospitals were studied to evaluate existing and new sepsis criteria."
Dr. Manu Shankar-Hari, from Guy's and St. Thomas' NHS Foundation Trust, London, UK, and colleagues reviewed 44 studies of septic shock involving 166,479 patients and used a Delphi process to arrive at the new consensus definition: "septic shock is defined as a subset of sepsis in which underlying circulatory, cellular, and metabolic abnormalities are associated with a greater risk of mortality than sepsis alone."
Dr. Shankar-Hari told Reuters Health by email, "The proposed definition for septic shock is a paradigm shift in illness concept. We wanted to provide consistency in diagnosing septic shock. The epidemiology of this illness as we measure currently is messy."
After examining six possible sets of clinical criteria, the group identified two criteria that proved most consistent with the proposed septic shock definition: hypotension requiring use of vasopressors to maintain mean blood pressure of 65 mm Hg or greater and having a serum lactate level greater than 2 mmol/L persisting after adequate fluid resuscitation.
In their summary report, Dr. Clifford S. Deutschman, from Hofstra-Northwell School of Medicine, Feinstein Institute for Medical Research, New Hyde Park, New York, and colleagues on the Task Force write, "The proposed criteria should aid diagnostic categorization once initial assessment and immediate management are completed. qSOFA or SOFA may at some point be used as entry criteria for clinical trials."
"Greater clarity and consistency will also facilitate research and more accurate coding," they add.
Dr. Edward Abraham, from Wake Forest School of Medicine, Winston Salem, North Carolina, who wrote an editorial related to these reports, told Reuters Health by email, "While the new definitions advance the field, particularly from an epidemiologic viewpoint and potentially in helping to identify the economic impact associated with sepsis and septic shock, they are only of limited help in defining care for an individual patient or in designing clinical trials to examine new therapies for sepsis."
"As noted in the editorial, more discriminatory definitions, based on specific cellular and genomic alterations, are necessary to truly affect care for individual patients and to assist in the development of novel therapeutic approaches to sepsis and septic shock," he said.
A number of organizations supported this research and a number of coauthors reported disclosures.
NEW YORK (Reuters Health) - The Sepsis Definitions Task Force, using expanded quantitative information, has updated its definitions for sepsis and septic shock and the clinical criteria underlying them.
Two reports and one summary communication published in JAMA February 23 detail the processes used to reach the consensus
definitions that have remained largely unchanged for more than two decades.
"The new definitions and clinical criteria of sepsis and septic shock are aimed to help clinicians at the bedside recognize these deadly syndromes and start therapy promptly," Dr. Christopher W. Seymour, from the University of Pittsburgh School of Medicine in Pennsylvania, told Reuters Health by email.
"After two years of deliberations and research, we were surprised to uncover the broad differences in how clinicians approach sepsis, and variety of criteria used in septic shock trials in the past decade. This mandated a re-examination of the criteria, strong efforts to speak a common language, and generate simple, easy to use criteria," Dr. Seymour said.
Dr. Seymour and colleagues recommended elimination of the terms sepsis syndrome, septicemia, and severe sepsis and settled on the definition of sepsis as "life-threatening organ dysfunction due to a dysregulated host response to infection."
They explored several sets of clinical criteria and their predictive validity for hospital mortality, including the Sequential Organ Function Assessment (SOFA), Logistic Organ Dysfunction System (LODS), systemic inflammatory response syndrome (SIRS), and a simplified qSOFA model that included Glasgow Coma Scale (GCS) score of 13 or less, systolic blood pressure of 100 mm Hg or less, and respiratory rate of 22/min or more (1 point each; score range, 0-3).
For intensive care unit encounters with suspected infection, SOFA came out on top, whereas for encounters with suspected infection outside of the ICU, qSOFA offered the best predictive validity for in-hospital mortality.
"Sepsis has no gold standard for diagnosis," Dr. Seymour said. "Given its complex pathophysiology and our evolving knowledge base, the current definition and criteria for sepsis represent a first step. Our field will need to continue to embark on improvements in the practicality, validity, and scientific rationale for sepsis definitions/criteria in future iterations."
He added,"We also hope that physicians recognize that, for the first time, these criteria derive from new data analyses in real patients. More than 700,000 encounters in 170 hospitals were studied to evaluate existing and new sepsis criteria."
Dr. Manu Shankar-Hari, from Guy's and St. Thomas' NHS Foundation Trust, London, UK, and colleagues reviewed 44 studies of septic shock involving 166,479 patients and used a Delphi process to arrive at the new consensus definition: "septic shock is defined as a subset of sepsis in which underlying circulatory, cellular, and metabolic abnormalities are associated with a greater risk of mortality than sepsis alone."
Dr. Shankar-Hari told Reuters Health by email, "The proposed definition for septic shock is a paradigm shift in illness concept. We wanted to provide consistency in diagnosing septic shock. The epidemiology of this illness as we measure currently is messy."
After examining six possible sets of clinical criteria, the group identified two criteria that proved most consistent with the proposed septic shock definition: hypotension requiring use of vasopressors to maintain mean blood pressure of 65 mm Hg or greater and having a serum lactate level greater than 2 mmol/L persisting after adequate fluid resuscitation.
In their summary report, Dr. Clifford S. Deutschman, from Hofstra-Northwell School of Medicine, Feinstein Institute for Medical Research, New Hyde Park, New York, and colleagues on the Task Force write, "The proposed criteria should aid diagnostic categorization once initial assessment and immediate management are completed. qSOFA or SOFA may at some point be used as entry criteria for clinical trials."
"Greater clarity and consistency will also facilitate research and more accurate coding," they add.
Dr. Edward Abraham, from Wake Forest School of Medicine, Winston Salem, North Carolina, who wrote an editorial related to these reports, told Reuters Health by email, "While the new definitions advance the field, particularly from an epidemiologic viewpoint and potentially in helping to identify the economic impact associated with sepsis and septic shock, they are only of limited help in defining care for an individual patient or in designing clinical trials to examine new therapies for sepsis."
"As noted in the editorial, more discriminatory definitions, based on specific cellular and genomic alterations, are necessary to truly affect care for individual patients and to assist in the development of novel therapeutic approaches to sepsis and septic shock," he said.
A number of organizations supported this research and a number of coauthors reported disclosures.
NEW YORK (Reuters Health) - The Sepsis Definitions Task Force, using expanded quantitative information, has updated its definitions for sepsis and septic shock and the clinical criteria underlying them.
Two reports and one summary communication published in JAMA February 23 detail the processes used to reach the consensus
definitions that have remained largely unchanged for more than two decades.
"The new definitions and clinical criteria of sepsis and septic shock are aimed to help clinicians at the bedside recognize these deadly syndromes and start therapy promptly," Dr. Christopher W. Seymour, from the University of Pittsburgh School of Medicine in Pennsylvania, told Reuters Health by email.
"After two years of deliberations and research, we were surprised to uncover the broad differences in how clinicians approach sepsis, and variety of criteria used in septic shock trials in the past decade. This mandated a re-examination of the criteria, strong efforts to speak a common language, and generate simple, easy to use criteria," Dr. Seymour said.
Dr. Seymour and colleagues recommended elimination of the terms sepsis syndrome, septicemia, and severe sepsis and settled on the definition of sepsis as "life-threatening organ dysfunction due to a dysregulated host response to infection."
They explored several sets of clinical criteria and their predictive validity for hospital mortality, including the Sequential Organ Function Assessment (SOFA), Logistic Organ Dysfunction System (LODS), systemic inflammatory response syndrome (SIRS), and a simplified qSOFA model that included Glasgow Coma Scale (GCS) score of 13 or less, systolic blood pressure of 100 mm Hg or less, and respiratory rate of 22/min or more (1 point each; score range, 0-3).
For intensive care unit encounters with suspected infection, SOFA came out on top, whereas for encounters with suspected infection outside of the ICU, qSOFA offered the best predictive validity for in-hospital mortality.
"Sepsis has no gold standard for diagnosis," Dr. Seymour said. "Given its complex pathophysiology and our evolving knowledge base, the current definition and criteria for sepsis represent a first step. Our field will need to continue to embark on improvements in the practicality, validity, and scientific rationale for sepsis definitions/criteria in future iterations."
He added,"We also hope that physicians recognize that, for the first time, these criteria derive from new data analyses in real patients. More than 700,000 encounters in 170 hospitals were studied to evaluate existing and new sepsis criteria."
Dr. Manu Shankar-Hari, from Guy's and St. Thomas' NHS Foundation Trust, London, UK, and colleagues reviewed 44 studies of septic shock involving 166,479 patients and used a Delphi process to arrive at the new consensus definition: "septic shock is defined as a subset of sepsis in which underlying circulatory, cellular, and metabolic abnormalities are associated with a greater risk of mortality than sepsis alone."
Dr. Shankar-Hari told Reuters Health by email, "The proposed definition for septic shock is a paradigm shift in illness concept. We wanted to provide consistency in diagnosing septic shock. The epidemiology of this illness as we measure currently is messy."
After examining six possible sets of clinical criteria, the group identified two criteria that proved most consistent with the proposed septic shock definition: hypotension requiring use of vasopressors to maintain mean blood pressure of 65 mm Hg or greater and having a serum lactate level greater than 2 mmol/L persisting after adequate fluid resuscitation.
In their summary report, Dr. Clifford S. Deutschman, from Hofstra-Northwell School of Medicine, Feinstein Institute for Medical Research, New Hyde Park, New York, and colleagues on the Task Force write, "The proposed criteria should aid diagnostic categorization once initial assessment and immediate management are completed. qSOFA or SOFA may at some point be used as entry criteria for clinical trials."
"Greater clarity and consistency will also facilitate research and more accurate coding," they add.
Dr. Edward Abraham, from Wake Forest School of Medicine, Winston Salem, North Carolina, who wrote an editorial related to these reports, told Reuters Health by email, "While the new definitions advance the field, particularly from an epidemiologic viewpoint and potentially in helping to identify the economic impact associated with sepsis and septic shock, they are only of limited help in defining care for an individual patient or in designing clinical trials to examine new therapies for sepsis."
"As noted in the editorial, more discriminatory definitions, based on specific cellular and genomic alterations, are necessary to truly affect care for individual patients and to assist in the development of novel therapeutic approaches to sepsis and septic shock," he said.
A number of organizations supported this research and a number of coauthors reported disclosures.
EMA initiative aims to accelerate drug development

Photo courtesy of the FDA
The European Medicines Agency (EMA) has launched PRIME (PRIority MEdicines), an initiative intended to accelerate the development of drugs that target unmet medical needs.
These “priority medicines” may offer a major therapeutic advantage over existing treatments or benefit patients who currently have no treatment options in the European Union (EU).
Through PRIME, the EMA will offer early support to drug developers to optimize the generation of robust data on a treatment’s benefits and risks and enable accelerated assessment of an application for marketing authorization.
By engaging with developers early, the EMA aims to strengthen the design of clinical trials to facilitate the generation of high quality data to support an application for marketing authorization.
PRIME builds on the existing regulatory framework and available tools such as scientific advice and accelerated assessment.
To be accepted for PRIME, a treatment has to show the potential to benefit patients with unmet medical needs based on early clinical data.
Once a candidate medicine has been selected for PRIME, the EMA:
- Appoints a rapporteur from the Committee for Medicinal Products for Human Use (CHMP), or from the Committee on Advanced Therapies (CAT) in the case of an advanced therapy, to provide continuous support and help to build knowledge before a company submits an application for marketing authorization
- Organizes a kick-off meeting with the CHMP/CAT rapporteur and a multidisciplinary group of experts from relevant EMA scientific committees and working parties, and provides guidance on the overall development plan and regulatory strategy
- Assigns a dedicated EMA contact point
- Provides scientific advice at key development milestones, involving additional stakeholders such as health technology assessment bodies to facilitate quicker access to the new drug
- Confirms potential for accelerated assessment when an application for marketing authorization is submitted.
PRIME is open to all drug companies on the basis of preliminary clinical evidence. However, micro-, small- and medium-sized enterprises and applicants from the academic sector can apply earlier on the basis of compelling non-clinical data and tolerability data from initial clinical trials. They may also request fee waivers for scientific advice.
The EMA has released guidance documents on PRIME as well as a comprehensive overview of the EU early access regulatory tools—ie, accelerated assessment, conditional marketing authorization, and compassionate use.
The agency has also published revised guidelines on the implementation of accelerated assessment and conditional marketing authorization. These tools are reserved for treatments addressing major public health needs, and the revised guidelines provide more detailed information based on past experience.
Although PRIME is specifically designed to promote accelerated assessment, the EMA said the initiative will also help drug developers make the best use of other EU early access tools and initiatives, which can be combined whenever a drug fulfills the respective criteria.
PRIME was developed in consultation with the EMA’s scientific committees, the European Commission and its expert group on Safe and Timely Access to Medicines for Patients, as well as the European medicines regulatory network.
The main principles of PRIME were released for a 2-month public consultation in 2015, and the comments received were taken into account in the final version. ![]()
Photo courtesy of the FDA
The European Medicines Agency (EMA) has launched PRIME (PRIority MEdicines), an initiative intended to accelerate the development of drugs that target unmet medical needs.
These “priority medicines” may offer a major therapeutic advantage over existing treatments or benefit patients who currently have no treatment options in the European Union (EU).
Through PRIME, the EMA will offer early support to drug developers to optimize the generation of robust data on a treatment’s benefits and risks and enable accelerated assessment of an application for marketing authorization.
By engaging with developers early, the EMA aims to strengthen the design of clinical trials to facilitate the generation of high quality data to support an application for marketing authorization.
PRIME builds on the existing regulatory framework and available tools such as scientific advice and accelerated assessment.
To be accepted for PRIME, a treatment has to show the potential to benefit patients with unmet medical needs based on early clinical data.
Once a candidate medicine has been selected for PRIME, the EMA:
- Appoints a rapporteur from the Committee for Medicinal Products for Human Use (CHMP), or from the Committee on Advanced Therapies (CAT) in the case of an advanced therapy, to provide continuous support and help to build knowledge before a company submits an application for marketing authorization
- Organizes a kick-off meeting with the CHMP/CAT rapporteur and a multidisciplinary group of experts from relevant EMA scientific committees and working parties, and provides guidance on the overall development plan and regulatory strategy
- Assigns a dedicated EMA contact point
- Provides scientific advice at key development milestones, involving additional stakeholders such as health technology assessment bodies to facilitate quicker access to the new drug
- Confirms potential for accelerated assessment when an application for marketing authorization is submitted.
PRIME is open to all drug companies on the basis of preliminary clinical evidence. However, micro-, small- and medium-sized enterprises and applicants from the academic sector can apply earlier on the basis of compelling non-clinical data and tolerability data from initial clinical trials. They may also request fee waivers for scientific advice.
The EMA has released guidance documents on PRIME as well as a comprehensive overview of the EU early access regulatory tools—ie, accelerated assessment, conditional marketing authorization, and compassionate use.
The agency has also published revised guidelines on the implementation of accelerated assessment and conditional marketing authorization. These tools are reserved for treatments addressing major public health needs, and the revised guidelines provide more detailed information based on past experience.
Although PRIME is specifically designed to promote accelerated assessment, the EMA said the initiative will also help drug developers make the best use of other EU early access tools and initiatives, which can be combined whenever a drug fulfills the respective criteria.
PRIME was developed in consultation with the EMA’s scientific committees, the European Commission and its expert group on Safe and Timely Access to Medicines for Patients, as well as the European medicines regulatory network.
The main principles of PRIME were released for a 2-month public consultation in 2015, and the comments received were taken into account in the final version. ![]()
Photo courtesy of the FDA
The European Medicines Agency (EMA) has launched PRIME (PRIority MEdicines), an initiative intended to accelerate the development of drugs that target unmet medical needs.
These “priority medicines” may offer a major therapeutic advantage over existing treatments or benefit patients who currently have no treatment options in the European Union (EU).
Through PRIME, the EMA will offer early support to drug developers to optimize the generation of robust data on a treatment’s benefits and risks and enable accelerated assessment of an application for marketing authorization.
By engaging with developers early, the EMA aims to strengthen the design of clinical trials to facilitate the generation of high quality data to support an application for marketing authorization.
PRIME builds on the existing regulatory framework and available tools such as scientific advice and accelerated assessment.
To be accepted for PRIME, a treatment has to show the potential to benefit patients with unmet medical needs based on early clinical data.
Once a candidate medicine has been selected for PRIME, the EMA:
- Appoints a rapporteur from the Committee for Medicinal Products for Human Use (CHMP), or from the Committee on Advanced Therapies (CAT) in the case of an advanced therapy, to provide continuous support and help to build knowledge before a company submits an application for marketing authorization
- Organizes a kick-off meeting with the CHMP/CAT rapporteur and a multidisciplinary group of experts from relevant EMA scientific committees and working parties, and provides guidance on the overall development plan and regulatory strategy
- Assigns a dedicated EMA contact point
- Provides scientific advice at key development milestones, involving additional stakeholders such as health technology assessment bodies to facilitate quicker access to the new drug
- Confirms potential for accelerated assessment when an application for marketing authorization is submitted.
PRIME is open to all drug companies on the basis of preliminary clinical evidence. However, micro-, small- and medium-sized enterprises and applicants from the academic sector can apply earlier on the basis of compelling non-clinical data and tolerability data from initial clinical trials. They may also request fee waivers for scientific advice.
The EMA has released guidance documents on PRIME as well as a comprehensive overview of the EU early access regulatory tools—ie, accelerated assessment, conditional marketing authorization, and compassionate use.
The agency has also published revised guidelines on the implementation of accelerated assessment and conditional marketing authorization. These tools are reserved for treatments addressing major public health needs, and the revised guidelines provide more detailed information based on past experience.
Although PRIME is specifically designed to promote accelerated assessment, the EMA said the initiative will also help drug developers make the best use of other EU early access tools and initiatives, which can be combined whenever a drug fulfills the respective criteria.
PRIME was developed in consultation with the EMA’s scientific committees, the European Commission and its expert group on Safe and Timely Access to Medicines for Patients, as well as the European medicines regulatory network.
The main principles of PRIME were released for a 2-month public consultation in 2015, and the comments received were taken into account in the final version. ![]()
CDC quantifies threat of resistant HAIs in US

in the intensive care unit
New data from the US Centers for Disease Control and Prevention (CDC) suggest the incidence of certain healthcare-associated infections (HAIs) has fallen in recent years, but antibiotic-resistant bacteria remain a threat.
Therefore, the CDC is advising healthcare workers to use a combination of infection control recommendations to better protect patients from these infections.
“New data show that far too many patients are getting infected with dangerous, drug-resistant bacteria in healthcare settings,” said CDC Director Tom Frieden, MD.
The facts and figures are available in the CDC’s latest Vital Signs report and the agency’s annual progress report on HAI prevention.
The data indicate that 1 in 7 catheter- and surgery-related HAIs in acute care hospitals can be caused by 6 types of antibiotic-resistant bacteria. That number increases to 1 in 4 infections in long-term acute care hospitals.
The 6 antibiotic-resistant threats are carbapenem-resistant Enterobacteriaceae (CRE), methicillin-resistant Staphylococcus aureus (MRSA), ESBL-producing Enterobacteriaceae (extended-spectrum β-lactamases), vancomycin-resistant Enterococcus (VRE), multidrug-resistant Pseudomonas aeruginosa, and multidrug-resistant Acinetobacter.
Prevention and resistance
According to the CDC’s data, acute care hospitals saw a 50% decrease in central line-associated bloodstream infections between 2008 and 2014. But 1 in 6 remaining central line-associated bloodstream infections is caused by urgent or serious antibiotic-resistant bacteria.
Between 2008 and 2014, acute care hospitals saw a 17% decrease in surgical site infections related to 10 procedures that were tracked in previous HAI progress reports. One in 7 remaining surgical site infections is caused by urgent or serious antibiotic-resistant bacteria.
Acute care hospitals saw no change in the incidence of catheter-associated urinary tract infections (CAUTIs) between 2009 and 2014. However, there was a reduction in CAUTIs between 2013 and 2014. One in 10 CAUTIs is caused by urgent or serious antibiotic-resistant bacteria.
The Vital Signs report also examines Clostridium difficile, which caused almost half a million infections in the US in 2011 alone. The CDC’s annual progress report shows that hospital-onset C difficile infections decreased by 8% between 2011 and 2014.
In addition to the reports, the CDC has released a web app with interactive data on HAIs caused by antibiotic-resistant bacteria.
The tool, known as the Antibiotic Resistance Patient Safety Atlas, provides national, regional, and state map views of superbug/drug combinations showing percent resistance over time. The Atlas uses data reported to the CDC’s National Healthcare Safety Network from 2011 to 2014 from more than 4000 healthcare facilities. ![]()
in the intensive care unit
New data from the US Centers for Disease Control and Prevention (CDC) suggest the incidence of certain healthcare-associated infections (HAIs) has fallen in recent years, but antibiotic-resistant bacteria remain a threat.
Therefore, the CDC is advising healthcare workers to use a combination of infection control recommendations to better protect patients from these infections.
“New data show that far too many patients are getting infected with dangerous, drug-resistant bacteria in healthcare settings,” said CDC Director Tom Frieden, MD.
The facts and figures are available in the CDC’s latest Vital Signs report and the agency’s annual progress report on HAI prevention.
The data indicate that 1 in 7 catheter- and surgery-related HAIs in acute care hospitals can be caused by 6 types of antibiotic-resistant bacteria. That number increases to 1 in 4 infections in long-term acute care hospitals.
The 6 antibiotic-resistant threats are carbapenem-resistant Enterobacteriaceae (CRE), methicillin-resistant Staphylococcus aureus (MRSA), ESBL-producing Enterobacteriaceae (extended-spectrum β-lactamases), vancomycin-resistant Enterococcus (VRE), multidrug-resistant Pseudomonas aeruginosa, and multidrug-resistant Acinetobacter.
Prevention and resistance
According to the CDC’s data, acute care hospitals saw a 50% decrease in central line-associated bloodstream infections between 2008 and 2014. But 1 in 6 remaining central line-associated bloodstream infections is caused by urgent or serious antibiotic-resistant bacteria.
Between 2008 and 2014, acute care hospitals saw a 17% decrease in surgical site infections related to 10 procedures that were tracked in previous HAI progress reports. One in 7 remaining surgical site infections is caused by urgent or serious antibiotic-resistant bacteria.
Acute care hospitals saw no change in the incidence of catheter-associated urinary tract infections (CAUTIs) between 2009 and 2014. However, there was a reduction in CAUTIs between 2013 and 2014. One in 10 CAUTIs is caused by urgent or serious antibiotic-resistant bacteria.
The Vital Signs report also examines Clostridium difficile, which caused almost half a million infections in the US in 2011 alone. The CDC’s annual progress report shows that hospital-onset C difficile infections decreased by 8% between 2011 and 2014.
In addition to the reports, the CDC has released a web app with interactive data on HAIs caused by antibiotic-resistant bacteria.
The tool, known as the Antibiotic Resistance Patient Safety Atlas, provides national, regional, and state map views of superbug/drug combinations showing percent resistance over time. The Atlas uses data reported to the CDC’s National Healthcare Safety Network from 2011 to 2014 from more than 4000 healthcare facilities. ![]()
in the intensive care unit
New data from the US Centers for Disease Control and Prevention (CDC) suggest the incidence of certain healthcare-associated infections (HAIs) has fallen in recent years, but antibiotic-resistant bacteria remain a threat.
Therefore, the CDC is advising healthcare workers to use a combination of infection control recommendations to better protect patients from these infections.
“New data show that far too many patients are getting infected with dangerous, drug-resistant bacteria in healthcare settings,” said CDC Director Tom Frieden, MD.
The facts and figures are available in the CDC’s latest Vital Signs report and the agency’s annual progress report on HAI prevention.
The data indicate that 1 in 7 catheter- and surgery-related HAIs in acute care hospitals can be caused by 6 types of antibiotic-resistant bacteria. That number increases to 1 in 4 infections in long-term acute care hospitals.
The 6 antibiotic-resistant threats are carbapenem-resistant Enterobacteriaceae (CRE), methicillin-resistant Staphylococcus aureus (MRSA), ESBL-producing Enterobacteriaceae (extended-spectrum β-lactamases), vancomycin-resistant Enterococcus (VRE), multidrug-resistant Pseudomonas aeruginosa, and multidrug-resistant Acinetobacter.
Prevention and resistance
According to the CDC’s data, acute care hospitals saw a 50% decrease in central line-associated bloodstream infections between 2008 and 2014. But 1 in 6 remaining central line-associated bloodstream infections is caused by urgent or serious antibiotic-resistant bacteria.
Between 2008 and 2014, acute care hospitals saw a 17% decrease in surgical site infections related to 10 procedures that were tracked in previous HAI progress reports. One in 7 remaining surgical site infections is caused by urgent or serious antibiotic-resistant bacteria.
Acute care hospitals saw no change in the incidence of catheter-associated urinary tract infections (CAUTIs) between 2009 and 2014. However, there was a reduction in CAUTIs between 2013 and 2014. One in 10 CAUTIs is caused by urgent or serious antibiotic-resistant bacteria.
The Vital Signs report also examines Clostridium difficile, which caused almost half a million infections in the US in 2011 alone. The CDC’s annual progress report shows that hospital-onset C difficile infections decreased by 8% between 2011 and 2014.
In addition to the reports, the CDC has released a web app with interactive data on HAIs caused by antibiotic-resistant bacteria.
The tool, known as the Antibiotic Resistance Patient Safety Atlas, provides national, regional, and state map views of superbug/drug combinations showing percent resistance over time. The Atlas uses data reported to the CDC’s National Healthcare Safety Network from 2011 to 2014 from more than 4000 healthcare facilities. ![]()
Inhibitor exhibits activity against myeloma

A dual kinase inhibitor has shown early promise as a potential treatment for multiple myeloma (MM), according to investigators.
The inhibitor, ON123300, targets both AMPK-related protein kinase 5 (ARK5) and cyclin-dependent kinase 4 (CDK4), proteins responsible for maintaining energy balance within the cell.
Investigators found that ON123300 can induce apoptosis in MM cells in vitro and halt tumor growth in mouse models of MM.
The team reported these findings in Cancer Research.
“ARK5 is critical for myeloma survival, and this study suggests a novel function for ARK5 in bridging the mTOR and MYC pathways,” said study author Deepak Perumal, PhD, of the Icahn School of Medicine at Mount Sinai in New York, New York.
“Given that MYC is critically overexpressed in myeloma, we sought to determine whether selective inhibition of ARK5 and CDK4 could be an effective way to target MYC-driven proliferation in myeloma.”
The team at Mount Sinai developed ON123300 in collaboration with Onconova Therapeutics, Inc. And they tested the drug in MM cell lines and primary samples from patients with recurring MM, as well as human HS-5 bone marrow stromal cells.
ON123300 induced rapid cell-cycle arrest and apoptosis in MM cells but was not toxic to normal peripheral blood cells.
In mouse models of MM, ON123300 decreased tumor growth without causing significant toxicity.
The investigators also discovered that MM cells that are sensitive to ON123300 have a unique genomic signature, which could guide the clinical development of the drug.
“Our study results show that ON123300 induces cell death and negatively regulates key oncogenic pathways in multiple myeloma cells,” said Samir Parekh, MD, also of the Icahn School of Medicine at Mount Sinai.
“This is the first report showing potent cytotoxicity of CDK4/ARK5 inhibition in MM and provides the foundation for further clinical trials using CDK4/ARK5 inhibitors to improve outcomes for MM patients.” ![]()
A dual kinase inhibitor has shown early promise as a potential treatment for multiple myeloma (MM), according to investigators.
The inhibitor, ON123300, targets both AMPK-related protein kinase 5 (ARK5) and cyclin-dependent kinase 4 (CDK4), proteins responsible for maintaining energy balance within the cell.
Investigators found that ON123300 can induce apoptosis in MM cells in vitro and halt tumor growth in mouse models of MM.
The team reported these findings in Cancer Research.
“ARK5 is critical for myeloma survival, and this study suggests a novel function for ARK5 in bridging the mTOR and MYC pathways,” said study author Deepak Perumal, PhD, of the Icahn School of Medicine at Mount Sinai in New York, New York.
“Given that MYC is critically overexpressed in myeloma, we sought to determine whether selective inhibition of ARK5 and CDK4 could be an effective way to target MYC-driven proliferation in myeloma.”
The team at Mount Sinai developed ON123300 in collaboration with Onconova Therapeutics, Inc. And they tested the drug in MM cell lines and primary samples from patients with recurring MM, as well as human HS-5 bone marrow stromal cells.
ON123300 induced rapid cell-cycle arrest and apoptosis in MM cells but was not toxic to normal peripheral blood cells.
In mouse models of MM, ON123300 decreased tumor growth without causing significant toxicity.
The investigators also discovered that MM cells that are sensitive to ON123300 have a unique genomic signature, which could guide the clinical development of the drug.
“Our study results show that ON123300 induces cell death and negatively regulates key oncogenic pathways in multiple myeloma cells,” said Samir Parekh, MD, also of the Icahn School of Medicine at Mount Sinai.
“This is the first report showing potent cytotoxicity of CDK4/ARK5 inhibition in MM and provides the foundation for further clinical trials using CDK4/ARK5 inhibitors to improve outcomes for MM patients.” ![]()
A dual kinase inhibitor has shown early promise as a potential treatment for multiple myeloma (MM), according to investigators.
The inhibitor, ON123300, targets both AMPK-related protein kinase 5 (ARK5) and cyclin-dependent kinase 4 (CDK4), proteins responsible for maintaining energy balance within the cell.
Investigators found that ON123300 can induce apoptosis in MM cells in vitro and halt tumor growth in mouse models of MM.
The team reported these findings in Cancer Research.
“ARK5 is critical for myeloma survival, and this study suggests a novel function for ARK5 in bridging the mTOR and MYC pathways,” said study author Deepak Perumal, PhD, of the Icahn School of Medicine at Mount Sinai in New York, New York.
“Given that MYC is critically overexpressed in myeloma, we sought to determine whether selective inhibition of ARK5 and CDK4 could be an effective way to target MYC-driven proliferation in myeloma.”
The team at Mount Sinai developed ON123300 in collaboration with Onconova Therapeutics, Inc. And they tested the drug in MM cell lines and primary samples from patients with recurring MM, as well as human HS-5 bone marrow stromal cells.
ON123300 induced rapid cell-cycle arrest and apoptosis in MM cells but was not toxic to normal peripheral blood cells.
In mouse models of MM, ON123300 decreased tumor growth without causing significant toxicity.
The investigators also discovered that MM cells that are sensitive to ON123300 have a unique genomic signature, which could guide the clinical development of the drug.
“Our study results show that ON123300 induces cell death and negatively regulates key oncogenic pathways in multiple myeloma cells,” said Samir Parekh, MD, also of the Icahn School of Medicine at Mount Sinai.
“This is the first report showing potent cytotoxicity of CDK4/ARK5 inhibition in MM and provides the foundation for further clinical trials using CDK4/ARK5 inhibitors to improve outcomes for MM patients.” ![]()
System could aid assessment of sickle cell disease

and a normal one
Image by Betty Pace
A microfluidic system can measure the deformability and adhesion of red blood cells (RBCs) in samples from patients with sickle cell disease (SCD), according to research published in Technology.
The researchers noted that RBC deformability has been associated with vaso-occlusion in SCD, but we have limited knowledge on deformation characteristics of RBCs adhered to endothelium-associated proteins in microphysiological fluid flow conditions.
In the past, various approaches have been used to measure RBC deformability, including optical tweezers, micropipette aspiration, and atomic force microscopy. These methods have enabled sensitive and controlled measurement of RBC mechanical properties, but they are typically performed in open environments without fluid flow.
“Microfluidic techniques allow incorporation of physiological flow conditions, as well as biologically relevant adhesion surfaces in a closed setting, which better mimic the natural physiological environment of the RBCs in blood flow,” said study author Umut Gurkan, PhD, of the Case Western Reserve University in Cleveland, Ohio.
For their system, Dr Gurkan and his colleagues integrated a microfluidic approach with a cell-dimensioning algorithm.
They introduced a new parameter to assess the deformability of RBCs. It is known as the dynamic deformability index (DDI), which they defined as the time-dependent change of the cell’s aspect ratio in response to fluid flow shear stress.
The researchers assessed the deformability and adhesion of RBCs containing healthy hemoglobin A (HbA) and homozygous sickle hemoglobin (HbS). And they found the DDI of HbS-containing RBCs was significantly lower than the DDI of HbA-containing RBCs.
The team also found they could divide HbS-containing RBCs into 2 groups—deformable and non-deformable RBCs.
“We report, for the first time, on the subpopulations of RBCs in terms of dynamic deformation characteristics in SCD: deformable and non-deformable RBCs,” said Yunus Alapan, a PhD candidate at Case Western Reserve University.
“Furthermore, we analyzed adhesion of non-deformable RBCs, in comparison to deformable RBCs, quantitatively at physiological and above physiological flow shear stresses in blood samples obtained from SCD patients.”
“We observed significantly greater numbers of adhered non-deformable sickle RBCs than deformable sickle RBCs at flow shear stresses well above the physiological range, suggesting an interplay between dynamic deformability and increased adhesion of RBCs in vaso-occlusive events.”
Now, the researchers are working to further characterize deformability and adhesion of RBCs in a greater number of SCD patients to analyze their associations with clinical phenotypes and complications.
The team said their system may provide important biophysical insights into disease pathophysiology when widely applied in SCD.
They also believe the microfluidic platform has the potential to be used as an in vitro assay for monitoring disease activity at baseline, during clinical flux after treatment, during painful episodes, and in association with long-term complications. ![]()
and a normal one
Image by Betty Pace
A microfluidic system can measure the deformability and adhesion of red blood cells (RBCs) in samples from patients with sickle cell disease (SCD), according to research published in Technology.
The researchers noted that RBC deformability has been associated with vaso-occlusion in SCD, but we have limited knowledge on deformation characteristics of RBCs adhered to endothelium-associated proteins in microphysiological fluid flow conditions.
In the past, various approaches have been used to measure RBC deformability, including optical tweezers, micropipette aspiration, and atomic force microscopy. These methods have enabled sensitive and controlled measurement of RBC mechanical properties, but they are typically performed in open environments without fluid flow.
“Microfluidic techniques allow incorporation of physiological flow conditions, as well as biologically relevant adhesion surfaces in a closed setting, which better mimic the natural physiological environment of the RBCs in blood flow,” said study author Umut Gurkan, PhD, of the Case Western Reserve University in Cleveland, Ohio.
For their system, Dr Gurkan and his colleagues integrated a microfluidic approach with a cell-dimensioning algorithm.
They introduced a new parameter to assess the deformability of RBCs. It is known as the dynamic deformability index (DDI), which they defined as the time-dependent change of the cell’s aspect ratio in response to fluid flow shear stress.
The researchers assessed the deformability and adhesion of RBCs containing healthy hemoglobin A (HbA) and homozygous sickle hemoglobin (HbS). And they found the DDI of HbS-containing RBCs was significantly lower than the DDI of HbA-containing RBCs.
The team also found they could divide HbS-containing RBCs into 2 groups—deformable and non-deformable RBCs.
“We report, for the first time, on the subpopulations of RBCs in terms of dynamic deformation characteristics in SCD: deformable and non-deformable RBCs,” said Yunus Alapan, a PhD candidate at Case Western Reserve University.
“Furthermore, we analyzed adhesion of non-deformable RBCs, in comparison to deformable RBCs, quantitatively at physiological and above physiological flow shear stresses in blood samples obtained from SCD patients.”
“We observed significantly greater numbers of adhered non-deformable sickle RBCs than deformable sickle RBCs at flow shear stresses well above the physiological range, suggesting an interplay between dynamic deformability and increased adhesion of RBCs in vaso-occlusive events.”
Now, the researchers are working to further characterize deformability and adhesion of RBCs in a greater number of SCD patients to analyze their associations with clinical phenotypes and complications.
The team said their system may provide important biophysical insights into disease pathophysiology when widely applied in SCD.
They also believe the microfluidic platform has the potential to be used as an in vitro assay for monitoring disease activity at baseline, during clinical flux after treatment, during painful episodes, and in association with long-term complications. ![]()
and a normal one
Image by Betty Pace
A microfluidic system can measure the deformability and adhesion of red blood cells (RBCs) in samples from patients with sickle cell disease (SCD), according to research published in Technology.
The researchers noted that RBC deformability has been associated with vaso-occlusion in SCD, but we have limited knowledge on deformation characteristics of RBCs adhered to endothelium-associated proteins in microphysiological fluid flow conditions.
In the past, various approaches have been used to measure RBC deformability, including optical tweezers, micropipette aspiration, and atomic force microscopy. These methods have enabled sensitive and controlled measurement of RBC mechanical properties, but they are typically performed in open environments without fluid flow.
“Microfluidic techniques allow incorporation of physiological flow conditions, as well as biologically relevant adhesion surfaces in a closed setting, which better mimic the natural physiological environment of the RBCs in blood flow,” said study author Umut Gurkan, PhD, of the Case Western Reserve University in Cleveland, Ohio.
For their system, Dr Gurkan and his colleagues integrated a microfluidic approach with a cell-dimensioning algorithm.
They introduced a new parameter to assess the deformability of RBCs. It is known as the dynamic deformability index (DDI), which they defined as the time-dependent change of the cell’s aspect ratio in response to fluid flow shear stress.
The researchers assessed the deformability and adhesion of RBCs containing healthy hemoglobin A (HbA) and homozygous sickle hemoglobin (HbS). And they found the DDI of HbS-containing RBCs was significantly lower than the DDI of HbA-containing RBCs.
The team also found they could divide HbS-containing RBCs into 2 groups—deformable and non-deformable RBCs.
“We report, for the first time, on the subpopulations of RBCs in terms of dynamic deformation characteristics in SCD: deformable and non-deformable RBCs,” said Yunus Alapan, a PhD candidate at Case Western Reserve University.
“Furthermore, we analyzed adhesion of non-deformable RBCs, in comparison to deformable RBCs, quantitatively at physiological and above physiological flow shear stresses in blood samples obtained from SCD patients.”
“We observed significantly greater numbers of adhered non-deformable sickle RBCs than deformable sickle RBCs at flow shear stresses well above the physiological range, suggesting an interplay between dynamic deformability and increased adhesion of RBCs in vaso-occlusive events.”
Now, the researchers are working to further characterize deformability and adhesion of RBCs in a greater number of SCD patients to analyze their associations with clinical phenotypes and complications.
The team said their system may provide important biophysical insights into disease pathophysiology when widely applied in SCD.
They also believe the microfluidic platform has the potential to be used as an in vitro assay for monitoring disease activity at baseline, during clinical flux after treatment, during painful episodes, and in association with long-term complications. ![]()
Diet and Atopic Dermatitis
Atopic dermatitis (AD) is the leading diagnosis among pediatric dermatologists,1 and this condition is commonly seen worldwide by dermatologists and allergists.2 There is a widespread misconception held by many patients and their guardians who believe that AD is caused by a food allergy.3 Although AD is related to and part of the atopic complex of disorders associated with food allergies, the role of diet in AD is not well defined. Previously it was recommended to delay early exposure to foods, but now it is recommended to do the opposite in certain situations. In fact, delaying exposure to certain types of foods can increase the likelihood of food allergies (eg, early exposure to peanut butter lowers the statistical chance of developing peanut allergies). This article reviews recent data on the role of diet in AD regarding disease activity as well as new and emerging data on dietary modifications for prevention and intervention. Emerging data on the relationship between AD and food allergies also are presented.
Pathogenesis of AD
The skin barrier plays a vital role in the prevention of pathogens, allergen exposure, and sensitization. There is no solitary root cause of AD, rather it is a combination of inflammation and barrier dysfunction associated with allergic diathesis (eg, atopy). Many patients with AD, especially those with persistent disease, have an intrinsic barrier dysfunction as part of the root cause of their illness, which may be caused by genetically mediated filaggrin defects or alternative barrier dysfunction such as decreased ceramide content that predisposes to percutaneous and mucosal sensitization.4,5 Another source of percutaneous exposure to allergens is macroscopic breaks in the skin caused by scratching, which allows dendritic termini of Langerhans cells to be exposed to percutaneous antigens4,6 through binding to high-affinity IgE receptors.
Langerhans cells exposed to allergens can trigger either an immediate or delayed-type (type I or type II) reaction (sensitization phase) in the lymph node causing inflammatory activation (elicitation). Inflammatory activity in AD is broad and complex and includes the release of IL-4, elevated IgE levels, and eosinophilia, which trigger the helper T cell TH2 and TH17 cascade of cytokines, including IL-2, IL-4, IL-5, IL-8, IL-10, IL-13, IL-17α, tumor necrosis factor α, and IFN-γ,7-9 with the latter worsening barrier defect via downregulation of intercellular substances (eg, filaggrin) and intercellular adhesion expression (eg, claudin 1).6,7,10
Atopic dermatitis does not exist in isolation. The barrier dysfunction associated with AD allows for sensitization to allergens, including those found in food and/or the environment. The atopic march, which occurs via barrier abnormalities facilitating sensitization, can result in further atopy, such as food allergies, environmental allergies, asthma, and eosinophilic esophagitis.11
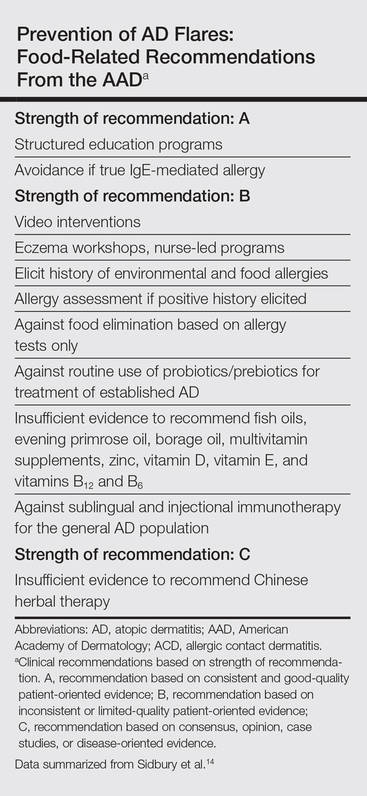
|
AD and Food Allergies
Many patients and guardians believe AD is caused by a food allergy and that diet restrictions will resolve the disease. Although the latter is not true, in reality many patients with AD do have food allergies. Approximately 40% of infants and young children with moderate to severe AD and 8% of the general population of children will manifest a specific IgE-based food allergy. Food-specific IgE can be triggered or exacerbated by AD through the induction of hives, cutaneous activation of mast cells, increased “spontaneous” basophil histamine release, and food-related lymphocyte-proliferative responses measurable by food patch testing.12 Allergists generally recommend avoidance of or use of heavily denatured food (in the case of a milk/egg allergy) in the setting of documented IgE-mediated allergens.13 Food allergies in AD can manifest with flares, hives, pruritus, and/or other cutaneous symptoms in the absence of flaring AD disease.
Guidelines from the American Academy of Dermatology (AAD)(Table) for the management of AD have recently recommended testing for food allergies in children younger than 5 years who have intractable AD or known food-induced reactions.14 This technique will largely identify children at risk for anaphylaxis but may not yield information contributing to AD improvement. Furthermore, withdrawal of allergens with known IgE-mediated response was classified by the AAD as having consistent good-quality patient-oriented evidence, and asking about allergic reactions as well as acting on a reported allergic history had inconsistent or limited-quality patient-oriented evidence. It is believed that atopy can progress, or march, into a food and/or environmental allergy at any point in life; therefore, testing for a food allergy should be considered in all patients with recent onset of severe and/or persistent AD and/or food-aggravated AD due to a lifetime risk of sensitization.14,15 A food introduction plan may require collaboration with an allergist, especially in high-risk patients (eg, those with known food reactions, family history of food allergies, severe atopy).
Prevention of AD Through Dietary Modification
The National Institute of Allergy and Infectious Diseases consensus group published guidelines on food allergies that affect AD management, including avoidance of proven allergens but not random elimination of food allergens in AD; the group identifies AD and family history of AD as risk factors for food allergies.16 The best data in support of avoidance of documented food allergens to reduce AD severity has been found for egg white allergy and avoidance. Active egg allergy also is linked to staphylococcal superantigen IgE sensitizations,17 but the reason for the link is not yet clear. For the pediatric population, exclusive breastfeeding until 4 to 6 months of age and introduction of solids within the first 4 to 6 months as well as avoidance of maternal dietary restriction during pregnancy and lactation was further endorsed, with use of hydrolyzed formulas as an alternative to exclusive breastfeeding in infants who are not exclusively breastfed (cost permitting).16,18
A Cochrane review of maternal dietary restrictions during pregnancy found no benefit of maternal prenatal dietary restriction on AD prevalence in the first 18 months of life but did note an association with lower mean gestational weight.19
There is currently an effort to produce foods, such as soybeans and corn, that are genetically modified to reduce exposure to the allergenic component, but it is possible that when large-scale challenges occur, these foods also will be allergenic.20,21 In the case of a modified apple, some promising reduction in allergy symptoms has been reported.22 Although genetically modified foods may benefit children with food allergies in the future, they are a source of some controversy.
Complementary and Alternative Medicine
The AAD guidelines do not recommend complementary and alternative medicine (CAM) to treat AD,14 but it remains a commonly used therapy in the United States. A 2014 analysis of data from the 2007 US-based national health interview survey of 9417 children (age range, 0–17 years) demonstrated that 46.9% of children used 1 or more CAM, of which 0.99% used CAM specifically for AD. In this study, herbal therapy, vitamins, homeopathy, diet, and movement techniques were associated with increased prevalence of AD.23 Although some herbals have been shown to be beneficial in AD,24 hepatotoxicity has been reported with some herbal therapies.25 Complementary techniques with evidence-based support include massage therapy,26 relocation to an alternative climate, acupuncture that rivals cetirizine in efficacy, and supportive nutritional advice.24,27
Factors Affecting the Incidence of AD
Atopic dermatitis is of greater prevalence in children in developed wealthy nations such as the United States, supporting the role of enhanced hygiene and overall good health through vaccination as a possible contributor to the rise in AD prevalence in the last 4 decades.28,29 Alternatively, viruses such as respiratory syncytial virus may trigger AD, suggesting vaccination against the virus may reduce the risk for AD.30 Overall, vaccination improves life expectancy and should be conducted on schedule without reservation. Other aspects of hygiene that could conceptually affect prevalence of AD are raw food ingestion and the effects of foodborne microbes on the intestinal microbiome in relationship to AD development. Probiotics have been tested for this purpose.
Probiotics and prebiotics have been theorized to work through a reduction in inflammation; these agents have some evidence in their favor, but they were not endorsed in the AAD guidelines14 despite showing promise in meta-analysis. In particular prenatal and postnatal (maternal and child) supplementation of Lactobacillus rhamnosus shows promise.31-33 Food elimination diets and supplements including vitamin D, selenium, fish oil, borage oil, and zinc were not found to be beneficial and were not recommended in the AAD guidelines.14,34
Percutaneous exposure to peanuts, possibly in household dust, may be the mechanism of peanut sensitization in AD27 via an inherent adjuvant effect of peanut protein.28 The recent LEAP (Learning Early About Peanut Allergy) trial randomized 530 infants aged 4 to 11 months to peanut-avoidant versus peanut-exposed diets for 60 months. The results showed statistically reduced (approximately one-twelfth of the risk) peanut allergy even in infants known to be sensitized (approximately one-third of the risk).35 It is now recommended in countries with a high prevalence of peanut allergies to introduce peanuts to an infant’s diet between 4 and 11 months of age (evidence level 1 [highest level of evidence]), with referral to an allergist for introduction in known sensitization cases and severe AD.36 In the setting of known or documented peanut allergy and for evaluation of potential food allergies, an allergist should be consulted.
Other interventions have been described as promising in mouse models. Those supplements include Lithospermum erythrorhizon,37Platycodon grandiflorus,38Hypsizygus marmoreous,39 fortified ginseng extract,40 polyunsaturated fatty acids,41 and galactooligosaccharide.42 Prebiotic oligosaccharides also are promising for early prevention of AD symptoms in infants, but otherwise these agents have remained largely untested in AD.43 None of these therapies have been endorsed by the AAD, and the long-term safety and efficacy in humans remains to be proven.
Risks of Dietary Restriction
Dietary restrictions in treating AD can have negative consequences, including reduced birth weight when initiated in pregnancy,19 osteomalacia from vitamin D deficiency,44 and nutritional deficiencies (eg, calcium, phosphorus, iron, vitamin K, vitamin D, zinc, vitamin A, B1, B2, B6, niacin, cholesterol, and/or vitamin C deficiencies).45 Excess dietary intake of vegetables in individuals with extensive food allergies can result in carotenemia.46 Protein-restricted diets from use of rice milk or dietary protein restriction can result in kwashiorkorlike protein malnutrition and marasmus.47-49 Nutritional counseling and/or supplementation is recommended for patients with food-restricted diets.
Avoiding Fragrance in Food
Food intolerance often is reported by AD patients. In allergies, food intolerance refers to side effects such as gastrointestinal symptoms; in dermatology, food intolerance can include itching, systemic flares of allergic contact dermatitis (eg, fragrance allergy), or true IgE-mediated allergies such as oral allergy syndrome. Oral allergy syndrome (pollen-food allergy syndrome) is an epitope-spread phenomenon related to an allergy to tree pollen, causing broad allergy to specific groups of fruits and nuts.50 Food triggers in AD include kiwi, milk, apple, tomato, citrus fruits, tree nuts, and peanuts. Oral allergy syndrome is common in food-sensitive AD patients (51.2%) followed by gastrointestinal symptoms (23.5%) and worsening AD (11.4%).51 Sensitization to fragrance can cross-react with foods (eg, balsam of Peru and tomatoes).52 A tomato allergy can be detected either by a skin-prick test or a food patch test in this setting.53 An allergist should be consulted if oral allergy syndrome is suspected.
Conclusion
Food allergies are more common in AD patients and patients should be referred to an allergist for evaluation and management. Strict dietary practice is not recommended, while avoiding proven food allergens in AD could be beneficial. Dermatologists should be aware that patients with dietary restrictions may lack key nutrients, manifesting with nutritional deficiencies in the skin; therefore, nutrition counseling may be needed in the most severe AD/allergy patients. This field is evolving; therefore, ongoing study and evaluation of interventions as they relate to AD will be needed to assess best practices for diet in AD over time.
1. Schachner L, Ling NS, Press S. A statistical analysis of a pediatric dermatology clinic. Pediatr Dermatol. 1983;1:157-164.
2. Kiprono SK, Muchunu JW, Masenga JE. Skin diseases in pediatric patients attending a tertiary dermatology hospital in Northern Tanzania: a cross-sectional study. BMC Dermatol. 2015;15:16.
3. Wensink M, Timmer C, Brand PL. Atopic dermatitis in infants not caused by food allergy [in Dutch]. Ned Tijdschr Geneeskd. 2008;152:4-9.
4. De Benedetto A, Kubo A, Beck LA. Skin barrier disruption: a requirement for allergen sensitization? J Invest Dermatol. 2012;132(3, pt 2):949-963.
5. Margolis DJ, Apter AJ, Gupta J, et al. The persistence of atopic dermatitis and filaggrin (FLG) mutations in a US longitudinal cohort. J Allergy Clin Immunol. 2012;130:912-917.
6. Hanifin JM. Evolving concepts of pathogenesis in atopic dermatitis and other eczemas. J Invest Dermatol. 2009;129:320-322.
7. Batista DI, Perez L, Orfali RL, et al. Profile of skin barrier proteins (filaggrin, claudins 1 and 4) and Th1/Th2/Th17 cytokines in adults with atopic dermatitis. J Eur Acad Dermatol Venereol. 2015;29:1091-1095.
8. Kondo H, Ichikawa Y, Imokawa G. Percutaneous sensitization with allergens through barrier-disrupted skin elicits a Th2-dominant cytokine response. Eur J Immunol. 1998;28:769-779.
9. Correa da Rosa J, Malajian D, Shemer A, et al. Patients with atopic dermatitis have attenuated and distinct contact hypersensitivity responses to common allergens in skin. J Allergy Clin Immunol. 2015;135:712-720.
10. Paller AS. Latest approaches to treating atopic dermatitis. Chem Immunol Allergy. 2012;96:132-140.
11. Cianferoni A, Spergel J. Eosinophilic esophagitis: a comprehensive review [published online July 22, 2015]. Clin Rev Allergy Immunol. doi:10.1111/all.12846.
12. Sicherer SH, Sampson HA. Food hypersensitivity and atopic dermatitis; pathophysiology, epidemiology, diagnosis, and management. J Allergy Clin Immunol. 1999;104(3, pt 2):S114-S122.
13. Sicherer SH, Sampson HA. Food allergy: epidemiology, pathogenesis, diagnosis, and treatment. J Allergy Clin Immunol. 2014;133:291-307.
14. Sidbury R, Tom WL, Bergman JN, et al. Guidelines of care for the management of atopic dermatitis: section 4. prevention of disease flares and use of adjunctive therapies and approaches. J Am Acad Dermatol. 2014;71:1218-1233.
15. Marenholz I, Rivera VA, Esparza-Gordillo J, et al. Association screening in the epidermal differentiation complex (EDC) identifies an SPRR3 repeat number variant as a risk factor for eczema. J Invest Dermatol. 2011;131:1644-1649.
16. Burks AW, Jones SM, Boyce JA, et al. NIAID-sponsored 2010 guidelines for managing food allergy: applications in the pediatric population. Pediatrics. 2011;128:955-965.
17. Ong PY. Association between egg and staphylococcal superantigen IgE sensitizations in atopic dermatitis. Allergy Asthma Proc. 2014;35:346-348.
18. Botteman M, Detzel P. Cost-effectiveness of partially hydrolyzed whey protein formula in the primary prevention of atopic dermatitis in high-risk urban infants in Southeast Asia. Ann Nutr Metab. 2015;66(suppl 1):26-32.
19. Kramer MS, Kakuma R. Maternal dietary antigen avoidance during pregnancy or lactation, or both, for preventing or treating atopic disease in the child. Cochrane Database Syst Rev. 2012;9:CD000133.
20. Yum HY, Lee SY, Lee KE, et al. Genetically modified and wild soybeans: an immunologic comparison. Allergy Asthma Proc. 2005;26:210-216.
21. Mathur C, Kathuria PC, Dahiya P, et al. Lack of detectable allergenicity in genetically modified maize containing “Cry” proteins as compared to native maize based on in silico & in vitro analysis. PLoS One. 2015;10:e0117340.
22. Dubois AE, Pagliarani G, Brouwer RM, et al. First successful reduction of clinical allergenicity of food by genetic modification: Mal d 1-silenced apples cause fewer allergy symptoms than the wild-type cultivar [published online July 24, 2015]. Allergy. 2015;70:1406-1412.
23. Silverberg JI, Lee-Wong M, Silverberg NB. Complementary and alternative medicines and childhood eczema: a US population-based study. Dermatitis. 2014;25:246-254.
24. Pfab F, Schalock PC, Napadow V, et al. Complementary integrative approach for treating pruritus. Dermatol Ther. 2013;26:149-156.
25. Stickel F, Shouval D. Hepatotoxicity of herbal and dietary supplements: an update. Arch Toxicol. 2015;89:851-865.
26. Schachner L, Field T, Hernandez-Reif M, et al. Atopic dermatitis symptoms decreased in children following massage therapy. Pediatr Dermatol. 1998;15:390-395.
27. Pfab F, Schalock PC, Napadow V, et al. Acupuncture for allergic disease therapy–the current state of evidence. Expert Rev Clin Immunol. 2014;10:831-841.
28. Silverberg JI, Hanifin JM. Adult eczema prevalence and associations with asthma and other health and demographic factors: a US population-based study. J Allergy Clin Immunol. 2013;132:1132-1138.
29. Silverberg JI, Norowitz KB, Kleiman E, et al. Association between varicella zoster virus infection and atopic dermatitis in early and late childhood: a case-control study. J Allergy Clin Immunol. 2010;126:300-305.
30. Welliver RC, Wong DT, Sun M, et al. The development of respiratory syncytial virus-specific IgE and the release of histamine in nasopharyngeal secretions after infection. N Engl J Med. 1981;305:841-846.
31. Foolad N, Brezinski EA, Chase EP, et al. Effect of nutrient supplementation on atopic dermatitis in children: a systematic review of probiotics, prebiotics, formula, and fatty acids. JAMA Dermatol. 2013;149:350-355.
32. Kalliomäki M, Salminen S, Arvilommi H, et al. Probiotics in primary prevention of atopic disease: a randomised placebo-controlled trial. Lancet. 2001;357:1076-1079.
33. Taylor AL, Dunstan JA, Prescott SL. Probiotic supplementation for the first 6 months of life fails to reduce the risk of atopic dermatitis and increases the risk of allergen sensitization in high-risk children: a randomized controlled trial. J Allergy Clin Immunol. 2007;119:184-191.
34. Bronsnick T, Murzaku EC, Rao BK. Diet in dermatology: part I: atopic dermatitis, acne, and nonmelanoma skin cancer. J Am Acad Dermatol. 2014;71:1039.e1-1039.e12.
35. Du Toit G, Roberts G, Sayre PH, et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med. 2015;372:803-813.
36. Fleischer DM, Sicherer S, Greenhawt M, et al. Consensus communication on early peanut introduction and the prevention of peanut allergy in high-risk infants [published online October 2015]. Allergy. 2015;70:1193-1195.
37. Kim J, Cho Y. Gromwell (Lithospermum erythrorhizon) supplementation enhances epidermal levels of cera-mides, glucosylceramides, β-glucocerebrosidase, and acidicsphingomyelinase in NC/Nga mice. J Med Food. 2013;16:927-933.
38. Choi JH, Jin SW, Han EH, et al. Platycodon grandiflorum root-derived saponins attenuate atopic dermatitis-like skin lesions via suppression of NF-κB and STAT1 and activation of Nrf2/ARE-mediated heme oxygenase-1. Phytomedicine. 2014;21:1053-1061.
39. Kim T, Park K, Jung HS, et al. Evaluation of anti-atopic dermatitis activity of Hypsizigus marmoreus extract. Phytother Res. 2014;28:1539-1546.
40. Kim JR, Choi J, Kim J, et al. 20-O-β-D-glucopyranosyl-20(S)-protopanaxadiol-fortified ginseng extract attenuates the development of atopic dermatitis-like symptoms in NC/Nga mice. J Ethnopharmacol. 2014;151:365-371.
41. Weise C, Ernst D, van Tol EA, et al. Dietary polyunsaturated fatty acids and non-digestible oligosaccharides reduce dermatitis in mice. Pediatr Allergy Immunol. 2013;24:361-367.
42. Tanabe S, Hochi S. Oral administration of a galactooligosaccharide preparation inhibits development of atopic dermatitis-like skin lesions in NC/Nga mice. Int J Mol Med. 2010;25:331-336.
43. Arslanoglu S, Moro GE, Boehm G, et al. Early neutral prebiotic oligosaccharide supplementation reduces the incidence of some allergic manifestations in the first 5 years of life. J Biol Regul Homeost Agents. 2012;26(3 suppl):49-59.
44. Shikino K, Ikusaka M, Yamashita T. Vitamin D-deficient osteomalacia due to excessive self-restrictions for atopic dermatitis [published online July 4, 2014] . BMJ Case Rep.
45. Kim J, Kwon J, Noh G, et al. The effects of elimination diet on nutritional status in subjects with atopic dermatitis. Nutr Res Pract. 2013;7:488-494.
46. Silverberg NB, Lee-Wong M. Generalized yellow discoloration of the skin. Cutis. 2014;93:E11-E12.
47. Hon KL, Nip SY, Cheung KL. A tragic case of atopic eczema: malnutrition and infections despite multivitamins and supplements. Iran J Allergy Asthma Immunol. 2012;11:267-270.
48. Diamanti A, Pedicelli S, D’Argenio P, et al. Iatrogenic kwashiorkor in three infants on a diet of rice beverages. Pediatr Allergy Immunol. 2011;22:878-879.
49. Pillai K, Acharya S. Iatrogenic kwashiorkar. Indian Pediatr. 2010;47:540-541.
50. Price A, Ramachandran S, Smith GP, et al. Oral allergy syndrome (pollen-food allergy syndrome). Dermatitis. 2015;26:78-88.
51. Mattila L, Kilpeläinen M, Terho EO, et al. Food hypersensitivity among Finnish university students: association with atopic diseases. Clin Exp Allergy. 2003;33:600-606.
52. Paulsen E, Christensen LP, Andersen KE. Tomato contact dermatitis. Contact Dermatitis. 2012;67:321-327.
53. Di Leo E, Nettis E, Cardinale F, et al. Tomato atopy patch test in adult atopic dermatitis: diagnostic value and comparison among different methods. Allergy. 2009;64:659-663.
Atopic dermatitis (AD) is the leading diagnosis among pediatric dermatologists,1 and this condition is commonly seen worldwide by dermatologists and allergists.2 There is a widespread misconception held by many patients and their guardians who believe that AD is caused by a food allergy.3 Although AD is related to and part of the atopic complex of disorders associated with food allergies, the role of diet in AD is not well defined. Previously it was recommended to delay early exposure to foods, but now it is recommended to do the opposite in certain situations. In fact, delaying exposure to certain types of foods can increase the likelihood of food allergies (eg, early exposure to peanut butter lowers the statistical chance of developing peanut allergies). This article reviews recent data on the role of diet in AD regarding disease activity as well as new and emerging data on dietary modifications for prevention and intervention. Emerging data on the relationship between AD and food allergies also are presented.
Pathogenesis of AD
The skin barrier plays a vital role in the prevention of pathogens, allergen exposure, and sensitization. There is no solitary root cause of AD, rather it is a combination of inflammation and barrier dysfunction associated with allergic diathesis (eg, atopy). Many patients with AD, especially those with persistent disease, have an intrinsic barrier dysfunction as part of the root cause of their illness, which may be caused by genetically mediated filaggrin defects or alternative barrier dysfunction such as decreased ceramide content that predisposes to percutaneous and mucosal sensitization.4,5 Another source of percutaneous exposure to allergens is macroscopic breaks in the skin caused by scratching, which allows dendritic termini of Langerhans cells to be exposed to percutaneous antigens4,6 through binding to high-affinity IgE receptors.
Langerhans cells exposed to allergens can trigger either an immediate or delayed-type (type I or type II) reaction (sensitization phase) in the lymph node causing inflammatory activation (elicitation). Inflammatory activity in AD is broad and complex and includes the release of IL-4, elevated IgE levels, and eosinophilia, which trigger the helper T cell TH2 and TH17 cascade of cytokines, including IL-2, IL-4, IL-5, IL-8, IL-10, IL-13, IL-17α, tumor necrosis factor α, and IFN-γ,7-9 with the latter worsening barrier defect via downregulation of intercellular substances (eg, filaggrin) and intercellular adhesion expression (eg, claudin 1).6,7,10
Atopic dermatitis does not exist in isolation. The barrier dysfunction associated with AD allows for sensitization to allergens, including those found in food and/or the environment. The atopic march, which occurs via barrier abnormalities facilitating sensitization, can result in further atopy, such as food allergies, environmental allergies, asthma, and eosinophilic esophagitis.11
|
AD and Food Allergies
Many patients and guardians believe AD is caused by a food allergy and that diet restrictions will resolve the disease. Although the latter is not true, in reality many patients with AD do have food allergies. Approximately 40% of infants and young children with moderate to severe AD and 8% of the general population of children will manifest a specific IgE-based food allergy. Food-specific IgE can be triggered or exacerbated by AD through the induction of hives, cutaneous activation of mast cells, increased “spontaneous” basophil histamine release, and food-related lymphocyte-proliferative responses measurable by food patch testing.12 Allergists generally recommend avoidance of or use of heavily denatured food (in the case of a milk/egg allergy) in the setting of documented IgE-mediated allergens.13 Food allergies in AD can manifest with flares, hives, pruritus, and/or other cutaneous symptoms in the absence of flaring AD disease.
Guidelines from the American Academy of Dermatology (AAD)(Table) for the management of AD have recently recommended testing for food allergies in children younger than 5 years who have intractable AD or known food-induced reactions.14 This technique will largely identify children at risk for anaphylaxis but may not yield information contributing to AD improvement. Furthermore, withdrawal of allergens with known IgE-mediated response was classified by the AAD as having consistent good-quality patient-oriented evidence, and asking about allergic reactions as well as acting on a reported allergic history had inconsistent or limited-quality patient-oriented evidence. It is believed that atopy can progress, or march, into a food and/or environmental allergy at any point in life; therefore, testing for a food allergy should be considered in all patients with recent onset of severe and/or persistent AD and/or food-aggravated AD due to a lifetime risk of sensitization.14,15 A food introduction plan may require collaboration with an allergist, especially in high-risk patients (eg, those with known food reactions, family history of food allergies, severe atopy).
Prevention of AD Through Dietary Modification
The National Institute of Allergy and Infectious Diseases consensus group published guidelines on food allergies that affect AD management, including avoidance of proven allergens but not random elimination of food allergens in AD; the group identifies AD and family history of AD as risk factors for food allergies.16 The best data in support of avoidance of documented food allergens to reduce AD severity has been found for egg white allergy and avoidance. Active egg allergy also is linked to staphylococcal superantigen IgE sensitizations,17 but the reason for the link is not yet clear. For the pediatric population, exclusive breastfeeding until 4 to 6 months of age and introduction of solids within the first 4 to 6 months as well as avoidance of maternal dietary restriction during pregnancy and lactation was further endorsed, with use of hydrolyzed formulas as an alternative to exclusive breastfeeding in infants who are not exclusively breastfed (cost permitting).16,18
A Cochrane review of maternal dietary restrictions during pregnancy found no benefit of maternal prenatal dietary restriction on AD prevalence in the first 18 months of life but did note an association with lower mean gestational weight.19
There is currently an effort to produce foods, such as soybeans and corn, that are genetically modified to reduce exposure to the allergenic component, but it is possible that when large-scale challenges occur, these foods also will be allergenic.20,21 In the case of a modified apple, some promising reduction in allergy symptoms has been reported.22 Although genetically modified foods may benefit children with food allergies in the future, they are a source of some controversy.
Complementary and Alternative Medicine
The AAD guidelines do not recommend complementary and alternative medicine (CAM) to treat AD,14 but it remains a commonly used therapy in the United States. A 2014 analysis of data from the 2007 US-based national health interview survey of 9417 children (age range, 0–17 years) demonstrated that 46.9% of children used 1 or more CAM, of which 0.99% used CAM specifically for AD. In this study, herbal therapy, vitamins, homeopathy, diet, and movement techniques were associated with increased prevalence of AD.23 Although some herbals have been shown to be beneficial in AD,24 hepatotoxicity has been reported with some herbal therapies.25 Complementary techniques with evidence-based support include massage therapy,26 relocation to an alternative climate, acupuncture that rivals cetirizine in efficacy, and supportive nutritional advice.24,27
Factors Affecting the Incidence of AD
Atopic dermatitis is of greater prevalence in children in developed wealthy nations such as the United States, supporting the role of enhanced hygiene and overall good health through vaccination as a possible contributor to the rise in AD prevalence in the last 4 decades.28,29 Alternatively, viruses such as respiratory syncytial virus may trigger AD, suggesting vaccination against the virus may reduce the risk for AD.30 Overall, vaccination improves life expectancy and should be conducted on schedule without reservation. Other aspects of hygiene that could conceptually affect prevalence of AD are raw food ingestion and the effects of foodborne microbes on the intestinal microbiome in relationship to AD development. Probiotics have been tested for this purpose.
Probiotics and prebiotics have been theorized to work through a reduction in inflammation; these agents have some evidence in their favor, but they were not endorsed in the AAD guidelines14 despite showing promise in meta-analysis. In particular prenatal and postnatal (maternal and child) supplementation of Lactobacillus rhamnosus shows promise.31-33 Food elimination diets and supplements including vitamin D, selenium, fish oil, borage oil, and zinc were not found to be beneficial and were not recommended in the AAD guidelines.14,34
Percutaneous exposure to peanuts, possibly in household dust, may be the mechanism of peanut sensitization in AD27 via an inherent adjuvant effect of peanut protein.28 The recent LEAP (Learning Early About Peanut Allergy) trial randomized 530 infants aged 4 to 11 months to peanut-avoidant versus peanut-exposed diets for 60 months. The results showed statistically reduced (approximately one-twelfth of the risk) peanut allergy even in infants known to be sensitized (approximately one-third of the risk).35 It is now recommended in countries with a high prevalence of peanut allergies to introduce peanuts to an infant’s diet between 4 and 11 months of age (evidence level 1 [highest level of evidence]), with referral to an allergist for introduction in known sensitization cases and severe AD.36 In the setting of known or documented peanut allergy and for evaluation of potential food allergies, an allergist should be consulted.
Other interventions have been described as promising in mouse models. Those supplements include Lithospermum erythrorhizon,37Platycodon grandiflorus,38Hypsizygus marmoreous,39 fortified ginseng extract,40 polyunsaturated fatty acids,41 and galactooligosaccharide.42 Prebiotic oligosaccharides also are promising for early prevention of AD symptoms in infants, but otherwise these agents have remained largely untested in AD.43 None of these therapies have been endorsed by the AAD, and the long-term safety and efficacy in humans remains to be proven.
Risks of Dietary Restriction
Dietary restrictions in treating AD can have negative consequences, including reduced birth weight when initiated in pregnancy,19 osteomalacia from vitamin D deficiency,44 and nutritional deficiencies (eg, calcium, phosphorus, iron, vitamin K, vitamin D, zinc, vitamin A, B1, B2, B6, niacin, cholesterol, and/or vitamin C deficiencies).45 Excess dietary intake of vegetables in individuals with extensive food allergies can result in carotenemia.46 Protein-restricted diets from use of rice milk or dietary protein restriction can result in kwashiorkorlike protein malnutrition and marasmus.47-49 Nutritional counseling and/or supplementation is recommended for patients with food-restricted diets.
Avoiding Fragrance in Food
Food intolerance often is reported by AD patients. In allergies, food intolerance refers to side effects such as gastrointestinal symptoms; in dermatology, food intolerance can include itching, systemic flares of allergic contact dermatitis (eg, fragrance allergy), or true IgE-mediated allergies such as oral allergy syndrome. Oral allergy syndrome (pollen-food allergy syndrome) is an epitope-spread phenomenon related to an allergy to tree pollen, causing broad allergy to specific groups of fruits and nuts.50 Food triggers in AD include kiwi, milk, apple, tomato, citrus fruits, tree nuts, and peanuts. Oral allergy syndrome is common in food-sensitive AD patients (51.2%) followed by gastrointestinal symptoms (23.5%) and worsening AD (11.4%).51 Sensitization to fragrance can cross-react with foods (eg, balsam of Peru and tomatoes).52 A tomato allergy can be detected either by a skin-prick test or a food patch test in this setting.53 An allergist should be consulted if oral allergy syndrome is suspected.
Conclusion
Food allergies are more common in AD patients and patients should be referred to an allergist for evaluation and management. Strict dietary practice is not recommended, while avoiding proven food allergens in AD could be beneficial. Dermatologists should be aware that patients with dietary restrictions may lack key nutrients, manifesting with nutritional deficiencies in the skin; therefore, nutrition counseling may be needed in the most severe AD/allergy patients. This field is evolving; therefore, ongoing study and evaluation of interventions as they relate to AD will be needed to assess best practices for diet in AD over time.
Atopic dermatitis (AD) is the leading diagnosis among pediatric dermatologists,1 and this condition is commonly seen worldwide by dermatologists and allergists.2 There is a widespread misconception held by many patients and their guardians who believe that AD is caused by a food allergy.3 Although AD is related to and part of the atopic complex of disorders associated with food allergies, the role of diet in AD is not well defined. Previously it was recommended to delay early exposure to foods, but now it is recommended to do the opposite in certain situations. In fact, delaying exposure to certain types of foods can increase the likelihood of food allergies (eg, early exposure to peanut butter lowers the statistical chance of developing peanut allergies). This article reviews recent data on the role of diet in AD regarding disease activity as well as new and emerging data on dietary modifications for prevention and intervention. Emerging data on the relationship between AD and food allergies also are presented.
Pathogenesis of AD
The skin barrier plays a vital role in the prevention of pathogens, allergen exposure, and sensitization. There is no solitary root cause of AD, rather it is a combination of inflammation and barrier dysfunction associated with allergic diathesis (eg, atopy). Many patients with AD, especially those with persistent disease, have an intrinsic barrier dysfunction as part of the root cause of their illness, which may be caused by genetically mediated filaggrin defects or alternative barrier dysfunction such as decreased ceramide content that predisposes to percutaneous and mucosal sensitization.4,5 Another source of percutaneous exposure to allergens is macroscopic breaks in the skin caused by scratching, which allows dendritic termini of Langerhans cells to be exposed to percutaneous antigens4,6 through binding to high-affinity IgE receptors.
Langerhans cells exposed to allergens can trigger either an immediate or delayed-type (type I or type II) reaction (sensitization phase) in the lymph node causing inflammatory activation (elicitation). Inflammatory activity in AD is broad and complex and includes the release of IL-4, elevated IgE levels, and eosinophilia, which trigger the helper T cell TH2 and TH17 cascade of cytokines, including IL-2, IL-4, IL-5, IL-8, IL-10, IL-13, IL-17α, tumor necrosis factor α, and IFN-γ,7-9 with the latter worsening barrier defect via downregulation of intercellular substances (eg, filaggrin) and intercellular adhesion expression (eg, claudin 1).6,7,10
Atopic dermatitis does not exist in isolation. The barrier dysfunction associated with AD allows for sensitization to allergens, including those found in food and/or the environment. The atopic march, which occurs via barrier abnormalities facilitating sensitization, can result in further atopy, such as food allergies, environmental allergies, asthma, and eosinophilic esophagitis.11
|
AD and Food Allergies
Many patients and guardians believe AD is caused by a food allergy and that diet restrictions will resolve the disease. Although the latter is not true, in reality many patients with AD do have food allergies. Approximately 40% of infants and young children with moderate to severe AD and 8% of the general population of children will manifest a specific IgE-based food allergy. Food-specific IgE can be triggered or exacerbated by AD through the induction of hives, cutaneous activation of mast cells, increased “spontaneous” basophil histamine release, and food-related lymphocyte-proliferative responses measurable by food patch testing.12 Allergists generally recommend avoidance of or use of heavily denatured food (in the case of a milk/egg allergy) in the setting of documented IgE-mediated allergens.13 Food allergies in AD can manifest with flares, hives, pruritus, and/or other cutaneous symptoms in the absence of flaring AD disease.
Guidelines from the American Academy of Dermatology (AAD)(Table) for the management of AD have recently recommended testing for food allergies in children younger than 5 years who have intractable AD or known food-induced reactions.14 This technique will largely identify children at risk for anaphylaxis but may not yield information contributing to AD improvement. Furthermore, withdrawal of allergens with known IgE-mediated response was classified by the AAD as having consistent good-quality patient-oriented evidence, and asking about allergic reactions as well as acting on a reported allergic history had inconsistent or limited-quality patient-oriented evidence. It is believed that atopy can progress, or march, into a food and/or environmental allergy at any point in life; therefore, testing for a food allergy should be considered in all patients with recent onset of severe and/or persistent AD and/or food-aggravated AD due to a lifetime risk of sensitization.14,15 A food introduction plan may require collaboration with an allergist, especially in high-risk patients (eg, those with known food reactions, family history of food allergies, severe atopy).
Prevention of AD Through Dietary Modification
The National Institute of Allergy and Infectious Diseases consensus group published guidelines on food allergies that affect AD management, including avoidance of proven allergens but not random elimination of food allergens in AD; the group identifies AD and family history of AD as risk factors for food allergies.16 The best data in support of avoidance of documented food allergens to reduce AD severity has been found for egg white allergy and avoidance. Active egg allergy also is linked to staphylococcal superantigen IgE sensitizations,17 but the reason for the link is not yet clear. For the pediatric population, exclusive breastfeeding until 4 to 6 months of age and introduction of solids within the first 4 to 6 months as well as avoidance of maternal dietary restriction during pregnancy and lactation was further endorsed, with use of hydrolyzed formulas as an alternative to exclusive breastfeeding in infants who are not exclusively breastfed (cost permitting).16,18
A Cochrane review of maternal dietary restrictions during pregnancy found no benefit of maternal prenatal dietary restriction on AD prevalence in the first 18 months of life but did note an association with lower mean gestational weight.19
There is currently an effort to produce foods, such as soybeans and corn, that are genetically modified to reduce exposure to the allergenic component, but it is possible that when large-scale challenges occur, these foods also will be allergenic.20,21 In the case of a modified apple, some promising reduction in allergy symptoms has been reported.22 Although genetically modified foods may benefit children with food allergies in the future, they are a source of some controversy.
Complementary and Alternative Medicine
The AAD guidelines do not recommend complementary and alternative medicine (CAM) to treat AD,14 but it remains a commonly used therapy in the United States. A 2014 analysis of data from the 2007 US-based national health interview survey of 9417 children (age range, 0–17 years) demonstrated that 46.9% of children used 1 or more CAM, of which 0.99% used CAM specifically for AD. In this study, herbal therapy, vitamins, homeopathy, diet, and movement techniques were associated with increased prevalence of AD.23 Although some herbals have been shown to be beneficial in AD,24 hepatotoxicity has been reported with some herbal therapies.25 Complementary techniques with evidence-based support include massage therapy,26 relocation to an alternative climate, acupuncture that rivals cetirizine in efficacy, and supportive nutritional advice.24,27
Factors Affecting the Incidence of AD
Atopic dermatitis is of greater prevalence in children in developed wealthy nations such as the United States, supporting the role of enhanced hygiene and overall good health through vaccination as a possible contributor to the rise in AD prevalence in the last 4 decades.28,29 Alternatively, viruses such as respiratory syncytial virus may trigger AD, suggesting vaccination against the virus may reduce the risk for AD.30 Overall, vaccination improves life expectancy and should be conducted on schedule without reservation. Other aspects of hygiene that could conceptually affect prevalence of AD are raw food ingestion and the effects of foodborne microbes on the intestinal microbiome in relationship to AD development. Probiotics have been tested for this purpose.
Probiotics and prebiotics have been theorized to work through a reduction in inflammation; these agents have some evidence in their favor, but they were not endorsed in the AAD guidelines14 despite showing promise in meta-analysis. In particular prenatal and postnatal (maternal and child) supplementation of Lactobacillus rhamnosus shows promise.31-33 Food elimination diets and supplements including vitamin D, selenium, fish oil, borage oil, and zinc were not found to be beneficial and were not recommended in the AAD guidelines.14,34
Percutaneous exposure to peanuts, possibly in household dust, may be the mechanism of peanut sensitization in AD27 via an inherent adjuvant effect of peanut protein.28 The recent LEAP (Learning Early About Peanut Allergy) trial randomized 530 infants aged 4 to 11 months to peanut-avoidant versus peanut-exposed diets for 60 months. The results showed statistically reduced (approximately one-twelfth of the risk) peanut allergy even in infants known to be sensitized (approximately one-third of the risk).35 It is now recommended in countries with a high prevalence of peanut allergies to introduce peanuts to an infant’s diet between 4 and 11 months of age (evidence level 1 [highest level of evidence]), with referral to an allergist for introduction in known sensitization cases and severe AD.36 In the setting of known or documented peanut allergy and for evaluation of potential food allergies, an allergist should be consulted.
Other interventions have been described as promising in mouse models. Those supplements include Lithospermum erythrorhizon,37Platycodon grandiflorus,38Hypsizygus marmoreous,39 fortified ginseng extract,40 polyunsaturated fatty acids,41 and galactooligosaccharide.42 Prebiotic oligosaccharides also are promising for early prevention of AD symptoms in infants, but otherwise these agents have remained largely untested in AD.43 None of these therapies have been endorsed by the AAD, and the long-term safety and efficacy in humans remains to be proven.
Risks of Dietary Restriction
Dietary restrictions in treating AD can have negative consequences, including reduced birth weight when initiated in pregnancy,19 osteomalacia from vitamin D deficiency,44 and nutritional deficiencies (eg, calcium, phosphorus, iron, vitamin K, vitamin D, zinc, vitamin A, B1, B2, B6, niacin, cholesterol, and/or vitamin C deficiencies).45 Excess dietary intake of vegetables in individuals with extensive food allergies can result in carotenemia.46 Protein-restricted diets from use of rice milk or dietary protein restriction can result in kwashiorkorlike protein malnutrition and marasmus.47-49 Nutritional counseling and/or supplementation is recommended for patients with food-restricted diets.
Avoiding Fragrance in Food
Food intolerance often is reported by AD patients. In allergies, food intolerance refers to side effects such as gastrointestinal symptoms; in dermatology, food intolerance can include itching, systemic flares of allergic contact dermatitis (eg, fragrance allergy), or true IgE-mediated allergies such as oral allergy syndrome. Oral allergy syndrome (pollen-food allergy syndrome) is an epitope-spread phenomenon related to an allergy to tree pollen, causing broad allergy to specific groups of fruits and nuts.50 Food triggers in AD include kiwi, milk, apple, tomato, citrus fruits, tree nuts, and peanuts. Oral allergy syndrome is common in food-sensitive AD patients (51.2%) followed by gastrointestinal symptoms (23.5%) and worsening AD (11.4%).51 Sensitization to fragrance can cross-react with foods (eg, balsam of Peru and tomatoes).52 A tomato allergy can be detected either by a skin-prick test or a food patch test in this setting.53 An allergist should be consulted if oral allergy syndrome is suspected.
Conclusion
Food allergies are more common in AD patients and patients should be referred to an allergist for evaluation and management. Strict dietary practice is not recommended, while avoiding proven food allergens in AD could be beneficial. Dermatologists should be aware that patients with dietary restrictions may lack key nutrients, manifesting with nutritional deficiencies in the skin; therefore, nutrition counseling may be needed in the most severe AD/allergy patients. This field is evolving; therefore, ongoing study and evaluation of interventions as they relate to AD will be needed to assess best practices for diet in AD over time.
1. Schachner L, Ling NS, Press S. A statistical analysis of a pediatric dermatology clinic. Pediatr Dermatol. 1983;1:157-164.
2. Kiprono SK, Muchunu JW, Masenga JE. Skin diseases in pediatric patients attending a tertiary dermatology hospital in Northern Tanzania: a cross-sectional study. BMC Dermatol. 2015;15:16.
3. Wensink M, Timmer C, Brand PL. Atopic dermatitis in infants not caused by food allergy [in Dutch]. Ned Tijdschr Geneeskd. 2008;152:4-9.
4. De Benedetto A, Kubo A, Beck LA. Skin barrier disruption: a requirement for allergen sensitization? J Invest Dermatol. 2012;132(3, pt 2):949-963.
5. Margolis DJ, Apter AJ, Gupta J, et al. The persistence of atopic dermatitis and filaggrin (FLG) mutations in a US longitudinal cohort. J Allergy Clin Immunol. 2012;130:912-917.
6. Hanifin JM. Evolving concepts of pathogenesis in atopic dermatitis and other eczemas. J Invest Dermatol. 2009;129:320-322.
7. Batista DI, Perez L, Orfali RL, et al. Profile of skin barrier proteins (filaggrin, claudins 1 and 4) and Th1/Th2/Th17 cytokines in adults with atopic dermatitis. J Eur Acad Dermatol Venereol. 2015;29:1091-1095.
8. Kondo H, Ichikawa Y, Imokawa G. Percutaneous sensitization with allergens through barrier-disrupted skin elicits a Th2-dominant cytokine response. Eur J Immunol. 1998;28:769-779.
9. Correa da Rosa J, Malajian D, Shemer A, et al. Patients with atopic dermatitis have attenuated and distinct contact hypersensitivity responses to common allergens in skin. J Allergy Clin Immunol. 2015;135:712-720.
10. Paller AS. Latest approaches to treating atopic dermatitis. Chem Immunol Allergy. 2012;96:132-140.
11. Cianferoni A, Spergel J. Eosinophilic esophagitis: a comprehensive review [published online July 22, 2015]. Clin Rev Allergy Immunol. doi:10.1111/all.12846.
12. Sicherer SH, Sampson HA. Food hypersensitivity and atopic dermatitis; pathophysiology, epidemiology, diagnosis, and management. J Allergy Clin Immunol. 1999;104(3, pt 2):S114-S122.
13. Sicherer SH, Sampson HA. Food allergy: epidemiology, pathogenesis, diagnosis, and treatment. J Allergy Clin Immunol. 2014;133:291-307.
14. Sidbury R, Tom WL, Bergman JN, et al. Guidelines of care for the management of atopic dermatitis: section 4. prevention of disease flares and use of adjunctive therapies and approaches. J Am Acad Dermatol. 2014;71:1218-1233.
15. Marenholz I, Rivera VA, Esparza-Gordillo J, et al. Association screening in the epidermal differentiation complex (EDC) identifies an SPRR3 repeat number variant as a risk factor for eczema. J Invest Dermatol. 2011;131:1644-1649.
16. Burks AW, Jones SM, Boyce JA, et al. NIAID-sponsored 2010 guidelines for managing food allergy: applications in the pediatric population. Pediatrics. 2011;128:955-965.
17. Ong PY. Association between egg and staphylococcal superantigen IgE sensitizations in atopic dermatitis. Allergy Asthma Proc. 2014;35:346-348.
18. Botteman M, Detzel P. Cost-effectiveness of partially hydrolyzed whey protein formula in the primary prevention of atopic dermatitis in high-risk urban infants in Southeast Asia. Ann Nutr Metab. 2015;66(suppl 1):26-32.
19. Kramer MS, Kakuma R. Maternal dietary antigen avoidance during pregnancy or lactation, or both, for preventing or treating atopic disease in the child. Cochrane Database Syst Rev. 2012;9:CD000133.
20. Yum HY, Lee SY, Lee KE, et al. Genetically modified and wild soybeans: an immunologic comparison. Allergy Asthma Proc. 2005;26:210-216.
21. Mathur C, Kathuria PC, Dahiya P, et al. Lack of detectable allergenicity in genetically modified maize containing “Cry” proteins as compared to native maize based on in silico & in vitro analysis. PLoS One. 2015;10:e0117340.
22. Dubois AE, Pagliarani G, Brouwer RM, et al. First successful reduction of clinical allergenicity of food by genetic modification: Mal d 1-silenced apples cause fewer allergy symptoms than the wild-type cultivar [published online July 24, 2015]. Allergy. 2015;70:1406-1412.
23. Silverberg JI, Lee-Wong M, Silverberg NB. Complementary and alternative medicines and childhood eczema: a US population-based study. Dermatitis. 2014;25:246-254.
24. Pfab F, Schalock PC, Napadow V, et al. Complementary integrative approach for treating pruritus. Dermatol Ther. 2013;26:149-156.
25. Stickel F, Shouval D. Hepatotoxicity of herbal and dietary supplements: an update. Arch Toxicol. 2015;89:851-865.
26. Schachner L, Field T, Hernandez-Reif M, et al. Atopic dermatitis symptoms decreased in children following massage therapy. Pediatr Dermatol. 1998;15:390-395.
27. Pfab F, Schalock PC, Napadow V, et al. Acupuncture for allergic disease therapy–the current state of evidence. Expert Rev Clin Immunol. 2014;10:831-841.
28. Silverberg JI, Hanifin JM. Adult eczema prevalence and associations with asthma and other health and demographic factors: a US population-based study. J Allergy Clin Immunol. 2013;132:1132-1138.
29. Silverberg JI, Norowitz KB, Kleiman E, et al. Association between varicella zoster virus infection and atopic dermatitis in early and late childhood: a case-control study. J Allergy Clin Immunol. 2010;126:300-305.
30. Welliver RC, Wong DT, Sun M, et al. The development of respiratory syncytial virus-specific IgE and the release of histamine in nasopharyngeal secretions after infection. N Engl J Med. 1981;305:841-846.
31. Foolad N, Brezinski EA, Chase EP, et al. Effect of nutrient supplementation on atopic dermatitis in children: a systematic review of probiotics, prebiotics, formula, and fatty acids. JAMA Dermatol. 2013;149:350-355.
32. Kalliomäki M, Salminen S, Arvilommi H, et al. Probiotics in primary prevention of atopic disease: a randomised placebo-controlled trial. Lancet. 2001;357:1076-1079.
33. Taylor AL, Dunstan JA, Prescott SL. Probiotic supplementation for the first 6 months of life fails to reduce the risk of atopic dermatitis and increases the risk of allergen sensitization in high-risk children: a randomized controlled trial. J Allergy Clin Immunol. 2007;119:184-191.
34. Bronsnick T, Murzaku EC, Rao BK. Diet in dermatology: part I: atopic dermatitis, acne, and nonmelanoma skin cancer. J Am Acad Dermatol. 2014;71:1039.e1-1039.e12.
35. Du Toit G, Roberts G, Sayre PH, et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med. 2015;372:803-813.
36. Fleischer DM, Sicherer S, Greenhawt M, et al. Consensus communication on early peanut introduction and the prevention of peanut allergy in high-risk infants [published online October 2015]. Allergy. 2015;70:1193-1195.
37. Kim J, Cho Y. Gromwell (Lithospermum erythrorhizon) supplementation enhances epidermal levels of cera-mides, glucosylceramides, β-glucocerebrosidase, and acidicsphingomyelinase in NC/Nga mice. J Med Food. 2013;16:927-933.
38. Choi JH, Jin SW, Han EH, et al. Platycodon grandiflorum root-derived saponins attenuate atopic dermatitis-like skin lesions via suppression of NF-κB and STAT1 and activation of Nrf2/ARE-mediated heme oxygenase-1. Phytomedicine. 2014;21:1053-1061.
39. Kim T, Park K, Jung HS, et al. Evaluation of anti-atopic dermatitis activity of Hypsizigus marmoreus extract. Phytother Res. 2014;28:1539-1546.
40. Kim JR, Choi J, Kim J, et al. 20-O-β-D-glucopyranosyl-20(S)-protopanaxadiol-fortified ginseng extract attenuates the development of atopic dermatitis-like symptoms in NC/Nga mice. J Ethnopharmacol. 2014;151:365-371.
41. Weise C, Ernst D, van Tol EA, et al. Dietary polyunsaturated fatty acids and non-digestible oligosaccharides reduce dermatitis in mice. Pediatr Allergy Immunol. 2013;24:361-367.
42. Tanabe S, Hochi S. Oral administration of a galactooligosaccharide preparation inhibits development of atopic dermatitis-like skin lesions in NC/Nga mice. Int J Mol Med. 2010;25:331-336.
43. Arslanoglu S, Moro GE, Boehm G, et al. Early neutral prebiotic oligosaccharide supplementation reduces the incidence of some allergic manifestations in the first 5 years of life. J Biol Regul Homeost Agents. 2012;26(3 suppl):49-59.
44. Shikino K, Ikusaka M, Yamashita T. Vitamin D-deficient osteomalacia due to excessive self-restrictions for atopic dermatitis [published online July 4, 2014] . BMJ Case Rep.
45. Kim J, Kwon J, Noh G, et al. The effects of elimination diet on nutritional status in subjects with atopic dermatitis. Nutr Res Pract. 2013;7:488-494.
46. Silverberg NB, Lee-Wong M. Generalized yellow discoloration of the skin. Cutis. 2014;93:E11-E12.
47. Hon KL, Nip SY, Cheung KL. A tragic case of atopic eczema: malnutrition and infections despite multivitamins and supplements. Iran J Allergy Asthma Immunol. 2012;11:267-270.
48. Diamanti A, Pedicelli S, D’Argenio P, et al. Iatrogenic kwashiorkor in three infants on a diet of rice beverages. Pediatr Allergy Immunol. 2011;22:878-879.
49. Pillai K, Acharya S. Iatrogenic kwashiorkar. Indian Pediatr. 2010;47:540-541.
50. Price A, Ramachandran S, Smith GP, et al. Oral allergy syndrome (pollen-food allergy syndrome). Dermatitis. 2015;26:78-88.
51. Mattila L, Kilpeläinen M, Terho EO, et al. Food hypersensitivity among Finnish university students: association with atopic diseases. Clin Exp Allergy. 2003;33:600-606.
52. Paulsen E, Christensen LP, Andersen KE. Tomato contact dermatitis. Contact Dermatitis. 2012;67:321-327.
53. Di Leo E, Nettis E, Cardinale F, et al. Tomato atopy patch test in adult atopic dermatitis: diagnostic value and comparison among different methods. Allergy. 2009;64:659-663.
1. Schachner L, Ling NS, Press S. A statistical analysis of a pediatric dermatology clinic. Pediatr Dermatol. 1983;1:157-164.
2. Kiprono SK, Muchunu JW, Masenga JE. Skin diseases in pediatric patients attending a tertiary dermatology hospital in Northern Tanzania: a cross-sectional study. BMC Dermatol. 2015;15:16.
3. Wensink M, Timmer C, Brand PL. Atopic dermatitis in infants not caused by food allergy [in Dutch]. Ned Tijdschr Geneeskd. 2008;152:4-9.
4. De Benedetto A, Kubo A, Beck LA. Skin barrier disruption: a requirement for allergen sensitization? J Invest Dermatol. 2012;132(3, pt 2):949-963.
5. Margolis DJ, Apter AJ, Gupta J, et al. The persistence of atopic dermatitis and filaggrin (FLG) mutations in a US longitudinal cohort. J Allergy Clin Immunol. 2012;130:912-917.
6. Hanifin JM. Evolving concepts of pathogenesis in atopic dermatitis and other eczemas. J Invest Dermatol. 2009;129:320-322.
7. Batista DI, Perez L, Orfali RL, et al. Profile of skin barrier proteins (filaggrin, claudins 1 and 4) and Th1/Th2/Th17 cytokines in adults with atopic dermatitis. J Eur Acad Dermatol Venereol. 2015;29:1091-1095.
8. Kondo H, Ichikawa Y, Imokawa G. Percutaneous sensitization with allergens through barrier-disrupted skin elicits a Th2-dominant cytokine response. Eur J Immunol. 1998;28:769-779.
9. Correa da Rosa J, Malajian D, Shemer A, et al. Patients with atopic dermatitis have attenuated and distinct contact hypersensitivity responses to common allergens in skin. J Allergy Clin Immunol. 2015;135:712-720.
10. Paller AS. Latest approaches to treating atopic dermatitis. Chem Immunol Allergy. 2012;96:132-140.
11. Cianferoni A, Spergel J. Eosinophilic esophagitis: a comprehensive review [published online July 22, 2015]. Clin Rev Allergy Immunol. doi:10.1111/all.12846.
12. Sicherer SH, Sampson HA. Food hypersensitivity and atopic dermatitis; pathophysiology, epidemiology, diagnosis, and management. J Allergy Clin Immunol. 1999;104(3, pt 2):S114-S122.
13. Sicherer SH, Sampson HA. Food allergy: epidemiology, pathogenesis, diagnosis, and treatment. J Allergy Clin Immunol. 2014;133:291-307.
14. Sidbury R, Tom WL, Bergman JN, et al. Guidelines of care for the management of atopic dermatitis: section 4. prevention of disease flares and use of adjunctive therapies and approaches. J Am Acad Dermatol. 2014;71:1218-1233.
15. Marenholz I, Rivera VA, Esparza-Gordillo J, et al. Association screening in the epidermal differentiation complex (EDC) identifies an SPRR3 repeat number variant as a risk factor for eczema. J Invest Dermatol. 2011;131:1644-1649.
16. Burks AW, Jones SM, Boyce JA, et al. NIAID-sponsored 2010 guidelines for managing food allergy: applications in the pediatric population. Pediatrics. 2011;128:955-965.
17. Ong PY. Association between egg and staphylococcal superantigen IgE sensitizations in atopic dermatitis. Allergy Asthma Proc. 2014;35:346-348.
18. Botteman M, Detzel P. Cost-effectiveness of partially hydrolyzed whey protein formula in the primary prevention of atopic dermatitis in high-risk urban infants in Southeast Asia. Ann Nutr Metab. 2015;66(suppl 1):26-32.
19. Kramer MS, Kakuma R. Maternal dietary antigen avoidance during pregnancy or lactation, or both, for preventing or treating atopic disease in the child. Cochrane Database Syst Rev. 2012;9:CD000133.
20. Yum HY, Lee SY, Lee KE, et al. Genetically modified and wild soybeans: an immunologic comparison. Allergy Asthma Proc. 2005;26:210-216.
21. Mathur C, Kathuria PC, Dahiya P, et al. Lack of detectable allergenicity in genetically modified maize containing “Cry” proteins as compared to native maize based on in silico & in vitro analysis. PLoS One. 2015;10:e0117340.
22. Dubois AE, Pagliarani G, Brouwer RM, et al. First successful reduction of clinical allergenicity of food by genetic modification: Mal d 1-silenced apples cause fewer allergy symptoms than the wild-type cultivar [published online July 24, 2015]. Allergy. 2015;70:1406-1412.
23. Silverberg JI, Lee-Wong M, Silverberg NB. Complementary and alternative medicines and childhood eczema: a US population-based study. Dermatitis. 2014;25:246-254.
24. Pfab F, Schalock PC, Napadow V, et al. Complementary integrative approach for treating pruritus. Dermatol Ther. 2013;26:149-156.
25. Stickel F, Shouval D. Hepatotoxicity of herbal and dietary supplements: an update. Arch Toxicol. 2015;89:851-865.
26. Schachner L, Field T, Hernandez-Reif M, et al. Atopic dermatitis symptoms decreased in children following massage therapy. Pediatr Dermatol. 1998;15:390-395.
27. Pfab F, Schalock PC, Napadow V, et al. Acupuncture for allergic disease therapy–the current state of evidence. Expert Rev Clin Immunol. 2014;10:831-841.
28. Silverberg JI, Hanifin JM. Adult eczema prevalence and associations with asthma and other health and demographic factors: a US population-based study. J Allergy Clin Immunol. 2013;132:1132-1138.
29. Silverberg JI, Norowitz KB, Kleiman E, et al. Association between varicella zoster virus infection and atopic dermatitis in early and late childhood: a case-control study. J Allergy Clin Immunol. 2010;126:300-305.
30. Welliver RC, Wong DT, Sun M, et al. The development of respiratory syncytial virus-specific IgE and the release of histamine in nasopharyngeal secretions after infection. N Engl J Med. 1981;305:841-846.
31. Foolad N, Brezinski EA, Chase EP, et al. Effect of nutrient supplementation on atopic dermatitis in children: a systematic review of probiotics, prebiotics, formula, and fatty acids. JAMA Dermatol. 2013;149:350-355.
32. Kalliomäki M, Salminen S, Arvilommi H, et al. Probiotics in primary prevention of atopic disease: a randomised placebo-controlled trial. Lancet. 2001;357:1076-1079.
33. Taylor AL, Dunstan JA, Prescott SL. Probiotic supplementation for the first 6 months of life fails to reduce the risk of atopic dermatitis and increases the risk of allergen sensitization in high-risk children: a randomized controlled trial. J Allergy Clin Immunol. 2007;119:184-191.
34. Bronsnick T, Murzaku EC, Rao BK. Diet in dermatology: part I: atopic dermatitis, acne, and nonmelanoma skin cancer. J Am Acad Dermatol. 2014;71:1039.e1-1039.e12.
35. Du Toit G, Roberts G, Sayre PH, et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med. 2015;372:803-813.
36. Fleischer DM, Sicherer S, Greenhawt M, et al. Consensus communication on early peanut introduction and the prevention of peanut allergy in high-risk infants [published online October 2015]. Allergy. 2015;70:1193-1195.
37. Kim J, Cho Y. Gromwell (Lithospermum erythrorhizon) supplementation enhances epidermal levels of cera-mides, glucosylceramides, β-glucocerebrosidase, and acidicsphingomyelinase in NC/Nga mice. J Med Food. 2013;16:927-933.
38. Choi JH, Jin SW, Han EH, et al. Platycodon grandiflorum root-derived saponins attenuate atopic dermatitis-like skin lesions via suppression of NF-κB and STAT1 and activation of Nrf2/ARE-mediated heme oxygenase-1. Phytomedicine. 2014;21:1053-1061.
39. Kim T, Park K, Jung HS, et al. Evaluation of anti-atopic dermatitis activity of Hypsizigus marmoreus extract. Phytother Res. 2014;28:1539-1546.
40. Kim JR, Choi J, Kim J, et al. 20-O-β-D-glucopyranosyl-20(S)-protopanaxadiol-fortified ginseng extract attenuates the development of atopic dermatitis-like symptoms in NC/Nga mice. J Ethnopharmacol. 2014;151:365-371.
41. Weise C, Ernst D, van Tol EA, et al. Dietary polyunsaturated fatty acids and non-digestible oligosaccharides reduce dermatitis in mice. Pediatr Allergy Immunol. 2013;24:361-367.
42. Tanabe S, Hochi S. Oral administration of a galactooligosaccharide preparation inhibits development of atopic dermatitis-like skin lesions in NC/Nga mice. Int J Mol Med. 2010;25:331-336.
43. Arslanoglu S, Moro GE, Boehm G, et al. Early neutral prebiotic oligosaccharide supplementation reduces the incidence of some allergic manifestations in the first 5 years of life. J Biol Regul Homeost Agents. 2012;26(3 suppl):49-59.
44. Shikino K, Ikusaka M, Yamashita T. Vitamin D-deficient osteomalacia due to excessive self-restrictions for atopic dermatitis [published online July 4, 2014] . BMJ Case Rep.
45. Kim J, Kwon J, Noh G, et al. The effects of elimination diet on nutritional status in subjects with atopic dermatitis. Nutr Res Pract. 2013;7:488-494.
46. Silverberg NB, Lee-Wong M. Generalized yellow discoloration of the skin. Cutis. 2014;93:E11-E12.
47. Hon KL, Nip SY, Cheung KL. A tragic case of atopic eczema: malnutrition and infections despite multivitamins and supplements. Iran J Allergy Asthma Immunol. 2012;11:267-270.
48. Diamanti A, Pedicelli S, D’Argenio P, et al. Iatrogenic kwashiorkor in three infants on a diet of rice beverages. Pediatr Allergy Immunol. 2011;22:878-879.
49. Pillai K, Acharya S. Iatrogenic kwashiorkar. Indian Pediatr. 2010;47:540-541.
50. Price A, Ramachandran S, Smith GP, et al. Oral allergy syndrome (pollen-food allergy syndrome). Dermatitis. 2015;26:78-88.
51. Mattila L, Kilpeläinen M, Terho EO, et al. Food hypersensitivity among Finnish university students: association with atopic diseases. Clin Exp Allergy. 2003;33:600-606.
52. Paulsen E, Christensen LP, Andersen KE. Tomato contact dermatitis. Contact Dermatitis. 2012;67:321-327.
53. Di Leo E, Nettis E, Cardinale F, et al. Tomato atopy patch test in adult atopic dermatitis: diagnostic value and comparison among different methods. Allergy. 2009;64:659-663.
Practice Points
- Test children younger than 5 years with moderate to severe atopic dermatitis (AD) for food allergies if they have persistently severe AD or known food-induced reactions.
- Food elimination diets are not recommended for management of AD.
- There is not enough evidence supporting the use of complementary and alternative medicine, probiotics/prebiotics, or supplements for the treatment of AD.
