User login
New Ideas Showcased in Research at RIV Competition
Standing adjacent Poster 391 in a loud, crowded meeting hall, Monika Wells, MD, MPH, a resident in internal medicine at Virginia Mason Medical Center in Seattle, chatted with a colleague. A few feet away, a group of doctors and healthcare professionals huddled dramatically, just barely out of earshot.
The fate of Dr. Wells’ scientific abstract hung in the balance.

Her study, a look at scheduling the start and stop times of hospitalist shifts around expected demand to reduce costs and patient wait times, was a short-list finalist in the Innovations category of HM16’s annual Research, Innovation, and Clinical Vignettes scientific abstract competition. With her work done—she had already made presentations to first a pair of semifinalist judges and then to a herd of all 10 of the category judges—Dr. Wells looked remarkably calm as she waited for the announcement of the winners.
Either way, she said, the competition had been an invigorating, exciting experience.
“I’m a doctor, so I like to compete,” she half-joked. “It definitely has been motivating.”
RIV ribbons this year were handed out to seven winners in four categories. The competition garnered 914 abstracts accepted for presentation.
Dr. Wells ended up being one of them. She was named Innovations’ trainee winner. In her study, researchers found that analyzing the flow of admissions and redistributing hospitalists to better conform to that flow reduced patient wait times and costs as well as improved the subjective experience of hospitalists even as volume increased.
The overall winner in the Innovations category also went to a trainee, Baely Crockett, PharmD, a resident at Eskenazi Health in Indianapolis. Her study looked at a pharmacist-managed rivaroxaban clinic for the treatment of venous thromboembolism (VTE). It was the first time, as far as the judges knew, that an award had gone to a pharmacist.
Dr. Crockett’s abstract showed that patients diagnosed in the ED with low-risk VTE are given a prescription scheduled to be seen in the follow-up clinic within two to five days, at which point the pharmacist sees the patients and reviews their case with them and determines treatment duration.
Dr. Crockett said the pharmacists involved are especially suitable for the role not only because of their expertise in the medication and the handling of time-consuming co-pay issues and other concerns but also because they shadowed ED physicians for six months to get training and experience.
“We’re able to fill in gaps that are true challenges to the patient’s success in finishing therapy,” she said.
One of the Innovations judges, Michael Craig, MD, MPH, FHM, associate professor of medicine at the University of North Carolina in Chapel Hill, said the research hit on an area of growing interest.
“The movement toward outpatient treatment of VTE is a pretty big topic that lots of people are working on,” he said. “It’s very relevant. The whole idea of having a pharmacist-driven intervention is unique; nobody had thought of or heard of before.”
The winner in the Research category was Vineet Chopra, MD, MSc, FHM, assistant professor at the University of Michigan in Ann Arbor, whose work set out to quantify how to prevent bloodstream infection and blood clots from the use of peripherally inserted central catheters, or PICC lines. Researchers created a simulation model, based on data from the literature, looking at what would happen to a hospital if the use of certain types of PICCs was increased while use of other types was decreased—the rationale being that PICCs with just one channel, or port, have a lower risk of infection or blood clots than those with multiple ports.
It is a risk that is often unrecognized, and PICC lines with multiple ports are often ordered as a just-in-case measure in the event that the first port gets clogged.
Chopra and colleagues found that, at the average hospital, about 75% of all PICCs used tend to be multichannel and 25% single-channel. They found every 5% increase in single-channel PICC use could prevent almost 1.5 infections per 1,000 patients, and 0.5 blood clots, with a corresponding cost savings of $13,000 per event. That can add up to hundreds of thousands of dollars a year at large hospitals.
And those calculations, Dr. Chopra noted, do not include penalties for infections or the financial effects of having those results publicly reported. Researchers are now creating an online tool— at improvepicc.com—that will allow users to calculate their own costs and potential savings.
“The hope of this is that it will give hospital administrators and hospital leadership and quality officers the momentum, perhaps, to overcome the inertia of not thinking actively,” said Dr. Chopra, who notched his first win after 10 years of participating in the RIV competition. “I think we don’t think actively about the choices we make when it comes to these devices.”
In the Clinical Vignettes category, winner Molly Kantor, MD, assistant clinical professor at the University of California, San Diego, recounted the case of a sickle-cell disease patient whose diagnosis, and hence treatment, was delayed and who ultimately died. She outlined a series of missteps, including taking at face-value a patient-reported past medical disease, which turned out to be wrong; making certain diagnoses based on lab tests and stopping there; and anchoring on the original diagnosis when the thought process was later reevaluated.
Dr. Kantor said the case is a caution flag to hospitalists, reinforcing the need for “a broad differential diagnosis.”
“[Make] sure that the data fits together and that you’re not using just one isolated piece of information to cinch everything, including the past medical history or a certain lab test, when the whole picture doesn’t quite fit together,” she said. “Looking back at this case, it’s pretty clear that the puzzle pieces probably weren’t quite fitting together, but there was enough that the easier thing to do was to make the diagnosis and move on.”
In the Pediatric Clinical Vignettes category, winner Jennifer Ladd, MD, a resident at Duke University, won for a study of a vexing case of a 2-year-old who was irritable and stalled on developmental milestones. At the hospital, the thought was that it could likely be a recurrence of herpes simplex (HSV) encephalitis, but the spinal fluid showed no signs of that and the acyclovir, which nearly always works for the disorder, was having no effect and the symptoms worsened.
The key in the case, said Alyssa Stephany, MD, then assistant professor at Duke University and now section chief of pediatric hospital medicine at Children’s Hospital of Wisconsin, who presented the case in Dr. Ladd’s absence, was that the team reopened the diagnosis and didn’t get ensnared in cognitive bias. A biopsy ultimately showed HSV in the brain tissue; it was a case of recurrence, despite signs to the contrary. Foscarnet was used to effectively treat the child; it is unknown why acyclovir didn’t work in this case.
“It kind of brings to the surface that that’s what a hospitalist is—a hospitalist is that person who sits and thinks, and really thinks, about the patient and doesn’t just do their rote work of input and output of a patient through the hospital system,” Dr. Stephany said. “When you get a case like this, it makes you take pause.”
The trainee winner in the Research category was N. Lance Downing, MD, of Stanford University School of Medicine, for work on an EHR-based severe sepsis alert. The trainee winner in Clinical Vignettes was Bhakti Shah, MD, of North Shore-LIJ Health System, now Northwell Health, on a rare case of autoimmune NMDA receptor encephalitis. TH
Thomas R. Collins is a freelance writer in South Florida.
2016 RIV Finalists, Winners
Research Category
WINNER:

Vineet Chopra, MD, MSc, FHM, LIMITING THE NUMBER OF LUMENS IN PERIPHERALLY INSERTED CENTRAL CATHETERS TO IMPROVE OUTCOMES AND REDUCE COST: A SIMULATION STUDY
TRAINEE WINNER:
N. Downing, MD, AN ELECTRONIC HEALTH RECORD-BASED SEVERE SEPSIS ALERT TO IMPROVE SEPSIS TREATMENT PERFORMANCE: RANDOMIZED EVALUATION
FINALISTS:
Waseem Khaliq, MD, MPH, PREVALENCE AND PREDICTORS OF NON-ADHERENCE TO BREAST CANCER SCREENING: PERSPECTIVE AND PREFERENCES OF HOSPITALIZED WOMEN
Dilli Poudel, MD, SYSTEMIC SCLEROSIS AS A RISK FACTOR OF ACUTE MYOCARDIAL INFARCTION: A US POPULATION BASED STUDY
Aiham Albaeni, MD, REGIONAL VARIATION IN RESOURCES UTILIZATION AND OUTCOMES FOLLOWING OUT-OF-HOSPITAL CARDIAC ARREST IN THE UNITED STATES
Poushali Bhattacharjee, MD, DETECTING SEPSIS: ARE TWO OPINIONS BETTER THAN ONE?
Vineet Chopra, MD, MSc, FHM, THE INFLUENCE OF RED BLOOD CELL TRANSFUSION ON VENOUS THROMBOEMBOLISM IN PATIENTS WITH PERIPHERALLY-INSERTED CENTRAL CATHETERS
Shaker Eid, MD, MBA, IMPACT OF HOSPITAL TEACHING STATUS ON OUT-OF-HOSPITAL CARDIAC ARREST OUTCOMES AND RESOURCE UTILIZATION IN THE UNITED STATES: 2000-2012
Tarun Jain, MD, CONTRAST-INDUCED NEPHROPATHY IN STEMI PATIENTS WITH AND WITHOUT CHRONIC KIDNEY DISEASE
Mona Beier, MD, CREATING A PATIENT SAFETY CULTURE ONE INCIDENT REPORT AT A TIME
Charles Pollack, MD, REINITIATION OF ANTITHROMBOTIC THERAPY AFTER EMERGENCY PROCEDURES OR AFTER AN EMERGENT BLEEDING EVENT: ADDITIONAL INTERIM EXPERIENCE FROM THE RE-VERSE AD TRIAL
Robert Boxer, MD, PhD, SAVING TIME: A TIME-MOTION ANALYSIS OF THE IMPACT OF REGIONALIZATION AND DAILY ADMITTING ON INTERN WORKFLOW
Kaleigh Evans, MD, THIRD TROPONIN ORDER OVERUSE IN THE SETTING OF CLINICAL STABILITY
David Paje, MD, SFHM, RISK OF VENOUS THROMBOEMBOLISM IN HOSPITALIZED PATIENTS WITH INFLAMMATORY BOWEL DISEASE
Rehan Qayyum, MD, COMPARISON OF TIME-TRENDS IN PATIENT SATISFACTION BETWEEN TEACHING AND NONTEACHING HOSPITAL
Joshua Rolnick, MD, VALIDATION OF TEST PERFORMANCE AND CLINICAL TIME ZERO FOR AN ELECTRONIC HEALTH RECORD-EMBEDDED SEVERE SEPSIS ALERT
Allison Louis, MD, BLIND SIDED: MISSING POOR VISUAL ACUITY AND DECREASED SELF-EFFICACY IN HOSPITALIZED PATIENTS WITH DIABETES
G. Randy Smith, MD, MS, SFHM, ASSOCIATION OF HOSPITAL ADMISSION SERVICE STRUCTURE WITH EARLY TRANSFER TO CRITICAL CARE, HOSPITAL READMISSION, AND LENGTH OF STAY
Kathleene Wooldridge, MD, R-VA-MARQUIS: IMPLEMENTING BEST PRACTICES IN MEDICATION RECONCILIATION FOR RURAL VETERANS
INNOVATION CATEGORY
WINNER:

Baely Crockett, PharmD, NOVEL PHARMACIST-MANAGED RIVAROXABAN CLINIC FOR OUTPATIENT TREATMENT OF VENOUS THROMBOEMBOLISM
TRAINEE WINNER:
Monika Wells, MD, MPH, DESIGNING HOSPITALIST SHIFTS AROUND ADMISSION DEMAND REDUCES PATIENT WAIT TIMES AND COST
FINALISTS:
Jessica Dong, WHO MOVED MY EHR CHEESE? A NEW APPROACH TO CURATING AND INDIVIDUALIZING COMMUNICATIONS TO PHYSICIANS ABOUT EHR SOFTWARE UPDATES
Stephanie Rennke, MD, MED REC: A SKILLS-BASED CURRICULUM ON MEDICATION SAFETY AND MEDICATION RECONCILIATION FOR MEDICAL STUDENTS
Jens Langsjoen, MD, DEVELOPING AN INPATIENT DELIRIUM PREVENTION PROTOCOL
Mark Goldin, MD, BUILDING PARALLEL CO-MANAGEMENT SERVICES IN A LARGE ACADEMIC HOSPITALIST GROUP
Brian Lichtenstein, MD, IMPROVING RISK-ADJUSTED OUTCOME MEASURES WITH PHYSICIAN-ORIENTED DOCUMENTATION INTERVENTIONS
Matthew Cerasale, MD, REAL-TIME PADUA: AN AUTOMATED EHR INTEGRATED VENOUS THROMBOEMBOLISM RISK ASSESSMENT TOOL
Franziska Jovin, MD, MMM, FHM, IMPLEMENTATION OF A PAY-FOR-PERFOMANCE STRUCTURE FOR HOSPITALIST-LED QUALITY IMPROVEMENT PROJECTS
Arpit Khandelwal, MD, MANAGING CHALLENGING PATIENTS: FROM CONFLICT TO TEACHING OPPORTUNITY
Justin Lotfi, MD, MAKING IT SIMPLE - PROCESS IMPROVEMENT FOR OUTSIDE MEDICAL RECORDS
David McCollum, MD, FIXING WHAT IS BROKEN: QUALITY IMPROVEMENT IN THE CRITICAL LAB VALUE PROCESS
Nidhi Rohatgi, MD, MS, A NOVEL MD-RN COLLABORATIVE PROTOCOL TO PREVENT AND MANAGE ACUTE DELIRIUM IN INPATIENT WARDS
Lesley Schmaltz, MD, UNNECESSARY TRANSFUSIONS: HOSPITAL MEDICINE LEADING INSTITUTION-WIDE CHANGE
Anuj Dalal, MD, FHM, IMPLEMENTATION OF A PATIENT-CENTERED ‘MICROBLOG' MESSAGING PLATFORM TO IMPROVE CARE TEAM COMMUNICATION
Willard Ellis, MD, PhD, FHM, INTENSIVE FOLLOW UP AFTER PALLIATIVE CARE CONSULTATIONS TO REDUCE READMISSIONS
Lakshmi Swaminathan, MD, MHSA, FHM, USING “MAGIC” TO FACILITATE APPROPRIATE PICC USE: RESULTS OF IMPLEMENTATION OF A PICC APPROPRIATENESS ASSESSMENT TOOL
Charles Coffey, MD, MSc, FHM, IMPLEMENTING GUIDELINE-BASED INDICATIONS FOR CARDIAC MONITORING AT CEDARS-SINAI MEDICAL CENTER
Erik Hoyer, MD, USE OF A HOSPITALIST CLINICAL COMMUNITY TO FACILITATE DISSEMINATION OF AN EARLY MOBILITY QUALITY IMPROVEMENT PROGRAM
Elizabeth Stewart, MD, A MULTIDISCIPLINARY APPROACH TO HIGH VALUE CARDIAC BIOMARKER
CLINICAL VIGNETTES CATEGORY
WINNER (ADULT):

Molly Kantor, MD, THE TIP OF THE ICEBERG: A RARE CAUSE OF ACUTE LIVER FAILURE
WINNER (PEDIATRIC):

Jennifer Ladd, MD, MORE THAN JUST THE “TERRIBLE TWOS”: A CASE OF RESISTANT HSV ENCEPHALITIS
TRAINEE WINNER:

Bhakti Shah, MD, UNMASKING THE TERATOMA
FINALISTS:
Weijen Chang, MD, SFHM, UNCOILING A PROBLEMATIC TICKLE IN THE THROAT
Kenton Dover, MD, KEEPING AN EYE OUT FOR THE DIAGNOSIS
Stephanie Royer, MD, THE YOUNGEST REPORTED CASE OF EOSINOPHILIC CHOLANGITIS
Oluremi Ajala, MD, ANGINA OF ABDOMINAL ORIGIN
Asana Anderson, MBBS, A PARATHYROID CRISIS BURIED IN A SEPTIC OTOMASTOIDITIS
Kyle Bennett, DO, BULLS-EYE MARKS THE SPOT: LYME CARDITIS PRESENTING AS RASH AND PRESYNCOPE
John Biebelhausen, MD, MBA, CROSSFIT CATASTROPHE: CHEST PAIN IN A HEALTHY YOUNG WOMAN
Xuan Gao, MD, A CASE OF THE UNSEEN: KLEBSIELLA PNEUMONIA PYOGENIC LIVER ABSCESS WITH PNEUMONIA AND SEPTIC ENDOPHTHALMITIS IN A NON-ASIAN U.S. RESIDENT
Sana Grover, MBBS, 'ABSTINENT AND INTOXICATED'. A RARE CASE OF AUTO-BREWERY SYNDROME
Andrew Hawrylak, MD, WHEN IT'S NOT AN ALLERGIC REACTION: AN UNUSUAL CASE OF ECTHYEMA GANGRENOSUM ASSOCIATED WITH PROTEUS BACTEREMIA
Rasheen Imtiaz, MD, LACTIC ACIDOSIS IN ASTHMA
Jessie King, MD, PhD, THE SMOKING WOMAN
Bradley Manning, MD, A SUPER-ANTIGEN-MEDIATED MIMIC OF ACUTE APPENDICITIS
Hiroki Matsuura, IMPAIRED CONSCIOUSNESS WITH INDOLENT BREAST MASS
Niharika Singh, MD, LOWER EXTREMITY NECROTIZING FASCIITIS: AN UNUSUAL PRESENTATION OF PERFORATED SIGMOID DIVERTICULITIS
Vivan Tran, DO, PUTTING THE PEE IN PREGNANCY: A CASE OF GESTATIONAL DIABETES INSIPIDUS YOU DON'T WANT TO MISS
Kristen Welch, THE MYSTERIOUS DANCE: A RARE CASE OF DELAYED ONSET DIABETIC STRIATOPATHY
Standing adjacent Poster 391 in a loud, crowded meeting hall, Monika Wells, MD, MPH, a resident in internal medicine at Virginia Mason Medical Center in Seattle, chatted with a colleague. A few feet away, a group of doctors and healthcare professionals huddled dramatically, just barely out of earshot.
The fate of Dr. Wells’ scientific abstract hung in the balance.
Her study, a look at scheduling the start and stop times of hospitalist shifts around expected demand to reduce costs and patient wait times, was a short-list finalist in the Innovations category of HM16’s annual Research, Innovation, and Clinical Vignettes scientific abstract competition. With her work done—she had already made presentations to first a pair of semifinalist judges and then to a herd of all 10 of the category judges—Dr. Wells looked remarkably calm as she waited for the announcement of the winners.
Either way, she said, the competition had been an invigorating, exciting experience.
“I’m a doctor, so I like to compete,” she half-joked. “It definitely has been motivating.”
RIV ribbons this year were handed out to seven winners in four categories. The competition garnered 914 abstracts accepted for presentation.
Dr. Wells ended up being one of them. She was named Innovations’ trainee winner. In her study, researchers found that analyzing the flow of admissions and redistributing hospitalists to better conform to that flow reduced patient wait times and costs as well as improved the subjective experience of hospitalists even as volume increased.
The overall winner in the Innovations category also went to a trainee, Baely Crockett, PharmD, a resident at Eskenazi Health in Indianapolis. Her study looked at a pharmacist-managed rivaroxaban clinic for the treatment of venous thromboembolism (VTE). It was the first time, as far as the judges knew, that an award had gone to a pharmacist.
Dr. Crockett’s abstract showed that patients diagnosed in the ED with low-risk VTE are given a prescription scheduled to be seen in the follow-up clinic within two to five days, at which point the pharmacist sees the patients and reviews their case with them and determines treatment duration.
Dr. Crockett said the pharmacists involved are especially suitable for the role not only because of their expertise in the medication and the handling of time-consuming co-pay issues and other concerns but also because they shadowed ED physicians for six months to get training and experience.
“We’re able to fill in gaps that are true challenges to the patient’s success in finishing therapy,” she said.
One of the Innovations judges, Michael Craig, MD, MPH, FHM, associate professor of medicine at the University of North Carolina in Chapel Hill, said the research hit on an area of growing interest.
“The movement toward outpatient treatment of VTE is a pretty big topic that lots of people are working on,” he said. “It’s very relevant. The whole idea of having a pharmacist-driven intervention is unique; nobody had thought of or heard of before.”
The winner in the Research category was Vineet Chopra, MD, MSc, FHM, assistant professor at the University of Michigan in Ann Arbor, whose work set out to quantify how to prevent bloodstream infection and blood clots from the use of peripherally inserted central catheters, or PICC lines. Researchers created a simulation model, based on data from the literature, looking at what would happen to a hospital if the use of certain types of PICCs was increased while use of other types was decreased—the rationale being that PICCs with just one channel, or port, have a lower risk of infection or blood clots than those with multiple ports.
It is a risk that is often unrecognized, and PICC lines with multiple ports are often ordered as a just-in-case measure in the event that the first port gets clogged.
Chopra and colleagues found that, at the average hospital, about 75% of all PICCs used tend to be multichannel and 25% single-channel. They found every 5% increase in single-channel PICC use could prevent almost 1.5 infections per 1,000 patients, and 0.5 blood clots, with a corresponding cost savings of $13,000 per event. That can add up to hundreds of thousands of dollars a year at large hospitals.
And those calculations, Dr. Chopra noted, do not include penalties for infections or the financial effects of having those results publicly reported. Researchers are now creating an online tool— at improvepicc.com—that will allow users to calculate their own costs and potential savings.
“The hope of this is that it will give hospital administrators and hospital leadership and quality officers the momentum, perhaps, to overcome the inertia of not thinking actively,” said Dr. Chopra, who notched his first win after 10 years of participating in the RIV competition. “I think we don’t think actively about the choices we make when it comes to these devices.”
In the Clinical Vignettes category, winner Molly Kantor, MD, assistant clinical professor at the University of California, San Diego, recounted the case of a sickle-cell disease patient whose diagnosis, and hence treatment, was delayed and who ultimately died. She outlined a series of missteps, including taking at face-value a patient-reported past medical disease, which turned out to be wrong; making certain diagnoses based on lab tests and stopping there; and anchoring on the original diagnosis when the thought process was later reevaluated.
Dr. Kantor said the case is a caution flag to hospitalists, reinforcing the need for “a broad differential diagnosis.”
“[Make] sure that the data fits together and that you’re not using just one isolated piece of information to cinch everything, including the past medical history or a certain lab test, when the whole picture doesn’t quite fit together,” she said. “Looking back at this case, it’s pretty clear that the puzzle pieces probably weren’t quite fitting together, but there was enough that the easier thing to do was to make the diagnosis and move on.”
In the Pediatric Clinical Vignettes category, winner Jennifer Ladd, MD, a resident at Duke University, won for a study of a vexing case of a 2-year-old who was irritable and stalled on developmental milestones. At the hospital, the thought was that it could likely be a recurrence of herpes simplex (HSV) encephalitis, but the spinal fluid showed no signs of that and the acyclovir, which nearly always works for the disorder, was having no effect and the symptoms worsened.
The key in the case, said Alyssa Stephany, MD, then assistant professor at Duke University and now section chief of pediatric hospital medicine at Children’s Hospital of Wisconsin, who presented the case in Dr. Ladd’s absence, was that the team reopened the diagnosis and didn’t get ensnared in cognitive bias. A biopsy ultimately showed HSV in the brain tissue; it was a case of recurrence, despite signs to the contrary. Foscarnet was used to effectively treat the child; it is unknown why acyclovir didn’t work in this case.
“It kind of brings to the surface that that’s what a hospitalist is—a hospitalist is that person who sits and thinks, and really thinks, about the patient and doesn’t just do their rote work of input and output of a patient through the hospital system,” Dr. Stephany said. “When you get a case like this, it makes you take pause.”
The trainee winner in the Research category was N. Lance Downing, MD, of Stanford University School of Medicine, for work on an EHR-based severe sepsis alert. The trainee winner in Clinical Vignettes was Bhakti Shah, MD, of North Shore-LIJ Health System, now Northwell Health, on a rare case of autoimmune NMDA receptor encephalitis. TH
Thomas R. Collins is a freelance writer in South Florida.
2016 RIV Finalists, Winners
Research Category
WINNER:
Vineet Chopra, MD, MSc, FHM, LIMITING THE NUMBER OF LUMENS IN PERIPHERALLY INSERTED CENTRAL CATHETERS TO IMPROVE OUTCOMES AND REDUCE COST: A SIMULATION STUDY
TRAINEE WINNER:
N. Downing, MD, AN ELECTRONIC HEALTH RECORD-BASED SEVERE SEPSIS ALERT TO IMPROVE SEPSIS TREATMENT PERFORMANCE: RANDOMIZED EVALUATION
FINALISTS:
Waseem Khaliq, MD, MPH, PREVALENCE AND PREDICTORS OF NON-ADHERENCE TO BREAST CANCER SCREENING: PERSPECTIVE AND PREFERENCES OF HOSPITALIZED WOMEN
Dilli Poudel, MD, SYSTEMIC SCLEROSIS AS A RISK FACTOR OF ACUTE MYOCARDIAL INFARCTION: A US POPULATION BASED STUDY
Aiham Albaeni, MD, REGIONAL VARIATION IN RESOURCES UTILIZATION AND OUTCOMES FOLLOWING OUT-OF-HOSPITAL CARDIAC ARREST IN THE UNITED STATES
Poushali Bhattacharjee, MD, DETECTING SEPSIS: ARE TWO OPINIONS BETTER THAN ONE?
Vineet Chopra, MD, MSc, FHM, THE INFLUENCE OF RED BLOOD CELL TRANSFUSION ON VENOUS THROMBOEMBOLISM IN PATIENTS WITH PERIPHERALLY-INSERTED CENTRAL CATHETERS
Shaker Eid, MD, MBA, IMPACT OF HOSPITAL TEACHING STATUS ON OUT-OF-HOSPITAL CARDIAC ARREST OUTCOMES AND RESOURCE UTILIZATION IN THE UNITED STATES: 2000-2012
Tarun Jain, MD, CONTRAST-INDUCED NEPHROPATHY IN STEMI PATIENTS WITH AND WITHOUT CHRONIC KIDNEY DISEASE
Mona Beier, MD, CREATING A PATIENT SAFETY CULTURE ONE INCIDENT REPORT AT A TIME
Charles Pollack, MD, REINITIATION OF ANTITHROMBOTIC THERAPY AFTER EMERGENCY PROCEDURES OR AFTER AN EMERGENT BLEEDING EVENT: ADDITIONAL INTERIM EXPERIENCE FROM THE RE-VERSE AD TRIAL
Robert Boxer, MD, PhD, SAVING TIME: A TIME-MOTION ANALYSIS OF THE IMPACT OF REGIONALIZATION AND DAILY ADMITTING ON INTERN WORKFLOW
Kaleigh Evans, MD, THIRD TROPONIN ORDER OVERUSE IN THE SETTING OF CLINICAL STABILITY
David Paje, MD, SFHM, RISK OF VENOUS THROMBOEMBOLISM IN HOSPITALIZED PATIENTS WITH INFLAMMATORY BOWEL DISEASE
Rehan Qayyum, MD, COMPARISON OF TIME-TRENDS IN PATIENT SATISFACTION BETWEEN TEACHING AND NONTEACHING HOSPITAL
Joshua Rolnick, MD, VALIDATION OF TEST PERFORMANCE AND CLINICAL TIME ZERO FOR AN ELECTRONIC HEALTH RECORD-EMBEDDED SEVERE SEPSIS ALERT
Allison Louis, MD, BLIND SIDED: MISSING POOR VISUAL ACUITY AND DECREASED SELF-EFFICACY IN HOSPITALIZED PATIENTS WITH DIABETES
G. Randy Smith, MD, MS, SFHM, ASSOCIATION OF HOSPITAL ADMISSION SERVICE STRUCTURE WITH EARLY TRANSFER TO CRITICAL CARE, HOSPITAL READMISSION, AND LENGTH OF STAY
Kathleene Wooldridge, MD, R-VA-MARQUIS: IMPLEMENTING BEST PRACTICES IN MEDICATION RECONCILIATION FOR RURAL VETERANS
INNOVATION CATEGORY
WINNER:
Baely Crockett, PharmD, NOVEL PHARMACIST-MANAGED RIVAROXABAN CLINIC FOR OUTPATIENT TREATMENT OF VENOUS THROMBOEMBOLISM
TRAINEE WINNER:
Monika Wells, MD, MPH, DESIGNING HOSPITALIST SHIFTS AROUND ADMISSION DEMAND REDUCES PATIENT WAIT TIMES AND COST
FINALISTS:
Jessica Dong, WHO MOVED MY EHR CHEESE? A NEW APPROACH TO CURATING AND INDIVIDUALIZING COMMUNICATIONS TO PHYSICIANS ABOUT EHR SOFTWARE UPDATES
Stephanie Rennke, MD, MED REC: A SKILLS-BASED CURRICULUM ON MEDICATION SAFETY AND MEDICATION RECONCILIATION FOR MEDICAL STUDENTS
Jens Langsjoen, MD, DEVELOPING AN INPATIENT DELIRIUM PREVENTION PROTOCOL
Mark Goldin, MD, BUILDING PARALLEL CO-MANAGEMENT SERVICES IN A LARGE ACADEMIC HOSPITALIST GROUP
Brian Lichtenstein, MD, IMPROVING RISK-ADJUSTED OUTCOME MEASURES WITH PHYSICIAN-ORIENTED DOCUMENTATION INTERVENTIONS
Matthew Cerasale, MD, REAL-TIME PADUA: AN AUTOMATED EHR INTEGRATED VENOUS THROMBOEMBOLISM RISK ASSESSMENT TOOL
Franziska Jovin, MD, MMM, FHM, IMPLEMENTATION OF A PAY-FOR-PERFOMANCE STRUCTURE FOR HOSPITALIST-LED QUALITY IMPROVEMENT PROJECTS
Arpit Khandelwal, MD, MANAGING CHALLENGING PATIENTS: FROM CONFLICT TO TEACHING OPPORTUNITY
Justin Lotfi, MD, MAKING IT SIMPLE - PROCESS IMPROVEMENT FOR OUTSIDE MEDICAL RECORDS
David McCollum, MD, FIXING WHAT IS BROKEN: QUALITY IMPROVEMENT IN THE CRITICAL LAB VALUE PROCESS
Nidhi Rohatgi, MD, MS, A NOVEL MD-RN COLLABORATIVE PROTOCOL TO PREVENT AND MANAGE ACUTE DELIRIUM IN INPATIENT WARDS
Lesley Schmaltz, MD, UNNECESSARY TRANSFUSIONS: HOSPITAL MEDICINE LEADING INSTITUTION-WIDE CHANGE
Anuj Dalal, MD, FHM, IMPLEMENTATION OF A PATIENT-CENTERED ‘MICROBLOG' MESSAGING PLATFORM TO IMPROVE CARE TEAM COMMUNICATION
Willard Ellis, MD, PhD, FHM, INTENSIVE FOLLOW UP AFTER PALLIATIVE CARE CONSULTATIONS TO REDUCE READMISSIONS
Lakshmi Swaminathan, MD, MHSA, FHM, USING “MAGIC” TO FACILITATE APPROPRIATE PICC USE: RESULTS OF IMPLEMENTATION OF A PICC APPROPRIATENESS ASSESSMENT TOOL
Charles Coffey, MD, MSc, FHM, IMPLEMENTING GUIDELINE-BASED INDICATIONS FOR CARDIAC MONITORING AT CEDARS-SINAI MEDICAL CENTER
Erik Hoyer, MD, USE OF A HOSPITALIST CLINICAL COMMUNITY TO FACILITATE DISSEMINATION OF AN EARLY MOBILITY QUALITY IMPROVEMENT PROGRAM
Elizabeth Stewart, MD, A MULTIDISCIPLINARY APPROACH TO HIGH VALUE CARDIAC BIOMARKER
CLINICAL VIGNETTES CATEGORY
WINNER (ADULT):
Molly Kantor, MD, THE TIP OF THE ICEBERG: A RARE CAUSE OF ACUTE LIVER FAILURE
WINNER (PEDIATRIC):
Jennifer Ladd, MD, MORE THAN JUST THE “TERRIBLE TWOS”: A CASE OF RESISTANT HSV ENCEPHALITIS
TRAINEE WINNER:
Bhakti Shah, MD, UNMASKING THE TERATOMA
FINALISTS:
Weijen Chang, MD, SFHM, UNCOILING A PROBLEMATIC TICKLE IN THE THROAT
Kenton Dover, MD, KEEPING AN EYE OUT FOR THE DIAGNOSIS
Stephanie Royer, MD, THE YOUNGEST REPORTED CASE OF EOSINOPHILIC CHOLANGITIS
Oluremi Ajala, MD, ANGINA OF ABDOMINAL ORIGIN
Asana Anderson, MBBS, A PARATHYROID CRISIS BURIED IN A SEPTIC OTOMASTOIDITIS
Kyle Bennett, DO, BULLS-EYE MARKS THE SPOT: LYME CARDITIS PRESENTING AS RASH AND PRESYNCOPE
John Biebelhausen, MD, MBA, CROSSFIT CATASTROPHE: CHEST PAIN IN A HEALTHY YOUNG WOMAN
Xuan Gao, MD, A CASE OF THE UNSEEN: KLEBSIELLA PNEUMONIA PYOGENIC LIVER ABSCESS WITH PNEUMONIA AND SEPTIC ENDOPHTHALMITIS IN A NON-ASIAN U.S. RESIDENT
Sana Grover, MBBS, 'ABSTINENT AND INTOXICATED'. A RARE CASE OF AUTO-BREWERY SYNDROME
Andrew Hawrylak, MD, WHEN IT'S NOT AN ALLERGIC REACTION: AN UNUSUAL CASE OF ECTHYEMA GANGRENOSUM ASSOCIATED WITH PROTEUS BACTEREMIA
Rasheen Imtiaz, MD, LACTIC ACIDOSIS IN ASTHMA
Jessie King, MD, PhD, THE SMOKING WOMAN
Bradley Manning, MD, A SUPER-ANTIGEN-MEDIATED MIMIC OF ACUTE APPENDICITIS
Hiroki Matsuura, IMPAIRED CONSCIOUSNESS WITH INDOLENT BREAST MASS
Niharika Singh, MD, LOWER EXTREMITY NECROTIZING FASCIITIS: AN UNUSUAL PRESENTATION OF PERFORATED SIGMOID DIVERTICULITIS
Vivan Tran, DO, PUTTING THE PEE IN PREGNANCY: A CASE OF GESTATIONAL DIABETES INSIPIDUS YOU DON'T WANT TO MISS
Kristen Welch, THE MYSTERIOUS DANCE: A RARE CASE OF DELAYED ONSET DIABETIC STRIATOPATHY
Standing adjacent Poster 391 in a loud, crowded meeting hall, Monika Wells, MD, MPH, a resident in internal medicine at Virginia Mason Medical Center in Seattle, chatted with a colleague. A few feet away, a group of doctors and healthcare professionals huddled dramatically, just barely out of earshot.
The fate of Dr. Wells’ scientific abstract hung in the balance.
Her study, a look at scheduling the start and stop times of hospitalist shifts around expected demand to reduce costs and patient wait times, was a short-list finalist in the Innovations category of HM16’s annual Research, Innovation, and Clinical Vignettes scientific abstract competition. With her work done—she had already made presentations to first a pair of semifinalist judges and then to a herd of all 10 of the category judges—Dr. Wells looked remarkably calm as she waited for the announcement of the winners.
Either way, she said, the competition had been an invigorating, exciting experience.
“I’m a doctor, so I like to compete,” she half-joked. “It definitely has been motivating.”
RIV ribbons this year were handed out to seven winners in four categories. The competition garnered 914 abstracts accepted for presentation.
Dr. Wells ended up being one of them. She was named Innovations’ trainee winner. In her study, researchers found that analyzing the flow of admissions and redistributing hospitalists to better conform to that flow reduced patient wait times and costs as well as improved the subjective experience of hospitalists even as volume increased.
The overall winner in the Innovations category also went to a trainee, Baely Crockett, PharmD, a resident at Eskenazi Health in Indianapolis. Her study looked at a pharmacist-managed rivaroxaban clinic for the treatment of venous thromboembolism (VTE). It was the first time, as far as the judges knew, that an award had gone to a pharmacist.
Dr. Crockett’s abstract showed that patients diagnosed in the ED with low-risk VTE are given a prescription scheduled to be seen in the follow-up clinic within two to five days, at which point the pharmacist sees the patients and reviews their case with them and determines treatment duration.
Dr. Crockett said the pharmacists involved are especially suitable for the role not only because of their expertise in the medication and the handling of time-consuming co-pay issues and other concerns but also because they shadowed ED physicians for six months to get training and experience.
“We’re able to fill in gaps that are true challenges to the patient’s success in finishing therapy,” she said.
One of the Innovations judges, Michael Craig, MD, MPH, FHM, associate professor of medicine at the University of North Carolina in Chapel Hill, said the research hit on an area of growing interest.
“The movement toward outpatient treatment of VTE is a pretty big topic that lots of people are working on,” he said. “It’s very relevant. The whole idea of having a pharmacist-driven intervention is unique; nobody had thought of or heard of before.”
The winner in the Research category was Vineet Chopra, MD, MSc, FHM, assistant professor at the University of Michigan in Ann Arbor, whose work set out to quantify how to prevent bloodstream infection and blood clots from the use of peripherally inserted central catheters, or PICC lines. Researchers created a simulation model, based on data from the literature, looking at what would happen to a hospital if the use of certain types of PICCs was increased while use of other types was decreased—the rationale being that PICCs with just one channel, or port, have a lower risk of infection or blood clots than those with multiple ports.
It is a risk that is often unrecognized, and PICC lines with multiple ports are often ordered as a just-in-case measure in the event that the first port gets clogged.
Chopra and colleagues found that, at the average hospital, about 75% of all PICCs used tend to be multichannel and 25% single-channel. They found every 5% increase in single-channel PICC use could prevent almost 1.5 infections per 1,000 patients, and 0.5 blood clots, with a corresponding cost savings of $13,000 per event. That can add up to hundreds of thousands of dollars a year at large hospitals.
And those calculations, Dr. Chopra noted, do not include penalties for infections or the financial effects of having those results publicly reported. Researchers are now creating an online tool— at improvepicc.com—that will allow users to calculate their own costs and potential savings.
“The hope of this is that it will give hospital administrators and hospital leadership and quality officers the momentum, perhaps, to overcome the inertia of not thinking actively,” said Dr. Chopra, who notched his first win after 10 years of participating in the RIV competition. “I think we don’t think actively about the choices we make when it comes to these devices.”
In the Clinical Vignettes category, winner Molly Kantor, MD, assistant clinical professor at the University of California, San Diego, recounted the case of a sickle-cell disease patient whose diagnosis, and hence treatment, was delayed and who ultimately died. She outlined a series of missteps, including taking at face-value a patient-reported past medical disease, which turned out to be wrong; making certain diagnoses based on lab tests and stopping there; and anchoring on the original diagnosis when the thought process was later reevaluated.
Dr. Kantor said the case is a caution flag to hospitalists, reinforcing the need for “a broad differential diagnosis.”
“[Make] sure that the data fits together and that you’re not using just one isolated piece of information to cinch everything, including the past medical history or a certain lab test, when the whole picture doesn’t quite fit together,” she said. “Looking back at this case, it’s pretty clear that the puzzle pieces probably weren’t quite fitting together, but there was enough that the easier thing to do was to make the diagnosis and move on.”
In the Pediatric Clinical Vignettes category, winner Jennifer Ladd, MD, a resident at Duke University, won for a study of a vexing case of a 2-year-old who was irritable and stalled on developmental milestones. At the hospital, the thought was that it could likely be a recurrence of herpes simplex (HSV) encephalitis, but the spinal fluid showed no signs of that and the acyclovir, which nearly always works for the disorder, was having no effect and the symptoms worsened.
The key in the case, said Alyssa Stephany, MD, then assistant professor at Duke University and now section chief of pediatric hospital medicine at Children’s Hospital of Wisconsin, who presented the case in Dr. Ladd’s absence, was that the team reopened the diagnosis and didn’t get ensnared in cognitive bias. A biopsy ultimately showed HSV in the brain tissue; it was a case of recurrence, despite signs to the contrary. Foscarnet was used to effectively treat the child; it is unknown why acyclovir didn’t work in this case.
“It kind of brings to the surface that that’s what a hospitalist is—a hospitalist is that person who sits and thinks, and really thinks, about the patient and doesn’t just do their rote work of input and output of a patient through the hospital system,” Dr. Stephany said. “When you get a case like this, it makes you take pause.”
The trainee winner in the Research category was N. Lance Downing, MD, of Stanford University School of Medicine, for work on an EHR-based severe sepsis alert. The trainee winner in Clinical Vignettes was Bhakti Shah, MD, of North Shore-LIJ Health System, now Northwell Health, on a rare case of autoimmune NMDA receptor encephalitis. TH
Thomas R. Collins is a freelance writer in South Florida.
2016 RIV Finalists, Winners
Research Category
WINNER:
Vineet Chopra, MD, MSc, FHM, LIMITING THE NUMBER OF LUMENS IN PERIPHERALLY INSERTED CENTRAL CATHETERS TO IMPROVE OUTCOMES AND REDUCE COST: A SIMULATION STUDY
TRAINEE WINNER:
N. Downing, MD, AN ELECTRONIC HEALTH RECORD-BASED SEVERE SEPSIS ALERT TO IMPROVE SEPSIS TREATMENT PERFORMANCE: RANDOMIZED EVALUATION
FINALISTS:
Waseem Khaliq, MD, MPH, PREVALENCE AND PREDICTORS OF NON-ADHERENCE TO BREAST CANCER SCREENING: PERSPECTIVE AND PREFERENCES OF HOSPITALIZED WOMEN
Dilli Poudel, MD, SYSTEMIC SCLEROSIS AS A RISK FACTOR OF ACUTE MYOCARDIAL INFARCTION: A US POPULATION BASED STUDY
Aiham Albaeni, MD, REGIONAL VARIATION IN RESOURCES UTILIZATION AND OUTCOMES FOLLOWING OUT-OF-HOSPITAL CARDIAC ARREST IN THE UNITED STATES
Poushali Bhattacharjee, MD, DETECTING SEPSIS: ARE TWO OPINIONS BETTER THAN ONE?
Vineet Chopra, MD, MSc, FHM, THE INFLUENCE OF RED BLOOD CELL TRANSFUSION ON VENOUS THROMBOEMBOLISM IN PATIENTS WITH PERIPHERALLY-INSERTED CENTRAL CATHETERS
Shaker Eid, MD, MBA, IMPACT OF HOSPITAL TEACHING STATUS ON OUT-OF-HOSPITAL CARDIAC ARREST OUTCOMES AND RESOURCE UTILIZATION IN THE UNITED STATES: 2000-2012
Tarun Jain, MD, CONTRAST-INDUCED NEPHROPATHY IN STEMI PATIENTS WITH AND WITHOUT CHRONIC KIDNEY DISEASE
Mona Beier, MD, CREATING A PATIENT SAFETY CULTURE ONE INCIDENT REPORT AT A TIME
Charles Pollack, MD, REINITIATION OF ANTITHROMBOTIC THERAPY AFTER EMERGENCY PROCEDURES OR AFTER AN EMERGENT BLEEDING EVENT: ADDITIONAL INTERIM EXPERIENCE FROM THE RE-VERSE AD TRIAL
Robert Boxer, MD, PhD, SAVING TIME: A TIME-MOTION ANALYSIS OF THE IMPACT OF REGIONALIZATION AND DAILY ADMITTING ON INTERN WORKFLOW
Kaleigh Evans, MD, THIRD TROPONIN ORDER OVERUSE IN THE SETTING OF CLINICAL STABILITY
David Paje, MD, SFHM, RISK OF VENOUS THROMBOEMBOLISM IN HOSPITALIZED PATIENTS WITH INFLAMMATORY BOWEL DISEASE
Rehan Qayyum, MD, COMPARISON OF TIME-TRENDS IN PATIENT SATISFACTION BETWEEN TEACHING AND NONTEACHING HOSPITAL
Joshua Rolnick, MD, VALIDATION OF TEST PERFORMANCE AND CLINICAL TIME ZERO FOR AN ELECTRONIC HEALTH RECORD-EMBEDDED SEVERE SEPSIS ALERT
Allison Louis, MD, BLIND SIDED: MISSING POOR VISUAL ACUITY AND DECREASED SELF-EFFICACY IN HOSPITALIZED PATIENTS WITH DIABETES
G. Randy Smith, MD, MS, SFHM, ASSOCIATION OF HOSPITAL ADMISSION SERVICE STRUCTURE WITH EARLY TRANSFER TO CRITICAL CARE, HOSPITAL READMISSION, AND LENGTH OF STAY
Kathleene Wooldridge, MD, R-VA-MARQUIS: IMPLEMENTING BEST PRACTICES IN MEDICATION RECONCILIATION FOR RURAL VETERANS
INNOVATION CATEGORY
WINNER:
Baely Crockett, PharmD, NOVEL PHARMACIST-MANAGED RIVAROXABAN CLINIC FOR OUTPATIENT TREATMENT OF VENOUS THROMBOEMBOLISM
TRAINEE WINNER:
Monika Wells, MD, MPH, DESIGNING HOSPITALIST SHIFTS AROUND ADMISSION DEMAND REDUCES PATIENT WAIT TIMES AND COST
FINALISTS:
Jessica Dong, WHO MOVED MY EHR CHEESE? A NEW APPROACH TO CURATING AND INDIVIDUALIZING COMMUNICATIONS TO PHYSICIANS ABOUT EHR SOFTWARE UPDATES
Stephanie Rennke, MD, MED REC: A SKILLS-BASED CURRICULUM ON MEDICATION SAFETY AND MEDICATION RECONCILIATION FOR MEDICAL STUDENTS
Jens Langsjoen, MD, DEVELOPING AN INPATIENT DELIRIUM PREVENTION PROTOCOL
Mark Goldin, MD, BUILDING PARALLEL CO-MANAGEMENT SERVICES IN A LARGE ACADEMIC HOSPITALIST GROUP
Brian Lichtenstein, MD, IMPROVING RISK-ADJUSTED OUTCOME MEASURES WITH PHYSICIAN-ORIENTED DOCUMENTATION INTERVENTIONS
Matthew Cerasale, MD, REAL-TIME PADUA: AN AUTOMATED EHR INTEGRATED VENOUS THROMBOEMBOLISM RISK ASSESSMENT TOOL
Franziska Jovin, MD, MMM, FHM, IMPLEMENTATION OF A PAY-FOR-PERFOMANCE STRUCTURE FOR HOSPITALIST-LED QUALITY IMPROVEMENT PROJECTS
Arpit Khandelwal, MD, MANAGING CHALLENGING PATIENTS: FROM CONFLICT TO TEACHING OPPORTUNITY
Justin Lotfi, MD, MAKING IT SIMPLE - PROCESS IMPROVEMENT FOR OUTSIDE MEDICAL RECORDS
David McCollum, MD, FIXING WHAT IS BROKEN: QUALITY IMPROVEMENT IN THE CRITICAL LAB VALUE PROCESS
Nidhi Rohatgi, MD, MS, A NOVEL MD-RN COLLABORATIVE PROTOCOL TO PREVENT AND MANAGE ACUTE DELIRIUM IN INPATIENT WARDS
Lesley Schmaltz, MD, UNNECESSARY TRANSFUSIONS: HOSPITAL MEDICINE LEADING INSTITUTION-WIDE CHANGE
Anuj Dalal, MD, FHM, IMPLEMENTATION OF A PATIENT-CENTERED ‘MICROBLOG' MESSAGING PLATFORM TO IMPROVE CARE TEAM COMMUNICATION
Willard Ellis, MD, PhD, FHM, INTENSIVE FOLLOW UP AFTER PALLIATIVE CARE CONSULTATIONS TO REDUCE READMISSIONS
Lakshmi Swaminathan, MD, MHSA, FHM, USING “MAGIC” TO FACILITATE APPROPRIATE PICC USE: RESULTS OF IMPLEMENTATION OF A PICC APPROPRIATENESS ASSESSMENT TOOL
Charles Coffey, MD, MSc, FHM, IMPLEMENTING GUIDELINE-BASED INDICATIONS FOR CARDIAC MONITORING AT CEDARS-SINAI MEDICAL CENTER
Erik Hoyer, MD, USE OF A HOSPITALIST CLINICAL COMMUNITY TO FACILITATE DISSEMINATION OF AN EARLY MOBILITY QUALITY IMPROVEMENT PROGRAM
Elizabeth Stewart, MD, A MULTIDISCIPLINARY APPROACH TO HIGH VALUE CARDIAC BIOMARKER
CLINICAL VIGNETTES CATEGORY
WINNER (ADULT):
Molly Kantor, MD, THE TIP OF THE ICEBERG: A RARE CAUSE OF ACUTE LIVER FAILURE
WINNER (PEDIATRIC):
Jennifer Ladd, MD, MORE THAN JUST THE “TERRIBLE TWOS”: A CASE OF RESISTANT HSV ENCEPHALITIS
TRAINEE WINNER:
Bhakti Shah, MD, UNMASKING THE TERATOMA
FINALISTS:
Weijen Chang, MD, SFHM, UNCOILING A PROBLEMATIC TICKLE IN THE THROAT
Kenton Dover, MD, KEEPING AN EYE OUT FOR THE DIAGNOSIS
Stephanie Royer, MD, THE YOUNGEST REPORTED CASE OF EOSINOPHILIC CHOLANGITIS
Oluremi Ajala, MD, ANGINA OF ABDOMINAL ORIGIN
Asana Anderson, MBBS, A PARATHYROID CRISIS BURIED IN A SEPTIC OTOMASTOIDITIS
Kyle Bennett, DO, BULLS-EYE MARKS THE SPOT: LYME CARDITIS PRESENTING AS RASH AND PRESYNCOPE
John Biebelhausen, MD, MBA, CROSSFIT CATASTROPHE: CHEST PAIN IN A HEALTHY YOUNG WOMAN
Xuan Gao, MD, A CASE OF THE UNSEEN: KLEBSIELLA PNEUMONIA PYOGENIC LIVER ABSCESS WITH PNEUMONIA AND SEPTIC ENDOPHTHALMITIS IN A NON-ASIAN U.S. RESIDENT
Sana Grover, MBBS, 'ABSTINENT AND INTOXICATED'. A RARE CASE OF AUTO-BREWERY SYNDROME
Andrew Hawrylak, MD, WHEN IT'S NOT AN ALLERGIC REACTION: AN UNUSUAL CASE OF ECTHYEMA GANGRENOSUM ASSOCIATED WITH PROTEUS BACTEREMIA
Rasheen Imtiaz, MD, LACTIC ACIDOSIS IN ASTHMA
Jessie King, MD, PhD, THE SMOKING WOMAN
Bradley Manning, MD, A SUPER-ANTIGEN-MEDIATED MIMIC OF ACUTE APPENDICITIS
Hiroki Matsuura, IMPAIRED CONSCIOUSNESS WITH INDOLENT BREAST MASS
Niharika Singh, MD, LOWER EXTREMITY NECROTIZING FASCIITIS: AN UNUSUAL PRESENTATION OF PERFORATED SIGMOID DIVERTICULITIS
Vivan Tran, DO, PUTTING THE PEE IN PREGNANCY: A CASE OF GESTATIONAL DIABETES INSIPIDUS YOU DON'T WANT TO MISS
Kristen Welch, THE MYSTERIOUS DANCE: A RARE CASE OF DELAYED ONSET DIABETIC STRIATOPATHY
Discovery could aid development of new sepsis therapies
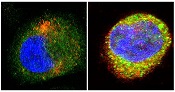
antibodies toward SHARPIN
(red) and caspase 1 (green).
Cell on right showing increase
in caspase 1 upon stimulation
with LPS and ATP and co-
localization with SHARPIN as
visualized by the merged
fluorescence (yellow). Nuclei
are stained blue with DAPI.
Image courtesy of The
American Journal of Pathology
A new study suggests that SHARPIN, a protein involved in regulating inflammation, has anti-septic effects.
Researchers believe this discovery, reported in The American Journal of Pathology, could spur the development of novel treatments for sepsis.
“Sepsis has been linked to enhanced activity of the enzyme caspase 1 and aberrant expression of pro-inflammatory interleukins 1β and 18,” said Liliana Schaefer, MD, of Goethe-Universität in Frankfurt, Germany.
“SHARPIN binds to caspase 1 and inhibits its activation. Our study proposes that the caspase 1/SHARPIN interaction may be a key pharmacological target in sepsis and perhaps in other inflammatory conditions where SHARPIN is involved.”
The researchers found that sepsis in mice bred to be deficient in SHARPIN resulted in enhanced levels of interleukins 1β and 18 and active caspase 1, as well as shortened survival.
Treatment with a caspase 1 inhibitor reversed these effects—reducing levels of interleukins 1β and 18, decreasing cell death in the spleen, and prolonging survival.
The researchers also found evidence to suggest this mechanism may be relevant to human sepsis.
“We found a decline in SHARPIN levels in septic patients correlating with enhanced activation of caspase 1 in circulating mononuclear cells and an increase of interleukin 1β/18 in the plasma,” Dr Schaefer said.
“Our findings suggest that using pharmacological caspase 1 inhibitors could be beneficial in septic patients with low SHARPIN levels, and these therapies may be more efficient than other anti-inflammatory therapies.” ![]()
antibodies toward SHARPIN
(red) and caspase 1 (green).
Cell on right showing increase
in caspase 1 upon stimulation
with LPS and ATP and co-
localization with SHARPIN as
visualized by the merged
fluorescence (yellow). Nuclei
are stained blue with DAPI.
Image courtesy of The
American Journal of Pathology
A new study suggests that SHARPIN, a protein involved in regulating inflammation, has anti-septic effects.
Researchers believe this discovery, reported in The American Journal of Pathology, could spur the development of novel treatments for sepsis.
“Sepsis has been linked to enhanced activity of the enzyme caspase 1 and aberrant expression of pro-inflammatory interleukins 1β and 18,” said Liliana Schaefer, MD, of Goethe-Universität in Frankfurt, Germany.
“SHARPIN binds to caspase 1 and inhibits its activation. Our study proposes that the caspase 1/SHARPIN interaction may be a key pharmacological target in sepsis and perhaps in other inflammatory conditions where SHARPIN is involved.”
The researchers found that sepsis in mice bred to be deficient in SHARPIN resulted in enhanced levels of interleukins 1β and 18 and active caspase 1, as well as shortened survival.
Treatment with a caspase 1 inhibitor reversed these effects—reducing levels of interleukins 1β and 18, decreasing cell death in the spleen, and prolonging survival.
The researchers also found evidence to suggest this mechanism may be relevant to human sepsis.
“We found a decline in SHARPIN levels in septic patients correlating with enhanced activation of caspase 1 in circulating mononuclear cells and an increase of interleukin 1β/18 in the plasma,” Dr Schaefer said.
“Our findings suggest that using pharmacological caspase 1 inhibitors could be beneficial in septic patients with low SHARPIN levels, and these therapies may be more efficient than other anti-inflammatory therapies.” ![]()
antibodies toward SHARPIN
(red) and caspase 1 (green).
Cell on right showing increase
in caspase 1 upon stimulation
with LPS and ATP and co-
localization with SHARPIN as
visualized by the merged
fluorescence (yellow). Nuclei
are stained blue with DAPI.
Image courtesy of The
American Journal of Pathology
A new study suggests that SHARPIN, a protein involved in regulating inflammation, has anti-septic effects.
Researchers believe this discovery, reported in The American Journal of Pathology, could spur the development of novel treatments for sepsis.
“Sepsis has been linked to enhanced activity of the enzyme caspase 1 and aberrant expression of pro-inflammatory interleukins 1β and 18,” said Liliana Schaefer, MD, of Goethe-Universität in Frankfurt, Germany.
“SHARPIN binds to caspase 1 and inhibits its activation. Our study proposes that the caspase 1/SHARPIN interaction may be a key pharmacological target in sepsis and perhaps in other inflammatory conditions where SHARPIN is involved.”
The researchers found that sepsis in mice bred to be deficient in SHARPIN resulted in enhanced levels of interleukins 1β and 18 and active caspase 1, as well as shortened survival.
Treatment with a caspase 1 inhibitor reversed these effects—reducing levels of interleukins 1β and 18, decreasing cell death in the spleen, and prolonging survival.
The researchers also found evidence to suggest this mechanism may be relevant to human sepsis.
“We found a decline in SHARPIN levels in septic patients correlating with enhanced activation of caspase 1 in circulating mononuclear cells and an increase of interleukin 1β/18 in the plasma,” Dr Schaefer said.
“Our findings suggest that using pharmacological caspase 1 inhibitors could be beneficial in septic patients with low SHARPIN levels, and these therapies may be more efficient than other anti-inflammatory therapies.” ![]()
FDA requires labeling changes to metformin-containing drugs
Metformin can be used safely in patients with mild impairment in kidney function and in some patients with moderate impairment in kidney function, according to the FDA’s recent review of several medical studies.
These findings have prompted the FDA to require manufacturers to change the labeling for metformin-containing drugs. These drugs’ labels now must include the results of the medical studies and new measures of kidney function for determining if a patient can use metformin, says a written statement from the FDA.
Metformin’s current labeling strongly recommends against its use in some patients with kidneys that do not work normally. The FDA is specifically requiring that new labels include the recommendation that the measure of kidney function used to determine whether a patient can receive metformin be changed from one based on a single laboratory parameter (blood creatinine concentration) to one that provides a better estimate of renal function (that is, the glomerular filtration rate estimating equation, eGFR).
The full labeling recommendations are available in the FDA’s written statement.
Additional information including a data summary and a list of metformin-containing drugs is available in the FDA Drug Safety Communication.
The FDA asks that healthcare professionals and patients report adverse events or side effects related to the use of metformin-containing drugs to the FDA’s MedWatch Safety Information and Adverse Event Reporting Program.
Metformin can be used safely in patients with mild impairment in kidney function and in some patients with moderate impairment in kidney function, according to the FDA’s recent review of several medical studies.
These findings have prompted the FDA to require manufacturers to change the labeling for metformin-containing drugs. These drugs’ labels now must include the results of the medical studies and new measures of kidney function for determining if a patient can use metformin, says a written statement from the FDA.
Metformin’s current labeling strongly recommends against its use in some patients with kidneys that do not work normally. The FDA is specifically requiring that new labels include the recommendation that the measure of kidney function used to determine whether a patient can receive metformin be changed from one based on a single laboratory parameter (blood creatinine concentration) to one that provides a better estimate of renal function (that is, the glomerular filtration rate estimating equation, eGFR).
The full labeling recommendations are available in the FDA’s written statement.
Additional information including a data summary and a list of metformin-containing drugs is available in the FDA Drug Safety Communication.
The FDA asks that healthcare professionals and patients report adverse events or side effects related to the use of metformin-containing drugs to the FDA’s MedWatch Safety Information and Adverse Event Reporting Program.
Metformin can be used safely in patients with mild impairment in kidney function and in some patients with moderate impairment in kidney function, according to the FDA’s recent review of several medical studies.
These findings have prompted the FDA to require manufacturers to change the labeling for metformin-containing drugs. These drugs’ labels now must include the results of the medical studies and new measures of kidney function for determining if a patient can use metformin, says a written statement from the FDA.
Metformin’s current labeling strongly recommends against its use in some patients with kidneys that do not work normally. The FDA is specifically requiring that new labels include the recommendation that the measure of kidney function used to determine whether a patient can receive metformin be changed from one based on a single laboratory parameter (blood creatinine concentration) to one that provides a better estimate of renal function (that is, the glomerular filtration rate estimating equation, eGFR).
The full labeling recommendations are available in the FDA’s written statement.
Additional information including a data summary and a list of metformin-containing drugs is available in the FDA Drug Safety Communication.
The FDA asks that healthcare professionals and patients report adverse events or side effects related to the use of metformin-containing drugs to the FDA’s MedWatch Safety Information and Adverse Event Reporting Program.
U.S. sepsis-related mortality rates differ based on data source
Despite challenges in estimating sepsis-related mortality in the U.S. because of its complex clinical nature and variety of underlying causes, estimates based on administrative claims data may be more accurate than those derived from death certificates, according to a report published April 8 in the Morbidity and Mortality Weekly Report.
Dr. Lauren Epstein of the division of healthcare quality promotion at the National Center for Emerging and Zoonotic Infectious Diseases, and her colleagues, compared U.S. sepsis-related mortality estimates from different sources. Deaths attributable to diagnoses corresponding to ICD-10 diagnosis codes A40 (streptococcal septicemia) and A41 (other septicemia) from 1999 to 2014 were extracted from the CDC WONDER (Wide-ranging Online Data for Epidemiologic Research) database. Administrative claims data using various combinations of the ICD-9-CM administrative codes for primary or secondary infection and organ dysfunction to identify severe sepsis from 2004 to 2009 were extracted from the largest all-payer, publicly available inpatient database in the United States, the Nationwide Inpatient Sample. (MMWR. 2016 Apr 8;65[13]:342-5).
Of the roughly 2.5 million death certificates listing sepsis as a cause of death, 22% identified sepsis as the underlying cause of death during the time period assessed. The results of the comparison demonstrated that the estimated range of sepsis-related mortality based on death certificate data was lower than that obtained using administrative claims data (ranges, 146,000-159,000 and 168,000-381,000, respectively). These results indicate that the annual estimate based on administrative claims data during the time period assessed was 15%-140% higher than the estimate based on death certificate data.
To explain the difference between the estimated sepsis-related mortality ranges, the authors said that while both death certificate and administrative claims data are important sources of public health information, they are each associated with limitations that can affect such estimates. For example, the authors said that death certificate certifiers may be more prone to record sepsis as an immediate cause of death, resulting in lower estimates of sepsis-related mortality based on underlying causes of death. Regarding administrative claims data, the authors said that such data cannot be all inclusive, as only those sepsis-related deaths occurring in health care facilities are captured.
The authors said that their results highlight the need for a better defined and more reliable sepsis surveillance system that should be based on objective clinical data. This approach would allow for increased accuracy in the tracking of sepsis trends in the United States, as well as an improved system for gauging the impact of sepsis awareness and prevention efforts.
No funding sources or conflicts of interest were reported.
Despite challenges in estimating sepsis-related mortality in the U.S. because of its complex clinical nature and variety of underlying causes, estimates based on administrative claims data may be more accurate than those derived from death certificates, according to a report published April 8 in the Morbidity and Mortality Weekly Report.
Dr. Lauren Epstein of the division of healthcare quality promotion at the National Center for Emerging and Zoonotic Infectious Diseases, and her colleagues, compared U.S. sepsis-related mortality estimates from different sources. Deaths attributable to diagnoses corresponding to ICD-10 diagnosis codes A40 (streptococcal septicemia) and A41 (other septicemia) from 1999 to 2014 were extracted from the CDC WONDER (Wide-ranging Online Data for Epidemiologic Research) database. Administrative claims data using various combinations of the ICD-9-CM administrative codes for primary or secondary infection and organ dysfunction to identify severe sepsis from 2004 to 2009 were extracted from the largest all-payer, publicly available inpatient database in the United States, the Nationwide Inpatient Sample. (MMWR. 2016 Apr 8;65[13]:342-5).
Of the roughly 2.5 million death certificates listing sepsis as a cause of death, 22% identified sepsis as the underlying cause of death during the time period assessed. The results of the comparison demonstrated that the estimated range of sepsis-related mortality based on death certificate data was lower than that obtained using administrative claims data (ranges, 146,000-159,000 and 168,000-381,000, respectively). These results indicate that the annual estimate based on administrative claims data during the time period assessed was 15%-140% higher than the estimate based on death certificate data.
To explain the difference between the estimated sepsis-related mortality ranges, the authors said that while both death certificate and administrative claims data are important sources of public health information, they are each associated with limitations that can affect such estimates. For example, the authors said that death certificate certifiers may be more prone to record sepsis as an immediate cause of death, resulting in lower estimates of sepsis-related mortality based on underlying causes of death. Regarding administrative claims data, the authors said that such data cannot be all inclusive, as only those sepsis-related deaths occurring in health care facilities are captured.
The authors said that their results highlight the need for a better defined and more reliable sepsis surveillance system that should be based on objective clinical data. This approach would allow for increased accuracy in the tracking of sepsis trends in the United States, as well as an improved system for gauging the impact of sepsis awareness and prevention efforts.
No funding sources or conflicts of interest were reported.
Despite challenges in estimating sepsis-related mortality in the U.S. because of its complex clinical nature and variety of underlying causes, estimates based on administrative claims data may be more accurate than those derived from death certificates, according to a report published April 8 in the Morbidity and Mortality Weekly Report.
Dr. Lauren Epstein of the division of healthcare quality promotion at the National Center for Emerging and Zoonotic Infectious Diseases, and her colleagues, compared U.S. sepsis-related mortality estimates from different sources. Deaths attributable to diagnoses corresponding to ICD-10 diagnosis codes A40 (streptococcal septicemia) and A41 (other septicemia) from 1999 to 2014 were extracted from the CDC WONDER (Wide-ranging Online Data for Epidemiologic Research) database. Administrative claims data using various combinations of the ICD-9-CM administrative codes for primary or secondary infection and organ dysfunction to identify severe sepsis from 2004 to 2009 were extracted from the largest all-payer, publicly available inpatient database in the United States, the Nationwide Inpatient Sample. (MMWR. 2016 Apr 8;65[13]:342-5).
Of the roughly 2.5 million death certificates listing sepsis as a cause of death, 22% identified sepsis as the underlying cause of death during the time period assessed. The results of the comparison demonstrated that the estimated range of sepsis-related mortality based on death certificate data was lower than that obtained using administrative claims data (ranges, 146,000-159,000 and 168,000-381,000, respectively). These results indicate that the annual estimate based on administrative claims data during the time period assessed was 15%-140% higher than the estimate based on death certificate data.
To explain the difference between the estimated sepsis-related mortality ranges, the authors said that while both death certificate and administrative claims data are important sources of public health information, they are each associated with limitations that can affect such estimates. For example, the authors said that death certificate certifiers may be more prone to record sepsis as an immediate cause of death, resulting in lower estimates of sepsis-related mortality based on underlying causes of death. Regarding administrative claims data, the authors said that such data cannot be all inclusive, as only those sepsis-related deaths occurring in health care facilities are captured.
The authors said that their results highlight the need for a better defined and more reliable sepsis surveillance system that should be based on objective clinical data. This approach would allow for increased accuracy in the tracking of sepsis trends in the United States, as well as an improved system for gauging the impact of sepsis awareness and prevention efforts.
No funding sources or conflicts of interest were reported.
FROM MMWR
Key clinical point: Sepsis surveillance should be based on objective clinical data rather than on data obtained from death certificates.
Major finding: Using administrative codes, the U.S. sepsis-related mortality estimate from 2004 to 2009 was 15%-140% higher than the estimate derived from the use of death certificates (ranges; 168,000-381,000 and 146,000-159,000, respectively).
Data source: Death certificate data from the CDC WONDER database and administrative claims data from a previously published report of sepsis mortality estimates based on the Nationwide Inpatient Sample, Healthcare Cost and Utilization Project, Agency for Healthcare Research and Quality.
Disclosures: No funding sources or conflicts of interest were reported.
Clazakizumab safe, effective for PsA treatment
Treatment with clazakizumab was well tolerated and effective at treating musculoskeletal stress in patients with psoriatic arthritis (PsA), Dr. Philip Mease and his associates reported in a phase IIB study published in Arthritis & Rheumatology.
After 16 weeks, American College of Rheumatology (ACR) 20 response rates were highest in the group that received 100-mg doses of clazakizumab at 52.4%, compared with 46.3% for the 25-mg group, 39% for the 200-mg group, and 29.3% for the placebo group. ACR 50/ACR 70 response rates were higher for clazakizumab than for placebo after 16 weeks and 24 weeks, without clear evidence of a dose response.

Adverse events were more common for patients taking clazakizumab and occurred most frequently in the 200-mg group. However, serious adverse events were no more common in the 25-mg and 100-mg groups, compared with the placebo group. Discontinuations due to adverse events were highest in the 200-mg group, and were similar in all other groups.
“Clazakizumab may be particularly suited for patients with PsA in whom skin disease is well controlled with topical agents, ultraviolet therapy, and/or oral systemic therapy such as MTX [methotrexate], but whose musculoskeletal manifestations, such as joint signs and symptoms, enthesitis, and dactylitis, require more potent systemic therapy. Furthermore, some PsA patients do not present with skin lesions at diagnosis; those patients may also benefit from clazakizumab treatment,” the investigators noted.
Find the full study in Arthritis & Rheumatology (doi: 10.1002/art.39700).
Treatment with clazakizumab was well tolerated and effective at treating musculoskeletal stress in patients with psoriatic arthritis (PsA), Dr. Philip Mease and his associates reported in a phase IIB study published in Arthritis & Rheumatology.
After 16 weeks, American College of Rheumatology (ACR) 20 response rates were highest in the group that received 100-mg doses of clazakizumab at 52.4%, compared with 46.3% for the 25-mg group, 39% for the 200-mg group, and 29.3% for the placebo group. ACR 50/ACR 70 response rates were higher for clazakizumab than for placebo after 16 weeks and 24 weeks, without clear evidence of a dose response.
Adverse events were more common for patients taking clazakizumab and occurred most frequently in the 200-mg group. However, serious adverse events were no more common in the 25-mg and 100-mg groups, compared with the placebo group. Discontinuations due to adverse events were highest in the 200-mg group, and were similar in all other groups.
“Clazakizumab may be particularly suited for patients with PsA in whom skin disease is well controlled with topical agents, ultraviolet therapy, and/or oral systemic therapy such as MTX [methotrexate], but whose musculoskeletal manifestations, such as joint signs and symptoms, enthesitis, and dactylitis, require more potent systemic therapy. Furthermore, some PsA patients do not present with skin lesions at diagnosis; those patients may also benefit from clazakizumab treatment,” the investigators noted.
Find the full study in Arthritis & Rheumatology (doi: 10.1002/art.39700).
Treatment with clazakizumab was well tolerated and effective at treating musculoskeletal stress in patients with psoriatic arthritis (PsA), Dr. Philip Mease and his associates reported in a phase IIB study published in Arthritis & Rheumatology.
After 16 weeks, American College of Rheumatology (ACR) 20 response rates were highest in the group that received 100-mg doses of clazakizumab at 52.4%, compared with 46.3% for the 25-mg group, 39% for the 200-mg group, and 29.3% for the placebo group. ACR 50/ACR 70 response rates were higher for clazakizumab than for placebo after 16 weeks and 24 weeks, without clear evidence of a dose response.
Adverse events were more common for patients taking clazakizumab and occurred most frequently in the 200-mg group. However, serious adverse events were no more common in the 25-mg and 100-mg groups, compared with the placebo group. Discontinuations due to adverse events were highest in the 200-mg group, and were similar in all other groups.
“Clazakizumab may be particularly suited for patients with PsA in whom skin disease is well controlled with topical agents, ultraviolet therapy, and/or oral systemic therapy such as MTX [methotrexate], but whose musculoskeletal manifestations, such as joint signs and symptoms, enthesitis, and dactylitis, require more potent systemic therapy. Furthermore, some PsA patients do not present with skin lesions at diagnosis; those patients may also benefit from clazakizumab treatment,” the investigators noted.
Find the full study in Arthritis & Rheumatology (doi: 10.1002/art.39700).
FROM ARTHRITIS & RHEUMATOLOGY

Persistent knee pain predicts structural osteoarthritis early
AMSTERDAM – Persistent knee pain is an important predictor of structural joint damage and could potentially be used to predict knee osteoarthritis (OA) earlier, according to Dutch research reported at the World Congress on Osteoarthritis.
The analysis found that women participating in the Rotterdam Study who had knee pain on most days of the preceding month were more than four times more likely to develop knee OA within 5 years on MRI (odds ratio, 4.53) than were those without frequent knee pain.

Other signs and symptoms predictive of later OA on MRI included a history of knee injury (OR, 2.52), pain on palpation (OR, 2.30) or during activity (OR, 2.13), the feeling of the knee giving way (OR, 2.13), joint line tenderness (OR, 2.04), crepitus (or grating sounds or sensations; OR, 1.85), and Heberden’s nodes (OR, 1.67).
“Signs and symptoms can predict structural knee OA in 5 years in women without knee OA at baseline,” said the presenting study author Dieuwke Schiphof, Ph.D., a postdoctoral researcher at Erasmus University Medical Center in Rotterdam, at the meeting sponsored by the Osteoarthritis Research Society International.
“Knee pain on most days of the last month is an important predictive symptom for all structural OA definitions,” she said, adding that crepitus was an important sign of patellofemoral OA, and the feeling of giving way and joint line tenderness were important signs for tibiofemoral OA.
The aim of their study was to try to determine the value of previously identified clinical signs and symptoms for determining the onset of structural knee OA. Around 600 women aged 45-60 years without OA at baseline were included from the population-based cohort Rotterdam study. Participants had completed a standard questionnaire and had physical, radiographic, and MRI examination of both knees at baseline and at a mean follow-up of 5 years later.
The mean age of women was 59.5 years and 33 of 1,137 knees had isolated patellofemoral OA and 69 had isolated tibiofemoral OA, 111 one or the other, and 22 had radiographic knee OA.
Results showed that knee pain on most days of the last month (OR, 7.57) and crepitus (OR, 3.05) were most predictive of isolated patellofemoral OA on MRI. The prevalence of patellofemoral OA was 3% but this increased to 20% if both these signs and symptoms were present.
Knee pain on most days of the last month (OR, 4.13) was also predictive of isolated tibiofemoral OA on MRI, together with a history of knee pain (OR, 2.48), knee pain during activities (OR, 2.04), and the feeling of the knee giving way (OR, 3.15). If two or three or more signs and symptoms were present, the predictive value increased from a prevalence of 6% to 12% to 18%.
Knee pain on most days of the last month was also highly predictive of radiographic OA (OR, 7.77), as was pain at palpation (OR, 4.36), prior injury (OR, 3.64), and the feeling of the knee giving way (OR, 2.75). Again, when additional signs or symptoms were present the prevalence increased from a prevalence of 3% at follow-up to 4% with one, 8% with two, and up to 14% for three or more.
These signs and symptoms could potentially be used to help identify patients that may benefit from preventive treatment for knee OA, the researchers believe.
The study was funded by The Netherlands Organisation for Health Research and Development and Reumafonds, the Dutch Arthritis Association. Dr. Schiphof had no financial disclosures.
AMSTERDAM – Persistent knee pain is an important predictor of structural joint damage and could potentially be used to predict knee osteoarthritis (OA) earlier, according to Dutch research reported at the World Congress on Osteoarthritis.
The analysis found that women participating in the Rotterdam Study who had knee pain on most days of the preceding month were more than four times more likely to develop knee OA within 5 years on MRI (odds ratio, 4.53) than were those without frequent knee pain.
Other signs and symptoms predictive of later OA on MRI included a history of knee injury (OR, 2.52), pain on palpation (OR, 2.30) or during activity (OR, 2.13), the feeling of the knee giving way (OR, 2.13), joint line tenderness (OR, 2.04), crepitus (or grating sounds or sensations; OR, 1.85), and Heberden’s nodes (OR, 1.67).
“Signs and symptoms can predict structural knee OA in 5 years in women without knee OA at baseline,” said the presenting study author Dieuwke Schiphof, Ph.D., a postdoctoral researcher at Erasmus University Medical Center in Rotterdam, at the meeting sponsored by the Osteoarthritis Research Society International.
“Knee pain on most days of the last month is an important predictive symptom for all structural OA definitions,” she said, adding that crepitus was an important sign of patellofemoral OA, and the feeling of giving way and joint line tenderness were important signs for tibiofemoral OA.
The aim of their study was to try to determine the value of previously identified clinical signs and symptoms for determining the onset of structural knee OA. Around 600 women aged 45-60 years without OA at baseline were included from the population-based cohort Rotterdam study. Participants had completed a standard questionnaire and had physical, radiographic, and MRI examination of both knees at baseline and at a mean follow-up of 5 years later.
The mean age of women was 59.5 years and 33 of 1,137 knees had isolated patellofemoral OA and 69 had isolated tibiofemoral OA, 111 one or the other, and 22 had radiographic knee OA.
Results showed that knee pain on most days of the last month (OR, 7.57) and crepitus (OR, 3.05) were most predictive of isolated patellofemoral OA on MRI. The prevalence of patellofemoral OA was 3% but this increased to 20% if both these signs and symptoms were present.
Knee pain on most days of the last month (OR, 4.13) was also predictive of isolated tibiofemoral OA on MRI, together with a history of knee pain (OR, 2.48), knee pain during activities (OR, 2.04), and the feeling of the knee giving way (OR, 3.15). If two or three or more signs and symptoms were present, the predictive value increased from a prevalence of 6% to 12% to 18%.
Knee pain on most days of the last month was also highly predictive of radiographic OA (OR, 7.77), as was pain at palpation (OR, 4.36), prior injury (OR, 3.64), and the feeling of the knee giving way (OR, 2.75). Again, when additional signs or symptoms were present the prevalence increased from a prevalence of 3% at follow-up to 4% with one, 8% with two, and up to 14% for three or more.
These signs and symptoms could potentially be used to help identify patients that may benefit from preventive treatment for knee OA, the researchers believe.
The study was funded by The Netherlands Organisation for Health Research and Development and Reumafonds, the Dutch Arthritis Association. Dr. Schiphof had no financial disclosures.
AMSTERDAM – Persistent knee pain is an important predictor of structural joint damage and could potentially be used to predict knee osteoarthritis (OA) earlier, according to Dutch research reported at the World Congress on Osteoarthritis.
The analysis found that women participating in the Rotterdam Study who had knee pain on most days of the preceding month were more than four times more likely to develop knee OA within 5 years on MRI (odds ratio, 4.53) than were those without frequent knee pain.
Other signs and symptoms predictive of later OA on MRI included a history of knee injury (OR, 2.52), pain on palpation (OR, 2.30) or during activity (OR, 2.13), the feeling of the knee giving way (OR, 2.13), joint line tenderness (OR, 2.04), crepitus (or grating sounds or sensations; OR, 1.85), and Heberden’s nodes (OR, 1.67).
“Signs and symptoms can predict structural knee OA in 5 years in women without knee OA at baseline,” said the presenting study author Dieuwke Schiphof, Ph.D., a postdoctoral researcher at Erasmus University Medical Center in Rotterdam, at the meeting sponsored by the Osteoarthritis Research Society International.
“Knee pain on most days of the last month is an important predictive symptom for all structural OA definitions,” she said, adding that crepitus was an important sign of patellofemoral OA, and the feeling of giving way and joint line tenderness were important signs for tibiofemoral OA.
The aim of their study was to try to determine the value of previously identified clinical signs and symptoms for determining the onset of structural knee OA. Around 600 women aged 45-60 years without OA at baseline were included from the population-based cohort Rotterdam study. Participants had completed a standard questionnaire and had physical, radiographic, and MRI examination of both knees at baseline and at a mean follow-up of 5 years later.
The mean age of women was 59.5 years and 33 of 1,137 knees had isolated patellofemoral OA and 69 had isolated tibiofemoral OA, 111 one or the other, and 22 had radiographic knee OA.
Results showed that knee pain on most days of the last month (OR, 7.57) and crepitus (OR, 3.05) were most predictive of isolated patellofemoral OA on MRI. The prevalence of patellofemoral OA was 3% but this increased to 20% if both these signs and symptoms were present.
Knee pain on most days of the last month (OR, 4.13) was also predictive of isolated tibiofemoral OA on MRI, together with a history of knee pain (OR, 2.48), knee pain during activities (OR, 2.04), and the feeling of the knee giving way (OR, 3.15). If two or three or more signs and symptoms were present, the predictive value increased from a prevalence of 6% to 12% to 18%.
Knee pain on most days of the last month was also highly predictive of radiographic OA (OR, 7.77), as was pain at palpation (OR, 4.36), prior injury (OR, 3.64), and the feeling of the knee giving way (OR, 2.75). Again, when additional signs or symptoms were present the prevalence increased from a prevalence of 3% at follow-up to 4% with one, 8% with two, and up to 14% for three or more.
These signs and symptoms could potentially be used to help identify patients that may benefit from preventive treatment for knee OA, the researchers believe.
The study was funded by The Netherlands Organisation for Health Research and Development and Reumafonds, the Dutch Arthritis Association. Dr. Schiphof had no financial disclosures.
AT OARSI 2016
Key clinical point: Several signs and symptoms could be used to help identify patients with osteoarthritis (OA) up to 5 years before joint damage occurs.
Major finding: Knee pain on most days of the last month was predictive of both MRI and radiographic knee damage.
Data source: 592 women from the Rotterdam Study without knee OA at baseline.
Disclosures: The study was funded by The Netherlands Organisation for Health Research and Development and Reumafonds, the Dutch Arthritis Association. Dr. Schiphof had no financial disclosures.
Onychomatricoma: A Rare Case of Unguioblastic Fibroma of the Fingernail Associated With Trauma
Onychomatricoma (OM) is a rare benign neoplasm of the nail matrix. Even less common is its possible association with both trauma to the nail apparatus and onychomycosis. This case illustrates both of these findings.
Case Report
A 72-year-old white man presented to the dermatology clinic with a 26-year history of a thickened nail plate on the right third finger that had developed soon after a baseball injury. The patient reported that the nail was completely normal prior to the trauma. According to the patient, the distal aspect of the finger was directly hit by a baseball and subsequently was wrapped by the patient for a few weeks. The nail then turned black and eventually fell off. When the nail grew back, it appeared abnormal and in its current state. The patient stated the lesion was asymptomatic at the time of presentation.

Physical examination revealed thickening, yellow discoloration, and transverse overcurvature of the nail plate on the right third finger with longitudinal ridging (Figure 1). A culture of the nail plate grew Chaetomium species. Application of topical clotrimazole for 3 months followed by a 6-week course of oral terbinafine produced no improvement. The patient then consented to a nail matrix incisional biopsy 6 months after initial presentation. After a digital nerve block was administered and a tourniquet of the proximal digit was applied, a nail avulsion was performed. Subsequently, a 3-mm punch biopsy was taken of the clinically apparent tumor in the nail matrix.
On microscopic examination of the removed tissue, a benign mixed epithelial and stromal proliferative lesion was noted. The basaloid epithelium, lacking a granular layer, arose from the surface epithelial layer and formed a reticulated pattern extending into the stromal component, which was moderately cellular with spindle to fusiform nuclei dissecting between collagen bundles arranged in parallel arrays (Figure 2). The stromal component predominated over the epithelial component in this neoplasm. The nail was preserved in formalin and underwent hematoxylin and eosin staining. It was thickened and grossly showed filiform fibrous projections extending into the nail plate. Histologically, the nail displayed prominent oval clear channels. Periodic acid–Schiff staining was negative for fungal organisms.
A diagnosis of unguioblastic fibroma–type OM was made. After receiving the diagnosis, expected course, and treatment options, the patient was offered conservative surgical excision but preferred clinical monitoring. At his last visit (6 months after the biopsy), the nail plate distal to the biopsy site had thinning and improvement, while the nail plate distal to the matrix that was not removed continued to show thickening, yellow discoloration, overcurvature, and longitudinal ridging (Figure 3).
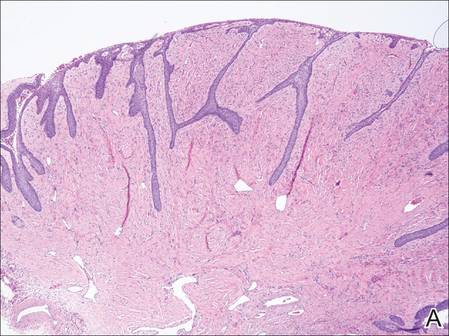
| 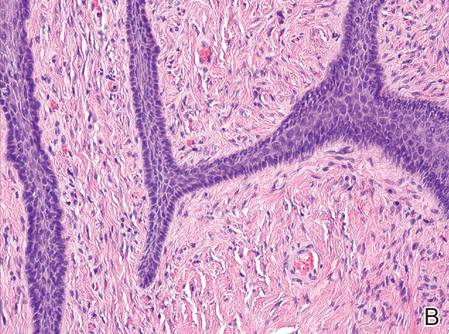
| |
Figure 2. The basaloid epithelium arose from the surface epithelial layer and formed a reticulated pattern extending into the stromal component (A)(H&E, original magnification ×2). At higher magnification, the stromal component was moderately cellular with spindle to fusiform nuclei dissecting between collagen bundles arranged in parallel arrays (B)(H&E, original magnification ×10). | ||
|
|

Comment
Onychomatricoma is a rare tumor originating from the nail matrix. The tumor was first described by Baran and Kint1 in 1992 using the term onychomatrixoma, but later the term onychomatricoma became more widely used.2 Onychomatricomas are more common in adults (mean age, 48 years) and white individuals with no gender predilection.3,4 Fingernail involvement is twice as common as toenail involvement.3 Onychomatricoma is the only tumor that actively produces a nail plate.4
Clinically, OM presents with yellow discoloration along the entire nail plate and proximal splinter hemorrhages. It has a tendency toward transverse overcurvature of the nail plate with prominent longitudinal ridging.4 Trauma has been associated in at least 3 cases reported in the literature, though the association was sometimes weak.3,4 Xanthonychia and onychodystrophy of the nail are common.3 Pterygium, melanonychia, nail bleeding, and cutaneous horns have been reported but are rare.3-5 The tumor typically is painless with no radiographic bone involvement.3 Onychomycosis can be present,3 which may either be a predisposing factor for the tumor or secondary due to the deformed nail plate.4
When the nail plate is avulsed and the proximal nail fold is turned back, the matrix tumor is exposed. This polypoid and filiform tumor has characteristic fingerlike fibrokeratogenous projections extending from the nail matrix into the nail plate.3
Histologically, the tumor is fibroepithelial or biphasic with stromal and epithelial components. It has a lobulated and papillary growth pattern with 2 distinct areas that correspond to 2 anatomic zones.3 The base of the tumor corresponds to the proximal anatomic zone, which begins at the root of the nail and extends to the cuticle. This area is composed of V-shaped keratinous zones similar to the normal matrix. If the nail is removed prior to excision, these areas can be avulsed, leaving clear clefts. The superficial aspect of the tumor corresponds to the distal anatomic zone, which is located in the region of the lunula. This area is composed of multiple digitate or fingerlike projections with a fibrous core and a thick matrical epithelial covering.3 These digitations extend into small cavities in the nail plate, which can be visualized as clear channels or woodwormlike holes in hematoxylin and eosin–stained specimens. A biphasic fibrous stroma also can be observed with the superficial dermis being cellular with fibrillary collagen and the deep dermis more hypocellular with thicker collagen bundles.3,4
An analysis of keratins in the nail matrix, bed, and isthmus showed that OM has the capacity to recapitulate the entire nail unit with differentiation toward the nail bed and isthmus.6 It appears that the mesenchymal component has an inductive effect that can lead to complete epithelial onychogenic differentiation.6
Due to the histological differences among the described cases of OM in the literature, a new classification based on the spectrum of epithelial to stromal ratio of stromal cellularity and the extent of nuclear pleomorphism was proposed in 2004.7 The prominent feature of the unguioblastoma type of OM is epithelial, while the cellular stroma is the prominent feature in the unguioblastic fibroma type. Atypical unguioblastic fibroma refers to a tumor with increased mitotic activity and nuclear pleomorphism among the stroma.7
Most OM tumors follow a benign clinical course; however, complete excision is advised to include the normal nail matrix proximal to the lesion, which may prevent recurrence and serves as a primary treatment.
Conclusion
Onychomatricoma is a benign neoplasm of the nail matrix that may be triggered by trauma; however, due to the weak association, further observations and studies should be conducted to substantiate this possibility. Patients with the classic clinical presentation possibly may be spared a nail avulsion and biopsy. Onychomycosis occurs in the setting of OM, and culture and treatment are unlikely to change the appearance or course of this nail condition.
1. Baran R, Kint A. Onychomatrixoma. filamentous tufted tumour in the matrix of a funnel-shaped nail: a new entity (report of three cases). Br J Dermatol. 1992;126:510-515.
2. Haneke E, Franken J. Onychomatricoma. Dermatol Surg. 1995;21:984-987.
3. Gaertner EM, Gordon M, Reed T. Onychomatricoma: case report of an unusual subungual tumor with literature review. J Cutan Pathol. 2009;36(suppl 1):66-69.
4. Cañueto J, Santos-Briz Á, García JL, et al. Onychomatricoma: genome-wide analyses of a rare nail matrix tumor. J Am Acad Dermatol. 2011;64:573-578.
5. Perrin C, Baran R. Onychomatricoma with dorsalpterygium: pathogenic mechanisms in 3 cases. J Am Acad Dermatol. 2008;59:990-994.
6. Perrin C, Langbein L, Schweizer J, et al. Onychomatricoma in the light of the microanatomy of the normal nail unit. Am J Dermatopathol. 2011;33:131-139.
7. Ko CJ, Shi L, Barr RJ, et al. Unguioblastoma and unguioblastic fibroma—an expanded spectrum of onychomatricoma. J Cutan Pathol. 2004;31:307-311.
Onychomatricoma (OM) is a rare benign neoplasm of the nail matrix. Even less common is its possible association with both trauma to the nail apparatus and onychomycosis. This case illustrates both of these findings.
Case Report
A 72-year-old white man presented to the dermatology clinic with a 26-year history of a thickened nail plate on the right third finger that had developed soon after a baseball injury. The patient reported that the nail was completely normal prior to the trauma. According to the patient, the distal aspect of the finger was directly hit by a baseball and subsequently was wrapped by the patient for a few weeks. The nail then turned black and eventually fell off. When the nail grew back, it appeared abnormal and in its current state. The patient stated the lesion was asymptomatic at the time of presentation.
Physical examination revealed thickening, yellow discoloration, and transverse overcurvature of the nail plate on the right third finger with longitudinal ridging (Figure 1). A culture of the nail plate grew Chaetomium species. Application of topical clotrimazole for 3 months followed by a 6-week course of oral terbinafine produced no improvement. The patient then consented to a nail matrix incisional biopsy 6 months after initial presentation. After a digital nerve block was administered and a tourniquet of the proximal digit was applied, a nail avulsion was performed. Subsequently, a 3-mm punch biopsy was taken of the clinically apparent tumor in the nail matrix.
On microscopic examination of the removed tissue, a benign mixed epithelial and stromal proliferative lesion was noted. The basaloid epithelium, lacking a granular layer, arose from the surface epithelial layer and formed a reticulated pattern extending into the stromal component, which was moderately cellular with spindle to fusiform nuclei dissecting between collagen bundles arranged in parallel arrays (Figure 2). The stromal component predominated over the epithelial component in this neoplasm. The nail was preserved in formalin and underwent hematoxylin and eosin staining. It was thickened and grossly showed filiform fibrous projections extending into the nail plate. Histologically, the nail displayed prominent oval clear channels. Periodic acid–Schiff staining was negative for fungal organisms.
A diagnosis of unguioblastic fibroma–type OM was made. After receiving the diagnosis, expected course, and treatment options, the patient was offered conservative surgical excision but preferred clinical monitoring. At his last visit (6 months after the biopsy), the nail plate distal to the biopsy site had thinning and improvement, while the nail plate distal to the matrix that was not removed continued to show thickening, yellow discoloration, overcurvature, and longitudinal ridging (Figure 3).
|
|
| |
Figure 2. The basaloid epithelium arose from the surface epithelial layer and formed a reticulated pattern extending into the stromal component (A)(H&E, original magnification ×2). At higher magnification, the stromal component was moderately cellular with spindle to fusiform nuclei dissecting between collagen bundles arranged in parallel arrays (B)(H&E, original magnification ×10). | ||
|
|
Comment
Onychomatricoma is a rare tumor originating from the nail matrix. The tumor was first described by Baran and Kint1 in 1992 using the term onychomatrixoma, but later the term onychomatricoma became more widely used.2 Onychomatricomas are more common in adults (mean age, 48 years) and white individuals with no gender predilection.3,4 Fingernail involvement is twice as common as toenail involvement.3 Onychomatricoma is the only tumor that actively produces a nail plate.4
Clinically, OM presents with yellow discoloration along the entire nail plate and proximal splinter hemorrhages. It has a tendency toward transverse overcurvature of the nail plate with prominent longitudinal ridging.4 Trauma has been associated in at least 3 cases reported in the literature, though the association was sometimes weak.3,4 Xanthonychia and onychodystrophy of the nail are common.3 Pterygium, melanonychia, nail bleeding, and cutaneous horns have been reported but are rare.3-5 The tumor typically is painless with no radiographic bone involvement.3 Onychomycosis can be present,3 which may either be a predisposing factor for the tumor or secondary due to the deformed nail plate.4
When the nail plate is avulsed and the proximal nail fold is turned back, the matrix tumor is exposed. This polypoid and filiform tumor has characteristic fingerlike fibrokeratogenous projections extending from the nail matrix into the nail plate.3
Histologically, the tumor is fibroepithelial or biphasic with stromal and epithelial components. It has a lobulated and papillary growth pattern with 2 distinct areas that correspond to 2 anatomic zones.3 The base of the tumor corresponds to the proximal anatomic zone, which begins at the root of the nail and extends to the cuticle. This area is composed of V-shaped keratinous zones similar to the normal matrix. If the nail is removed prior to excision, these areas can be avulsed, leaving clear clefts. The superficial aspect of the tumor corresponds to the distal anatomic zone, which is located in the region of the lunula. This area is composed of multiple digitate or fingerlike projections with a fibrous core and a thick matrical epithelial covering.3 These digitations extend into small cavities in the nail plate, which can be visualized as clear channels or woodwormlike holes in hematoxylin and eosin–stained specimens. A biphasic fibrous stroma also can be observed with the superficial dermis being cellular with fibrillary collagen and the deep dermis more hypocellular with thicker collagen bundles.3,4
An analysis of keratins in the nail matrix, bed, and isthmus showed that OM has the capacity to recapitulate the entire nail unit with differentiation toward the nail bed and isthmus.6 It appears that the mesenchymal component has an inductive effect that can lead to complete epithelial onychogenic differentiation.6
Due to the histological differences among the described cases of OM in the literature, a new classification based on the spectrum of epithelial to stromal ratio of stromal cellularity and the extent of nuclear pleomorphism was proposed in 2004.7 The prominent feature of the unguioblastoma type of OM is epithelial, while the cellular stroma is the prominent feature in the unguioblastic fibroma type. Atypical unguioblastic fibroma refers to a tumor with increased mitotic activity and nuclear pleomorphism among the stroma.7
Most OM tumors follow a benign clinical course; however, complete excision is advised to include the normal nail matrix proximal to the lesion, which may prevent recurrence and serves as a primary treatment.
Conclusion
Onychomatricoma is a benign neoplasm of the nail matrix that may be triggered by trauma; however, due to the weak association, further observations and studies should be conducted to substantiate this possibility. Patients with the classic clinical presentation possibly may be spared a nail avulsion and biopsy. Onychomycosis occurs in the setting of OM, and culture and treatment are unlikely to change the appearance or course of this nail condition.
Onychomatricoma (OM) is a rare benign neoplasm of the nail matrix. Even less common is its possible association with both trauma to the nail apparatus and onychomycosis. This case illustrates both of these findings.
Case Report
A 72-year-old white man presented to the dermatology clinic with a 26-year history of a thickened nail plate on the right third finger that had developed soon after a baseball injury. The patient reported that the nail was completely normal prior to the trauma. According to the patient, the distal aspect of the finger was directly hit by a baseball and subsequently was wrapped by the patient for a few weeks. The nail then turned black and eventually fell off. When the nail grew back, it appeared abnormal and in its current state. The patient stated the lesion was asymptomatic at the time of presentation.
Physical examination revealed thickening, yellow discoloration, and transverse overcurvature of the nail plate on the right third finger with longitudinal ridging (Figure 1). A culture of the nail plate grew Chaetomium species. Application of topical clotrimazole for 3 months followed by a 6-week course of oral terbinafine produced no improvement. The patient then consented to a nail matrix incisional biopsy 6 months after initial presentation. After a digital nerve block was administered and a tourniquet of the proximal digit was applied, a nail avulsion was performed. Subsequently, a 3-mm punch biopsy was taken of the clinically apparent tumor in the nail matrix.
On microscopic examination of the removed tissue, a benign mixed epithelial and stromal proliferative lesion was noted. The basaloid epithelium, lacking a granular layer, arose from the surface epithelial layer and formed a reticulated pattern extending into the stromal component, which was moderately cellular with spindle to fusiform nuclei dissecting between collagen bundles arranged in parallel arrays (Figure 2). The stromal component predominated over the epithelial component in this neoplasm. The nail was preserved in formalin and underwent hematoxylin and eosin staining. It was thickened and grossly showed filiform fibrous projections extending into the nail plate. Histologically, the nail displayed prominent oval clear channels. Periodic acid–Schiff staining was negative for fungal organisms.
A diagnosis of unguioblastic fibroma–type OM was made. After receiving the diagnosis, expected course, and treatment options, the patient was offered conservative surgical excision but preferred clinical monitoring. At his last visit (6 months after the biopsy), the nail plate distal to the biopsy site had thinning and improvement, while the nail plate distal to the matrix that was not removed continued to show thickening, yellow discoloration, overcurvature, and longitudinal ridging (Figure 3).
|
|
| |
Figure 2. The basaloid epithelium arose from the surface epithelial layer and formed a reticulated pattern extending into the stromal component (A)(H&E, original magnification ×2). At higher magnification, the stromal component was moderately cellular with spindle to fusiform nuclei dissecting between collagen bundles arranged in parallel arrays (B)(H&E, original magnification ×10). | ||
|
|
Comment
Onychomatricoma is a rare tumor originating from the nail matrix. The tumor was first described by Baran and Kint1 in 1992 using the term onychomatrixoma, but later the term onychomatricoma became more widely used.2 Onychomatricomas are more common in adults (mean age, 48 years) and white individuals with no gender predilection.3,4 Fingernail involvement is twice as common as toenail involvement.3 Onychomatricoma is the only tumor that actively produces a nail plate.4
Clinically, OM presents with yellow discoloration along the entire nail plate and proximal splinter hemorrhages. It has a tendency toward transverse overcurvature of the nail plate with prominent longitudinal ridging.4 Trauma has been associated in at least 3 cases reported in the literature, though the association was sometimes weak.3,4 Xanthonychia and onychodystrophy of the nail are common.3 Pterygium, melanonychia, nail bleeding, and cutaneous horns have been reported but are rare.3-5 The tumor typically is painless with no radiographic bone involvement.3 Onychomycosis can be present,3 which may either be a predisposing factor for the tumor or secondary due to the deformed nail plate.4
When the nail plate is avulsed and the proximal nail fold is turned back, the matrix tumor is exposed. This polypoid and filiform tumor has characteristic fingerlike fibrokeratogenous projections extending from the nail matrix into the nail plate.3
Histologically, the tumor is fibroepithelial or biphasic with stromal and epithelial components. It has a lobulated and papillary growth pattern with 2 distinct areas that correspond to 2 anatomic zones.3 The base of the tumor corresponds to the proximal anatomic zone, which begins at the root of the nail and extends to the cuticle. This area is composed of V-shaped keratinous zones similar to the normal matrix. If the nail is removed prior to excision, these areas can be avulsed, leaving clear clefts. The superficial aspect of the tumor corresponds to the distal anatomic zone, which is located in the region of the lunula. This area is composed of multiple digitate or fingerlike projections with a fibrous core and a thick matrical epithelial covering.3 These digitations extend into small cavities in the nail plate, which can be visualized as clear channels or woodwormlike holes in hematoxylin and eosin–stained specimens. A biphasic fibrous stroma also can be observed with the superficial dermis being cellular with fibrillary collagen and the deep dermis more hypocellular with thicker collagen bundles.3,4
An analysis of keratins in the nail matrix, bed, and isthmus showed that OM has the capacity to recapitulate the entire nail unit with differentiation toward the nail bed and isthmus.6 It appears that the mesenchymal component has an inductive effect that can lead to complete epithelial onychogenic differentiation.6
Due to the histological differences among the described cases of OM in the literature, a new classification based on the spectrum of epithelial to stromal ratio of stromal cellularity and the extent of nuclear pleomorphism was proposed in 2004.7 The prominent feature of the unguioblastoma type of OM is epithelial, while the cellular stroma is the prominent feature in the unguioblastic fibroma type. Atypical unguioblastic fibroma refers to a tumor with increased mitotic activity and nuclear pleomorphism among the stroma.7
Most OM tumors follow a benign clinical course; however, complete excision is advised to include the normal nail matrix proximal to the lesion, which may prevent recurrence and serves as a primary treatment.
Conclusion
Onychomatricoma is a benign neoplasm of the nail matrix that may be triggered by trauma; however, due to the weak association, further observations and studies should be conducted to substantiate this possibility. Patients with the classic clinical presentation possibly may be spared a nail avulsion and biopsy. Onychomycosis occurs in the setting of OM, and culture and treatment are unlikely to change the appearance or course of this nail condition.
1. Baran R, Kint A. Onychomatrixoma. filamentous tufted tumour in the matrix of a funnel-shaped nail: a new entity (report of three cases). Br J Dermatol. 1992;126:510-515.
2. Haneke E, Franken J. Onychomatricoma. Dermatol Surg. 1995;21:984-987.
3. Gaertner EM, Gordon M, Reed T. Onychomatricoma: case report of an unusual subungual tumor with literature review. J Cutan Pathol. 2009;36(suppl 1):66-69.
4. Cañueto J, Santos-Briz Á, García JL, et al. Onychomatricoma: genome-wide analyses of a rare nail matrix tumor. J Am Acad Dermatol. 2011;64:573-578.
5. Perrin C, Baran R. Onychomatricoma with dorsalpterygium: pathogenic mechanisms in 3 cases. J Am Acad Dermatol. 2008;59:990-994.
6. Perrin C, Langbein L, Schweizer J, et al. Onychomatricoma in the light of the microanatomy of the normal nail unit. Am J Dermatopathol. 2011;33:131-139.
7. Ko CJ, Shi L, Barr RJ, et al. Unguioblastoma and unguioblastic fibroma—an expanded spectrum of onychomatricoma. J Cutan Pathol. 2004;31:307-311.
1. Baran R, Kint A. Onychomatrixoma. filamentous tufted tumour in the matrix of a funnel-shaped nail: a new entity (report of three cases). Br J Dermatol. 1992;126:510-515.
2. Haneke E, Franken J. Onychomatricoma. Dermatol Surg. 1995;21:984-987.
3. Gaertner EM, Gordon M, Reed T. Onychomatricoma: case report of an unusual subungual tumor with literature review. J Cutan Pathol. 2009;36(suppl 1):66-69.
4. Cañueto J, Santos-Briz Á, García JL, et al. Onychomatricoma: genome-wide analyses of a rare nail matrix tumor. J Am Acad Dermatol. 2011;64:573-578.
5. Perrin C, Baran R. Onychomatricoma with dorsalpterygium: pathogenic mechanisms in 3 cases. J Am Acad Dermatol. 2008;59:990-994.
6. Perrin C, Langbein L, Schweizer J, et al. Onychomatricoma in the light of the microanatomy of the normal nail unit. Am J Dermatopathol. 2011;33:131-139.
7. Ko CJ, Shi L, Barr RJ, et al. Unguioblastoma and unguioblastic fibroma—an expanded spectrum of onychomatricoma. J Cutan Pathol. 2004;31:307-311.
Practice Points
- Onychomatricoma is a rare benign neoplasm of the nail matrix that actively produces a nail plate.
- Onychomatricoma should be in the differential diagnosis of a thickened discolored nail plate with transverse overcurvature.
- Onychomatricoma has been associated with onychomycosis and trauma to the nail apparatus.

Uterus transplant update: Fungal infection may have caused complication
The failure of the first U.S. uterus transplant may have been due a complication triggered by an infection of Candida, according to the Cleveland Clinic.
“Preliminary results suggest that the complication was due to an infection caused by an organism that is commonly found in a woman’s reproductive system,” officials at the Cleveland Clinic said in an April 8 statement. “The infection appears to have compromised the blood supply to the uterus, causing the need for its removal. There is an ongoing review of all the data and the team is modifying the protocol to reduce the chances of this complication occurring again in the future. The health of our patient is and has always been our primary concern.”
A team of surgeons at the Cleveland Clinic performed the first U.S. uterus transplant on a 26-year-old woman with uterine factor infertility on Feb. 24, but had to remove the transplanted uterus several days later following a sudden complication. The transplant is part of a study aimed at achieving pregnancy in women with uterine factor infertility. The study is still ongoing.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
The failure of the first U.S. uterus transplant may have been due a complication triggered by an infection of Candida, according to the Cleveland Clinic.
“Preliminary results suggest that the complication was due to an infection caused by an organism that is commonly found in a woman’s reproductive system,” officials at the Cleveland Clinic said in an April 8 statement. “The infection appears to have compromised the blood supply to the uterus, causing the need for its removal. There is an ongoing review of all the data and the team is modifying the protocol to reduce the chances of this complication occurring again in the future. The health of our patient is and has always been our primary concern.”
A team of surgeons at the Cleveland Clinic performed the first U.S. uterus transplant on a 26-year-old woman with uterine factor infertility on Feb. 24, but had to remove the transplanted uterus several days later following a sudden complication. The transplant is part of a study aimed at achieving pregnancy in women with uterine factor infertility. The study is still ongoing.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
The failure of the first U.S. uterus transplant may have been due a complication triggered by an infection of Candida, according to the Cleveland Clinic.
“Preliminary results suggest that the complication was due to an infection caused by an organism that is commonly found in a woman’s reproductive system,” officials at the Cleveland Clinic said in an April 8 statement. “The infection appears to have compromised the blood supply to the uterus, causing the need for its removal. There is an ongoing review of all the data and the team is modifying the protocol to reduce the chances of this complication occurring again in the future. The health of our patient is and has always been our primary concern.”
A team of surgeons at the Cleveland Clinic performed the first U.S. uterus transplant on a 26-year-old woman with uterine factor infertility on Feb. 24, but had to remove the transplanted uterus several days later following a sudden complication. The transplant is part of a study aimed at achieving pregnancy in women with uterine factor infertility. The study is still ongoing.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
VIDEO: More routine use of unilateral thyroidectomy advocated for papillary thyroid microcarcinoma
BOSTON – A study of over 60 years of patient data from the Mayo Clinic suggests a reconsideration of the routine use of unilateral thyroid lobectomy (UL) as the initial treatment for papillary thyroid microcarcinoma.
“Papillary thyroid microcarcinoma [PTM] patients have a normal life expectancy and typically are cured by adequate tumor resection. More than 99% of PTM patients are not at risk of either distant spread or mortality from cancer,” said Dr. Ian D. Hay of the Mayo Clinic, Rochester, Minn. Unilateral thyroid lobectomy is one treatment option for papillary thyroid microcarcinoma along with conventional bilateral nodal resection approaches of near-total thyroidectomy (NT) or total thyroidectomy (TT), or selective radioactive iodine remnant ablation (RRA).

Awareness of PTM is not new; examination of thyroid glands at autopsy going back decades has revealed their presence in 6%-36% of samples. A more recent development is the use of high-resolution ultrasound-guided biopsies of papillary thyroid carcinoma (PTC) lesions as small as 3 cm. For example, at the Mayo Clinic the diagnosis of PTM was about one annually from 1935 to 1944, while from 2005 to 2014 the average was close to one per day. “At Mayo, 34% of PTCs seen since 1995 are PTMs,” Dr. Hay said at the annual meeting of the Endocrine Society.
The best initial management of PTMs is disputed, with observation favored by some, TT and RRA favored by others, and ethanol ablation having been found to be effective by institutions including the Mayo Clinic. UL has been deemphasized, despite the 2015 American Thyroid Association Guidelines recommendation of UL as the usual surgical procedure for adults with PTM.
Dr. Hay and his colleagues sought to provide some clarity to the issue by taking advantage of the institute’s database of adult (18+ years) PTM patients who were consecutively treated from 1935 to 2014. The decades of data allowed a long-term look at patient outcomes. They examined data from 1,345 patients, 954 women and 391 men with a median age at surgery of 48 years. The mean follow-up was 15.4 years, representing almost 21,000 patient years. Data on tumor recurrence and cause-specific mortality were derived from a data base of over 4,300 PTC patients representing over 66,000 patient-years of observation.
Median tumor size was 7 mm (range, 0.08-1.0 cm). Extrathyroid invasion was evident in 18 (1.3%) cases and 298 tumors (26%) were multifocal. There were 399 (30%) node-positive tumors at diagnosis and 4 (0.3%) cases featuring initial distant metastases.
The mean MACIS (metastasis, age at presentation, completeness of surgical resection, invasion [extrathyroidal], size) score was 4.25 with little variation in score over time. Almost all (96%) patients had a MACIS score of under 6. Bilateral lobar resection was done in 1,132 (95%) patients, with NT or TT comprising 80% of the cases. UL was done in only 202 (15%) cases. The use of TT skyrocketed from 3% of the cases done in the first 2 decades to 40% in the last 2 decades. Regional nodes were removed at surgery in 743 (55%) cases, either by “node picking” (23%) or compartmental dissection (32%).
Overall survival following surgery in PTM patients was similar to age- and gender-matched controls (397 deaths observed, 431 deaths expected; P = .16). Only four (0.3%) patients died of PTM. The rates of locoregional recurrence were similar for the unilateral and bilateral approaches (P = .90). In 1,148 patients with potentially curable PTM, defined as the absence of metastasis at diagnosis and no gross residual disease, the rates of tumor recurrence 10, 20, and 40 years after surgery were 6%, 7%, and 10%, respectively. In these 1,148 patients, the 30-year locoregional recurrence rates after UL alone were similar to those seen after NT or TT followed by RRA (P = .99).
UL did not result in permanent unilateral vocal cord paresis or permanent hypoparathyroidism. These adversities were more likely to develop following bilateral lobectomy.
“Since [UL] produces comparable recurrence results when compared to bilateral surgery and is not associated with either cord paresis or hypoparathyroidism, then perhaps it is overdue for institutions like Mayo to individualize our treatment policies and more often employ UL when surgery, and not observation or ultrasound-guided percutaneous ethanol ablation, is chosen to treat PTM,” said Dr. Hay.
Dr. Hay was adamant on the overuse of ultrasound in the detection of small-diameter carcinomas in the decision for bilateral surgery. “It’s embarrassing how much we are wasting resources and doing too much ultrasound too often,” he said in an interview.
Dr. Hay had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
BOSTON – A study of over 60 years of patient data from the Mayo Clinic suggests a reconsideration of the routine use of unilateral thyroid lobectomy (UL) as the initial treatment for papillary thyroid microcarcinoma.
“Papillary thyroid microcarcinoma [PTM] patients have a normal life expectancy and typically are cured by adequate tumor resection. More than 99% of PTM patients are not at risk of either distant spread or mortality from cancer,” said Dr. Ian D. Hay of the Mayo Clinic, Rochester, Minn. Unilateral thyroid lobectomy is one treatment option for papillary thyroid microcarcinoma along with conventional bilateral nodal resection approaches of near-total thyroidectomy (NT) or total thyroidectomy (TT), or selective radioactive iodine remnant ablation (RRA).
Awareness of PTM is not new; examination of thyroid glands at autopsy going back decades has revealed their presence in 6%-36% of samples. A more recent development is the use of high-resolution ultrasound-guided biopsies of papillary thyroid carcinoma (PTC) lesions as small as 3 cm. For example, at the Mayo Clinic the diagnosis of PTM was about one annually from 1935 to 1944, while from 2005 to 2014 the average was close to one per day. “At Mayo, 34% of PTCs seen since 1995 are PTMs,” Dr. Hay said at the annual meeting of the Endocrine Society.
The best initial management of PTMs is disputed, with observation favored by some, TT and RRA favored by others, and ethanol ablation having been found to be effective by institutions including the Mayo Clinic. UL has been deemphasized, despite the 2015 American Thyroid Association Guidelines recommendation of UL as the usual surgical procedure for adults with PTM.
Dr. Hay and his colleagues sought to provide some clarity to the issue by taking advantage of the institute’s database of adult (18+ years) PTM patients who were consecutively treated from 1935 to 2014. The decades of data allowed a long-term look at patient outcomes. They examined data from 1,345 patients, 954 women and 391 men with a median age at surgery of 48 years. The mean follow-up was 15.4 years, representing almost 21,000 patient years. Data on tumor recurrence and cause-specific mortality were derived from a data base of over 4,300 PTC patients representing over 66,000 patient-years of observation.
Median tumor size was 7 mm (range, 0.08-1.0 cm). Extrathyroid invasion was evident in 18 (1.3%) cases and 298 tumors (26%) were multifocal. There were 399 (30%) node-positive tumors at diagnosis and 4 (0.3%) cases featuring initial distant metastases.
The mean MACIS (metastasis, age at presentation, completeness of surgical resection, invasion [extrathyroidal], size) score was 4.25 with little variation in score over time. Almost all (96%) patients had a MACIS score of under 6. Bilateral lobar resection was done in 1,132 (95%) patients, with NT or TT comprising 80% of the cases. UL was done in only 202 (15%) cases. The use of TT skyrocketed from 3% of the cases done in the first 2 decades to 40% in the last 2 decades. Regional nodes were removed at surgery in 743 (55%) cases, either by “node picking” (23%) or compartmental dissection (32%).
Overall survival following surgery in PTM patients was similar to age- and gender-matched controls (397 deaths observed, 431 deaths expected; P = .16). Only four (0.3%) patients died of PTM. The rates of locoregional recurrence were similar for the unilateral and bilateral approaches (P = .90). In 1,148 patients with potentially curable PTM, defined as the absence of metastasis at diagnosis and no gross residual disease, the rates of tumor recurrence 10, 20, and 40 years after surgery were 6%, 7%, and 10%, respectively. In these 1,148 patients, the 30-year locoregional recurrence rates after UL alone were similar to those seen after NT or TT followed by RRA (P = .99).
UL did not result in permanent unilateral vocal cord paresis or permanent hypoparathyroidism. These adversities were more likely to develop following bilateral lobectomy.
“Since [UL] produces comparable recurrence results when compared to bilateral surgery and is not associated with either cord paresis or hypoparathyroidism, then perhaps it is overdue for institutions like Mayo to individualize our treatment policies and more often employ UL when surgery, and not observation or ultrasound-guided percutaneous ethanol ablation, is chosen to treat PTM,” said Dr. Hay.
Dr. Hay was adamant on the overuse of ultrasound in the detection of small-diameter carcinomas in the decision for bilateral surgery. “It’s embarrassing how much we are wasting resources and doing too much ultrasound too often,” he said in an interview.
Dr. Hay had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
BOSTON – A study of over 60 years of patient data from the Mayo Clinic suggests a reconsideration of the routine use of unilateral thyroid lobectomy (UL) as the initial treatment for papillary thyroid microcarcinoma.
“Papillary thyroid microcarcinoma [PTM] patients have a normal life expectancy and typically are cured by adequate tumor resection. More than 99% of PTM patients are not at risk of either distant spread or mortality from cancer,” said Dr. Ian D. Hay of the Mayo Clinic, Rochester, Minn. Unilateral thyroid lobectomy is one treatment option for papillary thyroid microcarcinoma along with conventional bilateral nodal resection approaches of near-total thyroidectomy (NT) or total thyroidectomy (TT), or selective radioactive iodine remnant ablation (RRA).
Awareness of PTM is not new; examination of thyroid glands at autopsy going back decades has revealed their presence in 6%-36% of samples. A more recent development is the use of high-resolution ultrasound-guided biopsies of papillary thyroid carcinoma (PTC) lesions as small as 3 cm. For example, at the Mayo Clinic the diagnosis of PTM was about one annually from 1935 to 1944, while from 2005 to 2014 the average was close to one per day. “At Mayo, 34% of PTCs seen since 1995 are PTMs,” Dr. Hay said at the annual meeting of the Endocrine Society.
The best initial management of PTMs is disputed, with observation favored by some, TT and RRA favored by others, and ethanol ablation having been found to be effective by institutions including the Mayo Clinic. UL has been deemphasized, despite the 2015 American Thyroid Association Guidelines recommendation of UL as the usual surgical procedure for adults with PTM.
Dr. Hay and his colleagues sought to provide some clarity to the issue by taking advantage of the institute’s database of adult (18+ years) PTM patients who were consecutively treated from 1935 to 2014. The decades of data allowed a long-term look at patient outcomes. They examined data from 1,345 patients, 954 women and 391 men with a median age at surgery of 48 years. The mean follow-up was 15.4 years, representing almost 21,000 patient years. Data on tumor recurrence and cause-specific mortality were derived from a data base of over 4,300 PTC patients representing over 66,000 patient-years of observation.
Median tumor size was 7 mm (range, 0.08-1.0 cm). Extrathyroid invasion was evident in 18 (1.3%) cases and 298 tumors (26%) were multifocal. There were 399 (30%) node-positive tumors at diagnosis and 4 (0.3%) cases featuring initial distant metastases.
The mean MACIS (metastasis, age at presentation, completeness of surgical resection, invasion [extrathyroidal], size) score was 4.25 with little variation in score over time. Almost all (96%) patients had a MACIS score of under 6. Bilateral lobar resection was done in 1,132 (95%) patients, with NT or TT comprising 80% of the cases. UL was done in only 202 (15%) cases. The use of TT skyrocketed from 3% of the cases done in the first 2 decades to 40% in the last 2 decades. Regional nodes were removed at surgery in 743 (55%) cases, either by “node picking” (23%) or compartmental dissection (32%).
Overall survival following surgery in PTM patients was similar to age- and gender-matched controls (397 deaths observed, 431 deaths expected; P = .16). Only four (0.3%) patients died of PTM. The rates of locoregional recurrence were similar for the unilateral and bilateral approaches (P = .90). In 1,148 patients with potentially curable PTM, defined as the absence of metastasis at diagnosis and no gross residual disease, the rates of tumor recurrence 10, 20, and 40 years after surgery were 6%, 7%, and 10%, respectively. In these 1,148 patients, the 30-year locoregional recurrence rates after UL alone were similar to those seen after NT or TT followed by RRA (P = .99).
UL did not result in permanent unilateral vocal cord paresis or permanent hypoparathyroidism. These adversities were more likely to develop following bilateral lobectomy.
“Since [UL] produces comparable recurrence results when compared to bilateral surgery and is not associated with either cord paresis or hypoparathyroidism, then perhaps it is overdue for institutions like Mayo to individualize our treatment policies and more often employ UL when surgery, and not observation or ultrasound-guided percutaneous ethanol ablation, is chosen to treat PTM,” said Dr. Hay.
Dr. Hay was adamant on the overuse of ultrasound in the detection of small-diameter carcinomas in the decision for bilateral surgery. “It’s embarrassing how much we are wasting resources and doing too much ultrasound too often,” he said in an interview.
Dr. Hay had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT ENDO 2016
Key clinical point: Unilateral thryoidectomy should be reconsidered as a routine strategy in treatment of papillary thyroid microcarcinoma.
Major finding: Data compiled from over 80 years at a single institution indicates the value of unilateral thyroidectomy in terms of recurrence and morbidity.
Data source: Retrospective analysis of data from 1,153 adult patients.
Disclosures: Dr. Hay had no disclosures.

New vulvar cancer guidelines stress regional disease control
HOLLYWOOD, FLA. – The National Comprehensive Cancer Network has issued new guidelines for the diagnosis and management of vulvar cancer.
Vulvar cancers are rare neoplasms, with an estimated U.S. annual incidence of 5,950 cases, and 1,110 deaths. The majority of cases (about 90%) are of squamous cell histology.

Treatment of vulvar cancer has evolved from en bloc resections used throughout most of the 20th century, to more refined techniques, said Dr. Benjamin E. Greer, professor of gynecological oncology at the University of Washington in Seattle.
“In the 1980s, we started to modify treatment to reduce morbidity,” he said at the annual conference of the National Comprehensive Cancer Network.
With older, more radical techniques, groin breakdown, leg edema, and impaired sexual function were common post-surgery consequences. Current practice, however, is to perform regional lymph node management for unilateral cancers, radical local excision rather than en bloc resections, separate groin incisions, lymphatic mapping, radiation, chemotherapy, and, if necessary, exenteration, Dr. Greer noted.
The guidelines note that adequate surgical margins – 1 to 2 cm – at the time of primary surgery appear to be essential for reducing risk of local recurrence, and that if margins are within 8 mm of tumor, the surgeon should consider re-excision or adjuvant radiation.
Lymph node status is the most important determinant of survival, with historical reports showing overall survival following surgery of 70% to 80% among patients with negative nodes, compared with 30% to 40% of those with positive nodes, he said.
Evaluation of bilateral inguinofemoral groin nodes should be performed in patients with lesions in the vulvar midline, and ipsilateral groin node evaluation should be performed for those with lateral lesions lying more than 2 cm from the vulvar midline. Additionally, select patients may require sentinel lymph node biopsy, the guidelines state.
Unilateral carcinomas of the vulva can be treated with limited radical vulvectomy and ipsilateral inguinal femoral node dissection. Lymph node dissection can be performed through a separate incision. For patients with positive nodes, adjuvant radiation may aid in disease control. Patients with inoperable carcinomas are recommended to receive radiation and chemotherapy.
Radiation for vulvar cancer
“For early stage tumors, adjuvant radiotherapy is an effective treatment modality that significantly decreases recurrence, especially in surgically resected groins, and it leads to improvement in relapse-free and overall survival,” said Dr. Wui-Jin Koh, medical director for radiation oncology at the Fred Hutchinson Cancer Research Center in Seattle.
Concurrent chemotherapy and radiation may provide additional therapeutic benefit, especially for patients with advanced, unresectable tumors, and it may help to address systemic risk in patients with multiple positive lymph nodes, Dr. Koh said.

The guidelines state that radiation can be given with external beam radiation delivered via a 3D-conformal or intensity modulated (IMRT) technique, with brachytherapy boost for some tumors where the anatomy permits.
“Careful attention should be taken to ensure adequate tumor coverage by combining clinical examination, imaging findings, and appropriate nodal volumes at risk to define the target volume,” the guideline states.
For adjuvant therapy, doses of 50.4 Gy divided in 1.8 Gy fractions should be delivered once daily 5 days per week, with minimal treatment breaks.
For treatment of unresectable tumors, doses range from 59.4 Gy to 64.8 Gy in 1.8 Gy fractions, with a boost dose to approximately 70 Gy for large lymph nodes in select cases.
Residual disease
The decision to provide additional treatment following surgery is based on whether the patient is clinically negative for residual tumor at the primary site and nodes.
“If one has negative margins and negative nodes? Observation, absolutely,” Dr. Koh said. “If one has positive margins for invasive disease, our recommendation is to re-excise and not go straight to radiation, and if one can do it and get negative margins, again observe the majority of them.”
“Use radiation very judiciously,” he added. “Only if patients have positive margins or have unresectable primary disease do we routinely recommend radiation.”
Locally advanced disease
For patients who cannot be treated with conventional or sphincter-sparing, organ preserving surgery upfront, the recommendation is to provide chemoradiation, with initial radiation to the primary site, groins, and pelvis, and concurrent week cisplatin at a dose of 30-40 mg/m2 per week. The recommended radiation doses are 45 Gy to at-risk, microscopic clinical tumor volume, and 57.6 to 60 Gy to gross tumor volume (primary site and nodes).
“If one uses IMRT, you need to be very generous with the volumes,” Dr. Koh said.
The panelists also recommend re-imaging and re-evaluating patients 6 to 8 weeks after the completion of chemoradiation, with possible resection or biopsy of the primary tumor site, and limited groin resection of imaged residual disease.
For patients with clearly node-positive disease, “my general preference is to give upfront chemoradiation therapy to avoid delay of primary therapy, and then resect residual nodes after the chemoradiation is done,” he said.
HOLLYWOOD, FLA. – The National Comprehensive Cancer Network has issued new guidelines for the diagnosis and management of vulvar cancer.
Vulvar cancers are rare neoplasms, with an estimated U.S. annual incidence of 5,950 cases, and 1,110 deaths. The majority of cases (about 90%) are of squamous cell histology.
Treatment of vulvar cancer has evolved from en bloc resections used throughout most of the 20th century, to more refined techniques, said Dr. Benjamin E. Greer, professor of gynecological oncology at the University of Washington in Seattle.
“In the 1980s, we started to modify treatment to reduce morbidity,” he said at the annual conference of the National Comprehensive Cancer Network.
With older, more radical techniques, groin breakdown, leg edema, and impaired sexual function were common post-surgery consequences. Current practice, however, is to perform regional lymph node management for unilateral cancers, radical local excision rather than en bloc resections, separate groin incisions, lymphatic mapping, radiation, chemotherapy, and, if necessary, exenteration, Dr. Greer noted.
The guidelines note that adequate surgical margins – 1 to 2 cm – at the time of primary surgery appear to be essential for reducing risk of local recurrence, and that if margins are within 8 mm of tumor, the surgeon should consider re-excision or adjuvant radiation.
Lymph node status is the most important determinant of survival, with historical reports showing overall survival following surgery of 70% to 80% among patients with negative nodes, compared with 30% to 40% of those with positive nodes, he said.
Evaluation of bilateral inguinofemoral groin nodes should be performed in patients with lesions in the vulvar midline, and ipsilateral groin node evaluation should be performed for those with lateral lesions lying more than 2 cm from the vulvar midline. Additionally, select patients may require sentinel lymph node biopsy, the guidelines state.
Unilateral carcinomas of the vulva can be treated with limited radical vulvectomy and ipsilateral inguinal femoral node dissection. Lymph node dissection can be performed through a separate incision. For patients with positive nodes, adjuvant radiation may aid in disease control. Patients with inoperable carcinomas are recommended to receive radiation and chemotherapy.
Radiation for vulvar cancer
“For early stage tumors, adjuvant radiotherapy is an effective treatment modality that significantly decreases recurrence, especially in surgically resected groins, and it leads to improvement in relapse-free and overall survival,” said Dr. Wui-Jin Koh, medical director for radiation oncology at the Fred Hutchinson Cancer Research Center in Seattle.
Concurrent chemotherapy and radiation may provide additional therapeutic benefit, especially for patients with advanced, unresectable tumors, and it may help to address systemic risk in patients with multiple positive lymph nodes, Dr. Koh said.
The guidelines state that radiation can be given with external beam radiation delivered via a 3D-conformal or intensity modulated (IMRT) technique, with brachytherapy boost for some tumors where the anatomy permits.
“Careful attention should be taken to ensure adequate tumor coverage by combining clinical examination, imaging findings, and appropriate nodal volumes at risk to define the target volume,” the guideline states.
For adjuvant therapy, doses of 50.4 Gy divided in 1.8 Gy fractions should be delivered once daily 5 days per week, with minimal treatment breaks.
For treatment of unresectable tumors, doses range from 59.4 Gy to 64.8 Gy in 1.8 Gy fractions, with a boost dose to approximately 70 Gy for large lymph nodes in select cases.
Residual disease
The decision to provide additional treatment following surgery is based on whether the patient is clinically negative for residual tumor at the primary site and nodes.
“If one has negative margins and negative nodes? Observation, absolutely,” Dr. Koh said. “If one has positive margins for invasive disease, our recommendation is to re-excise and not go straight to radiation, and if one can do it and get negative margins, again observe the majority of them.”
“Use radiation very judiciously,” he added. “Only if patients have positive margins or have unresectable primary disease do we routinely recommend radiation.”
Locally advanced disease
For patients who cannot be treated with conventional or sphincter-sparing, organ preserving surgery upfront, the recommendation is to provide chemoradiation, with initial radiation to the primary site, groins, and pelvis, and concurrent week cisplatin at a dose of 30-40 mg/m2 per week. The recommended radiation doses are 45 Gy to at-risk, microscopic clinical tumor volume, and 57.6 to 60 Gy to gross tumor volume (primary site and nodes).
“If one uses IMRT, you need to be very generous with the volumes,” Dr. Koh said.
The panelists also recommend re-imaging and re-evaluating patients 6 to 8 weeks after the completion of chemoradiation, with possible resection or biopsy of the primary tumor site, and limited groin resection of imaged residual disease.
For patients with clearly node-positive disease, “my general preference is to give upfront chemoradiation therapy to avoid delay of primary therapy, and then resect residual nodes after the chemoradiation is done,” he said.
HOLLYWOOD, FLA. – The National Comprehensive Cancer Network has issued new guidelines for the diagnosis and management of vulvar cancer.
Vulvar cancers are rare neoplasms, with an estimated U.S. annual incidence of 5,950 cases, and 1,110 deaths. The majority of cases (about 90%) are of squamous cell histology.
Treatment of vulvar cancer has evolved from en bloc resections used throughout most of the 20th century, to more refined techniques, said Dr. Benjamin E. Greer, professor of gynecological oncology at the University of Washington in Seattle.
“In the 1980s, we started to modify treatment to reduce morbidity,” he said at the annual conference of the National Comprehensive Cancer Network.
With older, more radical techniques, groin breakdown, leg edema, and impaired sexual function were common post-surgery consequences. Current practice, however, is to perform regional lymph node management for unilateral cancers, radical local excision rather than en bloc resections, separate groin incisions, lymphatic mapping, radiation, chemotherapy, and, if necessary, exenteration, Dr. Greer noted.
The guidelines note that adequate surgical margins – 1 to 2 cm – at the time of primary surgery appear to be essential for reducing risk of local recurrence, and that if margins are within 8 mm of tumor, the surgeon should consider re-excision or adjuvant radiation.
Lymph node status is the most important determinant of survival, with historical reports showing overall survival following surgery of 70% to 80% among patients with negative nodes, compared with 30% to 40% of those with positive nodes, he said.
Evaluation of bilateral inguinofemoral groin nodes should be performed in patients with lesions in the vulvar midline, and ipsilateral groin node evaluation should be performed for those with lateral lesions lying more than 2 cm from the vulvar midline. Additionally, select patients may require sentinel lymph node biopsy, the guidelines state.
Unilateral carcinomas of the vulva can be treated with limited radical vulvectomy and ipsilateral inguinal femoral node dissection. Lymph node dissection can be performed through a separate incision. For patients with positive nodes, adjuvant radiation may aid in disease control. Patients with inoperable carcinomas are recommended to receive radiation and chemotherapy.
Radiation for vulvar cancer
“For early stage tumors, adjuvant radiotherapy is an effective treatment modality that significantly decreases recurrence, especially in surgically resected groins, and it leads to improvement in relapse-free and overall survival,” said Dr. Wui-Jin Koh, medical director for radiation oncology at the Fred Hutchinson Cancer Research Center in Seattle.
Concurrent chemotherapy and radiation may provide additional therapeutic benefit, especially for patients with advanced, unresectable tumors, and it may help to address systemic risk in patients with multiple positive lymph nodes, Dr. Koh said.
The guidelines state that radiation can be given with external beam radiation delivered via a 3D-conformal or intensity modulated (IMRT) technique, with brachytherapy boost for some tumors where the anatomy permits.
“Careful attention should be taken to ensure adequate tumor coverage by combining clinical examination, imaging findings, and appropriate nodal volumes at risk to define the target volume,” the guideline states.
For adjuvant therapy, doses of 50.4 Gy divided in 1.8 Gy fractions should be delivered once daily 5 days per week, with minimal treatment breaks.
For treatment of unresectable tumors, doses range from 59.4 Gy to 64.8 Gy in 1.8 Gy fractions, with a boost dose to approximately 70 Gy for large lymph nodes in select cases.
Residual disease
The decision to provide additional treatment following surgery is based on whether the patient is clinically negative for residual tumor at the primary site and nodes.
“If one has negative margins and negative nodes? Observation, absolutely,” Dr. Koh said. “If one has positive margins for invasive disease, our recommendation is to re-excise and not go straight to radiation, and if one can do it and get negative margins, again observe the majority of them.”
“Use radiation very judiciously,” he added. “Only if patients have positive margins or have unresectable primary disease do we routinely recommend radiation.”
Locally advanced disease
For patients who cannot be treated with conventional or sphincter-sparing, organ preserving surgery upfront, the recommendation is to provide chemoradiation, with initial radiation to the primary site, groins, and pelvis, and concurrent week cisplatin at a dose of 30-40 mg/m2 per week. The recommended radiation doses are 45 Gy to at-risk, microscopic clinical tumor volume, and 57.6 to 60 Gy to gross tumor volume (primary site and nodes).
“If one uses IMRT, you need to be very generous with the volumes,” Dr. Koh said.
The panelists also recommend re-imaging and re-evaluating patients 6 to 8 weeks after the completion of chemoradiation, with possible resection or biopsy of the primary tumor site, and limited groin resection of imaged residual disease.
For patients with clearly node-positive disease, “my general preference is to give upfront chemoradiation therapy to avoid delay of primary therapy, and then resect residual nodes after the chemoradiation is done,” he said.
AT THE NCCN ANNUAL CONFERENCE
Key clinical point: Nodal status is an important determinant of survival of patients with vulvar carcinomas.
Major finding: Historically, reported overall survival following surgery is 70% to 80% among patients with negative nodes, compared with 30% to 40% of those with positive nodes.
Data source: Review of new clinical guidelines for the management of patients with vulvar cancer.
Disclosures: Dr. Greer and Dr. Koh reported having no relevant clinical disclosures.
