User login
Clinical Characteristics and HLA Alleles of a Family With Simultaneously Occurring Alopecia Areata
Alopecia areata (AA) presents as sudden, nonscarring, recurrent hair loss characterized by well-circumscribed hairless patches. Although AA may be observed on any hair-bearing areas of the body, the most commonly affected sites are the scalp, beard area, eyebrows, and eyelashes.1 The incidence of AA is 1% to 2% in the general population and it is more common in males than females younger than 40 years.2 Although the majority of patients present with self-limited and well-circumscribed hairless patches that resolve within 2 years, 7% to 10% display a chronic and severe prognosis.3
The etiopathogenesis of AA is not clearly understood, but its occurrence and progression can involve immune dysfunction, genetic predisposition, infections, and physical and psychological trauma.2 Alopecia areata is observed to occur sporadically in most patients. Family history has been found in 3% to 42% of cases, but simultaneous occurrence of AA in family members is rare.4 In this case series, we present 4 cases of active AA lesions occurring simultaneously in a family who also had associated psychologic disorders.
Case Series
Patient 1 (Proband)
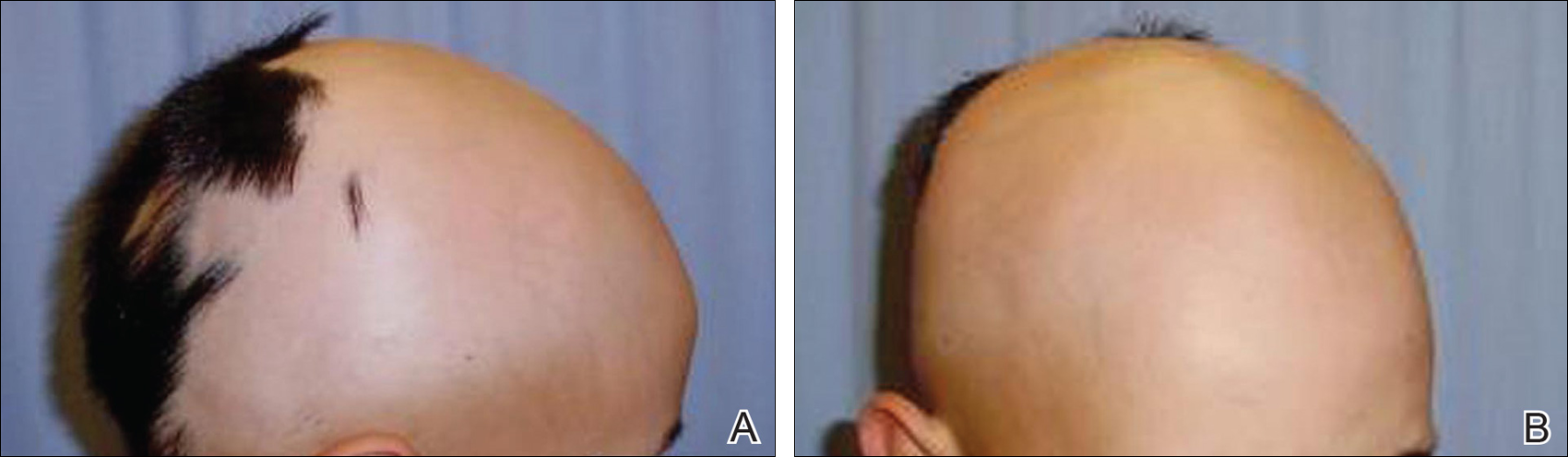
An 11-year-old boy presented with a 6-year history of ongoing AA with recurrent improvement and relapses on the scalp, eyebrows, and eyelashes. Various topical and oral medications had been prescribed by several outside dermatologists; however, these treatments provided minimal benefit and resulted in the recurrence of AA. Dermatologic examination revealed hair loss on the entire frontal, parietal, and temporal regions of the scalp, as well as half of the occipital region and one-third of the lateral side of the eyebrows (Figure 1). Psychological evaluation revealed introvert personality characteristics, lack of self-confidence, and signs of depression and anxiety.
Patient 2 (Proband’s Father)
A 38-year-old man presented with a 16-year history of recurrent loss and regrowth of hair on the scalp and beard area and white spots on the penis and arms. He previously had not undergone any treatments. Dermatologic examination revealed well-circumscribed, 1- to 4-cm, hairless patches on the occipital region of the scalp and in the beard area (Figure 2A) and multiple, 2- to 10-mm, vitiliginous lesions on both forearms (Figure 2B) and the penis. The patient had been unemployed for 6 months. Psychological evaluation revealed obsessive-compulsive disorder and obsessive-compulsive personality disorder.

Patient 3 (Proband’s Mother)
A 32-year-old woman presented with a 3-year history of chronic AA. She previously had not undergone any treatments. Dermatologic examination revealed 2 well-circumscribed, 3- to 4-cm patches of hair loss on the occipital and left temporal regions of the scalp (Figure 3). Psychological evaluation revealed obsessive-compulsive personality disorder and depression. The patient did not have any autoimmune diseases.

Patient 4 (Proband’s Sister)
A 10-year-old girl presented with a 6-year history of recurrent, self-limited AA on various areas of scalp. She previously had not undergone any treatments. Dermatologic examination revealed a 3-cm hairless patch on the occipital region of the scalp (Figure 4). Psychiatric evaluation revealed narcissistic personality disorder, anxiety, and lack of self-confidence.

Laboratory Evaluation and HLA Antigen DNA Typing
Laboratory testing including complete blood cell count; liver, kidney, and thyroid function; and vitamin B12, zinc, folic acid, and fasting blood sugar levels were performed in all patients.
HLA antigen DNA typing was performed by polymerase chain reaction with sequence-specific primers in all patients after informed consent was obtained.
Clinical and laboratory examinations revealed no symptoms or findings of Epstein-Barr virus and cytomegalovirus infections, cicatricial alopecia, or connective tissue diseases in any of the patients. HLA antigen DNA typing revealed the following HLA alleles: B*35/40, C*04/15, DRB1*08/10, and DQB1*03/05 in patient 1; B*04/13, C*06/15, DRB1*07/10, and DQB1*02/05 in patient 2; B*33/37, C*04/06, DRB1*08/15, and DQ*06/06 in patient 3; B*13/37, C*06/06, DRB1*07/15, and DQB1*02/06 in patient 4.
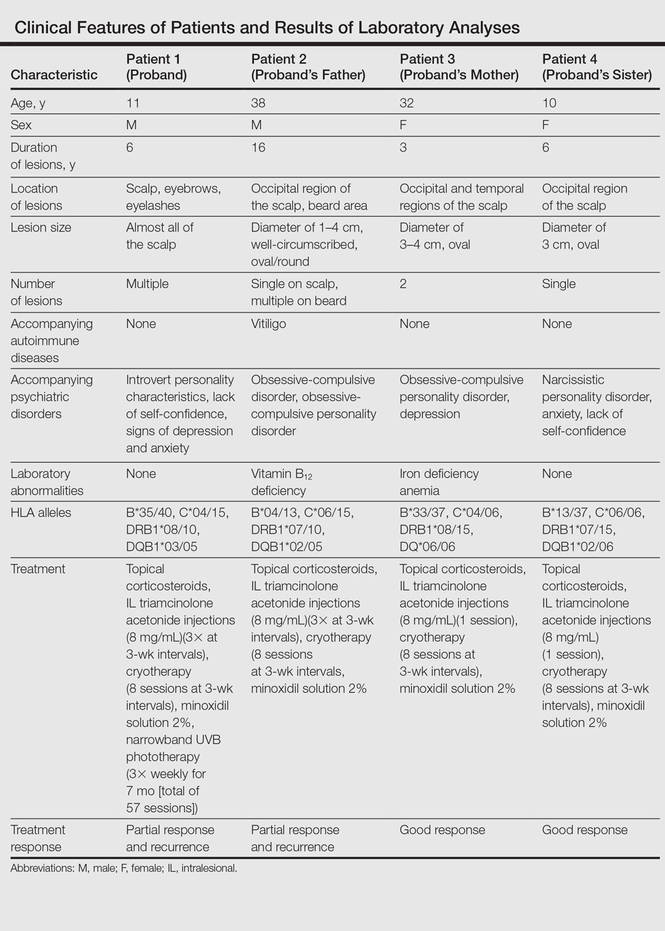
Laboratory testing revealed vitamin B12 deficiency in patient 2 and iron deficiency anemia in patient 3; all other laboratory tests were within reference range. Antithyroglobulin and antithyroid peroxidase autoantibodies were all negative. Clinical features and laboratory analyses for all patients are summarized in the Table.
Treatment
All patients were recommended psychiatric therapy and started on dermatologic treatments. Topical corticosteroids, intralesional triamcinolone acetonide (8 mg/mL) injections into areas of hair loss, 8 total sessions of cryotherapy administered at 3-week intervals, and minoxidil solution 2% were administered respectively to all 4 patients. Alopecia areata in patients 3 and 4 completely regressed; however, no benefit was observed in patients 1 and 2 after 1 year of treatment. Because there was no response to the prior interventions, patient 1 was started on treatment with cyclosporine 2.5 mg/kg twice daily. However, therapy was discontinued after 1 month and treatment with narrowband UVB (3 times per week for 7 months [total of 57 sessions]) and topical corticosteroids were initiated (Table). The patient partially benefited from these regimens and recurrence was observed during the course of the treatment.
Although it was recommended that all 4 patients undergo psychiatric treatment and follow-up regularly with a psychiatrist, the patients declined. After approximately 1 year of dermatologic treatment, all 4 patients were lost to follow-up.
Comment
The etiopathogenesis of AA is unclear, but there is strong evidence suggesting that it is a T-cell–mediated autoimmune disease targeting the hair follicles. Common association of AA with autoimmune diseases such as vitiligo and thyroiditis support the immunological origin of the disease.3 In our case, patient 2 had AA along with vitiligo, but no associated autoimmune diseases (eg, vitiligo, diabetes mellitus, pernicious anemia, thyroid diseases) were noted in the other patients. Genetic and environmental factors are known to be influential as much as immune dysfunction in the etiology of AA.2
The presence of family history in 20% of patients supports the genetic predisposition of AA.4 In a genetic study by Martinez-Mir et al,5 susceptibility loci for AA were demonstrated on chromosomes 6, 10, 16, and 18. HLA antigen alleles, which provide predisposition to AA, have been investigated and associations with many different HLA antigens have been described for AA. In these studies, a relationship between AA and HLA class I antigens was not determined. Notable results mainly focused on HLA class II antigens.6-8 Colombe et al7 and Marques Da Costa et al8 demonstrated that long-lasting alopecia totalis or alopecia universalis (AT/AU) patients had a strong relationship with HLA-DRB1*1104; DRB1*04/05 was reported to be the most frequent HLA group among all patients with AA.6-10 In contrast, we did not detect these alleles in our patients. Colombe et al7,11 noted that HLA-DQB1*03 is a marker for both patch-type AA and AT/AU. Colombe et al10 showed that HLA-DQB1*03 was present in more than 80% of patients (N=286) with long-lasting AA. Barahmani et al9 confirmed a strong association between HLA-DQB1*0301, DRB1*1104, and AT/AU. In our patients, we detected HLA-DQB1*03/05 in patient 1 who had the earliest onset and most severe presentation of AA. In some studies, HLA-DRB1*03 was found to be less frequent in patients with AA, and this allele was suggested to be a protective factor.6,12 However, this allele was not detected in any of our patients.
The association of HLA alleles and AA has been investigated in Turkish patients with AA.13-15 Akar et al13 and Kavak et al14 detected that the frequency of HLA-DQB1*03 allele was remarkably higher in patients with AA than in healthy controls. These results were consistent with Colombe et al.10 On the other hand, Kavak et al14 reported that the frequency of HLA-DR16 was decreased in the patient group with AA. In another study, the frequency of HLA-B62 was increased in patients with AA compared to healthy controls.15 The HLA-DQB1*03 allele was found to be associated with AA in only patient 1 in our case series, and HLA alleles were not commonly shared among the 4 patients. Additionally, lack of consanguinity between patients 2 and 3 (the parents) also suggested that genetic factors were not involved in our familial cases.
Blaumeiser et al16 reported a lifetime risk of 7.4% in parents and 7.1% in siblings of 206 AA patients; however, because these studies investigated the presence of AA in any given life period of the family members, their results do not reflect frequency of simultaneous AA presence within one family. In a literature search using PubMed, Google Scholar, and other national databases for the terms alopecia areata as well as family, sibling, concurrently, concomitant, co-existent, and simultaneously, only 2 cases involving a husband and wife and 1 case of 2 siblings who concurrently had AA have been previously reported.17,18 Simultaneous presence of AA in more than 3 members of the same family is rare, and these cases have been observed in different generations and time periods.19 Among our patients, despite different age of onset and duration, AA was simultaneously present in the entire family.
Moreover, Rodriguez et al20 reported that the concordance rate of AA in identical twins was 42% and dizygotic twins was 10%. Environmental factors and infections also have been implicated in the etiology of AA. Infections caused by viruses such as cytomegalovirus and Epstein-Barr virus have been thought to be potential triggering factors; however, no evidence has been found.21,22 The clinical and laboratory examinations in our study did not reveal any presence and/or history of any known infectious disease, and there was no history of contact with water infected by acrylamide or a similar chemical.
Various life events and intense psychological stress may play an important role in triggering AA. Depression, hysteria, psychopathic deviance, psychasthenia, schizophrenia, anxiety, health concerns, bizarre thoughts, and family problems were found to be more frequent in patients with AA than healthy controls.23 The most common psychological disorders associated with AA are generalized anxiety disorder, major depressive disorder, adjustment disorders, and phobias.1,24 Ruiz-Doblado et al25 determined the presence of psychiatric comorbidities in 66% (21/32) of AA cases. Chu et al26 reported that the differences in ages of onset of AA revealed differences in psychiatric comorbidities. The risk for depression was higher in patients with AA younger than 20 years. An increased rate of anxiety was detected with patients with an onset of AA between the ages of 20 and 39 years. Obsessive-compulsive disorder and anxiety were more common in patients aged 40 to 59 years. Interestingly, the investigators also observed that approximately 50% of psychiatric disorders occurred prior to onset of AA.26 One study showed higher rates of stressful life events in children than in controls.27 Ghanizadeh24 reported at least 1 psychiatric disorder in 78% (11/14) of children and adolescents with AA. In the same study, obsessive-compulsive disorder was found to be the second common condition following major depression in AA.24
In our patients, psychiatric evaluations revealed obsessive-compulsive personality disorder in patients 2 and 3, depression in patient 3, and symptoms of anxiety with a lack of self-confidence in patients 1 and 4. Psychiatric disorders affecting the entire family may stem from unemployment of the father. Similar to the results noted in prior studies, depression, the most commonly associated psychiatric disorder of AA, was present in 2 of 4 patients. Obsessive-compulsive disorder, the second most common psychiatric disorder among AA patients, was present in patients 2 and 3. These results indicate that AA may be associated with shared stressful events and psychiatric disorders. Therefore, in addition to dermatologic treatment, it was recommended that all patients undergo psychiatric treatment and follow-up regularly with a psychiatrist; however, the patients declined. At the end of a 1-year treatment period and follow-up, resistance to therapy with minimal recovery followed by a rapid recurrence was determined in patients 1 and 2.
Conclusion
This report demonstrated that familial AA was strongly associated with psychological disorders that were detected in all patients. In our patients, HLA alleles did not seem to have a role in the development of familial AA. These results suggest that HLA was not associated with AA triggered by psychological stress. We believe that psychological disorders and stressful life events may play an important role in the occurrence of AA and lead to the development of resistance against treatment in familial and resistant AA cases.
- García-Hernández MJ, Ruiz-Doblado S, Rodriguez-Pichardo A, et al. Alopecia areata, stress and psychiatric disorders: a review. J Dermatol. 1999;26:625-632.
- Bhat YJ, Manzoor S, Khan AR, et al. Trace element levels in alopecia areata. Indian J Dermatol Venereol Leprol. 2009;75:29-31.
- Alexis AF, Dudda-Subramanya R, Sinha AA. Alopecia areata: autoimmune basis of hair loss. Eur J Dermatol. 2004;14:364-370.
- Green J, Sinclair RD. Genetics of alopecia areata. Australas J Dermatol. 2000;41:213-218.
- Martinez-Mir A, Zlotogorski A, Gordon D, et al.Genomewide scan for linkage reveals evidence of several susceptibility loci for alopecia areata. Am J Hum Genet. 2007;80:316-328.
- Entz P, Blaumeiser B, Betz RC, et al. Investigation of the HLA-DRB1 locus in alopecia areata. Eur J Dermatol. 2006;16:363-367.
- Colombe BW, Price VH, Khoury EL, et al. HLA class II alleles in long-standing alopecia totalis/alopecia universalis and long-standing patchy alopecia areata differentiate these two clinical groups. J Invest Dermatol. 1995;104(suppl 5):4-5.
- Marques Da Costa C, Dupont E, Van der Cruys M, et al. Earlier occurrence of severe alopecia areata in HLA-DRB1*11-positive patients. Dermatology. 2006;213:12-14.
- Barahmani N, de Andrade M, Slusser JP, et al. Human leukocyte antigen class II alleles are associated with risk of alopecia areata. J Invest Dermatol. 2008;128:240-243.
- Colombe BW, Lou CD, Price VH. The genetic basis of alopecia areata: HLA associations with patchy alopecia areata versus alopecia totalis and alopecia universalis. J Investig Dermatol Symp Proc. 1999;4:216-219.
- Colombe BW, Price VH, Khoury EL, et al. HLA class II antigen associations help to define two types of alopecia areata. J Am Acad Dermatol. 1995;33(5, pt 1):757-764.
- Broniarczyk-Dyła G, Prusińska-Bratoś M, Dubla-Berner M, et al. The protective role of the HLA-DR locus in patients with various clinical types of alopecia areata. Arch Immunol Ther Exp (Warsz). 2002;50:333-336.
- Akar A, Orkunuglu E, Sengul A, et al. HLA class II alleles in patients with alopecia areata. Eur J Dermatol. 2002;12:236-239.
- Kavak A, Baykal C, Ozarmagan G, et al. HLA in alopecia areata. Int J Dermatol. 2000;30:589-592.
- Aliagaoglu C, Pirim I, Atasoy M, et al. Association between alopecia areata and HLA class I and II in Turkey. J Dermatol. 2005;32:711-714.
- Blaumeiser B, Goot I, Fimmers R, et al. Familial aggregation of alopecia areata. J Am Acad Dermatol. 2006;54:627-632.
- Zalka AD, Byarlay JA, Goldsmith LA. Alopecia a deux: simultaneous occurrence of alopecia in a husband and wife. Arch Dermatol. 1994;130:390-392.
- Menon R, Kiran C. Concomitant presentation of alopecia areata in siblings: a rare occurrence. Int J Trichology. 2012;4:86-88.
- Valsecchi R, Vicari O, Frigeni A, et al. Familial alopecia areata-genetic susceptibility or coincidence? Acta Derm Venereol (Stockh). 1985;65:175-177.
- Rodriguez TA, Fernandes KE, Dresser KL, et al. Concordance rate of alopecia areata in identical twins supports both genetic and environmental factors. J Am Acad Dermatol. 2010;62:525-527.
- Rodriguez TA, Duvic M. Onset of alopecia areata after Epstein Barr virus infectious mononucleosis. J Am Acad Dermatol. 2008;59:137-139.
- Offidani A, Amerio P, Bernardini ML, et al. Role of cytomegalovirus replication in alopecia areata pathogenesis. J Cutan Med Surg. 2000;4:63-65.
- Alfani S, Antinone V, Mozzetta A, et al. Psychological status of patients with alopecia areata. Acta Derm Venereol. 2012;92:304-306.
- Ghanizadeh A. Comorbidity of psychiatric disorders in children and adolescents with alopecia areata in a child and adolescent psychiatry clinical sample. Int J Dermatol. 2008;47:1118-1120.
- Ruiz-Doblado S, Carrizosa A, Garcia-Hernandez MJ. Alopecia areata: psychiatric comorbidity and adjustment to illness. Int J Dermatol. 2003;42:434-437.
- Chu SY, Chen YJ, Tseng WC, et al. Psychiatric comorbidities in patients with alopecia areata in Taiwan: a case-control study. Br J Dermatol. 2012;166:525-531.
- Manolache L, Petrescu-Seceleanu D, Benea V. Alopecia areata and stressful events in children. J Eur Acad Dermatol Venereol. 2009;23:107-109.
Alopecia areata (AA) presents as sudden, nonscarring, recurrent hair loss characterized by well-circumscribed hairless patches. Although AA may be observed on any hair-bearing areas of the body, the most commonly affected sites are the scalp, beard area, eyebrows, and eyelashes.1 The incidence of AA is 1% to 2% in the general population and it is more common in males than females younger than 40 years.2 Although the majority of patients present with self-limited and well-circumscribed hairless patches that resolve within 2 years, 7% to 10% display a chronic and severe prognosis.3
The etiopathogenesis of AA is not clearly understood, but its occurrence and progression can involve immune dysfunction, genetic predisposition, infections, and physical and psychological trauma.2 Alopecia areata is observed to occur sporadically in most patients. Family history has been found in 3% to 42% of cases, but simultaneous occurrence of AA in family members is rare.4 In this case series, we present 4 cases of active AA lesions occurring simultaneously in a family who also had associated psychologic disorders.
Case Series
Patient 1 (Proband)
An 11-year-old boy presented with a 6-year history of ongoing AA with recurrent improvement and relapses on the scalp, eyebrows, and eyelashes. Various topical and oral medications had been prescribed by several outside dermatologists; however, these treatments provided minimal benefit and resulted in the recurrence of AA. Dermatologic examination revealed hair loss on the entire frontal, parietal, and temporal regions of the scalp, as well as half of the occipital region and one-third of the lateral side of the eyebrows (Figure 1). Psychological evaluation revealed introvert personality characteristics, lack of self-confidence, and signs of depression and anxiety.
Patient 2 (Proband’s Father)
A 38-year-old man presented with a 16-year history of recurrent loss and regrowth of hair on the scalp and beard area and white spots on the penis and arms. He previously had not undergone any treatments. Dermatologic examination revealed well-circumscribed, 1- to 4-cm, hairless patches on the occipital region of the scalp and in the beard area (Figure 2A) and multiple, 2- to 10-mm, vitiliginous lesions on both forearms (Figure 2B) and the penis. The patient had been unemployed for 6 months. Psychological evaluation revealed obsessive-compulsive disorder and obsessive-compulsive personality disorder.
Patient 3 (Proband’s Mother)
A 32-year-old woman presented with a 3-year history of chronic AA. She previously had not undergone any treatments. Dermatologic examination revealed 2 well-circumscribed, 3- to 4-cm patches of hair loss on the occipital and left temporal regions of the scalp (Figure 3). Psychological evaluation revealed obsessive-compulsive personality disorder and depression. The patient did not have any autoimmune diseases.
Patient 4 (Proband’s Sister)
A 10-year-old girl presented with a 6-year history of recurrent, self-limited AA on various areas of scalp. She previously had not undergone any treatments. Dermatologic examination revealed a 3-cm hairless patch on the occipital region of the scalp (Figure 4). Psychiatric evaluation revealed narcissistic personality disorder, anxiety, and lack of self-confidence.
Laboratory Evaluation and HLA Antigen DNA Typing
Laboratory testing including complete blood cell count; liver, kidney, and thyroid function; and vitamin B12, zinc, folic acid, and fasting blood sugar levels were performed in all patients.
HLA antigen DNA typing was performed by polymerase chain reaction with sequence-specific primers in all patients after informed consent was obtained.
Clinical and laboratory examinations revealed no symptoms or findings of Epstein-Barr virus and cytomegalovirus infections, cicatricial alopecia, or connective tissue diseases in any of the patients. HLA antigen DNA typing revealed the following HLA alleles: B*35/40, C*04/15, DRB1*08/10, and DQB1*03/05 in patient 1; B*04/13, C*06/15, DRB1*07/10, and DQB1*02/05 in patient 2; B*33/37, C*04/06, DRB1*08/15, and DQ*06/06 in patient 3; B*13/37, C*06/06, DRB1*07/15, and DQB1*02/06 in patient 4.
Laboratory testing revealed vitamin B12 deficiency in patient 2 and iron deficiency anemia in patient 3; all other laboratory tests were within reference range. Antithyroglobulin and antithyroid peroxidase autoantibodies were all negative. Clinical features and laboratory analyses for all patients are summarized in the Table.
Treatment
All patients were recommended psychiatric therapy and started on dermatologic treatments. Topical corticosteroids, intralesional triamcinolone acetonide (8 mg/mL) injections into areas of hair loss, 8 total sessions of cryotherapy administered at 3-week intervals, and minoxidil solution 2% were administered respectively to all 4 patients. Alopecia areata in patients 3 and 4 completely regressed; however, no benefit was observed in patients 1 and 2 after 1 year of treatment. Because there was no response to the prior interventions, patient 1 was started on treatment with cyclosporine 2.5 mg/kg twice daily. However, therapy was discontinued after 1 month and treatment with narrowband UVB (3 times per week for 7 months [total of 57 sessions]) and topical corticosteroids were initiated (Table). The patient partially benefited from these regimens and recurrence was observed during the course of the treatment.
Although it was recommended that all 4 patients undergo psychiatric treatment and follow-up regularly with a psychiatrist, the patients declined. After approximately 1 year of dermatologic treatment, all 4 patients were lost to follow-up.
Comment
The etiopathogenesis of AA is unclear, but there is strong evidence suggesting that it is a T-cell–mediated autoimmune disease targeting the hair follicles. Common association of AA with autoimmune diseases such as vitiligo and thyroiditis support the immunological origin of the disease.3 In our case, patient 2 had AA along with vitiligo, but no associated autoimmune diseases (eg, vitiligo, diabetes mellitus, pernicious anemia, thyroid diseases) were noted in the other patients. Genetic and environmental factors are known to be influential as much as immune dysfunction in the etiology of AA.2
The presence of family history in 20% of patients supports the genetic predisposition of AA.4 In a genetic study by Martinez-Mir et al,5 susceptibility loci for AA were demonstrated on chromosomes 6, 10, 16, and 18. HLA antigen alleles, which provide predisposition to AA, have been investigated and associations with many different HLA antigens have been described for AA. In these studies, a relationship between AA and HLA class I antigens was not determined. Notable results mainly focused on HLA class II antigens.6-8 Colombe et al7 and Marques Da Costa et al8 demonstrated that long-lasting alopecia totalis or alopecia universalis (AT/AU) patients had a strong relationship with HLA-DRB1*1104; DRB1*04/05 was reported to be the most frequent HLA group among all patients with AA.6-10 In contrast, we did not detect these alleles in our patients. Colombe et al7,11 noted that HLA-DQB1*03 is a marker for both patch-type AA and AT/AU. Colombe et al10 showed that HLA-DQB1*03 was present in more than 80% of patients (N=286) with long-lasting AA. Barahmani et al9 confirmed a strong association between HLA-DQB1*0301, DRB1*1104, and AT/AU. In our patients, we detected HLA-DQB1*03/05 in patient 1 who had the earliest onset and most severe presentation of AA. In some studies, HLA-DRB1*03 was found to be less frequent in patients with AA, and this allele was suggested to be a protective factor.6,12 However, this allele was not detected in any of our patients.
The association of HLA alleles and AA has been investigated in Turkish patients with AA.13-15 Akar et al13 and Kavak et al14 detected that the frequency of HLA-DQB1*03 allele was remarkably higher in patients with AA than in healthy controls. These results were consistent with Colombe et al.10 On the other hand, Kavak et al14 reported that the frequency of HLA-DR16 was decreased in the patient group with AA. In another study, the frequency of HLA-B62 was increased in patients with AA compared to healthy controls.15 The HLA-DQB1*03 allele was found to be associated with AA in only patient 1 in our case series, and HLA alleles were not commonly shared among the 4 patients. Additionally, lack of consanguinity between patients 2 and 3 (the parents) also suggested that genetic factors were not involved in our familial cases.
Blaumeiser et al16 reported a lifetime risk of 7.4% in parents and 7.1% in siblings of 206 AA patients; however, because these studies investigated the presence of AA in any given life period of the family members, their results do not reflect frequency of simultaneous AA presence within one family. In a literature search using PubMed, Google Scholar, and other national databases for the terms alopecia areata as well as family, sibling, concurrently, concomitant, co-existent, and simultaneously, only 2 cases involving a husband and wife and 1 case of 2 siblings who concurrently had AA have been previously reported.17,18 Simultaneous presence of AA in more than 3 members of the same family is rare, and these cases have been observed in different generations and time periods.19 Among our patients, despite different age of onset and duration, AA was simultaneously present in the entire family.
Moreover, Rodriguez et al20 reported that the concordance rate of AA in identical twins was 42% and dizygotic twins was 10%. Environmental factors and infections also have been implicated in the etiology of AA. Infections caused by viruses such as cytomegalovirus and Epstein-Barr virus have been thought to be potential triggering factors; however, no evidence has been found.21,22 The clinical and laboratory examinations in our study did not reveal any presence and/or history of any known infectious disease, and there was no history of contact with water infected by acrylamide or a similar chemical.
Various life events and intense psychological stress may play an important role in triggering AA. Depression, hysteria, psychopathic deviance, psychasthenia, schizophrenia, anxiety, health concerns, bizarre thoughts, and family problems were found to be more frequent in patients with AA than healthy controls.23 The most common psychological disorders associated with AA are generalized anxiety disorder, major depressive disorder, adjustment disorders, and phobias.1,24 Ruiz-Doblado et al25 determined the presence of psychiatric comorbidities in 66% (21/32) of AA cases. Chu et al26 reported that the differences in ages of onset of AA revealed differences in psychiatric comorbidities. The risk for depression was higher in patients with AA younger than 20 years. An increased rate of anxiety was detected with patients with an onset of AA between the ages of 20 and 39 years. Obsessive-compulsive disorder and anxiety were more common in patients aged 40 to 59 years. Interestingly, the investigators also observed that approximately 50% of psychiatric disorders occurred prior to onset of AA.26 One study showed higher rates of stressful life events in children than in controls.27 Ghanizadeh24 reported at least 1 psychiatric disorder in 78% (11/14) of children and adolescents with AA. In the same study, obsessive-compulsive disorder was found to be the second common condition following major depression in AA.24
In our patients, psychiatric evaluations revealed obsessive-compulsive personality disorder in patients 2 and 3, depression in patient 3, and symptoms of anxiety with a lack of self-confidence in patients 1 and 4. Psychiatric disorders affecting the entire family may stem from unemployment of the father. Similar to the results noted in prior studies, depression, the most commonly associated psychiatric disorder of AA, was present in 2 of 4 patients. Obsessive-compulsive disorder, the second most common psychiatric disorder among AA patients, was present in patients 2 and 3. These results indicate that AA may be associated with shared stressful events and psychiatric disorders. Therefore, in addition to dermatologic treatment, it was recommended that all patients undergo psychiatric treatment and follow-up regularly with a psychiatrist; however, the patients declined. At the end of a 1-year treatment period and follow-up, resistance to therapy with minimal recovery followed by a rapid recurrence was determined in patients 1 and 2.
Conclusion
This report demonstrated that familial AA was strongly associated with psychological disorders that were detected in all patients. In our patients, HLA alleles did not seem to have a role in the development of familial AA. These results suggest that HLA was not associated with AA triggered by psychological stress. We believe that psychological disorders and stressful life events may play an important role in the occurrence of AA and lead to the development of resistance against treatment in familial and resistant AA cases.
Alopecia areata (AA) presents as sudden, nonscarring, recurrent hair loss characterized by well-circumscribed hairless patches. Although AA may be observed on any hair-bearing areas of the body, the most commonly affected sites are the scalp, beard area, eyebrows, and eyelashes.1 The incidence of AA is 1% to 2% in the general population and it is more common in males than females younger than 40 years.2 Although the majority of patients present with self-limited and well-circumscribed hairless patches that resolve within 2 years, 7% to 10% display a chronic and severe prognosis.3
The etiopathogenesis of AA is not clearly understood, but its occurrence and progression can involve immune dysfunction, genetic predisposition, infections, and physical and psychological trauma.2 Alopecia areata is observed to occur sporadically in most patients. Family history has been found in 3% to 42% of cases, but simultaneous occurrence of AA in family members is rare.4 In this case series, we present 4 cases of active AA lesions occurring simultaneously in a family who also had associated psychologic disorders.
Case Series
Patient 1 (Proband)
An 11-year-old boy presented with a 6-year history of ongoing AA with recurrent improvement and relapses on the scalp, eyebrows, and eyelashes. Various topical and oral medications had been prescribed by several outside dermatologists; however, these treatments provided minimal benefit and resulted in the recurrence of AA. Dermatologic examination revealed hair loss on the entire frontal, parietal, and temporal regions of the scalp, as well as half of the occipital region and one-third of the lateral side of the eyebrows (Figure 1). Psychological evaluation revealed introvert personality characteristics, lack of self-confidence, and signs of depression and anxiety.
Patient 2 (Proband’s Father)
A 38-year-old man presented with a 16-year history of recurrent loss and regrowth of hair on the scalp and beard area and white spots on the penis and arms. He previously had not undergone any treatments. Dermatologic examination revealed well-circumscribed, 1- to 4-cm, hairless patches on the occipital region of the scalp and in the beard area (Figure 2A) and multiple, 2- to 10-mm, vitiliginous lesions on both forearms (Figure 2B) and the penis. The patient had been unemployed for 6 months. Psychological evaluation revealed obsessive-compulsive disorder and obsessive-compulsive personality disorder.
Patient 3 (Proband’s Mother)
A 32-year-old woman presented with a 3-year history of chronic AA. She previously had not undergone any treatments. Dermatologic examination revealed 2 well-circumscribed, 3- to 4-cm patches of hair loss on the occipital and left temporal regions of the scalp (Figure 3). Psychological evaluation revealed obsessive-compulsive personality disorder and depression. The patient did not have any autoimmune diseases.
Patient 4 (Proband’s Sister)
A 10-year-old girl presented with a 6-year history of recurrent, self-limited AA on various areas of scalp. She previously had not undergone any treatments. Dermatologic examination revealed a 3-cm hairless patch on the occipital region of the scalp (Figure 4). Psychiatric evaluation revealed narcissistic personality disorder, anxiety, and lack of self-confidence.
Laboratory Evaluation and HLA Antigen DNA Typing
Laboratory testing including complete blood cell count; liver, kidney, and thyroid function; and vitamin B12, zinc, folic acid, and fasting blood sugar levels were performed in all patients.
HLA antigen DNA typing was performed by polymerase chain reaction with sequence-specific primers in all patients after informed consent was obtained.
Clinical and laboratory examinations revealed no symptoms or findings of Epstein-Barr virus and cytomegalovirus infections, cicatricial alopecia, or connective tissue diseases in any of the patients. HLA antigen DNA typing revealed the following HLA alleles: B*35/40, C*04/15, DRB1*08/10, and DQB1*03/05 in patient 1; B*04/13, C*06/15, DRB1*07/10, and DQB1*02/05 in patient 2; B*33/37, C*04/06, DRB1*08/15, and DQ*06/06 in patient 3; B*13/37, C*06/06, DRB1*07/15, and DQB1*02/06 in patient 4.
Laboratory testing revealed vitamin B12 deficiency in patient 2 and iron deficiency anemia in patient 3; all other laboratory tests were within reference range. Antithyroglobulin and antithyroid peroxidase autoantibodies were all negative. Clinical features and laboratory analyses for all patients are summarized in the Table.
Treatment
All patients were recommended psychiatric therapy and started on dermatologic treatments. Topical corticosteroids, intralesional triamcinolone acetonide (8 mg/mL) injections into areas of hair loss, 8 total sessions of cryotherapy administered at 3-week intervals, and minoxidil solution 2% were administered respectively to all 4 patients. Alopecia areata in patients 3 and 4 completely regressed; however, no benefit was observed in patients 1 and 2 after 1 year of treatment. Because there was no response to the prior interventions, patient 1 was started on treatment with cyclosporine 2.5 mg/kg twice daily. However, therapy was discontinued after 1 month and treatment with narrowband UVB (3 times per week for 7 months [total of 57 sessions]) and topical corticosteroids were initiated (Table). The patient partially benefited from these regimens and recurrence was observed during the course of the treatment.
Although it was recommended that all 4 patients undergo psychiatric treatment and follow-up regularly with a psychiatrist, the patients declined. After approximately 1 year of dermatologic treatment, all 4 patients were lost to follow-up.
Comment
The etiopathogenesis of AA is unclear, but there is strong evidence suggesting that it is a T-cell–mediated autoimmune disease targeting the hair follicles. Common association of AA with autoimmune diseases such as vitiligo and thyroiditis support the immunological origin of the disease.3 In our case, patient 2 had AA along with vitiligo, but no associated autoimmune diseases (eg, vitiligo, diabetes mellitus, pernicious anemia, thyroid diseases) were noted in the other patients. Genetic and environmental factors are known to be influential as much as immune dysfunction in the etiology of AA.2
The presence of family history in 20% of patients supports the genetic predisposition of AA.4 In a genetic study by Martinez-Mir et al,5 susceptibility loci for AA were demonstrated on chromosomes 6, 10, 16, and 18. HLA antigen alleles, which provide predisposition to AA, have been investigated and associations with many different HLA antigens have been described for AA. In these studies, a relationship between AA and HLA class I antigens was not determined. Notable results mainly focused on HLA class II antigens.6-8 Colombe et al7 and Marques Da Costa et al8 demonstrated that long-lasting alopecia totalis or alopecia universalis (AT/AU) patients had a strong relationship with HLA-DRB1*1104; DRB1*04/05 was reported to be the most frequent HLA group among all patients with AA.6-10 In contrast, we did not detect these alleles in our patients. Colombe et al7,11 noted that HLA-DQB1*03 is a marker for both patch-type AA and AT/AU. Colombe et al10 showed that HLA-DQB1*03 was present in more than 80% of patients (N=286) with long-lasting AA. Barahmani et al9 confirmed a strong association between HLA-DQB1*0301, DRB1*1104, and AT/AU. In our patients, we detected HLA-DQB1*03/05 in patient 1 who had the earliest onset and most severe presentation of AA. In some studies, HLA-DRB1*03 was found to be less frequent in patients with AA, and this allele was suggested to be a protective factor.6,12 However, this allele was not detected in any of our patients.
The association of HLA alleles and AA has been investigated in Turkish patients with AA.13-15 Akar et al13 and Kavak et al14 detected that the frequency of HLA-DQB1*03 allele was remarkably higher in patients with AA than in healthy controls. These results were consistent with Colombe et al.10 On the other hand, Kavak et al14 reported that the frequency of HLA-DR16 was decreased in the patient group with AA. In another study, the frequency of HLA-B62 was increased in patients with AA compared to healthy controls.15 The HLA-DQB1*03 allele was found to be associated with AA in only patient 1 in our case series, and HLA alleles were not commonly shared among the 4 patients. Additionally, lack of consanguinity between patients 2 and 3 (the parents) also suggested that genetic factors were not involved in our familial cases.
Blaumeiser et al16 reported a lifetime risk of 7.4% in parents and 7.1% in siblings of 206 AA patients; however, because these studies investigated the presence of AA in any given life period of the family members, their results do not reflect frequency of simultaneous AA presence within one family. In a literature search using PubMed, Google Scholar, and other national databases for the terms alopecia areata as well as family, sibling, concurrently, concomitant, co-existent, and simultaneously, only 2 cases involving a husband and wife and 1 case of 2 siblings who concurrently had AA have been previously reported.17,18 Simultaneous presence of AA in more than 3 members of the same family is rare, and these cases have been observed in different generations and time periods.19 Among our patients, despite different age of onset and duration, AA was simultaneously present in the entire family.
Moreover, Rodriguez et al20 reported that the concordance rate of AA in identical twins was 42% and dizygotic twins was 10%. Environmental factors and infections also have been implicated in the etiology of AA. Infections caused by viruses such as cytomegalovirus and Epstein-Barr virus have been thought to be potential triggering factors; however, no evidence has been found.21,22 The clinical and laboratory examinations in our study did not reveal any presence and/or history of any known infectious disease, and there was no history of contact with water infected by acrylamide or a similar chemical.
Various life events and intense psychological stress may play an important role in triggering AA. Depression, hysteria, psychopathic deviance, psychasthenia, schizophrenia, anxiety, health concerns, bizarre thoughts, and family problems were found to be more frequent in patients with AA than healthy controls.23 The most common psychological disorders associated with AA are generalized anxiety disorder, major depressive disorder, adjustment disorders, and phobias.1,24 Ruiz-Doblado et al25 determined the presence of psychiatric comorbidities in 66% (21/32) of AA cases. Chu et al26 reported that the differences in ages of onset of AA revealed differences in psychiatric comorbidities. The risk for depression was higher in patients with AA younger than 20 years. An increased rate of anxiety was detected with patients with an onset of AA between the ages of 20 and 39 years. Obsessive-compulsive disorder and anxiety were more common in patients aged 40 to 59 years. Interestingly, the investigators also observed that approximately 50% of psychiatric disorders occurred prior to onset of AA.26 One study showed higher rates of stressful life events in children than in controls.27 Ghanizadeh24 reported at least 1 psychiatric disorder in 78% (11/14) of children and adolescents with AA. In the same study, obsessive-compulsive disorder was found to be the second common condition following major depression in AA.24
In our patients, psychiatric evaluations revealed obsessive-compulsive personality disorder in patients 2 and 3, depression in patient 3, and symptoms of anxiety with a lack of self-confidence in patients 1 and 4. Psychiatric disorders affecting the entire family may stem from unemployment of the father. Similar to the results noted in prior studies, depression, the most commonly associated psychiatric disorder of AA, was present in 2 of 4 patients. Obsessive-compulsive disorder, the second most common psychiatric disorder among AA patients, was present in patients 2 and 3. These results indicate that AA may be associated with shared stressful events and psychiatric disorders. Therefore, in addition to dermatologic treatment, it was recommended that all patients undergo psychiatric treatment and follow-up regularly with a psychiatrist; however, the patients declined. At the end of a 1-year treatment period and follow-up, resistance to therapy with minimal recovery followed by a rapid recurrence was determined in patients 1 and 2.
Conclusion
This report demonstrated that familial AA was strongly associated with psychological disorders that were detected in all patients. In our patients, HLA alleles did not seem to have a role in the development of familial AA. These results suggest that HLA was not associated with AA triggered by psychological stress. We believe that psychological disorders and stressful life events may play an important role in the occurrence of AA and lead to the development of resistance against treatment in familial and resistant AA cases.
- García-Hernández MJ, Ruiz-Doblado S, Rodriguez-Pichardo A, et al. Alopecia areata, stress and psychiatric disorders: a review. J Dermatol. 1999;26:625-632.
- Bhat YJ, Manzoor S, Khan AR, et al. Trace element levels in alopecia areata. Indian J Dermatol Venereol Leprol. 2009;75:29-31.
- Alexis AF, Dudda-Subramanya R, Sinha AA. Alopecia areata: autoimmune basis of hair loss. Eur J Dermatol. 2004;14:364-370.
- Green J, Sinclair RD. Genetics of alopecia areata. Australas J Dermatol. 2000;41:213-218.
- Martinez-Mir A, Zlotogorski A, Gordon D, et al.Genomewide scan for linkage reveals evidence of several susceptibility loci for alopecia areata. Am J Hum Genet. 2007;80:316-328.
- Entz P, Blaumeiser B, Betz RC, et al. Investigation of the HLA-DRB1 locus in alopecia areata. Eur J Dermatol. 2006;16:363-367.
- Colombe BW, Price VH, Khoury EL, et al. HLA class II alleles in long-standing alopecia totalis/alopecia universalis and long-standing patchy alopecia areata differentiate these two clinical groups. J Invest Dermatol. 1995;104(suppl 5):4-5.
- Marques Da Costa C, Dupont E, Van der Cruys M, et al. Earlier occurrence of severe alopecia areata in HLA-DRB1*11-positive patients. Dermatology. 2006;213:12-14.
- Barahmani N, de Andrade M, Slusser JP, et al. Human leukocyte antigen class II alleles are associated with risk of alopecia areata. J Invest Dermatol. 2008;128:240-243.
- Colombe BW, Lou CD, Price VH. The genetic basis of alopecia areata: HLA associations with patchy alopecia areata versus alopecia totalis and alopecia universalis. J Investig Dermatol Symp Proc. 1999;4:216-219.
- Colombe BW, Price VH, Khoury EL, et al. HLA class II antigen associations help to define two types of alopecia areata. J Am Acad Dermatol. 1995;33(5, pt 1):757-764.
- Broniarczyk-Dyła G, Prusińska-Bratoś M, Dubla-Berner M, et al. The protective role of the HLA-DR locus in patients with various clinical types of alopecia areata. Arch Immunol Ther Exp (Warsz). 2002;50:333-336.
- Akar A, Orkunuglu E, Sengul A, et al. HLA class II alleles in patients with alopecia areata. Eur J Dermatol. 2002;12:236-239.
- Kavak A, Baykal C, Ozarmagan G, et al. HLA in alopecia areata. Int J Dermatol. 2000;30:589-592.
- Aliagaoglu C, Pirim I, Atasoy M, et al. Association between alopecia areata and HLA class I and II in Turkey. J Dermatol. 2005;32:711-714.
- Blaumeiser B, Goot I, Fimmers R, et al. Familial aggregation of alopecia areata. J Am Acad Dermatol. 2006;54:627-632.
- Zalka AD, Byarlay JA, Goldsmith LA. Alopecia a deux: simultaneous occurrence of alopecia in a husband and wife. Arch Dermatol. 1994;130:390-392.
- Menon R, Kiran C. Concomitant presentation of alopecia areata in siblings: a rare occurrence. Int J Trichology. 2012;4:86-88.
- Valsecchi R, Vicari O, Frigeni A, et al. Familial alopecia areata-genetic susceptibility or coincidence? Acta Derm Venereol (Stockh). 1985;65:175-177.
- Rodriguez TA, Fernandes KE, Dresser KL, et al. Concordance rate of alopecia areata in identical twins supports both genetic and environmental factors. J Am Acad Dermatol. 2010;62:525-527.
- Rodriguez TA, Duvic M. Onset of alopecia areata after Epstein Barr virus infectious mononucleosis. J Am Acad Dermatol. 2008;59:137-139.
- Offidani A, Amerio P, Bernardini ML, et al. Role of cytomegalovirus replication in alopecia areata pathogenesis. J Cutan Med Surg. 2000;4:63-65.
- Alfani S, Antinone V, Mozzetta A, et al. Psychological status of patients with alopecia areata. Acta Derm Venereol. 2012;92:304-306.
- Ghanizadeh A. Comorbidity of psychiatric disorders in children and adolescents with alopecia areata in a child and adolescent psychiatry clinical sample. Int J Dermatol. 2008;47:1118-1120.
- Ruiz-Doblado S, Carrizosa A, Garcia-Hernandez MJ. Alopecia areata: psychiatric comorbidity and adjustment to illness. Int J Dermatol. 2003;42:434-437.
- Chu SY, Chen YJ, Tseng WC, et al. Psychiatric comorbidities in patients with alopecia areata in Taiwan: a case-control study. Br J Dermatol. 2012;166:525-531.
- Manolache L, Petrescu-Seceleanu D, Benea V. Alopecia areata and stressful events in children. J Eur Acad Dermatol Venereol. 2009;23:107-109.
- García-Hernández MJ, Ruiz-Doblado S, Rodriguez-Pichardo A, et al. Alopecia areata, stress and psychiatric disorders: a review. J Dermatol. 1999;26:625-632.
- Bhat YJ, Manzoor S, Khan AR, et al. Trace element levels in alopecia areata. Indian J Dermatol Venereol Leprol. 2009;75:29-31.
- Alexis AF, Dudda-Subramanya R, Sinha AA. Alopecia areata: autoimmune basis of hair loss. Eur J Dermatol. 2004;14:364-370.
- Green J, Sinclair RD. Genetics of alopecia areata. Australas J Dermatol. 2000;41:213-218.
- Martinez-Mir A, Zlotogorski A, Gordon D, et al.Genomewide scan for linkage reveals evidence of several susceptibility loci for alopecia areata. Am J Hum Genet. 2007;80:316-328.
- Entz P, Blaumeiser B, Betz RC, et al. Investigation of the HLA-DRB1 locus in alopecia areata. Eur J Dermatol. 2006;16:363-367.
- Colombe BW, Price VH, Khoury EL, et al. HLA class II alleles in long-standing alopecia totalis/alopecia universalis and long-standing patchy alopecia areata differentiate these two clinical groups. J Invest Dermatol. 1995;104(suppl 5):4-5.
- Marques Da Costa C, Dupont E, Van der Cruys M, et al. Earlier occurrence of severe alopecia areata in HLA-DRB1*11-positive patients. Dermatology. 2006;213:12-14.
- Barahmani N, de Andrade M, Slusser JP, et al. Human leukocyte antigen class II alleles are associated with risk of alopecia areata. J Invest Dermatol. 2008;128:240-243.
- Colombe BW, Lou CD, Price VH. The genetic basis of alopecia areata: HLA associations with patchy alopecia areata versus alopecia totalis and alopecia universalis. J Investig Dermatol Symp Proc. 1999;4:216-219.
- Colombe BW, Price VH, Khoury EL, et al. HLA class II antigen associations help to define two types of alopecia areata. J Am Acad Dermatol. 1995;33(5, pt 1):757-764.
- Broniarczyk-Dyła G, Prusińska-Bratoś M, Dubla-Berner M, et al. The protective role of the HLA-DR locus in patients with various clinical types of alopecia areata. Arch Immunol Ther Exp (Warsz). 2002;50:333-336.
- Akar A, Orkunuglu E, Sengul A, et al. HLA class II alleles in patients with alopecia areata. Eur J Dermatol. 2002;12:236-239.
- Kavak A, Baykal C, Ozarmagan G, et al. HLA in alopecia areata. Int J Dermatol. 2000;30:589-592.
- Aliagaoglu C, Pirim I, Atasoy M, et al. Association between alopecia areata and HLA class I and II in Turkey. J Dermatol. 2005;32:711-714.
- Blaumeiser B, Goot I, Fimmers R, et al. Familial aggregation of alopecia areata. J Am Acad Dermatol. 2006;54:627-632.
- Zalka AD, Byarlay JA, Goldsmith LA. Alopecia a deux: simultaneous occurrence of alopecia in a husband and wife. Arch Dermatol. 1994;130:390-392.
- Menon R, Kiran C. Concomitant presentation of alopecia areata in siblings: a rare occurrence. Int J Trichology. 2012;4:86-88.
- Valsecchi R, Vicari O, Frigeni A, et al. Familial alopecia areata-genetic susceptibility or coincidence? Acta Derm Venereol (Stockh). 1985;65:175-177.
- Rodriguez TA, Fernandes KE, Dresser KL, et al. Concordance rate of alopecia areata in identical twins supports both genetic and environmental factors. J Am Acad Dermatol. 2010;62:525-527.
- Rodriguez TA, Duvic M. Onset of alopecia areata after Epstein Barr virus infectious mononucleosis. J Am Acad Dermatol. 2008;59:137-139.
- Offidani A, Amerio P, Bernardini ML, et al. Role of cytomegalovirus replication in alopecia areata pathogenesis. J Cutan Med Surg. 2000;4:63-65.
- Alfani S, Antinone V, Mozzetta A, et al. Psychological status of patients with alopecia areata. Acta Derm Venereol. 2012;92:304-306.
- Ghanizadeh A. Comorbidity of psychiatric disorders in children and adolescents with alopecia areata in a child and adolescent psychiatry clinical sample. Int J Dermatol. 2008;47:1118-1120.
- Ruiz-Doblado S, Carrizosa A, Garcia-Hernandez MJ. Alopecia areata: psychiatric comorbidity and adjustment to illness. Int J Dermatol. 2003;42:434-437.
- Chu SY, Chen YJ, Tseng WC, et al. Psychiatric comorbidities in patients with alopecia areata in Taiwan: a case-control study. Br J Dermatol. 2012;166:525-531.
- Manolache L, Petrescu-Seceleanu D, Benea V. Alopecia areata and stressful events in children. J Eur Acad Dermatol Venereol. 2009;23:107-109.
Practice Points
- The etiopathogenesis of alopecia areata (AA) is not clearly understood, but its occurrence and progression can involve immune dysfunction, genetic predisposition, infections, and physical and psychological trauma.
- Alopecia areata is observed to occur sporadically in most patients. Simultaneous presence of AA in more than 3 members of the same family is rare, and these cases have been observed in different generations and time periods.
- HLA antigen alleles, which provide predisposition to AA, have been investigated, and associations with many different HLA antigens have been described for AA. In previous studies, HLA-DQB1*03 allele was reported as the most common HLA allele in patients with AA.
- Psychological disorders and shared stressful life events may play an important role in the occurrence of AA and lead to the development of resistance against treatment in familial and resistant AA cases.

Dual immune checkpoint blockade found durable in melanoma
CHICAGO – Immune checkpoint blockade, especially with a combination of agents having complementary mechanisms of action, has durable efficacy when used as initial therapy for advanced melanoma, according to an update of the CheckMate 067 trial.
The trial randomized 945 treatment-naive patients with unresectable stage III or IV melanoma evenly to double-blind treatment with nivolumab, an antibody to the cell surface receptor programmed death 1 (PD-1); ipilimumab, an antibody to the T-cell receptor cytotoxic T-lymphocyte–associated antigen 4 (CTLA4); or the combination.

Initial results, after a median follow-up of about 12.4 months, showed that the risk of progression-free survival events was 58% lower with the combination and 43% lower with nivolumab alone as compared with ipilimumab alone (N Engl J Med. 2015;373[1]:23-34).
The update, now with a median follow-up of 20.7 months, showed that these results held up, with respective 58% and 45% reductions in the risk of events, researchers reported at the annual meeting of the American Society of Clinical Oncology. The combination was also superior to nivolumab alone, netting a 24% lower risk of events. Additionally, no cumulative or new toxicities were seen.
“Based on available evidence, the combination of nivolumab and ipilimumab represents a means to improve outcomes versus nivolumab alone,” said first author Jedd D. Wolchok, MD, PhD, chief of the Melanoma & Immunotherapeutics Service at the Memorial Sloan Kettering Cancer Center in New York. “Additional insights will be gained with the emergence of overall survival data.”
Neither tumor expression of PD-L1, a ligand of PD-1, nor presence of a BRAF mutation was very helpful in identifying patients who would benefit to a greater extent from these therapies.
The findings add to evidence establishing the efficacy of combination immunotherapy in melanoma, according to invited discussant Marc S. Ernstoff, MD, professor and chair of the department of medicine at the Roswell Park Cancer Institute in Buffalo, N.Y. At the same time, the trial left unanswered questions such as what strategy should be used after progression on either or both agents, and what are the appropriate doses and durations of therapy. Also unclear is which type of therapy to use first line in patients with BRAF mutations, he added. “Whether you start with immunotherapy or targeted therapy in BRAF-mutated patients is still in equipoise, and I would encourage everyone here to participate in the ECOG 6134 trial looking at the randomization of immune checkpoint therapy versus targeted therapy in BRAF-mutated patients,” he said. “The biomarker studies are still provocative, and we still need a lot more data to be able to preselect patients who might benefit from either of these therapies.”
“One has to recognize that these agents are costly,” Dr. Ernstoff maintained, with the acquisition cost of the checkpoint inhibitors ranging from roughly $140,000 to $290,000 per year depending on the agent(s) used. This issue will also have to be addressed going forward.
“The future is very bright. There are now 76 trials listed in PDQ [Physician Data Query] of combination PD-1 therapies in melanoma alone,” he concluded. “Immunotherapy continues to capture our imagination.”
The updated intent-to-treat analyses of CheckMate 067 – conducted after all patients had at least 18 months of follow-up – showed that median progression-free survival, one of the trial’s primary endpoints, was now 11.5 months with the combination of nivolumab (Opdivo) and ipilimumab (Yervoy), 6.9 months with nivolumab alone, and 2.9 months with ipilimumab alone, Dr. Wolchok reported at the meeting.
The differences translated to significantly better outcomes with the combination (hazard ratio, 0.42) and with nivolumab (HR, 0.55) as compared with ipilimumab. Moreover, the combination was superior to nivolumab (HR, 0.76).
The overall response rate, the trial’s other primary endpoint, was 57.6% with the combination and 43.7% with nivolumab alone, both of which were superior to the 19.0% with ipilimumab alone.
“While the response rates have not changed, some partial responses have evolved into complete responses over time,” Dr. Wolchok noted.
Findings were similar when patients were stratified by BRAF mutational status. And in exploratory analyses, outcomes were numerically better with the combination than with nivolumab alone regardless of whether tumors had high or low PD-L1 expression.
Safety results were much the same as previously reported. The rate of grade 3 or 4 treatment-related adverse events was 56.5% with the combination, 19.8% with nivolumab monotherapy, and 27.0% with ipilimumab monotherapy. There were no treatment-related deaths with the combination and one with each of the monotherapies.
“There is no common signature adverse event with this combination,” Dr. Wolchok pointed out. “The majority of grade 3 or 4 adverse events resolved in all of the groups with the use of established algorithms. However, as observed in prior studies, most of the endocrine events did not resolve and required hormone replacement.”
About 40% of the combination therapy group stopped treatment because of adverse events. “Interestingly, 68% of these patients who discontinued due to treatment-related adverse events developed a response, and 50% of these responses occurred after treatment had ended,” he reported. “This is very important information for us as we talk to patients and their families about the difficulties of stopping treatment.”
Dr. Wolchok disclosed that he is a consultant for Bristol-Myers Squibb, Genentech, Jounce Therapeutics, Medimmune, Merck, Polaris, Polynoma, Potenza, Tizona, Ziopharm, F-Star, Beigene, Lilly, Advaxis, and Sellas, and that he receives grant/research support from Bristol-Myers Squibb. The trial was sponsored by Bristol-Myers Squibb. Dako collaborated on development of the automated anti–PD-L1 immunohistochemistry assay.
CHICAGO – Immune checkpoint blockade, especially with a combination of agents having complementary mechanisms of action, has durable efficacy when used as initial therapy for advanced melanoma, according to an update of the CheckMate 067 trial.
The trial randomized 945 treatment-naive patients with unresectable stage III or IV melanoma evenly to double-blind treatment with nivolumab, an antibody to the cell surface receptor programmed death 1 (PD-1); ipilimumab, an antibody to the T-cell receptor cytotoxic T-lymphocyte–associated antigen 4 (CTLA4); or the combination.
Initial results, after a median follow-up of about 12.4 months, showed that the risk of progression-free survival events was 58% lower with the combination and 43% lower with nivolumab alone as compared with ipilimumab alone (N Engl J Med. 2015;373[1]:23-34).
The update, now with a median follow-up of 20.7 months, showed that these results held up, with respective 58% and 45% reductions in the risk of events, researchers reported at the annual meeting of the American Society of Clinical Oncology. The combination was also superior to nivolumab alone, netting a 24% lower risk of events. Additionally, no cumulative or new toxicities were seen.
“Based on available evidence, the combination of nivolumab and ipilimumab represents a means to improve outcomes versus nivolumab alone,” said first author Jedd D. Wolchok, MD, PhD, chief of the Melanoma & Immunotherapeutics Service at the Memorial Sloan Kettering Cancer Center in New York. “Additional insights will be gained with the emergence of overall survival data.”
Neither tumor expression of PD-L1, a ligand of PD-1, nor presence of a BRAF mutation was very helpful in identifying patients who would benefit to a greater extent from these therapies.
The findings add to evidence establishing the efficacy of combination immunotherapy in melanoma, according to invited discussant Marc S. Ernstoff, MD, professor and chair of the department of medicine at the Roswell Park Cancer Institute in Buffalo, N.Y. At the same time, the trial left unanswered questions such as what strategy should be used after progression on either or both agents, and what are the appropriate doses and durations of therapy. Also unclear is which type of therapy to use first line in patients with BRAF mutations, he added. “Whether you start with immunotherapy or targeted therapy in BRAF-mutated patients is still in equipoise, and I would encourage everyone here to participate in the ECOG 6134 trial looking at the randomization of immune checkpoint therapy versus targeted therapy in BRAF-mutated patients,” he said. “The biomarker studies are still provocative, and we still need a lot more data to be able to preselect patients who might benefit from either of these therapies.”
“One has to recognize that these agents are costly,” Dr. Ernstoff maintained, with the acquisition cost of the checkpoint inhibitors ranging from roughly $140,000 to $290,000 per year depending on the agent(s) used. This issue will also have to be addressed going forward.
“The future is very bright. There are now 76 trials listed in PDQ [Physician Data Query] of combination PD-1 therapies in melanoma alone,” he concluded. “Immunotherapy continues to capture our imagination.”
The updated intent-to-treat analyses of CheckMate 067 – conducted after all patients had at least 18 months of follow-up – showed that median progression-free survival, one of the trial’s primary endpoints, was now 11.5 months with the combination of nivolumab (Opdivo) and ipilimumab (Yervoy), 6.9 months with nivolumab alone, and 2.9 months with ipilimumab alone, Dr. Wolchok reported at the meeting.
The differences translated to significantly better outcomes with the combination (hazard ratio, 0.42) and with nivolumab (HR, 0.55) as compared with ipilimumab. Moreover, the combination was superior to nivolumab (HR, 0.76).
The overall response rate, the trial’s other primary endpoint, was 57.6% with the combination and 43.7% with nivolumab alone, both of which were superior to the 19.0% with ipilimumab alone.
“While the response rates have not changed, some partial responses have evolved into complete responses over time,” Dr. Wolchok noted.
Findings were similar when patients were stratified by BRAF mutational status. And in exploratory analyses, outcomes were numerically better with the combination than with nivolumab alone regardless of whether tumors had high or low PD-L1 expression.
Safety results were much the same as previously reported. The rate of grade 3 or 4 treatment-related adverse events was 56.5% with the combination, 19.8% with nivolumab monotherapy, and 27.0% with ipilimumab monotherapy. There were no treatment-related deaths with the combination and one with each of the monotherapies.
“There is no common signature adverse event with this combination,” Dr. Wolchok pointed out. “The majority of grade 3 or 4 adverse events resolved in all of the groups with the use of established algorithms. However, as observed in prior studies, most of the endocrine events did not resolve and required hormone replacement.”
About 40% of the combination therapy group stopped treatment because of adverse events. “Interestingly, 68% of these patients who discontinued due to treatment-related adverse events developed a response, and 50% of these responses occurred after treatment had ended,” he reported. “This is very important information for us as we talk to patients and their families about the difficulties of stopping treatment.”
Dr. Wolchok disclosed that he is a consultant for Bristol-Myers Squibb, Genentech, Jounce Therapeutics, Medimmune, Merck, Polaris, Polynoma, Potenza, Tizona, Ziopharm, F-Star, Beigene, Lilly, Advaxis, and Sellas, and that he receives grant/research support from Bristol-Myers Squibb. The trial was sponsored by Bristol-Myers Squibb. Dako collaborated on development of the automated anti–PD-L1 immunohistochemistry assay.
CHICAGO – Immune checkpoint blockade, especially with a combination of agents having complementary mechanisms of action, has durable efficacy when used as initial therapy for advanced melanoma, according to an update of the CheckMate 067 trial.
The trial randomized 945 treatment-naive patients with unresectable stage III or IV melanoma evenly to double-blind treatment with nivolumab, an antibody to the cell surface receptor programmed death 1 (PD-1); ipilimumab, an antibody to the T-cell receptor cytotoxic T-lymphocyte–associated antigen 4 (CTLA4); or the combination.
Initial results, after a median follow-up of about 12.4 months, showed that the risk of progression-free survival events was 58% lower with the combination and 43% lower with nivolumab alone as compared with ipilimumab alone (N Engl J Med. 2015;373[1]:23-34).
The update, now with a median follow-up of 20.7 months, showed that these results held up, with respective 58% and 45% reductions in the risk of events, researchers reported at the annual meeting of the American Society of Clinical Oncology. The combination was also superior to nivolumab alone, netting a 24% lower risk of events. Additionally, no cumulative or new toxicities were seen.
“Based on available evidence, the combination of nivolumab and ipilimumab represents a means to improve outcomes versus nivolumab alone,” said first author Jedd D. Wolchok, MD, PhD, chief of the Melanoma & Immunotherapeutics Service at the Memorial Sloan Kettering Cancer Center in New York. “Additional insights will be gained with the emergence of overall survival data.”
Neither tumor expression of PD-L1, a ligand of PD-1, nor presence of a BRAF mutation was very helpful in identifying patients who would benefit to a greater extent from these therapies.
The findings add to evidence establishing the efficacy of combination immunotherapy in melanoma, according to invited discussant Marc S. Ernstoff, MD, professor and chair of the department of medicine at the Roswell Park Cancer Institute in Buffalo, N.Y. At the same time, the trial left unanswered questions such as what strategy should be used after progression on either or both agents, and what are the appropriate doses and durations of therapy. Also unclear is which type of therapy to use first line in patients with BRAF mutations, he added. “Whether you start with immunotherapy or targeted therapy in BRAF-mutated patients is still in equipoise, and I would encourage everyone here to participate in the ECOG 6134 trial looking at the randomization of immune checkpoint therapy versus targeted therapy in BRAF-mutated patients,” he said. “The biomarker studies are still provocative, and we still need a lot more data to be able to preselect patients who might benefit from either of these therapies.”
“One has to recognize that these agents are costly,” Dr. Ernstoff maintained, with the acquisition cost of the checkpoint inhibitors ranging from roughly $140,000 to $290,000 per year depending on the agent(s) used. This issue will also have to be addressed going forward.
“The future is very bright. There are now 76 trials listed in PDQ [Physician Data Query] of combination PD-1 therapies in melanoma alone,” he concluded. “Immunotherapy continues to capture our imagination.”
The updated intent-to-treat analyses of CheckMate 067 – conducted after all patients had at least 18 months of follow-up – showed that median progression-free survival, one of the trial’s primary endpoints, was now 11.5 months with the combination of nivolumab (Opdivo) and ipilimumab (Yervoy), 6.9 months with nivolumab alone, and 2.9 months with ipilimumab alone, Dr. Wolchok reported at the meeting.
The differences translated to significantly better outcomes with the combination (hazard ratio, 0.42) and with nivolumab (HR, 0.55) as compared with ipilimumab. Moreover, the combination was superior to nivolumab (HR, 0.76).
The overall response rate, the trial’s other primary endpoint, was 57.6% with the combination and 43.7% with nivolumab alone, both of which were superior to the 19.0% with ipilimumab alone.
“While the response rates have not changed, some partial responses have evolved into complete responses over time,” Dr. Wolchok noted.
Findings were similar when patients were stratified by BRAF mutational status. And in exploratory analyses, outcomes were numerically better with the combination than with nivolumab alone regardless of whether tumors had high or low PD-L1 expression.
Safety results were much the same as previously reported. The rate of grade 3 or 4 treatment-related adverse events was 56.5% with the combination, 19.8% with nivolumab monotherapy, and 27.0% with ipilimumab monotherapy. There were no treatment-related deaths with the combination and one with each of the monotherapies.
“There is no common signature adverse event with this combination,” Dr. Wolchok pointed out. “The majority of grade 3 or 4 adverse events resolved in all of the groups with the use of established algorithms. However, as observed in prior studies, most of the endocrine events did not resolve and required hormone replacement.”
About 40% of the combination therapy group stopped treatment because of adverse events. “Interestingly, 68% of these patients who discontinued due to treatment-related adverse events developed a response, and 50% of these responses occurred after treatment had ended,” he reported. “This is very important information for us as we talk to patients and their families about the difficulties of stopping treatment.”
Dr. Wolchok disclosed that he is a consultant for Bristol-Myers Squibb, Genentech, Jounce Therapeutics, Medimmune, Merck, Polaris, Polynoma, Potenza, Tizona, Ziopharm, F-Star, Beigene, Lilly, Advaxis, and Sellas, and that he receives grant/research support from Bristol-Myers Squibb. The trial was sponsored by Bristol-Myers Squibb. Dako collaborated on development of the automated anti–PD-L1 immunohistochemistry assay.
AT THE 2016 ASCO ANNUAL MEETING
Key clinical point: Nivolumab-ipilimumab combination therapy and nivolumab monotherapy are more efficacious than ipilimumab monotherapy when used in the first line for advanced melanoma.
Major finding: The risk of progression-free survival events was lower with nivolumab plus ipilimumab (HR, 0.42) and with nivolumab alone (HR, 0.55) as compared with ipilimumab alone.
Data source: A phase III randomized trial among 945 treatment-naive patients with advanced melanoma (CheckMate 067).
Disclosures: Dr. Wolchok disclosed that he is a consultant for Bristol-Myers Squibb, Genentech, Jounce Therapeutics, Medimmune, Merck, Polaris, Polynoma, Potenza, Tizona, Ziopharm, F-Star, Beigene, Lilly, Advaxis, and Sellas, and that he receives grant/research support from Bristol-Myers Squibb. The trial was sponsored by Bristol-Myers Squibb. Dako collaborated on development of the automated anti-PD-L1 immunohistochemistry assay.

2017 Fellows Application Process Now Open
SHM Fellows designation is a prestigious way to differentiate yourself in the rapidly growing profession of hospital medicine. There are currently 2,000 hospitalists who have earned the FHM/SFHM designation by demonstrating core values of leadership, teamwork, and quality improvement.
The application process is now open. Apply by Sept. 15 to receive an early decision on or before Oct. 28. The regular decision application will remain open through Nov. 30, with a decision notification on or before Dec. 31. Apply now and learn how you can join other hospitalists who have earned this exclusive designation and recognition at www.hospitalmedicine.org/fellows.
SHM Fellows designation is a prestigious way to differentiate yourself in the rapidly growing profession of hospital medicine. There are currently 2,000 hospitalists who have earned the FHM/SFHM designation by demonstrating core values of leadership, teamwork, and quality improvement.
The application process is now open. Apply by Sept. 15 to receive an early decision on or before Oct. 28. The regular decision application will remain open through Nov. 30, with a decision notification on or before Dec. 31. Apply now and learn how you can join other hospitalists who have earned this exclusive designation and recognition at www.hospitalmedicine.org/fellows.
SHM Fellows designation is a prestigious way to differentiate yourself in the rapidly growing profession of hospital medicine. There are currently 2,000 hospitalists who have earned the FHM/SFHM designation by demonstrating core values of leadership, teamwork, and quality improvement.
The application process is now open. Apply by Sept. 15 to receive an early decision on or before Oct. 28. The regular decision application will remain open through Nov. 30, with a decision notification on or before Dec. 31. Apply now and learn how you can join other hospitalists who have earned this exclusive designation and recognition at www.hospitalmedicine.org/fellows.
Academic Hospitalist Academy Has New Location
The eighth annual Academic Hospitalist Academy (AHA) will be held Sept. 12–15 at the Lakeway Resort and Spa in Austin, Texas. This is a can’t-miss event for academic hospitalists. At AHA, you will:
- Gain valuable tools for career development
- Establish a national network
- Take advantage of an effective learning environment with a 1:10
faculty-to-student ratio
- Develop scholarly work and increase scholarly output
- Earn CME credit
Seats are limited. Reserve your spot now at www.academichospitalist.org.
The eighth annual Academic Hospitalist Academy (AHA) will be held Sept. 12–15 at the Lakeway Resort and Spa in Austin, Texas. This is a can’t-miss event for academic hospitalists. At AHA, you will:
- Gain valuable tools for career development
- Establish a national network
- Take advantage of an effective learning environment with a 1:10
faculty-to-student ratio
- Develop scholarly work and increase scholarly output
- Earn CME credit
Seats are limited. Reserve your spot now at www.academichospitalist.org.
The eighth annual Academic Hospitalist Academy (AHA) will be held Sept. 12–15 at the Lakeway Resort and Spa in Austin, Texas. This is a can’t-miss event for academic hospitalists. At AHA, you will:
- Gain valuable tools for career development
- Establish a national network
- Take advantage of an effective learning environment with a 1:10
faculty-to-student ratio
- Develop scholarly work and increase scholarly output
- Earn CME credit
Seats are limited. Reserve your spot now at www.academichospitalist.org.
EC extends marketing authorization for brentuximab vedotin

Photo from Business Wire
The European Commission (EC) has extended the current conditional marketing authorization of brentuximab vedotin (Adcetris) to include the treatment of adults with CD30+ Hodgkin lymphoma (HL) who are at an increased risk of relapse or progression following autologous stem cell transplant (ASCT).
Conditional marketing authorizations are valid for 1 year and are reviewed annually.
The company developing the drug is required to provide comprehensive data confirming the drug’s benefit-risk balance is positive. Once these data are available, the marketing authorization may be converted into a standard marketing authorization.
Drugs are eligible for conditional marketing authorization if they are designated as orphan medicines, intended for use in emergency situations, or designed to treat, prevent, or diagnose seriously debilitating or life-threatening diseases.
The EC previously granted brentuximab vedotin conditional marketing authorization for 2 indications:
- To treat adults with relapsed or refractory CD30+ HL after ASCT or following at least 2 prior therapies when ASCT or multi-agent chemotherapy is not a treatment option
- To treat adults with relapsed or refractory systemic anaplastic large-cell lymphoma (sALCL).
In January 2016, the EC approved a Type II variation to include data on the retreatment of adult patients with HL or sALCL who previously responded to brentuximab vedotin and later relapsed.
Brentuximab vedotin is under joint development by Seattle Genetics and Takeda Pharmaceutical Company Limited.
AETHERA trial
The EC’s decision to extend the conditional marketing authorization of brentuximab vedotin is based on results from the phase 3 AETHERA trial.
The trial was designed to compare brentuximab vedotin to placebo, both administered for up to 16 cycles (approximately 1 year) every 3 weeks following ASCT. Results from the trial were published in The Lancet in March 2015 and presented at the 2014 ASH Annual Meeting.
The study enrolled 329 HL patients at risk of relapse or progression, including 165 on the brentuximab vedotin arm and 164 on the placebo arm.
Patients were eligible for enrollment if they had a history of primary refractory HL, relapsed within a year of receiving frontline chemotherapy, and/or had disease outside of the lymph nodes at the time of pre-ASCT relapse.
Brentuximab vedotin conferred a significant increase in progression-free survival over placebo, with a hazard ratio of 0.57 (P=0.001). The median progression-free survival was 43 months for patients who received brentuximab vedotin and 24 months for those who received placebo.
The most common adverse events (≥20%), of any grade and regardless of causality, in the brentuximab vedotin arm were neutropenia (78%), peripheral sensory neuropathy (56%), thrombocytopenia (41%), anemia (27%), upper respiratory tract infection (26%), fatigue (24%), peripheral motor neuropathy (23%), nausea (22%), cough (21%), and diarrhea (20%).
The most common adverse events (≥20%), of any grade and regardless of causality, in the placebo arm were neutropenia (34%), upper respiratory tract infection (23%), and thrombocytopenia (20%).
In all, 67% of patients on the brentuximab vedotin arm experienced peripheral neuropathy. Of those patients, 85% had resolution (59%) or partial improvement (26%) in symptoms at the time of their last evaluation, with a median time to improvement of 23 weeks (range, 0.1-138). ![]()
Photo from Business Wire
The European Commission (EC) has extended the current conditional marketing authorization of brentuximab vedotin (Adcetris) to include the treatment of adults with CD30+ Hodgkin lymphoma (HL) who are at an increased risk of relapse or progression following autologous stem cell transplant (ASCT).
Conditional marketing authorizations are valid for 1 year and are reviewed annually.
The company developing the drug is required to provide comprehensive data confirming the drug’s benefit-risk balance is positive. Once these data are available, the marketing authorization may be converted into a standard marketing authorization.
Drugs are eligible for conditional marketing authorization if they are designated as orphan medicines, intended for use in emergency situations, or designed to treat, prevent, or diagnose seriously debilitating or life-threatening diseases.
The EC previously granted brentuximab vedotin conditional marketing authorization for 2 indications:
- To treat adults with relapsed or refractory CD30+ HL after ASCT or following at least 2 prior therapies when ASCT or multi-agent chemotherapy is not a treatment option
- To treat adults with relapsed or refractory systemic anaplastic large-cell lymphoma (sALCL).
In January 2016, the EC approved a Type II variation to include data on the retreatment of adult patients with HL or sALCL who previously responded to brentuximab vedotin and later relapsed.
Brentuximab vedotin is under joint development by Seattle Genetics and Takeda Pharmaceutical Company Limited.
AETHERA trial
The EC’s decision to extend the conditional marketing authorization of brentuximab vedotin is based on results from the phase 3 AETHERA trial.
The trial was designed to compare brentuximab vedotin to placebo, both administered for up to 16 cycles (approximately 1 year) every 3 weeks following ASCT. Results from the trial were published in The Lancet in March 2015 and presented at the 2014 ASH Annual Meeting.
The study enrolled 329 HL patients at risk of relapse or progression, including 165 on the brentuximab vedotin arm and 164 on the placebo arm.
Patients were eligible for enrollment if they had a history of primary refractory HL, relapsed within a year of receiving frontline chemotherapy, and/or had disease outside of the lymph nodes at the time of pre-ASCT relapse.
Brentuximab vedotin conferred a significant increase in progression-free survival over placebo, with a hazard ratio of 0.57 (P=0.001). The median progression-free survival was 43 months for patients who received brentuximab vedotin and 24 months for those who received placebo.
The most common adverse events (≥20%), of any grade and regardless of causality, in the brentuximab vedotin arm were neutropenia (78%), peripheral sensory neuropathy (56%), thrombocytopenia (41%), anemia (27%), upper respiratory tract infection (26%), fatigue (24%), peripheral motor neuropathy (23%), nausea (22%), cough (21%), and diarrhea (20%).
The most common adverse events (≥20%), of any grade and regardless of causality, in the placebo arm were neutropenia (34%), upper respiratory tract infection (23%), and thrombocytopenia (20%).
In all, 67% of patients on the brentuximab vedotin arm experienced peripheral neuropathy. Of those patients, 85% had resolution (59%) or partial improvement (26%) in symptoms at the time of their last evaluation, with a median time to improvement of 23 weeks (range, 0.1-138). ![]()
Photo from Business Wire
The European Commission (EC) has extended the current conditional marketing authorization of brentuximab vedotin (Adcetris) to include the treatment of adults with CD30+ Hodgkin lymphoma (HL) who are at an increased risk of relapse or progression following autologous stem cell transplant (ASCT).
Conditional marketing authorizations are valid for 1 year and are reviewed annually.
The company developing the drug is required to provide comprehensive data confirming the drug’s benefit-risk balance is positive. Once these data are available, the marketing authorization may be converted into a standard marketing authorization.
Drugs are eligible for conditional marketing authorization if they are designated as orphan medicines, intended for use in emergency situations, or designed to treat, prevent, or diagnose seriously debilitating or life-threatening diseases.
The EC previously granted brentuximab vedotin conditional marketing authorization for 2 indications:
- To treat adults with relapsed or refractory CD30+ HL after ASCT or following at least 2 prior therapies when ASCT or multi-agent chemotherapy is not a treatment option
- To treat adults with relapsed or refractory systemic anaplastic large-cell lymphoma (sALCL).
In January 2016, the EC approved a Type II variation to include data on the retreatment of adult patients with HL or sALCL who previously responded to brentuximab vedotin and later relapsed.
Brentuximab vedotin is under joint development by Seattle Genetics and Takeda Pharmaceutical Company Limited.
AETHERA trial
The EC’s decision to extend the conditional marketing authorization of brentuximab vedotin is based on results from the phase 3 AETHERA trial.
The trial was designed to compare brentuximab vedotin to placebo, both administered for up to 16 cycles (approximately 1 year) every 3 weeks following ASCT. Results from the trial were published in The Lancet in March 2015 and presented at the 2014 ASH Annual Meeting.
The study enrolled 329 HL patients at risk of relapse or progression, including 165 on the brentuximab vedotin arm and 164 on the placebo arm.
Patients were eligible for enrollment if they had a history of primary refractory HL, relapsed within a year of receiving frontline chemotherapy, and/or had disease outside of the lymph nodes at the time of pre-ASCT relapse.
Brentuximab vedotin conferred a significant increase in progression-free survival over placebo, with a hazard ratio of 0.57 (P=0.001). The median progression-free survival was 43 months for patients who received brentuximab vedotin and 24 months for those who received placebo.
The most common adverse events (≥20%), of any grade and regardless of causality, in the brentuximab vedotin arm were neutropenia (78%), peripheral sensory neuropathy (56%), thrombocytopenia (41%), anemia (27%), upper respiratory tract infection (26%), fatigue (24%), peripheral motor neuropathy (23%), nausea (22%), cough (21%), and diarrhea (20%).
The most common adverse events (≥20%), of any grade and regardless of causality, in the placebo arm were neutropenia (34%), upper respiratory tract infection (23%), and thrombocytopenia (20%).
In all, 67% of patients on the brentuximab vedotin arm experienced peripheral neuropathy. Of those patients, 85% had resolution (59%) or partial improvement (26%) in symptoms at the time of their last evaluation, with a median time to improvement of 23 weeks (range, 0.1-138). ![]()
NHL patients may have higher risk of second cancer

Photo courtesy of NIH
Compared to patients with other common cancers, patients with non-Hodgkin lymphoma (NHL) have a higher risk of developing a second, unrelated malignancy, according to a new study.
Researchers looked at data on more than 2.1 million patients with 10 of the most common cancers and found that patients with NHL or bladder cancer had the highest risk of developing a second malignancy.
The researchers reported these findings in Cancer.
For this study, Karim Chamie, MD, of the University of California, Los Angeles, and his colleagues looked at data from Surveillance, Epidemiology, and End Results database.
The team identified patients age 18 and older who were diagnosed with one of the 10 most common cancers—NHL, melanoma, and prostate, breast, lung, colon, rectal, bladder, uterine, and kidney cancers—between 1992 and 2008.
Of the 2,116,163 patients identified, 170,865 (8.1%) developed a second primary malignancy.
In multivariable analysis, patients with NHL or bladder cancer had the highest risk of developing a second malignancy.
The hazard ratios for patients with NHL were 2.70 for men and 2.88 for women. The hazard ratios for bladder cancer were 1.88 for men and 1.66 for women.
Lung cancer was a common second malignancy for both NHL and bladder cancer patients. NHL patients also tended to develop prostate and breast cancer.
Among patients with 2 incident cancers, 13% died of their initial cancer, and 55% died of their second primary malignancy. Lung cancer was the cause of death in 12% of the patients.
“As clinicians, we can become so focused on surveilling our patients to see if a primary cancer recurs that we sometimes may not be aware that patients can be at risk of developing a second, unrelated cancer,” Dr Chamie said.
He and his colleagues believe this study makes a case for monitoring cancer patients for second malignancies. ![]()
Photo courtesy of NIH
Compared to patients with other common cancers, patients with non-Hodgkin lymphoma (NHL) have a higher risk of developing a second, unrelated malignancy, according to a new study.
Researchers looked at data on more than 2.1 million patients with 10 of the most common cancers and found that patients with NHL or bladder cancer had the highest risk of developing a second malignancy.
The researchers reported these findings in Cancer.
For this study, Karim Chamie, MD, of the University of California, Los Angeles, and his colleagues looked at data from Surveillance, Epidemiology, and End Results database.
The team identified patients age 18 and older who were diagnosed with one of the 10 most common cancers—NHL, melanoma, and prostate, breast, lung, colon, rectal, bladder, uterine, and kidney cancers—between 1992 and 2008.
Of the 2,116,163 patients identified, 170,865 (8.1%) developed a second primary malignancy.
In multivariable analysis, patients with NHL or bladder cancer had the highest risk of developing a second malignancy.
The hazard ratios for patients with NHL were 2.70 for men and 2.88 for women. The hazard ratios for bladder cancer were 1.88 for men and 1.66 for women.
Lung cancer was a common second malignancy for both NHL and bladder cancer patients. NHL patients also tended to develop prostate and breast cancer.
Among patients with 2 incident cancers, 13% died of their initial cancer, and 55% died of their second primary malignancy. Lung cancer was the cause of death in 12% of the patients.
“As clinicians, we can become so focused on surveilling our patients to see if a primary cancer recurs that we sometimes may not be aware that patients can be at risk of developing a second, unrelated cancer,” Dr Chamie said.
He and his colleagues believe this study makes a case for monitoring cancer patients for second malignancies. ![]()
Photo courtesy of NIH
Compared to patients with other common cancers, patients with non-Hodgkin lymphoma (NHL) have a higher risk of developing a second, unrelated malignancy, according to a new study.
Researchers looked at data on more than 2.1 million patients with 10 of the most common cancers and found that patients with NHL or bladder cancer had the highest risk of developing a second malignancy.
The researchers reported these findings in Cancer.
For this study, Karim Chamie, MD, of the University of California, Los Angeles, and his colleagues looked at data from Surveillance, Epidemiology, and End Results database.
The team identified patients age 18 and older who were diagnosed with one of the 10 most common cancers—NHL, melanoma, and prostate, breast, lung, colon, rectal, bladder, uterine, and kidney cancers—between 1992 and 2008.
Of the 2,116,163 patients identified, 170,865 (8.1%) developed a second primary malignancy.
In multivariable analysis, patients with NHL or bladder cancer had the highest risk of developing a second malignancy.
The hazard ratios for patients with NHL were 2.70 for men and 2.88 for women. The hazard ratios for bladder cancer were 1.88 for men and 1.66 for women.
Lung cancer was a common second malignancy for both NHL and bladder cancer patients. NHL patients also tended to develop prostate and breast cancer.
Among patients with 2 incident cancers, 13% died of their initial cancer, and 55% died of their second primary malignancy. Lung cancer was the cause of death in 12% of the patients.
“As clinicians, we can become so focused on surveilling our patients to see if a primary cancer recurs that we sometimes may not be aware that patients can be at risk of developing a second, unrelated cancer,” Dr Chamie said.
He and his colleagues believe this study makes a case for monitoring cancer patients for second malignancies. ![]()
Study reveals global variations of P vivax
from patients in Thailand
Image by Wanlapa Roobsoong
Researchers say they have uncovered the global, evolving, and historic make-up of the malaria parasite Plasmodium vivax.
The group’s study revealed 4 genetically distinct populations of P vivax that provide insight into the movement of the parasite over time and
show how it is still adapting to regional variations in the mosquitoes that transmit P vivax, the humans infected with the parasite, and the drugs used to fight it.
“Our findings show it is evolving in response to antimalarial drugs and adapting to regional differences, indicating a wide range of approaches will likely be necessary to eliminate it globally,” said Jane Carlton, PhD, of New York University in New York, New York.
Dr Carlton and her colleagues reported these findings in Nature Genetics.
The researchers sequenced 182 DNA samples of P vivax collected from patients in 11 countries. The team said this provided new insights into the nature of P vivax as it exists today and also served as a “genetic history book” of the studied regions.
“The DNA data show that P vivax has clearly had a different history of association with global human populations than other malaria parasites, indicating that unique aspects of its biology may have influenced the ways in which it spread around the world,” said Daniel Neafsey, PhD, of the Broad Institute in Cambridge, Massachusetts.
Specifically, the researchers found that Central and South American P vivax populations are genetically diverse and distinct from all other contemporary P vivax populations. The team said this suggests that New World parasites may have been introduced by colonial seafarers and represent a now-eliminated European parasite population.
The researchers also found that contemporary African and South Asian P vivax populations are genetically similar. They said this suggests that South Asian P vivax populations may have genetically mingled with European lineages during the colonial era, or it may reflect ancient connections between human populations in the Eastern Mediterranean, Middle East, and Indian subcontinent.
Another finding was the relatively homogeneous genetic makeup of P vivax in Mexico, which reflects a steady decline of the disease in this country over the last decade.
By contrast, the Papua New Guinea population of P vivax was shown to be very diverse relative to other P vivax populations.
A similar study, which also illustrated the global variations of P vivax, was recently published in Nature Genetics in as well. ![]()
from patients in Thailand
Image by Wanlapa Roobsoong
Researchers say they have uncovered the global, evolving, and historic make-up of the malaria parasite Plasmodium vivax.
The group’s study revealed 4 genetically distinct populations of P vivax that provide insight into the movement of the parasite over time and
show how it is still adapting to regional variations in the mosquitoes that transmit P vivax, the humans infected with the parasite, and the drugs used to fight it.
“Our findings show it is evolving in response to antimalarial drugs and adapting to regional differences, indicating a wide range of approaches will likely be necessary to eliminate it globally,” said Jane Carlton, PhD, of New York University in New York, New York.
Dr Carlton and her colleagues reported these findings in Nature Genetics.
The researchers sequenced 182 DNA samples of P vivax collected from patients in 11 countries. The team said this provided new insights into the nature of P vivax as it exists today and also served as a “genetic history book” of the studied regions.
“The DNA data show that P vivax has clearly had a different history of association with global human populations than other malaria parasites, indicating that unique aspects of its biology may have influenced the ways in which it spread around the world,” said Daniel Neafsey, PhD, of the Broad Institute in Cambridge, Massachusetts.
Specifically, the researchers found that Central and South American P vivax populations are genetically diverse and distinct from all other contemporary P vivax populations. The team said this suggests that New World parasites may have been introduced by colonial seafarers and represent a now-eliminated European parasite population.
The researchers also found that contemporary African and South Asian P vivax populations are genetically similar. They said this suggests that South Asian P vivax populations may have genetically mingled with European lineages during the colonial era, or it may reflect ancient connections between human populations in the Eastern Mediterranean, Middle East, and Indian subcontinent.
Another finding was the relatively homogeneous genetic makeup of P vivax in Mexico, which reflects a steady decline of the disease in this country over the last decade.
By contrast, the Papua New Guinea population of P vivax was shown to be very diverse relative to other P vivax populations.
A similar study, which also illustrated the global variations of P vivax, was recently published in Nature Genetics in as well. ![]()
from patients in Thailand
Image by Wanlapa Roobsoong
Researchers say they have uncovered the global, evolving, and historic make-up of the malaria parasite Plasmodium vivax.
The group’s study revealed 4 genetically distinct populations of P vivax that provide insight into the movement of the parasite over time and
show how it is still adapting to regional variations in the mosquitoes that transmit P vivax, the humans infected with the parasite, and the drugs used to fight it.
“Our findings show it is evolving in response to antimalarial drugs and adapting to regional differences, indicating a wide range of approaches will likely be necessary to eliminate it globally,” said Jane Carlton, PhD, of New York University in New York, New York.
Dr Carlton and her colleagues reported these findings in Nature Genetics.
The researchers sequenced 182 DNA samples of P vivax collected from patients in 11 countries. The team said this provided new insights into the nature of P vivax as it exists today and also served as a “genetic history book” of the studied regions.
“The DNA data show that P vivax has clearly had a different history of association with global human populations than other malaria parasites, indicating that unique aspects of its biology may have influenced the ways in which it spread around the world,” said Daniel Neafsey, PhD, of the Broad Institute in Cambridge, Massachusetts.
Specifically, the researchers found that Central and South American P vivax populations are genetically diverse and distinct from all other contemporary P vivax populations. The team said this suggests that New World parasites may have been introduced by colonial seafarers and represent a now-eliminated European parasite population.
The researchers also found that contemporary African and South Asian P vivax populations are genetically similar. They said this suggests that South Asian P vivax populations may have genetically mingled with European lineages during the colonial era, or it may reflect ancient connections between human populations in the Eastern Mediterranean, Middle East, and Indian subcontinent.
Another finding was the relatively homogeneous genetic makeup of P vivax in Mexico, which reflects a steady decline of the disease in this country over the last decade.
By contrast, the Papua New Guinea population of P vivax was shown to be very diverse relative to other P vivax populations.
A similar study, which also illustrated the global variations of P vivax, was recently published in Nature Genetics in as well. ![]()
Results support INR self-monitoring/management

Results of a systematic review support self-monitoring and self-management for patients on long-term oral anticoagulation therapy.
Researchers found that both self-monitoring and self-management were associated with a reduction in thromboembolic events when compared to standard monitoring.
Self-management, but not self-monitoring, was associated with a reduction in all-cause mortality.
And neither practice appeared to have an effect on major bleeding.
These results were published in the Cochrane Database of Systematic Reviews.
Point-of-care testing has made it possible for patients on long-term oral anticoagulation therapy to monitor their own international normalized ratio (INR).
Patients can either adjust their own medication according to a pre-determined dose-INR schedule, which is known as self-management, or they can call into a clinic to be told the appropriate dose adjustment, which is known as self-monitoring.
For the current review, Carl Heneghan, BM BCh, DPhil, of the University of Oxford in the UK, and his colleagues evaluated data from 28 randomized trials including 8950 patients. The trials compared self-monitoring and self-management with standard monitoring.
The researchers said pooled estimates showed a reduction in thromboembolic events with both self-management and self-monitoring, compared to standard monitoring.
Eleven studies including 3497 patients showed the relative risk (RR) of thromboembolic events was 0.47 (95% CI 0.31 to 0.70) for self-management compared to standard monitoring.
Seven studies including 4097 patients showed the RR of thromboembolic events was 0.69 (95% CI 0.49 to 0.97) for self-monitoring compared to standard monitoring.
Eight studies including 3058 patients suggested that self-management caused a reduction in all-cause mortality (RR=0.55, 95% CI 0.36 to 0.84) when compared to standard monitoring.
But 3 studies of 3300 patients indicated that self-monitoring did not reduce all-cause mortality (RR=0.94, 95% CI 0.78 to 1.15).
In 20 trials of 8018 patients, neither self-monitoring nor self-management reduced major hemorrhage (RR=0.95, 95% CI, 0.80 to 1.12) when compared to standard monitoring.
For all of these analyses, the quality of evidence was moderate.
“Our review of the latest research finds that self-monitoring alone does indeed result in a statistically significant reduction in thromboembolic events, whereas our previous review did not find this effect,” Dr Heneghan said.
“Suitable patients still need to be identified and educated for self-monitoring as it is not feasible for everyone, but the evidence clearly demonstrates that self-monitoring can improve the quality of oral anticoagulation therapy and adds weight to the argument that more patients should be given the opportunity to benefit from this treatment approach.”
The current review is an update on a previous review carried out by the same researchers in 2010. It includes 10 new studies of 4227 participants. ![]()
Results of a systematic review support self-monitoring and self-management for patients on long-term oral anticoagulation therapy.
Researchers found that both self-monitoring and self-management were associated with a reduction in thromboembolic events when compared to standard monitoring.
Self-management, but not self-monitoring, was associated with a reduction in all-cause mortality.
And neither practice appeared to have an effect on major bleeding.
These results were published in the Cochrane Database of Systematic Reviews.
Point-of-care testing has made it possible for patients on long-term oral anticoagulation therapy to monitor their own international normalized ratio (INR).
Patients can either adjust their own medication according to a pre-determined dose-INR schedule, which is known as self-management, or they can call into a clinic to be told the appropriate dose adjustment, which is known as self-monitoring.
For the current review, Carl Heneghan, BM BCh, DPhil, of the University of Oxford in the UK, and his colleagues evaluated data from 28 randomized trials including 8950 patients. The trials compared self-monitoring and self-management with standard monitoring.
The researchers said pooled estimates showed a reduction in thromboembolic events with both self-management and self-monitoring, compared to standard monitoring.
Eleven studies including 3497 patients showed the relative risk (RR) of thromboembolic events was 0.47 (95% CI 0.31 to 0.70) for self-management compared to standard monitoring.
Seven studies including 4097 patients showed the RR of thromboembolic events was 0.69 (95% CI 0.49 to 0.97) for self-monitoring compared to standard monitoring.
Eight studies including 3058 patients suggested that self-management caused a reduction in all-cause mortality (RR=0.55, 95% CI 0.36 to 0.84) when compared to standard monitoring.
But 3 studies of 3300 patients indicated that self-monitoring did not reduce all-cause mortality (RR=0.94, 95% CI 0.78 to 1.15).
In 20 trials of 8018 patients, neither self-monitoring nor self-management reduced major hemorrhage (RR=0.95, 95% CI, 0.80 to 1.12) when compared to standard monitoring.
For all of these analyses, the quality of evidence was moderate.
“Our review of the latest research finds that self-monitoring alone does indeed result in a statistically significant reduction in thromboembolic events, whereas our previous review did not find this effect,” Dr Heneghan said.
“Suitable patients still need to be identified and educated for self-monitoring as it is not feasible for everyone, but the evidence clearly demonstrates that self-monitoring can improve the quality of oral anticoagulation therapy and adds weight to the argument that more patients should be given the opportunity to benefit from this treatment approach.”
The current review is an update on a previous review carried out by the same researchers in 2010. It includes 10 new studies of 4227 participants. ![]()
Results of a systematic review support self-monitoring and self-management for patients on long-term oral anticoagulation therapy.
Researchers found that both self-monitoring and self-management were associated with a reduction in thromboembolic events when compared to standard monitoring.
Self-management, but not self-monitoring, was associated with a reduction in all-cause mortality.
And neither practice appeared to have an effect on major bleeding.
These results were published in the Cochrane Database of Systematic Reviews.
Point-of-care testing has made it possible for patients on long-term oral anticoagulation therapy to monitor their own international normalized ratio (INR).
Patients can either adjust their own medication according to a pre-determined dose-INR schedule, which is known as self-management, or they can call into a clinic to be told the appropriate dose adjustment, which is known as self-monitoring.
For the current review, Carl Heneghan, BM BCh, DPhil, of the University of Oxford in the UK, and his colleagues evaluated data from 28 randomized trials including 8950 patients. The trials compared self-monitoring and self-management with standard monitoring.
The researchers said pooled estimates showed a reduction in thromboembolic events with both self-management and self-monitoring, compared to standard monitoring.
Eleven studies including 3497 patients showed the relative risk (RR) of thromboembolic events was 0.47 (95% CI 0.31 to 0.70) for self-management compared to standard monitoring.
Seven studies including 4097 patients showed the RR of thromboembolic events was 0.69 (95% CI 0.49 to 0.97) for self-monitoring compared to standard monitoring.
Eight studies including 3058 patients suggested that self-management caused a reduction in all-cause mortality (RR=0.55, 95% CI 0.36 to 0.84) when compared to standard monitoring.
But 3 studies of 3300 patients indicated that self-monitoring did not reduce all-cause mortality (RR=0.94, 95% CI 0.78 to 1.15).
In 20 trials of 8018 patients, neither self-monitoring nor self-management reduced major hemorrhage (RR=0.95, 95% CI, 0.80 to 1.12) when compared to standard monitoring.
For all of these analyses, the quality of evidence was moderate.
“Our review of the latest research finds that self-monitoring alone does indeed result in a statistically significant reduction in thromboembolic events, whereas our previous review did not find this effect,” Dr Heneghan said.
“Suitable patients still need to be identified and educated for self-monitoring as it is not feasible for everyone, but the evidence clearly demonstrates that self-monitoring can improve the quality of oral anticoagulation therapy and adds weight to the argument that more patients should be given the opportunity to benefit from this treatment approach.”
The current review is an update on a previous review carried out by the same researchers in 2010. It includes 10 new studies of 4227 participants. ![]()
Can Mindfulness Components Added To A Diet-Exercise Program Improve Weight Loss Outcomes?
Study Overview
Objective. To determine whether weight loss and cardiometabolic risk factors are improved when mindfulness training is added to a diet-exercise program.
Design. 2-arm randomized controlled trial.
Setting and participants. Study participants were recruited through fliers, newspaper advertisements, online postings, and referrals at University of California, San Francisco clinics, and were enrolled from July 2009 to February 2012. Inclusion criteria were body mass index (BMI) between 30 and 45.9, abdominal obesity (waist circumference > 102 cm for men and > 88 cm for women), and age 18 or older. Exclusion criteria were current involvement with diet program or diet mediation, diabetes mellitus, fasting glucose ≥ 126 mg/dL, or hemoglobin A1c (HbA1C) between 6.0% and 6.5% with abnormal oral glucose tolerance test. Participants were randomized in a 1:1 ratio to one of 2 weight loss program arms using a computer-generated randomization sequence.
Intervention. In both arms, participants received general diet and exercise guidelines prescribing healthy eating and frequent exercise delivered in 16 sessions lasting 2 to 2½ hours and one all-day session over 5.5 months. Participants in the mindfulness intervention additionally received mindfulness training for eating, physical activity, and stress management from mindfulness mediation instructors and a registered dietician. They also followed guidelines at home, which included practicing meditation for up to 30 minutes 6 days a week, mini-meditations, and eating mindfully. To control for the activities and attention inherent in the mindfulness arm (eg, social support, expectation of benefit, snacks provided during mindful eating exercises, at home practice), the control arm was an “active control” and included additional nutritional and physical activity information, snacks, strength training, home activities, conversations about society and weight loss, and low-dose progressive muscle relaxation and cognitive-behavioral training. Active control materials were delivered by one of 3 registered dieticians.
Main outcomes measures. The primary outcome was 18-month weight change. Participants’ weight, height, blood pressure, and weight circumference were measured at baseline and 3, 6, 12, and 18 months between 8 am and 10 am. Measurements were taken under fasting conditions and by arm-blinded staff. Blood samples were taken to assess secondary outcome changes in glucose, lipid, HbA1C, insulin, and C-reactive protein. Researchers also collected anonymous qualitative feedback from participants and supervisors to do a secondary analysis assessing differences in effectiveness and helpfulness of mindfulness teachings among instructors.
Main results. Of the potential participants that contacted the study team in response to recruitment efforts (n = 1485), 216 were fully eligible based on criteria and a screening visit. Participants that consented to participate (n = 194) were randomized. Participants across both groups were predominantly female, of European ethnic origin, and similar in age: mindfulness group, 47.2 years (13.0) and active control group, 47.8 years (12.4). At baseline, the mindfulness and active control arms had average BMIs of 35.4 (3.5) and 35.6 (3.8), respectively. Baseline characteristics, session attendance, and 18-month retention were similar for both arms. Participants in the mindfulness arm reported completing 70% (2.1 hours per week, SD = 1.2) of the recommended meditation time and eating 57% (SD = 29) of meals mindfully.
Weight loss outcomes between groups favored the mindfulness arms, but results were not significant. The largest difference of –1.9 kg (95% CI –4.5 to 0.8; P = 0.17) was at 12 months. The difference persisted at 18 months with –1.7 kg (95% CI –4.7 to 1.2 kg; P = 0.24). The mindfulness arm lost 4.2 kg (95% CI –6.2 to 2.2 kg) while the active control arm lost 2.4 kg (95% CI –4.5 to –0.3 kg).
Cardiometabolic outcomes at 12 months showed group differences in fasting glucose that favored the mindfulness arm, –3.1 mg/dL (95% CI 26.3 to 0.1; P = 0.06), while there was a significant group difference at 18 months, –4.1 mg/dL (95% CI –7.3 to –0.9; P = 0.01). Data at 18-months showed that normal glucose changed minimally in the mindfulness arm, –0.31 mg/dL (95% CI –2.5 to 1.9), but increased in the active control arm 3.8 mg/dL (95% CI 1.5 to 6.1). Other cardiometabolic outcomes (ie, triglyceride/HDL ratio and triglycerides) showed significance at 12 months, favoring the mindfulness arm, but not at 18 months. Although not all were statistically significant, 9 of 11 outcomes favored the mindfulness arm at 18 months.
Significant interactions (P < 0.05) were found between arm and enrollment rounds categorized by mindfulness instructor on weight, BMI, fasting glucose, homeostatic homeostasis model assessment of insulin resistance (defined as [glucose x insulin/{40 × 33.25}]), and HbA1c, with a marginally significant effect for waist circumference (P = 0.08). Qualitative feedback on mindfulness instructors showed that in the group with a lowly rated instructor, participants lost less weight at 18 months (–2.0 kg [95% CI –4.7 to 0.7]), compared to participants in groups with highly rated instructors (–6.3 kg [95% CI –9.1 to –3.6]; P = 0.02). Similar trends followed for reductions in BMI and waist circumference.
Conclusions. With regard to weight loss outcomes, a mindfulness-enhanced diet-exercise program and an active control arm did not show substantial differences. Some evidence, however, suggests modest benefit of added mindfulness components, which may lead to long-term maintenance of fasting glucose levels and improved atherogenic lipid profiles.
Commentary
Mindfulness, or nonjudgmental focus on the present moment, has been utilized by many interventions targeted at self-regulated behavior [1]. Mindfulness interventions aim to promote healthy behavior changes by encouraging careful monitoring of behavior reactivity. Weight loss and weight loss maintenance have been of particular interest with this approach because mindfulness-based interventions may promote long-term maintenance of weight loss [2]. This maintenance is achieved through a focus on modifying health behaviors, rather than a focus on weight loss alone [3]. Mindfulness has been incorporated into weight loss interventions through yoga practices [4] and mindfulness meditation [5].
Several studies have explored the relationship between mindfulness and weight loss in various populations, highlighting mindfulness’s role in weight loss and behavior change. Most notably, mindfulness interventions have shown improvements in fasting glucose levels [6], psychological distress [7], self-efficacy, weight loss, eating behaviors, and physical activity [8–10]. Despite being well designed, this study by Daubenmier et al did not find significant changes in weight loss. However, secondary outcomes related to weight, metabolic, syndrome, and cardiovascular risk showed modest improvements with mindfulness. These results may correlate to previous findings showing that lifestyle changes many not result in weight loss but can reverse or reduce disorders related to obesity [11].
The study was strengthened by randomization, intention-to-treat analysis, objective measures by arm-blinded staff, standardized measuring conditions, balanced participant allocation to each arm, 1-year follow-up, and qualitative feedback on instructors to assess whether weight loss may be instructor-dependent. In addition, the authors made an effort to mask their intention to test the effects of a mindfulness-enhanced intervention. They designed a rigorous active control intervention arm by controlling for attention, social support, expectations of benefit, diet-exercise guidelines, and elements of a mindfulness approach to stress management. An additional strength included a cost-analysis of adding mindfulness components. The generalizability of the results may be limited as the study population were predominantly white females and most had a bachelor’s degree. The study sample was also disproportionately menopausal women, a group that especially struggles with weight loss. This demographic factor may be responsible for the lack of significant weight loss. Other limitations of this study include participant dropout and variability between instructor styles, although the latter was explored in a secondary analysis of weight loss differences between instructors.
The researchers discussed how the active control intervention arm may have contributed to the lack of significant weight loss difference between groups. The researchers also highlighted that participants randomized to the mindfulness arm that were not interested in mindfulness practices may have benefitted less than those who were interested. This combined with the modest diet and exercise components of the intervention may also explain the lack of significance in results. It may also explain why some outcomes were significant at earlier months but attenuated by 18 months. Future studies should assess incorporating more intense exercise and diet approaches, as well as continuous contact throughout the 18-month time period.
Applications for Clinical Practice
This study demonstrated that mindfulness components added to a diet-exercise program can be helpful in promoting metabolic changes but not necessarily weight loss. Since metabolic changes can be protective against morbidities (eg, type 2 diabetes), mindfulness can be a powerful and cost-effective approach within clinical practice. Mindfulness practices can also be easily implemented in various settings and with diverse populations. Future studies should explore adding mindfulness components to more intensive weight loss interventions. Providers and health care settings should consider incorporating mindfulness practices into weight management counseling and programs.
—Michelle J. Williamson and Katrina F. Mateo, MPH
1. Caldwell KL, Baime MJ, Wolever RQ. Mindfulness based approaches to obesity and weight loss maintenance. J Ment Health Couns 2012;34:26982.
2. O’Reilly GA, Cook L, Spruijt-Metz D, Black DS. Mindfulness-based interventions for obesity-related eating behaviours: A literature review. Obes Rev 2014;15:453–61.
3. Robison J. Health at every size: Toward a new paradigm of weight and health. MedGenMed 2005;7:13.
4. Godsey J. The role of mindfulness based interventions in the treatment of obesity and eating disorders: An integrative review. Complement Ther Med 2013;21:430–9.
5. Keune PM, Forintos DP. Mindfulness meditation: A preliminary study on meditation practice during everyday life activities and its association with well-being. Psychol Top 2010;19:373–86.
6. Mason AE, Epel ES, Kristeller J, et al. Effects of a mindfulness-based intervention on mindful eating, sweets consumption, and fasting glucose levels in obese adults: data from the SHINE randomized controlled trial. J Behav Med 2016;39:201–13.
7. Dalen J, Smith BW, Shelley BM, et al. Pilot study: Mindful Eating and Living (MEAL): Weight, eating behavior, and psychological outcomes associated with a mindfulness-based intervention for people with obesity. Complement Ther Med 2010;18:260–64.
8. Kristeller JL, Wolever RQ, Sheets V. Mindfulness-based eating awareness training (MB-EAT) for binge eating: A randomized clinical trial. Mindfulness 2013;5:282–97.
9. Miller C, Kristeller JL, Headings A, Nagaraja H. Comparison of a mindful eating intervention to a diabetes self- management intervention among adults with type 2 diabetes: a randomized controlled trial. Health Educ Behav 2013;41:145–54.
10. Timmerman GM, Brown A. The effect of a mindful restaurant eating intervention on weight management in women. J Nutr Educ Behav 2012;44:22–8.
11. Bacon L, Stern JS, Van Loan MD, Keim NL. Size acceptance and intuitive eating improve health for obese, female chronic dieters. J Am Diet Assoc 2005;105:929–36.
Study Overview
Objective. To determine whether weight loss and cardiometabolic risk factors are improved when mindfulness training is added to a diet-exercise program.
Design. 2-arm randomized controlled trial.
Setting and participants. Study participants were recruited through fliers, newspaper advertisements, online postings, and referrals at University of California, San Francisco clinics, and were enrolled from July 2009 to February 2012. Inclusion criteria were body mass index (BMI) between 30 and 45.9, abdominal obesity (waist circumference > 102 cm for men and > 88 cm for women), and age 18 or older. Exclusion criteria were current involvement with diet program or diet mediation, diabetes mellitus, fasting glucose ≥ 126 mg/dL, or hemoglobin A1c (HbA1C) between 6.0% and 6.5% with abnormal oral glucose tolerance test. Participants were randomized in a 1:1 ratio to one of 2 weight loss program arms using a computer-generated randomization sequence.
Intervention. In both arms, participants received general diet and exercise guidelines prescribing healthy eating and frequent exercise delivered in 16 sessions lasting 2 to 2½ hours and one all-day session over 5.5 months. Participants in the mindfulness intervention additionally received mindfulness training for eating, physical activity, and stress management from mindfulness mediation instructors and a registered dietician. They also followed guidelines at home, which included practicing meditation for up to 30 minutes 6 days a week, mini-meditations, and eating mindfully. To control for the activities and attention inherent in the mindfulness arm (eg, social support, expectation of benefit, snacks provided during mindful eating exercises, at home practice), the control arm was an “active control” and included additional nutritional and physical activity information, snacks, strength training, home activities, conversations about society and weight loss, and low-dose progressive muscle relaxation and cognitive-behavioral training. Active control materials were delivered by one of 3 registered dieticians.
Main outcomes measures. The primary outcome was 18-month weight change. Participants’ weight, height, blood pressure, and weight circumference were measured at baseline and 3, 6, 12, and 18 months between 8 am and 10 am. Measurements were taken under fasting conditions and by arm-blinded staff. Blood samples were taken to assess secondary outcome changes in glucose, lipid, HbA1C, insulin, and C-reactive protein. Researchers also collected anonymous qualitative feedback from participants and supervisors to do a secondary analysis assessing differences in effectiveness and helpfulness of mindfulness teachings among instructors.
Main results. Of the potential participants that contacted the study team in response to recruitment efforts (n = 1485), 216 were fully eligible based on criteria and a screening visit. Participants that consented to participate (n = 194) were randomized. Participants across both groups were predominantly female, of European ethnic origin, and similar in age: mindfulness group, 47.2 years (13.0) and active control group, 47.8 years (12.4). At baseline, the mindfulness and active control arms had average BMIs of 35.4 (3.5) and 35.6 (3.8), respectively. Baseline characteristics, session attendance, and 18-month retention were similar for both arms. Participants in the mindfulness arm reported completing 70% (2.1 hours per week, SD = 1.2) of the recommended meditation time and eating 57% (SD = 29) of meals mindfully.
Weight loss outcomes between groups favored the mindfulness arms, but results were not significant. The largest difference of –1.9 kg (95% CI –4.5 to 0.8; P = 0.17) was at 12 months. The difference persisted at 18 months with –1.7 kg (95% CI –4.7 to 1.2 kg; P = 0.24). The mindfulness arm lost 4.2 kg (95% CI –6.2 to 2.2 kg) while the active control arm lost 2.4 kg (95% CI –4.5 to –0.3 kg).
Cardiometabolic outcomes at 12 months showed group differences in fasting glucose that favored the mindfulness arm, –3.1 mg/dL (95% CI 26.3 to 0.1; P = 0.06), while there was a significant group difference at 18 months, –4.1 mg/dL (95% CI –7.3 to –0.9; P = 0.01). Data at 18-months showed that normal glucose changed minimally in the mindfulness arm, –0.31 mg/dL (95% CI –2.5 to 1.9), but increased in the active control arm 3.8 mg/dL (95% CI 1.5 to 6.1). Other cardiometabolic outcomes (ie, triglyceride/HDL ratio and triglycerides) showed significance at 12 months, favoring the mindfulness arm, but not at 18 months. Although not all were statistically significant, 9 of 11 outcomes favored the mindfulness arm at 18 months.
Significant interactions (P < 0.05) were found between arm and enrollment rounds categorized by mindfulness instructor on weight, BMI, fasting glucose, homeostatic homeostasis model assessment of insulin resistance (defined as [glucose x insulin/{40 × 33.25}]), and HbA1c, with a marginally significant effect for waist circumference (P = 0.08). Qualitative feedback on mindfulness instructors showed that in the group with a lowly rated instructor, participants lost less weight at 18 months (–2.0 kg [95% CI –4.7 to 0.7]), compared to participants in groups with highly rated instructors (–6.3 kg [95% CI –9.1 to –3.6]; P = 0.02). Similar trends followed for reductions in BMI and waist circumference.
Conclusions. With regard to weight loss outcomes, a mindfulness-enhanced diet-exercise program and an active control arm did not show substantial differences. Some evidence, however, suggests modest benefit of added mindfulness components, which may lead to long-term maintenance of fasting glucose levels and improved atherogenic lipid profiles.
Commentary
Mindfulness, or nonjudgmental focus on the present moment, has been utilized by many interventions targeted at self-regulated behavior [1]. Mindfulness interventions aim to promote healthy behavior changes by encouraging careful monitoring of behavior reactivity. Weight loss and weight loss maintenance have been of particular interest with this approach because mindfulness-based interventions may promote long-term maintenance of weight loss [2]. This maintenance is achieved through a focus on modifying health behaviors, rather than a focus on weight loss alone [3]. Mindfulness has been incorporated into weight loss interventions through yoga practices [4] and mindfulness meditation [5].
Several studies have explored the relationship between mindfulness and weight loss in various populations, highlighting mindfulness’s role in weight loss and behavior change. Most notably, mindfulness interventions have shown improvements in fasting glucose levels [6], psychological distress [7], self-efficacy, weight loss, eating behaviors, and physical activity [8–10]. Despite being well designed, this study by Daubenmier et al did not find significant changes in weight loss. However, secondary outcomes related to weight, metabolic, syndrome, and cardiovascular risk showed modest improvements with mindfulness. These results may correlate to previous findings showing that lifestyle changes many not result in weight loss but can reverse or reduce disorders related to obesity [11].
The study was strengthened by randomization, intention-to-treat analysis, objective measures by arm-blinded staff, standardized measuring conditions, balanced participant allocation to each arm, 1-year follow-up, and qualitative feedback on instructors to assess whether weight loss may be instructor-dependent. In addition, the authors made an effort to mask their intention to test the effects of a mindfulness-enhanced intervention. They designed a rigorous active control intervention arm by controlling for attention, social support, expectations of benefit, diet-exercise guidelines, and elements of a mindfulness approach to stress management. An additional strength included a cost-analysis of adding mindfulness components. The generalizability of the results may be limited as the study population were predominantly white females and most had a bachelor’s degree. The study sample was also disproportionately menopausal women, a group that especially struggles with weight loss. This demographic factor may be responsible for the lack of significant weight loss. Other limitations of this study include participant dropout and variability between instructor styles, although the latter was explored in a secondary analysis of weight loss differences between instructors.
The researchers discussed how the active control intervention arm may have contributed to the lack of significant weight loss difference between groups. The researchers also highlighted that participants randomized to the mindfulness arm that were not interested in mindfulness practices may have benefitted less than those who were interested. This combined with the modest diet and exercise components of the intervention may also explain the lack of significance in results. It may also explain why some outcomes were significant at earlier months but attenuated by 18 months. Future studies should assess incorporating more intense exercise and diet approaches, as well as continuous contact throughout the 18-month time period.
Applications for Clinical Practice
This study demonstrated that mindfulness components added to a diet-exercise program can be helpful in promoting metabolic changes but not necessarily weight loss. Since metabolic changes can be protective against morbidities (eg, type 2 diabetes), mindfulness can be a powerful and cost-effective approach within clinical practice. Mindfulness practices can also be easily implemented in various settings and with diverse populations. Future studies should explore adding mindfulness components to more intensive weight loss interventions. Providers and health care settings should consider incorporating mindfulness practices into weight management counseling and programs.
—Michelle J. Williamson and Katrina F. Mateo, MPH
Study Overview
Objective. To determine whether weight loss and cardiometabolic risk factors are improved when mindfulness training is added to a diet-exercise program.
Design. 2-arm randomized controlled trial.
Setting and participants. Study participants were recruited through fliers, newspaper advertisements, online postings, and referrals at University of California, San Francisco clinics, and were enrolled from July 2009 to February 2012. Inclusion criteria were body mass index (BMI) between 30 and 45.9, abdominal obesity (waist circumference > 102 cm for men and > 88 cm for women), and age 18 or older. Exclusion criteria were current involvement with diet program or diet mediation, diabetes mellitus, fasting glucose ≥ 126 mg/dL, or hemoglobin A1c (HbA1C) between 6.0% and 6.5% with abnormal oral glucose tolerance test. Participants were randomized in a 1:1 ratio to one of 2 weight loss program arms using a computer-generated randomization sequence.
Intervention. In both arms, participants received general diet and exercise guidelines prescribing healthy eating and frequent exercise delivered in 16 sessions lasting 2 to 2½ hours and one all-day session over 5.5 months. Participants in the mindfulness intervention additionally received mindfulness training for eating, physical activity, and stress management from mindfulness mediation instructors and a registered dietician. They also followed guidelines at home, which included practicing meditation for up to 30 minutes 6 days a week, mini-meditations, and eating mindfully. To control for the activities and attention inherent in the mindfulness arm (eg, social support, expectation of benefit, snacks provided during mindful eating exercises, at home practice), the control arm was an “active control” and included additional nutritional and physical activity information, snacks, strength training, home activities, conversations about society and weight loss, and low-dose progressive muscle relaxation and cognitive-behavioral training. Active control materials were delivered by one of 3 registered dieticians.
Main outcomes measures. The primary outcome was 18-month weight change. Participants’ weight, height, blood pressure, and weight circumference were measured at baseline and 3, 6, 12, and 18 months between 8 am and 10 am. Measurements were taken under fasting conditions and by arm-blinded staff. Blood samples were taken to assess secondary outcome changes in glucose, lipid, HbA1C, insulin, and C-reactive protein. Researchers also collected anonymous qualitative feedback from participants and supervisors to do a secondary analysis assessing differences in effectiveness and helpfulness of mindfulness teachings among instructors.
Main results. Of the potential participants that contacted the study team in response to recruitment efforts (n = 1485), 216 were fully eligible based on criteria and a screening visit. Participants that consented to participate (n = 194) were randomized. Participants across both groups were predominantly female, of European ethnic origin, and similar in age: mindfulness group, 47.2 years (13.0) and active control group, 47.8 years (12.4). At baseline, the mindfulness and active control arms had average BMIs of 35.4 (3.5) and 35.6 (3.8), respectively. Baseline characteristics, session attendance, and 18-month retention were similar for both arms. Participants in the mindfulness arm reported completing 70% (2.1 hours per week, SD = 1.2) of the recommended meditation time and eating 57% (SD = 29) of meals mindfully.
Weight loss outcomes between groups favored the mindfulness arms, but results were not significant. The largest difference of –1.9 kg (95% CI –4.5 to 0.8; P = 0.17) was at 12 months. The difference persisted at 18 months with –1.7 kg (95% CI –4.7 to 1.2 kg; P = 0.24). The mindfulness arm lost 4.2 kg (95% CI –6.2 to 2.2 kg) while the active control arm lost 2.4 kg (95% CI –4.5 to –0.3 kg).
Cardiometabolic outcomes at 12 months showed group differences in fasting glucose that favored the mindfulness arm, –3.1 mg/dL (95% CI 26.3 to 0.1; P = 0.06), while there was a significant group difference at 18 months, –4.1 mg/dL (95% CI –7.3 to –0.9; P = 0.01). Data at 18-months showed that normal glucose changed minimally in the mindfulness arm, –0.31 mg/dL (95% CI –2.5 to 1.9), but increased in the active control arm 3.8 mg/dL (95% CI 1.5 to 6.1). Other cardiometabolic outcomes (ie, triglyceride/HDL ratio and triglycerides) showed significance at 12 months, favoring the mindfulness arm, but not at 18 months. Although not all were statistically significant, 9 of 11 outcomes favored the mindfulness arm at 18 months.
Significant interactions (P < 0.05) were found between arm and enrollment rounds categorized by mindfulness instructor on weight, BMI, fasting glucose, homeostatic homeostasis model assessment of insulin resistance (defined as [glucose x insulin/{40 × 33.25}]), and HbA1c, with a marginally significant effect for waist circumference (P = 0.08). Qualitative feedback on mindfulness instructors showed that in the group with a lowly rated instructor, participants lost less weight at 18 months (–2.0 kg [95% CI –4.7 to 0.7]), compared to participants in groups with highly rated instructors (–6.3 kg [95% CI –9.1 to –3.6]; P = 0.02). Similar trends followed for reductions in BMI and waist circumference.
Conclusions. With regard to weight loss outcomes, a mindfulness-enhanced diet-exercise program and an active control arm did not show substantial differences. Some evidence, however, suggests modest benefit of added mindfulness components, which may lead to long-term maintenance of fasting glucose levels and improved atherogenic lipid profiles.
Commentary
Mindfulness, or nonjudgmental focus on the present moment, has been utilized by many interventions targeted at self-regulated behavior [1]. Mindfulness interventions aim to promote healthy behavior changes by encouraging careful monitoring of behavior reactivity. Weight loss and weight loss maintenance have been of particular interest with this approach because mindfulness-based interventions may promote long-term maintenance of weight loss [2]. This maintenance is achieved through a focus on modifying health behaviors, rather than a focus on weight loss alone [3]. Mindfulness has been incorporated into weight loss interventions through yoga practices [4] and mindfulness meditation [5].
Several studies have explored the relationship between mindfulness and weight loss in various populations, highlighting mindfulness’s role in weight loss and behavior change. Most notably, mindfulness interventions have shown improvements in fasting glucose levels [6], psychological distress [7], self-efficacy, weight loss, eating behaviors, and physical activity [8–10]. Despite being well designed, this study by Daubenmier et al did not find significant changes in weight loss. However, secondary outcomes related to weight, metabolic, syndrome, and cardiovascular risk showed modest improvements with mindfulness. These results may correlate to previous findings showing that lifestyle changes many not result in weight loss but can reverse or reduce disorders related to obesity [11].
The study was strengthened by randomization, intention-to-treat analysis, objective measures by arm-blinded staff, standardized measuring conditions, balanced participant allocation to each arm, 1-year follow-up, and qualitative feedback on instructors to assess whether weight loss may be instructor-dependent. In addition, the authors made an effort to mask their intention to test the effects of a mindfulness-enhanced intervention. They designed a rigorous active control intervention arm by controlling for attention, social support, expectations of benefit, diet-exercise guidelines, and elements of a mindfulness approach to stress management. An additional strength included a cost-analysis of adding mindfulness components. The generalizability of the results may be limited as the study population were predominantly white females and most had a bachelor’s degree. The study sample was also disproportionately menopausal women, a group that especially struggles with weight loss. This demographic factor may be responsible for the lack of significant weight loss. Other limitations of this study include participant dropout and variability between instructor styles, although the latter was explored in a secondary analysis of weight loss differences between instructors.
The researchers discussed how the active control intervention arm may have contributed to the lack of significant weight loss difference between groups. The researchers also highlighted that participants randomized to the mindfulness arm that were not interested in mindfulness practices may have benefitted less than those who were interested. This combined with the modest diet and exercise components of the intervention may also explain the lack of significance in results. It may also explain why some outcomes were significant at earlier months but attenuated by 18 months. Future studies should assess incorporating more intense exercise and diet approaches, as well as continuous contact throughout the 18-month time period.
Applications for Clinical Practice
This study demonstrated that mindfulness components added to a diet-exercise program can be helpful in promoting metabolic changes but not necessarily weight loss. Since metabolic changes can be protective against morbidities (eg, type 2 diabetes), mindfulness can be a powerful and cost-effective approach within clinical practice. Mindfulness practices can also be easily implemented in various settings and with diverse populations. Future studies should explore adding mindfulness components to more intensive weight loss interventions. Providers and health care settings should consider incorporating mindfulness practices into weight management counseling and programs.
—Michelle J. Williamson and Katrina F. Mateo, MPH
1. Caldwell KL, Baime MJ, Wolever RQ. Mindfulness based approaches to obesity and weight loss maintenance. J Ment Health Couns 2012;34:26982.
2. O’Reilly GA, Cook L, Spruijt-Metz D, Black DS. Mindfulness-based interventions for obesity-related eating behaviours: A literature review. Obes Rev 2014;15:453–61.
3. Robison J. Health at every size: Toward a new paradigm of weight and health. MedGenMed 2005;7:13.
4. Godsey J. The role of mindfulness based interventions in the treatment of obesity and eating disorders: An integrative review. Complement Ther Med 2013;21:430–9.
5. Keune PM, Forintos DP. Mindfulness meditation: A preliminary study on meditation practice during everyday life activities and its association with well-being. Psychol Top 2010;19:373–86.
6. Mason AE, Epel ES, Kristeller J, et al. Effects of a mindfulness-based intervention on mindful eating, sweets consumption, and fasting glucose levels in obese adults: data from the SHINE randomized controlled trial. J Behav Med 2016;39:201–13.
7. Dalen J, Smith BW, Shelley BM, et al. Pilot study: Mindful Eating and Living (MEAL): Weight, eating behavior, and psychological outcomes associated with a mindfulness-based intervention for people with obesity. Complement Ther Med 2010;18:260–64.
8. Kristeller JL, Wolever RQ, Sheets V. Mindfulness-based eating awareness training (MB-EAT) for binge eating: A randomized clinical trial. Mindfulness 2013;5:282–97.
9. Miller C, Kristeller JL, Headings A, Nagaraja H. Comparison of a mindful eating intervention to a diabetes self- management intervention among adults with type 2 diabetes: a randomized controlled trial. Health Educ Behav 2013;41:145–54.
10. Timmerman GM, Brown A. The effect of a mindful restaurant eating intervention on weight management in women. J Nutr Educ Behav 2012;44:22–8.
11. Bacon L, Stern JS, Van Loan MD, Keim NL. Size acceptance and intuitive eating improve health for obese, female chronic dieters. J Am Diet Assoc 2005;105:929–36.
1. Caldwell KL, Baime MJ, Wolever RQ. Mindfulness based approaches to obesity and weight loss maintenance. J Ment Health Couns 2012;34:26982.
2. O’Reilly GA, Cook L, Spruijt-Metz D, Black DS. Mindfulness-based interventions for obesity-related eating behaviours: A literature review. Obes Rev 2014;15:453–61.
3. Robison J. Health at every size: Toward a new paradigm of weight and health. MedGenMed 2005;7:13.
4. Godsey J. The role of mindfulness based interventions in the treatment of obesity and eating disorders: An integrative review. Complement Ther Med 2013;21:430–9.
5. Keune PM, Forintos DP. Mindfulness meditation: A preliminary study on meditation practice during everyday life activities and its association with well-being. Psychol Top 2010;19:373–86.
6. Mason AE, Epel ES, Kristeller J, et al. Effects of a mindfulness-based intervention on mindful eating, sweets consumption, and fasting glucose levels in obese adults: data from the SHINE randomized controlled trial. J Behav Med 2016;39:201–13.
7. Dalen J, Smith BW, Shelley BM, et al. Pilot study: Mindful Eating and Living (MEAL): Weight, eating behavior, and psychological outcomes associated with a mindfulness-based intervention for people with obesity. Complement Ther Med 2010;18:260–64.
8. Kristeller JL, Wolever RQ, Sheets V. Mindfulness-based eating awareness training (MB-EAT) for binge eating: A randomized clinical trial. Mindfulness 2013;5:282–97.
9. Miller C, Kristeller JL, Headings A, Nagaraja H. Comparison of a mindful eating intervention to a diabetes self- management intervention among adults with type 2 diabetes: a randomized controlled trial. Health Educ Behav 2013;41:145–54.
10. Timmerman GM, Brown A. The effect of a mindful restaurant eating intervention on weight management in women. J Nutr Educ Behav 2012;44:22–8.
11. Bacon L, Stern JS, Van Loan MD, Keim NL. Size acceptance and intuitive eating improve health for obese, female chronic dieters. J Am Diet Assoc 2005;105:929–36.
Help for Active Surveillance Anxiety in Men with Prostate Cancer
Study Overview
Objective. To examine the feasibility, acceptability and benefits of mindfulness meditation training in men with low-grade prostate cancer on active surveillance.
Design. Randomized controlled pilot trial.
Setting and participants. Participants were men with low-risk localized prostate cancer who were on an IRB-approved active surveillance protocol within a medium-sized community hospital system in suburban Chicago. Enrolled patients were randomized to the active intervention or a control condition where participants received a book on mindfulness but no specific instructions to read it.
Intervention. Patients in the intervention arm attended an 8-week mindfulness-based stress reduction intervention, consisting of weekly sessions lasting 2½ hours held at their local primary hospital. Sessions were conducted by a trained and experienced mindfulness instructor. The intervention also included a half day retreat near the end of the intervention period to practice the skills that were taught.
Main outcome measures. Main outcome measures were prostate cancer anxiety (measured using the 18-item Memorial Anxiety Scale for Prostate Cancer), uncertainty tolerance (measured using the 12-item Intolerance of Uncertainty Short Form), mindfulness (measured via the 15-item Mindful Attention Awareness Scale), and health-related quality of life (measured using 10-item PROMIS Global Health-10). Researchers also measured “posttraumatic growth” using the Posttraumatic Growth Inventory, a 21-item self-report scale used to assess growth or benefits after a specific traumatic life event, such as a diagnosis of cancer. Participants completed instruments at baseline, 8 weeks, 6 months, and 12 months. At 12 months they also complete a brief feasibility and acceptance survey.
Main results. Over a 3-year period, 115 men were approached to participate and 54 enrolled. 11 withdrew prior to randomization citing lack of time as the primary reason. Ultimately, 24 men were randomized to the mindfulness arm and 19 to control. Average age was 70 years and 95% were white. Over 90% had never previously meditated or had never meditated on a regular basis. There were no significant differences between enrollees and decliners on baseline clinical or sociodemographic variables, and there were no significant differences between mindfulness and control patients on sociodemographic or clinical variables or outcome measures.
Participants in the intervention group reported decreased prostate cancer anxiety at 6 months (P = 0.02, effect size ([ES] 0.30) and uncertainty intolerance at 12 months (P = 0.02, ES 0.32) and increased quality of life at 8 weeks (P = 0.05, ES 0.17), mindfulness at 8 weeks (P < 0.04, ES 0.35) and 12 months (P < 0.01, ES 0.17), and posttraumatic growth (P < 0.05 for all follow-up measurements). When measuring changes between the groups, the only outcome that was significant was posttraumatic growth (P = 0.01, ES 0.73). Written responses to the open-ended survey questions regarding participants’ experience with the course cited increased emotional regulation and self-awareness and positive health behavior change.
Conclusion. An 8-week mindfulness training is feasible and acceptable to men with prostate cancer on active surveillance and may help men cope more effectively with stress and anxiety related to their cancer experience.
Commentary
Prostate cancer is the most common nonskin malignancy in men. More than 180,000 men are diagnosed per year, with over 26,000 prostate cancer deaths annually [1]. The optimal approach to treating newly diagnosed prostate cancer can be variable, but for most patients with low-risk (Gleason score ≤ 6) localized prostate cancer, active surveillance is the recommended disease management strategy [2]. Despite the favorable prognosis of low-risk prostate cancer, men who choose active surveillance may experience anxiety and uncertainty, which can cause many to request definitive therapy even when there is no tumor progression [3].
Mindfulness-based meditation is a practice that is increasingly being investigated for a wide array of health conditions. Mindfulness has been defined as being intentionally aware of internal and external experiences that occur at the present moment, without judgment. Behavioral interventions such as mindfulness training may lessen anxiety related to uncertainty intolerance and help maintain patient engagement in active surveillance [4].
This small pilot study by Victorson et al evaluated an 8-week mindfulness meditation intervention intended to help men in active surveillance manage cancer-related uncertainty intolerance. They found the meditation training to be generally feasible and acceptable among participants. Men in the active intervention demonstrated statistically significant within-group changes that included decreased prostate cancer anxiety and increased mental well-being and posttraumatic growth, but there were no differences between groups except for posttraumatic growth. Interestingly, the control group also reported a moderate increase in mindfulness at 12 months, which was found (in an exploratory follow-up analysis) to be unrelated to reading the mindfulness book they were given (eg, those who did not open the book had higher average mindfulness scores than those who read the book from cover to cover).
Limitations of the study include the small sample size and lack of diversity among the participants, who were 95% white and well educated. In addition, the response rate prior to randomization was low: out of 115 men approached, 43 were ultimately randomized. Retention rates at 12 months were similar: 71% for intervention and 74% for control.
Applications for Clinical Practice
A growing body of research demonstrates that mindfulness practice may aid in improving psychological well-being. Further research is necessary before a clinical recommendation can be offered regarding use of mindfulness instruction to alleviate anxiety in men with low-grade prostate cancer being managed with active surveillance.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin 2016;66:7-–30.
2. Chen RC, Rumble RB, Loblaw DA, et al. Active surveillance for the management of localized prostate cancer (Cancer Care Ontario Guideline): American Society of Clinical Oncology Clinical Practice Guideline Endorsement. J Clin Oncol 2016;34:2182–90.
3. Latini DM, Hart SL, Knight SJ, et al; CaPSURE Investigators. The relationship between anxiety and time to treatment for patients with prostate cancer on surveillance. J Urol 2007;178(3 Pt 1):826–31; discussion 831–2.
4. Tan HJ, Marks LS, Hoyt MA, et al. The relationship between intolerance of uncertainty and anxiety in men on active surveillance for prostate cancer. J Urol 2016;195:1724–30.
Study Overview
Objective. To examine the feasibility, acceptability and benefits of mindfulness meditation training in men with low-grade prostate cancer on active surveillance.
Design. Randomized controlled pilot trial.
Setting and participants. Participants were men with low-risk localized prostate cancer who were on an IRB-approved active surveillance protocol within a medium-sized community hospital system in suburban Chicago. Enrolled patients were randomized to the active intervention or a control condition where participants received a book on mindfulness but no specific instructions to read it.
Intervention. Patients in the intervention arm attended an 8-week mindfulness-based stress reduction intervention, consisting of weekly sessions lasting 2½ hours held at their local primary hospital. Sessions were conducted by a trained and experienced mindfulness instructor. The intervention also included a half day retreat near the end of the intervention period to practice the skills that were taught.
Main outcome measures. Main outcome measures were prostate cancer anxiety (measured using the 18-item Memorial Anxiety Scale for Prostate Cancer), uncertainty tolerance (measured using the 12-item Intolerance of Uncertainty Short Form), mindfulness (measured via the 15-item Mindful Attention Awareness Scale), and health-related quality of life (measured using 10-item PROMIS Global Health-10). Researchers also measured “posttraumatic growth” using the Posttraumatic Growth Inventory, a 21-item self-report scale used to assess growth or benefits after a specific traumatic life event, such as a diagnosis of cancer. Participants completed instruments at baseline, 8 weeks, 6 months, and 12 months. At 12 months they also complete a brief feasibility and acceptance survey.
Main results. Over a 3-year period, 115 men were approached to participate and 54 enrolled. 11 withdrew prior to randomization citing lack of time as the primary reason. Ultimately, 24 men were randomized to the mindfulness arm and 19 to control. Average age was 70 years and 95% were white. Over 90% had never previously meditated or had never meditated on a regular basis. There were no significant differences between enrollees and decliners on baseline clinical or sociodemographic variables, and there were no significant differences between mindfulness and control patients on sociodemographic or clinical variables or outcome measures.
Participants in the intervention group reported decreased prostate cancer anxiety at 6 months (P = 0.02, effect size ([ES] 0.30) and uncertainty intolerance at 12 months (P = 0.02, ES 0.32) and increased quality of life at 8 weeks (P = 0.05, ES 0.17), mindfulness at 8 weeks (P < 0.04, ES 0.35) and 12 months (P < 0.01, ES 0.17), and posttraumatic growth (P < 0.05 for all follow-up measurements). When measuring changes between the groups, the only outcome that was significant was posttraumatic growth (P = 0.01, ES 0.73). Written responses to the open-ended survey questions regarding participants’ experience with the course cited increased emotional regulation and self-awareness and positive health behavior change.
Conclusion. An 8-week mindfulness training is feasible and acceptable to men with prostate cancer on active surveillance and may help men cope more effectively with stress and anxiety related to their cancer experience.
Commentary
Prostate cancer is the most common nonskin malignancy in men. More than 180,000 men are diagnosed per year, with over 26,000 prostate cancer deaths annually [1]. The optimal approach to treating newly diagnosed prostate cancer can be variable, but for most patients with low-risk (Gleason score ≤ 6) localized prostate cancer, active surveillance is the recommended disease management strategy [2]. Despite the favorable prognosis of low-risk prostate cancer, men who choose active surveillance may experience anxiety and uncertainty, which can cause many to request definitive therapy even when there is no tumor progression [3].
Mindfulness-based meditation is a practice that is increasingly being investigated for a wide array of health conditions. Mindfulness has been defined as being intentionally aware of internal and external experiences that occur at the present moment, without judgment. Behavioral interventions such as mindfulness training may lessen anxiety related to uncertainty intolerance and help maintain patient engagement in active surveillance [4].
This small pilot study by Victorson et al evaluated an 8-week mindfulness meditation intervention intended to help men in active surveillance manage cancer-related uncertainty intolerance. They found the meditation training to be generally feasible and acceptable among participants. Men in the active intervention demonstrated statistically significant within-group changes that included decreased prostate cancer anxiety and increased mental well-being and posttraumatic growth, but there were no differences between groups except for posttraumatic growth. Interestingly, the control group also reported a moderate increase in mindfulness at 12 months, which was found (in an exploratory follow-up analysis) to be unrelated to reading the mindfulness book they were given (eg, those who did not open the book had higher average mindfulness scores than those who read the book from cover to cover).
Limitations of the study include the small sample size and lack of diversity among the participants, who were 95% white and well educated. In addition, the response rate prior to randomization was low: out of 115 men approached, 43 were ultimately randomized. Retention rates at 12 months were similar: 71% for intervention and 74% for control.
Applications for Clinical Practice
A growing body of research demonstrates that mindfulness practice may aid in improving psychological well-being. Further research is necessary before a clinical recommendation can be offered regarding use of mindfulness instruction to alleviate anxiety in men with low-grade prostate cancer being managed with active surveillance.
Study Overview
Objective. To examine the feasibility, acceptability and benefits of mindfulness meditation training in men with low-grade prostate cancer on active surveillance.
Design. Randomized controlled pilot trial.
Setting and participants. Participants were men with low-risk localized prostate cancer who were on an IRB-approved active surveillance protocol within a medium-sized community hospital system in suburban Chicago. Enrolled patients were randomized to the active intervention or a control condition where participants received a book on mindfulness but no specific instructions to read it.
Intervention. Patients in the intervention arm attended an 8-week mindfulness-based stress reduction intervention, consisting of weekly sessions lasting 2½ hours held at their local primary hospital. Sessions were conducted by a trained and experienced mindfulness instructor. The intervention also included a half day retreat near the end of the intervention period to practice the skills that were taught.
Main outcome measures. Main outcome measures were prostate cancer anxiety (measured using the 18-item Memorial Anxiety Scale for Prostate Cancer), uncertainty tolerance (measured using the 12-item Intolerance of Uncertainty Short Form), mindfulness (measured via the 15-item Mindful Attention Awareness Scale), and health-related quality of life (measured using 10-item PROMIS Global Health-10). Researchers also measured “posttraumatic growth” using the Posttraumatic Growth Inventory, a 21-item self-report scale used to assess growth or benefits after a specific traumatic life event, such as a diagnosis of cancer. Participants completed instruments at baseline, 8 weeks, 6 months, and 12 months. At 12 months they also complete a brief feasibility and acceptance survey.
Main results. Over a 3-year period, 115 men were approached to participate and 54 enrolled. 11 withdrew prior to randomization citing lack of time as the primary reason. Ultimately, 24 men were randomized to the mindfulness arm and 19 to control. Average age was 70 years and 95% were white. Over 90% had never previously meditated or had never meditated on a regular basis. There were no significant differences between enrollees and decliners on baseline clinical or sociodemographic variables, and there were no significant differences between mindfulness and control patients on sociodemographic or clinical variables or outcome measures.
Participants in the intervention group reported decreased prostate cancer anxiety at 6 months (P = 0.02, effect size ([ES] 0.30) and uncertainty intolerance at 12 months (P = 0.02, ES 0.32) and increased quality of life at 8 weeks (P = 0.05, ES 0.17), mindfulness at 8 weeks (P < 0.04, ES 0.35) and 12 months (P < 0.01, ES 0.17), and posttraumatic growth (P < 0.05 for all follow-up measurements). When measuring changes between the groups, the only outcome that was significant was posttraumatic growth (P = 0.01, ES 0.73). Written responses to the open-ended survey questions regarding participants’ experience with the course cited increased emotional regulation and self-awareness and positive health behavior change.
Conclusion. An 8-week mindfulness training is feasible and acceptable to men with prostate cancer on active surveillance and may help men cope more effectively with stress and anxiety related to their cancer experience.
Commentary
Prostate cancer is the most common nonskin malignancy in men. More than 180,000 men are diagnosed per year, with over 26,000 prostate cancer deaths annually [1]. The optimal approach to treating newly diagnosed prostate cancer can be variable, but for most patients with low-risk (Gleason score ≤ 6) localized prostate cancer, active surveillance is the recommended disease management strategy [2]. Despite the favorable prognosis of low-risk prostate cancer, men who choose active surveillance may experience anxiety and uncertainty, which can cause many to request definitive therapy even when there is no tumor progression [3].
Mindfulness-based meditation is a practice that is increasingly being investigated for a wide array of health conditions. Mindfulness has been defined as being intentionally aware of internal and external experiences that occur at the present moment, without judgment. Behavioral interventions such as mindfulness training may lessen anxiety related to uncertainty intolerance and help maintain patient engagement in active surveillance [4].
This small pilot study by Victorson et al evaluated an 8-week mindfulness meditation intervention intended to help men in active surveillance manage cancer-related uncertainty intolerance. They found the meditation training to be generally feasible and acceptable among participants. Men in the active intervention demonstrated statistically significant within-group changes that included decreased prostate cancer anxiety and increased mental well-being and posttraumatic growth, but there were no differences between groups except for posttraumatic growth. Interestingly, the control group also reported a moderate increase in mindfulness at 12 months, which was found (in an exploratory follow-up analysis) to be unrelated to reading the mindfulness book they were given (eg, those who did not open the book had higher average mindfulness scores than those who read the book from cover to cover).
Limitations of the study include the small sample size and lack of diversity among the participants, who were 95% white and well educated. In addition, the response rate prior to randomization was low: out of 115 men approached, 43 were ultimately randomized. Retention rates at 12 months were similar: 71% for intervention and 74% for control.
Applications for Clinical Practice
A growing body of research demonstrates that mindfulness practice may aid in improving psychological well-being. Further research is necessary before a clinical recommendation can be offered regarding use of mindfulness instruction to alleviate anxiety in men with low-grade prostate cancer being managed with active surveillance.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin 2016;66:7-–30.
2. Chen RC, Rumble RB, Loblaw DA, et al. Active surveillance for the management of localized prostate cancer (Cancer Care Ontario Guideline): American Society of Clinical Oncology Clinical Practice Guideline Endorsement. J Clin Oncol 2016;34:2182–90.
3. Latini DM, Hart SL, Knight SJ, et al; CaPSURE Investigators. The relationship between anxiety and time to treatment for patients with prostate cancer on surveillance. J Urol 2007;178(3 Pt 1):826–31; discussion 831–2.
4. Tan HJ, Marks LS, Hoyt MA, et al. The relationship between intolerance of uncertainty and anxiety in men on active surveillance for prostate cancer. J Urol 2016;195:1724–30.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin 2016;66:7-–30.
2. Chen RC, Rumble RB, Loblaw DA, et al. Active surveillance for the management of localized prostate cancer (Cancer Care Ontario Guideline): American Society of Clinical Oncology Clinical Practice Guideline Endorsement. J Clin Oncol 2016;34:2182–90.
3. Latini DM, Hart SL, Knight SJ, et al; CaPSURE Investigators. The relationship between anxiety and time to treatment for patients with prostate cancer on surveillance. J Urol 2007;178(3 Pt 1):826–31; discussion 831–2.
4. Tan HJ, Marks LS, Hoyt MA, et al. The relationship between intolerance of uncertainty and anxiety in men on active surveillance for prostate cancer. J Urol 2016;195:1724–30.