User login
VIDEO: Alzheimer’s anti-tau drug fails, but shows hint of effect when taken alone
TORONTO – A highly anticipated phase III trial of an anti-tau drug has posted negative topline results, conferring no cognitive or functional benefits when given in conjunction with standard-of-care Alzheimer’s disease medications.
The drug, LMTX (TauRx, Singapore), also did not slow the progression of brain atrophy on imaging in either of two doses tested, according to a company press release.
Although the study didn’t meet its clinical endpoints in the overall cohort of 891 patients with mild-moderate Alzheimer’s disease, TauRx promoted it as “promising,” based on a subgroup analysis of patients who took the drug as monotherapy. None of these patients were taking any standard-of-care Alzheimer’s medications; the press release did not say how many this group comprised. But it did imply that the group was small enough that the treatment effect was diluted in the pooled primary analysis.
In patients who took the drug as monotherapy, LMTX was associated with dose-dependent, statistically significant improvements in the Alzheimer’s Disease Assessment Scale measures of cognition (ADAS-cog) and Alzheimer’s Disease Cooperative Study Activities of Daily Living inventory (ADCS-ADL). The drug was also associated with a slowing of brain ventricular expansion, compared with controls, suggesting that it could be preserving brain mass.
ADAS-cog scores for patients taking LMTX monotherapy 75 mg twice a day declined 6.3 points less than did controls, indicating preserved cognition. Those taking LMTX monotherapy 125 mg twice a day declined 5.8 points less than did controls. On the ADCS-ADL, patients taking 75 mg twice a day scored 6.5 points higher than controls, indicating better function, and those taking 125 mg twice a day scored 6.9 points higher.
Lateral ventricular volume expansion on MRI was significantly less than that seen in controls. For those taking 75 mg twice a day, ventricular expansion was reduced by 38%, and for those taking 125 mg twice a day, expansion was reduced by 33%.
This indicates a decrease in the rate of brain atrophy, the press release said, and the finding was “confirmed by corresponding increases in the whole-brain volumes in the same patient groups.”
The press release also said that the imaging findings offer physiologic confirmation of the cognitive and functional findings. “This is the first treatment in which a clinical effect has been supported by evidence in delay of progression in brain atrophy shown by MRI scans.”
The missing number of patients who took LMTX monotherapy is key, however, in determining whether the positive effects in that group are real or a chance finding, according to Richard J. Caselli, MD, associate director and clinical core director of the Alzheimer’s Disease Center at the Mayo Clinic, Scottsdale, Ariz.
“Were the monotherapy results a fluke that washed out with bigger numbers or a meaningful effect? That needs to be clarified,” he said when asked to comment on the study. “Smaller ‘N’ trials can have skewed results due to random chances that mean nothing, and that is my fear. It’s unproven at this point but the burden of proof will rest on the investigators to replicate the positive outcome.”
The finding of a positive signal in monotherapy only is puzzling and also demands an explanation, said Michael Wolfe, PhD, a professor of neurology at Harvard University, Boston.
LMTX is a purified form of the dye methylene blue. Its method of action in preventing or dissolving tau tangles is not fully elucidated. A 2013 paper in a German chemistry journal, Angewandte Chemie, suggested that it works through oxidation to maintain the tau protein as a monomer, which prevents aggregation into filaments. There is no reason to think this pathway could intersect or interfere with any of the standard-of-care Alzheimer’s medications.
“There’s nothing obvious that comes to mind regarding interaction,” between the drug classes, Dr. Wolfe said in an interview. “We can’t say anything about this mechanistically. Any explanation here is just hand waving, I think.”
Dean Hartley, PhD, director of science initiatives at the Alzheimer’s Association, commented on the trial in a video interview at the Alzheimer’s Association International Conference 2016.
Neither Dr. Caselli nor Dr. Wolfe had relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
TORONTO – A highly anticipated phase III trial of an anti-tau drug has posted negative topline results, conferring no cognitive or functional benefits when given in conjunction with standard-of-care Alzheimer’s disease medications.
The drug, LMTX (TauRx, Singapore), also did not slow the progression of brain atrophy on imaging in either of two doses tested, according to a company press release.
Although the study didn’t meet its clinical endpoints in the overall cohort of 891 patients with mild-moderate Alzheimer’s disease, TauRx promoted it as “promising,” based on a subgroup analysis of patients who took the drug as monotherapy. None of these patients were taking any standard-of-care Alzheimer’s medications; the press release did not say how many this group comprised. But it did imply that the group was small enough that the treatment effect was diluted in the pooled primary analysis.
In patients who took the drug as monotherapy, LMTX was associated with dose-dependent, statistically significant improvements in the Alzheimer’s Disease Assessment Scale measures of cognition (ADAS-cog) and Alzheimer’s Disease Cooperative Study Activities of Daily Living inventory (ADCS-ADL). The drug was also associated with a slowing of brain ventricular expansion, compared with controls, suggesting that it could be preserving brain mass.
ADAS-cog scores for patients taking LMTX monotherapy 75 mg twice a day declined 6.3 points less than did controls, indicating preserved cognition. Those taking LMTX monotherapy 125 mg twice a day declined 5.8 points less than did controls. On the ADCS-ADL, patients taking 75 mg twice a day scored 6.5 points higher than controls, indicating better function, and those taking 125 mg twice a day scored 6.9 points higher.
Lateral ventricular volume expansion on MRI was significantly less than that seen in controls. For those taking 75 mg twice a day, ventricular expansion was reduced by 38%, and for those taking 125 mg twice a day, expansion was reduced by 33%.
This indicates a decrease in the rate of brain atrophy, the press release said, and the finding was “confirmed by corresponding increases in the whole-brain volumes in the same patient groups.”
The press release also said that the imaging findings offer physiologic confirmation of the cognitive and functional findings. “This is the first treatment in which a clinical effect has been supported by evidence in delay of progression in brain atrophy shown by MRI scans.”
The missing number of patients who took LMTX monotherapy is key, however, in determining whether the positive effects in that group are real or a chance finding, according to Richard J. Caselli, MD, associate director and clinical core director of the Alzheimer’s Disease Center at the Mayo Clinic, Scottsdale, Ariz.
“Were the monotherapy results a fluke that washed out with bigger numbers or a meaningful effect? That needs to be clarified,” he said when asked to comment on the study. “Smaller ‘N’ trials can have skewed results due to random chances that mean nothing, and that is my fear. It’s unproven at this point but the burden of proof will rest on the investigators to replicate the positive outcome.”
The finding of a positive signal in monotherapy only is puzzling and also demands an explanation, said Michael Wolfe, PhD, a professor of neurology at Harvard University, Boston.
LMTX is a purified form of the dye methylene blue. Its method of action in preventing or dissolving tau tangles is not fully elucidated. A 2013 paper in a German chemistry journal, Angewandte Chemie, suggested that it works through oxidation to maintain the tau protein as a monomer, which prevents aggregation into filaments. There is no reason to think this pathway could intersect or interfere with any of the standard-of-care Alzheimer’s medications.
“There’s nothing obvious that comes to mind regarding interaction,” between the drug classes, Dr. Wolfe said in an interview. “We can’t say anything about this mechanistically. Any explanation here is just hand waving, I think.”
Dean Hartley, PhD, director of science initiatives at the Alzheimer’s Association, commented on the trial in a video interview at the Alzheimer’s Association International Conference 2016.
Neither Dr. Caselli nor Dr. Wolfe had relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
TORONTO – A highly anticipated phase III trial of an anti-tau drug has posted negative topline results, conferring no cognitive or functional benefits when given in conjunction with standard-of-care Alzheimer’s disease medications.
The drug, LMTX (TauRx, Singapore), also did not slow the progression of brain atrophy on imaging in either of two doses tested, according to a company press release.
Although the study didn’t meet its clinical endpoints in the overall cohort of 891 patients with mild-moderate Alzheimer’s disease, TauRx promoted it as “promising,” based on a subgroup analysis of patients who took the drug as monotherapy. None of these patients were taking any standard-of-care Alzheimer’s medications; the press release did not say how many this group comprised. But it did imply that the group was small enough that the treatment effect was diluted in the pooled primary analysis.
In patients who took the drug as monotherapy, LMTX was associated with dose-dependent, statistically significant improvements in the Alzheimer’s Disease Assessment Scale measures of cognition (ADAS-cog) and Alzheimer’s Disease Cooperative Study Activities of Daily Living inventory (ADCS-ADL). The drug was also associated with a slowing of brain ventricular expansion, compared with controls, suggesting that it could be preserving brain mass.
ADAS-cog scores for patients taking LMTX monotherapy 75 mg twice a day declined 6.3 points less than did controls, indicating preserved cognition. Those taking LMTX monotherapy 125 mg twice a day declined 5.8 points less than did controls. On the ADCS-ADL, patients taking 75 mg twice a day scored 6.5 points higher than controls, indicating better function, and those taking 125 mg twice a day scored 6.9 points higher.
Lateral ventricular volume expansion on MRI was significantly less than that seen in controls. For those taking 75 mg twice a day, ventricular expansion was reduced by 38%, and for those taking 125 mg twice a day, expansion was reduced by 33%.
This indicates a decrease in the rate of brain atrophy, the press release said, and the finding was “confirmed by corresponding increases in the whole-brain volumes in the same patient groups.”
The press release also said that the imaging findings offer physiologic confirmation of the cognitive and functional findings. “This is the first treatment in which a clinical effect has been supported by evidence in delay of progression in brain atrophy shown by MRI scans.”
The missing number of patients who took LMTX monotherapy is key, however, in determining whether the positive effects in that group are real or a chance finding, according to Richard J. Caselli, MD, associate director and clinical core director of the Alzheimer’s Disease Center at the Mayo Clinic, Scottsdale, Ariz.
“Were the monotherapy results a fluke that washed out with bigger numbers or a meaningful effect? That needs to be clarified,” he said when asked to comment on the study. “Smaller ‘N’ trials can have skewed results due to random chances that mean nothing, and that is my fear. It’s unproven at this point but the burden of proof will rest on the investigators to replicate the positive outcome.”
The finding of a positive signal in monotherapy only is puzzling and also demands an explanation, said Michael Wolfe, PhD, a professor of neurology at Harvard University, Boston.
LMTX is a purified form of the dye methylene blue. Its method of action in preventing or dissolving tau tangles is not fully elucidated. A 2013 paper in a German chemistry journal, Angewandte Chemie, suggested that it works through oxidation to maintain the tau protein as a monomer, which prevents aggregation into filaments. There is no reason to think this pathway could intersect or interfere with any of the standard-of-care Alzheimer’s medications.
“There’s nothing obvious that comes to mind regarding interaction,” between the drug classes, Dr. Wolfe said in an interview. “We can’t say anything about this mechanistically. Any explanation here is just hand waving, I think.”
Dean Hartley, PhD, director of science initiatives at the Alzheimer’s Association, commented on the trial in a video interview at the Alzheimer’s Association International Conference 2016.
Neither Dr. Caselli nor Dr. Wolfe had relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
AT AAIC 2016
Key clinical point: Negative primary outcomes from a phase III trial of the anti-tau drug LMTX for Alzheimer’s disease were tempered by intriguing positive subanalysis data.
Major finding: ADAS-cog scores for patients taking LMTX monotherapy 75 mg twice a day declined 6.3 points less than did controls, indicating preserved cognition. Those for patients taking LMTX monotherapy 125 mg twice a day declined 5.8 points less than did controls.
Data source: A phase III trial of the anti-tau drug LMTX in 891 patients with mild-moderate Alzheimer’s disease.
Disclosures: The trial was sponsored by TauRx. Neither Dr. Caselli nor Dr. Wolfe had relevant disclosures.

Vegetarian diets 101
In the era where obesity is the No. 1 health crisis affecting people of all ages, physicians are often faced with questions regarding restricted diets or a patient may report that they are “vegetarian” in their history. Although new trendy diets appear all the time, “vegetarian inclined” diets are among the most common. A study conducted in 2008 identified that approximately 10% of Americans age 18 and older consumed a vegetarian diet.1 It is important to know the basics so that you can offer some guidance and look for possible deficiencies that may result from an altered diet.
Studies show that children who follow a vegetarian diet have normal growth and development but tend to be leaner than their omnivore counterparts.2 A healthy diet consumed in childhood lessens the risk for chronic diseases and promotes optimal growth and development. But altered or restricted diets in adolescents can be tricky because teens are actively growing and therefore usually need greater amounts of vital nutrients. So guidance is important to avoid common mistakes.

The simplest way to remember what is appropriate in a vegetarian diet is the restriction on intake of any food that once had a mother and a father. The vegetarian diet is further divided based on what it includes or excludes. Although the below list is not complete, it outlines the more common vegetarian diets:
• Vegan. This diet restricts intake of any animal product.
• Macrobiotics. This diet consists of whole grain, brown rice, fruits, and vegetables, and restricts intake of white meat or fish to twice a week.
• Lacto-vegetarian. This diet is one which allows milk products.
• Ovo vegetarian. – This diet allows eggs, but no meat, dairy, or fish.
• Pescitarian. This diet restricts meats, dairy, and eggs, but allows fish.
• Semi-vegetarian. This diet just restricts eating meat.
It is important to encourage anyone wishing to follow a vegetarian diet to fully research and understand what it entails. Health.gov under “dietary guidelines 2015-2020” is a wonderful reference to help understand how much of vital nutrients should be consumed to promote healthy eating habits and prevent deficiencies.
The key nutrients to discuss with patients are intake of protein, iron, calcium, vitamin B12, and vitamin D. Inadequate or incorrect intake can lead to deficiency of the vital nutrients that likely will result in disease.
Protein is a necessary nutrient because it provides the essential amino acids necessary for growth and repair. When animal protein breaks down, it provides all of the essential amino acids, unlike plant protein which can be deficient in some of the amino acids. Because each source of plant protein varies in the amino acid it is deficient in, it is important to have a mixed source of protein to ensure adequate intake. The soy bean has comparable amounts of protein to animal protein. Other sources of protein are legumes, grain, cereal, eggs, nuts, Greek yogurt, cottage cheese, but these are less digestible so greater consumption is needed to meet the daily requirements. Deficiency in protein can result in impaired growth.
Iron that is obtained from animals or meat sources has heme component, which makes it easier to absorb. Iron obtained from plants does not contain heme component and therefore is more difficult to absorb. Ascorbic acid (vitamin C) helps nonheme iron to be absorbed, but must be taken with an iron source to be effective. Therefore, vitamin C–containing foods such as fruits and vegetables should be consumed at every meal to assist in iron absorption. Deficiency in iron can lead to anemia and reduced energy.
Calcium is an important nutrient for bone formation, and deficiency can lead to increased risk for fracture and osteoporosis later in life. Its excretion and absorption can be affected by other nutrients, such as iron and zinc, present during digestion. Milk and dairy products are the most common source for calcium intake, but there are other calcium sources such as kale, broccoli, and food fortified with calcium such as cereal and orange juice. These foods can be better sources of calcium than supplements because they allow for better absorption.
Vitamin D is needed for calcium and phosphorus absorption, which is important for proper bone formation. Vitamin D is found in dairy products, fortified food and beverages, and exposure to the sun. Those living in colder climates and of darker pigmentation are at greater risk of deficiency so supplementation is usually necessary. Deficiency of vitamin D can lead to rickets.
Vitamin B12 is found in meat, fish, and dairy products, but not in plants. Intake of B12 is likely to be deficient in vegans because they do not consume most of those sources. Vegans are at a significant risk of vitamin B12 deficiency3 which can lead to macrocytosis, anemia, and decreased energy.
Educating families on healthy eating is essential at any visit. A good understanding of the possible deficiencies that can occur with restricted diets will allow for proper guidance and avoidable diseases.
References
1. Stahler C. “How Many Youth Are Vegetarian? The Vegetarian Resource Group Asks in a 2010 National Poll.”
2. Pediatrics. 1989 Sep;84(3):475-81.
3. J Am Diet Assoc. 2003 Jun;103(6):771-5.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
In the era where obesity is the No. 1 health crisis affecting people of all ages, physicians are often faced with questions regarding restricted diets or a patient may report that they are “vegetarian” in their history. Although new trendy diets appear all the time, “vegetarian inclined” diets are among the most common. A study conducted in 2008 identified that approximately 10% of Americans age 18 and older consumed a vegetarian diet.1 It is important to know the basics so that you can offer some guidance and look for possible deficiencies that may result from an altered diet.
Studies show that children who follow a vegetarian diet have normal growth and development but tend to be leaner than their omnivore counterparts.2 A healthy diet consumed in childhood lessens the risk for chronic diseases and promotes optimal growth and development. But altered or restricted diets in adolescents can be tricky because teens are actively growing and therefore usually need greater amounts of vital nutrients. So guidance is important to avoid common mistakes.
The simplest way to remember what is appropriate in a vegetarian diet is the restriction on intake of any food that once had a mother and a father. The vegetarian diet is further divided based on what it includes or excludes. Although the below list is not complete, it outlines the more common vegetarian diets:
• Vegan. This diet restricts intake of any animal product.
• Macrobiotics. This diet consists of whole grain, brown rice, fruits, and vegetables, and restricts intake of white meat or fish to twice a week.
• Lacto-vegetarian. This diet is one which allows milk products.
• Ovo vegetarian. – This diet allows eggs, but no meat, dairy, or fish.
• Pescitarian. This diet restricts meats, dairy, and eggs, but allows fish.
• Semi-vegetarian. This diet just restricts eating meat.
It is important to encourage anyone wishing to follow a vegetarian diet to fully research and understand what it entails. Health.gov under “dietary guidelines 2015-2020” is a wonderful reference to help understand how much of vital nutrients should be consumed to promote healthy eating habits and prevent deficiencies.
The key nutrients to discuss with patients are intake of protein, iron, calcium, vitamin B12, and vitamin D. Inadequate or incorrect intake can lead to deficiency of the vital nutrients that likely will result in disease.
Protein is a necessary nutrient because it provides the essential amino acids necessary for growth and repair. When animal protein breaks down, it provides all of the essential amino acids, unlike plant protein which can be deficient in some of the amino acids. Because each source of plant protein varies in the amino acid it is deficient in, it is important to have a mixed source of protein to ensure adequate intake. The soy bean has comparable amounts of protein to animal protein. Other sources of protein are legumes, grain, cereal, eggs, nuts, Greek yogurt, cottage cheese, but these are less digestible so greater consumption is needed to meet the daily requirements. Deficiency in protein can result in impaired growth.
Iron that is obtained from animals or meat sources has heme component, which makes it easier to absorb. Iron obtained from plants does not contain heme component and therefore is more difficult to absorb. Ascorbic acid (vitamin C) helps nonheme iron to be absorbed, but must be taken with an iron source to be effective. Therefore, vitamin C–containing foods such as fruits and vegetables should be consumed at every meal to assist in iron absorption. Deficiency in iron can lead to anemia and reduced energy.
Calcium is an important nutrient for bone formation, and deficiency can lead to increased risk for fracture and osteoporosis later in life. Its excretion and absorption can be affected by other nutrients, such as iron and zinc, present during digestion. Milk and dairy products are the most common source for calcium intake, but there are other calcium sources such as kale, broccoli, and food fortified with calcium such as cereal and orange juice. These foods can be better sources of calcium than supplements because they allow for better absorption.
Vitamin D is needed for calcium and phosphorus absorption, which is important for proper bone formation. Vitamin D is found in dairy products, fortified food and beverages, and exposure to the sun. Those living in colder climates and of darker pigmentation are at greater risk of deficiency so supplementation is usually necessary. Deficiency of vitamin D can lead to rickets.
Vitamin B12 is found in meat, fish, and dairy products, but not in plants. Intake of B12 is likely to be deficient in vegans because they do not consume most of those sources. Vegans are at a significant risk of vitamin B12 deficiency3 which can lead to macrocytosis, anemia, and decreased energy.
Educating families on healthy eating is essential at any visit. A good understanding of the possible deficiencies that can occur with restricted diets will allow for proper guidance and avoidable diseases.
References
1. Stahler C. “How Many Youth Are Vegetarian? The Vegetarian Resource Group Asks in a 2010 National Poll.”
2. Pediatrics. 1989 Sep;84(3):475-81.
3. J Am Diet Assoc. 2003 Jun;103(6):771-5.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
In the era where obesity is the No. 1 health crisis affecting people of all ages, physicians are often faced with questions regarding restricted diets or a patient may report that they are “vegetarian” in their history. Although new trendy diets appear all the time, “vegetarian inclined” diets are among the most common. A study conducted in 2008 identified that approximately 10% of Americans age 18 and older consumed a vegetarian diet.1 It is important to know the basics so that you can offer some guidance and look for possible deficiencies that may result from an altered diet.
Studies show that children who follow a vegetarian diet have normal growth and development but tend to be leaner than their omnivore counterparts.2 A healthy diet consumed in childhood lessens the risk for chronic diseases and promotes optimal growth and development. But altered or restricted diets in adolescents can be tricky because teens are actively growing and therefore usually need greater amounts of vital nutrients. So guidance is important to avoid common mistakes.
The simplest way to remember what is appropriate in a vegetarian diet is the restriction on intake of any food that once had a mother and a father. The vegetarian diet is further divided based on what it includes or excludes. Although the below list is not complete, it outlines the more common vegetarian diets:
• Vegan. This diet restricts intake of any animal product.
• Macrobiotics. This diet consists of whole grain, brown rice, fruits, and vegetables, and restricts intake of white meat or fish to twice a week.
• Lacto-vegetarian. This diet is one which allows milk products.
• Ovo vegetarian. – This diet allows eggs, but no meat, dairy, or fish.
• Pescitarian. This diet restricts meats, dairy, and eggs, but allows fish.
• Semi-vegetarian. This diet just restricts eating meat.
It is important to encourage anyone wishing to follow a vegetarian diet to fully research and understand what it entails. Health.gov under “dietary guidelines 2015-2020” is a wonderful reference to help understand how much of vital nutrients should be consumed to promote healthy eating habits and prevent deficiencies.
The key nutrients to discuss with patients are intake of protein, iron, calcium, vitamin B12, and vitamin D. Inadequate or incorrect intake can lead to deficiency of the vital nutrients that likely will result in disease.
Protein is a necessary nutrient because it provides the essential amino acids necessary for growth and repair. When animal protein breaks down, it provides all of the essential amino acids, unlike plant protein which can be deficient in some of the amino acids. Because each source of plant protein varies in the amino acid it is deficient in, it is important to have a mixed source of protein to ensure adequate intake. The soy bean has comparable amounts of protein to animal protein. Other sources of protein are legumes, grain, cereal, eggs, nuts, Greek yogurt, cottage cheese, but these are less digestible so greater consumption is needed to meet the daily requirements. Deficiency in protein can result in impaired growth.
Iron that is obtained from animals or meat sources has heme component, which makes it easier to absorb. Iron obtained from plants does not contain heme component and therefore is more difficult to absorb. Ascorbic acid (vitamin C) helps nonheme iron to be absorbed, but must be taken with an iron source to be effective. Therefore, vitamin C–containing foods such as fruits and vegetables should be consumed at every meal to assist in iron absorption. Deficiency in iron can lead to anemia and reduced energy.
Calcium is an important nutrient for bone formation, and deficiency can lead to increased risk for fracture and osteoporosis later in life. Its excretion and absorption can be affected by other nutrients, such as iron and zinc, present during digestion. Milk and dairy products are the most common source for calcium intake, but there are other calcium sources such as kale, broccoli, and food fortified with calcium such as cereal and orange juice. These foods can be better sources of calcium than supplements because they allow for better absorption.
Vitamin D is needed for calcium and phosphorus absorption, which is important for proper bone formation. Vitamin D is found in dairy products, fortified food and beverages, and exposure to the sun. Those living in colder climates and of darker pigmentation are at greater risk of deficiency so supplementation is usually necessary. Deficiency of vitamin D can lead to rickets.
Vitamin B12 is found in meat, fish, and dairy products, but not in plants. Intake of B12 is likely to be deficient in vegans because they do not consume most of those sources. Vegans are at a significant risk of vitamin B12 deficiency3 which can lead to macrocytosis, anemia, and decreased energy.
Educating families on healthy eating is essential at any visit. A good understanding of the possible deficiencies that can occur with restricted diets will allow for proper guidance and avoidable diseases.
References
1. Stahler C. “How Many Youth Are Vegetarian? The Vegetarian Resource Group Asks in a 2010 National Poll.”
2. Pediatrics. 1989 Sep;84(3):475-81.
3. J Am Diet Assoc. 2003 Jun;103(6):771-5.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.

Should Physicians Care about Costs?
The healthcare industry is under major stress from steady declines in all sources of revenue. The drivers are multifactorial but include declining reimbursement from payors, a shift from fee-for-service to pay-for-performance, and state-by-state variability in patients covered by Medicaid, by high-deductible plans, or by being uninsured. In academic medical centers, rising overhead costs coupled with a reticence to raise student tuition and declining research funding streams have further compounded the situation.
Regardless of the actual numbers, all healthcare institutions are feeling the financial pinch. Most are intensely focused on cost-reduction efforts. The question is, what do physicians think about their role in these efforts, and what efforts will be most effective?
A recent survey of a large physician group practice found that many physicians do not know what their cost drivers are or do not think it is their role to participate in cost-reduction efforts.1 Of note, the group practice in the survey is a Pioneer Medicare accountable care organization (ACO) and participates in a combination of fee-for-service and capitated contracts.
Within the survey, the researchers embedded a cost-consciousness scale, which is a validated survey tool designed to assess daily cost consciousness. They also embedded other survey items to determine the physicians’ concerns for malpractice, comfort with diagnostic uncertainty, and perception of patient-family pressure for utilization of services. The average overall cost-consciousness score was 29 out of 44, with higher scores indicating more cost consciousness.
Almost all physicians agreed that they need to reduce unnecessary testing (97%), need to adhere to guidelines (98%), and have a responsibility to control costs (92%). However, 33% felt it was unfair for them to have to be both cost-conscious and concerned with the welfare of their patients.
Approximately a third of respondents also felt that there was too much emphasis on cost and that physicians are too busy to worry about costs.
More than a third (37%) said they did not have good knowledge about test-procedure cost within their system.
More than half of physicians felt pressure from patients to perform tests and procedures (from 68% of primary-care physicians, 58% of medical specialists, and 56% of surgical specialists) and felt pressure to refer to consultants (from 65% of primary-care physicians, 35% of medical specialists, and 34% of surgical specialists).
Based on this survey and other literature about physicians’ perceptions of their role and their ability to control costs, it is clear that the first step in understanding how to engage physicians in cost-reducing efforts is to understand what the drivers are for utilization and what the concerns are for reducing cost. Many hypothesize that the drivers to support the status quo include a fear of litigation, fear of missing a diagnosis, and patient demands for services. Another major driver of current utilization is that there is ongoing support for the status quo, as the majority of reimbursement for providers is still based on fee-for-service.
Change Efforts
One cost-reducing effort that has gained widespread enthusiasm from medical societies is the Choosing Wisely campaign. This campaign is an effort originally driven by the American Board of Internal Medicine (ABIM) Foundation to help physicians become aware of and reduce unnecessary utilization of resources. Each Choosing Wisely list is generated and endorsed by the relevant medical society and widely advertised to physicians via a variety of mechanisms. More than 70 medical societies have participated in the effort to date.
The recommendations are often widely accepted by those in the specialty since they are evidence-based and derived and advertised by their own specialty societies. In the survey mentioned above, almost all physicians agreed that their Choosing Wisely was a good source of guidance (ranging from 92% of surgical specialties to 97% of primary-care physicians). In order to drive the movement from the patient perspective, Consumer Reports has developed educational materials aimed at the consumer side of healthcare (ie, patients and families).
As Consumer Reports suggests, the first step to implementing cost-conscious care is to measure awareness of cost and causes of overutilization. By first understanding behaviors, a group can then work to impact such behaviors. It is highly likely that the drivers are different based on the specialty of the physician, the patient population being served, and the local healthcare market drivers. As such, there will not be a single, across-the-board solution to reducing unnecessary utilization of services (and therefore cost), but interventions will need to be tailored to different groups depending on the drivers of cost locally.
Depending on the issues within a group, successful interventions could include:
- Decision support tools (for appropriate use of consultants and diagnostic tests)
- Display of testing costs (not just at the time of ordering)
- Efforts aimed at patient education (both as general consumers as well as at the point of care)
- Malpractice reform to support physicians trying to balance cost consciousness with patient welfare
In Sum
We have a long way to go in engaging physicians in efforts to reduce unnecessary utilization and cost. I recommend that hospitalist practices utilize the survey tool used in this study to understand the perceived barriers and drivers of cost within their practice and work with their local administrative teams to better understand patterns of overutilization among their group. Then interventions can be designed to be evidence-based, tailored to local workflow, and both reliable and sustainable.
If done well, hospitalists can have a huge impact on utilization and cost and position their groups and their hospitals well to succeed in this cost-constrained era of healthcare. TH
References
- Colla CH, Kinsella EA, Morden NE, Meyers DJ, Rosenthal MB, Sequist TD. Physician perception of Choosing Wisely and drivers of overuse. Am J Manag Care. 2016;22(5):337-343.

The healthcare industry is under major stress from steady declines in all sources of revenue. The drivers are multifactorial but include declining reimbursement from payors, a shift from fee-for-service to pay-for-performance, and state-by-state variability in patients covered by Medicaid, by high-deductible plans, or by being uninsured. In academic medical centers, rising overhead costs coupled with a reticence to raise student tuition and declining research funding streams have further compounded the situation.
Regardless of the actual numbers, all healthcare institutions are feeling the financial pinch. Most are intensely focused on cost-reduction efforts. The question is, what do physicians think about their role in these efforts, and what efforts will be most effective?
A recent survey of a large physician group practice found that many physicians do not know what their cost drivers are or do not think it is their role to participate in cost-reduction efforts.1 Of note, the group practice in the survey is a Pioneer Medicare accountable care organization (ACO) and participates in a combination of fee-for-service and capitated contracts.
Within the survey, the researchers embedded a cost-consciousness scale, which is a validated survey tool designed to assess daily cost consciousness. They also embedded other survey items to determine the physicians’ concerns for malpractice, comfort with diagnostic uncertainty, and perception of patient-family pressure for utilization of services. The average overall cost-consciousness score was 29 out of 44, with higher scores indicating more cost consciousness.
Almost all physicians agreed that they need to reduce unnecessary testing (97%), need to adhere to guidelines (98%), and have a responsibility to control costs (92%). However, 33% felt it was unfair for them to have to be both cost-conscious and concerned with the welfare of their patients.
Approximately a third of respondents also felt that there was too much emphasis on cost and that physicians are too busy to worry about costs.
More than a third (37%) said they did not have good knowledge about test-procedure cost within their system.
More than half of physicians felt pressure from patients to perform tests and procedures (from 68% of primary-care physicians, 58% of medical specialists, and 56% of surgical specialists) and felt pressure to refer to consultants (from 65% of primary-care physicians, 35% of medical specialists, and 34% of surgical specialists).
Based on this survey and other literature about physicians’ perceptions of their role and their ability to control costs, it is clear that the first step in understanding how to engage physicians in cost-reducing efforts is to understand what the drivers are for utilization and what the concerns are for reducing cost. Many hypothesize that the drivers to support the status quo include a fear of litigation, fear of missing a diagnosis, and patient demands for services. Another major driver of current utilization is that there is ongoing support for the status quo, as the majority of reimbursement for providers is still based on fee-for-service.
Change Efforts
One cost-reducing effort that has gained widespread enthusiasm from medical societies is the Choosing Wisely campaign. This campaign is an effort originally driven by the American Board of Internal Medicine (ABIM) Foundation to help physicians become aware of and reduce unnecessary utilization of resources. Each Choosing Wisely list is generated and endorsed by the relevant medical society and widely advertised to physicians via a variety of mechanisms. More than 70 medical societies have participated in the effort to date.
The recommendations are often widely accepted by those in the specialty since they are evidence-based and derived and advertised by their own specialty societies. In the survey mentioned above, almost all physicians agreed that their Choosing Wisely was a good source of guidance (ranging from 92% of surgical specialties to 97% of primary-care physicians). In order to drive the movement from the patient perspective, Consumer Reports has developed educational materials aimed at the consumer side of healthcare (ie, patients and families).
As Consumer Reports suggests, the first step to implementing cost-conscious care is to measure awareness of cost and causes of overutilization. By first understanding behaviors, a group can then work to impact such behaviors. It is highly likely that the drivers are different based on the specialty of the physician, the patient population being served, and the local healthcare market drivers. As such, there will not be a single, across-the-board solution to reducing unnecessary utilization of services (and therefore cost), but interventions will need to be tailored to different groups depending on the drivers of cost locally.
Depending on the issues within a group, successful interventions could include:
- Decision support tools (for appropriate use of consultants and diagnostic tests)
- Display of testing costs (not just at the time of ordering)
- Efforts aimed at patient education (both as general consumers as well as at the point of care)
- Malpractice reform to support physicians trying to balance cost consciousness with patient welfare
In Sum
We have a long way to go in engaging physicians in efforts to reduce unnecessary utilization and cost. I recommend that hospitalist practices utilize the survey tool used in this study to understand the perceived barriers and drivers of cost within their practice and work with their local administrative teams to better understand patterns of overutilization among their group. Then interventions can be designed to be evidence-based, tailored to local workflow, and both reliable and sustainable.
If done well, hospitalists can have a huge impact on utilization and cost and position their groups and their hospitals well to succeed in this cost-constrained era of healthcare. TH
References
- Colla CH, Kinsella EA, Morden NE, Meyers DJ, Rosenthal MB, Sequist TD. Physician perception of Choosing Wisely and drivers of overuse. Am J Manag Care. 2016;22(5):337-343.
The healthcare industry is under major stress from steady declines in all sources of revenue. The drivers are multifactorial but include declining reimbursement from payors, a shift from fee-for-service to pay-for-performance, and state-by-state variability in patients covered by Medicaid, by high-deductible plans, or by being uninsured. In academic medical centers, rising overhead costs coupled with a reticence to raise student tuition and declining research funding streams have further compounded the situation.
Regardless of the actual numbers, all healthcare institutions are feeling the financial pinch. Most are intensely focused on cost-reduction efforts. The question is, what do physicians think about their role in these efforts, and what efforts will be most effective?
A recent survey of a large physician group practice found that many physicians do not know what their cost drivers are or do not think it is their role to participate in cost-reduction efforts.1 Of note, the group practice in the survey is a Pioneer Medicare accountable care organization (ACO) and participates in a combination of fee-for-service and capitated contracts.
Within the survey, the researchers embedded a cost-consciousness scale, which is a validated survey tool designed to assess daily cost consciousness. They also embedded other survey items to determine the physicians’ concerns for malpractice, comfort with diagnostic uncertainty, and perception of patient-family pressure for utilization of services. The average overall cost-consciousness score was 29 out of 44, with higher scores indicating more cost consciousness.
Almost all physicians agreed that they need to reduce unnecessary testing (97%), need to adhere to guidelines (98%), and have a responsibility to control costs (92%). However, 33% felt it was unfair for them to have to be both cost-conscious and concerned with the welfare of their patients.
Approximately a third of respondents also felt that there was too much emphasis on cost and that physicians are too busy to worry about costs.
More than a third (37%) said they did not have good knowledge about test-procedure cost within their system.
More than half of physicians felt pressure from patients to perform tests and procedures (from 68% of primary-care physicians, 58% of medical specialists, and 56% of surgical specialists) and felt pressure to refer to consultants (from 65% of primary-care physicians, 35% of medical specialists, and 34% of surgical specialists).
Based on this survey and other literature about physicians’ perceptions of their role and their ability to control costs, it is clear that the first step in understanding how to engage physicians in cost-reducing efforts is to understand what the drivers are for utilization and what the concerns are for reducing cost. Many hypothesize that the drivers to support the status quo include a fear of litigation, fear of missing a diagnosis, and patient demands for services. Another major driver of current utilization is that there is ongoing support for the status quo, as the majority of reimbursement for providers is still based on fee-for-service.
Change Efforts
One cost-reducing effort that has gained widespread enthusiasm from medical societies is the Choosing Wisely campaign. This campaign is an effort originally driven by the American Board of Internal Medicine (ABIM) Foundation to help physicians become aware of and reduce unnecessary utilization of resources. Each Choosing Wisely list is generated and endorsed by the relevant medical society and widely advertised to physicians via a variety of mechanisms. More than 70 medical societies have participated in the effort to date.
The recommendations are often widely accepted by those in the specialty since they are evidence-based and derived and advertised by their own specialty societies. In the survey mentioned above, almost all physicians agreed that their Choosing Wisely was a good source of guidance (ranging from 92% of surgical specialties to 97% of primary-care physicians). In order to drive the movement from the patient perspective, Consumer Reports has developed educational materials aimed at the consumer side of healthcare (ie, patients and families).
As Consumer Reports suggests, the first step to implementing cost-conscious care is to measure awareness of cost and causes of overutilization. By first understanding behaviors, a group can then work to impact such behaviors. It is highly likely that the drivers are different based on the specialty of the physician, the patient population being served, and the local healthcare market drivers. As such, there will not be a single, across-the-board solution to reducing unnecessary utilization of services (and therefore cost), but interventions will need to be tailored to different groups depending on the drivers of cost locally.
Depending on the issues within a group, successful interventions could include:
- Decision support tools (for appropriate use of consultants and diagnostic tests)
- Display of testing costs (not just at the time of ordering)
- Efforts aimed at patient education (both as general consumers as well as at the point of care)
- Malpractice reform to support physicians trying to balance cost consciousness with patient welfare
In Sum
We have a long way to go in engaging physicians in efforts to reduce unnecessary utilization and cost. I recommend that hospitalist practices utilize the survey tool used in this study to understand the perceived barriers and drivers of cost within their practice and work with their local administrative teams to better understand patterns of overutilization among their group. Then interventions can be designed to be evidence-based, tailored to local workflow, and both reliable and sustainable.
If done well, hospitalists can have a huge impact on utilization and cost and position their groups and their hospitals well to succeed in this cost-constrained era of healthcare. TH
References
- Colla CH, Kinsella EA, Morden NE, Meyers DJ, Rosenthal MB, Sequist TD. Physician perception of Choosing Wisely and drivers of overuse. Am J Manag Care. 2016;22(5):337-343.
TV time linked to risk of death from PE

Photo courtesy of LG
The amount of TV a person watches each day may influence his risk of dying from pulmonary embolism (PE), according to research published in Circulation.
Researchers evaluated more than 80,000 people in Japan and found the risk of PE death rose as TV viewing time increased.
People who watched TV for 2.5 to 4.9 hours each day had a 70% greater risk of dying from PE than people who watched less than 2.5 hours of TV a day.
For each additional 2 hours of TV watched each day, a person’s risk of PE death increased by 40%.
“Pulmonary embolism occurs at a lower rate in Japan than it does in Western countries, but it may be on the rise,” said study author Hiroyasu Iso, MD, PhD, of Osaka University Graduate School of Medicine.
“The Japanese people are increasingly adopting sedentary lifestyles, which we believe is putting them at increased risk.”
To assess the link between TV viewing and PE death in Japan, Dr Iso and colleagues analyzed information on 86,024 subjects participating in the JACC study. This included 50,017 women and 36,007 men, ranging in age from 40 to 79.
From 1988 to 1990, the subjects completed a questionnaire that included information about average time spent watching TV each day.
The subjects were followed for a median of 19.2 years, until 2009. Mortality from PE was determined from death certificates. In all, 59 of the subjects died of PE.
The researchers calculated the risk of death from PE according to the amount of TV watched after adjusting for subjects’ age at baseline, sex, body mass index, history of hypertension, history of diabetes mellitus, smoking status, perceived mental stress, educational level, walking activity, and sports activity.
Compared to subjects who watched less than 2.5 hours of TV per day, those who watched 2.5 to 4.9 hours had an increased risk of PE death, with a hazard ratio of 1.7.
The risk was greater among subjects whose average TV viewing time was more than 5 hours per day, with a hazard ratio of 2.5.
The researchers said the actual risk of PE death may be higher because PE can be difficult to diagnose. They also pointed out that this study was conducted before computers, tablets, and smartphones became popular sources of information and entertainment.
“Nowadays, with online video streaming, the term ‘binge-watching’ to describe viewing multiple episodes of television programs in one sitting has become popular,” said study author Toru Shirakawa, MD, of Osaka University Graduate School of Medicine. “This popularity may reflect a rapidly growing habit.”
Earlier results from this study were presented at the ESC Congress 2015. ![]()
Photo courtesy of LG
The amount of TV a person watches each day may influence his risk of dying from pulmonary embolism (PE), according to research published in Circulation.
Researchers evaluated more than 80,000 people in Japan and found the risk of PE death rose as TV viewing time increased.
People who watched TV for 2.5 to 4.9 hours each day had a 70% greater risk of dying from PE than people who watched less than 2.5 hours of TV a day.
For each additional 2 hours of TV watched each day, a person’s risk of PE death increased by 40%.
“Pulmonary embolism occurs at a lower rate in Japan than it does in Western countries, but it may be on the rise,” said study author Hiroyasu Iso, MD, PhD, of Osaka University Graduate School of Medicine.
“The Japanese people are increasingly adopting sedentary lifestyles, which we believe is putting them at increased risk.”
To assess the link between TV viewing and PE death in Japan, Dr Iso and colleagues analyzed information on 86,024 subjects participating in the JACC study. This included 50,017 women and 36,007 men, ranging in age from 40 to 79.
From 1988 to 1990, the subjects completed a questionnaire that included information about average time spent watching TV each day.
The subjects were followed for a median of 19.2 years, until 2009. Mortality from PE was determined from death certificates. In all, 59 of the subjects died of PE.
The researchers calculated the risk of death from PE according to the amount of TV watched after adjusting for subjects’ age at baseline, sex, body mass index, history of hypertension, history of diabetes mellitus, smoking status, perceived mental stress, educational level, walking activity, and sports activity.
Compared to subjects who watched less than 2.5 hours of TV per day, those who watched 2.5 to 4.9 hours had an increased risk of PE death, with a hazard ratio of 1.7.
The risk was greater among subjects whose average TV viewing time was more than 5 hours per day, with a hazard ratio of 2.5.
The researchers said the actual risk of PE death may be higher because PE can be difficult to diagnose. They also pointed out that this study was conducted before computers, tablets, and smartphones became popular sources of information and entertainment.
“Nowadays, with online video streaming, the term ‘binge-watching’ to describe viewing multiple episodes of television programs in one sitting has become popular,” said study author Toru Shirakawa, MD, of Osaka University Graduate School of Medicine. “This popularity may reflect a rapidly growing habit.”
Earlier results from this study were presented at the ESC Congress 2015. ![]()
Photo courtesy of LG
The amount of TV a person watches each day may influence his risk of dying from pulmonary embolism (PE), according to research published in Circulation.
Researchers evaluated more than 80,000 people in Japan and found the risk of PE death rose as TV viewing time increased.
People who watched TV for 2.5 to 4.9 hours each day had a 70% greater risk of dying from PE than people who watched less than 2.5 hours of TV a day.
For each additional 2 hours of TV watched each day, a person’s risk of PE death increased by 40%.
“Pulmonary embolism occurs at a lower rate in Japan than it does in Western countries, but it may be on the rise,” said study author Hiroyasu Iso, MD, PhD, of Osaka University Graduate School of Medicine.
“The Japanese people are increasingly adopting sedentary lifestyles, which we believe is putting them at increased risk.”
To assess the link between TV viewing and PE death in Japan, Dr Iso and colleagues analyzed information on 86,024 subjects participating in the JACC study. This included 50,017 women and 36,007 men, ranging in age from 40 to 79.
From 1988 to 1990, the subjects completed a questionnaire that included information about average time spent watching TV each day.
The subjects were followed for a median of 19.2 years, until 2009. Mortality from PE was determined from death certificates. In all, 59 of the subjects died of PE.
The researchers calculated the risk of death from PE according to the amount of TV watched after adjusting for subjects’ age at baseline, sex, body mass index, history of hypertension, history of diabetes mellitus, smoking status, perceived mental stress, educational level, walking activity, and sports activity.
Compared to subjects who watched less than 2.5 hours of TV per day, those who watched 2.5 to 4.9 hours had an increased risk of PE death, with a hazard ratio of 1.7.
The risk was greater among subjects whose average TV viewing time was more than 5 hours per day, with a hazard ratio of 2.5.
The researchers said the actual risk of PE death may be higher because PE can be difficult to diagnose. They also pointed out that this study was conducted before computers, tablets, and smartphones became popular sources of information and entertainment.
“Nowadays, with online video streaming, the term ‘binge-watching’ to describe viewing multiple episodes of television programs in one sitting has become popular,” said study author Toru Shirakawa, MD, of Osaka University Graduate School of Medicine. “This popularity may reflect a rapidly growing habit.”
Earlier results from this study were presented at the ESC Congress 2015. ![]()
ASCO issues guideline on chronic pain management in adult cancer survivors

Photo courtesy of NIH
The American Society of Clinical Oncology (ASCO) has issued a new clinical practice guideline on the management of chronic pain in adult cancer survivors.
ASCO’s recommendations comprise both long-standing and new approaches, including routine screening for chronic pain, the use of alternative pain management approaches, the use of medical cannabis in certain settings where it is legal, and assessing the potential for opioid overuse.
“Many oncologists and primary care physicians are not trained to recognize or treat long-term pain associated with cancer,” said Judith A. Paice, PhD, RN, a co-chair of the ASCO expert panel that developed the guideline.
“This guideline will help clinicians identify pain early and develop comprehensive treatment plans, using a broad range of approaches.”
The guideline recommendations were developed by a multidisciplinary panel of experts in medical oncology, hematology/oncology, pain medicine, palliative care, hospice, radiation oncology, social work, symptom management research, rehabilitation, psychology, and anesthesiology, as well as a patient representative.
The panel conducted a systematic review of the medical literature published from 1996 to 2015. The resulting guideline includes the following key recommendations.
Clinicians should screen for pain at each encounter with a patient. Recurrent disease, second malignancy, or late-onset treatment effects should be evaluated, treated, and monitored.
Clinicians may prescribe non-pharmacologic interventions such as physical medicine and rehabilitation, integrative therapies (eg, acupuncture and massage), interventional therapies, and psychological approaches (eg, guided imagery, hypnosis, and meditation).
Systemic non-opioid analgesics (NSAIDS, acetaminophen) and adjuvant analgesics (selected antidepressants and anticonvulsants) may be prescribed to relieve chronic pain and/or improve physical function.
Clinicians may follow specific state regulations that allow access to medical cannabis or cannabinoids for patients with chronic pain after considering the potential benefits and risks of the available formulations.
Clinicians may prescribe a trial of opioids in carefully selected cancer patients who do not respond to more conservative pain management and who continue to experience pain-related distress or impairment of physical function.
Clinicians should assess the risk of adverse effects of opioids used in pain management and incorporate universal precautions to minimize abuse, addiction, and adverse consequences.
“Of great importance is the attention to appropriate assessment, not only of the individual’s pain, but also of their potential for over-reliance on opioids,” Dr Paice said. “This guideline outlines precautions that help ensure cancer survivors with persistent pain use opioids safely and effectively, while limiting access to those who are struggling with addiction.” ![]()
Photo courtesy of NIH
The American Society of Clinical Oncology (ASCO) has issued a new clinical practice guideline on the management of chronic pain in adult cancer survivors.
ASCO’s recommendations comprise both long-standing and new approaches, including routine screening for chronic pain, the use of alternative pain management approaches, the use of medical cannabis in certain settings where it is legal, and assessing the potential for opioid overuse.
“Many oncologists and primary care physicians are not trained to recognize or treat long-term pain associated with cancer,” said Judith A. Paice, PhD, RN, a co-chair of the ASCO expert panel that developed the guideline.
“This guideline will help clinicians identify pain early and develop comprehensive treatment plans, using a broad range of approaches.”
The guideline recommendations were developed by a multidisciplinary panel of experts in medical oncology, hematology/oncology, pain medicine, palliative care, hospice, radiation oncology, social work, symptom management research, rehabilitation, psychology, and anesthesiology, as well as a patient representative.
The panel conducted a systematic review of the medical literature published from 1996 to 2015. The resulting guideline includes the following key recommendations.
Clinicians should screen for pain at each encounter with a patient. Recurrent disease, second malignancy, or late-onset treatment effects should be evaluated, treated, and monitored.
Clinicians may prescribe non-pharmacologic interventions such as physical medicine and rehabilitation, integrative therapies (eg, acupuncture and massage), interventional therapies, and psychological approaches (eg, guided imagery, hypnosis, and meditation).
Systemic non-opioid analgesics (NSAIDS, acetaminophen) and adjuvant analgesics (selected antidepressants and anticonvulsants) may be prescribed to relieve chronic pain and/or improve physical function.
Clinicians may follow specific state regulations that allow access to medical cannabis or cannabinoids for patients with chronic pain after considering the potential benefits and risks of the available formulations.
Clinicians may prescribe a trial of opioids in carefully selected cancer patients who do not respond to more conservative pain management and who continue to experience pain-related distress or impairment of physical function.
Clinicians should assess the risk of adverse effects of opioids used in pain management and incorporate universal precautions to minimize abuse, addiction, and adverse consequences.
“Of great importance is the attention to appropriate assessment, not only of the individual’s pain, but also of their potential for over-reliance on opioids,” Dr Paice said. “This guideline outlines precautions that help ensure cancer survivors with persistent pain use opioids safely and effectively, while limiting access to those who are struggling with addiction.” ![]()
Photo courtesy of NIH
The American Society of Clinical Oncology (ASCO) has issued a new clinical practice guideline on the management of chronic pain in adult cancer survivors.
ASCO’s recommendations comprise both long-standing and new approaches, including routine screening for chronic pain, the use of alternative pain management approaches, the use of medical cannabis in certain settings where it is legal, and assessing the potential for opioid overuse.
“Many oncologists and primary care physicians are not trained to recognize or treat long-term pain associated with cancer,” said Judith A. Paice, PhD, RN, a co-chair of the ASCO expert panel that developed the guideline.
“This guideline will help clinicians identify pain early and develop comprehensive treatment plans, using a broad range of approaches.”
The guideline recommendations were developed by a multidisciplinary panel of experts in medical oncology, hematology/oncology, pain medicine, palliative care, hospice, radiation oncology, social work, symptom management research, rehabilitation, psychology, and anesthesiology, as well as a patient representative.
The panel conducted a systematic review of the medical literature published from 1996 to 2015. The resulting guideline includes the following key recommendations.
Clinicians should screen for pain at each encounter with a patient. Recurrent disease, second malignancy, or late-onset treatment effects should be evaluated, treated, and monitored.
Clinicians may prescribe non-pharmacologic interventions such as physical medicine and rehabilitation, integrative therapies (eg, acupuncture and massage), interventional therapies, and psychological approaches (eg, guided imagery, hypnosis, and meditation).
Systemic non-opioid analgesics (NSAIDS, acetaminophen) and adjuvant analgesics (selected antidepressants and anticonvulsants) may be prescribed to relieve chronic pain and/or improve physical function.
Clinicians may follow specific state regulations that allow access to medical cannabis or cannabinoids for patients with chronic pain after considering the potential benefits and risks of the available formulations.
Clinicians may prescribe a trial of opioids in carefully selected cancer patients who do not respond to more conservative pain management and who continue to experience pain-related distress or impairment of physical function.
Clinicians should assess the risk of adverse effects of opioids used in pain management and incorporate universal precautions to minimize abuse, addiction, and adverse consequences.
“Of great importance is the attention to appropriate assessment, not only of the individual’s pain, but also of their potential for over-reliance on opioids,” Dr Paice said. “This guideline outlines precautions that help ensure cancer survivors with persistent pain use opioids safely and effectively, while limiting access to those who are struggling with addiction.” ![]()
Lenalidomide maintenance doesn’t improve OS in DLBCL

Photo courtesy of Celgene
Initial results from the phase 3 REMARC study suggest that lenalidomide (Revlimid) maintenance does not prolong overall survival (OS) in patients with diffuse large B-cell lymphoma (DLBCL) who have responded to first-line treatment with R-CHOP.
Based on these results, Celgene Corporation, the company developing lenalidomide, said it does not plan to seek approval for the drug for this indication.
REMARC is a randomized, double-blind study designed to compare lenalidomide maintenance to placebo in 650 patients responding to induction therapy with R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone).
Patients in REMARC had received 6 to 8 cycles of the R-CHOP-14 regimen, 6 to 8 cycles of the R-CHOP-21 regimen, or 6 cycles of R-CHOP-14/R-CHOP-21 completed by 2 cycles of rituximab alone.
The primary endpoint of the study—a significant improvement in progression-free survival for patients receiving lenalidomide—was met.
However, the interim analysis of OS showed no benefit for patients in the lenalidomide arm.
Celgene said that, based on these results, the company is not planning to seek approval for lenalidomide as maintenance in this patient population.
“We are continuing to partner with LYSA [Lymphoma Study Association] to complete the analyses of the REMARC study,” said Michael Pehl, of Celgene.
“We remain committed to finishing the 4 ongoing phase 3 trials evaluating Revlimid and are confident about its potential as a treatment option across different settings in lymphoma.”
The REMARC study is part of a research program focused on non-Hodgkin lymphoma. In addition to the REMARC study, lenalidomide is also being evaluated in:
- The RELEVANCE study—in combination with rituximab in previously untreated follicular lymphoma (FL)
- The AUGMENT study—in combination with rituximab in relapsed/refractory FL and marginal zone lymphoma
- The MAGNIFY study—in combination with rituximab in relapsed/refractory FL, marginal zone lymphoma, and mantle cell lymphoma
- The ROBUST study—in combination with R-CHOP in previously untreated ABC-subtype DLBCL.
Data from RELEVANCE and AUGMENT are expected in the first and second half of 2017, respectively. ![]()
Photo courtesy of Celgene
Initial results from the phase 3 REMARC study suggest that lenalidomide (Revlimid) maintenance does not prolong overall survival (OS) in patients with diffuse large B-cell lymphoma (DLBCL) who have responded to first-line treatment with R-CHOP.
Based on these results, Celgene Corporation, the company developing lenalidomide, said it does not plan to seek approval for the drug for this indication.
REMARC is a randomized, double-blind study designed to compare lenalidomide maintenance to placebo in 650 patients responding to induction therapy with R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone).
Patients in REMARC had received 6 to 8 cycles of the R-CHOP-14 regimen, 6 to 8 cycles of the R-CHOP-21 regimen, or 6 cycles of R-CHOP-14/R-CHOP-21 completed by 2 cycles of rituximab alone.
The primary endpoint of the study—a significant improvement in progression-free survival for patients receiving lenalidomide—was met.
However, the interim analysis of OS showed no benefit for patients in the lenalidomide arm.
Celgene said that, based on these results, the company is not planning to seek approval for lenalidomide as maintenance in this patient population.
“We are continuing to partner with LYSA [Lymphoma Study Association] to complete the analyses of the REMARC study,” said Michael Pehl, of Celgene.
“We remain committed to finishing the 4 ongoing phase 3 trials evaluating Revlimid and are confident about its potential as a treatment option across different settings in lymphoma.”
The REMARC study is part of a research program focused on non-Hodgkin lymphoma. In addition to the REMARC study, lenalidomide is also being evaluated in:
- The RELEVANCE study—in combination with rituximab in previously untreated follicular lymphoma (FL)
- The AUGMENT study—in combination with rituximab in relapsed/refractory FL and marginal zone lymphoma
- The MAGNIFY study—in combination with rituximab in relapsed/refractory FL, marginal zone lymphoma, and mantle cell lymphoma
- The ROBUST study—in combination with R-CHOP in previously untreated ABC-subtype DLBCL.
Data from RELEVANCE and AUGMENT are expected in the first and second half of 2017, respectively. ![]()
Photo courtesy of Celgene
Initial results from the phase 3 REMARC study suggest that lenalidomide (Revlimid) maintenance does not prolong overall survival (OS) in patients with diffuse large B-cell lymphoma (DLBCL) who have responded to first-line treatment with R-CHOP.
Based on these results, Celgene Corporation, the company developing lenalidomide, said it does not plan to seek approval for the drug for this indication.
REMARC is a randomized, double-blind study designed to compare lenalidomide maintenance to placebo in 650 patients responding to induction therapy with R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone).
Patients in REMARC had received 6 to 8 cycles of the R-CHOP-14 regimen, 6 to 8 cycles of the R-CHOP-21 regimen, or 6 cycles of R-CHOP-14/R-CHOP-21 completed by 2 cycles of rituximab alone.
The primary endpoint of the study—a significant improvement in progression-free survival for patients receiving lenalidomide—was met.
However, the interim analysis of OS showed no benefit for patients in the lenalidomide arm.
Celgene said that, based on these results, the company is not planning to seek approval for lenalidomide as maintenance in this patient population.
“We are continuing to partner with LYSA [Lymphoma Study Association] to complete the analyses of the REMARC study,” said Michael Pehl, of Celgene.
“We remain committed to finishing the 4 ongoing phase 3 trials evaluating Revlimid and are confident about its potential as a treatment option across different settings in lymphoma.”
The REMARC study is part of a research program focused on non-Hodgkin lymphoma. In addition to the REMARC study, lenalidomide is also being evaluated in:
- The RELEVANCE study—in combination with rituximab in previously untreated follicular lymphoma (FL)
- The AUGMENT study—in combination with rituximab in relapsed/refractory FL and marginal zone lymphoma
- The MAGNIFY study—in combination with rituximab in relapsed/refractory FL, marginal zone lymphoma, and mantle cell lymphoma
- The ROBUST study—in combination with R-CHOP in previously untreated ABC-subtype DLBCL.
Data from RELEVANCE and AUGMENT are expected in the first and second half of 2017, respectively. ![]()
mAb granted breakthrough designation for MM

Photo courtesy of Janssen
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for daratumumab (Darzalex), a CD38-directed monoclonal antibody (mAb), as part of combination therapy for patients with multiple myeloma (MM).
The designation is for daratumumab in combination with lenalidomide and dexamethasone or bortezomib and dexamethasone for the treatment of MM patients who have received at least 1 prior therapy.
This is the second breakthrough designation the FDA has granted to daratumumab.
The FDA’s breakthrough designation is intended to expedite the development and review of new therapies for serious or life-threatening conditions.
To earn the designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need.
In May 2013, the FDA granted daratumumab breakthrough designation for the treatment of MM patients who have received at least 3 prior lines of therapy, including a proteasome inhibitor and an immunomodulatory agent, or who are double-refractory to a proteasome inhibitor and an immunomodulatory agent.
In November 2015, daratumumab received accelerated approval from the FDA for this indication. Continued approval of the mAb may be contingent upon verification and description of clinical benefit in a confirmatory trial.
Phase 3 trials
The newest breakthrough designation for daratumumab was based on data from two phase 3 studies—CASTOR (MMY3004) and POLLUX (MMY3003). Both studies were sponsored by Janssen Biotech, Inc., the company developing daratumumab.
In the CASTOR trial, researchers compared daratumumab-bortezomib-dexamethasone to bortezomib-dexamethasone in MM patients who had received at least 1 prior therapy.
The researchers said the addition of daratumumab significantly improved progression-free survival without increasing the cumulative toxicity or the toxicity of the bortezomib-dexamethasone combination.
Results from this trial were presented at the 2016 ASCO Annual Meeting.
In the POLLUX trial, researchers compared daratumumab-lenalidomide-dexamethasone to lenalidomide-dexamethasone in MM patients who had received at least 1 prior therapy.
According to the researchers, daratumumab-lenalidomide-dexamethasone conferred the highest response rate reported to date in the treatment of relapsed/refractory MM, significantly improved progression-free survival compared to lenalidomide-dexamethasone, and had a manageable safety profile.
These results were presented at the 21st Congress of the European Hematology Association. ![]()
Photo courtesy of Janssen
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for daratumumab (Darzalex), a CD38-directed monoclonal antibody (mAb), as part of combination therapy for patients with multiple myeloma (MM).
The designation is for daratumumab in combination with lenalidomide and dexamethasone or bortezomib and dexamethasone for the treatment of MM patients who have received at least 1 prior therapy.
This is the second breakthrough designation the FDA has granted to daratumumab.
The FDA’s breakthrough designation is intended to expedite the development and review of new therapies for serious or life-threatening conditions.
To earn the designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need.
In May 2013, the FDA granted daratumumab breakthrough designation for the treatment of MM patients who have received at least 3 prior lines of therapy, including a proteasome inhibitor and an immunomodulatory agent, or who are double-refractory to a proteasome inhibitor and an immunomodulatory agent.
In November 2015, daratumumab received accelerated approval from the FDA for this indication. Continued approval of the mAb may be contingent upon verification and description of clinical benefit in a confirmatory trial.
Phase 3 trials
The newest breakthrough designation for daratumumab was based on data from two phase 3 studies—CASTOR (MMY3004) and POLLUX (MMY3003). Both studies were sponsored by Janssen Biotech, Inc., the company developing daratumumab.
In the CASTOR trial, researchers compared daratumumab-bortezomib-dexamethasone to bortezomib-dexamethasone in MM patients who had received at least 1 prior therapy.
The researchers said the addition of daratumumab significantly improved progression-free survival without increasing the cumulative toxicity or the toxicity of the bortezomib-dexamethasone combination.
Results from this trial were presented at the 2016 ASCO Annual Meeting.
In the POLLUX trial, researchers compared daratumumab-lenalidomide-dexamethasone to lenalidomide-dexamethasone in MM patients who had received at least 1 prior therapy.
According to the researchers, daratumumab-lenalidomide-dexamethasone conferred the highest response rate reported to date in the treatment of relapsed/refractory MM, significantly improved progression-free survival compared to lenalidomide-dexamethasone, and had a manageable safety profile.
These results were presented at the 21st Congress of the European Hematology Association. ![]()
Photo courtesy of Janssen
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for daratumumab (Darzalex), a CD38-directed monoclonal antibody (mAb), as part of combination therapy for patients with multiple myeloma (MM).
The designation is for daratumumab in combination with lenalidomide and dexamethasone or bortezomib and dexamethasone for the treatment of MM patients who have received at least 1 prior therapy.
This is the second breakthrough designation the FDA has granted to daratumumab.
The FDA’s breakthrough designation is intended to expedite the development and review of new therapies for serious or life-threatening conditions.
To earn the designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need.
In May 2013, the FDA granted daratumumab breakthrough designation for the treatment of MM patients who have received at least 3 prior lines of therapy, including a proteasome inhibitor and an immunomodulatory agent, or who are double-refractory to a proteasome inhibitor and an immunomodulatory agent.
In November 2015, daratumumab received accelerated approval from the FDA for this indication. Continued approval of the mAb may be contingent upon verification and description of clinical benefit in a confirmatory trial.
Phase 3 trials
The newest breakthrough designation for daratumumab was based on data from two phase 3 studies—CASTOR (MMY3004) and POLLUX (MMY3003). Both studies were sponsored by Janssen Biotech, Inc., the company developing daratumumab.
In the CASTOR trial, researchers compared daratumumab-bortezomib-dexamethasone to bortezomib-dexamethasone in MM patients who had received at least 1 prior therapy.
The researchers said the addition of daratumumab significantly improved progression-free survival without increasing the cumulative toxicity or the toxicity of the bortezomib-dexamethasone combination.
Results from this trial were presented at the 2016 ASCO Annual Meeting.
In the POLLUX trial, researchers compared daratumumab-lenalidomide-dexamethasone to lenalidomide-dexamethasone in MM patients who had received at least 1 prior therapy.
According to the researchers, daratumumab-lenalidomide-dexamethasone conferred the highest response rate reported to date in the treatment of relapsed/refractory MM, significantly improved progression-free survival compared to lenalidomide-dexamethasone, and had a manageable safety profile.
These results were presented at the 21st Congress of the European Hematology Association. ![]()
1-800-Zap-My-Zits
ANSWERThe correct diagnosis is discoid lupus erythematosus (DLE; choice “c”). For those unfamiliar with DLE, it is often mistaken for the other items listed. Biopsy can distinguish among them.
Fungal infection (dermatophytosis; choice “a”) of the face is unusual and would have responded in some way to the antifungal cream. Likewise, the use of steroid creams would have markedly worsened a fungal infection.
Although this could have been psoriasis (choice “b”), it’s rare for that condition to be confined to the face. It almost always appears elsewhere—the scalp, elbows, knees, and/or nails.
Dermatomyositis (choice “d”), an autoimmune condition, can certainly present with a bimalar rash. However, it is usually accompanied by additional symptoms, such as progressive weakness and muscle pain.
DISCUSSION
DLE can represent a stand-alone diagnosis, or it can be a manifestation of systemic lupus erythematosus (SLE). When present in this bimalar form, the lesions are often mistaken for the “butterfly rash” commonly seen in SLE.
This patient was thoroughly tested for SLE, and no evidence of it was found. Biopsy did, however, show changes consistent with DLE (interface dermatitis with increased mucin formation, among others).
The treatment for DLE is rather simple: It consists of sun protection and oral hydroxychloroquine. This helps reduce inflammation, although the patient will still have residual scarring.
ANSWERThe correct diagnosis is discoid lupus erythematosus (DLE; choice “c”). For those unfamiliar with DLE, it is often mistaken for the other items listed. Biopsy can distinguish among them.
Fungal infection (dermatophytosis; choice “a”) of the face is unusual and would have responded in some way to the antifungal cream. Likewise, the use of steroid creams would have markedly worsened a fungal infection.
Although this could have been psoriasis (choice “b”), it’s rare for that condition to be confined to the face. It almost always appears elsewhere—the scalp, elbows, knees, and/or nails.
Dermatomyositis (choice “d”), an autoimmune condition, can certainly present with a bimalar rash. However, it is usually accompanied by additional symptoms, such as progressive weakness and muscle pain.
DISCUSSION
DLE can represent a stand-alone diagnosis, or it can be a manifestation of systemic lupus erythematosus (SLE). When present in this bimalar form, the lesions are often mistaken for the “butterfly rash” commonly seen in SLE.
This patient was thoroughly tested for SLE, and no evidence of it was found. Biopsy did, however, show changes consistent with DLE (interface dermatitis with increased mucin formation, among others).
The treatment for DLE is rather simple: It consists of sun protection and oral hydroxychloroquine. This helps reduce inflammation, although the patient will still have residual scarring.
ANSWERThe correct diagnosis is discoid lupus erythematosus (DLE; choice “c”). For those unfamiliar with DLE, it is often mistaken for the other items listed. Biopsy can distinguish among them.
Fungal infection (dermatophytosis; choice “a”) of the face is unusual and would have responded in some way to the antifungal cream. Likewise, the use of steroid creams would have markedly worsened a fungal infection.
Although this could have been psoriasis (choice “b”), it’s rare for that condition to be confined to the face. It almost always appears elsewhere—the scalp, elbows, knees, and/or nails.
Dermatomyositis (choice “d”), an autoimmune condition, can certainly present with a bimalar rash. However, it is usually accompanied by additional symptoms, such as progressive weakness and muscle pain.
DISCUSSION
DLE can represent a stand-alone diagnosis, or it can be a manifestation of systemic lupus erythematosus (SLE). When present in this bimalar form, the lesions are often mistaken for the “butterfly rash” commonly seen in SLE.
This patient was thoroughly tested for SLE, and no evidence of it was found. Biopsy did, however, show changes consistent with DLE (interface dermatitis with increased mucin formation, among others).
The treatment for DLE is rather simple: It consists of sun protection and oral hydroxychloroquine. This helps reduce inflammation, although the patient will still have residual scarring.

A 52-year-old man is referred to dermatology by his primary care provider for evaluation of facial lesions that first appeared almost a year ago. The patient, who works as a welder, has noticed that sun exposure tends to exacerbate the problem. He denies joint pain, fever, and malaise. He self-diagnosed the condition as acne and ordered a product from a TV ad, but this cream only made things worse. The asymptomatic lesions persist, despite application of a number of prescription products (2.5% hydrocortisone cream, adapalene gel, and antifungal creams, including tolnaftate and clotrimazole). The eruption—comprised of discrete, round, scaly lesions—covers a good portion of the bimalar areas of his face. The lesions are purplish red, and on closer inspection, you observe patulous follicular orifices. Some of the older lesions have focal atrophy. The rest of the examination is unremarkable.

An Exhausting Case of “Smoker’s Cough”
ANSWER
The correct interpretation includes sinus rhythm with complete heart block and a junctional rhythm, a rightward axis, and evidence of an anterior myocardial infarction (MI).
Sinus rhythm is evidenced by the regular rate and rhythm of the P waves.
Complete heart block is identified by the atrioventricular (AV) dissociation (QRS independent of the P wave), while the normal QRS duration—despite AV dissociation—confirms the existence of a junctional rhythm.
A positive R-wave axis slightly above the upper limit of normal, as seen with this patient, constitutes a rightward axis.
Finally, the posteriorly directed forces in the anterior precordial leads with poor R-wave progression denote an anterior MI.
ANSWER
The correct interpretation includes sinus rhythm with complete heart block and a junctional rhythm, a rightward axis, and evidence of an anterior myocardial infarction (MI).
Sinus rhythm is evidenced by the regular rate and rhythm of the P waves.
Complete heart block is identified by the atrioventricular (AV) dissociation (QRS independent of the P wave), while the normal QRS duration—despite AV dissociation—confirms the existence of a junctional rhythm.
A positive R-wave axis slightly above the upper limit of normal, as seen with this patient, constitutes a rightward axis.
Finally, the posteriorly directed forces in the anterior precordial leads with poor R-wave progression denote an anterior MI.
ANSWER
The correct interpretation includes sinus rhythm with complete heart block and a junctional rhythm, a rightward axis, and evidence of an anterior myocardial infarction (MI).
Sinus rhythm is evidenced by the regular rate and rhythm of the P waves.
Complete heart block is identified by the atrioventricular (AV) dissociation (QRS independent of the P wave), while the normal QRS duration—despite AV dissociation—confirms the existence of a junctional rhythm.
A positive R-wave axis slightly above the upper limit of normal, as seen with this patient, constitutes a rightward axis.
Finally, the posteriorly directed forces in the anterior precordial leads with poor R-wave progression denote an anterior MI.
One week ago, a 67-year-old African-American woman with a history of diabetes, hypertension, and smoking developed a nonproductive cough and chest discomfort. Over the past 24 hours, her symptoms have progressed, with increasing fatigue. She has delayed seeking care to spend time with visiting family, but this morning she calls for an appointment. At presentation, she describes her chest discomfort as a “vague, dull ache.” She denies sharp chest pain, radiation, syncope, near-syncope, and palpitations. She says her cough has resolved, aside from her usual early-morning “smoker’s cough.” However, she still experiences fatigue with exertion and must stop to rest after walking up one flight of stairs or about half a block on level ground. When asked about gardening, her favorite hobby, she tells you she stopped last week because she “didn’t have the energy” for it. Her medical history is remarkable for type 2 diabetes (for the past 10 years) and hypertension, for which she has been treated her entire adult life. She also has osteoarthritis. In the 20 years she has been in your patient panel, she has closely monitored her health and been vigilant about taking her medications. Her surgical history is remarkable for hysterectomy, cholecystectomy, and bilateral bunion resections. The patient retired two years ago after a 20-year career as a tax attorney. Her husband died of a myocardial infarction at age 56. She has two adult children, who also have hypertension. She has a 50–pack-year history of tobacco use and smokes up to one full pack of cigarettes per day. She denies alcohol and illicit drug use, aside from the occasional “nip” of brandy and infrequent marijuana use. Her medication list includes metformin, glyburide, hydrochlorothiazide, and lisinopril. She is allergic to sulfa. The review of systems is remarkable for hearing loss, diabetic neuropathy in both feet, and chronic loose stools. Vital signs include a blood pressure of 148/88 mm Hg—higher than measurements from her past three visits. Her pulse is 60 beats/min; respiratory rate, 14 breaths/min-1; and temperature, 98.8°F. On physical exam, her weight is 201 lb and her height is 68 in; her weight has remained stable over the past two years. The HEENT exam findings include corrective lenses, bilateral hearing aids, and extensive dental work (including veneers). The neck is supple, without thyromegaly or jugular venous distention. The lungs are clear in all fields, apart from occasional crackles in both bases that clear with coughing. Her cardiac exam reveals a regular rate with no extra heart sounds or rubs, but a soft, early diastolic murmur at the left lower sternal border. The abdomen is soft and nontender with well-healed surgical scars and no palpable masses. Osteoarthritis is present in both hands, and her left hip has decreased range of motion, compared to her right. Peripheral pulses are strong bilaterally, and her neurologic exam is intact. You draw laboratory specimens and order a chest x-ray and ECG, which reveals a ventricular rate of 56 beats/min; PR interval, unmeasurable; QRS duration, 106 ms; QT/QTc interval, 400/386 ms; P axis, 36°; R axis, 120°; and T axis, 7°. What is your interpretation of this ECG?
Terrorist Activity: Are You Ready?
I was relaxing after work in my local American Legion a few weeks ago when a quiet young man entered with a backpack. He set it down to use the restroom, and when he returned a few minutes later, he picked up the backpack and walked away. After he left, a group of us discussed how lax we were about this situation. Yes, it was probably innocent—but what if it wasn’t? A sign over the bar reads, “Don’t let anyone leave a stranger.” The purpose of that sign is, of course, to make everyone feel welcome, but these days I think it also means to be aware of your surroundings. I have seen too many American flags at half-staff this year to overlook a potential tragedy.
Today, clinicians must be prepared for all possible emergencies, including terrorism. Acts of terrorism (as the word implies) are designed to instill terror and panic, disrupt security and communication systems, destroy property, and kill or injure innocent civilians.
Recent terrorist attacks in 2016, while shocking in their brutality, were not inconceivable—public locations where large groups gather are logical targets. Terrorists often target high-traffic areas, such as airports or shopping malls, where they can quickly disappear into a crowd if necessary (hence the concern circling the Olympic Games to be held in Brazil this month).
Attacks at restaurants, airports, and other public “hot spots” are especially frightening. With terrorist attack locations in the past year ranging from nightclubs (the Pulse Nightclub shooting in Orlando, Florida, left 49 dead) to restaurants (a bomb in Dhaka, Bangladesh, killed 20) to conference rooms (a shooting in San Bernardino, California, left 14 dead and 21 injured), it’s clear that the fundamental message terrorists want to send is: You are not safe—anywhere!
While organized events and big crowds are a bull’s-eye for terrorists, our personal surroundings have risk factors, too. Because a terrorist attack can happen anywhere at any time, you need to be prepared by knowing what to do and how to maximize your chances of survival.
As this year’s attacks exemplify, we shouldn’t assume we understand the “logic” or thinking of terrorist organizations or individuals. Preparation for a terrorist attack boils down to being aware of the warning signs and being cautious and alert. Terrorists use a range of weapons and tactics, including bombs, arson, hijacking, and kidnapping (see Table).1,2
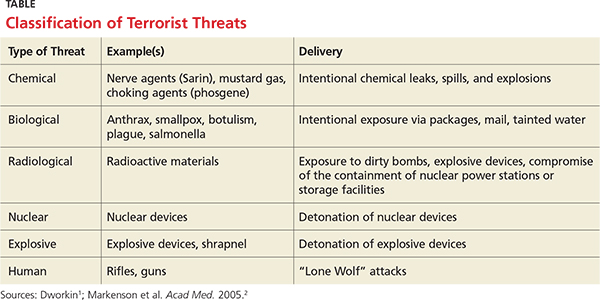
According to Dr. Howard Mell, an EMS director in North Carolina, the overwhelming majority of gunfire in the emergency department—or anywhere—is not the result of an active shooter. Most gunfire is targeted at a specific goal (ie, escaping or avoiding capture) or person. However, should there be an active shooter, he recommends three steps to take: Run (if the path is open), hide (if your exit is blocked), or fight (if there are no other alternatives).3
Wherever you are, always have multiple potential escape routes in mind. If you run, leave all belongings behind. Help others escape if possible, and take steps to prevent others from entering once you have left the area.
If you are unable to run, decide where to hide. If possible, barricade the area; if you are in a room, turn out the lights and stay away from the door. Be silent and put your cell phone on silent. While you are hiding, prepare to fight.
Fighting is the last resort. Act aggressively and improvise weapons to use against the assailant. If you have family, friends, or colleagues with you, put them to work!
When law enforcement officers arrive, understand that their job is to go right to the source and contain the danger. Keep your hands visible at all times, with fingers spread. Do not grab them for protection, and avoid yelling or pointing. Be prepared to give the authorities any pertinent information (eg, shooter description, last known location, direction of travel, or weapons seen).
Many health care facilities and organizations have valuable disaster and terrorism training programs, which include emergency evacuation procedures. I encourage you to take advantage of them, particularly if you travel internationally.4
Continue for personal preparedness >>
This is about personal preparedness. While I am not promoting paranoia, I do believe the risk for terrorist activity has increased in recent years.
I therefore urge you to have a healthy suspicion when you see or hear people
• Asking unusual questions about safety procedures at work
• Engaging in behaviors that provoke suspicion
• Loitering, parking, or standing in the same area over multiple days
• Attempting to disguise themselves from visit to visit
• Obtaining unusual quantities of weapons, ammunition, or explosive precursors
• Wearing clothing not appropriate for the season
• Leaving items, including backpacks or packages, unattended
• Leaving anonymous threats via telephone or e-mail
If after conducting a risk assessment of your surroundings, you believe you could (directly or indirectly) be impacted by terrorism, you must implement evacuation plans, notification of appropriate personnel, and personal safety measures.
In the event of a terrorist incident, remain calm, follow the advice of local emergency officials, and follow radio, television, and cell phone updates for news and instructions. 5
If an attack occurs near you or your home, here are practical steps you can take: Check for injuries. Give first aid and get help for seriously injured people. Check for damage using a flashlight—do not light matches or candles, or use electrical switches. Check for fires, fire hazards, and other household hazards. Sniff for gas leaks, starting at the water heater. If you smell gas or suspect a leak, turn off the main gas valve, open windows, and evacuate quickly. Shut off any damaged utilities, and confine or secure your pets. Call your family contact—but do not use the telephone again unless it is a life-threatening emergency. Cell phones may or may not be working. Check on your neighbors, especially those who are elderly or disabled.
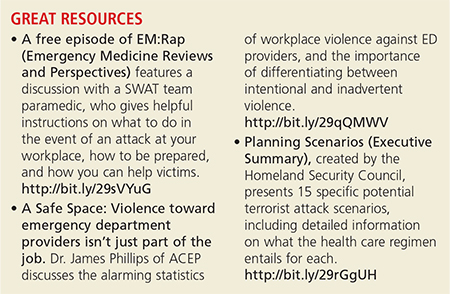
Terrorist attacks leave citizens concerned about future incidents of terrorism in the United States and their potential impact. They raise ambiguity about what might happen next and increase stress levels. You can take steps to prepare for terrorist attacks and reduce the stress you may feel, now and later, should an emergency arise. Taking preparatory action can reassure you, your family, and your children that you have a measure of control—even in the face of terrorism. If you have additional suggestions for terrorist defense preparation, you can email your ideas to PAEditor@frontlinemedcom.com.
References
1. Dworkin RW. Preparing hospitals, doctors, and nurses for a terrorist attack. Hudson Institute. www.hudson.org/content/researchattach ments/attachment/291/dworkin_white_paper.pdf. Accessed July 6, 2016.
2. Markenson F, DiMaggio C, Redlener I. Preparing health professions students for terrorism, disaster, and public health emergencies: core competencies. Acad Med. 2005;80(6):517-526.
3. Mell HK. Run, hide, fight: how to react when there’s gunfire in the emergency department. ACEP NOW. June 21, 2016. www.acepnow.com/react-theres-gunfire-emergency-department/?elq_mid=10369&elq_cid=5274988. Accessed July 6, 2016.
4. Uniformed Services University of the Health Sciences, Center for the Study of Traumatic Stress. Workplace preparedness for terrorism. www.cstsonline.org/assets/media/docu ments/CSTS_report_sloan_workplace_prepare_terrorism_preparedness.pdf. Accessed July 6, 2016.
5. American Red Cross. Terrorism Preparedness. www.redcross.org/prepare/disaster/terrorism. Accessed July 6, 2016.
I was relaxing after work in my local American Legion a few weeks ago when a quiet young man entered with a backpack. He set it down to use the restroom, and when he returned a few minutes later, he picked up the backpack and walked away. After he left, a group of us discussed how lax we were about this situation. Yes, it was probably innocent—but what if it wasn’t? A sign over the bar reads, “Don’t let anyone leave a stranger.” The purpose of that sign is, of course, to make everyone feel welcome, but these days I think it also means to be aware of your surroundings. I have seen too many American flags at half-staff this year to overlook a potential tragedy.
Today, clinicians must be prepared for all possible emergencies, including terrorism. Acts of terrorism (as the word implies) are designed to instill terror and panic, disrupt security and communication systems, destroy property, and kill or injure innocent civilians.
Recent terrorist attacks in 2016, while shocking in their brutality, were not inconceivable—public locations where large groups gather are logical targets. Terrorists often target high-traffic areas, such as airports or shopping malls, where they can quickly disappear into a crowd if necessary (hence the concern circling the Olympic Games to be held in Brazil this month).
Attacks at restaurants, airports, and other public “hot spots” are especially frightening. With terrorist attack locations in the past year ranging from nightclubs (the Pulse Nightclub shooting in Orlando, Florida, left 49 dead) to restaurants (a bomb in Dhaka, Bangladesh, killed 20) to conference rooms (a shooting in San Bernardino, California, left 14 dead and 21 injured), it’s clear that the fundamental message terrorists want to send is: You are not safe—anywhere!
While organized events and big crowds are a bull’s-eye for terrorists, our personal surroundings have risk factors, too. Because a terrorist attack can happen anywhere at any time, you need to be prepared by knowing what to do and how to maximize your chances of survival.
As this year’s attacks exemplify, we shouldn’t assume we understand the “logic” or thinking of terrorist organizations or individuals. Preparation for a terrorist attack boils down to being aware of the warning signs and being cautious and alert. Terrorists use a range of weapons and tactics, including bombs, arson, hijacking, and kidnapping (see Table).1,2
According to Dr. Howard Mell, an EMS director in North Carolina, the overwhelming majority of gunfire in the emergency department—or anywhere—is not the result of an active shooter. Most gunfire is targeted at a specific goal (ie, escaping or avoiding capture) or person. However, should there be an active shooter, he recommends three steps to take: Run (if the path is open), hide (if your exit is blocked), or fight (if there are no other alternatives).3
Wherever you are, always have multiple potential escape routes in mind. If you run, leave all belongings behind. Help others escape if possible, and take steps to prevent others from entering once you have left the area.
If you are unable to run, decide where to hide. If possible, barricade the area; if you are in a room, turn out the lights and stay away from the door. Be silent and put your cell phone on silent. While you are hiding, prepare to fight.
Fighting is the last resort. Act aggressively and improvise weapons to use against the assailant. If you have family, friends, or colleagues with you, put them to work!
When law enforcement officers arrive, understand that their job is to go right to the source and contain the danger. Keep your hands visible at all times, with fingers spread. Do not grab them for protection, and avoid yelling or pointing. Be prepared to give the authorities any pertinent information (eg, shooter description, last known location, direction of travel, or weapons seen).
Many health care facilities and organizations have valuable disaster and terrorism training programs, which include emergency evacuation procedures. I encourage you to take advantage of them, particularly if you travel internationally.4
Continue for personal preparedness >>
This is about personal preparedness. While I am not promoting paranoia, I do believe the risk for terrorist activity has increased in recent years.
I therefore urge you to have a healthy suspicion when you see or hear people
• Asking unusual questions about safety procedures at work
• Engaging in behaviors that provoke suspicion
• Loitering, parking, or standing in the same area over multiple days
• Attempting to disguise themselves from visit to visit
• Obtaining unusual quantities of weapons, ammunition, or explosive precursors
• Wearing clothing not appropriate for the season
• Leaving items, including backpacks or packages, unattended
• Leaving anonymous threats via telephone or e-mail
If after conducting a risk assessment of your surroundings, you believe you could (directly or indirectly) be impacted by terrorism, you must implement evacuation plans, notification of appropriate personnel, and personal safety measures.
In the event of a terrorist incident, remain calm, follow the advice of local emergency officials, and follow radio, television, and cell phone updates for news and instructions. 5
If an attack occurs near you or your home, here are practical steps you can take: Check for injuries. Give first aid and get help for seriously injured people. Check for damage using a flashlight—do not light matches or candles, or use electrical switches. Check for fires, fire hazards, and other household hazards. Sniff for gas leaks, starting at the water heater. If you smell gas or suspect a leak, turn off the main gas valve, open windows, and evacuate quickly. Shut off any damaged utilities, and confine or secure your pets. Call your family contact—but do not use the telephone again unless it is a life-threatening emergency. Cell phones may or may not be working. Check on your neighbors, especially those who are elderly or disabled.
Terrorist attacks leave citizens concerned about future incidents of terrorism in the United States and their potential impact. They raise ambiguity about what might happen next and increase stress levels. You can take steps to prepare for terrorist attacks and reduce the stress you may feel, now and later, should an emergency arise. Taking preparatory action can reassure you, your family, and your children that you have a measure of control—even in the face of terrorism. If you have additional suggestions for terrorist defense preparation, you can email your ideas to PAEditor@frontlinemedcom.com.
References
1. Dworkin RW. Preparing hospitals, doctors, and nurses for a terrorist attack. Hudson Institute. www.hudson.org/content/researchattach ments/attachment/291/dworkin_white_paper.pdf. Accessed July 6, 2016.
2. Markenson F, DiMaggio C, Redlener I. Preparing health professions students for terrorism, disaster, and public health emergencies: core competencies. Acad Med. 2005;80(6):517-526.
3. Mell HK. Run, hide, fight: how to react when there’s gunfire in the emergency department. ACEP NOW. June 21, 2016. www.acepnow.com/react-theres-gunfire-emergency-department/?elq_mid=10369&elq_cid=5274988. Accessed July 6, 2016.
4. Uniformed Services University of the Health Sciences, Center for the Study of Traumatic Stress. Workplace preparedness for terrorism. www.cstsonline.org/assets/media/docu ments/CSTS_report_sloan_workplace_prepare_terrorism_preparedness.pdf. Accessed July 6, 2016.
5. American Red Cross. Terrorism Preparedness. www.redcross.org/prepare/disaster/terrorism. Accessed July 6, 2016.
I was relaxing after work in my local American Legion a few weeks ago when a quiet young man entered with a backpack. He set it down to use the restroom, and when he returned a few minutes later, he picked up the backpack and walked away. After he left, a group of us discussed how lax we were about this situation. Yes, it was probably innocent—but what if it wasn’t? A sign over the bar reads, “Don’t let anyone leave a stranger.” The purpose of that sign is, of course, to make everyone feel welcome, but these days I think it also means to be aware of your surroundings. I have seen too many American flags at half-staff this year to overlook a potential tragedy.
Today, clinicians must be prepared for all possible emergencies, including terrorism. Acts of terrorism (as the word implies) are designed to instill terror and panic, disrupt security and communication systems, destroy property, and kill or injure innocent civilians.
Recent terrorist attacks in 2016, while shocking in their brutality, were not inconceivable—public locations where large groups gather are logical targets. Terrorists often target high-traffic areas, such as airports or shopping malls, where they can quickly disappear into a crowd if necessary (hence the concern circling the Olympic Games to be held in Brazil this month).
Attacks at restaurants, airports, and other public “hot spots” are especially frightening. With terrorist attack locations in the past year ranging from nightclubs (the Pulse Nightclub shooting in Orlando, Florida, left 49 dead) to restaurants (a bomb in Dhaka, Bangladesh, killed 20) to conference rooms (a shooting in San Bernardino, California, left 14 dead and 21 injured), it’s clear that the fundamental message terrorists want to send is: You are not safe—anywhere!
While organized events and big crowds are a bull’s-eye for terrorists, our personal surroundings have risk factors, too. Because a terrorist attack can happen anywhere at any time, you need to be prepared by knowing what to do and how to maximize your chances of survival.
As this year’s attacks exemplify, we shouldn’t assume we understand the “logic” or thinking of terrorist organizations or individuals. Preparation for a terrorist attack boils down to being aware of the warning signs and being cautious and alert. Terrorists use a range of weapons and tactics, including bombs, arson, hijacking, and kidnapping (see Table).1,2
According to Dr. Howard Mell, an EMS director in North Carolina, the overwhelming majority of gunfire in the emergency department—or anywhere—is not the result of an active shooter. Most gunfire is targeted at a specific goal (ie, escaping or avoiding capture) or person. However, should there be an active shooter, he recommends three steps to take: Run (if the path is open), hide (if your exit is blocked), or fight (if there are no other alternatives).3
Wherever you are, always have multiple potential escape routes in mind. If you run, leave all belongings behind. Help others escape if possible, and take steps to prevent others from entering once you have left the area.
If you are unable to run, decide where to hide. If possible, barricade the area; if you are in a room, turn out the lights and stay away from the door. Be silent and put your cell phone on silent. While you are hiding, prepare to fight.
Fighting is the last resort. Act aggressively and improvise weapons to use against the assailant. If you have family, friends, or colleagues with you, put them to work!
When law enforcement officers arrive, understand that their job is to go right to the source and contain the danger. Keep your hands visible at all times, with fingers spread. Do not grab them for protection, and avoid yelling or pointing. Be prepared to give the authorities any pertinent information (eg, shooter description, last known location, direction of travel, or weapons seen).
Many health care facilities and organizations have valuable disaster and terrorism training programs, which include emergency evacuation procedures. I encourage you to take advantage of them, particularly if you travel internationally.4
Continue for personal preparedness >>
This is about personal preparedness. While I am not promoting paranoia, I do believe the risk for terrorist activity has increased in recent years.
I therefore urge you to have a healthy suspicion when you see or hear people
• Asking unusual questions about safety procedures at work
• Engaging in behaviors that provoke suspicion
• Loitering, parking, or standing in the same area over multiple days
• Attempting to disguise themselves from visit to visit
• Obtaining unusual quantities of weapons, ammunition, or explosive precursors
• Wearing clothing not appropriate for the season
• Leaving items, including backpacks or packages, unattended
• Leaving anonymous threats via telephone or e-mail
If after conducting a risk assessment of your surroundings, you believe you could (directly or indirectly) be impacted by terrorism, you must implement evacuation plans, notification of appropriate personnel, and personal safety measures.
In the event of a terrorist incident, remain calm, follow the advice of local emergency officials, and follow radio, television, and cell phone updates for news and instructions. 5
If an attack occurs near you or your home, here are practical steps you can take: Check for injuries. Give first aid and get help for seriously injured people. Check for damage using a flashlight—do not light matches or candles, or use electrical switches. Check for fires, fire hazards, and other household hazards. Sniff for gas leaks, starting at the water heater. If you smell gas or suspect a leak, turn off the main gas valve, open windows, and evacuate quickly. Shut off any damaged utilities, and confine or secure your pets. Call your family contact—but do not use the telephone again unless it is a life-threatening emergency. Cell phones may or may not be working. Check on your neighbors, especially those who are elderly or disabled.
Terrorist attacks leave citizens concerned about future incidents of terrorism in the United States and their potential impact. They raise ambiguity about what might happen next and increase stress levels. You can take steps to prepare for terrorist attacks and reduce the stress you may feel, now and later, should an emergency arise. Taking preparatory action can reassure you, your family, and your children that you have a measure of control—even in the face of terrorism. If you have additional suggestions for terrorist defense preparation, you can email your ideas to PAEditor@frontlinemedcom.com.
References
1. Dworkin RW. Preparing hospitals, doctors, and nurses for a terrorist attack. Hudson Institute. www.hudson.org/content/researchattach ments/attachment/291/dworkin_white_paper.pdf. Accessed July 6, 2016.
2. Markenson F, DiMaggio C, Redlener I. Preparing health professions students for terrorism, disaster, and public health emergencies: core competencies. Acad Med. 2005;80(6):517-526.
3. Mell HK. Run, hide, fight: how to react when there’s gunfire in the emergency department. ACEP NOW. June 21, 2016. www.acepnow.com/react-theres-gunfire-emergency-department/?elq_mid=10369&elq_cid=5274988. Accessed July 6, 2016.
4. Uniformed Services University of the Health Sciences, Center for the Study of Traumatic Stress. Workplace preparedness for terrorism. www.cstsonline.org/assets/media/docu ments/CSTS_report_sloan_workplace_prepare_terrorism_preparedness.pdf. Accessed July 6, 2016.
5. American Red Cross. Terrorism Preparedness. www.redcross.org/prepare/disaster/terrorism. Accessed July 6, 2016.