User login
Influenza: A vaccine we love to hate
The Centers for Disease Control and Prevention, American Academy of Pediatrics, and American Academy of Family Physicians recommend that everyone 6 months of age and older get a seasonal flu vaccine. Emphasizing influenza vaccination in children recognizes the high burden of morbidity and significant mortality associated with influenza in young children as well as their role in transmission in the community.
In 2015-2016, the CDC reported 83 influenza deaths in children, and estimated the rate of hospitalization for children younger than 4 years of age to be 42/100,000 (at press time). In 2015-2016, the H1N1 strain was dominant in the community overall, with influenza B being most prevalent late in the season. The CDC estimates that nearly 75% of children less than 24 months and 68% between 2 and 4 years of age were immunized this year. Overall vaccine efficacy in children 6 months through 8 years was reported at 47% last season from a CDC study using a study design that compares vaccination odds among influenza reverse transcription polymerase chain reaction (RT-PCR)–positive cases and RT-PCR–negative controls.
Influenza virus vaccines are unique in that they are updated, often annually, to include the most current hemagglutinin (HA) antigens based on estimates from circulating strains. In the United States, influenza vaccine manufacturers submit a supplement to their license and obtain Food and Drug Administration approval. These applications require only a limited study of safety in approximately 300 adults, essentially to verify attenuation (Influenza Other Respir Viruses. 2016. doi: 10.111/irv.1283). They do not require clinical proof of efficacy or even a threshold of immunogenicity.

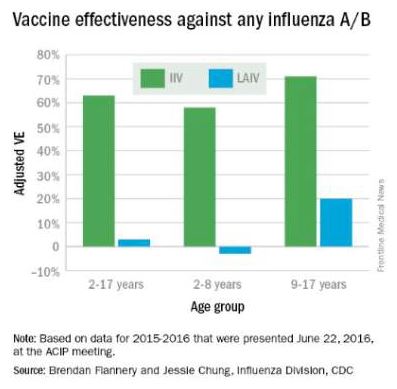
At the June 2016 CDC’s Advisory Committee on Immunization Practices (ACIP) meeting, data were presented comparing the efficacy of this season’s live attenuated influenza vaccine (LAIV) with inactivated influenza vaccine (IIV) by age and specific influenza type and subtype. Data from the U.S. Flu Vaccine Effectiveness (VE) Network, a consortium of five CDC-funded sites that conducts annual studies of influenza vaccine effectiveness, failed to demonstrate efficacy for LAIV in children aged 2-8 years. There was an absence of efficacy against the primary circulating strain, A(H1N1). This contrasted with the 62% efficacy report for IIV against A(H1N1).
The concern for efficacy for LAIV was not limited to 2015-2016; efficacy was poor in 2013-2014 during a year in which A(H1N1) was the dominant virus as well, and in 2014-2015 when the prevalent strain was a drifted A(H3N2). The lack of efficacy in 2015-2016 and 2013-2014 when A(H1N1) was the prevalent strain was especially enigmatic given its high efficacy against A(H1N1) between 2009 and 2011. Studies of LAIV from Astra Zeneca and the U.S. Department of Defense were consistent with those from the U.S. Flu VE Network; however, there were discordant data from Finland where vaccine efficacy was present. As a result of these studies, the ACIP voted that LAIV should not be used during the 2016-2017 flu season. This vote reinforces the importance of monitoring the effectiveness of annual flu vaccination and other public health interventions.
ACIP recommendations for 2016-2017
• Children younger than 2 years of age and those with chronic health problems such as asthma, diabetes, and disorders of the brain or nervous system are at especially high risk of developing serious flu complications.
• Annual influenza immunization, with either the IIV or recombinant influenza vaccine (RIV), for everyone 6 months and older, remains the only effective strategy for decreasing influenza disease in the community.
• LAIV should not be used during the 2016-2017 flu season.
ACIP recommendations must be reviewed and approved by the CDC’s director before becoming CDC policy. The final annual recommendations on the prevention and control of influenza with vaccines will be published in CDC Morbidity and Mortality Weekly Report (MMWR) Recommendations and Reports in late summer or early fall.
Flu vaccines available for children for 2016-2017
• The trivalent flu vaccine protects against three flu viruses; two influenza A viruses and an influenza B virus. Standard dose trivalent shots are manufactured with viruses grown in eggs. These are approved for children aged 6 months and older. There are different brands of this type of vaccine; each specific formulation has different age-based approvals.

• The quadrivalent flu vaccine protects against four flu viruses; two influenza A viruses and two influenza B viruses. A standard dose quadrivalent formulation is available for children; one brand is approved for children 6 months and older while others are approved for those 3 years and older.
• A cell-based vaccine, developed through a manufacturing process different from the traditional egg-based manufacturing process, was approved as a quadrivalent formulation for use in children 4 years of age and older.
Unanswered questions for the 2016-2017 influenza season
• Children 6 months to 8 years who are getting vaccinated for the first time need two doses. How should we consider influenza-naive children who received two doses of LAIV last year? The reason for the LAIV’s loss of efficacy in the years 2014 through 2016 is unknown, although it has been hypothesized that reduced immunogenicity is one possible cause for the lack of protection. Rather than speculate, we need to wait for ACIP to gather more data and then publish recommendations as to whether to consider such children vaccine naive (and therefore requiring two doses this season) or previously immunized (and therefore in need of only a single dose).
• Will supply be adequate this year? LAIV represents about 8% of the 171-176 million doses that were projected to be available during the 2016-2017 season; however, it represents nearly one-third of doses given to children. Thus, the potential for shortages in pediatric offices is real, and pediatricians and vaccine manufacturers need to work together to make sure sufficient pediatric formulation is available. The CDC is working with manufacturers to ensure there is sufficient supply to meet the demand.
Dr. Pelton is chief of pediatric infectious disease and coordinator of the maternal-child HIV program at Boston Medical Center. He has received honoraria from Sanofi Pasteur and Seqirus for participation in vaccine advisory boards in the prior 12 months. Email him at pdnews@frontlinemedcom.com.
The Centers for Disease Control and Prevention, American Academy of Pediatrics, and American Academy of Family Physicians recommend that everyone 6 months of age and older get a seasonal flu vaccine. Emphasizing influenza vaccination in children recognizes the high burden of morbidity and significant mortality associated with influenza in young children as well as their role in transmission in the community.
In 2015-2016, the CDC reported 83 influenza deaths in children, and estimated the rate of hospitalization for children younger than 4 years of age to be 42/100,000 (at press time). In 2015-2016, the H1N1 strain was dominant in the community overall, with influenza B being most prevalent late in the season. The CDC estimates that nearly 75% of children less than 24 months and 68% between 2 and 4 years of age were immunized this year. Overall vaccine efficacy in children 6 months through 8 years was reported at 47% last season from a CDC study using a study design that compares vaccination odds among influenza reverse transcription polymerase chain reaction (RT-PCR)–positive cases and RT-PCR–negative controls.
Influenza virus vaccines are unique in that they are updated, often annually, to include the most current hemagglutinin (HA) antigens based on estimates from circulating strains. In the United States, influenza vaccine manufacturers submit a supplement to their license and obtain Food and Drug Administration approval. These applications require only a limited study of safety in approximately 300 adults, essentially to verify attenuation (Influenza Other Respir Viruses. 2016. doi: 10.111/irv.1283). They do not require clinical proof of efficacy or even a threshold of immunogenicity.
At the June 2016 CDC’s Advisory Committee on Immunization Practices (ACIP) meeting, data were presented comparing the efficacy of this season’s live attenuated influenza vaccine (LAIV) with inactivated influenza vaccine (IIV) by age and specific influenza type and subtype. Data from the U.S. Flu Vaccine Effectiveness (VE) Network, a consortium of five CDC-funded sites that conducts annual studies of influenza vaccine effectiveness, failed to demonstrate efficacy for LAIV in children aged 2-8 years. There was an absence of efficacy against the primary circulating strain, A(H1N1). This contrasted with the 62% efficacy report for IIV against A(H1N1).
The concern for efficacy for LAIV was not limited to 2015-2016; efficacy was poor in 2013-2014 during a year in which A(H1N1) was the dominant virus as well, and in 2014-2015 when the prevalent strain was a drifted A(H3N2). The lack of efficacy in 2015-2016 and 2013-2014 when A(H1N1) was the prevalent strain was especially enigmatic given its high efficacy against A(H1N1) between 2009 and 2011. Studies of LAIV from Astra Zeneca and the U.S. Department of Defense were consistent with those from the U.S. Flu VE Network; however, there were discordant data from Finland where vaccine efficacy was present. As a result of these studies, the ACIP voted that LAIV should not be used during the 2016-2017 flu season. This vote reinforces the importance of monitoring the effectiveness of annual flu vaccination and other public health interventions.
ACIP recommendations for 2016-2017
• Children younger than 2 years of age and those with chronic health problems such as asthma, diabetes, and disorders of the brain or nervous system are at especially high risk of developing serious flu complications.
• Annual influenza immunization, with either the IIV or recombinant influenza vaccine (RIV), for everyone 6 months and older, remains the only effective strategy for decreasing influenza disease in the community.
• LAIV should not be used during the 2016-2017 flu season.
ACIP recommendations must be reviewed and approved by the CDC’s director before becoming CDC policy. The final annual recommendations on the prevention and control of influenza with vaccines will be published in CDC Morbidity and Mortality Weekly Report (MMWR) Recommendations and Reports in late summer or early fall.
Flu vaccines available for children for 2016-2017
• The trivalent flu vaccine protects against three flu viruses; two influenza A viruses and an influenza B virus. Standard dose trivalent shots are manufactured with viruses grown in eggs. These are approved for children aged 6 months and older. There are different brands of this type of vaccine; each specific formulation has different age-based approvals.
• The quadrivalent flu vaccine protects against four flu viruses; two influenza A viruses and two influenza B viruses. A standard dose quadrivalent formulation is available for children; one brand is approved for children 6 months and older while others are approved for those 3 years and older.
• A cell-based vaccine, developed through a manufacturing process different from the traditional egg-based manufacturing process, was approved as a quadrivalent formulation for use in children 4 years of age and older.
Unanswered questions for the 2016-2017 influenza season
• Children 6 months to 8 years who are getting vaccinated for the first time need two doses. How should we consider influenza-naive children who received two doses of LAIV last year? The reason for the LAIV’s loss of efficacy in the years 2014 through 2016 is unknown, although it has been hypothesized that reduced immunogenicity is one possible cause for the lack of protection. Rather than speculate, we need to wait for ACIP to gather more data and then publish recommendations as to whether to consider such children vaccine naive (and therefore requiring two doses this season) or previously immunized (and therefore in need of only a single dose).
• Will supply be adequate this year? LAIV represents about 8% of the 171-176 million doses that were projected to be available during the 2016-2017 season; however, it represents nearly one-third of doses given to children. Thus, the potential for shortages in pediatric offices is real, and pediatricians and vaccine manufacturers need to work together to make sure sufficient pediatric formulation is available. The CDC is working with manufacturers to ensure there is sufficient supply to meet the demand.
Dr. Pelton is chief of pediatric infectious disease and coordinator of the maternal-child HIV program at Boston Medical Center. He has received honoraria from Sanofi Pasteur and Seqirus for participation in vaccine advisory boards in the prior 12 months. Email him at pdnews@frontlinemedcom.com.
The Centers for Disease Control and Prevention, American Academy of Pediatrics, and American Academy of Family Physicians recommend that everyone 6 months of age and older get a seasonal flu vaccine. Emphasizing influenza vaccination in children recognizes the high burden of morbidity and significant mortality associated with influenza in young children as well as their role in transmission in the community.
In 2015-2016, the CDC reported 83 influenza deaths in children, and estimated the rate of hospitalization for children younger than 4 years of age to be 42/100,000 (at press time). In 2015-2016, the H1N1 strain was dominant in the community overall, with influenza B being most prevalent late in the season. The CDC estimates that nearly 75% of children less than 24 months and 68% between 2 and 4 years of age were immunized this year. Overall vaccine efficacy in children 6 months through 8 years was reported at 47% last season from a CDC study using a study design that compares vaccination odds among influenza reverse transcription polymerase chain reaction (RT-PCR)–positive cases and RT-PCR–negative controls.
Influenza virus vaccines are unique in that they are updated, often annually, to include the most current hemagglutinin (HA) antigens based on estimates from circulating strains. In the United States, influenza vaccine manufacturers submit a supplement to their license and obtain Food and Drug Administration approval. These applications require only a limited study of safety in approximately 300 adults, essentially to verify attenuation (Influenza Other Respir Viruses. 2016. doi: 10.111/irv.1283). They do not require clinical proof of efficacy or even a threshold of immunogenicity.
At the June 2016 CDC’s Advisory Committee on Immunization Practices (ACIP) meeting, data were presented comparing the efficacy of this season’s live attenuated influenza vaccine (LAIV) with inactivated influenza vaccine (IIV) by age and specific influenza type and subtype. Data from the U.S. Flu Vaccine Effectiveness (VE) Network, a consortium of five CDC-funded sites that conducts annual studies of influenza vaccine effectiveness, failed to demonstrate efficacy for LAIV in children aged 2-8 years. There was an absence of efficacy against the primary circulating strain, A(H1N1). This contrasted with the 62% efficacy report for IIV against A(H1N1).
The concern for efficacy for LAIV was not limited to 2015-2016; efficacy was poor in 2013-2014 during a year in which A(H1N1) was the dominant virus as well, and in 2014-2015 when the prevalent strain was a drifted A(H3N2). The lack of efficacy in 2015-2016 and 2013-2014 when A(H1N1) was the prevalent strain was especially enigmatic given its high efficacy against A(H1N1) between 2009 and 2011. Studies of LAIV from Astra Zeneca and the U.S. Department of Defense were consistent with those from the U.S. Flu VE Network; however, there were discordant data from Finland where vaccine efficacy was present. As a result of these studies, the ACIP voted that LAIV should not be used during the 2016-2017 flu season. This vote reinforces the importance of monitoring the effectiveness of annual flu vaccination and other public health interventions.
ACIP recommendations for 2016-2017
• Children younger than 2 years of age and those with chronic health problems such as asthma, diabetes, and disorders of the brain or nervous system are at especially high risk of developing serious flu complications.
• Annual influenza immunization, with either the IIV or recombinant influenza vaccine (RIV), for everyone 6 months and older, remains the only effective strategy for decreasing influenza disease in the community.
• LAIV should not be used during the 2016-2017 flu season.
ACIP recommendations must be reviewed and approved by the CDC’s director before becoming CDC policy. The final annual recommendations on the prevention and control of influenza with vaccines will be published in CDC Morbidity and Mortality Weekly Report (MMWR) Recommendations and Reports in late summer or early fall.
Flu vaccines available for children for 2016-2017
• The trivalent flu vaccine protects against three flu viruses; two influenza A viruses and an influenza B virus. Standard dose trivalent shots are manufactured with viruses grown in eggs. These are approved for children aged 6 months and older. There are different brands of this type of vaccine; each specific formulation has different age-based approvals.
• The quadrivalent flu vaccine protects against four flu viruses; two influenza A viruses and two influenza B viruses. A standard dose quadrivalent formulation is available for children; one brand is approved for children 6 months and older while others are approved for those 3 years and older.
• A cell-based vaccine, developed through a manufacturing process different from the traditional egg-based manufacturing process, was approved as a quadrivalent formulation for use in children 4 years of age and older.
Unanswered questions for the 2016-2017 influenza season
• Children 6 months to 8 years who are getting vaccinated for the first time need two doses. How should we consider influenza-naive children who received two doses of LAIV last year? The reason for the LAIV’s loss of efficacy in the years 2014 through 2016 is unknown, although it has been hypothesized that reduced immunogenicity is one possible cause for the lack of protection. Rather than speculate, we need to wait for ACIP to gather more data and then publish recommendations as to whether to consider such children vaccine naive (and therefore requiring two doses this season) or previously immunized (and therefore in need of only a single dose).
• Will supply be adequate this year? LAIV represents about 8% of the 171-176 million doses that were projected to be available during the 2016-2017 season; however, it represents nearly one-third of doses given to children. Thus, the potential for shortages in pediatric offices is real, and pediatricians and vaccine manufacturers need to work together to make sure sufficient pediatric formulation is available. The CDC is working with manufacturers to ensure there is sufficient supply to meet the demand.
Dr. Pelton is chief of pediatric infectious disease and coordinator of the maternal-child HIV program at Boston Medical Center. He has received honoraria from Sanofi Pasteur and Seqirus for participation in vaccine advisory boards in the prior 12 months. Email him at pdnews@frontlinemedcom.com.

Sleep Apnea in Later Life More Than Doubles Subsequent Alzheimer’s Disease Risk
DENVER—Obstructive sleep apnea (OSA) diagnosed later in life is associated with an increased likelihood of subsequent Alzheimer’s disease, Omonigho Bubu, MD, MPH, said at the 2016 Annual Meeting of the Associated Professional Sleep Societies.
He presented a retrospective cohort study in which a dose-response relationship was apparent. The more severe an individual’s OSA, as reflected in a higher apnea–hypopnea index on polysomnography, the greater the risk of later being diagnosed with Alzheimer’s disease, compared with matched controls during up to 13 years of follow-up.
Researchers identified several possible contributing factors for the observed relationship between OSA and Alzheimer’s disease. Patients with OSA and more severe sleep fragmentation, nocturnal hypoxia, and abnormal sleep duration were significantly more likely to subsequently develop Alzheimer’s disease than were patients with OSA and less severely disrupted sleep measures, added Dr. Bubu, a PhD candidate at the University of South Florida in Tampa.
The study included 756 patients age 65 and older with no history of cognitive decline when diagnosed with OSA by polysomnography at Tampa General Hospital during 2001–2005. They were matched by age, race, sex, BMI, and zip code to two control groups totaling 3,780 subjects. The controls, drawn from outpatient medical clinics at the hospital, had various medical problems, but no sleep disorders or cognitive impairment.
During a mean 10.5-year follow-up period, 513 subjects were diagnosed with Alzheimer’s disease, according to Medicare data. In a Cox proportional hazards analysis adjusted for age, sex, race, BMI, and education level, OSA was independently associated with a 2.2-fold increased risk of Alzheimer’s disease. Further adjustment for alcohol intake, smoking, use of sleep medications, and chronic medical conditions didn’t substantially change the results.
However, the investigators were not able to control for APOE ε4 allele status, which is a known risk factor for OSA and Alzheimer’s disease, so it remains unclear whether the association is “all related to APOE,” said Richard J. Caselli, MD, Professor of Neurology at the Mayo Clinic in Scottsdale, Arizona.
Time to onset of Alzheimer’s disease was shorter in patients with OSA. The mean time to diagnosis was 60.8 months after diagnosis of OSA, compared with 73 and 78 months in members of the two control groups who developed the dementia.
When the risk of developing Alzheimer’s disease was stratified according to baseline OSA severity, a dose-response effect was seen. Mild OSA, defined as 5–14 apnea–hypopnea events per hour of sleep, was associated with a 1.67-fold greater risk than in controls. The moderate OSA group, which had 15–29 events per hour, had a 1.81-fold increased risk. Patients with severe OSA, with 30 or more events per hour, had a 2.63-fold increased risk.
Gender, race, and education modified the relationship between OSA and Alzheimer’s disease, Dr. Bubu said. Women with OSA had a 2.28-fold greater risk of later developing the disease, compared with controls; men had a 1.42-fold increased risk. African-Americans with OSA were at 2.56-fold greater risk than were controls, while Hispanics with OSA were at 1.8-fold increased risk, and non-Hispanic whites were at 1.87-fold increased risk. Patients with OSA and a high school education or less were at 2.73 times greater risk of Alzheimer’s disease than were controls; those with at least some college or technical school were at 1.82-fold risk, and patients with OSA who had attended graduate school had a 1.31-fold increased risk.
“Our results definitely show that OSA precedes the onset of Alzheimer’s disease. But we cannot say that’s causation. That will be left to future research examining the potential mechanisms we’ve identified,” Dr. Bubu said.
A key missing link in establishing a causal relationship is the lack of data on how many of the older patients diagnosed with OSA accepted treatment for the condition, and what their response rates were. In other words, it remains to be seen whether OSA occurring later in life is a modifiable risk factor for Alzheimer’s disease, as opposed to an early expression of the dementing disease process, whereby treatment of the sleep disorder doesn’t affect the progressive cognitive decline.
Short sleep duration of less than six hours as well as a mean total sleep time greater than nine hours in patients with OSA were associated with significantly increased risk of Alzheimer’s disease, compared with a sleep time of six to nine hours. Patients with high sleep-onset latency in the sleep lab, a high REM latency from sleep onset, a low percentage of time spent in REM, an oxygen saturation level of less than 90% for at least 1% of sleep time, or a high number of arousals per hour of sleep were also at increased risk of subsequent Alzheimer’s disease.
The study was supported by the Byrd Alzheimer’s Institute. Dr. Bubu reported having no financial conflicts.
—Bruce Jancin
Suggested Reading
Kheirandish-Gozal L, Philby ME, Alonso-Álvarez ML, et al. Biomarkers of Alzheimer disease in children with obstructive sleep apnea: effect of adenotonsillectomty. Sleep. 2016;39(6):1225-1232.
DENVER—Obstructive sleep apnea (OSA) diagnosed later in life is associated with an increased likelihood of subsequent Alzheimer’s disease, Omonigho Bubu, MD, MPH, said at the 2016 Annual Meeting of the Associated Professional Sleep Societies.
He presented a retrospective cohort study in which a dose-response relationship was apparent. The more severe an individual’s OSA, as reflected in a higher apnea–hypopnea index on polysomnography, the greater the risk of later being diagnosed with Alzheimer’s disease, compared with matched controls during up to 13 years of follow-up.
Researchers identified several possible contributing factors for the observed relationship between OSA and Alzheimer’s disease. Patients with OSA and more severe sleep fragmentation, nocturnal hypoxia, and abnormal sleep duration were significantly more likely to subsequently develop Alzheimer’s disease than were patients with OSA and less severely disrupted sleep measures, added Dr. Bubu, a PhD candidate at the University of South Florida in Tampa.
The study included 756 patients age 65 and older with no history of cognitive decline when diagnosed with OSA by polysomnography at Tampa General Hospital during 2001–2005. They were matched by age, race, sex, BMI, and zip code to two control groups totaling 3,780 subjects. The controls, drawn from outpatient medical clinics at the hospital, had various medical problems, but no sleep disorders or cognitive impairment.
During a mean 10.5-year follow-up period, 513 subjects were diagnosed with Alzheimer’s disease, according to Medicare data. In a Cox proportional hazards analysis adjusted for age, sex, race, BMI, and education level, OSA was independently associated with a 2.2-fold increased risk of Alzheimer’s disease. Further adjustment for alcohol intake, smoking, use of sleep medications, and chronic medical conditions didn’t substantially change the results.
However, the investigators were not able to control for APOE ε4 allele status, which is a known risk factor for OSA and Alzheimer’s disease, so it remains unclear whether the association is “all related to APOE,” said Richard J. Caselli, MD, Professor of Neurology at the Mayo Clinic in Scottsdale, Arizona.
Time to onset of Alzheimer’s disease was shorter in patients with OSA. The mean time to diagnosis was 60.8 months after diagnosis of OSA, compared with 73 and 78 months in members of the two control groups who developed the dementia.
When the risk of developing Alzheimer’s disease was stratified according to baseline OSA severity, a dose-response effect was seen. Mild OSA, defined as 5–14 apnea–hypopnea events per hour of sleep, was associated with a 1.67-fold greater risk than in controls. The moderate OSA group, which had 15–29 events per hour, had a 1.81-fold increased risk. Patients with severe OSA, with 30 or more events per hour, had a 2.63-fold increased risk.
Gender, race, and education modified the relationship between OSA and Alzheimer’s disease, Dr. Bubu said. Women with OSA had a 2.28-fold greater risk of later developing the disease, compared with controls; men had a 1.42-fold increased risk. African-Americans with OSA were at 2.56-fold greater risk than were controls, while Hispanics with OSA were at 1.8-fold increased risk, and non-Hispanic whites were at 1.87-fold increased risk. Patients with OSA and a high school education or less were at 2.73 times greater risk of Alzheimer’s disease than were controls; those with at least some college or technical school were at 1.82-fold risk, and patients with OSA who had attended graduate school had a 1.31-fold increased risk.
“Our results definitely show that OSA precedes the onset of Alzheimer’s disease. But we cannot say that’s causation. That will be left to future research examining the potential mechanisms we’ve identified,” Dr. Bubu said.
A key missing link in establishing a causal relationship is the lack of data on how many of the older patients diagnosed with OSA accepted treatment for the condition, and what their response rates were. In other words, it remains to be seen whether OSA occurring later in life is a modifiable risk factor for Alzheimer’s disease, as opposed to an early expression of the dementing disease process, whereby treatment of the sleep disorder doesn’t affect the progressive cognitive decline.
Short sleep duration of less than six hours as well as a mean total sleep time greater than nine hours in patients with OSA were associated with significantly increased risk of Alzheimer’s disease, compared with a sleep time of six to nine hours. Patients with high sleep-onset latency in the sleep lab, a high REM latency from sleep onset, a low percentage of time spent in REM, an oxygen saturation level of less than 90% for at least 1% of sleep time, or a high number of arousals per hour of sleep were also at increased risk of subsequent Alzheimer’s disease.
The study was supported by the Byrd Alzheimer’s Institute. Dr. Bubu reported having no financial conflicts.
—Bruce Jancin
DENVER—Obstructive sleep apnea (OSA) diagnosed later in life is associated with an increased likelihood of subsequent Alzheimer’s disease, Omonigho Bubu, MD, MPH, said at the 2016 Annual Meeting of the Associated Professional Sleep Societies.
He presented a retrospective cohort study in which a dose-response relationship was apparent. The more severe an individual’s OSA, as reflected in a higher apnea–hypopnea index on polysomnography, the greater the risk of later being diagnosed with Alzheimer’s disease, compared with matched controls during up to 13 years of follow-up.
Researchers identified several possible contributing factors for the observed relationship between OSA and Alzheimer’s disease. Patients with OSA and more severe sleep fragmentation, nocturnal hypoxia, and abnormal sleep duration were significantly more likely to subsequently develop Alzheimer’s disease than were patients with OSA and less severely disrupted sleep measures, added Dr. Bubu, a PhD candidate at the University of South Florida in Tampa.
The study included 756 patients age 65 and older with no history of cognitive decline when diagnosed with OSA by polysomnography at Tampa General Hospital during 2001–2005. They were matched by age, race, sex, BMI, and zip code to two control groups totaling 3,780 subjects. The controls, drawn from outpatient medical clinics at the hospital, had various medical problems, but no sleep disorders or cognitive impairment.
During a mean 10.5-year follow-up period, 513 subjects were diagnosed with Alzheimer’s disease, according to Medicare data. In a Cox proportional hazards analysis adjusted for age, sex, race, BMI, and education level, OSA was independently associated with a 2.2-fold increased risk of Alzheimer’s disease. Further adjustment for alcohol intake, smoking, use of sleep medications, and chronic medical conditions didn’t substantially change the results.
However, the investigators were not able to control for APOE ε4 allele status, which is a known risk factor for OSA and Alzheimer’s disease, so it remains unclear whether the association is “all related to APOE,” said Richard J. Caselli, MD, Professor of Neurology at the Mayo Clinic in Scottsdale, Arizona.
Time to onset of Alzheimer’s disease was shorter in patients with OSA. The mean time to diagnosis was 60.8 months after diagnosis of OSA, compared with 73 and 78 months in members of the two control groups who developed the dementia.
When the risk of developing Alzheimer’s disease was stratified according to baseline OSA severity, a dose-response effect was seen. Mild OSA, defined as 5–14 apnea–hypopnea events per hour of sleep, was associated with a 1.67-fold greater risk than in controls. The moderate OSA group, which had 15–29 events per hour, had a 1.81-fold increased risk. Patients with severe OSA, with 30 or more events per hour, had a 2.63-fold increased risk.
Gender, race, and education modified the relationship between OSA and Alzheimer’s disease, Dr. Bubu said. Women with OSA had a 2.28-fold greater risk of later developing the disease, compared with controls; men had a 1.42-fold increased risk. African-Americans with OSA were at 2.56-fold greater risk than were controls, while Hispanics with OSA were at 1.8-fold increased risk, and non-Hispanic whites were at 1.87-fold increased risk. Patients with OSA and a high school education or less were at 2.73 times greater risk of Alzheimer’s disease than were controls; those with at least some college or technical school were at 1.82-fold risk, and patients with OSA who had attended graduate school had a 1.31-fold increased risk.
“Our results definitely show that OSA precedes the onset of Alzheimer’s disease. But we cannot say that’s causation. That will be left to future research examining the potential mechanisms we’ve identified,” Dr. Bubu said.
A key missing link in establishing a causal relationship is the lack of data on how many of the older patients diagnosed with OSA accepted treatment for the condition, and what their response rates were. In other words, it remains to be seen whether OSA occurring later in life is a modifiable risk factor for Alzheimer’s disease, as opposed to an early expression of the dementing disease process, whereby treatment of the sleep disorder doesn’t affect the progressive cognitive decline.
Short sleep duration of less than six hours as well as a mean total sleep time greater than nine hours in patients with OSA were associated with significantly increased risk of Alzheimer’s disease, compared with a sleep time of six to nine hours. Patients with high sleep-onset latency in the sleep lab, a high REM latency from sleep onset, a low percentage of time spent in REM, an oxygen saturation level of less than 90% for at least 1% of sleep time, or a high number of arousals per hour of sleep were also at increased risk of subsequent Alzheimer’s disease.
The study was supported by the Byrd Alzheimer’s Institute. Dr. Bubu reported having no financial conflicts.
—Bruce Jancin
Suggested Reading
Kheirandish-Gozal L, Philby ME, Alonso-Álvarez ML, et al. Biomarkers of Alzheimer disease in children with obstructive sleep apnea: effect of adenotonsillectomty. Sleep. 2016;39(6):1225-1232.
Suggested Reading
Kheirandish-Gozal L, Philby ME, Alonso-Álvarez ML, et al. Biomarkers of Alzheimer disease in children with obstructive sleep apnea: effect of adenotonsillectomty. Sleep. 2016;39(6):1225-1232.
Disordered sleep: Ask the right questions to reveal this hidden confounder
It seems like common sense: Sleeping poorly results in not feeling good. The truth is that many of our patients are sleep deprived but are either unaware of, or unwilling to acknowledge, their problem. The busy life that many patients have does not allow adequate time for sleep. In fact, I have encountered patients who think of sleep as an inconvenience that takes away time from other pursuits.
Sleep deprivation in psychiatric disorders
Sleep deprivation occurs when the duration or quality of sleep is inadequate. Inadequate sleep duration can be caused by insomnia or simply not allowing enough time for sleep (1 aspect of poor sleep hygiene). Poor sleep quality often is caused by sleep-disordered breathing.
Sleep deprivation can result in either sleepiness or fatigue. Sleepiness is a propensity to fall asleep; fatigue is a lack of energy that is not alleviated by additional sleep. Fatigue is more likely to be associated with a psychiatric disorder; sleepiness is more predominant in sleep disorders (although there is significant overlap). For example, patients with a major depressive disorder can experience fatigue as much as patients with sleep deprivation, but the latter also is more likely to result in sleepiness. Trouble concentrating is seen in anxiety, depression, attention-deficit/hyperactivity disorder (ADHD), and sleep deprivation.1
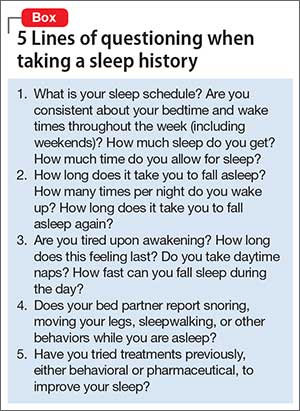
Insomnia or poor sleep hygiene can be diagnosed with a thorough sleep history. I take special care to consider sleep problems by presenting 5 groups of questions to the patient (Box).
Sleep-disordered breathing
A sleep study is required to accurately diagnose sleep-disordered breathing. Unless this diagnosis is specifically looked for, it remains hidden from both physicians and patients. Clues to the presence of sleep-disordered breathing include snorting, snoring, and gasping for air during sleep; witnessed apnea during sleep; nighttime awakening; daytime fatigue; nocturia; mouth breathing or dry mouth; acid reflux; irritability; morning headache; nighttime sweating; and low libido. Risk factors for sleep-disordered breathing include obesity; smoking; menopause; family history; increasing age; and anatomical factors (eg, deviation of the nasal septum; retrognathia; long face syndrome; high-arched narrow hard palate; large tonsils, uvula, or tongue).2
Measuring sleep quality
Some patients are unaware of the extent to which they are sleepy. The most widely used scale to measure sleepiness is the Epworth Sleepiness Scale.3 Sleep specialists view a score of ≥10 on the Epworth scale as indicative of daytime sleepiness. In addition, a patient’s daily consumption of caffeinated beverages can be a clue to excessive sleepiness or, at least, fatigue. If the degree of sleepiness cannot be determined subjectively, objective measures, such as the Multiple Sleep Latency Test (MSLT), can quantify it. In a randomly selected sample from the general population, 13.4% had excessive daytime sleepiness as measured by the MSLT.4
Adult ADHD and sleep deprivation
In my practice, sleep problems confound both the diagnosis and treatment of psychiatric disorders, especially ADHD. Often, patients who report ADHD symptoms have no clear history of ADHD during childhood. In these cases, I always consider the possibility that their ADHD symptoms are due to sleep deprivation. Sleep deprivation can mimic the poor executive function and difficulty concentrating that is often seen in ADHD, because such deprivation is associated with decreased activity in the prefrontal cortex during wakefulness.5
In patients who provide a clear history of ADHD symptoms during childhood, it is possible that inadequate sleep exacerbates ADHD symptoms as adults. Unless sleep deprivation is diagnosed and treated in these patients, they can end up taking a higher-than-necessary dosage of a stimulant. Also, patients who have ADHD might have a difficult time managing their sleep schedule because of poor executive functioning. This, in turn, can result in additional sleep deprivation, thus worsening their ADHD symptoms, creating a vicious circle.
Psychotropics and sedation
Many psychiatric medications list sedation as a side effect. Patients with untreated sleep problems might be more likely to notice this side effect because sleep problems contribute to their fatigue. I have had patients who were unable to tolerate sedative medications until their sleep apnea was treated.
In conclusion
It is important to consider sleep deprivation in your differential diagnosis of psychiatric patients. This will allow for more accurate diagnosis and treatment and, in some cases, can avoid treatment resistance.
1. Stahl SM. Excessive sleepiness. San Diego, CA: NEI Press; 2005.
2. Jordan AS, McSharry DG, Malhotra A. Adult obstructive sleep apnoea. Lancet. 2014;383(9918):736-747.
3. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540-545.
4. Drake CL, Roehrs TA, Richardson GS, et al. Epidemiology and morbidity of excessive daytime sleepiness. Sleep. 2002;25:A91-A92.
5. Thomas M, Sing H, Belenky G, et al. Neural basis of alertness and cognitive performance impairments during sleepiness. I. Effects of 24 h of sleep deprivation on waking human regional brain activity. J Sleep Res. 2000;9(4):335-352.
It seems like common sense: Sleeping poorly results in not feeling good. The truth is that many of our patients are sleep deprived but are either unaware of, or unwilling to acknowledge, their problem. The busy life that many patients have does not allow adequate time for sleep. In fact, I have encountered patients who think of sleep as an inconvenience that takes away time from other pursuits.
Sleep deprivation in psychiatric disorders
Sleep deprivation occurs when the duration or quality of sleep is inadequate. Inadequate sleep duration can be caused by insomnia or simply not allowing enough time for sleep (1 aspect of poor sleep hygiene). Poor sleep quality often is caused by sleep-disordered breathing.
Sleep deprivation can result in either sleepiness or fatigue. Sleepiness is a propensity to fall asleep; fatigue is a lack of energy that is not alleviated by additional sleep. Fatigue is more likely to be associated with a psychiatric disorder; sleepiness is more predominant in sleep disorders (although there is significant overlap). For example, patients with a major depressive disorder can experience fatigue as much as patients with sleep deprivation, but the latter also is more likely to result in sleepiness. Trouble concentrating is seen in anxiety, depression, attention-deficit/hyperactivity disorder (ADHD), and sleep deprivation.1
Insomnia or poor sleep hygiene can be diagnosed with a thorough sleep history. I take special care to consider sleep problems by presenting 5 groups of questions to the patient (Box).
Sleep-disordered breathing
A sleep study is required to accurately diagnose sleep-disordered breathing. Unless this diagnosis is specifically looked for, it remains hidden from both physicians and patients. Clues to the presence of sleep-disordered breathing include snorting, snoring, and gasping for air during sleep; witnessed apnea during sleep; nighttime awakening; daytime fatigue; nocturia; mouth breathing or dry mouth; acid reflux; irritability; morning headache; nighttime sweating; and low libido. Risk factors for sleep-disordered breathing include obesity; smoking; menopause; family history; increasing age; and anatomical factors (eg, deviation of the nasal septum; retrognathia; long face syndrome; high-arched narrow hard palate; large tonsils, uvula, or tongue).2
Measuring sleep quality
Some patients are unaware of the extent to which they are sleepy. The most widely used scale to measure sleepiness is the Epworth Sleepiness Scale.3 Sleep specialists view a score of ≥10 on the Epworth scale as indicative of daytime sleepiness. In addition, a patient’s daily consumption of caffeinated beverages can be a clue to excessive sleepiness or, at least, fatigue. If the degree of sleepiness cannot be determined subjectively, objective measures, such as the Multiple Sleep Latency Test (MSLT), can quantify it. In a randomly selected sample from the general population, 13.4% had excessive daytime sleepiness as measured by the MSLT.4
Adult ADHD and sleep deprivation
In my practice, sleep problems confound both the diagnosis and treatment of psychiatric disorders, especially ADHD. Often, patients who report ADHD symptoms have no clear history of ADHD during childhood. In these cases, I always consider the possibility that their ADHD symptoms are due to sleep deprivation. Sleep deprivation can mimic the poor executive function and difficulty concentrating that is often seen in ADHD, because such deprivation is associated with decreased activity in the prefrontal cortex during wakefulness.5
In patients who provide a clear history of ADHD symptoms during childhood, it is possible that inadequate sleep exacerbates ADHD symptoms as adults. Unless sleep deprivation is diagnosed and treated in these patients, they can end up taking a higher-than-necessary dosage of a stimulant. Also, patients who have ADHD might have a difficult time managing their sleep schedule because of poor executive functioning. This, in turn, can result in additional sleep deprivation, thus worsening their ADHD symptoms, creating a vicious circle.
Psychotropics and sedation
Many psychiatric medications list sedation as a side effect. Patients with untreated sleep problems might be more likely to notice this side effect because sleep problems contribute to their fatigue. I have had patients who were unable to tolerate sedative medications until their sleep apnea was treated.
In conclusion
It is important to consider sleep deprivation in your differential diagnosis of psychiatric patients. This will allow for more accurate diagnosis and treatment and, in some cases, can avoid treatment resistance.
It seems like common sense: Sleeping poorly results in not feeling good. The truth is that many of our patients are sleep deprived but are either unaware of, or unwilling to acknowledge, their problem. The busy life that many patients have does not allow adequate time for sleep. In fact, I have encountered patients who think of sleep as an inconvenience that takes away time from other pursuits.
Sleep deprivation in psychiatric disorders
Sleep deprivation occurs when the duration or quality of sleep is inadequate. Inadequate sleep duration can be caused by insomnia or simply not allowing enough time for sleep (1 aspect of poor sleep hygiene). Poor sleep quality often is caused by sleep-disordered breathing.
Sleep deprivation can result in either sleepiness or fatigue. Sleepiness is a propensity to fall asleep; fatigue is a lack of energy that is not alleviated by additional sleep. Fatigue is more likely to be associated with a psychiatric disorder; sleepiness is more predominant in sleep disorders (although there is significant overlap). For example, patients with a major depressive disorder can experience fatigue as much as patients with sleep deprivation, but the latter also is more likely to result in sleepiness. Trouble concentrating is seen in anxiety, depression, attention-deficit/hyperactivity disorder (ADHD), and sleep deprivation.1
Insomnia or poor sleep hygiene can be diagnosed with a thorough sleep history. I take special care to consider sleep problems by presenting 5 groups of questions to the patient (Box).
Sleep-disordered breathing
A sleep study is required to accurately diagnose sleep-disordered breathing. Unless this diagnosis is specifically looked for, it remains hidden from both physicians and patients. Clues to the presence of sleep-disordered breathing include snorting, snoring, and gasping for air during sleep; witnessed apnea during sleep; nighttime awakening; daytime fatigue; nocturia; mouth breathing or dry mouth; acid reflux; irritability; morning headache; nighttime sweating; and low libido. Risk factors for sleep-disordered breathing include obesity; smoking; menopause; family history; increasing age; and anatomical factors (eg, deviation of the nasal septum; retrognathia; long face syndrome; high-arched narrow hard palate; large tonsils, uvula, or tongue).2
Measuring sleep quality
Some patients are unaware of the extent to which they are sleepy. The most widely used scale to measure sleepiness is the Epworth Sleepiness Scale.3 Sleep specialists view a score of ≥10 on the Epworth scale as indicative of daytime sleepiness. In addition, a patient’s daily consumption of caffeinated beverages can be a clue to excessive sleepiness or, at least, fatigue. If the degree of sleepiness cannot be determined subjectively, objective measures, such as the Multiple Sleep Latency Test (MSLT), can quantify it. In a randomly selected sample from the general population, 13.4% had excessive daytime sleepiness as measured by the MSLT.4
Adult ADHD and sleep deprivation
In my practice, sleep problems confound both the diagnosis and treatment of psychiatric disorders, especially ADHD. Often, patients who report ADHD symptoms have no clear history of ADHD during childhood. In these cases, I always consider the possibility that their ADHD symptoms are due to sleep deprivation. Sleep deprivation can mimic the poor executive function and difficulty concentrating that is often seen in ADHD, because such deprivation is associated with decreased activity in the prefrontal cortex during wakefulness.5
In patients who provide a clear history of ADHD symptoms during childhood, it is possible that inadequate sleep exacerbates ADHD symptoms as adults. Unless sleep deprivation is diagnosed and treated in these patients, they can end up taking a higher-than-necessary dosage of a stimulant. Also, patients who have ADHD might have a difficult time managing their sleep schedule because of poor executive functioning. This, in turn, can result in additional sleep deprivation, thus worsening their ADHD symptoms, creating a vicious circle.
Psychotropics and sedation
Many psychiatric medications list sedation as a side effect. Patients with untreated sleep problems might be more likely to notice this side effect because sleep problems contribute to their fatigue. I have had patients who were unable to tolerate sedative medications until their sleep apnea was treated.
In conclusion
It is important to consider sleep deprivation in your differential diagnosis of psychiatric patients. This will allow for more accurate diagnosis and treatment and, in some cases, can avoid treatment resistance.
1. Stahl SM. Excessive sleepiness. San Diego, CA: NEI Press; 2005.
2. Jordan AS, McSharry DG, Malhotra A. Adult obstructive sleep apnoea. Lancet. 2014;383(9918):736-747.
3. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540-545.
4. Drake CL, Roehrs TA, Richardson GS, et al. Epidemiology and morbidity of excessive daytime sleepiness. Sleep. 2002;25:A91-A92.
5. Thomas M, Sing H, Belenky G, et al. Neural basis of alertness and cognitive performance impairments during sleepiness. I. Effects of 24 h of sleep deprivation on waking human regional brain activity. J Sleep Res. 2000;9(4):335-352.
1. Stahl SM. Excessive sleepiness. San Diego, CA: NEI Press; 2005.
2. Jordan AS, McSharry DG, Malhotra A. Adult obstructive sleep apnoea. Lancet. 2014;383(9918):736-747.
3. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540-545.
4. Drake CL, Roehrs TA, Richardson GS, et al. Epidemiology and morbidity of excessive daytime sleepiness. Sleep. 2002;25:A91-A92.
5. Thomas M, Sing H, Belenky G, et al. Neural basis of alertness and cognitive performance impairments during sleepiness. I. Effects of 24 h of sleep deprivation on waking human regional brain activity. J Sleep Res. 2000;9(4):335-352.
Is Chemotherapy a Good Choice for Neuroendocrine Tumors?
How effective is chemotherapy in treating neuroendocrine tumors (NETs)? Unfortunately, there is a lack of strong evidence from randomized trials, according to researchers from Gosford Hospital, University of Sydney; Royal North Shore Hospital, Northern Cancer Institute, and Macquarie University Hospitals, all in Australia; and Memorial Sloan Kettering Cancer Center in New York.
Related: Complex Malignancies: A Diagnostic and Therapeutic Trilemma
Few systematic reviews about chemotherapy for patients with NET have been published, and no meta-analyses have been done, the researchers say. They decided to rectify that deficiency and winnowed several hundred “potentially relevant” studies to 8 after examination.
Six studies compared one chemotherapy regimen against another (usually the standard streptozotocin [STZ] plus 5-fluorouracil [5FU]). Two studies compared chemotherapy with interferon (IFN). The researchers found no studies comparing chemotherapy with targeted therapy or somatostatin analogues and none comparing chemotherapy with best-supportive care.
Related: Harnessing Vaccines to Treat Cancers
Their analysis revealed no difference between STZ/5FU and other chemotherapies in response rate, progression-free survival (PFS), 1-year overall survival (OS), and OS. Response rates seemed to be higher for IFN, but no PFS or OS were demonstrated.
Any recommendations for chemotherapy as an option are “largely based on weak evidence,” the researchers charge. The problem, they say, is that the overall quality of the studies was poor. Only one met all features of a randomized trial with low risk of biases. The researchers cite inadequate randomization, lack of blinding, missing data, and selective reporting, among other flaws. In spite of the drawbacks of the studies they examined, their review remains the largest and most comprehensive review and appraisal of the existing evidence of chemotherapy in NET, the researchers say.
Related: Finding Synchronous Cancers
The past few years have seen the “evolution of an impressive array of systemic options,” they conclude, and “it remains to be seen whether chemotherapy shows enough efficacy compared to these options to warrant its side effect profile.” They point out that their review highlights not only the paucity of strong evidence, but also an urgent need of good randomized data—especially on the new, promising chemotherapeutic agents.
Source:
Wong MH, Chan DL, Lee A, et al. PLoS One. 2016;11(6):e0158140.
doi: 10.1371/journal.pone.0158140
How effective is chemotherapy in treating neuroendocrine tumors (NETs)? Unfortunately, there is a lack of strong evidence from randomized trials, according to researchers from Gosford Hospital, University of Sydney; Royal North Shore Hospital, Northern Cancer Institute, and Macquarie University Hospitals, all in Australia; and Memorial Sloan Kettering Cancer Center in New York.
Related: Complex Malignancies: A Diagnostic and Therapeutic Trilemma
Few systematic reviews about chemotherapy for patients with NET have been published, and no meta-analyses have been done, the researchers say. They decided to rectify that deficiency and winnowed several hundred “potentially relevant” studies to 8 after examination.
Six studies compared one chemotherapy regimen against another (usually the standard streptozotocin [STZ] plus 5-fluorouracil [5FU]). Two studies compared chemotherapy with interferon (IFN). The researchers found no studies comparing chemotherapy with targeted therapy or somatostatin analogues and none comparing chemotherapy with best-supportive care.
Related: Harnessing Vaccines to Treat Cancers
Their analysis revealed no difference between STZ/5FU and other chemotherapies in response rate, progression-free survival (PFS), 1-year overall survival (OS), and OS. Response rates seemed to be higher for IFN, but no PFS or OS were demonstrated.
Any recommendations for chemotherapy as an option are “largely based on weak evidence,” the researchers charge. The problem, they say, is that the overall quality of the studies was poor. Only one met all features of a randomized trial with low risk of biases. The researchers cite inadequate randomization, lack of blinding, missing data, and selective reporting, among other flaws. In spite of the drawbacks of the studies they examined, their review remains the largest and most comprehensive review and appraisal of the existing evidence of chemotherapy in NET, the researchers say.
Related: Finding Synchronous Cancers
The past few years have seen the “evolution of an impressive array of systemic options,” they conclude, and “it remains to be seen whether chemotherapy shows enough efficacy compared to these options to warrant its side effect profile.” They point out that their review highlights not only the paucity of strong evidence, but also an urgent need of good randomized data—especially on the new, promising chemotherapeutic agents.
Source:
Wong MH, Chan DL, Lee A, et al. PLoS One. 2016;11(6):e0158140.
doi: 10.1371/journal.pone.0158140
How effective is chemotherapy in treating neuroendocrine tumors (NETs)? Unfortunately, there is a lack of strong evidence from randomized trials, according to researchers from Gosford Hospital, University of Sydney; Royal North Shore Hospital, Northern Cancer Institute, and Macquarie University Hospitals, all in Australia; and Memorial Sloan Kettering Cancer Center in New York.
Related: Complex Malignancies: A Diagnostic and Therapeutic Trilemma
Few systematic reviews about chemotherapy for patients with NET have been published, and no meta-analyses have been done, the researchers say. They decided to rectify that deficiency and winnowed several hundred “potentially relevant” studies to 8 after examination.
Six studies compared one chemotherapy regimen against another (usually the standard streptozotocin [STZ] plus 5-fluorouracil [5FU]). Two studies compared chemotherapy with interferon (IFN). The researchers found no studies comparing chemotherapy with targeted therapy or somatostatin analogues and none comparing chemotherapy with best-supportive care.
Related: Harnessing Vaccines to Treat Cancers
Their analysis revealed no difference between STZ/5FU and other chemotherapies in response rate, progression-free survival (PFS), 1-year overall survival (OS), and OS. Response rates seemed to be higher for IFN, but no PFS or OS were demonstrated.
Any recommendations for chemotherapy as an option are “largely based on weak evidence,” the researchers charge. The problem, they say, is that the overall quality of the studies was poor. Only one met all features of a randomized trial with low risk of biases. The researchers cite inadequate randomization, lack of blinding, missing data, and selective reporting, among other flaws. In spite of the drawbacks of the studies they examined, their review remains the largest and most comprehensive review and appraisal of the existing evidence of chemotherapy in NET, the researchers say.
Related: Finding Synchronous Cancers
The past few years have seen the “evolution of an impressive array of systemic options,” they conclude, and “it remains to be seen whether chemotherapy shows enough efficacy compared to these options to warrant its side effect profile.” They point out that their review highlights not only the paucity of strong evidence, but also an urgent need of good randomized data—especially on the new, promising chemotherapeutic agents.
Source:
Wong MH, Chan DL, Lee A, et al. PLoS One. 2016;11(6):e0158140.
doi: 10.1371/journal.pone.0158140
Clinical value of costly ER/PR testing of ductal carcinoma biopsies questioned
Limiting hormone receptor testing of diagnostic core biopisies containing ductal carcinoma in situ (DCIS) could save up to $35 million in associated health care costs every year in the United States.
The results of a cost analysis conducted by researchers at Johns Hopkins University were so striking that the hospital has now eliminated reflex testing of core needle biopsies for DCIS, Christopher J. VandenBussche, MD, and his colleagues wrote in the American Journal of Surgical Pathology (2016;40:1090-9).
“We suggest that reflex [hormone receptor] testing of core needle biopsy specimens harboring DCIS should not be performed, as the results do not guide the next step in therapy,” wrote Dr. VandenBussche of Johns Hopkins University, Baltimore. “On the basis of this study, we have convinced our clinicians and no longer reflexively perform estrogen- and progesterone-receptor [ER/PR] testing on core needle biopsy specimens with DCIS at Hopkins and encourage other institutions to follow suit.”
Conducting expensive hormone receptor testing of these biopsy samples before surgery doesn’t make clinical or financial sense, for several reasons, the team said:
• Hormone receptor status at biopsy has no effect on the next treatment step, as DCIS patients always progress first to surgical excision, not neoadjuvant hormone therapy.
• Surgery sometimes reveals extensive breast cancer in patents with pure DCIS, and these cancers will always need ER/PR testing, rendering irrelevant biopsy testing.
• Because ER and PR labeling are often heterogeneous in DCIS, negative results for ER/PR on small core needle biopsy specimens would have to be repeated anyway on surgical excision specimens with larger amounts of DCIS, to be sure that the result is truly negative.
• Hormone therapy for DCIS does decrease recurrence, but it doesn’t impact survival – and it does carry significant adverse effects. Therefore, many women refuse hormone therapy if they do have ER/PR-positive tumors.
• The independent role of PR status in DCIS is unproven, so testing for it is not supported by clinical evidence.
To examine the costs associated with reflexive ER/PR testing, the investigators reviewed 58 core needle biopsies of pure DCIS followed by surgical excision. None of the patients had neoadjuvant hormone therapy. Of the 58 tumors, 76% were pure DCIS, and 16% were DCIS with invasive breast cancer. Most of the DCIS (47) tumors were ER+/PR+; 6 were ER-/PR-; and 5 were ER+/PR-.
The team reviewed the records of 49 patients who underwent surgical excision and ended up with a diagnosis of pure DCIS. These included 46 ER-positive cases, and 3 that were ER-negative in both biopsy and excision.
The findings suggested that ER/PR results from either the biopsy and the surgical excision samples were relevant to therapy in only a portion of these patients.
“We found that the ER/PR results after surgical excision impacted therapy in at most only 16 of 49 cases (33%),” they said. These included the 3 ER-/PR-negative cases, which would, in any case, not have triggered hormone therapy; 10 patients who chose hormone therapy despite a Hopkins oncologist’s neutral recommendation; 1 of 2 who took hormone therapy on a Hopkins oncologist’s recommendation; and 2 of 3 who took it after seeing a non-Hopkins oncologist.
“In contrast,” the authors wrote, “in 33 of the cases (67%), the ER/PR result of the DCIS after surgical excision did not impact therapy.” All of these were ER-positive cases, including 4 patients who opted for bilateral mastectomies (no subsequent role for neoadjuvant therapy), 8 who declined to meet with an oncologist, 1 for whom hormone therapy was contraindicated, 8 (of 8) who declined hormone therapy when their Hopkins oncologist did not recommend it, 10 (of 20) who declined hormone therapy when their Hopkins oncologist was neutral about its risk/benefit ratio, 1 (of 2) who declined hormone therapy when the Hopkins oncologist recommended it, and the 1 patient (of 3) who declined hormone therapy after visiting a non-Hopkins oncologist.
After reviewing the costs associated with these cases, “we found that ER testing … costing $20,685.72 ($357 per patient) had been performed unnecessarily,” the investigators said. In addition, if the PR testing – which has never been proven clinically important in DCIS – had been eliminated, there would have been an additional $86.46 savings per patient, a total savings of $5,014.
“Extrapolating the increased cost of $583 per DCIS diagnosis on core needle biopsy to 60,000 new cases of DCIS in the United States each year, reflex core needle biopsy ER/PR testing unnecessarily increases costs by approximately $35 million,” the authors said. “We recommend that ER/PR not be reflexively ordered on core needle biopsy specimens or surgical excision specimens containing DCIS, but instead that ER alone be performed on surgical excision specimens only when hormone therapy is a serious consideration after medical oncology consultation.”
The group noted that this total reflects the total amount billed, not typical reimbursement. “Regardless,” they said, “the cost of this testing is staggering.”
The authors did not mention the study’s funding source. They had no relevant financial disclosures.
On Twitter @Alz_Gal
It is important to note that the authors are not recommending hormone receptor testing be completely abandoned for ductal carcinoma in situ. They are simply suggesting that the testing should be deferred to being performed on the surgical resection specimen rather than the diagnostic core needle biopsy tissue.
The sample size used (58 cases) is clearly extremely small and cannot be used as the basis for sweeping recommendations for the many thousands of DCIS cases that are diagnosed in the United States annually. This study is from a major academic program; other programs may run the risk of patients not having the ER testing done at all if it is no longer a routine component of pathology testing on DCIS tissue.
The case is probably stronger for abandoning PR testing in DCIS, since this value is very unlikely to influence management decisions on its own.

|
Dr. Lisa Newman |
Other institutions should be encouraged to perform their own analyses to monitor the cost-effectiveness of ER/PR testing on core needle biopsies revealing DCIS. A study of this type should also be considered for large, multisite data sets, such as the American College of Surgeons’ National Cancer Database.
Lisa Newman, MD, FACS, is director of the breast oncology program for the Henry Ford Health System, and medical director for the Henry Ford International Center for the Study of Breast Cancer Subtypes, both in Detroit. She also serves as adjunct professor of health management and policy at the University of Michigan School of Public Health, Detroit. She has no relevant financial disclosures.
It is important to note that the authors are not recommending hormone receptor testing be completely abandoned for ductal carcinoma in situ. They are simply suggesting that the testing should be deferred to being performed on the surgical resection specimen rather than the diagnostic core needle biopsy tissue.
The sample size used (58 cases) is clearly extremely small and cannot be used as the basis for sweeping recommendations for the many thousands of DCIS cases that are diagnosed in the United States annually. This study is from a major academic program; other programs may run the risk of patients not having the ER testing done at all if it is no longer a routine component of pathology testing on DCIS tissue.
The case is probably stronger for abandoning PR testing in DCIS, since this value is very unlikely to influence management decisions on its own.
|
|
Dr. Lisa Newman |
Other institutions should be encouraged to perform their own analyses to monitor the cost-effectiveness of ER/PR testing on core needle biopsies revealing DCIS. A study of this type should also be considered for large, multisite data sets, such as the American College of Surgeons’ National Cancer Database.
Lisa Newman, MD, FACS, is director of the breast oncology program for the Henry Ford Health System, and medical director for the Henry Ford International Center for the Study of Breast Cancer Subtypes, both in Detroit. She also serves as adjunct professor of health management and policy at the University of Michigan School of Public Health, Detroit. She has no relevant financial disclosures.
It is important to note that the authors are not recommending hormone receptor testing be completely abandoned for ductal carcinoma in situ. They are simply suggesting that the testing should be deferred to being performed on the surgical resection specimen rather than the diagnostic core needle biopsy tissue.
The sample size used (58 cases) is clearly extremely small and cannot be used as the basis for sweeping recommendations for the many thousands of DCIS cases that are diagnosed in the United States annually. This study is from a major academic program; other programs may run the risk of patients not having the ER testing done at all if it is no longer a routine component of pathology testing on DCIS tissue.
The case is probably stronger for abandoning PR testing in DCIS, since this value is very unlikely to influence management decisions on its own.
|
|
Dr. Lisa Newman |
Other institutions should be encouraged to perform their own analyses to monitor the cost-effectiveness of ER/PR testing on core needle biopsies revealing DCIS. A study of this type should also be considered for large, multisite data sets, such as the American College of Surgeons’ National Cancer Database.
Lisa Newman, MD, FACS, is director of the breast oncology program for the Henry Ford Health System, and medical director for the Henry Ford International Center for the Study of Breast Cancer Subtypes, both in Detroit. She also serves as adjunct professor of health management and policy at the University of Michigan School of Public Health, Detroit. She has no relevant financial disclosures.
Limiting hormone receptor testing of diagnostic core biopisies containing ductal carcinoma in situ (DCIS) could save up to $35 million in associated health care costs every year in the United States.
The results of a cost analysis conducted by researchers at Johns Hopkins University were so striking that the hospital has now eliminated reflex testing of core needle biopsies for DCIS, Christopher J. VandenBussche, MD, and his colleagues wrote in the American Journal of Surgical Pathology (2016;40:1090-9).
“We suggest that reflex [hormone receptor] testing of core needle biopsy specimens harboring DCIS should not be performed, as the results do not guide the next step in therapy,” wrote Dr. VandenBussche of Johns Hopkins University, Baltimore. “On the basis of this study, we have convinced our clinicians and no longer reflexively perform estrogen- and progesterone-receptor [ER/PR] testing on core needle biopsy specimens with DCIS at Hopkins and encourage other institutions to follow suit.”
Conducting expensive hormone receptor testing of these biopsy samples before surgery doesn’t make clinical or financial sense, for several reasons, the team said:
• Hormone receptor status at biopsy has no effect on the next treatment step, as DCIS patients always progress first to surgical excision, not neoadjuvant hormone therapy.
• Surgery sometimes reveals extensive breast cancer in patents with pure DCIS, and these cancers will always need ER/PR testing, rendering irrelevant biopsy testing.
• Because ER and PR labeling are often heterogeneous in DCIS, negative results for ER/PR on small core needle biopsy specimens would have to be repeated anyway on surgical excision specimens with larger amounts of DCIS, to be sure that the result is truly negative.
• Hormone therapy for DCIS does decrease recurrence, but it doesn’t impact survival – and it does carry significant adverse effects. Therefore, many women refuse hormone therapy if they do have ER/PR-positive tumors.
• The independent role of PR status in DCIS is unproven, so testing for it is not supported by clinical evidence.
To examine the costs associated with reflexive ER/PR testing, the investigators reviewed 58 core needle biopsies of pure DCIS followed by surgical excision. None of the patients had neoadjuvant hormone therapy. Of the 58 tumors, 76% were pure DCIS, and 16% were DCIS with invasive breast cancer. Most of the DCIS (47) tumors were ER+/PR+; 6 were ER-/PR-; and 5 were ER+/PR-.
The team reviewed the records of 49 patients who underwent surgical excision and ended up with a diagnosis of pure DCIS. These included 46 ER-positive cases, and 3 that were ER-negative in both biopsy and excision.
The findings suggested that ER/PR results from either the biopsy and the surgical excision samples were relevant to therapy in only a portion of these patients.
“We found that the ER/PR results after surgical excision impacted therapy in at most only 16 of 49 cases (33%),” they said. These included the 3 ER-/PR-negative cases, which would, in any case, not have triggered hormone therapy; 10 patients who chose hormone therapy despite a Hopkins oncologist’s neutral recommendation; 1 of 2 who took hormone therapy on a Hopkins oncologist’s recommendation; and 2 of 3 who took it after seeing a non-Hopkins oncologist.
“In contrast,” the authors wrote, “in 33 of the cases (67%), the ER/PR result of the DCIS after surgical excision did not impact therapy.” All of these were ER-positive cases, including 4 patients who opted for bilateral mastectomies (no subsequent role for neoadjuvant therapy), 8 who declined to meet with an oncologist, 1 for whom hormone therapy was contraindicated, 8 (of 8) who declined hormone therapy when their Hopkins oncologist did not recommend it, 10 (of 20) who declined hormone therapy when their Hopkins oncologist was neutral about its risk/benefit ratio, 1 (of 2) who declined hormone therapy when the Hopkins oncologist recommended it, and the 1 patient (of 3) who declined hormone therapy after visiting a non-Hopkins oncologist.
After reviewing the costs associated with these cases, “we found that ER testing … costing $20,685.72 ($357 per patient) had been performed unnecessarily,” the investigators said. In addition, if the PR testing – which has never been proven clinically important in DCIS – had been eliminated, there would have been an additional $86.46 savings per patient, a total savings of $5,014.
“Extrapolating the increased cost of $583 per DCIS diagnosis on core needle biopsy to 60,000 new cases of DCIS in the United States each year, reflex core needle biopsy ER/PR testing unnecessarily increases costs by approximately $35 million,” the authors said. “We recommend that ER/PR not be reflexively ordered on core needle biopsy specimens or surgical excision specimens containing DCIS, but instead that ER alone be performed on surgical excision specimens only when hormone therapy is a serious consideration after medical oncology consultation.”
The group noted that this total reflects the total amount billed, not typical reimbursement. “Regardless,” they said, “the cost of this testing is staggering.”
The authors did not mention the study’s funding source. They had no relevant financial disclosures.
On Twitter @Alz_Gal
Limiting hormone receptor testing of diagnostic core biopisies containing ductal carcinoma in situ (DCIS) could save up to $35 million in associated health care costs every year in the United States.
The results of a cost analysis conducted by researchers at Johns Hopkins University were so striking that the hospital has now eliminated reflex testing of core needle biopsies for DCIS, Christopher J. VandenBussche, MD, and his colleagues wrote in the American Journal of Surgical Pathology (2016;40:1090-9).
“We suggest that reflex [hormone receptor] testing of core needle biopsy specimens harboring DCIS should not be performed, as the results do not guide the next step in therapy,” wrote Dr. VandenBussche of Johns Hopkins University, Baltimore. “On the basis of this study, we have convinced our clinicians and no longer reflexively perform estrogen- and progesterone-receptor [ER/PR] testing on core needle biopsy specimens with DCIS at Hopkins and encourage other institutions to follow suit.”
Conducting expensive hormone receptor testing of these biopsy samples before surgery doesn’t make clinical or financial sense, for several reasons, the team said:
• Hormone receptor status at biopsy has no effect on the next treatment step, as DCIS patients always progress first to surgical excision, not neoadjuvant hormone therapy.
• Surgery sometimes reveals extensive breast cancer in patents with pure DCIS, and these cancers will always need ER/PR testing, rendering irrelevant biopsy testing.
• Because ER and PR labeling are often heterogeneous in DCIS, negative results for ER/PR on small core needle biopsy specimens would have to be repeated anyway on surgical excision specimens with larger amounts of DCIS, to be sure that the result is truly negative.
• Hormone therapy for DCIS does decrease recurrence, but it doesn’t impact survival – and it does carry significant adverse effects. Therefore, many women refuse hormone therapy if they do have ER/PR-positive tumors.
• The independent role of PR status in DCIS is unproven, so testing for it is not supported by clinical evidence.
To examine the costs associated with reflexive ER/PR testing, the investigators reviewed 58 core needle biopsies of pure DCIS followed by surgical excision. None of the patients had neoadjuvant hormone therapy. Of the 58 tumors, 76% were pure DCIS, and 16% were DCIS with invasive breast cancer. Most of the DCIS (47) tumors were ER+/PR+; 6 were ER-/PR-; and 5 were ER+/PR-.
The team reviewed the records of 49 patients who underwent surgical excision and ended up with a diagnosis of pure DCIS. These included 46 ER-positive cases, and 3 that were ER-negative in both biopsy and excision.
The findings suggested that ER/PR results from either the biopsy and the surgical excision samples were relevant to therapy in only a portion of these patients.
“We found that the ER/PR results after surgical excision impacted therapy in at most only 16 of 49 cases (33%),” they said. These included the 3 ER-/PR-negative cases, which would, in any case, not have triggered hormone therapy; 10 patients who chose hormone therapy despite a Hopkins oncologist’s neutral recommendation; 1 of 2 who took hormone therapy on a Hopkins oncologist’s recommendation; and 2 of 3 who took it after seeing a non-Hopkins oncologist.
“In contrast,” the authors wrote, “in 33 of the cases (67%), the ER/PR result of the DCIS after surgical excision did not impact therapy.” All of these were ER-positive cases, including 4 patients who opted for bilateral mastectomies (no subsequent role for neoadjuvant therapy), 8 who declined to meet with an oncologist, 1 for whom hormone therapy was contraindicated, 8 (of 8) who declined hormone therapy when their Hopkins oncologist did not recommend it, 10 (of 20) who declined hormone therapy when their Hopkins oncologist was neutral about its risk/benefit ratio, 1 (of 2) who declined hormone therapy when the Hopkins oncologist recommended it, and the 1 patient (of 3) who declined hormone therapy after visiting a non-Hopkins oncologist.
After reviewing the costs associated with these cases, “we found that ER testing … costing $20,685.72 ($357 per patient) had been performed unnecessarily,” the investigators said. In addition, if the PR testing – which has never been proven clinically important in DCIS – had been eliminated, there would have been an additional $86.46 savings per patient, a total savings of $5,014.
“Extrapolating the increased cost of $583 per DCIS diagnosis on core needle biopsy to 60,000 new cases of DCIS in the United States each year, reflex core needle biopsy ER/PR testing unnecessarily increases costs by approximately $35 million,” the authors said. “We recommend that ER/PR not be reflexively ordered on core needle biopsy specimens or surgical excision specimens containing DCIS, but instead that ER alone be performed on surgical excision specimens only when hormone therapy is a serious consideration after medical oncology consultation.”
The group noted that this total reflects the total amount billed, not typical reimbursement. “Regardless,” they said, “the cost of this testing is staggering.”
The authors did not mention the study’s funding source. They had no relevant financial disclosures.
On Twitter @Alz_Gal
FROM THE AMERICAN JOURNAL OF SURGICAL PATHOLOGY
Key clinical point: Hormone receptor testing of diagnostic core needle biopsies should not be automatic.
Major finding: Limiting testing to excised surgical section specimens could save up to $35 million a year in the United States.
Data source: The cost analysis examined testing and treatment of 58 patients with ductal carcinoma in situ.
Disclosures: The authors had no relevant financial disclosures.

First-in-class agent shows early promise in treating clear cell renal cell carcinoma
CHICAGO – Investigational agent PT2385, an inhibitor of hypoxia-inducible factor 2-alpha (HIF-2alpha), appears safe and tolerable and demonstrated early evidence of clinical activity in heavily pretreated patients with advanced clear cell renal cell carcinoma, investigators reported at the annual meeting of the American Society of Clinical Oncology.
In a small, phase I dose-escalation study, 39% of patients in the study achieved complete response, partial response, or stable disease lasting at least 16 weeks.

PT2385 is a first-in-class, orally administered selective small molecule inhibitor of HIF-2alpha, a transcription factor with a role in clear cell renal cell carcinoma.
“Hypoxia-inducible factor 2-alpha is a key oncogenic driver of clear cell renal cell carcinoma,” Kevin Courtney, MD, PhD, of the University of Texas Southwestern Medical Center, Dallas, said at the meeting.
A total of 51 patients (n = 26 for dose escalation cohort and n = 25 in dose expansion cohort) met the study’s eligibility requirements of having a diagnosis of clear cell renal cell carcinoma, an Eastern Cooperative Oncology Group score ranging from 0 to 1, and at least one prior anticancer therapy. The median age of the cohort was 65 years with the youngest participant being 29 years and the oldest being 80 years old. The majority of patients were male (71%), had received four or more prior systemic therapies (53%), and had undergone vascular endothelial growth factor therapy (98%). Patients were treated with continuous twice-daily oral dosing of PT2385 until progression or toxicity. A total of three patients were treated at the 100-mg dose, three at the 200-mg dose, four at the 400-mg dose, seven at the 800-mg dose, six at a dose of 1,200 mg, and three at a dose of 1,800 mg.
“No dose-limiting toxicity was observed at any dose level,” Dr. Courtney said.
Based on safety, pharmokinetic and pharmodynamic data, 800 mg twice daily was the selected dose for the expansion cohort, he reported.
Of 51 patients treated, 1 patient had a complete response, 3 achieved partial responses, and 16 patients achieved stable disease for at least 16 weeks. The most common grade one or two adverse events were anemia (n = 18), peripheral edema (n = 18), fatigue (n = 18), nausea (n = 15), and back pain (n = 12). Only two grade four adverse events (low lymphocyte count) were reported.
“Notably, hypertension was not seen,” Dr. Courtney said.
At the time the study concluded, the four patients who achieved complete or partial responses remained on the treatment, and five had received treatment for a year or longer.
The study was funded by Peloton Therapeutics. Dr. Courtney reported having stock and ownership interest in, serving in advisory roles for, or receiving research funding from multiple companies. Several coinvestigators reported receiving research funding from or holding patents with multiple companies including Peloton Therapeutics.
On Twitter @jessnicolecraig
CHICAGO – Investigational agent PT2385, an inhibitor of hypoxia-inducible factor 2-alpha (HIF-2alpha), appears safe and tolerable and demonstrated early evidence of clinical activity in heavily pretreated patients with advanced clear cell renal cell carcinoma, investigators reported at the annual meeting of the American Society of Clinical Oncology.
In a small, phase I dose-escalation study, 39% of patients in the study achieved complete response, partial response, or stable disease lasting at least 16 weeks.
PT2385 is a first-in-class, orally administered selective small molecule inhibitor of HIF-2alpha, a transcription factor with a role in clear cell renal cell carcinoma.
“Hypoxia-inducible factor 2-alpha is a key oncogenic driver of clear cell renal cell carcinoma,” Kevin Courtney, MD, PhD, of the University of Texas Southwestern Medical Center, Dallas, said at the meeting.
A total of 51 patients (n = 26 for dose escalation cohort and n = 25 in dose expansion cohort) met the study’s eligibility requirements of having a diagnosis of clear cell renal cell carcinoma, an Eastern Cooperative Oncology Group score ranging from 0 to 1, and at least one prior anticancer therapy. The median age of the cohort was 65 years with the youngest participant being 29 years and the oldest being 80 years old. The majority of patients were male (71%), had received four or more prior systemic therapies (53%), and had undergone vascular endothelial growth factor therapy (98%). Patients were treated with continuous twice-daily oral dosing of PT2385 until progression or toxicity. A total of three patients were treated at the 100-mg dose, three at the 200-mg dose, four at the 400-mg dose, seven at the 800-mg dose, six at a dose of 1,200 mg, and three at a dose of 1,800 mg.
“No dose-limiting toxicity was observed at any dose level,” Dr. Courtney said.
Based on safety, pharmokinetic and pharmodynamic data, 800 mg twice daily was the selected dose for the expansion cohort, he reported.
Of 51 patients treated, 1 patient had a complete response, 3 achieved partial responses, and 16 patients achieved stable disease for at least 16 weeks. The most common grade one or two adverse events were anemia (n = 18), peripheral edema (n = 18), fatigue (n = 18), nausea (n = 15), and back pain (n = 12). Only two grade four adverse events (low lymphocyte count) were reported.
“Notably, hypertension was not seen,” Dr. Courtney said.
At the time the study concluded, the four patients who achieved complete or partial responses remained on the treatment, and five had received treatment for a year or longer.
The study was funded by Peloton Therapeutics. Dr. Courtney reported having stock and ownership interest in, serving in advisory roles for, or receiving research funding from multiple companies. Several coinvestigators reported receiving research funding from or holding patents with multiple companies including Peloton Therapeutics.
On Twitter @jessnicolecraig
CHICAGO – Investigational agent PT2385, an inhibitor of hypoxia-inducible factor 2-alpha (HIF-2alpha), appears safe and tolerable and demonstrated early evidence of clinical activity in heavily pretreated patients with advanced clear cell renal cell carcinoma, investigators reported at the annual meeting of the American Society of Clinical Oncology.
In a small, phase I dose-escalation study, 39% of patients in the study achieved complete response, partial response, or stable disease lasting at least 16 weeks.
PT2385 is a first-in-class, orally administered selective small molecule inhibitor of HIF-2alpha, a transcription factor with a role in clear cell renal cell carcinoma.
“Hypoxia-inducible factor 2-alpha is a key oncogenic driver of clear cell renal cell carcinoma,” Kevin Courtney, MD, PhD, of the University of Texas Southwestern Medical Center, Dallas, said at the meeting.
A total of 51 patients (n = 26 for dose escalation cohort and n = 25 in dose expansion cohort) met the study’s eligibility requirements of having a diagnosis of clear cell renal cell carcinoma, an Eastern Cooperative Oncology Group score ranging from 0 to 1, and at least one prior anticancer therapy. The median age of the cohort was 65 years with the youngest participant being 29 years and the oldest being 80 years old. The majority of patients were male (71%), had received four or more prior systemic therapies (53%), and had undergone vascular endothelial growth factor therapy (98%). Patients were treated with continuous twice-daily oral dosing of PT2385 until progression or toxicity. A total of three patients were treated at the 100-mg dose, three at the 200-mg dose, four at the 400-mg dose, seven at the 800-mg dose, six at a dose of 1,200 mg, and three at a dose of 1,800 mg.
“No dose-limiting toxicity was observed at any dose level,” Dr. Courtney said.
Based on safety, pharmokinetic and pharmodynamic data, 800 mg twice daily was the selected dose for the expansion cohort, he reported.
Of 51 patients treated, 1 patient had a complete response, 3 achieved partial responses, and 16 patients achieved stable disease for at least 16 weeks. The most common grade one or two adverse events were anemia (n = 18), peripheral edema (n = 18), fatigue (n = 18), nausea (n = 15), and back pain (n = 12). Only two grade four adverse events (low lymphocyte count) were reported.
“Notably, hypertension was not seen,” Dr. Courtney said.
At the time the study concluded, the four patients who achieved complete or partial responses remained on the treatment, and five had received treatment for a year or longer.
The study was funded by Peloton Therapeutics. Dr. Courtney reported having stock and ownership interest in, serving in advisory roles for, or receiving research funding from multiple companies. Several coinvestigators reported receiving research funding from or holding patents with multiple companies including Peloton Therapeutics.
On Twitter @jessnicolecraig
AT THE 2016 ASCO ANNUAL MEETING
Key clinical point: The first-in-class oral HIF-2alpha inhibitor PT2385 demonstrated early evidence of clinical activity in patients with advanced clear cell renal cell carcinoma. The drug also appears safe and tolerable.
Major finding: Overall, one patient had a complete response, three achieved partial responses, and 16 patients achieved stable disease for at least 16 weeks.
Data source: A phase I dose-escalation and expansion study of 51 heavily pretreated patients with advanced clear cell renal cell carcinoma.
Disclosures: The study was funded by Peloton Therapeutics. Dr. Courtney reported having stock and ownership interest in, serving in advisory roles for, or receiving research funding from multiple companies. Several coinvestigators reported receiving research funding from or holding patents with multiple companies including Peloton Therapeutics.

GERD and sleep disorders often go hand in glove
Gastroesophageal reflux disease (GERD) is fertile soil for medical and psychiatric comorbid conditions, with sleep disorders leading the way, according to Maurice M. Ohayon, MD, who presented the findings of a longitudinal, population-based study on GERD and its "fellow travelers" at the annual meeting of the Associated Professional Sleep Societies. Insomnia, obstructive sleep apnea, and restless legs syndrome were among the most prevalent comorbidities of GERD. However, one sleep disorder symptom was reported to be a problem in up to 46% of those with the digestive disease. To learn more, see Family Practice News at: http://www.familypracticenews.com/specialty-focus/pulmonary-sleep-medicine/single-article-page/gerd-and-sleep-disorders-often-go-hand-in-glove/1dc81a99b64d296e03b86aa28893fbc7.html.
Gastroesophageal reflux disease (GERD) is fertile soil for medical and psychiatric comorbid conditions, with sleep disorders leading the way, according to Maurice M. Ohayon, MD, who presented the findings of a longitudinal, population-based study on GERD and its "fellow travelers" at the annual meeting of the Associated Professional Sleep Societies. Insomnia, obstructive sleep apnea, and restless legs syndrome were among the most prevalent comorbidities of GERD. However, one sleep disorder symptom was reported to be a problem in up to 46% of those with the digestive disease. To learn more, see Family Practice News at: http://www.familypracticenews.com/specialty-focus/pulmonary-sleep-medicine/single-article-page/gerd-and-sleep-disorders-often-go-hand-in-glove/1dc81a99b64d296e03b86aa28893fbc7.html.
Gastroesophageal reflux disease (GERD) is fertile soil for medical and psychiatric comorbid conditions, with sleep disorders leading the way, according to Maurice M. Ohayon, MD, who presented the findings of a longitudinal, population-based study on GERD and its "fellow travelers" at the annual meeting of the Associated Professional Sleep Societies. Insomnia, obstructive sleep apnea, and restless legs syndrome were among the most prevalent comorbidities of GERD. However, one sleep disorder symptom was reported to be a problem in up to 46% of those with the digestive disease. To learn more, see Family Practice News at: http://www.familypracticenews.com/specialty-focus/pulmonary-sleep-medicine/single-article-page/gerd-and-sleep-disorders-often-go-hand-in-glove/1dc81a99b64d296e03b86aa28893fbc7.html.
Early sustained viral response linked to better outcomes among HCV patients
Patients with hepatitis C virus (HCV) infections may have the best long-term outcomes if they achieve sustained viral response (SVR) before they develop clinically significant portal hypertension, according to a study reported on in the July issue of Gastroenterology. On the other hand, patients in stage 2 cirrhosis were more likely than stage 1 patients to develop liver decompensation and to die of hepatocellular carcinoma, regardless of SVR. “The available evidence, including our own, suggests that it is opportune to treat HCV as early as possible, in order to reduce progression to stages of cirrhosis in which a viral cure may be less likely lead to ultimate achievement of a major benefit,” said Dr. Vito Di Marco and his associates from the University of Palermo, Italy. More on the study, and its limitations, is available at Family Practice News: http://www.familypracticenews.com/specialty-focus/infectious-diseases/single-article-page/early-sustained-viral-response-linked-to-better-outcomes-among-hcv-patients/5089546903e73ad3c6947ff3bd3f8dbc.html.
Patients with hepatitis C virus (HCV) infections may have the best long-term outcomes if they achieve sustained viral response (SVR) before they develop clinically significant portal hypertension, according to a study reported on in the July issue of Gastroenterology. On the other hand, patients in stage 2 cirrhosis were more likely than stage 1 patients to develop liver decompensation and to die of hepatocellular carcinoma, regardless of SVR. “The available evidence, including our own, suggests that it is opportune to treat HCV as early as possible, in order to reduce progression to stages of cirrhosis in which a viral cure may be less likely lead to ultimate achievement of a major benefit,” said Dr. Vito Di Marco and his associates from the University of Palermo, Italy. More on the study, and its limitations, is available at Family Practice News: http://www.familypracticenews.com/specialty-focus/infectious-diseases/single-article-page/early-sustained-viral-response-linked-to-better-outcomes-among-hcv-patients/5089546903e73ad3c6947ff3bd3f8dbc.html.
Patients with hepatitis C virus (HCV) infections may have the best long-term outcomes if they achieve sustained viral response (SVR) before they develop clinically significant portal hypertension, according to a study reported on in the July issue of Gastroenterology. On the other hand, patients in stage 2 cirrhosis were more likely than stage 1 patients to develop liver decompensation and to die of hepatocellular carcinoma, regardless of SVR. “The available evidence, including our own, suggests that it is opportune to treat HCV as early as possible, in order to reduce progression to stages of cirrhosis in which a viral cure may be less likely lead to ultimate achievement of a major benefit,” said Dr. Vito Di Marco and his associates from the University of Palermo, Italy. More on the study, and its limitations, is available at Family Practice News: http://www.familypracticenews.com/specialty-focus/infectious-diseases/single-article-page/early-sustained-viral-response-linked-to-better-outcomes-among-hcv-patients/5089546903e73ad3c6947ff3bd3f8dbc.html.
Statement warns of drugs causing or exacerbating heart failure
Many commonly used prescription drugs, over-the-counter agents, and several complimentary or alternative medications can either trigger heart failure or exacerbate the disease in patients with existing heart failure, according to a scientific statement written by a committee of the American Heart Association that was released on July 11. The comprehensive statement lists 88 distinct prescription drugs or drug classes. Read more about the statement at Cardiology News, available here: http://www.ecardiologynews.com/specialty-focus/heart-failure/single-article-page/statement-warns-of-drugs-causing-or-exacerbating-heart-failure/e62f58d7bf5e124f84a09242a258bfb5.html.
Many commonly used prescription drugs, over-the-counter agents, and several complimentary or alternative medications can either trigger heart failure or exacerbate the disease in patients with existing heart failure, according to a scientific statement written by a committee of the American Heart Association that was released on July 11. The comprehensive statement lists 88 distinct prescription drugs or drug classes. Read more about the statement at Cardiology News, available here: http://www.ecardiologynews.com/specialty-focus/heart-failure/single-article-page/statement-warns-of-drugs-causing-or-exacerbating-heart-failure/e62f58d7bf5e124f84a09242a258bfb5.html.
Many commonly used prescription drugs, over-the-counter agents, and several complimentary or alternative medications can either trigger heart failure or exacerbate the disease in patients with existing heart failure, according to a scientific statement written by a committee of the American Heart Association that was released on July 11. The comprehensive statement lists 88 distinct prescription drugs or drug classes. Read more about the statement at Cardiology News, available here: http://www.ecardiologynews.com/specialty-focus/heart-failure/single-article-page/statement-warns-of-drugs-causing-or-exacerbating-heart-failure/e62f58d7bf5e124f84a09242a258bfb5.html.
Alpha-1 antitrypsin deficiency: An underrecognized, treatable cause of COPD
Alpha-1 antitrypsin deficiency is a common but underrecognized genetic condition that increases the risk of chronic obstructive pulmonary disease (COPD) and liver disease. Because delayed diagnosis is thought to be associated with adverse outcomes, physicians are encouraged to follow available guidelines and test for the disease in all symptomatic adults with fixed airflow obstruction. This article from the Cleveland Clinic Journal of Medicine describes how to detect this genetic condition and the promising new therapies that are being investigated to treat it. The article is available at: http://www.ccjm.org/current-issue/issue-single-view/alpha-1-antitrypsin-deficiency-an-underrecognized-treatable-cause-of-copd/405de7ef6d4fcd6663e0af929c45b845.html.
Alpha-1 antitrypsin deficiency is a common but underrecognized genetic condition that increases the risk of chronic obstructive pulmonary disease (COPD) and liver disease. Because delayed diagnosis is thought to be associated with adverse outcomes, physicians are encouraged to follow available guidelines and test for the disease in all symptomatic adults with fixed airflow obstruction. This article from the Cleveland Clinic Journal of Medicine describes how to detect this genetic condition and the promising new therapies that are being investigated to treat it. The article is available at: http://www.ccjm.org/current-issue/issue-single-view/alpha-1-antitrypsin-deficiency-an-underrecognized-treatable-cause-of-copd/405de7ef6d4fcd6663e0af929c45b845.html.
Alpha-1 antitrypsin deficiency is a common but underrecognized genetic condition that increases the risk of chronic obstructive pulmonary disease (COPD) and liver disease. Because delayed diagnosis is thought to be associated with adverse outcomes, physicians are encouraged to follow available guidelines and test for the disease in all symptomatic adults with fixed airflow obstruction. This article from the Cleveland Clinic Journal of Medicine describes how to detect this genetic condition and the promising new therapies that are being investigated to treat it. The article is available at: http://www.ccjm.org/current-issue/issue-single-view/alpha-1-antitrypsin-deficiency-an-underrecognized-treatable-cause-of-copd/405de7ef6d4fcd6663e0af929c45b845.html.