User login
LETTER: The Value of a Structured On-Boarding Peer Mentorship Program
To demonstrate the impact of a structured peer mentorship program in a large size service-oriented hospitalist group with 71 full-time hospitalist and 21 full-time APPs serving a daily census of 400 patients, we piloted a structured peer mentorship project from June 2015 until December 2015 with 10 new hospitalist hires. Each new hire was paired with a senior hospitalist colleague for a total of four weeks over a period of two months and the outcomes were measured through a 10-question anonymous survey at the end of 90 days. The survey response rate was 80%. The questions pertained to the effectiveness of mentorship program, practice group culture orientation, adherence to high-yield patient satisfaction behaviors related to Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey, work efficiency, job satisfaction, navigating through various hospital floors, efficient clinical staff communication, hand of care sign-out process, understanding of various hospitalist shifts and open-ended feedback.
Our results revealed that 100% of the new hires recommended to continue the on-boarding mentorship program on a permanent basis and 95% of the responses on the Likert scale were either very positive or positive. The total cost of the mentorship program was estimated to be 2-3 moon-lighting shifts ($2400-$3600) for the group. This cost was mainly associated with extra staffing needed during the first half of the shadowing week since the mentor was carrying half of the daily census. The marginal benefits of the program were far more and long lasting than the short-term cost. The program assisted in early acclimatization to the practice group culture, provider engagement and satisfaction and early productivity. It also has the potential to increase retention in a high-turnover hospitalist work field. We conclude that effective peer mentorship can play an important role in the organizational success of a large hospitalist program. Successful mentoring programs require proper understanding, planning, resource allocation, implementation and evaluation. From increased morale to increased productivity, the benefits are numerous. Mentoring is a tangible way to show employees that they are valued and that the organization’s future includes them.
— Muhammad Nabeel, MD, FACP, Clinical Assistant Professor, College of Human Medicine, Michigan State University, GRMEP; Hospitalist, Spectrum Health Medical Group, Grand Rapids, MI
— Rashelle Ludolph, MHA, MBA (Second Author), Director Operations, Acute Care Medicine, Spectrum Health Medical Group, Grand Rapids, MI
To demonstrate the impact of a structured peer mentorship program in a large size service-oriented hospitalist group with 71 full-time hospitalist and 21 full-time APPs serving a daily census of 400 patients, we piloted a structured peer mentorship project from June 2015 until December 2015 with 10 new hospitalist hires. Each new hire was paired with a senior hospitalist colleague for a total of four weeks over a period of two months and the outcomes were measured through a 10-question anonymous survey at the end of 90 days. The survey response rate was 80%. The questions pertained to the effectiveness of mentorship program, practice group culture orientation, adherence to high-yield patient satisfaction behaviors related to Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey, work efficiency, job satisfaction, navigating through various hospital floors, efficient clinical staff communication, hand of care sign-out process, understanding of various hospitalist shifts and open-ended feedback.
Our results revealed that 100% of the new hires recommended to continue the on-boarding mentorship program on a permanent basis and 95% of the responses on the Likert scale were either very positive or positive. The total cost of the mentorship program was estimated to be 2-3 moon-lighting shifts ($2400-$3600) for the group. This cost was mainly associated with extra staffing needed during the first half of the shadowing week since the mentor was carrying half of the daily census. The marginal benefits of the program were far more and long lasting than the short-term cost. The program assisted in early acclimatization to the practice group culture, provider engagement and satisfaction and early productivity. It also has the potential to increase retention in a high-turnover hospitalist work field. We conclude that effective peer mentorship can play an important role in the organizational success of a large hospitalist program. Successful mentoring programs require proper understanding, planning, resource allocation, implementation and evaluation. From increased morale to increased productivity, the benefits are numerous. Mentoring is a tangible way to show employees that they are valued and that the organization’s future includes them.
— Muhammad Nabeel, MD, FACP, Clinical Assistant Professor, College of Human Medicine, Michigan State University, GRMEP; Hospitalist, Spectrum Health Medical Group, Grand Rapids, MI
— Rashelle Ludolph, MHA, MBA (Second Author), Director Operations, Acute Care Medicine, Spectrum Health Medical Group, Grand Rapids, MI
To demonstrate the impact of a structured peer mentorship program in a large size service-oriented hospitalist group with 71 full-time hospitalist and 21 full-time APPs serving a daily census of 400 patients, we piloted a structured peer mentorship project from June 2015 until December 2015 with 10 new hospitalist hires. Each new hire was paired with a senior hospitalist colleague for a total of four weeks over a period of two months and the outcomes were measured through a 10-question anonymous survey at the end of 90 days. The survey response rate was 80%. The questions pertained to the effectiveness of mentorship program, practice group culture orientation, adherence to high-yield patient satisfaction behaviors related to Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey, work efficiency, job satisfaction, navigating through various hospital floors, efficient clinical staff communication, hand of care sign-out process, understanding of various hospitalist shifts and open-ended feedback.
Our results revealed that 100% of the new hires recommended to continue the on-boarding mentorship program on a permanent basis and 95% of the responses on the Likert scale were either very positive or positive. The total cost of the mentorship program was estimated to be 2-3 moon-lighting shifts ($2400-$3600) for the group. This cost was mainly associated with extra staffing needed during the first half of the shadowing week since the mentor was carrying half of the daily census. The marginal benefits of the program were far more and long lasting than the short-term cost. The program assisted in early acclimatization to the practice group culture, provider engagement and satisfaction and early productivity. It also has the potential to increase retention in a high-turnover hospitalist work field. We conclude that effective peer mentorship can play an important role in the organizational success of a large hospitalist program. Successful mentoring programs require proper understanding, planning, resource allocation, implementation and evaluation. From increased morale to increased productivity, the benefits are numerous. Mentoring is a tangible way to show employees that they are valued and that the organization’s future includes them.
— Muhammad Nabeel, MD, FACP, Clinical Assistant Professor, College of Human Medicine, Michigan State University, GRMEP; Hospitalist, Spectrum Health Medical Group, Grand Rapids, MI
— Rashelle Ludolph, MHA, MBA (Second Author), Director Operations, Acute Care Medicine, Spectrum Health Medical Group, Grand Rapids, MI
Therapy can provide clinical benefit in haplo-HSCT, data suggest
![]()
Photo by Chad McNeeley
BARCELONA—Results from 2 studies suggest an immunogene therapy can provide a clinical benefit in adults with high-risk hematologic malignancies undergoing haploidentical hematopoietic stem cell transplant (haplo-HSCT).
When compared to historical controls, patients who received the immunogene therapy, Zalmoxis, had lower rates of non-relapse mortality (NRM) and chronic graft-vs-host disease (GVHD), as well as improved overall survival (OS).
The only adverse event related to Zalmoxis was GVHD, which was resolved.
These data were presented at the EBMT International Transplant Course. The studies were funded by MolMed S.p.A., the company developing Zalmoxis.
About the therapy
Zalmoxis is a treatment consisting of allogeneic, genetically modified T cells. The cells are intended to be given to haplo-HSCT recipients to help fight off infection, enhance the success of the transplant, and support long-lasting anticancer effects.
Because the genetically modified T cells can also cause GVHD, they are equipped with a suicide gene, which makes them susceptible to treatment with ganciclovir or valganciclovir. So if a patient develops GVHD, he or she can receive ganciclovir/valganciclovir, which should kill the modified T cells and prevent further development of GVHD.
Trial data
The data presented at the EBMT International Transplant Course were from the phase 1/2 TK007 trial and the ongoing phase 3 TK008 trial.
The TK007 trial included haplo-HSCT recipients with various high-risk hematologic malignancies, while the TK008 trial is enrolling patients with high-risk acute leukemia who are undergoing haplo-HSCT.
Researchers have compared 37 Zalmoxis-treated patients from these trials to 140 contemporaneous control patients from the database of the EBMT registry.
Results of this pair-matched analysis showed an OS improvement in Zalmoxis-treated patients, which was driven by a reduction in NRM. The OS was 49% in the Zalmoxis group and 37% in controls (P=0.01), and the NRM was 22% and 43%, respectively (P=0.014).
Among controls dying from non-relapse causes, the majority (78%) died from either infection (56%) or GVHD (22%), while the only adverse event related to Zalmoxis treatment was GVHD. And this GVHD was fully resolved by activating the suicide-gene system with ganciclovir treatment, without any GVHD-related death.
Furthermore, the incidence of chronic GVHD was lower in Zalmoxis-treated patients than in controls—6% and 25%, respectively (P=0.04).
Therefore, the researchers concluded that the protective effects of Zalmoxis in controlling infection and GVHD mainly drove the decreased NRM in the Zalmoxis group.
These data supported the European Commission’s recent decision to grant conditional marketing authorization for Zalmoxis. ![]()
![]()
Photo by Chad McNeeley
BARCELONA—Results from 2 studies suggest an immunogene therapy can provide a clinical benefit in adults with high-risk hematologic malignancies undergoing haploidentical hematopoietic stem cell transplant (haplo-HSCT).
When compared to historical controls, patients who received the immunogene therapy, Zalmoxis, had lower rates of non-relapse mortality (NRM) and chronic graft-vs-host disease (GVHD), as well as improved overall survival (OS).
The only adverse event related to Zalmoxis was GVHD, which was resolved.
These data were presented at the EBMT International Transplant Course. The studies were funded by MolMed S.p.A., the company developing Zalmoxis.
About the therapy
Zalmoxis is a treatment consisting of allogeneic, genetically modified T cells. The cells are intended to be given to haplo-HSCT recipients to help fight off infection, enhance the success of the transplant, and support long-lasting anticancer effects.
Because the genetically modified T cells can also cause GVHD, they are equipped with a suicide gene, which makes them susceptible to treatment with ganciclovir or valganciclovir. So if a patient develops GVHD, he or she can receive ganciclovir/valganciclovir, which should kill the modified T cells and prevent further development of GVHD.
Trial data
The data presented at the EBMT International Transplant Course were from the phase 1/2 TK007 trial and the ongoing phase 3 TK008 trial.
The TK007 trial included haplo-HSCT recipients with various high-risk hematologic malignancies, while the TK008 trial is enrolling patients with high-risk acute leukemia who are undergoing haplo-HSCT.
Researchers have compared 37 Zalmoxis-treated patients from these trials to 140 contemporaneous control patients from the database of the EBMT registry.
Results of this pair-matched analysis showed an OS improvement in Zalmoxis-treated patients, which was driven by a reduction in NRM. The OS was 49% in the Zalmoxis group and 37% in controls (P=0.01), and the NRM was 22% and 43%, respectively (P=0.014).
Among controls dying from non-relapse causes, the majority (78%) died from either infection (56%) or GVHD (22%), while the only adverse event related to Zalmoxis treatment was GVHD. And this GVHD was fully resolved by activating the suicide-gene system with ganciclovir treatment, without any GVHD-related death.
Furthermore, the incidence of chronic GVHD was lower in Zalmoxis-treated patients than in controls—6% and 25%, respectively (P=0.04).
Therefore, the researchers concluded that the protective effects of Zalmoxis in controlling infection and GVHD mainly drove the decreased NRM in the Zalmoxis group.
These data supported the European Commission’s recent decision to grant conditional marketing authorization for Zalmoxis. ![]()
![]()
Photo by Chad McNeeley
BARCELONA—Results from 2 studies suggest an immunogene therapy can provide a clinical benefit in adults with high-risk hematologic malignancies undergoing haploidentical hematopoietic stem cell transplant (haplo-HSCT).
When compared to historical controls, patients who received the immunogene therapy, Zalmoxis, had lower rates of non-relapse mortality (NRM) and chronic graft-vs-host disease (GVHD), as well as improved overall survival (OS).
The only adverse event related to Zalmoxis was GVHD, which was resolved.
These data were presented at the EBMT International Transplant Course. The studies were funded by MolMed S.p.A., the company developing Zalmoxis.
About the therapy
Zalmoxis is a treatment consisting of allogeneic, genetically modified T cells. The cells are intended to be given to haplo-HSCT recipients to help fight off infection, enhance the success of the transplant, and support long-lasting anticancer effects.
Because the genetically modified T cells can also cause GVHD, they are equipped with a suicide gene, which makes them susceptible to treatment with ganciclovir or valganciclovir. So if a patient develops GVHD, he or she can receive ganciclovir/valganciclovir, which should kill the modified T cells and prevent further development of GVHD.
Trial data
The data presented at the EBMT International Transplant Course were from the phase 1/2 TK007 trial and the ongoing phase 3 TK008 trial.
The TK007 trial included haplo-HSCT recipients with various high-risk hematologic malignancies, while the TK008 trial is enrolling patients with high-risk acute leukemia who are undergoing haplo-HSCT.
Researchers have compared 37 Zalmoxis-treated patients from these trials to 140 contemporaneous control patients from the database of the EBMT registry.
Results of this pair-matched analysis showed an OS improvement in Zalmoxis-treated patients, which was driven by a reduction in NRM. The OS was 49% in the Zalmoxis group and 37% in controls (P=0.01), and the NRM was 22% and 43%, respectively (P=0.014).
Among controls dying from non-relapse causes, the majority (78%) died from either infection (56%) or GVHD (22%), while the only adverse event related to Zalmoxis treatment was GVHD. And this GVHD was fully resolved by activating the suicide-gene system with ganciclovir treatment, without any GVHD-related death.
Furthermore, the incidence of chronic GVHD was lower in Zalmoxis-treated patients than in controls—6% and 25%, respectively (P=0.04).
Therefore, the researchers concluded that the protective effects of Zalmoxis in controlling infection and GVHD mainly drove the decreased NRM in the Zalmoxis group.
These data supported the European Commission’s recent decision to grant conditional marketing authorization for Zalmoxis. ![]()
FDA grants drug orphan designation for PNH

The US Food and Drug Administration (FDA) has granted orphan drug designation to Coversin as a treatment for paroxysmal nocturnal hemoglobinuria (PNH).
Coversin is a recombinant small protein (16,740 Da) derived from a native protein found in the saliva of the Ornithodoros moubata tick.
The drug is a second-generation complement inhibitor that acts on complement component C5, preventing release of C5a and formation of C5b-9 (also known as the membrane attack complex).
Coversin is being developed by Akari Therapeutics.
In vitro experiments have shown that Coversin inhibits red blood cell lysis in PNH, and Coversin can achieve full complement inhibition in the blood of PNH patients who are resistant to eculizumab.
In a phase 1a trial of healthy volunteers, Coversin completely inhibited complement C5 activity within 12 hours of administration.
Akari Therapeutics is currently conducting a phase 1b study of Coversin in healthy volunteers and is enrolling patients with eculizumab-resistant PNH in a phase 2 trial.
The company has also been administering Coversin to a patient with eculizumab-resistant PNH. Thus far, Coversin has prevented hemolytic episodes and improved disease symptoms in this patient. The only drug-related adverse event has been occasional local and transient irritation at the injection site.
“We have continued to see complete complement inhibition and symptom control in a PNH patient with resistance to eculizumab, who has been self-administering subcutaneous Coversin for over 7 months,” said Gur Roshwalb, MD, CEO of Akari Therapeutics.
“We believe that Coversin, when approved, could provide important benefits for all patients with PNH.”
Coversin is also being studied in atypical hemolytic uremic syndrome and Guillain Barré syndrome.
About orphan designation
The FDA grants orphan designation to drugs and biologics intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved. ![]()
The US Food and Drug Administration (FDA) has granted orphan drug designation to Coversin as a treatment for paroxysmal nocturnal hemoglobinuria (PNH).
Coversin is a recombinant small protein (16,740 Da) derived from a native protein found in the saliva of the Ornithodoros moubata tick.
The drug is a second-generation complement inhibitor that acts on complement component C5, preventing release of C5a and formation of C5b-9 (also known as the membrane attack complex).
Coversin is being developed by Akari Therapeutics.
In vitro experiments have shown that Coversin inhibits red blood cell lysis in PNH, and Coversin can achieve full complement inhibition in the blood of PNH patients who are resistant to eculizumab.
In a phase 1a trial of healthy volunteers, Coversin completely inhibited complement C5 activity within 12 hours of administration.
Akari Therapeutics is currently conducting a phase 1b study of Coversin in healthy volunteers and is enrolling patients with eculizumab-resistant PNH in a phase 2 trial.
The company has also been administering Coversin to a patient with eculizumab-resistant PNH. Thus far, Coversin has prevented hemolytic episodes and improved disease symptoms in this patient. The only drug-related adverse event has been occasional local and transient irritation at the injection site.
“We have continued to see complete complement inhibition and symptom control in a PNH patient with resistance to eculizumab, who has been self-administering subcutaneous Coversin for over 7 months,” said Gur Roshwalb, MD, CEO of Akari Therapeutics.
“We believe that Coversin, when approved, could provide important benefits for all patients with PNH.”
Coversin is also being studied in atypical hemolytic uremic syndrome and Guillain Barré syndrome.
About orphan designation
The FDA grants orphan designation to drugs and biologics intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved. ![]()
The US Food and Drug Administration (FDA) has granted orphan drug designation to Coversin as a treatment for paroxysmal nocturnal hemoglobinuria (PNH).
Coversin is a recombinant small protein (16,740 Da) derived from a native protein found in the saliva of the Ornithodoros moubata tick.
The drug is a second-generation complement inhibitor that acts on complement component C5, preventing release of C5a and formation of C5b-9 (also known as the membrane attack complex).
Coversin is being developed by Akari Therapeutics.
In vitro experiments have shown that Coversin inhibits red blood cell lysis in PNH, and Coversin can achieve full complement inhibition in the blood of PNH patients who are resistant to eculizumab.
In a phase 1a trial of healthy volunteers, Coversin completely inhibited complement C5 activity within 12 hours of administration.
Akari Therapeutics is currently conducting a phase 1b study of Coversin in healthy volunteers and is enrolling patients with eculizumab-resistant PNH in a phase 2 trial.
The company has also been administering Coversin to a patient with eculizumab-resistant PNH. Thus far, Coversin has prevented hemolytic episodes and improved disease symptoms in this patient. The only drug-related adverse event has been occasional local and transient irritation at the injection site.
“We have continued to see complete complement inhibition and symptom control in a PNH patient with resistance to eculizumab, who has been self-administering subcutaneous Coversin for over 7 months,” said Gur Roshwalb, MD, CEO of Akari Therapeutics.
“We believe that Coversin, when approved, could provide important benefits for all patients with PNH.”
Coversin is also being studied in atypical hemolytic uremic syndrome and Guillain Barré syndrome.
About orphan designation
The FDA grants orphan designation to drugs and biologics intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved. ![]()
FDA approves cord blood product

The US Food and Drug Administration (FDA) has issued a biologics license to the Cleveland Cord Blood Center (CCBC) for Clevecord™ (HPC, Cord Blood), a hematopoietic progenitor cell product derived from umbilical cord blood.
Under this license, CCBC is authorized to manufacture Clevecord at its facility in Warrensville Heights, Ohio.
Clevecord is indicated for use in unrelated donor transplant procedures, in conjunction with an appropriate preparative regimen.
The product can be used for hematopoietic and immunologic reconstitution in patients with disorders that affect the hematopoietic system, whether they are inherited, acquired, or result from myeloablative treatment.
Each Clevecord unit contains a minimum of 5 x 108 total nucleated cells with at least 1.25 x 106 viable CD34+ cells at the time of cryopreservation. The recommended minimum dose is 2.5 x 107 nucleated cells/kg at cryopreservation.
Clevecord has been approved with a black box warning, which states that use of the product may result in fatal infusion reactions, graft-vs-host disease, engraftment syndrome, and graft failure.
For more details on Clevecord, see the package insert on the FDA website.
“Obtaining FDA licensure for Clevecord is reflective of the Cleveland Cord Blood Center’s dedication to meeting the highest quality standards in the industry for distribution of our cord blood products to transplant centers throughout the US and around the world,” said Wouter Van’t Hof, cord blood bank director at CCBC.
CCBC collects, processes, stores, and distributes umbilical cord blood units for use in transplants and advanced research in cellular therapy.
The organization says its cord blood collections represent a diverse cross-section of donor ethnicity to support transplant needs, particularly in the underserved African-American population.
“Up to 50% of parents giving birth in our partner hospitals donate their baby’s umbilical cord blood, a rate well above the national average,” said Marcie Finney, executive director of CCBC.
CCBC cord blood units can be searched and accessed through registries, including the National Bone Marrow Donor Program and Bone Marrow Donors Worldwide. ![]()
The US Food and Drug Administration (FDA) has issued a biologics license to the Cleveland Cord Blood Center (CCBC) for Clevecord™ (HPC, Cord Blood), a hematopoietic progenitor cell product derived from umbilical cord blood.
Under this license, CCBC is authorized to manufacture Clevecord at its facility in Warrensville Heights, Ohio.
Clevecord is indicated for use in unrelated donor transplant procedures, in conjunction with an appropriate preparative regimen.
The product can be used for hematopoietic and immunologic reconstitution in patients with disorders that affect the hematopoietic system, whether they are inherited, acquired, or result from myeloablative treatment.
Each Clevecord unit contains a minimum of 5 x 108 total nucleated cells with at least 1.25 x 106 viable CD34+ cells at the time of cryopreservation. The recommended minimum dose is 2.5 x 107 nucleated cells/kg at cryopreservation.
Clevecord has been approved with a black box warning, which states that use of the product may result in fatal infusion reactions, graft-vs-host disease, engraftment syndrome, and graft failure.
For more details on Clevecord, see the package insert on the FDA website.
“Obtaining FDA licensure for Clevecord is reflective of the Cleveland Cord Blood Center’s dedication to meeting the highest quality standards in the industry for distribution of our cord blood products to transplant centers throughout the US and around the world,” said Wouter Van’t Hof, cord blood bank director at CCBC.
CCBC collects, processes, stores, and distributes umbilical cord blood units for use in transplants and advanced research in cellular therapy.
The organization says its cord blood collections represent a diverse cross-section of donor ethnicity to support transplant needs, particularly in the underserved African-American population.
“Up to 50% of parents giving birth in our partner hospitals donate their baby’s umbilical cord blood, a rate well above the national average,” said Marcie Finney, executive director of CCBC.
CCBC cord blood units can be searched and accessed through registries, including the National Bone Marrow Donor Program and Bone Marrow Donors Worldwide. ![]()
The US Food and Drug Administration (FDA) has issued a biologics license to the Cleveland Cord Blood Center (CCBC) for Clevecord™ (HPC, Cord Blood), a hematopoietic progenitor cell product derived from umbilical cord blood.
Under this license, CCBC is authorized to manufacture Clevecord at its facility in Warrensville Heights, Ohio.
Clevecord is indicated for use in unrelated donor transplant procedures, in conjunction with an appropriate preparative regimen.
The product can be used for hematopoietic and immunologic reconstitution in patients with disorders that affect the hematopoietic system, whether they are inherited, acquired, or result from myeloablative treatment.
Each Clevecord unit contains a minimum of 5 x 108 total nucleated cells with at least 1.25 x 106 viable CD34+ cells at the time of cryopreservation. The recommended minimum dose is 2.5 x 107 nucleated cells/kg at cryopreservation.
Clevecord has been approved with a black box warning, which states that use of the product may result in fatal infusion reactions, graft-vs-host disease, engraftment syndrome, and graft failure.
For more details on Clevecord, see the package insert on the FDA website.
“Obtaining FDA licensure for Clevecord is reflective of the Cleveland Cord Blood Center’s dedication to meeting the highest quality standards in the industry for distribution of our cord blood products to transplant centers throughout the US and around the world,” said Wouter Van’t Hof, cord blood bank director at CCBC.
CCBC collects, processes, stores, and distributes umbilical cord blood units for use in transplants and advanced research in cellular therapy.
The organization says its cord blood collections represent a diverse cross-section of donor ethnicity to support transplant needs, particularly in the underserved African-American population.
“Up to 50% of parents giving birth in our partner hospitals donate their baby’s umbilical cord blood, a rate well above the national average,” said Marcie Finney, executive director of CCBC.
CCBC cord blood units can be searched and accessed through registries, including the National Bone Marrow Donor Program and Bone Marrow Donors Worldwide. ![]()
Effects of caring for advanced cancer patients

SAN FRANCISCO—Family caregivers of patients with high-mortality cancers may often experience high levels of depression and anxiety, results of a survey suggest.
The survey showed that caregivers can spend more than 8 hours a day providing care.
And as caregiving time increases, self-care behaviors such as sleep and exercise decline, which may confer poorer mental health.
These findings were presented at the 2016 Palliative Care in Oncology Symposium (abstract 239).
“Caregivers and patients are faced with an enormous physical and emotional toll when dealing with advanced cancer,” said study investigator J. Nicholas Dionne-Odom, PhD, RN, of the University of Alabama at Birmingham.
“When they put their own health and well-being on the back burner, it can affect their care to the patient.”
Dr Dionne-Odom and his colleagues conducted a cross-sectional survey of 294 family caregivers of Medicare beneficiaries diagnosed with pancreatic, lung, brain, ovarian, head and neck, hematologic, or stage IV cancers.
The survey was fielded across 8 cancer centers in Alabama, Florida, and Tennessee. Survey questions explored measures of self-care behaviors and quality of life.
The caregivers had an average age of 66. They were mostly female (72.8%), white (91.2%), retired (54.4%), and the patient’s spouse/partner (60.2%). Nearly half of the caregivers lived in rural areas (46.9%), and more than half had annual incomes less than $50,000 (53.8%).
Most of the caregivers said they provided care 6 to 7 days a week (71%) for more than 1 year (68%).
Twenty-three percent of caregivers reported a high level of depressive symptoms, and 34% reported borderline or high levels of anxiety symptoms, associated with significantly lower scores for self-care.
Lower self-care behavior scores were associated with a longer overall duration of caregiving, more hours in the day spent caregiving, more days of the week spent caregiving, and with fair or poor patient health.
“We hope our research rallies the oncology palliative care communities to develop assessment tools and services that support caregivers,” Dr Dionne-Odom said. “These efforts would help ensure that caregivers are supported and healthy when they take on the important role of caring for an individual with advanced cancer.” ![]()
SAN FRANCISCO—Family caregivers of patients with high-mortality cancers may often experience high levels of depression and anxiety, results of a survey suggest.
The survey showed that caregivers can spend more than 8 hours a day providing care.
And as caregiving time increases, self-care behaviors such as sleep and exercise decline, which may confer poorer mental health.
These findings were presented at the 2016 Palliative Care in Oncology Symposium (abstract 239).
“Caregivers and patients are faced with an enormous physical and emotional toll when dealing with advanced cancer,” said study investigator J. Nicholas Dionne-Odom, PhD, RN, of the University of Alabama at Birmingham.
“When they put their own health and well-being on the back burner, it can affect their care to the patient.”
Dr Dionne-Odom and his colleagues conducted a cross-sectional survey of 294 family caregivers of Medicare beneficiaries diagnosed with pancreatic, lung, brain, ovarian, head and neck, hematologic, or stage IV cancers.
The survey was fielded across 8 cancer centers in Alabama, Florida, and Tennessee. Survey questions explored measures of self-care behaviors and quality of life.
The caregivers had an average age of 66. They were mostly female (72.8%), white (91.2%), retired (54.4%), and the patient’s spouse/partner (60.2%). Nearly half of the caregivers lived in rural areas (46.9%), and more than half had annual incomes less than $50,000 (53.8%).
Most of the caregivers said they provided care 6 to 7 days a week (71%) for more than 1 year (68%).
Twenty-three percent of caregivers reported a high level of depressive symptoms, and 34% reported borderline or high levels of anxiety symptoms, associated with significantly lower scores for self-care.
Lower self-care behavior scores were associated with a longer overall duration of caregiving, more hours in the day spent caregiving, more days of the week spent caregiving, and with fair or poor patient health.
“We hope our research rallies the oncology palliative care communities to develop assessment tools and services that support caregivers,” Dr Dionne-Odom said. “These efforts would help ensure that caregivers are supported and healthy when they take on the important role of caring for an individual with advanced cancer.” ![]()
SAN FRANCISCO—Family caregivers of patients with high-mortality cancers may often experience high levels of depression and anxiety, results of a survey suggest.
The survey showed that caregivers can spend more than 8 hours a day providing care.
And as caregiving time increases, self-care behaviors such as sleep and exercise decline, which may confer poorer mental health.
These findings were presented at the 2016 Palliative Care in Oncology Symposium (abstract 239).
“Caregivers and patients are faced with an enormous physical and emotional toll when dealing with advanced cancer,” said study investigator J. Nicholas Dionne-Odom, PhD, RN, of the University of Alabama at Birmingham.
“When they put their own health and well-being on the back burner, it can affect their care to the patient.”
Dr Dionne-Odom and his colleagues conducted a cross-sectional survey of 294 family caregivers of Medicare beneficiaries diagnosed with pancreatic, lung, brain, ovarian, head and neck, hematologic, or stage IV cancers.
The survey was fielded across 8 cancer centers in Alabama, Florida, and Tennessee. Survey questions explored measures of self-care behaviors and quality of life.
The caregivers had an average age of 66. They were mostly female (72.8%), white (91.2%), retired (54.4%), and the patient’s spouse/partner (60.2%). Nearly half of the caregivers lived in rural areas (46.9%), and more than half had annual incomes less than $50,000 (53.8%).
Most of the caregivers said they provided care 6 to 7 days a week (71%) for more than 1 year (68%).
Twenty-three percent of caregivers reported a high level of depressive symptoms, and 34% reported borderline or high levels of anxiety symptoms, associated with significantly lower scores for self-care.
Lower self-care behavior scores were associated with a longer overall duration of caregiving, more hours in the day spent caregiving, more days of the week spent caregiving, and with fair or poor patient health.
“We hope our research rallies the oncology palliative care communities to develop assessment tools and services that support caregivers,” Dr Dionne-Odom said. “These efforts would help ensure that caregivers are supported and healthy when they take on the important role of caring for an individual with advanced cancer.” ![]()
WHO updates ranking of critically important antimicrobials
In light of increasing antibiotic resistance among pathogens, the World Health Organization has revised its global rankings of critically important antimicrobials used in human medicine, designating quinolones, third- and fourth-generation cephalosporins, macrolides and ketolides, and glycopeptides as among the highest-priority drugs in the world.
Peter C. Collignon, MBBS, of Canberra (Australia) Hospital and his colleagues on the WHO Advisory Group on Integrated Surveillance of Antimicrobial Resistance, created the rankings for use in developing risk management strategies related to antimicrobial use in food production animals. According to Dr. Collignon and his coauthors, the rankings are intended to help regulators and other stakeholders know which types of antimicrobials used in animals present potentially higher risks to human populations and help inform how this use might be better managed (e.g. restriction to single-animal therapy or prohibition of mass treatment and extra-label use) to minimize the risk of transmission of resistance to the human population.

WHO studies previously suggested that antimicrobials which currently have no veterinary equivalent (for example, carbapenems) “as well as any new class of antimicrobial developed for human therapy should not be used in animals.” Dr. Collignon’s WHO Advisory Group followed two essential criteria to designate antimicrobials of utmost importance to human health in the new study: 1. antimicrobials that are the sole, or one of limited available therapies, to treat serious bacterial infections in people and 2. antimicrobials used to treat infections in people caused by either (a) bacteria that may be transmitted to humans from nonhuman sources or (b) bacteria that may acquire resistance genes from nonhuman sources.
The highest-priority and most critically important antimicrobials are those which meet the criteria listed above and that are used in greatest volume or highest frequency by humans. Another criteria for prioritization involves antimicrobial classes where evidence suggests that the “transmission of resistant bacteria or resistance genes from nonhuman sources is already occurring, or has occurred previously.” Quinolones, third- and fourth-generation cephalosporins, macrolides and ketolides, and glycopeptides were the only antimicrobials that met all criteria for prioritization.
“Antimicrobial resistance remains a threat to human health and drivers of resistance act in all sectors; human, animal, and the environment,” the WHO Advisory Group concluded. “Prioritizing the antimicrobials that are critically important for humans is a valuable and strategic risk-management tool and will be improved with the evidence-based approach which is currently underway.”
Read the full study in Clinical Infectious Diseases (doi: 10.1093/cid/ciw475).
In light of increasing antibiotic resistance among pathogens, the World Health Organization has revised its global rankings of critically important antimicrobials used in human medicine, designating quinolones, third- and fourth-generation cephalosporins, macrolides and ketolides, and glycopeptides as among the highest-priority drugs in the world.
Peter C. Collignon, MBBS, of Canberra (Australia) Hospital and his colleagues on the WHO Advisory Group on Integrated Surveillance of Antimicrobial Resistance, created the rankings for use in developing risk management strategies related to antimicrobial use in food production animals. According to Dr. Collignon and his coauthors, the rankings are intended to help regulators and other stakeholders know which types of antimicrobials used in animals present potentially higher risks to human populations and help inform how this use might be better managed (e.g. restriction to single-animal therapy or prohibition of mass treatment and extra-label use) to minimize the risk of transmission of resistance to the human population.
WHO studies previously suggested that antimicrobials which currently have no veterinary equivalent (for example, carbapenems) “as well as any new class of antimicrobial developed for human therapy should not be used in animals.” Dr. Collignon’s WHO Advisory Group followed two essential criteria to designate antimicrobials of utmost importance to human health in the new study: 1. antimicrobials that are the sole, or one of limited available therapies, to treat serious bacterial infections in people and 2. antimicrobials used to treat infections in people caused by either (a) bacteria that may be transmitted to humans from nonhuman sources or (b) bacteria that may acquire resistance genes from nonhuman sources.
The highest-priority and most critically important antimicrobials are those which meet the criteria listed above and that are used in greatest volume or highest frequency by humans. Another criteria for prioritization involves antimicrobial classes where evidence suggests that the “transmission of resistant bacteria or resistance genes from nonhuman sources is already occurring, or has occurred previously.” Quinolones, third- and fourth-generation cephalosporins, macrolides and ketolides, and glycopeptides were the only antimicrobials that met all criteria for prioritization.
“Antimicrobial resistance remains a threat to human health and drivers of resistance act in all sectors; human, animal, and the environment,” the WHO Advisory Group concluded. “Prioritizing the antimicrobials that are critically important for humans is a valuable and strategic risk-management tool and will be improved with the evidence-based approach which is currently underway.”
Read the full study in Clinical Infectious Diseases (doi: 10.1093/cid/ciw475).
In light of increasing antibiotic resistance among pathogens, the World Health Organization has revised its global rankings of critically important antimicrobials used in human medicine, designating quinolones, third- and fourth-generation cephalosporins, macrolides and ketolides, and glycopeptides as among the highest-priority drugs in the world.
Peter C. Collignon, MBBS, of Canberra (Australia) Hospital and his colleagues on the WHO Advisory Group on Integrated Surveillance of Antimicrobial Resistance, created the rankings for use in developing risk management strategies related to antimicrobial use in food production animals. According to Dr. Collignon and his coauthors, the rankings are intended to help regulators and other stakeholders know which types of antimicrobials used in animals present potentially higher risks to human populations and help inform how this use might be better managed (e.g. restriction to single-animal therapy or prohibition of mass treatment and extra-label use) to minimize the risk of transmission of resistance to the human population.
WHO studies previously suggested that antimicrobials which currently have no veterinary equivalent (for example, carbapenems) “as well as any new class of antimicrobial developed for human therapy should not be used in animals.” Dr. Collignon’s WHO Advisory Group followed two essential criteria to designate antimicrobials of utmost importance to human health in the new study: 1. antimicrobials that are the sole, or one of limited available therapies, to treat serious bacterial infections in people and 2. antimicrobials used to treat infections in people caused by either (a) bacteria that may be transmitted to humans from nonhuman sources or (b) bacteria that may acquire resistance genes from nonhuman sources.
The highest-priority and most critically important antimicrobials are those which meet the criteria listed above and that are used in greatest volume or highest frequency by humans. Another criteria for prioritization involves antimicrobial classes where evidence suggests that the “transmission of resistant bacteria or resistance genes from nonhuman sources is already occurring, or has occurred previously.” Quinolones, third- and fourth-generation cephalosporins, macrolides and ketolides, and glycopeptides were the only antimicrobials that met all criteria for prioritization.
“Antimicrobial resistance remains a threat to human health and drivers of resistance act in all sectors; human, animal, and the environment,” the WHO Advisory Group concluded. “Prioritizing the antimicrobials that are critically important for humans is a valuable and strategic risk-management tool and will be improved with the evidence-based approach which is currently underway.”
Read the full study in Clinical Infectious Diseases (doi: 10.1093/cid/ciw475).
FROM CLINICAL INFECTIOUS DISEASES

New ELISA better differentiates chronic, acute hepatitis E infection
While real-time polymerase chain reaction (PCR) testing is the standard test for hepatitis E virus infection, an anti-HEV-specific enzyme-linked immunosorbent assay (ELISA) is more effective than is PCR at distinguishing between acute and chronic HEV infections.
“A clinical challenge in the management of immunocompromised patients with HEV infection is to differentiate between the acute and chronic course of infection [as] approximately 60% of infected immunocompromised individuals experience a chronic infection, which might require treatment with ribavirin,” said lead author Patrick Behrendt, Dr.med., of Hannover (Germany) Medical School.
The anti-HEV antigen (Ag) ELISA has recently become commercially available, making it an even bigger matter of interest. Dr. Behrendt and his coinvestigators analyzed sera from 18 patients with acute and 21 patients with chronic HEV, whose samples were collected between 2008 and 2015. The sera were retrospectively analyzed via both real-time PCR and ELISA to compare the efficacy of each in identifying HEV – more specifically, HEV genotype 3 – in each subject. For the ELISA analysis, 100 mcL of serum were added to each well of an ELISA plate, which was subsequently incubated at 37 degrees Celsius for 1 hour.
The researchers analyzed sera from four individuals with chronic HEV using serial dilutions to compare sensitivity of real-time PCR and ELISA. In three out of those four sera (75%), ELISA showed negative results due to HEV RNA levels of fewer than 10,000 copies/mL; on the other hand, real-time PCR showed a “linear reduction in levels,” indicating that it is the better option in detecting HEV genotype 3 (J Infect Dis. 2016 May 27;214[3]:361-8).
ELISA was also used on 20 chronic HEV patients and 17 acute HEV patients to determine its sensitivity at distinguishing between the two types of infection. In this cohort, only 64.7% of RNA-positive patients were deemed positive according to the ELISA testing, while ELISA results were positive in all of the cases of chronic HEV infections. None of the patients with chronic infection registered a false-negative, which indicates “a high reliability of the assay for this cohort,” according to the investigators.
“Comparison of chronically infected individuals with acutely infected patients revealed drastically increased ODs in chronically infected patients, while most of the positive samples from acutely infected patients displayed significantly lower values [which] led to a sensitivity of 100% (20 of 20) [ELISA] results for chronically HEV infected individuals,” the authors concluded. “Our study demonstrates that [ELISA] has a sensitivity of 65% and a specificity of 92% in detecting an ongoing HEV infection in a real-life cohort.”
The German Center for Infection Research, the Helmholtz Center for Infection Research, and the German Ministry for Education and Research funded the study. The researchers reported no relevant financial disclosures.
While real-time polymerase chain reaction (PCR) testing is the standard test for hepatitis E virus infection, an anti-HEV-specific enzyme-linked immunosorbent assay (ELISA) is more effective than is PCR at distinguishing between acute and chronic HEV infections.
“A clinical challenge in the management of immunocompromised patients with HEV infection is to differentiate between the acute and chronic course of infection [as] approximately 60% of infected immunocompromised individuals experience a chronic infection, which might require treatment with ribavirin,” said lead author Patrick Behrendt, Dr.med., of Hannover (Germany) Medical School.
The anti-HEV antigen (Ag) ELISA has recently become commercially available, making it an even bigger matter of interest. Dr. Behrendt and his coinvestigators analyzed sera from 18 patients with acute and 21 patients with chronic HEV, whose samples were collected between 2008 and 2015. The sera were retrospectively analyzed via both real-time PCR and ELISA to compare the efficacy of each in identifying HEV – more specifically, HEV genotype 3 – in each subject. For the ELISA analysis, 100 mcL of serum were added to each well of an ELISA plate, which was subsequently incubated at 37 degrees Celsius for 1 hour.
The researchers analyzed sera from four individuals with chronic HEV using serial dilutions to compare sensitivity of real-time PCR and ELISA. In three out of those four sera (75%), ELISA showed negative results due to HEV RNA levels of fewer than 10,000 copies/mL; on the other hand, real-time PCR showed a “linear reduction in levels,” indicating that it is the better option in detecting HEV genotype 3 (J Infect Dis. 2016 May 27;214[3]:361-8).
ELISA was also used on 20 chronic HEV patients and 17 acute HEV patients to determine its sensitivity at distinguishing between the two types of infection. In this cohort, only 64.7% of RNA-positive patients were deemed positive according to the ELISA testing, while ELISA results were positive in all of the cases of chronic HEV infections. None of the patients with chronic infection registered a false-negative, which indicates “a high reliability of the assay for this cohort,” according to the investigators.
“Comparison of chronically infected individuals with acutely infected patients revealed drastically increased ODs in chronically infected patients, while most of the positive samples from acutely infected patients displayed significantly lower values [which] led to a sensitivity of 100% (20 of 20) [ELISA] results for chronically HEV infected individuals,” the authors concluded. “Our study demonstrates that [ELISA] has a sensitivity of 65% and a specificity of 92% in detecting an ongoing HEV infection in a real-life cohort.”
The German Center for Infection Research, the Helmholtz Center for Infection Research, and the German Ministry for Education and Research funded the study. The researchers reported no relevant financial disclosures.
While real-time polymerase chain reaction (PCR) testing is the standard test for hepatitis E virus infection, an anti-HEV-specific enzyme-linked immunosorbent assay (ELISA) is more effective than is PCR at distinguishing between acute and chronic HEV infections.
“A clinical challenge in the management of immunocompromised patients with HEV infection is to differentiate between the acute and chronic course of infection [as] approximately 60% of infected immunocompromised individuals experience a chronic infection, which might require treatment with ribavirin,” said lead author Patrick Behrendt, Dr.med., of Hannover (Germany) Medical School.
The anti-HEV antigen (Ag) ELISA has recently become commercially available, making it an even bigger matter of interest. Dr. Behrendt and his coinvestigators analyzed sera from 18 patients with acute and 21 patients with chronic HEV, whose samples were collected between 2008 and 2015. The sera were retrospectively analyzed via both real-time PCR and ELISA to compare the efficacy of each in identifying HEV – more specifically, HEV genotype 3 – in each subject. For the ELISA analysis, 100 mcL of serum were added to each well of an ELISA plate, which was subsequently incubated at 37 degrees Celsius for 1 hour.
The researchers analyzed sera from four individuals with chronic HEV using serial dilutions to compare sensitivity of real-time PCR and ELISA. In three out of those four sera (75%), ELISA showed negative results due to HEV RNA levels of fewer than 10,000 copies/mL; on the other hand, real-time PCR showed a “linear reduction in levels,” indicating that it is the better option in detecting HEV genotype 3 (J Infect Dis. 2016 May 27;214[3]:361-8).
ELISA was also used on 20 chronic HEV patients and 17 acute HEV patients to determine its sensitivity at distinguishing between the two types of infection. In this cohort, only 64.7% of RNA-positive patients were deemed positive according to the ELISA testing, while ELISA results were positive in all of the cases of chronic HEV infections. None of the patients with chronic infection registered a false-negative, which indicates “a high reliability of the assay for this cohort,” according to the investigators.
“Comparison of chronically infected individuals with acutely infected patients revealed drastically increased ODs in chronically infected patients, while most of the positive samples from acutely infected patients displayed significantly lower values [which] led to a sensitivity of 100% (20 of 20) [ELISA] results for chronically HEV infected individuals,” the authors concluded. “Our study demonstrates that [ELISA] has a sensitivity of 65% and a specificity of 92% in detecting an ongoing HEV infection in a real-life cohort.”
The German Center for Infection Research, the Helmholtz Center for Infection Research, and the German Ministry for Education and Research funded the study. The researchers reported no relevant financial disclosures.
FROM THE JOURNAL OF INFECTIOUS DISEASES
Key clinical point: An anti-HEV-specific enzyme-linked immunosorbent assay (ELISA) is more effective at identifying acute versus chronic HEV infection than is HEV RNA real-time PCR.
Major finding: ELISA detected significantly higher levels of HEV Ag in chronically infected subjects than in acutely affected ones, but was less sensitive at detecting HEV infection overall than real-time PCR.
Data source: Retrospective cohort study of 21 chronic and 18 acute HEV patients from 2008-2015.
Disclosures: The German Center for Infection Research, the Helmholtz Center for Infection Research, and the German Ministry for Education and Research funded the study. The researchers reported no relevant financial disclosures.

Colon cancer
Colorectal cancer (CRC) screening has become a focal point of the practice of gastroenterology. Successful screening leads to a reduction in cancer mortality and is one of the most impactful means by which we improve population health.
Rick Boland, MD, of the Baylor Center of Gastrointestinal Cancer Research in Dallas reminded us at the annual Digestive Disease Week that carcinogenesis in colorectal cancer is a multistep process and described several pathways of which clinicians should be aware. Germline mutations (inherited) vs. somatic mutations (acquired) may be driver mutations that confer selection advantage and become targets for therapy in contrast to passenger mutations that are not mechanistic targets. Germline mutations should be considered when there is a family history of CRC, especially in a young patient, and are characteristic of familial adenomatous polyposis (APC), attenuated polyposis (MYH-MUTYH), and nonadenomatous polyposis syndromes such as Peutz-Jeghers (STK11).

Microsatellite instability is an alternative pathway to cancer. Hereditary nonpolyposis colorectal cancer (Lynch syndrome) is representative of this pathway with common abnormalities in mismatch repair genes such as MLH1, MSH2, MSH6, or PMS2. Lynch syndrome patients are BRAF and CIMP negative. This is in contrast to a more recent pathway to cancer that arises from sessile serrated polyps that also display microsatellite instability, but are BRAF and CIMP positive.
The clinical importance of understanding the pathway through which cancer develops in an individual patient is that depending on the mechanism of tumorigenesis, different treatment strategies can prevent or treat cancer. For example, exciting novel therapies are being developed for microsatellite unstable cancers using immune checkpoint inhibitors. Aspirin can reduce CRC mortality, especially tumors that overexpress COX2 or harbor PIK3CA mutations, and have demonstrated benefit even postoperatively in patients receiving surgical resection of CRC.
I gave a talk focused on current guidelines for reducing mortality among individuals at average risk for developing CRC. The U.S. Preventive Services Task Force updated their recommendations this year and chose to focus on highlighting the importance of CRC screening between the ages of 50 and 75 years, tailored screening for those between the ages of 76 and 85 years, and stopping screening after age 85 years. However, the statement does not recommend specific tests and instead lists competing strategies of annual fecal immunochemical test (FIT) or highly sensitive fecal occult blood test (FOBT) with or without flexible sigmoidoscopy every 10 years, flexible sigmoidoscopy every 5 years, colonoscopy every 10 years, CT colonography every 5 years, and FIT-DNA every 1 or 3 years. The FIT-DNA adds a separate FIT to a stool exam for KRAS mutations, NDRG4 and BMP3 methylation, and beta-actin. There are no studies to determine whether CRC mortality is reduced, but one study demonstrated a higher sensitivity for CRC with the combined FIT-DNA, compared with FIT alone, but a lower specificity. The FDA also recently approved a blood-based CRC screening test that detects circulating methylated septin 9 gene DNA. Septin 9 is a gene that codes for GTP-binding protein and acts as a tumor suppressor that can be inactivated by methylation.
Irrespective of which strategy is pursued, colonoscopy is the final common pathway. Quality is important because there remains a disappointing rate of CRC after colonoscopy. Prior work has demonstrated significant differences in the adenoma detection rate (ADR) between endoscopists in the same practice. A recent Kaiser study found that for every 1% increase in the ADR there is a 3% decrease in the rate of cancer developing after colonoscopy.
Disruptive technology is emerging that may displace gastroenterologists from primary endoscopic screening. A self-propelled disposable colonoscope (Aer-O-Scope) has been developed that uses pneumatic pressure to advance a tethered camera through the colonic lumen guided by a joystick. Sedation is not required and the device does not need manual advancement, facilitating use by nongastroenterologists.
Uri Ladabaum, MD, of Stanford (Calif.) University presented the clinical impact of screening for hereditary and familial CRC. Lynch syndrome is characterized by a family history of cancer in at least three individuals spanning at least two generations including one with early cancer development. He reminded us that Lynch syndrome cancers are not limited to CRC but also include uterine, ovarian, gastric, small intestinal, urinary, biliary, pancreatic, and neurologic tumors. Microsatellite instability is likely present, mismatch repair gene abnormalities should be sought, and screening should include colonoscopy every 1-2 years. Aspirin chemoprophylaxis should be recommended, as should prophylactic hysterectomy and oophorectomy among affected women due to the uterine and ovarian cancer risk.
Polyposis syndromes constitute a separate group of hereditary cancers that includes familial adenomatous polyposis (FAP) arising from defects in the APC gene that may present as florid or attenuated FAP, and MYH-associated polyposis. If a patient presents with more than 10 adenomas, a polyposis syndrome should be considered. More rare syndromes include Cowden, juvenile polyposis, and Peutz-Jeghers.
Douglas Rex, MD, of Indiana University, Indianapolis, provided an array of highly clinically relevant tips to improve screening colonoscopy quality, which has been shown to reduce CRC mortality. Some of the basic concepts include using split-dose preparations and high-definition endoscopes, measuring and reporting adenoma detection rates, and using water immersion with carbon dioxide instead of air insufflation. Special attention was given to the diagnosis and removal of sessile lesions of the colon. Dr. Rex revealed many of his “tricks” to achieving high-quality colonoscopy, which include retroflexion to access polyps behind folds, using a stiff snare, and attaching a cap to the end of the colonoscope in order to facilitate visualization of polyps and assist in the mucosal resection of sessile lesions. Dr. Rex also presented data to support his recommendation to use “avulsion” with cold snare and forceps while limiting coagulative ablation for residual polyp tissue.
Finally, Rajeev Jain, MD, of Dallas presented the rapidly evolving area of reimbursement reform including the Medicare Access and CHIP Reauthorization Act (MACRA) that is driving payment away from fee-for-service and towards bundled payments, accountable care networks, and patient-centered medical homes. Key to this reform is the documentation and reporting of quality for procedural and cognitive patient encounters. There are limited performance measures specific to gastroenterology and hepatology, which currently include measures to both document appropriate CRC screening and reduce colonoscopy overuse, inflammatory bowel disease management, and hepatitis C management. However, there are many cost-cutting measures that can also be reported by gastroenterologists to fulfill these requirements. The Physician Quality Reporting System requires at least nine measures for at least 50% of Medicare patients in order to avoid penalties. It is not enough to track and document quality measures – results must also be reported through CMS-approved entities called qualified clinical data registries.
Dr. Jain described the movement toward payment bundles in which a single reimbursement is provided for services rendered by all providers and sites across a single episode of care. Screening colonoscopy was used as an example of how this could impact gastroenterology: a single payment would be provided for the preprocedure evaluation and education, the procedure itself (including endoscopy, anesthesia, pathology, facility), and postprocedure follow-up. Additional payments would not be provided for additional services such as repeating the colonoscopy because of a poor preparation or to treat postpolypectomy bleeding. Overall, health care reimbursement is moving to recognize value (quality/cost), reduce variation in care, and transfer more of the financial risk to health care providers and systems.
Dr. Inadomi, division of gastroenterology, department of medicine, University of Washington School of Medicine, department of health services, University of Washington School of Public Health, Seattle. He is on the clinical advisory committee for ChemImage and on the scientific advisory board for Epigenomics.
Colorectal cancer (CRC) screening has become a focal point of the practice of gastroenterology. Successful screening leads to a reduction in cancer mortality and is one of the most impactful means by which we improve population health.
Rick Boland, MD, of the Baylor Center of Gastrointestinal Cancer Research in Dallas reminded us at the annual Digestive Disease Week that carcinogenesis in colorectal cancer is a multistep process and described several pathways of which clinicians should be aware. Germline mutations (inherited) vs. somatic mutations (acquired) may be driver mutations that confer selection advantage and become targets for therapy in contrast to passenger mutations that are not mechanistic targets. Germline mutations should be considered when there is a family history of CRC, especially in a young patient, and are characteristic of familial adenomatous polyposis (APC), attenuated polyposis (MYH-MUTYH), and nonadenomatous polyposis syndromes such as Peutz-Jeghers (STK11).
Microsatellite instability is an alternative pathway to cancer. Hereditary nonpolyposis colorectal cancer (Lynch syndrome) is representative of this pathway with common abnormalities in mismatch repair genes such as MLH1, MSH2, MSH6, or PMS2. Lynch syndrome patients are BRAF and CIMP negative. This is in contrast to a more recent pathway to cancer that arises from sessile serrated polyps that also display microsatellite instability, but are BRAF and CIMP positive.
The clinical importance of understanding the pathway through which cancer develops in an individual patient is that depending on the mechanism of tumorigenesis, different treatment strategies can prevent or treat cancer. For example, exciting novel therapies are being developed for microsatellite unstable cancers using immune checkpoint inhibitors. Aspirin can reduce CRC mortality, especially tumors that overexpress COX2 or harbor PIK3CA mutations, and have demonstrated benefit even postoperatively in patients receiving surgical resection of CRC.
I gave a talk focused on current guidelines for reducing mortality among individuals at average risk for developing CRC. The U.S. Preventive Services Task Force updated their recommendations this year and chose to focus on highlighting the importance of CRC screening between the ages of 50 and 75 years, tailored screening for those between the ages of 76 and 85 years, and stopping screening after age 85 years. However, the statement does not recommend specific tests and instead lists competing strategies of annual fecal immunochemical test (FIT) or highly sensitive fecal occult blood test (FOBT) with or without flexible sigmoidoscopy every 10 years, flexible sigmoidoscopy every 5 years, colonoscopy every 10 years, CT colonography every 5 years, and FIT-DNA every 1 or 3 years. The FIT-DNA adds a separate FIT to a stool exam for KRAS mutations, NDRG4 and BMP3 methylation, and beta-actin. There are no studies to determine whether CRC mortality is reduced, but one study demonstrated a higher sensitivity for CRC with the combined FIT-DNA, compared with FIT alone, but a lower specificity. The FDA also recently approved a blood-based CRC screening test that detects circulating methylated septin 9 gene DNA. Septin 9 is a gene that codes for GTP-binding protein and acts as a tumor suppressor that can be inactivated by methylation.
Irrespective of which strategy is pursued, colonoscopy is the final common pathway. Quality is important because there remains a disappointing rate of CRC after colonoscopy. Prior work has demonstrated significant differences in the adenoma detection rate (ADR) between endoscopists in the same practice. A recent Kaiser study found that for every 1% increase in the ADR there is a 3% decrease in the rate of cancer developing after colonoscopy.
Disruptive technology is emerging that may displace gastroenterologists from primary endoscopic screening. A self-propelled disposable colonoscope (Aer-O-Scope) has been developed that uses pneumatic pressure to advance a tethered camera through the colonic lumen guided by a joystick. Sedation is not required and the device does not need manual advancement, facilitating use by nongastroenterologists.
Uri Ladabaum, MD, of Stanford (Calif.) University presented the clinical impact of screening for hereditary and familial CRC. Lynch syndrome is characterized by a family history of cancer in at least three individuals spanning at least two generations including one with early cancer development. He reminded us that Lynch syndrome cancers are not limited to CRC but also include uterine, ovarian, gastric, small intestinal, urinary, biliary, pancreatic, and neurologic tumors. Microsatellite instability is likely present, mismatch repair gene abnormalities should be sought, and screening should include colonoscopy every 1-2 years. Aspirin chemoprophylaxis should be recommended, as should prophylactic hysterectomy and oophorectomy among affected women due to the uterine and ovarian cancer risk.
Polyposis syndromes constitute a separate group of hereditary cancers that includes familial adenomatous polyposis (FAP) arising from defects in the APC gene that may present as florid or attenuated FAP, and MYH-associated polyposis. If a patient presents with more than 10 adenomas, a polyposis syndrome should be considered. More rare syndromes include Cowden, juvenile polyposis, and Peutz-Jeghers.
Douglas Rex, MD, of Indiana University, Indianapolis, provided an array of highly clinically relevant tips to improve screening colonoscopy quality, which has been shown to reduce CRC mortality. Some of the basic concepts include using split-dose preparations and high-definition endoscopes, measuring and reporting adenoma detection rates, and using water immersion with carbon dioxide instead of air insufflation. Special attention was given to the diagnosis and removal of sessile lesions of the colon. Dr. Rex revealed many of his “tricks” to achieving high-quality colonoscopy, which include retroflexion to access polyps behind folds, using a stiff snare, and attaching a cap to the end of the colonoscope in order to facilitate visualization of polyps and assist in the mucosal resection of sessile lesions. Dr. Rex also presented data to support his recommendation to use “avulsion” with cold snare and forceps while limiting coagulative ablation for residual polyp tissue.
Finally, Rajeev Jain, MD, of Dallas presented the rapidly evolving area of reimbursement reform including the Medicare Access and CHIP Reauthorization Act (MACRA) that is driving payment away from fee-for-service and towards bundled payments, accountable care networks, and patient-centered medical homes. Key to this reform is the documentation and reporting of quality for procedural and cognitive patient encounters. There are limited performance measures specific to gastroenterology and hepatology, which currently include measures to both document appropriate CRC screening and reduce colonoscopy overuse, inflammatory bowel disease management, and hepatitis C management. However, there are many cost-cutting measures that can also be reported by gastroenterologists to fulfill these requirements. The Physician Quality Reporting System requires at least nine measures for at least 50% of Medicare patients in order to avoid penalties. It is not enough to track and document quality measures – results must also be reported through CMS-approved entities called qualified clinical data registries.
Dr. Jain described the movement toward payment bundles in which a single reimbursement is provided for services rendered by all providers and sites across a single episode of care. Screening colonoscopy was used as an example of how this could impact gastroenterology: a single payment would be provided for the preprocedure evaluation and education, the procedure itself (including endoscopy, anesthesia, pathology, facility), and postprocedure follow-up. Additional payments would not be provided for additional services such as repeating the colonoscopy because of a poor preparation or to treat postpolypectomy bleeding. Overall, health care reimbursement is moving to recognize value (quality/cost), reduce variation in care, and transfer more of the financial risk to health care providers and systems.
Dr. Inadomi, division of gastroenterology, department of medicine, University of Washington School of Medicine, department of health services, University of Washington School of Public Health, Seattle. He is on the clinical advisory committee for ChemImage and on the scientific advisory board for Epigenomics.
Colorectal cancer (CRC) screening has become a focal point of the practice of gastroenterology. Successful screening leads to a reduction in cancer mortality and is one of the most impactful means by which we improve population health.
Rick Boland, MD, of the Baylor Center of Gastrointestinal Cancer Research in Dallas reminded us at the annual Digestive Disease Week that carcinogenesis in colorectal cancer is a multistep process and described several pathways of which clinicians should be aware. Germline mutations (inherited) vs. somatic mutations (acquired) may be driver mutations that confer selection advantage and become targets for therapy in contrast to passenger mutations that are not mechanistic targets. Germline mutations should be considered when there is a family history of CRC, especially in a young patient, and are characteristic of familial adenomatous polyposis (APC), attenuated polyposis (MYH-MUTYH), and nonadenomatous polyposis syndromes such as Peutz-Jeghers (STK11).
Microsatellite instability is an alternative pathway to cancer. Hereditary nonpolyposis colorectal cancer (Lynch syndrome) is representative of this pathway with common abnormalities in mismatch repair genes such as MLH1, MSH2, MSH6, or PMS2. Lynch syndrome patients are BRAF and CIMP negative. This is in contrast to a more recent pathway to cancer that arises from sessile serrated polyps that also display microsatellite instability, but are BRAF and CIMP positive.
The clinical importance of understanding the pathway through which cancer develops in an individual patient is that depending on the mechanism of tumorigenesis, different treatment strategies can prevent or treat cancer. For example, exciting novel therapies are being developed for microsatellite unstable cancers using immune checkpoint inhibitors. Aspirin can reduce CRC mortality, especially tumors that overexpress COX2 or harbor PIK3CA mutations, and have demonstrated benefit even postoperatively in patients receiving surgical resection of CRC.
I gave a talk focused on current guidelines for reducing mortality among individuals at average risk for developing CRC. The U.S. Preventive Services Task Force updated their recommendations this year and chose to focus on highlighting the importance of CRC screening between the ages of 50 and 75 years, tailored screening for those between the ages of 76 and 85 years, and stopping screening after age 85 years. However, the statement does not recommend specific tests and instead lists competing strategies of annual fecal immunochemical test (FIT) or highly sensitive fecal occult blood test (FOBT) with or without flexible sigmoidoscopy every 10 years, flexible sigmoidoscopy every 5 years, colonoscopy every 10 years, CT colonography every 5 years, and FIT-DNA every 1 or 3 years. The FIT-DNA adds a separate FIT to a stool exam for KRAS mutations, NDRG4 and BMP3 methylation, and beta-actin. There are no studies to determine whether CRC mortality is reduced, but one study demonstrated a higher sensitivity for CRC with the combined FIT-DNA, compared with FIT alone, but a lower specificity. The FDA also recently approved a blood-based CRC screening test that detects circulating methylated septin 9 gene DNA. Septin 9 is a gene that codes for GTP-binding protein and acts as a tumor suppressor that can be inactivated by methylation.
Irrespective of which strategy is pursued, colonoscopy is the final common pathway. Quality is important because there remains a disappointing rate of CRC after colonoscopy. Prior work has demonstrated significant differences in the adenoma detection rate (ADR) between endoscopists in the same practice. A recent Kaiser study found that for every 1% increase in the ADR there is a 3% decrease in the rate of cancer developing after colonoscopy.
Disruptive technology is emerging that may displace gastroenterologists from primary endoscopic screening. A self-propelled disposable colonoscope (Aer-O-Scope) has been developed that uses pneumatic pressure to advance a tethered camera through the colonic lumen guided by a joystick. Sedation is not required and the device does not need manual advancement, facilitating use by nongastroenterologists.
Uri Ladabaum, MD, of Stanford (Calif.) University presented the clinical impact of screening for hereditary and familial CRC. Lynch syndrome is characterized by a family history of cancer in at least three individuals spanning at least two generations including one with early cancer development. He reminded us that Lynch syndrome cancers are not limited to CRC but also include uterine, ovarian, gastric, small intestinal, urinary, biliary, pancreatic, and neurologic tumors. Microsatellite instability is likely present, mismatch repair gene abnormalities should be sought, and screening should include colonoscopy every 1-2 years. Aspirin chemoprophylaxis should be recommended, as should prophylactic hysterectomy and oophorectomy among affected women due to the uterine and ovarian cancer risk.
Polyposis syndromes constitute a separate group of hereditary cancers that includes familial adenomatous polyposis (FAP) arising from defects in the APC gene that may present as florid or attenuated FAP, and MYH-associated polyposis. If a patient presents with more than 10 adenomas, a polyposis syndrome should be considered. More rare syndromes include Cowden, juvenile polyposis, and Peutz-Jeghers.
Douglas Rex, MD, of Indiana University, Indianapolis, provided an array of highly clinically relevant tips to improve screening colonoscopy quality, which has been shown to reduce CRC mortality. Some of the basic concepts include using split-dose preparations and high-definition endoscopes, measuring and reporting adenoma detection rates, and using water immersion with carbon dioxide instead of air insufflation. Special attention was given to the diagnosis and removal of sessile lesions of the colon. Dr. Rex revealed many of his “tricks” to achieving high-quality colonoscopy, which include retroflexion to access polyps behind folds, using a stiff snare, and attaching a cap to the end of the colonoscope in order to facilitate visualization of polyps and assist in the mucosal resection of sessile lesions. Dr. Rex also presented data to support his recommendation to use “avulsion” with cold snare and forceps while limiting coagulative ablation for residual polyp tissue.
Finally, Rajeev Jain, MD, of Dallas presented the rapidly evolving area of reimbursement reform including the Medicare Access and CHIP Reauthorization Act (MACRA) that is driving payment away from fee-for-service and towards bundled payments, accountable care networks, and patient-centered medical homes. Key to this reform is the documentation and reporting of quality for procedural and cognitive patient encounters. There are limited performance measures specific to gastroenterology and hepatology, which currently include measures to both document appropriate CRC screening and reduce colonoscopy overuse, inflammatory bowel disease management, and hepatitis C management. However, there are many cost-cutting measures that can also be reported by gastroenterologists to fulfill these requirements. The Physician Quality Reporting System requires at least nine measures for at least 50% of Medicare patients in order to avoid penalties. It is not enough to track and document quality measures – results must also be reported through CMS-approved entities called qualified clinical data registries.
Dr. Jain described the movement toward payment bundles in which a single reimbursement is provided for services rendered by all providers and sites across a single episode of care. Screening colonoscopy was used as an example of how this could impact gastroenterology: a single payment would be provided for the preprocedure evaluation and education, the procedure itself (including endoscopy, anesthesia, pathology, facility), and postprocedure follow-up. Additional payments would not be provided for additional services such as repeating the colonoscopy because of a poor preparation or to treat postpolypectomy bleeding. Overall, health care reimbursement is moving to recognize value (quality/cost), reduce variation in care, and transfer more of the financial risk to health care providers and systems.
Dr. Inadomi, division of gastroenterology, department of medicine, University of Washington School of Medicine, department of health services, University of Washington School of Public Health, Seattle. He is on the clinical advisory committee for ChemImage and on the scientific advisory board for Epigenomics.
AT DDW 2016

Abstracts Presented at the 2016 AVAHO Annual Meeting

Veterans’ keratinocyte carcinoma, actinic keratosis care cost $356 million in 2012
Almost 4% of the 5.9 million veterans treated by the Veterans Health Administration in 2012 had a diagnosis of keratinocyte carcinoma (KC) or actinic keratosis (AK), and their treatment cost $356 million, according to an analysis of VHA-provided or -contracted outpatient encounters.
Treatment costs per patient for KCs, also known as nonmelanoma skin cancers, were $1,456 for basal cell carcinoma (BCC), $1,326 for squamous cell carcinoma (SCC), $1,016 for unspecified, nongenital invasive KCs, $971 for squamous cell carcinoma in situ, and $906 for genital skin cancer (not shown on graph), reported Jean Yoon, PhD, of Veterans Affairs Palo Alto Health Care System, Menlo Park, Calif., and her associates (Dermatol Surg. 2016;42:1041-7).
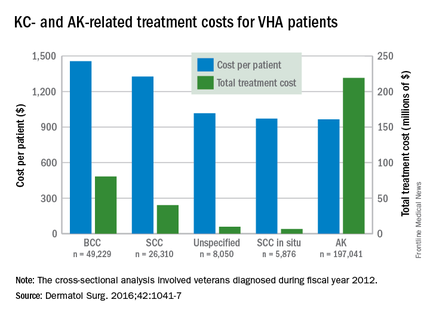
The VHA’s cost per patient for AK was relatively low – $965 per patient in 2012 – but the number of patients – 197,041 – was more than four times higher than any of the KCs. There were 49,229 veterans with BCC, 26,310 veterans with SCC, 8,050 veterans with unspecified KC, 5,876 veterans with SCC in situ, and 512 veterans with genital skin cancer, according to the analysis of administrative data on outpatient care and prescription drugs provided or paid by the VHA in fiscal year 2012. The total number of patients was 227,601, as some patients had more than one of the study diagnoses.
As a result of the high number of patients, actinic keratosis care totaled $219 million, compared with $80 million for BCC, $40 million for SCC, $9.6 million for nonspecified KC, $6.6 million for SCC in situ, and $582,000 for genital skin cancer, the investigators wrote.
The study was supported by a grant from the Department of Veterans Affairs. One of Dr. Yoon’s associates served as a consultant to several companies, but the remaining investigators had no conflicts to report.
Almost 4% of the 5.9 million veterans treated by the Veterans Health Administration in 2012 had a diagnosis of keratinocyte carcinoma (KC) or actinic keratosis (AK), and their treatment cost $356 million, according to an analysis of VHA-provided or -contracted outpatient encounters.
Treatment costs per patient for KCs, also known as nonmelanoma skin cancers, were $1,456 for basal cell carcinoma (BCC), $1,326 for squamous cell carcinoma (SCC), $1,016 for unspecified, nongenital invasive KCs, $971 for squamous cell carcinoma in situ, and $906 for genital skin cancer (not shown on graph), reported Jean Yoon, PhD, of Veterans Affairs Palo Alto Health Care System, Menlo Park, Calif., and her associates (Dermatol Surg. 2016;42:1041-7).
The VHA’s cost per patient for AK was relatively low – $965 per patient in 2012 – but the number of patients – 197,041 – was more than four times higher than any of the KCs. There were 49,229 veterans with BCC, 26,310 veterans with SCC, 8,050 veterans with unspecified KC, 5,876 veterans with SCC in situ, and 512 veterans with genital skin cancer, according to the analysis of administrative data on outpatient care and prescription drugs provided or paid by the VHA in fiscal year 2012. The total number of patients was 227,601, as some patients had more than one of the study diagnoses.
As a result of the high number of patients, actinic keratosis care totaled $219 million, compared with $80 million for BCC, $40 million for SCC, $9.6 million for nonspecified KC, $6.6 million for SCC in situ, and $582,000 for genital skin cancer, the investigators wrote.
The study was supported by a grant from the Department of Veterans Affairs. One of Dr. Yoon’s associates served as a consultant to several companies, but the remaining investigators had no conflicts to report.
Almost 4% of the 5.9 million veterans treated by the Veterans Health Administration in 2012 had a diagnosis of keratinocyte carcinoma (KC) or actinic keratosis (AK), and their treatment cost $356 million, according to an analysis of VHA-provided or -contracted outpatient encounters.
Treatment costs per patient for KCs, also known as nonmelanoma skin cancers, were $1,456 for basal cell carcinoma (BCC), $1,326 for squamous cell carcinoma (SCC), $1,016 for unspecified, nongenital invasive KCs, $971 for squamous cell carcinoma in situ, and $906 for genital skin cancer (not shown on graph), reported Jean Yoon, PhD, of Veterans Affairs Palo Alto Health Care System, Menlo Park, Calif., and her associates (Dermatol Surg. 2016;42:1041-7).
The VHA’s cost per patient for AK was relatively low – $965 per patient in 2012 – but the number of patients – 197,041 – was more than four times higher than any of the KCs. There were 49,229 veterans with BCC, 26,310 veterans with SCC, 8,050 veterans with unspecified KC, 5,876 veterans with SCC in situ, and 512 veterans with genital skin cancer, according to the analysis of administrative data on outpatient care and prescription drugs provided or paid by the VHA in fiscal year 2012. The total number of patients was 227,601, as some patients had more than one of the study diagnoses.
As a result of the high number of patients, actinic keratosis care totaled $219 million, compared with $80 million for BCC, $40 million for SCC, $9.6 million for nonspecified KC, $6.6 million for SCC in situ, and $582,000 for genital skin cancer, the investigators wrote.
The study was supported by a grant from the Department of Veterans Affairs. One of Dr. Yoon’s associates served as a consultant to several companies, but the remaining investigators had no conflicts to report.
FROM DERMATOLOGIC SURGERY