User login
Hydroxychloroquine dosage recommendations often ignored
Evidence continues to mount that some North American rheumatologists are not following practice recommendations for minimizing the retinal toxicity risk of patients on long-term hydroxychloroquine treatment.
An audit of 100 patients seen at any of nine Canadian rheumatology clinics during early 2016 showed that 30% of patients were not on appropriate weight-based hydroxychloroquine dosages, and 13% of patients on the drug had not received a baseline retinal assessment during their first year of treatment, Sahil Koppikar, MD, reported in a poster presented at the annual meeting of the Canadian Rheumatology Association in Ottawa in February.

In a second recently reported study, researchers from the Chicago area documented that roughly half of the 554 rheumatology patients on hydroxychloroquine (HCQ) in a regional health system and seen by an ophthalmologist during 2009-2016 received an excessive dosage of the drug (Ophthalmology. 2017 Jan 30. doi: 10.1016/j.ophtha.2016.12.021).
Although his study did not examine reasons for the compliance shortfall, Dr. Koppikar proposed some possible factors.
HCQ comes only as 200-mg tablets, and prescribing intermediate dosages can be a challenge (although veteran clinicians know that a safe and easy way to dial down a dosage is to have the patient periodically skip a dose). Also, “it is more convenient to prescribe 400 mg daily rather than calculate an exact dosage,” Dr. Koppikar said in an interview. In addition, rheumatologists may be unaware that the prevalence of retinopathy in patients on HCQ is fairly common (about 8% in one large recent study), assessment for risk factors that heighten sensitivity to the drug isn’t always done, and appointments for retinal screening can fall through the cracks.
“It behooves rheumatologists to adopt the [HCQ] recommendations of the American Academy of Ophthalmology [AAO] because there is more toxicity than we previously appreciated,” he added. A new version of the AAO’s recommendations came out in March 2016.
The Committee on Rheumatologic Care of the American College of Rheumatology (ACR) has regularly updated the ACR’s position statement on screening for HCQ retinopathy and appropriate dosages, with the most recent version out in August 2016. The August statement “is very similar” to the AAO’s 2016 recommendations, said Vinicius Domingues, MD, a member of the committee and an ACR spokesman for the revision. The ACR statement acknowledges and cites the AAO 2016 recommendations.

The ACR’s 2016 statement also does not fully endorse the AAO’s 2016 firm statement that “all patients using HCQ keep daily dosage less than 5.0 mg/kg real weight,” aside from “rare instances” when a higher dosage is needed to treat a “life-threatening disease.”
The ACR 2016 statement goes on to note that other authors have recommended a dosage of 6.5 mg/kg of actual body weight but capped at 400 mg/day and adjusted for renal insufficiency, and the ACR statement stops short of specifying which dosage strategy it recommends.
“The AAO recommendations are much more definitive and state more specifically what screening is recommended and what is a safe dosage,” commented Dr. Rosenbaum.
Dr. Domingues agreed that rheumatologist compliance with HCQ best practices has been spotty.
“In the past few years, more studies have used new ways to detect macular abnormalities and have identified a higher-than-expected incidence of maculopathy. Through lectures, CME, and articles, rheumatologists have received a tremendous amount of information with regard to screening and preventing retinal toxicity,” he said in an interview. “There are still gaps, and some rheumatologists still prescribe HCQ without taking into consideration the patient’s weight.”
That was a key finding in the poster presented at the Canadian Rheumatology Association by Dr. Koppikar and his collaborator on the study, Henry Averns, MD. The 100 patients assessed through the nine-clinic audit process averaged 58 years old, 81% were women, and patients had been taking HCQ for an average of just over 6 years, primarily for rheumatoid arthritis or systemic lupus erythematosus. Nearly two-thirds had a high risk for retinal toxicity. Based on the 2011 recommendations from the AAO and ACR, 17% of the patients were receiving an HCQ overdose that was more than 10% above the recommended dosage, and another 13% received a smaller overdose. If the 2016 dosage guidelines were applied, the extent of overdosing might be even greater, Dr. Koppikar said.
Dr. Koppikar and Dr. Averns said they believe that one way to address HCQ overdosing is by giving clinicians a dosing chart to easily find the right dosage for a patient’s weight. They have distributed these charts to the practices they audited and plan to do a follow-up audit to measure the effect of the intervention on HCQ prescribing.
Results from the initial clinical audit showed that “clinicians were not meeting standards, and we needed an intervention [a dosing chart] to implement a change,” Dr. Koppikar said. “Clinical audits are easy to implement, cost effective, and help improve patient care.”
Dr. Koppikar, Dr. Rosenbaum, Dr. Domingues, and Dr. Averns had no relevant financial disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
Evidence continues to mount that some North American rheumatologists are not following practice recommendations for minimizing the retinal toxicity risk of patients on long-term hydroxychloroquine treatment.
An audit of 100 patients seen at any of nine Canadian rheumatology clinics during early 2016 showed that 30% of patients were not on appropriate weight-based hydroxychloroquine dosages, and 13% of patients on the drug had not received a baseline retinal assessment during their first year of treatment, Sahil Koppikar, MD, reported in a poster presented at the annual meeting of the Canadian Rheumatology Association in Ottawa in February.
In a second recently reported study, researchers from the Chicago area documented that roughly half of the 554 rheumatology patients on hydroxychloroquine (HCQ) in a regional health system and seen by an ophthalmologist during 2009-2016 received an excessive dosage of the drug (Ophthalmology. 2017 Jan 30. doi: 10.1016/j.ophtha.2016.12.021).
Although his study did not examine reasons for the compliance shortfall, Dr. Koppikar proposed some possible factors.
HCQ comes only as 200-mg tablets, and prescribing intermediate dosages can be a challenge (although veteran clinicians know that a safe and easy way to dial down a dosage is to have the patient periodically skip a dose). Also, “it is more convenient to prescribe 400 mg daily rather than calculate an exact dosage,” Dr. Koppikar said in an interview. In addition, rheumatologists may be unaware that the prevalence of retinopathy in patients on HCQ is fairly common (about 8% in one large recent study), assessment for risk factors that heighten sensitivity to the drug isn’t always done, and appointments for retinal screening can fall through the cracks.
“It behooves rheumatologists to adopt the [HCQ] recommendations of the American Academy of Ophthalmology [AAO] because there is more toxicity than we previously appreciated,” he added. A new version of the AAO’s recommendations came out in March 2016.
The Committee on Rheumatologic Care of the American College of Rheumatology (ACR) has regularly updated the ACR’s position statement on screening for HCQ retinopathy and appropriate dosages, with the most recent version out in August 2016. The August statement “is very similar” to the AAO’s 2016 recommendations, said Vinicius Domingues, MD, a member of the committee and an ACR spokesman for the revision. The ACR statement acknowledges and cites the AAO 2016 recommendations.
The ACR’s 2016 statement also does not fully endorse the AAO’s 2016 firm statement that “all patients using HCQ keep daily dosage less than 5.0 mg/kg real weight,” aside from “rare instances” when a higher dosage is needed to treat a “life-threatening disease.”
The ACR 2016 statement goes on to note that other authors have recommended a dosage of 6.5 mg/kg of actual body weight but capped at 400 mg/day and adjusted for renal insufficiency, and the ACR statement stops short of specifying which dosage strategy it recommends.
“The AAO recommendations are much more definitive and state more specifically what screening is recommended and what is a safe dosage,” commented Dr. Rosenbaum.
Dr. Domingues agreed that rheumatologist compliance with HCQ best practices has been spotty.
“In the past few years, more studies have used new ways to detect macular abnormalities and have identified a higher-than-expected incidence of maculopathy. Through lectures, CME, and articles, rheumatologists have received a tremendous amount of information with regard to screening and preventing retinal toxicity,” he said in an interview. “There are still gaps, and some rheumatologists still prescribe HCQ without taking into consideration the patient’s weight.”
That was a key finding in the poster presented at the Canadian Rheumatology Association by Dr. Koppikar and his collaborator on the study, Henry Averns, MD. The 100 patients assessed through the nine-clinic audit process averaged 58 years old, 81% were women, and patients had been taking HCQ for an average of just over 6 years, primarily for rheumatoid arthritis or systemic lupus erythematosus. Nearly two-thirds had a high risk for retinal toxicity. Based on the 2011 recommendations from the AAO and ACR, 17% of the patients were receiving an HCQ overdose that was more than 10% above the recommended dosage, and another 13% received a smaller overdose. If the 2016 dosage guidelines were applied, the extent of overdosing might be even greater, Dr. Koppikar said.
Dr. Koppikar and Dr. Averns said they believe that one way to address HCQ overdosing is by giving clinicians a dosing chart to easily find the right dosage for a patient’s weight. They have distributed these charts to the practices they audited and plan to do a follow-up audit to measure the effect of the intervention on HCQ prescribing.
Results from the initial clinical audit showed that “clinicians were not meeting standards, and we needed an intervention [a dosing chart] to implement a change,” Dr. Koppikar said. “Clinical audits are easy to implement, cost effective, and help improve patient care.”
Dr. Koppikar, Dr. Rosenbaum, Dr. Domingues, and Dr. Averns had no relevant financial disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
Evidence continues to mount that some North American rheumatologists are not following practice recommendations for minimizing the retinal toxicity risk of patients on long-term hydroxychloroquine treatment.
An audit of 100 patients seen at any of nine Canadian rheumatology clinics during early 2016 showed that 30% of patients were not on appropriate weight-based hydroxychloroquine dosages, and 13% of patients on the drug had not received a baseline retinal assessment during their first year of treatment, Sahil Koppikar, MD, reported in a poster presented at the annual meeting of the Canadian Rheumatology Association in Ottawa in February.
In a second recently reported study, researchers from the Chicago area documented that roughly half of the 554 rheumatology patients on hydroxychloroquine (HCQ) in a regional health system and seen by an ophthalmologist during 2009-2016 received an excessive dosage of the drug (Ophthalmology. 2017 Jan 30. doi: 10.1016/j.ophtha.2016.12.021).
Although his study did not examine reasons for the compliance shortfall, Dr. Koppikar proposed some possible factors.
HCQ comes only as 200-mg tablets, and prescribing intermediate dosages can be a challenge (although veteran clinicians know that a safe and easy way to dial down a dosage is to have the patient periodically skip a dose). Also, “it is more convenient to prescribe 400 mg daily rather than calculate an exact dosage,” Dr. Koppikar said in an interview. In addition, rheumatologists may be unaware that the prevalence of retinopathy in patients on HCQ is fairly common (about 8% in one large recent study), assessment for risk factors that heighten sensitivity to the drug isn’t always done, and appointments for retinal screening can fall through the cracks.
“It behooves rheumatologists to adopt the [HCQ] recommendations of the American Academy of Ophthalmology [AAO] because there is more toxicity than we previously appreciated,” he added. A new version of the AAO’s recommendations came out in March 2016.
The Committee on Rheumatologic Care of the American College of Rheumatology (ACR) has regularly updated the ACR’s position statement on screening for HCQ retinopathy and appropriate dosages, with the most recent version out in August 2016. The August statement “is very similar” to the AAO’s 2016 recommendations, said Vinicius Domingues, MD, a member of the committee and an ACR spokesman for the revision. The ACR statement acknowledges and cites the AAO 2016 recommendations.
The ACR’s 2016 statement also does not fully endorse the AAO’s 2016 firm statement that “all patients using HCQ keep daily dosage less than 5.0 mg/kg real weight,” aside from “rare instances” when a higher dosage is needed to treat a “life-threatening disease.”
The ACR 2016 statement goes on to note that other authors have recommended a dosage of 6.5 mg/kg of actual body weight but capped at 400 mg/day and adjusted for renal insufficiency, and the ACR statement stops short of specifying which dosage strategy it recommends.
“The AAO recommendations are much more definitive and state more specifically what screening is recommended and what is a safe dosage,” commented Dr. Rosenbaum.
Dr. Domingues agreed that rheumatologist compliance with HCQ best practices has been spotty.
“In the past few years, more studies have used new ways to detect macular abnormalities and have identified a higher-than-expected incidence of maculopathy. Through lectures, CME, and articles, rheumatologists have received a tremendous amount of information with regard to screening and preventing retinal toxicity,” he said in an interview. “There are still gaps, and some rheumatologists still prescribe HCQ without taking into consideration the patient’s weight.”
That was a key finding in the poster presented at the Canadian Rheumatology Association by Dr. Koppikar and his collaborator on the study, Henry Averns, MD. The 100 patients assessed through the nine-clinic audit process averaged 58 years old, 81% were women, and patients had been taking HCQ for an average of just over 6 years, primarily for rheumatoid arthritis or systemic lupus erythematosus. Nearly two-thirds had a high risk for retinal toxicity. Based on the 2011 recommendations from the AAO and ACR, 17% of the patients were receiving an HCQ overdose that was more than 10% above the recommended dosage, and another 13% received a smaller overdose. If the 2016 dosage guidelines were applied, the extent of overdosing might be even greater, Dr. Koppikar said.
Dr. Koppikar and Dr. Averns said they believe that one way to address HCQ overdosing is by giving clinicians a dosing chart to easily find the right dosage for a patient’s weight. They have distributed these charts to the practices they audited and plan to do a follow-up audit to measure the effect of the intervention on HCQ prescribing.
Results from the initial clinical audit showed that “clinicians were not meeting standards, and we needed an intervention [a dosing chart] to implement a change,” Dr. Koppikar said. “Clinical audits are easy to implement, cost effective, and help improve patient care.”
Dr. Koppikar, Dr. Rosenbaum, Dr. Domingues, and Dr. Averns had no relevant financial disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
Key clinical point:
Major finding: A practice audit showed that 30% of rheumatology patients treated with hydroxychloroquine received an excessive dosage.
Data source: An audit of 100 rheumatology patients seen at any of nine rheumatology clinics in Eastern Ontario, Canada.
Disclosures: Dr. Koppikar, Dr. Rosenbaum, Dr. Domingues, and Dr. Averns had no relevant financial disclosures.
High Lead Levels From Old Bullet Fragments
Bullets and bullet fragments are not always removed if they don’t threaten the injured person’s life. But “retained” bullet fragments (RBFs) can lead to nonspecific symptoms of lead toxicity years later, such as, fatigue, abdominal pain, and memory loss.
Routine testing of adults with RBFs is infrequent, the CDC says. Usually, testing for blood levels of lead is done to monitor occupational exposure. But the number of people with RBFs who have toxic blood lead levels (BLLs) may be higher than thought. At BLLs ≥ 10 µg/dL, hypertension, kidney dysfunction, possible subclinical neurocognitive deficits, and adverse reproductive outcomes have been documented.
Related: The Long Legacy of Agent Orange
CDC researchers analyzed data from 41 states for 145,811 adults with elevated BLLs from all causes, reported by the Adult Blood Lead Epidemiology and Surveillance program from 2003 to 2012. Of those reported cases, 349 had levels ≥ 80 µg/dL. RBF-associated cases accounted for 0.3% of adults with elevated BLLs, but 4.9% of adults with BLLs ≥ 80 µg/dL. The maximum recorded RBF-associated BLL was 306 µg/dL. Further, RBF-associated cases were “overrepresented” among people with BLLs ≥ 80 µg/dL: 3.7%, compared with 0.2% of people without RBF-related elevated lead levels.
As of 2004, the researchers say, < 100 cases of lead toxicity caused by RBFs had been reported in the medical literature. They advise asking any patient who has elevated BLLs with an unknown lead exposure source about RBFs. A low index of suspicion could delay diagnosis or even contribute to an incorrect diagnosis.
Related: Cutting Down on Dialysis-Related Infections
Moreover, BLLs can fluctuate in people with RBFs, they note. A patient with a low BLL at the time of testing can have an increase in BLL and become symptomatic when RBFs migrate, such as into a joint space. The CDC researchers suggest baseline and intermittent BLL tests for people with a history of RBFs.
Bullets and bullet fragments are not always removed if they don’t threaten the injured person’s life. But “retained” bullet fragments (RBFs) can lead to nonspecific symptoms of lead toxicity years later, such as, fatigue, abdominal pain, and memory loss.
Routine testing of adults with RBFs is infrequent, the CDC says. Usually, testing for blood levels of lead is done to monitor occupational exposure. But the number of people with RBFs who have toxic blood lead levels (BLLs) may be higher than thought. At BLLs ≥ 10 µg/dL, hypertension, kidney dysfunction, possible subclinical neurocognitive deficits, and adverse reproductive outcomes have been documented.
Related: The Long Legacy of Agent Orange
CDC researchers analyzed data from 41 states for 145,811 adults with elevated BLLs from all causes, reported by the Adult Blood Lead Epidemiology and Surveillance program from 2003 to 2012. Of those reported cases, 349 had levels ≥ 80 µg/dL. RBF-associated cases accounted for 0.3% of adults with elevated BLLs, but 4.9% of adults with BLLs ≥ 80 µg/dL. The maximum recorded RBF-associated BLL was 306 µg/dL. Further, RBF-associated cases were “overrepresented” among people with BLLs ≥ 80 µg/dL: 3.7%, compared with 0.2% of people without RBF-related elevated lead levels.
As of 2004, the researchers say, < 100 cases of lead toxicity caused by RBFs had been reported in the medical literature. They advise asking any patient who has elevated BLLs with an unknown lead exposure source about RBFs. A low index of suspicion could delay diagnosis or even contribute to an incorrect diagnosis.
Related: Cutting Down on Dialysis-Related Infections
Moreover, BLLs can fluctuate in people with RBFs, they note. A patient with a low BLL at the time of testing can have an increase in BLL and become symptomatic when RBFs migrate, such as into a joint space. The CDC researchers suggest baseline and intermittent BLL tests for people with a history of RBFs.
Bullets and bullet fragments are not always removed if they don’t threaten the injured person’s life. But “retained” bullet fragments (RBFs) can lead to nonspecific symptoms of lead toxicity years later, such as, fatigue, abdominal pain, and memory loss.
Routine testing of adults with RBFs is infrequent, the CDC says. Usually, testing for blood levels of lead is done to monitor occupational exposure. But the number of people with RBFs who have toxic blood lead levels (BLLs) may be higher than thought. At BLLs ≥ 10 µg/dL, hypertension, kidney dysfunction, possible subclinical neurocognitive deficits, and adverse reproductive outcomes have been documented.
Related: The Long Legacy of Agent Orange
CDC researchers analyzed data from 41 states for 145,811 adults with elevated BLLs from all causes, reported by the Adult Blood Lead Epidemiology and Surveillance program from 2003 to 2012. Of those reported cases, 349 had levels ≥ 80 µg/dL. RBF-associated cases accounted for 0.3% of adults with elevated BLLs, but 4.9% of adults with BLLs ≥ 80 µg/dL. The maximum recorded RBF-associated BLL was 306 µg/dL. Further, RBF-associated cases were “overrepresented” among people with BLLs ≥ 80 µg/dL: 3.7%, compared with 0.2% of people without RBF-related elevated lead levels.
As of 2004, the researchers say, < 100 cases of lead toxicity caused by RBFs had been reported in the medical literature. They advise asking any patient who has elevated BLLs with an unknown lead exposure source about RBFs. A low index of suspicion could delay diagnosis or even contribute to an incorrect diagnosis.
Related: Cutting Down on Dialysis-Related Infections
Moreover, BLLs can fluctuate in people with RBFs, they note. A patient with a low BLL at the time of testing can have an increase in BLL and become symptomatic when RBFs migrate, such as into a joint space. The CDC researchers suggest baseline and intermittent BLL tests for people with a history of RBFs.
Survey: Patients largely unaware of docs’ industry ties

A survey of nearly 2000 people suggests many Americans may not know if their physician receives industry payments.
A majority of the individuals surveyed were treated by a doctor who received some form of industry payment in the last year, but few of the patients were aware of these payments.
In fact, more than half of the patients did not know that accepting industry payments is something physicians may do.
“The findings suggest that although physicians who accept industry payments are in the minority, they are caring for a very substantial portion of America’s adult patient population,” said Genevieve Pham-Kanter, PhD, of Drexel University’s Dornsife School of Public Health in Philadelphia, Pennsylvania.
She and her colleagues reported these findings in the Journal of General Internal Medicine.
Since 2013, the Sunshine Act, part of the Patient Protection and Affordable Care Act, has required pharmaceutical and medical device manufacturers to report gifts and payments they make to healthcare providers. This information is publicly available on the Centers for Medicare and Medicaid Services’ Open Payments website.
Dr Pham-Kanter and her colleagues conducted their survey shortly before the first release of the Open Payments data in September 2014. However, payment data were already publicly available in certain states, nationwide via the Pro Publica website, and through disclosures made by pharmaceutical and medical device firms themselves (who had been required to release payment information as part of legal settlements or did so voluntarily).
Survey results
The researchers conducted their online survey in 3542 adults. Respondents were asked whether they were aware of industry payments and to name the physicians they had seen most frequently in the previous year.
Physician names were then linked to the Open Payment data to ascertain how often patients saw doctors who accepted industry payments.
There were 1987 respondents who could be matched to a specific physician. Sixty-five percent of these individuals had visited a physician who accepted an industry payment in the last 12 months, but only 5% of the respondents actually knew if their doctors received industry payments.
Forty-five percent of respondents said they knew about the practice of doctors receiving industry payments, and 12% said information about such payments was publicly available.
“These findings tell us that if you thought that your doctor was not receiving any money from industry, you’re most likely mistaken,” Dr Pham-Kanter said. “Patients should be aware of the incentives that their physicians face that may lead them to not always act in their patients’ best interest.”
In Open Payments, all physicians averaged $193 in yearly payments and gifts. But when measuring only the doctors visited by participants in the survey, the median payment amount over the last year was $510, more than 2.5 times the US average.
“We may be lulled into thinking this isn’t a big deal because the average payment amount across all doctors is low,” Dr Pham-Kanter said. “But that obscures the fact that most people are seeing doctors who receive the largest payments.”
“Drug companies have long known that even small gifts to physicians can be influential,” added study author Michelle Mello, JD, PhD, of Stanford University School of Medicine and Stanford Law School in California. “And research validates the notion that they tend to induce feelings of reciprocity.” ![]()
A survey of nearly 2000 people suggests many Americans may not know if their physician receives industry payments.
A majority of the individuals surveyed were treated by a doctor who received some form of industry payment in the last year, but few of the patients were aware of these payments.
In fact, more than half of the patients did not know that accepting industry payments is something physicians may do.
“The findings suggest that although physicians who accept industry payments are in the minority, they are caring for a very substantial portion of America’s adult patient population,” said Genevieve Pham-Kanter, PhD, of Drexel University’s Dornsife School of Public Health in Philadelphia, Pennsylvania.
She and her colleagues reported these findings in the Journal of General Internal Medicine.
Since 2013, the Sunshine Act, part of the Patient Protection and Affordable Care Act, has required pharmaceutical and medical device manufacturers to report gifts and payments they make to healthcare providers. This information is publicly available on the Centers for Medicare and Medicaid Services’ Open Payments website.
Dr Pham-Kanter and her colleagues conducted their survey shortly before the first release of the Open Payments data in September 2014. However, payment data were already publicly available in certain states, nationwide via the Pro Publica website, and through disclosures made by pharmaceutical and medical device firms themselves (who had been required to release payment information as part of legal settlements or did so voluntarily).
Survey results
The researchers conducted their online survey in 3542 adults. Respondents were asked whether they were aware of industry payments and to name the physicians they had seen most frequently in the previous year.
Physician names were then linked to the Open Payment data to ascertain how often patients saw doctors who accepted industry payments.
There were 1987 respondents who could be matched to a specific physician. Sixty-five percent of these individuals had visited a physician who accepted an industry payment in the last 12 months, but only 5% of the respondents actually knew if their doctors received industry payments.
Forty-five percent of respondents said they knew about the practice of doctors receiving industry payments, and 12% said information about such payments was publicly available.
“These findings tell us that if you thought that your doctor was not receiving any money from industry, you’re most likely mistaken,” Dr Pham-Kanter said. “Patients should be aware of the incentives that their physicians face that may lead them to not always act in their patients’ best interest.”
In Open Payments, all physicians averaged $193 in yearly payments and gifts. But when measuring only the doctors visited by participants in the survey, the median payment amount over the last year was $510, more than 2.5 times the US average.
“We may be lulled into thinking this isn’t a big deal because the average payment amount across all doctors is low,” Dr Pham-Kanter said. “But that obscures the fact that most people are seeing doctors who receive the largest payments.”
“Drug companies have long known that even small gifts to physicians can be influential,” added study author Michelle Mello, JD, PhD, of Stanford University School of Medicine and Stanford Law School in California. “And research validates the notion that they tend to induce feelings of reciprocity.” ![]()
A survey of nearly 2000 people suggests many Americans may not know if their physician receives industry payments.
A majority of the individuals surveyed were treated by a doctor who received some form of industry payment in the last year, but few of the patients were aware of these payments.
In fact, more than half of the patients did not know that accepting industry payments is something physicians may do.
“The findings suggest that although physicians who accept industry payments are in the minority, they are caring for a very substantial portion of America’s adult patient population,” said Genevieve Pham-Kanter, PhD, of Drexel University’s Dornsife School of Public Health in Philadelphia, Pennsylvania.
She and her colleagues reported these findings in the Journal of General Internal Medicine.
Since 2013, the Sunshine Act, part of the Patient Protection and Affordable Care Act, has required pharmaceutical and medical device manufacturers to report gifts and payments they make to healthcare providers. This information is publicly available on the Centers for Medicare and Medicaid Services’ Open Payments website.
Dr Pham-Kanter and her colleagues conducted their survey shortly before the first release of the Open Payments data in September 2014. However, payment data were already publicly available in certain states, nationwide via the Pro Publica website, and through disclosures made by pharmaceutical and medical device firms themselves (who had been required to release payment information as part of legal settlements or did so voluntarily).
Survey results
The researchers conducted their online survey in 3542 adults. Respondents were asked whether they were aware of industry payments and to name the physicians they had seen most frequently in the previous year.
Physician names were then linked to the Open Payment data to ascertain how often patients saw doctors who accepted industry payments.
There were 1987 respondents who could be matched to a specific physician. Sixty-five percent of these individuals had visited a physician who accepted an industry payment in the last 12 months, but only 5% of the respondents actually knew if their doctors received industry payments.
Forty-five percent of respondents said they knew about the practice of doctors receiving industry payments, and 12% said information about such payments was publicly available.
“These findings tell us that if you thought that your doctor was not receiving any money from industry, you’re most likely mistaken,” Dr Pham-Kanter said. “Patients should be aware of the incentives that their physicians face that may lead them to not always act in their patients’ best interest.”
In Open Payments, all physicians averaged $193 in yearly payments and gifts. But when measuring only the doctors visited by participants in the survey, the median payment amount over the last year was $510, more than 2.5 times the US average.
“We may be lulled into thinking this isn’t a big deal because the average payment amount across all doctors is low,” Dr Pham-Kanter said. “But that obscures the fact that most people are seeing doctors who receive the largest payments.”
“Drug companies have long known that even small gifts to physicians can be influential,” added study author Michelle Mello, JD, PhD, of Stanford University School of Medicine and Stanford Law School in California. “And research validates the notion that they tend to induce feelings of reciprocity.” ![]()
Genetic variants linked to HSCT outcomes in ALL

ORLANDO, FL—Results of a genome-wide association study suggest that several genetic variants are associated with outcomes of allogeneic hematopoietic stem cell transplant (HSCT) in patients with acute lymphoblastic leukemia (ALL).
Investigators identified several single-nucleotide polymorphisms (SNPs) in ALL patients and their unrelated donors that were associated with disease-related death or progression-free survival (PFS) within 1 year of HSCT.
“We believe that these findings will lead to a better understanding of the biology of this disease,” said investigator Theresa Hahn, PhD, of Roswell Park Cancer Institute in Buffalo, New York.
“Additionally, we expect that this work will eventually help clinical teams to identify unrelated donors with genotypes that yield better survival in transplant patients and enhance the chances for successful blood and marrow transplants.”
Dr Hahn presented this work as a “Best Abstract” at the 2017 BMT Tandem Meetings (abstract 1).
For this study, she and her colleagues analyzed data on patients treated at more than 150 US transplant centers between 2000 and 2011. The investigators evaluated data on more than 3000 patients with acute leukemias or myelodysplastic syndromes, but Dr Hahn only presented findings in the ALL patients and their donors.
The patients and donors were divided into 2 cohorts. Cohort 1 included 483 ALL patients who underwent HSCT from 2000 to 2008 and 466 unrelated donors who were a 10/10 HLA match for the patients.
Cohort 2 included 94 ALL patients who received a transplant from a 10/10 HLA-matched donor between 2009 and 2011 or from an 8/8 HLA-matched donor between 2000 and 2011. There were 92 donors in this cohort.
The investigators sequenced blood samples from the recipients and donors to identify SNPs. The SNPs were then measured for association with disease-related death and PFS using Cox proportional hazards models adjusted for recipient age, disease status at HSCT (early, intermediate, or advanced), graft source (blood or marrow), and year of transplant.
SNPs in donors
The top 2 SNPs in donors that were associated with a significant increase in disease-related death were:
- rs79503405 in LRP2 on chromosome 2.
- rs77618918 in ASIC2 on chromosome 17.
Dr Hahn noted that rs79503405 is in complete linkage disequilibrium (r2=1.0) with a genotyped missense variant (rs17848149) and a synonymous coding variant (rs35114151) in LRP2.
She also pointed out that the other top SNP (rs77618918) associated with disease-related death is not in linkage disequilibrium with other SNPs of functional importance, so the significance of this SNP is unknown.
There were no SNPs in donors that were significantly associated with PFS.
SNPs in recipients
In HSCT recipients, there were 3 linked variants in NRG1 on chromosome 8 (rs79853417, rs6990973, and rs145488394) that were significantly associated with disease-related death.
Another SNP (rs60640657) on chromosome 2 (CTNNA3/LOC101928961/LRRTM3) was also significantly associated with ALL-related death.
In addition, Dr Hahn and her colleagues found that 1 region in recipient genomes contains multiple variants (rs113263921 and others) associated with PFS. The SNPs are located on chromosome 3 in MLH1 and TRANK1.
“The donor and recipient genetic variants contributed independently to death due to ALL,” Dr Hahn said in closing. “Genetic variants for PFS do not overlap with death due to ALL, and this is probably due to the inclusion of both non-fatal disease progression as well as transplant-related mortality in the definition of PFS.”
“Constitutional genetic variants in recipients and donors increase the risk of death due to ALL, and they warrant further study into the impact of these genes on disease and transplant-related biology.” ![]()
ORLANDO, FL—Results of a genome-wide association study suggest that several genetic variants are associated with outcomes of allogeneic hematopoietic stem cell transplant (HSCT) in patients with acute lymphoblastic leukemia (ALL).
Investigators identified several single-nucleotide polymorphisms (SNPs) in ALL patients and their unrelated donors that were associated with disease-related death or progression-free survival (PFS) within 1 year of HSCT.
“We believe that these findings will lead to a better understanding of the biology of this disease,” said investigator Theresa Hahn, PhD, of Roswell Park Cancer Institute in Buffalo, New York.
“Additionally, we expect that this work will eventually help clinical teams to identify unrelated donors with genotypes that yield better survival in transplant patients and enhance the chances for successful blood and marrow transplants.”
Dr Hahn presented this work as a “Best Abstract” at the 2017 BMT Tandem Meetings (abstract 1).
For this study, she and her colleagues analyzed data on patients treated at more than 150 US transplant centers between 2000 and 2011. The investigators evaluated data on more than 3000 patients with acute leukemias or myelodysplastic syndromes, but Dr Hahn only presented findings in the ALL patients and their donors.
The patients and donors were divided into 2 cohorts. Cohort 1 included 483 ALL patients who underwent HSCT from 2000 to 2008 and 466 unrelated donors who were a 10/10 HLA match for the patients.
Cohort 2 included 94 ALL patients who received a transplant from a 10/10 HLA-matched donor between 2009 and 2011 or from an 8/8 HLA-matched donor between 2000 and 2011. There were 92 donors in this cohort.
The investigators sequenced blood samples from the recipients and donors to identify SNPs. The SNPs were then measured for association with disease-related death and PFS using Cox proportional hazards models adjusted for recipient age, disease status at HSCT (early, intermediate, or advanced), graft source (blood or marrow), and year of transplant.
SNPs in donors
The top 2 SNPs in donors that were associated with a significant increase in disease-related death were:
- rs79503405 in LRP2 on chromosome 2.
- rs77618918 in ASIC2 on chromosome 17.
Dr Hahn noted that rs79503405 is in complete linkage disequilibrium (r2=1.0) with a genotyped missense variant (rs17848149) and a synonymous coding variant (rs35114151) in LRP2.
She also pointed out that the other top SNP (rs77618918) associated with disease-related death is not in linkage disequilibrium with other SNPs of functional importance, so the significance of this SNP is unknown.
There were no SNPs in donors that were significantly associated with PFS.
SNPs in recipients
In HSCT recipients, there were 3 linked variants in NRG1 on chromosome 8 (rs79853417, rs6990973, and rs145488394) that were significantly associated with disease-related death.
Another SNP (rs60640657) on chromosome 2 (CTNNA3/LOC101928961/LRRTM3) was also significantly associated with ALL-related death.
In addition, Dr Hahn and her colleagues found that 1 region in recipient genomes contains multiple variants (rs113263921 and others) associated with PFS. The SNPs are located on chromosome 3 in MLH1 and TRANK1.
“The donor and recipient genetic variants contributed independently to death due to ALL,” Dr Hahn said in closing. “Genetic variants for PFS do not overlap with death due to ALL, and this is probably due to the inclusion of both non-fatal disease progression as well as transplant-related mortality in the definition of PFS.”
“Constitutional genetic variants in recipients and donors increase the risk of death due to ALL, and they warrant further study into the impact of these genes on disease and transplant-related biology.” ![]()
ORLANDO, FL—Results of a genome-wide association study suggest that several genetic variants are associated with outcomes of allogeneic hematopoietic stem cell transplant (HSCT) in patients with acute lymphoblastic leukemia (ALL).
Investigators identified several single-nucleotide polymorphisms (SNPs) in ALL patients and their unrelated donors that were associated with disease-related death or progression-free survival (PFS) within 1 year of HSCT.
“We believe that these findings will lead to a better understanding of the biology of this disease,” said investigator Theresa Hahn, PhD, of Roswell Park Cancer Institute in Buffalo, New York.
“Additionally, we expect that this work will eventually help clinical teams to identify unrelated donors with genotypes that yield better survival in transplant patients and enhance the chances for successful blood and marrow transplants.”
Dr Hahn presented this work as a “Best Abstract” at the 2017 BMT Tandem Meetings (abstract 1).
For this study, she and her colleagues analyzed data on patients treated at more than 150 US transplant centers between 2000 and 2011. The investigators evaluated data on more than 3000 patients with acute leukemias or myelodysplastic syndromes, but Dr Hahn only presented findings in the ALL patients and their donors.
The patients and donors were divided into 2 cohorts. Cohort 1 included 483 ALL patients who underwent HSCT from 2000 to 2008 and 466 unrelated donors who were a 10/10 HLA match for the patients.
Cohort 2 included 94 ALL patients who received a transplant from a 10/10 HLA-matched donor between 2009 and 2011 or from an 8/8 HLA-matched donor between 2000 and 2011. There were 92 donors in this cohort.
The investigators sequenced blood samples from the recipients and donors to identify SNPs. The SNPs were then measured for association with disease-related death and PFS using Cox proportional hazards models adjusted for recipient age, disease status at HSCT (early, intermediate, or advanced), graft source (blood or marrow), and year of transplant.
SNPs in donors
The top 2 SNPs in donors that were associated with a significant increase in disease-related death were:
- rs79503405 in LRP2 on chromosome 2.
- rs77618918 in ASIC2 on chromosome 17.
Dr Hahn noted that rs79503405 is in complete linkage disequilibrium (r2=1.0) with a genotyped missense variant (rs17848149) and a synonymous coding variant (rs35114151) in LRP2.
She also pointed out that the other top SNP (rs77618918) associated with disease-related death is not in linkage disequilibrium with other SNPs of functional importance, so the significance of this SNP is unknown.
There were no SNPs in donors that were significantly associated with PFS.
SNPs in recipients
In HSCT recipients, there were 3 linked variants in NRG1 on chromosome 8 (rs79853417, rs6990973, and rs145488394) that were significantly associated with disease-related death.
Another SNP (rs60640657) on chromosome 2 (CTNNA3/LOC101928961/LRRTM3) was also significantly associated with ALL-related death.
In addition, Dr Hahn and her colleagues found that 1 region in recipient genomes contains multiple variants (rs113263921 and others) associated with PFS. The SNPs are located on chromosome 3 in MLH1 and TRANK1.
“The donor and recipient genetic variants contributed independently to death due to ALL,” Dr Hahn said in closing. “Genetic variants for PFS do not overlap with death due to ALL, and this is probably due to the inclusion of both non-fatal disease progression as well as transplant-related mortality in the definition of PFS.”
“Constitutional genetic variants in recipients and donors increase the risk of death due to ALL, and they warrant further study into the impact of these genes on disease and transplant-related biology.” ![]()
Combo prolongs OS in relapsed/refractory MM

NEW DEHLI—A 2-drug combination previously shown to prolong progression-free survival (PFS) in patients with relapsed/refractory multiple myeloma (MM) can prolong overall survival (OS) as well, according to researchers.
Updated results of the phase 3 ENDEAVOR trial showed that patients who received treatment with carfilzomib and dexamethasone had a 7.6-month benefit in median OS when compared to patients who received bortezomib and dexamethasone.
Previous results from this trial showed a 9.3-month benefit in median PFS with carfilzomib and dexamethasone.
“Based on these data, we now know that [carfilzomib] not only significantly extended progression-free survival compared to [bortezomib] but also overall survival, making it a clinically meaningful advance in the treatment of relapsed or refractory multiple myeloma,” said Meletios A. Dimopoulos, MD, of the University of Athens in Greece.
Dr Dimopoulos presented OS results from ENDEAVOR at the 16th International Myeloma Workshop. The trial was funded by Onyx Pharmaceuticals, Inc., a subsidiary of Amgen.
ENDEAVOR included 929 MM patients who had received 1 to 3 prior treatment regimens. The patients were randomized to receive carfilzomib and low-dose dexamethasone (n=464) or bortezomib and low-dose dexamethasone (n=465) until disease progression.
Baseline characteristics were similar between the treatment arms.
Detailed patient and treatment characteristics, as well as response and PFS data, have been previously reported.
OS and safety
The median OS was 47.6 months in the carfilzomib arm and 40.0 months in the bortezomib arm. All-cause mortality was significantly lower with the carfilzomib combination than the bortezomib combination (hazard ratio [HR]=0.791, 1-sided P=0.0100).
Researchers said there was an OS benefit with the carfilzomib combination whether or not patients received prior treatment with bortezomib and regardless of patients’ age, ECOG performance status at baseline, cytogenetic risk group, or the number of previous therapies they received.
The HR was 0.75 (carfilzomib vs bortezomib) for patients with no prior bortezomib and 0.84 for patients who received prior bortezomib. The HR was 0.85 for patients younger than 65, 0.71 for those ages 65 to 74, and 0.84 for patients age 75 and older.
The HR was 0.81 for patients with an ECOG status of 0, 0.80 for those with a status of 1, and 0.50 for those with a status of 2. The HR was 0.83 for patients with high-risk cytogenetics and 0.85 for those with standard-risk cytogenetics.
The HR was 0.83 for patients with 1 prior line of therapy and 0.76 for those with 2 to 3 prior lines of therapy.
The researchers said safety results in this analysis were comparable with previously reported results. The incidence of grade 3 or higher adverse events was 81.4% in the carfilzomib arm and 71.1% in the bortezomib arm.
The most common adverse events of any grade (in the carfilzomib and bortezomib arms, respectively) were anemia (42.5% and 28.3%), diarrhea (36.3% and 40.6%), pyrexia (32.4% and 15.4%), dyspnea (32.2% and 13.6%), fatigue (32.2% and 30.7%), and hypertension (32.2% and 9.9%). ![]()
NEW DEHLI—A 2-drug combination previously shown to prolong progression-free survival (PFS) in patients with relapsed/refractory multiple myeloma (MM) can prolong overall survival (OS) as well, according to researchers.
Updated results of the phase 3 ENDEAVOR trial showed that patients who received treatment with carfilzomib and dexamethasone had a 7.6-month benefit in median OS when compared to patients who received bortezomib and dexamethasone.
Previous results from this trial showed a 9.3-month benefit in median PFS with carfilzomib and dexamethasone.
“Based on these data, we now know that [carfilzomib] not only significantly extended progression-free survival compared to [bortezomib] but also overall survival, making it a clinically meaningful advance in the treatment of relapsed or refractory multiple myeloma,” said Meletios A. Dimopoulos, MD, of the University of Athens in Greece.
Dr Dimopoulos presented OS results from ENDEAVOR at the 16th International Myeloma Workshop. The trial was funded by Onyx Pharmaceuticals, Inc., a subsidiary of Amgen.
ENDEAVOR included 929 MM patients who had received 1 to 3 prior treatment regimens. The patients were randomized to receive carfilzomib and low-dose dexamethasone (n=464) or bortezomib and low-dose dexamethasone (n=465) until disease progression.
Baseline characteristics were similar between the treatment arms.
Detailed patient and treatment characteristics, as well as response and PFS data, have been previously reported.
OS and safety
The median OS was 47.6 months in the carfilzomib arm and 40.0 months in the bortezomib arm. All-cause mortality was significantly lower with the carfilzomib combination than the bortezomib combination (hazard ratio [HR]=0.791, 1-sided P=0.0100).
Researchers said there was an OS benefit with the carfilzomib combination whether or not patients received prior treatment with bortezomib and regardless of patients’ age, ECOG performance status at baseline, cytogenetic risk group, or the number of previous therapies they received.
The HR was 0.75 (carfilzomib vs bortezomib) for patients with no prior bortezomib and 0.84 for patients who received prior bortezomib. The HR was 0.85 for patients younger than 65, 0.71 for those ages 65 to 74, and 0.84 for patients age 75 and older.
The HR was 0.81 for patients with an ECOG status of 0, 0.80 for those with a status of 1, and 0.50 for those with a status of 2. The HR was 0.83 for patients with high-risk cytogenetics and 0.85 for those with standard-risk cytogenetics.
The HR was 0.83 for patients with 1 prior line of therapy and 0.76 for those with 2 to 3 prior lines of therapy.
The researchers said safety results in this analysis were comparable with previously reported results. The incidence of grade 3 or higher adverse events was 81.4% in the carfilzomib arm and 71.1% in the bortezomib arm.
The most common adverse events of any grade (in the carfilzomib and bortezomib arms, respectively) were anemia (42.5% and 28.3%), diarrhea (36.3% and 40.6%), pyrexia (32.4% and 15.4%), dyspnea (32.2% and 13.6%), fatigue (32.2% and 30.7%), and hypertension (32.2% and 9.9%). ![]()
NEW DEHLI—A 2-drug combination previously shown to prolong progression-free survival (PFS) in patients with relapsed/refractory multiple myeloma (MM) can prolong overall survival (OS) as well, according to researchers.
Updated results of the phase 3 ENDEAVOR trial showed that patients who received treatment with carfilzomib and dexamethasone had a 7.6-month benefit in median OS when compared to patients who received bortezomib and dexamethasone.
Previous results from this trial showed a 9.3-month benefit in median PFS with carfilzomib and dexamethasone.
“Based on these data, we now know that [carfilzomib] not only significantly extended progression-free survival compared to [bortezomib] but also overall survival, making it a clinically meaningful advance in the treatment of relapsed or refractory multiple myeloma,” said Meletios A. Dimopoulos, MD, of the University of Athens in Greece.
Dr Dimopoulos presented OS results from ENDEAVOR at the 16th International Myeloma Workshop. The trial was funded by Onyx Pharmaceuticals, Inc., a subsidiary of Amgen.
ENDEAVOR included 929 MM patients who had received 1 to 3 prior treatment regimens. The patients were randomized to receive carfilzomib and low-dose dexamethasone (n=464) or bortezomib and low-dose dexamethasone (n=465) until disease progression.
Baseline characteristics were similar between the treatment arms.
Detailed patient and treatment characteristics, as well as response and PFS data, have been previously reported.
OS and safety
The median OS was 47.6 months in the carfilzomib arm and 40.0 months in the bortezomib arm. All-cause mortality was significantly lower with the carfilzomib combination than the bortezomib combination (hazard ratio [HR]=0.791, 1-sided P=0.0100).
Researchers said there was an OS benefit with the carfilzomib combination whether or not patients received prior treatment with bortezomib and regardless of patients’ age, ECOG performance status at baseline, cytogenetic risk group, or the number of previous therapies they received.
The HR was 0.75 (carfilzomib vs bortezomib) for patients with no prior bortezomib and 0.84 for patients who received prior bortezomib. The HR was 0.85 for patients younger than 65, 0.71 for those ages 65 to 74, and 0.84 for patients age 75 and older.
The HR was 0.81 for patients with an ECOG status of 0, 0.80 for those with a status of 1, and 0.50 for those with a status of 2. The HR was 0.83 for patients with high-risk cytogenetics and 0.85 for those with standard-risk cytogenetics.
The HR was 0.83 for patients with 1 prior line of therapy and 0.76 for those with 2 to 3 prior lines of therapy.
The researchers said safety results in this analysis were comparable with previously reported results. The incidence of grade 3 or higher adverse events was 81.4% in the carfilzomib arm and 71.1% in the bortezomib arm.
The most common adverse events of any grade (in the carfilzomib and bortezomib arms, respectively) were anemia (42.5% and 28.3%), diarrhea (36.3% and 40.6%), pyrexia (32.4% and 15.4%), dyspnea (32.2% and 13.6%), fatigue (32.2% and 30.7%), and hypertension (32.2% and 9.9%). ![]()
Chlormethine gel approved to treat mycosis fungoides

The European Commission has granted marketing authorization for chlormethine gel (Ledaga®) as a treatment for adults with mycosis fungoides (MF), but the product is not expected to be available until next year.
Ledaga is a hybrid medicine of Caryolysine, which has been approved for use in the European Union since 1946.
Hybrid medicines have a different strength, are administered differently, or have a different indication from the reference medicine.
Ledaga contains the same active substance as Caryolysine—chlormethine, a bifunctional alkylating agent that inhibits rapidly proliferating cells—but Ledaga is a gel intended for cutaneous use.
Actelion Pharmaceuticals Ltd, the company developing Ledaga, has agreed to fulfill a list of post-approval measures for the product proposed by the European Medicines Agency’s Committee for Medicinal Products for Human Use.
Subject to fulfilling the agreed commitments and achieving market access in various countries, a potential first European launch of Ledaga is not expected before January 2018. When it is launched, Ledaga will be available as a 160 μg/g gel.
Phase 2 study
The authorization of hybrid medicines depends partly on the results of tests on the reference medicine and partly on new data from clinical trials.
The marketing authorization for Ledaga is based, in part, on results of a multicenter, randomized, observer-blinded, active-controlled study of patients with stage I and IIA MF. Results from this phase 2 study were published in JAMA Dermatology.
The study enrolled 260 MF patients who were randomized 1:1 to receive topical treatment with 0.02% chlormethine gel (Ledaga) or compounded control—0.02% chlormethine compounded in Aquaphor® ointment—once daily for up to 12 months.
A response was defined as at least a 50% improvement in the baseline Composite Assessment of Index Lesion Severity score.
In the intent-to-treat population, 59% (76/130) of patients who received Ledaga achieved a clinical response, compared to 48% (62/130) of patients treated with the compounded control. The rate of complete response was 14% (n=18) and 12% (n=15), respectively.
Patients who were treated for at least 6 months were included in the efficacy-evaluable population. In this population, 77% (69/90) of patients who received Ledaga achieved a clinical response, compared to 59% (56/95) of patients treated with the compounded control. The rate of complete response was 19% (n=17) and 15% (n=14), respectively.
Reductions in mean lesion severity were seen as early as 4 weeks into the study, with further reductions observed with continuing therapy. The time to first confirmed response favored Ledaga.
The most frequent adverse reactions reported with Ledaga were skin-related—dermatitis (55%; eg, skin irritation, erythema, rash, urticaria, skin-burning sensation, skin pain), pruritus (20%), skin infections (12%), skin ulceration and blistering (6%), and skin hyperpigmentation (6%).
No systemic absorption of chlormethine was detected with treatment. ![]()
The European Commission has granted marketing authorization for chlormethine gel (Ledaga®) as a treatment for adults with mycosis fungoides (MF), but the product is not expected to be available until next year.
Ledaga is a hybrid medicine of Caryolysine, which has been approved for use in the European Union since 1946.
Hybrid medicines have a different strength, are administered differently, or have a different indication from the reference medicine.
Ledaga contains the same active substance as Caryolysine—chlormethine, a bifunctional alkylating agent that inhibits rapidly proliferating cells—but Ledaga is a gel intended for cutaneous use.
Actelion Pharmaceuticals Ltd, the company developing Ledaga, has agreed to fulfill a list of post-approval measures for the product proposed by the European Medicines Agency’s Committee for Medicinal Products for Human Use.
Subject to fulfilling the agreed commitments and achieving market access in various countries, a potential first European launch of Ledaga is not expected before January 2018. When it is launched, Ledaga will be available as a 160 μg/g gel.
Phase 2 study
The authorization of hybrid medicines depends partly on the results of tests on the reference medicine and partly on new data from clinical trials.
The marketing authorization for Ledaga is based, in part, on results of a multicenter, randomized, observer-blinded, active-controlled study of patients with stage I and IIA MF. Results from this phase 2 study were published in JAMA Dermatology.
The study enrolled 260 MF patients who were randomized 1:1 to receive topical treatment with 0.02% chlormethine gel (Ledaga) or compounded control—0.02% chlormethine compounded in Aquaphor® ointment—once daily for up to 12 months.
A response was defined as at least a 50% improvement in the baseline Composite Assessment of Index Lesion Severity score.
In the intent-to-treat population, 59% (76/130) of patients who received Ledaga achieved a clinical response, compared to 48% (62/130) of patients treated with the compounded control. The rate of complete response was 14% (n=18) and 12% (n=15), respectively.
Patients who were treated for at least 6 months were included in the efficacy-evaluable population. In this population, 77% (69/90) of patients who received Ledaga achieved a clinical response, compared to 59% (56/95) of patients treated with the compounded control. The rate of complete response was 19% (n=17) and 15% (n=14), respectively.
Reductions in mean lesion severity were seen as early as 4 weeks into the study, with further reductions observed with continuing therapy. The time to first confirmed response favored Ledaga.
The most frequent adverse reactions reported with Ledaga were skin-related—dermatitis (55%; eg, skin irritation, erythema, rash, urticaria, skin-burning sensation, skin pain), pruritus (20%), skin infections (12%), skin ulceration and blistering (6%), and skin hyperpigmentation (6%).
No systemic absorption of chlormethine was detected with treatment. ![]()
The European Commission has granted marketing authorization for chlormethine gel (Ledaga®) as a treatment for adults with mycosis fungoides (MF), but the product is not expected to be available until next year.
Ledaga is a hybrid medicine of Caryolysine, which has been approved for use in the European Union since 1946.
Hybrid medicines have a different strength, are administered differently, or have a different indication from the reference medicine.
Ledaga contains the same active substance as Caryolysine—chlormethine, a bifunctional alkylating agent that inhibits rapidly proliferating cells—but Ledaga is a gel intended for cutaneous use.
Actelion Pharmaceuticals Ltd, the company developing Ledaga, has agreed to fulfill a list of post-approval measures for the product proposed by the European Medicines Agency’s Committee for Medicinal Products for Human Use.
Subject to fulfilling the agreed commitments and achieving market access in various countries, a potential first European launch of Ledaga is not expected before January 2018. When it is launched, Ledaga will be available as a 160 μg/g gel.
Phase 2 study
The authorization of hybrid medicines depends partly on the results of tests on the reference medicine and partly on new data from clinical trials.
The marketing authorization for Ledaga is based, in part, on results of a multicenter, randomized, observer-blinded, active-controlled study of patients with stage I and IIA MF. Results from this phase 2 study were published in JAMA Dermatology.
The study enrolled 260 MF patients who were randomized 1:1 to receive topical treatment with 0.02% chlormethine gel (Ledaga) or compounded control—0.02% chlormethine compounded in Aquaphor® ointment—once daily for up to 12 months.
A response was defined as at least a 50% improvement in the baseline Composite Assessment of Index Lesion Severity score.
In the intent-to-treat population, 59% (76/130) of patients who received Ledaga achieved a clinical response, compared to 48% (62/130) of patients treated with the compounded control. The rate of complete response was 14% (n=18) and 12% (n=15), respectively.
Patients who were treated for at least 6 months were included in the efficacy-evaluable population. In this population, 77% (69/90) of patients who received Ledaga achieved a clinical response, compared to 59% (56/95) of patients treated with the compounded control. The rate of complete response was 19% (n=17) and 15% (n=14), respectively.
Reductions in mean lesion severity were seen as early as 4 weeks into the study, with further reductions observed with continuing therapy. The time to first confirmed response favored Ledaga.
The most frequent adverse reactions reported with Ledaga were skin-related—dermatitis (55%; eg, skin irritation, erythema, rash, urticaria, skin-burning sensation, skin pain), pruritus (20%), skin infections (12%), skin ulceration and blistering (6%), and skin hyperpigmentation (6%).
No systemic absorption of chlormethine was detected with treatment. ![]()
Rising arthritis prevalence driven by obesity
Rising obesity is driving an increase in arthritis prevalence, and the association is not appreciated because the impact of body mass index on joint disease is not fully understood, according to a study spanning four generations.
The proportion of people in more recent birth cohorts reporting arthritis symptoms indicates a successively greater prevalence of arthritis compared to earlier generations, based on an 18-year longitudinal study conducted by Elizabeth M. Badley, PhD, of Dalla Lana School of Public Health, University of Toronto, and her colleagues. The researchers compared the prevalence of arthritis across four birth cohorts: World War II (1935-1944; n = 1,598), older baby boomers (1945-1954; n = 2,208), younger baby boomers (1955-1964; n = 2,781) and Generation Xers (1965-1974; n = 2,230).
“Although our results do not represent projections as such, extrapolation of the trajectories of arthritis with age and comparison of the trajectories across cohorts suggest that current projections of the prevalence of arthritis … may be too low for obese individuals,” they concluded.
Using the World War II cohort as the reference group for comparison, the odds ratio for arthritis in Gen Xers was 3.2; for younger baby boomers it was 2.14; for older baby boomers, it was 1.48.
Furthermore, in all cohorts the age of onset of arthritis in obese individuals was earlier compared to those of normal weight.
“This has implications for the targeting of public health messages for the control and management of arthritis,” the researchers wrote (Arthritis Care Res. 2017. doi: 10.1002/acr.23213).
The authors noted that although the study participants were asked about arthritis in general it was likely the overall findings reflected an increasing prevalence of osteoarthritis.
And while the researchers could only speculate about the reasons for the higher prevalence of arthritis seen in recent cohorts, it was possible there had been “unrecognized changes over time in environmental or biologic exposures.”
The study was funded in part by a CIHR operating grant. No conflicts of interest were declared.
Rising obesity is driving an increase in arthritis prevalence, and the association is not appreciated because the impact of body mass index on joint disease is not fully understood, according to a study spanning four generations.
The proportion of people in more recent birth cohorts reporting arthritis symptoms indicates a successively greater prevalence of arthritis compared to earlier generations, based on an 18-year longitudinal study conducted by Elizabeth M. Badley, PhD, of Dalla Lana School of Public Health, University of Toronto, and her colleagues. The researchers compared the prevalence of arthritis across four birth cohorts: World War II (1935-1944; n = 1,598), older baby boomers (1945-1954; n = 2,208), younger baby boomers (1955-1964; n = 2,781) and Generation Xers (1965-1974; n = 2,230).
“Although our results do not represent projections as such, extrapolation of the trajectories of arthritis with age and comparison of the trajectories across cohorts suggest that current projections of the prevalence of arthritis … may be too low for obese individuals,” they concluded.
Using the World War II cohort as the reference group for comparison, the odds ratio for arthritis in Gen Xers was 3.2; for younger baby boomers it was 2.14; for older baby boomers, it was 1.48.
Furthermore, in all cohorts the age of onset of arthritis in obese individuals was earlier compared to those of normal weight.
“This has implications for the targeting of public health messages for the control and management of arthritis,” the researchers wrote (Arthritis Care Res. 2017. doi: 10.1002/acr.23213).
The authors noted that although the study participants were asked about arthritis in general it was likely the overall findings reflected an increasing prevalence of osteoarthritis.
And while the researchers could only speculate about the reasons for the higher prevalence of arthritis seen in recent cohorts, it was possible there had been “unrecognized changes over time in environmental or biologic exposures.”
The study was funded in part by a CIHR operating grant. No conflicts of interest were declared.
Rising obesity is driving an increase in arthritis prevalence, and the association is not appreciated because the impact of body mass index on joint disease is not fully understood, according to a study spanning four generations.
The proportion of people in more recent birth cohorts reporting arthritis symptoms indicates a successively greater prevalence of arthritis compared to earlier generations, based on an 18-year longitudinal study conducted by Elizabeth M. Badley, PhD, of Dalla Lana School of Public Health, University of Toronto, and her colleagues. The researchers compared the prevalence of arthritis across four birth cohorts: World War II (1935-1944; n = 1,598), older baby boomers (1945-1954; n = 2,208), younger baby boomers (1955-1964; n = 2,781) and Generation Xers (1965-1974; n = 2,230).
“Although our results do not represent projections as such, extrapolation of the trajectories of arthritis with age and comparison of the trajectories across cohorts suggest that current projections of the prevalence of arthritis … may be too low for obese individuals,” they concluded.
Using the World War II cohort as the reference group for comparison, the odds ratio for arthritis in Gen Xers was 3.2; for younger baby boomers it was 2.14; for older baby boomers, it was 1.48.
Furthermore, in all cohorts the age of onset of arthritis in obese individuals was earlier compared to those of normal weight.
“This has implications for the targeting of public health messages for the control and management of arthritis,” the researchers wrote (Arthritis Care Res. 2017. doi: 10.1002/acr.23213).
The authors noted that although the study participants were asked about arthritis in general it was likely the overall findings reflected an increasing prevalence of osteoarthritis.
And while the researchers could only speculate about the reasons for the higher prevalence of arthritis seen in recent cohorts, it was possible there had been “unrecognized changes over time in environmental or biologic exposures.”
The study was funded in part by a CIHR operating grant. No conflicts of interest were declared.
FROM ARTHRITIS CARE & RESEARCH
Key clinical point: The prevalence of arthritis in the general population is growing and increasing obesity appears to be a factor.
Major finding: When researchers used the World War II cohort as the reference group for comparison, the odds ratio for arthritis in Gen Xers was 3.2; for younger baby boomers it was 2.14; for older baby boomers, it was 1.48.
Data source: A longitudinal analysis of data from the 1994/95 to 2010/11 National Population Health survey that included 8,817 participants in four birth cohorts.
Disclosures: The study was funded in part by a CIHR operating grant. No conflicts of interest were declared.
When Heart Problems Crop Up
ANSWER
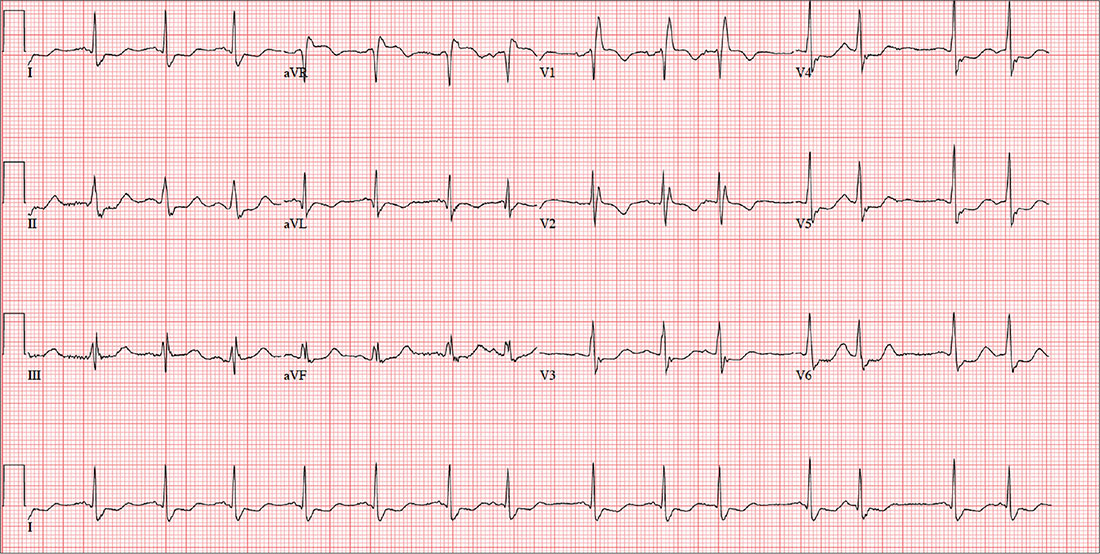
This ECG shows a sinus rhythm with premature atrial complexes, a normal axis, a right bundle branch block, and T-wave abnormalities consistent with lateral ischemia.
Sinus rhythm is evidenced by the P waves’ rate of ≥ 60 beats/min and ≤ 100 beats/min. The P waves that indicate premature atrial contractions have a different appearance than normal P waves, a result of the atrial activation from a site other than the sinus node. Because both the normal P wave and the premature atrial contraction conduct through the normal ventricular conduction system, the associated QRS complexes are identica
A right bundle branch block is identified by a QRS duration > 120 ms with a terminal broad S wave in lead I and an RSR’ complex in leads V1 and V2. The ST segment depressions in precordial leads V3 through V6 propagate the diagnosis of lateral ischemia.
The patient was not found to have atrial fibrillation, and his palpitations and evidence of lateral ischemia resolved when he resumed taking his ß-blocker.
ANSWER
This ECG shows a sinus rhythm with premature atrial complexes, a normal axis, a right bundle branch block, and T-wave abnormalities consistent with lateral ischemia.
Sinus rhythm is evidenced by the P waves’ rate of ≥ 60 beats/min and ≤ 100 beats/min. The P waves that indicate premature atrial contractions have a different appearance than normal P waves, a result of the atrial activation from a site other than the sinus node. Because both the normal P wave and the premature atrial contraction conduct through the normal ventricular conduction system, the associated QRS complexes are identica
A right bundle branch block is identified by a QRS duration > 120 ms with a terminal broad S wave in lead I and an RSR’ complex in leads V1 and V2. The ST segment depressions in precordial leads V3 through V6 propagate the diagnosis of lateral ischemia.
The patient was not found to have atrial fibrillation, and his palpitations and evidence of lateral ischemia resolved when he resumed taking his ß-blocker.
ANSWER
This ECG shows a sinus rhythm with premature atrial complexes, a normal axis, a right bundle branch block, and T-wave abnormalities consistent with lateral ischemia.
Sinus rhythm is evidenced by the P waves’ rate of ≥ 60 beats/min and ≤ 100 beats/min. The P waves that indicate premature atrial contractions have a different appearance than normal P waves, a result of the atrial activation from a site other than the sinus node. Because both the normal P wave and the premature atrial contraction conduct through the normal ventricular conduction system, the associated QRS complexes are identica
A right bundle branch block is identified by a QRS duration > 120 ms with a terminal broad S wave in lead I and an RSR’ complex in leads V1 and V2. The ST segment depressions in precordial leads V3 through V6 propagate the diagnosis of lateral ischemia.
The patient was not found to have atrial fibrillation, and his palpitations and evidence of lateral ischemia resolved when he resumed taking his ß-blocker.
A 72-year-old farmer presents with heart palpitations he has had for the past three weeks. He fears he may be in atrial fibrillation and at risk for a stroke, stating that a few months ago his neighbor complained of palpitations (later attributed to atrial fibrillation) and had an embolic stroke due to a clot in the left atrium. The patient denies any history of cardiac arrhythmias, chest pain, syncope, or near-syncope. He does report occasional bouts of lightheadedness, which have increased in frequency. He is more concerned, though, by the strong, intensified heartbeats that he can feel in his throat.
Past medical and surgical histories are positive for type 2 diabetes, hypertension, and hyperlipidemia, as well as an appendectomy and cholecystectomy. He has also had several upper extremity fractures in the past, all of which have healed well.
The patient’s wife died recently from complications following a hip replacement surgery, but he and his two sons continue to work on the 460-acre family farm he has owned all his life. A chronic smoker, he has smoked one to two packs of cigarettes per day since he was 15. He does not drink alcohol but does consume one to two pots of coffee per day.
His medication list includes metformin, atorvastatin, and metoprolol. He hasn’t taken his metoprolol for two months, because he switched pharmacies and the pills he received were a different color so he didn’t believe they were the right drug (despite the label on the bottle). He has no known drug allergies, but sulfa drugs induce nausea.
The review of systems is remarkable for arthritic pain in his hands, shoulders, hips, knees, and ankles. The patient complains of gastric reflux and occasional diarrhea. He states his mood is still down from the loss of his wife, but he denies being depressed.
His weight is 232 lb and his height, 70 in. Vital signs include a blood pressure of 168/92 mm Hg; pulse, 84 beats/min; respiratory rate, 14 breaths/min-1; and temperature, 99.2°F.
Physical exam reveals a weathered but otherwise healthy-looking male in no distress. He wears corrective lenses. The HEENT exam reveals surprisingly good dentition for a man his age. There are no carotid bruits. The lungs have expiratory crackles in both bases that change with coughing.
The cardiac exam reveals an irregular rate of 88 beats/min with a grade II/VI early systolic murmur at the left upper sternal border. There are no extra heart sounds or rubs. The abdomen is soft and nontender with old, well-healed cholecystectomy and appendectomy incision scars. The peripheral pulses are strong and equal bilaterally. Arthritic changes are evident in the hands and feet. The neurologic exam is grossly intact.
An ECG is performed; it reveals a ventricular rate of 87 beats/min; PR interval, 156 ms; QRS duration, 138 ms; QT/QTc interval, 440/529 ms; P axis, 58°; R axis, 26°; and T axis, 105°. What is your interpretation of this ECG?

Sneak Peek: The Hospital Leader Blog
Editor’s note: This article first appeared on “The Hospital Leader” blog. Read the full post at hospitalleader.org.
In December, I wrote a letter to hospital executives, urging them to deliberately invest their own personal time and effort in fostering hospitalist well-being. I suggested several actions that leaders can take to enhance hospitalist job satisfaction and reduce the risk of burnout and turnover.
Following publication of that post, I heard from several hospital executives and was pleasantly surprised that they all responded positively to my message. Several execs told me that they gained valuable new insights about their hospitalists’ challenges and needs; others said they planned to take action on one or more of my suggestions that had never occurred to them before.
Their feedback reinforced my belief that most hospital leaders actually do care a lot about promoting healthy, stable, and sustainable hospitalist programs, but the hospital leaders I talked with also had some messages for their hospitalist colleagues, and I think it’s important to share them in the spirit of fostering a healthy exchange of perspectives. Your hospital’s leaders would be delighted and encouraged if you engaged them in dialogue about these issues.
Help us help you
Several hospital leaders told me that their hospitalists grumble about being treated by the medical staff (and even nurses) like second-class citizens or glorified residents. Those same hospitalists, however, routinely show up for work dressed in scrubs and tennis shoes rather than professional attire. They rarely come in early when it’s busy or invest more time than is absolutely needed to see the patients on their list, making it easy for others to dismiss them as shift workers.
Hospitalists, they say, are unwilling to come in on their own time to attend a medical staff meeting, something other doctors do as a matter of course. And instead of interacting as social peers with other physicians when opportunity arises (i.e., in the cafeteria or doctors’ lounge), the hospitalists just grab food and head back to eat together in their work room.
The executives said they want to help enhance the stature of their hospitalists within the medical staff, but the Here’s a typical comment:
“[Hospitalists] also need to be willing to participate in hospital and system committees. Although this may require them to interrupt their workflow and stay late on some days they are working or come in on days off, they will never garner the respect of their colleagues if they are unwilling to do so.”
Read the full post at hospitalleader.org.
Leslie Flores is a hospital medicine consultant and member of SHM’s Practice Analysis Committee.
Also on The Hospital Leader. . .
• Creating Value through Crowdsourcing & Finding ‘Value’ in the New Year, by Vineet Arora, MD, MPP, FHM
• BREAKING NEWS: “Physicians Deemed Unnecessary”; Social Worker Promoted to Hospital CEO, by Jordan Messler, MD, SFHM
• ER Docs and Out-of-Network Billing: Are We in the Same Boat?, by Brad Flansbaum, DO, MPH, MHM
• The Best Way to Die?, by David Brabeck, MD
Editor’s note: This article first appeared on “The Hospital Leader” blog. Read the full post at hospitalleader.org.
In December, I wrote a letter to hospital executives, urging them to deliberately invest their own personal time and effort in fostering hospitalist well-being. I suggested several actions that leaders can take to enhance hospitalist job satisfaction and reduce the risk of burnout and turnover.
Following publication of that post, I heard from several hospital executives and was pleasantly surprised that they all responded positively to my message. Several execs told me that they gained valuable new insights about their hospitalists’ challenges and needs; others said they planned to take action on one or more of my suggestions that had never occurred to them before.
Their feedback reinforced my belief that most hospital leaders actually do care a lot about promoting healthy, stable, and sustainable hospitalist programs, but the hospital leaders I talked with also had some messages for their hospitalist colleagues, and I think it’s important to share them in the spirit of fostering a healthy exchange of perspectives. Your hospital’s leaders would be delighted and encouraged if you engaged them in dialogue about these issues.
Help us help you
Several hospital leaders told me that their hospitalists grumble about being treated by the medical staff (and even nurses) like second-class citizens or glorified residents. Those same hospitalists, however, routinely show up for work dressed in scrubs and tennis shoes rather than professional attire. They rarely come in early when it’s busy or invest more time than is absolutely needed to see the patients on their list, making it easy for others to dismiss them as shift workers.
Hospitalists, they say, are unwilling to come in on their own time to attend a medical staff meeting, something other doctors do as a matter of course. And instead of interacting as social peers with other physicians when opportunity arises (i.e., in the cafeteria or doctors’ lounge), the hospitalists just grab food and head back to eat together in their work room.
The executives said they want to help enhance the stature of their hospitalists within the medical staff, but the Here’s a typical comment:
“[Hospitalists] also need to be willing to participate in hospital and system committees. Although this may require them to interrupt their workflow and stay late on some days they are working or come in on days off, they will never garner the respect of their colleagues if they are unwilling to do so.”
Read the full post at hospitalleader.org.
Leslie Flores is a hospital medicine consultant and member of SHM’s Practice Analysis Committee.
Also on The Hospital Leader. . .
• Creating Value through Crowdsourcing & Finding ‘Value’ in the New Year, by Vineet Arora, MD, MPP, FHM
• BREAKING NEWS: “Physicians Deemed Unnecessary”; Social Worker Promoted to Hospital CEO, by Jordan Messler, MD, SFHM
• ER Docs and Out-of-Network Billing: Are We in the Same Boat?, by Brad Flansbaum, DO, MPH, MHM
• The Best Way to Die?, by David Brabeck, MD
Editor’s note: This article first appeared on “The Hospital Leader” blog. Read the full post at hospitalleader.org.
In December, I wrote a letter to hospital executives, urging them to deliberately invest their own personal time and effort in fostering hospitalist well-being. I suggested several actions that leaders can take to enhance hospitalist job satisfaction and reduce the risk of burnout and turnover.
Following publication of that post, I heard from several hospital executives and was pleasantly surprised that they all responded positively to my message. Several execs told me that they gained valuable new insights about their hospitalists’ challenges and needs; others said they planned to take action on one or more of my suggestions that had never occurred to them before.
Their feedback reinforced my belief that most hospital leaders actually do care a lot about promoting healthy, stable, and sustainable hospitalist programs, but the hospital leaders I talked with also had some messages for their hospitalist colleagues, and I think it’s important to share them in the spirit of fostering a healthy exchange of perspectives. Your hospital’s leaders would be delighted and encouraged if you engaged them in dialogue about these issues.
Help us help you
Several hospital leaders told me that their hospitalists grumble about being treated by the medical staff (and even nurses) like second-class citizens or glorified residents. Those same hospitalists, however, routinely show up for work dressed in scrubs and tennis shoes rather than professional attire. They rarely come in early when it’s busy or invest more time than is absolutely needed to see the patients on their list, making it easy for others to dismiss them as shift workers.
Hospitalists, they say, are unwilling to come in on their own time to attend a medical staff meeting, something other doctors do as a matter of course. And instead of interacting as social peers with other physicians when opportunity arises (i.e., in the cafeteria or doctors’ lounge), the hospitalists just grab food and head back to eat together in their work room.
The executives said they want to help enhance the stature of their hospitalists within the medical staff, but the Here’s a typical comment:
“[Hospitalists] also need to be willing to participate in hospital and system committees. Although this may require them to interrupt their workflow and stay late on some days they are working or come in on days off, they will never garner the respect of their colleagues if they are unwilling to do so.”
Read the full post at hospitalleader.org.
Leslie Flores is a hospital medicine consultant and member of SHM’s Practice Analysis Committee.
Also on The Hospital Leader. . .
• Creating Value through Crowdsourcing & Finding ‘Value’ in the New Year, by Vineet Arora, MD, MPP, FHM
• BREAKING NEWS: “Physicians Deemed Unnecessary”; Social Worker Promoted to Hospital CEO, by Jordan Messler, MD, SFHM
• ER Docs and Out-of-Network Billing: Are We in the Same Boat?, by Brad Flansbaum, DO, MPH, MHM
• The Best Way to Die?, by David Brabeck, MD

New Trump travel order could disrupt meetings, trainees
President’s Trump’s revised executive order blocking travelers from six Muslim-majority countries from entering the United States could land a damaging blow to global cooperation in scientific research and impede assemblies of the world’s top medical experts.
The executive order, signed March 6, bars citizens of Iran, Libya, Somalia, Sudan, Syria, and Yemen from obtaining visas for 90 days and blocks refugees from the affected countries from entering the U.S. for 120 days. The new executive measure, which takes effect March 16, supersedes President Trump’s original Jan. 27 travel ban that has been blocked by federal courts.
The new order clarifies that citizens of the six countries who are legal permanent U.S. residents or who have current visas to enter the country are exempt from the travel prohibition.
The revised travel ban could disrupt the exchange of medical knowledge by barring foreign experts from traveling to medical and scientific conferences in the United States, and leaves the status of medical trainees from those countries in limbo, according to American Medical Association President Andrew W. Gurman, MD.
“Hundreds of physicians from six countries are subject to the revised executive order and have applied to U.S. training programs and requested visa sponsorship,” he said in a statement. “The new executive order leaves them in limbo and without an explicit waiver, these foreign physicians will be unable to provide care in the U.S. when training programs begin on July 1.”
The new order is already being challenged in court. On March 7, the state of Hawaii filed a lawsuit seeking to block the order, saying that it subjects a portion of Hawaii’s population to “discrimination and second-class treatment.”
When the original ban took effect, thousands of academics from around the world, including physicians, researchers, and professors, vowed to boycott U.S.-based conferences. A Google Docs petition started shortly after the ban was announced garnered more than 5,000 signatures by professionals acting in solidarity with those affected by the travel restrictions. The academicians who signed the petition said they would not attend international conferences in the United States until those restricted from participating could rejoin their colleagues and freely share their ideas.
The new executive order comes nearly 2 months after President Trump’s original travel ban caused nationwide protests and led to a series of legal challenges. The states of Washington and Minnesota, which sued President Trump over his original ban, argued that such a ban harms the teaching and research missions of their universities and prevents students and faculty from traveling for research and academic collaboration. In addition, the executive order restricts universities from hiring attractive candidates from countries affected by the ban, state officials said.
A federal court temporarily blocked the original travel ban on Feb. 3, a decision upheld by the 9th U.S. Circuit Court of Appeals on Feb. 9.
The new executive order excludes Iraq this time around and also removes language that had indefinitely banned Syrian refugees. In a March 6 memorandum, the White House said the purpose of the ban is to prevent “foreign nationals who may aid, support, or commit violent, criminal, or terrorist acts,” while the administration enhances the screening and vetting protocols and procedures for granting visas and admission to the United States.
“This nation cannot delay the immediate implementation of additional heightened screening and vetting protocols and procedures for issuing visas to ensure that we strengthen the safety and security of our country,” the memo states.
This article was updated March 8, 2017.
agallegos@frontlinemedcom.com
On Twitter @legal_med
President’s Trump’s revised executive order blocking travelers from six Muslim-majority countries from entering the United States could land a damaging blow to global cooperation in scientific research and impede assemblies of the world’s top medical experts.
The executive order, signed March 6, bars citizens of Iran, Libya, Somalia, Sudan, Syria, and Yemen from obtaining visas for 90 days and blocks refugees from the affected countries from entering the U.S. for 120 days. The new executive measure, which takes effect March 16, supersedes President Trump’s original Jan. 27 travel ban that has been blocked by federal courts.
The new order clarifies that citizens of the six countries who are legal permanent U.S. residents or who have current visas to enter the country are exempt from the travel prohibition.
The revised travel ban could disrupt the exchange of medical knowledge by barring foreign experts from traveling to medical and scientific conferences in the United States, and leaves the status of medical trainees from those countries in limbo, according to American Medical Association President Andrew W. Gurman, MD.
“Hundreds of physicians from six countries are subject to the revised executive order and have applied to U.S. training programs and requested visa sponsorship,” he said in a statement. “The new executive order leaves them in limbo and without an explicit waiver, these foreign physicians will be unable to provide care in the U.S. when training programs begin on July 1.”
The new order is already being challenged in court. On March 7, the state of Hawaii filed a lawsuit seeking to block the order, saying that it subjects a portion of Hawaii’s population to “discrimination and second-class treatment.”
When the original ban took effect, thousands of academics from around the world, including physicians, researchers, and professors, vowed to boycott U.S.-based conferences. A Google Docs petition started shortly after the ban was announced garnered more than 5,000 signatures by professionals acting in solidarity with those affected by the travel restrictions. The academicians who signed the petition said they would not attend international conferences in the United States until those restricted from participating could rejoin their colleagues and freely share their ideas.
The new executive order comes nearly 2 months after President Trump’s original travel ban caused nationwide protests and led to a series of legal challenges. The states of Washington and Minnesota, which sued President Trump over his original ban, argued that such a ban harms the teaching and research missions of their universities and prevents students and faculty from traveling for research and academic collaboration. In addition, the executive order restricts universities from hiring attractive candidates from countries affected by the ban, state officials said.
A federal court temporarily blocked the original travel ban on Feb. 3, a decision upheld by the 9th U.S. Circuit Court of Appeals on Feb. 9.
The new executive order excludes Iraq this time around and also removes language that had indefinitely banned Syrian refugees. In a March 6 memorandum, the White House said the purpose of the ban is to prevent “foreign nationals who may aid, support, or commit violent, criminal, or terrorist acts,” while the administration enhances the screening and vetting protocols and procedures for granting visas and admission to the United States.
“This nation cannot delay the immediate implementation of additional heightened screening and vetting protocols and procedures for issuing visas to ensure that we strengthen the safety and security of our country,” the memo states.
This article was updated March 8, 2017.
agallegos@frontlinemedcom.com
On Twitter @legal_med
President’s Trump’s revised executive order blocking travelers from six Muslim-majority countries from entering the United States could land a damaging blow to global cooperation in scientific research and impede assemblies of the world’s top medical experts.
The executive order, signed March 6, bars citizens of Iran, Libya, Somalia, Sudan, Syria, and Yemen from obtaining visas for 90 days and blocks refugees from the affected countries from entering the U.S. for 120 days. The new executive measure, which takes effect March 16, supersedes President Trump’s original Jan. 27 travel ban that has been blocked by federal courts.
The new order clarifies that citizens of the six countries who are legal permanent U.S. residents or who have current visas to enter the country are exempt from the travel prohibition.
The revised travel ban could disrupt the exchange of medical knowledge by barring foreign experts from traveling to medical and scientific conferences in the United States, and leaves the status of medical trainees from those countries in limbo, according to American Medical Association President Andrew W. Gurman, MD.
“Hundreds of physicians from six countries are subject to the revised executive order and have applied to U.S. training programs and requested visa sponsorship,” he said in a statement. “The new executive order leaves them in limbo and without an explicit waiver, these foreign physicians will be unable to provide care in the U.S. when training programs begin on July 1.”
The new order is already being challenged in court. On March 7, the state of Hawaii filed a lawsuit seeking to block the order, saying that it subjects a portion of Hawaii’s population to “discrimination and second-class treatment.”
When the original ban took effect, thousands of academics from around the world, including physicians, researchers, and professors, vowed to boycott U.S.-based conferences. A Google Docs petition started shortly after the ban was announced garnered more than 5,000 signatures by professionals acting in solidarity with those affected by the travel restrictions. The academicians who signed the petition said they would not attend international conferences in the United States until those restricted from participating could rejoin their colleagues and freely share their ideas.
The new executive order comes nearly 2 months after President Trump’s original travel ban caused nationwide protests and led to a series of legal challenges. The states of Washington and Minnesota, which sued President Trump over his original ban, argued that such a ban harms the teaching and research missions of their universities and prevents students and faculty from traveling for research and academic collaboration. In addition, the executive order restricts universities from hiring attractive candidates from countries affected by the ban, state officials said.
A federal court temporarily blocked the original travel ban on Feb. 3, a decision upheld by the 9th U.S. Circuit Court of Appeals on Feb. 9.
The new executive order excludes Iraq this time around and also removes language that had indefinitely banned Syrian refugees. In a March 6 memorandum, the White House said the purpose of the ban is to prevent “foreign nationals who may aid, support, or commit violent, criminal, or terrorist acts,” while the administration enhances the screening and vetting protocols and procedures for granting visas and admission to the United States.
“This nation cannot delay the immediate implementation of additional heightened screening and vetting protocols and procedures for issuing visas to ensure that we strengthen the safety and security of our country,” the memo states.
This article was updated March 8, 2017.
agallegos@frontlinemedcom.com
On Twitter @legal_med