User login
FDA approves emergency use of saliva test to detect COVID-19
As the race to develop rapid testing for COVID-19 expands, the Food and Drug Administration has granted emergency approval for an approach that uses saliva as the primary test biomaterial.

According to a document provided to the FDA, the Rutgers Clinical Genomics Laboratory TaqPath SARS-CoV-2 Assay is intended for the qualitative detection of nucleic acid from SARS-CoV-2 in oropharyngeal (throat) swab, nasopharyngeal swab, anterior nasal swab, mid-turbinate nasal swab from individuals suspected of COVID-19 by their health care clinicians. To expand on this assay, Rutgers University–based RUCDR Infinite Biologics developed a saliva collection method in partnership with Spectrum Solutions and Accurate Diagnostic Labs.
The document states that Samples are transported for RNA extraction and are tested within 48 hours of collection. In saliva samples obtained from 60 patients evaluated by the researchers, all were in agreement with the presence of COVID-19.

“If shown to be as accurate as nasopharyngeal and oropharyngeal samples, saliva as a biomatrix offers the advantage of not generating aerosols or creating as many respiratory droplets during specimen procurement, therefore decreasing the risk of transmission to the health care worker doing the testing,” said Matthew P. Cheng, MDCM, of the division of infectious diseases at McGill University Health Centre, Montreal, who was not involved in development of the test but who has written about diagnostic testing for the virus.
“Also, it may be easy enough for patients to do saliva self-collection at home. However, it is important to note that SARS-CoV-2 tests on saliva have not yet undergone the more rigorous evaluation of full FDA authorization, and saliva is not a preferred specimen type of the FDA nor the [Centers for Disease Control and Prevention] for respiratory virus testing.”
In a prepared statement, Andrew I. Brooks, PhD, chief operating officer at RUCDR Infinite Biologics, said the saliva collection method enables clinicians to preserve personal protective equipment for use in patient care instead of testing. “We can significantly increase the number of people tested each and every day as self-collection of saliva is quicker and more scalable than swab collections,” he said. “All of this combined will have a tremendous impact on testing in New Jersey and across the United States.”
The tests are currently available to the RWJBarnabas Health network, based in West Orange, N.J., which has partnered with Rutgers University.
As the race to develop rapid testing for COVID-19 expands, the Food and Drug Administration has granted emergency approval for an approach that uses saliva as the primary test biomaterial.
According to a document provided to the FDA, the Rutgers Clinical Genomics Laboratory TaqPath SARS-CoV-2 Assay is intended for the qualitative detection of nucleic acid from SARS-CoV-2 in oropharyngeal (throat) swab, nasopharyngeal swab, anterior nasal swab, mid-turbinate nasal swab from individuals suspected of COVID-19 by their health care clinicians. To expand on this assay, Rutgers University–based RUCDR Infinite Biologics developed a saliva collection method in partnership with Spectrum Solutions and Accurate Diagnostic Labs.
The document states that Samples are transported for RNA extraction and are tested within 48 hours of collection. In saliva samples obtained from 60 patients evaluated by the researchers, all were in agreement with the presence of COVID-19.
“If shown to be as accurate as nasopharyngeal and oropharyngeal samples, saliva as a biomatrix offers the advantage of not generating aerosols or creating as many respiratory droplets during specimen procurement, therefore decreasing the risk of transmission to the health care worker doing the testing,” said Matthew P. Cheng, MDCM, of the division of infectious diseases at McGill University Health Centre, Montreal, who was not involved in development of the test but who has written about diagnostic testing for the virus.
“Also, it may be easy enough for patients to do saliva self-collection at home. However, it is important to note that SARS-CoV-2 tests on saliva have not yet undergone the more rigorous evaluation of full FDA authorization, and saliva is not a preferred specimen type of the FDA nor the [Centers for Disease Control and Prevention] for respiratory virus testing.”
In a prepared statement, Andrew I. Brooks, PhD, chief operating officer at RUCDR Infinite Biologics, said the saliva collection method enables clinicians to preserve personal protective equipment for use in patient care instead of testing. “We can significantly increase the number of people tested each and every day as self-collection of saliva is quicker and more scalable than swab collections,” he said. “All of this combined will have a tremendous impact on testing in New Jersey and across the United States.”
The tests are currently available to the RWJBarnabas Health network, based in West Orange, N.J., which has partnered with Rutgers University.
As the race to develop rapid testing for COVID-19 expands, the Food and Drug Administration has granted emergency approval for an approach that uses saliva as the primary test biomaterial.
According to a document provided to the FDA, the Rutgers Clinical Genomics Laboratory TaqPath SARS-CoV-2 Assay is intended for the qualitative detection of nucleic acid from SARS-CoV-2 in oropharyngeal (throat) swab, nasopharyngeal swab, anterior nasal swab, mid-turbinate nasal swab from individuals suspected of COVID-19 by their health care clinicians. To expand on this assay, Rutgers University–based RUCDR Infinite Biologics developed a saliva collection method in partnership with Spectrum Solutions and Accurate Diagnostic Labs.
The document states that Samples are transported for RNA extraction and are tested within 48 hours of collection. In saliva samples obtained from 60 patients evaluated by the researchers, all were in agreement with the presence of COVID-19.
“If shown to be as accurate as nasopharyngeal and oropharyngeal samples, saliva as a biomatrix offers the advantage of not generating aerosols or creating as many respiratory droplets during specimen procurement, therefore decreasing the risk of transmission to the health care worker doing the testing,” said Matthew P. Cheng, MDCM, of the division of infectious diseases at McGill University Health Centre, Montreal, who was not involved in development of the test but who has written about diagnostic testing for the virus.
“Also, it may be easy enough for patients to do saliva self-collection at home. However, it is important to note that SARS-CoV-2 tests on saliva have not yet undergone the more rigorous evaluation of full FDA authorization, and saliva is not a preferred specimen type of the FDA nor the [Centers for Disease Control and Prevention] for respiratory virus testing.”
In a prepared statement, Andrew I. Brooks, PhD, chief operating officer at RUCDR Infinite Biologics, said the saliva collection method enables clinicians to preserve personal protective equipment for use in patient care instead of testing. “We can significantly increase the number of people tested each and every day as self-collection of saliva is quicker and more scalable than swab collections,” he said. “All of this combined will have a tremendous impact on testing in New Jersey and across the United States.”
The tests are currently available to the RWJBarnabas Health network, based in West Orange, N.J., which has partnered with Rutgers University.
Learning about the curve
Empty shelves that once cradled toilet paper rolls; lines of shoppers, some with masks; waiting 6 feet or at least a shopping cart length apart to get into grocery stores; hazmat-suited workers loading body bags into makeshift mortuaries ... These are the images we have come to associate with the COVID-19 pandemic. But then there also are the graphs and charts, none of them bearing good news. Some are difficult to interpret because they may be missing a key ingredient, such as a scale. Day to day fluctuations in the timeliness of the data points can make valid comparisons impossible. In most cases, it is too early to look at the graphs and hope for the big picture. Whether you are concerned about the stock market or the number of new cases of the virus in your county, you are hoping to see some graphic depiction of a favorable trend.

We have suddenly learned about the urgency of a process called “flattening the curve.” Are we doing as good a job of flattening as we could be? Are we doing better than France or Spain? Or are we heading toward an Italianesque apocalypse? Who is going to tell us when the flattening is for real and not just a 2- or 3-day statistical aberration?
The curves we are obsessed with today are those showing us new cases and new deaths. But And we won’t be seeing this curve in four-color graphics on the front page of our newspapers. It is the learning curve, and we want it to be as steep as we can make it without any hint of flattening in the foreseeable future.
We need to learn more about corona-like viruses. Why are some of us more vulnerable? We need to learn more about contagion. Does the 6-foot guideline make any sense? How long are viral particles floating in the air capable of initiating disease? What about air flow and dilution? Can we build a cruise ship or airplane that will be less of a health hazard?
More importantly, we need to learn to be better prepared. Even before the pandemic there have been shortages in intravenous solutions and drugs of critical importance to common diseases. Can we learn how to create reliable and affordable supply chains that allow researchers and developers to make a reasonable profit? Can we relearn to value science? Can we learn to invest more heavily in epidemiology and make it a specialty that attracts our best thinkers and communicators? Then can we elect officials who will share our trust in their recommendations?
Can we do a better job of resolving the tension between those who believe in a strong federal government and those who believe in local autonomy because we are seeing every day that this is an issue of survival, not just coexistence? Can we learn that the globalization that has allowed this viral spread can also be leveraged to beat it into submission?

Over the last half century there has been an unfortunate flattening of the learning curve. Ironically we have seen exponential growth among hi-tech industries that have forced us to keep abreast of new developments. But along with this has been a growing skepticism about value of scientific investigation. It is time we climbed back on that steep learning curve. The view gets better the higher we climb.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Empty shelves that once cradled toilet paper rolls; lines of shoppers, some with masks; waiting 6 feet or at least a shopping cart length apart to get into grocery stores; hazmat-suited workers loading body bags into makeshift mortuaries ... These are the images we have come to associate with the COVID-19 pandemic. But then there also are the graphs and charts, none of them bearing good news. Some are difficult to interpret because they may be missing a key ingredient, such as a scale. Day to day fluctuations in the timeliness of the data points can make valid comparisons impossible. In most cases, it is too early to look at the graphs and hope for the big picture. Whether you are concerned about the stock market or the number of new cases of the virus in your county, you are hoping to see some graphic depiction of a favorable trend.
We have suddenly learned about the urgency of a process called “flattening the curve.” Are we doing as good a job of flattening as we could be? Are we doing better than France or Spain? Or are we heading toward an Italianesque apocalypse? Who is going to tell us when the flattening is for real and not just a 2- or 3-day statistical aberration?
The curves we are obsessed with today are those showing us new cases and new deaths. But And we won’t be seeing this curve in four-color graphics on the front page of our newspapers. It is the learning curve, and we want it to be as steep as we can make it without any hint of flattening in the foreseeable future.
We need to learn more about corona-like viruses. Why are some of us more vulnerable? We need to learn more about contagion. Does the 6-foot guideline make any sense? How long are viral particles floating in the air capable of initiating disease? What about air flow and dilution? Can we build a cruise ship or airplane that will be less of a health hazard?
More importantly, we need to learn to be better prepared. Even before the pandemic there have been shortages in intravenous solutions and drugs of critical importance to common diseases. Can we learn how to create reliable and affordable supply chains that allow researchers and developers to make a reasonable profit? Can we relearn to value science? Can we learn to invest more heavily in epidemiology and make it a specialty that attracts our best thinkers and communicators? Then can we elect officials who will share our trust in their recommendations?
Can we do a better job of resolving the tension between those who believe in a strong federal government and those who believe in local autonomy because we are seeing every day that this is an issue of survival, not just coexistence? Can we learn that the globalization that has allowed this viral spread can also be leveraged to beat it into submission?
Over the last half century there has been an unfortunate flattening of the learning curve. Ironically we have seen exponential growth among hi-tech industries that have forced us to keep abreast of new developments. But along with this has been a growing skepticism about value of scientific investigation. It is time we climbed back on that steep learning curve. The view gets better the higher we climb.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Empty shelves that once cradled toilet paper rolls; lines of shoppers, some with masks; waiting 6 feet or at least a shopping cart length apart to get into grocery stores; hazmat-suited workers loading body bags into makeshift mortuaries ... These are the images we have come to associate with the COVID-19 pandemic. But then there also are the graphs and charts, none of them bearing good news. Some are difficult to interpret because they may be missing a key ingredient, such as a scale. Day to day fluctuations in the timeliness of the data points can make valid comparisons impossible. In most cases, it is too early to look at the graphs and hope for the big picture. Whether you are concerned about the stock market or the number of new cases of the virus in your county, you are hoping to see some graphic depiction of a favorable trend.
We have suddenly learned about the urgency of a process called “flattening the curve.” Are we doing as good a job of flattening as we could be? Are we doing better than France or Spain? Or are we heading toward an Italianesque apocalypse? Who is going to tell us when the flattening is for real and not just a 2- or 3-day statistical aberration?
The curves we are obsessed with today are those showing us new cases and new deaths. But And we won’t be seeing this curve in four-color graphics on the front page of our newspapers. It is the learning curve, and we want it to be as steep as we can make it without any hint of flattening in the foreseeable future.
We need to learn more about corona-like viruses. Why are some of us more vulnerable? We need to learn more about contagion. Does the 6-foot guideline make any sense? How long are viral particles floating in the air capable of initiating disease? What about air flow and dilution? Can we build a cruise ship or airplane that will be less of a health hazard?
More importantly, we need to learn to be better prepared. Even before the pandemic there have been shortages in intravenous solutions and drugs of critical importance to common diseases. Can we learn how to create reliable and affordable supply chains that allow researchers and developers to make a reasonable profit? Can we relearn to value science? Can we learn to invest more heavily in epidemiology and make it a specialty that attracts our best thinkers and communicators? Then can we elect officials who will share our trust in their recommendations?
Can we do a better job of resolving the tension between those who believe in a strong federal government and those who believe in local autonomy because we are seeing every day that this is an issue of survival, not just coexistence? Can we learn that the globalization that has allowed this viral spread can also be leveraged to beat it into submission?
Over the last half century there has been an unfortunate flattening of the learning curve. Ironically we have seen exponential growth among hi-tech industries that have forced us to keep abreast of new developments. But along with this has been a growing skepticism about value of scientific investigation. It is time we climbed back on that steep learning curve. The view gets better the higher we climb.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Mother of pearl: The power of pearl powder
Because of its dense protein and mineral composition, it has been used to treat several skin and bone disorders, as well as palpitations, insomnia, and epilepsy.3,4 The pearl-farming industry itself was established in Japan and has existed for more than a century; today, pearls are cultured globally and continue to receive attention for conferring health benefits.5

Calcium carbonate is the primary component of mollusk shells (roughly 95%), with the remainder an organic matrix including proteins, glycoproteins, and polysaccharides.6 Pearl powder is known to have exhibited antiaging, antioxidant, antiradiative, and tonic activities; in recent years, it has been incorporated into health foods for such properties and used in the clinical setting to treat ulcers (aphthous, gastric, and duodenal).4,7 Consisting of multiple active proteins, pearl powder is thought to be conducive to skin cell growth and effective for wound repair.4 This column focuses on recent research into the dermatologic potential of the powder derived from mother of pearl.
Wound healing
A decade ago, Jian-Ping et al. showed in mice that the water-soluble matrix of pearl powder (Hyriopsis cumingii) could significantly induce oral fibroblast proliferation and collagen accumulation, suppress matrix metalloproteinase-2 activity, and significantly foster TIMP-1 synthesis. The investigators concluded that the wound healing facilitated by pearl powder derives, in part, from its capacity to promote fibroblast mitosis, collagen deposition, and production of TIMP-1.8
Two years later, Lee et al. evaluated the effects of water-soluble nacre (mother of pearl) on second-degree burn wound healing in porcine skin as a proxy for human skin. They found that its application quickly led to burn-induced granulation areas filling with collagen, with normal skin appearance restored to wounded dermis and epidermis. Angiogenesis was also promoted by water-soluble nacre as was wound recovery in areas with apoptotic and necrotic cellular damage. Murine fibroblast NIH3T3 cells treated with water-soluble nacre also demonstrated augmented proliferation and collagen production. The researchers cited the restoration of angiogenesis and fibroblast activity as the primary benefits of water-soluble nacre, suggesting its potential as a wound therapy, preferable to powdered nacre due to better biocompatibility with less discomfort.9
The next year, Li et al. found that mother of pearl extract promoted cell migration of fibroblasts in cell culture, demonstrating its potential as a wound healing model.7In 2019, Chen et al. studied the effects of pearl powders of varying particle sizes to treat wounds in vitro and in vivo. They found that micro- and nanosized pearl powders augmented proliferation and migration of skin cells and shortened wound closure time. All powders also improved the biomechanical strength of healed skin, enhanced collagen formation and deposition, and expanded cutaneous angiogenesis, with nanoscale pearl powder displaying greatest efficiency.4
Skin tone and atopic dermatitis
In 2000, Lopez et al. implanted powdered nacre (mother of pearl derived from Pinctada maxima), which can promote and regulate bone-forming cells, into rat dermis to evaluate its effects on skin fibroblasts. They noted that the implant yielded well-vascularized tissue and improved extracellular matrix production, synthesis of substances involved in cellular adhesion and communication, and tissue regeneration (such as collagen types I and III). The investigators concluded that the powdered nacre contributed to the conditions necessary for improved skin tone and proper physiologic functioning of the skin.10
Rousseau et al. extracted lipids from the nacre of the oyster P. margaritifera to test on artificially dehydrated skin explants with the intention of developing new treatments for atopic dermatitis. The researchers determined that the lipids spurred a reconstitution of the intercellular material of the stratum corneum, concluding that new products to treat atopic dermatitis might be based on the signaling activity of nacre lipids.11
Antifibrotic and anti-inflammatory activity
A 2015 study by Yang et al. showed that a room-temperature superextraction system to yield the main active constituents of pearl was successful in enhancing their anti-inflammatory and antiapoptotic activity in human keratinocyte cells (HaCaT) exposed to low-dose UVB. The investigators combined pearl extract and poly (gamma-glutamic acid) hydrogels and observed reductions in inflammation and apoptosis of HaCaT cells. They concluded that a marketed pearl extract may be able to suppress radiation dermatitis present in keratinocytes.12

Two years later, Latire et al. used human dermal fibroblasts in primary culture to assess the potential biological activities of the matrix macromolecular components extracted from the shells of two edible mollusks (the blue mussel Mytilus edulis and the Pacific oyster Crassostrea gigas). The investigators found that both extracts influenced metabolic functions of the cells and reduced type I collagen levels, with an associated rise in matrix metalloproteinase-1 activity. Given their findings implying the effectiveness of the extracts in facilitating the catabolic pathway of human dermal fibroblasts, the authors suggest that these shell matrices present the potential for use in treating fibrosis, especially for scleroderma.6
Antioxidant and antiaging activity
Shao et al. demonstrated 10 years ago that pearl powder provides a moisturizing effect on the skin, with ultramicro pearl powder delivering a more robust moisturizing result than water-soluble pearl powder. These two types of pearl powder, along with another one tested (ultranano pearl powder), also significantly diminished the activation of tyrosinase and free radicals. Water-soluble pearl powder did not perform as well as the other two formulations in free radical scavenging. The investigators suggested that their results support the use of pearl powder to combat aging and enhance beauty, and could be used in the clinical setting.13
In 2017, Yang et al. reported on the in vitro antihemolytic and antioxidant activity of pearl powder in shielding human erythrocytes against 2,2’-azobis(2-amidinopropane) dihydrochloride–induced oxidative damage to membrane proteins/lipids. The researchers contend that the strong antioxidant qualities of pearl powder could be applied to prevent or protect against various diseases resulting from free radical damage.2
Human trials: Antioxidant, antiaging, skin appearance
Chiu et al. studied the antioxidant activity of various pearl powder extracts in a randomized, placebo-controlled trial in 2018. They also investigated the life span–prolonging effects of the powders using wild-type Caenorhabditis elegans. Twenty healthy middle-aged subjects were separated into two groups (experimental and placebo), with 3 g of pearl powder administered in capsules to the former and 3 g of placebo to the latter over 8 weeks. Blood samples taken at the beginning and every 2 weeks during the trial and in the 10th week revealed maximum antioxidant activity of the pearl powder and prolongation of C. elegans lifespan by 18.87%. Subjects using pearl powder demonstrated significant increases in total antioxidant capacity, thiols, glutathione, and enzymic antioxidant activity, along with notably inhibited lipid peroxidation products. The investigators concluded that pearl powder extract acted as a potent antioxidant and its use may be warranted to treat degenerative conditions related to aging.3
A recent study of the perception of blue light on Korean women’s faces using blue pearl pigment revealed that the pigment does indeed elicit the perception of the blue-light effect, notably transparency and gloss, which is particularly valued in Korea.14
Conclusion
The use of mother of pearl and pearl powder in traditional Chinese medicine and as a cosmetic and food additive has a rich and lengthy history. Contemporary research clearly suggests interesting avenues for further investigation and some promising results. Much more research is necessary, though, to delineate the potential roles of pearl powder in the skin care arsenal.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014), and a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems. Write to her at dermnews@mdedge.com
References
1. Zhang J et al. J Sep Sci. 2015 May;38(9):1552-60.
2. Yang HL et al. J Food Drug Anal. 2017 Oct;25(4):898-907.
3. Chiu HF et al. J Food Drug Anal. 2018 Jan;26(1):309-17.
4. Chen X et al. Drug Dev Ind Pharm. 2019 Jun;45(6):1009-16.
5. Nagai K. Zoolog Sci. 2013 Oct;30(10):783-93.
6. Latire T et al. Cytotechnology. 2017 Oct;69(5):815-29.
7. Li YC et al. Pharm Biol. 2013 Mar;51(3):289-97.
8. Jian-Ping D et al. Pharm Biol. 2010 Feb;48(2):122-7.
9. Lee K et al. Mol Biol Rep. 2012 Mar;39(3):3211-8.
10. Lopez E et al. Tissue Cell. 2000 Feb;32(1):95-101.
11. Rousseau M et al. Comp Biochem Physiol B Biochem Mol Biol. 2006 Sep;145(1):1-9.
12. Yang YL et al. Biomed Mater Eng. 2015;26 Suppl 1:S139-45.
13. Shao DZ et al. J Cosmet Sci. 2010 Mar-Apr;61(2):133-45.
14. Lee M et al. Skin Res Technol. 2020 Jan;26(1):76-80.
Because of its dense protein and mineral composition, it has been used to treat several skin and bone disorders, as well as palpitations, insomnia, and epilepsy.3,4 The pearl-farming industry itself was established in Japan and has existed for more than a century; today, pearls are cultured globally and continue to receive attention for conferring health benefits.5
Calcium carbonate is the primary component of mollusk shells (roughly 95%), with the remainder an organic matrix including proteins, glycoproteins, and polysaccharides.6 Pearl powder is known to have exhibited antiaging, antioxidant, antiradiative, and tonic activities; in recent years, it has been incorporated into health foods for such properties and used in the clinical setting to treat ulcers (aphthous, gastric, and duodenal).4,7 Consisting of multiple active proteins, pearl powder is thought to be conducive to skin cell growth and effective for wound repair.4 This column focuses on recent research into the dermatologic potential of the powder derived from mother of pearl.
Wound healing
A decade ago, Jian-Ping et al. showed in mice that the water-soluble matrix of pearl powder (Hyriopsis cumingii) could significantly induce oral fibroblast proliferation and collagen accumulation, suppress matrix metalloproteinase-2 activity, and significantly foster TIMP-1 synthesis. The investigators concluded that the wound healing facilitated by pearl powder derives, in part, from its capacity to promote fibroblast mitosis, collagen deposition, and production of TIMP-1.8
Two years later, Lee et al. evaluated the effects of water-soluble nacre (mother of pearl) on second-degree burn wound healing in porcine skin as a proxy for human skin. They found that its application quickly led to burn-induced granulation areas filling with collagen, with normal skin appearance restored to wounded dermis and epidermis. Angiogenesis was also promoted by water-soluble nacre as was wound recovery in areas with apoptotic and necrotic cellular damage. Murine fibroblast NIH3T3 cells treated with water-soluble nacre also demonstrated augmented proliferation and collagen production. The researchers cited the restoration of angiogenesis and fibroblast activity as the primary benefits of water-soluble nacre, suggesting its potential as a wound therapy, preferable to powdered nacre due to better biocompatibility with less discomfort.9
The next year, Li et al. found that mother of pearl extract promoted cell migration of fibroblasts in cell culture, demonstrating its potential as a wound healing model.7In 2019, Chen et al. studied the effects of pearl powders of varying particle sizes to treat wounds in vitro and in vivo. They found that micro- and nanosized pearl powders augmented proliferation and migration of skin cells and shortened wound closure time. All powders also improved the biomechanical strength of healed skin, enhanced collagen formation and deposition, and expanded cutaneous angiogenesis, with nanoscale pearl powder displaying greatest efficiency.4
Skin tone and atopic dermatitis
In 2000, Lopez et al. implanted powdered nacre (mother of pearl derived from Pinctada maxima), which can promote and regulate bone-forming cells, into rat dermis to evaluate its effects on skin fibroblasts. They noted that the implant yielded well-vascularized tissue and improved extracellular matrix production, synthesis of substances involved in cellular adhesion and communication, and tissue regeneration (such as collagen types I and III). The investigators concluded that the powdered nacre contributed to the conditions necessary for improved skin tone and proper physiologic functioning of the skin.10
Rousseau et al. extracted lipids from the nacre of the oyster P. margaritifera to test on artificially dehydrated skin explants with the intention of developing new treatments for atopic dermatitis. The researchers determined that the lipids spurred a reconstitution of the intercellular material of the stratum corneum, concluding that new products to treat atopic dermatitis might be based on the signaling activity of nacre lipids.11
Antifibrotic and anti-inflammatory activity
A 2015 study by Yang et al. showed that a room-temperature superextraction system to yield the main active constituents of pearl was successful in enhancing their anti-inflammatory and antiapoptotic activity in human keratinocyte cells (HaCaT) exposed to low-dose UVB. The investigators combined pearl extract and poly (gamma-glutamic acid) hydrogels and observed reductions in inflammation and apoptosis of HaCaT cells. They concluded that a marketed pearl extract may be able to suppress radiation dermatitis present in keratinocytes.12
Two years later, Latire et al. used human dermal fibroblasts in primary culture to assess the potential biological activities of the matrix macromolecular components extracted from the shells of two edible mollusks (the blue mussel Mytilus edulis and the Pacific oyster Crassostrea gigas). The investigators found that both extracts influenced metabolic functions of the cells and reduced type I collagen levels, with an associated rise in matrix metalloproteinase-1 activity. Given their findings implying the effectiveness of the extracts in facilitating the catabolic pathway of human dermal fibroblasts, the authors suggest that these shell matrices present the potential for use in treating fibrosis, especially for scleroderma.6
Antioxidant and antiaging activity
Shao et al. demonstrated 10 years ago that pearl powder provides a moisturizing effect on the skin, with ultramicro pearl powder delivering a more robust moisturizing result than water-soluble pearl powder. These two types of pearl powder, along with another one tested (ultranano pearl powder), also significantly diminished the activation of tyrosinase and free radicals. Water-soluble pearl powder did not perform as well as the other two formulations in free radical scavenging. The investigators suggested that their results support the use of pearl powder to combat aging and enhance beauty, and could be used in the clinical setting.13
In 2017, Yang et al. reported on the in vitro antihemolytic and antioxidant activity of pearl powder in shielding human erythrocytes against 2,2’-azobis(2-amidinopropane) dihydrochloride–induced oxidative damage to membrane proteins/lipids. The researchers contend that the strong antioxidant qualities of pearl powder could be applied to prevent or protect against various diseases resulting from free radical damage.2
Human trials: Antioxidant, antiaging, skin appearance
Chiu et al. studied the antioxidant activity of various pearl powder extracts in a randomized, placebo-controlled trial in 2018. They also investigated the life span–prolonging effects of the powders using wild-type Caenorhabditis elegans. Twenty healthy middle-aged subjects were separated into two groups (experimental and placebo), with 3 g of pearl powder administered in capsules to the former and 3 g of placebo to the latter over 8 weeks. Blood samples taken at the beginning and every 2 weeks during the trial and in the 10th week revealed maximum antioxidant activity of the pearl powder and prolongation of C. elegans lifespan by 18.87%. Subjects using pearl powder demonstrated significant increases in total antioxidant capacity, thiols, glutathione, and enzymic antioxidant activity, along with notably inhibited lipid peroxidation products. The investigators concluded that pearl powder extract acted as a potent antioxidant and its use may be warranted to treat degenerative conditions related to aging.3
A recent study of the perception of blue light on Korean women’s faces using blue pearl pigment revealed that the pigment does indeed elicit the perception of the blue-light effect, notably transparency and gloss, which is particularly valued in Korea.14
Conclusion
The use of mother of pearl and pearl powder in traditional Chinese medicine and as a cosmetic and food additive has a rich and lengthy history. Contemporary research clearly suggests interesting avenues for further investigation and some promising results. Much more research is necessary, though, to delineate the potential roles of pearl powder in the skin care arsenal.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014), and a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems. Write to her at dermnews@mdedge.com
References
1. Zhang J et al. J Sep Sci. 2015 May;38(9):1552-60.
2. Yang HL et al. J Food Drug Anal. 2017 Oct;25(4):898-907.
3. Chiu HF et al. J Food Drug Anal. 2018 Jan;26(1):309-17.
4. Chen X et al. Drug Dev Ind Pharm. 2019 Jun;45(6):1009-16.
5. Nagai K. Zoolog Sci. 2013 Oct;30(10):783-93.
6. Latire T et al. Cytotechnology. 2017 Oct;69(5):815-29.
7. Li YC et al. Pharm Biol. 2013 Mar;51(3):289-97.
8. Jian-Ping D et al. Pharm Biol. 2010 Feb;48(2):122-7.
9. Lee K et al. Mol Biol Rep. 2012 Mar;39(3):3211-8.
10. Lopez E et al. Tissue Cell. 2000 Feb;32(1):95-101.
11. Rousseau M et al. Comp Biochem Physiol B Biochem Mol Biol. 2006 Sep;145(1):1-9.
12. Yang YL et al. Biomed Mater Eng. 2015;26 Suppl 1:S139-45.
13. Shao DZ et al. J Cosmet Sci. 2010 Mar-Apr;61(2):133-45.
14. Lee M et al. Skin Res Technol. 2020 Jan;26(1):76-80.
Because of its dense protein and mineral composition, it has been used to treat several skin and bone disorders, as well as palpitations, insomnia, and epilepsy.3,4 The pearl-farming industry itself was established in Japan and has existed for more than a century; today, pearls are cultured globally and continue to receive attention for conferring health benefits.5
Calcium carbonate is the primary component of mollusk shells (roughly 95%), with the remainder an organic matrix including proteins, glycoproteins, and polysaccharides.6 Pearl powder is known to have exhibited antiaging, antioxidant, antiradiative, and tonic activities; in recent years, it has been incorporated into health foods for such properties and used in the clinical setting to treat ulcers (aphthous, gastric, and duodenal).4,7 Consisting of multiple active proteins, pearl powder is thought to be conducive to skin cell growth and effective for wound repair.4 This column focuses on recent research into the dermatologic potential of the powder derived from mother of pearl.
Wound healing
A decade ago, Jian-Ping et al. showed in mice that the water-soluble matrix of pearl powder (Hyriopsis cumingii) could significantly induce oral fibroblast proliferation and collagen accumulation, suppress matrix metalloproteinase-2 activity, and significantly foster TIMP-1 synthesis. The investigators concluded that the wound healing facilitated by pearl powder derives, in part, from its capacity to promote fibroblast mitosis, collagen deposition, and production of TIMP-1.8
Two years later, Lee et al. evaluated the effects of water-soluble nacre (mother of pearl) on second-degree burn wound healing in porcine skin as a proxy for human skin. They found that its application quickly led to burn-induced granulation areas filling with collagen, with normal skin appearance restored to wounded dermis and epidermis. Angiogenesis was also promoted by water-soluble nacre as was wound recovery in areas with apoptotic and necrotic cellular damage. Murine fibroblast NIH3T3 cells treated with water-soluble nacre also demonstrated augmented proliferation and collagen production. The researchers cited the restoration of angiogenesis and fibroblast activity as the primary benefits of water-soluble nacre, suggesting its potential as a wound therapy, preferable to powdered nacre due to better biocompatibility with less discomfort.9
The next year, Li et al. found that mother of pearl extract promoted cell migration of fibroblasts in cell culture, demonstrating its potential as a wound healing model.7In 2019, Chen et al. studied the effects of pearl powders of varying particle sizes to treat wounds in vitro and in vivo. They found that micro- and nanosized pearl powders augmented proliferation and migration of skin cells and shortened wound closure time. All powders also improved the biomechanical strength of healed skin, enhanced collagen formation and deposition, and expanded cutaneous angiogenesis, with nanoscale pearl powder displaying greatest efficiency.4
Skin tone and atopic dermatitis
In 2000, Lopez et al. implanted powdered nacre (mother of pearl derived from Pinctada maxima), which can promote and regulate bone-forming cells, into rat dermis to evaluate its effects on skin fibroblasts. They noted that the implant yielded well-vascularized tissue and improved extracellular matrix production, synthesis of substances involved in cellular adhesion and communication, and tissue regeneration (such as collagen types I and III). The investigators concluded that the powdered nacre contributed to the conditions necessary for improved skin tone and proper physiologic functioning of the skin.10
Rousseau et al. extracted lipids from the nacre of the oyster P. margaritifera to test on artificially dehydrated skin explants with the intention of developing new treatments for atopic dermatitis. The researchers determined that the lipids spurred a reconstitution of the intercellular material of the stratum corneum, concluding that new products to treat atopic dermatitis might be based on the signaling activity of nacre lipids.11
Antifibrotic and anti-inflammatory activity
A 2015 study by Yang et al. showed that a room-temperature superextraction system to yield the main active constituents of pearl was successful in enhancing their anti-inflammatory and antiapoptotic activity in human keratinocyte cells (HaCaT) exposed to low-dose UVB. The investigators combined pearl extract and poly (gamma-glutamic acid) hydrogels and observed reductions in inflammation and apoptosis of HaCaT cells. They concluded that a marketed pearl extract may be able to suppress radiation dermatitis present in keratinocytes.12
Two years later, Latire et al. used human dermal fibroblasts in primary culture to assess the potential biological activities of the matrix macromolecular components extracted from the shells of two edible mollusks (the blue mussel Mytilus edulis and the Pacific oyster Crassostrea gigas). The investigators found that both extracts influenced metabolic functions of the cells and reduced type I collagen levels, with an associated rise in matrix metalloproteinase-1 activity. Given their findings implying the effectiveness of the extracts in facilitating the catabolic pathway of human dermal fibroblasts, the authors suggest that these shell matrices present the potential for use in treating fibrosis, especially for scleroderma.6
Antioxidant and antiaging activity
Shao et al. demonstrated 10 years ago that pearl powder provides a moisturizing effect on the skin, with ultramicro pearl powder delivering a more robust moisturizing result than water-soluble pearl powder. These two types of pearl powder, along with another one tested (ultranano pearl powder), also significantly diminished the activation of tyrosinase and free radicals. Water-soluble pearl powder did not perform as well as the other two formulations in free radical scavenging. The investigators suggested that their results support the use of pearl powder to combat aging and enhance beauty, and could be used in the clinical setting.13
In 2017, Yang et al. reported on the in vitro antihemolytic and antioxidant activity of pearl powder in shielding human erythrocytes against 2,2’-azobis(2-amidinopropane) dihydrochloride–induced oxidative damage to membrane proteins/lipids. The researchers contend that the strong antioxidant qualities of pearl powder could be applied to prevent or protect against various diseases resulting from free radical damage.2
Human trials: Antioxidant, antiaging, skin appearance
Chiu et al. studied the antioxidant activity of various pearl powder extracts in a randomized, placebo-controlled trial in 2018. They also investigated the life span–prolonging effects of the powders using wild-type Caenorhabditis elegans. Twenty healthy middle-aged subjects were separated into two groups (experimental and placebo), with 3 g of pearl powder administered in capsules to the former and 3 g of placebo to the latter over 8 weeks. Blood samples taken at the beginning and every 2 weeks during the trial and in the 10th week revealed maximum antioxidant activity of the pearl powder and prolongation of C. elegans lifespan by 18.87%. Subjects using pearl powder demonstrated significant increases in total antioxidant capacity, thiols, glutathione, and enzymic antioxidant activity, along with notably inhibited lipid peroxidation products. The investigators concluded that pearl powder extract acted as a potent antioxidant and its use may be warranted to treat degenerative conditions related to aging.3
A recent study of the perception of blue light on Korean women’s faces using blue pearl pigment revealed that the pigment does indeed elicit the perception of the blue-light effect, notably transparency and gloss, which is particularly valued in Korea.14
Conclusion
The use of mother of pearl and pearl powder in traditional Chinese medicine and as a cosmetic and food additive has a rich and lengthy history. Contemporary research clearly suggests interesting avenues for further investigation and some promising results. Much more research is necessary, though, to delineate the potential roles of pearl powder in the skin care arsenal.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014), and a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems. Write to her at dermnews@mdedge.com
References
1. Zhang J et al. J Sep Sci. 2015 May;38(9):1552-60.
2. Yang HL et al. J Food Drug Anal. 2017 Oct;25(4):898-907.
3. Chiu HF et al. J Food Drug Anal. 2018 Jan;26(1):309-17.
4. Chen X et al. Drug Dev Ind Pharm. 2019 Jun;45(6):1009-16.
5. Nagai K. Zoolog Sci. 2013 Oct;30(10):783-93.
6. Latire T et al. Cytotechnology. 2017 Oct;69(5):815-29.
7. Li YC et al. Pharm Biol. 2013 Mar;51(3):289-97.
8. Jian-Ping D et al. Pharm Biol. 2010 Feb;48(2):122-7.
9. Lee K et al. Mol Biol Rep. 2012 Mar;39(3):3211-8.
10. Lopez E et al. Tissue Cell. 2000 Feb;32(1):95-101.
11. Rousseau M et al. Comp Biochem Physiol B Biochem Mol Biol. 2006 Sep;145(1):1-9.
12. Yang YL et al. Biomed Mater Eng. 2015;26 Suppl 1:S139-45.
13. Shao DZ et al. J Cosmet Sci. 2010 Mar-Apr;61(2):133-45.
14. Lee M et al. Skin Res Technol. 2020 Jan;26(1):76-80.
Resources for LGBTQ youth during challenging times
If you are anything like me, March 1 came and went as just another first day of the month. Few of us could have imagined that our day-to-day way of life would soon be upended, and our country would be in the midst of the COVID-19 pandemic. While there is considerable anxiety around protecting our individual health, social distancing and the physical isolation that comes from it have cut off a vital source of support for many of our lesbian, gay, bisexual, transgender, and questioning (or queer) (LGBTQ) youth. Shared experiences with other young people like themselves provide these youth with a sense of community that they may not find in their schools, towns, etc.
LGBTQ youth already face increased rates of anxiety and depression compared with their heterosexual and cisgender peers. According to the 2017 Youth Risk Behavior Survey, 63% of LGB youth nationwide reported feeling sad or hopeless compared with 28% of their heterosexual peers. While quarantined at home, many of these youth now are stuck for many more hours per day with families who may not accept them for who they are. Previous research by Ryan et al. shows that LGB adolescents who have higher rates of family rejection are nearly six times more likely to have higher rates of depression and more than eight times more likely to attempt suicide than their peers who come from families with low or no levels of rejection (Pediatrics. 2009 Jan;123[1]:346-52). Going to school for roughly 8 hours a day allows some of these youth an escape from what is otherwise an unpleasant home situation. In addition, educators and other school staff may be among the only allies that a student has in his/her life, and school cancellations remove students from access to these important people.
Due to stay-at-home orders and physical distancing measures, lack of in-person access to medical and psychological care can be distressing for many LGBTQ youth. While many practices have been able to convert to audiovisual telemedicine visits, not all of them have the resources or capability to do so. Consequently, LGBTQ youth may have reduced access to support services that help to bolster their social and emotional health. In addition, many trans youth suffer from physical dysphoria that can make it distressing to see themselves on camera doing teletherapy and so they wish to avoid it for this reason.
This is not to say that everything is bleak. LGBTQ youth can also be resilient in times of stress and worry. “The LGBTQ community has a long history of overcoming adversity and utilizing challenges to build an even stronger sense of community. This pandemic will create yet another opportunity for us to highlight existing health disparities and to support our LGBTQ young people in finding creative responses,” said Heather Newby, LCSW, clinical social worker for the GENECIS (GENder Education and Care Interdisciplinary Support) Program at Children’s Medical Center Dallas. In addition, she reported that many LGBTQ advocacy groups have created excellent online support networks and resources to provide nationwide, regional, and local help.
During these challenging times, there are a number of resources that LGBTQ youth can turn to while trying to maintain their connection to their peers. First, many local LGBTQ service organizations have moved their in-person support groups to a virtual or online platform. Check with your local service organization to see what they are offering during these times. National organizations, such as Gender Spectrum, continue to have online groups as well that youth can participate in. Second, many virtual mental health helplines, such as those through the Trevor Project, remain staffed should LGBTQ youth need to access their services (1-866-488-7386, plus text and chat). They can be reached 24/7 to help those whose mental health has been affected during this pandemic. Third, youth can continue to stay connected to their friends through means such as Zoom, FaceTime, or other virtual audiovisual tools. Lastly, some youth have taken to meeting in school parking lots, mall parking lots, etc., and staying at least 6 feet apart so that they can still see their friends in person.

While the current times may be challenging, they will pass and we will be able to return to those activities that bring us joy. Do not hesitate to reach out if you need help. As Rainer Maria Rilke once said, “In the difficult, we must have our joys, our happiness, our dreams: There against the depth of this background, they stand out, there for the first time we see how beautiful they are.”
Dr. Cooper is assistant professor of pediatrics at University of Texas Southwestern, Dallas, and an adolescent medicine specialist at Children’s Medical Center Dallas. He has no relevant financial disclosures. Dr. Cooper is on Twitter @teendocmbc. Email him at pdnews@mdedge.com.
If you are anything like me, March 1 came and went as just another first day of the month. Few of us could have imagined that our day-to-day way of life would soon be upended, and our country would be in the midst of the COVID-19 pandemic. While there is considerable anxiety around protecting our individual health, social distancing and the physical isolation that comes from it have cut off a vital source of support for many of our lesbian, gay, bisexual, transgender, and questioning (or queer) (LGBTQ) youth. Shared experiences with other young people like themselves provide these youth with a sense of community that they may not find in their schools, towns, etc.
LGBTQ youth already face increased rates of anxiety and depression compared with their heterosexual and cisgender peers. According to the 2017 Youth Risk Behavior Survey, 63% of LGB youth nationwide reported feeling sad or hopeless compared with 28% of their heterosexual peers. While quarantined at home, many of these youth now are stuck for many more hours per day with families who may not accept them for who they are. Previous research by Ryan et al. shows that LGB adolescents who have higher rates of family rejection are nearly six times more likely to have higher rates of depression and more than eight times more likely to attempt suicide than their peers who come from families with low or no levels of rejection (Pediatrics. 2009 Jan;123[1]:346-52). Going to school for roughly 8 hours a day allows some of these youth an escape from what is otherwise an unpleasant home situation. In addition, educators and other school staff may be among the only allies that a student has in his/her life, and school cancellations remove students from access to these important people.
Due to stay-at-home orders and physical distancing measures, lack of in-person access to medical and psychological care can be distressing for many LGBTQ youth. While many practices have been able to convert to audiovisual telemedicine visits, not all of them have the resources or capability to do so. Consequently, LGBTQ youth may have reduced access to support services that help to bolster their social and emotional health. In addition, many trans youth suffer from physical dysphoria that can make it distressing to see themselves on camera doing teletherapy and so they wish to avoid it for this reason.
This is not to say that everything is bleak. LGBTQ youth can also be resilient in times of stress and worry. “The LGBTQ community has a long history of overcoming adversity and utilizing challenges to build an even stronger sense of community. This pandemic will create yet another opportunity for us to highlight existing health disparities and to support our LGBTQ young people in finding creative responses,” said Heather Newby, LCSW, clinical social worker for the GENECIS (GENder Education and Care Interdisciplinary Support) Program at Children’s Medical Center Dallas. In addition, she reported that many LGBTQ advocacy groups have created excellent online support networks and resources to provide nationwide, regional, and local help.
During these challenging times, there are a number of resources that LGBTQ youth can turn to while trying to maintain their connection to their peers. First, many local LGBTQ service organizations have moved their in-person support groups to a virtual or online platform. Check with your local service organization to see what they are offering during these times. National organizations, such as Gender Spectrum, continue to have online groups as well that youth can participate in. Second, many virtual mental health helplines, such as those through the Trevor Project, remain staffed should LGBTQ youth need to access their services (1-866-488-7386, plus text and chat). They can be reached 24/7 to help those whose mental health has been affected during this pandemic. Third, youth can continue to stay connected to their friends through means such as Zoom, FaceTime, or other virtual audiovisual tools. Lastly, some youth have taken to meeting in school parking lots, mall parking lots, etc., and staying at least 6 feet apart so that they can still see their friends in person.
While the current times may be challenging, they will pass and we will be able to return to those activities that bring us joy. Do not hesitate to reach out if you need help. As Rainer Maria Rilke once said, “In the difficult, we must have our joys, our happiness, our dreams: There against the depth of this background, they stand out, there for the first time we see how beautiful they are.”
Dr. Cooper is assistant professor of pediatrics at University of Texas Southwestern, Dallas, and an adolescent medicine specialist at Children’s Medical Center Dallas. He has no relevant financial disclosures. Dr. Cooper is on Twitter @teendocmbc. Email him at pdnews@mdedge.com.
If you are anything like me, March 1 came and went as just another first day of the month. Few of us could have imagined that our day-to-day way of life would soon be upended, and our country would be in the midst of the COVID-19 pandemic. While there is considerable anxiety around protecting our individual health, social distancing and the physical isolation that comes from it have cut off a vital source of support for many of our lesbian, gay, bisexual, transgender, and questioning (or queer) (LGBTQ) youth. Shared experiences with other young people like themselves provide these youth with a sense of community that they may not find in their schools, towns, etc.
LGBTQ youth already face increased rates of anxiety and depression compared with their heterosexual and cisgender peers. According to the 2017 Youth Risk Behavior Survey, 63% of LGB youth nationwide reported feeling sad or hopeless compared with 28% of their heterosexual peers. While quarantined at home, many of these youth now are stuck for many more hours per day with families who may not accept them for who they are. Previous research by Ryan et al. shows that LGB adolescents who have higher rates of family rejection are nearly six times more likely to have higher rates of depression and more than eight times more likely to attempt suicide than their peers who come from families with low or no levels of rejection (Pediatrics. 2009 Jan;123[1]:346-52). Going to school for roughly 8 hours a day allows some of these youth an escape from what is otherwise an unpleasant home situation. In addition, educators and other school staff may be among the only allies that a student has in his/her life, and school cancellations remove students from access to these important people.
Due to stay-at-home orders and physical distancing measures, lack of in-person access to medical and psychological care can be distressing for many LGBTQ youth. While many practices have been able to convert to audiovisual telemedicine visits, not all of them have the resources or capability to do so. Consequently, LGBTQ youth may have reduced access to support services that help to bolster their social and emotional health. In addition, many trans youth suffer from physical dysphoria that can make it distressing to see themselves on camera doing teletherapy and so they wish to avoid it for this reason.
This is not to say that everything is bleak. LGBTQ youth can also be resilient in times of stress and worry. “The LGBTQ community has a long history of overcoming adversity and utilizing challenges to build an even stronger sense of community. This pandemic will create yet another opportunity for us to highlight existing health disparities and to support our LGBTQ young people in finding creative responses,” said Heather Newby, LCSW, clinical social worker for the GENECIS (GENder Education and Care Interdisciplinary Support) Program at Children’s Medical Center Dallas. In addition, she reported that many LGBTQ advocacy groups have created excellent online support networks and resources to provide nationwide, regional, and local help.
During these challenging times, there are a number of resources that LGBTQ youth can turn to while trying to maintain their connection to their peers. First, many local LGBTQ service organizations have moved their in-person support groups to a virtual or online platform. Check with your local service organization to see what they are offering during these times. National organizations, such as Gender Spectrum, continue to have online groups as well that youth can participate in. Second, many virtual mental health helplines, such as those through the Trevor Project, remain staffed should LGBTQ youth need to access their services (1-866-488-7386, plus text and chat). They can be reached 24/7 to help those whose mental health has been affected during this pandemic. Third, youth can continue to stay connected to their friends through means such as Zoom, FaceTime, or other virtual audiovisual tools. Lastly, some youth have taken to meeting in school parking lots, mall parking lots, etc., and staying at least 6 feet apart so that they can still see their friends in person.
While the current times may be challenging, they will pass and we will be able to return to those activities that bring us joy. Do not hesitate to reach out if you need help. As Rainer Maria Rilke once said, “In the difficult, we must have our joys, our happiness, our dreams: There against the depth of this background, they stand out, there for the first time we see how beautiful they are.”
Dr. Cooper is assistant professor of pediatrics at University of Texas Southwestern, Dallas, and an adolescent medicine specialist at Children’s Medical Center Dallas. He has no relevant financial disclosures. Dr. Cooper is on Twitter @teendocmbc. Email him at pdnews@mdedge.com.
Oncologists need to advocate for scarce COVID-19 resources: ASCO
both at the institutional and regional level, according to new recommendations from the American Society for Clinical Oncology (ASCO).
“There was a lot of concern from the oncology community that if a patient had cancer, they would be arbitrarily excluded from consideration for critical care resources,” said Jonathan M. Marron, MD, chair-elect of ASCO’s Ethics Committee and lead author of the recommendations.
“The hope is that we’ll never have to make any of these decisions ... but the primary reason for putting together these recommendations was that if such decisions have to be made, we hope to inform them,” he told Medscape Medical News.
Marron, who is a pediatric hematologist at Boston Children’s Hospital, says ASCO’s main recommendation is that decisions about the allocation of resources must be separated from bedside clinical care, meaning that clinicians who are caring for individual patients should not also be the ones making the allocation decisions.
“Those dueling responsibilities are a conflict of interest and make that physician unable to make an unbiased decision,” he said.
“It’s also just an unbearable burden to try and do those two things simultaneously,” he added. “It’s an incredible burden to do them individually, but it’s multifold worse to try to do them both simultaneously.”
He said the vital role of oncologists who provide treatment is to offer the kind of personalized information that triage committees need in order to make appropriate decisions.
“They should be asked – maybe even must be asked – to provide the most high-quality evidence-based data about their patients’ diagnosis and prognosis,” Marron commented. “Because oncology is evolving so rapidly, and cancer is so many different diseases, it’s impossible for someone making these decisions to know everything they would need to know about why this patient is likely to survive their cancer and this patient is not.”
He says that during the COVID-19 pandemic, concerns regarding public health transcend the well-being of individual patients and that consideration must be given to providing the maximum benefit to the greatest number of people.
“That makes perfect sense and is the appropriate and laudable goal during a public health emergency like this ... but one of the challenges is that there is this belief that a diagnosis of cancer is uniformly fatal,” Marron said.
“It’s certainly conceivable that it would be a better use of resources to give the last ventilator to a young, otherwise healthy patient rather than a patient with multiply recurrent progressive metastatic cancer,” he continued. “However, we want to ensure that there is at least a discussion where that information is made available, rather than just saying, ‘She’s got cancer. She’s a lost cause.’ ”
Cancer patients are doing very well
Concerns about cancer misconceptions have been circulating in the oncology community since the start of the pandemic. “It’s really important that people understand that cancer patients are doing very well nowadays, and even with a diagnosis of cancer, they can potentially live for many years,” Anne Chiang, MD, PhD, from the Smilow Cancer Network, New Haven, Connecticut, told Medscape Medical News in a recent interview.
Thus far, even in hard-hit New York City, fears that cancer patients may not be receiving appropriate care have not materialized, according to Mark Robson, MD, a medical oncologist at Memorial Sloan Kettering Cancer Center (MSKCC). “I would emphasize that cancer patients are ABSOLUTELY getting the care they need, including patients with metastatic disease,” he recently tweeted. “NOONE at @sloan_kettering (or anywhere else) is being ‘triaged’ because of advanced cancer. Period.”
Robson told Medscape Medical News that although MSKCC continues to provide oncology care to patients with cancer, “we are [also] treating them if they develop COVID. ... I am trying to help pivot the institution towards care in this setting.”
He said he agrees with Craig Spencer, MD, MPH, director of global health in emergency medicine at the New York–Presbyterian/Columbia University Medical Center, who recently tweeted, “If you need a ventilator, you get a ventilator. Let’s be clear – this isn’t being ‘rationed.’ ”
Marron emphasized that an important safeguard against uninformed decision making is appropriate planning. For hospitalized patients, this means oncologists who provide treatment should offer information even before it is requested. But he said the “duty to plan” begins long before that.
“Clinicians haven’t always been great at talking about death and long-term outcomes with their patients, but this really cranks up the importance of having those conversations, and having them early, even though it’s incredibly hard. If someone has expressed that they would never want to be put on a ventilator, it’s important now even more so that is made clear,” he said.
He said early responses to the ASCO statement suggest that it has calmed some concerns in the oncology community, “but it still remains to be seen whether individual institutions will take this to heart, because this unto itself cannot enforce anything – it is up to individual institutions. I am hopeful this will get to the people it needs to get to.”
This article first appeared on Medscape.com.
both at the institutional and regional level, according to new recommendations from the American Society for Clinical Oncology (ASCO).
“There was a lot of concern from the oncology community that if a patient had cancer, they would be arbitrarily excluded from consideration for critical care resources,” said Jonathan M. Marron, MD, chair-elect of ASCO’s Ethics Committee and lead author of the recommendations.
“The hope is that we’ll never have to make any of these decisions ... but the primary reason for putting together these recommendations was that if such decisions have to be made, we hope to inform them,” he told Medscape Medical News.
Marron, who is a pediatric hematologist at Boston Children’s Hospital, says ASCO’s main recommendation is that decisions about the allocation of resources must be separated from bedside clinical care, meaning that clinicians who are caring for individual patients should not also be the ones making the allocation decisions.
“Those dueling responsibilities are a conflict of interest and make that physician unable to make an unbiased decision,” he said.
“It’s also just an unbearable burden to try and do those two things simultaneously,” he added. “It’s an incredible burden to do them individually, but it’s multifold worse to try to do them both simultaneously.”
He said the vital role of oncologists who provide treatment is to offer the kind of personalized information that triage committees need in order to make appropriate decisions.
“They should be asked – maybe even must be asked – to provide the most high-quality evidence-based data about their patients’ diagnosis and prognosis,” Marron commented. “Because oncology is evolving so rapidly, and cancer is so many different diseases, it’s impossible for someone making these decisions to know everything they would need to know about why this patient is likely to survive their cancer and this patient is not.”
He says that during the COVID-19 pandemic, concerns regarding public health transcend the well-being of individual patients and that consideration must be given to providing the maximum benefit to the greatest number of people.
“That makes perfect sense and is the appropriate and laudable goal during a public health emergency like this ... but one of the challenges is that there is this belief that a diagnosis of cancer is uniformly fatal,” Marron said.
“It’s certainly conceivable that it would be a better use of resources to give the last ventilator to a young, otherwise healthy patient rather than a patient with multiply recurrent progressive metastatic cancer,” he continued. “However, we want to ensure that there is at least a discussion where that information is made available, rather than just saying, ‘She’s got cancer. She’s a lost cause.’ ”
Cancer patients are doing very well
Concerns about cancer misconceptions have been circulating in the oncology community since the start of the pandemic. “It’s really important that people understand that cancer patients are doing very well nowadays, and even with a diagnosis of cancer, they can potentially live for many years,” Anne Chiang, MD, PhD, from the Smilow Cancer Network, New Haven, Connecticut, told Medscape Medical News in a recent interview.
Thus far, even in hard-hit New York City, fears that cancer patients may not be receiving appropriate care have not materialized, according to Mark Robson, MD, a medical oncologist at Memorial Sloan Kettering Cancer Center (MSKCC). “I would emphasize that cancer patients are ABSOLUTELY getting the care they need, including patients with metastatic disease,” he recently tweeted. “NOONE at @sloan_kettering (or anywhere else) is being ‘triaged’ because of advanced cancer. Period.”
Robson told Medscape Medical News that although MSKCC continues to provide oncology care to patients with cancer, “we are [also] treating them if they develop COVID. ... I am trying to help pivot the institution towards care in this setting.”
He said he agrees with Craig Spencer, MD, MPH, director of global health in emergency medicine at the New York–Presbyterian/Columbia University Medical Center, who recently tweeted, “If you need a ventilator, you get a ventilator. Let’s be clear – this isn’t being ‘rationed.’ ”
Marron emphasized that an important safeguard against uninformed decision making is appropriate planning. For hospitalized patients, this means oncologists who provide treatment should offer information even before it is requested. But he said the “duty to plan” begins long before that.
“Clinicians haven’t always been great at talking about death and long-term outcomes with their patients, but this really cranks up the importance of having those conversations, and having them early, even though it’s incredibly hard. If someone has expressed that they would never want to be put on a ventilator, it’s important now even more so that is made clear,” he said.
He said early responses to the ASCO statement suggest that it has calmed some concerns in the oncology community, “but it still remains to be seen whether individual institutions will take this to heart, because this unto itself cannot enforce anything – it is up to individual institutions. I am hopeful this will get to the people it needs to get to.”
This article first appeared on Medscape.com.
both at the institutional and regional level, according to new recommendations from the American Society for Clinical Oncology (ASCO).
“There was a lot of concern from the oncology community that if a patient had cancer, they would be arbitrarily excluded from consideration for critical care resources,” said Jonathan M. Marron, MD, chair-elect of ASCO’s Ethics Committee and lead author of the recommendations.
“The hope is that we’ll never have to make any of these decisions ... but the primary reason for putting together these recommendations was that if such decisions have to be made, we hope to inform them,” he told Medscape Medical News.
Marron, who is a pediatric hematologist at Boston Children’s Hospital, says ASCO’s main recommendation is that decisions about the allocation of resources must be separated from bedside clinical care, meaning that clinicians who are caring for individual patients should not also be the ones making the allocation decisions.
“Those dueling responsibilities are a conflict of interest and make that physician unable to make an unbiased decision,” he said.
“It’s also just an unbearable burden to try and do those two things simultaneously,” he added. “It’s an incredible burden to do them individually, but it’s multifold worse to try to do them both simultaneously.”
He said the vital role of oncologists who provide treatment is to offer the kind of personalized information that triage committees need in order to make appropriate decisions.
“They should be asked – maybe even must be asked – to provide the most high-quality evidence-based data about their patients’ diagnosis and prognosis,” Marron commented. “Because oncology is evolving so rapidly, and cancer is so many different diseases, it’s impossible for someone making these decisions to know everything they would need to know about why this patient is likely to survive their cancer and this patient is not.”
He says that during the COVID-19 pandemic, concerns regarding public health transcend the well-being of individual patients and that consideration must be given to providing the maximum benefit to the greatest number of people.
“That makes perfect sense and is the appropriate and laudable goal during a public health emergency like this ... but one of the challenges is that there is this belief that a diagnosis of cancer is uniformly fatal,” Marron said.
“It’s certainly conceivable that it would be a better use of resources to give the last ventilator to a young, otherwise healthy patient rather than a patient with multiply recurrent progressive metastatic cancer,” he continued. “However, we want to ensure that there is at least a discussion where that information is made available, rather than just saying, ‘She’s got cancer. She’s a lost cause.’ ”
Cancer patients are doing very well
Concerns about cancer misconceptions have been circulating in the oncology community since the start of the pandemic. “It’s really important that people understand that cancer patients are doing very well nowadays, and even with a diagnosis of cancer, they can potentially live for many years,” Anne Chiang, MD, PhD, from the Smilow Cancer Network, New Haven, Connecticut, told Medscape Medical News in a recent interview.
Thus far, even in hard-hit New York City, fears that cancer patients may not be receiving appropriate care have not materialized, according to Mark Robson, MD, a medical oncologist at Memorial Sloan Kettering Cancer Center (MSKCC). “I would emphasize that cancer patients are ABSOLUTELY getting the care they need, including patients with metastatic disease,” he recently tweeted. “NOONE at @sloan_kettering (or anywhere else) is being ‘triaged’ because of advanced cancer. Period.”
Robson told Medscape Medical News that although MSKCC continues to provide oncology care to patients with cancer, “we are [also] treating them if they develop COVID. ... I am trying to help pivot the institution towards care in this setting.”
He said he agrees with Craig Spencer, MD, MPH, director of global health in emergency medicine at the New York–Presbyterian/Columbia University Medical Center, who recently tweeted, “If you need a ventilator, you get a ventilator. Let’s be clear – this isn’t being ‘rationed.’ ”
Marron emphasized that an important safeguard against uninformed decision making is appropriate planning. For hospitalized patients, this means oncologists who provide treatment should offer information even before it is requested. But he said the “duty to plan” begins long before that.
“Clinicians haven’t always been great at talking about death and long-term outcomes with their patients, but this really cranks up the importance of having those conversations, and having them early, even though it’s incredibly hard. If someone has expressed that they would never want to be put on a ventilator, it’s important now even more so that is made clear,” he said.
He said early responses to the ASCO statement suggest that it has calmed some concerns in the oncology community, “but it still remains to be seen whether individual institutions will take this to heart, because this unto itself cannot enforce anything – it is up to individual institutions. I am hopeful this will get to the people it needs to get to.”
This article first appeared on Medscape.com.
Suicide increased 35% during 1999-2018 in the U.S.
Age-adjusted suicide rate rose from 10.5 per 100,000 to 14.2 from 1999 to 2018, according to trends reported by the Centers for Disease Control and Prevention in a data brief.
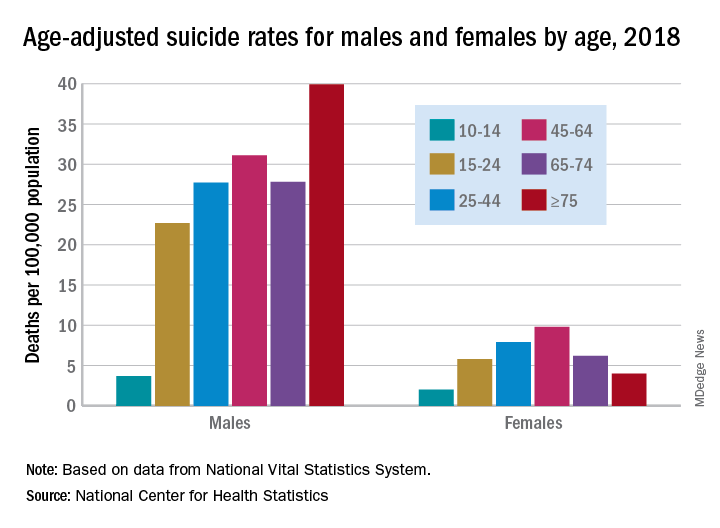
Holly Hedegaard, MD, and colleagues from the National Center for Health Statistics within the CDC analyzed final mortality data from the National Vital Statistics System. As the second most common cause of death among Americans aged 10-34 years and the fourth most common among those aged 35-54 years, suicide is a major contributer to premature mortality.
at 22.8 and 6.2 per 100,000, respectively. Young people aged 10-14 years among both genders had the lowest rates of completing suicide, but it was men aged 75 years and older and women aged 45-64 years who had the highest rates. All of these trends were consistent throughout the study period.
Drawing from the 2013 National Center for Health Statistics Urban-Rural Classification Scheme for Counties, the researchers found that rural counties had significantly higher rates of suicide than did urban counties in 2018, and this was true for men and women. That said, suicide rates were still 3.5-3.9 times higher among men than among women regardless of urbanicity or rurality that year.
The full data brief can be found on the CDC website.
Age-adjusted suicide rate rose from 10.5 per 100,000 to 14.2 from 1999 to 2018, according to trends reported by the Centers for Disease Control and Prevention in a data brief.
Holly Hedegaard, MD, and colleagues from the National Center for Health Statistics within the CDC analyzed final mortality data from the National Vital Statistics System. As the second most common cause of death among Americans aged 10-34 years and the fourth most common among those aged 35-54 years, suicide is a major contributer to premature mortality.
at 22.8 and 6.2 per 100,000, respectively. Young people aged 10-14 years among both genders had the lowest rates of completing suicide, but it was men aged 75 years and older and women aged 45-64 years who had the highest rates. All of these trends were consistent throughout the study period.
Drawing from the 2013 National Center for Health Statistics Urban-Rural Classification Scheme for Counties, the researchers found that rural counties had significantly higher rates of suicide than did urban counties in 2018, and this was true for men and women. That said, suicide rates were still 3.5-3.9 times higher among men than among women regardless of urbanicity or rurality that year.
The full data brief can be found on the CDC website.
Age-adjusted suicide rate rose from 10.5 per 100,000 to 14.2 from 1999 to 2018, according to trends reported by the Centers for Disease Control and Prevention in a data brief.
Holly Hedegaard, MD, and colleagues from the National Center for Health Statistics within the CDC analyzed final mortality data from the National Vital Statistics System. As the second most common cause of death among Americans aged 10-34 years and the fourth most common among those aged 35-54 years, suicide is a major contributer to premature mortality.
at 22.8 and 6.2 per 100,000, respectively. Young people aged 10-14 years among both genders had the lowest rates of completing suicide, but it was men aged 75 years and older and women aged 45-64 years who had the highest rates. All of these trends were consistent throughout the study period.
Drawing from the 2013 National Center for Health Statistics Urban-Rural Classification Scheme for Counties, the researchers found that rural counties had significantly higher rates of suicide than did urban counties in 2018, and this was true for men and women. That said, suicide rates were still 3.5-3.9 times higher among men than among women regardless of urbanicity or rurality that year.
The full data brief can be found on the CDC website.
Social distancing comes to the medicine wards
As the coronavirus pandemic has swept across America, so have advisories for social distancing. As of April 2, stay-at-home orders had been given in 38 states and parts of 7 more, affecting about 300 million people. Most of these people have been asked to maintain 6 feet of separation to anyone outside their immediate family and to avoid all avoidable contacts.

Typical hospital medicine patients at an academic hospital, however, traditionally receive visits from their hospitalist, an intern, a resident, and sometimes several medical students, pharmacists, and case managers. At University of California, San Diego, Health, many of these visits would occur during Focused Interdisciplinary Team rounds, with providers moving together in close proximity.
Asymptomatic and presymptomatic spread of coronavirus have been documented, which means distancing is a good idea for everyone. The risks of traditional patient visits during the coronavirus pandemic include spread to both patients (at high risk of complications) and staff (taken out of the workforce during surge times). Even if coronavirus were not a risk, visits to isolation rooms consume PPE, which is in short supply.

In response to the pandemic, UCSD Hospital Medicine drafted guidelines for the reduction of patient contacts. Our slide presentations and written guidelines were then distributed to physicians, nurses, pharmacists, and other staff by our pandemic response command center. Key points include the following:
- Target one in-person MD visit per day for stable patients. This means that attending reexaminations of patients seen by residents, nurse practitioners, physician assistants, and so on would not be done for billing or teaching purposes, only when clinically necessary.
- Use phone or video conferencing for follow-up discussions unless direct patient contact is needed.
- Consider skipping daily exams on patients who do not require them, such as patients awaiting placement or stably receiving long courses of antibiotics. Interview them remotely or from the door instead.
- Conduct team rounds, patient discussions, and handoffs with all members 6 feet apart or by telephone or video. Avoid shared work rooms. Substitute video conferences for in-person meetings. Use EMR embedded messaging to reduce face-to-face discussions.
- Check if a patient is ready for a visit before donning PPE to avoid waste.
- Explain to patients that distancing is being conducted to protect them. In our experience, when patients are asked about distancing, they welcome the changes.

We have also considered that most patient visits are generated by nurses and assistants. To increase distancing and reduce PPE waste, we have encouraged nurses and pharmacists to maximize their use of remote communication with patients and to suggest changes to care plans and come up with creative solutions to reduce traffic. We specifically suggested the following changes to routine care:
- Reduce frequency of taking vital signs, such as just daily or as needed, in stable patients (for example, those awaiting placement).
- Reduce checks for alcohol withdrawal and neurologic status as soon as possible, and stop fingersticks in patients with well-controlled diabetes not receiving insulin.
- Substitute less frequently administered medications where appropriate if doing so would reduce room traffic (such as enoxaparin for heparin, ceftriaxone for cefazolin, naproxen for ibuprofen, or patient-controlled analgesia for as needed morphine).
- Place intravenous pumps in halls if needed – luckily, our situation has not required these measures in San Diego.
- Explore the possibility of increased patient self-management (self-dosed insulin or inhalers) where medically appropriate.
- Eliminate food service and janitorial trips to isolation rooms unless requested by registered nurse.

There are clear downsides to medical distancing for hospital medicine patients. Patients might have delayed diagnosis of new conditions or inadequate management of conditions requiring frequent assessment, such as alcohol withdrawal. Opportunities for miscommunication (either patient-provider or provider-provider) may be increased with distancing. Isolation also comes with emotional costs such as stress and feelings of isolation or abandonment. Given the dynamic nature of the pandemic response, we are continually reevaluating our distancing guidelines to administer the safest and most effective hospital care possible as we approach California’s expected peak coronavirus infection period.
Dr. Jenkins is professor and chair of the Patient Safety Committee in the Division of Hospital Medicine at UCSD. Dr. Seymann is clinical professor and vice chief for academic affairs, UCSD division of hospital medicine. Dr. Horman and Dr. Bell are hospitalists and associate professors of medicine at UC San Diego Health.
As the coronavirus pandemic has swept across America, so have advisories for social distancing. As of April 2, stay-at-home orders had been given in 38 states and parts of 7 more, affecting about 300 million people. Most of these people have been asked to maintain 6 feet of separation to anyone outside their immediate family and to avoid all avoidable contacts.
Typical hospital medicine patients at an academic hospital, however, traditionally receive visits from their hospitalist, an intern, a resident, and sometimes several medical students, pharmacists, and case managers. At University of California, San Diego, Health, many of these visits would occur during Focused Interdisciplinary Team rounds, with providers moving together in close proximity.
Asymptomatic and presymptomatic spread of coronavirus have been documented, which means distancing is a good idea for everyone. The risks of traditional patient visits during the coronavirus pandemic include spread to both patients (at high risk of complications) and staff (taken out of the workforce during surge times). Even if coronavirus were not a risk, visits to isolation rooms consume PPE, which is in short supply.
In response to the pandemic, UCSD Hospital Medicine drafted guidelines for the reduction of patient contacts. Our slide presentations and written guidelines were then distributed to physicians, nurses, pharmacists, and other staff by our pandemic response command center. Key points include the following:
- Target one in-person MD visit per day for stable patients. This means that attending reexaminations of patients seen by residents, nurse practitioners, physician assistants, and so on would not be done for billing or teaching purposes, only when clinically necessary.
- Use phone or video conferencing for follow-up discussions unless direct patient contact is needed.
- Consider skipping daily exams on patients who do not require them, such as patients awaiting placement or stably receiving long courses of antibiotics. Interview them remotely or from the door instead.
- Conduct team rounds, patient discussions, and handoffs with all members 6 feet apart or by telephone or video. Avoid shared work rooms. Substitute video conferences for in-person meetings. Use EMR embedded messaging to reduce face-to-face discussions.
- Check if a patient is ready for a visit before donning PPE to avoid waste.
- Explain to patients that distancing is being conducted to protect them. In our experience, when patients are asked about distancing, they welcome the changes.
We have also considered that most patient visits are generated by nurses and assistants. To increase distancing and reduce PPE waste, we have encouraged nurses and pharmacists to maximize their use of remote communication with patients and to suggest changes to care plans and come up with creative solutions to reduce traffic. We specifically suggested the following changes to routine care:
- Reduce frequency of taking vital signs, such as just daily or as needed, in stable patients (for example, those awaiting placement).
- Reduce checks for alcohol withdrawal and neurologic status as soon as possible, and stop fingersticks in patients with well-controlled diabetes not receiving insulin.
- Substitute less frequently administered medications where appropriate if doing so would reduce room traffic (such as enoxaparin for heparin, ceftriaxone for cefazolin, naproxen for ibuprofen, or patient-controlled analgesia for as needed morphine).
- Place intravenous pumps in halls if needed – luckily, our situation has not required these measures in San Diego.
- Explore the possibility of increased patient self-management (self-dosed insulin or inhalers) where medically appropriate.
- Eliminate food service and janitorial trips to isolation rooms unless requested by registered nurse.
There are clear downsides to medical distancing for hospital medicine patients. Patients might have delayed diagnosis of new conditions or inadequate management of conditions requiring frequent assessment, such as alcohol withdrawal. Opportunities for miscommunication (either patient-provider or provider-provider) may be increased with distancing. Isolation also comes with emotional costs such as stress and feelings of isolation or abandonment. Given the dynamic nature of the pandemic response, we are continually reevaluating our distancing guidelines to administer the safest and most effective hospital care possible as we approach California’s expected peak coronavirus infection period.
Dr. Jenkins is professor and chair of the Patient Safety Committee in the Division of Hospital Medicine at UCSD. Dr. Seymann is clinical professor and vice chief for academic affairs, UCSD division of hospital medicine. Dr. Horman and Dr. Bell are hospitalists and associate professors of medicine at UC San Diego Health.
As the coronavirus pandemic has swept across America, so have advisories for social distancing. As of April 2, stay-at-home orders had been given in 38 states and parts of 7 more, affecting about 300 million people. Most of these people have been asked to maintain 6 feet of separation to anyone outside their immediate family and to avoid all avoidable contacts.
Typical hospital medicine patients at an academic hospital, however, traditionally receive visits from their hospitalist, an intern, a resident, and sometimes several medical students, pharmacists, and case managers. At University of California, San Diego, Health, many of these visits would occur during Focused Interdisciplinary Team rounds, with providers moving together in close proximity.
Asymptomatic and presymptomatic spread of coronavirus have been documented, which means distancing is a good idea for everyone. The risks of traditional patient visits during the coronavirus pandemic include spread to both patients (at high risk of complications) and staff (taken out of the workforce during surge times). Even if coronavirus were not a risk, visits to isolation rooms consume PPE, which is in short supply.
In response to the pandemic, UCSD Hospital Medicine drafted guidelines for the reduction of patient contacts. Our slide presentations and written guidelines were then distributed to physicians, nurses, pharmacists, and other staff by our pandemic response command center. Key points include the following:
- Target one in-person MD visit per day for stable patients. This means that attending reexaminations of patients seen by residents, nurse practitioners, physician assistants, and so on would not be done for billing or teaching purposes, only when clinically necessary.
- Use phone or video conferencing for follow-up discussions unless direct patient contact is needed.
- Consider skipping daily exams on patients who do not require them, such as patients awaiting placement or stably receiving long courses of antibiotics. Interview them remotely or from the door instead.
- Conduct team rounds, patient discussions, and handoffs with all members 6 feet apart or by telephone or video. Avoid shared work rooms. Substitute video conferences for in-person meetings. Use EMR embedded messaging to reduce face-to-face discussions.
- Check if a patient is ready for a visit before donning PPE to avoid waste.
- Explain to patients that distancing is being conducted to protect them. In our experience, when patients are asked about distancing, they welcome the changes.
We have also considered that most patient visits are generated by nurses and assistants. To increase distancing and reduce PPE waste, we have encouraged nurses and pharmacists to maximize their use of remote communication with patients and to suggest changes to care plans and come up with creative solutions to reduce traffic. We specifically suggested the following changes to routine care:
- Reduce frequency of taking vital signs, such as just daily or as needed, in stable patients (for example, those awaiting placement).
- Reduce checks for alcohol withdrawal and neurologic status as soon as possible, and stop fingersticks in patients with well-controlled diabetes not receiving insulin.
- Substitute less frequently administered medications where appropriate if doing so would reduce room traffic (such as enoxaparin for heparin, ceftriaxone for cefazolin, naproxen for ibuprofen, or patient-controlled analgesia for as needed morphine).
- Place intravenous pumps in halls if needed – luckily, our situation has not required these measures in San Diego.
- Explore the possibility of increased patient self-management (self-dosed insulin or inhalers) where medically appropriate.
- Eliminate food service and janitorial trips to isolation rooms unless requested by registered nurse.
There are clear downsides to medical distancing for hospital medicine patients. Patients might have delayed diagnosis of new conditions or inadequate management of conditions requiring frequent assessment, such as alcohol withdrawal. Opportunities for miscommunication (either patient-provider or provider-provider) may be increased with distancing. Isolation also comes with emotional costs such as stress and feelings of isolation or abandonment. Given the dynamic nature of the pandemic response, we are continually reevaluating our distancing guidelines to administer the safest and most effective hospital care possible as we approach California’s expected peak coronavirus infection period.
Dr. Jenkins is professor and chair of the Patient Safety Committee in the Division of Hospital Medicine at UCSD. Dr. Seymann is clinical professor and vice chief for academic affairs, UCSD division of hospital medicine. Dr. Horman and Dr. Bell are hospitalists and associate professors of medicine at UC San Diego Health.
Most e-consults not followed by specialist visit
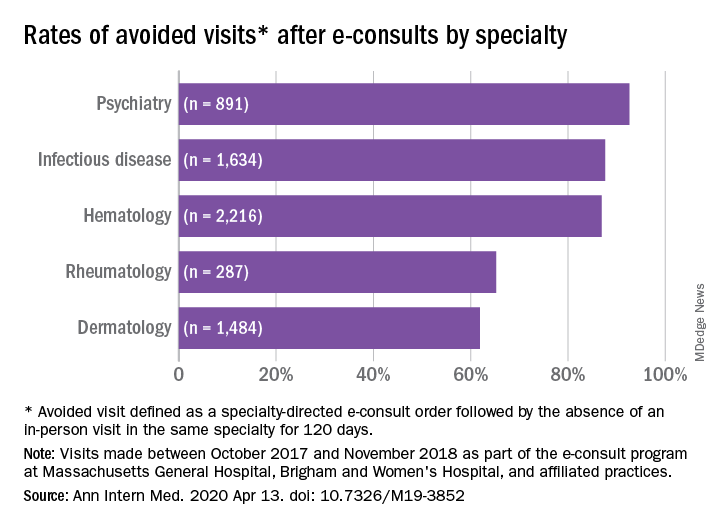
Studies have shown that e-consults increase access to specialist care and primary care physician (PCP) education, according to research published in the Annals of Internal Medicine (2020. Apr 14. doi: 10.7326/M19-3852) by Salman Ahmed, MD, and colleagues.
These resources are already being frequently used by physicians, but more often by general internists and hospitalists than by subspecialists, according to a recent survey by the American College of Physicians. That survey found that 42% of its respondents are using e-consults and that subspecialists’ use is less common primarily because of the lack of access to e-consult technology.
What hasn’t been widely researched are the effects of large-scale e-consult programs, said Dr. Ahmed, who is associate physician in the renal division at Brigham and Women’s Hospital, Boston, in an interview.
For frontline providers such as PCPs, e-consults are a way to quickly seek out answers to clinical questions from specialists. In turn, the specialist can help a wider pool of participants, he noted.
The findings of Dr. Ahmed’s study, which included several academic centers and hospitals affiliated with Partners HealthCare System, a nonprofit network in eastern Massachusetts that includes Brigham and Women’s Hospital, used several metrics to analyze the appropriateness and utility of e-consults across a range of specialties. An e-consult was considered useful if it resulted in the avoidance of a visit to a specialist, which was defined as the absence of an in-person visit to the type of specialist consulted electronically for 120 days. An e-consult was considered appropriate if it met the following four criteria.
- It could not be answered by referring to society guidelines or widely available, evidence-based summary sources.
- It did not seek logistic information, such as where to have a specific laboratory test done.
- It did not include a question of high urgency.
- The medical complexity of the clinical situation was not substantial enough to warrant an in-person consultation.
The investigators examined e-consult inquiries to mostly physician health care providers in five specialties – hematology, infectious disease, dermatology, rheumatology, and psychiatry – over a year.
High rates of appropriateness
The search spanned 6,512 eligible e-consults from 1,096 referring providers to 121 specialist consultants. Narrowing their search to 741 records with complete data, the investigators found that 70.2% of these consults met the criteria for appropriateness. In an analysis of four reviewers blinded to each other’s results, raters agreed on the appropriateness of 94% of e-consults.
Across specialties, more than 81% of e-consults were associated with avoided in-person visits.
The reasons for most e-consults were to seek answers to questions about diagnosis, therapeutics, or patient inquiries, or to request further education by PCPs.
“Across all specialties, the most common reasons an e-consult was not considered appropriate were failing the point-of-care resource test and asking a question of inappropriately high complexity,” the authors summarized.
Physicians and PCPs from tertiary care practices made up the majority of referring providers, with turnaround time for consults averaging 24 hours across specialties.
Rates of appropriateness, content, patient demographics, and timeliness of e-consult responses varied among the four specialties. Those with high avoidance of visits rates tended to have high appropriateness rates, indicating that some specialties may be more conducive to e-consults than others, the authors noted. Psychiatry and hematology had the highest proportion of appropriate e-consults (77.9% and 73.3% respectively). Rheumatology had the lowest proportion of appropriate e-consults and one of the lowest rates of avoided in-person visits, and dermatology had the lowest rate of avoided in-person visits, at 61.9%.
The majority (93%) of e-consults sought in psychiatry were therapy related, whereas 88.4% of the e-consult questions in rheumatology related to diagnosis.
“Questions about diagnosis were less likely to be answerable via e-consult, which suggests that to provide diagnoses, consultants may wish to engage with the patient directly,” Dr. Ahmed said in an interview.
Infectious disease specialists seemed to be the fastest responders, with nearly 90% of their consultations having been answered within a day. Dermatology specialists had the distinction of having the youngest e-consult patients (mean age, 38.6 years).
PCPs weigh in on results
Physicians said in interviews that the study data reflects their own positive experiences with e-consults.
“Although I don’t always think [an e-consult] is able to fully prevent the specialist visit, it does allow the specialist to provide recommendations for work-up that can be done prior to the specialist visit,” said Santina Wheat MD, a family physician at Erie Family Health Center in Chicago. This reduces the time in which the consult is placed to when effective treatment can take place.
Patients who may have to wait months or even years to see a specialty doctor, benefit from e-consults, said Dr. Wheat, who is also a member of the editorial advisory board of Family Practice News. “As part of an organization that does e-consults to another hospital with a different electronic medical record, the e-consult increases the likelihood that all of the clinical information reaches the specialists and prevents tests from being repeated.”
Starting an e-consult may also increase the likelihood that the patient quickly sees a specialist at the contracted hospital, she added.
Sarah G. Candler, MD, said in an interview that she also sees e-consults as an essential tool. “When patients present with rare, complex, or atypical pictures, I find it helpful to have specialists weigh in. The e-consult helps me ensure that I work to the top of my abilities as an internist,” said Dr. Candler, who is practice medical director and physician director of academic relations at Iora Primary Care, Northside Clinic, Houston. However, she did not agree with the study’s avoided in-person visits metric for assessing utility.
“In some cases, the end result of an e-consult is a referral for an in-person evaluation, and the role of the e-consult is to ensure that I have done my due diligence as a primary care doctor asking the correct questions, getting the appropriate work-up completed, and referring to the appropriate specialty for next steps, when necessary,” noted Dr. Candler, who also serves on the editorial advisory board of Internal Medicine News.
Financial considerations
The study’s authors suggested taking a closer look at standardizing payment for the use of e-consults and developing appropriateness criteria for them.
Health systems could use such criteria to study what makes an e-consult useful and how to best utilize this tool, Dr. Ahmed said in an interview.
“Compensation models that promote high-quality, effective, and efficient e-consults are needed to reinforce the ability of health systems to optimize the mix of e-consults and in-person visits,” Dr. Ahmed and colleagues suggested.
Because not all patient care requires e-consults, the model makes the most sense in practices that already participate in value-based payment programs. In these types of programs, the cost can be shared according to the variable risk and patient need for the service, Dr. Candler explained.
“I have been fortunate to work in two different systems that function in this way, which means that e-consults have been readily available and encouraged-both to improve patient care and decrease overall cost by decreasing unnecessary testing or specialist referral,” she said.
Dr. Wheat said that the managed care organization affiliated with her practice seems to be saving money with e-consults, as it decreases the need to pay for specialist visits in some instances and for repeated work-ups.
Future studies
The study’s cohort represented just one large health care system with a shared electronic health record. “Single-system descriptive studies, such as that of Ahmed and colleagues, are particularly useful for local evaluation and quality improvement efforts,” Varsha G. Vimalananda, MD, and B. Graeme Fincke, MD, both of the Center for Healthcare Organization and Implementation Research at Bedford (Mass.) Veterans Affairs Hospital, wrote in a related editorial.
“However, we need innovative approaches to evaluation that estimate the effect of e-consults on quality and cost of care across health care systems and over time. Implementation studies can help to identify key contributors to success,” the editorialists wrote.
One of the study authors, reported receiving personal fees from Bayer outside the submitted work. The other authors of the paper and the authors of the editorial reported no conflicts of interest. Dr. Candler said her employer contracts with an e-consult service, but that she is not compensated for use of the service. She is also a coeditor of Annals of Internal Medicine’s blog, “Fresh Look.”
SOURCE: Ahmed S et al. Ann Intern Med. 2020 Apr 14. doi: 10.7326/M19-3852.
Studies have shown that e-consults increase access to specialist care and primary care physician (PCP) education, according to research published in the Annals of Internal Medicine (2020. Apr 14. doi: 10.7326/M19-3852) by Salman Ahmed, MD, and colleagues.
These resources are already being frequently used by physicians, but more often by general internists and hospitalists than by subspecialists, according to a recent survey by the American College of Physicians. That survey found that 42% of its respondents are using e-consults and that subspecialists’ use is less common primarily because of the lack of access to e-consult technology.
What hasn’t been widely researched are the effects of large-scale e-consult programs, said Dr. Ahmed, who is associate physician in the renal division at Brigham and Women’s Hospital, Boston, in an interview.
For frontline providers such as PCPs, e-consults are a way to quickly seek out answers to clinical questions from specialists. In turn, the specialist can help a wider pool of participants, he noted.
The findings of Dr. Ahmed’s study, which included several academic centers and hospitals affiliated with Partners HealthCare System, a nonprofit network in eastern Massachusetts that includes Brigham and Women’s Hospital, used several metrics to analyze the appropriateness and utility of e-consults across a range of specialties. An e-consult was considered useful if it resulted in the avoidance of a visit to a specialist, which was defined as the absence of an in-person visit to the type of specialist consulted electronically for 120 days. An e-consult was considered appropriate if it met the following four criteria.
- It could not be answered by referring to society guidelines or widely available, evidence-based summary sources.
- It did not seek logistic information, such as where to have a specific laboratory test done.
- It did not include a question of high urgency.
- The medical complexity of the clinical situation was not substantial enough to warrant an in-person consultation.
The investigators examined e-consult inquiries to mostly physician health care providers in five specialties – hematology, infectious disease, dermatology, rheumatology, and psychiatry – over a year.
High rates of appropriateness
The search spanned 6,512 eligible e-consults from 1,096 referring providers to 121 specialist consultants. Narrowing their search to 741 records with complete data, the investigators found that 70.2% of these consults met the criteria for appropriateness. In an analysis of four reviewers blinded to each other’s results, raters agreed on the appropriateness of 94% of e-consults.
Across specialties, more than 81% of e-consults were associated with avoided in-person visits.
The reasons for most e-consults were to seek answers to questions about diagnosis, therapeutics, or patient inquiries, or to request further education by PCPs.
“Across all specialties, the most common reasons an e-consult was not considered appropriate were failing the point-of-care resource test and asking a question of inappropriately high complexity,” the authors summarized.
Physicians and PCPs from tertiary care practices made up the majority of referring providers, with turnaround time for consults averaging 24 hours across specialties.
Rates of appropriateness, content, patient demographics, and timeliness of e-consult responses varied among the four specialties. Those with high avoidance of visits rates tended to have high appropriateness rates, indicating that some specialties may be more conducive to e-consults than others, the authors noted. Psychiatry and hematology had the highest proportion of appropriate e-consults (77.9% and 73.3% respectively). Rheumatology had the lowest proportion of appropriate e-consults and one of the lowest rates of avoided in-person visits, and dermatology had the lowest rate of avoided in-person visits, at 61.9%.
The majority (93%) of e-consults sought in psychiatry were therapy related, whereas 88.4% of the e-consult questions in rheumatology related to diagnosis.
“Questions about diagnosis were less likely to be answerable via e-consult, which suggests that to provide diagnoses, consultants may wish to engage with the patient directly,” Dr. Ahmed said in an interview.
Infectious disease specialists seemed to be the fastest responders, with nearly 90% of their consultations having been answered within a day. Dermatology specialists had the distinction of having the youngest e-consult patients (mean age, 38.6 years).
PCPs weigh in on results
Physicians said in interviews that the study data reflects their own positive experiences with e-consults.
“Although I don’t always think [an e-consult] is able to fully prevent the specialist visit, it does allow the specialist to provide recommendations for work-up that can be done prior to the specialist visit,” said Santina Wheat MD, a family physician at Erie Family Health Center in Chicago. This reduces the time in which the consult is placed to when effective treatment can take place.
Patients who may have to wait months or even years to see a specialty doctor, benefit from e-consults, said Dr. Wheat, who is also a member of the editorial advisory board of Family Practice News. “As part of an organization that does e-consults to another hospital with a different electronic medical record, the e-consult increases the likelihood that all of the clinical information reaches the specialists and prevents tests from being repeated.”
Starting an e-consult may also increase the likelihood that the patient quickly sees a specialist at the contracted hospital, she added.
Sarah G. Candler, MD, said in an interview that she also sees e-consults as an essential tool. “When patients present with rare, complex, or atypical pictures, I find it helpful to have specialists weigh in. The e-consult helps me ensure that I work to the top of my abilities as an internist,” said Dr. Candler, who is practice medical director and physician director of academic relations at Iora Primary Care, Northside Clinic, Houston. However, she did not agree with the study’s avoided in-person visits metric for assessing utility.
“In some cases, the end result of an e-consult is a referral for an in-person evaluation, and the role of the e-consult is to ensure that I have done my due diligence as a primary care doctor asking the correct questions, getting the appropriate work-up completed, and referring to the appropriate specialty for next steps, when necessary,” noted Dr. Candler, who also serves on the editorial advisory board of Internal Medicine News.
Financial considerations
The study’s authors suggested taking a closer look at standardizing payment for the use of e-consults and developing appropriateness criteria for them.
Health systems could use such criteria to study what makes an e-consult useful and how to best utilize this tool, Dr. Ahmed said in an interview.
“Compensation models that promote high-quality, effective, and efficient e-consults are needed to reinforce the ability of health systems to optimize the mix of e-consults and in-person visits,” Dr. Ahmed and colleagues suggested.
Because not all patient care requires e-consults, the model makes the most sense in practices that already participate in value-based payment programs. In these types of programs, the cost can be shared according to the variable risk and patient need for the service, Dr. Candler explained.
“I have been fortunate to work in two different systems that function in this way, which means that e-consults have been readily available and encouraged-both to improve patient care and decrease overall cost by decreasing unnecessary testing or specialist referral,” she said.
Dr. Wheat said that the managed care organization affiliated with her practice seems to be saving money with e-consults, as it decreases the need to pay for specialist visits in some instances and for repeated work-ups.
Future studies
The study’s cohort represented just one large health care system with a shared electronic health record. “Single-system descriptive studies, such as that of Ahmed and colleagues, are particularly useful for local evaluation and quality improvement efforts,” Varsha G. Vimalananda, MD, and B. Graeme Fincke, MD, both of the Center for Healthcare Organization and Implementation Research at Bedford (Mass.) Veterans Affairs Hospital, wrote in a related editorial.
“However, we need innovative approaches to evaluation that estimate the effect of e-consults on quality and cost of care across health care systems and over time. Implementation studies can help to identify key contributors to success,” the editorialists wrote.
One of the study authors, reported receiving personal fees from Bayer outside the submitted work. The other authors of the paper and the authors of the editorial reported no conflicts of interest. Dr. Candler said her employer contracts with an e-consult service, but that she is not compensated for use of the service. She is also a coeditor of Annals of Internal Medicine’s blog, “Fresh Look.”
SOURCE: Ahmed S et al. Ann Intern Med. 2020 Apr 14. doi: 10.7326/M19-3852.
Studies have shown that e-consults increase access to specialist care and primary care physician (PCP) education, according to research published in the Annals of Internal Medicine (2020. Apr 14. doi: 10.7326/M19-3852) by Salman Ahmed, MD, and colleagues.
These resources are already being frequently used by physicians, but more often by general internists and hospitalists than by subspecialists, according to a recent survey by the American College of Physicians. That survey found that 42% of its respondents are using e-consults and that subspecialists’ use is less common primarily because of the lack of access to e-consult technology.
What hasn’t been widely researched are the effects of large-scale e-consult programs, said Dr. Ahmed, who is associate physician in the renal division at Brigham and Women’s Hospital, Boston, in an interview.
For frontline providers such as PCPs, e-consults are a way to quickly seek out answers to clinical questions from specialists. In turn, the specialist can help a wider pool of participants, he noted.
The findings of Dr. Ahmed’s study, which included several academic centers and hospitals affiliated with Partners HealthCare System, a nonprofit network in eastern Massachusetts that includes Brigham and Women’s Hospital, used several metrics to analyze the appropriateness and utility of e-consults across a range of specialties. An e-consult was considered useful if it resulted in the avoidance of a visit to a specialist, which was defined as the absence of an in-person visit to the type of specialist consulted electronically for 120 days. An e-consult was considered appropriate if it met the following four criteria.
- It could not be answered by referring to society guidelines or widely available, evidence-based summary sources.
- It did not seek logistic information, such as where to have a specific laboratory test done.
- It did not include a question of high urgency.
- The medical complexity of the clinical situation was not substantial enough to warrant an in-person consultation.
The investigators examined e-consult inquiries to mostly physician health care providers in five specialties – hematology, infectious disease, dermatology, rheumatology, and psychiatry – over a year.
High rates of appropriateness
The search spanned 6,512 eligible e-consults from 1,096 referring providers to 121 specialist consultants. Narrowing their search to 741 records with complete data, the investigators found that 70.2% of these consults met the criteria for appropriateness. In an analysis of four reviewers blinded to each other’s results, raters agreed on the appropriateness of 94% of e-consults.
Across specialties, more than 81% of e-consults were associated with avoided in-person visits.
The reasons for most e-consults were to seek answers to questions about diagnosis, therapeutics, or patient inquiries, or to request further education by PCPs.
“Across all specialties, the most common reasons an e-consult was not considered appropriate were failing the point-of-care resource test and asking a question of inappropriately high complexity,” the authors summarized.
Physicians and PCPs from tertiary care practices made up the majority of referring providers, with turnaround time for consults averaging 24 hours across specialties.
Rates of appropriateness, content, patient demographics, and timeliness of e-consult responses varied among the four specialties. Those with high avoidance of visits rates tended to have high appropriateness rates, indicating that some specialties may be more conducive to e-consults than others, the authors noted. Psychiatry and hematology had the highest proportion of appropriate e-consults (77.9% and 73.3% respectively). Rheumatology had the lowest proportion of appropriate e-consults and one of the lowest rates of avoided in-person visits, and dermatology had the lowest rate of avoided in-person visits, at 61.9%.
The majority (93%) of e-consults sought in psychiatry were therapy related, whereas 88.4% of the e-consult questions in rheumatology related to diagnosis.
“Questions about diagnosis were less likely to be answerable via e-consult, which suggests that to provide diagnoses, consultants may wish to engage with the patient directly,” Dr. Ahmed said in an interview.
Infectious disease specialists seemed to be the fastest responders, with nearly 90% of their consultations having been answered within a day. Dermatology specialists had the distinction of having the youngest e-consult patients (mean age, 38.6 years).
PCPs weigh in on results
Physicians said in interviews that the study data reflects their own positive experiences with e-consults.
“Although I don’t always think [an e-consult] is able to fully prevent the specialist visit, it does allow the specialist to provide recommendations for work-up that can be done prior to the specialist visit,” said Santina Wheat MD, a family physician at Erie Family Health Center in Chicago. This reduces the time in which the consult is placed to when effective treatment can take place.
Patients who may have to wait months or even years to see a specialty doctor, benefit from e-consults, said Dr. Wheat, who is also a member of the editorial advisory board of Family Practice News. “As part of an organization that does e-consults to another hospital with a different electronic medical record, the e-consult increases the likelihood that all of the clinical information reaches the specialists and prevents tests from being repeated.”
Starting an e-consult may also increase the likelihood that the patient quickly sees a specialist at the contracted hospital, she added.
Sarah G. Candler, MD, said in an interview that she also sees e-consults as an essential tool. “When patients present with rare, complex, or atypical pictures, I find it helpful to have specialists weigh in. The e-consult helps me ensure that I work to the top of my abilities as an internist,” said Dr. Candler, who is practice medical director and physician director of academic relations at Iora Primary Care, Northside Clinic, Houston. However, she did not agree with the study’s avoided in-person visits metric for assessing utility.
“In some cases, the end result of an e-consult is a referral for an in-person evaluation, and the role of the e-consult is to ensure that I have done my due diligence as a primary care doctor asking the correct questions, getting the appropriate work-up completed, and referring to the appropriate specialty for next steps, when necessary,” noted Dr. Candler, who also serves on the editorial advisory board of Internal Medicine News.
Financial considerations
The study’s authors suggested taking a closer look at standardizing payment for the use of e-consults and developing appropriateness criteria for them.
Health systems could use such criteria to study what makes an e-consult useful and how to best utilize this tool, Dr. Ahmed said in an interview.
“Compensation models that promote high-quality, effective, and efficient e-consults are needed to reinforce the ability of health systems to optimize the mix of e-consults and in-person visits,” Dr. Ahmed and colleagues suggested.
Because not all patient care requires e-consults, the model makes the most sense in practices that already participate in value-based payment programs. In these types of programs, the cost can be shared according to the variable risk and patient need for the service, Dr. Candler explained.
“I have been fortunate to work in two different systems that function in this way, which means that e-consults have been readily available and encouraged-both to improve patient care and decrease overall cost by decreasing unnecessary testing or specialist referral,” she said.
Dr. Wheat said that the managed care organization affiliated with her practice seems to be saving money with e-consults, as it decreases the need to pay for specialist visits in some instances and for repeated work-ups.
Future studies
The study’s cohort represented just one large health care system with a shared electronic health record. “Single-system descriptive studies, such as that of Ahmed and colleagues, are particularly useful for local evaluation and quality improvement efforts,” Varsha G. Vimalananda, MD, and B. Graeme Fincke, MD, both of the Center for Healthcare Organization and Implementation Research at Bedford (Mass.) Veterans Affairs Hospital, wrote in a related editorial.
“However, we need innovative approaches to evaluation that estimate the effect of e-consults on quality and cost of care across health care systems and over time. Implementation studies can help to identify key contributors to success,” the editorialists wrote.
One of the study authors, reported receiving personal fees from Bayer outside the submitted work. The other authors of the paper and the authors of the editorial reported no conflicts of interest. Dr. Candler said her employer contracts with an e-consult service, but that she is not compensated for use of the service. She is also a coeditor of Annals of Internal Medicine’s blog, “Fresh Look.”
SOURCE: Ahmed S et al. Ann Intern Med. 2020 Apr 14. doi: 10.7326/M19-3852.
FROM ANNALS OF INTERNAL MEDICINE
Preschoolers with higher BMI have elevated risk for fracture
Children with overweight or obese body mass index measures at preschool age were significantly more likely than were normal weight children to suffer upper- and lower-limb fractures before age 15 years, according to data from almost 470,000 children.
Previous studies of adults have shown associations between obesity and fractures, but the impact of higher BMI at preschool age on fracture incidence later in childhood has not been explored, according to Jennifer C.E. Lane, MD, of the University of Oxford (England), and colleagues. “A focused study of the association between preschool obesity and fracture risk offers the opportunity to better understand the impact of obesity in early life,” they wrote in the Journal of Bone and Mineral Research.
The researchers reviewed data from 466,997 children at 296 primary care centers using the Information System for Research in Primary Care, a Spanish national database, for the years 2003-2013. The children were assessed starting at age 4 years and followed until age 15 years or until they left the region or died, or until the study period ended, on Dec. 31, 2016. The average follow-up time was 4.9 years, and 49% of the children were girls. BMI categories were determined via the World Health Organization growth standards for calculating age- and sex-specific BMI z scores, and the categories were defined as underweight (< −2 BMI z score), normal weight (−2 to +2 BMI z score), overweight (> +2 BMI z score), and obese (> +3 BMI z score).
Overall, children with a BMI in the overweight or obese ranges at first assessment were significantly more likely than were their normal weight counterparts to suffer lower-limb fractures (adjusted hazard ratios, 1.42 and 1.74, respectively) and upper-limb fractures (aHRs, 1.10 and 1.19, respectively) during the follow-up period.
The total incidence of fractures during childhood for those in the study who were underweight, normal weight, overweight, or obese, was 9.20%, 10.06%, 11.28%, and 13.05% respectively.
In a secondary analysis, fracture risk varied by anatomic location and reflected previous findings showing an increased risk of distal limb fractures associated with high BMI, the researchers said.
The findings were limited by several factors, including the smaller-than-average proportion of children with overweight or obese BMI measures, the imprecise nature of the BMI z score as a predictor of obesity in children, and the lack of data on sports, medical issues, and general activity levels, the researchers noted.
However, the results were strengthened by the population-based sample and long-term follow-up, and the work “suggests that interventions to treat obesity in early childhood could have benefits for the primary or secondary prevention of fractures later in childhood, especially in the prevention of fractures within the forearm and hand or foot and ankle,” the authors concluded.
The study was supported in part by the NIHR Biomedical Research Centre, Oxford, and La Marató de TV3 Foundation. Dr. Lane disclosed funding from a Versus Arthritis Clinical Research Fellowship but had no financial conflicts to disclose. Some authors reported relationships with numerous pharmaceutical firms.
SOURCE: Lane JCE et al. J Bone Miner Res. 2020 Apr 7. doi: 10.1002/jbmr.3984
Children with overweight or obese body mass index measures at preschool age were significantly more likely than were normal weight children to suffer upper- and lower-limb fractures before age 15 years, according to data from almost 470,000 children.
Previous studies of adults have shown associations between obesity and fractures, but the impact of higher BMI at preschool age on fracture incidence later in childhood has not been explored, according to Jennifer C.E. Lane, MD, of the University of Oxford (England), and colleagues. “A focused study of the association between preschool obesity and fracture risk offers the opportunity to better understand the impact of obesity in early life,” they wrote in the Journal of Bone and Mineral Research.
The researchers reviewed data from 466,997 children at 296 primary care centers using the Information System for Research in Primary Care, a Spanish national database, for the years 2003-2013. The children were assessed starting at age 4 years and followed until age 15 years or until they left the region or died, or until the study period ended, on Dec. 31, 2016. The average follow-up time was 4.9 years, and 49% of the children were girls. BMI categories were determined via the World Health Organization growth standards for calculating age- and sex-specific BMI z scores, and the categories were defined as underweight (< −2 BMI z score), normal weight (−2 to +2 BMI z score), overweight (> +2 BMI z score), and obese (> +3 BMI z score).
Overall, children with a BMI in the overweight or obese ranges at first assessment were significantly more likely than were their normal weight counterparts to suffer lower-limb fractures (adjusted hazard ratios, 1.42 and 1.74, respectively) and upper-limb fractures (aHRs, 1.10 and 1.19, respectively) during the follow-up period.
The total incidence of fractures during childhood for those in the study who were underweight, normal weight, overweight, or obese, was 9.20%, 10.06%, 11.28%, and 13.05% respectively.
In a secondary analysis, fracture risk varied by anatomic location and reflected previous findings showing an increased risk of distal limb fractures associated with high BMI, the researchers said.
The findings were limited by several factors, including the smaller-than-average proportion of children with overweight or obese BMI measures, the imprecise nature of the BMI z score as a predictor of obesity in children, and the lack of data on sports, medical issues, and general activity levels, the researchers noted.
However, the results were strengthened by the population-based sample and long-term follow-up, and the work “suggests that interventions to treat obesity in early childhood could have benefits for the primary or secondary prevention of fractures later in childhood, especially in the prevention of fractures within the forearm and hand or foot and ankle,” the authors concluded.
The study was supported in part by the NIHR Biomedical Research Centre, Oxford, and La Marató de TV3 Foundation. Dr. Lane disclosed funding from a Versus Arthritis Clinical Research Fellowship but had no financial conflicts to disclose. Some authors reported relationships with numerous pharmaceutical firms.
SOURCE: Lane JCE et al. J Bone Miner Res. 2020 Apr 7. doi: 10.1002/jbmr.3984
Children with overweight or obese body mass index measures at preschool age were significantly more likely than were normal weight children to suffer upper- and lower-limb fractures before age 15 years, according to data from almost 470,000 children.
Previous studies of adults have shown associations between obesity and fractures, but the impact of higher BMI at preschool age on fracture incidence later in childhood has not been explored, according to Jennifer C.E. Lane, MD, of the University of Oxford (England), and colleagues. “A focused study of the association between preschool obesity and fracture risk offers the opportunity to better understand the impact of obesity in early life,” they wrote in the Journal of Bone and Mineral Research.
The researchers reviewed data from 466,997 children at 296 primary care centers using the Information System for Research in Primary Care, a Spanish national database, for the years 2003-2013. The children were assessed starting at age 4 years and followed until age 15 years or until they left the region or died, or until the study period ended, on Dec. 31, 2016. The average follow-up time was 4.9 years, and 49% of the children were girls. BMI categories were determined via the World Health Organization growth standards for calculating age- and sex-specific BMI z scores, and the categories were defined as underweight (< −2 BMI z score), normal weight (−2 to +2 BMI z score), overweight (> +2 BMI z score), and obese (> +3 BMI z score).
Overall, children with a BMI in the overweight or obese ranges at first assessment were significantly more likely than were their normal weight counterparts to suffer lower-limb fractures (adjusted hazard ratios, 1.42 and 1.74, respectively) and upper-limb fractures (aHRs, 1.10 and 1.19, respectively) during the follow-up period.
The total incidence of fractures during childhood for those in the study who were underweight, normal weight, overweight, or obese, was 9.20%, 10.06%, 11.28%, and 13.05% respectively.
In a secondary analysis, fracture risk varied by anatomic location and reflected previous findings showing an increased risk of distal limb fractures associated with high BMI, the researchers said.
The findings were limited by several factors, including the smaller-than-average proportion of children with overweight or obese BMI measures, the imprecise nature of the BMI z score as a predictor of obesity in children, and the lack of data on sports, medical issues, and general activity levels, the researchers noted.
However, the results were strengthened by the population-based sample and long-term follow-up, and the work “suggests that interventions to treat obesity in early childhood could have benefits for the primary or secondary prevention of fractures later in childhood, especially in the prevention of fractures within the forearm and hand or foot and ankle,” the authors concluded.
The study was supported in part by the NIHR Biomedical Research Centre, Oxford, and La Marató de TV3 Foundation. Dr. Lane disclosed funding from a Versus Arthritis Clinical Research Fellowship but had no financial conflicts to disclose. Some authors reported relationships with numerous pharmaceutical firms.
SOURCE: Lane JCE et al. J Bone Miner Res. 2020 Apr 7. doi: 10.1002/jbmr.3984
FROM THE JOURNAL OF BONE AND MINERAL RESEARCH