User login
By the numbers: Asthma-COPD overlap deaths
Death rates for combined asthma and chronic obstructive pulmonary disease declined during 1999-2016, but the risk remains higher among women, compared with men, and in certain occupations, according to a recent report from the Centers for Disease Control and Prevention.
There is also an association between mortality and nonworking status among adults aged 25-64 years, which “suggests that asthma-COPD overlap might be associated with substantial morbidity,” Katelynn E. Dodd, MPH, and associates at the CDC’s National Institute for Occupational Safety and Health said in the Morbidity and Mortality Weekly Report. “These patients have been reported to have worse health outcomes than do those with asthma or COPD alone.”
For females with asthma-COPD overlap, the age-adjusted death rate among adults aged 25 years and older dropped from 7.71 per million in 1999 to 4.01 in 2016, with corresponding rates of 6.70 and 3.01 per million for males, they reported.
In 1999-2016, a total of 18,766 U.S. decedents aged ≥25 years had both asthma and COPD assigned as the underlying or contributing cause of death (12,028 women and 6,738 men), for an overall death rate of 5.03 per million persons (women, 5.59; men, 4.30), data from the National Vital Statistics System show.
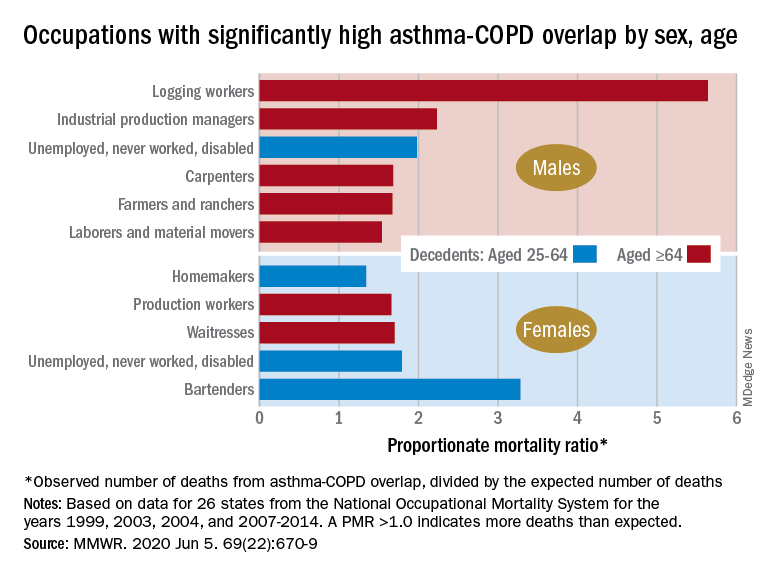
Additional analysis, based on the calculation of proportionate mortality ratios (PMRs), also showed that mortality varied by occupational status and age for both males and females, the investigators said, noting that workplace exposures, such as dusts and secondhand smoke, are known to cause both asthma and COPD.
The PMR represents the observed number of deaths from asthma-COPD overlap in a specified industry or occupation, divided by the expected number of deaths, so a value over 1.0 indicates that there were more deaths associated with the condition than expected, Ms. Dodd and her associates explained.
Among female decedents, the occupation with the highest PMR that was statistically significant was bartending at 3.28. For men, the highest significant PMR, 5.64, occurred in logging workers. Those rates, however, only applied to one of the two age groups: 25-64 years in women and ≥65 in men, based on data from the National Occupational Mortality Surveillance, which included information from 26 states for the years 1999, 2003, 2004, and 2007-2014.
Occupationally speaking, the one area of common ground between males and females was lack of occupation. PMRs for those aged 25-64 years “were significantly elevated among men (1.98) and women (1.79) who were unemployed, never worked, or were disabled workers,” they said. PMRs were elevated for nonworking older males and females but were not significant.
The elevated PMRs suggest “that asthma-COPD overlap might be associated with substantial morbidity resulting in loss of employment [because] retired and unemployed persons might have left the workforce because of severe asthma or COPD,” the investigators wrote.
SOURCE: Dodd KE et al. MMWR. 2020 Jun 5. 69(22):670-9.
Death rates for combined asthma and chronic obstructive pulmonary disease declined during 1999-2016, but the risk remains higher among women, compared with men, and in certain occupations, according to a recent report from the Centers for Disease Control and Prevention.
There is also an association between mortality and nonworking status among adults aged 25-64 years, which “suggests that asthma-COPD overlap might be associated with substantial morbidity,” Katelynn E. Dodd, MPH, and associates at the CDC’s National Institute for Occupational Safety and Health said in the Morbidity and Mortality Weekly Report. “These patients have been reported to have worse health outcomes than do those with asthma or COPD alone.”
For females with asthma-COPD overlap, the age-adjusted death rate among adults aged 25 years and older dropped from 7.71 per million in 1999 to 4.01 in 2016, with corresponding rates of 6.70 and 3.01 per million for males, they reported.
In 1999-2016, a total of 18,766 U.S. decedents aged ≥25 years had both asthma and COPD assigned as the underlying or contributing cause of death (12,028 women and 6,738 men), for an overall death rate of 5.03 per million persons (women, 5.59; men, 4.30), data from the National Vital Statistics System show.
Additional analysis, based on the calculation of proportionate mortality ratios (PMRs), also showed that mortality varied by occupational status and age for both males and females, the investigators said, noting that workplace exposures, such as dusts and secondhand smoke, are known to cause both asthma and COPD.
The PMR represents the observed number of deaths from asthma-COPD overlap in a specified industry or occupation, divided by the expected number of deaths, so a value over 1.0 indicates that there were more deaths associated with the condition than expected, Ms. Dodd and her associates explained.
Among female decedents, the occupation with the highest PMR that was statistically significant was bartending at 3.28. For men, the highest significant PMR, 5.64, occurred in logging workers. Those rates, however, only applied to one of the two age groups: 25-64 years in women and ≥65 in men, based on data from the National Occupational Mortality Surveillance, which included information from 26 states for the years 1999, 2003, 2004, and 2007-2014.
Occupationally speaking, the one area of common ground between males and females was lack of occupation. PMRs for those aged 25-64 years “were significantly elevated among men (1.98) and women (1.79) who were unemployed, never worked, or were disabled workers,” they said. PMRs were elevated for nonworking older males and females but were not significant.
The elevated PMRs suggest “that asthma-COPD overlap might be associated with substantial morbidity resulting in loss of employment [because] retired and unemployed persons might have left the workforce because of severe asthma or COPD,” the investigators wrote.
SOURCE: Dodd KE et al. MMWR. 2020 Jun 5. 69(22):670-9.
Death rates for combined asthma and chronic obstructive pulmonary disease declined during 1999-2016, but the risk remains higher among women, compared with men, and in certain occupations, according to a recent report from the Centers for Disease Control and Prevention.
There is also an association between mortality and nonworking status among adults aged 25-64 years, which “suggests that asthma-COPD overlap might be associated with substantial morbidity,” Katelynn E. Dodd, MPH, and associates at the CDC’s National Institute for Occupational Safety and Health said in the Morbidity and Mortality Weekly Report. “These patients have been reported to have worse health outcomes than do those with asthma or COPD alone.”
For females with asthma-COPD overlap, the age-adjusted death rate among adults aged 25 years and older dropped from 7.71 per million in 1999 to 4.01 in 2016, with corresponding rates of 6.70 and 3.01 per million for males, they reported.
In 1999-2016, a total of 18,766 U.S. decedents aged ≥25 years had both asthma and COPD assigned as the underlying or contributing cause of death (12,028 women and 6,738 men), for an overall death rate of 5.03 per million persons (women, 5.59; men, 4.30), data from the National Vital Statistics System show.
Additional analysis, based on the calculation of proportionate mortality ratios (PMRs), also showed that mortality varied by occupational status and age for both males and females, the investigators said, noting that workplace exposures, such as dusts and secondhand smoke, are known to cause both asthma and COPD.
The PMR represents the observed number of deaths from asthma-COPD overlap in a specified industry or occupation, divided by the expected number of deaths, so a value over 1.0 indicates that there were more deaths associated with the condition than expected, Ms. Dodd and her associates explained.
Among female decedents, the occupation with the highest PMR that was statistically significant was bartending at 3.28. For men, the highest significant PMR, 5.64, occurred in logging workers. Those rates, however, only applied to one of the two age groups: 25-64 years in women and ≥65 in men, based on data from the National Occupational Mortality Surveillance, which included information from 26 states for the years 1999, 2003, 2004, and 2007-2014.
Occupationally speaking, the one area of common ground between males and females was lack of occupation. PMRs for those aged 25-64 years “were significantly elevated among men (1.98) and women (1.79) who were unemployed, never worked, or were disabled workers,” they said. PMRs were elevated for nonworking older males and females but were not significant.
The elevated PMRs suggest “that asthma-COPD overlap might be associated with substantial morbidity resulting in loss of employment [because] retired and unemployed persons might have left the workforce because of severe asthma or COPD,” the investigators wrote.
SOURCE: Dodd KE et al. MMWR. 2020 Jun 5. 69(22):670-9.
FROM MMWR
Rapid changes to health system spurred by COVID might be here to stay
The U.S. health care system is famously resistant to government-imposed change. It took decades to create Medicare and Medicaid, mostly because of opposition from the medical-industrial complex. Then it was nearly another half-century before the passage of the Affordable Care Act.
“Health care is never going back to the way it was before,” said Gail Wilensky, a health economist who ran the Medicare and Medicaid programs for President George H.W. Bush in the early 1990s.
Ms. Wilensky is far from the only longtime observer of the American health care system to marvel at the speed of some long-sought changes. But experts warn that the breakthroughs may not all make the health system work better or make it less expensive.
That said, here are three trends that seem likely to continue.
Telehealth for all
Telehealth is not new; medical professionals have used it to reach patients in rural or remote settings since the late 1980s.
But even while technology has made video visits easier, it has failed to reach critical mass, largely because of political fights. Licensing has been one main obstacle – determining how a doctor in one state can legally treat a patient in a state where the doctor is not licensed.
The other obstacle, not surprisingly, is payment. Should a video visit be reimbursed at the same rate as an in-person visit? Will making it easier for doctors and other medical professionals to use telehealth encourage unnecessary care, thus driving up the nation’s $3.6 trillion health tab even more? Or could it replace care once provided free by phone?
Still, the pandemic has pushed aside those sticking points. Almost overnight, by necessity, every health care provider who can is delivering telemedicine. A new survey from Gallup found the number of patients reporting “virtual” medical visits more than doubled, from 12% to 27%, from late March to mid-May. That is attributable, at least in part, to Medicare having made it easier for doctors to bill for virtual visits.
It’s easy to see why many patients like video visits – there’s no parking to find and pay for, and it takes far less time out of a workday than going to an office.
Doctors and other practitioners seem more ambivalent. On one hand, it can be harder to examine a patient over video and some services just can’t be done via a digital connection. On the other hand, they can see more patients in the same amount of time and may need less support staff and possibly smaller offices if more visits are conducted virtually.
Of course, telemedicine doesn’t work for everyone. Many areas and patients don’t have reliable or robust broadband connections that make video visits work. And some patients, particularly the oldest seniors, lack the technological skills needed to connect.
Primary care doctors in peril
Another trend that has suddenly accelerated is worry over the nation’s dwindling supply of primary care doctors. The exodus of practitioners performing primary care has been a concern over the past several years, as baby boomer doctors retire and others have grown weary of more and more bureaucracy from government and private payers. Having faced a difficult financial crisis during the pandemic, more family physicians may move into retirement or seek other professional options.
At the same time, fewer current medical students are choosing specialties in primary care.
“I’ve been trying to raise the alarm about the kind of perilous future of primary care,” said Farzad Mostashari, MD, a top Department of Health & Human Services official in the Obama administration. Dr. Mostashari runs Aledade, a company that helps primary care doctors make the transition from fee-for-service medicine to new payment models.
The American Academy of Family Physicians reports that 70% of primary care physicians are reporting declines in patient volume of 50% or more since March, and 40% have laid off or furloughed staff. The AAFP has joined other primary care and insurance groups in asking HHS for an infusion of cash.
“This is absolutely essential to effectively treat patients today and to maintain their ongoing operations until we overcome this public health emergency,” the groups wrote.
One easy way to help keep primary care doctors afloat would be to pay them not according to what they do, but in a lump sum to keep patients healthy. This move from fee-for-service to what’s known as capitation or value-based care has unfolded gradually and was championed in the Affordable Care Act.
But some experts argue it needs to happen more quickly and they predict that the coronavirus pandemic could finally mark the beginning of the end for doctors who still charge for each service individually. Dr. Mostashari, who spends his time helping doctors make the transition, said in times like these, it would make more sense for primary care doctors to have “a steady monthly revenue stream, and [the doctor] can decide the best way to deliver that care: unlimited texts, phone calls, video calls. The goal is to give you satisfactory outcomes and a great patient experience.”
Still, many physicians, particularly those in solo or small practices, worry about the potential financial risk – especially the possibility of getting paid less if they don’t meet certain benchmarks that the doctors may not be able to directly control.
But with many practices now ground to a halt, or just starting to reopen, those physicians who get paid per patient rather than per service are in a much better position to stay afloat. That model may gain traction as doctors ponder the next pandemic, or the next wave of this one.
Hospitals on the decline?
The pandemic also might lead to less emphasis on hospital-based care. While hospitals in many parts of the country have obviously been full of very sick COVID patients, they have closed down other nonemergency services to preserve supplies and resources to fight the pandemic. People with other ailments have stayed away in droves even when services were available, for fear of catching something worse than what they already have.
Many experts predict that care won’t just snap back when the current emergency wanes. Mark Smith, MD, former president of the California Health Care Foundation, said among consumers, a switch has been flipped. “Overnight it seems we’ve gone from high-touch to no-touch.”
Which is not great for hospitals that have spent millions trying to attract patients to their labor-and-delivery units, orthopedic centers, and other parts of the facility that once generated lots of income.
Even more concerning is that hospitals’ ability to weather the current financial shock varies widely. Those most in danger of closing are in rural and underserved areas, where patients could wind up with even less access to care that is scarce already.
All of which underscores the point that not all these changes will necessarily be good for the health system or society. Financial pressures could end up driving more consolidation, which could push up prices as large groups of hospitals and doctors gain more bargaining clout.
But the changes are definitely happening at a pace few have ever seen, said Ms. Wilensky, “When you’re forced to find different ways of doing things, and you find out they are easier and more efficient, it’s going to be hard to go back to the old way.”
A version of this article originally appeared on Kaiser Health News, which is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
The U.S. health care system is famously resistant to government-imposed change. It took decades to create Medicare and Medicaid, mostly because of opposition from the medical-industrial complex. Then it was nearly another half-century before the passage of the Affordable Care Act.
“Health care is never going back to the way it was before,” said Gail Wilensky, a health economist who ran the Medicare and Medicaid programs for President George H.W. Bush in the early 1990s.
Ms. Wilensky is far from the only longtime observer of the American health care system to marvel at the speed of some long-sought changes. But experts warn that the breakthroughs may not all make the health system work better or make it less expensive.
That said, here are three trends that seem likely to continue.
Telehealth for all
Telehealth is not new; medical professionals have used it to reach patients in rural or remote settings since the late 1980s.
But even while technology has made video visits easier, it has failed to reach critical mass, largely because of political fights. Licensing has been one main obstacle – determining how a doctor in one state can legally treat a patient in a state where the doctor is not licensed.
The other obstacle, not surprisingly, is payment. Should a video visit be reimbursed at the same rate as an in-person visit? Will making it easier for doctors and other medical professionals to use telehealth encourage unnecessary care, thus driving up the nation’s $3.6 trillion health tab even more? Or could it replace care once provided free by phone?
Still, the pandemic has pushed aside those sticking points. Almost overnight, by necessity, every health care provider who can is delivering telemedicine. A new survey from Gallup found the number of patients reporting “virtual” medical visits more than doubled, from 12% to 27%, from late March to mid-May. That is attributable, at least in part, to Medicare having made it easier for doctors to bill for virtual visits.
It’s easy to see why many patients like video visits – there’s no parking to find and pay for, and it takes far less time out of a workday than going to an office.
Doctors and other practitioners seem more ambivalent. On one hand, it can be harder to examine a patient over video and some services just can’t be done via a digital connection. On the other hand, they can see more patients in the same amount of time and may need less support staff and possibly smaller offices if more visits are conducted virtually.
Of course, telemedicine doesn’t work for everyone. Many areas and patients don’t have reliable or robust broadband connections that make video visits work. And some patients, particularly the oldest seniors, lack the technological skills needed to connect.
Primary care doctors in peril
Another trend that has suddenly accelerated is worry over the nation’s dwindling supply of primary care doctors. The exodus of practitioners performing primary care has been a concern over the past several years, as baby boomer doctors retire and others have grown weary of more and more bureaucracy from government and private payers. Having faced a difficult financial crisis during the pandemic, more family physicians may move into retirement or seek other professional options.
At the same time, fewer current medical students are choosing specialties in primary care.
“I’ve been trying to raise the alarm about the kind of perilous future of primary care,” said Farzad Mostashari, MD, a top Department of Health & Human Services official in the Obama administration. Dr. Mostashari runs Aledade, a company that helps primary care doctors make the transition from fee-for-service medicine to new payment models.
The American Academy of Family Physicians reports that 70% of primary care physicians are reporting declines in patient volume of 50% or more since March, and 40% have laid off or furloughed staff. The AAFP has joined other primary care and insurance groups in asking HHS for an infusion of cash.
“This is absolutely essential to effectively treat patients today and to maintain their ongoing operations until we overcome this public health emergency,” the groups wrote.
One easy way to help keep primary care doctors afloat would be to pay them not according to what they do, but in a lump sum to keep patients healthy. This move from fee-for-service to what’s known as capitation or value-based care has unfolded gradually and was championed in the Affordable Care Act.
But some experts argue it needs to happen more quickly and they predict that the coronavirus pandemic could finally mark the beginning of the end for doctors who still charge for each service individually. Dr. Mostashari, who spends his time helping doctors make the transition, said in times like these, it would make more sense for primary care doctors to have “a steady monthly revenue stream, and [the doctor] can decide the best way to deliver that care: unlimited texts, phone calls, video calls. The goal is to give you satisfactory outcomes and a great patient experience.”
Still, many physicians, particularly those in solo or small practices, worry about the potential financial risk – especially the possibility of getting paid less if they don’t meet certain benchmarks that the doctors may not be able to directly control.
But with many practices now ground to a halt, or just starting to reopen, those physicians who get paid per patient rather than per service are in a much better position to stay afloat. That model may gain traction as doctors ponder the next pandemic, or the next wave of this one.
Hospitals on the decline?
The pandemic also might lead to less emphasis on hospital-based care. While hospitals in many parts of the country have obviously been full of very sick COVID patients, they have closed down other nonemergency services to preserve supplies and resources to fight the pandemic. People with other ailments have stayed away in droves even when services were available, for fear of catching something worse than what they already have.
Many experts predict that care won’t just snap back when the current emergency wanes. Mark Smith, MD, former president of the California Health Care Foundation, said among consumers, a switch has been flipped. “Overnight it seems we’ve gone from high-touch to no-touch.”
Which is not great for hospitals that have spent millions trying to attract patients to their labor-and-delivery units, orthopedic centers, and other parts of the facility that once generated lots of income.
Even more concerning is that hospitals’ ability to weather the current financial shock varies widely. Those most in danger of closing are in rural and underserved areas, where patients could wind up with even less access to care that is scarce already.
All of which underscores the point that not all these changes will necessarily be good for the health system or society. Financial pressures could end up driving more consolidation, which could push up prices as large groups of hospitals and doctors gain more bargaining clout.
But the changes are definitely happening at a pace few have ever seen, said Ms. Wilensky, “When you’re forced to find different ways of doing things, and you find out they are easier and more efficient, it’s going to be hard to go back to the old way.”
A version of this article originally appeared on Kaiser Health News, which is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
The U.S. health care system is famously resistant to government-imposed change. It took decades to create Medicare and Medicaid, mostly because of opposition from the medical-industrial complex. Then it was nearly another half-century before the passage of the Affordable Care Act.
“Health care is never going back to the way it was before,” said Gail Wilensky, a health economist who ran the Medicare and Medicaid programs for President George H.W. Bush in the early 1990s.
Ms. Wilensky is far from the only longtime observer of the American health care system to marvel at the speed of some long-sought changes. But experts warn that the breakthroughs may not all make the health system work better or make it less expensive.
That said, here are three trends that seem likely to continue.
Telehealth for all
Telehealth is not new; medical professionals have used it to reach patients in rural or remote settings since the late 1980s.
But even while technology has made video visits easier, it has failed to reach critical mass, largely because of political fights. Licensing has been one main obstacle – determining how a doctor in one state can legally treat a patient in a state where the doctor is not licensed.
The other obstacle, not surprisingly, is payment. Should a video visit be reimbursed at the same rate as an in-person visit? Will making it easier for doctors and other medical professionals to use telehealth encourage unnecessary care, thus driving up the nation’s $3.6 trillion health tab even more? Or could it replace care once provided free by phone?
Still, the pandemic has pushed aside those sticking points. Almost overnight, by necessity, every health care provider who can is delivering telemedicine. A new survey from Gallup found the number of patients reporting “virtual” medical visits more than doubled, from 12% to 27%, from late March to mid-May. That is attributable, at least in part, to Medicare having made it easier for doctors to bill for virtual visits.
It’s easy to see why many patients like video visits – there’s no parking to find and pay for, and it takes far less time out of a workday than going to an office.
Doctors and other practitioners seem more ambivalent. On one hand, it can be harder to examine a patient over video and some services just can’t be done via a digital connection. On the other hand, they can see more patients in the same amount of time and may need less support staff and possibly smaller offices if more visits are conducted virtually.
Of course, telemedicine doesn’t work for everyone. Many areas and patients don’t have reliable or robust broadband connections that make video visits work. And some patients, particularly the oldest seniors, lack the technological skills needed to connect.
Primary care doctors in peril
Another trend that has suddenly accelerated is worry over the nation’s dwindling supply of primary care doctors. The exodus of practitioners performing primary care has been a concern over the past several years, as baby boomer doctors retire and others have grown weary of more and more bureaucracy from government and private payers. Having faced a difficult financial crisis during the pandemic, more family physicians may move into retirement or seek other professional options.
At the same time, fewer current medical students are choosing specialties in primary care.
“I’ve been trying to raise the alarm about the kind of perilous future of primary care,” said Farzad Mostashari, MD, a top Department of Health & Human Services official in the Obama administration. Dr. Mostashari runs Aledade, a company that helps primary care doctors make the transition from fee-for-service medicine to new payment models.
The American Academy of Family Physicians reports that 70% of primary care physicians are reporting declines in patient volume of 50% or more since March, and 40% have laid off or furloughed staff. The AAFP has joined other primary care and insurance groups in asking HHS for an infusion of cash.
“This is absolutely essential to effectively treat patients today and to maintain their ongoing operations until we overcome this public health emergency,” the groups wrote.
One easy way to help keep primary care doctors afloat would be to pay them not according to what they do, but in a lump sum to keep patients healthy. This move from fee-for-service to what’s known as capitation or value-based care has unfolded gradually and was championed in the Affordable Care Act.
But some experts argue it needs to happen more quickly and they predict that the coronavirus pandemic could finally mark the beginning of the end for doctors who still charge for each service individually. Dr. Mostashari, who spends his time helping doctors make the transition, said in times like these, it would make more sense for primary care doctors to have “a steady monthly revenue stream, and [the doctor] can decide the best way to deliver that care: unlimited texts, phone calls, video calls. The goal is to give you satisfactory outcomes and a great patient experience.”
Still, many physicians, particularly those in solo or small practices, worry about the potential financial risk – especially the possibility of getting paid less if they don’t meet certain benchmarks that the doctors may not be able to directly control.
But with many practices now ground to a halt, or just starting to reopen, those physicians who get paid per patient rather than per service are in a much better position to stay afloat. That model may gain traction as doctors ponder the next pandemic, or the next wave of this one.
Hospitals on the decline?
The pandemic also might lead to less emphasis on hospital-based care. While hospitals in many parts of the country have obviously been full of very sick COVID patients, they have closed down other nonemergency services to preserve supplies and resources to fight the pandemic. People with other ailments have stayed away in droves even when services were available, for fear of catching something worse than what they already have.
Many experts predict that care won’t just snap back when the current emergency wanes. Mark Smith, MD, former president of the California Health Care Foundation, said among consumers, a switch has been flipped. “Overnight it seems we’ve gone from high-touch to no-touch.”
Which is not great for hospitals that have spent millions trying to attract patients to their labor-and-delivery units, orthopedic centers, and other parts of the facility that once generated lots of income.
Even more concerning is that hospitals’ ability to weather the current financial shock varies widely. Those most in danger of closing are in rural and underserved areas, where patients could wind up with even less access to care that is scarce already.
All of which underscores the point that not all these changes will necessarily be good for the health system or society. Financial pressures could end up driving more consolidation, which could push up prices as large groups of hospitals and doctors gain more bargaining clout.
But the changes are definitely happening at a pace few have ever seen, said Ms. Wilensky, “When you’re forced to find different ways of doing things, and you find out they are easier and more efficient, it’s going to be hard to go back to the old way.”
A version of this article originally appeared on Kaiser Health News, which is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Pandemic conditions can complicate care of patients with PAH
in these patients, according to a research article published in Pulmonary Circulation.
“The impetus for this manuscript was a recent discussion within the Pulmonary Hypertension Association (PHA) and [its] Scientific Leadership Council who expressed a need for guidelines from experts in the field,” wrote John J. Ryan, MD, of the University of Utah, Salt Lake City, and colleagues.
The authors highlight some of the unique challenges in caring for patients with pulmonary hypertension (PH), particularly pulmonary arterial hypertension (PAH), in the context of the COVID-19 pandemic.
Telemedicine and temporary visit schedules for new and returning PAH patients can help reduce risk of virus transmission, if patient accessibility to telemedicine is feasible. Protocols to reduce the risk of virus exposure or transmission in the office setting included less frequent echocardiography and 6-Minute Walk Tests (6MWTs) for patients in stable condition. In stable patients, “avoid pulmonary function of V/Q tests when possible,” the authors wrote.
New patients who have been referred for PAH present a challenge in conducting a thorough evaluation that would normally include measurement of invasive hemodynamics in keeping with current diagnostic guidelines. Clinicians will need to balance the potential risks of COVID-19 exposure during elective procedures against the benefits of full evaluations to plan PAH treatment, the authors noted.
For established patients who are clinically stable, remote visits may be an option, with a risk/benefit assessment of the need for in-person diagnostic tests at the current time, they said. However, telemedicine’s limitations include not only patient accessibility and understanding of audio and video technology, but also inability to accurately measure vital signs, they said.
As for routine testing such as echocardiograms, 6MWTs, and other laboratory testing, “it is important to consider the additive value of these sometimes comprehensive tests in the context of the risks associated with visiting the hospital or clinic to obtain them,” the authors said.
Patients who are unstable and experience worsening right heart failure (RHF) at home may have contracted a COVID-19 infection, but the differential diagnosis includes sepsis, ischemia, and PAH disease progression. “During the current pandemic, fever at home in a PAH patient should be assumed to represent a COVID-19 infection,” and patients with worsening respiratory symptoms that require hospitalization should be tested for COVID-19, the authors emphasized.
Use of ECMO or other intensive interventions should be considered in the context of risk assessment, the authors said. “As a general recommendation, practitioners should consider utilizing an established PAH-specific risk assessment tool to help identify patients who are more likely to survive heroic interventions during the COVID-19 outbreak,” they wrote.
Training and education of PH providers will continue to be limited by the pandemic, and many clinical trials and research programs have been suspended and will need to be restructured to minimize risk of transmission of the COVID-19 virus, the authors said. However, health care providers must continue to provide PAH patients and families with advice and updates in best practices, while “acknowledging that the situation changes rapidly,” they concluded.
Dr. Ryan disclosed participating on the speakers bureau, and provides consulting services for, Actelion and Bayer, as well as research support from the Reagan Corporation, the Gordon Family, and the Cushman Family.
SOURCE: Ryan JJ et al. Pulm Circ. 2020 Apr 29. doi: 10.1177/2045894020920153.
in these patients, according to a research article published in Pulmonary Circulation.
“The impetus for this manuscript was a recent discussion within the Pulmonary Hypertension Association (PHA) and [its] Scientific Leadership Council who expressed a need for guidelines from experts in the field,” wrote John J. Ryan, MD, of the University of Utah, Salt Lake City, and colleagues.
The authors highlight some of the unique challenges in caring for patients with pulmonary hypertension (PH), particularly pulmonary arterial hypertension (PAH), in the context of the COVID-19 pandemic.
Telemedicine and temporary visit schedules for new and returning PAH patients can help reduce risk of virus transmission, if patient accessibility to telemedicine is feasible. Protocols to reduce the risk of virus exposure or transmission in the office setting included less frequent echocardiography and 6-Minute Walk Tests (6MWTs) for patients in stable condition. In stable patients, “avoid pulmonary function of V/Q tests when possible,” the authors wrote.
New patients who have been referred for PAH present a challenge in conducting a thorough evaluation that would normally include measurement of invasive hemodynamics in keeping with current diagnostic guidelines. Clinicians will need to balance the potential risks of COVID-19 exposure during elective procedures against the benefits of full evaluations to plan PAH treatment, the authors noted.
For established patients who are clinically stable, remote visits may be an option, with a risk/benefit assessment of the need for in-person diagnostic tests at the current time, they said. However, telemedicine’s limitations include not only patient accessibility and understanding of audio and video technology, but also inability to accurately measure vital signs, they said.
As for routine testing such as echocardiograms, 6MWTs, and other laboratory testing, “it is important to consider the additive value of these sometimes comprehensive tests in the context of the risks associated with visiting the hospital or clinic to obtain them,” the authors said.
Patients who are unstable and experience worsening right heart failure (RHF) at home may have contracted a COVID-19 infection, but the differential diagnosis includes sepsis, ischemia, and PAH disease progression. “During the current pandemic, fever at home in a PAH patient should be assumed to represent a COVID-19 infection,” and patients with worsening respiratory symptoms that require hospitalization should be tested for COVID-19, the authors emphasized.
Use of ECMO or other intensive interventions should be considered in the context of risk assessment, the authors said. “As a general recommendation, practitioners should consider utilizing an established PAH-specific risk assessment tool to help identify patients who are more likely to survive heroic interventions during the COVID-19 outbreak,” they wrote.
Training and education of PH providers will continue to be limited by the pandemic, and many clinical trials and research programs have been suspended and will need to be restructured to minimize risk of transmission of the COVID-19 virus, the authors said. However, health care providers must continue to provide PAH patients and families with advice and updates in best practices, while “acknowledging that the situation changes rapidly,” they concluded.
Dr. Ryan disclosed participating on the speakers bureau, and provides consulting services for, Actelion and Bayer, as well as research support from the Reagan Corporation, the Gordon Family, and the Cushman Family.
SOURCE: Ryan JJ et al. Pulm Circ. 2020 Apr 29. doi: 10.1177/2045894020920153.
in these patients, according to a research article published in Pulmonary Circulation.
“The impetus for this manuscript was a recent discussion within the Pulmonary Hypertension Association (PHA) and [its] Scientific Leadership Council who expressed a need for guidelines from experts in the field,” wrote John J. Ryan, MD, of the University of Utah, Salt Lake City, and colleagues.
The authors highlight some of the unique challenges in caring for patients with pulmonary hypertension (PH), particularly pulmonary arterial hypertension (PAH), in the context of the COVID-19 pandemic.
Telemedicine and temporary visit schedules for new and returning PAH patients can help reduce risk of virus transmission, if patient accessibility to telemedicine is feasible. Protocols to reduce the risk of virus exposure or transmission in the office setting included less frequent echocardiography and 6-Minute Walk Tests (6MWTs) for patients in stable condition. In stable patients, “avoid pulmonary function of V/Q tests when possible,” the authors wrote.
New patients who have been referred for PAH present a challenge in conducting a thorough evaluation that would normally include measurement of invasive hemodynamics in keeping with current diagnostic guidelines. Clinicians will need to balance the potential risks of COVID-19 exposure during elective procedures against the benefits of full evaluations to plan PAH treatment, the authors noted.
For established patients who are clinically stable, remote visits may be an option, with a risk/benefit assessment of the need for in-person diagnostic tests at the current time, they said. However, telemedicine’s limitations include not only patient accessibility and understanding of audio and video technology, but also inability to accurately measure vital signs, they said.
As for routine testing such as echocardiograms, 6MWTs, and other laboratory testing, “it is important to consider the additive value of these sometimes comprehensive tests in the context of the risks associated with visiting the hospital or clinic to obtain them,” the authors said.
Patients who are unstable and experience worsening right heart failure (RHF) at home may have contracted a COVID-19 infection, but the differential diagnosis includes sepsis, ischemia, and PAH disease progression. “During the current pandemic, fever at home in a PAH patient should be assumed to represent a COVID-19 infection,” and patients with worsening respiratory symptoms that require hospitalization should be tested for COVID-19, the authors emphasized.
Use of ECMO or other intensive interventions should be considered in the context of risk assessment, the authors said. “As a general recommendation, practitioners should consider utilizing an established PAH-specific risk assessment tool to help identify patients who are more likely to survive heroic interventions during the COVID-19 outbreak,” they wrote.
Training and education of PH providers will continue to be limited by the pandemic, and many clinical trials and research programs have been suspended and will need to be restructured to minimize risk of transmission of the COVID-19 virus, the authors said. However, health care providers must continue to provide PAH patients and families with advice and updates in best practices, while “acknowledging that the situation changes rapidly,” they concluded.
Dr. Ryan disclosed participating on the speakers bureau, and provides consulting services for, Actelion and Bayer, as well as research support from the Reagan Corporation, the Gordon Family, and the Cushman Family.
SOURCE: Ryan JJ et al. Pulm Circ. 2020 Apr 29. doi: 10.1177/2045894020920153.
FROM PULMONARY CIRCULATION
American Cancer Society update: ‘It is best not to drink alcohol’
In its updated cancer prevention guidelines, the American Cancer Society now recommends that “it is best not to drink alcohol.”
Previously, ACS suggested that, for those who consume alcoholic beverages, intake should be no more than one drink per day for women or two per day for men. That recommendation is still in place, but is now accompanied by this new, stronger directive.
The revised guidelines also place more emphasis on reducing the consumption of processed and red meat and highly processed foods, and on increasing physical activity.
But importantly, there is also a call for action from public, private, and community organizations to work to together to increase access to affordable, nutritious foods and physical activity.
“Making healthy choices can be challenging for many, and there are strategies included in the guidelines that communities can undertake to help reduce barriers to eating well and physical activity,” said Laura Makaroff, DO, American Cancer Society senior vice president. “Individual choice is an important part of a healthy lifestyle, but having the right policies and environmental factors to break down these barriers is also important, and that is something that clinicians can support.”
The guidelines were published in CA: A Cancer Journal for Clinicians.
The link between cancer and lifestyle factors has long been established, and for the past 4 decades, both government and leading nonprofit health organizations, including the ACS and the World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR), have released cancer prevention guidelines and recommendations that focus on managing weight, diet, physical activity, and alcohol consumption.
In 2012, the ACS issued guidelines on diet and physical activity, and their current guideline is largely based on the WCRF/AICR systematic reviews and Continuous Update Project reports, which were last updated in 2018. The ACS guidelines also incorporated systematic reviews conducted by the International Agency on Cancer Research (IARC) and the U.S. Department of Agriculture and the Department of Health and Human Services (USDA/HHS) and other analyses that were published since the WCRF/AICR recommendations were released.
Emphasis on three areas
The differences between the old guidelines and the update do not differ dramatically, but Makaroff highlighted a few areas that have increased emphasis.
Time spent being physically active is critical. The recommendation has changed to encourage adults to engage in 150-300 minutes (2.5-5 hours) of moderate-intensity physical activity, or 75-150 minutes (1.25-2.5 hours) of vigorous-intensity physical activity, or an equivalent combination, per week. Achieving or exceeding the upper limit of 300 minutes is optimal.
“That is more than what we have recommended in the past, along with the continued message that children and adolescents engage in at least 1 hour of moderate- or vigorous-intensity activity each day,” she told Medscape Medical News.
The ACS has also increased emphasis on reducing the consumption of processed and red meat. “This is part of a healthy eating pattern and making sure that people are eating food that is high in nutrients that help achieve and maintain a healthy body weight,” said Makaroff.
A healthy diet should include a variety of dark green, red, and orange vegetables; fiber-rich legumes; and fruits with a variety of colors and whole grains, according to the guidelines. Sugar-sweetened beverages, highly processed foods, and refined grain products should be limited or avoided.
The revised dietary recommendations reflect a shift from a “reductionist or nutrient-centric” approach to one that is more “holistic” and that focuses on dietary patterns. In contrast to a focus on individual nutrients and bioactive compounds, the new approach is more consistent with what and how people actually eat, ACS points out.
The third area that Makaroff highlighted is alcohol, where the recommendation is to avoid or limit consumption. “The current update says not to drink alcohol, which is in line with the scientific evidence, but for those people who choose to drink alcohol, to limit it to one drink per day for women and two drinks per day for men.”
Thus, the change here is that the previous guideline only recommended limiting alcohol consumption, while the update suggests that, optimally, it should be avoided completely.
The ACS has also called for community involvement to help implement these goals: “Public, private, and community organizations should work collaboratively at national, state, and local levels to develop, advocate for, and implement policy and environmental changes that increase access to affordable, nutritious foods; provide safe, enjoyable, and accessible opportunities for physical activity; and limit alcohol for all individuals.”
No smoking guns
Commenting on the guidelines, Steven K. Clinton, MD, PhD, associate director of the Center for Advanced Functional Foods Research and Entrepreneurship at the Ohio State University, Columbus, explained that he didn’t view the change in alcohol as that much of an evolution. “It’s been 8 years since they revised their overall guidelines, and during that time frame, there has been an enormous growth in the evidence that has been used by many organizations,” he said.
Clinton noted that the guidelines are consistent with the whole body of current scientific literature. “It’s very easy to go to the document and look for the ‘smoking gun’ – but the smoking gun is really not one thing,” he said. “It’s a pattern, and what dietitians and nutritionists are telling people is that you need to orchestrate a healthy lifestyle and diet, with a diet that has a foundation of fruits, vegetables, whole grains, and modest intake of refined grains and meat. You are orchestrating an entire pattern to get the maximum benefit.”
Makaroff is an employee of the ACS. Clinton has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
In its updated cancer prevention guidelines, the American Cancer Society now recommends that “it is best not to drink alcohol.”
Previously, ACS suggested that, for those who consume alcoholic beverages, intake should be no more than one drink per day for women or two per day for men. That recommendation is still in place, but is now accompanied by this new, stronger directive.
The revised guidelines also place more emphasis on reducing the consumption of processed and red meat and highly processed foods, and on increasing physical activity.
But importantly, there is also a call for action from public, private, and community organizations to work to together to increase access to affordable, nutritious foods and physical activity.
“Making healthy choices can be challenging for many, and there are strategies included in the guidelines that communities can undertake to help reduce barriers to eating well and physical activity,” said Laura Makaroff, DO, American Cancer Society senior vice president. “Individual choice is an important part of a healthy lifestyle, but having the right policies and environmental factors to break down these barriers is also important, and that is something that clinicians can support.”
The guidelines were published in CA: A Cancer Journal for Clinicians.
The link between cancer and lifestyle factors has long been established, and for the past 4 decades, both government and leading nonprofit health organizations, including the ACS and the World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR), have released cancer prevention guidelines and recommendations that focus on managing weight, diet, physical activity, and alcohol consumption.
In 2012, the ACS issued guidelines on diet and physical activity, and their current guideline is largely based on the WCRF/AICR systematic reviews and Continuous Update Project reports, which were last updated in 2018. The ACS guidelines also incorporated systematic reviews conducted by the International Agency on Cancer Research (IARC) and the U.S. Department of Agriculture and the Department of Health and Human Services (USDA/HHS) and other analyses that were published since the WCRF/AICR recommendations were released.
Emphasis on three areas
The differences between the old guidelines and the update do not differ dramatically, but Makaroff highlighted a few areas that have increased emphasis.
Time spent being physically active is critical. The recommendation has changed to encourage adults to engage in 150-300 minutes (2.5-5 hours) of moderate-intensity physical activity, or 75-150 minutes (1.25-2.5 hours) of vigorous-intensity physical activity, or an equivalent combination, per week. Achieving or exceeding the upper limit of 300 minutes is optimal.
“That is more than what we have recommended in the past, along with the continued message that children and adolescents engage in at least 1 hour of moderate- or vigorous-intensity activity each day,” she told Medscape Medical News.
The ACS has also increased emphasis on reducing the consumption of processed and red meat. “This is part of a healthy eating pattern and making sure that people are eating food that is high in nutrients that help achieve and maintain a healthy body weight,” said Makaroff.
A healthy diet should include a variety of dark green, red, and orange vegetables; fiber-rich legumes; and fruits with a variety of colors and whole grains, according to the guidelines. Sugar-sweetened beverages, highly processed foods, and refined grain products should be limited or avoided.
The revised dietary recommendations reflect a shift from a “reductionist or nutrient-centric” approach to one that is more “holistic” and that focuses on dietary patterns. In contrast to a focus on individual nutrients and bioactive compounds, the new approach is more consistent with what and how people actually eat, ACS points out.
The third area that Makaroff highlighted is alcohol, where the recommendation is to avoid or limit consumption. “The current update says not to drink alcohol, which is in line with the scientific evidence, but for those people who choose to drink alcohol, to limit it to one drink per day for women and two drinks per day for men.”
Thus, the change here is that the previous guideline only recommended limiting alcohol consumption, while the update suggests that, optimally, it should be avoided completely.
The ACS has also called for community involvement to help implement these goals: “Public, private, and community organizations should work collaboratively at national, state, and local levels to develop, advocate for, and implement policy and environmental changes that increase access to affordable, nutritious foods; provide safe, enjoyable, and accessible opportunities for physical activity; and limit alcohol for all individuals.”
No smoking guns
Commenting on the guidelines, Steven K. Clinton, MD, PhD, associate director of the Center for Advanced Functional Foods Research and Entrepreneurship at the Ohio State University, Columbus, explained that he didn’t view the change in alcohol as that much of an evolution. “It’s been 8 years since they revised their overall guidelines, and during that time frame, there has been an enormous growth in the evidence that has been used by many organizations,” he said.
Clinton noted that the guidelines are consistent with the whole body of current scientific literature. “It’s very easy to go to the document and look for the ‘smoking gun’ – but the smoking gun is really not one thing,” he said. “It’s a pattern, and what dietitians and nutritionists are telling people is that you need to orchestrate a healthy lifestyle and diet, with a diet that has a foundation of fruits, vegetables, whole grains, and modest intake of refined grains and meat. You are orchestrating an entire pattern to get the maximum benefit.”
Makaroff is an employee of the ACS. Clinton has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
In its updated cancer prevention guidelines, the American Cancer Society now recommends that “it is best not to drink alcohol.”
Previously, ACS suggested that, for those who consume alcoholic beverages, intake should be no more than one drink per day for women or two per day for men. That recommendation is still in place, but is now accompanied by this new, stronger directive.
The revised guidelines also place more emphasis on reducing the consumption of processed and red meat and highly processed foods, and on increasing physical activity.
But importantly, there is also a call for action from public, private, and community organizations to work to together to increase access to affordable, nutritious foods and physical activity.
“Making healthy choices can be challenging for many, and there are strategies included in the guidelines that communities can undertake to help reduce barriers to eating well and physical activity,” said Laura Makaroff, DO, American Cancer Society senior vice president. “Individual choice is an important part of a healthy lifestyle, but having the right policies and environmental factors to break down these barriers is also important, and that is something that clinicians can support.”
The guidelines were published in CA: A Cancer Journal for Clinicians.
The link between cancer and lifestyle factors has long been established, and for the past 4 decades, both government and leading nonprofit health organizations, including the ACS and the World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR), have released cancer prevention guidelines and recommendations that focus on managing weight, diet, physical activity, and alcohol consumption.
In 2012, the ACS issued guidelines on diet and physical activity, and their current guideline is largely based on the WCRF/AICR systematic reviews and Continuous Update Project reports, which were last updated in 2018. The ACS guidelines also incorporated systematic reviews conducted by the International Agency on Cancer Research (IARC) and the U.S. Department of Agriculture and the Department of Health and Human Services (USDA/HHS) and other analyses that were published since the WCRF/AICR recommendations were released.
Emphasis on three areas
The differences between the old guidelines and the update do not differ dramatically, but Makaroff highlighted a few areas that have increased emphasis.
Time spent being physically active is critical. The recommendation has changed to encourage adults to engage in 150-300 minutes (2.5-5 hours) of moderate-intensity physical activity, or 75-150 minutes (1.25-2.5 hours) of vigorous-intensity physical activity, or an equivalent combination, per week. Achieving or exceeding the upper limit of 300 minutes is optimal.
“That is more than what we have recommended in the past, along with the continued message that children and adolescents engage in at least 1 hour of moderate- or vigorous-intensity activity each day,” she told Medscape Medical News.
The ACS has also increased emphasis on reducing the consumption of processed and red meat. “This is part of a healthy eating pattern and making sure that people are eating food that is high in nutrients that help achieve and maintain a healthy body weight,” said Makaroff.
A healthy diet should include a variety of dark green, red, and orange vegetables; fiber-rich legumes; and fruits with a variety of colors and whole grains, according to the guidelines. Sugar-sweetened beverages, highly processed foods, and refined grain products should be limited or avoided.
The revised dietary recommendations reflect a shift from a “reductionist or nutrient-centric” approach to one that is more “holistic” and that focuses on dietary patterns. In contrast to a focus on individual nutrients and bioactive compounds, the new approach is more consistent with what and how people actually eat, ACS points out.
The third area that Makaroff highlighted is alcohol, where the recommendation is to avoid or limit consumption. “The current update says not to drink alcohol, which is in line with the scientific evidence, but for those people who choose to drink alcohol, to limit it to one drink per day for women and two drinks per day for men.”
Thus, the change here is that the previous guideline only recommended limiting alcohol consumption, while the update suggests that, optimally, it should be avoided completely.
The ACS has also called for community involvement to help implement these goals: “Public, private, and community organizations should work collaboratively at national, state, and local levels to develop, advocate for, and implement policy and environmental changes that increase access to affordable, nutritious foods; provide safe, enjoyable, and accessible opportunities for physical activity; and limit alcohol for all individuals.”
No smoking guns
Commenting on the guidelines, Steven K. Clinton, MD, PhD, associate director of the Center for Advanced Functional Foods Research and Entrepreneurship at the Ohio State University, Columbus, explained that he didn’t view the change in alcohol as that much of an evolution. “It’s been 8 years since they revised their overall guidelines, and during that time frame, there has been an enormous growth in the evidence that has been used by many organizations,” he said.
Clinton noted that the guidelines are consistent with the whole body of current scientific literature. “It’s very easy to go to the document and look for the ‘smoking gun’ – but the smoking gun is really not one thing,” he said. “It’s a pattern, and what dietitians and nutritionists are telling people is that you need to orchestrate a healthy lifestyle and diet, with a diet that has a foundation of fruits, vegetables, whole grains, and modest intake of refined grains and meat. You are orchestrating an entire pattern to get the maximum benefit.”
Makaroff is an employee of the ACS. Clinton has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Aspirin and warfarin together leads to increased bleeding without reducing thrombotic events
Background: Current guidelines recommend against using aspirin in combination with warfarin for patients with AFib, unless the patient has another indication for aspirin such as recent percutaneous coronary intervention (PCI) or a mechanical heart valve. These recommendations are based on limited clinical trial data that showed an increased risk of adverse events with combination therapy without clinical benefit. Despite these recommendations, recent studies have shown that aspirin use without a clinical indication remains common in patients taking warfarin for AFib. The prevalence of aspirin use without a clinical indication in patients taking warfarin for VTE is less well studied.

Study design: Registry-based cohort study.
Setting: Six anticoagulation clinics in Michigan.
Synopsis: Of the 6,539 patients included in the study, 2,453 patients (37.5%) were taking both warfarin and aspirin without an indication for aspirin therapy; 3,688 propensity score–matched patients (1,844 in each group) were compared to assess rates of bleeding and rates of observed thrombosis at 1 year in patients taking warfarin alone versus warfarin plus aspirin. Patients treated with warfarin plus aspirin experienced more bleeding events than did patients on warfarin monotherapy (95% confidence interval, 23.8%-28.3% vs. 95% CI, 18.3%-22.3%; P less than .001). Rates of observed thrombosis were similar between the two groups (95% CI, 1.6%-3.1% vs. 95% CI, 2.0%-3.6%; P = .40). This study demonstrates that aspirin use without a clinical indication remains common in patients taking warfarin for AFib or VTE, and that reducing inappropriate aspirin use in this patient population may help prevent adverse outcomes.
Bottom line: Use of aspirin without a clinical indication in patients taking warfarin is common and is associated with an increased risk of bleeding without significant clinical benefit.
Citation: Schaefer JK et al. Association of adding aspirin to warfarin therapy without an apparent indication with bleeding and other adverse events. JAMA Intern Med. 2019 Mar 4;179(4):533-41.
Dr. Wachter is an associate medical director at Duke Regional Hospital and an assistant professor of medicine at Duke University.
Background: Current guidelines recommend against using aspirin in combination with warfarin for patients with AFib, unless the patient has another indication for aspirin such as recent percutaneous coronary intervention (PCI) or a mechanical heart valve. These recommendations are based on limited clinical trial data that showed an increased risk of adverse events with combination therapy without clinical benefit. Despite these recommendations, recent studies have shown that aspirin use without a clinical indication remains common in patients taking warfarin for AFib. The prevalence of aspirin use without a clinical indication in patients taking warfarin for VTE is less well studied.
Study design: Registry-based cohort study.
Setting: Six anticoagulation clinics in Michigan.
Synopsis: Of the 6,539 patients included in the study, 2,453 patients (37.5%) were taking both warfarin and aspirin without an indication for aspirin therapy; 3,688 propensity score–matched patients (1,844 in each group) were compared to assess rates of bleeding and rates of observed thrombosis at 1 year in patients taking warfarin alone versus warfarin plus aspirin. Patients treated with warfarin plus aspirin experienced more bleeding events than did patients on warfarin monotherapy (95% confidence interval, 23.8%-28.3% vs. 95% CI, 18.3%-22.3%; P less than .001). Rates of observed thrombosis were similar between the two groups (95% CI, 1.6%-3.1% vs. 95% CI, 2.0%-3.6%; P = .40). This study demonstrates that aspirin use without a clinical indication remains common in patients taking warfarin for AFib or VTE, and that reducing inappropriate aspirin use in this patient population may help prevent adverse outcomes.
Bottom line: Use of aspirin without a clinical indication in patients taking warfarin is common and is associated with an increased risk of bleeding without significant clinical benefit.
Citation: Schaefer JK et al. Association of adding aspirin to warfarin therapy without an apparent indication with bleeding and other adverse events. JAMA Intern Med. 2019 Mar 4;179(4):533-41.
Dr. Wachter is an associate medical director at Duke Regional Hospital and an assistant professor of medicine at Duke University.
Background: Current guidelines recommend against using aspirin in combination with warfarin for patients with AFib, unless the patient has another indication for aspirin such as recent percutaneous coronary intervention (PCI) or a mechanical heart valve. These recommendations are based on limited clinical trial data that showed an increased risk of adverse events with combination therapy without clinical benefit. Despite these recommendations, recent studies have shown that aspirin use without a clinical indication remains common in patients taking warfarin for AFib. The prevalence of aspirin use without a clinical indication in patients taking warfarin for VTE is less well studied.
Study design: Registry-based cohort study.
Setting: Six anticoagulation clinics in Michigan.
Synopsis: Of the 6,539 patients included in the study, 2,453 patients (37.5%) were taking both warfarin and aspirin without an indication for aspirin therapy; 3,688 propensity score–matched patients (1,844 in each group) were compared to assess rates of bleeding and rates of observed thrombosis at 1 year in patients taking warfarin alone versus warfarin plus aspirin. Patients treated with warfarin plus aspirin experienced more bleeding events than did patients on warfarin monotherapy (95% confidence interval, 23.8%-28.3% vs. 95% CI, 18.3%-22.3%; P less than .001). Rates of observed thrombosis were similar between the two groups (95% CI, 1.6%-3.1% vs. 95% CI, 2.0%-3.6%; P = .40). This study demonstrates that aspirin use without a clinical indication remains common in patients taking warfarin for AFib or VTE, and that reducing inappropriate aspirin use in this patient population may help prevent adverse outcomes.
Bottom line: Use of aspirin without a clinical indication in patients taking warfarin is common and is associated with an increased risk of bleeding without significant clinical benefit.
Citation: Schaefer JK et al. Association of adding aspirin to warfarin therapy without an apparent indication with bleeding and other adverse events. JAMA Intern Med. 2019 Mar 4;179(4):533-41.
Dr. Wachter is an associate medical director at Duke Regional Hospital and an assistant professor of medicine at Duke University.
SECTION 4: HEALTHCARE SYSTEMS: SUPPORTING AND ADVANCING CHILD HEALTH
Alvarez F, Alverson B, Balighian E, Beauchamp-Walters J, Biondi E, Blankenberg R, Bridgeman C, Brown J, Buchanan AO, Carlson D, Chang P, Coon E, Daud YN, Denniston S, DeWolfe CC, Deutsch SA, Doshi A, Fisher E, Gage S, Gallagher MP, Gill A, Goel Jones V, Grill J, Gupta A, Herbst BF Jr, Hershey D, Hoang K, Holmes AV, Hopkins A, Jones Y, Khan A, Lee V, Li ST, Lye, PS, Maginot T, Maloney C, Maniscalco J, Mannino Avila E, Markowsky A, Marks M, Matheny Antommaria AH, Maul E, McCulloh R, Melwani A, Miller C, Mittal V, Natt B, O'Toole J, Ottolini M, Percelay J, Phillips S, Pressel D, Quinonez R, Ralston S, Rappaport DI, Rauch D, Rhee K, Riese J, Roberts K, Rogers A, Rosenberg RE, Ruhlen M, Russell CJ, Russo C, Schwenk KM, Sekaran A, Shadman KA, Shah SS, Shen M, Simon T, Singh A, Smith K, Srinivas N Srivastava R, Sterni L, Thompson ED Jr, Thomson J, Tieder J, Tremoulet A, Wang ME, Williams R, Wu S. Name of Chapter. In: Pediatric Hospital Medicine Core Competencies: 2020 Revision. Section 4: Healthcare Systems: Supporting and Advancing Child Health. J Hosp Med. 2020;15(S1):xxx-xxx (insert page numbers). https://doi.org/jhm.3400
Alvarez F, Alverson B, Balighian E, Beauchamp-Walters J, Biondi E, Blankenberg R, Bridgeman C, Brown J, Buchanan AO, Carlson D, Chang P, Coon E, Daud YN, Denniston S, DeWolfe CC, Deutsch SA, Doshi A, Fisher E, Gage S, Gallagher MP, Gill A, Goel Jones V, Grill J, Gupta A, Herbst BF Jr, Hershey D, Hoang K, Holmes AV, Hopkins A, Jones Y, Khan A, Lee V, Li ST, Lye, PS, Maginot T, Maloney C, Maniscalco J, Mannino Avila E, Markowsky A, Marks M, Matheny Antommaria AH, Maul E, McCulloh R, Melwani A, Miller C, Mittal V, Natt B, O'Toole J, Ottolini M, Percelay J, Phillips S, Pressel D, Quinonez R, Ralston S, Rappaport DI, Rauch D, Rhee K, Riese J, Roberts K, Rogers A, Rosenberg RE, Ruhlen M, Russell CJ, Russo C, Schwenk KM, Sekaran A, Shadman KA, Shah SS, Shen M, Simon T, Singh A, Smith K, Srinivas N Srivastava R, Sterni L, Thompson ED Jr, Thomson J, Tieder J, Tremoulet A, Wang ME, Williams R, Wu S. Name of Chapter. In: Pediatric Hospital Medicine Core Competencies: 2020 Revision. Section 4: Healthcare Systems: Supporting and Advancing Child Health. J Hosp Med. 2020;15(S1):xxx-xxx (insert page numbers). https://doi.org/jhm.3400
Alvarez F, Alverson B, Balighian E, Beauchamp-Walters J, Biondi E, Blankenberg R, Bridgeman C, Brown J, Buchanan AO, Carlson D, Chang P, Coon E, Daud YN, Denniston S, DeWolfe CC, Deutsch SA, Doshi A, Fisher E, Gage S, Gallagher MP, Gill A, Goel Jones V, Grill J, Gupta A, Herbst BF Jr, Hershey D, Hoang K, Holmes AV, Hopkins A, Jones Y, Khan A, Lee V, Li ST, Lye, PS, Maginot T, Maloney C, Maniscalco J, Mannino Avila E, Markowsky A, Marks M, Matheny Antommaria AH, Maul E, McCulloh R, Melwani A, Miller C, Mittal V, Natt B, O'Toole J, Ottolini M, Percelay J, Phillips S, Pressel D, Quinonez R, Ralston S, Rappaport DI, Rauch D, Rhee K, Riese J, Roberts K, Rogers A, Rosenberg RE, Ruhlen M, Russell CJ, Russo C, Schwenk KM, Sekaran A, Shadman KA, Shah SS, Shen M, Simon T, Singh A, Smith K, Srinivas N Srivastava R, Sterni L, Thompson ED Jr, Thomson J, Tieder J, Tremoulet A, Wang ME, Williams R, Wu S. Name of Chapter. In: Pediatric Hospital Medicine Core Competencies: 2020 Revision. Section 4: Healthcare Systems: Supporting and Advancing Child Health. J Hosp Med. 2020;15(S1):xxx-xxx (insert page numbers). https://doi.org/jhm.3400
SECTION 3: SPECIALIZED SERVICES
How to cite articles within Section 2
Alvarez F, Alverson B, Balighian E, Beauchamp-Walters J, Biondi E, Blankenberg R, Bridgeman C, Brown J, Buchanan AO, Carlson D, Chang P, Coon E, Daud YN, Denniston S, DeWolfe CC, Deutsch SA, Doshi A, Fisher E, Gage S, Gallagher MP, Gill A, Goel Jones V, Grill J, Gupta A, Herbst BF Jr, Hershey D, Hoang K, Holmes AV, Hopkins A, Jones Y, Khan A, Lee V, Li ST, Lye, PS, Maginot T, Maloney C, Maniscalco J, Mannino Avila E, Markowsky A, Marks M, Matheny Antommaria AH, Maul E, McCulloh R, Melwani A, Miller C, Mittal V, Natt B, O'Toole J, Ottolini M, Percelay J, Phillips S, Pressel D, Quinonez R, Ralston S, Rappaport DI, Rauch D, Rhee K, Riese J, Roberts K, Rogers A, Rosenberg RE, Ruhlen M, Russell CJ, Russo C, Schwenk KM, Sekaran A, Shadman KA, Shah SS, Shen M, Simon T, Singh A, Smith K, Srinivas N Srivastava R, Sterni L, Thompson ED Jr, Thomson J, Tieder J, Tremoulet A, Wang ME, Williams R, Wu S. Name of Chapter. In: Pediatric Hospital Medicine Core Competencies: 2020 Revision. Section 3: Specialized Services. J Hosp Med. 2020;15(S1):xx-xxx (insert page numbers). https://doi.org/10.12788/jhm.3399
How to cite articles within Section 2
Alvarez F, Alverson B, Balighian E, Beauchamp-Walters J, Biondi E, Blankenberg R, Bridgeman C, Brown J, Buchanan AO, Carlson D, Chang P, Coon E, Daud YN, Denniston S, DeWolfe CC, Deutsch SA, Doshi A, Fisher E, Gage S, Gallagher MP, Gill A, Goel Jones V, Grill J, Gupta A, Herbst BF Jr, Hershey D, Hoang K, Holmes AV, Hopkins A, Jones Y, Khan A, Lee V, Li ST, Lye, PS, Maginot T, Maloney C, Maniscalco J, Mannino Avila E, Markowsky A, Marks M, Matheny Antommaria AH, Maul E, McCulloh R, Melwani A, Miller C, Mittal V, Natt B, O'Toole J, Ottolini M, Percelay J, Phillips S, Pressel D, Quinonez R, Ralston S, Rappaport DI, Rauch D, Rhee K, Riese J, Roberts K, Rogers A, Rosenberg RE, Ruhlen M, Russell CJ, Russo C, Schwenk KM, Sekaran A, Shadman KA, Shah SS, Shen M, Simon T, Singh A, Smith K, Srinivas N Srivastava R, Sterni L, Thompson ED Jr, Thomson J, Tieder J, Tremoulet A, Wang ME, Williams R, Wu S. Name of Chapter. In: Pediatric Hospital Medicine Core Competencies: 2020 Revision. Section 3: Specialized Services. J Hosp Med. 2020;15(S1):xx-xxx (insert page numbers). https://doi.org/10.12788/jhm.3399
How to cite articles within Section 2
Alvarez F, Alverson B, Balighian E, Beauchamp-Walters J, Biondi E, Blankenberg R, Bridgeman C, Brown J, Buchanan AO, Carlson D, Chang P, Coon E, Daud YN, Denniston S, DeWolfe CC, Deutsch SA, Doshi A, Fisher E, Gage S, Gallagher MP, Gill A, Goel Jones V, Grill J, Gupta A, Herbst BF Jr, Hershey D, Hoang K, Holmes AV, Hopkins A, Jones Y, Khan A, Lee V, Li ST, Lye, PS, Maginot T, Maloney C, Maniscalco J, Mannino Avila E, Markowsky A, Marks M, Matheny Antommaria AH, Maul E, McCulloh R, Melwani A, Miller C, Mittal V, Natt B, O'Toole J, Ottolini M, Percelay J, Phillips S, Pressel D, Quinonez R, Ralston S, Rappaport DI, Rauch D, Rhee K, Riese J, Roberts K, Rogers A, Rosenberg RE, Ruhlen M, Russell CJ, Russo C, Schwenk KM, Sekaran A, Shadman KA, Shah SS, Shen M, Simon T, Singh A, Smith K, Srinivas N Srivastava R, Sterni L, Thompson ED Jr, Thomson J, Tieder J, Tremoulet A, Wang ME, Williams R, Wu S. Name of Chapter. In: Pediatric Hospital Medicine Core Competencies: 2020 Revision. Section 3: Specialized Services. J Hosp Med. 2020;15(S1):xx-xxx (insert page numbers). https://doi.org/10.12788/jhm.3399
SECTION 2: CORE SKILLS
How to cite articles within Section 2
Alvarez F, Alverson B, Balighian E, Beauchamp-Walters J, Biondi E, Blankenberg R, Bridgeman C, Brown J, Buchanan AO, Carlson D, Chang P, Coon E, Daud YN, Denniston S, DeWolfe CC, Deutsch SA, Doshi A, Fisher E, Gage S, Gallagher MP, Gill A, Goel Jones V, Grill J, Gupta A, Herbst BF Jr, Hershey D, Hoang K, Holmes AV, Hopkins A, Jones Y, Khan A, Lee V, Li ST, Lye, PS, Maginot T, Maloney C, Maniscalco J, Mannino Avila E, Markowsky A, Marks M, Matheny Antommaria AH, Maul E, McCulloh R, Melwani A, Miller C, Mittal V, Natt B, O'Toole J, Ottolini M, Percelay J, Phillips S, Pressel D, Quinonez R, Ralston S, Rappaport DI, Rauch D, Rhee K, Riese J, Roberts K, Rogers A, Rosenberg RE, Ruhlen M, Russell CJ, Russo C, Schwenk KM, Sekaran A, Shadman KA, Shah SS, Shen M, Simon T, Singh A, Smith K, Srinivas N Srivastava R, Sterni L, Thompson ED Jr, Thomson J, Tieder J, Tremoulet A, Wang ME, Williams R, Wu S. Name of Chapter. In: Pediatric Hospital Medicine Core Competencies: 2020 Revision. Section 2: Core Skills. J Hosp Med. 2020;15(S1):XX-XX (insert page numbers). https://doi.org/10.12788/jhm.3398
How to cite articles within Section 2
Alvarez F, Alverson B, Balighian E, Beauchamp-Walters J, Biondi E, Blankenberg R, Bridgeman C, Brown J, Buchanan AO, Carlson D, Chang P, Coon E, Daud YN, Denniston S, DeWolfe CC, Deutsch SA, Doshi A, Fisher E, Gage S, Gallagher MP, Gill A, Goel Jones V, Grill J, Gupta A, Herbst BF Jr, Hershey D, Hoang K, Holmes AV, Hopkins A, Jones Y, Khan A, Lee V, Li ST, Lye, PS, Maginot T, Maloney C, Maniscalco J, Mannino Avila E, Markowsky A, Marks M, Matheny Antommaria AH, Maul E, McCulloh R, Melwani A, Miller C, Mittal V, Natt B, O'Toole J, Ottolini M, Percelay J, Phillips S, Pressel D, Quinonez R, Ralston S, Rappaport DI, Rauch D, Rhee K, Riese J, Roberts K, Rogers A, Rosenberg RE, Ruhlen M, Russell CJ, Russo C, Schwenk KM, Sekaran A, Shadman KA, Shah SS, Shen M, Simon T, Singh A, Smith K, Srinivas N Srivastava R, Sterni L, Thompson ED Jr, Thomson J, Tieder J, Tremoulet A, Wang ME, Williams R, Wu S. Name of Chapter. In: Pediatric Hospital Medicine Core Competencies: 2020 Revision. Section 2: Core Skills. J Hosp Med. 2020;15(S1):XX-XX (insert page numbers). https://doi.org/10.12788/jhm.3398
How to cite articles within Section 2
Alvarez F, Alverson B, Balighian E, Beauchamp-Walters J, Biondi E, Blankenberg R, Bridgeman C, Brown J, Buchanan AO, Carlson D, Chang P, Coon E, Daud YN, Denniston S, DeWolfe CC, Deutsch SA, Doshi A, Fisher E, Gage S, Gallagher MP, Gill A, Goel Jones V, Grill J, Gupta A, Herbst BF Jr, Hershey D, Hoang K, Holmes AV, Hopkins A, Jones Y, Khan A, Lee V, Li ST, Lye, PS, Maginot T, Maloney C, Maniscalco J, Mannino Avila E, Markowsky A, Marks M, Matheny Antommaria AH, Maul E, McCulloh R, Melwani A, Miller C, Mittal V, Natt B, O'Toole J, Ottolini M, Percelay J, Phillips S, Pressel D, Quinonez R, Ralston S, Rappaport DI, Rauch D, Rhee K, Riese J, Roberts K, Rogers A, Rosenberg RE, Ruhlen M, Russell CJ, Russo C, Schwenk KM, Sekaran A, Shadman KA, Shah SS, Shen M, Simon T, Singh A, Smith K, Srinivas N Srivastava R, Sterni L, Thompson ED Jr, Thomson J, Tieder J, Tremoulet A, Wang ME, Williams R, Wu S. Name of Chapter. In: Pediatric Hospital Medicine Core Competencies: 2020 Revision. Section 2: Core Skills. J Hosp Med. 2020;15(S1):XX-XX (insert page numbers). https://doi.org/10.12788/jhm.3398
SECTION 1: COMMON CLINICAL DIAGNOSES AND CONDITIONS
How to cite articles within Section 1
Alvarez F, Alverson B, Balighian E, Beauchamp-Walters J, Biondi E, Blankenberg R, Bridgeman C, Brown J, Buchanan AO, Carlson D, Chang P, Coon E, Daud YN, Denniston S, DeWolfe CC, Deutsch SA, Doshi A, Fisher E, Gage S, Gallagher MP, Gill A, Goel Jones V, Grill J, Gupta A, Herbst BF Jr, Hershey D, Hoang K, Holmes AV, Hopkins A, Jones Y, Khan A, Lee V, Li ST, Lye, PS, Maginot T, Maloney C, Maniscalco J, Mannino Avila E, Markowsky A, Marks M, Matheny Antommaria AH, Maul E, McCulloh R, Melwani A, Miller C, Mittal V, Natt B, O'Toole J, Ottolini M, Percelay J, Phillips S, Pressel D, Quinonez R, Ralston S, Rappaport DI, Rauch D, Rhee K, Riese J, Roberts K, Rogers A, Rosenberg RE, Ruhlen M, Russell CJ, Russo C, Schwenk KM, Sekaran A, Shadman KA, Shah SS, Shen M, Simon T, Singh A, Smith K, Srinivas N Srivastava R, Sterni L, Thompson ED Jr, Thomson J, Tieder J, Tremoulet A, Wang ME, Williams R, Wu S. Name of Chapter. In: Pediatric Hospital Medicine Core Competencies: 2020 Revision. Section 1: Common Clinical Diagnoses and Conditions. J Hosp Med. 2020;15(S1):xx-xx (insert page numbers). https://doi.org/10.12788/jhm.3397
How to cite articles within Section 1
Alvarez F, Alverson B, Balighian E, Beauchamp-Walters J, Biondi E, Blankenberg R, Bridgeman C, Brown J, Buchanan AO, Carlson D, Chang P, Coon E, Daud YN, Denniston S, DeWolfe CC, Deutsch SA, Doshi A, Fisher E, Gage S, Gallagher MP, Gill A, Goel Jones V, Grill J, Gupta A, Herbst BF Jr, Hershey D, Hoang K, Holmes AV, Hopkins A, Jones Y, Khan A, Lee V, Li ST, Lye, PS, Maginot T, Maloney C, Maniscalco J, Mannino Avila E, Markowsky A, Marks M, Matheny Antommaria AH, Maul E, McCulloh R, Melwani A, Miller C, Mittal V, Natt B, O'Toole J, Ottolini M, Percelay J, Phillips S, Pressel D, Quinonez R, Ralston S, Rappaport DI, Rauch D, Rhee K, Riese J, Roberts K, Rogers A, Rosenberg RE, Ruhlen M, Russell CJ, Russo C, Schwenk KM, Sekaran A, Shadman KA, Shah SS, Shen M, Simon T, Singh A, Smith K, Srinivas N Srivastava R, Sterni L, Thompson ED Jr, Thomson J, Tieder J, Tremoulet A, Wang ME, Williams R, Wu S. Name of Chapter. In: Pediatric Hospital Medicine Core Competencies: 2020 Revision. Section 1: Common Clinical Diagnoses and Conditions. J Hosp Med. 2020;15(S1):xx-xx (insert page numbers). https://doi.org/10.12788/jhm.3397
How to cite articles within Section 1
Alvarez F, Alverson B, Balighian E, Beauchamp-Walters J, Biondi E, Blankenberg R, Bridgeman C, Brown J, Buchanan AO, Carlson D, Chang P, Coon E, Daud YN, Denniston S, DeWolfe CC, Deutsch SA, Doshi A, Fisher E, Gage S, Gallagher MP, Gill A, Goel Jones V, Grill J, Gupta A, Herbst BF Jr, Hershey D, Hoang K, Holmes AV, Hopkins A, Jones Y, Khan A, Lee V, Li ST, Lye, PS, Maginot T, Maloney C, Maniscalco J, Mannino Avila E, Markowsky A, Marks M, Matheny Antommaria AH, Maul E, McCulloh R, Melwani A, Miller C, Mittal V, Natt B, O'Toole J, Ottolini M, Percelay J, Phillips S, Pressel D, Quinonez R, Ralston S, Rappaport DI, Rauch D, Rhee K, Riese J, Roberts K, Rogers A, Rosenberg RE, Ruhlen M, Russell CJ, Russo C, Schwenk KM, Sekaran A, Shadman KA, Shah SS, Shen M, Simon T, Singh A, Smith K, Srinivas N Srivastava R, Sterni L, Thompson ED Jr, Thomson J, Tieder J, Tremoulet A, Wang ME, Williams R, Wu S. Name of Chapter. In: Pediatric Hospital Medicine Core Competencies: 2020 Revision. Section 1: Common Clinical Diagnoses and Conditions. J Hosp Med. 2020;15(S1):xx-xx (insert page numbers). https://doi.org/10.12788/jhm.3397
Lessons From the COVID-19 Pandemic: It’s Time to Invest in Public Health
What have you been doing since you left the US Public Health Service?
RADM Boris D. Lushniak, MD, MPH. I retired in 2015 and spent a year at the Uniformed Services University for the Health Sciences in Bethesda, Maryland as the Chair of Preventive Medicine and Biostatistics before I took the opportunity to become the Dean of the School of Public Health at the University of Maryland in College Park. I was very intrigued with that position. It’s a large and young school of public health—just 13 years since its inception. And it functions at both the undergraduate and graduate school levels. We have 2,400 undergraduates in 4 different degree paths. The intriguing part of this is the ability to influence a young person’s educational pathway, and for them to look at all the opportunities in public health, and to focus on a mission, which falls into the mission of the US Public Health Service (PHS) Commissioned Corps: Protect, promote and advance the health and safety of our nation.
It has been a very intriguing transition; I have been the Dean there for 3 years. Who would have predicted that things would change drastically in that time, both at the academic level (ie, moving a school from being a normal college environment to an online environment) and now moving into the realm of preparing for the near future of that university in terms of a potential reopening. It is using all of my public health experiences and putting it at that culmination point, which is my community of 52,000 people—40,000 students at the University in College Park, and 12,000 faculty and staff members.
We are responsible for making sure that the return is as safe as possible. With so many unknowns in the world of COVID-19 and so many unpredictable components, it is quite an undertaking to be able to determine for that community of 52,000 whether it’s time to return, and under what circumstances do we return.
In addition, we’re part of a larger community. The University of Maryland in College Park is in Prince George’s County, which is the epicenter of disease and death in Maryland. The School of Public Health is working closely with county authorities. Some of our students are now contact tracers. It’s been interesting to see our faculty, staff, and students standing up as a volunteer support structure for Public Health.
We have incredible research going on at the school. One of my prime research physicians, Don Milton, MD, DrPH, has been studying the transmission of influenza. Now his work is priming on not just influenza, but also COVID-19. Our hope is to establish a community that will be safe and healthy for everyone, and so it’s been an incredible amount of work.
How would you describe the federal/ local public health cooperation?
RADM Lushniak. First and foremost, we have seen a major issue in terms of state and local response to the COVID-19 pandemic. I have to congratulate the state and the local officials for doing as best as they can under the strained circumstances that they’re in.
The first strained circumstance is that local and state health departments have lost nearly a quarter of their workforce: 50,000 jobs across the country since the recession of 2008. Part of the answer why it’s been such a struggle is that our nation as a whole hasn’t looked at public health and hasn’t looked at prevention as a key component of how our country works. We have seen a lack of support at the state and the local level, the shedding of jobs, and the lack of foresight in terms of saying that prevention works and public health is important for our cities, states, regions, and the nation. We need to reemphasize that in terms of public health.
In the State of Maryland, in general, the counties are doing as best as they can under the circumstances. They certainly started out with trying to do as much testing as possible. Testing is a critical component to this response, and obviously, we have a situation nationwide with the testing still trying to be put online to the extent that it needs to be. We need to be able to test more and more individuals to be able to determine the people who are positive. The curve ball that COVID-19 threw us is that 25 to 50% of individuals who may have a positive test may be asymptomatic. So, this isn’t simple. It’s not a matter of just saying, “Okay, you’re sick. You may then have it.” It may be: “Hey, you’re feeling healthy, you still may have it.”
But just as important as testing is what you do with those individuals who are tested. You need to have health departments turning to these individuals and providing them directions of what needs to be done. If one is COVID-19-positive, one goes into isolation for at least 14 days. And if ill, they need to be connected with a medical care system. That’s an important part of the state and local response is making sure the individuals are properly directed to the right pathway.
In addition, contact tracing is critical. The way we’re going to fight COVID-19 is the ability for us to go out there and determine if you are a positive, who did you come in contact with, and did you potentially spread this to others? You need to direct individuals who may have been in contact with the person who is now COVID- 19-positive, saying “You may have to quarantine yourself, watch out for symptoms, and you have to be really careful in the meantime.”
State and local officials took up the burden of making decisions in terms of communicating the directions given to the population. Is stay at home required? Is it the closure of businesses? Is it the wearing of masks? Certainly, the issue of physical distancing plays a role.
All that was implemented at the state and local level. Under the circumstances, it has been done as well as possible, but that now reflects on the issue of the federal response. And the federal response, I’ll admit, has been less than I had hoped for on several realms.
Number one, coordination and direction from the federal level has been rather piecemeal. State and local officials, I think, were waiting for further directions. What did federal officials think; what did they want us to do? State and local officials want independence to implement things, but what’s the right answer? I think this has been not handled well at the highest levels of the US government.
Secondly, obviously, there was an issue with testing, and the responsibility here lays with the Centers of Disease Control and Prevention (CDC), which had problems from the get-go with setting up their testing caches and getting them out. We’re still catching up from there. Now it’s unfolding that the tie in between the federal government and the private sector and academic centers are at least making some headway on that testing front.
Third, people rely on the federal officials not only for action but also for communication. It really boils down to: Who’s in charge, who’s telling me the information that I need to know, who’s honest with me and telling me what they don’t know, and who has the insight to say, “Here’s how we’re going to find out the things that we don’t know?” Who’s there empathizing with the population?
The reality is there’s been a mismatch between the communication channels for the federal government and getting down not just to the state and locals but, also, to the general population in this country.
How would you characterize the US Public Health Service Response?
RADM Lushniak. I’ll first start off with kudos and congratulations to the Commissioned Corps of the PHS for their response to date. I think the latest numbers that ADM Brett Giroir, MD, Assistant Secretary of Health, told Congress in May, was that at the time more than 3,100 of the 6,100 current officers at the PHS have been deployed over the last several months. The reality is that the Commissioned Corps is out there doing service to our nation and to the world. PHS teams were deployed initially to Japan and the Diamond Princess cruise ship. The Corps been out there internationally.
Nationally, the Corps was at the Javits Center in New York assisting in setting up that medical response. They have been assisting at the military bases initially where some of the individuals who were coming in from China and other places were being held in quarantine. They have been assisting with investigations at nursing homes across the country and meat packing plants where there have been outbreaks occurring. The Commissioned Corps has been out there, so that’s the good news.
The bad news is that the Corps is a small uniformed service. The reality is nobody still is seeing the Corps or knows about the Corps as they’re out there doing their thing. It was very nice that ADM Giroir put a plug in for them in his recent congressional testimony. That’s great that our leadership is out there acknowledging the Corps. But to a large extent, I still have an issue with the Commissioned Corps being an underfunded uniformed service of this country. The Commissioned Corps is the only uniformed service in the world whose only mission is public health. But, lack of support reflects the idea of the lack of importance that public health plays in the minds of policy makers.
To a large extent, we have had no dollars in the Corps recently for training of officers to prepare for this. For 10 years we’ve waited for a Ready Reserve to be set up. The Ready Reserve component was part of the Affordable Care Act. I was in the office of the Surgeon General as we were told to ramp this up. Now 10 years later, in the midst of this COVID-19 pandemic, Congress finally has passed legislation that sets a pathway for a Ready Reserve.
Why is the Ready Reserve important? In essence, we have incredible public health professionals out there in the civilian ranks who would be willing to assist the Commissioned Corps in their mission, either to backfill critical positions where Corps officers are currently stationed and need to be deployed, or as a Ready Reserve that’s ready to deploy itself. All this is happening right now. I hope for better days, and I hope this COVID-19 pandemic will wake our nation up to the need of a Public Health Service Commissioned Corps, a uniformed service, that's out there doing good.
What lessons are we learning about public health in this pandemic?
RADM Lushniak. We’ve just developed a new space force, the 8th uniformed US service. In reality they are talking about tens of thousands of people assigned to it. Excuse me if I’m going to be assertive. I’m a big fan of space exploration. I realize that space is the final frontier and that perhaps we have to be able to defend our country in that regard. But we’re already saying that space is worth investing in. Where is the wisdom that we’re not investing in battling on this planet against emerging threats like COVID-19? And why is it that to this date the Commissioned Corps of the Public Health Service does not have its own budget; does not have a line item anywhere; does not have money directed for training; and, in essence, only serves because its officers are stationed at other agencies who pay for these officers? It’s a personnel system and not really treated as a key and critical uniformed service of this country. That’s point number one in terms of lessons learned and what needs to be done.
In addition, it’s not just the people in uniform who serve at the federal level, civilians serve as well. These civilians work at the CDC, at the US Food and Drug Administration, at the National Institute of Health, at the Indian Health Service, and at many, many other agencies throughout the US government. Within those realms, we need to show support of those federal practitioners who are working very diligently and in a devoted fashion to fight this pandemic as well. Part of it is the moral support to recognize that there are multiple fronts to fighting this pandemic and the federal practitioner who is working out there, is a key component to this.
I don’t want everything to be money, money, money, but the fact is that CDC’s budget has been decreasing over the years. How are we supposed to set up the laboratories, how are we supposed to demand the high level of expertise when, in fact, everything has to be done on a shoestring?
Finally, we notice public health in the midst of a crisis, but public health matters each and every day. The idea that the pandemic certainly brings to light what needs to get done, but without a pandemic, what do we have? We still have cigarette smoking, the number 1 killer in this country. That’s a public health issue. We have cardiovascular diseases as an extreme killer in this country. That’s a public health issue. We have diabetes mellitus that is rampant. We have substance abuse, including the opioid epidemic. Those are public health issues. We have hypertension, we have overweight and obesity. Those are all public health issues that public health battles each and every day without the recognition.
What we need is a major shift in the philosophy of this country to really take the health and wellness of our society as a key component of how you’ll raise that on to a pedestal—the idea that health and wellness is critical to the functioning of this country.
How have recent public health emergencies influenced the Commissioned Corps?
RADM Lushniak. The key feature is that the Public Health Service Commissioned Corps has been growing in its mission over the years. The pre-9/11 Commissioned Corps, was a different life. The post-9/11 world is the first time that the Commissioned Corps really fell into this idea of being America’s public health responders. I think that we ramped it up; we started out strong.
This was shown not only in the World Trade Center and the 9/11 disasters that occurred, but in the anthrax scenario that unfolded shortly afterwards. We saw it further continue in Hurricane Katrina and the multiple hurricane responses.
Then the Ebola response, in my last year of serving in uniform, was another action of both the civilian sector of federal responders as well as the uniformed sector. The beauty of that in terms of what we learned from Ebola was that coordination is key. That was the first time that the PHS worked so closely with the US Department of Defense and our sister services to basically have an international mission unfold with that level of coordination.
We can use those changes that have gone on, the metamorphoses that have happened over the years, as a jumping off point, but they need to be fulfilled with further growth and support of the Commissioned Corps of the US Public Health Service. The numbers are the lowest they’ve been in recent times in terms of active duty officers. That’s not a good thing. As the mission expands, the idea of recruiting and retaining remains a problem. We have to deal with it.
Was your interest in taking the position at the University of Maryland in part to help build the future of public health?
RADM Lushniak. Certainly, I was so excited to be at the University of Maryland College Park exactly for that reason. The undergraduates are coming in from high school and their eyes are wide open. Two things are important at that stage. One is to teach them about the beauty of public health. That it’s a bold and noble mission. As I always tell our students, it’s about the 3 Ps: Promoting health and wellbeing, preventing disease and injury, and prolonging a high quality of life.
When you put all those things together, that’s an incredible mission. I want to tell them at that young age, “Be a part of this, figure out where you fit in.” But it’s not for everyone. I tell my students that one of the major attributes that I need to see in a student is optimism. Public health does not deal well with pessimism. If your character is pessimistic, I actually dissuade you from becoming a public health person because there are a lot of barriers in this incredible bold and noble mission, and optimism needs to be a key feature that keeps us all going.
Next is the realization that there’s so many different public health issues in our world, so many different problems to deal with. I mentioned some of them previously in terms of the public health issues we see each and every day.
Let me talk about one that’s, in particular, shining through in the midst of COVID-19, but also shines through each and every day. That’s the issue of health equity in our communities. A young person, who usually comes in and wants to help their community, needs to realize that part of the battle of public health is to make sure that we deal with the disparities that exist. We must make health equity a key component of our jobs. We are here to serve others.
There’s a saying at the University of Maryland College Park that we’re a “Do good university.” I would say that public health is a do-good profession. It is about compassion, it’s about love, it’s about caring. Those are the types of people that I try to bring into the school, and I try to mentor and support.
What have you been doing since you left the US Public Health Service?
RADM Boris D. Lushniak, MD, MPH. I retired in 2015 and spent a year at the Uniformed Services University for the Health Sciences in Bethesda, Maryland as the Chair of Preventive Medicine and Biostatistics before I took the opportunity to become the Dean of the School of Public Health at the University of Maryland in College Park. I was very intrigued with that position. It’s a large and young school of public health—just 13 years since its inception. And it functions at both the undergraduate and graduate school levels. We have 2,400 undergraduates in 4 different degree paths. The intriguing part of this is the ability to influence a young person’s educational pathway, and for them to look at all the opportunities in public health, and to focus on a mission, which falls into the mission of the US Public Health Service (PHS) Commissioned Corps: Protect, promote and advance the health and safety of our nation.
It has been a very intriguing transition; I have been the Dean there for 3 years. Who would have predicted that things would change drastically in that time, both at the academic level (ie, moving a school from being a normal college environment to an online environment) and now moving into the realm of preparing for the near future of that university in terms of a potential reopening. It is using all of my public health experiences and putting it at that culmination point, which is my community of 52,000 people—40,000 students at the University in College Park, and 12,000 faculty and staff members.
We are responsible for making sure that the return is as safe as possible. With so many unknowns in the world of COVID-19 and so many unpredictable components, it is quite an undertaking to be able to determine for that community of 52,000 whether it’s time to return, and under what circumstances do we return.
In addition, we’re part of a larger community. The University of Maryland in College Park is in Prince George’s County, which is the epicenter of disease and death in Maryland. The School of Public Health is working closely with county authorities. Some of our students are now contact tracers. It’s been interesting to see our faculty, staff, and students standing up as a volunteer support structure for Public Health.
We have incredible research going on at the school. One of my prime research physicians, Don Milton, MD, DrPH, has been studying the transmission of influenza. Now his work is priming on not just influenza, but also COVID-19. Our hope is to establish a community that will be safe and healthy for everyone, and so it’s been an incredible amount of work.
How would you describe the federal/ local public health cooperation?
RADM Lushniak. First and foremost, we have seen a major issue in terms of state and local response to the COVID-19 pandemic. I have to congratulate the state and the local officials for doing as best as they can under the strained circumstances that they’re in.
The first strained circumstance is that local and state health departments have lost nearly a quarter of their workforce: 50,000 jobs across the country since the recession of 2008. Part of the answer why it’s been such a struggle is that our nation as a whole hasn’t looked at public health and hasn’t looked at prevention as a key component of how our country works. We have seen a lack of support at the state and the local level, the shedding of jobs, and the lack of foresight in terms of saying that prevention works and public health is important for our cities, states, regions, and the nation. We need to reemphasize that in terms of public health.
In the State of Maryland, in general, the counties are doing as best as they can under the circumstances. They certainly started out with trying to do as much testing as possible. Testing is a critical component to this response, and obviously, we have a situation nationwide with the testing still trying to be put online to the extent that it needs to be. We need to be able to test more and more individuals to be able to determine the people who are positive. The curve ball that COVID-19 threw us is that 25 to 50% of individuals who may have a positive test may be asymptomatic. So, this isn’t simple. It’s not a matter of just saying, “Okay, you’re sick. You may then have it.” It may be: “Hey, you’re feeling healthy, you still may have it.”
But just as important as testing is what you do with those individuals who are tested. You need to have health departments turning to these individuals and providing them directions of what needs to be done. If one is COVID-19-positive, one goes into isolation for at least 14 days. And if ill, they need to be connected with a medical care system. That’s an important part of the state and local response is making sure the individuals are properly directed to the right pathway.
In addition, contact tracing is critical. The way we’re going to fight COVID-19 is the ability for us to go out there and determine if you are a positive, who did you come in contact with, and did you potentially spread this to others? You need to direct individuals who may have been in contact with the person who is now COVID- 19-positive, saying “You may have to quarantine yourself, watch out for symptoms, and you have to be really careful in the meantime.”
State and local officials took up the burden of making decisions in terms of communicating the directions given to the population. Is stay at home required? Is it the closure of businesses? Is it the wearing of masks? Certainly, the issue of physical distancing plays a role.
All that was implemented at the state and local level. Under the circumstances, it has been done as well as possible, but that now reflects on the issue of the federal response. And the federal response, I’ll admit, has been less than I had hoped for on several realms.
Number one, coordination and direction from the federal level has been rather piecemeal. State and local officials, I think, were waiting for further directions. What did federal officials think; what did they want us to do? State and local officials want independence to implement things, but what’s the right answer? I think this has been not handled well at the highest levels of the US government.
Secondly, obviously, there was an issue with testing, and the responsibility here lays with the Centers of Disease Control and Prevention (CDC), which had problems from the get-go with setting up their testing caches and getting them out. We’re still catching up from there. Now it’s unfolding that the tie in between the federal government and the private sector and academic centers are at least making some headway on that testing front.
Third, people rely on the federal officials not only for action but also for communication. It really boils down to: Who’s in charge, who’s telling me the information that I need to know, who’s honest with me and telling me what they don’t know, and who has the insight to say, “Here’s how we’re going to find out the things that we don’t know?” Who’s there empathizing with the population?
The reality is there’s been a mismatch between the communication channels for the federal government and getting down not just to the state and locals but, also, to the general population in this country.
How would you characterize the US Public Health Service Response?
RADM Lushniak. I’ll first start off with kudos and congratulations to the Commissioned Corps of the PHS for their response to date. I think the latest numbers that ADM Brett Giroir, MD, Assistant Secretary of Health, told Congress in May, was that at the time more than 3,100 of the 6,100 current officers at the PHS have been deployed over the last several months. The reality is that the Commissioned Corps is out there doing service to our nation and to the world. PHS teams were deployed initially to Japan and the Diamond Princess cruise ship. The Corps been out there internationally.
Nationally, the Corps was at the Javits Center in New York assisting in setting up that medical response. They have been assisting at the military bases initially where some of the individuals who were coming in from China and other places were being held in quarantine. They have been assisting with investigations at nursing homes across the country and meat packing plants where there have been outbreaks occurring. The Commissioned Corps has been out there, so that’s the good news.
The bad news is that the Corps is a small uniformed service. The reality is nobody still is seeing the Corps or knows about the Corps as they’re out there doing their thing. It was very nice that ADM Giroir put a plug in for them in his recent congressional testimony. That’s great that our leadership is out there acknowledging the Corps. But to a large extent, I still have an issue with the Commissioned Corps being an underfunded uniformed service of this country. The Commissioned Corps is the only uniformed service in the world whose only mission is public health. But, lack of support reflects the idea of the lack of importance that public health plays in the minds of policy makers.
To a large extent, we have had no dollars in the Corps recently for training of officers to prepare for this. For 10 years we’ve waited for a Ready Reserve to be set up. The Ready Reserve component was part of the Affordable Care Act. I was in the office of the Surgeon General as we were told to ramp this up. Now 10 years later, in the midst of this COVID-19 pandemic, Congress finally has passed legislation that sets a pathway for a Ready Reserve.
Why is the Ready Reserve important? In essence, we have incredible public health professionals out there in the civilian ranks who would be willing to assist the Commissioned Corps in their mission, either to backfill critical positions where Corps officers are currently stationed and need to be deployed, or as a Ready Reserve that’s ready to deploy itself. All this is happening right now. I hope for better days, and I hope this COVID-19 pandemic will wake our nation up to the need of a Public Health Service Commissioned Corps, a uniformed service, that's out there doing good.
What lessons are we learning about public health in this pandemic?
RADM Lushniak. We’ve just developed a new space force, the 8th uniformed US service. In reality they are talking about tens of thousands of people assigned to it. Excuse me if I’m going to be assertive. I’m a big fan of space exploration. I realize that space is the final frontier and that perhaps we have to be able to defend our country in that regard. But we’re already saying that space is worth investing in. Where is the wisdom that we’re not investing in battling on this planet against emerging threats like COVID-19? And why is it that to this date the Commissioned Corps of the Public Health Service does not have its own budget; does not have a line item anywhere; does not have money directed for training; and, in essence, only serves because its officers are stationed at other agencies who pay for these officers? It’s a personnel system and not really treated as a key and critical uniformed service of this country. That’s point number one in terms of lessons learned and what needs to be done.
In addition, it’s not just the people in uniform who serve at the federal level, civilians serve as well. These civilians work at the CDC, at the US Food and Drug Administration, at the National Institute of Health, at the Indian Health Service, and at many, many other agencies throughout the US government. Within those realms, we need to show support of those federal practitioners who are working very diligently and in a devoted fashion to fight this pandemic as well. Part of it is the moral support to recognize that there are multiple fronts to fighting this pandemic and the federal practitioner who is working out there, is a key component to this.
I don’t want everything to be money, money, money, but the fact is that CDC’s budget has been decreasing over the years. How are we supposed to set up the laboratories, how are we supposed to demand the high level of expertise when, in fact, everything has to be done on a shoestring?
Finally, we notice public health in the midst of a crisis, but public health matters each and every day. The idea that the pandemic certainly brings to light what needs to get done, but without a pandemic, what do we have? We still have cigarette smoking, the number 1 killer in this country. That’s a public health issue. We have cardiovascular diseases as an extreme killer in this country. That’s a public health issue. We have diabetes mellitus that is rampant. We have substance abuse, including the opioid epidemic. Those are public health issues. We have hypertension, we have overweight and obesity. Those are all public health issues that public health battles each and every day without the recognition.
What we need is a major shift in the philosophy of this country to really take the health and wellness of our society as a key component of how you’ll raise that on to a pedestal—the idea that health and wellness is critical to the functioning of this country.
How have recent public health emergencies influenced the Commissioned Corps?
RADM Lushniak. The key feature is that the Public Health Service Commissioned Corps has been growing in its mission over the years. The pre-9/11 Commissioned Corps, was a different life. The post-9/11 world is the first time that the Commissioned Corps really fell into this idea of being America’s public health responders. I think that we ramped it up; we started out strong.
This was shown not only in the World Trade Center and the 9/11 disasters that occurred, but in the anthrax scenario that unfolded shortly afterwards. We saw it further continue in Hurricane Katrina and the multiple hurricane responses.
Then the Ebola response, in my last year of serving in uniform, was another action of both the civilian sector of federal responders as well as the uniformed sector. The beauty of that in terms of what we learned from Ebola was that coordination is key. That was the first time that the PHS worked so closely with the US Department of Defense and our sister services to basically have an international mission unfold with that level of coordination.
We can use those changes that have gone on, the metamorphoses that have happened over the years, as a jumping off point, but they need to be fulfilled with further growth and support of the Commissioned Corps of the US Public Health Service. The numbers are the lowest they’ve been in recent times in terms of active duty officers. That’s not a good thing. As the mission expands, the idea of recruiting and retaining remains a problem. We have to deal with it.
Was your interest in taking the position at the University of Maryland in part to help build the future of public health?
RADM Lushniak. Certainly, I was so excited to be at the University of Maryland College Park exactly for that reason. The undergraduates are coming in from high school and their eyes are wide open. Two things are important at that stage. One is to teach them about the beauty of public health. That it’s a bold and noble mission. As I always tell our students, it’s about the 3 Ps: Promoting health and wellbeing, preventing disease and injury, and prolonging a high quality of life.
When you put all those things together, that’s an incredible mission. I want to tell them at that young age, “Be a part of this, figure out where you fit in.” But it’s not for everyone. I tell my students that one of the major attributes that I need to see in a student is optimism. Public health does not deal well with pessimism. If your character is pessimistic, I actually dissuade you from becoming a public health person because there are a lot of barriers in this incredible bold and noble mission, and optimism needs to be a key feature that keeps us all going.
Next is the realization that there’s so many different public health issues in our world, so many different problems to deal with. I mentioned some of them previously in terms of the public health issues we see each and every day.
Let me talk about one that’s, in particular, shining through in the midst of COVID-19, but also shines through each and every day. That’s the issue of health equity in our communities. A young person, who usually comes in and wants to help their community, needs to realize that part of the battle of public health is to make sure that we deal with the disparities that exist. We must make health equity a key component of our jobs. We are here to serve others.
There’s a saying at the University of Maryland College Park that we’re a “Do good university.” I would say that public health is a do-good profession. It is about compassion, it’s about love, it’s about caring. Those are the types of people that I try to bring into the school, and I try to mentor and support.
What have you been doing since you left the US Public Health Service?
RADM Boris D. Lushniak, MD, MPH. I retired in 2015 and spent a year at the Uniformed Services University for the Health Sciences in Bethesda, Maryland as the Chair of Preventive Medicine and Biostatistics before I took the opportunity to become the Dean of the School of Public Health at the University of Maryland in College Park. I was very intrigued with that position. It’s a large and young school of public health—just 13 years since its inception. And it functions at both the undergraduate and graduate school levels. We have 2,400 undergraduates in 4 different degree paths. The intriguing part of this is the ability to influence a young person’s educational pathway, and for them to look at all the opportunities in public health, and to focus on a mission, which falls into the mission of the US Public Health Service (PHS) Commissioned Corps: Protect, promote and advance the health and safety of our nation.
It has been a very intriguing transition; I have been the Dean there for 3 years. Who would have predicted that things would change drastically in that time, both at the academic level (ie, moving a school from being a normal college environment to an online environment) and now moving into the realm of preparing for the near future of that university in terms of a potential reopening. It is using all of my public health experiences and putting it at that culmination point, which is my community of 52,000 people—40,000 students at the University in College Park, and 12,000 faculty and staff members.
We are responsible for making sure that the return is as safe as possible. With so many unknowns in the world of COVID-19 and so many unpredictable components, it is quite an undertaking to be able to determine for that community of 52,000 whether it’s time to return, and under what circumstances do we return.
In addition, we’re part of a larger community. The University of Maryland in College Park is in Prince George’s County, which is the epicenter of disease and death in Maryland. The School of Public Health is working closely with county authorities. Some of our students are now contact tracers. It’s been interesting to see our faculty, staff, and students standing up as a volunteer support structure for Public Health.
We have incredible research going on at the school. One of my prime research physicians, Don Milton, MD, DrPH, has been studying the transmission of influenza. Now his work is priming on not just influenza, but also COVID-19. Our hope is to establish a community that will be safe and healthy for everyone, and so it’s been an incredible amount of work.
How would you describe the federal/ local public health cooperation?
RADM Lushniak. First and foremost, we have seen a major issue in terms of state and local response to the COVID-19 pandemic. I have to congratulate the state and the local officials for doing as best as they can under the strained circumstances that they’re in.
The first strained circumstance is that local and state health departments have lost nearly a quarter of their workforce: 50,000 jobs across the country since the recession of 2008. Part of the answer why it’s been such a struggle is that our nation as a whole hasn’t looked at public health and hasn’t looked at prevention as a key component of how our country works. We have seen a lack of support at the state and the local level, the shedding of jobs, and the lack of foresight in terms of saying that prevention works and public health is important for our cities, states, regions, and the nation. We need to reemphasize that in terms of public health.
In the State of Maryland, in general, the counties are doing as best as they can under the circumstances. They certainly started out with trying to do as much testing as possible. Testing is a critical component to this response, and obviously, we have a situation nationwide with the testing still trying to be put online to the extent that it needs to be. We need to be able to test more and more individuals to be able to determine the people who are positive. The curve ball that COVID-19 threw us is that 25 to 50% of individuals who may have a positive test may be asymptomatic. So, this isn’t simple. It’s not a matter of just saying, “Okay, you’re sick. You may then have it.” It may be: “Hey, you’re feeling healthy, you still may have it.”
But just as important as testing is what you do with those individuals who are tested. You need to have health departments turning to these individuals and providing them directions of what needs to be done. If one is COVID-19-positive, one goes into isolation for at least 14 days. And if ill, they need to be connected with a medical care system. That’s an important part of the state and local response is making sure the individuals are properly directed to the right pathway.
In addition, contact tracing is critical. The way we’re going to fight COVID-19 is the ability for us to go out there and determine if you are a positive, who did you come in contact with, and did you potentially spread this to others? You need to direct individuals who may have been in contact with the person who is now COVID- 19-positive, saying “You may have to quarantine yourself, watch out for symptoms, and you have to be really careful in the meantime.”
State and local officials took up the burden of making decisions in terms of communicating the directions given to the population. Is stay at home required? Is it the closure of businesses? Is it the wearing of masks? Certainly, the issue of physical distancing plays a role.
All that was implemented at the state and local level. Under the circumstances, it has been done as well as possible, but that now reflects on the issue of the federal response. And the federal response, I’ll admit, has been less than I had hoped for on several realms.
Number one, coordination and direction from the federal level has been rather piecemeal. State and local officials, I think, were waiting for further directions. What did federal officials think; what did they want us to do? State and local officials want independence to implement things, but what’s the right answer? I think this has been not handled well at the highest levels of the US government.
Secondly, obviously, there was an issue with testing, and the responsibility here lays with the Centers of Disease Control and Prevention (CDC), which had problems from the get-go with setting up their testing caches and getting them out. We’re still catching up from there. Now it’s unfolding that the tie in between the federal government and the private sector and academic centers are at least making some headway on that testing front.
Third, people rely on the federal officials not only for action but also for communication. It really boils down to: Who’s in charge, who’s telling me the information that I need to know, who’s honest with me and telling me what they don’t know, and who has the insight to say, “Here’s how we’re going to find out the things that we don’t know?” Who’s there empathizing with the population?
The reality is there’s been a mismatch between the communication channels for the federal government and getting down not just to the state and locals but, also, to the general population in this country.
How would you characterize the US Public Health Service Response?
RADM Lushniak. I’ll first start off with kudos and congratulations to the Commissioned Corps of the PHS for their response to date. I think the latest numbers that ADM Brett Giroir, MD, Assistant Secretary of Health, told Congress in May, was that at the time more than 3,100 of the 6,100 current officers at the PHS have been deployed over the last several months. The reality is that the Commissioned Corps is out there doing service to our nation and to the world. PHS teams were deployed initially to Japan and the Diamond Princess cruise ship. The Corps been out there internationally.
Nationally, the Corps was at the Javits Center in New York assisting in setting up that medical response. They have been assisting at the military bases initially where some of the individuals who were coming in from China and other places were being held in quarantine. They have been assisting with investigations at nursing homes across the country and meat packing plants where there have been outbreaks occurring. The Commissioned Corps has been out there, so that’s the good news.
The bad news is that the Corps is a small uniformed service. The reality is nobody still is seeing the Corps or knows about the Corps as they’re out there doing their thing. It was very nice that ADM Giroir put a plug in for them in his recent congressional testimony. That’s great that our leadership is out there acknowledging the Corps. But to a large extent, I still have an issue with the Commissioned Corps being an underfunded uniformed service of this country. The Commissioned Corps is the only uniformed service in the world whose only mission is public health. But, lack of support reflects the idea of the lack of importance that public health plays in the minds of policy makers.
To a large extent, we have had no dollars in the Corps recently for training of officers to prepare for this. For 10 years we’ve waited for a Ready Reserve to be set up. The Ready Reserve component was part of the Affordable Care Act. I was in the office of the Surgeon General as we were told to ramp this up. Now 10 years later, in the midst of this COVID-19 pandemic, Congress finally has passed legislation that sets a pathway for a Ready Reserve.
Why is the Ready Reserve important? In essence, we have incredible public health professionals out there in the civilian ranks who would be willing to assist the Commissioned Corps in their mission, either to backfill critical positions where Corps officers are currently stationed and need to be deployed, or as a Ready Reserve that’s ready to deploy itself. All this is happening right now. I hope for better days, and I hope this COVID-19 pandemic will wake our nation up to the need of a Public Health Service Commissioned Corps, a uniformed service, that's out there doing good.
What lessons are we learning about public health in this pandemic?
RADM Lushniak. We’ve just developed a new space force, the 8th uniformed US service. In reality they are talking about tens of thousands of people assigned to it. Excuse me if I’m going to be assertive. I’m a big fan of space exploration. I realize that space is the final frontier and that perhaps we have to be able to defend our country in that regard. But we’re already saying that space is worth investing in. Where is the wisdom that we’re not investing in battling on this planet against emerging threats like COVID-19? And why is it that to this date the Commissioned Corps of the Public Health Service does not have its own budget; does not have a line item anywhere; does not have money directed for training; and, in essence, only serves because its officers are stationed at other agencies who pay for these officers? It’s a personnel system and not really treated as a key and critical uniformed service of this country. That’s point number one in terms of lessons learned and what needs to be done.
In addition, it’s not just the people in uniform who serve at the federal level, civilians serve as well. These civilians work at the CDC, at the US Food and Drug Administration, at the National Institute of Health, at the Indian Health Service, and at many, many other agencies throughout the US government. Within those realms, we need to show support of those federal practitioners who are working very diligently and in a devoted fashion to fight this pandemic as well. Part of it is the moral support to recognize that there are multiple fronts to fighting this pandemic and the federal practitioner who is working out there, is a key component to this.
I don’t want everything to be money, money, money, but the fact is that CDC’s budget has been decreasing over the years. How are we supposed to set up the laboratories, how are we supposed to demand the high level of expertise when, in fact, everything has to be done on a shoestring?
Finally, we notice public health in the midst of a crisis, but public health matters each and every day. The idea that the pandemic certainly brings to light what needs to get done, but without a pandemic, what do we have? We still have cigarette smoking, the number 1 killer in this country. That’s a public health issue. We have cardiovascular diseases as an extreme killer in this country. That’s a public health issue. We have diabetes mellitus that is rampant. We have substance abuse, including the opioid epidemic. Those are public health issues. We have hypertension, we have overweight and obesity. Those are all public health issues that public health battles each and every day without the recognition.
What we need is a major shift in the philosophy of this country to really take the health and wellness of our society as a key component of how you’ll raise that on to a pedestal—the idea that health and wellness is critical to the functioning of this country.
How have recent public health emergencies influenced the Commissioned Corps?
RADM Lushniak. The key feature is that the Public Health Service Commissioned Corps has been growing in its mission over the years. The pre-9/11 Commissioned Corps, was a different life. The post-9/11 world is the first time that the Commissioned Corps really fell into this idea of being America’s public health responders. I think that we ramped it up; we started out strong.
This was shown not only in the World Trade Center and the 9/11 disasters that occurred, but in the anthrax scenario that unfolded shortly afterwards. We saw it further continue in Hurricane Katrina and the multiple hurricane responses.
Then the Ebola response, in my last year of serving in uniform, was another action of both the civilian sector of federal responders as well as the uniformed sector. The beauty of that in terms of what we learned from Ebola was that coordination is key. That was the first time that the PHS worked so closely with the US Department of Defense and our sister services to basically have an international mission unfold with that level of coordination.
We can use those changes that have gone on, the metamorphoses that have happened over the years, as a jumping off point, but they need to be fulfilled with further growth and support of the Commissioned Corps of the US Public Health Service. The numbers are the lowest they’ve been in recent times in terms of active duty officers. That’s not a good thing. As the mission expands, the idea of recruiting and retaining remains a problem. We have to deal with it.
Was your interest in taking the position at the University of Maryland in part to help build the future of public health?
RADM Lushniak. Certainly, I was so excited to be at the University of Maryland College Park exactly for that reason. The undergraduates are coming in from high school and their eyes are wide open. Two things are important at that stage. One is to teach them about the beauty of public health. That it’s a bold and noble mission. As I always tell our students, it’s about the 3 Ps: Promoting health and wellbeing, preventing disease and injury, and prolonging a high quality of life.
When you put all those things together, that’s an incredible mission. I want to tell them at that young age, “Be a part of this, figure out where you fit in.” But it’s not for everyone. I tell my students that one of the major attributes that I need to see in a student is optimism. Public health does not deal well with pessimism. If your character is pessimistic, I actually dissuade you from becoming a public health person because there are a lot of barriers in this incredible bold and noble mission, and optimism needs to be a key feature that keeps us all going.
Next is the realization that there’s so many different public health issues in our world, so many different problems to deal with. I mentioned some of them previously in terms of the public health issues we see each and every day.
Let me talk about one that’s, in particular, shining through in the midst of COVID-19, but also shines through each and every day. That’s the issue of health equity in our communities. A young person, who usually comes in and wants to help their community, needs to realize that part of the battle of public health is to make sure that we deal with the disparities that exist. We must make health equity a key component of our jobs. We are here to serve others.
There’s a saying at the University of Maryland College Park that we’re a “Do good university.” I would say that public health is a do-good profession. It is about compassion, it’s about love, it’s about caring. Those are the types of people that I try to bring into the school, and I try to mentor and support.