User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Finerenone: ‘Striking’ cut in pneumonia, COVID-19 risks
The nonsteroidal mineralocorticoid receptor antagonist finerenone (Kerendia) unexpectedly showed that it might protect against incident infective pneumonia and COVID-19. The finding was based on secondary analyses run on more than 13,000 people enrolled in the two pivotal trials for finerenone.
Finerenone was approved by the Food and Drug Administration in 2021 for slowing progressive renal dysfunction and preventing cardiovascular events in adults with type 2 diabetes and chronic kidney disease (CKD).
‘Striking reduction in the risk of pneumonia’
The “striking reduction in risk of pneumonia” in a new analysis suggests that “the propagation of pulmonary infection into lobar or bronchial consolidation may be reduced by finerenone,” write Bertram Pitt, MD, and coauthors in a report published on October 26 in JAMA Network Open.
They also suggest that if further studies confirm that finerenone treatment reduces complications from pneumonia and COVID-19, it would have “significant medical implications,” especially because of the limited treatment options now available for complications from COVID-19.
The new analyses used the FIDELITY dataset, a prespecified merging of results from the FIDELIO-DKD and FIGARO-DKD trials, which together enrolled 13,026 people with type 2 diabetes and CKD, as determined on the basis of the patients’ having a urine albumin-to-creatinine ratio of at least 30 mg/g.
The primary outcomes of these trials showed that treatment with finerenone led to significant slowing of the progression of CKD and a significant reduction in the incidence of cardiovascular events, compared with placebo during median follow-up of 3 years.
The new, secondary analyses focused on the 6.0% of participants in whom there was evidence of pneumonia and the 1.6% in whom there was evidence of having COVID-19. Pneumonia was the most common serious adverse event in the two trials, a finding consistent with the documented risk for pneumonia faced by people with CKD.
Finerenone linked with a 29% relative reduction in pneumonia
When analyzed by treatment, the incidence of pneumonia was 4.7% among those who received finerenone and 6.7% among those who received placebo. This translated into a significant relative risk reduction of 29% associated with finerenone treatment.
Analysis of COVID-19 adverse events showed a 1.3% incidence among those who received finerenone and a 1.8% incidence among those in the placebo group, which translated into a significant 27% relative risk reduction linked with finerenone treatment.
In contrast, the data showed no reduced incidence of several other respiratory infections among the finerenone recipients, including nasopharyngitis, bronchitis, and influenza. The data also showed no signal that pneumonia or COVID-19 was more severe among the people who did not receive finerenone, nor did finerenone treatment appear to affect pneumonia recovery.
Analysis based on adverse events reports
These secondary analyses are far from definitive. The authors relied on pneumonia and COVID-19 being reported as adverse events. Each investigator diagnosed pneumonia at their discretion, and the trials did not specify diagnostic criteria. The authors also acknowledge that testing for COVID-19 was “not widespread” and that one of the two pivotal trials largely ran prior to the onset of the COVID-19 pandemic so that only 6 participants developed COVID-19 symptoms out of more than 5,700 enrolled.
The authors hypothesize that several actions of finerenone might potentially help mediate an effect on pneumonia and COVID-19: improvements in pulmonary inflammation and fibrosis, upregulation of expression of angiotensin converting enzyme 2, and amelioration of right heart pressure and pulmonary congestion. Also, antagonizing the mineralocorticoid receptor on monocytes and macrophages may block macrophage infiltration and accumulation of active macrophages, which can mediate the pulmonary tissue damage caused by COVID-19.
The FIDELIO-DKD and FIGARO-DKD trials and the FIDELITY combined database were sponsored by Bayer, the company that markets finerenone (Kerendia). Dr. Pitt has received personal fees from Bayer and personal fees and stock options from numerous other companies. Several coauthors reported having a financial relationship with Bayer, as well as with other companies.
A version of this article first appeared on Medscape.com.
The nonsteroidal mineralocorticoid receptor antagonist finerenone (Kerendia) unexpectedly showed that it might protect against incident infective pneumonia and COVID-19. The finding was based on secondary analyses run on more than 13,000 people enrolled in the two pivotal trials for finerenone.
Finerenone was approved by the Food and Drug Administration in 2021 for slowing progressive renal dysfunction and preventing cardiovascular events in adults with type 2 diabetes and chronic kidney disease (CKD).
‘Striking reduction in the risk of pneumonia’
The “striking reduction in risk of pneumonia” in a new analysis suggests that “the propagation of pulmonary infection into lobar or bronchial consolidation may be reduced by finerenone,” write Bertram Pitt, MD, and coauthors in a report published on October 26 in JAMA Network Open.
They also suggest that if further studies confirm that finerenone treatment reduces complications from pneumonia and COVID-19, it would have “significant medical implications,” especially because of the limited treatment options now available for complications from COVID-19.
The new analyses used the FIDELITY dataset, a prespecified merging of results from the FIDELIO-DKD and FIGARO-DKD trials, which together enrolled 13,026 people with type 2 diabetes and CKD, as determined on the basis of the patients’ having a urine albumin-to-creatinine ratio of at least 30 mg/g.
The primary outcomes of these trials showed that treatment with finerenone led to significant slowing of the progression of CKD and a significant reduction in the incidence of cardiovascular events, compared with placebo during median follow-up of 3 years.
The new, secondary analyses focused on the 6.0% of participants in whom there was evidence of pneumonia and the 1.6% in whom there was evidence of having COVID-19. Pneumonia was the most common serious adverse event in the two trials, a finding consistent with the documented risk for pneumonia faced by people with CKD.
Finerenone linked with a 29% relative reduction in pneumonia
When analyzed by treatment, the incidence of pneumonia was 4.7% among those who received finerenone and 6.7% among those who received placebo. This translated into a significant relative risk reduction of 29% associated with finerenone treatment.
Analysis of COVID-19 adverse events showed a 1.3% incidence among those who received finerenone and a 1.8% incidence among those in the placebo group, which translated into a significant 27% relative risk reduction linked with finerenone treatment.
In contrast, the data showed no reduced incidence of several other respiratory infections among the finerenone recipients, including nasopharyngitis, bronchitis, and influenza. The data also showed no signal that pneumonia or COVID-19 was more severe among the people who did not receive finerenone, nor did finerenone treatment appear to affect pneumonia recovery.
Analysis based on adverse events reports
These secondary analyses are far from definitive. The authors relied on pneumonia and COVID-19 being reported as adverse events. Each investigator diagnosed pneumonia at their discretion, and the trials did not specify diagnostic criteria. The authors also acknowledge that testing for COVID-19 was “not widespread” and that one of the two pivotal trials largely ran prior to the onset of the COVID-19 pandemic so that only 6 participants developed COVID-19 symptoms out of more than 5,700 enrolled.
The authors hypothesize that several actions of finerenone might potentially help mediate an effect on pneumonia and COVID-19: improvements in pulmonary inflammation and fibrosis, upregulation of expression of angiotensin converting enzyme 2, and amelioration of right heart pressure and pulmonary congestion. Also, antagonizing the mineralocorticoid receptor on monocytes and macrophages may block macrophage infiltration and accumulation of active macrophages, which can mediate the pulmonary tissue damage caused by COVID-19.
The FIDELIO-DKD and FIGARO-DKD trials and the FIDELITY combined database were sponsored by Bayer, the company that markets finerenone (Kerendia). Dr. Pitt has received personal fees from Bayer and personal fees and stock options from numerous other companies. Several coauthors reported having a financial relationship with Bayer, as well as with other companies.
A version of this article first appeared on Medscape.com.
The nonsteroidal mineralocorticoid receptor antagonist finerenone (Kerendia) unexpectedly showed that it might protect against incident infective pneumonia and COVID-19. The finding was based on secondary analyses run on more than 13,000 people enrolled in the two pivotal trials for finerenone.
Finerenone was approved by the Food and Drug Administration in 2021 for slowing progressive renal dysfunction and preventing cardiovascular events in adults with type 2 diabetes and chronic kidney disease (CKD).
‘Striking reduction in the risk of pneumonia’
The “striking reduction in risk of pneumonia” in a new analysis suggests that “the propagation of pulmonary infection into lobar or bronchial consolidation may be reduced by finerenone,” write Bertram Pitt, MD, and coauthors in a report published on October 26 in JAMA Network Open.
They also suggest that if further studies confirm that finerenone treatment reduces complications from pneumonia and COVID-19, it would have “significant medical implications,” especially because of the limited treatment options now available for complications from COVID-19.
The new analyses used the FIDELITY dataset, a prespecified merging of results from the FIDELIO-DKD and FIGARO-DKD trials, which together enrolled 13,026 people with type 2 diabetes and CKD, as determined on the basis of the patients’ having a urine albumin-to-creatinine ratio of at least 30 mg/g.
The primary outcomes of these trials showed that treatment with finerenone led to significant slowing of the progression of CKD and a significant reduction in the incidence of cardiovascular events, compared with placebo during median follow-up of 3 years.
The new, secondary analyses focused on the 6.0% of participants in whom there was evidence of pneumonia and the 1.6% in whom there was evidence of having COVID-19. Pneumonia was the most common serious adverse event in the two trials, a finding consistent with the documented risk for pneumonia faced by people with CKD.
Finerenone linked with a 29% relative reduction in pneumonia
When analyzed by treatment, the incidence of pneumonia was 4.7% among those who received finerenone and 6.7% among those who received placebo. This translated into a significant relative risk reduction of 29% associated with finerenone treatment.
Analysis of COVID-19 adverse events showed a 1.3% incidence among those who received finerenone and a 1.8% incidence among those in the placebo group, which translated into a significant 27% relative risk reduction linked with finerenone treatment.
In contrast, the data showed no reduced incidence of several other respiratory infections among the finerenone recipients, including nasopharyngitis, bronchitis, and influenza. The data also showed no signal that pneumonia or COVID-19 was more severe among the people who did not receive finerenone, nor did finerenone treatment appear to affect pneumonia recovery.
Analysis based on adverse events reports
These secondary analyses are far from definitive. The authors relied on pneumonia and COVID-19 being reported as adverse events. Each investigator diagnosed pneumonia at their discretion, and the trials did not specify diagnostic criteria. The authors also acknowledge that testing for COVID-19 was “not widespread” and that one of the two pivotal trials largely ran prior to the onset of the COVID-19 pandemic so that only 6 participants developed COVID-19 symptoms out of more than 5,700 enrolled.
The authors hypothesize that several actions of finerenone might potentially help mediate an effect on pneumonia and COVID-19: improvements in pulmonary inflammation and fibrosis, upregulation of expression of angiotensin converting enzyme 2, and amelioration of right heart pressure and pulmonary congestion. Also, antagonizing the mineralocorticoid receptor on monocytes and macrophages may block macrophage infiltration and accumulation of active macrophages, which can mediate the pulmonary tissue damage caused by COVID-19.
The FIDELIO-DKD and FIGARO-DKD trials and the FIDELITY combined database were sponsored by Bayer, the company that markets finerenone (Kerendia). Dr. Pitt has received personal fees from Bayer and personal fees and stock options from numerous other companies. Several coauthors reported having a financial relationship with Bayer, as well as with other companies.
A version of this article first appeared on Medscape.com.
A special part of the brain lights up when we see food
“We eat first with our eyes.”
The Roman foodie Apicius is thought to have uttered those words in the 1st century A.D. Now, some 2,000 years later, scientists may be proving him right.
Dubbed the “ventral food component,” this part resides in the brain’s visual cortex, in a region known to play a role in identifying faces, scenes, and words.
The study, published in the journal Current Biology, involved using artificial intelligence (AI) technology to build a computer model of this part of the brain. Similar models are emerging across fields of research to simulate and study complex systems of the body. A computer model of the digestive system was recently used to determine the best body position for taking a pill.
“The research is still cutting-edge,” says study author Meenakshi Khosla, PhD. “There’s a lot more to be done to understand whether this region is the same or different in different individuals, and how it is modulated by experience or familiarity with different kinds of foods.”
Pinpointing those differences could provide insights into how people choose what they eat, or even help us learn what drives eating disorders, Dr. Khosla says.
Part of what makes this study unique was the researchers’ approach, dubbed “hypothesis neutral.” Instead of setting out to prove or disprove a firm hypothesis, they simply started exploring the data to see what they could find. The goal: To go beyond “the idiosyncratic hypotheses scientists have already thought to test,” the paper says. So, they began sifting through a public database called the Natural Scenes Dataset, an inventory of brain scans from eight volunteers viewing 56,720 images.
As expected, the software analyzing the dataset spotted brain regions already known to be triggered by images of faces, bodies, words, and scenes. But to the researchers’ surprise, the analysis also revealed a previously unknown part of the brain that seemed to be responding to images of food.
“Our first reaction was, ‘That’s cute and all, but it can’t possibly be true,’ ” Dr. Khosla says.
To confirm their discovery, the researchers used the data to train a computer model of this part of the brain, a process that takes less than an hour. Then they fed the model more than 1.2 million new images.
Sure enough, the model lit up in response to food. Color didn’t matter – even black-and-white food images triggered it, though not as strongly as color ones. And the model could tell the difference between food and objects that looked like food: a banana versus a crescent moon, or a blueberry muffin versus a puppy with a muffin-like face.
From the human data, the researchers found that some people responded slightly more to processed foods like pizza than unprocessed foods like apples. They hope to explore how other things, such as liking or disliking a food, may affect a person’s response to that food.
This technology could open up other areas of research as well. Dr. Khosla hopes to use it to explore how the brain responds to social cues like body language and facial expressions.
For now, Dr. Khosla has already begun to verify the computer model in real people by scanning the brains of a new set of volunteers. “We collected pilot data in a few subjects recently and were able to localize this component,” she says.
A version of this article first appeared on Medscape.com.
“We eat first with our eyes.”
The Roman foodie Apicius is thought to have uttered those words in the 1st century A.D. Now, some 2,000 years later, scientists may be proving him right.
Dubbed the “ventral food component,” this part resides in the brain’s visual cortex, in a region known to play a role in identifying faces, scenes, and words.
The study, published in the journal Current Biology, involved using artificial intelligence (AI) technology to build a computer model of this part of the brain. Similar models are emerging across fields of research to simulate and study complex systems of the body. A computer model of the digestive system was recently used to determine the best body position for taking a pill.
“The research is still cutting-edge,” says study author Meenakshi Khosla, PhD. “There’s a lot more to be done to understand whether this region is the same or different in different individuals, and how it is modulated by experience or familiarity with different kinds of foods.”
Pinpointing those differences could provide insights into how people choose what they eat, or even help us learn what drives eating disorders, Dr. Khosla says.
Part of what makes this study unique was the researchers’ approach, dubbed “hypothesis neutral.” Instead of setting out to prove or disprove a firm hypothesis, they simply started exploring the data to see what they could find. The goal: To go beyond “the idiosyncratic hypotheses scientists have already thought to test,” the paper says. So, they began sifting through a public database called the Natural Scenes Dataset, an inventory of brain scans from eight volunteers viewing 56,720 images.
As expected, the software analyzing the dataset spotted brain regions already known to be triggered by images of faces, bodies, words, and scenes. But to the researchers’ surprise, the analysis also revealed a previously unknown part of the brain that seemed to be responding to images of food.
“Our first reaction was, ‘That’s cute and all, but it can’t possibly be true,’ ” Dr. Khosla says.
To confirm their discovery, the researchers used the data to train a computer model of this part of the brain, a process that takes less than an hour. Then they fed the model more than 1.2 million new images.
Sure enough, the model lit up in response to food. Color didn’t matter – even black-and-white food images triggered it, though not as strongly as color ones. And the model could tell the difference between food and objects that looked like food: a banana versus a crescent moon, or a blueberry muffin versus a puppy with a muffin-like face.
From the human data, the researchers found that some people responded slightly more to processed foods like pizza than unprocessed foods like apples. They hope to explore how other things, such as liking or disliking a food, may affect a person’s response to that food.
This technology could open up other areas of research as well. Dr. Khosla hopes to use it to explore how the brain responds to social cues like body language and facial expressions.
For now, Dr. Khosla has already begun to verify the computer model in real people by scanning the brains of a new set of volunteers. “We collected pilot data in a few subjects recently and were able to localize this component,” she says.
A version of this article first appeared on Medscape.com.
“We eat first with our eyes.”
The Roman foodie Apicius is thought to have uttered those words in the 1st century A.D. Now, some 2,000 years later, scientists may be proving him right.
Dubbed the “ventral food component,” this part resides in the brain’s visual cortex, in a region known to play a role in identifying faces, scenes, and words.
The study, published in the journal Current Biology, involved using artificial intelligence (AI) technology to build a computer model of this part of the brain. Similar models are emerging across fields of research to simulate and study complex systems of the body. A computer model of the digestive system was recently used to determine the best body position for taking a pill.
“The research is still cutting-edge,” says study author Meenakshi Khosla, PhD. “There’s a lot more to be done to understand whether this region is the same or different in different individuals, and how it is modulated by experience or familiarity with different kinds of foods.”
Pinpointing those differences could provide insights into how people choose what they eat, or even help us learn what drives eating disorders, Dr. Khosla says.
Part of what makes this study unique was the researchers’ approach, dubbed “hypothesis neutral.” Instead of setting out to prove or disprove a firm hypothesis, they simply started exploring the data to see what they could find. The goal: To go beyond “the idiosyncratic hypotheses scientists have already thought to test,” the paper says. So, they began sifting through a public database called the Natural Scenes Dataset, an inventory of brain scans from eight volunteers viewing 56,720 images.
As expected, the software analyzing the dataset spotted brain regions already known to be triggered by images of faces, bodies, words, and scenes. But to the researchers’ surprise, the analysis also revealed a previously unknown part of the brain that seemed to be responding to images of food.
“Our first reaction was, ‘That’s cute and all, but it can’t possibly be true,’ ” Dr. Khosla says.
To confirm their discovery, the researchers used the data to train a computer model of this part of the brain, a process that takes less than an hour. Then they fed the model more than 1.2 million new images.
Sure enough, the model lit up in response to food. Color didn’t matter – even black-and-white food images triggered it, though not as strongly as color ones. And the model could tell the difference between food and objects that looked like food: a banana versus a crescent moon, or a blueberry muffin versus a puppy with a muffin-like face.
From the human data, the researchers found that some people responded slightly more to processed foods like pizza than unprocessed foods like apples. They hope to explore how other things, such as liking or disliking a food, may affect a person’s response to that food.
This technology could open up other areas of research as well. Dr. Khosla hopes to use it to explore how the brain responds to social cues like body language and facial expressions.
For now, Dr. Khosla has already begun to verify the computer model in real people by scanning the brains of a new set of volunteers. “We collected pilot data in a few subjects recently and were able to localize this component,” she says.
A version of this article first appeared on Medscape.com.
FROM CURRENT BIOLOGY
Droplet dispersal in sterile processing units far exceeds guideline limit
In the era of Ebola, COVID-19, and even Legionnaires, technicians and other staff working behind the scenes to ensure provider and patient safety continue to face a long-recognized but under addressed challenge: splashes and airborne droplets.
Granted, National Institute for Occupational Safety and Health (NIOSH) standards, industry standards, and professional guidelines are all in place to prevent unintentional exposure to pathogens. However, findings from a newly published study in the American Journal of Infection Control suggest they fall short.
In the study, researchers found that simulated manual cleaning of medical devices generated a drenching splash throughout the process with droplet dispersal exceeding 7 feet (2.1 meters).
Cori L. Ofstead, MSPH, lead author and president/CEO of Ofstead & Associates, Bloomington, Minn., told this news organization. “That’s the problem with having standards and guidelines that are not based on relevant evidence, [which] in this case, is a single study that was done in an intensive care area where they had an infection outbreak.”
Ms. Ofstead was referring to a report in the journal Infection Control and Hospital Epidemiology, detailing a Canadian investigation involving a multidrug-resistant Pseudomonas aeruginosa outbreak in an ICU. The report implicated the faucets over the hand hygiene sinks, with fluorescent dye showing droplet dispersal roughly 3 feet away from the sinks.
“Somehow it [the 3-feet rule] got implemented in guidelines in sterile processing decontamination areas, which are not the same as hand hygiene,’’ Ms. Ofstead explained.
With a goal of providing more current evidence on droplet generation and dispersal, as well as personal protection equipment (PPE) exposure/effectiveness, she and her colleagues simulated manual cleaning of a decommissioned colonoscope and transvaginal ultrasound probe, using for the study location a new academic sterile processing unit.
To detect droplet generation and dispersal as well as splash following common technician activities (for example, colonoscope brushing, scrubbing, rinsing and transport to an automated endoscope reprocessor [AER] for sterilization), the researchers affixed blue moisture-detection paper to environmental surfaces, on carts positioned 4 feet (1.2 meters) from the sink (to simulate observers), and along a 15-foot pathway between the sink and AER.
They observed droplets everywhere.
Technician activities such as running the faucet and rinsing the probe under running water generated substantial splashing overall. Instrument rinsing in particular produced small and large droplets and confluent puddles of water around the sink and in the broad area surrounding the workspace. Droplets were also dispersed on the floor 7.25 feet (2.2 meters) away and along the entire 15-foot path from the sink to the AER.
At the sink, the technician risked drenching exposure from head to toe during most activities, and even observers positioned 3-4 feet away were found to have droplets on their gowns. In addition, saturated shoe covers reportedly tracked moisture away from the sink to the unit door – a distance of 13 feet (4 meters) – and 2 feet (0.6 meters) farther out into the PPE foyer for donning and doffing.
Although PPE gowns effectively repelled moisture during cleaning of a single device, Ms. Ofstead emphasized that technicians typically handle up to 10 instruments during a normal, 2-hour shift, further increasing exposure risk with each subsequent cleaning.
However, perhaps one of the most surprising findings was that despite an optimal unit design, including physical separation of clean and dirty activities and pressurized air flow to protect workers, droplets were still broadly dispersed.
Current efforts, however well-intentioned, might not be offering the degree of protection (and consideration) that sterile processing technicians need.
“The study was conducted in a new sterile processing area that had an extra excellent kind of distancing and three separate rooms, something that I think most of our hospitals are working toward,” Stella Hines, MD, associate professor at the University of Maryland School of Medicine, Baltimore, explained. Dr. Hines was not directly involved in the study.
“But it also really kind of highlighted what’s happening to workers potentially,” she added. “For example, we want to know if that spray or splatter has a live microbe it in that could cause a problem or ... in a highly wet environment, if that water has some kind of chemical in it that could pose an occupational hazard to the worker based on skin or mucous membrane exposure.”
Ms. Ofstead agreed. “We need to be thinking about the exposure of critically important workers and the environment in an era where we are worried about aerosol-generating procedures and superbugs,” she explained.
Dr. Hines and Ms. Ofstead also noted that the majority of staff involved in front-line patient care have never actually ventured into the sterile processing units nor do they recognize the risks that technicians working in these units face on a daily, or even hourly, basis.
“The people who run these operations are very well trained and knowledgeable. I think that it would be helpful for them to know that they’re appreciated and for the people upstairs on the front lines using the equipment to see what goes on downstairs and all of the painstaking steps that need to be in place for the equipment to come out of sterile processing and be ready to go,” said Dr. Hines.
In the meantime, hospital leaders need to address the challenges and danger posed by migrating infectious droplets, especially for workers involved in processes that stir them up in the first place – workers who by the end of their shifts are unavoidably drenched with infectious blood and tissue secretions.
“I think that it’s going to take a much bigger kind of worldview from hospital leadership,” Dr. Hines said.
The study was supported in part by a grant from Healthmark Industries. Ms. Ofstead reports research grants or consulting fees through her organization with 3M Company, Ambu, Boston Scientific, Cleanis, Fortive/Advanced Sterilization Products, Healthmark Industries, Pentax, and Steris/Cantel/Medviators. Dr. Hines reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In the era of Ebola, COVID-19, and even Legionnaires, technicians and other staff working behind the scenes to ensure provider and patient safety continue to face a long-recognized but under addressed challenge: splashes and airborne droplets.
Granted, National Institute for Occupational Safety and Health (NIOSH) standards, industry standards, and professional guidelines are all in place to prevent unintentional exposure to pathogens. However, findings from a newly published study in the American Journal of Infection Control suggest they fall short.
In the study, researchers found that simulated manual cleaning of medical devices generated a drenching splash throughout the process with droplet dispersal exceeding 7 feet (2.1 meters).
Cori L. Ofstead, MSPH, lead author and president/CEO of Ofstead & Associates, Bloomington, Minn., told this news organization. “That’s the problem with having standards and guidelines that are not based on relevant evidence, [which] in this case, is a single study that was done in an intensive care area where they had an infection outbreak.”
Ms. Ofstead was referring to a report in the journal Infection Control and Hospital Epidemiology, detailing a Canadian investigation involving a multidrug-resistant Pseudomonas aeruginosa outbreak in an ICU. The report implicated the faucets over the hand hygiene sinks, with fluorescent dye showing droplet dispersal roughly 3 feet away from the sinks.
“Somehow it [the 3-feet rule] got implemented in guidelines in sterile processing decontamination areas, which are not the same as hand hygiene,’’ Ms. Ofstead explained.
With a goal of providing more current evidence on droplet generation and dispersal, as well as personal protection equipment (PPE) exposure/effectiveness, she and her colleagues simulated manual cleaning of a decommissioned colonoscope and transvaginal ultrasound probe, using for the study location a new academic sterile processing unit.
To detect droplet generation and dispersal as well as splash following common technician activities (for example, colonoscope brushing, scrubbing, rinsing and transport to an automated endoscope reprocessor [AER] for sterilization), the researchers affixed blue moisture-detection paper to environmental surfaces, on carts positioned 4 feet (1.2 meters) from the sink (to simulate observers), and along a 15-foot pathway between the sink and AER.
They observed droplets everywhere.
Technician activities such as running the faucet and rinsing the probe under running water generated substantial splashing overall. Instrument rinsing in particular produced small and large droplets and confluent puddles of water around the sink and in the broad area surrounding the workspace. Droplets were also dispersed on the floor 7.25 feet (2.2 meters) away and along the entire 15-foot path from the sink to the AER.
At the sink, the technician risked drenching exposure from head to toe during most activities, and even observers positioned 3-4 feet away were found to have droplets on their gowns. In addition, saturated shoe covers reportedly tracked moisture away from the sink to the unit door – a distance of 13 feet (4 meters) – and 2 feet (0.6 meters) farther out into the PPE foyer for donning and doffing.
Although PPE gowns effectively repelled moisture during cleaning of a single device, Ms. Ofstead emphasized that technicians typically handle up to 10 instruments during a normal, 2-hour shift, further increasing exposure risk with each subsequent cleaning.
However, perhaps one of the most surprising findings was that despite an optimal unit design, including physical separation of clean and dirty activities and pressurized air flow to protect workers, droplets were still broadly dispersed.
Current efforts, however well-intentioned, might not be offering the degree of protection (and consideration) that sterile processing technicians need.
“The study was conducted in a new sterile processing area that had an extra excellent kind of distancing and three separate rooms, something that I think most of our hospitals are working toward,” Stella Hines, MD, associate professor at the University of Maryland School of Medicine, Baltimore, explained. Dr. Hines was not directly involved in the study.
“But it also really kind of highlighted what’s happening to workers potentially,” she added. “For example, we want to know if that spray or splatter has a live microbe it in that could cause a problem or ... in a highly wet environment, if that water has some kind of chemical in it that could pose an occupational hazard to the worker based on skin or mucous membrane exposure.”
Ms. Ofstead agreed. “We need to be thinking about the exposure of critically important workers and the environment in an era where we are worried about aerosol-generating procedures and superbugs,” she explained.
Dr. Hines and Ms. Ofstead also noted that the majority of staff involved in front-line patient care have never actually ventured into the sterile processing units nor do they recognize the risks that technicians working in these units face on a daily, or even hourly, basis.
“The people who run these operations are very well trained and knowledgeable. I think that it would be helpful for them to know that they’re appreciated and for the people upstairs on the front lines using the equipment to see what goes on downstairs and all of the painstaking steps that need to be in place for the equipment to come out of sterile processing and be ready to go,” said Dr. Hines.
In the meantime, hospital leaders need to address the challenges and danger posed by migrating infectious droplets, especially for workers involved in processes that stir them up in the first place – workers who by the end of their shifts are unavoidably drenched with infectious blood and tissue secretions.
“I think that it’s going to take a much bigger kind of worldview from hospital leadership,” Dr. Hines said.
The study was supported in part by a grant from Healthmark Industries. Ms. Ofstead reports research grants or consulting fees through her organization with 3M Company, Ambu, Boston Scientific, Cleanis, Fortive/Advanced Sterilization Products, Healthmark Industries, Pentax, and Steris/Cantel/Medviators. Dr. Hines reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In the era of Ebola, COVID-19, and even Legionnaires, technicians and other staff working behind the scenes to ensure provider and patient safety continue to face a long-recognized but under addressed challenge: splashes and airborne droplets.
Granted, National Institute for Occupational Safety and Health (NIOSH) standards, industry standards, and professional guidelines are all in place to prevent unintentional exposure to pathogens. However, findings from a newly published study in the American Journal of Infection Control suggest they fall short.
In the study, researchers found that simulated manual cleaning of medical devices generated a drenching splash throughout the process with droplet dispersal exceeding 7 feet (2.1 meters).
Cori L. Ofstead, MSPH, lead author and president/CEO of Ofstead & Associates, Bloomington, Minn., told this news organization. “That’s the problem with having standards and guidelines that are not based on relevant evidence, [which] in this case, is a single study that was done in an intensive care area where they had an infection outbreak.”
Ms. Ofstead was referring to a report in the journal Infection Control and Hospital Epidemiology, detailing a Canadian investigation involving a multidrug-resistant Pseudomonas aeruginosa outbreak in an ICU. The report implicated the faucets over the hand hygiene sinks, with fluorescent dye showing droplet dispersal roughly 3 feet away from the sinks.
“Somehow it [the 3-feet rule] got implemented in guidelines in sterile processing decontamination areas, which are not the same as hand hygiene,’’ Ms. Ofstead explained.
With a goal of providing more current evidence on droplet generation and dispersal, as well as personal protection equipment (PPE) exposure/effectiveness, she and her colleagues simulated manual cleaning of a decommissioned colonoscope and transvaginal ultrasound probe, using for the study location a new academic sterile processing unit.
To detect droplet generation and dispersal as well as splash following common technician activities (for example, colonoscope brushing, scrubbing, rinsing and transport to an automated endoscope reprocessor [AER] for sterilization), the researchers affixed blue moisture-detection paper to environmental surfaces, on carts positioned 4 feet (1.2 meters) from the sink (to simulate observers), and along a 15-foot pathway between the sink and AER.
They observed droplets everywhere.
Technician activities such as running the faucet and rinsing the probe under running water generated substantial splashing overall. Instrument rinsing in particular produced small and large droplets and confluent puddles of water around the sink and in the broad area surrounding the workspace. Droplets were also dispersed on the floor 7.25 feet (2.2 meters) away and along the entire 15-foot path from the sink to the AER.
At the sink, the technician risked drenching exposure from head to toe during most activities, and even observers positioned 3-4 feet away were found to have droplets on their gowns. In addition, saturated shoe covers reportedly tracked moisture away from the sink to the unit door – a distance of 13 feet (4 meters) – and 2 feet (0.6 meters) farther out into the PPE foyer for donning and doffing.
Although PPE gowns effectively repelled moisture during cleaning of a single device, Ms. Ofstead emphasized that technicians typically handle up to 10 instruments during a normal, 2-hour shift, further increasing exposure risk with each subsequent cleaning.
However, perhaps one of the most surprising findings was that despite an optimal unit design, including physical separation of clean and dirty activities and pressurized air flow to protect workers, droplets were still broadly dispersed.
Current efforts, however well-intentioned, might not be offering the degree of protection (and consideration) that sterile processing technicians need.
“The study was conducted in a new sterile processing area that had an extra excellent kind of distancing and three separate rooms, something that I think most of our hospitals are working toward,” Stella Hines, MD, associate professor at the University of Maryland School of Medicine, Baltimore, explained. Dr. Hines was not directly involved in the study.
“But it also really kind of highlighted what’s happening to workers potentially,” she added. “For example, we want to know if that spray or splatter has a live microbe it in that could cause a problem or ... in a highly wet environment, if that water has some kind of chemical in it that could pose an occupational hazard to the worker based on skin or mucous membrane exposure.”
Ms. Ofstead agreed. “We need to be thinking about the exposure of critically important workers and the environment in an era where we are worried about aerosol-generating procedures and superbugs,” she explained.
Dr. Hines and Ms. Ofstead also noted that the majority of staff involved in front-line patient care have never actually ventured into the sterile processing units nor do they recognize the risks that technicians working in these units face on a daily, or even hourly, basis.
“The people who run these operations are very well trained and knowledgeable. I think that it would be helpful for them to know that they’re appreciated and for the people upstairs on the front lines using the equipment to see what goes on downstairs and all of the painstaking steps that need to be in place for the equipment to come out of sterile processing and be ready to go,” said Dr. Hines.
In the meantime, hospital leaders need to address the challenges and danger posed by migrating infectious droplets, especially for workers involved in processes that stir them up in the first place – workers who by the end of their shifts are unavoidably drenched with infectious blood and tissue secretions.
“I think that it’s going to take a much bigger kind of worldview from hospital leadership,” Dr. Hines said.
The study was supported in part by a grant from Healthmark Industries. Ms. Ofstead reports research grants or consulting fees through her organization with 3M Company, Ambu, Boston Scientific, Cleanis, Fortive/Advanced Sterilization Products, Healthmark Industries, Pentax, and Steris/Cantel/Medviators. Dr. Hines reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE AMERICAN JOURNAL OF INFECTION CONTROL
Is it flu, RSV, or COVID? Experts fear the ‘tripledemic’
Just when we thought this holiday season, finally, would be the back-to-normal one, some infectious disease experts are warning that a so-called “tripledemic” – influenza, COVID-19, and RSV – may be in the forecast.
The warning isn’t without basis.
The flu season has gotten an early start. As of Oct. 21, early increases in seasonal flu activity have been reported in most of the country, the Centers for Disease Control and Prevention said, with the southeast and south-central areas having the highest activity levels.
Children’s hospitals and EDs are seeing a surge in children with RSV.
COVID-19 cases are trending down, according to the CDC, but epidemiologists – scientists who study disease outbreaks – always have their eyes on emerging variants.
said Justin Lessler, PhD, a professor of epidemiology at the University of North Carolina at Chapel Hill. Dr. Lessler is on the coordinating team for the COVID-19 Scenario Modeling Hub, which aims to predict the course COVID-19, and the Flu Scenario Modeling Hub, which does the same for influenza.
For COVID-19, some models are predicting some spikes before Christmas, he said, and others see a new wave in 2023. For the flu, the model is predicting an earlier-than-usual start, as the CDC has reported.
While flu activity is relatively low, the CDC said, the season is off to an early start. For the week ending Oct. 21, 1,674 patients were hospitalized for flu, higher than in the summer months but fewer than the 2,675 hospitalizations for the week of May 15, 2022.
As of Oct. 20, COVID-19 cases have declined 12% over the last 2 weeks, nationwide. But hospitalizations are up 10% in much of the Northeast, The New York Times reports, and the improvement in cases and deaths has been slowing down.
As of Oct. 15, 15% of RSV tests reported nationwide were positive, compared with about 11% at that time in 2021, the CDC said. The surveillance collects information from 75 counties in 12 states.
Experts point out that the viruses – all three are respiratory viruses – are simply playing catchup.
“They spread the same way and along with lots of other viruses, and you tend to see an increase in them during the cold months,” said Timothy Brewer, MD, professor of medicine and epidemiology at UCLA.
The increase in all three viruses “is almost predictable at this point in the pandemic,” said Dean Blumberg, MD, a professor and chief of pediatric infectious diseases at the University of California Davis Health. “All the respiratory viruses are out of whack.”
Last year, RSV cases were up, too, and began to appear very early, he said, in the summer instead of in the cooler months. Flu also appeared early in 2021, as it has in 2022.
That contrasts with the flu season of 2020-2021, when COVID precautions were nearly universal, and cases were down. At UC Davis, “we didn’t have one pediatric admission due to influenza in the 2020-2021 [flu] season,” Dr. Blumberg said.
The number of pediatric flu deaths usually range from 37 to 199 per year, according to CDC records. But in the 2020-2021 season, the CDC recorded one pediatric flu death in the U.S.
Both children and adults have had less contact with others the past two seasons, Dr. Blumberg said, “and they don’t get the immunity they got with those infections [previously]. That’s why we are seeing out-of-season, early season [viruses].”
Eventually, he said, the cases of flu and RSV will return to previous levels. “It could be as soon as next year,” Dr. Blumberg said. And COVID-19, hopefully, will become like influenza, he said.
“RSV has always come around in the fall and winter,” said Elizabeth Murray, DO, a pediatric emergency medicine doctor at the University of Rochester (N.Y.) Medical Center and a spokesperson for the American Academy of Pediatrics. In 2022, children are back in school and for the most part not masking. “It’s a perfect storm for all the germs to spread now. They’ve just been waiting for their opportunity to come back.”
Self-care vs. not
RSV can pose a risk for anyone, but most at risk are children under age 5, especially infants under age 1, and adults over age 65. There is no vaccine for it. Symptoms include a runny nose, decreased appetite, coughing, sneezing, fever, and wheezing. But in young infants, there may only be decreased activity, crankiness, and breathing issues, the CDC said.
Keep an eye on the breathing if RSV is suspected, Dr. Murray tells parents. If your child can’t breathe easily, is unable to lie down comfortably, can’t speak clearly, or is sucking in the chest muscles to breathe, get medical help. Most kids with RSV can stay home and recover, she said, but often will need to be checked by a medical professional.
She advises against getting an oximeter to measure oxygen levels for home use. “They are often not accurate,” she said. If in doubt about how serious your child’s symptoms are, “don’t wait it out,” and don’t hesitate to call 911.
Symptoms of flu, COVID, and RSV can overlap. But each can involve breathing problems, which can be an emergency.
“It’s important to seek medical attention for any concerning symptoms, but especially severe shortness of breath or difficulty breathing, as these could signal the need for supplemental oxygen or other emergency interventions,” said Mandy De Vries, a respiratory therapist and director of education at the American Association for Respiratory Care. Inhalation treatment or mechanical ventilation may be needed for severe respiratory issues.
Precautions
To avoid the tripledemic – or any single infection – Timothy Brewer, MD, a professor of medicine and epidemiology at the University of California, Los Angeles, suggests some familiar measures: “Stay home if you’re feeling sick. Make sure you are up to date on your vaccinations. Wear a mask indoors.”
A version of this article first appeared on Medscape.com.
Just when we thought this holiday season, finally, would be the back-to-normal one, some infectious disease experts are warning that a so-called “tripledemic” – influenza, COVID-19, and RSV – may be in the forecast.
The warning isn’t without basis.
The flu season has gotten an early start. As of Oct. 21, early increases in seasonal flu activity have been reported in most of the country, the Centers for Disease Control and Prevention said, with the southeast and south-central areas having the highest activity levels.
Children’s hospitals and EDs are seeing a surge in children with RSV.
COVID-19 cases are trending down, according to the CDC, but epidemiologists – scientists who study disease outbreaks – always have their eyes on emerging variants.
said Justin Lessler, PhD, a professor of epidemiology at the University of North Carolina at Chapel Hill. Dr. Lessler is on the coordinating team for the COVID-19 Scenario Modeling Hub, which aims to predict the course COVID-19, and the Flu Scenario Modeling Hub, which does the same for influenza.
For COVID-19, some models are predicting some spikes before Christmas, he said, and others see a new wave in 2023. For the flu, the model is predicting an earlier-than-usual start, as the CDC has reported.
While flu activity is relatively low, the CDC said, the season is off to an early start. For the week ending Oct. 21, 1,674 patients were hospitalized for flu, higher than in the summer months but fewer than the 2,675 hospitalizations for the week of May 15, 2022.
As of Oct. 20, COVID-19 cases have declined 12% over the last 2 weeks, nationwide. But hospitalizations are up 10% in much of the Northeast, The New York Times reports, and the improvement in cases and deaths has been slowing down.
As of Oct. 15, 15% of RSV tests reported nationwide were positive, compared with about 11% at that time in 2021, the CDC said. The surveillance collects information from 75 counties in 12 states.
Experts point out that the viruses – all three are respiratory viruses – are simply playing catchup.
“They spread the same way and along with lots of other viruses, and you tend to see an increase in them during the cold months,” said Timothy Brewer, MD, professor of medicine and epidemiology at UCLA.
The increase in all three viruses “is almost predictable at this point in the pandemic,” said Dean Blumberg, MD, a professor and chief of pediatric infectious diseases at the University of California Davis Health. “All the respiratory viruses are out of whack.”
Last year, RSV cases were up, too, and began to appear very early, he said, in the summer instead of in the cooler months. Flu also appeared early in 2021, as it has in 2022.
That contrasts with the flu season of 2020-2021, when COVID precautions were nearly universal, and cases were down. At UC Davis, “we didn’t have one pediatric admission due to influenza in the 2020-2021 [flu] season,” Dr. Blumberg said.
The number of pediatric flu deaths usually range from 37 to 199 per year, according to CDC records. But in the 2020-2021 season, the CDC recorded one pediatric flu death in the U.S.
Both children and adults have had less contact with others the past two seasons, Dr. Blumberg said, “and they don’t get the immunity they got with those infections [previously]. That’s why we are seeing out-of-season, early season [viruses].”
Eventually, he said, the cases of flu and RSV will return to previous levels. “It could be as soon as next year,” Dr. Blumberg said. And COVID-19, hopefully, will become like influenza, he said.
“RSV has always come around in the fall and winter,” said Elizabeth Murray, DO, a pediatric emergency medicine doctor at the University of Rochester (N.Y.) Medical Center and a spokesperson for the American Academy of Pediatrics. In 2022, children are back in school and for the most part not masking. “It’s a perfect storm for all the germs to spread now. They’ve just been waiting for their opportunity to come back.”
Self-care vs. not
RSV can pose a risk for anyone, but most at risk are children under age 5, especially infants under age 1, and adults over age 65. There is no vaccine for it. Symptoms include a runny nose, decreased appetite, coughing, sneezing, fever, and wheezing. But in young infants, there may only be decreased activity, crankiness, and breathing issues, the CDC said.
Keep an eye on the breathing if RSV is suspected, Dr. Murray tells parents. If your child can’t breathe easily, is unable to lie down comfortably, can’t speak clearly, or is sucking in the chest muscles to breathe, get medical help. Most kids with RSV can stay home and recover, she said, but often will need to be checked by a medical professional.
She advises against getting an oximeter to measure oxygen levels for home use. “They are often not accurate,” she said. If in doubt about how serious your child’s symptoms are, “don’t wait it out,” and don’t hesitate to call 911.
Symptoms of flu, COVID, and RSV can overlap. But each can involve breathing problems, which can be an emergency.
“It’s important to seek medical attention for any concerning symptoms, but especially severe shortness of breath or difficulty breathing, as these could signal the need for supplemental oxygen or other emergency interventions,” said Mandy De Vries, a respiratory therapist and director of education at the American Association for Respiratory Care. Inhalation treatment or mechanical ventilation may be needed for severe respiratory issues.
Precautions
To avoid the tripledemic – or any single infection – Timothy Brewer, MD, a professor of medicine and epidemiology at the University of California, Los Angeles, suggests some familiar measures: “Stay home if you’re feeling sick. Make sure you are up to date on your vaccinations. Wear a mask indoors.”
A version of this article first appeared on Medscape.com.
Just when we thought this holiday season, finally, would be the back-to-normal one, some infectious disease experts are warning that a so-called “tripledemic” – influenza, COVID-19, and RSV – may be in the forecast.
The warning isn’t without basis.
The flu season has gotten an early start. As of Oct. 21, early increases in seasonal flu activity have been reported in most of the country, the Centers for Disease Control and Prevention said, with the southeast and south-central areas having the highest activity levels.
Children’s hospitals and EDs are seeing a surge in children with RSV.
COVID-19 cases are trending down, according to the CDC, but epidemiologists – scientists who study disease outbreaks – always have their eyes on emerging variants.
said Justin Lessler, PhD, a professor of epidemiology at the University of North Carolina at Chapel Hill. Dr. Lessler is on the coordinating team for the COVID-19 Scenario Modeling Hub, which aims to predict the course COVID-19, and the Flu Scenario Modeling Hub, which does the same for influenza.
For COVID-19, some models are predicting some spikes before Christmas, he said, and others see a new wave in 2023. For the flu, the model is predicting an earlier-than-usual start, as the CDC has reported.
While flu activity is relatively low, the CDC said, the season is off to an early start. For the week ending Oct. 21, 1,674 patients were hospitalized for flu, higher than in the summer months but fewer than the 2,675 hospitalizations for the week of May 15, 2022.
As of Oct. 20, COVID-19 cases have declined 12% over the last 2 weeks, nationwide. But hospitalizations are up 10% in much of the Northeast, The New York Times reports, and the improvement in cases and deaths has been slowing down.
As of Oct. 15, 15% of RSV tests reported nationwide were positive, compared with about 11% at that time in 2021, the CDC said. The surveillance collects information from 75 counties in 12 states.
Experts point out that the viruses – all three are respiratory viruses – are simply playing catchup.
“They spread the same way and along with lots of other viruses, and you tend to see an increase in them during the cold months,” said Timothy Brewer, MD, professor of medicine and epidemiology at UCLA.
The increase in all three viruses “is almost predictable at this point in the pandemic,” said Dean Blumberg, MD, a professor and chief of pediatric infectious diseases at the University of California Davis Health. “All the respiratory viruses are out of whack.”
Last year, RSV cases were up, too, and began to appear very early, he said, in the summer instead of in the cooler months. Flu also appeared early in 2021, as it has in 2022.
That contrasts with the flu season of 2020-2021, when COVID precautions were nearly universal, and cases were down. At UC Davis, “we didn’t have one pediatric admission due to influenza in the 2020-2021 [flu] season,” Dr. Blumberg said.
The number of pediatric flu deaths usually range from 37 to 199 per year, according to CDC records. But in the 2020-2021 season, the CDC recorded one pediatric flu death in the U.S.
Both children and adults have had less contact with others the past two seasons, Dr. Blumberg said, “and they don’t get the immunity they got with those infections [previously]. That’s why we are seeing out-of-season, early season [viruses].”
Eventually, he said, the cases of flu and RSV will return to previous levels. “It could be as soon as next year,” Dr. Blumberg said. And COVID-19, hopefully, will become like influenza, he said.
“RSV has always come around in the fall and winter,” said Elizabeth Murray, DO, a pediatric emergency medicine doctor at the University of Rochester (N.Y.) Medical Center and a spokesperson for the American Academy of Pediatrics. In 2022, children are back in school and for the most part not masking. “It’s a perfect storm for all the germs to spread now. They’ve just been waiting for their opportunity to come back.”
Self-care vs. not
RSV can pose a risk for anyone, but most at risk are children under age 5, especially infants under age 1, and adults over age 65. There is no vaccine for it. Symptoms include a runny nose, decreased appetite, coughing, sneezing, fever, and wheezing. But in young infants, there may only be decreased activity, crankiness, and breathing issues, the CDC said.
Keep an eye on the breathing if RSV is suspected, Dr. Murray tells parents. If your child can’t breathe easily, is unable to lie down comfortably, can’t speak clearly, or is sucking in the chest muscles to breathe, get medical help. Most kids with RSV can stay home and recover, she said, but often will need to be checked by a medical professional.
She advises against getting an oximeter to measure oxygen levels for home use. “They are often not accurate,” she said. If in doubt about how serious your child’s symptoms are, “don’t wait it out,” and don’t hesitate to call 911.
Symptoms of flu, COVID, and RSV can overlap. But each can involve breathing problems, which can be an emergency.
“It’s important to seek medical attention for any concerning symptoms, but especially severe shortness of breath or difficulty breathing, as these could signal the need for supplemental oxygen or other emergency interventions,” said Mandy De Vries, a respiratory therapist and director of education at the American Association for Respiratory Care. Inhalation treatment or mechanical ventilation may be needed for severe respiratory issues.
Precautions
To avoid the tripledemic – or any single infection – Timothy Brewer, MD, a professor of medicine and epidemiology at the University of California, Los Angeles, suggests some familiar measures: “Stay home if you’re feeling sick. Make sure you are up to date on your vaccinations. Wear a mask indoors.”
A version of this article first appeared on Medscape.com.
In childhood sickle cell disease stroke prevention is key
CINCINNATI – Sickle cell disease is well known for its associated anemia, but patients experience a range of other complications as well. These include vision and kidney problems, delayed growth, susceptibility to infection, and pain.
Another issue, not always as well recognized, is a considerably heightened risk for childhood stroke. “, and there’s also an elevated risk of five times the general population in adults with sickle cell disease,” said Lori Jordan, MD, PhD, in an interview.
At the 2022 annual meeting of the Child Neurology Society, Dr. Jordan spoke about stroke as a complication of sickle cell disease, and the role that neurologists can play in preventing primary or secondary strokes. “At least in children, studies have shown that if we screen and identify patients who are at highest risk of stroke, there are primary prevention therapies – usually implemented by hematologists, but that neurologists often are involved with – both monitoring for cognitive effects of silent cerebral infarct and also with treating patients who unfortunately still have an acute stroke,” said Dr. Jordan, who is an associate professor of pediatrics, neurology, and radiology at Vanderbilt University Medical Center, Nashville, Tenn. She also is director of the pediatric stroke program at Vanderbilt.
Time is of the essence
“In general, stroke in children is rare, but it’s more common in sickle cell disease, so it’s really important for providers to know that stroke risk is higher in those patients, particularly in those children, and then identify it and treat it earlier. Time is of the essence, and if we can give them the same therapeutics that we give the general stroke population, then time really becomes a factor, so it’s important that people know that it’s an issue for this population,” said Eboni Lance, MD, PhD, who coordinated the session where Dr. Jordan spoke.
Sickle cell disease is caused by a double mutation in the gene encoding the hemoglobin gene, producing the altered sickle hemoglobin (hemoglobin S). The change causes the hemoglobin proteins to tend to stick to one another, which can lead red blood cells to adopt a sickle-like shape. The sickle-shaped blood cells in turn have a tendency to aggregate and can block blood flow or lead to endothelial injury. Symptoms of stroke in children can include hemiparesis, aphasia, and seizure, but they can also be silent.
If no preventive is employed, one in nine with sickle cell disease will experience a stroke by the age of 19. Cerebrovascular symptoms are the most frequent debilitating complication of the condition. Nearly 40% of patients with sickle cell disease will have a silent cerebral infarct by age 18, as will 50% by age 30. Silent strokes have been associated with worse educational attainment and a greater need for educational special services.
Factors contributing to stroke in children with sickle cell disease include anemia and a low blood oxygen count, reduced oxygen affinity of hemoglobin variant, and cerebral vasculopathy. An estimated 10%-15% of young adults with sickle cell disease have severe intracranial stenosis.
Primary and secondary stroke prevention strategies
The dire consequences of stroke in this patient population underline the importance of primary stroke prevention, which requires the use of transcranial Doppler (TCD) ultrasound. It has been validated as a tool to screen for initial stroke risk in children with no history of stroke. High velocity measured on TCD indicates a narrowed blood vessel or elevated blood that is compensating for anemia. It adds up to a “struggling brain,” said Dr. Jordan, during her talk. If the TCD ultrasound velocity is greater than 200 cm/sec (or 170 cm/sec, depending on nonimaging versus imaging TCD), the TWiTCH trial showed that seven monthly transfusions is the number needed to treat to prevent one stroke. After 1 year, patients can be switched from transfusions to hydroxyurea if the patient has no significant intracranial stenosis. Hydroxyurea boosts both fetal and total hemoglobin, and also counters inflammation.
Following an acute stroke or transient ischemic attack, patients should receive a transfusion within 2 hours of presenting in the health care setting. American Society of Hematology guidelines recommend exchange transfusion rather than a simple transfusion. A simple transfusion can be initiated if an exchange transfusion is not available within 2 hours and hemoglobin values are less than 8.5 g/dL, to be followed by performance of exchange transfusion when available.
For chronic secondary stroke prevention, transfusions should be performed approximately monthly with the goal of maintaining hemoglobin above 9 g/dL at all times, as well as suppressing hemoglobin S levels to 30% or less of total hemoglobin.
Sudden, severe headache is a potential harbinger of complications like aneurysm, which occurs 10-fold more often among patients with sickle cell disease than the general population. It could also indicate increased intracranial pressure or cerebral venous sinus thrombosis.
Treatment of acute headache in sickle cell disease should avoid use of triptans, since vasoconstriction can counter the increased cerebral blood flow that compensates for anemia. Gabapentin and amitriptyline are good treatment choices.
New-onset seizures are a potential sign of stroke or posterior reversible leukoencephalopathy (PRES) in patients with sickle cell disease. Urgent MRI should be considered for all new-onset seizures. If blood pressure is high, PRES may be present. Seizures may also be an indicator of a previous brain injury.
Dr. Jordan has no relevant financial disclosures. Dr. Lance has served on an advisory board for Novartis.
CINCINNATI – Sickle cell disease is well known for its associated anemia, but patients experience a range of other complications as well. These include vision and kidney problems, delayed growth, susceptibility to infection, and pain.
Another issue, not always as well recognized, is a considerably heightened risk for childhood stroke. “, and there’s also an elevated risk of five times the general population in adults with sickle cell disease,” said Lori Jordan, MD, PhD, in an interview.
At the 2022 annual meeting of the Child Neurology Society, Dr. Jordan spoke about stroke as a complication of sickle cell disease, and the role that neurologists can play in preventing primary or secondary strokes. “At least in children, studies have shown that if we screen and identify patients who are at highest risk of stroke, there are primary prevention therapies – usually implemented by hematologists, but that neurologists often are involved with – both monitoring for cognitive effects of silent cerebral infarct and also with treating patients who unfortunately still have an acute stroke,” said Dr. Jordan, who is an associate professor of pediatrics, neurology, and radiology at Vanderbilt University Medical Center, Nashville, Tenn. She also is director of the pediatric stroke program at Vanderbilt.
Time is of the essence
“In general, stroke in children is rare, but it’s more common in sickle cell disease, so it’s really important for providers to know that stroke risk is higher in those patients, particularly in those children, and then identify it and treat it earlier. Time is of the essence, and if we can give them the same therapeutics that we give the general stroke population, then time really becomes a factor, so it’s important that people know that it’s an issue for this population,” said Eboni Lance, MD, PhD, who coordinated the session where Dr. Jordan spoke.
Sickle cell disease is caused by a double mutation in the gene encoding the hemoglobin gene, producing the altered sickle hemoglobin (hemoglobin S). The change causes the hemoglobin proteins to tend to stick to one another, which can lead red blood cells to adopt a sickle-like shape. The sickle-shaped blood cells in turn have a tendency to aggregate and can block blood flow or lead to endothelial injury. Symptoms of stroke in children can include hemiparesis, aphasia, and seizure, but they can also be silent.
If no preventive is employed, one in nine with sickle cell disease will experience a stroke by the age of 19. Cerebrovascular symptoms are the most frequent debilitating complication of the condition. Nearly 40% of patients with sickle cell disease will have a silent cerebral infarct by age 18, as will 50% by age 30. Silent strokes have been associated with worse educational attainment and a greater need for educational special services.
Factors contributing to stroke in children with sickle cell disease include anemia and a low blood oxygen count, reduced oxygen affinity of hemoglobin variant, and cerebral vasculopathy. An estimated 10%-15% of young adults with sickle cell disease have severe intracranial stenosis.
Primary and secondary stroke prevention strategies
The dire consequences of stroke in this patient population underline the importance of primary stroke prevention, which requires the use of transcranial Doppler (TCD) ultrasound. It has been validated as a tool to screen for initial stroke risk in children with no history of stroke. High velocity measured on TCD indicates a narrowed blood vessel or elevated blood that is compensating for anemia. It adds up to a “struggling brain,” said Dr. Jordan, during her talk. If the TCD ultrasound velocity is greater than 200 cm/sec (or 170 cm/sec, depending on nonimaging versus imaging TCD), the TWiTCH trial showed that seven monthly transfusions is the number needed to treat to prevent one stroke. After 1 year, patients can be switched from transfusions to hydroxyurea if the patient has no significant intracranial stenosis. Hydroxyurea boosts both fetal and total hemoglobin, and also counters inflammation.
Following an acute stroke or transient ischemic attack, patients should receive a transfusion within 2 hours of presenting in the health care setting. American Society of Hematology guidelines recommend exchange transfusion rather than a simple transfusion. A simple transfusion can be initiated if an exchange transfusion is not available within 2 hours and hemoglobin values are less than 8.5 g/dL, to be followed by performance of exchange transfusion when available.
For chronic secondary stroke prevention, transfusions should be performed approximately monthly with the goal of maintaining hemoglobin above 9 g/dL at all times, as well as suppressing hemoglobin S levels to 30% or less of total hemoglobin.
Sudden, severe headache is a potential harbinger of complications like aneurysm, which occurs 10-fold more often among patients with sickle cell disease than the general population. It could also indicate increased intracranial pressure or cerebral venous sinus thrombosis.
Treatment of acute headache in sickle cell disease should avoid use of triptans, since vasoconstriction can counter the increased cerebral blood flow that compensates for anemia. Gabapentin and amitriptyline are good treatment choices.
New-onset seizures are a potential sign of stroke or posterior reversible leukoencephalopathy (PRES) in patients with sickle cell disease. Urgent MRI should be considered for all new-onset seizures. If blood pressure is high, PRES may be present. Seizures may also be an indicator of a previous brain injury.
Dr. Jordan has no relevant financial disclosures. Dr. Lance has served on an advisory board for Novartis.
CINCINNATI – Sickle cell disease is well known for its associated anemia, but patients experience a range of other complications as well. These include vision and kidney problems, delayed growth, susceptibility to infection, and pain.
Another issue, not always as well recognized, is a considerably heightened risk for childhood stroke. “, and there’s also an elevated risk of five times the general population in adults with sickle cell disease,” said Lori Jordan, MD, PhD, in an interview.
At the 2022 annual meeting of the Child Neurology Society, Dr. Jordan spoke about stroke as a complication of sickle cell disease, and the role that neurologists can play in preventing primary or secondary strokes. “At least in children, studies have shown that if we screen and identify patients who are at highest risk of stroke, there are primary prevention therapies – usually implemented by hematologists, but that neurologists often are involved with – both monitoring for cognitive effects of silent cerebral infarct and also with treating patients who unfortunately still have an acute stroke,” said Dr. Jordan, who is an associate professor of pediatrics, neurology, and radiology at Vanderbilt University Medical Center, Nashville, Tenn. She also is director of the pediatric stroke program at Vanderbilt.
Time is of the essence
“In general, stroke in children is rare, but it’s more common in sickle cell disease, so it’s really important for providers to know that stroke risk is higher in those patients, particularly in those children, and then identify it and treat it earlier. Time is of the essence, and if we can give them the same therapeutics that we give the general stroke population, then time really becomes a factor, so it’s important that people know that it’s an issue for this population,” said Eboni Lance, MD, PhD, who coordinated the session where Dr. Jordan spoke.
Sickle cell disease is caused by a double mutation in the gene encoding the hemoglobin gene, producing the altered sickle hemoglobin (hemoglobin S). The change causes the hemoglobin proteins to tend to stick to one another, which can lead red blood cells to adopt a sickle-like shape. The sickle-shaped blood cells in turn have a tendency to aggregate and can block blood flow or lead to endothelial injury. Symptoms of stroke in children can include hemiparesis, aphasia, and seizure, but they can also be silent.
If no preventive is employed, one in nine with sickle cell disease will experience a stroke by the age of 19. Cerebrovascular symptoms are the most frequent debilitating complication of the condition. Nearly 40% of patients with sickle cell disease will have a silent cerebral infarct by age 18, as will 50% by age 30. Silent strokes have been associated with worse educational attainment and a greater need for educational special services.
Factors contributing to stroke in children with sickle cell disease include anemia and a low blood oxygen count, reduced oxygen affinity of hemoglobin variant, and cerebral vasculopathy. An estimated 10%-15% of young adults with sickle cell disease have severe intracranial stenosis.
Primary and secondary stroke prevention strategies
The dire consequences of stroke in this patient population underline the importance of primary stroke prevention, which requires the use of transcranial Doppler (TCD) ultrasound. It has been validated as a tool to screen for initial stroke risk in children with no history of stroke. High velocity measured on TCD indicates a narrowed blood vessel or elevated blood that is compensating for anemia. It adds up to a “struggling brain,” said Dr. Jordan, during her talk. If the TCD ultrasound velocity is greater than 200 cm/sec (or 170 cm/sec, depending on nonimaging versus imaging TCD), the TWiTCH trial showed that seven monthly transfusions is the number needed to treat to prevent one stroke. After 1 year, patients can be switched from transfusions to hydroxyurea if the patient has no significant intracranial stenosis. Hydroxyurea boosts both fetal and total hemoglobin, and also counters inflammation.
Following an acute stroke or transient ischemic attack, patients should receive a transfusion within 2 hours of presenting in the health care setting. American Society of Hematology guidelines recommend exchange transfusion rather than a simple transfusion. A simple transfusion can be initiated if an exchange transfusion is not available within 2 hours and hemoglobin values are less than 8.5 g/dL, to be followed by performance of exchange transfusion when available.
For chronic secondary stroke prevention, transfusions should be performed approximately monthly with the goal of maintaining hemoglobin above 9 g/dL at all times, as well as suppressing hemoglobin S levels to 30% or less of total hemoglobin.
Sudden, severe headache is a potential harbinger of complications like aneurysm, which occurs 10-fold more often among patients with sickle cell disease than the general population. It could also indicate increased intracranial pressure or cerebral venous sinus thrombosis.
Treatment of acute headache in sickle cell disease should avoid use of triptans, since vasoconstriction can counter the increased cerebral blood flow that compensates for anemia. Gabapentin and amitriptyline are good treatment choices.
New-onset seizures are a potential sign of stroke or posterior reversible leukoencephalopathy (PRES) in patients with sickle cell disease. Urgent MRI should be considered for all new-onset seizures. If blood pressure is high, PRES may be present. Seizures may also be an indicator of a previous brain injury.
Dr. Jordan has no relevant financial disclosures. Dr. Lance has served on an advisory board for Novartis.
FROM CNS 2022
‘Financial toxicity’: Harsh side effect of cancer care
When 32-year-old Brittany Dicks was diagnosed with stage II triple negative breast cancer in January 2022, she wasn’t worried about the cost of treatment. A medical assistant in Charleston, S.C., Ms. Dicks had full-time employment with health benefits.
But when she wasn’t able to work for several months because of chemotherapy and its side effects, Ms. Dicks lost her job. Her health insurance coverage ended in May. And although she filed for Medicaid at the beginning of June, it wasn’t approved until September.
Meanwhile, Ms. Dicks still needed treatment. She estimates that she ran up close to $20,000 in medical debt while finishing chemotherapy during the 4 months she was uninsured.
The surgeon she had seen since her diagnosis terminated her care when she could no longer pay her bills. That left her delaying a much-needed mastectomy.
“I don’t sleep at night,” said Ms. Dicks, a single mother of two young kids, ages 3 and 11. “Mentally, I’m drained. Just because I have cancer, doesn’t mean the bills aren’t due every month.”
As soon as she felt well enough over the summer, she started working as a part-time delivery driver for DoorDash to help pay for food and gas.
But that was just a Band-Aid. Even when her new insurance kicked in, covering the costs of daily life remained a struggle.
Ms. Dicks is still in deep medical debt. Her Medicaid has covered new medical expenses, and she hopes Medicaid will reimburse her for the debt she incurred over the summer while she waited for her coverage to kick in. So far, though, Medicaid has not touched her $20,000 debt.
“I fear that I’m not going to be able to dig out of this hole,” Ms. Dicks said.
Researchers who study the financial impacts of cancer have a term for Ms. Dicks’ experience: financial toxicity.
Financial toxicity is a catchall term for the burden many Americans with cancer experience.
“Financial toxicity is a multidimensional concept. There’s both a material burden and a psychosocial one,” said Grace Li Smith, MD, PhD, MPH, a radiation oncologist at the University of Texas MD Anderson Cancer Center, Houston.
Researchers are also now beginning to understand the psychological effects these financial burdens can have on patients and their family.
“Financial toxicity is not unique to the patient,” said Dr. Li Smith. It “very directly impacts the whole family or household.”
Stifling financial pressures
Early in her career, Dr. Li Smith was already seeing how her patients’ worries extended beyond their physical disease.
One of Dr. Li Smith’s first patients told her their greatest worry wasn’t whether the treatment would work or what physical toxicity to expect, it was how they would pay for their care.
“There was much more anxiety and true distress about the financial burden than about the treatment itself,” Dr. Li Smith recalled.
This fear about the costs of cancer care is well founded. In the United States, cancer treatment costs reached an estimated $150 billion in 2020 and continue to rise. Patients shoulder a significant portion of that burden – with one study estimating that patients paid $21 billion for their cancer care in 2019.
The burden is often compounded by decreased income. Between 40% and 85% of patients with cancer needed to take time off work or quit their jobs during treatment. And for those, like Dicks, who find themselves with no insurance, out-of-pocket costs can quickly skyrocket.
In fact, one study of newly diagnosed cancer patients over age 50 reported that more than 42% of patients fully depleted their financial assets and around 30% incurred debt by the second year of their diagnosis.
Younger adults may be even more financially vulnerable. A study of patients in Washington found that those under 65 – which represent about half of cancer cases – were two to five times more likely to declare bankruptcy than patients over 65.
Dr. Li Smith and colleagues have found that younger patients aged 18-64 experienced greater monetary hardships, which meant less money for food, worse adherence to medications, as well as greater distress and anxiety overall. In fact, younger adults were over 4.5 times more likely to encounter severe financial toxicity, compared with older adults, and about 4 times more likely to experience severe psychological effects from this burden.
The distress, if left unchecked, can spiral out of control.
Molly MacDonald had just gone through a financially devastating divorce in 2005 when she was diagnosed with breast cancer. Recently out of work and dealing with a $1,300 monthly COBRA premium, the mother of five had no financial safety net. She risked having her car repossessed and her utilities shut off.
“I gave tentative thought to how I could take my life and make it look like an accident,” said Ms. MacDonald. “I thought the kids would be better off without me.”
For some, the loss of income can be even more worrisome than the medical bills. Some patients may go back to work during treatment, often against medical advice.
When Stephanie Caputo, 43, of Monroe, N.J., began treatment for stage III breast cancer in 2021, her physician recommended she stop working. Treatment would make her immunocompromised, and her job in a medical clinic could expose her to harmful pathogens, including the coronavirus.
Ms. Caputo went on disability and received $900 every 2 weeks. But that wasn’t enough to pay her mortgage, let alone cover her other monthly expenses as a single mother of 4 teenagers.
After finishing chemotherapy, and during radiation, Ms. Caputo went back to work, part time, against her doctor’s advice.
“My doctor is telling me I can’t work, but I also can’t have my house go into default,” said Ms. Caputo.
But being on her feet through 12-hour shifts made treatment side effects, especially back and joint pain, kick into overdrive. “The physicality of my job was really difficult to tolerate,” she said.
The physical burden was too great to take on more work, but the extra money also wasn’t enough to keep her afloat. Fortunately, her brother stepped in and covered 6 months of her mortgage payments.
Financial toxicity impacts families
Although financial toxicity research to date has largely focused on the patient, researchers are also starting to understand that family members and caregivers often share in the burden.
“We are just at the beginning of realizing that this is a real problem,” said Fumiko Chino, MD, a radiation oncologist at Memorial Sloan Kettering Cancer Center, New York.
Dr. Chino and colleagues recently showed that family members of patients with cancer were more likely to delay or forgo medical care than family members of people without cancer. The study found the effect was greatest among family members of younger adults with cancer.
“The caregiver and family burden related to cancer diagnosis and treatment is really underappreciated,” said Dr. Chino. “Family members and caregivers are neglecting their own health concerns, passing up career opportunities, struggling with financial concerns.”
Dr. Chino speaks from personal experience. When her fiancé, later husband, was diagnosed with neuroendocrine carcinoma in 2005, Dr. Chino quit her job as art director at a television production company to take care of him.
The couple, both in their 20s, struggled to afford his care. Dr. Chino put her own dental, medical, and mental health care on hold. She never, for instance, went to physical therapy to address injuries sustained sleeping in hospital chairs and moving around her husband who was over 6 feet tall. At one point, she walked with a limp.
Dr. Chino’s husband passed away in 2007, and even 15 years later, her injury from sleeping in hospital chairs remains “a significant physical burden,” she said. But like many caregivers “I wasn’t really thinking about my own health.”
Danielle Hadfield, 35, an ED nurse in Rochester, N.Y., also delayed her own care when her mom got sick.
Ms. Hadfield quit her job shortly after her mom was diagnosed with cholangiocarcinoma in August 2020. Ms. Hadfield knew her mom, who lived 3.5 hours away in Albany, N.Y., would need a lot of care in the upcoming months.
“I knew this was going to be the last year or so of her life, and I wanted to be there for her,” said Ms. Hadfield.
When Ms. Hadfield quit her job, she and her husband – who was self-employed – purchased health insurance coverage through the New York state marketplace. The monthly insurance payments for Ms. Hadfield, who was pregnant with her second child, her husband, and their toddler cost as much as the family’s monthly mortgage payments.
In addition to providing childcare for her young daughter and making frequent trips to Albany, Ms. Hadfield began a side business as a legal nurse consultant, working mostly at night, to replace a portion of her lost income. During this time, she began to experience pain attacks that would migrate through her body along with intermittent tongue and facial numbness. She ignored these health issues for nearly a year, until after her mother died in November 2021.
Only after her mother passed away did Ms. Hadfield begin seeking answers to her own pain. In September 2022, she finally got them. She had a nerve condition called small-fiber sensory neuropathy.
But even with a diagnosis, she is still facing more tests to root out the cause and understand the best treatment.
Is help out there?
What can physicians do to help patients and families at risk for financial toxicity?
Specific guidelines for dealing with financial toxicity do not exist in most professional guidelines, nor are there standard screening tools to identify it, said Dr. Li Smith.
These gaps put pressure on physicians to ask about financial barriers and concerns, but most do not know how to broach the topic or how to help. “Physicians may not know how to fix the problem or what resources exist,” Dr. Li Smith said.
Patients and family members, on the other hand, are often reluctant to bring up cost with physicians. Some may be ashamed to talk about their financial problems while others may fear doing so will prevent them from being offered the best possible treatments, said Ms. MacDonald.
But, experts say, financial toxicity needs to be dealt with head on. That means involving financial navigators or counselors and social workers who can, for instance, help patients and families find financial support for their basic living expenses.
From a research perspective, more clinical trials should include financial toxicity outcomes, said Joshua Palmer, MD, a radiation oncologist at the University of Michigan, Ann Arbor.
Dr. Palmer and colleagues recently showed that the number of radiation therapy clinical trials including financial toxicity endpoints increased significantly from 2001 to 2020, though the absolute rate of inclusion remains low, at roughly 1.5% of radiation therapy-based clinical trials including financial toxicity endpoints from 2016 to 2020.
“Financial burden is part of the broader discussion about shared decision-making,” said Dr. Palmer.
In shared decision-making, physicians discuss the risks and benefits of different treatment options, empowering the patient to make an informed choice with the physician.
What we want to avoid is patients feeling like they will get inferior care, if they have financial barriers, said Dr. Palmer.
And every little bit can help. In 2006, Ms. MacDonald started the Pink Fund – a nonprofit to help patients with cancer cover nonmedical cost-of-living expenses. Both Ms. Caputo and Ms. Dicks received grants from the Pink Fund. For Ms. Caputo, the funds covered 2 months of car payments and for Ms. Dicks, it covered 2 months of rent.
While the one-time grant was a big help, said Ms. Dicks, “cancer is an everyday thing.” And “we all deserve peace of mind” when trying to heal.
A version of this article first appeared on WebMD.com.
When 32-year-old Brittany Dicks was diagnosed with stage II triple negative breast cancer in January 2022, she wasn’t worried about the cost of treatment. A medical assistant in Charleston, S.C., Ms. Dicks had full-time employment with health benefits.
But when she wasn’t able to work for several months because of chemotherapy and its side effects, Ms. Dicks lost her job. Her health insurance coverage ended in May. And although she filed for Medicaid at the beginning of June, it wasn’t approved until September.
Meanwhile, Ms. Dicks still needed treatment. She estimates that she ran up close to $20,000 in medical debt while finishing chemotherapy during the 4 months she was uninsured.
The surgeon she had seen since her diagnosis terminated her care when she could no longer pay her bills. That left her delaying a much-needed mastectomy.
“I don’t sleep at night,” said Ms. Dicks, a single mother of two young kids, ages 3 and 11. “Mentally, I’m drained. Just because I have cancer, doesn’t mean the bills aren’t due every month.”
As soon as she felt well enough over the summer, she started working as a part-time delivery driver for DoorDash to help pay for food and gas.
But that was just a Band-Aid. Even when her new insurance kicked in, covering the costs of daily life remained a struggle.
Ms. Dicks is still in deep medical debt. Her Medicaid has covered new medical expenses, and she hopes Medicaid will reimburse her for the debt she incurred over the summer while she waited for her coverage to kick in. So far, though, Medicaid has not touched her $20,000 debt.
“I fear that I’m not going to be able to dig out of this hole,” Ms. Dicks said.
Researchers who study the financial impacts of cancer have a term for Ms. Dicks’ experience: financial toxicity.
Financial toxicity is a catchall term for the burden many Americans with cancer experience.
“Financial toxicity is a multidimensional concept. There’s both a material burden and a psychosocial one,” said Grace Li Smith, MD, PhD, MPH, a radiation oncologist at the University of Texas MD Anderson Cancer Center, Houston.
Researchers are also now beginning to understand the psychological effects these financial burdens can have on patients and their family.
“Financial toxicity is not unique to the patient,” said Dr. Li Smith. It “very directly impacts the whole family or household.”
Stifling financial pressures
Early in her career, Dr. Li Smith was already seeing how her patients’ worries extended beyond their physical disease.
One of Dr. Li Smith’s first patients told her their greatest worry wasn’t whether the treatment would work or what physical toxicity to expect, it was how they would pay for their care.
“There was much more anxiety and true distress about the financial burden than about the treatment itself,” Dr. Li Smith recalled.
This fear about the costs of cancer care is well founded. In the United States, cancer treatment costs reached an estimated $150 billion in 2020 and continue to rise. Patients shoulder a significant portion of that burden – with one study estimating that patients paid $21 billion for their cancer care in 2019.
The burden is often compounded by decreased income. Between 40% and 85% of patients with cancer needed to take time off work or quit their jobs during treatment. And for those, like Dicks, who find themselves with no insurance, out-of-pocket costs can quickly skyrocket.
In fact, one study of newly diagnosed cancer patients over age 50 reported that more than 42% of patients fully depleted their financial assets and around 30% incurred debt by the second year of their diagnosis.
Younger adults may be even more financially vulnerable. A study of patients in Washington found that those under 65 – which represent about half of cancer cases – were two to five times more likely to declare bankruptcy than patients over 65.
Dr. Li Smith and colleagues have found that younger patients aged 18-64 experienced greater monetary hardships, which meant less money for food, worse adherence to medications, as well as greater distress and anxiety overall. In fact, younger adults were over 4.5 times more likely to encounter severe financial toxicity, compared with older adults, and about 4 times more likely to experience severe psychological effects from this burden.
The distress, if left unchecked, can spiral out of control.
Molly MacDonald had just gone through a financially devastating divorce in 2005 when she was diagnosed with breast cancer. Recently out of work and dealing with a $1,300 monthly COBRA premium, the mother of five had no financial safety net. She risked having her car repossessed and her utilities shut off.
“I gave tentative thought to how I could take my life and make it look like an accident,” said Ms. MacDonald. “I thought the kids would be better off without me.”
For some, the loss of income can be even more worrisome than the medical bills. Some patients may go back to work during treatment, often against medical advice.
When Stephanie Caputo, 43, of Monroe, N.J., began treatment for stage III breast cancer in 2021, her physician recommended she stop working. Treatment would make her immunocompromised, and her job in a medical clinic could expose her to harmful pathogens, including the coronavirus.
Ms. Caputo went on disability and received $900 every 2 weeks. But that wasn’t enough to pay her mortgage, let alone cover her other monthly expenses as a single mother of 4 teenagers.
After finishing chemotherapy, and during radiation, Ms. Caputo went back to work, part time, against her doctor’s advice.
“My doctor is telling me I can’t work, but I also can’t have my house go into default,” said Ms. Caputo.
But being on her feet through 12-hour shifts made treatment side effects, especially back and joint pain, kick into overdrive. “The physicality of my job was really difficult to tolerate,” she said.
The physical burden was too great to take on more work, but the extra money also wasn’t enough to keep her afloat. Fortunately, her brother stepped in and covered 6 months of her mortgage payments.
Financial toxicity impacts families
Although financial toxicity research to date has largely focused on the patient, researchers are also starting to understand that family members and caregivers often share in the burden.
“We are just at the beginning of realizing that this is a real problem,” said Fumiko Chino, MD, a radiation oncologist at Memorial Sloan Kettering Cancer Center, New York.
Dr. Chino and colleagues recently showed that family members of patients with cancer were more likely to delay or forgo medical care than family members of people without cancer. The study found the effect was greatest among family members of younger adults with cancer.
“The caregiver and family burden related to cancer diagnosis and treatment is really underappreciated,” said Dr. Chino. “Family members and caregivers are neglecting their own health concerns, passing up career opportunities, struggling with financial concerns.”
Dr. Chino speaks from personal experience. When her fiancé, later husband, was diagnosed with neuroendocrine carcinoma in 2005, Dr. Chino quit her job as art director at a television production company to take care of him.
The couple, both in their 20s, struggled to afford his care. Dr. Chino put her own dental, medical, and mental health care on hold. She never, for instance, went to physical therapy to address injuries sustained sleeping in hospital chairs and moving around her husband who was over 6 feet tall. At one point, she walked with a limp.
Dr. Chino’s husband passed away in 2007, and even 15 years later, her injury from sleeping in hospital chairs remains “a significant physical burden,” she said. But like many caregivers “I wasn’t really thinking about my own health.”
Danielle Hadfield, 35, an ED nurse in Rochester, N.Y., also delayed her own care when her mom got sick.
Ms. Hadfield quit her job shortly after her mom was diagnosed with cholangiocarcinoma in August 2020. Ms. Hadfield knew her mom, who lived 3.5 hours away in Albany, N.Y., would need a lot of care in the upcoming months.
“I knew this was going to be the last year or so of her life, and I wanted to be there for her,” said Ms. Hadfield.
When Ms. Hadfield quit her job, she and her husband – who was self-employed – purchased health insurance coverage through the New York state marketplace. The monthly insurance payments for Ms. Hadfield, who was pregnant with her second child, her husband, and their toddler cost as much as the family’s monthly mortgage payments.
In addition to providing childcare for her young daughter and making frequent trips to Albany, Ms. Hadfield began a side business as a legal nurse consultant, working mostly at night, to replace a portion of her lost income. During this time, she began to experience pain attacks that would migrate through her body along with intermittent tongue and facial numbness. She ignored these health issues for nearly a year, until after her mother died in November 2021.
Only after her mother passed away did Ms. Hadfield begin seeking answers to her own pain. In September 2022, she finally got them. She had a nerve condition called small-fiber sensory neuropathy.
But even with a diagnosis, she is still facing more tests to root out the cause and understand the best treatment.
Is help out there?
What can physicians do to help patients and families at risk for financial toxicity?
Specific guidelines for dealing with financial toxicity do not exist in most professional guidelines, nor are there standard screening tools to identify it, said Dr. Li Smith.
These gaps put pressure on physicians to ask about financial barriers and concerns, but most do not know how to broach the topic or how to help. “Physicians may not know how to fix the problem or what resources exist,” Dr. Li Smith said.
Patients and family members, on the other hand, are often reluctant to bring up cost with physicians. Some may be ashamed to talk about their financial problems while others may fear doing so will prevent them from being offered the best possible treatments, said Ms. MacDonald.
But, experts say, financial toxicity needs to be dealt with head on. That means involving financial navigators or counselors and social workers who can, for instance, help patients and families find financial support for their basic living expenses.
From a research perspective, more clinical trials should include financial toxicity outcomes, said Joshua Palmer, MD, a radiation oncologist at the University of Michigan, Ann Arbor.
Dr. Palmer and colleagues recently showed that the number of radiation therapy clinical trials including financial toxicity endpoints increased significantly from 2001 to 2020, though the absolute rate of inclusion remains low, at roughly 1.5% of radiation therapy-based clinical trials including financial toxicity endpoints from 2016 to 2020.
“Financial burden is part of the broader discussion about shared decision-making,” said Dr. Palmer.
In shared decision-making, physicians discuss the risks and benefits of different treatment options, empowering the patient to make an informed choice with the physician.
What we want to avoid is patients feeling like they will get inferior care, if they have financial barriers, said Dr. Palmer.
And every little bit can help. In 2006, Ms. MacDonald started the Pink Fund – a nonprofit to help patients with cancer cover nonmedical cost-of-living expenses. Both Ms. Caputo and Ms. Dicks received grants from the Pink Fund. For Ms. Caputo, the funds covered 2 months of car payments and for Ms. Dicks, it covered 2 months of rent.
While the one-time grant was a big help, said Ms. Dicks, “cancer is an everyday thing.” And “we all deserve peace of mind” when trying to heal.
A version of this article first appeared on WebMD.com.
When 32-year-old Brittany Dicks was diagnosed with stage II triple negative breast cancer in January 2022, she wasn’t worried about the cost of treatment. A medical assistant in Charleston, S.C., Ms. Dicks had full-time employment with health benefits.
But when she wasn’t able to work for several months because of chemotherapy and its side effects, Ms. Dicks lost her job. Her health insurance coverage ended in May. And although she filed for Medicaid at the beginning of June, it wasn’t approved until September.
Meanwhile, Ms. Dicks still needed treatment. She estimates that she ran up close to $20,000 in medical debt while finishing chemotherapy during the 4 months she was uninsured.
The surgeon she had seen since her diagnosis terminated her care when she could no longer pay her bills. That left her delaying a much-needed mastectomy.
“I don’t sleep at night,” said Ms. Dicks, a single mother of two young kids, ages 3 and 11. “Mentally, I’m drained. Just because I have cancer, doesn’t mean the bills aren’t due every month.”
As soon as she felt well enough over the summer, she started working as a part-time delivery driver for DoorDash to help pay for food and gas.
But that was just a Band-Aid. Even when her new insurance kicked in, covering the costs of daily life remained a struggle.
Ms. Dicks is still in deep medical debt. Her Medicaid has covered new medical expenses, and she hopes Medicaid will reimburse her for the debt she incurred over the summer while she waited for her coverage to kick in. So far, though, Medicaid has not touched her $20,000 debt.
“I fear that I’m not going to be able to dig out of this hole,” Ms. Dicks said.
Researchers who study the financial impacts of cancer have a term for Ms. Dicks’ experience: financial toxicity.
Financial toxicity is a catchall term for the burden many Americans with cancer experience.
“Financial toxicity is a multidimensional concept. There’s both a material burden and a psychosocial one,” said Grace Li Smith, MD, PhD, MPH, a radiation oncologist at the University of Texas MD Anderson Cancer Center, Houston.
Researchers are also now beginning to understand the psychological effects these financial burdens can have on patients and their family.
“Financial toxicity is not unique to the patient,” said Dr. Li Smith. It “very directly impacts the whole family or household.”
Stifling financial pressures
Early in her career, Dr. Li Smith was already seeing how her patients’ worries extended beyond their physical disease.
One of Dr. Li Smith’s first patients told her their greatest worry wasn’t whether the treatment would work or what physical toxicity to expect, it was how they would pay for their care.
“There was much more anxiety and true distress about the financial burden than about the treatment itself,” Dr. Li Smith recalled.
This fear about the costs of cancer care is well founded. In the United States, cancer treatment costs reached an estimated $150 billion in 2020 and continue to rise. Patients shoulder a significant portion of that burden – with one study estimating that patients paid $21 billion for their cancer care in 2019.
The burden is often compounded by decreased income. Between 40% and 85% of patients with cancer needed to take time off work or quit their jobs during treatment. And for those, like Dicks, who find themselves with no insurance, out-of-pocket costs can quickly skyrocket.
In fact, one study of newly diagnosed cancer patients over age 50 reported that more than 42% of patients fully depleted their financial assets and around 30% incurred debt by the second year of their diagnosis.
Younger adults may be even more financially vulnerable. A study of patients in Washington found that those under 65 – which represent about half of cancer cases – were two to five times more likely to declare bankruptcy than patients over 65.
Dr. Li Smith and colleagues have found that younger patients aged 18-64 experienced greater monetary hardships, which meant less money for food, worse adherence to medications, as well as greater distress and anxiety overall. In fact, younger adults were over 4.5 times more likely to encounter severe financial toxicity, compared with older adults, and about 4 times more likely to experience severe psychological effects from this burden.
The distress, if left unchecked, can spiral out of control.
Molly MacDonald had just gone through a financially devastating divorce in 2005 when she was diagnosed with breast cancer. Recently out of work and dealing with a $1,300 monthly COBRA premium, the mother of five had no financial safety net. She risked having her car repossessed and her utilities shut off.
“I gave tentative thought to how I could take my life and make it look like an accident,” said Ms. MacDonald. “I thought the kids would be better off without me.”
For some, the loss of income can be even more worrisome than the medical bills. Some patients may go back to work during treatment, often against medical advice.
When Stephanie Caputo, 43, of Monroe, N.J., began treatment for stage III breast cancer in 2021, her physician recommended she stop working. Treatment would make her immunocompromised, and her job in a medical clinic could expose her to harmful pathogens, including the coronavirus.
Ms. Caputo went on disability and received $900 every 2 weeks. But that wasn’t enough to pay her mortgage, let alone cover her other monthly expenses as a single mother of 4 teenagers.
After finishing chemotherapy, and during radiation, Ms. Caputo went back to work, part time, against her doctor’s advice.
“My doctor is telling me I can’t work, but I also can’t have my house go into default,” said Ms. Caputo.
But being on her feet through 12-hour shifts made treatment side effects, especially back and joint pain, kick into overdrive. “The physicality of my job was really difficult to tolerate,” she said.
The physical burden was too great to take on more work, but the extra money also wasn’t enough to keep her afloat. Fortunately, her brother stepped in and covered 6 months of her mortgage payments.
Financial toxicity impacts families
Although financial toxicity research to date has largely focused on the patient, researchers are also starting to understand that family members and caregivers often share in the burden.
“We are just at the beginning of realizing that this is a real problem,” said Fumiko Chino, MD, a radiation oncologist at Memorial Sloan Kettering Cancer Center, New York.
Dr. Chino and colleagues recently showed that family members of patients with cancer were more likely to delay or forgo medical care than family members of people without cancer. The study found the effect was greatest among family members of younger adults with cancer.
“The caregiver and family burden related to cancer diagnosis and treatment is really underappreciated,” said Dr. Chino. “Family members and caregivers are neglecting their own health concerns, passing up career opportunities, struggling with financial concerns.”
Dr. Chino speaks from personal experience. When her fiancé, later husband, was diagnosed with neuroendocrine carcinoma in 2005, Dr. Chino quit her job as art director at a television production company to take care of him.
The couple, both in their 20s, struggled to afford his care. Dr. Chino put her own dental, medical, and mental health care on hold. She never, for instance, went to physical therapy to address injuries sustained sleeping in hospital chairs and moving around her husband who was over 6 feet tall. At one point, she walked with a limp.
Dr. Chino’s husband passed away in 2007, and even 15 years later, her injury from sleeping in hospital chairs remains “a significant physical burden,” she said. But like many caregivers “I wasn’t really thinking about my own health.”
Danielle Hadfield, 35, an ED nurse in Rochester, N.Y., also delayed her own care when her mom got sick.
Ms. Hadfield quit her job shortly after her mom was diagnosed with cholangiocarcinoma in August 2020. Ms. Hadfield knew her mom, who lived 3.5 hours away in Albany, N.Y., would need a lot of care in the upcoming months.
“I knew this was going to be the last year or so of her life, and I wanted to be there for her,” said Ms. Hadfield.
When Ms. Hadfield quit her job, she and her husband – who was self-employed – purchased health insurance coverage through the New York state marketplace. The monthly insurance payments for Ms. Hadfield, who was pregnant with her second child, her husband, and their toddler cost as much as the family’s monthly mortgage payments.
In addition to providing childcare for her young daughter and making frequent trips to Albany, Ms. Hadfield began a side business as a legal nurse consultant, working mostly at night, to replace a portion of her lost income. During this time, she began to experience pain attacks that would migrate through her body along with intermittent tongue and facial numbness. She ignored these health issues for nearly a year, until after her mother died in November 2021.
Only after her mother passed away did Ms. Hadfield begin seeking answers to her own pain. In September 2022, she finally got them. She had a nerve condition called small-fiber sensory neuropathy.
But even with a diagnosis, she is still facing more tests to root out the cause and understand the best treatment.
Is help out there?
What can physicians do to help patients and families at risk for financial toxicity?
Specific guidelines for dealing with financial toxicity do not exist in most professional guidelines, nor are there standard screening tools to identify it, said Dr. Li Smith.
These gaps put pressure on physicians to ask about financial barriers and concerns, but most do not know how to broach the topic or how to help. “Physicians may not know how to fix the problem or what resources exist,” Dr. Li Smith said.
Patients and family members, on the other hand, are often reluctant to bring up cost with physicians. Some may be ashamed to talk about their financial problems while others may fear doing so will prevent them from being offered the best possible treatments, said Ms. MacDonald.
But, experts say, financial toxicity needs to be dealt with head on. That means involving financial navigators or counselors and social workers who can, for instance, help patients and families find financial support for their basic living expenses.
From a research perspective, more clinical trials should include financial toxicity outcomes, said Joshua Palmer, MD, a radiation oncologist at the University of Michigan, Ann Arbor.
Dr. Palmer and colleagues recently showed that the number of radiation therapy clinical trials including financial toxicity endpoints increased significantly from 2001 to 2020, though the absolute rate of inclusion remains low, at roughly 1.5% of radiation therapy-based clinical trials including financial toxicity endpoints from 2016 to 2020.
“Financial burden is part of the broader discussion about shared decision-making,” said Dr. Palmer.
In shared decision-making, physicians discuss the risks and benefits of different treatment options, empowering the patient to make an informed choice with the physician.
What we want to avoid is patients feeling like they will get inferior care, if they have financial barriers, said Dr. Palmer.
And every little bit can help. In 2006, Ms. MacDonald started the Pink Fund – a nonprofit to help patients with cancer cover nonmedical cost-of-living expenses. Both Ms. Caputo and Ms. Dicks received grants from the Pink Fund. For Ms. Caputo, the funds covered 2 months of car payments and for Ms. Dicks, it covered 2 months of rent.
While the one-time grant was a big help, said Ms. Dicks, “cancer is an everyday thing.” And “we all deserve peace of mind” when trying to heal.
A version of this article first appeared on WebMD.com.
Ivermectin for COVID-19: Final nail in the coffin
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
It began in a petri dish.
Ivermectin, a widely available, cheap, and well-tolerated drug on the WHO’s list of essential medicines for its critical role in treating river blindness, was shown to dramatically reduce the proliferation of SARS-CoV-2 virus in cell culture.
You know the rest of the story. Despite the fact that the median inhibitory concentration in cell culture is about 100-fold higher than what one can achieve with oral dosing in humans, anecdotal reports of miraculous cures proliferated.
Cohort studies suggested that people who got ivermectin did very well in terms of COVID outcomes.
A narrative started to develop online – one that is still quite present today – that authorities were suppressing the good news about ivermectin in order to line their own pockets and those of the execs at Big Pharma. The official Twitter account of the Food and Drug Administration clapped back, reminding the populace that we are not horses or cows.
And every time a study came out that seemed like the nail in the coffin for the so-called horse paste, it rose again, vampire-like, feasting on the blood of social media outrage.
The truth is that, while excitement for ivermectin mounted online, it crashed quite quickly in scientific circles. Most randomized trials showed no effect of the drug. A couple of larger trials which seemed to show dramatic effects were subsequently shown to be fraudulent.
Then the TOGETHER trial was published. The 1,400-patient study from Brazil, which treated outpatients with COVID-19, found no significant difference in hospitalization or ER visits – the primary outcome – between those randomized to ivermectin vs. placebo or another therapy.
But still, Brazil. Different population than the United States. Different health systems. And very different rates of Strongyloides infections (this is a parasite that may be incidentally treated by ivermectin, leading to improvement independent of the drug’s effect on COVID). We all wanted a U.S. trial.
And now we have it. ACTIV-6 was published Oct. 21 in JAMA, a study randomizing outpatients with COVID-19 from 93 sites around the United States to ivermectin or placebo.
A total of 1,591 individuals – median age 47, 60% female – with confirmed symptomatic COVID-19 were randomized from June 2021 to February 2022. About half had been vaccinated.
The primary outcome was straightforward: time to clinical recovery. The time to recovery, defined as having three symptom-free days, was 12 days in the ivermectin group and 13 days in the placebo group – that’s within the margin of error.
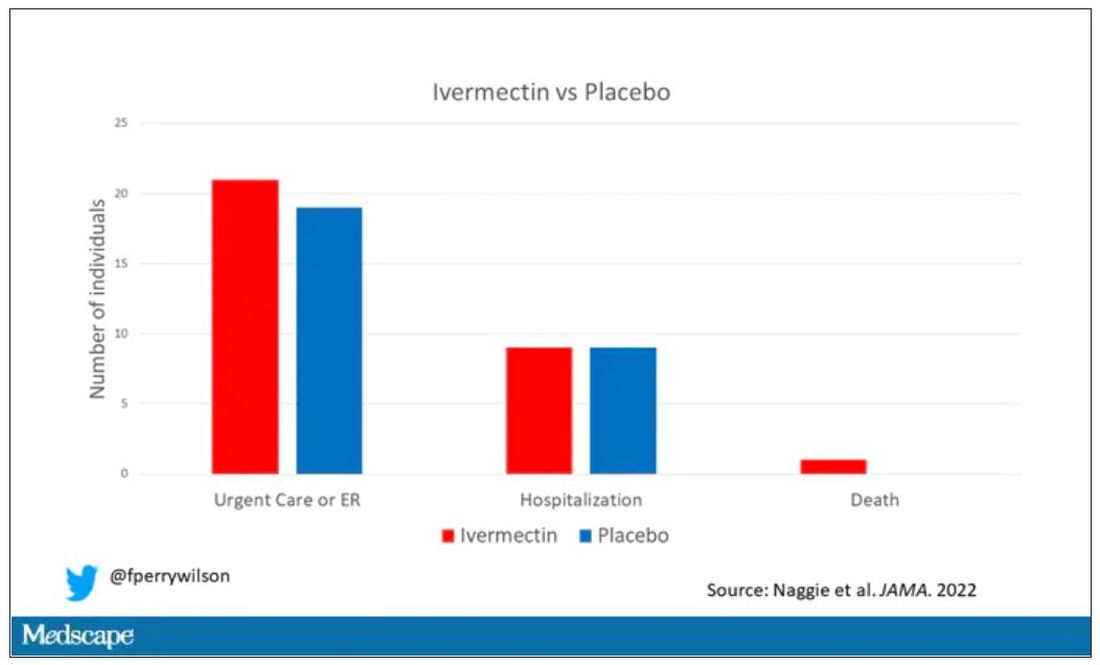
But overall, everyone in the trial did fairly well. Serious outcomes, like death, hospitalization, urgent care, or ER visits, occurred in 32 people in the ivermectin group and 28 in the placebo group. Death itself was rare – just one occurred in the trial, in someone receiving ivermectin.OK, are we done with this drug yet? Is this nice U.S. randomized trial enough to convince people that results from a petri dish don’t always transfer to humans, regardless of the presence or absence of an evil pharmaceutical cabal?
No, of course not. At this point, I can predict the responses. The dose wasn’t high enough. It wasn’t given early enough. The patients weren’t sick enough, or they were too sick. This is motivated reasoning, plain and simple. It’s not to say that there isn’t a chance that this drug has some off-target effects on COVID that we haven’t adequately measured, but studies like ACTIV-6 effectively rule out the idea that it’s a miracle cure. And you know what? That’s OK. Miracle cures are vanishingly rare. Most things that work in medicine work OK; they make us a little better, and we learn why they do that and improve on them, and try again and again. It’s not flashy; it doesn’t have that allure of secret knowledge. But it’s what separates science from magic.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator; his science communication work can be found in the Huffington Post, on NPR, and on Medscape.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
It began in a petri dish.
Ivermectin, a widely available, cheap, and well-tolerated drug on the WHO’s list of essential medicines for its critical role in treating river blindness, was shown to dramatically reduce the proliferation of SARS-CoV-2 virus in cell culture.
You know the rest of the story. Despite the fact that the median inhibitory concentration in cell culture is about 100-fold higher than what one can achieve with oral dosing in humans, anecdotal reports of miraculous cures proliferated.
Cohort studies suggested that people who got ivermectin did very well in terms of COVID outcomes.
A narrative started to develop online – one that is still quite present today – that authorities were suppressing the good news about ivermectin in order to line their own pockets and those of the execs at Big Pharma. The official Twitter account of the Food and Drug Administration clapped back, reminding the populace that we are not horses or cows.
And every time a study came out that seemed like the nail in the coffin for the so-called horse paste, it rose again, vampire-like, feasting on the blood of social media outrage.
The truth is that, while excitement for ivermectin mounted online, it crashed quite quickly in scientific circles. Most randomized trials showed no effect of the drug. A couple of larger trials which seemed to show dramatic effects were subsequently shown to be fraudulent.
Then the TOGETHER trial was published. The 1,400-patient study from Brazil, which treated outpatients with COVID-19, found no significant difference in hospitalization or ER visits – the primary outcome – between those randomized to ivermectin vs. placebo or another therapy.
But still, Brazil. Different population than the United States. Different health systems. And very different rates of Strongyloides infections (this is a parasite that may be incidentally treated by ivermectin, leading to improvement independent of the drug’s effect on COVID). We all wanted a U.S. trial.
And now we have it. ACTIV-6 was published Oct. 21 in JAMA, a study randomizing outpatients with COVID-19 from 93 sites around the United States to ivermectin or placebo.
A total of 1,591 individuals – median age 47, 60% female – with confirmed symptomatic COVID-19 were randomized from June 2021 to February 2022. About half had been vaccinated.
The primary outcome was straightforward: time to clinical recovery. The time to recovery, defined as having three symptom-free days, was 12 days in the ivermectin group and 13 days in the placebo group – that’s within the margin of error.
But overall, everyone in the trial did fairly well. Serious outcomes, like death, hospitalization, urgent care, or ER visits, occurred in 32 people in the ivermectin group and 28 in the placebo group. Death itself was rare – just one occurred in the trial, in someone receiving ivermectin.OK, are we done with this drug yet? Is this nice U.S. randomized trial enough to convince people that results from a petri dish don’t always transfer to humans, regardless of the presence or absence of an evil pharmaceutical cabal?
No, of course not. At this point, I can predict the responses. The dose wasn’t high enough. It wasn’t given early enough. The patients weren’t sick enough, or they were too sick. This is motivated reasoning, plain and simple. It’s not to say that there isn’t a chance that this drug has some off-target effects on COVID that we haven’t adequately measured, but studies like ACTIV-6 effectively rule out the idea that it’s a miracle cure. And you know what? That’s OK. Miracle cures are vanishingly rare. Most things that work in medicine work OK; they make us a little better, and we learn why they do that and improve on them, and try again and again. It’s not flashy; it doesn’t have that allure of secret knowledge. But it’s what separates science from magic.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator; his science communication work can be found in the Huffington Post, on NPR, and on Medscape.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
It began in a petri dish.
Ivermectin, a widely available, cheap, and well-tolerated drug on the WHO’s list of essential medicines for its critical role in treating river blindness, was shown to dramatically reduce the proliferation of SARS-CoV-2 virus in cell culture.
You know the rest of the story. Despite the fact that the median inhibitory concentration in cell culture is about 100-fold higher than what one can achieve with oral dosing in humans, anecdotal reports of miraculous cures proliferated.
Cohort studies suggested that people who got ivermectin did very well in terms of COVID outcomes.
A narrative started to develop online – one that is still quite present today – that authorities were suppressing the good news about ivermectin in order to line their own pockets and those of the execs at Big Pharma. The official Twitter account of the Food and Drug Administration clapped back, reminding the populace that we are not horses or cows.
And every time a study came out that seemed like the nail in the coffin for the so-called horse paste, it rose again, vampire-like, feasting on the blood of social media outrage.
The truth is that, while excitement for ivermectin mounted online, it crashed quite quickly in scientific circles. Most randomized trials showed no effect of the drug. A couple of larger trials which seemed to show dramatic effects were subsequently shown to be fraudulent.
Then the TOGETHER trial was published. The 1,400-patient study from Brazil, which treated outpatients with COVID-19, found no significant difference in hospitalization or ER visits – the primary outcome – between those randomized to ivermectin vs. placebo or another therapy.
But still, Brazil. Different population than the United States. Different health systems. And very different rates of Strongyloides infections (this is a parasite that may be incidentally treated by ivermectin, leading to improvement independent of the drug’s effect on COVID). We all wanted a U.S. trial.
And now we have it. ACTIV-6 was published Oct. 21 in JAMA, a study randomizing outpatients with COVID-19 from 93 sites around the United States to ivermectin or placebo.
A total of 1,591 individuals – median age 47, 60% female – with confirmed symptomatic COVID-19 were randomized from June 2021 to February 2022. About half had been vaccinated.
The primary outcome was straightforward: time to clinical recovery. The time to recovery, defined as having three symptom-free days, was 12 days in the ivermectin group and 13 days in the placebo group – that’s within the margin of error.
But overall, everyone in the trial did fairly well. Serious outcomes, like death, hospitalization, urgent care, or ER visits, occurred in 32 people in the ivermectin group and 28 in the placebo group. Death itself was rare – just one occurred in the trial, in someone receiving ivermectin.OK, are we done with this drug yet? Is this nice U.S. randomized trial enough to convince people that results from a petri dish don’t always transfer to humans, regardless of the presence or absence of an evil pharmaceutical cabal?
No, of course not. At this point, I can predict the responses. The dose wasn’t high enough. It wasn’t given early enough. The patients weren’t sick enough, or they were too sick. This is motivated reasoning, plain and simple. It’s not to say that there isn’t a chance that this drug has some off-target effects on COVID that we haven’t adequately measured, but studies like ACTIV-6 effectively rule out the idea that it’s a miracle cure. And you know what? That’s OK. Miracle cures are vanishingly rare. Most things that work in medicine work OK; they make us a little better, and we learn why they do that and improve on them, and try again and again. It’s not flashy; it doesn’t have that allure of secret knowledge. But it’s what separates science from magic.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator; his science communication work can be found in the Huffington Post, on NPR, and on Medscape.
A version of this article first appeared on Medscape.com.
Side effects from COVID vaccine show its effectiveness
It means your body had a greater antibody response than people who had just a little pain or rash at the injection site, or no reaction at all.
That’s according to new research published in the journal JAMA Network Open .
“These findings support reframing postvaccination symptoms as signals of vaccine effectiveness and reinforce guidelines for vaccine boosters in older adults,” researchers from Columbia University in New York, the University of Vermont, and Boston University wrote.
The vaccines provided strong protection regardless of the level of reaction, researchers said. Almost all the study’s 928 adult participants had a positive antibody response after receiving two doses of vaccine.
“I don’t want a patient to tell me that, ‘Golly, I didn’t get any reaction, my arm wasn’t sore, I didn’t have fever. The vaccine didn’t work.’ I don’t want that conclusion to be out there,” William Schaffner, MD, a professor in the division of infectious diseases at Vanderbilt University Medical Center, Nashville, Tenn., told CNN.
“This is more to reassure people who have had a reaction that that’s their immune system responding, actually in a rather good way, to the vaccine, even though it has caused them some discomfort,” said Dr. Schaffner, who was not involved in the study.
A version of this article first appeared on WebMD.com.
It means your body had a greater antibody response than people who had just a little pain or rash at the injection site, or no reaction at all.
That’s according to new research published in the journal JAMA Network Open .
“These findings support reframing postvaccination symptoms as signals of vaccine effectiveness and reinforce guidelines for vaccine boosters in older adults,” researchers from Columbia University in New York, the University of Vermont, and Boston University wrote.
The vaccines provided strong protection regardless of the level of reaction, researchers said. Almost all the study’s 928 adult participants had a positive antibody response after receiving two doses of vaccine.
“I don’t want a patient to tell me that, ‘Golly, I didn’t get any reaction, my arm wasn’t sore, I didn’t have fever. The vaccine didn’t work.’ I don’t want that conclusion to be out there,” William Schaffner, MD, a professor in the division of infectious diseases at Vanderbilt University Medical Center, Nashville, Tenn., told CNN.
“This is more to reassure people who have had a reaction that that’s their immune system responding, actually in a rather good way, to the vaccine, even though it has caused them some discomfort,” said Dr. Schaffner, who was not involved in the study.
A version of this article first appeared on WebMD.com.
It means your body had a greater antibody response than people who had just a little pain or rash at the injection site, or no reaction at all.
That’s according to new research published in the journal JAMA Network Open .
“These findings support reframing postvaccination symptoms as signals of vaccine effectiveness and reinforce guidelines for vaccine boosters in older adults,” researchers from Columbia University in New York, the University of Vermont, and Boston University wrote.
The vaccines provided strong protection regardless of the level of reaction, researchers said. Almost all the study’s 928 adult participants had a positive antibody response after receiving two doses of vaccine.
“I don’t want a patient to tell me that, ‘Golly, I didn’t get any reaction, my arm wasn’t sore, I didn’t have fever. The vaccine didn’t work.’ I don’t want that conclusion to be out there,” William Schaffner, MD, a professor in the division of infectious diseases at Vanderbilt University Medical Center, Nashville, Tenn., told CNN.
“This is more to reassure people who have had a reaction that that’s their immune system responding, actually in a rather good way, to the vaccine, even though it has caused them some discomfort,” said Dr. Schaffner, who was not involved in the study.
A version of this article first appeared on WebMD.com.
FROM JAMA NETWORK OPEN
Study reveals racial disparities in advanced HF therapies
A new study shows that Black Americans received ventricular assist devices (VADs) and heart transplants about half as often as White Americans, even when receiving care at an advanced heart failure (HF) center.
The analysis, drawn from 377 patients treated at one of 21 VAD centers in the United States as part of the RIVIVAL study, found that 22.3% of White adults received a heart transplant or VAD, compared with 11% of Black adults.
“That’s what is so concerning to us, that we’re seeing this pattern within this select population. I think it would be too reasonable to hypothesize that it very well could be worse in the general population,” study author Thomas Cascino, MD, MSc, University of Michigan, Ann Arbor, commented.
The study was published online in Circulation: Heart Failure, and it builds on previous work by the researchers, showing that patient preference for early VAD therapy is associated with higher New York Heart Association (NYHA) class and lower income level but not race.
In the present analysis, the number of Black and White participants who said they “definitely or probably” wanted VAD therapy was similar (27% vs. 29%), as was the number wanting “any and all life-sustaining therapies” (74% vs. 65%).
Two-thirds of the cohort was NYHA class III, the average EuroQoL visual analog scale (EQ-VAS) score was 64.6 among the 100 participants who identified as Black and 62.1 in the 277 White participants, and the average age was 58 and 61 years, respectively.
Death rates were also similar during the 2-year follow-up: 18% of Black patients and 13% of White patients.
After controlling for multiple clinical and social determinants of health, including age, Interagency Registry for Mechanically Assisted Circulator Support (INTERMACS) patient profile, EQ-VAS score, and level of education, Black participants had a 55% lower rate of VAD or transplant, compared with White participants (hazard ratio, 0.45; 95% confidence interval, 0.23-0.85). Adding VAD preference to the model did not affect the association.
“Our study suggests that we as providers may be making decisions differently,” Dr. Cascino said. “We can’t say for sure what the reasons are but certainly structural racism, discrimination, and provider biases are the things I worry about.”
“There’s an absolute need for us to look inwards, reflect, and acknowledge that we are likely playing a role in this and then start to be part of the change,” he added.
“The lives disabled or lost are simply too many,” coauthor Wendy Taddei-Peters, PhD, a clinical trials project official at the National Heart, Lung, and Blood Institute, said in an NIH statement. “An immediate step could be to require implicit bias training, particularly for transplant and VAD team members.”
Other suggestions are better tracking of underserved patients and the reasons why they do not receive VAD or become listed for transplant; inclusion of psychosocial components into decision-making about advanced therapy candidacy; and having “disparity experts” join in heart team meetings to help identify biases in real time.
Commenting on the study, Khadijah Breathett, MD, HF/transplant cardiologist and tenured associate professor of medicine, Indiana University Bloomington, said, “I’m glad there’s more push for awareness, because there’s still a population of people that don’t believe this is a real problem.”

Dr. Breathett, who is also a racial equity researcher, noted that the findings are similar to those of multiple studies suggesting racial disparities in HF care. In her own 2019 study of 400 providers shown identical clinical vignettes except for race, survey results and think-aloud interviews showed that decisions about advanced HF therapies are hierarchal and not democratic, social history and adherence are the most influential factors, and Black men are seen as not trustworthy and adherent, despite identical social histories, which ultimately led to White men being offered transplantation and Black men VAD implantation. The bias was particularly evident among older providers.
“This problem is real,” Dr. Breathett said. “The process of allocating life-saving therapies is not fair, and there is some level of discrimination that’s taking place towards persons of color, particularly Black patients. It’s time that we consider how we fix these issues.”
To see whether centers can move the needle and put systemic level changes into practice, Dr. Breathett and colleagues are launching the Seeking Objectivity in Allocation of Advanced Heart Failure (SOCIAL HF) Therapies Trial at 14 sites in the United States. It will measure the number of minority and female patients receiving advanced HF therapies at centers randomized to usual care or HF training, including evidence-based bias reduction training, use of objective measures of social support, and changes to facilitate group dynamics. The trial is set to start in January and be completed in September 2026.
“The main takeaway from this study is that it highlights and re-highlights the fact that racial disparities do exist in access to advanced therapy care,” Jaimin Trivedi, MD, MPH, associate professor of cardiothoracic surgery and director of clinical research and bioinformatics, University of Louisville, Ky., said in an interview.
He also called for education and training for all professionals, not just during residency or fellowship, to specifically identify issues with Black patients and encourage Black patients and their family members to get more involved in their HF care.
Dr. Trivedi said that further studies should examine why death rates were similar in the study despite the observed disparities in VAD implantation and transplantation.
He also pointed out that while patients in the study were treated from July 2015 to June 2016, a recent analysis by his team of the United Network for Organ Sharing (UNOS) database showed that 26% of transplants in 2019 were among Black patients, up from just 5% in 1987. “So, there are some encouraging signs as well.”
The study was funded by the National Institutes of Health/National Heart, Lung, and Blood Institute (NHLBI) and the National Center for Advancing Translational Sciences. Dr. Cascino reports having no relevant financial relationships. Four coauthors report financial relationships, including David Lanfear, who serves on the advisory board at Medscape. Dr. Breathett reported funding from multiple NHLBI grants.
A version of this article first appeared on Medscape.com.
A new study shows that Black Americans received ventricular assist devices (VADs) and heart transplants about half as often as White Americans, even when receiving care at an advanced heart failure (HF) center.
The analysis, drawn from 377 patients treated at one of 21 VAD centers in the United States as part of the RIVIVAL study, found that 22.3% of White adults received a heart transplant or VAD, compared with 11% of Black adults.
“That’s what is so concerning to us, that we’re seeing this pattern within this select population. I think it would be too reasonable to hypothesize that it very well could be worse in the general population,” study author Thomas Cascino, MD, MSc, University of Michigan, Ann Arbor, commented.
The study was published online in Circulation: Heart Failure, and it builds on previous work by the researchers, showing that patient preference for early VAD therapy is associated with higher New York Heart Association (NYHA) class and lower income level but not race.
In the present analysis, the number of Black and White participants who said they “definitely or probably” wanted VAD therapy was similar (27% vs. 29%), as was the number wanting “any and all life-sustaining therapies” (74% vs. 65%).
Two-thirds of the cohort was NYHA class III, the average EuroQoL visual analog scale (EQ-VAS) score was 64.6 among the 100 participants who identified as Black and 62.1 in the 277 White participants, and the average age was 58 and 61 years, respectively.
Death rates were also similar during the 2-year follow-up: 18% of Black patients and 13% of White patients.
After controlling for multiple clinical and social determinants of health, including age, Interagency Registry for Mechanically Assisted Circulator Support (INTERMACS) patient profile, EQ-VAS score, and level of education, Black participants had a 55% lower rate of VAD or transplant, compared with White participants (hazard ratio, 0.45; 95% confidence interval, 0.23-0.85). Adding VAD preference to the model did not affect the association.
“Our study suggests that we as providers may be making decisions differently,” Dr. Cascino said. “We can’t say for sure what the reasons are but certainly structural racism, discrimination, and provider biases are the things I worry about.”
“There’s an absolute need for us to look inwards, reflect, and acknowledge that we are likely playing a role in this and then start to be part of the change,” he added.
“The lives disabled or lost are simply too many,” coauthor Wendy Taddei-Peters, PhD, a clinical trials project official at the National Heart, Lung, and Blood Institute, said in an NIH statement. “An immediate step could be to require implicit bias training, particularly for transplant and VAD team members.”
Other suggestions are better tracking of underserved patients and the reasons why they do not receive VAD or become listed for transplant; inclusion of psychosocial components into decision-making about advanced therapy candidacy; and having “disparity experts” join in heart team meetings to help identify biases in real time.
Commenting on the study, Khadijah Breathett, MD, HF/transplant cardiologist and tenured associate professor of medicine, Indiana University Bloomington, said, “I’m glad there’s more push for awareness, because there’s still a population of people that don’t believe this is a real problem.”
Dr. Breathett, who is also a racial equity researcher, noted that the findings are similar to those of multiple studies suggesting racial disparities in HF care. In her own 2019 study of 400 providers shown identical clinical vignettes except for race, survey results and think-aloud interviews showed that decisions about advanced HF therapies are hierarchal and not democratic, social history and adherence are the most influential factors, and Black men are seen as not trustworthy and adherent, despite identical social histories, which ultimately led to White men being offered transplantation and Black men VAD implantation. The bias was particularly evident among older providers.
“This problem is real,” Dr. Breathett said. “The process of allocating life-saving therapies is not fair, and there is some level of discrimination that’s taking place towards persons of color, particularly Black patients. It’s time that we consider how we fix these issues.”
To see whether centers can move the needle and put systemic level changes into practice, Dr. Breathett and colleagues are launching the Seeking Objectivity in Allocation of Advanced Heart Failure (SOCIAL HF) Therapies Trial at 14 sites in the United States. It will measure the number of minority and female patients receiving advanced HF therapies at centers randomized to usual care or HF training, including evidence-based bias reduction training, use of objective measures of social support, and changes to facilitate group dynamics. The trial is set to start in January and be completed in September 2026.
“The main takeaway from this study is that it highlights and re-highlights the fact that racial disparities do exist in access to advanced therapy care,” Jaimin Trivedi, MD, MPH, associate professor of cardiothoracic surgery and director of clinical research and bioinformatics, University of Louisville, Ky., said in an interview.
He also called for education and training for all professionals, not just during residency or fellowship, to specifically identify issues with Black patients and encourage Black patients and their family members to get more involved in their HF care.
Dr. Trivedi said that further studies should examine why death rates were similar in the study despite the observed disparities in VAD implantation and transplantation.
He also pointed out that while patients in the study were treated from July 2015 to June 2016, a recent analysis by his team of the United Network for Organ Sharing (UNOS) database showed that 26% of transplants in 2019 were among Black patients, up from just 5% in 1987. “So, there are some encouraging signs as well.”
The study was funded by the National Institutes of Health/National Heart, Lung, and Blood Institute (NHLBI) and the National Center for Advancing Translational Sciences. Dr. Cascino reports having no relevant financial relationships. Four coauthors report financial relationships, including David Lanfear, who serves on the advisory board at Medscape. Dr. Breathett reported funding from multiple NHLBI grants.
A version of this article first appeared on Medscape.com.
A new study shows that Black Americans received ventricular assist devices (VADs) and heart transplants about half as often as White Americans, even when receiving care at an advanced heart failure (HF) center.
The analysis, drawn from 377 patients treated at one of 21 VAD centers in the United States as part of the RIVIVAL study, found that 22.3% of White adults received a heart transplant or VAD, compared with 11% of Black adults.
“That’s what is so concerning to us, that we’re seeing this pattern within this select population. I think it would be too reasonable to hypothesize that it very well could be worse in the general population,” study author Thomas Cascino, MD, MSc, University of Michigan, Ann Arbor, commented.
The study was published online in Circulation: Heart Failure, and it builds on previous work by the researchers, showing that patient preference for early VAD therapy is associated with higher New York Heart Association (NYHA) class and lower income level but not race.
In the present analysis, the number of Black and White participants who said they “definitely or probably” wanted VAD therapy was similar (27% vs. 29%), as was the number wanting “any and all life-sustaining therapies” (74% vs. 65%).
Two-thirds of the cohort was NYHA class III, the average EuroQoL visual analog scale (EQ-VAS) score was 64.6 among the 100 participants who identified as Black and 62.1 in the 277 White participants, and the average age was 58 and 61 years, respectively.
Death rates were also similar during the 2-year follow-up: 18% of Black patients and 13% of White patients.
After controlling for multiple clinical and social determinants of health, including age, Interagency Registry for Mechanically Assisted Circulator Support (INTERMACS) patient profile, EQ-VAS score, and level of education, Black participants had a 55% lower rate of VAD or transplant, compared with White participants (hazard ratio, 0.45; 95% confidence interval, 0.23-0.85). Adding VAD preference to the model did not affect the association.
“Our study suggests that we as providers may be making decisions differently,” Dr. Cascino said. “We can’t say for sure what the reasons are but certainly structural racism, discrimination, and provider biases are the things I worry about.”
“There’s an absolute need for us to look inwards, reflect, and acknowledge that we are likely playing a role in this and then start to be part of the change,” he added.
“The lives disabled or lost are simply too many,” coauthor Wendy Taddei-Peters, PhD, a clinical trials project official at the National Heart, Lung, and Blood Institute, said in an NIH statement. “An immediate step could be to require implicit bias training, particularly for transplant and VAD team members.”
Other suggestions are better tracking of underserved patients and the reasons why they do not receive VAD or become listed for transplant; inclusion of psychosocial components into decision-making about advanced therapy candidacy; and having “disparity experts” join in heart team meetings to help identify biases in real time.
Commenting on the study, Khadijah Breathett, MD, HF/transplant cardiologist and tenured associate professor of medicine, Indiana University Bloomington, said, “I’m glad there’s more push for awareness, because there’s still a population of people that don’t believe this is a real problem.”
Dr. Breathett, who is also a racial equity researcher, noted that the findings are similar to those of multiple studies suggesting racial disparities in HF care. In her own 2019 study of 400 providers shown identical clinical vignettes except for race, survey results and think-aloud interviews showed that decisions about advanced HF therapies are hierarchal and not democratic, social history and adherence are the most influential factors, and Black men are seen as not trustworthy and adherent, despite identical social histories, which ultimately led to White men being offered transplantation and Black men VAD implantation. The bias was particularly evident among older providers.
“This problem is real,” Dr. Breathett said. “The process of allocating life-saving therapies is not fair, and there is some level of discrimination that’s taking place towards persons of color, particularly Black patients. It’s time that we consider how we fix these issues.”
To see whether centers can move the needle and put systemic level changes into practice, Dr. Breathett and colleagues are launching the Seeking Objectivity in Allocation of Advanced Heart Failure (SOCIAL HF) Therapies Trial at 14 sites in the United States. It will measure the number of minority and female patients receiving advanced HF therapies at centers randomized to usual care or HF training, including evidence-based bias reduction training, use of objective measures of social support, and changes to facilitate group dynamics. The trial is set to start in January and be completed in September 2026.
“The main takeaway from this study is that it highlights and re-highlights the fact that racial disparities do exist in access to advanced therapy care,” Jaimin Trivedi, MD, MPH, associate professor of cardiothoracic surgery and director of clinical research and bioinformatics, University of Louisville, Ky., said in an interview.
He also called for education and training for all professionals, not just during residency or fellowship, to specifically identify issues with Black patients and encourage Black patients and their family members to get more involved in their HF care.
Dr. Trivedi said that further studies should examine why death rates were similar in the study despite the observed disparities in VAD implantation and transplantation.
He also pointed out that while patients in the study were treated from July 2015 to June 2016, a recent analysis by his team of the United Network for Organ Sharing (UNOS) database showed that 26% of transplants in 2019 were among Black patients, up from just 5% in 1987. “So, there are some encouraging signs as well.”
The study was funded by the National Institutes of Health/National Heart, Lung, and Blood Institute (NHLBI) and the National Center for Advancing Translational Sciences. Dr. Cascino reports having no relevant financial relationships. Four coauthors report financial relationships, including David Lanfear, who serves on the advisory board at Medscape. Dr. Breathett reported funding from multiple NHLBI grants.
A version of this article first appeared on Medscape.com.
Four commonly abused drugs linked with atrial fibrillation
Cocaine, methamphetamine, opioids, and cannabis may independently increase risk of atrial fibrillation (AFib), based on data from almost 24 million people.
While more work is needed to uncover causal links, physicians should be aware that these commonly abused substances could be driving new cases of AFib, reported investigators from the University of California, San Francisco.
“Though alcohol and tobacco smoking have each been associated with a heightened risk of [AFib], relationships between other drug use and [AFib] are poorly understood,” they wrote in European Heart Journal.
Some previous studies have ventured into this terrain, but most focused on fatal arrhythmias, or offered anecdotal evidence. This knowledge gap is particularly concerning for cannabis, the researchers noted, as medical and recreational use are on the rise.

The present analysis included data from 23.5 million adults in California who received care through a hospital, emergency department, or outpatient surgery center during 2005-2015. Based on ICD-9 diagnostic codes, 132,834 of these patients used cannabis, 98,271 used methamphetamines, 48,701 used cocaine, and 10,032 used opiates. Inclusion required lack of AFib at baseline.
Reliance on ICD-9 codes makes the data “quite specific,” but lacking sensitivity, according to principal author Gregory M. Marcus, MD, cardiologist and professor of medicine at UCSF.
“If they were designated as using these drugs, that is very likely true,” Dr. Marcus said in an interview. “But certainly, the absence of any mention of use of these drugs does not exclude the possibility that some people were still using them. That would not create spurious false-positive relationships; if anything, it attenuates existing relationships.”
In other words, using ICD-9 codes reduced the power to detect an association between each drug and AFib, meaning any relationship needed to be sufficiently strong enough to generate a significant result.
At the end of the decade-long study period, 998,747 patients (4.2%) had developed incident AFib. After adjusting for potential confounders and mediators, all four drugs showed significant, independent associations with AFib. Methamphetamines presented the greatest risk (hazard ratio, 1.86%), followed by opiates (HR, 1.74), cocaine (HR, 1.61), and cannabis (HR, 1.35).
“Our findings provide the first evidence utilizing a longitudinal cohort to demonstrate that cannabis use predicts the future onset of AFib,” Dr. Marcus and colleagues wrote.
Dose-response relationships were not detected for any of the substances; however, usage levels were also derived from ICD-9 codes, which may have been insufficient for this purpose, according to the investigators.
Causal mechanisms deserve a closer look
Causal links between AFib and each of the drugs remain unclear. Citing prior research, Dr. Marcus and colleagues explained how methamphetamines are capable of “significant cardiac electrical remodeling,” while cocaine may cause sodium channel dysregulation, and opioids can render atrial myocytes more susceptible to oxidative damage. Although cannabis has previously been linked with hospitalization for arrhythmia, a pharmacologic driver of this phenomenon remains largely unexamined.
“We don’t know for sure precisely what the constituents are that are responsible for our findings,” Dr. Marcus said. “It’s possible that there are some effects that are much more generic, such as inhaling a burned substance. There is good evidence that if you inhale pretty much any sort of particulate matter, that increases inflammation in the body. Inflammation is known to be a trigger for atrial fibrillation.”
Alternatively, all four drugs – whether stimulants or depressants – cause “quite dramatic and often rapid effects on the autonomic nervous system,” Dr. Marcus said, noting that these rapid swings are a known trigger for AFib.
Brian Olshansky, MD, emeritus professor of internal medicine-cardiovascular medicine at the University of Iowa, Iowa City, suggested that nonpharmacologic factors are likely also playing a role.

“All these drugs have slightly different mechanisms of action, so there’s not one mechanism that would explain why all of them would cause atrial fibrillation,” Dr. Olshansky said in an interview. “That does suggest that there’s something else going on, besides just the drug itself. It would be potentially concerning if we were to lay the blame totally on these drugs.”
Dr. Olshansky, who recently coauthored a review of stimulant drugs and arrhythmias, suggested that lifestyle, comorbidities, and drug impurities may have added to the risk of AF.
“[The investigators] did try to correct for that kind of stuff, but it’s very hard to correct for a lot of the issues that may be ongoing with individuals who partake in these drugs,” Dr. Olshansky said in an interview. “They may not be a healthy lot, in general.”
Still, considering previous data linking drugs of abuse with arrhythmias, he said the detected risks were “intriguing,” and deserved a closer look.
“It’s a nice groundbreaking study, with regard to the fact that they showed unique relationships that we don’t completely understand,” Dr. Olshansky said. “It opens up a new opportunity for further investigation.”
The investigators disclosed relationships with InCarda, Baylis Medical, Johnson & Johnson, and others. Dr. Olshansky disclosed no relevant competing interests.
Cocaine, methamphetamine, opioids, and cannabis may independently increase risk of atrial fibrillation (AFib), based on data from almost 24 million people.
While more work is needed to uncover causal links, physicians should be aware that these commonly abused substances could be driving new cases of AFib, reported investigators from the University of California, San Francisco.
“Though alcohol and tobacco smoking have each been associated with a heightened risk of [AFib], relationships between other drug use and [AFib] are poorly understood,” they wrote in European Heart Journal.
Some previous studies have ventured into this terrain, but most focused on fatal arrhythmias, or offered anecdotal evidence. This knowledge gap is particularly concerning for cannabis, the researchers noted, as medical and recreational use are on the rise.
The present analysis included data from 23.5 million adults in California who received care through a hospital, emergency department, or outpatient surgery center during 2005-2015. Based on ICD-9 diagnostic codes, 132,834 of these patients used cannabis, 98,271 used methamphetamines, 48,701 used cocaine, and 10,032 used opiates. Inclusion required lack of AFib at baseline.
Reliance on ICD-9 codes makes the data “quite specific,” but lacking sensitivity, according to principal author Gregory M. Marcus, MD, cardiologist and professor of medicine at UCSF.
“If they were designated as using these drugs, that is very likely true,” Dr. Marcus said in an interview. “But certainly, the absence of any mention of use of these drugs does not exclude the possibility that some people were still using them. That would not create spurious false-positive relationships; if anything, it attenuates existing relationships.”
In other words, using ICD-9 codes reduced the power to detect an association between each drug and AFib, meaning any relationship needed to be sufficiently strong enough to generate a significant result.
At the end of the decade-long study period, 998,747 patients (4.2%) had developed incident AFib. After adjusting for potential confounders and mediators, all four drugs showed significant, independent associations with AFib. Methamphetamines presented the greatest risk (hazard ratio, 1.86%), followed by opiates (HR, 1.74), cocaine (HR, 1.61), and cannabis (HR, 1.35).
“Our findings provide the first evidence utilizing a longitudinal cohort to demonstrate that cannabis use predicts the future onset of AFib,” Dr. Marcus and colleagues wrote.
Dose-response relationships were not detected for any of the substances; however, usage levels were also derived from ICD-9 codes, which may have been insufficient for this purpose, according to the investigators.
Causal mechanisms deserve a closer look
Causal links between AFib and each of the drugs remain unclear. Citing prior research, Dr. Marcus and colleagues explained how methamphetamines are capable of “significant cardiac electrical remodeling,” while cocaine may cause sodium channel dysregulation, and opioids can render atrial myocytes more susceptible to oxidative damage. Although cannabis has previously been linked with hospitalization for arrhythmia, a pharmacologic driver of this phenomenon remains largely unexamined.
“We don’t know for sure precisely what the constituents are that are responsible for our findings,” Dr. Marcus said. “It’s possible that there are some effects that are much more generic, such as inhaling a burned substance. There is good evidence that if you inhale pretty much any sort of particulate matter, that increases inflammation in the body. Inflammation is known to be a trigger for atrial fibrillation.”
Alternatively, all four drugs – whether stimulants or depressants – cause “quite dramatic and often rapid effects on the autonomic nervous system,” Dr. Marcus said, noting that these rapid swings are a known trigger for AFib.
Brian Olshansky, MD, emeritus professor of internal medicine-cardiovascular medicine at the University of Iowa, Iowa City, suggested that nonpharmacologic factors are likely also playing a role.
“All these drugs have slightly different mechanisms of action, so there’s not one mechanism that would explain why all of them would cause atrial fibrillation,” Dr. Olshansky said in an interview. “That does suggest that there’s something else going on, besides just the drug itself. It would be potentially concerning if we were to lay the blame totally on these drugs.”
Dr. Olshansky, who recently coauthored a review of stimulant drugs and arrhythmias, suggested that lifestyle, comorbidities, and drug impurities may have added to the risk of AF.
“[The investigators] did try to correct for that kind of stuff, but it’s very hard to correct for a lot of the issues that may be ongoing with individuals who partake in these drugs,” Dr. Olshansky said in an interview. “They may not be a healthy lot, in general.”
Still, considering previous data linking drugs of abuse with arrhythmias, he said the detected risks were “intriguing,” and deserved a closer look.
“It’s a nice groundbreaking study, with regard to the fact that they showed unique relationships that we don’t completely understand,” Dr. Olshansky said. “It opens up a new opportunity for further investigation.”
The investigators disclosed relationships with InCarda, Baylis Medical, Johnson & Johnson, and others. Dr. Olshansky disclosed no relevant competing interests.
Cocaine, methamphetamine, opioids, and cannabis may independently increase risk of atrial fibrillation (AFib), based on data from almost 24 million people.
While more work is needed to uncover causal links, physicians should be aware that these commonly abused substances could be driving new cases of AFib, reported investigators from the University of California, San Francisco.
“Though alcohol and tobacco smoking have each been associated with a heightened risk of [AFib], relationships between other drug use and [AFib] are poorly understood,” they wrote in European Heart Journal.
Some previous studies have ventured into this terrain, but most focused on fatal arrhythmias, or offered anecdotal evidence. This knowledge gap is particularly concerning for cannabis, the researchers noted, as medical and recreational use are on the rise.
The present analysis included data from 23.5 million adults in California who received care through a hospital, emergency department, or outpatient surgery center during 2005-2015. Based on ICD-9 diagnostic codes, 132,834 of these patients used cannabis, 98,271 used methamphetamines, 48,701 used cocaine, and 10,032 used opiates. Inclusion required lack of AFib at baseline.
Reliance on ICD-9 codes makes the data “quite specific,” but lacking sensitivity, according to principal author Gregory M. Marcus, MD, cardiologist and professor of medicine at UCSF.
“If they were designated as using these drugs, that is very likely true,” Dr. Marcus said in an interview. “But certainly, the absence of any mention of use of these drugs does not exclude the possibility that some people were still using them. That would not create spurious false-positive relationships; if anything, it attenuates existing relationships.”
In other words, using ICD-9 codes reduced the power to detect an association between each drug and AFib, meaning any relationship needed to be sufficiently strong enough to generate a significant result.
At the end of the decade-long study period, 998,747 patients (4.2%) had developed incident AFib. After adjusting for potential confounders and mediators, all four drugs showed significant, independent associations with AFib. Methamphetamines presented the greatest risk (hazard ratio, 1.86%), followed by opiates (HR, 1.74), cocaine (HR, 1.61), and cannabis (HR, 1.35).
“Our findings provide the first evidence utilizing a longitudinal cohort to demonstrate that cannabis use predicts the future onset of AFib,” Dr. Marcus and colleagues wrote.
Dose-response relationships were not detected for any of the substances; however, usage levels were also derived from ICD-9 codes, which may have been insufficient for this purpose, according to the investigators.
Causal mechanisms deserve a closer look
Causal links between AFib and each of the drugs remain unclear. Citing prior research, Dr. Marcus and colleagues explained how methamphetamines are capable of “significant cardiac electrical remodeling,” while cocaine may cause sodium channel dysregulation, and opioids can render atrial myocytes more susceptible to oxidative damage. Although cannabis has previously been linked with hospitalization for arrhythmia, a pharmacologic driver of this phenomenon remains largely unexamined.
“We don’t know for sure precisely what the constituents are that are responsible for our findings,” Dr. Marcus said. “It’s possible that there are some effects that are much more generic, such as inhaling a burned substance. There is good evidence that if you inhale pretty much any sort of particulate matter, that increases inflammation in the body. Inflammation is known to be a trigger for atrial fibrillation.”
Alternatively, all four drugs – whether stimulants or depressants – cause “quite dramatic and often rapid effects on the autonomic nervous system,” Dr. Marcus said, noting that these rapid swings are a known trigger for AFib.
Brian Olshansky, MD, emeritus professor of internal medicine-cardiovascular medicine at the University of Iowa, Iowa City, suggested that nonpharmacologic factors are likely also playing a role.
“All these drugs have slightly different mechanisms of action, so there’s not one mechanism that would explain why all of them would cause atrial fibrillation,” Dr. Olshansky said in an interview. “That does suggest that there’s something else going on, besides just the drug itself. It would be potentially concerning if we were to lay the blame totally on these drugs.”
Dr. Olshansky, who recently coauthored a review of stimulant drugs and arrhythmias, suggested that lifestyle, comorbidities, and drug impurities may have added to the risk of AF.
“[The investigators] did try to correct for that kind of stuff, but it’s very hard to correct for a lot of the issues that may be ongoing with individuals who partake in these drugs,” Dr. Olshansky said in an interview. “They may not be a healthy lot, in general.”
Still, considering previous data linking drugs of abuse with arrhythmias, he said the detected risks were “intriguing,” and deserved a closer look.
“It’s a nice groundbreaking study, with regard to the fact that they showed unique relationships that we don’t completely understand,” Dr. Olshansky said. “It opens up a new opportunity for further investigation.”
The investigators disclosed relationships with InCarda, Baylis Medical, Johnson & Johnson, and others. Dr. Olshansky disclosed no relevant competing interests.
FROM EUROPEAN HEART JOURNAL