User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Asymptomatic Umbilical Nodule
The Diagnosis: Sister Mary Joseph Nodule
Histopathologic analysis of the biopsy specimen revealed a dense infiltrate of large, hyperchromatic, mucin-producing cells exhibiting varying degrees of nuclear pleomorphism (Figure 1). Immunohistochemical (IHC) staining was negative for cytokeratin (CK) 20; however, CK7 was found positive (Figure 2), which confirmed the presence of a metastatic adenocarcinoma, consistent with the clinical diagnosis of a Sister Mary Joseph nodule (SMJN). Subsequent IHC workup to determine the site of origin revealed densely positive expression of both cancer antigen 125 and paired homeobox gene 8 (PAX-8)(Figure 3), consistent with primary ovarian disease. Furthermore, expression of estrogen receptor and p53 both were positive within the nuclei, illustrating an aberrant expression pattern. On the other hand, cancer antigen 19-9, caudal-type homeobox 2, gross cystic disease fluid protein 15, and mammaglobin were all determined negative, thus leading to the pathologic diagnosis of a metastatic ovarian adenocarcinoma. Additional workup with computed tomography of the abdomen and pelvis highlighted a large left ovarian mass with multiple omental nodules as well as enlarged retroperitoneal and pelvic lymph nodes.
.")
The SMJN is a rare presentation of internal malignancy that appears as a nodule that metastasizes to the umbilicus. It may be ulcerated or necrotic and is seen in up to 10% of patients with cutaneous metastases from internal malignancy.1 These nodules are named after Sister Mary Joseph, the surgical assistant of Dr. William Mayo who first described the relationship between umbilical nodules seen in patients with gastrointestinal and genitourinary cancer. The most common underlying malignancies include primary gastrointestinal and gynecologic adenocarcinomas. In a retrospective study of 34 patients by Chalya et al,2 the stomach was found to be the most common primary site (41.1%). The presence of an SMJN affords a poor prognosis, with a mean overall survival of 11 months from the time of diagnosis.3 The mechanism of disease dissemination remains unknown but is thought to occur through lymphovascular invasion of tumor cells and spread via the umbilical ligament.1,4
.")
Merkel cell carcinoma is a cutaneous neuroendocrine tumor that most commonly presents in elderly patients as red-violet nodules or plaques. Although Merkel cell carcinoma most frequently is encountered on sun-exposed skin, they also can arise on the trunk and abdomen. Positive IHC staining for CK20 would be expected; however, it was negative in our case.5
. B, Paired homeobox gene 8 (PAX-8) immunohistochemical staining displayed the uptake in the tumor cells")
Cutaneous endometriosis is a rare disease presentation and most commonly occurs as a secondary process due to surgical inoculation of the abdominal wall. Primary cutaneous endometriosis in which there is no history of abdominal surgery less frequently is encountered. Patients typically will report pain and cyclical bleeding with menses. Pathology demonstrates ectopic endometrial tissue with glands and uterine myxoid stroma.6
Amelanotic melanoma is an uncommon subtype of malignant melanoma that presents as nonpigmented nodules that have a propensity to ulcerate and bleed. Furthermore, the umbilicus is an exceedingly rare location for primary melanoma. However, one report does exist, and amelanotic melanoma should be considered in the differential for patients with umbilical nodules.7
Dermoid cysts are benign congenital lesions that typically present as a painless, slow-growing, and wellcircumscribed nodule, as similarly experienced by our patient. They most commonly are found on the testicles and ovaries but also are known to arise in embryologic fusion planes, and reports of umbilical lesions exist.8 Dermoid cysts are diagnosed based on histopathology, supporting the need for a biopsy to distinguish a malignant process from benign lesions.9
- Gabriele R, Conte M, Egidi F, et al. Umbilical metastases: current viewpoint. World J Surg Oncol. 2005;3:13.
- Chalya PL, Mabula JB, Rambau PF, et al. Sister Mary Joseph’s nodule at a university teaching hospital in northwestern Tanzania: a retrospective review of 34 cases. World J Surg Oncol. 2013;11:151.
- Leyrat B, Bernadach M, Ginzac A, et al. Sister Mary Joseph nodules: a case report about a rare location of skin metastasis. Case Rep Oncol. 2021;14:664-670.
- Yendluri V, Centeno B, Springett GM. Pancreatic cancer presenting as a Sister Mary Joseph’s nodule: case report and update of the literature. Pancreas. 2007;34:161-164.
- Uchi H. Merkel cell carcinoma: an update and immunotherapy. Front Oncol. 2018;8:48.
- Bittar PG, Hryneewycz KT, Bryant EA. Primary cutaneous endometriosis presenting as an umbilical nodule. JAMA Dermatol. 2021;157:1227.
- Kovitwanichkanont T, Joseph S, Yip L. Hidden in plain sight: umbilical melanoma [published online January 28, 2020]. Med J Aust. 2020;212:154-155.e1.
- Prior A, Anania P, Pacetti M, et al. Dermoid and epidermoid cysts of scalp: case series of 234 consecutive patients. World Neurosurg. 2018;120:119-124.
- Akinci O, Turker C, Erturk MS, et al. Umbilical dermoid cyst: a rare case. Cerrahpasa Med J. 2020;44:51-53.
The Diagnosis: Sister Mary Joseph Nodule
Histopathologic analysis of the biopsy specimen revealed a dense infiltrate of large, hyperchromatic, mucin-producing cells exhibiting varying degrees of nuclear pleomorphism (Figure 1). Immunohistochemical (IHC) staining was negative for cytokeratin (CK) 20; however, CK7 was found positive (Figure 2), which confirmed the presence of a metastatic adenocarcinoma, consistent with the clinical diagnosis of a Sister Mary Joseph nodule (SMJN). Subsequent IHC workup to determine the site of origin revealed densely positive expression of both cancer antigen 125 and paired homeobox gene 8 (PAX-8)(Figure 3), consistent with primary ovarian disease. Furthermore, expression of estrogen receptor and p53 both were positive within the nuclei, illustrating an aberrant expression pattern. On the other hand, cancer antigen 19-9, caudal-type homeobox 2, gross cystic disease fluid protein 15, and mammaglobin were all determined negative, thus leading to the pathologic diagnosis of a metastatic ovarian adenocarcinoma. Additional workup with computed tomography of the abdomen and pelvis highlighted a large left ovarian mass with multiple omental nodules as well as enlarged retroperitoneal and pelvic lymph nodes.
The SMJN is a rare presentation of internal malignancy that appears as a nodule that metastasizes to the umbilicus. It may be ulcerated or necrotic and is seen in up to 10% of patients with cutaneous metastases from internal malignancy.1 These nodules are named after Sister Mary Joseph, the surgical assistant of Dr. William Mayo who first described the relationship between umbilical nodules seen in patients with gastrointestinal and genitourinary cancer. The most common underlying malignancies include primary gastrointestinal and gynecologic adenocarcinomas. In a retrospective study of 34 patients by Chalya et al,2 the stomach was found to be the most common primary site (41.1%). The presence of an SMJN affords a poor prognosis, with a mean overall survival of 11 months from the time of diagnosis.3 The mechanism of disease dissemination remains unknown but is thought to occur through lymphovascular invasion of tumor cells and spread via the umbilical ligament.1,4
Merkel cell carcinoma is a cutaneous neuroendocrine tumor that most commonly presents in elderly patients as red-violet nodules or plaques. Although Merkel cell carcinoma most frequently is encountered on sun-exposed skin, they also can arise on the trunk and abdomen. Positive IHC staining for CK20 would be expected; however, it was negative in our case.5
Cutaneous endometriosis is a rare disease presentation and most commonly occurs as a secondary process due to surgical inoculation of the abdominal wall. Primary cutaneous endometriosis in which there is no history of abdominal surgery less frequently is encountered. Patients typically will report pain and cyclical bleeding with menses. Pathology demonstrates ectopic endometrial tissue with glands and uterine myxoid stroma.6
Amelanotic melanoma is an uncommon subtype of malignant melanoma that presents as nonpigmented nodules that have a propensity to ulcerate and bleed. Furthermore, the umbilicus is an exceedingly rare location for primary melanoma. However, one report does exist, and amelanotic melanoma should be considered in the differential for patients with umbilical nodules.7
Dermoid cysts are benign congenital lesions that typically present as a painless, slow-growing, and wellcircumscribed nodule, as similarly experienced by our patient. They most commonly are found on the testicles and ovaries but also are known to arise in embryologic fusion planes, and reports of umbilical lesions exist.8 Dermoid cysts are diagnosed based on histopathology, supporting the need for a biopsy to distinguish a malignant process from benign lesions.9
The Diagnosis: Sister Mary Joseph Nodule
Histopathologic analysis of the biopsy specimen revealed a dense infiltrate of large, hyperchromatic, mucin-producing cells exhibiting varying degrees of nuclear pleomorphism (Figure 1). Immunohistochemical (IHC) staining was negative for cytokeratin (CK) 20; however, CK7 was found positive (Figure 2), which confirmed the presence of a metastatic adenocarcinoma, consistent with the clinical diagnosis of a Sister Mary Joseph nodule (SMJN). Subsequent IHC workup to determine the site of origin revealed densely positive expression of both cancer antigen 125 and paired homeobox gene 8 (PAX-8)(Figure 3), consistent with primary ovarian disease. Furthermore, expression of estrogen receptor and p53 both were positive within the nuclei, illustrating an aberrant expression pattern. On the other hand, cancer antigen 19-9, caudal-type homeobox 2, gross cystic disease fluid protein 15, and mammaglobin were all determined negative, thus leading to the pathologic diagnosis of a metastatic ovarian adenocarcinoma. Additional workup with computed tomography of the abdomen and pelvis highlighted a large left ovarian mass with multiple omental nodules as well as enlarged retroperitoneal and pelvic lymph nodes.
The SMJN is a rare presentation of internal malignancy that appears as a nodule that metastasizes to the umbilicus. It may be ulcerated or necrotic and is seen in up to 10% of patients with cutaneous metastases from internal malignancy.1 These nodules are named after Sister Mary Joseph, the surgical assistant of Dr. William Mayo who first described the relationship between umbilical nodules seen in patients with gastrointestinal and genitourinary cancer. The most common underlying malignancies include primary gastrointestinal and gynecologic adenocarcinomas. In a retrospective study of 34 patients by Chalya et al,2 the stomach was found to be the most common primary site (41.1%). The presence of an SMJN affords a poor prognosis, with a mean overall survival of 11 months from the time of diagnosis.3 The mechanism of disease dissemination remains unknown but is thought to occur through lymphovascular invasion of tumor cells and spread via the umbilical ligament.1,4
Merkel cell carcinoma is a cutaneous neuroendocrine tumor that most commonly presents in elderly patients as red-violet nodules or plaques. Although Merkel cell carcinoma most frequently is encountered on sun-exposed skin, they also can arise on the trunk and abdomen. Positive IHC staining for CK20 would be expected; however, it was negative in our case.5
Cutaneous endometriosis is a rare disease presentation and most commonly occurs as a secondary process due to surgical inoculation of the abdominal wall. Primary cutaneous endometriosis in which there is no history of abdominal surgery less frequently is encountered. Patients typically will report pain and cyclical bleeding with menses. Pathology demonstrates ectopic endometrial tissue with glands and uterine myxoid stroma.6
Amelanotic melanoma is an uncommon subtype of malignant melanoma that presents as nonpigmented nodules that have a propensity to ulcerate and bleed. Furthermore, the umbilicus is an exceedingly rare location for primary melanoma. However, one report does exist, and amelanotic melanoma should be considered in the differential for patients with umbilical nodules.7
Dermoid cysts are benign congenital lesions that typically present as a painless, slow-growing, and wellcircumscribed nodule, as similarly experienced by our patient. They most commonly are found on the testicles and ovaries but also are known to arise in embryologic fusion planes, and reports of umbilical lesions exist.8 Dermoid cysts are diagnosed based on histopathology, supporting the need for a biopsy to distinguish a malignant process from benign lesions.9
- Gabriele R, Conte M, Egidi F, et al. Umbilical metastases: current viewpoint. World J Surg Oncol. 2005;3:13.
- Chalya PL, Mabula JB, Rambau PF, et al. Sister Mary Joseph’s nodule at a university teaching hospital in northwestern Tanzania: a retrospective review of 34 cases. World J Surg Oncol. 2013;11:151.
- Leyrat B, Bernadach M, Ginzac A, et al. Sister Mary Joseph nodules: a case report about a rare location of skin metastasis. Case Rep Oncol. 2021;14:664-670.
- Yendluri V, Centeno B, Springett GM. Pancreatic cancer presenting as a Sister Mary Joseph’s nodule: case report and update of the literature. Pancreas. 2007;34:161-164.
- Uchi H. Merkel cell carcinoma: an update and immunotherapy. Front Oncol. 2018;8:48.
- Bittar PG, Hryneewycz KT, Bryant EA. Primary cutaneous endometriosis presenting as an umbilical nodule. JAMA Dermatol. 2021;157:1227.
- Kovitwanichkanont T, Joseph S, Yip L. Hidden in plain sight: umbilical melanoma [published online January 28, 2020]. Med J Aust. 2020;212:154-155.e1.
- Prior A, Anania P, Pacetti M, et al. Dermoid and epidermoid cysts of scalp: case series of 234 consecutive patients. World Neurosurg. 2018;120:119-124.
- Akinci O, Turker C, Erturk MS, et al. Umbilical dermoid cyst: a rare case. Cerrahpasa Med J. 2020;44:51-53.
- Gabriele R, Conte M, Egidi F, et al. Umbilical metastases: current viewpoint. World J Surg Oncol. 2005;3:13.
- Chalya PL, Mabula JB, Rambau PF, et al. Sister Mary Joseph’s nodule at a university teaching hospital in northwestern Tanzania: a retrospective review of 34 cases. World J Surg Oncol. 2013;11:151.
- Leyrat B, Bernadach M, Ginzac A, et al. Sister Mary Joseph nodules: a case report about a rare location of skin metastasis. Case Rep Oncol. 2021;14:664-670.
- Yendluri V, Centeno B, Springett GM. Pancreatic cancer presenting as a Sister Mary Joseph’s nodule: case report and update of the literature. Pancreas. 2007;34:161-164.
- Uchi H. Merkel cell carcinoma: an update and immunotherapy. Front Oncol. 2018;8:48.
- Bittar PG, Hryneewycz KT, Bryant EA. Primary cutaneous endometriosis presenting as an umbilical nodule. JAMA Dermatol. 2021;157:1227.
- Kovitwanichkanont T, Joseph S, Yip L. Hidden in plain sight: umbilical melanoma [published online January 28, 2020]. Med J Aust. 2020;212:154-155.e1.
- Prior A, Anania P, Pacetti M, et al. Dermoid and epidermoid cysts of scalp: case series of 234 consecutive patients. World Neurosurg. 2018;120:119-124.
- Akinci O, Turker C, Erturk MS, et al. Umbilical dermoid cyst: a rare case. Cerrahpasa Med J. 2020;44:51-53.
A 64-year-old woman with no notable medical history was referred to our dermatology clinic with an intermittent eczematous rash around the eyelids of 3 months’ duration. While performing a total-body skin examination, a firm pink nodule with a smooth surface incidentally was discovered on the umbilicus. The patient was uncertain when the lesion first appeared and denied any associated symptoms including pain and bleeding. Additionally, a lymph node examination revealed right inguinal lymphadenopathy. Upon further questioning, she reported worsening muscle weakness, fatigue, night sweats, and an unintentional weight loss of 10 pounds. A 6-mm punch biopsy of the umbilical lesion was obtained for routine histopathology.


Children and COVID: Weekly cases fall to lowest level in over a year
With the third autumn of the COVID era now upon us, the discussion has turned again to a possible influenza/COVID twindemic, as well as the new-for-2022 influenza/COVID/respiratory syncytial virus tripledemic. It appears, however, that COVID may have missed the memo.
For the sixth time in the last 7 weeks, the number of new COVID cases in children fell, with just under 23,000 reported during the week of Oct. 14-20, according to the American Academy of Pediatrics and the Children’s Hospital Association. That is the lowest weekly count so far this year, and the lowest since early July of 2021, just as the Delta surge was starting. New pediatric cases had dipped to 8,500, the lowest for any week during the pandemic, a couple of weeks before that, the AAP/CHA data show.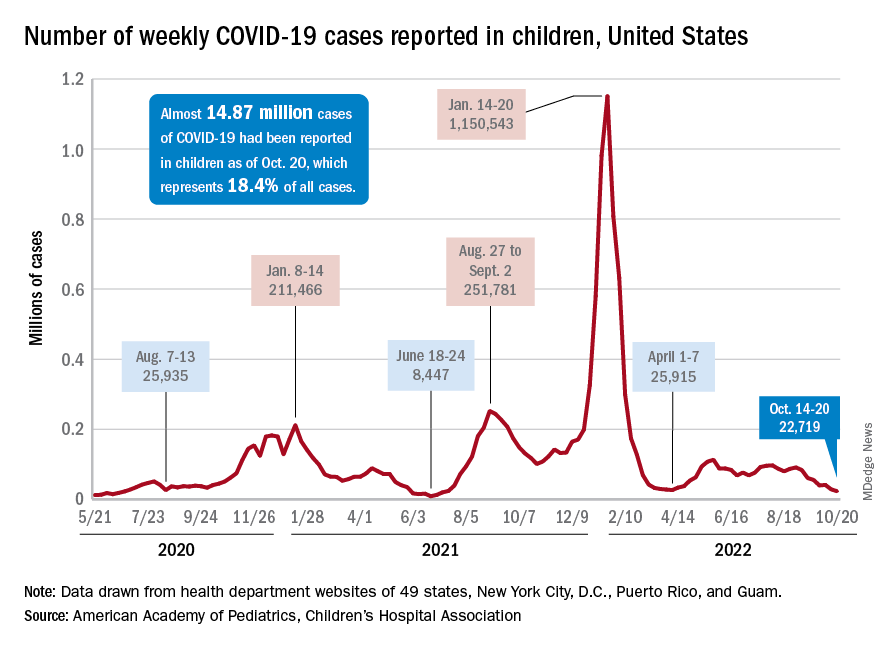
Weekly cases have fallen by almost 75% since over 90,000 were reported for the week of Aug. 26 to Sept. 1, even as children have returned to school and vaccine uptake remains slow in the youngest age groups. Rates of emergency department visits with diagnosed COVID also have continued to drop, as have new admissions, and both are nearing their 2021 lows, according to the Centers for Disease Control and Prevention.
New vaccinations in children under age 5 years were up slightly for the most recent week (Oct. 13-19), but total uptake for that age group is only 7.1% for an initial dose and 2.9% for full vaccination. Among children aged 5-11 years, 38.7% have received at least one dose and 31.6% have completed the primary series, with corresponding figures of 71.2% and 60.9% for those aged 12-17, the CDC said on its COVID Data Tracker.
Despite the low overall numbers, though, the youngest children are, in one respect, punching above their weight when it comes to vaccinations. In the 2 weeks from Oct. 6 to Oct. 19, children under 5 years of age, who represent 5.9% of the U.S. population, received 9.2% of the initial vaccine doses administered. Children aged 5-11 years, who represent 8.7% of the total population, got just 4.2% of all first doses over those same 2 weeks, while 12- to 17-year-olds, who make up 7.6% of the population, got 3.4% of the vaccine doses, the CDC reported.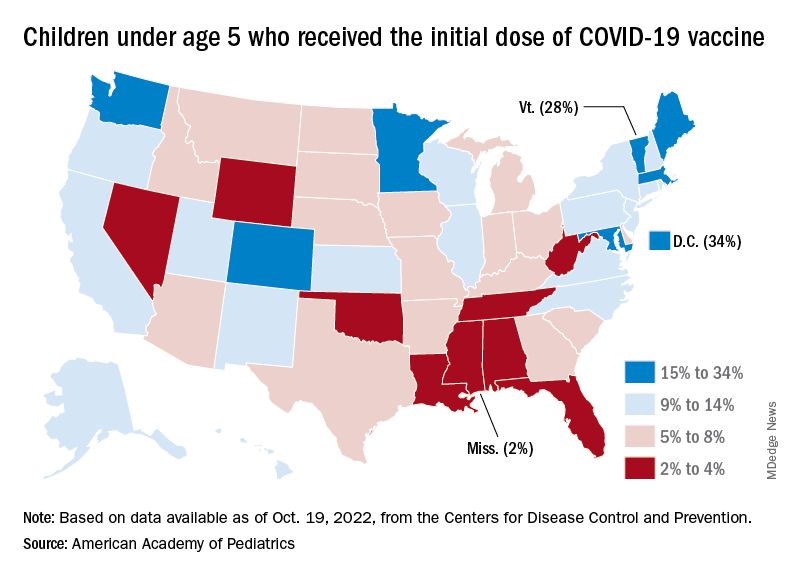
On the vaccine-approval front, the Food and Drug Administration recently announced that the new bivalent COVID-19 vaccines are now included in the emergency use authorizations for children who have completed primary or booster vaccination. The Moderna vaccine is authorized as a single-dose booster for children as young as 6 years and the Pfizer-BioNTech vaccine can be given as a single booster dose in children as young as 5 years, the FDA said.
“These bivalent COVID-19 vaccines include an mRNA component of the original strain to provide an immune response that is broadly protective against COVID-19 and an mRNA component in common between the omicron variant BA.4 and BA.5 lineages,” the FDA said.
With the third autumn of the COVID era now upon us, the discussion has turned again to a possible influenza/COVID twindemic, as well as the new-for-2022 influenza/COVID/respiratory syncytial virus tripledemic. It appears, however, that COVID may have missed the memo.
For the sixth time in the last 7 weeks, the number of new COVID cases in children fell, with just under 23,000 reported during the week of Oct. 14-20, according to the American Academy of Pediatrics and the Children’s Hospital Association. That is the lowest weekly count so far this year, and the lowest since early July of 2021, just as the Delta surge was starting. New pediatric cases had dipped to 8,500, the lowest for any week during the pandemic, a couple of weeks before that, the AAP/CHA data show.
Weekly cases have fallen by almost 75% since over 90,000 were reported for the week of Aug. 26 to Sept. 1, even as children have returned to school and vaccine uptake remains slow in the youngest age groups. Rates of emergency department visits with diagnosed COVID also have continued to drop, as have new admissions, and both are nearing their 2021 lows, according to the Centers for Disease Control and Prevention.
New vaccinations in children under age 5 years were up slightly for the most recent week (Oct. 13-19), but total uptake for that age group is only 7.1% for an initial dose and 2.9% for full vaccination. Among children aged 5-11 years, 38.7% have received at least one dose and 31.6% have completed the primary series, with corresponding figures of 71.2% and 60.9% for those aged 12-17, the CDC said on its COVID Data Tracker.
Despite the low overall numbers, though, the youngest children are, in one respect, punching above their weight when it comes to vaccinations. In the 2 weeks from Oct. 6 to Oct. 19, children under 5 years of age, who represent 5.9% of the U.S. population, received 9.2% of the initial vaccine doses administered. Children aged 5-11 years, who represent 8.7% of the total population, got just 4.2% of all first doses over those same 2 weeks, while 12- to 17-year-olds, who make up 7.6% of the population, got 3.4% of the vaccine doses, the CDC reported.
On the vaccine-approval front, the Food and Drug Administration recently announced that the new bivalent COVID-19 vaccines are now included in the emergency use authorizations for children who have completed primary or booster vaccination. The Moderna vaccine is authorized as a single-dose booster for children as young as 6 years and the Pfizer-BioNTech vaccine can be given as a single booster dose in children as young as 5 years, the FDA said.
“These bivalent COVID-19 vaccines include an mRNA component of the original strain to provide an immune response that is broadly protective against COVID-19 and an mRNA component in common between the omicron variant BA.4 and BA.5 lineages,” the FDA said.
With the third autumn of the COVID era now upon us, the discussion has turned again to a possible influenza/COVID twindemic, as well as the new-for-2022 influenza/COVID/respiratory syncytial virus tripledemic. It appears, however, that COVID may have missed the memo.
For the sixth time in the last 7 weeks, the number of new COVID cases in children fell, with just under 23,000 reported during the week of Oct. 14-20, according to the American Academy of Pediatrics and the Children’s Hospital Association. That is the lowest weekly count so far this year, and the lowest since early July of 2021, just as the Delta surge was starting. New pediatric cases had dipped to 8,500, the lowest for any week during the pandemic, a couple of weeks before that, the AAP/CHA data show.
Weekly cases have fallen by almost 75% since over 90,000 were reported for the week of Aug. 26 to Sept. 1, even as children have returned to school and vaccine uptake remains slow in the youngest age groups. Rates of emergency department visits with diagnosed COVID also have continued to drop, as have new admissions, and both are nearing their 2021 lows, according to the Centers for Disease Control and Prevention.
New vaccinations in children under age 5 years were up slightly for the most recent week (Oct. 13-19), but total uptake for that age group is only 7.1% for an initial dose and 2.9% for full vaccination. Among children aged 5-11 years, 38.7% have received at least one dose and 31.6% have completed the primary series, with corresponding figures of 71.2% and 60.9% for those aged 12-17, the CDC said on its COVID Data Tracker.
Despite the low overall numbers, though, the youngest children are, in one respect, punching above their weight when it comes to vaccinations. In the 2 weeks from Oct. 6 to Oct. 19, children under 5 years of age, who represent 5.9% of the U.S. population, received 9.2% of the initial vaccine doses administered. Children aged 5-11 years, who represent 8.7% of the total population, got just 4.2% of all first doses over those same 2 weeks, while 12- to 17-year-olds, who make up 7.6% of the population, got 3.4% of the vaccine doses, the CDC reported.
On the vaccine-approval front, the Food and Drug Administration recently announced that the new bivalent COVID-19 vaccines are now included in the emergency use authorizations for children who have completed primary or booster vaccination. The Moderna vaccine is authorized as a single-dose booster for children as young as 6 years and the Pfizer-BioNTech vaccine can be given as a single booster dose in children as young as 5 years, the FDA said.
“These bivalent COVID-19 vaccines include an mRNA component of the original strain to provide an immune response that is broadly protective against COVID-19 and an mRNA component in common between the omicron variant BA.4 and BA.5 lineages,” the FDA said.
Time to ditch clarithromycin for H. pylori?
Rates of resistance to clarithromycin among Helicobacter pylori isolates in the United States and Europe are high enough to warrant discontinuation of empiric use of proton pump inhibitor (PPI)–based triple therapy that includes the antibiotic in these regions, a new study has found.
Overall, 22.2% of participants were resistant to clarithromycin – a rate that is above the currently recommended threshold of 15% or higher for avoidance of PPI-based triple therapy that includes clarithromycin.
, study investigator William Chey, MD, professor and chief, Division of Gastroenterology and Hepatology, Michigan Medicine, Ann Arbor, said in an interview.
Judith Kim, MD, a gastroenterologist at NYU Langone Health and clinical instructor of medicine at NYU Grossman School of Medicine, who wasn’t involved in the study, agrees.
“The use of PPI-based triple therapy is still common practice despite recent recommendations to avoid clarithromycin in areas with high resistance rates,” Dr. Kim told this news organization.
“This study shows that multiple parts of the United States and Europe have high resistance rates,” rendering clarithromycin-based regimens “more likely to ineffectively eradicate H pylori,” Dr. Kim said.
The study was published online in The American Journal of Gastroenterology.
Better options now available
Guidelines advise against the use of PPI-based triple regimens with clarithromycin for H. pylori infection in areas where resistance is 15% or higher or for patients who have previously received macrolides. However, up-to-date information on H. pylori antimicrobial resistance patterns is limited, especially in the United States.
Dr. Chey and colleagues assessed resistance rates to antibiotics commonly used to treat H. pylori in isolates from 907 adults with the infection in the United States and Europe. They included four U.S. subregions and five participating European countries.
In all U.S. subregions and European countries, clarithromycin resistance rates were above 15% except possibly in the United Kingdom, where the sample size was too small to provide a reliable estimate.
Three-quarters of the clarithromycin-resistant isolates were also resistant to metronidazole.
The study also found that, overall, 1.2% of patients had isolates that were resistant to amoxicillin, and 69.2% had isolates resistant to metronidazole. Resistance patterns were similar in the United States and Europe; metronidazole resistance was the most common (50%-79% of isolates), and amoxicillin was the least common (≤ 5%).
“Overall, these data provide robust evidence to support a shift away from the default empiric prescription of triple combinations containing a PPI and clarithromycin for H. pylori infection in the United States and Europe,” the study team writes.
The high prevalence of resistance, including dual resistance, highlights the need for antibiotic stewardship and resistance surveillance, as well as novel treatment strategies for H. pylori infection, they add.
Last spring, as previously reported, the United States Food and Drug Administration approved two vonoprazan-based treatments for H. pylori: Voquezna Triple Pak (vonoprazan, amoxicillin, clarithromycin) and Voquezna Dual Pak (vonoprazan, amoxicillin), both from Phathom Pharmaceuticals.
“Vonoprazan-based treatment may be superior to standard PPI triple therapy for clarithromycin-resistant infections based on prior studies and is a potential good option,” Dr. Kim said.
Still, she added, she “would most likely first recommend regimens that do not have clarithromycin, such as bismuth quadruple therapy.”
Study’s importance
Because the study drew upon the largest dataset to date on U.S. resistance rates, it should be used to more precisely guide first-line therapy decisions, said Richard Peek, Jr., MD, professor of medicine and director of gastroenterology at Vanderbilt University Medical Center, Nashville, Tenn.
“To date, there has been a dearth of information in the United States regarding H. pylori resistance rates, which has often led to the use of ineffective empiric therapies and inappropriate exposure to antibiotics,” Dr. Peek, who wasn’t involved in the study, told this news organization.
“These data are particularly exciting when viewed within the context of new genomic sequencing tests that can determine H. pylori resistance patterns using DNA isolated from the stomach or the stool,” he said.
Dr. Peek agreed that the recent approval of vonoprazan-based therapies “adds another regimen to the therapeutic armamentarium available for eradicating H. pylori, and its value seems to be particularly beneficial for eradication failures.”
The research was funded by Phathom Pharmaceuticals. Dr. Chey is a board member of the American College of Gastroenterology, GI on Demand, the International Foundation of Functional GI Disorders, and the Rome Foundation. He has received compensation as a consultant from AbbVie, Alfasigma, Allakos, Alnylam, Bayer, BioAmerica, Cosmo, Intrinsic Medicine, Ironwood Pharmaceuticals, QOL Medical, Nestle, Phathom Pharmaceuticals, RedHill Biopharma, Salix/Valeant, Takeda, Urovant, and Vibrant; grant/research support from BioAmerica, Commonwealth Diagnostics International, QOL Medical, Salix, and Vibrant; owns stock/stock options in GI on Demand and Modify Health; and owns patents relating to methods and kits for identifying food sensitivities and intolerances, digital manometry, and a rectal expulsion device. Dr. Peek and Dr. Kim report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Rates of resistance to clarithromycin among Helicobacter pylori isolates in the United States and Europe are high enough to warrant discontinuation of empiric use of proton pump inhibitor (PPI)–based triple therapy that includes the antibiotic in these regions, a new study has found.
Overall, 22.2% of participants were resistant to clarithromycin – a rate that is above the currently recommended threshold of 15% or higher for avoidance of PPI-based triple therapy that includes clarithromycin.
, study investigator William Chey, MD, professor and chief, Division of Gastroenterology and Hepatology, Michigan Medicine, Ann Arbor, said in an interview.
Judith Kim, MD, a gastroenterologist at NYU Langone Health and clinical instructor of medicine at NYU Grossman School of Medicine, who wasn’t involved in the study, agrees.
“The use of PPI-based triple therapy is still common practice despite recent recommendations to avoid clarithromycin in areas with high resistance rates,” Dr. Kim told this news organization.
“This study shows that multiple parts of the United States and Europe have high resistance rates,” rendering clarithromycin-based regimens “more likely to ineffectively eradicate H pylori,” Dr. Kim said.
The study was published online in The American Journal of Gastroenterology.
Better options now available
Guidelines advise against the use of PPI-based triple regimens with clarithromycin for H. pylori infection in areas where resistance is 15% or higher or for patients who have previously received macrolides. However, up-to-date information on H. pylori antimicrobial resistance patterns is limited, especially in the United States.
Dr. Chey and colleagues assessed resistance rates to antibiotics commonly used to treat H. pylori in isolates from 907 adults with the infection in the United States and Europe. They included four U.S. subregions and five participating European countries.
In all U.S. subregions and European countries, clarithromycin resistance rates were above 15% except possibly in the United Kingdom, where the sample size was too small to provide a reliable estimate.
Three-quarters of the clarithromycin-resistant isolates were also resistant to metronidazole.
The study also found that, overall, 1.2% of patients had isolates that were resistant to amoxicillin, and 69.2% had isolates resistant to metronidazole. Resistance patterns were similar in the United States and Europe; metronidazole resistance was the most common (50%-79% of isolates), and amoxicillin was the least common (≤ 5%).
“Overall, these data provide robust evidence to support a shift away from the default empiric prescription of triple combinations containing a PPI and clarithromycin for H. pylori infection in the United States and Europe,” the study team writes.
The high prevalence of resistance, including dual resistance, highlights the need for antibiotic stewardship and resistance surveillance, as well as novel treatment strategies for H. pylori infection, they add.
Last spring, as previously reported, the United States Food and Drug Administration approved two vonoprazan-based treatments for H. pylori: Voquezna Triple Pak (vonoprazan, amoxicillin, clarithromycin) and Voquezna Dual Pak (vonoprazan, amoxicillin), both from Phathom Pharmaceuticals.
“Vonoprazan-based treatment may be superior to standard PPI triple therapy for clarithromycin-resistant infections based on prior studies and is a potential good option,” Dr. Kim said.
Still, she added, she “would most likely first recommend regimens that do not have clarithromycin, such as bismuth quadruple therapy.”
Study’s importance
Because the study drew upon the largest dataset to date on U.S. resistance rates, it should be used to more precisely guide first-line therapy decisions, said Richard Peek, Jr., MD, professor of medicine and director of gastroenterology at Vanderbilt University Medical Center, Nashville, Tenn.
“To date, there has been a dearth of information in the United States regarding H. pylori resistance rates, which has often led to the use of ineffective empiric therapies and inappropriate exposure to antibiotics,” Dr. Peek, who wasn’t involved in the study, told this news organization.
“These data are particularly exciting when viewed within the context of new genomic sequencing tests that can determine H. pylori resistance patterns using DNA isolated from the stomach or the stool,” he said.
Dr. Peek agreed that the recent approval of vonoprazan-based therapies “adds another regimen to the therapeutic armamentarium available for eradicating H. pylori, and its value seems to be particularly beneficial for eradication failures.”
The research was funded by Phathom Pharmaceuticals. Dr. Chey is a board member of the American College of Gastroenterology, GI on Demand, the International Foundation of Functional GI Disorders, and the Rome Foundation. He has received compensation as a consultant from AbbVie, Alfasigma, Allakos, Alnylam, Bayer, BioAmerica, Cosmo, Intrinsic Medicine, Ironwood Pharmaceuticals, QOL Medical, Nestle, Phathom Pharmaceuticals, RedHill Biopharma, Salix/Valeant, Takeda, Urovant, and Vibrant; grant/research support from BioAmerica, Commonwealth Diagnostics International, QOL Medical, Salix, and Vibrant; owns stock/stock options in GI on Demand and Modify Health; and owns patents relating to methods and kits for identifying food sensitivities and intolerances, digital manometry, and a rectal expulsion device. Dr. Peek and Dr. Kim report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Rates of resistance to clarithromycin among Helicobacter pylori isolates in the United States and Europe are high enough to warrant discontinuation of empiric use of proton pump inhibitor (PPI)–based triple therapy that includes the antibiotic in these regions, a new study has found.
Overall, 22.2% of participants were resistant to clarithromycin – a rate that is above the currently recommended threshold of 15% or higher for avoidance of PPI-based triple therapy that includes clarithromycin.
, study investigator William Chey, MD, professor and chief, Division of Gastroenterology and Hepatology, Michigan Medicine, Ann Arbor, said in an interview.
Judith Kim, MD, a gastroenterologist at NYU Langone Health and clinical instructor of medicine at NYU Grossman School of Medicine, who wasn’t involved in the study, agrees.
“The use of PPI-based triple therapy is still common practice despite recent recommendations to avoid clarithromycin in areas with high resistance rates,” Dr. Kim told this news organization.
“This study shows that multiple parts of the United States and Europe have high resistance rates,” rendering clarithromycin-based regimens “more likely to ineffectively eradicate H pylori,” Dr. Kim said.
The study was published online in The American Journal of Gastroenterology.
Better options now available
Guidelines advise against the use of PPI-based triple regimens with clarithromycin for H. pylori infection in areas where resistance is 15% or higher or for patients who have previously received macrolides. However, up-to-date information on H. pylori antimicrobial resistance patterns is limited, especially in the United States.
Dr. Chey and colleagues assessed resistance rates to antibiotics commonly used to treat H. pylori in isolates from 907 adults with the infection in the United States and Europe. They included four U.S. subregions and five participating European countries.
In all U.S. subregions and European countries, clarithromycin resistance rates were above 15% except possibly in the United Kingdom, where the sample size was too small to provide a reliable estimate.
Three-quarters of the clarithromycin-resistant isolates were also resistant to metronidazole.
The study also found that, overall, 1.2% of patients had isolates that were resistant to amoxicillin, and 69.2% had isolates resistant to metronidazole. Resistance patterns were similar in the United States and Europe; metronidazole resistance was the most common (50%-79% of isolates), and amoxicillin was the least common (≤ 5%).
“Overall, these data provide robust evidence to support a shift away from the default empiric prescription of triple combinations containing a PPI and clarithromycin for H. pylori infection in the United States and Europe,” the study team writes.
The high prevalence of resistance, including dual resistance, highlights the need for antibiotic stewardship and resistance surveillance, as well as novel treatment strategies for H. pylori infection, they add.
Last spring, as previously reported, the United States Food and Drug Administration approved two vonoprazan-based treatments for H. pylori: Voquezna Triple Pak (vonoprazan, amoxicillin, clarithromycin) and Voquezna Dual Pak (vonoprazan, amoxicillin), both from Phathom Pharmaceuticals.
“Vonoprazan-based treatment may be superior to standard PPI triple therapy for clarithromycin-resistant infections based on prior studies and is a potential good option,” Dr. Kim said.
Still, she added, she “would most likely first recommend regimens that do not have clarithromycin, such as bismuth quadruple therapy.”
Study’s importance
Because the study drew upon the largest dataset to date on U.S. resistance rates, it should be used to more precisely guide first-line therapy decisions, said Richard Peek, Jr., MD, professor of medicine and director of gastroenterology at Vanderbilt University Medical Center, Nashville, Tenn.
“To date, there has been a dearth of information in the United States regarding H. pylori resistance rates, which has often led to the use of ineffective empiric therapies and inappropriate exposure to antibiotics,” Dr. Peek, who wasn’t involved in the study, told this news organization.
“These data are particularly exciting when viewed within the context of new genomic sequencing tests that can determine H. pylori resistance patterns using DNA isolated from the stomach or the stool,” he said.
Dr. Peek agreed that the recent approval of vonoprazan-based therapies “adds another regimen to the therapeutic armamentarium available for eradicating H. pylori, and its value seems to be particularly beneficial for eradication failures.”
The research was funded by Phathom Pharmaceuticals. Dr. Chey is a board member of the American College of Gastroenterology, GI on Demand, the International Foundation of Functional GI Disorders, and the Rome Foundation. He has received compensation as a consultant from AbbVie, Alfasigma, Allakos, Alnylam, Bayer, BioAmerica, Cosmo, Intrinsic Medicine, Ironwood Pharmaceuticals, QOL Medical, Nestle, Phathom Pharmaceuticals, RedHill Biopharma, Salix/Valeant, Takeda, Urovant, and Vibrant; grant/research support from BioAmerica, Commonwealth Diagnostics International, QOL Medical, Salix, and Vibrant; owns stock/stock options in GI on Demand and Modify Health; and owns patents relating to methods and kits for identifying food sensitivities and intolerances, digital manometry, and a rectal expulsion device. Dr. Peek and Dr. Kim report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Psychiatric comorbidities in the pediatric neurology clinic
CINCINNATI – Neurology and psychiatry have an inherent kinship, as one often deals with the brain and the other always focuses on the mind. The two fields can be intertwined, since neurological conditions are often associated with psychiatric comorbidities amid complex relationships: For example, a young patient with a neurological disorder may experience anxiety due to life changes, his or her diagnosis, or altered biological pathways from the condition or medications used to treat it.
As a result, , according to Devin McNulty, PhD, who spoke on the topic at the 2022 annual meeting of the Child Neurology Society.
The ‘second pandemic’
Mental health conditions represent about 16% of the global burden of disease among people aged 10-19, and the COVID-19 pandemic has drastically worsened the problem, as shutdowns, school loss, and economic struggles have added to the burden. “I think we’ve really seen mental health as sort of the second pandemic. We’ve seen this in Chicago in our emergency room, and in outpatient clinics wait-lists are really high. I think adolescents are specifically at risk,” said Dr. McNulty during her talk. She is an assistant professor of psychiatry and behavioral sciences at Northwestern University and a child psychiatrist at Ann & Robert H. Lurie Children’s Hospital of Chicago.
Common diagnoses include major depressive order, social anxiety disorder, generalized anxiety disorder, post-traumatic stress disorder, obsessive-compulsive disorder, somatic symptom disorder, and functional neurological symptom disorder. The last can appear as neurological symptoms that are not consistent with neurological medical conditions, such as attacks or seizures, abnormal movements, sensory loss or gain, weakness or paralysis, or speech and swallowing issues. It is the second most commonly diagnosed disorder in neurology clinics and accounts for 10% of neurology hospitalizations, and it leads to high rates of health care utilization and functional impairment.
Overall, children with neurological conditions are at about a 5-fold increased risk for depression and anxiety disorders, with a range of contributing risk factors. These include biological factors like medication use, neurological dysfunction, and genetic vulnerability. Psychological factors include stressors, the child’s reaction to the diagnosis and illness, and the level of his or her coping skills. Psychiatric comorbidities may also be triggered by social factors such as familial stress, peer rejection and social isolation, and barriers to treatment for the neurological condition. As just one example, overprotective parenting behavior, while adaptive in moderation, can create a sort of feedback loop that can lead to separation anxiety.
A unique opportunity
“There’s an overlap,” Dr. McNulty said, “because the origin is often multifactorial.” A young patient has a medical condition, which can be chronic or disabling, and the age of onset and diagnosis comes during a critical developmental period. “Then we have issues such as the impact of treatments, whether that’s medication side effects or medical visits. And then disease-related environmental changes, such as family factors, social changes, and impact on school,” said Dr. McNulty.
Child neurologists are in a unique position to identify and ensure treatment of these psychiatric comorbidities, according to Dr. McNulty. “Child neurologists will see psychiatric symptoms in their patient population, and pediatric providers have a unique capacity and ability to treat these patients, especially when you’re seeing patients on a frequent basis. You get to know these patients and their families really well,” she said.
She specifically pointed to three areas: psychosocial screening, differential diagnosis, and treatment and management.
There are broad-based screening measures that can be useful, such as the Strengths and Difficulties Questionnaire and the Pediatric Symptom Checklist. Disorder-specific screening tools include the PHQ-9 (depression), GAD7 (anxiety), Vanderbilt (ADHD), and PROMIS measures for anxiety and depression. “The idea behind the screening measure is that all patients would fill this out and then if a patient screens positive, they would benefit from a more thorough evaluation and history,” said Dr. McNulty.
However, she noted that screening shouldn’t necessarily be a one-off effort. Research has shown that sequential screening is the most powerful strategy. “Then you can get a baseline of a patient’s emotional and behavioral functioning, and it’s actually the changes in some of these screening measures that might give them most clinical information,” said Dr. McNulty.
In fact, on October 11, 2022, the U.S. Preventive Services Task Force announced a recommendation that all children starting at age 8 should be screened for anxiety disorders. It is already recommended to screen children aged 12 and over for depressive disorders, although these documents are aimed primarily at pediatricians or primary care clinics. The American Academy of Neurology has also recommended routine screening of psychiatric and behavioral disorders among children with epilepsy.
A unique perspective
Once a disorder is identified, neurologists can bring a unique perspective to treatment. The neurologist can use his or her knowledge of the disease state to assess whether symptoms are due to poor adjustment to the neurological condition, a primary psychiatric disorder, or the biological underpinnings of the illness or prescribed medications. “I think their neurologist can sort of help tease that apart, [using] their knowledge of neurologic disorders and pathways and medications in a way that psychologists might not be able to do on their own,” said Dr. McNulty.
She also emphasized that there are effective treatments for psychiatric disorders, including cognitive behavioral therapy and various pharmacotherapy options. Other approaches for treating comorbid neurological and psychiatric disorders may include building adaptive coping skills, psychoeducation, and incorporating changes to the family or school environment.
During the Q&A period, one person commented that there should be more psychiatric training for neurology residents. “We do work with the same brain, so I completely agree with that,” said Dr. McNulty.
She was also asked how to identify psychiatric symptoms in nonverbal patients. “One thing that I pay close attention to when I ask parents about (their child) is changes in their physical (attributes). Oftentimes in anxiety in folks who are not severely impaired, if we’re feeling anxious we might be breathing a little faster, or we might get a little sweaty. So looking for physical manifestations is one thing. And then sometimes I’ll tell the parents, if we’re not quite sure, I’ll say ‘I’m not sure, but this is very common given the disorder that you have. Can we check?’ I’m always very clear that I may not be nailing it, but then when we go after it with targeted treatment and we see it getting better, we can say ‘Aha!’ ”
Dr. McNulty has no relevant financial disclosures.
CINCINNATI – Neurology and psychiatry have an inherent kinship, as one often deals with the brain and the other always focuses on the mind. The two fields can be intertwined, since neurological conditions are often associated with psychiatric comorbidities amid complex relationships: For example, a young patient with a neurological disorder may experience anxiety due to life changes, his or her diagnosis, or altered biological pathways from the condition or medications used to treat it.
As a result, , according to Devin McNulty, PhD, who spoke on the topic at the 2022 annual meeting of the Child Neurology Society.
The ‘second pandemic’
Mental health conditions represent about 16% of the global burden of disease among people aged 10-19, and the COVID-19 pandemic has drastically worsened the problem, as shutdowns, school loss, and economic struggles have added to the burden. “I think we’ve really seen mental health as sort of the second pandemic. We’ve seen this in Chicago in our emergency room, and in outpatient clinics wait-lists are really high. I think adolescents are specifically at risk,” said Dr. McNulty during her talk. She is an assistant professor of psychiatry and behavioral sciences at Northwestern University and a child psychiatrist at Ann & Robert H. Lurie Children’s Hospital of Chicago.
Common diagnoses include major depressive order, social anxiety disorder, generalized anxiety disorder, post-traumatic stress disorder, obsessive-compulsive disorder, somatic symptom disorder, and functional neurological symptom disorder. The last can appear as neurological symptoms that are not consistent with neurological medical conditions, such as attacks or seizures, abnormal movements, sensory loss or gain, weakness or paralysis, or speech and swallowing issues. It is the second most commonly diagnosed disorder in neurology clinics and accounts for 10% of neurology hospitalizations, and it leads to high rates of health care utilization and functional impairment.
Overall, children with neurological conditions are at about a 5-fold increased risk for depression and anxiety disorders, with a range of contributing risk factors. These include biological factors like medication use, neurological dysfunction, and genetic vulnerability. Psychological factors include stressors, the child’s reaction to the diagnosis and illness, and the level of his or her coping skills. Psychiatric comorbidities may also be triggered by social factors such as familial stress, peer rejection and social isolation, and barriers to treatment for the neurological condition. As just one example, overprotective parenting behavior, while adaptive in moderation, can create a sort of feedback loop that can lead to separation anxiety.
A unique opportunity
“There’s an overlap,” Dr. McNulty said, “because the origin is often multifactorial.” A young patient has a medical condition, which can be chronic or disabling, and the age of onset and diagnosis comes during a critical developmental period. “Then we have issues such as the impact of treatments, whether that’s medication side effects or medical visits. And then disease-related environmental changes, such as family factors, social changes, and impact on school,” said Dr. McNulty.
Child neurologists are in a unique position to identify and ensure treatment of these psychiatric comorbidities, according to Dr. McNulty. “Child neurologists will see psychiatric symptoms in their patient population, and pediatric providers have a unique capacity and ability to treat these patients, especially when you’re seeing patients on a frequent basis. You get to know these patients and their families really well,” she said.
She specifically pointed to three areas: psychosocial screening, differential diagnosis, and treatment and management.
There are broad-based screening measures that can be useful, such as the Strengths and Difficulties Questionnaire and the Pediatric Symptom Checklist. Disorder-specific screening tools include the PHQ-9 (depression), GAD7 (anxiety), Vanderbilt (ADHD), and PROMIS measures for anxiety and depression. “The idea behind the screening measure is that all patients would fill this out and then if a patient screens positive, they would benefit from a more thorough evaluation and history,” said Dr. McNulty.
However, she noted that screening shouldn’t necessarily be a one-off effort. Research has shown that sequential screening is the most powerful strategy. “Then you can get a baseline of a patient’s emotional and behavioral functioning, and it’s actually the changes in some of these screening measures that might give them most clinical information,” said Dr. McNulty.
In fact, on October 11, 2022, the U.S. Preventive Services Task Force announced a recommendation that all children starting at age 8 should be screened for anxiety disorders. It is already recommended to screen children aged 12 and over for depressive disorders, although these documents are aimed primarily at pediatricians or primary care clinics. The American Academy of Neurology has also recommended routine screening of psychiatric and behavioral disorders among children with epilepsy.
A unique perspective
Once a disorder is identified, neurologists can bring a unique perspective to treatment. The neurologist can use his or her knowledge of the disease state to assess whether symptoms are due to poor adjustment to the neurological condition, a primary psychiatric disorder, or the biological underpinnings of the illness or prescribed medications. “I think their neurologist can sort of help tease that apart, [using] their knowledge of neurologic disorders and pathways and medications in a way that psychologists might not be able to do on their own,” said Dr. McNulty.
She also emphasized that there are effective treatments for psychiatric disorders, including cognitive behavioral therapy and various pharmacotherapy options. Other approaches for treating comorbid neurological and psychiatric disorders may include building adaptive coping skills, psychoeducation, and incorporating changes to the family or school environment.
During the Q&A period, one person commented that there should be more psychiatric training for neurology residents. “We do work with the same brain, so I completely agree with that,” said Dr. McNulty.
She was also asked how to identify psychiatric symptoms in nonverbal patients. “One thing that I pay close attention to when I ask parents about (their child) is changes in their physical (attributes). Oftentimes in anxiety in folks who are not severely impaired, if we’re feeling anxious we might be breathing a little faster, or we might get a little sweaty. So looking for physical manifestations is one thing. And then sometimes I’ll tell the parents, if we’re not quite sure, I’ll say ‘I’m not sure, but this is very common given the disorder that you have. Can we check?’ I’m always very clear that I may not be nailing it, but then when we go after it with targeted treatment and we see it getting better, we can say ‘Aha!’ ”
Dr. McNulty has no relevant financial disclosures.
CINCINNATI – Neurology and psychiatry have an inherent kinship, as one often deals with the brain and the other always focuses on the mind. The two fields can be intertwined, since neurological conditions are often associated with psychiatric comorbidities amid complex relationships: For example, a young patient with a neurological disorder may experience anxiety due to life changes, his or her diagnosis, or altered biological pathways from the condition or medications used to treat it.
As a result, , according to Devin McNulty, PhD, who spoke on the topic at the 2022 annual meeting of the Child Neurology Society.
The ‘second pandemic’
Mental health conditions represent about 16% of the global burden of disease among people aged 10-19, and the COVID-19 pandemic has drastically worsened the problem, as shutdowns, school loss, and economic struggles have added to the burden. “I think we’ve really seen mental health as sort of the second pandemic. We’ve seen this in Chicago in our emergency room, and in outpatient clinics wait-lists are really high. I think adolescents are specifically at risk,” said Dr. McNulty during her talk. She is an assistant professor of psychiatry and behavioral sciences at Northwestern University and a child psychiatrist at Ann & Robert H. Lurie Children’s Hospital of Chicago.
Common diagnoses include major depressive order, social anxiety disorder, generalized anxiety disorder, post-traumatic stress disorder, obsessive-compulsive disorder, somatic symptom disorder, and functional neurological symptom disorder. The last can appear as neurological symptoms that are not consistent with neurological medical conditions, such as attacks or seizures, abnormal movements, sensory loss or gain, weakness or paralysis, or speech and swallowing issues. It is the second most commonly diagnosed disorder in neurology clinics and accounts for 10% of neurology hospitalizations, and it leads to high rates of health care utilization and functional impairment.
Overall, children with neurological conditions are at about a 5-fold increased risk for depression and anxiety disorders, with a range of contributing risk factors. These include biological factors like medication use, neurological dysfunction, and genetic vulnerability. Psychological factors include stressors, the child’s reaction to the diagnosis and illness, and the level of his or her coping skills. Psychiatric comorbidities may also be triggered by social factors such as familial stress, peer rejection and social isolation, and barriers to treatment for the neurological condition. As just one example, overprotective parenting behavior, while adaptive in moderation, can create a sort of feedback loop that can lead to separation anxiety.
A unique opportunity
“There’s an overlap,” Dr. McNulty said, “because the origin is often multifactorial.” A young patient has a medical condition, which can be chronic or disabling, and the age of onset and diagnosis comes during a critical developmental period. “Then we have issues such as the impact of treatments, whether that’s medication side effects or medical visits. And then disease-related environmental changes, such as family factors, social changes, and impact on school,” said Dr. McNulty.
Child neurologists are in a unique position to identify and ensure treatment of these psychiatric comorbidities, according to Dr. McNulty. “Child neurologists will see psychiatric symptoms in their patient population, and pediatric providers have a unique capacity and ability to treat these patients, especially when you’re seeing patients on a frequent basis. You get to know these patients and their families really well,” she said.
She specifically pointed to three areas: psychosocial screening, differential diagnosis, and treatment and management.
There are broad-based screening measures that can be useful, such as the Strengths and Difficulties Questionnaire and the Pediatric Symptom Checklist. Disorder-specific screening tools include the PHQ-9 (depression), GAD7 (anxiety), Vanderbilt (ADHD), and PROMIS measures for anxiety and depression. “The idea behind the screening measure is that all patients would fill this out and then if a patient screens positive, they would benefit from a more thorough evaluation and history,” said Dr. McNulty.
However, she noted that screening shouldn’t necessarily be a one-off effort. Research has shown that sequential screening is the most powerful strategy. “Then you can get a baseline of a patient’s emotional and behavioral functioning, and it’s actually the changes in some of these screening measures that might give them most clinical information,” said Dr. McNulty.
In fact, on October 11, 2022, the U.S. Preventive Services Task Force announced a recommendation that all children starting at age 8 should be screened for anxiety disorders. It is already recommended to screen children aged 12 and over for depressive disorders, although these documents are aimed primarily at pediatricians or primary care clinics. The American Academy of Neurology has also recommended routine screening of psychiatric and behavioral disorders among children with epilepsy.
A unique perspective
Once a disorder is identified, neurologists can bring a unique perspective to treatment. The neurologist can use his or her knowledge of the disease state to assess whether symptoms are due to poor adjustment to the neurological condition, a primary psychiatric disorder, or the biological underpinnings of the illness or prescribed medications. “I think their neurologist can sort of help tease that apart, [using] their knowledge of neurologic disorders and pathways and medications in a way that psychologists might not be able to do on their own,” said Dr. McNulty.
She also emphasized that there are effective treatments for psychiatric disorders, including cognitive behavioral therapy and various pharmacotherapy options. Other approaches for treating comorbid neurological and psychiatric disorders may include building adaptive coping skills, psychoeducation, and incorporating changes to the family or school environment.
During the Q&A period, one person commented that there should be more psychiatric training for neurology residents. “We do work with the same brain, so I completely agree with that,” said Dr. McNulty.
She was also asked how to identify psychiatric symptoms in nonverbal patients. “One thing that I pay close attention to when I ask parents about (their child) is changes in their physical (attributes). Oftentimes in anxiety in folks who are not severely impaired, if we’re feeling anxious we might be breathing a little faster, or we might get a little sweaty. So looking for physical manifestations is one thing. And then sometimes I’ll tell the parents, if we’re not quite sure, I’ll say ‘I’m not sure, but this is very common given the disorder that you have. Can we check?’ I’m always very clear that I may not be nailing it, but then when we go after it with targeted treatment and we see it getting better, we can say ‘Aha!’ ”
Dr. McNulty has no relevant financial disclosures.
FROM CNS 2022
Milk bad, cheese not? Dairy products tied to different CVD risks
The study, which analyzed a cohort from the Western Norway B-vitamin Intervention Trial (WENBIT), showed that higher dairy and milk consumption were associated with increased risk of mortality and stroke and butter was associated with an increased risk of acute myocardial infarction (AMI), but that cheese was associated with a decreased risk of AMI.
The findings are published in the European Journal of Preventive Cardiology.
“Dairy is a diverse food group, and different dairy products should be considered individually and not only in combination,” senior author Vegard Lysne, MSc, of the Centre for Nutrition, University of Bergen and the department of heart disease, Haukeland University Hospital, Bergen, Norway, said in an interview.
“Today’s dietary recommendations regarding dairy products are mainly based on the nutrient contents, with a focus on calcium, iodine, and saturated fat,” Dr. Lysne said.
Previous studies have indicated that different dairy products may influence cardiovascular health differently, even in opposite directions, but this has primarily been investigated in healthy populations, he noted.
“Data on CVD patients are scarce, and therefore, we wanted to investigate this in a population of patients with established CVD. Our primary aim in this study was to explore how the intake of different dairy products might be linked to cardiovascular outcomes and mortality in such a population,” he said.
The researchers analyzed 1,929 patients who had stable angina pectoris and were participants in WENBIT, a randomized, double-blind, placebo-controlled prospective secondary prevention study investigating the effect of vitamin B treatment on mortality and cardiovascular outcomes.
The majority, 80%, of the cohort were men, and the mean age of the patients was 61.8 years. In addition to stable angina pectoris, 47% of the cohort had hypertension, 31% had diabetes, and 29% were smokers. Most (90%) of the patients were taking acetylsalicylic acid, 90% were taking statins, and 77% were on beta-blockers.
Dietary data were obtained by a food frequency questionnaire that was given to patients at their first visit and returned either by mail or at a follow-up visit 1 month after the initial visit.
Frequency of consumption was given as times per day, week, month, or never consumed. Quantity was estimated using units such as slices, pieces, etc., or household measures.
The milk variable included high-fat, low-fat, skimmed, or unspecified milk. Cheese included brown cheese, which is a Norwegian caramel-like cheese made from whey, milk, and cream; white cheese; cream cheeses; cooked or processed cheeses; and boxed cheeses.
Total dairy was calculated as the sum, in grams, of milk, cheese, yogurt, cream, sour cream, ice cream, and butter.
Median follow-up times were 5.2 years for stroke, 7.8 years for AMI, and 14.1 years for mortality.
Patients who reported a higher intake of total dairy and milk had a higher risk of stroke and mortality.
Among those who reported a higher intake of total dairy, the hazard ratio for stroke was 1.4 (95% confidence interval [CI], 1.02-1.27).
Among those who reported a higher intake of milk, the HR for stroke was 1.13 (95% CI, 1.02-1.27).
Cardiovascular mortality appeared heightened in those who reported a higher intake of total dairy (HR, 1.06; 95% CI, 1.00-1.12) and in those who reported a higher intake of milk (HR, 1.07; 95% CI, 1.01-1.13).
Similarly, all-cause mortality was greater in those who reported higher total dairy consumption (HR, 1.07; 95% CI, 1.03-1.11) and in those who reported higher milk consumption (HR, 1.06; 95% CI, 1.03-1.10).
Higher cheese intake was inversely associated with AMI risk (HR, 0.92; 95% CI, 0.83-1.02).
Butter was associated with increased AMI risk (HR, 1.10; 95% CI, 0.97-1.24), as well as all-cause mortality (HR, 1.10; 95% CI, 1.00-1.20).
Dr. Lysne stressed that the results are from an observational study, and that doctors should not change what they tell their patients based on the results alone.
“There is a growing literature indicating that cheese might be linked to reduced cardiovascular risk, but if this is a causal effect, or if cheese is a marker of higher socioeconomic status and a healthier overall lifestyle remains unknown,” he said.
“I would like for future studies to evaluate dairy products on an individual basis, rather than a collective one. If the data suggest that different dairy products have distinct health effects, this should be implemented in dietary recommendations,” Dr. Lysne added.
Dairy a heterogeneous food group
“These results are not really surprising, because we have been hearing advice to consume low-fat milk, avoid whole milk, and so on, for a long time, so this study confirms what we already know,” Qi Sun, MD, ScD, associate professor in the departments of nutrition and epidemiology, Harvard T.H. Chan School of Public Health, Boston, told this news organization.
“However, I would be more specific about milk, and I don’t see any data regarding the fat content of the different types of milk. Their data only show the association for total milk. I would like to see data for low-fat milk versus high-fat milk in relation to heart disease,” Dr. Sun said.
“They also say in their conclusion that cheese was associated with a decreased risk of acute myocardial infarction, but as the hazard ratio shows, this is a nonsignificant association,” he said.
Dr. Sun agrees that dairy is a heterogeneous group of foods and that it is best to consider each type separately with regard to cardiovascular health.
“For example, heavy cream contains tons of saturated fat, butter contains a lot of saturated fat. Then there is yogurt, which also comes in regular, reduced-fat and low-fat varieties, which is a fantastic food. I would say it’s very healthy and is associated with a lower risk of heart disease and diabetes, so a good type of dairy. Yogurt and fermented dairy products should be beneficial, at least more so than full-fat milk or butter. I think butter and full-fat milk are still the primary dairy foods for people to avoid to reduce risk for cardiovascular disease,” he said.
Dr. Lysne and Dr. Sun have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The study, which analyzed a cohort from the Western Norway B-vitamin Intervention Trial (WENBIT), showed that higher dairy and milk consumption were associated with increased risk of mortality and stroke and butter was associated with an increased risk of acute myocardial infarction (AMI), but that cheese was associated with a decreased risk of AMI.
The findings are published in the European Journal of Preventive Cardiology.
“Dairy is a diverse food group, and different dairy products should be considered individually and not only in combination,” senior author Vegard Lysne, MSc, of the Centre for Nutrition, University of Bergen and the department of heart disease, Haukeland University Hospital, Bergen, Norway, said in an interview.
“Today’s dietary recommendations regarding dairy products are mainly based on the nutrient contents, with a focus on calcium, iodine, and saturated fat,” Dr. Lysne said.
Previous studies have indicated that different dairy products may influence cardiovascular health differently, even in opposite directions, but this has primarily been investigated in healthy populations, he noted.
“Data on CVD patients are scarce, and therefore, we wanted to investigate this in a population of patients with established CVD. Our primary aim in this study was to explore how the intake of different dairy products might be linked to cardiovascular outcomes and mortality in such a population,” he said.
The researchers analyzed 1,929 patients who had stable angina pectoris and were participants in WENBIT, a randomized, double-blind, placebo-controlled prospective secondary prevention study investigating the effect of vitamin B treatment on mortality and cardiovascular outcomes.
The majority, 80%, of the cohort were men, and the mean age of the patients was 61.8 years. In addition to stable angina pectoris, 47% of the cohort had hypertension, 31% had diabetes, and 29% were smokers. Most (90%) of the patients were taking acetylsalicylic acid, 90% were taking statins, and 77% were on beta-blockers.
Dietary data were obtained by a food frequency questionnaire that was given to patients at their first visit and returned either by mail or at a follow-up visit 1 month after the initial visit.
Frequency of consumption was given as times per day, week, month, or never consumed. Quantity was estimated using units such as slices, pieces, etc., or household measures.
The milk variable included high-fat, low-fat, skimmed, or unspecified milk. Cheese included brown cheese, which is a Norwegian caramel-like cheese made from whey, milk, and cream; white cheese; cream cheeses; cooked or processed cheeses; and boxed cheeses.
Total dairy was calculated as the sum, in grams, of milk, cheese, yogurt, cream, sour cream, ice cream, and butter.
Median follow-up times were 5.2 years for stroke, 7.8 years for AMI, and 14.1 years for mortality.
Patients who reported a higher intake of total dairy and milk had a higher risk of stroke and mortality.
Among those who reported a higher intake of total dairy, the hazard ratio for stroke was 1.4 (95% confidence interval [CI], 1.02-1.27).
Among those who reported a higher intake of milk, the HR for stroke was 1.13 (95% CI, 1.02-1.27).
Cardiovascular mortality appeared heightened in those who reported a higher intake of total dairy (HR, 1.06; 95% CI, 1.00-1.12) and in those who reported a higher intake of milk (HR, 1.07; 95% CI, 1.01-1.13).
Similarly, all-cause mortality was greater in those who reported higher total dairy consumption (HR, 1.07; 95% CI, 1.03-1.11) and in those who reported higher milk consumption (HR, 1.06; 95% CI, 1.03-1.10).
Higher cheese intake was inversely associated with AMI risk (HR, 0.92; 95% CI, 0.83-1.02).
Butter was associated with increased AMI risk (HR, 1.10; 95% CI, 0.97-1.24), as well as all-cause mortality (HR, 1.10; 95% CI, 1.00-1.20).
Dr. Lysne stressed that the results are from an observational study, and that doctors should not change what they tell their patients based on the results alone.
“There is a growing literature indicating that cheese might be linked to reduced cardiovascular risk, but if this is a causal effect, or if cheese is a marker of higher socioeconomic status and a healthier overall lifestyle remains unknown,” he said.
“I would like for future studies to evaluate dairy products on an individual basis, rather than a collective one. If the data suggest that different dairy products have distinct health effects, this should be implemented in dietary recommendations,” Dr. Lysne added.
Dairy a heterogeneous food group
“These results are not really surprising, because we have been hearing advice to consume low-fat milk, avoid whole milk, and so on, for a long time, so this study confirms what we already know,” Qi Sun, MD, ScD, associate professor in the departments of nutrition and epidemiology, Harvard T.H. Chan School of Public Health, Boston, told this news organization.
“However, I would be more specific about milk, and I don’t see any data regarding the fat content of the different types of milk. Their data only show the association for total milk. I would like to see data for low-fat milk versus high-fat milk in relation to heart disease,” Dr. Sun said.
“They also say in their conclusion that cheese was associated with a decreased risk of acute myocardial infarction, but as the hazard ratio shows, this is a nonsignificant association,” he said.
Dr. Sun agrees that dairy is a heterogeneous group of foods and that it is best to consider each type separately with regard to cardiovascular health.
“For example, heavy cream contains tons of saturated fat, butter contains a lot of saturated fat. Then there is yogurt, which also comes in regular, reduced-fat and low-fat varieties, which is a fantastic food. I would say it’s very healthy and is associated with a lower risk of heart disease and diabetes, so a good type of dairy. Yogurt and fermented dairy products should be beneficial, at least more so than full-fat milk or butter. I think butter and full-fat milk are still the primary dairy foods for people to avoid to reduce risk for cardiovascular disease,” he said.
Dr. Lysne and Dr. Sun have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The study, which analyzed a cohort from the Western Norway B-vitamin Intervention Trial (WENBIT), showed that higher dairy and milk consumption were associated with increased risk of mortality and stroke and butter was associated with an increased risk of acute myocardial infarction (AMI), but that cheese was associated with a decreased risk of AMI.
The findings are published in the European Journal of Preventive Cardiology.
“Dairy is a diverse food group, and different dairy products should be considered individually and not only in combination,” senior author Vegard Lysne, MSc, of the Centre for Nutrition, University of Bergen and the department of heart disease, Haukeland University Hospital, Bergen, Norway, said in an interview.
“Today’s dietary recommendations regarding dairy products are mainly based on the nutrient contents, with a focus on calcium, iodine, and saturated fat,” Dr. Lysne said.
Previous studies have indicated that different dairy products may influence cardiovascular health differently, even in opposite directions, but this has primarily been investigated in healthy populations, he noted.
“Data on CVD patients are scarce, and therefore, we wanted to investigate this in a population of patients with established CVD. Our primary aim in this study was to explore how the intake of different dairy products might be linked to cardiovascular outcomes and mortality in such a population,” he said.
The researchers analyzed 1,929 patients who had stable angina pectoris and were participants in WENBIT, a randomized, double-blind, placebo-controlled prospective secondary prevention study investigating the effect of vitamin B treatment on mortality and cardiovascular outcomes.
The majority, 80%, of the cohort were men, and the mean age of the patients was 61.8 years. In addition to stable angina pectoris, 47% of the cohort had hypertension, 31% had diabetes, and 29% were smokers. Most (90%) of the patients were taking acetylsalicylic acid, 90% were taking statins, and 77% were on beta-blockers.
Dietary data were obtained by a food frequency questionnaire that was given to patients at their first visit and returned either by mail or at a follow-up visit 1 month after the initial visit.
Frequency of consumption was given as times per day, week, month, or never consumed. Quantity was estimated using units such as slices, pieces, etc., or household measures.
The milk variable included high-fat, low-fat, skimmed, or unspecified milk. Cheese included brown cheese, which is a Norwegian caramel-like cheese made from whey, milk, and cream; white cheese; cream cheeses; cooked or processed cheeses; and boxed cheeses.
Total dairy was calculated as the sum, in grams, of milk, cheese, yogurt, cream, sour cream, ice cream, and butter.
Median follow-up times were 5.2 years for stroke, 7.8 years for AMI, and 14.1 years for mortality.
Patients who reported a higher intake of total dairy and milk had a higher risk of stroke and mortality.
Among those who reported a higher intake of total dairy, the hazard ratio for stroke was 1.4 (95% confidence interval [CI], 1.02-1.27).
Among those who reported a higher intake of milk, the HR for stroke was 1.13 (95% CI, 1.02-1.27).
Cardiovascular mortality appeared heightened in those who reported a higher intake of total dairy (HR, 1.06; 95% CI, 1.00-1.12) and in those who reported a higher intake of milk (HR, 1.07; 95% CI, 1.01-1.13).
Similarly, all-cause mortality was greater in those who reported higher total dairy consumption (HR, 1.07; 95% CI, 1.03-1.11) and in those who reported higher milk consumption (HR, 1.06; 95% CI, 1.03-1.10).
Higher cheese intake was inversely associated with AMI risk (HR, 0.92; 95% CI, 0.83-1.02).
Butter was associated with increased AMI risk (HR, 1.10; 95% CI, 0.97-1.24), as well as all-cause mortality (HR, 1.10; 95% CI, 1.00-1.20).
Dr. Lysne stressed that the results are from an observational study, and that doctors should not change what they tell their patients based on the results alone.
“There is a growing literature indicating that cheese might be linked to reduced cardiovascular risk, but if this is a causal effect, or if cheese is a marker of higher socioeconomic status and a healthier overall lifestyle remains unknown,” he said.
“I would like for future studies to evaluate dairy products on an individual basis, rather than a collective one. If the data suggest that different dairy products have distinct health effects, this should be implemented in dietary recommendations,” Dr. Lysne added.
Dairy a heterogeneous food group
“These results are not really surprising, because we have been hearing advice to consume low-fat milk, avoid whole milk, and so on, for a long time, so this study confirms what we already know,” Qi Sun, MD, ScD, associate professor in the departments of nutrition and epidemiology, Harvard T.H. Chan School of Public Health, Boston, told this news organization.
“However, I would be more specific about milk, and I don’t see any data regarding the fat content of the different types of milk. Their data only show the association for total milk. I would like to see data for low-fat milk versus high-fat milk in relation to heart disease,” Dr. Sun said.
“They also say in their conclusion that cheese was associated with a decreased risk of acute myocardial infarction, but as the hazard ratio shows, this is a nonsignificant association,” he said.
Dr. Sun agrees that dairy is a heterogeneous group of foods and that it is best to consider each type separately with regard to cardiovascular health.
“For example, heavy cream contains tons of saturated fat, butter contains a lot of saturated fat. Then there is yogurt, which also comes in regular, reduced-fat and low-fat varieties, which is a fantastic food. I would say it’s very healthy and is associated with a lower risk of heart disease and diabetes, so a good type of dairy. Yogurt and fermented dairy products should be beneficial, at least more so than full-fat milk or butter. I think butter and full-fat milk are still the primary dairy foods for people to avoid to reduce risk for cardiovascular disease,” he said.
Dr. Lysne and Dr. Sun have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM EUROPEAN JOURNAL OF PREVENTIVE CARDIOLOGY
Stroke management: There’s an app for that
“In clinical practice, guideline-driven patient care is very important in improving diagnosis and outcomes, and apps provide a very practical and easy way to check available guidelines,” senior author Fabio Pilato, MD, a neurologist at Università Campus Bio-Medico, Rome, told this news organization.
The review was published in the Journal of Stroke.
Reviewing the literature
“My colleagues and I wanted to discover whether smartphone apps, besides just facilitating communication between doctors and their patients, could improve patient care,” said Dr. Pilato. “We wanted to see if there were any apps that could guide clinical decisions according to guidelines and whether there were some being used in acute stroke management,” he added.
The investigators reviewed 43 studies of stroke-related mobile phone apps that were designed for the clinical management of stroke between June 1, 2007, when the first iPhone was introduced, and Jan. 31, 2022.
The apps were classified into the following three groups, according to their purpose: primary prevention apps, acute stroke management apps, and postacute stroke apps.
Prevention and management
The investigators found one primary prevention app, the Stroke Riskometer, that was based on an algorithm derived from the Framingham Stroke Risk Score and was designed to educate patients about diet, physical activity, and the warning signs of stroke. However, their review failed to show that the app was beneficial, compared with standard cardiovascular risk reduction.
Apps appeared to aid acute stroke management, according to the researchers. Prehospital apps, such as iLAMA, Smartphone-Assisted Pre-Hospital Medical Information System, FAST-ED, Egyptian Stroke Network, Act Fast, and the Mayo Clinic Acute Stroke Evaluation app were found to speed up stroke recognition, activate emergency medical services for speedier transport to the hospital, and facilitate communication with in-hospital stroke teams. All these prehospital apps reduced door-to-needle time.
The JOIN app also was shown to significantly reduce door-to-needle time, compared with no app support, in several studies. JOIN consists of a chat, a DICOM viewer, and an encrypted two-way video system for video calls between practitioners, as well as a milestones time stamp to record every step from home to hospital transportation to therapy onset.
StopStroke, another app that focuses on instant communication among physicians and allows real-time sharing of clinical data of stroke patients, reduced door-to-image and door-to-needle time, compared with no app.
Act Fast, which uses a National Institutes of Health Stroke Scale (NIHSS) calculator, a thrombolysis checklist, and a toolbox to share images and notes among practitioners involved in the decision-making process, decreased door-to-needle time by 16 minutes, compared with no app.
In a study of medical residents, adherence to guidelines was higher in participants who used the Mayo Clinic Acute Stroke Evaluation app, compared with those who did not. Door-to-needle time also was reduced by 16 minutes in the app-assisted group, compared with controls.
Postacute stroke apps
The Rehabilitation Guardian app, consisting of a health reminder, consultation, health information, and patient diary, gives medical information and provides rehabilitation exercises. Patients can enter their clinical information, and the medical staff can access it and assist with the rehab process remotely.
As for apps for chronic management and secondary prevention, Dr. Pilato and colleagues found that the PRESTRO app, which combines motivational support for a healthy lifestyle and tells patients to take their medications and measure their blood pressure, successfully got patients to be more physically active, compared with those who did not use the app.
Another app for secondary prevention, the Korea University Health Monitoring System for Stroke (KUHMS2), reduced blood pressure and glucose levels in patients who used it, compared with those who did not.
Lose It, a weight loss app, is an electronic food journal that shows the values of the macronutrients of foods that the patient consumes, as well as a daily calorie count. The Engaging Everyday Activities app effectively reminds patients who have had transient ischemic attacks about daily activities that can reduce their risk for a recurrent attack.
Movies4Stroke features educational videos about first aid, rehabilitation, how to improve swallowing, and stroke risk factors.
AFib 2gether allows patients to enter their clinical data and calculates their annual stroke risk scores. The information is provided to a health care provider before the next visit to help the patient make an informed decision about anticoagulation therapy.
“We believe that the widespread use of smartphones and apps may improve patient care in every part of the world and in particular in those parts where updated guideline consultation is not readily available. However, in our study we found that apps to implement guidelines by a clinical decision support system are still lacking. Our hope is that these apps will increase in the future,” said Dr. Pilato.
No panacea
Commenting on this review for this article, Amy Guzik, MD, associate professor of neurology at Wake Forest University School of Medicine, Winston-Salem, N.C., said that all physicians are looking for opportunities to use technology, especially in stroke, to diagnose and treat patients in the best way they can.
“Figuring out ways to increase efficiency and get the word out to our patients is very important to us and is probably why there are so many apps out there,” said Dr. Guzik.
“There are some ways such apps could be particularly useful. One is in remote hospitals that might not have a neurologist. Helping with the diagnosis and determining what is a bad stroke that needs to go to a higher level of medical care, or whether it is something the local hospital could take care of, would be useful,” said Dr. Guzik.
“Also helping EMS figure out which hospital to go to, or once they are on their way, being able to talk to the neurologist or neurosurgeon or the emergency room doctor and make a plan before the patient gets here, so we can expedite care when the patient arrives, is where apps can be particularly useful,” she added.
There are limitations to what apps can do, however. In the case of stroke, patients may often have important barriers that do not allow them to use apps at all, she said.
“Regardless of how they are being taken care of, a lot of our stroke patients will have problems with technology. A stroke can make texting difficult. Patients may have language difficulties, weakness, or cognitive impairment. They are relying on caregivers. All of this makes it difficult for a tech solution to be the automatic solution, unless things are done in a thoughtful way to make sure that it is appropriate for stroke patients.
“Also, there are a lot of elderly patients who may not necessarily be the most tech savvy and do not have as much digital literacy as younger patients. Another limitation to consider is that some people may not even have easy access to technology. So we must make sure that this is all done with an equity focus,” said Dr. Guzik.
The study was funded by the Associazione Nazionale fra le Imprese Assicuratrici (ANIA). Dr. Pilato and Dr. Guzik reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“In clinical practice, guideline-driven patient care is very important in improving diagnosis and outcomes, and apps provide a very practical and easy way to check available guidelines,” senior author Fabio Pilato, MD, a neurologist at Università Campus Bio-Medico, Rome, told this news organization.
The review was published in the Journal of Stroke.
Reviewing the literature
“My colleagues and I wanted to discover whether smartphone apps, besides just facilitating communication between doctors and their patients, could improve patient care,” said Dr. Pilato. “We wanted to see if there were any apps that could guide clinical decisions according to guidelines and whether there were some being used in acute stroke management,” he added.
The investigators reviewed 43 studies of stroke-related mobile phone apps that were designed for the clinical management of stroke between June 1, 2007, when the first iPhone was introduced, and Jan. 31, 2022.
The apps were classified into the following three groups, according to their purpose: primary prevention apps, acute stroke management apps, and postacute stroke apps.
Prevention and management
The investigators found one primary prevention app, the Stroke Riskometer, that was based on an algorithm derived from the Framingham Stroke Risk Score and was designed to educate patients about diet, physical activity, and the warning signs of stroke. However, their review failed to show that the app was beneficial, compared with standard cardiovascular risk reduction.
Apps appeared to aid acute stroke management, according to the researchers. Prehospital apps, such as iLAMA, Smartphone-Assisted Pre-Hospital Medical Information System, FAST-ED, Egyptian Stroke Network, Act Fast, and the Mayo Clinic Acute Stroke Evaluation app were found to speed up stroke recognition, activate emergency medical services for speedier transport to the hospital, and facilitate communication with in-hospital stroke teams. All these prehospital apps reduced door-to-needle time.
The JOIN app also was shown to significantly reduce door-to-needle time, compared with no app support, in several studies. JOIN consists of a chat, a DICOM viewer, and an encrypted two-way video system for video calls between practitioners, as well as a milestones time stamp to record every step from home to hospital transportation to therapy onset.
StopStroke, another app that focuses on instant communication among physicians and allows real-time sharing of clinical data of stroke patients, reduced door-to-image and door-to-needle time, compared with no app.
Act Fast, which uses a National Institutes of Health Stroke Scale (NIHSS) calculator, a thrombolysis checklist, and a toolbox to share images and notes among practitioners involved in the decision-making process, decreased door-to-needle time by 16 minutes, compared with no app.
In a study of medical residents, adherence to guidelines was higher in participants who used the Mayo Clinic Acute Stroke Evaluation app, compared with those who did not. Door-to-needle time also was reduced by 16 minutes in the app-assisted group, compared with controls.
Postacute stroke apps
The Rehabilitation Guardian app, consisting of a health reminder, consultation, health information, and patient diary, gives medical information and provides rehabilitation exercises. Patients can enter their clinical information, and the medical staff can access it and assist with the rehab process remotely.
As for apps for chronic management and secondary prevention, Dr. Pilato and colleagues found that the PRESTRO app, which combines motivational support for a healthy lifestyle and tells patients to take their medications and measure their blood pressure, successfully got patients to be more physically active, compared with those who did not use the app.
Another app for secondary prevention, the Korea University Health Monitoring System for Stroke (KUHMS2), reduced blood pressure and glucose levels in patients who used it, compared with those who did not.
Lose It, a weight loss app, is an electronic food journal that shows the values of the macronutrients of foods that the patient consumes, as well as a daily calorie count. The Engaging Everyday Activities app effectively reminds patients who have had transient ischemic attacks about daily activities that can reduce their risk for a recurrent attack.
Movies4Stroke features educational videos about first aid, rehabilitation, how to improve swallowing, and stroke risk factors.
AFib 2gether allows patients to enter their clinical data and calculates their annual stroke risk scores. The information is provided to a health care provider before the next visit to help the patient make an informed decision about anticoagulation therapy.
“We believe that the widespread use of smartphones and apps may improve patient care in every part of the world and in particular in those parts where updated guideline consultation is not readily available. However, in our study we found that apps to implement guidelines by a clinical decision support system are still lacking. Our hope is that these apps will increase in the future,” said Dr. Pilato.
No panacea
Commenting on this review for this article, Amy Guzik, MD, associate professor of neurology at Wake Forest University School of Medicine, Winston-Salem, N.C., said that all physicians are looking for opportunities to use technology, especially in stroke, to diagnose and treat patients in the best way they can.
“Figuring out ways to increase efficiency and get the word out to our patients is very important to us and is probably why there are so many apps out there,” said Dr. Guzik.
“There are some ways such apps could be particularly useful. One is in remote hospitals that might not have a neurologist. Helping with the diagnosis and determining what is a bad stroke that needs to go to a higher level of medical care, or whether it is something the local hospital could take care of, would be useful,” said Dr. Guzik.
“Also helping EMS figure out which hospital to go to, or once they are on their way, being able to talk to the neurologist or neurosurgeon or the emergency room doctor and make a plan before the patient gets here, so we can expedite care when the patient arrives, is where apps can be particularly useful,” she added.
There are limitations to what apps can do, however. In the case of stroke, patients may often have important barriers that do not allow them to use apps at all, she said.
“Regardless of how they are being taken care of, a lot of our stroke patients will have problems with technology. A stroke can make texting difficult. Patients may have language difficulties, weakness, or cognitive impairment. They are relying on caregivers. All of this makes it difficult for a tech solution to be the automatic solution, unless things are done in a thoughtful way to make sure that it is appropriate for stroke patients.
“Also, there are a lot of elderly patients who may not necessarily be the most tech savvy and do not have as much digital literacy as younger patients. Another limitation to consider is that some people may not even have easy access to technology. So we must make sure that this is all done with an equity focus,” said Dr. Guzik.
The study was funded by the Associazione Nazionale fra le Imprese Assicuratrici (ANIA). Dr. Pilato and Dr. Guzik reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“In clinical practice, guideline-driven patient care is very important in improving diagnosis and outcomes, and apps provide a very practical and easy way to check available guidelines,” senior author Fabio Pilato, MD, a neurologist at Università Campus Bio-Medico, Rome, told this news organization.
The review was published in the Journal of Stroke.
Reviewing the literature
“My colleagues and I wanted to discover whether smartphone apps, besides just facilitating communication between doctors and their patients, could improve patient care,” said Dr. Pilato. “We wanted to see if there were any apps that could guide clinical decisions according to guidelines and whether there were some being used in acute stroke management,” he added.
The investigators reviewed 43 studies of stroke-related mobile phone apps that were designed for the clinical management of stroke between June 1, 2007, when the first iPhone was introduced, and Jan. 31, 2022.
The apps were classified into the following three groups, according to their purpose: primary prevention apps, acute stroke management apps, and postacute stroke apps.
Prevention and management
The investigators found one primary prevention app, the Stroke Riskometer, that was based on an algorithm derived from the Framingham Stroke Risk Score and was designed to educate patients about diet, physical activity, and the warning signs of stroke. However, their review failed to show that the app was beneficial, compared with standard cardiovascular risk reduction.
Apps appeared to aid acute stroke management, according to the researchers. Prehospital apps, such as iLAMA, Smartphone-Assisted Pre-Hospital Medical Information System, FAST-ED, Egyptian Stroke Network, Act Fast, and the Mayo Clinic Acute Stroke Evaluation app were found to speed up stroke recognition, activate emergency medical services for speedier transport to the hospital, and facilitate communication with in-hospital stroke teams. All these prehospital apps reduced door-to-needle time.
The JOIN app also was shown to significantly reduce door-to-needle time, compared with no app support, in several studies. JOIN consists of a chat, a DICOM viewer, and an encrypted two-way video system for video calls between practitioners, as well as a milestones time stamp to record every step from home to hospital transportation to therapy onset.
StopStroke, another app that focuses on instant communication among physicians and allows real-time sharing of clinical data of stroke patients, reduced door-to-image and door-to-needle time, compared with no app.
Act Fast, which uses a National Institutes of Health Stroke Scale (NIHSS) calculator, a thrombolysis checklist, and a toolbox to share images and notes among practitioners involved in the decision-making process, decreased door-to-needle time by 16 minutes, compared with no app.
In a study of medical residents, adherence to guidelines was higher in participants who used the Mayo Clinic Acute Stroke Evaluation app, compared with those who did not. Door-to-needle time also was reduced by 16 minutes in the app-assisted group, compared with controls.
Postacute stroke apps
The Rehabilitation Guardian app, consisting of a health reminder, consultation, health information, and patient diary, gives medical information and provides rehabilitation exercises. Patients can enter their clinical information, and the medical staff can access it and assist with the rehab process remotely.
As for apps for chronic management and secondary prevention, Dr. Pilato and colleagues found that the PRESTRO app, which combines motivational support for a healthy lifestyle and tells patients to take their medications and measure their blood pressure, successfully got patients to be more physically active, compared with those who did not use the app.
Another app for secondary prevention, the Korea University Health Monitoring System for Stroke (KUHMS2), reduced blood pressure and glucose levels in patients who used it, compared with those who did not.
Lose It, a weight loss app, is an electronic food journal that shows the values of the macronutrients of foods that the patient consumes, as well as a daily calorie count. The Engaging Everyday Activities app effectively reminds patients who have had transient ischemic attacks about daily activities that can reduce their risk for a recurrent attack.
Movies4Stroke features educational videos about first aid, rehabilitation, how to improve swallowing, and stroke risk factors.
AFib 2gether allows patients to enter their clinical data and calculates their annual stroke risk scores. The information is provided to a health care provider before the next visit to help the patient make an informed decision about anticoagulation therapy.
“We believe that the widespread use of smartphones and apps may improve patient care in every part of the world and in particular in those parts where updated guideline consultation is not readily available. However, in our study we found that apps to implement guidelines by a clinical decision support system are still lacking. Our hope is that these apps will increase in the future,” said Dr. Pilato.
No panacea
Commenting on this review for this article, Amy Guzik, MD, associate professor of neurology at Wake Forest University School of Medicine, Winston-Salem, N.C., said that all physicians are looking for opportunities to use technology, especially in stroke, to diagnose and treat patients in the best way they can.
“Figuring out ways to increase efficiency and get the word out to our patients is very important to us and is probably why there are so many apps out there,” said Dr. Guzik.
“There are some ways such apps could be particularly useful. One is in remote hospitals that might not have a neurologist. Helping with the diagnosis and determining what is a bad stroke that needs to go to a higher level of medical care, or whether it is something the local hospital could take care of, would be useful,” said Dr. Guzik.
“Also helping EMS figure out which hospital to go to, or once they are on their way, being able to talk to the neurologist or neurosurgeon or the emergency room doctor and make a plan before the patient gets here, so we can expedite care when the patient arrives, is where apps can be particularly useful,” she added.
There are limitations to what apps can do, however. In the case of stroke, patients may often have important barriers that do not allow them to use apps at all, she said.
“Regardless of how they are being taken care of, a lot of our stroke patients will have problems with technology. A stroke can make texting difficult. Patients may have language difficulties, weakness, or cognitive impairment. They are relying on caregivers. All of this makes it difficult for a tech solution to be the automatic solution, unless things are done in a thoughtful way to make sure that it is appropriate for stroke patients.
“Also, there are a lot of elderly patients who may not necessarily be the most tech savvy and do not have as much digital literacy as younger patients. Another limitation to consider is that some people may not even have easy access to technology. So we must make sure that this is all done with an equity focus,” said Dr. Guzik.
The study was funded by the Associazione Nazionale fra le Imprese Assicuratrici (ANIA). Dr. Pilato and Dr. Guzik reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF STROKE
Pancreatic cancer screening appears safe, effective for high-risk patients
Pancreatic cancer screening appears to be safe and effective for certain patients with high-risk indications due to genetic susceptibility, according to a prospective multicenter study presented at the annual meeting of the American College of Gastroenterology.
Screening in high-risk patients detected high-risk lesions in 0.8% of patients, which was lower than the typical range found in the literature, at 3%, said Andy Silva-Santisteban, MD, a research fellow at Beth Israel Deaconess Medical Center at Harvard Medical School in Boston.
Pancreatic cancer is the third leading cause of cancer death in the U.S., which is estimated to become the second leading cause by 2030. About 15%-20% of patients are candidates for surgical resection at the time of diagnosis, with survival rates below 10%.
“These statistics have led pancreatic cancer screening to be studied with the goal of detecting earlier stages of the disease to improve survival,” Dr. Silva-Santisteban said. “However, pancreatic cancer screening is not recommended for the general population.”
Pancreatic cancer screening is recommended for patients with increased risk due to genetic susceptibility, yet recent studies have found that screening studies face limitations from factors like small sample sizes, single-center focus, retrospective nature, nonconsecutive accrual of patients, varied inclusion criteria, and use of nonstandardized screening protocols.
To overcome these limitations, Dr. Silva-Santisteban and colleagues conducted a prospective multicenter study of pancreatic cancer screening in consecutive high-risk patients at five centers in the United States between 2020 and 2022, also called the Pancreas Scan Study. Dr. Silva-Santisteban presented results from the first round of enrollment, which was awarded the Outstanding Research Award in the Biliary/Pancreas Category for Trainee.
The research team evaluated the yield (low-, moderate-, and high-risk pancreatic pathology), safety, and outcomes of screening. Low-risk pancreas pathology was categorized as fatty pancreas and chronic pancreatitis-like changes. Intermediate-risk was categorized as branch duct–intraductal papillary mucinous neoplasm or neuroendocrine tumor under 2 cm. High-risk was categorized as main duct–intraductal papillary mucinous neoplasm (MD-IPMN), pancreatic intraepithelial neoplasia grade III (PanIN-III)/dysplasia, neuroendocrine tumor over 2 cm, or pancreatic cancer.
Patients were included if they were 18 years or older and had at least one of the following: BRCA1, BRCA2, or PALB2 plus a family history of pancreatic cancer; Lynch syndrome plus a family history of pancreatic cancer; Peutz-Jeghers syndrome; familial atypical multiple mole melanoma (FAMMM); ataxia telangiectasia mutated plus family history of pancreatic cancer; hereditary pancreatitis; or familial pancreatic cancer (FPC) syndrome.
Screening was performed annually with either endoscopic ultrasound (EUS) or magnetic resonance cholangiopancreatography (MRCP). Fasting blood sugar was recorded annually to screen for new-onset diabetes.
Among 252 patients, 208 underwent EUS and 44 underwent MRCP. At the time of enrollment, 38.5% underwent their first screening, and 61.5% had a prior screening. The average age was 60, 69% were women, and 79% were White.
The most common indication was a BRCA1 or BRCA2 pathogenic variant in 93 patients (or 36.5%), followed by FPC syndrome in 80 patients (or 31.7%).
Low-risk pancreas pathology was noted in 23.4% of patients, with 17.5% having chronic pancreatitis-like changes. Intermediate risk was found in 31.7%, with nearly all detected as branch-duct IPMNs without worrisome features, Dr. Silva-Santisteban said.
Two patients (.8%) fell into the high-risk category with pancreatic adenocarcinoma. Both were positive for BRCA2 mutation and family history of pancreatic cancer.
In the first patient, who was compliant with screening, EUS showed a 3-cm adenocarcinoma (T2N1M0 stage IIB). The patient underwent neoadjuvant chemotherapy, followed by total pancreatectomy, and is currently in cancer remission. No complications from surgery were noted.
In the second patient, who was not compliant with screening and was lost to follow-up for 6 years, EUS showed a 2.5-cm adenocarcinoma and four metastatic lesions in the liver (T2N1M1 stage IV). The patient underwent palliative chemotherapy.
EUS was more likely to identify chronic pancreatitis-like changes, but MRCP was more likely to identify BD-IPMN. The two patients with pancreatic adenocarcinoma were identified with EUS. However, there wasn’t a significant difference between EUS and MRCP in identifying high-risk lesions.
In patients undergoing screening, new-onset prediabetes was noted in 18.2%, and new-onset diabetes was noted in 1.7%. However, there was no association between abnormal blood sugar and pancreas pathology.
Twelve patients (4.8%) underwent further pancreatic evaluation because of screening findings. None of the patients underwent low-yield pancreatic surgery, which was lower than reported in the literature, at 2.8%. Overall, there were no complications as a direct result of screening with EUS or MRI.
“Patients should be carefully counseled regarding benefits and harms from pancreatic cancer screening,” Dr. Silva-Santisteban said. “When feasible, such screening should be performed within the confines of a research study so more precise estimates of screening outcomes can be determined.”
The study funding was not disclosed. One author reported a consultant relationship with Pentax Medical, and the other authors indicated no relevant financial relationships.
Pancreatic cancer screening appears to be safe and effective for certain patients with high-risk indications due to genetic susceptibility, according to a prospective multicenter study presented at the annual meeting of the American College of Gastroenterology.
Screening in high-risk patients detected high-risk lesions in 0.8% of patients, which was lower than the typical range found in the literature, at 3%, said Andy Silva-Santisteban, MD, a research fellow at Beth Israel Deaconess Medical Center at Harvard Medical School in Boston.
Pancreatic cancer is the third leading cause of cancer death in the U.S., which is estimated to become the second leading cause by 2030. About 15%-20% of patients are candidates for surgical resection at the time of diagnosis, with survival rates below 10%.
“These statistics have led pancreatic cancer screening to be studied with the goal of detecting earlier stages of the disease to improve survival,” Dr. Silva-Santisteban said. “However, pancreatic cancer screening is not recommended for the general population.”
Pancreatic cancer screening is recommended for patients with increased risk due to genetic susceptibility, yet recent studies have found that screening studies face limitations from factors like small sample sizes, single-center focus, retrospective nature, nonconsecutive accrual of patients, varied inclusion criteria, and use of nonstandardized screening protocols.
To overcome these limitations, Dr. Silva-Santisteban and colleagues conducted a prospective multicenter study of pancreatic cancer screening in consecutive high-risk patients at five centers in the United States between 2020 and 2022, also called the Pancreas Scan Study. Dr. Silva-Santisteban presented results from the first round of enrollment, which was awarded the Outstanding Research Award in the Biliary/Pancreas Category for Trainee.
The research team evaluated the yield (low-, moderate-, and high-risk pancreatic pathology), safety, and outcomes of screening. Low-risk pancreas pathology was categorized as fatty pancreas and chronic pancreatitis-like changes. Intermediate-risk was categorized as branch duct–intraductal papillary mucinous neoplasm or neuroendocrine tumor under 2 cm. High-risk was categorized as main duct–intraductal papillary mucinous neoplasm (MD-IPMN), pancreatic intraepithelial neoplasia grade III (PanIN-III)/dysplasia, neuroendocrine tumor over 2 cm, or pancreatic cancer.
Patients were included if they were 18 years or older and had at least one of the following: BRCA1, BRCA2, or PALB2 plus a family history of pancreatic cancer; Lynch syndrome plus a family history of pancreatic cancer; Peutz-Jeghers syndrome; familial atypical multiple mole melanoma (FAMMM); ataxia telangiectasia mutated plus family history of pancreatic cancer; hereditary pancreatitis; or familial pancreatic cancer (FPC) syndrome.
Screening was performed annually with either endoscopic ultrasound (EUS) or magnetic resonance cholangiopancreatography (MRCP). Fasting blood sugar was recorded annually to screen for new-onset diabetes.
Among 252 patients, 208 underwent EUS and 44 underwent MRCP. At the time of enrollment, 38.5% underwent their first screening, and 61.5% had a prior screening. The average age was 60, 69% were women, and 79% were White.
The most common indication was a BRCA1 or BRCA2 pathogenic variant in 93 patients (or 36.5%), followed by FPC syndrome in 80 patients (or 31.7%).
Low-risk pancreas pathology was noted in 23.4% of patients, with 17.5% having chronic pancreatitis-like changes. Intermediate risk was found in 31.7%, with nearly all detected as branch-duct IPMNs without worrisome features, Dr. Silva-Santisteban said.
Two patients (.8%) fell into the high-risk category with pancreatic adenocarcinoma. Both were positive for BRCA2 mutation and family history of pancreatic cancer.
In the first patient, who was compliant with screening, EUS showed a 3-cm adenocarcinoma (T2N1M0 stage IIB). The patient underwent neoadjuvant chemotherapy, followed by total pancreatectomy, and is currently in cancer remission. No complications from surgery were noted.
In the second patient, who was not compliant with screening and was lost to follow-up for 6 years, EUS showed a 2.5-cm adenocarcinoma and four metastatic lesions in the liver (T2N1M1 stage IV). The patient underwent palliative chemotherapy.
EUS was more likely to identify chronic pancreatitis-like changes, but MRCP was more likely to identify BD-IPMN. The two patients with pancreatic adenocarcinoma were identified with EUS. However, there wasn’t a significant difference between EUS and MRCP in identifying high-risk lesions.
In patients undergoing screening, new-onset prediabetes was noted in 18.2%, and new-onset diabetes was noted in 1.7%. However, there was no association between abnormal blood sugar and pancreas pathology.
Twelve patients (4.8%) underwent further pancreatic evaluation because of screening findings. None of the patients underwent low-yield pancreatic surgery, which was lower than reported in the literature, at 2.8%. Overall, there were no complications as a direct result of screening with EUS or MRI.
“Patients should be carefully counseled regarding benefits and harms from pancreatic cancer screening,” Dr. Silva-Santisteban said. “When feasible, such screening should be performed within the confines of a research study so more precise estimates of screening outcomes can be determined.”
The study funding was not disclosed. One author reported a consultant relationship with Pentax Medical, and the other authors indicated no relevant financial relationships.
Pancreatic cancer screening appears to be safe and effective for certain patients with high-risk indications due to genetic susceptibility, according to a prospective multicenter study presented at the annual meeting of the American College of Gastroenterology.
Screening in high-risk patients detected high-risk lesions in 0.8% of patients, which was lower than the typical range found in the literature, at 3%, said Andy Silva-Santisteban, MD, a research fellow at Beth Israel Deaconess Medical Center at Harvard Medical School in Boston.
Pancreatic cancer is the third leading cause of cancer death in the U.S., which is estimated to become the second leading cause by 2030. About 15%-20% of patients are candidates for surgical resection at the time of diagnosis, with survival rates below 10%.
“These statistics have led pancreatic cancer screening to be studied with the goal of detecting earlier stages of the disease to improve survival,” Dr. Silva-Santisteban said. “However, pancreatic cancer screening is not recommended for the general population.”
Pancreatic cancer screening is recommended for patients with increased risk due to genetic susceptibility, yet recent studies have found that screening studies face limitations from factors like small sample sizes, single-center focus, retrospective nature, nonconsecutive accrual of patients, varied inclusion criteria, and use of nonstandardized screening protocols.
To overcome these limitations, Dr. Silva-Santisteban and colleagues conducted a prospective multicenter study of pancreatic cancer screening in consecutive high-risk patients at five centers in the United States between 2020 and 2022, also called the Pancreas Scan Study. Dr. Silva-Santisteban presented results from the first round of enrollment, which was awarded the Outstanding Research Award in the Biliary/Pancreas Category for Trainee.
The research team evaluated the yield (low-, moderate-, and high-risk pancreatic pathology), safety, and outcomes of screening. Low-risk pancreas pathology was categorized as fatty pancreas and chronic pancreatitis-like changes. Intermediate-risk was categorized as branch duct–intraductal papillary mucinous neoplasm or neuroendocrine tumor under 2 cm. High-risk was categorized as main duct–intraductal papillary mucinous neoplasm (MD-IPMN), pancreatic intraepithelial neoplasia grade III (PanIN-III)/dysplasia, neuroendocrine tumor over 2 cm, or pancreatic cancer.
Patients were included if they were 18 years or older and had at least one of the following: BRCA1, BRCA2, or PALB2 plus a family history of pancreatic cancer; Lynch syndrome plus a family history of pancreatic cancer; Peutz-Jeghers syndrome; familial atypical multiple mole melanoma (FAMMM); ataxia telangiectasia mutated plus family history of pancreatic cancer; hereditary pancreatitis; or familial pancreatic cancer (FPC) syndrome.
Screening was performed annually with either endoscopic ultrasound (EUS) or magnetic resonance cholangiopancreatography (MRCP). Fasting blood sugar was recorded annually to screen for new-onset diabetes.
Among 252 patients, 208 underwent EUS and 44 underwent MRCP. At the time of enrollment, 38.5% underwent their first screening, and 61.5% had a prior screening. The average age was 60, 69% were women, and 79% were White.
The most common indication was a BRCA1 or BRCA2 pathogenic variant in 93 patients (or 36.5%), followed by FPC syndrome in 80 patients (or 31.7%).
Low-risk pancreas pathology was noted in 23.4% of patients, with 17.5% having chronic pancreatitis-like changes. Intermediate risk was found in 31.7%, with nearly all detected as branch-duct IPMNs without worrisome features, Dr. Silva-Santisteban said.
Two patients (.8%) fell into the high-risk category with pancreatic adenocarcinoma. Both were positive for BRCA2 mutation and family history of pancreatic cancer.
In the first patient, who was compliant with screening, EUS showed a 3-cm adenocarcinoma (T2N1M0 stage IIB). The patient underwent neoadjuvant chemotherapy, followed by total pancreatectomy, and is currently in cancer remission. No complications from surgery were noted.
In the second patient, who was not compliant with screening and was lost to follow-up for 6 years, EUS showed a 2.5-cm adenocarcinoma and four metastatic lesions in the liver (T2N1M1 stage IV). The patient underwent palliative chemotherapy.
EUS was more likely to identify chronic pancreatitis-like changes, but MRCP was more likely to identify BD-IPMN. The two patients with pancreatic adenocarcinoma were identified with EUS. However, there wasn’t a significant difference between EUS and MRCP in identifying high-risk lesions.
In patients undergoing screening, new-onset prediabetes was noted in 18.2%, and new-onset diabetes was noted in 1.7%. However, there was no association between abnormal blood sugar and pancreas pathology.
Twelve patients (4.8%) underwent further pancreatic evaluation because of screening findings. None of the patients underwent low-yield pancreatic surgery, which was lower than reported in the literature, at 2.8%. Overall, there were no complications as a direct result of screening with EUS or MRI.
“Patients should be carefully counseled regarding benefits and harms from pancreatic cancer screening,” Dr. Silva-Santisteban said. “When feasible, such screening should be performed within the confines of a research study so more precise estimates of screening outcomes can be determined.”
The study funding was not disclosed. One author reported a consultant relationship with Pentax Medical, and the other authors indicated no relevant financial relationships.
FROM ACG 2022
Stopping levothyroxine in subclinical hypothyroidism safe, feasible
MONTREAL – Patients who discontinue levothyroxine for subclinical hypothyroidism may gravitate towards becoming mildly hypothyroid again, but they importantly show no differences in terms of symptoms and quality of life – and sometimes show even improvement – compared with those who continue treatment, new research shows.
“Our results show feasibility of patient enrollment and safety of discontinuing levothyroxine in patients with subclinical hypothyroidism,” said first author Spyridoula Maraka, MD, when presenting the findings at the American Thyroid Association annual meeting.

With evidence showing widespread overtreatment with levothyroxine for a variety of reasons, “a discontinuation study like this is important to understand the true need for life-long thyroxine therapy,” commented James V. Hennessey, MD, director of clinical endocrinology at Beth Israel Deaconess Medical Center, Boston.
Recommendations against levothyroxine for subclinical hypothyroidism
Subclinical hypothyroidism is commonly over-diagnosed, and treatment with thyroid hormone replacement, levothyroxine, has been shown to provide little, if any, benefit in terms of quality of life or relief of thyroid-related symptoms for these patients.
The treatment is meanwhile associated with burdens including cost and lifestyle adjustments, and one guideline panel recently issued a strong recommendation against routine levothyroxine use in most adults with subclinical hypothyroidism.
Nevertheless, levothyroxine treatment has soared in popularity and become one of the most commonly prescribed drugs in the United States.
With research lacking on one key solution of discontinuation of the therapy, Dr. Maraka, who is part of the Division of Endocrinology and Metabolism at the University of Arkansas for Medical Sciences, Little Rock, and colleagues conducted a double-blind, placebo-controlled trial at the Central Arkansas Veterans Healthcare System. In total, 50 patients treated for subclinical hypothyroidism were randomized 1:1 to continue receiving levothyroxine (25-75 mcg daily) or to discontinue treatment and receive a placebo instead, with a planned 6-month follow-up.
In the current interim analysis, Dr. Maraka reported results for the first 40 patients, including 20 randomized to levothyroxine and 20 to discontinuation.
There were no significant differences between the discontinuation and levothyroxine groups at baseline, which were of a similar age (66.2 vs. 70.8 years) and gender (75% women vs. 85% men).
The groups had similar baseline thyroid-stimulating hormone (TSH) levels (3.0 vs. 2.6 mIU/L), free T4 (both 0.9 ng/dL), thyroid peroxidase antibody positivity (17% vs. 11%), and similar clinical symptoms. All patients had at least one elevated TSH reading prior to starting levothyroxine.
With a follow-up of 6-8 weeks, 36.8% of patients in the discontinuation group had subclinical hypothyroidism, compared with 10% of patients who remained on levothyroxine (P = .0648), TSH levels were 5.5 versus 2.7 mIU/L (P = .001) and free T4 levels were 0.8 versus 0.9 ng/dL (P = .011).
No differences in symptoms, quality of life between groups
Importantly, there were no significant differences between the discontinuation versus levothyroxine groups in terms of symptoms, and even some improvements with discontinuation, including Thyroid-Specific Quality of Life Patient-Reported Outcome (ThyPRO)-Hypothyroid Symptoms score (4.6 reduction vs. 2.2 increase), tiredness (2.6 reduction vs. 1.1 increase), and EuroQoL 5-Dimension Self-Report Questionnaire (EQ-5D) quality of life score, for which there were no differences between groups.
There were no reports of overt hypothyroidism; hyperthyroidism; cardiovascular events including atrial fibrillation, stroke, or heart failure; osteoporotic fractures; or deaths.
One patient in the discontinuation group had a TSH level of 11 mIU/L at 6-8 weeks and switched to open-label levothyroxine 75 mcg daily. Another patient in the discontinuation group switched to open-label levothyroxine 75 mcg daily at 10 weeks due to fatigue; however, the patient was diagnosed with metastatic colon cancer 1 month later.
The finding that only about a third of patients who discontinued levothyroxine developed subclinical hypothyroidism was lower than expected, Dr. Maraka noted.
“This was ... unexpected ... for us,” she said. “We were expecting a larger number of patients to develop hypothyroidism, but to our surprise, that was not the case.”
“But what is more important is that there was no difference in the quality of life measures,” she added. “If anything, the placebo group was a little better, though the [differences] were not statistically significant.”
Dr. Maraka also noted that in further research and a final 6-month analysis, the authors will look at factors associated with developing subclinical hypothyroidism after treatment discontinuation, among other issues.
Discontinuation of levothyroxine is manageable
The results are encouraging, as they provide assurance that discontinuation of levothyroxine is manageable.
“This research will pave the way for initiatives to promote levothyroxine deprescription and implementation of evidence-based care for patients with subclinical hypothyroidism,” she said.
In further comments, Dr. Hennessey noted that the dilemma of having patients on levothyroxine who may not be benefitting from treatment is “significant,” with patients sometimes reluctant to discontinue treatment due to concerns of developing hypothyroidism-associated symptoms such as brain fog and weight gain.
He noted, however, that “many with mildly elevated TSH actually go on to normalize with time, so they are not really hypothyroid, [and] if we remove thyroxine from people with normal thyroid function, they will remain normal.”
Dr. Maraka has reported no relevant financial relationships. Dr. Hennessey has reported consulting for pharmaceutical companies to design clinical studies for thyroid medications.
A version of this article first appeared on Medscape.com.
MONTREAL – Patients who discontinue levothyroxine for subclinical hypothyroidism may gravitate towards becoming mildly hypothyroid again, but they importantly show no differences in terms of symptoms and quality of life – and sometimes show even improvement – compared with those who continue treatment, new research shows.
“Our results show feasibility of patient enrollment and safety of discontinuing levothyroxine in patients with subclinical hypothyroidism,” said first author Spyridoula Maraka, MD, when presenting the findings at the American Thyroid Association annual meeting.
With evidence showing widespread overtreatment with levothyroxine for a variety of reasons, “a discontinuation study like this is important to understand the true need for life-long thyroxine therapy,” commented James V. Hennessey, MD, director of clinical endocrinology at Beth Israel Deaconess Medical Center, Boston.
Recommendations against levothyroxine for subclinical hypothyroidism
Subclinical hypothyroidism is commonly over-diagnosed, and treatment with thyroid hormone replacement, levothyroxine, has been shown to provide little, if any, benefit in terms of quality of life or relief of thyroid-related symptoms for these patients.
The treatment is meanwhile associated with burdens including cost and lifestyle adjustments, and one guideline panel recently issued a strong recommendation against routine levothyroxine use in most adults with subclinical hypothyroidism.
Nevertheless, levothyroxine treatment has soared in popularity and become one of the most commonly prescribed drugs in the United States.
With research lacking on one key solution of discontinuation of the therapy, Dr. Maraka, who is part of the Division of Endocrinology and Metabolism at the University of Arkansas for Medical Sciences, Little Rock, and colleagues conducted a double-blind, placebo-controlled trial at the Central Arkansas Veterans Healthcare System. In total, 50 patients treated for subclinical hypothyroidism were randomized 1:1 to continue receiving levothyroxine (25-75 mcg daily) or to discontinue treatment and receive a placebo instead, with a planned 6-month follow-up.
In the current interim analysis, Dr. Maraka reported results for the first 40 patients, including 20 randomized to levothyroxine and 20 to discontinuation.
There were no significant differences between the discontinuation and levothyroxine groups at baseline, which were of a similar age (66.2 vs. 70.8 years) and gender (75% women vs. 85% men).
The groups had similar baseline thyroid-stimulating hormone (TSH) levels (3.0 vs. 2.6 mIU/L), free T4 (both 0.9 ng/dL), thyroid peroxidase antibody positivity (17% vs. 11%), and similar clinical symptoms. All patients had at least one elevated TSH reading prior to starting levothyroxine.
With a follow-up of 6-8 weeks, 36.8% of patients in the discontinuation group had subclinical hypothyroidism, compared with 10% of patients who remained on levothyroxine (P = .0648), TSH levels were 5.5 versus 2.7 mIU/L (P = .001) and free T4 levels were 0.8 versus 0.9 ng/dL (P = .011).
No differences in symptoms, quality of life between groups
Importantly, there were no significant differences between the discontinuation versus levothyroxine groups in terms of symptoms, and even some improvements with discontinuation, including Thyroid-Specific Quality of Life Patient-Reported Outcome (ThyPRO)-Hypothyroid Symptoms score (4.6 reduction vs. 2.2 increase), tiredness (2.6 reduction vs. 1.1 increase), and EuroQoL 5-Dimension Self-Report Questionnaire (EQ-5D) quality of life score, for which there were no differences between groups.
There were no reports of overt hypothyroidism; hyperthyroidism; cardiovascular events including atrial fibrillation, stroke, or heart failure; osteoporotic fractures; or deaths.
One patient in the discontinuation group had a TSH level of 11 mIU/L at 6-8 weeks and switched to open-label levothyroxine 75 mcg daily. Another patient in the discontinuation group switched to open-label levothyroxine 75 mcg daily at 10 weeks due to fatigue; however, the patient was diagnosed with metastatic colon cancer 1 month later.
The finding that only about a third of patients who discontinued levothyroxine developed subclinical hypothyroidism was lower than expected, Dr. Maraka noted.
“This was ... unexpected ... for us,” she said. “We were expecting a larger number of patients to develop hypothyroidism, but to our surprise, that was not the case.”
“But what is more important is that there was no difference in the quality of life measures,” she added. “If anything, the placebo group was a little better, though the [differences] were not statistically significant.”
Dr. Maraka also noted that in further research and a final 6-month analysis, the authors will look at factors associated with developing subclinical hypothyroidism after treatment discontinuation, among other issues.
Discontinuation of levothyroxine is manageable
The results are encouraging, as they provide assurance that discontinuation of levothyroxine is manageable.
“This research will pave the way for initiatives to promote levothyroxine deprescription and implementation of evidence-based care for patients with subclinical hypothyroidism,” she said.
In further comments, Dr. Hennessey noted that the dilemma of having patients on levothyroxine who may not be benefitting from treatment is “significant,” with patients sometimes reluctant to discontinue treatment due to concerns of developing hypothyroidism-associated symptoms such as brain fog and weight gain.
He noted, however, that “many with mildly elevated TSH actually go on to normalize with time, so they are not really hypothyroid, [and] if we remove thyroxine from people with normal thyroid function, they will remain normal.”
Dr. Maraka has reported no relevant financial relationships. Dr. Hennessey has reported consulting for pharmaceutical companies to design clinical studies for thyroid medications.
A version of this article first appeared on Medscape.com.
MONTREAL – Patients who discontinue levothyroxine for subclinical hypothyroidism may gravitate towards becoming mildly hypothyroid again, but they importantly show no differences in terms of symptoms and quality of life – and sometimes show even improvement – compared with those who continue treatment, new research shows.
“Our results show feasibility of patient enrollment and safety of discontinuing levothyroxine in patients with subclinical hypothyroidism,” said first author Spyridoula Maraka, MD, when presenting the findings at the American Thyroid Association annual meeting.
With evidence showing widespread overtreatment with levothyroxine for a variety of reasons, “a discontinuation study like this is important to understand the true need for life-long thyroxine therapy,” commented James V. Hennessey, MD, director of clinical endocrinology at Beth Israel Deaconess Medical Center, Boston.
Recommendations against levothyroxine for subclinical hypothyroidism
Subclinical hypothyroidism is commonly over-diagnosed, and treatment with thyroid hormone replacement, levothyroxine, has been shown to provide little, if any, benefit in terms of quality of life or relief of thyroid-related symptoms for these patients.
The treatment is meanwhile associated with burdens including cost and lifestyle adjustments, and one guideline panel recently issued a strong recommendation against routine levothyroxine use in most adults with subclinical hypothyroidism.
Nevertheless, levothyroxine treatment has soared in popularity and become one of the most commonly prescribed drugs in the United States.
With research lacking on one key solution of discontinuation of the therapy, Dr. Maraka, who is part of the Division of Endocrinology and Metabolism at the University of Arkansas for Medical Sciences, Little Rock, and colleagues conducted a double-blind, placebo-controlled trial at the Central Arkansas Veterans Healthcare System. In total, 50 patients treated for subclinical hypothyroidism were randomized 1:1 to continue receiving levothyroxine (25-75 mcg daily) or to discontinue treatment and receive a placebo instead, with a planned 6-month follow-up.
In the current interim analysis, Dr. Maraka reported results for the first 40 patients, including 20 randomized to levothyroxine and 20 to discontinuation.
There were no significant differences between the discontinuation and levothyroxine groups at baseline, which were of a similar age (66.2 vs. 70.8 years) and gender (75% women vs. 85% men).
The groups had similar baseline thyroid-stimulating hormone (TSH) levels (3.0 vs. 2.6 mIU/L), free T4 (both 0.9 ng/dL), thyroid peroxidase antibody positivity (17% vs. 11%), and similar clinical symptoms. All patients had at least one elevated TSH reading prior to starting levothyroxine.
With a follow-up of 6-8 weeks, 36.8% of patients in the discontinuation group had subclinical hypothyroidism, compared with 10% of patients who remained on levothyroxine (P = .0648), TSH levels were 5.5 versus 2.7 mIU/L (P = .001) and free T4 levels were 0.8 versus 0.9 ng/dL (P = .011).
No differences in symptoms, quality of life between groups
Importantly, there were no significant differences between the discontinuation versus levothyroxine groups in terms of symptoms, and even some improvements with discontinuation, including Thyroid-Specific Quality of Life Patient-Reported Outcome (ThyPRO)-Hypothyroid Symptoms score (4.6 reduction vs. 2.2 increase), tiredness (2.6 reduction vs. 1.1 increase), and EuroQoL 5-Dimension Self-Report Questionnaire (EQ-5D) quality of life score, for which there were no differences between groups.
There were no reports of overt hypothyroidism; hyperthyroidism; cardiovascular events including atrial fibrillation, stroke, or heart failure; osteoporotic fractures; or deaths.
One patient in the discontinuation group had a TSH level of 11 mIU/L at 6-8 weeks and switched to open-label levothyroxine 75 mcg daily. Another patient in the discontinuation group switched to open-label levothyroxine 75 mcg daily at 10 weeks due to fatigue; however, the patient was diagnosed with metastatic colon cancer 1 month later.
The finding that only about a third of patients who discontinued levothyroxine developed subclinical hypothyroidism was lower than expected, Dr. Maraka noted.
“This was ... unexpected ... for us,” she said. “We were expecting a larger number of patients to develop hypothyroidism, but to our surprise, that was not the case.”
“But what is more important is that there was no difference in the quality of life measures,” she added. “If anything, the placebo group was a little better, though the [differences] were not statistically significant.”
Dr. Maraka also noted that in further research and a final 6-month analysis, the authors will look at factors associated with developing subclinical hypothyroidism after treatment discontinuation, among other issues.
Discontinuation of levothyroxine is manageable
The results are encouraging, as they provide assurance that discontinuation of levothyroxine is manageable.
“This research will pave the way for initiatives to promote levothyroxine deprescription and implementation of evidence-based care for patients with subclinical hypothyroidism,” she said.
In further comments, Dr. Hennessey noted that the dilemma of having patients on levothyroxine who may not be benefitting from treatment is “significant,” with patients sometimes reluctant to discontinue treatment due to concerns of developing hypothyroidism-associated symptoms such as brain fog and weight gain.
He noted, however, that “many with mildly elevated TSH actually go on to normalize with time, so they are not really hypothyroid, [and] if we remove thyroxine from people with normal thyroid function, they will remain normal.”
Dr. Maraka has reported no relevant financial relationships. Dr. Hennessey has reported consulting for pharmaceutical companies to design clinical studies for thyroid medications.
A version of this article first appeared on Medscape.com.
AT ATA 2022
Healthy diet, less news helped prevent anxiety, depression during COVID
VIENNA –
Results from a longitudinal Spanish survey study of more than 1,000 adults showed that being outside, relaxing, participating in physical activities, and drinking plenty of water were also beneficial. However, social contact with friends and relatives, following a routine, and pursuing hobbies had no significant impact.
“This was a little surprising,” lead author Joaquim Radua, MD, PhD, August Pi i Sunyer Biomedical Research Institute (IDIBAPS), Barcelona, said in a release.
“Like many people, we had assumed that personal contact would play a bigger part in avoiding anxiety and depression during stressful times,” he added.
However, Dr. Radua said that because the study was conducted during the COVID-19 pandemic, “people who socialized may also have been anxious about getting infected.”
Consequently, “it may be that this specific behavior cannot be extrapolated to other times, when there is no pandemic,” he said.
The findings were presented at the 35th European College of Neuropsychopharmacology (ECNP) Congress.
Correlational versus longitudinal studies
Dr. Radua emphasized that individuals “should socialize,” of course.
“We think it’s important that people continue to follow what works for them and that if you enjoy seeing friends or following a hobby, you continue to do so,” he said.
“Our work was centered on COVID, but we now need to see if these factors apply to other stressful circumstances. These simple behaviors may prevent anxiety and depression, and prevention is better than cure,” he added.
The researchers note that, in “times of uncertainty” such as the COVID-19 pandemic, many individuals experience increases in both anxiety and depressive symptoms.
Although a range of behaviors are recommended to help people cope, the investigators add that some of the recommendations are based on correlational studies.
Indeed, the researchers previously identified a correlation between following a healthy/balanced diet, among other measures, and lower anxiety and depressive symptoms during the pandemic.
However, it is unclear from cross-sectional studies whether the behavior alters the symptoms, in which case the behavior could be considered “helpful,” or conversely whether the symptoms alter an individual’s behavior, in which case the behaviors “may be useless,” the investigators note.
The investigative team therefore set out to provide more robust evidence for making recommendations and conducted a prospective longitudinal study.
They recruited 1,049 adults online via social networks, matching them to the regional, age and sex, and urbanicity distribution of the overall Spanish population.
Every 2 weeks for 12 months, the researchers administered the General Anxiety Disorder (GAD)-7, the Patient Health Questionnaire (PHQ)-9, and a two-item ecological momentary assessment to minimize recall bias, among other measures. They also asked about 10 self-report coping behaviors.
Significant coping behaviors
The study was completed by 942 individuals, indicating a retention of 90%.
Among both completers and non-completers there was an over-representation of individuals aged 18-34 years and women, compared with the general population, and fewer participants aged at least 65 years.
Pre-recruitment, the mean baseline GAD-7 score among completers was 7.4, falling to around 5.5 at the time of the first questionnaire. Scores on the PHQ-9 were 7.6 and 5.6, respectively.
Performing population-weighted autoregressive moving average models to analyze the relationship between the current frequency of the coping behaviors and future changes in anxiety and depressive symptoms, the investigators found that the greatest effect was from following a healthy, balanced diet, with an impact size of 0.95.
This was followed by avoiding too much stressful news (impact size, 0.91), staying outdoors or looking outside (0.40), doing relaxing activities (0.33), participating in physical exercise (0.32), and drinking water to hydrate (0.25).
Overall, these coping behaviors were associated with a significant reduction in anxiety and depressive symptoms (all, P < .001).
On the other hand, there was no impact on future symptoms from socializing with friends and relatives, whether or not they lived in the same household. There was also no effect from following a routine, pursuing hobbies, or performing home tasks.
The researchers note that similar results were obtained when excluding participants with hazardous alcohol consumption, defined as a score on the Alcohol Use Disorders Identification Test of 8 or higher.
However, they point out that despite its prospective design and large cohort, the study was not interventional. Therefore, they “cannot rule out the possibility that decreasing the frequency of a behavior is an early sign of some mechanism that later leads to increased anxiety and depression symptoms.”
Nevertheless, they believe that possibility “seems unlikely.”
Reflective of a unique time?
Commenting on the findings, Catherine Harmer, PhD, director of the Psychopharmacology and Emotional Research Lab, department of psychiatry, University of Oxford (England), said in the release this was an “interesting study” that “provides some important insights as to which behaviors may protect our mental health during times of significant stress.”

She said the finding that social contact was not beneficial was “surprising” but may reflect the fact that, during the pandemic, it was “stressful even to have those social contacts, even if we managed to meet a friend outside.”
The results of the study may therefore be “reflective of the unique experience” of the COVID-19 pandemic, said Dr. Harmer, who was not involved with the research.
“I wouldn’t think that reading too much news would generally be something that has a negative impact on depression and anxiety, but I think it was very much at the time,” she said.
With the pandemic overwhelming one country after another, “the more you read about it, the more frightening it was,” she added, noting that it is “easy to forget how frightened we were at the beginning.”
Dr. Harmer noted that “it would be interesting” if the study was repeated and the same factors came out – or if they were unique to that time.
This would be “useful to know, as these times may come again. And the more information we have to cope with a pandemic, the better,” she concluded.
The research was supported by the AXA Research Fund via an AXA Award granted to Dr. Radua from the call for projects “mitigating risk in the wake of the COVID-19 pandemic.” The investigators and Dr. Harmer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
VIENNA –
Results from a longitudinal Spanish survey study of more than 1,000 adults showed that being outside, relaxing, participating in physical activities, and drinking plenty of water were also beneficial. However, social contact with friends and relatives, following a routine, and pursuing hobbies had no significant impact.
“This was a little surprising,” lead author Joaquim Radua, MD, PhD, August Pi i Sunyer Biomedical Research Institute (IDIBAPS), Barcelona, said in a release.
“Like many people, we had assumed that personal contact would play a bigger part in avoiding anxiety and depression during stressful times,” he added.
However, Dr. Radua said that because the study was conducted during the COVID-19 pandemic, “people who socialized may also have been anxious about getting infected.”
Consequently, “it may be that this specific behavior cannot be extrapolated to other times, when there is no pandemic,” he said.
The findings were presented at the 35th European College of Neuropsychopharmacology (ECNP) Congress.
Correlational versus longitudinal studies
Dr. Radua emphasized that individuals “should socialize,” of course.
“We think it’s important that people continue to follow what works for them and that if you enjoy seeing friends or following a hobby, you continue to do so,” he said.
“Our work was centered on COVID, but we now need to see if these factors apply to other stressful circumstances. These simple behaviors may prevent anxiety and depression, and prevention is better than cure,” he added.
The researchers note that, in “times of uncertainty” such as the COVID-19 pandemic, many individuals experience increases in both anxiety and depressive symptoms.
Although a range of behaviors are recommended to help people cope, the investigators add that some of the recommendations are based on correlational studies.
Indeed, the researchers previously identified a correlation between following a healthy/balanced diet, among other measures, and lower anxiety and depressive symptoms during the pandemic.
However, it is unclear from cross-sectional studies whether the behavior alters the symptoms, in which case the behavior could be considered “helpful,” or conversely whether the symptoms alter an individual’s behavior, in which case the behaviors “may be useless,” the investigators note.
The investigative team therefore set out to provide more robust evidence for making recommendations and conducted a prospective longitudinal study.
They recruited 1,049 adults online via social networks, matching them to the regional, age and sex, and urbanicity distribution of the overall Spanish population.
Every 2 weeks for 12 months, the researchers administered the General Anxiety Disorder (GAD)-7, the Patient Health Questionnaire (PHQ)-9, and a two-item ecological momentary assessment to minimize recall bias, among other measures. They also asked about 10 self-report coping behaviors.
Significant coping behaviors
The study was completed by 942 individuals, indicating a retention of 90%.
Among both completers and non-completers there was an over-representation of individuals aged 18-34 years and women, compared with the general population, and fewer participants aged at least 65 years.
Pre-recruitment, the mean baseline GAD-7 score among completers was 7.4, falling to around 5.5 at the time of the first questionnaire. Scores on the PHQ-9 were 7.6 and 5.6, respectively.
Performing population-weighted autoregressive moving average models to analyze the relationship between the current frequency of the coping behaviors and future changes in anxiety and depressive symptoms, the investigators found that the greatest effect was from following a healthy, balanced diet, with an impact size of 0.95.
This was followed by avoiding too much stressful news (impact size, 0.91), staying outdoors or looking outside (0.40), doing relaxing activities (0.33), participating in physical exercise (0.32), and drinking water to hydrate (0.25).
Overall, these coping behaviors were associated with a significant reduction in anxiety and depressive symptoms (all, P < .001).
On the other hand, there was no impact on future symptoms from socializing with friends and relatives, whether or not they lived in the same household. There was also no effect from following a routine, pursuing hobbies, or performing home tasks.
The researchers note that similar results were obtained when excluding participants with hazardous alcohol consumption, defined as a score on the Alcohol Use Disorders Identification Test of 8 or higher.
However, they point out that despite its prospective design and large cohort, the study was not interventional. Therefore, they “cannot rule out the possibility that decreasing the frequency of a behavior is an early sign of some mechanism that later leads to increased anxiety and depression symptoms.”
Nevertheless, they believe that possibility “seems unlikely.”
Reflective of a unique time?
Commenting on the findings, Catherine Harmer, PhD, director of the Psychopharmacology and Emotional Research Lab, department of psychiatry, University of Oxford (England), said in the release this was an “interesting study” that “provides some important insights as to which behaviors may protect our mental health during times of significant stress.”
She said the finding that social contact was not beneficial was “surprising” but may reflect the fact that, during the pandemic, it was “stressful even to have those social contacts, even if we managed to meet a friend outside.”
The results of the study may therefore be “reflective of the unique experience” of the COVID-19 pandemic, said Dr. Harmer, who was not involved with the research.
“I wouldn’t think that reading too much news would generally be something that has a negative impact on depression and anxiety, but I think it was very much at the time,” she said.
With the pandemic overwhelming one country after another, “the more you read about it, the more frightening it was,” she added, noting that it is “easy to forget how frightened we were at the beginning.”
Dr. Harmer noted that “it would be interesting” if the study was repeated and the same factors came out – or if they were unique to that time.
This would be “useful to know, as these times may come again. And the more information we have to cope with a pandemic, the better,” she concluded.
The research was supported by the AXA Research Fund via an AXA Award granted to Dr. Radua from the call for projects “mitigating risk in the wake of the COVID-19 pandemic.” The investigators and Dr. Harmer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
VIENNA –
Results from a longitudinal Spanish survey study of more than 1,000 adults showed that being outside, relaxing, participating in physical activities, and drinking plenty of water were also beneficial. However, social contact with friends and relatives, following a routine, and pursuing hobbies had no significant impact.
“This was a little surprising,” lead author Joaquim Radua, MD, PhD, August Pi i Sunyer Biomedical Research Institute (IDIBAPS), Barcelona, said in a release.
“Like many people, we had assumed that personal contact would play a bigger part in avoiding anxiety and depression during stressful times,” he added.
However, Dr. Radua said that because the study was conducted during the COVID-19 pandemic, “people who socialized may also have been anxious about getting infected.”
Consequently, “it may be that this specific behavior cannot be extrapolated to other times, when there is no pandemic,” he said.
The findings were presented at the 35th European College of Neuropsychopharmacology (ECNP) Congress.
Correlational versus longitudinal studies
Dr. Radua emphasized that individuals “should socialize,” of course.
“We think it’s important that people continue to follow what works for them and that if you enjoy seeing friends or following a hobby, you continue to do so,” he said.
“Our work was centered on COVID, but we now need to see if these factors apply to other stressful circumstances. These simple behaviors may prevent anxiety and depression, and prevention is better than cure,” he added.
The researchers note that, in “times of uncertainty” such as the COVID-19 pandemic, many individuals experience increases in both anxiety and depressive symptoms.
Although a range of behaviors are recommended to help people cope, the investigators add that some of the recommendations are based on correlational studies.
Indeed, the researchers previously identified a correlation between following a healthy/balanced diet, among other measures, and lower anxiety and depressive symptoms during the pandemic.
However, it is unclear from cross-sectional studies whether the behavior alters the symptoms, in which case the behavior could be considered “helpful,” or conversely whether the symptoms alter an individual’s behavior, in which case the behaviors “may be useless,” the investigators note.
The investigative team therefore set out to provide more robust evidence for making recommendations and conducted a prospective longitudinal study.
They recruited 1,049 adults online via social networks, matching them to the regional, age and sex, and urbanicity distribution of the overall Spanish population.
Every 2 weeks for 12 months, the researchers administered the General Anxiety Disorder (GAD)-7, the Patient Health Questionnaire (PHQ)-9, and a two-item ecological momentary assessment to minimize recall bias, among other measures. They also asked about 10 self-report coping behaviors.
Significant coping behaviors
The study was completed by 942 individuals, indicating a retention of 90%.
Among both completers and non-completers there was an over-representation of individuals aged 18-34 years and women, compared with the general population, and fewer participants aged at least 65 years.
Pre-recruitment, the mean baseline GAD-7 score among completers was 7.4, falling to around 5.5 at the time of the first questionnaire. Scores on the PHQ-9 were 7.6 and 5.6, respectively.
Performing population-weighted autoregressive moving average models to analyze the relationship between the current frequency of the coping behaviors and future changes in anxiety and depressive symptoms, the investigators found that the greatest effect was from following a healthy, balanced diet, with an impact size of 0.95.
This was followed by avoiding too much stressful news (impact size, 0.91), staying outdoors or looking outside (0.40), doing relaxing activities (0.33), participating in physical exercise (0.32), and drinking water to hydrate (0.25).
Overall, these coping behaviors were associated with a significant reduction in anxiety and depressive symptoms (all, P < .001).
On the other hand, there was no impact on future symptoms from socializing with friends and relatives, whether or not they lived in the same household. There was also no effect from following a routine, pursuing hobbies, or performing home tasks.
The researchers note that similar results were obtained when excluding participants with hazardous alcohol consumption, defined as a score on the Alcohol Use Disorders Identification Test of 8 or higher.
However, they point out that despite its prospective design and large cohort, the study was not interventional. Therefore, they “cannot rule out the possibility that decreasing the frequency of a behavior is an early sign of some mechanism that later leads to increased anxiety and depression symptoms.”
Nevertheless, they believe that possibility “seems unlikely.”
Reflective of a unique time?
Commenting on the findings, Catherine Harmer, PhD, director of the Psychopharmacology and Emotional Research Lab, department of psychiatry, University of Oxford (England), said in the release this was an “interesting study” that “provides some important insights as to which behaviors may protect our mental health during times of significant stress.”
She said the finding that social contact was not beneficial was “surprising” but may reflect the fact that, during the pandemic, it was “stressful even to have those social contacts, even if we managed to meet a friend outside.”
The results of the study may therefore be “reflective of the unique experience” of the COVID-19 pandemic, said Dr. Harmer, who was not involved with the research.
“I wouldn’t think that reading too much news would generally be something that has a negative impact on depression and anxiety, but I think it was very much at the time,” she said.
With the pandemic overwhelming one country after another, “the more you read about it, the more frightening it was,” she added, noting that it is “easy to forget how frightened we were at the beginning.”
Dr. Harmer noted that “it would be interesting” if the study was repeated and the same factors came out – or if they were unique to that time.
This would be “useful to know, as these times may come again. And the more information we have to cope with a pandemic, the better,” she concluded.
The research was supported by the AXA Research Fund via an AXA Award granted to Dr. Radua from the call for projects “mitigating risk in the wake of the COVID-19 pandemic.” The investigators and Dr. Harmer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ECNP 2022
Myocarditis after COVID vax rare and mild in teens
New data from Israel provide further evidence that myocarditis is a rare adverse event of vaccination with the Pfizer/BioNTech mRNA COVID-19 vaccine in adolescents – one that predominantly occurs in males and typically after the second dose.
The new data also indicate a “mild and benign” clinical course of myocarditis after vaccination, with “favorable” long-term prognosis based on cardiac imaging findings.
Guy Witberg, MD, MPH, Rabin Medical Center, Petah Tikva, Israel, and colleagues report their latest observations in correspondence in The New England Journal of Medicine, online.
The group previously reported in December 2021 that the incidence of myocarditis in Israel after receipt of the Pfizer/BioNTech BNT162b2 mRNA COVID-19 vaccine was highest among males between the ages of 16 and 29 (10.7 cases per 100,000).
The vaccine has since been approved for adolescents aged 12-15. Initial evidence for this age group, reported by Dr. Witberg and colleagues in March 2022, suggests a similar low incidence and mild course of myocarditis, although follow-up was limited to 30 days.
In their latest report, with follow-up out to 6 months, Dr. Witberg and colleagues identified nine probable or definite cases of myocarditis among 182,605 Israeli adolescents aged 12-15 who received the Pfizer/BioNTech mRNA vaccine – an incidence of 4.8 cases per 100,000.
Eight cases occurred after the second vaccine dose. All nine cases were mild.
Cardiac and inflammatory markers were elevated in all adolescent patients and electrocardiographic results were abnormal in two-thirds.
Eight patients had a normal ejection fraction, and four had a pericardial effusion. The patients spent 2-4 days hospitalized, and the in-hospital course was uneventful.
Echocardiographic findings were available a median of 10 days after discharge for eight patients. All echocardiograms showed a normal ejection fraction and resolution of pericardial effusion.
Five patients underwent cardiac MRI, including three scans performed at a median of 104 days after discharge. The scans showed “minimal evidence” of myocardial scarring or fibrosis, with evidence of late gadolinium enhancement ranging from 0% to 2%.
At a median of 206 days following discharge, all of the patients were alive, and none had been readmitted to the hospital, Dr. Witberg and colleagues report.
This research had no specific funding. Five authors have received research grants from Pfizer.
A version of this article first appeared on Medscape.com.
New data from Israel provide further evidence that myocarditis is a rare adverse event of vaccination with the Pfizer/BioNTech mRNA COVID-19 vaccine in adolescents – one that predominantly occurs in males and typically after the second dose.
The new data also indicate a “mild and benign” clinical course of myocarditis after vaccination, with “favorable” long-term prognosis based on cardiac imaging findings.
Guy Witberg, MD, MPH, Rabin Medical Center, Petah Tikva, Israel, and colleagues report their latest observations in correspondence in The New England Journal of Medicine, online.
The group previously reported in December 2021 that the incidence of myocarditis in Israel after receipt of the Pfizer/BioNTech BNT162b2 mRNA COVID-19 vaccine was highest among males between the ages of 16 and 29 (10.7 cases per 100,000).
The vaccine has since been approved for adolescents aged 12-15. Initial evidence for this age group, reported by Dr. Witberg and colleagues in March 2022, suggests a similar low incidence and mild course of myocarditis, although follow-up was limited to 30 days.
In their latest report, with follow-up out to 6 months, Dr. Witberg and colleagues identified nine probable or definite cases of myocarditis among 182,605 Israeli adolescents aged 12-15 who received the Pfizer/BioNTech mRNA vaccine – an incidence of 4.8 cases per 100,000.
Eight cases occurred after the second vaccine dose. All nine cases were mild.
Cardiac and inflammatory markers were elevated in all adolescent patients and electrocardiographic results were abnormal in two-thirds.
Eight patients had a normal ejection fraction, and four had a pericardial effusion. The patients spent 2-4 days hospitalized, and the in-hospital course was uneventful.
Echocardiographic findings were available a median of 10 days after discharge for eight patients. All echocardiograms showed a normal ejection fraction and resolution of pericardial effusion.
Five patients underwent cardiac MRI, including three scans performed at a median of 104 days after discharge. The scans showed “minimal evidence” of myocardial scarring or fibrosis, with evidence of late gadolinium enhancement ranging from 0% to 2%.
At a median of 206 days following discharge, all of the patients were alive, and none had been readmitted to the hospital, Dr. Witberg and colleagues report.
This research had no specific funding. Five authors have received research grants from Pfizer.
A version of this article first appeared on Medscape.com.
New data from Israel provide further evidence that myocarditis is a rare adverse event of vaccination with the Pfizer/BioNTech mRNA COVID-19 vaccine in adolescents – one that predominantly occurs in males and typically after the second dose.
The new data also indicate a “mild and benign” clinical course of myocarditis after vaccination, with “favorable” long-term prognosis based on cardiac imaging findings.
Guy Witberg, MD, MPH, Rabin Medical Center, Petah Tikva, Israel, and colleagues report their latest observations in correspondence in The New England Journal of Medicine, online.
The group previously reported in December 2021 that the incidence of myocarditis in Israel after receipt of the Pfizer/BioNTech BNT162b2 mRNA COVID-19 vaccine was highest among males between the ages of 16 and 29 (10.7 cases per 100,000).
The vaccine has since been approved for adolescents aged 12-15. Initial evidence for this age group, reported by Dr. Witberg and colleagues in March 2022, suggests a similar low incidence and mild course of myocarditis, although follow-up was limited to 30 days.
In their latest report, with follow-up out to 6 months, Dr. Witberg and colleagues identified nine probable or definite cases of myocarditis among 182,605 Israeli adolescents aged 12-15 who received the Pfizer/BioNTech mRNA vaccine – an incidence of 4.8 cases per 100,000.
Eight cases occurred after the second vaccine dose. All nine cases were mild.
Cardiac and inflammatory markers were elevated in all adolescent patients and electrocardiographic results were abnormal in two-thirds.
Eight patients had a normal ejection fraction, and four had a pericardial effusion. The patients spent 2-4 days hospitalized, and the in-hospital course was uneventful.
Echocardiographic findings were available a median of 10 days after discharge for eight patients. All echocardiograms showed a normal ejection fraction and resolution of pericardial effusion.
Five patients underwent cardiac MRI, including three scans performed at a median of 104 days after discharge. The scans showed “minimal evidence” of myocardial scarring or fibrosis, with evidence of late gadolinium enhancement ranging from 0% to 2%.
At a median of 206 days following discharge, all of the patients were alive, and none had been readmitted to the hospital, Dr. Witberg and colleagues report.
This research had no specific funding. Five authors have received research grants from Pfizer.
A version of this article first appeared on Medscape.com.