User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Drive, chip, and putt your way to osteoarthritis relief
Taking a swing against arthritis
Osteoarthritis is a tough disease to manage. Exercise helps ease the stiffness and pain of the joints, but at the same time, the disease makes it difficult to do that beneficial exercise. Even a relatively simple activity like jogging can hurt more than it helps. If only there were a low-impact exercise that was incredibly popular among the generally older population who are likely to have arthritis.
We love a good golf study here at LOTME, and a group of Australian and U.K. researchers have provided. Osteoarthritis affects 2 million people in the land down under, making it the most common source of disability there. In that population, only 64% reported their physical health to be good, very good, or excellent. Among the 459 golfers with OA that the study authors surveyed, however, the percentage reporting good health rose to more than 90%.
A similar story emerged when they looked at mental health. Nearly a quarter of nongolfers with OA reported high or very high levels of psychological distress, compared with just 8% of golfers. This pattern of improved physical and mental health remained when the researchers looked at the general, non-OA population.
This isn’t the first time golf’s been connected with improved health, and previous studies have shown golf to reduce the risks of cardiovascular disease, diabetes, and obesity, among other things. Just walking one 18-hole round significantly exceeds the CDC’s recommended 150 minutes of physical activity per week. Go out multiple times a week – leaving the cart and beer at home, American golfers – and you’ll be fit for a lifetime.
The golfers on our staff, however, are still waiting for those mental health benefits to kick in. Because when we’re adding up our scorecard after that string of four double bogeys to end the round, we’re most definitely thinking: “Yes, this sport is reducing my psychological distress. I am having fun right now.”
Battle of the sexes’ intestines
There are, we’re sure you’ve noticed, some differences between males and females. Females, for one thing, have longer small intestines than males. Everybody knows that, right? You didn’t know? Really? … Really?

Well, then, we’re guessing you haven’t read “Hidden diversity: Comparative functional morphology of humans and other species” by Erin A. McKenney, PhD, of North Carolina State University, Raleigh, and associates, which just appeared in PeerJ. We couldn’t put it down, even in the shower – a real page-turner/scroller. (It’s a great way to clean a phone, for those who also like to scroll, text, or talk on the toilet.)
The researchers got out their rulers, calipers, and string and took many measurements of the digestive systems of 45 human cadavers (21 female and 24 male), which were compared with data from 10 rats, 10 pigs, and 10 bullfrogs, which had been collected (the measurements, not the animals) by undergraduate students enrolled in a comparative anatomy laboratory course at the university.
There was little intestinal-length variation among the four-legged subjects, but when it comes to humans, females have “consistently and significantly longer small intestines than males,” the investigators noted.
The women’s small intestines, almost 14 feet long on average, were about a foot longer than the men’s, which suggests that women are better able to extract nutrients from food and “supports the canalization hypothesis, which posits that women are better able to survive during periods of stress,” coauthor Amanda Hale said in a written statement from the school. The way to a man’s heart may be through his stomach, but the way to a woman’s heart is through her duodenum, it seems.
Fascinating stuff, to be sure, but the thing that really caught our eye in the PeerJ article was the authors’ suggestion “that organs behave independently of one another, both within and across species.” Organs behaving independently? A somewhat ominous concept, no doubt, but it does explain a lot of the sounds we hear coming from our guts, which can get pretty frightening, especially on chili night.
Dog walking is dangerous business
Yes, you did read that right. A lot of strange things can send you to the emergency department. Go ahead and add dog walking onto that list.
Investigators from Johns Hopkins University estimate that over 422,000 adults presented to U.S. emergency departments with leash-dependent dog walking-related injuries between 2001 and 2020.
With almost 53% of U.S. households owning at least one dog in 2021-2022 in the wake of the COVID pet boom, this kind of occurrence is becoming more common than you think. The annual number of dog-walking injuries more than quadrupled from 7,300 to 32,000 over the course of the study, and the researchers link that spike to the promotion of dog walking for fitness, along with the boost of ownership itself.
The most common injuries listed in the National Electronic Injury Surveillance System database were finger fracture, traumatic brain injury, and shoulder sprain or strain. These mostly involved falls from being pulled, tripped, or tangled up in the leash while walking. For those aged 65 years and older, traumatic brain injury and hip fracture were the most common.
Women were 50% more likely to sustain a fracture than were men, and dog owners aged 65 and older were three times as likely to fall, twice as likely to get a fracture, and 60% more likely to have brain injury than were younger people. Now, that’s not to say younger people don’t also get hurt. After all, dogs aren’t ageists. The researchers have that data but it’s coming out later.
Meanwhile, the pitfalls involved with just trying to get our daily steps in while letting Muffin do her business have us on the lookout for random squirrels.
Taking a swing against arthritis
Osteoarthritis is a tough disease to manage. Exercise helps ease the stiffness and pain of the joints, but at the same time, the disease makes it difficult to do that beneficial exercise. Even a relatively simple activity like jogging can hurt more than it helps. If only there were a low-impact exercise that was incredibly popular among the generally older population who are likely to have arthritis.
We love a good golf study here at LOTME, and a group of Australian and U.K. researchers have provided. Osteoarthritis affects 2 million people in the land down under, making it the most common source of disability there. In that population, only 64% reported their physical health to be good, very good, or excellent. Among the 459 golfers with OA that the study authors surveyed, however, the percentage reporting good health rose to more than 90%.
A similar story emerged when they looked at mental health. Nearly a quarter of nongolfers with OA reported high or very high levels of psychological distress, compared with just 8% of golfers. This pattern of improved physical and mental health remained when the researchers looked at the general, non-OA population.
This isn’t the first time golf’s been connected with improved health, and previous studies have shown golf to reduce the risks of cardiovascular disease, diabetes, and obesity, among other things. Just walking one 18-hole round significantly exceeds the CDC’s recommended 150 minutes of physical activity per week. Go out multiple times a week – leaving the cart and beer at home, American golfers – and you’ll be fit for a lifetime.
The golfers on our staff, however, are still waiting for those mental health benefits to kick in. Because when we’re adding up our scorecard after that string of four double bogeys to end the round, we’re most definitely thinking: “Yes, this sport is reducing my psychological distress. I am having fun right now.”
Battle of the sexes’ intestines
There are, we’re sure you’ve noticed, some differences between males and females. Females, for one thing, have longer small intestines than males. Everybody knows that, right? You didn’t know? Really? … Really?
Well, then, we’re guessing you haven’t read “Hidden diversity: Comparative functional morphology of humans and other species” by Erin A. McKenney, PhD, of North Carolina State University, Raleigh, and associates, which just appeared in PeerJ. We couldn’t put it down, even in the shower – a real page-turner/scroller. (It’s a great way to clean a phone, for those who also like to scroll, text, or talk on the toilet.)
The researchers got out their rulers, calipers, and string and took many measurements of the digestive systems of 45 human cadavers (21 female and 24 male), which were compared with data from 10 rats, 10 pigs, and 10 bullfrogs, which had been collected (the measurements, not the animals) by undergraduate students enrolled in a comparative anatomy laboratory course at the university.
There was little intestinal-length variation among the four-legged subjects, but when it comes to humans, females have “consistently and significantly longer small intestines than males,” the investigators noted.
The women’s small intestines, almost 14 feet long on average, were about a foot longer than the men’s, which suggests that women are better able to extract nutrients from food and “supports the canalization hypothesis, which posits that women are better able to survive during periods of stress,” coauthor Amanda Hale said in a written statement from the school. The way to a man’s heart may be through his stomach, but the way to a woman’s heart is through her duodenum, it seems.
Fascinating stuff, to be sure, but the thing that really caught our eye in the PeerJ article was the authors’ suggestion “that organs behave independently of one another, both within and across species.” Organs behaving independently? A somewhat ominous concept, no doubt, but it does explain a lot of the sounds we hear coming from our guts, which can get pretty frightening, especially on chili night.
Dog walking is dangerous business
Yes, you did read that right. A lot of strange things can send you to the emergency department. Go ahead and add dog walking onto that list.
Investigators from Johns Hopkins University estimate that over 422,000 adults presented to U.S. emergency departments with leash-dependent dog walking-related injuries between 2001 and 2020.
With almost 53% of U.S. households owning at least one dog in 2021-2022 in the wake of the COVID pet boom, this kind of occurrence is becoming more common than you think. The annual number of dog-walking injuries more than quadrupled from 7,300 to 32,000 over the course of the study, and the researchers link that spike to the promotion of dog walking for fitness, along with the boost of ownership itself.
The most common injuries listed in the National Electronic Injury Surveillance System database were finger fracture, traumatic brain injury, and shoulder sprain or strain. These mostly involved falls from being pulled, tripped, or tangled up in the leash while walking. For those aged 65 years and older, traumatic brain injury and hip fracture were the most common.
Women were 50% more likely to sustain a fracture than were men, and dog owners aged 65 and older were three times as likely to fall, twice as likely to get a fracture, and 60% more likely to have brain injury than were younger people. Now, that’s not to say younger people don’t also get hurt. After all, dogs aren’t ageists. The researchers have that data but it’s coming out later.
Meanwhile, the pitfalls involved with just trying to get our daily steps in while letting Muffin do her business have us on the lookout for random squirrels.
Taking a swing against arthritis
Osteoarthritis is a tough disease to manage. Exercise helps ease the stiffness and pain of the joints, but at the same time, the disease makes it difficult to do that beneficial exercise. Even a relatively simple activity like jogging can hurt more than it helps. If only there were a low-impact exercise that was incredibly popular among the generally older population who are likely to have arthritis.
We love a good golf study here at LOTME, and a group of Australian and U.K. researchers have provided. Osteoarthritis affects 2 million people in the land down under, making it the most common source of disability there. In that population, only 64% reported their physical health to be good, very good, or excellent. Among the 459 golfers with OA that the study authors surveyed, however, the percentage reporting good health rose to more than 90%.
A similar story emerged when they looked at mental health. Nearly a quarter of nongolfers with OA reported high or very high levels of psychological distress, compared with just 8% of golfers. This pattern of improved physical and mental health remained when the researchers looked at the general, non-OA population.
This isn’t the first time golf’s been connected with improved health, and previous studies have shown golf to reduce the risks of cardiovascular disease, diabetes, and obesity, among other things. Just walking one 18-hole round significantly exceeds the CDC’s recommended 150 minutes of physical activity per week. Go out multiple times a week – leaving the cart and beer at home, American golfers – and you’ll be fit for a lifetime.
The golfers on our staff, however, are still waiting for those mental health benefits to kick in. Because when we’re adding up our scorecard after that string of four double bogeys to end the round, we’re most definitely thinking: “Yes, this sport is reducing my psychological distress. I am having fun right now.”
Battle of the sexes’ intestines
There are, we’re sure you’ve noticed, some differences between males and females. Females, for one thing, have longer small intestines than males. Everybody knows that, right? You didn’t know? Really? … Really?
Well, then, we’re guessing you haven’t read “Hidden diversity: Comparative functional morphology of humans and other species” by Erin A. McKenney, PhD, of North Carolina State University, Raleigh, and associates, which just appeared in PeerJ. We couldn’t put it down, even in the shower – a real page-turner/scroller. (It’s a great way to clean a phone, for those who also like to scroll, text, or talk on the toilet.)
The researchers got out their rulers, calipers, and string and took many measurements of the digestive systems of 45 human cadavers (21 female and 24 male), which were compared with data from 10 rats, 10 pigs, and 10 bullfrogs, which had been collected (the measurements, not the animals) by undergraduate students enrolled in a comparative anatomy laboratory course at the university.
There was little intestinal-length variation among the four-legged subjects, but when it comes to humans, females have “consistently and significantly longer small intestines than males,” the investigators noted.
The women’s small intestines, almost 14 feet long on average, were about a foot longer than the men’s, which suggests that women are better able to extract nutrients from food and “supports the canalization hypothesis, which posits that women are better able to survive during periods of stress,” coauthor Amanda Hale said in a written statement from the school. The way to a man’s heart may be through his stomach, but the way to a woman’s heart is through her duodenum, it seems.
Fascinating stuff, to be sure, but the thing that really caught our eye in the PeerJ article was the authors’ suggestion “that organs behave independently of one another, both within and across species.” Organs behaving independently? A somewhat ominous concept, no doubt, but it does explain a lot of the sounds we hear coming from our guts, which can get pretty frightening, especially on chili night.
Dog walking is dangerous business
Yes, you did read that right. A lot of strange things can send you to the emergency department. Go ahead and add dog walking onto that list.
Investigators from Johns Hopkins University estimate that over 422,000 adults presented to U.S. emergency departments with leash-dependent dog walking-related injuries between 2001 and 2020.
With almost 53% of U.S. households owning at least one dog in 2021-2022 in the wake of the COVID pet boom, this kind of occurrence is becoming more common than you think. The annual number of dog-walking injuries more than quadrupled from 7,300 to 32,000 over the course of the study, and the researchers link that spike to the promotion of dog walking for fitness, along with the boost of ownership itself.
The most common injuries listed in the National Electronic Injury Surveillance System database were finger fracture, traumatic brain injury, and shoulder sprain or strain. These mostly involved falls from being pulled, tripped, or tangled up in the leash while walking. For those aged 65 years and older, traumatic brain injury and hip fracture were the most common.
Women were 50% more likely to sustain a fracture than were men, and dog owners aged 65 and older were three times as likely to fall, twice as likely to get a fracture, and 60% more likely to have brain injury than were younger people. Now, that’s not to say younger people don’t also get hurt. After all, dogs aren’t ageists. The researchers have that data but it’s coming out later.
Meanwhile, the pitfalls involved with just trying to get our daily steps in while letting Muffin do her business have us on the lookout for random squirrels.

BMI is a flawed measure of obesity. What are alternatives?
“BMI is trash. Full stop.” This controversial tweet, which received thousands of likes and retweets, was cited in a recent article by one doctor on when physicians might stop using body mass index (BMI) to diagnose obesity.
BMI has for years been the consensus default method for assessing whether a person is overweight or has obesity, and is still widely used as the gatekeeper metric for treatment eligibility for certain weight-loss agents and bariatric surgery.
an important determinant of the cardiometabolic consequences of fat.
Alternative metrics include waist circumference and/or waist-to-height ratio (WHtR); imaging methods such as CT, MRI, and dual-energy x-ray absorptiometry (DXA); and bioelectrical impedance to assess fat volume and location. All have made some inroads on the tight grip BMI has had on obesity assessment.
Chances are, however, that BMI will not fade away anytime soon given how entrenched it has become in clinical practice and for insurance coverage, as well as its relative simplicity and precision.
“BMI is embedded in a wide range of guidelines on the use of medications and surgery. It’s embedded in Food and Drug Administration regulations and for billing and insurance coverage. It would take extremely strong data and years of work to undo the infrastructure built around BMI and replace it with something else. I don’t see that happening [anytime soon],” commented Daniel H. Bessesen, MD, a professor at the University of Colorado at Denver, Aurora, and chief of endocrinology for Denver Health.
“It would be almost impossible to replace all the studies that have used BMI with investigations using some other measure,” he said.
BMI Is ‘imperfect’
The entrenched position of BMI as the go-to metric doesn’t keep detractors from weighing in. As noted in a commentary on current clinical challenges surrounding obesity recently published in Annals of Internal Medicine, the journal’s editor-in-chief, Christine Laine, MD, and senior deputy editor Christina C. Wee, MD, listed six top issues clinicians must deal with, one of which, they say, is the need for a better measure of obesity than BMI.
“Unfortunately, BMI is an imperfect measure of body composition that differs with ethnicity, sex, body frame, and muscle mass,” noted Dr. Laine and Dr. Wee.
BMI is based on a person’s weight in kilograms divided by the square of their height in meters. A “healthy” BMI is between 18.5 and 24.9 kg/m2, overweight is 25-29.9, and 30 or greater is considered to represent obesity. However, certain ethnic groups have lower cutoffs for overweight or obesity because of evidence that such individuals can be at higher risk of obesity-related comorbidities at lower BMIs.
“BMI was chosen as the initial screening tool [for obesity] not because anyone thought it was perfect or the best measure but because of its simplicity. All you need is height, weight, and a calculator,” Dr. Wee said in an interview.
Numerous online calculators are available, including one from the Centers for Disease Control and Prevention where height in feet and inches and weight in pounds can be entered to generate the BMI.
BMI is also inherently limited by being “a proxy for adiposity” and not a direct measure, added Dr. Wee, who is also director of the Obesity Research Program of Beth Israel Deaconess Medical Center, Boston.
As such, BMI can’t distinguish between fat and muscle because it relies on weight only to gauge adiposity, noted Tiffany Powell-Wiley, MD, an obesity researcher at the National Heart, Lung, and Blood Institute in Bethesda, Md. Another shortcoming of BMI is that it “is good for distinguishing population-level risk for cardiovascular disease and other chronic diseases, but it does not help as much for distinguishing risk at an individual level,” she said in an interview.
These and other drawbacks have prompted researchers to look for other useful metrics. WHtR, for example, has recently made headway as a potential BMI alternative or complement.
The case for WHtR
Concern about overreliance on BMI despite its limitations is not new. In 2015, an American Heart Association scientific statement from the group’s Obesity Committee concluded that “BMI alone, even with lower thresholds, is a useful but not an ideal tool for identification of obesity or assessment of cardiovascular risk,” especially for people from Asian, Black, Hispanic, and Pacific Islander populations.
The writing panel also recommended that clinicians measure waist circumference annually and use that information along with BMI “to better gauge cardiovascular risk in diverse populations.”
Momentum for moving beyond BMI alone has continued to build following the AHA statement.
In September 2022, the National Institute for Health and Care Excellence, which sets policies for the United Kingdom’s National Health Service, revised its guidancefor assessment and management of people with obesity. The updated guidance recommends that when clinicians assess “adults with BMI below 35 kg/m2, measure and use their WHtR, as well as their BMI, as a practical estimate of central adiposity and use these measurements to help to assess and predict health risks.”
NICE released an extensive literature review with the revision, and based on the evidence, said that “using waist-to-height ratio as well as BMI would help give a practical estimate of central adiposity in adults with BMI under 35 kg/m2. This would in turn help professionals assess and predict health risks.”
However, the review added that, “because people with a BMI over 35 kg/m2 are always likely to have a high WHtR, the committee recognized that it may not be a useful addition for predicting health risks in this group.” The 2022 NICE review also said that it is “important to estimate central adiposity when assessing future health risks, including for people whose BMI is in the healthy-weight category.”
This new emphasis by NICE on measuring and using WHtR as part of obesity assessment “represents an important change in population health policy,” commented Dr. Powell-Wiley. “I expect more professional organizations will endorse use of waist circumference or waist-to-height ratio now that NICE has taken this step,” she predicted.
Waist circumference and WHtR may become standard measures of adiposity in clinical practice over the next 5-10 years.
The recent move by NICE to highlight a complementary role for WHtR “is another acknowledgment that BMI is an imperfect tool for stratifying cardiometabolic risk in a diverse population, especially in people with lower BMIs” because of its variability, commented Jamie Almandoz, MD, medical director of the weight wellness program at UT Southwestern Medical Center, Dallas.
WHtR vs. BMI
Another recent step forward for WHtR came with the publication of a post hoc analysis of data collected in the PARADIGM-HF trial, a study that had the primary purpose of comparing two medications for improving outcomes in more than 8,000 patients with heart failure with reduced ejection fraction.
The new analysis showed that “two indices that incorporate waist circumference and height, but not weight, showed a clearer association between greater adiposity and a higher risk of heart failure hospitalization,” compared with BMI.
WHtR was one of the two indices identified as being a better correlate for the adverse effect of excess adiposity compared with BMI.
The authors of the post hoc analysis did not design their analysis to compare WHtR with BMI. Instead, their goal was to better understand what’s known as the “obesity paradox” in people with heart failure with reduced ejection fraction: The recurring observation that, when these patients with heart failure have lower BMIs they fare worse, with higher rates of mortality and adverse cardiovascular outcomes, compared with patients with higher BMIs.
The new analysis showed that this paradox disappeared when WHtR was substituted for BMI as the obesity metric.
This “provides meaningful data about the superiority of WHtR, compared with BMI, for predicting heart failure outcomes,” said Dr. Powell-Wiley, although she cautioned that the analysis was limited by scant data in diverse populations and did not look at other important cardiovascular disease outcomes. While Dr. Powell-Wiley does not think that WHtR needs assessment in a prospective, controlled trial, she called for analysis of pooled prospective studies with more diverse populations to better document the advantages of WHtR over BMI.
The PARADIGM-HF post hoc analysis shows again how flawed BMI is for health assessment and the relative importance of an individualized understanding of a person’s body composition, Dr. Almandoz said in an interview. “As we collect more data, there is increasing awareness of how imperfect BMI is.”
Measuring waist circumference is tricky
Although WHtR looks promising as a substitute for or add-on to BMI, it has its own limitations, particularly the challenge of accurately measuring waist circumference.
Measuring waist circumference “not only takes more time but requires the assessor to be well trained about where to put the tape measure and making sure it’s measured at the same place each time,” even when different people take serial measurements from individual patients, noted Dr. Wee. Determining waist circumference can also be technically difficult when done on larger people, she added, and collectively these challenges make waist circumference “less reproducible from measurement to measurement.”
“It’s relatively clear how to standardize measurement of weight and height, but there is a huge amount of variability when the waist is measured,” agreed Dr. Almandoz. “And waist circumference also differs by ethnicity, race, sex, and body frame. There are significant differences in waist circumference levels that associate with increased health risks” between, for example, White and South Asian people.
Another limitation of waist circumference and WHtR is that they “cannot differentiate between visceral and abdominal subcutaneous adipose tissue, which are vastly different regarding cardiometabolic risk, commented Ian Neeland, MD, director of cardiovascular prevention at the University Hospitals Harrington Heart & Vascular Institute, Cleveland.
The imaging option
“Waist-to-height ratio is not the ultimate answer,” Dr. Neeland said in an interview. He instead endorsed “advanced imaging for body fat distribution,” such as CT or MRI scans, as his pick for what should be the standard obesity metric, “given that it is much more specific and actionable for both risk assessment and response to therapy. I expect slow but steady advancements that move away from BMI cutoffs, for example for bariatric surgery, given that BMI is an imprecise and crude tool.”
But although imaging with methods like CT and MRI may provide the best accuracy and precision for tracking the volume of a person’s cardiometabolically dangerous fat, they are also hampered by relatively high cost and, for CT and DXA, the issue of radiation exposure.
“CT, MRI, and DXA scans give more in-depth assessment of body composition, but should we expose people to the radiation and the cost?” Dr. Almandoz wondered.
“Height, weight, and waist circumference cost nothing to obtain,” creating a big relative disadvantage for imaging, said Naveed Sattar, MD, professor of metabolic medicine at the University of Glasgow.
“Data would need to show that imaging gives clinicians substantially more information about future risk” to justify its price, Dr. Sattar emphasized.
BMI’s limits mean adding on
Regardless of whichever alternatives to BMI end up getting used most, experts generally agree that BMI alone is looking increasingly inadequate.
“Over the next 5 years, BMI will come to be seen as a screening tool that categorizes people into general risk groups” that also needs “other metrics and variables, such as age, race, ethnicity, family history, blood glucose, and blood pressure to better describe health risk in an individual,” predicted Dr. Bessesen.
The endorsement of WHtR by NICE “will lead to more research into how to incorporate WHtR into routine practice. We need more evidence to translate what NICE said into practice,” said Dr. Sattar. “I don’t think we’ll see a shift away from BMI, but we’ll add alternative measures that are particularly useful in certain patients.”
“Because we live in diverse societies, we need to individualize risk assessment and couple that with technology that makes analysis of body composition more accessible,” agreed Dr. Almandoz. He noted that the UT Southwestern weight wellness program where he practices has, for about the past decade, routinely collected waist circumference and bioelectrical impedance data as well as BMI on all people seen in the practice for obesity concerns. Making these additional measurements on a routine basis also helps strengthen patient engagement.
“We get into trouble when we make rigid health policy and clinical decisions based on BMI alone without looking at the patient holistically,” said Dr. Wee. “Patients are more than arbitrary numbers, and clinicians should make clinical decisions based on the totality of evidence for each individual patient.”
Dr. Bessesen, Dr. Wee, Dr. Powell-Wiley, and Dr. Almandoz reported no relevant financial relationships. Dr. Neeland has reported being a consultant for Merck. Dr. Sattar has reported being a consultant or speaker for Abbott Laboratories, Afimmune, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Hanmi Pharmaceuticals, Janssen, MSD, Novartis, Novo Nordisk, Pfizer, Roche Diagnostics, and Sanofi.
A version of this article originally appeared on Medscape.com.
“BMI is trash. Full stop.” This controversial tweet, which received thousands of likes and retweets, was cited in a recent article by one doctor on when physicians might stop using body mass index (BMI) to diagnose obesity.
BMI has for years been the consensus default method for assessing whether a person is overweight or has obesity, and is still widely used as the gatekeeper metric for treatment eligibility for certain weight-loss agents and bariatric surgery.
an important determinant of the cardiometabolic consequences of fat.
Alternative metrics include waist circumference and/or waist-to-height ratio (WHtR); imaging methods such as CT, MRI, and dual-energy x-ray absorptiometry (DXA); and bioelectrical impedance to assess fat volume and location. All have made some inroads on the tight grip BMI has had on obesity assessment.
Chances are, however, that BMI will not fade away anytime soon given how entrenched it has become in clinical practice and for insurance coverage, as well as its relative simplicity and precision.
“BMI is embedded in a wide range of guidelines on the use of medications and surgery. It’s embedded in Food and Drug Administration regulations and for billing and insurance coverage. It would take extremely strong data and years of work to undo the infrastructure built around BMI and replace it with something else. I don’t see that happening [anytime soon],” commented Daniel H. Bessesen, MD, a professor at the University of Colorado at Denver, Aurora, and chief of endocrinology for Denver Health.
“It would be almost impossible to replace all the studies that have used BMI with investigations using some other measure,” he said.
BMI Is ‘imperfect’
The entrenched position of BMI as the go-to metric doesn’t keep detractors from weighing in. As noted in a commentary on current clinical challenges surrounding obesity recently published in Annals of Internal Medicine, the journal’s editor-in-chief, Christine Laine, MD, and senior deputy editor Christina C. Wee, MD, listed six top issues clinicians must deal with, one of which, they say, is the need for a better measure of obesity than BMI.
“Unfortunately, BMI is an imperfect measure of body composition that differs with ethnicity, sex, body frame, and muscle mass,” noted Dr. Laine and Dr. Wee.
BMI is based on a person’s weight in kilograms divided by the square of their height in meters. A “healthy” BMI is between 18.5 and 24.9 kg/m2, overweight is 25-29.9, and 30 or greater is considered to represent obesity. However, certain ethnic groups have lower cutoffs for overweight or obesity because of evidence that such individuals can be at higher risk of obesity-related comorbidities at lower BMIs.
“BMI was chosen as the initial screening tool [for obesity] not because anyone thought it was perfect or the best measure but because of its simplicity. All you need is height, weight, and a calculator,” Dr. Wee said in an interview.
Numerous online calculators are available, including one from the Centers for Disease Control and Prevention where height in feet and inches and weight in pounds can be entered to generate the BMI.
BMI is also inherently limited by being “a proxy for adiposity” and not a direct measure, added Dr. Wee, who is also director of the Obesity Research Program of Beth Israel Deaconess Medical Center, Boston.
As such, BMI can’t distinguish between fat and muscle because it relies on weight only to gauge adiposity, noted Tiffany Powell-Wiley, MD, an obesity researcher at the National Heart, Lung, and Blood Institute in Bethesda, Md. Another shortcoming of BMI is that it “is good for distinguishing population-level risk for cardiovascular disease and other chronic diseases, but it does not help as much for distinguishing risk at an individual level,” she said in an interview.
These and other drawbacks have prompted researchers to look for other useful metrics. WHtR, for example, has recently made headway as a potential BMI alternative or complement.
The case for WHtR
Concern about overreliance on BMI despite its limitations is not new. In 2015, an American Heart Association scientific statement from the group’s Obesity Committee concluded that “BMI alone, even with lower thresholds, is a useful but not an ideal tool for identification of obesity or assessment of cardiovascular risk,” especially for people from Asian, Black, Hispanic, and Pacific Islander populations.
The writing panel also recommended that clinicians measure waist circumference annually and use that information along with BMI “to better gauge cardiovascular risk in diverse populations.”
Momentum for moving beyond BMI alone has continued to build following the AHA statement.
In September 2022, the National Institute for Health and Care Excellence, which sets policies for the United Kingdom’s National Health Service, revised its guidancefor assessment and management of people with obesity. The updated guidance recommends that when clinicians assess “adults with BMI below 35 kg/m2, measure and use their WHtR, as well as their BMI, as a practical estimate of central adiposity and use these measurements to help to assess and predict health risks.”
NICE released an extensive literature review with the revision, and based on the evidence, said that “using waist-to-height ratio as well as BMI would help give a practical estimate of central adiposity in adults with BMI under 35 kg/m2. This would in turn help professionals assess and predict health risks.”
However, the review added that, “because people with a BMI over 35 kg/m2 are always likely to have a high WHtR, the committee recognized that it may not be a useful addition for predicting health risks in this group.” The 2022 NICE review also said that it is “important to estimate central adiposity when assessing future health risks, including for people whose BMI is in the healthy-weight category.”
This new emphasis by NICE on measuring and using WHtR as part of obesity assessment “represents an important change in population health policy,” commented Dr. Powell-Wiley. “I expect more professional organizations will endorse use of waist circumference or waist-to-height ratio now that NICE has taken this step,” she predicted.
Waist circumference and WHtR may become standard measures of adiposity in clinical practice over the next 5-10 years.
The recent move by NICE to highlight a complementary role for WHtR “is another acknowledgment that BMI is an imperfect tool for stratifying cardiometabolic risk in a diverse population, especially in people with lower BMIs” because of its variability, commented Jamie Almandoz, MD, medical director of the weight wellness program at UT Southwestern Medical Center, Dallas.
WHtR vs. BMI
Another recent step forward for WHtR came with the publication of a post hoc analysis of data collected in the PARADIGM-HF trial, a study that had the primary purpose of comparing two medications for improving outcomes in more than 8,000 patients with heart failure with reduced ejection fraction.
The new analysis showed that “two indices that incorporate waist circumference and height, but not weight, showed a clearer association between greater adiposity and a higher risk of heart failure hospitalization,” compared with BMI.
WHtR was one of the two indices identified as being a better correlate for the adverse effect of excess adiposity compared with BMI.
The authors of the post hoc analysis did not design their analysis to compare WHtR with BMI. Instead, their goal was to better understand what’s known as the “obesity paradox” in people with heart failure with reduced ejection fraction: The recurring observation that, when these patients with heart failure have lower BMIs they fare worse, with higher rates of mortality and adverse cardiovascular outcomes, compared with patients with higher BMIs.
The new analysis showed that this paradox disappeared when WHtR was substituted for BMI as the obesity metric.
This “provides meaningful data about the superiority of WHtR, compared with BMI, for predicting heart failure outcomes,” said Dr. Powell-Wiley, although she cautioned that the analysis was limited by scant data in diverse populations and did not look at other important cardiovascular disease outcomes. While Dr. Powell-Wiley does not think that WHtR needs assessment in a prospective, controlled trial, she called for analysis of pooled prospective studies with more diverse populations to better document the advantages of WHtR over BMI.
The PARADIGM-HF post hoc analysis shows again how flawed BMI is for health assessment and the relative importance of an individualized understanding of a person’s body composition, Dr. Almandoz said in an interview. “As we collect more data, there is increasing awareness of how imperfect BMI is.”
Measuring waist circumference is tricky
Although WHtR looks promising as a substitute for or add-on to BMI, it has its own limitations, particularly the challenge of accurately measuring waist circumference.
Measuring waist circumference “not only takes more time but requires the assessor to be well trained about where to put the tape measure and making sure it’s measured at the same place each time,” even when different people take serial measurements from individual patients, noted Dr. Wee. Determining waist circumference can also be technically difficult when done on larger people, she added, and collectively these challenges make waist circumference “less reproducible from measurement to measurement.”
“It’s relatively clear how to standardize measurement of weight and height, but there is a huge amount of variability when the waist is measured,” agreed Dr. Almandoz. “And waist circumference also differs by ethnicity, race, sex, and body frame. There are significant differences in waist circumference levels that associate with increased health risks” between, for example, White and South Asian people.
Another limitation of waist circumference and WHtR is that they “cannot differentiate between visceral and abdominal subcutaneous adipose tissue, which are vastly different regarding cardiometabolic risk, commented Ian Neeland, MD, director of cardiovascular prevention at the University Hospitals Harrington Heart & Vascular Institute, Cleveland.
The imaging option
“Waist-to-height ratio is not the ultimate answer,” Dr. Neeland said in an interview. He instead endorsed “advanced imaging for body fat distribution,” such as CT or MRI scans, as his pick for what should be the standard obesity metric, “given that it is much more specific and actionable for both risk assessment and response to therapy. I expect slow but steady advancements that move away from BMI cutoffs, for example for bariatric surgery, given that BMI is an imprecise and crude tool.”
But although imaging with methods like CT and MRI may provide the best accuracy and precision for tracking the volume of a person’s cardiometabolically dangerous fat, they are also hampered by relatively high cost and, for CT and DXA, the issue of radiation exposure.
“CT, MRI, and DXA scans give more in-depth assessment of body composition, but should we expose people to the radiation and the cost?” Dr. Almandoz wondered.
“Height, weight, and waist circumference cost nothing to obtain,” creating a big relative disadvantage for imaging, said Naveed Sattar, MD, professor of metabolic medicine at the University of Glasgow.
“Data would need to show that imaging gives clinicians substantially more information about future risk” to justify its price, Dr. Sattar emphasized.
BMI’s limits mean adding on
Regardless of whichever alternatives to BMI end up getting used most, experts generally agree that BMI alone is looking increasingly inadequate.
“Over the next 5 years, BMI will come to be seen as a screening tool that categorizes people into general risk groups” that also needs “other metrics and variables, such as age, race, ethnicity, family history, blood glucose, and blood pressure to better describe health risk in an individual,” predicted Dr. Bessesen.
The endorsement of WHtR by NICE “will lead to more research into how to incorporate WHtR into routine practice. We need more evidence to translate what NICE said into practice,” said Dr. Sattar. “I don’t think we’ll see a shift away from BMI, but we’ll add alternative measures that are particularly useful in certain patients.”
“Because we live in diverse societies, we need to individualize risk assessment and couple that with technology that makes analysis of body composition more accessible,” agreed Dr. Almandoz. He noted that the UT Southwestern weight wellness program where he practices has, for about the past decade, routinely collected waist circumference and bioelectrical impedance data as well as BMI on all people seen in the practice for obesity concerns. Making these additional measurements on a routine basis also helps strengthen patient engagement.
“We get into trouble when we make rigid health policy and clinical decisions based on BMI alone without looking at the patient holistically,” said Dr. Wee. “Patients are more than arbitrary numbers, and clinicians should make clinical decisions based on the totality of evidence for each individual patient.”
Dr. Bessesen, Dr. Wee, Dr. Powell-Wiley, and Dr. Almandoz reported no relevant financial relationships. Dr. Neeland has reported being a consultant for Merck. Dr. Sattar has reported being a consultant or speaker for Abbott Laboratories, Afimmune, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Hanmi Pharmaceuticals, Janssen, MSD, Novartis, Novo Nordisk, Pfizer, Roche Diagnostics, and Sanofi.
A version of this article originally appeared on Medscape.com.
“BMI is trash. Full stop.” This controversial tweet, which received thousands of likes and retweets, was cited in a recent article by one doctor on when physicians might stop using body mass index (BMI) to diagnose obesity.
BMI has for years been the consensus default method for assessing whether a person is overweight or has obesity, and is still widely used as the gatekeeper metric for treatment eligibility for certain weight-loss agents and bariatric surgery.
an important determinant of the cardiometabolic consequences of fat.
Alternative metrics include waist circumference and/or waist-to-height ratio (WHtR); imaging methods such as CT, MRI, and dual-energy x-ray absorptiometry (DXA); and bioelectrical impedance to assess fat volume and location. All have made some inroads on the tight grip BMI has had on obesity assessment.
Chances are, however, that BMI will not fade away anytime soon given how entrenched it has become in clinical practice and for insurance coverage, as well as its relative simplicity and precision.
“BMI is embedded in a wide range of guidelines on the use of medications and surgery. It’s embedded in Food and Drug Administration regulations and for billing and insurance coverage. It would take extremely strong data and years of work to undo the infrastructure built around BMI and replace it with something else. I don’t see that happening [anytime soon],” commented Daniel H. Bessesen, MD, a professor at the University of Colorado at Denver, Aurora, and chief of endocrinology for Denver Health.
“It would be almost impossible to replace all the studies that have used BMI with investigations using some other measure,” he said.
BMI Is ‘imperfect’
The entrenched position of BMI as the go-to metric doesn’t keep detractors from weighing in. As noted in a commentary on current clinical challenges surrounding obesity recently published in Annals of Internal Medicine, the journal’s editor-in-chief, Christine Laine, MD, and senior deputy editor Christina C. Wee, MD, listed six top issues clinicians must deal with, one of which, they say, is the need for a better measure of obesity than BMI.
“Unfortunately, BMI is an imperfect measure of body composition that differs with ethnicity, sex, body frame, and muscle mass,” noted Dr. Laine and Dr. Wee.
BMI is based on a person’s weight in kilograms divided by the square of their height in meters. A “healthy” BMI is between 18.5 and 24.9 kg/m2, overweight is 25-29.9, and 30 or greater is considered to represent obesity. However, certain ethnic groups have lower cutoffs for overweight or obesity because of evidence that such individuals can be at higher risk of obesity-related comorbidities at lower BMIs.
“BMI was chosen as the initial screening tool [for obesity] not because anyone thought it was perfect or the best measure but because of its simplicity. All you need is height, weight, and a calculator,” Dr. Wee said in an interview.
Numerous online calculators are available, including one from the Centers for Disease Control and Prevention where height in feet and inches and weight in pounds can be entered to generate the BMI.
BMI is also inherently limited by being “a proxy for adiposity” and not a direct measure, added Dr. Wee, who is also director of the Obesity Research Program of Beth Israel Deaconess Medical Center, Boston.
As such, BMI can’t distinguish between fat and muscle because it relies on weight only to gauge adiposity, noted Tiffany Powell-Wiley, MD, an obesity researcher at the National Heart, Lung, and Blood Institute in Bethesda, Md. Another shortcoming of BMI is that it “is good for distinguishing population-level risk for cardiovascular disease and other chronic diseases, but it does not help as much for distinguishing risk at an individual level,” she said in an interview.
These and other drawbacks have prompted researchers to look for other useful metrics. WHtR, for example, has recently made headway as a potential BMI alternative or complement.
The case for WHtR
Concern about overreliance on BMI despite its limitations is not new. In 2015, an American Heart Association scientific statement from the group’s Obesity Committee concluded that “BMI alone, even with lower thresholds, is a useful but not an ideal tool for identification of obesity or assessment of cardiovascular risk,” especially for people from Asian, Black, Hispanic, and Pacific Islander populations.
The writing panel also recommended that clinicians measure waist circumference annually and use that information along with BMI “to better gauge cardiovascular risk in diverse populations.”
Momentum for moving beyond BMI alone has continued to build following the AHA statement.
In September 2022, the National Institute for Health and Care Excellence, which sets policies for the United Kingdom’s National Health Service, revised its guidancefor assessment and management of people with obesity. The updated guidance recommends that when clinicians assess “adults with BMI below 35 kg/m2, measure and use their WHtR, as well as their BMI, as a practical estimate of central adiposity and use these measurements to help to assess and predict health risks.”
NICE released an extensive literature review with the revision, and based on the evidence, said that “using waist-to-height ratio as well as BMI would help give a practical estimate of central adiposity in adults with BMI under 35 kg/m2. This would in turn help professionals assess and predict health risks.”
However, the review added that, “because people with a BMI over 35 kg/m2 are always likely to have a high WHtR, the committee recognized that it may not be a useful addition for predicting health risks in this group.” The 2022 NICE review also said that it is “important to estimate central adiposity when assessing future health risks, including for people whose BMI is in the healthy-weight category.”
This new emphasis by NICE on measuring and using WHtR as part of obesity assessment “represents an important change in population health policy,” commented Dr. Powell-Wiley. “I expect more professional organizations will endorse use of waist circumference or waist-to-height ratio now that NICE has taken this step,” she predicted.
Waist circumference and WHtR may become standard measures of adiposity in clinical practice over the next 5-10 years.
The recent move by NICE to highlight a complementary role for WHtR “is another acknowledgment that BMI is an imperfect tool for stratifying cardiometabolic risk in a diverse population, especially in people with lower BMIs” because of its variability, commented Jamie Almandoz, MD, medical director of the weight wellness program at UT Southwestern Medical Center, Dallas.
WHtR vs. BMI
Another recent step forward for WHtR came with the publication of a post hoc analysis of data collected in the PARADIGM-HF trial, a study that had the primary purpose of comparing two medications for improving outcomes in more than 8,000 patients with heart failure with reduced ejection fraction.
The new analysis showed that “two indices that incorporate waist circumference and height, but not weight, showed a clearer association between greater adiposity and a higher risk of heart failure hospitalization,” compared with BMI.
WHtR was one of the two indices identified as being a better correlate for the adverse effect of excess adiposity compared with BMI.
The authors of the post hoc analysis did not design their analysis to compare WHtR with BMI. Instead, their goal was to better understand what’s known as the “obesity paradox” in people with heart failure with reduced ejection fraction: The recurring observation that, when these patients with heart failure have lower BMIs they fare worse, with higher rates of mortality and adverse cardiovascular outcomes, compared with patients with higher BMIs.
The new analysis showed that this paradox disappeared when WHtR was substituted for BMI as the obesity metric.
This “provides meaningful data about the superiority of WHtR, compared with BMI, for predicting heart failure outcomes,” said Dr. Powell-Wiley, although she cautioned that the analysis was limited by scant data in diverse populations and did not look at other important cardiovascular disease outcomes. While Dr. Powell-Wiley does not think that WHtR needs assessment in a prospective, controlled trial, she called for analysis of pooled prospective studies with more diverse populations to better document the advantages of WHtR over BMI.
The PARADIGM-HF post hoc analysis shows again how flawed BMI is for health assessment and the relative importance of an individualized understanding of a person’s body composition, Dr. Almandoz said in an interview. “As we collect more data, there is increasing awareness of how imperfect BMI is.”
Measuring waist circumference is tricky
Although WHtR looks promising as a substitute for or add-on to BMI, it has its own limitations, particularly the challenge of accurately measuring waist circumference.
Measuring waist circumference “not only takes more time but requires the assessor to be well trained about where to put the tape measure and making sure it’s measured at the same place each time,” even when different people take serial measurements from individual patients, noted Dr. Wee. Determining waist circumference can also be technically difficult when done on larger people, she added, and collectively these challenges make waist circumference “less reproducible from measurement to measurement.”
“It’s relatively clear how to standardize measurement of weight and height, but there is a huge amount of variability when the waist is measured,” agreed Dr. Almandoz. “And waist circumference also differs by ethnicity, race, sex, and body frame. There are significant differences in waist circumference levels that associate with increased health risks” between, for example, White and South Asian people.
Another limitation of waist circumference and WHtR is that they “cannot differentiate between visceral and abdominal subcutaneous adipose tissue, which are vastly different regarding cardiometabolic risk, commented Ian Neeland, MD, director of cardiovascular prevention at the University Hospitals Harrington Heart & Vascular Institute, Cleveland.
The imaging option
“Waist-to-height ratio is not the ultimate answer,” Dr. Neeland said in an interview. He instead endorsed “advanced imaging for body fat distribution,” such as CT or MRI scans, as his pick for what should be the standard obesity metric, “given that it is much more specific and actionable for both risk assessment and response to therapy. I expect slow but steady advancements that move away from BMI cutoffs, for example for bariatric surgery, given that BMI is an imprecise and crude tool.”
But although imaging with methods like CT and MRI may provide the best accuracy and precision for tracking the volume of a person’s cardiometabolically dangerous fat, they are also hampered by relatively high cost and, for CT and DXA, the issue of radiation exposure.
“CT, MRI, and DXA scans give more in-depth assessment of body composition, but should we expose people to the radiation and the cost?” Dr. Almandoz wondered.
“Height, weight, and waist circumference cost nothing to obtain,” creating a big relative disadvantage for imaging, said Naveed Sattar, MD, professor of metabolic medicine at the University of Glasgow.
“Data would need to show that imaging gives clinicians substantially more information about future risk” to justify its price, Dr. Sattar emphasized.
BMI’s limits mean adding on
Regardless of whichever alternatives to BMI end up getting used most, experts generally agree that BMI alone is looking increasingly inadequate.
“Over the next 5 years, BMI will come to be seen as a screening tool that categorizes people into general risk groups” that also needs “other metrics and variables, such as age, race, ethnicity, family history, blood glucose, and blood pressure to better describe health risk in an individual,” predicted Dr. Bessesen.
The endorsement of WHtR by NICE “will lead to more research into how to incorporate WHtR into routine practice. We need more evidence to translate what NICE said into practice,” said Dr. Sattar. “I don’t think we’ll see a shift away from BMI, but we’ll add alternative measures that are particularly useful in certain patients.”
“Because we live in diverse societies, we need to individualize risk assessment and couple that with technology that makes analysis of body composition more accessible,” agreed Dr. Almandoz. He noted that the UT Southwestern weight wellness program where he practices has, for about the past decade, routinely collected waist circumference and bioelectrical impedance data as well as BMI on all people seen in the practice for obesity concerns. Making these additional measurements on a routine basis also helps strengthen patient engagement.
“We get into trouble when we make rigid health policy and clinical decisions based on BMI alone without looking at the patient holistically,” said Dr. Wee. “Patients are more than arbitrary numbers, and clinicians should make clinical decisions based on the totality of evidence for each individual patient.”
Dr. Bessesen, Dr. Wee, Dr. Powell-Wiley, and Dr. Almandoz reported no relevant financial relationships. Dr. Neeland has reported being a consultant for Merck. Dr. Sattar has reported being a consultant or speaker for Abbott Laboratories, Afimmune, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Hanmi Pharmaceuticals, Janssen, MSD, Novartis, Novo Nordisk, Pfizer, Roche Diagnostics, and Sanofi.
A version of this article originally appeared on Medscape.com.
Hybrid ablation superior for persistent AFib: CEASE-AF
BARCELONA – Staged hybrid ablation provided superior freedom from atrial arrhythmias compared with endocardial catheter ablation alone, including the need for repeat ablations in patients with advanced atrial fibrillation (AF), new data show.
“We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase, so this is a huge difference,” concluded cardiac surgeon Nicholas Doll, MD, PhD, Schüchtermann Clinic, Bad Rothenfelde, Germany.
Dr. Doll presented the 12-month follow up results of the Combined Endoscopic Epicardial and Percutaneous Endocardial Ablation Versus Repeated Catheter Ablation in Persistent and Longstanding Persistent Atrial Fibrillation (CEASE-AF) trial at the European Heart Rhythm Association 2023 Congress, held recently in Barcelona and virtually.
He said CEASE-AF is the largest multicenter randomized clinical trial comparing these two approaches for control of atrial arrhythmias.
Safety outcomes were numerically higher in the hybrid ablation (HA) group of the trial but not statistically different from the catheter ablation (CA) group.
Unstable wavefront
As background, Dr. Doll explained that in advanced AF, there is a high degree of endocardial-epicardial dissociation with unstable wavefront propagation transitioning between the endocardial and epicardial surfaces. Endocardial mapping and ablation alone may be insufficient to address the mechanism of AF.
“So, the hypothesis of the CEASE-AF study was a minimally invasive hybrid ablation approach which combines endocardial and epicardial ablation to achieve superior effectiveness when compared to endocardial catheter ablation alone,” he said.
This prospective clinical trial randomized patients 2:1 at nine sites in five countries to HA (n = 102) or CA (n = 52). All had left atrial diameter of 4 cm to 6 cm and persistent AF for up to 1 year or longstanding persistent AF for greater than 1 year up to 10 years.
Any patient with a previous ablation procedure, BMI greater than 35 kg/m2, or left ventricular ejection fraction less than 30% was excluded.
For HA, stage 1 consisted of epicardial lesions for pulmonary vein isolation (PVI) plus the posterior wall box plus left atrial appendage exclusion using the AtriClip (AtriCure Inc.) left atrial appendage exclusion device. Stage 2 involved endocardial mapping and catheter ablation to address gaps.
For CA, the index procedure involved catheter-mediated PVI plus repeat endocardial ablation as clinically indicated. For both HA and CA, additional ablation techniques and lesions were allowed for nonparoxysmal AF.
The HA timeline was the first stage, index procedure at time 0 (n = 102), a 90-day blanking period, and then the second stage, endocardial procedure at 90 to 180 days from the index procedure (n = 93).
For the CA arm of the trial, endocardial catheter ablation was performed on a minimal endocardial lesion set at time 0. Then after a 90-day blanking period, repeat catheter ablation was performed if clinically indicated (6/52).
Repeat ablations and electrical or pharmaceutical cardioversions were allowed during the 12-month follow-up period from time 0.
The primary efficacy endpoint was freedom from AF, atrial flutter, or atrial tachycardia of greater than 30 seconds through 12 months in the absence of class I/III antiarrhythmic drugs except ones that previously had failed, at doses not exceeding those previously failed doses. The safety endpoint was a composite rate of major complications over the course of the study.
Even with relatively modest cohort sizes, the HA and CA arms of the trial were well matched at baseline for age (approximately 60 years), gender (75.5% and 73.1% male, respectively), BMI (29.7 and 29.8 kg/m2), and persistent AF (79.4% and 82.7%).
The groups had persistent AF for 2.94 ± 3.29 years and 3.34 ± 3.52 years, respectively. The mean left atrial size was 4.7 ± 0.5 cm for the HA group and 4.7 ± 0.4 cm for the CA group.
Outcomes favored hybrid ablation over catheter ablation, the researchers reported. “We never would have expected these huge differences,” Dr. Doll told the congress. “We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase.”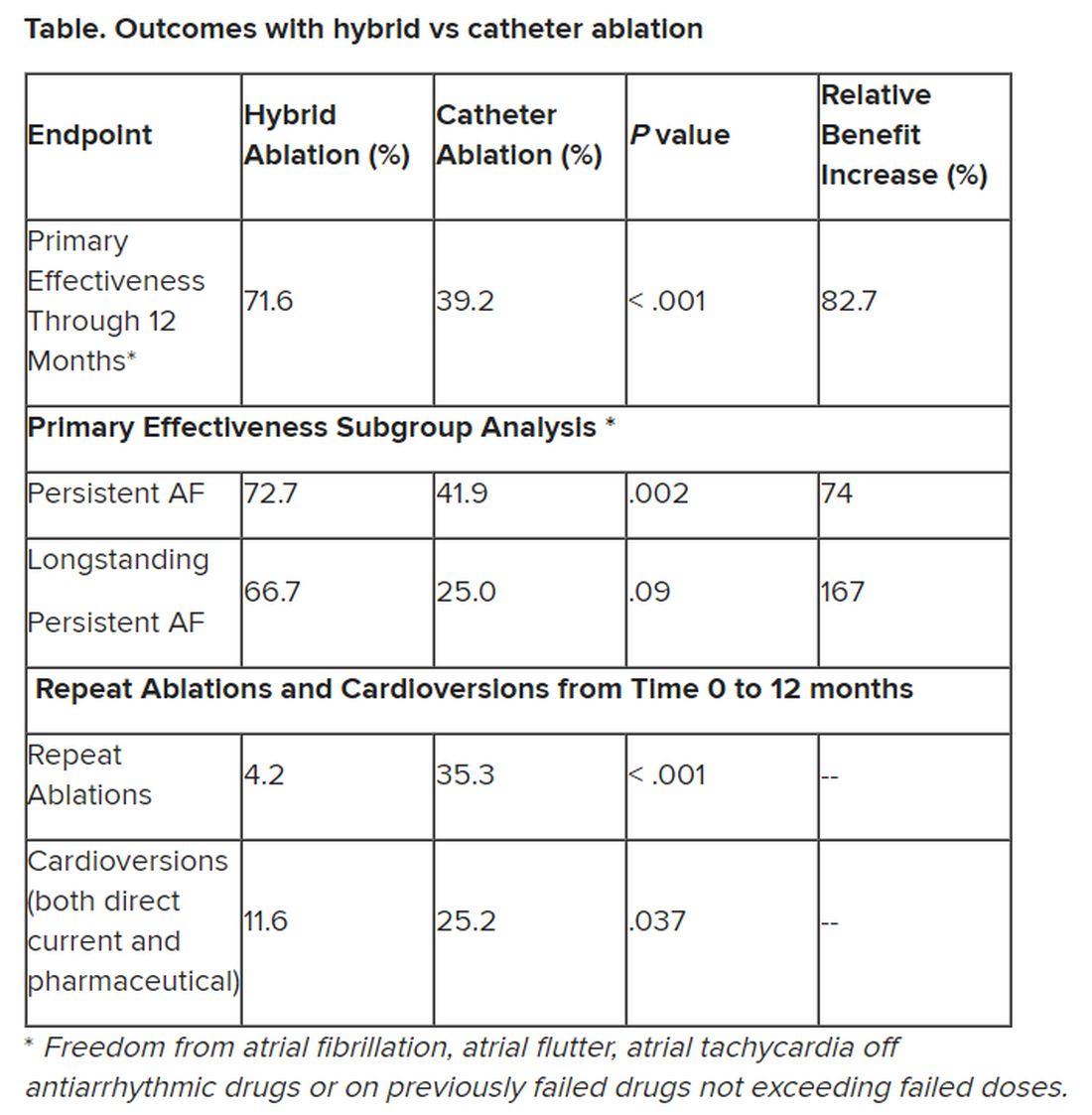
Subgroup analyses were consistent with the primary endpoint, but he said they would not be published because the trial was not powered for such comparisons.
Still, he noted that “there are only slightly reduced outcomes in the long-standing [persistent AF subgroup] in a really challenging patient arm, and we still have a success rate of 67%.” And the repeat ablations in about one-third of patients in the CA arm and need for cardioversions in about one quarter of them may have implications for reduced quality of life.
The total procedure duration was higher for the hybrid group at 336.4 ± 97 minutes, taking into account the index procedure plus the second stage procedure, vs. endocardial ablation at 251.9 ± 114 minutes, which includes the index procedure plus any repeat ablations (HA vs AF total duration, P < .001). Overall fluoroscopy time was approximately 8 minutes shorter for the HA arm.
Complications were assessed for 30 days post index procedure and 30 days post second stage procedure for the HA arm and for 30 days post index procedure and any repeat ablation for the CA arm.
The HA arm showed a complication rate of 7.8% vs. 5.8% for the CA arm (P = .751). Two patients in the former and three patients in the latter group had more than one major complication. There was one death in the HA group 93 days after the index procedure, and it was adjudicated as unrelated to the procedure.
“If you look back in the past, other studies showed a ... higher complication rate in the hybrid arm, so we feel very comfortable with these complication rates, which [are] very low and almost comparable,” Dr. Doll said.
Limitations of the study included symptom-driven electrocardiogram monitoring performed at unscheduled visits. Also, ablation beyond PVI in the CA arm and PVI/posterior box in the HA arm was not standardized and was performed according to standard practices in the participating countries.
“Success of epicardial-endocardial approach emphasizes the role of the collaborative heart team approach in the treatment of nonparoxysmal atrial fibrillation, and if I sum it up together, we can do it better” together, Dr. Doll advised.
‘Exceptional’ trial
After Dr. Doll’s presentation, appointed discussant Stylianos Tzeis, MD, PhD, head of the cardiology clinic and electrophysiology and pacing department at Mitera Hospital in Athens, congratulated the investigators and called CEASE-AF “an exceptional trial. It was really challenging to enroll patients in such a randomized controlled clinical trial.”
But Dr. Tzeis questioned whether pitting CA against HA was a fair comparison.
“Were the ablation targets similar between the two groups?” he asked. He noted that for the HA group, in the first stage the patients had PVI, posterior wall isolation, exclusion of the left atrial appendage, and additional lesions at the discretion of the operator. Ninety percent proceeded to the second stage, which was endocardial catheter ablation with verification of posterior wall isolation and PVI and additional lesions made if needed.
In the CA group, repeat catheter ablation could be performed after the 90-day blanking period if clinically indicated. “Please take note that only 10% were offered the second ablation. So at least in my perspective, this was a comparison of a two-stage approach versus a single-stage approach with a much more aggressive ablation protocol in the hybrid ablation group as compared to the endocardial group,” he said.
Seeing the higher success rate of the HA group in achieving the primary efficacy endpoint of freedom from all arrhythmias at 12 months, Dr. Tzeis asked, “Does this reflect the superiority of the epi-endo approach, or does it reflect the suboptimal performance of the catheter ablation approach?”
There was a 40% success rate in the CA patient population, a cohort that he deemed “not the most challenging persistent AF population in the world”: those with left atrial diameter of 47 millimeters and with 80% having an AF duration less than 12 months.
He also noted that “the average duration of the catheter ablation for the PVI in the vast majority of cases was 4 hours, which does not reflect what really happens in the everyday practice.”
All those critiques having been advanced, Dr. Tzeis said, “Definitely do not doubt my first comment that the authors should be congratulated, and I strongly believe that the main objective has been achieved to bring electrophysiologist and cardiac surgeons ... closer.”
The study sponsor was AtriCure Inc. with collaboration of Cardialysis BV. Doll has received consulting fees or royalties and/or has ownership or stockholder interest in AtriCure. Tzeis reports no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
BARCELONA – Staged hybrid ablation provided superior freedom from atrial arrhythmias compared with endocardial catheter ablation alone, including the need for repeat ablations in patients with advanced atrial fibrillation (AF), new data show.
“We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase, so this is a huge difference,” concluded cardiac surgeon Nicholas Doll, MD, PhD, Schüchtermann Clinic, Bad Rothenfelde, Germany.
Dr. Doll presented the 12-month follow up results of the Combined Endoscopic Epicardial and Percutaneous Endocardial Ablation Versus Repeated Catheter Ablation in Persistent and Longstanding Persistent Atrial Fibrillation (CEASE-AF) trial at the European Heart Rhythm Association 2023 Congress, held recently in Barcelona and virtually.
He said CEASE-AF is the largest multicenter randomized clinical trial comparing these two approaches for control of atrial arrhythmias.
Safety outcomes were numerically higher in the hybrid ablation (HA) group of the trial but not statistically different from the catheter ablation (CA) group.
Unstable wavefront
As background, Dr. Doll explained that in advanced AF, there is a high degree of endocardial-epicardial dissociation with unstable wavefront propagation transitioning between the endocardial and epicardial surfaces. Endocardial mapping and ablation alone may be insufficient to address the mechanism of AF.
“So, the hypothesis of the CEASE-AF study was a minimally invasive hybrid ablation approach which combines endocardial and epicardial ablation to achieve superior effectiveness when compared to endocardial catheter ablation alone,” he said.
This prospective clinical trial randomized patients 2:1 at nine sites in five countries to HA (n = 102) or CA (n = 52). All had left atrial diameter of 4 cm to 6 cm and persistent AF for up to 1 year or longstanding persistent AF for greater than 1 year up to 10 years.
Any patient with a previous ablation procedure, BMI greater than 35 kg/m2, or left ventricular ejection fraction less than 30% was excluded.
For HA, stage 1 consisted of epicardial lesions for pulmonary vein isolation (PVI) plus the posterior wall box plus left atrial appendage exclusion using the AtriClip (AtriCure Inc.) left atrial appendage exclusion device. Stage 2 involved endocardial mapping and catheter ablation to address gaps.
For CA, the index procedure involved catheter-mediated PVI plus repeat endocardial ablation as clinically indicated. For both HA and CA, additional ablation techniques and lesions were allowed for nonparoxysmal AF.
The HA timeline was the first stage, index procedure at time 0 (n = 102), a 90-day blanking period, and then the second stage, endocardial procedure at 90 to 180 days from the index procedure (n = 93).
For the CA arm of the trial, endocardial catheter ablation was performed on a minimal endocardial lesion set at time 0. Then after a 90-day blanking period, repeat catheter ablation was performed if clinically indicated (6/52).
Repeat ablations and electrical or pharmaceutical cardioversions were allowed during the 12-month follow-up period from time 0.
The primary efficacy endpoint was freedom from AF, atrial flutter, or atrial tachycardia of greater than 30 seconds through 12 months in the absence of class I/III antiarrhythmic drugs except ones that previously had failed, at doses not exceeding those previously failed doses. The safety endpoint was a composite rate of major complications over the course of the study.
Even with relatively modest cohort sizes, the HA and CA arms of the trial were well matched at baseline for age (approximately 60 years), gender (75.5% and 73.1% male, respectively), BMI (29.7 and 29.8 kg/m2), and persistent AF (79.4% and 82.7%).
The groups had persistent AF for 2.94 ± 3.29 years and 3.34 ± 3.52 years, respectively. The mean left atrial size was 4.7 ± 0.5 cm for the HA group and 4.7 ± 0.4 cm for the CA group.
Outcomes favored hybrid ablation over catheter ablation, the researchers reported. “We never would have expected these huge differences,” Dr. Doll told the congress. “We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase.”
Subgroup analyses were consistent with the primary endpoint, but he said they would not be published because the trial was not powered for such comparisons.
Still, he noted that “there are only slightly reduced outcomes in the long-standing [persistent AF subgroup] in a really challenging patient arm, and we still have a success rate of 67%.” And the repeat ablations in about one-third of patients in the CA arm and need for cardioversions in about one quarter of them may have implications for reduced quality of life.
The total procedure duration was higher for the hybrid group at 336.4 ± 97 minutes, taking into account the index procedure plus the second stage procedure, vs. endocardial ablation at 251.9 ± 114 minutes, which includes the index procedure plus any repeat ablations (HA vs AF total duration, P < .001). Overall fluoroscopy time was approximately 8 minutes shorter for the HA arm.
Complications were assessed for 30 days post index procedure and 30 days post second stage procedure for the HA arm and for 30 days post index procedure and any repeat ablation for the CA arm.
The HA arm showed a complication rate of 7.8% vs. 5.8% for the CA arm (P = .751). Two patients in the former and three patients in the latter group had more than one major complication. There was one death in the HA group 93 days after the index procedure, and it was adjudicated as unrelated to the procedure.
“If you look back in the past, other studies showed a ... higher complication rate in the hybrid arm, so we feel very comfortable with these complication rates, which [are] very low and almost comparable,” Dr. Doll said.
Limitations of the study included symptom-driven electrocardiogram monitoring performed at unscheduled visits. Also, ablation beyond PVI in the CA arm and PVI/posterior box in the HA arm was not standardized and was performed according to standard practices in the participating countries.
“Success of epicardial-endocardial approach emphasizes the role of the collaborative heart team approach in the treatment of nonparoxysmal atrial fibrillation, and if I sum it up together, we can do it better” together, Dr. Doll advised.
‘Exceptional’ trial
After Dr. Doll’s presentation, appointed discussant Stylianos Tzeis, MD, PhD, head of the cardiology clinic and electrophysiology and pacing department at Mitera Hospital in Athens, congratulated the investigators and called CEASE-AF “an exceptional trial. It was really challenging to enroll patients in such a randomized controlled clinical trial.”
But Dr. Tzeis questioned whether pitting CA against HA was a fair comparison.
“Were the ablation targets similar between the two groups?” he asked. He noted that for the HA group, in the first stage the patients had PVI, posterior wall isolation, exclusion of the left atrial appendage, and additional lesions at the discretion of the operator. Ninety percent proceeded to the second stage, which was endocardial catheter ablation with verification of posterior wall isolation and PVI and additional lesions made if needed.
In the CA group, repeat catheter ablation could be performed after the 90-day blanking period if clinically indicated. “Please take note that only 10% were offered the second ablation. So at least in my perspective, this was a comparison of a two-stage approach versus a single-stage approach with a much more aggressive ablation protocol in the hybrid ablation group as compared to the endocardial group,” he said.
Seeing the higher success rate of the HA group in achieving the primary efficacy endpoint of freedom from all arrhythmias at 12 months, Dr. Tzeis asked, “Does this reflect the superiority of the epi-endo approach, or does it reflect the suboptimal performance of the catheter ablation approach?”
There was a 40% success rate in the CA patient population, a cohort that he deemed “not the most challenging persistent AF population in the world”: those with left atrial diameter of 47 millimeters and with 80% having an AF duration less than 12 months.
He also noted that “the average duration of the catheter ablation for the PVI in the vast majority of cases was 4 hours, which does not reflect what really happens in the everyday practice.”
All those critiques having been advanced, Dr. Tzeis said, “Definitely do not doubt my first comment that the authors should be congratulated, and I strongly believe that the main objective has been achieved to bring electrophysiologist and cardiac surgeons ... closer.”
The study sponsor was AtriCure Inc. with collaboration of Cardialysis BV. Doll has received consulting fees or royalties and/or has ownership or stockholder interest in AtriCure. Tzeis reports no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
BARCELONA – Staged hybrid ablation provided superior freedom from atrial arrhythmias compared with endocardial catheter ablation alone, including the need for repeat ablations in patients with advanced atrial fibrillation (AF), new data show.
“We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase, so this is a huge difference,” concluded cardiac surgeon Nicholas Doll, MD, PhD, Schüchtermann Clinic, Bad Rothenfelde, Germany.
Dr. Doll presented the 12-month follow up results of the Combined Endoscopic Epicardial and Percutaneous Endocardial Ablation Versus Repeated Catheter Ablation in Persistent and Longstanding Persistent Atrial Fibrillation (CEASE-AF) trial at the European Heart Rhythm Association 2023 Congress, held recently in Barcelona and virtually.
He said CEASE-AF is the largest multicenter randomized clinical trial comparing these two approaches for control of atrial arrhythmias.
Safety outcomes were numerically higher in the hybrid ablation (HA) group of the trial but not statistically different from the catheter ablation (CA) group.
Unstable wavefront
As background, Dr. Doll explained that in advanced AF, there is a high degree of endocardial-epicardial dissociation with unstable wavefront propagation transitioning between the endocardial and epicardial surfaces. Endocardial mapping and ablation alone may be insufficient to address the mechanism of AF.
“So, the hypothesis of the CEASE-AF study was a minimally invasive hybrid ablation approach which combines endocardial and epicardial ablation to achieve superior effectiveness when compared to endocardial catheter ablation alone,” he said.
This prospective clinical trial randomized patients 2:1 at nine sites in five countries to HA (n = 102) or CA (n = 52). All had left atrial diameter of 4 cm to 6 cm and persistent AF for up to 1 year or longstanding persistent AF for greater than 1 year up to 10 years.
Any patient with a previous ablation procedure, BMI greater than 35 kg/m2, or left ventricular ejection fraction less than 30% was excluded.
For HA, stage 1 consisted of epicardial lesions for pulmonary vein isolation (PVI) plus the posterior wall box plus left atrial appendage exclusion using the AtriClip (AtriCure Inc.) left atrial appendage exclusion device. Stage 2 involved endocardial mapping and catheter ablation to address gaps.
For CA, the index procedure involved catheter-mediated PVI plus repeat endocardial ablation as clinically indicated. For both HA and CA, additional ablation techniques and lesions were allowed for nonparoxysmal AF.
The HA timeline was the first stage, index procedure at time 0 (n = 102), a 90-day blanking period, and then the second stage, endocardial procedure at 90 to 180 days from the index procedure (n = 93).
For the CA arm of the trial, endocardial catheter ablation was performed on a minimal endocardial lesion set at time 0. Then after a 90-day blanking period, repeat catheter ablation was performed if clinically indicated (6/52).
Repeat ablations and electrical or pharmaceutical cardioversions were allowed during the 12-month follow-up period from time 0.
The primary efficacy endpoint was freedom from AF, atrial flutter, or atrial tachycardia of greater than 30 seconds through 12 months in the absence of class I/III antiarrhythmic drugs except ones that previously had failed, at doses not exceeding those previously failed doses. The safety endpoint was a composite rate of major complications over the course of the study.
Even with relatively modest cohort sizes, the HA and CA arms of the trial were well matched at baseline for age (approximately 60 years), gender (75.5% and 73.1% male, respectively), BMI (29.7 and 29.8 kg/m2), and persistent AF (79.4% and 82.7%).
The groups had persistent AF for 2.94 ± 3.29 years and 3.34 ± 3.52 years, respectively. The mean left atrial size was 4.7 ± 0.5 cm for the HA group and 4.7 ± 0.4 cm for the CA group.
Outcomes favored hybrid ablation over catheter ablation, the researchers reported. “We never would have expected these huge differences,” Dr. Doll told the congress. “We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase.”
Subgroup analyses were consistent with the primary endpoint, but he said they would not be published because the trial was not powered for such comparisons.
Still, he noted that “there are only slightly reduced outcomes in the long-standing [persistent AF subgroup] in a really challenging patient arm, and we still have a success rate of 67%.” And the repeat ablations in about one-third of patients in the CA arm and need for cardioversions in about one quarter of them may have implications for reduced quality of life.
The total procedure duration was higher for the hybrid group at 336.4 ± 97 minutes, taking into account the index procedure plus the second stage procedure, vs. endocardial ablation at 251.9 ± 114 minutes, which includes the index procedure plus any repeat ablations (HA vs AF total duration, P < .001). Overall fluoroscopy time was approximately 8 minutes shorter for the HA arm.
Complications were assessed for 30 days post index procedure and 30 days post second stage procedure for the HA arm and for 30 days post index procedure and any repeat ablation for the CA arm.
The HA arm showed a complication rate of 7.8% vs. 5.8% for the CA arm (P = .751). Two patients in the former and three patients in the latter group had more than one major complication. There was one death in the HA group 93 days after the index procedure, and it was adjudicated as unrelated to the procedure.
“If you look back in the past, other studies showed a ... higher complication rate in the hybrid arm, so we feel very comfortable with these complication rates, which [are] very low and almost comparable,” Dr. Doll said.
Limitations of the study included symptom-driven electrocardiogram monitoring performed at unscheduled visits. Also, ablation beyond PVI in the CA arm and PVI/posterior box in the HA arm was not standardized and was performed according to standard practices in the participating countries.
“Success of epicardial-endocardial approach emphasizes the role of the collaborative heart team approach in the treatment of nonparoxysmal atrial fibrillation, and if I sum it up together, we can do it better” together, Dr. Doll advised.
‘Exceptional’ trial
After Dr. Doll’s presentation, appointed discussant Stylianos Tzeis, MD, PhD, head of the cardiology clinic and electrophysiology and pacing department at Mitera Hospital in Athens, congratulated the investigators and called CEASE-AF “an exceptional trial. It was really challenging to enroll patients in such a randomized controlled clinical trial.”
But Dr. Tzeis questioned whether pitting CA against HA was a fair comparison.
“Were the ablation targets similar between the two groups?” he asked. He noted that for the HA group, in the first stage the patients had PVI, posterior wall isolation, exclusion of the left atrial appendage, and additional lesions at the discretion of the operator. Ninety percent proceeded to the second stage, which was endocardial catheter ablation with verification of posterior wall isolation and PVI and additional lesions made if needed.
In the CA group, repeat catheter ablation could be performed after the 90-day blanking period if clinically indicated. “Please take note that only 10% were offered the second ablation. So at least in my perspective, this was a comparison of a two-stage approach versus a single-stage approach with a much more aggressive ablation protocol in the hybrid ablation group as compared to the endocardial group,” he said.
Seeing the higher success rate of the HA group in achieving the primary efficacy endpoint of freedom from all arrhythmias at 12 months, Dr. Tzeis asked, “Does this reflect the superiority of the epi-endo approach, or does it reflect the suboptimal performance of the catheter ablation approach?”
There was a 40% success rate in the CA patient population, a cohort that he deemed “not the most challenging persistent AF population in the world”: those with left atrial diameter of 47 millimeters and with 80% having an AF duration less than 12 months.
He also noted that “the average duration of the catheter ablation for the PVI in the vast majority of cases was 4 hours, which does not reflect what really happens in the everyday practice.”
All those critiques having been advanced, Dr. Tzeis said, “Definitely do not doubt my first comment that the authors should be congratulated, and I strongly believe that the main objective has been achieved to bring electrophysiologist and cardiac surgeons ... closer.”
The study sponsor was AtriCure Inc. with collaboration of Cardialysis BV. Doll has received consulting fees or royalties and/or has ownership or stockholder interest in AtriCure. Tzeis reports no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
AT EHRA 2023
Ablation for atrial fibrillation may protect the aging brain
BOSTON – , new research suggests.
Investigators found adults who had previously undergone catheter ablation were significantly less likely to be cognitively impaired during the 2-year study period, compared with those who receive medical management alone.
“Catheter ablation is intended to stop atrial fibrillation and restore the normal rhythm of the heart. By doing so, there is an improved cerebral hemodynamic profile,” said Bahadar S. Srichawla, DO, department of neurology, University of Massachusetts, Worcester.
“Thus, long-term cognitive outcomes may be improved due to improved blood flow to the brain by restoring the normal rhythm of the heart,” he added.
This research was presented at the 2023 annual meeting of the American Academy of Neurology.
Heart-brain connection
The study involved 887 older adults (mean age 75; 49% women) with atrial fibrillation participating in the SAGE-AF (Systematic Assessment of Geriatric Elements) study. A total of 193 (22%) participants underwent catheter ablation prior to enrollment. These individuals more frequently had an implantable cardiac device (46% vs. 28%, P < .001) and persistent atrial fibrillation (31% vs. 23%, P < .05).
Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA) tool at baseline and 1 and 2 years, with cognitive impairment defined as a MoCA score of 23 or below. Individuals who had catheter ablation had an average MoCA score of 25, compared with an average score of 23 in those who didn’t have catheter ablation.
After adjusting for potential confounding factors such as heart disease, renal disease, sleep apnea, and atrial fibrillation risk score, those who underwent catheter ablation were 36% less likely to develop cognitive impairment over 2 years than those who were treated only with medication (adjusted odds ratio, 0.64; 95% CI, 0.46-0.88).
During his presentation, Dr. Srichawla noted there is a hypothesis that individuals who are anticoagulated with warfarin may be prone to cerebral microbleeds and may be more cognitively impaired over time.
However, in a subgroup analysis, “cognitive function was similar at 2-year follow-up in those anticoagulated with warfarin, compared with all other anticoagulants. However, it should be noted that in this study, a direct head-to-head comparison was not done,” Dr. Srichawla told attendees.
“In patients with atrial fibrillation, catheter ablation should be discussed as a potential treatment strategy, particularly in patients who have or are at risk for cognitive decline and dementia,” Dr. Srichawla said.
Intriguing findings
Commenting on the research, Percy Griffin, PhD, Alzheimer’s Association director of scientific engagement, said the study is “intriguing and adds to what we know from previous research connecting cardiovascular and cognitive health.”
“However, there are limitations to this study,” Dr. Griffin said, “including its predominantly White cohort and the use of only neuropsychiatric testing to diagnose dementia. More research is needed to fully understand the impact of atrial fibrillation on cognitive outcomes in all people.”
“It’s well known that the heart and the brain are intimately connected. Individuals experiencing any cardiovascular issues should speak to their doctor,” Dr. Griffin added.
Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, agreed. “If you ever get up too quickly and feel woozy, that is your brain not getting enough blood flow and you are getting all the warning signs to correct that – or else! Similarly, with atrial fibrillation, the heart is contracting, but not effectively pumping blood to the brain,” he said.
“This line of research shows that correcting the abnormal heart rhythm by zapping the faulty circuit with a catheter is actually better for your brain health than just taking medications alone,” added Dr. Lakhan, who was not involved with the study.
The study had no commercial funding. Dr. Srichawla, Dr. Griffin, and Dr. Lakhan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
BOSTON – , new research suggests.
Investigators found adults who had previously undergone catheter ablation were significantly less likely to be cognitively impaired during the 2-year study period, compared with those who receive medical management alone.
“Catheter ablation is intended to stop atrial fibrillation and restore the normal rhythm of the heart. By doing so, there is an improved cerebral hemodynamic profile,” said Bahadar S. Srichawla, DO, department of neurology, University of Massachusetts, Worcester.
“Thus, long-term cognitive outcomes may be improved due to improved blood flow to the brain by restoring the normal rhythm of the heart,” he added.
This research was presented at the 2023 annual meeting of the American Academy of Neurology.
Heart-brain connection
The study involved 887 older adults (mean age 75; 49% women) with atrial fibrillation participating in the SAGE-AF (Systematic Assessment of Geriatric Elements) study. A total of 193 (22%) participants underwent catheter ablation prior to enrollment. These individuals more frequently had an implantable cardiac device (46% vs. 28%, P < .001) and persistent atrial fibrillation (31% vs. 23%, P < .05).
Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA) tool at baseline and 1 and 2 years, with cognitive impairment defined as a MoCA score of 23 or below. Individuals who had catheter ablation had an average MoCA score of 25, compared with an average score of 23 in those who didn’t have catheter ablation.
After adjusting for potential confounding factors such as heart disease, renal disease, sleep apnea, and atrial fibrillation risk score, those who underwent catheter ablation were 36% less likely to develop cognitive impairment over 2 years than those who were treated only with medication (adjusted odds ratio, 0.64; 95% CI, 0.46-0.88).
During his presentation, Dr. Srichawla noted there is a hypothesis that individuals who are anticoagulated with warfarin may be prone to cerebral microbleeds and may be more cognitively impaired over time.
However, in a subgroup analysis, “cognitive function was similar at 2-year follow-up in those anticoagulated with warfarin, compared with all other anticoagulants. However, it should be noted that in this study, a direct head-to-head comparison was not done,” Dr. Srichawla told attendees.
“In patients with atrial fibrillation, catheter ablation should be discussed as a potential treatment strategy, particularly in patients who have or are at risk for cognitive decline and dementia,” Dr. Srichawla said.
Intriguing findings
Commenting on the research, Percy Griffin, PhD, Alzheimer’s Association director of scientific engagement, said the study is “intriguing and adds to what we know from previous research connecting cardiovascular and cognitive health.”
“However, there are limitations to this study,” Dr. Griffin said, “including its predominantly White cohort and the use of only neuropsychiatric testing to diagnose dementia. More research is needed to fully understand the impact of atrial fibrillation on cognitive outcomes in all people.”
“It’s well known that the heart and the brain are intimately connected. Individuals experiencing any cardiovascular issues should speak to their doctor,” Dr. Griffin added.
Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, agreed. “If you ever get up too quickly and feel woozy, that is your brain not getting enough blood flow and you are getting all the warning signs to correct that – or else! Similarly, with atrial fibrillation, the heart is contracting, but not effectively pumping blood to the brain,” he said.
“This line of research shows that correcting the abnormal heart rhythm by zapping the faulty circuit with a catheter is actually better for your brain health than just taking medications alone,” added Dr. Lakhan, who was not involved with the study.
The study had no commercial funding. Dr. Srichawla, Dr. Griffin, and Dr. Lakhan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
BOSTON – , new research suggests.
Investigators found adults who had previously undergone catheter ablation were significantly less likely to be cognitively impaired during the 2-year study period, compared with those who receive medical management alone.
“Catheter ablation is intended to stop atrial fibrillation and restore the normal rhythm of the heart. By doing so, there is an improved cerebral hemodynamic profile,” said Bahadar S. Srichawla, DO, department of neurology, University of Massachusetts, Worcester.
“Thus, long-term cognitive outcomes may be improved due to improved blood flow to the brain by restoring the normal rhythm of the heart,” he added.
This research was presented at the 2023 annual meeting of the American Academy of Neurology.
Heart-brain connection
The study involved 887 older adults (mean age 75; 49% women) with atrial fibrillation participating in the SAGE-AF (Systematic Assessment of Geriatric Elements) study. A total of 193 (22%) participants underwent catheter ablation prior to enrollment. These individuals more frequently had an implantable cardiac device (46% vs. 28%, P < .001) and persistent atrial fibrillation (31% vs. 23%, P < .05).
Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA) tool at baseline and 1 and 2 years, with cognitive impairment defined as a MoCA score of 23 or below. Individuals who had catheter ablation had an average MoCA score of 25, compared with an average score of 23 in those who didn’t have catheter ablation.
After adjusting for potential confounding factors such as heart disease, renal disease, sleep apnea, and atrial fibrillation risk score, those who underwent catheter ablation were 36% less likely to develop cognitive impairment over 2 years than those who were treated only with medication (adjusted odds ratio, 0.64; 95% CI, 0.46-0.88).
During his presentation, Dr. Srichawla noted there is a hypothesis that individuals who are anticoagulated with warfarin may be prone to cerebral microbleeds and may be more cognitively impaired over time.
However, in a subgroup analysis, “cognitive function was similar at 2-year follow-up in those anticoagulated with warfarin, compared with all other anticoagulants. However, it should be noted that in this study, a direct head-to-head comparison was not done,” Dr. Srichawla told attendees.
“In patients with atrial fibrillation, catheter ablation should be discussed as a potential treatment strategy, particularly in patients who have or are at risk for cognitive decline and dementia,” Dr. Srichawla said.
Intriguing findings
Commenting on the research, Percy Griffin, PhD, Alzheimer’s Association director of scientific engagement, said the study is “intriguing and adds to what we know from previous research connecting cardiovascular and cognitive health.”
“However, there are limitations to this study,” Dr. Griffin said, “including its predominantly White cohort and the use of only neuropsychiatric testing to diagnose dementia. More research is needed to fully understand the impact of atrial fibrillation on cognitive outcomes in all people.”
“It’s well known that the heart and the brain are intimately connected. Individuals experiencing any cardiovascular issues should speak to their doctor,” Dr. Griffin added.
Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, agreed. “If you ever get up too quickly and feel woozy, that is your brain not getting enough blood flow and you are getting all the warning signs to correct that – or else! Similarly, with atrial fibrillation, the heart is contracting, but not effectively pumping blood to the brain,” he said.
“This line of research shows that correcting the abnormal heart rhythm by zapping the faulty circuit with a catheter is actually better for your brain health than just taking medications alone,” added Dr. Lakhan, who was not involved with the study.
The study had no commercial funding. Dr. Srichawla, Dr. Griffin, and Dr. Lakhan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2023
What new cardiovascular disease risk factors have emerged?
Cardiovascular disease (CVD) is the main cause of premature death and disability in the general population, and according to the World Health Organization, the incidence of CVD is increasing throughout the world. Conventional risk factors that contribute to the occurrence and worsening of CVD have been identified and widely studied. They include high cholesterol levels, high blood pressure, diabetes, obesity, smoking, and lack of physical activity. Despite the introduction of measures to prevent and treat these risk factors with lipid-lowering drugs, antihypertensives, antiplatelet drugs, and anticoagulants, the mortality rate related to CVD remains high.
Despite the effectiveness of many currently available treatment options, there are still significant gaps in risk assessment and treatment of CVD.
They are detailed in an editorial published in The American Journal of Medicine that describes their role and their impact on our cardiovascular health.
Systemic inflammation
The new coronary risk factors include the following diseases characterized by systemic inflammation:
- Gout – Among patients who have experienced a recent flare of gout, the probability of experiencing an acute cardiovascular event such as a myocardial infarction or stroke is increased.
- Rheumatoid arthritis and systemic lupus erythematous – Patients with one or both of these conditions are at higher odds of experiencing concomitant premature and extremely premature coronary artery disease.
- Inflammatory bowel disease (Crohn’s disease or ulcerative colitis) – Patients with this disease have increased odds of developing coronary artery disease.
- Psoriasis – Patients with psoriasis are up to 50% more likely to develop CVD.
Maternal and childhood factors
The following maternal and childhood factors are associated with an increased risk of developing coronary artery disease: gestational diabetes; preeclampsia; delivering a child of low birth weight; preterm delivery; and premature or surgical menopause. The factor or factors that increase the risk of coronary artery disease associated with each of these conditions are not known but may be the result of increased cytokine and oxidative stress.
An unusual and yet unexplained association has been observed between migraine headaches with aura in women and incident CVD.
Also of interest is the association of early life trauma and the risk of adverse cardiovascular outcomes in young and middle-aged individuals who have a history of myocardial infarction.
Transgender patients who present for gender-affirming care are also at increased cardiovascular risk. Among these patients, the increase in coronary artery disease risk may be related to high rates of anxiety and depression.
Environmental factors
Low socioeconomic status has emerged as a risk factor. Increased psychosocial stressors, limited educational and economic opportunities, and lack of peer influence favoring healthier lifestyle choices may be causative elements leading to enhanced coronary artery disease among individuals with low socioeconomic living conditions.
Air pollution was estimated to have caused 9 million deaths worldwide in 2019, with 62% due to CVD and 31.7% to coronary artery disease. Severely polluted environmental aerosols contain several toxic metals, such as lead, mercury, arsenic, and cadmium. Transient exposure to various air pollutants may trigger the onset of an acute coronary syndrome.
Lifestyle factors
Long working hours by patients who have experienced a first myocardial infarction increase the risk for a recurrent event, possibly because of prolonged exposure to work stressors.
Skipping breakfast has been linked to increased cardiovascular and all-cause mortality.
Long-term consumption of drinks containing sugar and artificial sweeteners has also been associated with increased cardiovascular mortality.
Recognizing the presence of one or more of these new risk factors could help prompt and improve behaviors for reducing more conventional CV risk factors to a minimum.
This article was translated from Univadis Italy, which is part of the Medscape Professional Network.
A version of this article first appeared on Medscape.com.
Cardiovascular disease (CVD) is the main cause of premature death and disability in the general population, and according to the World Health Organization, the incidence of CVD is increasing throughout the world. Conventional risk factors that contribute to the occurrence and worsening of CVD have been identified and widely studied. They include high cholesterol levels, high blood pressure, diabetes, obesity, smoking, and lack of physical activity. Despite the introduction of measures to prevent and treat these risk factors with lipid-lowering drugs, antihypertensives, antiplatelet drugs, and anticoagulants, the mortality rate related to CVD remains high.
Despite the effectiveness of many currently available treatment options, there are still significant gaps in risk assessment and treatment of CVD.
They are detailed in an editorial published in The American Journal of Medicine that describes their role and their impact on our cardiovascular health.
Systemic inflammation
The new coronary risk factors include the following diseases characterized by systemic inflammation:
- Gout – Among patients who have experienced a recent flare of gout, the probability of experiencing an acute cardiovascular event such as a myocardial infarction or stroke is increased.
- Rheumatoid arthritis and systemic lupus erythematous – Patients with one or both of these conditions are at higher odds of experiencing concomitant premature and extremely premature coronary artery disease.
- Inflammatory bowel disease (Crohn’s disease or ulcerative colitis) – Patients with this disease have increased odds of developing coronary artery disease.
- Psoriasis – Patients with psoriasis are up to 50% more likely to develop CVD.
Maternal and childhood factors
The following maternal and childhood factors are associated with an increased risk of developing coronary artery disease: gestational diabetes; preeclampsia; delivering a child of low birth weight; preterm delivery; and premature or surgical menopause. The factor or factors that increase the risk of coronary artery disease associated with each of these conditions are not known but may be the result of increased cytokine and oxidative stress.
An unusual and yet unexplained association has been observed between migraine headaches with aura in women and incident CVD.
Also of interest is the association of early life trauma and the risk of adverse cardiovascular outcomes in young and middle-aged individuals who have a history of myocardial infarction.
Transgender patients who present for gender-affirming care are also at increased cardiovascular risk. Among these patients, the increase in coronary artery disease risk may be related to high rates of anxiety and depression.
Environmental factors
Low socioeconomic status has emerged as a risk factor. Increased psychosocial stressors, limited educational and economic opportunities, and lack of peer influence favoring healthier lifestyle choices may be causative elements leading to enhanced coronary artery disease among individuals with low socioeconomic living conditions.
Air pollution was estimated to have caused 9 million deaths worldwide in 2019, with 62% due to CVD and 31.7% to coronary artery disease. Severely polluted environmental aerosols contain several toxic metals, such as lead, mercury, arsenic, and cadmium. Transient exposure to various air pollutants may trigger the onset of an acute coronary syndrome.
Lifestyle factors
Long working hours by patients who have experienced a first myocardial infarction increase the risk for a recurrent event, possibly because of prolonged exposure to work stressors.
Skipping breakfast has been linked to increased cardiovascular and all-cause mortality.
Long-term consumption of drinks containing sugar and artificial sweeteners has also been associated with increased cardiovascular mortality.
Recognizing the presence of one or more of these new risk factors could help prompt and improve behaviors for reducing more conventional CV risk factors to a minimum.
This article was translated from Univadis Italy, which is part of the Medscape Professional Network.
A version of this article first appeared on Medscape.com.
Cardiovascular disease (CVD) is the main cause of premature death and disability in the general population, and according to the World Health Organization, the incidence of CVD is increasing throughout the world. Conventional risk factors that contribute to the occurrence and worsening of CVD have been identified and widely studied. They include high cholesterol levels, high blood pressure, diabetes, obesity, smoking, and lack of physical activity. Despite the introduction of measures to prevent and treat these risk factors with lipid-lowering drugs, antihypertensives, antiplatelet drugs, and anticoagulants, the mortality rate related to CVD remains high.
Despite the effectiveness of many currently available treatment options, there are still significant gaps in risk assessment and treatment of CVD.
They are detailed in an editorial published in The American Journal of Medicine that describes their role and their impact on our cardiovascular health.
Systemic inflammation
The new coronary risk factors include the following diseases characterized by systemic inflammation:
- Gout – Among patients who have experienced a recent flare of gout, the probability of experiencing an acute cardiovascular event such as a myocardial infarction or stroke is increased.
- Rheumatoid arthritis and systemic lupus erythematous – Patients with one or both of these conditions are at higher odds of experiencing concomitant premature and extremely premature coronary artery disease.
- Inflammatory bowel disease (Crohn’s disease or ulcerative colitis) – Patients with this disease have increased odds of developing coronary artery disease.
- Psoriasis – Patients with psoriasis are up to 50% more likely to develop CVD.
Maternal and childhood factors
The following maternal and childhood factors are associated with an increased risk of developing coronary artery disease: gestational diabetes; preeclampsia; delivering a child of low birth weight; preterm delivery; and premature or surgical menopause. The factor or factors that increase the risk of coronary artery disease associated with each of these conditions are not known but may be the result of increased cytokine and oxidative stress.
An unusual and yet unexplained association has been observed between migraine headaches with aura in women and incident CVD.
Also of interest is the association of early life trauma and the risk of adverse cardiovascular outcomes in young and middle-aged individuals who have a history of myocardial infarction.
Transgender patients who present for gender-affirming care are also at increased cardiovascular risk. Among these patients, the increase in coronary artery disease risk may be related to high rates of anxiety and depression.
Environmental factors
Low socioeconomic status has emerged as a risk factor. Increased psychosocial stressors, limited educational and economic opportunities, and lack of peer influence favoring healthier lifestyle choices may be causative elements leading to enhanced coronary artery disease among individuals with low socioeconomic living conditions.
Air pollution was estimated to have caused 9 million deaths worldwide in 2019, with 62% due to CVD and 31.7% to coronary artery disease. Severely polluted environmental aerosols contain several toxic metals, such as lead, mercury, arsenic, and cadmium. Transient exposure to various air pollutants may trigger the onset of an acute coronary syndrome.
Lifestyle factors
Long working hours by patients who have experienced a first myocardial infarction increase the risk for a recurrent event, possibly because of prolonged exposure to work stressors.
Skipping breakfast has been linked to increased cardiovascular and all-cause mortality.
Long-term consumption of drinks containing sugar and artificial sweeteners has also been associated with increased cardiovascular mortality.
Recognizing the presence of one or more of these new risk factors could help prompt and improve behaviors for reducing more conventional CV risk factors to a minimum.
This article was translated from Univadis Italy, which is part of the Medscape Professional Network.
A version of this article first appeared on Medscape.com.
FROM THE AMERICAN JOURNAL OF MEDICINE
FDA okays latest artificial pancreas, the MiniMed 780G
The Food and Drug Administration has approved Medtronic Minimed’s 780G automated insulin delivery system with the Guardian 4 sensor.
The latest so-called artificial pancreas system is approved for people aged 7 years and older who have type 1 diabetes. Medtronic will begin taking preorders for the 780G on May 15, 2023. Users of the current MiniMed 770G will be eligible for no-cost remote software upgrades.
The 780G is currently available in 105 countries. It has been available in Europe since 2020 and in the United Kingdom since 2021. It is the first automated insulin delivery system to automatically administer bolus correction insulin doses every 5 minutes to correct meal-related hyperglycemia.
This so-called meal detection technology doesn’t replace manual premeal boluses but does provide extra insulin if the premeal bolus is skipped or is insufficient.
As with other automated systems, the 780G automatically adjusts basal insulin doses up or down based on glucose levels and trends and shuts off insulin delivery to prevent hypoglycemia. The insulin pump’s infusion set can be worn for 7 days, rather than 3 days as with the older system, and the glucose target level can be set as low as 100 mg/dL.
And in contrast to the older MiniMed 670G system, which tended to frequently boot users out of automated mode, with the 780G, users spent an average of 95% of the time in the automated “SmartGuard” mode.
In the pivotal U.S. trial, overall, patients who used the 780G spent 75% of the time in ideal glucose range (70-180 mg/dL) and 1.8% of the time below that range. Overnight, the figures were 82% and 1.5%, respectively. With the glucose target set at 100 mg/dL and active insulin time set to 2 hours, patients spent 78.8% of time in range without increased hyperglycemia.
In the ADAPT study, with the 780G, there was a 26% increase in time in ideal glucose range and a 1.4% reduction in A1c compared with results for patients who received multiple daily insulin injections with intermittently scanned continuous glucose monitoring, without an increase in hypoglycemia. Overnight, time in range increased 30.2%. The results were sustained at 1 year.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved Medtronic Minimed’s 780G automated insulin delivery system with the Guardian 4 sensor.
The latest so-called artificial pancreas system is approved for people aged 7 years and older who have type 1 diabetes. Medtronic will begin taking preorders for the 780G on May 15, 2023. Users of the current MiniMed 770G will be eligible for no-cost remote software upgrades.
The 780G is currently available in 105 countries. It has been available in Europe since 2020 and in the United Kingdom since 2021. It is the first automated insulin delivery system to automatically administer bolus correction insulin doses every 5 minutes to correct meal-related hyperglycemia.
This so-called meal detection technology doesn’t replace manual premeal boluses but does provide extra insulin if the premeal bolus is skipped or is insufficient.
As with other automated systems, the 780G automatically adjusts basal insulin doses up or down based on glucose levels and trends and shuts off insulin delivery to prevent hypoglycemia. The insulin pump’s infusion set can be worn for 7 days, rather than 3 days as with the older system, and the glucose target level can be set as low as 100 mg/dL.
And in contrast to the older MiniMed 670G system, which tended to frequently boot users out of automated mode, with the 780G, users spent an average of 95% of the time in the automated “SmartGuard” mode.
In the pivotal U.S. trial, overall, patients who used the 780G spent 75% of the time in ideal glucose range (70-180 mg/dL) and 1.8% of the time below that range. Overnight, the figures were 82% and 1.5%, respectively. With the glucose target set at 100 mg/dL and active insulin time set to 2 hours, patients spent 78.8% of time in range without increased hyperglycemia.
In the ADAPT study, with the 780G, there was a 26% increase in time in ideal glucose range and a 1.4% reduction in A1c compared with results for patients who received multiple daily insulin injections with intermittently scanned continuous glucose monitoring, without an increase in hypoglycemia. Overnight, time in range increased 30.2%. The results were sustained at 1 year.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved Medtronic Minimed’s 780G automated insulin delivery system with the Guardian 4 sensor.
The latest so-called artificial pancreas system is approved for people aged 7 years and older who have type 1 diabetes. Medtronic will begin taking preorders for the 780G on May 15, 2023. Users of the current MiniMed 770G will be eligible for no-cost remote software upgrades.
The 780G is currently available in 105 countries. It has been available in Europe since 2020 and in the United Kingdom since 2021. It is the first automated insulin delivery system to automatically administer bolus correction insulin doses every 5 minutes to correct meal-related hyperglycemia.
This so-called meal detection technology doesn’t replace manual premeal boluses but does provide extra insulin if the premeal bolus is skipped or is insufficient.
As with other automated systems, the 780G automatically adjusts basal insulin doses up or down based on glucose levels and trends and shuts off insulin delivery to prevent hypoglycemia. The insulin pump’s infusion set can be worn for 7 days, rather than 3 days as with the older system, and the glucose target level can be set as low as 100 mg/dL.
And in contrast to the older MiniMed 670G system, which tended to frequently boot users out of automated mode, with the 780G, users spent an average of 95% of the time in the automated “SmartGuard” mode.
In the pivotal U.S. trial, overall, patients who used the 780G spent 75% of the time in ideal glucose range (70-180 mg/dL) and 1.8% of the time below that range. Overnight, the figures were 82% and 1.5%, respectively. With the glucose target set at 100 mg/dL and active insulin time set to 2 hours, patients spent 78.8% of time in range without increased hyperglycemia.
In the ADAPT study, with the 780G, there was a 26% increase in time in ideal glucose range and a 1.4% reduction in A1c compared with results for patients who received multiple daily insulin injections with intermittently scanned continuous glucose monitoring, without an increase in hypoglycemia. Overnight, time in range increased 30.2%. The results were sustained at 1 year.
A version of this article first appeared on Medscape.com.
New ACC guidance on heart failure with preserved ejection fraction
The American College of Cardiology has released an Expert Consensus Decision Pathway (ECDP) on the management of heart failure with preserved ejection fraction (HFpEF).
The 44-page document highlights the “critical need” to accurately diagnose HFpEF to permit timely implementation of evidence- and guideline-based therapies to improve patient outcomes.
Although the incidence of overall HF in the United States appears to be stable or declining, the incidence of HFpEF continues to rise in tandem with increasing age and burdens of obesity, sedentary lifestyle, and cardiometabolic disorders.
HFpEF now accounts for more than one half of HF cases but remains “underrecognized” in everyday clinical practice, said the writing group, led by Michelle Kittleson, MD, PhD, professor of medicine, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles.
HFpEF is a complex condition, often with multiple overlapping comorbidities, including hypertension, diabetes, obesity, and sleep apnea; optimal management requires a multidisciplinary approach, the writing group said.
The ECDP on HFpEF lays out a structure for diagnosis, clinical decision-making, management of comorbidities, implementation of the latest guideline-directed medical therapy (pharmacologic and nonpharmacologic), and equitable delivery of care.
The document was published online in the Journal of the American College of Cardiology.
It aligns with and builds on recommendations from the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.
“HFpEF is one of the most pressing diagnostic and therapeutic challenges in clinical medicine today given its increasing prevalence, under diagnosis, poor prognosis, limited therapeutic options, and substantial burden on the health care system worldwide,” wrote the authors of a companion scientific statement on HFpEF.
Despite these challenges, the success of recent sodium-glucose cotransporter 2 inhibitor trials has shown that HFpEF is treatable, Barry Borlaug, MD, department of cardiovascular medicine, Mayo Clinic, Rochester, Minn., and coauthors pointed out.
They noted that “ongoing large-scale studies of HFpEF pathobiology, an increasing number of translational studies spanning the gap between the bedside and the bench, and numerous clinical trials of novel therapeutics in HFpEF offer a glimpse of hope toward a future of reduced prevalence, morbidity, and mortality associated with HFpEF, which would be a major advance for population health.”
A version of this article originally appeared on Medscape.com.
The American College of Cardiology has released an Expert Consensus Decision Pathway (ECDP) on the management of heart failure with preserved ejection fraction (HFpEF).
The 44-page document highlights the “critical need” to accurately diagnose HFpEF to permit timely implementation of evidence- and guideline-based therapies to improve patient outcomes.
Although the incidence of overall HF in the United States appears to be stable or declining, the incidence of HFpEF continues to rise in tandem with increasing age and burdens of obesity, sedentary lifestyle, and cardiometabolic disorders.
HFpEF now accounts for more than one half of HF cases but remains “underrecognized” in everyday clinical practice, said the writing group, led by Michelle Kittleson, MD, PhD, professor of medicine, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles.
HFpEF is a complex condition, often with multiple overlapping comorbidities, including hypertension, diabetes, obesity, and sleep apnea; optimal management requires a multidisciplinary approach, the writing group said.
The ECDP on HFpEF lays out a structure for diagnosis, clinical decision-making, management of comorbidities, implementation of the latest guideline-directed medical therapy (pharmacologic and nonpharmacologic), and equitable delivery of care.
The document was published online in the Journal of the American College of Cardiology.
It aligns with and builds on recommendations from the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.
“HFpEF is one of the most pressing diagnostic and therapeutic challenges in clinical medicine today given its increasing prevalence, under diagnosis, poor prognosis, limited therapeutic options, and substantial burden on the health care system worldwide,” wrote the authors of a companion scientific statement on HFpEF.
Despite these challenges, the success of recent sodium-glucose cotransporter 2 inhibitor trials has shown that HFpEF is treatable, Barry Borlaug, MD, department of cardiovascular medicine, Mayo Clinic, Rochester, Minn., and coauthors pointed out.
They noted that “ongoing large-scale studies of HFpEF pathobiology, an increasing number of translational studies spanning the gap between the bedside and the bench, and numerous clinical trials of novel therapeutics in HFpEF offer a glimpse of hope toward a future of reduced prevalence, morbidity, and mortality associated with HFpEF, which would be a major advance for population health.”
A version of this article originally appeared on Medscape.com.
The American College of Cardiology has released an Expert Consensus Decision Pathway (ECDP) on the management of heart failure with preserved ejection fraction (HFpEF).
The 44-page document highlights the “critical need” to accurately diagnose HFpEF to permit timely implementation of evidence- and guideline-based therapies to improve patient outcomes.
Although the incidence of overall HF in the United States appears to be stable or declining, the incidence of HFpEF continues to rise in tandem with increasing age and burdens of obesity, sedentary lifestyle, and cardiometabolic disorders.
HFpEF now accounts for more than one half of HF cases but remains “underrecognized” in everyday clinical practice, said the writing group, led by Michelle Kittleson, MD, PhD, professor of medicine, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles.
HFpEF is a complex condition, often with multiple overlapping comorbidities, including hypertension, diabetes, obesity, and sleep apnea; optimal management requires a multidisciplinary approach, the writing group said.
The ECDP on HFpEF lays out a structure for diagnosis, clinical decision-making, management of comorbidities, implementation of the latest guideline-directed medical therapy (pharmacologic and nonpharmacologic), and equitable delivery of care.
The document was published online in the Journal of the American College of Cardiology.
It aligns with and builds on recommendations from the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.
“HFpEF is one of the most pressing diagnostic and therapeutic challenges in clinical medicine today given its increasing prevalence, under diagnosis, poor prognosis, limited therapeutic options, and substantial burden on the health care system worldwide,” wrote the authors of a companion scientific statement on HFpEF.
Despite these challenges, the success of recent sodium-glucose cotransporter 2 inhibitor trials has shown that HFpEF is treatable, Barry Borlaug, MD, department of cardiovascular medicine, Mayo Clinic, Rochester, Minn., and coauthors pointed out.
They noted that “ongoing large-scale studies of HFpEF pathobiology, an increasing number of translational studies spanning the gap between the bedside and the bench, and numerous clinical trials of novel therapeutics in HFpEF offer a glimpse of hope toward a future of reduced prevalence, morbidity, and mortality associated with HFpEF, which would be a major advance for population health.”
A version of this article originally appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Meditation curbs stress, depression as adjunct to CAD rehab
Regular meditation reduced depression by roughly 44% in adults with coronary artery disease who were involved in a cardiovascular rehabilitation program.
An increasing body of research supports the impact of psychological risk factors including stress, personality type, anger, and hostility on conditions such as depression and anxiety, but also social isolation and low socioeconomic status, Ana Luisa Vitorino Monteiro, MD, of the University of Lisbon said in a presentation at the annual congress of the European Association of Preventive Cardiology. In addition, “stress, anxiety, and depression deteriorate the cardiovascular (CV) system through psycho-neuro-immunoendocrinology system and behavioral pathways.”
Meditation as a tool for stress management has been gaining popularity, but its use as part of a CV rehabilitation program as a complementary therapy has not been well studied, she added.
Dr. Monteiro and colleagues recruited 80 adults with CAD who were undergoing CV rehabilitation to join a meditation program. Of these, 48 accepted (60%) and 40% declined. Those who accepted were part of an exercise-based CV rehabilitation program that met three times a week for at least 6 months. The mean age of the participants was 65 years, and 80% were male.
Participants were randomized to an intervention group with a weekly 90-minute session that included breathing and meditation for 1 month in addition to usual care, or to usual care in the rehabilitation program. Over the next 3 months, the intervention patients were encouraged to practice daily meditation for 20 minutes alone or using video support material, with a weekly follow-up phone call. Assessments of stress, anxiety, and depression took place at baseline and after 4 months using the Perceived Stress Scale, Beck Anxiety Inventory, Beck Depression Inventory, and HeartQoL questionnaire.
At 4 months, individuals in the meditation group had reduced depression levels significantly, by 44%, compared with controls (P < .001). Anxiety and stress decreased significantly, by 30% (P = .04) and 31% (P = .05), respectively. After 4 months, individuals in the control group were offered the opportunity to follow the meditation protocol.
In addition, “the emotional dimension of quality of life increased by 60% in the intervention group,” Dr. Monteiro noted. However, physical QoL did not change between groups.
The study was limited by the small sample size, and more research is needed in larger and more diverse populations, Dr. Monteiro said. However, the results support the value of meditation as an adjunct component of care for CAD patients in a long-term rehabilitation program.
Motivation makes a difference
The current study is important as an exploration of “a straightforward, simple, low-risk approach that could be an adjunct to benefit patients with serious cardiovascular disease,” Brian Olshansky, MD, a cardiologist at the University of Iowa, Iowa City, said in an interview.

“We have moved into a time of polypharmacy and multiple interventions for patients with underlying cardiovascular disease which, in many cases, have proven benefit but also potential adverse effects,” he said. “Engaging patients to participate in their health care, when there is serious underlying cardiovascular disease, has potential beneficial impact in many ways. Meditation is a low-risk, low-cost, potentially beneficial adjunct to standard medical therapy that may enhance psychological outcomes as shown here in this small study.”
However, “patients often rely on high-cost, potentially high-risk therapeutic interventions, expecting complete control of their problems without their own collaborative intervention,” he noted.
Dr. Olshansky said he was not surprised by any of the findings, and would have been surprised if meditation had failed to show any benefit for the study population.
“I am very pleased to see these results and would encourage meditation practice to be part of cardiovascular rehabilitation for motivated individuals,” he said. “What did surprise me was the adherence to the meditation protocol for those who participated. This represents a highly motivated group and it may be difficult to expect the same results in less motivated individuals.”
The current study has several strengths, including the use of controls and high rates of adherence to the protocol, said Dr. Olshansky. Other strengths include the standardized approach and the reasonable quality of the outcome measures, which showed a substantial benefit.
However, “this is a small study of motivated individuals of whom 80% were male,” and generalizability to other populations is unclear, Dr. Olshansky said. In addition, the racial mix was not described, and the severity of the underlying coronary artery disease and the therapies provided to these individuals is not detailed. A sicker population may not fare as well.”
The reasons for the benefits of meditation remain uncertain, Dr. Olshansky said. “It could be, specifically, that the meditation itself has physiological effects that ultimately translate into psychosocial benefit. However, those who enrolled and were interested may have derived a placebo effect. In any case, benefit was achieved, but the crossover benefit to the control group is unclear.
“In other words, the statistical approach to benefit is uncertain as to when it was measured, but presumably before the control group was allowed to engage in a meditation practice,” and the follow-up was short term, said Dr. Olshansky.
Data support patient engagement
The message to clinicians and patients: “Patients should be engaged in their own health care when it comes to rehabilitation for cardiovascular disease,” said Dr. Olshansky. “Motivated individuals who are educated about a meditative practice performed in a standardized way will have improvement most likely in their quality of life, and when it comes to measurements of depression, stress and anxiety.”
Although the mechanisms behind the benefits remain unclear, “having a standardized credible prescription for which patients can become intimately engaged is beneficial,” he added.
The study received no outside funding. Neither Dr. Monteiro nor Dr. Olshansky had any financial conflicts to disclose.
Regular meditation reduced depression by roughly 44% in adults with coronary artery disease who were involved in a cardiovascular rehabilitation program.
An increasing body of research supports the impact of psychological risk factors including stress, personality type, anger, and hostility on conditions such as depression and anxiety, but also social isolation and low socioeconomic status, Ana Luisa Vitorino Monteiro, MD, of the University of Lisbon said in a presentation at the annual congress of the European Association of Preventive Cardiology. In addition, “stress, anxiety, and depression deteriorate the cardiovascular (CV) system through psycho-neuro-immunoendocrinology system and behavioral pathways.”
Meditation as a tool for stress management has been gaining popularity, but its use as part of a CV rehabilitation program as a complementary therapy has not been well studied, she added.
Dr. Monteiro and colleagues recruited 80 adults with CAD who were undergoing CV rehabilitation to join a meditation program. Of these, 48 accepted (60%) and 40% declined. Those who accepted were part of an exercise-based CV rehabilitation program that met three times a week for at least 6 months. The mean age of the participants was 65 years, and 80% were male.
Participants were randomized to an intervention group with a weekly 90-minute session that included breathing and meditation for 1 month in addition to usual care, or to usual care in the rehabilitation program. Over the next 3 months, the intervention patients were encouraged to practice daily meditation for 20 minutes alone or using video support material, with a weekly follow-up phone call. Assessments of stress, anxiety, and depression took place at baseline and after 4 months using the Perceived Stress Scale, Beck Anxiety Inventory, Beck Depression Inventory, and HeartQoL questionnaire.
At 4 months, individuals in the meditation group had reduced depression levels significantly, by 44%, compared with controls (P < .001). Anxiety and stress decreased significantly, by 30% (P = .04) and 31% (P = .05), respectively. After 4 months, individuals in the control group were offered the opportunity to follow the meditation protocol.
In addition, “the emotional dimension of quality of life increased by 60% in the intervention group,” Dr. Monteiro noted. However, physical QoL did not change between groups.
The study was limited by the small sample size, and more research is needed in larger and more diverse populations, Dr. Monteiro said. However, the results support the value of meditation as an adjunct component of care for CAD patients in a long-term rehabilitation program.
Motivation makes a difference
The current study is important as an exploration of “a straightforward, simple, low-risk approach that could be an adjunct to benefit patients with serious cardiovascular disease,” Brian Olshansky, MD, a cardiologist at the University of Iowa, Iowa City, said in an interview.
“We have moved into a time of polypharmacy and multiple interventions for patients with underlying cardiovascular disease which, in many cases, have proven benefit but also potential adverse effects,” he said. “Engaging patients to participate in their health care, when there is serious underlying cardiovascular disease, has potential beneficial impact in many ways. Meditation is a low-risk, low-cost, potentially beneficial adjunct to standard medical therapy that may enhance psychological outcomes as shown here in this small study.”
However, “patients often rely on high-cost, potentially high-risk therapeutic interventions, expecting complete control of their problems without their own collaborative intervention,” he noted.
Dr. Olshansky said he was not surprised by any of the findings, and would have been surprised if meditation had failed to show any benefit for the study population.
“I am very pleased to see these results and would encourage meditation practice to be part of cardiovascular rehabilitation for motivated individuals,” he said. “What did surprise me was the adherence to the meditation protocol for those who participated. This represents a highly motivated group and it may be difficult to expect the same results in less motivated individuals.”
The current study has several strengths, including the use of controls and high rates of adherence to the protocol, said Dr. Olshansky. Other strengths include the standardized approach and the reasonable quality of the outcome measures, which showed a substantial benefit.
However, “this is a small study of motivated individuals of whom 80% were male,” and generalizability to other populations is unclear, Dr. Olshansky said. In addition, the racial mix was not described, and the severity of the underlying coronary artery disease and the therapies provided to these individuals is not detailed. A sicker population may not fare as well.”
The reasons for the benefits of meditation remain uncertain, Dr. Olshansky said. “It could be, specifically, that the meditation itself has physiological effects that ultimately translate into psychosocial benefit. However, those who enrolled and were interested may have derived a placebo effect. In any case, benefit was achieved, but the crossover benefit to the control group is unclear.
“In other words, the statistical approach to benefit is uncertain as to when it was measured, but presumably before the control group was allowed to engage in a meditation practice,” and the follow-up was short term, said Dr. Olshansky.
Data support patient engagement
The message to clinicians and patients: “Patients should be engaged in their own health care when it comes to rehabilitation for cardiovascular disease,” said Dr. Olshansky. “Motivated individuals who are educated about a meditative practice performed in a standardized way will have improvement most likely in their quality of life, and when it comes to measurements of depression, stress and anxiety.”
Although the mechanisms behind the benefits remain unclear, “having a standardized credible prescription for which patients can become intimately engaged is beneficial,” he added.
The study received no outside funding. Neither Dr. Monteiro nor Dr. Olshansky had any financial conflicts to disclose.
Regular meditation reduced depression by roughly 44% in adults with coronary artery disease who were involved in a cardiovascular rehabilitation program.
An increasing body of research supports the impact of psychological risk factors including stress, personality type, anger, and hostility on conditions such as depression and anxiety, but also social isolation and low socioeconomic status, Ana Luisa Vitorino Monteiro, MD, of the University of Lisbon said in a presentation at the annual congress of the European Association of Preventive Cardiology. In addition, “stress, anxiety, and depression deteriorate the cardiovascular (CV) system through psycho-neuro-immunoendocrinology system and behavioral pathways.”
Meditation as a tool for stress management has been gaining popularity, but its use as part of a CV rehabilitation program as a complementary therapy has not been well studied, she added.
Dr. Monteiro and colleagues recruited 80 adults with CAD who were undergoing CV rehabilitation to join a meditation program. Of these, 48 accepted (60%) and 40% declined. Those who accepted were part of an exercise-based CV rehabilitation program that met three times a week for at least 6 months. The mean age of the participants was 65 years, and 80% were male.
Participants were randomized to an intervention group with a weekly 90-minute session that included breathing and meditation for 1 month in addition to usual care, or to usual care in the rehabilitation program. Over the next 3 months, the intervention patients were encouraged to practice daily meditation for 20 minutes alone or using video support material, with a weekly follow-up phone call. Assessments of stress, anxiety, and depression took place at baseline and after 4 months using the Perceived Stress Scale, Beck Anxiety Inventory, Beck Depression Inventory, and HeartQoL questionnaire.
At 4 months, individuals in the meditation group had reduced depression levels significantly, by 44%, compared with controls (P < .001). Anxiety and stress decreased significantly, by 30% (P = .04) and 31% (P = .05), respectively. After 4 months, individuals in the control group were offered the opportunity to follow the meditation protocol.
In addition, “the emotional dimension of quality of life increased by 60% in the intervention group,” Dr. Monteiro noted. However, physical QoL did not change between groups.
The study was limited by the small sample size, and more research is needed in larger and more diverse populations, Dr. Monteiro said. However, the results support the value of meditation as an adjunct component of care for CAD patients in a long-term rehabilitation program.
Motivation makes a difference
The current study is important as an exploration of “a straightforward, simple, low-risk approach that could be an adjunct to benefit patients with serious cardiovascular disease,” Brian Olshansky, MD, a cardiologist at the University of Iowa, Iowa City, said in an interview.
“We have moved into a time of polypharmacy and multiple interventions for patients with underlying cardiovascular disease which, in many cases, have proven benefit but also potential adverse effects,” he said. “Engaging patients to participate in their health care, when there is serious underlying cardiovascular disease, has potential beneficial impact in many ways. Meditation is a low-risk, low-cost, potentially beneficial adjunct to standard medical therapy that may enhance psychological outcomes as shown here in this small study.”
However, “patients often rely on high-cost, potentially high-risk therapeutic interventions, expecting complete control of their problems without their own collaborative intervention,” he noted.
Dr. Olshansky said he was not surprised by any of the findings, and would have been surprised if meditation had failed to show any benefit for the study population.
“I am very pleased to see these results and would encourage meditation practice to be part of cardiovascular rehabilitation for motivated individuals,” he said. “What did surprise me was the adherence to the meditation protocol for those who participated. This represents a highly motivated group and it may be difficult to expect the same results in less motivated individuals.”
The current study has several strengths, including the use of controls and high rates of adherence to the protocol, said Dr. Olshansky. Other strengths include the standardized approach and the reasonable quality of the outcome measures, which showed a substantial benefit.
However, “this is a small study of motivated individuals of whom 80% were male,” and generalizability to other populations is unclear, Dr. Olshansky said. In addition, the racial mix was not described, and the severity of the underlying coronary artery disease and the therapies provided to these individuals is not detailed. A sicker population may not fare as well.”
The reasons for the benefits of meditation remain uncertain, Dr. Olshansky said. “It could be, specifically, that the meditation itself has physiological effects that ultimately translate into psychosocial benefit. However, those who enrolled and were interested may have derived a placebo effect. In any case, benefit was achieved, but the crossover benefit to the control group is unclear.
“In other words, the statistical approach to benefit is uncertain as to when it was measured, but presumably before the control group was allowed to engage in a meditation practice,” and the follow-up was short term, said Dr. Olshansky.
Data support patient engagement
The message to clinicians and patients: “Patients should be engaged in their own health care when it comes to rehabilitation for cardiovascular disease,” said Dr. Olshansky. “Motivated individuals who are educated about a meditative practice performed in a standardized way will have improvement most likely in their quality of life, and when it comes to measurements of depression, stress and anxiety.”
Although the mechanisms behind the benefits remain unclear, “having a standardized credible prescription for which patients can become intimately engaged is beneficial,” he added.
The study received no outside funding. Neither Dr. Monteiro nor Dr. Olshansky had any financial conflicts to disclose.
FROM ESC PREVENTIVE CARDIOLOGY 2023
Proposed Medicare bill would raise docs’ pay with inflation
Introduced by four physician U.S. House representatives, HR 2474 would link Medicare fee schedule updates to the Medicare Economic Index, a measure of inflation related to physicians’ practice costs and wages.
That’s a long-sought goal of the American Medical Association, which is leading 120 state medical societies and medical specialty groups in championing the bill.
The legislation is essential to enabling physician practices to better absorb payment distributions triggered by budget neutrality rules, performance adjustments, and periods of high inflation, the groups wrote in a joint letter sent to the bill’s sponsors. The sponsors say they hope the legislation will improve access to care, as low reimbursements cause some physicians to limit their number of Medicare patients.
Physicians groups for years have urged federal lawmakers to scrap short-term fixes staving off Medicare pay cuts in favor of permanent reforms. Unlike nearly all other Medicare clinicians including hospitals, physicians’ Medicare payment updates aren’t currently tied to inflation.
Adjusted for inflation, Medicare payments to physicians have declined 26% between 2001 and 2023, including a 2% payment reduction in 2023, according to the AMA. Small and rural physician practices have been disproportionately affected by these reductions, as have doctors treating low-income or uninsured patients, the AMA said.
Last month, an influential federal advisory panel recommended permanently tying Medicare physician pay increases to inflation. Clinicians’ cost of providing services, measured by the Medicare Economic Index, rose by 2.6% in 2021 and are estimated to have risen 4.7% in 2022, significantly more than in recent years, the Medicare Payment Advisory Commission said.
A version of this article originally appeared on Medscape.com.
Introduced by four physician U.S. House representatives, HR 2474 would link Medicare fee schedule updates to the Medicare Economic Index, a measure of inflation related to physicians’ practice costs and wages.
That’s a long-sought goal of the American Medical Association, which is leading 120 state medical societies and medical specialty groups in championing the bill.
The legislation is essential to enabling physician practices to better absorb payment distributions triggered by budget neutrality rules, performance adjustments, and periods of high inflation, the groups wrote in a joint letter sent to the bill’s sponsors. The sponsors say they hope the legislation will improve access to care, as low reimbursements cause some physicians to limit their number of Medicare patients.
Physicians groups for years have urged federal lawmakers to scrap short-term fixes staving off Medicare pay cuts in favor of permanent reforms. Unlike nearly all other Medicare clinicians including hospitals, physicians’ Medicare payment updates aren’t currently tied to inflation.
Adjusted for inflation, Medicare payments to physicians have declined 26% between 2001 and 2023, including a 2% payment reduction in 2023, according to the AMA. Small and rural physician practices have been disproportionately affected by these reductions, as have doctors treating low-income or uninsured patients, the AMA said.
Last month, an influential federal advisory panel recommended permanently tying Medicare physician pay increases to inflation. Clinicians’ cost of providing services, measured by the Medicare Economic Index, rose by 2.6% in 2021 and are estimated to have risen 4.7% in 2022, significantly more than in recent years, the Medicare Payment Advisory Commission said.
A version of this article originally appeared on Medscape.com.
Introduced by four physician U.S. House representatives, HR 2474 would link Medicare fee schedule updates to the Medicare Economic Index, a measure of inflation related to physicians’ practice costs and wages.
That’s a long-sought goal of the American Medical Association, which is leading 120 state medical societies and medical specialty groups in championing the bill.
The legislation is essential to enabling physician practices to better absorb payment distributions triggered by budget neutrality rules, performance adjustments, and periods of high inflation, the groups wrote in a joint letter sent to the bill’s sponsors. The sponsors say they hope the legislation will improve access to care, as low reimbursements cause some physicians to limit their number of Medicare patients.
Physicians groups for years have urged federal lawmakers to scrap short-term fixes staving off Medicare pay cuts in favor of permanent reforms. Unlike nearly all other Medicare clinicians including hospitals, physicians’ Medicare payment updates aren’t currently tied to inflation.
Adjusted for inflation, Medicare payments to physicians have declined 26% between 2001 and 2023, including a 2% payment reduction in 2023, according to the AMA. Small and rural physician practices have been disproportionately affected by these reductions, as have doctors treating low-income or uninsured patients, the AMA said.
Last month, an influential federal advisory panel recommended permanently tying Medicare physician pay increases to inflation. Clinicians’ cost of providing services, measured by the Medicare Economic Index, rose by 2.6% in 2021 and are estimated to have risen 4.7% in 2022, significantly more than in recent years, the Medicare Payment Advisory Commission said.
A version of this article originally appeared on Medscape.com.
Surgeons, intensivists earn more than do colleagues from private insurance
General and orthopedic surgeons and intensivists earn the highest net reimbursements from private U.S. insurers, a new report estimates.
On average in 2021, they were paid $5.8 million, $4.9 million, and $3.3 million, respectively, according to figures compiled by AMN Healthcare, a Dallas-based health staffing company.
None of 15 other physician specialties topped $3 million in net reimbursement on average, and three – dermatology, pediatrics, and family medicine – didn’t reach $1 million.
The report doesn’t include data about reimbursement from Medicare and Medicaid, and its numbers assume that 50% of insurance claims are denied. Denial rates differ from practice to practice.
Still, the findings offer a “benchmark tool” to help clinicians understand how they rank against their peers, Linda Murphy, president of AMN Healthcare’s Revenue Cycle Solutions division, said in an interview.
This is the first year that the company has calculated physician reimbursement levels by using claim and clearinghouse data, Ms. Murphy said. Previously, a division of the firm compiled data by surveying chief financial officers from hospitals.
The report’s estimate that insurers deny 50% of claims is “conservative,” Ms. Murphy said. Miscoding is a significant factor behind that number.
The estimated 2021 net private insurance reimbursements by specialty for direct services, assuming a 50% denial rate:
- Anesthesiology: $1,665,510
- Cardiology: $1,703,013
- Critical Care (intensivist): $3,338,656
- Dermatology: $729,107
- Family medicine: $697,094
- Gastroenterology: $2,765,110
- Internal medicine: $1,297,200
- Neurology: $1,390,181
- Obstetrician/gynecology: $1,880,888
- Otolaryngology: $2,095,277
- Pediatrics: $661,552
- Psychiatry: $1,348,730
- Pulmonology: $1,561,617
- Radiology: $1,015,750
- Rheumatology: $1,705,140
- General surgery: $5,834,508
- Orthopedic surgery: $4,904,757
- Urology: $2,943,381
Among 18 physician specialties overall, the report estimated that the average net reimbursement in 2021 was $1.9 million.
The report also estimated that the net reimbursement amounts at $875,140 for certified registered nurse anesthetists and $388,696 for nurse practitioners.
Surprisingly, Ms. Murphy said, there’s “a really large swing” among reimbursement levels for individual specialties. The quartile of cardiologists with the lowest level of reimbursement, for example, submitted $2.1 million in claims in 2021, netting about $1 million at a 50% denial rate versus the $7.3 million made by those in the highest quartile, netting about $3.6 million.
The gap seems to be due to regional variations, she said, adding that a rural cardiologist will have different billing practices than does one practicing in New York City.
The quartile of general surgeons with the highest reimbursement levels billed for $21.1 million on average in 2021, making about $10.5 million at a 50% denial rate. The lowest quartile billed for $5.5 million, making about $2.7 million at a 50% denial rate.
The report noted that primary care physicians – that is, family medicine, internal medicine, and pediatrics specialists – have much lower levels of reimbursement, compared with most other specialties. But the work of primary care physicians “may lead to considerable ‘downstream revenue’ through the hospital admissions, tests and treatment they order.”
A previous analysis by a division of AMN Healthcare found that primary care physicians, on average, generate $2,113,273 a year in net annual revenue for their affiliated hospitals, nearing the $2,446,429 in net annual hospital revenue generated by specialists.
AMN Healthcare is preparing another report that will examine Medicare reimbursements, Ms. Murphy said. According to the new report, payments by nonprivate insurers amount to about one-third of the total amount of reimbursement by commercial insurers.
A version of this article originally appeared on Medscape.com.
General and orthopedic surgeons and intensivists earn the highest net reimbursements from private U.S. insurers, a new report estimates.
On average in 2021, they were paid $5.8 million, $4.9 million, and $3.3 million, respectively, according to figures compiled by AMN Healthcare, a Dallas-based health staffing company.
None of 15 other physician specialties topped $3 million in net reimbursement on average, and three – dermatology, pediatrics, and family medicine – didn’t reach $1 million.
The report doesn’t include data about reimbursement from Medicare and Medicaid, and its numbers assume that 50% of insurance claims are denied. Denial rates differ from practice to practice.
Still, the findings offer a “benchmark tool” to help clinicians understand how they rank against their peers, Linda Murphy, president of AMN Healthcare’s Revenue Cycle Solutions division, said in an interview.
This is the first year that the company has calculated physician reimbursement levels by using claim and clearinghouse data, Ms. Murphy said. Previously, a division of the firm compiled data by surveying chief financial officers from hospitals.
The report’s estimate that insurers deny 50% of claims is “conservative,” Ms. Murphy said. Miscoding is a significant factor behind that number.
The estimated 2021 net private insurance reimbursements by specialty for direct services, assuming a 50% denial rate:
- Anesthesiology: $1,665,510
- Cardiology: $1,703,013
- Critical Care (intensivist): $3,338,656
- Dermatology: $729,107
- Family medicine: $697,094
- Gastroenterology: $2,765,110
- Internal medicine: $1,297,200
- Neurology: $1,390,181
- Obstetrician/gynecology: $1,880,888
- Otolaryngology: $2,095,277
- Pediatrics: $661,552
- Psychiatry: $1,348,730
- Pulmonology: $1,561,617
- Radiology: $1,015,750
- Rheumatology: $1,705,140
- General surgery: $5,834,508
- Orthopedic surgery: $4,904,757
- Urology: $2,943,381
Among 18 physician specialties overall, the report estimated that the average net reimbursement in 2021 was $1.9 million.
The report also estimated that the net reimbursement amounts at $875,140 for certified registered nurse anesthetists and $388,696 for nurse practitioners.
Surprisingly, Ms. Murphy said, there’s “a really large swing” among reimbursement levels for individual specialties. The quartile of cardiologists with the lowest level of reimbursement, for example, submitted $2.1 million in claims in 2021, netting about $1 million at a 50% denial rate versus the $7.3 million made by those in the highest quartile, netting about $3.6 million.
The gap seems to be due to regional variations, she said, adding that a rural cardiologist will have different billing practices than does one practicing in New York City.
The quartile of general surgeons with the highest reimbursement levels billed for $21.1 million on average in 2021, making about $10.5 million at a 50% denial rate. The lowest quartile billed for $5.5 million, making about $2.7 million at a 50% denial rate.
The report noted that primary care physicians – that is, family medicine, internal medicine, and pediatrics specialists – have much lower levels of reimbursement, compared with most other specialties. But the work of primary care physicians “may lead to considerable ‘downstream revenue’ through the hospital admissions, tests and treatment they order.”
A previous analysis by a division of AMN Healthcare found that primary care physicians, on average, generate $2,113,273 a year in net annual revenue for their affiliated hospitals, nearing the $2,446,429 in net annual hospital revenue generated by specialists.
AMN Healthcare is preparing another report that will examine Medicare reimbursements, Ms. Murphy said. According to the new report, payments by nonprivate insurers amount to about one-third of the total amount of reimbursement by commercial insurers.
A version of this article originally appeared on Medscape.com.
General and orthopedic surgeons and intensivists earn the highest net reimbursements from private U.S. insurers, a new report estimates.
On average in 2021, they were paid $5.8 million, $4.9 million, and $3.3 million, respectively, according to figures compiled by AMN Healthcare, a Dallas-based health staffing company.
None of 15 other physician specialties topped $3 million in net reimbursement on average, and three – dermatology, pediatrics, and family medicine – didn’t reach $1 million.
The report doesn’t include data about reimbursement from Medicare and Medicaid, and its numbers assume that 50% of insurance claims are denied. Denial rates differ from practice to practice.
Still, the findings offer a “benchmark tool” to help clinicians understand how they rank against their peers, Linda Murphy, president of AMN Healthcare’s Revenue Cycle Solutions division, said in an interview.
This is the first year that the company has calculated physician reimbursement levels by using claim and clearinghouse data, Ms. Murphy said. Previously, a division of the firm compiled data by surveying chief financial officers from hospitals.
The report’s estimate that insurers deny 50% of claims is “conservative,” Ms. Murphy said. Miscoding is a significant factor behind that number.
The estimated 2021 net private insurance reimbursements by specialty for direct services, assuming a 50% denial rate:
- Anesthesiology: $1,665,510
- Cardiology: $1,703,013
- Critical Care (intensivist): $3,338,656
- Dermatology: $729,107
- Family medicine: $697,094
- Gastroenterology: $2,765,110
- Internal medicine: $1,297,200
- Neurology: $1,390,181
- Obstetrician/gynecology: $1,880,888
- Otolaryngology: $2,095,277
- Pediatrics: $661,552
- Psychiatry: $1,348,730
- Pulmonology: $1,561,617
- Radiology: $1,015,750
- Rheumatology: $1,705,140
- General surgery: $5,834,508
- Orthopedic surgery: $4,904,757
- Urology: $2,943,381
Among 18 physician specialties overall, the report estimated that the average net reimbursement in 2021 was $1.9 million.
The report also estimated that the net reimbursement amounts at $875,140 for certified registered nurse anesthetists and $388,696 for nurse practitioners.
Surprisingly, Ms. Murphy said, there’s “a really large swing” among reimbursement levels for individual specialties. The quartile of cardiologists with the lowest level of reimbursement, for example, submitted $2.1 million in claims in 2021, netting about $1 million at a 50% denial rate versus the $7.3 million made by those in the highest quartile, netting about $3.6 million.
The gap seems to be due to regional variations, she said, adding that a rural cardiologist will have different billing practices than does one practicing in New York City.
The quartile of general surgeons with the highest reimbursement levels billed for $21.1 million on average in 2021, making about $10.5 million at a 50% denial rate. The lowest quartile billed for $5.5 million, making about $2.7 million at a 50% denial rate.
The report noted that primary care physicians – that is, family medicine, internal medicine, and pediatrics specialists – have much lower levels of reimbursement, compared with most other specialties. But the work of primary care physicians “may lead to considerable ‘downstream revenue’ through the hospital admissions, tests and treatment they order.”
A previous analysis by a division of AMN Healthcare found that primary care physicians, on average, generate $2,113,273 a year in net annual revenue for their affiliated hospitals, nearing the $2,446,429 in net annual hospital revenue generated by specialists.
AMN Healthcare is preparing another report that will examine Medicare reimbursements, Ms. Murphy said. According to the new report, payments by nonprivate insurers amount to about one-third of the total amount of reimbursement by commercial insurers.
A version of this article originally appeared on Medscape.com.