User login
Teaching opportunities of live surgery broadcasts debated
SAN DIEGO – Two thoracic societies are being challenged to review their rejection of at medical meetings.
The American Association for Thoracic Surgery and Society of Thoracic Surgeons “should modify their stance on live surgery as an educational tool like almost all of their sister organizations,” said Joseph E. Bavaria, MD, FACS, of the University of Pennsylvania, Philadelphia. “Presently, it is effectively a ban on the practice. But there are no data to suggest that it does harm to patients if done with proper constraints.”

Live broadcasts of surgeries at medical meetings are both common and controversial. Dr. Bavaria listed numerous recent thoracic meetings in Europe and Canada that featured live broadcasts. But, he noted, the AATS and STS are not supportive of the trend.
In a policy amended in 2017, the AATS states, among other things, that “national and international cardiothoracic societies should consider prohibiting live surgery broadcasts to large audiences at their annual meetings.” The STS policy, amended in 2016, is nearly identical. However, it adds language specifying that “violation of these guidelines may lead to disciplinary action by the Society.”
Both the AATS and STS policies state that surgeons should not take part in live broadcasts of operations that are intended for the public. And both policies say “generally, recorded broadcasts, either edited or unedited, are preferable to live surgery broadcasts because recordings intended for later broadcast pose fewer risks of harm to patients.”
The policies don’t elaborate on how a live broadcast of an operation might be more harmful than one aired at a later time. “Where are the data to support this statement?” Dr. Bavaria asked. “Is this what we call the expert opinion of a few people with gray hair? Our European and Canadian colleagues certainly don’t agree with [the policies] and might take issue with our sanctimonious lecturing that’s not supported by any data whatsoever.”
He pointed to a 2011 study that examined 250 cardiac procedures that were broadcast live to 32 scientific meetings. Researchers found that “there is no evidence for an excess perioperative risk for patients operated under the conditions of live broadcasting” (Eur J Cardiothorac Surg. 2011;40[2]:367-71).
A member of the audience at the AATS session pointed out that the study may be misleading because only top surgeons may be willing to perform procedures live on television. Dr. Bavaria responded by noting that the outcomes of surgeries performed on live video were not worse.
Skeptics have also expressed concern about the potential for sensationalism in live broadcasts and the drive for participants to make a splash: “the demands of ‘the performance,’ including questions and discussion with the audience, may divert the surgeon’s attention and produce an inferior outcome,” wrote three physicians in 2011 (J Surg Educ. 2011 Jan-Feb; 68[1]:58-61).
The trio also expressed worry about safety risks posed by extra equipment and extra people in the operating room during a live broadcast. However, Dr. Bavaria said the crowded conditions of an operation observed in person – instead of via video – could be worse: “You don’t have a sterile environment, you have people hanging around all over. A moderated live session could be better for the surgeon and the patient, rather than having a bunch of people in the room.”
Dr. Bavaria was also asked why surgeries couldn’t be recorded for airing later instead of being broadcast live, as this approach “takes you out of the nexus of having two masters, the patient and the audience.” In response, Dr. Bavaria said editing takes extra time in order to capture the nuances of the live procedure.
Dr. Bavaria reports no relevant disclosures.

Peter Angelos, MD, FACS, is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics, chief of endocrine surgery, and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago. Dr. Angelos has no disclosures.
Peter Angelos, MD, FACS, is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics, chief of endocrine surgery, and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago. Dr. Angelos has no disclosures.
Peter Angelos, MD, FACS, is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics, chief of endocrine surgery, and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago. Dr. Angelos has no disclosures.
SAN DIEGO – Two thoracic societies are being challenged to review their rejection of at medical meetings.
The American Association for Thoracic Surgery and Society of Thoracic Surgeons “should modify their stance on live surgery as an educational tool like almost all of their sister organizations,” said Joseph E. Bavaria, MD, FACS, of the University of Pennsylvania, Philadelphia. “Presently, it is effectively a ban on the practice. But there are no data to suggest that it does harm to patients if done with proper constraints.”
Live broadcasts of surgeries at medical meetings are both common and controversial. Dr. Bavaria listed numerous recent thoracic meetings in Europe and Canada that featured live broadcasts. But, he noted, the AATS and STS are not supportive of the trend.
In a policy amended in 2017, the AATS states, among other things, that “national and international cardiothoracic societies should consider prohibiting live surgery broadcasts to large audiences at their annual meetings.” The STS policy, amended in 2016, is nearly identical. However, it adds language specifying that “violation of these guidelines may lead to disciplinary action by the Society.”
Both the AATS and STS policies state that surgeons should not take part in live broadcasts of operations that are intended for the public. And both policies say “generally, recorded broadcasts, either edited or unedited, are preferable to live surgery broadcasts because recordings intended for later broadcast pose fewer risks of harm to patients.”
The policies don’t elaborate on how a live broadcast of an operation might be more harmful than one aired at a later time. “Where are the data to support this statement?” Dr. Bavaria asked. “Is this what we call the expert opinion of a few people with gray hair? Our European and Canadian colleagues certainly don’t agree with [the policies] and might take issue with our sanctimonious lecturing that’s not supported by any data whatsoever.”
He pointed to a 2011 study that examined 250 cardiac procedures that were broadcast live to 32 scientific meetings. Researchers found that “there is no evidence for an excess perioperative risk for patients operated under the conditions of live broadcasting” (Eur J Cardiothorac Surg. 2011;40[2]:367-71).
A member of the audience at the AATS session pointed out that the study may be misleading because only top surgeons may be willing to perform procedures live on television. Dr. Bavaria responded by noting that the outcomes of surgeries performed on live video were not worse.
Skeptics have also expressed concern about the potential for sensationalism in live broadcasts and the drive for participants to make a splash: “the demands of ‘the performance,’ including questions and discussion with the audience, may divert the surgeon’s attention and produce an inferior outcome,” wrote three physicians in 2011 (J Surg Educ. 2011 Jan-Feb; 68[1]:58-61).
The trio also expressed worry about safety risks posed by extra equipment and extra people in the operating room during a live broadcast. However, Dr. Bavaria said the crowded conditions of an operation observed in person – instead of via video – could be worse: “You don’t have a sterile environment, you have people hanging around all over. A moderated live session could be better for the surgeon and the patient, rather than having a bunch of people in the room.”
Dr. Bavaria was also asked why surgeries couldn’t be recorded for airing later instead of being broadcast live, as this approach “takes you out of the nexus of having two masters, the patient and the audience.” In response, Dr. Bavaria said editing takes extra time in order to capture the nuances of the live procedure.
Dr. Bavaria reports no relevant disclosures.
SAN DIEGO – Two thoracic societies are being challenged to review their rejection of at medical meetings.
The American Association for Thoracic Surgery and Society of Thoracic Surgeons “should modify their stance on live surgery as an educational tool like almost all of their sister organizations,” said Joseph E. Bavaria, MD, FACS, of the University of Pennsylvania, Philadelphia. “Presently, it is effectively a ban on the practice. But there are no data to suggest that it does harm to patients if done with proper constraints.”
Live broadcasts of surgeries at medical meetings are both common and controversial. Dr. Bavaria listed numerous recent thoracic meetings in Europe and Canada that featured live broadcasts. But, he noted, the AATS and STS are not supportive of the trend.
In a policy amended in 2017, the AATS states, among other things, that “national and international cardiothoracic societies should consider prohibiting live surgery broadcasts to large audiences at their annual meetings.” The STS policy, amended in 2016, is nearly identical. However, it adds language specifying that “violation of these guidelines may lead to disciplinary action by the Society.”
Both the AATS and STS policies state that surgeons should not take part in live broadcasts of operations that are intended for the public. And both policies say “generally, recorded broadcasts, either edited or unedited, are preferable to live surgery broadcasts because recordings intended for later broadcast pose fewer risks of harm to patients.”
The policies don’t elaborate on how a live broadcast of an operation might be more harmful than one aired at a later time. “Where are the data to support this statement?” Dr. Bavaria asked. “Is this what we call the expert opinion of a few people with gray hair? Our European and Canadian colleagues certainly don’t agree with [the policies] and might take issue with our sanctimonious lecturing that’s not supported by any data whatsoever.”
He pointed to a 2011 study that examined 250 cardiac procedures that were broadcast live to 32 scientific meetings. Researchers found that “there is no evidence for an excess perioperative risk for patients operated under the conditions of live broadcasting” (Eur J Cardiothorac Surg. 2011;40[2]:367-71).
A member of the audience at the AATS session pointed out that the study may be misleading because only top surgeons may be willing to perform procedures live on television. Dr. Bavaria responded by noting that the outcomes of surgeries performed on live video were not worse.
Skeptics have also expressed concern about the potential for sensationalism in live broadcasts and the drive for participants to make a splash: “the demands of ‘the performance,’ including questions and discussion with the audience, may divert the surgeon’s attention and produce an inferior outcome,” wrote three physicians in 2011 (J Surg Educ. 2011 Jan-Feb; 68[1]:58-61).
The trio also expressed worry about safety risks posed by extra equipment and extra people in the operating room during a live broadcast. However, Dr. Bavaria said the crowded conditions of an operation observed in person – instead of via video – could be worse: “You don’t have a sterile environment, you have people hanging around all over. A moderated live session could be better for the surgeon and the patient, rather than having a bunch of people in the room.”
Dr. Bavaria was also asked why surgeries couldn’t be recorded for airing later instead of being broadcast live, as this approach “takes you out of the nexus of having two masters, the patient and the audience.” In response, Dr. Bavaria said editing takes extra time in order to capture the nuances of the live procedure.
Dr. Bavaria reports no relevant disclosures.
REPORTING FROM AATS
CMSC looks to increase advocacy efforts to address looming concerns
As patients with multiple sclerosis and their caregivers face various challenges in the American health care system, the Consortium of Multiple Sclerosis Centers (CMSC) is re-energizing its focus on advocacy. The 2018 annual meeting in Nashville, Tenn., will feature programming designed to teach MS professionals and researchers how to speak up and let their voices be heard.
“CMSC has re-engaged in advocacy, in a more focused and energized way, because of mounting concerns that there is inadequate advocacy pressure on some of the critical issues negatively impacting the quality and comprehensive nature of MS care required of people living with MS,” said Lisa Taylor Skutnik, a physical therapist and chief operating officer of the CMSC. “Both people living with MS and the clinicians dedicated to treating them are increasingly frustrated and powerless in attempts to facilitate the right care and resources for people living with MS. Our members are facing significant barriers and obstacles to ensure timely and seamless comprehensive care.”

The development of quality measures in MS is also a “huge concern,” she said, referring to the federal government’s efforts to develop new ways to measure whether health professionals are providing high-quality care. Physicians have expressed widespread concern about the measures, which are being linked to reimbursement from Medicare and Medicaid.
Among the highlights of the CMSC meeting will be an educational session that “will focus on the available resources within the MS community for MS professionals and researchers to access advocacy efforts and get involved,” Ms. Skutnik said.
Another educational session “will focus on helping MS clinicians and researchers to understand all of the various stakeholders and their respective perspectives related to access to comprehensive care services for those living with MS,” such as pharmacy benefit managers and insurers, she said.
As patients with multiple sclerosis and their caregivers face various challenges in the American health care system, the Consortium of Multiple Sclerosis Centers (CMSC) is re-energizing its focus on advocacy. The 2018 annual meeting in Nashville, Tenn., will feature programming designed to teach MS professionals and researchers how to speak up and let their voices be heard.
“CMSC has re-engaged in advocacy, in a more focused and energized way, because of mounting concerns that there is inadequate advocacy pressure on some of the critical issues negatively impacting the quality and comprehensive nature of MS care required of people living with MS,” said Lisa Taylor Skutnik, a physical therapist and chief operating officer of the CMSC. “Both people living with MS and the clinicians dedicated to treating them are increasingly frustrated and powerless in attempts to facilitate the right care and resources for people living with MS. Our members are facing significant barriers and obstacles to ensure timely and seamless comprehensive care.”
The development of quality measures in MS is also a “huge concern,” she said, referring to the federal government’s efforts to develop new ways to measure whether health professionals are providing high-quality care. Physicians have expressed widespread concern about the measures, which are being linked to reimbursement from Medicare and Medicaid.
Among the highlights of the CMSC meeting will be an educational session that “will focus on the available resources within the MS community for MS professionals and researchers to access advocacy efforts and get involved,” Ms. Skutnik said.
Another educational session “will focus on helping MS clinicians and researchers to understand all of the various stakeholders and their respective perspectives related to access to comprehensive care services for those living with MS,” such as pharmacy benefit managers and insurers, she said.
As patients with multiple sclerosis and their caregivers face various challenges in the American health care system, the Consortium of Multiple Sclerosis Centers (CMSC) is re-energizing its focus on advocacy. The 2018 annual meeting in Nashville, Tenn., will feature programming designed to teach MS professionals and researchers how to speak up and let their voices be heard.
“CMSC has re-engaged in advocacy, in a more focused and energized way, because of mounting concerns that there is inadequate advocacy pressure on some of the critical issues negatively impacting the quality and comprehensive nature of MS care required of people living with MS,” said Lisa Taylor Skutnik, a physical therapist and chief operating officer of the CMSC. “Both people living with MS and the clinicians dedicated to treating them are increasingly frustrated and powerless in attempts to facilitate the right care and resources for people living with MS. Our members are facing significant barriers and obstacles to ensure timely and seamless comprehensive care.”
The development of quality measures in MS is also a “huge concern,” she said, referring to the federal government’s efforts to develop new ways to measure whether health professionals are providing high-quality care. Physicians have expressed widespread concern about the measures, which are being linked to reimbursement from Medicare and Medicaid.
Among the highlights of the CMSC meeting will be an educational session that “will focus on the available resources within the MS community for MS professionals and researchers to access advocacy efforts and get involved,” Ms. Skutnik said.
Another educational session “will focus on helping MS clinicians and researchers to understand all of the various stakeholders and their respective perspectives related to access to comprehensive care services for those living with MS,” such as pharmacy benefit managers and insurers, she said.
Rehabilitation in MS is hot topic at CMSC 2018
This year’s annual meeting of the Consortium of Multiple Sclerosis Centers in Nashville, Tenn., will feature an intense focus on rehabilitation in MS. The topic is often a priority for patients but not necessarily at top of mind for health care providers, said rehabilitation therapist Patty Bobryk, secretary of the CMSC.
“This year, some of the Rehab Track topics include addressing respiratory issues in MS, exploring the impact of visual impairments on rehab, and recommending the proper orthotics, as well as discussing treatments that focus on mind-body understanding,” said Ms. Bobryk of MS Comprehensive Care Center of Central Florida, Orlando. She serves as cochair of the International Organization of MS Rehabilitation Therapists.

Rehabilitation in MS is a controversial topic. Two years ago, the CMSC endorsed a statement criticizing a 2015 report by the American Academy of Neurology that found limited evidence supporting MS rehabilitation (Neurology. 2015 Nov 24;85[21]:1896-903). The statement, also supported by the International Organization of MS Nurses and International Organization of MS Rehabilitation Therapists, declared that the AAN report “presents an incomplete review of the evidence published” (Neurol Clin Pract. 2016 Dec;6[6]:475-9).
However, the statement acknowledged that “larger studies with better research methodologies and higher-quality evidence are needed in rehabilitation.”
More recently, a 2017 systematic review of systematic reviews of rehabilitation in MS found that “strong” evidence only exists “for physical therapy for improved activity and participation, and for exercise-based educational programs for the reduction of patient-reported fatigue.” The review of reviews also found there’s “ ‘moderate’ evidence for multidisciplinary rehabilitation for longer-term gains at the levels of activity (disability) and participation, for cognitive-behavior therapy for the treatment of depression, and for information-provision interventions for improved patient knowledge” (Arch Phys Med Rehabil. 2017 Feb;98[2]:353-67).
In an interview, Ms. Bobryk said the MS rehabilitation community is evolving toward “a better understanding of neuroplasticity and the impact that rehab can have on maintaining and improving functional skills.”
In addition, she said, “more emphasis is being placed on early intervention and preventing the secondary effects of the disease versus providing only compensatory strategies.”
Highlights of this year’s rehab sessions at the CMSC conference include a 3-hour course on imbalance in MS that will “provide an intensive review of the anatomy of the balance system and educate the audience on evaluation and treatment interventions specific to retraining the balance system,” Ms. Bobryk said.
Another highlight: A half-day course that will “provide the rationale for including rehabilitation in a comprehensive model of care for people with severe MS,” she said. “Unique interventions such as the use of functional electrical stimulation cycling and body weight-supported treadmill training will be discussed.”
In the big picture, “clinicians who are working in the field of MS realize the benefits of rehab, but more education is needed to spread the word to the broader scope of health care providers,” Ms. Bobryk said. “Patients are often the ones that bring up rehab to their physicians to initiate a referral.”
This year’s annual meeting of the Consortium of Multiple Sclerosis Centers in Nashville, Tenn., will feature an intense focus on rehabilitation in MS. The topic is often a priority for patients but not necessarily at top of mind for health care providers, said rehabilitation therapist Patty Bobryk, secretary of the CMSC.
“This year, some of the Rehab Track topics include addressing respiratory issues in MS, exploring the impact of visual impairments on rehab, and recommending the proper orthotics, as well as discussing treatments that focus on mind-body understanding,” said Ms. Bobryk of MS Comprehensive Care Center of Central Florida, Orlando. She serves as cochair of the International Organization of MS Rehabilitation Therapists.
Rehabilitation in MS is a controversial topic. Two years ago, the CMSC endorsed a statement criticizing a 2015 report by the American Academy of Neurology that found limited evidence supporting MS rehabilitation (Neurology. 2015 Nov 24;85[21]:1896-903). The statement, also supported by the International Organization of MS Nurses and International Organization of MS Rehabilitation Therapists, declared that the AAN report “presents an incomplete review of the evidence published” (Neurol Clin Pract. 2016 Dec;6[6]:475-9).
However, the statement acknowledged that “larger studies with better research methodologies and higher-quality evidence are needed in rehabilitation.”
More recently, a 2017 systematic review of systematic reviews of rehabilitation in MS found that “strong” evidence only exists “for physical therapy for improved activity and participation, and for exercise-based educational programs for the reduction of patient-reported fatigue.” The review of reviews also found there’s “ ‘moderate’ evidence for multidisciplinary rehabilitation for longer-term gains at the levels of activity (disability) and participation, for cognitive-behavior therapy for the treatment of depression, and for information-provision interventions for improved patient knowledge” (Arch Phys Med Rehabil. 2017 Feb;98[2]:353-67).
In an interview, Ms. Bobryk said the MS rehabilitation community is evolving toward “a better understanding of neuroplasticity and the impact that rehab can have on maintaining and improving functional skills.”
In addition, she said, “more emphasis is being placed on early intervention and preventing the secondary effects of the disease versus providing only compensatory strategies.”
Highlights of this year’s rehab sessions at the CMSC conference include a 3-hour course on imbalance in MS that will “provide an intensive review of the anatomy of the balance system and educate the audience on evaluation and treatment interventions specific to retraining the balance system,” Ms. Bobryk said.
Another highlight: A half-day course that will “provide the rationale for including rehabilitation in a comprehensive model of care for people with severe MS,” she said. “Unique interventions such as the use of functional electrical stimulation cycling and body weight-supported treadmill training will be discussed.”
In the big picture, “clinicians who are working in the field of MS realize the benefits of rehab, but more education is needed to spread the word to the broader scope of health care providers,” Ms. Bobryk said. “Patients are often the ones that bring up rehab to their physicians to initiate a referral.”
This year’s annual meeting of the Consortium of Multiple Sclerosis Centers in Nashville, Tenn., will feature an intense focus on rehabilitation in MS. The topic is often a priority for patients but not necessarily at top of mind for health care providers, said rehabilitation therapist Patty Bobryk, secretary of the CMSC.
“This year, some of the Rehab Track topics include addressing respiratory issues in MS, exploring the impact of visual impairments on rehab, and recommending the proper orthotics, as well as discussing treatments that focus on mind-body understanding,” said Ms. Bobryk of MS Comprehensive Care Center of Central Florida, Orlando. She serves as cochair of the International Organization of MS Rehabilitation Therapists.
Rehabilitation in MS is a controversial topic. Two years ago, the CMSC endorsed a statement criticizing a 2015 report by the American Academy of Neurology that found limited evidence supporting MS rehabilitation (Neurology. 2015 Nov 24;85[21]:1896-903). The statement, also supported by the International Organization of MS Nurses and International Organization of MS Rehabilitation Therapists, declared that the AAN report “presents an incomplete review of the evidence published” (Neurol Clin Pract. 2016 Dec;6[6]:475-9).
However, the statement acknowledged that “larger studies with better research methodologies and higher-quality evidence are needed in rehabilitation.”
More recently, a 2017 systematic review of systematic reviews of rehabilitation in MS found that “strong” evidence only exists “for physical therapy for improved activity and participation, and for exercise-based educational programs for the reduction of patient-reported fatigue.” The review of reviews also found there’s “ ‘moderate’ evidence for multidisciplinary rehabilitation for longer-term gains at the levels of activity (disability) and participation, for cognitive-behavior therapy for the treatment of depression, and for information-provision interventions for improved patient knowledge” (Arch Phys Med Rehabil. 2017 Feb;98[2]:353-67).
In an interview, Ms. Bobryk said the MS rehabilitation community is evolving toward “a better understanding of neuroplasticity and the impact that rehab can have on maintaining and improving functional skills.”
In addition, she said, “more emphasis is being placed on early intervention and preventing the secondary effects of the disease versus providing only compensatory strategies.”
Highlights of this year’s rehab sessions at the CMSC conference include a 3-hour course on imbalance in MS that will “provide an intensive review of the anatomy of the balance system and educate the audience on evaluation and treatment interventions specific to retraining the balance system,” Ms. Bobryk said.
Another highlight: A half-day course that will “provide the rationale for including rehabilitation in a comprehensive model of care for people with severe MS,” she said. “Unique interventions such as the use of functional electrical stimulation cycling and body weight-supported treadmill training will be discussed.”
In the big picture, “clinicians who are working in the field of MS realize the benefits of rehab, but more education is needed to spread the word to the broader scope of health care providers,” Ms. Bobryk said. “Patients are often the ones that bring up rehab to their physicians to initiate a referral.”
Wide variety of MS topics on tap at CMSC 2018
More than 2,000 members of the multiple sclerosis care, advocacy, research, and patient communities will gather in Nashville, Tenn., May 30–June 2 for the annual meeting of the Consortium of Multiple Sclerosis Centers.
Dozens of topics will be discussed, ranging from complementary/alternative therapies, ethics, and neuropsychiatry to neuroimmunology and disease models, relapse management, and self-care. Clinicians also will tackle sensitive topics such as suicide, depression, and cognitive impairment.
“Accredited continuing education will be offered for MDs, registered nurses, pharmacists, occupational therapists, physical therapists, social workers, and psychologists,” said Gary Cutter, PhD, president of the CMSC. “Our offerings include beginner courses, advanced science sessions, rehab and mental health tracks, platform and poster sessions, and roundtables.”

“We’ll discuss meds for progressive forms of MS as well as targeted therapies based on new information from genetics,” Dr. Cutter said. Participants will also gain insight from registries and other data sources, he added.
Lecture topics will include the use of computerized screening for cognitive dysfunction in the MS clinic and new research into MS pathology.
Other sessions will explore the use of cannabis, infusion therapies, respiratory enhancement, and a new class of medications for blocking lipid metabolism. Rehabilitation will also be a major focus.
One session will examine MS in patients before conception, during pregnancy, and in the postpartum period. Another session will explore suicide in MS and discuss how clinics can identify and help patients at risk.
The annual CMSC conference stands apart because it’s a “relatively unique meeting where the entire MS treatment team, researchers, and persons with MS can interact and discuss the complex issues in MS care,” Dr. Cutter said. “Much of this takes place outside of the formal program but can still have major impact on all of us. The enthusiasm of the young attendees is always amazing. They are supported, involved, and encouraged.”
More than 2,000 members of the multiple sclerosis care, advocacy, research, and patient communities will gather in Nashville, Tenn., May 30–June 2 for the annual meeting of the Consortium of Multiple Sclerosis Centers.
Dozens of topics will be discussed, ranging from complementary/alternative therapies, ethics, and neuropsychiatry to neuroimmunology and disease models, relapse management, and self-care. Clinicians also will tackle sensitive topics such as suicide, depression, and cognitive impairment.
“Accredited continuing education will be offered for MDs, registered nurses, pharmacists, occupational therapists, physical therapists, social workers, and psychologists,” said Gary Cutter, PhD, president of the CMSC. “Our offerings include beginner courses, advanced science sessions, rehab and mental health tracks, platform and poster sessions, and roundtables.”
“We’ll discuss meds for progressive forms of MS as well as targeted therapies based on new information from genetics,” Dr. Cutter said. Participants will also gain insight from registries and other data sources, he added.
Lecture topics will include the use of computerized screening for cognitive dysfunction in the MS clinic and new research into MS pathology.
Other sessions will explore the use of cannabis, infusion therapies, respiratory enhancement, and a new class of medications for blocking lipid metabolism. Rehabilitation will also be a major focus.
One session will examine MS in patients before conception, during pregnancy, and in the postpartum period. Another session will explore suicide in MS and discuss how clinics can identify and help patients at risk.
The annual CMSC conference stands apart because it’s a “relatively unique meeting where the entire MS treatment team, researchers, and persons with MS can interact and discuss the complex issues in MS care,” Dr. Cutter said. “Much of this takes place outside of the formal program but can still have major impact on all of us. The enthusiasm of the young attendees is always amazing. They are supported, involved, and encouraged.”
More than 2,000 members of the multiple sclerosis care, advocacy, research, and patient communities will gather in Nashville, Tenn., May 30–June 2 for the annual meeting of the Consortium of Multiple Sclerosis Centers.
Dozens of topics will be discussed, ranging from complementary/alternative therapies, ethics, and neuropsychiatry to neuroimmunology and disease models, relapse management, and self-care. Clinicians also will tackle sensitive topics such as suicide, depression, and cognitive impairment.
“Accredited continuing education will be offered for MDs, registered nurses, pharmacists, occupational therapists, physical therapists, social workers, and psychologists,” said Gary Cutter, PhD, president of the CMSC. “Our offerings include beginner courses, advanced science sessions, rehab and mental health tracks, platform and poster sessions, and roundtables.”
“We’ll discuss meds for progressive forms of MS as well as targeted therapies based on new information from genetics,” Dr. Cutter said. Participants will also gain insight from registries and other data sources, he added.
Lecture topics will include the use of computerized screening for cognitive dysfunction in the MS clinic and new research into MS pathology.
Other sessions will explore the use of cannabis, infusion therapies, respiratory enhancement, and a new class of medications for blocking lipid metabolism. Rehabilitation will also be a major focus.
One session will examine MS in patients before conception, during pregnancy, and in the postpartum period. Another session will explore suicide in MS and discuss how clinics can identify and help patients at risk.
The annual CMSC conference stands apart because it’s a “relatively unique meeting where the entire MS treatment team, researchers, and persons with MS can interact and discuss the complex issues in MS care,” Dr. Cutter said. “Much of this takes place outside of the formal program but can still have major impact on all of us. The enthusiasm of the young attendees is always amazing. They are supported, involved, and encouraged.”
Hefty rewards pay off in smoking-cessation study
A new study finds it pays to pay people to stop lighting up: Smokers were more likely to quit if they had an opportunity to gain rewards worth $600 than if they simply received free cessation aids or free e-cigarettes.
The wide majority of the more than 6,000 smokers in the randomized study didn’t quit despite offers of various incentives. All the same, “programs that offered financial incentives tripled the rates of smoking cessation, reduced employers’ costs per successful quit, as compared with programs that offered cessation aids alone, and yielded total costs that compared favorably with the costs of employing smokers,” the study authors wrote.
The researchers reached out to employees and spouses at 54 companies that use wellness programs provided by the Vitality Institute, which supports research into health promotion. The institute provided grant support for the study.
Just over 6,000 employees and spouses who smoked were assigned to five groups. One group received usual care. The others received interventions: free smoking-cessation aids (nicotine replacement therapy, bupropion, or varenicline); free e-cigarettes; up to $600 worth of an unidentified “reward incentive” plus free cessation aids; and up to $600 via a redeemable deposit, plus free cessation aids.
Participants could only get the entire reward incentive or the full $600 redeemable deposit if they showed signs of sustained smoking cessation via blood or urine test at 1, 3, and 6 months.
The median age in the groups ranged from 43 to 45 years, and most were not college graduates. Just over half were women, and roughly 90% said they wanted to quit smoking.
Overall, 20% of the 6,006 participants logged onto the trial website, a sign that they were “engaged.” The number was highest in the free e-cigarette and reward groups (21%-23%) and lowest in the usual care group (16%).
The researchers focused on how many participants abstained from smoking – as confirmed by blood or urine test – for 6 months past the target quit date. The test data confirmed that just 1.3% of the total participants, 80 people, sustained cessation over 6 months.
Only 0.1% of the usual-care group sustained smoking cessation, and the number wasn’t much higher (0.5%) in the free cessation aids group.
One percent of those in the free e-cigarette group sustained cessation. However, the researchers noted there wasn’t a significant difference in the quit rates between the usual care, free cessation aid, and free e-cigarette groups.
“The observation of greater e-cigarette use in the free e-cigarette group than in the free cessation aids group, coupled with the absence of benefit of free e-cigarettes versus no intervention, supports the conclusion that offering free e-cigarettes does not promote smoking cessation,” they cautioned.
In the reward incentive and $600 redeemable-deposit groups, 2% and 2.9% of participants quit over a sustained period, respectively. Cessation rates in the $600 deposit group were superior to the free cessation aid group (P less than .001) and the free e-cigarette group (P = .008). Cessation rates in the incentive group were superior to those in the free cessation aid group (P = .006).
“Average costs per participant assigned to each intervention were lowest in the usual-care group ($0.82) and highest in the redeemable-deposit group ($100.96),” the researchers reported. “The overall cost of each program per participant who was abstinent for 6 months was lower in the rewards and redeemable-deposit groups than in the free e-cigarettes or free cessation aids groups.”
The study received grant support from the Vitality Institute. Most of the study authors reported no relevant disclosures. One author reported serving on the scientific advisory board of VAL Health, and another reported various grants and personal fees.
SOURCE: Halpern SD et al. N Engl J Med. 2018 May 23. doi: 10.1056/NEJMsa1715757.
A new study finds it pays to pay people to stop lighting up: Smokers were more likely to quit if they had an opportunity to gain rewards worth $600 than if they simply received free cessation aids or free e-cigarettes.
The wide majority of the more than 6,000 smokers in the randomized study didn’t quit despite offers of various incentives. All the same, “programs that offered financial incentives tripled the rates of smoking cessation, reduced employers’ costs per successful quit, as compared with programs that offered cessation aids alone, and yielded total costs that compared favorably with the costs of employing smokers,” the study authors wrote.
The researchers reached out to employees and spouses at 54 companies that use wellness programs provided by the Vitality Institute, which supports research into health promotion. The institute provided grant support for the study.
Just over 6,000 employees and spouses who smoked were assigned to five groups. One group received usual care. The others received interventions: free smoking-cessation aids (nicotine replacement therapy, bupropion, or varenicline); free e-cigarettes; up to $600 worth of an unidentified “reward incentive” plus free cessation aids; and up to $600 via a redeemable deposit, plus free cessation aids.
Participants could only get the entire reward incentive or the full $600 redeemable deposit if they showed signs of sustained smoking cessation via blood or urine test at 1, 3, and 6 months.
The median age in the groups ranged from 43 to 45 years, and most were not college graduates. Just over half were women, and roughly 90% said they wanted to quit smoking.
Overall, 20% of the 6,006 participants logged onto the trial website, a sign that they were “engaged.” The number was highest in the free e-cigarette and reward groups (21%-23%) and lowest in the usual care group (16%).
The researchers focused on how many participants abstained from smoking – as confirmed by blood or urine test – for 6 months past the target quit date. The test data confirmed that just 1.3% of the total participants, 80 people, sustained cessation over 6 months.
Only 0.1% of the usual-care group sustained smoking cessation, and the number wasn’t much higher (0.5%) in the free cessation aids group.
One percent of those in the free e-cigarette group sustained cessation. However, the researchers noted there wasn’t a significant difference in the quit rates between the usual care, free cessation aid, and free e-cigarette groups.
“The observation of greater e-cigarette use in the free e-cigarette group than in the free cessation aids group, coupled with the absence of benefit of free e-cigarettes versus no intervention, supports the conclusion that offering free e-cigarettes does not promote smoking cessation,” they cautioned.
In the reward incentive and $600 redeemable-deposit groups, 2% and 2.9% of participants quit over a sustained period, respectively. Cessation rates in the $600 deposit group were superior to the free cessation aid group (P less than .001) and the free e-cigarette group (P = .008). Cessation rates in the incentive group were superior to those in the free cessation aid group (P = .006).
“Average costs per participant assigned to each intervention were lowest in the usual-care group ($0.82) and highest in the redeemable-deposit group ($100.96),” the researchers reported. “The overall cost of each program per participant who was abstinent for 6 months was lower in the rewards and redeemable-deposit groups than in the free e-cigarettes or free cessation aids groups.”
The study received grant support from the Vitality Institute. Most of the study authors reported no relevant disclosures. One author reported serving on the scientific advisory board of VAL Health, and another reported various grants and personal fees.
SOURCE: Halpern SD et al. N Engl J Med. 2018 May 23. doi: 10.1056/NEJMsa1715757.
A new study finds it pays to pay people to stop lighting up: Smokers were more likely to quit if they had an opportunity to gain rewards worth $600 than if they simply received free cessation aids or free e-cigarettes.
The wide majority of the more than 6,000 smokers in the randomized study didn’t quit despite offers of various incentives. All the same, “programs that offered financial incentives tripled the rates of smoking cessation, reduced employers’ costs per successful quit, as compared with programs that offered cessation aids alone, and yielded total costs that compared favorably with the costs of employing smokers,” the study authors wrote.
The researchers reached out to employees and spouses at 54 companies that use wellness programs provided by the Vitality Institute, which supports research into health promotion. The institute provided grant support for the study.
Just over 6,000 employees and spouses who smoked were assigned to five groups. One group received usual care. The others received interventions: free smoking-cessation aids (nicotine replacement therapy, bupropion, or varenicline); free e-cigarettes; up to $600 worth of an unidentified “reward incentive” plus free cessation aids; and up to $600 via a redeemable deposit, plus free cessation aids.
Participants could only get the entire reward incentive or the full $600 redeemable deposit if they showed signs of sustained smoking cessation via blood or urine test at 1, 3, and 6 months.
The median age in the groups ranged from 43 to 45 years, and most were not college graduates. Just over half were women, and roughly 90% said they wanted to quit smoking.
Overall, 20% of the 6,006 participants logged onto the trial website, a sign that they were “engaged.” The number was highest in the free e-cigarette and reward groups (21%-23%) and lowest in the usual care group (16%).
The researchers focused on how many participants abstained from smoking – as confirmed by blood or urine test – for 6 months past the target quit date. The test data confirmed that just 1.3% of the total participants, 80 people, sustained cessation over 6 months.
Only 0.1% of the usual-care group sustained smoking cessation, and the number wasn’t much higher (0.5%) in the free cessation aids group.
One percent of those in the free e-cigarette group sustained cessation. However, the researchers noted there wasn’t a significant difference in the quit rates between the usual care, free cessation aid, and free e-cigarette groups.
“The observation of greater e-cigarette use in the free e-cigarette group than in the free cessation aids group, coupled with the absence of benefit of free e-cigarettes versus no intervention, supports the conclusion that offering free e-cigarettes does not promote smoking cessation,” they cautioned.
In the reward incentive and $600 redeemable-deposit groups, 2% and 2.9% of participants quit over a sustained period, respectively. Cessation rates in the $600 deposit group were superior to the free cessation aid group (P less than .001) and the free e-cigarette group (P = .008). Cessation rates in the incentive group were superior to those in the free cessation aid group (P = .006).
“Average costs per participant assigned to each intervention were lowest in the usual-care group ($0.82) and highest in the redeemable-deposit group ($100.96),” the researchers reported. “The overall cost of each program per participant who was abstinent for 6 months was lower in the rewards and redeemable-deposit groups than in the free e-cigarettes or free cessation aids groups.”
The study received grant support from the Vitality Institute. Most of the study authors reported no relevant disclosures. One author reported serving on the scientific advisory board of VAL Health, and another reported various grants and personal fees.
SOURCE: Halpern SD et al. N Engl J Med. 2018 May 23. doi: 10.1056/NEJMsa1715757.
FROM NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Smokers are more likely to sustain cessation if they receive incentives worth $600.
Major finding: Cessation rates for 6 months past target quit date reached as high as 2.9% in smokers who had the opportunity to gain rewards, while they didn’t top 1% in those who received free cessation aids or free e-cigarettes.
Study details: A randomized, prospective study of 6,006 smokers (employees of 54 companies and spouses) who were assigned to usual care or one of four intervention groups.
Disclosures: The study received grant support from the Vitality Institute. Most of the study authors reported no relevant disclosures. One reported serving on the scientific advisory board of VAL Health, and another reported various grants and personal fees.
Source: Halpern SD et al. N Engl J Med. 2018 May 23. doi: 10.1056/NEJMsa1715757.
Malignant pleural mesothelioma guidelines often are ignored
SAN DIEGO – National guidelines for the treatment of malignant pleural mesothelioma often are not followed, a new study showed, with fewer than one-third of patients receiving cancer-directed surgery.
Another 32% received no treatment, although that didn’t seem to have an impact on median months of survival.

Still, “there can be a wide variation in median survival time, depending on clinical factors and tumor characteristics,” said study coauthor Harmik Soukiasian, MD, of Cedars-Sinai Medical Center, Los Angeles. “Given the variation in prognosis, it is quite astonishing that over 30% of MPM patients are not receiving any form of treatment. As clinicians armed with these data, we need to investigate why that is.”
Dr. Soukiasian presented the study findings at the annual meeting of the American Association for Thoracic Surgery.
MPM, a rare cancer, is mainly linked to asbestos exposure. “MPM is almost always a fatal disease, and the prognosis can only be modestly influenced by oncological treatments,” according to the authors of guidelines released in 2013. “The diagnostic process can be complex, with highly specialized advice frequently required to arrive at a definite diagnosis. Treatment varies from therapeutic nihilism to radical combined-modality treatment approaches” (J Thorac Dis. 2013 Dec;5[6]:E254-E307).
Surgical resection is a controversial treatment for MPM, Dr. Soukiasian said. It is “based on the principle of macroscopic resection of solid tumor with adjuvant therapy to treat micrometastatic disease,” he explained. “Cancer-directed surgery for MPM is usually reserved for localized epithelial type histology and is associated with a 5-year survival rate of 15%.”
For the new study, the investigators tracked 3,834 patients in the National Cancer Database (2004-2014) diagnosed with MPM clinical stages I-III. Most had epithelioid MPM (69%), with sarcomatoid (17%) and mixed subtype (15%) making up the rest. They examined whether patient treatment complied with the National Comprehensive Cancer Network (NCCN) guidelines, which recommend surgery in resectable epithelioid MPM.
“Our study revealed significant lack of compliance with NCCN guidelines, as well as many disparities in the management of MPM,” Dr. Soukiasian said. “For the overall cohort, 32.3% of patients did not receive any treatment, 18.1% had surgery plus chemotherapy, 38.6% chemotherapy alone, and only 7% received trimodality therapy. In patients with epithelial histology, surgery was significantly underutilized, with only 30% of patients receiving cancer-directed surgery.”
In addition, he said, “our study reveals several disparities that affect compliance with NCCN guidelines. Treatment disparities were observed in women, octogenarians, the uninsured, the Medicaid-insured, and in patients with comorbidities. Guideline adherence was significantly increased in academic and high-volume hospitals with an associated increase in survival.”
But the study also found that median survival estimates were similar regardless of treatment: 10 months for no treatment, 15 months for chemotherapy only, 17 months for surgery only, and 22 months for surgery plus chemotherapy.
During the AATS presentation, an audience member asked about how performance status – a measure of a person’s ability to perform everyday activities – affects the eligibility for surgery.
“It’s quite common for low performance status to exclude someone from surgery,” the audience member said. “Some of these patients are very sick.”
Dr. Soukiasian acknowledged that performance status was not included in the data. The study was focused on the gap between guidelines and real-world practice, and generated questions of why and about the potential opportunity for improved treatment of these patients.
How do patient choices, cost, and quality of life factor in? “These are very important questions and concerns,” Dr. Soukiasian said. “Although our research does not provide data or conclusions on quality of life or cost, these topics will be important to address in follow-up studies to elucidate possible barriers in the treatment of MPM and the initiation of future educational opportunities for our patients.”
No disclosures and no study funding were reported.
SOURCE: Espinoza-Mercado F et al. General Thoracic Surgery Simultaneous Scientific Session. Abstract 18.
SAN DIEGO – National guidelines for the treatment of malignant pleural mesothelioma often are not followed, a new study showed, with fewer than one-third of patients receiving cancer-directed surgery.
Another 32% received no treatment, although that didn’t seem to have an impact on median months of survival.
Still, “there can be a wide variation in median survival time, depending on clinical factors and tumor characteristics,” said study coauthor Harmik Soukiasian, MD, of Cedars-Sinai Medical Center, Los Angeles. “Given the variation in prognosis, it is quite astonishing that over 30% of MPM patients are not receiving any form of treatment. As clinicians armed with these data, we need to investigate why that is.”
Dr. Soukiasian presented the study findings at the annual meeting of the American Association for Thoracic Surgery.
MPM, a rare cancer, is mainly linked to asbestos exposure. “MPM is almost always a fatal disease, and the prognosis can only be modestly influenced by oncological treatments,” according to the authors of guidelines released in 2013. “The diagnostic process can be complex, with highly specialized advice frequently required to arrive at a definite diagnosis. Treatment varies from therapeutic nihilism to radical combined-modality treatment approaches” (J Thorac Dis. 2013 Dec;5[6]:E254-E307).
Surgical resection is a controversial treatment for MPM, Dr. Soukiasian said. It is “based on the principle of macroscopic resection of solid tumor with adjuvant therapy to treat micrometastatic disease,” he explained. “Cancer-directed surgery for MPM is usually reserved for localized epithelial type histology and is associated with a 5-year survival rate of 15%.”
For the new study, the investigators tracked 3,834 patients in the National Cancer Database (2004-2014) diagnosed with MPM clinical stages I-III. Most had epithelioid MPM (69%), with sarcomatoid (17%) and mixed subtype (15%) making up the rest. They examined whether patient treatment complied with the National Comprehensive Cancer Network (NCCN) guidelines, which recommend surgery in resectable epithelioid MPM.
“Our study revealed significant lack of compliance with NCCN guidelines, as well as many disparities in the management of MPM,” Dr. Soukiasian said. “For the overall cohort, 32.3% of patients did not receive any treatment, 18.1% had surgery plus chemotherapy, 38.6% chemotherapy alone, and only 7% received trimodality therapy. In patients with epithelial histology, surgery was significantly underutilized, with only 30% of patients receiving cancer-directed surgery.”
In addition, he said, “our study reveals several disparities that affect compliance with NCCN guidelines. Treatment disparities were observed in women, octogenarians, the uninsured, the Medicaid-insured, and in patients with comorbidities. Guideline adherence was significantly increased in academic and high-volume hospitals with an associated increase in survival.”
But the study also found that median survival estimates were similar regardless of treatment: 10 months for no treatment, 15 months for chemotherapy only, 17 months for surgery only, and 22 months for surgery plus chemotherapy.
During the AATS presentation, an audience member asked about how performance status – a measure of a person’s ability to perform everyday activities – affects the eligibility for surgery.
“It’s quite common for low performance status to exclude someone from surgery,” the audience member said. “Some of these patients are very sick.”
Dr. Soukiasian acknowledged that performance status was not included in the data. The study was focused on the gap between guidelines and real-world practice, and generated questions of why and about the potential opportunity for improved treatment of these patients.
How do patient choices, cost, and quality of life factor in? “These are very important questions and concerns,” Dr. Soukiasian said. “Although our research does not provide data or conclusions on quality of life or cost, these topics will be important to address in follow-up studies to elucidate possible barriers in the treatment of MPM and the initiation of future educational opportunities for our patients.”
No disclosures and no study funding were reported.
SOURCE: Espinoza-Mercado F et al. General Thoracic Surgery Simultaneous Scientific Session. Abstract 18.
SAN DIEGO – National guidelines for the treatment of malignant pleural mesothelioma often are not followed, a new study showed, with fewer than one-third of patients receiving cancer-directed surgery.
Another 32% received no treatment, although that didn’t seem to have an impact on median months of survival.
Still, “there can be a wide variation in median survival time, depending on clinical factors and tumor characteristics,” said study coauthor Harmik Soukiasian, MD, of Cedars-Sinai Medical Center, Los Angeles. “Given the variation in prognosis, it is quite astonishing that over 30% of MPM patients are not receiving any form of treatment. As clinicians armed with these data, we need to investigate why that is.”
Dr. Soukiasian presented the study findings at the annual meeting of the American Association for Thoracic Surgery.
MPM, a rare cancer, is mainly linked to asbestos exposure. “MPM is almost always a fatal disease, and the prognosis can only be modestly influenced by oncological treatments,” according to the authors of guidelines released in 2013. “The diagnostic process can be complex, with highly specialized advice frequently required to arrive at a definite diagnosis. Treatment varies from therapeutic nihilism to radical combined-modality treatment approaches” (J Thorac Dis. 2013 Dec;5[6]:E254-E307).
Surgical resection is a controversial treatment for MPM, Dr. Soukiasian said. It is “based on the principle of macroscopic resection of solid tumor with adjuvant therapy to treat micrometastatic disease,” he explained. “Cancer-directed surgery for MPM is usually reserved for localized epithelial type histology and is associated with a 5-year survival rate of 15%.”
For the new study, the investigators tracked 3,834 patients in the National Cancer Database (2004-2014) diagnosed with MPM clinical stages I-III. Most had epithelioid MPM (69%), with sarcomatoid (17%) and mixed subtype (15%) making up the rest. They examined whether patient treatment complied with the National Comprehensive Cancer Network (NCCN) guidelines, which recommend surgery in resectable epithelioid MPM.
“Our study revealed significant lack of compliance with NCCN guidelines, as well as many disparities in the management of MPM,” Dr. Soukiasian said. “For the overall cohort, 32.3% of patients did not receive any treatment, 18.1% had surgery plus chemotherapy, 38.6% chemotherapy alone, and only 7% received trimodality therapy. In patients with epithelial histology, surgery was significantly underutilized, with only 30% of patients receiving cancer-directed surgery.”
In addition, he said, “our study reveals several disparities that affect compliance with NCCN guidelines. Treatment disparities were observed in women, octogenarians, the uninsured, the Medicaid-insured, and in patients with comorbidities. Guideline adherence was significantly increased in academic and high-volume hospitals with an associated increase in survival.”
But the study also found that median survival estimates were similar regardless of treatment: 10 months for no treatment, 15 months for chemotherapy only, 17 months for surgery only, and 22 months for surgery plus chemotherapy.
During the AATS presentation, an audience member asked about how performance status – a measure of a person’s ability to perform everyday activities – affects the eligibility for surgery.
“It’s quite common for low performance status to exclude someone from surgery,” the audience member said. “Some of these patients are very sick.”
Dr. Soukiasian acknowledged that performance status was not included in the data. The study was focused on the gap between guidelines and real-world practice, and generated questions of why and about the potential opportunity for improved treatment of these patients.
How do patient choices, cost, and quality of life factor in? “These are very important questions and concerns,” Dr. Soukiasian said. “Although our research does not provide data or conclusions on quality of life or cost, these topics will be important to address in follow-up studies to elucidate possible barriers in the treatment of MPM and the initiation of future educational opportunities for our patients.”
No disclosures and no study funding were reported.
SOURCE: Espinoza-Mercado F et al. General Thoracic Surgery Simultaneous Scientific Session. Abstract 18.
REPORTING FROM THE AATS ANNUAL MEETING
Key clinical point:
Major finding: Guidelines recommend surgery in epithelioid MPM, but only 30% of patients received it.
Study details: Analysis of 3,834 patients diagnosed with MPM clinical stages I-III during 2004-2014.
Disclosures: No disclosures and no study funding were reported.
Source: Espinoza-Mercado F et al. General Thoracic Surgery Simultaneous Scientific Session. Abstract 18.
Delay of NSCLC surgery can lead to worse prognosis
SAN DIEGO – Delaying
“There is significant upstaging with time from completion of clinical staging to surgical resection, with a 4% increase of upstaging per week for the overall study population,” said study coauthor Harmik J. Soukiasian, MD, FACS, of Cedars-Sinai Medical Center, Los Angeles, in an interview. “Upstaging impacts lung cancer prognosis as more advanced stages portend to a poorer prognosis.”

An estimated 80%-85% of lung cancer patients have NSCLC, according to the American Cancer Society, and Dr. Soukiasian said surgery offers a chance at a cure for those diagnosed at stage I.
“National Cancer Comprehensive Network (NCCN) Guidelines recommend surgery within 8 weeks of completed clinical staging for NSCLC to limit cancer progression or upstaging,” Dr. Soukiasian said. “Although these guidelines are well established and widely adopted, our study performs a more granular analysis, studying time as a predictor of upstaging for those patients diagnosed with stage I NSCLC.”
For the new study, Dr. Soukiasian and colleagues tracked 52,406 patients in a cancer database who had stage I NSCLC but had not undergone preoperative chemotherapy. The researchers tracked their clinical stages for up to 12 weeks from initial staging.
Researchers found that, while staging levels rose with each successive week, just 25% of patients underwent surgery by 1 week, and only 79% had surgery in accordance with NSCLC guidelines by week 8. At 12 weeks, 9% had still not undergone surgery.
Upstaging was common: 22% at 1 week, 32% after 8 weeks, and 33% after 12 weeks.
“We demonstrate that patients diagnosed with stage I NSCLC benefit from surgery sooner than the 8-week window recommended by the NCCN guidelines,” Dr. Soukiasian said. “Exclusive of the rate of progression and in addition to time to surgery, our study also demonstrated academic centers, higher lymph node yield during surgery, and left-sided tumors to be independent predictors of upstaging.”
The study design doesn’t provide insight into why surgery is often delayed. However, “we can theorize factors associated with delays to surgery may be due to patient factors (personal scheduling, availability of support systems, etc.), delays in follow up, operating room availability or scheduling, and issues with insurance approval,” Dr. Soukiasian said.
In his presentation, Dr. Soukiasian emphasized the role of the mediastinum. “Given the clinical impact of stage III disease, we analyzed upstaging rates of stage I NSCLC to stage IIIA and revealed a 1.3% increase per week of upstaging specifically to stage IIIA. Additionally, almost 5% of patients initially diagnosed with stage I NSCLC upstaged to IIIA disease. The significant rate of upstaging to IIIA disease makes the case for more accurate and aggressive mediastinal staging prior to surgical resection.”
No disclosures and no study funding are reported.
SOURCE: Soukiasian HJ et al. AATS 2018, Abstract 67.
SAN DIEGO – Delaying
“There is significant upstaging with time from completion of clinical staging to surgical resection, with a 4% increase of upstaging per week for the overall study population,” said study coauthor Harmik J. Soukiasian, MD, FACS, of Cedars-Sinai Medical Center, Los Angeles, in an interview. “Upstaging impacts lung cancer prognosis as more advanced stages portend to a poorer prognosis.”
An estimated 80%-85% of lung cancer patients have NSCLC, according to the American Cancer Society, and Dr. Soukiasian said surgery offers a chance at a cure for those diagnosed at stage I.
“National Cancer Comprehensive Network (NCCN) Guidelines recommend surgery within 8 weeks of completed clinical staging for NSCLC to limit cancer progression or upstaging,” Dr. Soukiasian said. “Although these guidelines are well established and widely adopted, our study performs a more granular analysis, studying time as a predictor of upstaging for those patients diagnosed with stage I NSCLC.”
For the new study, Dr. Soukiasian and colleagues tracked 52,406 patients in a cancer database who had stage I NSCLC but had not undergone preoperative chemotherapy. The researchers tracked their clinical stages for up to 12 weeks from initial staging.
Researchers found that, while staging levels rose with each successive week, just 25% of patients underwent surgery by 1 week, and only 79% had surgery in accordance with NSCLC guidelines by week 8. At 12 weeks, 9% had still not undergone surgery.
Upstaging was common: 22% at 1 week, 32% after 8 weeks, and 33% after 12 weeks.
“We demonstrate that patients diagnosed with stage I NSCLC benefit from surgery sooner than the 8-week window recommended by the NCCN guidelines,” Dr. Soukiasian said. “Exclusive of the rate of progression and in addition to time to surgery, our study also demonstrated academic centers, higher lymph node yield during surgery, and left-sided tumors to be independent predictors of upstaging.”
The study design doesn’t provide insight into why surgery is often delayed. However, “we can theorize factors associated with delays to surgery may be due to patient factors (personal scheduling, availability of support systems, etc.), delays in follow up, operating room availability or scheduling, and issues with insurance approval,” Dr. Soukiasian said.
In his presentation, Dr. Soukiasian emphasized the role of the mediastinum. “Given the clinical impact of stage III disease, we analyzed upstaging rates of stage I NSCLC to stage IIIA and revealed a 1.3% increase per week of upstaging specifically to stage IIIA. Additionally, almost 5% of patients initially diagnosed with stage I NSCLC upstaged to IIIA disease. The significant rate of upstaging to IIIA disease makes the case for more accurate and aggressive mediastinal staging prior to surgical resection.”
No disclosures and no study funding are reported.
SOURCE: Soukiasian HJ et al. AATS 2018, Abstract 67.
SAN DIEGO – Delaying
“There is significant upstaging with time from completion of clinical staging to surgical resection, with a 4% increase of upstaging per week for the overall study population,” said study coauthor Harmik J. Soukiasian, MD, FACS, of Cedars-Sinai Medical Center, Los Angeles, in an interview. “Upstaging impacts lung cancer prognosis as more advanced stages portend to a poorer prognosis.”
An estimated 80%-85% of lung cancer patients have NSCLC, according to the American Cancer Society, and Dr. Soukiasian said surgery offers a chance at a cure for those diagnosed at stage I.
“National Cancer Comprehensive Network (NCCN) Guidelines recommend surgery within 8 weeks of completed clinical staging for NSCLC to limit cancer progression or upstaging,” Dr. Soukiasian said. “Although these guidelines are well established and widely adopted, our study performs a more granular analysis, studying time as a predictor of upstaging for those patients diagnosed with stage I NSCLC.”
For the new study, Dr. Soukiasian and colleagues tracked 52,406 patients in a cancer database who had stage I NSCLC but had not undergone preoperative chemotherapy. The researchers tracked their clinical stages for up to 12 weeks from initial staging.
Researchers found that, while staging levels rose with each successive week, just 25% of patients underwent surgery by 1 week, and only 79% had surgery in accordance with NSCLC guidelines by week 8. At 12 weeks, 9% had still not undergone surgery.
Upstaging was common: 22% at 1 week, 32% after 8 weeks, and 33% after 12 weeks.
“We demonstrate that patients diagnosed with stage I NSCLC benefit from surgery sooner than the 8-week window recommended by the NCCN guidelines,” Dr. Soukiasian said. “Exclusive of the rate of progression and in addition to time to surgery, our study also demonstrated academic centers, higher lymph node yield during surgery, and left-sided tumors to be independent predictors of upstaging.”
The study design doesn’t provide insight into why surgery is often delayed. However, “we can theorize factors associated with delays to surgery may be due to patient factors (personal scheduling, availability of support systems, etc.), delays in follow up, operating room availability or scheduling, and issues with insurance approval,” Dr. Soukiasian said.
In his presentation, Dr. Soukiasian emphasized the role of the mediastinum. “Given the clinical impact of stage III disease, we analyzed upstaging rates of stage I NSCLC to stage IIIA and revealed a 1.3% increase per week of upstaging specifically to stage IIIA. Additionally, almost 5% of patients initially diagnosed with stage I NSCLC upstaged to IIIA disease. The significant rate of upstaging to IIIA disease makes the case for more accurate and aggressive mediastinal staging prior to surgical resection.”
No disclosures and no study funding are reported.
SOURCE: Soukiasian HJ et al. AATS 2018, Abstract 67.
AT THE AATS ANNUAL MEETING
Key clinical point: Clinical staging levels worsen in each successive surgery-free week after initial staging in certain NSCLC patients.
Major finding: There was a 1.3% increase per week of upstaging to stage IIIA.
Study details: Analysis of 52,406 patients with stage I NSCLC who were tracked for up to 12 weeks.
Disclosures: No disclosures and no funding were reported.
Source: Soukiasian HJ et al. AATS 2018, Abstract 67.
Do black women pay a price for hair care regimens?
A new analysis of 18 hair products used by black women finds that they contain 45 endocrine-disrupting or asthma-associated chemicals, a finding that could help explain why this population suffers from higher rates of chemical exposure and hormone-related health conditions.
“We found multiples of our targeted chemicals in all of our products,” said study lead author Jessica S. Helm, PhD, of the Silent Spring Institute, Newton, Mass., in an interview. “We’re concerned about the additive effect of multiple products being used together.”

According to the study, previous research has found that, compared with white women, U.S. black women have higher urinary levels of chemicals like phthalates and parabens. Black women also have higher rates of asthma and hormone-related health conditions like uterine fibroids and infertility, Dr. Helms said.
The researchers launched their study to better understand the possible role of hair care products in raising chemical levels in black women, Dr. Helm said.
The researchers tested 18 types of hair care products shown by a 2004-2005 survey to be popular among black women: hot oil treatments, anti-frizz products and polishes, leave-in conditioners, root stimulators, hair lotions, and relaxers. Researchers had purchased the products in 2008.
The researchers detected 45 of 66 target chemicals in the samples, including some that are banned in the European Union or regulated in California based on health concerns, according to Dr. Helms.
Most of the products contained parabens and phthalates (both 78%), UV filters (72%), and cyclosiloxanes (67%).
All products contained at least 1 of 19 targeted fragrances, while “hair lotions, root stimulators, and hair relaxers contained multiple fragrance chemicals per product, with an average of five to eight targeted fragrance chemicals detected per product versus an average of two in the anti-frizz products.”
How do the findings compare with previous research? “They’re roughly consistent with what’s been found before, but potentially on the higher end,” Dr. Helms said. “For some of these chemicals, there’s not a lot of data from the past.”
Most of the chemicals aren’t listed on product labels, Dr. Helm said. “It’s possible that some of the ingredients were unintentionally added as part of manufacturing or other processes.”
Dr. Helm urged physicians to consider the connections between hair care products and chemical exposure. “Maybe there’s an opportunity to use fewer products,” she said.
Dr. Helm acknowledged that it is difficult to find hair care products that don’t include fragrance. She recommends the use of products made from plants or organic ingredients, and she pointed to a Silver Spring Institute–affiliated app called DetoxMe that offers suggestions about reducing chemical exposure from consumer products.
The study was funded by the Rose Foundation, the Goldman Fund, and Hurricane Voices Breast Cancer Foundation. The authors report no relevant disclosures.
cenews@mdedge.com
SOURCE: Helm JS et al. Environ Res. 2018 Apr 25. doi: 10.1016/j.envres.2018.03.030.
A new analysis of 18 hair products used by black women finds that they contain 45 endocrine-disrupting or asthma-associated chemicals, a finding that could help explain why this population suffers from higher rates of chemical exposure and hormone-related health conditions.
“We found multiples of our targeted chemicals in all of our products,” said study lead author Jessica S. Helm, PhD, of the Silent Spring Institute, Newton, Mass., in an interview. “We’re concerned about the additive effect of multiple products being used together.”
According to the study, previous research has found that, compared with white women, U.S. black women have higher urinary levels of chemicals like phthalates and parabens. Black women also have higher rates of asthma and hormone-related health conditions like uterine fibroids and infertility, Dr. Helms said.
The researchers launched their study to better understand the possible role of hair care products in raising chemical levels in black women, Dr. Helm said.
The researchers tested 18 types of hair care products shown by a 2004-2005 survey to be popular among black women: hot oil treatments, anti-frizz products and polishes, leave-in conditioners, root stimulators, hair lotions, and relaxers. Researchers had purchased the products in 2008.
The researchers detected 45 of 66 target chemicals in the samples, including some that are banned in the European Union or regulated in California based on health concerns, according to Dr. Helms.
Most of the products contained parabens and phthalates (both 78%), UV filters (72%), and cyclosiloxanes (67%).
All products contained at least 1 of 19 targeted fragrances, while “hair lotions, root stimulators, and hair relaxers contained multiple fragrance chemicals per product, with an average of five to eight targeted fragrance chemicals detected per product versus an average of two in the anti-frizz products.”
How do the findings compare with previous research? “They’re roughly consistent with what’s been found before, but potentially on the higher end,” Dr. Helms said. “For some of these chemicals, there’s not a lot of data from the past.”
Most of the chemicals aren’t listed on product labels, Dr. Helm said. “It’s possible that some of the ingredients were unintentionally added as part of manufacturing or other processes.”
Dr. Helm urged physicians to consider the connections between hair care products and chemical exposure. “Maybe there’s an opportunity to use fewer products,” she said.
Dr. Helm acknowledged that it is difficult to find hair care products that don’t include fragrance. She recommends the use of products made from plants or organic ingredients, and she pointed to a Silver Spring Institute–affiliated app called DetoxMe that offers suggestions about reducing chemical exposure from consumer products.
The study was funded by the Rose Foundation, the Goldman Fund, and Hurricane Voices Breast Cancer Foundation. The authors report no relevant disclosures.
cenews@mdedge.com
SOURCE: Helm JS et al. Environ Res. 2018 Apr 25. doi: 10.1016/j.envres.2018.03.030.
A new analysis of 18 hair products used by black women finds that they contain 45 endocrine-disrupting or asthma-associated chemicals, a finding that could help explain why this population suffers from higher rates of chemical exposure and hormone-related health conditions.
“We found multiples of our targeted chemicals in all of our products,” said study lead author Jessica S. Helm, PhD, of the Silent Spring Institute, Newton, Mass., in an interview. “We’re concerned about the additive effect of multiple products being used together.”
According to the study, previous research has found that, compared with white women, U.S. black women have higher urinary levels of chemicals like phthalates and parabens. Black women also have higher rates of asthma and hormone-related health conditions like uterine fibroids and infertility, Dr. Helms said.
The researchers launched their study to better understand the possible role of hair care products in raising chemical levels in black women, Dr. Helm said.
The researchers tested 18 types of hair care products shown by a 2004-2005 survey to be popular among black women: hot oil treatments, anti-frizz products and polishes, leave-in conditioners, root stimulators, hair lotions, and relaxers. Researchers had purchased the products in 2008.
The researchers detected 45 of 66 target chemicals in the samples, including some that are banned in the European Union or regulated in California based on health concerns, according to Dr. Helms.
Most of the products contained parabens and phthalates (both 78%), UV filters (72%), and cyclosiloxanes (67%).
All products contained at least 1 of 19 targeted fragrances, while “hair lotions, root stimulators, and hair relaxers contained multiple fragrance chemicals per product, with an average of five to eight targeted fragrance chemicals detected per product versus an average of two in the anti-frizz products.”
How do the findings compare with previous research? “They’re roughly consistent with what’s been found before, but potentially on the higher end,” Dr. Helms said. “For some of these chemicals, there’s not a lot of data from the past.”
Most of the chemicals aren’t listed on product labels, Dr. Helm said. “It’s possible that some of the ingredients were unintentionally added as part of manufacturing or other processes.”
Dr. Helm urged physicians to consider the connections between hair care products and chemical exposure. “Maybe there’s an opportunity to use fewer products,” she said.
Dr. Helm acknowledged that it is difficult to find hair care products that don’t include fragrance. She recommends the use of products made from plants or organic ingredients, and she pointed to a Silver Spring Institute–affiliated app called DetoxMe that offers suggestions about reducing chemical exposure from consumer products.
The study was funded by the Rose Foundation, the Goldman Fund, and Hurricane Voices Breast Cancer Foundation. The authors report no relevant disclosures.
cenews@mdedge.com
SOURCE: Helm JS et al. Environ Res. 2018 Apr 25. doi: 10.1016/j.envres.2018.03.030.
Key clinical point: Endocrine-disrupting and asthma-associated chemicals are commonly found in hair care products used by black women.
Major finding: Of the 66 target chemicals, 45 were found in the 18 products tested.
Study details: Analysis of 18 hair care products purchased in 2008.
Disclosures: The study was funded by the Goldman Fund, Hurricane Voices Breast Cancer Foundation, and the Rose Foundation. The authors report no relevant disclosures.
Source: Helm JS et al. Environ Res. 2018 Apr 25. doi: 10.1016/j.envres.2018.03.030.
Objective compensation systems can eliminate gender pay gap
Innovative compensation systems aimed at achieving fairness, consistency, and transparency in
At the University of Alabama at Birmingham, research showed that a newly adopted compensation system – one not even designed to address gender disparities – boosted the salaries of female surgeons from 46% to 72% of the salaries of their male colleagues. A gender salary gap also narrowed at Oregon Health & Sciences University, Portland, after a new compensation policy was put into place.

The two studies were presented at the annual meeting of the American Surgical Association.
Recent studies have revealed significant gaps in the salaries of female physicians, compared with their male counterparts. The challenge in this kind of study is to fairly compare salaries by adjusting for hours worked, time taken for family obligations, negotiated starting salary, and other factors that play into salary level.
A 2016 analysis of 590 surgeons at 24 medical schools found that men made a mean of $323,000 a year, compared with $270,000 among women. The gap persisted after adjustment for factors like years of experience and publication history at $280,000 (women) and $312,000 (men). The pay gap among 744 surgical subspecialists was even wider at $343,000 (men) versus $267,000 (women). After adjustment, male surgical subspecialists made $329,000, while women made $285,000 (JAMA Intern Med. 2016;176[9]:1294-304).
In 2015, the administration at Oregon Health & Sciences University instituted a school-wide “Faculty First” compensation plan. It aligns faculty pay – based on specialty and academic rank – with 3-year rolling median salaries in the Western region as reported by the Association of American Medical Colleges.
A study of compensation at OHSU led by Heather E. Hoops, MD, examined the salaries earned by certain department of surgery faculty during 2009-2017 and promotion and retention rates during 1998-2007. The study excluded instructors, the chair of the department, and some other faculty members whose salaries were based on specific bonuses.
The researchers found that prior to the change in 2015, the 24 female faculty made significantly less than the 62 men (P = .004). After the “Faculty First” initiative was implemented in 2015, salaries for both genders grew significantly and gender salary gap was virtually closed after that time.
The researchers found no gender disparity in time to promotion among the faculty. No significant difference was found in the rate of departure between male and female faculty (P = .73), although women who were not promoted tended to leave more quickly than their male counterparts.
“Objective compensation plans may work by mitigating gender-based implicit bias in the salary negotiation process and differences in salary negotiation style between females and males,” Dr. Hoops and her coauthors wrote. “However, objective compensation plans do not supplant the need for other institutional interventions, such as implicit bias training and objective and transparent promotion criteria, to improve gender equality among surgeons.”
In the other study, University of Alabama at Birmingham researchers analyzed surgeon salaries earned during 2014-2017. In 2017, the university switched some surgeons to a new compensation system based on work revenue value units with incentives.

In an interview, study lead author Melanie Morris, MD, said the new pay system unexpectedly reduced the gender pay gap. “The rationale for this department compensation plan was to create a fair and transparent compensation system for all faculty,” she said. “In doing so, this plan unintentionally led to these described changes to equalize an unrecognized disparity. We are proud of the result and recognize there is still more work to do. Each institution should know their own data to see if a gender pay disparity exists and devise a plan to address it.”
OHSU Department of Surgery funded the Oregon study. The study authors report no disclosures. The University of Alabama at Birmingham study reports no funding. The study authors report no disclosures.
The complete manuscript of these studies and their presentation at the American Surgical Association’s 138th Annual Meeting, April 2018, in Phoenix, is anticipated to be published in the Annals of Surgery pending editorial review.
SOURCE: Morris MS et al. ASA Annual Meeting 2018, Abstract 4. Hoops HE et al. ASA Annual Meeting 2018, Abstract 9.
Innovative compensation systems aimed at achieving fairness, consistency, and transparency in
At the University of Alabama at Birmingham, research showed that a newly adopted compensation system – one not even designed to address gender disparities – boosted the salaries of female surgeons from 46% to 72% of the salaries of their male colleagues. A gender salary gap also narrowed at Oregon Health & Sciences University, Portland, after a new compensation policy was put into place.
The two studies were presented at the annual meeting of the American Surgical Association.
Recent studies have revealed significant gaps in the salaries of female physicians, compared with their male counterparts. The challenge in this kind of study is to fairly compare salaries by adjusting for hours worked, time taken for family obligations, negotiated starting salary, and other factors that play into salary level.
A 2016 analysis of 590 surgeons at 24 medical schools found that men made a mean of $323,000 a year, compared with $270,000 among women. The gap persisted after adjustment for factors like years of experience and publication history at $280,000 (women) and $312,000 (men). The pay gap among 744 surgical subspecialists was even wider at $343,000 (men) versus $267,000 (women). After adjustment, male surgical subspecialists made $329,000, while women made $285,000 (JAMA Intern Med. 2016;176[9]:1294-304).
In 2015, the administration at Oregon Health & Sciences University instituted a school-wide “Faculty First” compensation plan. It aligns faculty pay – based on specialty and academic rank – with 3-year rolling median salaries in the Western region as reported by the Association of American Medical Colleges.
A study of compensation at OHSU led by Heather E. Hoops, MD, examined the salaries earned by certain department of surgery faculty during 2009-2017 and promotion and retention rates during 1998-2007. The study excluded instructors, the chair of the department, and some other faculty members whose salaries were based on specific bonuses.
The researchers found that prior to the change in 2015, the 24 female faculty made significantly less than the 62 men (P = .004). After the “Faculty First” initiative was implemented in 2015, salaries for both genders grew significantly and gender salary gap was virtually closed after that time.
The researchers found no gender disparity in time to promotion among the faculty. No significant difference was found in the rate of departure between male and female faculty (P = .73), although women who were not promoted tended to leave more quickly than their male counterparts.
“Objective compensation plans may work by mitigating gender-based implicit bias in the salary negotiation process and differences in salary negotiation style between females and males,” Dr. Hoops and her coauthors wrote. “However, objective compensation plans do not supplant the need for other institutional interventions, such as implicit bias training and objective and transparent promotion criteria, to improve gender equality among surgeons.”
In the other study, University of Alabama at Birmingham researchers analyzed surgeon salaries earned during 2014-2017. In 2017, the university switched some surgeons to a new compensation system based on work revenue value units with incentives.
In an interview, study lead author Melanie Morris, MD, said the new pay system unexpectedly reduced the gender pay gap. “The rationale for this department compensation plan was to create a fair and transparent compensation system for all faculty,” she said. “In doing so, this plan unintentionally led to these described changes to equalize an unrecognized disparity. We are proud of the result and recognize there is still more work to do. Each institution should know their own data to see if a gender pay disparity exists and devise a plan to address it.”
OHSU Department of Surgery funded the Oregon study. The study authors report no disclosures. The University of Alabama at Birmingham study reports no funding. The study authors report no disclosures.
The complete manuscript of these studies and their presentation at the American Surgical Association’s 138th Annual Meeting, April 2018, in Phoenix, is anticipated to be published in the Annals of Surgery pending editorial review.
SOURCE: Morris MS et al. ASA Annual Meeting 2018, Abstract 4. Hoops HE et al. ASA Annual Meeting 2018, Abstract 9.
Innovative compensation systems aimed at achieving fairness, consistency, and transparency in
At the University of Alabama at Birmingham, research showed that a newly adopted compensation system – one not even designed to address gender disparities – boosted the salaries of female surgeons from 46% to 72% of the salaries of their male colleagues. A gender salary gap also narrowed at Oregon Health & Sciences University, Portland, after a new compensation policy was put into place.
The two studies were presented at the annual meeting of the American Surgical Association.
Recent studies have revealed significant gaps in the salaries of female physicians, compared with their male counterparts. The challenge in this kind of study is to fairly compare salaries by adjusting for hours worked, time taken for family obligations, negotiated starting salary, and other factors that play into salary level.
A 2016 analysis of 590 surgeons at 24 medical schools found that men made a mean of $323,000 a year, compared with $270,000 among women. The gap persisted after adjustment for factors like years of experience and publication history at $280,000 (women) and $312,000 (men). The pay gap among 744 surgical subspecialists was even wider at $343,000 (men) versus $267,000 (women). After adjustment, male surgical subspecialists made $329,000, while women made $285,000 (JAMA Intern Med. 2016;176[9]:1294-304).
In 2015, the administration at Oregon Health & Sciences University instituted a school-wide “Faculty First” compensation plan. It aligns faculty pay – based on specialty and academic rank – with 3-year rolling median salaries in the Western region as reported by the Association of American Medical Colleges.
A study of compensation at OHSU led by Heather E. Hoops, MD, examined the salaries earned by certain department of surgery faculty during 2009-2017 and promotion and retention rates during 1998-2007. The study excluded instructors, the chair of the department, and some other faculty members whose salaries were based on specific bonuses.
The researchers found that prior to the change in 2015, the 24 female faculty made significantly less than the 62 men (P = .004). After the “Faculty First” initiative was implemented in 2015, salaries for both genders grew significantly and gender salary gap was virtually closed after that time.
The researchers found no gender disparity in time to promotion among the faculty. No significant difference was found in the rate of departure between male and female faculty (P = .73), although women who were not promoted tended to leave more quickly than their male counterparts.
“Objective compensation plans may work by mitigating gender-based implicit bias in the salary negotiation process and differences in salary negotiation style between females and males,” Dr. Hoops and her coauthors wrote. “However, objective compensation plans do not supplant the need for other institutional interventions, such as implicit bias training and objective and transparent promotion criteria, to improve gender equality among surgeons.”
In the other study, University of Alabama at Birmingham researchers analyzed surgeon salaries earned during 2014-2017. In 2017, the university switched some surgeons to a new compensation system based on work revenue value units with incentives.
In an interview, study lead author Melanie Morris, MD, said the new pay system unexpectedly reduced the gender pay gap. “The rationale for this department compensation plan was to create a fair and transparent compensation system for all faculty,” she said. “In doing so, this plan unintentionally led to these described changes to equalize an unrecognized disparity. We are proud of the result and recognize there is still more work to do. Each institution should know their own data to see if a gender pay disparity exists and devise a plan to address it.”
OHSU Department of Surgery funded the Oregon study. The study authors report no disclosures. The University of Alabama at Birmingham study reports no funding. The study authors report no disclosures.
The complete manuscript of these studies and their presentation at the American Surgical Association’s 138th Annual Meeting, April 2018, in Phoenix, is anticipated to be published in the Annals of Surgery pending editorial review.
SOURCE: Morris MS et al. ASA Annual Meeting 2018, Abstract 4. Hoops HE et al. ASA Annual Meeting 2018, Abstract 9.
HIV infection linked to higher risk of non-melanoma skin cancer
A Danish cohort study provides more evidence of a significant link between HIV infection and two types of skin cancer.
, with incidence rate ratios (IRRs) of 1.79 and 5.40, respectively, when compared with a background population, who were HIV-negative.
“The risk of SCC seemed to increase with increasing level of immunosuppression while the increased risk of BCC was restricted to patients reporting MSM [men who have sex with men] as route of infection,” wrote the authors, led by Silje Haukali Omland, MD, PhD, of the department of dermato-venereology, Copenhagen University Hospital.
The Danish nationwide cohort study, which matched each HIV patient with 5 age- and sex-matched individuals from the background population, was published online March 26 in the Journal of the American Academy of Dermatology.
The results are similar to those published elsewhere, as is the finding that HIV-positive patients do not face a higher risk of malignant melanoma. “The results here confirm prior studies and support heightened vigilance for skin conditions, such as SCC and BCC in HIV patients,” said Michael J. Silverberg, PhD, of Kaiser Permanente Division of Research, in an interview after reviewing the study findings. He was not a study author.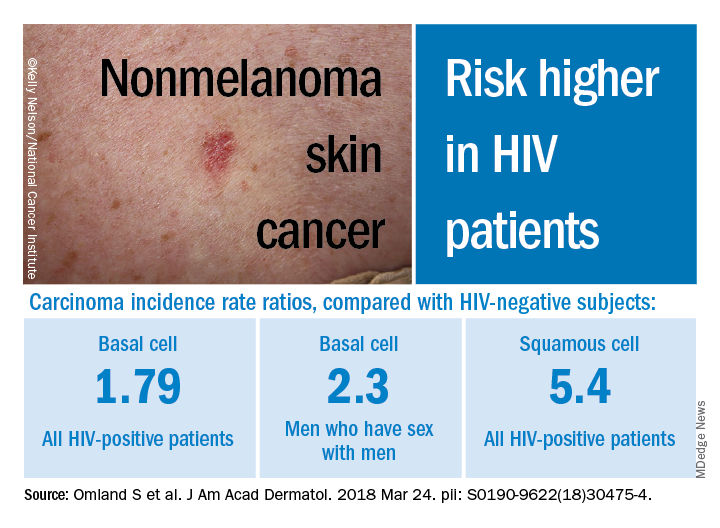
Researchers have long noted a connection between various types of cancer and HIV infection. But, as noted in a 2013 study led by Dr. Silverberg, research into links between HIV and non-melanoma skin cancers has been sparse and inconclusive. That study of white adults found higher adjusted rate ratios for SCC (2.6) and BCC (2.1) among those who were HIV-positive compared with those who were HIV-negative (J Natl Cancer Inst. 2013 Mar 6;105[5]:350-60).
In the Danish study, researchers tracked sex-and age-matched cohorts of HIV-infected (4,280) and non-HIV-infected patients (21,399) aged 16 years or older from study inclusion through as late as 2014. All the HIV-positive subjects had taken antiretroviral medications. The researchers also compared the HIV-positive patients to their non-HIV-infected siblings.
Overall, those who were HIV-positive were more likely to develop BCC (IRR, 1.79, 95% CI, 1.43-2.22), and males who reported sex with men had an even higher risk (IRR, 2.30, 95% CI, 1.76-3.02).
As for SCC, the IRR was 5.40 (95% CI, 3.07-9.52) among those who were HIV-positive, compared with the background population, and the researchers found evidence that risk increased with level of immunosuppression. Those who indicated heterosexual and male homosexual transmission had similar rates of SCC.
The rates of BCC or SCC were not higher among siblings of HIV-positive patients.
In addition, the risk of melanoma was not increased among those who were HIV-positive subjects or their siblings, when compared with the background group. However, the researchers noted that the study turned up a low number of HIV-positive subjects with melanoma, potentially throwing off the results.
The researchers noted that the inclusion of siblings in the study suggests that sun exposure in childhood was not a confounding factor. Presumably, they wrote, the siblings had similar levels of exposure as children, although exposure to sun bed tanning could differ between siblings.
“Study methods appear very strong and consistent with other work done in the area,” Dr. Silverberg said in the interview. As for possible causes of the disparities, he noted that exposure to the sun or to tanning beds could explain the greater risk of BCC among men who have sex with men. “For SCC, there may be a biological link, as studies have suggested a link with human papillomavirus for that particular cancer,” he added.
No study funding was reported. The study authors reported disclosures that included grants, research grants, speaker fees, and/or advisory board honoraria from several drug manufacturers. Dr. Silverberg has no relevant disclosures.
A Danish cohort study provides more evidence of a significant link between HIV infection and two types of skin cancer.
, with incidence rate ratios (IRRs) of 1.79 and 5.40, respectively, when compared with a background population, who were HIV-negative.
“The risk of SCC seemed to increase with increasing level of immunosuppression while the increased risk of BCC was restricted to patients reporting MSM [men who have sex with men] as route of infection,” wrote the authors, led by Silje Haukali Omland, MD, PhD, of the department of dermato-venereology, Copenhagen University Hospital.
The Danish nationwide cohort study, which matched each HIV patient with 5 age- and sex-matched individuals from the background population, was published online March 26 in the Journal of the American Academy of Dermatology.
The results are similar to those published elsewhere, as is the finding that HIV-positive patients do not face a higher risk of malignant melanoma. “The results here confirm prior studies and support heightened vigilance for skin conditions, such as SCC and BCC in HIV patients,” said Michael J. Silverberg, PhD, of Kaiser Permanente Division of Research, in an interview after reviewing the study findings. He was not a study author.
Researchers have long noted a connection between various types of cancer and HIV infection. But, as noted in a 2013 study led by Dr. Silverberg, research into links between HIV and non-melanoma skin cancers has been sparse and inconclusive. That study of white adults found higher adjusted rate ratios for SCC (2.6) and BCC (2.1) among those who were HIV-positive compared with those who were HIV-negative (J Natl Cancer Inst. 2013 Mar 6;105[5]:350-60).
In the Danish study, researchers tracked sex-and age-matched cohorts of HIV-infected (4,280) and non-HIV-infected patients (21,399) aged 16 years or older from study inclusion through as late as 2014. All the HIV-positive subjects had taken antiretroviral medications. The researchers also compared the HIV-positive patients to their non-HIV-infected siblings.
Overall, those who were HIV-positive were more likely to develop BCC (IRR, 1.79, 95% CI, 1.43-2.22), and males who reported sex with men had an even higher risk (IRR, 2.30, 95% CI, 1.76-3.02).
As for SCC, the IRR was 5.40 (95% CI, 3.07-9.52) among those who were HIV-positive, compared with the background population, and the researchers found evidence that risk increased with level of immunosuppression. Those who indicated heterosexual and male homosexual transmission had similar rates of SCC.
The rates of BCC or SCC were not higher among siblings of HIV-positive patients.
In addition, the risk of melanoma was not increased among those who were HIV-positive subjects or their siblings, when compared with the background group. However, the researchers noted that the study turned up a low number of HIV-positive subjects with melanoma, potentially throwing off the results.
The researchers noted that the inclusion of siblings in the study suggests that sun exposure in childhood was not a confounding factor. Presumably, they wrote, the siblings had similar levels of exposure as children, although exposure to sun bed tanning could differ between siblings.
“Study methods appear very strong and consistent with other work done in the area,” Dr. Silverberg said in the interview. As for possible causes of the disparities, he noted that exposure to the sun or to tanning beds could explain the greater risk of BCC among men who have sex with men. “For SCC, there may be a biological link, as studies have suggested a link with human papillomavirus for that particular cancer,” he added.
No study funding was reported. The study authors reported disclosures that included grants, research grants, speaker fees, and/or advisory board honoraria from several drug manufacturers. Dr. Silverberg has no relevant disclosures.
A Danish cohort study provides more evidence of a significant link between HIV infection and two types of skin cancer.
, with incidence rate ratios (IRRs) of 1.79 and 5.40, respectively, when compared with a background population, who were HIV-negative.
“The risk of SCC seemed to increase with increasing level of immunosuppression while the increased risk of BCC was restricted to patients reporting MSM [men who have sex with men] as route of infection,” wrote the authors, led by Silje Haukali Omland, MD, PhD, of the department of dermato-venereology, Copenhagen University Hospital.
The Danish nationwide cohort study, which matched each HIV patient with 5 age- and sex-matched individuals from the background population, was published online March 26 in the Journal of the American Academy of Dermatology.
The results are similar to those published elsewhere, as is the finding that HIV-positive patients do not face a higher risk of malignant melanoma. “The results here confirm prior studies and support heightened vigilance for skin conditions, such as SCC and BCC in HIV patients,” said Michael J. Silverberg, PhD, of Kaiser Permanente Division of Research, in an interview after reviewing the study findings. He was not a study author.
Researchers have long noted a connection between various types of cancer and HIV infection. But, as noted in a 2013 study led by Dr. Silverberg, research into links between HIV and non-melanoma skin cancers has been sparse and inconclusive. That study of white adults found higher adjusted rate ratios for SCC (2.6) and BCC (2.1) among those who were HIV-positive compared with those who were HIV-negative (J Natl Cancer Inst. 2013 Mar 6;105[5]:350-60).
In the Danish study, researchers tracked sex-and age-matched cohorts of HIV-infected (4,280) and non-HIV-infected patients (21,399) aged 16 years or older from study inclusion through as late as 2014. All the HIV-positive subjects had taken antiretroviral medications. The researchers also compared the HIV-positive patients to their non-HIV-infected siblings.
Overall, those who were HIV-positive were more likely to develop BCC (IRR, 1.79, 95% CI, 1.43-2.22), and males who reported sex with men had an even higher risk (IRR, 2.30, 95% CI, 1.76-3.02).
As for SCC, the IRR was 5.40 (95% CI, 3.07-9.52) among those who were HIV-positive, compared with the background population, and the researchers found evidence that risk increased with level of immunosuppression. Those who indicated heterosexual and male homosexual transmission had similar rates of SCC.
The rates of BCC or SCC were not higher among siblings of HIV-positive patients.
In addition, the risk of melanoma was not increased among those who were HIV-positive subjects or their siblings, when compared with the background group. However, the researchers noted that the study turned up a low number of HIV-positive subjects with melanoma, potentially throwing off the results.
The researchers noted that the inclusion of siblings in the study suggests that sun exposure in childhood was not a confounding factor. Presumably, they wrote, the siblings had similar levels of exposure as children, although exposure to sun bed tanning could differ between siblings.
“Study methods appear very strong and consistent with other work done in the area,” Dr. Silverberg said in the interview. As for possible causes of the disparities, he noted that exposure to the sun or to tanning beds could explain the greater risk of BCC among men who have sex with men. “For SCC, there may be a biological link, as studies have suggested a link with human papillomavirus for that particular cancer,” he added.
No study funding was reported. The study authors reported disclosures that included grants, research grants, speaker fees, and/or advisory board honoraria from several drug manufacturers. Dr. Silverberg has no relevant disclosures.
FROM JAAD
Key clinical point: HIV-positive patients are at an increased risk for basal cell carcinoma (BCC) and squamous cell carcinoma (SCC).
Major finding: Among HIV-infected patients, the risk of BCC was increased by almost twofold and the risk of BCC was increased by more than fivefold.
Study details: A Danish population-based cohort study of 4,280 HIV-infected patients and 21,399 age-and sex-matched subjects.
Disclosures: No study funding was reported. The authors reported disclosures that included research grants, speaker fees, and/or advisory board honoraria from several drug manufacturers.
Source: Omland S et al. J Am Acad Dermatol. 2018 Mar 24. pii: S0190-9622(18)30475-4. doi: 10.1016/j.jaad.2018.03.024.