User login
Early Strides Made in Personalized Refractory Asthma Care
KEYSTONE, COLO. – Six novel phenotypes have been defined that can be used to personalize therapy for difficult-to-treat, refractory asthma.
"There’s no doubt in my mind now, we need to identify the exact phenotype, so as to treat [refractory asthma] with personalized, directed therapy," Dr. Richard J. Martin said at an allergy and pulmonary diseases meeting. "This will improve asthma control and lung function."

Bronchoscopic evaluation of the upper and lower airways as well as reflux studies were used to identify the phenotypes, and prompted the researchers to develop a supraglottic index to visually score abnormalities in the upper airway.
"We think this is superior to any GI study for reflux," said Dr. Martin, chair of medicine and the Edelstein chair of pulmonary medicine at National Jewish Health in Denver, which sponsored the meeting. "So many GI studies are falsely negative because they provide only a snapshot in time, whereas the supraglottic index really shows you a history over a long period of time."
The supraglottic index (SGI) uses a scale to score for the presence of edema and erythema/hyperemia in the epiglottis, false vocal cords, and arytenoid cartilage, as well as secretions or mucosal thickening of the piriform recess and posterior commissure. A total score of 0-4 is normal, 5-9 is mild pathology, 10-16 is moderate, and 17-22 is severe pathology. A score of 10 or more is an important clue for clinicians because it is indicative of reflux that is high enough to produce aspiration or to hit the vocal cords.
The SGI was used in 58 patients who met American Thoracic Society criteria for refractory asthma and who had a 12% improvement after bronchial dilation or PC20 (the provocative concentration of methacholine inducing a 20% fall in FEV1 [forced expiratory volume in 1 second]) of 6 mg/mL or less. Patients with more than a 5 pack-years of smoking were excluded.
Notably, 20 patients initially received guideline-based evaluation and treatment with intensified therapy for 4 months, followed by bronchoscopy-directed therapy, and 38 went directly to bronchoscopy.
The cohort’s mean age was 55 years and the mean FEV1 was 60.7%, even on medication. They had very poorly controlled asthma and severe airway hyperresponsiveness, as indicated by a mean asthma control test (ACT) score of 11.5 and a mean PC20 of 1.6 mg/mL.
Based on bronchoscopic evaluation, five mutually exclusive phenotypes emerged: tissue eosinophilia in 4 patients, subacute bacterial infection in 13, gastroesophageal reflux in 22, combination (any two or all three of the above) in 13, and "nonspecific" in 6. A sixth phenotype (tissue mast cells) has since been identified and can be effectively treated with something as simple as cromolyn, Dr. Martin said.
In all, 44 of the 58 patients (76%) had an SGI of 10 or more. Of these, 43 also had reflux testing, and 34 had documented gastroesophageal reflux disease (GERD). Some 14 patients (24%) had an SGI less than 10, with 8 of the 9 patients who also underwent reflux testing being negative for GERD.
Patients with a positive GERD test had a significantly higher mean SGI score than did those with a negative GERD test (15.8 vs. 8.9; P less than .0001), he said, but later noted that bronchoscopists were blinded to some – but not all – of the reflux test results.
When the investigators looked at treatment outcomes, they found "absolutely no change" in FEV1 or ACT scores after 4 months of intensified, guideline-directed standard therapy in the 20 control patients. In contrast, after bronchoscopic-directed therapy, ACT improved almost into the well-controlled range, and FEV1 increased from 64% of predicted to 76% of predicted, Dr. Martin said.
"So this internal control group shows us we really have to phenotype and direct asthma therapy," he said.
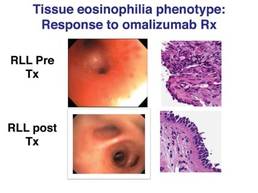
Among the 38 patients who went directly to bronchoscopic-directed evaluation and therapy, significant increases in ACT and FEV1 were observed 6 months post treatment among all but the nonspecific phenotype. Dr. Martin pointed out that patients in the tissue eosinophilia group experienced "tremendous improvement" in FEV1 with the use of omalizumab (Xolair), whereas no benefit was seen in the nonspecific group.
"You read the literature and it’s a 6%-7% improvement in FEV1 [with omalizumab], but we had a 43% improvement in FEV1 by selecting the correct patients," he remarked.
Omalizumab is approved in the United States for the treatment of moderate to severe persistent allergic asthma despite inhaled corticosteroids, but it is approved only as an add-on therapy in the European Union, due in part to the difficulty of predicting which patients will respond. A previous analysis of seven randomized omalizumab trials including the INNOVATE trial reported that baseline characteristics do not reliably predict benefit with omalizumab (Respir. Med. 2007;101:1483-92).
Further investigation is needed to determine the exact tissue eosinophil number that is important for treatment, Dr. Martin said. For the purpose of this preliminary work, which was described as a real-world study that took all comers, the phenotype was defined as more than 10 eosinophils per high-power field.
A study is now underway to validate the SGI, including intra- and interoperator variability. Further research is also needed to identify a noninvasive means of evaluation, to better understand the subacute bacterial infection phenotype and microbiome, and to determine how to treat the more problematic nonspecific phenotype. Dr. Martin stressed that for patients with the combination phenotype, each of the phenotypes must be treated to obtain maximum benefit.
During a discussion of the study, he said that lavage, biopsy, and brush evaluations are all needed to identify atypical bacteria, and that careful attention must be paid to the cleanliness of the endoscope to avoid cross-contamination of the airways during evaluation. Endobronchial biopsies were typically taken from the right lower lobe as well as from areas of abnormality.
Dr. Martin also noted that no association was identified between a specific phenotype and sinusitis, which was present in 71% of the patients, or with obesity. The mean body mass index of the cohort was 31 kg/m2.
Additional details of the study can be found online (Chest 2011 Aug. 11 [doi:10.1378/chest.11-0741]).
Dr. Martin reported no relevant conflicts of interest.
KEYSTONE, COLO. – Six novel phenotypes have been defined that can be used to personalize therapy for difficult-to-treat, refractory asthma.
"There’s no doubt in my mind now, we need to identify the exact phenotype, so as to treat [refractory asthma] with personalized, directed therapy," Dr. Richard J. Martin said at an allergy and pulmonary diseases meeting. "This will improve asthma control and lung function."
Bronchoscopic evaluation of the upper and lower airways as well as reflux studies were used to identify the phenotypes, and prompted the researchers to develop a supraglottic index to visually score abnormalities in the upper airway.
"We think this is superior to any GI study for reflux," said Dr. Martin, chair of medicine and the Edelstein chair of pulmonary medicine at National Jewish Health in Denver, which sponsored the meeting. "So many GI studies are falsely negative because they provide only a snapshot in time, whereas the supraglottic index really shows you a history over a long period of time."
The supraglottic index (SGI) uses a scale to score for the presence of edema and erythema/hyperemia in the epiglottis, false vocal cords, and arytenoid cartilage, as well as secretions or mucosal thickening of the piriform recess and posterior commissure. A total score of 0-4 is normal, 5-9 is mild pathology, 10-16 is moderate, and 17-22 is severe pathology. A score of 10 or more is an important clue for clinicians because it is indicative of reflux that is high enough to produce aspiration or to hit the vocal cords.
The SGI was used in 58 patients who met American Thoracic Society criteria for refractory asthma and who had a 12% improvement after bronchial dilation or PC20 (the provocative concentration of methacholine inducing a 20% fall in FEV1 [forced expiratory volume in 1 second]) of 6 mg/mL or less. Patients with more than a 5 pack-years of smoking were excluded.
Notably, 20 patients initially received guideline-based evaluation and treatment with intensified therapy for 4 months, followed by bronchoscopy-directed therapy, and 38 went directly to bronchoscopy.
The cohort’s mean age was 55 years and the mean FEV1 was 60.7%, even on medication. They had very poorly controlled asthma and severe airway hyperresponsiveness, as indicated by a mean asthma control test (ACT) score of 11.5 and a mean PC20 of 1.6 mg/mL.
Based on bronchoscopic evaluation, five mutually exclusive phenotypes emerged: tissue eosinophilia in 4 patients, subacute bacterial infection in 13, gastroesophageal reflux in 22, combination (any two or all three of the above) in 13, and "nonspecific" in 6. A sixth phenotype (tissue mast cells) has since been identified and can be effectively treated with something as simple as cromolyn, Dr. Martin said.
In all, 44 of the 58 patients (76%) had an SGI of 10 or more. Of these, 43 also had reflux testing, and 34 had documented gastroesophageal reflux disease (GERD). Some 14 patients (24%) had an SGI less than 10, with 8 of the 9 patients who also underwent reflux testing being negative for GERD.
Patients with a positive GERD test had a significantly higher mean SGI score than did those with a negative GERD test (15.8 vs. 8.9; P less than .0001), he said, but later noted that bronchoscopists were blinded to some – but not all – of the reflux test results.
When the investigators looked at treatment outcomes, they found "absolutely no change" in FEV1 or ACT scores after 4 months of intensified, guideline-directed standard therapy in the 20 control patients. In contrast, after bronchoscopic-directed therapy, ACT improved almost into the well-controlled range, and FEV1 increased from 64% of predicted to 76% of predicted, Dr. Martin said.
"So this internal control group shows us we really have to phenotype and direct asthma therapy," he said.
Among the 38 patients who went directly to bronchoscopic-directed evaluation and therapy, significant increases in ACT and FEV1 were observed 6 months post treatment among all but the nonspecific phenotype. Dr. Martin pointed out that patients in the tissue eosinophilia group experienced "tremendous improvement" in FEV1 with the use of omalizumab (Xolair), whereas no benefit was seen in the nonspecific group.
"You read the literature and it’s a 6%-7% improvement in FEV1 [with omalizumab], but we had a 43% improvement in FEV1 by selecting the correct patients," he remarked.
Omalizumab is approved in the United States for the treatment of moderate to severe persistent allergic asthma despite inhaled corticosteroids, but it is approved only as an add-on therapy in the European Union, due in part to the difficulty of predicting which patients will respond. A previous analysis of seven randomized omalizumab trials including the INNOVATE trial reported that baseline characteristics do not reliably predict benefit with omalizumab (Respir. Med. 2007;101:1483-92).
Further investigation is needed to determine the exact tissue eosinophil number that is important for treatment, Dr. Martin said. For the purpose of this preliminary work, which was described as a real-world study that took all comers, the phenotype was defined as more than 10 eosinophils per high-power field.
A study is now underway to validate the SGI, including intra- and interoperator variability. Further research is also needed to identify a noninvasive means of evaluation, to better understand the subacute bacterial infection phenotype and microbiome, and to determine how to treat the more problematic nonspecific phenotype. Dr. Martin stressed that for patients with the combination phenotype, each of the phenotypes must be treated to obtain maximum benefit.
During a discussion of the study, he said that lavage, biopsy, and brush evaluations are all needed to identify atypical bacteria, and that careful attention must be paid to the cleanliness of the endoscope to avoid cross-contamination of the airways during evaluation. Endobronchial biopsies were typically taken from the right lower lobe as well as from areas of abnormality.
Dr. Martin also noted that no association was identified between a specific phenotype and sinusitis, which was present in 71% of the patients, or with obesity. The mean body mass index of the cohort was 31 kg/m2.
Additional details of the study can be found online (Chest 2011 Aug. 11 [doi:10.1378/chest.11-0741]).
Dr. Martin reported no relevant conflicts of interest.
KEYSTONE, COLO. – Six novel phenotypes have been defined that can be used to personalize therapy for difficult-to-treat, refractory asthma.
"There’s no doubt in my mind now, we need to identify the exact phenotype, so as to treat [refractory asthma] with personalized, directed therapy," Dr. Richard J. Martin said at an allergy and pulmonary diseases meeting. "This will improve asthma control and lung function."
Bronchoscopic evaluation of the upper and lower airways as well as reflux studies were used to identify the phenotypes, and prompted the researchers to develop a supraglottic index to visually score abnormalities in the upper airway.
"We think this is superior to any GI study for reflux," said Dr. Martin, chair of medicine and the Edelstein chair of pulmonary medicine at National Jewish Health in Denver, which sponsored the meeting. "So many GI studies are falsely negative because they provide only a snapshot in time, whereas the supraglottic index really shows you a history over a long period of time."
The supraglottic index (SGI) uses a scale to score for the presence of edema and erythema/hyperemia in the epiglottis, false vocal cords, and arytenoid cartilage, as well as secretions or mucosal thickening of the piriform recess and posterior commissure. A total score of 0-4 is normal, 5-9 is mild pathology, 10-16 is moderate, and 17-22 is severe pathology. A score of 10 or more is an important clue for clinicians because it is indicative of reflux that is high enough to produce aspiration or to hit the vocal cords.
The SGI was used in 58 patients who met American Thoracic Society criteria for refractory asthma and who had a 12% improvement after bronchial dilation or PC20 (the provocative concentration of methacholine inducing a 20% fall in FEV1 [forced expiratory volume in 1 second]) of 6 mg/mL or less. Patients with more than a 5 pack-years of smoking were excluded.
Notably, 20 patients initially received guideline-based evaluation and treatment with intensified therapy for 4 months, followed by bronchoscopy-directed therapy, and 38 went directly to bronchoscopy.
The cohort’s mean age was 55 years and the mean FEV1 was 60.7%, even on medication. They had very poorly controlled asthma and severe airway hyperresponsiveness, as indicated by a mean asthma control test (ACT) score of 11.5 and a mean PC20 of 1.6 mg/mL.
Based on bronchoscopic evaluation, five mutually exclusive phenotypes emerged: tissue eosinophilia in 4 patients, subacute bacterial infection in 13, gastroesophageal reflux in 22, combination (any two or all three of the above) in 13, and "nonspecific" in 6. A sixth phenotype (tissue mast cells) has since been identified and can be effectively treated with something as simple as cromolyn, Dr. Martin said.
In all, 44 of the 58 patients (76%) had an SGI of 10 or more. Of these, 43 also had reflux testing, and 34 had documented gastroesophageal reflux disease (GERD). Some 14 patients (24%) had an SGI less than 10, with 8 of the 9 patients who also underwent reflux testing being negative for GERD.
Patients with a positive GERD test had a significantly higher mean SGI score than did those with a negative GERD test (15.8 vs. 8.9; P less than .0001), he said, but later noted that bronchoscopists were blinded to some – but not all – of the reflux test results.
When the investigators looked at treatment outcomes, they found "absolutely no change" in FEV1 or ACT scores after 4 months of intensified, guideline-directed standard therapy in the 20 control patients. In contrast, after bronchoscopic-directed therapy, ACT improved almost into the well-controlled range, and FEV1 increased from 64% of predicted to 76% of predicted, Dr. Martin said.
"So this internal control group shows us we really have to phenotype and direct asthma therapy," he said.
Among the 38 patients who went directly to bronchoscopic-directed evaluation and therapy, significant increases in ACT and FEV1 were observed 6 months post treatment among all but the nonspecific phenotype. Dr. Martin pointed out that patients in the tissue eosinophilia group experienced "tremendous improvement" in FEV1 with the use of omalizumab (Xolair), whereas no benefit was seen in the nonspecific group.
"You read the literature and it’s a 6%-7% improvement in FEV1 [with omalizumab], but we had a 43% improvement in FEV1 by selecting the correct patients," he remarked.
Omalizumab is approved in the United States for the treatment of moderate to severe persistent allergic asthma despite inhaled corticosteroids, but it is approved only as an add-on therapy in the European Union, due in part to the difficulty of predicting which patients will respond. A previous analysis of seven randomized omalizumab trials including the INNOVATE trial reported that baseline characteristics do not reliably predict benefit with omalizumab (Respir. Med. 2007;101:1483-92).
Further investigation is needed to determine the exact tissue eosinophil number that is important for treatment, Dr. Martin said. For the purpose of this preliminary work, which was described as a real-world study that took all comers, the phenotype was defined as more than 10 eosinophils per high-power field.
A study is now underway to validate the SGI, including intra- and interoperator variability. Further research is also needed to identify a noninvasive means of evaluation, to better understand the subacute bacterial infection phenotype and microbiome, and to determine how to treat the more problematic nonspecific phenotype. Dr. Martin stressed that for patients with the combination phenotype, each of the phenotypes must be treated to obtain maximum benefit.
During a discussion of the study, he said that lavage, biopsy, and brush evaluations are all needed to identify atypical bacteria, and that careful attention must be paid to the cleanliness of the endoscope to avoid cross-contamination of the airways during evaluation. Endobronchial biopsies were typically taken from the right lower lobe as well as from areas of abnormality.
Dr. Martin also noted that no association was identified between a specific phenotype and sinusitis, which was present in 71% of the patients, or with obesity. The mean body mass index of the cohort was 31 kg/m2.
Additional details of the study can be found online (Chest 2011 Aug. 11 [doi:10.1378/chest.11-0741]).
Dr. Martin reported no relevant conflicts of interest.
FROM A MEETING ON ALLERGY AND RESPIRATORY DISEASES
Major Finding: Six phenotypes have been identified using bronchoscopy and a supraglottic index that can be used to evaluate and direct therapy for refractory asthma.
Data Source: Data were taken from an observational treatment study of 58 patients with difficult to treat, refractory asthma.
Disclosures: Dr. Martin and his coauthors reported no relevant conflicts of interest.
Early Thrombolysis Improves Long-term Outcomes After DVT
SAN DIEGO – Catheter-directed thrombolysis added to standard therapy for deep vein thrombosis reduced the risk of post-thrombotic syndrome by 14.5%, but at an increased cost of bleeding among 209 patients in a randomized, controlled trial.
At 2 years, 55.6% of patients receiving standard treatment with anticoagulation and compression stockings developed post-thrombotic syndrome (PTS), compared with 41.1% receiving catheter-directed thrombolysis (CDT) plus standard therapy (P = .047) in the multicenter CaVenT study.
The number needed to treat to prevent one PTS was seven, Dr. Per Morten Sandset and his colleagues will report in a late-breaking abstract to be presented Dec. 13 at the annual meeting of the American Society of Hematology. About one in four patients is still at risk for developing PTS after adequate treatment with anticoagulation and compression stockings.
The CaVenT (Catheter-Directed Thrombolysis for Acute Iliofemoral Deep Vein Thrombosis) trial provides much-needed prospective, randomized data on CDT, and is unique in that it focuses on functional rather than surrogate outcomes used in previous trials and case series, Dr. Sandset said at a press briefing in which he discussed the findings.
Still, the study is small and unlikely to change practice or resolve the controversy that has surrounded the use of early fibrinolysis since systemic thrombolytic therapy was introduced decades ago.
"For the first time, we have the evidence to support this type of treatment for centers that have developed this methodology, but I also believe we need further study," said Dr. Sandset, a professor in the division of specialized medicine and surgery at Oslo University in Oslo, Norway.
Briefing moderator Dr. Charles Abrams, associate chief of hematology-oncology at the University of Pennsylvania School of Medicine in Philadelphia, said CaVenT provides the best randomized data to date, but that many clinicians, particularly in the United States, have been hesitant to adopt early fibrinolysis because of the increased risk of a serious bleeding complication.
"This is a tantalizing trial, but I don’t think ... when I’m back at my own institution that the next patient I see with a deep vein thrombosis is probably going to get it," he said.
Both men said results are eagerly awaited from the ongoing phase III, randomized ATTRACT trial evaluating CDT with blood-thinning drugs in 692 patients with proximal DVT. The cohort is three times larger than that of the CaVenT trial, but results from the North American trial are not expected possibly until 2015.
CaVenT randomized 209 patients who presented at 20 hospitals in Norway with their first acute iliofemoral DVT and symptoms present for up to 21 days to CDT with alteplase (Activase) followed by standard treatment or standard treatment alone. In all, 189 patients were evaluable for analysis. Their average age was 51.5 years (range 18-75 years), and 36% were women.
CDT significantly increased the rate of iliofemoral patency at six months from 47.4% with standard therapy to 65.9% (P = .012), Dr. Sandset said.
Importantly, patients who regained iliofemoral patency at six months had significantly less PTS at 2 years than those who experienced insufficient recanalization (36.9% vs. 61.3%, P less than .001). In all, 80 of the 90 patients in the CDT arm had successful lysis.
Bleeding complications were reported in 20 patients in the CDT arm and none in the control arm. Five bleeding events were clinically relevant and three were major, including compartment syndrome of the calf requiring surgery, abdominal wall hematoma requiring transfusion, and an inguinal puncture site hematoma.
No deaths, pulmonary embolisms, strokes or other complications with a permanently reduced outcome were reported, Dr. Sandset said.
"CDT should be considered in patients with acute iliofemoral DVT and no apparent risk of bleeding," he said, adding that the results should be taken into account when guidelines are revised.
One of the problems for clinicians managing patients with DVT is that PTS can vary from simple heaviness in the leg to a constantly swollen leg that can impair the patient’s ability to walk or hold a steady job, Dr. Abrams said.
"Patients with bigger clots and clots higher up in their thigh get more persistent symptoms, but you really can’t predict all that well who will have a bad long-term complication," he said in an interview. "And the downside of this is that the administration of this drug in other trials has led to bleeding complications in 5% of patients, and 2% of that 5% are either strokes or retroperitoneal bleeding."
PTS was identified using the Villalta clinical scale (J Thromb. Haemost. 2009;7:884-8) comprised of five patient-related venous symptoms (pain, cramps, heaviness, paraesthesia and pruritus) and six clinician-rated physical signs (pretibial edema, skin induration, hyperpigmentation, pain during calf compression, venous ectasia and redness). Using a 4-point scale in which 0 was none and 3 was severe, a total score of less than 5 indicated no PTS, 5-14 was mild/moderate PTS and a score of at least 15 or the presence of venous ulcer was severe PTS.
Dr. Abrams noted that older patients are also at greater risk of a bleeding complication than younger patients, and that clinicians will have to weigh the pros and cons of the current findings in this context with their patients.
Dr. Sandset and Dr. Abrams reported no conflicts of interest.☐
The presentation of these data on catheter directed thrombolysis by hematologists represents an example of the impact of investigator bias on the interpretation of scientific findings. The authors report a series of over 200 patients with acute iliofemoral DVT randomized to either catheter directed thrombolysis (CDT) plus standard therapy or standard therapy alone. The
| Cynthia K. Shortell, M.D. |
important findings were a 14.5% reduction in post thrombotic syndrome (PTS, as measured by the Villalta scale) at two years in patients receiving CDT and a 2% incidence (3 patients) of major bleeding in the CDT group compared to no major bleeding in the standard therapy group.
Several issues with this abstract deserve discussion; first, the follow up period is relatively short, as the development of PTS often occurs more than two years following the initial clot; in addition, the incidence of PTS reported in the CDT group is significantly higher than previously reported in the literature, and the difference between the two groups is less than reported in work by Comerota and others in prior analyses. Lastly, although perhaps not substantive, the authors claim that prior reports use surrogate, rather than functional endpoints, which is simply incorrect.
While it is encouraging that hematologists are investigating the use of CDT to prevent the long term consequences of DVT, both their interpretation and lack of acceptance of their own data is discouraging. Even a 14% decrease in the incidence of PTS is of potential benefit given the morbidity of this disorder, and a 2% major bleeding risk is actually quite small. Hence, the statements by Dr. Sandset that "for the first time we have evidence to support this type of treatment", followed by Dr. Abrams "I don’t think the next patient I see is going to get this therapy" leaves one somewhat puzzled. Perhaps the results of the ATTRACT trial will change their minds, but in the meantime we are left to fight the battle at an institutional level.
Cynthia K. Shortell, M.D., is a professor of surgery, chief of vascular surgery, and program director of vascular residency at Duke University Medical Center, Durham, N.C., as well as an associate medical editor of Vascular Specialist. She had no disclosures.
The presentation of these data on catheter directed thrombolysis by hematologists represents an example of the impact of investigator bias on the interpretation of scientific findings. The authors report a series of over 200 patients with acute iliofemoral DVT randomized to either catheter directed thrombolysis (CDT) plus standard therapy or standard therapy alone. The
| Cynthia K. Shortell, M.D. |
important findings were a 14.5% reduction in post thrombotic syndrome (PTS, as measured by the Villalta scale) at two years in patients receiving CDT and a 2% incidence (3 patients) of major bleeding in the CDT group compared to no major bleeding in the standard therapy group.
Several issues with this abstract deserve discussion; first, the follow up period is relatively short, as the development of PTS often occurs more than two years following the initial clot; in addition, the incidence of PTS reported in the CDT group is significantly higher than previously reported in the literature, and the difference between the two groups is less than reported in work by Comerota and others in prior analyses. Lastly, although perhaps not substantive, the authors claim that prior reports use surrogate, rather than functional endpoints, which is simply incorrect.
While it is encouraging that hematologists are investigating the use of CDT to prevent the long term consequences of DVT, both their interpretation and lack of acceptance of their own data is discouraging. Even a 14% decrease in the incidence of PTS is of potential benefit given the morbidity of this disorder, and a 2% major bleeding risk is actually quite small. Hence, the statements by Dr. Sandset that "for the first time we have evidence to support this type of treatment", followed by Dr. Abrams "I don’t think the next patient I see is going to get this therapy" leaves one somewhat puzzled. Perhaps the results of the ATTRACT trial will change their minds, but in the meantime we are left to fight the battle at an institutional level.
Cynthia K. Shortell, M.D., is a professor of surgery, chief of vascular surgery, and program director of vascular residency at Duke University Medical Center, Durham, N.C., as well as an associate medical editor of Vascular Specialist. She had no disclosures.
The presentation of these data on catheter directed thrombolysis by hematologists represents an example of the impact of investigator bias on the interpretation of scientific findings. The authors report a series of over 200 patients with acute iliofemoral DVT randomized to either catheter directed thrombolysis (CDT) plus standard therapy or standard therapy alone. The
| Cynthia K. Shortell, M.D. |
important findings were a 14.5% reduction in post thrombotic syndrome (PTS, as measured by the Villalta scale) at two years in patients receiving CDT and a 2% incidence (3 patients) of major bleeding in the CDT group compared to no major bleeding in the standard therapy group.
Several issues with this abstract deserve discussion; first, the follow up period is relatively short, as the development of PTS often occurs more than two years following the initial clot; in addition, the incidence of PTS reported in the CDT group is significantly higher than previously reported in the literature, and the difference between the two groups is less than reported in work by Comerota and others in prior analyses. Lastly, although perhaps not substantive, the authors claim that prior reports use surrogate, rather than functional endpoints, which is simply incorrect.
While it is encouraging that hematologists are investigating the use of CDT to prevent the long term consequences of DVT, both their interpretation and lack of acceptance of their own data is discouraging. Even a 14% decrease in the incidence of PTS is of potential benefit given the morbidity of this disorder, and a 2% major bleeding risk is actually quite small. Hence, the statements by Dr. Sandset that "for the first time we have evidence to support this type of treatment", followed by Dr. Abrams "I don’t think the next patient I see is going to get this therapy" leaves one somewhat puzzled. Perhaps the results of the ATTRACT trial will change their minds, but in the meantime we are left to fight the battle at an institutional level.
Cynthia K. Shortell, M.D., is a professor of surgery, chief of vascular surgery, and program director of vascular residency at Duke University Medical Center, Durham, N.C., as well as an associate medical editor of Vascular Specialist. She had no disclosures.
SAN DIEGO – Catheter-directed thrombolysis added to standard therapy for deep vein thrombosis reduced the risk of post-thrombotic syndrome by 14.5%, but at an increased cost of bleeding among 209 patients in a randomized, controlled trial.
At 2 years, 55.6% of patients receiving standard treatment with anticoagulation and compression stockings developed post-thrombotic syndrome (PTS), compared with 41.1% receiving catheter-directed thrombolysis (CDT) plus standard therapy (P = .047) in the multicenter CaVenT study.
The number needed to treat to prevent one PTS was seven, Dr. Per Morten Sandset and his colleagues will report in a late-breaking abstract to be presented Dec. 13 at the annual meeting of the American Society of Hematology. About one in four patients is still at risk for developing PTS after adequate treatment with anticoagulation and compression stockings.
The CaVenT (Catheter-Directed Thrombolysis for Acute Iliofemoral Deep Vein Thrombosis) trial provides much-needed prospective, randomized data on CDT, and is unique in that it focuses on functional rather than surrogate outcomes used in previous trials and case series, Dr. Sandset said at a press briefing in which he discussed the findings.
Still, the study is small and unlikely to change practice or resolve the controversy that has surrounded the use of early fibrinolysis since systemic thrombolytic therapy was introduced decades ago.
"For the first time, we have the evidence to support this type of treatment for centers that have developed this methodology, but I also believe we need further study," said Dr. Sandset, a professor in the division of specialized medicine and surgery at Oslo University in Oslo, Norway.
Briefing moderator Dr. Charles Abrams, associate chief of hematology-oncology at the University of Pennsylvania School of Medicine in Philadelphia, said CaVenT provides the best randomized data to date, but that many clinicians, particularly in the United States, have been hesitant to adopt early fibrinolysis because of the increased risk of a serious bleeding complication.
"This is a tantalizing trial, but I don’t think ... when I’m back at my own institution that the next patient I see with a deep vein thrombosis is probably going to get it," he said.
Both men said results are eagerly awaited from the ongoing phase III, randomized ATTRACT trial evaluating CDT with blood-thinning drugs in 692 patients with proximal DVT. The cohort is three times larger than that of the CaVenT trial, but results from the North American trial are not expected possibly until 2015.
CaVenT randomized 209 patients who presented at 20 hospitals in Norway with their first acute iliofemoral DVT and symptoms present for up to 21 days to CDT with alteplase (Activase) followed by standard treatment or standard treatment alone. In all, 189 patients were evaluable for analysis. Their average age was 51.5 years (range 18-75 years), and 36% were women.
CDT significantly increased the rate of iliofemoral patency at six months from 47.4% with standard therapy to 65.9% (P = .012), Dr. Sandset said.
Importantly, patients who regained iliofemoral patency at six months had significantly less PTS at 2 years than those who experienced insufficient recanalization (36.9% vs. 61.3%, P less than .001). In all, 80 of the 90 patients in the CDT arm had successful lysis.
Bleeding complications were reported in 20 patients in the CDT arm and none in the control arm. Five bleeding events were clinically relevant and three were major, including compartment syndrome of the calf requiring surgery, abdominal wall hematoma requiring transfusion, and an inguinal puncture site hematoma.
No deaths, pulmonary embolisms, strokes or other complications with a permanently reduced outcome were reported, Dr. Sandset said.
"CDT should be considered in patients with acute iliofemoral DVT and no apparent risk of bleeding," he said, adding that the results should be taken into account when guidelines are revised.
One of the problems for clinicians managing patients with DVT is that PTS can vary from simple heaviness in the leg to a constantly swollen leg that can impair the patient’s ability to walk or hold a steady job, Dr. Abrams said.
"Patients with bigger clots and clots higher up in their thigh get more persistent symptoms, but you really can’t predict all that well who will have a bad long-term complication," he said in an interview. "And the downside of this is that the administration of this drug in other trials has led to bleeding complications in 5% of patients, and 2% of that 5% are either strokes or retroperitoneal bleeding."
PTS was identified using the Villalta clinical scale (J Thromb. Haemost. 2009;7:884-8) comprised of five patient-related venous symptoms (pain, cramps, heaviness, paraesthesia and pruritus) and six clinician-rated physical signs (pretibial edema, skin induration, hyperpigmentation, pain during calf compression, venous ectasia and redness). Using a 4-point scale in which 0 was none and 3 was severe, a total score of less than 5 indicated no PTS, 5-14 was mild/moderate PTS and a score of at least 15 or the presence of venous ulcer was severe PTS.
Dr. Abrams noted that older patients are also at greater risk of a bleeding complication than younger patients, and that clinicians will have to weigh the pros and cons of the current findings in this context with their patients.
Dr. Sandset and Dr. Abrams reported no conflicts of interest.☐
SAN DIEGO – Catheter-directed thrombolysis added to standard therapy for deep vein thrombosis reduced the risk of post-thrombotic syndrome by 14.5%, but at an increased cost of bleeding among 209 patients in a randomized, controlled trial.
At 2 years, 55.6% of patients receiving standard treatment with anticoagulation and compression stockings developed post-thrombotic syndrome (PTS), compared with 41.1% receiving catheter-directed thrombolysis (CDT) plus standard therapy (P = .047) in the multicenter CaVenT study.
The number needed to treat to prevent one PTS was seven, Dr. Per Morten Sandset and his colleagues will report in a late-breaking abstract to be presented Dec. 13 at the annual meeting of the American Society of Hematology. About one in four patients is still at risk for developing PTS after adequate treatment with anticoagulation and compression stockings.
The CaVenT (Catheter-Directed Thrombolysis for Acute Iliofemoral Deep Vein Thrombosis) trial provides much-needed prospective, randomized data on CDT, and is unique in that it focuses on functional rather than surrogate outcomes used in previous trials and case series, Dr. Sandset said at a press briefing in which he discussed the findings.
Still, the study is small and unlikely to change practice or resolve the controversy that has surrounded the use of early fibrinolysis since systemic thrombolytic therapy was introduced decades ago.
"For the first time, we have the evidence to support this type of treatment for centers that have developed this methodology, but I also believe we need further study," said Dr. Sandset, a professor in the division of specialized medicine and surgery at Oslo University in Oslo, Norway.
Briefing moderator Dr. Charles Abrams, associate chief of hematology-oncology at the University of Pennsylvania School of Medicine in Philadelphia, said CaVenT provides the best randomized data to date, but that many clinicians, particularly in the United States, have been hesitant to adopt early fibrinolysis because of the increased risk of a serious bleeding complication.
"This is a tantalizing trial, but I don’t think ... when I’m back at my own institution that the next patient I see with a deep vein thrombosis is probably going to get it," he said.
Both men said results are eagerly awaited from the ongoing phase III, randomized ATTRACT trial evaluating CDT with blood-thinning drugs in 692 patients with proximal DVT. The cohort is three times larger than that of the CaVenT trial, but results from the North American trial are not expected possibly until 2015.
CaVenT randomized 209 patients who presented at 20 hospitals in Norway with their first acute iliofemoral DVT and symptoms present for up to 21 days to CDT with alteplase (Activase) followed by standard treatment or standard treatment alone. In all, 189 patients were evaluable for analysis. Their average age was 51.5 years (range 18-75 years), and 36% were women.
CDT significantly increased the rate of iliofemoral patency at six months from 47.4% with standard therapy to 65.9% (P = .012), Dr. Sandset said.
Importantly, patients who regained iliofemoral patency at six months had significantly less PTS at 2 years than those who experienced insufficient recanalization (36.9% vs. 61.3%, P less than .001). In all, 80 of the 90 patients in the CDT arm had successful lysis.
Bleeding complications were reported in 20 patients in the CDT arm and none in the control arm. Five bleeding events were clinically relevant and three were major, including compartment syndrome of the calf requiring surgery, abdominal wall hematoma requiring transfusion, and an inguinal puncture site hematoma.
No deaths, pulmonary embolisms, strokes or other complications with a permanently reduced outcome were reported, Dr. Sandset said.
"CDT should be considered in patients with acute iliofemoral DVT and no apparent risk of bleeding," he said, adding that the results should be taken into account when guidelines are revised.
One of the problems for clinicians managing patients with DVT is that PTS can vary from simple heaviness in the leg to a constantly swollen leg that can impair the patient’s ability to walk or hold a steady job, Dr. Abrams said.
"Patients with bigger clots and clots higher up in their thigh get more persistent symptoms, but you really can’t predict all that well who will have a bad long-term complication," he said in an interview. "And the downside of this is that the administration of this drug in other trials has led to bleeding complications in 5% of patients, and 2% of that 5% are either strokes or retroperitoneal bleeding."
PTS was identified using the Villalta clinical scale (J Thromb. Haemost. 2009;7:884-8) comprised of five patient-related venous symptoms (pain, cramps, heaviness, paraesthesia and pruritus) and six clinician-rated physical signs (pretibial edema, skin induration, hyperpigmentation, pain during calf compression, venous ectasia and redness). Using a 4-point scale in which 0 was none and 3 was severe, a total score of less than 5 indicated no PTS, 5-14 was mild/moderate PTS and a score of at least 15 or the presence of venous ulcer was severe PTS.
Dr. Abrams noted that older patients are also at greater risk of a bleeding complication than younger patients, and that clinicians will have to weigh the pros and cons of the current findings in this context with their patients.
Dr. Sandset and Dr. Abrams reported no conflicts of interest.☐
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF HEMATOLOGY
Major Finding: At 2 years, 55.6% of patients receiving standard DVT treatment developed post-thrombotic syndrome vs. 41.1% receiving catheter-directed thrombolysis plus standard therapy (P = .047).
Data Source: Prospective, randomized trial in 209 patients with an acute iliofemoral deep vein thrombosis.
Disclosures: Dr. Sandset and Dr. Abrams reported no conflicts of interest.
Emergency Surgical Service Enhances Resident Education
LAKE BUENA VISTA, FLA. – An emergency surgical service rotation delivers more than half of ACGME requirements for laparoscopic surgery in just 2 months of training, a retrospective analysis shows.
"Emergency surgery has the potential to reduce the need for hospital hopping and will increase the time residents spend under their program director," Dr. Hesham Ahmed said at the annual meeting of the Eastern Association for the Surgery of Trauma.
His analysis compared ACGME (Accreditation Council for Graduate Medical Education) requirements before and after the creation of an ESS (emergency surgical service) at Robert Wood Johnson University Hospital in New Brunswick, N.J. Case loads were tabulated for the last four graduating classes (two pre-ESS and two post-ESS) using the hospital’s prospectively accrued ESS database.
More than 70 different types of procedures were recorded in the ESS registry, including multispecialty approaches, reoperations, delayed abdominal closures, urgent surgical airway management, and seldom performed operations such as vagotomy and repair of perforated peptic ulcers.
Residents rotating on the ESS completed 816 cases between 2010 and 2011, 39% of which were laparoscopic, said Dr. Ahmed, a trauma and critical care surgeon at the hospital. This included 109 laparoscopic appendectomies, 99 laparoscopic cholecystectomies, and 14 advanced laparoscopic cases.
ESS significantly increased the total number of laparoscopic appendectomy cases performed by residents compared with the pre-ESS classes of 2008 and 2009 (P value less than .001).
Similar results were found for laparoscopic cholecystectomy cases (P less than .003), notably without a significant increase in conversion to open cholecystectomy (P less than .09), he said.
Within a 2-month period, residents that rotated on the ESS achieved on average 61% of the 60 ACGME required cases for laparoscopy.
ESS faculty supervised 24% of all chief resident major operative and endoscopy cases performed at the academic hospital for the class of 2011.
ESS also increased the total surgical volume at the institution from an almost even split with its participating sites during the two pre-ESS graduating classes of 48% and 50% to 63% and 68% during the two post-ESS graduating classes, Dr. Ahmed said. The increase in volume was statistically significant (P less than .001).

Invited discussant Dr. Jeannette Capella, a surgeon with the department of emergency medicine and trauma service at Altoona (Pa.) Regional Medical Center, said there are numerous financial and practical advantages to including emergency general surgery under the acute care surgery umbrella.
"However, in the struggle to make our specialty financially secure and professionally appealing, we need to make sure that the education of our general surgery residents does not suffer," she said. "To my knowledge, this is the first study to look at how our new practice model is affecting our residents."
Dr. Capella agreed with Dr. Ahmed that shifting residents from affiliated hospital rotations to the ESS at the primary institution would improve residents’ education, but said specific measures such as improved board scores or patient outcomes are needed to demonstrate the quality of education during such a shift.
Anecdotally, Dr. Ahmed said that in the last 2 years, three students went on to critical care or acute care fellowships and that previously "everyone wanted to go to plastic surgery. So there is a big change in the residents."
Dr. Capella then asked how residents’ exposure to other areas of general surgery had been affected and whether the increased workload posed any problems for the hospital in complying with resident work-hour rules. Dr. Ahmed said that no deficiencies arose in the residents’ exposure to other surgical areas, nor were problems encountered with work hours.
Finally, audience members questioned where the cases came from that were filtered to the new ESS. Dr. Ahmed said that they did not do outreach and that prior to the development of the ESS, trauma surgeons would perform the acute care procedures now handled by the ESS.
Dr. Ahmed and his coauthors reported no conflicts of interest.
LAKE BUENA VISTA, FLA. – An emergency surgical service rotation delivers more than half of ACGME requirements for laparoscopic surgery in just 2 months of training, a retrospective analysis shows.
"Emergency surgery has the potential to reduce the need for hospital hopping and will increase the time residents spend under their program director," Dr. Hesham Ahmed said at the annual meeting of the Eastern Association for the Surgery of Trauma.
His analysis compared ACGME (Accreditation Council for Graduate Medical Education) requirements before and after the creation of an ESS (emergency surgical service) at Robert Wood Johnson University Hospital in New Brunswick, N.J. Case loads were tabulated for the last four graduating classes (two pre-ESS and two post-ESS) using the hospital’s prospectively accrued ESS database.
More than 70 different types of procedures were recorded in the ESS registry, including multispecialty approaches, reoperations, delayed abdominal closures, urgent surgical airway management, and seldom performed operations such as vagotomy and repair of perforated peptic ulcers.
Residents rotating on the ESS completed 816 cases between 2010 and 2011, 39% of which were laparoscopic, said Dr. Ahmed, a trauma and critical care surgeon at the hospital. This included 109 laparoscopic appendectomies, 99 laparoscopic cholecystectomies, and 14 advanced laparoscopic cases.
ESS significantly increased the total number of laparoscopic appendectomy cases performed by residents compared with the pre-ESS classes of 2008 and 2009 (P value less than .001).
Similar results were found for laparoscopic cholecystectomy cases (P less than .003), notably without a significant increase in conversion to open cholecystectomy (P less than .09), he said.
Within a 2-month period, residents that rotated on the ESS achieved on average 61% of the 60 ACGME required cases for laparoscopy.
ESS faculty supervised 24% of all chief resident major operative and endoscopy cases performed at the academic hospital for the class of 2011.
ESS also increased the total surgical volume at the institution from an almost even split with its participating sites during the two pre-ESS graduating classes of 48% and 50% to 63% and 68% during the two post-ESS graduating classes, Dr. Ahmed said. The increase in volume was statistically significant (P less than .001).
Invited discussant Dr. Jeannette Capella, a surgeon with the department of emergency medicine and trauma service at Altoona (Pa.) Regional Medical Center, said there are numerous financial and practical advantages to including emergency general surgery under the acute care surgery umbrella.
"However, in the struggle to make our specialty financially secure and professionally appealing, we need to make sure that the education of our general surgery residents does not suffer," she said. "To my knowledge, this is the first study to look at how our new practice model is affecting our residents."
Dr. Capella agreed with Dr. Ahmed that shifting residents from affiliated hospital rotations to the ESS at the primary institution would improve residents’ education, but said specific measures such as improved board scores or patient outcomes are needed to demonstrate the quality of education during such a shift.
Anecdotally, Dr. Ahmed said that in the last 2 years, three students went on to critical care or acute care fellowships and that previously "everyone wanted to go to plastic surgery. So there is a big change in the residents."
Dr. Capella then asked how residents’ exposure to other areas of general surgery had been affected and whether the increased workload posed any problems for the hospital in complying with resident work-hour rules. Dr. Ahmed said that no deficiencies arose in the residents’ exposure to other surgical areas, nor were problems encountered with work hours.
Finally, audience members questioned where the cases came from that were filtered to the new ESS. Dr. Ahmed said that they did not do outreach and that prior to the development of the ESS, trauma surgeons would perform the acute care procedures now handled by the ESS.
Dr. Ahmed and his coauthors reported no conflicts of interest.
LAKE BUENA VISTA, FLA. – An emergency surgical service rotation delivers more than half of ACGME requirements for laparoscopic surgery in just 2 months of training, a retrospective analysis shows.
"Emergency surgery has the potential to reduce the need for hospital hopping and will increase the time residents spend under their program director," Dr. Hesham Ahmed said at the annual meeting of the Eastern Association for the Surgery of Trauma.
His analysis compared ACGME (Accreditation Council for Graduate Medical Education) requirements before and after the creation of an ESS (emergency surgical service) at Robert Wood Johnson University Hospital in New Brunswick, N.J. Case loads were tabulated for the last four graduating classes (two pre-ESS and two post-ESS) using the hospital’s prospectively accrued ESS database.
More than 70 different types of procedures were recorded in the ESS registry, including multispecialty approaches, reoperations, delayed abdominal closures, urgent surgical airway management, and seldom performed operations such as vagotomy and repair of perforated peptic ulcers.
Residents rotating on the ESS completed 816 cases between 2010 and 2011, 39% of which were laparoscopic, said Dr. Ahmed, a trauma and critical care surgeon at the hospital. This included 109 laparoscopic appendectomies, 99 laparoscopic cholecystectomies, and 14 advanced laparoscopic cases.
ESS significantly increased the total number of laparoscopic appendectomy cases performed by residents compared with the pre-ESS classes of 2008 and 2009 (P value less than .001).
Similar results were found for laparoscopic cholecystectomy cases (P less than .003), notably without a significant increase in conversion to open cholecystectomy (P less than .09), he said.
Within a 2-month period, residents that rotated on the ESS achieved on average 61% of the 60 ACGME required cases for laparoscopy.
ESS faculty supervised 24% of all chief resident major operative and endoscopy cases performed at the academic hospital for the class of 2011.
ESS also increased the total surgical volume at the institution from an almost even split with its participating sites during the two pre-ESS graduating classes of 48% and 50% to 63% and 68% during the two post-ESS graduating classes, Dr. Ahmed said. The increase in volume was statistically significant (P less than .001).
Invited discussant Dr. Jeannette Capella, a surgeon with the department of emergency medicine and trauma service at Altoona (Pa.) Regional Medical Center, said there are numerous financial and practical advantages to including emergency general surgery under the acute care surgery umbrella.
"However, in the struggle to make our specialty financially secure and professionally appealing, we need to make sure that the education of our general surgery residents does not suffer," she said. "To my knowledge, this is the first study to look at how our new practice model is affecting our residents."
Dr. Capella agreed with Dr. Ahmed that shifting residents from affiliated hospital rotations to the ESS at the primary institution would improve residents’ education, but said specific measures such as improved board scores or patient outcomes are needed to demonstrate the quality of education during such a shift.
Anecdotally, Dr. Ahmed said that in the last 2 years, three students went on to critical care or acute care fellowships and that previously "everyone wanted to go to plastic surgery. So there is a big change in the residents."
Dr. Capella then asked how residents’ exposure to other areas of general surgery had been affected and whether the increased workload posed any problems for the hospital in complying with resident work-hour rules. Dr. Ahmed said that no deficiencies arose in the residents’ exposure to other surgical areas, nor were problems encountered with work hours.
Finally, audience members questioned where the cases came from that were filtered to the new ESS. Dr. Ahmed said that they did not do outreach and that prior to the development of the ESS, trauma surgeons would perform the acute care procedures now handled by the ESS.
Dr. Ahmed and his coauthors reported no conflicts of interest.
FROM THE ANNUAL MEETING OF THE EASTERN ASSOCIATION FOR THE SURGERY OF TRAUMA
Foundation Takes Bold Approach to Psoriasis Management
The new National Psoriasis Foundation consensus guidelines on the management of plaque psoriasis take a practical approach to helping physicians manage the disease beyond topical treatment.
The guidelines feature a table summarizing the latest consensus on eight systemic medications, and they hone in on specific forms of psoriasis in a way that is more quickly understandable than in the past, according to lead author Dr. Sylvia Hsu, chief of Ben Taub Dermatology Service and a dermatology professor at Baylor College of Medicine in Houston.

"The aim is to simplify and clarify when to use these drugs for patients whose psoriasis is beyond topical treatment," she said. "A lot of the drugs can be used first line, so it’s not like a treatment algorithm."
Dr. Hsu acknowledged that the guidelines are a bit bold because they directly state, for example, that acitretin doesn’t work well for plaque psoriasis, and that evidence is scant to support the use of alefacept to achieve full clearance. The latter position was devised well before Astellas announced in December 2011 that it was pulling alefacept from the market, she said in an interview.
Physicians may also be surprised that the guidelines, published in Archives of Dermatology (2012;148:95-102), recommend cyclosporine as a short-term solution for up to 12 weeks to control a psoriasis flare.
"We know that you can use cyclosporine for up to a year because it’s FDA-approved for up to 12 months, but the typical use is as a quick-fix to transition to other agents that are slower acting," she said. "It’s a practical table."

Established drugs such as etanercept (Enbrel) and adalimumab (Humira) are recommended as first-line therapies for plaque psoriasis, but so is the newer monoclonal antibody ustekinumab (Stelara), so avoid the misconception that dermatologists need to prescribe systemic medications in a particular order based upon time on the market, Dr. Hsu noted.
The National Psoriasis Foundation (NPF) guidelines, however, do not provide a formula for how to treat patients, said coauthor Dr. Steven R. Feldman, professor of dermatology at Wake Forest Baptist Medical Center in Winston-Salem, N.C.
"They don’t say if you have this patient, this must be done first and then if that doesn’t work, do this second, and that third," he said. "There is no guideline of that type for psoriasis because no one treatment is better than all the other treatments in every way and patients weigh the various variables differently."
The new guidelines were adapted from the Canadian Guidelines for the Management of Plaque Psoriasis to reflect United States practice patterns, and are very similar to those published on the subject by the American Academy of Dermatology (AAD), Dr. Feldman said.
"I think these guidelines are clearly consensus guidelines, getting the experts together and deciding what they feel is best, whereas the AAD made a special effort to create evidence-based guidelines based on the available data," he said. "In the end, I think the recommendations are basically the same thing. Neither one tells physicians exactly what to do in a given situation; it’s more about describing the reasonable options that a patient and physician could choose in any situation."
NPF and AAD guidelines coauthor Dr. Mark Lebwohl, professor and chair of the department dermatology at Mount Sinai School of Medicine in New York, said the AAD guidelines are superb, but that "having this second set of guidelines allows us to answer even more questions."

He noted that there is often information in one guideline that is missing from another because new psoriasis developments happen so quickly. For example, a section recommending that physicians consider withholding tumor necrosis factor antagonists in psoriasis patients undergoing elective surgery was borrowed from the Canadian guidelines, but does not appear in the AAD guidelines, he said. The section discusses the controversy over the potential for increased risk of postsurgical infection in patients on biologics, and provides guidance on when specific agents should be withheld.
Conversely, the NPF guidelines discuss the pros and cons of the excimer laser, but this discussion is missing from the Canadian guidelines because the laser is not approved there.
"In a year, the guidelines will all be out of date again; they are a work in progress," said Dr. Lebwohl, who added that the NPF is trying to find a mechanism to update the guidelines in real time as new developments arise.
What the NPF/Canadian guidelines offer physicians is a rigorous evaluation of the literature with a patient-focused approach to psoriasis treatment, said Dr. Kim A. Papp, director of research at Probity Medical Research, Waterloo, Ont., who helped coauthor both sets of guidelines.
"We all appreciate that the art of medicine incorporates habit, consensus, experience, and hopefully sound data," he said. "Consequently, a second and perhaps equally important offering of the guidelines to physicians is an independent affirmation or an independent negation of one’s art in treating psoriasis."
Where the NPF guidelines may prove particularly helpful is in supporting that therapeutic choice with insurers. If a physician thought that a particular biologic agent was the best treatment option for a patient, that physician could point to the guidelines as a way to let insurers know that what is being recommended is within the standard of care, said Dr. Feldman.
The new guidelines could also push physicians to be more aggressive in using some of the available systemic agents. He pointed out that one of the "major enthusiasms" for creating the guidelines was a 2009 National Psoriasis Foundation survey finding that 57% of patients with severe psoriasis were receiving treatment insufficient to achieve adequate control (J. Am. Acad. Dermatol. 2007;57:957-62).

"There needed to be guidelines that would encourage physicians to provide patients treatment that met the severity of their illness," said Dr. Feldman, who suggested that safety concerns, dated training, and a perception that psoriasis isn’t such a bad disease, all played into the lack of aggressive treatment.
The NPF guidelines clearly detail the safety risks associated with each agent, and have a specific section on special populations, including pregnant women, patients with HIV, and those with hepatitis B or C.
For the purpose of the new guidelines, patients are considered to have moderate to severe psoriasis if they cannot achieve or would not be expected to achieve adequate control using topical agents, with adequacy defined by the patient’s own perception of the disease and its burdens. Cutoffs based on clinical metrics, such as the Psoriasis Area and Severity Index, percentage of body surface area affected, and the Dermatological Life Quality Index are necessary in clinical trials, but "have little value in daily practice," the authors noted.
Strict numeric cutoffs can also cause problems with insurers and reimbursement.
"This [document] provides the insurers and other regulators the opportunity to set more meaningful standards for their policies," Dr. Feldman said. "When they see guidelines published in the Archives and supported by the National Psoriasis Foundation, it lends a lot of weight to doing things the way doctors do things in the patient’s best interest."
The physicians interviewed for this story all disclosed consultancies and research arrangements with multiple companies that manufacture psoriasis treatments.
The new National Psoriasis Foundation consensus guidelines on the management of plaque psoriasis take a practical approach to helping physicians manage the disease beyond topical treatment.
The guidelines feature a table summarizing the latest consensus on eight systemic medications, and they hone in on specific forms of psoriasis in a way that is more quickly understandable than in the past, according to lead author Dr. Sylvia Hsu, chief of Ben Taub Dermatology Service and a dermatology professor at Baylor College of Medicine in Houston.
"The aim is to simplify and clarify when to use these drugs for patients whose psoriasis is beyond topical treatment," she said. "A lot of the drugs can be used first line, so it’s not like a treatment algorithm."
Dr. Hsu acknowledged that the guidelines are a bit bold because they directly state, for example, that acitretin doesn’t work well for plaque psoriasis, and that evidence is scant to support the use of alefacept to achieve full clearance. The latter position was devised well before Astellas announced in December 2011 that it was pulling alefacept from the market, she said in an interview.
Physicians may also be surprised that the guidelines, published in Archives of Dermatology (2012;148:95-102), recommend cyclosporine as a short-term solution for up to 12 weeks to control a psoriasis flare.
"We know that you can use cyclosporine for up to a year because it’s FDA-approved for up to 12 months, but the typical use is as a quick-fix to transition to other agents that are slower acting," she said. "It’s a practical table."
Established drugs such as etanercept (Enbrel) and adalimumab (Humira) are recommended as first-line therapies for plaque psoriasis, but so is the newer monoclonal antibody ustekinumab (Stelara), so avoid the misconception that dermatologists need to prescribe systemic medications in a particular order based upon time on the market, Dr. Hsu noted.
The National Psoriasis Foundation (NPF) guidelines, however, do not provide a formula for how to treat patients, said coauthor Dr. Steven R. Feldman, professor of dermatology at Wake Forest Baptist Medical Center in Winston-Salem, N.C.
"They don’t say if you have this patient, this must be done first and then if that doesn’t work, do this second, and that third," he said. "There is no guideline of that type for psoriasis because no one treatment is better than all the other treatments in every way and patients weigh the various variables differently."
The new guidelines were adapted from the Canadian Guidelines for the Management of Plaque Psoriasis to reflect United States practice patterns, and are very similar to those published on the subject by the American Academy of Dermatology (AAD), Dr. Feldman said.
"I think these guidelines are clearly consensus guidelines, getting the experts together and deciding what they feel is best, whereas the AAD made a special effort to create evidence-based guidelines based on the available data," he said. "In the end, I think the recommendations are basically the same thing. Neither one tells physicians exactly what to do in a given situation; it’s more about describing the reasonable options that a patient and physician could choose in any situation."
NPF and AAD guidelines coauthor Dr. Mark Lebwohl, professor and chair of the department dermatology at Mount Sinai School of Medicine in New York, said the AAD guidelines are superb, but that "having this second set of guidelines allows us to answer even more questions."
He noted that there is often information in one guideline that is missing from another because new psoriasis developments happen so quickly. For example, a section recommending that physicians consider withholding tumor necrosis factor antagonists in psoriasis patients undergoing elective surgery was borrowed from the Canadian guidelines, but does not appear in the AAD guidelines, he said. The section discusses the controversy over the potential for increased risk of postsurgical infection in patients on biologics, and provides guidance on when specific agents should be withheld.
Conversely, the NPF guidelines discuss the pros and cons of the excimer laser, but this discussion is missing from the Canadian guidelines because the laser is not approved there.
"In a year, the guidelines will all be out of date again; they are a work in progress," said Dr. Lebwohl, who added that the NPF is trying to find a mechanism to update the guidelines in real time as new developments arise.
What the NPF/Canadian guidelines offer physicians is a rigorous evaluation of the literature with a patient-focused approach to psoriasis treatment, said Dr. Kim A. Papp, director of research at Probity Medical Research, Waterloo, Ont., who helped coauthor both sets of guidelines.
"We all appreciate that the art of medicine incorporates habit, consensus, experience, and hopefully sound data," he said. "Consequently, a second and perhaps equally important offering of the guidelines to physicians is an independent affirmation or an independent negation of one’s art in treating psoriasis."
Where the NPF guidelines may prove particularly helpful is in supporting that therapeutic choice with insurers. If a physician thought that a particular biologic agent was the best treatment option for a patient, that physician could point to the guidelines as a way to let insurers know that what is being recommended is within the standard of care, said Dr. Feldman.
The new guidelines could also push physicians to be more aggressive in using some of the available systemic agents. He pointed out that one of the "major enthusiasms" for creating the guidelines was a 2009 National Psoriasis Foundation survey finding that 57% of patients with severe psoriasis were receiving treatment insufficient to achieve adequate control (J. Am. Acad. Dermatol. 2007;57:957-62).
"There needed to be guidelines that would encourage physicians to provide patients treatment that met the severity of their illness," said Dr. Feldman, who suggested that safety concerns, dated training, and a perception that psoriasis isn’t such a bad disease, all played into the lack of aggressive treatment.
The NPF guidelines clearly detail the safety risks associated with each agent, and have a specific section on special populations, including pregnant women, patients with HIV, and those with hepatitis B or C.
For the purpose of the new guidelines, patients are considered to have moderate to severe psoriasis if they cannot achieve or would not be expected to achieve adequate control using topical agents, with adequacy defined by the patient’s own perception of the disease and its burdens. Cutoffs based on clinical metrics, such as the Psoriasis Area and Severity Index, percentage of body surface area affected, and the Dermatological Life Quality Index are necessary in clinical trials, but "have little value in daily practice," the authors noted.
Strict numeric cutoffs can also cause problems with insurers and reimbursement.
"This [document] provides the insurers and other regulators the opportunity to set more meaningful standards for their policies," Dr. Feldman said. "When they see guidelines published in the Archives and supported by the National Psoriasis Foundation, it lends a lot of weight to doing things the way doctors do things in the patient’s best interest."
The physicians interviewed for this story all disclosed consultancies and research arrangements with multiple companies that manufacture psoriasis treatments.
The new National Psoriasis Foundation consensus guidelines on the management of plaque psoriasis take a practical approach to helping physicians manage the disease beyond topical treatment.
The guidelines feature a table summarizing the latest consensus on eight systemic medications, and they hone in on specific forms of psoriasis in a way that is more quickly understandable than in the past, according to lead author Dr. Sylvia Hsu, chief of Ben Taub Dermatology Service and a dermatology professor at Baylor College of Medicine in Houston.
"The aim is to simplify and clarify when to use these drugs for patients whose psoriasis is beyond topical treatment," she said. "A lot of the drugs can be used first line, so it’s not like a treatment algorithm."
Dr. Hsu acknowledged that the guidelines are a bit bold because they directly state, for example, that acitretin doesn’t work well for plaque psoriasis, and that evidence is scant to support the use of alefacept to achieve full clearance. The latter position was devised well before Astellas announced in December 2011 that it was pulling alefacept from the market, she said in an interview.
Physicians may also be surprised that the guidelines, published in Archives of Dermatology (2012;148:95-102), recommend cyclosporine as a short-term solution for up to 12 weeks to control a psoriasis flare.
"We know that you can use cyclosporine for up to a year because it’s FDA-approved for up to 12 months, but the typical use is as a quick-fix to transition to other agents that are slower acting," she said. "It’s a practical table."
Established drugs such as etanercept (Enbrel) and adalimumab (Humira) are recommended as first-line therapies for plaque psoriasis, but so is the newer monoclonal antibody ustekinumab (Stelara), so avoid the misconception that dermatologists need to prescribe systemic medications in a particular order based upon time on the market, Dr. Hsu noted.
The National Psoriasis Foundation (NPF) guidelines, however, do not provide a formula for how to treat patients, said coauthor Dr. Steven R. Feldman, professor of dermatology at Wake Forest Baptist Medical Center in Winston-Salem, N.C.
"They don’t say if you have this patient, this must be done first and then if that doesn’t work, do this second, and that third," he said. "There is no guideline of that type for psoriasis because no one treatment is better than all the other treatments in every way and patients weigh the various variables differently."
The new guidelines were adapted from the Canadian Guidelines for the Management of Plaque Psoriasis to reflect United States practice patterns, and are very similar to those published on the subject by the American Academy of Dermatology (AAD), Dr. Feldman said.
"I think these guidelines are clearly consensus guidelines, getting the experts together and deciding what they feel is best, whereas the AAD made a special effort to create evidence-based guidelines based on the available data," he said. "In the end, I think the recommendations are basically the same thing. Neither one tells physicians exactly what to do in a given situation; it’s more about describing the reasonable options that a patient and physician could choose in any situation."
NPF and AAD guidelines coauthor Dr. Mark Lebwohl, professor and chair of the department dermatology at Mount Sinai School of Medicine in New York, said the AAD guidelines are superb, but that "having this second set of guidelines allows us to answer even more questions."
He noted that there is often information in one guideline that is missing from another because new psoriasis developments happen so quickly. For example, a section recommending that physicians consider withholding tumor necrosis factor antagonists in psoriasis patients undergoing elective surgery was borrowed from the Canadian guidelines, but does not appear in the AAD guidelines, he said. The section discusses the controversy over the potential for increased risk of postsurgical infection in patients on biologics, and provides guidance on when specific agents should be withheld.
Conversely, the NPF guidelines discuss the pros and cons of the excimer laser, but this discussion is missing from the Canadian guidelines because the laser is not approved there.
"In a year, the guidelines will all be out of date again; they are a work in progress," said Dr. Lebwohl, who added that the NPF is trying to find a mechanism to update the guidelines in real time as new developments arise.
What the NPF/Canadian guidelines offer physicians is a rigorous evaluation of the literature with a patient-focused approach to psoriasis treatment, said Dr. Kim A. Papp, director of research at Probity Medical Research, Waterloo, Ont., who helped coauthor both sets of guidelines.
"We all appreciate that the art of medicine incorporates habit, consensus, experience, and hopefully sound data," he said. "Consequently, a second and perhaps equally important offering of the guidelines to physicians is an independent affirmation or an independent negation of one’s art in treating psoriasis."
Where the NPF guidelines may prove particularly helpful is in supporting that therapeutic choice with insurers. If a physician thought that a particular biologic agent was the best treatment option for a patient, that physician could point to the guidelines as a way to let insurers know that what is being recommended is within the standard of care, said Dr. Feldman.
The new guidelines could also push physicians to be more aggressive in using some of the available systemic agents. He pointed out that one of the "major enthusiasms" for creating the guidelines was a 2009 National Psoriasis Foundation survey finding that 57% of patients with severe psoriasis were receiving treatment insufficient to achieve adequate control (J. Am. Acad. Dermatol. 2007;57:957-62).
"There needed to be guidelines that would encourage physicians to provide patients treatment that met the severity of their illness," said Dr. Feldman, who suggested that safety concerns, dated training, and a perception that psoriasis isn’t such a bad disease, all played into the lack of aggressive treatment.
The NPF guidelines clearly detail the safety risks associated with each agent, and have a specific section on special populations, including pregnant women, patients with HIV, and those with hepatitis B or C.
For the purpose of the new guidelines, patients are considered to have moderate to severe psoriasis if they cannot achieve or would not be expected to achieve adequate control using topical agents, with adequacy defined by the patient’s own perception of the disease and its burdens. Cutoffs based on clinical metrics, such as the Psoriasis Area and Severity Index, percentage of body surface area affected, and the Dermatological Life Quality Index are necessary in clinical trials, but "have little value in daily practice," the authors noted.
Strict numeric cutoffs can also cause problems with insurers and reimbursement.
"This [document] provides the insurers and other regulators the opportunity to set more meaningful standards for their policies," Dr. Feldman said. "When they see guidelines published in the Archives and supported by the National Psoriasis Foundation, it lends a lot of weight to doing things the way doctors do things in the patient’s best interest."
The physicians interviewed for this story all disclosed consultancies and research arrangements with multiple companies that manufacture psoriasis treatments.
Frequent Respiratory Infections? Rule Out Bronchiectasis
KEYSTONE, COLO. – Despite claims to the contrary, bronchiectasis is alive and unwell.
"One of the things that I hear time and time again is, ‘I just don’t see much bronchiectasis in my practice,’ but I think it’s because we’re not looking," Dr. Gwen A. Huitt remarked at an allergy and pulmonary diseases meeting.

She advised clinicians that if they are prescribing antibiotics for respiratory exacerbations more than twice a year, and possibly even more than once a year, they should consider underlying bronchiectasis as a possible etiology. By the time bronchiectasis is suspected, it is often too late and the patient has developed resistance to an antibiotic, particularly quinolones and macrolides because they are easy to give patients with recurrent respiratory infections.
A noncontrast CT scan – and not a chest x-ray – is the method of choice to diagnosis bronchiectasis, because it allows proper visualization of dilated bronchi and bronchioles, said Dr. Huitt, director of the adult infectious disease unit at National Jewish Health in Denver, which sponsored the meeting. Her service also screens all patients for cystic fibrosis (CF) and alpha-1-antitrypsin deficiency (Alpha-1) both for levels and phenotype because they’ve found that even phenotypic MZ heterozygotes do not clear infection well.
Once bronchiectasis has been determined, it is important to identify the etiology. In one study involving 150 adults with bronchiectasis, however, the cause was idiopathic in 53% (Am. J. Respir. Crit. Care Med. 2000;162:1277-84). That percentage has fallen only slightly since the study was published, she said.
Treatment goals should aim to reduce or eliminate the underlying host deficiency and improve secretion clearance with any and all mechanisms possible. Secretions can be modified with nebulized hypertonic saline starting at 3%, and even nebulized normal saline to get the heavy secretions out, Dr. Huitt said. Acetylcysteine (Mucomyst) and guaifenesin are also helpful, but dornase alfa (Pulmozyme) is not indicated in non-CF patients and was actually harmful in one study.
Clinicians also need to be diligent about controlling infections rationally.
"That means if you have a gram-negative organism, don’t keep throwing cipro [ciprofloxacin] at it because you are going to lose cipro after the fifth or sixth time you give it," she said. "These organisms are going to develop drug resistance.
"This is where using dual therapy with oral antibiotics and inhaled antibiotics, I think, is going to be the cornerstone."
Approval of inhaled ciprofloxacin is right around the corner, and clinical trials of inhaled mannitol and aztreonam are now underway in non-CF bronchiectasis. Inhaled tobramycin (TOBI), amikacin (Amikin), and colistin are established in clinical practice but can be difficult to obtain for non-CF patients, and the brand-name versions can be cost prohibitive out of pocket at about $5,000 a month, Dr. Huitt observed.
"As we expand some off-label uses, and that’s what many of us do when we have very difficult patients to manage and your back is against the wall, you’re going to try some of these things if they are available to you," she said.
Although guidelines do not recommend obtaining sputum cultures in patients with acute exacerbations, she suggests this is for "garden variety" bronchiectasis.
"Again, if someone is coming into your office two times or more a year with a respiratory tract infection, you should really do a sputum culture to see what you’re dealing with," Dr. Huitt insisted.
Clinicians also should think about prevention in the form of immunizations, early treatment of infection and smoking cessation, and get respiratory therapists involved to evaluate patients to see what type of airway hygiene can be utilized.
Although the Flutter valve is a durable and easy-to-use device, National Jewish has drifted away from it because patients with poor lung function cannot lift the ball bearing on it and it can only be used in the upright position, whereas the Acapella valve can be used in multiple positions, Dr. Huitt said.
Inhaled corticosteroids and long-acting bronchodilators can be used for management, but azithromycin (Zithromax) should be used only if there are no nontuberculosis mycobacteria (NTM) on culture.
"Azithromycin is being used like water today and I think it is going to come back and haunt us in the future because we are seeing a huge rise in our service of macrolide-resistant nontuberculosis mycobacteria patients who have been on chronic macrolides as an anti-inflammatory that never had a culture done," Dr. Huitt said. "By the time we see them, they’ve lost the macrolide and that is a cornerstone drug for the treatment of NTMs."
Finally, lung resection surgery should always be considered as an adjunctive treatment option in patients with very focal bronchiectasis. With a skilled surgeon, most resections can be accomplished with the video-assisted thorascopic approach, which avoids spreading the rib cage, reduces the risk of rib fractures, and minimizes postoperative pain, she said.
Dr. Huitt is an advisory board member for Hill-Rom.
KEYSTONE, COLO. – Despite claims to the contrary, bronchiectasis is alive and unwell.
"One of the things that I hear time and time again is, ‘I just don’t see much bronchiectasis in my practice,’ but I think it’s because we’re not looking," Dr. Gwen A. Huitt remarked at an allergy and pulmonary diseases meeting.
She advised clinicians that if they are prescribing antibiotics for respiratory exacerbations more than twice a year, and possibly even more than once a year, they should consider underlying bronchiectasis as a possible etiology. By the time bronchiectasis is suspected, it is often too late and the patient has developed resistance to an antibiotic, particularly quinolones and macrolides because they are easy to give patients with recurrent respiratory infections.
A noncontrast CT scan – and not a chest x-ray – is the method of choice to diagnosis bronchiectasis, because it allows proper visualization of dilated bronchi and bronchioles, said Dr. Huitt, director of the adult infectious disease unit at National Jewish Health in Denver, which sponsored the meeting. Her service also screens all patients for cystic fibrosis (CF) and alpha-1-antitrypsin deficiency (Alpha-1) both for levels and phenotype because they’ve found that even phenotypic MZ heterozygotes do not clear infection well.
Once bronchiectasis has been determined, it is important to identify the etiology. In one study involving 150 adults with bronchiectasis, however, the cause was idiopathic in 53% (Am. J. Respir. Crit. Care Med. 2000;162:1277-84). That percentage has fallen only slightly since the study was published, she said.
Treatment goals should aim to reduce or eliminate the underlying host deficiency and improve secretion clearance with any and all mechanisms possible. Secretions can be modified with nebulized hypertonic saline starting at 3%, and even nebulized normal saline to get the heavy secretions out, Dr. Huitt said. Acetylcysteine (Mucomyst) and guaifenesin are also helpful, but dornase alfa (Pulmozyme) is not indicated in non-CF patients and was actually harmful in one study.
Clinicians also need to be diligent about controlling infections rationally.
"That means if you have a gram-negative organism, don’t keep throwing cipro [ciprofloxacin] at it because you are going to lose cipro after the fifth or sixth time you give it," she said. "These organisms are going to develop drug resistance.
"This is where using dual therapy with oral antibiotics and inhaled antibiotics, I think, is going to be the cornerstone."
Approval of inhaled ciprofloxacin is right around the corner, and clinical trials of inhaled mannitol and aztreonam are now underway in non-CF bronchiectasis. Inhaled tobramycin (TOBI), amikacin (Amikin), and colistin are established in clinical practice but can be difficult to obtain for non-CF patients, and the brand-name versions can be cost prohibitive out of pocket at about $5,000 a month, Dr. Huitt observed.
"As we expand some off-label uses, and that’s what many of us do when we have very difficult patients to manage and your back is against the wall, you’re going to try some of these things if they are available to you," she said.
Although guidelines do not recommend obtaining sputum cultures in patients with acute exacerbations, she suggests this is for "garden variety" bronchiectasis.
"Again, if someone is coming into your office two times or more a year with a respiratory tract infection, you should really do a sputum culture to see what you’re dealing with," Dr. Huitt insisted.
Clinicians also should think about prevention in the form of immunizations, early treatment of infection and smoking cessation, and get respiratory therapists involved to evaluate patients to see what type of airway hygiene can be utilized.
Although the Flutter valve is a durable and easy-to-use device, National Jewish has drifted away from it because patients with poor lung function cannot lift the ball bearing on it and it can only be used in the upright position, whereas the Acapella valve can be used in multiple positions, Dr. Huitt said.
Inhaled corticosteroids and long-acting bronchodilators can be used for management, but azithromycin (Zithromax) should be used only if there are no nontuberculosis mycobacteria (NTM) on culture.
"Azithromycin is being used like water today and I think it is going to come back and haunt us in the future because we are seeing a huge rise in our service of macrolide-resistant nontuberculosis mycobacteria patients who have been on chronic macrolides as an anti-inflammatory that never had a culture done," Dr. Huitt said. "By the time we see them, they’ve lost the macrolide and that is a cornerstone drug for the treatment of NTMs."
Finally, lung resection surgery should always be considered as an adjunctive treatment option in patients with very focal bronchiectasis. With a skilled surgeon, most resections can be accomplished with the video-assisted thorascopic approach, which avoids spreading the rib cage, reduces the risk of rib fractures, and minimizes postoperative pain, she said.
Dr. Huitt is an advisory board member for Hill-Rom.
KEYSTONE, COLO. – Despite claims to the contrary, bronchiectasis is alive and unwell.
"One of the things that I hear time and time again is, ‘I just don’t see much bronchiectasis in my practice,’ but I think it’s because we’re not looking," Dr. Gwen A. Huitt remarked at an allergy and pulmonary diseases meeting.
She advised clinicians that if they are prescribing antibiotics for respiratory exacerbations more than twice a year, and possibly even more than once a year, they should consider underlying bronchiectasis as a possible etiology. By the time bronchiectasis is suspected, it is often too late and the patient has developed resistance to an antibiotic, particularly quinolones and macrolides because they are easy to give patients with recurrent respiratory infections.
A noncontrast CT scan – and not a chest x-ray – is the method of choice to diagnosis bronchiectasis, because it allows proper visualization of dilated bronchi and bronchioles, said Dr. Huitt, director of the adult infectious disease unit at National Jewish Health in Denver, which sponsored the meeting. Her service also screens all patients for cystic fibrosis (CF) and alpha-1-antitrypsin deficiency (Alpha-1) both for levels and phenotype because they’ve found that even phenotypic MZ heterozygotes do not clear infection well.
Once bronchiectasis has been determined, it is important to identify the etiology. In one study involving 150 adults with bronchiectasis, however, the cause was idiopathic in 53% (Am. J. Respir. Crit. Care Med. 2000;162:1277-84). That percentage has fallen only slightly since the study was published, she said.
Treatment goals should aim to reduce or eliminate the underlying host deficiency and improve secretion clearance with any and all mechanisms possible. Secretions can be modified with nebulized hypertonic saline starting at 3%, and even nebulized normal saline to get the heavy secretions out, Dr. Huitt said. Acetylcysteine (Mucomyst) and guaifenesin are also helpful, but dornase alfa (Pulmozyme) is not indicated in non-CF patients and was actually harmful in one study.
Clinicians also need to be diligent about controlling infections rationally.
"That means if you have a gram-negative organism, don’t keep throwing cipro [ciprofloxacin] at it because you are going to lose cipro after the fifth or sixth time you give it," she said. "These organisms are going to develop drug resistance.
"This is where using dual therapy with oral antibiotics and inhaled antibiotics, I think, is going to be the cornerstone."
Approval of inhaled ciprofloxacin is right around the corner, and clinical trials of inhaled mannitol and aztreonam are now underway in non-CF bronchiectasis. Inhaled tobramycin (TOBI), amikacin (Amikin), and colistin are established in clinical practice but can be difficult to obtain for non-CF patients, and the brand-name versions can be cost prohibitive out of pocket at about $5,000 a month, Dr. Huitt observed.
"As we expand some off-label uses, and that’s what many of us do when we have very difficult patients to manage and your back is against the wall, you’re going to try some of these things if they are available to you," she said.
Although guidelines do not recommend obtaining sputum cultures in patients with acute exacerbations, she suggests this is for "garden variety" bronchiectasis.
"Again, if someone is coming into your office two times or more a year with a respiratory tract infection, you should really do a sputum culture to see what you’re dealing with," Dr. Huitt insisted.
Clinicians also should think about prevention in the form of immunizations, early treatment of infection and smoking cessation, and get respiratory therapists involved to evaluate patients to see what type of airway hygiene can be utilized.
Although the Flutter valve is a durable and easy-to-use device, National Jewish has drifted away from it because patients with poor lung function cannot lift the ball bearing on it and it can only be used in the upright position, whereas the Acapella valve can be used in multiple positions, Dr. Huitt said.
Inhaled corticosteroids and long-acting bronchodilators can be used for management, but azithromycin (Zithromax) should be used only if there are no nontuberculosis mycobacteria (NTM) on culture.
"Azithromycin is being used like water today and I think it is going to come back and haunt us in the future because we are seeing a huge rise in our service of macrolide-resistant nontuberculosis mycobacteria patients who have been on chronic macrolides as an anti-inflammatory that never had a culture done," Dr. Huitt said. "By the time we see them, they’ve lost the macrolide and that is a cornerstone drug for the treatment of NTMs."
Finally, lung resection surgery should always be considered as an adjunctive treatment option in patients with very focal bronchiectasis. With a skilled surgeon, most resections can be accomplished with the video-assisted thorascopic approach, which avoids spreading the rib cage, reduces the risk of rib fractures, and minimizes postoperative pain, she said.
Dr. Huitt is an advisory board member for Hill-Rom.
EXPERT ANALYSIS FROM A MEETING ON ALLERGY AND PULMONARY DISEASES
Skipping Antibiotic Guidelines Ups Trauma Surgical Infections
LAKE BUENA VISTA, FLA. – Just 49.3% of patients undergoing emergency trauma laparotomy received antibiotics in accordance with the Surgical Care Improvement Project guidelines in a multicenter, retrospective analysis of 306 patients.
"Many of the non-SCIP patients received the wrong antibiotic or antibiotics for too long after their index operation," lead author Brian P. Smith said at the annual meeting of the Eastern Association for the Surgery of Trauma.
Moreover, compliance with the guidelines slashed surgical site infection rates from 32.9% among patients with noncompliant antibiotic management to 16.6% (P less than .001).
The Surgical Care Improvement Project (SCIP) established surgical antibiotic prophylaxis guidelines as part of a collaborative effort by the Centers for Medicare and Medicaid Services and the Centers for Disease Control and Prevention to reduce surgical complications. While these antibiotic prophylaxis guidelines have become well established in patients undergoing elective operative procedures, they have never been studied in trauma patients undergoing emergency surgery, said Dr. Smith, a surgical resident at Temple University Hospital in Philadelphia.*
He reported on an analysis involving 306 trauma patients who survived for more than 4 days after undergoing emergency laparotomy within 2 hours of admission at two level 1 trauma centers during 2007 and 2008. Patients were compared on the basis of adherence to the following SCIP guidelines: prophylactic antibiotic given, antibiotic received within 1 hour prior to incision, correct antibiotic selection, and discontinuation of antibiotic within 24 hours after surgery.

Their mean age was 32 years, 70% had penetrating wounds, 44% had enteric injuries, and 20% had preoperative hypotension.
In all, 155 patients received noncompliant perioperative antibiotic management. Of these, 55% received no prophylaxis or incorrect antibiotics, 46% received antibiotics outside of the recommended 60-minute window, and 54% received them beyond the 24-hour limit, Dr. Smith said.
"It’s important to note these because they represent simple practice maneuvers that can be changed to help improve antibiotic stewardship in our trauma patients," he said.
The SCIP group spent significantly fewer days than the non-SCIP group in the ICU (mean 4 days vs. 7 days; P = .02) and in the hospital (mean 14 days vs. 19 days; P = .01), although no significant difference in mortality was detected (3% vs. 6%; P = .41).
Notably, Injury Severity Score was higher at admission in the non-SCIP group at 16 vs. 13 in the SCIP group (P = .03). Prehospital transfer time, which could influence the prolongation of antibiotics before surgery, was not available.
In a multivariate regression analysis that adjusted for such confounding factors as age, Injury Severity Score, shock, presence of enteric injury, transfusion requirements, damage control surgery, surgery duration, and hospital, complete adherence to the four SCIP guidelines independently decreased the risk of a surgical site infection (odds ratio, 0.448).
The non-SCIP group had significantly more enteric injuries than the SCIP group (52% vs. 35%; P = .027), and the rate of prolonged antibiotics was higher in patients with enteric injuries, compared with those without enteric injuries (38.6% vs. 19.4%; P = .001), Dr. Smith pointed out.
"This suggests the possibility that the extent of antibiotics rather than the enteric injuries themselves explained the wound infection rates in these two groups," he said.
Discussant Dr. John Santaniello, a critical care surgeon from Loyola University Chicago, Maywood, Ill., said the authors need to further elucidate antibiotic usage in patients with enteric injuries to distinguish true SCIP prophylaxis violations from empiric treatment for contamination.

He also questioned why the authors included only four of the six SCIP measures, omitting preoperative skin preparation and intraoperative normothermia maintenance, which have been shown to reduce surgical wound infections.
Dr. Smith said missing data and difficulty in abstracting data from handwritten records kept them from analyzing these two measures.
Attendee Dr. Patrick Reilly, chief of traumatology, surgical critical care, and emergency surgery at the University of Pennsylvania in Philadelphia, questioned how SCIP compliance was defined in a damage-control patient, and asked whether the investigators have a routine way of closing the skin when the fascia can be closed in these patients.
"For a number of years, we have had a practice – we don’t really call it a practice management guideline because we don’t really have any evidence for it – where we leave the skin open if we close the fascia, at least initially, because we’ve realized a high incidence of wound infections regardless of what antibiotic regimen we use," Dr. Reilly said.
Dr. Smith responded that they used the time from the index operation as the cut-point for SCIP compliance in the damage-control setting, but acknowledged that in many practices, patients receive another dose of antibiotics when they return to the operating room for a second look or washout.
Preliminary data on skin management in damage-control patients is being analyzed, but "we suspect, as you do at your institution, that it is probably the management of the skin in the setting of the fascial closure that may contribute to surgical site infections and are looking at a future study," he said.
Finally, when asked how the results have changed practice at Temple University, Dr. Smith said they’d like to believe they are using only 24 hours’ worth of antibiotics in the setting of prophylaxis but lack the evidence to confirm this. He pointed out that although more than a decade has passed since the Eastern Association for the Surgery of Trauma published its own antibiotic guidelines, more than 50% of surgeons in the study were not in compliance.
"Certainly, there is always room for improvement in how we treat our patients," he added.
Dr. Smith and Dr. Santaniello reported no conflicts of interest. Conflict of interest information for Dr. Reilly was not available.
*Correction, 2/22/2012: An earlier version of this article misidentified the lead author of the study.
LAKE BUENA VISTA, FLA. – Just 49.3% of patients undergoing emergency trauma laparotomy received antibiotics in accordance with the Surgical Care Improvement Project guidelines in a multicenter, retrospective analysis of 306 patients.
"Many of the non-SCIP patients received the wrong antibiotic or antibiotics for too long after their index operation," lead author Brian P. Smith said at the annual meeting of the Eastern Association for the Surgery of Trauma.
Moreover, compliance with the guidelines slashed surgical site infection rates from 32.9% among patients with noncompliant antibiotic management to 16.6% (P less than .001).
The Surgical Care Improvement Project (SCIP) established surgical antibiotic prophylaxis guidelines as part of a collaborative effort by the Centers for Medicare and Medicaid Services and the Centers for Disease Control and Prevention to reduce surgical complications. While these antibiotic prophylaxis guidelines have become well established in patients undergoing elective operative procedures, they have never been studied in trauma patients undergoing emergency surgery, said Dr. Smith, a surgical resident at Temple University Hospital in Philadelphia.*
He reported on an analysis involving 306 trauma patients who survived for more than 4 days after undergoing emergency laparotomy within 2 hours of admission at two level 1 trauma centers during 2007 and 2008. Patients were compared on the basis of adherence to the following SCIP guidelines: prophylactic antibiotic given, antibiotic received within 1 hour prior to incision, correct antibiotic selection, and discontinuation of antibiotic within 24 hours after surgery.
Their mean age was 32 years, 70% had penetrating wounds, 44% had enteric injuries, and 20% had preoperative hypotension.
In all, 155 patients received noncompliant perioperative antibiotic management. Of these, 55% received no prophylaxis or incorrect antibiotics, 46% received antibiotics outside of the recommended 60-minute window, and 54% received them beyond the 24-hour limit, Dr. Smith said.
"It’s important to note these because they represent simple practice maneuvers that can be changed to help improve antibiotic stewardship in our trauma patients," he said.
The SCIP group spent significantly fewer days than the non-SCIP group in the ICU (mean 4 days vs. 7 days; P = .02) and in the hospital (mean 14 days vs. 19 days; P = .01), although no significant difference in mortality was detected (3% vs. 6%; P = .41).
Notably, Injury Severity Score was higher at admission in the non-SCIP group at 16 vs. 13 in the SCIP group (P = .03). Prehospital transfer time, which could influence the prolongation of antibiotics before surgery, was not available.
In a multivariate regression analysis that adjusted for such confounding factors as age, Injury Severity Score, shock, presence of enteric injury, transfusion requirements, damage control surgery, surgery duration, and hospital, complete adherence to the four SCIP guidelines independently decreased the risk of a surgical site infection (odds ratio, 0.448).
The non-SCIP group had significantly more enteric injuries than the SCIP group (52% vs. 35%; P = .027), and the rate of prolonged antibiotics was higher in patients with enteric injuries, compared with those without enteric injuries (38.6% vs. 19.4%; P = .001), Dr. Smith pointed out.
"This suggests the possibility that the extent of antibiotics rather than the enteric injuries themselves explained the wound infection rates in these two groups," he said.
Discussant Dr. John Santaniello, a critical care surgeon from Loyola University Chicago, Maywood, Ill., said the authors need to further elucidate antibiotic usage in patients with enteric injuries to distinguish true SCIP prophylaxis violations from empiric treatment for contamination.
He also questioned why the authors included only four of the six SCIP measures, omitting preoperative skin preparation and intraoperative normothermia maintenance, which have been shown to reduce surgical wound infections.
Dr. Smith said missing data and difficulty in abstracting data from handwritten records kept them from analyzing these two measures.
Attendee Dr. Patrick Reilly, chief of traumatology, surgical critical care, and emergency surgery at the University of Pennsylvania in Philadelphia, questioned how SCIP compliance was defined in a damage-control patient, and asked whether the investigators have a routine way of closing the skin when the fascia can be closed in these patients.
"For a number of years, we have had a practice – we don’t really call it a practice management guideline because we don’t really have any evidence for it – where we leave the skin open if we close the fascia, at least initially, because we’ve realized a high incidence of wound infections regardless of what antibiotic regimen we use," Dr. Reilly said.
Dr. Smith responded that they used the time from the index operation as the cut-point for SCIP compliance in the damage-control setting, but acknowledged that in many practices, patients receive another dose of antibiotics when they return to the operating room for a second look or washout.
Preliminary data on skin management in damage-control patients is being analyzed, but "we suspect, as you do at your institution, that it is probably the management of the skin in the setting of the fascial closure that may contribute to surgical site infections and are looking at a future study," he said.
Finally, when asked how the results have changed practice at Temple University, Dr. Smith said they’d like to believe they are using only 24 hours’ worth of antibiotics in the setting of prophylaxis but lack the evidence to confirm this. He pointed out that although more than a decade has passed since the Eastern Association for the Surgery of Trauma published its own antibiotic guidelines, more than 50% of surgeons in the study were not in compliance.
"Certainly, there is always room for improvement in how we treat our patients," he added.
Dr. Smith and Dr. Santaniello reported no conflicts of interest. Conflict of interest information for Dr. Reilly was not available.
*Correction, 2/22/2012: An earlier version of this article misidentified the lead author of the study.
LAKE BUENA VISTA, FLA. – Just 49.3% of patients undergoing emergency trauma laparotomy received antibiotics in accordance with the Surgical Care Improvement Project guidelines in a multicenter, retrospective analysis of 306 patients.
"Many of the non-SCIP patients received the wrong antibiotic or antibiotics for too long after their index operation," lead author Brian P. Smith said at the annual meeting of the Eastern Association for the Surgery of Trauma.
Moreover, compliance with the guidelines slashed surgical site infection rates from 32.9% among patients with noncompliant antibiotic management to 16.6% (P less than .001).
The Surgical Care Improvement Project (SCIP) established surgical antibiotic prophylaxis guidelines as part of a collaborative effort by the Centers for Medicare and Medicaid Services and the Centers for Disease Control and Prevention to reduce surgical complications. While these antibiotic prophylaxis guidelines have become well established in patients undergoing elective operative procedures, they have never been studied in trauma patients undergoing emergency surgery, said Dr. Smith, a surgical resident at Temple University Hospital in Philadelphia.*
He reported on an analysis involving 306 trauma patients who survived for more than 4 days after undergoing emergency laparotomy within 2 hours of admission at two level 1 trauma centers during 2007 and 2008. Patients were compared on the basis of adherence to the following SCIP guidelines: prophylactic antibiotic given, antibiotic received within 1 hour prior to incision, correct antibiotic selection, and discontinuation of antibiotic within 24 hours after surgery.
Their mean age was 32 years, 70% had penetrating wounds, 44% had enteric injuries, and 20% had preoperative hypotension.
In all, 155 patients received noncompliant perioperative antibiotic management. Of these, 55% received no prophylaxis or incorrect antibiotics, 46% received antibiotics outside of the recommended 60-minute window, and 54% received them beyond the 24-hour limit, Dr. Smith said.
"It’s important to note these because they represent simple practice maneuvers that can be changed to help improve antibiotic stewardship in our trauma patients," he said.
The SCIP group spent significantly fewer days than the non-SCIP group in the ICU (mean 4 days vs. 7 days; P = .02) and in the hospital (mean 14 days vs. 19 days; P = .01), although no significant difference in mortality was detected (3% vs. 6%; P = .41).
Notably, Injury Severity Score was higher at admission in the non-SCIP group at 16 vs. 13 in the SCIP group (P = .03). Prehospital transfer time, which could influence the prolongation of antibiotics before surgery, was not available.
In a multivariate regression analysis that adjusted for such confounding factors as age, Injury Severity Score, shock, presence of enteric injury, transfusion requirements, damage control surgery, surgery duration, and hospital, complete adherence to the four SCIP guidelines independently decreased the risk of a surgical site infection (odds ratio, 0.448).
The non-SCIP group had significantly more enteric injuries than the SCIP group (52% vs. 35%; P = .027), and the rate of prolonged antibiotics was higher in patients with enteric injuries, compared with those without enteric injuries (38.6% vs. 19.4%; P = .001), Dr. Smith pointed out.
"This suggests the possibility that the extent of antibiotics rather than the enteric injuries themselves explained the wound infection rates in these two groups," he said.
Discussant Dr. John Santaniello, a critical care surgeon from Loyola University Chicago, Maywood, Ill., said the authors need to further elucidate antibiotic usage in patients with enteric injuries to distinguish true SCIP prophylaxis violations from empiric treatment for contamination.
He also questioned why the authors included only four of the six SCIP measures, omitting preoperative skin preparation and intraoperative normothermia maintenance, which have been shown to reduce surgical wound infections.
Dr. Smith said missing data and difficulty in abstracting data from handwritten records kept them from analyzing these two measures.
Attendee Dr. Patrick Reilly, chief of traumatology, surgical critical care, and emergency surgery at the University of Pennsylvania in Philadelphia, questioned how SCIP compliance was defined in a damage-control patient, and asked whether the investigators have a routine way of closing the skin when the fascia can be closed in these patients.
"For a number of years, we have had a practice – we don’t really call it a practice management guideline because we don’t really have any evidence for it – where we leave the skin open if we close the fascia, at least initially, because we’ve realized a high incidence of wound infections regardless of what antibiotic regimen we use," Dr. Reilly said.
Dr. Smith responded that they used the time from the index operation as the cut-point for SCIP compliance in the damage-control setting, but acknowledged that in many practices, patients receive another dose of antibiotics when they return to the operating room for a second look or washout.
Preliminary data on skin management in damage-control patients is being analyzed, but "we suspect, as you do at your institution, that it is probably the management of the skin in the setting of the fascial closure that may contribute to surgical site infections and are looking at a future study," he said.
Finally, when asked how the results have changed practice at Temple University, Dr. Smith said they’d like to believe they are using only 24 hours’ worth of antibiotics in the setting of prophylaxis but lack the evidence to confirm this. He pointed out that although more than a decade has passed since the Eastern Association for the Surgery of Trauma published its own antibiotic guidelines, more than 50% of surgeons in the study were not in compliance.
"Certainly, there is always room for improvement in how we treat our patients," he added.
Dr. Smith and Dr. Santaniello reported no conflicts of interest. Conflict of interest information for Dr. Reilly was not available.
*Correction, 2/22/2012: An earlier version of this article misidentified the lead author of the study.
FROM THE ANNUAL MEETING OF THE EASTERN ASSOCIATION FOR THE SURGERY OF TRAUMA
Major Finding: Surgical site infection rates were 32.9% in the SCIP noncompliant group vs. 16.6% in the SCIP-compliant group (P less than .001).
Data Source: Researchers conducted a multicenter, retrospective analysis of 306 patients who underwent emergency trauma laparotomy.
Disclosures: Dr. Smith and Dr. Santaniello reported no conflicts of interest. Conflict of interest information for Dr. Reilly was not available.
Team-Based Geriatric Protocol Cuts Trauma Mortality
LAKE BUENA VISTA, FLA. – Mortality was sharply reduced in elderly patients undergoing trauma care with an aggressive protocol marked by multidisciplinary teamwork and prompt identification of occult shock.
The survival benefit was significant even among patients older than 75 years, a group with notoriously high mortality rates, Dr. Eric Bradburn said at the annual meeting of the Eastern Association for the Surgery of Trauma.

Injured geriatric patients pose unique challenges to the trauma team because of their abnormal responses to shock and injury and frequent polypharmacy. They are also increasing in numbers with today’s active geriatric population, comprising 36% of all admissions at his own level II trauma center, said Dr. Bradburn, an acute care surgeon at Lancaster General Hospital in Hershey, Pa.
With the protocol, patients older than 65 years were screened on admission for high-risk injuries, comorbidities, and/or physiologic parameters associated with increased geriatric mortality in the literature. If one or more high-risk indicator was present, a high-risk protocol was initiated that included:
• ICU admission.
• STAT arterial blood gas (ABG).
• An ABG every 4 hours, if base deficit is –6 mmol/L or more, until base deficit is –2 mmol/L.
• STAT echocardiogram (EKG).
• Basic metabolic profile; magnesium and phosphorus tests in morning.
• Prothrombin time, partial thromboplastin time, and international normalized ratio in morning.
• Neurologic checks every hour for 24 hours.
• For unexplained hemodynamic instability, obtain a STAT EKG.
• Geriatric medicine consult.
The protocol was initiated in January 2006, with all 4,534 geriatric trauma patients admitted from 2000 to 2010 included in the analysis. Of these, 309 patients died for an overall mortality rate of 6.8%, Dr. Bradburn said.
Mortality rates increased sharply at age 75 years – consistent with the literature – from less than 4% to more than 6% and rose steadily to more than 11% by age 95 years.
In multivariate adjusted analysis of 3,902 patients with full data available, mortality significantly improved for geriatric patients on the protocol (odds ratio, 0.63), he said. The receiver operating curve was 0.86. Variables includes in the analysis were Injury Severity Score (ISS), trauma level, Revised Trauma Score (RTS), and age.
Patients on the protocol had significantly lower mortality rates regardless of whether they were 75-84 years (OR, 2.72), older than 85 years (OR, 4.62), had an Injury Severity Score of 17-25 (OR, 6.45) or ISS greater than 25 (OR, 15.93).
Furthermore, mortality was significantly lower among patients who received the full protocol even at the highest ISS categories, compared with those who did not receive the protocol or received either the protocol or the geriatric consult, "demonstrating the synergy and impact our full protocol has on this population," Dr. Bradburn said.
"We believe the implications of this study demonstrate that an aggressive approach to the geriatric trauma patient can result in a positive outcome in this population," he concluded.
Invited discussant Dr. Carl Schulman, a trauma and burn surgeon at the University of Miami’s Ryder Trauma Center, pointed out that geriatric consultations alone have been shown to improve mortality.
"Can you really show that your protocol added anything to this?" he asked. "Maybe all the results you have shown are from the geriatric consult alone, and this geriatric protocol is unnecessary. This would save a lot of unnecessary testing and improve the cost/benefit ratio, by simply having the geriatric consult."
The audience also questioned what services the geriatricians provided.
Dr. Bradburn said the geriatricians assisted most with social, rehabilitative, and end-of-life issues and medication issues, but also managed some comorbidities. He said the combined approach goes beyond these issues by alerting the trauma team early on to abnormal values "rather than waiting until the reserves are tapped." He noted that elderly trauma patients often present with occult hypotension leading to bias and that the literature is replete with data showing that not enough attention is paid to this population until it is too late.
Later, in a interview following the meeting, Dr. Bradburn explained that his trauma team managed the patients "from the bay to discharge."

Additional input from the geriatric team included recommendations continuing/discontinuing certain medications; assisting with management of delirium; and addressing DNR status, preinjury functional assessments, as well as social and rehab needs, he said.
"They were key in addressing the polypharmacy issue removing many of those medications that might lead to falls or increased risk for delirium."
Geriatricians’ direction on appropriate rehabilitation can boost measures such as 30-day mortality or 6-month mortality, he said. For example, in the case of an elderly fall resulting in a traumatic brain injury and extremity fractures, aggressive focused rehab to address the preexisting physical deficits that led to the fall, as well as the deficits acquired by the fall, would certainly improve the quality of life for that individual and potentially prevent additional falls.
At the meeting, Dr. Schulman also asked whether the high DNR rate of 20% could have contributed to the results. Dr. Bradburn responded that if a DNR is put into the regression model, it actually makes the results better, changing the odds ratio from 0.63 to 0.36.
Dr. Bradburn said his team had hoped to investigate functional outcomes, but that these data were not complete.
He noted that the current study is limited by its retrospective design and acknowledged that "from our data you cannot fully attribute its success solely to one part of our protocol." Still, he said, the benefits are "clear."
"This study lays the groundwork for a prospective multi-institutional study – in which we can potentially tease if one part of our protocol is more effective than any other."
The protocol should be replicable beyond Lancaster General Hospital, he said. "We think the approach is unique, but believe with further study we can show this can be applied at other institutions with equivalent successes."
Dr. Bradburn and Dr. Schulman reported no relevant conflicts of interest.
LAKE BUENA VISTA, FLA. – Mortality was sharply reduced in elderly patients undergoing trauma care with an aggressive protocol marked by multidisciplinary teamwork and prompt identification of occult shock.
The survival benefit was significant even among patients older than 75 years, a group with notoriously high mortality rates, Dr. Eric Bradburn said at the annual meeting of the Eastern Association for the Surgery of Trauma.
Injured geriatric patients pose unique challenges to the trauma team because of their abnormal responses to shock and injury and frequent polypharmacy. They are also increasing in numbers with today’s active geriatric population, comprising 36% of all admissions at his own level II trauma center, said Dr. Bradburn, an acute care surgeon at Lancaster General Hospital in Hershey, Pa.
With the protocol, patients older than 65 years were screened on admission for high-risk injuries, comorbidities, and/or physiologic parameters associated with increased geriatric mortality in the literature. If one or more high-risk indicator was present, a high-risk protocol was initiated that included:
• ICU admission.
• STAT arterial blood gas (ABG).
• An ABG every 4 hours, if base deficit is –6 mmol/L or more, until base deficit is –2 mmol/L.
• STAT echocardiogram (EKG).
• Basic metabolic profile; magnesium and phosphorus tests in morning.
• Prothrombin time, partial thromboplastin time, and international normalized ratio in morning.
• Neurologic checks every hour for 24 hours.
• For unexplained hemodynamic instability, obtain a STAT EKG.
• Geriatric medicine consult.
The protocol was initiated in January 2006, with all 4,534 geriatric trauma patients admitted from 2000 to 2010 included in the analysis. Of these, 309 patients died for an overall mortality rate of 6.8%, Dr. Bradburn said.
Mortality rates increased sharply at age 75 years – consistent with the literature – from less than 4% to more than 6% and rose steadily to more than 11% by age 95 years.
In multivariate adjusted analysis of 3,902 patients with full data available, mortality significantly improved for geriatric patients on the protocol (odds ratio, 0.63), he said. The receiver operating curve was 0.86. Variables includes in the analysis were Injury Severity Score (ISS), trauma level, Revised Trauma Score (RTS), and age.
Patients on the protocol had significantly lower mortality rates regardless of whether they were 75-84 years (OR, 2.72), older than 85 years (OR, 4.62), had an Injury Severity Score of 17-25 (OR, 6.45) or ISS greater than 25 (OR, 15.93).
Furthermore, mortality was significantly lower among patients who received the full protocol even at the highest ISS categories, compared with those who did not receive the protocol or received either the protocol or the geriatric consult, "demonstrating the synergy and impact our full protocol has on this population," Dr. Bradburn said.
"We believe the implications of this study demonstrate that an aggressive approach to the geriatric trauma patient can result in a positive outcome in this population," he concluded.
Invited discussant Dr. Carl Schulman, a trauma and burn surgeon at the University of Miami’s Ryder Trauma Center, pointed out that geriatric consultations alone have been shown to improve mortality.
"Can you really show that your protocol added anything to this?" he asked. "Maybe all the results you have shown are from the geriatric consult alone, and this geriatric protocol is unnecessary. This would save a lot of unnecessary testing and improve the cost/benefit ratio, by simply having the geriatric consult."
The audience also questioned what services the geriatricians provided.
Dr. Bradburn said the geriatricians assisted most with social, rehabilitative, and end-of-life issues and medication issues, but also managed some comorbidities. He said the combined approach goes beyond these issues by alerting the trauma team early on to abnormal values "rather than waiting until the reserves are tapped." He noted that elderly trauma patients often present with occult hypotension leading to bias and that the literature is replete with data showing that not enough attention is paid to this population until it is too late.
Later, in a interview following the meeting, Dr. Bradburn explained that his trauma team managed the patients "from the bay to discharge."
Additional input from the geriatric team included recommendations continuing/discontinuing certain medications; assisting with management of delirium; and addressing DNR status, preinjury functional assessments, as well as social and rehab needs, he said.
"They were key in addressing the polypharmacy issue removing many of those medications that might lead to falls or increased risk for delirium."
Geriatricians’ direction on appropriate rehabilitation can boost measures such as 30-day mortality or 6-month mortality, he said. For example, in the case of an elderly fall resulting in a traumatic brain injury and extremity fractures, aggressive focused rehab to address the preexisting physical deficits that led to the fall, as well as the deficits acquired by the fall, would certainly improve the quality of life for that individual and potentially prevent additional falls.
At the meeting, Dr. Schulman also asked whether the high DNR rate of 20% could have contributed to the results. Dr. Bradburn responded that if a DNR is put into the regression model, it actually makes the results better, changing the odds ratio from 0.63 to 0.36.
Dr. Bradburn said his team had hoped to investigate functional outcomes, but that these data were not complete.
He noted that the current study is limited by its retrospective design and acknowledged that "from our data you cannot fully attribute its success solely to one part of our protocol." Still, he said, the benefits are "clear."
"This study lays the groundwork for a prospective multi-institutional study – in which we can potentially tease if one part of our protocol is more effective than any other."
The protocol should be replicable beyond Lancaster General Hospital, he said. "We think the approach is unique, but believe with further study we can show this can be applied at other institutions with equivalent successes."
Dr. Bradburn and Dr. Schulman reported no relevant conflicts of interest.
LAKE BUENA VISTA, FLA. – Mortality was sharply reduced in elderly patients undergoing trauma care with an aggressive protocol marked by multidisciplinary teamwork and prompt identification of occult shock.
The survival benefit was significant even among patients older than 75 years, a group with notoriously high mortality rates, Dr. Eric Bradburn said at the annual meeting of the Eastern Association for the Surgery of Trauma.
Injured geriatric patients pose unique challenges to the trauma team because of their abnormal responses to shock and injury and frequent polypharmacy. They are also increasing in numbers with today’s active geriatric population, comprising 36% of all admissions at his own level II trauma center, said Dr. Bradburn, an acute care surgeon at Lancaster General Hospital in Hershey, Pa.
With the protocol, patients older than 65 years were screened on admission for high-risk injuries, comorbidities, and/or physiologic parameters associated with increased geriatric mortality in the literature. If one or more high-risk indicator was present, a high-risk protocol was initiated that included:
• ICU admission.
• STAT arterial blood gas (ABG).
• An ABG every 4 hours, if base deficit is –6 mmol/L or more, until base deficit is –2 mmol/L.
• STAT echocardiogram (EKG).
• Basic metabolic profile; magnesium and phosphorus tests in morning.
• Prothrombin time, partial thromboplastin time, and international normalized ratio in morning.
• Neurologic checks every hour for 24 hours.
• For unexplained hemodynamic instability, obtain a STAT EKG.
• Geriatric medicine consult.
The protocol was initiated in January 2006, with all 4,534 geriatric trauma patients admitted from 2000 to 2010 included in the analysis. Of these, 309 patients died for an overall mortality rate of 6.8%, Dr. Bradburn said.
Mortality rates increased sharply at age 75 years – consistent with the literature – from less than 4% to more than 6% and rose steadily to more than 11% by age 95 years.
In multivariate adjusted analysis of 3,902 patients with full data available, mortality significantly improved for geriatric patients on the protocol (odds ratio, 0.63), he said. The receiver operating curve was 0.86. Variables includes in the analysis were Injury Severity Score (ISS), trauma level, Revised Trauma Score (RTS), and age.
Patients on the protocol had significantly lower mortality rates regardless of whether they were 75-84 years (OR, 2.72), older than 85 years (OR, 4.62), had an Injury Severity Score of 17-25 (OR, 6.45) or ISS greater than 25 (OR, 15.93).
Furthermore, mortality was significantly lower among patients who received the full protocol even at the highest ISS categories, compared with those who did not receive the protocol or received either the protocol or the geriatric consult, "demonstrating the synergy and impact our full protocol has on this population," Dr. Bradburn said.
"We believe the implications of this study demonstrate that an aggressive approach to the geriatric trauma patient can result in a positive outcome in this population," he concluded.
Invited discussant Dr. Carl Schulman, a trauma and burn surgeon at the University of Miami’s Ryder Trauma Center, pointed out that geriatric consultations alone have been shown to improve mortality.
"Can you really show that your protocol added anything to this?" he asked. "Maybe all the results you have shown are from the geriatric consult alone, and this geriatric protocol is unnecessary. This would save a lot of unnecessary testing and improve the cost/benefit ratio, by simply having the geriatric consult."
The audience also questioned what services the geriatricians provided.
Dr. Bradburn said the geriatricians assisted most with social, rehabilitative, and end-of-life issues and medication issues, but also managed some comorbidities. He said the combined approach goes beyond these issues by alerting the trauma team early on to abnormal values "rather than waiting until the reserves are tapped." He noted that elderly trauma patients often present with occult hypotension leading to bias and that the literature is replete with data showing that not enough attention is paid to this population until it is too late.
Later, in a interview following the meeting, Dr. Bradburn explained that his trauma team managed the patients "from the bay to discharge."
Additional input from the geriatric team included recommendations continuing/discontinuing certain medications; assisting with management of delirium; and addressing DNR status, preinjury functional assessments, as well as social and rehab needs, he said.
"They were key in addressing the polypharmacy issue removing many of those medications that might lead to falls or increased risk for delirium."
Geriatricians’ direction on appropriate rehabilitation can boost measures such as 30-day mortality or 6-month mortality, he said. For example, in the case of an elderly fall resulting in a traumatic brain injury and extremity fractures, aggressive focused rehab to address the preexisting physical deficits that led to the fall, as well as the deficits acquired by the fall, would certainly improve the quality of life for that individual and potentially prevent additional falls.
At the meeting, Dr. Schulman also asked whether the high DNR rate of 20% could have contributed to the results. Dr. Bradburn responded that if a DNR is put into the regression model, it actually makes the results better, changing the odds ratio from 0.63 to 0.36.
Dr. Bradburn said his team had hoped to investigate functional outcomes, but that these data were not complete.
He noted that the current study is limited by its retrospective design and acknowledged that "from our data you cannot fully attribute its success solely to one part of our protocol." Still, he said, the benefits are "clear."
"This study lays the groundwork for a prospective multi-institutional study – in which we can potentially tease if one part of our protocol is more effective than any other."
The protocol should be replicable beyond Lancaster General Hospital, he said. "We think the approach is unique, but believe with further study we can show this can be applied at other institutions with equivalent successes."
Dr. Bradburn and Dr. Schulman reported no relevant conflicts of interest.
FROM THE ANNUAL MEETING OF THE EASTERN ASSOCIATION FOR THE SURGERY OF TRAUMA
Trauma Surgeons on Par With Neurosurgeons for Small ICHs
LAKE BUENA VISTA, Fla.– Score one for the trauma surgeons. Outcomes are no different for patients with small intracranial hemorrhages managed by a trauma surgeon rather than a neurosurgeon, a new study shows.
Investigators at the JPS Health Network in Fort Worth, Tex., compared trauma activations for 124 patients before and 199 patients after a protocol was instituted at the level 1 trauma center allowing trauma surgeons to manage patients with a traumatic brain injury due to a fall resulting in a 1-cm or less intracranial hemorrhage (ICH). Patients with penetrating wounds or who were transferred to other acute care facilities were excluded from the analysis.
After the protocol was initiated, neurosurgery consults significantly decreased from 93.5% to 83.4% (P less than .01), Ms. Tiffany Littleton, trauma services research associate, and her colleagues reported at the annual meeting of the Eastern Association for the Surgery of Trauma.
No significant differences at discharge were observed pre- and postprotocol for patient age (61.5 years vs. 58 years), sex (71% male vs. 65%), race (69.4% white vs. 70.4%), Glasgow Coma Scale scores (median 14.5 vs. 15), or Injury Severity Score (both median 20).
Additionally, there were no differences in outcomes such as length of stay (median 4 days for both; P = .86), condition on discharge (P = .57), where patients were discharged to (P = .14), or Glasgow Outcome Scale (GOS) scores (P = .18), she reported.
At discharge, most patients pre- and postprotocol had moderate disability (70.2% vs. 50.3%), went home without the need for professional assistance (59.7% vs. 49.2%), and were GOS classified as "good recovery" (50% vs. 60%).
"Due to the demand placed on neurosurgeons for more severe brain injuries, these data suggest patients managed by trauma surgeons could have comparable outcomes to those managed by neurosurgeons," the authors concluded.
The results are particularly relevant, as the literature is scant regarding the management of ICHs of 1 cm or less. Moreover, the number of trauma activations resulting from falls is expected to increase with the aging American population, the investigators noted.
Falls are the second leading cause of trauma activations, and half of fall fatalities and associated costs are related to traumatic brain injury. Falls also constitute 52% of emergency department visits for adults aged 75 years or older.
Despite the potential for turf wars when departmental duties are shifted, "neurosurgeons were delighted" with the new protocol, senior author and JPS medical director of trauma services Dr. Rajesh Gandhi said in an interview. In fact, it was two neurosurgeons who developed and initiated the protocol change.
The researchers are currently acquiring data from the National Trauma Bank to examine differences in ICH outcomes in a larger sample.
"Additionally, we want to look at the range in which trauma surgeons can effectively manage ICH, and determine the point at which neurosurgeon management results in significant differences in outcome," said Ms. Littleton. "This can also translate to rural health care in terms of transferring these types of patients to trauma centers."
Ms. Littleton and her coauthors reported no financial conflicts of interest. Dr. Gandhi serves as a speaker for LifeCell and KCI.
LAKE BUENA VISTA, Fla.– Score one for the trauma surgeons. Outcomes are no different for patients with small intracranial hemorrhages managed by a trauma surgeon rather than a neurosurgeon, a new study shows.
Investigators at the JPS Health Network in Fort Worth, Tex., compared trauma activations for 124 patients before and 199 patients after a protocol was instituted at the level 1 trauma center allowing trauma surgeons to manage patients with a traumatic brain injury due to a fall resulting in a 1-cm or less intracranial hemorrhage (ICH). Patients with penetrating wounds or who were transferred to other acute care facilities were excluded from the analysis.
After the protocol was initiated, neurosurgery consults significantly decreased from 93.5% to 83.4% (P less than .01), Ms. Tiffany Littleton, trauma services research associate, and her colleagues reported at the annual meeting of the Eastern Association for the Surgery of Trauma.
No significant differences at discharge were observed pre- and postprotocol for patient age (61.5 years vs. 58 years), sex (71% male vs. 65%), race (69.4% white vs. 70.4%), Glasgow Coma Scale scores (median 14.5 vs. 15), or Injury Severity Score (both median 20).
Additionally, there were no differences in outcomes such as length of stay (median 4 days for both; P = .86), condition on discharge (P = .57), where patients were discharged to (P = .14), or Glasgow Outcome Scale (GOS) scores (P = .18), she reported.
At discharge, most patients pre- and postprotocol had moderate disability (70.2% vs. 50.3%), went home without the need for professional assistance (59.7% vs. 49.2%), and were GOS classified as "good recovery" (50% vs. 60%).
"Due to the demand placed on neurosurgeons for more severe brain injuries, these data suggest patients managed by trauma surgeons could have comparable outcomes to those managed by neurosurgeons," the authors concluded.
The results are particularly relevant, as the literature is scant regarding the management of ICHs of 1 cm or less. Moreover, the number of trauma activations resulting from falls is expected to increase with the aging American population, the investigators noted.
Falls are the second leading cause of trauma activations, and half of fall fatalities and associated costs are related to traumatic brain injury. Falls also constitute 52% of emergency department visits for adults aged 75 years or older.
Despite the potential for turf wars when departmental duties are shifted, "neurosurgeons were delighted" with the new protocol, senior author and JPS medical director of trauma services Dr. Rajesh Gandhi said in an interview. In fact, it was two neurosurgeons who developed and initiated the protocol change.
The researchers are currently acquiring data from the National Trauma Bank to examine differences in ICH outcomes in a larger sample.
"Additionally, we want to look at the range in which trauma surgeons can effectively manage ICH, and determine the point at which neurosurgeon management results in significant differences in outcome," said Ms. Littleton. "This can also translate to rural health care in terms of transferring these types of patients to trauma centers."
Ms. Littleton and her coauthors reported no financial conflicts of interest. Dr. Gandhi serves as a speaker for LifeCell and KCI.
LAKE BUENA VISTA, Fla.– Score one for the trauma surgeons. Outcomes are no different for patients with small intracranial hemorrhages managed by a trauma surgeon rather than a neurosurgeon, a new study shows.
Investigators at the JPS Health Network in Fort Worth, Tex., compared trauma activations for 124 patients before and 199 patients after a protocol was instituted at the level 1 trauma center allowing trauma surgeons to manage patients with a traumatic brain injury due to a fall resulting in a 1-cm or less intracranial hemorrhage (ICH). Patients with penetrating wounds or who were transferred to other acute care facilities were excluded from the analysis.
After the protocol was initiated, neurosurgery consults significantly decreased from 93.5% to 83.4% (P less than .01), Ms. Tiffany Littleton, trauma services research associate, and her colleagues reported at the annual meeting of the Eastern Association for the Surgery of Trauma.
No significant differences at discharge were observed pre- and postprotocol for patient age (61.5 years vs. 58 years), sex (71% male vs. 65%), race (69.4% white vs. 70.4%), Glasgow Coma Scale scores (median 14.5 vs. 15), or Injury Severity Score (both median 20).
Additionally, there were no differences in outcomes such as length of stay (median 4 days for both; P = .86), condition on discharge (P = .57), where patients were discharged to (P = .14), or Glasgow Outcome Scale (GOS) scores (P = .18), she reported.
At discharge, most patients pre- and postprotocol had moderate disability (70.2% vs. 50.3%), went home without the need for professional assistance (59.7% vs. 49.2%), and were GOS classified as "good recovery" (50% vs. 60%).
"Due to the demand placed on neurosurgeons for more severe brain injuries, these data suggest patients managed by trauma surgeons could have comparable outcomes to those managed by neurosurgeons," the authors concluded.
The results are particularly relevant, as the literature is scant regarding the management of ICHs of 1 cm or less. Moreover, the number of trauma activations resulting from falls is expected to increase with the aging American population, the investigators noted.
Falls are the second leading cause of trauma activations, and half of fall fatalities and associated costs are related to traumatic brain injury. Falls also constitute 52% of emergency department visits for adults aged 75 years or older.
Despite the potential for turf wars when departmental duties are shifted, "neurosurgeons were delighted" with the new protocol, senior author and JPS medical director of trauma services Dr. Rajesh Gandhi said in an interview. In fact, it was two neurosurgeons who developed and initiated the protocol change.
The researchers are currently acquiring data from the National Trauma Bank to examine differences in ICH outcomes in a larger sample.
"Additionally, we want to look at the range in which trauma surgeons can effectively manage ICH, and determine the point at which neurosurgeon management results in significant differences in outcome," said Ms. Littleton. "This can also translate to rural health care in terms of transferring these types of patients to trauma centers."
Ms. Littleton and her coauthors reported no financial conflicts of interest. Dr. Gandhi serves as a speaker for LifeCell and KCI.
FROM THE ANNUAL MEETING OF THE EASTERN ASSOCIATION FOR THE SURGERY OF TRAUMA
Trauma Risk in Oral Anticoagulant Users Prompt Search for Antidotes
LAKE BUENA VISTA, FLA. – Patients on one of the powerful new oral anticoagulants are left without a good antidote for bleeding if they experience a traumatic injury.
The use of these agents is climbing as baby boomers age and the number of patients with atrial fibrillation continues its steady rise from 2.0 million in 1995 to a projected 4.34 million by 2030.

"If you think it’s an epidemic now, it will become even more so in the coming years," Dr. Mark Cipolle, medical director of trauma and neurocritical care at Christiana Care Health System in Wilmington, Del., said at the annual meeting of the Eastern Association for the Surgery of Trauma.
Currently, no specific antidote is available for dabigatran (Pradaxa) or the factor Xa inhibitor rivaroxaban (Xarelto), both of which are approved for stroke prevention in nonvalvular atrial fibrillation and for deep vein thrombosis following hip or knee replacement surgery.
The oral Xa inhibitor apixaban (Eliquis) is under priority review for stroke and DVT prevention in atrial fibrillation and will likely move, sans antidote, into the marketplace later this year based on robust results from the recent ARISTOTLE trial.
Vitamin K and protamine sulfate are not expected to affect the anticoagulant activity of the new oral anticoagulants. Some centers have had anectodal success in reversing dabigatran with activated prothrombin complex concentrates (aPCCs), but this has not been widely adopted, according to Dr. Cipolle.
"Some of my colleagues in pharmacy think this may be the drug to help us reverse dabigatran ... but our blood bank hematologists aren’t thrilled about going to this because of the development of antibodies for the new agents," he said.
The two aPCCs available in the United States are factor eight inhibitor binding activity (FEIBA) and anti-inhibitor coagulant complex, heat treated (Autoplex T); both are indicated for bypass therapy in patients with acquired inhibitors and contain the coagulation factors II, VII, IX, and X.

One of the first randomized trials to look at a specific PCC (Cofact) showed that a single bolus immediately and completely reversed the anticoagulation effect of rivaroxaban in 12 healthy volunteers who were taking 20 mg twice daily, but the PCC had no influence on the effect of dabigatran 150 mg twice daily (Circulation 2011;124:1573-9), said copanelist John Gallagher, clinical nurse specialist for the surgical/trauma ICU at the Hospital of the University of Pennsylvania in Philadelphia.
Recombinant activated factor VIIa has been widely studied in trauma, but not for this specific indication. Early research on antibody monoclonal development is showing promise, Dr. Cipolle said. A recent study described a monoclonal mouse antibody with a high and specific affinity to inhibit dabigatran in both human plasma and whole blood and in a rat in vivo model (J. Am. Coll. Cardiol. 2011;57:E1130).
The package insert for dabigatran recommends emergency dialysis as a reversal strategy, stating that about 60% of dabigatran is removed over 2-3 hours. "This [strategy] may work," said Dr. Cipolle, observing that about 80% of dabigatran is renally excreted, compared with 66% of rivaroxaban and only 25% of apixaban.
Although not trivial, the half-lives of dabigatran (14-17 hours), rivaroxaban (9 hours), and apixaban (9-14 hours) are shorter than that of warfarin (40 hours), which means that "if you can wait and just not give them the drug, you are probably going to be okay," he said.
Dr. Cipolle cautioned, however, that reversal of labs may not indicate loss of anticoagulant effects. Also, clotting factors and continued prolongation of anticoagulation assays do not indicate lack of effect.
"The drug industry has spent years developing a drug that we could take orally that you don’t have to measure, and all we want to do is measure it," he said. "We would like to know just how much anticoagulant effect is present, and if our reversal strategies are working.
"A normal PTT [partial thromboplastin time] is very helpful, but other than that, the classic anticoagulation studies aren’t terribly helpful."
This point was also referenced in a recent letter to the New England Journal of Medicine penned by two trauma surgeons and an emergency physician who treated several injured patients on dabigatran, all of whom had poor outcomes (N. Engl. J. Med. 2011;365:2039-40). Although their values for activated clotting time on rapid thromboelastography (rTEG) were grossly abnormal at the time of admission, all of the patients had normal results on conventional anticoagulation studies.
"Unfortunately, even with the aid of rTEG, supportive care is all that is available in the emergency setting," wrote the authors, who strongly urged that hemorrhagic complications and death resulting from trauma be included as part of routine surveillance of all newly approved oral anticoagulants. The authors also argued that "the ability to perform rapid dialysis in patients with bleeding whose condition is unstable or in those with large intracranial hemorrhages will present an incredible challenge, even at level 1 trauma centers."
Both Dr. Cipolle and Mr. Gallagher emphasized that institutions should have a protocol in place for anticoagulant reversal. The protocol should be based on evidence and practice guidelines, be transparent and modifiable, and identify specific anticoagulant agents, triggers for reversal such as intracranial hemorrhage or solid organ injury, and reversal strategies and methods for monitoring both the use of anticoagulants and reversal strategies, Mr. Gallagher said.
During a discussion of the study, attendees asked how to address anticoagulation at discharge in, for example, a 72-year-old man with early Alzheimer’s disease and a fourth admission for a fall. Dr. Cipolle replied that a recommendation would be placed in his chart based on his initial risk and that a hospitalist or cardiologist would also be called in. He observed that trauma surgeons typically overestimate the fall risk, compared with the stroke risk, and often feel that making such a recommendation may be out of their purview.

Audience member Dr. Ronald Gross, chief of trauma and emergency surgery at Baystate Medical Center in Springfield, Mass., said trauma surgeons need to play a more active role in anticoagulation. He added that physicians at his center have a conversation prior to discharge with every single fall patient about the risks and benefits of anticoagulation, and also contact their prescribing physicians.
Session moderator Dr. Lewis Kaplan, a trauma and critical care surgeon at Yale University, New Haven, Conn., said the nurse practitioners at his center call primary care physicians when trauma patients are admitted and make a follow-up call upon discharge. The trauma surgeon makes an anticoagulation recommendation at discharge, although half the time, despite the conversation, patients are back on their anticoagulants in a matter of weeks, Dr. Kaplan said.
Dr. Cipolle and Mr. Gallagher reported no conflicts of interest. Dr. Lewis serves as a consultant to Pfizer.
LAKE BUENA VISTA, FLA. – Patients on one of the powerful new oral anticoagulants are left without a good antidote for bleeding if they experience a traumatic injury.
The use of these agents is climbing as baby boomers age and the number of patients with atrial fibrillation continues its steady rise from 2.0 million in 1995 to a projected 4.34 million by 2030.
"If you think it’s an epidemic now, it will become even more so in the coming years," Dr. Mark Cipolle, medical director of trauma and neurocritical care at Christiana Care Health System in Wilmington, Del., said at the annual meeting of the Eastern Association for the Surgery of Trauma.
Currently, no specific antidote is available for dabigatran (Pradaxa) or the factor Xa inhibitor rivaroxaban (Xarelto), both of which are approved for stroke prevention in nonvalvular atrial fibrillation and for deep vein thrombosis following hip or knee replacement surgery.
The oral Xa inhibitor apixaban (Eliquis) is under priority review for stroke and DVT prevention in atrial fibrillation and will likely move, sans antidote, into the marketplace later this year based on robust results from the recent ARISTOTLE trial.
Vitamin K and protamine sulfate are not expected to affect the anticoagulant activity of the new oral anticoagulants. Some centers have had anectodal success in reversing dabigatran with activated prothrombin complex concentrates (aPCCs), but this has not been widely adopted, according to Dr. Cipolle.
"Some of my colleagues in pharmacy think this may be the drug to help us reverse dabigatran ... but our blood bank hematologists aren’t thrilled about going to this because of the development of antibodies for the new agents," he said.
The two aPCCs available in the United States are factor eight inhibitor binding activity (FEIBA) and anti-inhibitor coagulant complex, heat treated (Autoplex T); both are indicated for bypass therapy in patients with acquired inhibitors and contain the coagulation factors II, VII, IX, and X.
One of the first randomized trials to look at a specific PCC (Cofact) showed that a single bolus immediately and completely reversed the anticoagulation effect of rivaroxaban in 12 healthy volunteers who were taking 20 mg twice daily, but the PCC had no influence on the effect of dabigatran 150 mg twice daily (Circulation 2011;124:1573-9), said copanelist John Gallagher, clinical nurse specialist for the surgical/trauma ICU at the Hospital of the University of Pennsylvania in Philadelphia.
Recombinant activated factor VIIa has been widely studied in trauma, but not for this specific indication. Early research on antibody monoclonal development is showing promise, Dr. Cipolle said. A recent study described a monoclonal mouse antibody with a high and specific affinity to inhibit dabigatran in both human plasma and whole blood and in a rat in vivo model (J. Am. Coll. Cardiol. 2011;57:E1130).
The package insert for dabigatran recommends emergency dialysis as a reversal strategy, stating that about 60% of dabigatran is removed over 2-3 hours. "This [strategy] may work," said Dr. Cipolle, observing that about 80% of dabigatran is renally excreted, compared with 66% of rivaroxaban and only 25% of apixaban.
Although not trivial, the half-lives of dabigatran (14-17 hours), rivaroxaban (9 hours), and apixaban (9-14 hours) are shorter than that of warfarin (40 hours), which means that "if you can wait and just not give them the drug, you are probably going to be okay," he said.
Dr. Cipolle cautioned, however, that reversal of labs may not indicate loss of anticoagulant effects. Also, clotting factors and continued prolongation of anticoagulation assays do not indicate lack of effect.
"The drug industry has spent years developing a drug that we could take orally that you don’t have to measure, and all we want to do is measure it," he said. "We would like to know just how much anticoagulant effect is present, and if our reversal strategies are working.
"A normal PTT [partial thromboplastin time] is very helpful, but other than that, the classic anticoagulation studies aren’t terribly helpful."
This point was also referenced in a recent letter to the New England Journal of Medicine penned by two trauma surgeons and an emergency physician who treated several injured patients on dabigatran, all of whom had poor outcomes (N. Engl. J. Med. 2011;365:2039-40). Although their values for activated clotting time on rapid thromboelastography (rTEG) were grossly abnormal at the time of admission, all of the patients had normal results on conventional anticoagulation studies.
"Unfortunately, even with the aid of rTEG, supportive care is all that is available in the emergency setting," wrote the authors, who strongly urged that hemorrhagic complications and death resulting from trauma be included as part of routine surveillance of all newly approved oral anticoagulants. The authors also argued that "the ability to perform rapid dialysis in patients with bleeding whose condition is unstable or in those with large intracranial hemorrhages will present an incredible challenge, even at level 1 trauma centers."
Both Dr. Cipolle and Mr. Gallagher emphasized that institutions should have a protocol in place for anticoagulant reversal. The protocol should be based on evidence and practice guidelines, be transparent and modifiable, and identify specific anticoagulant agents, triggers for reversal such as intracranial hemorrhage or solid organ injury, and reversal strategies and methods for monitoring both the use of anticoagulants and reversal strategies, Mr. Gallagher said.
During a discussion of the study, attendees asked how to address anticoagulation at discharge in, for example, a 72-year-old man with early Alzheimer’s disease and a fourth admission for a fall. Dr. Cipolle replied that a recommendation would be placed in his chart based on his initial risk and that a hospitalist or cardiologist would also be called in. He observed that trauma surgeons typically overestimate the fall risk, compared with the stroke risk, and often feel that making such a recommendation may be out of their purview.
Audience member Dr. Ronald Gross, chief of trauma and emergency surgery at Baystate Medical Center in Springfield, Mass., said trauma surgeons need to play a more active role in anticoagulation. He added that physicians at his center have a conversation prior to discharge with every single fall patient about the risks and benefits of anticoagulation, and also contact their prescribing physicians.
Session moderator Dr. Lewis Kaplan, a trauma and critical care surgeon at Yale University, New Haven, Conn., said the nurse practitioners at his center call primary care physicians when trauma patients are admitted and make a follow-up call upon discharge. The trauma surgeon makes an anticoagulation recommendation at discharge, although half the time, despite the conversation, patients are back on their anticoagulants in a matter of weeks, Dr. Kaplan said.
Dr. Cipolle and Mr. Gallagher reported no conflicts of interest. Dr. Lewis serves as a consultant to Pfizer.
LAKE BUENA VISTA, FLA. – Patients on one of the powerful new oral anticoagulants are left without a good antidote for bleeding if they experience a traumatic injury.
The use of these agents is climbing as baby boomers age and the number of patients with atrial fibrillation continues its steady rise from 2.0 million in 1995 to a projected 4.34 million by 2030.
"If you think it’s an epidemic now, it will become even more so in the coming years," Dr. Mark Cipolle, medical director of trauma and neurocritical care at Christiana Care Health System in Wilmington, Del., said at the annual meeting of the Eastern Association for the Surgery of Trauma.
Currently, no specific antidote is available for dabigatran (Pradaxa) or the factor Xa inhibitor rivaroxaban (Xarelto), both of which are approved for stroke prevention in nonvalvular atrial fibrillation and for deep vein thrombosis following hip or knee replacement surgery.
The oral Xa inhibitor apixaban (Eliquis) is under priority review for stroke and DVT prevention in atrial fibrillation and will likely move, sans antidote, into the marketplace later this year based on robust results from the recent ARISTOTLE trial.
Vitamin K and protamine sulfate are not expected to affect the anticoagulant activity of the new oral anticoagulants. Some centers have had anectodal success in reversing dabigatran with activated prothrombin complex concentrates (aPCCs), but this has not been widely adopted, according to Dr. Cipolle.
"Some of my colleagues in pharmacy think this may be the drug to help us reverse dabigatran ... but our blood bank hematologists aren’t thrilled about going to this because of the development of antibodies for the new agents," he said.
The two aPCCs available in the United States are factor eight inhibitor binding activity (FEIBA) and anti-inhibitor coagulant complex, heat treated (Autoplex T); both are indicated for bypass therapy in patients with acquired inhibitors and contain the coagulation factors II, VII, IX, and X.
One of the first randomized trials to look at a specific PCC (Cofact) showed that a single bolus immediately and completely reversed the anticoagulation effect of rivaroxaban in 12 healthy volunteers who were taking 20 mg twice daily, but the PCC had no influence on the effect of dabigatran 150 mg twice daily (Circulation 2011;124:1573-9), said copanelist John Gallagher, clinical nurse specialist for the surgical/trauma ICU at the Hospital of the University of Pennsylvania in Philadelphia.
Recombinant activated factor VIIa has been widely studied in trauma, but not for this specific indication. Early research on antibody monoclonal development is showing promise, Dr. Cipolle said. A recent study described a monoclonal mouse antibody with a high and specific affinity to inhibit dabigatran in both human plasma and whole blood and in a rat in vivo model (J. Am. Coll. Cardiol. 2011;57:E1130).
The package insert for dabigatran recommends emergency dialysis as a reversal strategy, stating that about 60% of dabigatran is removed over 2-3 hours. "This [strategy] may work," said Dr. Cipolle, observing that about 80% of dabigatran is renally excreted, compared with 66% of rivaroxaban and only 25% of apixaban.
Although not trivial, the half-lives of dabigatran (14-17 hours), rivaroxaban (9 hours), and apixaban (9-14 hours) are shorter than that of warfarin (40 hours), which means that "if you can wait and just not give them the drug, you are probably going to be okay," he said.
Dr. Cipolle cautioned, however, that reversal of labs may not indicate loss of anticoagulant effects. Also, clotting factors and continued prolongation of anticoagulation assays do not indicate lack of effect.
"The drug industry has spent years developing a drug that we could take orally that you don’t have to measure, and all we want to do is measure it," he said. "We would like to know just how much anticoagulant effect is present, and if our reversal strategies are working.
"A normal PTT [partial thromboplastin time] is very helpful, but other than that, the classic anticoagulation studies aren’t terribly helpful."
This point was also referenced in a recent letter to the New England Journal of Medicine penned by two trauma surgeons and an emergency physician who treated several injured patients on dabigatran, all of whom had poor outcomes (N. Engl. J. Med. 2011;365:2039-40). Although their values for activated clotting time on rapid thromboelastography (rTEG) were grossly abnormal at the time of admission, all of the patients had normal results on conventional anticoagulation studies.
"Unfortunately, even with the aid of rTEG, supportive care is all that is available in the emergency setting," wrote the authors, who strongly urged that hemorrhagic complications and death resulting from trauma be included as part of routine surveillance of all newly approved oral anticoagulants. The authors also argued that "the ability to perform rapid dialysis in patients with bleeding whose condition is unstable or in those with large intracranial hemorrhages will present an incredible challenge, even at level 1 trauma centers."
Both Dr. Cipolle and Mr. Gallagher emphasized that institutions should have a protocol in place for anticoagulant reversal. The protocol should be based on evidence and practice guidelines, be transparent and modifiable, and identify specific anticoagulant agents, triggers for reversal such as intracranial hemorrhage or solid organ injury, and reversal strategies and methods for monitoring both the use of anticoagulants and reversal strategies, Mr. Gallagher said.
During a discussion of the study, attendees asked how to address anticoagulation at discharge in, for example, a 72-year-old man with early Alzheimer’s disease and a fourth admission for a fall. Dr. Cipolle replied that a recommendation would be placed in his chart based on his initial risk and that a hospitalist or cardiologist would also be called in. He observed that trauma surgeons typically overestimate the fall risk, compared with the stroke risk, and often feel that making such a recommendation may be out of their purview.
Audience member Dr. Ronald Gross, chief of trauma and emergency surgery at Baystate Medical Center in Springfield, Mass., said trauma surgeons need to play a more active role in anticoagulation. He added that physicians at his center have a conversation prior to discharge with every single fall patient about the risks and benefits of anticoagulation, and also contact their prescribing physicians.
Session moderator Dr. Lewis Kaplan, a trauma and critical care surgeon at Yale University, New Haven, Conn., said the nurse practitioners at his center call primary care physicians when trauma patients are admitted and make a follow-up call upon discharge. The trauma surgeon makes an anticoagulation recommendation at discharge, although half the time, despite the conversation, patients are back on their anticoagulants in a matter of weeks, Dr. Kaplan said.
Dr. Cipolle and Mr. Gallagher reported no conflicts of interest. Dr. Lewis serves as a consultant to Pfizer.
EXPERT OPINION FROM THE ANNUAL MEETING OF THE EASTERN ASSOCIATION FOR THE SURGERY OF TRAUMA
Less May Be More in Treating High-Risk Myeloma
SAN DIEGO – A provocative analysis suggests that a sequence of bortezomib and lenalidomide provides a better survival advantage than regimens with three or more agents in patients with multiple myeloma and high-risk cytogenetics.*
"While the limitations of this retrospective study limit drawing definitive conclusions, it appears that poor cytogenetics and biology trump treatment intensification," Dr. Rachid Baz and his colleagues stated in a poster presentation at the annual meeting of the American Society of Hematology.

The investigators reported on 208 patients with multiple myeloma who received bortezomib (Velcade) and lenalidomide (Revlimid), nonconcurrently between January 2004 and August 2010 at the H. Lee Moffitt Cancer Center and Research Institute in Tampa. The patients were stratified by treatment into six groups: lenalidomide with or without dexamethasone (lenalidomide A) or lenalidomide in combination with two or more agents (lenalidomide B); bortezomib with or with dexamethasone (bortezomib A) or bortezomib in combination with two or more agents (bortezomib B); and finally, only doublets or single agents (nonintensive therapy) or three or more agents in combination (intensive therapy).
No differences were observed between the lenalidomide A and B, bortezomib A and B, or intensive and nonintensive therapy groups in the baseline characteristics of age, International Staging System (ISS) and Durie/Salmon stage, beta2microglobulin or renal function, presence of poor-risk cytogenetics, and frequency of high-dose therapy.
Poor-risk cytogenetics, an increasingly fluid term in the context of growing success with novel myeloma agents, included deletions 13q and 17p, translocations, (4;14) and (14;16) or hypodiploidy.
Lenalidomide A patients had a trend toward improved median overall survival at 72 months, compared with 57 months for the lenalidomide B group receiving more complex regimens (P = .07), reported Dr. Baz, with Moffitt’s hematologic malignancies and experimental therapeutics departments.
Median overall survival, the study’s primary end point, however, was significantly improved in the bortezomib A group at 72 months vs. 45 months in the bortezomib B group (P = .02).
Similarly, the nonintensive therapy group lived significantly longer for 74 months vs. 57 months for the intensive therapy group (P = .03).
Notably, patients with high-risk cytogenetics had significantly worse survival if they received intensive therapy rather than nonintensive therapy (median 44 months vs. 72 months; P = .01), he noted. In contrast, patients without high-risk cytogenetics had similar overall survival regardless of whether they belonged to the intensive therapy or nonintensive therapy groups (median 76 months vs. 75 months).
On multivariate analysis that adjusted for known covariates linked to myeloma survival such as ISS stage and high-dose therapy, the only features predictive of poor outcome were renal failure at baseline and intensive therapy.
Dr. Baz said the investigators were surprised by the counterintuitive results and that they could be due to bias from an unidentified confounding factor. For example, it’s possible that high-risk patients who appeared more ill were more likely to be given more intensive therapy by the practicing physician and may have had poor outcomes nonetheless, whereas high-risk patients who appeared more stable were more likely to be given less intensive therapy, but did well because of more indolent disease characteristics.
A potential biologic explanation for the finding might be related to genomic instabilities more commonly seen in high-risk myeloma.
"Patients with high-risk disease have myeloma cells that are more likely to acquire drug resistance faster," he said in an interview. "As a result, if you expose those myeloma cells to many drugs at once, they may acquire resistance to them faster and you get less mileage than if you spread out the drugs."
Dr. Baz said further study at the molecular level is needed to see how drug resistance develops in myeloma in the context of combination therapy with three or four drugs versus treatment with one or two drugs.
"I think the finding is hypothesis generating," he said. "It doesn’t change my practice with the patients I see today, but it needs more study."
Baseline characteristics of the non-intensive and intensive therapy groups were: age (58.9 years, 58.5 years), heavy chain IgG (60%, 63%), light chain Kappa (58%, 67%), ISS stage II (40%, 38%), ISS III (24%, 33%), Durie/Salmon stage III (75%, 85%), creatinine at least 2.0 mg/dL (12%, 13%), presence of bone disease (67%, 80%), poor-risk cytogenetics (43%, 36%), prior high-dose therapy (64%, 66%), and thalidomide use (59%, 47%).
The only significant difference between two groups was the presence of more males in the intensive group (73% vs. 52%; P = .01).
Dr. Baz reported research funding from Celgene and membership on an entity’s board of directors or advisory committee and research funding from Millennium Pharmaceuticals. His coauthors reported similar relationships with Celgene, Millennium, Novartis, and Allergan.
*CLARIFICATION 1/23/12 The status of bortezomib and lenalidomide in treatment for multiple myeloma was clarified in this sentence.
"This is an intriguing observation," Dr. Martha Q. Lacy said in a separate interview. "The author points out that it is a retrospective study, and results could be confounded by a number of variables, so I agree that one cannot take this as the definitive word on this subject. This should be studied in well-designed prospective studies. It also underscores the need to design trials with overall survival as the primary end point.
"Increasingly, myeloma studies have used remission rates and progression-free survival as primary end points," she said. "If studies are not designed with overall survival as the end point, we risk missing potentially critical insights into the best treatment strategies."
Dr. Lacy is with the hematology division at the Mayo Clinic in Rochester, Minn.
"This is an intriguing observation," Dr. Martha Q. Lacy said in a separate interview. "The author points out that it is a retrospective study, and results could be confounded by a number of variables, so I agree that one cannot take this as the definitive word on this subject. This should be studied in well-designed prospective studies. It also underscores the need to design trials with overall survival as the primary end point.
"Increasingly, myeloma studies have used remission rates and progression-free survival as primary end points," she said. "If studies are not designed with overall survival as the end point, we risk missing potentially critical insights into the best treatment strategies."
Dr. Lacy is with the hematology division at the Mayo Clinic in Rochester, Minn.
"This is an intriguing observation," Dr. Martha Q. Lacy said in a separate interview. "The author points out that it is a retrospective study, and results could be confounded by a number of variables, so I agree that one cannot take this as the definitive word on this subject. This should be studied in well-designed prospective studies. It also underscores the need to design trials with overall survival as the primary end point.
"Increasingly, myeloma studies have used remission rates and progression-free survival as primary end points," she said. "If studies are not designed with overall survival as the end point, we risk missing potentially critical insights into the best treatment strategies."
Dr. Lacy is with the hematology division at the Mayo Clinic in Rochester, Minn.
SAN DIEGO – A provocative analysis suggests that a sequence of bortezomib and lenalidomide provides a better survival advantage than regimens with three or more agents in patients with multiple myeloma and high-risk cytogenetics.*
"While the limitations of this retrospective study limit drawing definitive conclusions, it appears that poor cytogenetics and biology trump treatment intensification," Dr. Rachid Baz and his colleagues stated in a poster presentation at the annual meeting of the American Society of Hematology.
The investigators reported on 208 patients with multiple myeloma who received bortezomib (Velcade) and lenalidomide (Revlimid), nonconcurrently between January 2004 and August 2010 at the H. Lee Moffitt Cancer Center and Research Institute in Tampa. The patients were stratified by treatment into six groups: lenalidomide with or without dexamethasone (lenalidomide A) or lenalidomide in combination with two or more agents (lenalidomide B); bortezomib with or with dexamethasone (bortezomib A) or bortezomib in combination with two or more agents (bortezomib B); and finally, only doublets or single agents (nonintensive therapy) or three or more agents in combination (intensive therapy).
No differences were observed between the lenalidomide A and B, bortezomib A and B, or intensive and nonintensive therapy groups in the baseline characteristics of age, International Staging System (ISS) and Durie/Salmon stage, beta2microglobulin or renal function, presence of poor-risk cytogenetics, and frequency of high-dose therapy.
Poor-risk cytogenetics, an increasingly fluid term in the context of growing success with novel myeloma agents, included deletions 13q and 17p, translocations, (4;14) and (14;16) or hypodiploidy.
Lenalidomide A patients had a trend toward improved median overall survival at 72 months, compared with 57 months for the lenalidomide B group receiving more complex regimens (P = .07), reported Dr. Baz, with Moffitt’s hematologic malignancies and experimental therapeutics departments.
Median overall survival, the study’s primary end point, however, was significantly improved in the bortezomib A group at 72 months vs. 45 months in the bortezomib B group (P = .02).
Similarly, the nonintensive therapy group lived significantly longer for 74 months vs. 57 months for the intensive therapy group (P = .03).
Notably, patients with high-risk cytogenetics had significantly worse survival if they received intensive therapy rather than nonintensive therapy (median 44 months vs. 72 months; P = .01), he noted. In contrast, patients without high-risk cytogenetics had similar overall survival regardless of whether they belonged to the intensive therapy or nonintensive therapy groups (median 76 months vs. 75 months).
On multivariate analysis that adjusted for known covariates linked to myeloma survival such as ISS stage and high-dose therapy, the only features predictive of poor outcome were renal failure at baseline and intensive therapy.
Dr. Baz said the investigators were surprised by the counterintuitive results and that they could be due to bias from an unidentified confounding factor. For example, it’s possible that high-risk patients who appeared more ill were more likely to be given more intensive therapy by the practicing physician and may have had poor outcomes nonetheless, whereas high-risk patients who appeared more stable were more likely to be given less intensive therapy, but did well because of more indolent disease characteristics.
A potential biologic explanation for the finding might be related to genomic instabilities more commonly seen in high-risk myeloma.
"Patients with high-risk disease have myeloma cells that are more likely to acquire drug resistance faster," he said in an interview. "As a result, if you expose those myeloma cells to many drugs at once, they may acquire resistance to them faster and you get less mileage than if you spread out the drugs."
Dr. Baz said further study at the molecular level is needed to see how drug resistance develops in myeloma in the context of combination therapy with three or four drugs versus treatment with one or two drugs.
"I think the finding is hypothesis generating," he said. "It doesn’t change my practice with the patients I see today, but it needs more study."
Baseline characteristics of the non-intensive and intensive therapy groups were: age (58.9 years, 58.5 years), heavy chain IgG (60%, 63%), light chain Kappa (58%, 67%), ISS stage II (40%, 38%), ISS III (24%, 33%), Durie/Salmon stage III (75%, 85%), creatinine at least 2.0 mg/dL (12%, 13%), presence of bone disease (67%, 80%), poor-risk cytogenetics (43%, 36%), prior high-dose therapy (64%, 66%), and thalidomide use (59%, 47%).
The only significant difference between two groups was the presence of more males in the intensive group (73% vs. 52%; P = .01).
Dr. Baz reported research funding from Celgene and membership on an entity’s board of directors or advisory committee and research funding from Millennium Pharmaceuticals. His coauthors reported similar relationships with Celgene, Millennium, Novartis, and Allergan.
*CLARIFICATION 1/23/12 The status of bortezomib and lenalidomide in treatment for multiple myeloma was clarified in this sentence.
SAN DIEGO – A provocative analysis suggests that a sequence of bortezomib and lenalidomide provides a better survival advantage than regimens with three or more agents in patients with multiple myeloma and high-risk cytogenetics.*
"While the limitations of this retrospective study limit drawing definitive conclusions, it appears that poor cytogenetics and biology trump treatment intensification," Dr. Rachid Baz and his colleagues stated in a poster presentation at the annual meeting of the American Society of Hematology.
The investigators reported on 208 patients with multiple myeloma who received bortezomib (Velcade) and lenalidomide (Revlimid), nonconcurrently between January 2004 and August 2010 at the H. Lee Moffitt Cancer Center and Research Institute in Tampa. The patients were stratified by treatment into six groups: lenalidomide with or without dexamethasone (lenalidomide A) or lenalidomide in combination with two or more agents (lenalidomide B); bortezomib with or with dexamethasone (bortezomib A) or bortezomib in combination with two or more agents (bortezomib B); and finally, only doublets or single agents (nonintensive therapy) or three or more agents in combination (intensive therapy).
No differences were observed between the lenalidomide A and B, bortezomib A and B, or intensive and nonintensive therapy groups in the baseline characteristics of age, International Staging System (ISS) and Durie/Salmon stage, beta2microglobulin or renal function, presence of poor-risk cytogenetics, and frequency of high-dose therapy.
Poor-risk cytogenetics, an increasingly fluid term in the context of growing success with novel myeloma agents, included deletions 13q and 17p, translocations, (4;14) and (14;16) or hypodiploidy.
Lenalidomide A patients had a trend toward improved median overall survival at 72 months, compared with 57 months for the lenalidomide B group receiving more complex regimens (P = .07), reported Dr. Baz, with Moffitt’s hematologic malignancies and experimental therapeutics departments.
Median overall survival, the study’s primary end point, however, was significantly improved in the bortezomib A group at 72 months vs. 45 months in the bortezomib B group (P = .02).
Similarly, the nonintensive therapy group lived significantly longer for 74 months vs. 57 months for the intensive therapy group (P = .03).
Notably, patients with high-risk cytogenetics had significantly worse survival if they received intensive therapy rather than nonintensive therapy (median 44 months vs. 72 months; P = .01), he noted. In contrast, patients without high-risk cytogenetics had similar overall survival regardless of whether they belonged to the intensive therapy or nonintensive therapy groups (median 76 months vs. 75 months).
On multivariate analysis that adjusted for known covariates linked to myeloma survival such as ISS stage and high-dose therapy, the only features predictive of poor outcome were renal failure at baseline and intensive therapy.
Dr. Baz said the investigators were surprised by the counterintuitive results and that they could be due to bias from an unidentified confounding factor. For example, it’s possible that high-risk patients who appeared more ill were more likely to be given more intensive therapy by the practicing physician and may have had poor outcomes nonetheless, whereas high-risk patients who appeared more stable were more likely to be given less intensive therapy, but did well because of more indolent disease characteristics.
A potential biologic explanation for the finding might be related to genomic instabilities more commonly seen in high-risk myeloma.
"Patients with high-risk disease have myeloma cells that are more likely to acquire drug resistance faster," he said in an interview. "As a result, if you expose those myeloma cells to many drugs at once, they may acquire resistance to them faster and you get less mileage than if you spread out the drugs."
Dr. Baz said further study at the molecular level is needed to see how drug resistance develops in myeloma in the context of combination therapy with three or four drugs versus treatment with one or two drugs.
"I think the finding is hypothesis generating," he said. "It doesn’t change my practice with the patients I see today, but it needs more study."
Baseline characteristics of the non-intensive and intensive therapy groups were: age (58.9 years, 58.5 years), heavy chain IgG (60%, 63%), light chain Kappa (58%, 67%), ISS stage II (40%, 38%), ISS III (24%, 33%), Durie/Salmon stage III (75%, 85%), creatinine at least 2.0 mg/dL (12%, 13%), presence of bone disease (67%, 80%), poor-risk cytogenetics (43%, 36%), prior high-dose therapy (64%, 66%), and thalidomide use (59%, 47%).
The only significant difference between two groups was the presence of more males in the intensive group (73% vs. 52%; P = .01).
Dr. Baz reported research funding from Celgene and membership on an entity’s board of directors or advisory committee and research funding from Millennium Pharmaceuticals. His coauthors reported similar relationships with Celgene, Millennium, Novartis, and Allergan.
*CLARIFICATION 1/23/12 The status of bortezomib and lenalidomide in treatment for multiple myeloma was clarified in this sentence.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF HEMATOLOGY
Major Finding: Patients with high-risk cytogenetics treated with intensive therapy had a median overall survival of 46 months vs. 71 months if treated with nonintensive therapy (P = .01).
Data Source: Retrospective analysis of 208 patients with multiple myeloma.
Disclosures: Dr. Baz reported research funding from Celgene and membership on an entity’s board of directors or advisory committee and research funding from Millennium Pharmaceuticals. His coauthors reported similar relationships with Celgene, Millennium, Novartis, and Allergan. Dr. Lacy reports research funding from Celgene.